
Increasing relevance of Gram‐positive cocci in urinary tract ...
Upload
khangminh22Category
view
0download
0
Clinical Nutrition
Lower urinary Tract Disease in Cats—New Problems,New Paradigms1
C. A. TONY BUFFIHGTON
Department of Veterinary Clinical Sciences, College of Veterinary Medicine, The Ohio State University,Columbus, OH 432 Ì0-1089
ABSTRACT Companion animal diets may be relatedto prevention, pathogenesis and/or treatment of diseases of the lower urinary tract. For example, urolithia-sis can be either diet induced or nutrient sensitive. Oneof the most interesting developments in veterinary uro-lithiasis research has been the recent change in thecomposition of stones recovered from cats. In 1984,88% of stones analyzed by quantitative methods were>70% struvite, whereas <1% were calcium oxalate. In1992, the percentage of struvite had dropped to 62,whereas the percentage of calcium oxalate had increased to 24. Another recent development in lowerurinary tract disease of cats is the recognition that urolithiasis appears to be a minor cause of the signs offrequency, urgency and hematuria for which patientsare presented. This suggests that diet may no longerbe involved, or be involved in previously unrecognizedways, in many current cases of this disease. Some ofthese feline patients may have a disease similar to interstitial cystitis, a disease of humans that appears tobe of neuroepithelial origin. Our laboratory has beenstudying this possibility recently, and many similaritiesbetween the two diseases have been found. J. Nutr.124: 2643S-2651S, 1994.
INDEXING KEY WORDS:
•cat •lower urinary tract disease•urolithiasis •interstitial cystitis •substance P
Lower urinary tract diseases (LUTD) occur commonly in cats. Signs of LUTD may be caused by urolithiasis, urinary tract infection, neoplasia, congenitalanomalies, and inflammation. In 1985, an overall incidence of lower urinary tract disease of ~0.85% inthe United States cat population was reported (Lawleret al. 1985). Historically, struvite urolithiasis waspresent in many cats suffering LUTD. Components ofthe diet that have been investigated as causative agentsof struvite include, but are not limited to, ash, magnesium and ingredients that influence acid-base status(Buffington 1992).
0022-3166/94 $3.00 ©1994 American Institute of Nutrition.
Although LUTD has been blamed on the ash contentof diets (Blount 1931), experimental confirmation ofthis assertion is lacking. One group (Dickinson andScott 1956) failed to produce urinary calculi in growingcats fed diets containing bone ash concentrations of8, 22 or 30%. Thus, whereas mineral components ofash may influence struvite formation, the ash contentof the diet per se cannot be blamed.
Several studies conducted during the 1970s confirmed that urolithiasis and urinary tract obstructioncould be induced in cats by feeding diets containinglarge quantities of magnesium (Jackson 1971, Kallfelzet al. 1980, Lewis et al. 1978, Rich et al. 1974). Forexample, one study (Lewis et al. 1978) found that calculi developed in cats fed diets containing 0.75 or 1.0%magnesium carbonate. The investigators reported average urine pH values of 7.3-8.3 in all groups fed thehigh magnesium diets. A more recent study (Finco etal. 1985) examined the role of magnesium on struviteurolithiasis by feeding five diets varying in moistureand magnesium content to cats. When canned dietscontaining 0.46 or 0.72% magnesium were fed, six ofeight cats in each group experienced obstruction.When dry food containing 0.45% magnesium oxidewas fed, six of eight cats developed urethral obstruction or a stone. One of four cats fed the same dry dietcontaining 0.17% magnesium developed urethral obstruction from struvite crystals, and at the time of obstruction this cat's urine was alkaline. Urine pH values
of most cats were <7.0, but measurements were madeafter 12 h of food deprivation. These investigators alsoreported that, within diet groups, urine magnesiumconcentration in cats with urethral obstruction wasnot higher than in those that did not obstruct. They
1Presented as part of the Waltham Symposium on the Nutritionof Companion Animals in association with the 15th InternationalCongress of Nutrition at Adelaide, SA,Australia, on September 23-25, 1993. Guest editors for this symposium were Kay Earle, JohnMercer and D'Ann Finley.
2643S
by on May 8, 2007
jn.nutrition.orgD
ownloaded from

2644S SUPPLEMENT
concluded that factor(s) other than urine magnesiumconcentration were important in urethral obstruction.
The relevance of the pH of the urine reported inthe above-mentioned studies has more recently become apparent (Buffington et al. 1990) but was demonstrated in previous studies. Addition of 1.5% ammonium chloride to a diet containing 0.44% magnesium oxide (Taton et al. 1984a, Taton et al. 1984b)reduced the pH of the urine of cats fed the diet from7.0 to 5.9. When cats fed the dry food without ammonium chloride developed obstruction or struvitecalculi, they were switched to the diet containing ammonium chloride. No further obstructions occurredin these cats, and existing struvite calculi dissolved,demonstrating the effectiveness of urine acidificationin dissolving struvite uroliths even in cats fed largeamounts of magnesium.
Because many previous studies had used alkaliniz-ing salts of magnesium, we fed adult male cats purifieddiets with 0.05% magnesium or 0.5% magnesium,added either as the oxide (MgO) or chloride (MgCl2)salt (Buffington et al. 1985). Mean urine pH values of6.9 (basal), 7.7 (MgO) and 5.7 (MgCl2) resulted, andstruvite crystals commonly occurred in the urine ofcats fed the basal and MgO-containing diets but notin the urine of cats fed the MgCl2-containing diet. Onecat fed the basal diet developed hematuria, and onecat fed the MgO-containing diet developed urethralobstruction with struvite crystals.
It thus appears that the early conclusion that "excessive" dietary magnesium causes struvite urolithia-sis resulted from an experimental design error in thechoice of magnesium salt added and a disregard forurine pH. If magnesium chloride had been added todiets in earlier studies, magnesium might have beenthought to actually prevent struvite formation (asphosphorus, currently added to many diets as phosphoric acid, currently is thought to). Moreover, commercial cat foods reportedly (Lewis and Morris 1984)contain average magnesium concentrations of 0.16%for canned, 0.14% for semimoist and 0.16% for drycat foods. These quantities are much lower than thoseused in most of the experimental studies describedabove. The magnesium content of commercial catfoods also has been reported to be reasonably consistent (Graser and Lewis 1981).
Although struvite crystal formation is inhibited ata urine pH of ~6.4, further reduction of urine pH isnot without risk, because metabolic acidosis occurswhen acid intake exceeds output. Acidosis can causea variety of adverse results, including direct toxicityof the acids, and detrimental effects on renal function,bone homeostasis and mineral balance. Low urine pHand magnesium concentrations also might increase therisk of calcium oxalate urolithiasis.
Both methionine and ammonium chloride havebeen used to acidify the urine, and both can be toxic.Excessive methionine consumption has decreased food
intake and weight gain in kittens (Fau et al. 1983) andhas caused hemolytic anemia, methemoglobinemiaand Heinz body formation (Maede et al. 1987). Ingestion of ammonium chloride may result in anorexia,vomiting and diarrhea (Lloyd and Sullivan 1984). Incontrast, addition of ammonium chloride (300 mg/kgbody weight) to a commercial dry cat food that normally resulted in 4-h postprandial urine pH of nearly8.0 did not decrease 4-h postprandial urine pH below6.7, nor did it significantly alter venous blood pH,pCO2 or bicarbonate concentration (Finco et al. 1986a).A higher dosage reduced 4-h postprandial urine pH to~6.0 and significantly decreased blood bicarbonateconcentration during the course of the study. Neitherdosage had significant effects on appetite, body weight,urine specific gravity or blood ammonia concentrations 30 min after feeding, and no adverse gastrointestinal signs were observed. These studies demonstrate that the acidifying effects and the safety of aurinary acidifier depends on the diet to which it isadded.
In addition to inducing chronic metabolic acidosis,ingestion of an acidifying diet that is marginal in potassium content can deplete body potassium stores.Potassium depletion and hypokalemia in turn may leadto chronic tubulointerstitial nephritis and increasedurinary fractional excretion of potassium, further aggravating potassium depletion (Fettman 1989). Dowet al. (1987) reported a clinical syndrome of hypoka-lemic nephropathy in cats fed an acidifying diet lowin potassium; several of the cats had metabolic acidosis. More recently, we (DiBartola et al. 1993) reported that three of nine cats fed a diet high in protein(40% of dry matter) and acid content, but marginallyreplete in potassium, developed chronic renal failureduring a 2-y study. Problems of inadequate dietarypotassium in cat foods may have resulted from thelow requirement published by the NRC, which wasbased on studies (Hills et al. 1982) wherein cats thatwere fed an amount of potassium that permitted normal growth still had low circulating potassium concentrations. Also, the variance among analyses of potassium in complex matrices, such as pet foods, canbe large, as much as 25% in some cases (author's personal experience), so that less potassium may havebeen present in some diets than manufacturers believed.
When acid intake exceeds output, carbonate andphosphate from bone buffer the higher acid load. Inone study (Buffington 1988), addition of 3% ammonium chloride to the diet slowed growth, decreasedblood pH and bicarbonate concentrations, loweredurine pH, increased urine calcium excretion and promoted bone demineralization of caudal vertebrae ofyoung cats. Similar changes in blood and urine havebeen reported in older cats fed diets containing 1.5%ammonium chloride (Ching et al. 1989). Recent studies (Fettman et al. 1992) also suggest that the type of
by on May 8, 2007
jn.nutrition.orgD
ownloaded from
LOWER URINARY TRACT DISEASE IN CATS 2645S
acidifying ingredient is not an important determinantof the effect of acidification. Cat foods acidified bytwo methods had similar adverse effects on acid-base,mineral and bone homeostasis. One of the diets wasnaturally acidified, whereas the other was acidified byaddition of phosphoric acid. Both diets induced un-compensated chronic metabolic acidosis, significantlydecreased whole-body balances of calcium, phosphorus, potassium and magnesium, and decreased boneformation.
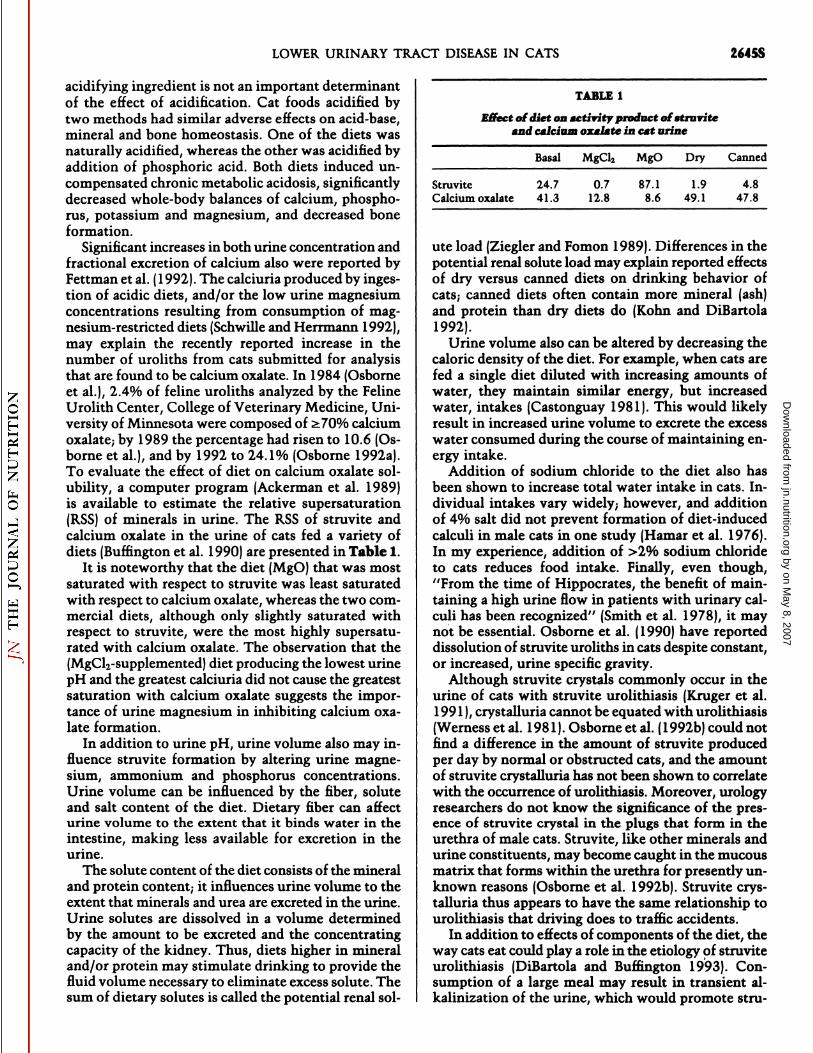
Significant increases in both urine concentration andfractional excretion of calcium also were reported byFettman et al. (1992). The calciuria produced by ingestion of acidic diets, and/or the low urine magnesiumconcentrations resulting from consumption of magnesium-restricted diets (Schwüleand Herrmann 1992),may explain the recently reported increase in thenumber of uroliths from cats submitted for analysisthat are found to be calcium oxalate. In 1984 (Osborneet al.), 2.4% of feline uroliths analyzed by the FelineUrolith Center, College of Veterinary Medicine, University of Minnesota were composed of >70% calciumoxalate; by 1989 the percentage had risen to 10.6 (Osborne et al.), and by 1992 to 24.1% (Osborne 1992a).To evaluate the effect of diet on calcium oxalate solubility, a computer program (Ackerman et al. 1989)is available to estimate the relative supersaturation(RSS) of minerals in urine. The RSS of struvite andcalcium oxalate in the urine of cats fed a variety ofdiets (Buffington et al. 1990) are presented in Table 1.
It is noteworthy that the diet (MgO) that was mostsaturated with respect to struvite was least saturatedwith respect to calcium oxalate, whereas the two commercial diets, although only slightly saturated withrespect to struvite, were the most highly supersaturated with calcium oxalate. The observation that the(MgCl2-supplemented) diet producing the lowest urinepH and the greatest calciuria did not cause the greatestsaturation with calcium oxalate suggests the importance of urine magnesium in inhibiting calcium oxalate formation.
In addition to urine pH, urine volume also may influence struvite formation by altering urine magnesium, ammonium and phosphorus concentrations.Urine volume can be influenced by the fiber, soluteand salt content of the diet. Dietary fiber can affecturine volume to the extent that it binds water in theintestine, making less available for excretion in theurine.
The solute content of the diet consists of the mineraland protein content; it influences urine volume to theextent that minerals and urea are excreted in the urine.Urine solutes are dissolved in a volume determinedby the amount to be excreted and the concentratingcapacity of the kidney. Thus, diets higher in mineraland/or protein may stimulate drinking to provide thefluid volume necessary to eliminate excess solute. Thesum of dietary solutes is called the potential renal sol-
TABLE 1
Effect of diet on activity product of struviteand calcium oxalate in cat urine
Basal MgCl2 MgO Dry Canned
StruviteCalcium oxalate24.7 41.30.7 12.887.1 8.61.949.14.8 47.8
ute load (Ziegler and Fomon 1989). Differences in thepotential renal solute load may explain reported effectsof dry versus canned diets on drinking behavior ofcats,- canned diets often contain more mineral (ash)and protein than dry diets do (Kohn and DiBartola1992).
Urine volume also can be altered by decreasing thecaloric density of the diet. For example, when cats arefed a single diet diluted with increasing amounts ofwater, they maintain similar energy, but increasedwater, intakes (Castonguay 1981). This would likelyresult in increased urine volume to excrete the excesswater consumed during the course of maintaining energy intake.
Addition of sodium chloride to the diet also hasbeen shown to increase total water intake in cats. Individual intakes vary widely; however, and additionof 4% salt did not prevent formation of diet-inducedcalculi in male cats in one study (Hamar et al. 1976).In my experience, addition of >2% sodium chlorideto cats reduces food intake. Finally, even though,"From the time of Hippocrates, the benefit of maintaining a high urine flow in patients with urinary calculi has been recognized" (Smith et al. 1978), it maynot be essential. Osborne et al. (1990) have reporteddissolution of struvite uroliths in cats despite constant,or increased, urine specific gravity.
Although struvite crystals commonly occur in theurine of cats with struvite urolithiasis (Kruger et al.1991), crystalluria cannot be equated with urolithiasis(Werness et al. 1981). Osborne et al. (1992b) could notfind a difference in the amount of struvite producedper day by normal or obstructed cats, and the amountof struvite crystalluria has not been shown to correlatewith the occurrence of urolithiasis. Moreover, urologyresearchers do not know the significance of the presence of struvite crystal in the plugs that form in theurethra of male cats. Struvite, like other minerals andurine constituents, may become caught in the mucousmatrix that forms within the urethra for presently unknown reasons (Osborne et al. 1992b). Struvite crystalluria thus appears to have the same relationship tourolithiasis that driving does to traffic accidents.
In addition to effects of components of the diet, theway cats eat could play a role in the etiology of struviteurolithiasis (DiBartola and Buffington 1993). Consumption of a large meal may result in transient al-kalinization of the urine, which would promote stru-
by on May 8, 2007
jn.nutrition.orgD
ownloaded from
2646S SUPPLEMENT
vite crystal formation (Finke and Litzenberger 1992).Cats do not commonly eat large meals when food iscontinuously available; however, generally consuming10-20 small meals over a 24-h period (DiBartola andBuffington 1993). This feeding pattern attenuatespostprandial alkalinization of the urine.
Recent evidence suggests that struvite urolithiasismay no longer be a common cause of lower urinarytract disease in cats. Of 141 cats presented to the University of Minnesota Veterinary hospital between1982 and 1985 with signs of lower urinary tract disease(Kruger et al. 1991 ), only 23% had struvite calculi. Nodiagnosis could be made in 58% of female and 79%of unobstructed male cats, based on absence of evidence of infection (bacterial, mycoplasmal or viral),urolithiasis, neoplasia or congenital abnormality.Moreover, the frequency of calculi submitted foranalysis that are struvite apparently has been decliningsince 1985 (Osborne 1992).
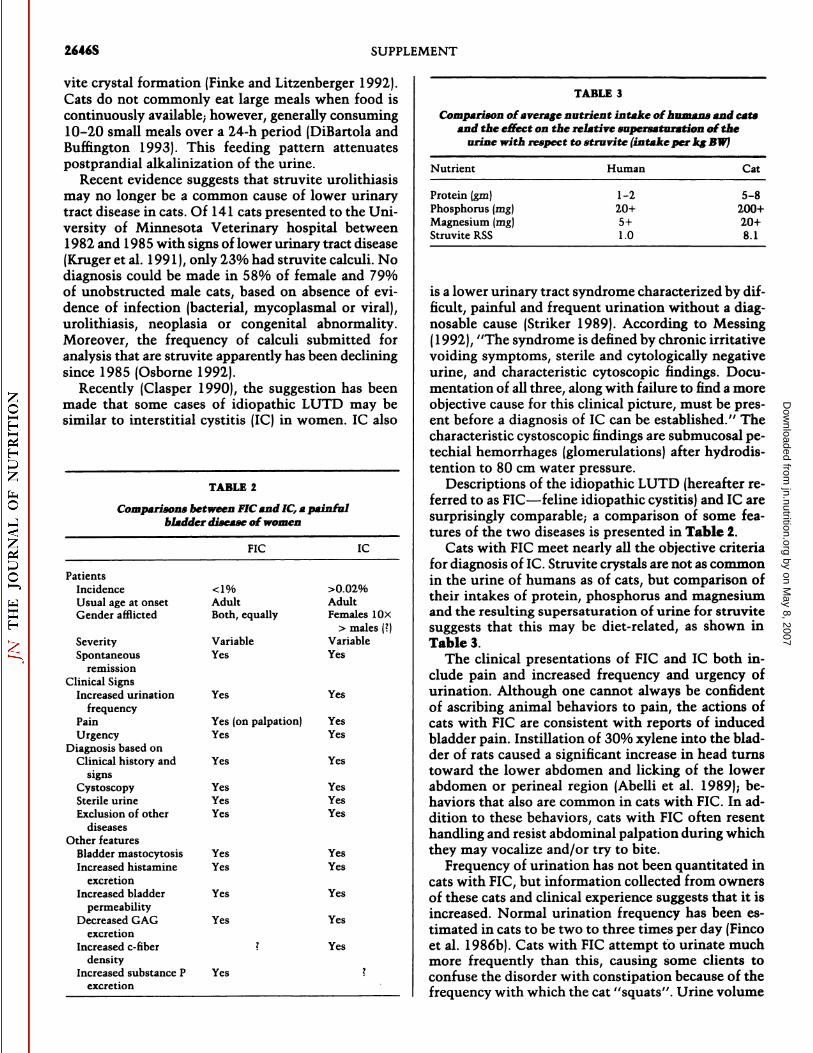
Recently (Clasper 1990), the suggestion has beenmade that some cases of idiopathic LUTD may besimilar to interstitial cystitis (1C) in women. 1C also
TABLE 2
Comparisons between FIC and 1C, a painfulbladder disease of women
FIC 1C
PatientsIncidenceUsual
age atonsetGenderafflictedSeveritySpontaneous<1%AdultBoth,equallyVariableYes>0.02%AdultFemales10X>
males(?)VariableYes
remissionClinical Signs
Increased urinationfrequency
PainUrgency
Diagnosis based onClinical history and
signsCystoscopySterile urineExclusion of other
diseasesOther features
Bladder mastocytosisIncreased histamine
excretionIncreased bladder
permeabilityDecreased GAG
excretionIncreased c-fiber
densityIncreased substance P
excretion
Yes Yes
Yes (on palpation) YesYes Yes
Yes Yes
Yes YesYes YesYes Yes
Yes YesYes Yes
Yes Yes
Yes Yes
? Yes
Yes
TABLE 3
Comparison of average nutrient intake of humans and catsand the effect on the relative supersaturation of the
urine with respect to struvite (intake per kg BW)
Nutrient Human Cat
Protein (gru)Phosphorus (mg)Magnesium (mg)Struvite RSS
1-220+5+1.0
5-8200+20+8.1
is a lower urinary tract syndrome characterized by difficult, painful and frequent urination without a diag-nosable cause (Striker 1989). According to Messing(1992), "The syndrome is defined by chronic irritativevoiding symptoms, sterile and cytologically negativeurine, and characteristic cytoscopic findings. Documentation of all three, along with failure to find a moreobjective cause for this clinical picture, must be present before a diagnosis of 1C can be established." Thecharacteristic cystoscopic findings are submucosal pe-techial hemorrhages (glomerulations) after hydrodis-tention to 80 cm water pressure.
Descriptions of the idiopathic LUTD (hereafter referred to as FIC—feline idiopathic cystitis) and 1C aresurprisingly comparable; a comparison of some features of the two diseases is presented in Table 2.
Cats with FIC meet nearly all the objective criteriafor diagnosis of 1C.Struvite crystals are not as commonin the urine of humans as of cats, but comparison oftheir intakes of protein, phosphorus and magnesiumand the resulting supersaturation of urine for struvitesuggests that this may be diet-related, as shown inTable 3.
The clinical presentations of FIC and 1C both include pain and increased frequency and urgency ofurination. Although one cannot always be confidentof ascribing animal behaviors to pain, the actions ofcats with FIC are consistent with reports of inducedbladder pain. Instillation of 30% xylene into the bladder of rats caused a significant increase in head turnstoward the lower abdomen and licking of the lowerabdomen or perineal region (Abelli et al. 1989); behaviors that also are common in cats with FIC. In addition to these behaviors, cats with FIC often resenthandling and resist abdominal palpation during whichthey may vocalize and/or try to bite.
Frequency of urination has not been quantitated incats with FIC, but information collected from ownersof these cats and clinical experience suggests that it isincreased. Normal urination frequency has been estimated in cats to be two to three times per day (Fincoet al. 1986b). Cats with FIC attempt to urinate muchmore frequently than this, causing some clients toconfuse the disorder with constipation because of thefrequency with which the cat "squats". Urine volume
by on May 8, 2007
jn.nutrition.orgD
ownloaded from
LOWER URINARY TRACT DISEASE IN CATS 2647S
produced during these episodes usually is <2 ml. Urgency to urinate also occurs in cats with the disease,sometimes resulting in urination outside the litterbox(Houpt 1991). This behavior does not appear to beincontinence because of the small volumes of urineusually produced during these efforts. Interestingly,one of the promising treatments for 1C, amitriptyline,(Hanno et al. 1989) also is prescribed with some success for inappropriate urination in cats (Marder 1991).The mechanism of action of amitriptyline, if it is trulyeffective, currently is unknown, and a variety of possibilities exist (Max et al. 1987). Amitriptyline can inhibit histamine release from (rat peritoneal) mast cellsin vitro (Theoharides et al. 1982), inhibit segmentaltransmission of wide dynamic range and nociceptiveneurons in the cat trigeminal nucleus (Fromm et al.1991), and increase synaptic serotonin content by inhibiting axon reuptake (Eschalier 1990). Amitriptylinealso has anticholinergic effects and tends to increasebladder capacity (Hanno et al. 1989).
Results of urinalysis and culture of patients suffering from FIC or 1C also are similar; in both diseases,urine is sterile and cytologically nondescript. Microscopic hematuria is reported more commonly in catsthan it is in women, although it occurs in both patientgroups (Holm-Bentzen et al. 1987, Kruger étal.1991).This may be because of etiologic differences betweenthe two diseases, presentation at different stages ofthe disease or to the fact that veterinarians commonlycollect urine by antepubic cystocentesis; hematuria hasbeen reported (Kruger et al. 1991) in 46% of urinalysesof normal cats (and >90% of cats with LUTD).
Radiographie studies may be conducted in womento exclude the presence of other disorders but are nothelpful in diagnosing 1C. Radiographie studies of catsfor diagnosis of lower urinary tract disease are muchmore common because of the limited access of cys-toscopy in veterinary medicine and are needed to ruleout the primary differential diagnosis, which is uro-lithiasis.
Cystoscopy is required for diagnosis of 1C, althoughthe typical cystoscopic findings of prominent vascu-larity and submucosal petechial hemorrhages (glo-merulations) after a second distention are shared withother bladder diseases (Messing 1992). Moreover, appearance of glomerulations has been suggested to result from "overdistention" of any bladder that is notroutinely stretched to this degree (Messing 1992). Weand others (McCarthy and McDermaid 1990) havefound similar lesions in cats with FIC.
The diagnosis of FIC thus rests upon the same criteria as does 1C, "chronic irritative voiding symptoms,sterile and cytologically negative urine, and characteristic cystoscopic findings . . . along with failure tofind a more objective cause for this clinical picture"(Messing 1992).
Unfortunately, because the etiology of both diseasesis unknown, any similarities between them may be
coincidental. To further examine the association andto permit formulation of a hypothesis to explain someof the signs, we have examined a number of other parameters of these diseases. To date, we have collectedpreliminary data for histopathology, histamine, substance P and glycosaminoglycan excretion and bladderpermeability.
The histopathologic findings in patients with 1Cvary (Messing 1992); the common findings of a relatively normal epithelium and muscularis with submucosal edema and vasodilation without remarkableinflammatory infiltrate (Messing 1992) is consistentwith findings in many cats with FIC. Mast cells alsohave been found in bladder biopsy specimens of some,but not all, women with 1C (Messing 1992) and catswith FIC (author's unpublished results). Problems withthe study of mast cells include the presence of differentsubsets of mast cells that affect their detection bystandard histologie techniques and the fact that theirgranules, to which commonly used stains bind, maybe released by the distention that occurs before thebiopsy specimen is collected.
Recently, the presence of mast cells in the bladderwall of 1C sufferers was suggested by the demonstration of increased histamine release into the cystoscopyfluid after hydrodistention of patients compared tonon-IC controls (Yun 1989). Using the same assay, wefound that the histamine concentration of the 80-cmeffluent was twice that found in the 10-cm effluent oftwo cats with FIC.
The increased nerve fiber density has been found inthe bladder of patients with 1C (Christmas et al. 1990),Hamid et al. 1988), suggesting a role for neurogenicinflammation in the pathophysiology of 1C. Based onincreased numbers of neurons positive for vasoactiveintestinal polypeptide and neuropeptide Y immuno-reactivity, the enhanced innervation of the bladder hasbeen suggested to represent an increase of sympatheticneurons (Hohenfellner et al. 1992). The number ofneurons positive for substance P and calcitonin-gene-related peptide immunoreactivity was not found to besignificantly different from patients with stress incontinence or vesicovaginal fistula. The absence of effecton for substance P and calcitonin-gene-related peptideimmunoreactivity was offered as evidence of the lackof effect of sensory afferent nerve involvement in 1C.They supported this conclusion by reference to similarresults reported from analysis of synovial fluid fromknee joints in patients suffering from rheumatoid arthritis (Larrson et al. 1991); Larrsonetal. (1991) however, came to a different conclusion from their results.They, and others (Donnerer et al. 1992), have suggested that reduced staining could result from a disease-induced increase in neuropeptide release (or decreased storage) from sensory afferent fibers. Moreover, Hohenfellner et al. (1992) collected tissues from1C patients after hydrodistention, whereas controlsamples were collected from (presumably undistended)
by on May 8, 2007
jn.nutrition.orgD
ownloaded from

2648S SUPPLEMENT
bladders during repair of stress incontinence. Bladderdistention is known to cause release of neuropeptidesfrom sensory afferent fibers (Maggi 1991), which mightexplain Hohenfellner's inability to find differences infor substance P and calcitonin-gene-related peptideimmunoreactivity between the groups.
To begin to evaluate the role of substance P in catswith FIC, we examined the cystoscopy effluent of threecats with FIC for substance P immunoreactivity. Allsubstance P concentrations were below the limit ofdetection of the assay, 2.9 pg/ml, except for one 80-cm H2O pressure-distended sample, in which 3.3 pg/ml was found. Further studies will be necessary toevaluate the role of substance P and other neuropeptides in inflammatory bladder diseases.
Further support for sensory afferent fiber involvement in the pathogenesis of 1C comes from studies ofthe effects of capsaicin on bladder function (Maggi andMeli 1986, Maggi and Meli 1988). Instillation of capsaicin, a pungent ingredient in hot peppers that stimulates a specific population of sensory afferent fibers,into the bladders of five patients with hypersensitivebladders produced a concentration-dependent reduction in capacity and pressure threshold for micturition.Moreover, all patients reported disappearance ormarked attenuation of their symptoms for a few daysafter capsaicin treatment, suggesting that capsaicin-sensitive sensory neurons (CSSN) are present in thehuman bladder. The urinary bladder of cats also contains a population of unmyelinated visceral afférentsthat responded to high intravesical pressure (80 cmwater) and to intraluminal application of chemical irritants (Habler et al. 1990), indicating that CSSN occurin the bladder of cats as well.
In addition to generation of an action potential,stimulation of CSSN also induces local release of neu-rotransmitters, even in the absence of a propagatedaction potential; a phenomenon referred to as the"axon reflex" (Maggi and Meli 1988). This reflex appears to provide protection of normal skin (Maggi etal. 1987), stomach (Holzer et al. 1991) and bladder(Maggi et al. 1988) epithelium and also to play a rolein neurogenic inflammatory processes in a variety oftissues, including skin (Breneman et al. 1992), intestine (Eysselein et al. 1992), lung (Barnes 1991), joints(Larsson et al. 1991) and bladder (Maggi 1991b, Maggi1991b).
Although neuropeptides are required for normalbladder function, neuropeptides released locally byCSSN after chemical or mechanical stimulation candilate microvessels and increase vascular permeability,which may appear as glomerulations in the bladderwall (Maggi 1991a). Neuropeptides also can degranulate mast cells (Dray 1992), which may explain thefinding of increased histamine concentrations in bladder effluent of 1C patients after distention (Yun et al.1992). Additionally, the depletion of neuropeptidesshortly after distension may explain the reduction in
pain reported by some 1C patients after distensiontherapy.
The most consistent finding in some patients with1C is a functional defect of the urothelial glycos-aminoglycan (GAG) layer (Hurst et al. 1993, Parsonset al. 1990). Such a defect might permit urine to penetrate the urothelium and induce inflammation. Studies (Hurst et al. 1987) have found that urinary GAGexcretion in 1C patients is lower than it is in normalhumans, which they attributed to increased bindingof GAG to the damaged urothelium. Some qualitativedifferences also have been reported (Holm-Bentzen etal. 1986). We have found decreased GAG excretion incats with FIC (Buffington et al. 1993). The GAG concentration (mean ±SD) in 24-h urine samples fromnormal cats was 41.6 ±21.9, and the GAG/Cr ratio(mg GAG/mg Cr) was 13.2 ±6.1. These values weresignificantly (P < 0.05) greater than the GAG concentration of 17.1 ±5.9, and GAG/Cr ratio of 6.0 ±1.5found in the urine of cats with FIC. In spot urine samples from normal cats, the GAG concentration was38.8 ±12.3 and the GAG/Cr ratio was 7.1 ±2.0.Theseresults also were significantly (P < 0.05) greater thanthe GAG concentration of 10.6 ±7.4 and GAG/Crratio of 3.5 ±2.6 found in spot samples of urine ofcats with FIC. Interestingly, both parameters were reduced in cats with FIC whether or not they were exhibiting signs of the disease at the time of urine collection. If this observation is confirmed by furtherstudy, it would suggest that some GAG-related abnormality might predispose to this disease.
As discussed above, one consequence of defects inthe urothelial GAG layer is thought to be increasedpermeability (Lilly and Parsons 1990, Parsons et al.1991 ). The response variable used in these studies, theamount of instilled urea missing after 45 min, canprovide only indirect evidence of differences in permeability, however. Moreover, the increased "loss"
of urea in 1C patients compared to normal controlsmay have been because of the fact that patients, butnot controls, underwent cystoscopy before the ureastudy. If greater bladder filling occurred in these patients, the outcome of the study might have been affected; Tammela et al. (1993) have shown that increasing intravesicular pressure to ~20 cm waterpressure can significantly increase bladder permeability.
Increased SP release from stimulated c-fibers alsocould influence bladder permeability. Although SPmay, under normal physiological conditions, have arole in the maintenance of epithelial barrier function(De Sanctis et al. 1990), it also has been shown to increase pulmonary epithelial permeability (Peterssonand Svensjo 1990). These findings provide an alternative explanation for the increased bladder permeability found in women with 1C. To study epithelialpermeability more directly, we have measured bladderepithelial permeability using sodium salicylate (SS)and
by on May 8, 2007
jn.nutrition.orgD
ownloaded from
LOWER URINARY TRACT DISEASE IN CATS 2649S
have found significant differences between normal catsand those with FIC.
In summary, review of research conducted withinthe last ten years suggests that the view of LUTD assynonymous with struvite urolithiasis must be reconsidered. Possibly because of changes in compositionof cat foods, the incidence of struvite-related urolithiasis and urethral obstruction have declined. The morerecently recognized problems related to potassium,acidosis and calcium oxalate urolithiasis suggest thatacidification of some diets may be excessive and mightbe decreased without a resurgence of struvite urolithiasis. A moderate approach might be to remove asmuch alkalinizing potential as possible before addingacid. Moreover, the decline in struvite urolithiasis mayhave unmasked another disease of the "feline urologiesyndrome", interstitial cystitis. If accurate, FIC wouldbe the first naturally-occurring model of 1C to be recognized and could be exploited to test a number ofhypotheses concerning the etiology of this disease.
LITERATURE CITED
Abelli, L., Conte, B., Somma, V., Maggi, C. A., Guiliani, S. & Meli,A. (1989) A method for studying pain arising from the urinarybladder in conscious, freely-moving rats. J. Urol. 141: 148-151.
Ackermann, D., Brown, C., Dunthorn, M., Purich, D. L. & Finlayson,B. (1989) Use of the computer program EQUIL to estimatepH in model solutions and human urine. Urol. Res. 17: 157-161.
Barnes, P. J. (1991) Neuropeptides and asthma. Am. Rev. Respir.Dis. 143: S28-S32.
Blount, W. P. (1931) Urinary calculi. Vet. J. 87: 561-576.Breneman, D. L., Cardone, J. S., Blumsack, R. F., Lather, R. M.,
Searle, E. A. & Pollack, V. E. (1992) Topical capsaicin fortreatment of hemodialysis-related pruritus. J. Am. Acad. Der-matol. 26: 91-94.
Buffington, C. A. (1988) Effects of Diet on the Feline StruviteUrolithiasis Syndrome, PhD thesis, University of California,Davis, California.
Buffington, C. A. T. (1992) Nutritional aspects of struvite urolithiasis. In: Proceedings Kal Kan Symposium for Treatment ofDog and Cat Diseases, pp. 51-57, Kal Kan Foods Inc., Vernon,CA.
Buffington, C. A. T., Blaisdell, J. L., Binns, S. P. & Woodworth,B. E. (1993) Decreased urine glycosaminoglycan excretion incats with inflammatory bladder syndrome. J. Urol. 149: 509A.
Buffington, C. A., Rogers, Q. R. & Morris, J. G. (1990) Effect ofdiet on struvite activity product in feline urine. Am. J. Vet. Res.51: 2025-2030.
Buffington, C. A., Rogers, Q. R., Morris, J. G. &.Cook, N. E. (1985)Feline struvite urolithiasis: magnesium effect depends on urinarypH. Feline Pract. 15:29-33.
Castonguay, T. W. (1981) Dietary dilution and intake in the cat.Physiol. Behav. 27: 547-549.
Ching, S. V., Fettman, M. J., Hamar, D. W., Nagode, L. A. & Smith,K. R. (1989) The effect of chronic dietary acidification usingammonium chloride on acid-base and mineral metabolism in theadult cat. J. Nutr. 119: 902-915.
Christmas, T. J., Rode, J., Chappie, C. R., Milroy, E. J. G. & Turner-Warwick, R. T. (1990) Nerve fibre proliferation in interstitialcystitis. Virchows Arch. A Path. Anat. 416: 447-451.
Clasper, M. (1990) A case of interstitial cystitis and Hunner'sulcer in a domestic shorthaired cat. N. Z. Vet. J. 38: 158-160.
De Sanctis, G. T., App, E. M., Trask, J. K., De Sanctis, B. I., Remmers,J. E., Green, F. H., Man, S. F. & King, M. (1990) Resorptiveclearance and transepithelial potential difference in capsaicin-treated F344 rats. J. Appi. Physiol. 68: 1826-1832.
DiBartola, S. P. & Buffington, C. A. (1993) Feline urologie syndrome. In: Textbook of Small Animal Surgery (Slatter, D. H.,ed), 2nd ed., pp. 1473-1487, Saunders, Philadelphia, PA.
Dibartola, S. P., Buffington, C. A., Chew, D. J., Mcloughlin, M. A.finSparks, R. A. (1993) Development of chronic renal diseasein cats fed a commercial diet. J. Am. Vet. Med. Assoc. 202: 744-
751.Dickinson, C. D. & Scott, P. P. (1956) Failure to produce urinary
calculi in kittens by the addition of mineral salts derived frombone-meal to the diet. Vet. Ree. 68: 858-859.
Donnerer, J., Schuligoi, R. & Stein, C. (1992) Increased contentand transport of substance P and calcitonin gene-related peptidein sensory nerves innervating inflamed tissue: evidence for a regulatory function of nerve growth factor in vivo. Neuroscience49: 693-698.
Dow, S. W., Fettman, M. J. & LeCouteur, R. S. (1987) Potassiumdepletion in cats: renal and dietary influences. J. Am. Vet. Med.Assoc. 191: 1569-1575.
Dray, A. (1992) Neuropharmacological mechanisms of capsaicinand related substances. Biochem. Pharmacol. 44: 611-615.
Eschalier, A. (1990) Antidepressants and pain management. In:Serotonin and Pain (Besson, J. M., éd.),pp. 305-325, Elsevier
Science, New York, NY.Eysselein, V. E., Reinshagen, M., Patel, A., Davis, W., Nast, C. &
Sternini, C. (1992) Calcitonin gene-related peptide in inflammatory bowel disease and experimentally induced colitis. Ann.N. Y. Acad. Sci. 657: 319-327.
Fau, D., Smalley, D. A. Si Rogers, Q. R. (1983) (Abstract) Effectsof excess methionine in the kitten. Fed. Proc. 42: 542.
Fettman, M. J. (1989) Feline kaliopenic polymyopathy/nephrop-athy syndrome. Vet. Clin. North Am. 19: 415-432.
Fettman, M. J., Coble, J. M., Hamar, Norrdin, R. W., Seim, H. B.,Kealy, R. D., Rogers, Q. R., McCrea, K. & Moffat, K. (1991)Effect of dietary phosphoric acid supplementation on acid-basebalance and mineral and bone metabolism in adult cats. Am. J.Vet. Res. 53: 2125-2135.
Finco, D. R., Adams, D., Crowell, W. A., Stattleman, A. J., Brown,S. A. &.Barsanti, J. A. (1986b) Food and water intake and urinecomposition in cats: influence of continuous versus periodicfeeding. Am. J. Vet. Res. 47: 1638-1642.
Finco, D. R., Barsanti, J. A. & Brown, S. A. (1986a|) Ammoniumchloride as a urinary acidifier in cats: efficacy, safety and rationalefor its use. Mod. Vet. Pract. 67: 537-541.
Finco, D. R., Barsanti, J. A. & Crowell, W. A. (1985) Characterization of magnesium-induced urinary disease in the cat andcomparison with feline urologie syndrome. Am. J. Vet. Res. 46:391-400.
Finke, M. D. &. Litzenberger, B. A. (1992) Effects of food intakeon urine pH in cats. J. Small Anim. Pract. 33: 261-265.
Fromm, G. H., Nakata, M. & Kondo, T. (1990) Differential actionof amitriptyline on neurons in the trigeminal nucleus. Neurology41: 1932-1936.
Graser, D. H. & Lewis, L. D. (1981) The consistency of dietaryminerals in commercial cat foods and their relationship to felineurolithiasis. Feline Pract. 11: 41-47.
Habler, H. J., Janig, W. & Koltzenburg, M. (1990) Activation ofunmyelinated afferent fibres by mechanical stimuli and inflammation of the urinary bladder in the cat. J. Physiol. 425: 545-562.
Hamar, D., Chow, F. H. C., Dysart, M. I. &. Rich, L. J. (1976)Effect of sodium chloride in prevention of experimentally produced phosphate uroliths in male cats. J. Am. Anim. Hosp. Assoc.12: 514-517.
Hamid, Q. A., Rode, J., Flanagan, A. M., Dhillon, A. P., Bishop,A. E., Stratton, M., Evans, D. J. &.Polak, J. M. (1988) Endocrine
by on May 8, 2007
jn.nutrition.orgD
ownloaded from

2650S SUPPLEMENT
differentiation in inflamed urinary bladder epithelium withmetaplastic changes. Virchows Arch. Path. Anat. Histopath. 412:267-272.
Hanno, P.M., Buehler, J.& Wein, A. J. (1989) Use of amitriptylinein the treatment of interstitial cystitis. J. Urol. 141: 846-848.
Hills, D. L., Morris, J. G. & Rogers, Q. R. (1982) Potassium requirement of kittens as affected by dietary protein. J. Nutr. 112:216-222.
Hohenfellner, M., Nunes, L., Schmidt, R. A., Lampel, A., Thuroff,J. W. & Tanagho, E. A. (1992) Interstitial cystitis: increasedsympathetic innervation and related neuropeptide synthesis. J.Urol. 147:587-591.
Holm-Bentzen, M., Ammitzboll, T. & Hald, T. (1986) Glycos-aminoglycans on the surface of the human urothelium: a preliminary report. Neurourol. Urodynam. 5: 519-523.
Holm-Bentzen, M., Jacobsen, F., Nerstrom, B., Lose, G., Kristensen,J. K., Pedersen, R. H., Krarup, T., Feggetter, J., Bates, P., Barnard,R., Larsen, S. & Hald, T. (1987) Painful bladder disease: clinicaland pathoanatomical differences in 115 patients. J. Urol. 138:500-502.
Holzer, P., Livingston, E. H., Saria, A. & Guth, P. H. (1991) Sensory neurons mediate protective vasodilatation in rat gastricmucosa. Am. J. Physiol. 260: G363-G370.
Houpt, K. A. (1991) Housesoiling: treatment of a common felineproblem. Vet. Med. 86: 1000-1006.
Hurst,R. E., Parsons, C.L., Roy, J.B.& Young, J.L. (1993) Urinaryglycosaminoglycan excretion as a laboratory marker in the diagnosis of interstitial cystitis. J. Urol. 149: 31-35.
Hurst, R. E., Rhodes, S. W., Adamson, P. B., Parsons, C. L. & Roy,J. B. (1987) Functional and structural characteristics of theglycosaminoglycans of the bladder luminal surface. J. Urol. 138:433-437.
Jackson, O. F. (1971) The treatment and subsequent preventionof struvite urolithiasis in cats. J. Small Anim. Pract. 12: 555-
568.Kallfelz, F. A., Bresselt, J. D. &. Wallace, R. J. (1980) Urethral
obstruction in random source and SPF male cats induced by highlevels of dietary magnesium and phosphorus. Feline Pract. 10:25-35.
Kohn, C. W. & DiBartola, S. P. (1992) Composition and distribution of body fluids in dogs and cats. In: Fluid Therapy in SmallAnimal Practice (DiBartola, S. P., éd.),pp. 1-34, Saunders, Philadelphia, PA.
Kruger, J. M., Osborne, C. A. &. Goyal, S. M. (1991) Clinicalevaluation of cats with lower urinary tract disease. J. Am. Vet.Med. Assoc. 199:211-216.
Larsson, J., Ekblom, A., Henriksson, K., Lundberg, T. & Theodors-son, E. (1991) Concentration of Substance P, neurokinin A,CGRP, NPY, and VIP in synovial fluid from knee joints in patients suffering from rheumatoid arthritis. Scand.}. Rheum. 20:326-335.
Lawler, D. F., Sjolin, D. W., Collins, J. E. (1985) Incidence rateof feline lower urinary tract disease in the United States. FelinePract. 15: 13-16.
Lewis, L. D., Chow, F. H. C., Taton, G. F. & Hamar, W. (1978)Effects of various dietary mineral concentrations on the occurrence of feline urolithiasis. J. Am. Vet. Med. Assoc. 172: 559-
564.Lewis, L. D. Si Morris, M. L. (1984) Treatment and prevention
of feline struvite urolithiasis. Vet. Clin. North Am. 14: 649-
660.Lilly, J. D. & Parsons, C. L. (1990) Bladder surface glycosami
noglycans: A human epithelial permeability barrier. Surg. Gy-necol. Obstet. 171: 493-496.
Lloyd, W. E. & Sullivan, D. J. (1984) Effects of orally administeredammonium chloride and methionine on feline urinary acidity.Vet. Med. 80: 773-778.
Maede, Y., Hoshino, T, Inaba, M. & Namioka, S. (1987) Methi-onine-induced hemolytic anemia with methemoglobinemia and
Heinz body formation in erythrocytes in cats. Amer. J. Vet. Res.48: 289-292.
Maggi, C. A. (199la) The role of peptides in the regulation of themicturition reflex: an update. Gen. Pharmacol. 22: 1-24.
Maggi, C. A. (199Ib) Capsaicin and primary afferent neurons,from basic science to human therapy. J. Auton. Nerv. Syst. 33:1-14.
Maggi, C. A., Abelli, L., Guiliani, S., Santicioli, P. & Meli, A. (1988)The contribution of sensory nerves to xylene-induced cystitis inrats. Neuroscience 26: 709-723.
Maggi, C. A., Borsini, F., Santicioli, P., Geppetti, P., Abelli, L.,Evangelista, S., Manzini, S., Theodorsson-Norheim, E., Somma,
V., Amenta, F., Bacciarelli, C. & Meli, A. (1987) Cutaneouslesions in capsaicin-pretrested rats—a trophic role of capsaicin-sensitive afférents?Naunyn-Schmiedebergs Arch. Pharmakol.336: 538-545.
Maggi, C. A., Guiliani, S., Del Bianco, E., Geppetti, P., Theodorsson,E. & Santicioli, P. Calcitonin gene-related peptide in the regulation of urinary tract motility. Ann. N. Y. Acad. Sci. 657: 328-343.
Maggi, C. A. & Meli, A. (1986) The role of neuropeptides in theregulation of micturition reflex. J. Autonom. Pharmacol. 6: 133-162.
Maggi, C. A. & Meli, A. (1988) The sensory-efferent function ofcapsaicin-sensitive nerves. Gen. Pharmacol. 19: 1-43.
Marder, A. (1991) Vet Clin of North Amer: Psychotropic drugsand behavioral therapy. Small Anim. Pract. 21: 329-342.
Max, M. B., Culnane, M., Schafer, S. C., Gracely, R. H., Walther,D. J., Smoller, B. &. Dubner, R. (1987) Amitriptyline relievesdiabetic neuropathy pain in patients with normal or depressedmood. Neurology 37: 589-596.
McCarthy, T. C. & McDermaid, S. L. (1990) Cystoscopy. Vet.Clin. North Am. Small Anim. Pract. 20: 1315-1339.
Messing, E. M. (1992) Interstitial cystitis and related syndromes.In: Campbell's Urology, 3rd ed., pp. 982-1005, W. B. Saunders,
Philadelphia, PA.Osborne, C. A., Clinton, C. W., Brunkow, H. C., Frost, A. P. & Johnston,
G. R. (1984) Epidemiology of naturally occurring feline uorlithsand urethral plugs. Vet. Clin. North Am. 14: 481-491.
Osborne, C. A., Kruger, J. M., Lulich, J. P., Beauclair, K. D., Unger,L. K., Bird, K. A., Koehler, L. A., Bartges, J. W., Felice, L. J.,Molitor, T., Polzin, D. J., Hall, C. L. & O'Brien, T. D. (1992a)
Feline lower urinary tract diseases: state of the science. In: Proceedings of the Kal Kan Symposium for Treatment of Dog andCat Diseases, pp. 89-98, Kal Kan Foods Inc., Vernon, CA.
Osborne, C. A., Kruger, J. P., Lulich, J. P., Bartges, J. W., Polzin,D. J., Molitor, T., Beauclair, K. D., &Onffroy, J. (1992b) Felinematrix-crystalline urethral plugs: a unifying hypothesis of causes.J. Small Anim. Pract. 33: 172-177.
Osborne, C. A., Lulich, J. P., Kruger, J. M., Polzin, D. J., Johnston,G. R. & Kroll, R. A. (1990) Medical dissolution of feline struvite urocystoliths. J. Am. Vet. Med. Assoc. 196: 1053-1063.
Osborne, C. A., Sann, J. J., Unger, L. K., Clinton, C. W. &.Davenport,M. P. (1989) Mineral composition of 4500 uroliths from dogs,cats, horses, cattle, sheep, goats, and pigs. Vet. Med. 84: 750-
764.Parsons, C. L., Boychuk, D., Jones, S., Hurst, R. E. & Calaban, H.
(1990) Bladder surface glycosaminoglycans: an epithelial permeability barrier. J. Urol. 143: 139-142.
Parsons, C. L., Lilly, J. D. &.Stein, P. (1991) Epithelial dysfunctionin nonbacterial cystitis. J. Urol. 145: 732-735.
Rich, L. J., Dysart, M. I., Chow, F. H. C. & Hamar, D. W. (1974)Urethral obstruction in male cats: experimental production byaddition of magnesium and phosphate to the diet. Feline Pract.4: 44-47.
Schwüle,P. O. & Herrmann, U. (1992) Environmental factors in »the pathophysiology of recurrent idiopathic calcium urolithiasis(RCU), with emphasis on nutrition. Urol. Res. 20: 72-83.
Smith, L. H., Van Den Berg, C. J. & Wilson, D. M. (1978) Nutrition and urolithiasis. N. Engl. J. Med. 298: 87-89.
by on May 8, 2007
jn.nutrition.orgD
ownloaded from

LOWER URINARY TRACT DISEASE IN CATS 2651S
Striker, G. E. (1989) KUH notes. J. Urol. 142: 139.Tammela, T., Wein, A. J., Monson, F. C. &. Levin, R. M. (1993)
Urothielial permeability of the isolated whole bladder. Neu-rourol. Urodyn. 12: 39-47.
Taton, G. F., Ramar, D. W. &. Lewis, L. D. (1984a) Evaluationof ammonium chloride as a urinary acidifier in the cat. J. Am.Vet. Med. Assoc. 184: 433-436.
Taton, G. F., Hamar, D. W. & Lewis, L. D. (1984b) Urinary acidification in the prevention and treatment of feline struvite uro-lithiasis. J. Am. Vet. Med. Assoc. 184: 437-443.
Theoharides, T. C., Bondy, P. K., Tsakalos, N. D. &. Askenase,P. W. (1982) Differential release of serotonin and histaminefrom mast cells. Nature 297: 229-231.
Werness, P. G., Bergeri, J. H. & Smith, L. H. (1981) Crystalluria.J. Crystal Growth 53: 166-181.
Yun, S. A., Laub, D. J., Weese, D. L., Lad, P. M., Leach, G. E. &Zimmern, P. E. (1992) Stimulated release of urine histaminein interstitial cystitis patients. J. Urol. 148: 1145-1148.
Ziegler, E. E. & Fomon, S. J. (1989) Potential renal solute load ofinfant formulas. J. Nutr. 119: 1785-1788.
by on May 8, 2007
jn.nutrition.orgD
ownloaded from
Copyright © 2022 FDOKUMEN




















