High-dose imatinib mesylate therapy in newly diagnosed Philadelphia chromosome-positive chronic...
7
doi:10.1182/blood-2003-11-3800 Prepublished online December 24, 2003; 2004 103: 2873-2878 Alessandra Ferrajoli and Jorge Cortes Francis Giles, Mary Beth Rios, Jianqin Shan, Laurie Letvak, Deborah Thomas, Stefan Faderl, Hagop Kantarjian, Moshe Talpaz, Susan O'Brien, Guillermo Garcia-Manero, Srdan Verstovsek, positive chronic phase chronic myeloid leukemia - chromosome High-dose imatinib mesylate therapy in newly diagnosed Philadelphia http://bloodjournal.hematologylibrary.org/content/103/8/2873.full.html Updated information and services can be found at: (372 articles) Plenary Papers (795 articles) Oncogenes and Tumor Suppressors (4217 articles) Neoplasia (3716 articles) Clinical Trials and Observations Articles on similar topics can be found in the following Blood collections http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requests Information about reproducing this article in parts or in its entirety may be found online at: http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprints Information about ordering reprints may be found online at: http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtml Information about subscriptions and ASH membership may be found online at: Copyright 2011 by The American Society of Hematology; all rights reserved. Washington DC 20036. by the American Society of Hematology, 2021 L St, NW, Suite 900, Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly For personal use only. by guest on June 5, 2013. bloodjournal.hematologylibrary.org From
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of High-dose imatinib mesylate therapy in newly diagnosed Philadelphia chromosome-positive chronic...

doi:10.1182/blood-2003-11-3800Prepublished online December 24, 2003;2004 103: 2873-2878
Alessandra Ferrajoli and Jorge CortesFrancis Giles, Mary Beth Rios, Jianqin Shan, Laurie Letvak, Deborah Thomas, Stefan Faderl, Hagop Kantarjian, Moshe Talpaz, Susan O'Brien, Guillermo Garcia-Manero, Srdan Verstovsek,
positive chronic phase chronic myeloid leukemia−chromosomeHigh-dose imatinib mesylate therapy in newly diagnosed Philadelphia
http://bloodjournal.hematologylibrary.org/content/103/8/2873.full.htmlUpdated information and services can be found at:
(372 articles)Plenary Papers � (795 articles)Oncogenes and Tumor Suppressors �
(4217 articles)Neoplasia � (3716 articles)Clinical Trials and Observations �
Articles on similar topics can be found in the following Blood collections
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
Copyright 2011 by The American Society of Hematology; all rights reserved.Washington DC 20036.by the American Society of Hematology, 2021 L St, NW, Suite 900, Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly
For personal use only. by guest on June 5, 2013. bloodjournal.hematologylibrary.orgFrom

Plenary paper
High-dose imatinib mesylate therapy in newly diagnosed Philadelphiachromosome–positive chronic phase chronic myeloid leukemiaHagop Kantarjian, Moshe Talpaz, Susan O’Brien, Guillermo Garcia-Manero, Srdan Verstovsek, Francis Giles, Mary Beth Rios,Jianqin Shan, Laurie Letvak, Deborah Thomas, Stefan Faderl, Alessandra Ferrajoli, and Jorge Cortes
Imatinib mesylate (STI571) is effective inchronic phase chronic myelogenous leu-kemia (CML). However, most patientstreated with 400 mg imatinib daily havevariable levels of residual molecular dis-ease. We treated 114 patients with newlydiagnosed chronic phase CML with 400mg imatinib twice daily. Overall, 109 pa-tients (96%) had a major cytogenetic re-sponse (Philadelphia chromosome [Ph] <35%), and 103 (90%) had a complete re-sponse (Ph 0%). With a median follow-upof 15 months, no patient has progressed
to accelerated or blastic phase. The esti-mated 2-year survival rate was 94%. Byquantitative polymerase chain reaction(QPCR) studies, 71 (63%) of 112 patientsshowed BCR-ABL/ABL percentage ratiosdecrease to less than 0.05%, and 31 (28%)to undetectable levels. Compared withstandard-dose imatinib, high-dose ima-tinib was associated with significantlybetter complete cytogenetic response(P � .0005), major molecular response(QPRC < 0.05%; P � .00001), and com-plete molecular response (undetectable
BCR-ABL; P � .001). High-dose imatinibwas well tolerated but resulted in morefrequent myelosuppression; 82% of pa-tients continue to receive 600 mg or moreof imatinib daily. In conclusion, high-doseimatinib induced higher rates of completecytogenetic response and of molecularresponse in patients with newly diag-nosed chronic phase CML. (Blood. 2004;103:2873-2878)
© 2004 by The American Society of Hematology
Introduction
Imatinib mesylate (STI571, Gleevec; Novartis Pharmaceuticals,East Hanover, NJ) is a selective Bcr-Abl protein tyrosine kinaseinhibitor against c-abl, bcr/abl, c-kit, and platelet-derived growthfactor receptor (PDGF-R).1,2 Imatinib has demonstrated signifi-cant activity in all phases of Philadelphia chromosome (Ph)–positive chronic myeloid leukemia (CML).3-12 The recom-mended dosage is 400 mg daily for chronic phase CML and 600mg daily for CML in transformation. In patients with previouslyuntreated early chronic phase CML, 400 mg imatinib orallydaily has produced complete hematologic responses (CHRs) inmore than 95% of patients, and complete cytogenetic responsesin 60% to 75%.11,12 However, patients with undetectable levelsof BCR-ABL assessed by polymerase chain reaction (PCR)studies (complete molecular response) represented only 5% to15%. Achievement of a complete cytogenetic response withinterferon alpha (IFN-�) has been associated with 10-yearsurvival rates of 70% to 85%.13-17 Patients with undetectableBCR-ABL levels after IFN-� have not relapsed after long-termfollow-up.13,15 Thus, while achievement of a complete cytoge-netic response is an important short-term goal in CML therapy,reaching undetectable levels of BCR-ABL may improve long-term event-free survival.
Several observations suggest that higher dosages of imatinibmay be more effective. The initial phase 1 trial showed a clear
dose-response relationship.3 Complete hematologic responserates were 98% with daily imatinib doses of 300 mg or higher,compared with 56% with 200 or 250 mg daily, and lower rateswith dosages less than 200 mg. Cytogenetic responses were 54%with dosages 300 mg/day or higher, but were rare at lowerdosages. In accelerated phase CML, patients treated with 600mg imatinib daily had higher response rates, and longerresponse and survival durations.7 In chronic phase CML afterIFN-� failure, imatinib dosage escalation to 800 mg daily afterCML relapse at 400 mg daily recaptured CHR in 60% of patientsand improved cytogenetic response to a major one in 40%.18
Amplification of the BCR-ABL gene or overexpression of itsprotein product are known mechanisms of resistance. Severalmutations within the Abl structure in Bcr-Abl result in relativerather than absolute resistance to imatinib. Some resistancemechanisms may be overcome with imatinib dosageescalation.19-22
We have recently treated 36 patients in late chronic CML afterIFN-� failure with 400 mg imatinib orally twice daily. Thecomplete cytogenetic response rate was 89%, and 41% hadundetectable levels of BCR-ABL.23 These results appear to besignificantly better than with 400 mg imatinib daily in chronicphase CML after IFN-�failure.5,6 In this study, we investigated theefficacy and toxicity of high-dose imatinib (800 mg daily) in newly
From the Departments of Leukemia and Bioimmunotherapy, The Universityof Texas, M. D. Anderson Cancer Center, Houston, TX; and NovartisPharmaceuticals, East Hanover, NJ.
Submitted November 12, 2003; accepted December 13, 2003. Prepublishedonline as Blood First Edition Paper, December 24, 2003; DOI 10.1182/blood-2003-11-3800.
Supported in part by the Betty Foster Leukemia Research Fund and the CMLPO1 CA49639. J.C. is a Clinical Research Scholar of the Leukemia andLymphoma Society.
L.L. is employed by Novartis Pharmaceuticals, whose potential product was
studied in the present work.
An Inside Blood analysis of this article appears in the front of this issue.
Reprints: Hagop Kantarjian, Department of Leukemia, M. D. Anderson CancerCenter, 1515 Holcombe Blvd, Box 428, Houston, TX 77030; e-mail:[email protected].
The publication costs of this article were defrayed in part by page chargepayment. Therefore, and solely to indicate this fact, this article is herebymarked ‘‘advertisement’’ in accordance with 18 U.S.C. section 1734.
© 2004 by The American Society of Hematology
2873BLOOD, 15 APRIL 2004 � VOLUME 103, NUMBER 8
For personal use only. by guest on June 5, 2013. bloodjournal.hematologylibrary.orgFrom

diagnosed CML, and compared the results with standard-doseimatinib (400 mg daily) in a similar CML population.
Patients and methods
Study group
Patients with newly diagnosed Ph-positive CML in early chronic phase(diagnosis to therapy � 12 months) were eligible for our institutionalinvestigational new drug (IND) study (ID-01_151). Patients wererequired to be 15 years or older and to have adequate performance status(Eastern Cooperative Oncology Group [ECOG], 0 to 2), serum creati-nine less than 176.8 �M (2 mg/dL), total bilirubin less than 34.2 �M (2mg/dL), and normal cardiac function (New York Heart Association class3-4 cardiac disease excluded). Patients previously treated with imatinibwere not eligible; prior therapy with hydroxyurea was allowed, but priortherapy with IFN-� or cytarabine was allowed only for a month or less.Women of childbearing age were required to have a negative pregnancytest before starting imatinib, and all patients at risk were required to usecontraception during therapy. Patients provided written informed con-sent before entry into the study; the study was reviewed and approved bythe internal review board of our institution (M.D. Anderson CancerCenter) and performed in accordance with the Declaration of Helsinki.
Patients with accelerated or blastic phase CML were excluded.24,25
Patients with cytogenetic clonal evolution were eligible if there were noother criteria of accelerated phase CML.
Treatment and dose modifications
Imatinib was given orally at 400 mg twice daily. Hydroxyurea was allowedfor debulking during the first 4 weeks of therapy. Anagrelide was permittedfor up to 3 weeks.
Dose reductions of imatinib for nonhematologic or hematologic toxiceffects were as follows. For persistent grade 2 nonhematologic toxic effects,therapy was interrupted until recovery to grade 1 or less and resumed at theoriginal dosage level. If grade 2 toxicity recurred, treatment was interruptedagain until recovery and resumed at a daily dosage of 600 mg. For grade 3or 4 nonhematologic toxicity, therapy was interrupted until recovery tograde 1 or less and resumed at a daily dosage of 600 mg. For severehematologic toxicity (granulocyte count of � 0.5 � 109/L or a plateletcount of � 40 � 109/L), therapy was interrupted until the neutrophilsrecovered to 109/L or higher and/or platelets to 60 � 109/L or higher. If thetoxicity resolved within 2 weeks, treatment was resumed at the originaldosage. If toxicity resolved after more than 2 weeks, or if it recurred afterresuming therapy, the dosage was reduced to 600 mg. Further dose reductions to400 mg or 300 mg daily were allowed using the same guidelines for hematologicand nonhematologic toxicity. Patients developing anemia received packed redblood cell transfusions or blood products at the discretion of the investigator, or40 000 units erythropoietin subcutaneously once a week until the hemoglobinlevel increased to 120 g/L (12 g/dL) or more.
Monitoring
Complete blood counts and serum chemistry were done weekly duringthe first 4 weeks, then every 6 to 8 weeks thereafter. Bone marrowstudies, including morphologic and cytogenetic or fluorescent in situhybridization (iFISH) analysis, and quantitative PCR studies, wereperformed every 3 months in the first year, then every 3 to 6 months.Patients were followed for survival at least every 3 months. Drug safetyparameters were evaluated at each visit and graded according to theNational Cancer Institute Common Toxicity Criteria (NCI CTC),version 2.0.
Statistical considerations
Response criteria were as previously described.26 A CHR was defined as awhite blood cell count of less than 10 � 109/L, a platelet count of less than450 � 109/L, no immature cells (blasts, promyelocytes, myelocytes) in the
peripheral blood, and disappearance of all signs and symptoms related toleukemia (including palpable splenomegaly) lasting for at least 4 weeks.Response was further categorized by the best cytogenetic response:complete, 0% Ph-positive cells; partial, 1% to 34% Ph-positive cells; andminor, 35% to 90% Ph-positive cells. Major cytogenetic response includedcomplete plus partial cytogenetic responses (Ph-positive cells 0%-34%).Cytogenetic response was judged by standard cytogenetic analysis ofmetaphase spreads. Patients were categorized by their best cytogenetic ormolecular response. Differences among variables were compared by thechi-square test. Time to disease transformation was calculated from the timetreatment began until appearance of accelerated or blastic phase disease.Survival was calculated from the time treatment began until death from anycause. Survival and time to event curves were estimated by the Kaplan-Meier method and compared by the log rank test.
Cytogenetic and PCR analysis
Cytogenetic analysis was performed by the G-banding technique. Marrowspecimens were examined on direct or short-term (24-hour) cultures; atleast 20 metaphases were analyzed. PCR was done by real-time reversetranscriptase–PCR, and negative results (ie, undetectable transcript) wereconfirmed by nested PCR as previously reported.27 The sensitivity of thetest is 1:100 000.The quantitative PCR (QPCR) analysis measured the BCR-ABL/ABL percentage ratio. For the purpose of this analysis, a complete molecularresponse was defined as negative (undetectable) BCR-ABL levels. A majormolecular response was defined as BCR-ABL/ABL values less than 0.05%. Thiswas based on previous studies identifying BCR-ABL/ABL values of 0.045% to0.1% to be prognostically important.28,29 A BCR-ABL/ABL ratio of 0.05% isroughly equivalent to a 3-log reduction in disease.30
Historical control group
For comparative purposes, 50 patients with newly diagnosed Ph-positiveCML treated on an institutional IND study (ID01-015) with 400 mgimatinib orally daily were analyzed. All patients were entered in the studyfrom April to May 2001.11 The study of the historical control groupimmediately preceded the current study (which entered patients from June2001 until April 2003).
Results
Study group
From June 2001 until April 2003, 114 patients were enrolled on theinstitutional IND study (ID-01_151). Their median age was 48years (range, 17-84 years). Risk group (Sokal) stratification for 99patients with evaluable data was as follows: good, 41%; intermedi-ate, 37%; and poor, 21%. Their characteristics are summarized inTable 1. There were 50 patients (44%) who had received othertherapies (IFN-�, 1; hydrea, 49). There were 6 patients (5%) whohad cytogenetic clonal evolution (other than complex Ph transloca-tions or loss of chromosome Y): 3 with double Ph, 3 with otherabnormalities. The median follow-up of the study group was 15months and of the historical control group 31 months.
Response
Of the patients, 112 (98%) achieved CHR (Table 2). A majorcytogenetic response was noted in 109 patients (96%): complete in103 (90%) and partial in 6 (5%). Complete cytogenetic responsewas achieved in 59 patients (52%) at 3 months of therapy, and in 94(82%) at 6 months. Compared with standard-dose imatinib, high-dose imatinib was associated with achievement of significantlybetter complete cytogenetic responses (P � .0005; Figure 1).Patients with Sokal high risk had a lower complete cytogeneticresponse rate (76% versus 95%; P � .03). There were no other
2874 KANTARJIAN et al BLOOD, 15 APRIL 2004 � VOLUME 103, NUMBER 8
For personal use only. by guest on June 5, 2013. bloodjournal.hematologylibrary.orgFrom

significant differences in the incidence of complete cytogeneticresponse by known prognostic factors (eg, older age, spleno-megaly, thrombocytosis) within the small numbers involved. All 6patients with clonal evolution achieved a complete cytogeneticresponse (and disappearance of cytogenetic clonal evolution).
Figure 2 shows the values of BCR-ABL/ABL percentage ratioduring imatinib therapy. There was a consistent and significantdecline of these ratios over time. The median BCR-ABL/ABLpercentage ratio decreased from 0.90% (range, 0%-107%) after 3months to 0.030% (range, 0%-51%) after 12 months of therapy. Of112 patients evaluable for molecular response, 71 (63%) achievedratios of less than 0.05%, including 31 patients (28%) who hadundetectable transcripts (confirmed by nested PCR). There were 48patients who had at least 2 consecutive PCR values less than0.05%, and 10 patients had at least 2 consecutive analyses withundetectable transcripts. Compared with standard-dose imatinib,patients receiving high-dose imatinib achieved significantly better
major (BCR-ABL/ABL ratio � 0.05%; Figure 3; P � .00001) andcomplete (BCR-ABL/ABL negative ratio; Figure 4; P � .001)molecular responses. The estimated cumulative 18-month inci-dence of complete molecular response was 28% with high-doseimatinib versus 7% with standard-dose imatinib.
Time to progression and survival
Of the 114 patients treated, 96 (84%) remain alive in chronic phaseon imatinib therapy. The other 18 patients stopped therapy becauseof noncompliance (n � 4), insurance issues (n � 3), toxicity(n � 7), cytogenetic refractoriness (n � 3), and death unrelated toimatinib (n � 1). After a median follow-up of 15 months (range,3-27 months), 112 patients (98%) are alive in chronic phase.Among all patients, 2 died—one from complications of allogeneicstem cell transplantation done in chronic phase (100% Ph-positiveat 6 months) and the second of unrelated causes. None of the 114patients have transformed; transformation-free status was betterwith high-dose imatinib (Figure 5; P � .004). Only 3 of 167patients on either study have died (Figure 6). No patient in thecurrent study group has developed chromosomal abnormalities inthe emerging Ph-negative cells (2 did so in the historical group).
Response duration
Of the 109 patients with a major cytogenetic response, 11 weretaken off therapy for issues not related to response (noncompliance,
Table 1. Characteristics of the study and historical control groups
Parameter
No. (%)
Studygroup
Historicalgroup P
Age, 60 y or older [median age, y] 31 (27)[48] 13 (26)[48] 1.0
Female sex 44 (39) 24 (48) .34
Performance status 2 2 (2) 0 (0) 1.0
Splenomegaly 31 (27) 11 (22) .56
Diagnosis to therapy, mo
[median time, mo] [1] [2]
0 19 (17) 5 (10) .34
1 to 11 95 (83) 45 (90)
Hemoglobin level [median
level, g/L] [123] [125]
Less than 100 g/L 3 (3) 3 (6) .37
WBC count, � 109/L [median
count, � 109/L] [32.2] [22.5]
50 or higher 41 (36) 11 (22) .1
Platelet count, � 109/L [median
count, � 109/L] [375] [382]
450 to 700 27 (24) 11 (22) .76
Higher than 700 18 (16) 6 (12)
Peripheral blasts, any 42 (37) 14 (28) .29
Peripheral basophils, 7% or more 29 (25) 10 (20) .55
Marrow blasts, more than 5% 6 (5) 0 (0) .18
Marrow basophils, 5% or more 26 (23) 7 (14) .21
Clonal evolution present 6 (5) 0 (0) .18
Sokal risk group .14
Low 41 (36) 24 (48)
Intermediate 37 (32) 12 (24)
High 21 (18) 12 (24)
Unknown 15 (13) 2 (4)
Populations are as follows: study group, N � 114; historical group, N � 50.
Table 2. Response to imatinib mesylate therapy
Response
No. (%)
PStudygroup
Historicalgroup
Complete hematologic 112 (98) 49 (98) —
Cytogenetic 110 (96) 49 (98) —
Complete 103 (90) 37 (74) .01
Partial 6 (5) 9 (18) —
Minor 1 (1) 3 (6) —
Populations are as follows: study group, N � 114; historical group, N � 50. —indicates lack of statistical significance.
Figure 1. Estimated cumulative incidence of complete cytogenetic response inthe study and historical control groups. CR indicates complete response.
Figure 2. BCR-ABL/ABL percentage ratio over the course of therapy. Results areexpressed for each evaluable patient at each 3-month period. Number of evaluablepatients is shown on top. The dotted line represents a percentage ratio of 0.05%.Percentages shown under this line represent the proportion of patients below thisthreshold at each time point.
HIGH-DOSE IMATINIB IN Ph-POSITIVE CML 2875BLOOD, 15 APRIL 2004 � VOLUME 103, NUMBER 8
For personal use only. by guest on June 5, 2013. bloodjournal.hematologylibrary.orgFrom
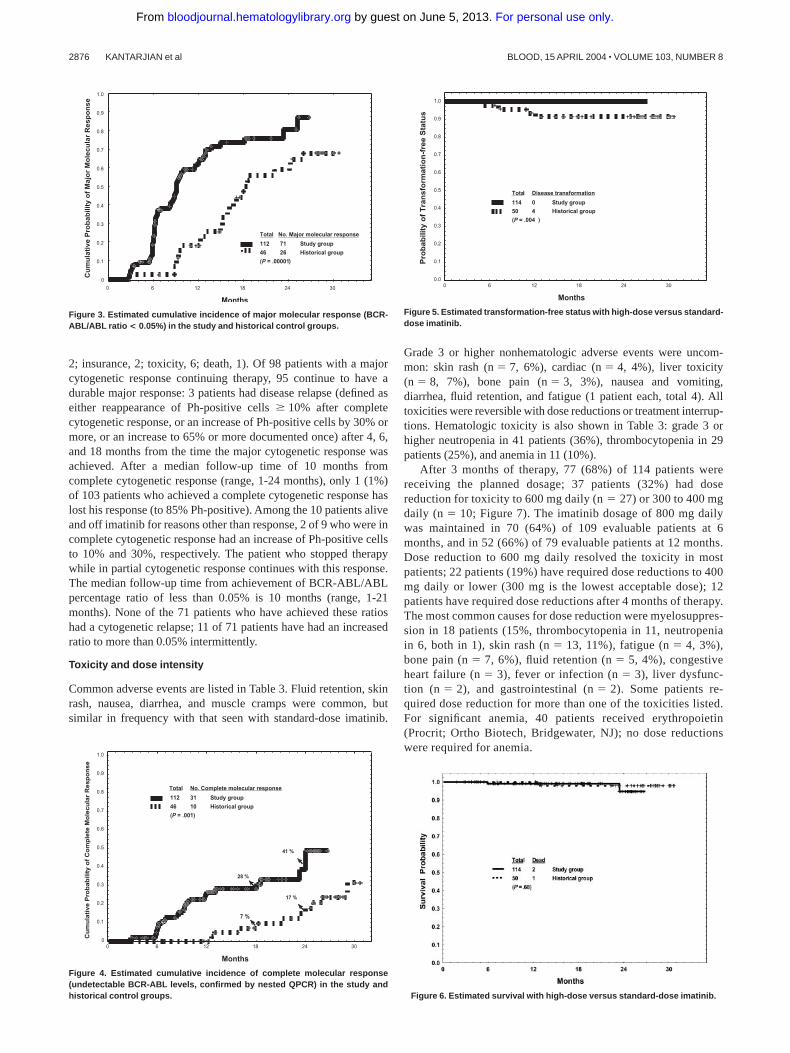
2; insurance, 2; toxicity, 6; death, 1). Of 98 patients with a majorcytogenetic response continuing therapy, 95 continue to have adurable major response: 3 patients had disease relapse (defined aseither reappearance of Ph-positive cells � 10% after completecytogenetic response, or an increase of Ph-positive cells by 30% ormore, or an increase to 65% or more documented once) after 4, 6,and 18 months from the time the major cytogenetic response wasachieved. After a median follow-up time of 10 months fromcomplete cytogenetic response (range, 1-24 months), only 1 (1%)of 103 patients who achieved a complete cytogenetic response haslost his response (to 85% Ph-positive). Among the 10 patients aliveand off imatinib for reasons other than response, 2 of 9 who were incomplete cytogenetic response had an increase of Ph-positive cellsto 10% and 30%, respectively. The patient who stopped therapywhile in partial cytogenetic response continues with this response.The median follow-up time from achievement of BCR-ABL/ABLpercentage ratio of less than 0.05% is 10 months (range, 1-21months). None of the 71 patients who have achieved these ratioshad a cytogenetic relapse; 11 of 71 patients have had an increasedratio to more than 0.05% intermittently.
Toxicity and dose intensity
Common adverse events are listed in Table 3. Fluid retention, skinrash, nausea, diarrhea, and muscle cramps were common, butsimilar in frequency with that seen with standard-dose imatinib.
Grade 3 or higher nonhematologic adverse events were uncom-mon: skin rash (n � 7, 6%), cardiac (n � 4, 4%), liver toxicity(n � 8, 7%), bone pain (n � 3, 3%), nausea and vomiting,diarrhea, fluid retention, and fatigue (1 patient each, total 4). Alltoxicities were reversible with dose reductions or treatment interrup-tions. Hematologic toxicity is also shown in Table 3: grade 3 orhigher neutropenia in 41 patients (36%), thrombocytopenia in 29patients (25%), and anemia in 11 (10%).
After 3 months of therapy, 77 (68%) of 114 patients werereceiving the planned dosage; 37 patients (32%) had dosereduction for toxicity to 600 mg daily (n � 27) or 300 to 400 mgdaily (n � 10; Figure 7). The imatinib dosage of 800 mg dailywas maintained in 70 (64%) of 109 evaluable patients at 6months, and in 52 (66%) of 79 evaluable patients at 12 months.Dose reduction to 600 mg daily resolved the toxicity in mostpatients; 22 patients (19%) have required dose reductions to 400mg daily or lower (300 mg is the lowest acceptable dose); 12patients have required dose reductions after 4 months of therapy.The most common causes for dose reduction were myelosuppres-sion in 18 patients (15%, thrombocytopenia in 11, neutropeniain 6, both in 1), skin rash (n � 13, 11%), fatigue (n � 4, 3%),bone pain (n � 7, 6%), fluid retention (n � 5, 4%), congestiveheart failure (n � 3), fever or infection (n � 3), liver dysfunc-tion (n � 2), and gastrointestinal (n � 2). Some patients re-quired dose reduction for more than one of the toxicities listed.For significant anemia, 40 patients received erythropoietin(Procrit; Ortho Biotech, Bridgewater, NJ); no dose reductionswere required for anemia.
Figure 5. Estimated transformation-free status with high-dose versus standard-dose imatinib.
Figure 6. Estimated survival with high-dose versus standard-dose imatinib.
Figure 3. Estimated cumulative incidence of major molecular response (BCR-ABL/ABL ratio < 0.05%) in the study and historical control groups.
Figure 4. Estimated cumulative incidence of complete molecular response(undetectable BCR-ABL levels, confirmed by nested QPCR) in the study andhistorical control groups.
2876 KANTARJIAN et al BLOOD, 15 APRIL 2004 � VOLUME 103, NUMBER 8
For personal use only. by guest on June 5, 2013. bloodjournal.hematologylibrary.orgFrom

Discussion
A body of evidence suggested that higher dosages of imatinib maybe associated with better disease control and with overcomingrelative CML resistance to imatinib.18-23 Initiation of high-doseimatinib early in the course of CML may also reduce the emergenceof imatinib-resistant CML clones. In this study, we treated 114patients with newly diagnosed Ph-positive CML in chronic phasewith 400 mg imatinib orally twice daily. The overall completecytogenetic response rate was 90%. Molecular responses wereexcellent: 63% of patients achieved a major molecular response,which was complete in 28%. The 12-month cumulative incidenceof complete cytogenetic response was 95%, of a major molecularresponse 60%, and of a complete molecular response 26%. Thesecomplete cytogenetic and molecular response rates are unprec-edented. With a median follow-up time of 15 months, the estimated2-year survival rate is 94%. Compared with standard-dose ima-tinib, high-dose imatinib was associated with better completecytogenetic and major/complete molecular responses (Figures 2-4).Progression-free survival was also better (Figure 5), although thenumber of events is very small.
In previous studies with IFN-� regimens, the complete cytoge-netic response rates were 5% to 25%.16,17,26,31-33 Patients whoachieved a complete cytogenetic response had estimated 10-yearsurvival rates of 70% to 80%,13-15 which made achievement of acomplete cytogenetic response an early surrogate end point forlong-term survival, and a major therapeutic objective. The com-plete cytogenetic response rate of 90% in this study is encouragingin relation to long-term prognosis, assuming the prognostic signifi-cance of a complete cytogenetic response achieved with imatinib issimilar to that achieved with IFN-� therapy. Except for Sokal riskgroup, no pretreatment characteristics have predicted for differ-ences in the incidence of complete cytogenetic response. All 6patients with cytogenetic clonal evolution achieved a completecytogenetic response. No chromosomal abnormalities have so farbeen observed in the Ph-negative cells.34
Achievement of a major molecular response (reduction ofBCR-ABL/ABL ratio by 3-log or more, or to � 0.05%) hasbecome the focus of newer regimens. Hochhaus et al previouslyreported that patients who attained BCR-ABL/ABL ratios of0.045% or less with IFN-� therapy had an estimated 3-year relapserate of 0% versus 80% for those having lesser degrees of molecular
response.28 Molecular remissions have been reported infrequentlywith standard-dose imatinib. In a study by Hochhaus et al, all 55patients with CML in complete cytogenetic remission after ima-tinib therapy remained PCR-positive with median follow-up of 1.3years.35 In the International Randomized Study of Interferon versusSTI571 (IRIS trial) in newly diagnosed CML, patients achieving3-log or more reductions of BCR-ABL/ABL (about 38% ofpatients) currently have an estimated 2-year progression-freesurvival rate of 100%.30 In our analysis of patients in chronic phaseCML who achieved a complete cytogenetic response with imatinib,29% of patients achieved BCR-ABL/ABL ratios of 0.05% or lesson imatinib, and 13% had undetectable transcripts. Patients whohad major molecular responses had a progression rate of 3% versus21% for those who had fewer degrees of disease reduction(P � .001).36 In the present study, the incidence of major molecularresponse (BCR-ABL/ABL ratio � 0.05%, roughly equivalent to3-log reduction) was 63%, and of complete molecular response28%. The 18-month cumulative incidence of major molecularresponse was 72% with high-dose imatinib versus 42% withstandard-dose imatinib (Figure 3). The 18-month cumulativeincidence of complete molecular response was 28% with high-doseimatinib versus 7% with standard-dose imatinib (Figure 4). Ofnote, the incidences of major molecular response (42%) and ofundetectable BCR-ABL (7%) at 18 months in the historical group(standard-dose imatinib) were similar to those reported in the IRISstudy.12,30 None of our patients who had a major molecularresponse have had a cytogenetic relapse. The methodology formolecular analysis varies in different studies, and some techniquesreported in the literature may be more sensitive.37 However, usingthe identical molecular technique at our institution, we demon-strated better quality molecular response with high-dose versusstandard-dose imatinib, as well as similar incidences of majormolecular responses and undetectable BCR-ABL levels withstandard-dose imatinib as was reported in the IRIS study.12,30
Several investigations now aim to increase the frequency ofPCR negativity with CML therapy. Most are resorting to combiningimatinib with IFN-� or cytarabine (ara-C) as frontline therapy, insingle-arm or randomized designs. These combinations may intro-duce early toxicity (often not palatable to patients) and synergisticmyelosuppression (compromising imatinib dose delivery). Analternative would be to introduce additional therapy at the time ofmaximal stable response achieved with imatinib (short of aPCR-negative status). In our study, the cumulative incidence ofPCR negativity continues to increase with therapy (Figure 4). Thisshould be considered in strategies that implement additionaltherapeutic strategies (such as vaccines, interferon, decitabine,
Figure 7. Imatinib dose delivery over time.
Table 3. Severe side effects with high-dose versusstandard-dose imatinib
Toxicity
No. (%) with grades 3-4 toxicity
Studygroup
Historicalcontrol
Fluid retention 1 (1) 0 (0)
Bone pain 3 (3) 1 (2)
Skin rash 7 (6) 3 (6)
Fatigue 1 (1) 1 (2)
Nausea/vomiting 1 (1) 0
Diarrhea 1 (1) 0
Abnormal liver function tests 8 (7) 5 (10)
Cardiac 4 (4) 1 (2)
Anemia* 11 (10) 2 (4)
Neutropenia 41 (36) 10 (20)
Thrombocytopenia 29 (25) 6 (12)
Populations are as follows: study group, N � 114; historical control, N � 50.*P values for differences were as follows: anemia, P � .35; neutropenia,
P � .05; and thrombocytopenia, P � .06.
HIGH-DOSE IMATINIB IN Ph-POSITIVE CML 2877BLOOD, 15 APRIL 2004 � VOLUME 103, NUMBER 8
For personal use only. by guest on June 5, 2013. bloodjournal.hematologylibrary.orgFrom

homoharringtonine, or others) to evaluate their effect on increasingthe rate of PCR-negative response.
High-dose imatinib was associated with more hematologictoxicity. In a phase 1 study of imatinib in chronic phase CML,patients were treated with escalating dosages of 25 mg to 1000 mgdaily. A maximum tolerated dosage was not defined, and furtherdose escalations were not pursued because of evidence of biologicand clinical activity. In patients with accelerated phase CML, therewas no difference in the incidence of severe hematologic ornonhematologic toxicity among patients treated with 400 mg or600 mg daily. In our previous study of high-dose imatinib inchronic phase CML after IFN-� failure, fluid retention was morelikely to require therapy (ie, grade 2 according to the NCI CTC),but grade 3 edema was rare.23 Severe skin rashes were more
common. This was partly confirmed in the current study, whichshowed a similar incidence of severe extramedullary side effectswith 400 mg versus 800 mg of imatinib daily. Myelosuppressionwas more frequent with 800 mg, although manageable with dosereductions or with growth factor support (erythropoietin, filgras-tim). After 12 months of therapy, 66% of patients continued toreceive 800 mg imatinib daily, and 16% were receiving 600 mgdaily. Thus, higher imatinib dosages could be delivered to mostpatients in early chronic phase CML.
In summary, high-dose imatinib 800 mg daily resulted inunprecedented high rates of complete cytogenetic and molecularresponses. If such responses have similar long-term significance asseen in previous studies, they may translate into major improve-ment in the prognosis of CML.
References
1. Druker BJ, Tamuira S, Buchdunger E, et al. Ef-fects of a selective inhibitor of the Abl tyrosinekinase on the growth of Bcr-Abl positive cells. NatMed. 1996;2:561-566.
2. Beran M, Cao X, Estrov Z, et al. Detection of chi-meric BCR-ABL genes on bone marrow samplesand blood smears in chronic myeloid and acutelymphoblastic leukemia by in situ hybridization.Blood. 1994;83:1922-1928.
3. Druker BJ, Talpaz M, Resta DJ, et al. Efficacy andsafety of a specific inhibitor of the BCR-ABL ty-rosine kinase in chronic myeloid leukemia. N EnglJ Med. 2001;344:1031-1037.
4. Druker BJ, Lydon NB. Lessons learned from thedevelopment of an abl tyrosine kinase inhibitor forchronic myelogenous leukemia. J Clin Invest.2000;105:3-7.
5. Kantarjian H, Sawyers C, Hochhaus A, et al. He-matologic and cytogenetic responses to imatinibmesylate in chronic myelogenous leukemia.N Engl J Med. 2002;346:645-652.
6. Kantarjian HM, Talpaz M, O’Brien S, et al. Ima-tinib mesylate for Philadelphia chromosome-posi-tive, chronic-phase myeloid leukemia after failureof interferon-alpha: follow-up results. Clin CancerRes. 2002;8:2177-2187.
7. Talpaz M, Silver RT, Druker BJ, et al. Imatinib in-duces durable hematologic and cytogenetic re-sponses in patients with accelerated phasechronic myeloid leukemia: results of a phase 2study. Blood. 2002;99:1928-1937.
8. Kantarjian HM, O’Brien S, Cortes JE, et al. Treat-ment of Philadelphia chromosome-positive, ac-celerated-phase chronic myelogenous leukemiawith imatinib mesylate. Clin Cancer Res. 2002;8:2167-2176.
9. Sawyers CL, Hochhaus A, Feldman E, et al. Ima-tinib induces hematologic and cytogenetic re-sponses in patients with chronic myelogenousleukemia in myeloid blast crisis: results of aphase II study. Blood. 2002;99:3530-3539.
10. Kantarjian HM, Cortes J, O’Brien S, et al. Imatinibmesylate (STI571) therapy for Philadelphia chro-mosome-positive chronic myelogenous leukemiain blast phase. Blood. 2002;99:3547-3553.
11. Kantarjian HM, Cortes JE, O’Brien S, et al. Ima-tinib mesylate therapy in newly diagnosed pa-tients with Philadelphia chromosome-positivechronic myelogenous leukemia: high incidence ofearly complete and major cytogenetic responses.Blood. 2003;101:97-100.
12. O’Brien SG, Guilhot F, Larson RA, et al. Imatinibcompared with interferon and low-dose cytara-bine for newly diagnosed chronic-phase chronicmyeloid leukemia. N Engl J Med. 2003;348:994-1004.
13. Mahon F, Delbrel X, Cony-Makhoul P, et al. Fol-low-up of complete cytogenetic remission in pa-tients with chronic myeloid leukemia-like syn-
drome in mice with v-abl and BCR/ABL. J ClinOncol. 2003;20:214-220.
14. Bonifazi F, de Vivo A, Gianantonio R, et al.Chronic myeloid leukemia and interferon-a: astudy of complete cytogenetic responders. Blood.2001;98:3074-3081.
15. Kantarjian H, O’Brien S, Cortes J, et al. Completecytogenetic and molecular responses to inter-feron-a based therapy for chronic myelogenousleukemia are associated with excellent long-termprognosis. Cancer. 2003;97:1033-1041.
16. Garcia-Manero G, Faderl S, O’Brien S, Cortes J,Talpaz M, Kantarjian H. Chronic myelogenousleukemia: a review and update of therapeuticstrategies. Cancer. 2003;98:437-457.
17. Faderl S, Talpaz M, Estrov Z, Kantarjian HM.Chronic myelogenous leukemia: biology andtherapy. Ann Intern Med. 1999;131:207-219.
18. Kantarjian HM, Talpaz M, O’Brien S, et al. Doseescalation of imatinib mesylate can overcomeresistance to standard-dose therapy in patientswith chronic myelogenous leukemia. Blood. 2003;101:473-475.
19. Weisberg E, Griffin JD. Mechanism of resistanceto the ABL tyrosine kinase inhibitor STI571 inBCR/ABL-transformed hematopoietic cell lines.Blood. 2000;95:3498-3505.
20. Mahon FX, Deininger MW, Schultheis B, et al.Selection and characterization of BCR-ABL posi-tive cell lines with differential sensitivity to the ty-rosine kinase inhibitor STI571: diverse mecha-nisms of resistance. Blood. 2000;96:1070-1079.
21. le Coutre P, Tassi E, Varella-Garcia M, et al. In-duction of resistance to the Abelson inhibitorSTI571 in human leukemic cells through geneamplification. Blood. 2000;95:1758-1766.
22. Hochhaus A. Cytogenetic and molecular mecha-nisms of resistance to imatinib. Semin Hematol.2003;40:69-79.
23. Cortes J, Giles F, O’Brien S, et al. Result of high-dose imatinib mesylate in patients with Philadel-phia chromosome-positive chronic myeloid leuke-mia after failure of interferon-a. Blood. 2003;102:83-86.
24. Kantarjian H, Dixon D, Keating MJ, et al. Charac-teristics of accelerated disease in chronic my-elogenous leukemia. Cancer. 1988;61:1441-1446.
25. Kantarjian HM, Keating MJ, Talpaz M, et al.Chronic myelogenous leukemia in blast crisis:analysis of 242 patients. Am J Med. 1987;83:445-454.
26. Kantarjian HM, Smith T, O’Brien S, Beran M,Pierce S, Talpaz M, The Leukemia Service. Pro-longed survival in chronic myelogenous leukemiaafter cytogenetic response to interferon-alphatherapy. Ann Intern Med. 1995;122:254-261.
27. Kantarjian HM, Talpaz M, Cortes J, et al. Quanti-
tative polymerase chain reaction monitoring ofBCR-ABL during therapy with imatinib mesylate(STI571; Gleevec) in chronic-phase chronic my-elogenous leukemia. Clin Cancer Res. 2003;9:160-166.
28. Hochhaus A, Reiter A, Saussele S, et al. Molecu-lar heterogeneity in complete cytogenetic re-sponders after interferon-alpha therapy forchronic myelogenous leukemia: low levels ofminimal residual disease are associated with con-tinuing remission. Blood. 2000;95:62-66.
29. Paschka P, Muller M, Merx K, et al. Molecularmonitoring of response to imatinib (Glivec) inCML patients pretreated with interferon-alpha:low levels of residual disease are associated withcontinuous remission. Leukemia. 2003;17:1687-1694.
30. Hughes T, Kaeda J, Branford S, et al. Frequencyof major molecular responses to imatinib or inter-feron alfa plus cytarabine in newly diagnosedchronic myeloid leukemia. N Engl J Med. 2003;349:1423-1432.
31. Kantarjian HM, O’Brien S, Smith TL, et al. Treat-ment of Philadelphia chromosome-positive earlychronic phase chronic myelogenous leukemiawith daily doses of interferon alpha and low-dosecytarabine. J Clin Oncol. 1999;17:284-292.
32. Guilhot F, Chastang C, Michallet M, et al. Inter-feron alfa-2b combined with cytarabine versusinterferon alone in chronic myelogenous leuke-mia. French Chronic Myeloid Leukemia StudyGroup. N Engl J Med. 1997;337:223-229.
33. Interferon alfa-2a as compared with conventionalchemotherapy for the treatment of chronic my-eloid leukemia. The Italian Cooperative StudyGroup on Chronic Myeloid Leukemia. N EnglJ Med. 1994;330:820-825.
34. Medina J, Kantarjian H, Talpaz, et al. Chromo-somal abnormalities in Philadelphia chromo-some-negative metaphases appearing duringimatinib mesylate therapy in patients with Phila-delphia chromosome-positive chronic myelog-enous leukemia in chronic phase. Cancer. 2003;98:1905-1911.
35. Hochhaus A, Lahaye T, Kreil S, et al. Interim anal-ysis of imatinib treatment in 300 patients withchronic myelogenous leukemia (CML): evaluationof response and resistance [abstract]. Proceed-ings ASCO. 2002;21:262a.
36. Cortes J, O’Brien S, Talpaz M, et al. Clinical sig-nificance of molecular response in chronic my-eloid leukemia (CML) after imatinib mesylate(Gleevec) therapy: low levels of residual diseasepredict for response duration [abstract]. Blood.2003;102:416a.
37. Merx K, Muller MC, Kreil S, et al. Early reductionof BCR-ABL mRNA transcript levels predicts cyto-genetic response in chronic phase CML patientstreated with imatinib after failure of interferon al-pha. Leukemia. 2002;16:1579-1583.
2878 KANTARJIAN et al BLOOD, 15 APRIL 2004 � VOLUME 103, NUMBER 8
For personal use only. by guest on June 5, 2013. bloodjournal.hematologylibrary.orgFrom