The chemical form of metallic debris in tissues surrounding metal-on-metal hips with unexplained...
9
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright
Transcript of The chemical form of metallic debris in tissues surrounding metal-on-metal hips with unexplained...
This article appeared in a journal published by Elsevier. The attached
copy is furnished to the author for internal non-commercial research
and education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling or
licensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of the
article (e.g. in Word or Tex form) to their personal website or
institutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies are
encouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
The chemical form of metallic debris in tissues surrounding metal-on-metalhips with unexplained failure
Alister J. Hart a,*, Paul D. Quinn b, Barry Sampson c, Ann Sandison d, Kirk D. Atkinson e, John A. Skinner f,Jonathan J. Powell g, J. Fred W. Mosselmans b
aDepartment of Orthopaedic Surgery, Imperial College and Imperial College Healthcare NHS Trust, Charing Cross Hospital Campus, Fulham Palace Road, London W6 8RF, UKb Science Division, Diamond Light Source, Harwell Science and Innovation Campus, Didcot, Oxon OX11 0DE, UKcDepartment of Clinical Chemistry, Imperial College and Imperial College Healthcare NHS Trust, Charing Cross Hospital Campus, Fulham Palace Road, London W6 8RF, UKdDepartment of Histopathology, Imperial College Healthcare NHS Trust, Charing Cross Hospital Campus, Fulham Palace Road, London W6 8RF, UKeNuclear Department, Defence Academy College of Management and Technology, HMS Sultan, Military Road, Gosport PO12 3BY, UKfDepartment of Orthopaedics, Royal National Orthopaedic Hospital, Stanmore HA7 4LP, UKgMedical Research Council Human Nutrition Research Centre, Cambridge CB1 9NL, UK
a r t i c l e i n f o
Article history:Received 2 March 2010Received in revised form 2 June 2010Accepted 7 June 2010Available online 10 June 2010
Keywords:Metal ion toxicityHip arthroplastyElectron beamCorrosion productWear debris
a b s t r a c t
Implant-derived material from metal-on-metal (MOM) hip arthroplasties may be responsible for anunexplained tissue inflammatory response. The chemical form of the metal species in the tissues is pre-dominantly chromium (Cr), but the currently used techniques have not been able to determine whetherthis is Cr(III) phosphate or Cr(III) oxide. The analytical challenge must overcome the fact that the metal inthe tissues is at a relatively low concentration and tissue preparation or the microscopy beam used canaffect the results. Microfocus X-ray spectroscopy using a synchrotron beam is useful in addressing boththese issues. Using this technique we compared tissue from failed MOM hips with: (1) tissue from metal-on-polyethylene (MOP) hips; (2) chemical standards; (3) metal discs cut from MOM hips. The most abun-dant implant-related species in all MOM hip tissues contained Cr. Comparison with standards revealedthe chemical form was Cr(III) phosphate, which did not vary with manufacturer type (four types ana-lysed) or level of blood metal ions. Cobalt (Co) and molybdenum (Mo) were occasionally present in areasof high Cr. Co was normally found in a metallic state in the tissue, while Mo was found in an oxidizedstate. The variety of metallic species may have arisen from corrosion, wear or a combination of both.No evidence of Cr(VI) was seen in the tissues examined.
! 2010 Acta Materialia Inc. Published by Elsevier Ltd. All rights reserved.
1. Introduction
Metal-on-metal (MOM) hip arthroplasty now represent 35% ofall hip arthroplasties performed per annum in the USA [1]. Recentreports found unexplained periprosthetic soft tissue reactions [2]and systemic genotoxicity [3] in patients with MOM hips. The com-monestmode of failure ofMOMhips is unexplained (43% of failures)according to theUKNational Joint Registry. This is in contrast tome-tal-on-polyethylene (MOP) hips, where the commonest mode offailure is aseptic loosening. MOM hip replacements have beenshown to work well in the medium term [4], even for highly activepatients. However, sometimes the device has to be removed due topoor biocompatibility, at a rate ranging between 1% and 10% [5,6]depending on the type of prosthesis. A better understanding of themechanism of poor biocompatibility may help surgeons select the
longest lasting device for each patient and engineers to design im-plants with improved human biocompatibility. Biocompatibilitycan de defined as the ability of a material to performwith an appro-priate host response in a specific application [7]. In one type ofMOMhip the inflammatory changeswere so severe [8] that the devicewaswithdrawn from the UK healthcare market by the Medicines andHealthcare Products Regulatory Agency [9].
Histological investigations have shown that irrespective of thefailure mode there are commonly seen scattered fine black parti-cles that are associated with macrophages in superficial and deeptissue [10]. However, there is confusion as to what these particlesare; Mahendra et al. [10] referred to them as cobalt (Co)–chro-mium (Cr) metal particles and aggregates. The properties of wearand corrosion products from ASTM F75 Co–Cr–Mo orthopaedic im-plants have been studied for some years [11,12] and it has gener-ally been found that the wear debris and corrosion products in thetissue are abundant in Cr, however, relatively few studies haveinvestigated the metal speciation of the debris.
1742-7061/$ - see front matter ! 2010 Acta Materialia Inc. Published by Elsevier Ltd. All rights reserved.doi:10.1016/j.actbio.2010.06.006
* Corresponding author. Tel./fax: +44 2088467332.E-mail address: [email protected] (A.J. Hart).
Acta Biomaterialia 6 (2010) 4439–4446
Contents lists available at ScienceDirect
Acta Biomaterialia
journal homepage: www.elsevier .com/locate /actabiomat

Author's personal copy
There are six reports that investigated the chemical speciationof implant-derived metallic species in human periprosthetic tis-sues. These are summarized in Table 1. All of these studies usedformalin-preserved tissue. Synchrotron analysis was used in onlyone of these reports, investigating tissue from a single MOP hip[13]. Only two of these studies investigated tissues fromMOM hipsand neither were able to match spectra from the tissue with metalcontrols. These two studies disagree with the speciation of themain metallic species found: Huber et al. found Cr phosphate[14] and Catelas et al. found Cr oxide [15]. Characterization of im-plant-derived metallic species that are present in the tissues sur-rounding these hips in humans is a logical first step inunderstanding their biocompatibility. This can be in terms of phys-ical (i.e. particulate or soluble) and chemical (valence state andother atoms bound) forms.
These previous analyses relied on combinations of techniques,such as energy dispersive X-ray spectroscopy (EDX) and Fouriertransform infrared spectroscopy. These can give either stoichiome-tric or chemical information, but not both simultaneously orunambiguous chemical species determination. To determine thespeciation of these particles we used microfocus X-ray spectros-copy. This is a method that can determine both the valence stateand the chemical structure of nano- and microscale materialswithin tissue specimens. It uses a high intensity X-ray beam thatis produced by a synchrotron. This technique neither requires inva-sive sample preparation, such as staining, nor any special condi-tions, such as a vacuum. Thus, the sample can be looked at in asnear to the ‘‘in vivo” state as possible. Hence, the aim of this studywas to definitively identify the chemical form of the main metal-containing species in the periprosthetic tissues of current genera-tion MOM hips using a direct method. We have previouslyreported data from two patients in a preliminary report [16],where we showed that the effect of fixation did not apparently af-fect the amount of Cr and Co seen and in those two patients thatmost of the metal-containing debris was Cr phosphate. Here we re-port the results of the full study on seven MOM patients and haveexamined the state of Cr- and Co-containing particles.
2. Patients and methods
2.1. Patients and controls
The research ethics committee approved the study on 25 Febru-ary 2008 and all patients consented to the use of their tissue. Inorder to check that there was no influence of the hip type, we ana-lysed tissue from seven patients with current generation MOMhips (three ASR, two BHR, one Biomet and one Cormet). The med-ian age of the patients was 49 years at primary implantation andthe median number of months between primary and revision oper-ations was 26.5. We chose to examine capsular tissue frompatients where the mode of failure was unexplained following
clinical examination and assessment by plain radiographic, micro-biological and intra-operative methods.
As control samples we used tissue from two patients with failedMOP hips. These hips failed due to aseptic loosening. Comparisonwas also made with Cr standards [16] and Co(II) acetate, Co(II) pht-alocyanine, Co metal and metal discs cut from two MOM hips, anASR (DePuy International, Leeds, UK) and a Durom (Zimmer GmbH,Winterthur, Switzerland). These hips were manufactured fromCoCrMo ASTM F75.
2.2. Preparation of patient hip tissue
Hip capsule tissue from nine patients with two types of failedhips (MOM and MOP) was analysed. The results are summarizedin Table 2. We used three methods of tissue preparation to exam-ine the effect of preparation on the chemical species present in thetissue: formalin fixed; fresh frozen; metal contamination avoid-ance (MCA). The formalin fixed tissue was processed in paraffinwax, 3–4 lm thick sections were cut and stained with haematoxy-lin and eosin (H&E). This enabled histological examination of thetissue so that the joint surface edge could be found and cell fea-tures identified. This also enabled the architecture of the sectionto be determined so that we could reliably chose the area to bemapped by the synchrotron beam (because unstained sectionswere aligned in the beam before analysis). For synchroton analysiswe used sequential 10 lm sections to increase any potential signal.The sections were dewaxed by immersion in xylene. We usedquartz slides to reduce the signal from the variable iron back-ground in many regular glass slides.
There were concerns that the process of fixing and sectioningcould contaminate the tissue or alter the distribution and chemis-try of the implant-derived wear debris, so a MCA procedure wasadapted from the work of Collingwood et al. [17], who investigatedmetal-based particles in brain tissue. This involved sectioning withpolytetrafluroethylene-coated blades, spreading epoxy gluearound the sections on the slides and covering with 25 lm thickKapton (a polyamide film, Du Pont, Stevenage, UK), cut to sizeusing plastic scissors.
In addition, the MCA procedure was used to prepare snap frozensections from two patients. One section was cut at 5 lm thicknessfor H&E staining and sequential sections cut at 10 lms were pickedup onto silica slides and brought to room temperature. The cryostatand blade were cleaned with absolute alcohol between specimens.
2.3. Synchrotron methods
The synchrotron work was conducted in the microfocus spec-troscopy beamline (I18) at the Diamond Light Source (Harwell Sci-ence and Innovation Campus, UK) [18]. Two types of experimentswere performed: X-ray Fluorescence (XRF) mapping of the sample
Table 1Reports of chemical characterization of implant-derived metallic species in tissue surrounding hip replacements.
Author & date Hip type and number Specimen type Analysis technique Findings
Huber (2009) [13] 11 MOM, Sikomet smalldiameter Ti stem and cup
Periprosthetic tissue EDXA & FTIR All showed chromium Phosphate
Catelas (2006) [28] All MOM 15 currentgeneration; 4 Mckee–Farrar
Digested periprosthetic tissue EDXA Cr oxide and Co–Cr–Mo metallic particles
Chassot (2004) [29] 5 MOP, 1 COP Periprosthetic tissue Van De Grafaccelerator
Co, Cr, Fe, Ni but no speciation
Ektessabi (2001) [27] 1 MOP Periprosthetic tissue Synchrotron XRF andXANES
Cr species, but not chromium oxide orchromium metallic
Shahgaldi (1995) [11] 7 MOM, 2 MOP Periprosthetic tissue EDXA Mainly CrUrban (1994) [10] 15 MOP Periprosthetic tissue and scrapings
from prosthesisFTIR Cr phosphate
4440 A.J. Hart et al. / Acta Biomaterialia 6 (2010) 4439–4446

Author's personal copy
and X-ray absorption spectroscopy (XAS) with a typical beam sizeof 4 ! 4 lm.
2.3.1. Synchrotron micro-XRFSynchrotron micro-XRF has significantly better detection limits
(2–3 orders of magnitude) than electron microprobing and doesnot require special sample preparations. The typical detection limitof electron probe micro analysis is 100 p.p.m., although this can beimproved to 10 p.p.m. for ‘‘ideal” samples [19]. For transition metalatoms in tissue synchrotron XRF has a detection limit of hundredsof parts per billion [20]. The highest sensitivity can be achievedwith an incident energy of about 500 eV above the absorption edgeof the element being looked at, and is dependent of the photon fluxand the detector system of the beamline. In Diamond beamline I18there are about 1 ! 1012 photons at 8.0 keV and 1 ! 1011 at20.2 keV. The X-rays typically have sufficient energy to penetratethe whole of the sample (10–20 lm of tissue), thus with a4 ! 4 lm beam the effective sample volume is 320 lm for a10 lm thick slice as the sample is at 45" with respect to the inci-dent beam. There is little effect on the results from large (i.e. sev-eral micron) particles as opposed to nanoparticles, especially forsemi-quantitative studies. XRF at these incident photon energiesis not a surface sensitive technique as it sees the whole of the tis-sue core. Hence, synchrotron XRF is increasingly being used tostudy metal in human tissues [21,22].
Two-dimensional maps of the elemental distribution in thesamples were produced for all patient samples, typically coveringa 400 ! 400 lm region in 4 lm steps. The majority of maps wereproduced using an incident energy of 8 keV, which is sufficient toobserve the residual Cr and Co in the tissue. For one patient bothfrozen and dewaxed sections were mapped by XRF at 20.2 keV toobserve the Mo in the tissue. The absorption cross-section, whichdetermines the amount of fluorescence observed, is energy depen-dent. At 20.2 keV the Cr X-ray absorption cross-section is seventimes smaller than at 8.0 keV, reducing the overall sensitivity toCr in maps at this energy compared with 8 keV.
2.3.2. Micro-XASXAS was used to determine the chemical form of the metals in
the tissues [23], as the high intensity of synchrotron X-rays makesit possible to detect elements present in very low concentrations.At characteristic wavelengths the X-ray absorption of an elementchanges dramatically, these are called absorption edges. Near theabsorption edge the spectra may contain fine structure that revealsthe electronic and geometrical environment of the absorbing atom.This technique is termed X-ray absorption near edge structure(XANES) spectroscopy. Further from the edge extended X-rayabsorption fine structure (EXAFS) spectoscopy reveals the localatomic environment of the element. In the XANES region, whichis the energy region near the edge, the absorption spectrum is
dominated by electronic transitions to bound states and multiplescattering of the ejected electron. Information on the oxidationstate, electronic configuration and site symmetry around theabsorbing atom can be gleaned from this part of the spectrum.XANES spectroscopy can also be used as a fingerprint to identifyphases by comparison with known standards. Single scatteringprocesses are normally the primary cause of modulations in the ex-tended region away from the edge, referred to as EXAFS, which canbe used to determine the distances, coordination number and spe-cies of the neighbors of the absorbing atom. XANES/EXAFS spec-troscopy of the Co, Cr and Mo edges were measured at points ofinterest selected from the XRF map.
The tuneability of synchrotron radiation allows XAS spectra ofmost elements to be collected. Combining the high brightness withthe small spot size available makes possible the examination ofsamples at high spatial resolution. X-ray absorption spectra weretypically collected to 400 eV beyond the absorption edge and tookaround 25 min to collect. These spectra represent the average spe-ciation of the metal studied within the sample volume. At somepoints multiple spectra were collected to improve data qualityand to investigate possible beam damage to the sample. Datareduction and XANES analysis were done using the programs Athe-na [24] and PySpline [25], while EXAFS spectra fitting was doneusing DL-EXCURVE [26].
XANES spectra were recorded for the Cr and Co standards intransmission mode. Full EXAFS data were collected from the twotypes of MOM hips using 10 mm discs cut from the femoral headusing a diamond saw. The Co and Cr spectra were recorded usingelectron yield, while the Mo spectrum was recorded in fluores-cence mode.
2.4. Transmission electron microscopy (TEM) and energy dispersiveX-ray spectroscopy
Tissue was fixed with osmic acid, embedded in an epoxy resinand microtomed to 60–80 nm thick. This tissue was unstained.Sections were examined by bright field TEM in a JEOL 2000FXmicroscope at 120 keV. The chemical composition of electron-dense particles was determined using an INCA X-sight energy dis-persive X-ray detector.
3. Results
3.1. XRF analysis
All the XRF maps from six of the seven MOM patients showedthat Cr was the most abundant and widely distributed elementin the tissues surrounding MOM hip arthroplasties. The MOP con-trol samples (n = 2) displayed negligible levels of Cr and Co in theXRF maps.
Table 2Summary data for the tissues analysed by synchrotron micro-XRF.
Patient Hip type Age atprimary
Monthsto failure
Failuremode
Preparationmethods
Predominant metallic species Blood Co level(nmol/L)
Blood Cr level(nmol/L)
1 MOM (ASR) 56 30 U F, FF Cr phosphate 770 8092 MOM (ASR) 50 36 U F Cr phosphate 229 2103 MOM (BHR) 54 74 U F Cr phosphate 1685 11394 MOM (BHR) 45 23 U F Cr phosphate 1262 7005 MOM (Biomet) 48 16 U F, FF, MCA Cr phosphate 576 8126 MOM (Cormet) 45 12 U F, FF, MCA – 65 157 MOM (ASR) 50 45 U F Cr phosphate 5600 30768 MOP 75 12 L F Co & Cr in very small amounts Not measured Not measured9 MOP 70 102 L F Co & Cr in very small amounts Not measured Not measured
U, unexplained: exclusion of other possible causes: infection excluded by low CRP or negative microbiology cultures; no loosening at operation or radiographically; nodislocation. L, loosening; F, formalin; FF, fresh frozen; MCA, metal contamination avoidance.
A.J. Hart et al. / Acta Biomaterialia 6 (2010) 4439–4446 4441

Author's personal copy
An XRF map at an excitation energy of 8.0 keV of the Cr and Codistribution in fixed tissue taken from patient 2, along with theassociated light microscopy image of a stained section, are dis-played in Fig. 1. In the MOM hips Co was found in discrete locationsand the concentration levels with respect to Cr varied greatlyacross the samples, but did not reflect the MOM alloy composition(the Co:Cr ratio in these high Co pixels varied over the range Co:Cr1:9–1:3 compared with the alloy composition of 2:1). There is aclear correlation between the dark macrophage areas and Cr.
3.2. Effect of different preparation methods
As mentioned above, to exclude processing and contaminationartefacts a subset of specimens was also carefully prepared by fro-zen sectioning. Comparison of fixed and frozen tissue sectionsshowed similar distributions and relative concentrations of Mo,Co and Cr, indicating that, for this system, the fixing process didnot appear to affect the location of metals. Fig. 2, an XRF map(patient 5) recorded at 20.2 keV, shows that Co, Mo and Cr wereassociated at some discrete locations, but again Cr was most abun-dant and widely distributed.
3.3. XAS of Cr in tissues
We recorded Cr K-edge XAS spectra at 33 separate points fromtissue samples of six of the seven patients with MOM hips (the data
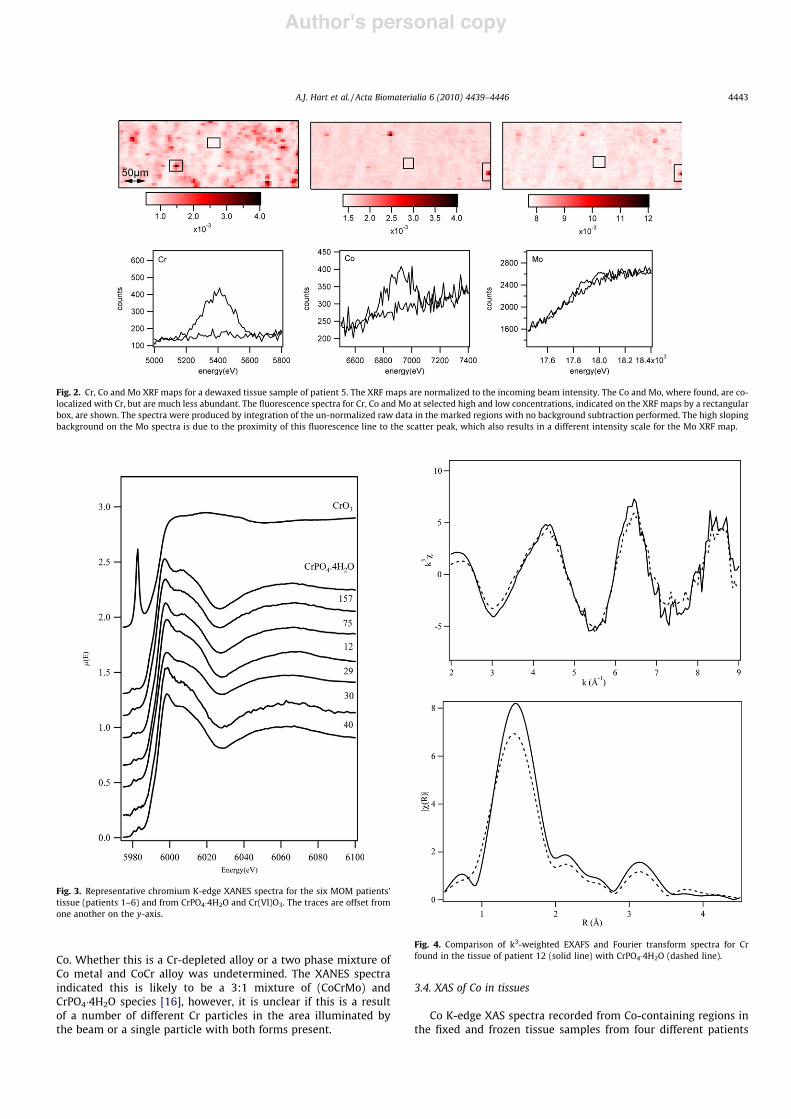
collection time at each point to generate spectra for identificationwas around 45 min). No XAS spectra were recorded from the MOPsamples as there was no detectable level of Cr or Co found in them.In one patient (No. 6), whose case is discussed below, there was aminimal amount of Cr present and XAS was not carried out on thispatient. XANES/EXAFS Cr spectra from different regions and differ-ent samples, both fixed and frozen, were collected and at all buttwo of the 33 points very similar Cr spectra were observed. InFig. 3 a representative Cr XANES spectrum is shown from each ofthese six patients and compared with the XANES spectra ofCr(PO4)"4H2O and Cr2O3, a Cr(VI) standard. The sharp pre-peak at5991 eV in the Cr(VI)O3 spectrum is a characteristic feature ofCr(VI) XANES spectra [27]. This makes XANES spectroscopy anexcellent method for identifying Cr(VI) as in a particular sampleonly #5% of the total Cr needs be Cr(VI) to be detectable. We didnot observe any evidence of this peak in any of the Cr spectra takenfrom the tissue samples. Comparison of both the EXAFS and Fouriertransform of a representative tissue spectrum and CrPO4"4H2O(Fig. 4) showed excellent agreement.
At one point we saw evidence of a second form of Cr wherethere was a very high Co concentration. Examination of the fluores-cence signal showed that at this position in the tissue the ratio ofCo to Cr was approximately 3:1, which is higher than the compo-sition of the MOM hip, however, given the arguments on the for-mation of CrPO4 it is likely that CoCr wear particles would bedepleted of Cr. The Co spectrum at this point indicates metallic
Fig. 1. (A) Comparison between a light microscopy image and XRF maps of a region from the same tissue section from patient 2. The XRF map shows the distribution ofchromium (maximum count above baseline 4960) and Co (maximum count above baseline 3150) while the image of the H&E stained section shows aggregates of pigmentedmacrophages. The light microscope image is a view of the unstained section within the synchrotron beamline. The edge of the tissue was included to create a cleardemarcation between tissue and non-tissue areas and to enable localization of areas of interest in the output of the XRF data. (B) A further comparison is shown (taken fromHart et al. [16]) from patient 4. A light microscopy image (bottom) shows the cellular areas and the XRF map shows the distribution of Cr (red colour in top image) and Co(yellow colour in top image). The Cr distribution exactly mirrors the contour of the macrophage aggregates, with no Cr visible in the fatty connective tissue. Co, where found,is co-localised with Cr, but is clearly much less abundant. (For interpretation of the references to colours in this figure legend, the reader is referred to the web version of thispaper.)
4442 A.J. Hart et al. / Acta Biomaterialia 6 (2010) 4439–4446
Author's personal copy
Co. Whether this is a Cr-depleted alloy or a two phase mixture ofCo metal and CoCr alloy was undetermined. The XANES spectraindicated this is likely to be a 3:1 mixture of (CoCrMo) andCrPO4"4H2O species [16], however, it is unclear if this is a resultof a number of different Cr particles in the area illuminated bythe beam or a single particle with both forms present.
3.4. XAS of Co in tissues
Co K-edge XAS spectra recorded from Co-containing regions inthe fixed and frozen tissue samples from four different patients
Fig. 2. Cr, Co and Mo XRF maps for a dewaxed tissue sample of patient 5. The XRF maps are normalized to the incoming beam intensity. The Co and Mo, where found, are co-localized with Cr, but are much less abundant. The fluorescence spectra for Cr, Co and Mo at selected high and low concentrations, indicated on the XRF maps by a rectangularbox, are shown. The spectra were produced by integration of the un-normalized raw data in the marked regions with no background subtraction performed. The high slopingbackground on the Mo spectra is due to the proximity of this fluorescence line to the scatter peak, which also results in a different intensity scale for the Mo XRF map.
Fig. 3. Representative chromium K-edge XANES spectra for the six MOM patients’tissue (patients 1–6) and from CrPO4"4H2O and Cr(VI)O3. The traces are offset fromone another on the y-axis.
Fig. 4. Comparison of k3-weighted EXAFS and Fourier transform spectra for Crfound in the tissue of patient 12 (solid line) with CrPO4"4H2O (dashed line).
A.J. Hart et al. / Acta Biomaterialia 6 (2010) 4439–4446 4443
Author's personal copy
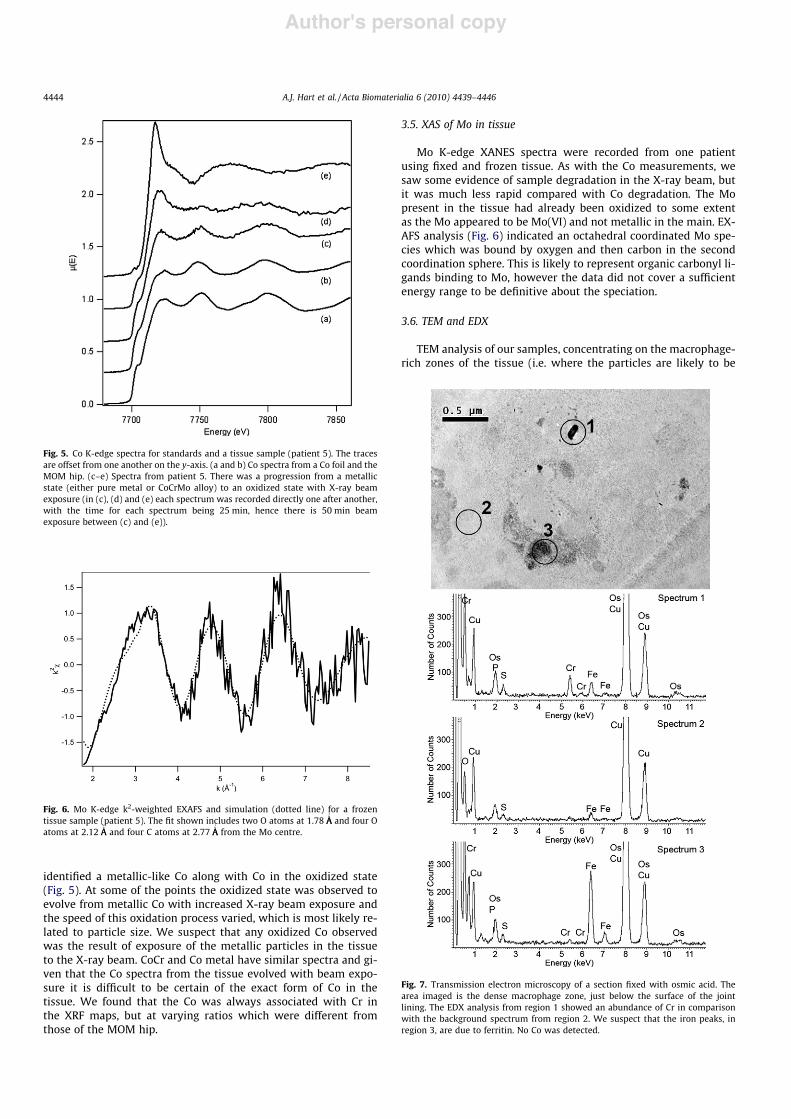
identified a metallic-like Co along with Co in the oxidized state(Fig. 5). At some of the points the oxidized state was observed toevolve from metallic Co with increased X-ray beam exposure andthe speed of this oxidation process varied, which is most likely re-lated to particle size. We suspect that any oxidized Co observedwas the result of exposure of the metallic particles in the tissueto the X-ray beam. CoCr and Co metal have similar spectra and gi-ven that the Co spectra from the tissue evolved with beam expo-sure it is difficult to be certain of the exact form of Co in thetissue. We found that the Co was always associated with Cr inthe XRF maps, but at varying ratios which were different fromthose of the MOM hip.
3.5. XAS of Mo in tissue
Mo K-edge XANES spectra were recorded from one patientusing fixed and frozen tissue. As with the Co measurements, wesaw some evidence of sample degradation in the X-ray beam, butit was much less rapid compared with Co degradation. The Mopresent in the tissue had already been oxidized to some extentas the Mo appeared to be Mo(VI) and not metallic in the main. EX-AFS analysis (Fig. 6) indicated an octahedral coordinated Mo spe-cies which was bound by oxygen and then carbon in the secondcoordination sphere. This is likely to represent organic carbonyl li-gands binding to Mo, however the data did not cover a sufficientenergy range to be definitive about the speciation.
3.6. TEM and EDX
TEM analysis of our samples, concentrating on the macrophage-rich zones of the tissue (i.e. where the particles are likely to be
Fig. 5. Co K-edge spectra for standards and a tissue sample (patient 5). The tracesare offset from one another on the y-axis. (a and b) Co spectra from a Co foil and theMOM hip. (c–e) Spectra from patient 5. There was a progression from a metallicstate (either pure metal or CoCrMo alloy) to an oxidized state with X-ray beamexposure (in (c), (d) and (e) each spectrum was recorded directly one after another,with the time for each spectrum being 25 min, hence there is 50 min beamexposure between (c) and (e)).
Fig. 6. Mo K-edge k2-weighted EXAFS and simulation (dotted line) for a frozentissue sample (patient 5). The fit shown includes two O atoms at 1.78 ÅA
0
and four Oatoms at 2.12 ÅA
0
and four C atoms at 2.77 ÅA0
from the Mo centre.
Fig. 7. Transmission electron microscopy of a section fixed with osmic acid. Thearea imaged is the dense macrophage zone, just below the surface of the jointlining. The EDX analysis from region 1 showed an abundance of Cr in comparisonwith the background spectrum from region 2. We suspect that the iron peaks, inregion 3, are due to ferritin. No Co was detected.
4444 A.J. Hart et al. / Acta Biomaterialia 6 (2010) 4439–4446
Author's personal copy
found) revealed relatively few particulate structures, and EDX re-vealed Cr peaks but no Co (Fig. 7).
4. Discussion
This is the first study to chemically characterize the implant-de-rived metal species from a number of human tissue samples sur-rounding different current generation MOM hip arthroplasties. Weused synchrotron radiation to achieve this, a technique that hasnot been previously used for current generation MOM hips andhas several advantages over other methods. First, it is possible toproduce a metal map of a relatively large area (400 ! 400 lm). Sec-ond, the beam causes less damagewhen comparedwith other X-raysources (e.g. EDX during TEM). Third, it is able to produce high qual-ity spectra, capable of determining the chemical form, despite rela-tively low concentrations of the material of interest. Finally, it ispossible, in the case of frozen sectioning, to analyse the tissue withno preparation other than sectioning (electronmicroscopy for com-parison requires coating and insertion into a vacuum). The disad-vantage of this technology is that it is only available in specializedfacilities, forwhich there is competitive demand.Hence, the numberof samples that can be analysed will always be somewhat limited.
We can see that the tissue surrounding MOM hips contains avariety of metal species, including Co in a metallic state andMo(VI). However, in all the patients where there were significantamounts of metal in the tissue we found Cr(III)PO4 was much themost abundant and we observed no Cr(VI). The depletion of cobaltis of clinical relevance in that elevated blood concentrations of Coand Cr very probably cannot be assigned to particulate matter inthe bloodstream. The solubility of corrosion products in the biolog-ical environment (depletion and enrichment) and the possibility ofrenal elimination are of clinical relevance if immunological effectsare to be considered (e.g. in cases of unexplained failure). The lackof Cr(VI) is also clinically relevant because Cr(VI) causes cancer[28]. These results were obtained by the analysis of 33 separatespectral points in six patients. With XANES spectroscopy it isimpossible to prove the total absence of Cr(VI). First, our detectionlimit for Cr(VI) was #5% of the total Cr at any one spot we sampled,i.e. if 2% of the total Cr in a sampled volume (#160 lm3) was Cr(VI)we would not see it. However, we have no reason to believe thatthe speciation should vary greatly for Cr within the tissue, as weonly saw evidence of two types of Cr containing species. Secondwe cannot record XANES spectra from every point in the tissue,but only collect from a reasonable number of points from differentsamples. Potentially, intracellular chemicals such as peroxidescould oxidize Cr(III) into Cr(VI), which might be reversed on expo-sure to air. However, these limitations apply to any non ‘‘in vitro”technique and we are not aware of an instrument or preparationmethod that would overcome this. Further, if there was rapidreduction of Cr(VI) to Cr(III) then we would expect to see Crhydroxides or oxide rather than Cr(III)PO4 as the end product,and we did not see any evidence of either of these.
Our EDX data were concordant with the abundance of Cr. Therelative absence of Co is interesting because both bearing surfacesof a MOM hip are made from Co–Cr–Mo, present at 60%, 30% and7%, respectively, and it is known that the ratio Co:Cr in the bloodand urine of patients with MOM hips is at least 1:1 and at high cir-culating metal levels is usually 2:1 [29].
Our findings are robust as they are invariant within the sampleset and fitted well to the spectroscopic curves generated by theCrPO4 standard. Furthermore, the XAS results did not change fol-lowing a variety of preparation methods, including frozen section-ing. Previous in vitro studies suggested that Cr(VI) may be acorrosion product of MOM hips [30]. Our finding of no Cr(VI) isreassuring for patients and doctors.
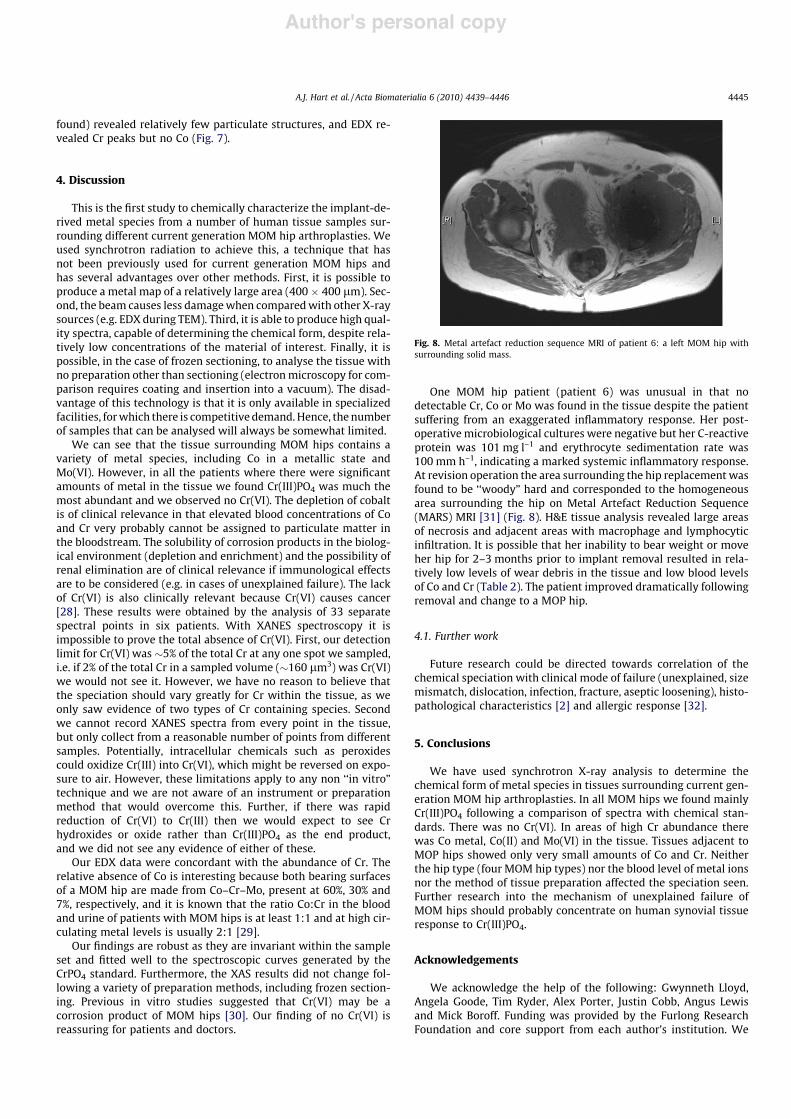
One MOM hip patient (patient 6) was unusual in that nodetectable Cr, Co or Mo was found in the tissue despite the patientsuffering from an exaggerated inflammatory response. Her post-operativemicrobiological cultures were negative but her C-reactiveprotein was 101 mg l–1 and erythrocyte sedimentation rate was100 mm h–1, indicating a marked systemic inflammatory response.At revision operation the area surrounding the hip replacement wasfound to be ‘‘woody” hard and corresponded to the homogeneousarea surrounding the hip on Metal Artefact Reduction Sequence(MARS) MRI [31] (Fig. 8). H&E tissue analysis revealed large areasof necrosis and adjacent areas with macrophage and lymphocyticinfiltration. It is possible that her inability to bear weight or moveher hip for 2–3 months prior to implant removal resulted in rela-tively low levels of wear debris in the tissue and low blood levelsof Co and Cr (Table 2). The patient improved dramatically followingremoval and change to a MOP hip.
4.1. Further work
Future research could be directed towards correlation of thechemical speciation with clinical mode of failure (unexplained, sizemismatch, dislocation, infection, fracture, aseptic loosening), histo-pathological characteristics [2] and allergic response [32].
5. Conclusions
We have used synchrotron X-ray analysis to determine thechemical form of metal species in tissues surrounding current gen-eration MOM hip arthroplasties. In all MOM hips we found mainlyCr(III)PO4 following a comparison of spectra with chemical stan-dards. There was no Cr(VI). In areas of high Cr abundance therewas Co metal, Co(II) and Mo(VI) in the tissue. Tissues adjacent toMOP hips showed only very small amounts of Co and Cr. Neitherthe hip type (four MOM hip types) nor the blood level of metal ionsnor the method of tissue preparation affected the speciation seen.Further research into the mechanism of unexplained failure ofMOM hips should probably concentrate on human synovial tissueresponse to Cr(III)PO4.
Acknowledgements
We acknowledge the help of the following: Gwynneth Lloyd,Angela Goode, Tim Ryder, Alex Porter, Justin Cobb, Angus Lewisand Mick Boroff. Funding was provided by the Furlong ResearchFoundation and core support from each author’s institution. We
Fig. 8. Metal artefact reduction sequence MRI of patient 6: a left MOM hip withsurrounding solid mass.
A.J. Hart et al. / Acta Biomaterialia 6 (2010) 4439–4446 4445

Author's personal copy
thank the Diamond Light Source for the provision of synchrotronbeam time.
Appendix A. Figures with essential colour discrimination
Certain figures in this article, particularly Figs. 1 and 2 are diffi-cult to interpret in black and white. The full colour images can befound in the on-line version, at doi:10.1016/j.actbio.2010.06.006.
References
[1] Bozic KJ, Kurtz S, Lau E, Ong K, Chiu V, Vail TP, et al. The epidemiology ofbearing surface usage in total hip arthroplasty in the United States. J Bone JointSurg Am 2009;91:1614.
[2] Willert HG, Buchhorn GH, Fayyazi A, Flury R, Windler M, Koster G, et al. Metal-on-metal bearings and hypersensitivity in patients with artificial hip joints. Aclinical and histomorphological study. J Bone Joint Surg Am 2005;87:28.
[3] Dunstan E, Ladon D, Whittingham-Jones P, Carrington R, Briggs TW.Chromosomal aberrations in the peripheral blood of patients with metal-on-metal hip bearings. J Bone Joint Surg Am 2008;90:517.
[4] Treacy RB, McBryde CW, Pynsent PB. Birmingham hip resurfacing arthroplasty.A minimum follow-up of five years. J Bone Joint Surg Br 2005;87:167.
[5] Medicines and Healthcare Products Regulatory Agency. Medical Device AlertMDA/2010/033: all metal-on-metal (MOM) hip replacements. London: MHRA;2010.
[6] Pandit H, Glyn-Jones S, McLardy-Smith P, Gundle R, Whitwell D, Gibbons CL,et al. Pseudotumours associated with metal-on-metal hip resurfacings. J BoneJoint Surg Br 2008;90:847.
[7] Williams DF. On the mechanisms of biocompatibility. Biomaterials2008;29:2941.
[8] Toms AP, Marshall TJ, Cahir J, Darrah C, Nolan J, Donell ST, et al. MRI of earlysymptomatic metal-on-metal total hip arthroplasty: a retrospective review ofradiological findings in 20 hips. Clin Radiol 2008;63:49.
[9] Medicines and Healthcare Products Regulatory Agency. Medical Device AlertMDA/2007/054: total hip replacement: DePuy Ultima TPS femoral stem usedin combination with Ultima metal-on-metal articulation. London: MHRA;2007.
[10] Mahendra G, Pandit H, Kliskey K, Murray D, Gill HS, Athanasou N. Necrotic andinflammatory changes in metal-on-metal resurfacing hip arthroplasties. ActaOrthop 2009;80:653.
[11] Shahgaldi BF, Heatley FW, Dewar A, Corrin B. In vivo corrosion of cobalt–chromium and titanium wear particles. J Bone Joint Surg Br 1995;77:962.
[12] Urban RM, Jacobs JJ, Gilbert JL, Galante JO. Migration of corrosion productsfrom modular hip prostheses. Particle microanalysis and histopathologicalfindings. J Bone Joint Surg Am 1994;76:1345.
[13] Shettlemore MG, Bundy KJ. Examination of in vivo influences onbioluminescent microbial assessment of corrosion product toxicity.Biomaterials 2001;22:2215.
[14] Huber M, Reinisch G, Trettenhahn G, Zweymuller K, Lintner F. Presence ofcorrosion products and hypersensitivity-associated reactions in periprosthetic
tissue after aseptic loosening of total hip replacements with metal bearingsurfaces. Acta Biomater 2009;5:172.
[15] Catelas I, Campbell PA, Bobyn JD, Medley JB, Huk OL. Wear particles frommetal-on-metal total hip replacements: effects of implant design andimplantation time. Proc Inst Mech Eng H 2006;220:195.
[16] Hart AJ, Sandison A, Quinn P, Sampson B, Atkinson K, Skinner JA, et al.Microfocus study of metal distribution and speciation in tissue extracted fromrevised metal on metal hip implants. J Phys Conf Ser 2009;190:012208.
[17] Collingwood J, Dobson J. Mapping and characterization of iron compounds inAlzheimer’s tissue. J Alzheimers Dis 2006;10:215.
[18] Mosselmans JF, Quinn PD, Dent AJ, Cavill SA, Moreno SD, Peach A, et al. JSynchrotron Radiat 2009;16:818.
[19] Goldstein J, Newbury DE, Joy DC, Lyman CE, Echlin P, Lifshin E, et al. Scanningelectron microscopy and X-ray microanalysis. New York: Kluwer/Plenum;2002.
[20] Geraki K, Farquharson MJ, Bradley DA. Concentrations of Fe, Cu and Zn inbreast tissue: a synchrotron XRF study. Phys Med Biol 2002;47:2327.
[21] Collingwood JF, Chong RK, Kasama T, Cervera-Gontard L, Dunin-Borkowski RE,Perry G, et al. J Alzheimers Dis 2008;14:235.
[22] Osterode W, Falkenberg G, Höftberger R, Wrba F. Iron, copper, zinc andbromine mapping in cirrhotic liver slices from patients with hemochromatosisstudied by microscopic synchrotron radiation X-ray fluorescence analysis incontinuous scanning mode. Spectrochim Acta B Atomic Spectrosc2007;62:682–8.
[23] Koningsberger DC, Prins R. X-absorption, principles applications techniques ofEXAFS, Sexafs and XANES. New York: Wiley; 1988.
[24] Ravel B, Newville M. ATHENA, ARTEMIS, HEPHAESTUS: data analysis for X-rayabsorption spectroscopy using IFEFFIT. J Synchrotron Radiat 2005;12:537.
[25] Tenderholt A, Hedman B, Hodgson KO. PySpline: a modern, cross-platformprogram for the processing of raw averaged XAS edge and EXAFS data. In:Hedman B, Pianetta P, editors. X-ray Absorption Fine Structure – XAFS13. NewYork: Springer; 2007. p. 105.
[26] Tomic S, Scarle B, Wander A, Harrison NM, Dent AJ, Mosselmans JFW, et al.New tools for the analysis of EXAFS: the DL EXCURV Package. Council for theCentral Laboratory of the Research Councils; 2005.
[27] Bajt S, Clarck S, Sutton SR, Rivers ML, Smith JV. Synchrotron X-ray microprobedetermination of chromate content using X-ray absorption near-edgestructure. Anal Chem 1993;65:1800.
[28] Norseth T. The carcinogenicity of chromium. Environ Health Perspect1981;40:121.
[29] Hart AJ, Skinner JA, Winship P, Faria N, Kulinskaya E, Webster D, et al.Circulating levels of cobalt and chromium from metal-on-metal hipreplacement are associated with CD8+ T-cell lymphopenia. J Bone Joint SurgBr 2009;91-B:835.
[30] Ektessabi AM, Kitamura N, Takada K, Hakamada S, Yoshida S, Hayakawa S,et al. X-ray fluorescence spectroscopy imaging and X-ray absorption finestructure spectroscopy using the synchrotron radiation microbeam. Radiat Res2000;153:232.
[31] Sabah S, Mitchell A, Henckel J, Sandison A, Skinner J, Hart AJ. Magneticresonance imaging findings in painful metal-on-metal hips: a prospectivestudy. J Arthroplasty 2010. doi:10.1016/j.arth.2009.11.008.
[32] Thomas P, Braathen LR, Dorig M, Aubock J, Nestle F, Werfel T, et al. Increasedmetal allergy in patients with failed metal-on-metal hip arthroplasty and peri-implant T-lymphocytic inflammation. Allergy 2009;64:1157.
4446 A.J. Hart et al. / Acta Biomaterialia 6 (2010) 4439–4446