The ???Primary??? Antiphospholipid Syndrome: Major Clinical and Serological Features
Upload
independentCategory
view
2download
0
Antiphospholipid Antibodies and RetinalThrombosis in Patients Without Risk Factors:
A Prospective Case-control Study
ROSARIO COBO-SORIANO, MD, PHD, SILVIA SANCHEZ-RAMON, MD,M. JESUS APARICIO, MD, M. ANGELES TEIJEIRO, MD, PILAR VIDAL, MD,
MARTA SUAREZ-LEOZ, MD, PHD, MARGARITA RODRIGUEZ-MAHOU, MD, PHD,ANA RODRIGUEZ-HUERTA, MD, EDUARDO FERNANDEZ-CRUZ, MD, PHD,
AND CARLOS CORTES, MD, PHD
● PURPOSE: To determine the prevalence of antiphos-pholipid antibodies and other immunologic abnormalitiesin patients with occlusive retinal vascular events, exemptfrom conventional risk factors of retinal thrombosis.● METHODS: Forty patients with retinal vascular occlu-sion (26 with retinal vein occlusions, eight with arterialocclusions, two with combined venous and arterial oc-clusions, and four with venous occlusions plus vasculi-tis), free of main accepted risk factors for retinalthrombosis, were prospectively screened for antiphos-pholipid antibodies (anticardiolipin-antibodies and lupusanticoagulant) and other immunologic abnormalities.Fourteen patients were younger than 50 years. Preva-lence and mean values of antiphospholipid antibodies(aPL) were compared with those in a homogeneouscontrol group of 40 patients.● RESULTS: The prevalence of antiphospholipid antibod-ies in the study group was 22.5% (nine of 40). Compar-ison with control group prevalence (5% [two of 40])showed a statistically significant difference (P 5 .04).Six patients in the study group disclosed positivity forIgG-anticardiolipin antibodies, one patient for IgM anti-cardiolipin antibodies, and two patients for both isotypesIgG and IgM anticardiolipin antibodies. The antibodyassay for lupus anticoagulant was negative for all pa-tients. Three patients were diagnosed as having primaryantiphospholipid antibody syndrome and are undergoing
systemic anticoagulant therapy. Relevant immunologicabnormalities were also found (27.5% with antinuclearantibodies, 35% with elevation of circulating immunecomplexes, 35% with complement deficiency, 30% withpositive rheumatoid factor, and 17.5% with positiveC-reactive protein). Thirteen patients (32.5%) had morethan four parameters altered. No significant associationwas found between prevalence or mean values of anticar-diolipin antibody and patients younger than 50 years.● CONCLUSIONS: The high prevalence of anticardiolipinantibodies in patients with vaso-occlusive retinopathyexempt from conventional risk factors, and the relevantdiagnostic and therapeutic implications, lead us to rec-ommend a systematic search for specific antiphospholipidantibodies in such patients. (Am J Ophthalmol 1999;128:725–732. © 1999 by Elsevier Science Inc. Allrights reserved.)
R ETINAL THROMBOSIS IS CONSIDERED A DISEASE OF THE
elderly, with more than 90% of cases in patients morethan 50 years of age, with associated systemic vascular
disease.1 More than 50% to 70% of patients suffer fromarterial hypertension, cardiovascular atherosclerotic disease,or diabetes mellitus, and the vast majority of the vascularocclusions have been attributed to degenerative changes ofthe vessel wall.2–5 Traditionally, for this reason, no medicaltreatment has been found to be effective in the managementof these conditions,3 and most cases are not investigated as tocause or treated, limiting the ophthalmologist’s role to pre-vention of further ocular complications.
Antiphospholipid antibodies are recently recognizedvascular risk factors that have been increasingly identifiedas causative agents in multiple thromboembolic events.They are circulating serum polyclonal immunoglobulinsthat bind anionic membrane phospholipids and coagula-
Accepted for publication Aug 11, 1999.From the Departments of Ophthalmology (Drs Cobo-Soriano, Apari-
cio, Teijeiro, Vidal, Suarez-Leoz, and Cortes), Immunology (Drs Sanchez-Ramon, Rodriguez-Mahou, and Fernandez-Cruz), and Hematology (DrRodriguez-Huerta), Hospital General Universitario “Gregorio Maranon,”Area 1 Atencion Especializada, Universidad Complutense de Madrid,Madrid, Spain.
Reprint requests to Rosario Cobo-Soriano, MD, PhD, C/Cuesta BlancaNo. 154, Alcobendas, 28100, Madrid, Spain; fax: 34-91-527-44-76;e-mail: [email protected]
© 1999 BY ELSEVIER SCIENCE INC. ALL RIGHTS RESERVED.0002-9394/99/$20.00 725PII S0002-9394(99)00311-6

tion plasmatic proteins (autoantibodies), leading to ahypercoagulable state and recurrent thrombosis.
The clinical importance of detection of antiphospho-lipid antibodies stems from their association with a syn-drome characterized by the triad of arterial or venousthrombosis, recurrent abortions caused by placental vascu-lar insufficiency, and thrombocytopenia, known as theantiphospholipid syndrome, that requires long-term anti-coagulation therapy. Antiphospholipid syndrome may befound associated with underlying systemic autoimmunedisorders, particularly systemic lupus erythematosus and“lupus-like” syndromes, or may appear isolated withoutmanifestations of systemic disease (primary antiphospho-lipid syndrome).6
Ophthalmologic manifestations described in associationwith antiphospholipid antibodies include amaurosis fugaxepisodes, transient diplopia and visual field loss, ischemicoptic neuropathy, retinal and choroidal vascular occlu-sions, and peripheral proliferative retinopathy.7–14 In ad-dition, a high rate (88%) of retinal abnormalities has beenfound in patients with primary antiphospholipid syn-drome.15 However, the incidence of antiphospholipid an-tibodies among patients suffering from retinal vascularocclusions is still uncertain, and most publications to dateare either case reports or small series. Few prospectivestudies have been performed on the overall group of retinalthrombosis (patients older than 50 years with associatedrisk factors), reporting low rates of prevalence of antiphos-pholipid antibodies (0% to 9%); most authors concludetheir manuscripts by emphasizing the importance of deter-mining the frequency of these antibodies in the youngerpatients without evident risk factors.7,16–18
We performed a prospective case-control study to ascer-tain the prevalence of antiphospholipid antibodies inpatients free of conventional risk factors and to determinewhether other immunologic abnormalities are involved.
PATIENTS AND METHODS
OURS IS A LARGE TEACHING AND REFERRAL INSTITUTION
serving a population of 650,000 inhabitants in a large city.During a 24-month period between September 1996 andSeptember 1998, we were able to enroll 40 consecutiveoutpatients at the Retina Clinic who had an acute episodeof retinal vascular occlusion (venous, arterial, or both) andwho did not have five accepted risk factors for thrombosis.
All patients with the following recognized systemicdisorders were excluded at the initial examination: sys-temic arterial hypertension, diabetes mellitus, hyperlipid-emia, embolizating cardiopathy, and significant carotidatherosclerosis. Patients were then referred to the InternalMedicine Service, where a complete general medicalexamination was performed, and the absence of the afore-mentioned diseases was objectively proven. Specific atten-tion was paid to the presence of arterial hypertension
(blood pressure greater than 140 mm Hg systolic and 90mm Hg diastolic on more than one occasion), diabetesmellitus (considered present if repeated fasting serumglucose levels were elevated), and hyperlipidemia (definedas repeated increased serum total cholesterol or triglyceridelevels, or atherogenic index greater than 5). Heart diseasewas investigated when necessary by the internist, searchingfor electrocardiographic or echocardiographic signs of val-vular disease, myocardial infarction, atrial fibrillation,conduction blocks, ventricular arrythmias, or atrial en-largement. Significant atherosclerosis on carotid echo-Doppler examination was considered to be present if flowreduction was greater than 60%.
Later, patients underwent a thorough laboratory studyby the Immunology and Hematology Services, with par-ticular attention to the detection of antiphospholipidantibodies (anticardiolipin antibodies by the ImmunologyService and lupus anticoagulant by the Hematology Ser-vice). In addition, all patients were investigated for clinicalcriteria for connective-tissue disease or consumption oflupus-related drugs, and tested for human immunodefi-ciency virus antibodies, hepatitis B surface antigen, andhepatitis C virus antibodies, all of which were confirmed tobe negative. Informed consent was obtained from allpatients.
The ophthalmologic evaluation included, when feasible,questioning to ascertain whether the patient had experi-enced previous thrombotic episodes, best-corrected visualacuity, visual field assesment of arterial occlusions, slit-lamp biomicroscopy, applanation tonometry, binocularophthalmoscopy, and fluorescein angiography. Retinalphotographs were taken in all patients during the acutethrombotic event. Retinal vascular findings were dividedinto venous occlusions (central, hemispheric, majorbranch, and macular branch), arterial occlusions (central,hemispheric, major branch, and distal branch), combinedvenous and arterial occlusions, and a fourth group in whichvenous occlusion was associated with ophthalmoscopic orangiographic signs of vasculitis.
Specific immunologic investigations obtained in allpatients included detection of antiphospholipid antibod-ies, lupus anticoagulant, and possible associated autoim-mune disease. Anticardiolipin antibodies, isotypes IgG andIgM, were measured by means of an enzyme-linked immu-nosorbent assay (Fresenius; Gull Diagnostics, Bad Hom-burg, Germany). Immunoglobulin G and IgM results wereclassified as negative (0 to 5), low positive (5 to 15),moderately positive (15 to 60), or high positive (greaterthan 60) in GPL and MPL units/ml, respectively.
Lupus anticoagulant refers to prolonged phospholipid-dependent coagulation tests carried out by the followingthree procedures: activated partial thromboplastin time,tissue thromboplastin inhibition performed by increasingdilutions of thromboplastin from 1:100 to 1:1,000, and asimplified dilute Russell viper venom time (normal value,less than 30 to 40 minutes). If any of these test results was
AMERICAN JOURNAL OF OPHTHALMOLOGY726 DECEMBER 1999

abnormal, correction by mixture of activated partial throm-boplastin time test with control plasma at 50% dilution andconfirmatory tests (platelet neutralization test and confirma-tory-Russell dilute viper venom time), were performed. False-positive tests for syphilis were investigated by the rapidplasma reagin test; positive results were confirmed by meansof the treponemic microagglutination test.
To investigate possible associated autoimmune disease,we determined the following parameters: by nephelometry,we measured serum immunoglobulins (IgG, IgM, IgA),complement factors (C3, C4 y FB), circulating immunecomplexes, C-reactive protein, and rheumatoid factor.Total hemolytic complement activity was detected by theradial immunodiffusion technique. Serum samples werealso screened by indirect immunofluorescence to detectantinuclear antibodies on rat liver, stomach, and kidneysections and HEp-2 cell slides. Anti–native DNA andanti-extraible nuclear antibodies were both evaluated byenzyme-linked immunosorbent assay when presence ofantinuclear antibodies was observed. In patients sufferingfrom vasculitis, HLA-B27 was also determined.
In addition, all patients underwent routine laboratorystudies (standard hematologic blood cell count, erythro-cyte sedimentation rate, standard serum chemistries, and acomplete lipid profile). Ophthalmologic and immunologicfollow-up was performed in all cases, and determinations ofthose values were made at 3-month to 6-month intervals.
Anticardiolipin antibodies and lupus anticoagulant werecompared with those of a control group comprising 40consecutive outpatients who had ophthalmopathy otherthan vaso-occlusive retinopathy (10 patients with refrac-tive disturbances, nine patients with conjunctivitis, onepatient with episcleritis, three patients with age-relatedmacular degeneration, two patients with ocular trauma,three patients with open-angle glaucoma, eight patientswith cataracts, and four patients with uveitis). They were
also investigated for the previously mentioned systemicdiseases. The control group included only those who werewithout risk factors and accepted the immunologic study.
Data were initially registered in a database (MicrosoftExcel 97; Microsoft Corporation, Redmond, Washington).The statistical analysis was performed with the programEpi-Info (Division of Surveillance and Epidemiology Pro-gram Office, Centers for Disease Control and Prevention,Bethesda, Maryland). Descriptive analysis included meanand SD for quantitative variables, and for qualitativevariables, absolute and relative frequency (percentage).The bivariant comparative analysis included Fisher exacttest for qualitative variables when n less than 20 or when25% of theoretic values were less than five. We also usedthe Student t test to compare means of quantitativevariables between two independent groups. The level ofstatistical significance was fixed at P , .05.
RESULTS
THE STUDY GROUP CONSISTED OF 40 PATIENTS, 19 MEN
(47.5%) and 21 women (52.5%), with a mean (6SD) ageof 53 6 14.3 years (range, 26 to 79 years). Fourteenpatients were younger than 50 years.
Table 1 summarizes sample distribution by type ofvascular occlusion: 26 cases (65%) were venous occlusions,eight cases (20%) arterial occlusions, two cases (5%)combined arterial and venous occlusions, and four cases(10%) venous occlusions plus vasculitis. Laterality wasdistributed as follows: right eye in 15 cases, left eye in 24cases, and both eyes in one case.
The prevalence of antiphospholipid antibodies in thestudy group was 22.5% (nine of 40). Comparison withcontrol group prevalence (5% [two of 40]), showed astatistically significant difference (P 5 .04). Nine patients
TABLE 1. Types of Retinal Vascular Occlusion in 40 Patients
Type of Retinal Vascular
Occlusion
No. (%) of
Patients Description No.
Venous occlusion 26 (65) Central vein occlusion
Hemispheric branch vein occlusion
Major branch vein occlusion
Macular branch vein occlusion
8
1
11
6*
Venous plus arterial
occlusion
2 (5) Distal venous plus arterial occlusion 2
Arterial occlusion 8 (20) Central artery occlusion
Major branch artery occlusion
Distal branch artery occlusion
Distal branch artery plus choroidal occlusion
1
5
1
1
Vasculitis plus
venous occlusion
4 (10) Central vein occlusion plus vasculitis
Major branch vein occlusion plus vasculitis
2
2
*One case bilateral.
ANTIPHOSPHOLIPID ANTIBODIES AND RETINAL THROMBOSISVOL. 128, NO. 6 727

in the study group presented positive titers of anticardio-lipin antibodies: six cases of IgG isotype, one case of IgMisotype, and two cases of both IgG and IgM isotypes. Theyall had negative results on the rapid plasma reagent test.Two patients had negative values on first determinationand positive values in later measurements (Cases 4 and 5).No case showed positivity for lupus anticoagulant assay,although in 10 patients two coagulation tests were altered.Summaries of the key clinical and laboratory features ofpositive cases are presented in Table 2. Two of them hadprevious occlusive vascular events (retinal in Case 3 andcerebral in Case 9), and Case 2 had an obstetric anteced-ent (two abortions).
Three patients (Cases 1, 2, and 3) met the criteria forprimary antiphospholipid syndrome after two positive titermeasurements in a 3-month period, all of them actuallyreceiving oral anticoagulation therapy. Figures 1 through 6represent some of these patients’ acute thrombotic events.The clinical form and evolution of retinal vascular occlu-sions in these patients did not seem to be more severe thanin the rest of the study group with negative antiphospho-lipid antibodies. Thirty-one patients scored below thethreshold of positivity for anticardiolipin antibodies: theanticardiolipin antibody IgG and IgM mean (6SD) valuesin the series were 10.1 6 20 GPL units/ml and 7.6 6 12.3MPL units/ml.
As mentioned, the control group consisted of 40 pa-tients without retinal vascular occlusive disease and with-out conventional risk factors. Ages ranged between 35 and67 years (mean, 57 years). Two control subjects (5%) hadpositive anticardiolipin antibody titers (one patient withpenetrating ocular trauma with an intraocular foreign bodyhad an IgG value of 28 GPL units/ml, and one patient with
related macular degeneration had anticardiolipin antibodyIgM titers of 15 MPL units/ml). However, most values inthe control group were negative (less than 5 units/ml),with mean values of anticardiolipin antibody IgG of3.37 6 5 GPL units/ml, and IgM, 4.42 6 3.4 MPLunits/ml. Comparative analysis study showed a statisticaldifference between both groups when relative frequenciesof anticardiolipin antibodies were compared (P 5 .04,Fisher exact test), but mean levels did not reach statisticalsignificance: anticardiolipin antibody IgG (P 5 .056, ttest) and anticardiolipin antibody IgM (P 5 .1, t test).
We also determined the frequencies of other immuno-
FIGURE 1. Case 1. Fluorescein angiography of an eye withtemporoinferior branch retinal vein occlusion, showing fovealand temporal hemorrhages with nonperfusion of involved ves-sels, in a 29-year-old man with previous episodes of peripheralhemorrhages and vasculitis.
TABLE 2. Ophthalmologic and Immunologic Data in Positive Cases
Patient No.,
Age (yrs), Sex Vascular Occlusion
aCL IgG/IgM
(GPL/MPL units/ml)* LA*
Associated Immunological
Abnormalities (Titers)*
1, 29, M BRVO temporoinferior
LE plus vasculitis
46.4/1.3, PAPS Negative CIC (5,15 mg/ml), CH100 (52 UCH100/ml)
2, 47, F Hemispheric superior BVRO RE 15/18, PAPS Negative C3 (79 mg/dl), CH100 (47 UCH100/ml), CIC (3.5 mg/ml)
3, 53, M BRAO temporoinferior RE 20/11, PAPS Negative C4 (16 mg/dl), CH100 (46 UCH100/ml), ANA1 (1/40 H)
4, 43, F CRVO LE 30/9 Negative CH100 (54 UCH100/ml)
5, 74, F MBRVO RE 18/13 Negative C4 (20 mg/dl), ANA1 (1/40 H)
6, 70, M CRVO LE 20/2.5 Negative No immunologic parameters altered
7, 52, F MBRVO LE 16.7/1.7 Negative No immunologic parameters altered
8, 49, F BRVO temporoinferior LE 17/3.8 Negative ANA1 (1/60 H)
9, 55, F BRVO temporosuperior RE 120/78 Negative C4 (16 mg/dl), CH100 (31 UCH100/ml),
CRP1, ANA1, RF1
BRVO 5 branch retinal vein occlusion; BRAO 5 branch retinal artery occlusion; CRVO 5 central retinal vein occlusion; MBRVO 5 macular
branch retinal vein occlusion; PAPS 5 primary antiphospholipids antibody syndrome.
*Reference values: aCL (anticardiolipin antibodies) IgG, IgM 5 0–15 GPL/MPL U/ml; LA (lupus anticoagulant) 5 negative; CIC (circulating
immune complexes) 5 0–1.5 mg/ml; C3, C4 (complement factors), C3 5 83–177 mg/dl, C4 5 20–60 mg/dl, CH100 (total hemolytic
complement activity) 5 70–200 UCH100/ml; CRP (C-reactive protein) , 3.2; RF (rheumatoid factor), ANA (antinuclear antibodies) 5 negative.
AMERICAN JOURNAL OF OPHTHALMOLOGY728 DECEMBER 1999
logic abnormalities. Eleven patients had positive antinu-clear antibodies (27.5%), 14 had increased titers ofcirculating immune complexes (35%), 14 had decreasedlevels of complement (C3, C4, or total hemolytic comple-ment; 35%), 12 had positive rheumatoid factor (30%), andseven had positive C-reactive protein (17.5%). Thirteenpatients (32.5%) had more than four simultaneous immu-nologic parameters altered. No patient met criteria forconnective-tissue disorder or systemic lupus erythemato-sus, although three patients had a positive antibody assayfor anti–native DNA antibodies.
To determine whether younger patients with retinalthrombosis had higher mean levels or prevalence of anti-cardiolipin antibodies, or more associated immunologicabnormalities, we divided the series into two age groups:younger and older than 50 years. Table 3 shows anticar-diolipin antibody percentages, mean values, and otherimmunologic parameters, and a comparison between the
groups. Differences in anticardiolipin antibody prevalencesand mean values between patients younger and older than50 years did not reach statistical significance. Regardingother immunologic parameters, we found no statisticaldifferences between the two groups other than a significantprevalence of rheumatoid factor in the older group.
DISCUSSION
WE CARRIED OUT AN IMMUNOLOGIC STUDY ON 40 PA-
tients suffering from an acute episode of retinal vascularocclusion who had no conventional risk factors, to learnwhether this subpopulation would present a significantlyhigher prevalence of antiphospholipid antibodies than thatreported in the general retinal thrombosis population.
Studies on the prevalence of antiphospholipid antibod-ies in ocular vascular events are scarce, mostly retrospec-
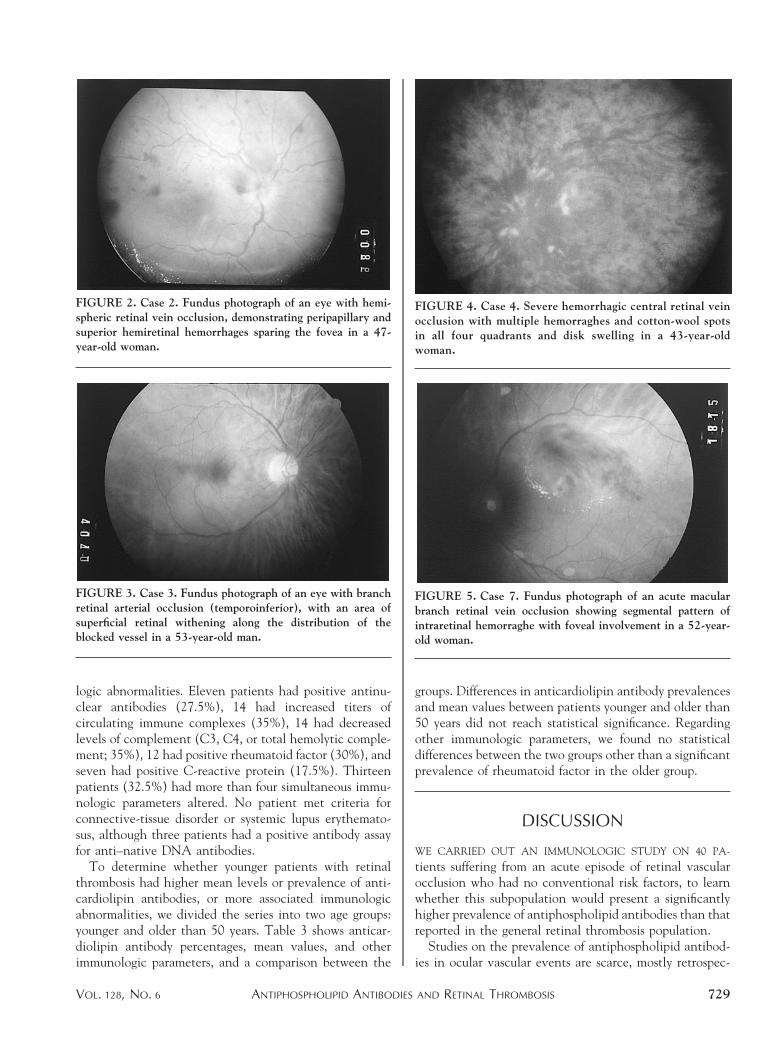
FIGURE 2. Case 2. Fundus photograph of an eye with hemi-spheric retinal vein occlusion, demonstrating peripapillary andsuperior hemiretinal hemorrhages sparing the fovea in a 47-year-old woman.
FIGURE 3. Case 3. Fundus photograph of an eye with branchretinal arterial occlusion (temporoinferior), with an area ofsuperficial retinal withening along the distribution of theblocked vessel in a 53-year-old man.
FIGURE 4. Case 4. Severe hemorrhagic central retinal veinocclusion with multiple hemorraghes and cotton-wool spotsin all four quadrants and disk swelling in a 43-year-oldwoman.
FIGURE 5. Case 7. Fundus photograph of an acute macularbranch retinal vein occlusion showing segmental pattern ofintraretinal hemorraghe with foveal involvement in a 52-year-old woman.
ANTIPHOSPHOLIPID ANTIBODIES AND RETINAL THROMBOSISVOL. 128, NO. 6 729

tive, and performed in the oldest patients with risk factors.Therefore, reported prevalence data are low, ranging from0% to 9%.7,16–18 Our data support a significantly higherrate (22.5%) for the group of patients with retinal throm-bosis exempt from the main conventional risk factors forthrombosis. We are unaware of previous reports of preva-lence data for this subgroup and could find no reference toit in a computerized search using MEDLINE. Furthermore,a statistically significant difference was demonstrated com-pared with a homogeneous control group.
Anticardiolipin IgG isotype was significantly more fre-quent than the IgM isotype, consistent with previousworks on antiphospholipid antibodies mediating othertypes of vascular events, in which IgG isotype class seemedto correlate best with clinical disease.10,19
We were unable to demonstrate that younger patientswith retinal vascular events had a higher incidence ofantiphospholipid antibodies or other immunologic abnor-malities, probably because of the size of the sample.However, seven of nine positive cases were in patientsyounger than 55 years. Interestingly, Glacet-Bernard andassociates7 highlighted the low frequency of antiphospho-lipid antibodies in the under-50 age group (one of 16cases), even in patients with vasculitis in whom highervalues might be expected. In fact, in that study,7 three ofthe four positive cases occurred in patients older than 60years with more than two risk factors. Watts and associ-ates10 found an increased frequency of anticardiolipinantibody (37%) in a series of anterior ischemic opticneuropathy in which 100% of patients were older than 60years. However, antiphospholipid syndrome has tradition-ally been associated with cerebrovascular events in youngindividuals. Angellini and associates20 reported a highprevalence of antiphospholipid antibodies (76%) in chil-dren with transient cerebral ischemia episodes, and mostreports of isolated cases of stroke associated with antiphos-
pholipid antibodies have been in patients younger than 50years.11–14,20–23
Lupus anticoagulant was negative in all cases, althoughin nine patients two coagulation tests were altered. How-ever, previous reports show a strong association betweenthrombotic phenomena and the presence of lupus antico-agulant; Derksen and Kater24 indicated that 46% of pa-tients with systemic lupus erythematosus and positive lupusanticoagulant develop thrombosis, compared with 4.5% to18% of patients with systemic lupus in general. Anotherreview stated that 30% of patients who are positive forlupus anticoagulant develop thromboses.25 Literature ref-erences to an association of lupus anticoagulant withocular vascular events are isolated cases,11,12,14,26–28 and, toour knowledge, there are no larger and conclusive series.
The pathogenic mechanism by which antiphospholipidantibodies mediate thrombosis is undefined. In vitro, theyare anticoagulant, but in vivo, their effect is paradoxicallyto promote a thrombotic tendency, probably because ofaction on phospholipid components of platelet membrane,vascular endothelium, and coagulation factors.29–31
Regarding the type of affected vessel, in our study, veinspredominated over arteries. However, arterial occlusionsseem to be more commonly associated with antiphospho-lipid syndrome than venous occlusive disease in theliterature.7,27–30
Our data show a relevant number of immunologicaltered values, although we have not found statisticalcorrelation with age or presence of antiphospholipid anti-bodies. These alterations, although nonspecific at the timeof the study, could be the first signs of further connective-tissue disease. It is generally accepted that partial orcomplete deficiency of C4 can predispose to diseases such
FIGURE 6. Case 9. Fundus photograph of an eye with branchretinal vein occlusion with hemorrhages and cotton-wool spotsin the superotemporal retinal quadrant in a 55-year-old womanwith high levels of IgG anticardiolipin antibodies.
TABLE 3. Comparison of Relative Frequencies of aCL,Mean Values of aCL, and Other Immunologic Parameters
Between Age Groups
Parameters
,50 yrs
(n 5 14)
.50 yrs
(n 5 26) P Value
aCL (no. [%]) 4/14 (28.6) 5/26 (19) .7*
aCL IgG (mean 6 SD) 11.4 6 13 10.1 6 23 .6†
aCL IgM (mean 6 SD) 7.09 6 5 7.98 6 15 .6†
ANA1 (no. [%]) 3/14 (21) 8/26 (30.7) .7*
Complement decrease
(CH100) (no. [%])
6/14 (43) 8/26 (30.7) .5*
Rheumatoid factor (no. [%]) 1/14 (7) 11/26 (42) .03*
CRP1 (no. [%]) 4/14 (28) 3/26 (11.5) .2*
CIC elevation (no. [%]) 5/14 (36) 9/26 (34.6) 1.0*
aCL 5 anticardiolipin antibodies; ANA 5 antinuclear antibody;
CH100 5 total hemolytic complement; CRP 5 C-reactive pro-
tein; CIC 5 circulating immune complex.
*Fisher exact test.†Student t test.
AMERICAN JOURNAL OF OPHTHALMOLOGY730 DECEMBER 1999

as systemic lupus erythematosus. In addition, patients withprimary antiphospholipid antibody syndrome have a sig-nificantly lower prevalence of antinuclear antibodies thanpatients with antiphospholipid syndrome plus systemiclupus erythematosus.33 Therefore, these two parametersmay help to locate patients with primary antiphospholipidantibody syndrome who subsequently may develop featuresof systemic lupus erythematosus. Asherson and Harris32
reported that a subpopulation of patients with systemiclupus erythematosus had a thrombophilic tendency, in whichvaso-occlusive retinopathy was more frequent than the typi-cal vasculitic picture in systemic lupus erythematosus ofcotton-wool spots and hemorrhages; in this subgroup theyfound an important presence of lupus anticoagulant or anti-cardiolipin antibodies that showed significant associationwith cerebrovascular disease.
The identification of antiphospholipid antibodies is oftremendous interest and relevance in ophthalmology be-cause it can provide a new overview of the pathogenesis ofretinal vascular diseases, particularly in patients withoutevident risk factors. In addition, detection of antiphospho-lipid antibodies has important diagnostic and therapeuticimplications: diagnosis of a possible underlying autoim-mune disease or primary antiphospholipid antibody syn-drome with subsequent indication for anticoagulationtherapy and further close monitoring of their immunologicsituation.
Moreover, identification of such autoantibodies opensnew modes of treatment for certain vascular disorders bythe reduction of antiphospholipid antibody activity. Somevascular occlusions in systemic lupus erythematosus arecaused by direct interference with the coagulation systemmediated by antiphospholipid antibodies, rather than bycirculating immune complexes8; consequently, the correcttreatment is anticoagulant therapy rather than systemiccorticosteroids.34 Finally, prompt detection of antiphos-pholipid antibodies and therapeutic intervention can pre-vent not only future thrombotic ocular episodes but alsosuch episodes in other vital anatomic organs.
In conclusion, our data demonstrate that patients withvaso-occlusive retinopathy who are free of the main riskfactors have a significantly higher prevalence of antiphos-pholipid antibodies than that reported for the overallthrombosis population (22.5%). Moreover, important im-munologic alterations have been found, and we havediagnosed and treated three cases of primary antiphospho-lipid syndrome, all of them with antecedents of previousdifferent ischemic attacks. Because of the important diag-nostic and therapeutic implications of the syndrome,antiphospholipid antibodies should be systematicallysearched for in this group of patients. We believe thatscreening in these selected patients may reveal additionalspecific treatable thrombotic syndromes. Prospective stud-ies of this question with larger series of patients will help toclarify the importance of antiphospholipid antibodies inthis population.
ACKNOWLEDGMENTS
We greatly appreciate the assistance of Javier Carbone,MD, Elena Seoane, MD, and Carmen Rodriguez-Perez,MD, from the Immunology Service in the follow-up ofpatients, and Cristina Pascual, MD, PhD, from the Hema-tology Service in performing studies for lupus anticoagu-lant. Thomas O’Boyle assisted with English in themanuscript.
REFERENCES
1. Gupta A, Agarwal A, Bansal RK, Agarwal A. Ischaemiccentral retinal vein occlusion in the young. Eye 1993;7:138–142.
2. Brown GC. Retinal arterial obstructive disease. In: Ryan SJ,Schachat AP, Murphy RB, editors. Retina, 2nd ed. St Louis:Mosby-Year Book Inc, 1994:1361–1377.
3. Clarkson JC. Central retinal vein occlusion. In: Ryan SJ,Schachat AP, Murphy RB, editors. Retina, 2nd ed. St. Louis:Mosby-Year Book Inc, 1994:1379–1385.
4. Hayreh SS, Zimmerman MB, Podhajsky BSN. Incidence ofvarious types of retinal vein occlusion and their recurrenceand demographic characteristics. Am J Ophthalmol 1994;117:429–441.
5. Vine AK, Samama MM. The role of abnormalities in theanticoagulant and fibrinolytic systems in retinal vascularocclusions. Surv Ophthalmol 1993;37:283–289.
6. Finazzi G, Brancaccio V, Moia M, et al. The Italian registryof antiphospholipid antibodies: advances in basic, laboratoryand clinical aspects of thromboembolic diseases. Haemato-logica 1997;82:101–105.
7. Glacet-Bernard A, Bayani N, Chretien P, Cochard C, LelongF, Coscas G. Antiphospholipid antibodies in retinal vascularocclusions. Arch Ophthalmol 1994;112:790–795.
8. Acheson JF, Gregson RM, Schulenburg WE. Vaso-occlusiveretinopathy in the primary antiphospholipid syndrome. Eye1991;5:48–55.
9. Snyers B, Lambert M, Hardy JP. Retinal and choroidalvaso-occlusive disease in systemic lupus erythematosus asso-ciated with antiphospholipid antibodies. Retina 1990;10:255–260.
10. Watts MT, Greaves M, Clearkin LG. Antiphospholipidantibodies in the aetiology of ischaemic optic neuropathy.Eye 1991;5:75–79.
11. Levine SR, Crofts JW, Lesser GR, Floberg J, Welch KMA.Visual symptoms associated with the presence of a lupusanticoagulant. Ophthalmology 1988;95:686–692.
12. Garcıa-Vicente C, Belmonte J, Ramirez J, Castellano J.Retinopatıa proliferante y anticoagulante lupico. Arch SocEsp Oftalmol 1988;55:387–392.
13. Pulido JS, Ward LM, Fishman GA, Goodwin JA, FroelichCJ, Sanghvi JP. Antiphospholipid antibodies associated withretinal vascular disease. Retina 1987;7:215–218.
14. Kleiner RC, Najarian LV, Schatten S, Jabs DA, Patz A,Kaplan HJ. Vaso-occlusive retinopathy associated with an-tiphospholipid antibodies (lupus anticoagulant retinopathy).Ophthalmology 1989;96:896–904.
15. Castanon C, Amigo MC, Banales JL, Nava A, Reyes PA.Ocular vaso-occlusive disease in primary antiphospholipidsyndrome. Ophthalmology 1995;102:256–262.
16. Chabanel A, Horellou MH, Conrad J, Samama MM. Retinalvein occlusions: hemorrheology and hemostasis. ThrombHaemost 1993;69:996.
ANTIPHOSPHOLIPID ANTIBODIES AND RETINAL THROMBOSISVOL. 128, NO. 6 731

17. Bertram B, Haase G, Remky A, Reim M. Anticardiolipinantibodies in vascular occlusions of the eye. Ophthalmology1994;91:768–771.
18. Merry P, Acheson JF. Management of retinal vein occlusion.BMJ 1988;296:294.
19. Gharavi AE, Harris EN, Asherson RA, Hughes GRV.Anticardiolipin antibodies: isotype distribution and an-tiphospholipid specificity. Ann Rheum Dis 1987;46:1–6.
20. Angellini L, Ravelli A, Caporall R, Rumi V, Nardocci N,Martini A. High prevalence of antiphospholipid antibodiesin children with idiopathic cerebral ischemia. Pediatrics1994;94:500–503.
21. Brown GC, Magargal LE, Shields JA, Goldberg RE, WalshPN. Retinal arterial obstructions in children and youngadults. Ophthalmology 1988;88:18–25.
22. Levine SR, Deegan MJ, Futrell N, Welch KMA. Cerebro-vascular and neurologic disease associated with antiphospho-lipid antibodies: 48 cases. Neurology 1990;40:1181–1189.
23. Tietjen GE, Levine SR, Brown E, Mascha E, Welch KMA.Factors that predict antiphospholipid immunoreactivity inyoung people with transient focal neurological events. ArchNeurol 1993;50:833–836.
24. Derksen RHWM, Kater L. Lupus anticoagulant: revival of anold phenomenon. Clin Exp Rheum 1984;3:349–357.
25. Lechner K, Pabinger-Fasching I. Lupus anticoagulant andthrombosis: a study of 25 cases and review of literature.Haemostasis 1985;15:254–262.
26. Sanabria MR, Pascual P, Gonzalez JC. Oclusion vascular
retiniana periferica y sındrome antifosfolıpido primario. StOphthal 1998;17:41–43.
27. Saiz JA, Monotlio S, Olcina L, Valls B, Gonzalez A, MarcoM. Anticoagulante lupico y lupus eritematoso sistemico:oclusion arterial retiniana aguda. Arch Soc Esp Oftalmol1994;67:299–304.
28. Reisin LH, Reisin I, Darwshi A, Aviel E. Central retinalartery occlusion in a patient with circulating lupus antico-agulant. Ann Ophthalmol 1989;21:269–271.
29. Levine SR, Brey RL, Joseph CLM, Havstad S. Risk ofrecurrent thromboembolic events in patients with focalcerebral ischemia and antiphospholipid antibodies. Stroke1992;23:129–131.
30. Klasmashta MA, Hughes GRH. Antiphospholipid antibodiesand antiphospholipid syndrome. Curr Opin Rheumatol1995;7:389–394.
31. Cuadrado MJ, Amengual O, Klasmashta MA. Anticuerposantifosfolıpido. Rev Esp Reumatol 1996;23:389–395.
32. Asherson RA, Harris EN. Anticardiolipin antibodies: clini-cal associations. Postgrad Med J 1986;48:1081–1087.
33. Vianna JL, Klasmashta MA, Ordi-Ros J, et al. Comparison ofthe primary and secondary antiphospholipid syndrome: aEuropean multicenter study of 114 patients. Am J Med1994;96:2–9.
34. Jabs DA, Fine SL, Hochberg MC, Newman SA, Heiner GG,Stevens MB. Severe retinal vaso-occlusive disease in systemiclupus erythematosus. Arch Ophthalmol 1986;104:558–563.
The full-text of AJO is now available online at www.ajo.com. AuthorsInteractivet, currently available in limited form, is undergoing an upgrade.
AMERICAN JOURNAL OF OPHTHALMOLOGY732 DECEMBER 1999
Copyright © 2022 FDOKUMEN