
Exercise intervention attenuates emotional distress and natural killer cell decrements following...
14
Biofeedback and Self-Regulation, VoL 15, No. 3, 1990 Exercise Intervention Attenuates Emotional Distress and Natural Killer Cell Decrements Following Notification of Positive Serologic Status for HIV-11 Arthur R. LaPerriere, Michael H. Antoni, Neil Schneiderman, 2 Gaff Ironson, Nancy Klimas, Panagiota Caralis, and Mary Ann Fletcher Center for the Biopsychosocial Studies of AIDS, University of Miami The impact of aerobic exercise training as a buffer of the affective distress and immune decrements which accompany the notification of HIV-1 antibody status in an AIDS risk group was studied. Fifty asymptomatic gay males with a pretraining fitness level of average or below (determined by predicted VO2 max) were randomly assigned to either an aerobic exercise training program or a no-contact control condition. After five weeks of training, at a point 72 hours before serostatus notification, psychometric, fitness and immunologic data were collected on all subjects. Psychometric and immunologic measures were again collected one-week postnotification. Seropositive controls showed significant in- creases in anxiety and depression, as well as decrements in natural killer cell number following notification whereas, seropositive exercisers showed no similar changes and in fact, resembled both seronegative groups. These findings suggest that concurrent changes in some affective and immunologic measures in response to an acute stressor might be attenuated by an experimentally manipulated aerobic exercise training intervention. Descriptor Key'Words: aerobic exercise; AIDS risk group; emotional distress; HIV-1, HIV-1 diag- nosis; psychoneuroimmunology. IThe research was supported by NIMH grant No. P50MH43455. 2Address all correspondence to Neil Schneidennan, Department of Psychology, P.O. Box 248185, University of Miami, Coral Gables, Florida 33124. 229 0363-3586/90/09(0-0229506.00/0 © 1990Plenum Publishing Corporation
Transcript of Exercise intervention attenuates emotional distress and natural killer cell decrements following...

Biofeedback and Self-Regulation, VoL 15, No. 3, 1990
Exercise Intervention Attenuates Emotional Distress and Natural Killer Cell Decrements Following Notification of Positive Serologic Status for HIV-11
Arthur R. LaPerriere, Michael H. Antoni, Neil Schneiderman, 2 Gaff Ironson, Nancy Klimas, Panagiota Caralis, and Mary Ann Fletcher Center for the Biopsychosocial Studies of AIDS, University of Miami
The impact of aerobic exercise training as a buffer of the affective distress and immune decrements which accompany the notification of HIV-1 antibody status in an AIDS risk group was studied. Fifty asymptomatic gay males with a pretraining fitness level of average or below (determined by predicted VO 2 max) were randomly assigned to either an aerobic exercise training program or a no-contact control condition. After five weeks of training, at a point 72 hours before serostatus notification, psychometric, fitness and immunologic data were collected on all subjects. Psychometric and immunologic measures were again collected one-week postnotification. Seropositive controls showed significant in- creases in anxiety and depression, as well as decrements in natural killer cell number following notification whereas, seropositive exercisers showed no similar changes and in fact, resembled both seronegative groups. These findings suggest that concurrent changes in some affective and immunologic measures in response to an acute stressor might be attenuated by an experimentally manipulated aerobic exercise training intervention.
Descriptor Key'Words: aerobic exercise; AIDS risk group; emotional distress; HIV-1, HIV-1 diag- nosis; psychoneuroimmunology.
IThe research was supported by NIMH grant No. P50MH43455. 2Address all correspondence to Neil Schneidennan, Department of Psychology, P.O. Box 248185, University of Miami, Coral Gables, Florida 33124.
229
0363-3586/90/09(0-0229506.00/0 © 1990 Plenum Publishing Corporation

230 LaPerriere et al.
The Centers for Disease Control (1988) and others (Ostrow, 1987; Sherer, 1988) have raised a concern about the potential adverse psychological sequelae that follow a positive diagnosis for the human immunodeficiency virus (HIV-1) an- tibody test. Such phenomena may range from increases in anxiety and depres- sion levels (Goodkin, 1988; Kelly & St. Lawrence, 1988; Ostrow et al., 1989) and incidence of reactive adjustment disorders to full-blown DSM-III, Axis I depression and anxiety diagnoses (Kelly & St. Lawrence, 1988; Tross, 1987) and suicidal ideation (Goodkin, 1988), related perhaps to the known increased risk of suicide in persons with AIDS (Marzuk et al., 1988). In one longitudinal study of asymptomatic gay males who were assessed both psychologically and immunologically before and after learning their HIV-1 antibody status, we have shown a significant increase in anxiety and other distress scores following notification of a seropositive diagnosis (Ironson et al., 1990).
Evidence has accrued associating affective factors with the progression of HIV-1 infection (Cecchi, 1984; Coates, Temoshok, & Mandel, 1984; Donlou, Wolcott, Gottlieb, & Landsverk, 1985; Solomon & Temoshok, 1987). In fact, Goodkin (1988) suggests that increases in anxiety and depression should be viewed as potential psychological risk factors for the progression of HIV-1 in- fection from asymptomatic (CDC-Stage II) to later stages displaying symptomatology (i.e., CDC-Stage III and beyond). This view is supported by a growing psychoneuroimmunologic literature suggesting that affective symptomatology may also impact cell-mediated immunity (Calabrese, Kling, & Gold, 1987; Irwin, Daniels, Bloom, Smith, & Wiener, 1987)--an important determinant of clinical course in the HIV-infected individual (DeMartini et aL, 1988). Therefore, it is reasonable to suggest that among recently diagnosed HIV-1 seropositive individuals, anxiety and depression might exacerbate the immune suppression induced by the HIV-1 infection potentiating a faster clini- cal deterioration.
Behavioral stress management interventions that decrease emotional dis- tress may produce immunomodulatory effects, which may favor a restoration of competence and a resultant retardation of HIV-1 disease promotion (Antoni et al., 1990). One such intervention is aerobic exercise training. Improvements in aerobic fitness level achieved in exercise training programs have been related to reductions in anxiety (Morgan, 1984) and depression (Greist et al., 1979); enhanced self-esteem (Morgan, 1982), and increased perception of psychologic well-being (Morgan, 1985); as well as increases in T-lymphocyte percentages (Watson et aL, 1986), number of mature natural killer (NK) cells (Targan, Brit- van, & Dorey, 1981), and NK cell cytotoxicity (Hanson & Flaherty, 1981; for review see LaPerriere, Schneiderman, Antoni, & Fletcher, 1989).
Here we report the psychological and immunological buffering effects of an aerobic exercise group training program. We chose to investigate these ef- fects with a group exercise protocol, which due to the social reinforcement

Exercise Training in AIDS Risk Group 231
component, has repeatedly been found to optimize exercise adherence (Dish- man, 1984; Dishman, 1987; Oldridge, 1982). Psychometric and blood measures were assessed among asymptomatic HIV-1 seropositive and seronegative gay males before and after they learned of their antibody status.
M E T H O D
Participants
Fifty gay males never tested and therefore unaware of their HIV-1 status were recruited into this study from the Health Crisis Network Center (a com- munity outreach program) as well as from newspaper advertisements. Each sub- ject completed an informed consent and indicated his willingness to be tested for and receive the results of an HIV-1 antibody test as part of the study. In addition, a complete physical examination, including an aerobic fitness evalua- tion and a medical history questionnaire, was conducted and a measure of dis- positional anxiety was administered at study entry. Exclusion criteria were: (1) having a diagnosis of CDC-Stage II, III, or IV; (2) unexplained weight loss of greater than 10% or 15 lb. within the previous 3 months; (3) mucocutaneous oral candidiasis; (4) lymphadenopathy other than inguinal or anterior cervical; (5) fever of unexplained origin; (6) unexplained night sweats or diarrhea; (7) herpes zoster within the previous 3 months; (8) drug or ethanol abuse; (9) use of anabolic steroids; (10) regular use of antihistamines; (11) being younger than 18 or older than 40; (12) engagement in regular aerobic exercise, either as a participant in a group exercise program or on an individual basis; and (13) a predicted maximum oxygen consumption (PVO 2 max) greater than 53 ml/kg/min if age 18-29 or 49 rnl/kg/min if age 30-40. Subjects meeting these requirements were thus asymptomatic and relatively healthy, while of average or below- average fitness. Because all subjects were asymptomatic, those shown ultimately to be HIV-1 seropositive were presumed to be very early in the disease process and could potentially derive maximum benefit from this behavioral intervention.
Procedure
Subjects were randomly assigned (prior to serologic testing for HIV-1 antibodies) to either an aerobic exercise training or an assessment-only control group) Subjects in the aerobic exercise training condition were exercised three
3The randomization procedure actually involved randomizing to either the aerobic training condition, a cognitive stress management condition, or the assessment-only control group. The results of the cognitive stress management group are not reported in this paper.

232 LaPerriere et al.
times per week utilizing a bicycle ergometer. Each 45-minute session consisted of repeated 3-min bouts of exercise at approximately 80% age predicted max- imum heart rate (PMHR; 220 minus each subject's age), alternated with 2-min periods of less intense exercise (e.g., 60-79% PMHR). This type of exercise, termed Interval Training, has been shown to be a more effective method of increasing aerobic capacity than more traditional modes of exercise (Perry, Mosher, LaPerriere, Roalstad, & Ostrovsky, 1988).
Aerobic fitness evaluations were performed for all subjects at entry into the study and again five weeks later in order to assess training effects. These evaluations consisted of 5 min of bicycle exercise, producing a 5th-minute sub- maximal heart rate. This heart rate was then substituted into the Fox equation to yield a predicted maximum oxygen uptake (PVO 2 max; Fox, Billings, Bartels, Bason, & Mathews, 1973). VO 2 max is considered to be the best overall indicator of aerobic fitness level (Saltin & Astrand, 1967).
Psychometric and immune measures were assessed after five weeks of training and constituted the prediagnosis test point (pre). All subjects received notification of their HIV-1 antibody status 72 hours later with psychometric and immune measures assessed again one week following serologic notification (post). The study was a 2 x 4 split plot design with time (pre and post) as the within-subjects factor and group (seronegative exercisers IN = 20], seropositive exercisers [N = 10], seronegative controls [N = 13], and seropositive controls IN = 7]) as the between-subjects factor.
Measures
Control Measures. Potential immunomodulatory confounds such as sleep, physical activity, nutritional status, and hematocrit were assessed at the pre and post measurement points to determine if any differences existed between any of the four groups at either time point or if differential changes occurred in any of these control variables across the observation period. Number of hours of sleep per day and times engaged in vigorous physical activity (outside the treatment condition) were assessed using self-report questionnaires. Nutritional status and total blood volume were estimated by measurement of serum levels of albumin and hematocrit, respectively.
Emotional Distress Measures. The Profile of Mood States (POMS; Mc- Nair, Lorr, & Droppleman, 1981), a 65-item pencil-and-paper self-report test with subscales measuring several mood states was administered at pre and post time points. Because the existing literature indicates an increase in anxiety and depression following a diagnosis of HIV-1 seropositivity, the subscales of in- terest in the present study were Tension-Anxiety and Depression-Dejection. This measure has been designed for and standardized on a normal non-

Exercise Training in AIDS Risk Group 233
psychiatric sample (McNair et aL, 1981) and was previously used in studies of affective functioning in AIDS populations (Donlou et al., 1985; Namir et al., 1987). The trait version of the State-Trait Anxiety Inventory (STAI; Spiel- berger et aL, 1970) was administered at entry into the study to assess baseline differences in dispositional anxiety.
Immunologic Measures. Measurements of lymphocyte phenotype were chosen for their known sensitivity to aerobic exercise training (Watson et aL, 1986; Hanson & Flaherty) and/or their clinical relevance to HIV-1 infection (DeMartini et aL, 1988). These included enumerations of T-helper/inducer (CD4) and NK (CD56) cells as determined by a whole blood two-color direct immunofluorescence procedure (Fletcher et aL, 1987) and NK cell cytotoxicity using a whole blood staining technique (Baron et aL, 1985), Briefly, commer- cially available monoclonal antibodies conjugated with either phycoerythrin or fluorescein isothiocynate were used to identify CD4 and CD56 cells. Aliquots of blood were incubated with the appropriate monoclonal antibody or isotopic control for 15 min at 4°C. Erythrocytes were lysed with an ammonium chloride- potassium bicarbonate-ethylenediaminetetraacetic acid (EDTA) solution. After washing, the percent and absolute counts of positive cells was determined by flow cytometric techniques.
Natural killer cell cytotoxicity against the K562 cell target was determined in triplicate at four effector-to-target cell ratios. A chromium release whole blood assay was used and results were expressed as percent cytotoxicity at an effector-to-target cell ratio of 1:1. Effector cells were defined as those express- ing the CD56 cell surface marker as measured using NKH.1 monoclonal an- tibody (Coulter Immunology). A detailed explanation of the methods used to determine these immune measures can be found in our previous work (Fletcher et al., 1987). Immune measures were assessed at pre and post time points.
HIV-I Antibody Test
HIV-1 antibody was determined with the Abbott Laboratory ELISA pro- cedure to confirm seropositivity status. Those samples that were positive by ELISA were repeated. Samples that were repeatedly positive by ELISA were confirmed by immunoblot using the methods described by the Centers for Dis- ease Control.
Data Analysis
Control variables were analyzed utilizing a repeated-measures split plot analysis of variance (ANOVA). Prior to specific hypothesis testing, means and standard deviations were calculated for PVO 2 max" Changes in fitness for exer-

234 LaPerriere et aL
cisers vs. controls were evaluated utilizing repeated measures ANOVA. Means and standard deviations were calculated for the POMS scales for each group and differences were investigated using repeated-measures multiple analysis of variance (MANOVA) and planned post hoe comparisons.
Because the immunological data were not normally distributed and also violated the assumption of homogeneity of variance (between groups), non- parametric tests were used; Mann-Whitney U (M-W) tests for independent samples assessed differences between groups at both the pre and post time points. One-way repeated-measures ANOVAs were computed between the pre and post time points separately within each group to assess changes in immune variables because there were no violations of within-group parametric test as- sumptions.
RESULTS
Demographic Information
The sociodemographic characteristics of the four study groups are in- cluded in Table I. There were no significant differences in age, F(3, 48) = .68, p > .10, nor ethnicity, Z2(9) = 13.46, p > .10. All but two subjects (one seronegative control and one seropositive exerciser) were college educated and there were no significant differences is the distributions of education, Z2(12) = 10.49, p > .10, employment status, ~z(12) = 15.33, p > .10, or annual income, Z2(18) = 10.96, p > .10. There were no differences in declared sexual orientation among groups, %2(9) = 5.35, p > .10, with the majority of subjects identifying themselves as either exclusively or predominately homosexual. In addition, there were no differences among the groups in self-reported current living ar- rangements, Z2(12) = 17.64, p > .10.
Control Measures
Analyses of behavioral and serum-derived control variables indicated no significant differences among any of the four groups in sleep, physical activity, serum albumin, or hematocrit at either the pre- or postnotification time points (p's > .10, except hematocrit p > .08). In addition, within-subjects analyses showed that none of these markers changed significantly across the evaluation period for any group (p's > .10, except hematocrit p > .07). The means and standard deviations for each of these variables are presented in Table II.

Exercise Training in AIDS Risk Group 235
Table I. Demographic Characteristics of the Sample at Entry into the Study
HIV-I negative HIV-1 positive
Exercise Control Exercise Control
Age 30.9 (5.4) 32.6 (4.4) 31.2 (5.4) 29.0 (5.0) Ethnicity
Caucasian 17 10 07 03 Black American 00 00 00 01 Hispanic 01 03 03 03 Other 0i 00 00 00
Education High school 00 01 01 00 Some college 06 04 04 03 College graduate 09 07 03 01 Graduate degree 04 01 02 02
Employment status Full time 14 09 09 05 Part time 01 02 00 00 Student 03 01 00 00 Unemployed 01 01 01 02
Modal annual income 20,000 25,000 25,000 20,000 Sexual orientation Exclusively homosexual 1 t 08 08 05 Predominantly homosexual 07 03 02 02 Bisexual 01 01 00 00 Predominantly heterosexual 00 01 00 00
Current living arrangement Live alone 09 07 04 05 Live with lover 01 02 00 01 Live with nonlover 02 00 00 01 Live with parents 07 03 04 00 Other 00 01 02 00
Table I1. Means (and Standard Deviations) for Control Variables Measured 72 Hours Pre- and 1 Week Postnotification of Serologic Status for HIV-1
HIV-1 negative HIV-1 positive Control Time variable point Exercise Control Exercise Control
Sleep Pre 6.8 (0.9) 7.9 (1.6) 7.1 (0.8) 7.4 (1.0) (hours/night) Post 7.2 (1.2) 6.5 (1.1) 7.4 (0.8) 7.1 (0.4)
Physical Activity Pre 2.2 (2.1) 1.8 (2.1) t.2 (1.8) 2.3 (2.6) (times/week) Post 1.1 (0.3) 1.7 (0.5) 1.0 (0.2) 1.8 (0.5)
Albumin Pre 4.6 (0.4) 4.7 (0.4) 4.5 (0.3) 4.6 (0.2) (g/100 dl) Post 4.6 (0.4) 4.6 (0.3) 4.4 (0.3) 4.4 (0.4)
Hematocrit Pre 49.3 (2.6) 48.0 (2.1) 45.6 (3.0) 46.3 (3.7) (g/100 dl) Post 47.4 (3.0) 47.4 (2.8) 45.6 (2.4) 46.0 (2.4)

236 LaPerriere et al.
Fitness Evaluation
Subjects randomly assigned to the aerobic exercise training group showed a significant improvement in fitness level, as measured by the change in PVO2 max, from entry into the study (39.4 ml/kg/min) until 72 hours prior to serostatus notification (week 5) (43.0 mllkg/min), F(1, 26) = 5.77, p < .05. Furthermore, both seronegative and seropositive exercisers averaged more than a 10% increase in their fitness level. Conversely, those subjects assigned to the assessment-only control group showed no significant changes in PVO 2 m,x (41.0 vs. 42.5 ml/kg/min) over the same time period. In fact, both seronegative and seropositive controls averaged less than a 3% change in their fitness levels.
Emotional Distress
Before examining changes in situational distress, baseline differences in dispositional anxiety among groups were first assessed. Because the STAI Trait scores showed marginally significant differences among the four groups at baseline, F(3, 46) = 2.48, p = .07, we decided to control for the contribution of individual differences in dispositional anxiety, by using STAI-Trait scores as a covariate in all subsequent analyses of emotional distress. Subjects were able to predict their serostatus (response to the statement "I think my HIV-1 test result will be: positive or negative" at baseline) with 75% accuracy, )~2 = 4.02, p < .05.
Means and standard deviations for the POMS (anxiety and depression subscales) are presented in Table III. A repeated-measures M A N C O V A includ- ing the tension-anxiety (anxiety) and depression-dejection (depression) sub- scales of the POMS showed a significant group-by-t ime interaction, F(6, 90) = 3.01, p < .01. A univariate repeated-measures A N C O V A confirmed a significant group-by-t ime interaction for both anxiety, F(3, 46) = 3.16, p < .05, and depres- sion subscales, F(3, 46) = 5.63, p < .01. A follow-up one-way A N O V A of
Table III. Means (and Standard Deviations) for Anxiety and Depression Subscales of the Profile of Mood States Measured 72 h Pre- and 1 Week Postnotification of Serologic Status
for HIV-1
HIV-1 negative HIV-1 positive Time Subscale point Exercise Control Exercise Control
Anxiety Pre 7.7 (1.1) 8.5 (1.4) 12.8 (2.0) 11.3 (1.6) Post 6.0 (1.4) 3.8 (0.7) 12.9 (2.5) 16.3 (3.8) a
Depression Pre 5.0 (0.9) 5.3 (1.3) 10.9 (1.7) 10.0 (1.6) Post 3.9 (1.3) 2.8 (1.4) 14.0 (3.7) 23.8 (7.9) a
~p < .05 (magnitude of change significantly different from all groups).
Exercise Training in AIDS Risk Group 237
Q- 10 C l
o
-10 i I
6"
4" 7_= x 2-
0- c e= ~2"
-4"
o
- 8 "
HIV HJV~ HIV- EXERCISE I
HIV- CONTROL
i
P r e Post
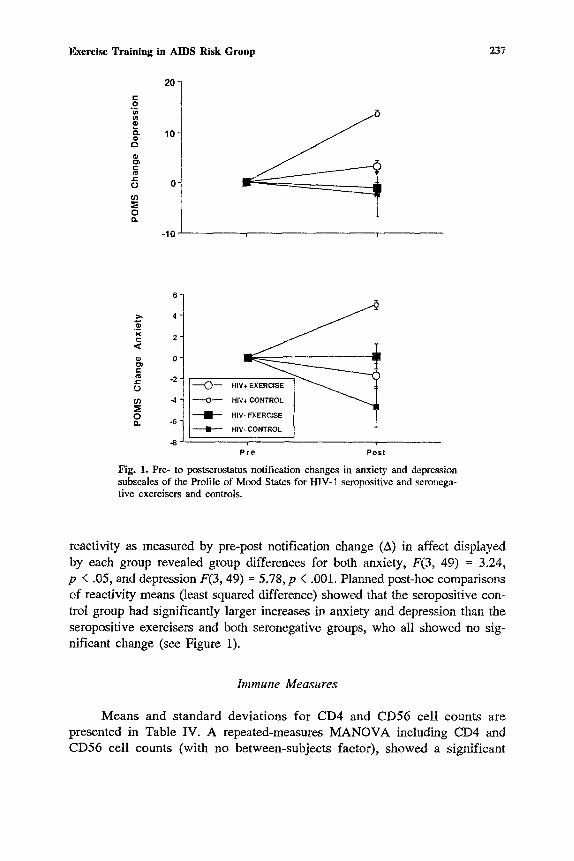
Fig. 1. Pre- to postserostatus notification changes in anxiety and depression subscales of the Profile of Mood States for HIV-1 seropositive and seronega- tive exercisers and controls.
reactivity as measured by pre-post notification change (A) in affect displayed by each group revealed group differences for both anxiety, F(3, 49) = 3.24, p < .05, and depression F(3, 49) = 5.78, p < .001. Planned post-hoc comparisons of reactivity means (least squared difference) showed that the seropositive con- trol group had significantly larger increases in anxiety and depression than the seropositive exercisers and both seronegative groups, who all showed no sig- nificant change (see Figure 1).
Immune Measures
Means and standard deviations for CD4 and CD56 cell counts are presented in Table IV. A repeated-measures MANOVA including CD4 and CD56 cell counts (with no between-subjects factor), showed a significant

HIV-1 negative HIV-1 positive Lymphocyte Time phenotype point Exercise Control Exercise Control
CD56 Pre 375 (26) 476 (28) 400 (39) 473 (86) (mm 3) Post 337 (28) 406 (45) 379 (64) 294 (47)"
CD4 Pre 962 (60) 1112 (87) 860 (92) 889 (136) (mm 3) Post 964 (54) 1267 (92) 898 (72) 828 (077)
~p < .05 (pre- vs. postnotification).
CO I.O a o
change from pre to postnotification, F(2, 48) = 4.19, p < .05. A simple effect paired repeated measures A N O V A , examining each group separately, revealed
that the seroposit ive controls displayed a significant decrease in CD56 cells across this period, F(1, 6) = 4.26, p < .01. However , s imilar changes were not observed in the seroposi t ive exercisers nor in either seronegative group. Mann- Whi tney tests indicated that the seroposit ive controls had significantly greater
p re -pos t notification decrements in CD56 cells than seroposit ive exercisers (Z = 2.1, p < .05) as well as in comparison with both seronegative groups (p 's < .05) (see Figure 2). There were no significant p re -pos t changes in NK cell cytotoxici ty in any of the four groups nor were there significant differences noted between any group at either t ime point on this measure. Although the differences in the magni tude of reactivity for CD4 counts among groups were nonsignificant, it is noteworthy that on average, the seroposit ive exercisers in-
-50
o t-- t~ t- O
- 100
-150
- - - (>-
- - - o - - - - - I I - -
m m
HIV
HIV+ CONTROL
HIV- EXERCISE X ~
HIV- CONTROL
238 LaPerriere et al.
Table IV. Means (and Standard Deviations) for CD56 and CD4 Lymphocyte Phenotypic Counts Measured 72 h Pre- and 1 Week Postnotification of Serologic Status for HIV-1
- 200 , , P r e P o s t
Fig. 2. Pre- to postserostatus notification change in natural killer cell (CD56) count for HIV-1 seropositive and seronegative exercisers and controls.

Exercise Training in AIDS Risk Group 239
creased their CD4 counts by 38 cells/ram 3 while seropositive controls decreased their counts by 61 eells/mm 3.
DISCUSSION
The primary goal of this study was to assess the efficacy of a behavioral stress management intervention (i.e., aerobic exercise group training) as a buffer of emotional distress and immune decrements that accompany news of a life- threatening diagnosiswHIV-1 seropositivity. To test this hypothesis we utilized a standardized, aerobic training program (conducted in a group setting) in a randomized experimental design.
The decision to study the buffering effects of aerobic training with this sample resulted from the convergence of several contemporary findings. First, psychosocial stressors involving personal loss (e.g., bereavement), and]or a loss of perceived control are accompanied by concurrent impairments in psychologi- cal and immunological functioning (see Antoni et al., 1990, for review). Second, recently diagnosed HIV-1 seropositive individuals have been found to display large, significant increases in affective distress, especially in the period immediately following antibody testing (Ironson et aL, i990). Third, one be- havioral stress management intervention (aerobic exercise) has been shown to reduce anxiety and depression on the one hand and to enhance certain aspects of cellular immunity on the other (Morgan, 1985; Watson et aL, 1986; see Laperriere et al., 1989, for review). We reasoned that such a behavioral treat- ment might attenuate the affective and immunological sequelae of HIV-1 seropositivity notification among members of an AIDS high risk group--gay males.
The aerobic training program did result in a significant improvement in fitness, which was attained in five weeks. To test our affective distress buffering hypothesis we were interested in two major questions. First, does notification of HIV-1 serostatus possess potency and specificity as a psychosocial stressor? And second, does aerobic exercise training buffer affective distress responses and immunologic decrements at one week postnotification among seropositives, and are these effects specific to seropositive exercisers (vs. seronegative exer- cisers)? Our findings provide support for both these hypotheses. First, the seropositive control subjects revealed postnotification depression scores that were within the range of psychiatric outpatients (McNair et aL, 1981), suggest- ing some degree of affective disturbance in the immediate postnotification period. Moreover, seropositive controls showed significantly larger changes in POMS anxiety and depression scores at one week postnotification as compared to seropositive exercisers, who showed scores equivalent to college sample norms (McNair et aL, 1981) and virtually no change pre- to postnotification.

240 LaPerriere et al.
It should be noted, however, that seropositive individuals in both the treatment and control group were more anxious and depressed at prediagnosis than either seronegative group. We wondered if these differences were due to perceived risk of infectivity between the seropositive and seronegative subjects. At entry into the study each individual was asked if they thought their HIV-1 test would be negative or positive. A statistically significant 75% accurately categorized their eventual HIV-1 status. It is important to remember that all subjects were completely asymptomatie at all time points (verified by an intensive physical exam, medical interview, and self-report questionnaire). Although not the focus of the study, one possible explanation for the accuracy of their predictions was that those who predicted their HIV-1 serologic status to be positive were en- gaging in more risky behavior and therefore perceived themselves to be at greater risk for HIV-1 infection. This predictive accuracy may account for the specificity of affective distress buffering effects to seropositives.
In line with our immunologic buffering hypothesis, seropositive controls showed a sharp decline in NK cell number after learning their antibody status whereas seropositive exercisers showed a negligible change over the same period of time. Although NK cell cytotoxicity--expressed on a per effector (CD56) cell basismshowed no such change, the significant drop in CD56 cell counts observed in the seropositive controls could result in a significant decre- ment in an important element of innate immune function--natural cell mediated cytotoxicity (Herberman et al., 1986). The buffering effect of exercise appeared to be specific to the NK cell population; helper[inducer cell counts did not vary significantly. The pattern of results in this study could not be explained by sociodemographic differences, as all groups were equivalent in age, ethnicity, socioeconomic status, and sexual orientation. In addition, no group differences or changes were observed in biobehavioral variables such as sleep, physical activity, nutritional status, or total blood volume. Taken together, the two sets of buffering effects noted herein suggest parallel movement in affective and immunological "response" systems that are affected by an experimentally manipulated aerobic training intervention. It is possible that individual differen- ces in affective response dispositions may contribute, beyond this experimental effect, to psychoimmunologic associations. Our attempt to control for disposi- tional differences in "anxiousness" among subjects in the present study reflects, to some degree, this concern. It is possible that some of the buffering effects observed may be attributed to the fact that these individuals were engaged in an active coping task and also had the benefit of the social support component of the group format. One way to begin to determine the specific effects at- tributable to exercise may be to have low versus high-intensity exercise groups. If exercise-induced fitness change is accounting for the observed buffering ef- fects, then exercise intensity should be related to the magnitude of these effects.

Exercise Training in AIDS Risk Group 241
Another way to get at the specificity issue would be to have exercisers practice in an individual as opposed to a group format.
Beyond providing evidence for the covadance of psychological and im- munological processes, the present findings support the efficacy of a particular behavioral stress management intervention--aerobic exercise--as a useful strategy for attenuating postnotification psychological impairments among HIV- 1 infected individuals. Illumination of the psychologic and physiologic mechanisms accounting for these effects will require a larger panel of im- munological, psychological, and neuroendocrine measures collected over shorter intervals before and after serostatus notification.
REFERENCES
Antoifi, M. H., Schneiderman, N., Fletcher, M., LaPerriere, A., Goldstein, D., & Ironson, G. (1990). Psychoneuroimmunology and HIV-1. Journal of Consulting and Clinical Psychology, 58(1), 38-49.
Antoni, M. H., Schneiderrnan, N., LaPerriere, A., Baggett, H. L., August, S., & Fletcher, M. A. (1988). Stress management and immune function. Proceedings from NIMH conference on priorities in stress research. Washington, DC: NIMH, Government Printing Office.
Baron, G. C., Klimas, N. G., Fischl, M. A., & Fletcher, M. A. (1985). Decreased natural ceil- mediated eytotoxicity per effector cell in acquired immunodeficiency syndrome. Diagnostic Immunology, 3, 197-204.
Calabrese, J., Kling, M., & Gold, P. (1987). Alterations in immunocompetence during stress, bereavement, and depression: Focus on neuroendoerine regulation. American Journal of Psychiatry, 144, 1123-1134.
Centers for Disease Control (1988). Update: Serologic testing for antibody to human im- munodeficiency virus. Morbidity and Mortality Weekly Report, 36, 834-845.
Dishman, R. K. (1984). Motivation and exercise adherence. In J. M., Silva, III, & R. S. Weinberg (Eds.), Psychological foundations of sport. Champaign, IL: Human Kinetics.
Dishman, R. K. (1987). Exercise adherence and habitual physical activity. In W. P. Morgan & S. E. Goldston (Eds.), Exercise and mental health. Champaign, NY: Hemisphere.
Donlou, J. N., Wolcott, M. S., Gottlieb, M. S., & Landsverk, J. (1985). Psychosocial aspects of AIDS and AIDS-related complex: A pilot study. Journal ofPsychosocial Oncology, 3, 39-55.
Fletcher, M. A., Baron, G. C., Ashman, M. R., Fischl, M. A., & Klimas, N. G. (i987). Use of whole blood methods in assessment of immune parameters in immuno:leficieney states. Diag- nostic and Clinical Immunology, 5, 69-81.
Fox, E., Billings, C., Barrels, R., Bason, R., & Mathews, D. (1973). Fitness standards for male college students. International Zeitschrift J~r Angewandte Physiologic Einschiiesslich Ar- beitsphysiologie, 31, 231-236.
Goodkin, K. (1988). Psychiatric aspects of HIV infection. Texas Medicine, 84, 55-61. Greist, J. H., Klein, M. H., Eischens, R. R., Faris, J., Gurman, A. S., & Morgan, W. P. (1979).
Running as treatment for depression. Comparative Psychiatry, 20, 41-53. Hanson, P., & Flaherty, D. (1981). Immunological responses to training in conditioned runners.
Clinical Science, 60, 225-228. Herberman, R. B., Reynolds, C. W., & Ortaldo, J. R. (1986). Mechanism of cytotoxicity by natural
killer (NK) cells. Annual Review of Immunology, 4, 651-680. Ironson, G., LaPerriere, A., Antoni, M.,, Klimas, N., Fletcher, M. A., & Schneiderman, N. (1990).
Changes in immunologic and psychological measures as a function of anticipation and reaction to news of HIV-I antibody status. Psychosomatic Medicine, 52, 247-270.
242 LaPerriere et al.
Irwin, M., Daniels, M., Bloom, E., Smith, T., & Weiner, H. (1987). Life events, depressive symptoms, and immune function. American Journal of Psychiatry, 144, 437-441.
Kelly, J. A., & St. Lawrence, J. S. (1988). The AIDS health crisis: Psychological and social in- terventions. New York: Plenum.
Kiecolt-Glaser, J., Glaser, R., Williger, D., Stout, J., Messick, G., Sheppard, S., Ricker, D., Romisher, S., Briner, W., Bonnell, G., & Donnerberg, R. (1985). Psychosocial enhancement of immunocompetence in a geriatric population. Health Psychology, 4, 25-41.
LaPerriere, A., Schneiderman, N., Antoni, M. H., & Fletcher, M. A. (1989). Aerobic exercise train- ing and psychoneuroimmunology in AIDS research. In A. Baum & L. Temoshok (Eds.), Psychological aspects of AIDS (pp. 259-286). Hillsdale, NJ: Erlbaum.
Marzuk, P. M., Tierney, H., Tarfidd, K., Gross, E. M., Morgan, E. B., Hsu, M. A., & Mann, J. G. (1988). Increased risk of suicide in persons with AIDS. Journal of the American Medical Association, 259, 1332-1333.
McNair, D. M., Lorr, M., & Dropplemen, L. F. (1981). EITS manual for the Profile of Mood States. San Diego: Educational and Industrial Testing Service.
Morgan, W. P. (1982). Psychological effects of exercise. Behavioral Medicine Update, 4, 25-30. Morgan, W. P. (1984). Physical activity and mental health. In H. Eckert & H. J. MonToye, Exercise
and health (pp. 133-145). Champaign, IL: Human Kinetics. Morgan, W. P. (1985). Affective benefits of vigorous physical activity. Medicine and Science in
Sports and Exercise, 17, 94-100. Namir, S., Wolcott, D., Fawzy, I., & Alumbaugh, M. (1987). Coping with AIDS: Psychological
and health implications. Journal of Applied Social Psychology, 17(3), 309-328. Oldridge, N. B. (1982). Compliance and exercise in primary and secondary prevention of coronary
heart disease: A review. Preventive Medicine, 11, 56-70. Ostrow, D. G. (1987). Medical and psychological implications of HTLV-III testing. In D. G. Ostrow
(Ed.), Biobehavioral control of AIDS (pp. 19-26). New York: Irvington Press. Ostrow, D. G., Joseph, J., Kessler, R., Soucy, J., Tal, M., Eller, M., Chmiel, J., & Phair, J. (1989).
Disclosure of HIV antibody status: Behavioral and mental health correlates. AIDS Education and Prevention, I(I), 1-11.
Perry, A. C., Mosher, P. E., LaPerriere, A. R., Roalstad, M., & Ostrovsky, P. (1988). Comparison of training responses to interval vs. continuous aerobic dance. Journal of Sports Medicine and Physical Fitness, 28(3), 274-279.
Saltin, B., & Astrand, P. (1967). Maximal oxygen uptake in athletes. Journal of Applied Physiology, 23, 353-358.
Sherer, R. (1988). Physician use of the HIV antibody test: The need for consent, counseling, con- fidentiality, and caution. Journal of the American Medical Association, 259, 264-265.
Spielberger, C., Gorusch, R., & Lushene, R. (1970). State-Trait Anxiety Inventory manual. Palo Alto: Consulting Psychologists Press.
Targan, S., Britvan, L., & Dorey, F. (1981). Activation of human NKCC by moderate exercise: Increased frequency of NK cells with enhanced capability of effector-target lytie interactions. Clinical Experimental Immunology, 45, 352-360.
Tross, S. (1987, March). Psychological response to AIDS and HIV disease. Proceedings of con- ference on Current concepts in psycho-oncology and AIDS, New York: Memorial Sloan-Ket- tering Cancer Center.
Watson, R. R., Mofiguchi, S., Jackson, J. C., Werner, L., Wilmore, J. H., & Freund, B. J. (1986). Modifications of cellular immune functions in humans by endurance exercise training during 13-adrenergic blockade with atenolol or propranolol. Medicine and Science in Sports and Ex- ercise, 18, 95-100.
Wolpe, J. (1958). Psychotherapy by reciprocal inhibition. Stanford: Stanford University Press.




















