Autologous Pancreatic Islet Transplantation in Human Bone Marrow
Upload
khangminh22Category
view
0download
0
Concise Review: Guidance in Developing
Commercializable Autologous/Patient-Specific Cell
Therapy Manufacturing
Shannon Eaker, Myriam Armant, Harvey Brandwein, Scott Burger, Andrew
Campbell, Carmine Carpenito, Dominic Clarke, Timothy Fong, Ohad Karnieli,
Knut Niss, Wouter Van't Hof, Ravenska Wagey
Dow
nloaded from https://academ
ic.oup.com/stcltm
/article/2/11/871/6386175 by guest on 22 June 2022

®
Concise Review: Guidance in DevelopingCommercializable Autologous/Patient-Specific CellTherapy Manufacturing
SHANNON EAKER,a,b MYRIAM ARMANT,a,c HARVEY BRANDWEIN,a,d SCOTT BURGER,a,e
ANDREW CAMPBELL,a,f CARMINE CARPENITO,a,g DOMINIC CLARKE,a,h TIMOTHY FONG,a,i
OHAD KARNIELI,a,j KNUT NISS,a,k WOUTER VAN’T HOF,a,l RAVENSKA WAGEYa,m
Key Words. Cellular therapy • Stem cells • Stem cell culture • Clinical translation
aInternational Society forCellular Therapy; bGEHealthcare, Knoxville,Tennessee, USA; cHarvardUniversity, Boston,Massachusetts, USA;dPall Corporation, PortWashington, New York, USA;eAdvanced Cell and GeneTherapy, Chapel Hill, NorthCarolina, USA; fLifeTechnologies, Grand Island,New York, USA; gLonza,Walkersville, Maryland, USA;hCharter Medical, Ltd.,Winston-Salem, NorthCarolina, USA; iProgenitorCell Therapy, Allendale, NewJersey, USA; jPluristemTherapeutics, Haifa, Israel;kNovartis PharmaceuticalsCorp., Morris Plains, NewJersey, USA; lAthersys,Cleveland, Ohio, USA;mStemCell Technologies,Vancouver, British Columbia,Canada
Correspondence: Shannon Eaker,Ph.D., GE Healthcare, 1104Potterstone Drive, Knoxville,Tennessee 37922, USA.Telephone: 865-274-1159;E-Mail: [email protected]
Received March 19, 2013;accepted for publication June 24,2013; first published online inSCTM EXPRESS October 7, 2013.
©AlphaMed Press1066-5099/2013/$20.00/0
http://dx.doi.org/10.5966/sctm.2013-0050
ABSTRACT
Cell therapy is poised to play an enormous role in regenerativemedicine. However, little guidance isbeing made available to academic and industrial entities in the start-up phase. In this technicalreview, members of the International Society for Cell Therapy provide guidance in developing com-mercializable autologous and patient-specificmanufacturing strategies from the perspective of pro-cess development. Special emphasis is placed on providing guidance to small academic or biotechresearchers as towhat simple questions canbe addressedor answered at the bench in order tomaketheir cell therapy productsmore feasible for commercial-scale production.We discuss the processesthat are required for scale-out at the manufacturing level, and how many questions can be ad-dressed at the bench level. The goal of this review is to provide guidance in the form of topics thatcan be addressed early in the process of development to better the chances of the product beingsuccessful for future commercialization. STEM CELLS TRANSLATIONAL MEDICINE 2013;2:871–883
INTRODUCTION
This review focuses on providing guidance to thesmall academic or biotech researcher in an effortto aid in cell therapy product development.Items to be addressed include typical good man-ufacturing practice (GMP) processes, technologytransfer, cell sources, isolation procedures, bio-and cryopreservation,media, cytokines, sera, se-rum-free media, scalable platforms, matrices,cell densities, harvesting, genetic alterations,characterization/phenotypic assays, and safetyassays (Fig. 1). Although each process is not stan-dard for all cell types, we compare multiple celltypes and propose alternate methods whereavailable. Although cell therapy manufacturinghas relied heavily on biologicmanufacturing/bio-process, we compare and contrast how sharedprocesses might be beneficial. For example, ad-herent cells are commonly used for biologic pro-duction; however, the cells are normally notrecovered. In the case of cell therapy, manufac-turing adherent mesenchymal stem cells(MSCs) becomes a serious scalability issue. Al-ternative adherent scale-up/scale-out systemsare available. Alternatively, some groups havesuccessfully adapted MSCs to suspension cul-tures.
GMP Processes, Definition, and CellTherapy-Specific Processes
Overview of GMPWhat is GMP and how does one implement it formanufacturing autologous cell therapies?GMP isdefined by Medicines and Healthcare ProductsRegulatory Agency (MHRA) in the United King-dom as “that part of quality assurance which en-sures that medicinal products are consistentlyproduced and controlled to the quality standardsappropriate to their intended use and as requiredby the marketing authorization or product specifi-cation. GMP is concerned with both productionand quality control.” Both the U.S. Food and DrugAdministration (FDA) and the EuropeanMedicinesAgency (EMA) have similar definitions.
As defined, GMP guidelines cover not onlythe actual physical process of making the drugbut also the quality assurance that the drug isproduced under conditions that are consistent,safe, and effective for their intended use. Withthis intent, GMP guidelines include nearly allaspects of drug manufacturing, including butnot limited to the quality control and assur-ance system, manufacturing facilities, equip-ment and devices used in the process, rawmaterials, media and medium supplements,storage, and shipping. In the United States,
STANDARDS, POLICIES, PROTOCOLS, AND REGULATIONSFOR CELL-BASED THERAPIES
STEM CELLS TRANSLATIONAL MEDICINE 2013;2:871–883 www.StemCellsTM.com ©AlphaMed Press 2013
Dow
nloaded from https://academ
ic.oup.com/stcltm
/article/2/11/871/6386175 by guest on 22 June 2022

guidelines for cell-based therapeutics are regulated by theFDA (http://www.fda.gov) and are encompassed in the drugmanufacturing regulations as described in Title 21 of the Codeof Federal Regulations (CFR) in several sections (21CFR210,211, 610, and 820), including the use of human tissue and cellproducts (21CFR1271). The EMA (http://www.ema.europa.eu/ema) for the European Union and theMHRA (http://www.mhra.gov.uk) publishes similar guidelines. Both the EMA and MHRAconsider cell therapy products to be advanced-therapy medici-nal products and reviewed by the Committee for Advanced Ther-apies. Additional guidance for cell and gene therapies may befound in Regulation (EC) No. 1394/2007. It is important to under-stand these regulations early in the product development phasein order to ensure that compliance can be achieved. If issuesarise, they can be addressed prior to production. The intent ofthis review is not to provide specific guidance on how to navigatethrough the regulatory approval process but rather to pointreaders to sources of information so that they may become fa-miliar with regulations and guidance specific to their products asthey develop their cell therapies.
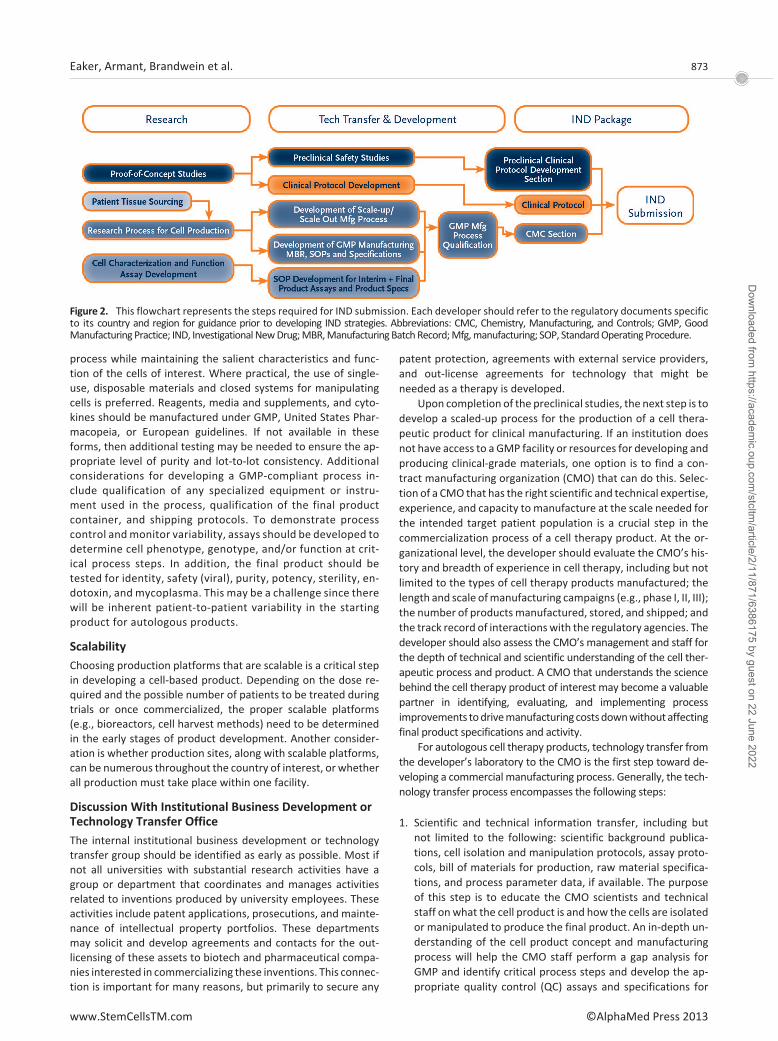
The overall process for preparing to initiate a phase I safetyclinical trial in the United States is depicted in Figure 2. There arethree major stages of activities in the process to apply for ap-proval to conduct a phase I clinical trial: Research, TechnologyTransfer and Development, and the Investigational New Drug(IND) application. The Research stage is where the initial charac-terization, isolation, and production of the cell therapeutic prod-uct are identified and generated. Most, if not all, of these activi-ties occur in the research laboratory of the inventor, and the celltherapy product generated in this setting is used in proof-of-
concept studies in animal models of disease showing the poten-tial clinical application of the cell therapy. If the proof-of-conceptstudies show promise and testing in human disease is indicated,the program moves into the Technology Transfer and Develop-ment stage, where formal preclinical studies in appropriate ani-mal models to characterize the safety of the product are per-formed. This stage also includes process scale-up or scale-out,development of initial process and product specifications, andgeneration of documentation to support manufacturing andproduct quality testing. The activities in these areas are the basisof the Chemistry, Manufacturing, and Controls (CMC) section ofthe IND application. The clinical protocol is also developed in thisstage. Lastly, these three major components (preclinical, CMC,and clinical protocol) are assembled into the IND application forregulatory agency review and approval. Both the EMA and theMHRA have similar processes to apply for a phase I trial, butdevelopers should refer to specific regulatory documents fortheir countries and regions for guidance.
Considerations in Designing a GMP-Compliant ProcessTo implement GMP guidelines for the production of autologouscell therapy products, the approach begins at themanufacturingprocess design stage. It is necessary to perform a gap analysis forGMP compliance from incoming rawmaterial quality and sourceto the validation of final product shipping containers. For eachprocess step, whether it involves cell isolation or enrichment, invitro culture, genetic modification, or final product fill and finish,the overall approach should be to reduce risk of contaminationof the product, establish documentation to verify that the entireprocess is correctly performed, and minimize variability in the
Figure 1. This flowchart represents a typical cell therapy product process and production layout. Each step has multiple steps within it andcan be variable depending on the cell type.
872 Cell Therapy, Manufacturing, and Commercialization
©AlphaMed Press 2013 STEM CELLS TRANSLATIONAL MEDICINE
Dow
nloaded from https://academ
ic.oup.com/stcltm
/article/2/11/871/6386175 by guest on 22 June 2022
process while maintaining the salient characteristics and func-tion of the cells of interest. Where practical, the use of single-use, disposable materials and closed systems for manipulatingcells is preferred. Reagents, media and supplements, and cyto-kines should be manufactured under GMP, United States Phar-macopeia, or European guidelines. If not available in theseforms, then additional testing may be needed to ensure the ap-propriate level of purity and lot-to-lot consistency. Additionalconsiderations for developing a GMP-compliant process in-clude qualification of any specialized equipment or instru-ment used in the process, qualification of the final productcontainer, and shipping protocols. To demonstrate processcontrol andmonitor variability, assays should be developed todetermine cell phenotype, genotype, and/or function at crit-ical process steps. In addition, the final product should betested for identity, safety (viral), purity, potency, sterility, en-dotoxin, and mycoplasma. This may be a challenge since therewill be inherent patient-to-patient variability in the startingproduct for autologous products.
ScalabilityChoosing production platforms that are scalable is a critical stepin developing a cell-based product. Depending on the dose re-quired and the possible number of patients to be treated duringtrials or once commercialized, the proper scalable platforms(e.g., bioreactors, cell harvest methods) need to be determinedin the early stages of product development. Another consider-ation is whether production sites, along with scalable platforms,can be numerous throughout the country of interest, or whetherall production must take place within one facility.
Discussion With Institutional Business Development orTechnology Transfer OfficeThe internal institutional business development or technologytransfer group should be identified as early as possible. Most ifnot all universities with substantial research activities have agroup or department that coordinates and manages activitiesrelated to inventions produced by university employees. Theseactivities include patent applications, prosecutions, and mainte-nance of intellectual property portfolios. These departmentsmay solicit and develop agreements and contacts for the out-licensing of these assets to biotech and pharmaceutical compa-nies interested in commercializing these inventions. This connec-tion is important for many reasons, but primarily to secure any
patent protection, agreements with external service providers,and out-license agreements for technology that might beneeded as a therapy is developed.
Upon completion of the preclinical studies, the next step is todevelop a scaled-up process for the production of a cell thera-peutic product for clinical manufacturing. If an institution doesnot have access to a GMP facility or resources for developing andproducing clinical-grade materials, one option is to find a con-tract manufacturing organization (CMO) that can do this. Selec-tion of a CMO that has the right scientific and technical expertise,experience, and capacity to manufacture at the scale needed forthe intended target patient population is a crucial step in thecommercialization process of a cell therapy product. At the or-ganizational level, the developer should evaluate the CMO’s his-tory and breadth of experience in cell therapy, including but notlimited to the types of cell therapy products manufactured; thelength and scale ofmanufacturing campaigns (e.g., phase I, II, III);the number of productsmanufactured, stored, and shipped; andthe track record of interactionswith the regulatory agencies. Thedeveloper should also assess the CMO’s management and staff forthe depth of technical and scientific understanding of the cell ther-apeutic process and product. A CMO that understands the sciencebehind the cell therapy product of interest may become a valuablepartner in identifying, evaluating, and implementing processimprovements todrivemanufacturingcostsdownwithoutaffectingfinal product specifications and activity.
For autologous cell therapy products, technology transfer fromthe developer’s laboratory to the CMO is the first step toward de-veloping a commercial manufacturing process. Generally, the tech-nology transfer process encompasses the following steps:
1. Scientific and technical information transfer, including butnot limited to the following: scientific background publica-tions, cell isolation and manipulation protocols, assay proto-cols, bill of materials for production, raw material specifica-tions, and process parameter data, if available. The purposeof this step is to educate the CMO scientists and technicalstaff onwhat the cell product is and how the cells are isolatedor manipulated to produce the final product. An in-depth un-derstanding of the cell product concept and manufacturingprocess will help the CMO staff perform a gap analysis forGMP and identify critical process steps and develop the ap-propriate quality control (QC) assays and specifications for
Figure 2. This flowchart represents the steps required for IND submission. Each developer should refer to the regulatory documents specificto its country and region for guidance prior to developing IND strategies. Abbreviations: CMC, Chemistry, Manufacturing, and Controls; GMP, GoodManufacturing Practice; IND, InvestigationalNewDrug;MBR,ManufacturingBatchRecord;Mfg,manufacturing; SOP, StandardOperating Procedure.
873Eaker, Armant, Brandwein et al.
www.StemCellsTM.com ©AlphaMed Press 2013
Dow
nloaded from https://academ
ic.oup.com/stcltm
/article/2/11/871/6386175 by guest on 22 June 2022

process control, from procurement of rawmaterials and sup-plies to the final product container for patient administration.A process that lacks appropriate process controls will intro-duce manufacturing variability to an autologous cell productthat will likely begin with cells thatmay already have inherentpatient-to-patient variability. An educated CMO staff will en-able better troubleshooting if interim product or in-processtesting falls outside of expected specifications.
2. Training of the process development (PD) staff. If the manu-facturing process has already been used in clinical-scale man-ufacturing and has final Standard Operating Procedures(SOPs), Manufacturing Batch Records (MBRs), raw materialsacceptance criteria and specifications, and other documenta-tion, then this step may be skipped and the technology trans-fer may proceed directly to training the CMO QC and manu-facturing staff. This transfer will be smooth and relativelyseamless if the manufacturing and quality documents havethe details and rigor needed for commercial industrial manu-facturing. But for many developers moving from preclinicalphase to a phase I clinical trial, the protocols used to generatethe cell product may have been performed only at the re-search scale for proof-of-concept or toxicity studies in animalmodels andmay not be sufficient for producing clinical doses.In this step, the role of the PD staff is to learn the process fromthe developer through direct observation and hands-on train-ing of the laboratory process so that they can then design aGMP-compliant process at the appropriate scale needed forclinical doses. The PD staff may also need to develop QC as-says for process control and convert research protocols into aformat that facilitates GMP compliance (e.g., SOPs andMBRs)for proper documentation during clinical manufacturing. Acollaborative effort between the developer and PD staff dur-ing this step will help ensure that the process is faithfullytransferred to generate the cell product with the desiredidentity, purity, and activity.
3. Training of the QC and operations manufacturing staff. Thefinal step in the technology transfer process is the training ofthe technical staff thatwill perform the clinicalmanufacturingprocess and testing of interim and final products. If the CMOperformeddevelopmentwork to scale up andmodify the pro-cess for GMP compliance, then the trainers are normally theCMO’s PD staff, although the developer may also be involvedin the training process. As with the previous steps, classroomeducation of the operations staff on the nature of the cellproduct and process is recommended before hands-on train-ing so that the staff understands the critical process parame-ters in production. The training should include engineeringruns performed in a clean-room environment. Since thesesessions are typically performed by the full complement ofmanufacturing operators, process verifiers, and QC test per-sonnel, these training runs often help identify potential ma-terials and personnel workflow issues that may introduce riskof product contamination, other process variability not evi-dent during development, or areas where information flow isconfusing or incomplete between QC and operations. TheMBR should incorporate any process changes or improve-ments found in the engineering runs prior to process qualifi-cation runs. Lastly, documentation of successful trainingdemonstrating that the staff is proficient and competent tomanufacture the product should be included in the technol-ogy transfer process.
In summary, the technology transfer process involves thetransfer of both knowledge and methodology from the devel-oper to the CMOor other interested parties (investors). Technol-ogy transfer may include classroom education and hands-ontraining but should be designed to ensure faithful replication ofthe process used to produce the therapeutic cell product. It isalso important to identify local translational centers, either in-dustry- or government-derived. Translational centers help facil-itate research and innovative science in order to reach clinicaldiagnostic and therapeutic use as quickly and as productively aspossible. These centers can help with funding opportunities andadvise on business initiative directions, and some offer in-houseresearch facilities. These include, for example, the National Cen-ter for Advancing Translational Sciences in the United States, theMedical Research Council in theUnited Kingdom, andMedicen inFrance.
PROCESSES
Cell Sources and Isolation ProcessesCell sources and isolation processes vary greatly, and it is best toaddress any concerns early in development. As an example, wewill discuss the isolation and sourcing for MSCs. Despite the vastvariety of source tissues such as bone marrow, adipose, peri-odontal, and others, MSCs show some common characteristicsthat include fibroblast-like shape in culture, multipotent differ-entiation, extensive proliferation capacity, plastic adherence,and a common surface marker profile (e.g., CD34�, CD45�,CD31�, CD44�, CD90�, CD166�, and CD105�). However,there is no single surfacemarker that uniquely definesMSCs. Thecommon characteristics of MSCs are the basis for the isolationtechniques. The techniques can be gathered in to three maingroups: size/weight separation, plastic adhesion, and CDmarkerselection.
It is important to note that, if available, control material orcells (not primary patient-derived) should be considered for allprocess development work. For instance, K562 cells (an immor-talized human erythroleukemic cell line) are ideal for T-cell pro-cess optimization.
The first and most commonly used isolation technologyis Ficoll-Paque gradients. Ficoll (GE Healthcare, Little Chalf-ont, U.K., http://www.gehealthcare.com) is a neutral, highlybranched, high-mass, hydrophilic polysaccharide that dissolvesreadily in aqueous solutions. It is prepared by reaction of thepolysaccharide with epichlorohydrin. Ficoll is part of Ficoll-Paque, which is used in laboratories to separate blood or bonemarrow to its components (erythrocytes, leukocytes, etc.). Fi-coll-Paque is normally placed at the bottomof a conical tube, andthe aspirate is then slowly layered above Ficoll-Paque. After cen-trifugation, the following layers are visible: upper layer of plasmaand other constituents, a layer of mononuclear cells called buffycoat (peripheral bloodmononuclear cells [PBMCs]/mononuclearcells [MNCs]/MSCs), Ficoll-Paque, and erythrocytes and granulo-cytes, which should be present in pellet form. Once separatingthe layer, the cell mixture can be further processed using selec-tive adherence or CD marker selection. Many devices (suchas the Cobe 2991 [Terumo BCT, Lakewood, CO, http://www.terumobct.com], Cell Saver [Haemonetics, Braintree, MA,http://www.haemonetics.com], and Sepax [BioSafe, Eysins,Switzerland, http://www.biosafe.ch] devices) have separate
874 Cell Therapy, Manufacturing, and Commercialization
©AlphaMed Press 2013 STEM CELLS TRANSLATIONAL MEDICINE
Dow
nloaded from https://academ
ic.oup.com/stcltm
/article/2/11/871/6386175 by guest on 22 June 2022

protocols for closed-system use with Ficoll. Several develop-ments based on Ficoll-Paque have evolved over the years, fromprepacked tubes with a polymer layer that separates the Ficoll-Paque and the buffy coat layer, all the way to prepacked col-umns.
One such product is the SepMate-50 (StemCell Technologies,Vancouver, BC, Canada, http://www.stemcell.com), a special-ized tube containing a porous insert that forms a physical barrierbetween the Ficoll-Paque and sample. Although the product islabeled for research use only, this barrier allows the sample to berapidly pipetted onto the insert, avoiding the need for overlayingit directly onto Ficoll-Paque. The SepMate insert also reduces theduration of the centrifugation step, and after centrifugation, thetop layer containing plasmaandPBMCs canbepoured into a newtube. Other devices include a column containing a porous, high-density polyethylene barrier. These products allow blood to belayered on much more quickly without mixing polysaccharideand blood.
An alternate method of isolating MSCs and other progenitorcells on the basis of physical properties involves the use of filtra-tion-based systems. One such product is the Purecell Select Sys-tem (Pall Corporation, Port Washington, NY, http://www.pall.com), which can be usedwith blood, bonemarrow, and umbilicalcord blood to prepare MSCs based on their entrapment in andadsorption to a fibrous polyester filter matrix [1, 2]. Followingthe filtration/collection step, cells are then recovered by retro-grade rinsing of the filter with an appropriate harvest solution,such as PlasmaLyte-A (Baxter Healthcare, Deerfield, IL, http://www.baxter.com) or saline/dextran solutions. This method canbe completed in a short period of time (15–30 minutes) andprovides levels ofMNCs and CD34� cells that are comparable toor higher than those of Ficoll-based methods, albeit with some-what higher levels of granulocytes. Filter-based separations havethe advantage of being rapid and easy to use without the needfor a centrifuge, and they can be done at the point of care withina disposable closed system to minimize contamination risk.
Another device for point-of-care extraction of adipose-de-rived MSC is the Celution System (Cytori, San Diego, CA, http://www.cytori.com). The Celution System consists of an electro-mechanical software-driven device, a presterilized single-useconsumable set, and a proprietary processing reagent. The adi-pose-derived regenerative cells are isolated from the adiposetissue matrix in a highly optimized automated process using en-zymatic digestion, gravity-based separation, and centrifugalconcentration.
Phenotypic isolation can be achieved by selection of plasticadhesion in which cells after gradient separation are placed oncoated cell culture dishes. MSCs adhere to plastic; therefore,once theMSCs have been seeded for 4–24 hours, the media canbe replaced and adherent cells will colonize. Some laboratoriesskip the separation steps and seed the aspirate directly, relyingonly on the adherence for isolation of theMSCs. Additionally, cellsorting technologies that can sort cells by size or shape can beused. Such technologies include fluorescence-activated cell sort-ing (FACS) using selective marker labeling or size exclusion. Thistechnique is limited by sample size, cost, and aseptic handling.
An additional option for MSC isolation is based on selectionusing antibodies against the common MSC CD markers by cellsorters. One example of magnetic sorting technology is theMACS (magnetic-activated cell sorter; Miltenyi Biotec, BergischGladbach, Germany, http://www.miltenyibiotec.com). The prin-
ciple behind this technology is the use of CD antibodies that areattached to magnetic beads. The aspirate or cells are incubatedwith the beads, allowing specific binding between the antibodyand CDmarker on the cell. Once bound, the mixture is placed ona magnetic column, and the beads with the bound cells stick tothe column because of the magnetic nature of the bead. Theretained, antibody-bound cells can then be washed out by re-moving the magnet and washing out the cells. It should be de-termined whether the cell source will be obtained fresh or fro-zen. Issues regarding cryopreservation, logistics, and so forthmust be thought of prior to product development.
Cryopreservation for Cellular TherapiesCryopreservation of cells and long-term storage options permitcompletion of safety and quality control testing, along withtransport from the collection site to the processing facility andsubsequently to the clinical site [3–5]. Although the basic con-cepts surrounding cell cryopreservation are the same, no singlemethod is universally applied for a variety of reasons—the basicreason is that no cell therapy product is essentially the same. Thegeneral processes are typically established on the basis of a num-ber of standard parameters, including the following:
● Harvesting and processing of cells● Addition of the cryopreservation media● Cooling protocol● Storage temperature and container● Warming/thawing● Post-thaw assessment
The current understanding and practice of cryopreservationfor cells and more specifically cell therapy have been well docu-mented, and suboptimal cryopreservation techniques can se-verely impact cell/product stability [6]. Modifying any of thesesteps can impact cell utility and cell therapy development. Herewe highlight some of the critical aspects and provide additionalsupport when considering cryopreservation protocol develop-ment for cell therapies. Raw material and finished product sta-bility, or shelf life, is very important when working with cells [6].To maximize cell stability, recovery, and function, each of thesteps should be considered.
Cell Harvesting/ProcessingFollowing cell/tissue harvest, cells are processed and pelleted(centrifugation) to concentrate and remove any excess growthmedia. Further processing may be performed to remove growthfactors, serum, and so forth. Once concentrated, cells should beresuspended in an appropriate medium as soon as possible tolimit any undue stress. Several assessment methods are avail-able, and the best method will depend in part on the cell model,but oftentimes the use of multiple methods will provide a betteroverall assessment of the population. Standard cell counts—using trypan blue or live/dead assays, for example—can providean overall cell number, but additional functional assays shouldbe included [3, 7, 8]. Once prefreeze counts are determined, cellscan be prepared for cryopreservation.
Cryopreservation MediaThe cryopreservation media used for freezing cells have numer-ous variations, but typically include culture media or balancedsalt solution, cryoprotective agent (CPA), and proteins. Manystudies have been performed to determine the optimal CPA and
875Eaker, Armant, Brandwein et al.
www.StemCellsTM.com ©AlphaMed Press 2013
Dow
nloaded from https://academ
ic.oup.com/stcltm
/article/2/11/871/6386175 by guest on 22 June 2022

concentration for preserving cells, and standard protocols in-clude a 5%–10% dimethyl sulfoxide (DMSO) solution [3–5]. Al-though certain perceived standard protocols exist, it is importantthat each cell product be evaluated for the optimal basemediumsolution and DMSO concentration used. Although culture mediahave typically been used as the base solution, more optimizedbalanced salt solutions are available and may provide enhancedbuffering and stability thereby reducing cell stress [7, 9]. Sincesome cells are highly sensitive to DMSO, studies should be per-formed to determine the optimal concentration [9]. Twenty-four-hour post-thaw viability is a more reliable parameter thanthe viability at time of thaw, which can differ quite dramaticallydepending on the solution and the freezing protocol.
Cooling and StorageAlthough the influence of cooling rate on post-thaw survival hasbeen documented for various cell types, standard protocol formost therapeutic cell models is performedwith a controlled ratefreezing (CRF) device having a rate of 1°C–2°C per minute [3–5].Manual techniques, such as using the Nalgene Mr. Frosty (Nal-gene, Rochester, NY, http://www.nalgene.com), are effective al-ternatives if a CRF device is not available. One drawback to man-ual protocols is that these methods are suitable only for cryovialcontainers and are not conducive to larger scale production.Cells are then transferred to storage in either the liquid (�196°C)or vapor (�156°C) phase of nitrogen. Although storage at�80°Ccan be used, long-term storage is typically performed at temper-atures below �150°C—the temperature at which all enzymaticactivity is suppressed [3, 5]. Cells and products can essentially bepreserved indefinitely if these temperatures are maintained.
Thawing and Post-Thaw AssessmentThawing of cryopreserved cells is typically performed as rapidlyas possible, and standard practice uses a water bath at 37°C.Rapid warming rates are commonly achieved by agitating thesample in a water bath until all visible ice crystals have melted.Once thawed, samples should be immediately removed from thewater bath and slowly diluted with media and washed [3–5].DMSO can be toxic to cells, so limiting their exposure to higherconcentrations and temperatures above 2°C–8°C is recom-mended. Dilution and washing requirements will be dependentupon the intended use of the cells or product and should bedetermined. Following the freeze/thaw process, cells can befragile, and care should be takenwhen handling cells tominimizepotential cell loss.
Post-thaw viability and recovery testing is critical to assess-ing the health of the cell population and developing cryopreser-vation protocols. Using the wrong assays or testing at the wrongtime can significantly impact efficacy and subsequent utility ofthe cells. Assessment is often performed immediately post-thaw, but the literature has shown that this can lead to inaccu-rate results [3, 8]. Ideally, assessment studies should be per-formed immediately, as well as over a 24–48-hour post-thawrecovery period to determine the true recovery profile. Just asimportant are the assays used to assess the recovery and viabil-ity. Viability and recovery assays can be divided into multiplecategories consisting of physical/membrane integrity, metabolicactivity, mechanical activity, proliferation, and functional/en-graftment potential. Typically, more than onemeasure is used todetermine the post-thaw viability of cells. The functional activityis often very critical to overall efficacy.
Cryopreservation ContainersAlthough overlooked at times, especially earlier in the develop-ment process, the freezing/storage container used is important.The use of cryovials for cryopreservation storage is standardpractice, especially for research and development uses. Theseproducts are not idealwhere clinical and larger scale applicationsare intended. Cryovials often cannot support large volumes(greater than 5 ml) and rely on open processing. If clinical appli-cations are anticipated, disposable closed-system cell freezingbags should be considered. These specialized containers allowfor aseptic filling and removal and reliable sterile containment.Other considerations should include information on the cell con-tact material of the container, potential leachables and extract-ables, and particulate levels.
Maintaining thequality of the startingmaterial, or cell sourcematerial, will impact the cryopreservation and post-thaw re-sults—essentially, what you put in is what you get out. Each ofthe aspects discussed above is critical when developing an effec-tive cell therapy cryopreservation strategy and protocol. Al-though general processes exist, minor modifications can andshould be performed to create an optimal protocol.
Media, Cytokines, Sera, and Serum-Free MediaThere are many important factors in a cell culture process, butthe cell culture medium is arguably the most critical. In the mostbasic sense, cell culture media supply critical nutrients to thecells and allow them to grow and remain viable. Generally, cellculturemedia contain energy sources, amino acids, vitamins, lip-ids, inorganic metals, salts, and buffering agents. These compo-nents are designed and balanced to present a physiological en-vironment for the specific cell of interest [10]. The quality of thecomponents used and the consistency of manufacture of thesefactors are critical to the performance of the medium.
Serum is commonly added to cell culture media. It is oftenderived from bovine, human, or horse sources and is processedand treated in various ways (irradiated, heat inactivated, etc.).Serum is a relatively undefinedmaterial that varies by source andlot. It contains a rich mixture of lipids, growth factors, proteins,metabolites, inorganic minerals, and other nutrients that caninduce cell growth in various culture systems. Serum also con-tains extracellular matrix proteins that promote the attachmentof cells to tissue culture plates. Although there are benefits tousing serum, there are also some drawbacks. Serum presentslot-to-lot variability. This is a problem when the consistency ofmanufacturing is a goal. Often lots of serummust be qualified toensure that performance meets specifications. This involves aconsiderable amount of labor and validation. Serum can alsopresent a regulatory risk since it may be a source of risk foradventitious agent contamination. Finally, cost and limited lotsizes are additional negative aspects of using serum, as well asdemand on a limited supply of serum. In addition, human plate-let lysate can be used to replace fetal bovine serum (FBS), possi-bly in autologous applications.
For these reasons, the use of serum-free medium (SFM) hasbeen increasingly preferred [11]. SFM presents a greater degreeof definition, reproducibility, and manufacturability than tradi-tional serum-supplemented formulations. To replace serum,SFM often include proteins, lipids, trace metals, and growth fac-tors at empirically determined concentrations for the specificcell type and application of interest. The components chosen
876 Cell Therapy, Manufacturing, and Commercialization
©AlphaMed Press 2013 STEM CELLS TRANSLATIONAL MEDICINE
Dow
nloaded from https://academ
ic.oup.com/stcltm
/article/2/11/871/6386175 by guest on 22 June 2022

may be synthetic, recombinant, or from native tissue extracts(serum albumin, transferrin, etc.). Recombinant growth factorsand cytokines are available and may be included in media topromote cell growth or to drive cellular responses according to aspecific signaling pathway. Similar to serum, the incorporation ofrecombinant proteins adds a degree of cost and complexity tothe formulation.
Regardless of the components used, one challenge in thedesign of cell culture media for cell therapy applications is toproduce a formulation that delivers consistent results for multi-ple donors. In a patient-specific autologous therapy, themediumideally will provide predictable results for each patient. It is im-portant during the development of a cell culture medium thatmultiple donor pools are evaluated.
Adherence Versus SuspensionIf the cell product requires ex vivo culture for expansion, activa-tion, differentiation, or genetic or othermanipulation, the devel-oper must consider the type of device in which to culture thecells. Two basic cell culture systems exist: vessels for adherentcells and vessels for cells that grow in suspension. Each typeof cell type presents different technical issues for scaling up andscaling out. For adherent cells, one must provide a solid sub-strate or surface onwhich the cellsmust attach to grow. Thismaybe accomplished by simply providing a flat surface as found withtraditional cell culture flasks or through the use of beads sus-pended in media. Traditional flat-surface vessels allow the cellsto be visualized during culture to assess the relative health, mor-phology, and density of the cells. Scaling up or scaling out, how-ever, may become logistically challenging if large numbers ofcells are required per dose or per lot. Several manufacturershave developed large and small flasks with multiple layers thathelp reduce the number of flasks needed per lot. Additionally,manipulating adherent cells in multiple flasks may increase therisk of contamination. Device manufacturers have designed anddeveloped robotic systems to automate the handling of flasksand closed devices with large surface areas that allow easierscale-up and scale-out processes.
Another solution to the scaling of an adherent cell product isthe use of beads in suspension cultures. Growing adherent cellson beads may also reduce manufacturing logistics by allowingone to manipulate the cells in vessels as if they were nonadher-ent cells. Technical issues with scaling up and scaling out arereduced, but visualization of the cells during culture may be dif-ficult or impossible. Because many adherent cell products usepercentage of confluence as an important parameter for cellhealth and function, bead-based systemsmay not be suitable forall adherent cell types.
There are many devices and vessels for culturing cells thatgrow in suspension already available to cell therapy developersfrom the pharmaceutical and biotech fields. Systems for growingcells to produce recombinant proteins and antibodies may beadapted for growing stem cells, T cells and other lymphocytepopulations, dendritic cells, and many other types of cells.
Scalable Platforms: Scale-Up Versus Scale-OutTo provide for the increased cell numbers or patient doses re-quired for clinical trials and commercialization of cell-based ther-apies, the need to expand or increase the manufacturing capac-ity becomes “mission critical” for a successful new therapeuticproduct.
The term “scale-up” typically refers to increasing the manu-facturing output or capacity, which is achieved by increasing thenumber of cells or volume processed for each manufacturing lotperformed. The term “scale-out” refers to the alternate ap-proach of keeping the manufacturing lot size the same but in-creasing or expanding out the number of manufacturing lines orunit operations that can be run concurrently. Considerations forwhether to scale up or scale out a manufacturing process haveseveral aspects, including the type of cells, the total number ofcells or patient doses needed per manufactured lot, and thepracticality of manufacturing increased cell numbers or volumein a GMP-compliant process, preferably with a closed manufac-turing process to minimize contamination risk.
For allogeneic products, it is most often a scaling up of theprocess that is used to provide between 5 billion and 50 billioncells per manufactured lot. For such scale-ups, the current ap-proach is to use either more cell culture flasks, cell factories/hyperstacks, or larger scale single-use bioreactors for adherentor suspension cells.
For autologous products, the goal is to be able to produce asuitable number of cells for one to five patient doses of cells,typically in the 1–5 billion range per manufactured run, and tothen be able to scale out the number of manufactured runs thatcan be performed on a regular (daily or weekly) basis. In thesescale-out cases, the choices are again to use conventional cellculture flasks, cell factories or static-bags, and bioreactors.
BioreactorsThere are several different types of bioreactors that can be usedto generate large quantities of cells for the production of thera-peutic proteins, viral vaccines, tissue engineering, or cell therapyapplications. The advantage of using bioreactor technology isthat variables such as temperature, pH, dissolved gasses, andagitation can bemonitored and closely controlled at a large scalein a closed environment. This can help maintain a process that isconsistent and reproducible at various scales. Bioreactor tech-nology can be generally separated by size,modeof agitation, andcell type (suspension, adherent, etc.). The most common typesof vessel designs include stirred-tank, packed-bed, hollow-fiber,and cellbag bioreactors.
The simplest form of a stirred-tank bioreactor is the spinnerflask. These vessels have a limited operating volume and aremostly used for process optimization. On the other end of thespectrum, stirred-tank bioreactors for the processing of mam-malian cells can reach up to 20,000 liters in scale.
Stirred-tank bioreactors are defined by an internal impellerthat provides the mixing of the medium and gases. In addition,the impeller provides the needed uplift to keep the cells in sus-pension. Thus, cells are floating freely in the reactor. A majoradvantage of these bioreactors is that they allow for the closemonitoring of critical process parameters, such as oxygen, pH,and temperature. In addition, sampling can be performed at anystage of the process without major interruption (e.g., via sterilesampling ports such asMillipore’s NovaSeptum system [Billerica,MA, http://www.millipore.com]). This allows for a close in-lineor off-line monitoring of the cells (e.g., via FACS analysis). Al-though stirred-tank systems have been used routinely for pro-tein/monoclonal antibody manufacturing for decades, their usefor the production of cell therapy products is in the early stages.For one thing, traditional stainless steel tanks require an inten-sive cleaning procedure between runs and in addition have to be
877Eaker, Armant, Brandwein et al.
www.StemCellsTM.com ©AlphaMed Press 2013
Dow
nloaded from https://academ
ic.oup.com/stcltm
/article/2/11/871/6386175 by guest on 22 June 2022

validated for each new run. Sincemany cell therapy applications,such as expansion of patient-specific T cells, do not require largequantities of cells, the cost and labor associated with the clean-ing procedure and validation are not justified for these tradi-tional systems. However, in recent years various single-use bio-reactor systems have been developed and introduced to themarketplace. These systems are commercially available at differ-ent sizes ranging from 2 to 250 liters and allow for convenientcost-effective manufacturing of cell therapy products.
A special case in stirred-tank reactors is the growth of an-chorage-dependent cells. Since these bioreactors do not providea surface on which cells can grow, the addition of microcarriersto the bioreactor is needed. These particles range in size from100 to 300 �m and provide the surface area needed for celladherence and growth. Several microcarriers are available in arange of sizes, core materials, and surface structures, and theappropriate carrier has to be determined for each cell type inde-pendently.
Independent of how the cells are grown, either in suspensionor onmicrocarriers, one attribute of stirred-tank bioreactors thatneeds to be considered are the shear forces that are introducedinto the system through the agitation. Thus, in the process de-velopment phase, the impact of shear forces on the cells needsto be analyzed. This is especially critical for processes involvingstemcells as various studies have shown that a high level of shearforces could influence the cell potency.
Although stirred vessels rely on an internal impeller to driveagitation of the culture medium, cellbag bioreactors instead usea rocking motion to agitate the fluid [12, 13]. This provides agentle mixing that greatly reduces shear stress compared withother agitated systems. Because of this, wave motion bioreac-tors are popular cell typeswhere theminimization of shear stressis necessary. The most well-known system is the WAVE Bioreac-tor (GE Healthcare), which has been used in many different ap-plications and to generate material for many clinical trials. Cell-bag reactors are single-use systems and eliminate the need fortank sterilization and complex setup schemes, which makes theprocess less laborious and reduces the need for cleaning valida-tion.Wavemotion bioreactors are popular options for expansionof patient-specific T cells and anchorage-dependent cells used incell therapy applications (grownonmicrocarriers), and they havebeen used for the production of monoclonal antibodies for clin-ical-scale productions. These systems offer control of mixingrate, temperature, and oxygenation at a scale-up to 500 liters.
Packed-bed bioreactors are systems designed to expandcells that are immobilized on a growth surface that may includebeads, porous matrices, or mesh structures [14]. The growthsurfaces are packed into the bioreactor vessel in a tight configu-ration that allows for a very high cell density (more than 1� 108
cells per milliliter). Cell culture media can be perfused throughthe system at a controlled rate to provide sufficient nutritionaland growth requirements for the cells. These systems are ame-nable to the production of expressed proteins because the spentmedium containing the molecule of interest can be removedwithout disturbing the cells. Recently, packed-bed systems havebeen used more commonly for the production of cell productssuch as adherent adult stem cells and human embryonic stemcells. The advantages of this system include the potential for veryhigh density cultures, very low shear stress, and extensive pro-cess parameter control. Although the potential for growing largenumbers of cells is high, the efficient and effective harvest of the
cells presents a substantial challenge. Cell harvest in a packed-bed process will require optimization of dissociation and wash-ing steps to reach a high yield. Currently, there are availablepacked-bed systems on the market such as the Quantum (Beck-man Coulter, Fullerton, CA, http://www.beckmancoulter.com),iCELLis (ATMI, Danbury, CT, http://www.atmi.com), and theCelligen PBR system (New Brunswick, Enfield, CT, http://newbrunswick.eppendorf.com).
Monitoring of bioreactor runs, regardless of the type of sys-tem used, is a critical activity to ensure run consistency and op-timal performance. Parameters such as dissolved oxygen, pH,temperature, mixing rate, and gassing rate are typically mea-sured in real time using in-line sensors placed within the reactorvessel. Additional variables such as lactate, glutamine, gluta-mate, glucose, cell number, and cell viability can be measuredthrough off-line devices (such as the BioProfile Analyzer; NovaBiomedical, Waltham, MA, http://www.novabiomedical.com).Taken together these variables can be tracked andused tomodelspecific processes. These data can be used to optimize cell out-put and process yield. Real-time monitoring can also be used toquickly identify problems and allow the scientist to adjust con-trols to avoid scrapping an expensive run [15].
Although most in-line parameters are measured by tradi-tional sensor technology that is either chemical- or optical-based, there is notable research being conducted on next gener-ationmonitoring technology [15]. Raman spectroscopy has beenapplied to generate sensors that are capable of analyzing a cul-ture to predict glutamine, glutamate, glucose, lactate, ammo-nium, and viable cell density simultaneously. This would repre-sent a significant advancement by reducing the need forextensive offline analysis and the subsequent delayed responsein parameter control.
Batch, Fed-Batch, and PerfusionPrimarily driven by bioprocess applications, there are three dif-ferent modes of operation for primary cell culture process:batch, fed-batch, and perfusion. Batch refers to inoculating a cellculture system with a predetermined quantity of medium and cellconcentration and allowing the culture to run with no feeds orme-dium exchange until harvest. Fed-batch refers to inoculating a cellculture system and adding media, cytokines/growth factors, nutri-ents,orapH-controllingbuffer to increasethecelldensityandmain-tain high viability for the majority of the culture time. Perfusionrefers to inoculating a cell culture system and continuously feedingandharvesting tomaintainhealth, viability, andproductivity as longas possible (significantly longer than a batch or fed-batch process).Perfusion removes and replaces media within a container, leavingthe cells in the original cell culture system, without compromisingthe sterility of the cell culture system [16]. Theprocess is performedthrough controlled cycles of harvesting spent media out of the cellculture system (the cells remaining in the container or bag), whilefeeding in fresh media. Perfusion is typically done using either astand-alonebioreactor (for adherent cells) or a cellbag-basedbiore-actor (for suspension cells). Harvesting of spentmedia is performedusing either a hollow fiber ormembrane sheet type filters. It allowsfor high cell densities to be achieved and is scalable for a wide vari-ety of volumes. Perfusion is a highly efficient way of culturing cellswith higher cell viability than batch or fed-batch systems, and it canproduce much greater cell numbers from the same size container.This is ideal for autologous therapies where high cell densities are
878 Cell Therapy, Manufacturing, and Commercialization
©AlphaMed Press 2013 STEM CELLS TRANSLATIONAL MEDICINE
Dow
nloaded from https://academ
ic.oup.com/stcltm
/article/2/11/871/6386175 by guest on 22 June 2022

neededwhile reducing the overall of cost of themedia and supple-ments.
AntibioticsIn general, most cell therapy laboratories and production facili-ties do not use antibiotics. The introduction of antibiotics addsadditional nonhuman components to the product. Carryover ofantibiotics into the final cell product may also have serious con-sequences for patient safety, such as an allergic reaction to pen-icillin. It also increases the possibility of false-negative resultsduring sterility/bacterial testing prior to patient treatment.
Matrices/CoatingsIn vivo, many cell types depend on the surrounding extracellularmatrix (ECM) and associated cell signaling components forgrowth and proper function. In cell culture, adherent cell lines orprimary cells require ECM for attachment to cell growth surfacessuch as flasks, plates, microcarriers, and scaffolds. ECM consistsof components such as proteins (such as laminin, collagen, fi-bronectin, and elastin) and proteoglycans. Certain cell types thatare grown in culture are not able to produce sufficient ECM forproper cell attachment. Several strategies have been developedto overcome this. Serum-supplemented media are widely usedfor many cell types because of their growth-promoting proper-ties, as well as the broad complement of cellular attachmentsubstrates that are contained in serum. For serum-free systems,ECMmolecules can be used to treat cultureware to promote cellattachment. Additionally, recombinant molecules or syntheticchemical processes can be incorporated into themanufacture ofculture surfaces to facilitate cell attachment without any pre-treatment. These precoated products are commercially availablefrom many vendors and present a convenient option. For manytissue engineering applications, the use of a three-dimensionallattice (such as collagen scaffolds) for cell growth may provide amore physiologically relevant environment to encourage tissue-forming properties [17].
Seed DensitiesOptimization of an efficient expansion protocol is a crucial part ofmanufacturing and process development. Researchers have re-ported the lack of standardization of expansion protocols, in-cluding cell seeding density for cell therapy [18]. The initial plat-ing of cells in cultureware containing a specific mediumformulation marks the beginning of cell expansion for thescale-up process. Seeding density can significantly affect cellquality and cell yield and thus requires optimization at an earlystage of the process. Determining optimal seeding density is,however, highly dependent onparameters such asmediumcom-position (e.g., serum-free formulation, FBS-containing formula-tion, cytokine composition, glucose level), tissue source, qualityof donor (age, medical history), culture method (low oxygen,two-dimensional [2D] culture, bioreactor, scaffolds, enzymes fordissociation), and culture flasks [19–22]. Seeding density can beoptimized once medium composition, tissue source, and culturemethod have been determined. Both initial cell seeding density(from primary tissue) and passaging cell density will determinethe output of a scale-up procedure in terms of cell yield and cost(time of culture, labor and materials). In some practices, cells arepurchased from a supplier where cells are isolated and culture-ex-panded in one particular medium formulation and then cryopre-served. Following freeze-thaw, cells could be culture-expanded in a
different formulationwith amodified protocol. Changing of culturemedium and protocol require further optimization of seeding den-sity post-thaw for long-term cell expansion.
Researchers have reported in tissue engineering applica-tions, certain biomechanical properties of hyaluronic acid hydro-gels showed improvement with higher MSC seeding densities[23], although others have reported that lower seeding densitiesof MSCs favor a higher proliferation rate and maintenance ofstemness properties in a 2D culture system [21, 24]. However, anincreased cell proliferation rate does not necessarily translate tooptimal cell yield. Optimization of seeding density strategiesneed to be established to find a balance between time, labor,andmaterials cost andoptimal cell yield. Every scale-up system isunique, and therefore seeding density needs to be optimizedaccording to each system.
HarvestingThe harvesting of expanded cells is a critical step in themanufac-turing of cell therapy products, as this is often the final process-ing step prior to patient infusion or cryopreservation. Cell har-vesting can be a laborious and time-intensive process, and as thevolume of cells being processed increases, this step can quicklybecome a process bottleneck [14]. The objective in the harvest-ing process is to achieve a reduction in volume or an increase incell concentration with high yield and recovery while maintain-ing the integrity and functionality of the cells.
It is important early on in the development of a cell therapyproduct to estimate what scale of commercial production will beneeded, so that in initial preclinical and process developmentand phase I efforts one works with a method that can be scaledupor scaled out tomeet the product requirements for later stagetrials and commercialization. For most autologous cell productsthat are grown in suspension culture, such as antigen-specific Tcells, dendritic cells, and natural killer (NK) cells, a typical produc-tion volume is in the 2–10-liter range, whereas CD34� hemato-poietic stems cells and tumor-infiltrating lymphocytes are oftenin the 10–15-liter range, and in some cases as high as 50–70liters. For adherent cells, such as bonemarrow-derivedMSCs thevolume of cells harvested from cell culture vessels are typicallyproduced in 5–10 liters of culture fluid.
Several technology choices exist for cell harvesting depend-ing on the volume of cells and the available infrastructure andpersonnel resources. The most commonly or widely usedmethod is centrifugation with 250- or 500-ml centrifuge bottles,althoughwith harvest volumes greater than 5 liters, manual cen-trifugation becomes increasingly time-consuming and labor-in-tensive and can be a significant driver of the cost of goods. An-other drawback of centrifugation is that it involvesmultiple openmanipulations in the decanting and resuspending of the cells,which introduces contamination risk and therefore requires a fullclean-room facility. For these reasons, other “closed” technolo-gies are also being adapted for use with cellular therapies, suchas blood processing equipment/cell processors and tangentialflow filtration devices available from several suppliers.
Gas ConditionsAlthough most mammalian cell culture uses 5% CO2 as the de-sired agent, it is important to note that variations in the concen-trations of both CO2 and O2 might provide positive growth con-ditions and must be explored. For example, hypoxic conditions
879Eaker, Armant, Brandwein et al.
www.StemCellsTM.com ©AlphaMed Press 2013
Dow
nloaded from https://academ
ic.oup.com/stcltm
/article/2/11/871/6386175 by guest on 22 June 2022

could possibly provide better pH and overall medium stabiliza-tion, as well as increased growth.
Feeder Cells and Antigen-Presenting CellsMany cell therapy products require feeder cells or antigen-present-ing cells to aid in cell production. Although each cellular product isdifferent, we discuss this application for T-cell production.
T cells are optimally activated/stimulated by professional an-tigen-presenting cells (APCs), or dendritic cells (DCs). These APCsprovide the antigen-specific primary signal and the secondarycostimulatory signal to the T cells. However, the manufacturingof personalizedDCs is expensive, labor-intensive, and highly vari-able. In addition, DCs from disease-state patients may be im-paired in their ability to properly activate T cells. Bulk T cells canbe activated using irradiated allogeneic PBMCs and OKT3 anti-body (a monoclonal antibody that blocks the function of CD3 onT cells, rapid expansion protocol). This process can also be costlyand have inconsistent/irregular results because of the donor-to-donor variability of the PBMCs, aswell as limited supply. Artificialactivationmodalities with definedmolecular profiles are a highlydesired alternative to the DCs and allo-PBMC feeder cell schema.The CD3/CD28 DynaBeads (Life Technologies, Rockville, MD,http://www.lifetech.com) are an alternative to DCs and allo-PBMC activation/stimulation. The paramagnetic beads arecoated with anti-CD3 and anti-CD28 antibodies and deliver ro-bust signals capable of activating and expanding bulk T cellsthrough the T cell receptor (TcR) complex and the CD28 costimu-latorymolecule. However, these beads are capable of expandingonly a subset of T cells, which may not necessarily represent thecomplete population of desired cells. A more consistent andcomprehensive tool is the K562-based artificial APC system. TheK562 erythroleukemic cell line provides an excellent platformbecause it does not express human leukocyte antigen (HLA)mol-ecules, therebymitigating allogeneic responses. The cell line alsoexpresses adhesion molecules that facilitate APC:T-cell interac-tions. In addition, the cell can be genetically modified to expressHLA molecules, costimulatory molecules, and cytokines. Expres-sion of the high affinity Fc receptor on K562 cells also allows thepresentation of antibodies such as anti-CD3 and anti-CD28 to theT cells, making it an attractive off-the-shelf product that can beused for expansion of any clinical sample. HLA-expressing K562cells canalsobeusedtoselectivelyexpandantigen-specificTcellsbypulsing with specific peptides. The ability to manufacture a robust/consistent APC product for the activation and expansion of a T-cellsample is critical for the commercialization of an autologous T-cellproduct.
Genetic Alterations and Vector DesignAlthough the frequency of any given subset of cells in the body oran isolated procedure can be extremely low, advances in geneticengineering have allowed the production of well-defined pheno-typic cell subpopulations from a bulk starting material. Cells canbe genetically modified in a transient manner (via RNA electro-poration) or a durable permanent fashion (viral, plasmid). Thegeneticmodificationsmade to these cellsmay also be coupled toan ex vivo expansion phase, with the transient alterations occur-ring at the end of the amplification whereas the permanentchanges typically occur near the onset of the culture. Although Tcells and DCs are the twomost common types of cells poised forgenetic modification, hematopoietic stem cells (HSCs) and NKcells can also be a potential source. The cell type and amount of
starting material will have a dramatic impact on the culture timeand cell divisions required to achieve the desired output.
The cell product can be transiently modified using a large-scale GMP electroporation system, such as a MaxCyte system(MaxCyte, Gaithersburg, MD, http://www.maxcyte.com), andRNA or plasmid. Although the expression is temporary, modifica-tions to enhance stability of the genetic material can maintain ex-pression for extended periods of time. Permanently modified cellstypically involve viral vectors (lentivirus, retrovirus, adenovirus) orplasmidDNAmaintainedbyselectionorepisomal replication.Tcellscanbemodified toexpress a variety of genes that impact their func-tion and phenotype, including cytokines, cell surface molecules forredirected specificity (TcRs and chimeric antigen receptors), intra-cellular modulators, and DNA-modifying enzymes (zinc-finger nu-cleases). DCs can be altered to express target antigens (Provenge;Dendreon,Seattle,WA,http://www.dendreon.com), costimulatorymolecules, andmaturationmolecules.
The choice and design of vector for the geneticmodificationsis also a critical component for the cell product. The virus encod-ing the gene of interest must be able to efficiently transducetarget cells with minimal toxicity; if long-term engraftment ofcells is required, minimal immunogenicity is also imperative. Ex-pression of the gene is driven by an internal promoter thatshould maintain stable expression in the cell. Typically, the pro-moters are chosen to be ubiquitously active (elongation factor-1�, cyclic GMP-dependent protein kinase [PKG]) in all cell types;however, promoters may also be cell type-specific or expressionmay be regulated by environmental cues, such as hypoxia, ordrug-induced (e.g., tet-on and tet-off). The potential for in vivotoxicity is of great concern, and safety mechanisms to addressthe potential need also be considered for the vector design. Sui-cide switches/genes can also be incorporated into the vectorallowing for the immediate removal of the cells. Insertional acti-vation of oncogenes is a concern for safety, as is the potential forgenerating recombinant replicating virus. The safety require-ments are key components that need to be factored into therelease of the final product.
STABILITY AND REPRODUCIBILITY ASSAYS
A critical step is to determine how stable each product isthroughout the production process. It is advised that during eachstep, characterization be performed initially. This will determinehow each process step could potentially alter a cell’s phenotype.It is also suggested that as the process or materials within itchange, cell characterization assays be performed to determinehow or whether the change affected the product. In addition, ifcomponents of the assay itself change (by the end user or man-ufacturer), product changes must also be determined.
Variability in Processes and Cellular Raw MaterialAlthough determining variations in the overall process, includingevaluation of raw materials and supply management, is the spe-cialty of the CMO, it is important to understand how critical thisprocess is. Variations, such as cell potency and patient-specificproperties, should be addressed. Factors that can minimize suchvariations can be identified as alternatives, allowing the down-stream process individuals to be aware prior to determining theoverall risk assessment road map. Are there lot-to-lot variationsin any materials, including sera? Items to be assessed at the
880 Cell Therapy, Manufacturing, and Commercialization
©AlphaMed Press 2013 STEM CELLS TRANSLATIONAL MEDICINE
Dow
nloaded from https://academ
ic.oup.com/stcltm
/article/2/11/871/6386175 by guest on 22 June 2022

bench scale are starting/source materials (cell lines, viral/bacte-rial stocks, media, chemicals, serum, water) and in-process ma-terials (resins, buffers, filters, columnhousings, tubing, reagents)[25]. Packaging and device/delivery components will be ad-dressed by the CMO.
Phenotypic Assays
A defined characterization profile ensures that the manufactur-ing process reproducibly yields the intended product. It is anevolving process from laboratory research and across clinical de-velopment. Among the arsenal of assays that are available tocharacterize cell therapy products, cell phenotyping by multipa-rametric flow cytometry has been the premier tool to identifyand enumerate cell subsets [26]. Over the last decade, progressat the level of hardware technology (lasers, fluidics, optics, elec-tronics), fluorochrome chemistry (greater variety of antibody-fluorochrome conjugates), and software interface has led to theadvent of polychromatic flow cytometry where more than 5 andup to 20 parameters can be analyzed simultaneously at the sin-gle-cell level [27]. This remarkable technology hasmade its markin the diagnostic world, where it has been used to dissect thecomplexities of the hematopoietic and immune system. Thisplatform is ideally suited to interrogating and defining the inher-ent heterogeneity of cell therapy products, through the develop-ment of a product-specific phenotype assay.
The fundamentals of phenotyping assays are reagent choice,panel design, and instrument calibration. Starting early in prod-uct and process development with a broad screening of cell sur-facemarkers is a goodway to gain in-depth knowledge about theproduct phenotype and choose appropriate markers. The nextstep is to distinguish the critical phenotypic attributes from lessrelevant markers. The diversity of cell therapy products is suchthat there are no commercially available optimized panels (witha few exceptions), so validating the selected antibody cocktail(s)has to be done for each type of product. It is a labor-intensiveiterative process that involves antibody titration (to optimize thesignal-to-noise ratio), antibody pairing with fluorochromes (dimmarkers with high stain index fluorochrome and vice versa), andmaking sure that single stain performances are not compro-mised by spectral overlap [28, 29]. At this stage, proper controls,compensation matrix, and acquisition templates can be defined.At the instrument level, a comprehensive quality assurance andquality control program must be in place to calibrate, optimize,and maintain cytometer performance [30]. The development ofa phenotype assay has to be completed by putting in place a dataanalysis plan to manage the high-content information and ex-tract the interrogated product profile.
The product’s ultimate signature profile delivers informationabout its identity (what the product is, which can include positiveand negative markers), purity (what are the cellular contami-nants, if any), and release criteria (expressed as percentage ofcells as well as mean fluorescence intensity). In some cases, sur-face markers with inducible or regulated expression can be partof a potency assay as well. Part or all of the profile can also beused in process testing and in comparability studies. Polychro-matic flow cytometry can bring a wealth of information about aproduct and fits in as part of a matrix of analytical assays for celltherapy product characterization.
Potency, Safety Assays, Toxicity, ImmunodeficientMice, and Animal ImagingThe ability to generate large numbers of phenotypically andfunctionally defined cells provides a promising strategy for thetreatment of numerous diseases. Given the recent success ofautologous cell therapy in the treatment of cancer, it is poised tobecome a standard care for many malignancies. Each manufac-tured lot is patient-specific and will need to meet numerous cri-teria for release. This section describes the assays to be imple-mented in order to address identity, safety, and potency. It alsodiscusses the use of animal models to assess in vivo efficacy anddifferent imaging systems to monitor trafficking and engraft-ment of the infused cells. The International Society for CellularTherapy (ISCT) has recently published a position paper on po-tency assays for the cell therapy industry [31].
Large-scale manufacturing of patient-specific lots will re-quire a robust identity testing to ensure that each lot is matchedwith the intended patient. The most accurate method for thistesting will be polymerase chain reaction (PCR)-based. The pro-duction/expansion of the cells will require significant culture pe-riods and assays that can address the purity and phenotype needto also be implemented. In the case of T cells, the expanded cellswill need to be assessed for a “rested” phenotype, thereby min-imizing potential toxicities. In the case of dendritic cells, theywould need to be examined for the presence of immature DCs,which could pose hurdles for vaccine efficacy. Assays to addresstoxicities and off-target effects of transgene expressing T cellscan be examined in multiparameter tests. The final T-cell productcanbetestedagainst target-negativeandtarget-positivecontrolsorartificial target cells (K562). This system can be used to measuretoxicity and off-target effects against the negative controls and effi-cacy/potency against the positive controls. For the case of geneti-cally modified T cells (viral vectors), two major concerns are theinsertional transformation of the T cells and the production of rep-lication-competent virus. For theoncogenic transformation compo-nent, long-termor chronic stimulationof themodifiedTcells shouldnot result in the outgrowth of a clonal subpopulation of cells. Theassay for recombinant virus can be assessed by a p24-enzyme-linked immunosorbent assay or either a PCR-based or cell-basedamplification assay of the T-cell supernatant.
These assays provide valuable information regarding in vitrofunction; however, they do not necessarily correlate with in vivofunction. Immunodeficient mice models can help answer somequestions regarding in vivo functions such as trafficking, biodis-tribution, and organ-specific nesting. The NSG mouse (NOD.Cg-Prkdcscid Il2rgtm1Wjl/SzJ) is a severely immunocompromisedmouse strain that supports the engraftment of a wide variety ofprimary human cells. Xenografted cells can include primary tu-mor cells, T cells, DCs, hematopoietic stem cells, and skin cellsand can be transferred into the mice by multiple routes (intra-vascular, intraperitoneal, subcutaneous). The biodistribution ofthe cells is an important component to assess since it may di-rectly influence both efficacy and toxicity in nondisease organs.Historically, complete organ/tissue harvest of engrafted micecan be performed at various timepoints, and a full necropsy of alltissues and organs can be performed. Critical organs and tissuesinclude blood, spleen, lymph nodes, and bone marrow; otherimportant tissues include the liver, lung, kidney, brain, gonads,heart, and skin. Engrafted cells can be detected by flow cytom-etry, PCR, and immunohistochemistry. Both the presence and
881Eaker, Armant, Brandwein et al.
www.StemCellsTM.com ©AlphaMed Press 2013
Dow
nloaded from https://academ
ic.oup.com/stcltm
/article/2/11/871/6386175 by guest on 22 June 2022

absolute amounts of engrafted cells can be determined withtime, providing a detailed kinetic profile of their distribution.Long-term persistence in these organs may be an indicator oftoxicities and off-target effects.
Noninvasive imaging of xenografted mice allows for longitu-dinal tracking of the cells without terminating the study. Intrave-nous infusion of cells is usually followed by a temporary resi-dence in the lung tissue for �24 hours, after which the cellsdistribute throughout the body. If an immediate placement ofthe cells is required, then alternate routes of entry may be re-quired, such as intraperitoneal or direct intraorgan placement.Intraperitoneal infusion is also an option for delivery; however,trafficking may favor the lymphatic system rather than a moresystemic distribution, and imaging studies can address the distri-bution as well as the magnitude of the cell dose. Several modesof imaging can be used to track and follow the xenografted cells.Luciferase-tagged cells can be located and quantitated with theaddition of luciferin substrate using a charge-coupled devicecamera (Xenogen system; STTARR, Toronto, ON, Canada, http://www.sttarr.com). Cells can also be tracked using fluorescentproteins. For cells located deep in the mouse, proteins such asTurboFP635 or tdTomato may be more applicable for in vivo usebecause of their ability to emit through tissue. However, fluores-cence is diminished in a hypoxic environment such as a tumor,whichmay limit its use in certainmodels. Cells can also be loadedwith nanoparticles and tracked in mouse models; however, di-viding cells will dilute the signal and may provide tracking/trace-ability only for several population doublings.
The development of assays that address safety and toxicityas well as in vivo trafficking and propagation will establish animportant basis for the cellular product. It may also provide im-portant details that may be correlated to clinical outcome.
More traditional tumorigenicity assessment includes subcu-taneous or intramuscular administration of cells, followed by as-sessment of growth of the injection area relative to tumorgrowth after injection of known tumorigenic cell types, such asHT-1080 cells. However, intravenous injection is a commonroute of administration for cell therapy products, and the objec-tive of this section is to describe safety study designs to evaluate
tumorigenicity after intravenous administration of a cell therapyproduct in a nude mouse model. This type of assessment hasbeen used in FDA-approved INDs and may therefore serve as ageneral example. Still, for each product, agreement with regula-tory agencies should be sought for the experimental designbased on the specifics of the product driving the controls, timeframes, and specific endpoints that should be used, in the in-tended mode of administration in the clinic [32].
CONCLUSIONDetermining the factors that can enhance the success of a celltherapy product early in development is critical to the overallsuccess of the product. Even if all of the processes describedabove are not achievable, addressing them in the developmentstage will benefit downstream interested parties. Making dataavailable,whether positive or negative, is a critical component tosuccess. Processes for each cell product vary greatly, but the fieldwill benefit greatly from the establishment of a roadmap for celltherapy process variations and options.
ACKNOWLEDGMENTS
We thank the ISCT, the Alliance for Regenerative Medicine, theCalifornia Institute for Regenerative Medicine, and the NIH Cen-ter for Regenerative Medicine for their input and advice.
AUTHOR CONTRIBUTIONS
S.E., M.A., H.B., S.B., A.C., C.C., D.C., T.F., O.K., K.N., W.V.H., andR.W.: manuscript writing.
DISCLOSURE OF POTENTIAL CONFLICTS OF INTEREST
A.C. has compensated employmentwith Life Technologies. T.F. hascompensated employment and compensated stock options withPCT Cell Therapy Services. K.N. has compensated employmentwithNovartis.W.V.H. has compensated employment, is a patent holder,and holds stock options with Athersys, Inc. R.W. has compensatedemployment with StemCell Technologies, Inc.
REFERENCES1 HibinoN,NalbandianA,Devine L et al. Com-
parison of human bone marrow mononuclearcell isolation methods for creating tissue-engi-neered vascular grafts: Novel filter systemversustraditional density centrifugationmethod. TissueEng Part CMethods 2011;17:993–998.2 Sowemimo-Coker SO, Andrade F, Kim A et
al. A simple filtration system for red blood celldepletion and volume reduction in routine pro-cessing of human umbilical cord blood. VoxSang 2009;96:138–145.3 Hubel A. Advancing the preservation of
cellular therapy products. Transfusion 2011;51(suppl 4):82S–86S.4 Hunt CJ. Cryopreservation of human stem
cells for clinical application: A review. TransfusMed Hemother 2011;38:107–123.5 Thirumala S, Goebel WS, Woods EJ. Clini-
cal grade adult stem cell banking. Organogen-esis 2009;5:143–154.6 Burger S. Biopreservation stability con-
siderations for cell therapy development and
commercialization. BioPreservation Today2009;1:4 –5.7 Clarke DM. Optimizing biopreservation
yield: Steps to improving cryopreservation out-comes. BioPreservation Today 2009;1:6.8 Mathew AJ. What is your viability assay
really saying? BioPreservation Today 2009;1:8.9 Clarke DM, Yadock DJ, Nicoud IB et al. Im-
proved post-thaw recovery of peripheral bloodstem/progenitor cells using a novel intracellu-lar-like cryopreservation solution. Cytotherapy2009;11:472–479.10 Gorfien SF, Campbell A, Vemuri MC. De-
sign of culturemedia. In:MurrayM-Y, ed. Com-prehensive Biotechnology. 2nd ed. Burlington,VT: Academic Press; 2011:205–215.11 Jayme DW. Serum-free and protein-free
media. In: Stacey GN, Davis J, eds. BiologicalMedicines from Cell Culture. London, U.K.: Wi-ley; 2007:29–44.12 Eibl R, Werner S, Eibl D. Bag bioreactor
based on wave-induced motion: Characteris-
tics and applications. Adv Biochem Eng Bio-technol 2010;115:55–87.13 Singh V. Disposable bioreactor for cell
culture using wave-induced agitation. Cyto-technology 1999;30:149–158.14 Rowley J, Abraham E, Campbell A et al.
Meeting lot-size challenges of manufacturingadherent cells for therapy. BioProcess Int2012;10:16–22.15 Abu-Absi NR, Kenty BM, CuellarME et al.
Real timemonitoring ofmultiple parameters inmammalian cell culture bioreactors using anin-line Raman spectroscopy probe. BiotechnolBioeng 2011;108:1215–1221.16 Tran CA, Burton L, Russom D et al. Man-
ufacturing of large numbers of patient-specificT cells for adoptive immunotherapy: An ap-proach to improving product safety, composi-tion, and production capacity. J Immunother2007;30:644–654.17 Artym VV,Matsumoto K. Imaging cells in
three-dimensional collagenmatrix. Curr ProtocCell Biol 2010;Chapter 10:Unit 10.18.1–18.20.
882 Cell Therapy, Manufacturing, and Commercialization
©AlphaMed Press 2013 STEM CELLS TRANSLATIONAL MEDICINE
Dow
nloaded from https://academ
ic.oup.com/stcltm
/article/2/11/871/6386175 by guest on 22 June 2022

18 Fekete N, Rojewski MT, Furst D et al.GMP-compliant isolation and large-scale ex-pansion of bone marrow-derived MSC. PLoSOne 2012;7:e43255.19 Fossett E, Khan WS. Optimising human
mesenchymal stem cell numbers for clinicalapplication: A literature review. Stem Cells Int2012;2012:465259.20 Fossett E, Khan WS, Longo UG et al. Ef-
fect of age and gender on cell proliferation andcell surface characterization of synovial fat padderived mesenchymal stem cells. J Orthop Res2012;30:1013–1018.21 Sekiya I, Larson BL, Smith JR et al. Expan-
sion of human adult stem cells from bonemar-row stroma: Conditions that maximize theyields of early progenitors and evaluate theirquality. STEM CELLS 2002;20:530–541.22 Sotiropoulou PA, Perez SA, Salagianni M
et al. Characterization of the optimal culture
conditions for clinical scale production of hu-man mesenchymal stem cells. STEM CELLS 2006;24:462–471.23 Erickson IE, Kestle SR, Zellars KH et al.
High mesenchymal stem cell seeding densitiesin hyaluronic acid hydrogels produce engi-neered cartilage with native tissue properties.Acta Biomater 2012;8:3027–3034.24 Colter DC, Sekiya I, Prockop DJ. Identifi-
cation of a subpopulation of rapidly self-re-newing and multipotential adult stem cells incolonies of human marrow stromal cells. ProcNatl Acad Sci USA 2001;98:7841–7845.25 Beck G, Schenerman M, Dougherty J et
al. Raw material control strategies for biopro-cesses. BioProcess Int 2009;7:18–33.26 Shapiro HM. Practical Flow Cytometry.
4th ed. Hoboken, NJ: Wiley-Liss, 2003.27 Chattopadhyay PK, Hogerkorp CM, Roe-
derer M. A chromatic explosion: The develop-
ment and future of multiparameter flow cy-tometry. Immunology 2008;125:441–449.28 Maecker H, Trotter J. Selecting reagents
for multicolor flow cytometry. Becton Dickin-son Application Note 23-9538-01. FranklinLakes, NJ: Becton Dickinson, 2008.29 Mahnke YD, Roederer M. Optimizing a
multicolor immunophenotyping assay. Clin LabMed 2007;27:469–485, v.30 Perfetto SP, Ambrozak D, Nguyen R et al.
Quality assurance for polychromatic flow cy-tometry. Nat Protoc 2006;1:1522–1530.31 Bravery CA, Carmen J, Fong T et al. Po-
tency assay development for cellular therapyproducts: An ISCT review of the requirementsand experiences in the industry. Cytotherapy2013;15:9–19 e19.32 Bailey AM. Balancing tissue and tumor
formation in regenerative medicine. Sci TranslMed 2012;4:147fs28.
883Eaker, Armant, Brandwein et al.
www.StemCellsTM.com ©AlphaMed Press 2013
Dow
nloaded from https://academ
ic.oup.com/stcltm
/article/2/11/871/6386175 by guest on 22 June 2022
Copyright © 2022 FDOKUMEN