Human Central Nervous System Distribution of c/s-Diamminedichloroplatinum and Use as a...
7
[CANCER RESEARCH 42, 2474-2479, June 1982] 0008-5472/82/0042-OOOOS02.00 Human Central Nervous System Distribution of c/s-Diamminedichloroplatinum and Use as a Radiosensitizer in Malignant Brain Tumors1 David J. Stewart,2 Milam Leavens, Moshe Maor, Lyn Feun, Mario Luna, Jeanne Bonura, Richard Caprioli, Ti Li Loo, and Robert S. Benjamin3 Departments of Developmental Therapeutics ¡D J. S., L. F., T. L. L., R. S. B.], Surgery [M. Le.], Radiotherapy ¡M.M.], and Pathology [M. Lu.]. The University of Texas System Cancer Center M.D. Anderson Hospital and Tumor Institute, and Department of Analytical Chemistry ¡J. B., R. C.], University of Texas, Houston, Texas 77030 ABSTRACT The human central nervous system pharmacology of c/'s- diamminedichloroplatinum (CDDP) was studied, and trials were initiated of CDDP as a radiosensitizer in the treatment of malignant primary brain tumors. Samples were assayed for platinum using X-ray-dispersive fluorescence spectrometry. Platinum was barely detectable in cerebrospinal fluid from two patients and was not detectable (<0.10 ftg/ml) in cerebrospinal fluid from three patients receiving CDDP, 100 to 120 mg/sq m. Six patients were given CDDP, 20 to 25 mg/sq m i.V., during or before resection of intracerebral tumor. Potentially cytotoxic and radiosensitizing tumor platinum concentrations were attained. Autopsy tissue samples were obtained from two patients who had received CDDP, 20 to 120 mg/sq m i.V., and two who had received intracarotid (i.e.) CDDP, 60 to 100 mg/ sq m, therapeutically 0 hr to 102 days antemortem, and surgical tissue specimens were obtained from one patient who had received CDDP, 120 mg/sq m i.v., 180 days previously and from one who had received i.e. CDDP, 75 mg/sq m, 2 days previously. Platinum was quantifiable at concentrations from 0.33 to 2.97 ¡jLg/g. Platinum concentrations in edematous brain tissue adjacent to tumor were generally lower than platinum concentrations in intracerebral tumor. Brain platinum concen tration decreased with increasing distance from intracerebral tumor, and platinum varied from undetectable to 0.63 ftg/g (median, 0.33 ¿ig/g)in autopsy brain tissue from five patients who had received CDDP, 50 to 120 mg/sq m i.V., 2 to 165 days antemortem. The extent to which central nervous system pharmacology of an antineoplastic agent affects its activity against intracerebral neoplasms remains unclear. Fifteen patients with malignant brain tumors received CDDP, 40 mg/sq m/week i.v., during cranial irradiation, and some received 105 to 120 mg/sq m every 3 weeks after cranial irradiation. Close follow-up was necessary, and some weekly treatments needed to be omitted in individual patients. During the weekly CDDP, gastrointestinal, scalp, and renal toxicities and hypomagnesemia were noted but were tolerable. Only one patient developed myelosuppression. Ototoxicity may have been enhanced. Postirradiation CDDP, 105 to 120 mg/sq m every 3 weeks, caused substantially more gastrointestinal tox- icity and may have caused central nervous system toxicity in ' Supported in part by Grant 14528 from the National Cancer Institute, NIH, Bethesda, Md. Presented at the 17th Annual Meeting of the American Society of Clinical Oncology, Washington, D. C.. April 1981 (23). 2 Present address: Ontario Cancer Foundation, Ottawa General Hospital. Ottawa, Ontario, Canada K1G 8L6. 3To whom requests for reprints should be addressed, at Department of Developmental Therapeutics, M. D. Anderson Hospital, Houston, Texas 77030. Received June 18, 1981; accepted February 25. 1982. four patients, although other factors probably contributed. It is too early to evaluate effect on survival. INTRODUCTION Glioblastoma multiforme and brain métastasesfrom systemic cancers continue to carry a poor prognosis (19, 24). Nitrosou- reas remain the most effective chemotherapeutic agents in glioblastoma (4), but chemotherapy rarely results in long-term survival (2). Brain métastases rarely respond to systemic chemotherapy and may appear or progress despite response of extracerebral disease (3). The role of the pharmacology of a drug in determining whether it will be effective against intracerebral tumors is unknown. Lipid-insoluble, high-molec ular-weight compounds that are incapable of crossing the intact blood-brain barrier are nevertheless able to gain ready access to intracerebral tumors (12), because of the abnormal vascu- lature that is present (8). It has been argued that only those agents that are capable of crossing the blood-brain barrier will be able to penetrate into edematous brain adjacent to tumor, where the blood-brain barrier is relatively intact and where the most actively growing tumor cells reside (11). This postulate might explain the inability to cure intracerebral tumors with chemotherapy but does not explain why even the central part of ¡ntracerebral tumors does not shrink in response to treat ment. Moreover, some drugs that do not cross the blood-brain barrier to a very large extent, such as 4'-demethyl-1-O-(4,6- O-2-thenylidene-/}-D-glycopyranosyl)epipodophyllotoxin (VM- 26), have been shown to have activity against intracerebral tumors (20). Over the past 4 years, we have been studying the uptake of a number of antineoplastic agents into the human central nervous system and intracerebral tumors. It is hoped that, once the central nervous system pharmacology of a number of agents has been defined, we will be in a better position to judge whether there is truly a correlation between pharmaco- kinetic behavior and activity against intracerebral tumors. This report deals with the human central nervous system pharma cology of CDDP.4 Despite the very limited penetration of CDDP into animal brain and CSF (7, 13), we were interested in this drug because of its high degree of activity against a number of cancers, at least limited activity against the murine ependy- moblastoma (26), and reports of both primary and metastatic human intracerebral tumors responding to CDDP (9, 10, 16). In addition, it is known that CDDP is a radiosensitizer (6, 15) and that it has been shown to be synergistic with cranial irradiation in a rat intracerebral tumor model (5). Because of its * The abbreviations used are: CDDP, c/s-diamminedichloroplatinum; CSF, cerebrospinal fluid: i.e., intracarotid: i.a., intraarterial. 2474 CANCER RESEARCH VOL. 42 on June 27, 2015. © 1982 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Human Central Nervous System Distribution of c/s-Diamminedichloroplatinum and Use as a...

[CANCER RESEARCH 42, 2474-2479, June 1982]0008-5472/82/0042-OOOOS02.00
Human Central Nervous System Distribution of c/s-Diamminedichloroplatinumand Use as a Radiosensitizer in Malignant Brain Tumors1
David J. Stewart,2 Milam Leavens, Moshe Maor, Lyn Feun, Mario Luna, Jeanne Bonura, Richard Caprioli,Ti Li Loo, and Robert S. Benjamin3
Departments of Developmental Therapeutics ¡D J. S., L. F., T. L. L., R. S. B.], Surgery [M. Le.], Radiotherapy ¡M.M.], and Pathology [M. Lu.]. The University ofTexas System Cancer Center M.D. Anderson Hospital and Tumor Institute, and Department of Analytical Chemistry ¡J. B., R. C.], University of Texas,Houston, Texas 77030
ABSTRACT
The human central nervous system pharmacology of c/'s-
diamminedichloroplatinum (CDDP) was studied, and trials wereinitiated of CDDP as a radiosensitizer in the treatment ofmalignant primary brain tumors. Samples were assayed forplatinum using X-ray-dispersive fluorescence spectrometry.
Platinum was barely detectable in cerebrospinal fluid from twopatients and was not detectable (<0.10 ftg/ml) in cerebrospinalfluid from three patients receiving CDDP, 100 to 120 mg/sqm. Six patients were given CDDP, 20 to 25 mg/sq m i.V.,during or before resection of intracerebral tumor. Potentiallycytotoxic and radiosensitizing tumor platinum concentrationswere attained. Autopsy tissue samples were obtained from twopatients who had received CDDP, 20 to 120 mg/sq m i.V., andtwo who had received intracarotid (i.e.) CDDP, 60 to 100 mg/sq m, therapeutically 0 hr to 102 days antemortem, and surgicaltissue specimens were obtained from one patient who hadreceived CDDP, 120 mg/sq m i.v., 180 days previously andfrom one who had received i.e. CDDP, 75 mg/sq m, 2 dayspreviously. Platinum was quantifiable at concentrations from0.33 to 2.97 ¡jLg/g.Platinum concentrations in edematous braintissue adjacent to tumor were generally lower than platinumconcentrations in intracerebral tumor. Brain platinum concentration decreased with increasing distance from intracerebraltumor, and platinum varied from undetectable to 0.63 ftg/g(median, 0.33 ¿ig/g)in autopsy brain tissue from five patientswho had received CDDP, 50 to 120 mg/sq m i.V., 2 to 165days antemortem. The extent to which central nervous systempharmacology of an antineoplastic agent affects its activityagainst intracerebral neoplasms remains unclear.
Fifteen patients with malignant brain tumors received CDDP,40 mg/sq m/week i.v., during cranial irradiation, and somereceived 105 to 120 mg/sq m every 3 weeks after cranialirradiation. Close follow-up was necessary, and some weekly
treatments needed to be omitted in individual patients. Duringthe weekly CDDP, gastrointestinal, scalp, and renal toxicitiesand hypomagnesemia were noted but were tolerable. Only onepatient developed myelosuppression. Ototoxicity may havebeen enhanced. Postirradiation CDDP, 105 to 120 mg/sq mevery 3 weeks, caused substantially more gastrointestinal tox-icity and may have caused central nervous system toxicity in
' Supported in part by Grant 14528 from the National Cancer Institute, NIH,
Bethesda, Md. Presented at the 17th Annual Meeting of the American Society ofClinical Oncology, Washington, D. C.. April 1981 (23).
2 Present address: Ontario Cancer Foundation, Ottawa General Hospital.Ottawa, Ontario, Canada K1G 8L6.
3To whom requests for reprints should be addressed, at Department ofDevelopmentalTherapeutics, M. D. Anderson Hospital, Houston, Texas 77030.
Received June 18, 1981; accepted February 25. 1982.
four patients, although other factors probably contributed. It istoo early to evaluate effect on survival.
INTRODUCTION
Glioblastoma multiforme and brain métastasesfrom systemiccancers continue to carry a poor prognosis (19, 24). Nitrosou-reas remain the most effective chemotherapeutic agents inglioblastoma (4), but chemotherapy rarely results in long-termsurvival (2). Brain métastases rarely respond to systemicchemotherapy and may appear or progress despite responseof extracerebral disease (3). The role of the pharmacologyof a drug in determining whether it will be effective againstintracerebral tumors is unknown. Lipid-insoluble, high-molecular-weight compounds that are incapable of crossing the intactblood-brain barrier are nevertheless able to gain ready accessto intracerebral tumors (12), because of the abnormal vascu-
lature that is present (8). It has been argued that only thoseagents that are capable of crossing the blood-brain barrier will
be able to penetrate into edematous brain adjacent to tumor,where the blood-brain barrier is relatively intact and where the
most actively growing tumor cells reside (11). This postulatemight explain the inability to cure intracerebral tumors withchemotherapy but does not explain why even the central partof ¡ntracerebral tumors does not shrink in response to treatment. Moreover, some drugs that do not cross the blood-brainbarrier to a very large extent, such as 4'-demethyl-1-O-(4,6-O-2-thenylidene-/}-D-glycopyranosyl)epipodophyllotoxin (VM-
26), have been shown to have activity against intracerebraltumors (20).
Over the past 4 years, we have been studying the uptake ofa number of antineoplastic agents into the human centralnervous system and intracerebral tumors. It is hoped that, oncethe central nervous system pharmacology of a number ofagents has been defined, we will be in a better position tojudge whether there is truly a correlation between pharmaco-
kinetic behavior and activity against intracerebral tumors. Thisreport deals with the human central nervous system pharmacology of CDDP.4 Despite the very limited penetration of CDDP
into animal brain and CSF (7, 13), we were interested in thisdrug because of its high degree of activity against a number ofcancers, at least limited activity against the murine ependy-moblastoma (26), and reports of both primary and metastatichuman intracerebral tumors responding to CDDP (9, 10, 16).In addition, it is known that CDDP is a radiosensitizer (6, 15)and that it has been shown to be synergistic with cranialirradiation in a rat intracerebral tumor model (5). Because of its
* The abbreviations used are: CDDP, c/s-diamminedichloroplatinum; CSF,
cerebrospinal fluid: i.e., intracarotid: i.a., intraarterial.
2474 CANCER RESEARCH VOL. 42
on June 27, 2015. © 1982 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
CDDP: Central Nervous System Pharmacology and Use in Brain Tumors
ability to radiosensitize, because of its ability to produce responses in human intracerebral tumors, and because we wereable to document the presence of high concentrations of platinum in human intracerebral tumors after systemic administration of CDDP, we initiated a clinical trial in patients with malignant primary brain tumors using weekly i.v. CDDP during cranial irradiation. Along with the central nervous system pharmacology of CDDP, we report our initial experience usingCDDP as a radiosensitizer.
MATERIALS AND METHODS
All patients participating in this study gave informed consent. CDDPwas obtained from the New Drug Development Branch of the NationalCancer Institute or was purchased from Bristol Laboratories, Syracuse,N. Y. Single CSF samples were collected by lumbar puncture from 4patients receiving CDDP, 100 mg/sq m i.v., and on Day 1 from 3patients receiving CDDP, 15 mg/sq m/day, for 4 days. Multiple CSFsamples were obtained by Ommaya reservoir puncture from a patientreceiving CDDP, 120 mg/sq m i.v. All patients from whom CSF wasobtained were receiving the drug for therapeutic purposes. Duration ofdrug infusion was 2 to 4 hr. Only the patient with the Ommaya reservoirin place had intracerebral tumor.
Six patients undergoing surgical resection of intracerebral tumorwere given CDDP, 20 to 25 mg/sq m i.v., over 1 hr either immediatelybefore or during surgery. Resected tumor was collected at surgery forpharmacology studies. The dose administered was not intended to betherapeutic. Small fragments of edematous brain dislodged duringsurgery from the area adjacent to tumor were obtained from 4 of thesepatients. In addition, resected frontal lobe was collected from onepatient undergoing a lobectomy for metastatic malignant melanoma.Tumor was also obtained from a patient who underwent partial surgicalresection of a glioblastoma multiforme 48 hr after he had received atherapeutic i.e. infusion of CDDP, 75 mg/sq m. Samples were alsocollected from a patient undergoing resection of an ¡ntracerebral metastasis from testicular carcinoma several months after having receivedCDDP i.v. Tissue specimens were obtained at autopsy from 9 patientswho had received CDDP therapeutically at various time intervals ante-
mortem. Four of these patients had intracerebral tumors, of whom 2had received CDDP by i.e. infusion. Temporalis muscle was obtainedfrom 6 patients as an extracerebral control.
Platinum Assay Method. Samples were assayed for platinum usingX-ray-dispersive fluorescence spectrometry, as described previously
(18). Some tissues were analyzed by macerating them, drying a standard amount on Mylar film cemented onto nonpigmented 35-mm slide
mounts, and comparing the results to standard curves generated byadding variable amounts of CDDP to control tissues. Other tissuesamples were lyophilized resuspended in a standard zirconium solution, air dried on Mylar film, and assayed using the zirconium as aninternal standard. Once dried, samples were excited with an X-raybeam from a silver anode X-ray tube (40 kV, 20 ma) filtered with 200
firn of silver plus 50 ¡imof aluminum. Samples were counted for 600sec (live time). A Kevex Model 0600 Ultra Trace X-ray tube subsystemequipped with a 2 kilowatt X-ray generator, Mark AAA silicon (lithium)detector-cryostat, and a Model 7000 Micro-X universal spectrometer
(Kevex Corporation, Foster City, Calif.) was used. Quantitative measurements of platinum were performed using the platinum L a emission(weighted average, 9.43 keV). To correct for the interfering zinc Kaemission (weighted average, 9.57 keV), the spectrum of pure zinc wasnormalized to the zinc Ka peak (weighted average 8.63 keV) of thesample spectrum, and the normalized pure zinc Ka peak was subtracted from the sample spectrum. The area of the platinum L a-peak
(platinum window, 9.20 to 9.72 keV) was then mass normalized bydividing it by the area of an arbitrarily defined window (17.74 to 20.28keV) on the inelastic scatter peak of the exciting silver Ka emission.This inelastic scatter is proportional to the mass of the sample, and
therefore by determining the ratio of the area of the platinum L a-peak
to this scatter peak, the area is mass normalized and is a measure ofthe concentration of platinum in the sample.
Therapeutic Studies. Fourteen patients with glioblastoma multi-
forme and one patient with a meningeal sarcoma were entered on astudy to evaluate the feasibility of using CDDP as a radiosensitizer inpatients with malignant intracerebral tumors. Patients were givenCDDP, 40 mg/sq m/week, during the course of cranial radiation. Iftoxicity developed, radiotherapy was continued, but CDDP was withheld until toxicity had resolved. Following completion of cranial irradiation, CDDP administration was changed to every 3 weeks as a matterof convenience. Initially, this postirradiation CDDP was given as 120mg/sq m i.v. on a single day. Subsequently, the schedule was changedto 35 to 40 mg/sq m/day for 3 days. All patients received i.v. mannitoland hydration prior to and during CDDP infusions. Cranial irradiationwas delivered by a megavoltage apparatus with a minimum target(source)-skin or axis distance of 80 cm. Opposed lateral fields were
used with care taken to include the entire brain. Both fields weretreated daily with delivery of 5 fractions/week separated by approximately 24 hr. The tumor dose was calculated on the central axis of thetreatment field at the midplane of the skull. Patients received either6000 rads to the whole brain over a period of 7 weeks (35 fractions)or 5000 rads whole-brain irradiation followed by an additional 1500rads to a coned-down field covering the initial tumor site. Patients were
followed by weekly blood counts, blood urea nitrogen, and serumcreatinine. Computerized axial tomograms of the brain, audiograms,and electroencephalograms were repeated as clinically indicated. Cor-
ticosteroids were administered during the period of cranial irradiation,and an attempt was made to taper them once irradiation was finished.
RESULTS
CSF Platinum. In CSF, the lower limit of detection of platinumwas 0.10 jug/ml. Platinum CSF concentration was 0.12 /ig/mlin 2 patients who had received i.v. CDDP, 100 mg/sq m, 30min and 3 hr prior to CSF collection. Platinum was not detectable in the CSF collected from 3 patients who had received i.v.CDDP, 15 mg/sq m, 2 to 24 hr earlier, nor in the CSF from 2patients who had received i.v. CDDP, 100 mg/sq m, 30 minprior to lumbar puncture, nor in CSF samples collected from asingle patient by multiple Ommaya reservoir punctures 0, 40,120, and 220 min and 24, 52, and 99 hr following i.v. CDDP,120 mg/sq m.
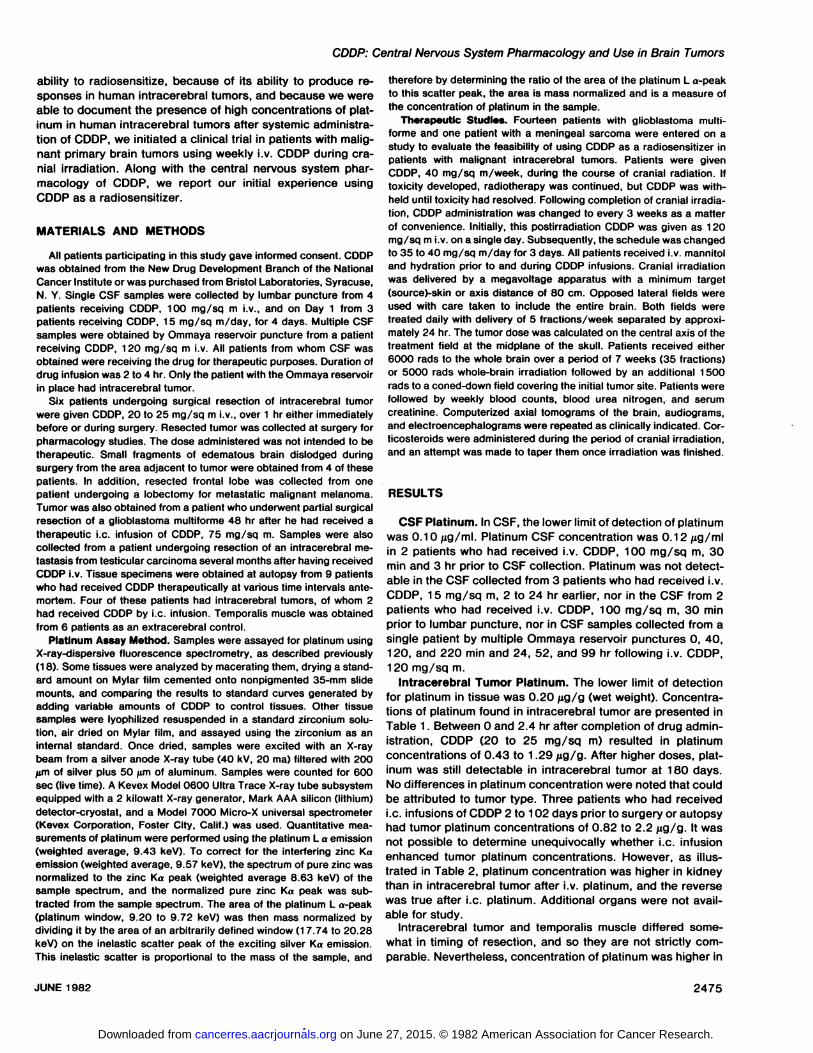
Intracerebral Tumor Platinum. The lower limit of detectionfor platinum in tissue was 0.20 ¿ig/g(wet weight). Concentrations of platinum found in intracerebral tumor are presented inTable 1. Between 0 and 2.4 hr after completion of drug administration, CDDP (20 to 25 mg/sq m) resulted in platinumconcentrations of 0.43 to 1.29 jug/g. After higher doses, platinum was still detectable in intracerebral tumor at 180 days.No differences in platinum concentration were noted that couldbe attributed to tumor type. Three patients who had receivedi.e. infusions of CDDP 2 to 102 days prior to surgery or autopsyhad tumor platinum concentrations of 0.82 to 2.2 jug/g. It wasnot possible to determine unequivocally whether i.e. infusionenhanced tumor platinum concentrations. However, as illustrated in Table 2, platinum concentration was higher in kidneythan in intracerebral tumor after i.v. platinum, and the reversewas true after i.e. platinum. Additional organs were not available for study.
Intracerebral tumor and temporalis muscle differed somewhat in timing of resection, and so they are not strictly comparable. Nevertheless, concentration of platinum was higher in
JUNE 1982 2475
on June 27, 2015. © 1982 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
D. J. Stewart et al.
Table 1
Platinum concentrations in intracerebral tumor, brain adjacent to tumor, and muscle after i.v. or i.e. CDDP
IntracerebraltumorPatient123456789101112Dose
ofCDDP(mg/sqm/course)2025252525252040/day
for3days120756060-100No.
ofcourses211111121213Routei.v.i.v.I.V.I.V.i.V.i.V.i.V.I.V.i.V.i.e.i.e.i.e.SourceoftissueAutopsySurgerySurgerySurgerySurgerySurgerySurgeryAutopsySurgerySurgeryAutopsyAutopsyTypeGlioblastomaGlioblastomaCyst
fluidCystwallMelanomaLungOropharyngealMelanomaThyroidGlioblastomaCenterPeripheryTesticularGlioblastomaGlioblastomaLungTime
fromlastcourseOhr0.1
hr0.4hr1.0hr1.1
hr1.5hr1.5hr2.4
hr48
hr48hr180days48hr6
days102 daysPlatinum(fig/
gwetwt)0.430.79s1.291.120.741.170.890.562.971.350.330.832.201.51Brain
adjacent totumorTime
(Ohr1.3hr1.3hr1.0hr1.3hr2.4
hr48
hr1
80days6
days102 daysPlatinum¿ig/g
wetwt)0.650.630.470.360.250.431.11<0.200.740.50MuscleTimeOhr1.3hr2.3hr2.0
hr2.5
hr2.4hrPlatinum(fig/g
wetwt)1.160.590.750.630.520.37
intracerebral tumor than in muscle in 5 of the 6 patients fromwhom muscle was obtained.
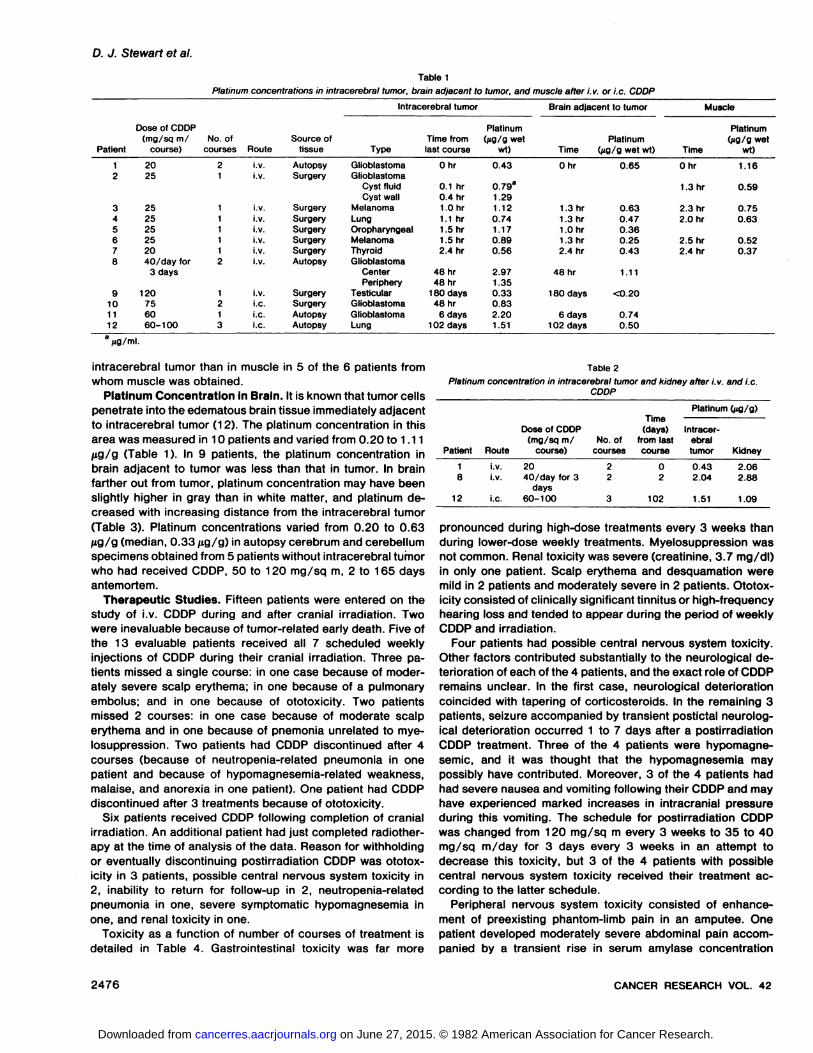
Platinum Concentration in Brain. It is known that tumor cellspenetrate into the edematous brain tissue immediately adjacentto intracerebral tumor (12). The platinum concentration in thisarea was measured in 10 patients and varied from 0.20 to 1.11HQ/Q (Table 1). In 9 patients, the platinum concentration inbrain adjacent to tumor was less than that in tumor. In brainfarther out from tumor, platinum concentration may have beenslightly higher in gray than in white matter, and platinum decreased with increasing distance from the intracerebral tumor(Table 3). Platinum concentrations varied from 0.20 to 0.63fig/g (median, 0.33 jug/g) in autopsy cerebrum and cerebellumspecimens obtained from 5 patients without intracerebral tumorwho had received CDDP, 50 to 120 mg/sq m, 2 to 165 daysantemortem.
Therapeutic Studies. Fifteen patients were entered on thestudy of i.v. CDDP during and after cranial irradiation. Twowere inevaluable because of tumor-related early death. Five of
the 13 évaluable patients received all 7 scheduled weeklyinjections of CDDP during their cranial irradiation. Three patients missed a single course: in one case because of moderately severe scalp erythema; in one because of a pulmonaryembolus; and in one because of ototoxicity. Two patientsmissed 2 courses: in one case because of moderate scalperythema and in one because of pnemonia unrelated to mye-
losuppression. Two patients had CDDP discontinued after 4courses (because of neutropenia-related pneumonia in onepatient and because of hypomagnesemia-related weakness,
malaise, and anorexia in one patient). One patient had CDDPdiscontinued after 3 treatments because of ototoxicity.
Six patients received CDDP following completion of cranialirradiation. An additional patient had just completed radiotherapy at the time of analysis of the data. Reason for withholdingor eventually discontinuing postirradiation CDDP was ototoxicity in 3 patients, possible central nervous system toxicity in2, inability to return for follow-up in 2, neutropenia-related
pneumonia in one, severe symptomatic hypomagnesemia inone, and renal toxicity in one.
Toxicity as a function of number of courses of treatment isdetailed in Table 4. Gastrointestinal toxicity was far more
Table 2
Platinum concentration in intracerebral tumor and kidney after i.v. and i.e.CDDP
Patient1812RouteI.V.
i.V.i.e.Dose
of CDDP(mg/sq m/
course)20
40/day for 3days
60-100No.
ofcourses2
23Time
(days)from lastcourse02102Platinum
(pg/g)Intracer
ebraltumor0.43
2.041.51Kidney2.062.881.09
pronounced during high-dose treatments every 3 weeks thanduring lower-dose weekly treatments. Myelosuppression was
not common. Renal toxicity was severe (creatinine, 3.7 mg/dl)in only one patient. Scalp erythema and desquamation weremild in 2 patients and moderately severe in 2 patients. Ototoxicity consisted of clinically significant tinnitus or high-frequencyhearing loss and tended to appear during the period of weeklyCDDP and irradiation.
Four patients had possible central nervous system toxicity.Other factors contributed substantially to the neurological deterioration of each of the 4 patients, and the exact role of CDDPremains unclear. In the first case, neurological deteriorationcoincided with tapering of corticosteroids. In the remaining 3patients, seizure accompanied by transient postictal neurological deterioration occurred 1 to 7 days after a postirradiationCDDP treatment. Three of the 4 patients were hypomagne-
semic, and it was thought that the hypomagnesemia maypossibly have contributed. Moreover, 3 of the 4 patients hadhad severe nausea and vomiting following their CDDP and mayhave experienced marked increases in intracranial pressureduring this vomiting. The schedule for postirradiation CDDPwas changed from 120 mg/sq m every 3 weeks to 35 to 40mg/sq m/day for 3 days every 3 weeks in an attempt todecrease this toxicity, but 3 of the 4 patients with possiblecentral nervous system toxicity received their treatment according to the latter schedule.
Peripheral nervous system toxicity consisted of enhancement of preexisting phantom-limb pain in an amputee. One
patient developed moderately severe abdominal pain accompanied by a transient rise in serum amylase concentration
2476 CANCER RESEARCH VOL. 42
on June 27, 2015. © 1982 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
CDDP: Central Nervous System Pharmacology and Use in Brain Tumors
Table 3
Platinum concentrations in autopsy brain specimens as a function of distance from intracerebral tumor
Dose of CDDPPatient (mg/sq m)Route1
20i.V.6
25i.v.8
40/day for 3i.v.days11
60 i.e.Type
ofbrain tis-
Time (hr)sue0
WhiteWhite1
.5WhiteWhiteGray48
WhiteWhiteGrayWhiteWhiteGrayWhiteGray144
WhiteWhiteDistance
fromtumor(cm)0-0.50.5-1.5AdjacentIpsilateralIpsilateral0-0.50.5-1.00.5-1.01.0-2.02.0-3.02.0-3.03.0-4.53.0-5.0IpsilateralContralateralBrain
platinum (fig/g wetwt)0.650.370.250.210.291.111.171.290.590.220.400.340.450.740.50Brain
platinumas% oftumor
platinum151862824333739432071311153423
Table 4
Toxicity of CDDP in combination with cranial irradiation
ToxicityTotal
no. ofcoursesNo.of courses withtoxicityGastrointestinalMildModerateSevereMyelosuppressionRenalScalpAuditoryCentral
nervoussystem"PeripheralnervoussystemHypomagnesemiaPancreatitisPneumoniaNeutropenia-relatedNormal
WBCCDDP
(40 mg/sq m/wk74121212441211CDDPa(105-
120 mg/sq mevery 3wk)131234421
a Insufficient follow-up information was available on 3 courses given to one
patient to assess gastrointestinal toxicity or myelosuppression.b Apparent central nervous system toxicity may have been more due to the
tumor itself than to the treatment but followed severe CDDP-induced nausea andvomiting in 3 cases, which was probably accompanied by a rise in intracranialpressure.
consistent with mild pancreatitis. Two patients, one of whomwas neutropenic, developed pneumonia.
It is too early to evaluate the effect of this treatment onsurvival.
DISCUSSION
Various studies with animals have demonstrated only smallquantities of platinum in brain and CSF after administration ofCDDP (7, 13). Our data indicate a comparable situation inhumans. Platinum was barely detectable in the CSF of somepatients and not detectable in the CSF of others after i.v.CDDP. Similarly, only low concentrations of platinum could bedemonstrated in autopsy brain samples from patients withoutintracerebral tumors who had received CDDP 2 to 165 daysantemortem. Thus, CDDP does not readily penetrate the intacthuman blood-brain and blood-CSF barriers. Despite this, high
concentrations of platinum were found in intracerebral tumorand edematous brain adjacent to tumor. This is not surprisingsince the vasculature within intracerebral tumors is completelydifferent from that in normal brain, with a marked disruption ofthe blood-brain barrier (8). It has been demonstrated previouslythat lipid-insoluble materials may attain high concentrations in
intracerebral tumor and that the concentration will decrease asa function of distance into brain from the tumor (12). Platinumconcentrations followed a pattern consistent with this observation. We have demonstrated previously that this is also truefor another antineoplastic agent, phosphonacetyl-L-aspartate
(22).The low concentrations of platinum found in normal brain,
brain distant from intracerebral tumor, and CSF coupled withthe recent observation that CDDP has activity against primarybrain tumors (9, 10) tend to detract from the hypothesis thatdrugs must be able to penetrate into brain as well as intointracerebral tumor to be effective (11 ). It is possible that it isstrictly fortuitous that lipid-soluble agents have thus far been
most effective against brain tumors. The role of the centralnervous system pharmacology of a drug in determining itsantitumor activity against intracranial tumors remains unclear.Other possibilities should be explored. For example, in vitrosensitivity studies should be performed on intracerebral andextracerebral tumor deposits from the same patient to determine whether clones of tumor cells particularly suited to survival in the central nervous system might also be inherentlymore resistant to chemotherapeutic agents.
It has been shown that concentrations of CDDP at least aslow as 1 /¿g/ml are radiopotentiating (1, 6, 15). Platinumconcentrations in this range were attained in intracerebraltumor with doses of 20 to 25 mg/sq m, and it is possible toadminister doses many times higher than this. Moreover, platinum was still detectable in intracerebral tumor several monthsafter administration of CDDP. It should be stressed that ourmethod measures total platinum, does not differentiate betweenvarious molecular species, and does not define the subcellularlocalization of the platinum. The method by which CDDP radi-
osensitizes and the maximum time after drug administrationthat it still radiosensitizes have not been fully defined (14).
JUNE 1982 2477
on June 27, 2015. © 1982 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
D. J. Stewart et al.
If only low concentrations of platinum had been found, itcould have been surmised that radiosensitizing and cytotoxicconcentrations were not attained. In view of the concentrationsfound, it is quite possible but not unequivocally proven thatsufficiently high concentrations of the radiosensitizing specieswere attained, and the data provide a pharmacological rationaleto investigate CDDP as a radiosensitizing agent for intracere-
bral tumors. CDDP has been shown previously to be synergisticwith cranial irradiation in a rat glioma model (5). This combination is particularly attractive since CDDP is also cytotoxicagainst many human tumors, including primary brain tumors(9, 10), tumors that frequently metastasize to the brain, suchas testicular carcinoma (25), and malignant melanoma (25).Moreover, since relatively little platinum penetrates into normalbrain tissue remote from the tumor, one would expect at mostslight potentiation of radiotoxicity to brain.
In this study, no comparison was made between intracerebraltumor and plasma platinum concentrations. However, tumorplatinum concentrations after CDDP, 20 to 25 mg/sq m, weresimilar to the peak plasma platinum concentrations of 0.4 to1.2 (median, 0.6) jtig/ml attained in a different group of patientswho received CDDP, 15 mg/sq m,5 and 48 hr after CDDP, 40
mg/sq m/day for 3 days, Patient 8 had tumor platinum concentrations similar to peak plasma platinum concentrationsnoted previously by us after CDDP, 100 to 120 mg/sq m (21).Moreover, platinum concentration was higher in intracerebraltumor than in temporalis muscle for 5 of the 6 patients fromwhom muscle was obtained.
Our initial clinical experience indicates that CDDP, 40 mg/sq m/week, during cranial irradiation is tolerable and feasible,although close follow-up of patients is necessary in case the
CDDP has to be temporarily interrupted. Ototoxicity may begreater than expected with CDDP or cranial irradiation alone,although further experience will be necessary to confirm this.We recommend discontinuing the CDDP but completing thecranial irradiation if clinically significant hearing loss or tinnitusoccurs. Gastrointestinal, bone marrow, renal, and scalp toxic-
ities are tolerable. The high rate of possible central nervoussystem toxicity in patients receiving postirradiation CDDP isdisconcerting, but much greater experience will be necessaryto determine whether this truly represented toxicity or whetherthe transient neurological deterioration was due solely to tapering corticosteroids and to treatment-related seizures. It ispossible that a continuation of the weekly CDDP schedule aftercompletion of the irradiation would prove more tolerable. It ispossible that hypomagnesemia was an important contributingfactor. Hypomagnesemia was common in our patients and hasbeen noted previously by others (17). It is too early to determinewhether this combination offers any therapeutic advantageover cranial irradiation alone. Additional patients are beingentered, and a complete report will follow.
Only limited data were obtained on platinum concentrationsin brain and intracerebral tumor after i.e. administration ofCDDP. No conclusions can be drawn, although we have demonstrated previously that peak platinum concentrations and CX f during drug infusion are higher in veins draining an areareceiving an ¡.a.infusion of CDDP than in peripheral veins (21 ).In addition, the differences in intracerebral tumor and kidneyplatinum concentrations after i.e. versus i.v. CDDP somewhat
5 D. J. Stewart, unpublished data.
support the contention that ¡.a.administration results in higherlocal tissue concentrations, but differences in drug doses,tumor types, and timing could also explain the observed results.
In summary, platinum attains potentially therapeutic and ra-diopotentiating concentrations in human intracerebral tumorand adjacent edematous brain after i.v. administration of CDDP.Concentrations of platinum in CSF, brain distant from intracerebral tumor, and brain from patients without intracerebral tumorare very low. Additional studies with a variety of chemothera-
peutic agents will be necessary to determine whether thecentral nervous system pharmacology of a drug plays a majorrole in its activity against intracerebral tumors. Weekly CDDP,40 mg/sq m/week, appears tolerable during cranial irradiation, but more experience is needed to assess toxicity andtherapeutic efficacy.
REFERENCES
1. Alverez, M. V., Cobreros, G . Heras, A., and Lopez Zumel, M. C. Studies onc/s-dichlorodiammineplatinum(ll) as a radiosensitizer. Br. J. Cancer, 37<Suppl. 3). 68-72. 1978.
2. Avellanóse, A.M., West, C. R., and Madajewicz, S. Five-year survival of non-irradiated malignant gliomas treated with chemotherapy alone. Proc. Am.Assoc. Cancer Res., 22. 531, 1981.
3. Benjamin, R. S., Weirnik, P. H.. and Bachur, N. R. Adriamycin chemotherapy—efficacy, safety, and pharmacologie basis of an intermittent singlehigh dosage schedule. Cancer (Phila.), 33. 19-27, 1974.
4. Crafts, D. C.. and Wilson. C. B. Basis and results of chemotherapeutictreatment of gliomas. Bull. Cancer (Paris). 64. 101-114, 1977.
5. Douple, E. B., and Richmond, R. C. Platinum complexes as radiosensitizersof hypoxic mammalian cells. Br. J. Cancer, 37(Suppl. 3). 98-102, 1978.
6. Dritschilo, A., Piro, A. J., and Kelman, A. D. The effect of c/s-platinum on therepair of radiation damage in plateau phase Chinese hamster (V-79) cells.Int. J. Radiât.Oncol. Biol. Phys., 5. 1345-1349, 1979.
7. Gormley, P., Poplack, D., and Pizzo, P. The cerebrospinal fluid (CSF)pharmacokinetics of c/s-diamminedichloroplatinum(ll) (DDP) and severalplatinum analogues. Proc. Am. Assoc. Cancer Res., 20. 279, 1979.
8. Mirano, A., and Matsui, T. Vascular structures in brain tumors. Hum. Pathol.,6:611. 1975.
9. Khan, A., McCullough. D., Borts, F., and Sinks, L. F. Update on use of c/s-platinum in CMS malignancies. Proc. Am. Assoc. Cancer Res., 21: 390,1980.
10. Leventhal, B. G., and Freeman, A. c/s-Diammine dichloroplatinum—a Phase
II study in pediatrie malignancies. Proc. Am. Assoc. Cancer Res., 20: 197,1979.
11. Levin, V. A. A pharmacologie basis for brain tumor chemotherapy. Semin.Oncol., 2. 57, 1975.
12. Levin, V. A., Freeman-Dove, M., and Landahl, H. D. Permeability characteristics of brain adjacent to tumor in rats. Arch. Neurol.. 32: 785, 1975.
13. Litters!, C. L , Le Roy, A. F., and Guarino, A. M. Disposition and distributionof platinum following parenteral administration of c/s-dichlorodiamminepla-tinum(ll) to animals. Cancer Treat. Rep., 63: 1485-1492, 1979.
14. Muggia, F. M., and Glatstein, E. Summary of investigations on platinumcompounds and radiation interactions. Int. J. Radiât.Oncol. Biol. Phys., 5.1407-1409. 1979.
15. Murthy, A. K.. Rossof, A. H., Anderson, K. M., and Hendrickson, F. R.Cytotoxicity and influence on radiation dose response curve of cis-diammi-nedichloroplatinum(ll)(cis-DDP). Int. J. Radiât.Oncol. Biol. Phys., 5: 1411-
1415. 1979.16. Rozencweig. M., Von Hoff, D. D.. Slavik, M., and Muggia, F. cis-Diammine-
dichloroplatinum: a new anticancer drug. Ann. Intern. Med., 86. 803-812,
1977.17. Schilsky, R. L., Anderson, T., and Weiss, R. B. Hypomagnesemia and renal
magnesium wasting in patients receiving c/s-diamminedichloroplatinum(ll)(DDP). Proc. Am. Assoc. Cancer Res., 20: 354, 1979.
18. Seifert, W., Caprioli, R.. Benjamin, R., and Hester, J. P. Energy dispersiveX-ray fluorescence determination of platinum in plasma, urine, and cerebrospinal fluid of patients administered c/s-diamminedichloroplatinum(ll) (DDP).Proc. Am. Assoc. Cancer Res., 20: 168, 1979.
19. Sharr, M. M., and Garfield, J. S. Management of intracranial métastases.Br.Med. J., f: 1535-1537, 1978.
20. Sklansky, B. D., Mann-Kaplan, R. S.. Reynolds, A. F., Rosenblum, M. L.,and Walker, M. D. 4'Demethyl-epipodophyllotoxin-/î-D-thenylidene-gluco-
side (PTG) in the treatment of malignant intracranial neoplasms. Cancer(Phila.). 33: 460. 1974.
21. Stewart, D. J., Benjamin, R. S., Seifert, W., Wallace, S., Gutterman, J. U.,Part, Y.. Calvo. D.. Ill, Samuels, M., and Loo, T. L. Clinical pharmacology ofintraarterial (IA) c/s-diamminedichloroplatinum II (DDP). Proc. Am. Assoc.
2478 CANCER RESEARCH VOL. 42
on June 27, 2015. © 1982 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
CDDP: Central Nervous System Pharmacology and Use in Brain Tumors
Cancer Res., 21: 337, 1980. Brooks, W. H.. Hunt, W. E. MacCarty. C. S.. Mahaley, M. S., Mealey, J., Jr..22. Stewart, D. J., Leavens, M., Friedman, J., Benjamin, R. S.. Moore. E. C.. Owens, G., Ransohoff, J.. II, Robertson, J. T., Shapiro, W. R., Smith. K. R.,
Bodey, G. P.. Valdivieso, M., Burgess, M. A., Wiseman, C., and Loo, T. L. Jr., Wilson, C. B., and Strike, T. A. Randomized comparisons of radiotherapyPenetration of N-<phosphonacetyl)-L-aspartate into human central nervous and nitrosoureas for the treatment of malignant glioma after surgery. N.system and intracerebral tumor. Cancer Res., 40: 3163-3166, 1980. Engl. J. Med., 303, 1323-1329, 1980.
23. Stewart, D. J., Leavens, M., Luna, M., Seifert, W., Loo, T. L., and Benjamin, 25. Williams, C. J., and Whitehouse, J. M. A. cis-Platinum: a new anticancerR. S. Human central nervous system pharmacology of c/s-diamminedichlo- agent. Br. Med. J., 1: 1689-1691, 1979.roplatinum (DDP). Proc. Am. Assoc. Cancer Res., 22. 359, 1981. 26. Wolpert-De Filippes. M. K. Antitumor activity of c/s-dichlorodiamminepla-
24. Walker, M. D., Green, S. B.. Byar, D. P., Alexander, E., Jr.. Batzdorf, U., tinum(ll). Cancer Treat. Rep., 63: 1453-1458. 1979.
JUNE 1982 2479
on June 27, 2015. © 1982 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
1982;42:2474-2479. Cancer Res David J. Stewart, Milam Leavens, Moshe Maor, et al. Malignant Brain Tumors-Diamminedichloroplatinum and Use as a Radiosensitizer in
cisHuman Central Nervous System Distribution of
Updated version
http://cancerres.aacrjournals.org/content/42/6/2474
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
To request permission to re-use all or part of this article, contact the AACR Publications
on June 27, 2015. © 1982 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from