HPV and Upper Aerodigestive Tract Cancers - OHSU
115
HPV and Upper Aerodigestive Tract Cancers Joshua Schindler, MD Slides not provided
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of HPV and Upper Aerodigestive Tract Cancers - OHSU

HPV and Upper
Aerodigestive Tract
Cancers Joshua Schindler, MD
Slides not provided



















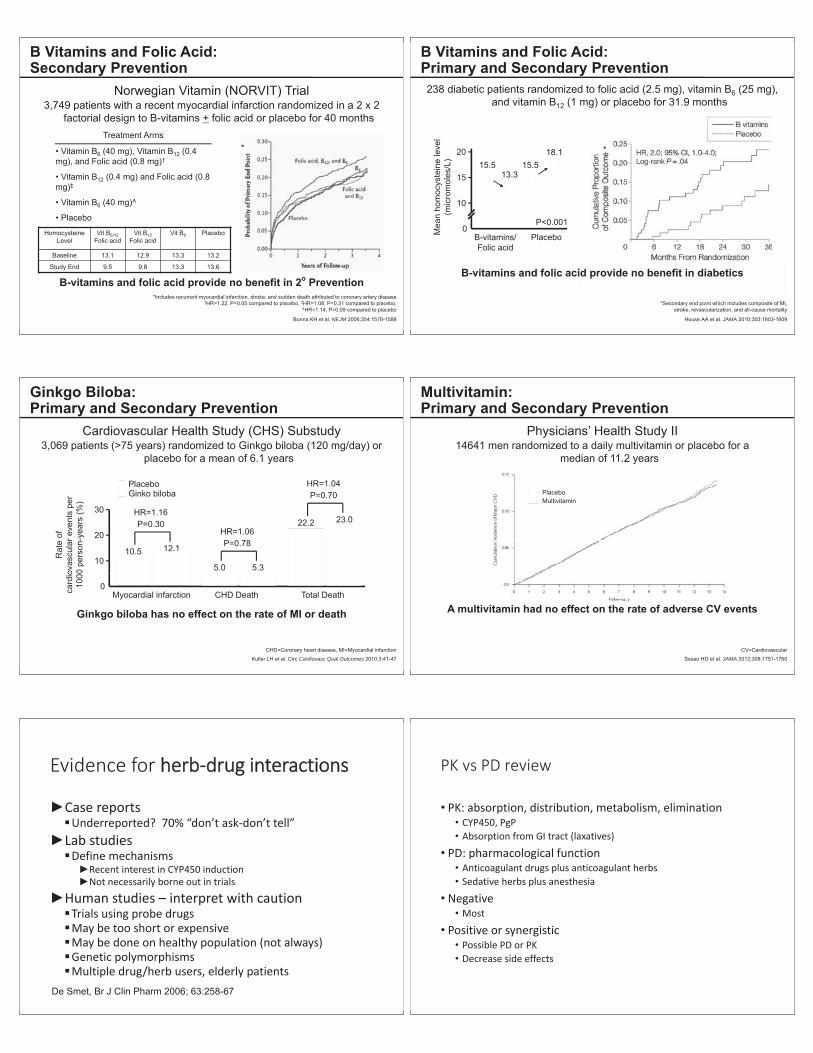
TThe Evidence for Current Cardiovascular Disease Prevention Guidelines:
Ineffective Therapies in Cardiovascular Disease
NEJMJACC
NEJMEpidemiology
Arch Intern Med Lancet Lancet NEJM
NEJMNEJM
Lancet Lancet JAMA
J Natl Cancer Inst

Arch Intern Med
NEJM BMJ
JAMA NEJM
NEJM JAMA
Cardiovasc Qual Outcomes JAMA





Carlo Patrono, Barry Coller, Garret A. FitzGerald, Jack Hirsh, and Gerald Roth





Financial Wellness:
Loan Repayment
Strategies for Medical
Professionals Justin Kribs, MS, CFP
Slides not provided

o
oo















CirculationLancet Circulation
Lancet


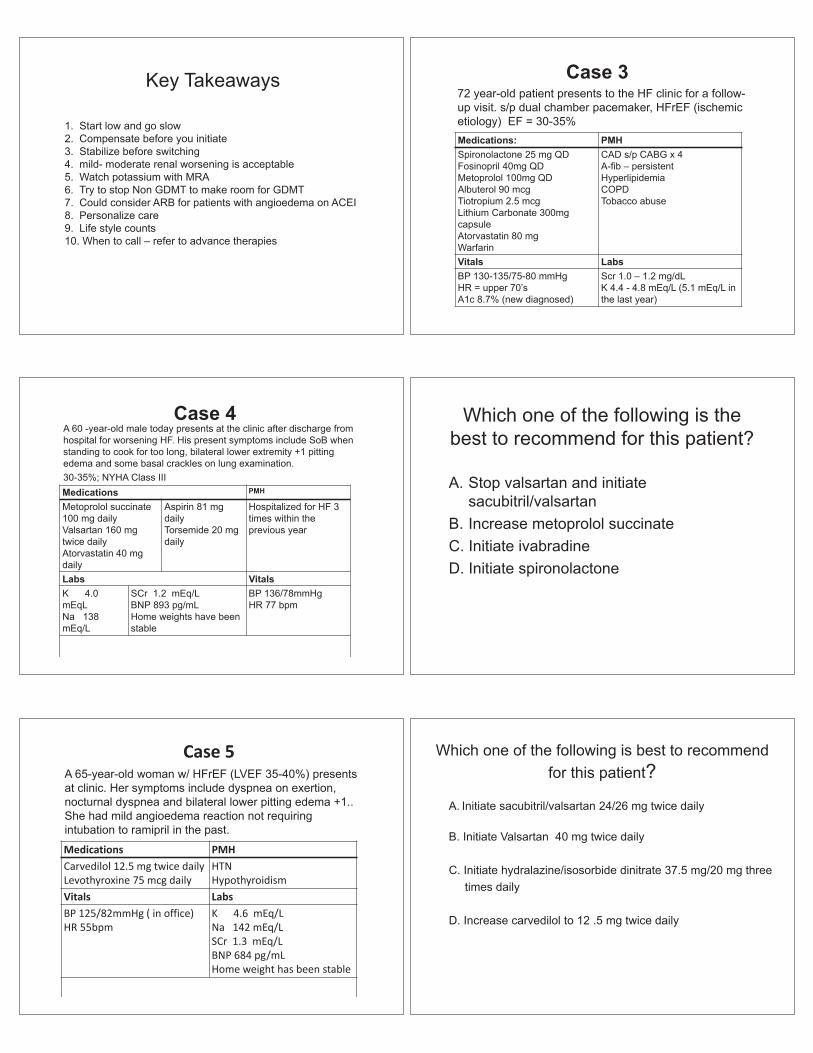
When to initiate ARNI?
Initiation of an ARNI de novo without prior exposure to ACEI or ARB
Is use of aldosterone antagonistmandatory prior to using ARNI?

Circ Cardiovasc Qual Outcomes





Vaping, Nicotine
Addiction and Lung
Injury: The Smoke is
Lifting
Holger Link, MD
Slides not provided

on >/= 2 occasions”
Hypertension
Hypertension

remains above goal
BP achieves target values on 4 medications
Hypertension

Sem Nephrol
De La Sierra: 8295 pts out of 68045 pts in Spain with > 140/90 on 3 meds12% with
37.5% White Coat Resistant

P=0.008
P=0.001
SBP DBP
P=0.054-15
-12
-9
-6
-3
0
*Different from control, p<0.05
Hypertension

Hypertension
Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-
blind, crossover trial
The Lancet

The Lancet Diabetes & Endocrinology
BP 150/100 mmHg. HR 80, BMI 38

HCTZ 12.5 mg qd
chlorthalidone 12.5 mg qd
spironolactone 12.5 qd or eplerenone 25 bid
chlorthalidone 25 mg qdLisinopril 20 mg qdspironolactone 12.5 mg qdcarvedilol 3.125 mg bid to start



. 325




Unexpected Career Paths in MedicinePrimary Care Conference 2020
Portland, OR
Jessica Walter, M.A. | Steve Kinder, [email protected] | [email protected]
OHSU Division of Managementwww.ohsu.edu/management
What did you want to be when you were
six years old?
EDUCATION EXPERIENCE YOU!
Goals
You will leave here today withconcrete TOOLS
that you can start usingTODAY
to CREATE your futureand make better DECISIONS
Licensure AcademicAppointments
PositionRequirements
Licensure AcademicAppointments
PositionRequirements

Keep learning
Blind tasting Blind tasting

Informational interviews
Informational [email protected]
What are your strengths?What are my strengths?
When do you see me do my best work?
When are you energized?

Seek Opportunity Seek Opportunity
See Opportunity Run experiments
ProjectsCommitteesInterim roleSchoolVolunteer

Network Density
Ibarra, H. (2015). Act like a leader. Think like a leader. Harvard Business Press. pp 94 – 95.

Network Density
Ibarra, H. (2015). Act like a leader. Think like a leader. Harvard Business Press. pp 94 – 95.
Who is going to speak for me?
Carla Harris
https://www.ted.com/talks/carla_harris_how_to_find_the_person_who_can_help_you_get_ahead_at_work
Photo from
Grow Others
J K J

C K J D C K J
D C K J Ghttps://www.bobsutton.net/books
Summary
1. Focus on purpose2. Find your gaps3. See(k) opportunities4. Build your team5. Build others
1. Meet three new people2. Conduct 1 informational
interview3. Craft 1 experiment 4. Connect 1 person to an
opportunity
To doVote now!
Finance 101Leadership StylesDesign ThinkingChange LeadershipPersonal Effectiveness

2019 ACC/AHA Primary Prevention
Guidelines SEAN ROBINSON, MD
OREGON HEALTH & SCIENCE UNIVERSITY
ASSISTANT PROFESSOR SPORTS & FAMILY MEDICINE
No conflict of interests
Preview Evidence
Patient Centered Approach to Comprehensive ASVCD Prevention
Team based Approach (COR I, LOE A) Shared decision making should guide discussions about best strategies to reduce ASCVD risk (COR I, LOE B-R)Social determinants of health should inform treatment recommendations (COR I, LOE B-NR)

Social Determinants of Health Income levelEducational opportunitiesOccupation, employment status, and workplace safetyGender inequityRacial segregationFood insecurity and inaccessibility of nutritious food choicesAccess to housing and utility servicesEarly childhood experiences and developmentSocial support and community inclusivityCrime rates and exposure to violent behaviorAvailability of transportationNeighborhood conditions and physical environment
Access to safe drinking water, clean air, and toxin-free environmentsRecreational and leisure opportunities
*Advanced age generally refers to age 75 years.ASCVD indicates atherosclerotic cardiovascular disease.
Assessment of Cardiovascular Risk
40-75 yo, routinely assess traditional cardiovascular risk factors and calculate 10-year risk of ASCVD using pooled cohort equations (COR I, LOE B-NR)20-39 yo, reasonable to assess traditional ASCVD risk every 4-6 years (COR IIa, LOE B-NR) Borderline risk (5%-7.5%) or intermediate risk ( 7.5% to 20%) reasonable to use risk-enhancing factors to guide therapy (COR IIa, LOE B-NR)In intermediate risk or selected adults at borderline risk, if risk-based discussion is uncertain, Coronary Calcium score is reasonable (COR IIa, LOE B-NR) 20-39 yo and 40-59 yo with ASCVD 7.5%, estimating lifetime risk may be considered (COR IIb, LOE B-NR)
Cohort equations
ASCVD Risk Estimator MESAFramingham CVD risk Reynolds SCORE QRISK/JBS3
Characterize Risk:
Low 5%
Borderline 5% to 7.5%
Intermediate 7.5% to 20%
High 20%

Summation
Coronary Calcium Score
Not a screening tool Helps further risk stratification/clarification
Intermediate risk Select borderline risk
CAC = 0 -> downward classification CAC 1-99 -> repeat risk discussion, ? Repeat test in 5 years CAC 100 (or 75% age/sex/race percentile) -> upward reclassification
My Take Away Points
10-year Risk assessment is the start of the conversation, not the end all be all Remember statins are not the only tool we have
Exercise, diet, sleep Use life-time risk as a tool to further the discussion (positive reinforcement or motivation to improve) Use risk-enhancers Use CAC to help clarify, demonstrate need/no need for therapy
Nutrition and Diet
Emphasize vegetables, fruits, legumes, nuts, whole grains, and fish (COR I, LOE B-R) Replace saturated fat with dietary mono/polyunsaturated fats (COR IIa, LOE B-NR)Reduce cholesterol and sodium in the diet (COR IIa, LOE B-NR) Minimize processed meats, refined carbohydrates, and sweetened beverages (COR IIa, LOE B-NR) AVOID trans fats (COR III, LOE B-NR)
Saturated vs Mono/polyunsaturated

Trans Fat
Eat real food
Exercise and Physical Activity
Counsel patients on optimization of living a physically active lifestyle (COR I, LOE B-R) Engage in 150 min/week of accumulated moderate intense exercise or 75 min/week of vigorous exercise in the form of aerobic exercise (COR I, LOE B-NR) Unable to meet the minimum abount above, engage in some moderate or vigorous intense exercise. This still can be beneficial. (COR IIa, LOE B-NR) Decreasing sedentary behavior may be reasonable to reduce ASCVD risk (COR IIb, LOE C-LD)
Intensity METs Examples
Sedentary behavior* 1–1.5 Sitting, reclining, or lying; watching television
Light 1.6–2.9 Walking slowly, cooking, light housework
Moderate 3.0–5.9
Brisk walking (2.4–4 mph), biking (5–9 mph), ballroom dancing, active yoga, recreational swimming
Vigorous 6Jogging/running, biking ( 10 mph), singles tennis, swimming laps
Sedentary behavior is defined as any waking behavior
characterized by an energy expenditure 1.5 METs while in
a sitting, reclining, or lying posture. Standing is a
sedentary activity in that it involves 1.5 METs, but it is not considered a component of
sedentary behavior.MET indicates metabolic
equivalent; and mph, miles per hour.

My Take Away
Please move Adults with Overweight and Obesity
Weight loss is recommended if overweight or obese (COR I, LOE B-R) Counseling and comprehensive lifestyle interventions, including calorie restriction, are recommended for achieving and maintaining weight loss (COR I, LOE B-R)Calculate BMI at least annually (COR I, LOE C-EO) Reasonable to measure waist circumference to identify those at higher cardiometabolic risk (COR IIa, LOE B_NR)
My Thoughts This can feel difficult to bring up and explore
Non-judgmental tone and listen to the patient and their prior failures
Ensure sleep is normal, I now rarely put much time and focus on weight loss if sleep is not buttoned up Everybody who is overweight knows they need to lose weight Stay away from fads Do not overload with recommendations or suggestions
Chose low hanging fruit, first Make goals reasonable and doable
Use motivational interviewing skills
Adults with Type 2 Diabetes Mellitus (DMII)
A tailored nutrition plan focusing on a heart-healthy dietary pattern is recommended to improve glycemic control, achieve weight loss if needed, and improve other ASCVD risk factors (COR I, LOE A) Exercise at least 150 minutes per week of moderate-intensity physical activity or 75 minutes of vigorous-intensity physical activity (COR I, LOE A) Initiate metformin as first-line therapy along with lifestyle therapies at the time of diagnosis to improve glycemic control and reduce ASCVD risk (COR IIa, LOE B-R)Reasonable to initiate a sodium-glucose cotransporter 2 (SGLT-2) inhibitor or a glucagon-like peptide-1 receptor (GLP-1R) agonist to improve glycemic control if above does not help (COR ILb, LOE B-R)

Risk-Enhancers in Diabetic Patients
Long duration ( 10 years for T2DM or 20 years for type 1 diabetes mellitus) Albuminuria 30 mcg albumin/mg creatinine eGFR <60 mL/min/1.73 m2 Retinopathy Neuropathy ABI <0.9
My Thoughts
DMII can be reversed!!Use diet, exercise and sleep to helpMetformin is first line pharmacologic treatment Use and know the risk-enhancers for DMIISodium-glucose cotransporter 2 (SGLT-2) inhibitor or a glucagon-like peptide-1 receptor (GLP-1R) for second line pharmacologic treatment
Adults with High Cholesterol
Intermediate risk ( 7.5% to <20% 10-year ASCVD risk) a moderate-intensity statin should be recommended (COR I, LOE A)In intermediate risk ( 7.5% to <20% 10-year ASCVD risk) patients, LDL-C levels should be reduced by 30% or more, and for optimal ASCVD risk reduction, especially in patients at high risk ( 20% 10-year ASCVD risk), levels should be reduced by 50% or more (COR I, LOE A)40 to 75 yo with DMII, regardless of estimated 10-year ASCVD risk, moderate-intensity statin therapy is indicated (COR I, LOE A)20 to 75 yo with an LDL-C level of 190 mg/dL or higher, maximally tolerated statin therapy is recommended (COR I, LOE B-R)DMII who have multiple ASCVD risk factors, it is reasonable to prescribe high-intensity statin therapy with the aim to reduce LDL-C levels by 50% or more (COR IIa, LOE B-R)Intermediate-risk ( 7.5% to <20% 10-year ASCVD risk) adults, risk-enhancing factors favor initiation or intensification of statin therapy (COR IIa, LOE B-R)
In intermediate-risk ( 7.5% to <20% 10-year ASCVD risk) adults or selected borderline-risk (5% to <7.5% 10-year ASCVD risk) adults in whom a CAC score is measured for the purpose of making a treatment decision, AND
CAC = zero, it is reasonable to withhold statin therapy and reassess in 5 to 10 years, as long as higher-risk conditions are absent (e.g., diabetes, family history of premature CHD, cigarette smoking); CAC = 1 to 99, it is reasonable to initiate statin therapy for patients 55 years of age; CAC = 100 or higher or in the 75th percentile or higher, it is reasonable to initiate statin therapy (COR IIa, LOE B-NR)
Borderline risk (5% to <7.5% 10-year ASCVD risk), the presence of risk- enhancing factors may justify initiation of moderate-intensity statin therapy (COR IIb, LOE B-R)

My Thoughts
Use a 10-year risk calculator for most patients Print/easy access to the flowsheetStatins are our friendsCAC can be helpful Patient-centered discussion are key to help communicate risk
Adults with Hypertension
Elevated blood pressure (BP) or hypertension, including those requiring antihypertensive medications nonpharmacological interventions are recommended to reduce BP. These include:
weight loss heart-healthy dietary pattern sodium reduction dietary potassium supplementationincreased physical activity with a structured exercise programlimited alcohol (COR I, LOE A)
10-year ASCVD risk of 10% or higher and an average systolic BP (SBP) of 130 mm Hg or higher or an average diastolic BP (DBP) of 80 mm Hg or higher, use of BP-lowering medications is recommended (COR I, LOE SBP: A, DBP: C-EO)In adults with confirmed hypertension and a 10-year ASCVD event risk of 10% or higher, a BP target of less than 130/80 mm Hg is recommended (COR I, LOE SBP: B-R, DBP: C-EO)In adults with hypertension and chronic kidney disease, treatment to a BP goal of less than 130/80 mm Hg is recommended (COR I, LOE SBP: B-R, DBP: C-EO)
In adults with T2DM and hypertension, antihypertensive drug treatment should be initiated at a BP of 130/80 mm Hg or higher, with a treatment goal of less than 130/80 mm Hg (COR I, LOE SBP: B-R, DBP: C-EO)In adults with an estimated 10-year ASCVD risk <10% and an SBP of 140 mm Hg or higher or a DBP of 90 mm Hg or higher, initiation and use of BP-lowering medication are recommended (COR I, LOE C-LD)
In adults with confirmed hypertension without additional markers of increased ASCVD risk, a BP target of less than 130/80 mm Hg may be reasonable (COR IIb, LOE SBP: B-NR, DBP: C-EO)

Table 7. Best Proven Nonpharmacological Interventions for Prevention and Treatment of Hypertension*
Nonpharmacological Intervention Goal
Approximate Impact on SBP
Hypertension Normotension
Weight loss Weight/body fat
Best goal is ideal body weight, but aim for at least a 1-kg reduction in body weight for most adults who are overweight. Expect about 1 mm Hg for every 1-kg reduction in body weight.
-5 mm Hg -2/3 mm Hg
Healthy diet DASH dietary pattern†
Consume a diet rich in fruits, vegetables, whole grains, and low-fat dairy products, with reduced content of saturated and total fat.
-11 mm Hg -3 mm Hg
Reduced intake of dietary sodium Dietary sodium
Optimal goal is <1500 mg/d,, but aim for at least a 1000-mg/d reduction in most adults.
-5/6 mm Hg -2/3 mm Hg
Enhanced intake of dietary potassium Dietary potassium Aim for 3500–5000 mg/d, preferably by
consumption of a diet rich in potassium. -4/5 mm Hg -2 mm Hg
Physical activity
Aerobic 90–150 min/wk65%–75% heart rate reserve -5/8 mm Hg -2/4 mm Hg
Dynamic resistance90–150 min/wk50%–80% 1 rep maximum6 exercises, 3 sets/exercise, 10 repetitions/set
-4 mm Hg -2 mm Hg
Isometric resistance
4 × 2 min (hand grip), 1 min rest between exercises, 30%–40% maximum voluntary contraction, 3 sessions/wk8–10 wk
-5 mm Hg -4 mm Hg
Moderation in alcohol intake
Alcohol consumption
In individuals who drink alcohol, reduce alcohol‡to:Men: 2 drinks dailyWomen: 1 drink daily
-4 mm Hg -3 mm Hg
My Thoughts
Lifestyle changes help120-129/ is Elevated Blood Pressure – formally known as Prehypertension Calculate ASCVD risk if found to have Hypertension (10% is cut off for medications)
140/90 -> Start medication
Treatment of Tobacco Use
Assess tobacco use at every visit and their tobacco use status; record as a vital sign to facilitate tobacco cessation (COR I, LOE A) Firmly advised to quit tobacco use (COE I, LOE A) A combination of behavioral interventions plus pharmacotherapy is recommended to maximize quit rates (COE I, LOE A) Tobacco abstinence is recommended to reduce ASCVD risk (COE I, LOE A) It is reasonable to dedicate trained staff to tobacco treatment in every healthcare system (COE IIa, LOE B-R) All adults and adolescents should avoid secondhand smoke exposure to reduce ASCVD risk (COE III, LOE B-NR)
My Thoughts
Tobacco is still REALLY bad for you Help your patient quit, bring it up often (every visit) Many options out there to help 1-800-Quit-Now
Aspirin (ASA) Use

Low-dose aspirin (75-100 mg orally daily) might be considered for the primary prevention of ASCVD among select adults 40 to 70 years of age who are at higher ASCVD risk but not at increased bleeding risk (COR IIb, LOE A) Low-dose aspirin (75-100 mg orally daily) should not be administered on a routine basis for the primary prevention of ASCVD among adults >70 years of age (COR III, LOE B-R) Low-dose aspirin (75-100 mg orally daily) should not be administered for the primary prevention of ASCVD among adults of any age who are at increased risk of bleeding (COR III, LOE C-LD)
My Thoughts
Avoid ASA usuallyThere still is a place for ASA in certain low risk patients These guidelines are for PRIMARY not secondary prevention
Simple 7
Top 10 Messages 1. Healthy lifestyle promotion is KEY to prevent ASCVD, heart
failure, atrial fibrillation 2. Use a TEAM and social determinants of health should help
guide informed treatment decisions. 3. 40-75 yo should undergo a 10 yr ASCVD risk estimation.
Followed by a risk discussion before starting medications. Risk -enhancing factor may help in this conversation.
4. CONSUME A HEALTHY DIET! Mostly Plants and real food. Weight loss strategies through calorie restriction should be applied for obese patients.
5. MOVE! 150 min/week of moderate intense exercise (75 min/week for vigorous)
6. DMII -> LIFESTYLE change. Metformin first followed by SGLT2 or GLP-1
7. Assess TOBACCO at every visit and advise to QUIT8. ASA for primary prevention should be used seldom9. STATIN is first line Tx for LDL >190, DMII, and at high risk for
ASCVD10. Target BLOOD PRESSURE is <130/80 mm Hg, Lifestyle is
first line treatment
Thank You



NEONATAL CHOLESTASIS GUIDELINES




DATE: 8 Nov 2019 PRESENTED BY: Jonathan Q. Purnell, MDProfessor, Knight Cardiovascular InstituteOregon Health & Science UniversityPortland, Oregon
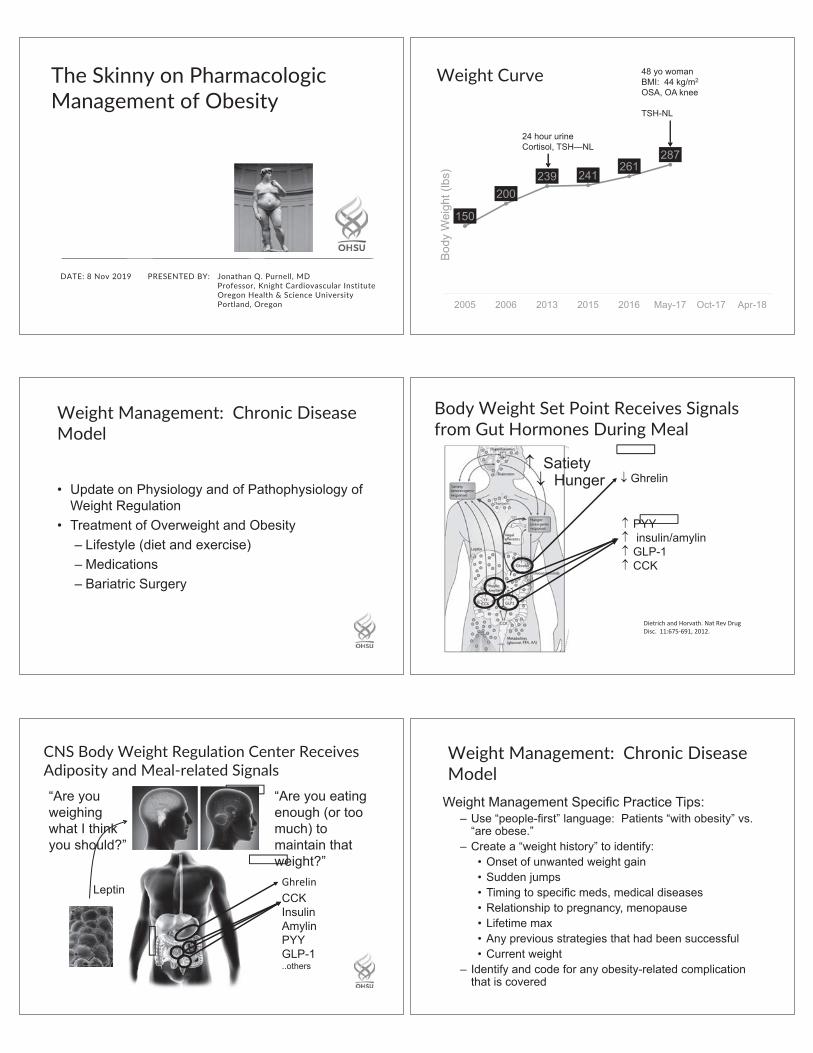
The Skinny on PharmacologicManagement of Obesity
Weight Curve
Weight Management: Chronic DiseaseModel
Body Weight Set Point Receives Signalsfrom Gut Hormones During Meal
CNS Body Weight Regulation Center ReceivesAdiposity and Meal related Signals
Weight Management: Chronic DiseaseModel

Obesity is associated with >230 complications
Yuen et al. Obesity Week 2016; Poster T-P-3166
Weight Management: Chronic DiseaseModel
Question
Weight LossComparison of“Named Diets.”Dansinger, et al. JAMA2005;293:43 53.
Diabetes Prevention Program: Modest Effecton Weight (Low fat Diet + Exercise)N Engl J Med 346:393–403, 2002.

Diabetes Incidence Best Lowered by Lifestyle(Low fat Diet + Exercise)N Engl J Med 346:393–403, 2002.
Lifestyle Recommendations
Weight Management: Chronic DiseaseModel
Recommendation For Consideration ofPharmacological Weight Management
Pharmacological Weight Management Pharmacological Weight Management

Weight Loss Medications Enhance CNSSignaling to Meal related Signals
Weight Loss With PhentermineMonroe, et al. BMJ. 1:352 54. 1968. Phentermine: Side Effects and Precautions
Weight Loss with Phentermine + Topiramate(Qsymia)Garvey WT, et al. Am J Clin Nutr. 2012;95:297 308.
Cardiovascular Safety During and After Use ofPhentermine and TopiramateRitchey ME, et al. J Clin Endocrinol Metab. 2019, 104(2):513–522

Weight Loss With Lorcaserin (5 HT2C agonist)Bohula EA et al. N Engl J Med 2018;379:1107 1117
Non inferiority of Lorcaserin (5 HT2C agonist) onMACEBohula EA et al. N Engl J Med 2018;379:1107 1117
Weight Loss With Buproprion + Naltrexon (Contrave)Nissen SE, et al. JAMA. 2016;315(10):990 1004.
Effect of Buproprion + Naltrexon (Contrave) on MACENissen SE, et al. JAMA. 2016;315(10):990 1004.
Liraglutide 3.0 for Weight Management and Type2 Diabetes Risk Reduction in Pre diabetesle Roux, et al. Lancet 2017; 389: 1399–409

Liraglutide 3.0 for Weight Management andType 2 Diabetes Risk Reduction in Pre diabetesle Roux, et al. Lancet 2017; 389: 1399–409
LEADER: Liraglutide 1.8 mg Improves CardiovascularOutcomes and All Cause Mortality in Type 2 DiabetesMarso SP et al. N Engl J Med 2016;375:311 322.
Weight Curve Weight Curve
Weight Curve: Next Steps Weight Curve: Next Steps

Question Weight Curve: Example of Using Rx forWeight Stability
Weight Curve: Example of Using Rx forWeight Stability
Weight Curve: Example of Using Rx forWeight Stability
Think management of hypercholesterolemia before statins and hypertension before ACEI
Patient is a non-responder (a “responder” may maintain weight)
Side effect(s) emerge
BMI 35 kg/m2 + comorbidityBMI 40 kg/m2
Reasons for Underutilization ofWeight Management Medications

Thank You

Nat Nev Cardiol. Eur Heart J

Eur Heart J
Eur Heart J
J Am Coll Cardiol. J Am Coll Cardiol. J Clin Lipidol N Engl J Med N Engl J Med

N Engl J Med N Engl J Med
Lancet Lancet N Engl J Med N Engl J Med N Engl J MedN Engl J Med. N Engl J Med. N Engl J Med
N Engl J Med N Engl J Med


J Clin Lipidol.

J Clin Lipidol Pharmacist's Letter.
J Clin Lipidol J Clin Lipidol J Am Coll Cardiol Arterioscler Thromb Vasc Biol. Mayo Clin Proc J Clin Lipidol J Am Coll Cardiol
J Clin Lipidol J Clin Lipidol J Clin Lipidol J Clin Lipidol J Am Heart Assoc

J Clin Lipidol J Clin LipidiolJ Clin Lipidol Am J Health-Syst Pharm Am Heart J J Am Coll Cardiol.
Ann Inter Med
(may increase with high TG)
(may increase with high TG)
J Clin Lipidol N Engl J Med
not
above

trans


Mayo Clin Proc.
N Engl J Med.

Thank You