Circulating Natriuretic Peptides in Cats with Heart Disease
10
Circulating Natriuretic Peptides in Cats with Heart Disease D.J. Connolly, R.J. Soares Magalhaes, H.M. Syme, A. Boswood, V. Luis Fuentes, L. Chu, and M. Metcalf Background: Circulating natriuretic peptide concentrations are increased in cats with myocardial dysfunction. Hypothesis: Serum N-terminal fragment of proatrial natriuretic peptide (NT-proANP) and NT-probrain natriuretic pep- tide (proBNP) concentrations may predict the presence of heart disease (HD) and congestive heart failure (CHF). A positive relationship is also predicted among natriuretic peptide (NP) concentrations, a noninvasive estimate of left ventricular filling pressure (E/E a ), and an echocardiographic measure of left atrial (LA) size (LA/aortic diameter [Ao]). Methods: Serum NP concentrations were measured in 28 healthy control and 50 study cats using sandwich enzyme immunoassays. The study group comprised cats, with HD but no CHF (HD CHF, n 5 17) and cats with CHF (HD 1 CHF, n 5 33). The relationship among NP concentrations, LA size, and E/E a was examined. The ability of NP to distinguish control from study cats, and HD CHF from HD 1 CHF cats, was explored using receiver operator curve analysis. Results: NP concentrations were significantly lower in control than in study cats (P 5 .0001). The NT-proBNP concentra- tions were positively correlated with LA/Ao ratio (r 5 0.34; P 5 .02) and with E/E a ratio (r 5 0.68; P o .05). An NT-proBNP concentration of 49 fmol/mL gave a sensitivity and specificity of 100 and 89.3%, respectively, for correctly distinguishing 96.2% of control from study cats. Pairwise comparisons of the areas under the curve identified a statistically significant difference (P 5 .011) between NT-proANP and NT-proBNP to distinguish control from study cats. NT-proANP and NT-proBNP concentra- tions were significantly higher in HD 1 CHF cats than in HD CHF cats (P 5 .0023 and .0001, respectively). Conclusions: Serum concentrations of NT-proANP and particularly NT-proBNP were different in healthy control cats, asymptomatic cats with HD, and cats with CHF, suggesting that measurement of NP concentrations may prove clinically useful as an initial screening test for cats with suspected cardiac disease. Key words: Diastolic dysfunction; Doppler tissue imaging; Feline cardiomyopathy; Left atrial pressure. N atriuretic peptides (NP) are a group of hormones synthesized by cardiomyocytes, and include atrial natriuretic peptide (ANP) and brain natriuretic peptide (BNP). They are released into the circulation as a result of myocardial stretch of the atria and ventricles, respec- tively, and are responsible for the regulation of body fluid homeostasis and blood pressure. 1 In human patients, they are increasingly being used as markers for the diag- nosis and prognosis of cardiac disease. 2–5 They also have a potential role in treatment of heart disease. 6 The primary stimulus for ANP release is increased atrial transmural pressure; however, its synthesis is also upregulated in hypertrophied cardiac myocytes. 7,8 ANP is encoded as a 126-amino acid precursor, which on re- lease is cleaved to the physiologically active 28-amino acid carboxy-terminal fragment and a 98-amino acid amino- terminal fragment (NT-proANP), both of which circulate in plasma. Usually, circulating NT-proANP is measured because it is far more stable at room temperature than ANP, making it more suitable as a diagnostic test. 9 BNP undergoes similar posttranslational modifica- tion. In healthy humans, cats, and dogs, circulating BNP probably originates from storage granules in the atria, allowing a rapid increase in plasma concentrations in response to sudden atrial wall stretch. Sustained in- creases in circulating BNP, as seen in patients with chronic heart failure, are facilitated by increased protein synthesis with the major site of BNP production switch- ing from the atria to the ventricles. 10 BNP concentrations therefore are principally regulated by ventricular wall stress and pressure load. 11 Increased circulating concentrations of these hor- mones have been identified in human patients with hypertrophic cardiomyopathy (HCM), 2,12 and NT-pro- BNP has been shown to correlate positively with the severity of hypertrophy. 2 HCM is the most prevalent cardiac disease in the adult cat and, similar to other feline cardiomyopathies, causes diastolic dysfunction, which frequently results in left atrial (LA) enlargement and congestive heart failure (CHF). 13,14 Increased concentra- tions of NPs might therefore be expected in affected cats. Plasma NT-proANP immunoreactivity has been previ- ously compared in cats with and without HCM. No significant difference was found between the 2 study groups, but the majority of cats in the HCM group were asymptomatic. The study identified a positive correlation between NT-ANP and echocardiographic parameters of LA size and left ventricular wall thickness. 15 Plasma BNP concentrations in cats with myocardial disease and CHF were found to be 10 times greater than those of control animals, and increased expression of myocardial BNP was identified in the atria and ventricles of cats with HCM. 3, a In studies of humans and dogs, a positive correlation between the presence and severity of CHF and NP con- centrations has been recognized. 16–21 Increased BNP concentrations in cats with HCM and CHF have also been reported. a Circulating NP concentrations have been shown to be positively correlated with disease severity and pulmonary capillary wedge pressure in canine and human pa- tients 17,21–24 and in experimental studies of dogs. 25 In veterinary cardiology, LA size is sometimes used as an From the Department of Veterinary Clinical Sciences, The Royal Veterinary College, Hatfield, Herts, UK. Corresponding author: D. J. Connolly, Department of Veterinary Clinical Sciences, The Royal Veterinary College, Hawkshead Lane, North Mymms, Hatfield, Herts AL9 7TA, UK; e-mail: dconnolly@ rvc.ac.uk. Submitted January 5, 2007; Revised March 11, 2007; Accepted July 23, 2007. Copyright r 2008 by the American College of Veterinary Internal Medicine 10.1111/j.1939-1676.2007.0024.x J Vet Intern Med 2008;22:96–105
Transcript of Circulating Natriuretic Peptides in Cats with Heart Disease

Circulat ing Natriuret ic Peptides in Cats with Heart Disease
D.J. Connolly, R.J. Soares Magalhaes, H.M. Syme, A. Boswood, V. Luis Fuentes, L. Chu, and M. Metcalf
Background: Circulating natriuretic peptide concentrations are increased in cats with myocardial dysfunction.
Hypothesis: Serum N-terminal fragment of proatrial natriuretic peptide (NT-proANP) and NT-probrain natriuretic pep-
tide (proBNP) concentrations may predict the presence of heart disease (HD) and congestive heart failure (CHF). A positive
relationship is also predicted among natriuretic peptide (NP) concentrations, a noninvasive estimate of left ventricular filling
pressure (E/Ea), and an echocardiographic measure of left atrial (LA) size (LA/aortic diameter [Ao]).
Methods: Serum NP concentrations were measured in 28 healthy control and 50 study cats using sandwich enzyme
immunoassays. The study group comprised cats, with HD but no CHF (HD� CHF, n 5 17) and cats with CHF (HD 1 CHF,
n 5 33). The relationship among NP concentrations, LA size, and E/Ea was examined. The ability of NP to distinguish control
from study cats, and HD � CHF from HD 1 CHF cats, was explored using receiver operator curve analysis.
Results: NP concentrations were significantly lower in control than in study cats (P 5 .0001). The NT-proBNP concentra-
tions were positively correlated with LA/Ao ratio (r 5 0.34; P 5 .02) and with E/Ea ratio (r 5 0.68; Po .05). An NT-proBNP
concentration of 49 fmol/mL gave a sensitivity and specificity of 100 and 89.3%, respectively, for correctly distinguishing 96.2%
of control from study cats. Pairwise comparisons of the areas under the curve identified a statistically significant difference (P 5
.011) between NT-proANP and NT-proBNP to distinguish control from study cats. NT-proANP and NT-proBNP concentra-
tions were significantly higher in HD 1 CHF cats than in HD � CHF cats (P 5 .0023 and .0001, respectively).
Conclusions: Serum concentrations of NT-proANP and particularly NT-proBNP were different in healthy control cats,
asymptomatic cats with HD, and cats with CHF, suggesting that measurement of NP concentrations may prove clinically useful
as an initial screening test for cats with suspected cardiac disease.
Key words: Diastolic dysfunction; Doppler tissue imaging; Feline cardiomyopathy; Left atrial pressure.
Natriuretic peptides (NP) are a group of hormonessynthesized by cardiomyocytes, and include atrial
natriuretic peptide (ANP) and brain natriuretic peptide(BNP). They are released into the circulation as a resultof myocardial stretch of the atria and ventricles, respec-tively, and are responsible for the regulation of body fluidhomeostasis and blood pressure.1 In human patients,they are increasingly being used as markers for the diag-nosis and prognosis of cardiac disease.2–5 They also havea potential role in treatment of heart disease.6
The primary stimulus for ANP release is increasedatrial transmural pressure; however, its synthesis is alsoupregulated in hypertrophied cardiac myocytes.7,8 ANPis encoded as a 126-amino acid precursor, which on re-lease is cleaved to the physiologically active 28-amino acidcarboxy-terminal fragment and a 98-amino acid amino-terminal fragment (NT-proANP), both of which circulatein plasma. Usually, circulating NT-proANP is measuredbecause it is far more stable at room temperature thanANP, making it more suitable as a diagnostic test.9
BNP undergoes similar posttranslational modifica-tion. In healthy humans, cats, and dogs, circulatingBNP probably originates from storage granules in theatria, allowing a rapid increase in plasma concentrationsin response to sudden atrial wall stretch. Sustained in-creases in circulating BNP, as seen in patients with
chronic heart failure, are facilitated by increased proteinsynthesis with the major site of BNP production switch-ing from the atria to the ventricles.10 BNP concentrationstherefore are principally regulated by ventricular wallstress and pressure load.11
Increased circulating concentrations of these hor-mones have been identified in human patients withhypertrophic cardiomyopathy (HCM),2,12 and NT-pro-BNP has been shown to correlate positively with theseverity of hypertrophy.2 HCM is the most prevalentcardiac disease in the adult cat and, similar to other felinecardiomyopathies, causes diastolic dysfunction, whichfrequently results in left atrial (LA) enlargement andcongestive heart failure (CHF).13,14 Increased concentra-tions of NPs might therefore be expected in affected cats.Plasma NT-proANP immunoreactivity has been previ-ously compared in cats with and without HCM. Nosignificant difference was found between the 2 studygroups, but the majority of cats in the HCM group wereasymptomatic. The study identified a positive correlationbetween NT-ANP and echocardiographic parameters ofLA size and left ventricular wall thickness.15 PlasmaBNP concentrations in cats with myocardial disease andCHF were found to be 10 times greater than those ofcontrol animals, and increased expression of myocardialBNP was identified in the atria and ventricles of cats withHCM.3, a
In studies of humans and dogs, a positive correlationbetween the presence and severity of CHF and NP con-centrations has been recognized.16–21 Increased BNPconcentrations in cats with HCM and CHF have alsobeen reported.a
Circulating NP concentrations have been shown to bepositively correlated with disease severity and pulmonarycapillary wedge pressure in canine and human pa-tients17,21–24 and in experimental studies of dogs.25 Inveterinary cardiology, LA size is sometimes used as an
From the Department of Veterinary Clinical Sciences, The RoyalVeterinary College, Hatfield, Herts, UK.
Corresponding author: D. J. Connolly, Department of VeterinaryClinical Sciences, The Royal Veterinary College, Hawkshead Lane,North Mymms, Hatfield, Herts AL9 7TA, UK; e-mail: [email protected].
Submitted January 5, 2007; Revised March 11, 2007; AcceptedJuly 23, 2007.
Copyright r 2008 by the American College of Veterinary InternalMedicine
10.1111/j.1939-1676.2007.0024.x
J Vet Intern Med 2008;22:96–105

indicator of disease severity.14,17 More sophisticatednoninvasive estimates of left ventricular filling pressureusing Doppler echocardiography have also been de-scribed.26–29 Studies in humans have shown acorrelation between various echocardiographic mea-sures, including the ratio (E/Ea) of early mitral inflowvelocity (E) to the longitudinal velocity of the mitralvalve annulus during early diastole (Ea) with invasivemeasures of mean LA pressure. Ea behaves as an index ofleft ventricular relaxation that is less preload dependentthan traditional echo-Doppler variables, and, when in-cluded in the ratio with E, can compensate for thenumerous influences on ventricular diastolic function,explaining why this ratio has a much stronger correlationwith left ventricular filling pressure than E alone.30 A re-cent report using dogs with experimentally induced acutemitral valve insufficiency also confirmed a high correla-tion between the E/Ea ratio and mean LA pressure.29 TheE/Ea ratio has also been shown to correlate well with leftheart filling pressures in human HCM patients.31 Similarstudies have not been reported for cats with HCM, de-spite the fact that mitral inflow and Doppler tissueimaging (DTI) waveforms are frequently measured incats.26,32,33
The aims of this study were to:
(1) Investigate the ability of serum NT-proANP andNT-proBNP concentrations to distinguish controlcats from study cats, and to distinguish cats with HDbut without CHF (HD � CHF) from those withCHF (HD 1 CHF).
(2) Investigate the relationship among serum NT-proANP and NT-proBNP concentrations, E/Ea,and LA/aortic diameter (Ao).
The hypothesis of the study was that serum NT-proANP and NT-proBNP concentrations could be usedto distinguish HD � CHF from HD 1 CHF cats, and todistinguish both groups from healthy control cats.
Materials and Methods
Animals and Diagnostic Tests
Healthy control cats consisted of animals seen at 2 private prac-
tices. Most cats were being screened as part of an annual health
check before vaccination or elective surgery such as neutering or
dental procedures. Five of the 28 control cats were being treated for
conditions unlikely to affect ANP or BNP concentrations: ear mite
infestation (2), tail trauma (1), impacted anal glands (1), and skin
laceration (1). All cats received thorough physical examinations by
veterinarians with postgraduate qualifications in cardiology or in-
ternal medicine (Royal College of Veterinary Surgeons Certificate in
Veterinary Cardiology or Diploma of the European College of Vet-
erinary Internal Medicine). Cats were excluded if they had
concurrent renal disease, thyroid disease, neoplasia, hematologic
disturbances, palpable goiter, or heart disease. Inclusion was deter-
mined by the absence of clinical signs (eg, absence of murmur,
gallop rhythm, tachypnea, and arrhythmia), previous history, CBC,
and biochemistry analysis, and in older cats, serum total T4 con-
centration.
Study cats were referred to the Royal Veterinary College cardi-
ology service for further assessment of cardiac dysfunction. Thirty-
five of 50 cats had received medication before referral. Medications
included 1 or more of the following: furosemide, spironolactone,
angiotensin converting enzyme inhibitor, atenolol, aspirin, and
diltiazem. All affected cats received thorough physical examina-
tions, echocardiography (two-dimensional [2D], M-mode, and
Doppler) with simultaneous electrocardiogram (ECG) recording.
One or more of the following tests were also performed: ECG, se-
rum biochemistry, CBC, thoracic radiography, systolic blood
pressure analysis using a Doppler flow detector,b serum cardiac
troponin I concentration, or serum total T4 concentration. Cats
were classified as having CHF on the basis of clinical signs and tho-
racic radiographic evidence consistent with pulmonary edema or
pleural effusion, or ultrasonographic evidence of pleural fluid, in the
presence of structural heart disease.
Standard echocardiographic studies34 were performed using a 7S
phased array probe (3.0–6.7MHz) with harmonic imaging.c The
frame rate generally used was 87 frames/s, although it varied from
43 to 97 frames/s. An ECG was recorded simultaneously in all cats.
For each variable, 3 measurements were averaged from 3 consecu-
tive cardiac cycles. The LA to Ao ratio (LA/Ao) was obtained using
2D echocardiography from the right parasternal short-axis heart
base view. Measurements were made at the first diastolic frame just
after aortic valve closure. LA/Ao was measured using the method
described byHansson et al35 (Fig 1). A ratio of41.5 was considered
consistent with LA enlargement.36
M-mode measurements of thickness of the interventricular sep-
tum in diastole, left ventricular internal diameter in diastole and
systole, and left ventricular freewall in diastole were made at the
level of the chordae tendineae in the short-axis view. Where asym-
metrical hypertrophy was identified, the maximum thickness of the
hypertrophied wall in diastole was measured from the 2D right pa-
rasternal long- and short-axis views. Papillary muscle size and wall
motion (hypokinesis and asymmetry) were judged subjectively, and
all images were reviewed by the principal author. The right para-
sternal long-axis view was used to identify systolic anterior motion
of the mitral valve.
Doppler echocardiography (color, pulsed wave, and continuous
wave) was used to characterize flow disturbances, including dynam-
ic right ventricular outflow tract obstruction and dynamic
left ventricular outflow tract obstruction with associated mitral
insufficiency. The specific diagnosis for the type of myocardial dis-
ease or congenital disease was made with regard to previous
publications.14,37,38
Fig 1. The left atrial (LA)/aortic diameter (Ao) ratio was mea-
sured as shown. Ao is measured from the midpoint of the right
coronary cusp to the commisures of the left and noncoronary cusps
(inside edge to inside edge). LA is measured by continuing this line,
from inside edge to inside edge of the LA.
97Natriuretic Peptides in Cats

To obtain the E/Ea ratio, Doppler studies were performed from
the left apical 4-chamber view as previously described,29 except that
the data were analyzed off-line.d Ea was measured by placing the
pulsed wave cursor over the interventricular septumwith the sample
volume at the level of the mitral annulus. A vagal maneuver was
attempted in all cats (briefly occluding the cat’s nares with a finger)
to aid separation of early and late waveforms of mitral inflow and
mitral annulus motion (Fig 2a,b). When this was achieved (defined
as E velocity at the onset of the A wave o0.2m/s26), the E and Ea
wave velocities were used to calculate the ratio. If both transmitral
and DTI E and A waves were fused (summed E/A and Ea/Aa), then
the summated E/A and Ea/Aa waveform velocities were used to cal-
culate E/Ea, as described previously.29 The E/Ea ratio was not
calculated in cats in which there was discordance between transmi-
tral and DTI E/A waveforms (ie, where transmitral E/A waves were
fused but DTI Ea/Aa were separated), because summation is likely
to result in higher velocities.
One milliliter of blood was collected by jugular venipuncture into
serum gel tubes. The samples were left at room temperature for 20
minutes and then centrifuged. After separation, serum was stored at
�20 1C for between 1 and 6 weeks and then at �80 1C for a variable
period up to 6 months until analysis. SerumNT-proANP and serum
NT-proBNP concentrations were measured using sandwich enzyme
immunoassays utilizing horseradish peroxidase (HRP) colorimetric
end points for the quantitative determination of ANP and BNP in
serum.e,f The BNP assay uses immunoaffinity-purified sheep anti-
body for feline NT-proBNP. The sandwich comprises anti–
NT-proBNP (1–20) bound to the wells of the plate and anti–
NT-proBNP (60–80) conjugated to HRP. The ANP assay uses poly-
clonal sheep anti-human NT-proANP antibody. The sandwich
comprises anti–NT-proANP (10–19) precoated to the wells of the
plate and anti–NT-proANP (85–90) conjugated to HRP. Samples
were run as duplicates with the mean value used for the study.
Assay Validation
Serum samples from cats with known NP concentrations were
pooled to provide samples with low, medium, and high NP concen-
trations. These samples were then used to calculate intra- and
interassay coefficients of variation (CV) and to determine the preci-
sion and reproducibility of the assay. Serum samples were diluted by
the addition of sample diluent and the resulting measured NP con-
centration compared with the predicted concentration to evaluate
dilutional parallelism. The analytical sensitivity (minimum detec-
tion limit) was determined by reading the 1 3 standard deviation
(SD) response from 10 replicate measurements of the zero standard.
In addition, feline NT-proANP serum samples were spiked
with synthetic human NT-proANP and the recovery of the peptide
measured.
Statistical Analysis
The results were analyzed using a commercially available statis-
tical software package.g The age distribution of the 3 groups was
compared by the Kruskal–Wallis equality-of-populations rank test.
A w2 test was used to assess the difference of proportions of sex in
the 3 groups.
The concentrations of NT-proANP and NT-proBNP were not
normally distributed across groups, and the Kruskal–Wallis
equality-of-populations rank test was used. The strength of the
relationship between NT-proANP and NT-proBNP and their cor-
relations with E/Ea and LA/Ao ratio were assessed by Spearman’s
rank correlation coefficient (r). Receiver operator curves (ROC)
were derived for each of the natriuretic hormone concentrations and
the areas under the curve were calculated for each. ROC analysis
was performed for all possible pair combinations to assess the ca-
pacity of pro-ANP and pro-BNP concentrations to discriminate
cats in each of 3 clinical outcomes (healthy, HD � CHF, HD 1
CHF). These ROC analyses enabled estimation of the concentration
of hormone cut-off that would best classify cats correctly. Cut-off
concentrations for both NT-proANP and NT-proBNP were esti-
mated based on the highest percentage of correctly classified
observations. Other reported results were the AUC and the sensi-
tivity and specificity of correct classification. Pairwise comparisons
of the AUCs were made by testing the equality of 2 ROC areas ob-
tained. A logistic regression model was used to assess the effect of
the concentrations of urea and creatinine on the concentrations of
natriuretic hormones. A maximum logistic regression model was
specified that included disease status as a binary outcome variable
and hormone, urea, and creatinine concentrations as explanatory
variables. The effect of retaining or dropping variables from the
model was assessed using Akaike’s Information Criteria (AIC)
scores. The AIC scores are statistical criteria that enable logistic re-
gression model comparisons; the smaller the AIC score, the better
the model.
Results
Animals
There were 78 cats of 11 breeds; they included 56 do-mestic short hair, 8 domestic long hair, 3 Persian, and 3Siamese cats. The groups comprised healthy control cats(n 5 28), HD� CHF cats (n 5 17), and HD 1 CHF cats(n 5 33). The mean age � SD of all cats in the study was
Fig 2. (a) Doppler pulse wave interrogation of mitral inflow show-
ing the E (passive ventricular filling) and A (active ventricular
filling) waveforms. (b) Interrogation of longitudinal septal mitral
annulus motion using pulse wave Doppler tissue imaging. The 2
waveforms Ea and Aa that represent tissue motion in early and late
diastole are visible.
98 Connolly et al

7.2 � 4.5 years (range, 1–19 years). The mean age for thecontrol group was 7.0 � 5.0 years (range, 6 months – 19years), for HD � CHF cats 6.3 � 3.6 years (range, 1–14years), and for HD 1 CHF cats 7.6� 4.6 years (range, 1–15 years). There were no significant differences in ageamong the 3 groups (P � .05).There were 54 male cats, with a higher proportion of
male cats in the study group (40) than in the controlgroup (14) (P4.05). The mean body weight of normalcats was similar in all 3 groups (P4.05) at 4.3 kg (95%CI: 3.97–4.6) for control cats, 4.4 kg (95% CI: 3.82–4.94)for HD � CHF cats, and 4.6 kg (95% CI: 4.25–4.98) forHD 1 CHF cats.The diagnoses in the study group included HCM, hy-
pertrophic obstructive cardiomyopathy, or both (n536);restrictive cardiomyopathy (RCM, n510); dilated card-iomyopathy (n51); mitral dysplasia (n51); double-chambered right ventricle (n51); and idiopathic third-degree atrio-ventricular block (n51). Of the HD � CHFcats, 4 had RCM and 13 had HCM. In the HD 1 CHFgroup, 6 cats had RCM and 23 had HCM.Cats were classified according to the International Re-
nal Interest Society classification of chronic renalinsufficiency.39 Of the 33 HD 1 CHF cats, 6 (18.2%)were classified as stage II (mild azotemia) with serumcreatinine concentration o2.8mg/dL (reference range,1.21–2.18) and 5 (15.2%) were classified as stage III(moderate azotemia) with serum creatinine concentra-tion between 2.8 and 5.0mg/dL.39
Serum total T4 concentration was measured in 5 of thecontrol cats, and was within the reference range for thelaboratories used by the 2 different practices. Serum totalT4 concentration was measured in 15 cats in the studygroup, with results from 8.3 to 61 nmol/L (referencerange, 19–65 nmol/L). Five of the cats had a T4 concen-tration below the normal reference range; 3 of these catshad CHF. Systolic blood pressure was measured in 31 ofthe study cats (range, 85–190mmHg) and was increased(systolic arterial pressure4175mmHg)40 in 2 of the cats.Blood pressure was not measured in any of the controlcats.
Diagnostic Tests
The limit of detection of the NT-proANP assay was145 fmol/mL. The intra-assay CVs (n 5 6) were 8.1, 7.5,and 4.9% and the interassay CVs (n 5 6) were 13.6, 8.7,and 20.7% for samples with low (274 fmol/mL), medium(791 fmol/mL), and high (2,584 fmol/mL) NT-proANPconcentrations, respectively. Spiking feline plasma sam-ples (n 5 6) with 1,095 fmol/mL human NT-proANPyielded an average recovery of 100% (range, 92–107%).The limit of detection of the NT-proBNP assay was
7.0 fmol/mL. The intra-assay CVs (n 5 20) were 13.1,10.1, and 7.0%, and the interassay CVs (n 5 3) were 15.3,12.2, and 7.7% for samples with low (112.2 fmol/mL),medium (276.0 fmol/mL), and high (854.1 fmol/mL) NT-proBNP concentrations, respectively. The NT-proBNPdilution parallelism indicated a mean recovery of 148%.Spiking of feline serum with humanNT-proBNP was notperformed.
Serum NT-proANP and NT-proBNP Concentrations
The mean and ranges of NT-proANP and NT-pro-BNP concentrations in the 3 groups are shown in Table 1and Figure 3a,b. We found a positive linear relationship
Table 1. The mean and the 95% CI of serumNT-proANP and serum NT-proBNP concentrationsobtained for cats in the control group, for cats with HDwithout heart failure (HD � CHF cats), and cats withheart failure (HD 1 CHF cats).
Group of cats
NT-proANP (fmol/mL) NT-proBNP (fmol/mL)
Median (95% CI) Median (95% CI)
Control 682 (530.2–833.8) 33.6 (11.2–56.1)
HD � CHF 1176.4 (809.96–1542.85) 184.1 (111.03–257.08)
HD 1 CHF 1865.03 (1499.3–2230.7) 524.7 (437.2–612.3)
95% CI, 95% confidence interval; NT-proANP, N-terminal frag-
ment of proatrial natriuretic peptide; NT-proBNP, NT-probrain
natriuretic peptide; HD, heart disease; CHF, congestive heart failure.
5,000
1,000
800
600
400
200
0
4,000
3,000
2,000
NT
-pro
BN
P (
fmo
l/ml)
NT
-pro
BN
P (
fmo
l/ml)
Control group Study group
Control group Study group
1,000
0
a
b
Fig 3. (a) Box-and-whiskers plots for the distribution of serum
N-terminal fragment of proatrial natriuretic peptide (NT-proANP)
concentration in 28 control cats and 50 study cats, showing lowest
observations, lower quartiles, medians, upper quartiles, lowest
scores (1.5 times the length of the interquartile range), and outliers.
(b) Box-and-whiskers plots for the distribution of serum N-terminal
probrain natriuretic peptide (NT-proBNP) concentration in 28 con-
trol cats and 50 study cats, showing lowest observations, lower
quartiles, medians, upper quartiles, lowest scores (1.5 times the
length of the inter-quartile range), upper observation, and outliers.
99Natriuretic Peptides in Cats
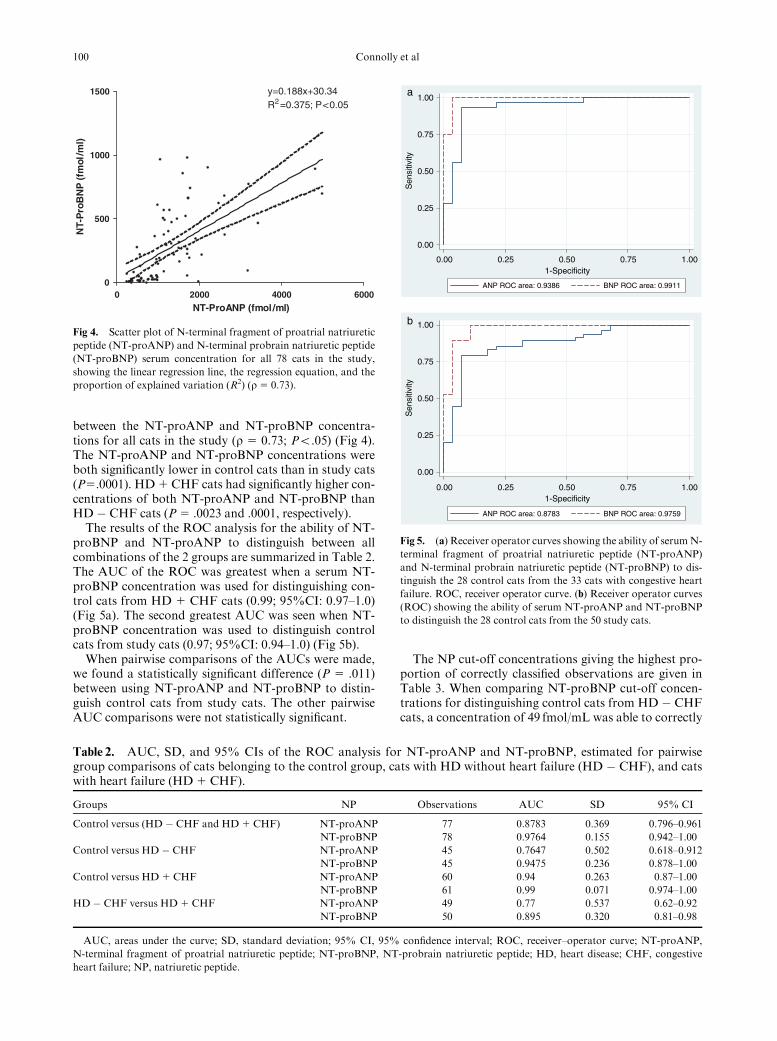
between the NT-proANP and NT-proBNP concentra-tions for all cats in the study (r 5 0.73; Po.05) (Fig 4).The NT-proANP and NT-proBNP concentrations wereboth significantly lower in control cats than in study cats(P5.0001). HD 1 CHF cats had significantly higher con-centrations of both NT-proANP and NT-proBNP thanHD � CHF cats (P 5 .0023 and .0001, respectively).The results of the ROC analysis for the ability of NT-
proBNP and NT-proANP to distinguish between allcombinations of the 2 groups are summarized in Table 2.The AUC of the ROC was greatest when a serum NT-proBNP concentration was used for distinguishing con-trol cats from HD 1 CHF cats (0.99; 95%CI: 0.97–1.0)(Fig 5a). The second greatest AUC was seen when NT-proBNP concentration was used to distinguish controlcats from study cats (0.97; 95%CI: 0.94–1.0) (Fig 5b).When pairwise comparisons of the AUCs were made,
we found a statistically significant difference (P 5 .011)between using NT-proANP and NT-proBNP to distin-guish control cats from study cats. The other pairwiseAUC comparisons were not statistically significant.
The NP cut-off concentrations giving the highest pro-portion of correctly classified observations are given inTable 3. When comparing NT-proBNP cut-off concen-trations for distinguishing control cats from HD � CHFcats, a concentration of 49 fmol/mL was able to correctly
0 2000 4000 60000
500
1000
1500 y=0.188x+30.34R =0.375; P<0.05
NT-ProANP (fmol /ml)
NT-
Pro
BN
P (
fmol
/ml)
Fig 4. Scatter plot of N-terminal fragment of proatrial natriuretic
peptide (NT-proANP) and N-terminal probrain natriuretic peptide
(NT-proBNP) serum concentration for all 78 cats in the study,
showing the linear regression line, the regression equation, and the
proportion of explained variation (R2) (r 5 0.73).
Table 2. AUC, SD, and 95% CIs of the ROC analysis for NT-proANP and NT-proBNP, estimated for pairwisegroup comparisons of cats belonging to the control group, cats with HD without heart failure (HD � CHF), and catswith heart failure (HD 1 CHF).
Groups NP Observations AUC SD 95% CI
Control versus (HD � CHF and HD 1 CHF) NT-proANP 77 0.8783 0.369 0.796–0.961
NT-proBNP 78 0.9764 0.155 0.942–1.00
Control versus HD � CHF NT-proANP 45 0.7647 0.502 0.618–0.912
NT-proBNP 45 0.9475 0.236 0.878–1.00
Control versus HD 1 CHF NT-proANP 60 0.94 0.263 0.87–1.00
NT-proBNP 61 0.99 0.071 0.974–1.00
HD � CHF versus HD 1 CHF NT-proANP 49 0.77 0.537 0.62–0.92
NT-proBNP 50 0.895 0.320 0.81–0.98
AUC, areas under the curve; SD, standard deviation; 95% CI, 95% confidence interval; ROC, receiver–operator curve; NT-proANP,
N-terminal fragment of proatrial natriuretic peptide; NT-proBNP, NT-probrain natriuretic peptide; HD, heart disease; CHF, congestive
heart failure; NP, natriuretic peptide.
0.00
0.25
0.50
0.75
1.00
Sen
sitiv
ity
0.00 0.25 0.50 0.75 1.001-Specificity
0.00 0.25 0.50 0.75 1.001-Specificity
a
b
0.00
0.25
0.50
0.75
1.00
Sen
sitiv
ity
Fig 5. (a) Receiver operator curves showing the ability of serumN-
terminal fragment of proatrial natriuretic peptide (NT-proANP)
and N-terminal probrain natriuretic peptide (NT-proBNP) to dis-
tinguish the 28 control cats from the 33 cats with congestive heart
failure. ROC, receiver operator curve. (b) Receiver operator curves
(ROC) showing the ability of serum NT-proANP and NT-proBNP
to distinguish the 28 control cats from the 50 study cats.
100 Connolly et al

classify 96.2% of the observations with a sensitivity andspecificity of 100 and 89.3%, respectively. Using a cut-offof 10 fmol/mL, the sensitivity was 100% but the specific-ity decreased to 14.3%; with a cut-off of 468 fmol/mL,the specificity increased to 100% but the sensitivitydecreased to 11.8%.A statistically significant positive correlation was seen
between the LA/Ao and the E/Ea ratio obtained for allstudy cats (r 5 0.57; Po.05) (Fig 6). The LA/Ao ratiowas significantly higher (Po.05) in HD 1 CHF cats at2.21 (range, 2.02–2.39) compared with 1.70 (range, 1.53–1.87) in HD � CHF cats. The E/Ea ratio was also higherin HD 1 CHF cats at 24.12 (range, 19.9–28.34) and at12.1 (range, 10.2–13.9) than in HD� CHF cats (Po.05).Both the NT-proANP and NT-proBNP concentra-
tions were significantly positively correlated with theLA/Ao and E/Ea ratios (Fig 7a,b). The correlation be-tween NT-proBNP concentration and LA/Ao and E/Ea
ratios was greater than that for NT-proANP concentra-
Table 3. Sensitivity and specificity of classification for the NT-proANP and NT-proBNP cut-off values with thehighest percentage of correct classification estimated for pairwise group comparisons of cats belonging to the controlgroup, cats with HD without heart failure (HD � CHF), and cats with heart failure (HD 1 CHF).
Groups NP
Cut-off value
(fmol/mL)
Correctly
classified (%)
Sensitivity
(%)
Specificity
(%)
Control versus (HD � CHF and
HD 1 CHF)
NT-proANP 960 83.12 83.67 82.14
NT-proBNP 49 96.15 100.0 89.29
Control versus HD � CHF NT-proANP 828 67.86 76.47 71.11
NT-proBNP 49 93.33 100.0 89.29
Control versus HD 1 CHF NT-proANP 919 88.33 96.88 78.57
NT-proBNP 148 96.43 96.97 96.72
HD � CHF versus HD 1 CHF NT-proANP 1250 73.47 75.00 70.59
NT-proBNP 220 86.00 93.94 70.59
NT-proANP, N-terminal fragment of proatrial natriuretic peptide; NT-proBNP, NT-probrain natriuretic peptide; HD, heart disease;
CHF, congestive heart failure; NP, natriuretic peptide.
0 10 20 30 40 500
1
2
3
4 y=6.399x+5.59R =0.148; P<0.05
E/Ea ratio
LA
/Ao
rat
io
Fig 6. Scatter plot of 36 paired measurements of left atrial (LA)/
aortic diameter (Ao) ratio and the Doppler-derived E/Ea ratio in
study cats, showing the linear regression line, the regression equa-
tion, and the proportion of explained variation (R2) (r 5 0.57).
0 2000 4000 60000
10
20
30
40
50 y=0.0034x+13.82R =0.096; P<0.05
NT-ProANP (fmol/ml)
E/E
a ra
tio
0 200 400 600 800 1000 12000
10
20
30
40
50 y=0.0237x+10.07R =0.4904 P<0.05
NT-ProBNP (fmol/ml)
E/E
a ra
tio
a
b
Fig 7. (a) Scatter plot of 35 paired measurements in study cats of
N-terminal fragment of proatrial natriuretic peptide (NT-proANP)
concentration and the E/Ea ratio, showing the regression line and
95% CIs of the line, the regression equation, and the proportion of
explained variation (R2) (r 5 0.59). (b) Scatter plot of 36 paired
measurements in study cats of N-terminal probrain natriuretic pep-
tide (NT-proBNP) concentration and the E/Ea ratio, showing the
regression line, regression equation, and the proportion of ex-
plained variation (R2) (r 5 0.68).
101Natriuretic Peptides in Cats

tions. The highest correlation was seen between NT-pro-BNP and the E/Ea ratio (r 5 0.68; P o .05) (Fig 7b).The concentrations of urea and creatinine were found
to act as potential confounding factors on the circulatingconcentrations of both hormones as expressed by a re-duction of the AIC score from 23.5 to 8.9 after inclusionof both variables in the logistic regression model.
Discussion
The results of this study indicate that both serum NT-proANP and serum NT-proBNP concentrations can beused to distinguish cats with HD from healthy controls.The increase in serum NT-proANP and NT-proBNPconcentrations with HD shown in Fig 3a,b suggests thatboth tests may be clinically useful. These findings areconsistent with previously published studies in dogs andhumans.17,20,21 The pairwise comparisons of the AUCsidentified a statistically significant difference (P 5 .011)between NT-proANP and NT-proBNP to distinguishcontrol cats from study cats (Fig 5b) in favor of NT-pro-BNP. Although the other pairwise AUC comparisonswere not statistically significant, this may be a conse-quence of the small group numbers. If a larger number ofcats had been available, a statistical difference in theAUC between NT-proANP and NT-proBNP for theother ROC curves may have been observed.One possible reason as to why NT-pro-BNP appears
to perform better is that the BNP assay uses antibodyraised against feline-specific NT-ProBNP peptide, where-as the ANP assay uses antibody raised against the humanpeptide. Although the ANP sequence is highly conservedacross mammalian species, amino acid differences arepresent between feline and human NT-proANP, and it ispossible that this difference may reduce the sensitivityand specificity of the test.10 An alternative explanationmay be that myocardial disease in cats frequently resultsin marked diastolic dysfunction and substantial remod-eling of the left ventricle, especially in cats with HCM.Indeed, previous studies have shown that this remodelingis accompanied by sufficient myocardial cell damage tocause an associated increase in serum cardiac troponin Iconcentrations.41,42 This chronic left ventricular remod-eling is likely to induce increased BNP protein synthesisin the ventricles as a result of increased left ventricularend-diastolic pressure, which would be detectable bymeasuring NT-proBNP in the serum of affected cats. Infact, immunohistochemistry of ANP and BNP in the fe-line myocardium has confirmed upregulation of BNP butnot ANP in cats with HCM.3
With regard to distinguishing cats with CHF fromcontrols, both assays performed well. The most likely ex-planation for the improved performance of ANP in thisparticular analysis is that cats in CHF invariably haveenlarged left atria, and the associated left atrial wallstress acts as a stimulus for ANP release. This stimuluswill be decreased or absent in cats with HD but no signsof CHF, which would explain why NT-proANP per-formed less well than NT-proBNP in distinguishing HD� CHF cats from controls. Furthermore, the ability ofserum NT-proBNP to outperform NT-proANP with
respect to this cohort may be related to its increasedsynthesis as a result of increased left ventricular diastolicpressure. This would support the use of NT-proBNP as apotential initial screening test to identify HD in breedinganimals, but additional trials are required beforedefinitive recommendations can be made. A cut-off con-centration of 49 fmol/mL for serum NT-proBNPcorrectly classified 96% of control and study cats with asensitivity of 100% and a specificity of 89.3%. Theseresults suggest that using this concentration in a screen-ing test rigorously identifies diseased animals, and alsoidentifies some false positives. Consequently, it would beprudent to follow up positive cats with a more specifictest such as echocardiography to confirm their diseasestatus. Interestingly, it has been shown in dogs that BNPcan detect occult myocardial disease before the onset ofobvious hemodynamic disturbances. This was demon-strated in a colony of Golden retrievers with occultmuscular dystrophy cardiomyopathy in which increasedcirculating BNP concentrations were identified in dogswith occult disease than in controls.43 In the presentstudy, serum NT-proBNP was used to distinguish catswith cardiac disease from healthy controls rather thanfrom cats with other conditions such as primary respira-tory disease. It is possible that if the test were used todistinguish cats with HD from healthy cats as well asthose with other noncardiac diseases, the accuracy maynot be as high as reported here.
The significant increase in serum NT-proANP andNT-proBNP in study cats over controls in this study issimilar to the finding of a previous study using both anenzyme-linked immunoassay and a radioimmunoassayfor ANP and a radioimmunoassay for BNP, but ROCanalysis was not reported.a In a recent report, plasmaNT-proANP immunoreactivity was compared betweencats with and without HCM. No significant differencewas identified between the 2 study groups, but unlike thepresent study, the majority of the HCM group wereasymptomatic.15
The E/Ea ratio has been used as an estimate of leftventricular filling pressure in studies of dogs and hu-mans,26–29 including human patients with HCM.31 Asignificant positive correlation was identified betweenthe E/Ea and LA/Ao ratios in the study group (Fig 6).This indicates that cats with increased left ventricular enddiastolic pressure estimated by E/Ea also have enlargedLA, and suggests that both ratios may be useful indica-tors of left ventricular diastolic dysfunction and diseaseseverity in the cat. However, these results do not allowthe E/Ea ratio to be properly validated in cats with HCMbecause no direct pressure measurements were recorded.Furthermore, validation also requires the inclusion ofthese measurements from the control group, which wasnot done in this study.
The NT fragments of ANP and BNP are at least inpart excreted by the kidneys; circulating concentrationsof these peptides therefore may be influenced by renalfunction. One study determined that dogs with chronicrenal failure have a 2-fold higher plasma carboxy-termi-nal ANP concentration than healthy dogs.16 Humanpatients with renal disease were found to have increased
102 Connolly et al

BNP concentrations,44 and in humans, glomerular filtra-tion rate has been shown to be negatively correlated withboth ANP and BNP.45 The effect of renal function onNP concentrations in the cat has not been reported andwas not evaluated in the present study. Therefore, theobserved higher NP concentrations in HD 1 CHF catsthan in HD � CHF cats may be explained (at least inpart) by impairment of renal function. This impairmentmay be treatment-induced in some cases. At present, it isnot possible to separate the effect of renal function onserum NT-proANP and NT-proBNP concentrationsfrom the effect of worsening HD, nor is it possible toquantify the effect of renal impairment on NP concen-trations. Nevertheless, the results indicate that NT-proBNP, and to a lesser extent NT-proANP, can clearlydistinguish HD � CHF cats (all but 1 of which hadserum urea and creatinine concentrations within thenormal range) from controls. It therefore is likely thatprogression of HD in cats with CHF is the main stimulusfor NP secretion.
Study Limitations
The samples were stored at �20 1C for a variable peri-od no longer than 2 weeks, and at �80 1C for a variableperiod up to 6 months. Unpublished studies performedby 1 of the authors (L.C.) indicate that both peptidesappear stable at �20 1C for 4 6 months. With regard tothe storage of NT-proBNP, these finding are similarto a previous publication46; hence, it is unlikely that thestorage method used in this study would have had amajor effect on the serum concentrations measured.The dilution parallelism for the NT-proBNP assay
indicates a greater than expected recovery. Repeat anal-ysis gave the same results, and may suggest that inaddition to the test peptide, other related peptides arebeing detected. However, the results from the ROC anal-ysis strongly imply that the test remains clinically usefulwith a high degree of accuracy, despite the suboptimaldilution parallelism analysis.A single NT-proANP/NT-proBNP measurement was
made for each cat during the study, and no attempt wasmade to assess the effect of daily variation in concentra-tions, stage of disease, or severity of myocardialremodeling. Furthermore, the influence of medicationon peptide concentrations was not analyzed.The echocardiographic studies were performed by
3 different but equally experienced clinicians working inthe referral clinic. This may have introduced someadditional study variation, although all images and mea-surements were reviewed by the principal author.The E and Ea Doppler measurements were taken from
different echocardiographic time frames. Breathing andintrinsic cardiac forces result in translational movementsof the heart within the thorax, and such movementcan lead to some variation in the amplitude of the DTIwaveforms.The control group of cats did not undergo an echocar-
diographic examination, and although no abnormalitieswere detected on thorough physical and careful cardiacexaminations, HD cannot be completely ruled out. In the
same way, hypertensive HD cannot be ruled out, becauseblood pressure was not measured in any of the controlcats.
E/Ea and LA/Ao measurements were not performed inthe control group, and it is likely that if we had includedthese measurements, the correlation coefficient would bedifferent. Interpretation of this analysis therefore is validonly for the diseased cats (HD � CHF and HD 1 CHFgroups).
Two study cats had a systolic blood pressure 4175mmHg. Both resented having the procedure per-formed and unfortunately were lost to follow-up, andrepeat measurements were not obtained. Neither cat un-derwent a retinal examination. Furthermore, bloodpressure was measured in only 31/50 of the study catsand it is possible that some of these cats had hypertensivecardiomyopathy rather than HCM.
In conclusion, despite these limitations, we found thatmeasurement of serum NT-proANP and NT-proBNPconcentrations allowed cats with HD to be clearly distin-guished from normal controls. Furthermore, both NPsclearly differentiated HD � CHF from HD 1 CHF cats.In addition, measurement of serum NT-proBNP also al-lowed HD � CHF cats to be differentiated from healthycontrols. Serum NT-proBNP may prove useful as aninitial screening test for HCM in cats.
Footnotes
a Sisson DD, Oyama MA, Solter PF. Plasma levels of ANP, BNP,
epinephrine, norepinephrine, serum aldosterone, and plasma ren-
nin activity in healthy cats and cats with myocardial disease. J Vet
Intern Med 2003; 17: 483bUltrasonic Doppler flow detector model 811-B, Parks Medical
Electronics, Aloha, ORcVivid 7, GE Vingmed Ultrasound A/S, Horten, NorwaydEcho Pac 7 for Vivid 7, GE Vingmed Ultrasound A/Se proANP(1-98) Guildhay Ltd, Biomedica Guildford, Surrey, UKfFeline Cardioscreen NT-proBNP Guildhay Ltd, Biomedica Guild-
fordg Stata Statistical Software: Release 9, StataCorp LP, College
Station, TX
Acknowledgments
We acknowledge Andria Cauvin, Anita Notenboom,Simon Dennis, and Simon Swift.
References
1. Wilkins MR, Redondo J, Brown LA. The natriuretic-peptide
family. Lancet 1997;349:1307–1310.
2. Arteaga E, Araujo AQ, Buck P, et al. Plasma amino-terminal
pro–B-type natriuretic peptide quantification in hypertrophic card-
iomyopathy. Am Heart J 2005;150:1228–1232.
3. Biondo AW, Ehrhart EJ, Sisson DD, et al. Immunohisto-
chemistry of atrial and brain natriuretic peptides in control cats
and cats with hypertrophic cardiomyopathy. Vet Pathol 2003;40:
501–506.
103Natriuretic Peptides in Cats

4. Tsutamoto T, Wada A, Maeda K, et al. Attenuation of com-
pensation of endogenous cardiac natriuretic peptide system in
chronic heart failure: Prognostic role of plasma brain natriuretic
peptide concentration in patients with chronic symptomatic left
ventricular dysfunction. Circulation 1997;96:509–516.
5. Maisel A, Hollander JE, Guss D, et al. Primary results of the
Rapid Emergency Department Heart Failure Outpatient Trial
(REDHOT). A multicenter study of B-type natriuretic peptide lev-
els, emergency department decision making, and outcomes in
patients presenting with shortness of breath. J Am Coll Cardiol
2004;44:1328–1333.
6. Jefferies JL, Denfield SW, Price JF, et al. A prospective eval-
uation of nesiritide in the treatment of pediatric heart failure.
Pediatr Cardiol 2006;27:402–407.
7. McGrath MF, de Bold ML, de Bold AJ. The endocrine func-
tion of the heart. Trends Endocrinol Metab 2005;16:469–477.
8. Yasue H, Yoshimura M, Sumida H, et al. Localization and
mechanism of secretion of B-type natriuretic peptide in comparison
with those of A-type natriuretic peptide in normal subjects and pa-
tients with heart failure. Circulation 1994;90:195–203.
9. Buckley MG, Marcus NJ, Yacoub MH. Cardiac peptide sta-
bility, aprotinin and room temperature: Importance for assessing
cardiac function in clinical practice. Clin Sci (London) 1999;97:689–
695.
10. Sisson DD. Neuroendocrine evaluation of cardiac disease.
Vet Clin North Am Small Anim Pract 2004;34:1105–1126.
11. Moro C, Berlan M. Cardiovascular and metabolic effects of
natriuretic peptides. Fundam Clin Pharmacol 2006;20:41–49.
12. Poutanen T, Tikanoja T, Jaaskelainen P, et al. Diastolic dys-
function without left ventricular hypertrophy is an early finding in
children with hypertrophic cardiomyopathy-causing mutations in
the beta-myosin heavy chain, alpha-tropomyosin, and myosin-
binding protein C genes. Am Heart J 2006;151:725 e721–725 e729.
13. Buchanan J. Prevalence of cardiovascular disorders. In: Fox
P, Sisson D, Moise N, eds. Textbook of Canine and Feline Cardi-
ology, 2nd ed. Philadelphia, PA: WB Saunders; 1999:457–470.
14. Fox P. Feline cardiomyopathies. In: Fox P, Sisson D, Moise
N, eds. Textbook of Canine and Feline Cardiology, 2nd ed. Phila-
delphia, PA: WB Saunders; 1999:621–678.
15. MacLean HN, Abbott JA, Ward DL, et al. N-terminal atrial
natriuretic peptide immunoreactivity in plasma of cats with hyper-
trophic cardiomyopathy. J Vet Intern Med 2006;20:284–289.
16. Vollmar AM, Reusch C, Kraft W, et al. Atrial natriuretic
peptide concentration in dogs with congestive heart failure, chronic
renal failure, and hyperadrenocorticism. Am J Vet Res 1991;52:
1831–1834.
17. Haggstrom J, Hansson K, Karlberg BE, et al. Plasma con-
centration of atrial natriuretic peptide in relation to severity of
mitral regurgitation in Cavalier King Charles Spaniels. Am J Vet
Res 1994;55:698–703.
18. Yoshimura M, Yasue H, Ogawa H. Pathophysiological sig-
nificance and clinical application of ANP and BNP in patients with
heart failure. Can J Physiol Pharmacol 2001;79:730–735.
19. Yoshimura M, Yasue H, Okumura K, et al. Different secre-
tion patterns of atrial natriuretic peptide and brain natriuretic
peptide in patients with congestive heart failure. Circulation 1993;
87:464–469.
20. Clerico A, Iervasi G, Del ChiccaMG, et al. Circulating levels
of cardiac natriuretic peptides (ANP and BNP) measured by highly
sensitive and specific immunoradiometric assays in normal subjects
and in patients with different degrees of heart failure. J Endocrinol
Invest 1998;21:170–179.
21. MacDonald KA, Kittleson MD, Munro C, et al. Brain nat-
riuretic peptide concentration in dogs with heart disease and
congestive heart failure. J Vet Intern Med 2003;17:172–177.
22. Haggstrom J, Hansson K, Kvart C, et al. Effects of naturally
acquired decompensated mitral valve regurgitation on the renin–
angiotensin–aldosterone system and atrial natriuretic peptide
concentration in dogs. Am J Vet Res 1997;58:77–82.
23. Raine AE, Erne P, Burgisser E, et al. Atrial natriuretic
peptide and atrial pressure in patients with congestive heart failure.
N Engl J Med 1986;315:533–537.
24. Parsonage WA, Galbraith AJ, Koerbin GL, et al. Value of
B-type natriuretic peptide for identifying significantly elevated
pulmonary artery wedge pressure in patients treated for established
chronic heart failure secondary to ischemic or idiopathic dilated
cardiomyopathy. Am J Cardiol 2005;95:883–885.
25. Asano K, Masuda K, Okumura M, et al. Plasma atrial and
brain natriuretic peptide levels in dogs with congestive heart failure.
J Vet Med Sci 1999;61:523–529.
26. Schober KE, Fuentes VL, Bonagura JD. Comparison be-
tween invasive hemodynamic measurements and noninvasive
assessment of left ventricular diastolic function by use of Doppler
echocardiography in healthy anesthetized cats. Am J Vet Res 2003;
64:93–103.
27. Ommen SR, Nishimura RA, Appleton CP, et al. Clinical
utility of Doppler echocardiography and tissue Doppler imaging in
the estimation of left ventricular filling pressures: A comparative
simultaneous Doppler-catheterization study. Circulation 2000;102:
1788–1794.
28. Kim YJ, SohnDW.Mitral annulus velocity in the estimation
of left ventricular filling pressure: Prospective study in 200 patients.
J Am Soc Echocardiogr 2000;13:980–985.
29. OyamaMA, Sisson DD, Bulmer BJ, et al. Echocardiograph-
ic estimation of mean left atrial pressure in a canine model
of acute mitral valve insufficiency. J Vet Intern Med 2004;18:
667–672.
30. Nagueh SF, Middleton KJ, Kopelen HA, et al. Doppler tis-
sue imaging: A noninvasive technique for evaluation of left
ventricular relaxation and estimation of filling pressures. J Am Coll
Cardiol 1997;30:1527–1533.
31. Nagueh SF, Lakkis NM, Middleton KJ, et al. Doppler esti-
mation of left ventricular filling pressures in patients with
hypertrophic cardiomyopathy. Circulation 1999;99:254–261.
32. Koffas H, Dukes-McEwan J, Corcoran BM, et al. Pulsed
tissue Doppler imaging in normal cats and cats with hypertrophic
cardiomyopathy. J Vet Intern Med 2006;20:65–77.
33. Carlos Sampedrano C, Chetboul V, Gouni V, et al. Systolic
and diastolic myocardial dysfunction in cats with hypertrophic
cardiomyopathy or systemic hypertension. J Vet Intern Med 2006;
20:1106–1115.
34. ThomasWP, Gaber CE, Jacobs GJ, et al. Recommendations
for standards in transthoracic two-dimensional echocardiography
in the dog and cat. Echocardiography Committee of the Specialty of
Cardiology, American College of Veterinary Internal Medicine. J
Vet Intern Med 1993;7:247–252.
35. Hansson K, Haggstrom J, Kvart C, et al. Left atrial to aortic
root indices using two dimensional and M-mode echocardiography
in Cavalier King Charles spaniels with and without left atrial en-
largement. Vet Radiol Ultrasound 2002;43:568–575.
36. Kienle RD Echocardiography. In: Kittleson MD, Kienle
RD, eds. Small Animal Cardiovascular Medicine. St Louis, MO:
Mosby Inc; 1998:95–117.
37. Fox PR. Hypertrophic cardiomyopathy. Clinical and patho-
logic correlates. J Vet Cardiol 2003;5:39–44.
38. Fox PR. Endomyocardial fibrosis and restrictive card-
iomyopathy: Pathologic and clinical features. J Vet Cardiol
2004;6:25–31.
39. Syme HM, Markwell PJ, Pfeiffer D, et al. Survival of cats
with naturally occurring chronic renal failure is related to severity of
proteinuria. J Vet Intern Med 2006;20:528–535.
40. Syme HM, Barber PJ, Markwell PJ, et al. Prevalence of sys-
tolic hypertension in cats with chronic renal failure. J Am Vet Med
Assoc 2002;220:1799–1804.
104 Connolly et al

41. ConnollyDJ, Cannata J, BoswoodA, et al. Cardiac troponin I
in cats with hypertrophic cardiomyopathy. J Feline Med Surg 2003;
5:209–216.
42. Herndon WE, Kittleson MD, Sanderson K, et al. Cardiac
troponin I in feline hypertrophic cardiomyopathy. J Vet InternMed
2002;16:558–564.
43. Chetboul V, Tessier-Vetzel D, Escriou C, et al. Diagnostic
potential of natriuretic peptides in the occult phase of Golden re-
triever muscular dystrophy cardiomyopathy. J Vet Intern Med
2004;18:845–850.
44. Mueller C, Laule-KilianK, Scholer A, et al. B-type natriuretic
peptide for acute dyspnoea in patients with kidney disease: Insights
from a randomized comparison. Kidney Int 2005;67:278–284.
45. Mark PB, Stewart GA, Gansevoort RT, et al. Diagnostic
potential of circulating natriuretic peptides in chronic kidney dis-
ease. Nephrol Dial Transplant 2006;21:402–410.
46. Meuller T, Gegenhuber A, Dieplinger B, et al. Long-term
stability of endogenous B-type natriuretic peptide (BNP) and amino
terminal proBNP (NT-proBNP) in frozen plasma samples. Clin
Chem Lab Med 2004;42:942–944.
105Natriuretic Peptides in Cats