
Expression, purification and characterization of flavin reductase from Citrobacter freundii A1
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
Available online at wwwsciencedirectcom
(2008) xxxndashxxx
CLB-06993 No of pages 7 4C
ARTICLE IN PRESS
Clinical Biochemistry xx
ROOF
Association of parental hyperhomocysteinemia and C677T Methylenetetrahydrofolate reductase (MTHFR) polymorphism with recurrent
pregnancy loss
Vinukonda Govindaiah a Shaik Mohammad Naushad b Krishnamurthy Prabhakara cPrasad Chintakindi Krishna b Akella Radha Rama Devi b
a Dept of pathology New York Medical College Valhalla NY 10595 USAb Diagnostics Division Centre for DNA Fingerprinting and Diagnostics (CDFD) 7-18 ECIL Road Nacharam Hyderabad
^ndash 500076 India
c Cytogenetics Laboratory VCGS Pathology Royal Childrens Hospital Melbourne Victoria Australia
Received 14 August 2008 received in revised form 27 November 2008 accepted 7 December 2008
P
RECT
EDAbstract
Objectives To investigate the association of parental hyperhomocysteinemia C677T Methylene tetrahydrofolate reductase (MTHFR)polymorphism and DNA damage with recurrent pregnancy loss (RPL)
Design and^methods A case-control study Reverse phase HPLC PCR-RFLP and Cytokinesis blocked micronuclei assay were used to assess
total plasma homocysteine C677T MTHFR polymorphism and DNA damage respectively Student t-test^ ANOVA and Fisher exact test were
used for statistical analysisResults Maternal [mean 116plusmn50 versus 86plusmn42 μmolL odds ratio (OR) 448] and paternal [
^mean 196plusmn95 versus 142plusmn74 μmolL
OR 692] hyperhomocysteinemia paternal age [OR 116] paternal MTHFR 677T allele [OR 230] and DNA damage were found to increase therisk for RPL DNA damage showed positive correlation with plasma homocysteine and MTHFR 677
^T allele
Conclusions Parental hyperhomocysteinemia paternal age paternal C677T MTHFR polymorphism and DNA damage are risk factors forRPL DNA damage showed positive correlation with plasma homocysteine and MTHFR 677T allelecopy 2008 The Canadian Society of Clinical Chemists Published by Elsevier Inc All rights reserved
RKeywords Homocysteine Recurrent pregnancy loss Methylene tetrahydrofolate reductase Polymorphism DNA damage
O
36
37
38
39
40
41
42
43
44
45
UNCIntroduction
The miscarriage of three or more consecutive pregnancies inthe first or early second trimester termed as recurrent pregnancyloss (RPL) was observed in b5 women according to the factsheet of American Society of Reproductive Medicine Parentalchromosomal anomalies uterine anomalies cervical incompe-tence endocrine disorders immunological factors coagulationdisorders infections maternal chronic diseases and otherfactors such as exposure to toxic chemicals contribute to
46
47
48
49
Corresponding author Fax +91 40 27155610E-mail addresses naushadsmgmailcom naushadscdfdorgin
(SM Naushad)
0009-9120$ - see front matter copy 2008 The Canadian Society of Clinical Chemistsdoi101016jclinbiochem200812003
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
approximately 50 cases in the remaining 50 cases theetiology is unexplained [1]
Aberrations in folate pathway such as maternal folatedeficiency maternal hyperhomocysteinemia and 677TT geno-type of Methylene tetrahydrofolate reductase (MTHFR)C677T polymorphism were found to contribute to etiologyof RPL in different populations [2] However there are a veryfew studies that have taken paternal risk factors as well intoaccount Several hypotheses were proposed to explain the roleof hyperhomocysteinemia in RPL Homocysteine by itself canbe embryo toxic [3] or it can potentially interact withhaemostatic genetic determinants there by increasing thethrombogenic potential [45] or it can alter the S-adenosylmethionine (SAM)
^S-adenosyl homocysteine (SAH) ratio [6]
Published by Elsevier Inc All rights reserved
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
C
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126^
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
2 V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
UNCO
RRE
or by causing uracil misincorporation in DNA causingmutations chromosomal breaks and micronuclei formation[7] SAM is a universal methyl donor that donates methylmoieties to DNA proteins neurotransmitters etc SAH is afeedback inhibitor of SAM Thus SAMSAH ratio serves as anindicator of cellular methylation status Trkova et al
^have
reported increased micronuclei frequencies in couples withreproductive failures [8]
In view of ethnic and population-level variations in thedistribution of MTHFR C677T polymorphism [9] lowfrequency MTHFR C677T polymorphism in Indian population[10] high incidence of deficiencies of B6 B12 and folateamong Indians [1112] lack of strategies for pre-conceptionalfolate supplementation and fortification of food grains withfolate hyperhomocysteinemia might be an important contri-butor for RPL among Indians The rationale behind this studywas to address the role of maternal as well as paternalhyperhomocysteinemia MTHFR C677T polymorphism andDNA damage in RPL and to deduce the role of hyperhomo-cysteinemia in DNA damage
Materials and methods
Subjects
Recruitment of the subjects was carried out during the periodof 1999 to 2006 A total of 140 couples with history of three ormore unexplained recurrent pregnancy losses were enrolled ascases in the study None of the couples with RPL had any livebirth (nulliparous) Among these 140 couples 100 couples hadfirst trimester pregnancy loss (between 8 to 12 weeks ofgestation) where as 40 couples had first trimester (8 to12 weeks) as well as second trimester (13 to 20 weeks)pregnancy losses Cases were screened for previous history ofthromboembolism anti-phospholipid syndrome uterineabnormalities chromosomal anomalies diabetes mellitusradiation exposure known erythrocyte antibody anti-P syn-drome pregnancy losses due to documented fetal malformationand indication for anticoagulant treatment during pregnancyand those with these risk factors were excluded from the studyEach patient was completely evaluated for recognized causes ofRPL by a panel of tests hysteroscopy hysterosalpingographyserial ultrasonography TIFFA scan during the pregnancykaryotyping fasting and post-prandial blood glucose anti-phospholipid antibodies (anti cardiolipin antibodies and lupusanticoagulant) lutheal phase insufficiency (by repeated serumprogesterone measurements and endometrial biopsy) prolactindosage thyroid hormones toxoplasmosis cytomegalovirusrubella HIV Group B streptococci chlamydia trachomatosishepatitis B and
^C and bacterial vaginosis Apart from these tests
a questionnaire was designed to record history of thromboem-bolism radiation exposure and anticoagulant treatment duringpregnancy From the initial 151 couples screened for the abovementioned tests one had uterus bicarnate one had highprolactin six maternal subjects [22p+ 9qh+ One cell Xqdelt^(613) (p25q22) in each and Inv 9 in two] and three paternalsubjects [Inv 9 small Y and t
^(114)] had chromosomal
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPR
OOF
anomalies Hence these eleven couples were excluded from thisstudy At the time of enrollment none of the subjects werepregnant Paternal age ranged from 22 yr to
^42 yr and maternal
age ranged from 19 yr to 35 yrA total of 140 couples with normal reproductive history
(having 2 or more children and no history of miscarriages)who also meet the same exclusion criteria were enrolled ascontrols Paternal age ranged from 23 yr to 42 yr and maternalage ranged from 18 yr to 34 yr None of the subjects weretaking supplements of vitamins or folic acid at the time ofsample collection
All the cases were referred from different Gynecologists forchromosomal evaluation Control group consisted of laboratorycontrols and subjects who visited the out patient unit for minorcomplications Recruitment took place during the period of1999ndash
^2007 Informed consent was obtained from all the
subjects Bioethical committee of Center approved the studyfor DNA Fingerprinting and Diagnostics Hyderabad Indiawhich also serves as Institutional Review Board
Whole blood samples were collected in EDTA and Sodiumheparin vaccutainers after overnight fasting EDTA plasmasamples were separated immediately after centrifugation at700 times
^g for 10 min and stored at
^minus20 degC until the analysis Buffy
coat was used for DNA isolation using phenol-chloroformextraction method Heparin samples freshly drawn were usedfor cell cultures
Plasma homocysteine analysis
For the determination of total plasma homocysteine 100^mL
sample was treated with 10 mL^of 10 tri-n-butyl phosphine in
dimethyl formamide for 30 min at 4 degC The solution was mixedwith 05
^mL chilled 10
^trichloroacetic acid containing 1 mM
EDTA followed by centrifugation at^1000 times
^g for 5 min 02
^mL
aliquot of the clear supernatant was taken and vigorously mixedwith 04 mL
^of 25 M-borate buffer (pH 105) containing 4 mM
EDTA and 02 mL^of SBD-F in 25 M Borate buffer (pH 95)
The mixture was filtered through a 045 mmMillipore filter andan aliquot of 10 mL
^final reaction mixture was subjected to
HPLC analysisHichrom C18 250times46 mm column (Hichrom Ltd
Berkshire UK) was used as a stationary phase and 0^1 mol
L potassium dihydrogen phosphate buffer (pH 21) containing4
^acetonitrile was used as mobile phase at a flow rate of
20 mL^min in the isocratic separation Fluorescence inten-
sities were measured with ex385 nmem515 nm withFluorescence detector attached to HPLC system (Watersmodel 510 Milford MA USA) Homocysteine in plasmasamples was quantified by comparing the peaks with the peaksof the pure standard [13] The 95th percentile of homocysteinelevels in male and female controls were used as the thresholdto define hyperhomocysteinemia
MTHFR C677T polymorphism
PCR amplification using F-5primeTTT GAG GCT GAC CTGAAG CAC TTG AAG GAG-3prime and R-5primeGAG TGG TAG
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
Table 1 t11
Allelic and genotypic differences for MTHFR C677T polymorphism betweenRPL cases and controls t12
t13MTHFR 677 Cases () Controls () OR 95 CI p value
t14Maternal 140 140t15CC 111 (793) 112 (800) 1 referencet16CT 25 (179) 28 (200) 090 050ndash163 085t17TT 4 (29) 0 (00) Inf 103ndashinf 013t18C allele 247 (882) 252 (900) 1 referencet19T allele (Crude) 33 (118) 28 (100) 120 071ndash204 059t110(Adjusted) 105 061ndash182 010t111Paternal 140 140t112CC 111 (793) 126 (900) 1 referencet113CT 27 (193) 14 (100) 219 110ndash434 004t114TT 2 (14) 0 (00) Inf 058ndashinf 045t115C allele 249 (889) 266 (950) 1 referencet116T allele (Crude) 31 (111) 14 (50) 237 124ndash451 001t117(Adjusted) 230 117ndash453 002
Note reference-Wild genotype was used as a reference Inf-infinity Odds ratiosfor T allele frequencies in cases and controls were adjusted for maternal agepaternal age number of pregnancy losses and MTHFR genotype of each otherusing conditional logistic regression t118
3V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
UNCO
RREC
CCC TGG ATG GGA AAG ATC CCG-3prime primers (SigmaGenosys 80-51127272 St Louis MO USA) was carried outin a total volume of 25 mL
^containing 012 mM of each
primer 02 mM each dNTP (MBI Fermantas Glen BurnieMD USA) 25 μl of 10
^times PCR buffer [10 mM Tris HClL (pH
83) 15 mM MgCl2 50 mM KCl] and 1^25 U Taq
polymerase (Bangalore Genie MME5J Bangalore KarnatakaIndia) and 100 ng template DNA The reaction conditionswere as follows initial denaturation at 95 degC for 15 min and30 subsequent cycles at denaturation at 94 degC for 60 sannealing at 61 degC for 60 s and extension at 72 degC for 2 minPCR product (173-bp) was subjected to restriction digestionwith 1U of HinfI enzyme (New England Biolabs IpswichMA USA) MTHFR C677T mutation creates the Hinf Irestriction site resulting in the cleavage of 173-bp fragmentinto 125-bp and 48-bp [14]
Cytokinesis-blocked human lymphocytes micronuclei assay
Peripheral blood cultures were set-up according to standardcell culture protocols In brief 05 mL
^of whole blood was
introduced into sterile culture vial containing 5 mL^RPMI-1640
medium (GIBCO India) supplemented with 10^fetal calf
serum and 01^phytohaemagglutinin (GIBCO India) were
grown at 37 degC After the completion of 68 h^culturing
Cytochalasin B (made up in a stock solution of 2 mgmL^in
dimethyl-sulfoxide) was added to make the final concentrationof 3 mgmL
^ After 28 h
^of further culturing cells were
transferred to centrifuge tubes and centrifuged for 10 min at1000 rpm The supernatant was discarded and the pellet wasresuspended in 0075 M KCL for 18 min About 2ndash
^3^mL of
chilled 13 acetone methanol was added to the hypotonicsolution and mixed for gentle fixation The tubes werecentrifuged and the pellet was resuspended in fresh fixativeThe total period of fixation was not more than
^2 h
^ as this
fixation preserves the cytoplasm around the nucleus The cellsuspension was gently dropped on to chilled slides and air-dried The slides were stained with 5
^phosphate buffered
Giemsa and visualized in oil immersion at 100^times high-power
objective lens and scanned for micronuclei in binucleates Onlybinucleates cells showing the cytoplasm around the nuclei wereincluded in the scoring 1000 binucleates were scored for eachindividual and the proportion of binucleates with micronucleiwas recorded [15]
In vitro analysis to study the impact of homocysteine onDNA damage
Peripheral blood of a control with normal homocysteinelevel (40 μmolL) was made into 10 aliquots and made intotwo batches of five each Peripheral blood cultures were set-upaccording to protocols described earlier After 24 h
^incubation
to each aliquot of a batch homocysteine was addedexogenously to a final concentration of 0 10 20 50 and100 μmolL and after 44 h
^culturing Cytochalsin B was added
and cytokinesis blocked human lymphocytes micronucleiassay was performed as described in the previous section
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPR
OOF
Average micronuclei frequency for each concentration wastaken for statistical calculations
Statistical analysis
Continuous variables were assessed using Student t-test^and ANOVA and were presented as meanplusmnstandard devia-
tion Categorical variables were computed in 2times2 contin-gency table based on presence or absence of variable in casesand controls and were subjected to Fisher exact test Oddsratios 95 confidence intervals and p value
^s were computed
using the software Multiple logistic regression analysis wasdone to investigate the individual effects of each variable aftercontrolling for potential confounders such as maternal agepaternal age number of pregnancy losses and MTHFRgenotype of one another A lsquoPrsquo
^value of b005 was
considered statistically significant Spearmans rank correla-tion coefficient was used to assess the correlation betweenplasma homocysteine and micronuclei frequency All thestatistical tests were performed using the software providedby wwwstatpagesorg
Results
After controlling for known confounding variables maternalage showed no significant association (OR 091 95 CI081ndash
^102) where as paternal age showed statistically sig-
nificant association (OR 116 95 CI 104ndash^130
^p=001)
with RPLThe 95 percentiles of homocysteine levels in male and
female controls were 196 μmolL and 140 μmolL respec-tively which were used as threshold values to definehyperhomocysteinemia Mean maternal homocysteine levelsand mean paternal homocysteine levels were higher in casesthan controls with 448 (95 CI 230ndash
^870) and 692 (95 CI
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
C
OOF
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288
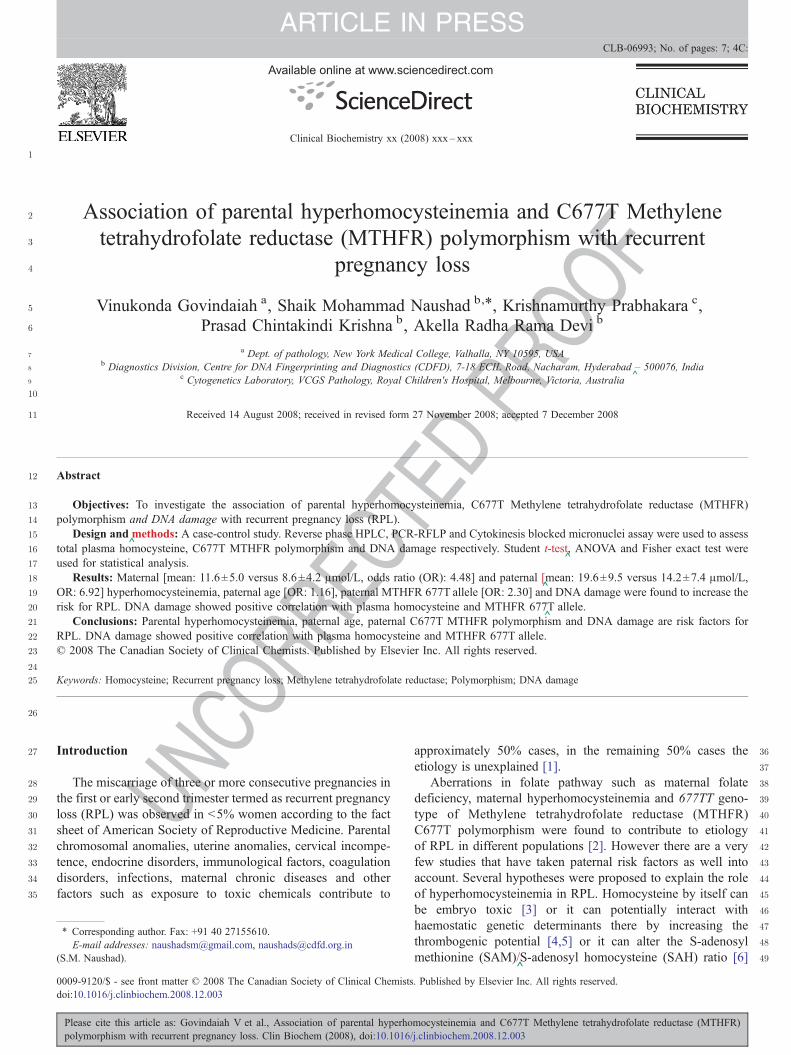
Fig 1 Plasma homocysteine scatter plot of RPL cases and controls according togender and MTHFR 677 genotype A RPL females with MTHFR 677 CCgenotype B RPL females with MTHFR 677 CT genotype C RPL females withMTHFR 677 TT genotype D RPL males with MTHFR 677 CC genotype ERPL males with MTHFR 677 CT genotype G Control females with MTHFR677 CC genotype H Control females with MTHFR 677 CT genotype IControl males with MTHFR 677 CC genotype J Control males with MTHFR677 CT genotype
t21
t22
t23
t24
t25
t26
t27
Fig 2 In vitro assay to study the impact of homocysteine gradient on DNAdamage X-axis Exogenous homocysteine concentration (in μmolL) Y-axisMicronuclei frequency (per thousand binucleated cells)
4 V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
NCOR
RE390ndash
^1229) fold increased risk for RPL (p
^b00001) There was
a correlation between maternal and paternal homocysteinelevels with a correlation coefficient of 019 The combinedelevated levels were observed in ten RPL couples and none ofthe control couples
The distribution of MTHFR C677T polymorphism wasfound to be in accordance with Hardy-Weinberg equilibriumin RPL mothers (p
^=023) control mothers (p
^=050) RPL
fathers (p^=100) and control fathers (p
^=077) Maternal and
paternal MTHFR 677 T-alleles were associated with 105(95 CI 061ndash
^182) and 230 (95 CI 117ndash
^453) fold-
increased risk for RPL after controlling for known confound-ing factors Statistical significance was observed only forpaternal T allele (p
^b005) (Table 1) Four RPL mothers and
two RPL fathers had MTHFR TT genotype and none of thecontrols had this genotype
MTHFR genotype was found to be one genetic determinantfor homocysteine however its impact was more prominent inmen than women Men with CT genotype showed homo-cysteine elevation greater than 95th percentile of controls(N196 μmolL) where as women with CT genotype althoughshowed significant increase in homocysteine compared to
U 289
290
291
292
293
294
295
296
297
298
299
300
Table 2Micronuclei frequency (Meanplusmnstandard deviation) distribution in cases andcontrols
Micronuclei frequency Cases Controls p value
Maternal 28plusmn25 23plusmn16 b005Paternal 43plusmn30 34plusmn25 0007
Spearmans correlation coefficient with plasma homocysteine (r)=046pb00001Spearmans correlation coefficient with MTHFR C677T polymorphism (r)=011pb001
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPRwomen with CC genotype the increase was lesser than 95th
percentile of controls (b140 μmolL) (Fig 1)Maternal as well as paternal RPL subjects showed higher
micronuclei frequency compared to respective controlsindicating significant DNA damage in RPL group Miconucleifrequency was positively correlated with plasma homocys-teine (r
^=046) and MTHFR C677T polymorphism (r
^=011)
(Table 2) In vitro assay showed dose dependent increase inthe micronuclei frequency with increasing homocysteineconcentration (Fig 2)
Discussion
Hyperhomocysteinemia and homozygosity for MTHFRC677T polymorphism were reported to be maternal risk factorsfor RPL Little is known about the role of paternal risk factors inRPL The current study was undertaken to examine theassociation between both maternal and paternal hyperhomo-cysteinemia and RPL No association was observed betweenmaternal age and RPL which could be due to age-matchedcontrols An association was observed between paternal age andRPL after controlling for the effect of maternal age The meanhomocysteine levels in RPL mothers and RPL fathers werehigher than control mothers and control fathers Maternal andpaternal hyperhomocysteinemia were found to increase the riskfor RPL by 448 fold (230 870) and 692 fold (390 1229)respectively Hyperhomocysteinemia in both the parents wasobserved in ten RPL couples where as none of the controlcouples had this combination These results indicate thatparental hyperhomocysteinemia may be an independent riskfactor for RPL
Paternal MTHFR 677 T-allele was associated with 237 foldrisk where as maternal T-allele did not show any statisticallysignificant risk for RPL Among the individual genotypesMTHFRTT-genotype was present only in cases not in controlsDespite the small numbers the results indicate an associationwith MTHFR 677TT and RPL
MTHFR genotype was found to influence the plasmahomocysteine levels in both the genders and hence a majorgenetic determinant of hyperhomocysteinemia Comparing the
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
5V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
UNCO
RREC
genotype and gender matched cases with controls showedevidence to suggest that cases have higher homocysteine thancontrols and hence apart from MTHFR genotype somegenetic or non-genetic determinant also plays a role inincreasing the homocysteine and might play an importantrole in the etiology of RPL However men with CT genotypeshowed homocysteine elevation greater than the 95thpercentile of controls where as women with CT genotypeshowed homocysteine levels lesser than the 95th percentile ofcontrols These gender differences in homocysteine mightexplain the risk associated with paternal T-allele The mostprofound associations between hyperhomocysteinemia andRPL were found in fathers who were heterozygous for the677T allele This is extremely common in Caucasians (40)and is not considered to be a risk factor for hyperhomocys-teinemia (in contrast to homozygotes) This discrepancy couldbe due to differences in the diet and also the possibility of anyother allele from a different loci co-segregating with MTHFR677T allele cannot be ruled out The gender differences inplasma homocysteine levels could be due to protective role ofestrogens (in females) [1617] stoichiometric synthesis ofhomocysteine with creatinecreatinine ratio proportional tomuscle mass [18] differences in the rates of remethylation andtranmethylation among males and females [19]
^Significant DNA damage was observed in RPL couplescompared to control couples which was found to havepositive association with homocysteine To strengthen thisassociation further in vitro assay was performed on peripheralblood cultures with exogenous addition of homocysteine invarying concentrations which showed dose-dependentincrease in the frequency of micronuclei This is a strongevidence to suggest that hyperhomocysteinemia induces DNAdamage DNA damage can be caused by many factors apartfrom hyperhomocysteinemia and hence there is a need toconduct another study focusing on the causes of DNA damagein RPL subjects
Our study is in agreement with Remy Slama et al^in showing
increased risk of RPL with increase in paternal age with asuggestion that the association is stronger for first trimesterpregnancy loss [20] This increased risk may be a consequenceof an increasing frequency of chromosomal anomalies in thespermatozoa with male age [2122] or due to increased DNAdamage [23] or due to increased chromosomal replications ofmale stem cells [24] Apart from our study several researchershave shown positive association of maternal hyperhomocystei-nemia and maternal MTHFR 677 TT genotype with RPL Highprevalence of hyperhomocysteinemia was observed in parouswomen (33) compared to nulliparous women (14) byWouters MG et al Five consecutive fetal deaths were reportedin a woman with MTHFR 677TT genotype and elevatedhomocysteine and high prevalence of hyperhomocysteinemia(12) folate deficiency (15) and C677T MTHFR CT and TTgenotypes (20) were reported in 100 consecutive women withRPL by Quere et al
^[25] Hyperhomocysteinemia and folate
deficiency were found to be associated with 36 and 21 fold riskfor RPL by Nelen et al [26] Smaller median chorionic vasculararea and perimeter were observed in women with hyperhomo-
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPR
OOF
cysteinemia by Nelen et al^suggesting that hyperhomocystei-
nemia is associated with defective chorionic vasculature [27]Meta-analysis of case-control studies conducted during theperiod of 1992ndash
^1999 showed that hyperhomocysteinemia and
MTHFRTT-genotype were associated with 27 fold and 14 foldrisk for RPL respectively [28] Another meta-analysis based onTwenty-six studies with 2120 RPL cases and 2949 controlsshowed that MTHFR TT-genotype was associated with nostatistically significant risk with an odds ratio of 121 (95 CI104 140) [29] Zetterberg et al
^have observed increased
frequency of combined MTHFR C677T and A1298C mutatedalleles in spontaneously aborted fetuses (OR 142 95 CI178ndash
^113) indicating that the MTHFR polymorphisms may
have a major impact on fetal survival [30] A pilot studyconducted on 24 South Indian women by Kumar et al
^has
shown high prevalence of hyperhomocysteinemia and red cellfolate deficiency in RPL [31] Candito et al
^reported four
consecutive pregnancy losses in a woman with hyperhomocys-teinemia (259 μmolL) B12 deficiency (b150 pgmL
^) and the
MTHFR 677 TT-genotype who got benefited with vitamin B12supplementation [32] DUva M et al
^have reported Hyperho-
mocysteinemia and MTHFR TT-genotype as risk factors forunexplained female sterility and recurrent pregnancy loss [33]
Apart from the study by Trkova et al^that showed increased
micronuclei frequency in couples with RPL several studieshave also explored the relationship between sperm quality andunexplained RPL Increased percentage of sperm stainingpositive for DNA fragmentation was observed in the RPL groupcompared to donor or general population by Carrell et al
^[34]
In a separate study they also showed that the mean aneuploidyrate in RPL group was significantly higher than the generalpopulation (277plusmn022 vs 148plusmn012 Pzb0005) [35] Bene-ficial effects of folate supplementation were observed bySteegers-Theunissen et al
^[36] and Nelen et al
^[37] who
reported increase in maternal plasmaamniotic fluid folate andlowering of fasting plasma homocysteine levels in theirrespective studies
The risk associated with maternal hyperhomocysteinemiacould be due to embryo toxicity or due to ability of highhomocysteine to activate factor V [38] and to inactivate proteinC thrombomodulin [39] heparan sulphate [40] tissueplasminogen activator binding to human endothelial cells [41]or due to impaired cellular methylation that alters geneexpression or due to uracil misincorporation in DNA resultingin DNA damage The risk associated with paternal hyperho-mocysteinemia could be due to its effect on sperm quality byincreasing DNA damage
The strength of the current study is the assessment of notonly maternal but also paternal hyperhomocysteinemia inrelation to RPL In order to strengthen our hypothesis furtherwe have initiated a pilot study to assess DNA damage in thesemen samples of subjects with recurrent pregnancy loss andobserved significant DNA damage in sperms of RPL fathersusing Fluorescence activated cell sorter technique A modifiedcytokinesis block micronucleus cytome assay for morecomprehensive measurement of DNA damage developedby Fenech et al that measures micronuclei frequency
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
C
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539
6 V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
UNCO
RRE
along with other DNA damage biomarkers such as nuclearbuds nucleoplasmic bridges as well as cytotoxic markersincluding apoptosis and necrosis can be incorporated infuture studies [42]
Our study projects paternal age as an independent riskfactor for RPL Impact of maternal age was controlled in thestudy design (using age-matched controls) as well as in theregression model This study projects that not only maternalhyperhomocysteinemia but also paternal hyperhomocysteine-mia is a risk factor for RPL at least among South IndiansSignificant DNA damage was observed in both maternal andpaternal RPL subjects Our study is in agreement with the twometa-analyses in showing that maternal MTHFR genotypemay not be a significant risk factor for RPL The impact ofpaternal MTHFR genotype on RPL could be due to elevatedhomocysteine levels that in turn result in DNA damage Thisstudy further shows a direct association between homocysteineelevation and DNA damage using in vivo and in vitro assaysHowever the mechanism by which homocysteine causes DNAdamage needs to be elucidated further There is a need forlarge case-control studies to explore the role of other geneticand nutritional factors that are likely to influence homo-cysteine levels in the pathophysiology of RPL
Acknowledgments
We thank Mr Ram Prakash Singh Mr R Sudheer KumarMr G Srinivas and Mr V Murali Mohan for the technicalassistance We thank all the families participated in this studyWe thank Department of Biotechnology Government of Indiafor its financial support
References
[1] Strobino B Fox HE Kline J Stein Z Susser M Warburton DCharacteristics of women with recurrent spontaneous abortions andwomen with favourable reproductive histories Am J Public Health198276(8)986ndash91
[2] Wouters MG Boers GH Blom HJ et al Hyperhomocysteinemia a riskfactor in women with unexplained recurrent early pregnancy loss FertilSteril 199360(5)820ndash5
[3] Greene ND Dunlevy LE Copp AJ Homocysteine is embryotoxic butdoes not cause neural tube defects in mouse embryos Anat Embryol2003206(3)185ndash91 (Berl)
[4] Durand P Lussier-Cacan S Blache D Acute methionine load-inducedhyperhomocysteinemia enhances platelet aggregation thromboxanebiosynthesis and macrophage-derived tissue factor activity in ratsFASEB J 199711(13)1157ndash68
[5] Nishinaga M Ozawa T Shimada K Homocysteine a thrombogenic agentsuppresses anticoagulant heparan sulfate expression in cultured porcineaortic endothelial cells J Clin Invest 199392(3)1381ndash6
[6] Isa Y Mishima T Tsuge H Hayakawa T Increase in S-adenosylhomo-cysteine content and its effect on the S-adenosylhomocysteine hydrolaseactivity under transient high plasma homocysteine levels in rats J Nutr SciVitaminol 200652(6)479ndash82 (Tokyo)
[7] Fenech MF Dreosti IE Rinaldi JR Folate vitamin B12 homocysteinestatus and chromosome damage rate in lymphocytes of older menCarcinogenesis 199718(7)1329ndash36
[8] Trkova M Kapras J Bobkova K Stankova J Mejsnarova B Increasedmicronuclei frequencies in couples with reproductive failure ReprodToxicol 200014(4)331ndash5
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPR
OOF
[9] Schneider JA Rees DC Liu YT et al A worldwide distribution of acommon MTHFR Mutation Am J Hum Genet 199862(5)1258ndash60
[10] Radha Rama Devi A Govindaiah V Ramakrishna G Naushad SMPrevalence of
^methylene tetrahydrofolate reductase polymorphism in
South Indian population Curr Sci 200486(3)440ndash3[11] Neela J Raman L The relationship between maternal nutritional status and
spontaneous abortion Natl Med J India 199710(1)15ndash6[12] Refsum H Yajnik CS Gadkari M et al Hyperhomocysteinemia and
elevated methylmalonic acid indicate a high prevalence of cobalamindeficiency in Asian Indians Am J Clin Nutr 200174(2)233ndash41
[13] Ubbink JB Hayward Vermaak WJ Bissbort S Rapid high-performanceliquid chromatographic assay for total homocysteine levels in humanserum J Chromatogr 1991565(1ndash
^2)441ndash6
[14] Frosst P Blom HJ Milos R et al A candidate genetic risk factor forvascular disease a common mutation in methylenetetrahydrofolatereductase Nat Genet 199510(1)111ndash3
[15] Nath CJ Ong T Micronuclei assay in cytokinesis-blocked binucleated andconventional mononucleated methods in human peripheral lymphocytesTeratog Carcinog Mutagen 199010(3)273ndash9
[16] Giri S Thompson PD Taxel P et al Oral estrogen improves serum lipidshomocysteine and fibrinolysis in elderly men Atherosclerosis 1998137359ndash66
[17] Kim MH Kim E Passon EL et al Cortisol and estradiol^non-genetic
factors for hyperhomocyst(e)inemia Metabolism 199746247ndash9[18] Brattstrom L Lindgren A Israelsson B Andersson A Hultberg B
Homocysteine and cysteine Determinants of plasma levels in middle-agedand elderly subjects J Inter-Am Med 1994236(6)633ndash41
[19] Fukagawa NK Martin JM Wurthmann A Prue AH Ebenstein DORourke B Sex-related differences in methionine metabolism and plasmahomocysteine concentrations Am J Clin Nutr 200072(1)22ndash9
[20] Slama R Bouyer J Windham G Fenster L Werwatz A Swan SHInfluence of paternal age on the risk of spontaneous abortion Am JEpidemiol 2005161816ndash23
[21] Bosch M Rajmil O Martinez-Pasarell O et al Linear increase of diploidyin human sperm with age a four-colour FISH study Eur J Hum Genet20019533ndash8
[22] Griffin DK Abruzzo MA Millie EA et al Non-disjunction in humansperm evidence for an effect of increasing paternal age Hum Mol Genet199542227ndash32
[23] Singh NP Muller CH Berger RE Effects of age on DNA double-strandbreaks and apoptosis in human sperm Fertil Steril 2003801420ndash30
[24] Crow J The origins patterns and implications of human spontaneousabortion Nat Rev Genet 2000140ndash7
[25] Quere I Bellet H Hoffet M Janbon C Mares P Gris JC A woman withfive consecutive fetal deaths case report and retrospective analysis ofhyperhomocysteinemia prevalence in 100 consecutive women withrecurrent miscarriages Fertil Steril 199869(1)152ndash4
[26] Nelen WL Blom HJ Steegers EA den Heijer M Thomas CM Eskes TKHomocysteine and folate levels as risk factors for recurrent earlypregnancy loss Obstet Gynecol 200095(4)519ndash24
[27] Nelen WL Bulten J Steegers EA Blom HJ Hanselaar AG Eskes TKMaternal homocysteine and chorionic vascularization in recurrent earlypregnancy loss Hum Reprod 200015(4)954ndash60
[28] Nelen WL Blom HJ Steegers EA den Heijer M Eskes TKHyperhomocysteinemia and recurrent early pregnancy loss a meta-analysis Fertil Steril 200074(6)1196ndash9
[29] Ren A Wang J Methylenetetrahydrofolate reductase C677T polymorph-ism and the risk of unexplained recurrent pregnancy loss a meta-analysisFertil Steril 200686(6)1716ndash22
[30] Zetterberg H Regland B Palmeacuter M et al Increased frequency ofcombined methylenetetrahydrofolate reductase C677T and A1298Cmutated alleles in spontaneously aborted embryos Eur J Hum Genet200210(2)113ndash8
[31] Kumar KS Govindaiah V Naushad SE Devi RR Jyothy A Plasmahomocysteine levels correlated to interactions between folate status andmethylene tetrahydrofolate reductase gene mutation in women withunexplained recurrent pregnancy loss J Obstet Gynaecol 200323(1)55ndash8
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
540
541
542
543
544
545
546
547
548
549
550
551
552
553
554
555
556
557
558
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573
574
7V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
[32] Candito M Magnaldo S Bayle J et al Clinical B12 deficiency in one caseof recurrent spontaneous pregnancy loss Clin Chem Lab Med 200341(8)1026ndash7
[33] DUva M Di Micco P Strina I et al Hyperhomocysteinemia in womenwith unexplained sterility or recurrent early pregnancy loss from SouthernItaly a preliminary report Thromb J 2007115ndash10
[34] Carrell DT Liu L Peterson CM et al Sperm DNA fragmentation isincreased in couples with unexplained recurrent pregnancy loss ArchAndrol 200349(1)49ndash55
[35] Carrell DT Wilcox AL Lowy L et al Elevated sperm chromosomeaneuploidy and apoptosis in patients with unexplained recurrent pregnancyloss Obstet Gynecol 2003101(6)1229ndash35
[36] Steegers-Theunissen RP Steegers EA de Boer R Thomas CM Klooster-man MD Eskes TK Elevated folate levels in amniotic fluid after oralsupplementation Eur J Obstet Gynecol Reprod Biol 199036(3)283ndash91
[37] Nelen WL Blom HJ Thomas CM Steegers EA Boers GH Eskes TKMethylenetetrahydrofolate reductase polymorphism affects the change in
UNCO
RREC
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
OF
homocysteine and folate concentrations resulting from low dose folic acidsupplementation in women with unexplained recurrent miscarriagesJ Nutr 1998128(8)1336ndash41
[38] Rodgers GM Kane WH Activation of endogenous Factor V by ahomocysteine-induced vascular endothelial cell activator J Clin Invest198677(6)1909ndash16
[39] Lentz SR Sadler JE Inhibition of thrombomodulin surface expression andprotein C activation by the thrombogenic agent homocysteine J ClinInvest 199188(6)1906ndash14
[40] Nishinaga M Ozawa T Shimada K Homocysteine a thrombogenic agentsuppresses anticoagulant heparan sulfate expression in cultured porcineaortic endothelial cells J Clin Invest 199392(3)1381ndash6
[41] Hajjar KA Mauri L Jacovina AT et al Tissue plasminogen activatorbinding to the annexin II tail domain Direct modulation by homocysteineJ Biol Chem 1998273(16)9987ndash93
[42] Fenech M Cytokinesis-block micronucleus cytome assay Nat Protoc20072(5)1084ndash104
TEDPR
O
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003

C
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126^
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
2 V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
UNCO
RRE
or by causing uracil misincorporation in DNA causingmutations chromosomal breaks and micronuclei formation[7] SAM is a universal methyl donor that donates methylmoieties to DNA proteins neurotransmitters etc SAH is afeedback inhibitor of SAM Thus SAMSAH ratio serves as anindicator of cellular methylation status Trkova et al
^have
reported increased micronuclei frequencies in couples withreproductive failures [8]
In view of ethnic and population-level variations in thedistribution of MTHFR C677T polymorphism [9] lowfrequency MTHFR C677T polymorphism in Indian population[10] high incidence of deficiencies of B6 B12 and folateamong Indians [1112] lack of strategies for pre-conceptionalfolate supplementation and fortification of food grains withfolate hyperhomocysteinemia might be an important contri-butor for RPL among Indians The rationale behind this studywas to address the role of maternal as well as paternalhyperhomocysteinemia MTHFR C677T polymorphism andDNA damage in RPL and to deduce the role of hyperhomo-cysteinemia in DNA damage
Materials and methods
Subjects
Recruitment of the subjects was carried out during the periodof 1999 to 2006 A total of 140 couples with history of three ormore unexplained recurrent pregnancy losses were enrolled ascases in the study None of the couples with RPL had any livebirth (nulliparous) Among these 140 couples 100 couples hadfirst trimester pregnancy loss (between 8 to 12 weeks ofgestation) where as 40 couples had first trimester (8 to12 weeks) as well as second trimester (13 to 20 weeks)pregnancy losses Cases were screened for previous history ofthromboembolism anti-phospholipid syndrome uterineabnormalities chromosomal anomalies diabetes mellitusradiation exposure known erythrocyte antibody anti-P syn-drome pregnancy losses due to documented fetal malformationand indication for anticoagulant treatment during pregnancyand those with these risk factors were excluded from the studyEach patient was completely evaluated for recognized causes ofRPL by a panel of tests hysteroscopy hysterosalpingographyserial ultrasonography TIFFA scan during the pregnancykaryotyping fasting and post-prandial blood glucose anti-phospholipid antibodies (anti cardiolipin antibodies and lupusanticoagulant) lutheal phase insufficiency (by repeated serumprogesterone measurements and endometrial biopsy) prolactindosage thyroid hormones toxoplasmosis cytomegalovirusrubella HIV Group B streptococci chlamydia trachomatosishepatitis B and
^C and bacterial vaginosis Apart from these tests
a questionnaire was designed to record history of thromboem-bolism radiation exposure and anticoagulant treatment duringpregnancy From the initial 151 couples screened for the abovementioned tests one had uterus bicarnate one had highprolactin six maternal subjects [22p+ 9qh+ One cell Xqdelt^(613) (p25q22) in each and Inv 9 in two] and three paternalsubjects [Inv 9 small Y and t
^(114)] had chromosomal
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPR
OOF
anomalies Hence these eleven couples were excluded from thisstudy At the time of enrollment none of the subjects werepregnant Paternal age ranged from 22 yr to
^42 yr and maternal
age ranged from 19 yr to 35 yrA total of 140 couples with normal reproductive history
(having 2 or more children and no history of miscarriages)who also meet the same exclusion criteria were enrolled ascontrols Paternal age ranged from 23 yr to 42 yr and maternalage ranged from 18 yr to 34 yr None of the subjects weretaking supplements of vitamins or folic acid at the time ofsample collection
All the cases were referred from different Gynecologists forchromosomal evaluation Control group consisted of laboratorycontrols and subjects who visited the out patient unit for minorcomplications Recruitment took place during the period of1999ndash
^2007 Informed consent was obtained from all the
subjects Bioethical committee of Center approved the studyfor DNA Fingerprinting and Diagnostics Hyderabad Indiawhich also serves as Institutional Review Board
Whole blood samples were collected in EDTA and Sodiumheparin vaccutainers after overnight fasting EDTA plasmasamples were separated immediately after centrifugation at700 times
^g for 10 min and stored at
^minus20 degC until the analysis Buffy
coat was used for DNA isolation using phenol-chloroformextraction method Heparin samples freshly drawn were usedfor cell cultures
Plasma homocysteine analysis
For the determination of total plasma homocysteine 100^mL
sample was treated with 10 mL^of 10 tri-n-butyl phosphine in
dimethyl formamide for 30 min at 4 degC The solution was mixedwith 05
^mL chilled 10
^trichloroacetic acid containing 1 mM
EDTA followed by centrifugation at^1000 times
^g for 5 min 02
^mL
aliquot of the clear supernatant was taken and vigorously mixedwith 04 mL
^of 25 M-borate buffer (pH 105) containing 4 mM
EDTA and 02 mL^of SBD-F in 25 M Borate buffer (pH 95)
The mixture was filtered through a 045 mmMillipore filter andan aliquot of 10 mL
^final reaction mixture was subjected to
HPLC analysisHichrom C18 250times46 mm column (Hichrom Ltd
Berkshire UK) was used as a stationary phase and 0^1 mol
L potassium dihydrogen phosphate buffer (pH 21) containing4
^acetonitrile was used as mobile phase at a flow rate of
20 mL^min in the isocratic separation Fluorescence inten-
sities were measured with ex385 nmem515 nm withFluorescence detector attached to HPLC system (Watersmodel 510 Milford MA USA) Homocysteine in plasmasamples was quantified by comparing the peaks with the peaksof the pure standard [13] The 95th percentile of homocysteinelevels in male and female controls were used as the thresholdto define hyperhomocysteinemia
MTHFR C677T polymorphism
PCR amplification using F-5primeTTT GAG GCT GAC CTGAAG CAC TTG AAG GAG-3prime and R-5primeGAG TGG TAG
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
Table 1 t11
Allelic and genotypic differences for MTHFR C677T polymorphism betweenRPL cases and controls t12
t13MTHFR 677 Cases () Controls () OR 95 CI p value
t14Maternal 140 140t15CC 111 (793) 112 (800) 1 referencet16CT 25 (179) 28 (200) 090 050ndash163 085t17TT 4 (29) 0 (00) Inf 103ndashinf 013t18C allele 247 (882) 252 (900) 1 referencet19T allele (Crude) 33 (118) 28 (100) 120 071ndash204 059t110(Adjusted) 105 061ndash182 010t111Paternal 140 140t112CC 111 (793) 126 (900) 1 referencet113CT 27 (193) 14 (100) 219 110ndash434 004t114TT 2 (14) 0 (00) Inf 058ndashinf 045t115C allele 249 (889) 266 (950) 1 referencet116T allele (Crude) 31 (111) 14 (50) 237 124ndash451 001t117(Adjusted) 230 117ndash453 002
Note reference-Wild genotype was used as a reference Inf-infinity Odds ratiosfor T allele frequencies in cases and controls were adjusted for maternal agepaternal age number of pregnancy losses and MTHFR genotype of each otherusing conditional logistic regression t118
3V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
UNCO
RREC
CCC TGG ATG GGA AAG ATC CCG-3prime primers (SigmaGenosys 80-51127272 St Louis MO USA) was carried outin a total volume of 25 mL
^containing 012 mM of each
primer 02 mM each dNTP (MBI Fermantas Glen BurnieMD USA) 25 μl of 10
^times PCR buffer [10 mM Tris HClL (pH
83) 15 mM MgCl2 50 mM KCl] and 1^25 U Taq
polymerase (Bangalore Genie MME5J Bangalore KarnatakaIndia) and 100 ng template DNA The reaction conditionswere as follows initial denaturation at 95 degC for 15 min and30 subsequent cycles at denaturation at 94 degC for 60 sannealing at 61 degC for 60 s and extension at 72 degC for 2 minPCR product (173-bp) was subjected to restriction digestionwith 1U of HinfI enzyme (New England Biolabs IpswichMA USA) MTHFR C677T mutation creates the Hinf Irestriction site resulting in the cleavage of 173-bp fragmentinto 125-bp and 48-bp [14]
Cytokinesis-blocked human lymphocytes micronuclei assay
Peripheral blood cultures were set-up according to standardcell culture protocols In brief 05 mL
^of whole blood was
introduced into sterile culture vial containing 5 mL^RPMI-1640
medium (GIBCO India) supplemented with 10^fetal calf
serum and 01^phytohaemagglutinin (GIBCO India) were
grown at 37 degC After the completion of 68 h^culturing
Cytochalasin B (made up in a stock solution of 2 mgmL^in
dimethyl-sulfoxide) was added to make the final concentrationof 3 mgmL
^ After 28 h
^of further culturing cells were
transferred to centrifuge tubes and centrifuged for 10 min at1000 rpm The supernatant was discarded and the pellet wasresuspended in 0075 M KCL for 18 min About 2ndash
^3^mL of
chilled 13 acetone methanol was added to the hypotonicsolution and mixed for gentle fixation The tubes werecentrifuged and the pellet was resuspended in fresh fixativeThe total period of fixation was not more than
^2 h
^ as this
fixation preserves the cytoplasm around the nucleus The cellsuspension was gently dropped on to chilled slides and air-dried The slides were stained with 5
^phosphate buffered
Giemsa and visualized in oil immersion at 100^times high-power
objective lens and scanned for micronuclei in binucleates Onlybinucleates cells showing the cytoplasm around the nuclei wereincluded in the scoring 1000 binucleates were scored for eachindividual and the proportion of binucleates with micronucleiwas recorded [15]
In vitro analysis to study the impact of homocysteine onDNA damage
Peripheral blood of a control with normal homocysteinelevel (40 μmolL) was made into 10 aliquots and made intotwo batches of five each Peripheral blood cultures were set-upaccording to protocols described earlier After 24 h
^incubation
to each aliquot of a batch homocysteine was addedexogenously to a final concentration of 0 10 20 50 and100 μmolL and after 44 h
^culturing Cytochalsin B was added
and cytokinesis blocked human lymphocytes micronucleiassay was performed as described in the previous section
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPR
OOF
Average micronuclei frequency for each concentration wastaken for statistical calculations
Statistical analysis
Continuous variables were assessed using Student t-test^and ANOVA and were presented as meanplusmnstandard devia-
tion Categorical variables were computed in 2times2 contin-gency table based on presence or absence of variable in casesand controls and were subjected to Fisher exact test Oddsratios 95 confidence intervals and p value
^s were computed
using the software Multiple logistic regression analysis wasdone to investigate the individual effects of each variable aftercontrolling for potential confounders such as maternal agepaternal age number of pregnancy losses and MTHFRgenotype of one another A lsquoPrsquo
^value of b005 was
considered statistically significant Spearmans rank correla-tion coefficient was used to assess the correlation betweenplasma homocysteine and micronuclei frequency All thestatistical tests were performed using the software providedby wwwstatpagesorg
Results
After controlling for known confounding variables maternalage showed no significant association (OR 091 95 CI081ndash
^102) where as paternal age showed statistically sig-
nificant association (OR 116 95 CI 104ndash^130
^p=001)
with RPLThe 95 percentiles of homocysteine levels in male and
female controls were 196 μmolL and 140 μmolL respec-tively which were used as threshold values to definehyperhomocysteinemia Mean maternal homocysteine levelsand mean paternal homocysteine levels were higher in casesthan controls with 448 (95 CI 230ndash
^870) and 692 (95 CI
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
C
OOF
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288
Fig 1 Plasma homocysteine scatter plot of RPL cases and controls according togender and MTHFR 677 genotype A RPL females with MTHFR 677 CCgenotype B RPL females with MTHFR 677 CT genotype C RPL females withMTHFR 677 TT genotype D RPL males with MTHFR 677 CC genotype ERPL males with MTHFR 677 CT genotype G Control females with MTHFR677 CC genotype H Control females with MTHFR 677 CT genotype IControl males with MTHFR 677 CC genotype J Control males with MTHFR677 CT genotype
t21
t22
t23
t24
t25
t26
t27
Fig 2 In vitro assay to study the impact of homocysteine gradient on DNAdamage X-axis Exogenous homocysteine concentration (in μmolL) Y-axisMicronuclei frequency (per thousand binucleated cells)
4 V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
NCOR
RE390ndash
^1229) fold increased risk for RPL (p
^b00001) There was
a correlation between maternal and paternal homocysteinelevels with a correlation coefficient of 019 The combinedelevated levels were observed in ten RPL couples and none ofthe control couples
The distribution of MTHFR C677T polymorphism wasfound to be in accordance with Hardy-Weinberg equilibriumin RPL mothers (p
^=023) control mothers (p
^=050) RPL
fathers (p^=100) and control fathers (p
^=077) Maternal and
paternal MTHFR 677 T-alleles were associated with 105(95 CI 061ndash
^182) and 230 (95 CI 117ndash
^453) fold-
increased risk for RPL after controlling for known confound-ing factors Statistical significance was observed only forpaternal T allele (p
^b005) (Table 1) Four RPL mothers and
two RPL fathers had MTHFR TT genotype and none of thecontrols had this genotype
MTHFR genotype was found to be one genetic determinantfor homocysteine however its impact was more prominent inmen than women Men with CT genotype showed homo-cysteine elevation greater than 95th percentile of controls(N196 μmolL) where as women with CT genotype althoughshowed significant increase in homocysteine compared to
U 289
290
291
292
293
294
295
296
297
298
299
300
Table 2Micronuclei frequency (Meanplusmnstandard deviation) distribution in cases andcontrols
Micronuclei frequency Cases Controls p value
Maternal 28plusmn25 23plusmn16 b005Paternal 43plusmn30 34plusmn25 0007
Spearmans correlation coefficient with plasma homocysteine (r)=046pb00001Spearmans correlation coefficient with MTHFR C677T polymorphism (r)=011pb001
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPRwomen with CC genotype the increase was lesser than 95th
percentile of controls (b140 μmolL) (Fig 1)Maternal as well as paternal RPL subjects showed higher
micronuclei frequency compared to respective controlsindicating significant DNA damage in RPL group Miconucleifrequency was positively correlated with plasma homocys-teine (r
^=046) and MTHFR C677T polymorphism (r
^=011)
(Table 2) In vitro assay showed dose dependent increase inthe micronuclei frequency with increasing homocysteineconcentration (Fig 2)
Discussion
Hyperhomocysteinemia and homozygosity for MTHFRC677T polymorphism were reported to be maternal risk factorsfor RPL Little is known about the role of paternal risk factors inRPL The current study was undertaken to examine theassociation between both maternal and paternal hyperhomo-cysteinemia and RPL No association was observed betweenmaternal age and RPL which could be due to age-matchedcontrols An association was observed between paternal age andRPL after controlling for the effect of maternal age The meanhomocysteine levels in RPL mothers and RPL fathers werehigher than control mothers and control fathers Maternal andpaternal hyperhomocysteinemia were found to increase the riskfor RPL by 448 fold (230 870) and 692 fold (390 1229)respectively Hyperhomocysteinemia in both the parents wasobserved in ten RPL couples where as none of the controlcouples had this combination These results indicate thatparental hyperhomocysteinemia may be an independent riskfactor for RPL
Paternal MTHFR 677 T-allele was associated with 237 foldrisk where as maternal T-allele did not show any statisticallysignificant risk for RPL Among the individual genotypesMTHFRTT-genotype was present only in cases not in controlsDespite the small numbers the results indicate an associationwith MTHFR 677TT and RPL
MTHFR genotype was found to influence the plasmahomocysteine levels in both the genders and hence a majorgenetic determinant of hyperhomocysteinemia Comparing the
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
5V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
UNCO
RREC
genotype and gender matched cases with controls showedevidence to suggest that cases have higher homocysteine thancontrols and hence apart from MTHFR genotype somegenetic or non-genetic determinant also plays a role inincreasing the homocysteine and might play an importantrole in the etiology of RPL However men with CT genotypeshowed homocysteine elevation greater than the 95thpercentile of controls where as women with CT genotypeshowed homocysteine levels lesser than the 95th percentile ofcontrols These gender differences in homocysteine mightexplain the risk associated with paternal T-allele The mostprofound associations between hyperhomocysteinemia andRPL were found in fathers who were heterozygous for the677T allele This is extremely common in Caucasians (40)and is not considered to be a risk factor for hyperhomocys-teinemia (in contrast to homozygotes) This discrepancy couldbe due to differences in the diet and also the possibility of anyother allele from a different loci co-segregating with MTHFR677T allele cannot be ruled out The gender differences inplasma homocysteine levels could be due to protective role ofestrogens (in females) [1617] stoichiometric synthesis ofhomocysteine with creatinecreatinine ratio proportional tomuscle mass [18] differences in the rates of remethylation andtranmethylation among males and females [19]
^Significant DNA damage was observed in RPL couplescompared to control couples which was found to havepositive association with homocysteine To strengthen thisassociation further in vitro assay was performed on peripheralblood cultures with exogenous addition of homocysteine invarying concentrations which showed dose-dependentincrease in the frequency of micronuclei This is a strongevidence to suggest that hyperhomocysteinemia induces DNAdamage DNA damage can be caused by many factors apartfrom hyperhomocysteinemia and hence there is a need toconduct another study focusing on the causes of DNA damagein RPL subjects
Our study is in agreement with Remy Slama et al^in showing
increased risk of RPL with increase in paternal age with asuggestion that the association is stronger for first trimesterpregnancy loss [20] This increased risk may be a consequenceof an increasing frequency of chromosomal anomalies in thespermatozoa with male age [2122] or due to increased DNAdamage [23] or due to increased chromosomal replications ofmale stem cells [24] Apart from our study several researchershave shown positive association of maternal hyperhomocystei-nemia and maternal MTHFR 677 TT genotype with RPL Highprevalence of hyperhomocysteinemia was observed in parouswomen (33) compared to nulliparous women (14) byWouters MG et al Five consecutive fetal deaths were reportedin a woman with MTHFR 677TT genotype and elevatedhomocysteine and high prevalence of hyperhomocysteinemia(12) folate deficiency (15) and C677T MTHFR CT and TTgenotypes (20) were reported in 100 consecutive women withRPL by Quere et al
^[25] Hyperhomocysteinemia and folate
deficiency were found to be associated with 36 and 21 fold riskfor RPL by Nelen et al [26] Smaller median chorionic vasculararea and perimeter were observed in women with hyperhomo-
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPR
OOF
cysteinemia by Nelen et al^suggesting that hyperhomocystei-
nemia is associated with defective chorionic vasculature [27]Meta-analysis of case-control studies conducted during theperiod of 1992ndash
^1999 showed that hyperhomocysteinemia and
MTHFRTT-genotype were associated with 27 fold and 14 foldrisk for RPL respectively [28] Another meta-analysis based onTwenty-six studies with 2120 RPL cases and 2949 controlsshowed that MTHFR TT-genotype was associated with nostatistically significant risk with an odds ratio of 121 (95 CI104 140) [29] Zetterberg et al
^have observed increased
frequency of combined MTHFR C677T and A1298C mutatedalleles in spontaneously aborted fetuses (OR 142 95 CI178ndash
^113) indicating that the MTHFR polymorphisms may
have a major impact on fetal survival [30] A pilot studyconducted on 24 South Indian women by Kumar et al
^has
shown high prevalence of hyperhomocysteinemia and red cellfolate deficiency in RPL [31] Candito et al
^reported four
consecutive pregnancy losses in a woman with hyperhomocys-teinemia (259 μmolL) B12 deficiency (b150 pgmL
^) and the
MTHFR 677 TT-genotype who got benefited with vitamin B12supplementation [32] DUva M et al
^have reported Hyperho-
mocysteinemia and MTHFR TT-genotype as risk factors forunexplained female sterility and recurrent pregnancy loss [33]
Apart from the study by Trkova et al^that showed increased
micronuclei frequency in couples with RPL several studieshave also explored the relationship between sperm quality andunexplained RPL Increased percentage of sperm stainingpositive for DNA fragmentation was observed in the RPL groupcompared to donor or general population by Carrell et al
^[34]
In a separate study they also showed that the mean aneuploidyrate in RPL group was significantly higher than the generalpopulation (277plusmn022 vs 148plusmn012 Pzb0005) [35] Bene-ficial effects of folate supplementation were observed bySteegers-Theunissen et al
^[36] and Nelen et al
^[37] who
reported increase in maternal plasmaamniotic fluid folate andlowering of fasting plasma homocysteine levels in theirrespective studies
The risk associated with maternal hyperhomocysteinemiacould be due to embryo toxicity or due to ability of highhomocysteine to activate factor V [38] and to inactivate proteinC thrombomodulin [39] heparan sulphate [40] tissueplasminogen activator binding to human endothelial cells [41]or due to impaired cellular methylation that alters geneexpression or due to uracil misincorporation in DNA resultingin DNA damage The risk associated with paternal hyperho-mocysteinemia could be due to its effect on sperm quality byincreasing DNA damage
The strength of the current study is the assessment of notonly maternal but also paternal hyperhomocysteinemia inrelation to RPL In order to strengthen our hypothesis furtherwe have initiated a pilot study to assess DNA damage in thesemen samples of subjects with recurrent pregnancy loss andobserved significant DNA damage in sperms of RPL fathersusing Fluorescence activated cell sorter technique A modifiedcytokinesis block micronucleus cytome assay for morecomprehensive measurement of DNA damage developedby Fenech et al that measures micronuclei frequency
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
C
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539
6 V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
UNCO
RRE
along with other DNA damage biomarkers such as nuclearbuds nucleoplasmic bridges as well as cytotoxic markersincluding apoptosis and necrosis can be incorporated infuture studies [42]
Our study projects paternal age as an independent riskfactor for RPL Impact of maternal age was controlled in thestudy design (using age-matched controls) as well as in theregression model This study projects that not only maternalhyperhomocysteinemia but also paternal hyperhomocysteine-mia is a risk factor for RPL at least among South IndiansSignificant DNA damage was observed in both maternal andpaternal RPL subjects Our study is in agreement with the twometa-analyses in showing that maternal MTHFR genotypemay not be a significant risk factor for RPL The impact ofpaternal MTHFR genotype on RPL could be due to elevatedhomocysteine levels that in turn result in DNA damage Thisstudy further shows a direct association between homocysteineelevation and DNA damage using in vivo and in vitro assaysHowever the mechanism by which homocysteine causes DNAdamage needs to be elucidated further There is a need forlarge case-control studies to explore the role of other geneticand nutritional factors that are likely to influence homo-cysteine levels in the pathophysiology of RPL
Acknowledgments
We thank Mr Ram Prakash Singh Mr R Sudheer KumarMr G Srinivas and Mr V Murali Mohan for the technicalassistance We thank all the families participated in this studyWe thank Department of Biotechnology Government of Indiafor its financial support
References
[1] Strobino B Fox HE Kline J Stein Z Susser M Warburton DCharacteristics of women with recurrent spontaneous abortions andwomen with favourable reproductive histories Am J Public Health198276(8)986ndash91
[2] Wouters MG Boers GH Blom HJ et al Hyperhomocysteinemia a riskfactor in women with unexplained recurrent early pregnancy loss FertilSteril 199360(5)820ndash5
[3] Greene ND Dunlevy LE Copp AJ Homocysteine is embryotoxic butdoes not cause neural tube defects in mouse embryos Anat Embryol2003206(3)185ndash91 (Berl)
[4] Durand P Lussier-Cacan S Blache D Acute methionine load-inducedhyperhomocysteinemia enhances platelet aggregation thromboxanebiosynthesis and macrophage-derived tissue factor activity in ratsFASEB J 199711(13)1157ndash68
[5] Nishinaga M Ozawa T Shimada K Homocysteine a thrombogenic agentsuppresses anticoagulant heparan sulfate expression in cultured porcineaortic endothelial cells J Clin Invest 199392(3)1381ndash6
[6] Isa Y Mishima T Tsuge H Hayakawa T Increase in S-adenosylhomo-cysteine content and its effect on the S-adenosylhomocysteine hydrolaseactivity under transient high plasma homocysteine levels in rats J Nutr SciVitaminol 200652(6)479ndash82 (Tokyo)
[7] Fenech MF Dreosti IE Rinaldi JR Folate vitamin B12 homocysteinestatus and chromosome damage rate in lymphocytes of older menCarcinogenesis 199718(7)1329ndash36
[8] Trkova M Kapras J Bobkova K Stankova J Mejsnarova B Increasedmicronuclei frequencies in couples with reproductive failure ReprodToxicol 200014(4)331ndash5
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPR
OOF
[9] Schneider JA Rees DC Liu YT et al A worldwide distribution of acommon MTHFR Mutation Am J Hum Genet 199862(5)1258ndash60
[10] Radha Rama Devi A Govindaiah V Ramakrishna G Naushad SMPrevalence of
^methylene tetrahydrofolate reductase polymorphism in
South Indian population Curr Sci 200486(3)440ndash3[11] Neela J Raman L The relationship between maternal nutritional status and
spontaneous abortion Natl Med J India 199710(1)15ndash6[12] Refsum H Yajnik CS Gadkari M et al Hyperhomocysteinemia and
elevated methylmalonic acid indicate a high prevalence of cobalamindeficiency in Asian Indians Am J Clin Nutr 200174(2)233ndash41
[13] Ubbink JB Hayward Vermaak WJ Bissbort S Rapid high-performanceliquid chromatographic assay for total homocysteine levels in humanserum J Chromatogr 1991565(1ndash
^2)441ndash6
[14] Frosst P Blom HJ Milos R et al A candidate genetic risk factor forvascular disease a common mutation in methylenetetrahydrofolatereductase Nat Genet 199510(1)111ndash3
[15] Nath CJ Ong T Micronuclei assay in cytokinesis-blocked binucleated andconventional mononucleated methods in human peripheral lymphocytesTeratog Carcinog Mutagen 199010(3)273ndash9
[16] Giri S Thompson PD Taxel P et al Oral estrogen improves serum lipidshomocysteine and fibrinolysis in elderly men Atherosclerosis 1998137359ndash66
[17] Kim MH Kim E Passon EL et al Cortisol and estradiol^non-genetic
factors for hyperhomocyst(e)inemia Metabolism 199746247ndash9[18] Brattstrom L Lindgren A Israelsson B Andersson A Hultberg B
Homocysteine and cysteine Determinants of plasma levels in middle-agedand elderly subjects J Inter-Am Med 1994236(6)633ndash41
[19] Fukagawa NK Martin JM Wurthmann A Prue AH Ebenstein DORourke B Sex-related differences in methionine metabolism and plasmahomocysteine concentrations Am J Clin Nutr 200072(1)22ndash9
[20] Slama R Bouyer J Windham G Fenster L Werwatz A Swan SHInfluence of paternal age on the risk of spontaneous abortion Am JEpidemiol 2005161816ndash23
[21] Bosch M Rajmil O Martinez-Pasarell O et al Linear increase of diploidyin human sperm with age a four-colour FISH study Eur J Hum Genet20019533ndash8
[22] Griffin DK Abruzzo MA Millie EA et al Non-disjunction in humansperm evidence for an effect of increasing paternal age Hum Mol Genet199542227ndash32
[23] Singh NP Muller CH Berger RE Effects of age on DNA double-strandbreaks and apoptosis in human sperm Fertil Steril 2003801420ndash30
[24] Crow J The origins patterns and implications of human spontaneousabortion Nat Rev Genet 2000140ndash7
[25] Quere I Bellet H Hoffet M Janbon C Mares P Gris JC A woman withfive consecutive fetal deaths case report and retrospective analysis ofhyperhomocysteinemia prevalence in 100 consecutive women withrecurrent miscarriages Fertil Steril 199869(1)152ndash4
[26] Nelen WL Blom HJ Steegers EA den Heijer M Thomas CM Eskes TKHomocysteine and folate levels as risk factors for recurrent earlypregnancy loss Obstet Gynecol 200095(4)519ndash24
[27] Nelen WL Bulten J Steegers EA Blom HJ Hanselaar AG Eskes TKMaternal homocysteine and chorionic vascularization in recurrent earlypregnancy loss Hum Reprod 200015(4)954ndash60
[28] Nelen WL Blom HJ Steegers EA den Heijer M Eskes TKHyperhomocysteinemia and recurrent early pregnancy loss a meta-analysis Fertil Steril 200074(6)1196ndash9
[29] Ren A Wang J Methylenetetrahydrofolate reductase C677T polymorph-ism and the risk of unexplained recurrent pregnancy loss a meta-analysisFertil Steril 200686(6)1716ndash22
[30] Zetterberg H Regland B Palmeacuter M et al Increased frequency ofcombined methylenetetrahydrofolate reductase C677T and A1298Cmutated alleles in spontaneously aborted embryos Eur J Hum Genet200210(2)113ndash8
[31] Kumar KS Govindaiah V Naushad SE Devi RR Jyothy A Plasmahomocysteine levels correlated to interactions between folate status andmethylene tetrahydrofolate reductase gene mutation in women withunexplained recurrent pregnancy loss J Obstet Gynaecol 200323(1)55ndash8
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
540
541
542
543
544
545
546
547
548
549
550
551
552
553
554
555
556
557
558
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573
574
7V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
[32] Candito M Magnaldo S Bayle J et al Clinical B12 deficiency in one caseof recurrent spontaneous pregnancy loss Clin Chem Lab Med 200341(8)1026ndash7
[33] DUva M Di Micco P Strina I et al Hyperhomocysteinemia in womenwith unexplained sterility or recurrent early pregnancy loss from SouthernItaly a preliminary report Thromb J 2007115ndash10
[34] Carrell DT Liu L Peterson CM et al Sperm DNA fragmentation isincreased in couples with unexplained recurrent pregnancy loss ArchAndrol 200349(1)49ndash55
[35] Carrell DT Wilcox AL Lowy L et al Elevated sperm chromosomeaneuploidy and apoptosis in patients with unexplained recurrent pregnancyloss Obstet Gynecol 2003101(6)1229ndash35
[36] Steegers-Theunissen RP Steegers EA de Boer R Thomas CM Klooster-man MD Eskes TK Elevated folate levels in amniotic fluid after oralsupplementation Eur J Obstet Gynecol Reprod Biol 199036(3)283ndash91
[37] Nelen WL Blom HJ Thomas CM Steegers EA Boers GH Eskes TKMethylenetetrahydrofolate reductase polymorphism affects the change in
UNCO
RREC
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
OF
homocysteine and folate concentrations resulting from low dose folic acidsupplementation in women with unexplained recurrent miscarriagesJ Nutr 1998128(8)1336ndash41
[38] Rodgers GM Kane WH Activation of endogenous Factor V by ahomocysteine-induced vascular endothelial cell activator J Clin Invest198677(6)1909ndash16
[39] Lentz SR Sadler JE Inhibition of thrombomodulin surface expression andprotein C activation by the thrombogenic agent homocysteine J ClinInvest 199188(6)1906ndash14
[40] Nishinaga M Ozawa T Shimada K Homocysteine a thrombogenic agentsuppresses anticoagulant heparan sulfate expression in cultured porcineaortic endothelial cells J Clin Invest 199392(3)1381ndash6
[41] Hajjar KA Mauri L Jacovina AT et al Tissue plasminogen activatorbinding to the annexin II tail domain Direct modulation by homocysteineJ Biol Chem 1998273(16)9987ndash93
[42] Fenech M Cytokinesis-block micronucleus cytome assay Nat Protoc20072(5)1084ndash104
TEDPR
O
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
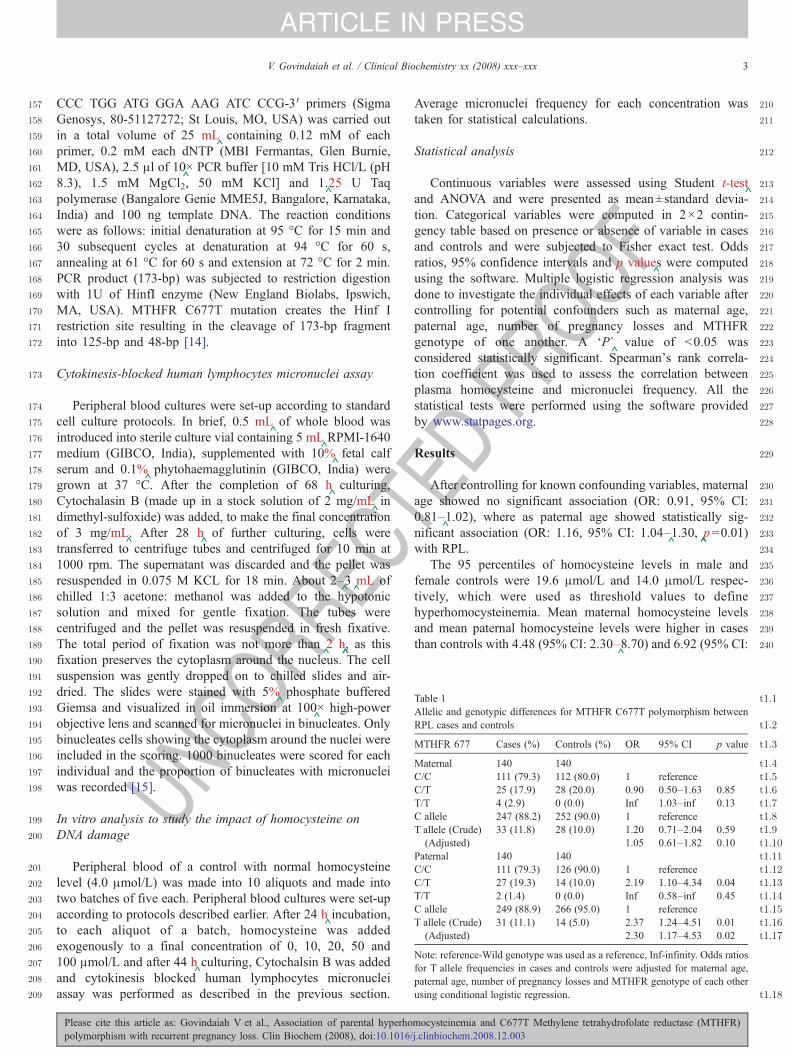
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
Table 1 t11
Allelic and genotypic differences for MTHFR C677T polymorphism betweenRPL cases and controls t12
t13MTHFR 677 Cases () Controls () OR 95 CI p value
t14Maternal 140 140t15CC 111 (793) 112 (800) 1 referencet16CT 25 (179) 28 (200) 090 050ndash163 085t17TT 4 (29) 0 (00) Inf 103ndashinf 013t18C allele 247 (882) 252 (900) 1 referencet19T allele (Crude) 33 (118) 28 (100) 120 071ndash204 059t110(Adjusted) 105 061ndash182 010t111Paternal 140 140t112CC 111 (793) 126 (900) 1 referencet113CT 27 (193) 14 (100) 219 110ndash434 004t114TT 2 (14) 0 (00) Inf 058ndashinf 045t115C allele 249 (889) 266 (950) 1 referencet116T allele (Crude) 31 (111) 14 (50) 237 124ndash451 001t117(Adjusted) 230 117ndash453 002
Note reference-Wild genotype was used as a reference Inf-infinity Odds ratiosfor T allele frequencies in cases and controls were adjusted for maternal agepaternal age number of pregnancy losses and MTHFR genotype of each otherusing conditional logistic regression t118
3V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
UNCO
RREC
CCC TGG ATG GGA AAG ATC CCG-3prime primers (SigmaGenosys 80-51127272 St Louis MO USA) was carried outin a total volume of 25 mL
^containing 012 mM of each
primer 02 mM each dNTP (MBI Fermantas Glen BurnieMD USA) 25 μl of 10
^times PCR buffer [10 mM Tris HClL (pH
83) 15 mM MgCl2 50 mM KCl] and 1^25 U Taq
polymerase (Bangalore Genie MME5J Bangalore KarnatakaIndia) and 100 ng template DNA The reaction conditionswere as follows initial denaturation at 95 degC for 15 min and30 subsequent cycles at denaturation at 94 degC for 60 sannealing at 61 degC for 60 s and extension at 72 degC for 2 minPCR product (173-bp) was subjected to restriction digestionwith 1U of HinfI enzyme (New England Biolabs IpswichMA USA) MTHFR C677T mutation creates the Hinf Irestriction site resulting in the cleavage of 173-bp fragmentinto 125-bp and 48-bp [14]
Cytokinesis-blocked human lymphocytes micronuclei assay
Peripheral blood cultures were set-up according to standardcell culture protocols In brief 05 mL
^of whole blood was
introduced into sterile culture vial containing 5 mL^RPMI-1640
medium (GIBCO India) supplemented with 10^fetal calf
serum and 01^phytohaemagglutinin (GIBCO India) were
grown at 37 degC After the completion of 68 h^culturing
Cytochalasin B (made up in a stock solution of 2 mgmL^in
dimethyl-sulfoxide) was added to make the final concentrationof 3 mgmL
^ After 28 h
^of further culturing cells were
transferred to centrifuge tubes and centrifuged for 10 min at1000 rpm The supernatant was discarded and the pellet wasresuspended in 0075 M KCL for 18 min About 2ndash
^3^mL of
chilled 13 acetone methanol was added to the hypotonicsolution and mixed for gentle fixation The tubes werecentrifuged and the pellet was resuspended in fresh fixativeThe total period of fixation was not more than
^2 h
^ as this
fixation preserves the cytoplasm around the nucleus The cellsuspension was gently dropped on to chilled slides and air-dried The slides were stained with 5
^phosphate buffered
Giemsa and visualized in oil immersion at 100^times high-power
objective lens and scanned for micronuclei in binucleates Onlybinucleates cells showing the cytoplasm around the nuclei wereincluded in the scoring 1000 binucleates were scored for eachindividual and the proportion of binucleates with micronucleiwas recorded [15]
In vitro analysis to study the impact of homocysteine onDNA damage
Peripheral blood of a control with normal homocysteinelevel (40 μmolL) was made into 10 aliquots and made intotwo batches of five each Peripheral blood cultures were set-upaccording to protocols described earlier After 24 h
^incubation
to each aliquot of a batch homocysteine was addedexogenously to a final concentration of 0 10 20 50 and100 μmolL and after 44 h
^culturing Cytochalsin B was added
and cytokinesis blocked human lymphocytes micronucleiassay was performed as described in the previous section
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPR
OOF
Average micronuclei frequency for each concentration wastaken for statistical calculations
Statistical analysis
Continuous variables were assessed using Student t-test^and ANOVA and were presented as meanplusmnstandard devia-
tion Categorical variables were computed in 2times2 contin-gency table based on presence or absence of variable in casesand controls and were subjected to Fisher exact test Oddsratios 95 confidence intervals and p value
^s were computed
using the software Multiple logistic regression analysis wasdone to investigate the individual effects of each variable aftercontrolling for potential confounders such as maternal agepaternal age number of pregnancy losses and MTHFRgenotype of one another A lsquoPrsquo
^value of b005 was
considered statistically significant Spearmans rank correla-tion coefficient was used to assess the correlation betweenplasma homocysteine and micronuclei frequency All thestatistical tests were performed using the software providedby wwwstatpagesorg
Results
After controlling for known confounding variables maternalage showed no significant association (OR 091 95 CI081ndash
^102) where as paternal age showed statistically sig-
nificant association (OR 116 95 CI 104ndash^130
^p=001)
with RPLThe 95 percentiles of homocysteine levels in male and
female controls were 196 μmolL and 140 μmolL respec-tively which were used as threshold values to definehyperhomocysteinemia Mean maternal homocysteine levelsand mean paternal homocysteine levels were higher in casesthan controls with 448 (95 CI 230ndash
^870) and 692 (95 CI
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
C
OOF
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288
Fig 1 Plasma homocysteine scatter plot of RPL cases and controls according togender and MTHFR 677 genotype A RPL females with MTHFR 677 CCgenotype B RPL females with MTHFR 677 CT genotype C RPL females withMTHFR 677 TT genotype D RPL males with MTHFR 677 CC genotype ERPL males with MTHFR 677 CT genotype G Control females with MTHFR677 CC genotype H Control females with MTHFR 677 CT genotype IControl males with MTHFR 677 CC genotype J Control males with MTHFR677 CT genotype
t21
t22
t23
t24
t25
t26
t27
Fig 2 In vitro assay to study the impact of homocysteine gradient on DNAdamage X-axis Exogenous homocysteine concentration (in μmolL) Y-axisMicronuclei frequency (per thousand binucleated cells)
4 V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
NCOR
RE390ndash
^1229) fold increased risk for RPL (p
^b00001) There was
a correlation between maternal and paternal homocysteinelevels with a correlation coefficient of 019 The combinedelevated levels were observed in ten RPL couples and none ofthe control couples
The distribution of MTHFR C677T polymorphism wasfound to be in accordance with Hardy-Weinberg equilibriumin RPL mothers (p
^=023) control mothers (p
^=050) RPL
fathers (p^=100) and control fathers (p
^=077) Maternal and
paternal MTHFR 677 T-alleles were associated with 105(95 CI 061ndash
^182) and 230 (95 CI 117ndash
^453) fold-
increased risk for RPL after controlling for known confound-ing factors Statistical significance was observed only forpaternal T allele (p
^b005) (Table 1) Four RPL mothers and
two RPL fathers had MTHFR TT genotype and none of thecontrols had this genotype
MTHFR genotype was found to be one genetic determinantfor homocysteine however its impact was more prominent inmen than women Men with CT genotype showed homo-cysteine elevation greater than 95th percentile of controls(N196 μmolL) where as women with CT genotype althoughshowed significant increase in homocysteine compared to
U 289
290
291
292
293
294
295
296
297
298
299
300
Table 2Micronuclei frequency (Meanplusmnstandard deviation) distribution in cases andcontrols
Micronuclei frequency Cases Controls p value
Maternal 28plusmn25 23plusmn16 b005Paternal 43plusmn30 34plusmn25 0007
Spearmans correlation coefficient with plasma homocysteine (r)=046pb00001Spearmans correlation coefficient with MTHFR C677T polymorphism (r)=011pb001
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPRwomen with CC genotype the increase was lesser than 95th
percentile of controls (b140 μmolL) (Fig 1)Maternal as well as paternal RPL subjects showed higher
micronuclei frequency compared to respective controlsindicating significant DNA damage in RPL group Miconucleifrequency was positively correlated with plasma homocys-teine (r
^=046) and MTHFR C677T polymorphism (r
^=011)
(Table 2) In vitro assay showed dose dependent increase inthe micronuclei frequency with increasing homocysteineconcentration (Fig 2)
Discussion
Hyperhomocysteinemia and homozygosity for MTHFRC677T polymorphism were reported to be maternal risk factorsfor RPL Little is known about the role of paternal risk factors inRPL The current study was undertaken to examine theassociation between both maternal and paternal hyperhomo-cysteinemia and RPL No association was observed betweenmaternal age and RPL which could be due to age-matchedcontrols An association was observed between paternal age andRPL after controlling for the effect of maternal age The meanhomocysteine levels in RPL mothers and RPL fathers werehigher than control mothers and control fathers Maternal andpaternal hyperhomocysteinemia were found to increase the riskfor RPL by 448 fold (230 870) and 692 fold (390 1229)respectively Hyperhomocysteinemia in both the parents wasobserved in ten RPL couples where as none of the controlcouples had this combination These results indicate thatparental hyperhomocysteinemia may be an independent riskfactor for RPL
Paternal MTHFR 677 T-allele was associated with 237 foldrisk where as maternal T-allele did not show any statisticallysignificant risk for RPL Among the individual genotypesMTHFRTT-genotype was present only in cases not in controlsDespite the small numbers the results indicate an associationwith MTHFR 677TT and RPL
MTHFR genotype was found to influence the plasmahomocysteine levels in both the genders and hence a majorgenetic determinant of hyperhomocysteinemia Comparing the
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
5V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
UNCO
RREC
genotype and gender matched cases with controls showedevidence to suggest that cases have higher homocysteine thancontrols and hence apart from MTHFR genotype somegenetic or non-genetic determinant also plays a role inincreasing the homocysteine and might play an importantrole in the etiology of RPL However men with CT genotypeshowed homocysteine elevation greater than the 95thpercentile of controls where as women with CT genotypeshowed homocysteine levels lesser than the 95th percentile ofcontrols These gender differences in homocysteine mightexplain the risk associated with paternal T-allele The mostprofound associations between hyperhomocysteinemia andRPL were found in fathers who were heterozygous for the677T allele This is extremely common in Caucasians (40)and is not considered to be a risk factor for hyperhomocys-teinemia (in contrast to homozygotes) This discrepancy couldbe due to differences in the diet and also the possibility of anyother allele from a different loci co-segregating with MTHFR677T allele cannot be ruled out The gender differences inplasma homocysteine levels could be due to protective role ofestrogens (in females) [1617] stoichiometric synthesis ofhomocysteine with creatinecreatinine ratio proportional tomuscle mass [18] differences in the rates of remethylation andtranmethylation among males and females [19]
^Significant DNA damage was observed in RPL couplescompared to control couples which was found to havepositive association with homocysteine To strengthen thisassociation further in vitro assay was performed on peripheralblood cultures with exogenous addition of homocysteine invarying concentrations which showed dose-dependentincrease in the frequency of micronuclei This is a strongevidence to suggest that hyperhomocysteinemia induces DNAdamage DNA damage can be caused by many factors apartfrom hyperhomocysteinemia and hence there is a need toconduct another study focusing on the causes of DNA damagein RPL subjects
Our study is in agreement with Remy Slama et al^in showing
increased risk of RPL with increase in paternal age with asuggestion that the association is stronger for first trimesterpregnancy loss [20] This increased risk may be a consequenceof an increasing frequency of chromosomal anomalies in thespermatozoa with male age [2122] or due to increased DNAdamage [23] or due to increased chromosomal replications ofmale stem cells [24] Apart from our study several researchershave shown positive association of maternal hyperhomocystei-nemia and maternal MTHFR 677 TT genotype with RPL Highprevalence of hyperhomocysteinemia was observed in parouswomen (33) compared to nulliparous women (14) byWouters MG et al Five consecutive fetal deaths were reportedin a woman with MTHFR 677TT genotype and elevatedhomocysteine and high prevalence of hyperhomocysteinemia(12) folate deficiency (15) and C677T MTHFR CT and TTgenotypes (20) were reported in 100 consecutive women withRPL by Quere et al
^[25] Hyperhomocysteinemia and folate
deficiency were found to be associated with 36 and 21 fold riskfor RPL by Nelen et al [26] Smaller median chorionic vasculararea and perimeter were observed in women with hyperhomo-
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPR
OOF
cysteinemia by Nelen et al^suggesting that hyperhomocystei-
nemia is associated with defective chorionic vasculature [27]Meta-analysis of case-control studies conducted during theperiod of 1992ndash
^1999 showed that hyperhomocysteinemia and
MTHFRTT-genotype were associated with 27 fold and 14 foldrisk for RPL respectively [28] Another meta-analysis based onTwenty-six studies with 2120 RPL cases and 2949 controlsshowed that MTHFR TT-genotype was associated with nostatistically significant risk with an odds ratio of 121 (95 CI104 140) [29] Zetterberg et al
^have observed increased
frequency of combined MTHFR C677T and A1298C mutatedalleles in spontaneously aborted fetuses (OR 142 95 CI178ndash
^113) indicating that the MTHFR polymorphisms may
have a major impact on fetal survival [30] A pilot studyconducted on 24 South Indian women by Kumar et al
^has
shown high prevalence of hyperhomocysteinemia and red cellfolate deficiency in RPL [31] Candito et al
^reported four
consecutive pregnancy losses in a woman with hyperhomocys-teinemia (259 μmolL) B12 deficiency (b150 pgmL
^) and the
MTHFR 677 TT-genotype who got benefited with vitamin B12supplementation [32] DUva M et al
^have reported Hyperho-
mocysteinemia and MTHFR TT-genotype as risk factors forunexplained female sterility and recurrent pregnancy loss [33]
Apart from the study by Trkova et al^that showed increased
micronuclei frequency in couples with RPL several studieshave also explored the relationship between sperm quality andunexplained RPL Increased percentage of sperm stainingpositive for DNA fragmentation was observed in the RPL groupcompared to donor or general population by Carrell et al
^[34]
In a separate study they also showed that the mean aneuploidyrate in RPL group was significantly higher than the generalpopulation (277plusmn022 vs 148plusmn012 Pzb0005) [35] Bene-ficial effects of folate supplementation were observed bySteegers-Theunissen et al
^[36] and Nelen et al
^[37] who
reported increase in maternal plasmaamniotic fluid folate andlowering of fasting plasma homocysteine levels in theirrespective studies
The risk associated with maternal hyperhomocysteinemiacould be due to embryo toxicity or due to ability of highhomocysteine to activate factor V [38] and to inactivate proteinC thrombomodulin [39] heparan sulphate [40] tissueplasminogen activator binding to human endothelial cells [41]or due to impaired cellular methylation that alters geneexpression or due to uracil misincorporation in DNA resultingin DNA damage The risk associated with paternal hyperho-mocysteinemia could be due to its effect on sperm quality byincreasing DNA damage
The strength of the current study is the assessment of notonly maternal but also paternal hyperhomocysteinemia inrelation to RPL In order to strengthen our hypothesis furtherwe have initiated a pilot study to assess DNA damage in thesemen samples of subjects with recurrent pregnancy loss andobserved significant DNA damage in sperms of RPL fathersusing Fluorescence activated cell sorter technique A modifiedcytokinesis block micronucleus cytome assay for morecomprehensive measurement of DNA damage developedby Fenech et al that measures micronuclei frequency
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
C
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539
6 V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
UNCO
RRE
along with other DNA damage biomarkers such as nuclearbuds nucleoplasmic bridges as well as cytotoxic markersincluding apoptosis and necrosis can be incorporated infuture studies [42]
Our study projects paternal age as an independent riskfactor for RPL Impact of maternal age was controlled in thestudy design (using age-matched controls) as well as in theregression model This study projects that not only maternalhyperhomocysteinemia but also paternal hyperhomocysteine-mia is a risk factor for RPL at least among South IndiansSignificant DNA damage was observed in both maternal andpaternal RPL subjects Our study is in agreement with the twometa-analyses in showing that maternal MTHFR genotypemay not be a significant risk factor for RPL The impact ofpaternal MTHFR genotype on RPL could be due to elevatedhomocysteine levels that in turn result in DNA damage Thisstudy further shows a direct association between homocysteineelevation and DNA damage using in vivo and in vitro assaysHowever the mechanism by which homocysteine causes DNAdamage needs to be elucidated further There is a need forlarge case-control studies to explore the role of other geneticand nutritional factors that are likely to influence homo-cysteine levels in the pathophysiology of RPL
Acknowledgments
We thank Mr Ram Prakash Singh Mr R Sudheer KumarMr G Srinivas and Mr V Murali Mohan for the technicalassistance We thank all the families participated in this studyWe thank Department of Biotechnology Government of Indiafor its financial support
References
[1] Strobino B Fox HE Kline J Stein Z Susser M Warburton DCharacteristics of women with recurrent spontaneous abortions andwomen with favourable reproductive histories Am J Public Health198276(8)986ndash91
[2] Wouters MG Boers GH Blom HJ et al Hyperhomocysteinemia a riskfactor in women with unexplained recurrent early pregnancy loss FertilSteril 199360(5)820ndash5
[3] Greene ND Dunlevy LE Copp AJ Homocysteine is embryotoxic butdoes not cause neural tube defects in mouse embryos Anat Embryol2003206(3)185ndash91 (Berl)
[4] Durand P Lussier-Cacan S Blache D Acute methionine load-inducedhyperhomocysteinemia enhances platelet aggregation thromboxanebiosynthesis and macrophage-derived tissue factor activity in ratsFASEB J 199711(13)1157ndash68
[5] Nishinaga M Ozawa T Shimada K Homocysteine a thrombogenic agentsuppresses anticoagulant heparan sulfate expression in cultured porcineaortic endothelial cells J Clin Invest 199392(3)1381ndash6
[6] Isa Y Mishima T Tsuge H Hayakawa T Increase in S-adenosylhomo-cysteine content and its effect on the S-adenosylhomocysteine hydrolaseactivity under transient high plasma homocysteine levels in rats J Nutr SciVitaminol 200652(6)479ndash82 (Tokyo)
[7] Fenech MF Dreosti IE Rinaldi JR Folate vitamin B12 homocysteinestatus and chromosome damage rate in lymphocytes of older menCarcinogenesis 199718(7)1329ndash36
[8] Trkova M Kapras J Bobkova K Stankova J Mejsnarova B Increasedmicronuclei frequencies in couples with reproductive failure ReprodToxicol 200014(4)331ndash5
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPR
OOF
[9] Schneider JA Rees DC Liu YT et al A worldwide distribution of acommon MTHFR Mutation Am J Hum Genet 199862(5)1258ndash60
[10] Radha Rama Devi A Govindaiah V Ramakrishna G Naushad SMPrevalence of
^methylene tetrahydrofolate reductase polymorphism in
South Indian population Curr Sci 200486(3)440ndash3[11] Neela J Raman L The relationship between maternal nutritional status and
spontaneous abortion Natl Med J India 199710(1)15ndash6[12] Refsum H Yajnik CS Gadkari M et al Hyperhomocysteinemia and
elevated methylmalonic acid indicate a high prevalence of cobalamindeficiency in Asian Indians Am J Clin Nutr 200174(2)233ndash41
[13] Ubbink JB Hayward Vermaak WJ Bissbort S Rapid high-performanceliquid chromatographic assay for total homocysteine levels in humanserum J Chromatogr 1991565(1ndash
^2)441ndash6
[14] Frosst P Blom HJ Milos R et al A candidate genetic risk factor forvascular disease a common mutation in methylenetetrahydrofolatereductase Nat Genet 199510(1)111ndash3
[15] Nath CJ Ong T Micronuclei assay in cytokinesis-blocked binucleated andconventional mononucleated methods in human peripheral lymphocytesTeratog Carcinog Mutagen 199010(3)273ndash9
[16] Giri S Thompson PD Taxel P et al Oral estrogen improves serum lipidshomocysteine and fibrinolysis in elderly men Atherosclerosis 1998137359ndash66
[17] Kim MH Kim E Passon EL et al Cortisol and estradiol^non-genetic
factors for hyperhomocyst(e)inemia Metabolism 199746247ndash9[18] Brattstrom L Lindgren A Israelsson B Andersson A Hultberg B
Homocysteine and cysteine Determinants of plasma levels in middle-agedand elderly subjects J Inter-Am Med 1994236(6)633ndash41
[19] Fukagawa NK Martin JM Wurthmann A Prue AH Ebenstein DORourke B Sex-related differences in methionine metabolism and plasmahomocysteine concentrations Am J Clin Nutr 200072(1)22ndash9
[20] Slama R Bouyer J Windham G Fenster L Werwatz A Swan SHInfluence of paternal age on the risk of spontaneous abortion Am JEpidemiol 2005161816ndash23
[21] Bosch M Rajmil O Martinez-Pasarell O et al Linear increase of diploidyin human sperm with age a four-colour FISH study Eur J Hum Genet20019533ndash8
[22] Griffin DK Abruzzo MA Millie EA et al Non-disjunction in humansperm evidence for an effect of increasing paternal age Hum Mol Genet199542227ndash32
[23] Singh NP Muller CH Berger RE Effects of age on DNA double-strandbreaks and apoptosis in human sperm Fertil Steril 2003801420ndash30
[24] Crow J The origins patterns and implications of human spontaneousabortion Nat Rev Genet 2000140ndash7
[25] Quere I Bellet H Hoffet M Janbon C Mares P Gris JC A woman withfive consecutive fetal deaths case report and retrospective analysis ofhyperhomocysteinemia prevalence in 100 consecutive women withrecurrent miscarriages Fertil Steril 199869(1)152ndash4
[26] Nelen WL Blom HJ Steegers EA den Heijer M Thomas CM Eskes TKHomocysteine and folate levels as risk factors for recurrent earlypregnancy loss Obstet Gynecol 200095(4)519ndash24
[27] Nelen WL Bulten J Steegers EA Blom HJ Hanselaar AG Eskes TKMaternal homocysteine and chorionic vascularization in recurrent earlypregnancy loss Hum Reprod 200015(4)954ndash60
[28] Nelen WL Blom HJ Steegers EA den Heijer M Eskes TKHyperhomocysteinemia and recurrent early pregnancy loss a meta-analysis Fertil Steril 200074(6)1196ndash9
[29] Ren A Wang J Methylenetetrahydrofolate reductase C677T polymorph-ism and the risk of unexplained recurrent pregnancy loss a meta-analysisFertil Steril 200686(6)1716ndash22
[30] Zetterberg H Regland B Palmeacuter M et al Increased frequency ofcombined methylenetetrahydrofolate reductase C677T and A1298Cmutated alleles in spontaneously aborted embryos Eur J Hum Genet200210(2)113ndash8
[31] Kumar KS Govindaiah V Naushad SE Devi RR Jyothy A Plasmahomocysteine levels correlated to interactions between folate status andmethylene tetrahydrofolate reductase gene mutation in women withunexplained recurrent pregnancy loss J Obstet Gynaecol 200323(1)55ndash8
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
540
541
542
543
544
545
546
547
548
549
550
551
552
553
554
555
556
557
558
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573
574
7V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
[32] Candito M Magnaldo S Bayle J et al Clinical B12 deficiency in one caseof recurrent spontaneous pregnancy loss Clin Chem Lab Med 200341(8)1026ndash7
[33] DUva M Di Micco P Strina I et al Hyperhomocysteinemia in womenwith unexplained sterility or recurrent early pregnancy loss from SouthernItaly a preliminary report Thromb J 2007115ndash10
[34] Carrell DT Liu L Peterson CM et al Sperm DNA fragmentation isincreased in couples with unexplained recurrent pregnancy loss ArchAndrol 200349(1)49ndash55
[35] Carrell DT Wilcox AL Lowy L et al Elevated sperm chromosomeaneuploidy and apoptosis in patients with unexplained recurrent pregnancyloss Obstet Gynecol 2003101(6)1229ndash35
[36] Steegers-Theunissen RP Steegers EA de Boer R Thomas CM Klooster-man MD Eskes TK Elevated folate levels in amniotic fluid after oralsupplementation Eur J Obstet Gynecol Reprod Biol 199036(3)283ndash91
[37] Nelen WL Blom HJ Thomas CM Steegers EA Boers GH Eskes TKMethylenetetrahydrofolate reductase polymorphism affects the change in
UNCO
RREC
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
OF
homocysteine and folate concentrations resulting from low dose folic acidsupplementation in women with unexplained recurrent miscarriagesJ Nutr 1998128(8)1336ndash41
[38] Rodgers GM Kane WH Activation of endogenous Factor V by ahomocysteine-induced vascular endothelial cell activator J Clin Invest198677(6)1909ndash16
[39] Lentz SR Sadler JE Inhibition of thrombomodulin surface expression andprotein C activation by the thrombogenic agent homocysteine J ClinInvest 199188(6)1906ndash14
[40] Nishinaga M Ozawa T Shimada K Homocysteine a thrombogenic agentsuppresses anticoagulant heparan sulfate expression in cultured porcineaortic endothelial cells J Clin Invest 199392(3)1381ndash6
[41] Hajjar KA Mauri L Jacovina AT et al Tissue plasminogen activatorbinding to the annexin II tail domain Direct modulation by homocysteineJ Biol Chem 1998273(16)9987ndash93
[42] Fenech M Cytokinesis-block micronucleus cytome assay Nat Protoc20072(5)1084ndash104
TEDPR
O
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
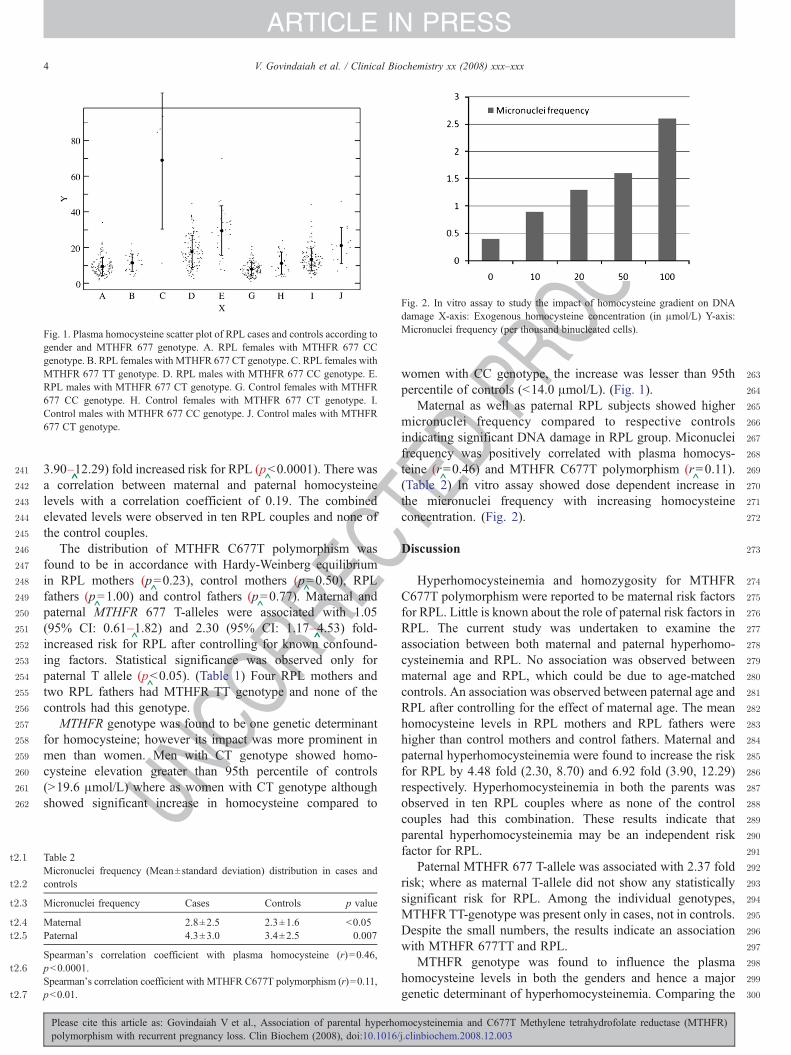
C
OOF
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288
Fig 1 Plasma homocysteine scatter plot of RPL cases and controls according togender and MTHFR 677 genotype A RPL females with MTHFR 677 CCgenotype B RPL females with MTHFR 677 CT genotype C RPL females withMTHFR 677 TT genotype D RPL males with MTHFR 677 CC genotype ERPL males with MTHFR 677 CT genotype G Control females with MTHFR677 CC genotype H Control females with MTHFR 677 CT genotype IControl males with MTHFR 677 CC genotype J Control males with MTHFR677 CT genotype
t21
t22
t23
t24
t25
t26
t27
Fig 2 In vitro assay to study the impact of homocysteine gradient on DNAdamage X-axis Exogenous homocysteine concentration (in μmolL) Y-axisMicronuclei frequency (per thousand binucleated cells)
4 V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
NCOR
RE390ndash
^1229) fold increased risk for RPL (p
^b00001) There was
a correlation between maternal and paternal homocysteinelevels with a correlation coefficient of 019 The combinedelevated levels were observed in ten RPL couples and none ofthe control couples
The distribution of MTHFR C677T polymorphism wasfound to be in accordance with Hardy-Weinberg equilibriumin RPL mothers (p
^=023) control mothers (p
^=050) RPL
fathers (p^=100) and control fathers (p
^=077) Maternal and
paternal MTHFR 677 T-alleles were associated with 105(95 CI 061ndash
^182) and 230 (95 CI 117ndash
^453) fold-
increased risk for RPL after controlling for known confound-ing factors Statistical significance was observed only forpaternal T allele (p
^b005) (Table 1) Four RPL mothers and
two RPL fathers had MTHFR TT genotype and none of thecontrols had this genotype
MTHFR genotype was found to be one genetic determinantfor homocysteine however its impact was more prominent inmen than women Men with CT genotype showed homo-cysteine elevation greater than 95th percentile of controls(N196 μmolL) where as women with CT genotype althoughshowed significant increase in homocysteine compared to
U 289
290
291
292
293
294
295
296
297
298
299
300
Table 2Micronuclei frequency (Meanplusmnstandard deviation) distribution in cases andcontrols
Micronuclei frequency Cases Controls p value
Maternal 28plusmn25 23plusmn16 b005Paternal 43plusmn30 34plusmn25 0007
Spearmans correlation coefficient with plasma homocysteine (r)=046pb00001Spearmans correlation coefficient with MTHFR C677T polymorphism (r)=011pb001
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPRwomen with CC genotype the increase was lesser than 95th
percentile of controls (b140 μmolL) (Fig 1)Maternal as well as paternal RPL subjects showed higher
micronuclei frequency compared to respective controlsindicating significant DNA damage in RPL group Miconucleifrequency was positively correlated with plasma homocys-teine (r
^=046) and MTHFR C677T polymorphism (r
^=011)
(Table 2) In vitro assay showed dose dependent increase inthe micronuclei frequency with increasing homocysteineconcentration (Fig 2)
Discussion
Hyperhomocysteinemia and homozygosity for MTHFRC677T polymorphism were reported to be maternal risk factorsfor RPL Little is known about the role of paternal risk factors inRPL The current study was undertaken to examine theassociation between both maternal and paternal hyperhomo-cysteinemia and RPL No association was observed betweenmaternal age and RPL which could be due to age-matchedcontrols An association was observed between paternal age andRPL after controlling for the effect of maternal age The meanhomocysteine levels in RPL mothers and RPL fathers werehigher than control mothers and control fathers Maternal andpaternal hyperhomocysteinemia were found to increase the riskfor RPL by 448 fold (230 870) and 692 fold (390 1229)respectively Hyperhomocysteinemia in both the parents wasobserved in ten RPL couples where as none of the controlcouples had this combination These results indicate thatparental hyperhomocysteinemia may be an independent riskfactor for RPL
Paternal MTHFR 677 T-allele was associated with 237 foldrisk where as maternal T-allele did not show any statisticallysignificant risk for RPL Among the individual genotypesMTHFRTT-genotype was present only in cases not in controlsDespite the small numbers the results indicate an associationwith MTHFR 677TT and RPL
MTHFR genotype was found to influence the plasmahomocysteine levels in both the genders and hence a majorgenetic determinant of hyperhomocysteinemia Comparing the
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
5V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
UNCO
RREC
genotype and gender matched cases with controls showedevidence to suggest that cases have higher homocysteine thancontrols and hence apart from MTHFR genotype somegenetic or non-genetic determinant also plays a role inincreasing the homocysteine and might play an importantrole in the etiology of RPL However men with CT genotypeshowed homocysteine elevation greater than the 95thpercentile of controls where as women with CT genotypeshowed homocysteine levels lesser than the 95th percentile ofcontrols These gender differences in homocysteine mightexplain the risk associated with paternal T-allele The mostprofound associations between hyperhomocysteinemia andRPL were found in fathers who were heterozygous for the677T allele This is extremely common in Caucasians (40)and is not considered to be a risk factor for hyperhomocys-teinemia (in contrast to homozygotes) This discrepancy couldbe due to differences in the diet and also the possibility of anyother allele from a different loci co-segregating with MTHFR677T allele cannot be ruled out The gender differences inplasma homocysteine levels could be due to protective role ofestrogens (in females) [1617] stoichiometric synthesis ofhomocysteine with creatinecreatinine ratio proportional tomuscle mass [18] differences in the rates of remethylation andtranmethylation among males and females [19]
^Significant DNA damage was observed in RPL couplescompared to control couples which was found to havepositive association with homocysteine To strengthen thisassociation further in vitro assay was performed on peripheralblood cultures with exogenous addition of homocysteine invarying concentrations which showed dose-dependentincrease in the frequency of micronuclei This is a strongevidence to suggest that hyperhomocysteinemia induces DNAdamage DNA damage can be caused by many factors apartfrom hyperhomocysteinemia and hence there is a need toconduct another study focusing on the causes of DNA damagein RPL subjects
Our study is in agreement with Remy Slama et al^in showing
increased risk of RPL with increase in paternal age with asuggestion that the association is stronger for first trimesterpregnancy loss [20] This increased risk may be a consequenceof an increasing frequency of chromosomal anomalies in thespermatozoa with male age [2122] or due to increased DNAdamage [23] or due to increased chromosomal replications ofmale stem cells [24] Apart from our study several researchershave shown positive association of maternal hyperhomocystei-nemia and maternal MTHFR 677 TT genotype with RPL Highprevalence of hyperhomocysteinemia was observed in parouswomen (33) compared to nulliparous women (14) byWouters MG et al Five consecutive fetal deaths were reportedin a woman with MTHFR 677TT genotype and elevatedhomocysteine and high prevalence of hyperhomocysteinemia(12) folate deficiency (15) and C677T MTHFR CT and TTgenotypes (20) were reported in 100 consecutive women withRPL by Quere et al
^[25] Hyperhomocysteinemia and folate
deficiency were found to be associated with 36 and 21 fold riskfor RPL by Nelen et al [26] Smaller median chorionic vasculararea and perimeter were observed in women with hyperhomo-
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPR
OOF
cysteinemia by Nelen et al^suggesting that hyperhomocystei-
nemia is associated with defective chorionic vasculature [27]Meta-analysis of case-control studies conducted during theperiod of 1992ndash
^1999 showed that hyperhomocysteinemia and
MTHFRTT-genotype were associated with 27 fold and 14 foldrisk for RPL respectively [28] Another meta-analysis based onTwenty-six studies with 2120 RPL cases and 2949 controlsshowed that MTHFR TT-genotype was associated with nostatistically significant risk with an odds ratio of 121 (95 CI104 140) [29] Zetterberg et al
^have observed increased
frequency of combined MTHFR C677T and A1298C mutatedalleles in spontaneously aborted fetuses (OR 142 95 CI178ndash
^113) indicating that the MTHFR polymorphisms may
have a major impact on fetal survival [30] A pilot studyconducted on 24 South Indian women by Kumar et al
^has
shown high prevalence of hyperhomocysteinemia and red cellfolate deficiency in RPL [31] Candito et al
^reported four
consecutive pregnancy losses in a woman with hyperhomocys-teinemia (259 μmolL) B12 deficiency (b150 pgmL
^) and the
MTHFR 677 TT-genotype who got benefited with vitamin B12supplementation [32] DUva M et al
^have reported Hyperho-
mocysteinemia and MTHFR TT-genotype as risk factors forunexplained female sterility and recurrent pregnancy loss [33]
Apart from the study by Trkova et al^that showed increased
micronuclei frequency in couples with RPL several studieshave also explored the relationship between sperm quality andunexplained RPL Increased percentage of sperm stainingpositive for DNA fragmentation was observed in the RPL groupcompared to donor or general population by Carrell et al
^[34]
In a separate study they also showed that the mean aneuploidyrate in RPL group was significantly higher than the generalpopulation (277plusmn022 vs 148plusmn012 Pzb0005) [35] Bene-ficial effects of folate supplementation were observed bySteegers-Theunissen et al
^[36] and Nelen et al
^[37] who
reported increase in maternal plasmaamniotic fluid folate andlowering of fasting plasma homocysteine levels in theirrespective studies
The risk associated with maternal hyperhomocysteinemiacould be due to embryo toxicity or due to ability of highhomocysteine to activate factor V [38] and to inactivate proteinC thrombomodulin [39] heparan sulphate [40] tissueplasminogen activator binding to human endothelial cells [41]or due to impaired cellular methylation that alters geneexpression or due to uracil misincorporation in DNA resultingin DNA damage The risk associated with paternal hyperho-mocysteinemia could be due to its effect on sperm quality byincreasing DNA damage
The strength of the current study is the assessment of notonly maternal but also paternal hyperhomocysteinemia inrelation to RPL In order to strengthen our hypothesis furtherwe have initiated a pilot study to assess DNA damage in thesemen samples of subjects with recurrent pregnancy loss andobserved significant DNA damage in sperms of RPL fathersusing Fluorescence activated cell sorter technique A modifiedcytokinesis block micronucleus cytome assay for morecomprehensive measurement of DNA damage developedby Fenech et al that measures micronuclei frequency
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
C
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539
6 V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
UNCO
RRE
along with other DNA damage biomarkers such as nuclearbuds nucleoplasmic bridges as well as cytotoxic markersincluding apoptosis and necrosis can be incorporated infuture studies [42]
Our study projects paternal age as an independent riskfactor for RPL Impact of maternal age was controlled in thestudy design (using age-matched controls) as well as in theregression model This study projects that not only maternalhyperhomocysteinemia but also paternal hyperhomocysteine-mia is a risk factor for RPL at least among South IndiansSignificant DNA damage was observed in both maternal andpaternal RPL subjects Our study is in agreement with the twometa-analyses in showing that maternal MTHFR genotypemay not be a significant risk factor for RPL The impact ofpaternal MTHFR genotype on RPL could be due to elevatedhomocysteine levels that in turn result in DNA damage Thisstudy further shows a direct association between homocysteineelevation and DNA damage using in vivo and in vitro assaysHowever the mechanism by which homocysteine causes DNAdamage needs to be elucidated further There is a need forlarge case-control studies to explore the role of other geneticand nutritional factors that are likely to influence homo-cysteine levels in the pathophysiology of RPL
Acknowledgments
We thank Mr Ram Prakash Singh Mr R Sudheer KumarMr G Srinivas and Mr V Murali Mohan for the technicalassistance We thank all the families participated in this studyWe thank Department of Biotechnology Government of Indiafor its financial support
References
[1] Strobino B Fox HE Kline J Stein Z Susser M Warburton DCharacteristics of women with recurrent spontaneous abortions andwomen with favourable reproductive histories Am J Public Health198276(8)986ndash91
[2] Wouters MG Boers GH Blom HJ et al Hyperhomocysteinemia a riskfactor in women with unexplained recurrent early pregnancy loss FertilSteril 199360(5)820ndash5
[3] Greene ND Dunlevy LE Copp AJ Homocysteine is embryotoxic butdoes not cause neural tube defects in mouse embryos Anat Embryol2003206(3)185ndash91 (Berl)
[4] Durand P Lussier-Cacan S Blache D Acute methionine load-inducedhyperhomocysteinemia enhances platelet aggregation thromboxanebiosynthesis and macrophage-derived tissue factor activity in ratsFASEB J 199711(13)1157ndash68
[5] Nishinaga M Ozawa T Shimada K Homocysteine a thrombogenic agentsuppresses anticoagulant heparan sulfate expression in cultured porcineaortic endothelial cells J Clin Invest 199392(3)1381ndash6
[6] Isa Y Mishima T Tsuge H Hayakawa T Increase in S-adenosylhomo-cysteine content and its effect on the S-adenosylhomocysteine hydrolaseactivity under transient high plasma homocysteine levels in rats J Nutr SciVitaminol 200652(6)479ndash82 (Tokyo)
[7] Fenech MF Dreosti IE Rinaldi JR Folate vitamin B12 homocysteinestatus and chromosome damage rate in lymphocytes of older menCarcinogenesis 199718(7)1329ndash36
[8] Trkova M Kapras J Bobkova K Stankova J Mejsnarova B Increasedmicronuclei frequencies in couples with reproductive failure ReprodToxicol 200014(4)331ndash5
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPR
OOF
[9] Schneider JA Rees DC Liu YT et al A worldwide distribution of acommon MTHFR Mutation Am J Hum Genet 199862(5)1258ndash60
[10] Radha Rama Devi A Govindaiah V Ramakrishna G Naushad SMPrevalence of
^methylene tetrahydrofolate reductase polymorphism in
South Indian population Curr Sci 200486(3)440ndash3[11] Neela J Raman L The relationship between maternal nutritional status and
spontaneous abortion Natl Med J India 199710(1)15ndash6[12] Refsum H Yajnik CS Gadkari M et al Hyperhomocysteinemia and
elevated methylmalonic acid indicate a high prevalence of cobalamindeficiency in Asian Indians Am J Clin Nutr 200174(2)233ndash41
[13] Ubbink JB Hayward Vermaak WJ Bissbort S Rapid high-performanceliquid chromatographic assay for total homocysteine levels in humanserum J Chromatogr 1991565(1ndash
^2)441ndash6
[14] Frosst P Blom HJ Milos R et al A candidate genetic risk factor forvascular disease a common mutation in methylenetetrahydrofolatereductase Nat Genet 199510(1)111ndash3
[15] Nath CJ Ong T Micronuclei assay in cytokinesis-blocked binucleated andconventional mononucleated methods in human peripheral lymphocytesTeratog Carcinog Mutagen 199010(3)273ndash9
[16] Giri S Thompson PD Taxel P et al Oral estrogen improves serum lipidshomocysteine and fibrinolysis in elderly men Atherosclerosis 1998137359ndash66
[17] Kim MH Kim E Passon EL et al Cortisol and estradiol^non-genetic
factors for hyperhomocyst(e)inemia Metabolism 199746247ndash9[18] Brattstrom L Lindgren A Israelsson B Andersson A Hultberg B
Homocysteine and cysteine Determinants of plasma levels in middle-agedand elderly subjects J Inter-Am Med 1994236(6)633ndash41
[19] Fukagawa NK Martin JM Wurthmann A Prue AH Ebenstein DORourke B Sex-related differences in methionine metabolism and plasmahomocysteine concentrations Am J Clin Nutr 200072(1)22ndash9
[20] Slama R Bouyer J Windham G Fenster L Werwatz A Swan SHInfluence of paternal age on the risk of spontaneous abortion Am JEpidemiol 2005161816ndash23
[21] Bosch M Rajmil O Martinez-Pasarell O et al Linear increase of diploidyin human sperm with age a four-colour FISH study Eur J Hum Genet20019533ndash8
[22] Griffin DK Abruzzo MA Millie EA et al Non-disjunction in humansperm evidence for an effect of increasing paternal age Hum Mol Genet199542227ndash32
[23] Singh NP Muller CH Berger RE Effects of age on DNA double-strandbreaks and apoptosis in human sperm Fertil Steril 2003801420ndash30
[24] Crow J The origins patterns and implications of human spontaneousabortion Nat Rev Genet 2000140ndash7
[25] Quere I Bellet H Hoffet M Janbon C Mares P Gris JC A woman withfive consecutive fetal deaths case report and retrospective analysis ofhyperhomocysteinemia prevalence in 100 consecutive women withrecurrent miscarriages Fertil Steril 199869(1)152ndash4
[26] Nelen WL Blom HJ Steegers EA den Heijer M Thomas CM Eskes TKHomocysteine and folate levels as risk factors for recurrent earlypregnancy loss Obstet Gynecol 200095(4)519ndash24
[27] Nelen WL Bulten J Steegers EA Blom HJ Hanselaar AG Eskes TKMaternal homocysteine and chorionic vascularization in recurrent earlypregnancy loss Hum Reprod 200015(4)954ndash60
[28] Nelen WL Blom HJ Steegers EA den Heijer M Eskes TKHyperhomocysteinemia and recurrent early pregnancy loss a meta-analysis Fertil Steril 200074(6)1196ndash9
[29] Ren A Wang J Methylenetetrahydrofolate reductase C677T polymorph-ism and the risk of unexplained recurrent pregnancy loss a meta-analysisFertil Steril 200686(6)1716ndash22
[30] Zetterberg H Regland B Palmeacuter M et al Increased frequency ofcombined methylenetetrahydrofolate reductase C677T and A1298Cmutated alleles in spontaneously aborted embryos Eur J Hum Genet200210(2)113ndash8
[31] Kumar KS Govindaiah V Naushad SE Devi RR Jyothy A Plasmahomocysteine levels correlated to interactions between folate status andmethylene tetrahydrofolate reductase gene mutation in women withunexplained recurrent pregnancy loss J Obstet Gynaecol 200323(1)55ndash8
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
540
541
542
543
544
545
546
547
548
549
550
551
552
553
554
555
556
557
558
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573
574
7V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
[32] Candito M Magnaldo S Bayle J et al Clinical B12 deficiency in one caseof recurrent spontaneous pregnancy loss Clin Chem Lab Med 200341(8)1026ndash7
[33] DUva M Di Micco P Strina I et al Hyperhomocysteinemia in womenwith unexplained sterility or recurrent early pregnancy loss from SouthernItaly a preliminary report Thromb J 2007115ndash10
[34] Carrell DT Liu L Peterson CM et al Sperm DNA fragmentation isincreased in couples with unexplained recurrent pregnancy loss ArchAndrol 200349(1)49ndash55
[35] Carrell DT Wilcox AL Lowy L et al Elevated sperm chromosomeaneuploidy and apoptosis in patients with unexplained recurrent pregnancyloss Obstet Gynecol 2003101(6)1229ndash35
[36] Steegers-Theunissen RP Steegers EA de Boer R Thomas CM Klooster-man MD Eskes TK Elevated folate levels in amniotic fluid after oralsupplementation Eur J Obstet Gynecol Reprod Biol 199036(3)283ndash91
[37] Nelen WL Blom HJ Thomas CM Steegers EA Boers GH Eskes TKMethylenetetrahydrofolate reductase polymorphism affects the change in
UNCO
RREC
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
OF
homocysteine and folate concentrations resulting from low dose folic acidsupplementation in women with unexplained recurrent miscarriagesJ Nutr 1998128(8)1336ndash41
[38] Rodgers GM Kane WH Activation of endogenous Factor V by ahomocysteine-induced vascular endothelial cell activator J Clin Invest198677(6)1909ndash16
[39] Lentz SR Sadler JE Inhibition of thrombomodulin surface expression andprotein C activation by the thrombogenic agent homocysteine J ClinInvest 199188(6)1906ndash14
[40] Nishinaga M Ozawa T Shimada K Homocysteine a thrombogenic agentsuppresses anticoagulant heparan sulfate expression in cultured porcineaortic endothelial cells J Clin Invest 199392(3)1381ndash6
[41] Hajjar KA Mauri L Jacovina AT et al Tissue plasminogen activatorbinding to the annexin II tail domain Direct modulation by homocysteineJ Biol Chem 1998273(16)9987ndash93
[42] Fenech M Cytokinesis-block micronucleus cytome assay Nat Protoc20072(5)1084ndash104
TEDPR
O
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
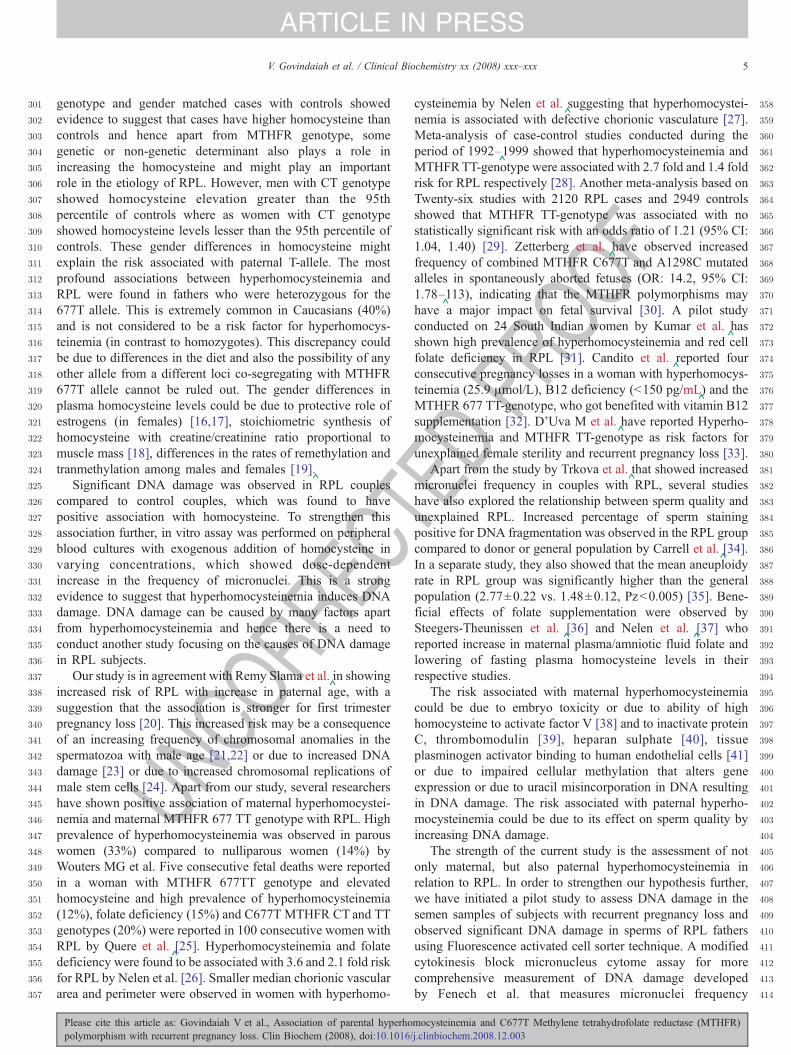
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
5V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
UNCO
RREC
genotype and gender matched cases with controls showedevidence to suggest that cases have higher homocysteine thancontrols and hence apart from MTHFR genotype somegenetic or non-genetic determinant also plays a role inincreasing the homocysteine and might play an importantrole in the etiology of RPL However men with CT genotypeshowed homocysteine elevation greater than the 95thpercentile of controls where as women with CT genotypeshowed homocysteine levels lesser than the 95th percentile ofcontrols These gender differences in homocysteine mightexplain the risk associated with paternal T-allele The mostprofound associations between hyperhomocysteinemia andRPL were found in fathers who were heterozygous for the677T allele This is extremely common in Caucasians (40)and is not considered to be a risk factor for hyperhomocys-teinemia (in contrast to homozygotes) This discrepancy couldbe due to differences in the diet and also the possibility of anyother allele from a different loci co-segregating with MTHFR677T allele cannot be ruled out The gender differences inplasma homocysteine levels could be due to protective role ofestrogens (in females) [1617] stoichiometric synthesis ofhomocysteine with creatinecreatinine ratio proportional tomuscle mass [18] differences in the rates of remethylation andtranmethylation among males and females [19]
^Significant DNA damage was observed in RPL couplescompared to control couples which was found to havepositive association with homocysteine To strengthen thisassociation further in vitro assay was performed on peripheralblood cultures with exogenous addition of homocysteine invarying concentrations which showed dose-dependentincrease in the frequency of micronuclei This is a strongevidence to suggest that hyperhomocysteinemia induces DNAdamage DNA damage can be caused by many factors apartfrom hyperhomocysteinemia and hence there is a need toconduct another study focusing on the causes of DNA damagein RPL subjects
Our study is in agreement with Remy Slama et al^in showing
increased risk of RPL with increase in paternal age with asuggestion that the association is stronger for first trimesterpregnancy loss [20] This increased risk may be a consequenceof an increasing frequency of chromosomal anomalies in thespermatozoa with male age [2122] or due to increased DNAdamage [23] or due to increased chromosomal replications ofmale stem cells [24] Apart from our study several researchershave shown positive association of maternal hyperhomocystei-nemia and maternal MTHFR 677 TT genotype with RPL Highprevalence of hyperhomocysteinemia was observed in parouswomen (33) compared to nulliparous women (14) byWouters MG et al Five consecutive fetal deaths were reportedin a woman with MTHFR 677TT genotype and elevatedhomocysteine and high prevalence of hyperhomocysteinemia(12) folate deficiency (15) and C677T MTHFR CT and TTgenotypes (20) were reported in 100 consecutive women withRPL by Quere et al
^[25] Hyperhomocysteinemia and folate
deficiency were found to be associated with 36 and 21 fold riskfor RPL by Nelen et al [26] Smaller median chorionic vasculararea and perimeter were observed in women with hyperhomo-
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPR
OOF
cysteinemia by Nelen et al^suggesting that hyperhomocystei-
nemia is associated with defective chorionic vasculature [27]Meta-analysis of case-control studies conducted during theperiod of 1992ndash
^1999 showed that hyperhomocysteinemia and
MTHFRTT-genotype were associated with 27 fold and 14 foldrisk for RPL respectively [28] Another meta-analysis based onTwenty-six studies with 2120 RPL cases and 2949 controlsshowed that MTHFR TT-genotype was associated with nostatistically significant risk with an odds ratio of 121 (95 CI104 140) [29] Zetterberg et al
^have observed increased
frequency of combined MTHFR C677T and A1298C mutatedalleles in spontaneously aborted fetuses (OR 142 95 CI178ndash
^113) indicating that the MTHFR polymorphisms may
have a major impact on fetal survival [30] A pilot studyconducted on 24 South Indian women by Kumar et al
^has
shown high prevalence of hyperhomocysteinemia and red cellfolate deficiency in RPL [31] Candito et al
^reported four
consecutive pregnancy losses in a woman with hyperhomocys-teinemia (259 μmolL) B12 deficiency (b150 pgmL
^) and the
MTHFR 677 TT-genotype who got benefited with vitamin B12supplementation [32] DUva M et al
^have reported Hyperho-
mocysteinemia and MTHFR TT-genotype as risk factors forunexplained female sterility and recurrent pregnancy loss [33]
Apart from the study by Trkova et al^that showed increased
micronuclei frequency in couples with RPL several studieshave also explored the relationship between sperm quality andunexplained RPL Increased percentage of sperm stainingpositive for DNA fragmentation was observed in the RPL groupcompared to donor or general population by Carrell et al
^[34]
In a separate study they also showed that the mean aneuploidyrate in RPL group was significantly higher than the generalpopulation (277plusmn022 vs 148plusmn012 Pzb0005) [35] Bene-ficial effects of folate supplementation were observed bySteegers-Theunissen et al
^[36] and Nelen et al
^[37] who
reported increase in maternal plasmaamniotic fluid folate andlowering of fasting plasma homocysteine levels in theirrespective studies
The risk associated with maternal hyperhomocysteinemiacould be due to embryo toxicity or due to ability of highhomocysteine to activate factor V [38] and to inactivate proteinC thrombomodulin [39] heparan sulphate [40] tissueplasminogen activator binding to human endothelial cells [41]or due to impaired cellular methylation that alters geneexpression or due to uracil misincorporation in DNA resultingin DNA damage The risk associated with paternal hyperho-mocysteinemia could be due to its effect on sperm quality byincreasing DNA damage
The strength of the current study is the assessment of notonly maternal but also paternal hyperhomocysteinemia inrelation to RPL In order to strengthen our hypothesis furtherwe have initiated a pilot study to assess DNA damage in thesemen samples of subjects with recurrent pregnancy loss andobserved significant DNA damage in sperms of RPL fathersusing Fluorescence activated cell sorter technique A modifiedcytokinesis block micronucleus cytome assay for morecomprehensive measurement of DNA damage developedby Fenech et al that measures micronuclei frequency
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
C
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539
6 V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
UNCO
RRE
along with other DNA damage biomarkers such as nuclearbuds nucleoplasmic bridges as well as cytotoxic markersincluding apoptosis and necrosis can be incorporated infuture studies [42]
Our study projects paternal age as an independent riskfactor for RPL Impact of maternal age was controlled in thestudy design (using age-matched controls) as well as in theregression model This study projects that not only maternalhyperhomocysteinemia but also paternal hyperhomocysteine-mia is a risk factor for RPL at least among South IndiansSignificant DNA damage was observed in both maternal andpaternal RPL subjects Our study is in agreement with the twometa-analyses in showing that maternal MTHFR genotypemay not be a significant risk factor for RPL The impact ofpaternal MTHFR genotype on RPL could be due to elevatedhomocysteine levels that in turn result in DNA damage Thisstudy further shows a direct association between homocysteineelevation and DNA damage using in vivo and in vitro assaysHowever the mechanism by which homocysteine causes DNAdamage needs to be elucidated further There is a need forlarge case-control studies to explore the role of other geneticand nutritional factors that are likely to influence homo-cysteine levels in the pathophysiology of RPL
Acknowledgments
We thank Mr Ram Prakash Singh Mr R Sudheer KumarMr G Srinivas and Mr V Murali Mohan for the technicalassistance We thank all the families participated in this studyWe thank Department of Biotechnology Government of Indiafor its financial support
References
[1] Strobino B Fox HE Kline J Stein Z Susser M Warburton DCharacteristics of women with recurrent spontaneous abortions andwomen with favourable reproductive histories Am J Public Health198276(8)986ndash91
[2] Wouters MG Boers GH Blom HJ et al Hyperhomocysteinemia a riskfactor in women with unexplained recurrent early pregnancy loss FertilSteril 199360(5)820ndash5
[3] Greene ND Dunlevy LE Copp AJ Homocysteine is embryotoxic butdoes not cause neural tube defects in mouse embryos Anat Embryol2003206(3)185ndash91 (Berl)
[4] Durand P Lussier-Cacan S Blache D Acute methionine load-inducedhyperhomocysteinemia enhances platelet aggregation thromboxanebiosynthesis and macrophage-derived tissue factor activity in ratsFASEB J 199711(13)1157ndash68
[5] Nishinaga M Ozawa T Shimada K Homocysteine a thrombogenic agentsuppresses anticoagulant heparan sulfate expression in cultured porcineaortic endothelial cells J Clin Invest 199392(3)1381ndash6
[6] Isa Y Mishima T Tsuge H Hayakawa T Increase in S-adenosylhomo-cysteine content and its effect on the S-adenosylhomocysteine hydrolaseactivity under transient high plasma homocysteine levels in rats J Nutr SciVitaminol 200652(6)479ndash82 (Tokyo)
[7] Fenech MF Dreosti IE Rinaldi JR Folate vitamin B12 homocysteinestatus and chromosome damage rate in lymphocytes of older menCarcinogenesis 199718(7)1329ndash36
[8] Trkova M Kapras J Bobkova K Stankova J Mejsnarova B Increasedmicronuclei frequencies in couples with reproductive failure ReprodToxicol 200014(4)331ndash5
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPR
OOF
[9] Schneider JA Rees DC Liu YT et al A worldwide distribution of acommon MTHFR Mutation Am J Hum Genet 199862(5)1258ndash60
[10] Radha Rama Devi A Govindaiah V Ramakrishna G Naushad SMPrevalence of
^methylene tetrahydrofolate reductase polymorphism in
South Indian population Curr Sci 200486(3)440ndash3[11] Neela J Raman L The relationship between maternal nutritional status and
spontaneous abortion Natl Med J India 199710(1)15ndash6[12] Refsum H Yajnik CS Gadkari M et al Hyperhomocysteinemia and
elevated methylmalonic acid indicate a high prevalence of cobalamindeficiency in Asian Indians Am J Clin Nutr 200174(2)233ndash41
[13] Ubbink JB Hayward Vermaak WJ Bissbort S Rapid high-performanceliquid chromatographic assay for total homocysteine levels in humanserum J Chromatogr 1991565(1ndash
^2)441ndash6
[14] Frosst P Blom HJ Milos R et al A candidate genetic risk factor forvascular disease a common mutation in methylenetetrahydrofolatereductase Nat Genet 199510(1)111ndash3
[15] Nath CJ Ong T Micronuclei assay in cytokinesis-blocked binucleated andconventional mononucleated methods in human peripheral lymphocytesTeratog Carcinog Mutagen 199010(3)273ndash9
[16] Giri S Thompson PD Taxel P et al Oral estrogen improves serum lipidshomocysteine and fibrinolysis in elderly men Atherosclerosis 1998137359ndash66
[17] Kim MH Kim E Passon EL et al Cortisol and estradiol^non-genetic
factors for hyperhomocyst(e)inemia Metabolism 199746247ndash9[18] Brattstrom L Lindgren A Israelsson B Andersson A Hultberg B
Homocysteine and cysteine Determinants of plasma levels in middle-agedand elderly subjects J Inter-Am Med 1994236(6)633ndash41
[19] Fukagawa NK Martin JM Wurthmann A Prue AH Ebenstein DORourke B Sex-related differences in methionine metabolism and plasmahomocysteine concentrations Am J Clin Nutr 200072(1)22ndash9
[20] Slama R Bouyer J Windham G Fenster L Werwatz A Swan SHInfluence of paternal age on the risk of spontaneous abortion Am JEpidemiol 2005161816ndash23
[21] Bosch M Rajmil O Martinez-Pasarell O et al Linear increase of diploidyin human sperm with age a four-colour FISH study Eur J Hum Genet20019533ndash8
[22] Griffin DK Abruzzo MA Millie EA et al Non-disjunction in humansperm evidence for an effect of increasing paternal age Hum Mol Genet199542227ndash32
[23] Singh NP Muller CH Berger RE Effects of age on DNA double-strandbreaks and apoptosis in human sperm Fertil Steril 2003801420ndash30
[24] Crow J The origins patterns and implications of human spontaneousabortion Nat Rev Genet 2000140ndash7
[25] Quere I Bellet H Hoffet M Janbon C Mares P Gris JC A woman withfive consecutive fetal deaths case report and retrospective analysis ofhyperhomocysteinemia prevalence in 100 consecutive women withrecurrent miscarriages Fertil Steril 199869(1)152ndash4
[26] Nelen WL Blom HJ Steegers EA den Heijer M Thomas CM Eskes TKHomocysteine and folate levels as risk factors for recurrent earlypregnancy loss Obstet Gynecol 200095(4)519ndash24
[27] Nelen WL Bulten J Steegers EA Blom HJ Hanselaar AG Eskes TKMaternal homocysteine and chorionic vascularization in recurrent earlypregnancy loss Hum Reprod 200015(4)954ndash60
[28] Nelen WL Blom HJ Steegers EA den Heijer M Eskes TKHyperhomocysteinemia and recurrent early pregnancy loss a meta-analysis Fertil Steril 200074(6)1196ndash9
[29] Ren A Wang J Methylenetetrahydrofolate reductase C677T polymorph-ism and the risk of unexplained recurrent pregnancy loss a meta-analysisFertil Steril 200686(6)1716ndash22
[30] Zetterberg H Regland B Palmeacuter M et al Increased frequency ofcombined methylenetetrahydrofolate reductase C677T and A1298Cmutated alleles in spontaneously aborted embryos Eur J Hum Genet200210(2)113ndash8
[31] Kumar KS Govindaiah V Naushad SE Devi RR Jyothy A Plasmahomocysteine levels correlated to interactions between folate status andmethylene tetrahydrofolate reductase gene mutation in women withunexplained recurrent pregnancy loss J Obstet Gynaecol 200323(1)55ndash8
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
540
541
542
543
544
545
546
547
548
549
550
551
552
553
554
555
556
557
558
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573
574
7V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
[32] Candito M Magnaldo S Bayle J et al Clinical B12 deficiency in one caseof recurrent spontaneous pregnancy loss Clin Chem Lab Med 200341(8)1026ndash7
[33] DUva M Di Micco P Strina I et al Hyperhomocysteinemia in womenwith unexplained sterility or recurrent early pregnancy loss from SouthernItaly a preliminary report Thromb J 2007115ndash10
[34] Carrell DT Liu L Peterson CM et al Sperm DNA fragmentation isincreased in couples with unexplained recurrent pregnancy loss ArchAndrol 200349(1)49ndash55
[35] Carrell DT Wilcox AL Lowy L et al Elevated sperm chromosomeaneuploidy and apoptosis in patients with unexplained recurrent pregnancyloss Obstet Gynecol 2003101(6)1229ndash35
[36] Steegers-Theunissen RP Steegers EA de Boer R Thomas CM Klooster-man MD Eskes TK Elevated folate levels in amniotic fluid after oralsupplementation Eur J Obstet Gynecol Reprod Biol 199036(3)283ndash91
[37] Nelen WL Blom HJ Thomas CM Steegers EA Boers GH Eskes TKMethylenetetrahydrofolate reductase polymorphism affects the change in
UNCO
RREC
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
OF
homocysteine and folate concentrations resulting from low dose folic acidsupplementation in women with unexplained recurrent miscarriagesJ Nutr 1998128(8)1336ndash41
[38] Rodgers GM Kane WH Activation of endogenous Factor V by ahomocysteine-induced vascular endothelial cell activator J Clin Invest198677(6)1909ndash16
[39] Lentz SR Sadler JE Inhibition of thrombomodulin surface expression andprotein C activation by the thrombogenic agent homocysteine J ClinInvest 199188(6)1906ndash14
[40] Nishinaga M Ozawa T Shimada K Homocysteine a thrombogenic agentsuppresses anticoagulant heparan sulfate expression in cultured porcineaortic endothelial cells J Clin Invest 199392(3)1381ndash6
[41] Hajjar KA Mauri L Jacovina AT et al Tissue plasminogen activatorbinding to the annexin II tail domain Direct modulation by homocysteineJ Biol Chem 1998273(16)9987ndash93
[42] Fenech M Cytokinesis-block micronucleus cytome assay Nat Protoc20072(5)1084ndash104
TEDPR
O
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
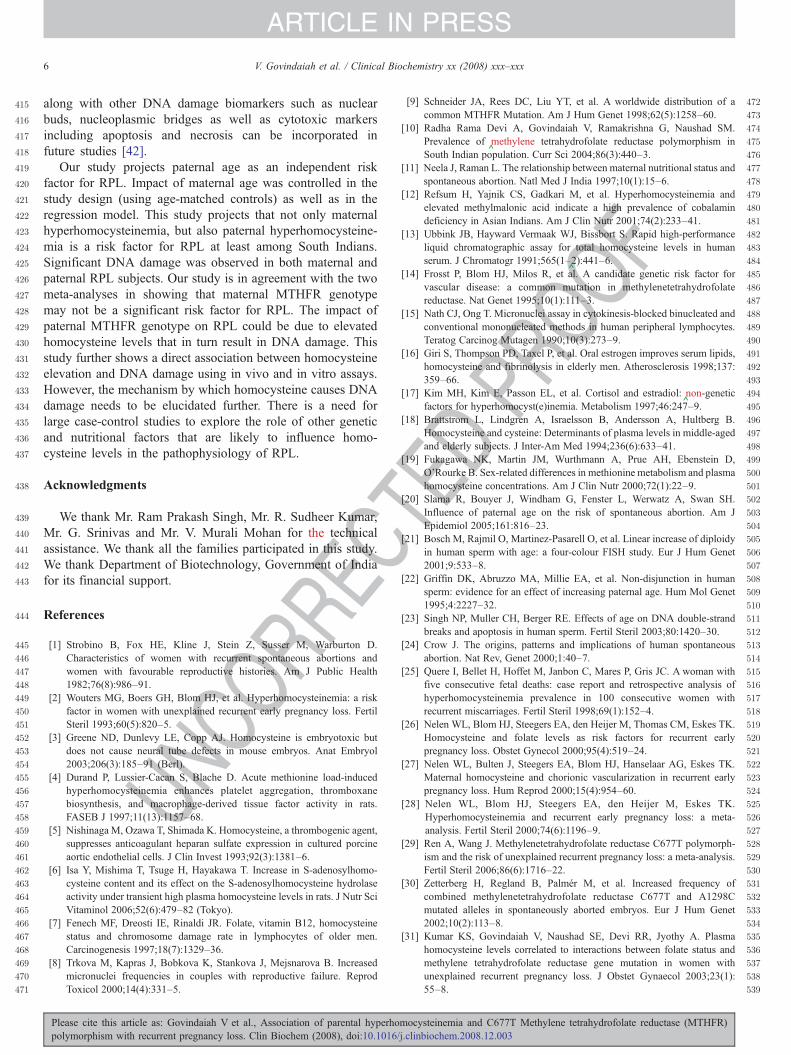
C
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539
6 V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
UNCO
RRE
along with other DNA damage biomarkers such as nuclearbuds nucleoplasmic bridges as well as cytotoxic markersincluding apoptosis and necrosis can be incorporated infuture studies [42]
Our study projects paternal age as an independent riskfactor for RPL Impact of maternal age was controlled in thestudy design (using age-matched controls) as well as in theregression model This study projects that not only maternalhyperhomocysteinemia but also paternal hyperhomocysteine-mia is a risk factor for RPL at least among South IndiansSignificant DNA damage was observed in both maternal andpaternal RPL subjects Our study is in agreement with the twometa-analyses in showing that maternal MTHFR genotypemay not be a significant risk factor for RPL The impact ofpaternal MTHFR genotype on RPL could be due to elevatedhomocysteine levels that in turn result in DNA damage Thisstudy further shows a direct association between homocysteineelevation and DNA damage using in vivo and in vitro assaysHowever the mechanism by which homocysteine causes DNAdamage needs to be elucidated further There is a need forlarge case-control studies to explore the role of other geneticand nutritional factors that are likely to influence homo-cysteine levels in the pathophysiology of RPL
Acknowledgments
We thank Mr Ram Prakash Singh Mr R Sudheer KumarMr G Srinivas and Mr V Murali Mohan for the technicalassistance We thank all the families participated in this studyWe thank Department of Biotechnology Government of Indiafor its financial support
References
[1] Strobino B Fox HE Kline J Stein Z Susser M Warburton DCharacteristics of women with recurrent spontaneous abortions andwomen with favourable reproductive histories Am J Public Health198276(8)986ndash91
[2] Wouters MG Boers GH Blom HJ et al Hyperhomocysteinemia a riskfactor in women with unexplained recurrent early pregnancy loss FertilSteril 199360(5)820ndash5
[3] Greene ND Dunlevy LE Copp AJ Homocysteine is embryotoxic butdoes not cause neural tube defects in mouse embryos Anat Embryol2003206(3)185ndash91 (Berl)
[4] Durand P Lussier-Cacan S Blache D Acute methionine load-inducedhyperhomocysteinemia enhances platelet aggregation thromboxanebiosynthesis and macrophage-derived tissue factor activity in ratsFASEB J 199711(13)1157ndash68
[5] Nishinaga M Ozawa T Shimada K Homocysteine a thrombogenic agentsuppresses anticoagulant heparan sulfate expression in cultured porcineaortic endothelial cells J Clin Invest 199392(3)1381ndash6
[6] Isa Y Mishima T Tsuge H Hayakawa T Increase in S-adenosylhomo-cysteine content and its effect on the S-adenosylhomocysteine hydrolaseactivity under transient high plasma homocysteine levels in rats J Nutr SciVitaminol 200652(6)479ndash82 (Tokyo)
[7] Fenech MF Dreosti IE Rinaldi JR Folate vitamin B12 homocysteinestatus and chromosome damage rate in lymphocytes of older menCarcinogenesis 199718(7)1329ndash36
[8] Trkova M Kapras J Bobkova K Stankova J Mejsnarova B Increasedmicronuclei frequencies in couples with reproductive failure ReprodToxicol 200014(4)331ndash5
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
TEDPR
OOF
[9] Schneider JA Rees DC Liu YT et al A worldwide distribution of acommon MTHFR Mutation Am J Hum Genet 199862(5)1258ndash60
[10] Radha Rama Devi A Govindaiah V Ramakrishna G Naushad SMPrevalence of
^methylene tetrahydrofolate reductase polymorphism in
South Indian population Curr Sci 200486(3)440ndash3[11] Neela J Raman L The relationship between maternal nutritional status and
spontaneous abortion Natl Med J India 199710(1)15ndash6[12] Refsum H Yajnik CS Gadkari M et al Hyperhomocysteinemia and
elevated methylmalonic acid indicate a high prevalence of cobalamindeficiency in Asian Indians Am J Clin Nutr 200174(2)233ndash41
[13] Ubbink JB Hayward Vermaak WJ Bissbort S Rapid high-performanceliquid chromatographic assay for total homocysteine levels in humanserum J Chromatogr 1991565(1ndash
^2)441ndash6
[14] Frosst P Blom HJ Milos R et al A candidate genetic risk factor forvascular disease a common mutation in methylenetetrahydrofolatereductase Nat Genet 199510(1)111ndash3
[15] Nath CJ Ong T Micronuclei assay in cytokinesis-blocked binucleated andconventional mononucleated methods in human peripheral lymphocytesTeratog Carcinog Mutagen 199010(3)273ndash9
[16] Giri S Thompson PD Taxel P et al Oral estrogen improves serum lipidshomocysteine and fibrinolysis in elderly men Atherosclerosis 1998137359ndash66
[17] Kim MH Kim E Passon EL et al Cortisol and estradiol^non-genetic
factors for hyperhomocyst(e)inemia Metabolism 199746247ndash9[18] Brattstrom L Lindgren A Israelsson B Andersson A Hultberg B
Homocysteine and cysteine Determinants of plasma levels in middle-agedand elderly subjects J Inter-Am Med 1994236(6)633ndash41
[19] Fukagawa NK Martin JM Wurthmann A Prue AH Ebenstein DORourke B Sex-related differences in methionine metabolism and plasmahomocysteine concentrations Am J Clin Nutr 200072(1)22ndash9
[20] Slama R Bouyer J Windham G Fenster L Werwatz A Swan SHInfluence of paternal age on the risk of spontaneous abortion Am JEpidemiol 2005161816ndash23
[21] Bosch M Rajmil O Martinez-Pasarell O et al Linear increase of diploidyin human sperm with age a four-colour FISH study Eur J Hum Genet20019533ndash8
[22] Griffin DK Abruzzo MA Millie EA et al Non-disjunction in humansperm evidence for an effect of increasing paternal age Hum Mol Genet199542227ndash32
[23] Singh NP Muller CH Berger RE Effects of age on DNA double-strandbreaks and apoptosis in human sperm Fertil Steril 2003801420ndash30
[24] Crow J The origins patterns and implications of human spontaneousabortion Nat Rev Genet 2000140ndash7
[25] Quere I Bellet H Hoffet M Janbon C Mares P Gris JC A woman withfive consecutive fetal deaths case report and retrospective analysis ofhyperhomocysteinemia prevalence in 100 consecutive women withrecurrent miscarriages Fertil Steril 199869(1)152ndash4
[26] Nelen WL Blom HJ Steegers EA den Heijer M Thomas CM Eskes TKHomocysteine and folate levels as risk factors for recurrent earlypregnancy loss Obstet Gynecol 200095(4)519ndash24
[27] Nelen WL Bulten J Steegers EA Blom HJ Hanselaar AG Eskes TKMaternal homocysteine and chorionic vascularization in recurrent earlypregnancy loss Hum Reprod 200015(4)954ndash60
[28] Nelen WL Blom HJ Steegers EA den Heijer M Eskes TKHyperhomocysteinemia and recurrent early pregnancy loss a meta-analysis Fertil Steril 200074(6)1196ndash9
[29] Ren A Wang J Methylenetetrahydrofolate reductase C677T polymorph-ism and the risk of unexplained recurrent pregnancy loss a meta-analysisFertil Steril 200686(6)1716ndash22
[30] Zetterberg H Regland B Palmeacuter M et al Increased frequency ofcombined methylenetetrahydrofolate reductase C677T and A1298Cmutated alleles in spontaneously aborted embryos Eur J Hum Genet200210(2)113ndash8
[31] Kumar KS Govindaiah V Naushad SE Devi RR Jyothy A Plasmahomocysteine levels correlated to interactions between folate status andmethylene tetrahydrofolate reductase gene mutation in women withunexplained recurrent pregnancy loss J Obstet Gynaecol 200323(1)55ndash8
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
540
541
542
543
544
545
546
547
548
549
550
551
552
553
554
555
556
557
558
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573
574
7V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
[32] Candito M Magnaldo S Bayle J et al Clinical B12 deficiency in one caseof recurrent spontaneous pregnancy loss Clin Chem Lab Med 200341(8)1026ndash7
[33] DUva M Di Micco P Strina I et al Hyperhomocysteinemia in womenwith unexplained sterility or recurrent early pregnancy loss from SouthernItaly a preliminary report Thromb J 2007115ndash10
[34] Carrell DT Liu L Peterson CM et al Sperm DNA fragmentation isincreased in couples with unexplained recurrent pregnancy loss ArchAndrol 200349(1)49ndash55
[35] Carrell DT Wilcox AL Lowy L et al Elevated sperm chromosomeaneuploidy and apoptosis in patients with unexplained recurrent pregnancyloss Obstet Gynecol 2003101(6)1229ndash35
[36] Steegers-Theunissen RP Steegers EA de Boer R Thomas CM Klooster-man MD Eskes TK Elevated folate levels in amniotic fluid after oralsupplementation Eur J Obstet Gynecol Reprod Biol 199036(3)283ndash91
[37] Nelen WL Blom HJ Thomas CM Steegers EA Boers GH Eskes TKMethylenetetrahydrofolate reductase polymorphism affects the change in
UNCO
RREC
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
OF
homocysteine and folate concentrations resulting from low dose folic acidsupplementation in women with unexplained recurrent miscarriagesJ Nutr 1998128(8)1336ndash41
[38] Rodgers GM Kane WH Activation of endogenous Factor V by ahomocysteine-induced vascular endothelial cell activator J Clin Invest198677(6)1909ndash16
[39] Lentz SR Sadler JE Inhibition of thrombomodulin surface expression andprotein C activation by the thrombogenic agent homocysteine J ClinInvest 199188(6)1906ndash14
[40] Nishinaga M Ozawa T Shimada K Homocysteine a thrombogenic agentsuppresses anticoagulant heparan sulfate expression in cultured porcineaortic endothelial cells J Clin Invest 199392(3)1381ndash6
[41] Hajjar KA Mauri L Jacovina AT et al Tissue plasminogen activatorbinding to the annexin II tail domain Direct modulation by homocysteineJ Biol Chem 1998273(16)9987ndash93
[42] Fenech M Cytokinesis-block micronucleus cytome assay Nat Protoc20072(5)1084ndash104
TEDPR
O
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
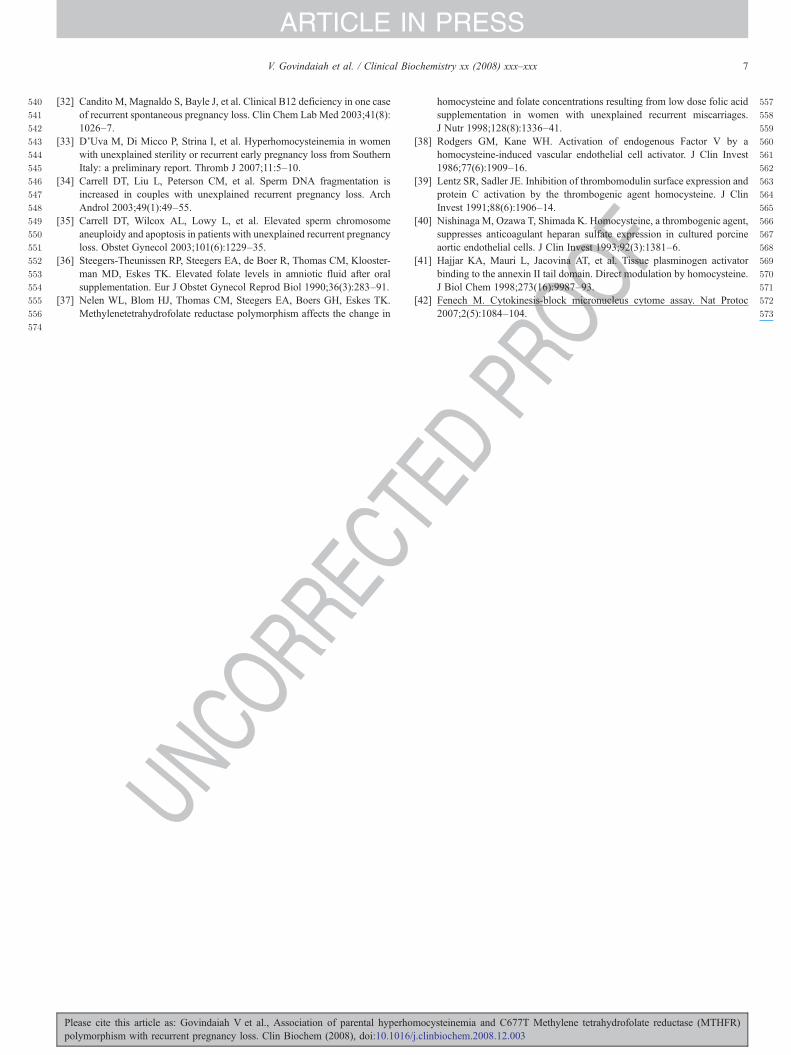
540
541
542
543
544
545
546
547
548
549
550
551
552
553
554
555
556
557
558
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573
574
7V Govindaiah et al Clinical Biochemistry xx (2008) xxxndashxxx
ARTICLE IN PRESS
[32] Candito M Magnaldo S Bayle J et al Clinical B12 deficiency in one caseof recurrent spontaneous pregnancy loss Clin Chem Lab Med 200341(8)1026ndash7
[33] DUva M Di Micco P Strina I et al Hyperhomocysteinemia in womenwith unexplained sterility or recurrent early pregnancy loss from SouthernItaly a preliminary report Thromb J 2007115ndash10
[34] Carrell DT Liu L Peterson CM et al Sperm DNA fragmentation isincreased in couples with unexplained recurrent pregnancy loss ArchAndrol 200349(1)49ndash55
[35] Carrell DT Wilcox AL Lowy L et al Elevated sperm chromosomeaneuploidy and apoptosis in patients with unexplained recurrent pregnancyloss Obstet Gynecol 2003101(6)1229ndash35
[36] Steegers-Theunissen RP Steegers EA de Boer R Thomas CM Klooster-man MD Eskes TK Elevated folate levels in amniotic fluid after oralsupplementation Eur J Obstet Gynecol Reprod Biol 199036(3)283ndash91
[37] Nelen WL Blom HJ Thomas CM Steegers EA Boers GH Eskes TKMethylenetetrahydrofolate reductase polymorphism affects the change in
UNCO
RREC
Please cite this article as Govindaiah V et al Association of parental hyperhopolymorphism with recurrent pregnancy loss Clin Biochem (2008) doi101016
OF
homocysteine and folate concentrations resulting from low dose folic acidsupplementation in women with unexplained recurrent miscarriagesJ Nutr 1998128(8)1336ndash41
[38] Rodgers GM Kane WH Activation of endogenous Factor V by ahomocysteine-induced vascular endothelial cell activator J Clin Invest198677(6)1909ndash16
[39] Lentz SR Sadler JE Inhibition of thrombomodulin surface expression andprotein C activation by the thrombogenic agent homocysteine J ClinInvest 199188(6)1906ndash14
[40] Nishinaga M Ozawa T Shimada K Homocysteine a thrombogenic agentsuppresses anticoagulant heparan sulfate expression in cultured porcineaortic endothelial cells J Clin Invest 199392(3)1381ndash6
[41] Hajjar KA Mauri L Jacovina AT et al Tissue plasminogen activatorbinding to the annexin II tail domain Direct modulation by homocysteineJ Biol Chem 1998273(16)9987ndash93
[42] Fenech M Cytokinesis-block micronucleus cytome assay Nat Protoc20072(5)1084ndash104
TEDPR
O
mocysteinemia and C677T Methylene tetrahydrofolate reductase (MTHFR)jclinbiochem200812003
Copyright © 2022 FDOKUMEN




















