
Ral Overactivation in Malignant Peripheral Nerve Sheath Tumors
Upload
independentCategory
view
0download
0
[CANCER RESEARCH 52, 6716-6721, December 1, 1992]
Advances in Brief
Evidence for the Involvement of a Potential Second Tumor Suppressor Gene on Chromosome 17 Distinct from p53 in Malignant Astrocytomas
Abha Saxena, W. C r a i g C l a r k , J a m e s T. Robertson, Barbara Ikejiri, Edward H. Oldfield, and Iqba l U n n i s a Ali 1
Surgical Neurology Branch, National Institute of Neurological Disorder and Stroke, N/H, Bethesda, Maryland 20892 [.4. S., B. I., E. H. 0., I. U. .4.], and Department of Neurosurgery, University of Tennessee, Memphis, Tennessee 38119 [W. C. C., J. T. R.]
Abstract
Molecular analysis of malignant astrocytomas demonstrated three distinct groups of tumors with chromosome 17p abnormalities, which include (a) deletion of the p53 locus (17p13.1) and mutations in the remaining allele, (b) deletion of the p53 locus but no detectable muta- tions in the remaining allele, and (c) deletions not including the p53 locus but mutations in one of the alleles. Furthermore, deletion mapping analysis demonstrated allelic loss of genes distal to DI7S28/D17S5 markers (17p13.3) in group C tumors. The loss of heterozygosity of genes on chromosome 17 without detectable mutation (group B) or de- letion (group C) in the p53 gene implies the presence of a second tumor suppressor gene in the telomeric region of 17p, the homozygous func- tional inactivation of which may play a role, either alone or in conjunc- tion with p53, in the initiation and/or progression of astrocytic neo- plasms.
Introduction
Deregulated cell growth associated with neoplasia is a con- sequence of multiple genetic aberrancies accumulated over time. Mutations in protooncogenes, which facilitate cell prolif- eration, as well as in tumor suppressor genes, which prevent or suppress cell proliferation, contribute to the emergence of a malignant phenotype (1). There is persuasive evidence for the functional inactivation of tumor suppressor genes in many hu- man neoplasms (2, 3). Homozygous functional inactivation of a tumor suppressor gene is often accomplished by mutations in one copy of the gene combined with physical loss of the chro- mosomal region harboring the remaining allele of the gene. Comparison of the constitutional and tumor genotypes by RFLP 2 analysis has demonstrated allelic deletions on specific chromosomes in many human malignancies, suggesting shared chromosomal lesions in diverse cancers. For example, deletion of sequences on chromosome 17 occurs in a broad spectrum of human neoplasms, including cancers of the colon, lung, breast, bone, ovary, and brain (4-12). It is widely believed that the target of these deletions is the p53 gene on chromosome 17p 13.1 (13). Loss of one allele of the p53 gene and mutations in the remaining allele represent the most frequent molecular genetic abnormalities of human cancers (14-16). Although a single tumor suppressor gene plays a crucial role in many can- cers, multiple suppressor genes may be affected in the same tumor (17-21). There is little doubt that most human cancers represent multigenic diseases, where genes on multiple chro-
Received 9/29/92; accepted 10/23/92. The costs of publication of this article were defrayed in part by the payment of
page charges. This article must therefore be hereby marked advertisement in accord- ance with 18 U.S.C. Section 1734 solely to indicate this fact.
1 To whom requests for reprints should be addressed, at Surgical Neurology Branch, Building 10/5D37, National Institute of Neurological Disorder and Stroke, NIH, Bethesda, MD 20892.
2 The abbreviations used are: RFLP, restriction fragment length polymorphism; PCR, polymerase chain reaction.
mosomes are altered. Furthermore, there is also evidence for the presence of more than one tumor suppressor gene on a single chromosome in some cancers (22-28).
In human glial tumors, reduction to homozygosity of genes is detected frequently on chromosomes 10 and 17 (10-12, 29-36). The former alteration is believed to be associated with the most malignant form of the disease, glioblastoma multiforme (20, 29-31), whereas allelic losses of genes on chromosome 17 and mutations of the p53 gene have been reported to be associated with low- and high-grade astrocytomas (32-34, 36, 37). Our analysis of 40 glial tumors for gene losses on chromosome 17 and for mutations of the p53 gene suggests a crucial role for the p53 gene in the evolution of glioblastomas. Furthermore, in addition to p53, our data indicate the presence of at least one other target gene in the telomeric region of the short arm of chromosome 17.
Materials and Methods
Tumor Specimens and Histopathology. At surgery tumors were care- fully separated from the surrounding normal brain, and the central part of the tumor was quickly frozen in liquid nitrogen and stored at -g0*c. T h e t u m o r s were g raded accord in 8 to the guidel ines o f the W H O (38),
Of the 40 tumors analyzed in this study, 34 were grade IV glioblastoma multiforme (24 primary and 10 recurrent), three were grade III ana- plastic astrocytoma (2 primary and 1 recurrent), and three were oli- goastrocytoma. Blood samples, obtained at surgery, were used to isolate lymphocyte DNA and served as normal controls.
RFLP Analysis. DNA was isolated from the peripheral blood lym- phocytes and frozen tumor tissues by sodium dodecyl sulfate-proteinase K digestion followed by phenol/chloroform extraction according to established methods (39). Ten ~tg of DNAs from matching lymphocytes and tumors were digested with appropriate restriction enzymes, elec- trophoretically separated in 0.8% agarose gels, and transferred to Ny- tran membranes. The following probes (obtained from the American Type Culture Collection, Rockville, MD) were used for the RFLP analysis: D17S34 (p13.3); D17S28 (p13.3); D17S5 (p13.3); D17S31 (p13.1-pll.2); p53 (p13.1); D17S71 (pll.2); and D17S4 (q23-25.3). Southern hybridization was performed using random primed radiola- beled insert probes (specific activity, >10 s cpm/ag of DNA). Hybrid- ization, subsequent washing of the filters, and autoradiography were performed as previously described (40). In some cases where the pa- tients were constitutionally homozygous for BamHI and ScaI polymor- phism at the p53 locus, PCR-based amplification of a 250-base pair genomic fragment containing the Thai polymorphism (41) at codon 72 of exon 4 of the p53 gene was used.
PCR Amplification and Sequencing of the p53 Gene. A 1.9-kilobase fragment of the p53 gene covering exons 5-9 was amplified using 200 ng of the genomic DNA and 1 ~tM concentration of the 5'-CAT- CGAATTCGTAGGAATTCACTTGTGCCCTGACTT-3' (sense) and 5'-CATCGAATTCTGGAAACTTTCCACTTGAT-3' (antisense) pri- mers (42), which contained EcoRI restriction sites at the 5' ends to facilitate cloning of the PCR products. The amplified double-stranded
6716
Research. on January 15, 2015. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from
A P O T E N T I A L S E C O N D T U M O R S U P P R E S S O R G E N E O N 1 7 p I N A S T R O C Y T O M A S
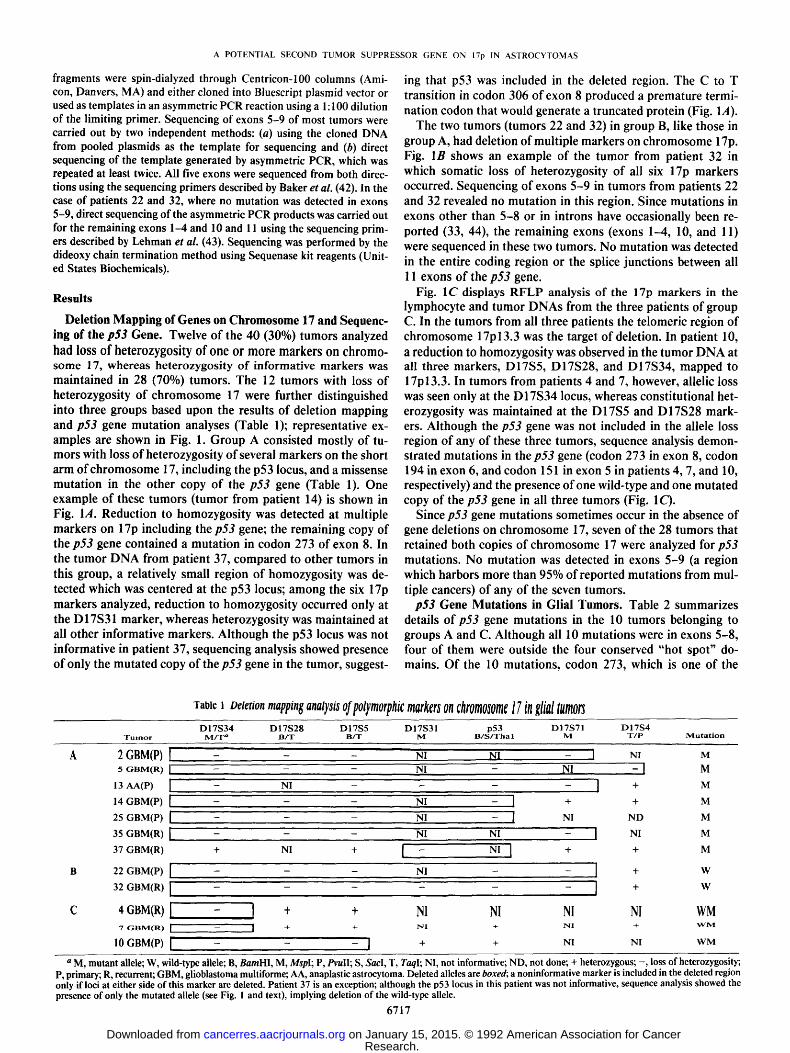
fragments were spin-dialyzed through Centricon-100 columns (Ami- con, Danvers, MA) and either cloned into Bluescript plasmid vector or used as templates in an asymmetric PCR reaction using a 1:100 dilution of the limiting primer. Sequencing of exons 5-9 of most tumors were carried out by two independent methods: (a) using the cloned DNA from pooled plasmids as the template for sequencing and (b) direct sequencing of the template generated by asymmetric PCR, which was repeated at least twice. All five exons were sequenced from both direc- tions using the sequencing primers described by Baker et al. (42). In the case of patients 22 and 32, where no mutation was detected in exons 5-9, direct sequencing of the asymmetric PCR products was carried out for the remaining exons 1-4 and 10 and 11 using the sequencing prim- ers described by Lehman et al. (43). Sequencing was performed by the dideoxy chain termination method using Sequenase kit reagents (Unit- ed States Biochemicals).
Results
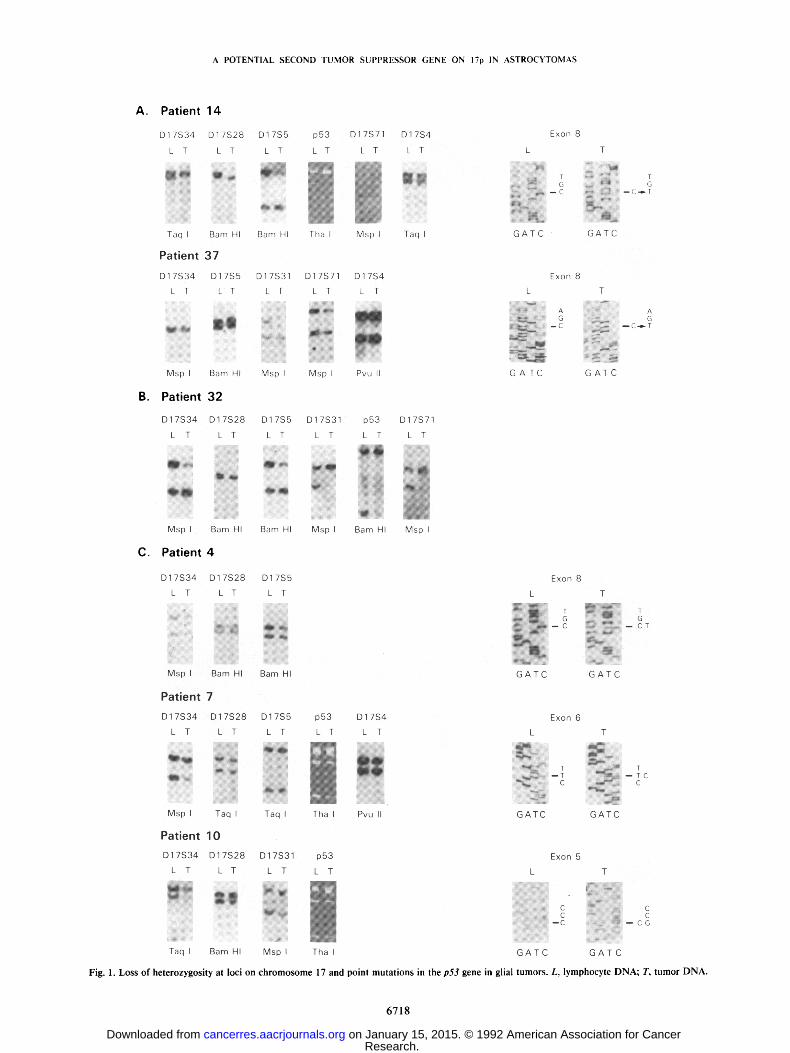
Deletion Mapping of Genes on Chromosome 17 and Sequenc- ing of the p53 Gene. Twelve of the 40 (30%) tumors analyzed had loss of heterozygosity of one or more markers on chromo- some 17, whereas heterozygosity of informative markers was maintained in 28 (70%) tumors. The 12 tumors with loss of heterozygosity of chromosome 17 were further distinguished into three groups based upon the results of deletion mapping and p53 gene mutation analyses (Table 1); representative ex- amples are shown in Fig. 1. Group A consisted mostly of tu- mors with loss of heterozygosity of several markers on the short arm of chromosome 17, including the p53 locus, and a missense mutation in the other copy of the p53 gene (Table 1). One example of these tumors (tumor from patient 14) is shown in Fig. 1A. Reduction to homozygosity was detected at multiple markers on 17p including the p53 gene; the remaining copy of the p53 gene contained a mutation in codon 273 of exon 8. In the tumor DNA from patient 37, compared to other tumors in this group, a relatively small region of homozygosity was de- tected which was centered at the p53 locus; among the six 17p markers analyzed, reduction to homozygosity occurred only at the D17S31 marker, whereas heterozygosity was maintained at all other informative markers. Although the p53 locus was not informative in patient 37, sequencing analysis showed presence of only the mutated copy of the p53 gene in the tumor, suggest-
ing that p53 was included in the deleted region. The C to T transition in codon 306 of exon 8 produced a premature termi- nation codon that would generate a truncated protein (Fig. 1A).
The two tumors (tumors 22 and 32) in group B, like those in group A, had deletion of multiple markers on chromosome 17p. Fig. 1B shows an example of the tumor from patient 32 in which somatic loss of heterozygosity of all six 17p markers occurred. Sequencing of exons 5-9 in tumors from patients 22 and 32 revealed no mutation in this region. Since mutations in exons other than 5-8 or in introns have occasionally been re- ported (33, 44), the remaining exons (exons 1-4, 10, and 11) were sequenced in these two tumors. No mutation was detected in the entire coding region or the splice junctions between all 11 exons of the p53 gene.
Fig. 1C displays RFLP analysis of the 17p markers in the lymphocyte and tumor DNAs from the three patients of group C. In the tumors from all three patients the telomeric region of chromosome 17p13.3 was the target of deletion. In patient 10, a reduction to homozygosity was observed in the tumor DNA at all three markers, D17S5, D17S28, and D17S34, mapped to 17p13.3. In tumors from patients 4 and 7, however, allelic loss was seen only at the D17S34 locus, whereas constitutional het- erozygosity was maintained at the D17S5 and D17S28 mark- ers. Although the p53 gene was not included in the allele loss region of any of these three tumors, sequence analysis demon- strated mutations in the p53 gene (codon 273 in exon 8, codon 194 in exon 6, and codon 151 in exon 5 in patients 4, 7, and 10, respectively) and the presence of one wild-type and one mutated copy of the p53 gene in all three tumors (Fig. 1C).
Since p53 gene mutations sometimes occur in the absence of gene deletions on chromosome 17, seven of the 28 tumors that retained both copies of chromosome 17 were analyzed for p53 mutations. No mutation was detected in exons 5-9 (a region which harbors more than 95% of reported mutations from mul- tiple cancers) of any of the seven tumors.
p53 Gene Mutations in Glial Tumors. Table 2 summarizes details of p53 gene mutations in the 10 tumors belonging to groups A and C. Although all 10 mutations were in exons 5-8, four of them were outside the four conserved "hot spot" do- mains. Of the 10 mutations, codon 273, which is one of the
Table 1 Deletion mapping analysis of polymorphic markers on chromosome 17 in glial tumors D17S34 D17S28 D17S5 D17S31 p53 D17S71 D17S4
T u m o r M / T a B / T B / T M B / S / T h a I M T / P M u t a t i o n
A 2 GBM(P) [ - - - N I N I - [ NI M 5 GBM(R) ] - - - - - N I - NI - ] M
13 AA(P) ] - NI - - - ] + M
14 GBM(P) [ - - - NI - I + + M
25 GBM(P) [ - - - NI - ] NI N D M
35 GBM(R) [ - - - N I NI - I NI M
37 GBM(R) + NI + [ - NI I + + M
B 22 GBM(P) [ - - - - NI - - ] + W
32 GBM(R) L, - . . . . . ] + W
C 4 GBM(R) [ - ] + + NI NI NI NI WM 7 G B M ( R ) [ - - [ + + N I + S l + W M
10 GBM(P) [ - - ] + + NI NI W M
a M, mutant allele; W, wild-type allele; B, BamHl, M, Mspl; P, PvulI; S, SacI, T, Taql; NI, not informative; ND, not done; + heterozygous; - , loss of heterozygosity; P, primary; R, recurrent; GBM, glioblastoma multiforme; AA, anaplastic astrocytoma. Deleted alleles are boxed; a noninformative marker is included in the deleted region only if loci at either side o f this marker are deleted. Patient 37 is an exception; although the p53 locus in this patient was not informative, sequence analysis showed the presence o f only the mutated allele (see Fig. 1 and text), implying deletion of the wild-type allele.
6 7 1 7
Research. on January 15, 2015. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from
A POTENTIAL SECOND TUMOR SUPPRESSOR GENE ON 17p IN ASTROCYTOMAS
A. Patient 14
D17S34 D17S28
L T L T
S m i.
Taq Barn HI
Patient 37
D17S5 p53 D17S71 D17S4 Exon 8
L T L T L T L T L
Bam HI Tha I Msp I Taq I G AT C
T
G ~,,4 - -C - ' ~ T
GATC
B.
D17S34 D17S5 D17S31
L T L T L T
O k D S ~
M s p I Barn HI
Patient 32
M s p I
D17S71 D17S4
L T L T L - w
" W " .="=-i
M s p I P v u II G A T C
Exon 8
A G
- C
T
G A T C
A
G -- C..-- T
C.
D17S34 D17S28 D17S5
L T L T L T
m ~ O O O
O m - - e
Msp I Bam HI Bam HI
Patient 4
D17S34 D17S28 D17S5
L T L T L T
Msp Bam HI Bam HI
D17S31 p53
L T L T
~ U
Msp I Barn HI
D17S71
L T
i �84 ~
Msp I
Exon 8
L
~ C 4 G A I C
T
!--CT
- : io G A T C
Patient 7
D17S34 D17528
L T L T
l l l ! e e
Msp I Taq I
Patient 10
D17S34 D17S28
L T L T
ze
D17S5 p53
L T L T
~ o D E I i i
~ Q
Taq I Tha I
D17S4 Fx0n 6
L T L
--~ : c
Pvu II G A T C
T
-Tc c
G A T C
D17S31 p53
L T L T
Exon 5 L T
B ~
" g
~ C C ~ C
- C ~ - - C
T a q I B a m HI M s p I T h a I G A T C G A T C
Fig. 1. Loss of heterozygosity at loci on ch romosome 17 and point mutat ions in the p53 gene in glial tumors. L, lymphocyte DNA; T, tumor DNA.
6 7 1 8
Research. on January 15, 2015. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from

A POTENTIAL SECOND TUMOR SUPPRESSOR GENE ON 17p IN ASTROCYTOMAS
Table 2 Mutations of the p53 gene in glial tumors
Conserved Tumor Allele Exon Codon Mutation AA changes region Conversion
A 2 M a 8 270 TTT~TTC Phe~Leu N TV 5 M 8 273 CGT~CAT Arg~His Y TS
13 M 5 145 CTG--.CCG Leu--Arg Y TV 14 M 8 273 CGT--~TGT Arg~Cys Y TS 25 M 7 248 CGG-.CAG Arg~Gln Y TS 35 M 5 145 CTG-,CCG Leu-,Pro Y TS 37 M 8 306 CGA-~TGA Arg-~Stop N TS
C 4 WM 8 273 CGT-~TGT Arg-~Cys Y TS 7 WM 6 194 CTT--.CCT Leu-~Pro N TS
10 WM 5 151 CCC-~GCC Pro~Ala N TV a M, mutant; W, wild type; Y, yes; N, no; TS, transition; TV, transversion.
three most frequently mutated codons of the p53 gene in mul- tiple human cancers (16), was the target of mutations in three tumors. Transitions, mostly on CpG dinucleotides, were more prevalent (7 of 10 mutations), but transversions were also de- tected (3 of 10 tumors). Of the seven transitions, two were T to C conversions and five occurred as C:G to T:A substitutions at the CpG sites.
Discussion
Mutational inactivation of the p53 gene occurs in many hu- man neoplasms. The data presented here support the crucial involvement of the p53 gene in the tumorigenic process of as- trocytomas and suggest the potential contribution of another tumor suppressor gene on the short arm of chromosome 17 in glial tumors. In 7 of 12 tumors (58%) that sustained somatic deletions on chromosome 17, we detected homozygous inacti- vation of the wild-type p53 gene through loss of one copy and mutation in the other (group A tumors), a pattern that con- forms to the classical paradigm of tumor suppressor genes. However, the remaining 42% of tumors with loss of heterozy- gosity on chromosome 17 had either no detectable mutation (group B tumors) or deletion (group C tumors) of the p53 gene. In these tumors as well as in the 28 tumors without gene losses on chromosome 17 or mutation in the p53 gene, the oncogenic process may have still targeted the p53 gene by other mecha- nisms. Sequestering of the wild-type p53 protein, observed in the cytoplasm of a significant number of breast tumors, may represent one such mechanism (45). Amplification of the MDM2 gene, whose protein product binds to the p53 protein (46), has been observed in many sarcomas (47), suggesting that complexing of the M D M 2 protein with p53 may provide yet another mechanism of its inactivation. Analysis for possible genetic alterations of the MDM2 gene in all 40 glial tumors examined in this study showed no evidence of amplification or other rearrangements (data not shown). It is conceivable that in some glioblastomas the negative regulatory function of the p53 gene is compromised by similar or heretofore unidentified mechanisms. Alternatively, mechanisms other than the inacti- vation of the p53 gene may exist on chromosome 17 involving other tumor suppressor genes. The latter possibility has been suggested for some breast tumors that sustain gene losses on chromosome 17 and retain a single wild-type p53 allele (25).
The data from group B and group C tumors in our study support the presence of another tumor suppressor gene on chro- mosome 17 distinct from p53 in glial tumors. In the two group B tumors, which lost one copy of the p53 gene, there was no mutation in exons 5-9, and the search for rare mutations in the rest of the exons and the intron/exon boundaries of all 11 exons
was unsuccessful. Although mutations in the intronic sequences affecting the transcription of the p53 gene cannot be ruled out, in these tumors deletions may be targeting a gene other than p53 on chromosome 17.
The presence of another potential tumor suppressor gene on chromosome 17 in glioblastomas is further suggested, and its map position defined, by somatic deletions in tumors of group C. The p53 locus was not included in the region of allele loss in the three tumors (tumors 4, 7, and 10) of this group. Further- more, retention of constitutional heterozygosity attwo 17pl 3.3 loci, D17S5 and D17S28, but reduction to homozygosity at another 17p13.3 locus, D17S34, in tumors 4 and 7,define the proximal boundary of the deleted region harboring a poten- tial tumor suppressor gene between the D17S5/D17S28 and D 17S34 markers. The unavailability of polymorphic markers in the telomeric region distal to the D17S34 locus (13) did not allow definition of the distal boundary of the deleted region.
All three tumors of group C contained one normal and one mutated copy of the p53 gene. The hypothesis that tumors with one wild-type and one mutant allele of the p53 gene may rep- resent an intermediate stage during tumor progression, eventu- ally leading to the loss of the remaining wild-type copy (42), may not be relevant in the case of glioblastomas, which are very advanced and malignant tumors at presentation. Furthermore, two of these tumors, from patients 4 and 7, were recurrent tumors, whereas the tumor from patient 10 was a primary tu- mor. This tumor recurred 8 months after surgery, and the 17p deletions and p53 mutation profile of the recurrent tumor was identical to that of the primary tumor (data not shown).
The role of the p53 gene in tumors of group C, however, remains speculative at the present time. Several mutant forms of p53 protein have been proposed to confer growth advantage on cells and function in a dominant negative fashion (15), pre- sumably by blocking the physiological function of the wild-type form by oligomerization (48). Normal p53, on the other hand, seems to negatively regulate the cell growth probably by virtue of its transcriptional regulatory activity (49). Furthermore, the phenotypic dominance of the normal p53 gene over its mutant form in a two-allele configuration has been demonstrated (50). The functions of wild-type and/or mutant forms of p53 may be modulated by the nature of the p53 mutation as well as by the microenvironment resulting from various patterns of genetic mutations in a particular tumor type. It is conceivable that in glioblastomas the homozygous functional loss of a gene in the telomeric region of chromosome 17 may enhance the dominant negative action of the mutant form of p53 in the presence of its normal allele. This notion is further supported by the fact that the region distal to the D17S5/D17S28 markers was always
6719
Research. on January 15, 2015. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from

A POTENTIAL SECOND TUMOR SUPPRESSOR GENE ON 17p IN ASTROCYTOMAS
included in chromosome 17 deletions in all of the tumors ana- 18. lyzed here except for one tumor (patient 37) from group A.
The tumorigenic process involves many mutational steps on multiple chromosomes and considerable interactions between 19. various mutant products. For example, in Wilms' tumor (22, 23), neurofibrosarcoma (24), breast cancer (25-26), renal can- 20. cer (27), and lung cancer (28), single chromosomes seem to be
21. the site of multiple independent mutations, which may either cooperate with each other or provide alternative genetic mech- anisms for tumor development. Here we provide evidence for 22. the presence of another potential tumor suppressor gene dis- tinct from p53 on chromosome 17 in glioblastomas and define 23. its map position in the telomeric region of the short arm of chromosome 17. This gene may act alone or in conjunction 24. with the p53 gene. Future studies aimed at the cloning and characterization of this gene should provide a better under- standing of the various mutational mechanisms involved in glioblastomas.
Acknowledgments
We are grateful to Dr. Bert Vogelstein for the generous gift o f the human M D M 2 probe. We are also grateful to Cheryl Null for very valuable assistance in providing the relevant clinical information on patients and to William Reinhold for expert technical assistance.
25.
26.
27. References
1. Bishop, J. M. Molecular themes in oncogenesis. Cell, 64: 235-248, 1991. 28. 2. Stanbridge, E. J. Human tumor suppressor genes. Annu. Rev. Genet., 24:
615-657, 1990. 3. Marshall, C. J. Tumor suppressor genes. Cell, 64: 313-326, 1991. 4. Nigro, J. M., Baker, S. J., Preisinger, A. C., Jessup, J. M., Hostetter, R., 29.
Cleary, K., Bigner, S. H., Davidson, N., Baylin, S., Devilee, P., Glover, T., Collins, F. C., Weston, A., Modali, R., Harris, C. C., and Vogelstein, B. Mutations in the p53 gene occur in diverse tumor types. Nature (Lond.), 342: 30. 705-708, 1989.
5. Baker, S. J., Fearon, E. R., Nigro, J. M., Hamilton, S. R., Preisinger, A. C., Jessup, J. M., vanTuinen, P., Ledbetter, D. H., Barker, D. F., Nakamura, Y., White, R., and Vogelstein, B. Chromosome 17 deletions and p53 gene mu- 31. tations in colorectal carcinomas. Science (Washington DC), 244:217-221, 1989.
6. Takahashi, T., Nau, M., Chiba, I., Birrer, M. J., Rosenberg, R. K., Vinocour, M., Levitt, M., Pass, H., Gazdar, A. F., and Minna, J. D. p53: a frequent target for genetic abnormalities in lung cancer. Science (Washington DC), 32. 246:491-494, 1989.
7. Toguchida, J., Ishizaki, K., Nakamura, Y., Sasaki, M. S., Ikanaga, M., Kato, M., Sujimoto, M., Kotoura, Y., and Yamamuro, T. Assignment of common allele loss in osteosarcoma to the subregion 17p13. Cancer Res., 49: 6247- 33. 6251, 1989.
8. Okamoto, A., Sameshima, Y., Yokoyama, S., Terashima, Y., Sugimura, T., Terada, M., and Yokta, J. Frequent allelic losses and mutations of the p53 gene in human ovarian cancer. Cancer Res., 51: 5171-5176, 1991. 34.
9. Mackay, J., Steel, C. M., Elder, P. A., Forrest, A. P. M., and Evans, H. J. Allele loss on short arm of chromosome 17 in breast cancers. Lancet, 2: 1384-1385, 1988. 35.
10. James, D. C., Carlbom, E., Nordenskjold, M., Collins, V. P., and Cavenee, W. K. Mitotic recombination of chromosome 17 in astrocytomas. Proc. Natl. Acad. Sci. USA, 86: 2858-2862, 1989. 36.
11. EI-Azouzi, M., Chung, R. Y., Farmer, G. E., Martuza, R. L., Black, P. McL., Rouleau, G. A., Hettlich, C., Hedley-Whyte, E. T., Zervas, N. T., Panagop- oulos, K., Nakamura, Y., Gusella, J. F., and Seizinger, B. R. Loss of distinct regions on the short arm of chromosome 17 associated with tumorigenesis of 37. human astrocytomas. Proc. Natl. Acad. Sci. USA, 86: 7186-7189, 1989.
12. Fults, D., Tippets, R. H., Thomas, G. A., Nakamura, Y., and White, R. Loss of heterozygosity for loci on chromosome 17p in human malignant astrocy- 38. toma. Cancer Res., 49: 6572-6577, 1989.
13. Fain, P. R. Third international workshop on human chromosome 17 map- 39. ping. Cytogenet. Cell Genet., 60: 178-186, 1992.
14. Vogelstein, B. A deadly inheritance. Nature (Lond.), 348: 681-682, 1990. 15. Levine, A. J., Momand, J., and Finlay, C. A. The p53 tumour suppressor 40.
gene. Nature (Lond.), 351: 453-456, 1991. 16. Hollstein, M., Sidransky, D., Vogelstein, B., and Harris, C. C. p53 mutations
in human cancers. Science (Washington DC), 253: 49-53, 1991. 41. 17. Vogelstein, B., Fearon, E. R., Kern, S. E., Hamilton, S. R., Preisinger, A. C.,
Nakamura, Y., and White, R. Allelotype of colorectal carcinomas. Science (Washington DC), 244: 207-211, 1989. 42.
6720
Devilee, P., van den Broek, M., Kuipers-Dijkshoorn, N., Kolluri, R., Meera Khan, P., Pearson, P., and Cornelisse, C. At least four different chromosomal regions are involved in loss of heterozygosity in human breast carcinoma. Genomics, 5: 554-560, 1989. Tsai, Y. C., Nichols, P. W., Hiti, A. L., Skinner, D. G., and Jones, P. A. Allelic losses of chromosome 9, 11, and 17 in human bladder cancer. Cancer Res., 50: 44-47, 1990. Fults, D., Pedone, C. A., Thomas, G. A., and White, R. Allelotype of human malignant astrocytoma. Cancer Res., 50: 5784-5789, 1990. Morita, M., Ishikawa, J., Tsutsumi, M., Hijiki, K., Tsukada, Y., Kamidono, S., Maeda, S., and Nakamura, Y. Allelotype of renal cell carcinoma. Cancer Res., 51: 820-823, 1991. Grundy, P., Koufos, A., Morgan, K., Li, F. P., Meadows, A. T., and Cavenee, W. K. Familial predisposition to Wilm's tumour does not map to the short arm of chromosome 11. Nature (Lond.), 336: 374-376, 1988. Huff, V., Compton, D. A., Chap, L., Stong, L. C., Geiser, C. F., and Saun- ders, G. F. Lack of linkage of familial Wilms' tumour to chromosomal band 1 lp13. Nature (Lond.), 366: 377-378, 1988. Menon, A. G., Anderson, K. M., Riccardi, V. M., Chung, R. Y., Whaley, J. M., Yandell, D. E., Farmer, G. E., Freiman, R. N., Lee, J. K., Li, F. P., Barker, D. F., Ledbetter, D. H., Kleider, A., Martuza, R. L., Gusella, J. F., and Siezinger, B. R. Chromosome 17p deletions and p53 gene mutations associated with the formation of malignant neurofibrosarcomas in von Reck- linghausen neurofibromatosis. Proc. Natl. Acad. Sci. USA, 87: 5435-5439, 1990. Coles, C., Thompson, A. M., Elder, P. A., Cohen, B. B., Mackenzie, I. M., Cranston, G., Chetty, U., Mackay, J., MacDonald, M., Nakamura, Y., Hoy- heim, B., and Steel, C. M. Evidence implicating at least two genes on chro- mosome 17p in breast carcinogenesis. Lancet, 336:761-763, 1990. Cropp, C. S., Lidereau, R., Campbell, G., Champene, M. H., and Callahan, R. Loss of heterozygosity on chromosome 17 and 18 in breast carcinoma: two additional regions identified. Proc. Natl. Acad. Sci. USA, 87: 7737-7741, 1990. Yamakawa, K., Morita, R., Takahashi, E., Hori, T., Ishikawa, J., and Naka- mura, Y. A detailed deletion mapping of the short arm of chromosome 3 in sporadic renal cell carcinoma. Cancer Res., 51:4707-4711, 1991. Hibi, K., Takahashi, T., Yamakawa, K., Ueda, R., Sekido, Y., Ariyoshi, Y., Suyama, M., Takagi, H., Nakamura, Y., and Takahashi, T. Three distinct regions involved in 3p deletion in human lung cancer. Oncogene, 7" 445-459, 1992. James, C. D., Carlbom, E., Dumanski, J. P., Hausen, M., Nordenskjold, M., Collins, V. P., and Cavanee, W. K. Clonal genomic alterations in glioma malignancy stages. Cancer Res., 48." 5546-5551, 1988. Fujimoto, M., Fults, D. W., Thomas, G. A., Nakamura, Y., Heilbrun, M. P., White, R., Story, J. L., Nayior, S. L., Kagan-Hallet, K. S., and Sheridan, P. J. Loss of heterozygosity on chromosome 10 in human glioblastoma multi- forme. Genomics, 4: 210-214, 1989. yon Deimling, A., Louis, D. N., yon Ammon, K., Peterson, I., Hoell, T., Chung, R. Y., Martuza, R. L., Schoenfeld, D. A., Yasargil, M. G., Wiestler, O. D., and Seizinger, B. R. Epidermal growth factor receptor gene amplifi- cation in human glioblastoma multiforme is invariably associated with loss of chromosome 10. J. Neurosurg., 77: 295-301, 1992. Mashiyama, S., Murakami, Y., Yoshimoto, T., Sekiya, T., and Hayashi, K. Detection of p53 gene mutations in human brain tumors by single-strand conformation polymorphismanalysis of polymerase chain reaction products. Oncogenes, 6: 1313-1318, 1991. Chung, R. Y., Whaley, J., Kley, N., Anderson, K., Louis, D., Menon, A., Hettlich, C., Freiman, R., Hedley-Whyte, E. T., Martuza, R., Jenkins, R., Yandell, D., and Seizinger, B. R. TP53 gene mutations and 17p deletions in human astrocytomas. Genes Chromosomes Cancer, 3:323-331, 1991. Fults, D., Brockmeyer, D., Tullous, M. W., Pedone, C. A., and Cawthon, R. M. p53 mutation and loss of heterozygosity on chromosomes 17 and 10 during human astrocytoma progression. Cancer Res., 52: 674-679, 1992. Frankel, R. H., Bayona, W., Koslow, M., and Newcomb, E. W. p53 muta- tions in human malignant gliomas: comparison of loss of heterozygosity with mutation frequency. Cancer Res., 52: 1427-1433, 1992. von Deimling, A., Eibl, R. H., Ohgaki, H., Louis, D. N., von Ammon, K., Petersen, I., Kleihues, P., Chung, R. Y:, Wiestler, O. D., and Seizinger, B. R. p53 mutations are associated with 17p allelic loss in grade II and grade III astrocytoma. Cancer Res., 52: 2987-2990, 1992. Sidransky, D., Mikkelsen, T., Schwechheimer, K., Rosenblum, M. L., Cave- nee, W., and Vogelstein, B. Clonal expansion of p53 mutant cells is associ- ated with brain tumour progression. Nature (Lond.), 355: 846-847, 1992. Kleihues, P., Burger, P. C., and Scheithauer, B. W. Histological Typing of Tumors of the Central Nervous System. Berlin: Springer-Verlag, 1992. Sambrook, J., Fritsch, E. F., and Maniatis, T. Molecular Cloning: A Labo- ratory Manual. Cold Spring Harbor, NY: Cold Spring Harbor Laboratory, 1989. Berkman, R. A., Clark, W. C., Saxena, A., Robertson, J. T., Oidfield, E. H., and Ali, I. U. Clonal composition of glioblastoma multiforme. J. Neurosurg., 77: 432-437, 1992. Meltzer, S. J., Yin, J., Huang, Y., McDaniel, T. K., Newkirk, C., Iseri, O., Volgelstein, B., and Resau, J. H. Proc. Natl. Acad. Sci. USA, 88: 4976-4980, 1991. Baker, S. J., Preisinger, A. C., Jessup, J. M., Paraskeva, C., Markowitz, S.,
Research. on January 15, 2015. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from

A POTENTIAL SECOND TUMOR SUPPRESSOR GENE ON 17p IN ASTROCYTOMAS
Wilson, J. K. V., Hamilton, S. R., and Vogelstein, B. p53 gene mutation occur in combination with 17p allele deletions as late events in colorectal tumorigenesis. Cancer Res., 50: 7717-7722, 1990.
43. Lehman, T. A., Bennett, W. P., Metcalf, R. A., Welsh, J. A., Ecker, J., Modali, R. V., Ullrich, S., Romano, J. W., Appella, E., Testa, J. R., Gerwin, B. I., and Harris, C. C. p53 mutations, ras mutations, and p53-heat shock 70 protein complexes in human lung carcinoma cell lines. Cancer Res., 51: 4090-4096, 1991.
44. Takahashi, T., D'Amico, D., Chiba, I., Buchhagen, D. L., and Minna, J. D. Identification of intronic point mutations as an alternative mechanisms for p53 inactivation in lung cancer. J. Clin. Invest., 86: 363-369, 1990.
45. Moll, U. M., Riou, G. Levine, A. J. Two distinct mechanisms alter p53 in breast cancer: mutation and nuclear exclusion. Proc. Natl. Acad. Sci. USA, 89: 7262-7266, 1992.
46. Momand, J., Zambetti, G. P., Olson, D. C., George, D., and Levine, A. J. The mdm-2 oncogene product forms a complex with the p53 protein and inhibits p53-mediated transactivation. Cell, 69: 1237-1245, 1992.
47. Oliner, J. D., Kinzler, K. W., Meltzer, P. S., George, D. L., and Vogelstein, B. Amplification of a gene encoding a p53-associated protein in human sarcomas. Nature (Lond.), 358: 80-83, 1992.
48. Kraiss, S., Quaiser, A., Oren, M., and Montenarh, M. Oligomerization of oncoprotein p53. J. Virol., 62: 4737-4744, 1988.
49. Farmer, G., Bargonetti, J., Zhu, H., Friedman, P., Prywes, R., and Prives, C. Wild-type p53 activates transcription in vitro. Nature (Lond.), 358: 83-86, 1992.
50. Chen, P-L., Chen, Y., Bookstein, R., and Lee, W-H. Genetic mechanisms of tumor suppression by the human p53 gene. Science (Washington DC), 250: 1576-1580, 1990.
6721
Research. on January 15, 2015. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from
1992;52:6716-6721. Cancer Res Abha Saxena, W. Craig Clark, James T. Robertson, et al. Malignant Astrocytomas
inp53Suppressor Gene on Chromosome 17 Distinct from Evidence for the Involvement of a Potential Second Tumor
Updated version
http://cancerres.aacrjournals.org/content/52/23/6716
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
To request permission to re-use all or part of this article, contact the AACR Publications
Research. on January 15, 2015. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from
Copyright © 2022 FDOKUMEN




















