Drug-Induced Movement Disorders
25
PHARMACOEPIDEMIOLOGY Drug Safety 1997 Mar: 16 (3): 180-204 © Adis International Limited. All rights reserved. Drug-Induced Movement Disorders Felix Javier Jimenez-Jimenez,l Pedro Jose Garcia-Ruiz 2 and Jose Antonio Molina 3 1 Department of Neurology of Hospital Universitario 'Principe de Asturias', Alcala de Henares, Madrid, Spain 2 Department of Neurology of Fundaci6n Jimenez Diaz, Madrid, Spain 3 Department of Neurology of Hospital Universitario Doce de Octubre, Madrid, Spain Contents Summary 1. Parkinsonism .. 1 .1 Frequency. 1.2 Implicated Drugs 1.3 Clinical Features and Prognosis. 1.4 Prevention 1.5 Therapy ... . 2. Tremor ..... . 2.1 Antipsychotics. 2.2 Calcium Antagonists . 2.3 Other Drugs ..... . 3. Chorea ......... . 3.1 Antiparkinsonian Drugs. 3.2 Anticonvulsant Drugs. 4. Dystonia .......... . 4.1 Antipsychotic Drugs . . 4.2 Orthopramides and Substituted Benzamides . 4.3 Antiparkinsonian Drugs. 5. Tardive Dyskinesia .. 6. Myoclonus. . . . . . . . . . . 6.1 Dopamine Antagonists 6.2 Antidepressant Drugs and Lithium 6.3 Antiparkinsonian Drugs. 6.4 Bismuth Salts . 7. Tics or Tourettism ...... . 8. Akathisia ........ . 8.1 Dopamine Antagonists 8.2 Antidepressant Drugs 9. Conclusion ......... . 180 181 181 181 183 183 184 184 184 184 185 185 185 186 186 186 187 187 187 188 188 188 189 189 189 189 190 190 190 Summary Parkinsonism, tremor, chorea-ballismus, dystonia, tardive dyskinesia, myoc- lonus, tics and akathisia can be induced by many drugs. The drugs that are most frequently implicated in movement disorders are antipsychotics, calcium antag- onists, orthopramides and substituted benzamides (e.g. metoclopramide, sulpir- ide, clebopride, domperidone), eNS stimulants, antidepressants, anticonvulsants, antiparkinsonian drugs and lithium. It is possible for a single drug to induce 2 or
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Drug-Induced Movement Disorders

PHARMACOEPIDEMIOLOGY Drug Safety 1997 Mar: 16 (3): 180-204 0114~5916/97/0003-0180/$12.50/O
© Adis International Limited. All rights reserved.
Drug-Induced Movement Disorders Felix Javier Jimenez-Jimenez,l Pedro Jose Garcia-Ruiz2 and Jose Antonio Molina3
1 Department of Neurology of Hospital Universitario 'Principe de Asturias', Alcala de Henares, Madrid, Spain
2 Department of Neurology of Fundaci6n Jimenez Diaz, Madrid, Spain 3 Department of Neurology of Hospital Universitario Doce de Octubre, Madrid, Spain
Contents Summary 1. Parkinsonism ..
1 .1 Frequency. 1.2 Implicated Drugs 1.3 Clinical Features and Prognosis. 1.4 Prevention 1.5 Therapy ... .
2. Tremor ..... . 2.1 Antipsychotics. 2.2 Calcium Antagonists . 2.3 Other Drugs ..... .
3. Chorea ......... . 3.1 Antiparkinsonian Drugs. 3.2 Anticonvulsant Drugs.
4. Dystonia .......... . 4.1 Antipsychotic Drugs . . 4.2 Orthopramides and Substituted Benzamides . 4.3 Antiparkinsonian Drugs.
5. Tardive Dyskinesia .. 6. Myoclonus. . . . . . . . . . .
6.1 Dopamine Antagonists 6.2 Antidepressant Drugs and Lithium 6.3 Antiparkinsonian Drugs. 6.4 Bismuth Salts .
7. Tics or Tourettism ...... . 8. Akathisia ........ .
8.1 Dopamine Antagonists 8.2 Antidepressant Drugs
9. Conclusion ......... .
180 181 181 181 183 183 184 184 184 184 185 185 185 186 186 186 187 187 187 188 188 188 189 189 189 189 190 190 190
Summary Parkinsonism, tremor, chorea-ballismus, dystonia, tardive dyskinesia, myoclonus, tics and akathisia can be induced by many drugs. The drugs that are most frequently implicated in movement disorders are antipsychotics, calcium antagonists, orthopramides and substituted benzamides (e.g. metoclopramide, sulpiride, clebopride, domperidone), eNS stimulants, antidepressants, anticonvulsants, antiparkinsonian drugs and lithium. It is possible for a single drug to induce 2 or

Drug-Induced Movement Disorders 181
more types of movement disorders in the same patient. Movement disorders are not always reversible after drug withdrawal.
Drug-induced movement disorders include parkinsonism, tremor, chorea-ballismus, dystonia, tardive dyskinesia, myoclonus, tics, or akathisia. Such disorders can be caused by a wide variety of drugs, with parkinsonism, tardive dyskinesia and dystonia being the most frequent iatrogenic movement disorders found in clinical practice. Not infrequently, 2 or more types of drug-induced movement disorder coexist in the same patient. This article focuses on the distinct types of iatrogenic movement disorders and their associations with various drugs.
1. Parkinsonism
Major signs of parkinsonism include resting tremor, cogwheel rigidity, akinesia and postural instability. Until recently, the term drug-induced parkinsonism was nearly synonymous with antipsychotic-induced parkinsonism. However, druginduced parkinsonism is a frequent adverse effect of numerous drugs that interfere with dopamine function in the basal ganglia,[I-4) including calcium antagonists, orthopramides and substituted benzamides.[2,5-8) Table I summarises the drugs that have been associated with induction or aggravation of parkinsonism.
1.1 Frequency
In Spain, several studies have reported that drug-induced parkinsonism accounts for 24 to 35% of parkinsonian syndromesp,5,7,8) The prevalence of drug-induced parkinsonism in a door-to-door survey conducted in Italy was 32.7 per 100 000 individuals, in other words, approximately 8 times less than that of idiopathic Parkinson's disease.[9) Another door-to-door survey conducted in Germany, but restricted to individuals older than 65 years, showed a prevalence of 0.41 % for druginduced parkinsonism and 0.71 % for Parkinson's disease.! 10)
© Adls Internaflonal Umited. All rights reserved.
Table I. Drugs associated with induction or aggravation of parkinsonism
Drug Antipsychotics[l-l7]
Calcium antagonists: flunarizine, cinnarizine[7,8,18-31]
diltiazem,!32-34] verapamil,[33,35,38] amlodipine,!37] manidipine[38]
Orthopramides and substituted benzamides: metoclopramide[39-48] sulpiride,[1,7,8] clebopride[l,7,8,49-51]
cisapride,[52] domperidone,[53] veralipride!54,55]
Dopamine storage and transport inhibitors: reserpine, [56] tetrabenazine!57]
Antiemeticlantivertiginous agents: thiethylperazine!8,58,59] prochlorperazine[48]
Methyldopa[8,60,61]
Antidepressants:
Evidence
././
././
?
././
./
?
././
././
./
fluoxetine[62-69], paroxetine,!70,71] trazodone[72] ?
phenelzine[73] ?
amfebutomone (bupropion)[74] ? Lithium[75-79] ?
Diazepam[60] ?
Anticonvulsants: valproic acid (sodium valproate),[81-84] phenytoin[85] ?
Cholinergic agents bethanechol, [86] pyridostigmine!87] ?
Other agents: amiodarone,[88-91] procaine,[92] pethidine ? (meperidine),193,94] amphotericin B,[95,96] cefaloridine,[97] naproxen,[98] ethanol,[99] oral contraceptives, [1 DD] indeloxazine, [1 01,102] captopril,[103] cytarabine[104]
Symbols: ././ = well documented or frequent; ./ = relatively well documented or relatively frequent; ? = not well documented or anecdotal reports_
1 ,2 Implicated Drugs
1.2. 1 Antlpsychotlcs Parkinsonism has been a well known adverse
effect of antipsychotic drugs since their introduction for the treatment of patients with psychiatric illnesses.! 11,12) Development of parkinsonism is not infrequent in antipsychotic users, especially in older individuals.[13-17) In our series of patients
Drug Safely 1997 Mar; 16 (3)

182
with drug-induced parkinsonism, based on patients who were referred to a Movement Disorders Unit, 'typical' antipsychotic drugs were implicated in 27.6% of those with parkinsonism.[8] Psychiatrists do not usually refer patients with mild parkinsonism to neurological clinics and, in addition, iatrogenic parkinsonism is not always recognised.[105,106] These 2 reasons may explain the relatively low frequency. In a lO-year series at a regional pharmacovigilance centre in France, antipsychotics were the offending drug in 39% of 53 patients with druginduced parkinsonism.l6]
Antipsychotics act as dopamine receptor antagonists. The development of drug-induced parkinsonism is usually dose-dependent for each drug, and seems to be related to the blockade of dopamine D2 receptors, and with the degree of D2 receptor occupancy in the striatum.l 107] Halogenated and piperazine phenothiazines, and butyrophenones, are the antipsychotics with the greatest likelihood of producing this complication.l12,15, 108, 109] The phenothiazine derivatives thiethylperazine[8,58,59] and prochlorperazine,[46] which are used for the treatment of vertigo, may also induce parkinsonism.
Although comparisons of absolute prevalence levels for parkinsonism and other movement disorders are difficult to make, the risk of developing these movement disorders with the newer 'atypical' antipsychotics (risperidone, remoxipride, clozapine) seems to be lower than that of the 'typical' ones.[lIO-1l71 This is probably linked with a lower affinity for D2 receptors: risperidone binds to serotonin (5-hydroxytryptamine; 5-HThA receptors with 20 times greater affinity than it binds to D2 receptors; remoxipride binds selectively, but weakly, to D2 receptors; and clozapine preferentially binds to D4 receptors.[l17]
Early age at onset of schizophrenia,[118] high ventricle: brain ratio,l1l8,119] and severity of negative symptoms of schizophrenia[l19,120] seem to be related to an increased risk and severity of antipsychoticinduced parkinsonism.
In a number of patients, the onset or aggravation of parkinsonian signs has occurred following anti-
© Adis International Lirnited. All rights reserved.
Jimenez-Jimenez et al.
psychotic withdrawaI.lI21,122] Melamed et al,l 1221 suggested that the antipsychotic may precipitate degeneration of vulnerable nigrostriatal neurons by generating cytotoxic free radicals or accelerating neuronal firing rates. Besides the blockade of dopamine receptors, antipsychotics inhibit complex I of the mitochondrial electron-transport chain in vitro, and patients with antipsychotic-induced parkinsonism showed decreased complex I activity in platelets.[123] This is a potentially interesting finding, since it is known that complex I activity is reduced in the substantia nigra of patients with Parkinson's disease.[124,125]
1.2.2 Calcium Antagonists Since the original description of cinnarizine
induced parkinsonism by Marti-Masso et al. in 1985,[18] many authors have indicated that calcium antagonists, mainly cinnarizine and flunarizine, are a frequent cause of drug-induced parkinsonism, at least in Europe and South America,[7,8,19-30] where their use is common; cinnarizine was used by 5 to 7% of the elderly Spanish popUlation in 1985.[31] Cinnarizine and flunarizine, taken alone or with other drugs, were the most frequently reported causes of drug-induced parkinsonism in several Spanish series.l5,7,81 Other calcium antagonists have been associated with induction or aggravation of parkinsonism in anecdotal reports (table I).
Calcium antagonists were implicated in 58.1 % of cases of drug-induced parkinsonism in our own series,[8] and were the offending drug in 30% of cases of drug-induced parkinsonism in a lO-year series at a regional pharmacovigilance centre in France.l6] Old age and a family history of essential tremor seem to predispose to calcium antagonistinduced drug-induced parkinsonism.[29,30,126]
Garcia-Ruiz et al,l127] described an experimental model of parkinsonism induced by cinnarizine in aged monkeys. Cinnarizine produced a persistent reduction of homo vanillic acid and 5-hydroxyindoleacetic acid (5-HIAA) levels in the CSF. The authors suggested that this effect is the result of a predominant presynaptic effect of cinnarizine on dopaminergic and serotonergic neurons - resulting
Drug Safety 1997 Mar; 16 (3)

Drug-Induced Movement Disorders
in inhibition of synthesis or release of their respective neurotransmitters - or a possible toxic effect.l127]
Several in vitro studies have shown that calcium antagonists decrease the synthesisl128] and releaseI129-13I] of dopamine from the striatum, inhibit [3H]spiperone binding to postsynaptic D2 receptors in the striatum,I13I,132] and reduce the levels of catecholamines and [3H] dopamine uptake, without neurotoxicity in dopamine-rich neuroblastoma cells.1133] The binding of metabolites offlunarizine and cinnarizine to striatal D2 receptors is higher than that of the parent drug,l134] In addition, like antipsychotics (section 1.2.1), flunarizine and cinnarizine inhibit mitochondrial complex 1,1135]
1.2.3 Orthopramides and Substituted Benzamides Several orthopramides and substituted benza
mides can induce or aggravate parkinsonism (table I). Like antipsychotics, these drugs block striatal D2 receptors.
1.2.4 Dopamine Storage and Transport Inhibitors Methyldopa has been reported to induce parkin
sonism in individual patients.18,60,61] Drug-induced parkinsonism is a well known adverse effect of drugs that interfere with the intraneuronal storage of dopamine, such as reserpinel56] and tetrabenazine.l57] Tetrabenazine also may also block postsynaptic dopamine receptors.
1 .3 Clinical Features and Prognosis
The clinical manifestations of drug-induced parkinsonism are often indistinguishable from those of idiopathic Parkinson's disease, although drug-induced parkinsonism more frequently causes postural tremor and bilateral symptoms,I136] and often coexists with tardive dyskinesia, tardive dystonia and/or akathisia,l8,15,19,21,28,137-139]
It has been traditionally assumed that druginduced parkinsonism was reversible; however, in many patients with parkinsonism-induced by antipsychoticsl12l ,138,139] or other antidopaminergic drugs, such as flunarizine or cinnarizine,18,25,29,121] the parkinsonian symptoms and signs do not completely disappear, despite withdrawal of the offending drug. The persistence of parkinsonian
© Adis International Umited. All rights reserved.
183
symptoms might reflect the fact that the patients have subclinical idiopathic parkinsonism, a condition that was unmasked by the offending drug. On the other hand, this could also represent the onset of Parkinson's disease in the patients while they were taking the drug, and a direct toxic effect on the dopaminergic system cannot be ruled out.
1 .4 Prevention
The best prevention of drug-induced parkinsonism (and other drug-induced movement disorders) is to avoid the inappropriate use of drugs that are capable of inducing these adverse effects. The prolonged and, in many cases, unnecessary use of cinnarizine or flunarizine in elderly patients in Spainl31] resulted in a high frequency of parkinsonism induced by these drugs.l5,7,8,18,25,29,30] In our own
drug-induced parkinsonism series, many patients were taking drugs to treat 'vertigo' or 'dyspepsia' for months or even years;18] also, there was frequent use of the antipsychotic drug flupenthixol, a thioxanthene that is marketed in combination with a benzodiazepine, with a trade name that could lead general physicians to suppose that he or she is prescribing an anxiolytic drug.
The choice and dosage of antipsychotic drugs in the treatment of patients with psychiatric disorders are crucial. It seems reasonable that the dosage of antipsychotic should be kept to the minimum required to achieve and maintain a therapeutic response, and that those antipsychotics (risperidone, remoxipride and clozapine) with a lower risk of inducing drug-induced parkinsonism (or other movement disorders) should be preferred.
The use of adjunctive anticholinergic drugs to prevent the development of parkinsonism is controversial. A consensus statement by the World Health Organization did not recommend the use of these compounds because of their adverse effects, the potentially increased risk of developing tardive dyskinesia, and the fact that many patients taking antipsychotic therapy do not develop drug-induced parkinsonism. I 140,141]
Drug Safety 1997 Mar; 16 (3)

184
1.5 Therapy
The first therapeutic measure for patients with drug-induced parkinsonism should be the discontinuation of the offending drug, whenever possible. In those patients with persistent parkinsonian signs, especially elderly individuals with presumed subclinical idiopathic parkinsonism that has been unmasked by the offending drug, management should be similar to that of Parkinson's disease.
In psychiatric patients with antipsychoticinduced parkinsonism, the first approach should be to reduce the antipsychotic dosage or switch to another antipsychotic with a lower incidence of this adverse effect. If these measures are ineffective, it may be necessary to consider pharmacological treatment, including anticholinergics[l40,141] or amantadine.[140] Levodopa or direct dopamine agonists could increase psychotic symptomsY09] and are not useful in many patients.[142]
2. Tremor
Tremor is defined as a rhythmic oscillation of a body part, produced by either alternating or synchronous contractions of reciprocally innervated antagonistic muscles. Tremor is a common adverse effect of a wide variety of drugs (table II).
Although drugs that induce parkinsonism can produce a typical parkinsonian resting tremor, more characteristically, drug-induced tremors are postural. [I 64] Antipsychotic drugs produce a lowfrequency postural tremor, anticonvulsant drugs and lithium produce a high-frequency low-amplitude tremor, while other drugs may enhance physiological tremor.
2.1 Antipsychotics
Miller and Jankovic[15] reported that 2% of patients with antipsychotic-induced movement disorders have postural tremor. Stacy and JankoviC[143] described 5 patients with a predominantly postural tremor ('tardive tremor') that had a frequency range of 3 to 5Hz (a type oftremor that is usually accompanied by other tardive movement disorders). Moreover, tremor recordings in psychiatric pa-
© Adis internalionai Umited. All rights reserved.
Jimenez-Jimenez et al.
Table II. Drugs associated with induction or aggravation of postural tremor
Drug Antipsychotics[143-147J Lithium[76.146.149]
Anticonvulsant drugs[l50] Tricyclic antidepressants[151.152]
~-Adrenergic agonists[l53] Theophylline[l54] Levodopa[l54]
Amphetamines[l54] Thyroxine[154]
Antihyperglycaemic drugs[154] Caffeine[l54]
Corticosteroids[l54]
Calcium antagonists: flunarizine, cinnarizine[30]
Amiodarone[l54]
Anticonvulsants: phenytoin,1155] zonisamide,[156]lamotrigine[157J
Selective serotonin reuptake inhibitors[l56-160]
Histamine Hl antagonists[161]
Pentavalent antimonials[l62]
Evidence
.1.1 ,/,/
,/,/
,/,/
,/,/
,/,/
.1.1 ,/,/
,/,/
,/,/
,/,/
,/,/
,/
,/
? ?
?
? Cocaine[163] ?
Symbols: ,/,/ = well documented or not infrequent; ,/ = relatively well documented or relatively frequent; ? = not well documented or anecdotal reports.
tients treated with antipsychotics have shown that many of these patients had postural tremor of low frequency.[145] There have been reports of single cases of tongue tremor[l44] and rubral like tremor[146] in patients exposed to antipsychotics. Finally, antipsychotics can induce postural tremor in all 4 limbs of guinea-pigs)l47]
2.2 Calcium Antagonists
Postural tremor seems to be a frequent clinical feature of calcium antagonist-induced parkinsonism. In our experience, this type of parkinsonism improves after withdrawal of the offending drug, but a coarse mixed tremor persists for many months, despite disappearance of parkinsonism. [30] We suggest that this persistent tremor is the equivalent of the antipsychotic-induced 'tardive tremor' reported by Stacy and Jankovic (section 2.1))143] A
Drug Safety 1997 Mar; 16 (3)

Drug-Induced Movement Disorders
case of tongue tremor has been reported in a patient treated with flunarizine.[145]
2.3 Other Drugs
Tremor is a common problem in patients taking lithiump6] Studies show a wide range of incidences of lithium-induced tremor - from 4 to 65% - as a result of differences in defining and reporting this adverse effect.[l48] Tremor often decreases as duration of lithium therapy increases.[l49]
Postural tremor appears in 20 to 25% of patients treated with valproic acid (sodium valproate),[145] and more infrequently, in patients treated with other anticonvulsant drugs (table II).
3. Chorea
Chorea refers to irregular, unpredictable, brief, jerky movements that flit from one part of the body to another in a random sequence. Table III summarises the drugs that can induce chorea. The choreiform movements induced by dopamine antagonists are part of the spectrum of tardive dyskinesia, and are discussed in section 5.
3.1 Antiparkinsonian Drugs
Choreiform dyskinesias are a well known adverse effect of levodopa,[165-171] dopamine agonists[l72-176] and, less frequently, of anticholinergic drugS[l85-188] and amantadineP26] Choreiform dyskinesias associated with levodopa therapy in patients with Parkinson's disease usually follow 2 patterns: 'peak-dose' and 'diphasic' (at the onset and the end of the beneficial effect).
3.1.1 Peak-Dose Dyskineslas Peak-dose dyskinesias can improve after reduc
tion of the levodopa dosage, but this measure results in increased parkinsonismP45.246] The redistribution of the total dose of levodopa to more frequent and lower individual doses, together with the addition of a dopamine agonist, or a change to a liquid formulation of levodopa, should be useful for the treatment of this pattern of dyskinesiasP47]
When the patient is treated simultaneously with anticholinergics, reduction of dosage or withdrawal
© Adis Internafional Umited. All rights reserved.
185
of these drugs should contribute to improvement of the dyskinesias. Recently, improvement of dyskinesias has been reported with the addition of clozapine,[248] buspirone,[249.250] and fluoxetine}251] In contrast, cholinergic agents[252.253] and drugs that are active at y-aminobutyric acid (GAB A) sites[254.255] do not improve dyskinesias, and the latter can aggravate parkinsonism.l256]
Isoniazid can improve dyskinesias, but also aggravates parkinsonian signs.l257] Improvement of levodopa-induced dyskinesias is one of the most important benefits of posteroventral pallidotomy. [258-260]
3.1.2 Diphasic Dysklnesias Diphasic dyskinesias, which can be choreiform
or dystonic, are present at the beginning and at the end of the levodopa response cycle, coinciding
Table III. Drugs associated with induction of chorea
Drugs
Dopamine antagonists (including antipsychotics)
Dopamine agonists: levodopa,[165-171] direct dopamine agonists]172-176]
eNS stimulants:
Evidence ,/,/
,/,/
amphetamines,[177-180] pemoline.]181] ,/,/ methylphenidate, [182] cocaine, [163.183] xanthines]184]
Anticholinergics]185-188] ,/
H1 antihistamines]189] ,/
H2 antihistamines[190] ,/ Oral contraceptives[191-201] ,/
Anticonvulsants: phenytoin[202-209] ,/
phenobarbital (phenobarbitone),[202] ? carbamazepine,[210,211] ethosuximide,[212] valproic acid (sodium valproate),[213] felbamate,[214] gabapentin[215]
Withdrawal of diazepam + pentobarbital[216] ?
Antidepressants: tricyclic antidepressants,[217-219] fluoxetine[220] ?
Lithium[221-225] ?
Other drugs: amantadine,[226] anabolic steroids,[227] ? methadone,[228] baclofen,[229] benzodiazepines,[230] methyldopa, [231,232] digoxin, [233.234] diazoxide,l235] gold salts,1236-238] cyproheptadine,1239] cyclosporin,[240] sulfasalazine,[241] aciclovir,[242] propofol[243.244]
Symbols: ,/,/ = well documented or frequent; ,/ = relatively well documented or relatively frequent; ? = not well documented or anecdotal reports_
Drug Safety 1997 Mar: 16 (3)

186
with the rise and fall of plasma levodopa concentrationsP61,262] The management ofthis pattern of dyskinesias is very difficult. The best measure is to administer more frequent doses of levodopa, in an attempt to overlap the end-of-dose period with the beginning of the levodopa response cycle, and the addition of a dopamine agonist.[246,247,262] Admin-istration of subcutaneous apomorphine at the beginning of the levodopa response cycle decreases the duration, but not the intensity of the dyskinesiasP63,264]
3.2 Anticonvulsant Drugs
Patients who are treated with anticonvulsant drugs, usually at toxic concentrations, can develop chorea. The anticonvulsant drug that has most frequently been associated with chorea is phenytoin,[202-209] although this adverse effect has been also reported with phenobarbital (phenobarbitone), [202] carbamazepine, [210,211] ethosuximide, [212] valproic acid,[213] felbamate[214] and gabapentin,[215] and after withdrawal of combined therapy with pentobarbital and diazepamPl6]
4. Dystonia
Dystonia is a syndrome dominated by sustained muscle contractions, frequently causing twisting and repetitive movements or abnormal postures. Acute and tardive (or chronic) dystonia can be induced by the drugs that are listed in table IV.
4.1 Antipsychotic Drugs
Antipsychotic drugs can induce acute and, less frequently, tardive dystonia. First reported by Burke et al. in 1982,[265] tardive dystonia usually develops within 6 years of starting antipsychotic treatment, [266] although it can appear after a short period of exposure. Miller and lankovicf l5] reported that 24% of patients with antipsychotic-induced movement disorders have dystonia. The frequency of development of antipsychotic-induced acute and tardive dystonia has been reported to range from 5.3 to 66.7%,[267-271] and 0.4 to 21 %,[272-276] respec-
© Adls International Limited. All rlghts reserved.
Jimenez-Jimenez et al.
tively. These wide ranges result from the various diagnostic criteria that are used.
Butyrophenones, and halogenated and piperazine phenothiazines, are the antipsychotics with the greatest likelihood of producing these complications, but the newer 'atypical' antipsychotics, such as risperidone and clozapine, are not devoid of this adverse effect.[117,339-345] The phenothiazine thi
ethylperazine, which is used for the therapy of vertigo,[298,346,347] and the butyrophenone droperidol,
used in epidural anaesthesia,[348] can also induce dystonia.
Table IV. Drugs associated with induction of acute and/or tardive dystonia
Drug Evidence Antipsychotic drugs[lS.265.276] ,/,/
Orthopramides and substituted benzamides: metoclopramide[45-47,2n] ,/,/
su]piride,[278-28l] tiapride,[279] cisapride,[282] ? domperidone, [283,284] vera]ipride[28S]
Dopamine agonists: ]evodopa[170,17l ,286-289] ,/ ,/
Direct dopamine agonists[290] ,/
Antidepressants: selective serotonin reuptake inhibitors[291-301] ,/
tricyclic antidepressants,[302.303] monoamine oxidase inhibitors[304,30S]
Anticonvu]sants:
?
carbamazepine,[306-308] phenytoin[309] ,/
phenobarbital (phenobarbitone)[310] ?
Anticholinergics[311] ?
Anxiolytics: buspirone,[293.300,3l2] diazepam,[3l3] ? bromazepam,[314] midazolam[31S]
CNS stimulants: amphetamines,[3l6.3l7] methylphenidate,[3l8] ? cocaine (and cocaine withdrawal)[163.319-323]
anti migraine drugs ergotamine,[324,32S] sumatriptan[326] ?
Calcium antagonists: cinnarizine,[8.28] flunarizine,[8.28] nifedipine[327] ?
Histamine antagonists (H1 and H2)[328-332] ?
Other drugs: a-Methylparatyrosine,[333] tetrabenazine,[S7] ? bethanechol chloride,[334] flecainide,[33S] chloroquine,[338] etoposide,[337] alfentanil[338]
Symbols: ,/,/ = well documented or frequent; ,/ = relatively well documented or relatively frequent; ? = not well documented or anecdotal reports.
Drug Safely 1997 Mar; 16 (3)

Drug-Induced Movement Disorders
Risk factors for the development of acute and tardive dystonia in patients receiving antipsychotic treatment include younger age,l240,245,246,265,270,27 1,349-352] male gender, [271,349,353] severity of schizophrenia, [271] and the presence of negative symptoms of schizophrenia at baseline.l271 ] Although some authors have reported that patients with mania were more likely to develop antipsychotic-induced dystonia than those with schizophrenia,[267,269] others have found no such differences.[267] Concomitant treatment with anticholinergics seems to prevent the development of dystonia. [270]
4.2 Orthopramides and Substituted Benzamides
Several orthopramides and substituted benz arnides, such as sulpiride,[278-281] tiapride,[279] metocloprarnide,[45,47,277] cisapride,[282] domperidone,[283,284]
and veralipride, a drug used in the treatment of postmenopausal symptoms, can induce tardive dystonia. [285]
4.3 Antiparkinsonian Drugs
Dystonia can be induced by levodopa,[170,171,286-289] anticholinergic agents[311] and dopamine agonists.[290] Dystonias associated with levodopa therapy can follow 3 patterns: 'early morning', 'peak-dose' and 'off-period' dystonias. The therapy of peak-dose dystonia is similar to that previously described for peak-dose choreiform dyskinesias (section 3.1).
Off-period dystonias usually affect the toes or legs, and less frequently, the face and neck.[260,289] They are usually painful, are asscciated with low plasma levodopa concentrations and coincide with the 'off' periods of motor fluctuationsP60]
In certain patients, painful dystonia of the lower extremities is a particular problem on waking in the morning (early morning dystonia). Early morning dystonia can be avoided by administering a dose of sustained-release carbidopa/levodopa or a longacting dopamine agonist at bedtime, or a dose of standard carbidopa/levodopa in the early morning or on waking.[246] Subcutaneous apomorphine,[354] oral lithium,[355,356] baclofen,[356] anticholinergics[356] or benzodiazepines, or (if dystonia is sus-
© Adis International Limited. All rights reserved.
187
tained) botulinum toxin injections,[356] can be useful alternatives.
5. Tardive Dyskinesia
The term 'tardive dyskinesia' is used to describe all persistent, occasionally reversible, abnormal involuntary movements caused by prolonged exposure to anti psychotics or other dopamine antagonists. The most common form of tardive dyskinesia presents as orofacial stereotypy ('buccolinguomasticatory syndrome'), at times associated with choreatic movements of the extremities and trunkJ357] In this section, we will review the data regarding this common form of tardive dyskinesia. Other tardive syndromes such as tremor (section 2), dystonia (section 4), myoclonus (section 6) and akathisia (section 8) are described elsewhere in this review.
Tardive dyskinesia was first described by Faurbye et al. in 1964.[358] It usually develops after a minimum of 1 to 2 years of antipsychotic therapy. Tardive dyskinesia accounted for 14% of patients with drug-induced movement disorders in a French study at a regional pharmacovigilance centre[359] and 63% of such patients referred to a Movement Disorders Unit in the US.[15]
The prevalence of tardi ve dyskinesia is reported to range from 3.7% and 60%, depending on demographic factors, inclusion criteria, and study designP76,360-384] Studies in Asiatic countries have shown low prevalence ratesP76,369,370]
The newer atypical anti psychotics risperidone, remoxipride, and clozapine, are associated with a lower incidence of tardive dyskinesia than typical anti psychotics, but are not devoid of this adverse effect. [114, 117,342,385-390] The anti vertiginous pheno-
thiazine thiethylperazine can also induce tardive dyskinesia.l59] Besides antipsychotics, other drugs can induce tardive dyskinesia (table V).
Proposed risk factors for tardive dyskinesia include: • advanced age[36I,362,368,382,384,435-437] • female gender[365,369,380,437-439]
• prolonged duration of exposure to antipsychotics[362,363,365,381]
Drug Safety 1997 Mar: 16 (3)
188
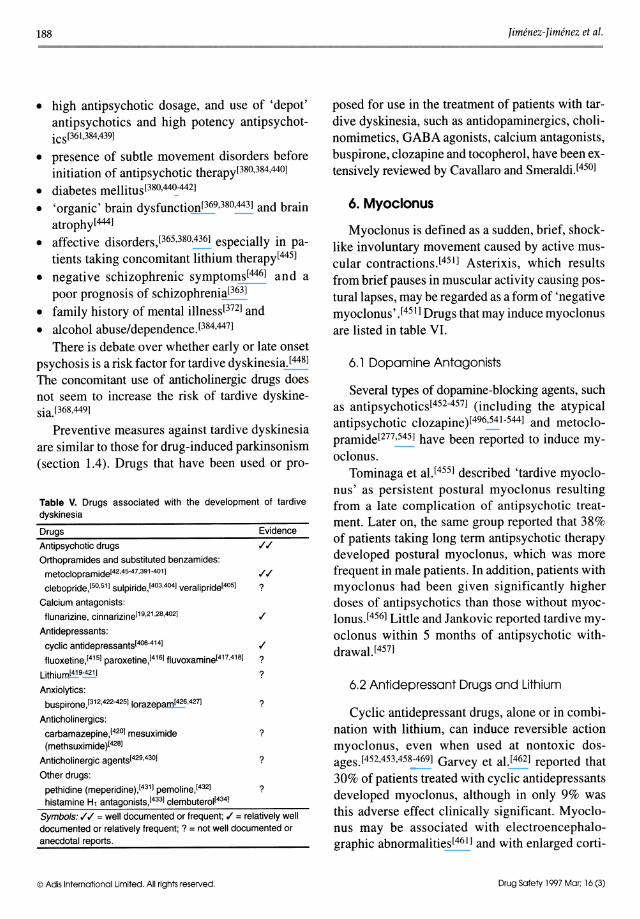
• high antipsychotic dosage, and use of 'depot' antipsychotics and high potency antipsychotiCS[361,384,439]
• presence of subtle movement disorders before initiation of antipsychotic therapy[380,384,440]
• diabetes mellitus[380,440-442] • 'organic' brain dysfunction[369,380,443] and brain
atrophy [444]
• affective disorders,[365,380,436] especially in patients taking concomitant lithium therapy[445]
• negative schizophrenic symptoms[446] and a poor prognosis of schizophrenia[363]
• family history of mental illness[372] and • alcohol abuse/dependence)384,447]
There is debate over whether early or late onset psychosis is a risk factor for tardive dyskinesia.[448] The concomitant use of anticholinergic drugs does not seem to increase the risk of tardive dyskinesia. [368.449]
Preventive measures against tardive dyskinesia are similar to those for drug-induced parkinsonism (section 1.4). Drugs that have been used or pro-
Table V. Drugs associated with the development of tardive dyskinesia
Drugs Evidence
Antipsychotic drugs
Orthopramides and substituted benzamides: metoclopramideI42,4S-47,391-401] ,(,(
clebopride,[SO,Sl] su[piride,[403,404J veralipride[40SJ ?
Calcium antagonists: flunarizine, cinnarizine[19,21 ,28,402J ,(
Antidepressants:
cyclic antidepressants[406-414J ,(
fluoxetine,[41S] paroxetine,[416] fluvoxamine[417,418] ? Lithium[419-421]
Anxiolytics: buspirone,[312,422-42S] lorazepam[426,427]
Anticholinergics:
carbamazepine, [420J mesuximide (methsuximide )[428J
Anticholinergic agents[429,430]
Other drugs:
?
?
?
?
pethidine (meperidine),1431] pemoline,1432] ? histamine Hl antagonists,[433] clembuterol1434]
Symbols: ,( ,( = well documented or frequent; ,( = relatively well documented or relatively frequent; ? = not well documented or anecdotal reports_
© Adis International Limited. All rights reserved,
Jimenez-Jimenez et al.
posed for use in the treatment of patients with tardive dyskinesia, such as antidopaminergics, cholinomimetics, GABA agonists, calcium antagonists, buspirone, clozapine and tocopherol, have been extensively reviewed by Cavallaro and Smeraldi.[450]
6. Myoclonus
Myoclonus is defined as a sudden, brief, shocklike involuntary movement caused by active muscular contractions.l45 ]] Asterixis, which results from brief pauses in muscular activity causing posturallapses, may be regarded as a form of 'negative myoclonus' .[451] Drugs that may induce myoclonus are listed in table VI.
6,1 Dopamine Antagonists
Several types of dopamine-blocking agents, such as antipsychotics[452-457] (including the atypical antipsychotic clozapine)[496,541-544] and metoclopramide[277,545] have been reported to induce myoclonus.
Tominaga et aI,[455] described 'tardive myoclonus' as persistent postural myoclonus resulting from a late complication of antipsychotic treatment. Later on, the same group reported that 38% of patients taking long term antipsychotic therapy developed postural myoclonus, which was more frequent in male patients. In addition, patients with myoclonus had been given significantly higher doses of antipsychotics than those without myoclonus.[456] Little and Jankovic reported tardive myoclonus within 5 months of antipsychotic withdrawal.[457]
6.2 Antidepressant Drugs and Lithium
Cyclic antidepressant drugs, alone or in combination with lithium, can induce reversible action myoclonus, even when used at nontoxic dosages.l452,453,458-469] Garvey et aI,[462] reported that
30% of patients treated with cyclic antidepressants developed myoclonus, although in only 9% was this adverse effect clinically significant. Myoclonus may be associated with electroencephalographic abnormalities[461] and with enlarged corti-
Drug Safety J 997 Mar: 16 (3)
Drug-Induced Movement Disorders
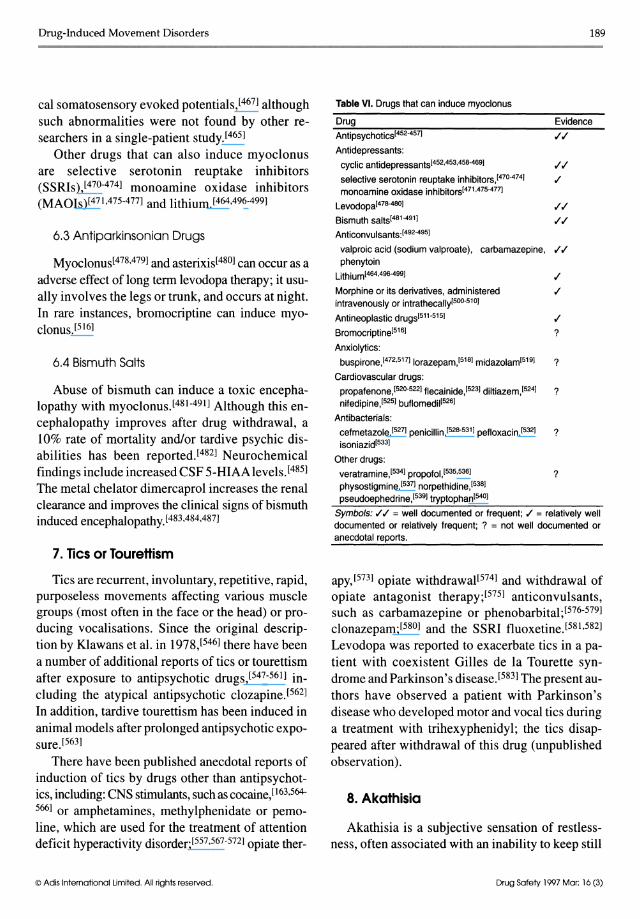
cal somatosensory evoked potentials,[467] although such abnormalities were not found by other researchers in a single-patient study.[465]
Other drugs that can also induce myoclonus are selective serotonin reuptake inhibitors (SSRIs),[470-474] monoamine oxidase inhibitors (MAOIs)[471,475-477] and lithium.[464,496-499]
6.3 Antiparkinsonian Drugs
Myoclonus[478,479] and asterixis[480] can occur as a
adverse effect of long term levodopa therapy; it usually involves the legs or trunk, and occurs at night. In rare instances, bromocriptine can induce myoclonus.[516]
6.4 Bismuth Salts
Abuse of bismuth can induce a toxic encephalopathy with myoclonus.l481-491] Although this encephalopathy improves after drug withdrawal, a 10% rate of mortality and/or tardive psychic disabilities has been reported.l482] Neurochemical findings include increased CSF 5-HIAAlevels.[485] The metal chelator dimercaprol increases the renal clearance and improves the clinical signs of bismuth induced encephalopathy.l483,484,487]
7. Tics or Tourettism
Tics are recurrent, involuntary, repetitive, rapid, purposeless movements affecting various muscle groups (most often in the face or the head) or producing vocalisations. Since the original description by Klawans et al. in 1978,[546] there have been a number of additional reports of tics or tourettism after exposure to antipsychotic drugs,[547-561] including the atypical antipsychotic clozapine.l562] In addition, tardive tourettism has been induced in animal models after prolonged antipsychotic exposure.l563]
There have been published anecdotal reports of induction of tics by drugs other than antipsychotics, including: CNS stimulants, such as cocaine,[163.564-566] or amphetamines, methylphenidate or pemoline, which are used for the treatment of attention deficit hyperactivity disorder;[557,567-5721 opiate ther-
© Adls Internofionol Umlted. All rights reserved.
189
Table VI. Drugs that can induce myoclonus
Drug Evidence Antipsychotics[452-457]
Antidepressants: cyclic antidepressantsI452,453,45B-469]
selective serotonin reuptake inhibitors,[470-474] monoamine oxidase inhibitors[471,475-477]
Levodopa[478-480]
Bismuth salts[481-491]
Anticanvulsants:[492-495]
.1.1
.1.1
.1.1
valproic acid (sodium valproate), carbamazepine, .!.! phenytoin
Lithium[464,496.499] .!
Morphine or its derivatives, administered .! intravenously or intrathecallyl500-510]
Antineoplastic drugs[511.515] .!
Bromocriptine[516] ?
Anxiolytics: buspirone,[472,517] lorazepam,[518] midazolam[519] ?
Cardiovascular drugs: propafenone,[520.522] flecainide,[523] diltiazem,[524] ? nifedipine,[525] buflomedil[526]
Antibacterials: cefmetazole,[527] penicillin,[528-531] pefloxacin,[532] ? isoniazid[533]
Other drugs: veratramine,[534] propofol,[535,536] ? physostigmine,[537] norpethidine,[538] pseudoephedrine,[539] tryptophan[540]
Symbols: .!.! = well documented or frequent; .! = relatively well documented or relatively frequent; ? = not well documented or anecdotal reports,
apy,[5731 opiate withdrawal[5741 and withdrawal of opiate antagonist therapy;[5751 anticonvulsants, such as carbamazepine or phenobarbital;[576-5791 clonazepam;[580] and the SSRI fluoxetine.l581,5821 Levodopa was reported to exacerbate tics in a patient with coexistent Gilles de la Tourette syndrome and Parkinson's disease.[5831 The present authors have observed a patient with Parkinson's disease who developed motor and vocal tics during a treatment with trihexyphenidyl; the tics disappeared after withdrawal of this drug (unpublished observation).
8. Akathisia
Akathisia is a subjective sensation of restlessness, often associated with an inability to keep still
Drug Safety 1997 Mor; 16 (3)
190
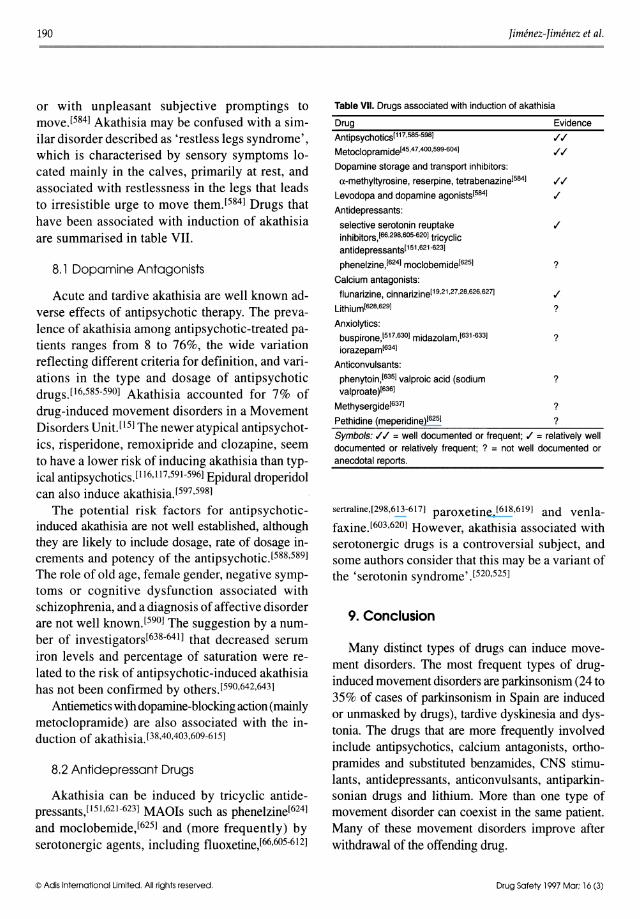
or with unpleasant subjective promptings to moveJ584] Akathisia may be confused with a similar disorder described as 'restless legs syndrome' , which is characterised by sensory symptoms located mainly in the calves, primarily at rest, and associated with restlessness in the legs that leads to irresistible urge to move themJ584] Drugs that have been associated with induction of akathisia are summarised in table VII.
8.1 Dopamine Antagonists
Acute and tardive akathisia are well known adverse effects of antipsychotic therapy. The prevalence of akathisia among antipsychotic-treated patients ranges from 8 to 76%, the wide variation reflecting different criteria for definition, and variations in the type and dosage of antipsychotic drugs.[l6,585-590] Akathisia accounted for 7% of drug-induced movement disorders in a Movement Disorders Unit.115] The newer atypical antipsychotics, risperidone, remoxipride and clozapine, seem to have a lower risk of inducing akathisia than typical antipsychotics.11l6,1l7,591-596] Epidural droperidol can also induce akathisiaJ597,598]
The potential risk factors for antipsychoticinduced akathisia are not well established, although they are likely to include dosage, rate of dosage increments and potency of the antipsychoticJ588,589] The role of old age, female gender, negative symptoms or cognitive dysfunction associated with schizophrenia, and a diagnosis of affective disorder are not well known.1590] The suggestion by a number of investigatorsI638-64I] that decreased serum iron levels and percentage of saturation were related to the risk of antipsychotic-induced akathisia has not been confirmed by others.1590,642,643]
Antiemetics with dopamine-blocking action (mainly metoclopramide) are also associated with the induction of akathisia.£38,4o,403,609-615]
8.2 Antidepressant Drugs
Akathisia can be induced by tricyclic antidepressants,1151,621-623] MAOIs such as phenelzinel624] and moclobemide,1625] and (more frequently) by serotonergic agents, including fluoxetine,I66,605-6l2]
© Adis Intematlonal Limited. All rights reserved.
Jimenez-Jimenez et al.
Table VII. Drugs associated with induction of akathisia
Drug Evidence Antipsychotics[117.585.5981 .1.1 Metoc[opramide[45,47,400,599-6041 .1.1
Dopamine storage and transport inhibitors:
a-methyltyrosine, reserpine, tetrabenazine[584] .1.1 Levodopa and dopamine agonists[584] .I
Antidepressants:
selective serotonin reuptake inhibitors, [66,298,605-620] tricyclic antidepressants[151,621-623]
phene[zine,[624] moc[obemide[625]
Calcium antagonists: f[unarizine, cinnarizine[19,21,27,28,626,627]
Lithium[628,629]
Anxio[ytics: buspirone,[517.630] midazolam,[631-633] iorazepam[634]
Anticonvu[sants: phenytoin,[635] va[proic acid (sodium va[proate )[6361
Methysergide[637]
Pethidine (meperidine)[625]
?
.I ?
?
?
?
?
Symbols: .1.1 = well documented or frequent; .I = relatively well documented or relatively frequent; ? = not well documented or anecdotal reports.
sertraline,[298,613-617] paroxetine,[618,619] and venla
faxine.l603,620] However, akathisia associated with serotonergic drugs is a controversial subject, and some authors consider that this may be a variant of the 'serotonin syndrome' J520,525]
9. Conclusion
Many distinct types of drugs can induce movement disorders. The most frequent types of druginduced movement disorders are parkinsonism (24 to 35% of cases of parkinsonism in Spain are induced or unmasked by drugs), tardive dyskinesia and dystonia. The drugs that are more frequently involved include antipsychotics, calcium antagonists, orthoprarnides and substituted benzarnides, eNS stimulants, antidepressants, anticonvulsants, antiparkinsonian drugs and lithium. More than one type of movement disorder can coexist in the same patient. Many of these movement disorders improve after withdrawal of the offending drug.
Drug Safety 1997 Mar: 16 (3)

Drug-Induced Movement Disorders
Acknowledgements
This work was supported in part by grant FIS 95/0269.
References I. Marti-Masso JF. Carrera N, Urtasun M. Newer drugs inducing
parkinsonism [abstract]. 9th International Symposium on Parkinson's disease: 1988 Jun 5-9; Jerusalem, Israel: 137
2. Marti-Masso JF, Carrera N, Urtasun M. Drug-induced parkinsonism: a growing list [letter]. Mov Disord 1993; 8: 125
3. Gershanik OS. Drug-induced movement disorders. Curr Opin Neurol Neurosurg 1993; 6: 369-76
4. Gershanik OS. Drug-induced parkinsonism in the aged: recognition and prevention. Drugs Aging 1994; 5: 127-32
5. Perez-Gilabert Y, Mateo D, Gimenez-Roldan S. Actividad asistencial en una consulta hospital aria especializada en enfermedad de Parkinson y transtornos del movimiento: un estudio prospectivo durante anos. Neurologia (Spain) 1994; 9: 317-23
6. Llau ME, Nguyen L, Senard JM, et al. Syndromes parkinsoniens d'origine medicamenteuse: experience d'un centre regional de pharmacovigilance sur dix ans. Rev Neurol (Paris) 1994; 150: 757-76
7. Marti-Masso JF, Poza J1. Parkinsonismo inducido 0 agravado por farrnacos: caracteristicas clinicas y evolucion historica de los farrnacos implicados. Neurologia (Spain) 1996; II: 10-5
8. Jimenez-Jimenez FJ, Orti-Pareja M, Ayuso-Peralta L, et al. Drug-induced parkinsonism in a movement disorders unit. A four-year survey. Parkinsonism Rei Disord 1996; 2: 145-9
9. Morgante L, Rocca WA, Di Rosa AE, et al. Prevalence of parkinson's disease and other types of parkinsonism: a door-todoor survey in three Sicilian municipalities. The Sicilian neuro-epidemiologic study (SNES) group. Neurology 1992; 42: 1901-7
10. Trenkwalder C, Schwarz J, Gebhard J, et al. Starnberg trial on epidemiology of parkinsonism and hypertension in the elderly. Prevalence of parkinson's disease and related disorders assessed by a door-to-door survey of inhabitants older than 65 years. Arch Neurol 1995; 52: 1017-22
II. Hubble JP. Drug-induced parkinsonism. In: Stern MB, Koller WC, editors. Parkinsonian syndromes. New York: Marcel Dekker Inc., 1993: 111-22
12. Ayd Jr FJ. A survey of drug-induced extrapyramidal reactions. JAMA 1961; 175: 1054-60
13. Murphy JE, Stewart RB. Efficacy of antiparkinsonian agents in preventing antipsychotic-induced extrapyramidal symptoms. Am J Hosp Pharm 1979; 36: 641-4
14. Binder RL, Kazamatsuri H, Nishimura T, et al. Tardive dyskinesia and neuroleptic-induced parkinsonism in Japan. Am J Psychiatry 1987; 144: 1494-6
15. Miller LG, Jankovic J. Neurologic approach to drug-induced movement disorders: a study of 125 patients. South Med J 1990; 8: 525-32
16. Ganzini L, Heintz R, Hoffman WF, et al. Acute extrapyramidal syndromes in neuroleptic-treated elders: a pilot study. J Geriatr Psychiatry Neuro11991; 4: 222-5
17. Avorn J, Bohn RL, Mogun H, et al. Neuroleptic drug exposure and treatment of parkinsonism in the elderly: a case-control study. Am J Med 1995; 99: 48-54
18. Marti-Masso JF, Carrera N, de la Puente E. Posible parkinsonismo por cinaricina. Med Clin (Barc) 1985; 85: 614-6
© Adis International limited. All rights reserved.
191
19. Chouza C, Scarameli A, Caamano JL, et al. Parkinsonism, tardive dyskinesia, akathisia, and depression-induced by flunarizine. Lancet 1986; I: 1300-4
20. Di Rosa AE, Morgante L, Meduri M, et al. Parkinson-like side effects during prolonged treatment with flunarizine. Funct Neurol 1987; 2: 47-50
21. Micheli F, Pardal MF, Gatto M, et al. Flunarizine- and cinnarizine-induced extrapyramidal reactions. Neurology 1987; 7: 881-4
22. De Michele G, Filla A, Coppola N, et al. Extrapyramidal sideeffects of flunarizine. Acta Neurol [Quad] (Napoli) 1987; 9: 230-3
23. Fernandez-Pardal M, Fernandez-Pardal J, Micheli F. Aggravation of parkinson's disease by cinnarizine [letter]. J Neurol Neurosurg Psychiatry 1988; 51: 158-9
24. Moretti A, Lucantoni C. Flunarizine-induced parkinsonism: clinical report. Ital J Neurol Sci 1988; 9: 295-7
25. Capella D, Laporte JR, Castel JM, et al. Parkinsonism, tremor, and depression-induced by cinnarizine and flunarizine [letter]. BMJ 1988; 297: 722-3
26. Benvenutti F, Baroni A, Bandinelli S, et al. Flunarizine-induced parkinsonism in the elderly. J Clin Pharmacol 1988; 28: 600-8
27. Kuzuhara S, Kohara N, Ohkawa Y, et al. Parkinsonism, depression and akathisia-induced by flunarizine, a calcium entry blockade. Report of 31 cases. Rinsho Shinkeigaku 1989; 29: 681-6
28. Micheli FE, Fernandez Pardal M, Giannaula R, et al. Movement disorders and depression due to flunarizine and cinnarizine. Mov Disord 1989; 4: 139-46
29. Gimenez-Roldan S, Mateo D. Cinnarizine-induced parkinsonism. Susceptibility related to aging and essential tremor. Clin Neuropharmacol 1991; 14: 156-64
30. Garcia-Ruiz P, Garcia de Wbenes J, Jimenez-Jimenez FJ, et al. Parkinsonism associated to calcium channel blockers (CCB). A prospective follow-up study. Clin Neuropharmacol 1992; 15: 19-26
31. Laporte JR, Capella D. Useless drugs are not placebos: lessons from flunarizine and cinnarizine [letter]. Lancet 1986; I: 853-4
32. Dick RS, Barold SS. Diltiazem-induced parkinsonism [letter]. Am J Med 1989; 87: 95-6
33. Malaterre HR, Lauribe P, Paganelli F, et al. Syndrome parkinsonien, effet indesirable possible des inhibiteurs calciques. Arch Mal Coeur Vaiss 1992; 85: 1335-7
34. Graham DF, Stewart-Wynne EG. Diltiazem-induced acute parkinsonism. Aust N Z J Med 1994; 24: 70
35. Garcia-Albea E, Jimenez-Jimenez FJ, Ayuso-Peralta L, et al. Parkinsonism unmasked by verapamil. Clin Neuropharmacol 1993; 16: 263-5
36. Padrell MD, Navarro M, Faura CC, et al. Verapamil-induced parkinsonism [letter]. Am J Med 1995; 99: 436
37. Sempere AP, Duarte J, Cabezas C, et al. Parkinsonism-induced by amlodipine. Mov Disord 1995; 10: 115-6
38. Nakashima K, Shimoda M, Kuno N, et al. Temporary symptom worsening caused by manidipine hydrochloride in two patients with parkinson's disease. Mov Disord 1994; 9: 106-7
39. Grimes JD. Parkinsonism and tardive dyskinesia associated with long-term metoclopramide therapy. N Engl J Med 1981; 305: 1417
40. Grimes JD, Hassan MN, Preston DN. Adverse neurologic effects of me to clop rami de. Can Med Assoc J 1982; 126: 23-5
41. Indo T, Ando K. Metoc1opramide-induced parkinsonism. Clinical characteristics of ten cases. Arch Neurol 1982; 39: 494-6
42. Bateman DN, Rawlins MD, Simpson JM. Extrapyramidal reactions with metoclopramide. BMJ 1985; 291: 930-2
Drug Safety 1997 Mar: 16 (3)

192
43. Yamamoto M, Ujike H, Ogawa N. Metoclopramide-induced parkinsonism. Clin Neuropharmacol1987; 10: 287-9
44. Sethi KD, Patel B, Meador KJ. Metoclopramide-induced parkinsonism [letter). South Med J 1989; 82: 1581-2
45. Miller LG, Jankovic J. Metoclopramide-induced movement disorders. Clinical findings with a review of the literature. Arch Intern Med 1989; 149: 2486-92
46. Bateman DN, Darling WM, Boys R, et al. Extrapyramidal reactions to metoclopramide and prochlorperazine. Q J Med 1989; 71: 307-11
47. Ganzini L, Casey DE, Hoffman WF, et al. The prevalence of metoclopramide-induced tardive dyskinesia and acute extrapyramidal movement disorders. Arch Intern Med 1993; 153: 1469-75
48. Avorn J, Gurwitz JH, Bohn RL, et al. Increased incidence of levodopa therapy following metoclopramide use. JAMA 1995; 274: 1780-2
49. Montagna P, Gabellini AS, Monari L, et al. Parkinsonian syndrome after long-term treatment with clebopride. Mov Disord 1992; 7: 89-90
50. Jimenez-Jimenez FJ, Cabrera-Valdivia F, Ayuso-Peralta L, et al. Persistent parkinsonism and tardive dyskinesia-induced by clebopride. Mov Disord 1993; 8: 246-7
51. Sempere AP, Duarte J, Palomares JM, et al. Parkinsonism and tardive dyskinesia after chronic use of clebopride. Mov Disord 1994; 9: 114-5
52. Naito Y, Kuzuhara S. Parkinsonism-induced or worsened by cisapride. Nippon Ronen Igakkai Zasshi 1994; 31: 899-902
53. Micheli F, Gatto E, Fermindez-Pardal M, et al. Domperidona y enfermedad de parkinson [letter). Medicina (B Aires) 1988; 48:218
54. Milandre L, Ali-Cherif A, Khalil R. Syndrome parkinsonien au cours d'un traitement par Ie veralipride. Rev Med Interne 1991; 12: 157-8
55. Franchignoni FP, Tesio L. Sindrome parkinsoniana indotta da veralipride. Minerva Ginecol 1995; 47: 277-9
56. North RR. Drug-induced movement disorders. Postgrad Med 1971; 97: 882
57. Jankovic J, Orman J. Tetrabenazine therapy of dystonia, chorea, tics, and dyskinesias. Neurology 1988; 38: 391-4
58. Prusinski A, Kozubski W, Szymanska R, et al. Neurological side effects after using thietylperazine. Pol Tyg Lek 1983; 38: 1227-8
59. Bremnum J. Extrapyramidal side effects after long-term treatment with thiethylperazine. Ugeskr Laeger 1988; 150: 2827
60. Rosenblum AM, Montgomery EB. Exacerbation of parkinsonism by methyldopa [letter). JAMA 1980; 244: 2727-8
61. Gillman MA, Sandyk R. Parkinsonism-induced by methyldopa. S Afr Med J 1984; 65: 194
62. Bouchard RH, Pourcher E, Vincent P. Fluoxetine and extrapyramidal side effects [letter). Am J Psychiatry 1989; 146: 1352-3
63. Tate JL. Extrapyramidal symptoms in a patient taking haloperidol and fluoxetine. Am J Psychiatry 1989; 146: 399
64. Gernaat HBPE, Van de Woude J, Touw DJ. Fluoxetine and parkinsonism in patients taking carbamazepine [letter]. Am J Psychiatry 1991; 141: 118-9
65. Jansen Steur ENH. Increase of parkinson disability after fluoxetine medication. Neurology 1993; 43: 211-3
66. Daric C, Dollfus S, Mihout B, et al. Fluoxetine et symptomes extrapyramidaux. A propos de deux observations. Encephale 1993; 19: 61-2
© Adis International Umited. All rights reserved.
Jimenez-Jimenez et al.
67. Gatto EM, Fernandez-Pardal M, Micheli F. Agravacion del parkinsonismo por fluoxetina [letter). Medicina (B Aires) 1994;54: 182
68. Caley CF, Friedman JH. Does fluoxetine exacerbate parkinson's disease? J Clin Psychiatry 1992; 53: 278-82
69. Montastruc JL, Fabre N, Blin 0, etal. Does fluoxetine aggravate parkinson's disease? A pilot prospective study. Mov Disord 1995; 10: 355-7
70. Jimenez-Jimenez FJ, Tejeiro J, Martfnez-Junquera G, et al. Parkinsonism exacerbated by paroxetine. Neurology 1995; 45: 2406
71. Malek-Ahmadi P, Allen SA. Paroxetine-molindone interaction [letter). J Clin Psychiatry 1995; 56: 82-3
72. Albanese A, Rossi P, Altavista MC. Can trazodone induce parkinsonism? Clin Neuropharmacol1988; ll: 180-2
73. Teusink JP, Alexopoulos GS, Shamoian CA. Parkinsonian side effects-induced by a monoamine oxidase inhibitor [letter). Am J Psychiatry 1984; 141: 118-9
74. Strouse TB, Salehmoghaddam S, Spar JE. Acute delirium and parkinsonism in a bupropion-treated liver transplant recipient [letter). J Clin Psychiatry 1993; 54: 489-90
75. Lutz EG. Acute lithium-induced parkinsonism precipitated by liquid protein diet [letter). J Med Soc N J 1978; 75: 165-6
76. Kane J, Rifkin A, Quitkin F, et al. Extrapyramidal side effects with lithium therapy. Am J Psychiatry 1978; 135: 851-3
77. Tyrer P, Alexander MS, Regan A, et al. An extrapyramidal syndrome after lithium therapy. Br J Psychiatry 1980; 136: 191-4
78. Gajkowski K, Werkowicz-Pelczyk D, Masiak I, et al. Neurologic symptoms in lithium poisoning. Neurol Neurochir Pol 1987; 21: 412-4
79. Holroyd S, Smith D. Disabling parkinsonism due to lithium: a case report [letter). J Geriatr Psychiatry Neuro11995; 8: 118-9
80. Suranyi-Cadotte BE, Nestoros IN, Nair NPV, et al. Parkinsonism-induced by high doses of diazepam. Bioi Psychiatry 1985; 20: 451-60
81. van der Zwan Jr A. Transient parkinson syndrome and tremor caused by the use of sodium valproate. Ned Tijdschr Geneeskd 1989; 133: 1230-2
82. Alvarez-GomezMJ, Vaamonde J, NarbonaJ, et al. Parkinsonian syndrome in childhood after sodium valproate administration. Clin Neuropharmacol1993; 16: 451-5
83. Sasso E, Delsoldato S, Negrotti A, et al. Reversible valproateinduced extrapyramidal disorders. Epilepsia 1994; 35: 391-3
84. Froomes PR, Stewart MR. A reversible parkinsonian syndrome and hepatotoxocity following addition of carbamazepine to sodium valproate. Aust N Z J Med 1994; 24: 413-4
85. Goiii M, Jimenez M, Seijoo M. Parkinsonism-induced by phenytoin. Clin Neuropharmacol1985; 8: 383-4
86. Fox JH, Bennett DA, Goetz CG, et al. Induction of parkinsonism by intraventricular bethanechol in a patient with Alzheimer's disease. Neurology 1989; 9: 1265
87. Iwasaki Y, Wakata N, Kinoshita M. Parkinsonism-induced by pyridostigmine. Acta Neurol Scand 1988; 78: 236
88. LeMarie JF, Autret A, Biziere K, et al. Amiodarone neuropathy. Further arguments for human drug-induced neurolipidosis. Eur Neuro11987; 147: 881-4
89. Palakurthy PR, Iyer V, Meckler RJ. Unusual neurotoxicity associated with amiodarone therapy. Arch Intern Med 1987; 147: 881-4
90. Werner EG, Olanow CWo Parkinsonism and amiodarone therapy. Ann Neurol 1989; 25: 630-2
91. Dotti MT, Federico A. Amiodarone-induced parkinsonism: a case report and pathogenetic discussion. Mov Disord 1995; 10: 233-4
Drug Safety 1997 Mar; 16 (3)

Drug-Induced Movement Disorders
92. Gjerris F. Transitory procaine-induced parkinsonism. J Neurol Neurosurg Psychiatry 1971; 34: 20-2
93. Lieberman AN, Goldstein M. Reversible parkinsonism related to meperidine [letter]. N Engl J Med 1985; 8: 509
94. Olive JM, Masana L, Gonzalez J. Meperidine and reversible parkinsonism. Mov Disord 1994; 9: 115-6
95. Fisher JF, Dewald J. Parkinsonism associated with intra-ventricular amphotericine B. J Antimicrob Ther 1983; 12: 97-9
96. Balmaceda CM, Walker RW, Castro-Malaspina H, et al. Reversal of amphotericin-B-related encephalopathy. Neurology 1994; 44: 1183-4
97. Mintz V, Liberman VA, Vries A. Parkinsonism syndrome due to cephaloridine [letter]. JAMA 1971; 216: 1200
98. Shaunak S, Brown P, Morgan-Hughes JA. Exacerbation of idiopathic Parkinson's disease by naproxen [letter]. BMJ 1995; 311: 422
99. Fernandez W, Lees AJ. Temporary deterioration in parkinsonian signs after modest alcohol intake. Mov Disord 1992; 7: 284-5
100. Yasui M, Kihira T, Ota K, et al. A case of parkinsonism-induced by an oral contraceptive. No To Shinkei 1992; 44: 163-6
10 I. Fujisawa Y, Tsuji T, Sasaki K. Parkinsonism-induced by indeloxazine hydrochloride. Clin Ther 1989; 11: 807-11
102. Ogawa N. Parkinsonism-induced by indeloxazine hydrochloride in the elderly. Clin Ther 1989; II: 802-6
103. Shimoda K, Hikasa C, Nishikawa S, et al. A case report of captopril-induced parkinsonism. Rinsho Shinkeigaku 1987; 27: 366-8
104. Luque FA, Selhorst JB, Petruska P. Parkinsonism-induced by high-dose cytosine arabinoside. Mov Disord 1987; 2: 219-22
105. Weiden PJ, Mann n, Haas G, et al. Clinical nonrecognition of neuroleptic-induced movement disorders: a cautionary study. Am J Psychiatry 1987; 144: 1148-53
106. Hansen TE, Brown WL, Weigel RM, et al. Vnderrecognition of tardive dyskinesia and drug-induced parkinsonism by psychiatric residents. Gen Hosp Psychiatry 1992; 14: 340-4
107. Farde L, Nordstrom AL, Wiesel AL, et al. Positron emission tomographic analysis of central D I and D2 dopamine receptor occupancy in patients treated with classical neuroleptics and cIozapine. J Clin Psychiatry 1992; 9: 538-44
108. Grohmann R, Koch R, Schmidt LG. Extrapyramidal symptoms in neuroleptic recipients. Agents Actions 1990; 29 Suppl.: 71-82
109. Weiner WJ, Lang AE. Drug-induced movement disorders (not including tardive dyskinesia). In: Weiner WJ, Lang AE, editors. Movement disorders. A comprehensive survey. Mount Kisco, New York: Futura Publishing Co., 1989: 599-644
110. Chouinard G. Early phase II clinical trial of remoxipride in treatment of schizophrenia with measurements of prolactin and neuroleptic activity. J Clin Psychopharmacol 1987; 7: 159-64
Ill. Laux G, Klieser E, Schroder HG, et al. A double-blind multicentre study comparing remoxipride, two and three times daily, with haloperidol in schizophrenia. Acta Psychiatr Scand 1990; 358 Suppl.: 125-9
112. Lindstrom LH, Wieselgren 1M, Struwe G, et al. A double- blind comparative multicentre study of remoxipride and haloperidol in schizophrenia. Acta Psychiatr Scand 1990; 358 Suppl.: 130-5
113. Kane JM, Safferman AZ, Pollack S, et al. Clozapine, negative symptoms, and extrapyramidal side effects. J Clin Psychiatry 1994: 55 Suppl. B: 74-7
114. Gerlach J, Peacock L. Motor and mental side effects of c1ozapine. J Clin Psychiatry 1994: 55 Suppl. B: 107-9
© Adis Intemational Umited. All rights reserved.
193
115. Bezchlibnyk-Butler KZ, Remington GJ. Antiparkinsonian drugs in the treatment of neuroleptic-induced extrapyramidal symptoms. Can J Psychiatry 1994; 39: 74-84
116. Kurz M, Hummer M, Oberbauer H, et al. Extrapyramidal side effects of cIozapine and haloperidol. Psychopharmacology (BerJ) 1995; 118: 52-6
117. Owens DGC. Adverse effects of antipsychotic agents. Do newer agents offer advantages? Drugs 1996; 51: 895-930
118. Sandyk R, Kay SR. Drug-induced parkinsonism: relationship to age at onset of schizophrenia. Funct Neuro11991; 6: 151-7
119. Hoffman WF, Labs SM, Casey DE. Neuroleptic-induced parkinsonism in older schizophrenics. BioI Psychiatry 1987; 22: 427-39
120. Prosser ES, Csernansky JG, Kaplan J, et al. Depression, parkinsonian symptoms, and negative symptoms in schizophrenics treated with neuroleptics. J Nerv Ment Dis 1987; 175: 100-5
121. Nelli AC, Yarden PE, Guazzelli M, et al. Parkinsonism following neuroleptic withdrawal. Arch Gen Psychiatry 1989; 46: 383-4
122. Melamed E, Achiron A, Shapira A, et al. Persistent and progressive parkinsonism after discontinuation of chronic neuroleptic therapy: an additional tardive syndrome? Clin Neuropharrnacoll991; 14: 273-8
123. Burkhardt C, Kelly JP, Lim YH, et al. Neuroleptic medications inhibit complex I of the electron transport chain. Ann Neurol 1993; 33: 512-7
124. Schapira AHV, Cooper JM, Dexter D, et al. Mitochondrial complex I deficiency in Parkinson's disease [letter]. Lancet 1989; I: 1269
125. Mizuno Y, Ohta S, Tanaka S, et al. Deficiencies in complex I subunits of the respiratory chain in Parkinson's disease. Biochem Biophys Res Commun 1989; 163: 1450-5
126. Negrotti A, Ca1zetti S, Sasso E. Calcium-entry blockers--induced parkinsonism: possible role of inherited susceptibility. Neurotoxicology 1992; 13: 261-4
127. Garcia-Ruiz PJ, Mena MA, Pefiafiel N, et al. Cinnarizine-induced parkinsonism in primates. Clin Neuropharmacol 1992; 15: 152-4
128. Pileblad E, Carlsson A. The Ca2+ antagonist nimodipine decreases and the Ca2+ agonist BAY K 8644 increases catecholamine synthesis in mouse brain. Neuropharmacology 1987; 26: 101-5
129. Yarom M, Zurgil N, Zisapel N. Calcium permeability changes and neurotransmitter release in cultured brain neurons. II. Temporal analysis of neurotransmitter release. J BioI Chern 1985;260: 16294-302
130. Barochovsky 0, Bradford HF. Development of transmitter- releasing capacity in neuron-enriched tissue cultures. J Neurochem 1987; 48: 787-97
131. Pardo B, Casarejos MJ, Tabernero C, etal. Farmacologfade los antagonistas del calcio sobre el sistema dopaminergico [abstract]. Neurologfa (Spain) 1989; 4: 160
132. De Vries DJ, Beart PM. Competitive inhibition of [3H]spiperone binding to D-2 dopamine receptors in striatal homogenates by organic calcium-channel antagonists and polivalent cations. Eur J Pharmacol1985; 106: 133-9
133. De Yebenes MJG, Casarejos MJ, Mena MA, et al. Effects of calcium antagonists on dopamine-rich human neuroblastoma cells, NB69 [abstract]. Mov Disord 1992; 7 Suppl. 1: 61
134. Kariya S, Isozaki S, Masubuchi Y, et al. Possible pharmacokinetic and pharmacodynamic factors affecting parkinsonism inducement by cinnarizine and flunarizine. Biochem Pharmaco11995; 50: 1645-50
Drug Safety 1997 Mar: 16 (3)

194
135. Veitch K, Hue L. Flunarizine and cinnarizine inhibit mitochondrial complexes I and II: possible implication for parkinsonism. Mol Pharmacol1994; 45: 158-63
136. Montastruc JL, Llau ME, Rascol 0, et al. Drug-induced parkinsonism: a review. Fundam Clin Pharmacol1994; 8: 293-306
137. Richardson MA, Craig TJ. The coexistence of parkinsonismlike symptoms and tardive dyskinesia. Am J Psychiatry 1982; 19: 341-3
138. Jankovic J, Casabona J. Coexistent tardive dyskinesia and parkinsonism. Clin Neuropharmacol1987; 10: 511-21
139. Stephen PJ, Williamson 1. Drug-induced parkinsonism in the elderly. Lancet 1984; II: 1082-3
140. Remington G, Bezchlibnyk-Butler K. Management of acute antipsychotic-induced extrapyramidal syndromes. CNS Drugs 1996; 5 Suppl. I: 21-35
141. Barnes TRE, McPhillips MA. Antipsychotic-induced extrapyramidal symptoms. Role of anticholinergic drugs in treatment. CNS Drugs 1996; 6: 315-30
142. Hardie RJ, Lees AJ. Neuroleptic-induced Parkinson's syndrome: clinical features and results of treatment with levodopa. J Neurol Neurosurg Psychiatry 1988; 51: 850-4
143. Stacy M, Jankovic 1. Tardive tremor. Mov Disord 1992; 7: 53-7 144. Arblaster LA, Lakie M, Mutch WJ, et al. A study of the early
signs of drug-induced parkinsonism. J Neurol Neurosurg Psychiatry 1993; 56: 301-3
145. Gabellini AS, Martinelli P, Coccagna G. Drug-induced tremor of the tongue. Ital J Neurol Sci 1989; 10: 89-91
146. Friedman JH. 'Rubral' tremor-induced by a neuroleptic drug. Mov Disord 1992; 7: 281-2
147. Tan U, Gepdiremen A, Banoglu N, et al. Intermittent tremorbursts-induced by chlorpromazine and pentobarbitone in guinea pigs: a new tremor model. Int J Neurosci 1991; 61: 221-8
148. Gelenberg AJ, Jefferson JW. Lithium tremor. J Clin Psychiatry 1995; 56: 283-7
149. Schou M, Baastrup PC, GrofP, et al. Pharmacological and clinical problems of lithium prophylaxis. Br J Psychiatry 1970; 116: 615-9
150. Karas BJ, Wilder BJ, Hammond EJ, et al. Valproate tremors. Neurology 1982; 2: 428-32
151. Lejoyeux M, Rouillon F, Ades J, et al. Neural symptoms-induced by tricyclic antidepressants: phenomenology and pathophysiology. Acta Psychiatr Scand 1992; 85: 249-56
152. Lejoyeux M, Rouillon F, Ades J. Prospective evaluation of the serotonin syndrome in depressed inpatients treated with clomipramine. Acta Psychiatr Scand 1993; 88: 369-71
153. Larsen K, Schmekel B. Tremor in healthy volunteers after bambuterol and terbutaline CR tablets. Eur J Clin Pharmacol 1993; 45: 303-5
154. Weiner WJ, Lang AE. Tremor. In: Weiner WJ, Lang AE, editors. Movement disorders. A comprehensive survey. Mount Kisco, NY: Futura Publishing Co., 1989: 221-56
155. Logan WJ, Freeman JM. Pseudodegenerative disease due to diphenylhydantoin intoxication. Arch Neuro11969; 21: 631-7
156. Taira T. Zonisamide-induced tremor: report of two cases. No To Shinkei 1992; 44: 61-3
157. Reutens DC, Duncan JS, Patsalos PN. Disabling tremor after lamotrigine with sodium valproate [letter]. Lancet 1993; 42: 185-6
158. Kaminski CA, Robbins MS, Weibley RE. Sertraline intoxication in a child. Ann Emerg Med 1994; 23: 1371-4
159. Apseloff G, Wilner KD, von-Deutsch DA, et al. Sertraline does not alter steady-state concentrations or renal clearance oflithium in healthy volunteers. J Clin Pharmacol 1992; 32: 643-6
© Adis International Urnited. All rights reserved.
Jimenez-Jimenez et al.
160. Debattista C, Schatzberg AF. Physical symptoms associated with paroxetine withdrawal [letter]. Am J Psychiatry 1995; 152: 1234-5
161. Soto J, Sacristan JA, Alsar MJ, et al. Terfenadine-induced tremor. Ann Neuro11993; 33: 226
162. Laguna-del-Estal P, Calabrese S, Zabala JA, et al. Toxicidad neur610gica por antimoniales pentavalentes durante el tratamiento de la leishmaniasis visceral. Med Clin (Barc) 1994; 102: 276-7
163. Cardoso FE, Jankovic J. Cocaine-related movement disorders. Mov Disord 1993; 8: 175-8
164. Findley U. Tremors: differential diagnosis and pharmacology. In: Jankovic J, Tolosa E, editors. Parkinson's disease and movement disorders, 2nd ed. Baltimore: Williams & Wilkins, 1993: 293-313
165. Cotzias GC, Van Woert MH, Schiffer LM. Aromatic amino acids and modification of parkinsonism. N Engl J Med 1967; 276: 567-72
166. Papavasiliou PS, Cotzias GC, Duby SE, et al. Levodopa in parkinsonism: potentiation of central effects with a peripheral inhibitor. N Engl J Med 1972; 285: 8-14
167. Barbeau A. Treatment with levodopa and R04-4602: review and present status. Adv Neurol 1973; 2: 173-98
168. Martin WE, Tolosa ES, Loewenson RL, et al. The effect of combining carbidopa with levodopa for Parkinson's disease. Geriatrics 1975; 30: 39-44
169. Sage 11, Mark MH, McHale DM, et al. Benefits of monitoring plasma levodopa in Parkinson's disease patients with druginduced chorea. Ann Neuro11991; 29: 623-8
170. Marconi R, Lefebvre-Caparros D, Bonnet AM, et al. Levodopainduced dyskinesias in Parkinson's disease: phenomenology and pathophysiology. Mov Disord 1994; 9: 2-12
171. Zimmerman Jr TR, Sage 11, Lang AE, et al. Severe evening dyskinesias in advanced Parkinson's disease: clinical description, relation to plasma levodopa, and treatment. Mov Disord 1994; 9: 173-7
172. Caine DB, Techeyne PF, Claverfa LE, et al. Bromocriptine in Parkinson's disease. BMJ 1974; 4: 442-4
173. Cotzias GC, Papavasiliou PS, Tolosa E, et al. Treatment of Parkinson's disease with aporphines. Possible role of growth hormones. N Engl J Med 1976; 294: 567-72
174. Lieberman A, Goldstein M, Leibowitz M, et al. Treatment of advanced Parkinson's disease with pergolide. Neurology 1981; 31: 675-82
175. McDonald RJ, Horowski L. Lisuride in the treatment of parkinsonism. EurNeurol1983; 22: 240-55
176. LeWitt P. Clinical and pharmacological aspects of the antiparkinsonian ergoline lisuride. In: Fahn S, Marsden CD, Jenner P, et aI., editors. Recent developments in Parkinson's disease. New York: Raven Press, 1986: 347-54
177. Klawans HL, Weiner WJ. The effect of d-amphetamine on choreiform movement disorders. Neurology 1974; 24: 312-8
178. Lundh H, Tunving K. An extrapyramidal choreiform syndrome caused by amphetamine addiction. J Neurol Neurosurg Psychiatry 1981; 44: 728-30
179. Rhee KJ, Albertson TE, Douglas JC. Choreoathetoid disorder associated with amphetamine-like drugs. Am J Emerg Med 1988; 6: 131-3
180. Sperling LS, Horowitz JL. Methamphetamine-induced choreoathetosis and rhabdomyolysis. Ann Intern Med 1994; 34: 388-90
181. Nausieda PA, Coller WC, Weiner WJ, et al. Pemoline-induced chorea. Neurology 1981; 31: 356-60
Drug Safety 1997 Mar; 16 (3)

Drug-Induced Movement Disorders
182. Weiner WJ, Nausieda PA, Klawans HL. Methylphenidate-induced chorea: case report and pharmacologic implications. Neurology 1979; 29: 1041-4
183. Habal R, Sauter 0, Olowe 0, et al. Cocaine and chorea. Am J Emerg Med 1991; 9: 618-20
184. Stuart AM, Worley LM, Spillane J. Choreiform movements observed in an 8-year-old child following use of an oral theophylline preparation. Clin Pediatr Phila 1992; 1: 692-4
185. Birket-Smith E. Abnormal involuntary movements-induced by anticholinergic therapy. Acta Neurol Scand 1974; 50: 801-11
186. Warne RW, Gubbay SS. Choreiform movements-induced by anticholinergic therapy [letter]. Med J Aust 1979; 1: 465
187. Matsumoto K, Nogaki H, Morimatsu M. A case of choreo-athetoid movements-induced by anticholinergic drugs, tryhexyphenidyl HCI and dosulepin HCl. Nippon Ronen Igakkai Zasshi 1992; 29: 686-9
188. Nomoto M, Thompson PO, Sheehy MP, et al. Anticholinergicinduced chorea in the treatment of focal dystonia. Mov Disord 1987; 2: 53-6
189. Thach BT, Chase TN, Bosma J. Oral facial dyskinesia associated with prolonged use of antihistaminic decongestants [letter]. N Engl J Med 1975; 293: 486-7
190. Lehmann AB. Reversible chorea due to ranitidine and cimetidine [letter]. Lancet 1988; II: 158
191. Nausieda PA, Koller WC, Weiner WJ, et al. Chorea-induced by oral contraceptives. Neurology 1979; 29: 1605-9
192. Bedard P, Langelier P, Danbova J, et al. Estrogens, progesterone and the extrapyramidal system. Adv Neuro11979; 24: 411-22
193. Galimberti D. Chorea-induced by the use of oral contraceptives. Report of a case and review of the literature.ltal J Neurol Sci 1987; 8: 383-6
194. Leys 0, Destee A, Petit H, et al. Chorea associated with oral contraception. J Neurol 1987; 235: 46-8
195. Driesen JJ, Wolters EC. Oral contraceptive-induced paraballism. Clin Neurol Neurosurg 1987; 89: 49-51
196. Mathur AK, Gatter RA. Chorea as the initial presentation of oral contraceptive-induced systemic lupus erythematosus. J Rheumatol 1988; 15: 1042-3
197. Liedholm LJ, Barajas F. Oral contraceptives causing chorea in a young woman [letter]. Lakartidningen 1988; 85: 448
198. Cocito 0, Gallo G. Hemichorea-induced by oral contraceptive use. Ital J Neurol Sci 1989; 10: 217-8
199. Profumo R, Toce S, Kotagal S. Neonatal choreoathetosis following prenatal exposure to oral contraceptives. Pediatrics 1990; 86: 648-9
200. Caviness IN, Muenter MD. An unusual cause of recurrent chorea. Mov Disord 1991; 6: 355-7
201. Steiger MJ, Quinn NP. Hormone replacement therapy-induced chorea [letter]. BMJ 1991; 302: 762
202. Chadwick 0, Reynolds EG, Marsden CD. Anticonvulsant-induced dyskinesias: a comparison with dyskinesias-induced by neuroleptics. J Neurol Neurosurg Psychiatry 1976; 9: 1210-8
203. Filloux F, Thompson JA. Transient chorea-induced by phenytoin. J Pediatr 1987; 110: 639-41
204. Szczechowski L, Rosciszewska D. Choreoathetotic movements in a patient with epilepsy after treatment with diphenylhydantoin. Neurol Neurochir Pol 1987; 21: 255-7
205. Martin6n-Sanchez F, Viso-Lorenzo JA. Una observaci6n pediatrica de coreoatetosis por difenilhidantoina. An Esp Pediatr 1990; 32: 554-5
206. Martinez-Orgado J, Garcia-Aparicio J, Cabanillas-Vilaplana L, et al. Coreoatetosis inducida por difenilhidantoina en un
© Adis International Umited. All rights reserved.
195
lactante con sindrome CHARGE. An Esp Pediatr 1990; 33: 384-6
207. Haider Y, Abbott RJ. Phenytoin-induced choreoathetosis [letter]. Postgrad Med J 1990; 66: 1089
208. Harrison MD, Lyons GR, Landow ER. Phenytoin and dyskinesias: a report of two cases and review of the literature. Mov Disord 1993: 8: 19-27
209. Shulman LM, Singer C, Weiner WJ. Phenytoin-induced focal chorea. Mov Disord 1996; 11: 111-4
210. Weaver OF, Camfield P, Fraser A. Massive carbamazepine overdose: clinical and pharmacologic observations in five episodes. Neurology 1988; 38: 755-9
211. Mosquet B, Starace J, Madelaine S, et al. Syndrome choreoathetosique sous carbamazepine et viloxazine. Consequence d'une interaction medicamenteuse?Therapie 1994; 49: 513-4
212. Kirschberg GJ. Dyskinesia: an unusual reaction to ethosuximide. Arch Neurol 1975; 32: 137-8
213. Lancman ME, Asconape JJ, Penry JK. Choreiform movements associated with the use of valproate. Arch Neurol 1994; 51: 702-4
214. Kerrick JM, Kelley BJ, Maister BH, et al. Involuntary movement disorders associated with felbamate. Neurology 1995; 45: 185-7
215. Buetefisch CM, Gutierrez A, Gutmann L. Choreoathetotic movements: a possible side effect of gabapentin. Neurology 1996; 46: 851-2
216. Patrick SJ, Snelling LK, Ment LR. Infantile chorea following abrupt withdrawal of diazepam and pentobarbital therapy. J Toxicol Clin Toxicol1993; 31: 127-32
217. Fann WE, Sullivan JL, Richman BW. Dyskinesias associated with tricyclic antidepressants. Br J Psychiatry 1976; 128: 490-3
218. Sandyk R. Nomifensine-induced orofacial dyskinesia and Sydenham's chorea. Int J Neurosci 1987; 35: 91-2
219. Patterson JP. Amoxapine-induced chorea [letter]. South Med J 1983; 76: 1077
220. Marchioni E, Perucca E, Soragna 0, et al. Choreiform syndrome associated with fluoxetine treatment in a patient with deficient CYP2D6 activity. Neurology 1996; 46: 853
221. Zorumski CP, Bakris GL. Choreoathetosis associated with lithium: case report and literature review. Am J Psychiatry 1983; 140: 1621-2
222. Walevski A, Radwan M. Choreoathetosis as toxic effect of lithium treatment. Eur Neurol 1986; 25: 412-5
223. Matsis PP, Fisher RA, Tasman-Jones C. Acute lithium toxicity: chorea, hypercalcemia and hyperamylasemia. Aust N Z J Med 1989; 19: 718-20
224. Reed SM, Wise MG, Timmerman I. Choreoathetosis: a sign of lithium toxicity. J Neuropsychiatry Clin Neurosci 1989; I: 57-60
225. Helmuth 0, Ljaljevic Z, Ramirez L, et al. Choreoathetosis-induced by verapamil and lithium treatment. J Clin PsychopharmacoI1989;9:454-5
226. Tsuda N, Negoro K, Morimatsu M. A case of multiple cerebral infarctions associated with hemichorea-induced by amantadine hydrochloride. Rinsho Shinkeigaku 1994; 34: 388-90
227. Tilzey A, Heptonstall J, Hamblin T. Toxic confusional state and choreiform movements after treatment with anabolic steroids. BMJ 1981; 283: 343-50
228. Wasserman S, Yahr MD. Choreic movements-induced by the use of methadone. Arch Neuro11980; 37: 727-8
229. Crystal HA. Baclofen therapy may be associated with chorea in Alzheimer's disease. Ann Neuro11990; 28: 839
Drug Safety 1997 Mar; 16 (3)

196
230. Kaplan SR, Murkofsky C. Oral-buccal dyskinesia symptoms associated with low-dose benzodiazepine treatment [letter]. Am J Psychiatry 1978; 135: 1558-9
231. Neil EM, Waters AK. Generalized choreiform movements as a complication of methyldopa therapy in chronic renal failure. Postgrad Med J 1981; 57: 732-3
232. Kaminsky P, Cosmidis S, Debouverie M, et al. Syndrome choreiforme provoque par l'alpha-methyldopa [letter]. Therapie 1988; 43: 239
233. Wedzicha JA, Gibb WR, Lees AJ, et al. Chorea in digoxin toxicity [letter]. J Neurol Neurosurg Psychiatry 1984; 47: 419
234. Mulder LJ, Van der Mast RC, Meerwaldt JD. Generalised chorea due to digoxin toxicity [letter]. BMJ 1988; 296: 1262
235. Neary 0, Thurston H, Pohl JE. Development of extrapyramidal symptoms in hypertensive patients treated with diazoxide [letter]. BMJ 1973; 3: 474-5
236. Vernay D, Dubost n, Thevenet JP, et al. 'Choree fibrillaire de Morvan' followed by Guillain-Barre syndrome in a patient receiving gold therapy [letter]. Arthritis Rheum 1986; 29: 1413-4
237. Aumaitre 0, Vernay D, Marcheix JC, et al. Choree fibrillaire de Morvan secondaire 11 un traitement par sels d'or. Presse Med 1988; 17: 2140
238. Petiot P, Charles N, Vial C, et al. Complications neurologiques des sels d' or: discussion nosologique a propos d'un cas. Rev Neurol (Paris) 1993; 149: 562-5
239. Samie MR, Ashton AK. Choreoathetosis-induced by cyproheptadine. Mov Disord 1989; 4: 81-4
240. Combarros 0, Fabrega E, Polo JM, et al. Cyclosporine-induced chorea after liver transplantation for Wilson's disease. Ann Neurol 1993; 33: 108-9
241. Quinn AG, Ellis WR, Bum D, et al. Chorea precipitated by sulphasalazine [letter]. BMJ 1991; 302: 1025
242. Burguet A, Menget A, Fromentin C, et al. Effets neurologiques de I' aciclovir apres greffe de moelle allogenique. Arch Fr Pediatr 1988; 45: 343-5
243. McHugh P. Acute choreoathetoid reaction to propofol [letter]. Anaesthesia 1991; 46: 425
244. Borgeat A, Wilder-Smith 0. Acute choreoathetoid reaction to propofol [letter]. Anaesthesia 1991; 46: 797
245. Tanner CM, Melamed E, Lees AJ. Managing motor fluctuations, dyskinesias, and other adverse effects in Parkinson's disease. Neurology 1994; 44 Suppl. I: S12-S16
246. Shale H, Tanner C. Pharmacological options for the management of dyskinesias. Drugs 1996; 52: 849-60
247. Koller WC, Silver DE, Lieberman A. An algorithm for the management of Parkinson's disease. Neurology 1994; 44 Suppl. 10: SI-S52
248. Bennet JP, Landow ER, Schuh LA. Suppression of dyskinesias in advanced Parkinson's disease. II. Increasing daily clozapine doses suppress dyskinesias and improve parkinsonism symptoms. Neurology 199; 43: 1551-5
249. Kleerdorfer B, Lees AJ, Stem GM. Buspirone in the treatment of levodopa-induced dyskinesias [letter]. J Neurol Neurosurg Psychiatry 1991; 54: 376-7
250. Bonifati V, Fabrizio E, Cipriani R, et al. Buspirone in levodopainduced dyskinesias. Clin Neuropharmacol1994; 17: 99-102
251. DurifF. Vidailhet M, Bonnet AM, et al. Levodopa-induced dyskinesias are improved by fluoxetine. Neurology 1956; 45: 1855-8
252. Tarsy D, LeopoldN, Sax D. Physostigmine in choreiform movement disorders. Neurology 1974; 24: 28-34
253. Klawans HL, Topel JL, Bergen D. Deanol in the treatment of levodopa-induced dyskinesias. Neurology 1975; 25: 290-3
© Adis Interna~onal Umlted. All rights reserved.
Jimenez-Jimenez et al.
254. Price PA, Parkes JD, Marsden CD. Sodium valproate in the treatment of levodopa-induced dyskinesias. J Neurol Neurosurg Psychiatry 1978; 41: 702-6
255. Ziegler M, Fournier V, Bathien N, et al. Therapeutic response to progabide in neuroleptic and levodopa-induced dyskinesias. Clin Neuropharmacol1987; 10: 238-46
256. Turjanski N, Lees AJ. Gamma vinyl GABAin the treatment of levodopa-induced dyskinesias [letter]. J Neurol Neurosurg Psychiatry 1992; 55: 413
257. Gershanik OS, Luqnin MR, Scipioni 0, et al. Isoniazid therapy in Parkinson's disease. Mov Disord 1988; 3: 133-9
258. Laitinen LV, Bergenheim A, Hariz MI. Leksell's posteroventral pallidotomy in the treatment of Parkinson's disease. J Neurosurg 1992; 76: 53-61
259. Laitinen LV. Pallidotomy for Parkinson's disease. Neurosurg Clin North Am 1995; 6: 105-12
260. Iacono RP, Shima F, Lonser RR, et al. The results, indications, and physiology of posteroventral pallidotomy for patients with Parkinson's disease. Neurosurgery 1995; 36: 1118-25
261. Obeso JA, Grandas F, Vaamonde J, et al. Motor complications associated with chronic levodopa therapy in Parkinson's disease. Neurology 1989; 39 Suppl. 2: 11-9
262. Muenter MD, Sharpless NS, Tyce GM, et al. Patterns of dystonia ('I-D-I' and 'D-I-D') in response to I-dopa therapy for Parkinson's disease. Mayo Clin Proc 1977; 52: 163-74
263. Victor JF, Pollak P, Gervason CL, et al. Levodopa-induced diphasic dyskinesias improved by subcutaneous apomorphine. Mov Disord 1992; 7: 283-4
264. DurifF, Deffond D, Dordain G, et al. Apomorphine and diphasic dyskinesia. Clin Neuropharmacol1994; 17: 99-102
265. Burke RE, Falm S, Jankovic J, et al. Tardive dystonia: late onset and persistent dystonia caused by antipsychotic drugs. Neurology 1982; 32: 1335-46
266. Wojcik JD, Falk WE, Fink JS, et al. A review of 32 cases of tardive dystonia. Am J Psychiatry 1991; 148: 1055-9
267. Nasrallah HA, Churchill CM, Hamdan-Allan GA. Higher frequency of neuroleptic-induced dystonia in mania than in schizophrenia [letter]. Am J Psychiatry 1988; 145: 1455-6
268. Remington GJ, Voineskos G, Pollock B, et al. Prevalence of neuroleptic-induced dystonia in mania and schizophrenia. Am J Psychiatry 1990; 147: 1231-3
269. Khanna R, Das A, Damodaran SS. Prospective study of neuroleptic-induced dystonia in mania and schizophrenia. Am J Psychiatry 1992; 149: 511-3
270. Spina E, Sturiale V, Valvo S, et al. Prevalence of acute dystonic reactions associated with neuroleptic treatment with and without anticholinergic prophylaxis. Int Clin Psychopharmacol 1993; 8: 21-4
271. Aguilar EJ, Keshavan MS, Martinez-Quiles MD, et al. Predictors of acute dystonia in first-episode psychotic patients. Am J Psychiatry 1994; 151: 1819-21
272. Yassa R, Nair V, Dimitry R. Prevalence of tardive dystonia. Acta Psychiatr Scand 1986; 73: 629-33
273. Friedman JH, Kuchanski LT, Wagner RL. Tardive dystonia in a psychiatric hospital. J Neurol Neurosurg Psychiatry 1987; 50: 801-3
274. Sethi KD, Hess DC, Harp RJ. Prevalence of dystonia in veterans on chronic antipsychotic therapy. Mov Disord 1990; 5: 319-21
275. Chiu H, Shum P, Lau J, et al. Prevalence of tardive dyskinesia, tardive dystonia, and respiratory dyskinesia among Chinese psychiatric patients in Hong Kong. Am J Psychiatry 1992; 149: 1081-5
276. Sachdev P. Tardive and chronically recurrent OCUlogyric crises. Mov Disord 1993; 8: 93-7
Drug Safety 1997 Mar; 16 (3)

Drug-Induced Movement Disorders
277. Lu CS, Chu NS. Acute'dystonic reaction with asterixis and myoclonus following metoclopramide therapy [letter]. J Neurol Neurosurg Psychiatry 1988; 51: 1002-3
278. Perez N, Fernandez S, Legarda I, et al. Distonia aguda por neurolepticos en el tratamiento del vertigo: a prop6sito de dos casos. Acta Otorrinolaringol Esp 1992; 43: 287-9
279. Schott K, Ried S, Stevens I, et al. Neuroleptically-induced dystonia in Huntington's disease: a case report. Eur Neuro11989; 29: 39-40
280. Miller LG, Jankovic J. Sulpiride-induced tardive dystonia. Mov Disord 1990; 5: 83-4
281. Linazasoro G, Marti-Masso JF, Olasagasti B. Acute dystoniainduced by sulpiride. Clin Neuropharrnacol 1991; 14: 463-4
282. Bucci KK, Haverstick DE, Abercrombie SA. Dystonic-like reaction following cisapride therapy. J Fam Pract 1995; 40: 86-8
283. Shafrir Y, Levy Y, Steinherz R. Acute dystonic reaction due to domperidone in a infant. Harefuah 1986; 1I0: 237-8
284. Bonuccelli U, Nocchiero A, Napolitano A, et aI. Domperidoneinduced acute dystonia and polycystic ovary syndrome. Mov Disord 1991; 6: 79-81
285. Gabellini AS, Pezzoli A, De-Massis P, etal. Veralipride-induced tardive dystonia in a patient with bipolar psychosis. Ital J Neurol Sci 1992; 13: 621-3
286. Kidron D, Melamed E. Forms of dystonia in patients with Parkinson's disease. Neurology 1987; 37: 1009-11
287. McHale DM, Sage JI, Sonsalla PK, et aI. Complex dystonia of Parkinson's disease: clinical features and relation to plasma levodopa profile. Clin Neuropharmacol 1990; 13: 164-70
288. Mark MH, Sage JI. Levodopa-associated hemifacial dystonia. Mov Disord 1991; 6: 383
289. Poewe WHo Clinical aspects of motor fluctuations in Parkinson's disease. Neurology 1994; 44 Suppl. 6: S6-9
290. Leiguarda R, Merello M, Sabe L, et al. Bromocriptine-induced dystonia in patients with aphasia and hemiparesis. Neurology 199; 4: 219-22
291. Kramer MS, Marcus DJ, DiFerdinando J, et al. Atypical acute dystonia associated with trazodone treatment. J Clin Psychopharmacol1986; 6: 117-8
292. Reccoppa L, Welch WA, Ware MR. Acute dystonia and fluoxetine [letter]. J Clin Psychiatry 1990; 51: 487
293. Boylan K. Persistent dystonia associated with buspirone. Neurology 1990; 40: 1904
294. Stoukides JA, Stoukides CA. Extrapyramidal symptoms upon discontinuation offluoxetine [letter]. Am J Psychiatry 1991; 148: 126
295. Rio J, Molins A, Viguera ML, et al. Distonia aguda por fluoxetina. Med Clin (Barc) 1992; 99: 46-7
296. George MS, Trimble MR. Dystonic reaction associated with fluvoxamine [letter]. J Clin Psychopharmacol 1993; 1: 220-1
297. Dave M. Fluoxetine-associated dystonia [letter]. Am J Psychiatry 1994; 151: 149
298. Shihabuddin L, Rapport D. Sertraline and extrapyramidal side effects [letter]. Am J Psychiatry 1994; 151: 288
299. Chong SA. Fluvoxamine and mandibular dystonia [letter]. Can J Psychiatry 1995; 40: 430-1
300. Lauterbach EC. Fluoxetine, buspirone, myoclonus, and dystonia [letter]. Am J Psychiatry 1995; 152: 1697
301. Hoaken PC. An alert to extrapyramidal side-effects from SSRIs [letter]. Can J Psychiatry 1995; 40: 51
302. Ornadel D, Barnes EA, Dick DJ. Acute dystonia due to amitryptiline [letter]. J Neurol Neurosurg Psychiatry 1992; 55:414
303. Lee HK. Dystonic reactions to amitriptyline and doxepin [letter]. Am J Psychiatry 1988; 145: 649
© Adis Internatlonal Umited. All rights reserved.
197
304. Pande AC, Max P. A dystonic reaction occurring during treatment with tranylcypromine [letter]. J Clin Psychopharmacol 1989; 9: 229-30
305. Jarecke CR, Reid P1. Acute dystonic reaction-induced by a monoamine oxidase inhibitor. J Clin Psychopharmacol1990; 10: 144-5
306. Critchley EM, Phillips M. Unusual idiosyncratic reactions to carbamazepine [letter]. J Neurol Neurosurg Psychiatry 1988; 51: 1238
307. Lee Jw. Persistent dystonia associated with carbamazepine therapy: a case report. N Z Med J 1994; 107: 360-1
308. Soman P, Jain S, Rajsekbar V, et al. Dystonia: a rare manifestation of carbamazepine toxicity. Postgrad Med J 1994; 70: 54-5
309. Moss W, Ojukwu C, Chiriboga CA. Phenytoin-induced movement disorder. Unilateral presentation in a child and response to diphenhydramine. Clin Pediatr (Phila) 1994; 33: 364-8
310. Lacayo A, Mitra N. Report of a case of phenobarbital--induced dystonia [letter]. Clin Pediatr (Phila) 1992; 31: 252
311. Howrie DL, Rowley AH, Krenzelok EP. Benztropine-induced acute dystonic reaction. Ann Emerg Med 1986; 15: 594-6
312. LeWitt PA, Walters A, Hening W, et al. Persistent movement disorders-induced by buspirone. Mov Disord 1993; 8: 331-4
313. Hooker EA, Danzl DE Acute dystonic reaction due to diazepam. J Emerg Med 1988; 6: 491-3
314. Perez-Trollen JM, Modrego-Pardo PJ, Vazquez-Andre M, et al. Bromazepam-induced dystonia. Biomed Pharmacother 1992; 46: 375-6
315. Stolarek IH, Ford MJ. Acute dystonia-induced by midazolam and abolished by flumazenil [letter]. BMJ 1990; 300: 614
316. Capstick C, Checkley S, Gray J, et al. Dystonia-induced by amphetamine and haloperidol [letter]. Br J Psychiatry 1994; 165: 276
317. Thiel A, Dressler D. Dyskinesias possibly-induced by norpseudoephedrine. J Neuro11994; 241: 167-169
318. Gay CT, Ryan SG. Paroxysmal kinesigenic dystonia after methylphenidate administration. J Child Neurol 1994; 9: 45-6
319. Merab J. Acute dystonic reaction to cocaine [letter]. AmJ Med 1988;84:564
320. Choy-Kwong M, Lipton RB. Dystonia related to cocaine withdrawal: a case report and pathogenic hypothesis. Neurology 1989; 39: 996-7
321. Kumor K. Cocaine withdrawal dystonia. Neurology 1990; 40: 863-4
322. Hegarty AM, Lipton RB, Merriam AE, et al. Cocaine as a risk factor for acute dystonic reactions. Neurology 1991; 41: 1670-2
323. Farrel PE, Diehl AK. Acute dystonic reaction to crack cocaine [letter]. Ann Emerg Med 1991; 20: 322
324. Merello MJ, Nogues MA, Leiguarda RC, et aI. Dystonia and reflex sympathetic dystrophy-induced by ergotamine. Mov Disord 1991; 6: 263-4
325. Olson WL. Dystonia and reflex sympathetic dystrophy-induced by ergotamine. Mov Disord 1992; 7: 188-9
326. Garda G, Kaufman MB, Colucci RD. Dystonic reaction associated with sumatriptan [letter]. Ann Pharmacother 1994; 28: 1199
327. de Medina A, Biasini 0, Rivera A, et al. Nifedipine and myoclonic dystonia [letter]. Ann Intern Med 1986; 104: 125
328. Casteels-Van-Daele M, Eggermont E, Casaer P, et al. Acute dystonic reactions and long-lasting impaired consciousness associated with oxatomide in children [letter]. Lancet 1986; I: 1204-5
329. Santora J, Rozek S, Samie MR. Diphenhydramine-induced dystonia [letter]. Clin Pharm 1989; 8: 471
Drug Safety 1997 Mar; 16 (3)

198
330. Roila F, Donati D, Basurto C, et al. Diphenhydramine and acute dystonia [letter]. Ann Intern Med 1989; Ill: 92-3
331. Etzel JV. Diphenhydramine-induced acute dystonia. Pharmacotherapy 1994; 14: 492-6
332. Romisher S, Felter R, Dougherty J. Tagamet-induced acute dystonia. Ann Emerg Med 1987; 16: 1162-4
333. McCann UD, Penetar DM, Belenky G. Acute dystonic reaction in normal humans caused by catecholamine depletion. Clin Neuropharmacol1990; 13: 565-568
334. Shafrir Y, Levy Y, Beharab A, et al. Acute dystonic reaction to bethanechol: a direct acetylcholine receptor agonist. Dev Med Child Neuro11986; 28: 646-8
335. Miller LG, Jankovic J. Persistent dystonia possibly-induced by flecainide. Mov Disord 1992; 7: 62-3
336. Achumba n, Ette EI, Thomas WO, et al. Chloroquine-induced acute dystonic reactions in the presence of metronidazole. Drug Intell Clin Pharm 1988; 22: 308-10
337. Ascher DP, Delaney RA. Acute dystonia from etoposide. Drug Intell Clin Pharm 1988; 22: 41-2
338. Mets B. Acute dystonia after alfentanil in untreated Parkinson's disease [letter]. Anesth Analg 1991; 72: 557-8
339. Lamberti JS, Bellnier T. Clozapine and tardive dystonia. J Nerv Ment Dis 1993; 181: 137-8
340. Kastrup 0, Gastpar M, Schwarz M. Acute dystonia due to c1ozapine. J Neurol Neurosurg Psychiatry 1994; 57: 119
341. Thomas P, Lalaux N, Vaiva G, et al. Dose-dependent stuttering and dystonia in a patient taking c10zapine [letter]. Am J Psychiatry 1994; 151: 1096
342. Owens DG. Extrapyramidal side effects and tolerability of risperidone: a review. J Clin Psychiatry 1994; 55 Suppl.: 29-35
343. Dickson R, Williams R, Dalby JT. Dystonic reaction and relapse with c10zapine discontinuation and risperidone intiation [letter]. Can J Psychiatry 1994; 39: 184
344. Radford JM, Brown TM, Borison RL. Unexpected dystonia while changing from c10zapine to risperidone [letter]. J Clin Psychopharmacol 1995; 15: 225-6
345. Worrall R, Wilson A, Cullen M. Dystonia and drug-induced hepatitis in a patient treated with c10zapine [letter]. Am J Psychiatry 1995; 152: 647-8
346. Lupu V, Gheragosian G. Reactie distonica severa in intoxicatia acuta cu Torecan. Rev Pediatr Obstet Ginecol Pediatr 1989; 38: 277-81
347. Jimenez-Jimenez FJ, Vazquez A, Garcfa-Ruiz P, et al. Chronic hemidystonia following acute dystonic reaction to thiethylperazine [letter]. J Neurol Neurosurg Psychiatry 1991; 54: 562
348. Shimada J, Akama Y, Tase C, et al. Problems of epidural droperidol administration. Masui 1994; 43: 1248-50
349. Gimenez-Roldan S, Mateo D, Bartolome P. Tardive dystonia and severe tardive dyskinesia. Acta Psychiatr Scand 1985; 71 : 488-94
350. Kang UJ, Burke RE, Fahn S. Natural history and treatment of tardive dystonia. Mov Disord 1986; I: 193-208
351. Gardos GG, Cole JO, Salomon M, et al. Clinical forms of severe tardive dyskinesia. Am J Psychiatry 1987; 144: 895-902
352. Addonizio G, Alexopoulos GS. Drug-induced dystonia in young and elderly patients. Am J Psychiatry 1988; 145: 869-71
353. Yassa R, Nair V, Iskandar H. A comparison of severe tardive dystonia and severe tardive dyskinesia. Acta Psychiatr Scand 1989; 80: 155-9
354. Bosch MF, Ludin HP. Apomorphin als adjuvante behandlung beim idiopathischen parkinsonsyndrom. Schweiz Arch Neurol Psychiatr 1994; 145: 8-13
355. Poewe WH, Lees AJ. The pharmacology of foot dystonia in parkinsonism. Clin Neuropharmacol1987; 10: 47-56
© Adis International Umited. All rights reserved.
Jimenez-Jimenez et al.
356. Pacchetti C, Albani G, Martignoni E, et al. 'Off' painful dystonia in Parkinson's disease treated with botulinum toxin. Mov Disord 1995; 10: 333-6
357. Tolosa E, Alom J, Marti MJ. Drug-induced dyskinesias. In: Jankovic J, Tolosa E, editors. Parkinson's disease and movement disorders. 2nd ed. Baltimore: William & Wilkins, 1993: 375-97
358. Faurbye A, Rasch PJ, Peterson PB, et al. Neurological symptoms in pharmacotherapy of psychoses. Acta Psychiatr Scand 1964; 40: 10-27
359. Llau ME, Senard JM, Rascol 0, et al. Mouvements anormaux d'origine medicamenteuse: l'experience d'un centre de pharmacovigilance sur cinq ans. Therapie 1995; 50: 425-7
360. Kolakowska T, Williams AO, Ardern M, et al. Tardive dyskinesia in schizophrenics under 60 years of age. Bioi Psychiatry 1986; 21: 161-9
361. Morgenstern H, Glazer WM, Gibowski LD, et al. Predictors of tardive dyskinesia: results of a cross-sectional study in an outpatient population. J Chronic Dis 1987; 40: 319-27
362. Gureje 0. Tardive dyskinesia in schizophrenics. Prevalence, distribution and relationship to neurological 'soft' signs in Nigerian patients. Acta Psychiatr Scand 1987; 76: 523-8
363. Chouinard G, Annable L, Ross-Chouinard A, et al. A 5-year prospective longitudinal study of tardive dyskinesia: factors predicting appearance of new cases. J Clin Psychopharmacol 1988; 8 (4 Suppl.): 21S-6S
364. Bourgeois M. Les dyskinesies tardives des neuroleptiques en France. Encephale 1988; 14 Spec No: 195-201
365. Moussaoui D, Douki S, Bentounsi B, et al. Epidemiologie des dyskinesies tardives au Maghreb. Encephale 1988; 14 Spec No: 203-8
366. Ko GN, Zhang LD, Yan WW, et al. The Shanghai 800: prevalence of tardive dyskinesia in a Chinese psychiatric hospital. Am J Psychiatry 1989; 146: 387-9
367. Yassa R, Nair NP, Iskander H, et al. Factors in the development of severe forms of tardive dyskinesia. Am J Psychiatry 1990; 147: 1156-63
368. Altamura AC, Cavallaro R, Regazzetti MG. Prevalence and risk factors for tardive dyskinesia: a study in an Italian population of chronic schizophrenics. Eur Arch Psychiatry Neurol Sci 1990; 240: 9-12
369. Tan CH, Tay LK. Tardive dyskinesia in elderly psychiatric patients in Singapore. Aust N Z J Psychiatry 1991; 25: 119-22
370. Inada T, Ohnishi K, Kamisada M, et al. A prospective study of tardive dyskinesia in Japan. Eur Arch Psychiatry Clin Neurosci 1991; 240: 250-4
371. Sramek J, Roy S, Ahrens T, et al. Prevalence of tardive dyskinesia among three ethnic groups of chronic psychiatric patients. Hosp Community Psychiatry 1991; 42: 590-2
372. Richardson MA, Haugland G, Craig TJ. Neuroleptic use, parkinsonian symptoms, tardive dyskinesia, and associated factors in child and adolescent psychiatric patients. Am J Psychiatry 1991; 148: 1322-8
373. Saltz BL, Woerner MG, Kane JM, et al. Prospective study of tardive dyskinesia incidence in the elderly. JAMA 1991; 266: 2402-6
374. Yassa R, Nastase C, Dupont D, et al. Tardive dyskinesia in elderly psychiatric patients: a 5-year study. Am J Psychiatry 1992; 149: 1206-11
375. Sweet RA, Mulsant BH, Rifai AH, et al. Dyskinesia and neuroleptic exposure in elderly psychiatric inpatients. J Geriatr Psychiatry NeuroI1992; 5: 156-61
Drug Safely 1997 Mar; 16 (3)

Drug-Induced Movement Disorders
376. Koshino Y, Madokoro S, Ito T, et al. A survey of tardive dyskinesia in psychiatric inpatients in Japan. Clin Neuropharmacol 1992; 15: 34-43
377. McCreadie RG. The Nithsdale schizophrenia surveys. An overview. Soc Psychiatry Psychiatr EpidemioI1992; 27: 40-5
378. Harris MJ, Panton D, Caligiuri MP, et al. High incidence of tardive dyskinesia in older outpatients on low doses of neuroleptics. Psychopharmacol Bull 1992; 28: 87-92
379. Chiu HF, Wing YK, Kwong PK, et al. Prevalence of tardive dyskinesia in samples of elderly people in Hong Kong. Acta Psychiatr Scand 1993; 87: 266-8
380. Jeste DV, Caligiuri MP. Tardive dyskinesia. Schizophr Bull 1993; 19: 303-15
381. Sweet RA, Mulsant BH, Gupta B, et al. Duration of neuroleptic treatment and prevalence of tardive dyskinesia in late life. Arch Gen Psychiatry 1995; 52: 478-86
382. Miller CH, Simioni I, Oberbauer H, et al. Tardive dyskinesia prevalence rates during a ten-year follow-up. J Nerv Ment Dis 1995; 183: 404-7
383. Dorevitch A, Meretyk I, Umansky Y, et al. Antipsychotic drugs and tardive dyskinesia: preliminary results in an adolescent psychiatric ward. J Clin Pharm Ther 1995; 20: 63-5
384. Jeste DV, Caligiuri MP, Paulsen JS, et al. Risk of tardive dyskinesia in older patients. A prospective longitudinal study of 266 outpatients. Arch Gen Psychiatry 1995; 52: 756-65
385. Ahlfors UG, Rimon R, AppeIberg B, et al. Remoxipride and haloperidol in schizophrenia: a double-blind multi centre study. Acta Psychiatr Scand 1990; 358 Suppl.: 99-103
386. Walinder J, Holm AC. Experiences oflong-term treatment with remoxipride: efficacy and tolerability. Acta Psychiatr Scand Suppl 1990; 358: 158-63
387. Kane JM, Woerner MG, Pollack S, et al. Does c\ozapine cause tardive dyskinesia? J Clin Psychiatry 1993; 54: 327-30
388. Tamminga CA, Thaker GK, Moran M, et al. Clozapine in tardive dyskinesia: observations from human and animal model studies. J Clin Psychiatry 1994; 55 Suppl. B: 102-6
389. Dave N. Clozapine-related tardive dyskinesia. Bioi Psychiatry 1994; 35: 886-7
390. Addington DE, Toews JA, Addington JM. Risperidone and tardive dyskinesia: a case report [letter]. J Clin Psychiatry 1995; 56: 484-5
391. Beuc\air L, Fontaine R. Tardive dyskinesia associated with metoc\opramide. Can Med Assoc J 1986; 134: 613-4
392. Lazzara RR, Stoudemire A, Manning D, et al. Metoc\opramideinduced tardive dyskinesia: a case report. Gen Hosp Psychiatry 1986; 8: 107-9
393. Patel M, Louis S. Long-term neurologic complications of me toc\opramide [letter]. N Y State J Med 1986; 86: 210
394. Breitbart W. Tardive dyskinesia associated with high-dose intravenous metoc\opramide [letter]. N Engl J Med 1986; 315: 518-9
395. Mahler Jr JC, Brown RP. More on metoclopramide and tardive dyskinesia [letter]. N Engl J Med 1987; 316: 412-3
396. Sewell DD, Jeste DY. Metoc\opramide-associated tardive dyskinesia. An analysis of 67 cases. Arch Fam Med 1992; 1: 271-8
397. Sewell DD, Yoshinobu BH, Caligiuri MP, et al. Metoclopramide-associated tardive dyskinesia in hemodialysis patients with diabetes mellitus. Two case reports. Gen Hosp Psychiatry 1992; 14: 416-9
398. Putnam PE, Orenstein SR, Wessel HB, et al. Tardive dyskinesia associated with use of metoc\opramide in a child. J Pediatr 1992; 121: 983-5
© Adis Internalional limited. All rights reserved.
199
399. Sewell DD, Kodsi AB, Caligiuri MP, et al. Metoc\opramide and tardive dyskinesia. Bioi Psychiatry 1994; 36: 630-2
400. Robinson D, Omar SJ, Dangel C, et al. Metoc\opramide-induced extrapyramidal symptoms in a diabetic patient [letter]. JAm Geriatr Soc 1994; 42: 1307-8
401. Macucci M, Dotti MT, Federico A. Familial acute dystonicdyskinetic syndrome with dominant inheritance after use of antidopaminergic antiemetic drugs. Mov Disord 1995; 10: 528-9
402. Assmann VC, Perquin WV, Touw DJ. Extrapyramidal movement disorders following the use of flunarizine. Ned Tijdschr Geneeskd 1988; 12: 1940-3
403. Sandyk R. Tardive dyskinesia-induced by sulpiride in a patient with hypothyroidism. Clin Neuropharmacol1986; 9: 100-1
404. Achiron A, Zoldan Y, Melamed E. Tardive dyskinesia-induced by sulpiride. Clin Neuropharmacol1990; 13: 248-52
405. Masmoudi K, Decocq G, Chetaille E, et al. Troubles extrapyramidaux induits par Ie veralipride (Agreal). A propos de cinq observations. Therapie 1995; 50: 451-4
406. Huang Cc. Persistent tardive dyskinesia associated with amoxapine therapy [letter]. Am J Psychiatry 1986; 143: 1069-70
407. Huang CC. Persistent tardive dyskinesia associated with amoxapine therapy: two case reports. Hillside J Clin Psychiatry 1986; 8: 209-13
408. Gangat AE, Luiz HA, Kajee AH, et al. TricyC\ic-induced acute tardive dyskinesia: a case report [letter]. S Afr Med J 1987; 71: 729
409. Yassa R, Camille Y, Belzile L. Tardive dyskinesia in the course of antidepressant therapy: a prevalence study and review of the literature. J Clin Psychopharmacol 1987; 7: 243-6
410. Otani K, Kaneko S, Fukushima Y, et al. Involuntary movements associated with mianserin treatment: a case report [letter]. Br J Psychiatry 1989; 154: 113-4
411. Golden RN, Miller H, Evans DL. Trimipramine and dopamine receptor blockade [letter]. J Clin Psychiatry 1989; 50: 392-3
412. Katz SE. Tardive dyskinesia associated with molindone treatment [letter]. Am J Psychiatry 1990; 147: 124-5
413. Sparring-Bjorksten K, Walinder J. Does mianserin induce involuntary movements in brain damaged patients? Int Clin Psychopharmacol 1993;8: 203-4
414. Gersten SP. Tardive dyskinesia-like syndromes with clomipramine [letter]. Am J Psychiatry 1993; 150: 165-6
415. Budman CL, Bruun RD. Persistent dyskinesia in a patient receiving fluoxetine [letter]. Am J Psychiatry 1991; 148: 1403
416. al-Adwani A. Brain damage and tardive dyskinesia [letter]. Br J Psychiatry 1995; 167: 410-1
417. Wils V. Extrapyramidal symptoms in a patient treated with fluvoxamine [letter]. J Neurol Neurosurg Psychiatry 1992; 55: 330-1
418. Arya DK, Szabadi E. DyskineSia associated with fluvoxamine. J Clin Psychopharmacol 1993; 13: 365-6
419. Sternbach H, Jordan S. Lithium-associated tardive dyskinesia. J Clin Psychopharmacol1990; 10: 143-4
420. Lazarus A. Tardive dyskinesia-like syndrome associated with lithium and carbamazepine. J Clin Psychopharmacol 1994; 14: 146-7
421. Ghadirian AM, Annable L, Belanger MC, et aI. A cross-sectional study of parkinsonism and tardive dyskinesia in lithium-treated affective disordered patients. J Clin Psychiatry 1996; 57: 22-8
422. Strauss A. Oral dyskinesia associated with buspirone use in an elderly woman [letter]. J Clin Psychiatry 1988; 49: 322-3
423. Simpson GM, Singh H. Buspirone and dyskinesia [letter]. J Clin Psychiatry 1988; 49: 50
Drug Safety 1997 Mar: 16 (3)

200
424. Lydiard RB. Buspirone revisited [letter]. 1 Clin Psychiatry 1989;50:308
425. Rock NL. Possible adverse effects of buspirone when used with other psychotropic drugs. 1 Clin Psychopharmacol 1990; 10: 80-1
426. Sandyk R. Orofacial dyskinesias associated with lorazepam therapy. Clin Pharm 1986; 5: 419-21
427. Sexson WR, Thigpen 1, Stajich GY. Stereotypic movements after lorazepam administration in premature neonates: a series and review of the literature. 1 Perinatol1995; 15: 146-149
428. Dooley 1, Camfield P, Buckley D, et al. Methsuximide-induced movement disorder. Pediatrics 1991; 88: 1291-2
429. Hauser RA, Olanow CWo Orobuccal dyskinesia associated with trihexyphenidyl therapy in a patient with Parkinson's disease. Mov Disord 1993; 8: 512-4
430. Linazasoro G. Anticholinergics and dyskinesia [letter]. Mov Disord 1994; 9: 689
431. Morisy L, Platt D. Hazards of high-dose meperidine [letter]. lAMA 1986; 255: 467-8
432. Merriam AE. Pemoline-induced abnormal involuntary movements. 1 Clin Psychopharmacol 1990; 10: 302-3
433. Schuller DE, Turkewitz D. Adverse effects of antihistamines. Postgrad Med 1986; 79: 75-86
434. Micheli F, Gatto E, Gene R, et al. Clenbuterol-induced tardive dyskinesia. Clin Neuropharmacol1991; 14: 427-31
435. Ramsay FM, Millard PH. Tardive dyskinesia in the elderly. Age Ageing 1986; 15: 145-50
436. Morgenstern H, Glazer WM, Niedzwiecki D, et al. The impact of neuroleptic medication on tardive dyskinesia: a meta-analysis of published studies. Am 1 Public Health 1987; 77: 717-24
437. Wolf ME, DeWolfe AS, Mosnaim AD. Risk factors for tardive dyskinesia according to primary psychiatric diagnosis. Hillside 1 Clin Psychiatry 1987; 9: 3-11
438. Yassa R, Jeste DY. Gender differences in tardive dyskinesia: a critical review of the literature. Schizophr Bull 1992; 18: 701-15
439. Muscettola G, Pampallona S, Barbato G, et al. Persistent tardive dyskinesia: demographic and pharmacological risk factors. Acta Psychiatr Scand 1993; 87: 29-36
440. Ganzini L, Heintz RT, Hoffman WF, et al. The prevalence of tardive dyskinesia in neuroleptic-treated diabetics. A controlled study. Arch Gen Psychiatry 1991; 48: 259-63
441. Ganzini L, Casey DE, Hoffman WF, et al. Tardive dyskinesia and diabetes mellitus. Psychopharmacol Bull 1992; 28: 281-6
442. Woerner MG, Saltz BL, Kane 1M, et al. Diabetes and development of tardive dyskinesia. Am 1 Psychiatry 1993; 150: 966-88
443. Pourcher E, Baruch P, Bouchard RH, et al. Neuroleptic associated tardive dyskinesias in young people with psychoses. Br 1 Psychiatry 1995; 166: 768-72
444. Ueyama K, Fukuzako H, Takeuchi K, et al. Brain atrophy and intellectual impairment in tardive dyskinesia. Ipn 1 Psychiatry Neuro11993; 47: 99-104
445. Dinan TG, Kohen D. Tardive dyskinesia in bipolar affective disorder: relationship to lithium therapy. Br J Psychiatry 1989; 155: 55-7
446. Waddington lL, Youssef HA. An unusual cluster of tardive dyskinesia in schizophrenia: association with cognitive dysfunction and negative symptoms. Am 1 Psychiatry 1986; 143: 1162-5
447. Dixon L, Weiden PI, Haas G, et al. Increased tardive dyskinesia in alcohol-abusing schizophrenic patients. Compr Psychiatry 1992; 33: 121-2
448. Yassa R, Nair V, Schwartz G. Early versus late onset psychosis and tardive dyskinesia. Bioi Psychiatry 1986; 21: 1291-7
© Adis International Limited. All rights reserved.
Jimenez-Jimenez et al.
449. Yassa R. Tardive dyskinesia and anticholinergic drugs. A critical review of the literature. Encephale 1988; 14 Spec No: 233-9
450. Cavallaro R, Smeraldi E. Antipsychotic-induced tardive dyskinesia: recognition, prevention and management. CNS Drugs 1995; 4: 278-293
451. Obeso lA, Artieda 1, Marsden CD. Different clinical presentations of myoclonus. In: lankovic 1, Tolosa E, editors. Parkinson's disease and movement disorders, 2nd ed. Baltimore: Williams & Wilkins: 315-28
452. Forstl H, Pohlmann-Eden B, Rothenberger A. Veranderungen somatosensibel evozierter Potentiale bei pharmakogener Myoklonie. Nervenarzt 1992; 63: 359-62
453. Brogmus KE, Lesch A. Psychopharmakainduzierte Myoklonien. Psychiatr Prax 1995; 22: 77-9
454. Drouet A, Valance J. Myoclonies de repos et d'action induites par la piperazine. Rev Med Interne 1994; 15: 364-5
455. Tominaga H, Fukuzako H, Izumi K, et al. Tardive myoclonus [letter]. Lancet 1987; I: 322
456. Fukuzako H, Tominaga H, Izumi K, et al. Postural myoclonus associated with long-term administration of neuroleptics in schizophrenic patients. Bioi Psychiatry 1990; 27: 1116-26
457. Little IT, lankovic 1. Tardive myoclonus. Mov Disord 1987; 2: 307-11
458. Noble 1, Matthew H. Acute poisoning by tricyclic antidepressants: clinical features and management of 100 patients. Clin Toxicol 1969; 2: 403-21
459. Burks IS, Walker JE, Rumack BH, et al. Tricyclic antidepressant poisoning; reversal of coma, choreoathetosis and myoclonus by physostigmine. lAMA 1974; 230: 1405-7
460. Darcourt G, Fadeuilhe A, Lavagna 1, et al. Trois cas de myoclonies d'action au cors de traitements par l'imipramine et l'amitriptyline. Rev Neurol (Paris) 1970; 122: 141-2
461. Lippmann S, Moskovitz R, O'Tuama L. Tricyclic-induced myoclonus [letter]. Am 1 Psychiatry 1977; 134: 90-1
462. Garvey MJ, Tollefson GD. Occurrence of myoclonus in patients treated with cyclic antidepressants. Arch Gen Psychiatry 1987; 44: 269-72
463. Casas M, Garcia-Ribera C, Alvarez E, et al. Myoclonic movements as a side-effect of treatment with therapeutic doses of clomipramine. Int Clin Psychopharmacol 1987; 2: 333-6
464. Devanand DP, Sackeim HA, Brown RP. Myoclonus during combined tricyclic antidepressant and lithium treatment. 1 Clin Psychopharmacol 1988; 8: 446-7
465. Fukuzako H, Hokazono Y, Tominaga H, et al. Jerk-locked averaging and somatosensory evoked potential in tricyclicinduced myoclonus: a case report. Ipn 1 Psychiatry Neurol 1989; 43: 645-9
466. Forstl H, Pohlmann-Eden B. Amplitudes of somatosensory evoked potentials reflect cortical hyperexcitability in antidepressant-induced myoclonus. Neurology 1990; 40: 924-6
467. Patterson IE Myoclonus caused by a tricyclic antidepressant. South Med 1 1990; 83: 463-5
468. Lejoyeux M, Ades 1, Rouillon E Myoclonies chez les patients traites par antidepresseurs tricycliques. Evaluation prospective [letter]. Presse Med 1994; 23: 447
469. Black Kl, Kilzieh N. Severe imipramine-induced myoclonus in a patient with psychotic bipolar depression, catatonia, and schizencephaly. Ann Clin Psychiatry 1994; 6: 45-9
470. Patel HC, Bruza D, Yeragani Y. Myoclonus with trazodone [letter].l Clin Psychopharmacol 1988; 8: 152
471. Feighner IP, Boyer WF, Tyler DL, et al. Adverse consequences of fluoxetine-MAOI combination therapy. 1 Clin Psychiatry 1990; 51: 222-5
Drug Safety 1997 Mar; 16 (3)

Drug-Induced Movement Disorders
472. Goldberg RJ, Huk M. Serotonin syndrome from trazodone and buspirone [letter]. Psychosomatics 1992; 33: 235-6
473. Jahr JS, Pisto JD, Gitlin MC, et al. The serotonin syndrome in a patient receiving sertraline after an ankle block. Anesth Analg 1994; 79: 189-91
474. Lauterbach EC. Reversible intermittent rhythmic myoclonus with fluoxetine in presumed Pick's disease. Mov Disord 1994; 9: 343-6
475. White PD. Myoclonus and episodic delirium associated with phenelzine: a case report [letter]. J Clin Psychiatry 1987; 48: 340-1
476. Naylor MW, Grunhaus L, Cameron O. Myoclonic seizures after abrupt withdrawal from phenelzine and alprazolam. J Nerv Ment Dis 1987; 175: 111-4
477. Askenasy JJ, Yahr MD. Is monoamine oxidase inhibitorinduced myoclonus serotoninergically mediated? J Neural Transm 1988; 72: 67-76
478. Klawans HL, Goetz C, Bergen D. Levodopa-induced myoclonus. Arch Neurol 1975; 32: 331-4
479. Hirschorn KA, Greenberg HS. Successful treatment of levodopa-induced myoclonus and levodopa withdrawal-induced neuroleptic malignant syndrome. A case report. Clin Neuropharmacol 1988; II: 278-81
480. Glantz R, Weiner WJ, Goetz CG, et al. Drug-induced asterixis in Parkinson's disease. Neurology 1982; 2: 553-5
481. Goule JP, Husson A, Fondimare A, et al. Encephalopatie aux sels insolubles de bismuth [letter]. Nouv Presse Med 1975; 4: 1366
482. Buge A, Rancurel G, Dechy H. Encephalopathies myocloniques bismuthiques. Formes evolutives, complications tardives, durables ou definitives. A propos de 41 cases. Rev Neurol (Paris) 1977; 133: 401-15
483. Nogue S, Mas A, Pares A, et al. Encefalopatia mioclonica y convulsiva por bismuto. Utilidad del tratamiento con dimercaprol. Med Clin (Bare) 1985; 84: 530-2
484. Vidailhet M, Le TH, Wechsler B, et al. L'encephalopathie au bismuth n'a pas disparu ... [letter]. Presse Med 1987; 16: 1054
485. Molina JA, Calandre L, Bermejo F. Myoclonic encephalopathy due to bismuth salts: treatment with dimercaprol and analysis ofCSF transmitters. Acta Neurol Scand 1989; 79: 200-3
486. Gomez-Jimenez J, Alvarez J, Boada-Rovira M, et al. Encelafopatia mioclonica por bismuto [letter]. Rev Clin Esp 1989; 184: 212
487. Molina JA, Calandre L, Bermejo F, et al. Encefalopatia mioclonica por sales de bismuto. Eficacia del tratamiento con dimercaprol. Med Clin (Barc) 1989; 93: 20-2
488. Mendelowitz PC, Hoffman RS, Weber S. Bismuth absorption and myoclonic encephalopathy during bismuth subsalicylate therapy [letter]. Ann Intern Med 1990; 112: 140-1
489. Nogue-Xarau S, Sanz-Gallen P. Encefalopatia mioclonica por bismuto [letter]. Rev Clin Esp 1990; 186: 145
490. Jungreis AC, Schaumburg HH. Encephalopathy from abuse of bismuth subsalicylate (Pepto-Bismol). Neurology 1993; 43: 1265
491. Gordon MF, Abrams RI, Rubin DB, et al. Bismuth subsalicylate toxicity as a cause of prolonged encephalopathy with myoclonus. Mov Disord 1995; 10: 220-2
492. Klawans HL, Carvey PM, Tanner CM, et al. Drug-induced myoclonus. Adv Neuro11986; 43: 251-64
493. Aguglia U, Zappia M, Quattrone A. Carbamazepine-induced nonepileptic myoclonus in a child with benign epilepsy. Epilepsia 1987; 28: 515-8
© Adis International Umited. All rights reserved.
201
494. Dhuna A, Pascual-Leone A, Talwar D. Exacerbation of partial seizures and onset of nonepileptic myoclonus with carbamazepine. Epilepsia 1991; 2: 275-8
495. AgugJia U, Gambardella A, Zappia M, et al. Negative myoclonus during valproate-related stupor. Neurophysiological evidence of a cortical non-epileptic origin. Electroencepha10gr Clin Neurophysiol1995; 94: 103-8
496. Lemus CZ, Lieberman JA, Johns CA. Myoclonus during treatment with clozapine and lithium: the role of serotonin. Hillside J Clin Psychiatry 1989; II: 127-30
497. Rosen PD, Stevens R. Action myoclonus in lithium toxicity. Ann Neuro11983; 13: 221-2
498. Julius SC, Brenner RP. Myoclonic seizures with lithium. Bioi Psychiatry 1987; 22: 1184-90
499. Prettyman R. Lithium neurotoxicity at subtherapeutic serum levels [letter]. Br J Psychiatry 1994; 164: 123
500. Glavina MJ, Robertshaw R. Myoclonic spasms following intrathecal morphine. Anaesthesia 1988; 43: 389-90
501. Potter JM, Reid DB, Shaw RJ, et al. Myoclonus associated with treatment with high doses of morphine: the role of supplemental drugs. BMJ 1989; 299: 150-3
502. Jayawardena B, Hill DJ. Myoclonic spasms after epidural diamorphine infusion. Anaesthesia 1991; 46: 473-4
503. De Conno F, Caraceni A, Martini C, et al. Hyperalgesia and myoclonus with intrathecal infusion of high-dose morphine. Pain 1991; 47: 337-9
504. Franco ML, Berro MJ, Saez JM, et al. Mioclonias de miembros inferiores como complicacion de la morfina espinal. Rev Esp Anestesiol Reanim 1992; 39: 192-3
505. Sjogren P, Jonsson T, Jensen NH, et al. Hyperalgesia and myoclonus in terminal cancer patients treated with continuous intravenous morphine. Pain 1993; 55: 93-7
506. Cartwright PD, Hesse C, Jackson AO. Myoclonic spasms following intrathecal diamorphine. J Pain Symptom Manage 1993; 8: 492-5
507. de-Armendi AJ, Fahey M, Ryan JF. Morphine-induced myoclonic movements in a pediatric pain patient. Anesth Analg 1993; 77: 191-2
508. Bowdle TA, Rooke GA. Postoperative myoclonus and rigidity after anesthesia with opioids. Anesth Analg 1994; 78: 783-6
509. Kloke M, Bingel U, Seeber S. Complications of spinal opioid therapy: myoclonus, spastic muscle tone and spinal jerking. Support Care Cancer 1994; 2: 249-52
510. Jacobsen LS, Olsen AK, Sjogren P, et al. Morphine-induced hyperalgesia, allodynia and myoclonus: new side-effects of morphine?UgeskrLaeger 1995; 157: 3307-10
511. Meloni G, Raucci U, Pinto RM, et al. Pretransplant conditioning with busulfan and cyclophosphamide in acute leukemia patients: neurological and electroencephalographic prospective study. Ann Oncol 1992; 3: 145-8
512. Martin M, Diaz-Rubio E, Casado A, et al. Prednimustine-induced myoclonus: a report of three cases. Acta Oncol 1994; 33: 81-2
513. Ammenti A, Reither B, Muller-Wiefel DE. Chlorambucil neurotoxicity: report of two cases. Helv Paediatr Acta 1980; 35: 281-7
514. Byrne TN Jr, Moseley TAE lll, Finer MA. Myoclonic seizures following chlorambucil overdose. Ann Neuro11981; 9: 191-4
515. LaDelfa I, Bayer N, Myers R, et al. Chlorambucil-induced myoclonic seizures in an adult. J Clin Onco11985; 3: 1691-2
516. Buchman AS, Bennett DA, Goetz CG. Bromocriptine-induced myoclonus. Neurology 1987; 37: 885
Drug Safety 1997 Mar: 16 (3)

202
517. Ritchie EC, Bridenbaugh RH, Jabbari B. Acute generalized myoclonus following buspirone administration. J Clin Psychiatry 1988; 49: 242-3
518. Lee DS, Wong HA, Knoppert DC. Myoclonus associated with lorazepam therapy in very-Iow-birth-weight infants. Bioi Neonate 1994; 66: 311-5
519. Magny JF, d'Allest AM, Nedelcoux H, et al. Midazolam and myoclonus in neonate. Eur J Pediatr 1994; 15: 389-90
520. Madigand M, Dien J, Pavin G, et al. Encephalopathie myoclonique probablement imputable 11 la propafenone [letter]. Presse Med 1988; 17: 538
521. Jeandel C, Bannwarth B, Trechot P, et al. Encephalopathie myoclonique 11 la propafenone. Therapie 1990; 45: 161-2
522. Chua TP, Farrell T, Lipkin DP. Myoclonus associated with propafenone [letter]. BMJ 1994; 308: 113
523. Ghika J, Goy 11, Naegeli C, et al. Acute reversible ataxomyoclonic encephalopathy with flecainide therapy. Schweiz Arch Neurol Psychiatr 1994; 145: 4-6
524. Jeret JS, Somasundaram M, Asaikar S. Diltiazem-induced myoclonus. N Y State J Med 1992; 92: 447-8
525. Pedro-Botet ML, Bonal J, Caralps A. Nifedipine and myoclonic disorders [letter]. Nephron 1989; 51: 281
526. Lucas C, Soetaert G, Leys D, et al. Myoclonies au cours d'un traitement par buflomedil. Acta Clin Belg 1989; 44: 360-1
527. Uchihara T, Tsukagoshi H. Myoclonic activity associated with cefmetazole, with a review of neurotoxicity of cephalosporins. Clin Neurol Neurosurg 1988; 90: 369-71
528. New PS, Wells CEo Cerebral toxicity associated with massive intravenous penicillin therapy. Neurology 1965; 15: 1052-8
529. Cohill DF, Pezzi PJ, Greenberg SR, Frobese AS. Central nervous system toxicity secondary to massive doses of penicillin 'G' in the treatment of overwhelming infections. Am J Med Sci 1967; 254: 692-4
530. Lerner PI, Smith N, Weinstein L. Penicillin neurotoxicity. Ann NY Acad Sci 1967; 145: 310-8
531. Conway N, Beck E, Somerville J. Penicillin encephalopathy. Postgrad Med J 1968; 44: 891-7
532. Durand JM, Telle H, Quiles N, et al. Syndrome confusionnel, myoclonies et traitement par la pefloxacine. Ann Med Interne (Paris) 1993; 144: 495-6
533. Yagi S, Moriya 0, Nakajima M, et al. A case of tuberculous pleurisy associated with myoclonus and Quincke's edema due to isoniazid and isoniazid sodium methanesulfonate. Kekkaku 1989;64:407-12
534. Fukuda T. Veratramine-induced myoclonus. Seishin Shinkeigaku Zasshi 1990; 92: 865-9
535. Bouly A, Nathan N, Feiss P. Propofol in myotonic dystrophy [letter]. Anaesthesia 1991; 46: 705
536. Hughes NJ, Lyons JB. Prolonged myoclonus and meningism following propofol. Can J Anaesth 1995; 42: 744-6
537. Mayeux R, Albert M, Jenike M. Physostigmine-induced myoclonus in Alzheimer's disease. Neurology. 1987; 7: 345-6
538. Reutens DC, Stewart-Wynne EG. Norpethidine-induced myoclonus in a patient with renal failure [letter]. J Neurol Neurosurg Psychiatry 1989; 52: 1450-1
539. Sica DA, Comstock TJ. Pseudoephedrine accumulation in renal failure. Am J Med Sci 1989; 298: 261-3
540. Korthals JK, Gieron-Korthals MA. Eosinophilia-myalgia syndrome with myoclonic jerks. J Fla Med Assoc 1990; 77: 1031-3
541. Berman I, Zalma A, Durand CJ, et al. Clozapine-induced myoclonic jerks and drop attacks [letter]. J Clin Psychiatry 1992; 53: 329-30
© Adis Internalional Limited. All rights reserved.
Jimenez-Jimenez et al.
542. Malow BA, Reese KB, Sato S, et al. Spectrum of EEG abnormalities during clozapine treatment. Electroencephalogr Clin Neurophysiol1994; 91: 205-11
543. Meltzer HY, Ranjan R. Valproic acid treatment of clozapine-induced myoclonus [letter]. Am J Psychiatry 1994; 151: 1246-7
544. Bak TH, Bauer M, Schaub RT, et al. Myoclonus in patients treated with clozapine: a case series. J Clin Psychiatry 1995; 56: 418-22
545. Eisele G. Neurologic complications of metoclopramide therapy [letter]. N Y State J Med 1988; 88: 332
546. Klawans HL, Falk DK, Nausieda PA, et al. Gilles de la Tourette syndrome after long-term chlorpromazine therapy. Neurology 1978; 28: 1064-8
547. De Veaugh-Geiss J. Tardive Tourette syndrome. Neurology 1980; 30: 562-3
548. Stahl SM. Tardive Tourette syndrome in an autistic patient after long-term neuroleptic administration [letter]. Am J Psychiatry 1980; 30: 562-3
549. Fog R, Pakkenberg H. Theoretical and clinical aspects of the Tourette syndrome (chronic multiple tic). J Neura! Transm 1980; 16 Suppl.: 211-5
550. Seeman MV, Patel J, Pyke J. Tardive dyskinesia with Tourettelike syndrome [letter]. J Clin Psychiatry 1981; 42: 357-8
551. Singer DW. Transient Gilles de la Tourette syndrome after chronic neuroleptic withdrawal. Dev Med Child Neuro11981; 23: 518-30
552. Mueller J, AminoffMA. Tourette-like syndrome after long-term neuroleptic drug treatment. Br J Psychiatry 1982; 141: 191-3
553. Klawans HL, Nausieda PA, Goetz CC, et al. Tourette-like symptoms following chronic neuroleptic therapy. Adv Neurol 1982; 35: 415-8
554. Jeste DV, Cutler NR, Kaufmann CA. Low-dose apomorphine and bromocriptine in neuroleptic-induced movement disorders. Bioi Psychiatry 1983; 18: 1085-91
555. Munetz MR, Slawsky RC, Neil JF. Tardive Tourette's syndrome treated with clonidine and mesoridazine. Psychosomatics 1985; 26: 254-7
556. La! S, Al Ansari E. Tourette-like syndrome following low dose short-term neuroleptic treatment. Can J Neurol Sci 1986; 13: 125-8
557. Casat CD, Wilson DC III. Tics with combined thioridazinemethylphenidate therapy: case report. J Clin Psychiatry 1986; 47: 44-5
558. Gualtieri CT, Patterson DR. Neuroleptic-induced tics in two hyperactive children. Am J Psychiatry 1986; 143: 1176-7
559. Karagianis JL, Nagpurkar R. A case of Tourette syndrome developing during haloperidol treatment. Can J Psychiatry 1990; 35: 228-32
560. Kuniyoshi M, Inanaga K, Arikawa K, et al. A case of tardive Tourette-like syndrome. Jpn J Psychiatry Neurol 1992; 46: 67-70
561. Bharucha KJ, Sethi KD. Tardive tourettism after exposure to neuroleptic therapy. Mov Disord 1995; 10: 791-3
562. Lindenmayer JP, Da-Silva D, Buendia A, et al. Tic-like syndrome after treatment with clozapine [letter]. Am J Psychiatry 1995; 152:649
563. Weinstein D, See RE, Ellison G. Delayed appearance of facial tics following chronic fluphenazine administration to guinea pigs. Pharmacol Biochem Behav 1989; 32: 1057-60
564. Factor SA, Sanchez-Ramos JR, Weiner WJ. Cocaine and Tourette's syndrome [letter]. Ann Neurol 1988; 23: 423-4
565. Pascual-Leone A, Dhuna A. Cocaine-associated multifocal tics. Neurology 1990; 40: 999-1000
Drug Safety 1997 Mar; 16 (3)

Drug-Induced Movement Disorders
566. Attig E, Amyot R, Botez T. Cocaine-induced chronic tics [letter]. J Neurol Neurosurg Psychiatry 1994; 57: 1143-4
567. Golden GS. The relationship between stimulant medication and tics. Pediatr Ann 1988; 17: 405-6
568. Sverd J, Gadow KD, Paolicelli LM. Methylphenidate treatment of attention-deficit hyperactivity disorder in boys with Tourette's syndrome. J Am Acad Child Adolesc Psychiatry 1989; 28: 574-9
569. Chandler ML, Barnhill JL, Gualtieri CT, et al. Tryptophan antagonism of stimulant-induced tics. J Clin Psychopharmacol 1989; 9: 69-70
570. Stevenson RD, Wolraich ML. Stimulant medication therapy in the treatment of children with attention deficit hyperactivity disorder. Pediatr Clin North Am 1989; 6: 1183-97
571. Borcherding BG, Keysor CS, Rapoport JL, et al. Motor/vocal tics and compulsive behaviors on stimulant drugs: is there a common vulnerability? Psychiatry Res 1990; 33: 83-94
572. Lipkin PH, Goldstein 11, Adesman AR. Tics and dyskinesias associated with stimulant treatment in attention-deficit hyperactivity disorder. Arch Pediatr Adolesc Med 1994; 148: 859-61
573. Bruun R, Kurian R. Opiate therapy and self-harming behavior in Tourette's syndrome. Mov Disord 1991; 6: 184-5
574. Lichter D, Majumdar L, Kurian R. Opiate withdrawal unmasks Tourette's syndrome. Clin Neuropharmacol1988; 11: 559-64
575. Sandyk R. Naloxone withdrawal exacerbates Tourette syndrome. J Clin Psychopharmacol 1986; 6: 58-9
576. Sandyk R: Phenobarbital-induced Tourette-Iike symptoms. Pediatr Neurol 1986; 2: 54-5
577. Burd L, Kerbeshian J, Fisher W, et al. Anticonvulsant medications: an iatrogenic cause of tic disorders. Can J Psychiatry 1986; 31: 419-23
578. Kurian R, Kersun J, Behr J, et al. Carbamazepine-induced tics. Clin Neuropharmacol1989; 12: 298-302
579. Robertson PL, Garofalo EA, Silverstein FS, et al. Carbamazepine-induced tics. Epilepsia 1993; 34: 965-8
580. Gillman MA, Sandyk R. Clonazepam-induced Tourette syndrome in a subject with hyperexplexia. Postgrad Med J 1987; 63: 311-2
581. Eisenhauer G, Jermain DM. Fluoxetine and tics in an adolescent. Ann Pharmacother 1993; 27: 725-6
582. Cunningham M, Cunningham K, Lydiard RB. Eye tics and subjective hearing impairment during fluoxetine therapy [letter]. Am J Psychiatry 1990; 147: 947-8
583. Shale H, Fabn S, Mayeux R. Tics in a patient with Parkinson's disease. Mov Disord 1986; 1: 79-83
584. Lang AE. Akathisia and the restless legs syndrome. In: Jankovic J, Tolosa E, editors. Parkinson's disease and movement disorders, 2nd ed. Baltimore: Williams & Wilkins: 399-418
585. Sandyk R, Kay SR. Relationship of neuroleptic-induced akathisia to drug-induced parkinsonism. Ital J Neurol Sci 1990; 11: 439-42
586. Barnes TR, Halstead SM, Little PW. Relationship between iron status and chronic akathisia in an in-patient population with chronic schizophrenia. Br J Psychiatry 1992; 161: 791-6
587. Berardi D, Zanfini R, Alessi S, et al. Effetti disforizzanti dei neurolettici in pazienti non schizofrenici. Minerva Psichiatr 1993; 34: 125-33
588. Sachdev P, Kruk J. Clinical characteristics and predisposing factors in acute drug-induced akathisia. Arch Gen Psychiatry 1994; 51: 963-74
589. Sachdev P. The epidemiology of drug-induced akathisia: Part I. Acute akathisia. Schizophr Bull 1995; 21: 431-49
© Adis International Umited. All rights reserved.
203
590. Sachdev P. The epidemiology of drug-induced akathisia: Part II. Chronic, tardive, and withdrawal akathisias. Schizophr Bull 1995; 21: 451-61
591. Cohen BM, Keck PE, Satlin A, et al. Prevalence and severity of akathisia in patients on c1ozapine. BioI Psychiatry 1991; 29: 1215-9
592. Fagan D, Scott DB, Mitchell M, et al. Effects of remoxipride on measures of psychological performance in healthy volunteers. Psychopharmacology (Berl) 1991; 105: 225-9
593. Safferman AZ, Lieberman JA, Pollack S, et al. Akathisia and c10zapine treatment. J Clin Psychopharmacol1993; 13: 286-7
594. Friedman JH. Akathisia with c10zapine [letter]. BioI Psychiatry 1993; 33: 852-3
595. Chengappa KN, Shelton MD, Baker RW, et al. The prevalence of akathisia in patients receiving stable doses of c1ozapine. J Clin Psychiatry 1994; 55: 142-5
596. Byerly MJ, Greer RA, Evans DL. Behavioral stimulation associated with risperidone initiation [letter]. Am J Psychiatry 1995; 152: 1096-7
597. Ward NG. Akathisia associated with droperidol during epidural anesthesia. Anesthesiology 1989; 71: 786-7
598. Athanassiadis C, Karamanis A. Akathisia after long-term epidural use of droperidol: a case report. Pain 1992; 50: 203-4
599. Hamilton PA. Metoclopramide-induced akathisia. Mil Med 1987; 152: 585-6
600. Sorbe B, Hallen C. Antiemetic treatment of chemotherapyinduced nausea in ovarian carcinoma patients. Gynecol Oncol 1989; 34: 141-4
601. Beightol RW, Coupal JJ, Shih WJ. Prevention ofmetoclopramide-induced akathisia during gastric emptying imaging. J Nucl Med 1991; 32: 1644-5
602. Cory DA. Adverse reaction to metocIopramide during enterocIysis [letter]. Am J Roentgenol1994; 163: 480
603. Fleishman SB, Lavin MR, Sattler M, et al. Antiemetic-induced akathisia in cancer patients receiving chemotherapy. Am J Psychiatry 1994; 151: 763-5
604. Weimer S. Akathisia in a cancer patient treated with antiemetics [letter]. Am J Psychiatry 1995; 152: 960-1
605. Lipinski Jr JF, Mallya G, Zimmerman P, et al. Fluoxetine-induced akathisia: clinical and theoretical implications. J Clin Psychiatry 1989; 50: 339-42
606. Maany I, Dhopesh V. Akathisia and fluoxetine. J Clin Psychiatry 1990; 51: 210-2
607. Friedman EH. Fluoxetine-induced akathisia in male OCD patients [letter]. J Clin Psychiatry 1990; 51: 212
608. Rothschild AJ, Locke CA. Reexposure to fluoxetine after serious suicide attempts by three patients: the role of akathisia. J Clin Psychiatry 1991; 52: 491-3
609. Fleischhacker WW. Propranolol for fluoxetine-induced akathisia [letter]. BioI Psychiatry 1991; 30: 531-2
610. Bertschy G, Vandel S. Fluoxetine-related indifference and akathisia. A case report. Therapie 1993; 48: 158-9
611. Marshall RD, Printz D, Cardenas D, et al. Adverse events in PTSD patients taking fluoxetine [letter]. Am J Psychiatry 1995; 152: 1238-9
612. Ketai R. Interaction between fluoxetine and neuroleptics [letter]. Am J Psychiatry 1993; ISO: 836-7
613. KIee B, Kronig MH. Case report of probable sertraline-induced akathisia [letter]. Am J Psychiatry 1993; 150: 986-7
614. LaPorta LD. Sertraline-induced akathisia. J Clin Psychopharmacol 1993; 13:219-20
615. Settle EC Jr. Akathisia and sertraline [letter]. J Clin Psychiatry 1993;54: 321
Drug Safety 1997 Mar: 16 (3)

204
616. Opler LA. Sertraline and akathisia [letter]. Am J Psychiatry 1994; 151: 620-1
617. Altshuler LL, Pierre JM, Wirshing WC, et al. Sertraline and akathisia. J Clin Psychopharmacol 1994; 14: 278-9
618. Phillips SD. A possible paroxetine withdrawal syndrome [letter]. Am J Psychiatry 1995; 152: 645-6
619. Adler LA, Angrist BM. Paroxetine and akathisia [letter]. Bioi Psychiatry 1995; 37: 336-7
620. Klysner R, Larsen JK, Sorensen P, et al. Toxic interaction of venlafaxine and isocarboxazide [letter]. Lancet 1995; 346: 1298-9
621. Zubenko GS, Cohen BM, Lipinski JF Jr. Antidepressant-related akathisia. J Clin Psychopharmacol 1987; 7: 254-7
622. Yeragani VK, Pohl R, Balon R. TricyC\ics, akathisia, and jitteriness [letter]. J Clin Psychopharmacol 1988; 8: 295
623. Sabaawi M, Richmond DR, Fragala MR. Akathisia in association with nortriptyline therapy. Am Fam Physician 1993; 48: 1024-6
624. Phillips SD, Ringo P. Phenelzine and venlafaxine interaction [letter]. Am J Psychiatry 1995; 152: 1400-1
625. Gillman PK. Possible serotonin syndrome with moclobemide and pethidine [letter]. Med J Aust 1995; 162: 554
626. Bakchine S, Lacomblez L, Soubrie C. Syndrome extrapyramidal au cours d'un traitement par la flunarizine. Rev Neurol (Paris) 1988; 144: 833-4
627. Rodriguez-Garda JL, Arechaga-Uriarte S. Akatisia inducida por flunarizina [letter]. Rev Clin Esp 1991; 188: 384
628. Price WA, Zimmer B. Lithium-induced akathisia [letter]. J Clin Psychiatry 1987; 48: 81
629. Patterson JE Lithium-induced akathisia [letter]. J Clin PsychopharmacoI1988;8:445
630. Patterson JF. Akathisia associated with buspirone. J Clin Psychopharmacol 1988; 8: 296-7
631. Lawrence K. Reversal of midazolam sedation. Crit Care Med 1993; 21: 1407-8
© Adis International Umited. All rights reserved.
Jimenez-Jimenez et al.
632. Honan VJ. Paradoxical reaction to midazolam and control with flumazenil. Gastrointest Endosc 1994; 40: 86-8
633. Hollman GA. Oral midazolam and emergence deli.rium. Ann Emerg Med 1995; 25: 853-4
634. Yassa R, Groulx B. Lorazepam in the treatment of lithiuminduced akathisia. J Clin Psychopharmacol 1989; 9: 70-1
635. Phelps S1, Baldree LA, Boucher BA, et al. Neuropsychiatric toxicity of phenytoin. Importance of monitoring phenytoin levels. Clin Pediatr (Phila) 1993; 32: 107-10
636. Riche H, Salord F, Jourdan C, et al. Neurological side effects related to valproate after neurosurgery [letter]. Acta Neurochir (Wien) 1994; 127: 240
637. Bernick C. Methysergide-induced akathisia. Clin Neuropharmacol 1988; 11:87-9
638. Brown KW, Glen SE, White T. Low serum iron status and akathisia. Lancet 1987; I: 1234-6
639. Barton A, Bowie J, Ebmeier K. Low plasma iron status and akathisia. J Neurol Neurosurg Psychiatry 1990; 53: 671-4
640. O'Loughlin V, Dickie AC, Ebmeier KP. Serum iron and transferrin in acute neuroleptic-induced akathisia [letter]. J Neurol Neurosurg Psychiatry 1991; 54: 363-4
641. Horiguchi J. Low serum iron in patients with neuroleptic-induced akathisia and dystonia under antipsychotic drug treatment. Acta Psychiatr Scand 1991; 84: 301-3
642. Sachdev P, Loneragan C. Acute drug-induced akathisia is not associated with low serum iron status. Psychopharmacology (Berl) 1991; 103: 138-9
643. Soni SD, Tench D, Routledge RC. Serum iron abnormalities in neuroleptic-induced akathisia in schizophrenic patients. Br J Psychiatry 1993; 163: 669-72
Correspondence and reprints: Dr Felix Javier JimenezJimenez, C/ Corregidor Jose de Pasamonte 24, 3° D, E-28030 Madrid, Spain.
Drug Safely 1997 Mar: 16 (3)