Validation of a Pseudomonas aeruginosa porcine model of septic shock
7
Validation of a Pseudomonas aeruginosa porcine model of septic shock ThomasRimmele´ a, *, Abdulnasser Assadi b , Farida Benatir a , Emmanuel Boselli a , Catherine Kaminski a , Florence Arnal b , Corinne Lambert b ,Joe¨lleGoudable b , Dominique Chassard a , Bernard Allaouchiche a a Department of Anaesthesiology and Intensive Care Medicine, Pavilion P, Edouard Herriot Hospital, Lyon, France b Laboratory of Pathophysiology, EA 18/96, Claude Bernard University, Lyon, France Accepted 25 October 2005 Available online 15 December 2005 KEYWORDS Septic shock; Intensive care; Porcine model; Cytokines; Pseudomonas aeruginosa; Pig Summary Objectives: To develop a standardized bacteraemic porcine model of septic shock with cardiovascular and immunological profiles similar to those observed in human clinical states. Methods: Sepsis was induced by an intravenous challenge of 18 anaesthetized pigs with live Pseudomonas aeruginosa. The pulmonary arterial pressure was monitored and the bacterial infusion was stopped when the systolic pulmonary arterial pres- sure reached 45 mm Hg. Septic shock was treated with fluid resuscitation and epi- nephrine infusion. The haemodynamic parameters and the rate of different inflammatory cytokines were recorded during 6 h of observation. Results: The mean SD cardiac output increased from 2.4 1.2 to 5.7 2.1 L/min while the mean SD systemic vascular resistance index decreased from 1957 744 to 709 221 dyn/s/cm 5 /m 2 . The pharmacokinetic profile of the inflammatory cyto- kines was similar to the one observed in human studies. Conclusions: The control of the systolic pulmonary arterial pressure during a P. aeruginosa infusion leads to a hyperdynamic, reproducible cardiovascular profile similar to the one observed in human septic shock. Since the immunological profile of the inflammatory cytokines is also similar to the human one, this standardized por- cine model appears to be appropriate for experimental research concerning sepsis. ª 2005 The British Infection Society. Published by Elsevier Ltd. All rights reserved. * Corresponding author. De ´partement d’Anesthe ´sie-Re ´animation, Pavillon P Re ´animation, Ho ˆpital Edouard Herriot, place d’Arsonval, 69003 Lyon, France. Tel.: þ33 472 110 217; fax: þ33 472 110 278. E-mail address: [email protected] (T. Rimmele ´). 0163-4453/$30 ª 2005 The British Infection Society. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.jinf.2005.10.023 Journal of Infection (2006) 53, 199e205 www.elsevierhealth.com/journals/jinf
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Validation of a Pseudomonas aeruginosa porcine model of septic shock

Journal of Infection (2006) 53, 199e205
www.elsevierhealth.com/journals/jinf
Validation of a Pseudomonas aeruginosaporcine model of septic shock
Thomas Rimmele a,*, Abdulnasser Assadi b, Farida Benatir a,Emmanuel Boselli a, Catherine Kaminski a, Florence Arnal b,Corinne Lambert b, Joelle Goudable b, Dominique Chassard a,Bernard Allaouchiche a
a Department of Anaesthesiology and Intensive Care Medicine, Pavilion P,Edouard Herriot Hospital, Lyon, Franceb Laboratory of Pathophysiology, EA 18/96, Claude Bernard University, Lyon, France
Accepted 25 October 2005Available online 15 December 2005
KEYWORDSSeptic shock;Intensive care;Porcine model;Cytokines;Pseudomonasaeruginosa;Pig
Summary Objectives: To develop a standardized bacteraemic porcine modelof septic shock with cardiovascular and immunological profiles similar to thoseobserved in human clinical states.Methods: Sepsis was induced by an intravenous challenge of 18 anaesthetized pigswith live Pseudomonas aeruginosa. The pulmonary arterial pressure was monitoredand the bacterial infusion was stopped when the systolic pulmonary arterial pres-sure reached 45 mm Hg. Septic shock was treated with fluid resuscitation and epi-nephrine infusion. The haemodynamic parameters and the rate of differentinflammatory cytokines were recorded during 6 h of observation.Results: The mean� SD cardiac output increased from 2.4� 1.2 to 5.7� 2.1 L/minwhile the mean� SD systemic vascular resistance index decreased from 1957� 744to 709� 221 dyn/s/cm5/m2. The pharmacokinetic profile of the inflammatory cyto-kines was similar to the one observed in human studies.Conclusions: The control of the systolic pulmonary arterial pressure during aP. aeruginosa infusion leads to a hyperdynamic, reproducible cardiovascular profilesimilar to the one observed in human septic shock. Since the immunological profile ofthe inflammatory cytokines is also similar to the human one, this standardized por-cine model appears to be appropriate for experimental research concerning sepsis.ª 2005 The British Infection Society. Published by Elsevier Ltd. All rights reserved.
* Corresponding author. Departement d’Anesthesie-Reanimation, Pavillon P Reanimation, Hopital Edouard Herriot, placed’Arsonval, 69003 Lyon, France. Tel.: þ33 472 110 217; fax: þ33 472 110 278.
E-mail address: [email protected] (T. Rimmele).
0163-4453/$30 ª 2005 The British Infection Society. Published by Elsevier Ltd. All rights reserved.doi:10.1016/j.jinf.2005.10.023

200 T. Rimmele et al.
Introduction
Despite both the availability of powerful anti-biotics and the improvement in the delivery ofcritical care medicine, sepsis and systemic inflam-matory response syndrome still remain the leadingcauses of death in intensive care units.1e3 There isa need for development of animal models that arerelevant for conducting experimental research incritical care medicine. Animal models for investi-gating complex disease states are decisive toolsfor researchers, because they provide a biologicalsystem that is similar in complexity to that of thehuman, although important differences in physiol-ogy do exist. In regards to understanding sepsis andsystemic inflammatory responses, many encourag-ing results from animal studies have been pub-lished.4 However interesting these preclinicalresults might be, they were followed by disap-pointing clinical trials.5 In many preclinical stud-ies, the use of inappropriate models might wellbe the limiting factor.6 For example, most ofanimal studies are performed on young healthyanimals made acutely ill, whereas in humans, sep-sis usually occurs gradually and in patients whomight be old or suffering from diabetes, cancer,organ failure, high blood pressure or immunesuppression.7 Thus, the debate over the relevanceand validity of various animal models of sepsis isongoing.6,8 Models of septic shocks are numerous,with each one having its advantages and draw-backs. Currently they all present some compro-mise between clinical realism and experimentalsimplification.
Although the Pseudomonas aeruginosa porcinemodel of septic shock is widely used throughoutthe world,8e10 its validity is highly controversialowing to the quick onset of an acute pulmonaryhypertension. Such hypertension is caused bya severe pulmonary arterial vasoconstriction dueto the release of inflammatory mediators suchas tumor necrosis factor-a (TNF-a) and endothe-lin-1.9 This results in right heart failure witha drop of cardiac output, which does not reflectthe hyperdynamic state observed in humanstudies.11
Our study aims at validating a well standardizedporcine model of septic shock in order to assesswhether the control of pulmonary arterial hyper-tension observed during P. aeruginosa infusioncould lead to a hyperdynamic state without anyright heart dysfunction. In addition, the immuno-logically induced response is monitored in thismodel by recording the pharmacokinetic profileof different inflammatory cytokines.
Materials and methods
Following approval of the local animal researchreview committee, a total of 18 healthy young pigswere studied. All of the animals were female, issuedfrom the Landras Pietrain race, and were 3 monthsold with a mean weight of 35 kg. The principles oflaboratory animal care were followed during thestudy. The animals were pre-anaesthetized with10 mg/kg of intramuscular ketamine (Panpharmalaboratories, Fougeres, France) before being anaes-thetized with 3 mg/kg of intravenous propofol(AstraZeneca laboratories, Rueil-Malmaison, France).Afterwards, the pigs were intubated with a 6.5 Frintraoral tube and placed on mechanical venti-lation performed by using a 50% fraction of inspiredoxygen. The tidal volume was 15 mL/kg and therespiratory frequency was adjusted to producea PaCO2 of 40 mm Hg during the investigation. Themaintenance of anaesthesia was performed by usingsevoflurane (Abbott laboratories, Rungis, France) ata minimal alveolar concentration of 1 and sufentanil(Janssen-Cilag laboratories, Issy-les-Moulineaux,France) 10 mg/h.12,13 A warming blanket maintainedthe animal body temperature at 37� 0.5 �C.
An arterial catheter was introduced into theright internal carotid artery to monitor the sys-temic arterial pressure, determine arterial bloodgas and withdraw blood samples. A pulmonaryarterial catheter was inserted via the right exter-nal jugular vein to measure pulmonary arterialpressure (PAP), pulmonary capillary wedge pres-sure (PCWP), central venous pressure (CVP) andthermodilution cardiac output (CO). A centralvenous catheter was also introduced through theleft external jugular vein to infuse the pigs.
Sepsis was induced with an intravenous infusionof live P. aeruginosa through the central ven-ous catheter (5� 108 CFU/mL at 0.3 mL/20 kg/min).9,12,13 The P. aeruginosa strain (no. HH02332100) used in this study was obtained from a patientat the hospital. It was kept in a glycerolized heart/brain (AES laboratories, Combourg, France) broth ate80 �C at the microbiology laboratory. All pigs wereinfused with bacteria which came from this bacterialstrain in order to avoid any variation of virulence.Twenty-four hours before the experiment, the P.aeruginosa suspension was defrosted and prickedout in heart/brain broth and cultivated at 37 �Cfor 6 h. Then, the broth was reseeded on bloodagar plate media (Biomerieux laboratories, MarcyL’Etoile, France) and cultivated at 37 �C for 18 h.Then, 40 mL of a bacterial suspension was preparedon the day of the investigation. The antibiogramrevealed that the strain was sensitive to all

Validation of a Pseudomonas aeruginosa porcine model of septic shock 201
anti-pseudomonas antibiotics except aztreonam,ticarcillin/clavulanate and fosfomycin. During theinfusion of the P. aeruginosa suspension, the systolicpulmonary arterial pressure (SPAP) was monitored.When the SPAP reached 45 mm Hg, the infusionwas stopped so as to limit the increase of the rightventricular afterload.
A mean arterial pressure (MAP) of 65 mm Hg anda PCWP of 10 mm Hg were maintained by a contin-uous infusion of epinephrine and fluid loading inorder to get a normotensive septic shock. Fluidloading was composed of both an isotonic salinesolution and hydroxyethylstarch. Hydroxyethyl-starch was added as soon as a major relative hypo-volaemia was observed.
The haemodynamic parameters such as heartrate (HR), MAP, CVP, SPAP, mean pulmonary arterialpressure (MPAP), PCWP, CO and cardiac index (CI)were recorded at regular intervals for 6 h. The sys-temic vascular resistance index (SVRI) and the pul-monary vascular resistance index (PVRI) werecalculated from standard formulae. The cardiacindex was calculated by dividing CO by the bodysurface area. The body surface area was calculatedas followed: body surface area¼ 0.087� (bodyweight)2/3.14 The systemic vascular resistance indexwas calculated as followed: SVRI¼ (MAP�CVP)�80/CI and the pulmonary vascular resistance indexwas calculated as followed: PVRI¼ (MPAP�PCWP)�80/CI.14
Epinephrine and fluid loading requirementswere also recorded each hour after the P. aerugi-nosa infusion over a period of 6 h. The beginningand the end of the P. aeruginosa infusion were,respectively, named T0 and Tep and each hourafter the beginning of the P. aeruginosa infusionwas given a number from T1 to T6. Blood gas anal-ysis and lactate level withdrawn in peripheralblood on the invasive arterial catheter wererecorded hourly. Finally, samples of blood werewithdrawn each hour in order to record the rateof different cytokines such as TNF-a, interleukin(IL)-1b, IL-6, IL-1ra. At the end of the investiga-tion, at T6, the animals were sacrificed with anintravenous injection of potassium chloride 2 g.
Data are expressed as mean� standard devia-tion (SD). The statistical differences were calculatedusing a repeated measures analysis of variancewith the StatView� 5.0 software (SAS Inst., Cary,NC, USA). A p value< 0.05 was considered statisti-cally significant.
Results
The mean� SD volume of P. aeruginosa suspen-sion infused was 19� 7 mL and the infusion lasted
40� 8 min. No pig died prematurely before theend of the experiment. The haemodynamic para-meters, lactate level, fluid loading and epineph-rine requirements during the experiment areshown in Table 1. The mean� SD cardiac outputincreased from 2.4� 1.2 to 5.7� 2.1 L/min whilethe systemic vascular resistance index decreasedfrom 1957� 744 to 709� 221 dyn/s/cm5/m2. Themean� SD total volume of crystalloids was5306� 1429 mL and the total volume of hydroxye-thylstarch was 1625� 437 mL. The mean� SDcumulative requirement of epinephrine was 1.9�1.7 mg. The immunological parameters such asthe rates of the different inflammatory cytokinesare shown in Table 2.
Discussion
Many animal models of sepsis have been described,but none has been accepted as generally superiorto another.6 Small mammals are often preferredfor sepsis models, because they are inexpensive,genetically homogeneous, and pathogen-free.6
Large mammals are also widely used, particularlyfor studies requiring invasive monitoring. In theseexperiments, pigs are usually chosen becauseboth their cardiovascular, renal and gastrointesti-nal anatomy and physiology are similar to thoseof human beings.6
Sepsis can be induced in animals either byadministering an infectious bolus or by the infusionof live bacteria.8,15 The models that use an infec-tious bolus are thought to be very close to clinicalreality.6 For example, the peritoneal cavity can becontaminated by inoculated bacteria or faeces andthe bowel can also be surgically perforated tocause massive contamination of the body with en-dogenous bacteria.6,16 Alternatively, the subcuta-neous tissue and the lung can also be infected toinduce sepsis.15 Although these models appear tobe very representative of clinical situations andappear to successfully reproduce pathophysiologicand immunological features, they are difficult toperform and are often poorly reproducible.
By way of contrast, endotoxemia and bacteremiarepresent models that have as their basis a lowinfectious dose, in which bacteria and/or theirassociated lipopolysaccharide (LPS) molecules, orendotoxins, are parenterally encountered by thehost. They reproduce many characteristics of sepsisand lead to a better control of sepsis and standard-ized investigations.8 However, they reflectaprimarilysystemic challenge and do not create any infectiousfocus. In other respects, the immune reaction thatcharacterizes sepsis is known to be perturbed.8
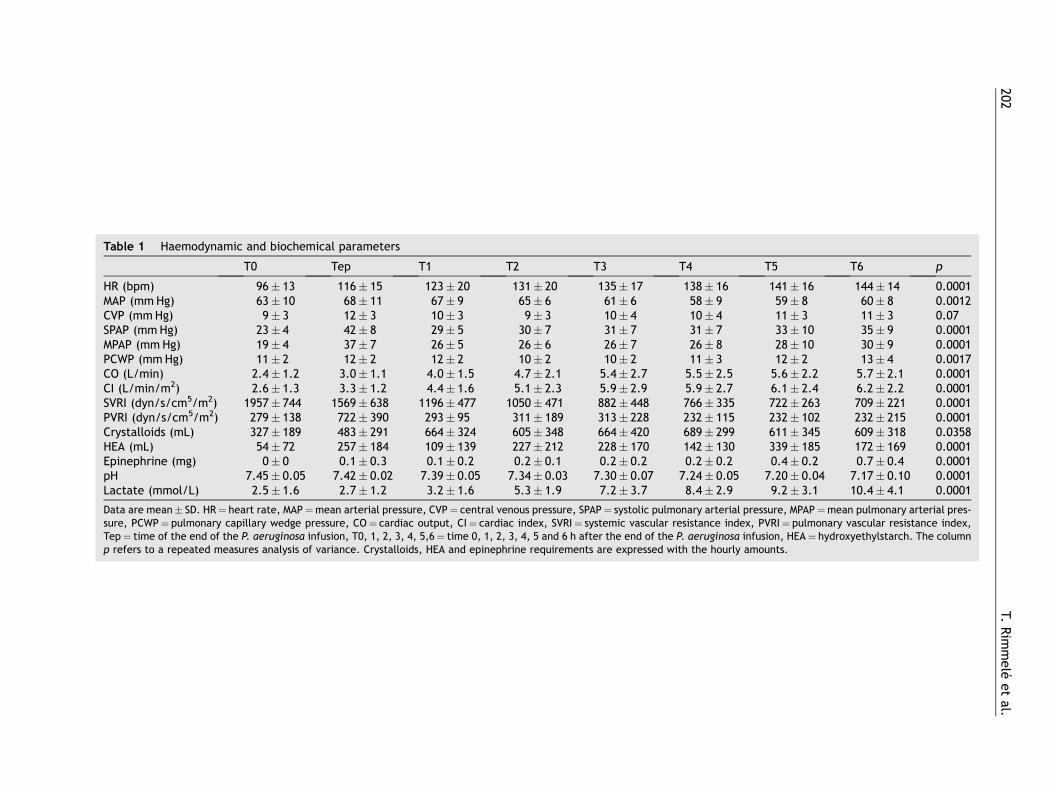
Table 1 Haemodyna
T3 T4 T5 T6 p
HR (bpm) 135� 17 138� 16 141� 16 144� 14 0.0001MAP (mm Hg) 61� 6 58� 9 59� 8 60� 8 0.0012CVP (mm Hg) 10� 4 10� 4 11� 3 11� 3 0.07SPAP (mm Hg) 31� 7 31� 7 33� 10 35� 9 0.0001MPAP (mm Hg) 26� 7 26� 8 28� 10 30� 9 0.0001PCWP (mm Hg) 10� 2 11� 3 12� 2 13� 4 0.0017CO (L/min) 5.4� 2.7 5.5� 2.5 5.6� 2.2 5.7� 2.1 0.0001CI (L/min/m2) 5.9� 2.9 5.9� 2.7 6.1� 2.4 6.2� 2.2 0.0001SVRI (dyn/s/cm5/m2) 882� 448 766� 335 722� 263 709� 221 0.0001PVRI (dyn/s/cm5/m2) 313� 228 232� 115 232� 102 232� 215 0.0001Crystalloids (mL) 664� 420 689� 299 611� 345 609� 318 0.0358HEA (mL) 228� 170 142� 130 339� 185 172� 169 0.0001Epinephrine (mg) 0.2� 0.2 0.2� 0.2 0.4� 0.2 0.7� 0.4 0.0001pH 7.30� 0.07 7.24� 0.05 7.20� 0.04 7.17� 0.10 0.0001Lactate (mmol/L) 7.2� 3.7 8.4� 2.9 9.2� 3.1 10.4� 4.1 0.0001
Data are mean� SD. HR¼ SPAP¼ systolic pulmonary arterial pressure, MPAP¼mean pulmonary arterial pres-sure, PCWP¼ pulmonary systemic vascular resistance index, PVRI¼ pulmonary vascular resistance index,Tep¼ time of the end of t after the end of the P. aeruginosa infusion, HEA¼ hydroxyethylstarch. The columnp refers to a repeated me nts are expressed with the hourly amounts.
202T.
Rim
mele
et
al.
mic and biochemical parameters
T0 Tep T1 T2
96� 13 116� 15 123� 20 131� 2063� 10 68� 11 67� 9 65� 69� 3 12� 3 10� 3 9� 3
23� 4 42� 8 29� 5 30� 719� 4 37� 7 26� 5 26� 611� 2 12� 2 12� 2 10� 2
2.4� 1.2 3.0� 1.1 4.0� 1.5 4.7� 2.12.6� 1.3 3.3� 1.2 4.4� 1.6 5.1� 2.3
1957� 744 1569� 638 1196� 477 1050� 471279� 138 722� 390 293� 95 311� 189327� 189 483� 291 664� 324 605� 34854� 72 257� 184 109� 139 227� 2120� 0 0.1� 0.3 0.1� 0.2 0.2� 0.1
7.45� 0.05 7.42� 0.02 7.39� 0.05 7.34� 0.032.5� 1.6 2.7� 1.2 3.2� 1.6 5.3� 1.9
heart rate, MAP¼mean arterial pressure, CVP¼ central venous pressure,capillary wedge pressure, CO¼ cardiac output, CI¼ cardiac index, SVRI¼he P. aeruginosa infusion, T0, 1, 2, 3, 4, 5,6¼ time 0, 1, 2, 3, 4, 5 and 6 hasures analysis of variance. Crystalloids, HEA and epinephrine requireme

Validation of a Pseudomonas aeruginosa porcine model of septic shock 203
Table 2 Immunological parameters
T0 Tep T1 T2 T3 T4 T5 T6 p
IL-1b (pg/mL) 0 9� 37 148� 132 215� 167 246� 175 220� 159 216� 140 202� 131 0.0001IL-6 (pg/mL) 0 113� 296 873� 667 1216� 2410 522� 670 325� 428 243� 318 189� 189 0.002TNF-a (pg/mL) 0 2876� 2726 6295� 3924 1977� 958 635� 200 448� 220 331� 163 264� 130 0.0001IL-1ra (pg/mL) 0 132� 348 1519� 489 1825� 401 1751� 436 1569� 408 1334� 321 1207� 387 0.0001
Data are mean� SD. IL¼ interleukin, TNF¼ tumor necrosis factor. The column p refers to a repeated measures analysis ofvariance.
Although animal models are essential for exper-imental studies, they are not devoid of drawbacks.Indeed, the failure to extrapolate the results fromanimals to humans is due to several factors such asdifferences in age, drug dosages or infectiveagents in human studies, existence of co-morbid-ities in patients, lack of intensive care in animalstudies, hyper-inflammatory states in animals andhypo-inflammatory states in patients at the timeof treatment.7 Therefore, it is no wonder thateach animal model of sepsis appears to be a com-promise between five conflicting parameters whichare clinical reality, experimental simplification,technical feasibility, manpower and financialresources.
The infusion of live bacteria represents one ofthe easiest sepsis models. The animals are usuallychallenged by an intravascular administration ofEscherichia coli or, less frequently, by a P. aerugi-nosa or Staphylococcus aureus infusion. This modelis quite attractive because it is very simple, con-venient, inexpensive and both perfectly standard-ized and reproducible. Despite its positive aspects,this model is controversial because of its lack ofrelevance to the hypodynamic cardiovascular stateoften reported.8
Indeed, in human beings, at its early phase,septic shock is characterized by a hyperdynamicstate with a decrease in SVR, an increase in CO anda modest increase in PVR. This classical haemody-namic profile of septic shock is also reported insome human experimental studies during whichthe administration of bacterial LPS endotoxin orP. aeruginosa leads to such cardiopulmonary hyper-dynamic manifestations.6
By way of contrast, induced septic shock in pigsis characterized by a severe pulmonary hyperten-sion with a reduced cardiac output; thus, it doesnot reflect the human situation. The increase inthe right ventricular afterload, due to the impor-tance of the SPAP, appears during the first minutesafter the beginning of the bacterial or the endo-toxin infusion.14 In this respect, such a phenome-non is well described in the medical literatureand should be attributed to the release of pro-
inflammatory mediators such as TNF-a and immu-noreactive endothelin-1 which are strong vasocon-strictors on pulmonary vessels.9,11
The hypodynamic cardiovascular state observedin many septic animal models is extremely signif-icant when the duration of the bacteria infusion isvery short. Indeed, Wyler et al. reported thata high-dose bolus injection of LPS produces a rapidcardiovascular collapse and early death.17 Basically,a prolonged infusion of a low dose of bacteria lim-its the appearance of the cardiovascular collapsein small or large animals.
During our experiment, septic shock was rapidlyobtained. Indeed, the mean� SD lactate levelincreased immediately after the infusion of P. aer-uginosa and reached 10.4� 4.1 mmol/L at T6.Moreover, fluid loading and epinephrine infusionwere immediately required after the end of theinfusion: 5306� 1429 mL of crystalloids, 1625�437 mL of hydroxyethylstarch and 1.9� 1.7 mg ofepinephrine were necessary to reach the resuscita-tion goals which were 65 mm Hg of PAM and10 mm Hg of PCWP. Very few data are availablein the medical literature that addresses fluid load-ing and the catecholamines requirement in suchmodels of sepsis. In addition, it is very difficult tocompare data from differing models performed ina large variety of conditions.
In regards to the haemodynamic profile of theseptic shock we obtained, we could notice a signif-icant hyperdynamic state. Indeed, the mean� SDsystemic vascular resistance index decreased rap-idly from 1957� 744 to 709� 221 dyn/s/cm5/m2
(p< 0.05) and cardiac output increased slowlyfrom 2.4� 1.2 to 5.7� 2.1 L/min (p< 0.05). Sucha cardiovascular profile was due to the slow admin-istration of P. aeruginosa (which was 0.3 mL/20 kg/min) and to the control of the pulmonary arterialhypertension during the P. aeruginosa infusion. Thiswas stopped when the SPAP reached 45 mm Hg. Thecontrol of the pulmonary arterial hypertension isthe main difference between our model and themajority of the other septic models in the medicalliterature. In the well-known P. aeruginosa porcinemodel of sepsis-induced acute lung injury from

204 T. Rimmele et al.
Fowler et al., a right heart dysfunction is presentbecause of the acute lung injury, and the haemody-namic state clearly moves with a decrease of thecardiac index.18
Our porcine model is a short-term model ofseptic shock since pigs were sacrificed 6 h after thebeginning of the bacterial infusion. Several chronicmodels also exist.19e22 Indeed, Trager et al.described a few years ago a clinically long-termrelevant model, during which pulmonary arterialpressure was controlled and continually adjustedto result in a moderate pulmonary hypertensionwith MPAP between 35 and 40 mm Hg.21,22
What is worth mentioning is that when sepsisoccurs, the immune system generates differentcytokines which are both the modulators of theinflammatory response and are responsible forthe metabolic and the haemodynamic response.23
In the research field of sepsis, the modulation ofthe action of such cytokines has been pointedout in many studies in the last few de-cades.19,20,23e25 When carrying out our experiment,we observed an increase in TNF-a level during thefollowing minutes after the P. aeruginosa infusionbegan with a peak at 60 min. Interleukin-1b levelrose after TNF-a with a maximum at 3 h. Apeak of IL-6 took place during the first hoursof the septic shock (Table 2). Although the TNF-a levels observed in our experiment are higherthan human data,26,27 probably due to the differ-ence of species, these findings are in totalaccordance with previous results reported in ex-perimental and human clinical studies performedin healthy volunteers.23 As for the anti-inflamma-tory cytokines, small quantities of LPS lead tothe appearance of IL-1ra in a period of 210e280 min after the LPS infusion.23 In human studies,the serum peak of IL-1ra is 100 times more signifi-cant than the peak of IL-1b.23 Our results men-tioned an early increase in the IL-1ra level butthe IL-1ra/IL-1b ratio only remained around 10.Thus, in the light of all these elements, we mayconclude that the inflammatory profile of the cyto-kines is relatively close to the one observed in clin-ical studies although the anti-inflammatory/pro-inflammatory cytokines ratio appears to bemuch lower in our porcine model than in humanstudies.
Conclusion
The main objective of our study was to demon-strate that a P. aeruginosa porcine model of septicshock develops a hyperdynamic state if the rightventricular afterload is tightly controlled by
limiting the systolic pulmonary arterial pressureduring the P. aeruginosa infusion. This was impor-tant to determine, because this haemodynamicprofile is similar to the one observed in humanstudies, and in addition, it had similar pharmacoki-netics for the inflammatory cytokines. It appearsthat the P. aeruginosa porcine model of septicshock as described has experimental benefits, be-cause it is both relatively inexpensive andreproducible.
References
1. Ronco C, Brendolan A, Lonnemann G, Bellomo R, Piccinni P,Digito A, et al. A pilot study of coupled plasma filtration withadsorption in septic shock. Crit Care Med 2002;30:1250e5.
2. Teramoto K, Nakamoto Y, Kunitomo T, Shoji H, Tani T,Hanazawa K, et al. Removal of endotoxin in blood by poly-myxin B immobilized polystyrene-derivative fiber. TherApher 2002;6:103e8.
3. Schoenberg MH, Weiss M, Radermacher P. Outcome of pa-tients with sepsis and septic shock after ICU treatment.Langenbecks Arch Surg 1998;383:44e8.
4. Ridings PC, Blocher CR, Fisher BJ, Fowler 3rd AA,Sugerman HJ. Beneficial effects of a bradykinin antagonistin a model of gram-negative sepsis. J Trauma 1995;39:81e8 [discussion 8e9].
5. Bone RC. Why sepsis trials fail. JAMA 1996;276:565e6.6. Parker SJ, Watkins PE. Experimental models of gram-nega-
tive sepsis. Br J Surg 2001;88:22e30.7. Esmon CT. Why do animal models (sometimes) fail to mimic
human sepsis? Crit Care Med 2004;32:S219e22.8. Freise H, Bruckner UB, Spiegel HU. Animal models of sepsis.
J Invest Surg 2001;14:195e212.9. Han JJ, Windsor A, Drenning DH, Leeper-Woodford S,
Mullen PG, Bechard DE, et al. Release of endothelin in rela-tion to tumor necrosis factor-alpha in porcine Pseudomonasaeruginosa-induced septic shock. Shock 1994;1:343e6.
10. Kadletz M, Dignan RJ, Mullen PG, Windsor AC, Sugerman HJ,Wechsler AS. Pulmonary artery endothelial cell function inswine pseudomonas sepsis. J Surg Res 1996;60:186e92.
11. Herity NA, Allen JD, Silke B, Adgey AA. Inhaled nitric oxidein combination with volume resuscitation refines a porcinemodel of endotoxic shock. Ir J Med Sci 2001;170:172e5.
12. Allaouchiche B, Duflo F, Tournadre JP, Debon R, Chassard D.Influence of sepsis on sevoflurane minimum alveolar con-centration in a porcine model. Br J Anaesth 2001;86:832e6.
13. Allaouchiche B, Duflo F, Debon R, Tournadre JP, Chassard D.Influence of sepsis on minimum alveolar concentration ofdesflurane in a porcine model. Br J Anaesth 2001;87:280e3.
14. MurpheyED, TraberDL. Pretreatment with tumornecrosis fac-tor-alpha attenuates arterial hypotension and mortality in-duced by endotoxin in pigs. Crit Care Med 2000;28:2015e21.
15. Deitch EA. Animal models of sepsis and shock: a review andlessons learned. Shock 1998;9:1e11.
16. Ritter C, Andrades M, Frota Junior ML, Bonatto F, Pinho RA,Polydoro M, et al. Oxidative parameters and mortality insepsis induced by cecal ligation and perforation. IntensiveCare Med 2003;29:1782e9.
17. Wyler F, Neutze JM, Rudolph AM. Effects of endotoxin ondistribution of cardiac output in unanesthetized rabbits.Am J Physiol 1970;219:246e51.
18. Ridings PC, Holloway S, Bloomfield GL, Phillips ML,Fisher BJ, Blocher CR, et al. Protective role of synthetic

Validation of a Pseudomonas aeruginosa porcine model of septic shock 205
sialylated oligosaccharide in sepsis-induced acute lung inju-ry. J Appl Physiol 1997;82:644e51.
19. Haberstroh J, Wiese K, Geist A, Dursunoglu GB, Gippner-Steppert C, et al. Effect of delayed treatment with re-combinant human granulocyte colony-stimulating factoron survival and plasma cytokine levels in a non-neutropenicporcine model of Pseudomonas aeruginosa sepsis. Shock1998;9:128e34.
20. Haberstroh J, Breuer H, Lucke I, Massarrat K, Fruh R, Mand U,et al. Effect of recombinant human granulocyte colony-stimu-lating factor on hemodynamic and cytokine response in a por-cine model of Pseudomonas sepsis. Shock 1995;4:216e24.
21. Trager K, Radermacher P, Rieger KM, Vlatten A, Vogt J,Iber T, et al. Norepinephrine and nomega-monomethyl-L-arginine in porcine septic shock: effects on hepatic O2
exchange and energy balance. Am J Respir Crit Care Med1999;159:1758e65.
22. Santak B, Radermacher P, Adler J, Iber T, Rieger KM,Wachter U, et al. Effect of increased cardiac output on liver
blood flow, oxygen exchange and metabolic rate duringlongterm endotoxin-induced shock in pigs. Br J Pharmacol1998;124:1689e97.
23. Girardin E, Dayer JM. Cytokines and antagonists in septicshock. Schweiz Med Wochenschr 1993;123:480e91.
24. Michie HR, Manogue KR, Spriggs DR, Revhaug A, O’Dwyer S,Dinarello CA, et al. Detection of circulating tumor necrosisfactor after endotoxin administration. N Engl J Med 1988;318:1481e6.
25. Tetta C, Bellomo R, D’Intini V, De Nitti C, Inguaggiato P,Brendolan A, et al. Do circulating cytokines really matterin sepsis? Kidney Int Suppl 2003;84:S69e71.
26. Casey LC, Balk RA, Bone RC. Plasma cytokine and endotoxinlevels correlate with survival in patients with the sepsissyndrome. Ann Intern Med 1993;119:771e8.
27. Riche FC, Cholley BP, Panis YH, Laisne MJ, Briard CG,Graulet AM, et al. Inflammatory cytokine response in pa-tients with septic shock secondary to generalized peritoni-tis. Crit Care Med 2000;28:433e7.