
SubLingual Immunotherapy: World Allergy Organization Position Paper 2009
Upload
independentCategory
view
1download
0
Immunotherapy
IL-2-based immunotherapy after autologous transplantation for lymphoma
and breast cancer induces immune activation and cytokine release:
a phase I/II trial
LJ Burns1, DJ Weisdorf1, TE DeFor1, DH Vesole3, TL Repka1, BR Blazar1, SR Burger2,A Panoskaltsis-Mortari1, CA Keever-Taylor3, M-J Zhang3 and JS Miller1
1Blood and Marrow Transplant Program and Cancer Center, Minneapolis, MN, USA; 2Laboratory Medicine and Pathology,University of Minnesota, Minneapolis, MN, USA; and 3Medical College of Wisconsin, Milwaukee, WI, USA
Summary:
We determined the safety, immune activating effects, andpotential efficacy of i.v. infusion of ex vivo interleukin-2(IL-2) activated natural killer (NK) cells (part I) or IL-2boluses (part II) during daily s.c. IL-2 administrationfollowing hematopoietic recovery from autologous trans-plantation. In all, 57 patients with relapsed lymphoma(n¼ 29) or metastatic breast cancer (n¼ 28) wereenrolled. In part I of the study, 34 patients were enrolledat three dose levels of ex vivo IL-2-activated NK cells.Lymphaphereses were performed on days 28 and 42 of s.c.IL-2 administration. Following overnight ex vivo IL-2activation of the pheresis product, the cells were reinfusedthe following day. In part II, 23 patients were enrolled atthree dose levels of supplemental i.v. IL-2 bolus infusions,given on days 28 and 35 during s.c. IL-2 administration.Toxicities were generally mild, and no patient requiredhospitalization. Lytic function was markedly enhanced forfresh peripheral blood mononuclear cells (PBMNCs)obtained 1 day postinfusion of either IL-2-activated cellsor IL-2 boluses. IL-2 boluses transiently increased thelevels of IL-6, IFN-c, TNF-a and IL1-b, with increases inIL-6 and IFN-c being dose dependent. A total of 37patients (19 patients with lymphoma, 18 with breastcancer) treated with an optimum dose of post-transplantimmunotherapy (defined as having received 1.75� 106 IU/m2/day of s.c. IL-2 plus at least one of the planned ex vivoIL-2-activated cell infusions/IL-2 boluses) could bematched with controls from the Autologous Blood andMarrow Transplant Registry database. The matched-pairs analysis demonstrated no improvement in diseaseoutcomes of survival and relapse. We conclude that IL-2-activated cells/IL-2 boluses can be safely administered,generate PBMNCs with enhanced cytotoxicity againstNK-resistant targets, and increase cytokine levels. Withthis dose and schedule of administration of IL-2, noimprovement in patient disease outcomes was noted.
Alternative strategies will be needed to exploit theimmunotherapeutic potential of IL-2-activated NK cells.Bone Marrow Transplantation (2003) 32, 177–186.doi:10.1038/sj.bmt.1704086Keywords: immunotherapy; NK cells; IL-2
High-dose chemotherapy with autologous stem cell supporthas been widely employed in the treatment for relapsedlymphoma and metastatic breast cancer. In chemotherapy-sensitive lymphoma and metastatic breast cancer patients,autologous transplantation can result in high remissionrates.1,2 However, many patients who achieve a completeremission following transplantation will relapse and die oftheir disease. Most patients relapse at sites of previous bulkdisease, suggesting that one reason for treatment failure isinability to eradicate chemotherapy-resistant clonogenictumor. An inadequately functioning immune system mayalso contribute to early relapse.Human natural killer (NK) cells represent a population
of large granular lymphocytes that express the CD56+/CD3� phenotype. Recombinant interleukin-2 (IL-2) sti-mulates both NK expansion and cytotoxic activity againsttumor targets in vivo and in vitro, including lymphoma andbreast cancer.3,4 Theoretically, IL-2-activated NK cells,functioning as short-term antitumor therapy, would bemost efficacious in a minimal residual disease setting suchas that induced by autologous transplantation. Followinginitial reports of the feasibility and immunologic potentialof post-transplant IL-2 immunotherapy,5–7 many investi-gators explored IL-2 and/or IL-2-activated effectors for avariety of malignancies with encouraging but inconclusiveresults.8–27
We previously reported the results of a phase I trial ofpost-autologous transplant s.c. IL-2 (Amgen Inc., Thou-sand Oaks, CA, USA).4 In all, 12 patients (six lymphoma,six breast cancer) were enrolled on a dose-escalation studyof s.c. IL-2 given for 84 days; the best-tolerated dose was0.25� 106U/m2/day. Patients receiving at least 28 days ofs.c. IL-2 exhibited a greater than 10-fold incrementin circulating NK cells. In addition, lytic function wasincreased against the NK-resistant targets Raji (lymphoma)Received 10 September 2002; accepted 21 January 2003
Correspondence: Dr LJ Burns, University of Minnesota, Mayo MailCode 286, Minneapolis, MN 55455, USA
Bone Marrow Transplantation (2003) 32, 177–186& 2003 Nature Publishing Group All rights reserved 0268-3369/03 $25.00
www.nature.com/bmt

and MCF-7 (breast cancer). In vivo IL-2-primed NK cellsobtained by lymphapheresis were activated in large-scale exvivo incubation in high-dose IL-2 (1000U/ml), with furtherenhancement of NK lytic function against Raji and MCF-7targets. We concluded that low-dose s.c. IL-2, althoughsafe and easily administered in the outpatient setting,resulted in submaximal NK lytic function against tumortargets, and hypothesized that ex vivo incubation in IL-2could be used to generate NK cells with potent antitumoreffects. In the current study, we sought to extend theseobservations by performing a phase I/II trial of infusion ofex vivo IL-2-activated NK cells to determine if this strategywould generate NK cells with sustained and potentantitumor effects. We subsequently evaluated whether i.v.boluses of IL-2 could be substituted for the ex vivo IL-2-activated cell infusions, while maintaining the same degreeof immune activation.
Patients and methods
Patient characteristics and eligibility criteria
In all, 34 patients between 18 and 65 years of age who hadundergone an autologous stem cell transplant for non-Hodgkin’s lymphoma, Hodgkin’s disease, or metastaticbreast cancer with no evidence of disease progression wereenrolled on the ex vivo IL-2 activation part of the study(Table 1). A total of 23 additional patients were enrolled onthe IL-2 bolus part of the study. Patients with T-cellimmunophenotype non-Hodgkin’s disease were not eligi-ble. Conditioning regimens were as previously described.1,28
Patients had to be between 30 and 180 days fromtransplant, transfusion independent, without need forgrowth factor support, and have an unsupported plateletcountX80 000� 109/l, hemoglobinX9 gm/dl, and an ANCX1.0� 109/l. The protocol received institutional reviewboard approval and all patients exercised written informedconsent when eligible for IL-2 therapy. Of the 28 patientswith breast cancer, 18 (64%) also received s.c. IL-2 as partof pretransplant stem cell mobilization as previouslydescribed.28
s.c. IL-2 therapy
Amgen IL-2 had been used in our previous phase I trialof s.c. IL-2.4 As Amgen IL-2 was no longer available, IL-2was provided and manufactured by Chiron (Emeryville,CA, USA) for the current study. Hence, it was necessaryto first establish the maximum tolerated dose (MTD) ofChiron-IL-2. Acetaminophen 650mg, ibuprofen 400mg,and diphenhydramine 50mg were self-administered as oralpremedications to IL-2, and repeated 4 h following eachself-injection. In part I of the study, IL-2 doses of 0.25,0.75, 1.25, 1.75, and 2.25� 106 IU/m2/day for 56 days weretested, within a range of Chiron IL-2 previously reported toexpand NK cells in vivo without significant toxicity.29
Patients were enrolled in cohorts of 3. Patients were notenrolled to the next dose level until a minimum of twopatients had completed therapy at an IL-2 dose level withno dose limiting toxicity (DLT) attributable to IL-2administration. DLT was defined by the Cancer andLeukemia Group B (CALGB) expanded common toxicitycriteria as Grade 3 toxicity. Toxicity was first formallyassessed at day 14 of IL-2 therapy, then every 14 days until7–14 days after IL-2 was stopped. If no DLT had occurredby day 14, the patient could escalate to the next dose levelfor the duration of therapy. IL-2 was discontinued inpatients experiencing DLT, then restarted at the next lowerdose level once toxicity had resolved. The MTD of IL-2 wasdefined as the dose below that in which 33% of patientsexperienced DLT. The MTD was used as the daily s.c. doseof IL-2, administered for 42 days, in part II of the study.
Lymphapheresis and ex vivo IL-2 activation (part I)
Minimal laboratory values required prior to lymphapher-esis included platelets450 000� 109/l, hemoglobinX9 gm/dl, ANC X1.0� 109/l, and normal renal and liverfunctions. Prior to the first lymphapheresis (day 28 of IL-2 therapy), patients must have received IL-2 for at least 21of the first 28 days and for five of the 7 days immediatelyprior to the planned apheresis. Prior to the secondlymphapheresis (day 42), patients must have received IL-2for at least 28 of the first 42 days and five of the 7 daysimmediately prior to apheresis. Patients not meeting thecriteria for apheresis continued on s.c. IL-2 alone. Avolume of 10–12 l leukaphereses were performed using aCS3000 cell sorter (Baxter, Deerfield, IL, USA). Thelymphapheresis product was cultured in AIM-V serum-freemedium (Gibco) supplemented with 1000 IU/ml IL-2 inpolyolefin gas permeable bags (Lifecell Tissue CultureFlask, Fenwal-Baxter) for 16 h, a time period previouslyshown to result in sustained induction of cytolytic activityagainst MCF-7 and Raji cell targets.4 All patients receivedpremedications 1 h prior to cell infusion and again 3–4 hlater. IL-2-activated lymphocytes were infused over 1–2 hthrough a 170mm blood administration filter the dayfollowing apheresis (days 29 and 43) in the outpatientclinic. Cell doses were based on mononuclear cells with thetotal cell count determined just prior to infusion. Patientswere enrolled in cohorts of 3 patients each with doseescalation to a maximum of a full lymphapheresis product.Cohort 1 received 4.0� 107 cells/kg and cohort 2 received
Table 1 Patient characteristics
IL-2 treatment
Part I Part II
IL-2+IL-2-activatedcells
IL-2+IL-2boluses
Number of patients 34 23Age in years, median (range) 46 (19–62) 43 (27–60)GenderMale 14 4Female 20 19
DiseaseNon-Hodgkin’s lymphoma 15 5Follicular 8 0Diffuse large cell 7 5
Hodgkin’s disease 5 4Metastatic breast cancer 14 14
IL-2=interleukin-2.
IL-2 based immunotherapy after autologous transplantationLJ Burns et al
178
Bone Marrow Transplantation

8.0� 107 cells/kg. If the planned cell dose was greater thanthe actual number of cells collected, then the dose infusedwas the full lymphapheresis product. Cohort 3 received afull lymphapheresis product. The median cell dose in a fulllymphapheresis product was 7.8� 107 cells/kg, with a rangeof 0.33–2.09� 108 cells/kg. Until the s.c. IL-2 dose escala-tion was completed and the MTD of daily IL-2 determinedto be 1.75� 106 IU/m2/day, all patients received the lowestcell dose of 4.0� 107 cells/kg. Cell dose escalation thenproceeded only after all patients at a given dose wereevaluated through day 56 of therapy (the last day of s.c. IL-2) with no DLT attributable to administration of IL-2 orIL-2-activated lymphocytes. Patients received the infusionson an outpatient basis and were observed for toxicity for aminimum of 4 h following infusion. Patients were formallyassessed for toxicity the day prior to apheresis, during andfollowing infusion of activated cells, and the day after cellinfusion. DLT was defined as Grade 2 or greater toxicity byCALGB criteria except for the following where Grade 3toxicity was dose limiting: liver, neurologic, hematologic,infection, pulmonary, dermatologic, allergy, performancestatus. A platelet count of o30 000� 109/l was considereddose-limiting. After the MTD of IL-2 in combination witha full lymphapheresis was shown to be safe, accrual wasextended to both ascertain safety and until part II of thestudy utilizing bolus IL-2 infusions could be initiated.
i.v. bolus IL-2 (part II)
The eligibility requirements for part II of the study wereidentical to part I of the study. All patients initiated s.c.IL-2 at the MTD established in part I of the study of1.75� 106 IU/m2/day. If no DLT had occurred after 14days, the patient continued at that dose for a total of 42days of therapy. Patients who developed intolerableconstitutional symptoms that did not constitute DLTdecreased their IL-2 dose to 1.25� 106 IU/m2/day for theremainder of the study. Patients received the same pre- andpost- medications for IV boluses of IL-2 as for the infusionsof IL-2-activated cells. The IL-2 boluses were given as anoutpatient over 2 h on days 28 and 35, with dose escalationper cohort of three patients each of 2.0, 4.0, and6.0� 106 IU/m2 per infusion. The dose of bolus IL-2 wasnot escalated until all patients in a given cohort hadcompleted the entire course of IL-2 therapy. Hence, morethan three patients were ultimately enrolled in the secondand third cohorts. Prior to receiving bolus IL-2, patientsmust have received IL-2 for at least 21 of the first 28 daysand for five of 7 days immediately prior to the plannedinfusion. Patients not meeting these criteria continued ondaily s.c. IL-2 alone. The IL-2 was infused over 2 h on anoutpatient basis and patients were monitored for aminimum of 4 h for complications. Patients were formallyassessed for toxicity the day prior to the IL-2 bolusinfusion, during and following the infusion and the dayafter infusion. The definition of DLT for bolus IL-2 was thesame as for ex vivo IL-2-activated cell infusions.
Cytolytic activity
Heparinized peripheral blood, serum, and plasma wereobtained at each clinic visit. Peripheral blood mononuclear
cells (PBMNCs) were prepared from peripheral blood byFicoll–Hypaque (sp. grav. 1.077) (Sigma, St Louis, MO,USA) density gradient centrifugation as described.4 Cellsurface antigens were determined by direct staining of cellswith mouse monoclonal antibodies. Fluorescein isothio-cyanate (FITC)- or phycoerythrin (PE)-coupled antibodies(Becton Dickinson, Mountain View, CA, USA) weredirected at CD3, CD25, CD56, and HLA-DR. FITC-and PE-coupled isotype-matched immunoglobulins wereused as controls. All analyses were performed withFACSCalibur (Becton Dickenson) and CELLQuest soft-ware (Becton Dickenson). Cytotoxicity assays wereperformed in triplicate using fresh PBMNC or 16 hIL-2-activated PBMNC against the NK-resistant B-celllymphoma line Raji (American Tissue Culture Collection(ATCC), Rockville) and the breast cancer cell line MCF-7(ATCC) in a 4-hour 51Cr release assay.4 To control fortarget variability, frozen targets (expanded from the samebatch) were thawed every 4–6 weeks.
Cytokine levels
Serum or plasma was stored at �701C and later assayed forcytokine levels using ELISA kits for interleukin-1b (IL-1b),interleukin-6 (IL-6), tumor necrosis factor-a (TNF-a), andinterferon-g (IFN-g). Assays were performed using themanufacturer’s recommendations (R&D Systems, Minnea-polis, MN, USA). Normal cytokine values for 495% ofhealthy individuals are considered by the University ofMinnesota Cytokine Reference Laboratory to be asfollows: IL-1b (o0.9 pg/ml), IL-6 (o3.0 pg/ml), TNF-a(o3.0 pg/ml), and IFN-g (o3.0 pg/ml).
Statistics
Results of experimental points were reported as mean7standard error of the mean (s.e.m.). Statistical comparisonsof experimental points between independent groups werecompleted with the two-sided Student’s t-test. Comparisonsof values at different time points but within the samepopulation were made with a two-sided paired-comparisont-test.30
Patients enrolled at the MTD of s.c. IL-2 and whoreceived at least one of the planned ex vivo IL-2-activatedcell infusions or IL-2 boluses (20 patients with lymphoma,20 with breast cancer) were eligible to be matched to amaximum of three controls from the Autologous Bloodand Marrow Transplant Registry (ABMTR) database.Controls were selected from 1726 potentially eligiblepatients from the database who had received an autologoustransplant for lymphoma or breast cancer, had not receivedany post-transplant immunotherapy, were not transplantedat one of the study institutions, and had similar follow-uptime. IL-2-treated patients were matched to controls for thefollowing variables: disease (NHL, HD, metastatic breastcancer), histologic subtype at diagnosis or those patientswith NHL or HD (Working Formulation subtype forNHL, nodular sclerosis/mixed cellularity/unknown forHD), disease status at time of transplant (primaryinduction failure with chemosensitive disease, clinicalremission, or chemosensitive/resistant relapse for
IL-2 based immunotherapy after autologous transplantationLJ Burns et al
179
Bone Marrow Transplantation

lymphoma; clinical remission, clinical remission except forbone abnormalities, or chemosensitive relapse for breastcancer), year of transplant (within 5 years), age attransplant (within 10 years), and time from diagnosis totransplant (within1.5 years). Patients with breast cancerwere also matched to controls for the presence of visceralmetastases and hormone receptor status. The case cohortincluded only patients who were in remission long enoughto receive the IL-2 therapy after autologous transplanta-tion, whereas the control cohort included all similarpatients who were not treated with IL-2 therapy afterautologous transplantation from the ABMTR. The IL-2-treated case cohort therefore excluded patients who diedearly or had an early relapse. This could introduce a biasfavoring IL-2-treated cases. To adjust this potential waitingtime bias, the controls in each match pair were selectedfrom among the patients with a complete remission aftertransplantation at least as long as the interval between thetransplantation and initial IL-2 therapy for the IL-2recipient. If more than three controls were eligible formatching with an IL-2-treated patient, then the threecontrols closest in age to the case patient were chosen.Cox’s regression model stratified on each matched pair wasused to analyze the effect of IL-2 therapy on the end pointsof survival and relapse. The proportionality assumption ofthe Cox model was tested by adding a time-dependentcovariate.
Results
Clinical tolerability of subcutaneous IL-2 therapy
Of nine patients enrolled at dose levels of 0.25 to1.25� 106 IU/m2/day, all but two were able to have theirdose of IL-2 increased by one dose level at day 14 of IL-2treatment. One patient enrolled at 0.75� 106 IU/m2/daydid not dose escalate secondary to thrombocytopenia; onepatient enrolled at 1.25� 106 IU/m2/day did not doseescalate because of fatigue and nausea. Toxicities wereotherwise mild, including Grade I fatigue, nausea, rash,cough, fever, myalgias, and sweats. The majority ofpatients developed transient induration and erythemaaround the s.c. injection sites.A total of 25 patients began IL-2 at 1.75� 106 IU/m2/
day. In all, 15 (60%) of the 25 patients were able to doseescalate to 2.25� 106 IU/m2/day on day 14. Of these, 13were able to remain on the higher dose for the durationof treatment, whereas the other two patients required asubsequent decrease back to the 1.75� 106 IU/m2/day doselevel because of either anemia or thrombocytopenia. In all,10 (40%) of the patients, however, were unable to havetheir dose escalated at day 14 because of side effects, andseven of these patients ultimately were removed from study.Toxicities included: severe swelling of the tongue and face(n¼ 1); thrombocytopenia (n¼ 2); nausea and vomiting(n¼ 1); intolerable fatigue (n¼ 5); edema (n¼ 1); andbacterial infection (n¼ 1). In all, eighteen (72%) of the 25patients who began IL-2 at 1.75� 106 IU/m2/day receivedX95% of the total number of planned injections. Nopatient required hospitalization; and all toxicity resolved
within 1 week of discontinuation of IL-2. The MTD of IL-2was thus established at 1.75� 106 IU/m2/day; therefore, nopatients were enrolled at a starting dose of 2.25� 106 IU/m2/day.
Clinical tolerability of ex vivo IL-2-activated cell infusions
All patients who received s.c. IL-2 at less than the MTD(0.25–1.25� 106 IU/m2/day) received a cell dose of4.0� 107 cells/kg. Grade I toxicities observed infrequentlyat this dose level included fever and chills at time of theinfusion. At the MTD of s.c. IL-2, 1.75� 106 IU/m2/day,four patients received a cell dose of 4.0� 107 cells/kg (onepatient underwent one apheresis, the remaining patientstwo aphereses); six patients received 8.0� 107 cells/kg(two patients underwent one apheresis, the remainingfour patients two aphereses); 10 patients underwent twolymphaphereses with reinfusion of the full product. GradeI–II toxicities included wheezing (n¼ 1), mild fever (37.1–38.01C) (n¼ 4), chills (n¼ 4), transient decrease in oxygensaturation to 88% during chills (n¼ 1), and transientdecrease of systolic blood pressure to 80–85mmHg (n¼ 1).No patient required hospitalization. Two patients wereremoved from study after the first apheresis (one for facialswelling, one for a bacterial infection). A third patientdeclined the second apheresis secondary to difficulties withvenous access.
Clinical tolerability of IL-2 boluses
All 23 patients received s.c. IL-2 at the MTD of1.75� 106 IU/m2/day. Three patients made up the firstcohort, and all three received 42 days of s.c. IL-2 injectionsand both planned i.v. IL-2 boluses of 2� 106 IU/m2. Six(50%) of the 12 patients enrolled at the 4� 106 IU/m2 doselevel received both i.v. boluses. Boluses were not infusedbecause of thrombocytopenia (n¼ 2), Clostridium difficileinfection (n¼ 1), rash (n¼ 1), insomnia (n¼ 1), andneutropenia (n¼ 1). Of the 12 patients, eight received all41–42 doses of s.c. IL-2; four patients receivedp23 days ofs.c. IL-2. Grade I toxicities occurring at the IL-2 bolus doseof 4� 106 IU/m2 included fever (n¼ 2), chills (n¼ 3), andshortness of breath (n¼ 1). Orthostatic hypotensionoccurred in two patients–one patient responded to intra-venous normal saline, the other had spontaneous resolutionof symptoms. All eight patients enrolled at the highest doseof bolus IL-2, 6� 106 IU/m2, received all 42 days of s.c. IL-2 injections and both infusions. Grade II toxicities of feverand chills were noted in all patients during the bolusinfusions, and thus this dose was felt to be the MTD of IL-2boluses. Three patients experienced a X10mmHg declinein systolic blood pressure and required infusion of normalsaline for blood pressure support.
Immune activation after IL-2 therapy
Laboratory tests were performed every 2 weeks to monitorimmune activation. There was a significant increase in thetotal white blood cell count, peaking at day 14 and aftereach activated cell infusion or IL-2 bolus infusion,analogous to our previously reported findings with
IL-2 based immunotherapy after autologous transplantationLJ Burns et al
180
Bone Marrow Transplantation

post transplant subcutaneous IL-2.4 The increase in totalWBC was primarily because of an increase in the number ofcirculating lymphocytes and eosinophils; the absolutenumber of circulating monocytes did not change with IL-2 therapy. The lymphocyte increase included a greaterthan 10-fold increase in circulating CD56+ bright/CD3�NK cells, which was sustained throughout the IL-2treatment period. The majority of the NK cells wereCD56+ bright/CD16+/CD3�. Less than 2% of CD56+cells expressed CD3 at any time point. In contrast to theincrease in NK cells, the absolute number of T cellsremained fairly stable throughout IL-2 administration,consistent with our previous finding.4 The phenotype ofthe mononuclear cells was unaltered by ex vivo incubationin IL-2. After 28 days of s.c. IL-2, 4474.6% (n¼ 20) ofPBMNC were CD56+/CD3� NK cells, which did notchange after overnight incubation in IL-2 (4374.4%),again in agreement with our previous findings.4
We tested the lytic function of PBMNC obtained atstudy entry prior to any s.c. IL-2 administration, pre- andpost infusion of IL-2-activated cells, and pre- and postinfusion of IL-2 boluses, as well as that of the IL-2-activated NK-cell infusion product against Raji and MCF-7 cells (Figure 1). Prior to s.c. IL-2, fresh nonactivatedPBMNC had no lytic activity (o5%) against either target.In vitro cytotoxicity was modestly enhanced following 28days of s.c. IL-2, prior to infusion of either IL-2-activatedcells or i.v. IL-2 boluses (about 10% at effector:target ratioof 20:1). In contrast, cytotoxicity was markedly enhancedfor fresh PBMNC obtained the day postinfusion of IL-2-activated cells or i.v. IL-2 boluses (25–45% at effector:targetratio of 20:1), as well as for the first IL-2-activated NK-cellinfusion product (40–60% at effector:target ratio of 20:1).The enhancement in cytotoxicity following the second IL-2-
activated cell infusion or IL-2 bolus was as potent as thefirst (data not shown).
Cytokines induced by IL-2
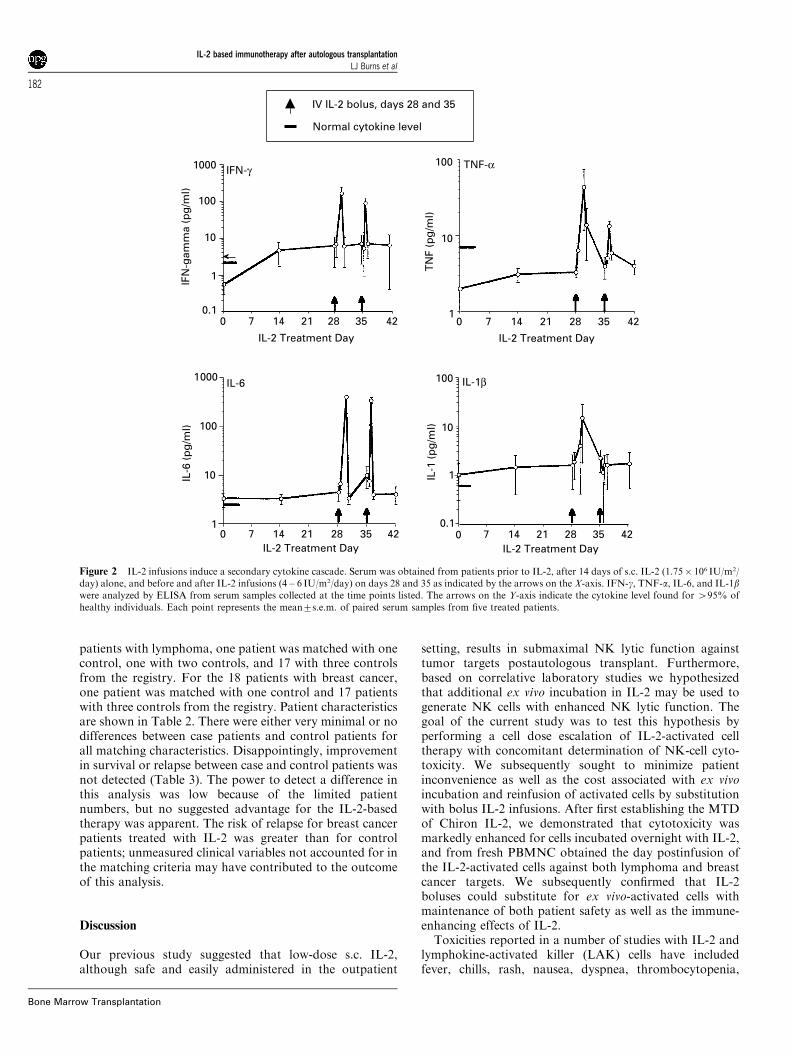
We previously reported that s.c. administration of IL-2 inthe post-transplant setting induced the release of solubleIL-2Ra and IFN-g.4 In contrast, neither IL-12, TNF-a,IL1-b nor IL-6 was significantly augmented compared tobaseline levels. In the current study, we determined thecirculating cytokine levels of IL-6, IFN-g, TNF-a, and IL1-b in patients at day 0, day 14, and throughout their courseof bolus IL-2 infusions. As shown in Figure 2, IL-2 bolusestransiently increased the levels of all four cytokines,although the increase in the level of IL-1b was minimal.Peak levels of IL-6, IFN-g, and TNF-a were noted 2 h aftereach IL-2 infusion. The peak level for IL1-b occurred 24 hafter infusion; a second peak was not noted after the secondIL-2 bolus. There was a dose-dependent increase in IL-6and IFN-g. Patients who received 4–6� 106 IU/m2 had astatistically significant greater increase in peak cytokinelevels of IL-6 and IFN-g compared to patients who received2� 106 IU/m2 of IL-2 (data not shown).
Clinical outcome following IL-2 immunotherapy: matched-pairs analysis
Patients enrolled at the MTD of s.c. IL-2 and who receivedat least one of the planned ex vivo IL-2-activated cellinfusions/IL-2 boluses (n¼ 40, 20 lymphoma and 20 breastcancer) were eligible to be matched to controls from theABMTR database. In all, 19 of the 20 patients withlymphoma and 18 of the 20 patients with metastatic breastcancer could be matched with control patients. For the 19
60 20 6.6 2.2 0.750
20
40
60
80 Pre-studyPre-cell infusionPost-cell infusionPre-IV IL-2Post-IV IL-2Product
Effector : Target Ratio
% S
pec
ific
Lys
is
Raji
60 20 6.6 2.2 0.750
20
40
60
80
Effector : Target Ratio
MCF-7
% S
pec
ific
Lys
is
Figure 1 Ex vivo IL-2-activated cell infusions or i.v. IL-2 boluses enhance NK-cell lytic activity against Raji (lymphoma) and MCF-7 (breast cancer)targets. Peripheral blood mononuclear cells (PBMNC) from patients receiving 1.75� 106 IU/m2/day of s.c. IL-2 were studied before and after starting post-transplant immunotherapy in a 4-h chromium release cytotoxicity assay against Raji (left panel) and MCF-7 (right panel) targets. Patient PBMNC weretested prior to study entry (x, n¼ 16 for Raji, n¼ 10 for MCF-7), after 28 days of s.c. IL-2 alone prior to either cell (J) or bolus infusions (&) (n¼ 18 forRaji, n¼ 18 for MCF-7) and 24 h after ex vivo IL-2-activated NK cell infusions (�, n¼ 11 for Raji, n¼ 15 for MCF-7) or IV IL-2 (’, n¼ 9 for both targets).The activity of the first infusion product is also shown (�–, n¼ 13 for Raji, n¼ 15 for MCF-7).
IL-2 based immunotherapy after autologous transplantationLJ Burns et al
181
Bone Marrow Transplantation
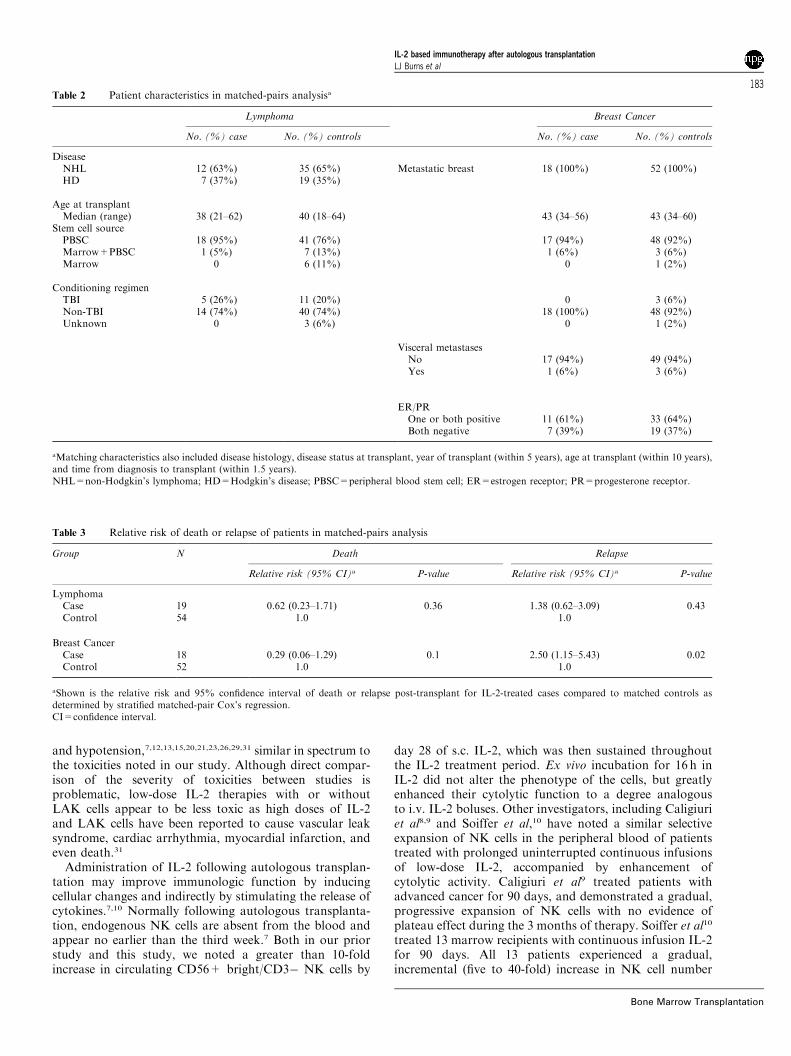
patients with lymphoma, one patient was matched with onecontrol, one with two controls, and 17 with three controlsfrom the registry. For the 18 patients with breast cancer,one patient was matched with one control and 17 patientswith three controls from the registry. Patient characteristicsare shown in Table 2. There were either very minimal or nodifferences between case patients and control patients forall matching characteristics. Disappointingly, improvementin survival or relapse between case and control patients wasnot detected (Table 3). The power to detect a difference inthis analysis was low because of the limited patientnumbers, but no suggested advantage for the IL-2-basedtherapy was apparent. The risk of relapse for breast cancerpatients treated with IL-2 was greater than for controlpatients; unmeasured clinical variables not accounted for inthe matching criteria may have contributed to the outcomeof this analysis.
Discussion
Our previous study suggested that low-dose s.c. IL-2,although safe and easily administered in the outpatient
setting, results in submaximal NK lytic function againsttumor targets postautologous transplant. Furthermore,based on correlative laboratory studies we hypothesizedthat additional ex vivo incubation in IL-2 may be used togenerate NK cells with enhanced NK lytic function. Thegoal of the current study was to test this hypothesis byperforming a cell dose escalation of IL-2-activated celltherapy with concomitant determination of NK-cell cyto-toxicity. We subsequently sought to minimize patientinconvenience as well as the cost associated with ex vivoincubation and reinfusion of activated cells by substitutionwith bolus IL-2 infusions. After first establishing the MTDof Chiron IL-2, we demonstrated that cytotoxicity wasmarkedly enhanced for cells incubated overnight with IL-2,and from fresh PBMNC obtained the day postinfusion ofthe IL-2-activated cells against both lymphoma and breastcancer targets. We subsequently confirmed that IL-2boluses could substitute for ex vivo-activated cells withmaintenance of both patient safety as well as the immune-enhancing effects of IL-2.Toxicities reported in a number of studies with IL-2 and
lymphokine-activated killer (LAK) cells have includedfever, chills, rash, nausea, dyspnea, thrombocytopenia,
4235282114700.1
1
IFN-γ
4235282114701
10
100
1000 IL-6
IFN
-gam
ma
(pg
/ml)
TN
F (p
g/m
l)
IL-6
(p
g/m
l)
IL-1
(p
g/m
l)
4235282114700.1
1
10
100 IL-1β
IL-2 Treatment Day
1000
100
10
IL-2 Treatment Day IL-2 Treatment Day
IV IL-2 bolus, days 28 and 35
Normal cytokine level
4235282114701
10
100 TNF-α
IL-2 Treatment Day
Figure 2 IL-2 infusions induce a secondary cytokine cascade. Serum was obtained from patients prior to IL-2, after 14 days of s.c. IL-2 (1.75� 106 IU/m2/day) alone, and before and after IL-2 infusions (4 – 6 IU/m2/day) on days 28 and 35 as indicated by the arrows on the X-axis. IFN-g, TNF-a, IL-6, and IL-1bwere analyzed by ELISA from serum samples collected at the time points listed. The arrows on the Y-axis indicate the cytokine level found for 495% ofhealthy individuals. Each point represents the mean7s.e.m. of paired serum samples from five treated patients.
IL-2 based immunotherapy after autologous transplantationLJ Burns et al
182
Bone Marrow Transplantation
and hypotension,7,12,13,15,20,21,23,26,29,31 similar in spectrum tothe toxicities noted in our study. Although direct compar-ison of the severity of toxicities between studies isproblematic, low-dose IL-2 therapies with or withoutLAK cells appear to be less toxic as high doses of IL-2and LAK cells have been reported to cause vascular leaksyndrome, cardiac arrhythmia, myocardial infarction, andeven death.31
Administration of IL-2 following autologous transplan-tation may improve immunologic function by inducingcellular changes and indirectly by stimulating the release ofcytokines.7,10 Normally following autologous transplanta-tion, endogenous NK cells are absent from the blood andappear no earlier than the third week.7 Both in our priorstudy and this study, we noted a greater than 10-foldincrease in circulating CD56+ bright/CD3� NK cells by
day 28 of s.c. IL-2, which was then sustained throughoutthe IL-2 treatment period. Ex vivo incubation for 16 h inIL-2 did not alter the phenotype of the cells, but greatlyenhanced their cytolytic function to a degree analogousto i.v. IL-2 boluses. Other investigators, including Caligiuriet al8,9 and Soiffer et al,10 have noted a similar selectiveexpansion of NK cells in the peripheral blood of patientstreated with prolonged uninterrupted continuous infusionsof low-dose IL-2, accompanied by enhancement ofcytolytic activity. Caligiuri et al9 treated patients withadvanced cancer for 90 days, and demonstrated a gradual,progressive expansion of NK cells with no evidence ofplateau effect during the 3 months of therapy. Soiffer et al10
treated 13 marrow recipients with continuous infusion IL-2for 90 days. All 13 patients experienced a gradual,incremental (five to 40-fold) increase in NK cell number
Table 2 Patient characteristics in matched-pairs analysisa
Lymphoma Breast Cancer
No. (%) case No. (%) controls No. (%) case No. (%) controls
DiseaseNHL 12 (63%) 35 (65%) Metastatic breast 18 (100%) 52 (100%)HD 7 (37%) 19 (35%)
Age at transplantMedian (range) 38 (21–62) 40 (18–64) 43 (34–56) 43 (34–60)
Stem cell sourcePBSC 18 (95%) 41 (76%) 17 (94%) 48 (92%)Marrow+PBSC 1 (5%) 7 (13%) 1 (6%) 3 (6%)Marrow 0 6 (11%) 0 1 (2%)
Conditioning regimenTBI 5 (26%) 11 (20%) 0 3 (6%)Non-TBI 14 (74%) 40 (74%) 18 (100%) 48 (92%)Unknown 0 3 (6%) 0 1 (2%)
Visceral metastasesNo 17 (94%) 49 (94%)Yes 1 (6%) 3 (6%)
ER/PROne or both positive 11 (61%) 33 (64%)Both negative 7 (39%) 19 (37%)
aMatching characteristics also included disease histology, disease status at transplant, year of transplant (within 5 years), age at transplant (within 10 years),and time from diagnosis to transplant (within 1.5 years).NHL=non-Hodgkin’s lymphoma; HD=Hodgkin’s disease; PBSC=peripheral blood stem cell; ER=estrogen receptor; PR=progesterone receptor.
Table 3 Relative risk of death or relapse of patients in matched-pairs analysis
Group N Death Relapse
Relative risk (95% CI)a P-value Relative risk (95% CI)a P-value
LymphomaCase 19 0.62 (0.23–1.71) 0.36 1.38 (0.62–3.09) 0.43Control 54 1.0 1.0
Breast CancerCase 18 0.29 (0.06–1.29) 0.1 2.50 (1.15–5.43) 0.02Control 52 1.0 1.0
aShown is the relative risk and 95% confidence interval of death or relapse post-transplant for IL-2-treated cases compared to matched controls asdetermined by stratified matched-pair Cox’s regression.CI=confidence interval.
IL-2 based immunotherapy after autologous transplantationLJ Burns et al
183
Bone Marrow Transplantation

during IL-2 treatment, and the majority of NK cells wereCD56 bright+CD16+CD3�. A minor increase in T-cellnumber was noted in only four of 13 patients. Thedifferences in the time course and degree of NK-cellexpansion in these studies may be related to the differencesin IL-2 source, dose, route of delivery, type of disease, ortreatment setting (transplant or nontransplant).Other investigators have explored the administration of
IL2 with IL-2-activated NK cells or LAK cells in thepostautologous.12,13,16 Lister et al13 reported 11 patientswith lymphoma and metastatic breast cancer who, 2 daysfollowing autologous transplantation, received an infusionof IL-2-activated NK cells, followed by additional IL-2 atvarying doses for over 90 days. The cells were generatedpretransplant after 6 days of low-dose IL-2 priming with3� 106/IU/m2 IL-2 (Chiron) by continuous infusion,leukapheresis for 4 days, followed by IL-2 ex vivo culturefor 14–18 days. In the Benyunes et al12 study of 16 patientsfollowing autologous transplantation for malignant lym-phoma, patients were initially treated with IL-2 (Roche) at3.0� 106U/m2/day by continuous infusion for 5 days.Patients then underwent three consecutive lymphaphereses,for LAK cell generation. Following 5 days of culture withIL-2, a median of 65, 61, and 43% of the infused LAK cellsexpressed CD3, CD8 or CD56, respectively. The LAK cellslysed the Daudi target in vitro with a median lysis of 54% atan effector to target ratio of 25:1, not dissimilar to theresults in the current study.NK cells constitutively express receptors for mono-
cyte-derived cytokines (monokines) and produce criticalcytokines (including IFN-g, TNF-a, and granulocyte–macrophage colony-stimulating factor (GM-CSF)) in res-ponse to monokine stimulation.32 In addition to theirpresumed role in the constitutional symptoms observedwith IL-2 administration,33 theoretically cytokines may beeither important mediators or suppressors of IL-2 cellactivation.34–36 Several studies have attempted to define thenature of the complex cytokine cascade following IL-2administration. IL-6, granulocyte colony-stimulating factor(G-CSF), and GM-CSF are induced in the blood afteradministration of IL-2.37 Bonig et al38 demonstrated aconsistent and early rise of IL-10, IL-5, and GM-CSFduring IL-2 therapy. TNF-a, IFN-g, and IL-6 are producedin significant amounts in supernatants of marrow mono-nuclear cells cultured in IL-2.39 In the current study, IL-2boluses transiently increased the levels of IL-6, IFN-g,TNF-a and IL1-b, with a dose-dependent increase in IL-6and IFN-g.Several trials with differing eligibility and design have
been performed with the aim of evaluating the safety andefficacy of immunotherapy with IL-2 in lymphoma.Benyunes et al12 treated 17 patients with IL-2 with orwithout LAK cells after autologous transplantation. Theclinical outcomes compared favorably with institutionalcontrols. Nagler et al18 conducted a clinical trial involving56 lymphoma patients with minimal residual diseasefollowing autologous stem cell transplantation utilizing acombination of s.c. IL-2 and INF-a in an outpatient settingand compared the results with 61 matched historicalcontrols. The overall survival, disease-free survival andrelapse rate of treated patients were significantly improved
compared with historical controls. In a phase I/II study,Robinson et al15 treated 19 patients with lymphoma withescalating doses of ’induction’ IL-2; following a 4-day restperiod, maintenance IL-2 was given by continuous i.v.infusion for 10 days. Encouragingly, 58% of the non-Hodgkin’s lymphoma patients in the phase II trialremained in clinical remission with a minimum follow-upof 1 year. Margolin et al22 reported 24 patients withlymphoma who received bone marrow and/or G-CSF-mobilized autologous peripheral blood stem cells that hadbeen exposed to IL-2 for 24 h ex vivo. Patients subsequentlyreceived IL-2 by low-dose continuous i.v. infusion untilhematologic reconstitution and then intermediate-dosecontinuous i.v. infusion for six maintenance cycles. Amongthe 24 lymphoma patients, nine were in continuous CRfrom 18 to 48 months, and 15 had died (12 due to relapseand three to therapy-related toxicities).Other investigators have attempted to determine if IL-2
therapy is efficacious in patients with metastatic breastcancer. Gravis et al25 noted no clinical beneficial effectfor 21 advanced heavily pretreated breast cancer patientstreated with either i.v. high-dose IL-2 or s.c. low-doseIL-2 following autologous transplantation. Toh et al26
reported a prospective phase II trial of 33 patients withchemosensitive metastatic breast cancer, who underwenttransplantation with autologous peripheral blood stem cellscultured in IL-2, followed by post-transplant low-dose IL-2. Compared to historical controls group, the Kaplan–Meier-estimated 2-year progression-free survival was 35%for IL-2-treated patients, compared with 17% in thecontrol arm (P¼ 0.73) and the estimated 2-year survivalwas 78%, compared with 61% in the control arm (P¼ 0.22).As no prior study has reported a matched-pairs analysis
of postautologous transplantation IL-2 therapy alone, weperformed one to assess the possible efficacy of the immuneactivation we observed. Although there was no trendtowards an advantage to IL-2-based immunotherapy, thepower to detect a difference in this matched-pairs analysiswas low because of limited patient numbers. In order toachieve narrow enough confidence intervals to showstatistical significance for the observed estimates of relativerisk of death, the study would require approximately 35lymphoma cases and 25 breast cancer cases with acorresponding increase in the number of controls. Patientheterogeneity may also have obscured a clinical benefit.Thus, a larger and more uniform, prospective randomizedstudy at the MTD of s.c. IL-2- and ex vivo-activated cells ori.v. bolus IL-2 would be needed to clarify the potential forclinical benefit. Enhancement of the potency of IL-2-activated NK cytotoxicity may require the use of moreinfusions of ex vivo-activated cells or IL-2 boluses,utilization of highly purified NK cells or NK-cell subsets,a combination of IL-2 with tumor-reactive monoclonalantibodies to induce effective antibody-dependent cellularcytotoxicity,40 combinations of NK-cell immunotherapywith chemotherapy or other cytokines such as IL-12,41 oraugmentation by NK-cell inhibitory receptor blockade.42
Indeed, as malignant cells may have multiple mechanismsby which they escape from immune control, more thanone immunotherapeutic intervention may be necessary toachieve clinical benefit. Further study is clearly needed to
IL-2 based immunotherapy after autologous transplantationLJ Burns et al
184
Bone Marrow Transplantation

take advantage of the immunotherapeutic potential of IL-2-activated NK cells.
Acknowledgements
We thank RN Juliette Gay and RN Cindy Steele for providingassistance in patient care, RN Roby Nicklow, RN EvaGallagher, Victoria Johnson, and Melissa Walker for datamanagement, MD Fred Sanchez for patient care, and MauriceWolin and Priscilla Ayers (Chiron). LJB is the recipient of aDepartment of Defense grant, and is also supported by the JanieLymphoma Research Fund and the Minnesota MedicalFoundation. This work was supported in part by NationalInstitute of Health Grant PO1-CA-65493 (JSM), R21CA78904(DJW) and Grant M01-RR00400 from the National Center forResearch Resources. We also acknowledge the support of theBone Marrow Transplant Research Fund of the University ofMinnesota and the Masonic Order of the Eastern Star.
References
1 Weisdorf DJ, Verfaillie CM, Miller WJ et al. Autologous bonemarrow versus non-mobilized peripheral blood stem celltransplantation for lymphoid malignancies: a prospective,comparative trial. Am J Hematol 1997; 54: 202–208.
2 Antman KH, Rowlings PA, Vaughan WP et al. High-dosechemotherapy with autologous hematopoietic stem-cell sup-port for breast cancer in North America. J Clin Oncol 1992; 15:1870–1879.
3 Verma UN, Areman E, Dickerson SA et al. Interleukin-2activation of chemotherapy and growth factor-mobilizedperipheral blood stem cells for generation of cytotoxiceffectors. Bone Marrow Transplant 1995; 15: 199–206.
4 Miller JS, Tessmer-Tuck J, Pierson BA et al. Low dosesubcutaneous interleukin-2 after autologous transplantationgenerates sustained in vivo natural killer cell activity. Biol BloodMarrow Transplant 1997; 3: 34–44.
5 Gottlieb DJ, Brenner MK, Heslop HE et al. A phase I clinicaltrial of recombinant interleukin 2 following high dose chemo-radiotherapy for haematological malignancy: applicability tothe elimination of minimal residual disease. Br J Cancer 1989;60: 610.
6 Blaise D, Olive D, Stoppa AM et al. Hematologic andimmunologic effects of the systemic administration of recom-binant interleukin-2 after autologous bone marrow transplan-tation. Blood 1990; 76: 1092–1097.
7 Higuchi CM, Thompson JA, Petersen FB et al. Toxicity andimmunomodulatory effects of interleukin-2 after autologousbone marrow transplantation for hematologic malignancies.Blood 1991; 77: 2561–2568.
8 Caligiuri MA, Murray C, Soiffer RJ et al. Extendedcontinuous infusion low-dose recombinant interleukin-2 inadvanced cancer: prolonged immunomodulation withoutsignificant toxicity. J Clin Oncol 1991; 9: 2110–2119.
9 Caligiuri MA, Murray C, Robertson MJ et al. Selectivemodulation of human natural killer cells in vivo afterprolonged infusion of low dose recombinant interleukin 2.J Clin Invest 1993; 91: 123–132.
10 Soiffer RJ, Murray C, Cochran K et al. Clinical andimmunologic effects of prolonged infusion of low doserecombinant interleukin-2 after autologous and T-celldepleted allogeneic bone marrow transplantation. Blood 1992;79: 517–526.
11 Weisdorf DJ, Anderson PM, Blazar BR et al. Interleukin-2immediately after autologous bone marrow transplantation foracute lymphoblastic leukemia: a phase I study. Transplantation1993; 55: 61–66.
12 Benyunes MC, Higuchi C, York A et al. Immunotherapy withinterleukin-2 with or without lymphokine-activated killer cellsafter autologous bone marrow transplantation for malignantlymphoma: a feasibility trial. Bone Marrow Transplant 1995;16: 283–288.
13 Lister J, Rybka WB, Donnenberg AD et al. Autologousperipheral blood stem cell transplantation and adoptiveimmunotherapy with activated natural killer cells in theimmediate posttransplant period. Clin Cancer Res 1995; 6:607–614.
14 Mazumder A. Experimental evidence of interleukin-2 activityin bone marrow transplantation. Cancer J Sci Am 1997; 3
(Suppl. 1): S37–S42.15 Robinson N, Benyunes MC, Thompson JA et al. Interleukin-2after autologous stem cell transplantation for hematologicmalignancy: a phase I/II study. Bone Marrow Transplant 1997;19: 435–442.
16 Benyunes MC, Massumoto C, York A et al. Interleukin-2 withor without lymphokine-activated killer cells as consolidativeimmunotherapy after autologous bone marrow transplant-ation for acute myelogenous leukemia. Bone Marrow Trans-plant 1993; 12: 159–163.
17 Meloni G, Vignetti M , Pogliani E et al. Interleukin-2 therapyin relapsed acute myelogenous leukemia. Cancer J Sci Am1997; 3 (Suppl. 1): S43–S47.
18 Nagler A, Ackerstein A, Or R et al. Immunotherapy withrecombinant human interleukin-2 and recombinant interferon-alpha in lymphoma patients post-autologous marrow or stemcell transplantation. Blood 1997; 89: 3951–3959.
19 Blaise D, Attal M, Pico JL et al. The use of a sequential highdose recombinant interleukin 2 regimen after autologous bonemarrow transplantation does not improve the disease freesurvival of patients with acute leukemia transplanted in firstcomplete remission. Leukemia Lymphoma 1997; 25: 469–478.
20 Van Besien K, Margolin K, Champlin R, Forman S. Activityof interleukin-2 in non-Hodgkin’s lymphoma following trans-plantation of interleukin-2-activated autologous bone marrowor stem cells. Cancer J Sci Am 1997; 3 (Suppl. 1): S54–S58.
21 Meehan KR, Arun B, Gehan EA et al. Immunotherapy withinterleukin-2 and alpha-interferon after IL-2-activated hema-topoietic stem cell transplantation for breast cancer. BoneMarrow Transplant 1999; 23: 667–673.
22 Margolin KA, Van Besien K, Wright C et al. Interleukin-2-activated autologous bone marrow and peripheral blood stemcells in the treatment of acute leukemia and lymphoma. BiolBlood Marrow Transplant 1999; 5: 36–45.
23 DeMagalhaes-Silverman M, Donnenberg A, Lembersky Bet al. Posttransplant adoptive immunotherapy with activatednatural killer cells in patients with metastatic breast cancer.J Immunother 1999; 23: 154–160.
24 Blaise D, Attal M, Reiffers J et al. Randomized study ofrecombinant interleukin-2 after autologous bone marrowtransplantation for acute leukemia in first complete remission.Eur Cytokine Net 2000; 11: 91–98.
25 Gravis G, Viens P, Vey N et al. Pilot study of immuno-therapy with interleukin-2 after autologous stem cell trans-plantation in advanced breast cancers. Anticancer Res 2000;20: 3987–3991.
26 Toh HC, McAfee SL, Sackstein R et al. High-dose cyclopho-sphamide + carboplatin and interleukin-2 (IL-2) activatedautologous stem cell transplantation followed by maintenanceIL-2 therapy in metastatic breast carcinoma – a phase II study.Bone Marrow Transplant 2000; 25: 19–24.
IL-2 based immunotherapy after autologous transplantationLJ Burns et al
185
Bone Marrow Transplantation

27 Toren A, Nagler A, Rozenfeld-Granot G et al. Amplificationof immunological functions by subcutaneous injection ofintermediate-high dose interleukin-2 for 2 years after auto-logous stem cell transplantation in children with stage IVneuroblastoma. Transplantation 2000; 70: 1100–1104.
28 Burns LJ, Weisdorf DJ, DeFor TE et al. Enhancement of theantitumor activity of a peripheral blood progenitor cell graftby mobilization with interleukin 2 plus granulocyte colony-stimulating factor in patients with advanced breast cancer.Exp Hematol 2000; 28: 96–103.
29 Meropol NJ, Porter M, Blumenson LE et al. Daily sub-cutaneous injection of low-dose interleukin 2 expands naturalkiller cells in vivo without significant toxicity. Clin Cancer Res1996; 2: 669–677.
30 Snedecor G, Cocharn W. Statistical Methods. Iowa StateUniversity Press: Iowa, 1989.
31 Rosenberg SA, Lotze MT, Muul LM et al. A progressreport on the treatment of 157 patients with advancedcancer using lymphokine-activated killer cells and inter-leukin-2 or high-dose interleukin-2 alone. N Engl J Med1987; 316: 889–897.
32 Cooper MA, Fehniger TA, Turner SC et al. Human naturalkiller cells: a unique innate immunoregulatory role for theCD56bright subset. Blood 2001; 97: 3146–3151.
33 Gemlo BT, Palladino MA, Jaffe HS et al. Circulatingcytokines in patients with metastatic cancer treated withrecombinant interleukin 2 and lymphokine-activated killercells. Cancer Res 1988; 48: 5864–5867.
34 Holter W, Goldman CK, Casabo L et al. Expressionof functional IL-2 receptors by lipopolysaccharide and
interferon-gamma stimulated human monocytes. J Immunol1987; 138: 2917–2922.
35 Greenbaum LA, Horowitz JB, Woods A et al. Autocrinegrowth of CD4+ T cells. Differential effects of IL-1 on helperand inflammatory T cells. J Immunol 1988; 140: 1555–1560.
36 Mills CD. Molecular basis of ‘suppressor’ macrophages:arginine metabolism via the nitric oxide synthesis pathway.J Immunol 1991; 46: 2719–2723.
37 Tritarelli E, Rocca E, Testa U et al. Adoptive immunotherapywith high-dose interleukin-2: kinetics of circulating progenitorscorrelate with interleukin-6, granulocyte colony-stimulatingfactor level. Blood 1991; 77: 741–749.
38 Bonig H, Laws HJ, Wundes A et al. In vivo cytokine responsesto interleukin-2 immunotherapy after autologous stem celltransplantation in children with solid tumors. Bone MarrowTransplant 2000; 26: 91–96.
39 Klingemann HG, Neerunjun J, Schwulera U, Ziltener HJ.Culture of normal and leukemic bone marrow in interleukin-2:analysis of cell activation, cell proliferation, and cytokineproduction. Leukemia 1993; 7: 1389–1393.
40 Sondel PM, Hank JA. Combination therapy with interleukin-2and antitumor monoclonal antibodies. Cancer J Sci Am 1997;3 (Suppl. 1): S121–S127.
41 Wigginton JM, Komschlies KL, Back TC et al. Administrationof IL-12 with pulse interleukin 2 and the rapid and completeeradication of murine renal carcinoma. J Natl Cancer Inst1996; 88: 38–43.
42 Koh CY, Blazar BR, George T et al. Augmentation ofantitumor effects by NK cell inhibitory receptor blockade invitro and in vivo. Blood 2001; 97: 3132–3137.
IL-2 based immunotherapy after autologous transplantationLJ Burns et al
186
Bone Marrow Transplantation
Copyright © 2022 FDOKUMEN




















