
Malignant triton tumors of the spine: Report of 2 cases
7
HE MTT is a variant of MPNST that shows rhabdo- myosarcomatous differentiation. This entity was originally described by Masson and Martin 5 in 1938, who suggested that the neural elements induced skeletal muscle differentiation, as was believed to occur in skeletal muscle of the Triton salamander. Three criteria were pro- posed to define a tumor as an MTT: 1) genesis within a peripheral nerve or ganglioneuroma in a patient with NF1, or a metastasis from such a tumor; 2) Schwann cell tumor- like growth characteristics; and 3) the presence of rhabdo- myoblasts within the mass of the tumor. 10 Malignant triton tumors have been described in a wide variety of anatomi- cal sites, including the head and neck, and the trunk and up- per and lower limbs. 13 Malignant triton tumors arising in and around the spine pose special difficulties in diagnosis and management, and MTTs of the spine, trunk, and but- tocks have a poorer prognosis than those in the head, neck, and extremities, 13 possibly due to the particular difficulties encountered in radical resection. Previous reports have noted that total macroscopic excision is more challenging due to intradural extension of the MTT. 6,9 In addition, these tumors have been noted as locally highly aggressive. 7 When arising from spinal nerves, MTTs can originate either extra- or intradurally, and can locally infiltrate both into or out of the thecal sac. In the present study we discuss the MTTs that come to the attention of the spinal or neuro- surgeon, regardless of intra- or extraaxial origin. We report 2 new cases of spinal MTTs from our own center and re- view all previously published cases, with a particular em- phasis on the surgical management of this lesion. J. Neurosurg.: Spine / Volume 8 / June 2008 J Neurosurg Spine 8:567–573, 2008 Malignant triton tumors of the spine Report of 2 cases GREG JAMES, M.R.C.S., PH.D., 1 MATTHEW CROCKER, M.R.C.S., 2 ANDREW KING, F.R.C.P ATH., 3 ISTVAN BODI, F.R.C.P ATH., 3 AHMED IBRAHIM, M.R.C.S., 2 AND BHUPAL P. CHITNAVIS, F.R.C.S.(SN) 2 1 Department of Neurosurgery, Barts & The London National Health Service Trust; and Departments of 2 Neurosurgery and 3 Clinical Neuropathology, King’s College Hospital, London, United Kingdom Malignant triton tumors (MTTs) are malignant peripheral nerve sheath tumors with rhabdomyosarcomatous differ- entiation. Malignant triton tumors affecting the spine are rare but present special challenges to the neurosurgeon. The authors report on 2 new cases of spinal MTTs, and analyze the 8 previously reported cases found via database search. The patients include a 15-year-old girl with thoracic MTT, and a 24-year-old man with lumbosacral MTT; both pa- tients underwent radical resection with spinal stabilization. When these cases were combined with the literature results there was a male/female ratio of 6:4, and an age range of 15–67 years (median 37.5). Nine patients presented with symptoms related to the spinal cord, cauda equina, or nerve root compression. Four patients had undergone previous radiotherapy, and 2 had neurofibromatosis Type 1. Five cases of MTT were lumbosacral, 4 were thoracic, and 1 was cervical. Seven patients had intradural extension of tumor. All patients underwent some form of surgery, with 8 hav- ing total macroscopic excision. However, 6 patients required subsequent operations. In the 8 patients for which sur- vival data was available, median time from diagnosis to death was 12 months (range 3–16). Malignant triton tumors are rare but should be included in the differential diagnosis of spinal tumors, particularly in patients who have undergone previous radiotherapy or who have neurofibromatosis. The authors suggest roles for rad- ical surgery and multidisciplinary management. (DOI: 10.3171/SPI/2008/8/6/567) KEY WORDS • literature review • malignant triton tumor • spine • surgical management T 567 Abbreviations used in this paper: CT = computed tomography; MPNST = malignant peripheral nerve sheath tumor; MR = magnet- ic resonance; MTT = malignant triton tumor; NF1 = neurofibro- matosis Type 1; PS = pedicle screw. This article contains some figures that are displayed in color online but in black and white in the print edition.
-
Upload
independent -
Category
Documents
-
view
7 -
download
0
Transcript of Malignant triton tumors of the spine: Report of 2 cases

HE MTT is a variant of MPNST that shows rhabdo-myosarcomatous differentiation. This entity wasoriginally described by Masson and Martin5 in 1938,
who suggested that the neural elements induced skeletalmuscle differentiation, as was believed to occur in skeletalmuscle of the Triton salamander. Three criteria were pro-posed to define a tumor as an MTT: 1) genesis within aperipheral nerve or ganglioneuroma in a patient with NF1,or a metastasis from such a tumor; 2) Schwann cell tumor-like growth characteristics; and 3) the presence of rhabdo-myoblasts within the mass of the tumor.10 Malignant tritontumors have been described in a wide variety of anatomi-cal sites, including the head and neck, and the trunk and up-per and lower limbs.13 Malignant triton tumors arising in
and around the spine pose special difficulties in diagnosisand management, and MTTs of the spine, trunk, and but-tocks have a poorer prognosis than those in the head, neck,and extremities,13 possibly due to the particular difficultiesencountered in radical resection. Previous reports havenoted that total macroscopic excision is more challengingdue to intradural extension of the MTT.6,9 In addition, thesetumors have been noted as locally highly aggressive.7When arising from spinal nerves, MTTs can originateeither extra- or intradurally, and can locally infiltrate bothinto or out of the thecal sac. In the present study we discussthe MTTs that come to the attention of the spinal or neuro-surgeon, regardless of intra- or extraaxial origin. We report2 new cases of spinal MTTs from our own center and re-view all previously published cases, with a particular em-phasis on the surgical management of this lesion.
J. Neurosurg.: Spine / Volume 8 / June 2008
J Neurosurg Spine 8:567–573, 2008
Malignant triton tumors of the spine
Report of 2 cases
GREG JAMES, M.R.C.S., PH.D.,1 MATTHEW CROCKER, M.R.C.S.,2
ANDREW KING, F.R.C.PATH.,3 ISTVAN BODI, F.R.C.PATH.,3 AHMED IBRAHIM, M.R.C.S.,2
AND BHUPAL P. CHITNAVIS, F.R.C.S.(SN)2
1Department of Neurosurgery, Barts & The London National Health Service Trust; and Departmentsof 2Neurosurgery and 3Clinical Neuropathology, King’s College Hospital, London, United Kingdom
PPMalignant triton tumors (MTTs) are malignant peripheral nerve sheath tumors with rhabdomyosarcomatous differ-entiation. Malignant triton tumors affecting the spine are rare but present special challenges to the neurosurgeon. Theauthors report on 2 new cases of spinal MTTs, and analyze the 8 previously reported cases found via database search.
The patients include a 15-year-old girl with thoracic MTT, and a 24-year-old man with lumbosacral MTT; both pa-tients underwent radical resection with spinal stabilization. When these cases were combined with the literature resultsthere was a male/female ratio of 6:4, and an age range of 15–67 years (median 37.5). Nine patients presented withsymptoms related to the spinal cord, cauda equina, or nerve root compression. Four patients had undergone previousradiotherapy, and 2 had neurofibromatosis Type 1. Five cases of MTT were lumbosacral, 4 were thoracic, and 1 wascervical. Seven patients had intradural extension of tumor. All patients underwent some form of surgery, with 8 hav-ing total macroscopic excision. However, 6 patients required subsequent operations. In the 8 patients for which sur-vival data was available, median time from diagnosis to death was 12 months (range 3–16).
Malignant triton tumors are rare but should be included in the differential diagnosis of spinal tumors, particularly inpatients who have undergone previous radiotherapy or who have neurofibromatosis. The authors suggest roles for rad-ical surgery and multidisciplinary management. (DOI: 10.3171/SPI/2008/8/6/567)
KEY WORDS • literature review • malignant triton tumor • spine •surgical management
T
567
Abbreviations used in this paper: CT = computed tomography;MPNST = malignant peripheral nerve sheath tumor; MR = magnet-ic resonance; MTT = malignant triton tumor; NF1 = neurofibro-matosis Type 1; PS = pedicle screw.
This article contains some figures that are displayed incolor online but in black and white in the print edition.
Case Reports
Case 1
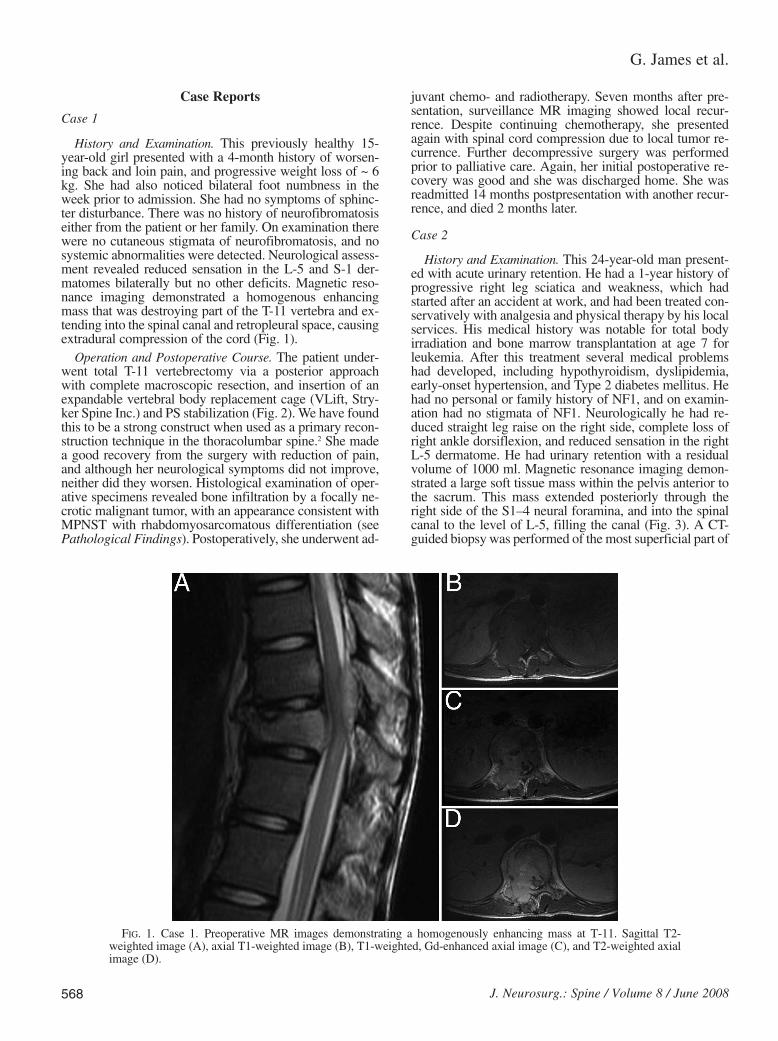
History and Examination. This previously healthy 15-year-old girl presented with a 4-month history of worsen-ing back and loin pain, and progressive weight loss of ~ 6kg. She had also noticed bilateral foot numbness in theweek prior to admission. She had no symptoms of sphinc-ter disturbance. There was no history of neurofibromatosiseither from the patient or her family. On examination therewere no cutaneous stigmata of neurofibromatosis, and nosystemic abnormalities were detected. Neurological assess-ment revealed reduced sensation in the L-5 and S-1 der-matomes bilaterally but no other deficits. Magnetic reso-nance imaging demonstrated a homogenous enhancingmass that was destroying part of the T-11 vertebra and ex-tending into the spinal canal and retropleural space, causingextradural compression of the cord (Fig. 1).
Operation and Postoperative Course. The patient under-went total T-11 vertebrectomy via a posterior approachwith complete macroscopic resection, and insertion of anexpandable vertebral body replacement cage (VLift, Stry-ker Spine Inc.) and PS stabilization (Fig. 2). We have foundthis to be a strong construct when used as a primary recon-struction technique in the thoracolumbar spine.2 She madea good recovery from the surgery with reduction of pain,and although her neurological symptoms did not improve,neither did they worsen. Histological examination of oper-ative specimens revealed bone infiltration by a focally ne-crotic malignant tumor, with an appearance consistent withMPNST with rhabdomyosarcomatous differentiation (seePathological Findings). Postoperatively, she underwent ad-
juvant chemo- and radiotherapy. Seven months after pre-sentation, surveillance MR imaging showed local recur-rence. Despite continuing chemotherapy, she presentedagain with spinal cord compression due to local tumor re-currence. Further decompressive surgery was performedprior to palliative care. Again, her initial postoperative re-covery was good and she was discharged home. She wasreadmitted 14 months postpresentation with another recur-rence, and died 2 months later.
Case 2
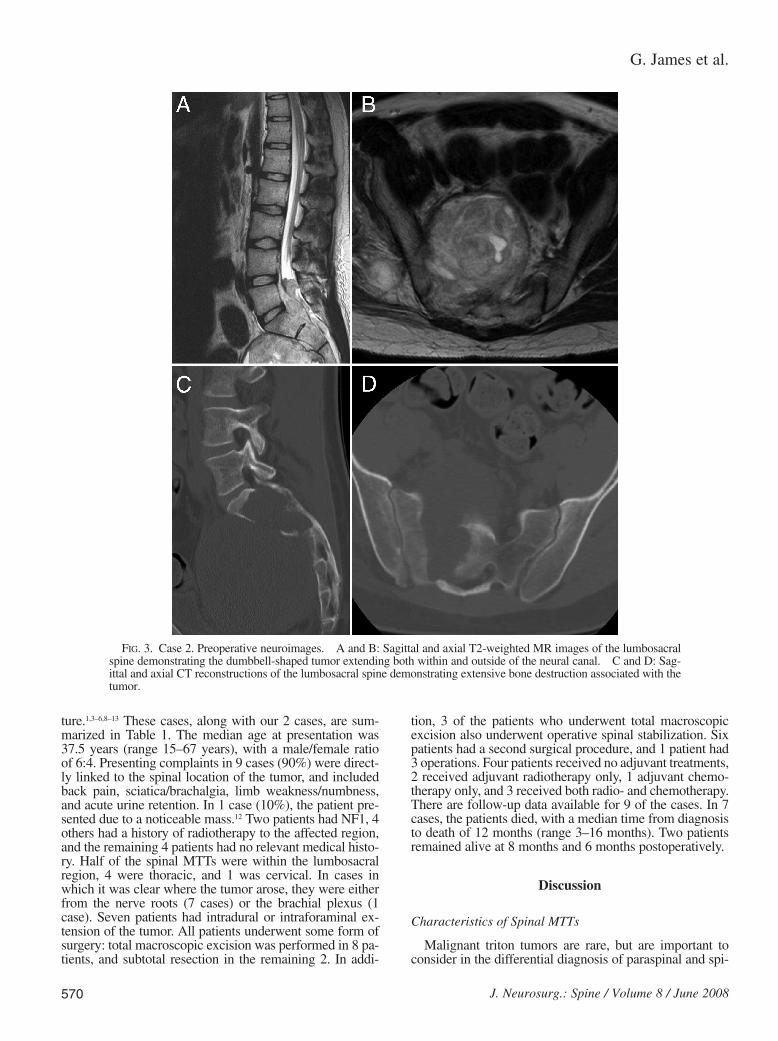
History and Examination. This 24-year-old man present-ed with acute urinary retention. He had a 1-year history ofprogressive right leg sciatica and weakness, which hadstarted after an accident at work, and had been treated con-servatively with analgesia and physical therapy by his localservices. His medical history was notable for total bodyirradiation and bone marrow transplantation at age 7 forleukemia. After this treatment several medical problemshad developed, including hypothyroidism, dyslipidemia,early-onset hypertension, and Type 2 diabetes mellitus. Hehad no personal or family history of NF1, and on examin-ation had no stigmata of NF1. Neurologically he had re-duced straight leg raise on the right side, complete loss ofright ankle dorsiflexion, and reduced sensation in the rightL-5 dermatome. He had urinary retention with a residualvolume of 1000 ml. Magnetic resonance imaging demon-strated a large soft tissue mass within the pelvis anterior tothe sacrum. This mass extended posteriorly through theright side of the S1–4 neural foramina, and into the spinalcanal to the level of L-5, filling the canal (Fig. 3). A CT-guided biopsy was performed of the most superficial part of
G. James et al.
568 J. Neurosurg.: Spine / Volume 8 / June 2008
FIG. 1. Case 1. Preoperative MR images demonstrating a homogenously enhancing mass at T-11. Sagittal T2-weighted image (A), axial T1-weighted image (B), T1-weighted, Gd-enhanced axial image (C), and T2-weighted axialimage (D).

the lesion, extending into the gluteal region, and a diagno-sis of MPNST was made.
Operation and Postoperative Course. The patient under-went a combined neurosurgical and colorectal procedure,which consisted of total macroscopic resection of the tu-mor, including sacrectomy, opening of the dura mater to re-sect the intradural extension, resection of the right sacralnerve roots (from which the tumor was seen to arise), anda defunctioning loop colostomy. Stabilization was achievedby insertion of lumbosacral PSs, iliac bolts, and a Moss–Miami cage filled with a mixture of bone autograft ma-terial and calcium triphosphate paste (Fig. 4). The patientmade an excellent recovery from the operation, and wasable to walk with the aid of a cane on discharge 3 weekspostoperatively. Currently (6 months postpresentation), thepatient remains well and is undergoing adjunctive chemo-radiotherapy.
Results
Pathological Findings
Specimens obtained from both patients were subjected tothorough histological examination, including immunohis-tochemistry for S-100 protein, smooth muscle actin, epithe-lial membrane antigen, glial fibrillary acidic protein, synap-tophysin, CD34, MNF116, CD99, and desmin. Geneticanalysis was performed in the patient in Case 1 (the 15-year-old girl) for STT/SSX, EWS/FLI-1, EWS/ERG, andG6PD. Cellular proliferation was examined by use of theKi 67 antibody.
Case 1. The histological characteristics of the 2 resectionspecimens were similar, and revealed a malignant spindle-cell tumor. There was a vague herringbone-like pattern insome areas, and brisk mitotic activity and geographical ne-crosis (Fig. 5A). The tumor infiltrated bone and soft tissue.The tumor showed focal positivity for S-100 protein, and
scattered positivity for desmin (Fig. 5B). Stains withsmooth muscle actin, glial fibrillary acidic protein, synap-tophysin, CD34, MNF116, and CD99 were negative. Stain-ing with Ki 67 revealed a proliferation index of ~ 80%.Genetic test results were negative for SYT/SSX, EWS/FLI-1, and EWS/ERG, and positive for G6PD (86,141.200 bp).The overall features of the lesion supported those of anMPNST with rhabdomyosarcomatous differentiation(MTT).
Case 2. The histological results in this patient revealed amalignant spindle cell tumor with areas with a herring-bone-like pattern (Fig. 6A). Glandular areas were also seen(Fig. 6B), and a focal collection of larger eosinophilic cells.Mitotic figures were abundant, and there was extensive ne-crosis. The tumor invaded skeletal muscle but no invasionof bone was seen. Although there was strong immunopos-itivity for vimentin, and focal positivity for S-100 protein inthe spindle cells, the eosinophilic cells were positive fordesmin (Fig. 6C). Stains for epithelial membrane antigen,smooth muscle actin, and CD34 were negative. The fea-tures were those of a MPNST with rhabdomyosarcomatousand epithelial differentiation (malignant glandular tritontumor).
Literature Review
A thorough literature search was performed using MED-LINE and EMBASE to identify publications containingkeywords including “malignant triton tumor/tumour,”“malignant peripheral nerve sheath tumor/tumour,”“MPNST,” “rhabdomyoblastic/rhabdomyosarcomatousdifferentiation,” “spine,” “spinal nerve/nerves,” “paraspi-nal,” “paravertebral,” and “vertebral.” In addition, the bib-liographies of retrieved papers were further scrutinized toidentify other publications. Retrieved papers were thenanalyzed according to a preprepared proforma.
Eight cases of spinal MTTs were identified in the litera-
J. Neurosurg.: Spine / Volume 8 / June 2008
Malignant triton tumors of the spine
569
FIG. 2. Case 1. Postoperative radiological images. Sagittal CT reconstruction demonstrating the VLift prosthesis insitu (A), and anteroposterior radiograph showing the appearance of the VLift cage and associated PSs (B).
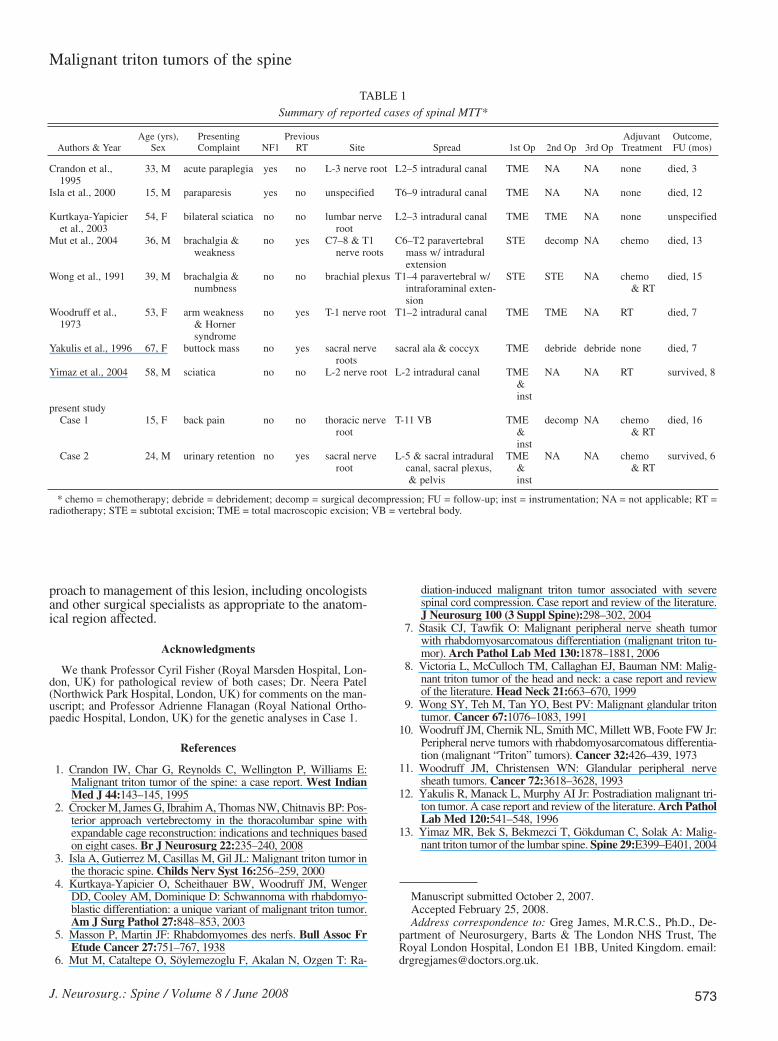
ture.1,3–6,8–13 These cases, along with our 2 cases, are sum-marized in Table 1. The median age at presentation was37.5 years (range 15–67 years), with a male/female ratio of 6:4. Presenting complaints in 9 cases (90%) were direct-ly linked to the spinal location of the tumor, and includedback pain, sciatica/brachalgia, limb weakness/numbness,and acute urine retention. In 1 case (10%), the patient pre-sented due to a noticeable mass.12 Two patients had NF1, 4others had a history of radiotherapy to the affected region,and the remaining 4 patients had no relevant medical histo-ry. Half of the spinal MTTs were within the lumbosacralregion, 4 were thoracic, and 1 was cervical. In cases inwhich it was clear where the tumor arose, they were eitherfrom the nerve roots (7 cases) or the brachial plexus (1case). Seven patients had intradural or intraforaminal ex-tension of the tumor. All patients underwent some form ofsurgery: total macroscopic excision was performed in 8 pa-tients, and subtotal resection in the remaining 2. In addi-
tion, 3 of the patients who underwent total macroscopicexcision also underwent operative spinal stabilization. Sixpatients had a second surgical procedure, and 1 patient had3 operations. Four patients received no adjuvant treatments,2 received adjuvant radiotherapy only, 1 adjuvant chemo-therapy only, and 3 received both radio- and chemotherapy.There are follow-up data available for 9 of the cases. In 7cases, the patients died, with a median time from diagnosisto death of 12 months (range 3–16 months). Two patientsremained alive at 8 months and 6 months postoperatively.
Discussion
Characteristics of Spinal MTTs
Malignant triton tumors are rare, but are important toconsider in the differential diagnosis of paraspinal and spi-
G. James et al.
570 J. Neurosurg.: Spine / Volume 8 / June 2008
FIG. 3. Case 2. Preoperative neuroimages. A and B: Sagittal and axial T2-weighted MR images of the lumbosacralspine demonstrating the dumbbell-shaped tumor extending both within and outside of the neural canal. C and D: Sag-ittal and axial CT reconstructions of the lumbosacral spine demonstrating extensive bone destruction associated with thetumor.
nal tumors, especially in patients with NF1 or in those whohave previously undergone radiotherapy. Spinal MTTs areknown to have a poor outcome in comparison to moreperipheral tumors,13 possibly due to the special surgicalchallenges posed. In the present study we present 2 newcases of spinal MTTs and analyze their characteristics,along with those of the 8 previously reported cases. Epide-miologically, spinal MTTs are not strongly associated witheither age or sex, with an approximately equal sex distrib-ution and a wide range of ages affected (15–67 years). Inall but 1 case, the patients presented with back pain, com-pressive radiculopathy or cauda equina syndrome, and noparticular clinical features to differentiate more benigncauses of these symptoms. More than half (60%) of thepatients had a history of either NF1 (in 2 patients) or radio-therapy to the anatomical site where the MTT arose (in 4
patients). This finding highlights the importance of includ-ing these factors in the assessment of a patient with a spinalmass. Malignant triton tumors appear to favor the lum-bosacral and thoracic spine, and tend to arise in the nerveroots before invading proximally via the neural foraminae,piercing the dura mater, and forming an intradural mass. Inall cases the patients underwent some form of resection.Total macroscopic resection was possible in the majority,although some surgeons favored subtotal resection due tothe lesion’s close relationship with neural structures. Inboth new cases we report, radical surgery with resection ofall macroscopic tumor was performed, including the in-tradural elements. En bloc excision of the tumor was notpossible due to the axial location and advanced local stageof the MTT and this may have had an impact on the out-come in these patients. In both patients, the invaded bone
J. Neurosurg.: Spine / Volume 8 / June 2008
Malignant triton tumors of the spine
571
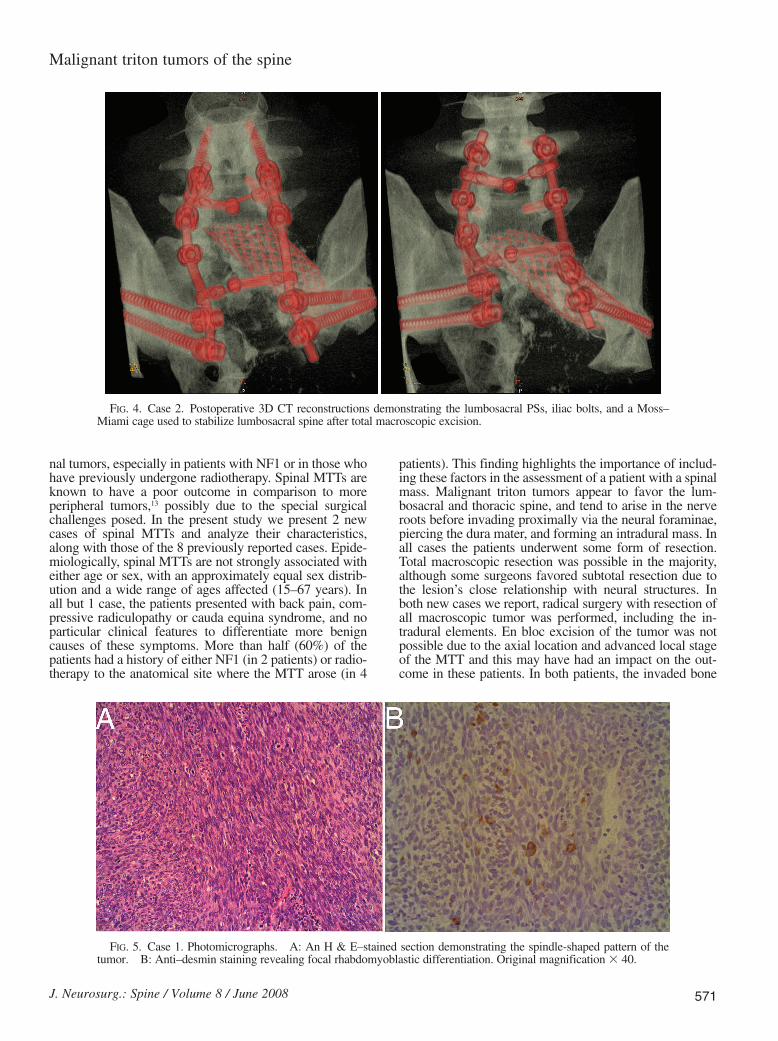
FIG. 4. Case 2. Postoperative 3D CT reconstructions demonstrating the lumbosacral PSs, iliac bolts, and a Moss–Miami cage used to stabilize lumbosacral spine after total macroscopic excision.
FIG. 5. Case 1. Photomicrographs. A: An H & E–stained section demonstrating the spindle-shaped pattern of thetumor. B: Anti–desmin staining revealing focal rhabdomyoblastic differentiation. Original magnification 3 40.
structures were removed (a vertebrectomy was performedin Case 1, and a sacrectomy in Case 2) and appropriateprostheses were inserted to achieve stabilization. The pre-senting symptoms in both patients resolved after surgeryand the patients were discharged home. Because MTTs areso rare, no large trials have been completed to judge theefficacy of adjuvant therapy. The authors of a report on aseries of head and neck MTTs indicated benefit fromchemo- and radiotherapy,8 although the small number ofpatients preclude making firm conclusions. In both newcases we report, the patients were referred to specialist on-cologists for adjuvant treatment. In the patient in Case 2,histological examination revealed both rhabdomyosarco-matous and glandular differentiation. Previous evidencesuggests that this type of tumor has a particularly poorprognosis, with a mean survival time from diagnosis of ,2 years and resistance to adjuvant therapies.9,11 Identifi-cation of glandular elements on the histopathologicalexamination is therefore of prognostic value and should besought.
Surgical Management of Spinal MTTs
Based on our review of cases, the median survival timefrom diagnosis of MTT was 1 year. This is probably relat-ed to late presentation; in the majority of cases the tumorwas large with wide local spread at initial assessment, pre-cluding en bloc resection. Despite the highly malignantnature of spinal MTTs and the poor prognosis of thesepatients, we believe that radical surgery has an importantrole in the palliation of symptoms. It is possible that symp-tom-free survival is improved, but our series is too small tomake conclusions on this point. Local recurrence rates andthe rate of further surgical procedures were both high in ouranalysis, and this may suggest that aggressive resectionwith removal of the affected nerve roots is appropriate. Thepatient in Case 2 underwent radical resection of sacralnerve roots and had a good functional outcome. Due to theextensive intrapelvic spread of the tumor in the patient inCase 2, colorectal and urological surgeons were consultedpreoperatively and the surgery was carried out as a jointprocedure with a coloproctologist who has a special inter-est in pelvic malignancy. Operatively, good radiologicaland clinical spinal stability was achieved despite radicalbone resection (vertebrectomy in Case 1 and sacrectomy inCase 2), which demonstrates that extensive tumor spreaddoes not necessarily compromise instrumentation of theadjacent spine. Indeed, without the use of appropriate pros-theses and reconstructive techniques, total macroscopicexcision and rehabilitation would have been impossibledue to subsequent spinal instability.
Conclusions
We have discussed the presentation, management, andprognosis of all reported spinal MTTs and included 2 newcases from our own center. Malignant triton tumor is a rarediagnosis but important to consider in patients who presentwith new compressive spinal symptoms, in particular thosewith a history of NF1 or radiotherapy. Despite the poorprognosis associated with this condition we suggest a rolefor radical surgery both from oncological and quality of lifestandpoints. We strongly advocate a multidisciplinary ap-
G. James et al.
572 J. Neurosurg.: Spine / Volume 8 / June 2008
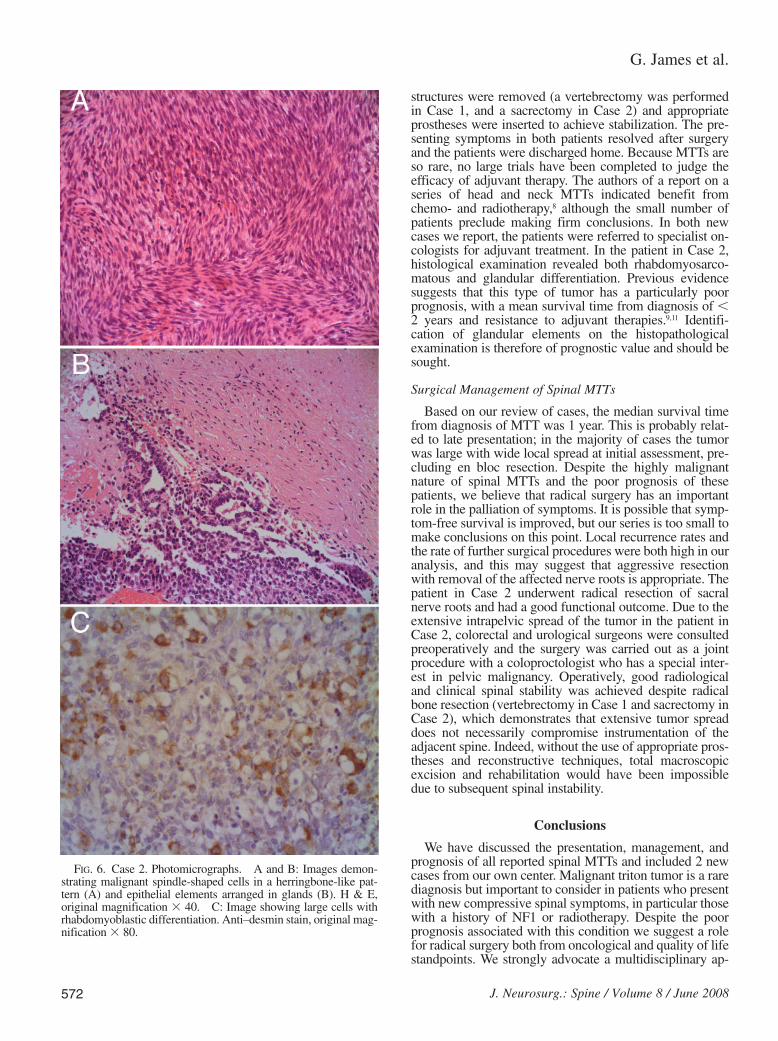
FIG. 6. Case 2. Photomicrographs. A and B: Images demon-strating malignant spindle-shaped cells in a herringbone-like pat-tern (A) and epithelial elements arranged in glands (B). H & E,original magnification 3 40. C: Image showing large cells withrhabdomyoblastic differentiation. Anti–desmin stain, original mag-nification 3 80.
proach to management of this lesion, including oncologistsand other surgical specialists as appropriate to the anatom-ical region affected.
Acknowledgments
We thank Professor Cyril Fisher (Royal Marsden Hospital, Lon-don, UK) for pathological review of both cases; Dr. Neera Patel(Northwick Park Hospital, London, UK) for comments on the man-uscript; and Professor Adrienne Flanagan (Royal National Ortho-paedic Hospital, London, UK) for the genetic analyses in Case 1.
References
1. Crandon IW, Char G, Reynolds C, Wellington P, Williams E:Malignant triton tumor of the spine: a case report. West IndianMed J 44:143–145, 1995
2. Crocker M, James G, Ibrahim A, Thomas NW, Chitnavis BP: Pos-terior approach vertebrectomy in the thoracolumbar spine withexpandable cage reconstruction: indications and techniques basedon eight cases. Br J Neurosurg 22:235–240, 2008
3. Isla A, Gutierrez M, Casillas M, Gil JL: Malignant triton tumor inthe thoracic spine. Childs Nerv Syst 16:256–259, 2000
4. Kurtkaya-Yapicier O, Scheithauer BW, Woodruff JM, WengerDD, Cooley AM, Dominique D: Schwannoma with rhabdomyo-blastic differentiation: a unique variant of malignant triton tumor.Am J Surg Pathol 27:848–853, 2003
5. Masson P, Martin JF: Rhabdomyomes des nerfs. Bull Assoc FrEtude Cancer 27:751–767, 1938
6. Mut M, Cataltepe O, Söylemezoglu F, Akalan N, Ozgen T: Ra-
diation-induced malignant triton tumor associated with severespinal cord compression. Case report and review of the literature.J Neurosurg 100 (3 Suppl Spine):298–302, 2004
7. Stasik CJ, Tawfik O: Malignant peripheral nerve sheath tumorwith rhabdomyosarcomatous differentiation (malignant triton tu-mor). Arch Pathol Lab Med 130:1878–1881, 2006
8. Victoria L, McCulloch TM, Callaghan EJ, Bauman NM: Malig-nant triton tumor of the head and neck: a case report and reviewof the literature. Head Neck 21:663–670, 1999
9. Wong SY, Teh M, Tan YO, Best PV: Malignant glandular tritontumor. Cancer 67:1076–1083, 1991
10. Woodruff JM, Chernik NL, Smith MC, Millett WB, Foote FW Jr:Peripheral nerve tumors with rhabdomyosarcomatous differentia-tion (malignant “Triton” tumors). Cancer 32:426–439, 1973
11. Woodruff JM, Christensen WN: Glandular peripheral nervesheath tumors. Cancer 72:3618–3628, 1993
12. Yakulis R, Manack L, Murphy AI Jr: Postradiation malignant tri-ton tumor. A case report and review of the literature. Arch PatholLab Med 120:541–548, 1996
13. Yimaz MR, Bek S, Bekmezci T, Gökduman C, Solak A: Malig-nant triton tumor of the lumbar spine. Spine 29:E399–E401, 2004
Manuscript submitted October 2, 2007.Accepted February 25, 2008.Address correspondence to: Greg James, M.R.C.S., Ph.D., De-
partment of Neurosurgery, Barts & The London NHS Trust, TheRoyal London Hospital, London E1 1BB, United Kingdom. email:[email protected].
J. Neurosurg.: Spine / Volume 8 / June 2008
Malignant triton tumors of the spine
573
TABLE 1Summary of reported cases of spinal MTT*
Age (yrs), Presenting Previous Adjuvant Outcome, Authors & Year Sex Complaint NF1 RT Site Spread 1st Op 2nd Op 3rd Op Treatment FU (mos)
Crandon et al., 33, M acute paraplegia yes no L-3 nerve root L2–5 intradural canal TME NA NA none died, 31995
Isla et al., 2000 15, M paraparesis yes no unspecified T6–9 intradural canal TME NA NA none died, 12
Kurtkaya-Yapicier 54, F bilateral sciatica no no lumbar nerve L2–3 intradural canal TME TME NA none unspecifiedet al., 2003 root
Mut et al., 2004 36, M brachalgia & no yes C7–8 & T1 C6–T2 paravertebral STE decomp NA chemo died, 13weakness nerve roots mass w/ intradural
extensionWong et al., 1991 39, M brachalgia & no no brachial plexus T1–4 paravertebral w/ STE STE NA chemo died, 15
numbness intraforaminal exten- & RTsion
Woodruff et al., 53, F arm weakness no yes T-1 nerve root T1–2 intradural canal TME TME NA RT died, 71973 & Horner
syndromeYakulis et al., 1996 67, F buttock mass no yes sacral nerve sacral ala & coccyx TME debride debride none died, 7
rootsYimaz et al., 2004 58, M sciatica no no L-2 nerve root L-2 intradural canal TME NA NA RT survived, 8
& inst
present studyCase 1 15, F back pain no no thoracic nerve T-11 VB TME decomp NA chemo died, 16
root & & RTinst
Case 2 24, M urinary retention no yes sacral nerve L-5 & sacral intradural TME NA NA chemo survived, 6root canal, sacral plexus, & & RT
& pelvis inst
* chemo = chemotherapy; debride = debridement; decomp = surgical decompression; FU = follow-up; inst = instrumentation; NA = not applicable; RT =radiotherapy; STE = subtotal excision; TME = total macroscopic excision; VB = vertebral body.




















