
Staphylococcus aureus infective endocarditis and septic pulmonary embolism after septic abortion
20
INTRODUCTION Infective endocarditis (IE) is one of the most devastating manifestations of S. aureus infection. It can occur in previously well individuals with no pre-existing cardiac abnormality. Between 20% and 65% of cases of S. aureus infective endocarditis (SAIE) are fatal, and a significant proportion of survivors are left with permanent sequelae due to local invasion of cardiac structures, embolization of vegetations, or metastatic infection. Prosthetic valve endocarditis caused by S. aureus is associated with a very high mortality, and surgery is often required for a successful outcome. EPIDEMIOLOGY OF S. AUREUS INFECTIVE ENDOCARDITIS A retrospective study of SAIE in Denmark over 5 years estimated the incidence of the disease at four cases per million people per year. 1 Several prospective and retro- spective studies have documented an increase in the inci- dence of both S. aureus bacteraemia (SAB) and SAIE worldwide, 2,3 and the proportion of all endocarditis cases that are due to S. aureus also appears to be increasing. For example, in one prospective study at a large US insti- tution, the proportion of endocarditis cases due to S. aureus increased almost 7-fold between 1993 and 1999. 4 In recent reports (including one from the large International Collaboration on Endocarditis), S. aureus was found to be responsible for 25% to 68% of cases of native valve endocarditis in adults, 5–10 and it was the causative organism in 10% to 30% cases of prosthetic valve endocarditis. 7,8,10 Possible reasons for the increase in the incidence of SAIE include the increased use of invasive procedures and intravascular devices, an increase in the prevalence of intravenous drug use (IVDU), and improvements in diagnostic techniques. 3 The proportion of SAIE that is acquired in the healthcare setting also appears to be increasing; 1,2,4,11 however, community-acquired SAIE still comprises the majority of cases in most recent studies. 1,12–14 Risk factors for SAIE identified in prospective studies include intravenous drug use, diabetes mellitus, hospital- ization, increasing age, prior cardiac surgery, pre-existing valvular heart disease, previous endocarditis, the presence of an intravascular device and male gender. 15 S. aureus has been identified as an independent risk factor for mortality in large prospective studies of infec- tive endocarditis due to all causes. 4 Endocarditis in patients with S. aureus bacteraemia (SAB) Reported rates of endocarditis in patients with SAB have varied between 0% and 64%, due to variations in study populations, case definitions, imaging modalities, autopsy rates and reporting bias. 11,16–29 In earlier studies, endocarditis was considered to be uncommon when SAB was acquired in hospital or when a primary focus for the bacteraemia (such as an intravascular catheter) was present. 17,21–23 However, more recent prospective Abstract S. aureus infective endocarditis (SAIE) is a serious infec- tion associated with considerable morbidity and mortality.There is evidence that the incidence of SAIE is increasing. As its clinical features are non-specific, SAIE must be suspected in every case of S. aureus bacteraemia, whether it is associated with an obvious source or not. The optimal antimicrobial agent(s) and duration of treat- ment for SAIE are currently not known, but on the basis of present evidence, a minimum of 2 weeks of antimicro- bial therapy is recommended for ‘right-sided’ SAIE, a minimum of 4 weeks for uncomplicated ‘left-sided’ SAIE, and a minimum of 6 weeks for complicated ‘left- sided’ or prosthetic valve SAIE. Although there is no evidence to suggest that combination therapy with a cell- wall active agent (e.g. flucloxacillin) and an aminogly- coside decreases mortality in SAIE, combination therapy should be considered during the initial 3–5 days of therapy as it can shorten the duration of bacteraemia. In complicated or prosthetic valve SAIE, early and close liaison with cardiology and cardiothoracic surgery services is essential. Rapid identification and suscepti- bility testing of the infecting organism are important in determining the choice of definitive antimicrobial therapy. (Intern Med J 2005; 35: S25–S44) Key words: Staphylococcus aureus, infective endocarditis, endocarditis, evidenced-based guidelines. Internal Medicine Journal 2005; 35: S25–S44 Staphylococcus aureus infective endocarditis: diagnosis and management guidelines R. J. MURRAY Department of Microbiology and Infectious Diseases, Royal Perth Hospital, Perth,Western Australia,Australia Correspondence to: Ronan J. Murray, Department of Microbiology and Infectious Diseases, Royal Perth Hospital, GPO Box X2213, Perth,WA 6847,Australia. Email: [email protected]
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Staphylococcus aureus infective endocarditis and septic pulmonary embolism after septic abortion

INTRODUCTION
Infective endocarditis (IE) is one of the most devastatingmanifestations of S. aureus infection. It can occur inpreviously well individuals with no pre-existing cardiacabnormality. Between 20% and 65% of cases of S. aureusinfective endocarditis (SAIE) are fatal, and a significantproportion of survivors are left with permanent sequelaedue to local invasion of cardiac structures, embolizationof vegetations, or metastatic infection. Prosthetic valveendocarditis caused by S. aureus is associated with a veryhigh mortality, and surgery is often required for asuccessful outcome.
EPIDEMIOLOGY OF S. AUREUSINFECTIVE ENDOCARDITIS
A retrospective study of SAIE in Denmark over 5 yearsestimated the incidence of the disease at four cases permillion people per year.1 Several prospective and retro-spective studies have documented an increase in the inci-dence of both S. aureus bacteraemia (SAB) and SAIEworldwide,2,3 and the proportion of all endocarditis casesthat are due to S. aureus also appears to be increasing.For example, in one prospective study at a large US insti-tution, the proportion of endocarditis cases due toS. aureus increased almost 7-fold between 1993 and1999.4 In recent reports (including one from the large
International Collaboration on Endocarditis), S. aureuswas found to be responsible for 25% to 68% of cases ofnative valve endocarditis in adults,5–10 and it was thecausative organism in 10% to 30% cases of prostheticvalve endocarditis.7,8,10
Possible reasons for the increase in the incidence ofSAIE include the increased use of invasive proceduresand intravascular devices, an increase in the prevalenceof intravenous drug use (IVDU), and improvements indiagnostic techniques.3 The proportion of SAIE that isacquired in the healthcare setting also appears to beincreasing;1,2,4,11 however, community-acquired SAIEstill comprises the majority of cases in most recentstudies.1,12–14
Risk factors for SAIE identified in prospective studiesinclude intravenous drug use, diabetes mellitus, hospital-ization, increasing age, prior cardiac surgery, pre-existingvalvular heart disease, previous endocarditis, thepresence of an intravascular device and male gender.15
S. aureus has been identified as an independent riskfactor for mortality in large prospective studies of infec-tive endocarditis due to all causes.4
Endocarditis in patients with S. aureus bacteraemia(SAB)Reported rates of endocarditis in patients with SAB havevaried between 0% and 64%, due to variations in studypopulations, case definitions, imaging modalities,autopsy rates and reporting bias.11,16–29 In earlier studies,endocarditis was considered to be uncommon whenSAB was acquired in hospital or when a primary focusfor the bacteraemia (such as an intravascular catheter)was present.17,21–23 However, more recent prospective
AbstractS. aureus infective endocarditis (SAIE) is a serious infec-tion associated with considerable morbidity andmortality.There is evidence that the incidence of SAIE isincreasing. As its clinical features are non-specific, SAIEmust be suspected in every case of S. aureus bacteraemia,whether it is associated with an obvious source or not.The optimal antimicrobial agent(s) and duration of treat-ment for SAIE are currently not known, but on the basisof present evidence, a minimum of 2 weeks of antimicro-bial therapy is recommended for ‘right-sided’ SAIE, aminimum of 4 weeks for uncomplicated ‘left-sided’SAIE, and a minimum of 6 weeks for complicated ‘left-sided’ or prosthetic valve SAIE. Although there is no
evidence to suggest that combination therapy with a cell-wall active agent (e.g. flucloxacillin) and an aminogly-coside decreases mortality in SAIE, combination therapyshould be considered during the initial 3–5 days oftherapy as it can shorten the duration of bacteraemia. Incomplicated or prosthetic valve SAIE, early and closeliaison with cardiology and cardiothoracic surgeryservices is essential. Rapid identification and suscepti-bility testing of the infecting organism are important indetermining the choice of definitive antimicrobialtherapy. (Intern Med J 2005; 35: S25–S44)
Key words: Staphylococcus aureus, infectiveendocarditis, endocarditis, evidenced-based guidelines.
Internal Medicine Journal 2005; 35: S25–S44
Staphylococcus aureus infective endocarditis: diagnosis andmanagement guidelines
R. J. MURRAY
Department of Microbiology and Infectious Diseases, Royal Perth Hospital, Perth,Western Australia, Australia
Correspondence to: Ronan J. Murray, Department ofMicrobiology and Infectious Diseases, Royal PerthHospital, GPO Box X2213, Perth,WA 6847, Australia.Email: [email protected]

MurrayS26
Internal Medicine Journal 2005; 35: S25–S44
studies of SAB using echocardiography and well-validated diagnostic criteria have demonstrated thatendocarditis is present in up to 25% of all cases of SAB,regardless of whether a portal of entry is identified orwhere the bacteraemia is acquired.11,24,25,27,28 In onerecent study, 52% of cases of SAIE were associated witha removable focus of infection and 46% were nosocomi-ally acquired.13 Because of the relationship between SABand SAIE, it has been proposed that S. aureus bacter-aemia be added to major criteria for the diagnosis ofinfective endocarditis as a modification to the existingDuke criteria (see further below).30
The incidence of SAIE in patients with SAB inAustralasia is not known. In three recent Australianstudies that included a total of 435 patients with SAB,endocarditis was reported in 2% to 32% of cases.31–33 Inone of these studies, it was noted that transoesophagealechocardiography was performed in only 23% of cases ofSAB, suggesting that SAIE may be underdiagnosed.33
S. aureus infective endocarditis in intravenous drugusersInfective endocarditis is a common cause of morbidityand mortality in intravenous drug users (IVDUs),34,35
and S. aureus is the most common cause of infectiveendocarditis in this patient group.7,34–38 The proportionof all cases of SAIE that occurs in IVDUs varies between0% and 65% depending on the population studied.7,10,22,39
The high rate of SAIE in this population is likely due toSAB resulting from unhygienic injection practices inindividuals colonized with S. aureus.40–42
Most IVDUs who develop SAIE have no underlyingcardiac abnormality.7,38,43 SAIE in these patients is morelikely to affect the tricuspid or pulmonary valves (‘right-sided’ infective endocarditis) than the aortic or mitralvalves (‘left-sided endocarditis’), although involvementof both sides of the heart can occur simultaneously.7,22,38
HIV infection is associated with a significantlyincreased risk of endocarditis in IVDUs, but not in thenon-IVDU population.44,45 This risk increases with thedegree of immune suppression, and mortality from
infective endocarditis is significantly higher in HIV-infected patients with CD4+ T-cell counts of ≤200/mm3
or AIDS.44 In non-immunosuppressed HIV-infectedpatients, the clinical course of SAIE and its response toantimicrobial therapy is similar to that in IVDUs withoutHIV infection.46,47
CLINICAL FEATURES OF S. AUREUSINFECTIVE ENDOCARDITIS
The common symptoms and signs of SAIE are shown inTable 1. Splinter haemorrhages, Osler’s nodes, Janewaylesions and Roth’s spots are uncommon findings, butperipheral embolic lesions are common (Fig. 1A–D).34
In patients with SAB, clinical features are neither sensi-tive nor specific for SAIE.13 In large retrospective studiesof SAB, endocarditis was only found at postmortemstudy in a significant percentage of cases.1,48
Early studies of SAIE found that an identifiable portalof entry for S. aureus was apparent in only a minority ofcases.17,23 However, a more recent study suggested that94% of patients with SAIE had an identifiable portal ofentry.11 Intravenous vascular access devices (IVADs)have been implicated as a frequent portal of entry forS. aureus.11,13,18,24,25,49
Cardiac manifestationsS. aureus produces extracellular toxins which can resultin rapid and extensive tissue damage and abscess forma-tion. The typical feature of infective endocarditis, theendocardial vegetation, consists of aggregates of plate-lets, fibrin and organisms which adhere to heart valves orto endocardium in the path of regurgitant jets of blood.Progression of the infection can result in a number ofdeleterious sequelae. Acute valvular dysfunction due toperforation or dehiscence results in acute severe conges-tive cardiac failure, which is the most common cause ofdeath from SAIE. Perivalvular abscesses can originatefrom parts of the prosthetic valve attached to the heartand can rapidly extend into the myocardium, resulting inconduction abnormalities or aneurysmal dilatation.
Table 1 Symptoms and signs of S. aureus infective endocarditis
Involvement Symptoms Signs
• Either left- or right-sided Fever Inflammation/pus at entry siteRigors TachycardiaMyalgias HypotensionArthralgias Metastatic infection (bone, joint, visceral)
• Left-sided Dyspnoea Heart blockCentral nervous system symptoms Oslerian manifestations†
(e.g. syncope, meningism, hemiparesis) Aortic or mitral valve regurgitationManifestations of arterial emboli (cerebral, visceral,
limb)• Right-sided Dyspnoea Tricuspid or pulmonary regurgitation
Pleuritic chest pain Lung consolidationCough with sputum EffusionHaemoptysis
†Osler’s nodes, Janeway lesions, splinter haemorrhages, Roth’s spots.

S27S. aureus infective endocarditis
Fistulae due to extension of the infection into the sinusesof Valsalva, aorta or pulmonary arteries can result inhaemodynamically significant intracardiac shunting.These events may have already occurred at the timeof diagnosis or develop at any time during the course oftherapy, and are associated with a high mortality ratewithout surgery.50
‘Right-sided’ SAIE runs a much more benign coursethan ‘left-sided’ SAIE, leading to significantly betteroutcomes from shorter treatment durations.38,51,52
Extracardiac manifestationsEmbolization of a vegetation may result in ischaemia ofthe region distal to the embolus and/or the establishmentof a metastatic focus of infection. In addition, excessiveimmune complex formation in the setting of a high-grade intravascular infection may result in organdysfunction (e.g. glomerulonephritis).
‘Left-sided’ SAIE
Embolization from the left side of the heart can affectvirtually any part of the body, but is especially seriouswhen it involves the central nervous system. In one retro-spective study, neurological events occurred in 35% ofpatients with SAIE, the most frequent of which wereunilateral hemiparesis, aphasia and meningitis. Mortalityfrom SAIE was significantly higher in patients who had
any neurological event compared with those who did nothave a neurological event (74% vs 56%, respectively),and most of these events had occurred prior to the diag-nosis of SAIE.53 Other common sites of embolizationinclude the kidneys, spleen (see Fig. 2), limbs, vertebralcolumn, epidural space and skeletal muscle (particularlythe iliopsoas complex).
Mycotic aneurysms result from metastatic infectioninvolving the arterial wall. These are most commonlyrecognized in the cerebral circulation when they rupture(resulting in intracranial haemorrhage) or thrombose(resulting in ischaemia). Most cerebral mycoticaneurysms occur in the territory of the middle cerebralartery and they may be multiple.54
Renal complications are seen in up to 50% of cases ofSAIE and occur as a result of embolic phenomena orimmune complex-medicated disease.6,7,55 Common patho-logic findings include infarction, glomerulonephritis,acute interstitial nephritis and cortical necrosis.56
‘Right-sided’ SAIE
Septic pulmonary emboli are usually multiple, small andperipheral and are rarely of haemodynamic significance.However, they can enlarge and cavitate to form lungabscesses, or rupture into the pleural space resulting inempyema formation.
PATHOLOGY TESTING
Readers are referred to the review on S. aureus bacter-aemia in this issue for details regarding blood culturecollection and result interpretation.
Serum bactericidal titre testA systematic review of the use of the serum bactericidaltitre (SBT) test in infective endocarditis found that there
Internal Medicine Journal 2005; 35: S25–S44
Figure 1 Peripheral stigmata of infective endocarditis. (A)Splinter haemorrhage. (B) Janeway lesions. (C) Osler’s nodes.(D) Embolic lesions typical of Staphylococcus aureus. Splinterhaemorrhages and Osler’s nodes are due to antigen/antibodycomplex deposition, whereas Janeway lesions are due tomicroemboli. Frequently in S. aureus endocarditis as opposedto endocarditis due to other bacterial species, the emboli andtherefore the lesions are bigger, and splinter haemorrhages,Osler’s nodes and Janeway lesions are less frequently seen.Osler’s nodes are typically painful whereas the others are not.♣(Photographs [A]–[C] courtesy of Dr Bryan Speed,Fairfield historical collection, photograph [D] from author’scollection.)
Figure 2 Computerized tomographic scan of abdomen,showing splenic abscess in case of Staphylococcus aureusendocarditis. (Photograph courtesy of A/Prof Iain Gosbell,Department of Microbiology and Infectious Diseases,South-western Area Pathology Service, Liverpool, NSW).

MurrayS28
was no significant association between the test resultand either survival or bacteriological outcome, and thatsignificant variations in methodology made interpre-tation of such assays problematic.57 Consequently,measurement of the SBT is not recommended in themanagement of patients with SAIE.
Serology testsEarly studies suggested that the demonstration of anti-bodies to teichoic acid (a component of the cell wall ofstaphylococci) in serum was useful as diagnostic markerof SAIE.58 However, it was subsequently reported thatthis test is neither sensitive nor specific for SAIE.22 Thus,measurement of antistaphylococcal antibodies is notrecommended in the diagnosis or management of SAIE.
Nucleic acid detectionRecent studies have demonstrated the potential utility ofnucleic acid detection methods such as real-time poly-merase chain reaction (PCR) and peptide nucleic acidfluorescence in situ hybridization (PNA-FISH) for thedetection of S. aureus directly from positive bloodcultures.59,60 Additionally, resistance to methicillin canalso be determined on the same sample simultaneously.59
S. aureus DNA has been identified directly from heartvalves by amplification and sequencing of bacterial 16SrDNA in cases of known or suspected SAIE.61,62
Although nucleic acid detection of S. aureus is notcurrently performed routinely in most clinical labora-tories, it may become more widely available in the futureand may be a valuable adjunct in the diagnosis andmanagement of SAIE.
IMAGING PROCEDURES
EchocardiographyThe advent of echocardiography represented a signifi-cant advance in the management of infective endo-carditis. Transthoracic echocardiography (TTE) allowsdirect visualization of valvular and endocardial struc-tures, is non-invasive, rapid, widely available and can beperformed by suitably trained non-medical personnel. Inan early study of the use of TTE in patients with SAB,unsuspected infective endocarditis was found in 11% of36 hospital-acquired SAB cases.22 Although TTE hasexcellent specificity for the detection of cardiac vegeta-tions in infective endocarditis (98%), its sensitivity isonly 40% to 80%;11,63,64 therefore, a negative TTEcannot exclude infective endocarditis in patients withSAB.
Transoesophageal echocardiography (TOE) canproduce higher quality images of the heart than TTEbecause the transducers use higher ultrasonic frequen-cies, imaging in multiple planes is readily obtainable andinterference from air-filled lungs or the chest wall iseliminated. Diagnostic sensitivities of 87% to 100% andspecificities of 89% to 100% have been reported for theuse of TOE in the diagnosis of SAIE.11,63,65–69 TOE isparticularly useful in detecting small vegetations,70
‘right-sided’ endocarditis,71 non-valvular endocarditis,72
prosthetic valve endocarditis,73 and complications ofendocarditis such as paravalvular abscesses,67 papillarymuscle rupture74 and valvular perforation.75 The highnegative predicative value of TOE is of importancebecause it may allow earlier cessation of antimicrobialtherapy,24,68 a strategy that is more cost-effective thanlong-course therapy for possible SAIE in catheter-associated SAB.76 Although TOE is invasive and usuallyrequires intravenous sedation, major complications arerare.77
Echocardiography may also be useful in predictingthe outcome of treatment in patients with SAIE.Although persistence of vegetations following successfultherapy of SAIE is not predictive of late complicationssuch as recurrence or emboli,78 an increase in vegetationsize over the course of therapy may predict a groupof patients at risk for complications, independently ofpersistent bacteraemia or ongoing embolic phenom-ena.79 One prospective study showed that vegetationsvisible by TTE were more likely to embolize than vege-tations visible only by TOE.13 In studies of IVDUs withtricuspid valve SAIE, patients with vegetations that weredetectable by TTE were more likely to have a prolongedfever, develop right heart failure, and/or require tricuspidvalve surgery than those in whom vegetations were notvisible.36,80
All patients with SAB should undergo echocardio-graphy within the first 5–7 days of therapy. In addition,TOE should be performed when the TTE is suboptimaland/or non-diagnostic in community-acquired orprolonged SAB, in prosthetic valve endocarditis (PVE)or infection associated with other intracardiac devices, ifnew-onset cardiac conduction disturbance occurs, orwhere short-course therapy (2 weeks) is being consid-ered. If the clinical suspicion of infective endocarditis ishigh, but initial echocardiography is negative, it shouldbe repeated in 7–10 days.
Other imaging proceduresPulmonary metastatic complications are common inpatients with ‘right-sided’ SAIE (see Fig. 3A,B).They donot in themselves dictate a change in management, butthey can progress to cavitation or rupture into the
Internal Medicine Journal 2005; 35: S25–S44
Figure 3 Pulmonary abscesses secondary to tricuspidendocarditis due to community MRSA. (A) Chest X-ray. (B).Computerized tomographic scan of chest. (Photographcourtesy of A/Prof Iain Gosbell, Department of Microbiologyand Infectious Diseases, South-western Area PathologyService, Liverpool, NSW).

S29S. aureus infective endocarditis
pleural space resulting in empyema. All patients with‘right-sided’ SAIE should therefore undergo chest radio-graphy (CXR) at the time of diagnosis, and this shouldbe repeated if symptoms or signs of pulmonaryembolism develop during or after therapy. If the CXRdoes not show any abnormality in a patient withsymptoms and signs suggestive of pulmonary embolism,computerized tomography (CT) of the chest should beperformed as it is a more sensitive (though more expen-sive and less widely available) test for the demonstrationof septic embolic lesions.81
Imaging to detect systemic metastatic complicationsshould be performed according to any symptoms andsigns that are elicited on patient history and examina-tion. A CT scan of the brain should be performed onpatients with focal neurological signs. Patients withsymptoms and signs of meningitis should have a cere-brospinal fluid examination once space-occupyingcerebral lesions or raised intracranial pressure have beenexcluded by clinical examination and cerebral imaging.
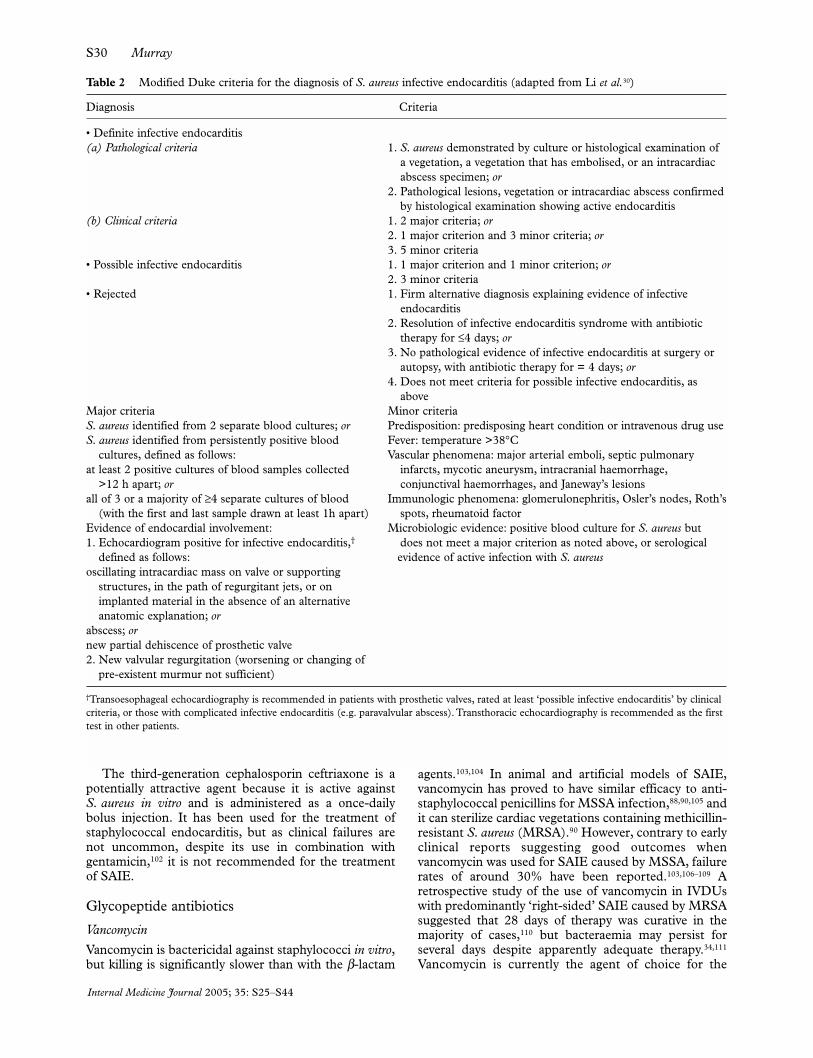
USE OF THE DUKE CRITERIA FORDIAGNOSIS OF S. AUREUSINFECTIVE ENDOCARDITIS
In 1994, a set of diagnostic criteria (known as the Dukecriteria) were developed for the diagnosis of infectiveendocarditis.82 The Duke criteria have been validated ina wide variety of populations and settings, and have beenshown to be both sensitive (>80%) and highly specific(>98%) for the diagnosis of infective endocarditis incomparison with the ‘gold standard’ of pathologicalconfirmation.3,30,82,83 Recently, several modifications havebeen proposed to increase the sensitivity of the Dukecriteria for detecting infective endocarditis (Table 2),including making SAB a major criterion.30
ANTIMICROBIAL THERAPY OFS. AUREUS INFECTIVEENDOCARDITIS
Recently published guidelines on the management ofSAIE provide differing recommendations regardingthe choice and dosages of antimicrobial agents and theduration of treatment.83–86 In the main, these recommen-dations are based largely on expert opinion or consensusrather than high-quality evidence from randomised,controlled clinical trials. Animal models are commonlyused in the evaluation of antimicrobial agents of poten-tial value for the treatment of SAIE, but efficacy in thesemodels does not always correlate with clinical outcomeswhen these agents are used in humans.
Although a number of prospective, randomisedcontrolled trials have compared various antimicrobialagents (alone or in combination) for the treatment ofSAIE, many of these trials are of limited value because ofnon-uniform definitions of endocarditis, small samplesizes, high dropout rates, and variations in drug dosages,administration routes, therapy duration and outcomemeasures. Because no prospective, randomised controlledtrials have determined the optimal duration of therapy for
SAIE, recommendations regarding treatment duration arelargely derived from retrospective studies, consensusopinion, or previously published recommendations.
β-Lactam antibiotics
Penicillins
Over 90% of S. aureus isolates in Australia are resistantto penicillin due to the production of penicillinase.87
When an isolate of S. aureus obtained from a patientwith infective endocarditis is susceptible to penicillin,benzylpenicillin (penicillin G) is considered the agent ofchoice, despite the lack of controlled clinical trials demon-strating its efficacy.
The semisynthetic antistaphylococcal β-lactamsnafcillin and oxacillin are bactericidal in animal modelsof S. aureus endocarditis.88–92 Flucloxacillin anddicloxacillin are the only agents from this group that areavailable in Australasia and are the agents of choice forthe treatment of SAIE due to penicillinase-producingmethicillin-susceptible S. aureus (MSSA) (Tables 3,4),although it should be emphasized that they have notbeen as thoroughly studied as other agents of thisantimicrobial group.Traditionally, they are administeredby bolus injection, but continuous infusion therapy isbeing increasingly utilized, particularly in the outpatientsetting93,94 (see section on outpatient antimicrobialtherapy for SAIE below). As peripheral vein thrombo-phlebitis is common with the use of intravenousdicloxacillin, it should always be administered via acentral venous catheter.
Because penicillins are more active against suscep-tible staphylococci than other cell-wall active agents (e.g.cephalosporins and glycopeptides), they should beconsidered first-line agents for susceptible isolates,except for patients with penicillin hypersensitivity.Patients who report an unconfirmed history of hyper-sensitivity to penicillins should be considered forimmediate-type hypersensitivity skin testing if this isavailable.95
Cephalosporins
The first-generation cephalosporins cephalothin andcephazolin demonstrate bactericidal activity againstMSSA in vitro. In animal models of SAIE, these agentswere of similar efficacy to the semisynthetic peni-cillins.91,92,96 While neither has been systematicallystudied in clinical trials, they are often used for the treat-ment of SAIE caused by MSSA in patients with non-immediate hypersensitivity to penicillins. Some in vitrostudies have shown that cephazolin is more susceptible toenzymatic hydrolysis by type A β-lactamases producedby some strains of S. aureus, particularly when highnumbers of organism are present (as is the case in acardiac vegetation),97,98 and clinical failures of cephazolintreatment of SAIE have been reported.99–101 Cephalothinis therefore preferred to cephazolin for the treatment ofSAIE, but if ‘high inoculum’ MIC testing or molecularcharacterization of the β-lactamase genes of the infectingstrain of S. aureus demonstrate that cephazolin is activeagainst that strain, then cephazolin may be used.101
Internal Medicine Journal 2005; 35: S25–S44
MurrayS30
The third-generation cephalosporin ceftriaxone is apotentially attractive agent because it is active againstS. aureus in vitro and is administered as a once-dailybolus injection. It has been used for the treatment ofstaphylococcal endocarditis, but as clinical failures arenot uncommon, despite its use in combination withgentamicin,102 it is not recommended for the treatmentof SAIE.
Glycopeptide antibiotics
Vancomycin
Vancomycin is bactericidal against staphylococci in vitro,but killing is significantly slower than with the β-lactam
agents.103,104 In animal and artificial models of SAIE,vancomycin has proved to have similar efficacy to anti-staphylococcal penicillins for MSSA infection,88,90,105 andit can sterilize cardiac vegetations containing methicillin-resistant S. aureus (MRSA).90 However, contrary to earlyclinical reports suggesting good outcomes whenvancomycin was used for SAIE caused by MSSA, failurerates of around 30% have been reported.103,106–109 Aretrospective study of the use of vancomycin in IVDUswith predominantly ‘right-sided’ SAIE caused by MRSAsuggested that 28 days of therapy was curative in themajority of cases,110 but bacteraemia may persist forseveral days despite apparently adequate therapy.34,111
Vancomycin is currently the agent of choice for the
Internal Medicine Journal 2005; 35: S25–S44
Table 2 Modified Duke criteria for the diagnosis of S. aureus infective endocarditis (adapted from Li et al.30)
Diagnosis Criteria
• Definite infective endocarditis(a) Pathological criteria 1. S. aureus demonstrated by culture or histological examination of
a vegetation, a vegetation that has embolised, or an intracardiac abscess specimen; or
2. Pathological lesions, vegetation or intracardiac abscess confirmed by histological examination showing active endocarditis
(b) Clinical criteria 1. 2 major criteria; or2. 1 major criterion and 3 minor criteria; or3. 5 minor criteria
• Possible infective endocarditis 1. 1 major criterion and 1 minor criterion; or2. 3 minor criteria
• Rejected 1. Firm alternative diagnosis explaining evidence of infective endocarditis
2. Resolution of infective endocarditis syndrome with antibiotic therapy for ≤4 days; or
3. No pathological evidence of infective endocarditis at surgery or autopsy, with antibiotic therapy for = 4 days; or
4. Does not meet criteria for possible infective endocarditis, as above
Major criteria Minor criteriaS. aureus identified from 2 separate blood cultures; or Predisposition: predisposing heart condition or intravenous drug useS. aureus identified from persistently positive blood Fever: temperature >38°C
cultures, defined as follows: Vascular phenomena: major arterial emboli, septic pulmonary at least 2 positive cultures of blood samples collected infarcts, mycotic aneurysm, intracranial haemorrhage,
>12 h apart; or conjunctival haemorrhages, and Janeway’s lesionsall of 3 or a majority of ≥4 separate cultures of blood Immunologic phenomena: glomerulonephritis, Osler’s nodes, Roth’s
(with the first and last sample drawn at least 1h apart) spots, rheumatoid factorEvidence of endocardial involvement: Microbiologic evidence: positive blood culture for S. aureus but 1. Echocardiogram positive for infective endocarditis,† does not meet a major criterion as noted above, or serological
defined as follows: evidence of active infection with S. aureusoscillating intracardiac mass on valve or supporting
structures, in the path of regurgitant jets, or onimplanted material in the absence of an alternative anatomic explanation; or
abscess; ornew partial dehiscence of prosthetic valve2. New valvular regurgitation (worsening or changing of
pre-existent murmur not sufficient)
†Transoesophageal echocardiography is recommended in patients with prosthetic valves, rated at least ‘possible infective endocarditis’ by clinicalcriteria, or those with complicated infective endocarditis (e.g. paravalvular abscess). Transthoracic echocardiography is recommended as the firsttest in other patients.

S31S. aureus infective endocarditis
treatment of SAIE caused by MRSA, or for the minorityof cases of SAIE caused by MSSA when the patient hasdemonstrated intolerance of or severe hypersensitivity toβ-lactam agents. However, as treatment failure in SAIEhas recently been described in association with the emer-gence of S. aureus with reduced vancomycin suscepti-bility (SA-RVS) while on vancomycin therapy, closeobservation and surveillance blood cultures should beperformed if it is used in the treatment of SAIE.112,113
Vancomycin has been administered by continuousinfusion in small studies that included patients withserious infections caused by Gram-positive cocci,including S. aureus.114,115 Continuous infusion vanco-mycin therapy may be considered in patients who do notrespond to bolus therapy and in those who are suitablefor outpatient intravenous antimicrobial therapy.
Teicoplanin
Teicoplanin has bactericidal activity against S. aureus invitro. In animal models of SAIE, teicoplanin was inferiorto nafcillin and cloxacillin in MSSA infection andinferior to vancomycin for MRSA infection,90,116 and inanother study, resistance emerged during therapy insome animals.117 Teicoplanin penetrates poorly into the
centre of vegetations in comparison with β-lactams andaminoglycosides,118 and an artificial model of SAIEdemonstrated sterilization only with very high doses.105
Uncontrolled, non-randomised studies of teicoplaninin the treatment of SAIE have reported unacceptablefailure rates, particularly when low doses were used.119–123
In a randomised, double-blind trial comparingvancomycin (30 mg/kg/day) with teicoplanin (12 mg/kgfor the first day, then 6 mg/kg/day) for the treatment ofSAB, all four patients with ‘left-sided’ SAIE in theteicoplanin group failed on therapy, resulting in discontin-uation of the trial.124 In another small trial that comparedhigh-dose teicoplanin (up to 20 mg/kg/day) withcloxacillin and gentamicin for the treatment of ‘right-sided’ SAIE in IVDUs, four of six patients receivingteicoplanin failed on therapy.122 Similarly, in a retrospec-tive study, the use of teicoplanin as ‘salvage therapy’ forSAIE resulted in only six of 13 patients achieving cure.123
Adverse effects of teicoplanin such as rash and fever werecommon in some of these studies, particularly whenhigher doses were used.121,123,125 In addition, resistance toteicoplanin has emerged during therapy for SAIE.117
Teicoplanin should only be used in rare cases of SAIEwhere patients are intolerant of both β-lactam agents
Internal Medicine Journal 2005; 35: S25–S44
Table 3 Recommendations for the treatment of ‘right-sided’ native valve endocarditis caused by S. aureus
Clinical setting Recommended antimicrobial therapy†
• Methicillin-susceptible S. aureus Flucloxacillin/dicloxacillin 2 g IV q4h for 14 days plusgentamicin 1 mg/kg IV q8h for the first 3 to 5 days
If isolate is susceptible to penicillin Substitute for flucloxacillin/dicloxacillin: Benzylpenicillin 1.8 g IV q4h
If non-severe penicillin hypersensitivity‡ Substitute for flucloxacillin/dicloxacillin: Cephalothin 2 g IV q4h • Severe penicillin hypersensitivity‡ or methicillin-resistant Vancomycin 15 mg/kg IV q12h for 28 days plus gentamicin
S. aureus 1 mg/kg IV q8h for the first 3 to 5 days• Intravenous therapy not possible; compliance with oral Rifampicin 300 mg PO q12h plus ciprofloxacin 750 mg
therapy can be assured PO q12h for 28 days• Intolerance of or hypersensitivity to vancomycin Discuss therapy with an Infectious Diseases Physician/Clinical
(for methicillin-resistant S. aureus) or to both β-lactams Microbiologist. Possible alternatives to β-lactams/ and vancomycin (for methicillin-susceptible S. aureus) vancomycin include:
Teicoplanin 800 mg IV q12h for first 24h, then 800 mg daily;orLinezolid 600 mg IV/PO q12h; orQuinupristin/dalfopristin 7.5 mg/kg IV q8h
• Outpatient intravenous antimicrobial therapy Discuss therapy with an Infectious Diseases Physician/Clinical Microbiologist. Options include:
Flucloxacillin 8–12 g/day by continuous infusion; orVancomycin 2 g/day by continuous infusion
Note: if any exclusion criteria are present (see footnote), treatment duration is as for ‘left-sided’ endocarditis (refer Table 4).Exclusion criteria for ‘short-course’ treatment of ‘right-sided’ native valve endocarditis caused by S. aureus include: (1) infectioncaused by methicillin-resistant S. aureus; (2) hypersensitivity to (or intolerance of) penicillins and cephalosporins; (3) prosthetic valve infection;(4) co-existent ‘left-sided’ infective endocarditis; (5) extrapulmonary metastatic infection (e.g. meningitis, osteomyelitis, septic arthritis,empyema); or (6) polymicrobial infection.†Doses and dose intervals of the following antimicrobial agents should be adjusted according to the patient’s renal function and therapeutic drugmonitoring results:
– gentamicin: aim for a trough serum concentration of <1 mg/L– vancomycin: aim for a trough serum concentration of 15-20 mg/L (intermittent dosing) or at least 20 mg/L (continuous infusion)– teicoplanin: aim for a trough serum concentration of >20 mg/L– flucloxacillin: as there are significant variations in methodology, refer to local laboratory data for interpretation.
‡Immediate-type hypersensitivity skin testing for penicillins should be considered when there is no clearly documented history of hypersensitivity.

MurrayS32
and vancomycin. If it is used for the treatment of SAIE,trough serum concentrations must be regularly measuredand a level of >20 mg/L should be maintained.126
Other antimicrobial agents
Clindamycin
Clindamycin demonstrates bacteriostatic activity againstS. aureus in vitro. Animal model data have indicated thatpersistent bacteraemia and relapse are common withclindamycin therapy, and that relapses are often associ-ated with an increase in the minimum inhibitory concen-tration (MIC) for this agent.88 High failure rates werereported when clindamycin was administered via intra-muscular injection in IVDUs with ‘right-sided’SAIE.127,128 Consequently, this agent is not recom-mended, either alone or in combination, for the treat-ment of SAIE.
Fluoroquinolones
Ciprofloxacin, moxifloxacin and gatifloxacin have bacte-ricidal activity against S. aureus in vitro, penetrate wellinto tissues, and are active against stationary phasebacteria. Animal models of SAIE have demonstrated thatciprofloxacin is as effective as nafcillin for MSSA, and aseffective as vancomycin for MRSA infection.129–131
However, resistance emerges rapidly when it is used asmonotherapy for the treatment of S. aureus infection.132
There are limited animal model or human data for thenewer fluoroquinolones (e.g. moxifloxacin, gatifloxacin)
in the treatment of SAIE.133,134 Currently, these agentsare not recommended as single agent therapy for thetreatment of SAIE.
Rifampicin
Rifampicin has rapid bactericidal activity againstS. aureus in vitro, good bioavailability after oral dosing,penetrates into cardiac vegetations, and has demon-strated bactericidal activity against organisms associatedwith foreign material.135 However, resistance emergedrapidly when it was used as monotherapy for SAIE inanimal models.88,136 Thus, monotherapy with rifampicinis not recommended for the treatment of SAIE.
Fusidic acid
Fusidic acid has bactericidal activity against S. aureus invitro and has good oral bioavailability. However, resis-tance emerges rapidly when this agent is used asmonotherapy for staphylococcal infection.137 There havebeen no prospective, randomised clinical trials of the useof fusidic acid, either alone or in combination, in thetreatment of SAIE.138 Some retrospective studies havesuggested that its use in combination with a β-lactamagent results in better outcomes in SAIE,20,139,140 but asingle large retrospective study of SAB did not demon-strate a significant survival benefit with this combinationin comparison with flucloxacillin monotherapy.141
The intravenous formulation of fusidic acid commonlycauses jaundice and elevated hepatic enzyme levels, whichlimits its usefulness.140 Fusidic acid should not be used
Internal Medicine Journal 2005; 35: S25–S44
Table 4 Recommendations for the treatment of ‘left-sided’ native valve endocarditis caused by S. aureus
Clinical setting Recommended antimicrobial therapy†
• Methicillin-susceptible S. aureus Flucloxacillin/dicloxacillin 2 g IV q4h for 28–42 days plus gentamicin 1 mg/kg IV q8h for the first 3 to 5 days
If isolate is susceptible to penicillin Substitute for flucloxacillin/dicloxacillin:Benzylpenicillin 1.8 g IV q4h
If non-severe penicillin hypersensitivity‡ Substitute for flucloxacillin/dicloxacillin:Cephalothin 2 g IV q4h
• Severe penicillin hypersensitivity‡ or Vancomycin 15 mg/kg IV q12h for 28–42 days plus gentamicin 1 mg/kg IV methicillin-resistant S. aureus q8h for the first 3 to 5 days
• Intolerance of or hypersensitivity to vancomycin Discuss therapy with an Infectious Diseases(formethicillin-resistant S. aureus) or to both Physician/Clinical Microbiologist.β-lactams andvancomycin (for methicillin- Alternatives to β-lactams/vancomycin include:susceptible S. aureus) Teicoplanin 800 mg IV q8h for first 24 h, then 800 mg daily; or
Linezolid 600 mg IV/PO q12h; orQuinupristin/dalfopristin 7.5 mg/kg IV q8h
• Outpatient intravenous antimicrobial therapy Discuss therapy with an Infectious Diseases Physician/Clinical Microbiologist.
Options include:Flucloxacillin 8–12 g/day by continuous infusionVancomycin 2 g/day by continuous infusion
†Doses and dose intervals of the following antimicrobial agents should be adjusted according to the patient’s renal function and therapeutic drugmonitoring results:
– gentamicin: aim for a trough serum concentration of <1 mg/L– vancomycin: aim for a trough serum concentration of 15-20 mg/L (intermittent dosing) or at least 20 mg/L (continuous infusion)– teicoplanin: aim for a trough serum concentration of >20 mg/L– flucloxacillin: as there are significant variations in methodology, refer to local laboratory data for interpretation.
‡Immediate-type hypersensitivity skin testing for penicillins should be considered when there is no clearly documented history of hypersensitivity.

S33S. aureus infective endocarditis
as monotherapy for SAIE and there is no convincingevidence to suggest that its addition to β-lactam therapyconfers benefit.
Co-trimoxazole (trimethoprim/sulfamethoxazole;TMP-SMX)
Co-trimoxazole has bactericidal activity against most(but not all) strains of S. aureus in vitro.142 In animalmodels of SAIE, cotrimoxazole was inferior tocloxacillin, vancomycin and teicoplanin for both MSSAand MRSA, with valve sterilization rates and mortalitycomparable to untreated animals.116 In a prospective,randomised controlled trial comparing co-trimoxazolewith vancomycin for the treatment of IVDUs withserious S. aureus infection (almost half of which were dueto MRSA), co-trimoxazole was found to be inferior tovancomycin in the group as a whole, with most clinicalfailures occurring in those patients who had ‘right-sided’SAIE due to MSSA. In addition, there was a non-significant trend towards a longer duration of bacteraemiaand increased adverse events in the co-trimoxazole-treated group.143 At present therefore there is insufficientevidence to recommend the use of co-trimoxazole for thetreatment of SAIE.
Quinupristin/dalfopristin
Quinupristin/dalfopristin demonstrates bacteriostaticactivity against staphylococci, including most strains thatare resistant to macrolides and lincosamides.144 Animalmodel data have suggested that quinupristin/dalfopristinmay be effective for the treatment of SAIE,144,145 andsynergistic bactericidal activity has been demonstratedwhen it was combined with β-lactams,146 vancomycin,147
or rifampicin148 in experimental MRSA endocarditis.There are currently no prospective randomised,controlled clinical trials of quinupristin/dalfopristin forthe treatment of SAIE. Although a multicentre,randomised, controlled trial that compared quinupristin/dalfopristin with vancomycin for the treatment ofcatheter-related bacteraemia due to MRSA suggestedequivalence,149 a multinational, non-randomised studyof the use of quinupristin/dalfopristin for the treatmentof MRSA infection refractory to standard therapydescribed clinical failure in five of 11 patients with endo-carditis, including two with proven bacteriologicalfailure.150
Quinupristin/dalfopristin is not currently recom-mended for the first-line treatment of SAIE, but may beconsidered in those patients with SAIE due to MRSAwho are intolerant of vancomycin, who have persistentbacteraemia despite appropriate first-line therapy, or inpatients with endocarditis due to SA-RVS, vancomycin-intermediate S. aureus (VISA), or vancomycin-resistantS. aureus (VRSA).
Linezolid
Linezolid belongs to the oxazolidinone class of antimi-crobial agents and is active against virtually all strains ofS. aureus in vitro. Linezolid was able to sterilize vege-tations as effectively as vancomycin in some studies of
animal models of methicillin-susceptible and methicillin-resistant SAIE,151,152 but not in others.153 It was notsynergistic with rifampicin in an animal model studyof MSSA infective endocarditis,154 or with vancomycinfor MRSA infective endocarditis.153 There are norandomised, controlled clinical trials of linezolid inSAIE, and only limited non-controlled clinical experi-ence has been reported in the literature.155–157 There havealready been reports of linezolid treatment failure inSAIE155,156 and resistance has developed during thecourse of treatment for serious MRSA infection.158
Currently, there is insufficient evidence to recom-mend the use of linezolid as first-line therapy in thetreatment of SAIE, but its use may be considered inthose patients with SAIE due to MRSA who are refrac-tory to or intolerant of vancomycin, or in patients withendocarditis due to SA-RVS, vancomycin-intermediateS. aureus (VISA) or vancomycin-resistant S. aureus(VRSA).
Combination antimicrobial therapyBased on in vitro and animal model evidence of syner-gistic bactericidal activity, combination therapy with twoor more antimicrobial agents has been used in SAIE withthe aim of improving outcomes and/or shortening theduration of treatment. In a New Zealand study of152 cases of staphylococcal endocarditis (mostly due toS. aureus) that involved valve surgery, there was no signif-icant difference in the rate of valve sterilization whensingle-agent therapy was compared with any combina-tion therapy in native valve endocarditis. However, anykind of combination therapy was six times more likely toresult in valve sterilization in prosthetic valve staphylo-coccal endocarditis when compared with single-agenttherapy.159
Cell-wall active agents plus aminoglycosides
Aminoglycosides are frequently used in combinationwith cell-wall active agents (β-lactams and glyco-peptides) in the treatment of serious staphylococcalinfections. Various combinations of agents have provedsynergistic against S. aureus in in vitro studies,105,160,161
and have demonstrated enhanced killing of organismswithin vegetations when compared with monotherapywith cell-wall active agents in animal models ofSAIE.88,89,162,163 An early retrospective study did not showany reduction in mortality when gentamicin was addedto an antistaphylococcal β-lactam agent for the treat-ment of SAIE.39 Although a multicentre, prospective,randomised clinical trial of nafcillin (for 6 weeks) versuscombination therapy with nafcillin (for 6 weeks) andgentamicin (for 2 weeks) for SAIE demonstrated that theaddition of gentamicin significantly reduced the durationof bacteraemia, there was no significant difference incure rates or mortality, and more nephrotoxicity wasseen with the combination regimen.164
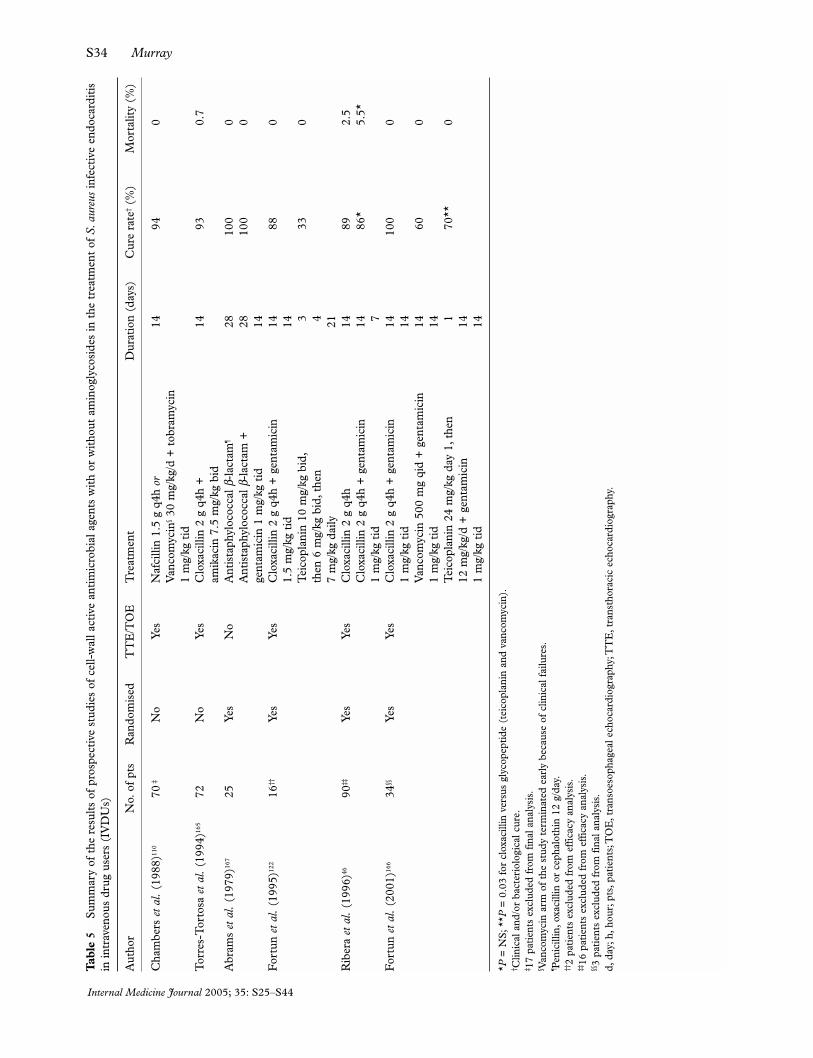
Several clinical trials have compared combinationantistaphylococcal β-lactam/aminoglycoside therapyto antistaphylococcal β-lactam monotherapy for SAIEin IVDUs with predominantly ‘right-sided’ disease(Table 5).46,109,122,164–167 There were significant variations
Internal Medicine Journal 2005; 35: S25–S44
MurrayS34
Internal Medicine Journal 2005; 35: S25–S44
Tabl
e5
Sum
mar
y of
the
res
ults
of
pros
pect
ive
stud
ies
of c
ell-
wal
l act
ive
antim
icro
bial
age
nts
with
or
with
out
amin
ogly
cosi
des
in t
he t
reat
men
t of
S.a
ureu
sin
fect
ive
endo
card
itis
in in
trav
enou
s dr
ug u
sers
(IV
DU
s)
Aut
hor
No.
of p
tsR
ando
mis
edT
TE
/TO
ET
reat
men
tD
urat
ion
(day
s)C
ure
rate
†(%
)M
orta
lity
(%)
Cha
mbe
rs e
tal.
(198
8)11
070
‡N
oYe
sN
afci
llin
1.5
g q4
h or
1494
0V
anco
myc
in§30
mg/
kg/d
+to
bram
ycin
1m
g/kg
tid
Tor
res-
Tor
tosa
eta
l.(1
994)
165
72N
oYe
sC
loxa
cilli
n 2
g q4
h +
1493
0.7
amik
acin
7.5
mg/
kg b
idA
bram
s et
al.
(197
9)16
725
Yes
No
Ant
ista
phyl
ococ
cal β
-lac
tam
¶28
100
0A
ntis
taph
yloc
occa
l β-l
acta
m+
2810
00
gent
amic
in 1
mg/
kg t
id14
For
tun
etal
.(1
995)
122
16††
Yes
Yes
Clo
xaci
llin
2g
q4h
+ge
ntam
icin
14
880
1.5
mg/
kg t
id14
Tei
copl
anin
10
mg/
kg b
id,
333
0th
en 6
mg/
kg b
id,t
hen
47
mg/
kg d
aily
21R
iber
a et
al.
(199
6)46
90‡‡
Yes
Yes
Clo
xaci
llin
2g
q4h
1489
2.5
Clo
xaci
llin
2g
q4h
+ge
ntam
icin
14
86*
5.5*
1m
g/kg
tid
7F
ortu
n et
al.
(200
1)16
634
§§Ye
sYe
sC
loxa
cilli
n 2
g q4
h+
gent
amic
in
1410
00
1m
g/kg
tid
14V
anco
myc
in 5
00m
g qi
d+
gent
amic
in
1460
01
mg/
kg t
id14
Tei
copl
anin
24
mg/
kg d
ay 1
,the
n 1
70**
012
mg/
kg/d
+ge
ntam
icin
14
1m
g/kg
tid
14
*P=
NS;
**P
=0.
03 f
or c
loxa
cilli
n ve
rsus
gly
cope
ptid
e (t
eico
plan
in a
nd v
anco
myc
in).
† Clin
ical
and
/or
bact
erio
logi
cal c
ure.
‡ 17
patie
nts
excl
uded
fro
m f
inal
ana
lysi
s.§ V
anco
myc
in a
rm o
f th
e st
udy
term
inat
ed e
arly
bec
ause
of
clin
ical
fai
lure
s.¶ P
enic
illin
,oxa
cilli
n or
cep
halo
thin
12
g/da
y.††
2 pa
tient
s ex
clud
ed f
rom
eff
icac
y an
alys
is.
‡‡16
pat
ient
s ex
clud
ed f
rom
eff
icac
y an
alys
is.
§§3
patie
nts
excl
uded
fro
m f
inal
ana
lysi
s.d,
day;
h,ho
ur;p
ts,p
atie
nts;
TO
E,t
rans
oeso
phag
eal e
choc
ardi
ogra
phy;
TT
E,t
rans
thor
acic
ech
ocar
diog
raph
y.

S35S. aureus infective endocarditis
in design, inclusion and exclusion criteria, and choiceand duration of antimicrobial therapy in these trials, butoverall, they suggest that the addition of an aminoglyco-side to a cell-wall active agent does not appear to be ofbenefit, and that antistaphylococcal β-lactams appearsuperior to glycopeptides (alone or in combination withaminoglycosides) for the treatment of SAIE caused byMSSA.
Once-daily aminoglycoside therapy is commonly usedfor infections due to Gram-negative organisms. However,as the efficacy and safety of once-daily dosing has notbeen directly compared with traditional three-times-daily dosing in the treatment of SAIE, it is currently notrecommended. Because of an increased potential fornephro- and ototoxicity when vancomycin is adminis-tered in combination with an aminoglycoside, thiscombination should be used with caution.168
Ciprofloxacin plus rifampicin
The combination of ciprofloxacin with rifampicin hasproved effective in animal models of SAIE, despiteconcerns regarding in vitro antagonism.131,169 A regimenconsisting of ciprofloxacin 300 mg twice daily intra-venously for up to 7 days followed by 750 mg twice dailyorally plus rifampicin 300 mg twice daily orally for a totalof 28 days achieved a 100% cure rate in a small prospec-tive, non-randomised study of 10 IVDUs with ‘right-sided’ SAIE.170 A prospective, open, randomised trialthat compared oral ciprofloxacin 750 mg twice daily andoral rifampicin 300 mg twice daily with intravenousoxacillin or vancomycin for 2 weeks combined withgentamicin 2 mg/kg three times daily for the first 5 daysfor the treatment of ‘right-sided’ SAIE in 85 IVDUsreported fewer clinical failures and significantly lesstoxicity in the group receiving ciprofloxacin andrifampicin.47 However, clinical failure associated withresistance to both agents has been reported with the useof this combination.171,172
At present, the combination of ciprofloxacin andrifampicin should be reserved for patients with uncom-plicated ‘right-sided’ SAIE who are unwilling or unableto receive intravenous therapy, and who will becompliant with oral therapy (or be willing to receive oraltherapy under direct supervision).
Vancomycin plus rifampicin
An early report described favourable outcomes followingthe addition of rifampicin to vancomycin in patients withSAIE who were failing therapy.173 Subsequently, arandomised, controlled clinical trial that comparedvancomycin (1 g twice daily) to vancomycin (1 g twicedaily) plus rifampicin (600 mg once daily orally) for4 weeks in 42 patients with SAIE caused by MRSA (themajority of whom were IVDUs with probable ‘right-sided’ disease) demonstrated no difference in outcomebetween the two groups.111 The emergence of rifampicinresistance has been described with this combination.174
Cell-wall active agents plus aminoglycosides plus rifampicin
The combination of vancomycin, rifampicin andgentamicin proved more effective than vancomycin
alone, vancomycin and gentamicin, or vancomycin andrifampicin in an animal model of endocarditis caused byS. epidermidis.175 A retrospective study of S. epidermidisprosthetic valve endocarditis suggested that therapy witha cell-wall active agent combined with an aminoglyco-side and/or rifampicin was more likely to be curativethan therapy with a cell-wall active agent alone, whethersurgery was performed during therapy or not.176 Theseresults have been extrapolated to the management ofprosthetic valve infective endocarditis caused byS. aureus in previously published guidelines. In theabsence of evidence from prospective, randomisedcontrolled trials, and given the significant mortality asso-ciated with this infection, both gentamicin andrifampicin should be given in combination with anantistaphylococcal β-lactam (for MSSA) or vancomycin(for MRSA) in prosthetic valve endocarditis caused byS. aureus.
Treatment of prosthetic valve S. aureus infectiveendocarditisProsthetic valve endocarditis (PVE) due to S. aureus isassociated with mortality rates of more than 40%.15,177–179
Intracardiac and extracardiac complications arecommon. ‘Early’ PVE caused by S. aureus occurs lessthan 12 months after valve surgery, and is usually theresult of contamination of the surgical field at the time ofor shortly after surgery. ‘Late’ PVE occurs more than12 months after valve surgery and results from seeding ofthe prosthesis from bacteraemia originating at a distantsite (e.g. an intravascular catheter). Both types of PVEoccur equally on bioprosthetic or mechanical valves.Close and early consultation with a cardiologist, cardio-thoracic surgeon and an infectious disease physician orclinical microbiologist is essential in PVE due toS. aureus. Transoesophageal echocardiography shouldalways be performed, as it is more sensitive for the detec-tion of intracardiac complications than TTE and allowsplanning of subsequent surgery.
No randomised, controlled clinical trials have beenperformed to determine the optimal antimicrobial treat-ment or the timing of surgery in prosthetic valve SAIE.Although data from clinical trials are lacking, there isgeneral agreement that combination antimicrobialtherapy using agents with bactericidal activity and withgood activity in association with prosthetic materialshould be used for the treatment of prosthetic valveSAIE (Table 6). If surgical specimens are negative onculture, the total duration of therapy should be at least6 weeks. If surgical specimens are culture-positive forS. aureus, or if an active intracardiac infection is found(e.g. myocardial abscess, annulus infection or pseudo-aneurysm), then treatment should continue for aminimum of 6 weeks following surgery. A large retro-spective study of ‘left-sided’ prosthetic valve SAIEsuggested that early valve replacement surgery lessenedmortality, even in the absence of intracardiac or extrac-ardiac complications,15 and similar findings were seen ina small prospective study which reported that four offour patients who had surgery for prosthetic valve SAIE
Internal Medicine Journal 2005; 35: S25–S44

MurrayS36
survived compared with two of 11 who did not.177
However, these studies would have been biased towardsfavourable outcomes in patients who underwent surgery,since patients with a poor prognosis at presentation maynot have been selected for surgery.
Outpatient parenteral antimicrobial therapy(OPAT) for S. aureus infective endocarditisThere have been no randomised, controlled clinical trialscomparing the efficacy and safety of OPAT to inpatienttherapy for SAIE. Several studies of OPAT for deep-seated staphylococcal infections have included smallnumbers of patients with SAIE.93,94,180–184 However, someauthorities have advised against OPAT for SAIE becauseof the significant risk of complications related to theinfection.185 The likelihood of an embolic event in SAIEis significantly higher than in streptococcal infectiveendocarditis.186 The risk of endocarditis-related compli-cations is considered to be highest in the first 2 weeks oftherapy, and the risk of line or antimicrobial-relatedadverse effects is highest between 2 and 6 weeks oftherapy.187 However, hospitalization does not preventcomplications from SAIE, and it is not known whetheroutcomes are worse if complications occur when thepatient is not hospitalized.184
A variety of antimicrobial regimes have been used forOPAT of SAIE with reported success, including ceftri-axone and gentamicin, teicoplanin and continuousinfusion flucloxacillin.93,94,180,182,188 The optimal choice ofagent and method of delivery varies significantlybetween institutions, but it is important that the choice
of antimicrobial agent is not compromised for the sakeof earlier hospital discharge and healthcare savings. Ifcontinuous infusion therapy is to be given, the stabilityof the antimicrobial agent at conditions in which it isto be stored and administered must be known.Flucloxacillin is stable in solution for up to 7 days at 4°C;however, dicloxacillin is unstable in solution at roomtemperature and is therefore unsuitable for OPAT. Asserum flucloxacillin concentrations may vary signifi-cantly when it is administered by infusion (due to varia-tions in renal function and other factors), measurementof serum flucloxacillin concentrations may be useful inguiding dosing during therapy.93,189 Vancomycin is alsostable in solution for several days and may be given as aninfusion or bolus therapy for OPAT. Continuous infusiontherapy should always be administered via a centralvenous catheter.
Careful selection of patients for OPAT is critical.185
Contraindications include active cardiac infection oruntreated metastatic infection, congestive cardiac failure,uncontrolled arrhythmias, a previous arterial embolicevent, inability to establish central venous access, no tele-phone at home, no ready access to the hospital or patientunwillingness to receive outpatient therapy. Relativecontraindications include prosthetic valve endocarditis, ahistory of intravenous drug use, and lack of reliable trans-portation. Patients with SAIE being considered for OPATshould receive at least the initial 10–14 days of therapy inhospital and should be assessed by a cardiologist, acardiothoracic surgeon, and an infectious diseases physi-cian or clinical microbiologist prior to discharge.
Internal Medicine Journal 2005; 35: S25–S44
Table 6 Recommendations for the treatment of prosthetic valve endocarditis caused by S. aureus
Clinical setting Recommended antimicrobial therapy†
• Methicillin-susceptible S. aureus Flucloxacillin/dicloxacillin 2 g IV q4h for 42 days plus rifampicin 600 mg IV/PO daily for 42 days plus gentamicin 1 mg/kg IV q8h for the first 14 days
If isolate is susceptible to penicillin Substitute for flucloxacillin/dicloxacillin:Benzylpenicllin 1.8 g IV q4h
If non-severe penicillin hypersensitivity‡ Substitute for flucloxacillin/dicloxacillin:Cephalothin 2 g IV q4h
• Severe penicillin hypersensitivity‡ or Vancomycin 15 mg/kg IV q12h for 42 days plus rifampicin 600 mg methicillin-resistant IV/PO S. aureus daily for 42 days plus gentamicin 1 mg/kg
IV q8h for the first 14 days• Intolerance of or hypersensitivity to vancomycin (for Discuss therapy with an Infectious Diseases
methicillin-resistant S. aureus) or to both β-lactams Physician/Clinical Microbiologist. Alternatives to and vancomycin (for methicillin-susceptible S. aureus) β-lactams/vancomycin include:
Teicoplanin 800 mg IV q12h for first 24 h, then 800 mg daily; orLinezolid 600 mg IV/PO q12h; orQuinupristin/dalfopristin 7.5 mg/kg IV q8h
• Outpatient intravenous antimicrobial therapy Not currently recommended
Note: urgent transoesophageal echocardiography and early referral to a cardiothoracic surgeon is essential.†Doses and dose intervals of the following antimicrobial agents should be adjusted according to the patient’s renal function and therapeutic drugmonitoring results:
– gentamicin: aim for a trough serum concentration of <1 mg/L– vancomycin: aim for a trough serum concentration of 15-20 mg/L (intermittent dosing) or at least 20 mg/L (continuous infusion)– teicoplanin: aim for a trough serum concentration of >20 mg/L– flucloxacillin: as there are significant variations in methodology, refer to local laboratory data for interpretation.
‡Immediate-type hypersensitivity skin testing for penicillins should be considered when there is no clearly documented history of hypersensitivity.

S37S. aureus infective endocarditis
TREATMENT OF CARDIAC ANDEXTRACARDIAC COMPLICATIONSOF S. AUREUS INFECTIVEENDOCARDITIS
Cardiac complicationsRegular and careful serial clinical examination of allpatients with SAIE is essential to detect the onset ofcomplications that may need surgical intervention. Serialechocardiography should be performed in patients withclinical and/or initial echocardiographic evidence ofcomplications, particularly in aortic valve SAIE wheresudden onset of severe valvular regurgitation may resultin acute severe pulmonary oedema requiring emergencysurgery.
Because intraventricular conduction disturbancesare common in patients with SAIE complicated byparavalvular infection,190 electrocardiography (ECG)should be performed at diagnosis and serially in patientswith persistent fever, heart failure or arrhythmias.191
Paravalvular extension of the infection is an indicationfor urgent surgical intervention. In prosthetic valveSAIE, small paravalvular leaks or other abnormalitieson echocardiography may predate the onset of endo-carditis; therefore, a comparison of echocardiographicfindings with previous results should be performedwhenever possible to establish their significance. Aspersistent bacteraemia may be the only indicator ofparavalvular infection, patients with bacteraemiapersisting for 7 days or more following the commence-ment of appropriate therapy should be evaluated forcardiac complications with transoesophageal echocardio-graphy, so that any surgically remediable cardiac lesionsare identified.
Extracardiac complicationsThe management of embolic events in ‘left-sided’ SAIEdepends on the site and size of the embolus. Such eventsare managed conservatively, unless there is occlusion ofan artery that perfuses a critical structure such as a limbor the heart, in which case immediate intervention maybe required.
Patients with SAIE who have neurological symptomsor signs at the time of diagnosis or during the course oftherapy should undergo imaging to determine the cause,location and extent of any lesion. The initial imagingmodality is usually computerized tomography (CT)because it is readily available in most institutions, can beperformed rapidly, and provides reliable informationregarding the nature and location of cerebral lesions inmost cases. In certain circumstances, magnetic reso-nance (MR) imaging (with or without MR angiography)may be indicated instead of or subsequent to CTimaging. As valve replacement surgery is relativelycontraindicated in the presence of a recent large cerebralembolic event (particularly if there is haemorrhagictransformation), most surgeons delay surgery for at least7–14 days to lessen the likelihood of precipitating orworsening the neurological deficit with subsequent anti-coagulant therapy. However, the consequences of
delaying surgery in patients with congestive cardiacfailure caused by SAIE are not insignificant and must bebalanced against this risk.
Mycotic aneurysms usually present with intracerebralor subarachnoid haemorrhage or as a stroke.54 Onereport has suggested that mycotic aneurysms causedby S. aureus are more likely to rupture.192 If cerebralimaging demonstrates a subarachnoid or intracerebralhaemorrhage, or clinical signs that suggest possibleaneurysm formation are present (e.g. headache orcranial nerve palsies without identifiable cause), thencerebral angiography should be considered. If ananeurysm is demonstrated, the patient should bereferred to a neurosurgeon or an interventional neuro-radiologist for consideration of surgical or percutaneousintervention.191
Embolization of vegetations into the pulmonarycirculation rarely requires surgical intervention.However, secondary infective complications such as lungabscess or empyema may require percutaneous and/oropen surgical drainage in addition to prolongation ofantimicrobial therapy longer than the recommended2 weeks for uncomplicated disease. Serial pulmonaryimaging (using chest X-ray and/or CT) may be requiredin patients with these complications or in those who donot respond as expected to antimicrobial therapy.
Significant metastatic infective foci such as visceralabscesses, empyemata or septic arthritis should betreated by percutaneous or open drainage withoutdelay to prevent further complications, increase thelikelihood of therapeutic success, and decrease the like-lihood of recurrence. Patients who may be at higher riskfor metastatic infection include those with prostheticjoints and those in whom the period of bacteraemia isprolonged.
SURGERY FOR S. AUREUS INFECTIVEENDOCARDITIS
The role of surgery in native or prosthetic valve SAIE hasnot been examined in randomised clinical trials. Severalretrospective studies have reported more favourableoutcomes in patients with SAIE who underwent surgerycompared with those that did not.193–199 However, thesestudies may have been biased towards better outcomesfor surgically treated patients, because patients with ahigher likelihood of survival and fewer comorbiditiesmay be more likely to be operated on. The need forsurgical intervention in SAIE needs to be individualizedfor each patient and should be reviewed if the clinicalstate deteriorates. All resected tissue from surgery shouldbe submitted for pathological and microbiological exam-ination to confirm the diagnosis of SAIE and to deter-mine the activity and extent of the infection at the timeof surgery.
The operative technique and choice of prosthesisemployed for the surgical treatment of SAIE depends onseveral factors, including the site and extent of the infec-tion, the availability of homografts or xenografts, and theexpertise of the surgeon. Specific recommendations arebeyond the scope of this review.
Internal Medicine Journal 2005; 35: S25–S44

MurrayS38
‘Left-sided’ SAIEIn patients with ‘left-sided’ SAIE, surgery should beconsidered in the presence of haemodynamically signifi-cant valvular regurgitation (New York Heart Associationstage III or IV congestive cardiac failure), large and/orhighly mobile vegetations, vegetations of ≥1 cm on theanterior mitral valve leaflet, paravalvular extension of theinfection, rupture of the sinus of Valsalva, mechanicalobstruction of a valve by vegetations, or duration ofbacteraemia ≥7 days despite appropriate therapy.Surgery may also be considered for those patients whohave experienced one or more embolic significant events.Vegetectomy combined with valve repair may be possiblewhen a single leaflet of the mitral valve is involved.200
‘Right-sided’ SAIE‘Right-sided’ SAIE generally has a more benign coursethan ‘left-sided’ disease, and vegetation size does notappear to correlate with failure of antimicrobialtherapy.80 There is, however, a high rate of recurrenceof ‘right-sided’ endocarditis in IVDUs who continueto inject drugs.38 Therefore, a conservative approach tosurgical management in ‘right-sided’ SAIE is oftenfollowed. Surgery may be considered for patients with‘right-sided’ SAIE who have persistent or recurrentbacteraemia or ongoing significant septic emboli despiteadequate therapy. Valvulectomy is usually performed ifthe patient is able to tolerate the resulting severetricuspid regurgitation.38,201,202 Subsequent prosthesisinsertion may be required in patients who develop severechronic tricuspid regurgitation.201
Prosthetic valve S. aureus endocarditisSurgery should be considered in all cases of prostheticvalve endocarditis caused by S. aureus and should beperformed as early as possible.191
ANTITHROMBOTIC THERAPY INS. AUREUS INFECTIVE ENDOCARDITIS
Animal models of SAIE have suggested that antiplateletagents such as aspirin and/or ticlodipine can significantlyreduce vegetation size and, when given with vancomycin,can sterilize vegetations more quickly.203–205 Administra-tion of aspirin to animals prior to the establishment ofSAIE resulted in decreased adherence of S. aureus tovegetations, fibrin and platelets, in addition to reductionsin vegetation size and bacterial density within thevegetation and the kidneys.203 However, as there havebeen no clinical trials of antiplatelet therapy in SAIE todate, it is not currently recommended.
Continuation of anticoagulation therapy in patientswith prosthetic valve SAIE is controversial. A smallretrospective study of ‘left-sided’ SAIE that comparedpatients with PVE (90% of whom were on anticoagulanttherapy) with patients with native valve endocarditis(none of whom were on anticoagulant therapy) foundthat there was no difference in the proportion of patientswho suffered from cerebral embolic events between the
groups. However, mortality was significantly higher inpatients with PVE (71% vs 31%), and most deaths inthis group were due to cerebral embolic complications,most commonly intracerebral haemorrhage.The authorsrecommended that anticoagulant therapy be withheldfor 7 days in patients with prosthetic valve SAIE.206
Other groups have recommended continuation of long-term anticoagulant therapy in patients with PVE, butdelaying valve surgery for at least 7 days if a CT scan ofthe brain demonstrates a large infarction.207
ACKNOWLEDGEMENTSThe author would like to thank: the Australian Society for Antimicro-bials and Australasian Society for Infectious Diseases, who provided allthe financial support for the costs of production and publication of thiswork; Professor John Turnidge and Associate Professor Keryn Chris-tiansen of the Australian Society for Antimicrobials, for devising theconcept of writing guidelines for the treatment of deep-seated staphy-lococcal infections and for assistance with various aspects of publica-tion; Associate Professor Iain Gosbell, Department of Microbiologyand Infectious Diseases, South-western Area Pathology Service, Liver-pool, NSW, for convening the ASA Staphylococcus aureusWorking Partyand co-ordinating the writing of the body of manuscripts, editing thismanuscript, and providing the photographs used in Figs 2 and 3A,B;Dr Bryan Speed, for providing the photographs from the FairfieldHospital Historical Collection, used in Fig. 1A–C; Mr Trevor Speight,Medical Editor, Medicines Information Co. Ltd, Auckland, NZ, forfinal editing and formatting of this manuscript; and the members of theAustralasian Society for Infectious Diseases who provided peer reviewof this work.
REFERENCES1 Espersen F, Frimodt-Moller N. Staphylococcus aureus
endocarditis: a review of 119 cases. Arch Intern Med 1986;146: 1118–21.
2 Steinberg JP, Clark CC, Hackman BO. Nosocomial andcommunity-acquired Staphylococcus aureus bacteremias from1980 to 1993: impact of intravascular devices and methicillinresistance. Clin Infect Dis 1996; 23: 255–9.
3 Petti CA, Fowler VG Jr. Staphylococcus aureus bacteremiaand endocarditis. Infect Dis Clin North Am 2002; 16:413–35.
4 Cabell CH, Jollis JG, Peterson GE, Corey GR, Anderson DJ,Sexton DJ et al. Changing patient characteristics and theeffect on mortality in endocarditis. Arch Intern Med 2002;162: 90–4.
5 Sanabria TJ, Alpert JS, Goldberg R, Pape LA, Cheeseman SH.Increasing frequency of staphylococcal infective endocarditis:experience at a university hospital, 1981 through 1988. ArchIntern Med 1990; 150: 1305–9.
6 Watanakunakorn C, Burkert T. Infective endocarditis at alarge community teaching hospital, 1980–1990: a review of210 episodes. Medicine (Baltimore) 1993; 72: 90–102.
7 Sandre RM, Shafran SD. Infective endocarditis: review of135 cases over 9 years. Clin Infect Dis 1996; 22: 276–86.
8 Mylonakis E, Calderwood SB. Infective endocarditis inadults. N Engl J Med 2001; 345: 1318–30.
9 Cabell CH, Abutryn E. Progress towards a globalunderstanding of infective endocarditis: early lessons fromthe International Collaboration on Endocarditisinvestigation. Infect Dis Clin North Am 2002; 16: 255–72.
10 Mouly S, Ruimy R, Launay O, Arnoult F, Brochet E,Trouillet J et al. The changing clinical aspects of infectiveendocarditis: descriptive review of 90 episodes in a Frenchteaching hospital and risk factors for death. J Infect 2002;45: 246–56.
Internal Medicine Journal 2005; 35: S25–S44
S39S. aureus infective endocarditis
11 Fowler VG Jr, Li J, Corey GR, Boley J, Marr KA, Gopal AKet al. Role of echocardiography in evaluation of patients withStaphylococcus aureus bacteremia: experience in 103 patients.J Am Coll Cardiol 1997; 30: 1072–8.
12 Watanakunakorn C. Staphylococcus aureus endocarditis at acommunity teaching hospital, 1980–1991. Arch Intern Med1994; 154: 2330–5.
13 Fowler VG Jr, Sanders LL, Kong LK, McClelland RS,Gottlieb GS, Li J et al. Infective endocarditis due toStaphylococcus aureus: 59 prospectively identified cases withfollow-up. Clin Infect Dis 1999; 28: 106–14.
14 Roder BL, Wandall DA, Frimodt-Moller N, Espersen F,Skinhoj P, Rosdahl VT. Clinical features of Staphylococcusaureus endocarditis: a 10-year experience in Denmark. ArchIntern Med 1999; 159: 462–9.
15 John MDV, Hibberd PL, Karchmer AW, Sleeper LA,Calderwood SB. Staphylococcus aureus prosthetic valveendocarditis: optimal management and risk factors for death.Clin Infect Dis 1998; 26: 1302–9.
16 Wilson R, Hamburger M. Fifteen year’s experience withStaphylococcus septicemia in a large city hospital: analysis of55 cases in the Cincinnati General Hospital 1940–1955. AmJ Med 1957; 22: 437–57.
17 Nolan CM, Beatty HN. Staphylococcus aureus bacteremia:current clinical patterns. Am J Med 1976; 60: 495–500.
18 Watanakunakorn C, Baird IM. Staphylococcus aureusbacteremia and endocarditis associated with a removableinfected intravenous device. Am J Med 1977; 63: 253–6.
19 Mirimanoff RO, Glauser MP. Endocarditis duringStaphylococcus aureus septicemia in a population of non-drugaddicts. Arch Intern Med 1982; 142: 1311–13.
20 Gransden WR, Eykeyn SJ, Phillips I. Staphylococcus aureusbacteraemia: 400 episodes in St. Thomas’s Hospital. BMJ1984; 288: 300–3.
21 Mylotte JM, McDermott C, Spooner JA. Prospective studyof 114 consecutive episodes of Staphylococcus aureusbacteremia. Rev Infect Dis 1987; 9: 891–907.
22 Bayer AS, Lam K, Ginzton L, Norman DC, Chiu CY, WardJI. Staphylococcus aureus bacteremia: clinical, serologic, andechocardiographic findings in patients with and withoutendocarditis. Arch Intern Med 1987; 147: 457–62.
23 Lautenschlager S, Herzog C, Zimmerli W. Course andoutcome of bacteremia due to Staphylococcus aureus:evaluation of different clinical case definitions. Clin InfectDis 1993; 16: 567–73.
24 Fowler VG Jr, Sanders LL, Sexton DJ, Kong L, Marr KA,Gopal AK et al. Outcome of Staphylococcus aureus bacteremiaaccording to compliance with recommendations of infectiousdiseases specialists: experience with 244 patients. Clin InfectDis 1998; 27: 478–86.
25 Marr KA, Kong LK, Fowler VG Jr, Gopal A, Sexton DJ,Conlon PJ et al. Incidence and outcome of Staphylococcusaureus bacteremia in hemodialysis patients. Kidney Int 1998;54: 1684–9.
26 Mylotte JM, Tayara A. Staphylococcus aureus bacteremia:predictors of 30-day mortality in a large cohort. Clin InfectDis 2000; 31: 1170–4.
27 Jensen AG,Wachmann CH, Espersen F, Scheibel J, Skinhoj P,Frimodt-Moller N. Treatment and outcome of Staphylococcusaureus bacteremia: a prospective study of 278 cases. ArchIntern Med 2002; 162: 25–32.
28 Fowler VG Jr, Olsen MK, Corey R, Woods CW, Cabell CH,Reller B et al. Clinical identifiers of complicatedStaphylococcus aureus bacteremia. Arch Intern Med 2003;163: 2066–72.
29 Chang FY, MacDonald BB, Peacock JE Jr, Musher DM,Triplett P, Mylotte JM et al. A prospective multicenter study
of Staphylococcus aureus bacteremia: incidence of endocarditis,risk factors for mortality, and clinical impact of methicillinresistance. Medicine (Baltimore) 2003; 82: 322–32.
30 Li JS, Sexton DJ, Mick N, Nettles R, Fowler VG Jr, Ryan Tet al. Proposed modifications to the Duke criteria for thediagnosis of infective endocarditis. Clin Infect Dis 2000; 30:633–8.
31 Kainer M, Slavin M, Chua J, Goutzmanis J, Kucers A.Community-acquired Staphylococcus aureus bacteremia:clinical features and complications [abstract K206]. 35thInterscience Conference on Antimicrobial Agents andChemotherapy; 1995; San Francisco, CA. Washington DC:American Society for Microbiology; 1995: 325.
32 O’Kane GM, Gottlieb T, Bradbury R. Staphylococcalbacteraemia: the hospital or the home? A review ofStaphylococcus aureus bacteraemia at Concord Hospital in1993. Aust NZ J Med 1998; 28: 23–7.
33 Blyth CC, Darragh H, Whelan A, O’Shea JP, Beaman MH,McCarthy JS. Evaluation of guidelines for the managementof Staphylococcus aureus bacteraemia. Intern Med J 2002; 32:224–32.
34 Levine DP, Crane LR, Zervos MJ. Bacteremia in narcoticaddicts at the Detroit Medical Center. II. Infectiousendocarditis: a prospective comparative study. Rev Infect Dis1986; 8: 374–96.
35 Marantz PR, Linzer M, Feiner CJ, Feinstein SA, Kozin AM,Friedland GH. Inability to predict diagnosis in febrileintravenous drug abusers. Ann Intern Med 1987; 106:823–8.
36 Hecht SR, Berger M. Right-sided endocarditis in intravenousdrug users: prognostic features in 102 episodes. Ann InternMed 1992; 117: 560–6.
37 Mathew J, Addai T, Anand A, Morrobel A, Maheshwari P,Freels S. Clinical features, site of involvement, bacteriologicfindings and outcome of infective endocarditis in intravenousdrug users. Arch Intern Med 1995; 155: 1641–8.
38 Miro JM, del Rio A, Mestres CA. Infective endocarditis andcardiac surgery in intravenous drug abusers and HIV-1infected patients. Cardiol Clin 2003; 21: 167–84.
39 Watanakunakorn C, Baird IM. Prognostic factors inStaphylococcus aureus endocarditis and results of therapy witha penicillin and gentamicin. Am J Med Sci 1977; 273: 133–9.
40 Tuazon CU, Sheagran JN. Increased staphylococcal carrierrate among narcotic addicts. J Infect Dis 1974; 129: 725–7.
41 Tuazon CU, Sheagren JN. Staphylococcal endocarditis inparenteral drug abusers: source of the organism. Ann InternMed 1975; 82: 788–90.
42 Crane LR, Levine DP, Zervos MJ, Cummings G. Bacteremiain narcotic addicts at the Detroit Medical Center:microbiology, epidemiology, risk factors and empiric therapy.Rev Infect Dis 1986; 8: 364–73.
43 Reisberg B. Infective endocarditis in the narcotic addict. ProgCardiovasc Dis 1979; 22: 193–204.
44 Manoff SB, Vhlahov D, Herskowitz A, Solomon L, Munoz A,Cohn S et al. Human immunodeficiency virus infection andinfective endocarditis among injecting drug users.Epidemiology 1996; 7: 563–5.
45 Spijkerman IJ, van Ameijden EJ, Mientjes GH, Coutinho RA,van den Hoek A. Human immunodeficiency virus infectionand other risk factors for skin abscesses and endocarditisamong injection drug users. J Clin Epidemiol 1996; 49:1149–54.
46 Ribera E, Gomez-Jiminez J, Cortes E, del Valle O, Planes A,Gonzales-Alujas MT et al. Effectiveness of cloxacillin withand without gentamicin in short term therapy for right-sidedStaphylococcus aureus endocarditis. Ann Intern Med 1996;125: 969–74.
Internal Medicine Journal 2005; 35: S25–S44

MurrayS40
47 Heldman AW, Hartert TV, Ray SC, Dauod EG, Kowalski TE,Pompili VJ et al. Oral antibiotic treatment of right-sidedstaphylococcal endocarditis in intravenous drug users:prospective randomized comparison with parenteral therapy.Am J Med 1996; 101: 68–76.
48 Frimodt-Moller N, Espersen F, Rosdahl VT. Antibiotictreatment of Staphylococcus aureus endocarditis. A review of119 cases. Acta Med Scand 1987; 222: 175–82.
49 Fernandez-Guerrero ML,Verdejo C, Azofra J, de Gorgolas M.Hospital-acquired infectious endocarditis not associated withcardiac surgery: an emerging problem. Clin Infect Dis 1995;20: 16–23.
50 Rohmann S, Erbel R, Mohr-Kahaly S, Meyer J. Use oftransesophageal echocardiography in the diagnosis of abscessin infective endocarditis. Eur Heart J 1995; 16: 54–62.
51 Bayer AS, Norman DC. Valve site-specific pathogeneticdifferences between right-sided and left-sided bacterialendocarditis. Chest 1990; 98: 200–5.
52 Di Nubile MJ. Short-course antibiotic therapy for right-sidedendocarditis caused by Staphylococcus aureus in intravenousdrug users. Ann Intern Med 1994; 121: 873–6.
53 Roder BL, Wandall DA, Espersen F, Frimodt-Moller N,Skinhoj P, Rosdahl VT. Neurologic manifestations inStaphylococcus aureus endocarditis: a review of 260 bacteremiccases in nondrug addicts. Am J Med 1997; 102: 379–86.
54 Corr P, Wright M, Handler LC. Endocarditis-related cerebralaneurysms: radiologic changes with treatment. AJNR Am JNeuroradiol 1995; 16: 745–8.
55 Von Reyn CF, Levy BS, Arbeit RD, Friedland G,Crumpacker CS. Infective endocarditis: an analysis based onstrict case definitions. Ann Intern Med 1981; 94: 505–18.
56 Majumdar A, Chowdhary S, Ferreira MA, Hammond LA,Howie AJ, Lipkin GW et al. Renal pathological findings ininfective endocarditis. Nephrol Dial Transplant 2000; 15:1782–7.
57 Coleman DL, Horwitz RI, Andriole VT. Association betweenserum inhibitory and bactericidal concentrations andtherapeutic outcome in bacterial endocarditis. Am J Med1982; 73: 260–7.
58 Tuazon CU, Sheagren JN. Teichoic acid antibodies in thediagnosis of serious infections with Staphylococcus aureus. AnnIntern Med 1976; 84: 543–6.
59 Shrestha NK, Tuohy MJ, Hall GS, Isada CM, Procop GW.Rapid identification of Staphylococcus aureus and the mecAgene from BacT/ALERT blood culture bottles by using theLightCycler system. J Clin Microbiol 2002; 40: 2659–61.
60 Oliveira K, Procop GW, Wilson D, Coull J, Stender H. Rapididentification of Staphylococcus aureus directly from bloodcultures by fluorescence in situ hybridization with peptidenucleic acid probes. J Clin Microbiol 2002; 40: 247–51.
61 Millar B, Moore J, Mallon P, Xu J, Crowe M, Mcclurg Ret al. Molecular diagnosis of infective endocarditis – a newDuke’s criterion. Scand J Infect Dis 2001; 33: 673–80.
62 Bosshard PP, Kronenberg A, Zbinden R, Ruef C, Bottger EC,Altwegg M. Etiologic diagnosis of infective endocarditis bybroad-range polymerase chain reaction: a 3-year experience.Clin Infect Dis 2003; 37: 167–72.
63 Shively BK, Gurule FT, Roldan CA, Leggett JH, SchillerNB. Diagnostic value of transesophageal compared withtransthoracic echocardiography in infective endocarditis.J Am Coll Cardiol 1991; 18: 391–7.
64 Purnell PW, O’Brien DP, Appelbe AF, Athan E. NosocomialStaphylococcus aureus bacteraemia: a high incidence ofendocarditis found on transesophageal echocardiography.Intern Med J 2001; 31: A23.
65 Erbel R, Rohmann S, Drexler M, Mohr-Kahaly S,Gerharz CD, Iversen S et al. Improved diagnostic value of
echocardiography in patients with infective endocarditis bytransesophageal approach: a prospective study. Eur Heart J1988; 9: 43–53.
66 Mugge A, Daniel WG, Frank G, Lichtlen PR.Echocardiography in infective endocarditis: reassessment ofprognostic implications of vegetation size determined by thetransthoracic and the transesophageal approach. J Am CollCardiol 1989; 14: 631–8.
67 Daniel WG, Mugge A, Martin RP, Lindert O, Hausmann D,Nonnast-Daniel B et al. Improvement in the diagnosis ofabscesses associated with endocarditis by transesophagealechocardiography. N Engl J Med 1991; 324: 795–800.
68 Lowry RW, Zoghbi WA, Baker WB, Wray RA, Quinones MA.Clinical impact of transesophageal echocardiography in thediagnosis and management of infective endocarditis. Am JCardiol 1994; 73: 1089–91.
69 Shapiro SM,Young E, De Guzman S, Ward J, Chiu CY,Ginzton LE et al. Transesophageal echocardiography indiagnosis of infective endocarditis. Chest 1994; 105: 377–82.
70 Birmingham GD, Rahko PS, Ballantyne F. Improveddetection of infective endocarditis with transesophagealechocardiography. Am Heart J 1992; 123: 774–81.
71 San Roman JA, Vilacosta I, Zamorano JL, Almeria C,Sanchez-Harguindey L. Transesophageal echocardiographyin right-sided endocarditis. J Am Coll Cardiol 1993;21: 1226.
72 Georgeson R, Liu M, Bansal RC. Transesophagealechocardiographic diagnosis of eustachian valve endocarditis.J Am Soc Echocardiogr 1996; 9: 206–8.
73 Daniel WG, Mugge A, Grote J, Hausmann D, Nikutta P,Laas J et al. Comparison of transthoracic andtransesophageal echocardiography for the detection ofabnormalities of prosthetic and bioprosthetic valves in themitral and aortic positions. Am J Cardiol 1993; 71: 210–15.
74 Habib G, Guidon C, Tricoire E, Djiane V, Monties JR,Luccioni R. Papillary muscle rupture caused by bacterialendocarditis: role of transesophageal echocardiography. J AmSoc Echocardiogr, 1994; 7: 79–81.
75 De Castro S, d’Amati G, Cartoni D, Venditti M, Magni G,Gallo P et al. Valvular perforation in left-sided infectiveendocarditis: a prospective echocardiographic evaluation andclinical outcome. Am Heart J 1997; 134: 656–64.
76 Rosen AB, Fowler VG Jr, Corey GR, Downs SM, Biddle AK,Li J et al. Cost-effectiveness of transesophagealechocardiography to determine the duration of therapy forintravascular catheter-associated Staphylococcus aureusbacteremia. Ann Intern Med 1999; 130: 810–20.
77 Daniel WG, Erbel R, Kasper W, Visser CA, Engberding R,Sutherland GR et al. Safety of transesophagealechocardiography: a multicenter survey of 10 419examinations. Circulation 1991; 83: 817–21.
78 Vuille C, Nidorf M, Weyman AE, Picard MH. Naturalhistory of vegetations during successful treatment ofendocarditis. Am Heart J 1994; 128: 1200–9.
79 Rohmann S, Erbel R, Darius H, George G, Makowski T,Zotz R et al. Prediction of rapid versus prolonged healing ofinfective endocarditis by monitoring vegetation size. J AmSoc Echocardiogr 1991; 4: 465–74.
80 Bayer AS, Blomquist IK, Bello E, Chiu CY, Ward JI,Ginzton LE. Tricuspid valve endocarditis due toStaphylococcus aureus: correlation of two-dimensionalechocardiography with clinical outcome. Chest 1988; 93:247–53.
81 Han D, Lee KS, Franquet T, Muller NL, Kim TS, Kim Het al. Thrombotic and nonthrombotic pulmonary arterialembolism: spectrum of imaging findings. Radiographics2003; 23: 1521–39.
Internal Medicine Journal 2005; 35: S25–S44

S41S. aureus infective endocarditis
82 Durack DT, Lukes AS, Bright DK. Duke EndocarditisService. New criteria for diagnosis of infective endocarditis:utilization of specific echocardiographic findings. Am J Med1994; 96: 200–9.
83 Bayer AS, Bolger AF, Taubert KA, Wilson W, Steckelberg J,Karchmer AW et al. Diagnosis and management of infectiveendocarditis and its complications. Circulation 1998; 98:2936–48.
84 Wilson WR, Karchmer AW, Dajani AS, Taubert KA, Bayer A,Kaye D et al. Antibiotic treatment of adults with infectiveendocarditis due to streptococci, enterococci, staphylococciand HACEK organisms. JAMA 1995; 274: 1703–13.
85 Rubinstein E, Carbon C, the Endocarditis Working Group ofthe International Society of Chemotherapy. Staphylococcalendocarditis – recommendations for therapy. Clin MicrobiolInfect 1998; 4 Suppl 3: S27–33.
86 Simmons NA, Ball AP, Eykeyn SJ, Littler WA, McGowan DA,Oakley CM et al. Antibiotic treatment of streptococcal,enterococcal and staphylococcal endocarditis. Heart 1998;79: 207–10.
87 Nimmo GR, Bell JM, Mitchell D, Gosbell IB, Pearman JW,Turnidge JD et al. Antimicrobial resistance in Staphylococcusaureus in teaching hospitals, 1989–1999. Microb Drug Resist2003; 9: 155–60.
88 Sande MA, Johnson ML. Antimicrobial therapy ofexperimental endocarditis caused by Staphylococcus aureus.J Infect Dis 1975; 131: 367–75.
89 Sande MA, Courtney KB. Nafcillin-gentamicin synergism inexperimental staphylococcal endocarditis. J Clin Lab Med1976; 88: 118–24.
90 Chambers HF, Sande MA. Teicoplanin versus nafcillin andvancomycin in the treatment of experimental endocarditiscaused by methicillin-susceptible or -resistant Staphylococcusaureus. Antimicrob Agents Chemother 1984; 26: 61–4.
91 Carrizosa J, Kobasa WD, Kaye D. Comparison of ceforanide,cefazolin, methicillin and nafcillin in S. aureus endocarditistherapy in rabbits. Antimicrob Agents Chemother 1980; 18:562–5.
92 Carrizosa J, Santoro J, Kaye D. Treatment of experimentalStaphylococcus aureus endocarditis: comparison ofcephalothin, cephazolin and methicillin. Antimicrob AgentsChemother 1978; 13: 74–7.
93 Leder K, Turnidge JD, Korman TM, Grayson ML. Theclinical efficacy of continuous-infusion flucloxacillin inserious staphylococcal sepsis. J Antimicrob Chemother 1999;43: 113–18.
94 Howden BP, Richards MJ. The efficacy of continuousinfusion flucloxacillin in home based therapy for seriousstaphylococcal infections and cellulitis. J AntimicrobChemother 2001; 48: 311–14.
95 Dodek P, Phillips P. Questionable history of immediate-typehypersensitivity to penicillin in staphylococcal endocarditis:treatment based on skin-test results versus empiricalalternative treatment – a decision analysis. Clin Infect Dis1999; 29: 1251–6.
96 Carrizosa J, Kobasa W, Kaye D. Effectiveness of nafcillin,methicillin, and cephalothin in experimental Staphylococcusaureus endocarditis. Antimicrob Agents Chemother 1979; 15:735–7.
97 Fong IW, Engelking ER, Kirby WMM. Relative inactivationby Staphylococcus aureus of eight cephalosporin antibiotics.Antimicrob Agents Chemother 1976; 9: 939–44.
98 Goldman PL, Petersdorf RG. Importance of β-lactamaseinactivation in treatment of experimental endocarditis causedby Staphylococcus aureus. J Infect Dis 1980; 141: 331–7.
99 Quinn EL, Pohlod D, Madhavan T, Burch K, Fisher E, Cox F.Clinical experiences with cephazolin and other
cephalosporins in bacterial endocarditis. J Infect Dis 1973;1328 Suppl: S386–9.
100 Bryant RE, Alford RH. Unsuccessful treatment ofstaphylococcal endocarditis with cephazolin. JAMA 1977;237: 569–70.
101 Nannini EC, Singh KV, Murray BE. Relapse of type A beta-lactamase-producing Staphylococcus aureus native valveendocarditis during cefazolin therapy: revisiting the issue.Clin Infect Dis 2003; 37: 1194–8.
102 Demin AA, Drobysheva VP. [Ceftriaxone in the treatment ofstaphylococcal endocarditis]. Antibiot Khimother 1998; 43:12–15.
103 Small PM, Chambers HF. Vancomycin for Staphylococcusaureus endocarditis in intravenous drug users. AntimicrobAgents Chemother 1990; 34: 1227–31.
104 Gentry CA, Rodvold KA, Novak RM, Hershow RC,Naderer OJ. Retrospective evaluation of therapies forStaphylococcus aureus endocarditis. Pharmacotherapy 1997;17: 990–7.
105 McGrath BJ, Kang SL, Kaatz GW, Rybak MJ. Bactericidalactivities of teicoplanin, vancomycin and gentamicin aloneand in combination against Staphylococcus aureus in an in vitro pharmacodynamic model of endocarditis. AntimicrobAgents Chemother 1994; 38: 2034–40.
106 Kirby WMM. Vancomycin therapy in severe staphylococcalinfections. Rev Infect Dis 1981; 3 Suppl 1: S236–9.
107 Geraci JE, Wilson WR. Vancomycin therapy for infectiveendocarditis. Rev Infect Dis 1981; 3 Suppl 1: S250–8.
108 Sorrell TC, Packham DR, Shanker S, Foldes M, Munro R.Vancomycin therapy for methicillin-resistant Staphylococcusaureus. Ann Intern Med 1982; 97: 344–50.
109 Chambers HF, Miller RT, Newman MD. Right-sidedStaphylococcus aureus endocarditis in intravenous drugabusers: two-week combination therapy. Ann Intern Med1988; 109: 619–24.
110 Levine DP, Cushing RD, Jui J, Brown WJ. Community-acquired methicillin-resistant Staphylococcus aureusendocarditis in the Detroit Medical Center. Ann Intern Med1982; 97: 330–8.
111 Levine DP, Fromm B, Reddy BR. Slow response tovancomycin or vancomycin plus rifampin in methicillin-resistant Staphylococcus aureus endocarditis. Ann Intern Med1991; 115: 674–80.
112 Moore MR, Perdreau-Remington F, Chambers HF.Vancomycin treatment failure associated with heterogeneousvancomycin-intermediate Staphylococcus aureus in a patientwith endocarditis and in the rabbit model of endocarditis.Antimicrob Agents Chemother 2003; 47: 1262–6.
113 Woods CW, Cheng AC, Fowler VG Jr, Moorefield M,Frederick J, Sakoulas G et al. Endocarditis caused byStaphylococcus aureus with reduced susceptibility tovancomycin. Clin Infect Dis 2004; 38: 1189–91.
114 Wysocki M, Delatour F, Faurisson F, Rauss A, Pean Y, Misset Bet al. Continuous versus intermittent infusion of vancomycinin severe staphylococcal infections: prospective multicenterrandomized study. Antimicrob Agents Chemother 2001; 45:2460–7.
115 James JK, Palmer SM, Levine DP, Rybak MJ. Comparison ofconventional dosing versus continuous infusion vancomycintherapy for patients with suspected or documented Gram-positive infections. Antimicrob Agents Chemother 1996; 40:696–700.
116 De Gorgolas M, Aviles P,Verdejo C, Fernandez Guerrero ML.Treatment of experimental endocarditis due to methicillin-susceptible or methicillin-resistant Staphylococcus aureus withtrimethoprim-sulfamethoxazole and antibiotics that inhibit cellwall synthesis. Antimicrob Agents Chemother 1995; 39: 953–7.
Internal Medicine Journal 2005; 35: S25–S44

MurrayS42
117 Kaatz GW, Seo SM, Dorman NJ, Lerner SA. Emergence ofteicoplanin resistance during therapy of Staphylococcus aureusendocarditis. J Infect Dis 1990; 162: 103–8.
118 Cremieux AC, Maziere B,Vallois JM, Ottaviani M, Azancot A,Raffoul H et al. Evaluation of antibiotic diffusion into cardiacvegetations by quantitative autoradiography. J Infect Dis1989; 159: 938–44.
119 Glupczynski Y, Lagast H, Van der Auwera P, Thys JP,Crokaert F,Yourassowsky E et al. Clinical evaluation ofteicoplanin for therapy of severe infections caused by Gram-positive bacteria. Antimicrob Agents Chemother 1986; 29:52–7.
120 Martino P, Venditti M, Micozzi A, Brandimatre C, Gentile G,Santini C et al. Teicoplanin in the treatment of Gram-positivebacterial endocarditis. Antimicrob Agents Chemother 1989;33: 1329–34.
121 Leport C, Perronne C, Massip P, Canton P, LeClercq P,Bernard E et al. Evaluation of teicoplanin for treatment ofendocarditis caused by Gram-positive cocci in 20 patients.Antimicrob Agents Chemother 1989; 33: 871–6.
122 Fortun J, Perez-Molina JA, Anon MT, Martinez-Beltran J,Loza E, Guerrero A. Right-sided endocarditis caused byStaphylococcus aureus in drug abusers. Antimicrob AgentsChemother 1995; 39: 525–8.
123 Wilson AP, Gaya H. Treatment of endocarditis withteicoplanin: a retrospective analysis of 104 cases.J Antimicrob Chemother 1996; 38: 507–21.
124 Gilbert DN, Wood CA, Kimbrough RC. The InfectiousDiseases Consortium of Oregon. Failure of treatment withteicoplanin at 6 milligrams/kilogram/day in patients withStaphylococcus aureus intravascular infection. AntimicrobAgents Chemother 1991; 35: 79–87.
125 Greenberg RN. Treatment of bone, joint, and vascular-accessassociated Gram-positive bacterial infections with teicoplanin.Antimicrob Agents Chemother 1990; 34: 2392–7.
126 Wilson APR, Gruneberg RN, Neu H. Dosagerecommendations for teicoplanin. J Antimicrob Chemother1993; 32: 792–6.
127 Burch KH, Quinn EL, Cox F, Madhavan T, Fisher E,Romig D. Intramuscular clindamycin for therapy of infectiveendocarditis. Report of 23 cases and review of the literature.Am J Cardiol 1976; 38: 929–33.
128 Cherubin CE, Nair R. Clindamycin in infective endocarditis.JAMA 1978; 239: 626–7.
129 Carpenter TC, Hackbarth CJ, Chambers HF, Sande MA.Efficacy of ciprofloxacin for experimental endocarditiscaused by methicillin-susceptible or -resistant strains ofStaphylococcus aureus. Antimicrob Agents Chemother 1986;30: 382–4.
130 Fernandez-Guerrero M, Rouse M, Henry N, Wilson W.Ciprofloxacin therapy of experimental endocarditis caused bymethicillin-susceptible or methicillin-resistant Staphylococcusaureus. Antimicrob Agents Chemother 1988; 32: 747–51.
131 Kaatz GW, Seo SM, Barriere SL, Albrecht LM, Rybak MJ.Ciprofloxacin and rifampin, alone and in combination, fortherapy of experimental staphylococcal endocarditis.Antimicrob Agents Chemother 1989; 33: 1184–7.
132 Mulligan ME, Ruane PJ, Johnston L, Wong P, Wheelock JP,MacDonald K et al. Ciprofloxacin for eradication ofmethicillin-resistant Staphylococcus aureus colonization. Am JMed 1987; 82: 215–19.
133 Entenza JM, Que YA, Vouillamoz J, Glauser MP, Moreillon P.Efficacies of moxifloxacin, ciprofloxacin, and vancomycinagainst experimental endocarditis due to methicillin-resistantStaphylococcus aureus expressing various degrees ofciprofloxacin resistance. Antimicrob Agents Chemother2001; 45: 3076–83.
134 Berrington AW, Koerner RJ, Perry JD, Bain HH, Gould FK.Treatment of Staphylococcus aureus endocarditis usingmoxifloxacin. Int J Med Microbiol 2001; 291: 237–9.
135 Chuard C, Herrmann M, Vadaux P, Waldvogel FA, Lew DP.Treatment of experimental foreign-body infection due tomethicillin-resistant Staphylococcus aureus by antimicrobialcombinations. Antimicrob Agents Chemother 1991; 35:2611–16.
136 Zak O, Scheld WM, Sande MA. Rifampin in experimentalendocarditis due to Staphylococcus aureus in rabbits. RevInfect Dis 1983; 5: S481–90.
137 Turnidge J, Collingnon P. Resistance to fusidic acid. Int JAntimicrob Agents 1999; 12 Suppl 2: S35–44.
138 Whitby M. Fusidic acid in septicaemia and endocarditis. IntJ Antimicrob Agents 1999; 12 Suppl 2: S17–22.
139 Humble MW, Eykeyn SJ, Phillips I. Staphylococcalbacteraemia, fusidic acid and jaundice. BMJ 1980; 280:1495–8.
140 Eykyn SJ. Staphylococcal bacteraemia and endocarditis andfusidic acid. J Antimicrob Chemother 1990; 25: 33–8.
141 Gosden PE, Reeves BC, Osbourne JRS, Turner A, Millar M.Retrospective study of outcome in patients treated forStaphylococcus aureus bacteremia. Clin Microbiol Infect 1997;3: 32–40.
142 Yeldandi V, Strodtman R, Lentino JR. In vitro and in vivostudies of trimethoprim-sulfamethoxazole against multiple-resistant Staphylococcus aureus. J Antimicrob Chemother1988; 22: 873–80.
143 Markowitz N, Quinn EL, Saravolatz LD. Trimethoprim-sulfamethoxazole compared with vancomycin for thetreatment of Staphylococcus aureus infection. Ann Intern Med1992; 117: 390–8.
144 Batard E, Jacqueline C, Boutoille D, Hamel A, Drugeon HB,Asseray N et al. Combination of quinupristin-dalfopristinand gentamicin against methicillin-resistant Staphylococcusaureus: experimental rabbit endocarditis study. AntimicrobAgents Chemother 2002; 46: 2174–8.
145 Carbon C. Quinupristin/dalfopristin: a review of its activityin experimental animal models of infection. J AntimicrobChemother 1997; 39 Suppl A: 115–19.
146 Vouillamoz J, Entenza JM, Feger C, Glauser MP, MoreillonP. Quinupristin-dalfopristin combined with beta-lactams fortreatment of experimental endocarditis due to Staphylococcusaureus constitutively resistant to macrolide-lincosamide-streptogramin B antibiotics. Antimicrob Agents Chemother2000; 44: 1789–95.
147 Pavie J, Lefort A, Zarrouk V, Chau F, Garry L, Leclercq Ret al. Efficacies of quinupristin-dalfopristin combined withvancomycin in vitro and in experimental endocarditis due tomethicillin-resistant Staphylococcus aureus in relation to cross-resistance to macrolides, lincosamides, and streptograminB-type antibiotics. Antimicrob Agents Chemother 2002; 46:3061–4.
148 Zarrouk V, Bozdogan B, Leclercq R, Garry L, Feger C,Carbon C et al. Activities of the combination of quinupristin-dalfopristin with rifampin in vitro and in experimentalendocarditis due to Staphylococcus aureus strains with variousphenotypes of resistance to macrolide-lincosamide-streptogramin antibiotics. Antimicrob Agents Chemother2001; 45: 1244–8.
149 Raad I, Bompart F, Hachem R. Prospective, randomizeddose-ranging open phase II pilot study ofquinupristin/dalfopristin versus vancomycin in the treatmentof catheter-related staphylococcal bacteremia. Eur J ClinMicrobiol Infect Dis 1999; 18: 199–202.
150 Drew RH, Perfect JR, Srinath L, Kurkimilis E, Dowzicky M,Talbot GH. For the Synercid Emergency-Use Study Group.
Internal Medicine Journal 2005; 35: S25–S44

S43S. aureus infective endocarditis
Treatment of methicillin-resistant Staphylococcus aureusinfections with quinupristin-dalfopristin in patients intolerantof or failing prior therapy. J Antimicrob Chemother 2000; 46:775–80.
151 Dailey CF, Dileto-Fang CL, Buchanan LV, Oramas-Shirey MP,Batts DH, Ford CW et al. Efficacy of linezolid in treatmentof experimental endocarditis caused by methicillin-resistantStaphylococcus aureus. Antimicrob Agents Chemother 2001;45: 2304–8.
152 Oramas-Shirey MP, Buchanan LV, Dileto-Fang CL, Dailey CF,Ford CW, Batts DH et al. Efficacy of linezolid in astaphylococcal endocarditis rabbit model. J AntimicrobChemother 2001; 47: 349–52.
153 Chiang FY, Climo M. Efficacy of linezolid alone or incombination with vancomycin for treatment of experimentalendocarditis due to methicillin-resistant Staphylococcusaureus. Antimicrob Agents Chemother 2003; 47: 3002–4.
154 Dailey CF, Pagano PJ, Buchanan LV, Paquette JA, Haas JV,Gibson JK. Efficacy of linezolid plus rifampicin in anexperimental model of methicillin-susceptible Staphylococcusaureus endocarditis. Antimicrob Agents Chemother 2003; 47:2655–8.
155 Ruiz ME, Guerrero IC, Tuazon CU. Endocarditis caused bymethicillin-resistant Staphylococcus aureus: treatment failurewith linezolid. Clin Infect Dis 2002; 35: 1018–20.
156 Moise PA, Forrest A, Birmingham MC, Schentag JJ. Theefficacy and safety of linezolid as treatment for Staphylococcusaureus infections in compassionate use patients who areintolerant of, or who have failed to respond to, vancomycin.J Antimicrob Chemother 2002; 50: 1017–26.
157 Andrade-Baiocchi S, Tognim MC, Baiocchi OC, Sader HS.Endocarditis due to glycopeptide-intermediate Staphylococcusaureus: case report and strain characterization. Diagn MicroInfect Dis 2003; 45: 149–52.
158 Tsiodras S, Gold HS, Sakoulas G, Eliopoulos GM,Wennersten C, Venkataraman L et al. Linezolid resistance ina clinical isolate of Staphylococcus aureus. Lancet 2001; 358:207–8.
159 Drinkovic D, Morris AJ, Pottumarthy S, MacCulloch D,West T. Bacteriological outcome of combination versussingle-agent treatment for staphylococcal endocarditis.J Antimicrob Chemother 2003; 52: 820–5.
160 Watanakunakorn C, Glotzbecker C. Enhancement of theeffects of antistaphylococcal antibiotics by aminoglycosides.Antimicrob Agents Chemother 1974; 6: 802–6.
161 Graham JC, Gould FK. Role of aminoglycosides in thetreatment of bacterial endocarditis. J Antimicrob Chemother2002; 49: 437–44.
162 Kaatz GW, Seo SM, Reddy VN, Bailey EM, Rybak MJ.Daptomycin compared with teicoplanin and vancomycin fortherapy of experimental Staphylococcus aureus endocarditis.Antimicrob Agents Chemother 1990; 34: 2081–5.
163 Apellaniz G, Valdes M, Perez R, Martin F, Soria F, Garcia Aet al. Comparison of the effectiveness of various antibiotics inthe treatment of methicillin-susceptible Staphylococcus aureusexperimental infective endocarditis. J Chemother 1991; 3:91–7.
164 Korzeniowski O, Sande MA, and the National CollaborativeEndocarditis Study Group. Combination antimicrobialtherapy for Staphylococcus aureus endocarditis in patientsaddicted to parenteral drugs and in non-addicts. Ann InternMed 1982; 97: 496–503.
165 Torres-Tortosa M, de Cueto M, Veegara A, Sanchez-Porto A,Perez-Guzman EP, Gonzalez-Serrano M et al. Prospectiveevaluation of a two-week course of intravenous antibiotics inintravenous drug addicts with infective endocarditis. Eur JClin Microbiol Infect Dis 1994; 13: 559–64.
166 Fortun J, Navas E, Martinez-Beltran J, Perez-Molina J,Martin-Davila P, Guerrero A et al. Short-course therapy forright-side endocarditis due to Staphylococcus aureus in drugabusers: cloxacillin versus glycopeptides in combination withgentamicin. Clin Infect Dis 2001; 33: 120–5.
167 Abrams B, Sklaver A, Hoffman T, Greenman R. Single orcombination therapy of staphylococcal endocarditis inintravenous drug abusers. Ann Intern Med 1979; 90:789–91.
168 Pittet D, Harding I. Infective endocarditis and glycopeptides.J Infect 1998; 37: 127–35.
169 Henry NK, Rouse MS, Whitesell AL, McConnell ME,Wilson WR. Treatment of methicillin-resistant Staphylococcusaureus experimental osteomyelitis with ciprofloxacin orvancomycin alone or in combination with rifampin. Am JMed 1987; 82 Suppl 4A: 73–5.
170 Dworkin RJ, Sande MA, Lee BL, Chambers HF. Treatmentof right-sided Staphylococcus aureus endocarditis inintravenous drug users with ciprofloxacin and rifampicin.Lancet, 1989; 2: 1071–3.
171 Peterson L, Quick J, Jensen B, Homann S, Johnson S,Tenquist J et al. Emergence of ciprofloxacin resistance innosocomial methicillin-resistant Staphylococcus aureus isolates:resistance during ciprofloxacin plus rifampin therapy formethicillin-resistant S. aureus colonization. Arch Intern Med1990; 150: 2151–5.
172 Tebas P, Martinez Ruiz R, Roman F, Mendaza P, RodriguezDiaz JC, Daza R et al. Early resistance to rifampin andciprofloxacin in the treatment of right-sided Staphylococcusaureus endocarditis. J Infect Dis 1991; 163: 204–5.
173 Faville RJ Jr, Zaske DE, Kaplan EL, Crossley K, Sabath LD,Quie PG. Staphylococcus aureus endocarditis. Combinedtherapy with vancomycin and rifampin. JAMA 1978; 240:1963–5.
174 Simon GL, Smith RH, Sande MA. Emergence of rifampin-resistant strains of Staphylococcus aureus during combinationtherapy with vancomycin and rifampin: a report of two cases.Rev Infect Dis 1983; 5: S507–8.
175 Kobasa WD, Kaye KL, Shapiro D, Kaye D. Therapy forexperimental endocarditis due to Staphylococcus epidermidis.Rev Infect Dis 1983; 5: S533–7.
176 Karchmer AW, Archer GL, Dismukes WE. Staphylococcusepidermidis causing prosthetic valve endocarditis:microbiological and clinical observations as guides totherapy. Ann Intern Med 1983; 98: 447–55.
177 Yu VL, Fang G, Keys TF, Harris AA, Gentry LO, Fuchs PCet al. Prosthetic valve endocarditis: superiority of surgicalvalve replacement versus medical therapy only. Ann ThoracSurg 1994; 58: 1073–7.
178 Tornos P, Sanz E, Permanyer-Miralda G, Almirante B,Planes AM, Soler-Soler J. Late prosthetic valveendocarditis: immediate and long term prognosis. Chest1992; 101: 37–41.
179 Chirouze C, Cabell CH, Fowler VG Jr, Khayat N, Olaison L,Miro JM et al. Prognostic factors in 61 cases ofStaphylococcus aureus prosthetic valve endocarditis from theInternational Collaboration on Endocarditis MergedDatabase. Clin Infect Dis 2004; 38: 1323–7.
180 Francioli PB. Ceftriaxone and outpatient treatment ofinfective endocarditis. Infect Dis Clin North Am 1993; 267:279–80.
181 Stamboulian D. Outpatient treatment of endocarditis in aclinic-based program in Argentina. Eur J Clin MicrobiolInfect Dis 1995; 14: 648–54.
182 Graninger W, Presterl E, Wenisch C, Schwameis E, Breyer S,Vukovich T. Management of serious staphylococcal infectionsin the outpatient setting. Drugs 1997; 54: 21–8.
Internal Medicine Journal 2005; 35: S25–S44

MurrayS44
183 Huminer D, Bishara J, Pitlik S. Home intravenous antibiotictherapy for patients with infective endocarditis. Eur J ClinMicrobiol Infect Dis 1999; 18: 330–4.
184 Tice AD. Safety of outpatient parenteral antimicrobialtherapy for endocarditis. Clin Infect Dis 2002; 34: 419–20.
185 Andrews MM, von Reyn CF. Patient selection criteria andmanagement guidelines for outpatient parenteral antibiotictherapy for native valve infective endocarditis. Clin Infect Dis2001; 33: 203–9.
186 Steckelberg JM, Murphy JG, Ballard D, Bailey K, Tajik AJ,Taliercio CP et al. Emboli in infective endocarditis: theprognostic value of echocardiography. Ann Intern Med 1991;114: 635–40.
187 Williams DN, Rehm SJ, Tice AD, Bradley JS, Kind AC,Craig WA. Practice guidelines for community-based anti-infective therapy. Clin Infect Dis 1997; 25: 787–801.
188 Rehm SJ. Outpatient intravenous antibiotic therapy forendocarditis. Infect Dis Clin North Am 1998; 12: 879–901.
189 Visser LG, Arnouts P, van Furth R, Mattie H, van denBroek PJ. Clinical pharmacokinetics of continuousintravenous administration of penicillins. Clin Infect Dis1993; 17: 491–5.
190 Meine TJ, Nettles RE, Anderson TJ, Cabell CH, Corey GR,Sexton DJ et al. Cardiac conduction abnormalities inendocarditis defined by the Duke criteria. Am Heart J 2001;142: 280–5.
191 Sexton DJ, Spelman D. Current best practice and guidelines:assessment and management of complications in infectiveendocarditis. Infect Dis Clin North Am 2002; 16: 507–21.
192 Weinstein L. Life-threatening complications of infectiveendocarditis and their management. Arch Intern Med 1986;146: 953–7.
193 Richardson JV, Karp RB, Kirklin JW, Dismukes WE.Treatment of infective endocarditis: a 10-year comparativeanalysis. Circulation 1978; 58: 589–97.
194 Croft CH, Woodward W, Elliott A, Commerford PJ,Barnard CN, Beck W. Analysis of surgical versus medicaltherapy in active complicated native valve endocarditis. Am JCardiol 1983; 51: 1650–5.
195 Aguado J, Gonzalez-Vilchez F, Martin-Duran R, Arjona R,Vazquez de Prada JA. Perivavlular abscesses associated withendocarditis. Clinical features and diagnostic accuracy oftwo-dimensional echocardiography. Chest 1993; 104: 88–93.
196 Mathew J, Abreo G, Namburi K, Narra L, Franklin C.Results of surgical treatment for infective endocarditis inintravenous drug users. Chest 1995; 108: 73–7.
197 Roder BL, Wandall DA, Espersen F, Frimodt-Moller N,Skinhoj P, Rosdahl VT. A study of 47 bacteremicStaphylococcus aureus endocarditis cases: 23 with native valvestreated surgically and 24 with prosthetic valves. ScandCardiovasc J 1997; 31: 305–9.
198 Langley SM, Alexiou C, Stafford HM, Dalrymple-Hay MJ,Haw MP, Livesey SA et al. Aortic valve replacement forendocarditis: determinants of early and late outcome. J HeartValve Dis 2000; 9: 697–704.
199 Bishara J, Leibovicci L, Gartman-Israel D, Sagie A, Kazakov A,Miroshnik E et al. Long-term outcome of infectiveendocarditis: the impact of surgical intervention. Clin InfectDis 2001; 33: 1636–43.
200 Hendren WG, Morris AS, Rosenkranz ER, Lyttle BW,Taylor PC, Stewart WJ et al. Mitral valve repair for bacterialendocarditis. J Thorac Cardiovasc Surg 1992; 103: 124–9.
201 Arbulu A, Holmes RJ, Asfaw I. Tricuspid valvulectomywithout replacement. Twenty years experience. J ThoracCardiovasc Surg 1991; 102: 917–22.
202 Arbulu A, Holmes RJ, Asfaw I. Surgical treatment ofintractable right-sided endocarditis in drug addicts: 25 years’experience. J Heart Valve Dis 1993; 2: 129–37.
203 Kupferwasser LI,Yeaman MR, Shapiro SM, Nast CC,Sullam PM, Filler SG et al. Acetylsalicylic acid reducesvegetation bacterial density, haematogenous bacterialdissemination, and frequency of embolic events inexperimental Staphylococcus aureus endocarditis throughantiplatelet and antibacterial effects. Circulation 1999; 99:2791–7.
204 Nicolau DP, Tessier PR, Nightingale CH, Quintiliani R.Influence of adjunctive ticlodipine on the treatment ofexperimental Staphylococcus aureus endocarditis. Int JAntimicrob Agents 1998; 9: 227–9.
205 Nicolau DP, Tessier PR, Nightingale CH. Beneficial effect ofcombination antiplatelet therapy on the development ofexperimental Staphylococcus aureus endocarditis. Int JAntimicrob Agents 1999; 11: 159–61.
206 Tornos P, Almirante B, Mirabet S, Permanyer G, Pahissa A,Soler-Soler J. Infective endocarditis due to Staphylococcusaureus: deleterious effect of anticoagulant therapy. ArchIntern Med 1999; 159: 473–5.
207 Salem DN, Daudelin D, Levine HJ, Pauker SG, Eckman MH,Riff J. Antithrombotic therapy in valvular heart disease. Chest2001; 119: 207S–219S.
Internal Medicine Journal 2005; 35: S25–S44




















