
Impact of high levels of progesterone on α1-integrin distribution in the endometrium of patients...
8
Acta histochemica 110 (2008) 363—370 Impact of high levels of progesterone on a 1 -integrin distribution in the endometrium of patients with unexplained infertility Sevtap Kilic a, , Tahir Hatipoglu b , Deniz Erdogan b , Cigdem Elmas b , Beril Yuksel a , Nicel Tasdemir a , Nafiye Yilmaz a , Sertac Batioglu a a Department of Reproductive Endocrinology, Dr. Zekai Tahir Burak Women’s Health and Research Hospital, Su ¨leymanbey Sok. 29, 10 Maltepe, Ankara 06570, Turkey b Department of Histology and Embryology, Faculty of Medicine, Gazi University, Ankara, Turkey Received 10 July 2007; received in revised form 23 November 2007; accepted 28 November 2007 KEYWORDS Integrins; Adhesion molecules; Endometrium; Infertility; Ovarian stimulation; Estrogen; Progesterone Summary Irregular or low expression of integrins, which are cell adhesion molecules, may be associated with infertility. We conducted a prospective controlled study evaluating the effects of supraphysiological levels of estrogen and progesterone created by human menopausal gonadotropins (HMG) and progesterone support on a 1 -integrin immunolocalisation in the endometrium. Three groups were enrolled in the study. The first group of patients (group 1) had unexplained infertility and had been treated with HMG and progesterone (n ¼ 27). The second group of patients (group 2) was an untreated fertile group (n ¼ 24). The third group (group 3) consisted of patients who had unexplained infertility and had received no treatment (n ¼ 11). Endometrial biopsy specimens were taken from individuals from each group during the ovulation induction period. a 1 -integrin immunohistochemistry was performed. Serum estradiol and progesterone levels were also measured in parallel with histological dating of endometrial biopsies. Group 1 showed no statistical difference from group 2 in a 1 - integrin or histological dating. Group 3 showed less a 1 -integrin in the glandular epithelium in the secretory phase. We observed that a 1 -integrin was specific to the secretory phase. Its localization was denser in group 2 when compared with group 3, which supports the conclusion that a 1 -integrin may be a useful marker for luteal phase quality. Moreover, the supraphysiological estrogen and progesterone levels created by HMG and progesterone support may affect the a 1 -integrin in the endometrium in the secretory phase in the case of unexplained infertile patients. & 2007 Elsevier GmbH. All rights reserved. ARTICLE IN PRESS www.elsevier.de/acthis 0065-1281/$ - see front matter & 2007 Elsevier GmbH. All rights reserved. doi:10.1016/j.acthis.2007.11.008 Corresponding author. Tel.: +90 312 230 65 85; fax: +90 312 430 07 18. E-mail address: [email protected] (S. Kilic).
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Impact of high levels of progesterone on α1-integrin distribution in the endometrium of patients...
ARTICLE IN PRESS
Acta histochemica 110 (2008) 363—370
0065-1281/$ - sdoi:10.1016/j.
�CorrespondE-mail addr
www.elsevier.de/acthis
Impact of high levels of progesterone on a1-integrindistribution in the endometrium of patients withunexplained infertility
Sevtap Kilica,�, Tahir Hatipoglub, Deniz Erdoganb, Cigdem Elmasb,Beril Yuksela, Nicel Tasdemira, Nafiye Yilmaza, Sertac Batioglua
aDepartment of Reproductive Endocrinology, Dr. Zekai Tahir Burak Women’s Health and Research Hospital,Suleymanbey Sok. 29, 10 Maltepe, Ankara 06570, TurkeybDepartment of Histology and Embryology, Faculty of Medicine, Gazi University, Ankara, Turkey
Received 10 July 2007; received in revised form 23 November 2007; accepted 28 November 2007
KEYWORDSIntegrins;Adhesion molecules;Endometrium;Infertility;Ovarian stimulation;Estrogen;Progesterone
ee front matter & 2007acthis.2007.11.008
ing author. Tel.: +90 312ess: sevtapkilic@gmail.
SummaryIrregular or low expression of integrins, which are cell adhesion molecules, may beassociated with infertility. We conducted a prospective controlled study evaluatingthe effects of supraphysiological levels of estrogen and progesterone created byhuman menopausal gonadotropins (HMG) and progesterone support on a1-integrinimmunolocalisation in the endometrium. Three groups were enrolled in the study.The first group of patients (group 1) had unexplained infertility and had been treatedwith HMG and progesterone (n ¼ 27). The second group of patients (group 2) was anuntreated fertile group (n ¼ 24). The third group (group 3) consisted of patients whohad unexplained infertility and had received no treatment (n ¼ 11). Endometrialbiopsy specimens were taken from individuals from each group during the ovulationinduction period. a1-integrin immunohistochemistry was performed. Serum estradioland progesterone levels were also measured in parallel with histological dating ofendometrial biopsies. Group 1 showed no statistical difference from group 2 in a1-integrin or histological dating. Group 3 showed less a1-integrin in the glandularepithelium in the secretory phase. We observed that a1-integrin was specific to thesecretory phase. Its localization was denser in group 2 when compared with group 3,which supports the conclusion that a1-integrin may be a useful marker for lutealphase quality. Moreover, the supraphysiological estrogen and progesterone levelscreated by HMG and progesterone support may affect the a1-integrin in theendometrium in the secretory phase in the case of unexplained infertile patients.& 2007 Elsevier GmbH. All rights reserved.
Elsevier GmbH. All rights reserved.
230 65 85; fax: +90 312 430 07 18.com (S. Kilic).
ARTICLE IN PRESS
S. Kilic et al.364
Introduction Burak Women’s Health Research and Training
a and b integrins are cell surface glycoproteinsbelonging to the family of cell adhesion molecules(Williams et al., 1989). Various studies haverevealed the role and function of integrin mole-cules throughout the menstrual cycle (Lessey andArnold, 1998). Recently, our understanding ofendometrial physiology has advanced markedlyfollowing extensive research into the moleculesinvolved in its development and function. Severalphysiological signals expressed in the endometriumduring the luteal phase have been investigated,including secreted proteins, cell surface receptors,nuclear transcription factors and changes in cellsurface morphology (Ordi et al., 2003).
Proteins, including a1, a4, av and b3 integrins areexpressed in a cyclic manner in the human endome-trium according to the phase of the menstrual cycle(Damsky et al., 1993; Ilesanmi et al., 1993; Suther-land et al., 1988). Histological appearance ofendometrial tissue is not helpful in determiningthe luteal timing as important functional abnormal-ities may not be reflected in obvious morphologicalchanges (Lessey et al., 2000); however, changes inlevels of marker proteins may be detected in theluteal phase using immunohistochemistry. The ex-pression of a1-integrin, which is a progesterone-dependent molecule, occurs on days 15–28 of thecycle. Several drugs used for ovarian stimulationaffect levels of expression in the endometriumresulting in estrogen and progesterone synthesis atsupraphysiological levels.
The purpose of the study reported here was toinvestigate whether estrogen and progesterone atsupraphysiological levels change a1-integrin expres-sion in the endometrium in patients treated withhuman menopausal gonadotropins (HMG) and pro-gesterone. In addition, we compared traditionalhistological dating criteria of the endometrium intreated and untreated groups. For this purpose, a1-integrin immunolocalisation was studied compara-tively on endometrial tissue samples taken frominfertile patients treated with HMG and progester-one, untreated fertile patients with normal men-strual cycle in the control group, and untreatedpatients with unexplained infertility.
Patients and methods
Source of tissues
This was a prospective controlled study con-ducted in the infertility clinic of the Dr. Zekai Tahir
Hospital between October 2003 and May 2006.Approval for the protocol was received from theEthics Committee of the Dr. Zekai Tahir BurakWomen’s Health Research and Training Hospital andinformed consent was given by all patients.Patients with diagnosis of polycystic ovary syn-drome, endometriosis, hydrosalpinx and with folli-cle stimulating hormone levels above 10mIU/mlwere excluded from the study. All patients withunexplained infertility (n ¼ 38) were examinedwith ultrasonography, hysterosalpinography, semenanalysis, hormone profile and laparoscopy, toprovide the diagnosis. Group 1 (n ¼ 27) wascomposed of patients with unexplained infertilityand who had HMG and progesterone treatment;group 2 (n ¼ 24) was composed of healthy fertilewomen with regular menstrual cycles and withouttreatment. Group 3 (n ¼ 11) was composed ofpatients with unexplained infertility and who hadno treatment. None of the patients had chronicdiseases and none were taking any medication.
The patients in group 1 had ovarian stimulationinduced by HMG (Menogon, Ferring Germany), asfollows. When 2–3 follicles of X17mm diameterwere observed, 10,000 units of human chorionicgonadotropin (HCG) (Profasi, Serono, Istanbul,Turkey) were administered subcutaneously. 8%crinone vaginal gel (Sereno, Istanbul, Turkey) wasapplied daily to all patients vaginally for lutealsupport for 12 days after ovulation. Transvaginalultrasonographic evaluation of follicular growthwas performed using a 5MHz vaginal transducerattached to a General Electric Scanner (model logic200, Waukesha, WI, USA). The average folliculardiameter was measured in all patients. Two orthree endometrial biopsies were performed duringa single menstrual cycle in each patient. Ultra-sonographic monitoring of ovulation was per-formed. Ultrasonographic studies have shown thatthe accuracy of histological endometrial dating isbest determined when ovulation is detected by thismethod (Shoupe et al., 1989). Ovulation wasdetected when clear demarcation of the folliclewall disappeared. HCG was not administered to thefertile group, but was administered at a dose of10,000 units of HCG (Profasi, Serono, Istanbul,Turkey) when 2–3 follicles of X17mm diameterwere observed to the treated infertile group inorder to trigger ovulation. The first sample ofendometrial tissue was taken from the front wall ofuterine fundus by pipelle (Ori, endometrial sam-pler, Orifice Medical AB, Ystand, Sweden) on days1–3 or days 9–12 of the menstrual bleeding of 27patients treated with HMG. The other samples weretaken from the back wall of the uterine fundus.
ARTICLE IN PRESS
Progesterone and a1-integrin in endometrium 365
Luteal phase endometrial samples were taken onday 7 post-ovulation from all groups. Forty en-dometrial samples from group 1, 40 endometrialsamples from group 2 and 18 endometrial samplesfrom group 3 were investigated. Due to the factthat some patients rejected sampling as toopainful; only two endometrial samples were takenfrom some patients. Table 1 summarizes the biopsytiming and numbers for the study group and thecontrol groups. Table 2 gives body-mass indices(BMI) and ages of patients.
Immunohistochemical method
All endometrial tissues were fixed for 72 h in 10%neutral buffered formalin. The tissues were sub-jected to routine histological processing andembedded in paraffin wax (Shadon, Pittsburg,USA). 4 mm thick sections were cut, mounted onpolylysine-coated sides (Menzel-Glaser, Braunsch-weig, Germany) and incubated overnight at 37 1Cthen for 1 h at 60 1C. Wax was removed with twochanges of xylene (15min each). The slides werethen placed in 96% ethanol and 80% ethanol for10min each, followed by two 5min changes ofdistilled water. Sections were boiled in a 650Wmicrowave oven in 10% 1M citrate buffer for
Table 1. Biopsy timing and number of endometrialsamples for control and study groups (n ¼ total numberof endometrial samples)
Biopsy (day) Group 1(n ¼ 40)
Group 2(n ¼ 40)
Group 3(n ¼ 18)
Days 1–3 7 9 0Days 9–12 13 12 7Day 7 post-ovulation 20 19 11
In group 1, samples were taken from five patients on days 1–3,from two patients on days 9–10 days of the menstrual cycle,from seven patients on post-ovulation day 7, from two patientsboth on days 1–3 and post-ovulation day 7, from 11 patients bothon days 9–12 and on post-ovulation day 7. In group 2, we tooksamples from three patients on days 1–3, from two patients ondays 9–10 of cycle, from three patients on post-ovulation day 7,from six patients both on days 1–3 days and post-ovulation day 7,from 10 patients both on days 9–12 and on post-ovulation day 7.In group 3, we took samples from four patients on post-ovulationday 7, and from seven patients both on days 9–12 and on post-ovulation day 7.
Table 2. Characteristics of control and study groups
Group 1
Age in years (range) 35 (29–39)Body-mass index (kg/m2) 25.573.90
�p-value o0.05 is significant.
20min. They were allowed to cool at roomtemperature for 20min and then tissues werecircumscribed with a hydrophobic pen. After wash-ing with distilled water and phosphate-bufferedsaline (PBS), 1.5% hydrogen peroxide was addeddropwise. Ultra V block (Labvision Corporation, SanFrancisco, CA, USA) was applied for 20min.Sections were then incubated with a 1:50 dilutionof rabbit polyclonal a1-integrin primary antibody(Lot 2091400501 Quartett, Immunodiagnostica andBiotechnologica GmbH, Berlin, Germany) in block-ing serum Ultra V block (Labvision Corporation, SanFrancisco, CA, USA), for 1 h. Sections were thenincubated with biotinylated goat anti-rabbit (Lot300402630 Quartett, Immunodiagnostica and Bio-technologica GmbH, Berlin, Germany), suppliedready to use, for 25 min. Slides were then exposedto a 1:300 dilution of streptavidin peroxidase (LotSHR 70731 Labvision Corporation, San Francisco,CA, USA), for 20min. Labeling was revealed byincubation with 30,3 diaminobenzidine (DAB), (Lab-vision Corp., San Francisco, CA, USA, one tabletdissolved in 20ml PBS/5% 0.3 H2O2 and used fresh)for 10min. All dilutions and thorough washesbetween steps were performed using PBS unlessotherwise specified. Finally, the section was coun-terstained with Mayer’s hematoxylin for 5min.Then sections were dehydrated through a gradedseries of ethanol, cleared with xylol and mountedwith Entellan (Merck, Darmstadt, Germany). Nega-tive controls were performed exactly as describedabove except that incubation with the primaryantibody was omitted.
Histological dating of endometrium was evalu-ated according to histopathological criteria ofNoyes et al. (1975).
All slides were evaluated using an Olympus BH-2photomicroscope (Olympus Corp., Hamburg, Ger-many). The following semi-quantitative scoringsystem was used to assess the immunolabelingintensity: (1) weak, (2) moderate and (3) stronglabeling. Two independent observers who wereblind to the treatment protocol performed theimmunolabeling score evaluations independently.The HSCORE was calculated using the followingequation: HSCORE ¼ _Pi(i+1), where i is the in-tensity of labeling with a value of 1, 2 or 3 and Pi isthe percentage of labeled epithelial and stromal
Group 2 Group 3 p�
34 (26–39) 32 (26–38) 0.09726.773.71 26.872.44 0.375
ARTICLE IN PRESS
S. Kilic et al.366
cells for each intensity, varying from 0% to 100%(McCarty et al., 1985). Results were expressed asthe mean7SD.
Hormone assay
Serum hormone levels were measured usingcommercially available kits. Estradiol and proges-terone were measured by an electrochemicalluminassay (ECL) technique (Roche, E 170 ELECSYS,Mannheim, Germany). The analysis sensitivity ofassay for estradiol was 5 pg/ml and linear intervalof test was 5.00–4300 pg/ml. The analysis sensitiv-ity of assay for progesterone was 0.03 ng/ml andlinear interval of the test was 0.03–60 ng/ml.
Statistical analysis
Data were analyzed using SPSS statistical soft-ware (Release 11.0, SPSS Inc., Chicago, IL, USA).The Kruskal–Wallis test was used to compare thethree groups. Mann–Whitney U test was used forthe comparison of two groups. Repeated measureswere evaluated by using the Friedman test withingroups. When p-values from Friedman test statis-tics were statistically significant, multiple compar-ison tests were used to determine which frequencyband differed from the others. A p-value o0.05was considered statistically significant.
Results
All patients included in our study were ovulatoryaccording to ultrasonographic criteria. Post-ovula-tory day 7 serum progestin levels of all patientswere above 10 ng/ml. In total, 98 specimens werestudied. No inflammatory or reactive changesrelated to the initial sampling were detected inany specimen.
Table 3. Hormonal values of control and study groups
1st measurement
Estradiol (pg/ml)Group 1 3379.0Group 2 28713Group 3 31.478.5p 0.076
Progesterone (ng/ml)Group 1 0.570.1Group 2 0.470.13�
Group 3 0.3570.17�
p o0.001
�Difference between study and control groups were significant (po0
Serum estradiol and progesterone concentrationsfor group 1 were compared with groups 2 and 3 forthe same days of endometrial sampling (Table 3).No significant differences between groups wereobserved for age, BMI, days 1–3 estradiol levels anddays 9–12 progesterone levels. A statisticallysignificant difference in days 1–3 and post-ovula-tory day 7 progesterone levels was observed(po0.001 for both). A statistically significantdifference between days 9 and 12 and post-ovulatory day 7 estradiol levels (po0.001 for both)was also noted (Table 3).
Forty endometrial specimens from group 1, 40endometrial specimens from group 2 and 18endometrial specimens from group 3 were takenin proliferative and secretory phases. Histologicalassessment of samples of proliferative endometrialtissue from all groups revealed normal structuralappearance of the surface and gland epithelium(GE). The endometrial stroma between the glandswas clear and normal. No a1-integrin labeling wasdetected in the GE and stroma of the three groupsin the proliferative phase (p ¼ 0.867, p ¼ 0.824).These observations are illustrated in Figures 1a–c.
When the secretory endometrium was investi-gated, apparent differences in a1-integrin immu-nolabeling among the groups (Figures 1d–f) werenoted. The semi-quantitative data and Hscorevalues are shown in Table 4. Stromal and glandularimmunoreactivity in group 3 was less than the othertwo groups in the secretory phase (Figures 1d–f).GE and stroma of secretory endometrium in group 1showed weak positive immunolabeling (Figure 1d).The most intense labeling was observed in groups 1and 2 (Figures 1d and f).
When group 1 was compared with group 3 andgroup 2 was compared with group 3, the differ-ences were statistically significant (Table 4). Thea1-integrin immunoreactivity in the stroma insecretory phase in group 3 did not differ from
2nd measurement 3rd measurement
15287228 9267103336724� 213733�
357.0729.8� 223.2725.7�
o0.001 o0.001
0.970.2 48.2713.11.070.1 16.375.0�
1.070.1 17.876.4�
0.100 o0.001
.001).
ARTICLE IN PRESS
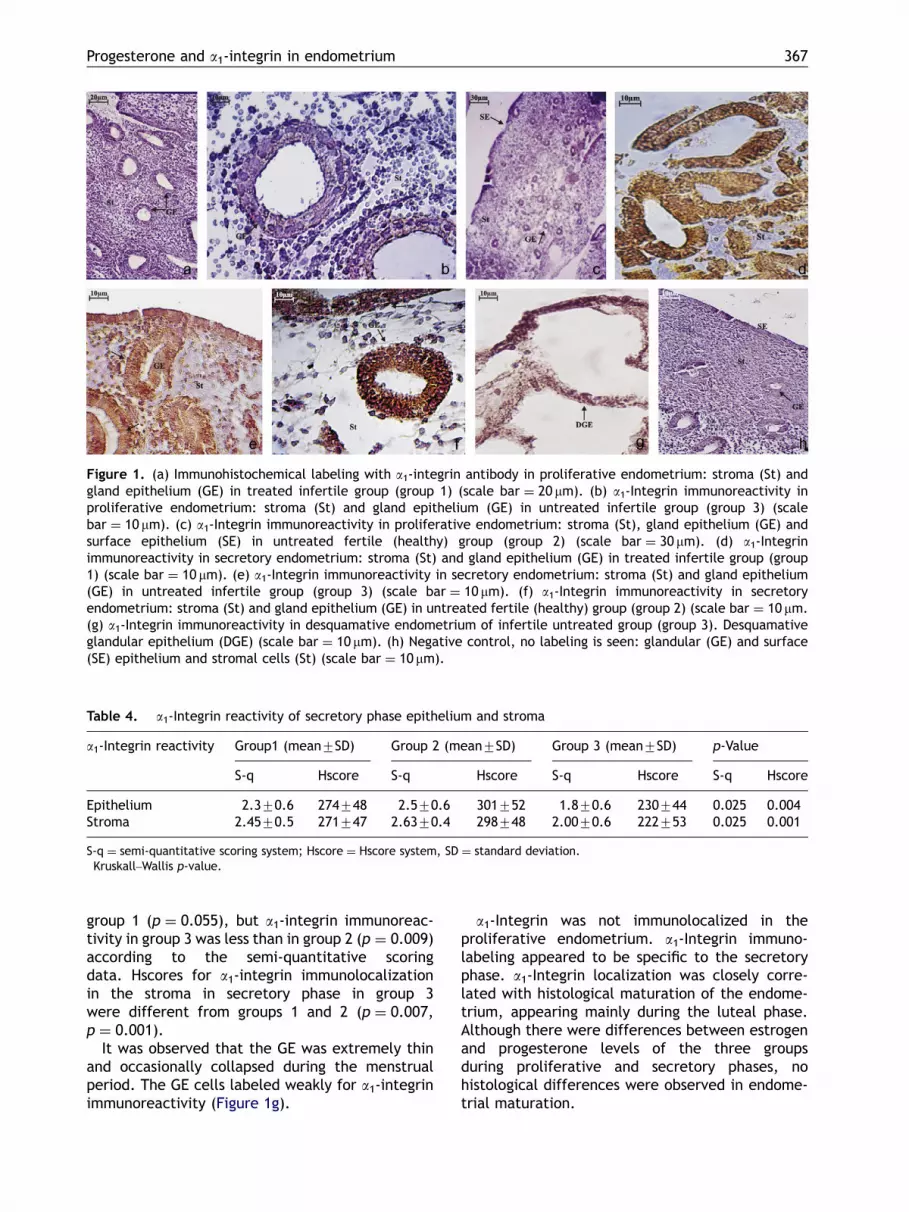
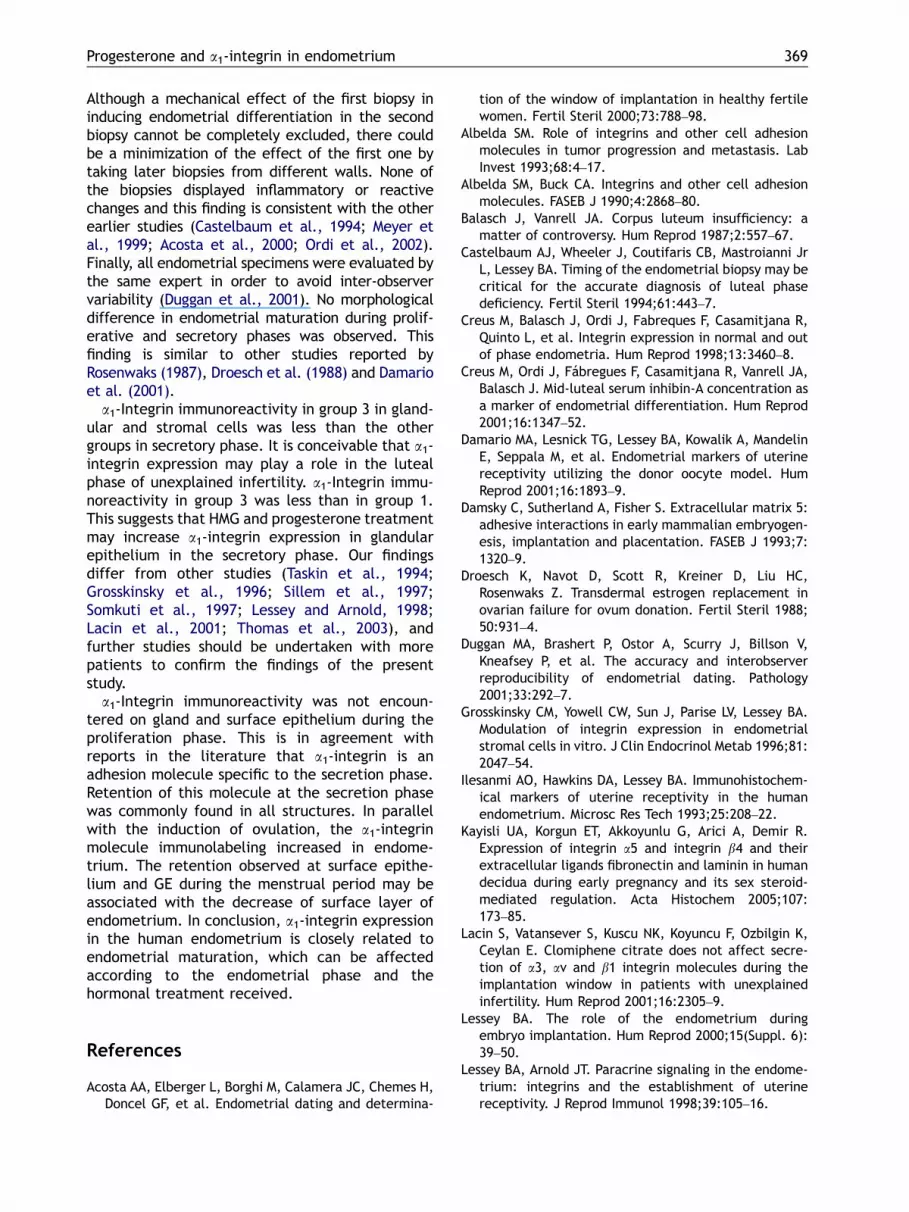
Figure 1. (a) Immunohistochemical labeling with a1-integrin antibody in proliferative endometrium: stroma (St) andgland epithelium (GE) in treated infertile group (group 1) (scale bar ¼ 20 mm). (b) a1-Integrin immunoreactivity inproliferative endometrium: stroma (St) and gland epithelium (GE) in untreated infertile group (group 3) (scalebar ¼ 10 mm). (c) a1-Integrin immunoreactivity in proliferative endometrium: stroma (St), gland epithelium (GE) andsurface epithelium (SE) in untreated fertile (healthy) group (group 2) (scale bar ¼ 30 mm). (d) a1-Integrinimmunoreactivity in secretory endometrium: stroma (St) and gland epithelium (GE) in treated infertile group (group1) (scale bar ¼ 10 mm). (e) a1-Integrin immunoreactivity in secretory endometrium: stroma (St) and gland epithelium(GE) in untreated infertile group (group 3) (scale bar ¼ 10 mm). (f) a1-Integrin immunoreactivity in secretoryendometrium: stroma (St) and gland epithelium (GE) in untreated fertile (healthy) group (group 2) (scale bar ¼ 10 mm.(g) a1-Integrin immunoreactivity in desquamative endometrium of infertile untreated group (group 3). Desquamativeglandular epithelium (DGE) (scale bar ¼ 10 mm). (h) Negative control, no labeling is seen: glandular (GE) and surface(SE) epithelium and stromal cells (St) (scale bar ¼ 10 mm).
Table 4. a1-Integrin reactivity of secretory phase epithelium and stroma
a1-Integrin reactivity Group1 (mean7SD) Group 2 (mean7SD) Group 3 (mean7SD) p-Value�
S-q Hscore S-q Hscore S-q Hscore S-q Hscore
Epithelium 2.370.6 274748 2.570.6 301752 1.870.6 230744 0.025 0.004Stroma 2.4570.5 271747 2.6370.4 298748 2.0070.6 222753 0.025 0.001
S-q ¼ semi-quantitative scoring system; Hscore ¼ Hscore system, SD ¼ standard deviation.�Kruskall–Wallis p-value.
Progesterone and a1-integrin in endometrium 367
group 1 (p ¼ 0.055), but a1-integrin immunoreac-tivity in group 3 was less than in group 2 (p ¼ 0.009)according to the semi-quantitative scoringdata. Hscores for a1-integrin immunolocalizationin the stroma in secretory phase in group 3were different from groups 1 and 2 (p ¼ 0.007,p ¼ 0.001).
It was observed that the GE was extremely thinand occasionally collapsed during the menstrualperiod. The GE cells labeled weakly for a1-integrinimmunoreactivity (Figure 1g).
a1-Integrin was not immunolocalized in theproliferative endometrium. a1-Integrin immuno-labeling appeared to be specific to the secretoryphase. a1-Integrin localization was closely corre-lated with histological maturation of the endome-trium, appearing mainly during the luteal phase.Although there were differences between estrogenand progesterone levels of the three groupsduring proliferative and secretory phases, nohistological differences were observed in endome-trial maturation.

ARTICLE IN PRESS
S. Kilic et al.368
Discussion
Integrins belong to the family of cell adhesionmolecules and play widespread roles in physiologicalevents including: embryogenesis, wound healing,immune responses and behavior of malignancies(Albelda and Buck, 1990; Albelda, 1993). Manystudies have used immunohistochemical methods toinvestigate the cyclic changes in the endometrium(Lessey et al., 1992; Ordi et al., 2003; Ilesanmi et al.,1993; Tabibzadeh, 1991). Extracellular matrix com-ponents such as integrins may promote embryoattachment (Lessey, 2000). Kayisli et al. (2005) foundthat sex hormones regulate extracellular matrixremodeling and integrin switching mechanisms,which may play role in implantation. Lessey et al.(1994, 1996, 2000), in their studies of humanendometrium, found that a1, a4 and b3-integrinshad weak retention during the proliferation period inthe GE and stroma; however, the retention becamedenser during the secretory period and cyclicchanges of the retention of a1, a4 and b3-integrinsin the gland tissue were apparent. The abnormalrelease of some integrins, which change cyclically ininfertile patients may be significant (Lessey et al.,1992, 1995; Meyer et al., 1997).
The most important function of corpora lutea isprogesterone secretion. The clinical concept ofluteal phase insufficiency presumes that sub-threshold progesterone stimulation of the uterusmay cause failure of endometrial development.How different serum progesterone levels affect theendometrium is still open to debate. Histologicaldelay can be presented at physiological or supra-physiological progesterone levels. Few previousprospective studies have investigated hormonaleffects on the expression of integrins in the humanendometrium.
Histology may not be a good method to deter-mine the timing of the luteal phase. Importantfunctional abnormalities may not be reflected inobvious morphological changes (Lessey et al., 2000;Noyes et al., 1975; Duggan et al., 2001). It isconceivable that a histologically normal appear-ance may conceal an endometrium with inadequateintegrin expression and this may be influencingendometrial function.
Integrin molecules are among the importantparameters in endometrial retention, though theseshow variable dynamics and cyclical distributionand changes may be induced as a result oftreatment with steroid preparations, gonadotropinsand chlomiphene molecules used externally. Otherfactors that may affect integrin release may beparacrine and endocrine molecules. Some studiesexamined integrin distribution in endometrial cells
in vitro, though no changes in integrin release werefound in such endometrial cells after addition ofestrogen, progesterone, diethylstilbesterol, pro-megesterone. Consequently, it was considered thatintegrin release was dominantly regulated bycytokines and growth factors, and decidual forma-tion might be regulated by steroid hormones(Grosskinsky et al., 1996; Sillem et al., 1997).
Previous studies by several groups have alsoshown no relationship between the expression ofendometrial integrins and the expression of estro-gen and progesterone receptors in the humanendometrium or in serum levels of ovarian steroids.Despite some studies which argue that integrinexpression does not vary with externally adminis-tered steroids, the study by Lessey and Arnold(1998) noted in particular that avb3 integrinincreased with externally administered estrogenand progesterone during the implantation windowphase.
It has been reported that gland-stromal desyn-chronization does not change in the endometriumin the same group treatment (Rosenwaks, 1987;Lessey and Arnold, 1998; Droesch et al., 1988;Damario et al., 2001). However, in some studies,the avb3 expression decreased in patients who weresubject to ovulation induction. It has been arguedthat supraphysiological levels of estrogen maydisrupt the harmony of stromal and gland structure(Balasch and Vanrell, 1987; Creus et al., 1998,2001; Somkuti et al., 1997; Meyer et al., 1999).Thomas et al. (2003), examined the a1b1, a4b1, avb3release, which is cyclic and specific to the lutealphase on day 6 following ovulation in the patientswho used gonadotropins for in vitro fertilization(IVF) purposes, and demonstrated that these threeintegrins decreased in GE in patients who haddonated oocytes. This may have been due to thesupraphysiological levels of estrogen.
Lacin et al. (2001), differing from Meyer et al.(1997) and Thomas et al. (2003), administeredchlomiphene citrate, oral contraceptive, estrogenor progesterone to patients, and reported thatthere was no change in integrin secretion despitethe decrease in endometrial thickness (Taskin et al.,1994). These various studies showed that during theluteal phase there are many different resultsregarding different integrin molecules.
Our study was a prospective and controlled studydesign where patients were investigated duringstimulated cycles with HMG and progesterone sup-port. One of the control groups (group 2) wasinvestigated during spontaneous cycles. An averageof two endometrial biopsies was taken during a singlemenstrual cycle from each woman. It could beargued that this might have affected the results.
ARTICLE IN PRESS
Progesterone and a1-integrin in endometrium 369
Although a mechanical effect of the first biopsy ininducing endometrial differentiation in the secondbiopsy cannot be completely excluded, there couldbe a minimization of the effect of the first one bytaking later biopsies from different walls. None ofthe biopsies displayed inflammatory or reactivechanges and this finding is consistent with the otherearlier studies (Castelbaum et al., 1994; Meyer etal., 1999; Acosta et al., 2000; Ordi et al., 2002).Finally, all endometrial specimens were evaluated bythe same expert in order to avoid inter-observervariability (Duggan et al., 2001). No morphologicaldifference in endometrial maturation during prolif-erative and secretory phases was observed. Thisfinding is similar to other studies reported byRosenwaks (1987), Droesch et al. (1988) and Damarioet al. (2001).
a1-Integrin immunoreactivity in group 3 in gland-ular and stromal cells was less than the othergroups in secretory phase. It is conceivable that a1-integrin expression may play a role in the lutealphase of unexplained infertility. a1-Integrin immu-noreactivity in group 3 was less than in group 1.This suggests that HMG and progesterone treatmentmay increase a1-integrin expression in glandularepithelium in the secretory phase. Our findingsdiffer from other studies (Taskin et al., 1994;Grosskinsky et al., 1996; Sillem et al., 1997;Somkuti et al., 1997; Lessey and Arnold, 1998;Lacin et al., 2001; Thomas et al., 2003), andfurther studies should be undertaken with morepatients to confirm the findings of the presentstudy.
a1-Integrin immunoreactivity was not encoun-tered on gland and surface epithelium during theproliferation phase. This is in agreement withreports in the literature that a1-integrin is anadhesion molecule specific to the secretion phase.Retention of this molecule at the secretion phasewas commonly found in all structures. In parallelwith the induction of ovulation, the a1-integrinmolecule immunolabeling increased in endome-trium. The retention observed at surface epithe-lium and GE during the menstrual period may beassociated with the decrease of surface layer ofendometrium. In conclusion, a1-integrin expressionin the human endometrium is closely related toendometrial maturation, which can be affectedaccording to the endometrial phase and thehormonal treatment received.
References
Acosta AA, Elberger L, Borghi M, Calamera JC, Chemes H,Doncel GF, et al. Endometrial dating and determina-
tion of the window of implantation in healthy fertilewomen. Fertil Steril 2000;73:788–98.
Albelda SM. Role of integrins and other cell adhesionmolecules in tumor progression and metastasis. LabInvest 1993;68:4–17.
Albelda SM, Buck CA. Integrins and other cell adhesionmolecules. FASEB J 1990;4:2868–80.
Balasch J, Vanrell JA. Corpus luteum insufficiency: amatter of controversy. Hum Reprod 1987;2:557–67.
Castelbaum AJ, Wheeler J, Coutifaris CB, Mastroianni JrL, Lessey BA. Timing of the endometrial biopsy may becritical for the accurate diagnosis of luteal phasedeficiency. Fertil Steril 1994;61:443–7.
Creus M, Balasch J, Ordi J, Fabreques F, Casamitjana R,Quinto L, et al. Integrin expression in normal and outof phase endometria. Hum Reprod 1998;13:3460–8.
Creus M, Ordi J, Fabregues F, Casamitjana R, Vanrell JA,Balasch J. Mid-luteal serum inhibin-A concentration asa marker of endometrial differentiation. Hum Reprod2001;16:1347–52.
Damario MA, Lesnick TG, Lessey BA, Kowalik A, MandelinE, Seppala M, et al. Endometrial markers of uterinereceptivity utilizing the donor oocyte model. HumReprod 2001;16:1893–9.
Damsky C, Sutherland A, Fisher S. Extracellular matrix 5:adhesive interactions in early mammalian embryogen-esis, implantation and placentation. FASEB J 1993;7:1320–9.
Droesch K, Navot D, Scott R, Kreiner D, Liu HC,Rosenwaks Z. Transdermal estrogen replacement inovarian failure for ovum donation. Fertil Steril 1988;50:931–4.
Duggan MA, Brashert P, Ostor A, Scurry J, Billson V,Kneafsey P, et al. The accuracy and interobserverreproducibility of endometrial dating. Pathology2001;33:292–7.
Grosskinsky CM, Yowell CW, Sun J, Parise LV, Lessey BA.Modulation of integrin expression in endometrialstromal cells in vitro. J Clin Endocrinol Metab 1996;81:2047–54.
Ilesanmi AO, Hawkins DA, Lessey BA. Immunohistochem-ical markers of uterine receptivity in the humanendometrium. Microsc Res Tech 1993;25:208–22.
Kayisli UA, Korgun ET, Akkoyunlu G, Arici A, Demir R.Expression of integrin a5 and integrin b4 and theirextracellular ligands fibronectin and laminin in humandecidua during early pregnancy and its sex steroid-mediated regulation. Acta Histochem 2005;107:173–85.
Lacin S, Vatansever S, Kuscu NK, Koyuncu F, Ozbilgin K,Ceylan E. Clomiphene citrate does not affect secre-tion of a3, av and b1 integrin molecules during theimplantation window in patients with unexplainedinfertility. Hum Reprod 2001;16:2305–9.
Lessey BA. The role of the endometrium duringembryo implantation. Hum Reprod 2000;15(Suppl. 6):39–50.
Lessey BA, Arnold JT. Paracrine signaling in the endome-trium: integrins and the establishment of uterinereceptivity. J Reprod Immunol 1998;39:105–16.

ARTICLE IN PRESS
S. Kilic et al.370
Lessey BA, Damjanovich L, Coutifaris C, Castelbaum A,Albelda SM, Buck CA. Integrin adhesion molecules inthe human endometrium. Correlation with the normaland abnormal menstrual cycle. J Clin Invest 1992;90:188–95.
Lessey BA, Castelbaum AJ, Buck CA, Lei Y, Yowell CW, SunJ. Further characterization of endometrial integrinsduring the menstrual cycle and in pregnancy. FertilSteril 1994;62:497–506.
Lessey BA, Castelbaum AJ, Sawin SW, Sun J. Integrins asmarkers of uterine receptivity in women with un-explained infertility. Fertil Steril 1995;63:535–42.
Lessey BA, Yeh I, Castelbaum AJ, Fritz MA, Ilesanmi AO,Korzeniowski P, et al. Endometrial progesteronereceptors and markers of uterine receptivity in thewindow of implantation. Fertil Steril 1996;65:477–83.
Lessey BA, Castelbaum AJ, Wolf L, Greene W, Paulson M,Meyer WR, et al. Use of integrins to date theendometrium. Fertil Steril 2000;73:779–87.
McCarty Jr KS, Miller LS, Cox EB, Konrath J, McCarty SrKS. Estrogen receptor analyses. Correlation of bio-chemical and immunohistochemical methods usingmonoclonal antireceptor antibodies. Arch Pathol LabMed 1985;109:716–21.
Meyer WR, Castelbaum AJ, Somkuti S, Sagoskin AW, DoyleM, Harris JE, et al. Hydrosalpinges adversely affectmarkers of endometrial receptivity. Hum Reprod 1997;12:1393–8.
Meyer WR, Novotny DB, Fritz MA, Beyler SA, Wolf LJ,Lessey BA. Effect of exogenous gonadotropins onendometrial maturation in oocyte donors. Fertil Steril1999;71(1):109–14.
Noyes RW, Hertig AT, Rock J. Dating the endometrialbiopsy. Am J Obstet Gynecol 1975;122:262–3.
Ordi J, Creus M, Ferrer B, Fabregues F, Carmona F,Casamitjana R, et al. Midluteal endometrial biopsyand avb3 integrin expression in the evaluation of theendometrium in infertility: implications for fecundity.Int J Gynecol Pathol 2002;21:231–8.
Ordi J, Creus M, Quinto L, Casamitjana R, Cardesa A,Balasch J. Within-subject between cycle variability ofhistological dating, alpha v beta 3 integrin expressionand pinopod formation in the human endometrium.J Clin Endocrinol Metab 2003;88:2119–25.
Rosenwaks Z. Donor eggs: their application in modernreproductive technologies. Fertil Steril 1987;47:895–909.
Shoupe D, Mishell Jr DR, Lacarra M, Lobo RA, HorensteinJ, d’Ablaing G, et al. Correlation of endometrialmaturation with four methods of estimating day ofovulation. Obstet Gynecol 1989;73:88–92.
Sillem M, Prifti S, Schmidt M, Rabe T, Runnebaum B.Endometrial integrin expression is independent ofestrogen or progestin treatment in vitro. Fertil Steril1997;67(5):877–82.
Somkuti SG, Yuan L, Fritz MA, Lessey BA. Epidermalgrowth factor and sex steroids dynamically regulate amarker of endometrial receptivity in Ishikawa cells.J Clin Endocrinol Metab 1997;82(7):2192–7.
Sutherland AE, Calarco PG, Damsky CH. Expression andfunction of cell surface extracellular matrix receptorsin mouse blastocyst attachment and outgrowth. J CellBiol 1988;106:1331–48.
Tabibzadeh S. Human endometrium: an active site ofcytokine production and action. Endocr Rev 1991;12:272–90.
Taskin O, Brown RW, Young DC, Poindexter AN, Wiehle RD.High doses of oral contraceptives do not alterendometrial a1 and avb3 integrins in the lateimplantation window. Fertil Steril 1994;61:850–5.
Thomas K, Thomson A, Wood S, Kingsland C, Vince G,Lewis-Jones I. Endometrial integrin expression inwomen undergoing in vitro fertilization and theassociation with subsequent treatment outcome.Fertil Steril 2003;80:502–7.
Williams PL, Warwick R, Dyson M, Bannister LH. Gray’sanatomy. London/New York: Churchill Livingstone;1989.




















