Why study sympathetic nervous system?
14
M. SINSKI 1 , J. LEWANDOWSKI 1 , P. ABRAMCZYK 1 , K. NARKIEWICZ 2 , Z. GACIONG 1 WHY STUDY SYMPATHETIC NERVOUS SYSTEM? 1 Department of Internal Diseases, Hypertension and Vascular Disease, Warsaw Medical University, Warsaw, Poland, 2 Department of Hypertension and Diabetology, Medical University of Gdansk, Gdansk, Poland Cardiovascular diseases are the most frequent causes of morbidity and mortality around the world. However, during last decades, an improvement was made in diagnosis and therapy of cardiovascular diseases, there was still a need for better understanding of their pathophysiology. Among neurohormonal systems, SNS plays a central role in cardiovascular regulation in both health and disease. Involvement of SNS in pathogenesis of hypertension, coronary artery disease or heart failure is well known and proved. Methods such as microneurography, direct catecholamine measurements, heart rate variability or baroreflex sensitivity assessment allowed studying sympathetic activity and its influence on cardiovascular disorders. Although introduced into scientific practice methods of SNS evaluation are not commonly used in the clinic. However, two of the methods: analysis of heart rate variability (HRV) and baroreflex sensitivity (BRS) were recommended as the diagnostic tools and can be found in clinical guidelines as basic assessment methods. Key words: sympathetic nervous system, noradrenaline, microneurography, HRV, BRS INTRODUCTION The aim of this article is to summarize the role of sympathetic nervous system (SNS) in cardiovascular pathophysiology and describe how methods for studying sympathetic activity influence clinical practice. There is no doubt about the great increase in the knowledge on neuroregulation of cardiovascular system during last 3 decades. Methods such as microneurography, direct catecholamine measurements, heart rate variability or baroreflex sensitivity assessment allowed studying pathophysiology of cardiovascular diseases. What is most important, JOURNAL OF PHYSIOLOGY AND PHARMACOLOGY 2006, 57, Suppl 11, 79`92 www.jpp.krakow.pl
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Why study sympathetic nervous system?

M. SINSKI1, J. LEWANDOWSKI1, P. ABRAMCZYK1, K. NARKIEWICZ2, Z. GACIONG1
WHY STUDY SYMPATHETIC NERVOUS SYSTEM?
1Department of Internal Diseases, Hypertension and Vascular Disease, Warsaw Medical University,Warsaw, Poland, 2Department of Hypertension and Diabetology, Medical University of Gdansk,
Gdansk, Poland
Cardiovascular diseases are the most frequent causes of morbidity and mortalityaround the world. However, during last decades, an improvement was made indiagnosis and therapy of cardiovascular diseases, there was still a need for betterunderstanding of their pathophysiology. Among neurohormonal systems, SNS playsa central role in cardiovascular regulation in both health and disease. Involvement ofSNS in pathogenesis of hypertension, coronary artery disease or heart failure is wellknown and proved. Methods such as microneurography, direct catecholaminemeasurements, heart rate variability or baroreflex sensitivity assessment allowedstudying sympathetic activity and its influence on cardiovascular disorders.Although introduced into scientific practice methods of SNS evaluation are notcommonly used in the clinic. However, two of the methods: analysis of heart ratevariability (HRV) and baroreflex sensitivity (BRS) were recommended as thediagnostic tools and can be found in clinical guidelines as basic assessment methods.
K e y w o r d s : sympathetic nervous system, noradrenaline, microneurography, HRV, BRS
INTRODUCTION
The aim of this article is to summarize the role of sympathetic nervous system(SNS) in cardiovascular pathophysiology and describe how methods for studyingsympathetic activity influence clinical practice. There is no doubt about the greatincrease in the knowledge on neuroregulation of cardiovascular system duringlast 3 decades. Methods such as microneurography, direct catecholaminemeasurements, heart rate variability or baroreflex sensitivity assessment allowedstudying pathophysiology of cardiovascular diseases. What is most important,
JOURNAL OF PHYSIOLOGY AND PHARMACOLOGY 2006, 57, Suppl 11, 79�92
www.jpp.krakow.pl

data obtained using those methods changed clinical practice. Some of them werealso introduced into clinic as a diagnostic tool.
Studies on SNS changed clinical practice
Cardiovascular diseases are the most frequent causes of morbidity and mortalityaround the world. However, during last decades, an improvement was made indiagnosis and therapy of cardiovascular diseases, there was still a need for betterunderstanding of their pathophysiology. Among neurohormonal systems, SNSplays a central role in cardiovascular regulation in both health and disease (1 - 5).Activation of SNS can increase peripheral vascular resistance and cardiac output toraise blood pressure. Arteriolar vasoconstriction, as well as sympathetic mediatedvenoconstriction with consequent central redistribution of blood, both acts toincrease blood pressure. Cardiac sympathetic chronotropic and inotropic effectsalso increase blood pressure, particularly in the setting of increased vascularresistance. Thus, increased sympathetic traffic to the peripheral vasculature andsympathetic discharge to the heart exert complementary effects on blood pressure.Activation of SNS may also contribute to blood pressure levels in the long term byother mechanisms. Effects of sympathetic activation on the kidney, renin-angiotensin system, blood vessel growth and permeability as well as resetting of thearterial baroreflex should be mentioned.
In a few past decades, convincing data were collected to support theory thatenhanced sympathetic activity was involved in pathogenesis of manycardiovascular diseases. Numerous data from various observationsoverwhelmingly attest to the importance of the SNS in essential hypertension,particularly in its early stages (2, 3). Increased sympathetic tone was also provedto promote development and progression of hypertension related complicationsthat led to increased cardiovascular morbidity and mortality. Different techniqueswere involved to quantify sympathetic cardiovascular effects in humans withessential hypertension. First, tachycardia is the simplest and probably the mostreliable marker of sympathetic overactivity in humans with hypertension. Anassociation of tachycardia with higher blood pressure has been found in numerousinvestigations and both a simultaneous elevation of the heart rate and plasmacatecholamines were reported in hypertensives. In some observations, it wasdescribed that in normotensive subjects tachycardia might predict development offuture hypertension. Also, an association of tachycardia and increased cardiacoutput was found as a characteristic feature of early stages of essentialhypertension. Secondly, important information regarding sympathetic activity inhypertension has come from techniques that assay in a sensitive fashion plasmalevel of sympathetic neurotransmitter - noradrenaline. Although a number of earlycomparisons between normotensive and hypertensive individuals led to equivocalresults, a meta-analyses of published data did show that essential hypertensivepatients displayed greater plasma noradrenaline values than normotensives (6).
80

Thirdly, other biochemical and neurophysiological approaches, such as thenoradrenaline radiolabeled technique and the microneurography, have providedfurther evidence of sympathetic overactivity in hypertensive individuals. In somestudies, use of the noradrenaline - radiolabeled tracer, which estimates thesecretion of noradrenaline from the sympathetic nerve terminals, confirmed agreater sympathetic activity in young hypertensive subjects as compared to age-matched normotensive individuals (7). An introduction of the microneurographyto scientific routine has provided further data that showed an increase ofsympathetic drive in essential hypertension. Microneurography was also used todemonstrate sympathetic enhancement during subsequent stages of hypertension.It was confirmed that sympathetic activity might be increased in normotensivesubjects with a family history of hypertension and especially in subjects withborderline hypertension as compared to normotensive subjects (8, 9) and mightprogressively increase. In addition, an increase in sympathetic traffic waspresented also in older patients with isolated systolic hypertension (10).
Knowledge regarding enhanced sympathetic activity in patients with essentialhypertension has many practical implementations and is currently employed indaily clinical routine. Common use of antiadrenergic agents in therapy ofhypertension might be an example.
Apart of hypertension, sympathetic overactivity has been implicated in thepathogenesis of other diseases as metabolic disorders, coronary artery disease,cardiac arrhythmias or heart failure. Studies using microneurography haveconsistently shown increased muscle sympathetic nerve activity in obese subjects.Earlier data based on plasma catecholamine measurements and whole-body andregional noradrenaline release revealed inconsistient results (11, 12). However,recent observations suggest that obesity in humans is associated with increasedsympathetic outflow and that body fat is a major determinant of sympathetic neuraldischarge. Moreover, sympathetic overactivity is also involved in pathogenesis ofmetabolic syndrome. Primarily enhanced sympathetic drive can producevasoconstriction, diminish the regional blood flow and tissue glucose delivery, andthus generate insulin resistance, a key phenomenon in pathogenesis of manymetabolic and cardiovascular disorders. Some other mechanisms of sympatheticinfluence on insulin resistance are also described. Activation of adrenergicperipheral ß-receptors changes proportion between slow and fast twitch musclefibers and decreases number of small blood vessels in the skeletal muscles (13).
Increased sympathetic drive in hypertensive subjects may be independentlyimplicated in atherosclerotic vascular disease, especially coronary artery diseaseand associated fatal cardiovascular events. Although coronary artery disease hasa multifactorial origin sympathetic overdrive can be crucial for its development.Increased sympathetic activity induces vascular and cardiac hypertrophy,produces coronary vasoconstriction and increases cardiac oxygen consumption.Procoagulative state, activation of platelets, increased hematocrit level andendothelial dysfunction are also well recognized results of sympathetic
81

overactivity (13). In addition an imbalance between sympathetic andparasympathetic system as well as sympathetically mediated disturbances inelectrolytes may exert proarrhytmic action and induce life frighteningarrhythmias. Another evidence for a role of sympathetic overactivity in ischemicheart disease is the efficacy of pharmacological ß-blockade in decreasing cardiacdeath in patients after myocardial infarction (14). Numerous studies clearlyshowed that sympathetic activity was more pronounced after myocardialinfarction than after unstable angina, while sympathetic activity in patients withstable angina did not differ from that in control subjects (15). This observationmay at least in part explain why patients with both myocardial infarction andunstable ischemic syndromes are at increased risk of sudden cardiac death.
There is also a growing body of evidence that elevated sympathetic activityplays an important role in the pathophysiology of congestive heart failure. Earlystudies has shown an increased plasma noradrenalin concentration and total,cardiac and renal noradrenaline spillover in patients with congestive heart failure(16). Later studies demonstrated that prognosis in cardiac failure was directlylinked to the level of activation of the SNS and most strongly with that in the highsympathetic outflow to the heart (17, 18). Finally, one of the major advances incardiology of the past years has been the successful introduction of ß-adrenergicdrugs to the therapy of cardiac failure, which has substantially improved theclinical outcome in patients with congestive heart failure.
METHODS OF EVALUATION OF THE SYMPATHETIC NERVOUS SYSTEM
Measurements of urine and plasma noradrenaline
Traditionally, activity of the SNS was assessed using measurements of urinenoradrenaline and adrenaline or their precursors and metabolites. However, this"static" approach cannot provide reliable assessment of short-term changes insympathetic activity and, therefore, has been replaced by measurement of plasmanoradrenaline concentration. These measurements provide useful information,but also have significant limitations (19). First, circulating noradrenalinerepresents only a small fraction (5 - 10%) of the amount of neurotransmittersecreted from nerve terminals. Second, plasma levels of noradrenaline areinfluenced, in addition to the level of sympathetic neural outflow, byprejunctional modulation of neurotransmitter release, as well as the clearance,metabolism and uptake of noradrenaline from the circulation. Thus, plasmameasurements do not allow discrimination between central (increased secretion)and peripheral (reduced clearance) mechanisms of inreased levels of theneurotransmitter (5). Third, the use of plasma noradrenaline is based on theassumption that these measurements reflect "overall" sympathetic activity.Contrary to this assumption, there are profound regional differences in theactivity and control of sympathetic function. Furthermore, the reproducibility and
82

sensitivity of plasma noradrenaline values are lower than those ofmicroneurographic recordings (20).
Value of plasma catecholamines measurement is increased if it is combinedwith assessment of responses to adrenergic antagonists and agonists. Using thisapproach, it has been shown that mildly hypertensive individuals had elevatedplasma noradrenaline levels, augmented decreases in vascular resistance inresponse to α-adrenergic blockade, and no increase in α-receptor sensitivity asestimated by responses to noradrenaline (21). This study demonstratedaugmented sympathetic vasoconstrictor activity in young mildly hypertensivehumans, suggesting that increased sympathetic vasoconstriction results fromenhanced sympathetic neural release of noradrenaline, and not from augmentedα-adrenergic response to the neurotransmitter.
Noradrenaline spillover rate measurements
The noradrenaline radiolabeled method is based on intravenous infusion ofsmall amounts of tritiated noradrenaline, which allows tissue clearance of thissubstance to be subtracted from plasma noradrenaline values and to make theremainder a marker of the neurotransmitter "spillover" from the neuroeffectorjunctions. This "spillover" in steady-state conditions mirrors the secretion ofnoradrenaline from the sympathetic nerve terminals. The noradrenaline"spillover" technique avoids the confounding influence of neurotransmitterclearance and permits assessment of noradrenaline release from specific targetorgans (22). Hypertension, in particular "early" hypertension, may becharacterized by increased sympathetic traffic not only to the heart and bloodvessels, but also to the kidneys. Using measurements of noradrenaline spillover,Esler et al. (23) found that noradrenaline release was elevated in hypertensivepatients, particularly in young hypertensives, and that the increased spilloveroccurred mainly from the heart and kidneys.
Using jugular vein noradrenaline spillover measurements, Ferrier et al. (24)have reported that higher sympathetic activity in hypertension may be explainedby increased cerebral noradrenaline release, mostly from subcortical forebrainregions. The same group of investigators subsequently reported that subcorticalnoradrenaline release was linked with both total body noradrenaline spillover aswell as renal noradrenaline spillover (25). Since the forebrain is involved in theemotional responses (especially the defense reaction) it has been suggested thatincreased noradrenaline spillover from certain subcortical regions may representa neurochemical manifestation of stress.
Quantitative assessment of tritiated noradrenaline uptake from plasmademonstrated impairment of noradrenaline transporter function in essentialhypertension (26). The potential role of impaired neuronal noradrenaline reuptakecan be directly assessed by infusion of the noradrenaline transport inhibitordesipramine (27). Finally, noradrenaline stores in the human heart could be
83

estimated by quantifying the processing inside sympathetic nerves of tritiatednoradrenaline to its intraneuronal metabolite, dihydroxyphenylglycol (DHPG),coupled with measurement of DHPG in coronary sinus plasma (28, 29).
Microneurography
Direct intraneural recordings using microneurography provide a moment-to-moment measure of central sympathetic neural outflow independent of theinfluence of the neuro-effector junction. This technique involves the recording ofmultiunit sympathetic nerve discharge from a peripheral nerve, usually theperoneal nerve (30, 31). Sympathetic nerve activity is recorded using tungstenmicroelectrodes (shaft diameter 200 µm, tapering to an uninsulated tip of 1 - 5µm) inserted selectively into muscle or skin fascicles. Recently,micronuerographic approach allowed also quantification of single-fibre musclesympathetic nerve traffic (32, 33).
Microneurography permits separate recordings of sympathetic nerve activityto muscle (MSNA) vessels or skin (SSNA). MSNA reflects the vasoconstrictorsignal to the skeletal muscle vasculature, is acutely sensitive to blood pressurechanges, and is closely regulated by the arterial and cardiopulmonary
84
7:
SSNA
MSNA
7:
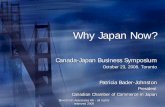
Fig. 1. Recordings of skin and muscle sympathetic nerve activity in a normal subject. Duration ofeach muscle sympathetic nerve activity burst is limited by the cardiac cycle; skin sympathetic nerveactivity bursts are broad based and may extend over several cardiac cycles. Both Recordings wereperformed in the young patient with essential hypertension.

baroreflexes. SSNA is not altered by either arterial or cardiopulmonarybaroreflexes. At rest, in a room temperature environment, SSNA reflectsvasomotor neural traffic to skin blood vessels with little if any sudomotoractivities present (34). MSNA and SSNA differ markedly with regard tomorphology (Fig. 1). SSNA bursts are broad based and may extend over severalcardiac cycles. The duration of each MSNA burst is limited by the cardiac cycle.
Measurement of sympathetic nerve activity from peripheral nerves inhumans has been shown to be safe, accurate, quantifiable and reproducible (35).Also important is that simultaneous measurements of sympathetic nerveactivity from different limbs show identical profiles in terms of burst frequencyand morphology. Thus, recordings in one limb can be reliably assumed toreflect recordings of sympathetic nerve activity to the muscle vascular bedthroughout the body (36).
The neural signals are amplified, filtered, rectified, and integrated to obtain avoltage display of sympathetic nerve activity. Sympathetic bursts are identified bya careful visual inspection of the voltage neurogram or by dedicated software.Muscle sympathetic nerve activity can be expressed as bursts per minute andburst per 100 heart beats, which allows comparison of sympathetic dischargebetween individuals (Fig. 2). The amplitude of each burst can also be determinedand sympathetic activity may be calculated as bursts/minute multiplied by meanburst amplitude and expressed as units/minute. Measurements of nerve activity atbaseline before each intervention are expressed as 100%. Changes in integrated
85
Low MSNA
High MSNA
Fig. 2. Recordings of muscle sympathetic nerve activity illustrating low (top) and high (bottom)activity. Recordings were performed in the young patient before and after 1minute apnea.

MSNA allow evaluation of within subject changes in sympathetic traffic inresponse to different stressors during the same recording session.
The introduction of microneurography has enabled a direct evaluation of thereflex sympathetic neural response to chemoreflex stimulation. These studieshave documented that the peripheral and central chemoreflexes have powerfuleffects on sympathetic activity in both health and disease and may contributeimportantly to disease pathophysiology, particularly in conditions such ashypertension (37), obstructive sleep apnea (38) and heart failure (39).
Although introduced into scientific practice methods of SNS evaluationdescribed above are not commonly used in the clinic. Limitations anddisadvantages of the various techniques has been reviewed in greater detailselsewhere (19). However two of the methods: analysis of heart rate variability(HRV) and baroreflex sensitivity (BRS) were recommended as the diagnostictools and can be found in clinical guidelines as basic assessment methods.
Heart rate variability
For more than 20 years spectral analysis of heart rate variability was used toassess autonomic control of the heart (40). Assessment of heart rate variability(HRV) is based on the analysis of consecutive sinus rhythm R-R intervals andmay provide quantitative information about the modulation of cardiac vagal andsympathetic nerve activities. HRV measurements can be derived from short term(2 to 5 minutes) or long-term ECG recordings (24 to 48 hours). It can bequantified in a number of ways but techniques of conventional time domain(statistical and geometrical) and frequency domain measurements (power spectraldensity) remain predominantly utilized. Recently (41), analysis of heart ratedynamics by methods based on non-linear system theory has been introduced,which may be an alternative way for studying the abnormalities in heart rate.
In normal humans, short term RR interval variability occurs predominantly ata low frequency (0.04 to 0.14 Hz) and a high frequency (±0.25 Hz, synchronouswith the respiratory frequency) (Fig. 3). The respiratory-related HF component isattributed mainly to vagal mechanisms. By contrast, different hypotheses havebeen proposed for the LF oscillation of RR interval variability. In several studies,LF component was not related to rates of noradrenaline spillover from the heartand or muscle sympathetic nerve traffic (19). Thus, while the LF/HF ratio may beconsidered as a marker of sympatho-vagal balance, it is unjustified to consider thelow frequency power as a surrogate measure of sympathetic nerve firing.
HRV as an independent cardiovascular risk factor
The closely monitored elderly population from the Framingham Heart Studywas assessed using HRV calculated from 2-hour ambulatory ECG recordings. Itwas found that HRV was significantly associated with all-cause mortality andprovided additional assessment of cardiovascular risk regardless traditional
86

cardiovascular risk factors. A later study showed that HRV was also anindependent risk factor in the healthy cohort of the Framingham study (42).
HRV in sudden cardiac death (SCD) and coronary heart disease riskassessment
HRV analysis was found useful in risk stratification for SCD in patients withheart failure. High LF values obtained during controlled breathing were foundpredictive of sudden cardiac death (43). HRV analysis was also classified asrecommendation Class I A for risk assessment by the Task Force on SuddenCardiac Death of European Society of Cardiology (44). It was also found that lowHRV predicts risk in coronary heart disease (45).
HRV in diabetes
Diabetic autonomic neuropathy is one of major complication of diabetescontributing significantly to the morbidity and mortality of the disease. Althoughtraditional measures and symptoms of autonomic function like resting
87
Fig. 3. Spectral analysis of simultaneous recordings of RR variability in a patient with heart failure(low) and in a control subject (high). There is a relative predominance of the LF component overthe HF component of RR interval in the patient with heart failure.

tachycardia, exercise intolerance, orthostatic hypotension, constipation,gastroparesis, erectile dysfunction, sudomotor dysfunction, impairedneurovascular function or hypoglycemic autonomic failure are able to documentthe presence of neuropathy, usually they are abnormal when there is severeclinical symptomatology. Thus by the time changes in function are evident, thenatural course of autonomic neuropathy is well established. HRV analysisdetermines the relative powers of the sympathetic and parasympathetic activities,is a very sensitive and early measure of autonomic neuropathy, and allowsmonitoring of disease progression. American Diabetes Association recommendsHRV analysis as a part of the diagnosis of autonomic neuropathy (46).
Baroreflex sensitivity
Baroreflex sensitivity measurement is based on the principle that the increasein blood pressure stimulates baroreceptors of the carotid sinus and aortic arch andresults in the activation of vagal fibers. As a result decrease in heart rate occurs.Sensitivity of baroreflex is defined as proportion of heart rate decrease due toblood pressure increase. Impaired baroreflex sensitivity is characterized bydecreased HVR and increased BP variability. As a result, normal buffering of BPincreases by HR decreases is lost.
In last decades neck suction (47) or pharmacological stimulation (48) wereused to activate baroreceptors and evoke heart rate changes. Advances in beat-by-beat blood pressure (BP) monitoring methods have now made possiblenoninvasive estimation of baroreflex sensitivity from the RR interval changesassociated with spontaneous fluctuations in BP. This new methodology offersclear advantages over traditional techniques of assessing baroreflex control.
88
BA
Fig. 4. Two methods of baroreflex sensitivity analysis-spectral (A) and sequence (B). Recordingswere made in the young patient with high-normal blood pressure.

Noninvasive estimates of baroreflex sensitivity are obtained from beat-to-beat BPand heart rate recordings by one of two methods to extract concordantly changingsystolic BP (SBP) and RR interval. Power spectral analysis provides a baroreflexestimate based on the RR interval changes associated with rhythmic BPoscillations over a range of frequencies reported to be associated with baroreflexfunction (Fig. 4). Second, recently developed method extracts covarying pressureand RR interval based on the magnitude of the changes occurring acrosssequential beats. In this technique, beat-by-beat BP and RR interval recordingsare scanned for sequences in which SBP and RR interval concurrently increase ordecrease for at least three consecutive beats. Baroreflex sensitivity is thenassessed from the relationship between SBP and RR interval across thesesequences (Fig. 4). Positive correlation was reported between baroreflexsensitivity estimates obtained by the frequency-domain-based and sequencemethod and from pharmacological manipulations of BP and RR interval (49).
Spontaneous baroreflex sensitivity is a very important marker for riskstratification particularly in patients who suffered from myocardial infarction (50- 53). A low BRS in patients with ischemic heart disease and impaired leftventricular function is the important prognostic parameter (54, 55). The Task Forceon Sudden Cardiac Death of European Society of Cardiology also classified BRSanalysis as a recommendation Class I A for cardiovascular risk assessment (44).
CONCLUSIONS
This brief review indicates that SNS is involved in pathophysiology of manycardiovascular disorders and points out an importance of its investigation for bothclinical and experimental research. Many aspects of the role of sympathetic systemare still controversial or remain a matter of debate. However, wider implementationof objective methods like microneurography, may contribute to better understandingof the role of SNS in cardiovascular disease and translate into better patient care.
REFERENCES
1. Mark AL. The sympathetic nervous system in hypertension: a potential long-term regulator ofarterial pressure. J Hypertens 1996; 14(suppl 5): 159-165.
2. Mancia G. Bjorn Folkow Award Lecture: the sympathetic nervous system in hypertension. JHypertens 1997; 15: 1553-1565.
3. Julius S, Nesbitt S. Sympathetic overactivity in hypertension. A moving target. Am J Hypertens1996; 9: 113-120.
4. Esler M, Lambert G, Brunner-La Rocca HP, Vaddadi G, Kaye D. Sympathetic nerve activity andneurotransmitter release in humans: translation from pathophysiology into clinical practice.Acta Physiol Scand 2003; 177: 275-284.
5. Narkiewicz K. Sympathetic nervous system and hypertension. Via Medica Press, Gdansk 2001.
89

6. Goldstein DS. Plasma catecholamines and essential hypertension: an analytical review.Hypertension 1983; 5: 86-99.
7. Esler MD, Lambert G, Jennings G. Regional norepinephrine turnover in human hypertension.Clin Exp Hypertens 1989; 11 (suppl 1): 75-89.
8. Anderson EA, Sinkey CA, Lawton WJ, Mark AL. Elevated sympathetic nerve activity inborderline hypertensive humans: evidence from direct intraneural recordings. Hypertension1988; 14: 1277-1283.
9. Floras JS, Hara K. Sympathoneural and haemodynamic characteristics of young subjects withmild essential hypertension. J Hypertens 1993; 11: 647-655.
10. Grassi G, Dell'Oro R, Bertinieri G, Turri C, Stella ML, Mancia G. Sympathetic nerve traffic andbaroreflex control of circulation in systodiastolic and isolated systolic hypertension of theelderly. J Hypertens 1999; 17 (suppl 3): 45-46.
11. Peterson HR, Rothschild M, Weinberg CR, et al. Body fat and the activity of the autonomicnervous system. N Engl J Med 1988; 318: 1077-1083.
12. Young JB, MacDonald IA. Sympathoadrenal activity in human obesity: heterogeneity offindings since 1980. Int J Obes Relat Metab Disord 1992; 16: 959-967.
13. Julius S.Corcoran Lecture. Sympathetic hyperactivity and coronary risk in hypertension.Hypertension 1993; 21: 886-893.
14. Gottlieb SS, McCarter RJ, Vogel RA. Effect of ß-blockade on mortality among high-risk andlow-risk patients after myocardial infarction. N Eng J Med 1998; 339: 489-97.
15. Graham LN, Smith PA, Stoker JB, Mackintosh AF, Mary DA. Sympathetic neural hyperactivityand its normalization following unstable angina and acute myocardial infarction. Clin Sci 2004;106: 605-611.
16. Hasking GJ, Esler MD, Jennings GL, Burton D, Johns JA, Korner PI. Norepinephrine spilloverto plasma in patients with congestive heart failure: evidence of increased overall and cardiorenalsympathetic nervous activity. Circulation 1986; 73: 615-621.
17. Cohn JN, Levine TB, Olivari MT, et al. Plasma norepinephrine as a guide to prognosis inpatients, with chronic congestive heart failure. N Engl J Med 1984; 311: 819-823.
18. Kaye DM, Lefkovits J, Jennings GL, Bergin P, Broughton A, Esler MD. Adverse consequencesof high sympathetic nervous activity in the failing human heart. J Am Coll Cardiol 1995; 26:1257-1263.
19. Grassi G, Esler M. How to assess sympathetic activity in humans. J Hypertens 1999; 7: 719-734.20. Grassi G, Bolla GB, Seravalle G, Turri C, Lanfranchi A, Mancia G. Comparison between
reproducibility and sensitivity of muscle sympathetic nerve traffic and plasma noradrenaline inman. Clin Sci 1997; 92: 285-289.
21. Egan B, Panis R, Hinderliter A, Schork N, Julius S. Mechanism of increased alpha adrenergicvasoconstriction in human essential hypertension. J Clin Invest 1987: 80: 812-817.
22. Esler M, Jennings G, Korner P, et al. Assessment of human sympathetic nervous system activityfrom measurements of norepinephrine turnover. Hypertension 1988; 11: 3-20.
23. Esler M, Jennings G, Lambert G. Noradrenaline release and the pathophysiology of primaryhuman hypertension. Am J Hypertens 1989; 2: 140-146.
24. Ferrier C, Essler MD, Eisenhofer G, et al. Increased norepinephrine spillover into the jugularveins in essential hypertension. Hypertension 1992; 19: 62-69.
25. Essler MD, Lambert GW, Ferrier C, et al. Central nervous system noradrenergic control ofsympathetic outflow in normotensive and hypertensive humans. Clin Exp Hypertens 1995; 17:409-423.
26. Rumantir MS, Kaye DM, Jennings GL, Vaz M, Hastings JA, Esler MD. Phenotypic evidence offaulty neuronal noradrenaline reuptake in essential hypertension. Hypertension 2000; 36: 824-829.
90

27. Schlaich MP, Lambert E, Kaye DM, et al. Sympathetic augmentation in hypertension: roleof nerve firing, norepinephrine reuptake, and angiotensin neuromodulation. Hypertension2004; 43: 169-175.
28. Eisenhofer G, Friberg P, Rundqvist B. et al. Cardiac sympathetic nerve function in congestiveheart failure. Circulation 1996; 93: 1667-1676.
29. Brunner-La Rocca HP, Esler MD, Jennings GL, Kaye DM. Effect of cardiac sympatheticnervous activity on mode of death in congestive heart failure. Eur Heart J 2003; 22: 1136-1143.
30. Wallin G. Intraneural recording and autonomic function in man. In Autonomic Failure R.Banister (ed.) London, UK: Oxford University Press 1983: pp. 36-51.
31. Mark AL, Victor RG, Nerhed G, Wallin BG: Microneurographic studies of the mechanisms ofsympathetic nerve responses to static exercise in humans. Circ Res 1985; 57: 461-469.
32. Macefield VG, Wallin BG, Vallbo AB. The discharge behaviour of single vasoconstrictor motorneurones in human muscle nerves. J Physiol (Lond) 1994; 481: 799-809.
33. Huggett RJ, Scott EM, Gilbey SG, Stoker JB, Mackintosh AF, Mary DA. Impact of type 2diabetes mellitus on sympathetic neural mechanisms in hypertension. Circulation 2003; 108:3097-3101.
34. Hagbarth KE, Hallin RG, Hongell A, Torebjork HE, Wallin BG. General characteristics ofsympathetic activity in human skin nerves. Acta Physiol Scand 1972; 84: 164-172.
35. van de Borne P, Montano M, Pagani N, Zimmerman B, Somers VK. Relationship betweenrepeated measures of hemodynamics, muscle sympathetic nerve activity and their spectraloscillations. Circulation 1997; 96: 4326-4332.
36. Wallin BG, Victor RG, Mark AL. Sympathetic outflow to resting muscles in arm and leg duringisometric handgrip and post-handgrip muscle ischemia. Am J Physiol 1989; 256: 105-110.
37. Somers VK, Mark AL, Abboud FM. Potentiation of sympathetic nerve responses to hypoxia inborderline hypertensive subjects. Hypertension 1988; 11: 608-612.
38. Narkiewicz K, van de Borne PJH, Pesek CA, Dyken ME, Montano N, Somers VK. Selectivepotentiation of peripheral chemoreflex sensitivity in obstructive sleep apnea. Circulation 1999;99: 1183-1189.
39. Narkiewicz K, Pesek CA, van de Borne PJH, Kato M, Somers VK. Enhanced sympatheticand ventilatory responses to central chemoreflex activation in heart failure. Circulation1999; 100: 262-267.
40. Malik M, Bigger JT, Camm AJ, et al. Task Force of the European Society of Cardiology an theNorth American Society of Pacing and Electrophysiology - Heart Rate Variability: Standard ofmeasurement, physiological interpretation and clinical use. Circulation 1996; 93: 1043-1065.
41. Makikallio TH, Tapanainen JM, Tulppo MP, et al. Clinical applicability of heart rate variabilityanalysis by methods based on nonlinear dynamics. Card Electrophysiol Rev 2002; 6: 250-255.
42. Tsuji H, Venditti FJ, Manders ES, et al. Reduced heart rate variability and mortality risk in anelderly cohort. The Framingham heart study. Circulation 1994; 90: 878-883.
43. La Rovera MT, Pinna GD, Maestri R, et al. Short term heart rate variability strongly predictssudden cardiac death in chronic heart failure patients. Circulation 2003; 107: 565-570.
44. Priori SG, Aliot E, Blomstron-Lundqvist C, et al. Task Force on Sudden Cardiac Death ofEuropean Society of Cardiology. Eur Heart J 2001; 22: 16.
45. Dekker JM, Crow RS, Folsom AR, et al. Low Heart Rate Variability in a 2-Minute RhythmStrip Predicts Risk of Coronary Heart Disease and Mortality From Several Causes : The ARICStudy. Circulation 2000; 102: 1239-1244.
46. Diabetic Neuropathies: A Statement by the ADA Diabetes Care. 2005; 28 (4): 956-962.47. Eckberg DL, Cavanaugh MS, Mark AL, Abboud FM. A simplified neck suction device for
activation of carotid baroreceptors. J Lab Clin Med 1975; 85: 167-173.
91

48. Smyth HS, Sleight P, Pickering GW. Reflex regulation of arterial pressure during sleep in man:a quantitative method of assessing baroreflex sensitivity. Circ Res 1969; 24: 109-121.
49. Robbe HW, Mulder LJ, Ruddel H, et al. Assessment of baroreceptor reflex sensitivity by meansof spectral analysis Hypertension 1987; 10; 538-543.
50. Barron H V and Lesh MD Autonomic nervous system and sudden cardiac death. J Am CollCardiol 1996; 27: 1053-1060.
51. Hartikainen JEK, Camm AJ. Baroreflex sensitivity in patients with myocardial infarction. EditCardiol 1995; 1: 72- 80.
52. Thames MD, Kinugawa T, Smith ML, Dibner Dunlap ME. Abnormalities of baroreflex controlin heart failure. J Am Coll Cardiol 1993; 22: 56-60.
53. LaRovere MT, Bigger Jr JT, Marcus FI, et al. Baroreflex sensitivity and heart-rate variability inprediction of total cardiac mortality after myocardial infarction. ATRAMI (Autonomic Toneand Reflexes After Myocardial Infarction). Lancet 1998; 351: 478-484.
54. La Rovere MT, Pinna GD, Hohnloser SH, et al. Baroreflex sensitivity and heart rate variabilityin the identification of patients at risk for life-threatening arrhythmias: implications for clinicaltrials. Circulation 2001; 103: 2072- 2077.
55. Mortara A, LaRovere MT, Pinna GD, et al. Arterial baroreflex modulation of heart rate inchronic heart failure, clinical and hemodynamic correlates and prognostic implications.Circulation 1997; 96: 3450-3458.
R e c e i v e d : November 21, 2006A c c e p t e d : November 24, 2006
Author�s address: Zbigniew Gaciong, Department of Internal Diseases, Hypertension andVascular Disease, Medical University of Warsaw, Banacha 1a, 02-097 Warsaw, Poland. Phone: + 48 22 599 2828, Fax: + 48 22 599 1928; e-mail: [email protected]
92