From diffusion tractography to quantitative white matter tract measures: a reproducibility study
12
From diffusion tractography to quantitative white matter tract measures: a reproducibility study O. Ciccarelli, a G.J.M. Parker, b A.T. Toosy, a C.A.M. Wheeler-Kingshott, a G.J. Barker, a P.A. Boulby, c D.H. Miller, a and A.J. Thompson a, * a NMR Research Unit, Institute of Neurology, University College London, Queen Square, London, WC1N 3BG, UK b Imaging Science and Biomedical Engineering, University of Manchester, Oxford Road, Manchester M13 9PT, UK c MRI Unit, National Society for Epilepsy, Chalfont St. Peter, Gerrards Cross, Buckinghanshire, SL9 0RJ, UK Received 13 March 2002; revised 12 September 2002; accepted 21 October 2002 Abstract The aim of this study is to propose methods for assessing the reproducibility of diffusion tractography algorithms in future clinical studies and to show their application to the tractography algorithm developed in our unit, fast marching tractography (FMT). FMT estimates anatomical connectivity between brain regions using the information provided by diffusion tensor imaging. Three major white-matter pathways were investigated in 11 normal subjects—anterior callosal fibers, optic radiations, and pyramidal tracts. FMT was used to generate maps of connectivity metric, and regions of voxels with highest connectivity metric to an anatomically defined starting point were identified for each tract under investigation. The reproducibilities of tract-“normalized” volume (NV) and fractional anisotropy (FA) measurements were assessed over such regions. The values of tract volumes are consistent with the postmortem data. Coefficients of variation (CVs) for FA and NV ranged from 1.7 to 7.1% and from 2.2 to 18.6%, respectively. CVs were lowest in the anterior callosal fibers (range: 1.7– 7.8%), followed by the optic radiations (range: 1.2–18.6%) and pyramidal tracts (range: 2.6 –15.5%), suggesting that fiber organization plays a role in determining the level of FMT reproducibility. In conclusion, these findings underline the importance of assessing the reliability of diffusion tractography before investigating white matter pathology. © 2003 Elsevier Science (USA). All rights reserved. Introduction Diffusion tensor imaging (DTI) is an MRI technique that provides information about the random thermal motion of water molecules in vivo (Basser et al., 1994). In human tissues, water diffusion is not free in all directions but hindered and restricted by the presence of barriers, includ- ing cell cytostructure and membranes. For example, in the white matter regions of the brain, where the neuronal pro- jections or axons are similarly aligned, water diffusion is generally greater in the direction parallel to axons than perpendicular to them. This property is termed diffusion anisotropy (Moseley et al., 1990; Chenevert et al., 1990). In contrast, in the gray matter regions, which are characterized by a less ordered tissue structure, diffusion tends to be less anisotropic and more uniform in all directions. Therefore, DTI allows in vivo identification of white matter and gray matter regions and it has been used in these areas to study pathological changes, including those occurring in multiple sclerosis (Horsfield et al., 1998; Tievsky et al., 1999; Wer- ring et al., 1999; Ciccarelli et al., 2001), tumors (Wiesh- mann et al., 1999; Bastin et al., 1999; Inglis et al., 1999), amyotrophic lateral sclerosis (Ellis et al., 1999), cerebral ischemia (Chabriat et al., 1999; Sorensen et al., 1999; Jones et al., 1999b; Helenius et al., 2002), and developmental malformations of the cortex (Eriksson et al., 2001). Since DTI is able to detect at the macroscopic scale of a voxel the extent of directional bias of diffusion occurring at the microscopic level, it can distinguish between regions where fibers are highly aligned in the voxel from those where fibers are less coherent. However, although DTI provides directional information at the voxel level, it pro- vides no explicit information about the connection between * Corresponding author. Fax: 44-207-8136505. E-mail address: [email protected] (A.J. Thompson). R Available online at www.sciencedirect.com NeuroImage 18 (2003) 348 –359 www.elsevier.com/locate/ynimg 1053-8119/03/$ – see front matter © 2003 Elsevier Science (USA). All rights reserved. doi:10.1016/S1053-8119(02)00042-3
-
Upload
manchester -
Category
Documents
-
view
1 -
download
0
Transcript of From diffusion tractography to quantitative white matter tract measures: a reproducibility study

From diffusion tractography to quantitative white matter tract measures:a reproducibility study
O. Ciccarelli,a G.J.M. Parker,b A.T. Toosy,a C.A.M. Wheeler-Kingshott,a G.J. Barker,a
P.A. Boulby,c D.H. Miller,a and A.J. Thompsona,*a NMR Research Unit, Institute of Neurology, University College London, Queen Square, London, WC1N 3BG, UKb Imaging Science and Biomedical Engineering, University of Manchester, Oxford Road, Manchester M13 9PT, UK
c MRI Unit, National Society for Epilepsy, Chalfont St. Peter, Gerrards Cross, Buckinghanshire, SL9 0RJ, UK
Received 13 March 2002; revised 12 September 2002; accepted 21 October 2002
Abstract
The aim of this study is to propose methods for assessing the reproducibility of diffusion tractography algorithms in future clinical studiesand to show their application to the tractography algorithm developed in our unit, fast marching tractography (FMT). FMT estimatesanatomical connectivity between brain regions using the information provided by diffusion tensor imaging. Three major white-matterpathways were investigated in 11 normal subjects—anterior callosal fibers, optic radiations, and pyramidal tracts. FMT was used to generatemaps of connectivity metric, and regions of voxels with highest connectivity metric to an anatomically defined starting point were identifiedfor each tract under investigation. The reproducibilities of tract-“normalized” volume (NV) and fractional anisotropy (FA) measurementswere assessed over such regions. The values of tract volumes are consistent with the postmortem data. Coefficients of variation (CVs) forFA and NV ranged from 1.7 to 7.1% and from 2.2 to 18.6%, respectively. CVs were lowest in the anterior callosal fibers (range: 1.7– 7.8%),followed by the optic radiations (range: 1.2–18.6%) and pyramidal tracts (range: 2.6–15.5%), suggesting that fiber organization plays a rolein determining the level of FMT reproducibility. In conclusion, these findings underline the importance of assessing the reliability ofdiffusion tractography before investigating white matter pathology.© 2003 Elsevier Science (USA). All rights reserved.
Introduction
Diffusion tensor imaging (DTI) is an MRI technique thatprovides information about the random thermal motion ofwater molecules in vivo (Basser et al., 1994). In humantissues, water diffusion is not free in all directions buthindered and restricted by the presence of barriers, includ-ing cell cytostructure and membranes. For example, in thewhite matter regions of the brain, where the neuronal pro-jections or axons are similarly aligned, water diffusion isgenerally greater in the direction parallel to axons thanperpendicular to them. This property is termed diffusionanisotropy (Moseley et al., 1990; Chenevert et al., 1990). Incontrast, in the gray matter regions, which are characterizedby a less ordered tissue structure, diffusion tends to be less
anisotropic and more uniform in all directions. Therefore,DTI allows in vivo identification of white matter and graymatter regions and it has been used in these areas to studypathological changes, including those occurring in multiplesclerosis (Horsfield et al., 1998; Tievsky et al., 1999; Wer-ring et al., 1999; Ciccarelli et al., 2001), tumors (Wiesh-mann et al., 1999; Bastin et al., 1999; Inglis et al., 1999),amyotrophic lateral sclerosis (Ellis et al., 1999), cerebralischemia (Chabriat et al., 1999; Sorensen et al., 1999; Joneset al., 1999b; Helenius et al., 2002), and developmentalmalformations of the cortex (Eriksson et al., 2001).
Since DTI is able to detect at the macroscopic scale of avoxel the extent of directional bias of diffusion occurring atthe microscopic level, it can distinguish between regionswhere fibers are highly aligned in the voxel from thosewhere fibers are less coherent. However, although DTIprovides directional information at the voxel level, it pro-vides no explicit information about the connection between
* Corresponding author. Fax:�44-207-8136505.E-mail address: [email protected] (A.J. Thompson).
R
Available online at www.sciencedirect.com
NeuroImage 18 (2003) 348–359 www.elsevier.com/locate/ynimg
1053-8119/03/$ – see front matter © 2003 Elsevier Science (USA). All rights reserved.doi:10.1016/S1053-8119(02)00042-3

neighboring voxels. A number of different tractographymethods, which use the information provided by the diffu-sion tensor concerning the orientation of fibres within avoxel, have recently been developed in order to determinethe pathways of cerebral connections in vivo (Conturo et al.,1999; Xue et al., 1999; Mori et al., 1999; Jones et al., 1999c;Basser et al., 2000; Poupon et al., 2000; Mori et al., 2000;Stieltjes et al., 2001; Gossl et al., 2002). The possibility ofa noninvasive assessment of anatomical connectivity1 hasimportant clinical implications and may increase our under-standing of neurological diseases and psychiatric condi-tions, in which connections between brain regions areknown to be disrupted (Mori et al., 2002; Steel et al., 2001).
Fast marching tractography (FMT) (Parker, 2000; Parkeret al., 2002a,b) is a recently developed method that is ableto detect possible connection pathways in the human brainand has been validated, in part, by application to animal data(Parker et al., 2002a) and by comparison with standardatlases (Parker et al., 2002b). This technique has the advan-tages that branching tracts can be traced, allowing recon-struction of the whole pathway, and providing the potentialfor quantification of white matter tracts via the generation ofmaps of a specific connectivity metric.
One of the ultimate goals for all tractography techniquesis to define quantitative and reproducible parameters formeasuring anatomical connectivity. As a first step towardthis, our study aimed to develop an in vivo method to assessthe reliability of diffusion tractography by using two differ-ent quantitative measurements along the tracts generated byFMT: fractional anisotropy (Pierpaoli and Basser, 1996)and “normalized” volume of the reconstructed tracts. Wefocused this initial investigation on three major pathways:the anterior callosal fibers, the optic radiations, and thepyramidal tracts. These pathways have a number of advan-tages: (1) They show different fiber organization, whichallows the testing of FMT reproducibility under differentconditions. (2) They have well-known anatomy, thus mak-ing the assessment of identified connections possible. (3)They are large, which makes the identification of connec-tivity more convenient than other fiber tracts of finer ormore intricate structure. (4) They are clinically relevantpathways in pathological conditions, such as multiple scle-rosis and stroke.
Methods
Subjects
Eleven normal subjects were studied (8 female and 3male). The mean age was 37.5 � 9.7 years.
MRI protocol
All scans were performed on a 1.5-T Signa EchospeedMRI system (GE Medical Systems, Milwaukee, WI). Allsubjects had a conventional dual-echo spin-echo set of im-ages acquired prior to DTI, providing proton density (PD)and T2-weighted images [TR 2000, TE 30/120 ms, FOV 240mm, matrix 256 � 256; 28 contiguous axial slices; 5-mmslice thickness].
The diffusion protocol consisted of a single-shot diffu-sion-weighted (DW) echo-planar imaging (EPI) sequence.The diffusion acquisition parameters were TE 95 ms; ac-quisition matrix 96 � 96 reconstructed as 128 � 128; FOV240 mm; 3 b � 0 smm�2 images; 60 diffusion-weightedimages, with diffusion gradients applied along 60 optimizeddiffusion directions (Jones et al., 1999a), diffusion times of� � 32 ms and � � 40 ms, and max gradient amplitude of22 � 10�3 T m�1, giving a maximum b factor b � 1000 smm�2; 42 contiguous axial slices; 2.5-mm slice thickness;diffusion data acquisition time � 20–30 min, dependentupon heart rate. Cardiac gating was used to reduce motionartifacts due to pulsation of blood and CSF. Correction ofeddy-current distortions in DW-EPI was performed using atwo-dimensional image registration technique (Symms etal., 1997), which also minimized the effect of any slighthead motion during acquisition. The data were then pro-cessed to determine the diffusion tensor on a pixel-by-pixelbasis (Basser et al., 1994). Fractional anisotropy (FA), eig-envector, and eigenvalue maps were calculated (Pierpaoliand Basser, 1996; Basser and Pierpaoli, 1996). The infor-mation contained in these maps was then used by FMT toobtain connectivity metrics which give an estimate of theconnectivity between brain regions.
Data analysis
The FMT algorithm (Parker, 2000; Parker et al., 2002a,b) was used to trace anterior callosal fibers, optic radiations,and pyramidal tracts.
Starting voxel definition criteriaSingle voxels were used as starting points for the FMT
method, using the following anatomical guidelines.
1. Anterior callosal fibers:
● We first selected the lowest axial slice where both thegenu and the splenium of corpus callosum were fullyvisible.
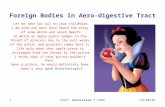
● We then selected a voxel on the midline in the anteriorpart of the genu, with its associated principal eigen-vector, when projected onto the axial plane, orientatedleft-right. In particular, on the axial slice, a voxel inthe first or second row from the anterior edge that didnot show apparent partial volume effects was chosen(Fig. 1).
1 We use the terms connection and connectivity as in Parker et al.,Neuroimage, 2002, to describe the presence of axonal projections betweenareas of the brain. We do not use the terms in a functional context, eitherat the interaxonal or at the interregional level.
349O. Ciccarelli et al. / NeuroImage 18 (2003) 348–359

2. Optic radiation:
● We selected the axial slice where the transition fromthe posterior limb of the internal capsule to the cere-bral peduncle was visible.
● A voxel close to the lateral geniculate nucleus andwithin the optic radiation at the apex of the arc aroundthe lateral ventricle, with the main eigenvector in an
anterior-medial to posterior-lateral orientation in axialprojection, was then chosen (Fig. 1).
3. Pyramidal tract:
● We selected the first axial slice below the most infe-rior slice where both optic tracts are fully visible.
Fig. 1. Principal eigenvector maps overlaid onto FA maps in one subject. The starting points are shown in the anterior genu of the corpus callosum (top row),in the optic radiations (middle row), and in the pyramidal tracts (bottom row).
350 O. Ciccarelli et al. / NeuroImage 18 (2003) 348–359

● A voxel in the middle third of the cerebral pedunclewith the projection of the principal eigenvector ontothe coronal plane oriented inferior-medial to superior-lateral was chosen. In particular, on the axial slice themost external voxel in this region was selected (Fig. 1).
All starting voxels used had an FA value �0.5, meaningthat there was a high degree of directional coherence, andtherefore implying that they were located within white mat-ter tissue. In the selection of the starting points, particularcare was taken regarding possible partial volume contami-nation. Placement was also checked with visual reference tothe corresponding slices of the PD and T2-weighted images.
Calculation of connectivity metric using the fiber trackingalgorithm
We subsequently applied the FMT method to estimatethe connectivity between each starting point and other brainregions. The connectivity metric is designed to rank possi-ble routes of connection through the dataset by assessinghow well they match the directional information providedby the principal eigenvector of diffusion at each voxel. A setof possible routes of connection are first generated via aregion-growing step that exploits the local directional co-herence of the eigenvectors; the regions therefore growrapidly along white matter pathways, and more slowly inregions lacking directional coherence (such as cortical graymatter). All possible routes of connection generated by thisstep are then ranked by defining a connectivity metric that
measures the alignment of the paths with the principaleigenvector at all points along their lengths (using the scalarproduct between the tangent to the path and the principaleigenvector). (More details can be found in Parker, 2000;Parker et al., 2002a,b).
To speed up the FMT analysis a restricted brain volumewas used which was defined depending on the expectedwhite matter pathway locations. For the analysis of thepyramidal tract, the hemisphere of interest was included,and the inferior extent of the volume of interest was re-stricted to two slices below the slice containing the startingpoint. For the optic radiation, the analysis was again re-stricted to the hemisphere of interest and limited to theregion posterior to the third ventricle. For tracing the cal-losal fibers, both hemispheres anterior to the central sulciwere selected. All studies were performed with a thresholdof FA � 0.1, to ensure that the paths detected would noterroneously enter areas of cerebrospinal fluid while retain-ing all the other tissues of potential clinical interest; theauthors acknowledge that this choice may have the possibleinconvenience of extending the tracts into gray matter re-gions.
Tract regions of interest: quantitative measurementsFor each FMT experiment, a histogram of the connectivity
metric within the defined regions of the restricted brain wasobtained and a threshold which defined voxels with the highestconnectivity metric to the start point was identified (Fig. 2).Although all the histograms obtained had similar shapes, the
Fig. 2. Histogram of connectivity metric of the right pyramidal tract that has been obtained in one subject by choosing the starting point displayed in Fig.1 On the y axis the total number of voxels is represented while on the x axis the value of the connectivity metric is represented in arbitrary units (axis scaledto look at highest connectivity values only). A threshold of 0.82, as defined by the last peak of the histogram (see arrow), has been selected in this case todefine voxels with the highest connectivity to the starting point.
351O. Ciccarelli et al. / NeuroImage 18 (2003) 348–359

threshold was specific to each connectivity metric, derived bythe FMT algorithm (see figure caption).
The connectivity threshold was applied to the maps ofthe connectivity metric to define regions of interest (ROI)identifying the areas of highest connectivity metric. TheseROIs were then overlaid on the FA maps and they wereinterpreted as regions defining the white matter pathwaysconnected to the start point. From these ROIs two parame-ters were calculated: (1) the mean FA; (2) the total tractvolume.
Since the size of the brain differs between subjects, the“normalized” volume (NV) of the tract was calculated bydividing the total tract volume by total intracranial volume(TIV), calculated as follows: the T2-weighted images wereautomatically segmented using SPM99 [Wellcome Depart-ment of Cognitive Neurology, Institute of Neurology, Lon-don, UK] (Ashburner and Friston 1997) into gray matter(GM), white matter (WM), and CSF and other tissue (notfurther subclassified), and mask images corresponding to
each class were generated; the spinal cord cutoff locationwas defined as the most rostral slice not containing cerebel-lum and was determined manually; in-house software wasthen used to calculate tissue volume from the segmentedimages rostral to the spinal cord cutoff level; the TIV wasdetermined by adding the GM, WM, and CSF volumes(Chard et al., 2002).
Postprocessing timeThe time for each step of the analysis was: (1) the
selection of the starting point and the application of FMTalgorithm required about 15 min (on a Sun MicrosystemsSunBlade 100); (2) plotting the histogram of the connectiv-ity metric and choosing the threshold required about 5 min;(3) the application of the threshold to the map of the con-nectivity metric to define voxels with the highest connec-tivity required about 10 min; (4) calculating the tract FA andtotal volume required 3 min; (5) calculating the TIV andsubsequently the NV required about 30 min. The acquisition
Table 1The image coordinates (x � right (R)-left (L), y � anterior-posterior, z � superior-inferior) of two adjacent starting points selected in each of the 11subjects are listed for each white matter tract under investigation
Subjects Callosal fibers Optic radiations Pyramidal tracts
CS1st point 63, 44, 21 R: 48, 68, 26 L: 82, 68, 26 R: 48, 68, 29 L: 71, 70, 292nd point 63, 45, 21 R: 48, 69, 26 L: 82, 69, 26 R: 48, 69, 29 L: 72, 70, 29
BD1st point 61, 42, 22 R: 45, 70, 26 L: 83, 70, 26 R: 55, 68, 29 L: 69, 68, 292nd point 62, 42, 22 R: 45, 71, 26 L: 83, 71, 26 R: 56, 68, 29 L: 69, 69, 29
SA1st point 63, 35, 18 R: 46, 66, 24 L: 83, 68, 24 R: 58, 66, 27 L: 71, 65, 272nd point 64, 35, 18 R: 46, 65, 24 L: 83, 67, 24 R: 58, 65, 27 L: 71, 66, 27
HG1st point 64, 41, 23 R: 44, 68, 28 L: 85, 69, 28 R: 56, 67, 30 L: 71, 67,302nd point 65, 41, 23 R: 43, 68, 28 L: 85, 68, 28 R: 56, 66, 30 L: 72, 67, 30
GI1st point 64, 45, 22 R: 45, 76, 27 L: 84, 75, 27 R: 57, 68, 30 L: 71, 68, 302nd point 63, 45, 22 R: 44, 76, 27 L: 84, 74, 27 R: 57, 69, 30 L: 71, 69, 30
AT1st point 64, 44, 22 R: 44, 70, 25 L: 82, 71, 25 R: 57, 67, 29 L: 71, 67, 292nd point 65, 44, 22 R: 44, 71, 25 L: 82, 70, 25 R: 56, 67, 29 L: 70, 67, 29
NL1st point 61, 46, 18 R: 44, 73, 25 L: 81, 72, 25 R: 56, 70, 27 L: 70, 70, 272nd point 62, 46, 18 R: 44, 72, 25 L: 81, 73, 25 R: 56, 71, 27 L: 69, 70, 27
RL1st point 67, 43, 17 R: 49, 70, 24 L: 83, 69, 24 R: 57, 66, 26 L: 76, 66, 262nd point 67, 44, 17 R: 49, 69, 24 L: 84, 70, 24 R: 58, 66, 26 L: 75, 66, 26
MO1st point 65, 44, 21 R: 47, 70, 23 L: 82, 71, 23 R: 47, 70, 23 L: 82, 70, 232nd point 66, 44, 21 R: 47, 71, 23 L: 82, 70, 23 R: 47, 71, 23 L: 82, 71, 23
OC1st point 62, 39, 21 R: 45, 64, 24 L: 84, 64, 24 R: 54, 59, 29 L: 71, 60, 292nd point 61, 39, 21 R: 45, 65, 24 L: 84, 65, 24 R: 54, 60, 29 L: 72, 60, 29
SB1st point 62, 44, 18 R: 46, 75, 21 L: 85, 75, 21 R: 57, 67, 25 L: 71, 67, 252nd point 63, 44, 18 R: 46, 76, 21 L: 85, 76, 21 R: 56, 66, 25 L: 71, 66, 25
The coordinate that has changed between the two trials is displayed in bold. Note that the second starting point was selected always on the same slice andmoved either along the x or y coordinates according to the guidelines described in the text. The connectivity metrics obtained by FMT using these seed voxelswere used to calculate the sensitivity of the method to adjacent starting points on the same slice within subjects.
352 O. Ciccarelli et al. / NeuroImage 18 (2003) 348–359

time, the image transfer and reconstruction times, the timefor the diffusion tensor calculation, and the time for subse-quent statistical analysis must also be added.
Statistical analysis
To compare the FA and NV between the left and rightoptic radiation and pyramidal tract the Wilcoxon test wasused.
The coefficient of variation (CV) for tract FA and NVwas calculated using the following formula (Bland andAltman, 1996a, b):
CV � �mean of the variance of a given measurement/mean measurement values.
Sensitivity of FMT to adjacent starting points withinsubjects assessed by using CV
In order to assess the effect on the FMT results ofdeliberately selecting a starting voxel adjacent to the start-ing point chosen in the baseline experiment, a second trialwas performed by the first observer (O.C.) in all subjects.For the optic radiations and pyramidal tracts, one adjacentstarting point was selected for each side of the brain, whilefor the analysis of the callosal fibers one adjacent voxelfrom the midline was chosen for each subject (Table 1). Theadjacent voxel was selected using the following criteria: ithad to share one face with the baseline starting voxel, it had
to be on the same axial slice, and it had to satisfy the startingvoxel definition criteria (as accurately as possible but obvi-ously excluding the voxel used at baseline). The FMT con-nectivity metrics obtained by using these two adjacent vox-els were used to calculate tract FA and NV, which were thenconsidered for the calculation of the CV.
Intraobserver CVA new FMT experiment was run after 3 weeks on the
data from 6 subjects (no rescan) by the same observer(O.C.), who was blind to all the details of the baseline FMTanalysis, including the coordinates of the starting points (forreproducibility of the starting points selection in these twoexperiments see Table 2). FMT experiments were per-formed once for each side of the brain for the optic radia-tions and pyramidal tracts and once for the callosal fibers.The mean FA and the NV obtained by this new evaluationwere used together with those provided by the baselineexperiments to calculate the tract variability in the samesubject when FMT experiments are repeated by the sameobserver.
Interobserver CVA new FMT experiment was performed in the same 6
subjects by a second observer (A.T.T.) (to see the selectionof the starting points performed by the second observer seeTable 3). The mean tract FA and the NV, obtained sepa-
Table 2The starting points selected in two different occasions by the same observer in 6 subjects are summarized by showing the difference between the voxelscoordinates (�x, �y, �z, where x � right (R)-left (L), y � anterior-posterior, z � superior–inferior) of the second experiment and those of the first one
Subjects Callosal fibers Optic radiations Pyramidal tracts
CS �1, 1, 0 R: 0, 1, 0; L: 0, 0, 0 R: 1, 1, 0; L: 1, 0, 0BD 0, 0, 0 R: 0, 1, 0; L: �1, �2, 0 R: 0, 0, 0; L: 0, 2, 0SA 1, 0, 0 R: 0, �1, 0; L: 0, �3, 0 R: 1, 0, 0; L: �1, 0, 0HG 0, 0, 0 R: �1, 1, 0; L: 1, 0, 0 R: �1, �1, 0; L: 0, 0, 0GI �2, 0, 0 R: 0, 0, 0; L: 0, 1, 0 R: �1, 1, 0; L: 1, 1, 0AT 1, �1, 0 R: 0, 1, 0; L: 0, 1, 0 R: �1, 1, 0; L: 1, 0, 0Mean 0.83, 0.33, 0 R: 0.16, 0.83, 0 L: 0.33, 1.16, 0 R: 0.83, 0.66, 0 L:0.66, 0.5,0
The last row shows the mean of the absolute differences for each white matter tract under investigation. The connectivity metrics obtained by FMT usingthese seed voxels were used to calculate the intraobserver CVs.
Table 3The starting points selected by two different observers in 6 subjects are summarized by showing the difference between the voxels coordinates (�x, �y,�z, where x � right (R)-left (L), y � anterior-posterior, z � superior-inferior) chosen by the second observer and those chosen by the first one
Subjects Callosal fibers Optic radiations Pyramidal tracts
CS 1, 1, 0 R: �1, 4, 0; L: 1, 4, 0 R: �1, 2, 0; L: 0, �1, 0BD 1, 1, 0 R: �1, 4, 0 L: �1, �3, 0 R: 1, �1, 0 L: 0, 1, 0SA 1, 0, 0 R: 0, �3, 1; L: 3, 5, 1 R: 1, 0, 0; L: �1, 0, 0HG 0, 0, 0 R: �1, 1, 0 L: 0, �1, 0 R: 1, �1, 0; L: 0, 0, 0GI 0, 0, 0 R: 0, 0, 0 L: 0, �2, 0 R: 0, 1, 0; L: 1, 2, 0AT 1, �1, �1 R: �1, 2, 0; L: 1, 3, 0 R: 0, 0, 0; L: 0, 1, 0Mean 0.66, 0.5, 0.16 R: 0.66, 2.33, 0.16 L: 1, 3, 0.16 R: 0.66, 0.83,0 L: 0.33, 0.83, 0
The last row shows the mean of the absolute differences for each white matter tract under investigation. The connectivity metrics obtained by FMT usingthese starting points were used to calculate the interobserver CVs.
353O. Ciccarelli et al. / NeuroImage 18 (2003) 348–359

354 O. Ciccarelli et al. / NeuroImage 18 (2003) 348–359

rately by two different observers using FMT in the samesubject, were considered for the calculation of the interob-server CV.
Test-retest CVFour subjects had a second scan after 3 to 6 months and
the whole process of data acquisition, tensor estimation,
Fig. 3. Map of connectivity metric of the anterior callosal fibers of a normal subject overlaid on a FA map. Color scale reflects the degree of connectivity(arbitrary units). The callosal fibers pass through the genu of corpus callosum and interconnect corresponding areas of each frontal lobe.Fig. 4. Map of connectivity metric of the right optic radiation of a normal subject overlaid on a FA map. Color scale reflects the degree of connectivity(arbitrary units). The optic tract shows posterior connections to the visual areas and medial connections to the lateral geniculate nuclei (yellow arrow). Whitearrows show the false positive connections.
Fig. 5. Map of connectivity metric of the right pyramidal tract of a normal subject overlaid on a FA map. Color scale reflects the degree of connectivity(arbitrary units). The pyramidal tracts travel from the middle portion of the cerebral peduncles (a) to the motor cortices (d), passing through the posteriorlimb of the internal capsule (b) and the corona radiata (c).
355O. Ciccarelli et al. / NeuroImage 18 (2003) 348–359

starting point selection, FMT processing, and ROI analysiswas performed again. The mean FA and the NV obtained bythis retest were used for the calculation of the test-retest CV.
Results
The maps of connectivity metric derived from FMT areconsistent with known anatomy of the tracts studied(Crosby et al., 1962). In particular, most of the callosalfibers that pass through the genu of the corpus callosuminterconnect corresponding areas of each frontal lobe (Fig.3). The optic radiations show posterior connections to thevisual areas and medial connections to the lateral geniculatenuclei (Fig. 4). The pyramidal tracts travel from the middleportion of the cerebral peduncles (where the starting pointswere placed) to the motor cortices, passing through theposterior limb of the internal capsule and the corona radiata(Fig. 5). False positive connections have been detected inthe course of the analysis, such as anterior projections fromthe optic radiations (Fig. 4). There was no significant dif-ference in mean FA, total uncorrected tract volume, and NVobtained from the baseline FMT experiment between the leftand the right optic radiation and pyramidal tract (Table 4).
Coefficients of variation for FA and NV in the white-matter pathways are shown in Table 5 (in case of bilateraltracts, they are given as mean of the CV of the right and leftside). The CVs for FA (ranging from 1.7 to 7.1%) aregenerally lower than the CVs for NV (ranging from 2.2 to18.6%). For both FA and NV, the interobserver CVs weregenerally higher than the intraobserver CVs, and the test-retest CVs were the highest. The lowest CVs were found inthe callosal fibers (range: 1.7–7.8%), followed by those inthe optic radiations (range: 1.2–18.6%) and in the pyramidaltracts (range: 2.6–15.5%).
Discussion
We have investigated the reproducibility of quantitativewhite matter tract measures derived using FMT, a recentlydeveloped tractography method that uses DTI data. Wefocused our investigation on three major pathways: theanterior callosal fibers, the optic radiations, and the pyra-
midal tracts. Since they are different in length, location,trajectory, and fiber organization, they provide the oppor-tunity to test FMT under different conditions. Moreover,these pathways are of considerable clinical interest, andcharacterization of the variability that may be expected intheir examination will form the basis for future comparativestudies between normal subjects and patients groups. Weshall first discuss the ability of FMT to reconstruct maps ofa connectivity metric, from which the white matter path-ways can be inferred. This will be followed by an evaluationof the reproducibility of mean FA and tract volume mea-surements. Finally, the future potential of FMT to constructgroup connectivity maps will be discussed.
The localization and course of the white matter pathwaysidentified on the connectivity maps as the voxels with thehighest connectivity to the start point are consistent withknown anatomy. Although FMT is able, in many cases, toelucidate branching fibers, some problems arise when mul-tiple tracts or orientations are present within a voxel. DTIprovides information concerning the average orientation offibers at the voxel level, and if this volume-averaged infor-mation is used to reconstruct a pathway, false positiveprojections may, on occasion, be observed. For example, theanterior projections from the optic radiations detected at thelevel of the Meyer loop (Fig. 4) may reflect the inferioroccipitofrontal fibers, which are known to accompany theoptic radiations for a short distance (Crosby et al., 1962;Burgel et al., 1999). A solution to this problem could beprovided by alternative approaches to DT-MRI, such asdiffusion spectrum analysis (Wedeen et al., 2000; Tseng etal., 2002), which, in combination with the use of a moreadvanced MRI scanner technology (e.g., higher magneticfield), may be able to resolve intersecting white matter tractswithin one voxel.
We have demonstrated the reproducibility of two quan-titative measures, i.e., mean tract FA and NV, using DTItractography information to bypass subjective determinationof regions of interest. Other studies have also focused onthese tract parameters (Virta et al., 1999; and Stieltjes et al.,
Table 4Mean fractional anisotropy, total uncorrected volume, and normalizedvolumes of the white matter pathways obtained from the baseline FMTexperiment in 11 normal subjects
FA (mean;� SD)
Total uncorrectedvolume (cm3)(mean; � SD)
Normalized volume(mean; � SD)
Callosal fibers 0.30 (0.02) 3.4 (0.9) 2.4 (0.05)Optic radiations 0.33 (0.03) 5.03 (1.49) 3.6 (1.07)Pyramidal tracts 0.34 (0.02) 9.89 (1.89) 7.06 (1.68)
Table 5Coefficients of variation (CVs) for fractional anisotropy (FA) andnormalized volume (NV) of white matter pathways
CallosalfibersCV %
OpticradiationsCV %
Pyramidaltracts CV%
Numberofsubjects
FA NV FA NV FA NV
Adjacent starting points 1.7 2.2 2.5 6.3 3.5 13 11Intraobserver 2.9 7.2 1.2 6.6 2.6 11.6 6Interobserver 3.7 6 2.6 13.9 3.8 15.3 6Test–retest 6.2 7.8 7.1 18.6 5 15.5 4
CVs lower than 5% are displayed in bold, those between 5 and 8% aredisplayed in italic, and those higher than 8% are shown in black.
CV, coefficient of variation; FA, fractional anisotropy; NV, normalizedvolume. (The CVs of the optic radiation and pyramidal tract are given asmean of the CV of the right and left side).
356 O. Ciccarelli et al. / NeuroImage 18 (2003) 348–359

2001, both studies in the brainstem), showing the impor-tance of assessing the reproducibility of such measures.However, direct comparisons between studies are not pos-sible because of the different aims, anatomical regions stud-ied, and methodologies used. The anisotropy of the tractsgives information about the degree of fiber tract directionalcoherence within an imaging voxel. The relatively lowvalue of FA in the white matter pathways suggests thatsome gray matter regions, which contain the points of originand termination of the fibers, were also included in theconnected regions. Consequently, it might be thought thatunrelated white matter tracts that share the same gray matterareas could be included into the reconstructed pathways.However, the risk of this happening is low, because theFMT algorithm follows only highly directionally coherenteigenvectors from the starting point. Moreover, the lowvalue of tract mean FA might be due to the presence ofcrossing fibers from other tracts, and of angulating fiberswithin a voxel. We also examined the total tract volume,which was obtained using a threshold defined on the histo-gram of the connectivity metric maps. The total tract vol-umes of the optic radiations and pyramidal tracts obtainedare strikingly consistent with data derived from postmortemhuman brains (Burgel et al., 1999; Rademacher et al., 2001),suggesting that the FMT method enables for the first time invivo quantification of tract volume without morphology-based segmentation, or postmortem analysis.
A comparison between the CVs obtained for FA and NVshows that FA is more reproducible. Different startingpoints within the same tract produce different, but closelyrelated, subsamples of the tract itself. The ROIs for thequantitative measurement of FA and NV are determined byapplying a tract-dependent threshold to the connectivitymetric. These ROIs have different volumes, generatingtherefore different tract volumes, but show similar meanFA. This indicates that the degree of fiber coherence islikely to be approximately constant on subsampling of thesame tract.
The values of mean FA of the three tracts under inves-tigation have a narrow range, and therefore it could beargued that mean FA is not the best measure to spatiallydistinguish between tracts. However, it has the potential todetect pathological conditions that are known to cause FAchanges. The values of NV, on the other hand, which havehigher within-subject CVs and higher within-subject stan-dard deviations than FA, have relatively small between-subject standard deviations, an important factor in powerand sample size calculations (Fisher and van Belle, 1993).For example, in the specific case of the left pyramidal tract,the between-subject standard deviation on the first measure-ment was 1.4 cm3. Consequently, group differences shouldbe detectable in pathological situations where a change inNV of 10% is expected with group sizes of about 55 in eachgroup (for 80% power and alpha of 0.05). Moreover, NVcould be used as a discriminative factor to select whitematter diseases that can be investigated using FMT. For
example, in FMT studies of multiple sclerosis or stroke,which show marked degeneration of white matter fibers,both mean FA and NV could be used to detect pathologicalchanges.
The differences in fiber pathway volumes obtained whenchoosing two adjacent starting points within the same sub-ject may in part reflect the anatomical mapping differencesof fibers that pass through different regions of the brain.This hypothesis is supported by the evidence that the high-est CV for adjacent starting points is seen in the pyramidaltracts, which show complex fiber organization and a widemapping volume. The pyramidal fibers are closely alignedand tightly packed in the cerebral peduncles, where thestarting points are placed, but spread in multiple branches inthe corona radiata and to the motor cortex, thus inducing theestimated tract volume to be sensitive to the starting pointlocation. Conversely, the lowest CV for NV for adjacentstarting points is reported in the anterior callosal fibers,which interconnect the less extensive medial prefrontal re-gions (Barbas and Pandya, 1984).
The lists of the starting point coordinates used for theFMT experiments by the same observer and by two differ-ent observers show that the placement of the seed point isfairly consistent with a mean distance between trials of lessthan a voxel; it can be observed, though, that it is morereproducible in the same observer than between observers.This is reflected in the fact that when the FMT analysis isperformed by a second observer the CVs for FA and NV areslightly higher than the intraobserver CVs. Therefore, thedevelopment of new guidelines to better define the startingpoints may further improve both the intraobserver and in-terobserver CVs. Also, future development of the DTI ac-quisition technique and higher field scanners, as noted ear-lier, could improve resolution, possibly allowing narrowerdefinition of the starting point of the tracts.
The lowest reproducibility for our quantitative measure-ments was found in the (intraobserver) test-retest analysis,suggesting that factors related to the data acquisition andreconstruction may play a role in inducing extra variability.In the present study the diffusion tensor calculation andFMT algorithm were performed in each subject’s nativespace. The development of registration algorithms able todeal correctly with the diffusion tensor (Pautler et al., 1998)may allow transformation of the data into a normalizedspace before applying tractography algorithms, possibly im-proving the test-retest CV.
An exciting future development of FMT would be theconstruction of group maps of white matter pathways in apopulation of subjects, which would compensate for theanatomical variability between individuals. With a largedatabase of subjects, it may be possible to construct MRIdiffusion tract tracing-based normal atlases, which can thenbe compared with pathological conditions, where the whitematter pathways are primarily or secondarily affected.
In conclusion, we have investigated in vivo anisotropyand volumetric quantification of FMT-derived white matter
357O. Ciccarelli et al. / NeuroImage 18 (2003) 348–359

tracts within the brain and shown that tract FA has betterreproducibility than NV. The highest reproducibility wasfound in the frontal callosal fibers, followed by the opticradiations and pyramidal tracts, suggesting that the fiberorganization and the length of the pathway are importantfactors in determining the level of reproducibility. Futuredevelopments of the FMT algorithm and DTI acquisitiontechniques should improve the reproducibility of FMT andallow more detailed and robust investigations of white mat-ter pathways.
It is important to assess the reliability of any tractogra-phy technique before moving on to investigate white matterpathology. In this study we described a method by which thereproducibility of FMT can be assessed; ideally all tractog-raphy techniques should be validated in a similar way be-fore being clinically applied. In particular, informationabout the reproducibility of the quantitative measurementsderived from tractography and the variability between thereconstructed tracts should always be obtained before inter-preting clinical data.
Acknowledgments
The authors thank D.G. MacManus for technical assis-tance with the MR scans, Prof. T. Yousry and D. Altman fortheir comments, and the subjects for kindly agreeing to takepart in this study. The NMR Unit is supported by a generousgrant from the MS Society of Great Britain and NorthernIreland. Dr. O. Ciccarelli is supported by TEVA Pharma-ceutical Ltd.
References
Ashburner, J., Friston, K., 1997. Multimodal image coregistration andpartitioning—A unified framework. NeuroImage 6, 209–217.
Barbas, H., Pandya, D.N., 1984. Topography of commissural fibers of theprefrontal cortex in the rhesus monkey. Exp. Brain Res. 55, 187–191.
Basser, P.J., Mattiello, J., LeBihan, D., 1994. Estimation of the effectiveself-diffusion tensor from the NMR spin echo. J. Magn Reson. B 103,247–254.
Basser, P.J., Pajevic, S., Pierpaoli, C., Duda, J., Aldroubi, A., 2000. In vivofiber tractography using DT-MRI data. Magn Reson. Med. 44, 625–632.
Basser, P.J., Pierpaoli, C., 1996. Microstructural and physiological featuresof tissues elucidated by quantitative-diffusion-tensor MRI. J. MagnReson. B 111, 209–219.
Bastin, M.E., Delgado, M., Whittle, I.R., Cannon, J., Wardlaw, J.M., 1999.The use of diffusion tensor imaging in quantifying the effect of dexa-methasone on brain tumours. NeuroReport 10, 1385–1391.
Bland, J.M., Altman, D.G., 1996a. Measurement error. Br. Med. J. 313,744.
Bland, J.M., Altman, D.G., 1996b. Measurement error proportional to themean. Br. Med. J. 313, 106.
Burgel, U., Schormann, T., Schleicher, A., Zilles, K., 1999. Mapping ofhistologically identified long fiber tracts in human cerebral hemispheresto the MRI volume of a reference brain: Position and spatial variabilityof the optic radiation. NeuroImage 10, 489–499.
Chabriat, H., Pappata, S., Poupon, C., Clark, C.A., Vahedi, K., Poupon, F.,Mangin, J.F., Pachot-Clouard, M., Jobert, A., Le Bihan, D., Bousser,M.G., 1999. Clinical severity in CADASIL related to ultrastructuraldamage in white matter: in vivo study with diffusion tensor MRI.Stroke 30, 2637–2643.
Chard, D.T., Parker, G.J., Griffin, C.M., Thompson, A.J., Miller, D.H.,2002. The reproducibility and sensitivity of brain tissue volume mea-surements derived from an SPM based segmentation methodology. J.Magn Reson. Imaging 15, 259–267.
Chenevert, T.L., Brunberg, J.A., Pipe, J.G., 1990. Anisotropic diffusion inhuman white matter: demonstration with MR techniques in vivo. Ra-diology 177, 401–405.
Ciccarelli, O., Werring, D.J., Wheeler-Kingshott, C.A., Barker, G.J.,Parker, G.J., Thompson, A.J., Miller, D.H., 2001. Investigation of MSnormal-appearing brain using diffusion tensor MRI with clinical cor-relations. Neurology 56, 926–933.
Conturo, T.E., Lori, N.F., Cull, T.S., Akbudak, E., Snyder, A.Z., Shimony,J.S., McKinstry, R.C., Burton, H., Raichle, M.E., 1999. Tracking neu-ronal fiber pathways in the living human brain. Proc. Natl. Acad. Sci.USA 96, 10422–10427.
Crosby, E.C., Humprey, T., Laver, E.W., 1962. Correlative Anatomy of theNervous System. Macmillan, New York.
Ellis, C.M., Simmons, A., Jones, D.K., Bland, J., Dawson, J.M., Horsfield,M.A., Williams, S.C., Leigh, P.N., 1999. Diffusion tensor MRI as-sesses corticospinal tract damage in ALS. Neurology 53, 1051–1058.
Eriksson, S.H., Rugg-Gunn, F.J., Symms, M.R., Barker, G.J., Duncan, J.S.,2001. Diffusion tensor imaging in patients with epilepsy and malfor-mations of cortical development. Brain 124, 617–626.
Fisher L.D. and van Belle G. Sample sizes for observational studies, in:Biostatistics. A Methodology for the Health Sciences, Wiley-Inter-science, New York, 1993, pp. 844–865.
Gossl, C., Fahrmeir, L., Putz, B., Auer, L.M., Auer, D.P., 2002. Fibertracking from DTI using linear state space models: detectability of thepyramidal tract. NeuroImage 16, 378–388.
Helenius, J., Soinne, L., Salonen, O., Kaste, M., Tatlisumak, T., 2002.Leukoaraiosis, ischemic stroke, and normal white matter on diffusion-weighted MRI. Stroke 33, 45–50.
Horsfield, M.A., Larsson, H.B., Jones, D.K., Gass, A., 1998. Diffusionmagnetic resonance imaging in multiple sclerosis. J. Neurol. Neuro-surg. Psychiatry 64, S80–S84.
Inglis, B.A., Neubauer, D., Yang, L., Plant, D., Mareci, T.H., Muir, D.,1999. Diffusion tensor MR imaging and comparative histology ofglioma engrafted in the rat spinal cord. AJNR Am. J. Neuroradiol. 20,713–716.
Jones, D.K., Horsfield, M.A., Simmons, A., 1999a. Optimal strategies formeasuring diffusion in anisotropic systems by magnetic resonanceimaging. Magn Reson. Med. 42, 515–525.
Jones, D.K., Lythgoe, D., Horsfield, M.A., Simmons, A., Williams, S.C.,Markus, H.S., 1999b. Characterization of white matter damage inischemic leukoaraiosis with diffusion tensor MRI. Stroke 30, 393–397.
Jones, D.K., Simmons, A., Williams, S.C., Horsfield, M.A., 1999c. Non-invasive assessment of axonal fiber connectivity in the human brain viadiffusion tensor MRI. Magn Reson. Med. 42, 37–41.
Mori, S., Crain, B.J., Chacko, V.P., van Zijl, P.C., 1999. Three-dimen-sional tracking of axonal projections in the brain by magnetic reso-nance imaging. Ann. Neurol. 45, 265–269.
Mori, S., Kaufmann, W.E., Pearlson, G.D., Crain, B.J., Stieltjes, B., So-laiyappan, M., van Zijl, P.C., 2000. In vivo visualization of humanneural pathways by magnetic resonance imaging. Ann. Neurol. 47,412–414.
Mori, S., Kaufmann, W.E., Davatzikos, C., Stieltjes, B., Amodei, L.,Fredericksen, K., Pearlson, G.D., Melhem, E.R., Solaiyappan, M.,Raymond, G.V., Moser, H.W., van Zijl, P.C., 2002. Imaging corticalassociation tracts in the human brain using diffusion- tensor-basedaxonal tracking. Magn Reson. Med. 47, 215–223.
Moseley, M.E., Cohen, Y., Kucharczyk, J., Mintorovitch, J., Asgari, H.S.,Wendland, M.F., Tsuruda, J., Norman, D., 1990. Diffusion-weighted
358 O. Ciccarelli et al. / NeuroImage 18 (2003) 348–359

MR imaging of anisotropic water diffusion in cat central nervoussystem. Radiology 176, 439–445.
Parker G.J. 2000. Tracing fibre tracts using fast marching. Proc. Int. Soc.Magn. Reson. Med. 85.
Parker, G.J., Stephan, K.E., Barker, G.J., Rowe, J.B., MacManus, D.G.,Wheeler-Kingshott, C.A., Ciccarelli, O., Passingham, R.E., Lemon,R.N., Turner, R., 2002a. Initial demonstration of in vivo tracing ofaxonal projections in the Macaque brain and comparison with thehuman brain using diffusion tensor imaging and fast marching tractog-raphy. NeuroImage 15, 797–809.
Parker, G.J., Wheeler-Kingshott, C.A., Barker, G.J., 2002b. Estimatingdistributed anatomical brain connectivity using fast marching methodsand diffusion tensor imaging. IEEE Trans. Med. Imaging 21, 505–512.
Pautler, R.G., Silva, A.C., Koretsky, A.P., 1998. In vivo neuronal tracttracing using manganese-enhanced magnetic resonance imaging. MagnReson. Med. 40, 740–748.
Pierpaoli, C., Basser, P.J., 1996. Toward a quantitative assessment ofdiffusion anisotropy. Magn. Reson. Med. 36, 893–906.
Poupon, C., Clark, C.A., Frouin, V., Regis, J., Bloch, I., Le Bihan, D.,Mangin, J., 2000. Regularization of diffusion-based direction mapsfor the tracking of brain white matter fascicles. NeuroImage 12,184 –195.
Rademacher, J., Burgel, U., Geyer, S., Schormann, T., Schleicher, A.,Freund, H.J., Zilles, K., 2001. Variability and asymmetry in the humanprecentral motor system: a cytoarchitectonic and myeloarchitectonicbrain mapping study. Brain 124, 2232–2258.
Sorensen, A.G., Wu, O., Copen, W.A., Davis, T.L., Gonzalez, R.G., Ko-roshetz, W.J., Reese, T.G., Rosen, B.R., Wedeen, V.J., Weisskoff,R.M., 1999. Human acute cerebral ischemia: detection of changes inwater diffusion anisotropy by using MR imaging. Radiology 212,785–792.
Steel, R.M., Bastin, M.E., McConnell, S., Marshall, I., Cunningham-Owens, D.G., Lawrie, S.M., Johnstone, E.C., Best, J.J., 2001. Diffusiontensor imaging (DTI) and proton magnetic resonance spectroscopy (1H
MRS) in schizophrenic subjects and normal controls. Psychiatry Res.106, 161–170.
Stieltjes, B., Kaufmann, W.E., van Zijl, P.C., Fredericksen, K., Pearlson,G.D., Solaiyappan, M., Mori, S., 2001. Diffusion tensor imaging andaxonal tracking in the human brainstem. NeuroImage 14, 723–735.
Symms, M.R., Barker, G.J., Franconi, F., Clark, C.A., 1997. Correction ofeddy-current distortions in diffusion-weighted echo-planar images witha two-dimensional registration technique. Proc. Int. Soc. Magn. Reson.Med., 1723.
Tievsky, A.L., Ptak, T., Farkas, J., 1999. Investigation of apparent diffu-sion coefficient and diffusion tensor anisotrophy in acute and chronicmultiple sclerosis lesions. AJNR Am. J. Neuroradiol. 20, 1491–1499.
Tseng, W-Y.I., Lin, C-P., Chen, J-H., Wedeen, V.J., 2002. diffusion spec-trum imaging of complex cortical cytoarchitecture in adult rats. Int.Soc. Magn. Reson. Med., 441.
Wedeen, V.J., Reese, T.G., Tuch, D.S., Weigel, M.R., Dou, J-G., Weiss-koff, R.M., Chesler, D., 2000. Mapping fiber orientation spectra incerebral white matter with fourier transform diffusion MRI. Int. Soc.Magn. Reson. Med., 82.
Virta, A., Branett, A., Pierpaoli, C., 2001. Visualizing and characterizingwhite matter fiber structure and architecture in the human pyramidaltract using diffusion tensor MRI. Magn. Reson. Imaging 17, 1121–1133.
Werring, D.J., Clark, C.A., Barker, G.J., Thompson, A.J., Miller, D.H.,1999. Diffusion tensor imaging of lesions and normal-appearing whitematter in multiple sclerosis. Neurology 52, 1626–1632.
Wieshmann, U.C., Clark, C.A., Symms, M.R., Franconi, F., Barker, G.J.,Shorvon, S.D., 1999. Reduced anisotropy of water diffusion in struc-tural cerebral abnormalities demonstrated with diffusion tensor imag-ing. Magn Reson. Imaging 17, 1269–1274.
Xue, R., van Zijl, P.C., Crain, B.J., Solaiyappan, M., Mori, S., 1999. Invivo three-dimensional reconstruction of rat brain axonal projectionsby diffusion tensor imaging. Magn Reson. Med. 42, 1123–1127.
359O. Ciccarelli et al. / NeuroImage 18 (2003) 348–359