Fluid, Electrolyte, and Acid–Base Disorders
21
Fluid, Electrolyte, and Acid–Base Disorders Stephen Horras, Jennifer Bepko, and Nicholas Longstreet Contents Volume Depletion .................................... 1 Volume Excess ........................................ 3 Sodium Disorders .................................... 4 Hyponatremia ......................................... 4 Hypernatremia ......................................... 8 Potassium Disorders ................................. 9 Hypokalemia .......................................... 9 Hyperkalemia ......................................... 11 Acid–Base Disorders ................................. 12 Metabolic Acidosis .................................... 12 Respiratory Alkalosis ................................. 14 Metabolic Alkalosis ................................... 14 Respiratory Acidosis .................................. 15 Mixed Acid–Base Disturbances ...................... 16 Misc. Electrolyte Disturbances ..................... 17 Magnesium ............................................ 17 Phosphate ............................................. 18 Calcium ............................................... 18 References ............................................ 19 Fluid, electrolyte, and acid–base disorders are frequently encountered in family medicine. Detecting and treating these disorders is impera- tive due to effects on organ perfusion [1]. These disorders present in all age-groups and various clinical settings; but those with chronic diseases are particularly vulnerable to serious complica- tions [2, 3]. Volume Depletion Volume depletion occurs with both actual volume loss and with relative volume loss by fluid redis- tribution (such as third spacing). Actual volume loss occurs through various losses: hemorrhage, the gastrointestinal (GI) tract (i.e., poor intake, vomiting, diarrhea), kidneys (urination), and evaporation (through sweating and breathing). Relative volume loss results in decreased intra- vascular volume without a decrease of total fluid in the body. Whether actual or relative, volume depletion results in decreased “effective circulat- ing volume” (ECV) causing a cascade of multiple compensatory mechanisms. In response to a decreased ECV, cardiac and cerebral blood flow is compromised. Accordingly cardiac and arterial baroreceptors sense the change in mean arterial pressure. This drop in mean arterial pressure trig- gers a norepinephrine-induced increase in heart rate and heart contractility with peripheral arterial vasoconstriction. Concurrently decreased renal blood flow due to decreased ECV triggers S. Horras (*) • N. Longstreet David Grant Family Medicine Residency Program, David Grant Medical Center, Travis AFB, USA e-mail: [email protected]; [email protected] J. Bepko DGMC Family Medicine Residency, David Grant USAF Medical Center, Nellis AFB, NV, USA e-mail: [email protected] # Springer International Publishing Switzerland (outside the USA) 2015 P. Paulman, R. Taylor (eds.), Family Medicine, DOI 10.1007/978-1-4939-0779-3_103-1 1
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Fluid, Electrolyte, and Acid–Base Disorders

Fluid, Electrolyte, and Acid–BaseDisorders
Stephen Horras, Jennifer Bepko, and Nicholas Longstreet
ContentsVolume Depletion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Volume Excess . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Sodium Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Hyponatremia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Hypernatremia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Potassium Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Hypokalemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Hyperkalemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Acid–Base Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Metabolic Acidosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Respiratory Alkalosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Metabolic Alkalosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Respiratory Acidosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Mixed Acid–Base Disturbances . . . . . . . . . . . . . . . . . . . . . . 16
Misc. Electrolyte Disturbances . . . . . . . . . . . . . . . . . . . . . 17Magnesium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Phosphate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Calcium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Fluid, electrolyte, and acid–base disorders arefrequently encountered in family medicine.Detecting and treating these disorders is impera-tive due to effects on organ perfusion [1]. Thesedisorders present in all age-groups and variousclinical settings; but those with chronic diseasesare particularly vulnerable to serious complica-tions [2, 3].
Volume Depletion
Volume depletion occurs with both actual volumeloss and with relative volume loss by fluid redis-tribution (such as third spacing). Actual volumeloss occurs through various losses: hemorrhage,the gastrointestinal (GI) tract (i.e., poor intake,vomiting, diarrhea), kidneys (urination), andevaporation (through sweating and breathing).Relative volume loss results in decreased intra-vascular volume without a decrease of total fluidin the body. Whether actual or relative, volumedepletion results in decreased “effective circulat-ing volume” (ECV) causing a cascade of multiplecompensatory mechanisms. In response to adecreased ECV, cardiac and cerebral blood flowis compromised. Accordingly cardiac and arterialbaroreceptors sense the change in mean arterialpressure. This drop in mean arterial pressure trig-gers a norepinephrine-induced increase in heartrate and heart contractility with peripheral arterialvasoconstriction. Concurrently decreased renalblood flow due to decreased ECV triggers
S. Horras (*) • N. LongstreetDavid Grant Family Medicine Residency Program,David Grant Medical Center, Travis AFB, USAe-mail: [email protected];[email protected]
J. BepkoDGMC Family Medicine Residency, David Grant USAFMedical Center, Nellis AFB, NV, USAe-mail: [email protected]
# Springer International Publishing Switzerland (outside the USA) 2015P. Paulman, R. Taylor (eds.), Family Medicine,DOI 10.1007/978-1-4939-0779-3_103-1
1

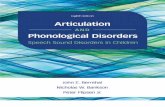
antidiuretic hormone (ADH) release and activatesthe renin-angiotensin-aldosterone system (RAAS).Once activated, renal sodium is retained and vaso-constriction further promoted. ADH secretion con-tributes to vasoconstriction and decreased renalwater clearance in an attempt to restore the ECV.Intrarenal prostaglandins are released with ADHstimulation and activation of RAAS. These prosta-glandins blunt the hypovolemia-induced vasocon-striction in the renal vasculature, therebydisproportionately preserving renal blood flowand glomerular filtration. This physiologicalresponse to volume depletion is illustrated inFig. 1. These vasoconstrictor mechanisms are trig-gered by volume depletion to protect cardiac andcerebral blood flow. Use of nonsteroidal anti-inflammatory drugs (NSAIDs) and angiotensin-converting enzyme inhibitors (ACE-I) may dimin-ish this renoprotective response [4–6].
Determining true volume status can bechallenging even for an experienced physician.Accurate volume status can be especially difficultwith the young, elderly, or disoriented patient.Clinically, volume depletion can manifest withlow blood pressure, palpitations, dizziness,decreased urine output, and lightheadedness.Objective findings in volume depletion includeresting tachycardia, orthostatic hypotension, rest-ing hypotension, however some patients withhypovolemia may not exhibit abnormal vitalsigns. Chronic hypotension manifests more subtlefindings such as general malaise, weakness,anorexia, and mental status changes. Volume sta-tus is also difficult when patients appear fluidoverloaded (e.g., congestive heart failure [CHF],cirrhosis, and nephrosis) due to excessive renalsodium and water conservation that drives volumedisproportionately to the interstitial fluid space
GI, Renal, Skin and/or RespiratoryVolume Loss
Decreased LV FunctionDecreased Oncotic Pressure Decreased Cardiac Output
Absolute Volume Depletion Hemorrhage
Third SpacingVasodilation
Increased AtrialNaturetic Hormone
Renin Release
Angiotensin I
Angiotensin |I
Increased Renal*
Prostaglandins
Renal H2ORetention
IncreasedUsg and Uosm
*Norepinephrine in addition in Angiotensin II and ADHstimulates Renal Prostaglandins production
AldosteroneRelease
Decreased Effective Circulating Volume
ADH ReleaseNorepinephrine
Increased Peripheral Vasoconstriction
Increased Heart RateIncreased Cardiac Contractility
PHYSIOLOGICAL RESPONSE TO VOLUMEDEPLETION IN ORDER TO PRESERVEEFFECTIVE CIRCULATING VOLUME
RenalVasodilation
Renal Na+
Retention
UNa< 20 mEq/L
RenalHypoperfusion
Fig. 1 Physiological response to volume depletion.GI gastrointestinal, LV left ventricle, UNa urine sodiumconcentration, Uosm urine osmolality, Usg urine specificgravity, ADH antidiuretic hormone, SIADH syndrome of
inappropriate ADH secretion (Originally appearedin: Taylor R, David A, Fields S, Phillips M, Scherger J,editors. Family medicine (Taylor). New York: Springer;2003)
2 S. Horras et al.

which is known as third spacing. Third spacingrefers to the interstitial space between skin andfascia that is not normally perfused with fluids.Third spacing can occur with increased fluid vol-ume (fluid replacement, renal dysfunction),increased capillary hydrostatic pressure (CHF),decreased sodium level (due to sodium loss),lowered albumin (malnutrition, liver disease,protein-losing enteropathy), increased capillarypermeability (burns, trauma, disseminated intra-vascular coagulation, infections), or lymphaticobstruction (iatrogenic removal). Regardless ofthe cause, third spacing results in decreased intra-vascular volume. Physical exam findings can bevaried due to differing etiologies, however edemais generally present.
Laboratory data can help determine fluid statussuch as serum osmolality (SOSM), blood ureanitrogen (BUN), urine osmolality (UOSM), andurine specific gravity. With volume depletion theurine specific gravity and UOSM are high (i.e.,>1.015 and >350 mOsm/kg, respectively) as aresult of ADH-induced renal water conservationleading to concentrated urine. In volume-depletedstates, renal hypoperfusion results in prerenal azo-temia and functional or nonintrinsic acute renalfailure causing BUN to be retained such that thenormal 10:1 BUN/creatinine ratio is elevated(e.g., to >20:1). When volume loss is due tohemorrhage, a hematocrit/hemoglobin can below, however concentration can occur with signif-icant third spacing. Generally with hypovolemia,an increased SOSM, increased serum sodium, andcorresponding decreased urine sodium (UNa) isseen, however inappropriate responses can beseen with certain comorbidities.
Volume depletion is treated according to theclinical situation and etiology. Treatment for mildvolume depletion occurs with slow restoration ofthe ECV such as using oral electrolyte solutions.Treatment escalates to infusion of isotonic fluid inmore severe settings. In addition to replacingexcess fluid loss, volume repletion must alsoinclude the replacement of daily obligate fluidlosses. The rate of volume replacement dependson the clinical situation. Restoration of ECVresults in normalization of postural blood pres-sure, pulse changes, and urinary excretion of
sodium [5]. Once the volume status has beenrestored, treatment can be directed to restoringelectrolyte loss and imbalances.
Volume Excess
Volume excess, or hypervolemia can be caused byexcessive fluid intake, excessive sodiumintake, chronic hepatic or renal failure, steroidtherapy, transfusion reaction, decreased cardiacoutput, head injury, medications, malnutrition, andmineralocorticoid excess. Volume overload can alsobe caused by decreased ECV, as discussed previ-ously, which results in renal sodium and waterconservation and edema formation (e.g.,hypoalbuminemia and left ventricular dysfunction).
Total body volume excess caused by decreasedECV and edema formation may cause symptomsof vital organ hypoperfusion (e.g., syncope, unsta-ble angina, decreased urine output, mental statuschanges). Depending on the etiology of volumeexcess, physical findings of CHF, hepatic cirrho-sis, and nephrosis might be present. Weight gainmay reflect the quantity of the volume retention,and monitoring weight gain can be clinically use-ful. Evidence of edema may be found in the lowerextremities in an ambulatory patient but may bemore evident in the presacral area in a recumbentpatient. Volume excess may present as pulmonaryedema, elevated jugular venous pressure, orprolonged hepatojugular reflux in CHF. Addition-ally, volume excess may not be readily evident onclinical exam as in a patient with bowel walledema [7]. Hypervolemia associated withincreased ECV causes urine sodium (UNa)wasting (UNa >20 mEq/L) and no excessivewater retention (assuming normal osmolality).
Treating volume excess caused by decreasedECV involves increasing cardiac output in heartfailure patients and restoring intravascular oncoticforces in patients with cirrhosis andhypoalbuminemia. Removal of some edema bydiuretics may be required, typically in the formof intravenous furosemide, especially if theretained fluid compromises ventilation. Whenthird-spaced fluid is significant it should beremoved with caution, as removal of large
Fluid, Electrolyte, and Acid–Base Disorders 3

amounts can cause rapid reaccumulationsextracted from the circulating volume, resultingin hypotension. With states of aldosterone excess,an aldosterone antagonist (i.e., spironolactone,eplerenone) is used to decrease sodiumreabsorption and edema, but ideally the sourceof the hyperaldosteronism is removed. In renalfailure, diuresis with potent loop diuretics maybe required to remove excess volume that maybe causing renal hypoperfusion. Careful anddeliberate diuresis is very important in CHF.
Sodium Disorders
Appreciating a patient’s fluid status is crucialwhen disorders of sodium concentration are pre-sent. Hyponatremia ([Na+] <135 mEq/L) andhypernatremia ([Na+] >145 mEq/L) should beapproached in terms of free water level status. Afirm understanding of tonicity is required whenapproaching sodium disorders.
Tonicity is the measure of the osmotic pressuregradient between the intracellular fluid compart-ment (ICF) and extracellular compartment (ECF).Tonicity is affected only by solutes that cannotcross the membrane (cellular membrane) whileosmolality is the property of a particular solution.These compartmentalized solutes create an osmoticgradient across the cell membrane [8]. In effectiveplasma osmolality, which is typically normalwithinthe range of 275–300 mOsm/kg H2O, only solutesthat predominantly do not pass between the ECFand ICF contribute to creating osmotic gradientsand effecting flow of water between the ECF andICF. Sodium is amajor plasma solute, and thereforewhen evaluating hyponatremia, the osmolalityshould be evaluated.
The plasma osmolality (POSM) is the totalosmolality of the solutes in the plasma and canbe calculated as
Posm ¼ 2 Naþ½ � þ glucose½ �18
þ BUN½ �2:8
Calculating the effective POSM can be helpfuland when different from measured (osmolalitygap) can indicate the presence of ethanol,
methanol, isopropanol, ethylene glycol, propyl-ene glycone, or acetone. Therefore, evaluatingplasma osmolality, effective and measured,would be the first step when approaching sodiumdisorders. Determining osmolality is also neededwhen approaching metabolic acidosis disorderswhich will be discussed later.
Hyponatremia
Hyponatremia (Table 2) and hypoosmolality (i.e.,plasma osmolality <275 mOsm/kg) indicateexcess water content relative to sodium causedby renal retention of ingested water such ashypovolemic-induced ADH release, SIADH, andexcess water ingestion greater than renalfree water clearance. Hyponatremia occurswithout hypoosmolality (i.e., pseudohypo-natremia) in the presence of hyperproteinemiaand hyperlipidemia. Pseudohyponatremia canoccur with severe hyperlipidemia (hypercholes-terolemia and hypertriglyceridemia) andhyperproteinemia (such as multiple myeloma),causing relatively lower proportions of sodiumin plasma but maintaining normal osmolality andtonicity between 275 and 300 mOsm/kg H2O[9–11].
Hyperglycemia is discussed more completelyin chapter “▶Diabetes Mellitus”; however, it isalso important to consider its impact on fluid andelectrolyte abnormalities. In states where serumglucose is highly elevated, fluid shifts can beprofound and electrolyte imbalance substantial.Excessive hyperglycemia obligates large amountsof additional water to extracellular spaces byosmotic-induced intracellular water loss (i.e., cel-lular dehydration). When evaluating hyperglyce-mia, the correct sodium should be calculated.
Corrected sodium = Measured sodium +0.024 � (serum glucose – 100) [12]Hyperglycemia causes an osmotic diuresis
leading both to salt and water losses, total bodyvolume depletion, or decreased renal perfusion.As kidney perfusion decreases, renal ability toexcrete glucose is impaired further contributingto hyperglycemia. The hyperglycemic diuresiscontributes to total body potassium losses through
4 S. Horras et al.

urine, though overt hypokalemia may not be evi-dent until fluid loss is replaced and insulin given.Potassium deficits can inhibit cellular glucoseuptake and cause cardiac dysrhythmias.
Volume repletion is paramount in treating hyper-glycemic episodes and leads to decrease in serumglucose and improved glomerular filtration rate.Isotonic saline is initially preferred, attendingto possible hemodynamic instability, and shouldbe started at 15–20 mL/kg/h decreasing to4–14 mL/kg/h once patient has stabilized [13]. Inhyperosmolar hyperglycemic nonketotic syndrome,insulin is a required therapy, though it should not begiven until fluid resuscitation is initiated since insu-lin drives glucose, potassium, and water into cellspotentially causing vascular collapse. In diabeticketoacidosis, higher doses of insulin via continuousinfusion are usually required. In order to avoidcerebral edema, fluid should be switched to0.45 % normal saline when sodium is greater than135 mmol/L with 5 % dextrose added once plasmaglucose is 200 mmol/L [14].
Hypernatremia (see Fig. 3) and hyperosmolality(i.e., plasma osmolality >300 mOsm/kg) reflect awater deficit relative to sodium caused by excesswater loss, decreased water intake, decreased waterretention, or excess intake of sodium salts.
Understanding osmolality and tonicity is cru-cial to understanding hyponatremia (Fig. 2),which is the most common occurring electrolyteabnormality [15]. Clinically, hyponatremia can befurther categorized by determining volume status[16]; there are three types of hyponatremia:hypovolemic, euvolemic, and hypervolemic.Common causes for hyponatremia are shown inTable 1.
Low-volume hyponatremia occurs in relationof solute to total body water, and sodium loss ismediated either by the kidneys or via extrarenalloss of sodium with water retention [8]. UNaconcentration can be a helpful measure of thesemechanisms as UNa >20 mmol/L representssodium loss mediated by the kidneys [17].In hypovolemic hyponatremia, ingested free
Relative and AbsoluteVolume Loss
Decreased EffectiveCirculating Volume
ADH Release
Access to H2O
Renal H2O Retention
Water intake > Renal H2O Excretion
Volume Expansion
Una+ < 20 mEq/L
Una+ > 20 mEq/L
AldosteroneRelease
HypoosmolarHyponatremia
AldosteroneSuppression
ADHSuppression
Elevated UsgElevated Uosm
Decreased UosmDecreased Usg
Renal Na+
Retention
PATHOGENESIS OFHYPONATREMIA
SIADHSecretion
Excess ADH Secretion
Renal H2O Retention
Volume Expansion Elevated UsgElevated Uosm
Una+ > 20 mEq/L
Fig. 2 Pathogenesis of hyponatremia. UNa urine sodiumconcentration, Uosm urine osmolality, Usg urine specificgravity, ADH antidiuretic hormone, SIADH syndrome of
inappropriate ADH secretion (Originally appeared in:Taylor R, David A, Fields S, Phillips M, Scherger J, edi-tors. Family medicine (Taylor). NewYork: Springer; 2003)
Fluid, Electrolyte, and Acid–Base Disorders 5

water is retained because of the nonosmotic (i.e.,hypovolemia-induced vasoconstriction) presenceof ADH acting in the distal convoluted tubule andcollecting duct [18–21]. With hypovolemichyponatremia from diuretic use, most commonlythiazide diuretics, the dilutional mechanism in thetubules is inhibited, but UNa concentration is not[21–25]. Thiazide-induced hyponatremia is morecommon in elderly women than men [26,27]. Mineralocorticoid deficiency from adrenalgland destruction or inherited deficiencies leadsto renal sodium wasting, causing a hypovolemicstate and activating vasopressin to further concen-trate urine sodium. Elevated serum potassiumwith hypovolemic hyponatremia should lead tofurther investigation of mineralocorticoid insuffi-ciency. Cerebral salt wasting is another cause ofhypovolemic hyponatremia. After neurologicalsurgery or head injury, a baroreceptor-mediatedvasopressin release is activated by urine sodiumand chloride loss, though etiology of this processis not well established. Chronic use of protonpump inhibitor-induced hyponatremia is increas-ingly being elucidated in literature and adds fur-ther concerns to long-term proton-pumpinhibitors (PPI) use [28]. The PPI-mediatedhyponatremia mechanism is unclear but likelyrelated to SIADH or sodium-losing nephropathy[29]. Extrarenal losses leading to hypovolemichyponatremia include GI losses (i.e., vomiting
and diarrhea) and third-space sequestration (i.e.,bowel obstruction, pancreatitis, peritonitis, asci-tes, massive tissue injury, venous congestion).Urine sodium concentrations in these causes areusually <20 mEq/L.
Euvolemic hyponatremia can be thought of asdilutional hyponatremia and is related to fluidintake above the kidneys’ ability to excrete water(Table 1, Fig. 2) [15, 30]. SIADH is the mostcommon form of euvolemic hyponatremia andoccurs when excess ADH is secreted in theabsence of volume or osmotic stimuli, resultingin water excess and hyponatremia caused by avariety of disorders including central nervous sys-tem and pulmonary diseases (Table 2). Euvolemichyponatremia can occur in exercise-associatedhyponatremia. Interestingly, long-distance run-ning athletes who consumed excessive amountsof water during competition in conjunction withADH-stimulatory effects of exercise intensity andduration led to hyponatremia [35]. Primary poly-dipsia [30] (i.e., ingestion of large quantities ofwater 10–15 L in 24 h) leads to hyponatremiasince intake exceeds the kidneys’ ability toexcrete free water.
Diseases that increase ECF volume throughelevated ADH and frequently reduced glomulelarfiltration rate (GFR) (e.g., CHF, cirrhosis,nephrotic syndrome, severe renal insufficiency)can lead to hypervolemic hyponatremia [36, 37].
Table 1 Main causes of hyponatremia
Hypovolemic states Euvolemic states Hypervolemic states
Osmotic (e.g., glucosuria, bicarbonaturia,ketonuria)
Hypothyroidism Congestive heart failure
Diuretics SIADH (see Table 2) Renal failure
Mineralocorticoid deficiency Severe pain and/orstress
Cirrhosis
Salt losing nephropathies Glucocorticoiddeficiency
Nephrosis
Cerebral salt wasting Primary polydipsia Decreased vascular integrity (e.g., sepsis,anaphylaxis)
GI volume losses (e.g., diarrhea, vomiting) Beer potomonia Acute or chroni renal failure
Sweat losses Dilute formula intake
Third-space sequestration Dilute tube-feeding
References used: [1, 17, 36]ADH antidiuretic hormone, GI gastrointestinal, SIADH syndrome of inappropriate secretion of ADH, ECV effectivecirculating volume, UNa urine sodium concentration
6 S. Horras et al.

ADH secretion increases in left heart function anddecreases due to baroreceptor mechanisms. [37]Low levels of circulating protein in both cirrhosisand nephrotic syndrome lead to hyponatremiathrough an ultimate decrease in intravascular vol-ume, leading to release of ADH. Edematouscauses of hyponatremia from aforementionedconditions are associated with weight gain andedema formation.
Hyponatremia-related symptoms varydepending on the cause of hyponatremia. Patientsmay be asymptomatic depending on the cause orpresent with confusion, weakness, irritability,
nausea, vomiting, postural dizziness, syncope,and falls, with seizures and coma less common.[38] Symptoms are usually present when serumsodium approaches <120 mEq/L. In severehyponatremia, neurological symptoms mayinclude seizures and coma. The severity of symp-toms depends not only on the level but the rapidityof decline. Patients who develop hyponatremiaover time may remain asymptomatic at relativelylower levels of plasma sodium concentrationbecause of brain cell adaptation tohypoosmolality [39].
Treatment of hyponatremia is dependent on theexpected cause. In hypoosmolar hyponatremiafrom volume loss, sodium replacement shouldalmost always be with oral or intravenous isotonicvolume repletion. In patients with neurologicalsymptoms or plasma sodium <110 mEq/L infu-sion of hypertonic saline with free water fluidrestriction are often both required. Physicianscomfortable with intensive or emergent medicineshould direct this treatment. Goal of treatment inthese cases is to restore ECV and normalizeplasma osmolality. For patients withhyponatremia caused by SIADH and those withsevere renal failure, re-equilibrating plasmaosmolality is done via fluid restriction. Identifyingand removing the source of SIADH secretion isalso key. Plasma sodium concentration correctionfor asymptomatic patients with SIADH should beincreased at a rate of 0.5 mEq/L/h until a level of120 mEq/L is reached; however, more rapidsodium correction might be necessary for thosepatients with severe neurological symptoms(1.0–1.5 mEq/L/h for the first 10 mEq/L elevationin the plasma sodium concentration). Avoidingexcessively rapid correction of hyponatremiadecreases the possibility of potentially devastatingcentral pontine demyelinization [40–49]. Withhypervolemic hyponatremia, focus of therapy ison restoring ECV by improving ventricular dys-function in patients with CHF and increasingoncotic pressures in those with nephrosis andcirrhosis. Tolvaptan, a V2 receptor antagonist,has been approved for treatment of euvolemicand hypervolemic hyponatremia for serumsodium <125 mEq/L or hyponatremia resistantto fluid restriction. This therapy must be done in
Table 2 Causes of syndrome of inappropriate antidiuretichormone secretion
Central nervous system disorders causing increasedhypothalamic production of antidiuretic hormone
Infections (e.g., meningitis, HIV infection)
Vascular problems (e.g., subdural hemorrhage)
Primary and metastatic cancers
Psychosis
Post pituitary surgery
Hypothalamic infiltrative disease (e.g., sarcoidosis)
Others (e.g., Guillain-Barré syndrome)
Pharmacologic agents
Stimulants of hypothalamic antidiuretic hormonesecretion- Haloperidol, Amitriptyline, Thioridazine,Thiothixene, Carbamazepine, Fluoxetine and sertraline,Monoamine oxidase inhibitors, and others
Potentiators of antidiuretic hormone effect-Chlorpropamide, Tolbutamide, Carbamazepine
Exogenous antidiuretic hormone preparations-Vasopressin, Oxytocin
Pulmonary disorders causing increased antidiuretichormone production
Pneumonias
Tuberculosis
Acute respiratory failure
Others (e.g., asthma, pneumothorax)
Ectopic production of antidiuretic hormone (e.g.,bronchogenic carcinoma, oat cell carcinoma of thelung, pancreatic carcinoma)
Pancreatic carcinoma
Prolactinoma
Others
Postoperative patient
Severe nausea
Adapted from: [1, 31–34]
Fluid, Electrolyte, and Acid–Base Disorders 7

a hospital setting and fluid restriction not be initi-ated. Tolvaptan dosing remains controversial inpreventing the overall disease progression in heartfailure [50].
Hypernatremia
Hypernatremia, serum sodium concentration>145mmol/L (Fig. 3), is caused by increased hypo-tonic fluid loss (i.e., GI losses, renal loss, insensiblelosses, or diabetes insipidus where ADH activity orsecretion is reduced) exceeding hypotonic fluidintake [31–34, 51–53]. Approximately 1–3 % ofall hospitalized patients are found to havehypernatremia [53, 54]. Thirst and access to waterare the two most important aspects in preventinghypernatremia [55]. Excessive oral intake of sodiumsalts and hypertonic volume expansion can also leadto hypernatremia [56] (Table 3).
In hypernatremia, plasma osmolality is>300 mOsm/kg. Urine sodium concentration of<20 mEq/L can be seen in a hypernatremicpatient with GI or insensible losses with
Table 3 Causes of hypernatremia
Primary Hypodipsia (defect of thirst)
Primary or metastatic tumor, granulomatous disease,vascular disease, trauma
Diabetes Inspidius
Central, nephrogenic
Pure Hypertonic Solute Gain
Ingestion of hypertonic solutions
Ingestion of salt-tablets
Inadequate Fluid Intake with increased free-waterloss
Increase sweating, fever
GI losses
Osmotic diuresis
Diuretics
Relative and AbsoluteVolume Loss
Decreased EffectiveCirculating Volume
ADH Release
Lack of H2O Replacement
UNa+ < 20 mEq/L
UNa+ > 20 mEq/L
Angiotensin II
Aldosterone
AldosteroneSuppression
Increased Uosm
Renal Na+
Retention
PATHOGENESIS OFHYPERNATREMIA
Renal H2O Retention
Volume Expansion
Hypernatremia
ADHRelease
Elevated Uosm
DI
Lack of ADH or ADH Effect
Renal H2O Loss
Volume Loss Decreased Uosm
SmallUNa+ > 20 mEq/L
Excess Hypertonic Na+ Intake
LargeUNa+ < 20 mEq/L
Fig. 3 Pathogenesis of hypernatremia. DI diabetes insipidus. (See Fig. 2 for other abbreviations.) (Originally appearedin: Taylor R, David A, Fields S, Phillips M, Scherger J, editors. Family medicine (Taylor). New York: Springer; 2003)
8 S. Horras et al.

inadequate hypotonic volume replacement. Addi-tionally, high urine osmolality (e.g.,>600 mOsm/kg) is observed in these patients as the kidneysattempt to maintain stable fluid and sodium bal-ance through renal water conservation. Whenhypernatremia is caused by renal volume lossesfrom diuretics or osmotic diuresis with inadequatehypotonic volume replacement urine sodium con-centration is >20 mEq/L, while urine osmolalitymay be <350 mOsm/kg and is less than plasmaosmolality. With the addition of sodium salts forvolume expansion, hypernatremia is associatedwith urine osmolality >350 mOsm/kg and urinesodium concentration >20 mEq/L. Patients withsevere hypernatremia (serum sodium concentra-tion >155 mEq/L) without maximum concen-trated urine (i.e., 800–1200 mOsm/kg) suggestsdiabetes insipidus, intrinsic renal disease, osmoticdiuresis, or diuretic use [52, 53, 57].
The symptoms of hypernatremia occur due tohyperosmolality of ECF shifting volume out ofcells. The rate and severity at which this processoccurs dictates symptom development. The mostdangerous symptoms are nonspecific weaknessand agitation, which signal changes in centralnervous system. As hypernatremia increases fallsand syncope from disorientation and somnolenceare more common. [58] Polyuria can reveal a renalloss of pure water (e.g., diabetes insipidus),osmotic diuresis (e.g., glycosuria), or diureticuse, especially in medications altering ADH func-tion. Also, hypertonic volume expansion or otheraddition of sodium salts can lead to a patient withthe appearance of clinical volume overload (i.e.,shortness of breath, pulmonary and peripheraledema, weight gain, systemic and venous hyper-tension, and S3 gallop).
Treating hypernatremia depends on the cause.Correction of asymptomatic or chronichypernatremia that develops over greater than48 h or previously unknown hypernatremia mustproceed slowly (i.e., [Na+] reduction of 0.5 mEq/L/h) to avoid cerebral edema and resultant neuro-logical dysfunction [59]. In cases whenhypernatremia has developed in less than 48 h,or acute hypernatremia, correction can proceed atup to 1 mEq/L/h [59]. Hypernatremia correction
that is too slow can also cause complications[60]. When ECV is diminished by hypotonic vol-ume loss, volume expansion with isotonic salineis initially used until signs of hypovolemia haveresolved. An added benefit of isotonic saline infu-sion is that it can contribute to equilibratingplasma osmolality in patients withhyperosmolality. Once euvolemia isre-established, hypotonic fluids (e.g., 0.45 % nor-mal saline or dextrose 5 % in water [D5W]) can beadministered in order to decrease plasma osmo-lality in pure water losses from the skin or kidneys[3, 60]. Hypernatremia caused by the addition ofNa+ salts is treated with D5W and diuretics. Cal-culating free water deficit can be helpful for man-agement; however, total body water and freewater loss are grossly underestimated with themost commonly used equation: total body waterdeficit = correction factor x premorbid weight �(1–140/Na+) [61]. Previously, treatment of centraldiabetes insipidus was with administration ofADH preparation (e.g., aqueous vasopressin,vasopressin in oil, and vasopressin nasal sprays);however, DDAVP (desmopressin) is preferred dueto the side effect profile and variable efficacy ofADH preparations [62, 63]. Correcting other elec-trolyte abnormalities and removing the offendingagent, which is frequently drug induced, treatnephrogenic diabetes insipidus. Thiazides and alow-sodium diet can be helpful in treatment aswell.
Potassium Disorders
Hypokalemia
Plasma potassium levels are typically maintainedat 3.5–5.0 mmol/L, with hypokalemia describedby potassium levels <3.5 mmol/L. Hypokalemiais a common electrolyte abnormality and com-monly the result of non-potassium sparingdiuretics. As with hyponatremia (Table 4), plasmahypokalemia can occur due to nonrenal causeswith urine potassium (UK) <25 mEq/L (e.g.,excessive GI, skin potassium losses) and due torenal causes with UK >25 mEq/L (e.g., sodium-
Fluid, Electrolyte, and Acid–Base Disorders 9

losing nephropathies, mineralocorticoid excess,vomiting, diuretics, and hypomagnesemia).However, hypokalemia may be more easily cate-gorized by potassium excreted via kidneys orpotassium loss through GI tract or cellular shifts(i.e., potassium driven intracellularly).
Potassium is typically passively reabsorbed inthe proximal tubule of the kidney with the move-ment of sodium and chloride, while being activelyreabsorbed in the thick ascending loop of Henle inthe medulla via Na-K-2Cl (NKCC2)cotransporter. Increased flow to the distal nephronthat occurs in diuretics that are effective moreproximally (e.g., loop and thiazide diuretics)lead to increased potassium loss. Additionally,volume depletion activates RAAS causing anincrease in potassium excretion. In fact, anythingthat leads to increases in mineralocorticoid activ-ity and subsequent aldosterone activity will alsolead to renal potassium loss.
Potassium can be lost through the GI tract aswell with diarrhea often associated with ahyperchloremic metabolic acidosis. Upper GIpotassium loss from vomiting is mediated byhypovolemic-induced RAAS activation, alongwith high levels of sodium bicarbonate andincreased distal flow to nephron where potassiumis excreted. Also, vomiting causes chloride deficitthat leads to metabolic alkalosis that may causeintracellular movement of potassium. The Na-K-ATPase pump in skeletal muscle and hepatocytesregulates most of the total body potassium and canbe a source of hypokalemia with pump derange-ment (reference number here). Increased insulinactivity drives potassium intracellularly by increas-ing pump activity, while β-adrenergic agonists areactive at the Na-K-ATPase pump, as well as in theNa-K-2Cl (NKCC2) cotransporter [64, 65].
Metabolic and respiratory alkalosis, hypother-mia, and hypokalemic periodic paralysis are alsorelated to extracellular potassium moving intra-cellularly. As alkalotic states may drive potassiuminto cells, acidotic states like diabetic ketoacidosisand renal tubular acidosis (RTA) associated withincreased UK loss and total body potassiumdepletion may cause an acidosis-induced increasein plasma potassium and corrected by treatingacidotic state.
Hypokalemia coexisting with hypertensionshould be further evaluated by checking renallevels. If the renin levels are low, the aldosteronelevel should be measured to evaluate for primaryhyperaldosteronism (i.e., high aldosterone levels)or exogenous mineralocorticoid (i.e., low
Table 4 Causes of hypokalemia
Renal potassium loss
Diuretics, current use
Vomiting and nasogastric tube drainage
Magnesium depletion
Mineralocorticoid excess (e.g., primary and secondaryhyperaldosteronism, Cushing’s disease, licoriceingestion, hyperreninism, Bartter syndrome, AdrenalAdenoma)
Diabetic ketoacidosis
Renal tubular acidosis
Ureterosigmoidostomy
Polyuria
Osmotic diuresis
Correction of chronic hypercapnia
Gastrointestinal loss
Diarrhea
Excess sweating
Intestinal fistulas
Rectal villous adenoma
Geophagia (i.e., clay ingestion)
Laxative abuse
Chloride-losing diarrhea
Intracellular K+ sequestration
Metabolic and respiratory alkalosis
Excess insulin
Treatment of megaloblastic anemias
Granulocyte-macrophage colony-stimulating factor(GM-CSF)
β-adrenergic agonist
Hypothermia
Catecholamine excess
Hypokalemic periodic paralysis
Pseudohypokalemia
Prolonged standing of collected blood with extremelyhigh WBC count
Blood specimen collected immediately after insulinadministration
Decreased K+ intake
Starvation
Adapted from Taylor R, David A, Fields S, Phillips M,Scherger J, editors. Family medicine (Taylor). New York:Springer; 2003
10 S. Horras et al.

aldosterone levels as in licorice ingestion). Highor normal renin levels can be associated withrenovascular hypertension and Cushing’s disease.Inadequate potassium intake alone can also causehypokalemia [66]. Treatment of severe megalo-blastic anemias or use of granulocyte-macrophagecolony-stimulating factor induces cell productionthat leads to uptake of hypokalemia [67].
Hemolysis during collection of blood productscan lead to spuriously elevated levels of plasmapotassium, while also conveying normal plasmapotassium when there is true hypokalemia.
Symptoms associated with hypokalemiainclude generalized weakness, musculoskeletalcomplaints (muscle cramps, muscle tenderness),GI complaints (anorexia, nausea, vomiting, con-stipation), polyuria, polydipsia, and cardiac com-plaints (palpitations, syncope). In skeletal muscleinjury and rhabdomyolysis, potassium releasefrom contracting skeletal muscle that would nor-mally cause vasodilation and improved bloodflow regionally is blunted in severe hypokalemia[68]. Potassium is also involved in cardiac musclerepolarization allowing for appropriate cardiacmuscle relaxation and diastolic filling. With hypo-kalemia, cardiac repolarization is prolonged lead-ing to classic electrocardiogram (EKG) changes.First noted is decreased magnitude of T waves,then U wave formation, and finally ST segmentdepression on EKG.
Oral replacement with potassium chloride orpotassium bicarbonate and underlying correctionof the cause are the mainstays of initial treatment.Intravenous potassium chloride may be used solelyor with oral therapy. Typically, 10 mEq of potas-sium supplementation will increase plasma potas-sium level by about 0.1 mEq/L with the potassiumgoal of 4.0 mEq/L to minimize untoward effects ofhypokalemia. Foods rich in potassium are less use-ful in treatment of hypokalemia since potassium inthese sources is in the form of potassium citrate orpotassium phosphate, which is about 60 % lessretained thanpotassiumchloride [69].Hypokalemiacan be corrected intravenously via peripheral line atabout 10 mEq/h since higher concentrations causelocal irritation along with venous sclerosis. A cen-tral line can avoid these adverse effects when aninfusion rate of 20 mEq/h or greater is required. In
all cases of potassium repletion, frequent plasmapotassium measurements should be monitored forefficacy of therapy [70]. Low magnesium must becorrected to ensure potassium is not lost renallyduring repletion [71]. Diuretics that work in thedistal convoluted tubule and antagonize aldoste-rone receptors (i.e., spironolactone) can decreasekaluresis that is caused by loop and thiazidediuretics.
Hyperkalemia
Hyperkalemia (see Table 5) is less well toleratedby the body than hypokalemia and occurs whenextracellular potassium levels are elevated beyondthe ability of kidneys, skin, and GI tract to excretepotassium. Extracellular potassium concentrationcan be affected by potassium shift from intracel-lular space to extracellular, potassium intake andpotassium excretion [72]. The kidneys performmost potassium excretion. Many medicationscan lead to hyperkalemia. Spironolactone,ACE-I, ARBs decrease aldosterone production,
Table 5 Causes of hyperkalemia
Increased K+ intake
Decreased K+ excretion
Acute and chronic renal failure
Decreased effective circulating volume
Hypoaldosteronism- K+-sparing diuretics, Hyporeninhypoaldosteronism in mild renal disease, NSAIDs, ACEinhibitors, Adrenal insufficiency
Intracellular K+ extrusion
Metabolic and respiratory acidosis
Tissue injury (e.g., crush, rhabdomyolysis, hematomaresorption)
Insulin deficiency in diabetic ketoacidosis, prolongedfasting; hyperosmolality from hyperglycemia
Drugs (e.g., digitalis intoxication, succinylcholine, andarginine HCI, β-adrenergic blockers)
Hyperkalemic periodic paralysis (from excessiveexercise, fasting)
Measurement error
Thrombocytosis
Leukocytosis
Hemolysis of blood sample (i.e., delay after blood draw,cell destruction from vigorous sample shaking
Blood collection from ischemic extremity
References used [1, 75–78]
Fluid, Electrolyte, and Acid–Base Disorders 11

which can lead to hyperkalemia. Medicationssuch as triamterene, amiloride, and the antibiotictrimethoprim decrease potassium excretion byblocking sodium channels. Other medications(e.g., nonselective beta-blockers, NSAIDs) canincrease extracellular potassium by inhibitingNa-K ATPase pump, causing potassium to remainin extracellular fluid space and decreasing aldo-sterone production [73]. Avoiding a combinationof these medications in patients with coexistentrenal failure is important [73]. Kidney dysfunc-tion (RTA type 4, CHF, and other causes ofhypoaldosteronism) can inhibit potassium excre-tion [72]. Additional conditions and ingestionsaffect transcellular movement of potassium lead-ing to hyperkalemia such as metabolic acidosis(0.2–1.7 mEq/L increase in [K+] for every 0.1decrease in pH), hypertonicity from hyperglyce-mia or hypernatremia, insulin deficiency in diabe-tes mellitus or from starvation, rhabdomyolysisand hematoma resorption or other forms of cellu-lar destruction, digitalis intoxication, andhyperkalemic periodic paralysis from intenseexercise or fasting. Hyperkalemia due to measure-ment error is also quite common and can becaused by hemolysis of red blood cells as a resultof collection (i.e., prolonged tourniquet use, fistclenching leading to minor ischemia) [74] or stor-age, release of K+ during coagulation of bloodsamples with increased WBCs (e.g., WBCs>100,000/mm2 in leukemia) (or increased plate-lets (i.e., >1,000,000/mm2) [74–76].
Hyperkalemia can cause nonspecific symptomssuch as muscle weakness, fatigue, malaise, nausea,vomiting, and paresthesias. Peaked T waves arehallmark EKG findings in hyperkalemia, thoughflattened Pwaves, increased PR interval, prolongedQRS duration with shortened QT interval may alsobe present. Uncorrected hyperkalemia can lead tosine wave development with resultant ventricularfibrillation and asystole. Bradycardia, dysrhyth-mias, and paralysis can also occur.
Treatment of acute hyperkalemia can be done byenhancing potassium cellular entry using insulin,glucose, and inhaled beta-agonists (i.e., albuterol orlevalbuterol) [77]. If hyperkalemia is associatedwith life-threatening dysrhythmias, calcium is
used to decrease the threshold of myocardial tissueexcitability induced by hyperkalemia, thereby min-imizing risk of serious cardiac events. Calciumchloride has more elemental calcium and greaterbioavailability than calcium gluconate but is typi-cally associated with tissue necrosis and thereforecannot be infused as rapidly; however, one salt hasnot been proven more effective over the other [78].Sodium bicarbonate has not shown to be moreeffective than placebo [78]. Loop diuretics areeffective for excreting total body potassium inpatients who make urine and kayexalate. Sodiumpolystyrene was previously shown to be effective[72], but new data shows no difference compared tostool softeners alone and is associated withincreased risk of intestinal necrosis [77, 79, 80].In patients refractory to these treatments, hemodi-alysis may prove necessary [78].
Acid–Base Disorders
Metabolic Acidosis
Metabolic acidosis is a primary reduction inplasma bicarbonate concentration leading tohypobicarbonatemia (Table 6), which stimulatescompensatory hyperventilation and hypocapnia(i.e., decreased pCO2). In metabolic acidosis, thecompensatory hyperventilation can be determinedwith the following formula. Full compensationmay take several hours.
Calculation for expected pCO2
pCO2 ¼ 1:5 � HCO3½ � þ 8
The limit of compensatory hyperventilation inmetabolic acidosis is 10 mmHg that may be moredifficult to achieve in acute versus acute process.If the rate of the pCO2 decrease is less or morethan predicted, a mixed acid–base disturbanceoccurs [81–84]. If the actual pCO2 is too highthen an additional respiratory acidosis is present;conversely if the pCO2 is too low then an addi-tional respiratory alkalosis is present. The clinicalscenario must be taken into account when
12 S. Horras et al.

approaching acid–base disorders. The etiology forthe bicarbonate loss must be determined. Lossescan occur with GI bicarbonate loss(e.g., diarrhea), renal bicarbonate loss (e.g., renaltubular acidosis), or bicarbonate titration withfixed endogenous acids (e.g., ketoacidosis) andexogenous acids (e.g., salicylate intoxication).Metabolic acidosis caused by pure bicarbonateloss is characterized by hyperchloremia and anormal anion gap. However, when metabolic aci-dosis is caused by the addition (e.g., methanolingestion), retention (e.g., renal failure) [85], orexcess production (e.g., lactic acidosis) of fixedacids that titrate bicarbonate, acidic anionsremaining in extracellular body fluids causeexpansion of the anion gap and a normal chlorideconcentration [86–88]. In reference to a calculatedanion gap, a result of 20–30 has a high chance ofmetabolic acidosis while a result >30 reflectsmetabolic acidosis. The anion gap is calculatedusing serum values with the following formula;
Anion Gap ¼ Sodium½ � � Chloride½ �� HCO3½ �
Metabolic acidosis can be divided into threecategories: increased anion gap, normal aniongap, and decreased anion gap. Increased anion
Table 6 Causes of hypobicarbonatemiaa
Metabolic acidosis (i.e., decreased pH, decreasedb anddecreased pCO2
c)
Hyperchloremia, normal anion gap
Bicarbonate loss (hypokalemia and urine pH < 5.5)
GI tract bicarbonate loss (e.g., diarrhea,ureterosigmoidostomy, fistulas, tube drainage)
Renal bicarbonate loss and production failure(e.g., RTAType 2, RTAType 1, RTAType 4, carbonicanhydrase inhibitors)
HCl addition (e.g., NH3Cl and somehyperalimentation fluids)
Hypoaldosteronism (hyperkalemia, submaximalurinary acidification)
Primary adrenal insufficiency
Hyporeninemic hypoaldosteronism (e.g., duringearly chronic renal failure, acute renal failure interstitialnephritis, angiotensin-converting enzyme inhibition, andnonsteroidal antiinflammatory drug use)
Aldosterone resistance (e.g., spironolactone,amiloride, triamterene)
Intestinal nephritis
Early renal failure
Acute renal failure
Initial recovery from organic acidosis (variable [K+]and urine pH)
Normochloremia, large anion gap (urine pH < 5.5)
Excessive production of endogenously generatedorganic acids
Diabetic ketoacidosis (i.e., excessive β-hydroxybutyrate and acetoacetate)
Starvation ketosis
Alcoholic ketosis
Lactic acidosis
Muscle necrosis
Decreased excretion of endogenous acidmetabolites
Renal failure
Ingestion of exogenous agents causing organicacidosis
Methanol
Ethylene glycol
Paraldehyde
Salicylates
Respiratory alkalosis (i.e., increased pH, decreased[HCO3
�]c and decreased pCO2b)
Increased CNS stimulation
Physiologic and psychogenic hyperventilation
CNS disease (e.g., infectious, trauma, infarct,bleeding, tumors, heat stroke)
Pregnancy
(continued)
Table 6 (continued)
Progesterone-producing tumors
Hepatic encephalopathy
Methylxanthines, nicotine, salicylates
Sepsis
Hypoxia
High altitude
Anemia, severe
Pulmonary embolus, pulmonary edema,pneumothorax
Carbon monoxide poisoning
Mechanical overventilation
Originally appeared in: Taylor R, David A, Fields S,Phillips M, Scherger J, editors. Family medicine (Taylor).New York: Springer; 2003aHypobicarbonatemia = decreased [HCO3
�]bPrimary acid–base eventcSecondary or compensatory acid–base event
Fluid, Electrolyte, and Acid–Base Disorders 13

gap metabolic acidosis is caused by ingestion oforganic acids (salicylates, methanol, ethylene gly-col, paraldehyde, propylene glycol), increasedorganic acid production (lactic acidosis,ketoacidosis), renal failure (phosphates, sulfates),or errors of metabolism (lipid metabolism errors,urea cycle disorders). Normal anion gap meta-bolic acidosis is due to intake of chloride salts(total parental nutrition, normal saline infusion),GI bicarbonate loss (diarrhea, colostomy,ileostomy, enteric fistula), urological procedures(ureterosigmoidostomy, ureteroileal conduit),ingestions (acetazolamide, magnesium sulfate),and renal bicarbonate loss (RTA, tubulointerstitialrenal disease, hyperparathyroidism).
Metabolic acidosis causes extracellularhyperkalemia due to cellular buffering of hydrogenions (failure of acidosis-induced hyperkalemia sug-gests total body potassium depletion), but becausesignificant volume loss is a frequent complication(e.g., diabetic ketoacidosis), total body hypokalemiamust always be expected (chronic renal failure andhypoaldosteronism may be an exception) [74]. Theingestion of acid toxins (e.g., paraldehyde, metha-nol, ethylene glycol, and salicylates) is associatednot only with the distinct acid metabolite but alsolactic acid as vascular collapse ensues [89].
Generally, compensatory responses will not beable to restore pH back to the normal value. Someof the most dangerous effects of acidosis on thebody include hyperventilation, depression ofmyocardial contractility, sympathetic overactiv-ity, peripheral arteriolar vasodilation,hyperkalemia, and cerebral vasodilation withresultant increased intracranial pressure. Many ofthese conditions can be deleterious and deadly.Therapy for metabolic acidosis is initially directedat restoration of the systemic pH to levels that donot compromise cardiac function or predispose tocardiac dysrhythmias. Dangerous pH levels differdepending on the etiology of the acidosis; in gen-eral, however, safe systemic pH exists at 7.2.Severe forms of metabolic acidosis thereforerequire administration of sodium bicarbonate inamounts necessary to restore the pH to this safelevel, with care taken to avoid volume excess andpost-treatment metabolic alkalosis byoveraggressive alkali therapy [90]. If the
metabolic acidosis is severe enough to warrantalkali therapy, physician comfortable with useshould manage it [89, 90].
Respiratory Alkalosis
Respiratory alkalosis is a primary reduction in thepCO2 (i.e., hypocapnia), which stimulates a com-pensatory cellular and renal reduction in bicarbon-ate concentration [1]. With primary acute andchronic respiratory alkalosis, the compensatorybicarbonate loss occurs at a rate of 2.0 mEq/L or5.0 mEq/L for every 10 mmHg decrease in thepCO2. The limits of these metabolic compensa-tions in acute and chronic respiratory alkalosis are18 and 12 mEq/L, respectively. If the rate ofcompensatory bicarbonate loss is less or morethan predicted, a mixed acid–base disturbance ispresent which is discussed later. Respiratory alka-losis is caused by central causes, hypoxia, pulmo-nary causes, and iatrogenically (excessivecontrolled ventilation) (Table 6).
Acute hypocapnia may be associated withcircumoral and digital paresthesias,lightheadedness, carpopedal spasm, and tetany.The associated hyperventilation is obvious, as itis mostly rate driven.With chronic hypocapnia therespiratory rate may be normal, and the depth ofrespiration may predominate as the mechanism ofpCO2 removal. Treatment is directed to the under-lying cause.
Metabolic Alkalosis
Metabolic alkalosis is a primary increase in plasmabicarbonate concentration (i.e., hyperbicar-bonatemia) that causes a compensatory reductionin ventilation and relative hypercapnia (i.e.,increased pCO2) [1]. The bicarbonate accumulationis due to acid loss, alkali administration, intracellularshifts, or bicarbonate retention. With primary meta-bolic alkalosis the compensatory hypoventilationoccurs at a rate of 0.7 mmHg increase in the pCO2
for every 1.0 mEq/L increase in the bicarbonateconcentration. The limit of this compensatoryhypoventilation is 55 mmHg because of hypoxia-
14 S. Horras et al.

induced ventilation. If the rate of pCO2 increase isless or more than predicted, a mixed acid–basedisturbance consisting of metabolic alkalosis andrespiratory alkalosis or acidosis is present. The listof potential causes for metabolic alkalosis is exten-sive, but most common reasons include loss ofgastric acid, renal acid loss, hypovolemia, hypoka-lemia, and diuretic use (Table 7).
Signs and symptoms associated with metabolicalkalosis relate to underlying cause. Metabolicalkalosis caused by volume depletion is character-ized by a urinary chloride concentration of less than10 mEq/L (i.e., saline-responsive), whereas meta-bolic alkalosis due to a primary increase in distalrenal tubule activity (e.g., mineralocorticoidexcess) and increased alkali ingestion is character-ized by a urinary chloride concentration higher than10 mEq/L (i.e., saline-resistant). Paradoxically, theurinary pH is usually acidic except when the disor-der is caused by excessive alkali ingestion.
Treatment of saline-responsive metabolicalkalosis requires volume repletion with isotonicnormal saline, which inhibits the volumedepletion-induced retention of bicarbonate,resulting in an alkaline diuresis. With saline-resistant metabolic alkalosis, the source of theexcess alkali ingestion must be removed orinhibited. Potassium deficits should also bereplete using potassium chloride.
Respiratory Acidosis
Respiratory acidosis is a primary increase in thepCO2 (i.e., hypercapnia), which stimulates com-pensatory cellular and renal retention of bicarbon-ate [1]. With primary acute and chronicrespiratory acidosis, the compensatory bicarbon-ate retention occurs at a rate of 1.0 mEq/L or4.0 mEq/L for every 10 mmHg increase in thepCO2. The limits of the metabolic compensationsduring acute and chronic respiratory acidosis are30 and 45 mEq/L, respectively. If the rate ofcompensatory bicarbonate retention is less ormore than predicted, a mixed acid–base distur-bance consisting of respiratory acidosis and met-abolic acidosis or alkalosis is present. Respiratoryacidosis occurs through three mechanisms:
Table 7 Causes of hyperbicarbonatemiaa
Metabolic alkalosis (i.e., increased [HCO3�]b increased
pCO2, increased pH)
Hypovolemia and chloride depletion (i.e., hypochloremia,hypokalemia: urine Na+ <10 mEq/L, Cl� <10 mEq/L,pH < 6, K+ < 10 mEq/L
Vomiting
Postdiuretic use
Congenital chloride diarrhea
Bartter syndrome
Acute correction of hypercapnia in hypovolemia
Hypervolemia (i.e., hypochloremia, hypokalemia; urineNa+ > 10 mEq/L, Cl� >10 mEq/L, pH < 6.0)
Mineralocorticoid excess
Renal artery stenosis
Primary aldosteronism
Adrenal hyperplasia
Excessive alkali (hypochloremia, hypokalemia; urineNa+ > 10 mEq/L, Cl� > 10 mEq/L, pH > 7.0)
Excessive exogenous alkali (e.g., absorbable antacids,milk-alkali syndrome, excessive infusion of NaHCO3)
Excessive endogenous alkali (e.g., NaHCO3)
Acute correction of chronic hypercapnia in euvolemia
Metabolism of β-hydroxybutyrate, acetoacetate, lactate,and citrate
Severe hypokalemia
Hypercalcemia (e.g., primary hyperparathyroidism)
Respiratory acidosis (i.e., lactate, increased pCO2,b increased
[HCO3�]
Suppression of CNS respiratory center
Drugs (e.g., sedatives
Oxygen-induced acute pCO2 retention in chronicobstructive pulmonary disease (COPD)
Sleep apnea
Disorders of respiratory muscles
Obstructed airway
Extrinsic foreign body
Aspiration
Laryngeal edema or spasm
Bronchospasm
Disturbances of gas exchange across alveolar membrane
Pulmonary edema
Adult respiratory distress syndrome
Diffuse pneumonia
COPD
Loss of ventilatory volume
Pneumothorax
Hemothorax
Pleural effusions
Originally appeared in: Taylor R, David A, Fields S,Phillips M, Scherger J, editors. Family medicine (Taylor).New York: Springer; 2003aHyperbicarbonatemia = increased [HCO3
�]bPrimary acid–base event
Fluid, Electrolyte, and Acid–Base Disorders 15

(1) excess CO2 in the inhaled gas, (2) decreasedalveolar ventilation, (3) increased production ofCO2. The most likely cause is inadequate alveolarventilation. A list of etiologies is provided in(Table 7).
Symptoms of respiratory acidosis includeshortness of breath and the mental status changesassociated with progressive acute and chronichypercapnia. The treatment of respiratory acidosisis directed to the primary cause to increase theeffectiveness of ventilation and pulmonary gasexchange.
Mixed Acid–Base Disturbances
The presence of a mixed acid–base disturbance isusually detected when a primary acid–base event
fails to demonstrate the expected compensation.This failure of compensation can predict the pres-ence of a respiratory and metabolic acid–baseevent occurring concurrently but does not predictthe presence of mixed metabolic events or mixedrespiratory events. Acid–base maps have similardiagnostic limitations. The mixture of more thantwo events can be determined by other laboratoryevidence but is best detected when historicalevaluations suggest multiple acid–base events.Although laboratory data may be the firstevidence of acid–base disturbances, utilization ofthese tools to predict primary and mixedacid–base disturbances must be related withclinical data to ensure that the information isappropriately interpreted (Table 8).
The presence of a mixed acid–base disturbanceis best detected by anticipating its presence in
Table 8 Common mixed acid–base disturbances
Disorder Examples
Predicted by rules of compensation
Metabolic acidosis and respiratory alkalosis (partial pressure of carbondioxide reduction greater than predicted for metabolic acidosis)
Chronic renal failure and septicemia
Metabolic alkalosis and respiratory acidosis (partial pressure of carbondioxide reduction less than predicted for metabolic acidosis)
Lactic acidosis and chronicobstructive pulmonary disease
Metabolic and respiratory alkalosis (partial pressure of carbon dioxideelevation less than predicted for metabolic alkalosis)
Diuretic overuse and psychogenichyperventilation
Metabolic alkalosis and respiratory acidosis (partial pressure of carbondioxide elevation greater than predicted for metabolic alkalosis)
Vomiting and adult respiratorydistress syndrome
Not predicted by rules of compensation
Hyperchloremia and large anion gap metabolic acidosis (nonequivalentchanges in chloride and bicarbonate concentrations and an elevated anion gap
Diarrhea and chronic renal disease
Metabolic alkalosis and large anion gap acidosis (nonequivalent changes inchloride bicarbonate concentrations and an elevated anion gap)
Vomiting and chronic renal failure
Acute and chronic respiratory alkalosis ([HCO3�] reduction greater than
predicted for acute respiratory alkalosis and less than predicted for chronicrespiratory alkalosis)
Septicemia and psychogenichyperventilation
Acute and chronic respiratory acidosis ([HCO3�] elevation greater than
predicted for acute respiratory acidosis and less than predicted for chronicrespiratory acidosis)
Acute respiratory failure and COPD
Chronic respiratory acidosis and acute respiratory alkalosis ([HCO3�]
elevation or reduction inconsistent with expected pCO2 elevation or reductionfor either of these disorders, respectively)
COPD and pulmonary embolus
Metabolic alkalosis and nonanion gap metabolic acidosis (difficult torecognize because [Cl�] and [HCO3
�] changes depend on which disorderpredominates; if each disorder is of equal magnitude, then [Cl�], [HCO3
�],pCO2, and pH are normal)
Chronic diuretic overuse and diarrhea
Originally appeared in: Taylor R, David A, Fields S, Phillips M, Scherger J, editors. Family medicine (Taylor). New York:Springer; 2003COPD chronic obstructive pulmonary disease
16 S. Horras et al.

clinical settings, although some laboratory find-ings can be helpful. The compensation inacid–base disturbances minimizes changes insystemic pH but never totally corrects the pH(the possible exception is chronic hypocapnia inpersons living at high altitudes). Therefore, thepresence of a normal pH with normal [HCO3
�]and pCO2 indicates the presence of a mixedacid–base disturbance. Likewise, with primaryacid–base disturbances the compensatory eventis in the same direction as the primary event;therefore, acid–base disturbances where the com-pensatory event and the primary event are inopposite directions also indicate the presence ofa mixed acid–base disturbance. A large anion gapmetabolic acidosis occurring concurrently with ahyperchloremia metabolic acidosis (e.g., a patientwith diabetic ketoacidosis and diarrhea) isdetected when the anion gap does not accountfor the amount of [HCO3
�] concentration reduc-tion. An example of this mixed disturbance is asign of recovery during the appropriate treatmentof diabetic ketoacidosis as β-hydroxybutyrate andacetoacetate (ketone bodies) are hepaticallyconverted to [HCO3
�], resulting in a transitionfrom the original large anion gap metabolic aci-dosis to a hyperchloremia metabolic acidosis withless severe systemic pH reductions. The presenceof a large anion gap, regardless of the systemicpH, indicates the presence of metabolic acidosis.For example, a patient with plasma metabolicalkalosis caused by diuretic use may have a[HCO3
�] of 36 mEq/L, and if the hypovolemiabecomes severe enough lactic acidosis may ensue.However, an 8 mEq/L drop in [HCO3
�] caused bytitration of lactic acid would result in a [HCO3
�]of 28 mEq/L, essentially no change in [Cl�], andan appropriate pCO2 response with the pH stillslightly alkalemic. This process can be detectedearly based on the concurrent increase in the aniongap as [HCO3
�] is consumed in the titration withlactic acid and elevated plasma lactic acid – if thepotential for this disorder had been anticipatedclinically.
The limits of compensation are important fac-tors to consider especially when suspecting respi-ratory acidosis in a patient with metabolicalkalosis. Although the compensation for
metabolic alkalosis is pCO2 retention, pCO2
values higher than 55mmHg do not occur becausethe resulting hypoxia stimulates ventilation.Therefore, in patients with metabolic alkalosisand a pCO2 higher than 55 mmHg, primaryimpairment of ventilation causing respiratory aci-dosis must also be present. Because the limits ofcompensation in chronic respiratory alkalosis is a[HCO3
�] of 14 mEq/L, [HCO3�] less than that
implies the additional presence of metabolic aci-dosis. Likewise, the limits of compensation forchronic respiratory acidosis is renal HCO3 reten-tion to 45 mEq/L, and higher [HCO3
�] concen-trations imply the additional presence ofmetabolic alkalosis. Because chronic renal dis-ease in its end stages results in a [HCO3
�] of12–14 mEq/L, greater [HCO3
�] reductionswould suggest additional causes of metabolic aci-dosis (e.g., vomiting).
Mixtures of acute and chronic respiratory aci-dosis as well as acute and chronic respiratoryalkalosis can be detected using the rules of com-pensation for primary acid–base disorders and byplotting pCO2 and [HCO3
�] on acid–base maps.Points that define mixtures of acute and chronicrespiratory alkalosis or respiratory acidosis mayalso be consistent with a mixture of acute respira-tory and metabolic alkalosis or acute respiratoryacidosis and metabolic alkalosis. Mixtures ofrespiratory acidosis and respiratory alkalosispose special problems. The more profoundevent may alter the pCO2 enough to leave therespiratory-induced metabolic compensationunopposed for hours to days (e.g., a patient withchronic obstructive pulmonary disease who ismechanically hyperventilated, thereby decreasingthe pCO2 and leaving the pCO2-induced [HCO3
�]elevation until renal [HCO3
�] excretion occursover the following hours to days).
Misc. Electrolyte Disturbances
Magnesium
Hypomagnesemia (Mg2+ < 1.5 mEq/L) associ-ated with urinary magnesium (UMg) conservation(UMg < 10 mg/day) can be caused by decreased
Fluid, Electrolyte, and Acid–Base Disorders 17

magnesium intake (e.g., protein calorie malnutri-tion), decreased magnesium absorption, andextrarenal magnesium loss [1]. Hypomagnesemiaassociated with urinary magnesium excretion(UMg > 10 mg/day) can be caused by excessiverenal magnesium loss (e.g., diuretic use, hypoka-lemia, hypercalciuria, hypervolemia, and hyper-thyroidism). Hypomagnesemia is also caused bychronic magnesium wasting and treatment-induced intracellular magnesium redistribution(e.g., diabetic ketoacidosis and alcoholism).
Hypermagnesemia (Mg2+ > 2.5 mEq/L)results when magnesium intake exceeds renalexcretion (UMg > 20 mg/day) and when thereis decreased renal excretion (UMg < 20 mg/day) caused by excessive renal magnesium tubu-lar reabsorption (e.g., hyperparathyroidism,hypovolemia, hypocalcemia, and hypothyroid-ism) and GFR (e.g., acute and chronic renal failureand hypovolemia).
Phosphate
Hypophosphatemia (plasma phosphorus<2.5 mg/dL) is caused by increased phosphaterenal excretion (i.e., UPO4 > 100 mg/24 h) indiabetic ketoacidosis, hypokalemia, and phos-phate deficiency (UPO4 < 100 mg/24 h) in hypo-parathyroidism and decreased phosphate intake(e.g., alcoholism, vitamin D deficiency, and useof phosphate binders), as well as intracellularphosphate shifts (UPO4 < 100 mg/24 h) in met-abolic and respiratory alkalosis [1]. Hyperpho-sphatemia (phosphorus >4.8 mg/dL) associatedwith UPO4 > 1500 mg/24 h is caused byincreased release of phosphates into the extracel-lular fluid by cell lysis (e.g., rhabdomyolysis) andinitial anionic redistribution of metabolic acidosis(e.g., diabetic ketoacidosis and lactic acidosis).
Hyperphosphatemia associated with UPO4 <
1500 mg/24 h is caused by decreased renal phos-phate excretion (e.g., volume depletion, acute andchronic renal failure, and hyperparathyroidism).Clinical manifestations vary depending on timecourse and mechanism. Symptom presentation ismore severe with acute versus chronic. Symptoms
may be mild if from intracellular shift as intracel-lular phosphate levels are enough for ATP produc-tion. Clinically patients may develop respiratorymuscle dysfunction, decreased contractility ofheart, hemolysis, insulin resistance, myopathy,rhabdomyolysis, and seizures. These symptomsare largely caused by adenosine triphosphatedepletion in hypophosphatemia. Treatment isphosphate repletion and may be done either orallyor intravenously.
Calcium
Hypocalcemia (Ca2+ < 8.5 mg/dL or ionizedCa2+ < 4.1 mg/dL) associated with normal orsubnormal parathyroid hormone (PTH) is causedby PTH-deficient hypoparathyroidism and severehypomagnesemia. Since 40 % of Ca is bound toplasma proteins, it is important to adjust for lowalbumin by adding 0.8 mg/dL for every 10 g/Ldecrease in normal albumin [1]. Calcium is regu-lated by parathyroid hormone. When levels ofCa2+ are low, PTH is secreted from the parathy-roid resulting in increased renal reabsorption aswell as increased renal vitamin D production,which stimulates increased intestinal absorptionof calcium. Hypocalcemia associated with ele-vated PTH is caused by chronic renal failure,vitamin D deficiency, malabsorption, drug-induced microsomal enzyme induction (e.g.,mithramycin and phenytoin), osteomalacia, andcauses of severe acute hyperphosphatemia suchas acute pancreatitis, hepatic failure, and othercauses of massive tissue necrosis.
Hypercalcemia (total [Ca2+] > 10.5 mg/DL orionized [Ca2+] > 5.1) with elevated PTH iscaused by primary hyperparathyroidism (i.e.,excessive production of PTH) and severe second-ary hyperparathyroidism of chronic renal failure.Hypercalcemia associated with normal PTH iscaused by vitamin D excess, sarcoidosis, hyper-thyroidism, increased bone calcium release (e.g.,immobilization and bony metastasis), extracellu-lar fluid depletion, thiazides, or milk-alkali syn-drome. Clinical manifestations includenephrolithiasis, bone pain, abdominal pain from
18 S. Horras et al.

constipation, nausea, vomiting, and psychiatricsymptoms. Asymptomatic patients with mildhypercalcemia do not need treatment, however if>14 mg/DL or if >12 mg/DL with symptomsshould be treated with aggressive saline rehydra-tion followed by furosemide diuresis, calcitonin,and bisphosphonates. Surgery would be indicatedfor primary hyperparathyroidism.
References
1. Fluid HJ. Electrolyte, and acid–base disorders. In:Taylor R, David A, Fields S, Phillips M, Scherger J,editors. Family medicine (Taylor). New York:Springer; 2003.
2. Hobbs J. Acid–base disorders. Postgrad Med. 1988;83suppl 2:91–8.
3. Beck LH. The aging kidney. Defending a delicatebalance of fluid and electrolytes. Geriatrics. 2000;55(4):26–8, 31–2.
4. Rose BD. Regulation of the effective circulating vol-ume. In: Rose BD, editor. Clinical physiology ofacid–base and electrolyte disturbances. 5th ed. -New York: McGraw-Hill; 2001. p. 258–84.
5. Rose BD. Hypovolemic states. In: Rose BD, editor.Clinical physiology of acid–base and electrolyte dis-turbances. 5th ed. New York: McGraw-Hill; 2001.p. 415–46.
6. Brady HR, Brenner BM. Acute renal failure. In:Isselbacher KJ, Braunwalde E, editors. Harrison’s prin-ciples of internal medicine. 13th ed. New York:McGraw-Hill; 1996. p. 1265–74.
7. Von Haehling S, Doehner W, Anker SD. Nutrition,metabolism, and the complex pathophysiology ofcachexia in chronic heart failure. Cardiovasc Res.2007;73(2):298–309.
8. Verbalis JG, Goldsmith SR, Greenberg A, Schrier RW,Sterns RH. Hyponatremia treatment guidelines 2007:expert panel recommendations. Am J Med. 2007;120(11 Suppl 1):S1.
9. Worth HGJ. Plasma sodium concentration: bearer offalse prophecies? BMJ. 1983;287:567.
10. Vaswani SK, Sprague R. Pseudohyponatremia in mul-tiple myeloma. South Med J. 1993;86 suppl 2:251–2.
11. Weisberg L. Pseudohyponatremia: a reappraisal. Am JMed. 1989;86(3):315–8.
12. Hillier TA, Abbott RD, Barrett EJ. Hyponatremia:evaluating the correction factor for hyperglycemia.Am J Med. 1999;106(4):399.
13. Westerberg D. Diabetic ketoacidosis: evaluation andtreatment. Am Fam Physician. 2013;87(5):337–46.
14. Kitabchi AE, Umpierrez GE, Miles JM, FisherJN. Hyperglycemic crisis in adult patients with diabe-tes. Diabetes Care. 2009;32(7):1335–43.
15. Upadhyay A, Jaber BL, Madias NE. Incidence andprevalence of hyponatremia. Am J Med. 2006;119(7 Suppl 1):S30–5.
16. Goh KP. Management of hyponatremia. Am Fam Phy-sician. 2004;69(10):2387–94.
17. Patel GP, Balk RA. Recognition and treatment ofhyponatremia in acutely ill hospitalized patients. ClinTher. 2007;29(2):211–29.
18. Keating JP, Schears GJ, Dodge PR. Oral water intoxi-cation in infants: an American epidemic. Am J DisChild. 1991;145:985–90.
19. Wattad A, Chiang ML, Hill LL. Hyponatremia in hospi-talized children. Clin Pediatr. 1992;31 suppl 3:153–7.
20. Kleinfeld M, Casimir M, Borra S. Hyponatremia asobserved in a chronic disease facility. J Am GeriatrSoc. 1979;27:156–61.
21. Ashouri OS. Severe diuretic-induced hyponatremia inthe elderly. Arch Intern Med. 1986;146:1355.
22. Anderson OK, Gudbrandsson T, Jamerson K. Meta-bolic adverse effects of thiazide diuretics: the impor-tance of normokalemia. J Intern Med Suppl.1991;735:89–96.
23. Friedman E, Shadel M, Halkin H, Farfel Z. Thiazideinduced hyponatremia: reproducibility by single doserechallenge and an analysis of pathogenesis. AnnIntern Med. 1989;110:24–30.
24. Ayus JC. Diuretic-induced hyponatremia. Arch InternMed. 1986;146:1295–6.
25. Sonnenblick M, Algur N, Rosin A. Thiazide inducedhyponatremia and vasopressin release. Ann InternMed. 1989;110:751.
26. Shapiro DS, Sonnenblick M, Galperin I, Melkonyan L,Munter G. Severe hyponatraemia in elderly hospital-ized patients: prevalence, aetiology and outcome.Intern Med J. 2010;40(8):574–80.
27. Sharabi Y, Illan R, Kamari Y, Cohen H, Nadler M,Messerli FH, Grossman E. Diuretic inducedhyponatraemia in elderly hypertensive women. J HumHypertens. 2002;16(9):631–5.
28. Correia L, Ferreira R, Correia I, Lebre A, Carda J,Monteiro R, Costa N. Severe hyponatremia in olderpatients at admission in an internal medicine depart-ment. Arch Gerontol Geriatr. 2014;59(3):642–7.
29. Liamis G, Milionis H, Elisaf M. A review of drug-induced hyponatremia. Am J Kidney Dis.2008;52(1):144–53.
30. Hew-Butler T. Arginine vasopressin, fluid balance andexercise: is exercise-associated hyponatraemia a disor-der of arginine vasopressin secretion? Sports Med.2010;40(6):459–79.
31. Jackson C, Carson W, Markowitz J, Mintzer J. SIADHassociated with fluoxetine and sertraline therapy. Am JPsychiatry. 1995;152:809.
32. ten Holt WL, van Iperen CE, Schrijver G, BartelinkAK. Severe hyponatremia during therapy with fluoxe-tine. Arch Intern Med. 1996;156:681.
33. Liu BA, Mittmann N, Knowles SR, ShearNH. Hyponatremia and the syndrome of inappropriate
Fluid, Electrolyte, and Acid–Base Disorders 19

secretion of antidiuretic hormone associated with theuse of selective serotonin reuptake inhibitors: a reviewof spontaneous reports. Can Med AssocJ. 1996;155:519.
34. Peterson JC, Pollack RW, Mahoney JJ, FullerRJ. Inappropriate antidiuretic hormone secondary to amonoamine oxidase inhibitor. JAMA. 1978;239:1422.
35. Rose BD. Hypoosmolal states-hyponatremia. In: RoseBD, editor. Clinical physiology of acid–base and elec-trolytes disorders. 5th ed. New York: McGraw-Hill;2001. p. 696–745.
36. Verbalis JG. Disorders of body water homeostasis. BestPract Res Clin Endocrinol Metab. 2003;17(4):471.
37. Wong L, Verbalis JG. Vasopressin V2 receptor antag-onists. Cardiovasc Res. 2001;51(3):391.
38. Porush JG. Disorders of water and salt metabolism. In:Faugert PF, Porush JG, editors. Renal disease in theaged. Boston: Little, Brown; 1991. p. 15–33.
39. Trachtman H, Futterweit S, Hammer E, Siegel TW,Oates P. The role of polyols in cerebral cell volumeregulation in hypernatremic and hyponatremic states.Life Sci. 1991;49:677–88.
40. Mickel HS, Oliver CN, Starke-Reed PE. Protein oxi-dation and myelinolysis occur in brain following rapidcorrection of hyponatremia. Biochem Biophys ResCommun. 1990;172:92–7.
41. Norenberg MD. Treatment of hyponatremia: the casefor a more conservative approach. In: Narins RG, edi-tor. Controversies in nephrology and hypertension.New York: Churchill-Livingstone; 1984. p. 379–91.
42. Ayus JC, Krothapalli RK, Arieff AL. Changing con-cepts in treatment of severe symptomatichyponatremia: rapid correction and possible relationto central pontine myelinolysis. Am J Med.1985;78:897–902.
43. Sterns RH, Riggs JE, Schochet Jr SS. Osmotic demy-elination syndrome following correction ofhyponatremia. N Engl J Med. 1986;314:1535.
44. Narins RG. Therapy of hyponatremia: does haste makewaste? N Engl J Med. 1986;314:1573.
45. Vieweg WV. Treatment strategies in the polydipsia-hyponatremia syndrome. J Clin Psychiatry. 1994;55suppl 4:154–60.
46. Karp BI, Laureno R. Pontine and extra pontinemyelinolysis: a neurologic disorder following rapidcorrection of hyponatremia. Medicine. 1993;72 suppl6:359–73.
47. Harris CP, Townsend JJ, Baringer JR. Symptomatichyponatremia: can myelinolysis be prevented by treat-ment? J Neurol Neurosurg Psychiatry. 1993;56 suppl6:626–32.
48. Pirzada NA, Ali II. Central pontine myelinolysis.Mayo Clin Proc. 2001;76(5):559–62.
49. Gross P, Reimann D, Henschkowski J, DamianM. Treatment of severe hyponatremia: conventionaland novel aspects. J Am Soc Nephrol. 2001;12 Suppl17:S10–4.
50. Nemerovsk C, Hutchinson DJ. Treatment ofhypervolemic or euvolemic hyponatremia associatedwith heart failure, cirrhosis, or the syndrome of inap-propriate antidiuretic hormone with tolvaptan: a clini-cal review. Clin Ther. 2010;32(6):1015–32.
51. Snyder NA, Feigal DW, Arieff AL. Hypernatremia inelderly patients: a heterogeneous, morbid and iatro-genic entity. Ann Intern Med. 1987;107:309–19.
52. Rose BD. Hyperosmolal states – hypernatremia. In:Rose BD, editor. Clinical physiology of acid–baseand electrolytes disorders. 5th ed. New York:McGraw-Hill; 2001. p. 746–93.
53. Phillips PA, Rolls BJ, Ledingham JG, Forsling ML,Morton JJ, Crowe MJ, Wollner L. Reduced thirst afterwater deprivation in healthy elderly men. N Engl JMed. 1984;311(12):753–9.
54. Palevsky PM, Bhagrath R, GreenbergA. Hypernatremia in hospitalized patients. Ann InternMed. 1996;124(2):197.
55. Adrogue H, Madias N. Hypernatremia. N Engl J Med.2000;342(20):1493–9.
56. Moder RG, Hurley DL. Fatal hypernatremia fromexogenous salt intake: report of a case and review ofthe literature. Mayo Clin Proc. 1990;65:1587–94.
57. Briggs JP, Singh IIJ, Sawaya BE, Schnermann J.Disorders of salt balance. In: Kokko JP, Tannen RL,editors. Fluids and electrolytes. 3rd ed. Philadelphia:WB Saunders; 1996. p. 3–62.
58. Arampatzis S, Frauchiger B, Fiedler GM, Leichtle AB,Buhl D, Schwarz C, Lindner G. Characteristics, symp-toms, and outcome of severe dysnatremias present onhospital admission. Am J Med. 2012;125(11):1125.e1.
59. Alshayeb HM, Showkat A, Babar F, Mangold T, WallBM. Severe hypernatremia correction rate and mortal-ity in hospitalized patients. Am J Med Sci.2011;341(5):356–60.
60. Bataille S, Baralla C, Torro D, Buffat C, Berland Y,Alazia M, Vacher-Coponat H. Undercorrection ofhypernatremia is frequent and associated with mortal-ity. BMC Nephrol. 2014;15:37.
61. Cheuvront SN, Kenefick R, Sollanek KJ, Ely BR,SawkaMN.Water-deficit equation: systematic analysisand improvement. Am J Clin Nutr. 2013;97(1):79.
62. Lam KS, Wat MS, Choi KL, Ip TP, Pang RW, KumanaCR. Pharmacokinetics, pharmacodynamics, long-termefficacy and safety of oral. Br J Clin Pharmacol.1996;42(3):379–85.
63. Makaryus AN, McFarlane SI. Diabetes insipidus: diag-nosis and treatment of a complex disease. Cleve Clin JMed. 2006;73(1):65.
64. Clausen T. Hormonal and pharmacological modifica-tion of plasma potassium homeostasis. Fundam ClinPharmacol. 2010;24(5):595–605.
65. Gosmanov AR,Wong JA, Thomason DB. Duality of Gprotein-coupled mechanisms for beta-adrenergic acti-vation of NKCC activity in skeletal muscle. Am JPhysiol Cell Physiol. 2002;283(4):C1025.
20 S. Horras et al.

66. Gallen IW, Rosa RM, Esparaz DY, Young JB, Robert-son GL, Batlle D, Epstein FH, Landsberg L. On themechanism of the effects of potassium restriction onblood pressure and renal sodium retention. Am J Kid-ney Dis. 1998;31(1):19.
67. Rose BD. Meaning and application of urine chemis-tries. In: Rose BD, editor. Clinical physiology ofacid–base and electrolyte disorders. 5th ed. New York:McGraw-Hill; 2001. p. 836.
68. Knochel JP, Schlein EM. On the mechanism of rhab-domyolysis in potassium depletion. J Clin Invest.1972;51(7):1750.
69. Paltiel O, Salakhov E, Ronen I, Berg D,Israeli A. Management of severe hypokalemia inhospitalized patients: a study of quality of care basedon computerized databases. Arch Intern Med.2001;161(8):1089–95.
70. Schaefer T, Wolford RW. Disorders of potassium.Emerg Med Clin North Am. 2005;23(3):723–47,viii–ix.
71. Medford-Davis RZ. Derangements of potassium.Emerg Med Clin North Am. 2014;32(2):329–47.
72. Alfonzo AVM, Isles C, Deighan C, GeddesC. Potassium disorders–clinical spectrum and emer-gency management. Resuscitation. 2006;70(1):10.
73. Mount DB, Zandi-Nejad K. Disorders of potassiumbalance. In: Brenner BM, Levine SA, editors. Brennerand Rector’s the kidney. 8th ed. Philadelphia: SaundersElsevier; 2007. p. 547–87.
74. Adrogue HJ, Madias NE. Changes in plasma potas-sium concentration during acute acid–base distur-bances. Am J Med. 1981;71:456.
75. Tannen RL. Potassium disorders. In: Kokko JP,Tannen RL, editors. Fluids and electrolytes. 3rded. Philadelphia: WB Saunders; 1996. p. 111–99.
76. Hobbs J. Acid–base, fluid and electrolyte disorders. In:Rakel RE, editor. Textbook of family practice. 4thed. Philadelphia: WB Saunders; 1990.
77. Mahoney BA, Smith WAD, Lo DS, Tsoi K, Tonelli M,Clase CM. Emergency interventions forhyperkalaemia. Cochrane Database Syst Rev. 2005;(2).
78. Putcha N, Allon M. Management of hyperkalemia indialysis patients. Semin Dial. 2007;20(5):431–9.
79. McGowan CE, Saha S, Chu G, Resnick MB, MossSF. Intestinal necrosis due to sodium polystyrene sul-fonate (Kayexalate) in sorbitol. South MedJ. 2009;102(5):493–7.
80. Weisberg LS. Management of severe hyperkalemia.Crit Care Med. 2008;36(12):3246–51.
81. Narins RG, Jones ER, Stom MC, Rudnick MR, BastlCP. Diagnostic strategies in disorders of fluid, electro-lyte and acid–base homeostasis. Am J Med.1982;72:496–504.
82. Narins RG, Emmett M. Simple and mixed acid–basedisorders: a practical approach. Medicine.1980;59:161–87.
83. Rose BD. Introduction to simple and mixed acid–basedisorders. In: Rose BD, editor. Clinical physiology ofacid–base and electrolytes disorders. 5th ed. NewYork:McGraw-Hill; 2001. p. 535–50.
84. Rose BD. Metabolic acidosis. In: Rose BD, editor.Clinical physiology of acid–base and electrolytes dis-orders. 5th ed. New York: McGraw-Hill; 2001.p. 578–646.
85. Prough DS. Physiologic acid–base and electrolytechanges in acute and chronic renal failure patients.Anesthesiol Clin North America. 2000;18(4):809–33, ix.
86. Oster JR, Perez GO, Materson BJ. Use of the anion gapin clinical medicine. South Med J. 1988;81:225–37.
87. Emmett M, Narins RG. Clinical use of the anion gap.Medicine. 1977;56:38.
88. Gabow PA, Kaehny WD, Fennessey PV, GoodmanMD, Gross P, Schrier RW. Diagnostic importanceof an increased anion gap. N Engl J Med.1980;303:854.
89. Rice M, Ismail B, Pillow MT. Approach to metabolicacidosis in the emergency department. Emerg MedClin North Am. 2014;32(2):403–20.
90. Fidkowski C, Helstrom J. Diagnosing metabolicacidosis in the critically ill: bridging the anion gapand base excess methods. Can J Anaesth.2009;56:247–56.
Fluid, Electrolyte, and Acid–Base Disorders 21