
Multiple Roles of Biosurfactants in Structural Biofilm Development by Pseudomonas aeruginosa
Journal of Critical Care (2009) 24, 625.e9–625.e14
Imipenem-resistant Pseudomonas aeruginosa infection ata medical-surgical intensive care unit: Risk factorsand mortalityGuilherme H.C. Furtado MD⁎, Maria D. Bergamasco MD,Fernando G. Menezes MD, Daniel Marques RN, Adriana Silva RN,Luciana B. Perdiz RN, Sérgio B. Wey MD, Eduardo A.S. Medeiros MD
Hospital Epidemiology Committee, Division of Infectious Diseases, Federal University of São Paulo,São Paulo-SP 04037-004, Brazil
0d
Keywords:Pseudomonas aeruginosa;Imipenem resistance;Nosocomial infection;Risk factors;Mortality;Intensive care unit
AbstractObjectives: The aim of this study was to evaluate the risk factors and attributable mortality associatedwith imipenem-resistant Pseudomonas aeruginosa (IRPA) infections in a medical-surgical intensivecare unit (ICU).Methods: A retrospective case-control study was carried out at a 16-bed medical-surgical ICU in a 780-bed, university-affiliated hospital. All patients admitted from January 1, 2003, to December 31, 2004,who had nosocomial infection caused by IRPA, were included in the study.Results: Imipenem-resistant P. aeruginosa was recovered from 63 patients during the study period. Onehundred eighty-two controls were matched with cases by period of admission, age, and time at risk.Urinary tract (34.9%) and respiratory tract (22.2%) were the main sources of IRPA isolation. Inmultivariate analysis, a previous stay in the ICU (odds ratio, 3.54; 95% confidence interval [CI], 1.29-9.73;P = .03) was the only independent risk factor for IRPA infection. The in-hospital mortality rate among casepatients was 49% (31 of 63) compared with 33% (61 of 182) for control patients (odds ratio, 1.92; 95%CI,1.07-3.44; P = .02). Thus, we had an attributable mortality of 16% (95% CI, 9.74%-22.3%; P = .03).Conclusions: Our study suggests that IRPA infections are strongly related to previous ICU stay, and thatIRPA infections significantly increase mortality in those critical patients.© 2009 Elsevier Inc. All rights reserved.
America [1]. The resistance of P. aeruginosa to imipenem is
1. IntroductionPseudomonas aeruginosa is a major cause of nosocomialpneumonia, wound, and urinary tract infections in Latin
⁎ Corresponding author. Tel.: +55 11 55718935; fax: +55 11 55718935.E-mail address: [email protected] (G.H.C. Furtado).
883-9441/$ – see front matter © 2009 Elsevier Inc. All rights reserved.oi:10.1016/j.jcrc.2009.03.006
increasing worldwide, especially in intensive care units(ICUs) [2-4]. The National Nosocomial Infection Surveil-lance [5] reported a 15% increase in 2003 compared with theperiod between 1998 and 2002.
The resistance of P. aeruginosa to carbapenems is oftenassociated with resistance to other drugs, making it difficultto treat infections caused by this pathogen [6].
625.e10 G.H.C. Furtado et al.
Identification of the risk factors associated with anti-microbial resistance in P. aeruginosa infections could guideappropriate empirical antibiotic therapy, thus, reducingunfavorable outcomes and morbidity. It is also importantthat the epidemiology of imipenem resistance in P. aerugi-nosa be understood to implement adequate measures.
Previous hospital-wide studies have tried to identify therisk factors associated with acquisition of imipenem-resistantP. aeruginosa (IRPA) [7-11]. However, few studies sought toidentify these risk factors in specific units [12].
A high endemic incidence rate of IRPA has beenobserved at our medical center over the last 7 years [13].Thus, we conducted this study to assess the risk factorsassociated with acquisition of IRPA infection at our largestmedical-surgical ICU.
2. Materials and methods
2.1. Hospital setting
A retrospective case-control study was carried out at amedical-surgical ICU with 16 beds at Hospital São Paulo, a750-bed university-affiliated hospital in São Paulo, Brazil.This hospital had an average of 14 955 patient-days permonth during the study period. The medical-surgical unit isthe largest ICU in the hospital. It had an average of 475patient-days per month during the study period. Only rectalswab surveillance for vancomycin-resistant enterococci wasperformed during the study period. Alcohol-based hand gelhas been used at the ICU since 2002.
There was an antimicrobial stewardship program thatanalyzed requests for controlled antimicrobial treatmentsdaily. This program was composed of 3 infectious diseasephysicians and a pharmacist. The following antibiotics wereconsidered controlled: fourth-generation cephalosporins,piperacillin-tazobactam, carbapenems, vancomycin, linezo-lid, ciprofloxacin, and polymyxin B.
2.2. Case and control definitions
All patients admitted to this ICU from January 1, 2003, toDecember 31, 2004 (24-month period), who had nosocomialinfection with IRPA isolated from any site more than 48hours after admission, were included in the study. Theearliest P. aeruginosa isolate recovered from each patientduring the study period was included in the analysis.Nosocomial infection was defined according to the diag-nostic criteria from the Centers for Diseases Control andPrevention [14].
We managed to rule out colonization because ourobjective is to assess IRPA infections. All patients wereevaluated by experienced infection control nurses from theInfection Control Committee. In addition, the controversialcases were thoroughly discussed with the study group.
Control patients were selected from patients hospitalizedin the same unit and matched to case patients (ratio, 3:1) bytime (within a 30-day interval), age (within a 10-yearinterval), and time at risk. Briefly, for the case patients,time at risk was the period between admission to the ICUand the first culture positive for IRPA. For each matchedcontrol patient, the time at risk was the length of stay in theICU. Control patients did not have IRPA infections duringthe study period. Only patients older than 14 years oldwere included.
The study was approved by the institutional ethicscommittee.
2.3. Microbiologic testing
All P. aeruginosa strains were isolated and identified atthe microbiology laboratory using conventional biochemicalmethods [15].
Antibiotic susceptibility was determined by the diskdiffusion method and interpreted according to the guidelinesof the Clinical and Laboratory Standards Institute, formerlyNational Committee for Clinical Laboratory Standards [16].
2.4. Data collection
Data were collected from medical records using astandardized questionnaire for case and control patients.There was no censoring.
Variables analyzed as risk factors included: age, sex,previous stay in ICU within 3 months, prior hospitalizationwithin 3 months, length of hospital stay, diagnosis, proximityto patient with IRPA infection or colonization, comorbidity,use of immunosuppressive drugs, surgery, corticosteroid use,invasive procedures (central line, mechanical ventilation andFoley catheter),duration of mechanical ventilation, use ofsedative drugs, number and class of antibiotics used, theAcute Physiology and Chronic Health Evaluation II(APACHE II) score [17], and presence of shock septic.The anatomical site of infection was also noted.
With regard to antimicrobial data, only antimicrobialdrugs administered for at least 48 hours within 3 weeks ofisolation of IRPA were analyzed. For control patients,antimicrobial drug treatment administered during thehospitalization was included in the analysis.
2.5. Statistical analysis
Potential risk factors were analyzed by univariate andmultivariate analysis. The χ2 test or Fishers' exact test wereused for categorical variables and Wilcoxon test forcontinuous variables.
Variables for which the P value was less than .05 inunivariate analysis were included in a multivariate logisticregression analysis model using the stepwise forward method.
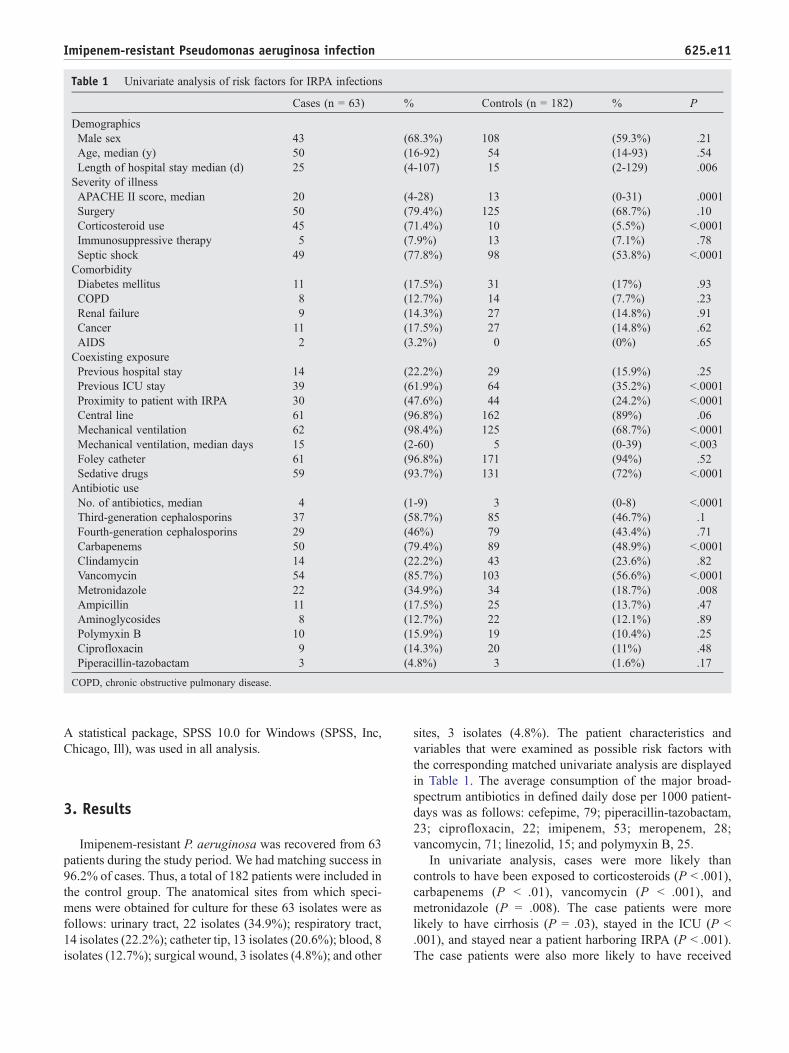
Table 1 Univariate analysis of risk factors for IRPA infections
Cases (n = 63) % Controls (n = 182) % P
DemographicsMale sex 43 (68.3%) 108 (59.3%) .21Age, median (y) 50 (16-92) 54 (14-93) .54Length of hospital stay median (d) 25 (4-107) 15 (2-129) .006
Severity of illnessAPACHE II score, median 20 (4-28) 13 (0-31) .0001Surgery 50 (79.4%) 125 (68.7%) .10Corticosteroid use 45 (71.4%) 10 (5.5%) b.0001Immunosuppressive therapy 5 (7.9%) 13 (7.1%) .78Septic shock 49 (77.8%) 98 (53.8%) b.0001ComorbidityDiabetes mellitus 11 (17.5%) 31 (17%) .93COPD 8 (12.7%) 14 (7.7%) .23Renal failure 9 (14.3%) 27 (14.8%) .91Cancer 11 (17.5%) 27 (14.8%) .62AIDS 2 (3.2%) 0 (0%) .65
Coexisting exposurePrevious hospital stay 14 (22.2%) 29 (15.9%) .25Previous ICU stay 39 (61.9%) 64 (35.2%) b.0001Proximity to patient with IRPA 30 (47.6%) 44 (24.2%) b.0001Central line 61 (96.8%) 162 (89%) .06Mechanical ventilation 62 (98.4%) 125 (68.7%) b.0001Mechanical ventilation, median days 15 (2-60) 5 (0-39) b.003Foley catheter 61 (96.8%) 171 (94%) .52Sedative drugs 59 (93.7%) 131 (72%) b.0001Antibiotic useNo. of antibiotics, median 4 (1-9) 3 (0-8) b.0001Third-generation cephalosporins 37 (58.7%) 85 (46.7%) .1Fourth-generation cephalosporins 29 (46%) 79 (43.4%) .71Carbapenems 50 (79.4%) 89 (48.9%) b.0001Clindamycin 14 (22.2%) 43 (23.6%) .82Vancomycin 54 (85.7%) 103 (56.6%) b.0001Metronidazole 22 (34.9%) 34 (18.7%) .008Ampicillin 11 (17.5%) 25 (13.7%) .47Aminoglycosides 8 (12.7%) 22 (12.1%) .89Polymyxin B 10 (15.9%) 19 (10.4%) .25Ciprofloxacin 9 (14.3%) 20 (11%) .48Piperacillin-tazobactam 3 (4.8%) 3 (1.6%) .17
COPD, chronic obstructive pulmonary disease.
625.e11Imipenem-resistant Pseudomonas aeruginosa infection
A statistical package, SPSS 10.0 for Windows (SPSS, Inc,Chicago, Ill), was used in all analysis.
3. Results
Imipenem-resistant P. aeruginosa was recovered from 63patients during the study period. We had matching success in96.2% of cases. Thus, a total of 182 patients were included inthe control group. The anatomical sites from which speci-mens were obtained for culture for these 63 isolates were asfollows: urinary tract, 22 isolates (34.9%); respiratory tract,14 isolates (22.2%); catheter tip, 13 isolates (20.6%); blood, 8isolates (12.7%); surgical wound, 3 isolates (4.8%); and other
sites, 3 isolates (4.8%). The patient characteristics andvariables that were examined as possible risk factors withthe corresponding matched univariate analysis are displayedin Table 1. The average consumption of the major broad-spectrum antibiotics in defined daily dose per 1000 patient-days was as follows: cefepime, 79; piperacillin-tazobactam,23; ciprofloxacin, 22; imipenem, 53; meropenem, 28;vancomycin, 71; linezolid, 15; and polymyxin B, 25.
In univariate analysis, cases were more likely thancontrols to have been exposed to corticosteroids (P b .001),carbapenems (P b .01), vancomycin (P b .001), andmetronidazole (P = .008). The case patients were morelikely to have cirrhosis (P = .03), stayed in the ICU (P b.001), and stayed near a patient harboring IRPA (P b .001).The case patients were also more likely to have received
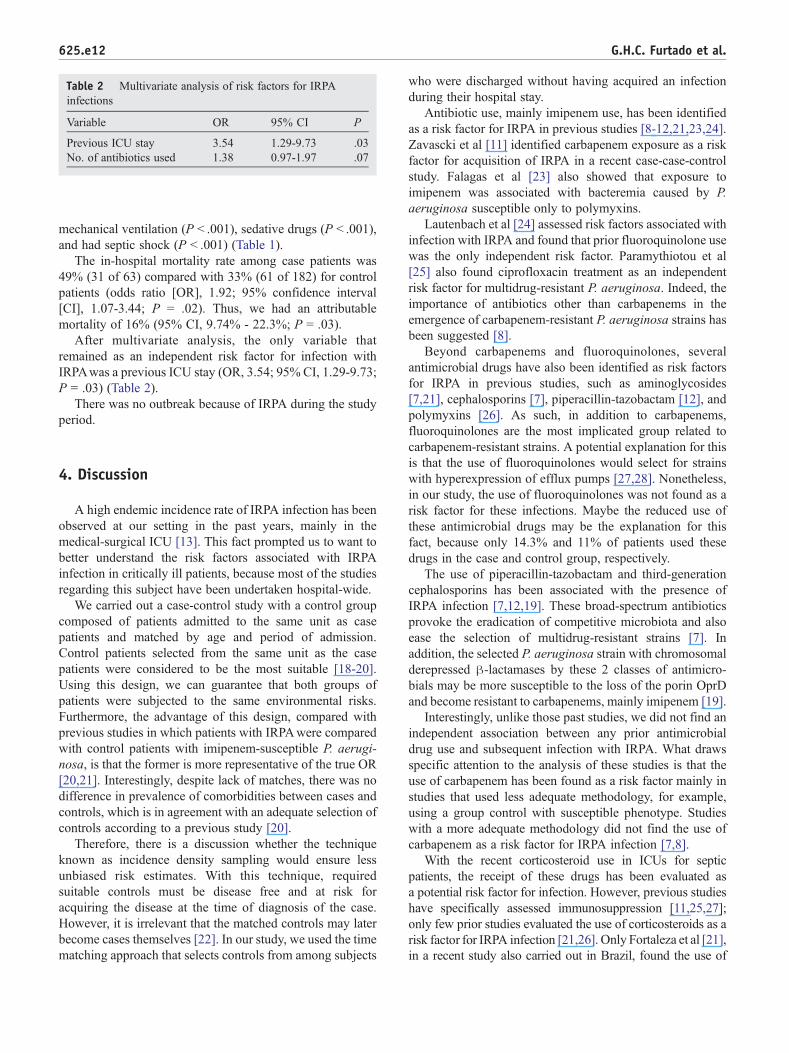
Table 2 Multivariate analysis of risk factors for IRPAinfections
Variable OR 95% CI P
Previous ICU stay 3.54 1.29-9.73 .03No. of antibiotics used 1.38 0.97-1.97 .07
625.e12 G.H.C. Furtado et al.
mechanical ventilation (P b .001), sedative drugs (P b .001),and had septic shock (P b .001) (Table 1).
The in-hospital mortality rate among case patients was49% (31 of 63) compared with 33% (61 of 182) for controlpatients (odds ratio [OR], 1.92; 95% confidence interval[CI], 1.07-3.44; P = .02). Thus, we had an attributablemortality of 16% (95% CI, 9.74% - 22.3%; P = .03).
After multivariate analysis, the only variable thatremained as an independent risk factor for infection withIRPAwas a previous ICU stay (OR, 3.54; 95% CI, 1.29-9.73;P = .03) (Table 2).
There was no outbreak because of IRPA during the studyperiod.
4. Discussion
A high endemic incidence rate of IRPA infection has beenobserved at our setting in the past years, mainly in themedical-surgical ICU [13]. This fact prompted us to want tobetter understand the risk factors associated with IRPAinfection in critically ill patients, because most of the studiesregarding this subject have been undertaken hospital-wide.
We carried out a case-control study with a control groupcomposed of patients admitted to the same unit as casepatients and matched by age and period of admission.Control patients selected from the same unit as the casepatients were considered to be the most suitable [18-20].Using this design, we can guarantee that both groups ofpatients were subjected to the same environmental risks.Furthermore, the advantage of this design, compared withprevious studies in which patients with IRPAwere comparedwith control patients with imipenem-susceptible P. aerugi-nosa, is that the former is more representative of the true OR[20,21]. Interestingly, despite lack of matches, there was nodifference in prevalence of comorbidities between cases andcontrols, which is in agreement with an adequate selection ofcontrols according to a previous study [20].
Therefore, there is a discussion whether the techniqueknown as incidence density sampling would ensure lessunbiased risk estimates. With this technique, requiredsuitable controls must be disease free and at risk foracquiring the disease at the time of diagnosis of the case.However, it is irrelevant that the matched controls may laterbecome cases themselves [22]. In our study, we used the timematching approach that selects controls from among subjects
who were discharged without having acquired an infectionduring their hospital stay.
Antibiotic use, mainly imipenem use, has been identifiedas a risk factor for IRPA in previous studies [8-12,21,23,24].Zavascki et al [11] identified carbapenem exposure as a riskfactor for acquisition of IRPA in a recent case-case-controlstudy. Falagas et al [23] also showed that exposure toimipenem was associated with bacteremia caused by P.aeruginosa susceptible only to polymyxins.
Lautenbach et al [24] assessed risk factors associated withinfection with IRPA and found that prior fluoroquinolone usewas the only independent risk factor. Paramythiotou et al[25] also found ciprofloxacin treatment as an independentrisk factor for multidrug-resistant P. aeruginosa. Indeed, theimportance of antibiotics other than carbapenems in theemergence of carbapenem-resistant P. aeruginosa strains hasbeen suggested [8].
Beyond carbapenems and fluoroquinolones, severalantimicrobial drugs have also been identified as risk factorsfor IRPA in previous studies, such as aminoglycosides[7,21], cephalosporins [7], piperacillin-tazobactam [12], andpolymyxins [26]. As such, in addition to carbapenems,fluoroquinolones are the most implicated group related tocarbapenem-resistant strains. A potential explanation for thisis that the use of fluoroquinolones would select for strainswith hyperexpression of efflux pumps [27,28]. Nonetheless,in our study, the use of fluoroquinolones was not found as arisk factor for these infections. Maybe the reduced use ofthese antimicrobial drugs may be the explanation for thisfact, because only 14.3% and 11% of patients used thesedrugs in the case and control group, respectively.
The use of piperacillin-tazobactam and third-generationcephalosporins has been associated with the presence ofIRPA infection [7,12,19]. These broad-spectrum antibioticsprovoke the eradication of competitive microbiota and alsoease the selection of multidrug-resistant strains [7]. Inaddition, the selected P. aeruginosa strain with chromosomalderepressed β-lactamases by these 2 classes of antimicro-bials may be more susceptible to the loss of the porin OprDand become resistant to carbapenems, mainly imipenem [19].
Interestingly, unlike those past studies, we did not find anindependent association between any prior antimicrobialdrug use and subsequent infection with IRPA. What drawsspecific attention to the analysis of these studies is that theuse of carbapenem has been found as a risk factor mainly instudies that used less adequate methodology, for example,using a group control with susceptible phenotype. Studieswith a more adequate methodology did not find the use ofcarbapenem as a risk factor for IRPA infection [7,8].
With the recent corticosteroid use in ICUs for septicpatients, the receipt of these drugs has been evaluated asa potential risk factor for infection. However, previous studieshave specifically assessed immunosuppression [11,25,27];only few prior studies evaluated the use of corticosteroids as arisk factor for IRPA infection [21,26]. Only Fortaleza et al [21],in a recent study also carried out in Brazil, found the use of

625.e13Imipenem-resistant Pseudomonas aeruginosa infection
corticosteroids as a significant variable, but only in theunivariate analysis. Interestingly, this variable was indepen-dently associated to nosocomial pneumonia caused by IRPA ina recent study undertaken by our group (nonpublished data).
Multivariate analysis showed that a previous ICU staywas the sole independent risk factor for IRPA infection in ourstudy. An ICU stay has been identified as a risk factor for thepresence of IRPA in previous studies [7,9,29,30]. Staying inan ICU is hypothesized to be a risk factor for IRPA because itcould represent an indirect measure of disease severity. Theintensive care support given to these patients and theplacement of several invasive devices introduce multipleopportunities infection control measures to fail. Moreover,the intensity of selective pressure by broad-spectrumantibiotics is higher in the ICU [7,31].
No underlying disease was associated with increased riskfor acquisition of IRPA in our study. Fortaleza et al [21]recently identified hemodialysis as an independent risk factorfor IRPA in a hospital-wide study also undertaken in Brazil.
Regarding invasive procedures, recent studies have foundmechanical ventilation as a risk factor for IRPA [7,10,11,30].In our study, mechanical ventilation was not identified as apotential risk factor for IRPA infection. Aloush et al [7]found that a high invasive device score was a risk factorfor multidrug-resistant P. aeruginosa. This score was basedon the use of mechanical ventilation, Foley catheter, andcentral line.
Mechanical ventilation is hypothesized to be a risk factorfor multidrug-resistant P. aeruginosa infection becausecolonization in the lungs of patients who have undergoneintubation is more common and may predispose the patientto pneumonia [30].
Nosocomial infections caused by IRPA are difficult totreat. The in-hospital mortality rate among patients infectedwith IRPAwas 49%, compared with 33% for control patients(OR, 1.92; 95% CI, 1.07-3.44; P = .02). Thus, theattributable mortality for IRPA infections was 16%. Thecrude mortality for urinary tract infections and non–urinarytract infections was 40% and 54%, respectively. Thus, theattributable mortality for urinary tract infections and non–urinary tract infections was 7% and 21%, respectively.
The case patients had higher APACHE II scores (P =.0001) and had more septic shock (P = .0001) than controlpatients. This can suggest that case patients were moreseriously ill than controls. Otherwise, these variables were notstatistically significant in multivariable analysis. In addition,none study has found APACHE II score as an independentrisk factor for IRPA infection to date. Despite this, thepredominance of urinary tract infections might justify therelatively low attributable mortality rate of patients with IRPAinfections since this kind of infection has commonly lowermortality rates.
The study has several limitations. First, we were unable toassess the role of patient-to-patient transmission. On the otherhand, we evaluated whether proximity to a patient harboringIRPA could be a potential risk factor for acquisition of IRPA.
This variable was significant in univariate analysis but not inmultivariate analysis. Nonetheless, recent studies haveshown lower rates of cross-transmission in ICUs [32-34].Multidrug resistance has usually been described as develop-ing in a susceptible strain of P. aeruginosa exposedsequentially to various antimicrobial agents [35].
Second, because active surveillance was not performedover the study period, we cannot ensure that control patientsdid not harbor IRPA. Otherwise, our aim was to assess riskfactors associated with IRPA infection, not colonization.Third, time-dependent information may have been compro-mised by using logistic regression analysis instead ofsurvival techniques like the Cox regression model. Fourth,several cases could have represented colonization rather thaninfection. Finally, our study was conducted in a medical-surgical ICU of a large university-affiliated hospital, and theresults may not be generalized to other patient populations.
In conclusion, this study sought to analyze the epidemiol-ogy of IRPA in a medical-surgical ICU with a high incidenceof infections caused by this pathogen. We found that aprevious stay in the ICU was the only significant risk factorfor acquisition of IRPA. This may suggest a greater role forICU stay over antimicrobial use as a risk factor for IRPAinfection. Despite this, our antimicrobial stewardshipprogram was reinforced in the ICU aiming at reducing themisuse of antimicrobial drugs. In addition, our results alsodemonstrated a significantly higher mortality rate related toIRPA infections in those critically ill patients.
References
[1] Andrade SS, Jones RN, Gales AC, Sader HS. Increasing prevalence ofantimicrobial resistance among Pseudomonas aeruginosa isolates inLatin America medical centers: 5 year report of the SENTRYAntimicrobial Surveillance Program (1997-2001). J Antimicrob Che-mother 2003;52:140-1.
[2] Goossens H. Susceptibility of multi-drug–resistant Pseudomonasaeruginosa in intensive care units: results from the European MYSTICstudy group. Clin Microbiol Infect 2003;9:980-3.
[3] Fridkin SK, Gaynes RP. Antimicrobial resistance in intensive careunits. Clin Chest Med 1999;20:303-16.
[4] Deshpande LM, Fritsce TR, Jones RN. Molecular epidemiology ofselected multidrug-resistant bacteria: a global report of the SENTRYAntimicrobial Surveillance Program. Diagn Microbiol Infect Dis2004;49(4):231-6.
[5] National Nosocomial Infections Surveillance (NNIS) System Report,data summary from January 1992 through June 2004, issued October2004. Am J Infect Control 2004;32(8):470-85.
[6] Livermore DM. Of Pseudomonas, porins, pumps and carbapenems.J Antimiccrob Chemother 2001;47:247-50.
[7] Aloush V, Navon-Venezia S, Seigman-Igra Y, Cabili S, Carmeli Y.Multidrug-resistant Pseudomonas aeruginosa: risk factors and clinicalimpact. Antimicrob Agents Chemother 2006;50(1):43-8.
[8] Harris AD, Smith D, Johnson JA, Bradham DD, Roghmann MC. Riskfactors for imipenem-resistant Pseudomonas aeruginosa in hospita-lized patients. Clin Infect Dis 2002;34(3):340-5.
[9] Troillet N, Samore MH, Carmeli Y. Imipenem-resistant Pseudomonasaeruginosa: risk factors and antibiotic susceptibility patterns. ClinInfect Dis 1997;25(5):1094-8.
625.e14 G.H.C. Furtado et al.
[10] Cao B, Whang H, Sun H, Zhu Y, Chen M. Risk factors and clinicaloutcomes of nosocomial multi-drug resistant Pseudomonas aerugi-nosa infections. J Hosp Infect 2004;57:112-8.
[11] Zavascki AP, Cruz RP, Goldani LZ. Risk factors for imipenem-resistant Pseudomonas aeruginosa: a comparative analysis of twocase-control studies in hospitalized patients. J Hosp Infect 2005;59(2):96-101.
[12] Ozkurt Z, Ertek M, Erol S, Altoparlak U, Akcay MN. The imipenem-resistant Pseudomonas aeruginosa in the burn unit. Burns 2005;31:870-3.
[13] Furtado GH, Martins ST, Machado AM, Wey SB, Medeiros EA.Clinical culture surveillance of carbapenem-resistant Pseudomonasaeruginosa and Acinetobacter species in a teaching hospital in SaoPaulo, Brazil. A 7-year study. Infect Control Hosp Epidemiol 2006;27(11):1270-3.
[14] Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM. CDCdefinitions for nosocomial infections. Am J Infect Control 1988;16:128-40.
[15] Kiska DL, Gilligan PH. Pseudomonas and Burkholderia. In: MurrayPR, Baron EJ, Pfaller MA, et al, editors. Manual of clinicalmicrobiology. Washington, DC: American Society for Microbiology;1995. p. 517-25.
[16] National Committee for Clinical Laboratory Standards. Performancestandards for antimicrobial disk susceptibility tests. Approved standard.NCCLS document M2-A5. 6th ed. Wayne, PA: NCCCLS; 2000.
[17] Knaus WA, Draper EA, Wagner DP, Zimmermann JE. APACHE II: aseverity of disease classification system. Crit Care Med 1985;13:818-29.
[18] Paterson DL. Looking for risk factors for acquisition of antibioticresistance. A 21st century approach. Clin Infect Dis 2002;34:1564-7.
[19] Harris AD, Karchmer TB, Carmeli Y, Samore MH. Methodologicalprinciples of case-control studies that analyzed risk factors forantibiotic resistance: a systematic review. Clin Infect Dis 2001;32:1055-61.
[20] Harris AD, Samore MH, Lipsitch M, Kaye KS, Perencevich E,Carmeli Y. Control-group selection importance in studies ofantimicrobial resistance: examples applied to Pseudomonas aerugi-nosa, enterococci, and Escherichia coli. Clin Infect Dis 2002;34:1558-63.
[21] Fortaleza CM, Freire MP, Filho D de C, de Carvalho Ramos M. Riskfactors for recovery of Imipenem- or ceftazidime-resistant Pseudo-monas aeruginosa among patients admitted to a teaching hospital inBrazil. Infect Control Hosp Epidemiol 2006;27:901-6.
[22] Schulgen G, Kropec A, Kappstein I, Daschner F, Schumacher M.Estimation of extra hospital stay attributable to nosocomial infec-tions: heterogeneity and timing of events. J Clin Epidemiol 2000;53:409-17.
[23] Falagas ME, Koletsi PK, Kopterides P, Michalopoulos A. Risk factorsfor isolation of strains susceptible only to polymyxins in patients withPseudomonas aeruginosa bacteremia. Antimicrob Agents Chemother2006;50(7):2541-3.
[24] Lautenbach E, Weiner MG, Nachamkin I, Bilker W, Sheridan A,Fishman N. Imipenem resistance among Pseudomonas aeruginosaisolates: risk factors for infection and impact of resistance on clinicaland economic outcomes. Infect Control Hosp Epidemiol 2006;27:893-900.
[25] Paramythioutou E, Lucet JC, Timsit JF, et al. Acquisition of multidrug-resistant Pseudomonas aeruginosa in patients in intensive care units:role of antibiotics with antipseudomonal activity. Clin Infect Dis2004;38:670-7.
[26] Mentzelopoulos SD, Pratikaki M, Platsouka E, Kraniotaki H, ZervakisD, Koutsoukou A, et al. Prolonged use of carbapenems and colistinpredisposes to ventilator-associated pneumonia by pandrug-resistantPseudomonas aeruginosa. Intensive Care Med 2007;33(9):1524-32.
[27] Peña C, Guzmán A, Suarez C, Dominguez MA, Tubau F, Pujol M,et al. Effects of carbapenem exposure on the risk for digestive tractcarriage of intensive care unit-endemic carbapenem-resistant Pseudo-monas aeruginosa strains in critically ill patients. Antimicrob AgentsChemother 2007;51(6):1967-71.
[28] Defez C, Fabbro-Peray P, Bouziges N, Gouby A, Mahamat A, DaurèsJP, et al. Risk factors for multidrug-resistant Pseudomonas aeruginosanosocomial infection. J Hosp Infect 2004;57(3):209-16.
[29] Gaynes RP, Culver DH. Resistance to imipenem among selected gram-negative bacilli in the United States. Infect Control Hosp Epidemiol1992;13:10-4.
[30] Gulay Z, Atay T, Amyes SG. Clonal spread of imipenem-resistantPseudomonas aeruginosa in the intensive care unit of a Turkishhospital. J Chemother 2001;13(5):546-54.
[31] Bergmans D. Cross-colonization with Pseudomonas aeruginosa ofpatients in an intensive care unit. Thorax 1998;53:1053-8.
[32] Weist K, Pollege K, Schulz I, Ruden H, Gastmeier P. How manynosocomial infections are associated with cross-transmission? Aprospective cohort study in a surgical intensive care unit. InfectControl Hosp Epidemiol 2002;23(3):127-32.
[33] Grundmann H, Barwolff S, Tami A, et al. How many infections arecaused by patient-to-patient transmission in intensive care unit? CritCare Med 2005;33(5):946-51.
[34] Halwani M, Solaymani-DodaranM, Grundmann H, Coupland C, SlackR. Cross-transmission of nosocomial pathogens in an adult intensivecare unit: incidence and risk factors. J Hosp Infect 2006;63(1):39-46.
[35] Carmeli Y, Trouillet N, Eliopoulos G, Samore MH. Emergence ofantibiotic-resistant Pseudomonas aeruginosa: comparison of risksassociated with different antipseudomonal agents. Antimicrob AgentsChemother 1999;43:1379-82.
Copyright © 2022 FDOKUMEN




















