
Post-mortem forensic neuroimaging: Correlation of MSCT and MRI findings with autopsy results
Upload
khangminh22Category
view
0download
0
Yale UniversityEliScholar – A Digital Platform for Scholarly Publishing at Yale
Yale Medicine Thesis Digital Library School of Medicine
1960
Chronic pyelonephritis at autopsySusan KleemanYale University
Follow this and additional works at: http://elischolar.library.yale.edu/ymtdl
This Open Access Thesis is brought to you for free and open access by the School of Medicine at EliScholar – A Digital Platform for ScholarlyPublishing at Yale. It has been accepted for inclusion in Yale Medicine Thesis Digital Library by an authorized administrator of EliScholar – A DigitalPlatform for Scholarly Publishing at Yale. For more information, please contact [email protected].
Recommended CitationKleeman, Susan, "Chronic pyelonephritis at autopsy" (1960). Yale Medicine Thesis Digital Library. 2798.http://elischolar.library.yale.edu/ymtdl/2798

YALE MEDICAL LIBRARY
3 9002 01069 4629
MUDD
LIBRARY
Medical





Digitized by the Internet Archive in 2017 with funding from
The National Endowment for the Humanities and the Arcadia Fund
https://archive.org/details/chronicpyelonephOOklee

CHRONIC PYELONEPHRITIS AT AUTOPSY
Susan Emily Thurman Kleeman
ABryn Mawr College
A thesis presented to the faculty of the
Yale University School of Medicine
in partial fulfillment of the
requirements for the Degree of
Doctor of Medicine
Department of Internal Medicine
I960

A* Nf y JU, 1960
v- UBRbK\
TH3 YU 2.30 6

To Frank

«*■
ACKNOWLEDGMENT
I wish to express rny gratitude to Dr» Lawrence R,
Freedman for his kind guidance, encouragement and patienc
in the preparation of this thesis,
I am also indebted to Dr* Averill A. Liebow for
his permission to study the pathological protocols and
microscopic slides*
Furthermore I wish to acknowledge the kind help of
Mrs* Jeanette Gardner and Mrs„ Leah West in obtaining
clinical records for me*


TABLE OF CONTENTS
I.
II.
III.
IV.
Vo
VI.
VII.
Introduction ..
Method and Materials ..
Results o.o............
Discussion ............
Summary and Conclusions
Appendix
Bibliography ..........
© <9
Page
1
3
8
32
50
52
54


TABLES AND FIGURES Page
Table 1, Chronic Pyelonephritis at Autopsy at G.N.H.C.H. January, 1957-January, 1959 ..».• 9
Table 2. Group I A - Chronic Pyelonephritis in the Absence of Genitourinary Tract Ab¬ normality in Males ....*.. . . .. .. . * .. . „.. .. *• 11
Table 3» Group I A - Chronic Pyelonephritis in the Absence of Genitourinary Tract Ab¬ normality in Females ................ 14
Table 4. Clinical and Pathological Correlates in Chronic Pyelonephritis in the Absence of Obstruction (Group I A) .................... 18
Table 5® Scarred Kidneys at Autopsy at G.N.H8C.H, January, 1957 - January, 1959 .. • * . ... •..,.. 23
Table 6. Group II A Scarred Kidneys with N.P.N.'s Greater than 85 rag. % and/or Contracted Kidneys in the Absence of Genitourinary Tract Abnormality in Males .................. 25
Table 7® Group II A Scarred Kidneys with N.P.N.’s Greater than 85 rag. % and/or Contracted Kidneys in the Absence of Genitourinary Tract Abnormality in Females ............... 26
Table 8. Clinical and Pathological Correlates in Scarred Kidney Group II A .................. 27
Table 9® Chronic Pyelonephritis at Autopsy .......... 34
Table 10. Hypertension in Chronic Pyelonephritis ..... 39
Table 11. Clinical Pyelonephritis .................... 44
Figure 1. Age Distrituion in Chronic Pyelonephritis- Group 1 A .................................. 36
Figure 2. Age Distribution in Scarred Kidneys - Group II A ................................. 37


-1-
INTRODUCTION
It is generally agreed that clinical pyelonephritis
in the absence of obstruction of the urinary tract is
primarily a disease of women (2, 33, 32, 1?, 10, 14).
A review of published cases, however, shows that
there has not been adequate documentation of this„ The
reported series suffer from one or more of the following
defects: a) obstructive disease of the urinary tract was
not excluded, b) bacteriologic evidence was derived from
broth cultures of urine, a procedure now known to be in¬
adequate for the diagnosis of urinary tract infection, and
c) many series do not distinguish the sexes or consider only
women.
In a recent study on the medical service of the Grace
New Haven Community Hospital where cases were selected on the
basis of quantitative urine bacteriology, clinical urinary
tract infection in the absence of obstruction was ten times
more frequent in women than in men thus documenting the prior-
noted impressions of most authors„
Chronic pyelonephritis is considered by most authors
to result from bacterial infection of the kidney (22, 42, 3,
17). If bacterial infection of the urinary tract is related
to chronic pyelonephritis at autopsy, one might expect to
find the sex incidence similar in the clinical and autopsy


-2-
studies. There Is reason to suspect from published data
(32, 14) that the sex incidence of chronic pyelonephritis at
autopsy in the absence of obstruction differs markedly from
the predicted ten to one. If this is indeed the case it would
necessitate a re-evaluation of the relationship between
clinical urinary tract infection and chronic pyelonephritis
at autopsy. The current impressions of chronic pyelonephritis
at autopsy are based upon relatively few studies, most of
which have not rigidly excluded from consideration cases
with obstruction of the genitourinary tract.
The present study was undertaken to examine the sex
incidence of chronic pyelonephritis at autopsy, observing
the precautions described above. During the course of the
study an attempt was made to examine other factors of interest
such as hypertension, family history for cardiovascular
disease, and renal disfunction as measured by elevation of
N.P.N.


-3-
METHOD AND MATERIALS
Collection of Data *
Of the 1,526 consecutive autopsies (57«^$ males and
42.6$ females) at the Grace New Haven Community Hospital over
the period from January, 1957 to January, 1959* ** two groups
of cases were selected for further study.
Group I — All cases with the final pathological
diagnosis of chronic pyelonephritis and pyelitis.
ft ft Group II All cases diagnosed as "scarred,”
"markedly scarred," "grossly scarred," and "scarring of the
kidneys." Cases diagnosed as "fine scarring of the kidney
with Kimraelstiel-Wilson Disease" and "focal scar of the
kidney" were not included. There were approximately three
cases in the former category and three in the latter. The
sex incidence was approximately one to one.
The scarred group (Group II) was included in this
study of chronic pyelonephritis so as to avoid the pitfall
of individual variation in pathological Interpretation and
* Autopsy numbers 12200 - 13780. (There were 5^ cases missing when all slips between 12200 and 13780 were counted. Therefore the series comprises 1,526 cases and not the expected 1,580 cases between numbers 12200 and 13780).
** To be referred to as "scarred kidneys" throughout the rest of this paper.


_4~
thus not overlook what others might consider changes compatible
with the diagnosis of chronic pyelonephritis.
The autopsy protocols were used at the source of in¬
formation for the pathological description of the kidneys
and genitourinary tract. From the clinical record, the past
history of genitourinary disease, diabetes, and hyperten¬
sion, was obtained, as well as the occurrence of a family
history of cardiovascular disease.
Information was collected on urine cultures, i.e.,
positive and negative and quantitative bacteriology, Hoivever,
the records of these cultures were for the most part in¬
adequate and only a minority had been quantitatively evaluated.
Therefore, the urine culture data is probably not valid in
the group considered "positive.M Sterile cultures ("negative")
are considered valid irrespective of the application of
quantitative techniques.
From Group I (chronic pyelonephritis and pyelitis)
all cases with evidence of primary genitourinary tract
abnormality were eliminated. This consisted of cases with
prostatic hypertrophy (including prostatic carcinoma),
urethral stricture, extraparenchymal stones (those below
the renal parenchyma -- in the calyces, pelves and ureters),
carcinomatous obstruction, cystocele and exstrophy of the
bladder. The remaining cases of Group I, those without
evidence of primary genitourinary tract abnormality, were
further studied for evidence of obstruction by looking for


trabeculation of the bladder; no additional cases were found
by this technique. Thus a group (Group I A) had been selected
for further study which contained all cases of chronic
pyelonephritis in the absence of primary genitourinary tract
abnormality.
Prom Group II (scarred kidneys), cases with N.P.N.’s
greater than 85 mg. % and/or contracted kidneys (one or both
kidneys weighing less than 100 grams, or described in the
pathological protocol as ’‘small") were selected. Again, as
in Group I (chronic pyelonephritis) cases with evidence of
primary genitourinary tract abnormality were excluded from
this group of cases with N.P.N.'s greater than 85 mg. %
and/or contracted kidney. Thus a group (Group II A) of cases
with significant renal disease in the absence of urinary
tract obstruction In which the pathological diagnosis of
chronic pyelonephritis might have been overlooked, was
selected from Group II (scarred kidneys) with N.P.N.’s
greater than 85 mg. % and/or contracted kidney.
Groups I A and II A were studied in detail. The
frequency of findings such as hypertension, positive and
negative urine cultures, diabetes, N.P.N.'s greater than
85 mg. /, past history of urinary tract infection, family
history of cardiovascular disease, were correlated for each
sex within each group (see Tables M,?).


-6-
Histologic Classification
The microscopic slides of the kidney sections of
patients diagnosed pathologically as chronic pyelonephritis,
pyelitis and scarred kidney, were reviewed with Dr. Lawrence
R. Freedman without prior knowledge of the pathological
classifications or sex. They were histologically classified
into 6 groups as follows:
1. Non specific scars (N.S.)
2. Minimal focal pyelonephritis (M.F.P.)
These were kidneys with lesions similar
to those described as "typical focal
pyelonephritis" present to a lesser degree.
3. Typical focal pyelonephritis (T.F.P.)
These kidneys had large focal scars, crowding
of glomeruli, some of which were hyalinized,
dilated and atophic tubules with and without
colloid, casts, interstitial fibrosis, and.
infiltration with round cells, separated by
areas of normal kidney.
4. Diffuse pyelonephritis-like scarring of the kidney
or diffuse scarred end-stage kidney (D.E.K.)
These kidneys contained most of the elements
of the typical chronic pyelonephritis but they
were in such an advanced stage of disease
that the ability to make this diagnosis with


-7-
certainty might he questioned by some
investigators.
5. Pyelitis (Pye.)
These kidneys had. inflammatory changes limited
to the mucous membranes of the pelves,
6. No abnormality seen (No0)
The histological classifications were correlated with the
sex in each group.


-8-
RESULTS
Group I - Chronic Pyelonephritis and Pyelitis (Table 1)
1,526 consecutive autopsies at the Grace New Haven
Community Hospital from January, 1957 to January, 1959 were
reviewedo The autopsy group was composed of 57.4$ males and
42.6$ females* There were 97 cases (6.34$ of the total
autopsy series) with the pathological diagnosis of chronic
pyelonephritis. This group consisted of 63 males (65$) and
34 females (35$)® 5 cases (0.33$ of total autopsy series)
had the pathological diagnosis of pyelitis. Two were males
(4o$) and three were females (60$). Thus the total group of
chronic pyelonephritis and pyelitis (Group I) consisted of
102 cases (6.67$ of the total autopsy series), of which
there were 65 males (63.7$) and 37 females (36.3$).
■ From Group I all cases with obstructive disease of the
genitourinary tract were excluded. This amounted to 49
cases (48$) of the total chronic pyelonephritis group), of
which 4o were males (81.6$ of the males of Group I) and 9
were females (18.4$ of the females of Group I). Thus it
can be seen that many more males are found with primary
abnormality of the genitourinary tract in association with
pyelonephritis than are females. Prostatic hypertrophy,
including carcinoma of the prostate, was the greatest single
cause of primary genitourinary tract abnormality. It was


TA
BL
E
1.
CH
RO
NIC
PY
EL
ON
EP
HR
ITIS
AT
AU
TO
PS
Y
AT
G.N
.H.C
VL
JAN
UA
RY
, 1957
- JA
NU
AR
Y,
19
59
„Q_ s
V5.
CQ ©
0
VO O o CM nt O o CO 4> o o o o « 9
CM *m o VO co o O o o o CM cm VO CM H VO O o vn o VO,
H fH pH
o ■£" cm CN- On CM H rH CM rH CO VM CM CM CM M3
o o £>- VO O o CM O 9 » <9 9 9 9
ev¬ vn, o CM rH o O O O o M- en, vo VO co ©
rH O tH
vm o rH
H-
CQ 0 VO CM CM VM o CM CM CM CM rH vn, fH IM- VO VO Hj- CM CM a5 00 S
Ht CM O- O o O o O CM cm VO o CM O O CM CM fH CM CM O
9 ♦ <3 9 O » o O 9 o 9 O VO o VO co en, ■d- o CM CM CM CM CM CM
-£■ VO fH rH vn,
H VO o- vn, CM c\ CM CM vn, rH pH VO rH rH CM 05 CM Ov O -d- CM vn, -P VM r—I o
Eh H 0 O c (D CQ L cO
CQ
P 42 bO -H P £ £ •H •H £ £ X3 ft £ 0 CQ H £ <H £*5 O o P P £
rH •H *H 0 rH rH >5 0 05
CM >> e >5 CM in 43
© O SH £ rO £ O £ £ 43 £ O 05 05 P
£ CQ CQ P 0 0
•H o •H O p,P P P 05 £>s 05 ■H CQ H £ S3 P £ 0 £ H m j£ m co 43 o o Of 05 *H CXD •H £
CQ CD O P 0 P CX- 0 £ £ O 05 •H o rH rH O +3 o CQ 1—1 tH 0 H CQ 0 O, 0 < >i 0 £ O O O CM >5 Gj £ P Pm 1 CM E CM £ CQ •H < o •H H S3 O £
•H P o5 *H CX 1—1 c *H CX £ Oj o rH O p £ 0 O £ o 42 t>S £ 43
Eh O CM o O
0 43 -P
£ >5 •X p
£ •H £ O CQ H
£ •H «H H ■H 05 O CQ P CO P 6 ■H £ O E *H £ P 05 £ >s £ O O O £ O 42 43 £ £ P 0 O £ CX 43 £ o CQ S £ 0 0 CO
0 P P L 0 tO £ £ CQ £ O H £ ■£ O P £ rO <3 c3 CO cO rH O P o o o ex H 0 05 0 H «H H co CQ >s £
■H Ul tO > CQ £ CM Eh £ £ £ H © P <H P O 0 0 > X O O t© CO P cd P, 0 •H
05 o © 0 >5 £ O H S P £ £ rH 43 O 05 o £ © £ •H 0 ex £ J>> £ £ CO P P H O O 42 £ 43 £ 0 O £ o £ O CO P o £ £ O p P 6 0 £ 0 £ £ H CQ CQ 9 »H £ 0 L> P CO >s X £ £> O C CO O O W <o ex
H O
O £ o


-10-
found in 32 cases comprising 65.2# of the cases with primary
genitourinary tract abnormality. Extraparenchymal caluli (those
calculi below the renal parenchyma - in the calyces, pelves,
and ureters) was the next largest group. There were 6 cases
(12.1#), composed of three males and three females. Third
in order of frequency was carcinomatous obstruction of the
urinary tract which was found in 5 cases (10#). Two were in
females/ three in males. Fourth in order of frequency was
urethral stricture of which there were two cases (4#) both
in males. The remaining factors were each found in one cases
stricture of the vesical neck, aberrant renal artery causing
ureteropelvie obstruction, and cystocele, which were all
found in females, and exstrophy of the bladder found, in a
male.
Group I A » Chronic Pyelonephritis In the Absence of Primary
Genitourinary Tract Abnormality (Tables 2, 3_)
There were 53 cases of chronic pyelonephritis in the
absence of primary genitourinary tract abnormality. This
was of the total number of cases of chronic pyelonephritis
diagnosed at autopsy at the Grace New Haven Community Hospital
from January, 1957 to January, 1959® Of these there were 25
males (47.2#) and 28 females (52.8#). Applying the Chi square
formula to this group, one finds no significant difference
between the ratio of males to females at the 5# level. Further¬
more if one assumes that the male to female distribution in


-11
o Ph G Ph Ph Ph Ph Ph Ph Ph Ph Ph
EH o fo Ph Eh Ph Ph Ph Ph Ph Ph O «H Eh Eh Eh Eh Eh Eh £ S <3 s CP Eh
X o * CP ^3 *0 * O mo O mo o o o o o o o o o mo mo mo O O <3 vo C- P-5>- MOvO CM CO co oo p- CM <o- rH rH vo -p VO MO is x is iH Cm rH pH CM rH i—1 rH rH rH rH rH rH rH rH i—1 H CP Co o o & Eh ° 0 H bO «h X SS Q W o
0 pH «m 0 o G HO 4 » <9 o
«H rH CQ CQ CQ CQ © w G G O O O o bO o G> O P^ P. PH Pi G
w tn * <9 - CQ <D Eh <3 •Eh
Ph CO W 0 ffi X EH rp is -p- o CO CO O OV CM
Ph VO Ov p- VO CM co O 3S is pH rH rH & H * 4) ro
O o Oh &4 {—i 40 -P <T* =H ra G O
H •H d <3 0 9 O ® 40 © CP PP 0 > X HO X -P 40 40 X « 40 CP CP O £> P P (P 4h P V} Ph O O o o o w e o D S 0 -P -P 40 40 b) 40 g O Ph Ph o X o X o o 0 O i-Q W _ e c G G G G G
© pH CO Ph w
t-Q o < H S3 is O is M H
ffi L O X
. M < x M <d
Ph P3 G> O o is W CQ O <3
rO
O
ctf
CQ CQ
• Ph tu cp
o ICO
MOlO ■cr b- f-i I
CM x>
: t* Ph
0 0 O bO 03
<3 CP
co tv-is
VO co vo is
o co
CM -P- is
Ov VO S
X
co vo is
VO vrv:
vo C'- vo:
•H
&
bO
0
"O
CM
a CQ
-I X 0 CQ rH Pj ro CM co ctf O CM nt 00 S 40 CO co rv
G CM CM CM <3 rH 1—i rH
CO VO rH rH ot O 4j- rH vo 00 C0 O CM CM CM 0^ rH rH ■rH rH
9
O
o
0 MO rH co rH ot • CM co co cd CO co CO rH rH rH *
(conti
nued
on
next
page)


TA
BL
E
2.
GR
OU
P
IA
CH
RO
NIC
PY
EL
ON
EP
HR
ITIS
IN
TH
E
AB
SE
NC
E
OF
GE
NIT
OU
RIN
AR
Y
TR
AC
T
AB
NO
RM
AL
ITY
IN
MA
LE
S
(conti
nued)
12
o X X X X X X X Ph 0 « £ X M X W X w x fin >>
*H O
s
e Q Eh Q Eh o Q Eh P-f
• rp ° o o O O O O UV, O O uv o v> o o O vv X *H p r-l rH CM CM 0-0- 0-00 00 (N- o c- 0-0 VO vv
X x H rH pH rH 1—1 rH rH pH rH
o
Q
<m a) C *
•H H bD P 3 C X O
m • O bD P, £
bD £
0 X H • Eh
X 1=)
• X oo o OV O rH o UV O •H rp Ph CO C- o uv CM rH ov o n3
X OV OV C\! rH rH ov £ 0 p. X
® -P <n P £ a © w 0 C X o X X 9 0 •H 0 > 9 -P a -P • X P 0 x x o Cm X X X 9 X to
« o o Cm o e © o O « 0 bD -p bD -p bD bD p 8 X X 0 o X 0 X o 0 0 o
X £ £ £ c £ £ c Hr 9
•H
©>> •
X • X ojo OjuV o jo o|o CO o o o o|o
X X oo Ko X CO -3- |0V nb o Cm ov Cm wo rH | CD JrH nh rH CM rH rH |H O
bn
« * X 0 X X
• e* X
x x x x Cm
0 0 O VO ov fcuO 0 IN-!S OVX < x
CO OVX
o (H |2
ov ovX
VO vo X
VO rH |S
oo cm^
o- VV 3
0
9
rp
Hfc
0 CQ rH P ■ct Ov VO C\i ON 0 O ov W VO CM W S P w W w HT CM
£ ov ov ov CM CM <tj i—1 rH rH rH rH
a
9
rO
-a- Cm Ov Ov CM W O CM a
ov ov CM OV 0 CM CM OV ov i—! X rH rH *
(conti
nued
on next
page)


13
© o Pw X Ph X Ph Ph <*H £h pH pH Ph W Ph Ph
EH o Eh EH Eh Q Eh S
X Eh
Ph X Hd ° o o O O o o o o VT\ O O O < ■H -p VO On O—ct o o ovco CM CO ev £>- E X 5s rH X c\] <M rH X X rH rH rH H Ph X O • E Eh hD 05 H -H X E W o
Q
Ph • 0 O «M C -P
•H s—1 w ?H 2 o X O E w CO O 9 E (D E H < 4 Eh
Ph E W E Eh 4 E CM U~\
X Ph £>- i—1 S E CM H
CO O * -P H P 4-3 5h Eh 0 w o3 <! © H 3 ■H 0 > X cp a E E O © E *H Ph -P W C B <s E O CCS fc>0 o o Ph Ph 0 X X ' e c W X CO
o < H S o E E Ph O E E g H
O X Eh « « Ph
- M 05 E E < X M < E^
X
s Ph « X O O E 0 ffj E 0 0 cx VO 00 -X O < ED 05 OvE vO S E\E CM
<J Pm
X
(T\ EV -x e
©
•H
E
bl)
«w
0)
9
TO
E
a =ffc E < X Eh 0 CO
X ft vr> VO E rH co E- 05 O ev X VA VO o X S 4-3 -X vo X vrx VO
PS E E E EV Ex E\ C i—1 i—1 rH X X X
05
*
see
Ap
pen
dix


-14-
Eh O < ca EH
a
§ M CQ
O EH H S W O
An o M O S W C/3 CQ <
w
£h
X M
cn H Eh H CQ ffi Ph M S3 O i-Q GO w w >H hJ p-t <q
s o w H An S O X g H
O X Eh
. H < X
o P X Ph Ph X X Ph X X O W Ah Ah Ah w w Ah W w m
«H Q Eh Eh Q Q Q Eh Q Q X s
«o • unun un o O O O O ❖
MN«N O UN o o
• P B O o o
<H 4-3 X O- e on ON o MNMN ON O ON 00 CM UN O CM ON CM X ^
o p
Q
rH f—1
X
iH rH rH C\i rH
X
rH rH
X
O rH CM CM
hO
o 0 o X C -P * 0 o •» » o • •
•H pH TO TO TO TO TO TO TO TO U P o o O o O O o O by X o p. p. P. p PE P. p- Pn p
® « 0 X H
•EH X X X X X Ph 1=)
• X JN- o ON P- CM o CM o P- ON •H X Ph ON H± CM rH ON NO CM UN
X rH CM CM rH rO s 0
0 « PH
O HP -P c O o Pj <4 TO P > X X X X X rC 0 9 .Q
*H 0 O O o -p* 4-> a 0 0 TO
X 0 Cm & P X
« • • o O
o s bO to 4-3 -P be s 0 P; Pr. o SH
0 c*
0 C“!
o c-1
O r>
0 r~*
b 8
CQ e
P-: 0
CQ
fl3 E A:
o o 43- o»
o o CM rH CM H
O O On i—I r—I H
O CN- rH
UN O O O rH CM
olo NOON rH I
OjO o NO rH
UN X)
H C <B O X X X X S Ph PQ
Ph Pi X> o o x CQ CQ O <3 0
0 o o rH O 00 o hQ- ON •4t 43- NO 6o 0 MNS: P~iS ■3- ^ »4N^ nC i2 NO ^ oo :s O-^g NO 13
« < CQ ON
a PQ
X Eh 0 TO
r-H Pj ON 03 ON ON ON 03 CM NO MN UN 0 O o- ON ON CM O un O pH UN ON S -P CM -4 o- 00 O O i—I rH CM ON 0 0 CM CM 04 CM O'! ON ON ON ON ON
Ah <J i—1 i—1 i—1 rH rH i—! rH rH rH rH
•H
O0
0
&
et o
0
$
(continued
on
nex
t
page)


15
Eh O
Eh
X
§
H P3 X O X H X
« o «H Sh Ph Ph Ph X
o X Ph X X <H X Eh X X X
•
X P •
*
vo O O vo O O VO vo •H -P coco COCO rH rH CO CO X X rH r-( rH rH rH rH
o
• P bO CO
«H
p X
Ph X X X 0 Ph X X X X X X Eh Eh Eh Eh X Eh
o o =5=
VO vo o o O VO vo vo VOC0 CM VC 00 c CM f—1 vo O CM CO too- CM X (—1 rH rH CM X rH rH
X
X o 9 0 ®
PGP X •H pH o P 3 X X O X CO o <a
X 0 X H < ° Eh
X X X X Eh O X
X X X X H
X CO 0 0 a
H 3 O-PHC Eh C CQ Sh > H <H •H 030 X P X 0 X C X X O 9 X O E X - 03 X: O X a X CO ffl X X
Ph <
o x 9 hH X * X; X X O X PQ P3 M SC
. M n 0 9 0 <! p 03 X X H < <9 9
S X X X M x o o x X PQ
<-
O < 0 0 O bO 03 0
<r\ <J X
« • © o o a
co CO CQ CO CO CO o o O o o o X p< X X. Ph X
x X X
-=J- -=3- -3" co
vo ro cm vo
-=3- vo VO CN-
vo CM
O n3' vo to VO CO
X •H
*0 G <v
X a <
X 0 X 9 X o X © X 0 <9 p 9 P p p 0
X p Gj X X X to o O o o
© 9 8 bO p bO P p p 0 0 X o 0 o X o O c G C G G G •> o
•H
O O XIO 00 o CM O o o o CM X CM kO o Cv- O o CO sO VO CM rH 1 <—1 CM X X 1—1
o fe CO »
o!o VO O- H|
o o O-Ov X
op CM b> CM H
£
06* <9
bO
X X X X X o
0
-3- VO vo :s
nfr o-x
O-
o-s o- VO^
vo ts-X
O- C'-X
vo vo x
OV VO X
X
CN-X
<o
*0
a CQ < Eh <D w
x X vo VO co 03 o vo vo o E P CM vo tN- 0 3 CM CM CM X <3 X i—i X
CM o t>- vo O- x- CM £>- CO o\ X CM CM CM CO CO X X X i—1
G
«=* O
X
CO X vo ©V
vo o vo e CO o- CM CO CO CM CM X X X *
(conti
nued
on n
ex
t page)

rt
<*

-16-
o •H ?h 0 0 PH Ph Ph Ph
O X Ph Oh Ph Xfl fc Ph Ph Eh EH Eh X Eh
s
Eh O o ©
<J X D • PD «H Hp
EH X X
X Ph •
< • ^jD
X bO 03 H •H M Q X O X o <D ® H X C P X X rH W G 3 O X O
X o /> »
<D X H w * Eh o X X X w CO X <* X <3 X X
X w X Eh © o
O p P <3 X^ CO U > H X •H (35 O
<D X 0 CO 3 X M C ©
Eh *h E • H P 05 X w c (L
X O CQ X G <r H — X O X co 9 O w w X X X X ©
x <c X X
o X H fc X o X © © o
X H 05 X X X © *
o x X PQ Eh *r
j H < X m <;
S 0 Ph M (DO DO PQ CD OX <xj M ID PQ O C
P X &
o o O O O vx cx o o o o o o O VX Dr vo X X vx o\ X X O CO COD CX VX X rH X X X c x X X CM X H X
X
o © 0 CO m CO o o o X X pH
><:
iH .a-
X- O- CO cx vr\ cx CM
X X p p X X O O
X p X O
-P -P o o c s
P o c
o o o o o jo o X x- -D x- X j~X 1—1 X X CM (X X
X X X
o vo X
00 co x
o
P-X cm o-D
ON VO X
cx X-X
CM vo X
VO 00 X
8 I
•H
X
oO
Cm
0
X
o
©
(X t>s
P4 0 CO X Ph vo Ov vo
i-4 X
05 O o -D 1—1 -D 6 P CM CM X X
< 0 3 CM cx (X (X X X <5 X X X X
€>
X
in o VO, vo CM co CM vo o cx cx -D -D 0 cx cx (X cx X 1—1 X X ❖
see
Appendix

-17-
the general population is 50:50, one finds no significant
difference between the autopsy population and that of the
general population at the level,.
The frequency of the following factors was studied
in the males and females with chronic pyelonephritis in the
absence of primary genitourinary tract abnormality (Table 4).
Hypertention, family history of hypertension, heart disease
or cerebrovascular disease, past history of diabetes,
finding of positive and negative urine cultures, N.P.N.'s
greater than 85 mg. %t presence of contracted kidney (those
weighing 100 grams or less, or being described as "small''
at autopsy), past history of urinary tract infection, and
history of catheterizations and pregnancies.
Hypertension
Of 25 males, 6 had a past history of hypertension
and two additional cases had diastolic pressures greater
than 100 ramo Hg. on their las t hospital admission with no
past history of hypertension noted in the chart. Thus 8
men, or 57^ of the 14 men on whom blood pressure inforraation
was obtained, had hypertension.
Of 28 females, 12 had a past history of hypertension
and three had diastolic pressures greater than 100mm. Hg.
on their last hospital admission, with no past history of
hypertension noted in the clinical chart. Thus 15 women,
or 62.5$ of the 24 women on whom blood pressure information


18
TABLE 4* CLINICAL AND PATHOLOGICAL CORRELATES IN CHRONIC PYELONEPHRITIS IN THE ABSENCE OF OBSTRUCTION (I A)
Males % Females %
Total
P.H. tB0P.a° 8 of
25
14 57.1 15 of
28
24 62.5
Fam. Hist.c *
Negative 6 of 14 42.8 5 of 17 29.2
'fr BP 5 of 14 38.4 3 of 17 17.6
CVA Heart 4 of 14 28 o3 10 of 17 58.8
Diab. g* 3 of 25 12.0 7 of 28 25.0
f. Urine Cult.
Positive 5 of 9 55.5 17 of 18 94.5
Negative ■ 4 of 9 44.5 1 of 18 5.5 do
N.P.N. greater 85 mg. % 11 of 18 63 *4 7 of 24 29.I
Contracted kidney 6 of 23 26.1 11 of 27 40.8
P.H. U.T.I. e° 0 of 25 0 9 of 28 32.2
HISTOLOGIC CLASSIFICATION lo
Males % Females %
N.So 0 of 24 0 2 of 27 7.^1
M.F.Po 3 Of 24 12.5 2 of 27 7.^1
T.F.P. 15 of 24 63.0 14 of 27 51.9
d.e.k. 5 of 24 20.4 6 of 27 22.2
Pye. 1 of 24 4.1 3 of 27 11.1
No. 0 of 24 0 0 of 27 0
* a., c„9 d.s e03) f.,g., 1., -- see Appendix

-19-
was obtained, had hypertension.
Family History of Hypertension, Heart Disease, or Cerebrovas-
cular Disease
Of the 14 males from whom a family history was
obtained, 6 (42.8$) had a negative family history of hyper¬
tension, heart disease, or cerebrovascular disease. 5 (38%)
had a positive family history of hypertension; and 4 (28$)
had a positive family history of heart disease or cerebro¬
vascular disease. Thus 66.7% had a positive family history
for cardiovascular disease.
Of the 17 females from whom a family history was'ob¬
tained, 5 (29/0 had a negative family history for hyper¬
tension, heart disease, or cerebrovascular disease; 3 (18$)
had a positive family history of hypertension; and 10 (39%)
had a positive family history of heart disease or cerebro¬
vascular disease. Thus 77$ of women had a positive family
history for cardiovascular disease.
Diabetes
Of the 25 males, there were 3 cases of diabetes (12$)
and of the 28 females there were 7 cases (25$).
Urine Cultures: Positive or Negative
Of the 9 males who had urine cultures done, 5 (53%)
were positive and 4 (44$) were negative.
Of the 17 women who had urine cultures, 16 (94$) were

-20-
positive and one {6%) was negative0 These positive cultures
were difficult to evaluate since quantitative studies were
performed on only a few. The negative cultures, however,
are considered to have been properly obtained0
N.P.N. Greater than 85 mg, %
Of the 18 men who had N.P.N. reported, 11 (63.^)
had N.P.N. greater than 85 mg. %% and of the 24 women on
whom N.P.N.'s were recorded, 7 (29/0 were greater than
85 mg. %.
Presence of Contracted Kidney
Of the 23 men on whom kidney size and weight were
obtained, 6 (26%) had contracted kidneys (one or both kidney
weighing 100 grams or less, or described in the pathological
protocol as "small").
Of the 27 women on whom information on kidney size
and weight were obtained, 10 (37^) had contracted kidneys.
Past History of Urinary Tract Infection
Of the 25 males, there was no record of the diagnosis
of urinary tract infection ever having been made. However,
one male (12259) had "frequency" in 195^ and alpha street,
was obtained on urine culture. This, however, was not
quantitatively evaluated. On his last admission the culture
was negative. There were several other cases with symptoms
which were difficult to evaluate. They are case 12323 --
dysuria and dribbling, 12374 -- frequency and nocturia, and


-21-
12259} 13209 -- nocturia, however, the symptoms of these
cases were not considered sufficient evidence to state that
the patient had a urinary tract infection.
Of the 28 females, there was a history in 9 (32%)
of urinary tract infection. One of these, 13102, was
diagnosed as cystitis; one, 12665s was diagnosed as "chronic
urinary tract disease"; and the remaining 7 were diagnosed
as having had pyelonephritis at some time in the past. As
in the male group there was one female case with symptoms
which were difficult to evaluate, 132?5 -- frequency and
nocturia.
Catheterization
Information on this is difficult to collect but it
appears that of 18 males, 5 males had single catheteriza¬
tions. One male had an Indwelling Foley catheter for an
undetermined amount of time. Of 23 women, 12 had single
catheterization at one time.
Pregnancy
Of 28 women, there was a history of at least one
pregnancy in 11 women. In three cases there were no
pregnancies; and in 14 cases there is no mention of the
patient having been, or having not been, pregnant.
Pregnancy and Catheterization
Of 28 women, there is a history of 1? women having been
pregnant and/or catheterized at some time in the past.


-22-
Group II - Scarred Kidneys (Table 5)
Of the 1,526 consecutive autopsies, 66 cases of
scarred kidney (4.3$ of the total autopsy series) were
found* 39 (59.1/0 were male and 27 (40.9$) were female.
In order to examine those cases with significant
renal disease in which the pathological diagnosis of chronic
pyelonephritis might have been overlooked, scarred kidneys
with N.P.N.’s greater than 85 mgc $ and/or contracted kidney
were selected* There were 26 cases (39.4$ of the total
scarred group); 14 were men (53.8$) and 12 were women
(46.2$); from this group all cases with primary genitourinary
tract abnormality were excluded. This amounted to 7 cases
(26.9$ of the total scarred group), of which 5 were male
(71$) and 2 were female (28$). As in the chronic pyelo¬
nephritis group, the percent of males with primary genito¬
urinary tract abnormality is much greater than that of
females and again, prostatic hypertrophy (including carcinoma
of the prostate) was the greatest single factor of primary
genitourinary tract abnormality. It was found in 4 cases
(51$). Urethral stricture was found in one male and one
female and carcinomatous obstruction of the urinary tract
was found In one female.
* Scarred kidney includes all kidneys with the pathological diagnosis of ’'scarred,'’ "grossly scarred.," "markedly scarred," and "scarring of the kidney(s)."


-23-
TABLE 5. SCARRED KIDNEYS AT AUTOPSY AT G.N.H.C.H. JANUARY, 1957 ~ JANUARY, 1959
Total % i Hale of /° Female %
Total Autopsies 1,526 8 ?6 57.4 650 42.6
Group II - Scarred Kidneys 66 4.3 39 59.1 2? 40.9
Scarred kidneys with N.P.N. greater than 85 mg. % and/or contracted kidney 26 39.4 14 53.8 12 46.2
Scarred kidneys with N.P.N. greater than 85 mg* % and/or con¬ tracted kidney with primary G U tract abnormalities 7 26.9 5 71.5 2 28.5
Prostatic Hyper¬ trophy (in¬ cludes carcinoma prostate) 4 4
Urethral stricture 2 1 1
Carcinomatous ob¬ struction 1 1
Group II A - Scarred Kidneys with N.P.N. greater than 85 mg. % and/or contracted kidneys without 1° G-U tract abnormality 19 73.1 9 4y .4 10 52 06

-24-
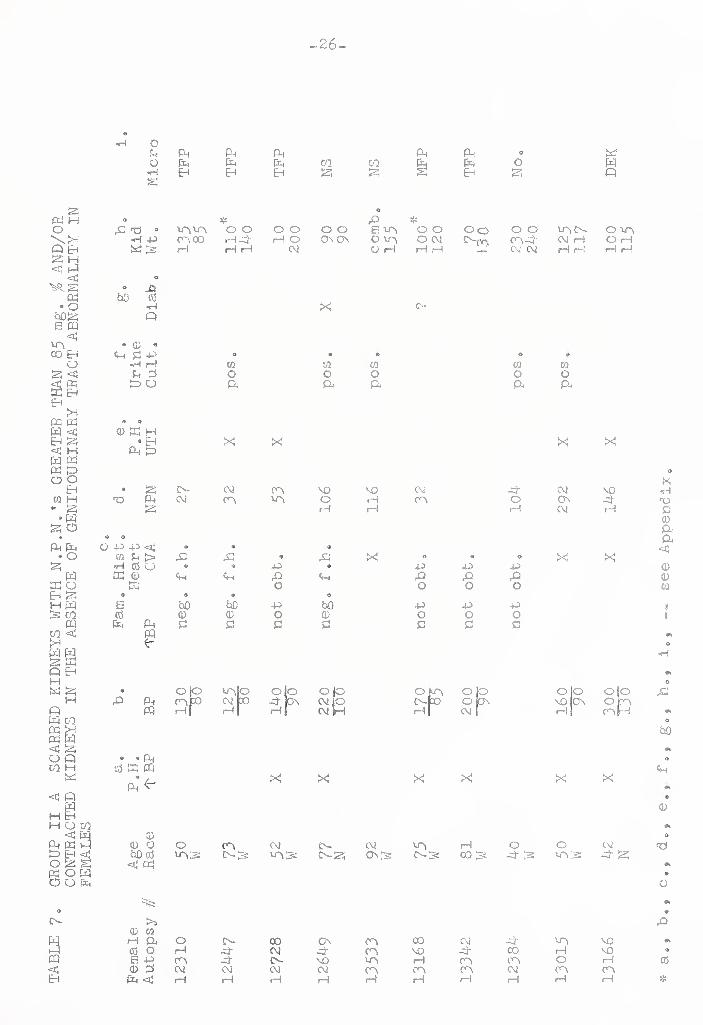
Group II A Scarred Kidneys With N,P,N. Greater Than 85 mg, /
And/or Contracted Kidney in the Absence of Primary Genito¬
urinary Tract Abnormality (Tables 6, J)
There were 19 cases of scarred kidney with N.P.N.'s
greater than 85 mg. / and/or contracted kidneys, in the
absence of primary genitourinary tract abnormality. This
was 73.1/ of the total number of cases of scarred kidney with
N.P.N.'s greater than 85 rag. / and/or contracted kidney.
Of these there were 9 males (4//) and 10 females (53/).
Applying the Chi square formula to this group (Group 11 A)
one finds no significant difference between the ratio of
males to females at the 5/ level.
The frequency of the following factors were studied
in Group II A (see Table 8). Hypertension, family history
of hypertension, heart disease or cerebrovascular disease,
past history of diabetes, the finding of positive or negative
urine culture, N.P.N.’s greater than 85 mg® /, the presence
of contracted, kidney and past history of urinary tract in¬
fections .
Hypertension
Of the 9 men, there was hypertension in 5 (55/)® Of
the 10 females, blood pressure information was only obtained
in 8. Of these, 6 (75/) had hypertension.


TA
BL
E 6
. G
BO
UP II
A
SC
AB
BE
D
KID
NE
YS
WIT
H N
.P.N
.'s
GB
EA
TE
B
TH
AN
85
mg*
%
AN
D/O
B
CO
NT
RA
CT
ED
KID
NE
YS
IN
TH
E
AB
SE
NC
E
OP
GE
NIT
OU
RIN
AR
Y
TR
AC
T
AB
NO
RM
AL
ITY
IN
MA
LE
S
-25-
•H G X P-< X Ph Ph X X X Q H X H X X H XI m X
s X gr Q EH EH O Q X s
* Hi* X'd • -H- O O O O co O co O CO 6 O O CO o o o o
•H -p On ON C\! CM XCM co o- On £>~ O X COCO X CM cO-H X is X X pH O CM X X i—! X X X
O X
° CS X
Q
» CD 9 9 <M G -P W CO
•H i—i QD o GO o G 3 X O
G X C X
9 a <D 5C H
• EH X Pi X
° X X On On X CO X X X '■o X X CO X- o CO X On X
X CM CM X
o 0 o x x < o
CO X > 9 0 o 6 ® 9 • o X x «3 O X -P X 4-} X X -p 4-> 9
X 0) X X X X X X X X X X o o o o o o o Q
S X X X X X X X X GO G3 o o o o o o o O 0) X Pi G C G c G G c G G
cq
° o jo X P-i iN-[X
W X jrH
O O O X I—I
o jo o wb x CM JrH i—i
o o jo On <r\h-
cm H
o jo XPO I—11
coho _3- o -H to o x X | rH
olo £
to
• ® P' ( GS X PQ
Ph*^
X X X X X Cm
<li
CD CD O CO co On ON rH 0- X X CM GO CO MO is: x is x is X' is X- 53 CN~is x is o-is X 3 » < Pd
<d to X CM X CM o- o CM CM -H X
o
e X
0*
0 cO O X X X X CM X X X H- a S X X On On o ON X X X o-
3 CM CM CM X CM X X CM CM * < X i—1 X 1—1 i—1 X X X X
see
Appendix

TA
BL
E
7,
GR
OU
P II
A
SC
AR
RE
D
KID
NE
YS
WIT
H N
.P.N
.'s
GR
EA
TE
R
TH
AN
85
mg.
%
AN
D/O
R
CO
NT
RA
CT
ED
KID
NE
YS
IN
TH
E
AB
SE
NC
E
OF
GE
NIT
OU
RIN
AR
Y
TR
AC
T
AB
NO
RM
AL
ITY
IN
FE
MA
LE
S
26
«H O SQ Pm PQ PQ PQ PQ 0 X a Pm Pm Pm m tQ Pm o w
•H Eh Eh Eh X X § Eh X Q s
o
O * X * X X » Mb Mb o o O O o o e Mb o o Oo o o IAN O Mb
•H -P Ob 00 rH ft rH O On On O Mb O CM Obft CM rH O rH X S rH rH rH CM O H rH rH CM CM rH rH rH rH
hO X
G5 •H Q
X c~
® 0 « Cm S3 -P O <s> ®
•H rH CO oo W w oo SQ 3 o o o o o X O ft ft ft ft ft
0) X H •Eh X
PQ X
• IS JN- CM ra PQ cm cb
S
o o
■P -P ft 02 Pi > X •H C5 O ® ®
PQ 4) X
Cm Cm
0 O 9
s bO bO CO <D <D X PQ
PQ kr
S3 S3
X
0b NO VO Mb O pH
rH rH
•» ©
X X -P •» X Gw o
o ■p bO o 0 S3 a
<\i cb
-P
X O
-P X o
X X
ft CM NO o On ft rH CM rH
o X X -p X o
-p -p -p o o o S3 S3 S3
o
02
8 8
•H
PQ PQ
• • Pm 05 Hi PQ
PQ ^
SI
to UbjO o o o jo Ofb o jo o O Of' to cm to ft ON CM jO o-to OpN NO ON Of 1 H| i—1 CM H rH| CM 1 rH Obf
X X X X X X
bQ
Cm
<D
0 0 o O Ob CM e- CM Mb H O O CM
O X
bo 05 VMS £b- Is Mbs o-X 0\S O-S 00 IS ft S MbS ft X ft X
X 0 00 rH Pj O CO 00 ON Ob CO CM ft '•b NO
© a
s* ©
X
05 o rH ft CM ft- rn, NO ft CO H NO 9
S P 0b ft {>- NO Mb 1—1 0b Ob O H cd 0 3 CM CM CM CM Ob Ob Ob OH cb Ob X ft X rH i—1 rH H H H H i—i H *
ee A
pp
en
dix


-27-
TABLE 8, CLINICAL AND PATHOLOGICAL CORRELATES IN SCARRED KIDNEY GROUP II A
Males % Females %
Total 9 10 a .
P.H* 'TB.P* 5 of 9 55.5 6 of 8 75 o0 c.
Fam. Hist.
Negative 1 of 1 100 * 3 of 6 50.0
1\B.P. 0 of 1. 0 0 of 6 0
CVA Heart 0 of 1 0 • 3 of 6 50*0
Dlab*
Urine cult*
1 of 9 ii*l '1 of 10 10*0
Positive 2 of 4 50*0 5 of 5 100.
Negative 2 of 4 5o*o 0 of 5 0 d*
N.P.N. greater 85 3
» ON
o
»-+>
00
75 o0 5 of 9 55 o5
Contracted kidney 6 of 9 66*6 8 of 10 80*0
e * 4 40.0
I
P.H. -U0T .1 „ 1 of 9 11.1 of 10
io HISTOLOGIC CLASSIFICATION
Males % Females a/ /o
N*S. 1 of 9 11*1 2 of 9 22*2
M.F.P0 2 of 9 22,2 1 of 9 11.1
t.f*p9 2 of 9 22*2 4 of 9 44*5
D*E.K. 4 of 9 44,5 1 of 9 11*1
Pye. 0 of 9 0 0 of 9 0
No* 0 of 9 0 1 of 9 11*1
* a *, cOJ dOJ e„, f., go, I*, — see i Appendix*


-28-
Family History of Hypertension, Heart Disease, or Cerebro¬
vascular Disease
Only in one of the 9 men was a family history obtained,
and it was negative for the above. Of the 10 women, 6 family
histories were obtained. Three were negative and three had
a positive history for heart disease or cerebrovascular
disease, ■
Diabetes
Of the 9 men, there was a history of diabetes in
one (11$) and of the 10 women there was a history of diabetes
in one (10$),
Urine Cultures: Positive or Negative
Of the 9 men, 4 had urine cultures. Two were positive
and two were negative. Of the 10 women, 5 had urine cultures.
All were positive. Once again, the positive cultures are
difficult to interpret since quantitative studies were
performed on only a few. The negative cultures however are-
considered to have been properly obtained,
N,P»N,fs Greater than 85 mg. $
Of the 9 men, N.P.N. was recorded in 8, Of these
6 (75$) had N.P.N.'s greater than 85 mg. $. Of the 9 women
on whom N.P.N,*s were recorded, 5 (55$) bad N.P.N.*s greater
than 85 mg. $„


Presence of Contracted Kidneys
Of the 9 men, 5 i55%) had contracted kidneys and
of the 10 women, 7 (70$) had contracted kidneys0
Past History of Urinary Tract Infection
Of the 9 men, only one (11%) had a past history of
urinary tract infection. Of the 10 women, 4 (40%) had a
past history of urinary tract infection.
Many of the figures in this section on Group II A
(scarred kidney) comprise very few patients and caution must *
therefore be exercised in drawing conclusions from them.
However, they agree with those obtained earlier In the study
on Group 1 A (chronic pyelonephritis) and it is felt that
they tend to confirm the general thesis that the incidence
of lesions called chronic pyelonephritis or perhaps due to
chronic pyelonephritis (Group II A) is the same in both sexes
Histologic Classification of Kidney Sections
The slides were reviewed without prior knowledge of
the autopsy diagnosis or sex for both the pyelonephritis
group and the scarred kidney group. They were histologically
classified into 6 groups as follows: Non specific Scars,
Minimal Focal Pyelonephritis, Typical. Focal Pyelonephritis,
Diffuse Pyelonephritis -like Scarred End stage Kidney, Pyeliti
No abnormality seen. (See Method for definition of groups).


-30-
a. Group I A - Chronic Pyelonephritis In the
Absence of Primary Gen11ourinary Tract Abnormality (Table 4)
Of the 24 men on whom microscopic slides of the
kidney were obtained, there were no cases of nonspecific
scars of the kidney0 There were three (12$) that were placed
In the category of minimal focal pyelonephritis. 15 cases
(63$) had typical focal pyelonephritis. There were 5 cases
(20$) with diffuse end stage pyelonephritis-like kidneys,
and one case of pyelitis.
Of the 27 women on whom microscopic slides of the
kidney were obtained, there were 2 cases (7$), with non¬
specific scars of the kidney. There were also 2 cases (7$)
with minimal focal pyelonephritis. 14 cases (5 2$) had
typical focal pyelonephritis and 6 cases (22$) had diffuse
end stage pyelonephritis-like kidneys. There were three
cases in the category of pyelitis. All three cases in the
histologic category of pyelitis were in agreement with the
cases of pyelitis diagnosed at autopsy. (It will be noted
that 5 cases were diagnosed at autopsy and only 4 cases, 3
women and one man, are noted in Group 1 A, since one man had
primary genitourinary tract abnormality and was excluded.)
b. Group II A - Scarred Kidneys with N.P.N.* s Greater 't'han 85 mg. $ and/or Contracted Kidney in the Absence of Primary Genitourinary Tract Abnormality (Table 8j~ ‘ ~ .
Of the 9 men, there was one (11$) with nonspecific
scars of the kidney. There were two cases (22$) in the


category of minimal focal pyelonephritis, and two cases
(22$) in the category of typical focal pyelonephritis 0 4
cases (44$) were diffuse end stage pyelonephritis-like
kidneys,
Of the 9 females on whom microscopic slides were
obtained, there were two cases (22$) of nonspecific scars of
the kidneyo One case (11$) was in the category of minimal
focal pyelonephritis, and 4 cases (44$) were In the category
of typical focal pyelonephritis. There was one case of diffuse
end stage pyelonephritis-like kidney, and one case (11$)
with no apparent pathology. Thus 4 of the 9 scarred males
appeared to have either minimal or typical pyelonephritis
as did 5 of the 9 scarred females.
It is felt that there were no significant differences
between the two sexes in the histological evaluation which
was carried out within the pathological groups selected for
study.

-32-
DISCUSSION
This study has demonstrated that chronic pyelonephritis
as seen at autopsy in the absence of obstructive disease of
the genitourinary tract occurs with equal frequency in males
and females.
In a review of the 1,526 consecutive autopsies at the
Grace New Haven Community Hospital from January, 195? to
January, 1959 there were 97 cases with the pathological
diagnosis of chronic pyelonephritis0 This overall incidence
of 6.34$ compares favorably with previous surveys reported
in the literature.
REFERENCE
Shure (39)
Eaaschou (32)
Jackson et ah (15)
Kinney and Mallory (20)
Keefer (1?)
Schreiner (37)
FREQUENCY OF CHRONIC PYELONEPHRITIS
2„5^ of 11,898 autopsies
5o6% of 3,6o? autopsies
9% of 4,425 autopsies
14fo of 1,000 autopsies
15-20^ of "all autopsies"
20/£ of random autopsies
In order not to overlook any cases of chronic pyelo¬
nephritis this study has also included in a separate group
(Group II) those cases in which a pathologic diagnosis of
"scarred kidneys" was made. This was done because the
etiologic factors causing renal scarring are not always


^33-
certain and scarring may be due to chronic pyelonephritis.
In the scarred kidney group (Group II) the male to female
ratio was found to be approximately one to one. From the
scarred kidney group cases with N.P.N.’s greater than 85 mg,
% and/or contracted kidneys were selected and analyzed
(Group II A), so that one might study those cases with
significant renal disease. Again, as in the chronic pyelo¬
nephritis group (Group I A), the number of males and females
were approximately equal, in the absence of obstructive
disease of the genitourinary tract.
In the literature opinions differ as to the sex
Incidence of chronic pyelonephritis at autopsy (Table 9).
This issue is greatly obscured since most of these investiga¬
tors did not rigidly exclude pyelonephritis in the presence
of obstructive disease (14, 1, 39$ 19)• Therefore, from
these studies one can get little idea of the true sex
Incidence of chronic pyelonephritis In the absence of ob¬
structive disease of the genitourinary tract. Three studies,
however, did delineate pyelonephritis in the absence of
obstruction. One of these (Likely et al,) is difficult to
evaluate since “nonobstractive pyelonephritis11 is not
defined. The remaining two studies (2, 32) where all of the
obstructive disease of the urinary tract is defined and
cases with obstruction are excluded, each have the Incidence
of two females to one male. These results are not dissimilar
from those in the present study showing an equal frequency


TA
BL
E
9„
CH
RO
NIC
PY
EL
ON
EP
HR
ITIS
AT
AU
TO
PS
Y
34,
CD H 03 V\ a VO o a 4- a a 6 H GO H a H co —p
CO <D 1—1 <D pH CO 03 O
0 ^—! rH o 0$ a Ov oo o a CM a a
S o VO H i—1 H CM P H H f—1 03 4 S R i—1 4 03 CM -3- -£T o CM VO CM VO
P CM Ov CM a CM CM O VO O H CM CM H
6 O E
4 0 P P P C O P -P >> 0 *H a o •H •H P 0 CO P s O a, O 03 03 P G
•H ♦ o o 0 0 o R CO -P o -p H «H p p R P CD o f—1 R 0 03 O 0 P P CO o R 0 0 >5 0 P CO 03 03 P >5 0 ftP H E CO 4
C O CD -P a'P -P 0 0 O 03 4 O o -P £0 0 0 O 41 CO *H 0 O
•H 03 4 G 4 P P co 03 H -P o c O •H R © 4 >s P R H O CO -H 4 H o O CO CO 0 H o 0 CD 0 6 a o H 0 ap O CO H CO -H <5 O X 0 £0 o p X 0 P 0) 03 H CO p 0 K3^ 0 0 p 0 0 CO R
CO G 0 0 -p Ph > O r a 0 4 CO 0 -P * •H 0 >s 4-0 o
<D -4- 0 cd o « <4 •P a 41 O 0 CO VO Ph o « E P 0 O a p P a b» cd O 03 P 4 03 R 0 P o O O ss 4 4 e o R P B e P vo 4
CSV >5 a o o rH p o ® 0 o 6* 0 P a4 pH •H 03 O co p O c H a O P> 03 p 0 X 4 a i—1 EDP CO
Cm Cm Cd 4h 0 o CO 0 o 0 *H o Cm 0 o p, o eo R O p 03 R O
03 o O P s p o 0 o a 0 P CO ° & Ph IS E -P PO o c p a E 4-^ £ © 03
P 0 R 0 EO co 0 P r o © co 0 « •H 0 0) «H •H rp 0 4 •H 0 ' c P a 4* <H 03 P 03 -P > 0 > 0 «H O 03 C Cm H £5 4 0 0 > 0 0 R •H 0 > 0 03 03 O O 0 a o 0 03 co H P-r PI «H Pd 0 CO *H co s CO od R G O -P H co ® 0 P CO CO 0 o H 0 X
>1 o >5 o 0 >> CO O 0 0 CO >5 G E 0 CO R CO X CO CO 0 R CO £0 0 co cd CO co X 0 P, P a 0 0 Pr a p 0 Q-i «H 0 O a a 0 CO CO O P o O O p o o s o o o 0
-P CO P -P -P O CO p 0 a p P 4P 0 CO R 4 R O 4- R a 4 CM R P VO CM R R O 4 0 c o < P CM 0 CM o CM 0 R CM H 0 <d P Eh G
CO p 0 -p o
H 1—1 H 4 a /-N 0 0 0 P H CM CM
Is •rH ®—■" a a P •R .—- g v_^
<D 0 P a P CO • O 0 a 0 1 H R R E CM c w 03 0 O O <D —' O^r P — t>a H •H 4 4 Ph co H 0 H 0 r—1 CM 0 P O G CD H dsi p 0 G 0 CO CO
Cm i—1 O P R Rd P 0 0 (D 0 0 0 4 •H <H 0 0
Ph m m CO i-l 14 Pd Pd


-35-
of males and females with chronic pyelonephritis in the
absence of obstruction.
To be certain that there was no histologic pattern
typical of one sex, the slides of the present series were
reviewed without prior knowledge of the autopsy diagnosis or
the sex, for both the chronic pyelonephritis group and the
scarred kidney group. The histologic changes seen within
the two groups did not differ significantly between the two
sexes.
The age incidence of pyelonephritis in males and
females was analyzed (see Figures 1 and 2) to see if there
was any particular difference between the distribution of
ages in the two sexes. The peak distributions were similar
but there were proportionately more males in the younger age
groups. The difference between these results and others
where there was a preponderance of males In the age group
over 60 years (28, 39) is most likely due to the inclusion
of prostatic hypertrophy in their series, and its exclusion
In this series.
The incidence of hypertension (diastolic pressure
greater than 100 mm. Hg.) was determined in the groups with
chronic pyelonephritis and scarred kidney in the absence of
obstruction (Groups I A and II A). In the former, the males
and females have a 57»and a 62.5$ incidence respectively.
Similarly in the latter, the incidence of hypertension for
males and females was 55.5$ ana 75$ respectively. It is


~3k-
flGE D\STR\&UT\OH \N GROUP Xft
CHRon\C LOflEPHRmS
□ MALE'S H=as
PEMPkLES
on LXJ cn <x o
cr U-) OQ z:
»Oi
«
\.
d» $ a* £ <*• ^ cT £cf* £ $
o-\o n-ao a.1-30 ai-no mi-so s\-<>o 6»-io
d* $. cf g cf £
~ll-«0 si-^o e\\-\oo
RG-E 1M VERRS
FIGURE #1


NU
MB
ER
Of
CR
5ES
-31-
RGE D\STR\fcvn\Ott Itt 6"ROUP HR SCftRRfcU KVDHE'VS
D MR^S
■ ftMftues n= \o
RGE IH ‘YEfiftS
FIGURE#2


-38-
apparent that the two sexes are approximately equally
affected. Since these groups are without matched control
patients, nothing definite can be said about the incidence
of hypertension in pyelonephritis„ However, it is of interest
to compare this data with that of others (Table 10)„
Since Longcope (21) first described the association
between pyelonephritis and hypertension and Weiss and
Parker (43) demonstrated the histological lesions in chronic
pyelonephritis which were associated with hypertension,
many have written on the relationship between the two diseases.
Unlike most investigators Bell (2) felt that hypertension is
seldom related to "uncomplicated chronic pyelonephritis" and
Goldring and Chasis (13) have produced evidence from which
they deduce that there is no correlation between the two
diseases. However most authors (Table 10) believe that the
incidence of hypertension is significantly higher in patients
with chronic pyelonephritis than in those without. The
evidence in the literature of an increased incidence of
hypertension in the presence of pyelonephritis is difficult
to evaluate due to the following factors:
1) Not all studies had control groups of the same
age distribution as the group of pyelonephritis patients.
2) Some studies were done on clinical cases, others
on autopsy cases.
3) The criteria for the diagnosis of clinical pyelo¬
nephritis are questionable, or not given.


TA
BL
E
10o
HY
PE
RT
EN
SIO
N
IN
CH
RO
NIC
PY
EL
ON
EP
HR
ITIS
-39-
* * ,P • ^ *
ftp ft O- 3 P « P Ov Ov o £ pq a o 9 3 / ON O- O 3-
OO CO 03
i—! O 3 *3 P » O- c o Ov c JS o
>$> o CO 03 VO VTV -L VO
JC ft. V. 9 O o o o o p o o -3- VO vo vrvco ■3- 03 o •H PQ -3- 03 P CO -3" vo -3 VO V3
C/3 o 0 3 & o
CO ,C & # 3 3 o o CO Ov P o o P P G o CO JN- P vo CO VftCO Ov P P
rC H P P p CO • p 0
O P >3
p » CO « p
>5 b CQ o P p p 3 P G o P
3 * O M O 3 P p P 0 3 S *H O PPG 3 0 P
CQ P 0 3 P 3 CQ P 3 ft • 3 0 0 p x a xi P £ 3 O 3 ft 3 CO p P 0 N ft 3 P 3 0 ft cd P P P 0 P CQ P 3 o 0 ® o s PH P C >3 O 3 3 3 3 p 50
P 0 3 0 0 P p o P 3 • o 3 C i—) > O P 3 p Cm G G 3 p P ft o » 0 •H (Dd 3 3 O p 0 0 O p CO W 5QrC >3 0 N • P CQ 3 >3 P P p 0 0 P Q ft ,3 CQ p 6 CD 0 3 ft * P X o CO 3 CO P 3 0 3 3 0 P CQ P CO 3 CO 0 0 0 cd 0 0 0 3 P 0 3 CQ O 3 G 3 P G 03 e P a P 45 O 50ft 50 3 P O P 0 P P 0
p 0 50ft <—1 3 0 0 G P *H P P 4_i p CO Xi 3 3 3 w •h 3 3 G o 3 3 P o
VO P P CP 3 3 Q P 3 -3- 3 Ov p 0 £ 3 3 3 0 o cd Q 0 P 3 CO 3 CO o 3 ft 0 o
CO - ft. 3 P 3 O 3 P p 0 > 0 cd ON O • O 0 O .« p ft CQ ft p ft P CQ 3 o Vft 3 O 3 p O P 3 O 3 o o O O >5 s P
3 P >3 3 3 P 3 o 3 P CQ 3 P 3 P 0 X O 0 3 ~ CQ CQ 3 w 0 ft, 3 P o O 0 £>5 ft-, >3 >> 0 3 P P p p >5 O 50 P ft > ft 3 rQ o ftp P CQ • CQ CQ CQ ftP O
!5 P 3 P 0 3 O CQ O 3 o 3 V3 G cd 0 P ° 503 o 3 3 P P P O c • 3 3-3 •H P 0 3 0 00 3 3 >> 50P 50 50 3 P 3 3 > 3 ,3 P CQ CO 3 ft. 3 p 3 3 ,P ON 50 OP 0 0 3 O 0 o O *> ft 3 P o P G P O p 3 P >3 P • • e p 3 3 Q CQ 3 P CQ •H CO P ft 50 Vi 3 P 3 3 3 ft, p ,—! CQ rP 3 CQ 3 >3,0 3 3^0 3 3 3 0 >5 0 >>ft >5 3 0 50 3 3 o CO O O EH 3 O 50 0 3 CQ P CQ P G CQ P 0 3
a •HPdP 3 POP3 0. O ft 3 ft P 3 0 >30 o & p 3 P P P 3 P O P O 3 O C G § >3 p p p^v?. P O P CQ P G p 0 P ft P P o 3 p p o o 0 x p >1 p p 3 >5 3 0 3 P CO 03 3,0 < 5 O CO CO Pn 0 O G rO P <t3 ft C P <3 o co >3 VT'*
0 3 P 0 3 3 3 0 P P >
CO W 3 O -—' 3 vo CO
■3 CO P'~' 3 P Vft 0 P CO 3 P Ov 3 co O o --- 3 v—' P 3 03 rH v—* 0 3 * * p CO 3 O CQ —• <D ft * 0 '— p 3 O CQ 3 3 *H o o 3 P 0 CQ 3 0 0 0 ft p G 0 i—! 3 50 3 O Os! P 3 CQ 3 50 ft H CQ p 3 G 3 P 3 p p 0 0 0 O 3 3 3 3 3 3 P o ft! PQ S o PQ 3 PQ 3 C/1 S 0 t-Q


TA
BL
E
10.
HY
PE
RT
EN
SIO
N
IN
CH
RO
NIC
PY
EL
ON
EP
HR
ITIS
(conti
nued)
40-
PrG • Vb V. V? 3 43 PL, O O o O Vi. O *H 0 CP CP cu 0 P £ PQ G CM O . 43 0 Vi V. 1
«H rH <M rH vp i—1 5 0 cc CO G o Sr p 43 0 up
'G p..
G o IP- O S o
On
0 «PQ
S * PQ
o V. >s V. W r 42 p; 0s- up up up 0 <r -P * V. • © a o V. CO •H PQ VO ON G CP vo 00 O 0 » 0 G- & . VO V\ 00 G G vo C\i O bO up co
•H rH Vb 0 rH
0 0 S B
CO 0 P Is co g 0 05 O 0 H o o CO
G G vp CV! CP 00 J2 “P (!) G‘ CP 3t CP PQ G
O G S rH G 0 O S £ PQ ) pi «H •H
to 0 W s CO 0 p CM 0 G
«H 0 M p 0 P G PC 3 43
0 EH P co Ei C 0
« S «H »3j P ® rd < S
Cm G co O G *H O G pi*— O c 9 43 Cm O rH H 0
05 Pi C G 0 G ■H -P 03 0 co co >* < G ■G 0 0 PQ *H 0 C S 0
G CO Pi
kr
43 03 0 43 43 G C o 05 © 0 0 43 O a 0 O bO G o PQ Pr O P G M G "H •H -P 0 43 03 H o vn, 4h G 13 P.O CO C 0 0 G CO O co 0 >5 P H £0 0 E r~l •H c Cm VO 43 G 0 EH 43 43 0 «m -P o O a 0* o M G P co co O *H G PQ rH 0 rH CO ed 0 0 0
P -P o « S rH 0 0 ffi *H G, CO 0 CO G o PQ G fe <M P ©•HP a, 43 s 0 CO ♦H £li 0 * i—1 O 0 coPG W 0 G 0 05 CO 0 rH o O bO © bO !s P-i O o c 0 G rH P S 43 «H O 43 G-
C 0 CO 0 CO G PS GPP G O G C\1 S P b£)G f» p G PS 03 3 0 H VP 0 G G O 05 0 Cm G 0 43 43 43 0 >H G 0
Cm •H S O p 0 G CO i—1 CO C CO PQ Cm bO <H 43 G Pj G S 5 0 Si 0 O *H O CO
05 op CO rH G rH O G O rH G S O o o o P 05 0 0 C 43 H S 0 S S P CO «H G PrG 0 O P O brf is co E CO £0 0 & c 43 bQ •H G *• O Pr Pr P,
■P o o 0 G P G C G G G © Pd O E O O G 43 P e 43 0 3 ®H 4-^ G 43 p PC 43 O 43 43 P 3 G ♦H J> O rH *H H *H O 0 3 P 3 3 O < a Q™ 5 o >5 o £ O S Cm <d Cm <! <5
,.,v 00 rH —
G G -P 43 G -—V r—v •H r—v £ ,— cm O- G vo E 0\ P]
0 CO Cm G G iH C cp CO H G G- o ! <—- -— C M- W 0 1 —• G ^ g G 00 G 0 G 0 0 G »—• o • P P p p «H 0 p p 0 CO (H co 0 0 •H O 0 G CO 0 0 O G 0 0 co Pd Cm G rH O 0 CO 0*2
Cm C Q 0 •H p 0 Cd s G G p 0 G U P 43 0 0 0 0 0 •H 43 0 0
Pd w PQ PQ © S Ph Ed CO EH S 0 S PL,


-41-
4) The definition of hypertension is not uniform
throughout the literature,
5) In many autopsy studies, investigators have
divided chronic pyelonephritis into various forms, e.gc,
atrophic, nonatrophic, and have only studied the incidence
of hypertension in one form or the other and thus have not
Included all cases of chronic pyelonephritis in their series.
It is apparent from this brief revieiv that the relation of
pyelonephritis to hypertension remains to be definitely
demonstrated.
In the present study 67/^ of the men and 76% of the
women with chronic pyelonephritis in the absence of obstruc¬
tion (Group I A) had a positive family history of cardio¬
vascular disease. Again one sees that the two sexes are
equally affected. The role of heredity in essential hyper¬
tension has been discussed at great length. The majority
of opinion seems to favor some sort of genetic mechanism in
hypertension, though the basis of inheritance is thought to
be multifactorial (30, 29, 4l, 4o),
In the hypertension of chronic pyelonephritis as well
as in essential hypertension, genetic factors may be im¬
portant. Kincaid-Smith et al. (19) and Sowry (40) found a
positive family history for hypertension present as fre¬
quently in a group of patients with pyelonephritis as in a
group of patients with essential hypertension, Brod (8)


-42-
found that the Incidence of hypertension in patients with
pyelonephritis over 40 years old, who had a family history
of hypertension, was 84.5^, whereas in a group of pyelonephritic
patients where there was no mention of family history the
incidence of hypertension was 59.7$» and further that the in¬
cidence of hypertension in a nonpyelonephritic control group
with a family history of hypertension was 30%a Thus it appears
that heredity and perhaps pyelonephritis both have roles in
the etiology of hypertension and that inheritance which is
believed to be a significant factor in the etiology of
essential hypertension is perhaps equally significant in the
hypertension of chronic pyelonephritis0 It has furthermore
been suggested that patients with essential hypertension are
more likely to develop chronic pyelonephritis (34, 40)o
Pertinent to this Is the study of Woods (44) which has shown
in animals that desoxycorticosterone acetate induced hyper¬
tension predisposes to renal infection,. The critical control
of this study was omitted, however, when the author neglected
to test the susceptibility of infection of rats given
desoxycorticosterone acetate before they developed hyper¬
tension 0 It can be seen that the exact interrelationship
of hypertension, heredity, and pyelonephritis are not yet
clearly defined,.
Thus this study has demonstrated that chronic pyelo¬
nephritis at autopsy in the absence of obstruction has an


^43-
equal incidence in men and women and further that there is no
histologic pattern typical of one sex or any characteristic
age distribution for either sex. Neither is there any dif¬
ference in the incidence of hypertension or positive family
history for cardiovascular disease between men and. women„
In contrast to the one to one ratio of males to
females at autopsy, the clinical incidence of urinary tract
infection heavily favors women. On reviewing the literature
(Table 11) very few studies of clinical pyelonephritis in the
absence of obstruction have been made. In Raaschou's (32)
study of 31 clinical cases of chronic pyelonephritis, there
were 14 cases in the absence of obstruction. It appears that
of the 14, 13 were female and only one was male. In a recent (11)
clinical study of urinary tract infection in the absence of
obstruction in all patients treated by the medical service
over one and a half years at the Grace New Haven Community
Hospital, the female to male ratio was ten to one. The
diagnosis of urinary tract infection in this study was based
on quantitative methods for evaluating urine bacteriology.
The discrepancy between the ten females to one male
clinically and the one female to one male at autopsy requires
an explanation. Perhaps the following can in part explain
the marked difference of the sex incidence in clinical and
pathological pyelonephritis.


-44
4 CD CD P P c- VO o 00 VC CO rH CG 4 0 vo o a VO rH tp CVI rH £ E rH VO rH -p CD rH CO Ph
0 CD e 03 i—! cm VO a CVi 4- 00 O P
0 cd CM VO CM rH H o s 00 r-l
g CD rH
4 cd E p ON CM a O CV VO P -4 £ o o- o- VO CO CVi 00 CG rH
Eh 1—1 a rH P CM
CO 0 >3 P
4m rH £ 4 £ rH Ph O 4-3 G cd rH 0 O 3t •FV O £ P O G £ 4 P £ P ON CO G £ 0 G £ 4 P O CO P •H CO £
o r*a ,P rH rH Cd P 44 8 p CO o O r-l rG 4 0 cd G 4 N P O 0 4- o p p P 05 0 Ph G G X 0 P G P 4 CG 0 p CO P -P 4 P £ 0 CO G £ £ £ On G 0 >3 G
£ P £ G O o 0 G 0 P i—! P £ G £ o a i—i b£ i PP P £ P P G 4 P G P 0 G O 4 O So 0 CO On X e P 0 G *>» P •P O X P < D £ cd 4 4 0 o G 4 £ C/1 CO G 41 0 0 ro C\2 p- P o *>. G 0 £ E 4 CD >3 , 0 £ 4 0 CO P a £ p «*■> 0 O rH O P a CO 0 O G E 0 o P G CO G CD 4-3 o o CO P CO cd 0 £ p G X E bD o
C/0 £ p £ cd P •r-1 P G cd cd £ 0 o O £ rO 4 bo i 0 G P Cd bQ G £ p p P O
CD 0 c cd CO 4 £ P G O O p a p a 0 P 0 P o •H p 0 G G 0 G CM P a o o E 1>3 P
C/1 cd 43 P o 4 4 P 4 P £ CM P CO £ >3 a 0 H o P p CO £ CO a 0 G O p CO LM Eh E G |H P 4 0 G £ £ 4 a £ P H G rO £ £ o cd G O £ £ cd P G 0 O >3 CO G « o cd G P CM £ X o p P 0 G P 4 p 0 3 P 0 0 p G (0 CO P 0 P CO P a 0 CO 4 o 03 ♦ 0 E £ p 4 4 G 'O 0 0 a cd p 4 0 E CO £ p 0 P P o ■o ♦H £ 0 P 4 4 P £ O p 0 0 p 0 a G a p 0 G CO p o G 0 • -s a X £ CO > bO G P •> P o £ 0 a 0 •H 0 p 0 O o p • C p 4 • p CO £ o G w 4-3 P P G P G bD G P cd a co p 4 bD p P Ph
P cd P 0 P P 4 4 CO G 4 0 £ E O 0 p i—1 g Pr P > P cd a cd O >5 0 0 £ C 4 P G cd
a o 4 G N 0 *H G P 4 O P £ • 4 £ G
«M 4 CO P P £ G P cd £ P P £ £ 0 o <S?J o a p bO G o 0 0 p P 0 cd CO O CO a P 4 o 0 CO O 0 G P G rO p G >1 G P P 0 0 0 H CO £ o P P 4 •H 0 G 4 X a p £ P CO >3 G 4 4 0 o £ cd © G P O 0 a 0 o G 0 0 £ £ fH •H rH bO '4 4 4 G cd P 4 a .H P 0 G £ P 41 G 0 cd p P 1—1 CO P P G G P G a 4 4 G O 0 >3 p cd cd G O p p p O 4 0 0 O £ i—1 P C X
C/1 a Q a G O 4 PQ 4 5 £ O > a a p CG 4 0 0
/—- o a
f—l p G 1—I -- 0
Q0 a o £ a 1—1 O -—- -—- a 0 o CM <—- CM <! 4 no CM CG CG P p 4 £'— —- CM
0 0 £ r-3 0 w G 0 ON £ 0 £ £ £ '— 4 O PH p O 0 O P G CO O >3 4 G co P 4 w 4 G £ G 0 4 4 — P 0 O bD Ph CO a O 0 CO £ 0 G £ o 0 0 0 0 CM 0 G 0 O o 0 a 4 4 O a 4 a a a R
aaschou
(32
) T
he
sam
e serie
s
as
ab
ov
e
- obstr
ucti
on
cases
ex
clu
ded
.


-45-
1. Urinary tract infection as seen in the clinic
bears no etiologic relationship to chronic pyelonephritis at
autopsy. This view does not seem likely because:
a) It must be kept in mind that most pyelo¬
nephritis at autopsy is found in association with obstruction,
a procedure well known to predispose the kidney to infec¬
tion. The following chart demonstrates the incidence of
pyelonephritis in association with obstruction.
Nesbit and Conger (28) 4o;£ of 1?2 cases had obstruction
Bell (2) Obstructive chronic pyelo¬ nephritis 12 times as common as nonobstructive chronic pyelonephritis
Haaschou (32) 63% of 202 cases had ob¬ struction.
Rhoads (34) 15*5% of 5^-8 cases had. obstruction.
Sanjuro (35) 98,^ of 256 cases had ob¬ struction .
The present study also demonstrates the large number
of cases of chronic pyelonephritis that are associated, with
obstruction of the genitourinary tract. It was found that
48/£ of 102 cases were associated with obstruction (see
Table 1). As obstruction is well known to predispose the
kidney to infection, it is highly probable that In a large
majority of cases, chronic pyelonephritis at autopsy is on
the basis of prior urinary tract Infection; and
b) Experimental studies have demonstrated


-46-
unequivocably that the histologic characteristics of chronic-
pyelonephritis in man can be reproduced by bacterial infec¬
tion of the kidneys in animals (24).
2. Infections in males are more easily overlooked
than infections in females. Are there a large number of men
who have clinically in apparent urinary tract infection in
which case do they have fewer or different symptoms? If this
is true, why are there fewer symptoms in men? Is this a
different kind of infection or does host response differ?
There is no definite evidence on these points but there is
no reason to support either of these possibilities. In the
present study the finding of N.P.N.'s greater than 85 mg. %
in 63^> of the men and in of the women certainly suggests
that kidney disfunction is at least as severe in men as in
women.
Since prostatitis is a common disease even in young
men one might ask whether this type of infection might be
equivalent to cystitis and posterior urethritis In women.
This could bring the clinical incidence of disease in the
sexes closer together. However no males in the present
study had a history of prostatis. (There was no information
on 4 patients.)
3. Clinical urinary tract infection in females results
in chronic pyelonephritis as seen at autopsy less frequently
than that in males. Although difficult to prove, It would
appear that many cases of urinary tract Infection in females
seem in Involve primarily the lower urinary tract and do not
result in chronic pyelonephritis. This explanation is


„4?-
reasonable and may account in part for the data obtained.
4. Although the pathologic changes called chronic
pyelonephritis may be the result of infection, they may
also result from other types of disease where the sex ratio
is closer to one to one, e.g., that associated with drugs
(phenacetin (27)), hypertension (19, 36), congenital dysplasia
(26).
5. In a further attempt to explain the discrepancy
between the ten to one ratio of females to males clinically
and the one to one ratio at autopsy, the clinical incidence
of ten to one might be questioned for as noted earlier, there
are very few clinical studies on urinary tract infection in
the absence of obstruction. Of note are Raaschou’s (32)
study on 31 patients, 14 of which were in the absence of ob¬
struction, and the recent study at the Grace New Haven Com¬
munity Hospital described previously. Both of these studies
were carried out on medical services. The incidence of
urinary tract infection in the absence of obstruction was
found to be from 10-13 females to one male in both studies.
It seems possible that some cases with this disease were
missed because they were treated on the urology service. If
this were so the clinical ratio of females to .males might be
altered. However it is not considered likely that the
number of cases that could have been missed in these studies
would be sufficient to alter the ratio of females to males

48-
from ten to one to one to one, especially since it is felt
that clinical urinary tract infection In the absence of
obstruction as seen on the urology service is much more common
in women (12). Further In support of the clinical difference
of the two sexes is the difference In incidence of a past
history of urinary tract infection in the males and females
with chronic pyelonephritis in the absence of obstruction
(see Table 4) where 0% of the men and 2>292% of the women
had a past history of urinary tract infection.
Thus 5 possibilities have been discussed in an attempt
to explain the marked difference of the ratio of males to
females with chronic pyelonephritis in the absence of obstruc¬
tion clinically and pathologically. Two of these seem reason¬
able in the light of present knowledge,
a) The frequently seen clinical urinary tract
infection In women does not invariably result in chronic
pyelonephritis as seen at autopsy,
b) The changes which we are calling pyelo¬
nephritis at autopsy are actually being produced by agents
other than infection, such as phenacetin, hypertension,
or congenital dysplasia; and that these are appearing more
frequently in the kidneys of men at autopsy, thus giving us
a false impression of the frequency of the disease we call
chronic pyelonephritis.
It is concluded that there is no thesis at the present


-49-
time which satisfactorily explains the discrepancy between
the incidence of clinical urinary tract infection and pyelo¬
nephritis at autopsy. It will remain for prospective in¬
vestigations fitted with proper controls to solve the many
unanswered questions which have been raised by the present
study.

-50-
SUMMARY AND CONCLUSIONS
Chronic pyelonephritis in the absence of obstructive
disease of the urinary tract was found in 53 instances upon
reviewing the autopsy material from January, 1957 to January,
1959 at the Grace New Haven Community Hospital, There was
an equal distribution of these cases between the sexes (^7%
were males and 53^ females). Kidneys with scars not specifically
one. called pyelonephritic demonstrated a similar one toAsex distribu¬
tion,
A review of this histologic material without prior-
knowledge of the pathologic diagnosis or the sex for both
the chronic pyelonephritic and scarred kidney groups did not
disclose any particular histologic features characteristic of
one or the other sex. Neither was there any particular age
distribution for one sex or the other. Similarly, there was
no difference between the sexes in incidence of hypertension,
family history of hypertensive vascular disease, or extent of
renal damage as measured by elevation of N.P.N. The major
difference between the sexes was the lower frequency with
which a past history of urinary tract infection was elicited
from the males as compared to the females.
The incidence of clinical urinary tract infection in
the absence of obstruction was approximately ten to one in
favor of the females. An attempt has been made to explain

-51-
the discrepancy between the sex incidence of clinical urinary-
tract infection and the sex incidence of chronic pyelonephritis
at autopsy.


-52-
APPENDIX
Footnotes for Tables 2, 3 j 6, 7> 8
a. ?0H,-TBP Past history of hypertension obtained — from the clinical records or a diastolic
pressure of 100 mm, Hg. or higher in the past.
b0 BoP. Blood Pressure, This refers to the blood pressure obtained on the patient’s last admission to the hospital, (Space blank when record of blood pressure on last admission not obtained.)
Co Fam» Hist«
'"'tBP Heart CVA
Family history of hypertension, heart disease or cerebrovascular disease. This refers to the history of one or more of these diseases In the patient’s parents or siblings.
do N.P.N. N.P.N. in mg. %„ This data was obtained by taking the highest N.P.N. on the last admission. If no N.P.N. was determined on the last admission, the highest N.P.N. of the most recent hospital admission prior to the last was recorded.
e. P.H. Past history of urinary tract infection. ~~ P-'PoPo This refers to the finding of the diagnosis
of pyelonephritis (acute or chronic), "urinary tract infection," or cystitis, in the clinical record.
f. Urine^ pos. = positive and ng = no growth or Cult. negative. Urine culture - many of these
were not evaluated o u'vi- see Method. This data was taken from the clinical record. The most recent results were recorded. In only 1 case was there a change from positive to negative and since the positive was not evaluated quantitatively, it is felt that the negative is more valid. This Is recorded as neg.

-53-
APPENDIX
(continued.)
g. Diab. Diabetes, Data obtained, from clinical record of this diagnosis at any time prior to death.
h. Kid Wt.
Kidney weight. The weight of the left kidney is expressed over the weight of the right kidney. These weights were obtained at autopsy and are in grams.
1. Micro Microscopic classification of the kidney (See Method).
NS = Nonspecific scar MFP = Minimal focal pyelonephritis TFP = Typical focal pyelonephritis DEK = Diffuse endstage kidney, pyelo¬
nephritis-like . Pye = Pyelitis No. = No abnormal tissue
*
X
This refers to a kidney weighing more than 100 grams but being described as "small" in the pathological protocol.
This refers to the presence of what¬ ever factor it IS listed under.

BIBLIOGRAPHY
1. Barker, N.W. and Walters, W„: Hypertension and chronic atrophic pyelonephritis, J.A.M.A, 115:912 , 19^0.
2. Bell, E.T.: Renal Diseases, 2nd Ed., Philadelphia, Lea and Febiger, 19p"0.
3. Birchall, R„ and Alexander, J.: Medical aspects of pyelonephritis, Medicine 29yl, 1950®
4. Boyd, W.: Changing concepts of pyelonephritis, Canadian Medical Assoc 0 -J. 47:128, 1942,
5. Braasch, W.F.: Atrophic pyelonephritis, J, Urol, ?:247, 1922.
6. Braasch, WoF0 and Jacobson, C.E0*. Chronic bilateral pyelonephritis and hypertension, JB Urol, 44:571? 19^0.
7„ Braasch, W.F., Walters, W. and Hammer, H.J.: Hyper- tension and the surgical kidney, J.A.M.A. 115:1637, 1940.
8. Brod, J.; Chronic pyelonephritis, Lancet 270:973, 19560
9. Caulk, J.R.: Pyelonephritis, its incidence, engendering elements and impelling Influences, J.Urol. 16:117, 1926.
10. Fishberg, A.E.: Hypertension and Nephritis, 5th ed., Philadelphia, Lea”and™Febiger, 19J0.
11o Freedman, L.R.: Observations on patients with acute urinary tract infection, Presented at the International Symposium: The Biology of Pyelonephritis, Henry Ford Hospital, October, 1959®
12. Glenn, J.F.: Personal communication.'
13® Goldring, W. and Chasis, H.: Hypertension and Hyper¬ tensive Disease, New York Commonwealth Fund", T9447
14. Jackson, G.G., Dallenbach, F.D0, Kipnls, G.P.: Pyelo- nephritis, correlation of clinical and pathologic observations in the antibiotic era, M. Clin. N. Am.
39:297, 1955®
15® Jackson, G.G., Poirier, K.P., and Grieble, H.C.: Con¬ cepts of pyelonephritis: experience with renal biopsies and long term clinical observations, Ann. Int. Med. 47:1165, 1957®


-55-
16o Jawetz, E.s Urinary Tract Infections, Disease-a-Month, November, 1954.
17, Keefer, C.S.: Pyelonephritis - its natural history and course, Bull, Johns Hopkins Hospc 100:107, 1957.
18, Kincaid-Smith, P.s Vascular obstruction in chronic pyelonephritic kidneys and its relationship to hyper¬ tension, Lancet 269:1263 , 1955*
19, Kincaid-Smith, P. , McMichael, J., and Murphy, E.A.: The clinical course and pathology of hypertension with oapilloedema (malignant hypertension), Quart, J. Med, 275117, 1958,
20, Kinney, T'.D. and Mallory, G.K.: Personal communication cited by Mansfield, J.S., Mallory, G.X., and Ellis, L.B, The differential diagnosis of chronic Bright’s Disease: A clinicooathological correlation, New England J. Med.
29:387, 1943.
21. Likely, D.S., Lisa, J.R., and Solomon, C.: Pyelo¬ nephritis with death in uremia, J.A.M.A. 119:397, 1942.
22. Longcope, W.T.: Chronic bilateral pyelonephritis -- its origin and its association with hypertension, Ann. Int, Med. 11:149,1937.
23. Loopuyt, L.: Infections of the urinary tract, II. Therapeutic results, Acta Med. Scandinav. 125:357, 1946.
24. Mallory, G.K., Crane, A.S., and Edwards, J.E.: Pathology of acute and of healed experimental pyelo¬ nephritis, Arch. Path. 30:330,1940.
25. Mansfield, J.S., Mallory, G.K., and Ellis, L.B.: The differential diagnosis of chronic Bright's Disease: A clinicopathological correlation, New England. J. Med. 229:387, 1943.
26. Marshall, A.G.: Scars of the renal cortex, J. Path. Bact. 71: 1956o
27. Moclten, S.E., and Smith, I.B.: Fatal nephritis in chronic phenacetin poisoning, Am. J. Med. 215:127, i960.
28. Nesbit, R.M., and Conger, K.B.: Chronic pyelonephritis, .New York State J. Med. 42:225, 1942.
29. Pickering, G.W.: Genetic factors In essential hyper¬ tension, Ann. Int. Med. 43:457, 1955.


-56-
30. Platt, R.: Heredity in hypertension, Quart. -J. Med. 16:111, 1947.
31. Putschar, W.: Some aspects of the pathology of pyelonephritis, J. Urol. 43_:793? 1940.
32. Raaschou, F„: Studies of Chronic Pyelonephritis, Copenhagen, Ejnar Munksgaard, 1948.
33. Rantz, L.A.; Infections of the urinary tract, Adv.nb-K Med. 1:137, 1942.
34. Rhoads, P.S.: The incidence and clinical importance of pyelonephritis in patients with hypertension, Hypertension2 The first Hahnemann symposium on hypertensive disease. Philadelphia, W.B. Saunders, 1959*
35® Sanjuro, L.A. and Fortuno, R.F.: Clinical and pathological study of pyelonephritis in Puerto Rico. Review of 2,800 autopsies, 1,887 clinical records, J. Urol. 77 039? 1957®
36. Saphir, 0. and Taylor, B0: Pyelonephritis lenta, Ann. Int. Med. 36:1017, 1952.
37® Schreiner, G.E.: The clinical and histologic spectrum of pyelonephritis, A.M.A. Arch. Int. Med. 102:32, 1958.
38. Schroeder, H.A. and Steele, J.M.: Studies on "essentlaln hypertension II. The association of hypertension with organic renal disease, Arch. Int, Med. 68_:26l, 1941.
39. Shure, N.M0: Pyelonephritis and hypertension, A study of their relation in 11,898 necropsies. Arch. Int. Med. 70:284, 1942.
4o„ Sowry, G.S.C.: Hypertension the coincidence of conditions, Part I. Post graduate Medical Journal (London) 34:39-48, 82-88, 1958.
41. Thomas, C.B.: The heritage of hypertension, Tr. A. Am. Physicians 65.: 121, 1952.
42. Weiss, S. and Parker, F., Jr.: Pyelonephritis -- its relation to vascular lesions and to arterial hyperten¬ sion, Medicine 1.8:222, 1939®
43. Weiss, S. and Parker, F.5 Jr.: Relation of pyelonephritis and otter urinary tract Infections to arterial hyper¬ tension, New England J. Med. 223:959» 1940.
44. Woods, J.W.; Susceptibility of rats with hormonal hyper¬ tension to experimental pyelonephritis, J. Clin. Investiga¬ tion, 37:1686, 1958.






\


YALE MEDICAL LIBRARY
Manuscript Theses
Unpublished theses submitted for the Master's and Doctor's degrees and
deposited in the Yale Medical Library are to be used only with due regard to the
rights of the authors. Bibliographical references may be noted, but passages
must not be copied without permission of the authors, and without proper credit
being given in subsequent written or published work.
This thesis by has been
used by the following persons, whose signatures attest their acceptance of the
above restrictions.
NAME AND ADDRESS DATE

Copyright © 2022 FDOKUMEN




















