
Follow-up Study on the Utility of von Willebrand Factor Levels in the Diagnosis of Cardiac Allograft...
7
Follow-up Study on the Utility of von Willebrand Factor Levels in the Diagnosis of Cardiac Allograft Vasculopathy Luis Martínez-Dolz, MD, PhD, a Luis Almenar, MD, PhD, a Eldemiro Reganon, PhD, b Virtudes Vila, PhD, b Carlos Chamorro, MD, a Luis Andrés, MD, a Vicenta Martínez-Sales, PhD, b Jose Moro, MD, a Jaime Agüero, MD, a Ignacio Sánchez-Lázaro, MD, a and Antonio Salvador, MD, PhD a Background: Cardiac allograft vasculopathy (CAV) is the major cause of late death in patients undergoing heart transplantation (HT). The most validated method for its diagnosis is intravascular ultrasound (IVUS), and there are no sufficiently reliable non-invasive methods. von Willebrand factor (vWF) is a marker of endothelial dysfunction/activity that is rarely studied in the context of CAV. The purpose of this study was to determine whether patients with higher levels of vWF in the first year post-transplant will develop a greater degree of CAV. Methods: A prospective study of 113 consecutive cardiac transplant recipients was initiated in January 2002. vWF determinations were performed at 1, 2, 4, 6, 9 and 12 months post-transplant, at the same time as biopsies. Coronary arteriography and IVUS were performed on the first and last follow-up visits. Heart–lung transplants, retransplants and pediatric transplants were excluded from the study. Patients who died in the first month and those who refused consent were also excluded. The final analysis included 72 patients and 405 vWF determinations. CAV was defined as an intimal thickening of 0.5 mm on follow-up versus baseline IVUS. Patients with CAV (n 41) and without CAV (n 31) after 1 year of follow-up were compared. Results: Patients who developed CAV had a higher prevalence of prior dyslipidemia, ischemic heart disease as the cause of HT, and rate of rejection, as well as higher vWF levels (321 122 vs 243 100%, p 0.05). The receiver– operator characteristic (ROC) curve showed that vWF values of 150% provided a sensitivity of 91%, and values of 400% a specificity of 91% (p 0.0001). The variables associated with CAV in the multivariate analysis were prior dyslipidemia, rejections and vWF, both linearly and by groups. vWF levels of 300% to 400% increased the probability of developing CAV by 390%, and levels 400% by 500%, versus levels 200%. Conclusions: vWF levels determined in the first year post-transplant help to distinguish a subgroup of patients with a higher incidence of CAV. J Heart Lung Transplant 2008;27:760 – 6. Copyright © 2008 by the International Society for Heart and Lung Transplantation. Cardiac allograft vasculopathy (CAV) and malignancy are the major causes of death in heart transplant (HT) patients after the early post-transplant period. 1 CAV is caused by an endothelial dysfunction in the coronary arteries of the implanted heart that is believed to be multifactorial in origin (brain death, ischemia–reperfusion injury, immu- nology, infection, cardiovascular risk factors). 2 The most validated method for diagnosis of this disease is intravascular ultrasound (IVUS), which as- sesses intimal proliferation and vessel remodeling. 3–6 There are no sufficiently reliable non-invasive methods to identify with precision which patients will develop the disease. The hypothesis of this study was that von Willebrand factor (vWF), as a marker of endothelial dysfunction/ activity, would be elevated in patients who develop the disease. Our objective was to conduct a follow-up study during the first year post-transplant to determine whether patients with higher vWF levels develop a greater degree of CAV. METHODS Study Design Inclusion and Exclusion Criteria A study on endothelial dysfunction/activity was initi- ated at our center in January 2002. The study protocol was approved by the hospital’s ethics committee and patients gave their consent to be included. The study ended in December 2006. From the a Heart Failure and Transplant Unit, Department of Cardiol- ogy, and b Center for Investigation (Biochemistry), La Fe University Hospital, Valencia, Spain. Submitted January 22, 2008; revised April 13, 2008; accepted April 21, 2008. Reprint requests: Luis Martínez Dolz, MD, Heart Failure and Trans- plant Unit, Department of Cardiology, La Fe University Hospital, Cavanilles 26-11, 46010 Valencia, Spain. Telephone: 0034-96-386- 2759. Fax: 0034-96-197-3314. E-mail: [email protected] Copyright © 2008 by the International Society for Heart and Lung Transplantation. 1053-2498/08/$–see front matter. doi:10.1016/ j.healun.2008.04.010 760 ALLOGRAFT VASCULOPATHY
Transcript of Follow-up Study on the Utility of von Willebrand Factor Levels in the Diagnosis of Cardiac Allograft...

FtLCI
B
M
R
C
Ctaeion
FoH
2
pC2CTj
7
ALLOGRAFT VASCULOPATHY
ollow-up Study on the Utility of von Willebrand Factor Levels inhe Diagnosis of Cardiac Allograft Vasculopathyuis Martínez-Dolz, MD, PhD,a Luis Almenar, MD, PhD,a Eldemiro Reganon, PhD,b Virtudes Vila, PhD,b
arlos Chamorro, MD,a Luis Andrés, MD,a Vicenta Martínez-Sales, PhD,b Jose Moro, MD,a Jaime Agüero, MD,a
gnacio Sánchez-Lázaro, MD,a and Antonio Salvador, MD, PhDa
ackground: Cardiac allograft vasculopathy (CAV) is the major cause of late death in patients undergoing hearttransplantation (HT). The most validated method for its diagnosis is intravascular ultrasound (IVUS),and there are no sufficiently reliable non-invasive methods. von Willebrand factor (vWF) is a markerof endothelial dysfunction/activity that is rarely studied in the context of CAV. The purpose of thisstudy was to determine whether patients with higher levels of vWF in the first year post-transplantwill develop a greater degree of CAV.
ethods: A prospective study of 113 consecutive cardiac transplant recipients was initiated in January 2002.vWF determinations were performed at 1, 2, 4, 6, 9 and 12 months post-transplant, at the same timeas biopsies. Coronary arteriography and IVUS were performed on the first and last follow-up visits.Heart–lung transplants, retransplants and pediatric transplants were excluded from the study.Patients who died in the first month and those who refused consent were also excluded. The finalanalysis included 72 patients and 405 vWF determinations. CAV was defined as an intimal thickeningof �0.5 mm on follow-up versus baseline IVUS. Patients with CAV (n � 41) and without CAV (n �31) after 1 year of follow-up were compared.
esults: Patients who developed CAV had a higher prevalence of prior dyslipidemia, ischemic heart diseaseas the cause of HT, and rate of rejection, as well as higher vWF levels (321 � 122 vs 243 � 100%,p � 0.05). The receiver–operator characteristic (ROC) curve showed that vWF values of 150%provided a sensitivity of 91%, and values of 400% a specificity of 91% (p � 0.0001). The variablesassociated with CAV in the multivariate analysis were prior dyslipidemia, rejections and vWF, bothlinearly and by groups. vWF levels of 300% to 400% increased the probability of developing CAV by390%, and levels �400% by 500%, versus levels �200%.
onclusions: vWF levels determined in the first year post-transplant help to distinguish a subgroup of patientswith a higher incidence of CAV. J Heart Lung Transplant 2008;27:760–6. Copyright © 2008 by the
International Society for Heart and Lung Transplantation.dsTtt
faddwg
MS
Aawp
ardiac allograft vasculopathy (CAV) and malignancy arehe major causes of death in heart transplant (HT) patientsfter the early post-transplant period.1 CAV is caused by anndothelial dysfunction in the coronary arteries of themplanted heart that is believed to be multifactorial inrigin (brain death, ischemia–reperfusion injury, immu-ology, infection, cardiovascular risk factors).2
The most validated method for diagnosis of this
rom the aHeart Failure and Transplant Unit, Department of Cardiol-gy, and bCenter for Investigation (Biochemistry), La Fe Universityospital, Valencia, Spain.Submitted January 22, 2008; revised April 13, 2008; accepted April
1, 2008.Reprint requests: Luis Martínez Dolz, MD, Heart Failure and Trans-
lant Unit, Department of Cardiology, La Fe University Hospital,avanilles 26-11, 46010 Valencia, Spain. Telephone: 0034-96-386-759. Fax: 0034-96-197-3314. E-mail: [email protected] © 2008 by the International Society for Heart and Lungransplantation. 1053-2498/08/$–see front matter. doi:10.1016/
e.healun.2008.04.010
60
isease is intravascular ultrasound (IVUS), which as-esses intimal proliferation and vessel remodeling.3–6
here are no sufficiently reliable non-invasive methodso identify with precision which patients will develophe disease.
The hypothesis of this study was that von Willebrandactor (vWF), as a marker of endothelial dysfunction/ctivity, would be elevated in patients who develop theisease. Our objective was to conduct a follow-up studyuring the first year post-transplant to determinehether patients with higher vWF levels develop a
reater degree of CAV.
ETHODStudy Design Inclusion and Exclusion Criteria
study on endothelial dysfunction/activity was initi-ted at our center in January 2002. The study protocolas approved by the hospital’s ethics committee andatients gave their consent to be included. The study
nded in December 2006.
abw
Hpwwttwsa
iptisictd
c
S
VnfabcTaalr
72sap
apaaswAwpav
S
QqmptMb(wqwacs
RC
P3f
The Journal of Heart and Lung Transplantation Martínez-Dolz et al. 761Volume 27, Number 7
vWF determinations were performed at 1, 2, 4, 6, 9nd 12 months post-transplant, at the same time asiopsies. Standard coronary arteriography and IVUSere performed on the first and last follow-up visits.Inclusion of the transplant patients was consecutive.
eart–lung transplants, retransplants, pediatric trans-lants, patients who died in the first month and patientsho refused consent were excluded. Also excludedere patients with fewer than four determinations. The
otal number of patients included was 72. Determina-ions were not considered for analysis if they coincidedith active infection or a biopsy with an insufficient
ample for analysis. The total number of determinationsnalyzed was 405.
The protocol of immunosuppression at our hospitalncludes antibody induction therapy with OKT3 (inrevious phases) or anti-CD25 in combination withriple maintenance therapy, usually with a calcineurinnhibitor � mycophenolate mofetil � steroids. Epi-odes of acute cellular rejection were treated with threentravenous doses of methylprednisolone 500 mg. Theytomegalovirus (CMV) prophylaxis regimen includedherapy with ganciclovir or valganciclovir in standardoses for 3 weeks in CMV-seronegative recipients.Figure 1 shows the study design, the patients in-
luded and determinations performed.
tudy Parameters and IVUS
enous blood samples were drawn by qualified person-el after the patients had rested overnight, after lyingor at least 30 minutes in a supine position, and beforeny oral intake of food or medication. A total of 5 ml oflood was collected into tubes containing an anti-oagulant solution of 0.13 mol/liter trisodium citrate.he ratio of anti-coagulant to blood was 1/9 (v/v). vWFntigen plasma level was measured with a researchnalyzer (ACL 6000; Instrumentation Laboratory) usingatex particles coated with a polyclonal antibody di-ected against vWF. The coefficient of variation was
Figure 1. Study design and d
.5%. Each sample was immediately centrifuged at,000g for 30 minutes at 4°C to obtain plasma. Theamples were tested immediately or frozen in aliquotst �80°C until use. vWF plasma levels are expressed asercentage over normal value.Conventional coronary angiography was performed
nd, during the procedure, a guiding catheter wasositioned in the ostium of the left main coronary arterynd an angioplasty guide-wire inserted through thenterior descending coronary artery to its most distalegment. Automated pullback was then performedhile acquiring video images for subsequent analysis.ll the images were interpreted by the same physicianho was blinded to the laboratory results and theatient’s clinical condition. Significant CAV was defineds an intimal thickening of �0.5 mm in the follow-upersus baseline IVUS in any area of the vessel lumen.
tatistical Analysis
ualitative variables are expressed as percentages anduantitative variables as mean � standard deviation oredian and interquartile range (Kolmogorov–Smirnov,� 0.05). Comparisons were made with the chi-square
est, Student’s t-test for independent samples and theann–Whitney U-test. The data were represented usingoxplot charts. The receiver–operator characteristicROC) area under the curve was used to determinehether a specific vWF value classified patients ade-uately. A multivariate analysis using logistic regressionas performed to check the association between vWF
nd CAV. p � 0.05 was considered statistically signifi-ant. SPSS v12.0 (SPSS, Inc., Chicago, IL) statisticaloftware was used.
ESULTSlinical Profile of Patients
atients with CAV (n � 41) and without CAV (n �1) were compared. Significant differences wereound for prevalence of prior dyslipidemia, ischemic
eterminations performed.

htw(
C
vtF
wlCTe
R
Tc
762 Martínez-Dolz et al. The Journal of Heart and Lung TransplantationJuly 2008
eart disease as the etiology of heart failure, rejec-ions during follow-up and vWF levels. All differencesere more prevalent in patients who developed CAV
Table 1).
hange in von Willebrand Factor Levels
WF levels remained stable on all follow-up visits afterransplant, without a tendency to increase or decrease.ifty percent of values were between 200% and 400%,
Table 1. Clinical Profile of Patients
Pre-transplant variablesAge (years)MaleBody mass index (kg/m2)Insulin-dependent diabetes mellitus (%)Arterial hypertension (%)Dyslipidemiaa (%)Smoking (%)Etiology of heart failurea
Ischemic heart disease (%)Idiopathic dilated cardiomyopathy (%)Valvular disease (%)Other (%)
CMV serology (recipient/donor)R�/D�
R�/D�
R�/D�
R�/D�
Induction immunosuppressionOKT3 (%)Anti-CD25 (%)
Maintenance immunosuppressionCyclosporine (%)Tacrolimus (%)Azathioprine (%)Mycophenolate mofetil (%)Everolimus (%)Steroids (%)
Other follow-up drugsCalcium channel blockers (%)ACE inhibitors (%)Anti-coagulants (%)Anti-aggregants (%)Statins (%)Insulin (%)
Rejection during follow-upa (%)Infection during follow-up (%)Creatinine at 1 year (mg/dl)sGOT/sGPT at 1 year (mg/dl)Hemoglobin at 1 year (mg/dl)von Willebrand factora (%)
Values expressed as percentages and mean � stadonor; ACE, angiotensin-converting enzyme; sGOT, sglutamic pyruvic transaminase.
aP � 0.05.
ithout significant changes during follow-up. When vWFevels were separated between patients with and withoutAV, higher levels were observed in patients with CAV.hese differences were significant on all follow-up visitsxcept the third (Month 4) (Figure 2 and Table 2).
OC Curve
he ROC curve showed a significant area under theurve (0.689, p � 0.0001). vWF values of 150% pro-
CAV(n � 41)
No CAV(n � 31)
53 � 8 50 � 1093 94
27 � 5 25 � 410 1323 3468 4277 67
61 3629 395 135 12
61 6520 1915 104 6
20 1080 90
85 8117 1910 1090 925 3
100 100
44 4626 244 2
32 3088 8528 3044 19
5 61.6 � 1.0 1.5 � 0.9
24 � 17/48 � 24 25 � 16/38 � 2311.9 � 1.5 12.4 � 1.6321 � 122 243 � 100
rd deviation. CMV, cytomegalovirus; R/D, recipient/m glutamic oxaloacetic transaminase; sGPT, serum
ndaeru

vfi
M
Aithadaoip
D
Cpdsftaimypt
dspsa
bjlfhr
odbp(mi
tlCfhdb
FaWT hird
T
N
C
p
C
The Journal of Heart and Lung Transplantation Martínez-Dolz et al. 763Volume 27, Number 7
ided a sensitivity of 91%, and values of 400% a speci-city of 91% (Figure 3).
ultivariate Analysis
multivariate analysis model was carried out thatncluded the following variables: diabetes mellitus; ar-erial hypertension; dyslipidemia; smoking; etiology ofeart failure; induction immunosuppression; rejection;nd vWF. The variables associated with CAV were prioryslipidemia, presence of rejections during follow-upnd vWF, both linearly and by groups. Thus, vWF levelsf 300% to 400% increased the probability of develop-
ng CAV by 390%, and levels �400% increased therobability by 500%, vs levels �200% (Table 3).
ISCUSSION
ardiac transplantation is the definitive therapy foratients with end-stage heart failure without contrain-ications for this procedure. The major limitations tourvival in the first year post-transplant are acute graftailure, multiple-organ failure, acute rejection and infec-ion.1 After this period, cardiac allograft vasculopathynd malignancy are the most common causes of deathn these patients. In angiographic studies, approxi-
ately 32% of patients have allograft vasculopathy at 5ears and 53% at 10 years, with the incidence increasingrogressively over time.1 However, angiography tendso underestimate the severity of the disease due to the
igure 2. Change in von Willebrand factor (vWF) levels. (Left) vWF levetendency to increase or decrease. Fifty percent of values were betwehen vWF levels were separated between patients with (lightgray) and
hese differences were significant on all follow-up visits except the t
able 2. Change in von Willebrand Factor (vWF) Levels
1 2
o CAV 218 � 147 234 � 71 22No. of patients 31 30
AV 349 � 177 358 � 204 33No. of patients 41 41
0.001 0.001
AV, cardiac allograft vasculopathy.
iffuse narrowing characteristic of CAV in its earlytages. Thus, IVUS has become the most accuraterocedure for its diagnosis and has been found ineveral studies to have value in predicting both CAVnd other cardiovascular end-points.3–6
CAV seems to have a multifactorial etiology in whichoth immunologic (cellular rejection,7–11 humoral re-
ection12–14 and HLA mismatch7,15) and non-immuno-ogic factors (hyperlipidemia,16–18 cytomegalovirus in-ection,19,20 dysglycemia and insulin resistance,21 or aistory of a coronary artery disease in the donor22 orecipient1,10) have been implicated.
There are no sufficiently reliable non-invasive meth-ds to identify with precision which patients willevelop the disease, although procedures such as do-utamine stress echocardiography,23–25 dipyridamoleerfusion studies26–29 or computerized tomographyCT) or positron emission tomography (PET) scans30,31
ay play an adjuvant role in the detection of myocardialschemia.
Several studies have shown that endothelial dysfunc-ion, as detected by an abnormal response to acetylcho-ine, is associated with the development of significantAV and suggest that serial studies of endothelial
unction might have clinical utility.6,32 On the otherand, monitoring of plasma markers of myocardialamage, inflammation and early endothelial injury haseen shown to be of great value for evaluating the
emained stable on all follow-up assessments after transplant, without200% and 400%, without significant changes during follow-up. (Right)hout CAV (darkgray), higher levels were observed in patients with CAV.(Month 4).
vWF (%) assessments
3 4 5 6
192 230 � 128 200 � 83 210 � 1060 30 25 25
208 309 � 201 250 � 39 367 � 1291 41 39 31
.18 0.02 0.015 0.0001
ls renwit
8 �3
4 �4
0
epectephCpscp
meoldddvTeiicC
llt
aw
iatm1rwwathC
slptdlpiasapHo
oi0esbCer
Fva
TV
DRLv
v
764 Martínez-Dolz et al. The Journal of Heart and Lung TransplantationJuly 2008
fficacy of therapeutic interventions and surveillance ofatients with CAV.33,34 Thus, patients with a persistentlevation in troponin I levels, as a marker of microvas-ular damage, during the first year after heart transplan-ation (post-HT) have greater progression of CAV andarlier graft dysfunction.35 Elevated levels of C-reactiverotein, a sensitive marker of systemic inflammation,ave been associated with the development ofAV36–38 and predict graft dysfunction.37,39 Elevatedlasma levels of BNP, which reflect wall stress andtructural remodeling of the graft, have also beenorrelated with the development of CAV in the lateost-HT phase.40
The hypothesis of this study was that vWF, as aarker of endothelial dysfunction/activity, would be
levated in patients who develop the disease. Thebjective of our investigation was to conduct a fol-
ow-up study during the first year post-transplant toetermine whether patients with higher vWF levelsevelop a greater degree of CAV. Significant CAV wasefined as intimal thickening of �0.5 mm follow-upersus baseline IVUS in any area of the vessel lumen.he parameter of an increase in maximal intimal thick-ning of �0.5 mm at 1 year of HT has been referred ton previous studies as prognostically relevant (becausets reproducibly has been associated with major adverseardiac events) or indicative of rapidly progressiveAV.41–43
When the clinical profile of the patients was ana-yzed, significant differences were found in the preva-ence of prior dyslipidemia, ischemic heart disease as
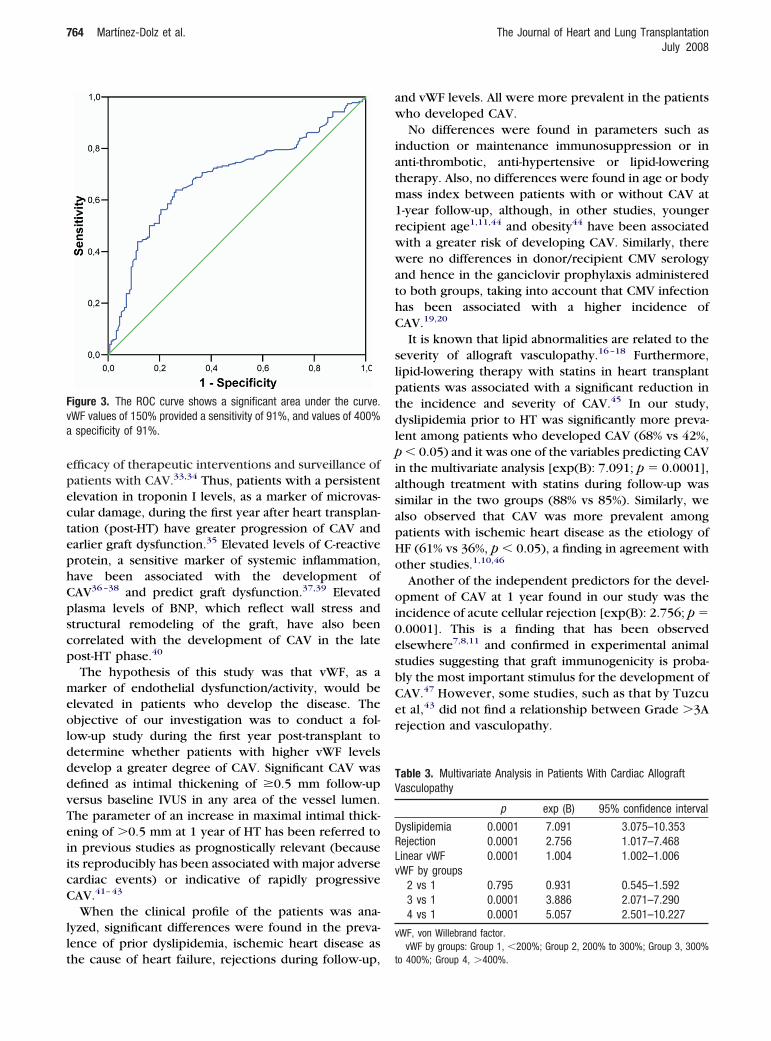
igure 3. The ROC curve shows a significant area under the curve.WF values of 150% provided a sensitivity of 91%, and values of 400%specificity of 91%.
he cause of heart failure, rejections during follow-up, t
nd vWF levels. All were more prevalent in the patientsho developed CAV.No differences were found in parameters such as
nduction or maintenance immunosuppression or innti-thrombotic, anti-hypertensive or lipid-loweringherapy. Also, no differences were found in age or bodyass index between patients with or without CAV at
-year follow-up, although, in other studies, youngerecipient age1,11,44 and obesity44 have been associatedith a greater risk of developing CAV. Similarly, thereere no differences in donor/recipient CMV serology
nd hence in the ganciclovir prophylaxis administeredo both groups, taking into account that CMV infectionas been associated with a higher incidence ofAV.19,20
It is known that lipid abnormalities are related to theeverity of allograft vasculopathy.16–18 Furthermore,ipid-lowering therapy with statins in heart transplantatients was associated with a significant reduction inhe incidence and severity of CAV.45 In our study,yslipidemia prior to HT was significantly more preva-
ent among patients who developed CAV (68% vs 42%,� 0.05) and it was one of the variables predicting CAV
n the multivariate analysis [exp(B): 7.091; p � 0.0001],lthough treatment with statins during follow-up wasimilar in the two groups (88% vs 85%). Similarly, welso observed that CAV was more prevalent amongatients with ischemic heart disease as the etiology ofF (61% vs 36%, p � 0.05), a finding in agreement withther studies.1,10,46
Another of the independent predictors for the devel-pment of CAV at 1 year found in our study was the
ncidence of acute cellular rejection [exp(B): 2.756; p �.0001]. This is a finding that has been observedlsewhere7,8,11 and confirmed in experimental animaltudies suggesting that graft immunogenicity is proba-ly the most important stimulus for the development ofAV.47 However, some studies, such as that by Tuzcut al,43 did not find a relationship between Grade �3Aejection and vasculopathy.
able 3. Multivariate Analysis in Patients With Cardiac Allograftasculopathy
p exp (B) 95% confidence interval
yslipidemia 0.0001 7.091 3.075–10.353ejection 0.0001 2.756 1.017–7.468inear vWF 0.0001 1.004 1.002–1.006WF by groups
2 vs 1 0.795 0.931 0.545–1.5923 vs 1 0.0001 3.886 2.071–7.2904 vs 1 0.0001 5.057 2.501–10.227
WF, von Willebrand factor.vWF by groups: Group 1, �200%; Group 2, 200% to 300%; Group 3, 300%
o 400%; Group 4, �400%.

avaldtsecwpsHtHiasdtwCd
tfltamso4vtgp�
aopr
pirhalbptt
ds
R
1
1
1
1
1
1
1
1
1
The Journal of Heart and Lung Transplantation Martínez-Dolz et al. 765Volume 27, Number 7
With regard to vWF, there have been very few studiesnalyzing its relationship to the presence of allograftasculopathy in the heart transplant population. vWF ismediator of platelet adhesion to damaged endothe-
ium and has been shown to play a critical role in theevelopment of vascular disease in general,48,49 al-hough its specific relationship to CAV has been rarelytudied. Cooke et al50 analyzed the presence of differ-nt atherogenic markers in 93 post-HT recipients andompared them to a population with advanced HF (48%ith ischemic heart disease) and a healthy controlopulation. They found that mean vWF levels wereimilar in the transplanted (207.9 � 65%) and advancedF groups (209.5 � 100%) and elevated above that of
he healthy control group (113 � 44.2%, p � 0.0005).owever, mean vWF values did not differ significantly
n transplanted patients with severe, mild or no CAV. Inny case, it was not a prospective but rather a cross-ectional study; furthermore, assessment of CAV wasone by standard coronary arteriography and post-ransplant duration was significantly longer in patientsith severe CAV (2,249 � 791 days) vs those withoutAV (1,186 � 869 days) or with mild CAV (1,620 � 627ays).In our study, we observed higher mean vWF levels in
he subgroup of patients who developed CAV at 1-yearollow-up (321 � 122% vs 243 � 100%, p � 0.05). vWFevels remained stable on all follow-up visits afterransplant, without a tendency to increase or decrease,nd these differences were significant on all assess-ents except the third (Month 4). The ROC curve
howed a significant area under the curve. vWF valuesf 150% provided a sensitivity of 91%, and values of00% a specificity of 91%. In the multivariate analysis,WF levels were the third independent predictive fac-or for the development of CAV, both linearly and byroups. Thus, vWF levels of 300% to 400% increased therobability of developing CAV by 390%, and levels400% by 500%, versus levels �200%.No other study in the literature has prospectively
nalyzed the relationship between vWF and the devel-pment of CAV, and the findings suggest that thisarameter, whose determination is simple and doneoutinely in most laboratories, has clinical utility.
Despite the limitations that may result from onlyerforming IVUS on the left main and anterior descend-
ng coronary arteries for diagnosis of CAV, as well as theelatively limited number of patients studied and notaving analyzed other parameters presumably associ-ted with the development of CAV (such as humaneukocyte antigen mismatch or humoral rejection), weelieve that vWF levels determined in the first yearost-HT could help to distinguish a subgroup of pa-ients with a greater incidence of CAV. For such pa-
ients, more aggressive pharmacologic treatments orifferent immunosuppressive regimens that have beenhown to be effective for reducing CAV are warranted.
EFERENCES
1. Taylor DO, Edwards LB, Boucek MM, et al. Registry of theInternational Society for Heart and Lung Transplantation: twenty-fourth official adult heart transplant report—2007. J Heart LungTransplant 2007;26:769–807.
2. Mehra MR. Contemporary concepts in prevention and treat-ment of cardiac allograft vasculopathy. Am J Transplant 2006;6:1248 –56.
3. Mehra MR, Ventura HO, Stapleton DD, et al. Presence of severeintimal thickening by intravascular ultrasonography predicts car-diac events in cardiac allograft vasculopathy. J Heart Lung Trans-plant 1995;14:632–9.
4. Rickenbacher PR, Pinto FJ, Lewis NP, et al. Prognostic impor-tance of intimal thickness as measured by intracoronary ultra-sound after cardiac transplantation. Circulation 1995;92:3445–52.
5. Kapadia SR, Nissen SE, Tuzcu EM. Impact of intravascular ultra-sound in understanding transplant coronary artery disease. CurrOpin Cardiol 1999;14:140–50.
6. Kofoed KF, Czernin J, Johnson J, et al. Effects of cardiac allograftvasculopathy on myocardial blood flow, vasodilatory capacity,and coronary vasomotion. Circulation 1997;95:600–6.
7. Uretsky BF, Murali S, Reddy PS, et al. Development of coronaryartery disease in cardiac transplant patients receiving immuno-suppressive therapy with cyclosporine and prednisone. Circula-tion 1987;76:827–34.
8. Radovancevic B, Poindexter S, Birovljev S, et al. Risk factors fordevelopment of accelerated coronary artery disease in cardiactransplant recipients. Eur J Cardiothorac Surg 1990;4:309–12.
9. Zerbe T, Uretsky B, Kormos R, et al. Graft atherosclerosis: effectsof cellular rejection and human lymphocyte antigen. J Heart LungTransplant 1992;11(suppl):S104–10.
0. Lindelow B, Bergh C, Lamm C, Andersson B, Waagstein F. Graftcoronary artery disease is strongly related to the aetiology of heartfailure and cellular rejections. Eur Heart J 1999;20:1326–34.
1. Stoica SC, Cafferty F, Pauriah M, et al. Allograft vasculopathy: thecumulative effect of acute rejection on development of cardiacallograft vasculopathy. J Heart Lung Transplant 2006;25:420–5.
2. Reed EF, Demetris AJ, Hammond E, et al. Acute antibody-mediated rejection of cardiac transplants. J Heart Lung Transplant2006;25:153–9.
3. Cherry R, Nielsen H, Reed E, et al. Vascular (humoral) rejection incardiac allograft biopsies: relation to circulating anti-HLA antibod-ies. J Heart Lung Transplant 1992;11:24–9.
4. Fredrich R, Toyoda M, Czer LS, et al. The clinical significance ofantibodies to human vascular endothelial cells after cardiactransplantation. Transplantation 1999;67:385–91.
5. Cocanougher B, Ballantyne CM, Pollack MS, et al. Degree of HLAmismatch as a predictor of death from allograft arteriopathy afterheart transplant. Transplant Proc 1993;25:233–6.
6. Escobar A, Ventura HO, Stapleton DD, et al. Cardiac allograftvasculopathy assessed by intravascular ultrasonography and non-immunologic risk factors. Am J Cardiol 1994;74:1042–6.
7. Kapadia SR, Nissen SE, Ziada KM, et al. Impact of lipid abnormal-ities in development and progression of transplant coronarydisease: a serial intravascular ultrasound study. J Am Coll Cardiol2001;38:206–13.
8. Holvoet P, Van Cleemput J, Collen D, Vanhaecke J. Oxidized lowdensity lipoprotein is a prognostic marker of transplant-associ-ated coronary artery disease. Arterioscler Thromb Vasc Biol
2000;20:698–702.
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
766 Martínez-Dolz et al. The Journal of Heart and Lung TransplantationJuly 2008
9. Fateh-Moghadam S, Bocksch W, Wessely R, et al. Cytomegalovi-rus infection status predicts progression of heart-transplant vas-culopathy. Transplantation 2003;76:1470–4.
0. Bonaros NE, Kocher A, Dunkler D, et al. Comparison of com-bined prophylaxis of cytomegalovirus hyperimmune globulinplus ganciclovir versus cytomegalovirus hyperimmune globulinalone in high-risk heart transplant recipients. Transplantation2004;77:890–7.
1. Kato T, Chan MC, Gao SZ, et al. Glucose intolerance, as reflectedby hemoglobin A1c level, is associated with the incidence andseverity of transplant coronary artery disease. J Am Coll Cardiol2004;43:1034–41.
2. Gao SZ, Hunt SA, Alderman EL, et al. Relation of donor age andpreexisting coronary artery disease on angiography and intra-coronary ultrasound to later development of accelerated allograftcoronary artery disease. J Am Coll Cardiol 1997;29:623–9.
3. Akosah KO, Mohanty PK, Funai JT, et al. Noninvasive detection oftransplant coronary artery disease by dobutamine stress echocar-diography. J Heart Lung Transplant 1994;13:1024–38.
4. Akosah KO, McDaniel S, Hanrahan JS, Mohanty PK. Dobutaminestress echocardiography early after heart transplantation predictsdevelopment of allograft coronary artery disease and outcome.J Am Coll Cardiol 1998;31:1607–14.
5. Spes CH, Klauss V, Mudra H, et al. Diagnostic and prognosticvalue of serial dobutamine stress echocardiography for noninva-sive assessment of cardiac allograft vasculopathy: a comparisonwith coronary angiography and intravascular ultrasound. Circula-tion 1999;100:509–15.
6. Carlsen J, Toft JC, Mortensen SA, et al. Myocardial perfusionscintigraphy as a screening method for significant coronary arterystenosis in cardiac transplant recipients. J Heart Lung Transplant2000;19:873–8.
7. Tse KK, Alavi A, Eisen HJ. Noninvasive diagnosis of cardiactransplant arteriopathy with dipyridamole thallium scintigraphy.J Nucl Med 1993;34:2049–52.
8. Elhendy A, Sozzi FB, van Domburg RT, et al. Accuracy ofdobutamine tetrofosmin myocardial perfusion imaging for thenoninvasive diagnosis of transplant coronary artery stenosis.J Heart Lung Transplant 2000;19:360–6.
9. Elhendy A, van Domburg RT, Vantrimpont P, et al. Prediction ofmortality in heart transplant recipients by stress technetium-99mtetrofosmin myocardial perfusion imaging. Am J Cardiol 2002;89:964–8.
0. Barbir M, Lazem F, Bowker T, et al. Determinants of transplant-related coronary calcium detected by ultrafast computed tomog-raphy scanning. Am J Cardiol 1997;79:1606–9.
1. Allen-Auerbach M, Schoder H, Johnson J, et al. Relationship betweencoronary function by positron emission tomography and temporalchanges in morphology by intravascular ultrasound (IVUS) in trans-plant recipients. J Heart Lung Transplant 1999;18:211–9.
2. Hollenberg SM, Klein LW, Parrillo JE, et al. Changes in coronaryendothelial function predict progression of allograft vasculopathyafter heart transplantation. J Heart Lung Transplant 2004;23:265–71.
3. Mehra MR, Benza R, Deng MC, Russell S, Webber S. Surrogatemarkers for late cardiac allograft survival. Am J Transplant2004;4:1184–91.
4. Pethig K, Heublein B, Wahlers T, et al. Mycophenolate mofetil for
secondary prevention of cardiac allograft vasculopathy: influenceon inflammation and progression of intimal hyperplasia. J HeartLung Transplant 2004;23:61–6.
5. Labarrere CA, Nelson DR, Cox CJ, et al. Cardiac-specifictroponin I levels and risk of coronary artery disease and graftfailure following heart transplantation. JAMA 2000;284:457– 64.
6. Pethig K, Heublein B, Kutschka I, Haverich A. Systemic inflam-matory response in cardiac allograft vasculopathy: high-sensitiveC-reactive protein is associated with progressive luminal obstruc-tion. Circulation 2000;102(suppl):III-233–6.
7. Labarrere CA, Lee JB, Nelson DR, et al. C-reactive protein,arterial endothelial activation, and development of transplantcoronary artery disease: a prospective study. Lancet 2002;360:1462–7.
8. Raichlin ER, McConnell JP, Lerman A, et al. Systemic inflamma-tion and metabolic syndrome in cardiac allograft vasculopathy.J Heart Lung Transplant 2007;26:826–33.
9. Eisenberg MS, Chen HJ, Warshofsky MK, et al. Elevated levels ofplasma C-reactive protein are associated with decreased graftsurvival in cardiac transplant recipients. Circulation 2000;102:2100–4.
0. Mehra MR, Uber PA, Potluri S, et al. Usefulness of an elevatedB-type natriuretic peptide to predict allograft failure, cardiacallograft vasculopathy, and survival after heart transplantation.Am J Cardiol 2004;94:454–8.
1. Mehra MR, Ventura HO, Chambers R, et al. Predictive model toassess risk for cardiac allograft vasculopathy: an intravascularultrasound study. J Am Coll Cardiol 1995;26:1537–44.
2. Kobashigawa JA, Tobis JM, Starling RC, et al. Multicenter intra-vascular ultrasound validation study among heart transplantrecipients: outcomes after five years. J Am Coll Cardiol 2005;45:1532–7.
3. Tuzcu EM, Kapadia SR, Sachar R, et al. Intravascular ultrasoundevidence of angiographically silent progression in coronary ath-erosclerosis predicts long-term morbidity and mortality aftercardiac transplantation. J Am Coll Cardiol 2005;45:1538–42.
4. Johnson MR. Transplant coronary disease: nonimmunologic riskfactors. J Heart Lung Transplant 1992;11(suppl):S124–32.
5. Kobashigawa JA, Katznelson S, Laks H, et al. Effect of pravastatinon outcomes after cardiac transplantation. N Engl J Med 1995;333:621–7.
6. Valantine H, Rickenbacker P, Kemna M, et al. Metabolic abnor-malities characteristic of dysmetabolic syndrome predict thedevelopment of transplant coronary artery disease: a prospectivestudy. Circulation 2001;103:2144–52.
7. Schmid C, Heemann U, Tilney N. Factors contributing to thedevelopment of chronic rejection in heterotopic rat heart trans-plantation. Transplantation 1997;64:222.
8. Montalescot G, Ankri A, Vicaut E, et al. Fibrinogen after coronaryangioplasty as a risk factor for restenosis. Circulation 1995;92:31–8.
9. Fuster V, Fass DN, Kaye MP, et al. Arteriosclerosis in normal andvon Willebrand pigs: long-term prospective study and aortictransplantation study. Circ Res 1982;51:587–93.
0. Cooke GE, Eaton GM, Whitby G, et al. Plasma atherogenicmarkers in congestive heart failure and posttransplant (heart)
patients. J Am Coll Cardiol 2000;36:509–16.



















