
Autopsy Validation Study of the Academic Research Consortium Stent Thrombosis Definition
MBC/200176; Total nos of Pages: 5;
Original article 1MBC 200176
AQ2
Hyperhomocysteinemia and the compound heterozygousstate for methylene tetrahydrofolate reductase areindependent risk factors for deep vein thrombosis amongSouth IndiansS.M. Naushad, Md Nurul Jain Jamal, R. Angalena, C. Krishna Prasadand A. Radha Rama Devi
AQ1
AQ3
Objective To investigate the role of methylene
tetrahydrofolate reductase (MTHFR) (677 C!T and 1298
A!C), factor V (1691 G!A), factor II (20210 G!A) genetic
polymorphisms and hyperhomocysteinemia in the aetiology
of deep vein thrombosis (DVT) in 163 cases and 163
controls.
Methods Polymerase chain reaction-restriction fragment
length polymorphism was used for genotyping, reverse-
phase high-performance liquid chromatography for plasma
homocysteine, and Student’s t-test and Fisher exact tests
were used for statistical analysis.
Results Elevated mean plasma homocysteine levels were
observed in DVT cases irrespective of gender differences.
Homocysteine elevation above the 95th percentile of the
control group associated with 9.4-fold and 7.6-fold
increased risk for DVT in men and women, respectively.
Genotyping showed the MTHFR 677CT/1298AC genotype
(i.e. compound heterozygosity) is associated with 3.5-fold
risk for thrombosis. The factor V Leiden mutation frequency
was higher in DVT cases, but not statistically significant;
however, genetic predisposition to this mutation was
0957-5235 � 2006 Lippincott Williams & Wilkins
associated with early age of DVT onset. Factor II mutation
was absent in cases and controls. Co-segregation of two or
more risk factors was associated with 11.7-fold increased
risk for thrombosis.
Conclusions This study projects that
hyperhomocysteinemia and compound heterozygous state
for MTHFR are independent risk factors for DVT among
South Indians. Blood Coagul Fibrinolysis 17:00–00 � 2006
Lippincott Williams & Wilkins.
Blood Coagulation and Fibrinolysis 2006, 17:00–00
Keywords: deep vein thrombosis, factor V, factor II, homocysteine,methylene tetrahydrofolate reductase
Center for DNA Fingerprinting and Diagnostics, Hyderabad, India
Correspondence and requests for reprints to Dr A. Radha Rama Devi, Head,Diagnostic Division, Center for DNA Fingerprinting and Diagnostics (CDFD),7–18 Nacharam, Hyderabad 500076, Andhra Pradesh, IndiaTel: +91 40 27171462; e-mail: [email protected]
Sponsorship: The Department of Biotechnology, Government of India funded thisstudy.
Received ?? ?? Revised ?? ??Accepted ?? ??
IntroductionGenetic and environmental factors can alter the procoa-
gulant and anticoagulant mechanisms and cause venous
thrombosis. Venous thrombosis has variable clinical
manifestations depending on the site and extent of
thrombus formation and the underlying cause. Deep
vein thrombosis (DVT) is one of the most common
causes of morbidity and mortality in the western world
[1,2], Pulmonary embolism is the most serious compli-
cation of the disease. Different genetic polymorphisms
both in haemostatic and non-haemostatic genes have
been reported to be risk factors [3,4] and include protein
C [5,6], protein S [7], factor V Leiden, prothrombin,
antithrombin III [8], methylene tetrahydrofolate reduc-
tase (MTHFR) and dysfibrinogenemia.
Factor V Leiden (G1691A) mutation confers activated
protein C resistance [9,10], altered anticoagulant function
and loss of efficiency to serve as a cofactor in activated
factor VIII degradation [11,12]. Hence its inheritance
increases the risk for occurrence and recurrence of venous
thrombosis [13].
The G20210A mutation in the 30-untranslated region of
prothrombin is identified as a risk factor for DVT, causing
elevated prothrombin levels, and this appears to be respon-
sible for the increased risk for thrombosis. The precise
mechanism by which prothrombin levels are altered is yet
to be determined. Increased efficiency of polyadenylation
of mRNA transcripts, however, has been suggested [14].
Among the range of nonhaemostatic factors that can
interact with haemostatic determinants, plasma homo-
cysteine is of prime importance. In recent years hyper-
homocysteinemia has attracted much interest as a
potential risk factor for both venous and arterial throm-
botic disease [15,16]. By stimulating the procoagulant
mechanism or by inhibiting anticoagulant mechanism,
homocysteine exerts its effect on thrombus formation.
One of the two enzymatic pathways of remethylation of

MBC/200176; Total nos of Pages: 5;
2 Blood Coagulation and Fibrinolysis 2006, Vol ?? No??
Table 1 Genotype frequencies in deep vein thrombosis cases andcontrols
Group WW WM MM MOdds ratio (95%
confidence interval) P value
MTHFR 677 CC CT TT T 1.53 (1.46–1.60) 0.19Cases 133 29 1 31/326Controls 142 21 0 21/326
MTHFR 1298 AA AC CC C 0.86 (0.84–0.88) 0.41Cases 57 105 1 107/326Controls 63 82 18 118/326
Factor V GG GA AA A 1.52 (1.43–1.64) 0.42Cases 149 13 1 15/326Controls 153 10 0 10/326
AQ4
AQ7
AQ5
AQ6
homocysteine to methionine involves MTHFR. An
MTHFR deficiency blocks this remethylation process,
resulting in hyperhomocysteinemia. Two common poly-
morphisms in MTHFR (i.e. C677T and A1298C) were
found to cause mild to moderate hyperhomocysteinemia.
The former mutation has greater clinical impact than the
latter. These two mutations occur in catalytic and regu-
latory domains, respectively. Inconsistent results have
been observed about the possible association of C677T
mutation in the aetiology of DVT [17,18].
There are fewer studies on the genetic risk factor evalu-
ation for DVT from India [19–22,24] and no comparable
studies from South India. The main aim of this study is to
determine the role of MTHFR, factor V, factor II genetic
polymorphisms and hyperhomocysteinemia in the aetiol-
ogy of DVT among South Indians.
Materials and methodsParticipantsAll of the 163 DVT patients (105 men and 58 women)
referred to our centre between October 1999 and
February 2004 agreed to participate in this study. The
diagnosis of DVT was based on impedance plethysmo-
graphy, Doppler ultrasonography, compression ultraso-
nography or contrast venography. Informed consent was
taken from each patient. The study protocol was
approved by bioethical committee of Center for DNA
Fingerprinting and Diagnostics. The control group com-
prised of 105 men and 58 women. Age, sex, and race or
ethnic group matched controls were selected.
MethodsFasting ethylenediamine tetraacetic acid anticoagulated
blood samples were collected on ice, and plasma was
separated immediately and frozen until the time of
analysis. Genomic DNA was isolated from the buffycoat
using the phenol–chloroform extraction method.
Total plasma homocysteine analysisSulfur-containing amino acids were derivatized using
ammonium 7-fluorobenzo-2-oxa-1,3-diazole-4-sulphonate
after treatment with tributyl N-phosphine. Reverse-phase
high-performance liquid chromatography with isocratic
separation was performed on an ODS 3v column using
0.1 mol/l KH2PO4:acetonitrile (96:4) as the mobile phase.
The standard calibration curve for concentrations ranging
from 5 to 200mmol/l was found to be linear (r¼ 0.999). This
method was validated against an enzyme-linked immun-
sorbent assay-based kit using Bland and Altman analysis.
Study of genetic polymorphisms:Factor V (G1691A), factor II (G20210A), MTHFR
(C677T) and MTHFR (A1298C) genetic polymor-
phisms were detected using polymerase chain reaction-
restriction fragment length polymorphism approaches
using MnlI, HindIII, HinfI and MboII restriction enzymes
[11,14,25].
Statistical analysisAs homocysteine levels were skewed, log-transformation
of the values was carried out and Grubb’s test was
performed to detect significant outliers. After correcting
for skewness and outliers, the 5th, 50th and 95th per-
centiles were calculated using an Excel datasheet and the
values were converted back to normal. Student’s t-test
was performed both on log-transformed data and cor-
rected data. Mean and SD values were obtained from
these statistics along with the P values. Graphpad soft-
ware was used for this analysis. For categorical variables,
Fisher’s exact test was performed using Vassarstats soft-
ware and the genotype frequencies, odds ratio and Pvalues were obtained. For all variables, a P value less than
0.05 was taken as statistically significant.
ResultsThe mean age of onset for DVT in men was 37.4�13.7 years and in women was 32.4� 13.8 (P< 0.05).
The frequencies of factor V, MTHFR C677T, MTHFR
A1298C mutations and hyperhomocysteinemia in cases
were 8.6%, 18.4%, 65% and 17.8% and the frequencies in
controls were 6.1%, 12.9%, 61.3% and 2.6%, respectively.
A total of 0.6% cases were homozygous for each mutation
and none of the controls were homozygous mutant for
the first two mutations. Eleven per cent of controls
were homozygous for the MTHFR A1298C mutation.
Factor II mutation was absent in both cases and controls
(Table 1).
MTHFR compound heterozygosity was observed in
11.7% of cases and 3.7% of controls; 1.2% of cases were
heterozygous for factor V, MTHFR C677T and MTHFR
A1298C, and none of the controls showed this combi-
nation. Co-segregation of MTHFR 677 C!T with factor
V/homocysteine or factor V with homocysteine was
associated with an 11.7-fold increased risk for thrombosis
(Table 2).
The total plasma homocysteine data was segregated
according to gender, and cut-off values were obtained
MBC/200176; Total nos of Pages: 5;
Hyperhomocysteinemia, MTHFR and DVT Naushad et al. 3
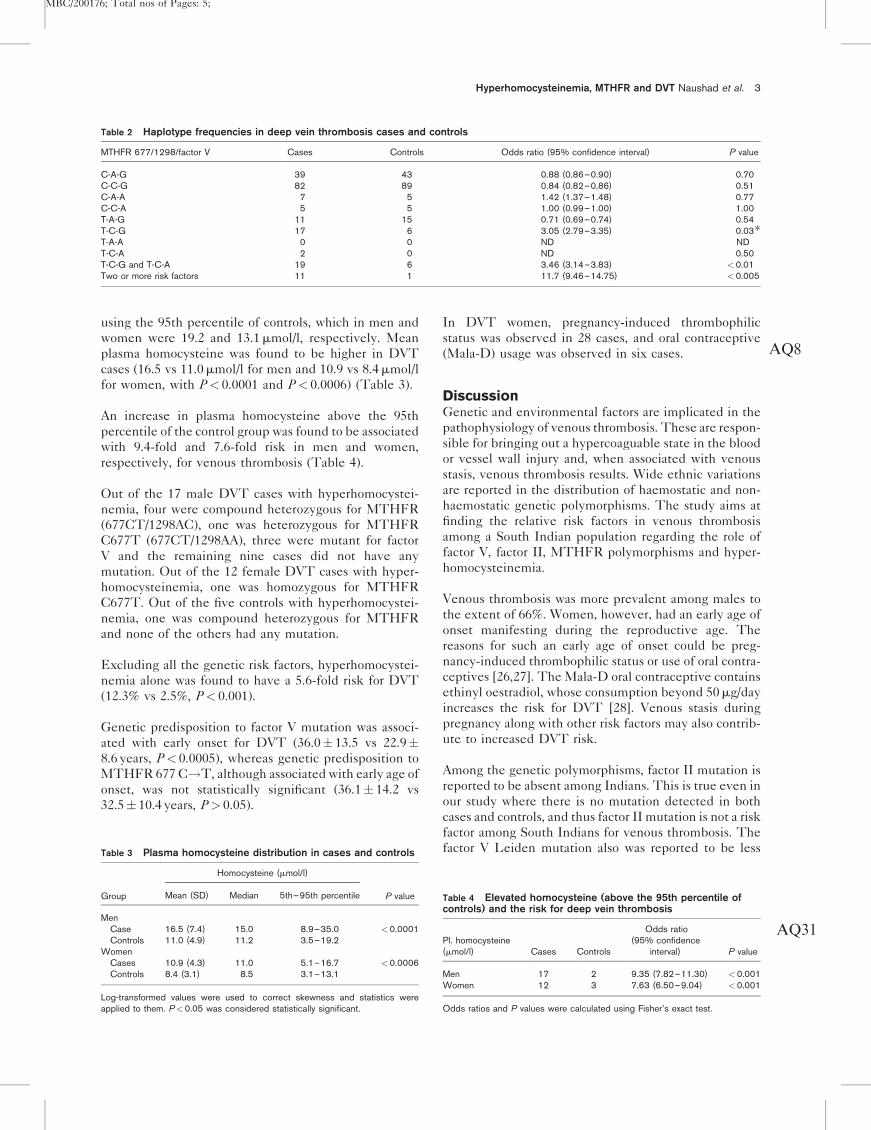
Table 2 Haplotype frequencies in deep vein thrombosis cases and controls
MTHFR 677/1298/factor V Cases Controls Odds ratio (95% confidence interval) P value
C-A-G 39 43 0.88 (0.86–0.90) 0.70C-C-G 82 89 0.84 (0.82–0.86) 0.51C-A-A 7 5 1.42 (1.37–1.48) 0.77C-C-A 5 5 1.00 (0.99–1.00) 1.00T-A-G 11 15 0.71 (0.69–0.74) 0.54T-C-G 17 6 3.05 (2.79–3.35) 0.03�T-A-A 0 0 ND NDT-C-A 2 0 ND 0.50T-C-G and T-C-A 19 6 3.46 (3.14–3.83) <0.01Two or more risk factors 11 1 11.7 (9.46–14.75) <0.005
AQ8
using the 95th percentile of controls, which in men and
women were 19.2 and 13.1mmol/l, respectively. Mean
plasma homocysteine was found to be higher in DVT
cases (16.5 vs 11.0mmol/l for men and 10.9 vs 8.4mmol/l
for women, with P< 0.0001 and P< 0.0006) (Table 3).
An increase in plasma homocysteine above the 95th
percentile of the control group was found to be associated
with 9.4-fold and 7.6-fold risk in men and women,
respectively, for venous thrombosis (Table 4).
Out of the 17 male DVT cases with hyperhomocystei-
nemia, four were compound heterozygous for MTHFR
(677CT/1298AC), one was heterozygous for MTHFR
C677T (677CT/1298AA), three were mutant for factor
V and the remaining nine cases did not have any
mutation. Out of the 12 female DVT cases with hyper-
homocysteinemia, one was homozygous for MTHFR
C677T. Out of the five controls with hyperhomocystei-
nemia, one was compound heterozygous for MTHFR
and none of the others had any mutation.
Excluding all the genetic risk factors, hyperhomocystei-
nemia alone was found to have a 5.6-fold risk for DVT
(12.3% vs 2.5%, P< 0.001).
Genetic predisposition to factor V mutation was associ-
ated with early onset for DVT (36.0� 13.5 vs 22.9�8.6 years, P< 0.0005), whereas genetic predisposition to
MTHFR 677 C!T, although associated with early age of
onset, was not statistically significant (36.1� 14.2 vs
32.5� 10.4 years, P> 0.05).
Table 3 Plasma homocysteine distribution in cases and controls
Group
Homocysteine (mmol/l)
P valueMean (SD) Median 5th–95th percentile
MenCase 16.5 (7.4) 15.0 8.9–35.0 <0.0001Controls 11.0 (4.9) 11.2 3.5–19.2
WomenCases 10.9 (4.3) 11.0 5.1–16.7 <0.0006Controls 8.4 (3.1) 8.5 3.1–13.1
Log-transformed values were used to correct skewness and statistics wereapplied to them. P<0.05 was considered statistically significant.
In DVT women, pregnancy-induced thrombophilic
status was observed in 28 cases, and oral contraceptive
(Mala-D) usage was observed in six cases.
DiscussionGenetic and environmental factors are implicated in the
pathophysiology of venous thrombosis. These are respon-
sible for bringing out a hypercoaguable state in the blood
or vessel wall injury and, when associated with venous
stasis, venous thrombosis results. Wide ethnic variations
are reported in the distribution of haemostatic and non-
haemostatic genetic polymorphisms. The study aims at
finding the relative risk factors in venous thrombosis
among a South Indian population regarding the role of
factor V, factor II, MTHFR polymorphisms and hyper-
homocysteinemia.
Venous thrombosis was more prevalent among males to
the extent of 66%. Women, however, had an early age of
onset manifesting during the reproductive age. The
reasons for such an early age of onset could be preg-
nancy-induced thrombophilic status or use of oral contra-
ceptives [26,27]. The Mala-D oral contraceptive contains
ethinyl oestradiol, whose consumption beyond 50mg/day
increases the risk for DVT [28]. Venous stasis during
pregnancy along with other risk factors may also contrib-
ute to increased DVT risk.
Among the genetic polymorphisms, factor II mutation is
reported to be absent among Indians. This is true even in
our study where there is no mutation detected in both
cases and controls, and thus factor II mutation is not a risk
factor among South Indians for venous thrombosis. The
factor V Leiden mutation also was reported to be less
Table 4 Elevated homocysteine (above the 95th percentile ofcontrols) and the risk for deep vein thrombosis
Pl. homocysteine(mmol/l) Cases Controls
Odds ratio(95% confidence
interval) P value
Men 17 2 9.35 (7.82–11.30) <0.001Women 12 3 7.63 (6.50–9.04) <0.001
Odds ratios and P values were calculated using Fisher’s exact test.
AQ31

MBC/200176; Total nos of Pages: 5;
4 Blood Coagulation and Fibrinolysis 2006, Vol ?? No??
AQ11
AQ9
AQ10
frequent among the Indian population. Certain endoga-
mous populations like Parsis have high prevalence up to
10%, indicating a wide ethnic variation among different
groups in India [19–24]. The relative risk associated with
factor V mutation in the current study is 1.5, which is not
statistically significant (P¼ 0.42).
The other important genetic variant in venous thrombo-
sis is the enzyme involved in methionine metabolism,
MTHFR, which is important in the remethylation of
homocysteine to methionine as it supplies 5-methyl
tetrahydrofolate as the co-substrate. The C677T
mutation in MTHFR gene is known to induce thermol-
ability, thereby lowering its activity. The A1298C
mutation does not induce thermolability, however; it
reduces the enzyme activity and can act in an additive
manner in combination with C677T [29]. The resultant
block in the conversion of homocysteine to methionine
causes homocysteine accumulation. Homocysteine is
now widely accepted to be involved in the integrity of
the vascular endothelium causing its damage. A meta-
analysis comprising of 3439 DVT cases and 5063 controls
from different parts of the world showed that MTHFR
mutants with a 5mmol/l increase in homocysteine exert
1.6-fold risk, which is reduced to 25% when there is a
3mmol/l decrease in homocysteine [18]. Mutation fre-
quencies vary from region to region and ethnicity. A study
from western India reported 14.9% C677T MTHFR
mutants among young patients of venous thrombosis
[20]. The current study from South India showed an
18.4% mutation frequency among cases and 12.9% among
controls. No statistical significance was observed in DVT
when there is a single mutation, either C677T or A1298C.
Compound heterozygosity, however, increased the risk
by 3.5-fold for DVT irrespective of the gender. The
homocysteine concentration among compound heterozy-
gous individuals was high among men and surprisingly
normal among women.
The mean homocysteine levels in DVT cases were
significantly higher than their controls (age-matched
and sex-matched). Furthermore, homocysteine levels
in men were significantly higher than women in geno-
type-matched cases and controls. The gender differences
observed could be explained on the basis of reproductive
hormones and stoichiometric formation of homocysteine
in connection with the creatine/creatinine synthesis that
is proportional to muscle mass [30–33]. Hyperhomocys-
teinemia was defined as the concentration of homocys-
teine above the 95th percentile of the control group,
which is 19.2 and 13.1mmol/l for men and women,
respectively, in the current study. In men a 9.4-fold
increased risk was observed in participants with homo-
cysteine above 19.2mmol/l, whereas in women the risk is
7.6-fold with homocysteine greater than 13.1mmol/l,
suggesting strongly that hyperhomocysteinemia is a risk
factor for DVT in both men and women.
The pathophysiology of homocysteine-related vascular
thrombosis is that high concentrations of homocysteine
activate factor V [34], reduce protein C activation, inac-
tivate the cofactor activity of thrombomodulin [35], sup-
press thrombomodulin and anticoagulant heparan sulfate
expression [36] and block tissue plasminogen activator
binding to human endothelial cells [37]. It therefore
affects both the vascular endothelium as well as the
haemostatic factors leading to thrombosis. Hyperhomo-
cysteinemia has emerged as an independent risk factor
after excluding other genetic risk factors. There is, how-
ever, a need to evaluate whether elevated plasma homo-
cysteine, itself a risk factor, or genetic or nutritional
factors influencing homocysteine have any direct impact
on thrombosis. Cattaneo et al. have shown positive associ-
ation of low vitamin B6 with the risk of DVT indepen-
dent of fasting and post-methionine-load homocysteine
levels [38]. Quere et al. have shown that methionine
levels below the median value were independently
associated with risk for DVT [39]. Oger et al. have shown
elevated plasma homocysteine, low serum folate and low
vitamin B12 as independent risk factors associated with
1.48-fold, 3.14-fold and 1.42-fold increased risk for DVT,
respectively [40]. Several studies have reported a high
prevalence of B vitamin (folate, vitamins B6 and B12)
deficiencies in Indians, which could be partly due to a
vegetarian diet [41–43]. There is a need to evaluate
whether the plasma homocysteine elevation observed
in this study is nutritional or genetic.
Genetic predisposition to MTHFR or factor V, or
both, was found associated with early onset of DVT. Co-
existence of two or more risk factors pronounced the risk
for DVT and may require prolonged anticoagulation [44].
To conclude, hyperhomocysteinemia due to nutritional
or genetic causes and compound heterozygous status for
MTHFR are independent risk factors for DVT among
South Indians. Co-segregation of two or more risk factors
inflates the risk for DVT.
AcknowledgementsThe authors thank all the patients who participated in
this study. They thank Mr Ram Prakash Singh and Mr G.
Srinivas for technical support.
References1 Nordstrom M, Lindblad B, et al. A prospective study of the incidence of
deep vein thrombosis with a defined population. J Intern Med 1992;232:150–160.
2 Rubinstein I, Murray D, et al. Fatal pulmonary emboli in hospitalizedpatients: an autopsy study. Arch Intern Med 1998; 148:1425–1426.
3 Rosendal FR. Thrombosis in the young: epidemiology and risk factors, afocus on venous thrombosis. Thromb Haemost 1997; 78:1–6.
4 Ridker PM. Inherited risk factors for venous thromboembolism: implicationfor clinical practice. Clin Cornerstone 2002; 4:18–30.
5 Griffn JH, Evatt B, Zimmerman TS, et al. Deficiency of protein C incongenital thrombotic disease. J Clin Invest 1981; 68:1370–1373.
6 Marciniak E, Wilson HD, Marlar RA. Neonatal purpura fulminas: a geneticdisorder related to theabsenceofprotein C inblood.Blood1985;65:15–20.

MBC/200176; Total nos of Pages: 5;
Hyperhomocysteinemia, MTHFR and DVT Naushad et al. 5
AQ28
AQ29
AQ30
AQ27
AQ26
AQ24
AQ25
AQ18AQ19AQ20AQ21
AQ12
AQ14
AQ13
AQ15
AQ16
AQ17
AQ22
AQ23
7 Mahasandana C, Suvatte V, Marlar RA, et al. Neonatal purpura fulminasassociated with protein S deficiency. Lancet 1990; 1:61–62.
8 Lane DA, Caso R. Anti thrombin: structure, genomic organization, functionand Inherited deficiency. The molecular biology of coagulation. BaillieresBest Pract Res Clin Haematol 1989;961.
9 Swenson PJ, Dahl Back B. Resistance to activated protein C as a basis forvenous thrombosis. N Engl J Med 1994; 343:1536–1538.
10 Koster T, Rosendaal FR, de Ronde H, Briet E, Vandenbroucke JP, BertinaRM. Venous thrombosis due to poor anticoagulant response to activatedprotein C: Leiden Thrombophilia Study. Lancet 1993; 342:1503.
11 Bertina RM, Koeleman BPC, Koster T, Rosendaal FR, Dirven RJ, de RondeH, et al. Mutation in blood coagulation Factor V associated with resistanceto activated protein C [letter]. Nature 1994; 369:64–67.
12 Simioni P, Prandonip, Lensing AW, et al. The risk of recurrent venousthromboembolism in patients with an Arg 506-gln mutation in the gene forFactor V (Factor V Leiden). N Engl J Med 1997; 336:399–403.
13 Martinelli I, Landi G, Merati G, Cella R, Tosetta A, Mannucci PM. Factor Vgene mutation is a risk factor for cerebral venous thrombosis. ThrombHaemost 1996; 75:393.
14 Poort SR, Rosendaal FR, Reitsma PH, Bertina RM. A common geneticvariation in the 30-untranslated region of the prothrombin gene is associatedwith elevated plasma prothrombin levels and an increase in venousthrombosis. Blood 1996; 88:3698.
15 Cattaneo M. Hyperhomocysteinemia, atherosclerosis and thrombosis.Thromb Haemost 1999; 81:165.
16 den Heijer M, Koster T, Blom HJ, et al. Hyperhomocysteinemia as a riskfactor for deep vein thrombosis. N Engl J Med 1996; 334:759.
17 Cattaneo M, Tsai MY, Bucciarelli P, et al. A common mutation in theMethylenetetrahydrofolate reductase gene (C677T) increases the risk fordeep vein thrombosis in patients with mutant factor V (factor V: Q506).Arterioscler Thromb Vasc Biol 1997; 17:1662.
18 Wald DS, Law M, Morris JK. Homocysteine and cardiovascular disease:evidence on causality from a meta-analysis. Br Med J (Clin Res Ed) 2002;325:1202.
19 Mohanty D, Shetty S, Ghosh K, Pawar A, Abraham P. Hereditarythrombophilia as a cause of Budd–Chiari syndrome: a study from WesternIndia. Hepatology 2001; 34:666–670.
20 Ghosh K, Shetty S, Madkaikar M, Pawar A, Nair S, Khare A, et al. Venousthromboembolism in young patients from western India: a study. Clin ApplThromb Hemost 2001; 7:158–165.
21 Saxena R, Mohanty S, Srivastava A, Choudhry VP, Kotwal J. Pathogeneticfactors underlying juvenile deep vein thrombosis (DVT) in Indians.Eur J Haematol 1999; 63:26–28.
22 Herrmann FH, Koesling M, Schroder W, Altman R, Jimenez Bonilla R,Lopaciuk S, et al. Prevalence of factor V Leiden mutation in variouspopulations. Genet Epidemiol 1997; 14:403–411.
23 Pawar A, Ghosh K, Shetty S, Colah R, Mohanty D. High frequency of factorV Leiden mutation in Parsis – a highly endogamous population in India.Thromb Haemost 2000; 83:965.
24 Castoldi E, Lunghi B, Mingozzi F, Ioannou P, Marchetti G, Bernardi F. Newcoagulation Factor V gene polymorphisms define a single and infrequenthaplotype underlying the factor V Leiden mutation in Mediterraneanpopulations and Indians. Thromb Haemost 1997; 78:1037–1041.
25 Van der Put NM, Gabreels F, Stevens EM, Smeitink JA, Trijbels FJ, EskesTK, et al. A second common mutation in the methylenetetrahydrofolatereductase gene: an additional risk factor for neural-tube defects?Am J Hum Genet 1998; 62:1044–1051.
26 Nishiguchi T, Matsuyama K, Kobayashi T, Kanayama N. Des-gamma-carboxyprothrombin (PIVKA-II) levels in maternal serum throughoutgestation. Semin Thromb Hemost 2005; 31:351–355.
27 Aznar J, Vaya A, Estelles A, et al. Risk of venous thrombosis in carriers of theprothrombin G20210A variant and factor V Leiden and their interactionwith oral contraceptives. Haematologica 2000; 85:1271–1276.
28 Bloemenkamp KWM, Rosendaal FR, Helmerhorst FM, Vandenbroucke JP.Higher risk of venous thrombosis during early use of oral contraceptives inwomen with inherited clotting defects. Arch Intern Med 2000; 160:49–52.
29 Yamanda K, et al. Effects of common polymorphisms on the properties ofrecombinant human methylene tetrahydrofolate reductase. Nat Genet1995; 10:111–113.
30 Lussier-cacan S, Xhignesse M, Piolot A, et al. Plasma total homocysteine inhealthy subjects: sex-specific relation with biological traits. Am J Clin Nutr1996; 64:587–593.
31 Andersson A, Brattstrom L, Israelsson B, et al. Plasma homocysteine beforeand after methionine loading with regard to age, gender, and menopausalstatus. Eur J Clin Invest 1992; 22:79–87.
32 Selhub J, Jacques PF, Wilson PWF, et al. Vitamin status and intake asprimary determinants of homocysteinemia in an elderly population. JAMA1993; 270:2693.
33 Mudd SH, Poole JR. Labile methyl balances for normal humans on variousdietary regimens. Metabolism 1975; 24:721–735.
34 Rodgers GM, Kane WH. Activation of endogenous Factor V by ahomocysteine-induced vascular endothelial cell activator. J Clin Invest1986; 77:1909–1916.
35 Lentz SR, Sadler JE. Inhibition of thrombomodulin surface expression andprotein C activation by the thrombogenic agent homocysteine. J Clin Invest1991; 88:1906–1914.
36 Nishinaga M, Ozawa T, Shimada K. Homocysteine, a thrombogenic agent,suppresses anticoagulant heparan sulfate expression in cultured porcineaortic endothelial cells. J Clin Invest 1993; 92:1381–1386.
37 Hajjar KA, Mauri L, Jacovina AT, Zhong F, Mirza UA, Padovan JC, Chait BT.Tissue plasminogen activator binding to the annexin II tail domain. Directmodulation by homocysteine. J Biol Chem 1998; 273:9987–9993.
38 Cattaneo M, Lombardi R, Lecchi A, Bucciarelli P, Mannucci PM. Lowplasma levels of vitamin B(6) are independently associated with aheightened risk of deep-vein thrombosis. Circulation 2001; 104:2442–2446.
39 Quere I, Perneger TV, Zittoun J, Bellet H, Gris JC, Daures JP, et al. Redblood cell methylfolate and plasma homocysteine as risk factors for venousthromboembolism: a matched case–control study. Lancet 2002;359:747–752.
40 Oger E, Lacut K, Le Gal G, Couturaud F, Guenet D, Abalain JH, et al.,EDITH Collaborative Study Group. Hyperhomocysteinemia and low Bvitamin levels are independently associated with venous thromboembolism:results from the EDITH study: a hospital-based case–control study.J Thromb Haemost 2006; 4:793–799.
41 Refsum H, Yajnik CS, Gadkari M, Schneede J, Vollset SE, Orning L, et al.Hyperhomocysteinemia and elevated methylmalonic acid indicate a highprevalence of cobalamin deficiency in Asian Indians. Am J Clin Nutr 2001;74:233–241.
42 Lakshmi AV, Maniprabha C, Krishna TP. Plasma homocysteine level inrelation to folate and vitamin B6 status in apparently normal men. Asia PacJ Clin Nutr 2001; 10:194–196.
43 Khanduri U, Sharma A, Joshi A. Occult cobalamin and folate deficiency inIndians. Natl Med J India 2005; 18:182–183.
44 Mandel H, Brenner B, Bernant M. Coexistence of hereditary homocystinuriaand factor V Leiden. Effect on thrombosis. N Engl J Med 1996; 334:763–768.
MBC Manuscript No. 200176
Blood Coagulation & Fibrinolysis Typeset by Thomson Digital
for Lippincott Williams & Wilkins
Dear Author, During the preparation of your manuscript for typesetting, some queries have arisen. These are listed below. Please check your typeset proof carefully and mark any corrections in the margin as neatly as possible or compile them as a separate list. This form should then be returned with your marked proof/list of corrections to the Production Editor.
QUERIES: to be answered by AUTHOR/EDITOR
AUTHOR: The following queries have arisen during the editing of your manuscript. Please answer the queries by marking the requisite corrections at the appropriate positions in the text.
QUERY NO.
QUERY DETAILS
<AQ1>
<AQ2>
<AQ3>
<AQ4>
<AQ5>
<AQ6>
<AQ7>
<AQ8>
<AQ9>
Please provide history date. Confirm author names are correctly stated Provide fax number Should reference [23] also be cited here? If not, references must be renumbered so first citations are numerical Provide name, city, state and country of supplier Provide name of kit and name, city, state and country of supplier Provide name, city, state and country of supplier Provide name, city, state and country of supplier Provide names and initials of first 6 authors et al.
<AQ10>
<AQ11>
<AQ12>
<AQ13>
<AQ14>
<AQ15>
<AQ16>
<AQ17>
<AQ18>
<AQ19>
<AQ20>
<AQ21>
<AQ22>
<AQ23>
Provide names and initials of first 6 authors et al. Provide names and initials of first 6 authors et al. Provide names and initials of first 6 authors et al. Provide volume number and full page span Provide full page span or state if letter/abstract etc Provide names and initials of first 6 authors et al. Provide full page span or state if letter/abstract etc Provide full page span or state if letter/abstract etc Provide full page span or state if letter/abstract etc Provide names and initials of first 6 authors et al. Provide full page span or state if letter/abstract etc Provide names and initials of first 6 authors et al. Provide full page span or state if letter/abstract etc Provide full page span or state if letter/abstract etc
<AQ24>
<AQ25>
<AQ26>
<AQ27>
<AQ28>
<AQ29>
<AQ30>
<AQ31>
Provide full page span or state if letter/abstract etc Provide names and initials of first 6 authors et al. Provide names and initials of first 6 authors et al. Provide names and initials of first 6 authors et al. Provide names and initials of first 6 authors et al. Provide names and initials of first 6 authors et al. Provide full page span or state if letter/abstract etc Replace Pl. in full - plasma?
Copyright © 2022 FDOKUMEN




















