
Evidence for naive T-cell repopulation despite thymus irradiation after autologous transplantation...
23
doi:10.1182/blood-2002-06-1929 Prepublished online October 24, 2002; Jean-Pierre Marolleau, Patrice Debre, Jean-Claude Brouet, Jean-Paul Fermand and Brigitte Autran Marion Malphettes, Guislaine Carcelain, Pierre Saint-Mezard, Veronique Leblond, Hester Korthals Altes, CD34+ selection and age autologous transplantation in adults with multiple myeloma: role of ex-vivo Evidence for naive T-cell repopulation despite thymus irradiation after (1880 articles) Transplantation (4217 articles) Neoplasia (5019 articles) Immunobiology Articles on similar topics can be found in the following Blood collections http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requests Information about reproducing this article in parts or in its entirety may be found online at: http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprints Information about ordering reprints may be found online at: http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtml Information about subscriptions and ASH membership may be found online at: digital object identifier (DOIs) and date of initial publication. the indexed by PubMed from initial publication. Citations to Advance online articles must include final publication). Advance online articles are citable and establish publication priority; they are appeared in the paper journal (edited, typeset versions may be posted when available prior to Advance online articles have been peer reviewed and accepted for publication but have not yet Copyright 2011 by The American Society of Hematology; all rights reserved. 20036. the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.org From
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Evidence for naive T-cell repopulation despite thymus irradiation after autologous transplantation...

doi:10.1182/blood-2002-06-1929Prepublished online October 24, 2002;
Jean-Pierre Marolleau, Patrice Debre, Jean-Claude Brouet, Jean-Paul Fermand and Brigitte AutranMarion Malphettes, Guislaine Carcelain, Pierre Saint-Mezard, Veronique Leblond, Hester Korthals Altes, CD34+ selection and ageautologous transplantation in adults with multiple myeloma: role of ex-vivo Evidence for naive T-cell repopulation despite thymus irradiation after
(1880 articles)Transplantation � (4217 articles)Neoplasia �
(5019 articles)Immunobiology �Articles on similar topics can be found in the following Blood collections
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
digital object identifier (DOIs) and date of initial publication. theindexed by PubMed from initial publication. Citations to Advance online articles must include
final publication). Advance online articles are citable and establish publication priority; they areappeared in the paper journal (edited, typeset versions may be posted when available prior to Advance online articles have been peer reviewed and accepted for publication but have not yet
Copyright 2011 by The American Society of Hematology; all rights reserved.20036.the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

1
Evidence for naive T-cell repopulation despite thymus irradiation after autologous
transplantation in adults with multiple myeloma. Role of ex-vivo CD34+ selection and
age.
Marion Malphettes, Guislaine Carcelain, Pierre Saint-Mezard, Véronique Leblond, Hester Korthals
Altes, Jean-Pierre Marolleau, Patrice Debré, Jean-Claude Brouet, Jean-Paul Fermand, and Brigitte
Autran.
From the Laboratoire d'Immunologie Cellulaire et Tissulaire URA CNRS 625, Hôpital de la Pitié-
Salpêtrière, Paris, France; the Service d’Immuno-Hématologie, Hôpital Saint-Louis, Paris, France; and
the Service d'Hématologie, Hôpital de la Pitié-Salpêtrière, Paris, France.
Supported by a grant from the Ligue Nationale Contre le Cancer.
Reprint requests : Brigitte Autran, M.D., Ph.D.,
Laboratoire d'Immunologie Cellulaire et Tissulaire
URA CNRS 625
CERVI, Hôpital Pitié-Salpétrière,
47 Boulevard de l’Hôpital, 75013 Paris, France.
Fax number : (33) 1 42 17 74 90
Email : [email protected]
Copyright (c) 2002 American Society of Hematology
Blood First Edition Paper, prepublished online October 24, 2002; DOI 10.1182/blood-2002-06-1929 For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

2
ABSTRACT Immunodeficiency following autologous CD34+ purified peripheral blood stem cell (PBSC)
transplantation could be related to T-cell depletion of the graft and/or impaired T-cell reconstitution
due to thymus irradiation. Aiming to assess the role of irradiated thymus in T-cell repopulation, we
studied 32 adults with multiple myeloma, randomly assigned to receive high dose therapy including
total body irradiation (TBI) followed by autologous transplantation with either unselected or CD34+
selected PBSC. The median number of reinfused CD3+ cells was lower in the selected group (0.03
versus 14 x 106/kg; p=0.002). Lymphocyte subset counts were evaluated from Month 3 to 24 post-
graft. Naive CD4+ T-cells were characterized both by phenotype and by T-cell receptor rearrangement
excision circles (TRECs) quantification. The reconstitution of CD3+ and CD4+ T-cells was
significantly delayed in the CD34+ selected group, but eventually led to similar counts than in the
unselected group after Month 12. Mechanism of reconstitution differed, however, between both
groups. Indeed, a marked increase in the naive CD62L+CD45RA+CD4+ subset was observed in the
selected group, but not in the unselected group in which half of CD45RA+CD4+ T-cells appear to be
CD62L-negative. Age was identified as an independent adverse factor for CD4+ and CD62L+
CD45RA+CD4+ T-cell reconstitution. Our results provide evidence that infusing T-cell depleted
PBSCs after TBI in adults delays T-cell reconstitution but accelerates thymic regeneration.
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

3
INTRODUCTION
Advances in the treatment of hematological malignancies have been reported with the use of high-dose
myeloablative therapy including or not body irradiation and followed by hematopoietic stem cell
transplantation (HSCT). Immunodeficiency is an important clinical problem in patients treated with
such intensive approaches.1,2 The incidence of severe infectious adverse events and second cancers
may be high,3-5 responsible for a significant treatment-related mortality.
Of all hematopoietic lineages, T-lineage lymphocytes (T-cells) undergo the most extensive post-
marrow maturation process. Thymic T-cell precursors maturation includes T-cell receptor (TCR) gene
rearrangement followed by negative and positive selection, T-cells entering then the peripheral pool as
naive T-cells. Numerous studies of T-cell regeneration after myeloablative therapy followed by HSCT
have shown that T-cells may be regenerated through two different pathways.6 One is thymus-
dependent and might be considered as a recapitulation of ontogeny. In addition, when the activity of
the thymus is low, the T-cell pool can be repopulated through peripheral expansion of reinfused
mature T-cells. Some studies suggest that the thymus dependent pathway is age-dependent and
becomes limited after childhood, presumably due to thymic involution.7,8
In an autologous setting, ex vivo treatment of hematopoietic stem cells has been proposed as a mean of
reducing contamination of the graft by residual tumoral cells.9 The positive selection of peripheral
blood stem cells (PBSCs) expressing the CD34 antigen has been used with this aim.10-12 The
enrichment of the graft in CD34+ cells is accompanied by a profound T-cell depletion that may
compromise the peripheral expansion of reinfused T-cells following HSCT.
The combination of high-dose therapy (HDT) including a thymic irradiation with the reinfusion of
CD34+ enriched autologous cells might thus be potentially responsible for a profound induced
immunodeficiency, as both T-cell regeneration pathways might be altered in these patients. As a
matter of fact, recent works provide evidence that adult thymus may contributes substantially to
immune reconstitution in some cases.13,14 However, the effect of thymic irradiation on thymic function
in autologous setting has not yet been evaluated.
In the present study, we report an evaluation of T-cell repopulation kinetics and mechanisms in
patients with multiple myeloma treated with HDT including total body irradiation (TBI) followed by
reinfusion of autologous stem cells, using either unselected or CD34+ selected PBSCs. The primary
objective of the study was to assess the capacity of irradiated adult thymus in T-cell repopulation in
such setting and factors influencing this function. To measure thymic output and to characterize naïve
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

4
T-cells, we used both phenotype and molecular criterias, namely CD45RA+CD62L+ phenotype and
quantification of excisional DNA products of T-cell receptor gene rearrangement.15
METHODS
Patients and treatments
All the 32 patients included in the present study (17 males and 15 females; median age, 50 years;
range, 36 to 56 years) were treated in a multicenter prospective trial where patients aged under 56 with
newly-diagnosed symptomatic multiple myeloma were randomly assigned up-front to receive either a
single HDT (HDT1 arm) or two sequential HDT (HDT2 arm). In addition, all patients were
independently randomized to be transplanted with CD34+ selected PBSCs (CD34+ selected group) or
unselected PBSCs (unselected group).
All patients first received one or two courses of high dose steroïd containing regimens and PBSCs
were thereafter mobilized by cytoxan (4g/m²) and lenograstim granulocyte colony-stimulating factor
(10 ìg/kg/d). When appropriate (CD34+ selected group), part of collected PBSCs were CD34+
selected using the Isolex®300i system (Baxter). The selection procedure resulted in a median purity of
95% (65-100%) and in a significant tumor cell depletion. In the HDT1 arm, HDT was preceded by 3
monthly courses of a VAD-like regimen and combined a multi-drug regimen (carmustine, etoposide,
melphalan 140 mg/m² and cytoxan 60 mg/kg) with a TBI (12 grays in 6 fractions). Patients treated in
the HDT2 arm received melphalan 140 mg/m² alone, always supported by unmanipulated PBSCs,
followed 2 to 3 months later by a second course of melphalan 140 mg/m² combined with etoposide (30
mg/kg) and 12-grays TBI. In both HDT groups, TBI-containing HDT were supported with unselected
or CD34+ selected PBSCs, according to the randomization procedure. No maintenance therapy was
planned after TBI-containing HDT. After a pneumonia related to Pneumocystis Carinii infection
occurred 4 months after HDT in Patient 9, all patients received oral cotrimoxazole as prophylactic
post-HDT treatment. All patients gave informed consent and the trial was approved by an institutional
ethics committee.
Blood samples for immunological studies
Heparinized blood samples were collected at Month 1, 3, 6, 9, 12, 15, 18, and 24 after the last PBSC
reinfusion. In addition, blood samples from diagnosis were available for 22 patients (12 from the
CD34+ selected group and 10 from the unselected group). Peripheral blood mononuclear cells (MNC)
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

5
were separated from blood on Ficoll-Hypaque density gradients (Pharmacia, Uppsala, Sweden).
Mononuclear cells were washed twice with RPMI 1640 (Gibco, Paisley, G.B.).
Flow cytometry
Lymphocyte subset analysis
Absolute CD4+ and CD8+ cell counts were performed on fresh blood samples by four-colour flow-
cytometry analysis of cells positive for CD45, CD3, CD4, or CD8, using fluorescent beads as an
internal standard (Coulter, Margency, France). The flow cytometry analysis of lymphocyte
subpopulations was performed on the same whole blood specimen in three color immunofluorescence,
using a panel of monoclonal antibodies to the following cell surface proteins: CD3 (PercP), CD4
(FITC, PE, or PerCP), CD8 (PE), CD45 (FITC)/CD14 (PE) (Becton Dickinson, Pont de Clay, France)
and CD8 (PC5), CD45RA (PE), CD45RO (FITC), CD62L (FITC), CD16 (FITC)/CD56 (PE)
(Immunotech, Marseille-Luminy, France). Irrelevant antibodies of respective isotype were used to
ascertain background staining. All antibodies were incubated with 100 µl of whole blood for 20 min at
20°C before red cell lysis. After washings with PBS, 5,000 lymphocytes defined by FSC/SSC gate
combined to CD14- CD45+ staining were acquired into the FACScan cytometer and analyzed
according to Cell Quest (Becton Dickinson, San Jose, California). The mean values +/- SEM in
healthy people are : 900 ± 185/mm3 for CD4+ cells; 482 ± 70/ mm3 for CD45RO+CD4+ cells; 420 ±
150/mm3 for CD62L+CD45RA+CD4+ cells, 649 ± 202/ mm3 for CD8+CD3+ cells, and 243 ±
95/mm3 for CD3-CD16+CD56+ cells.
Ki67 staining This antibody recognizes an unknown nuclear antigen present on proliferating cells. This antigen is
specifically expressed during the end of G1, S, G2 and M phases of the cell cycle. Surface staining
was performed on whole blood, as described above. After red cell lysis, cells were washed with PBS,
0.5% BSA (Sigma, St Quentin, France) and then fixed with PBS, 4% PFA (Sigma) for ten minutes at
room temperature. Cells were permeabilized in a PBS, 0.1% Saponin solution (Sigma) and stained
with an anti-Ki67-FITC monoclonal antibody for 20 min. Fifty thousand lymphocytes were acquired
into the FACScan cytometer and analysed according Cell Quest. The mean value of the expression of
the Ki67 antigen within the CD4+ and CD8+ T lymphocyte population established in 10 healthy
people is 1.6 ± 0.04%. After Ki67 intracellular staining, cells were washed and incubated with 10
mg/ml Topro-3-Iodide (Molecular probe, Leiden, Netherland) and 5 mg/ml Rnase (Sigma) for 45 min
at 4°C. Topro-3-Iodide is excited at 633 nm and emit at 675 nm. One hundred fifty thousand
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom
6
lymphocytes defined by FSC/SSC gate are acquired into a FACScalibur cytometerfitted with an
double Helium-Neon (633 nm)/Argon (488 nm) laser.
T-cell receptor rearrangement excisional circles (TRECs).
TRECs quantification was performed at Month 24 of follow-up on purified cell subsets, when
sufficient amounts of CD45RA+CD4+ T-cells were reached. CD45RA+CD4+ and CD45RA-CD4+ T-
cells were purified from fresh PBMC by magnetic separation over columns, using the MiniMACS
multisort kit according to manufacturer’s instructions (Miltenyi Biotec Inc, Sunnyval, CA). Briefly,
after 15 min incubation with 20 µl CD4 conjugated magnetic beads per 107 cells, CD4+ T-cells were
isolated from PBMC by positive selection over MiniMACS separation columns. Magnetic beads were
then released, cells were incubated with CD45RA-conjugated magnetic beads and passed over
columns. With this technique, at least 90% purity of the fractions was achieved. Truly naive T-cell are
better defined by the co-expression of CD45RA and CD62L antigens. However, due to practical
reasons, TREC analysis was performed in purified CD45RA+CD4+ T-cells as well as in the
CD45RA-CD4+ T-cell counterpart. DNA was purified using the DNAzol technic (Life Technologies).
Real-time PCR assay (Taqman, Perkin Elmer) for Signal joint (Sj) TRECs was performed in 50 ml
containing 100-400 ng DNA, 25 ml of Universal Master Mix (Perkin Elmer Biosystem), 400nM
forward (5’-CACATCCCTTTCAACCATGCTGACA-3’) and reverse primers (5’-
AGAACGGTGAATGAAGAGCGACA-3’) and 200 nM specific probe (5’-
TGCCCACTCCTGTGCACGGGTG-3’) under the following conditions : 50°C for 2 min, 95°C for 10
min, followed by 45 cycles of amplification (95°C for 15 sec, 60°C for 1 min).16 A non repeated
region of the GAPDH gene was amplified in every sample test as an internal control measurement for
imput DNA (forward primer 5'-CTCCCCACACACATGCACTTAC-3', reverse primer 5'-
CCTAGTCCCAGGGCTTTGATT-3', and the probe 5'-
AAAAGAGCTAGGAAGGGAAAGGACAGGCAACTTGGC-3'). For each sample the number of Sj
TREC copies was determined using a dilution series of the pGTH310 clone containing the Sj fragment
in the Sac I site of a pGEM 4 vector.
Statistical methods
The Fisher's exact test was used for binary variable comparison. The Mann-Whitney test was used for
continuous variable comparison, such as T-cell subset counts (median comparison). In addition, the
kinetics of T-cell subsets recovery per unit time were evaluated through the slope of the line fitted to
the data over time (simple linear regression). For that, we assumed that the rate of disappearance of
cells is negligible at the time scale of the study. Correlation between kinetics of recovery and age at
the moment of transplant was tested by the correlation t-test. Multivariate comparison were performed
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

7
using logistic regression and tested by the likelihood-ratio test. A P value less than 0.05 was
considered to indicate statistical significance. All calculations were performed using the STATA
software, version 7.0 (Stata Corporation, College Station, TX, USA) .
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom
8
RESULTS
Patient population
The distribution of the 32 patients included in the present study within the four randomization groups
was as follow: HDT1-unmanipulated arm, 10 patients; HDT1-CD34 arm, 8 patients; HDT2-
unmanipulated arm, 6 patients; HDT2-CD34 arm, 8 patients. The impact of the CD34+ selection was
assessed on the comparison of the group of 16 patients receiving CD34+ selected PBSC to the group
of 16 patients receiving unselected PBSC after the last course of HDT. The median age was similar in
both groups (49 years, range 36-56 in the selected group; 51 years, range 38-56 in the unselected
group; P=0.89). There was no difference in the one versus two courses of HDT distribution between
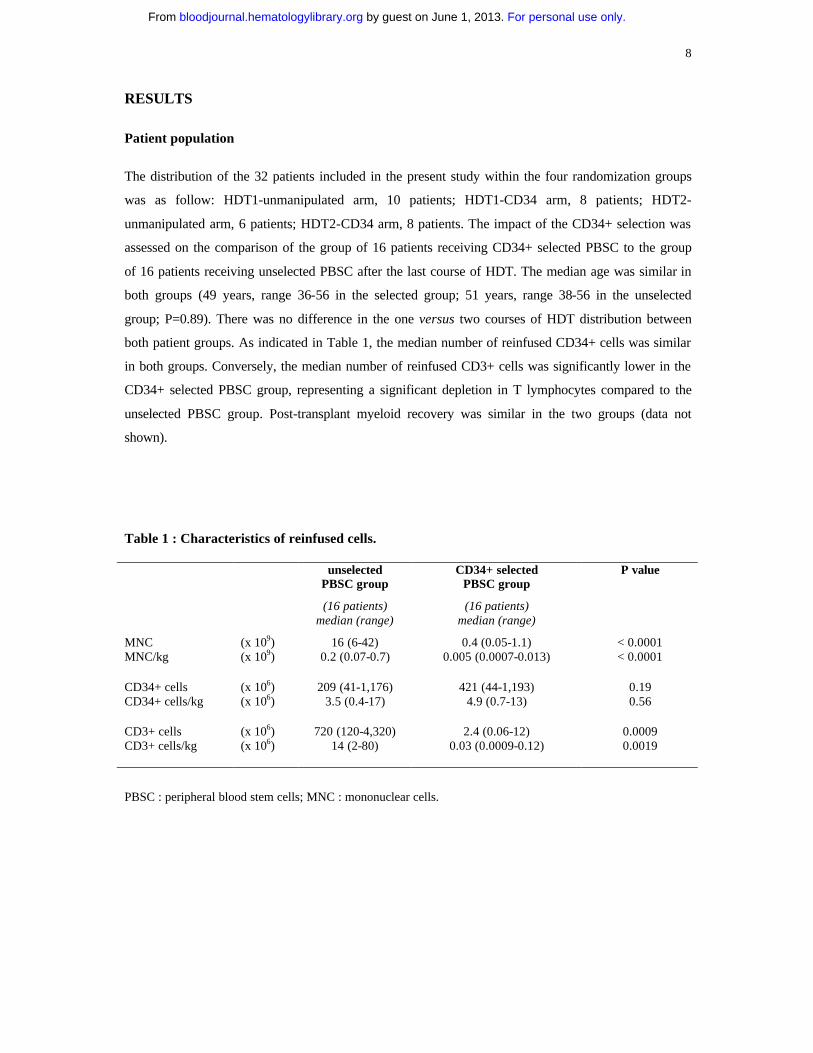
both patient groups. As indicated in Table 1, the median number of reinfused CD34+ cells was similar
in both groups. Conversely, the median number of reinfused CD3+ cells was significantly lower in the
CD34+ selected PBSC group, representing a significant depletion in T lymphocytes compared to the
unselected PBSC group. Post-transplant myeloid recovery was similar in the two groups (data not
shown).
PBSC : peripheral blood stem cells; MNC : mononuclear cells.
Table 1 : Characteristics of reinfused cells. unselected
PBSC group CD34+ selected
PBSC group P value
(16 patients) median (range)
(16 patients) median (range)
MNC (x 109) 16 (6-42) 0.4 (0.05-1.1) < 0.0001 MNC/kg (x 109) 0.2 (0.07-0.7) 0.005 (0.0007-0.013) < 0.0001 CD34+ cells (x 106) 209 (41-1,176) 421 (44-1,193) 0.19 CD34+ cells/kg (x 106) 3.5 (0.4-17) 4.9 (0.7-13) 0.56 CD3+ cells (x 106) 720 (120-4,320) 2.4 (0.06-12) 0.0009 CD3+ cells/kg (x 106) 14 (2-80) 0.03 (0.0009-0.12) 0.0019
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

9
Consequences of CD34+ selection
T-cell subset reconstitution
The CD3+ depletion in the reinfused cells associated with the CD34+ selection led to a significant
delay in T-cell reconstitution (Figure 1). The median number of CD3+ (Figure 1A), CD4+CD3+
(Figure 1B), and CD8+CD3+ (Figure 1C) cells detected in the peripheral blood was generally lower in
patients grafted after ex vivo CD34+ selection than in those grafted without ex vivo manipulation,
especially during the early follow-up. For the CD3+ and CD4+CD3+ T-cell subsets, median
comparisons showed statistically significant differences until Month 9. The mean number of
CD4+CD3+ T-cells remained below 200 cells/mm3 until Month 9 in the selected group, while not in
the unselected group. The CD34+ selection had, however, no influence on long-term T-cell
reconstitution after one year of follow-up since similar levels were reached in both groups. Baseline T-
cell subset evaluation (CD3+, CD4+CD3+, and CD8+CD3+ subsets) could be performed at diagnosis
in 22 of the 32 patients (12 from the CD34+ selected group and 10 from the unselected group). These
cell subset counts did not significantly differ from normal controls, without any differences between
patients from both selected and unselected groups (data not shown).
Figure 1 : Recovery of CD3+, CD4+CD3+, and CD8+CD3+ T-cells.
A : m e d i a n C D 3 + T-c e ll c o u n t
0
200
400
600
800
1000
1200
1400
M o n t h 3 M o n t h 6 M o n t h 9 M o n t h 1 2 M o n t h 1 5 M o n t h 1 8 M o n t h 2 4
cells
/mm
3
P=0.005 0.03 0.01 0.48 0.11 0.52 0.46
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

10
B : m e d i a n C D 4 + C D 3 + T - c e l l c o u n t
0
100
200
300
400
500
600
M o n t h 3 M o n t h 6 M o n t h 9 M o n t h 1 2 M o n t h 1 5 M o n t h 1 8 M o n t h 2 4
cells
/mm
3
C : m e d i a n C D 8 +CD3 + T - c e l l c o u n t
0
100
200
300
400
500
600
700
800
M o n t h 3 M o n t h 6 M o n t h 9 M o n t h 1 2 M o n t h 1 5 M o n t h 1 8 M o n t h 2 4
cells
/mm
3
Sequential assessments of median T-cell counts (at Month 3, 6, 9, 12, 15, 18, and 24) are shown for the whole CD3+ (A), the CD4+CD3+ (B), and the CD8+CD3+ (C) T-cell subsets, respectively. P values for median comparisons between the unselected (�) and CD34+ selected (�) groups are given at each time of follow -up. The Table included in the CD4+CD3+ section sequentially indicates the percentages of CDR5RO+ cells within the CD4+CD3+ T-cell subset in tested patients from both unselected and CD34+ selected groups. We also studied the pattern of expression of the CD45 isoforms in the CD4+ T-cell population. As
indicated in Figure 1B, CD45RO+ cells contribute almost exclusively to CD4+ T-cell reconstitution
P=0.07 0.02 0.002 0.11 0.62 0.52 0.60
Percentages of CD45R0+ cells (N patients tested) : Unselected group: 97% 92% 95% 92% 85% 84% 85% (10) (7) (12) (9) (9) (3) (7) CD34+ group: 99% 96% 83% 83% 84% 70% 74% (10) (9) (11) (13) (10) (7) (8)
P=0.005 0.08 0.03 0.57 0.04 0.34 0.53
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

11
for the first year in the unselected group but for the first 6 months only in the selected group. In the
two groups, early CD4+ T-cell reconstitution was accompanied by increased Ki67 staining. We
confirmed that the Ki67+CD4+ T-cells were CD45RO+ (data not shown). At Month 1, 19% of the
CD4+ and 24% of the CD8+ T-cells exhibit the Ki67 antigen. These percentages decreased as soon as
the third month post-graft and remained at values slightly above normal range (2 to 5%) until Month
15 without any difference between the CD4+ and CD8+ subsets neither between the selected and
unselected groups. The distribution of Ki67+CD4+ T-cells throughout the cell cycle was determined
by analyzing DNA content with TOPRO3iodide staining. The Ki67 antigen was distributed through all
cell cycle phases, i.e. G0/G1 as well as G2+M phases like in healthy individuals.
Naive CD4+ T-cell reconstitution
CD45RA+ cells steadily increased during the post-transplant follow-up and were detectable as soon as
month 6 in the unselected group but only at month 9 in the selected group. The median number of
CD45RA+CD4+ T-cells was lower in the selected group as compared to the unselected group during
the short-term follow-up only (p=0.01 and 0.02 at Month 3 and 6, respectively) (Figure 2). No
differences were observed at Month 9 and after. As indicated on Figure 2, almost half of the
CD45RA+ cells did not exhibit the CD62L in the unselected group, at any time of the follow-up.
Conversely, most of the CD4+CD45RA+ cells co-express the CD62L in the selected group.
Accordingly, a higher median number of CD62L+CD45RA+ CD4+ T-cells was observed in the
selected group as compared to the unselected from Month 9. This difference reached the statistically
significant level at Month 9 and 12 (p=0.02 and 0.02 , respectively).
Figure 2 : Recovery of naive CD4+ T-cells.
M e d i a n C D 4 5 R A + C D 4 + C D 3 + T - c e ll c o u n t
0
50
100
150
Month
3
Month
6
Month
9
Month
12
Month
15
Month
18
Month
24
cell
s/m
m3
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

12
Sequential assessments of median CD45RA+CD4+CD3+ T-cell counts (at Month 3, 6, 9, 12, 15, 18, and 24) are shown for both unselected (in gray) and CD34+ selected (in black) groups. P values for median comparisons between both groups are given at each time of follow-up. Fractions of CD62L+ T-cells are represented in plain areas.
To confirm that cells expressing CD45RA+CD4+ phenotype were enriched in naïve CD4T -cells, we
measured the number of TRECs in the selected CD45RA+CD4+ and CD45RA-CD4+ subpopulations
at Month 24 in 9 patients (5 patients from the CD34+ selected and 4 patients from the unselected
group) (Figure 3). We found that the number of TREC in these phenotypically designed naive
CD45RA+ cells was ten fold higher than in the CD45RA- counterpart (median TREC number, 18
versus 1.8 x 103/106 cells, P<0.001), without marked differences between patients from the selected or
unselected group. In both CD45RA- and CD45RA+ subpopulations, results obtained in normal
controls were in similar ranges (not shown). At Month 24, CD45RA+CD62L+ cells accounted for at
least 75% of the whole CD45RA+ T-cell population in each individual patient studied for TRECs. In
addition, there was a positive correlation between the number of TRECs measured and the percentage
of CD62L+ cells within the CD45RA+CD4+ T-cell subset tested (R = 0.91; p=0.001).
Figure 3 : T-cell Receptor Rearrangement Excision Circles (TRECs).
0
10000
20000
30000
40000
50000
60000
1 2 3 4 5 6 7 8 9
P a t i e n t s
TR
EC
s p
er 1
mil
lion
cel
ls
C D 4 5 R A - C D 4 + c e l l s C D 4 5 R A + C D 4 + c e l l s
Numbers of TRECs in both CD45RA-CD4+ and CD45RA+CD4+ T-cell subsets are indicated in white and gray, respectively, for the 9 tested patients. Patients n°1 to 5 belonged to the CD34+ selected group and patients n°6 to 9 belonged to the unselected group. Median number of TRECs was ten fold higher in the CD45RA+ as compared to the CD45RA- subset in patients receiving CD34+ selected graft, as well as in those receiving unselected graft (18 versus 1.8 x 103/106 cells in the whole population of patients tested, P<0.001).
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

13
Non T-cell subset reconstitution
Reconstitution of CD45+CD14+ and CD3-CD16+CD56+ cell subsets has been followed-up until
Month 15. During this period, CD45+CD14+ cell counts remained in the normal ranges in all patients
from the unselected as well as from the CD34+ selected group. Concerning the natural killer subset, a
significant difference between both patient groups was observed at Month 3 only. At that time, the
mean number of CD3-CD16+CD56+ cells (+/- SEM) was higher in patients from the CD34+ selected
group as compared to those from the unselected group (229 +/- 57 versus 113 +/- 22 /mm3; P=0.004).
This difference was not longer observed after this early period, as CD3-CD16+CD56+ cell counts
were within the normal ranges in both patient groups.
Role of age
T-cell subset reconstitution
Age had no impact on T-cell reconstitution until Month 15, but a negative impact on long-term CD3+
and CD4+CD3+ cells reconstitution was observed. At Month 18 and Month 24, the mean number of
CD3+ cells (+/- SEM) was 1310 +/- 222 and 1250 +/- 128 /mm3 in the 16 patients aged less than 50
years versus 729 +/- 208 and 893 +/- 133 /mm3 in the 16 patients aged more than 50 years (p=0.05 and
0.04, respectively). At Month 18 and Month 24, the mean number of CD4+ CD3+ cells was 508 +/-
184 and 558 +/- 66/mm3 in the 16 patients aged less than 50 years versus 259 +/- 128 and 357 +/-
59/mm3 in the 16 patients aged more than 50 years (p=0.01 and 0.02, respectively). These differences
remained significant after adjustment on the CD34+ selection criteria. Even when considered as a
continuous variable in a logistic regression analysis including the CD34+ selection criteria, age was
still an independent predictive factor of bad reconstitution at Month 24 (p=0.045 and 0.04, for CD3+
and CD4+CD3+ T-cells, respectively).
When kinetics of CD4+ T-cell recovery were correlated with age using a correlation t-test, we found a
negative correlation between advanced age and recovery of the whole CD4+ population in patients
from the CD34-selected group (R = -0.58; P=0.014) (Figure 4A) while not in those from the
unselected group (not shown). Age had no significant influence on CD8+ T-cell long-term
reconstitution.
Naive CD4+ T-cell reconstitution
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

14
As indicated on Figure 4B, we also found a negative correlation between age and CD62L+CD45RA+
CD4+ T-cell recovery either in patients from the CD34-selected group or in those from the unselected
group (R = -0.66 and –0.78; p=0.005 and 0.001, respectively). At Month 18 and Month 24, the mean
number of these naive CD62L+CD45RA+CD4+ cells (+/- SEM) was 98 +/- 21 and 163 +/- 40/mm3 in
the 16 patients aged less than 50 years versus 23 +/- 8 and 38 +/- 9/mm3 in the 16 patients aged more
than 50 years. Of note, the kinetics of recovery of the whole CD45RA+CD4+ T-cell population was
significantly affected by age in patients from the CD34-selected group only (R = -0.8; p=0.0001).
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

15
Figure 4 : Recovery of CD4+ T-cell versus age.
A
Recovery o f CD4+ T-ce lls versus a g e
in pat ien ts fro m the CD34+ sele c ted group
0
1
2
3
4
5
6
7
3 5 4 0 4 5 5 0 5 5 6 0
Age
Rec
over
y C
D4
(cel
ls/m
m3/
wee
k)
R =-0.58, P=0.014
B
Recovery o f CD62L+ CD45RA+ CD4+ T-ce l l s versus age
0
0,5
1
1,5
2
2,5
3
35 40 45 50 55 60
A g e
Rec
over
y (c
ells
/mm
3/w
eek)
CD34+ se lected group
R =-0.66; P=0.005
unse lec ted g roup
R =-0.78; P=0.001
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

16
Role of previous treatment
The role of the two treatment arms (HDT1 versus HDT2) on immune reconstitution was analyzed in
the whole patient population as well as in CD34+ selected and unselected patients separately. No
significant difference was found with the exception of a late transient deficiency in CD3+ and
CD8+CD3+ cells observed at Month 18 in patients who received two HDT as compared to those who
received one HDT (p=0.02 and 0.02 for the CD3+ and CD8+CD3+ subset, respectively by the Mann-
Whitney test). Of note, this transient deficiency in CD8+CD3+ cells associated with the HDT2 arm
appeared to be mainly observed in patients from the unselected PBSC group. This lack of marked
difference in immune reconstitution between both treatment arms and the fact that both selected and
unselected patient groups were well-balanced for these two treatment arms allow to eliminate a
potential bias introduced by a significant impact of previous therapy.
Role of intercurrent events
Opportunistic infections
As the immune reconstitution may have been influenced by the occurrence and treatment of
intercurrent infections in some patients, we retrospectively registered all opportunistic infections
which occurred during the 2-year follow-up in the 32 patients studied. We did not observe any
significant difference in opportunistic infection incidence between both patient groups in this limited
population of patients (6 events in 5 patients from the CD34+ selected group as compared to 3 events
in 3 patients from the unselected group). As indicated in Table 2, the 3 patients from the unselected
group who experienced opportunistic infections had quite normal CD4+CD3+ cell levels at the time of
the infection. In the CD34+ selected group, patients who experienced opportunistic infections had low
CD4+CD3+ cell levels at the time of infection. However, these levels were not significantly lower in
these patients as compared to those who had no infection at the corresponding times (p=0.43, 0.64, and
0.28 at Month 3, 9, and 24, respectively).
Table 2 : Occurrence of opportunistic infections. Type of infection Date of onset CD4+ CD3+ cells* Treatment (cells/mm3) CD34+ selected group
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

17
Patient 4 VZV pancreatitis Month 24 234 Acyclovir Patient 9 PCC pneumonia Month 4 149 Cotrimoxazole Patient 9 HSV oesophagitis Month 4 149 Acyclovir Patient 11 VZV varicella Month 9 308 Acyclovir Patient 14 VZV varicella Month 3 81 Acyclovir Patient 22 VZV retinitis Month 8 163 Acyclovir Unselected group Patient 13 CNS toxoplasmosis Month 9 480 Pyrimethamine- Sulfadiazine Patient 17 HSV pneumonia Month 4 444 Acyclovir Patient 28 VZV zoster Month 4 508 Acyclovir *: evaluated at the time or in the month before the onset of infection; VZV: Varicella Zoster virus; PCC: Pneumocystis Carinii; HSV: Herpes Simplex virus; CNS: central nervous system.
In patients who had opportunistic infection, no significant changes in the immune reconstitution
profile was noted after the occurrence of the infection and its treatment (data not shown). Of note,
these patients did not experience further opportunistic events, with the exception of one patient
(Patient 4) who developed secondary Hodgkin's disease associated with autoimmune hemolytic
anemia 4 years after transplantation.
Myeloma progression
During the 2-year follow-up of the study no patient had significant myeloma progression. As a
consequence, no patient received additional therapy such as chemotherapeutic agents, interferon, or
thalidomide that could have interacted with their immune reconstitution profile during the study
period.
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

18
DISCUSSION In the present study, we evaluated the mechanisms of T-cell reconstitution occurring after autologous
transplantation of CD34+ selected versus unselected PBSC grafts reinfused after TBI-containing HDT
in adults with multiple myeloma. We showed that overall the CD4+ T-cell reconstitution was
significantly delayed during the first year in the selected group, but eventually led to similar counts as
in the unselected group. This reconstitution rapidly involves the residual mature memory T-cells after
unselected grafts that might negatively regulate the thymic differentiation in that setting. In contrast,
the immune reconstitution of thymic origin was enhanced in the selected group as compared to the
unselected group, demonstrating that TBI in adults does not impair thymic function which is regulated
by peripheral lymphocyte emptiness. Age was identified as an independent adverse factor for CD4+
and naive CD4+ T-cell reconstitution.
In this limited population of patients, differences observed in immune reconstitution did not translate
into significant difference in the incidence of opportunistic infections. Analysis of the whole study
clinical parameters is in progress. Preliminary results appeared to show a higher rate of opportunistic
infections in the CD34+ selected group (data not shown here).16 This would suggest that not restoring
rapidly protective memory T-cells against pathogens would be associated with a higher incidence of
infections, despite further recovery of T-cell pool from thymic emigrants observed in this patient
group.
Post-transplant immunodeficiency has been described after allogeneic transplantation, especially after
T-cell depletion of the graft.17 However, in the allogeneic setting, immunological conflict and
immunosuppressive therapy are likely to impair not only thymic production, but also T-cell
proliferation. Of interest, very long-term T-cell reconstitution (20 to 27 years after allogeneic
transplantation) was evaluated using TRECs quantification.18 The main result was that a late and not
clinically relevant deficiency in the naive T-cell pool was only observed in patients transplanted in
adulthood and not in those transplanted in childhood. Autologous setting remains, however, preferable
to study thymic activity, especially when using CD34-selected graft in which purging procedure has
eliminated mature T-cells that could undergo peripheral expansion.
Our results confirm that both known regeneration pathways account for T-cell reconstitution in these
patients. The initial rapid increase in CD4+ T-cell count appears to involve peripheral T-cell
expansion in both groups. Indeed, proliferation of mature T-cells was evidenced by the high level of
Ki67+CD4+ T-cells, as well as the high proportion of memory type cells within the CD4+ T-cell
subset. A second mechanism takes place after 6 months, with differences between both groups,
however. Indeed, naïve CD62L+ CD45RA+CD4+ T-cells were restored faster in the selected group
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

19
compared to the unselected one. Of note, we found a very high proportion of CD45RA+CD4+ T-cells,
which did not express the CD62L antigen in patients from the unselected group. This was not
observed in patients from the CD34-selected group. Such high proportions are quite exceptional and
has not been observed in normal controls or during HIV infection. One explanation might be the
reversion of the CD45RO phenotype after peripheral expansion of the mature CD45R0+ memory T-
cells reinfused with unselected graft.19 These CD62L- CD45RA+CD4+ T-cells should therefore
belong to the memory rather than to the naïve subset. Our results were corroborated by our TRECs
findings which were correlated to the CD62L expression. Altogether, these results show that thymic
production in the selected group might be stimulated by some feed-back mechanisms from the
periphery where the mature T-cell infused with the graft were unable at reconstituting a sufficient T-
cell pool. Thus, a relative emptiness of the peripheral pool secondary to T-cell depleted HSCT
reinfusion is capable to promote naïve T -cell production. This has to be related to the “thymic rebond”
described after chemotherapy in children.7 A delay is, however, observed and might be due to transient
thymic dysfunction after thymic irradiation. Another explanation could be that, even if few naïve T -
cells are early generated, they undergo rapid peripheral expansion due to T-cell pool emptiness.
Immune reconstitution after autologous HSCT has already been evaluated by several groups.2,13,20 In
the study of Bromberger et al., immune reconstitution was reported in 9 patients with poor-risk non
Hodgkin lymphomas receiving autologous CD34+ selected cells.2 Immunoaffinity purification
followed by high speed FACS sorting was used to enrich the CD34+-selected graft. As in the present
study, a delayed CD4+ T-cell reconstitution was observed. Surprisingly, in this study, CD4+ T-cell
reconstitution was deeply impaired in both groups and remained below 200/mm3 at 6 months even in
the unmanipulated group. This could be due to alteration of progenitors by prior chemotherapy before
PBSCs harvesting. In our study, reinfused T-cell progenitors were not previously exposed to high
cumulative dosage of chemotherapy that may impair their ability to mature. In the study of Douek et
al., the ability of the thymus to generate naive T-cells was already shown in 40 patients with multiple
myeloma who underwent autologous transplantation with CD34+ enriched PBSC.13 The main
difference with the design of our present study was the lack of total body irradiation (TBI). The main
non-concordant result was the lack of significant delay in CD4+CD3+ T-cell reconstitution compared
to patients receiving unmanipulated PBSC, while we found a significant delay from Month 3 to 9 in
our study. As peripheral expansion of residual and/or reinfused mature T-cells is proposed as the main
mechanism for initial T-cell pool reconstitution, this non-concordant result thus suggests that TBI
exposure could lead to a reduced post-graft peripheral expansion through alterations of the host’s
microenvironment and/or residual mature T-cells. In the study of Rutella et al. conducted in patients
with various lymphoid malignancies (probably heavily preteated, as suggested by the reduced baseline
level in CD4+ cells), the very short-term T-cell reconstitution was evaluated for 4 months only after
non TBI-containing autologous CD34+ enriched PBSC transplants.20 A transient and very early
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

20
deficiency in CD4+CD3+ (and at a lower degree in CD8+CD3+) cells was observed when compared
to patients who received unselected transplants. Again, an inverse relationship between the number of
mature T-cells reinfused and the duration of the post-graft deficiency strongly supported the major role
of peripheral expansion of reinfused mature T-cells. As mentioned above, the lack of TBI may explain
that no deficiency in immune reconstitution was observed in these patients after Month 2.
Thymic irradiation has been proposed to deeply exacerbate post-transplant immunodeficiency after
CD34+ selected HSCT.3,21 We insist here on the ability of the thymus to produce naïve T -cells in
grafted adults despite irradiation since the TRECs proportions observed in the CD45RA+ subset were
identical to that of normal donors. Therefore our results are the first to demonstrate that thymic
production of new naïve T -cells can occur in adults after thymic irradiation. In addition we show it is
positively influenced by low peripheral blood T-cell numbers when the peripheral expansion of mature
residual T-cells is limited due to T-cell graft depletion. One can also suggest that depletion of NK cells
and monocytes might influence the rate and mechanism of T-cell reconstitution after TBI in adults
receiving CD34+ positively selected grafts. Interestingly, the earlier NK cell reconstitution observed
after CD34+ selected grafts suggests a de novo production of NK cells rather than an expansion of
residual NK cells from unselected grafts. Such phenomenon does not alter thymic regeneration, but
might also reflect the influence of the peripheral emptiness on the mechanism of immune
reconstitution.
In addition to peripheral emptiness, age is a major factor influencing restoration of naïve CD4+ T -cell
production, as already proposed in the allogeneic as well as in the autologous setting.13,18 The
influence of age also suggests that this naïve T -cell production comes from the thymus.22,23
Altogether, our results demonstrate that infusing T-cell depleted PBSCs in irradiated adults delays the
overall T-cell reconstitution in the early period, but accelerates the thymic regeneration process and
eventually leads to similar levels of CD4+ T-cell reconstitution than in unmanipulated HSCT.
AKNOWLEDGMENTS
We are indebted to Dr. Sabine Bréchignac for assistance in blood sample collection and to Dr. Hervé
Dombret for careful revision of the manuscript and editorial assistance.
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

21
REFERENCES
1. Keever CA, Small TN, Flomenberg N, et al. Immune reconstitution following bone marrow transplantation: Comparison of recipients of T-cell depleted marrow with recipients of conventionnal marrow grafts. Blood. 1989;73:1340-1350.
2. Bomberger C, Singh-Jairam M, Rodey G, et al. Lymphoid reconstitution after autologous PBSC
transplantation with FACS-sorted CD34+ hematopoietic progenitors. Blood. 1998;91:2588-2600.
3. Homberg LA, Boeckh M, Hooper H, et al. Increased incidence of cytomegalovirus disease after
autologous CD34-selected peripheral blood stem cell transplantation. Blood. 1999;94:4029-4035.
4. Anderson KC, Soiffer R, Delage R, et al. T-cell-depleted autologous bone marrow
transplantation therapy : Analysis of immune deficiency and late complications. Blood. 1990;76:235-244.
5. Divine M, Boutolleau D, Delfau-Larue MH, et al. Poor lymphocyte recovery following CD34-
selected autologous peripheral blood stem cell transplantation for non-Hodgkin's lymphoma. Br J Haematol. 1999 May;105(2):349-360.
6. Mackall C, Hakim FT, Gress RE, et al. T-Cell regeneration: all repertoires are not created equal.
Immunol Today. 1997;18: 245-251. 7. Mackall C, Fleisher T, Brown M et al. Age, thymopoiesis, and CD4+T-lymphocyte regeneration
after intensive chemotherapy. N Engl J Med. 1995;332:143-149. 8. Hakim F, Cepeda R, Kamei S, et al. Constraints on CD4 recovery postchemotherapy in adults:
thymic insufficiency and apopoptotic decline of expanded peripheral CD4 cells. Blood. 1997;90:3789-3798.
9. Vescio R, Cao J, Hong C, et al. CD34+ ceprate selection leads to a 4-5 log reduction in tumor
burden in myeloma PBC autografts based on PCR and Poisson distribution analysis. Blood. 1994;84(suppl 1):399a.
10. Berenson RJ, Bensinger WI, Hills RS, et al. Engraftment after infusion of CD34+ marrow cells
in patients with breast cancer or neuroblastoma. Blood. 1991;77:1717-1722. 11. Gribben J, Freedman A, Neuberg D, et al. Immunologic purging of marrow assessed by PCR
before autologous bone marrow transplantation for B-cell lymphoma. N Engl J Med. 1991;325:1525-1533.
12. Vescio R, Schiller G, Stewart AK, et al. Multicenter phase III trial to evaluate CD34+ selected
versus unselected autologous peripheral blood progenitor cell transplantation in multiple myeloma. Blood. 1999;93:1858-1868.
13. Douek DC, Vescio RA, Betts MR, et al. Assessment of thymic output in adults after
haematopoietic stem-cell transplantation and prediction of T-cell reconstitution. Lancet. 2000;355:1875-1881.
14. Weinberg K, Blazar BR, Wagner JE, et al. Factors affecting thymic function after allogenic
hematopoietic stem cell transplantation. Blood. 2001;97:1458-1466.
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

22
15. Livak F, Schatz D. T-cell receptor alpha locus V(D)J recombination by-products are abundant in thymocytes and mature T cells. Moll. Cell Biol. 1996;16:609-18.
16. Fermand JP, Marolleau JP, Alberti C, et al. In single versus tandem high dose therapy (HDT)
supported with autologous blood stem cell (ABSC) transplantation using unselected or CD34 enriched ABSC : Preliminary results of a two by two designed randomized trial in 230 young patients with multiple myeloma (MM) [abstract]. Blood. 2001;98:815a.
17. Roux E, Helg C, Dumont-Girard F, et al. Analysis of T-cell repopulation after allogenic bone marrow transplantation: significant differences between recipients of T-cell depleted and unmanipulated graft. Blood. 1996;87:3984-92.
18. Storek J, Joseph A, Espino G, et al. Immunity of patients surviving 20 to 30 years after
allogeneic or syngeneic bone marrow transplantation. Blood. 2001;98:3505-12. 19. Young JL, Ramage JM, Gaston JS, et al. In vitro responses of human CD45RobrightRA- and
CD45RO-Rabright T-cell subsets and their relationship to memory and naïve T -cells. Eur. J. Immunol. 1997;27:2383-90.
20. Rutella S, Rumi C, Laurenti L, et al. Immune reconstitution after transplantation of autologous
peripheral CD34+ cells: analysis of predictive factors and comparison with unselected progenitor transplants. Br. J. Haematol. 2000;108:105-15.
21. Schiller GJ, Vescio R, Berenson J. Cytomegalovirus infection following transplantation of
autologous CD34-selected progenitor cells. Blood. 2000;96:1194. 22. Mackall C, Punt J, Morgan P. Thymic function in young/old chimeras: substantial T-cell
regenerative capacity despite irreversible age-associated thymic involution. Eur. J. Immunol. 1998;28:1886-93.
23. Douek DC, Mc Farland RD, Keiser PH, et al. Changes in thymic function with age and during
the treatment of HIV infection. Nature. 1998;396:690-95.
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom


















![Free Indirect Discourse for the Naive [Edited transcript of talk, 2013]](https://static.fdokumen.com/doc/165x107/63128fbb3ed465f0570a4970/free-indirect-discourse-for-the-naive-edited-transcript-of-talk-2013.jpg)

