Fluid���structure interaction analysis of a patient���specific right coronary artery...
16
COMMUNICATIONS IN NUMERICAL METHODS IN ENGINEERING Commun. Numer. Meth. Engng 2009; 25:565–580 Published online 27 February 2009 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/cnm.1231 Fluid–structure interaction analysis of a patient-specific right coronary artery with physiological velocity and pressure waveforms Ryo Torii 1, ∗, † , Nigel B. Wood 1 , Nearchos Hadjiloizou 2 , Andrew W. Dowsey 3 , Andrew R. Wright 4 , Alun D. Hughes 2 , Justin Davies 2 , Darrel P. Francis 2 , Jamil Mayet 2 , Guang-Zhong Yang 3 , Simon A. McG. Thom 2 and X. Yun Xu 1 1 Department of Chemical Engineering, Imperial College London, London, U.K. 2 International Centre for Circulatory Health, St. Mary’s Hospital and Imperial College London, London, U.K. 3 Royal Society/Wolfson Medical Image Computing Laboratory, Imperial College London, London, U.K. 4 Department of Radiology, St. Mary’s Hospital and Imperial College NHS Trust, London, U.K. SUMMARY Coupled fluid–structure interaction (FSI) analysis of the human right coronary artery (RCA) has been carried out to investigate the effects of wall compliance on coronary hemodynamics. A 3-D model of a stenosed RCA was reconstructed based on multislice computerized tomography images. A velocity waveform in the proximal RCA and a pressure waveform in the distal RCA of a patient with a severe stenosis were acquired with a catheter delivered wire probe and applied as boundary conditions. The arterial wall was modeled as a Mooney–Rivlin hyperelastic material. The predicted maximum wall displacement (3.85 mm) was comparable with the vessel diameter (∼ 4mm), but the diameter variation was much smaller, 0.134 mm at the stenosis and 0.486 mm in the distal region. Comparison of the computational results between the FSI and rigid-wall models showed that the instantaneous wall shear stress (WSS) distributions were affected by diameter variation in the arterial wall; increasing systolic blood pressure dilated the vessel and consequently lowered WSS, whereas the opposite occurred when pressure started to decrease. However, the effects of wall compliance on time-averaged WSS (TAWSS) and oscillatory shear index (OSI) were insignificant (4.5 and 2.7% difference in maximum TAWSS and OSI, respectively). Copyright 2009 John Wiley & Sons, Ltd. Received 22 August 2008; Revised 6 January 2009; Accepted 12 January 2009 KEY WORDS: coronary atherosclerosis; fluid–structure interaction; physiological waveform ∗ Correspondence to: Ryo Torii, Department of Chemical Engineering, Imperial College London, South Kensington Campus, London SW7 2AZ, U.K. † E-mail: [email protected] Contract/grant sponsor: British Heart Foundation; contract/grant numbers: PG/04/078, FS/05/034 Contract/grant sponsor: Foundation for Circulatory Health; contract/grant number: ICCH/07/5015 Contract/grant sponsor: NIHR Biomedical Research Centre Funding Scheme Copyright 2009 John Wiley & Sons, Ltd.
Transcript of Fluid���structure interaction analysis of a patient���specific right coronary artery...

COMMUNICATIONS IN NUMERICAL METHODS IN ENGINEERINGCommun. Numer. Meth. Engng 2009; 25:565–580Published online 27 February 2009 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/cnm.1231
Fluid–structure interaction analysis of a patient-specific rightcoronary artery with physiological velocity and pressure
waveforms
Ryo Torii1,∗,†, Nigel B. Wood1, Nearchos Hadjiloizou2, Andrew W. Dowsey3,Andrew R. Wright4, Alun D. Hughes2, Justin Davies2, Darrel P. Francis2,
Jamil Mayet2, Guang-Zhong Yang3, Simon A. McG. Thom2 and X. Yun Xu1
1Department of Chemical Engineering, Imperial College London, London, U.K.2International Centre for Circulatory Health, St. Mary’s Hospital and Imperial College London, London, U.K.
3Royal Society/Wolfson Medical Image Computing Laboratory, Imperial College London, London, U.K.4Department of Radiology, St. Mary’s Hospital and Imperial College NHS Trust, London, U.K.
SUMMARY
Coupled fluid–structure interaction (FSI) analysis of the human right coronary artery (RCA) has beencarried out to investigate the effects of wall compliance on coronary hemodynamics. A 3-D model ofa stenosed RCA was reconstructed based on multislice computerized tomography images. A velocitywaveform in the proximal RCA and a pressure waveform in the distal RCA of a patient with a severestenosis were acquired with a catheter delivered wire probe and applied as boundary conditions. The arterialwall was modeled as a Mooney–Rivlin hyperelastic material. The predicted maximum wall displacement(3.85mm) was comparable with the vessel diameter (∼4mm), but the diameter variation was muchsmaller, 0.134mm at the stenosis and 0.486mm in the distal region. Comparison of the computationalresults between the FSI and rigid-wall models showed that the instantaneous wall shear stress (WSS)distributions were affected by diameter variation in the arterial wall; increasing systolic blood pressuredilated the vessel and consequently lowered WSS, whereas the opposite occurred when pressure started todecrease. However, the effects of wall compliance on time-averaged WSS (TAWSS) and oscillatory shearindex (OSI) were insignificant (4.5 and 2.7% difference in maximum TAWSS and OSI, respectively).Copyright q 2009 John Wiley & Sons, Ltd.
Received 22 August 2008; Revised 6 January 2009; Accepted 12 January 2009
KEY WORDS: coronary atherosclerosis; fluid–structure interaction; physiological waveform
∗Correspondence to: Ryo Torii, Department of Chemical Engineering, Imperial College London, South KensingtonCampus, London SW7 2AZ, U.K.
†E-mail: [email protected]
Contract/grant sponsor: British Heart Foundation; contract/grant numbers: PG/04/078, FS/05/034Contract/grant sponsor: Foundation for Circulatory Health; contract/grant number: ICCH/07/5015Contract/grant sponsor: NIHR Biomedical Research Centre Funding Scheme
Copyright q 2009 John Wiley & Sons, Ltd.

566 R. TORII ET AL.
1. INTRODUCTION
Atherosclerotic coronary artery disease is a major cause of mortality and morbidity in the developedand developing world, of which one of the outcomes is heart attack. Atherosclerosis shows afocal distribution, suggesting that mechanical factors related to blood flow may contribute toits development. There is considerable evidence implicating mechanical forces resulting fromintravascular pressure and flow (e.g. circumferential tensile stress and wall shear stress (WSS)) inthe regulation of blood vessel structure under physiological or pathological circumstances [1–4].However, there is a complex question regarding the precise relationship between hemodynamics,mechanical factors and atherosclerotic changes in the arterial wall. Addressing these questions ismade difficult as it is not possible to measure local flow patterns and mechanical forces in vivowith sufficient accuracy using imaging techniques alone, although evidence has been building forthe responses to WSS of arterial wall (endothelial and smooth muscle) cells and their internalmolecules, including atherogenic processes [5].
We have been investigating coronary hemodynamics using computational fluid dynamics (CFD)combined with medical imaging to determine detailed patterns of blood flow and WSS in anatom-ically realistic coronary arteries. Coronary hemodynamics has unique characteristics in the humancardiovascular system owing to diastolic-dominant flow [6] and cardiac-induced dynamic vesselmotion. Myers et al. [7] investigated the effects of arterial geometry, pulsatile flow condition anddynamic vessel motion on flow patterns in a realistic model of the right coronary artery (RCA).They concluded that arterial geometry was the dominant factor and flow pulsatility came second.Dynamic vessel motion was found to be less important than the other two factors. However,their model did not include the effect of arterial wall compliance. Recent advances in computingresources and numerical algorithms have made it possible for more complicated physics suchas fluid–structure interactions (FSI) to be included in computational simulations. FSI has beenapplied to a large number of cardiovascular problems since it is essential in some of those, e.g.motion of the natural/artificial heart valves [8]. FSI is also considered important in parts of thearterial system such as abdominal/thoracic aortas [9] including aortic aneurysms [10], carotidartery bifurcations [11, 12], cerebral aneurysms [13, 14] and coronary arteries [15–17]. Conversely,there is also a study indicating that the effect of arterial wall deformation on arterial flow can beinsignificant [18]. Experimental data showed that wall motion of non-stenosed coronary arterieswas approximately less than 8.4% of the vessel diameter (5.4±2% [19] and 2% [20] in terms ofstrain, 8.4% in diameter [21]). However, studies on stenosis and plaque structure [22–25] havedemonstrated the importance of FSI in stenosed arteries. FSI analyses of coronary arteries arestill sparse, largely due to lack of in vivo information such as subject-specific material properties,flow and pressure waveforms. The aim of the present study was to determine the effect of wallcompliance on blood flow patterns and WSS in a human RCA using computational FSI analysiswith in vivo anatomical, flow and pressure information.
2. COMPUTATIONAL METHOD
2.1. Vascular geometry reconstruction
A 3-D model of the RCA of a patient with a mild stenosis was reconstructed based on multislicecomputerized tomography (CT) images acquired at mid-diastole, 75% into the duration of the
Copyright q 2009 John Wiley & Sons, Ltd. Commun. Numer. Meth. Engng 2009; 25:565–580DOI: 10.1002/cnm

FSI ANALYSIS OF AN RCA 567
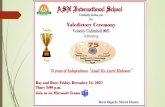
Figure 1. The RCA model reconstructed from CT images (left) and close-up view around the stenosis(in the box). The inlet and outlet were extended to minimize the effects of boundary conditions. The
extensions are shown in darker color.
cardiac cycle, using a Philips Mx8000 IDT 16-detector multi-slice CT scanner (Philips ElectronicsU.K. Ltd, Guildford, U.K.). The in-plane image resolution was approximately 0.43mm/pixel andthe slice interval was 0.5mm. The RCA was first delineated with CMRtools (CVIS, London, U.K.).The planes perpendicular to the centerline were computed at 1mm intervals and used to re-slicethe data set with cubic B-spline resampling [26]. The RCA was then semi-automatically segmentedfrom the resulting stack of cross-sectional images [27]. The lumenal surface was constructed byinterpolation of the extracted cross-sectional outlines using cubic B-splines. Because it is difficultto obtain the outer boundary of the RCA wall from the CT images, the wall was artificiallyconstructed based on the lumenal surface. First, a lumenal surface without stenosis was constructedby eliminating the stenosis and interpolating the lumenal surface assuming smooth variation indiameter along the centerline. Then the surface without the stenosis was extruded outward by0.5mm to obtain the outer wall surface based on wall thickness measurement made with anintravascular ultrasound probe [28]. The RCA model, which has a 62% stenosis (area reduction),is shown in Figure 1. The wall thickness at the stenosis throat is approximately 1.2mm. Theinlet and outlet were extended in length by five diameters in the direction normal to the in/outletcross sections to prevent interactions between boundary conditions and region of interest. Thereconstructed geometries were meshed using ICEM CFD (ANSYS, Inc.) with hexahedral elementsfor both the fluid and wall domains. The number of nodes and elements were 113 715 and 106 760for the fluid domain, 63 000 and 50 240 for the wall domain, respectively.
2.2. Computational fluid–structure interactions
The dynamic coupling of blood flow and wall motion was achieved using a commercial computa-tional mechanics suite ANSYS and ANSYS CFX (ANSYS Inc.). ANSYS is finite-element-basedsoftware for structural mechanics analysis and ANSYS CFX is finite-volume-based software forfluid mechanics computations. These are coupled and solved iteratively within each time step byapplying appropriate kinematic and dynamic conditions at the fluid–structure interface until theresidual of the system is below a specified tolerance. For fluid mechanics computations, the 3-DNavier–Stokes equations for incompressible flow with treatment of moving domain,
d
dt
∫V (t)
�dV +∫s�(Uj −Wj )dn j = 0 (1)
d
dt
∫V (t)
�Ui dV +∫s�(Uj −Wj )Ui dn j = −
∫sP dn j +
∫s�
(�Ui
�x j+ �Uj
�xi
)dn j (2)
Copyright q 2009 John Wiley & Sons, Ltd. Commun. Numer. Meth. Engng 2009; 25:565–580DOI: 10.1002/cnm

568 R. TORII ET AL.
Table I. Computational schemes used for fluid and structural mechanics computations,in ANSYS CFX and ANSYS mechanics.
Fluid Structure
Spatial discretization Finite volume method (FVM) Finite element method (FEM)Mesh configuration HexahedralInterpolation function∗ TrilinearPressure–velocity coupling Modified SIMPLE scheme†Time-marching scheme Second-order implicit backward
EulerNewmark method
Stabilization High resolution scheme‡ Integration parameter � inNewmark method is set to 0.6.
Linearized system solver Algebraic multi grid Wavefront direct solver
∗Numerical integration in FVM is implemented with finite element interpolation function and hence interpolationfunction is needed.†Velocity prediction method in SIMPLE scheme is modified to avoid ‘checkerboard’ numerical oscillation dueto collocated grid [29].
‡Second-order central difference and first-order upwind are blended; blending parameters are determined locallyto avoid numerical oscillation and to minimize the effects of upwinding [30].
were solved with time-dependent physiological velocity and pressure boundary conditions. HereUj and Wj are the flow velocity and the velocity of the control volume boundary, and P is pressure.V and s respectively denote volume and surface regions of integration, and dn j are the differentialCartesian components of the outward normal surface vector. Density and dynamic viscosity ofthe fluid are denoted as � and �. For structural mechanics, momentum balance equations weresolved with stress boundary conditions at the fluid–structure interface and constraint conditions.The computational mesh for fluid mechanics was updated with respect to boundary displacementby solving the Laplace equation so that the wall boundary displacement could be propagatedthrough all nodes within the domain. The numerical schemes used in fluid and structural mechanicscomputations are summarized in Table I.
2.3. Material properties
The arterial wall was modeled as a nine parameter Mooney–Rivlin hyperelastic material in thisstudy. Although arterial wall is known to have heterogeneous and anisotropic structure owingto multiple compositions including collagen fibers [31], the homogeneous and isotropic materialmodel was adopted due to lack of in vivo data on heterogeneity and fiber direction, which governsanisotropic behavior of the tissue. The strain energy function is
W = c10( I1−3)+c01( I2−3)+c20( I1−3)2+c11( I1−3)( I2−3)+c02( I2−3)2
+c30( I1−3)3+c21( I1−3)2( I2−3)+c12( I1−3)( I2−3)2+c03( I2−3)3+ 1
d(J−1)2 (3)
where I1 and I2 are the first and second deviatoric strain invariants and J is the determinant of theelastic deformation gradient tensor. The model parameters were set to c10=0.070,c20=3.2,c21=0.07160MPa and ci j =0.0MPa for the others, following the FSI analysis of the human RCA
Copyright q 2009 John Wiley & Sons, Ltd. Commun. Numer. Meth. Engng 2009; 25:565–580DOI: 10.1002/cnm

FSI ANALYSIS OF AN RCA 569
by Koshiba et al. [16]. The material incompressibility parameter d (=2/K , K is bulk modulus)was set to 1.0×10−5 Pa−1. Plaque components and residual stress were not considered in thisstudy for the sake of simplicity. The blood was assumed to be Newtonian because the flow is notstagnant and shear rate is consequently large enough to maintain a flow regime with nearly constantviscosity (shear rate �>100s−1). The density and viscosity of the blood were set to 1050kg/m3
and 4.0×10−3 Pas [6].
2.4. Physiological boundary conditions
Time-dependent velocity profiles were prescribed at the inlet of the RCA as the inflow boundaryconditions. The conditions at the outlet were time-dependent pressure, which was assumed tobe uniform over the cross section. Both the inflow and outflow boundary conditions were basedon in vivo measurements. The velocity and pressure waveforms were simultaneously acquiredwith an electrocardiography (ECG)-gated intravascular ultrasound Doppler and pressure probe(ComboWire, VolcanoTM Corporation) [32, 33] in the proximal and distal RCA of a patient with asevere stenosis during percutaneous coronary intervention (PCI), i.e. balloon angioplasty followedby stent insertion. The acquisition was made in addition to standard clinical protocol for PCI,but the additional risk is minimal because a catheter insertion is necessary in PCI procedure inorder to deliver a balloon and stent, and waveform acquisition requires an additional 0.356mmdiameter probe. The patient was well consented by a clinician, was fully aware of the risk andagreed with the waveform acquisition. Although the procedure is invasive, this is the only wayto obtain coronary pressure waveform that is one of the key pieces of information in this study.The acquired data were aligned with reference to the ECG R-wave. The velocity and pressurewaveforms were first decomposed using Fourier transform. The Fourier coefficients obtained wereused in functions prescribing pulsatile velocities at the inlet [34] and pressure at the outlet:
w(r, t) = B0
[1−
( rR
)2]+N∑
n=1
B0
2
⎡⎢⎣ 1− J0
(�n
r
Ri3/2
)/J0(�ni3/2)
1−2J1(�ni3/2)/(�ni3/2 J0(�ni3/2))
⎤⎥⎦e−2�niwt (4)
p(t) =N∑
n=0Cne
−2�niwt (5)
where Bn and Cn are Fourier coefficients, r is the cylindrical coordinate and t is the time.R denotes the radius of the inlet cross section. Here J0 and J1 are the Bessel functions of thefirst kind of order 0 and 1 and �n = R
√n�/v, where �=2�/T , is based on one cardiac cycle
(=1.0s). The Womersley parameter �= R√
�/v is 2.60 and the Reynolds number is 531 at peakflow and 276 based on the cycle-averaged velocity. The velocity and pressure waveforms appliedin the simulations are shown in Figure 2. In the actual computation, pulse pressure, p(t)− pref(pref=70mmHg=9310Pa) was specified at the outlet since the reconstructed RCA geometrycorresponded to a diastolic state (i.e. subject to diastolic pressure). The reference pressure (pref)was determined as the minimum pressure during the cardiac cycle. Wall boundary condition wasno-slip, i.e. velocities at the lumen-wall interface in the wall domain were the same as those inthe fluid domain. The proximal and distal ends of the artery were fixed with no axial or transaxialmotion. Cardiac-induced dynamic vessel motion was not considered in this study in order to isolatethe effects of wall compliance on coronary hemodynamics.
Copyright q 2009 John Wiley & Sons, Ltd. Commun. Numer. Meth. Engng 2009; 25:565–580DOI: 10.1002/cnm

570 R. TORII ET AL.
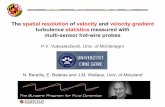
Figure 2. The velocity (left) and pressure (right) waveforms. The waveforms were acquired simultaneouslywith an intravascular ultrasound Doppler/pressure probe in the proximal site of the right coronary artery
of a patient with a severe stenosis.
3. RESULTS AND DISCUSSION
The wall deformation patterns were examined first. Figure 3 shows the displacement contours,caused by the internal pressure, on the lumen-wall interface at three time points during the cardiaccycle. At peak flow in systole, the maximum displacement, 3.50mm, occurs in the middle ofthe RCA distal to the stenosis. The maximum displacement increases to 3.85mm when peakpressure is reached in mid-cycle, but occurs at a location more distal than that at peak flow.In diastole, the displacement pattern remains similar to that at peak pressure but the maximumdisplacement, 1.48mm, is much smaller. Ding et al. [19] reported a maximum displacement of60mm for the RCA using biplane cineangiograms, while Zeng et al. [17, 21] showed transaxialRCA motion larger than several vessel diameters (RCA diameter ∼4mm), also based on biplanecineangiograms. The RCA displacement observed in vivo is much larger than that found in thisstudy, but it is unclear how much of the measured displacement is owing to coronary complianceand how much to cardiac wall motion. Our results show that the contribution of arterial complianceto the total RCA wall motion is small. With more realistic conditions such as tethering effectsof the surrounding myocardium and pericardium, the wall displacement would be restricted evenfurther. One of the other parameters of interest in RCA physiology is the temporal variation ofvessel diameter. Figure 4 shows changes in RCA diameter at three different locations: at thethroat of the stenosis (L1), in the post-stenotic region (L2) and in the distal region (L3). Theresults show that the temporal variation of RCA diameter is nearly in phase with pressure, whichis consistent with previous experimental and computational studies [11, 35]. Diameter variationsduring a cardiac cycle are 0.134, 0.266 and 0.486mm at L1-3, respectively. By normalizing thechanges with their corresponding initial diameters, the diameter variation ratios were calculated as4.71, 5.94 and 13.6% at L1-3, respectively. These values can be compared with previous data ontissue strain and temporal variation of cross-sectional area. For instance, Zeng et al. [21] presented8.4% of temporal radius variation (15% variation in cross-sectional area averaged along the RCAcenterline) using multi-slice CT. Ding et al. [19] reported the total wall strain of 5.4% usingbiplanar angiograms and Schaar et al. [20] reported a less than 2% circumferential strain using
Copyright q 2009 John Wiley & Sons, Ltd. Commun. Numer. Meth. Engng 2009; 25:565–580DOI: 10.1002/cnm

FSI ANALYSIS OF AN RCA 571
Figure 3. Predicted displacement patterns on the lumen-wall interface at peak flow (top left), peak pressure(top right) and in mid-diastole (bottom). The displacement is superimposed onto the original geometry,which is also displayed (transparent). The corresponding time point in each panel is indicated by the
vertical line in the velocity and pressure curves.
ultrasound-based intravascular palpography. Because the circumferential strain in a pressurizedvessel is approximately ε� =u/r , where u is radial displacement, the corresponding diametervariation is estimated to be 1–2%. Our FSI simulation results show comparable diameter variationsto experimental findings in the proximal region, but larger in the distal region particularly whencompared with the palpography measurement. One reason could be that the pressure waveform usedin the model was acquired from a patient who was also hypertensive; the pressure variation during
Copyright q 2009 John Wiley & Sons, Ltd. Commun. Numer. Meth. Engng 2009; 25:565–580DOI: 10.1002/cnm

572 R. TORII ET AL.
Figure 4. Variation of vessel diameter at the throat of the stenosis (L1, top right), distal to the stenosis(L2, bottom left) and in the distal region (L3, bottom right).
the cardiac cycle is 84.0mmHg, which is twice as large as normotensive pulse pressure. Anotherreason is the lack of surrounding tissue such as myocardium and pericardium in our model, whichwould restrict the radial motion. However, when compared with the total displacement (maximum3.85mm), the diameter variation, 0.486mm at a maximum, is one order of magnitude smaller,implying that the effect of wall displacement on RCA hemodynamics is likely to be small.
Since low and oscillatory WSS plays an important role in atherogenesis, WSS-related hemody-namic parameters such as time-averaged WSS (TAWSS) and oscillatory shear index (OSI) need tobe examined [2, 36, 37]. These parameters were compared between the FSI and rigid-wall modelsto assess the importance of FSI in determining coronary hemodynamics. As shown in Figure 5, theTAWSS is focally high at the throat of the stenosis for both cases, due to flow acceleration at thethroat causing high velocity gradient near the wall. Dilatation of the throat due to pulsating bloodpressure (cf. Figure 4) causes reduction in blood velocity at the throat and consequently slightlylower WSS (8.62 Pa for rigid wall and 8.23 Pa for FSI). This can be seen in the velocity contoursand vectors around the stenosis shown in Figure 6. For the rigid-wall case at peak flow, the areaof high velocity persists far downstream, and the post-stenotic flow is slightly curved and skewedtoward the upper wall. Conversely, the high velocity jet attenuates more rapidly in the post-stenoticregion with the FSI model, and the downstream flow remains straighter because of the dilated
Copyright q 2009 John Wiley & Sons, Ltd. Commun. Numer. Meth. Engng 2009; 25:565–580DOI: 10.1002/cnm

FSI ANALYSIS OF AN RCA 573
Figure 5. Comparison of TAWSS contours between the FSI (top) and rigid-wall models (bottom).
Figure 6. Comparison of velocity field between the FSI and rigid-wall models at three time points duringthe cardiac cycle. The time points are the same as in Figure 3. The velocity vectors are projected onto
the longitudinal section: (a) FSI and (b) rigid wall.
throat. The same trend is observed at peak pressure and mid-diastole. It is also notable that the flowrecirculation in the post-stenotic region, which causes low and oscillatory WSS, is not affected bywall distensibility. As a result, the overall TAWSS distributions for the FSI and rigid-wall casesare almost identical. The effect of wall compliance on instantaneous WSS distributions is alsoexamined. Figures 7 and 8 show comparison of instantaneous WSS contours between the FSIand rigid-wall models at five different time points. It is presented in Figure 7 that WSS patternsfor the two models are similar but quantitatively different at all time points except mid systole
Copyright q 2009 John Wiley & Sons, Ltd. Commun. Numer. Meth. Engng 2009; 25:565–580DOI: 10.1002/cnm

574 R. TORII ET AL.
Figure 7. Comparison of instantaneous WSS contours at five time points during the cardiac cycle. Eachcontour is unwrapped from the RCA surface and mapped onto a rectangle. L4 is on the pericardium-facingside (along outer wall) and L5 is on the epicardium-facing side (along inner wall): (a) reference lines; (b)at peak flow (t=0.14s); (c) mid systole (t=0.20s); (d) at peak pressure (t=0.40s); (e) early diastole
(t=0.50s); and (f ) mid diastole (t=0.70s).
Copyright q 2009 John Wiley & Sons, Ltd. Commun. Numer. Meth. Engng 2009; 25:565–580DOI: 10.1002/cnm

FSI ANALYSIS OF AN RCA 575
Peak flow(t = 0.14 s)
Mid systole(t = 0.20 s)
Peak pressure(t = 0.40 s)
Early diastole(t = 0.50 s)
Mid diastole(t = 0.70 s)
Figure 8. Comparison of instantaneous WSS profiles along L5 (inner wall, in the left panels) and L4(outer wall, in the right panels). The locations of L4 and L5 are shown in Figure 7. The distance from
the proximal end is normalized by the total length of the line.
Copyright q 2009 John Wiley & Sons, Ltd. Commun. Numer. Meth. Engng 2009; 25:565–580DOI: 10.1002/cnm

576 R. TORII ET AL.
Figure 9. Temporal WSS profiles at the throat of the stenosis (P1, top right), distal to thestenosis (P2, bottom left) and in the distal region (P3, bottom right). P1 and P3 are the
intersections of L1, L3 and L5 (cf. Figure 4).
(t=0.20s). The difference at mid systole is more pronounced in the distal region. Figure 8 enablesdetailed comparison along the inner and outer walls (L4 and L5). Before peak pressure (t=0.4s),WSS for the FSI model is lower than that in the rigid-wall case over the entire RCA, whereasWSS for the FSI model is higher than the rigid-wall model after peak pressure. This is becausethe increasing pressure dilates the vessel and WSS is consequently lowered before t=0.4s, andthe opposite occurs when pressure starts to decrease. The difference between FSI and rigid-wallmodels is more pronounced in the region distal to the stenosis (normalized distance=0.25) andlarger in the distal region in diastole (t=0.50, 0.70 s). These observations are consistent with Zenget al. [21] who reported more significant influence of RCA compliance on WSS. In the presentstudy, the reason for larger WSS difference between the FSI and rigid-wall models in the distalregion can be explained by the larger diameter variation (13.6%). Temporal variations of WSS atthree different locations were also examined (Figure 9). At the throat of the stenosis, the peak WSSvalues are almost the same for the two models, although WSS magnitude is generally lower for theFSI case before peak pressure (t=0.40s) and the relationship is inverted after peak pressure. Thisopposing effect of wall compliance on WSS results in almost identical TAWSS contours betweenthe two models. However, difference in WSS temporal variations is more significant in the distal
Copyright q 2009 John Wiley & Sons, Ltd. Commun. Numer. Meth. Engng 2009; 25:565–580DOI: 10.1002/cnm

FSI ANALYSIS OF AN RCA 577
Figure 10. Comparison of OSI contours between the FSI (top) and rigid-wall models (bottom). P2 andP3 are the same as those in Figure 9.
region of the RCA, especially at P3. The results show differences in oscillatory nature of WSSdue to wall compliance.
The OSI profiles are shown in Figure 10. OSI is defined as
OSI=0.5
(1− |∫ T
0 sdt |∫ T0 |s|dt
)(6)
where T is the period of a cardiac cycle and s is WSS as a vector. It tends to be high where thedirection of WSS varies in time. It can be seen that OSI is high in the post-stenotic region and atthe inside of the relatively sharp bend in the distal RCA (vicinity of L3 in Figure 4), approaching0.5 for both the FSI and rigid-wall cases. In these regions the flow is likely to be highly disturbedand the results show that the flow disturbance is present regardless of how the wall is modeled.Although the profiles for the two cases look similar, quantitative differences can be observed.OSI values for the FSI case are slightly higher than for the rigid wall, particularly in the distalregion. The local maxima at several locations is extracted for quantitative comparison. At P4, P5,P2 and P3 (from proximal to distal, cf. Figure 10), OSI values are 0.129, 0.473, 0.234 and 0.439for the FSI model, and 0.0968, 0.486, 0.156 and 0.381 for the rigid-wall model, respectively. Thecomparison shows that the maximum difference occurs at P6, middle of the distal section. Thisis consistent with data shown in Figures 7, 8 and 9 where larger WSS temporal variation in thedistal region was found.
The main focus of this study was to determine the influence of FSI on coronary artery hemody-namics. Hence the arterial wall was modeled as a simple homogeneous isotropic material and theresults were analyzed mostly in terms of hemodynamics rather than structural mechanics. Imple-mentation of more sophisticated material models and more realistic boundary conditions to accountfor the effects of surrounding tissue would be desirable. Indeed, anisotropic arterial stiffness was
Copyright q 2009 John Wiley & Sons, Ltd. Commun. Numer. Meth. Engng 2009; 25:565–580DOI: 10.1002/cnm

578 R. TORII ET AL.
observed in a number of studies, e.g. in human abdominal aortas and abdominal aortic aneurysms[38], although similar information on the coronary artery is not available. Anisotropic materialmodels have been proposed to represent such anisotropic behavior [38] including incorporation ofcollagenous fiber [39]. Studies on the sensitivity of wall stress to the material model for abdominalaortic aneurysms [40] and coronary artery with atherosclerotic lesion [41] showed that anisotropicmaterial models predicted higher wall stress (up to 30%) than that assuming an isotropic material,but no qualitative difference was noted in the stress distribution. This suggests that incorporatingthe anisotropic material model is likely to make the artery less deformable and would emphasizethe insignificance of FSI on coronary hemodynamics. Moreover, it is extremely difficult to obtainfiber orientation and detailed distribution of material compositions in vivo using clinical imagingtechniques. More elaborate wall models are important for wall stress analysis, which is anotherinteresting topic related to rupture of vulnerable plaques [15] and will be investigated in the nextstage of this study.
4. CONCLUSIONS
Coupled FSI analysis of the human RCA has been carried out in conjunction with physiolog-ical velocity and pressure waveforms to investigate the effects of wall compliance on coronaryhemodynamics. Comparison of the computational results between the FSI and rigid-wall modelsshowed insignificant difference in TAWSS and OSI, although the predicted wall displacement wascomparable with the vessel diameter. However, differences in instantaneous WSS profiles werenoticeable, especially in the distal region of the artery.
ACKNOWLEDGEMENTS
This study was supported by the British Heart Foundation (PG/04/078, FS/05/034) and Foundation forCirculatory Health (ICCH/07/5015). The authors are also grateful for support from the NIHR BiomedicalResearch Centre Funding Scheme.
REFERENCES
1. Caro CG, Fitz-Gerald JM, Schroter RC. Arterial wall shear and distribution of early atheroma in man. Nature1969; 223:1159–1161.
2. Ku DN, Giddens DP, Zarins CK, Glagov S. Pulsatile flow and atherosclerosis in the human carotid bifurcation,positive correlation between plaque location and low and oscillating shear stress. Arteriosclerosis 1985; 5(3):293–302.
3. Malek AM, Alper SL, Izumo S. Hemodynamic shear stress and its role in atherosclerosis. Journal of the AmericanMedical Association 1999; 2035–2042.
4. Slager CJ, Wentzel JJ, Gijsen FJH, Thury A, van der Wal AC, Schaar JA, Serruys PW. The role of shearstress in the destabilization of vulnerable plaques and related therapeutic implications. Nature Clinical Practice,Cardiovascular Medicine 2005; 2(9):456–464.
5. Stone PH, Coskun AU, Kinlay S, Popma JJ, Sonka M, Wahle A, Yeghiazarians Y, Maynard C, Kuntz RE,Feldman CL. Regions of low endothelial shear stress ar the sites where coronary plaque progresses and vascularremodeling occurs in humans: an in vivo serial study. European Heart Journal 2007; 28:705–710.
6. Nichols WW, O’Rourke MF. McDonald’s Blood Flow in Arteries (5th edn). Hodder Arnold: London, 2005.7. Myers JG, Moore JA, Ojha M, Johnston KW, Ethier CR. Factors influencing blood flow patterns in the human
right coronary artery. Annals of Biomedical Engineering 2001; 29:12.
Copyright q 2009 John Wiley & Sons, Ltd. Commun. Numer. Meth. Engng 2009; 25:565–580DOI: 10.1002/cnm

FSI ANALYSIS OF AN RCA 579
8. Ge L, Jones SC, Sotiropoulos F, Healy TM, Yoganathan AP. Numerical simulation of flow in mechanical heartvalves: grid resolution and flow symmetry. Transactions of ASME, Journal of Biomechanical Engineering 2003;125:709–718.
9. Figueroa CA, Vignon-Clementel IE, Jansen KE, Hughes TJR, Taylor CA. A coupled momentum method formodeling blood flow in three-dimensional deformable arteries. Computer Methods in Applied Mechanics andEngineering 2006; 195:5685–5706.
10. Scotti CM, Jimenez J, Muluk SC, Finol EA. Wall stress and flow dynamics in abdominal aortic aneurysms: finiteelement analysis vs. fluid–structure interaction. Computer Methods in Biomechanics and Biomedical Engineering2008; 11(3):301–322.
11. Tada S, Tarbell JM. A computational study of flow in a compliant carotid bifurcation—stress phase anglecorrelation with shear stress. Annals of Biomedical Engineering 2005; 33(9):1202–1212.
12. Karner G, Perktold K, Hofer M, Liepsch D. Flow characteristics in an anatomically realistic compliant carotidartery bifurcation model. Computer Methods in Biomechanics and Biomedical Engineering 1999; 2(3):171–185.
13. Torii R, Oshima M, Kobayashi T, Takagi K, Tezduyar TE. Fluid–structure interaction modeling of aneurysmalconditions with high and normal blood pressures. Computational Mechanics 2006; 38:482–490.
14. Tezduyar TE, Sathe S, Schwaab M, Conklin BS. Arterial fluid mechanics modeling with the stablized space–timefluid–structure interaction technique. International Journal for Numerical Methods in Fluids 2008; 57:601–629.
15. Tang D, Yang C, Zheng J, Woodard PK, Sicard GA, Saffitz JE, Yuan C. 3D MRI-based multicomponent FSImodels for atherosclerotic plaques. Annals of Biomedical Engineering 2004; 32(7):947–960.
16. Koshiba N, Ando J, Chen X, Hisada T. Multiphysics simulation of blood flow and LDL transport in aporohyperelastic arterial wall model. Transactions of the ASME, Journal of Biomechanical Engineering 2007;129:374–385.
17. Zeng D, Boutsianis E, Ammann M, Boomsma K, Wildermuth S, Poulikakos D. A study on the compliance of aright coronary artery and its impact on wall shear stress. Transactions of the ASME, Journal of BiomechanicalEngineering 2008; 130:041014-1–041014-11.
18. Dempere-Marco L, Oubel E, Castro M, Putman C, Frangi A, Cebral J. CFD Analysis Incorporating the Influenceof Wall Motion: Application to Intracranianl Aneurysms. Lecture Notes in Computer Science, vol. 4191. Springer:Berlin, 2006; 4191:438–445.
19. Ding Z, Zhu H, Friedman MH. Coronary artery dynamics in vivo. Annals of Biomedical Engineering 2002;30(4):419–429.
20. Schaar AJ, de Korte CL, Mastik F, van Damme LCA, Krams R, Serruys PW, van der Steen AFW. Three-dimensional palpography of human coronary arteries. Herz 2005; 30:125–133.
21. Zeng D, Ding Z, Friedman MH, Ethier CR. Effects of cardiac motion on right coronary artery hemodynamics.Annals of Biomedical Engineering 2003; 31(4):420–429.
22. Kock SA, Nygaard JV, Eldrup N, Frund ET, Klaerke A, Paaske WP, Falk E, Yong Kim W. Mechanical stresses incarotid plaques using MRI-based fluid–structure interaction models. Journal of Biomechanics 2008; 41:1651–1658.
23. Bluestein D, Alemu Y, Avrahami I, Gharib M, Dumont K, Ricotta JJ, Einav S. Influence of microcalcificationson vulnerable plaque mechanics using FSI modeling. Journal of Biomechanics 2008; 41:1111–1118.
24. Li MX, Beech-Brandt JJ, John LR, Hoskins PR, Easson WJ. Numerical analysis of pulsatile blood flow andvessel wall mechanics in different degrees of stenosis. Journal of Biomechanics 2007; 40:3715–3724.
25. Tang D, Yang C, Kobayashi S, Zheng J, Vito RP. Effect of stenosis asymmetry on blood flow and arterycompression: a three-dimensional fluid–structure interaction model. Annals of Biomedical Engineering 2003;31(10):1182–1193.
26. Thevenaz P. Interpolation revisited. IEEE Transactions on Medical Imaging 2000; 19(7):739–758.27. Varghese A, Merrifield RD, Crowe LA, Collins SA, Keenan NGJ, Firmin DN, Yang GZ, Pennell DJ. Evaluation
of carotid artery wall volume measurement using novel semiautomated analysis software. Journal of MagneticResonance Imaging 2006; 24:1401–1408.
28. Zhu H, Friedman MH. Relationship between the dynamic geometry and wall thickness of a human coronaryartery. Arteriosclerosis, Thrombosis and Vascular Biology 2003; 23:2260–2265.
29. Rhie CM, Chow WL. A numerical study of the turbulent flow past an isolated airfoil with trailing edge separation.AIAA Paper, 1982; 82-0998.
30. Barth TJ, Jesperson DC. The design and application of upwind schemes on unstructured meshes. AIAA Paper,1989; 89-0366.
31. Holzapfel GA, Ogden RW. Mechanics of Biological Tissue. Springer: Berlin, 2006.
Copyright q 2009 John Wiley & Sons, Ltd. Commun. Numer. Meth. Engng 2009; 25:565–580DOI: 10.1002/cnm

580 R. TORII ET AL.
32. Davies JE, Whinnett ZI, Francis DP, Manisty CH, Aguado-Sierra J, Willson K, Foale RA, Malik IS, Hughes AD,Parker KH, Mayet J. Evidence of a dominant backward-propagating ‘suction’ wave responsible for diastoliccoronary filling in humans, attenuated in left ventricular hypertrophy. Circulation 2006; 113:1768–1778.
33. Hadjiloizou N, Davies JE, Malik IS, Aguado-Sierra J, Willson K, Foale RA, Parker KH, Hughes AD, FrancisDP, Mayet J. Differences in cardiac microcirculatory wave patterns between the proximal left mainstem andproximal right coronary artery. American Journal of Physiology, Heart and Circulatory Physiology 2008; 295:H1198–H1205.
34. Womersley JR. Method for the calculation of velocity, rate of flow and viscous drag in arteries when the pressuregradient is known. Journal of Physiology 1955; 127(3):553–563.
35. Haluska BA, Jeffriess L, Mottam PM, Carlier SG, Marwick TH. A new technique for assessing arterial pressurewave forms and central pressure with tissue Doppler. Cardiovascular Ultrasound 2007; 5:6.
36. Glor FP, Long Q, Hughes AD, Augst AD, Ariff B, Thom SA, Verdonck PR, Xu XY. Reproducibility study ofmagnetic resonance image-based computational fluid dynamics prediction of carotid bifurcation flow. Annals ofBiomedical Engineering 2003; 31:142–151.
37. Kleinstreuer C, Hyun S, Buchanan JRJ, Longest PW, Archie JPJ, Truskey GA. Hemodynamic parameters andearly intimal thickening in branching blood vessels. Critical Reviews in Biomedical Engineering 2001; 29(1):1–64.
38. Vande Geest JP, Sacks MS, Vorp DA. The effects of aneurysm on the biaxial mechanical behavior of humanabdominal aorta. Journal of Biomechanics 2006; 39:1324–1334.
39. Holzapfel GA, Gasser TC. A new constitutive framework for arterial wall mechanics and a comparative studyof material models. Journal of Elasticity 2000; 61:1–48.
40. Vorp DA. Biomechanics of abdominal aortic aneurysm. Journal of Biomechanics 2007; 40:1887–1902.41. Williamson SD, Lam Y, Younis HF, Huang H, Patel S, Kaazenpur-Mofrad MR, Kamm RD. On the sensitivity of
wall stress in diseased arteries to variable material properties. Transactions of ASME, Journal of BiomechanicalEngineering 2003; 125:147–155.
Copyright q 2009 John Wiley & Sons, Ltd. Commun. Numer. Meth. Engng 2009; 25:565–580DOI: 10.1002/cnm