
Heart failure in patients with aortic stenosis: Clinical and prognostic significance of carbohydrate...
7
Heart failure in patients with aortic stenosis: Clinical and prognostic significance of carbohydrate antigen 125 and brain natriuretic peptide measurement Francesco Antonini-Canterin a, ⁎ , Bogdan A. Popescu b , Andreea C. Popescu c , Carmen C. Beladan b , Renata Korcova a , Rita Piazza a , Piero Cappelletti a , Daniela Rubin a , Matteo Cassin a , Pompilio Faggiano a , Gian Luigi Nicolosi a a Cardiologia, ARC, Azienda Ospedaliera S. Maria degli Angeli, Via Montereale, 24 33170 Pordenone, Italy b “Prof. Dr. C. C. Iliescu” Institute of Cardiovascular Diseases Bucharest, Romania c Cardiology Department, Elias Hospital Bucharest, Romania Received 11 October 2006; received in revised form 17 May 2007; accepted 26 May 2007 Available online 26 July 2007 Abstract Background: Brain natriuretic peptide (BNP) is related to symptomatic status and outcome in aortic stenosis (AS) patients. Carbohydrate antigen 125 (CA125) demonstrated recently a BNP-like behaviour in patients with congestive heart failure (CHF) but has never been studied in AS patients. We aimed to assess the role of CA125 and BNP in AS patients. Methods: CA125 and BNP blood levels, transthoracic echocardiography and independent evaluation of CHF symptoms were obtained in 64 consecutive patients (76 ± 9 years; 35 males) with AS (valve area 0.9 ± 0.3 cm 2 ). A pre-specified combined end-point consisting of cardiac mortality, urgent aortic valve replacement and hospitalization for CHF was considered. The median follow-up was 8 months (interquartile range 4.5–10 months). Results: Both CA125 and BNP have accurately identified patients with III–IV NYHA class: area under the ROC curve was 0.85 for CA125 and 0.78 for BNP (best cut-offs of 10.3 U/mL and 254.64 pg/mL respectively) and were independently correlated to left ventricular ejection fraction. Fifty-two percent of patients with CA125 ≥ 10.3 U/mL vs. 13% with CA125 b 10.3 U/mL (p b 0.01) and 65% patients with BNP ≥ 254 pg/mL vs. 7% with BNP b 254 pg/mL (p b 0.001) have reached the end-point. Conclusions: Both CA125 and BNP levels are significantly correlated with NYHA class and outcome in patients with AS. CA125 blood level assessment (less expensive) may improve the clinical management in this setting. © 2007 Elsevier Ireland Ltd. All rights reserved. Keywords: Aortic stenosis; Echocardiography; BNP; Carbohydrate antigen 125 1. Introduction The natural history of aortic stenosis changes dramati- cally after the onset of symptoms with an extremely high mortality rate on medical therapy within 3 years [1,2]. Therefore, there is a general agreement on the recommen- dation of aortic valve replacement in clearly symptomatic patients [3,4]. Symptoms assessment, however, is frequently difficult, especially in elderly patients with aortic stenosis because of reduction of physical activity or under-reporting by the patients themselves. Furthermore, there is a wide overlap in all echocardiographic and hemodynamic mea- surements between symptomatic and asymptomatic patients [5–7]. Recent studies have shown that plasma levels of natriuretic peptides, well recognized markers of left ventricular hypertrophy and dysfunction in patients with congestive heart failure [8,9], are also related to disease International Journal of Cardiology 128 (2008) 406 – 412 www.elsevier.com/locate/ijcard ⁎ Corresponding author. Tel.: +39 0434 399462; fax: +39 0434 399197. E-mail address: [email protected] (F. Antonini-Canterin). 0167-5273/$ - see front matter © 2007 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ijcard.2007.05.039
Transcript of Heart failure in patients with aortic stenosis: Clinical and prognostic significance of carbohydrate...

logy 128 (2008) 406–412www.elsevier.com/locate/ijcard
International Journal of Cardio
Heart failure in patients with aortic stenosis: Clinical andprognostic significance of carbohydrate antigen 125 and
brain natriuretic peptide measurement
Francesco Antonini-Canterin a,⁎, Bogdan A. Popescu b, Andreea C. Popescu c,Carmen C. Beladan b, Renata Korcova a, Rita Piazza a, Piero Cappelletti a,Daniela Rubin a, Matteo Cassin a, Pompilio Faggiano a, Gian Luigi Nicolosi a
a Cardiologia, ARC, Azienda Ospedaliera S. Maria degli Angeli, Via Montereale, 24 33170 Pordenone, Italyb “Prof. Dr. C. C. Iliescu” Institute of Cardiovascular Diseases Bucharest, Romania
c Cardiology Department, Elias Hospital Bucharest, Romania
Received 11 October 2006; received in revised form 17 May 2007; accepted 26 May 2007Available online 26 July 2007
Abstract
Background: Brain natriuretic peptide (BNP) is related to symptomatic status and outcome in aortic stenosis (AS) patients. Carbohydrateantigen 125 (CA125) demonstrated recently a BNP-like behaviour in patients with congestive heart failure (CHF) but has never been studiedin AS patients. We aimed to assess the role of CA125 and BNP in AS patients.Methods: CA125 and BNP blood levels, transthoracic echocardiography and independent evaluation of CHF symptoms were obtained in 64consecutive patients (76±9 years; 35 males) with AS (valve area 0.9±0.3 cm2). A pre-specified combined end-point consisting of cardiacmortality, urgent aortic valve replacement and hospitalization for CHF was considered. The median follow-up was 8 months (interquartilerange 4.5–10 months).Results: Both CA125 and BNP have accurately identified patients with III–IV NYHA class: area under the ROC curve was 0.85 for CA125and 0.78 for BNP (best cut-offs of 10.3 U/mL and 254.64 pg/mL respectively) and were independently correlated to left ventricular ejectionfraction. Fifty-two percent of patients with CA125≥10.3 U/mL vs. 13% with CA125b10.3 U/mL (pb0.01) and 65% patients withBNP≥254 pg/mL vs. 7% with BNPb254 pg/mL (pb0.001) have reached the end-point.Conclusions: Both CA125 and BNP levels are significantly correlated with NYHA class and outcome in patients with AS. CA125 bloodlevel assessment (less expensive) may improve the clinical management in this setting.© 2007 Elsevier Ireland Ltd. All rights reserved.
Keywords: Aortic stenosis; Echocardiography; BNP; Carbohydrate antigen
1251. Introduction
The natural history of aortic stenosis changes dramati-cally after the onset of symptoms with an extremely highmortality rate on medical therapy within 3 years [1,2].Therefore, there is a general agreement on the recommen-dation of aortic valve replacement in clearly symptomatic
⁎ Corresponding author. Tel.: +39 0434 399462; fax: +39 0434 399197.E-mail address: [email protected] (F. Antonini-Canterin).
0167-5273/$ - see front matter © 2007 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.ijcard.2007.05.039
patients [3,4]. Symptoms assessment, however, is frequentlydifficult, especially in elderly patients with aortic stenosisbecause of reduction of physical activity or under-reportingby the patients themselves. Furthermore, there is a wideoverlap in all echocardiographic and hemodynamic mea-surements between symptomatic and asymptomatic patients[5–7]. Recent studies have shown that plasma levels ofnatriuretic peptides, well recognized markers of leftventricular hypertrophy and dysfunction in patients withcongestive heart failure [8,9], are also related to disease

Table 1Patients' characteristics
All(n=64)
NYHA I–II(n=40)
NYHA III–IV(n=24)
p value
Age (years) 76±9 74±9 79±8 b0.05Female (%) 54.7 55.0 54.2 NSAortic peak
velocity (m/s)3.8±0.8 3.8±0.8 3.8±0.9 NS
Peak gradient(mm Hg)
61±27 61±25 61±30 NS
Mean gradient(mm Hg)
36±17 36±16 35±18 NS
Aortic valve area(cm2)
0.92±0.31
0.96±0.33 0.84±0.27 NS
Ejection fraction(%)
54±10 59±6 47±11 b0.001
Coronary arterydisease (%)
28.0 25.0 33.3 NS
Hypertension(%)
54.7 47.5 66.7 NS
Diabetes mellitus(%)
17.2 12.5 25.0 NS
Values are presented as mean±standard deviation or n (%) of patients.
407F. Antonini-Canterin et al. / International Journal of Cardiology 128 (2008) 406–412
severity [10–13] and to symptoms [14,15] in patients withAS. In addition, it has been reported that natriuretic peptidelevels predict symptom-free survival and postoperativeoutcome in patients with severe aortic stenosis [16–18].An increase of serum levels of carbohydrate antigen 125(CA125), a tumoural marker traditionally related to ovariancancer, has been recently observed in patients with chroniccongestive heart failure [19–22]. There is no information todate about the clinical usefulness of CA125 measurement inaortic stenosis patients. The purpose of the present study isthen to evaluate the clinical and prognostic significance ofboth brain natriuretic peptide (BNP) and CA125 in patientswith AS, correlating their blood levels with NYHA class,echocardiographic parameters and outcome.
2. Materials and methods
A total of 64 consecutive patients with isolated aorticstenosis referred to our adult echocardiography laboratorywere enrolled in this prospective study. The exclusioncriteria included more than mild associated aortic regurgi-tation, recent acute coronary syndrome (b1 month), priorcardiac surgery, chronic renal failure with a creatinine levelN2 mg/dL. Patients with known malignant diseases werealso excluded. The study protocol was approved by the localethics committee, and all patients gave written informedconsent.
Symptoms were assessed by experienced cardiologistsblinded to echocardiographic results and CA125/BNP levels.Patients were grouped according to the New York HeartAssociation (NYHA) classification. The presence of coro-nary artery disease was defined as history of myocardialinfarction or significant stenosis (N70% in a major epicardialcoronary artery) in a previous coronary angiogram. Thepresence of angina and exertional syncope was alsorecorded. All patients were followed-up by means ofscheduled clinical visits, by consulting the Regional HealthDatabase and by phone call interviews. A pre-specifiedcomposite end-point consisting of cardiac death, urgentvalve replacement and hospitalization for heart failure wasconsidered to evaluate the prognostic value of CA125 andBNP levels. Echocardiographic data were obtained usingcommercially available ultrasound systems (Hewlett PackardSonos 5500, Philips; Vivid 7, General Electric Inc.). Allpatients underwent a comprehensive examination includingM-mode and 2-D echocardiography and continuous-wave,pulsed-wave and Color Doppler. Measurements were madeaccording to the American Society of Echocardiographyguidelines [23] and averaged from 3 to 5 cardiac cycles. M-mode echocardiograms were derived from 2-dimensionalimages and recorded at 50 mm/s. An optimized parasternalshort-axis view at the mid-left ventricular level, just belowthe mitral valve leaflets was used to measure the followingparameters: left ventricular end-systolic and end-diastolicdimensions, ventricular septum and left ventricular posteriorwall thicknesses, and relative wall thickness. Left ventricular
mass and LVMI (left ventricular mass indexed by bodysurface area) were measured with M-mode echocardiogra-phy using the Devereux formula [24]. Left ventricularvolumes and ejection fraction were determined from amaximized apical 4-chamber view by measuring the end-systolic and end-diastolic volumes using the modified singleplane Simpson's method or area-length method. Peak aorticvelocity was obtained using continuous-wave Doppler fromthe window yielding the highest velocity signal. Mean aorticvalve gradient was derived by the modified Bernoulliequation tracing the continuous-wave flow envelope acrossthe aortic valve. The aortic valve area was calculated usingcontinuity equation [25]. The assessment of left ventriculardiastolic function was made from transmitral and pulmonaryvenous flow parameters, in patients in sinus rhythm, andclassified as normal, impaired relaxation, pseudonormal, orrestrictive pattern, as previously described [26]. Mitral andaortic regurgitation were evaluated by Doppler color-flowmapping [27,28]. All echocardiographic data were stored onhigh-quality S-VHS videotape for off-line analysis. BothCA125 and BNP levels were determined using commerciallyavailable kits (Bayer, ADVIA Centaur, chemiluminescentimmunoassay). Venous blood samples were taken from anantecubital vein at the time of the echocardiogram from allpatients into appropriate vacutainer test tubes, according tothe manufacturer's instructions. Plasma samples were frozenat −70 °C until assay.
2.1. Statistical analysis
Continuous variables are presented as mean±standarddeviation. Skewed data (such as CA125 and BNP values)were logarithmically transformed (ln), and the ln values werethen used in analyses. Comparisons between groups for
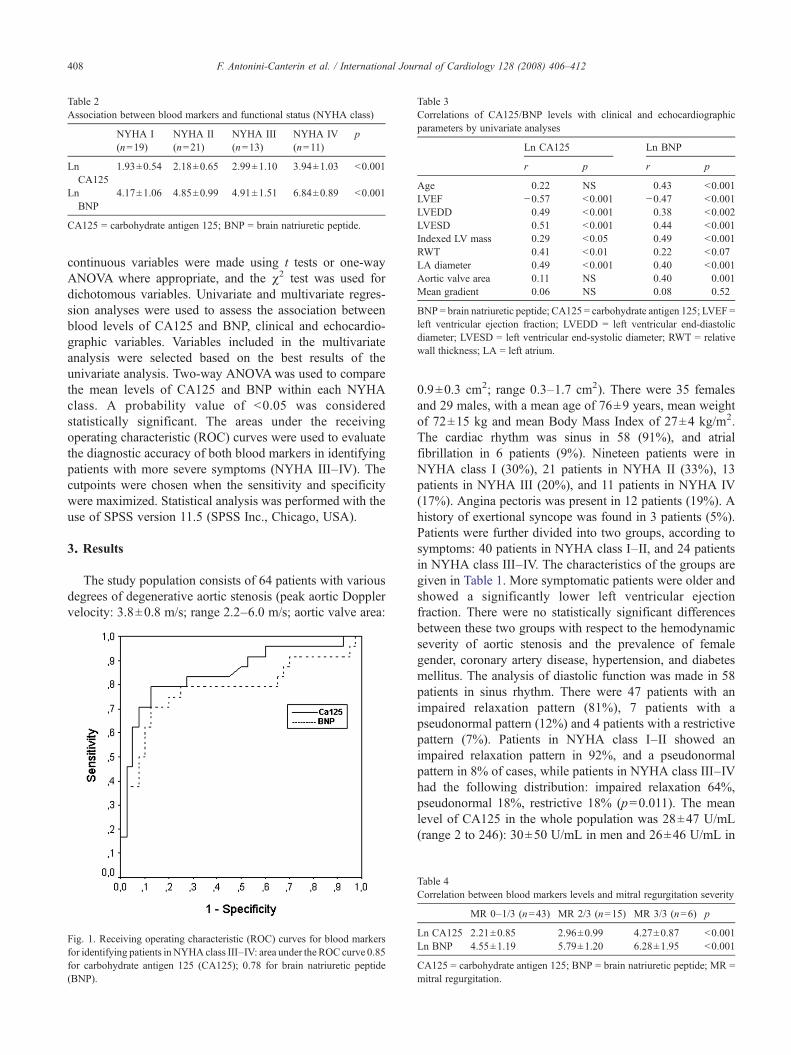
Table 2Association between blood markers and functional status (NYHA class)
NYHA I(n=19)
NYHA II(n=21)
NYHA III(n=13)
NYHA IV(n=11)
p
LnCA125
1.93±0.54 2.18±0.65 2.99±1.10 3.94±1.03 b0.001
LnBNP
4.17±1.06 4.85±0.99 4.91±1.51 6.84±0.89 b0.001
CA125 = carbohydrate antigen 125; BNP = brain natriuretic peptide.
Table 3Correlations of CA125/BNP levels with clinical and echocardiographicparameters by univariate analyses
Ln CA125 Ln BNP
r p r p
Age 0.22 NS 0.43 b0.001LVEF −0.57 b0.001 −0.47 b0.001LVEDD 0.49 b0.001 0.38 b0.002LVESD 0.51 b0.001 0.44 b0.001Indexed LV mass 0.29 b0.05 0.49 b0.001RWT 0.41 b0.01 0.22 b0.07LA diameter 0.49 b0.001 0.40 b0.001Aortic valve area 0.11 NS 0.40 0.001Mean gradient 0.06 NS 0.08 0.52
BNP = brain natriuretic peptide; CA125 = carbohydrate antigen 125; LVEF =left ventricular ejection fraction; LVEDD = left ventricular end-diastolicdiameter; LVESD = left ventricular end-systolic diameter; RWT = relativewall thickness; LA = left atrium.
408 F. Antonini-Canterin et al. / International Journal of Cardiology 128 (2008) 406–412
continuous variables were made using t tests or one-wayANOVA where appropriate, and the χ2 test was used fordichotomous variables. Univariate and multivariate regres-sion analyses were used to assess the association betweenblood levels of CA125 and BNP, clinical and echocardio-graphic variables. Variables included in the multivariateanalysis were selected based on the best results of theunivariate analysis. Two-way ANOVAwas used to comparethe mean levels of CA125 and BNP within each NYHAclass. A probability value of b0.05 was consideredstatistically significant. The areas under the receivingoperating characteristic (ROC) curves were used to evaluatethe diagnostic accuracy of both blood markers in identifyingpatients with more severe symptoms (NYHA III–IV). Thecutpoints were chosen when the sensitivity and specificitywere maximized. Statistical analysis was performed with theuse of SPSS version 11.5 (SPSS Inc., Chicago, USA).
3. Results
The study population consists of 64 patients with variousdegrees of degenerative aortic stenosis (peak aortic Dopplervelocity: 3.8±0.8 m/s; range 2.2–6.0 m/s; aortic valve area:
Fig. 1. Receiving operating characteristic (ROC) curves for blood markersfor identifying patients inNYHAclass III–IV: area under the ROC curve 0.85for carbohydrate antigen 125 (CA125); 0.78 for brain natriuretic peptide(BNP).
0.9±0.3 cm2; range 0.3–1.7 cm2). There were 35 femalesand 29 males, with a mean age of 76±9 years, mean weightof 72±15 kg and mean Body Mass Index of 27±4 kg/m2.The cardiac rhythm was sinus in 58 (91%), and atrialfibrillation in 6 patients (9%). Nineteen patients were inNYHA class I (30%), 21 patients in NYHA II (33%), 13patients in NYHA III (20%), and 11 patients in NYHA IV(17%). Angina pectoris was present in 12 patients (19%). Ahistory of exertional syncope was found in 3 patients (5%).Patients were further divided into two groups, according tosymptoms: 40 patients in NYHA class I–II, and 24 patientsin NYHA class III–IV. The characteristics of the groups aregiven in Table 1. More symptomatic patients were older andshowed a significantly lower left ventricular ejectionfraction. There were no statistically significant differencesbetween these two groups with respect to the hemodynamicseverity of aortic stenosis and the prevalence of femalegender, coronary artery disease, hypertension, and diabetesmellitus. The analysis of diastolic function was made in 58patients in sinus rhythm. There were 47 patients with animpaired relaxation pattern (81%), 7 patients with apseudonormal pattern (12%) and 4 patients with a restrictivepattern (7%). Patients in NYHA class I–II showed animpaired relaxation pattern in 92%, and a pseudonormalpattern in 8% of cases, while patients in NYHA class III–IVhad the following distribution: impaired relaxation 64%,pseudonormal 18%, restrictive 18% (p=0.011). The meanlevel of CA125 in the whole population was 28±47 U/mL(range 2 to 246): 30±50 U/mL in men and 26±46 U/mL in
Table 4Correlation between blood markers levels and mitral regurgitation severity
MR 0–1/3 (n=43) MR 2/3 (n=15) MR 3/3 (n=6) p
Ln CA125 2.21±0.85 2.96±0.99 4.27±0.87 b0.001Ln BNP 4.55±1.19 5.79±1.20 6.28±1.95 b0.001
CA125 = carbohydrate antigen 125; BNP = brain natriuretic peptide; MR =mitral regurgitation.
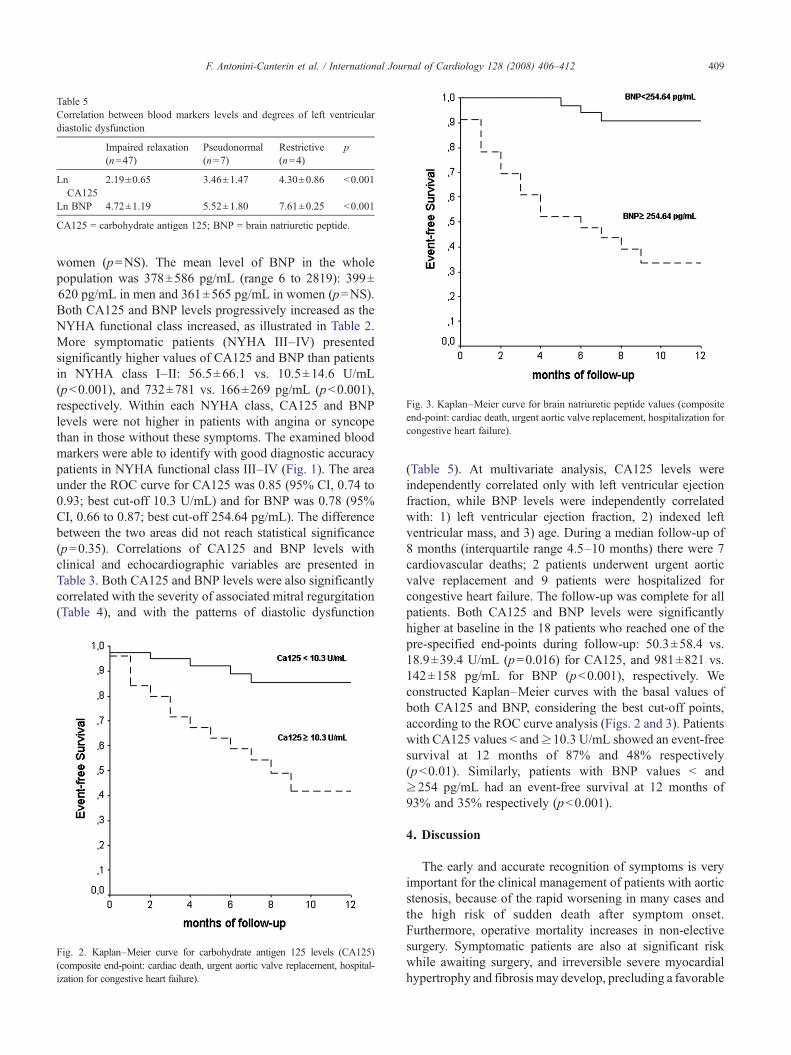
Table 5Correlation between blood markers levels and degrees of left ventriculardiastolic dysfunction
Impaired relaxation(n=47)
Pseudonormal(n=7)
Restrictive(n=4)
p
LnCA125
2.19±0.65 3.46±1.47 4.30±0.86 b0.001
Ln BNP 4.72±1.19 5.52±1.80 7.61±0.25 b0.001
CA125 = carbohydrate antigen 125; BNP = brain natriuretic peptide.
Fig. 3. Kaplan–Meier curve for brain natriuretic peptide values (compositeend-point: cardiac death, urgent aortic valve replacement, hospitalization forcongestive heart failure).
409F. Antonini-Canterin et al. / International Journal of Cardiology 128 (2008) 406–412
women (p=NS). The mean level of BNP in the wholepopulation was 378±586 pg/mL (range 6 to 2819): 399±620 pg/mL in men and 361±565 pg/mL in women (p=NS).Both CA125 and BNP levels progressively increased as theNYHA functional class increased, as illustrated in Table 2.More symptomatic patients (NYHA III–IV) presentedsignificantly higher values of CA125 and BNP than patientsin NYHA class I–II: 56.5±66.1 vs. 10.5±14.6 U/mL(pb0.001), and 732±781 vs. 166±269 pg/mL (pb0.001),respectively. Within each NYHA class, CA125 and BNPlevels were not higher in patients with angina or syncopethan in those without these symptoms. The examined bloodmarkers were able to identify with good diagnostic accuracypatients in NYHA functional class III–IV (Fig. 1). The areaunder the ROC curve for CA125 was 0.85 (95% CI, 0.74 to0.93; best cut-off 10.3 U/mL) and for BNP was 0.78 (95%CI, 0.66 to 0.87; best cut-off 254.64 pg/mL). The differencebetween the two areas did not reach statistical significance(p=0.35). Correlations of CA125 and BNP levels withclinical and echocardiographic variables are presented inTable 3. Both CA125 and BNP levels were also significantlycorrelated with the severity of associated mitral regurgitation(Table 4), and with the patterns of diastolic dysfunction
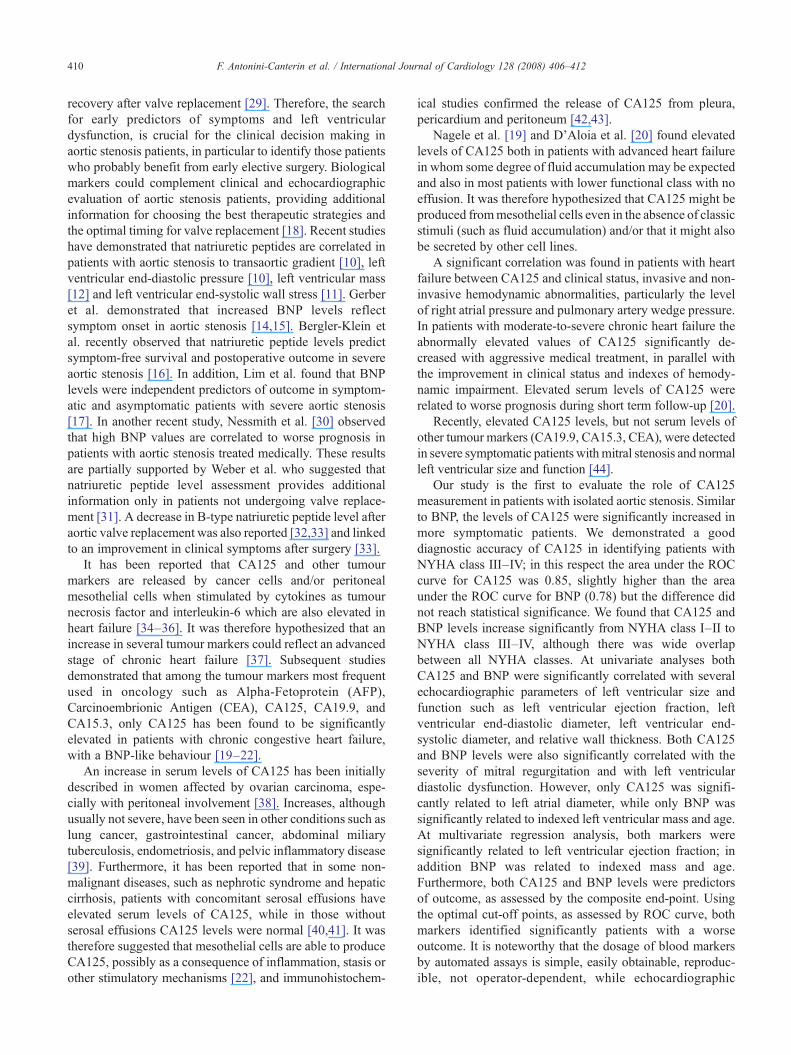
Fig. 2. Kaplan–Meier curve for carbohydrate antigen 125 levels (CA125)(composite end-point: cardiac death, urgent aortic valve replacement, hospital-ization for congestive heart failure).
(Table 5). At multivariate analysis, CA125 levels wereindependently correlated only with left ventricular ejectionfraction, while BNP levels were independently correlatedwith: 1) left ventricular ejection fraction, 2) indexed leftventricular mass, and 3) age. During a median follow-up of8 months (interquartile range 4.5–10 months) there were 7cardiovascular deaths; 2 patients underwent urgent aorticvalve replacement and 9 patients were hospitalized forcongestive heart failure. The follow-up was complete for allpatients. Both CA125 and BNP levels were significantlyhigher at baseline in the 18 patients who reached one of thepre-specified end-points during follow-up: 50.3±58.4 vs.18.9±39.4 U/mL (p=0.016) for CA125, and 981±821 vs.142±158 pg/mL for BNP (pb0.001), respectively. Weconstructed Kaplan–Meier curves with the basal values ofboth CA125 and BNP, considering the best cut-off points,according to the ROC curve analysis (Figs. 2 and 3). Patientswith CA125 values b and≥10.3 U/mL showed an event-freesurvival at 12 months of 87% and 48% respectively(pb0.01). Similarly, patients with BNP values b and≥254 pg/mL had an event-free survival at 12 months of93% and 35% respectively (pb0.001).
4. Discussion
The early and accurate recognition of symptoms is veryimportant for the clinical management of patients with aorticstenosis, because of the rapid worsening in many cases andthe high risk of sudden death after symptom onset.Furthermore, operative mortality increases in non-electivesurgery. Symptomatic patients are also at significant riskwhile awaiting surgery, and irreversible severe myocardialhypertrophy and fibrosis may develop, precluding a favorable
410 F. Antonini-Canterin et al. / International Journal of Cardiology 128 (2008) 406–412
recovery after valve replacement [29]. Therefore, the searchfor early predictors of symptoms and left ventriculardysfunction, is crucial for the clinical decision making inaortic stenosis patients, in particular to identify those patientswho probably benefit from early elective surgery. Biologicalmarkers could complement clinical and echocardiographicevaluation of aortic stenosis patients, providing additionalinformation for choosing the best therapeutic strategies andthe optimal timing for valve replacement [18]. Recent studieshave demonstrated that natriuretic peptides are correlated inpatients with aortic stenosis to transaortic gradient [10], leftventricular end-diastolic pressure [10], left ventricular mass[12] and left ventricular end-systolic wall stress [11]. Gerberet al. demonstrated that increased BNP levels reflectsymptom onset in aortic stenosis [14,15]. Bergler-Klein etal. recently observed that natriuretic peptide levels predictsymptom-free survival and postoperative outcome in severeaortic stenosis [16]. In addition, Lim et al. found that BNPlevels were independent predictors of outcome in symptom-atic and asymptomatic patients with severe aortic stenosis[17]. In another recent study, Nessmith et al. [30] observedthat high BNP values are correlated to worse prognosis inpatients with aortic stenosis treated medically. These resultsare partially supported by Weber et al. who suggested thatnatriuretic peptide level assessment provides additionalinformation only in patients not undergoing valve replace-ment [31]. A decrease in B-type natriuretic peptide level afteraortic valve replacement was also reported [32,33] and linkedto an improvement in clinical symptoms after surgery [33].
It has been reported that CA125 and other tumourmarkers are released by cancer cells and/or peritonealmesothelial cells when stimulated by cytokines as tumournecrosis factor and interleukin-6 which are also elevated inheart failure [34–36]. It was therefore hypothesized that anincrease in several tumour markers could reflect an advancedstage of chronic heart failure [37]. Subsequent studiesdemonstrated that among the tumour markers most frequentused in oncology such as Alpha-Fetoprotein (AFP),Carcinoembrionic Antigen (CEA), CA125, CA19.9, andCA15.3, only CA125 has been found to be significantlyelevated in patients with chronic congestive heart failure,with a BNP-like behaviour [19–22].
An increase in serum levels of CA125 has been initiallydescribed in women affected by ovarian carcinoma, espe-cially with peritoneal involvement [38]. Increases, althoughusually not severe, have been seen in other conditions such aslung cancer, gastrointestinal cancer, abdominal miliarytuberculosis, endometriosis, and pelvic inflammatory disease[39]. Furthermore, it has been reported that in some non-malignant diseases, such as nephrotic syndrome and hepaticcirrhosis, patients with concomitant serosal effusions haveelevated serum levels of CA125, while in those withoutserosal effusions CA125 levels were normal [40,41]. It wastherefore suggested that mesothelial cells are able to produceCA125, possibly as a consequence of inflammation, stasis orother stimulatory mechanisms [22], and immunohistochem-
ical studies confirmed the release of CA125 from pleura,pericardium and peritoneum [42,43].
Nagele et al. [19] and D'Aloia et al. [20] found elevatedlevels of CA125 both in patients with advanced heart failurein whom some degree of fluid accumulation may be expectedand also in most patients with lower functional class with noeffusion. It was therefore hypothesized that CA125 might beproduced frommesothelial cells even in the absence of classicstimuli (such as fluid accumulation) and/or that it might alsobe secreted by other cell lines.
A significant correlation was found in patients with heartfailure between CA125 and clinical status, invasive and non-invasive hemodynamic abnormalities, particularly the levelof right atrial pressure and pulmonary artery wedge pressure.In patients with moderate-to-severe chronic heart failure theabnormally elevated values of CA125 significantly de-creased with aggressive medical treatment, in parallel withthe improvement in clinical status and indexes of hemody-namic impairment. Elevated serum levels of CA125 wererelated to worse prognosis during short term follow-up [20].
Recently, elevated CA125 levels, but not serum levels ofother tumour markers (CA19.9, CA15.3, CEA), were detectedin severe symptomatic patients withmitral stenosis and normalleft ventricular size and function [44].
Our study is the first to evaluate the role of CA125measurement in patients with isolated aortic stenosis. Similarto BNP, the levels of CA125 were significantly increased inmore symptomatic patients. We demonstrated a gooddiagnostic accuracy of CA125 in identifying patients withNYHA class III–IV; in this respect the area under the ROCcurve for CA125 was 0.85, slightly higher than the areaunder the ROC curve for BNP (0.78) but the difference didnot reach statistical significance. We found that CA125 andBNP levels increase significantly from NYHA class I–II toNYHA class III–IV, although there was wide overlapbetween all NYHA classes. At univariate analyses bothCA125 and BNP were significantly correlated with severalechocardiographic parameters of left ventricular size andfunction such as left ventricular ejection fraction, leftventricular end-diastolic diameter, left ventricular end-systolic diameter, and relative wall thickness. Both CA125and BNP levels were also significantly correlated with theseverity of mitral regurgitation and with left ventriculardiastolic dysfunction. However, only CA125 was signifi-cantly related to left atrial diameter, while only BNP wassignificantly related to indexed left ventricular mass and age.At multivariate regression analysis, both markers weresignificantly related to left ventricular ejection fraction; inaddition BNP was related to indexed mass and age.Furthermore, both CA125 and BNP levels were predictorsof outcome, as assessed by the composite end-point. Usingthe optimal cut-off points, as assessed by ROC curve, bothmarkers identified significantly patients with a worseoutcome. It is noteworthy that the dosage of blood markersby automated assays is simple, easily obtainable, reproduc-ible, not operator-dependent, while echocardiographic
411F. Antonini-Canterin et al. / International Journal of Cardiology 128 (2008) 406–412
measurements are often technically difficult to obtain andrequire skilled and experienced sonographers. In addition,CA125 is relatively inexpensive as compared with natriureticpeptide measurements [19]. Nevertheless, the need forcaution in evaluating serial changes of CA125 in patientswith a previous history of malignancy should be emphasized[45]. The main limitation of this study is the relatively smallnumber of patients. Nevertheless, we are able to demonstratea significant relation between CA125 and symptoms, leftventricular function and outcome.
5. Conclusions
Although our study does not allow definitive conclusions asto which blood marker is the best predictor of functional statusand clinical outcome in aortic stenosis patients, the relativelycheaperCA125 appears to be comparable toBNP in this clinicalsetting as a simple and reliable test to identify high-risk patients.Further studies are needed to better define the pathophysiologyof CA125 production and release in aortic stenosis and toevaluate the relevance of serial assessment for the optimalclinical decision making in patients with aortic stenosis.
Acknowledgement
Dr. B.A. Popescu, Dr. A.C. Popescu and Dr. C.C. Beladanwere supported by Research Fellowships granted by theAssociation for Research in Cardiology, A.R.C., Pordenone,Italy.
References
[1] Ross Jr J, Braunwald E. Aortic stenosis. Circulation 1968;38(Suppl1):61–7.
[2] Turina J, Hess O, Sepulcri F, Krayenbuehl HP. Spontaneous course ofaortic valve disease. Eur Heart J 1987;8:471–83.
[3] Bonow RO, Carabello BA, de Leon Jr AC, et al. ACC/AHA guidelinesfor the management of patients with valvular heart disease: a report ofThe American College of Cardiology/American Heart AssociationTask Force on Practice Guidelines(Committee on Management ofPatients with Valvular Heart Disease). J Am Coll Cardiol 1998;32:1486–588.
[4] Iung B, Gohlke-Barwolf C, Tornos P, et al. Recommendations on themanagement of the asymptomatic patient with valvular heart disease.Eur Heart J 2002;23:1253–66.
[5] Rosenhek R, Maurer G, Baumgartner H. Should early elective surgerybe performed in patients with severe but asymptomatic aortic stenosis?Eur Heart J 2002;23:1417–21.
[6] Otto CM, Burwash IG, Legget ME, et al. Prospective study ofasymptomatic valvular aortic stenosis: clinical, echocardiographic andexercise predictors of outcome. Circulation 1997;95:2262–70.
[7] Antonini-Canterin F, Huang G, Cervesato E, et al. Relation of the totalejection isovolume index to symptoms in aortic stenosis. Am J Cardiol2002;90:665–8.
[8] Yasue H, Yoshimura M, Sumida H, et al. Localization and mechanismof secretion of B-type natriuretic peptide in comparison with those ofA-type natriuretic peptide in normal subjects and patients with heartfailure. Circulation 1994;90:195–203.
[9] Yamamoto K, Burnett Jr JC, Jougasaki M, et al. Superiority of brainnatriuretic peptide as a hormonalmarker of ventricular systolic and diastolicdysfunction and ventricular hypertrophy. Hypertension 1996;28:988–94.
[10] Prasad N, Bridges AB, Lang CC, et al. Brain natriuretic peptideconcentrations in patients with aortic stenosis. Am Heart J 1997;133:477–9.
[11] Ikeda T, Matsuda K, Itoh H, et al. Plasma levels of brain and atrialnatriuretic peptides elevate in proportion to left ventricular end-systolicwall stress in patients with aortic stenosis. AmHeart J 1997;133:307–14.
[12] Qi W, Mathisen P, Kjekshus J, et al. Natriuretic peptides in patientswith aortic stenosis. Am Heart J 2001;142:725–32.
[13] Weber M, Arnold R, Rau M, et al. Relation of N-terminal pro-B-Typenatriuretic peptide to severity of valvular aortic stenosis. Am J Cardiol2004;94:740–5.
[14] Gerber IL, Stewart RA, Legget ME, et al. Increased plasma natriureticpeptides reflect symptom onset in aortic stenosis. Circulation 2003;107:1884–90.
[15] Gerber IL, Legget ME,West TM, Richards AM, Stewart RA. Usefulnessof serial measurement of N-terminal pro-brain natriuretic peptide plasmalevels in asymptomatic patients with aortic stenosis to predictsymptomatic deterioration. Am J Cardiol 2005;95:898–901.
[16] Bergler-Klein J, Klaar U, Heger M, et al. Natriuretic pepetides predictsymptom-free survival and postoperative outcome in severe aorticstenosis. Circulation 2004;109:2302–8.
[17] Lim P, Monin JL, Monchi M, et al. Predictors of outcome of patientswith severe aortic stenosis and normal left ventricular function: role ofB-type natriuretic peptide. Eur Heart J 2004;25:2048–53.
[18] Watanabe M, Murakami M, Furukawa H, et al. Is measurement ofplasma brain natriuretc peptide levels a useful test to detect for surgicaltiming of valve disease? Int J Cardiol 2004;96:21–4.
[19] Nagele H, BahloM, Klapdor R, Schaeperkoetter D, RodigerW. CA125and its relation to cardiac function. Am Heart J 1999;137:1044–9.
[20] D'Aloia A, Faggiano P, Aurigemma G, et al. Serum levels ofcarbohydrate antigen 125 in patients with chronic heart failure. J AmColl Cardiol 2003;41:1805–11.
[21] Kouris NT, Zacharos ID, Kontogianni DD, et al. The significance ofCA125 levels in patients with chronic congestive heart failure. Correlationwith clinical and echocardiographic parameters. Eur J Heart Fail2005;7:199–203.
[22] Varol E, Ozaydin M, Dogan A, Kosar F. Tumour marker levels inpatients with chronic heart failure. Eur J Heart Fail 2005;7:840–3.
[23] Schiller NB, Shah PM, Crawford M, et al. Recommendations forquantification of the left ventricle by two-dimensional echocardiogra-phy. American Society of Echocardiography Committee on Standards,Subcommittee on Quantification of Two-Dimensional Echocardio-grams. J Am Soc Echocardiogr 1989;2:358–67.
[24] Devereux RB, Alonso DR, Lutas EM, et al. Echocardiographicassessment of left ventricular hypertrophy: comparison with necropsyfindings. Am J Cardiol 1986;57:450–8.
[25] Zoghbi WA, Farmer KL, Soto JG, Nelson JG, Quinones MA. Accuratenoninvasive quantification of stenotic aortic valve area by Dopplerechocardiography. Circulation 1986;73:452–9.
[26] Lubien E, DeMaria A, Krishnaswamy P, et al. Utility of B-natriuretcpeptide in detecting diastolic dysfunction: comparison with Dopplervelocity recordings. Circulation 2002;105:595–601.
[27] Helmcke F, Nanda NC, Hsiung MC, et al. Color Doppler assessment ofmitral regurgitation with ortogonal planes. Circulation 1987;75:175–83.
[28] Perry GJ, Helmcke F, Nanda NC, Byard C, Soto B. Evaluation of aorticinsufficiency by Doppler color flow mapping. J Am Coll Cardiol1987;9:952–9.
[29] Hein S, Arnon E, Kostin S, et al. Progression from compensatedhypertrophy to failure in the pressure-overloaded human heart: structuraldeterioration and compensatorymechanisms.Circulation 2003;25:984–91.
[30] Nessmith MG, Fukuta H, Brucks S, Little WC. Usefulness of an elevatedB-type natriuretic peptide in predicting survival in patients with aorticstenosis treated without surgery. Am J Cardiol 2005;96:1445–8.
[31] Weber M, Hausen M, Arnold R, et al. The prognostic value of N-terminal pro B-type natriuretic peptide (NT-proBNP) for conserva-tively and surgically treated patients with aortic valve stenosis. Heart2006;92:1639–44.

412 F. Antonini-Canterin et al. / International Journal of Cardiology 128 (2008) 406–412
[32] Neverdal NO, Knudsen CW, Husebye T, et al. The effect of aortic valvereplacement on plasma B-type natriuretic peptide in patients with severeaortic stenosis— one year follow up. Eur J Heart Fail 2006;8:257–62.
[33] Weber M, Arnold R, Rau M, et al. Relation of N-terminal pro B-typenatriuretic peptide to progression of aortic valve disease. Eur Heart J2005;26:1023–30.
[34] Ferrari R, Bachetti T, Confortini R, et al. Tumor necrosis factor solublereceptors in patients with various degree of congestive heart failure.Circulation 1995;92:1479–86.
[35] MacGowan GA, Mann DL, Kormos RL, Feldman AM, Murali S.Circulating interleukin-6 in severe heart failure. Am J Cardiol1997;79:1128–31.
[36] Zeimet AG, Offner FA, Marth C, et al. Modulation of CA125 releaseby inflammatory cytokines in human peritoneal mesothelial andovarian cancer cells. Anticancer Res 1997;17:3129–31.
[37] Faggiano P, D'Aloia A, Brentana L, et al. Serum levels of differenttumour markers in patients with chronic heart failure. Eur J Heart Fail2005;7:57–61.
[38] Bast Jr RC, Klug TL, St John E, et al. A radioimmunoassay using amonoclonal antibody to monitor the course of epithelial ovarian cancer.N Engl J Med 1983;309:883–7.
[39] Sjovall K, Nilsson B, Einhorn N. The significance of serum CA125 inmalignant and nonmalignant diseases. Gynecol Oncol 2002;85:175–8.
[40] Bergmann JF, Bidart JM, George M, Beaugrand M, Levy VG, BohuonC. Elevation of CA125 in patients with benign and malignant ascites.Cancer 1987;59:213–7.
[41] Sevinc A, Buyukberber S, Sari R, Kiroglu Y, Turk HM, Ates M.Elevated serum CA125 in hemodialysis patients with peritoneal,pleural or pericardial fluids. Gynecol Oncol 2000;77:254–7.
[42] Epiney M, Bertussa C, Weil A, Campana A, Bishof P. CA 125production by peritoneum: in-vitro and in-vivo studies. Hum Reprod2000;15:1261–5.
[43] Gullu I, Yalcin S, Tekuzman G. Tumour markers in effusions: acomparative study of tumourmarker levels in sera and effusion. In: TravisCC, editor. Use of biomarkers in assessing health and environmentalimpacts of chemical pollutants. New York: Plenum; 1993. p. 265–72.
[44] Duman C, Ercan E, Tengiz I, Bozdemir H, Ercan HE, Nalbantgil I.Elevated serum CA 125 levels in mitral stenotic patients with heartfailure. Cardiology 2003;100:7–10.
[45] Faggiano P, D'Aloia A, Bignotti T, Dei Cas L. One biologic marker(carbohydrate antigen-CA125), two different diseases (ovarian cancerand congestive heart failure): practical implications of monitoringCA125 serum levels. A case report. Ital Heart J 2003;4:497–9.




















