Idiopathic, nonobstructive cardiomyopathy in children
13
The American Journal of Cardiology Volume 21 FEBRUARY 1968 Nunrber 2 Clinical Studies Idiopathic, Nonobstructive Cardiomyopathy in Children* LEONARD C. HARRIS, M.D., F.A.c.c., ALVIN E. RODIN, M.D. 7 AND QUANC X. NGHIEM, M.D. Galveston, Texas I DIOPATHIC, nonobstructive cardiomyopathy may be defined as a subacute or chronic disorder of the heart muscle of unknown or obscure etiology. It is often associated with hypertrophy, fibrosis, endocardial or even pericardial involvementl; atherosclerotic and valvular heart disease are absent. Examples of various synonyms are endomyocardial fibrosis.” cryp togenic heart disease,3 cardiovascular col- lagenosis with parietal endocardial thronlbosis,4 idiopathic mural endocardial disease5 and idio- pathic myocardial hypertrophy.‘j The term “primary myocardial hypertrophy with sub- endocardial fibroelastosis” refers to a condition characteristically manifesting signs and symp- toms in infancy and with an early fatal outcome. It appears to be a different entity from that presented here. In the past decade progress in understanding and managing idiopathic cardiomyopathies has not been comparable with advances in the study of congenital or even rheumatic heart disease. In the United States, with a few exceptions,“-10 more effort has been devoted to the study of idiopathic hypertrophic subaortic stenosis than to other types of cardiomyopathy for which no cause could be found. However, elsewhere, especially in Africa,2-5 ~--l~ Brit- ain’ *I4 and Colombia,15 idiopathic, nonobstruc- tive cardiomyopathy has attracted much notice. Becker5 drew attention to its sporadic occur- rence in the United States. He has examined the case report and histologic material of our first case and regards the abnormality as similar to the South African variety. In this report a modification of the physiologic classification of Goodwin et a1.14 is used, and cases are grouped as (1) congestive (pulsus alternans), (2) restrictive, or (3) obstructive. Only the first two types will be discussed. We wish to emphasize that we are not certain that the cases reported here represent examples of the same disease process, but similarities in the clinical, physiologic and pathologic features suggest that grouping them under the title idiopathic, nonobstructive cardiomyopathy is ap- propriate from a diagnostic viewpoint and may be of future importance in etiologic investi- gations. None of the cases presented with rnani- festations suggesting acute myocarditis. Since idiopathic, nonobstructive cardiomy- opathy has been reported uncommonly in * From the Division of Pediatric Cardiology, Department of Pediatrics, and the Department of Pathologyt, Uni- versity of Texas Medical Branch, Galveston, Tex. This study was supported in part by the Bay :Irea Heart Associa- tion. Address for reprints: Leonard C. Harris, M.D., Director, Pediatric Cardiology, Department of Pediatrics, Uni- versity of Texas Medical Branch, Galveston, Tex. 77551. 153
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Idiopathic, nonobstructive cardiomyopathy in children
The American Journal of Cardiology Volume 21 FEBRUARY 1968 Nunrber 2
Clinical Studies
Idiopathic, Nonobstructive Cardiomyopathy
in Children*
LEONARD C. HARRIS, M.D., F.A.c.c., ALVIN E. RODIN, M.D. 7 AND QUANC X. NGHIEM, M.D.
Galveston, Texas
I DIOPATHIC, nonobstructive cardiomyopathy may be defined as a subacute or chronic
disorder of the heart muscle of unknown or obscure etiology. It is often associated with hypertrophy, fibrosis, endocardial or even pericardial involvementl; atherosclerotic and valvular heart disease are absent. Examples of various synonyms are endomyocardial fibrosis.” cryp togenic heart disease,3 cardiovascular col- lagenosis with parietal endocardial thronlbosis,4 idiopathic mural endocardial disease5 and idio- pathic myocardial hypertrophy.‘j The term “primary myocardial hypertrophy with sub- endocardial fibroelastosis” refers to a condition characteristically manifesting signs and symp- toms in infancy and with an early fatal outcome. It appears to be a different entity from that presented here.
In the past decade progress in understanding and managing idiopathic cardiomyopathies has not been comparable with advances in the study of congenital or even rheumatic heart disease. In the United States, with a few exceptions,“-10 more effort has been devoted to the study of idiopathic hypertrophic subaortic stenosis than to other types of cardiomyopathy
for which no cause could be found. However, elsewhere, especially in Africa,2-5 ~--l~ Brit- ain’ *I4 and Colombia,15 idiopathic, nonobstruc- tive cardiomyopathy has attracted much notice. Becker5 drew attention to its sporadic occur- rence in the United States. He has examined the case report and histologic material of our first case and regards the abnormality as similar to the South African variety.
In this report a modification of the physiologic classification of Goodwin et a1.14 is used, and cases are grouped as (1) congestive (pulsus alternans), (2) restrictive, or (3) obstructive. Only the first two types will be discussed. We wish to emphasize that we are not certain that the cases reported here represent examples of the same disease process, but similarities in the clinical, physiologic and pathologic features suggest that grouping them under the title idiopathic, nonobstructive cardiomyopathy is ap- propriate from a diagnostic viewpoint and may be of future importance in etiologic investi- gations. None of the cases presented with rnani- festations suggesting acute myocarditis.
Since idiopathic, nonobstructive cardiomy- opathy has been reported uncommonly in
* From the Division of Pediatric Cardiology, Department of Pediatrics, and the Department of Pathologyt, Uni- versity of Texas Medical Branch, Galveston, Tex. This study was supported in part by the Bay :Irea Heart Associa- tion.
Address for reprints: Leonard C. Harris, M.D., Director, Pediatric Cardiology, Department of Pediatrics, Uni- versity of Texas Medical Branch, Galveston, Tex. 77551.
153
Harris, Rodin and Nghiem
children,16-18 the purpose of this paper is to report its occurrence and manifestations in 8 children.
CASE MATERIAL
The earlier clinical and hemodynamic findings of Cases 1 to 5 were reported in a previous communi- cation on pulsus alternans.17 All patients have had right heart catheterizations and Cases 1 to 4 and Case 8, left heart catheterizations. ‘l‘he present clinical status of the 8 cases is summarized in Table I, pressure and cardiac output data and electrocardio- graphic and vectorcardiographic data in ‘Tables II and III. Additional pertinent clinical and laboratory data are supplied.
Of the 8 patients, 6 were male; 5 were Negro, 1 was white and 2 were Latin American of unknown racial origin.
The diagnoses were confirmecl by pathologic findings in 4 patients, obtained at autopsy in 3 ancl by myo- cardial biopsy in 1 (Case 7). A sibling of 1 of the 3 autopsy patients died. Since the clinical findings were similar to those of his brother, his diagnosis appears to be soundly based. In the remaining 3 cases, the diagnosis was made on clinical and hemo- dynamic grounds.
CASE HISTORIES
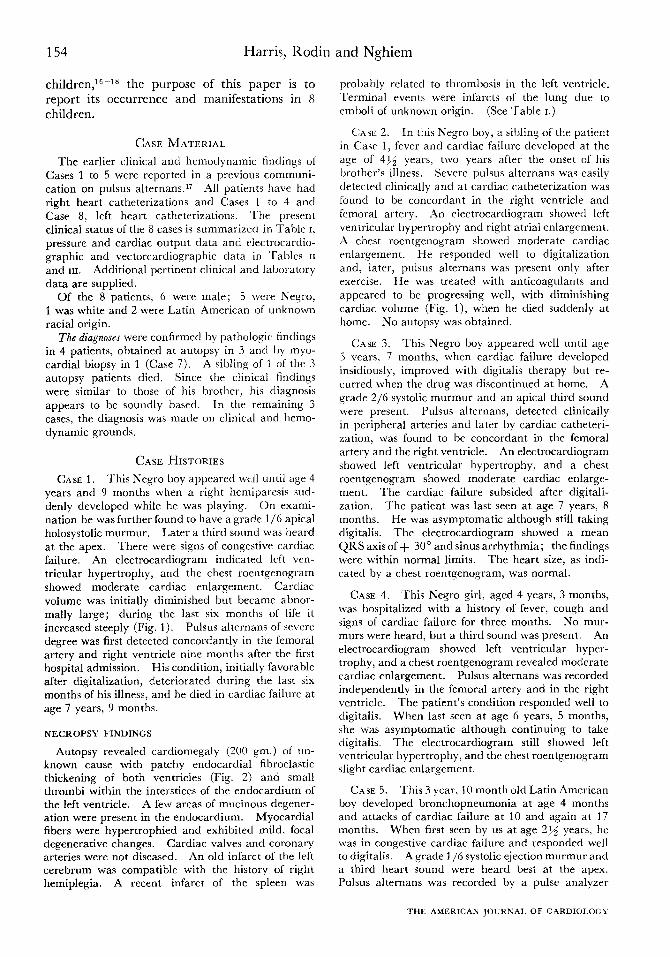
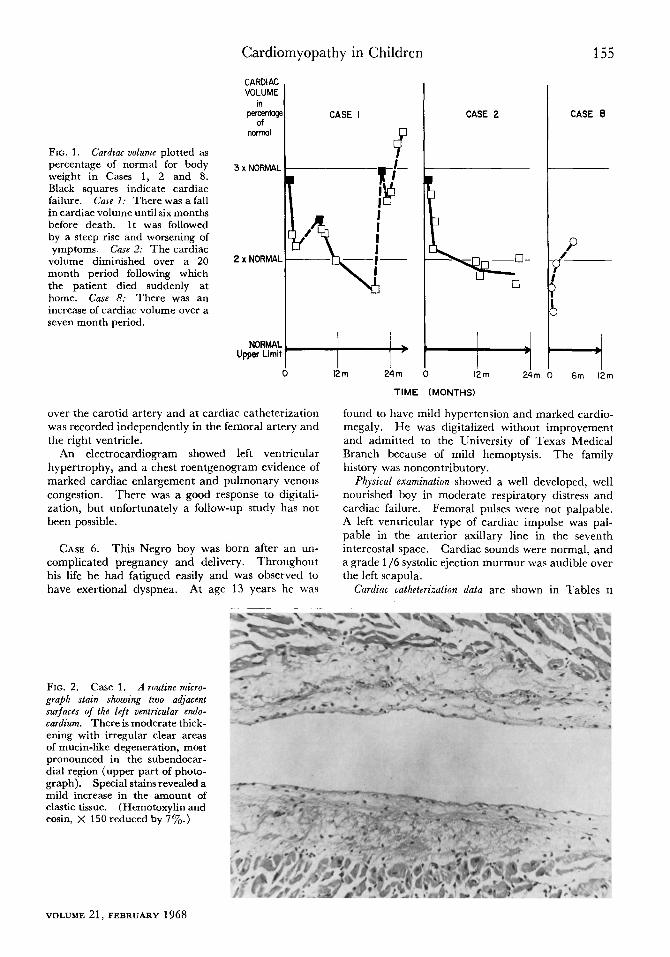
CASE 1. This Negro boy appeared well until age 4 years and 9 months when a right hemiparesis sud- denly developed while he was playing. On exami- nation he was further found to have a grade l/6 apical holosystolic murmur. Later a third sound was heard at the apex. There were signs of congestive cardiac failure. An electrocardiogram indicated left ven- tricular hypertrophy, and the chest roentgenogram showed moderate cardiac enlargement. Cardiac volume was initially diminished but became abnor- mally large; during the last six months of life it increased steeply (Fig. 1). Pulsus alternans of severe degree was first detected concordantly in the femoral artery and right ventricle nine months after the first hospital admission. His condition, initially favorable after digitalization, deteriorated during the last six months of his illness, and he died in cardiac failure at age 7 years, 9 months.
NECROPSY FINDINGS
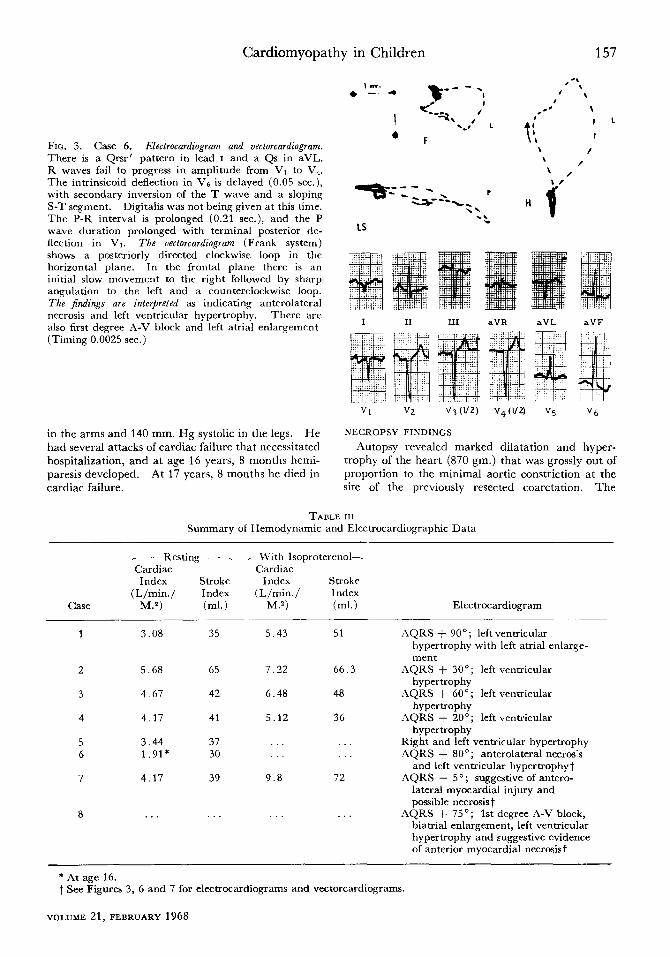
Autopsy revealed cardiomegaly (200 gm.) of un- known cause with patchy endocardial fibroelastic thickening of both ventricles (Fig. 2) and small thrombi within the interstices of the endocardium of the left ventricle. A few areas of mutinous degener- ation were present in the endocardium. Myocardial fibers were hypertrophied and exhibited mild, focal degenerative changes. Cardiac valves and coronary arteries were not diseased. An old infarct of the left cerebrum was compatible with the history of right hemiplegia. A recent infarct of the spleen was
probably related to thrombosis in the left ventricle. Terminal events were infarcts of the lung due to emboli of unknown origin. (See Table I.)
CASE 2. In this Negro boy, a sibling of the patient in Case 1, fever ancl carcliac failure developed at the age of 41~; years, two years after the onset of his brother’s illness. Severe pulsus alternans was easily cletectecl clinically and at cardiac catheterization was found to be concordant in the right ventricle and femoral artery. .4n electrocardiogram showecl left ventricular hypertrophy and right atria1 enlargement. A chest roentgenogram showed moderate cardiac enlargement. He responded well to digitalization and, later, pulsus alternans was present only after exercise. He was treated with anticoagulants and appeared to be progressing well, with diminishing cardiac volume (Fig. l), when he died suddenly at home. No autopsy was obtained.
CASE 3. This Negro boy appeared well until age 5 years. 7 months, when cardiac failure developed insidiously, improved with digitalis therapy but re- curred when the drug was discontinued at home. A grade 2/6 systolic murmur and an apical third sound were present. Pulsus alternans, detected clinically in peripheral arteries and later by cardiac catheteri- zation, was found to be concordant in the femoral artery and the right ventricle. .4n electrocardiogram showed left ventricular hypertrophy, and a chest roentgenogram showed moderate cardiac enlarge- ment. The cardiac failure subsided after digitali- zation. The patient was last seen at age 7 years, 8 months. He was asymptomatic although still taking digitalis. The electrocardiogram showed a mean QRS axis of + 30” and sinus arrhythmia; the findings were within normal limits. The heart size, as indi- cated by a chest roentgenogram, was normal.
CASE 4. This Negro girl, aged 4 years, 3 months, was hospitalized with a history of fever, cough and signs of cardiac failure for three months. No mur- murs were heard. but a third sound was present. An electrocardiogram showed left ventricular hyper- trophy, and a chest roentgenogram revealed moderate cardiac enlargement. Pulsus alternans was recorded independently in the femoral artery and in the right ventricle. The patient’s condition responded well to digitalis. When last seen at age 6 years, 5 months, she was asymptomatic although continuing to take digitalis. The electrocardiogram still showed left ventricular hypertrophy, and the chest roentgenogram slight cardiac enlargement.
CASE 5. This 3 year, 10 month old Latin American boy developed bronchopneumonia at age 4 months and attacks of cardiac failure at 10 and again at 17 months. When first seen by us at age 2pi years, he was in congestive cardiac failure and responded well to digitalis. A grade l/6 systolic ejection murmur and a third heart sound were heard best at the apex. P&us alternans was recorded by a pulse analyzer
THE AMERICAN ,JOURNAL OF CARDIoLOoT
Cardiomyopathy in Children 155
FIG. 1. Cardzac uolume plotted as percentage of normal for body weight in Cases 1, 2 and 8. Black squares indicate cardiac failure. Cake 7: There was a fall in cardiac volume until six months before death. It was followed by a steep rise and worsening of ymptoms. Case 2: The cardiac
volume diminished over a 20 month period following which the patient died suddenly at home. Case 8: There was an increase of cardiac volume over a seven month period.
CARDIAC VOLUME
in pereentagt
of n0W?d
3 x NORMAL
2 x NORMAL
NORMAL Upper Limil
CASE I
7
over the carotid artery and at cardiac catheterization was recorded independently in the femoral artery and the right ventricle.
An electrocardiogram showed left ventricular hypertrophy, and a chest roentgenogram evidence of marked cardiac enlargement and pulmonary venous congestion. There was a good response to digitali- zation, but unfortunately a follow-up study has not been possible.
CASE 6. This Negro boy was born after an un- complicated pregnancy and delivery. Throughout his life he had fatigued easily and was observed to have exertional dyspnea. At age 13 years he was
FIG. 2. Case 1. A routine micro- graph stain showing two adjacent surfaces of the left ventricular endo- cardium. There is moderate thick- ening with irregular clear areas of mucin-like degeneration, most pronounced in the subendocar- dial region (upper part of photo- graph). Special stains revealed a mild increase in the amount of elastic tissue. (Hemotoxylin and eosin, X 150 reduced by 7%.)
I 12 m Ai
CASE 2
km 24m
TIME (MONTHS)
CASE 8
I 6m 12m
found to have mild hypertension and marked cardio- megaly. He was digitalized without improvement and admitted to the University of Texas Medical Branch because of mild hemoptysis. The family history was noncontributory.
Physical examination showed a well developed, well nourished boy in moderate respiratory distress and cardiac failure. Femoral pulses were not palpable. A left ventricular type of cardiac impulse was pal- pable in the anterior axillary line in the seventh intercostal space. Cardiac sounds were normal, and a grade l/6 systolic ejection murmur was audible over the left scapula.
Cardiac catheterization data are shown in Tables II
VOLUME 21,FEBRUARY1968

156 Harris, Rodin and Nghiem
TABLE I
Summary of Clinical Findings
Age*
Case (yr.,
1 4%2
2t 4%2
j !Q 2
4
11 Ino
13
4-5 $
5x2
Pncum. wrlth
CF
Pnc,“n. 6 “11).
hefore onset. CF dt r,“srt
(:F
K~currcnr pncunr.. cnrdhc enlargrmvnt
from age 10 mrj.
Dyspnea, hcmoprvpriq, congestive CF
Exzrtinnal dyspnw,
.+bdominal disten-
tion, occnPion,*l vomirine
Pncum. ilt 1 h ? )‘.;
.‘asrhma” from 2-i
vr.; CF at 5Z{, vr.
CF
Puls. Embohc Fo Ilow-Up .\lr. Phenomens Other Findings
+ t tfzmip1rgi.l MI Died in CF iit 49{* proved hy .In+c.rd. nt 7x2 yrs. )r.
+ L’nknown, \\I1 Died suddenly no utops> excluded by .rngioc,ud. at 6%, y-r.
+ .X0”? hfl AS~“lpt.
rxcluded by ;unqoc*rd. 2 y-r. after
onset; ““rIndI
sized heart *~ NorI‘ hfl Asympt.
excluded hy ‘lrrgiocxd. 2412 Y’. sfter ““set; slightly en-
larged heart .t .\lxnt . . . Lost to followup
tir. 3 ,ipiul systolic
ejrctio” mwrnur + atrial sound; 2nd
sound single
:\t OnSet - Ilem~plegi.~ Cwrcution ot
;~t 16Rz iwrta
1’. resected
Mild .It .5 \r. + Transient Rt. ventricular hemipnresis biopsy; interstiri.d
(I dxy) at 5 fibrosis, myofibril1.r \ r. :!nd mitochondri,d
degeneration
\brrnr \hxr,t Little improvemrnt
with digitalis; t.dl (1
w”vcs in jug&r veins
Died in cnrdiac
failwe ;it 1731% Y’.
At 5Tfz yr. moderate
cardiac en-
largement ,I”d mild exertional
dyspnea Died in CF
at .59{, yr.
*At onset of symptoms.
t Sibling of child in Case I. $ Insidious onset.
5 Restrictive type. CF = cardiac failure; I’&. Air. = p&us dllernnnr, gr. = grad?; MI = “ncr.d InsuHiciency; angiocnrd. = .I”ginwrdiogr.lm; .uympt. =
asymptomatic; pneum. = pneumonin: ICS = intercostal spacr.
and III. The electrocardiogram and vectorcardlo- gram (Fig. 3) were interpreted as indicating antero- lateral myocardial necrosis. left ventricular hyper- trophy, left atria1 enlargement and first degree A-V block. A chest roentgenogram (Fig. 4) revealed gross cardiac enlargement, and pulmonary venous markings were increased.
Loboratory investigations disclosed serum glutamic oxalacetic transaminase (SGOT) 45 and serum glutamic pyruvic transaminase (SGPT) 32 units.
Hemoglobin was 13.1 gm./ 100 ml. Sickle cell prepar- ation gave a negative response.
Course of the Disease: Although there was evident coarctation of the aorta, the gross cardiac enlarge- ment was considered to be disproportionate to the degree of coarctation, thus suggesting that the patient had, in addition, primary myocardial disease. After surgical repair of the coarctation, cardiomegaly was still marked and symptomatic improvement was slight. At age 15 years, blood pressure was 120/84
TABLE 11
Pressures (mm. Hg)
_ Right Atrium - Right Ventricle Case 0 ” Mean S/D/EDP
- Pulmonary Artery _
Wedge S/D Mea” Mean
1 8.9 7.2
2 5.7 2.0 3 12.3 6.9 4 8.0 6.2 5.0 5 9.4 6.5 6 11.0 8.9 8.6 7 6.3 3.9 2.6 8 15.0 7.0 9.0
37/3.6/ 9.7 27/3.8/ 5.6
42/O /11.8 38/O / 4.5 40/3.2/ 7.8 46/6.0/ 9.0 31/x0/ 5 4 40/3.0.‘10.0
37/20 25 20.9 27/16 1’) 73 42;18 32 21 .o 38/13 24 65
31/18 26.4 20 3 40114 25
_ Left Atrium - Left Ventricle Femoral Artery n ” Mea” S/D/EDP S/D Mea”
95/14.2/27.3 tO2/57 73 120/12.8;23.0 122/76 86
95/64 77
133/74 89 97/58 72
114/58 72 9ti;47 65
45 25 26 105/15 134.0 lO6/54 78
S = systolic; D = diastolic; EDP = end-diastolic pressure.
THE AMERICAN .lOURNAL OF CARDIOLOGY
Cardiomyopathy in Children 157
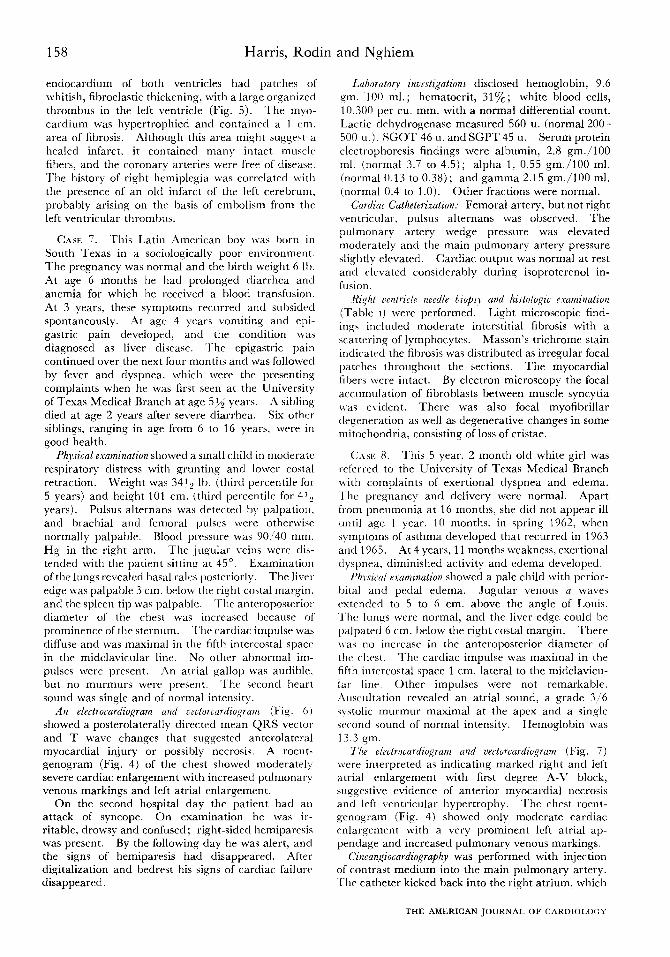
FIG. 3. Case 6. Electrocardiogram and vectorcardiogram. There is a Qrsr’ pattern in lead I and a Qs in aVL. R waves fail to progress in amplitude from VI to V:. The intrinsicoid deflection in Vs is delayed (0.05 sec.), with secondary inversion of the T wave and a sloping S-T segment. Digitalis was not being given at this time. The P-R interval is prolonged (0.21 sec.), and the P wave duration prolonged with terminal posterior de- flection in Vi. The vectorcardiogram (Frank system) shows a posteriorly directed clockwise loop in the horizontal plane. In the frontal plane there is an initial slow movement to the right followed by sharp angulation to the left and a counterclockwise loop. The jkdings are interpreted as indicating anterolateral necrosis and left ventricular hypertrophy. There are also first degree A-V block and left atria1 enlargement (Timing 0.0025 sec.)
in the arms and 140 mm. Hg systolic in the legs. He had several attacks of cardiac failure that necessitated hospitalization, and at age 16 years, 8 months hemi- paresis developed. At 17 years, 8 months he died in cardiac failure.
’ /
~=r-&.__ p ” ” \\ .\ 4
LS W
I II III aVR aVL aVF
Vl V2 V3 (1/21 V,(VZ) V5 V6
NECROPSY FINDINGS
Autopsy revealed marked dilatation and hyper- trophy of the heart (870 gm.) that was grossly out of proportion to the minimal aortic constriction at the site of the previously resected coarctation. The
TABLE III Summary of Hemodynamic and Electrocardiographic Data
Case
_ Resting --_ -With Isoproterenol- Cardiac Cardiac
Index Stroke Index SWOk?
(L/min./ Index (L/min./ Index M.2) (ml.) M.2) (ml.)
1 3.08 35 5.43 51
2 5.68 65 7.22 66.3
3 4.67 42 6.48 48
4 4.17 41 5.12 36
5 3.44 37 6 1.91* 30
7 4.17 39 9.8 72
8 . . .
Electrocardiogram
AQRS + 90”; left ventricular hypertrophy with left atria1 enlarge- ment
AQRS + 30’; left ventricular hypertrophy
AQRS + 60’; left ventricular hypertrophy
AQRS + 20’; left ventricular hypertrophy
Right and left ventricular hypertrophy AQRS + 80’; anterolateral necros%
and left ventricular hypertrophyt AQRS - 5O; suggestive of antero-
lateral myocardial injury and possible necrosist
AQRS + 75’; 1st degree A-V block, biatrial enlargement, left ventricular hypertrophy and suggestive evidence of anterior myocardial necrosist
* At age 16. t See Figures 3, 6 and 7 for electrocardiograms and vectorcardiograms.
VOLUME 21, FEBRUARY 1968
Harris, Rodin and Nghiem
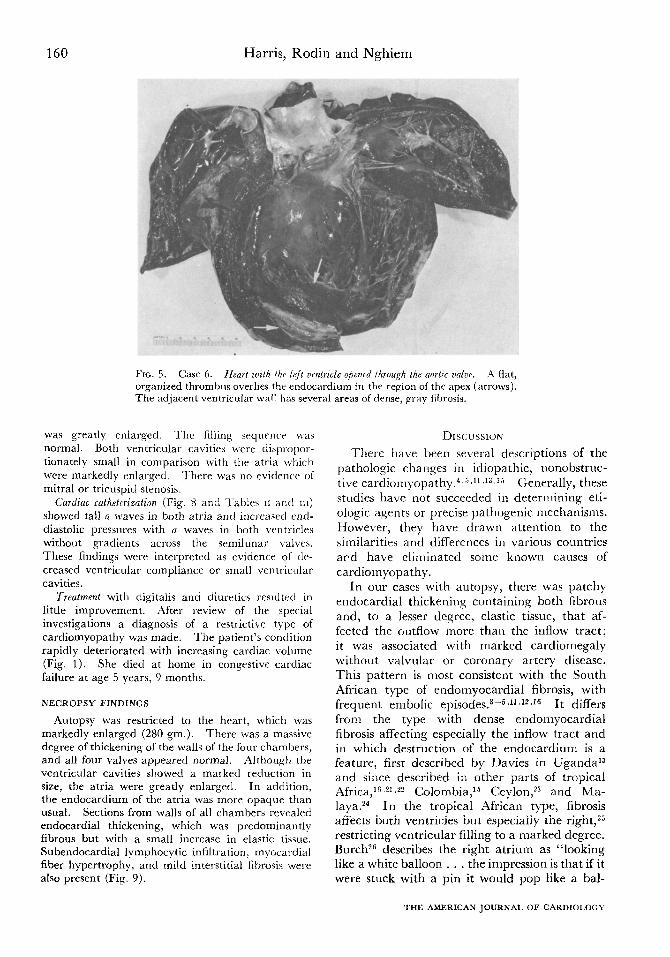
endocardium of both ventricles had patches ot
whitish, fibroelastic thickening, with a large organized
thrombus in the left ventricle (Fig. 5). The myo-
cardium was hypertrophied and contained a 1 cm.
area of fibrosis. Although this area might suggest a
healed infarct, it contained many intact muscle
fibers, and the coronary arteries were frrr of disease.
The history of right hemiplegia \vas correlated with
the presence of an old infarct of the left cerebrum.
probably arising on the basis of embolism from the
left ventricular thrombus.
CASE 7. This Latin American boy was Ijorn in
South Texas in a sociologically poor environment.
The pregnancy was normal and the birth weight 6 lb.
,4t age 6 months he had prolonged diarrhea and
anemia for which he received a blood transfusion.
At 3 years. these symptoms recurred and subsided
spontaneously. At age 4 years vomiting and epi-
gastric pain developed, and the condition was
diagnosed as liver disease. The epigastric pain
continued over the next four months and was followed
by fever and dyspnea. which were the presenting
complaints when he was first seen at the University
of Texas Medical Branch at age 55,’ years. A sibling
died at age 2 years after severe diarrhea. Six other
siblings, ranging in age from 6 to 16 years, were in
good health.
Physical examination showed a small child in moderate
respiratory distress with grunting and lower costal
retraction. Weight was 34l, lb. (third percentile for
5 years) and height 101 cm. (third percentile for 41,
years). Pulsus alternans was detected by palpation.
and brachial and femoral pulses were otherwise
normally palpable. Blood pressure was 90:40 mm.
Hg in the right arm. The jugular veins were dis-
tended with the patient sitting at 45’. Examination
of the lungs revealed basal ralrs posteriorly. The live1
edge \vas palpable 3 cm. below the right costal margin.
and the spleen tip was palpable. The anteroposteriol
diameter of the chest was increased because of
prominence of the sternum. ‘l’he cardiac impulse was
diffuse and \vas maximal in the fifth intercostal space
in the midclavicular linr. No other abnormal im-
pulses were present. An atria1 gallop was audible.
but no murmurs were present. The second heart
sound was single and of normal intensity.
An electrocardiogram und vectorcardiogram (Fig. 0)
showed a posterolaterally directed mean QRS vector
and T wave changes that suggested anterolateral
myocardial injury or possibly necrosis. A roent-
genogram (Fig. 4) of the chest showed moderateI>-
severe cardiac enlargement with increased pulmonary
venous markings and left atria1 enlargement.
On the second hospital day the patient had an
attack of syncope. On examination he was ir-
ritable, drowsy and confused; right-sided hemiparesis
was present. By the following day he was alert, and
the signs of hemiparesis had disappeared. After
digitalization and bedrest his signs of cardiac failure
disappeared.
Laboratorv invstigations disclosed hemoglobin, 9.6
Sm. 100 ml.; hematocrit, 3170; white blood cells,
10.300 per cu. mm. with a normal differential count.
Lactic dehydrogenase measured 560 u. (normal 2OO-
500 u.). SGOT 46 u. and SGPT 45 u. Serum protein
electrophoresis findings were albumin, 2.8 gm./lOO
ml. (normal 3.7 to 4.5); alpha 1. 0.55 gm./lOO ml.
(normal 0.13 to 0.38); and gamma 2.15 g-m./100 ml.
(normal 0.4 to 1.0). Other fractions were normal.
Card& Catheterization: Femoral artery, but not right
ventricular. pulsus alternans was observed. The
pulmonary artery wedge pressure was elevated
moderately and the main pulmonary artery pressure
slightly elevated. Cardiac output was normal at rest
and elevated considerably during isoproterenol in-
fusion.
Ri,ght ventricle needle biopq and histologic examination
(Table I) were performed. Light microscopic find-
ings included moderate interstitial fibrosis with a
scattering of lymphocytes. Masson’s trichrome stain
indicated the fibrosis was distributed as irregular focal
patches throughout the sections. The myocardial
fibers were intact. By electron microscopy the focal
accumulation of fibroblasts between muscle syncytia
was evident. There was also focal myofibriilar
degeneration as well as degenerative changes in some
mitochondria. consisting of loss of cristae.
C:ASI;. 8. This 5 year, 2 month old white girl was
referred to the University of Texas Medical Branch
with complaints of exertional dyspnea and edema.
‘l‘hr pregnancy and delivery were normal. Apart
from pneumonia at 16 months, she did not appear ill
until age 1 year. 10 months, in spring 1962, when
symptoms of asthma developed that recurred in 1963
and 1965. At 4 years, 11 months weakness. exertional
dyspnea. diminished activity and edema developed.
Phv.ricczl examination showed a pale child with perior-
Ijital and pedal edema. Jugular \‘enous a waves
extended to 5 to 6 cm. above the angle of Louis.
‘l‘hc llmqs were normal. and the liver edge could be
palpated 6 cm. below the right costal margin. There
was no increase in the antrroposterior diameter of
the chest. The cardiac impulse was maximal in the
fifth intercostal space 1 cm. lateral to the midclavicu-
lar line. Other impulses were not remarkable.
:Iuscultation revealed an atria1 sound, a grade 316
systolic murmur maximal at the apex and a single
second sound of normal intensity. Hemoglobin was
13.3 qm.
The electrocnrdiqram and vectorcardiogram (Fig. 7)
\verr interpreted as indicating marked right and left
atria1 enlargement with first degree A-V block,
suggesti\re evidence of anterior myocardial necrosis
and left ventricular hypertrophy. The chest roent-
genogram (Fig. 4) showed only moderate cardiac
enlargement with a very prominent left atria1 ap-
pendage and increased pulmonary venous markings.
Cineangiocardiography was performed with injection
of contrast medium into the main pulmonary artery.
‘l‘hr catheter kicked back into the right atrium, which
THE AMERICAN JOURNAL OF CARDIOLOGY
Cardiomyopathy in Children
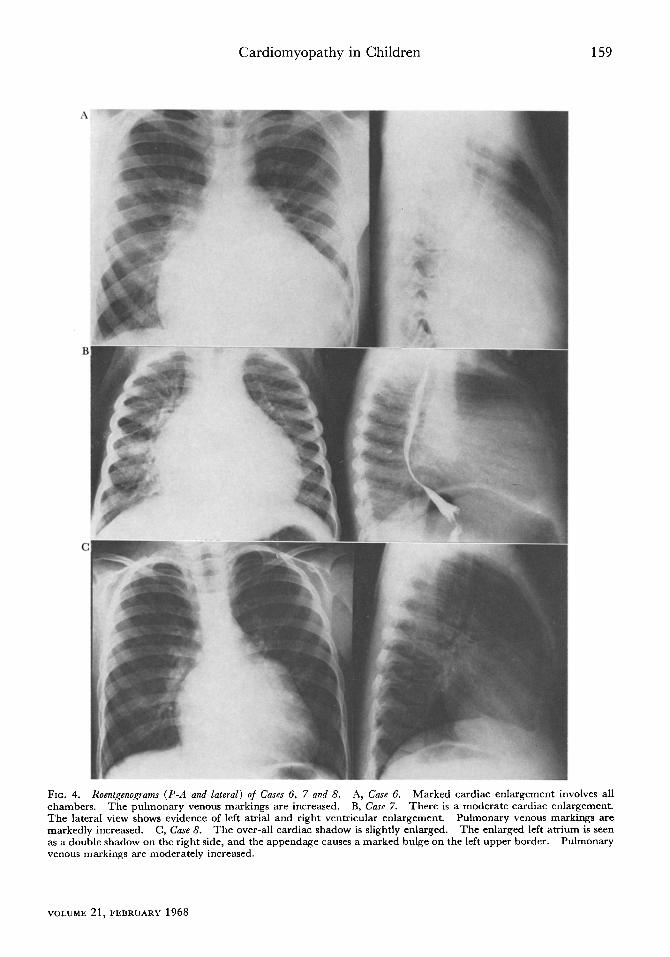
FIG. 4. Roentgenograms (P-A and lateral) of Cares 6, 7 and 8. A, Case 6. Marked cardiac enlargement involves
char nbers. The pulmonary venous markings are increased. B, Case 7. There is a moderate cardiac enlargema The lateral view shows evidence of left atria1 and right ventricular enlargement. Pulmonary venous markings mar kedly increased. C, Case 8. The over-all cardiac shadow is slightly enlarged. The enlarged left atrium is s as a double shadow on the right side, and the appendage causes a marked bulge on the left upper border. Pulmon vent IUS markings are moderately increased.
all snt. are een
ar y
VOLUME 21, FEBRUARY 1968
160 Harris, Rodin and Nghiem
FIG. 5. Case 6. Heurt mth the lefi uentrde ol,ened through the mrtzc ualue. A flat, organized thrombus overlies the endocardium in the region of the apex (arrows). The adjacent ventricular wall has several arras of dense, gray fibrosis.
was greatly enlarged. ‘l‘he filling srquencc \vas normal. Both ventricular cavities were cliapropor- tionately small in comparison with the atria which were markedly enlarged. There was no evidence of mitral or tricuspid stenosis.
Cardiac cathetnGzt&m (Fig. 8 and ‘l’abics II and III) showed tall a waves in both atria and increased rnd- diastolic pressures with a waves in both ventricles without gradients across the semilunar valves. These findings were interpreted as evidence of de- creased ventricular compliance or small ventricular cavities.
Treutment with digitalis and diuretics resulted in little improvement. .4fter review of the special investigations a diagnosis of a restrictive type of cardiomyopathy was made. The patient’s condition rapidly deteriorated with increasing cardiac volume (Fig. 1). She died at home in congestive cardiac failure at age 5 years, 9 months.
NECROPSY FINDINGS
Autopsy was restricted to the heart, which was markedly enlarged (280 gm.). There was a massive degree of thickening of the walls of the four chambers, and all four valves appeared normal. Although the ventricular cavities showed a marked reduction in size, the atria were greatly enlarged. In addition, the endocardium of the atria was more opaque than usual. Sections from walls of all chambers revealed endocardial thickening, which was predominantly fibrous but with a small increase in elastic tissue. Subendocardial lymphocytic infiltration: myocardial fiber hypertrophy, and mild interstitial fibrosis were also present (Fig. 9).
DISCUSSION
There have been several descriptions of the
pathologic changes in idiopathic, nonobstruc-
tive cardiomyopathy.4,5 ,‘I .I3 ,I5 Generally, these
studies have not succeeded in determining eti-
ologic agents or precise pathogenic mechanisms.
However, they have drawn attention to the
similarities and differences in various countries
ard have eliminated some known causes of
cardiomyopathy.
In our cases with autopsy, there was patchy
endocardial thickening containina both fibrous
and, to a lesser degree, elastic tissue, that af-
fected the outflow more than the inflow tract;
it was associated with marked cardiomegaly
without valvular or coronary artery disease.
This pattern is most consistent with the South
African type of endoInyocardia1 fibrosis, with
frequent embolic episodes.Y-5~II~Iz~16 It differs
from the tvpe with dense endomyocardial
fibrosis affeciing especially the inflow tract and
in which destruction of the endocardium is a
feature, first described by Davies in UgandaI
and since described in other parts of tropical
Africa,Ix~21~22 Colombia,15 Ceylon,2” and Ma-
laya. In the tropical African type, fibrosis
affects both ventricles but especially the right,*j
restricting ventricular filling to a marked degree.
Burchz6 describes the right atrium as “looking
like a white balloon . . . the impression is that if it
were stuck with a pin it would pop like a bal-
THE AMERICAN JOURNAL OF CARDIOLOGY

Cardiomyopathy in Children 161
6 -_ it - - _ <; _--_-
Frontal
l _._ ._
1 mv
UH# 78090-P
-
3 - - - - x 1
w-v_ _ - - e :>I E
P
\
Left srgittal y p.- :.
t_ _ *
c - -. Pro”t.1
.(
i ;
I II III aVR aVL aVF
V4R V3R V1 vz V3 v4 V5 Vb
6
lh*,ter,or
FIG. 6. Case 7. Electrocardiogram and vectorcardiogram. There is low amplitude in the limb leads. R waves from
VP to Vb are rudimentary. T waves in I, Vg and Vs are of low amplitude. There are deep S waves in VIR to Vi. On the vectorcardiogram. (Frank system) the clockwise horizontal loop is directed to the left and posteriorly. The findings
suggest anterolateral myocardial injury and possible necrosis. (Timing 0.0025 sec.)
FIG. 7. Case 8. Electrocardiogram and vectorcardiogram. P waves in lead II are tall and peaked, and the terminal portions are markedly posteriorly directed in Vi and VZ. The P-R interval is 0.24 sec. in duration. There is failure
of progression of R waves in Vi to Vt. S-T and T wave changes are conspicuous in Vs and Vs. In the vectorcardiogram
(Frank system) the predominantly clockwise figure-of-eight loop in the horizontal plane has initial and terminal slowing and is directed posteriorly with markedly increased voltage. The findings indicate marked right and left atria1 enlargement with first degree A-V block. In addition, there is evidence of left ventricular hypertrophy with marked secondary S-T and T changes. Although Q waves are absent in Vs and the horizontal loop is predominantly clockwise. the absence of sienificant ORS widening and slurring mitigates against associated left bundle branch block.
” .
(Timing 0.0025 sec.)
loon,” and the endocardial fibrosis as appearing to restrict ventricular dilatation as with con- strictive pericarditis. Physiologically, then, this tropical African type is primarily a restrictive cardiomyopathy (restricting ventricular filling) due to dense fibrosis of the endocardium, but the fibrosis also affects the contractile properties of the heart. This is in contrast with the single restrictive case in our series (Case 8) in which impaired ventricular compliance and diminu- tion of the size of the ventricular cavities appear to have resulted from marked ventricular hyper- trophy.
CONGESTIVE CARDIOMYOPATHY
Our remaining cases, with perhaps the excep-
VOLUME 21, FEBRUARY 1968
tion of Case 6, the patient with coarctation of the aorta, resemble the South African type of cardio- myopathy. Unlike Davies,13 who firmly op- poses this view, Edington and Jackson2’ believe that the South African type could represent a less severe manifestation of the tropical African type. Becker5 has suggested that in South Africa there are three stages in the development of the histologic changes-acute, subacute and chronic. In the acute stage mutinous edema, fibrinous necrosis and focal degeneration are present; in the subacute stage, cellular infiltra- tion, granulation tissue and organization; and in the chronic stage, endocardial sclerosis, elas- tic tissue hyperplasia and myocardial fibrosis. Tissues from our 4 cases have shown varying
162 Harris, Rodin and Nghiem
mm. : _ ..
A
mm. Hg.
160-
50-
487
IS-
‘oo- -
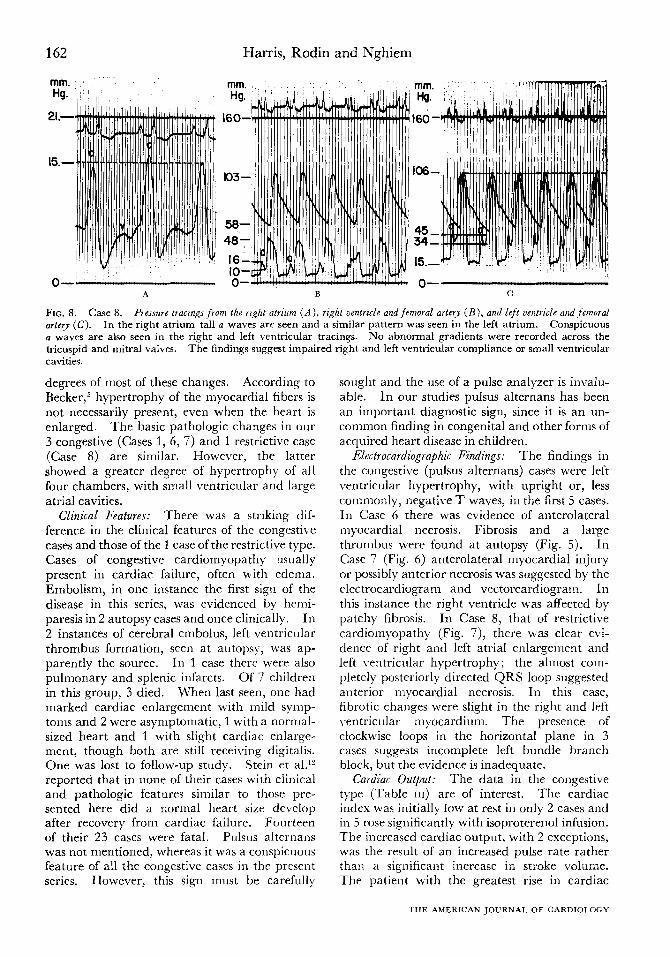
FIG. 8. Case 8. Pressure tracings from the right atrium (A), right ventricle and femoral artery (B), and left centricle and foxoral
arfe?y (C). In the right atrium tall D waves are seen and a similar pattern was seen in the left atrium. Conspicuous D waves are also seen in the right and left ventricular tracings. No abnormal gradients were recorded across the tricuspid and mitral valves. The findings suggest impaired right and left ventricular compliance or small ventricular cavities.
degrees of most of these changes. According to Becker,5 hypertrophy of the myocardial fibers is not necessarily present, even when the heart is enlarged. The basic pathologic changes in our 3 congestive (Cases 1, 6, 7) and 1 restrictive case (Case 8) are similar. However, the latter showed a greater degree of hypertrophy of all four chambers, with small ventricular and large atria1 cavities.
Clinical Features: There was a striking dif- ference in the clinical features of the congestive cases and those of the 1 case of the restrictive type. Cases of congestive cardiomyopathy usually present in cardiac failure, often with edema. Embolism, in one instance the first sign of the disease in this series, was evidenced by hemi- paresis in 2 autopsy cases and once clinically. In 2 instances of cerebral embolus, left \-entricular thrombus formation, seen at autopsy, was ap- parently the source. In 1 case there were also pulmonary and splenic infarcts. Of 7 children in this group, 3 died. When last seen, one had marked cardiac enlargement with mild symp- toms and 2 were asymptomatic, 1 with a normal- sized heart and 1 with slight cardiac enlarge- ment, though both are still receiving digitalis. One was lost to follow-up study. Stein et al.‘? reported that in none of their cases with clinical and pathologic features similar to those pre- sented here did a normal heart size develop after recovery from cardiac failure. Fourteen of their 23 cases were fatal. Pulsus alternans was not mentioned, whereas it was a conspicuous feature of all the congestive cases in the present series. However, this sign must be carefully
sought and the use of a pulse analyzer is invalu- able. In our studies pulsus alternans has been an important diagnostic sign, since it is an un- common finding in congenital and other forms of acquired heart disease in children.
Electrocardiographic Findings: The findings in the congestive (p&us alternans) cases were left ventricular hypertrophy, with upright or, less commonly, negative T waves, in the first 5 cases. In Case 6 there was evidence of anterolateral myocardial necrosis. Fibrosis and a large thrombus were found at autopsy (Fig. 5). In Case 7 (Fig. 6) anterolateral myocardial injury or possibly anterior necrosis was suggested by the electrocardiogram and vectorcardiogram. Ill this instance the right ventricle was affected by patchy fibrosis. In Case 8, that of restrictive cardiomyopathy (Fig. 7), there was clear evi- dence of right and left atria1 enlargement and left ventricular hypertrophy; the almost com- pletely posteriorly directed QRS loop suggested anterior myocardial necrosis. In this case, fibrotic changes were slight in the right and left ventricular myocardium. The presence of clockwise loops in the horizontal plane in 3 cases suggests incomplete left bundle branch block, but the evidence is inadequate.
Cardiac Output: The data in the congestive ty-pe (Table III) are of interest. The cardiac index was initially low at rest in only 2 cases and in 5 rose significantly with isoproterenol infusion. The increased cardiac output, with 2 exceptions, was the result of an increased pulse rate rather than a significant increase in stroke volume. The patient with the greatest rise in cardiac
THE .-ZMERICAN JOURNAI, OF CARDIOLOGY
Cardiomyopathy in Children 163
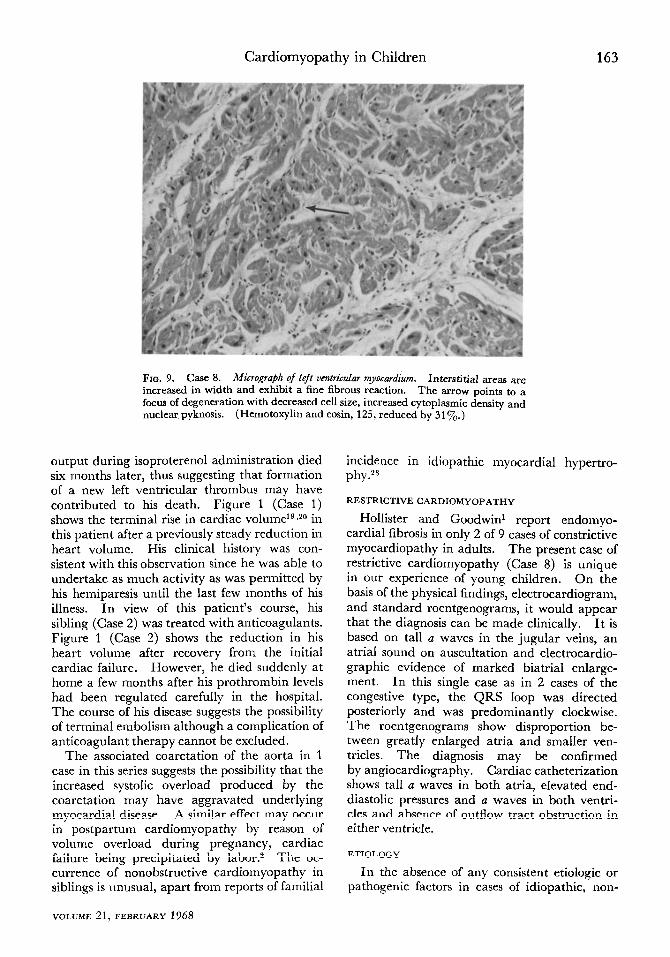
FIG. 9. Case 8. Micrograph of left vetiriGular myocardium. Interstitial areas are increased in width and exhibit a fine fibrous reaction. The arrow points to a focus of degeneration with decreased cell size, increased cytoplasmic density and nuclear pyknosis. (Hemotoxylin and eosin, 125, reduced by 31%.)
output during isoproterenol administration died six months later, thus suggesting that formation of a new left ventricular thrombus may have contributed to his death. Figure 1 (Case 1) shows the terminal rise in cardiac volume1g*20 in this patient after a previously steady reduction in heart volume. His clinical history was con- sistent with this observation since he was able to undertake as much activity as was permitted by his hemiparesis until the last few months of his illness. In view of this patient’s course, his sibling (Case 2) was treated with anticoagulants. Figure 1 (Case 2) shows the reduction in his heart volume after recovery from the initial cardiac failure. However, he died suddenly at home a few months after his prothrombin levels had been regulated carefully in the hospital. The course of his disease suggests the possibility of terminal embolism although a complication of anticoagulant therapy cannot be excluded.
The associated coarctation of the aorta in 1 case in this series suggests the possibility that the increased systolic overload produced by the coarctation may have aggravated underlying myocardial disease. A similar effect may occur in postpartum cardiomyopathy by reason of volume overload during pregnancy, cardiac failure being precipitated by labor.2 The oc- currence of nonobstructive cardiomyopathy in siblings is unusual, apart from reports of familial
VOLUME 21, FEBRUARY 1968
incidence in idiopathic myocardial hypertro- phy.28
RESTRICTIVE CARIX~MY~P,~THY
Hollister and Goodwin’ report endomyo- cardial fibrosis in only 2 of 9 cases of constrictive myocardiopathy in adults. The present case of restrictive cardiomyopathy (Case 8) is unique in our experience of young children. On the basis of the physical findings, electrocardiogram, and standard roentgenograms, it would appear that the diagnosis can be made clinically. It is based on tall a waves in the jugular veins, an atria1 sound on auscultation and electrocardio- graphic evidence of marked biatrial enlarge- ment. In this single case as in 2 cases of the congestive type, the QRS loop was directed posteriorly and was predominantly clockwise. The roentgenograms show disproportion be- tween greatly enlarged atria and smaller ven- tricles. The diagnosis may be confirmed by angiocardiography. Cardiac catheterization shows tall a waves in both atria, elevated end- diastolic pressures and a waves in both ventri- cles and absence of outflow tract obstruction in either ventricle.
ETIOLOGY
In the absence of any consistent etiologic or pathogenic factors in cases of idiopathic, non-
164 Harris, Rodin
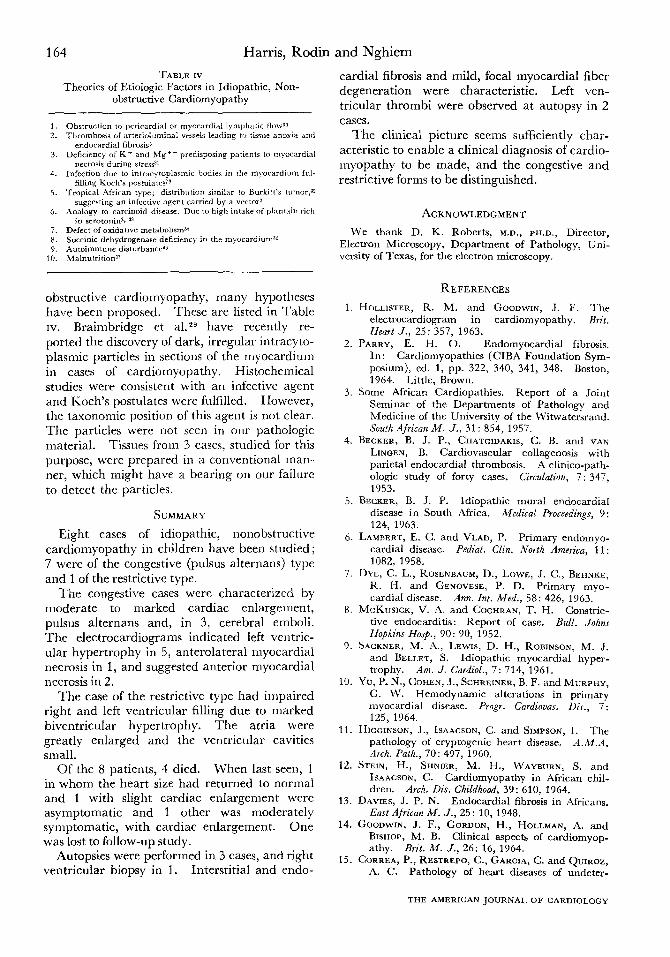
TABLE IV Theories of Etiologic Factors in Idiopathic, Non-
obstructive Cardiomyopathy
1. 2.
3.
4.
5.
6.
7. 8. 9.
10.
Obstruction to pericardi.4 or myocardial lymphatic flowan Thrombosis of arterioluminal vessels leading TV tissue anoxia and
endocardial fibrosis5 Deficiency of K ’ and Mg ’ + predisposing patients to myocardial
necrosis during stressa’ Infection due m intracytoplarmir bodies in rhe myocardium ful-
filling Koch’s postulates’g Tropical African type; distribution similar to Burkitt’s tumor.32
suggesting an infective agent carried by a vector? Annlogy to rarcinoid diarase. Due to high intake of plantain rich
in scrotonin% 33 Defect of oxidative metabolism* Succinic dehydrogenase deficiency in the myocardrum3a Autoimmune disturbanc+ Malnutrition37
obstructive cardiomyopathy, many hypotheses have been proposed. These are listed in Table IV. Braimbridge et a1.2s have recently re- ported the discovery of dark, irregular intracyto- plasmic particles in sections of the myocardium in cases of cardiomyopathy. Histochemical studies were consistent with an infective agent and Koch’s postulates were fulfilled. However, the taxonomic position of this agent is not clear. The particles were not seen in our pathologic material. Tissues from 3 cases, studied for this purpose, were prepared in a conventional man.- ner, which might have a bearing on our failure to detect the particles.
SUMMARY
Eight cases of idiopathic, nonobstructive cardiomyopathy in children have been studied ; 7 were of the congestive (pulsus alternans) type and 1 of the restrictive type.
The congestive cases were characterized by moderate to marked cardiac enlargement, pulsus alternans and, in 3, cerebral emboli. The electrocardiograms indicated left ventric- ular hypertrophy in 5, anterolateral myocardial necrosis in 1, and suggested anterior myocardial necrosis in 2.
The case of the restrictive type had impaired right and left ventricular filling due to marked biventricular hypertrophy. The atria were greatly enlarged and the ventricular cavities small.
Of the 8 patients, 4 died. When last seen, 1 in whom the heart size had returned to normal and 1 with slight cardiac enlargement were asymptomatic and 1 other was moderately symptomatic, with cardiac enlargement. One was lost to follow-up study.
Autopsies were performed in 3 cases, and right ventricular biopsy in 1. interstitial and endo-
and Nghiem
cardial fibrosis and mild, focal myocardial fiber degeneration were characteristic. Left ven- tricular thrombi were observed at autopsy in 2 cases.
The clinical picture seems sufficiently char- acteristic to enable a clinical diagnosis of cardio- myopathy to be made, and the congestive and restrictive forms to be distinguished.
ACKNOWLEDGMENT
We thank D. K. Roberts, M.D., PH.D., Director, Electron Microscopy, Department of Pathology, Uni- versity of Texas, for the electron microscopy.
REFERENCES
1. HCILLISTER, R. M. and GOODWIN, J. F. The eiectrocardiogram in cardiomyopathy. Brit. Heart J., 25: 357, 1963.
2. PARRY, E. H. 0. Endomyocardial fibrosis. In: Cardiomyopathies (CIBA Foundation Sym- posium), ed. 1, pp. 322, 340, 341, 348. Boston, 1964. Little, Brown.
3. Some African Cardiopathies. Report of a Joint Seminar of the Departments of Pathology and Medicine of the University of the Witwatersrand. Souih African M. J., 31: 854, 1957.
4. BECKER, B. J. P., CHATGIDAKIS, C. B. and VAN LINDEN, B. Cardiovascular collagenosis with parietal endocardial thrombosis. A clinico-path- ologic study of forty cases. Circulation, 7: 347, 1953.
5. BECKER, B. J. P. Idiopathic mural endocardial disease in South Africa. Medical Proceedings, 9: 124, 1963.
6. LAMBERT, E. C. and VLAD, P. Primary endomyo- cardial disease. Pediat. Clin. North America, 11: 1082, 1958.
7. DYE, C. L., ROSENBAUM, D., LOWE, J. C., BEHNKE, R. H. and GENOVESE, P. D. Primary myo- cardial disease. Ann. Int. Med., 58: 426, 1963.
8. MCKUSICK, V. A. and COCHRAN, T. H. Constric- tive endocarditis: Report of case. Bull. Johns Hopkins Hosp., 90: 90, 1952.
9. SACKNER, M. A., LEWIS, D. H., ROBINSON, M. J. and BELLET, S. Idiopathic myocardial hyper- trophy. Am. J. Cardial., 7: 714, 1961.
10. Yu, P. N., COHEN, J., SCHREINER, B. F. and MURPHY, G. W. Hemodynamic alterations in primary myocardial disease. Progr. Curdiovas. Dis., 7: 125, 1964.
11. HIGGINSON, J., ISAACSON, C. and SIMPSON, I. The pathology of cryptogenic heart disease. A.M.‘4. Arch. Path., 70: 497, 1960.
12. STEIN, H., SHNIER, M. I-I., WAYBURN, S. and ISAACSON, C. Cardiomyopathy in African chil- dren. Arch. Dis. Childhood, 39: 610, 1964.
13. DAVIES, J. P. N. Endocardial fibrosis in Africans. East African M. J., 25: 10, 1948.
14. GOODWIN, J. F., GORDON, H., HOLLMAN, A. and BISHOP, M. B. Clinical aspects of cardiomyop- athy. Brit. M. J., 26: 16, 1964.
15. CORREA, P., RESTREPO, C., GARCIA, C. and QUIROZ, A. C. Pathology of heart diseases of undeter-
THE AMERICAN JOURNAL OF CARDIOLOGY
Cardiomyopathy in Children 165
mined etiology which occur in Cali, Colombia. Am. Heart J., 66: 584, 1963.
16. ALTMAN, H. and STEIN, H. Idiopathic hypertrophy of the heart in African children; a report of 4 cases. Brit. M. J., 1: 1207, 1956.
17. HARRIS, L. C., NGHIEM, Q. X., SCHREIBER, M. H. and WALLACE, J. M. Severe pulsus alternans associated with primary myocardial disease in children. Circulation, 34: 948, 1966.
18. CADELL, J. L., WARLEY, A., CONNOR, D. H., D’ARBELA, P. G. and BILLINGHURST, J. R. Ac- quired heart disease in Ugandan children. Brit. Heart J. 28: 759, 1966.
19. SCHREIBER, M. H. The volume of the heart-a roentgenographic determination. Arizona Med., 21: 551, 1964.
20. NGHIEM, Q. X., SCHREIBER, M. H. and HARRIS, L. C. Cardiac volume in normal children and adolescents. Its application to patients with mitral insufficiency. Circulation, 35: 509, 1967.
21. TURNER, P. P. and MANSON-BAHR, P. E. C. Endo- myocardial fibrosis in Kenya and Tanganyika Africans. Brit. Heart J., 22: 305, 1960.
22. COELHO, E. and PIMENTEL, J. C. Diffuse endomyo- cardial fibrosis. Am. J. Med., 35: 569, 1963.
23. NAGARATNAM, N. and DISSANAYAKE, R. V. P. Endomyocardial fibrosis in the Ceylonese. Brit. Heart J., 21: 167, 1959.
24. LA BROOY, E. B. Endomyocardial fibrosis. Proc. Alumni A. Malaya, 10: 303, 1957.
25. ABRAHAMS, D. G. Endomyocardial fibrosis of the right ventricle. Quart. J. Med., 31: 1, 1962.
26. BURGH, G. E. Discussion-endomyocardial fibro- sis. In: Cardiomyopathies (CIBA Foundation Symposium), ed. 1, p. 348. Boston, 1964. Little, Brown.
27. EDINGTON, G. M. and JACKSON, J. G. The pa- thology of heart muscle disease and endomyo- cardial fibrosis in Nigeria. J. Path. @ Bact., 86: 333, 1963.
28. LAMBERT, E. C. and VLAD, P. Primary endomyo- cardial disease. Pediat. Clin. North America, 11, 1057, 1958.
29. BRAIMBRIDGE, M. V., DARRACOTT, S., CHAYEN, J., BITENSKY, L. and POWLTER, L. W. Possibility of a new infective aetiological agent in congestive cardiomyopathy. Lancet, 1: 172, 1967.
30. MILLER, A. J., PICK, R. and KATZ, L. N. Ven- tricular endomyocardial changes after impair- ment of cardiac lymph flow in dogs. Brit. Heart J., 25: 182, 1963.
31. SELYE, H. The Chemical Prevention of Cardiac Necroses, p. 1345. New York, 1958. The Ronald Press.
32. BURKITT, D. Determining the climatic limitations of a children’s cancer common in Africa. Brit. Med. J., 2: 1019, 1962.
33. CRAWFORD, M. A. Endomyocardial fibrosis and carcinoidosis. A common denominator? Am. Heart J., 66: 273, 1963.
34. WENDT, V. E. et al. The hemodynamics and cardiac metabolism in cardiomyopathies. M. Clin. North America, 46: 1445, 1962.
35. KOBERNICK, S. D., MANDELL, G. H., ZIRKIN, R. M. and HASHIMOTO, Y. Succinic dehydrogenase deficiency in idiopathic cardiomyopathy. Am J. Path., 43: 661, 1963.
36. BARRITT, D. W. and AL-SHAMMA’A, M. Heart failure from unexplained cardiomyopathy. Brit. Heart J., 28: 674, 1966.
37. GILLANDERS, A. D. Nutritional heart disease. Brit. Heart J., 13: 177, 1951.
VOLUME 21, FEBRUARY 1968