
Retinal Prosthesis:An Overview
14
Retinal Prosthesis An Overview Mauli Dalal
Transcript of Retinal Prosthesis:An Overview

Retinal Prosthesis An Overview
Mauli Dalal
Retinal Prosthesis: An Overview
1
Physiology and Anatomy of Eye:
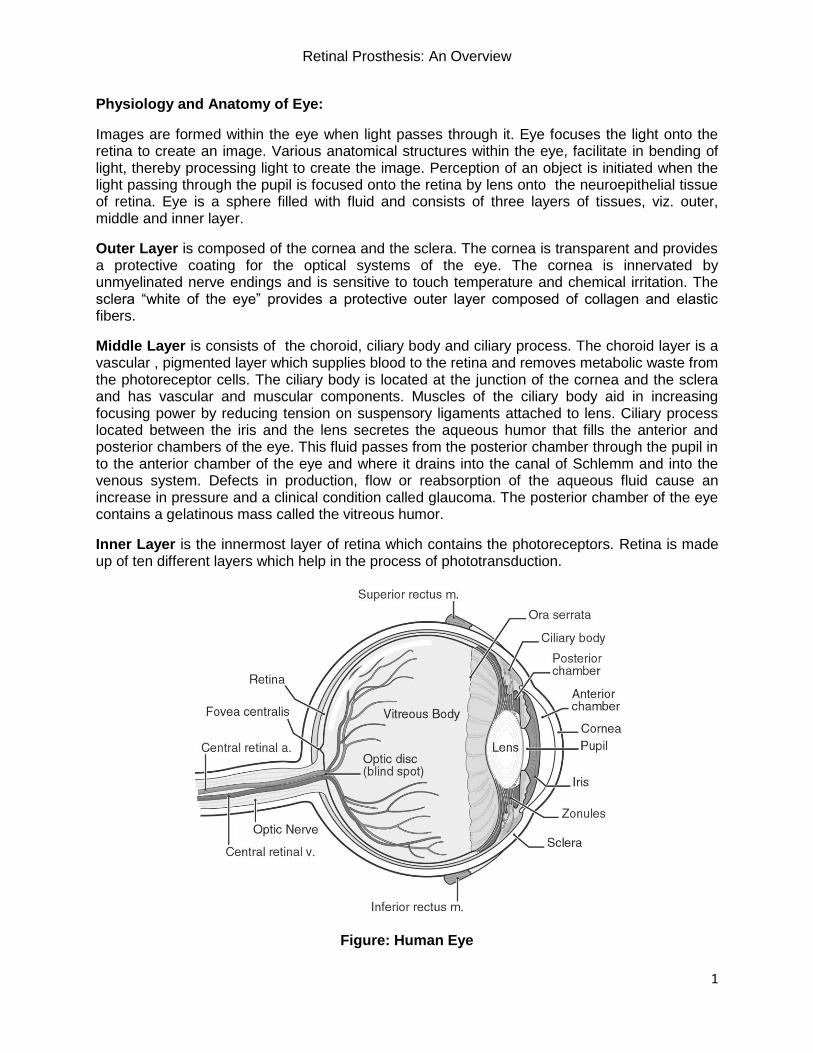
Images are formed within the eye when light passes through it. Eye focuses the light onto the retina to create an image. Various anatomical structures within the eye, facilitate in bending of light, thereby processing light to create the image. Perception of an object is initiated when the light passing through the pupil is focused onto the retina by lens onto the neuroepithelial tissue of retina. Eye is a sphere filled with fluid and consists of three layers of tissues, viz. outer, middle and inner layer.
Outer Layer is composed of the cornea and the sclera. The cornea is transparent and provides a protective coating for the optical systems of the eye. The cornea is innervated by unmyelinated nerve endings and is sensitive to touch temperature and chemical irritation. The sclera “white of the eye” provides a protective outer layer composed of collagen and elastic fibers.
Middle Layer is consists of the choroid, ciliary body and ciliary process. The choroid layer is a vascular , pigmented layer which supplies blood to the retina and removes metabolic waste from the photoreceptor cells. The ciliary body is located at the junction of the cornea and the sclera and has vascular and muscular components. Muscles of the ciliary body aid in increasing focusing power by reducing tension on suspensory ligaments attached to lens. Ciliary process located between the iris and the lens secretes the aqueous humor that fills the anterior and posterior chambers of the eye. This fluid passes from the posterior chamber through the pupil in to the anterior chamber of the eye and where it drains into the canal of Schlemm and into the venous system. Defects in production, flow or reabsorption of the aqueous fluid cause an increase in pressure and a clinical condition called glaucoma. The posterior chamber of the eye contains a gelatinous mass called the vitreous humor.
Inner Layer is the innermost layer of retina which contains the photoreceptors. Retina is made up of ten different layers which help in the process of phototransduction.
Figure: Human Eye

Retinal Prosthesis: An Overview
2
Layers of Retina: Retina is composed of ten different layers. These layers subsequently from the outermost to innermost lining are arranged as: Pigment cell layer, photoreceptor layer, external limiting membrane, outer nuclear layer, outer plexiform layer, inner nuclear layer, inner plexiform layer, ganglion cell layer, optic nerve layer and limiting membrane.
Sr. No Name of Layer: Summary:
1 Pigment Cell Layer Supporting cells containing melanin reduce the scattering of light
2 Photoreceptor Layer Contains the outer and inner segments viz. rods and cones
3 External Limiting Membrane
4 Outer Nuclear Layer Contains cell bodies of rods and cones
5 Outer Plexiform Layer Rod and cone axons, Horizontal cell dendrites and polar dendrites.
6 Inner Nuclear Layer Contains nuclei of horizontal, bipolar and amacrine cells.
7 Inner Plexiform Layer Contains axons of bipolars and amacrines as well as dendrites of ganglion cells.
8 Ganglion Cell Layer Nuclei of ganglion cells and displaced amacrine cells.
9 Optic Nerve Layer Fibers from ganglion transversing the retina leave eyeball and enter into optic disc.
10 Limiting Membrane Basement membrane consisting mainly of Muller Cells

Retinal Prosthesis: An Overview
3
Photoreceptors in the retina consist of rods and cones. Both of these cell types have an outer segment, and inner segment, and a synaptic process that connects to bipolar cells.
Outer segments are formed by an in folding of plasma membrane so as to produce stacks of disc like structures, rich in light sensitive photopigments. Rods are longer than cones. Discs of rods become detached from plasma membrane to form floating discs. Because of high density of photopigment molecules in rod receptors, a single photon of light can activate rod receptor cell. Cone cells are less sensitive to light; hence require hundreds of photons.
Inner segments of rods and cones are connected to outer segments by modified cilium which contains the classic ring of nine pairs of microtubules but lack a central pair. The photoreceptor photopigment is initially synthesized in inner segment, incorporated into plasma membrane and makes its way to outer segment membrane discs.
Figure : Variation in density of rods and cones
In Phototransduction, Light is absorbed by pigments in the outer segments of photoreceptors and initiates a process called photoisomerization. Rhodopsin (opsin+retinal) is converted from the 11-cis to an “all trans” form of rhodopsin. Additional conformational changes in opsin generate Metarhodopsin II. This Metarhodopsin II activates a G protein (transducin) that results in the breakdown of cyclic GMP (decreased levels of cGMP). In the dark cGMP gated Na channels are open and lead to a depolarization (dark current) of receptor cells. When cGMP levels are decreased, in response to light, Na channels close which leads to a hyperpolarization of the visual receptor cells. Photoreceptor release a neurotransmitter (glutamate) that can have an inhibitory effect or an excitatory effect on the bipolar or horizontal cells depending on the postsynaptic receptors.
Hyperpolarization of receptor cells by light decreases the release of glutamate. That can either hyperpolarize bipolar and horizontal cells (ones that have ionotropic receptors) or depolarized bipolar and horizontal cells (ones that have metabotropic receptors).These interactions provide the framework for the on-off patterns observed for visual fields.

Retinal Prosthesis: An Overview
4
Retinal Prosthesis is a device used to replace the lost photoreceptor cells' functions and images processed using computer via electrodes placed on the retina. These images are transmitted by stimulating the retina electrically or by means of neurotransmitters. There are two diseases namely Age Related Macular Degeneration(AMD) and Retinitis Pigmentosa which on progression result into blindness. As a result, there is a need of using retinal prosthesis.
Age Related Macular Degeneration(AMD) is classified into two types: Dry AMD and Wet AMD. This disease is generally found in individuals of 65 years and above. The primary cause of occurrence of AMD is drusen, a yellow colored accumulation between the innermost layer of choroid and retina's pigment cell layer. Consequently, it affects the light sensitivity of retina. The drusen accumulation is referred to as Dry AMD.
In Wet AMD, additionally to drusen accumulation, there is an ingrowth of blood vessels under macula which are present behind the retina. The leakage of blood and fluid from these blood vessels affects the light sensitivity of retina.

Retinal Prosthesis: An Overview
5
Retinitis Pigmentosa is a degenerative disease that primarily causes visual impairment ultimately resulting into blindness. It is observed in infancy as well as in aged individuals. It affects the individuals' adaptation to change in light sensitivity i.e. difficulty to adapt from light to dark or dark to light changes. The disease is diagnosed by dilating the eye. Ideally, the healthy retina is orangish- red in color. During dilation the orange-red color observed to be broken into dark brown and/or red spots caused by the breaking down of primary epithelial cells; signifies the presence of this disease.
Other tests that are carried out to test the person suspected of suffering from this disorder are: visual acuity, color testing, peripheral vision and refraction.
Retinitis Pigmentosa
Considering the previously discussed physiology and anatomy of retina, the biomaterials being used in the retinal prosthesis must have these properties: highly biocompatible, not susceptible to corrosion, should not cause inflammation or infections in eye, ductile, good conductor of electricity and not result in heating effect thereby damaging the surrounding tissues probably resulting into scar tissue formation.
Two types of retinal prosthesis have been designed till date which are Subretinal and Epiretinal Prosthesis. Both of these prosthesis are different in terms of the positions where they re implanted. Epiretinal prosthesis are placed on the retina whereas the subretinal prosthesis are placed on the outer surface of the retina, between the photoreceptor layer and retinal pigment epithelium.

Retinal Prosthesis: An Overview
6
Subretinal Prosthesis directly stimulate the retinal cells and relying on the normal processing of the inner and middle retinal layers. They tend to replace the functioning of degenerated photoreceptors in individuals suffering from AMD and/or retinitis pigmentosa. It is easy to adhere the implant in place as the implant is mechanically constrained by small distance between the outer retina and the retinal pigment epithelium. It primarily consists of a silicon wafer containing light sensitive micro-photodiodes, which generate signals by external excitation from the incoming light. The other components used are driver circuit, photovoltaic cell, micro-electrode array and transistors. Induction coupling is generally used to couple the circuitry and power regulation is done using zener diodes. The incident light passing through the retina generates current within these micro-photodiodes, which is then directly injected into the underlying retinal cells. This injection of current takes place due to the arrangement of array of micro-electrodes. The pattern of activation of micro-photodiodes by incident light further stimulates distinct pattern of bipolar, amacrine, ganglion and horizontal cells of retina. Hence; this leads to a visual perception which represents the actual incident image. These implants do not require external hardware other than the implanted micro-photodiodes array. Some key features of this device are: it moves within the eye, contains heat dissipating element, micro-electrode array being used do not cause retinal detachment post surgery (implantation). Certain subretinal implants being designed now require stimulation from external power source. Electrodes conductivity ranges from few micro-amperes to 1.55 mA.
Biomaterials which have been used in designing of these implants include Silicon Dioxide (SiO2), Iridium (Ir),Silicon Nitride (Si3N4) and Titanium Nitride (TiN). Of the mentioned biomaterials, TiN showed negative effects. It affected the cell culture of surrounding tissues. Hence, it is not biocompatible.

Retinal Prosthesis: An Overview
7
Further testing for biocompatibility has been carried out on animals as well as six individuals. The six individuals underwent subretinal implantation in their right eye (Chow et Al) and were observed for a period of eighteen months. They were implanted an artificial silicon chip (ASR).
Artificial Silicon Chip (ASR) is does not require external power source but can be stimulated by incident light within the range of 500-1100 nm. It contains 3500 micro-photodiodes with stimulating electrode. This stimulating electrode stimulates the functional cells of photoreceptors by providing them with electrical impulses. Thus, these artificial solar cells function analogous to photoreceptors within the retina and stimulate other cells. Specifications of this micro-electronic chip include: diameter is 2 mm and 25 micrometer thick, it contains 5000 negative intrinsic layer and positive micro-photodiode pixels which are arranged at a distance of 5 micrometer from one another. It is important to note that the chip is fabricated within Teflon sleeve, secured intra-operatively to saline filled syringe injector. Each pixel is of 400 micrometer square; fabricated with 9x9 micrometer IrOx electrode deposited and electrically bonded to each pixel.
Adjoining figure shows the
effect of biomaterials on cell
culture.
ASR Chip and its internal arrangement

Retinal Prosthesis: An Overview
8
Fabrication of Micro-electrodes: Various steps are followed to fabricate them. Firstly, spin coating and curing of 12 micrometer thick base coating on 100 mm diameter silicon wafer with polyamide. Then Ti/Au/Ti layer is deposited upon polyamide by physical vapor deposition, pattern is made. 3 micrometer polyamide is spun over the metalized polyamide. Later electrode sites and contact pads are formed by patterning wafer with O2 reactive ion etching (RIE).
It is interesting to know that none of these individuals experienced implant rejection, inflammation, erosion, neovascularization or migration. Drawbacks for this implant are: it can only be used if the individuals' neuronal cells are not damaged. Also, the heat produced must not be higher than that generated by heat dissipating elements. If so, it will result in burning the surrounding tissues. In-vivo experiments studied so far show the deposition of SiO2 on the surface of micro-photodiodes which causes the gold coating to disintegrate. The long term durability of this implant is yet needs testing by encapsulating it in a bio-inert polymer.
Data collected for six individuals
Epiretinal Prosthesis is implanted inside the retina. It provides direct stimulation to the stimulating ganglion cells and bypassing all other layers of retina. They consist of silicon-platinum electrode array mounted onto inner layer of retina. Array is stabilized using micro tacks along with slight mechanical pressures provided by vitreous humor. This implant needs an external video camera to capture images. The camera receives image of surrounding environment, processes it and the image formation is communicated to the implanted electrode array wirelessly via telemetry. External transmitter is also used so as to provide continuous power to the implant using radio-frequency induction coils or infrared lasers. The external camera as well as the image processing chip are mounted on the patient's eye-glasses. Image processing here involves reduction of image's resolution, conversion of image into spatial and temporal stimulation pattern so as to activate appropriate cells of retina. The system as a whole is capable to work in real time so that delays between the camera input and retina's stimulation do not affect the visual perception.
Research has begun with a first generation, 16-electrode device (e.g., the ArgusTM 16), which will permit the distinction between the presence and absence of light, and the second generation (e.g., ArgusTM II), which has 60 electrodes. It is hoped that further generation devices, containing up to 1,000 electrodes, will provide more useful vision. The first-generation device is currently being studied in 2 Investigational New Device Trials approved by the U.S. Food and Drug Administration (FDA). Second Sight Medical Products and the National Institutes of Health are partnering sponsors for these feasibility studies.
The Argus II device received commercial approval in Europe in March 2011. In 2013, the U.S. Food and Drug Administration (FDA) approved a humanitarian use device exemption (HDE) for the Argus II retinal prosthesis by Second Sight Medical. It is the gold standard for epiretinal

Retinal Prosthesis: An Overview
9
implants. This device has been designed by Mark S. Humayun, professor at University of Southern California. This device uses 60 platinum electrodes, inductive coil consisting of receiver and transmitter; coated with Silicone to wirelessly rely data and power to extra-ocular driver circuitry, external Visual Processing Unit (VPU) and video camera mounted upon eye glass. The platinum gray material used in the electrodes, is capable of covering 20 degrees of visual angle. HDE approval is limited to those devices that treat or diagnose fewer than 4000 people in the United States each year. The Argus II system is intended for use in adults, age 25 years or older, with severe to profound retinitis pigmentosa who have bare light perception (can perceive light, but not the direction from which it is coming) or no light perception in both eyes, evidence of intact inner layer retina function, and a previous history of the ability to see forms. Patients must also be willing and able to receive the recommended post implant clinical follow-up, device fitting, and visual rehabilitation.
Argus-II Design
The experimental conditions for this device considered : tasks performed with residual vision and the performance mapped with normal mapping. Fifteen subjects were able to perform better after undergoing epiretinal implantation. All patients were available for regular follow-ups, of which two patients had better performance with their residual vision, and ten showed significant improvement in performance. Of the other two subjects, trial on one had to be withdrawn as the patient complained of conjuctival erosion. The individuals undergone trials also showed promising results as they could identify short words, numbers, letters, differentiate between the sidewalls and obstacles. Also the visual acuity of these individuals was improved.
Using 60 electrodes has helped in sampling the resolution to 6x10 grid.

Retinal Prosthesis: An Overview
10
Biomaterials useful for Retinal Prosthesis:
Biomaterials that have been used for developing retinal prosthesis can be divided into 2 categories viz. permanent implants and absorbable devices. At present, most of the retinal implants that are used comprise of silicon whereas the absorbable devices' use has decreased. The reason absorbable (degradable) implants' use has reduced is because they have been found to have harmful effects post-implantation and cause complications. Polyviol is an example of absorbable device that was used two decades back. After surgery, it was found to expand internally ultimately leading to retinal breaks and retinal detachment but at the same time it had adverse reactions on the ocular tissues. Other materials whose use has then gradually decreased include polyethylene, nylon threads, solid PTFE, polyester, solid PTFE, hydrogels, porous PTFE and PTFE coated silicon. Polyethylene fulfilled all of the requirements for the purpose but it caused scleral erosion and increase in intra-ocular pressure post implantation. whereas nylon thread was causing only scleral erosion. Hydrogels sometimes cause friability viz unwanted movement of the tissue. Hence their use specifically for this purpose has decreased. Silicon PTFE upon implantation showed similar effects as polyethylene, and hence they were not used anymore. Porous expanded PTFE (e-PTFE) is being used as buckling bands as well as an outer layer of coating on silicone implants. Its use is now being considered as a substitute for silicone based implants.
Permanent Implant Materials:
Most of the implants that are being used today are made up of silicone. The properties of silicone include: it is a synthetic rubber compound, stable over a range of temperature. it is hydrophobic. it is soft and flexible, hence there are no chances of scleral erosion taking place the first silicone implant used was in 1959 ; a scleral buckle and till date over 70 varieties of silicone implants have been designed because of it is smoothness, it is used as a collagenous capsule encircling the implant. So primarily the implant is vascularized and gradually over time the layer of capsule becomes avascular, and translucent. Silicone sponge buckles are used for treating the cases of retinal tears. It is interesting to note that these buckles have the same properties as mentioned above for silicone. But at the same time, they are more elastic, show good buckling post operation and can also be injected with antibiotics so as to prevent infection. Silicone implants are usually considered as the "gold standard" for buckling but they do show some undesired effects discussed in above section.
Absorbable Implant Materials:
Absorbable buckles are being developed for experimentation purpose. The main idea behind their development is over time they tend to replace the scar tissue which is formed upon implantation. The problem with this buckle elements is: once reabsorbed it is difficult to ascertain whether their implantation has resulted in successful surgery of retinal reattachment. Experiments are being performed by using grafting procedure. For this procedure, the patient's tendons and tissues are used so as to overcome the risk of graft being rejected. The experiments seem to be successful but that increases the extra surgery procedures. Allografts and xenografts after being treated with Gelatin were experimented upon. But they were in most cases being rejected by the host cell. Gelatin sheets were then introduced but they also showed effects similar to allografts and xenografts. Poly glycolic acid (PGA) , polyurethanes and poly lactic acid (PLA) have showed promising results during various studies carried out on rabbits
Retinal Prosthesis: An Overview
11
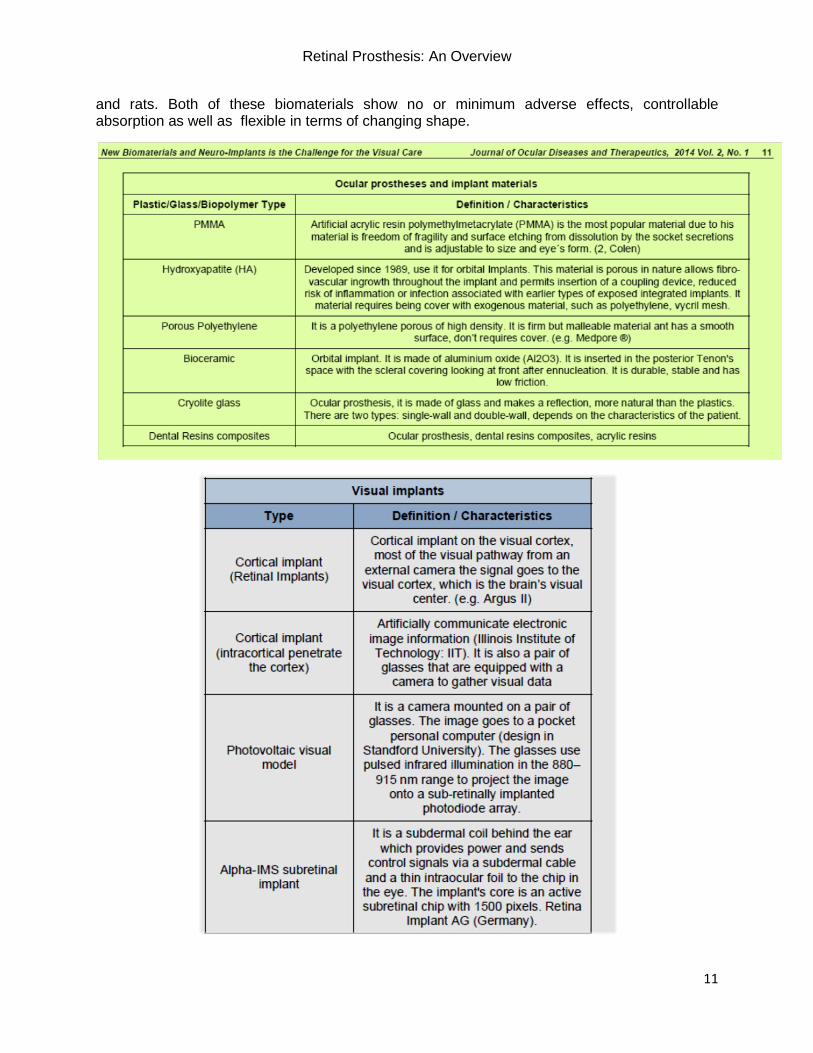
and rats. Both of these biomaterials show no or minimum adverse effects, controllable absorption as well as flexible in terms of changing shape.

Retinal Prosthesis: An Overview
12
Future Developments:
Clinical reports to date have demonstrated mixed success, with all patients report at least some sensation of light from the electrodes, and a smaller proportion gaining more detailed visual function, such as identifying patterns of light and dark areas. The clinical reports indicate that, even with low resolution, retinal implants are potentially useful in providing crude vision to individuals who otherwise would not have any visual sensation. However, clinical testing in implanted subjects is somewhat limited and the majority of spatial resolution simulation experiments have been conducted in normal controls. It remains unclear whether the low level vision provided by current retinal implants is sufficient to balance the risks associated with the surgical procedure, especially for subjects with intact peripheral vision. Several other aspects of retinal implants need to be addressed in future research, including the long term stability of the implants and the possibility of retinal neuron plasticity in response to prolonged stimulation. Currently sixty electrodes used in epiretinal prosthesis are capable of generating visual acuity, assist in mobility, identify characters, numbers and short words. Incorporating more number of electrodes approximately 1000 in the array will help in can be used to enhance residual vision. Stem cell therapy to generate 3D Retinal disk is being investigated upon at John Hopkins school of Medicine and it seems to show promising results for the future.

Retinal Prosthesis: An Overview
13
References:
[1] B.A. Berkowitz, J. Gorgis, A. Patel, F. Baameur, V.V. Gurevich, C.M. Craft, V.J. Kefalov, R. Roberts: Development of an MRI biomarker sensitive to tetrameric visual arrestin 1 and its reduction via light-evoked translocation in vivo. The FASEB Journal, 2014.
[2] Alan Y. Chow, MD; Vincent Y. Chow, BS; Kirk H. Packo, MD; John S. Pollack, MD; Gholam A. Peyman, MD; Ronald Schuchard, PHD: The Artificial Silicon Retina Microchip for the Treatment of VisionLoss From Retinitis Pigmentosa, Arch Ophthalmol. 2004;122(4):460-469. doi:10.1001/archopht.122.4.460
[3] Francesa Baino, Materials Science and Chemical Engineering Department, Politecnico di Torino, Corso Duca degli Abruzzi 24, 10129 Torino, Italy The use of polymers in the treatment of retinal detachment: current trends and future perspectives.
[4] Patricia Duran Ospina, Mayra Cacaeres Diaz and Jhonny Pena Plaza A Review in
Ocular Prosthesis and Vicual Implants: New Biomaterials and Neuro-Implants is the Challenge of Visual Care Journal of Ocular Disease and Therapeutics, 2014, 2,9-16.
[5] E. Zrenner, Will retinal implants restore vision? Science, Vol. 295, No. 5597 Feb. 2002, pp. 1022 – 1025
[6] H.G. Graf, C. Harendt, T. Engelhardt, C. Scherjon, K. Warkentin, H. Richter, J. N. Burghartz, High dynamic range CMOS imager technologies for biomedical applications IEEE Journal of Solid-State Circuits, Vol. 44, No. 1, Jan. 2009, pp. 281 – 289
[7] Sheila Nirenberg1 and Chethan Pandarinath, “Retinal prosthetic strategy with the capacity to restore normal vision” Department of Physiology and Biophysics, Weill Medical College of Cornell University, New York, NY 10065 Edited* by Norma Graham, Columbia University, New York, NY, and approved July 9, 2012 (received for review May 7, 2012)
[8] Mark S. Humayun, Eugene de Juan, Jr.,Robert J. Greenberg Visual Prosthesis and method of using same, US 5935155A, August 10, 1999
[9] Alan Y. Chow, Artificial Retina Device, US 5016633A, May 21 1991
[10] Doug Shiro, Joseph Rizzo, John Wyatt, Chronically Implantable Retinal Prosthesis, US 6324429B1, November27,2001
[11] The BRS Handbook for Physiology by Dr. L. Costanzo.




















