
Educating Student Registered Nurse Anesthetist on Malignant ...
Upload
independentCategory
view
1download
0
Eccrine Porocarcinoma (Malignant Eccrine Poroma)A Clinicopathologic Study of 69 Cases
A. Robson, M.R.C.Path., J. Greene, M.D., N. Ansari, M.R.C.Path.,B. Kim, M.D., P. T. Seed, M.Sc., C Stat, P. H. McKee, F.R.C.Path., andE. Calonje, M.D.
The clinicopathologic characteristics of 69 cases of eccrineporocarcinoma (EP) have been studied. Seven cases of purelyin situ disease are included. Forty patients were female, 29male with ages ranging from 29 to 91 years (mean 73 years).The lower extremity represented the single most common site(44%). Other common sites were the trunk (15 cases, 24%) andhead (11 cases, 18%). The histologic diagnosis of EP waspredicated on the basis of an irregular tumor at least partlyformed of characteristic poromatous basaloid epithelial cellsdisplaying ductal differentiation, and significant cytologic atyp-ia. Forty-seven tumors (68%) contained mature well-formedeccrine ducts having an eosinophilic luminal cuticle, with theremaining tumors containing small ill-formed ducts and/or in-tracytoplasmic lumina. All ducts were discernible via light mi-croscopy and in 49 cases were highlighted with DPAS stainand/or CEA/EMA immunocytochemistry. A variant with abroad pushing tumor margin and marked nuclear pleomor-phism showed some resemblance to proliferative bowenoiddysplasia. In 11 cases (18%) the tumors appeared to arise incontinuity with a benign preexistent poroma. A variety of his-tologic patterns were displayed including clear, squamous, andspindle cell differentiation, mucus cell metaplasia, and coloni-zation by melanocytes. Lymphovascular invasion was presentin 9 cases (15%). Three cases showed pagetoid extension ofmalignant cells (epidermotropism) and appeared to be multifo-cal. Follow-up was available in 54 patients (78%) with 9 (17%)experiencing local recurrence, 10 developing lymph node me-tastases (19%), and 6 (11%) experiencing distant metastases ordeath. Mitoses, the presence of lymphovascular invasion, andtumor depth >7 mm were associated with a poorer prognosis.Dividing tumors into those with a “pushing” or “infiltrating”advancing margin was also predictive of outcome with thelatter having an increased risk of local recurrence. This report,
the largest series of EP to date, suggests that the incidence ofaggressive behavior is less than popularly believed. Further-more, EP can display a wide variety of histologic patterns thatmay lead to diagnostic error in the unwary. The large numberof cases in this series enables a reliable evaluation of prognosticparameters. A more aggressive clinical course may be indicatedby more than 14 mitoses per high power field (hazard ratio[HR] for death 17.0, 95% confidence interval [CI] 2.71–107),lymphovascular invasion by tumor (HR 4.41, CI 1.13–17.2),and depth >7 mm (HR 5.49, CI 1.0–30.3). Thus, mitoses, lym-phovascular invasion, and tumor depth should be evaluated inthese tumors. We also suggest that tumors presenting an “in-filtrative” advancing margin are particularly prone to local re-currence and require wide excision with close attention to thesurgical margins by the reporting pathologist.Key Words: Eccrine porocarcinoma (malignant eccrineporoma)—Prognosis.
Am J Surg Pathol 25(6): 710–720, 2001.
In 1963 Pinkus and Mehregan described a glycogen-rich malignant tumor in an 82-year-old woman whichshowed multiple epidermotropic metastases and lymphnode deposits, subsequently killing the patient.22 Fromthe marked pagetoid extension and cytologic character-istics of the tumor cells, i.e., glycogen containing, ab-sence of tonofibrils, and their relationship to the sur-rounding epidermis, the authors concluded the tumor waslikely to be eccrine in origin. Since this original casereport of eccrine porocarcinoma (EP) there have beennumerous examples of EP described in the literature.Most of these have been either isolated cases or smallseries and frequently detail aggressive tumors. Of 44cases reported in the literature with follow-up, 26 had apoor outcome with locally aggressive disease, lymphnode, or distant metastases or death. By contrast, thelargest series of 27, 24, and 18 cases suggest such ag-gressive behavior may be the exception.3,18,31 We pre-sent and discuss the clinical and pathologic features of 69previously unreported primary EPs in the light of thesereports and discuss those histologic parameters that mayprovide a guide to prognosis.
From the Nuffield Department of Clinical Laboratory Sciences(A.R.), University of Oxford; the Department of Pathology (N.A.), St.Thomas’ Hospital, London, U.K.; the Department of Haematopathology(B.K.), University of Pittsburgh School of Medicine, Pittsburgh,Pennsylvania, U.S.A.; Fetal Health Research Group, Department ofObstetrics and Gynaecology (P.T.S.), King’s College, London, U.K.;the Department of Pathology (P.H.M.), Brigham’s and Women’sHospital, Boston, Massachusetts, U.S.A.; and the Department ofDermatopathology (J.G., E.C.), St. John’s Institute of Dermatology,St. Thomas’ Hospital, London, U.K.
Address correspondence and reprint requests to E. Calonje, MD,Department of Dermatopathology, St. John’s Institute of Dermatology,St. Thomas’ Hospital, Lambeth Palace Road, London, SE 1 7EI, U.K.;e-mail: [email protected]
The American Journal of Surgical Pathology 25(6): 710–720, 2001 © 2001 Lippincott Williams & Wilkins, Inc., Philadelphia
710

MATERIALS AND METHODS
Eighty-four cases diagnosed as EP were retrievedfrom the archives of St. John’s and St. Thomas’s Hos-pital and included consultation cases from two of theauthors (E.C. and P.H.M.). Fifteen of these were dis-carded through insufficient material, missing slides, or,upon review, were not considered acceptable by the au-thors’ criteria of EP. The hematoxylin and eosin-stainedsections were reexamined. In some cases special stains(Periodic Acid Schiff [PAS] and Diastase Periodic AcidSchiff [DPAS], n � 44) and immunocytochemical stud-ies (n � 29) had been carried out (for epithelial mem-brane antigen [EMA], 1:80, no antigen retrieval, Dako,Ely, UK, and carcinoembryonic antigen [CEA], 1:100,no antigen retrieval, Biogenics, San Ramon, CA, USA),and these slides were also examined. Table 1 lists thehistologic parameters evaluated in all tumors.
Evidence of ductal differentiation was invariably pres-ent. In situ lesions were diagnosed if the lesion containedmarkedly atypical cells showing duct formation withoutdermal invasion. Duct differentiation may vary from in-tracytoplasmic lumina to mature ducts with an eosino-philic cuticle bordered by cuboidal but clearly malignantepithelial cells. The cytologic pleomorphism of these ep-ithelial cells together with nuclear atypia indicates thatthe ducts are an integral part of the neoplasm and nottrapped “bystanders.” The intracytoplasmic lumina aresmaller, ill formed, and irregular in shape. Care wastaken not to misinterpret degenerative vacuolation of tu-mor cells as evidence of ductal differentiation. Duct mor-phology cannot distinguish between apocrine and eccrinetumors. However, no tumor displayed large eosinophilicgranular cells displaying decapitation secretion, hall-marks of apocrine glandular differentiation. Tumorswere classified as invasive if there were clear extensionof separate islands of atypical epithelial cells into thedermis. The nature of the tumor margin was categorizedas “pushing” or “infiltrative” according to broad advanc-ing islands of cells or small irregular groups and strandsof cells, respectively. A variant of invasive tumor havinga broad pushing advancing edge with focal dyskerato-sis and often-bizarre cytonuclear atypia reminiscent ofBowen’s disease (squamous carcinoma [SCC] in situ)was identified and termed “bowenoid” pattern. To ascer-tain whether EP can supervene on a preexisting lesion,the presence of a benign component was noted. The basisfor establishing part of the tumor as benign used ac-cepted diagnostic criteria of eccrine poroma, namely, asubstantial portion of the tumor formed of regular smallbasaloid epithelial cells with mature ducts lined by aneosinophilic cuticle and lacking any cytologic atypia. Inaddition to the usual histologic pattern of malignantsmall basaloid or amphophilic epithelial cells, other pat-terns of differentiation were recorded if present. Clear,
spindle, mucus, and squamous cell differentiation werenoted. Colonization of the tumor by melanocytes, as hasbeen reported previously in eccrine tumors, was re-corded. Despite established criteria for the accurate clas-sification of eccrine neoplasms, it is well recognized thatmany tumors are not infrequently encountered that defyrigorous categorization. Thus, tumors were also evalu-ated for morphologic characteristics of other types ofeccrine neoplasia.
Further to the nature of the advancing tumor margin,several other parameters were specifically evaluated forpossible prognostic significance: These included thepresence of lymphovascular and perineural invasion, mi-totic count, host response, and necrosis. Mitoses werecounted per 10 high power fields. Since it has been sug-gested that the host immune response may be importantin the defense against some malignancies (e.g., mela-noma), this was evaluated by assessing the presence oftumor infiltrating lymphocytes (TILs). TILs were classi-fied as “brisk,” “nonbrisk,” or “absent”. Brisk denotesthe permeation throughout the tumor by host lympho-cytes with death of tumor cells. Nonbrisk reflects similarchanges restricted to only part of the tumor, while absentdenotes the lack of any mononuclear cells within thesubstance of the tumor, even if a marked chronic inflam-matory response lies in the underlying dermis. Necrosiswas divided into comedo or diffuse. In comedonecrosis,islands of tumor cells contained central areas of tumorcell death with inflammatory debris in a pattern similarto that of comedo type, ductal carcinoma in situ of thebreast. Diffuse necrosis was represented by more wide-spread cell death. Comedonecrosis and/or generalizednecrosis were combined with the degree of nuclear atyp-ia to define two subjective categories, “high” and “low”grade malignancies. Low-grade tumors lacked necrosisand displayed less nuclear pleomorphism. Finally, themaximum depth of tumor invasion was measured using
TABLE 1. Histological parameters evaluated
In situ or invasiveDuct formationPresence of a benign poromatous componentNecrosisComedo necrosisClear cell )Spindle cell ) differentiationSquamous cell )Mucus cell )Other admixed adnexal patterns of differentiationColonization by melanocytesTumor-infiltrating lymphocytesBowenoid patternLymphovascular invasionPerineural invasionAdvancing tumor marginRegression“High” or “low” gradeDepth of invasionMitotic count
ECCRINE POROCARCINOMA (MALIGNANT ECCRINE POROMA) 711
Am J Surg Pathol, Vol. 25, No. 6, 2001
the Vernier scale. This represented the vertical distancefrom the granular layer (or ulcerated surface of the tu-mor) to the deepest point of invasion at the thickest re-gion of tumor. In fragmented specimens the thickest re-gion on the slide measurable was noted.
Survival analysis was used to assess time to death,lymph node involvement, or local recurrence and to re-late it to the observed histologic features that might beuseful in assessing prognosis of tumors. The log-rank testwas used for single variables, dividing continuous mea-sures at the quintiles; and Cox’s proportional hazardsregression with robust standard errors for adjusted esti-mates was also used. Results are presented as HR with95% CI. Statistical significance at the 5% level isclaimed where the interval does not include “no effect”(HR of 1). All analyses were in the computer packageStata version 6.0 (Stata Corp. College Station, TX).
The clinical data were reviewed and follow-up detailswere requested from the clinician or referring pathologist(see Acknowledgments).
RESULTS
Of the 69 patients within the study, 7 had in situ ec-crine carcinoma and 62 had invasive disease. Of the lat-ter 43 were female (69%) and 19 male (31%) with an agerange of 29–91 years (mean 73 years, median 78 years).In comparison, the 7 in situ cases comprised 5 femaleand 2 male patients with an age range of 52–87 years(mean 71 years, median 77 years). Table 2 presents theclinical details of patients with invasive disease, the legrepresenting the single most common location.
Four of the in situ cases arose on the leg with a further1 each on the foot, thigh, and head. Three patients hadmultiple invasive cutaneous nodules at presentation. Thepreoperative duration of the lesion was established in 34patients (49%) and varied from 2 weeks to 60 years(mean 9 years, median 4 years) but in numerous caseswas merely stated to be “many years.” Tumor size variedfrom 0.4 to 20.0 cm in the invasive cases (mean 2.2 cm,
median 2.0 cm). The in situ lesions varied from 0.5 to 3.0cm (mean 1.4 cm, median 1.2 cm).
The clinical diagnosis was never correct where thisinformation was supplied, and lesions were often be-lieved to be SCC, SCC in situ, or pyogenic granuloma.Fifty-five tumors underwent local excision, 4 were cu-retted, and 6 were biopsied. Of these, 27 had wider ex-cision due to involved surgical margins or the reportingpathologist deemed the margin of excision too close. Onepatient had a forequarter amputation due to multiplerecurrences/tumor deposits on the arm. Chemotherapy,radiotherapy, and laser therapy were each administeredto one patient.
Outcome was established in 54 patients (78%).Twenty-nine (54%) patients remain alive and well. Nine(17%) experienced local recurrence, one repeatedly, whotogether with one additional patient subsequently devel-oped lymph node metastases. Ten (19%) suffered lymphnode metastases. Two (4%) patients remain alive withmetastatic disease while 4 patients (7%) died with dis-seminated malignancy. Table 3 lists the histologic find-ings in all tumors.
The diagnosis of EP in these cases was based on thefinding of either an invasive architectural pattern and/orsignificant cytologic pleomorphism in a tumor showingeccrine differentiation. Thus, a tumor with an irregularadvancing margin and at least focal significant cytologicatypia is considered malignant; similarly, tumors havinga relatively broad advancing front that displayed markedcytologic atypia and prominent mitotic activity are in-cluded. Most tumors had a typically lobular morphologyin at least part of the lesion and were composed of some-what basaloid epithelial cells showing variable degreesof cytologic pleomorphism, sometimes with necrosis(Fig. 1). Of the 69 cases in this series, 47 contained easilyrecognizable ducts lined by cuboidal epithelial cells of-
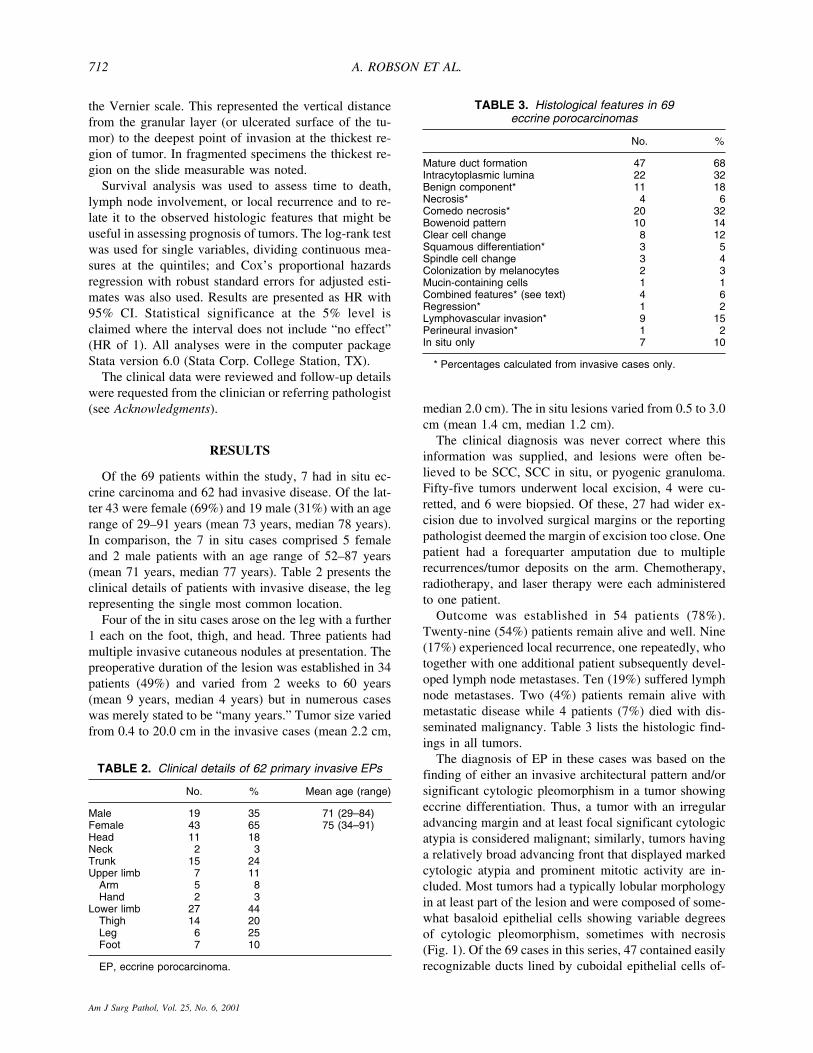
TABLE 3. Histological features in 69eccrine porocarcinomas
No. %
Mature duct formation 47 68Intracytoplasmic lumina 22 32Benign component* 11 18Necrosis* 4 6Comedo necrosis* 20 32Bowenoid pattern 10 14Clear cell change 8 12Squamous differentiation* 3 5Spindle cell change 3 4Colonization by melanocytes 2 3Mucin-containing cells 1 1Combined features* (see text) 4 6Regression* 1 2Lymphovascular invasion* 9 15Perineural invasion* 1 2In situ only 7 10
* Percentages calculated from invasive cases only.
TABLE 2. Clinical details of 62 primary invasive EPs
No. % Mean age (range)
Male 19 35 71 (29–84)Female 43 65 75 (34–91)Head 11 18Neck 2 3Trunk 15 24Upper limb 7 11
Arm 5 8Hand 2 3
Lower limb 27 44Thigh 14 20Leg 6 25Foot 7 10
EP, eccrine porocarcinoma.
A. ROBSON ET AL.712
Am J Surg Pathol, Vol. 25, No. 6, 2001

ten having an eosinophilic luminal cuticle. The remain-der contained less well-developed ducts, having irregularand poorly formed structures and/or intracytoplasmic lu-mina. In 46 cases of invasive and 3 cases of in situporocarcinoma, the presence of ducts or intracytoplasmiclumina was highlighted with PAS/DPAS staining (n �44) or immunocytochemistry (n � 29). The luminal duc-tal border stained positive with antibodies to EMAand/or CEA (Fig. 2).
Eleven (18%) EPs had residual foci of benign eccrineporoma (BEP). These foci displayed the typical architec-tural and cytologic features of eccrine poroma (Fig. 3);regular collections of uniform small cuboidal basaloidepithelial cells with a broad pushing tumor margin and
well-formed ducts having an eosinophilic luminalcuticle.
Necrosis was present within 24 tumors (39%) either asdiffuse and generalized tumor cell death (4 tumors, 6%)or as comedo type (20 cases, 32%) (Fig. 4). Most tumorshad an endophytic growth pattern with invasion into thedeep reticular dermis or beyond, of either broad collec-tions of tumor cells or small irregular infiltrating cords ofcells at the advancing edge.
In the bowenoid variant broad tongues of tumor in-vaded the dermis and consisted of markedly pleomorphicepithelial cells. Bizarre multinucleate tumor cells andfocal keratinization enhanced the likeness to proliferativebowenoid dysplasia (Fig. 5A). The presence of ductswithin the lesion lined by tumor cells, however, excludedthis diagnosis (Fig. 5B). Two in situ tumors showedsimilar bowenoid features.
Tumors growing with an expansile lower border caneasily be mistaken for benign lesions, particularly if thecytologic details are missed. However, one patient withthis pattern experienced metastatic spread and subse-quently died of disease.
FIG. 1. A typical example of an eccrine porocarcinoma;an infiltrative tumor connected to the epidermis witha lobulated architecture and necrosis, showing ductaldifferentiation.
FIG. 2. A tumor showing variable cytologic atypia, con-taining small poorly formed ducts highlighted by CEAimmunohistochemistry.
FIG. 3. Porocarcinoma with adjacent benign eccrineporoma.
FIG. 4. Note comedonecrosis.
ECCRINE POROCARCINOMA (MALIGNANT ECCRINE POROMA) 713
Am J Surg Pathol, Vol. 25, No. 6, 2001
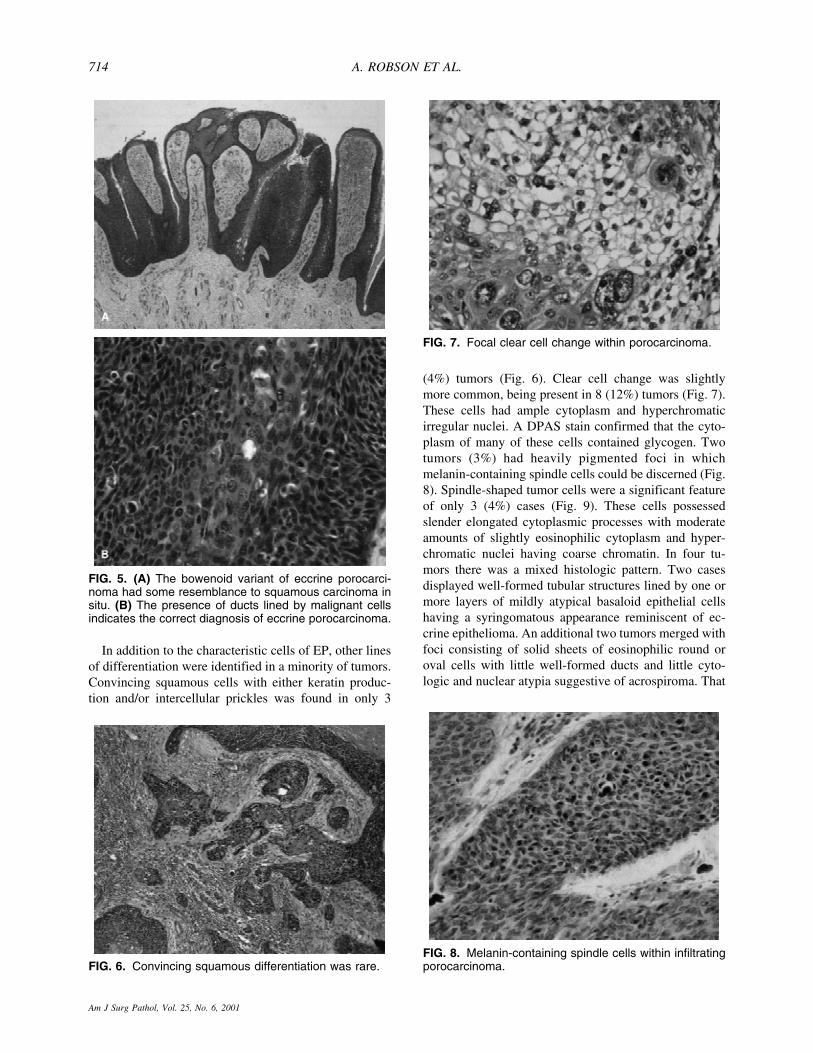
In addition to the characteristic cells of EP, other linesof differentiation were identified in a minority of tumors.Convincing squamous cells with either keratin produc-tion and/or intercellular prickles was found in only 3
(4%) tumors (Fig. 6). Clear cell change was slightlymore common, being present in 8 (12%) tumors (Fig. 7).These cells had ample cytoplasm and hyperchromaticirregular nuclei. A DPAS stain confirmed that the cyto-plasm of many of these cells contained glycogen. Twotumors (3%) had heavily pigmented foci in whichmelanin-containing spindle cells could be discerned (Fig.8). Spindle-shaped tumor cells were a significant featureof only 3 (4%) cases (Fig. 9). These cells possessedslender elongated cytoplasmic processes with moderateamounts of slightly eosinophilic cytoplasm and hyper-chromatic nuclei having coarse chromatin. In four tu-mors there was a mixed histologic pattern. Two casesdisplayed well-formed tubular structures lined by one ormore layers of mildly atypical basaloid epithelial cellshaving a syringomatous appearance reminiscent of ec-crine epithelioma. An additional two tumors merged withfoci consisting of solid sheets of eosinophilic round oroval cells with little well-formed ducts and little cyto-logic and nuclear atypia suggestive of acrospiroma. That
FIG. 6. Convincing squamous differentiation was rare.
FIG. 7. Focal clear cell change within porocarcinoma.
FIG. 8. Melanin-containing spindle cells within infiltratingporocarcinoma.
FIG. 5. (A) The bowenoid variant of eccrine porocarci-noma had some resemblance to squamous carcinoma insitu. (B) The presence of ducts lined by malignant cellsindicates the correct diagnosis of eccrine porocarcinoma.
A. ROBSON ET AL.714
Am J Surg Pathol, Vol. 25, No. 6, 2001

these cases adjoined the malignant component suggestedthat these foci represented part of the tumor rather than acoincidental benign lesion.
A single tumor had foci interpreted as regression. Thehistologic features were similar to those well establishedin malignant melanomas exhibiting this phenomenon.Thus, within the substance of the lesion, malignant tumorcells were replaced by connective tissue showing vascu-lar ectasia, inflammation, and fibrosis.
Death was predicted independently by mitoses abovethe 80th centile (>14 mitoses per high power field; hazardratio [HR] 17.0, 95% confidence interval [CI] 2.71–107),lymphovascular invasion by tumor (HR 4.41, CI 1.13–17.2) (Fig. 10), and depth >7 mm (HR 5.49, CI 1.0–30.3). Death or lymph node involvement was predictedby >14 mitoses (HR 8.5, CI 2.1–34.2) and marginally bydepth >7 mm (HR 2.5, CI 0.78–2.1). Perineural invasion,identified in only one case, did not achieve significance.After adjusting for mitosis and depth, the designation oftumor margin as “infiltrative” (Fig. 11) was strongly pre-dictive of local recurrence (HR 6.8, CI 2.1–21.9), sug-
gesting that the nature of the tumor margin should beevaluated in all EPs and commented upon in the surgicalreport. The presence of a benign component or other celltypes within the tumor, necrosis, categorizing the tumorsas high or low grade, and categorizing TILs as brisk,nonbrisk, or absent did not achieve statistical signifi-cance with regard to patient outcome. Interestingly, thepatients with apparently multiple cutaneous primary EPdid not fare worse in comparison to solitary tumors.
DISCUSSION
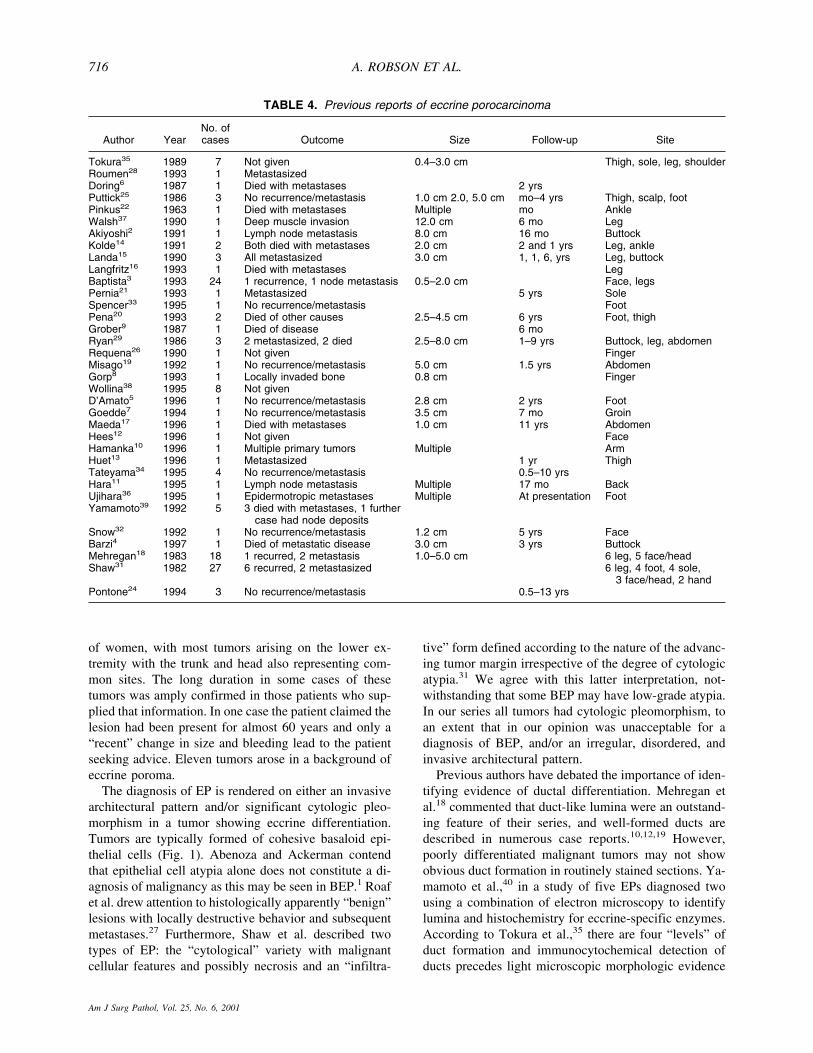
Since the first description of EP in 1963, numerousreports have appeared in the literature. These are listed inTable 4.2–22,24–26,28,29,31–39 Accurate data on the inci-dence of EP are difficult to obtain. Mehregan et al.18 andWick et al.38 quoted EP incidences of 0.01% and0.005%, respectively, of cutaneous tumors, with EP rep-resenting the most prevalent of malignant eccrine tu-mors. Although cases have been reported years after ra-diotherapy, the etiology of the majority of these tumorsremains unknown.7 EP is chiefly a tumor of elderlyadults 50–80 years of age,18,25,31,39 although it has beenreported in young adults1,15 as well as in a 12-year-oldboy with xeroderma pigmentosa.3 There is a suggestionof a male bias in the literature,7,32 although some indicatea preference for females.1 Unlike BEP, which is oftenfound on the palms and soles, the site of predilectiondoes not correlate with these areas of highest concentra-tion of eccrine glands; EP shows a preference for thetrunk or head and neck and lower extremity.1,18 Tumorsvary greatly in size from <1 cm to 10 cm. A longstandinghistory is often encountered (up to 50 years) partly re-flecting that some of these tumors arise from a preexist-ing BEP.15,25,31 Nonetheless, rapid development over afew months is also well documented.40 The findings inour series are in accord with these clinical features. Thus,the average age is 73 years with a slight preponderance
FIG. 9. Spindle cell differentiation.
FIG. 10. Lymphovascular invasion.
FIG. 11. An infiltrative growth pattern.
ECCRINE POROCARCINOMA (MALIGNANT ECCRINE POROMA) 715
Am J Surg Pathol, Vol. 25, No. 6, 2001
of women, with most tumors arising on the lower ex-tremity with the trunk and head also representing com-mon sites. The long duration in some cases of thesetumors was amply confirmed in those patients who sup-plied that information. In one case the patient claimed thelesion had been present for almost 60 years and only a“recent” change in size and bleeding lead to the patientseeking advice. Eleven tumors arose in a background ofeccrine poroma.
The diagnosis of EP is rendered on either an invasivearchitectural pattern and/or significant cytologic pleo-morphism in a tumor showing eccrine differentiation.Tumors are typically formed of cohesive basaloid epi-thelial cells (Fig. 1). Abenoza and Ackerman contendthat epithelial cell atypia alone does not constitute a di-agnosis of malignancy as this may be seen in BEP.1 Roafet al. drew attention to histologically apparently “benign”lesions with locally destructive behavior and subsequentmetastases.27 Furthermore, Shaw et al. described twotypes of EP: the “cytological” variety with malignantcellular features and possibly necrosis and an “infiltra-
tive” form defined according to the nature of the advanc-ing tumor margin irrespective of the degree of cytologicatypia.31 We agree with this latter interpretation, not-withstanding that some BEP may have low-grade atypia.In our series all tumors had cytologic pleomorphism, toan extent that in our opinion was unacceptable for adiagnosis of BEP, and/or an irregular, disordered, andinvasive architectural pattern.
Previous authors have debated the importance of iden-tifying evidence of ductal differentiation. Mehregan etal.18 commented that duct-like lumina were an outstand-ing feature of their series, and well-formed ducts aredescribed in numerous case reports.10,12,19 However,poorly differentiated malignant tumors may not showobvious duct formation in routinely stained sections. Ya-mamoto et al.,40 in a study of five EPs diagnosed twousing a combination of electron microscopy to identifylumina and histochemistry for eccrine-specific enzymes.According to Tokura et al.,35 there are four “levels” ofduct formation and immunocytochemical detection ofducts precedes light microscopic morphologic evidence
TABLE 4. Previous reports of eccrine porocarcinoma
Author YearNo. ofcases Outcome Size Follow-up Site
Tokura35 1989 7 Not given 0.4–3.0 cm Thigh, sole, leg, shoulderRoumen28 1993 1 MetastasizedDoring6 1987 1 Died with metastases 2 yrsPuttick25 1986 3 No recurrence/metastasis 1.0 cm 2.0, 5.0 cm mo–4 yrs Thigh, scalp, footPinkus22 1963 1 Died with metastases Multiple mo AnkleWalsh37 1990 1 Deep muscle invasion 12.0 cm 6 mo LegAkiyoshi2 1991 1 Lymph node metastasis 8.0 cm 16 mo ButtockKolde14 1991 2 Both died with metastases 2.0 cm 2 and 1 yrs Leg, ankleLanda15 1990 3 All metastasized 3.0 cm 1, 1, 6, yrs Leg, buttockLangfritz16 1993 1 Died with metastases LegBaptista3 1993 24 1 recurrence, 1 node metastasis 0.5–2.0 cm Face, legsPernia21 1993 1 Metastasized 5 yrs SoleSpencer33 1995 1 No recurrence/metastasis FootPena20 1993 2 Died of other causes 2.5–4.5 cm 6 yrs Foot, thighGrober9 1987 1 Died of disease 6 moRyan29 1986 3 2 metastasized, 2 died 2.5–8.0 cm 1–9 yrs Buttock, leg, abdomenRequena26 1990 1 Not given FingerMisago19 1992 1 No recurrence/metastasis 5.0 cm 1.5 yrs AbdomenGorp8 1993 1 Locally invaded bone 0.8 cm FingerWollina38 1995 8 Not givenD’Amato5 1996 1 No recurrence/metastasis 2.8 cm 2 yrs FootGoedde7 1994 1 No recurrence/metastasis 3.5 cm 7 mo GroinMaeda17 1996 1 Died with metastases 1.0 cm 11 yrs AbdomenHees12 1996 1 Not given FaceHamanka10 1996 1 Multiple primary tumors Multiple ArmHuet13 1996 1 Metastasized 1 yr ThighTateyama34 1995 4 No recurrence/metastasis 0.5–10 yrsHara11 1995 1 Lymph node metastasis Multiple 17 mo BackUjihara36 1995 1 Epidermotropic metastases Multiple At presentation FootYamamoto39 1992 5 3 died with metastases, 1 further
case had node depositsSnow32 1992 1 No recurrence/metastasis 1.2 cm 5 yrs FaceBarzi4 1997 1 Died of metastatic disease 3.0 cm 3 yrs ButtockMehregan18 1983 18 1 recurred, 2 metastasis 1.0–5.0 cm 6 leg, 5 face/headShaw31 1982 27 6 recurred, 2 metastasized 6 leg, 4 foot, 4 sole,
3 face/head, 2 handPontone24 1994 3 No recurrence/metastasis 0.5–13 yrs
A. ROBSON ET AL.716
Am J Surg Pathol, Vol. 25, No. 6, 2001

of duct formation. In our view the presence of eccrine-type ducts is a prerequisite for the reliable diagnosis ofEP. Thus, all the tumors described herein contained rec-ognizable ducts or intracytoplasmic lumina. Althoughthese were often highlighted by DPAS staining or im-munochemistry for CEA/EMA, no tumor was found tohave ducts using these ancillary techniques that had notbeen visible on light microscopy. However, as in othermalignancies with specific lines of differentiation, theextent of duct formation is variable. Of the 69 cases inthis series, 47 contained easily recognizable ducts linedby cuboidal epithelial cells having an eosinophilic lumi-nal cuticle. The remainder contained less well-developedducts mainly identified as intracytoplasmic lumina withclearly defined eosinophilic cuticles. Clearly, using rec-ognizable ducts as a major criterion for diagnosis im-plies that some poorly differentiated tumors may well beoverlooked.
The cells of EP are epithelioid and often appear ba-saloid, akin to those found in BEP. The basaloid cytol-ogy is superficially striking at low magnification. Highermagnification typically reveals the cells to have moreabundant and paler cytoplasm than is usual for BEP,although not as eosinophilic as is seen in squamous ke-ratinocytes. Furthermore, cytologic pleomorphism andnuclear atypia are invariably present. Pagetoid extensionof epithelial cells, which usually do not contain mucin, isa well-documented histologic pattern in EP. Other celltypes recorded within EP include squamous cells, spindlecells, clear cells, mucin-producing cells, and melano-cytes. The extent of squamous differentiation reported isvariable. Cited evidence has included individual cell dys-keratosis,3,25 more generalized keratinization,3,15,31 con-spicuous intercellular bridges,15,20 and keratohyalingranules.20,35,40 In some instances the basis for identifi-cation of squamous cells is not detailed.5,7 Conversely, indescribing 18 cases, Mehregan et al.18 commented thatthere was no tendency for keratinization or dyskeratosis.Several other reports make similar claims.2,14 The pres-ence of squamous cells is not surprising in eccrine neo-plasia because the luminal cells of the acrosyringium aresquamous in type. Using the strict criteria above, how-ever, we are more inclined to concur with Mehregan etal.18 having found convincing squamous cells in onlythree tumors. A spindle cell variant of porocarcinoma isrecognized and in three cases focal spindle cell differen-tiation was noted. These cells, which formed compactfascicles and islands, had elongated amphophilic cyto-plasm and similar nuclear characteristics to nearby epi-thelioid cells. No melanin or keratin production wasidentified within these portions of the tumor. Thus, aspectrum may exist between a pure spindle cell porocar-cinoma and tumors with more classical morphology.
Clear cell change is well described in a variety oftumor types including porocarcinoma. This was apparent
either focally or diffusely in eight tumors but neverformed a dominant population. The cells had cytoplas-mic clearing to variable degrees, highlighted by DPAShistochemistry, and were intimately connected with therest of the malignant tumor.
Melanocytes have been reported as “colonizing” a va-riety of tumors both benign and malignant. Wollina et al.reported the presence of S-100-positive dendritic mela-nocytes in BEP but not EP.39 Pique et al. described S-100dendritic melanocytes within a malignant hidroacan-thoma simplex,23 whereas Hara and Kamiya11 andMaeda et al.17 reported one case each of pigmented EPwith melanin pigment also being present in the metasta-ses of the former case. In the latter the tumor was exten-sively pigmented leading to an initial misdiagnosis ofmalignant melanoma, a clinical diagnosis also renderedin one of our tumors colonized by melanocytes. Pigmentor melanocyte-containing benign eccrine tumors are welldocumented, possibly more prevalent in dark-skinnedpeople, may be multiple, and may be grossly pigmented.Melanosomes are also described within EP analyzed ul-trastructurally. Although the mechanism of recruitmentof these organelles or cells remains unclear, melanocytesare present within the sweat duct anlagen in the first 14weeks of embryonic development, and the reappearanceof these cells in EP may reflect regression to a moreprimitive phenotype.
Mucin-producing cells visible by light microscopyhave only been described in a single tumor to our knowl-edge.19 In this report Paget’s disease was described aris-ing from an EP. Intraepidermal cells containing glycogenand sialomucin had microvilli and small lumina ultra-structurally. Well-formed ducts were immunopositive forCEA and EMA. The authors cited reports that sweatducts can undergo mucinous metaplasia. Yamamoto etal. reported that one of their five EPs contained mucousgranules on electron microscopy indicative of glandulardifferentiation.40 In the single tumor containing mucin-producing cells in this series, the cells displayed ampleclear cytoplasm, which stained positive with DPAS, andeccentric, irregular, and hyperchromatic nuclei. Theseatypical cells formed a cohesive, localized portion of thetumor and were intimately admixed with the remainingtumor cells indicating a common origin.
The complexity of the sweat gland apparatus is re-flected in the range of tumor types that may arise fromthis structure. Because “overlap” tumors are well knownto occur in a variety of neoplasms, care was taken toidentify any tumor with morphologic features of otheradnexal neoplasms. Previous patterns encountered in EPinclude an overlapping phenotype with syringoid eccrinecarcinoma in a metastasis40 and eccrine syringofibro-adenoma-like foci toward the periphery of a tumor.5 Inthis series two tumors showed focal eccrine epithelioma-like features, namely, tubules lined by several layers of
ECCRINE POROCARCINOMA (MALIGNANT ECCRINE POROMA) 717
Am J Surg Pathol, Vol. 25, No. 6, 2001

cuboidal epithelial cells associated with a desmoplasticstroma merging with more typical porocarcinomatoushistology. In another two cases the tumors displayed focireminiscent of nodular hidradenoma (acrospiroma) beingcomposed of monomorphic epithelial cells showing con-spicuous ductal differentiation. The ability of eccrineneoplasms to show several morphologic patterns within asingle tumor, albeit rarely, has implications for thoroughsampling of these tumors and careful attention in ap-praising their features in routine surgical pathology.
A long history before removal of EP, sometimes up to40–50 years, is very well established in the literature.2,31
In many tumors in this series, there was a long intervalbetween the patient noticing the lesion and its eventualremoval. Thus, it is possible that a significant proportionof EP follows a preexisting BEP, which undergoes ma-lignant transformation. The association between BEPand EP within a single tumor has also been well docu-mented. Shaw at al. contended that all 27 of the cases ofEP in their series arose alongside a BEP.31 Other authorsreported the common concurrence between the two.Thus, Abenoza and Ackerman stated that 30–50% ofporocarcinomas have admixed poroma,1 and Puttick etal. reported three poromas that had been present formany years before “transforming” into porocarcinoma.25
In our series 11 EPs had adjacent features typical of BEP.The benign component was conspicuous by its contrastwith the carcinomatous foci and strongly suggested apreexisting benign lesion rather than a well-differen-tiated area to the tumor.
In nine cases the tumor cells had a particularly pleo-morphic cytologic appearance similar to the markedpleomorphism commonly seen in SSC in situ. These tu-mors contained multinucleate cells having markedly ir-regular and hyperchromatic nuclei with plentiful mitoses,some of which were abnormal. These morphologic fea-tures have been described previously.2,29,31,35,40 Al-though the cytologic similarities between SCC in situand bowenoid EP may be superficially striking, the pres-ence of ductal differentiation readily establishes the cor-rect diagnosis. In addition, the bowenoid malignant EPhas a verrucous architecture rarely seen in SSC in situ.Furthermore, dyskeratotic cells are less prevalent in bo-wenoid EP in comparison with SCC in situ, which, wheninvasive, typically shows keratinization. Nevertheless,on a small biopsy, in the absence of ducts lined by atypi-cal cells, accurate distinction between the two may beimpossible. One of our cases subsequently metastasized,and similarly Langfritz et al. reported metastatic EP,which had previously been misdiagnosed as a “solarkeratosis.”16 Kolde et al.14 described metastasizing EP,which had previously been diagnosed as “Bowen’sdisease.”
The prognosis of EP is commonly held to be poor witha significant proportion of tumors metastasizing and
causing death. Akiyoshi et al. summarized the Japaneseexperience with 10 cases of 21 metastasizing2 and Landaand Winkelmann commented that in EP the prognosis ispoor and most die of disease.15 That this may reflectreporting bias is supported by the individual case reportsdetailed in Table 4. Most anecdotal cases pursued anaggressive course and perhaps was a factor leading to thecase being reported. However, the few large series pre-sent a different view. Of 24 tumors described by Baptistaet al., only two followed an aggressive course with onelocal recurrence and one lymph node metastasis.3 Simi-larly, of 18 tumors reported by Mehregan et al. only twospread to lymph nodes or distant sites and one tumorrecurred locally.18 Shaw et al.31 described the clinico-pathologic features of 27 cases in which 10 had follow-up. Of these, six recurred locally, some repeatedly, butonly two metastasized.31 Tumor stage appears to behighly significant in predicting prognosis. Thus, withpositive regional lymph node involvement mortality is65%,32 and 28% of patients reviewed by Goedde et al.had distant metastases, most of whom died of their dis-ease.7 Santa Cruz further stated that epidermotropism isa poor prognostic factor.30 However, it may be impos-sible to distinguish primary multifocal tumors from epi-dermotropic metastases in some cases. Because of theanecdotal nature of the bulk of literature reports, therehas been no clear consensus on those factors in primarylocalized EP that may portend a more aggressive clinicalcourse. Length of history, lymphovascular invasion, ex-tensive pleomorphism and mitoses, and advanced patientage have all been suggested to increase the chance of anegative outcome.29,32,40 Of 54 invasive malignancieswith follow-up described herein, 9 (17%) locally re-curred, 10 (19%) spread to regional lymph nodes, and 6(11%) metastasized to distant sites and/or caused thedeath of the patient. In an attempt to identify those fac-tors that may indicate the likely behavior of a tumor, weobserved and recorded a number of parameters that mayinfluence or predict tumor behavior and then analyzedthese data in terms of patient outcome using a statisticalpackage.
TILs have been found by several groups to be a pow-erful prognosticator in primary cutaneous malignantmelanoma. Thus, each tumor was appraised for the na-ture of the host response and classified into brisk, non-brisk, and absent using the same criteria laid down forevaluating melanoma. Although each category was rep-resented, there was no relationship between any groupand patient outcome. Interestingly, a single tumorshowed histologic evidence of regression manifest byinterruption of the tumor mass by inflammatory cells,fibrosis, and vascular ectasia in the stroma. Other param-eters specifically recorded with a view to possible prog-nostic indicators included mitotic index, lymphovascularand perineurial invasion, necrosis, tumor size, and depth
A. ROBSON ET AL.718
Am J Surg Pathol, Vol. 25, No. 6, 2001

and character of tumor margin. Mitoses were counted in10 high-power fields and were strongly predictive ofdeath (HR 17.0) or lymph node involvement (HR 8.5).Lymphovascular invasion (in 9 cases, 15%)(Fig. 10) wasassociated with death (HR 4.41). Necrosis was present in24 cases (39%) either as a relatively defined zone sur-rounded by viable tumor cells (comedo-type, 20 cases,32%) or widespread and diffuse (4 cases, 6%). Neithercomedo nor diffuse necrosis had any prognostic importon analysis. Although the gross size of tumor had nosignificant relationship to prognosis, tumor depth >7 mmpredicted death or lymph node involvement (HR 2.5).Finally, an “infiltrative” tumor margin had a dramaticinfluence on local recurrence (HR 6.8). Cutaneous EP israrely diagnosed preoperatively; thus, initial surgicalmanagement is not usually specifically planned. Al-though wide local excision of any cutaneous tumor is tobe recommended, our results from this series suggest EPswith an infiltrative pattern may benefit from further sur-gery if doubt exists regarding completeness of excision.Similarly, once this diagnosis has been made, then extracare should be taken by the surgical pathologist to evalu-ate resection margins.
Sentinel lymph node sampling has become standardpractice in the management of malignant melanoma. Ourdata suggest that the prevalence of positive sentinellymph nodes in EP is likely to be low; nevertheless, ifconfirmed by other studies, they also indicate that thisprocedure may be justified in those tumors >7 mm indepth or with high mitotic counts.
In the original case report, Pinkus and Mehregan22
described a tumor with marked pagetoid extension ofmalignant cells, a feature that has since been well docu-mented. Primary malignancies may be apparently multi-focal and have a significant intraepidermal component.Furthermore, primary EP may metastasize with epider-motropic deposits, sometimes in a “stepping-stone” dis-tribution. Abenoza and Ackerman1 stated that distin-guishing a primary tumor from a metastasis with signifi-cant pagetoid extension is impossible. In our study thehistomorphology of the multifocal lesions did not differsignificantly from the other tumors in the series. Inter-estingly, the patients in our study with multifocal tumorsdid not fare worse in comparison with single primarylesions. This suggests that the multiple lesions representtrue initial multifocality of the tumor rather than meta-static spread.
CONCLUSION
This series of malignant eccrine poromas is the largestreported to date in the literature. The clinicopathologicfeatures are largely in accord with those previously re-ported. This study also confirms other large series thatthe prognosis of EP is not as dismal as often believed
from literature case reports. Mitoses, lymphovascular in-vasion, and tumor depth �7 mm emerge as importantprognostic indicators. The presence of an infiltratingmargin should alert the surgical pathologist to recom-mend conservative wider excision if there is doubt re-garding completeness of excision. �
Acknowledgments
The authors thank the following: Dr. K. L. Agarwal, Epping,Dr. M. S. Al-Izzi, Welwyn Garden City, Dr. N. Aluwihare,Sutton Coldfield, Dr. E. J. Aps, Kent, Dr. T. G. AshworthCoventry, Dr. N. J. Ball Great Yarmouth, Dr. H. Barnes,London, Dr. A. Bell, London, Mr. P. Bird, London, Dr. M. M.Black, London, Dr. W. K. Blenkinsopp, Watford, Dr. C. Blow,Surrey, Dr. M. Botle, London, Dr. S. Boyle, London, Dr. S. M.Breathnach, London, Dr. Yoon Chia, High Wycombe, Dr. J.Chow, London, Dr. J. V. Clark, Northampton, Dr. T. J. Clark,Plymouth, Dr. B. Conroy, Chichester, Dr. D. J. Cooper,Worthing, Dr. M. J. Coppen, London, Mr. K. Cronin,Northampton, Dr. N. Dansie, Welwyn, Mr. T. W. Davies, Kent,Dr. D. W. Day, Torquay, Dr. K. R. Dempster, Windsor, Dr. K.J. Denton, Bristol, Mr. G. H. Dickson, Worthing, Dr. J. Dove,Luton, Dr. J. El-Jabbour, Barnet, Dr. H. A. Ellis, Newcastleupon Tyne, Dr. A. T. Evans, Dundee, Dr. Fernando,Bournemouth, Dr. J. Fsadni, Dunstable, Dr. J. J. Grant,Worthing, Dr. B. Green, Winchester, Dr. W. A. D. Griffiths,Epsom, Dr. P. B. Hamal, Wakefield, Dr. C. Hay, Torquay, Dr.S. Hill, St. Albans, Dr. K. J. Holley, Warwick, Dr. K. A.Hussein, Poole, Dr. P. D. James, Nottingham, Dr. C. Jameson,London, Dr. C. Jenkins, London, Dr. R. A. Jones,Middlesborough, Dr. T. J. Jones, Shrewsbury, Dr. P. A. Judd,Ipswich, Dr. A. R. Kittermaster, Kent, Dr. T. A. Leslie, Barnet,Dr. M. Lesna, Bournemouth, Dr. A. M. Light, Sutton Coldfield,Dr. B. A. Lyons, Plymouth, Dr. J. Madders, Stevenage, Dr.Madziwa, Worthing, Dr. P. D. L. Maurice, St. Albans, Dr. B.G. McCann, Norwich, Dr. D. McCormick, Portsmouth, Dr. J.M. F. McClement, Lincoln, Dr. J. Mckenzie, Epping, Dr. W.Merchant, Leeds, Mr. D. M. Z. Mercer, Bromley, Dr. K. Munis,Bromley, Dr. E. Munn, Kent, Dr. P. J. O’Donnell, Canterbury,Dr. S. C. Parker, Ashford, Dr. D. J. Parish, Bournemouth, Dr.A. W. Popple, Carlisle, Dr. D. I. Porter, Rugby, Dr. A. M.Ranken, London, Dr. A. Rikabi, Bristol, Dr. D. B. Rimmer,Bedford, Dr. A. Roberts, Windsor, Dr. K. Roberts, Worthing,Dr. J. R. Salisbury, London, Dr. E. Sawyer, London, Dr. K.Schafler, London, Dr. K. Shah, London, Dr. S. Shousha,Wanstead, Dr. N. Smith, London, Dr. R. Smith, London, Dr. G.Soosay, Essex, Dr. J. Southgate, Leicester, Dr. M. Spittle,London, Dr. P. J. Stevens, Sussex, Dr. S. M. Thomas, Surrey,Dr. P. A. Thorpe, Isleworth, Dr. Z. Twaij, Welwyn GardenCity, Dr. H. Vazir, Barnet, Dr. A. C. Vincenti, Winchester,Prof. E. Wilson-Jones, London, U.K., Dr. W. Grayson,Johannesburg, South Africa, Dr. S. Henzen-Logmans,Rotterdam, The Netherlands, Dr. B. J. Leppard, Tanzania, Dr.M. P. G. Little, Galway, Ireland, Dr. Sim Chee Seng,Singapore, Dr. G. Zimmer, Lausanne, Switzerland.
REFERENCES
1. Abenoza P, Ackerman BA. Porocarcinomas. In: Abenoza P,Ackerman BA, eds. Neoplasms With Eccrine Differentiation.Philadelphia: Lea & Febiger, 1990:415–31.
2. Akiyoshi E, Nogita T, Yamaguchi R, et al. Eccrine porocarcinoma.Dermatologica 1991;182:239–42.
ECCRINE POROCARCINOMA (MALIGNANT ECCRINE POROMA) 719
Am J Surg Pathol, Vol. 25, No. 6, 2001

3. Baptista AP, Tellechea O, Reis JP, et al. Eccrine porocarcinoma: areview of 24 cases. Ann Dermatol Venereol 1993;120:107–15.
4. Barzi AS, Ruggeri S, Recchia F, et al. Malignant metastatic eccrineporoma. Dermatol Surg 1997;23:267–72.
5. D’Amato MS, Patterson RH, Guccion JC, et al. Porocarcinoma ofthe heel. Cancer 1996;78:751–7.
6. Doring HF, Seifert HW. Eccrine porocarcinoma (malignant eccrineporoma)—a follow-up study. Z Hautkrankheiten 1987;62:1051–2.
7. Goedde TA, Bumpers H, Fiscella JA, et al. Eccrine porocarcinoma.J Surg Oncol 1994;55:261–4.
8. Van Gorp J, van der Putte SCJ. Periungual eccrine porocarcinoma.Dermatology 1993;187:67–70.
9. Grober A, Goldberg I, Rotem A. Malignant eccrine poroma withmetastatic involvement of the long bones. Clin Orthop 1987;223:303–7.
10. Hamanka S, Otsuka F. Multiple malignant eccrine poroma and alinear epidermal naevus. J Dermatol 1996;23:471–9.
11. Hara K, Kamiya S. Pigmented eccrine porocarcinoma: a mimic ofmalignant melanoma. Histopathology 1995;27:86–8.
12. Van Hees CLM, van Duinen CM, Bruijin JA, et al. Malignanteccrine poroma in a patient with Rothmund-Thomson syndrome.Br J Dermatol 1996;134:813–4.
13. Huet P, Dandurand M, Pignodel C, et al. Metastasizing eccrineporocarcinoma: report of a case and review of the literature. J AmAcad Dermatol 1996;35:860–4.
14. Kolde G, Macher E, Grundmann E. Metastasizing eccrine poro-carcinoma. Path Res Pract 1991;187:477–81.
15. Landa NG, Winkelmann RK. Epidermotropic eccrine porocarci-noma. J Am Acad Dermatol 1991;24:27–31.
16. Langfritz K, Grabbe S, Kovacs G, et al. Metastasizing eccrineporocarcinoma Hautarzt 1993;44:176–9.
17. Maeda T, Mori H, Matsuo T, et al. Malignant eccrine poroma withmultiple visceral metastases: report of a case with autopsy find-ings. J Cutan Pathol 1996;23:566–70.
18. Mehregan AH, Hashimoto K, Rahbari H. Eccrine adenocarcinoma.Arch Dermatol 1983;119:104–14.
19. Misago N, Toda S, Hikichi Y, et al. A unique case of extramam-mary Paget’s disease. Am J Dermatopathol 1992;14:553–9.
20. Pena J, Suster S. Squamous differentiation in malignant eccrineporoma. Am J Dermatopathol 1993;15:492–6.
21. Pernia LR, Guzman-Stein G, Miller HL. Surgical treatment of anaggressive metastasized eccrine poroma. Ann Plast Surg 1993;30:257–9.
22. Pinkus H, Mehregan AH. Epidermotropic eccrine carcinoma. ArchDermatol 1963;88:597–606.
23. Pique E, Olivares M, Espinel ML, et al. Malignant hidroacanthomasimplex. Dermatology 1995;190:72–6.
24. Pontone M, Potter GK, Berlin SJ, et al. Malignant eccrine neo-plasms of the foot. J Foot Ankle Surg 1994;33:486–91.
25. Puttick L, Ince P, Comaish JS. Three cases of eccrine porocarci-noma. Br J Dermatol 1986;115:111–6.
26. Requena L, Sanchez M, Aguilar A, et al. Periungual porocarci-noma. Dermatologica 1990;180:177–80.
27. Roaf V, Chin N, Lynfield Y. Pigmented sweat gland tumor mim-icking melanoma. Cutis 1997;59:43–6.
28. Roumen RM, Wobbes T, Pruszczynski M, et al. Malignant eccrineporoma with lymph node metastasis followed by multiple basalcarcinomas in a young female patient. Eur J Surg Oncol 1993;19:198–202.
29. Ryan JF, Barley CR, Pollock DJ. Malignant eccrine poroma: reportof three cases. J Clin Pathol 1986;39:1099–104.
30. Santa Cruz DJ. Sweat gland carcinomas: a comprehensive review.Semin Diag Pathol 1987;4:38–74.
31. Shaw M, McKee PH, Lowe D, et al. Malignant eccrine poroma: astudy of twenty-seven cases. Br J Dermatol 1982;107:675–80.
32. Snow SN, Reizner GT. Eccrine porocarcinoma of the face. J AmAcad Dermatol 1992;27:306–11.
33. Spencer DM, Bigler LR, Hearne DW, et al. Pedal papule: eccrineporocarcinoma (EPC) in association with poroma. Arch Dermatol1995;131:211–4.
34. Tateyama H, Eimoto T, Tada T, et al. P53 protein and proliferatingcell nuclear antigen in eccrine poroma and porocarcinoma. Am JDermatopathol 1995;17:457–64.
35. Tokura Y, Yoshikuni K, Teraki Y, et al. Immunohistochemicallydetectable duct-like structures in benign and malignant eccrineporoma: CEA and involucrin immunostaining. J Dermatol 1989;16:133–41.
36. Ujihara M, Hamanka S, Hamanka Y, et al. A case of multipleeccrine porocarcinoma with stepping-stone distribution on the foot.J Dermatol 1995;22:450–7.
37. Walsh MS. A case of eccrine porocarcinoma. J R Soc Med 1990;83:529–30.
38. Wick MR, Goellner JR, Wolfe JT III, et al. Adnexal carcinomas ofthe skin. I: Eccrine carcinomas. Cancer 1985;56:1147–62.
39. Wollina U, Castelli E, Rulke D. Immunohistochemistry of eccrineporoma and porocarcinoma—more than acrosyringeal tumors? Re-cent Results Cancer Res 1995;139:303–16.
40. Yamamoto O, Haratake J, Yokoyama S, et al. A histopathologicand ultrastructural study of eccrine porocarcinoma with specialreference to its subtypes. Virchows Arch 1992;420:395–401.
A. ROBSON ET AL.720
Am J Surg Pathol, Vol. 25, No. 6, 2001
Copyright © 2022 FDOKUMEN




















