
Malignant hypertension in children in India
6
Nephrol Dial Transplant (1996) 11: 1261-1266 Original Article Nephrology Dialysis Transplantation Malignant hypertension in children in India P. Kumar, P. Arora, V. Kher, P. K. Rai, S. Gulati, S. S. Baijal and S. Kumar Departments of Nephrology and Radiology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, UP, India Abstract Background. Malignant hypertension is now an uncommon entity in the western world but still remains a significant problem in India. Therefore we studied the aetiological spectrum, management, and outcome of these patients. Methods. Forty consecutive children (< 16 years) with malignant hypertension were admitted and investigated to exclude or confirm the secondary causes of hyperten- sion. For acute control of blood pressure sublingual nifedipine was used in dosage of 0.3-0.6 mg/kg, failing which intravenous nitroglycerin was used. In patients with aortoarteritis with active disease, steroids were used. Angioplasty was carried out for renal artery stenosis whenever possible. Results. Renoparenchymal disease was the commonest cause of malignant hypertension, and was seen in 25 cases, renovascular hypertension in 13 cases (11 aor- toarteritis and two fibromuscular dysplasia), and two had essential hypertension. For acute control of severe hypertension, sublingual nifedipine was effective in 92.5% of patients. Of the patients with renoparenchy- mal disease five became normotensive with treatment of the underlying disease, four received renal allograft, seven died, and nine are stable on antihypertensive drugs. Renal angioplasty was carried out in seven patients with renovascular hypertension (4 cured, 3 improved) and six are controlled on drugs. Conclusions. We conclude that apart from renoparen- chymal disease, aortoarteritis is a common cause of malignant hypertension in children. Sublingual nifedip- ine is effective for the rapid control of severe hyperten- sion, and angioplasty is effective in aortoarteritis for short-term preservation of renal function and control of hypertension. Key words: aortoarteritis; renovascular hypertension; treatment Correspondence and offprint requests to: Prof. Vijay Kher, Department of Nephrology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow 226014, UP, India. Introduction Malignant hypertension (MHT) has been a well- recognized entity since the beginning of this century [1]. MHT has been defined as severe elevation of blood pressure with grade III (bilateral haemorrhage and exudates) or grade IV (bilateral papilloedema) hyper- tensive retinopathy and the presence of end-organ damage [2-4]. Hypertension is common in the general population, but the development of a malignant phase is now a rare event. In earlier studies the incidence of malignant hypertension varied from 1 to 7% and the average survival of patients with malignant hyperten- sion was 10.5 months [5,6]. In the past two decades early recognition and prompt treatment with effective antihypertensive drugs has led to a true reduction in the number of patients developing malignant hyperten- sion, and a dramatic improvement in survival. Most of the earlier studies on hypertension in chil- dren have included those with severe persistent hyper- tension [7-11]. We report here the aetiological spectrum, management, and outcome of 40 children admitted with malignant hypertension. Subjects and methods In the last 6 years 40 consecutive paediatric patients (^16 years) admitted with the malignant or accelerated form of hypertension were studied. There were 27 males and 13 females with a mean age of 12 years (range 3-16 years). In all cases the diagnosis of malignant hypertension was based on the presence of grade III (bilateral exudates or haemor- rhage) or grade IV (bilateral papilloedema) hypertensive changes in the fundus and severe hypertension (definition given by Second Task Force on Control of Blood Pressure in Children) (Table 1) [12]. All the patients underwent investigations to exclude or confirm secondary hypertension. The investigations included complete haemogram, erythrocyte sedimentation rate (ESR), creatinine, blood urea nitrogen (BUN), serum electrolytes, calcium, phosphorus, alkaline phosphatase, triglycerides, and cholesterol. Urine was examined microscopically and 24-h urinary protein, creatinine, urinary electrolytes, and vanil- mandelic acid (VMA) excretion was also estimated. The radiological investigations were chest X-ray, ultrasonogram of abdomen (USG), and intravenous urogram (IVU). © 1996 European Dialysis and Transplant Association-European Renal Association by guest on August 30, 2014 http://ndt.oxfordjournals.org/ Downloaded from
Transcript of Malignant hypertension in children in India

Nephrol Dial Transplant (1996) 11: 1261-1266
Original Article
NephrologyDialysis
Transplantation
Malignant hypertension in children in India
P. Kumar, P. Arora, V. Kher, P. K. Rai, S. Gulati, S. S. Baijal and S. Kumar
Departments of Nephrology and Radiology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, UP,India
AbstractBackground. Malignant hypertension is now anuncommon entity in the western world but still remainsa significant problem in India. Therefore we studiedthe aetiological spectrum, management, and outcomeof these patients.Methods. Forty consecutive children (< 16 years) withmalignant hypertension were admitted and investigatedto exclude or confirm the secondary causes of hyperten-sion. For acute control of blood pressure sublingualnifedipine was used in dosage of 0.3-0.6 mg/kg, failingwhich intravenous nitroglycerin was used. In patientswith aortoarteritis with active disease, steroids wereused. Angioplasty was carried out for renal arterystenosis whenever possible.Results. Renoparenchymal disease was the commonestcause of malignant hypertension, and was seen in 25cases, renovascular hypertension in 13 cases (11 aor-toarteritis and two fibromuscular dysplasia), and twohad essential hypertension. For acute control of severehypertension, sublingual nifedipine was effective in92.5% of patients. Of the patients with renoparenchy-mal disease five became normotensive with treatmentof the underlying disease, four received renal allograft,seven died, and nine are stable on antihypertensivedrugs. Renal angioplasty was carried out in sevenpatients with renovascular hypertension (4 cured, 3improved) and six are controlled on drugs.Conclusions. We conclude that apart from renoparen-chymal disease, aortoarteritis is a common cause ofmalignant hypertension in children. Sublingual nifedip-ine is effective for the rapid control of severe hyperten-sion, and angioplasty is effective in aortoarteritis forshort-term preservation of renal function and controlof hypertension.
Key words: aortoarteritis; renovascular hypertension;treatment
Correspondence and offprint requests to: Prof. Vijay Kher,Department of Nephrology, Sanjay Gandhi Post Graduate Instituteof Medical Sciences, Lucknow 226014, UP, India.
Introduction
Malignant hypertension (MHT) has been a well-recognized entity since the beginning of this century[1]. MHT has been defined as severe elevation of bloodpressure with grade III (bilateral haemorrhage andexudates) or grade IV (bilateral papilloedema) hyper-tensive retinopathy and the presence of end-organdamage [2-4]. Hypertension is common in the generalpopulation, but the development of a malignant phaseis now a rare event. In earlier studies the incidence ofmalignant hypertension varied from 1 to 7% and theaverage survival of patients with malignant hyperten-sion was 10.5 months [5,6]. In the past two decadesearly recognition and prompt treatment with effectiveantihypertensive drugs has led to a true reduction inthe number of patients developing malignant hyperten-sion, and a dramatic improvement in survival.
Most of the earlier studies on hypertension in chil-dren have included those with severe persistent hyper-tension [7-11]. We report here the aetiologicalspectrum, management, and outcome of 40 childrenadmitted with malignant hypertension.
Subjects and methods
In the last 6 years 40 consecutive paediatric patients (^16years) admitted with the malignant or accelerated form ofhypertension were studied. There were 27 males and 13females with a mean age of 12 years (range 3-16 years). Inall cases the diagnosis of malignant hypertension was basedon the presence of grade III (bilateral exudates or haemor-rhage) or grade IV (bilateral papilloedema) hypertensivechanges in the fundus and severe hypertension (definitiongiven by Second Task Force on Control of Blood Pressurein Children) (Table 1) [12].
All the patients underwent investigations to exclude orconfirm secondary hypertension. The investigations includedcomplete haemogram, erythrocyte sedimentation rate (ESR),creatinine, blood urea nitrogen (BUN), serum electrolytes,calcium, phosphorus, alkaline phosphatase, triglycerides, andcholesterol. Urine was examined microscopically and 24-hurinary protein, creatinine, urinary electrolytes, and vanil-mandelic acid (VMA) excretion was also estimated. Theradiological investigations were chest X-ray, ultrasonogramof abdomen (USG), and intravenous urogram (IVU).
© 1996 European Dialysis and Transplant Association-European Renal Association
by guest on August 30, 2014
http://ndt.oxfordjournals.org/D
ownloaded from
1262 P. Kumar el al.
Table 1. Blood pressure values (mm Hg)
Age groups Present series Severe hypertension*
3-5 years6-9 years
10-12 years13-15 years16-18 years
Systolic
157194190207201
Diastolic
113136130135141
Systolic
124130134144150
Diastolic
8486909298
* Second Task Force on Blood Pressure Control in Children [12].
Micturating cystourethrogram (MCU), captopril renogram,and intra-arterial digital substraction angiography (DSA)were done in patients with a high suspicion of reflux nephro-pathy and renovascular hypertension. Electrocardiography(ECG) and echocardiography was done to assess the cardiacstatus. Kidney biopsy and serological studies were done asand when required. The 40 patients were classified as follows:
Renal parenchymal disease (RPD)
The diagnosis of chronic glomerulonephritis (CGN) wasmade on kidney biopsy in patients with normal-sized kidneysand in the rest diagnosis was presumptive, based on theclinical picture and investigations (oedema, oliguria andsignificant proteinuria). Reflux nephropathy was diagnosedby demonstration of a renal scar on ultrasound or intraven-ous urogram and vesicoureteric reflux on micturating cystou-rethrogram. All four patients with post-streptococcalglomerulonephritis (PSGN) had clinical setting of the dis-ease, and diagnosis was confirmed by kidney biopsy. Thediagnosis of obstructive uropathy was based on intravenousurography and ultrasonographic findings.
Diagnosis of haemolytic-uraemic syndrome (HUS) wasbased on clinical features, thrombocytopenia, anaemia evid-ence of haemolysis on peripheral blood smear, such ascrenated red cells and/or target cells, schistocytes, and renalhistopathology. Likewise the diagnosis of systemic lupuserythmatosus (SLE) was based on renal histology and highdsDNA antibody titre, positive antinuclear antibody, andlow level of complement C3.
Renovascular hypertension (R VH)
Captopril renogram and intra-arterial digital subtractionangiography was carried out in patients with a high suspicionof renovascular disease (no evidence of renal parenchymaldisease, presence of abdominal or peripheral bruit, historyof claudication, and constitutional symptoms). The diagnosisof aortoarteritis (AO) was based on the presence of symptomsand signs of ischaemic, inflammatory large-vessel disease aswell as classical angiographic findings (multifocal areas ofstenosis, irregularity or aneurysm formation of the aorta orits primary branches (or both)). Management of the patientwith RVH, in addition to antihypertensive drugs, includedrevascularization or nephrectomy. Angioplasty is done as apreferred first intervention, as a policy, if the lesion onangiography is amenable to angioplasty. If angioplasty fails,then other options are considered.
In patients with aneurysms, surgical revascularization isconsidered as a preferred modality. If the kidney size on the
affected side was less than 3 cm than the normal side andwas contributing to less than 10% of the total function,nephrectomy was considered. Patients who had evidence ofactive disease were started on prednisolone 1 mg/kg for 3months, which was tapered to 0.5 mg/kg and ultimately0.25 mg/kg by the end of 6 months. These patients wereregularly followed up for control of blood pressure, andrenal function was monitored with 3-monthly serum ureaand creatinine and GFR estimation by 99m DTPA scan.
The blood pressure response to intervention was classifiedas 'cured' if diastolic pressure was normal for the age withoutmedication, 'improved' if diastolic blood pressure was normalfor the age but still required drugs, albeit less than thoserequired during pre-revascularization, or 'failed' if any oneof above criteria was not met.
Essential hypertension (EH)
The diagnosis of essential hypertension was made afterexclusion of relevant secondary causes of hypertension andpatients were treated with drugs.
For acute management of accelerated hypertension, nifedi-pine was given sublingually. Sublingual nifedipine was startedwith a dose of 0.3 mg/kg; if there was no improvement inblood pressure in 30 min, nifedipine was increased to0.4 mg/kg and subsequently to 0.6 mg/kg. The patients whofailed to respond to three consecutive doses of nifedipinewere given intravenous nitroglycerin (10-50ng/min). Side-effects of drugs were also noted. The patients were followedup 3-monthly for control of blood pressure and renalfunction.
Results
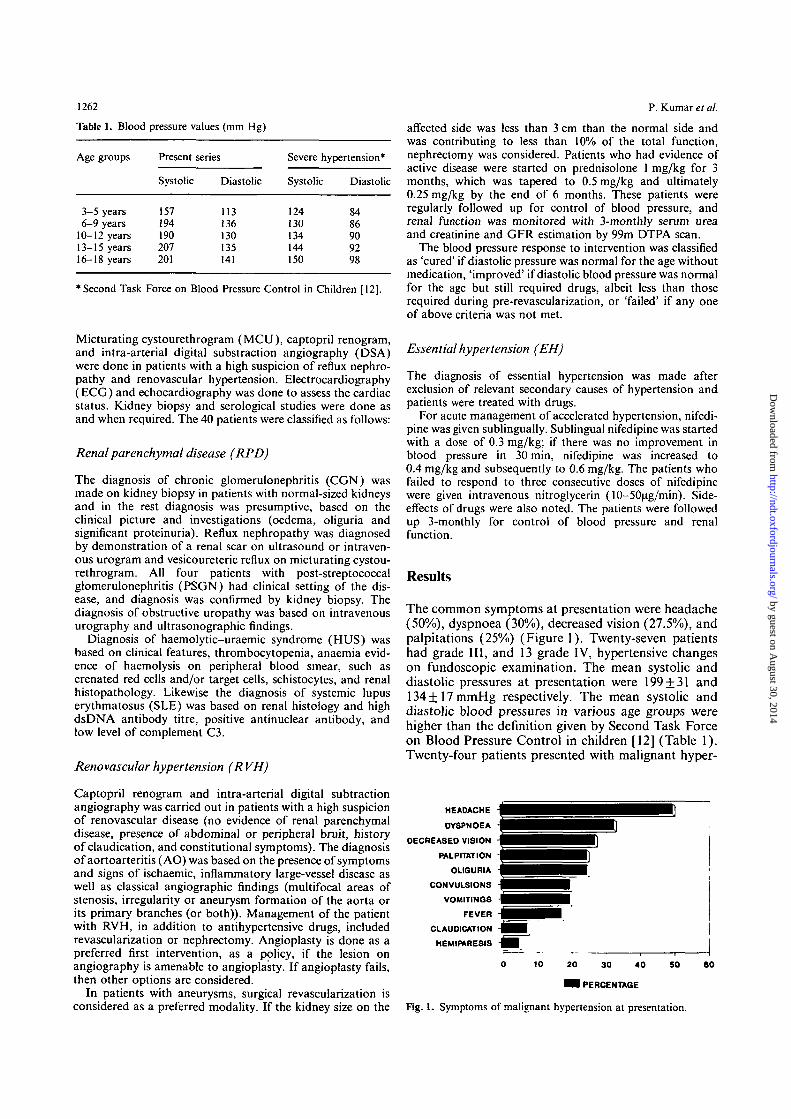
The common symptoms at presentation were headache(50%), dyspnoea (30%), decreased vision (27.5%), andpalpitations (25%) (Figure 1). Twenty-seven patientshad grade III, and 13 grade IV, hypertensive changeson fundoscopic examination. The mean systolic anddiastolic pressures at presentation were 199 + 31 and134+17mmHg respectively. The mean systolic anddiastolic blood pressures in various age groups werehigher than the definition given by Second Task Forceon Blood Pressure Control in children [12] (Table 1).Twenty-four patients presented with malignant hyper-
HEADACHE
DYSPNOEA
DECREASED VISION
PALPITATION
OLIGURIA
CONVULSIONS
VOMITINGS
FEVER
CLAUDICATION
HEMIPARESIS
10 SO20 30 40
H PERCENTAGE
Fig. 1. Symptoms of malignant hypertension at presentation.
80
by guest on August 30, 2014
http://ndt.oxfordjournals.org/D
ownloaded from
Malignant hypertension in children in India
tension as the initial manifestation, and 16 developedmalignant hypertension while on antihypertensivedrugs. The complications at presentation were renalfailure in 23 (mean serum creatinine 396 + 308 umol/1,heart failure in 12, and hypertensive encephalopathyin 12. Aetiologically the three main causes of malignanthypertension were renoparenchymal disease (62.5%),renovascular disease (32.5%), and essential hyperten-sion (5%).
Of the renoparenchymal disorders (Table 2) CGNwas the most common disease seen in 10 patients (5had biopsy-proven membranoproliferative glomerulo-nephritis). Renal failure was present in nine patientsand all of them required dialysis during follow-up.One patient had normal renal function at presentation.The mean creatinine at presentation was 500 +330 umol/1. At last follow up, six patients had died,three had received kidney transplant, and one is stableon drugs. Reflux nephropathy was present in fivepatients of which one received a kidney transplant andthe remaining four are stable on drugs. Of the fourpatients with PSGN, three became normotensive andone required antihypertensive drugs. One patient withobstructive uropathy died of renal failure and the otheris stable on antihypertensive drugs. One of the twopatients with HUS and the patient with SLE becamenormotensive. The mean serum creatinine at presenta-tion was significantly higher (P<0.01) in patients withrenal parenchymal diseases (376 ±316 umol/1) com-pared to patients with RVH (96.8 + 30 umol/1). Elevenpatients with RPD required haemodialysis. Threepatients with reflux nephropathy showed improvementin serum creatinine from 161+25 umol/1 to129+43 umol/1 with control of hypertension.
Renovascular hypertension was present in 13patients. Eleven had AO and two fibromuscular dyspla-sia (FMD). In patients of AO, intra-arterial DSA hadrevealed involvement of the abdominal aorta in 11(100%), renal-artery stenosis in 11 (100%), subclavianin four (36%), superior mesenteric artery in three(27%), and descending thoracic aorta and coeliac trunkin two each. Carotid and femoral artery involvementwas not seen. The renal artery showed bilateral involve-
1263
ment in five, while in six patients it was unilateral (4left, 2 right). Abdominal aorta showed either mild tomoderate stenosis or irregularity of the wall, onepatient showed aneurysm in the abdominal aorta inthe infrarenal part.
Of the 10 renal arteries in bilateral renal arterystenosis, two were occluded completely, six had sten-oses of more than 70%, and in two stenosis was lessthan 50%. In six unilateral stenoses, two were occludedcompletely and four had > 70% stenosis.
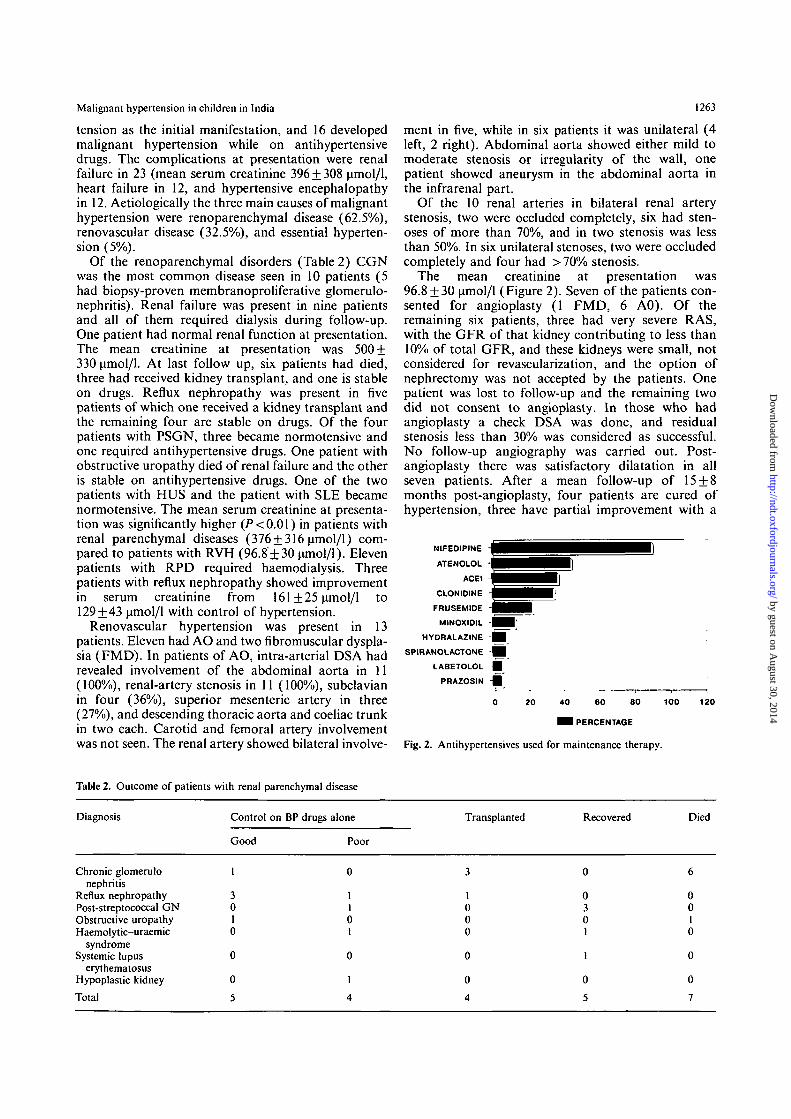
The mean creatinine at presentation was96.8 + 30 umol/1 (Figure 2). Seven of the patients con-sented for angioplasty (1 FMD, 6 A0). Of theremaining six patients, three had very severe RAS,with the GFR of that kidney contributing to less than10% of total GFR, and these kidneys were small, notconsidered for revascularization, and the option ofnephrectomy was not accepted by the patients. Onepatient was lost to follow-up and the remaining twodid not consent to angioplasty. In those who hadangioplasty a check DSA was done, and residualstenosis less than 30% was considered as successful.No follow-up angiography was carried out. Post-angioplasty there was satisfactory dilatation in allseven patients. After a mean follow-up of 15 + 8months post-angioplasty, four patients are cured ofhypertension, three have partial improvement with a
NIFEDIPINE - | | i HATENOLOL - • •
ACEI - ^ ^ HCLONIDINE ~ | ^ H
FRUSEMIDE ' • •MINOXIOIL - | ^ |
HYDRALAZINE H
SPIRANOLACTONE •
LABETOLOL |
PRAZOSIN •
0
•
20
H iI ]
40 60 80
• 1 PERCENTAGE
!
100 15
Fig. 2. Antihypertensives used for maintenance therapy.
Table 2. Outcome of patients with renal parenchymal disease
Diagnosis Control on BP drugs alone
Good Poor
Transplanted Recovered Died
Chronic glomerulonephritis
Reflux nephropathyPost-streptococcal GNObstructive uropathyHaemolytic-uraemic
syndromeSystemic lupus
erythematosusHypoplastic kidneyTotal
I
30I0
0
0
5
0301
1
0
5
0010
0
0
7
by guest on August 30, 2014
http://ndt.oxfordjournals.org/D
ownloaded from

P. Kumar et a/.
Table 3. Outcome of patients with RVH
Diagnosis On drugs alone BP control Angioplasty
Good Poor Cured Improved
Aortoarteritis* 2 2 4 2 Fibromuscular 0 1 0 1
dysplasia - - --
*One patient was lost to follow up.
care centre. Unlike most of the earlier studies which have taken children with severe persistent hypertension [7- 1 1 1, the present study includes children with grade 111 and grade IV hypertensive changes in the fundi along with severe hypertension at presentation.
The symptoms in children with severe hypertension are variable, ranging from none at all to classical symptoms of headache, convulsions, and cardiac fail- ure. In a series by Gill et al. [8], 17% patients were asymptomatic at detection of hypertension. All our patients were symptomatic at presentation and this could be explained by the severity of hypertension at
decrease in the requirement of drugs from three to one presentation (Table 1 ) [ 121. Three patients with aor- va able 3). The rest of the patients are on antihypertens- toarteritis presented with meningitis-like symptoms ives. The mean ueatinine at last was (abrupt onset headache, fever, vomiting, and altered 92.4 + 21.1 p o l l l . There was no significant difference mental state). TO the best of our knowledge such a in renal function at follow-up in those with angioplasty presentation of AO has not been reported. ~ ~ ~ i ~ g i ~ i ~ (S. treat 88.2 k 16.4 ~mol / l ) vs those without angio~la- presenting as hypertension has been reported in the sty (96.6 k20.8 p o l / l ) . literature [13]; however, our patients had no evidence
For rapid control of severe accelerated hypertension of meningitis on investigation. CI. scan of the head sublingual nifedipine (0.3-0.6 mg/kg) was effective in and CSF examination was normal. Sixty per cent of 37 patients (s~stolic from 199 k 31 to 120f 16 and our presented with MHT as the initial mani- diastolic from 134f l7 to 86*6 mHg). Three festation. Eight of I I cases of aortoarteritis had MHT patients required intravenous nitroglycerin at presentation. In a series of 88 patients by Almeida pdmin). Drugs used for maintenance
el 1141 more than 25% of them presented as were nifedipine, atenolol, clonidine, and ACE inhib- malignant hypertension. itors (Figure 3). Five patients required minoxidil. and
The renal parenchymal diseases were the most in two bilateral nephrectomy was done prior to trans- plantation. This was necessitated because of uncon- common cause of malignant hypertension in children,
trolled hypertension despite being on more than five accounting for 62.5% of cases in our series. Various
antihypertensive drugs in full doses. Twenty-three studies on severe hypertension in children have shown
patients were on antihypertensive drugs at last follow- that the renal parenchymal diseases account for up (8 with poor control of B~ and 15 with good 59-89%, and the conmumest cause is CGN 17-11]. control). The factors for poor control of BP were poor The majority of the patients with RPD had renal compliance and financial constraints. impairment at presentation and during follow-up.
Side-effects of antihypertensive drugs were seen in Eleven patients required dialysis (9 CGN, 1 RN, and eight patients. Palpitation and headache in four, severe urOpathy). hypotension in one, and hirsuitism in three. Renovascular hypertension accounts for 5-17% of
severe hypertension in children [7-1 I]. In most of the Asian countries, including ours, aortoarteritis is the
Discussion most common cause of renovascular hypertension, accounting for about two-thirds of all patients [15].
~h~ present study highlights the experience of child- The reasons for the higher prevalence of A 0 in India hood malignant hypertension in a tertiary nephrology- compared to western countries are not known- but
could be related to environmental or genetic factors. Tuberculosis was incriminated in earlier studies [16]
NO OI P ~ S but has not been confirmed by others [17]. None of our patients had tuberculosis. As A 0 is prevalent amongst Asians in the USA [I81 and is common in
- 8 Asian countries like Japan and China (HLA A9. A10, 7
6 B5, DW12 has been shown to be associated with A 0 in Japanese patients) genetic factors may be playing
5
4 - an important role in its pathogenesis. We have not
3
2 . I done HLA typing in our patients. In our study aonoar- teritis was the second most common cause of malignant -
1 - -
hypertension in children. Renal dysfunction was con- 0 -
CGN R N PSGNObs UIO HUS SLE Hyo Kna A 0 F W D EHT spicuously absent in these cases, both at presentation and during follow-up. Hence in children presenting
'1 4mg'b 15-3mgu .hngu with MHT, the presence of normal renal function is an important clue towards RVH or essential hyperten-
Fig. 3. Renal funct~on ( S creat ) at presentation sion as the underlying aetiology.
by guest on August 30, 2014
http://ndt.oxfordjournals.org/D
ownloaded from

Malignant hypertension in children in India
Percutaneous transluminal angioplasty (PTA) hasbeen an effective first-line procedure in restoring renalvascular flow and in alleviating or facilitating thecontrol of hypertension [19,20]. PTA has a reportedpatency rate as high as 80%. Restenosis is the mostfrequent complication and can occur within 1 to 2years [18]. In our study revascularization by percutan-eous transluminal angioplasty was successful in con-trolling hypertension. Of seven patients intervened fourwere off antihypertensive drugs and three haddecreased requirement of drugs at a mean follow upof 15 + 8 months. In a study by Kerr et al. [18], onlythree of seven PTA that were done for recanalizationof the renal artery were successful, and in two casessubsequent bypass procedure was required.
Essential hypertension was present in only 5% ofpatients of MHT, but this seems to be due to referralselection in our series, as in other studies [7, 8]. Mostpatients referred to our renal centre present with renalor renovascular disease and not essential hypertension.
The drugs normally used to treat acute hypertensionand hypertensive emergencies in the paediatric popula-tion include intravenous or intramuscular hydralazine,intravenous diazoxide, sodium nitroprusside, or labeta-lol [21]. All of these agents require parenteral adminis-tration, may cause unacceptable side-effects, especiallytachycardia, and require continuous monitoring. Mostof these drugs are not easily available in our country.Most centres in our country lack facilities for continu-ous monitoring of drug delivery and blood pressure.Fortunately sublingual nifedipine in a mean dose of0.3-0.6 mg/kg was effective in lowering acute severehypertension in 37 children. The major advantage ofnifedipine was its rapid onset of action, and this usuallymade parenteral drug administration unnecessary.Side-effects were seen on five occasions (4 patients hadpalpitations and headache, 1 patient developed severehypotension). Other studies in children have shown itto be effective on each occasion with a duration ofaction which lasts for 6h [22,23]. Since no majoradverse effects were encountered and the drug is welltolerated, we prefer this drug to intravenous drugs.Three patients required intravenous nitroglycerin(10-50 ug/min) to control severe hypertension. Noneof the patients required sodium nitroprusside.
In our series seven patients died, all with renalparenchymal disease as the underlying cause of malig-nant hypertension (6 CGN and 1 obstructive uropa-thy). All had advanced renal failure requiring dialysis.They died of uraemia because of the inability to affordrenal replacement therapy. The outcome was conspicu-ously superior in patients with RVH. Of the 23 patientson drug therapy 35% had poor control of bloodpressure at last follow-up because of poor compliancerelated mostly to non-availability of drugs from finan-cial constraints.
Thus we conclude that MHT is not an uncommonproblem in our country. Apart from renal parenchymaldiseases non-specific aortoarteritis is a common cause
1265
of malignant hypertension in children and it commonlypresents with MHT as the initial manifestation. Renalfunction remains normal and percutaneous translu-minal angioplasty is an effective method for short-termpreservation of renal function and control of hyperten-sion in aortoarteritis. The survival of children withMHT is better in patients with RVH compared toRPD. Sublingual nifedipine is effective and safe forrapid control of severe hypertension.
Acknowledgements. The authors appreciate the secretarial assistanceof Mr Santosh Kumar Verma. Data were presented in part at the1995 Annual Conference of the ERA at Athens, Greece.
References
1. Janeway TC. Nephritic hypertension: clinical and experimentalstudies. Am J Med Set 1913; 145: 625-656
2. Calhoun DA, Oparil S. Treatment of hypertensive crisis. N EnglJ Med 1990; 323: 1177-1183
3. Houston M. Pathophysiology, clinical aspects and treatment ofhypertensive crisis. Prog Cardiovasc Dis 1989; 32: 99-148
4. Keith NM, Wagener HP, Barker NW. Some different types ofessential hypertension: their course and prognosis. Am J MedSci 1939; 197: 332-343
5. Kincaid-Smith P, McMichael J, Murphy EA. Clinical courseand pathology of hypertension with papilloedema. Q J Med1958; 37: 117-153
6. Perera, GA. Hypertensive vascular disease, description andnatural history. J Chron Dis 1955; 1: 33-42
7. Still JL, Cottom D. Severe hypertension in childhood. Arch DisChild 1967; 42: 34-39
8. Gill DG, Mehdes da costa B, Cameron JS, Joseph MC, OggCS, Chantler C. Analysis of 100 children with severe andpersistent hypertension. Arch Dis Child 1976; 51: 951-956
9. Uhari M, Koskimies O. A survey of 164 Finnish children andadolescents with hypertension. Ada Paediatr Scand 1979; 68:193-198
10. Loirat C, Pillion G, Blum C. Hypertension in children: presentdata and problems. Adv Nephrol 1982; 11: 65-98
11. Dillon MJ. Investigation and management of hypertension inchildren. Pediatr Nephrol 1987; 1: 59-68
12. Report of the Second Task Force on Blood Pressure Control inChildren. Pediatrics 1987; 79: 3-27
13. Waters K, Gills J. Meningitis presenting as hypertension. ArchDis child 1987; 62: 191-193
14. Almeida AF, Bhiwalkar MG, Khanna UB et al. Malignanthypertension clinicopathological study of 88 patients. PostgradMedJ 1986; 34: 563-569
15. Sharma BK, Sagar S, Chugh KS, Sakhuja V, Rajchandran A,Malik N. Spectrum of renovascular hypertension in the youngin North India. A hospital based study on occurrence andclinical features. Angiology 1985; 36: 370-378
16. Sen PK, Kinare SG, Kelkar MD, Parulkar GB. Non specificaortoarteritis—A monograph based on a study of 101 cases.McGraw Hill Publishing Co, Bombay, 1972; 41-42
17. Chugh KS, Sakhuja V. Takayasu's arteritis as a cause ofrenovascular hypertension in Asian countries. Am J Nephrol1992; 12: 1-8
18. Kerr GS, Hallahan CW, Giordano J el al. Takayasu arteritis.Ann Intern Med 1994; 120: 919-929
19. Sharma S, Saxena A, Talwar KK, Kaul U. Mehta SN, Rajani M.Renal artery stenosis caused by non specific arteritis (Takayasudisease): results of treatment with percutaneous transluminalangioplasty in the management of Takayasu arteritis. Br J Radiol1992; 63: 517-522
20. Kumar S, Mandalam KR, Rao VRK et al. Percutaneoustransluminal angioplasty in non specific aortoarteritis (Takayasudisease). Experience of 16 cases. Cardiovasc Intervent Radiol1989; 12: 321-325
21. Dillon MJ. Modern management of hypertension. In Meadow R,
by guest on August 30, 2014
http://ndt.oxfordjournals.org/D
ownloaded from

1266 P. Kumar el al.
ed. Recent Advances in Paediatrics. No. 7. Churchill Livingstone, 23. Rascher W, Bonzel ICE, Ruder H, Muller Wiefel DE. Scharer K.Edinburgh, 1984: 35-55 Blood pressure and hormonal responses to sublingual nifedipine
22. Dilmen V, Cagler MK, Sewes DA, Kinik E. Nifedipine in in acute childhood hypertension. CIm Exp Hypertens (A) 1986:hypertensive emergencies of children. Am J Dis child 1983; 137: 8- 859-8691162-1165
Received for publication: 29.8.95Accepted in revised form: 1.2.96
by guest on August 30, 2014
http://ndt.oxfordjournals.org/D
ownloaded from




















