
Impaired Generation of Transit-Amplifying Progenitors in the ...
SchattemanOla Awad, Eduard I. Dedkov, Chunhua Jiao, Steven Bloomer, Robert J. Tomanek and Gina C.
Endothelial Cell Progenitors+ and CD14+Differential Healing Activities of CD34
Print ISSN: 1079-5642. Online ISSN: 1524-4636 Copyright © 2006 American Heart Association, Inc. All rights reserved.
Greenville Avenue, Dallas, TX 75231is published by the American Heart Association, 7272Arteriosclerosis, Thrombosis, and Vascular Biology
doi: 10.1161/01.ATV.0000203513.29227.6f2006;26:758-764; originally published online January 12, 2006;Arterioscler Thromb Vasc Biol.
http://atvb.ahajournals.org/content/26/4/758World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://atvb.ahajournals.org/content/suppl/2006/01/12/01.ATV.0000203513.29227.6f.DC1.htmlData Supplement (unedited) at:
http://atvb.ahajournals.org//subscriptions/
at: is onlineArteriosclerosis, Thrombosis, and Vascular Biology Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document. Question and AnswerPermissions and Rightspage under Services. Further information about this process is available in the
which permission is being requested is located, click Request Permissions in the middle column of the WebCopyright Clearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of theArteriosclerosis, Thrombosis, and Vascular Biologyin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from

Differential Healing Activities of CD34� and CD14�
Endothelial Cell ProgenitorsOla Awad, Eduard I. Dedkov, Chunhua Jiao, Steven Bloomer, Robert J. Tomanek, Gina C. Schatteman
Objective—Peripheral blood contains primitive (stem cell-like) and monocytic-like endothelial cell progenitors. Diabetesapparently converts these primitive progenitors, from a pro-angiogenic to anti-angiogenic phenotype. Monocyticprogenitors seem to be less affected by diabetes, but potential pro-angiogenic activities of freshly isolated monocyticprogenitors remain unexplored. We compared the ability of primitive and monocytic endothelial cell progenitors tostimulate vascular growth and healing in diabetes and investigated potential molecular mechanisms through which thecells mediate their in vivo effects.
Methods and Results—Human CD34� primitive progenitors and CD14� monocytic progenitors were injected locally intothe ischemic limbs of diabetic mice. CD14� cell therapy improved healing and vessel growth, although not as rapidlyor effectively as CD34� cell treatment. Western blot analysis revealed that cell therapy modulated expression ofmolecules in the VEGF, MCP-1, and angiopoietin pathways.
Conclusions—Injection of freshly isolated circulating CD14� cells improves healing and vascular growth indicating theirpotential for use in acute clinical settings. Importantly, CD14� cells could provide a therapeutic option for people withdiabetes, the function of whose CD34� cells may be compromised. At least some progenitor-induced healing probablyis mediated through increased sensitivity to VEGF and increases in MCP-1, and possibly modulation of angiopoietins.(Arterioscler Thromb Vasc Biol. 2006;26:758-764.)
Key Words: angiogenesis � CD34 � diabetes � endothelial progenitor cells � monocytes
Peripheral blood contains primitive (stem cell-like) andmonocytic endothelial cell (EC) progenitors that can
differentiate into ECs in vitro and integrate into the vascula-ture in vivo. However, in most situations, integration oflocally injected EC progenitors is rare. Nevertheless, ECprogenitors are of great clinical interest because they havebeen shown to promote vascular growth and tissue healing.
Among primitive EC progenitors are human CD34� pe-ripheral blood mononuclear cells (PBMCs) and mouse bonemarrow Sca-1�lin� cells.1–5 These cells leave the bone mar-row and enter the circulation at a very low rate, representing�0.1% of circulating cells. When injected locally, the freshlyisolated cells are potent stimulators of vessel growth inischemic tissue, although they rarely integrate into vessels.1–7
Human monocytes also differentiate into ECs in vitro8–13
and in vivo,9,11,14,15 and CD14� monocytes may be theprimary source of EC progenitors in the circulation.9 More-over, a recent study concluded that monocytes are thepredominant source of “EPCs,”12 that is, bone marrow-derived mononuclear cells that attach to fibronectin, bindUlex lectin, and take up acetylated low-density lipoproteinafter several days in culture.16,17 However, one study found
that CD14� and CD14� PBMCs have similar abilities todifferentiate into EC in vitro, although the CD14� populationcontained CD34� PBMCs.11
Surprisingly, little is known about the effect of freshlyisolated exogenous monocytic progenitors on revasculariza-tion in vivo. Locally injected freshly isolated CD34� PBMCs,which contain �10% monocytes, do not improve flowrestoration in ischemic limbs of nondiabetic and diabeticmice. However, because in vitro studies demonstrate thatCD34�CD14� cells inhibit CD14� cell responsiveness, this isnot unexpected.18 Intravenous injection of freshly isolatedCD14�, CD34�, or total PBMCs in the nondiabetic mousealso has no effect on healing, but because many thousand foldmore of the analogous cells are already present in the mouseblood stream, this should not be unexpected.11 In contrast,intravenous injection of cultured CD14�, CD34�, or totalPBMCs dramatically improved flow in the limbs relative tountreated controls, as did macrophages derived from CD14�
PBMCs, albeit to a lesser degree.11 These data suggest thatmonocytic progenitors require priming to differentiate intoEC and/or promote vascular growth. This should not besurprising because monocytes require activation to perform
Original received June 21, 2005; final version accepted January 4, 2006.From the Departments of Anatomy and Cell Biology (O.A., E.D., R.J.T.) and Exercise Science (C.J., S.B., G.C.S.), University of Iowa, Iowa City, Iowa.Consulting Editor for this article was Alan M. Fogelman, MD, Professor of Medicine and Executive Chair, Departments of Medicine and Cardiology,
UCLA School of Medicine, Los Angeles, Calif.O.A. and E.D. contributed equally to this work.Correspondence to Gina Schatteman, PhD, Exercise Science FH412, University of Iowa, Iowa City, IA 52242. E-mail [email protected]© 2006 American Heart Association, Inc.
Arterioscler Thromb Vasc Biol. is available at http://www.atvbaha.org DOI: 10.1161/01.ATV.0000203513.29227.6f
758 by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from

virtually every function with which they are associated.Apparently, tissue culture can provide such a stimulus.
From a therapeutic standpoint, the need to culture cellsbefore use is not ideal. However, earlier studies with freshlyisolated human CD34� and mouse Sca-1� cells indicate thatwhen injected directly into the tissue, primitive EC progeni-tors require no priming, or if they do, the ischemic tissueprovides the signal. The same might be true for CD14� cells.
Diabetes induces endothelial cell progenitor dysfunction,including in CD34� cells.1,4,5,19–21. We examined the abilityof freshly isolated CD14� cells to accelerate healing becausemonocytic progenitors appear to be less negatively affectedby this disease than primitive progenitors.4 Under basalconditions mouse diabetic and nondiabetic primitive progen-itors were indistinguishable with respect to their ability toproliferate and produce differentiated progeny. However,when subjected to oxidative stress or hypoxia, the primitivediabetic progenitors, but not their monocytic progeny, exhib-ited a reduced ability to produce endothelial cells relative totheir nondiabetic counterparts. Additional reasons for study-ing CD14� cells are that they are abundant in the blood andwould be easy to harvest clinically, and in vitro data suggestthat they may be more potent stimulators of vascular growththan whole PBMCs.18 Because CD34� and CD14� ECprogenitors have distinct in vitro characteristics, we alsotested whether the cells might cooperate to promote vasculargrowth and healing in vivo.
The data suggest that CD14� PBMCs may offer a thera-peutic alternative for people with diabetes, the function ofwhose CD34� PBMCs is compromised. Intramuscularly in-jected freshly isolated CD14� and CD34� EC progenitors, orthe combination of the 2 increased aggregate arteriolardensity and promoted muscle salvage in the diabetic mouseischemic hindlimb. All cell treatments also accelerated bloodflow restoration, but with different kinetics. Western blotanalysis showed distinct patterns of pro-angiogenic factorexpression in CD34� and CD14� cell-treated limbs, whichmay account for the different kinetics in blood flowrestoration.
Materials and MethodsDetailed procedures can be found in the online data supplement(http://atvb.ahajournals.org). P�0.05 was considered statisticallysignificant for all assays.
Isolation and Labeling of PBMCSBlood was collected from healthy adult volunteers according toUniversity of Iowa Institutional Review Board approved protocolswith informed consent. Cells were isolated as described.1 Briefly,mononuclear cells were collected by density centrifugation. CD34�
PBMCs were isolated using 2 rounds of anti-CD34� cell beadselection. Residual CD34� cells were used directly, or CD34�CD14�
PBMCs (hereafter referred to as CD14� PBMCs for clarity) wereisolated by 2 rounds of anti-CD14� cell bead selection. Some cellswere labeled with CM-DiI as described.9 Additional cells wereanalyzed for expression of the vascular endothelial cell growth factorreceptor 2 (VEGFR2) (Figure I, available online athttp://atvb.ahajournals.org)
AnimalsAnimal procedures were approved by the University of Iowa AnimalCare and Use Committee. Anesthesia was induced with 4% isoflu-
rane and maintained with 0.8% to 1.2% isoflurane. Euthanasia wasperformed by injection of 150 mg/kg sodium pentobarbital.
Diabetes was induced with streptozotocin in 8 to 12 weeks oldHFh11nu athymic mice male mice as described.22 Three to 4 weeksafter inducing diabetes, the left proximal femoral artery was ligatedas described.1 Two to 4 hours later, fresh human CD34� PBMCs(5�105, n�12 or 1�106; n�3), CD14� PBMCs (1�106, n�11), orthe combination of the 2 (5�105 CD34� and 1�106 CD14�; n�9)were injected intramuscularly into the ischemic limbs. (Figure 1A)Additional mice were injected with CD34- PBMCs (1�106; n�4),with vehicle (n�7), or nothing (n�5). We saw no additionalacceleration of or increase in blood flow restoration when 1�106
rather than 5�105 CD34�cells were used. Thus, we did all subse-quent experiments at the lower dose.
Blood Flow AnalysisLimb blood flow restoration distal to the ligation was analyzedimmediately before and after surgery and 2, 4, 6, 8, 10, and 12 daysafter surgery using scanning LASER Doppler analysis as de-scribed1,23 (Figure 1A). Flow comparisons over time among groupswere performed by repeated measures ANOVA with Tukey’s post-hoc analysis. Data are presented as percent mean blood flux in theoperated limb relative the unoperated limb.
Histology, Immunolabeling, and MorphometryControl and ischemic limb hamstring muscles, from �4 mm proxi-mal to 4 mm distal of the injection site (Figure 1A) were collected 5days after surgery (n�4 each group). Sections from 6 differentequally spaced levels were used for morphological examination andarteriolar density measurements. Hematoxylin and eosin stained
Figure 1. LASER Doppler analysis of blood flow in ischemic dia-betic mouse hindlimbs injected with PBMCs or vehicle on theday of femoral artery ligation. Data expressed as percent flux inischemic limb relative to contralateral control limb. A, Approxi-mate site of ligation (*) and PBMC injection (X). Outer tracingindicates typical region of the limbs analyzed for blood flow.Inner tracing approximates area of harvested muscle. B, Flowafter injection with vehicle (n�7), CD14� PBMCs (CD14�) (n�5),or a combination of CD14� and CD34� PBMCs (CD14�/CD34�)(n�5). Both CD14� injected groups differ from vehicle controlsbeginning at day 8 (P�0.05). C, Flow in ischemic limbs aftervehicle or CD34� PBMC injection. D, Effects of CD14� PBMCs(either singly or in combination) (n�10) on flow are intermediatebetween those of control (CD34� and vehicle) (n�11) andCD34� PBMC-injected mice (n�8). Flow in both the CD34� andCD14� PBMC-injected groups differ from controls (P�0.01 andP�0.05, respectively). P�0.075 for CD34� versus CD14� PBMCtreatment. Error bars�SEM.
Awad et al CD14� Endothelial Cell Progenitors Promote Healing 759
by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from

sections were scored for inflammation,24 and the area of necrotic andviable muscle measured. Data were analyzed by ANOVA with SNKpost-hoc analysis. The presence of mouse monocyte/macrophageswas assessed by incubation with anti-MMG lectin (Figure II,available online at http://atvb.ahajournals.org).
To analyze intramuscular arteriolar parameters, smooth musclecells were labeled with anti-smooth muscle actin and the borders ofmuscle fibers were delineated using rabbit anti-laminin antibodies.Measurements were made on digitized images of 3 to 5 cross-sections of the entire hamstring muscle group per animal in eachtreatment condition using a modification of a previously describedmethod.25 Numerical density (vessels per area), vessel diameter(external diameter), and vessels per muscle fiber were determined.The axial ratios of vessels were used to calculate length densityaccording to the relationship: Length density�(N/A) � (�a/b)/N.Where N is the number of vessels; a and b are the long and shortaxes, respectively; and A is the area of the muscle. Aggregate lengthdensity was calculated as the product of percent healthy muscle andlength density. Data were analyzed by ANOVA followed by Tukey’spost-hoc test. These sections also were examined for the presence ofCM-DiI labeled cells.
Western BlotsHamstring muscles (Figure 1A) from uninjected or PBMC treatedischemic limbs were collected 1 or 5 days after surgery; 50 �gprotein aliquots were separated by SDS-PAGE. After transfer,membranes were probed with anti- angiopoietin-1, angiopoietin-2,tie-2, vascular endothelial growth factor-A (VEGF-A), flk-1 (mouseVEGFR2), or monocyte chemoattractant protein-1 (MCP-1) antibod-ies. Data were normalized to GAPDH levels. Samples from 4 to 6mice in each group were analyzed 2 to 4 times each. Means werecompared by ANOVA with Tukey’s post-hoc analysis.
ResultsCD14� PBMCs Accelerate Blood Flow RestorationBone marrow and circulating cells have distinct in vivocharacteristics.15 Because circulating cells would actuallyenter sites of injury, and they are the ones most easilyharvested clinically, PBMCs were studied. Ischemic limbs ofdiabetic mice were injected with vehicle or a subset ofPBMCs, hindlimb blood flow followed for 12 days, and thepercentage of flow restored calculated1 (Figure 1).Meanblood glucose levels in diabetic mice were 435�35 mg/dL(range 257 to 560). Nondiabetic mice of the same strainaveraged 115�6 mg/dL (range, 94 to 135; n�9).
In the first 6 days, there were no significant differences inflow in limbs treated with CD14� PBMCs or the CD14�/CD34� combination compared with vehicle controls, butthere was a trend toward increased flow (Figure 1B). By 8days, both cell-treated groups showed increased flow relativeto vehicle treated controls (P�0.05), and this difference wasmaintained through 12 days for CD14� cell-treated limbs. Atno time did treatment with CD14� PBMCs or the CD14�/CD34� PBMC combination differ from one another.
Though some data suggest otherwise,9,12 it has been re-ported that CD14� and CD14� PBMCs have similar abilitiesto differentiate into EC in vitro.11 Thus, CD14� and CD34�
PBMCs, which contain �10% CD14� and �90% CD14�
PBMCs, could be equally potent in restoring blood flow.However, consistent with our previous work, injection ofCD34� PBMCs did not improve limb blood flow in thesemice (Figure 1C).
Flow restoration in limbs of mice that received CD14�
PBMCs either alone or in combination with CD34� PBMCs,
was intermediate between that of the poorly recoveringcontrols and rapidly healing CD34� PBMC-treated mice(Figure 1D). Also, CD14� PBMCs did not induce significantflow enhancement until day 8, whereas flow improved by day2 in CD34� PBMCs-treated limbs. Nevertheless, at 12 daysafter treatment, mice receiving CD14� PBMCs alone or incombination with CD34� cells exhibited a mean blood flowrestoration of 62% compared with 48% in controls, a 30%improvement in resting flow (Figure 1D). Thus, freshlyisolated CD14� cells potentiate blood flow restoration indiabetic mice.
CD34� and CD14� PBMCs PromoteMuscle HealingTo determine whether blood flow restoration correlates withincreased muscle salvage, we examined hematoxylin andeosin stained sections from 5 equally spaced regions forinflammation, muscle necrosis, and muscle repair.24 Differ-ences in inflammatory cell infiltration were not noticeablydifferent among groups, except in those co-injected withCD14� and CD34� PBMCs wherein inflammation was ex-tensive, even in regions where muscle was healthy (Table;Figure 2D).
Vehicle-treated limbs exhibited marked necrosis. In someareas, large segments of muscle were missing, resulting in asmall muscle mass. Regenerating muscle fibers with central-ized nuclei were rare in these limbs. In contrast, minimalnecrosis, fibrosis, and inflammation were seen in limbstreated with CD34� PBMCs. In many regions these limbswere indistinguishable from nonischemic controls (Figure 2Aand 2B). Even when single muscles were examined atmultiple levels, typically, the muscle was healthy with nosigns of necrosis (Figure 3A). Moreover, when entire cross-sections of the harvested muscle group were examined, onlysmall localized foci of necrosis were apparent in the limbs ofall but one animal (Figure 3B). Necrosis and more extensivefibrosis were apparent in limbs treated with CD14� PBMCsand in CD14�/CD34� PBMC co-injected limbs (Figure 2Cand 2D). The only notable difference between CD14� PBMCand CD14�/CD34� PBMC-treated limbs was the extensiveinflammation in the latter (Figure 2D). This appeared to becaused by recruitment of endogenous cells, because mousemonocytes, but few CM-DiI labeled cells, were present atsites of inflammation (Figure II). Muscles with regeneratingfibers, characterized by central nuclei, were observed in allcell treated groups (Figure 2E). CM-DiI labeled cells thatappeared to be integrated into capillaries could be seen, butthey were rare, consistent with previous reports of human-derived bone marrow cells in mouse vasculature.6,7,9
Inflammatory Assessment of Ischemic Muscle
Treatment
Vehicle CD14� CD14�/CD34� CD34�
Cellular infiltration/inflammation*
1.25�0.2 1.5�0.5 2.5�0.3 1.2�0.2
P (vs vehicle) 0.96 0.03 1.0
*Scale of 0 to 3 (no to extensive inflammatory infiltrate).Mean�SEM; n�4 per group.
760 Arterioscler Thromb Vasc Biol. April 2006
by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from
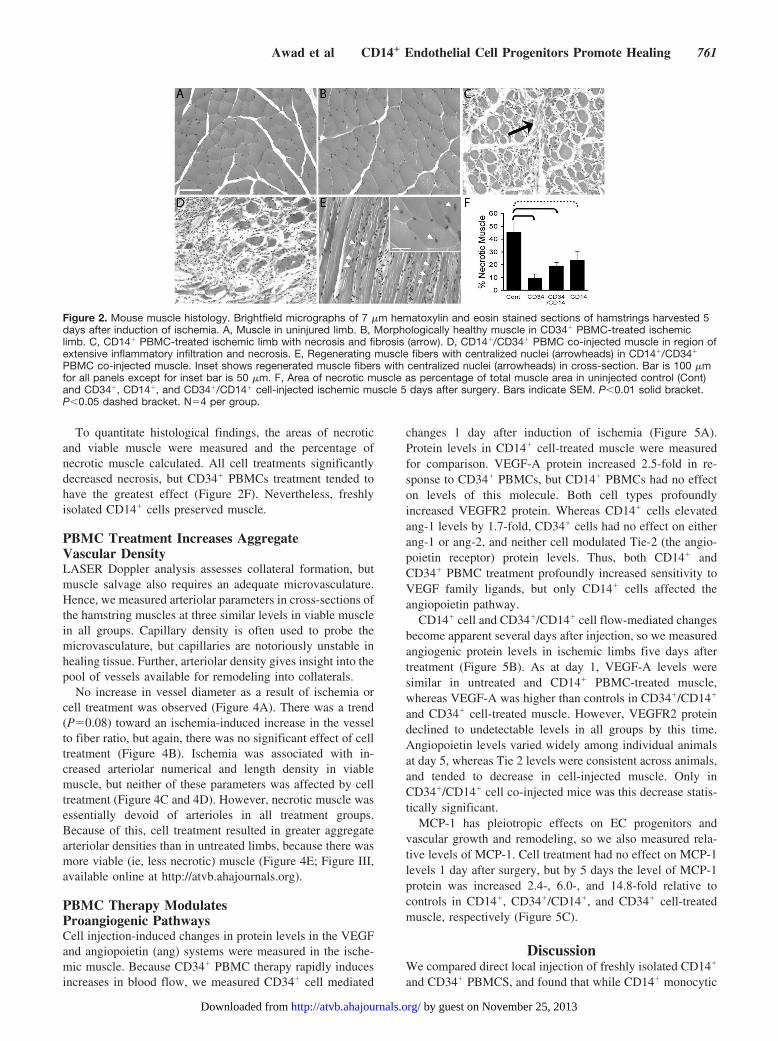
To quantitate histological findings, the areas of necroticand viable muscle were measured and the percentage ofnecrotic muscle calculated. All cell treatments significantlydecreased necrosis, but CD34� PBMCs treatment tended tohave the greatest effect (Figure 2F). Nevertheless, freshlyisolated CD14� cells preserved muscle.
PBMC Treatment Increases AggregateVascular DensityLASER Doppler analysis assesses collateral formation, butmuscle salvage also requires an adequate microvasculature.Hence, we measured arteriolar parameters in cross-sections ofthe hamstring muscles at three similar levels in viable musclein all groups. Capillary density is often used to probe themicrovasculature, but capillaries are notoriously unstable inhealing tissue. Further, arteriolar density gives insight into thepool of vessels available for remodeling into collaterals.
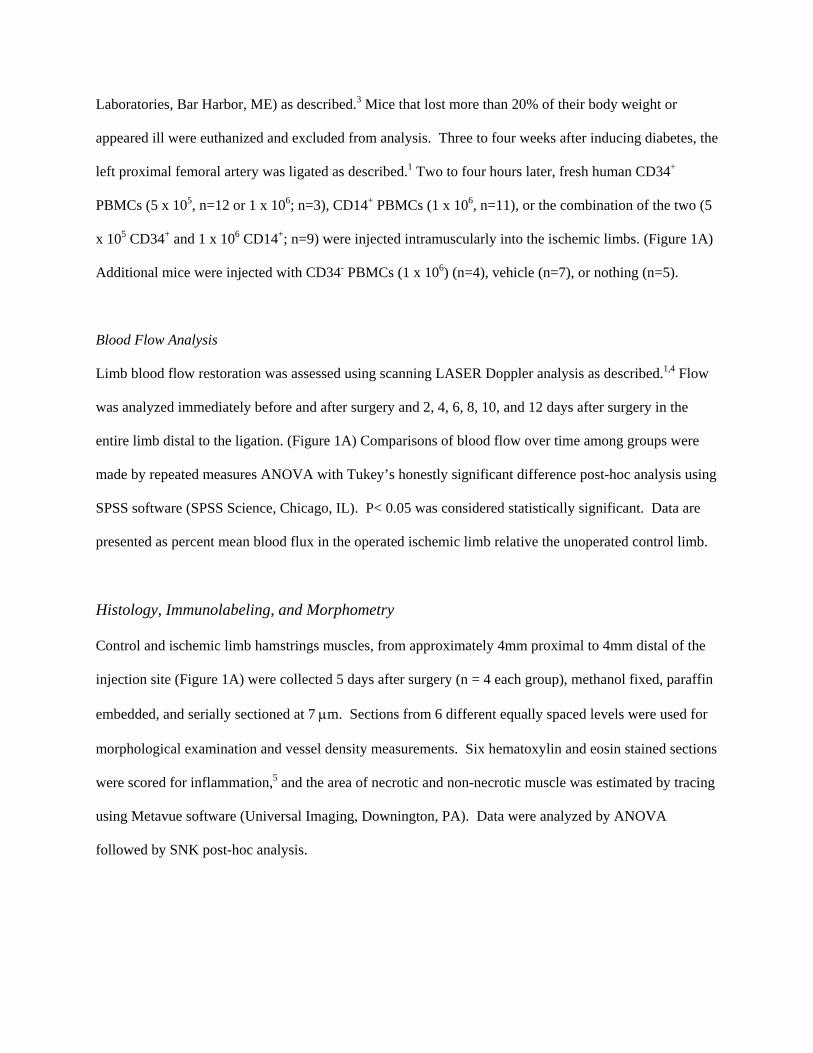
No increase in vessel diameter as a result of ischemia orcell treatment was observed (Figure 4A). There was a trend(P�0.08) toward an ischemia-induced increase in the vesselto fiber ratio, but again, there was no significant effect of celltreatment (Figure 4B). Ischemia was associated with in-creased arteriolar numerical and length density in viablemuscle, but neither of these parameters was affected by celltreatment (Figure 4C and 4D). However, necrotic muscle wasessentially devoid of arterioles in all treatment groups.Because of this, cell treatment resulted in greater aggregatearteriolar densities than in untreated limbs, because there wasmore viable (ie, less necrotic) muscle (Figure 4E; Figure III,available online at http://atvb.ahajournals.org).
PBMC Therapy ModulatesProangiogenic PathwaysCell injection-induced changes in protein levels in the VEGFand angiopoietin (ang) systems were measured in the ische-mic muscle. Because CD34� PBMC therapy rapidly inducesincreases in blood flow, we measured CD34� cell mediated
changes 1 day after induction of ischemia (Figure 5A).Protein levels in CD14� cell-treated muscle were measuredfor comparison. VEGF-A protein increased 2.5-fold in re-sponse to CD34� PBMCs, but CD14� PBMCs had no effecton levels of this molecule. Both cell types profoundlyincreased VEGFR2 protein. Whereas CD14� cells elevatedang-1 levels by 1.7-fold, CD34� cells had no effect on eitherang-1 or ang-2, and neither cell modulated Tie-2 (the angio-poietin receptor) protein levels. Thus, both CD14� andCD34� PBMC treatment profoundly increased sensitivity toVEGF family ligands, but only CD14� cells affected theangiopoietin pathway.
CD14� cell and CD34�/CD14� cell flow-mediated changesbecome apparent several days after injection, so we measuredangiogenic protein levels in ischemic limbs five days aftertreatment (Figure 5B). As at day 1, VEGF-A levels weresimilar in untreated and CD14� PBMC-treated muscle,whereas VEGF-A was higher than controls in CD34�/CD14�
and CD34� cell-treated muscle. However, VEGFR2 proteindeclined to undetectable levels in all groups by this time.Angiopoietin levels varied widely among individual animalsat day 5, whereas Tie 2 levels were consistent across animals,and tended to decrease in cell-injected muscle. Only inCD34�/CD14� cell co-injected mice was this decrease statis-tically significant.
MCP-1 has pleiotropic effects on EC progenitors andvascular growth and remodeling, so we also measured rela-tive levels of MCP-1. Cell treatment had no effect on MCP-1levels 1 day after surgery, but by 5 days the level of MCP-1protein was increased 2.4-, 6.0-, and 14.8-fold relative tocontrols in CD14�, CD34�/CD14�, and CD34� cell-treatedmuscle, respectively (Figure 5C).
DiscussionWe compared direct local injection of freshly isolated CD14�
and CD34� PBMCS, and found that while CD14� monocytic
Figure 2. Mouse muscle histology. Brightfield micrographs of 7 �m hematoxylin and eosin stained sections of hamstrings harvested 5days after induction of ischemia. A, Muscle in uninjured limb. B, Morphologically healthy muscle in CD34� PBMC-treated ischemiclimb. C, CD14� PBMC-treated ischemic limb with necrosis and fibrosis (arrow). D, CD14�/CD34� PBMC co-injected muscle in region ofextensive inflammatory infiltration and necrosis. E, Regenerating muscle fibers with centralized nuclei (arrowheads) in CD14�/CD34�
PBMC co-injected muscle. Inset shows regenerated muscle fibers with centralized nuclei (arrowheads) in cross-section. Bar is 100 �mfor all panels except for inset bar is 50 �m. F, Area of necrotic muscle as percentage of total muscle area in uninjected control (Cont)and CD34�, CD14�, and CD34�/CD14� cell-injected ischemic muscle 5 days after surgery. Bars indicate SEM. P�0.01 solid bracket.P�0.05 dashed bracket. N�4 per group.
Awad et al CD14� Endothelial Cell Progenitors Promote Healing 761
by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from
EC progenitors promote healing, accelerate blood flow res-toration, and induce vascular growth, they do so less wellthan their CD34� primitive EC progenitor counterparts.Nevertheless, because diabetes appears to have more delete-rious effects on primitive than monocytic progenitor function,CD14� PBMCS may provide an alternative therapeutic toolfor this large subset of patients. Moreover, CD14� therapy
may be feasible in an acute setting, because CD14� PBMCsare abundant and easy to isolate, and require no pre-activationwhen directly injected into the affected tissue.
Hematopoietic stem cells and monocytes both promotevascular growth.26,27 Thus, we expected that co-injection ofCD34� and CD14� PBMCs would lead to the greatest musclesalvage and tissue vascularization. The data do not show this(Figure 1), and our histological analysis suggests that exces-sive inflammation (Table) may be the reason. The cellularinfiltrate probably reduces the sensitivity of the Doppler flowmeasurements, leading to an underestimate of true bloodflow. More importantly, as the vascular density and musclesalvage data imply, although inflammation can be an angio-genic stimulus, excessive inflammation may have damped thelimbs’ ability to make new or remodel existing vessels.Interestingly, the inflammation does not appear to be causedby the presence of the human cells per se, because we foundfew human cells in the tissue at 5 days, when inflammationwas extensive. Rather, it seems that the exogenous cells act inconcert to attract endogenous cells, possibly through MCP-1.
The Doppler blood flow measurements indicate that celltherapy increases flow to collaterals (Figure 1). This could becaused in part by vasodilation initially, but as the blood flowremains elevated 12 days after induction of ischemia (bywhich time inflammation is largely absent), remodelingappears to occur ultimately. Arteriolar density and size alsoinfluence intramuscular limb blood flow, but these have notbeen examined previously in PBMC treated limbs. Ischemiainduces an increase in arteriolar density but not size, and,surprisingly, cell therapy does not further increase arteriolardensity or alter size in viable muscle (Figure 4). Apparently,once a critical arteriolar density necessary to preserve ische-mic muscle is reached, additional vessels are not assembled.However, because there is more viable muscle in PBMC thanvehicle-treated limbs, PBMC treatment results in an increasedaggregate vessel density (Figure 2F; Figure III). Thus, rapidand extensive vascular growth must occur in the PBMC-treated limbs.
CD34� and CD14� PBMCs might exert some of theireffects through modulation of pro-angiogenic molecules, andCD34� but not CD14� PBMCs increase VEGF-A protein(Figure 5A). We do not know if the VEGF detected wasproduced by the exogenous or endogenous cells. However,VEGF is a highly conserved protein across species, andhuman VEGF cross-reacts in the mouse.28 Whether producedby the injected human or by mouse cells the protein should be
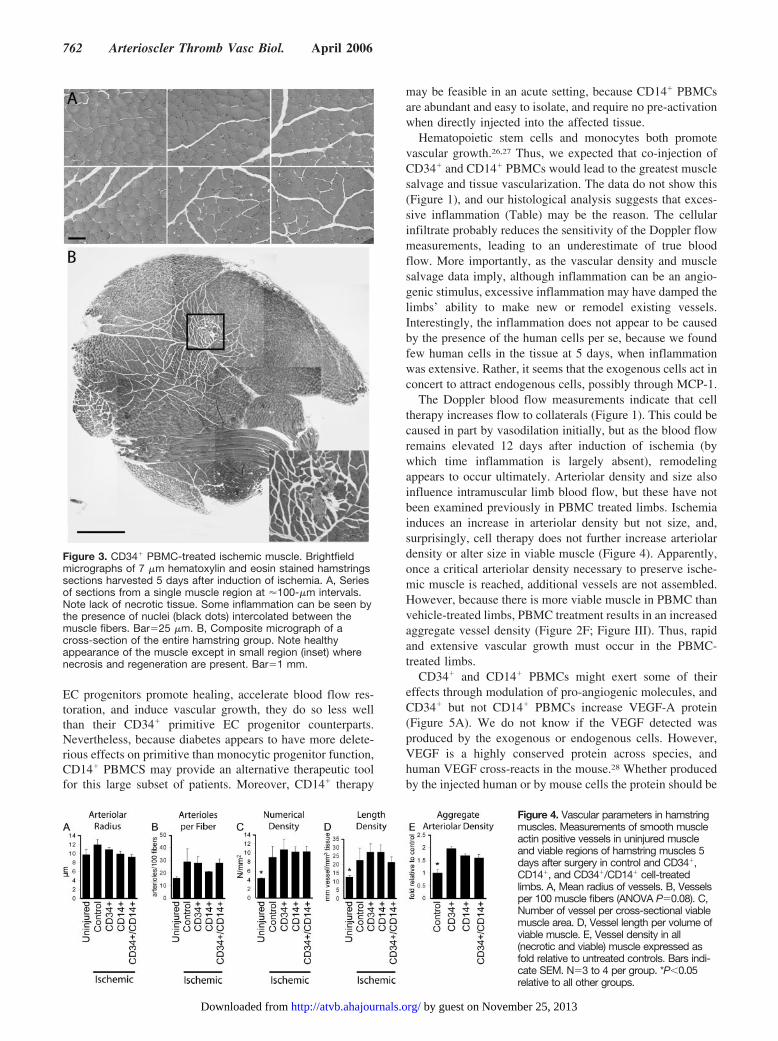
Figure 3. CD34� PBMC-treated ischemic muscle. Brightfieldmicrographs of 7 �m hematoxylin and eosin stained hamstringssections harvested 5 days after induction of ischemia. A, Seriesof sections from a single muscle region at �100-�m intervals.Note lack of necrotic tissue. Some inflammation can be seen bythe presence of nuclei (black dots) intercolated between themuscle fibers. Bar�25 �m. B, Composite micrograph of across-section of the entire hamstring group. Note healthyappearance of the muscle except in small region (inset) wherenecrosis and regeneration are present. Bar�1 mm.
Figure 4. Vascular parameters in hamstringmuscles. Measurements of smooth muscleactin positive vessels in uninjured muscleand viable regions of hamstring muscles 5days after surgery in control and CD34�,CD14�, and CD34�/CD14� cell-treatedlimbs. A, Mean radius of vessels. B, Vesselsper 100 muscle fibers (ANOVA P�0.08). C,Number of vessel per cross-sectional viablemuscle area. D, Vessel length per volume ofviable muscle. E, Vessel density in all(necrotic and viable) muscle expressed asfold relative to untreated controls. Bars indi-cate SEM. N�3 to 4 per group. *P�0.05relative to all other groups.
762 Arterioscler Thromb Vasc Biol. April 2006
by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from

active in vivo in the mouse. More significantly, both cellsaugment responsiveness to VEGF family proteins by dramat-ically increasing VEGFR2 protein. The potent induction ofVEGF-A and VEGFR2 may contribute to the strong earlyvascular growth response to CD34� PBMCs compared withCD14� PBMCs.
Although VEGF-A levels remained slightly elevated inlimbs treated with CD34� cells at day 5, we were unable todetect VEGFR2 protein (Figure 5B). This is not a technicalproblem as the same tissue samples were used for analyses ofother proteins, and VEGFR2 was detected in day 1 samples.The levels simply had declined, suggesting that most newvessel growth is completed by this time, and that subsequentimprovements in flow are caused by remodeling. This mayexplain why the greatest increases in limb blood flow occurwithin the first 6 days after induction of ischemia. This tooindicates that for acute events (such as myocardial infarction)PBMC-based therapies may be most effective when usedsoon after the event, emphasizing the importance of beingable to use freshly isolated cells therapeutically.
The angiopoietin data are more complex. CD34� cells haveno apparent immediate effect on the angiopoietins or theirreceptor, although CD14� cells induce an increase in angio-poietin 2, suggesting that these cells may have an earlyinfluence on remodeling (Figure 5A). The day 5 data werestriking because, although tie-2 receptor levels were consis-tent from animal to animal and cell therapy tended to depress
receptor levels, angiopoietin 1 and 2 protein levels variedwidely among cell-treated mice (Figure 5B). Protein levels inindividual mice were either similar to controls, or in the caseof angiopoietin 1, much lower, or angiopoietin 2, muchhigher. Thus, angiopoietin modulation seems to be dynamicat this point in time, consistent with vascular remodeling.
MCP-1 recruits monocytes, induces EC progenitor differ-entiation, and promotes arteriogenesis.14,15,29,30 Hence, thedramatic elevation in MCP-1 at day 5, but not at day 1, mayfurther explain why improvements in blood flow are notapparent in CD14� treated mice until day 6 (Figure 5C). Thatis, late elevation of MCP-1 may contribute to the increasedarteriogenesis. Additionally, MCP-1 could be recruiting en-dogenous EC progenitors and inducing their differentiation,thereby increasing microvascular growth.
In sum, our data indicate that local injection of smallnumbers of freshly isolated circulating cells can dramaticallyimpact healing and vascular growth, but that CD34� PBMCsare more effective than CD14� cells in doing so. Neverthe-less, CD14� cells could offer a therapeutic alternative forpeople with diabetes, the function of whose CD34� PBMCsmay be compromised.1,31 Finally, the data suggest that at leastsome PBMC induced healing is mediated through the VEGFand MCP-1 pathways, and possibly the angiopoietins.
AcknowledgmentsThis work was supported by grants from the Juvenile DiabetesResearch Foundation 1-2001 to 534 (G.S.), National Institutes of
Figure 5. Relative protein levels ofangiogenic factors and their receptors inischemic limbs. Fold change in proteinlevel in ischemic muscle in CD34�,CD14�, and CD34�/CD14� PBMC-treated relative to untreated ischemiccontrol (Cont) muscle. Changes in VEGFand the angiopoietin system (A) 1 dayand (B) 5 days after surgery and celltreatment. C, Changes in MCP-1 protein1 day (left) and 5 days (right) after sur-gery and cell treatment. Bars indicateSEM. P�0.01 solid bracket. P�0.05dashed bracket. N�4 to 6 mice pergroup.
Awad et al CD14� Endothelial Cell Progenitors Promote Healing 763
by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from

Health DK55965 (G.S.), and HL075446 (R.T.). The authors thankSonny Patel for technical assistance.
References1. Schatteman GC, Hanlon HD, Jiao C, Dodds SG, Christy BA. Blood-
derived angioblasts accelerate blood-flow restoration in diabetic mice.J Clin Invest. 2000;106:571–578.
2. Kocher AA, Schuster MD, Szabolcs MJ, Takuma S, Burkhoff D, WangJ, Homma S, Edwards NM, Itescu S. Neovascularization of ischemicmyocardium by human bone-marrow-derived angioblasts prevents car-diomyocyte apoptosis, reduces remodeling and improves cardiacfunction. Nat Med. 2001;7:430–436.
3. Sivan-Loukianova E, Awad O, Stepanovic V, Bickenbach JR,Schatteman GC. Circulating CD34� Cells Accelerate Vascularization andHealing of Diabetic Mouse Skin Wounds. J Vasc Res. 2003;40:368–377.
4. Awad O, Jiao C, Ma N, Dunnwald M, Schatteman GC. Obese diabeticmouse environment differentially affects primitive and monocytic endo-thelial cell progenitors. Stem Cells. 2005;23:575–583.
5. Stepanovic V, Awad O, Jiao C, Dunnwald M, Schatteman G. Leprdb
diabetic mouse bone marrow cells inhibit skin wound vascularization butpromote wound healing. Circ Res. 2003;92:1247–1253.
6. Yeh ET, Zhang S, Wu HD, Korbling M, Willerson JT, Estrov Z. Trans-differentiation of human peripheral blood CD34�-enriched cell popu-lation into cardiomyocytes, endothelial cells, and smooth muscle cells invivo. Circulation. 2003;108:2070–2073.
7. Ma N, Stamm C, Kaminski A, Li W, Kleine HD, Muller-Hilke B, ZhangL, Ladilov Y, Egger D, Steinhoff G. Human cord blood cells induceangiogenesis following myocardial infarction in NOD/scid-mice. Car-diovasc Res. 2005;66:45–54.
8. Fernandez Pujol B, Lucibello FC, Gehling UM, Lindemann K, WeidnerN, Zuzarte ML, Adamkiewicz J, Elsasser HP, Muller R, Havemann K.Endothelial-like cells derived from human CD14 positive monocytes.Differentiation. 2000;65:287–300.
9. Harraz M, Jiao C, Hanlon HD, Hartley RS, Schatteman GC. Cd34(-)blood-derived human endothelial cell progenitors. Stem Cells. 2001;19:304–312.
10. Schmeisser A, Garlichs CD, Zhang H, Eskafi S, Graffy C, Ludwig J,Strasser RH, Daniel WG. Monocytes coexpress endothelial and macroph-agocytic lineage markers and form cord-like structures in Matrigel underangiogenic conditions. Cardiovasc Res. 2001;49:671–680.
11. Urbich C, Heeschen C, Aicher A, Dernbach E, Zeiher AM, Dimmeler S.Relevance of monocytic features for neovascularization capacity of cir-culating endothelial progenitor cells. Circulation. 2003;108:2511–2516.
12. Rehman J, Li J, Orschell CM, March KL. Peripheral blood “endothelialprogenitor cells” are derived from monocyte/macrophages and secreteangiogenic growth factors. Circulation. 2003;107:1164–1169.
13. Zhao Y, Glesne D, Huberman E. A human peripheral blood monocyte-derived subset acts as pluripotent stem cells. Proc Natl Acad Sci U S A.2003;100:2426–2431.
14. Moldovan NI, Goldschmidt-Clermont PJ, Parker-Thornburg J, ShapiroSD, Kolattukudy PE. Contribution of monocytes/macrophages to com-pensatory neovascularization: the drilling of metalloelastase-positivetunnels in ischemic myocardium. Circ Res. 2000;87:378–384.
15. Fujiyama S, Amano K, Uehira K, Yoshida M, Nishiwaki Y, Nozawa Y,Jin D, Takai S, Miyazaki M, Egashira K, Imada T, Iwasaka T, MatsubaraH. Bone Marrow Monocyte Lineage Cells Adhere on Injured Endotheli-um in a Monocyte Chmeattractant Protein-1-Dependent Manner andAccelerate Reendothelialization as Endothelial Progenitor Cells. CircRes. 2003;2003:1–10.
16. Takahashi T, Kalka C, Masuda H, Chen D, Silver M, Kearney M, MagnerM, Isner JM, Asahara T. Ischemia- and cytokine-induced mobilization ofbone marrow-derived endothelial progenitor cells for neovascularization.Nat Med. 1999;5:434–438.
17. Murohara T, Ikeda H, Duan J, Shintani S, Sasaki K, Eguchi H, OnitsukaI, Matsui K, Imaizumi T. Transplanted cord blood-derived endothelialprecursor cells augment postnatal neovascularization. J Clin Invest. 2000;105:1527–1536.
18. Wang C, Jiao C, Hanlon HD, Zheng W, Tomanek RJ, Schatteman GC.Mechanical, cellular, and molecular factors interact to modulate circu-lating endothelial cell progenitors. Am J Physiol Heart Circ Physiol.2004;286:H1985–H1993.
19. Tepper OM, Galiano RD, Capla JM, Kalka C, Gagne PJ, Jacobowitz GR,Levine JP, Gurtner GC. Human endothelial progenitor cells from type IIdiabetics exhibit impaired proliferation, adhesion, and incorporation intovascular structures. Circulation. 2002;106:2781–2786.
20. Loomans CJM, de Koning EJP, Staal FJT, Rookmaaker MB, VerseydenC, de Boer HC, Verhaar MC, Braam B, Rabelink TJ, van Zonneveld AJ.Endothelial progenitor cell dysfunction - A novel concept in the patho-genesis of vascular complications of type 1 diabetes. Diabetes. 2004;53:195–199.
21. Tamarat R, Silvestre JS, Le Ricousse-Roussanne S, Barateau V, Lecomte-Raclet L, Clergue M, Duriez M, Tobelem G, Levy BI. Impairment inischemia-induced neovascularization in diabetes - Bone marrow mono-nuclear cell dysfunction and therapeutic potential of placenta growthfactor treatment. Am J Pathol. 2004;164:457–466.
22. Kunjathoor VV, Wilson DL, LeBoeuf RC. Increased atherosclerosis instreptozotocin-induced diabetic mice. J Clin Invest. 1996;97:1767–1773.
23. Couffinhal T, Silver M, Zheng LP, Kearney M, Witzenbichler B, IsnerJM. Mouse model of angiogenesis. Am J Pathol. 1998;152:1667–1679.
24. Akar H, Sarac A, Konuralp C, Yildiz L, Kolbakir F. Comparison ofhistopathologic effects of carnitine and ascorbic acid on reperfusioninjury. Eur J Cardiothorac Surg. 2001;19:500–506.
25. Zheng W, Weiss RM, Wang X, Zhou R, Arlen AM, Lei L, Lazartigues E,Tomanek RJ. DITPA stimulates arteriolar growth and modifies myo-cardial postinfarction remodeling. Am J Physiol Heart Circ Physiol.2004;286:H1994–H2000.
26. Minehata K, Mukouyama YS, Sekiguchi T, Hara T, Miyajima A. Mac-rophage colony stimulating factor modulates the development of hema-topoiesis by stimulating the differentiation of endothelial cells in theAGM region. Blood. 2002;99:2360–2368.
27. Arras M, Ito WD, Scholz D, Winkler B, Schaper J, Schaper W. Monocyteactivation in angiogenesis and collateral growth in the rabbit hindlimb.J Clin Invest. 1998;101:40–50.
28. Schuch G, Machluf M, Bartsch G, Jr., Nomi M, Richard H, Atala A,Soker S. In vivo administration of vascular endothelial growth factor(VEGF) and its antagonist, soluble neuropilin-1, predicts a role of VEGFin the progression of acute myeloid leukemia in vivo. Blood. 2002;100:4622–4628.
29. Hoefer IE, van Royen N, Buschmann IR, Piek JJ, Schaper W. Timecourse of arteriogenesis following femoral artery occlusion in the rabbit.Cardiovasc Res. 2001;49:609–617.
30. van Royen N, Hoefer I, Buschmann I, Kostin S, Voskuil M, Bode C,Schaper W, Piek JJ. Effects of local MCP-1 protein therapy on thedevelopment of the collateral circulation and atherosclerosis in Watanabehyperlipidemic rabbits. Cardiovasc Res. 2003;57:178–185.
31. Vasa M, Fichtlscherer S, Aicher A, Adler K, Urbich C, Martin H, ZeiherAM, Dimmeler S. Number and migratory activity of circulating endothe-lial progenitor cells inversely correlate with risk factors for coronaryartery disease. Circ Res. 2001;89:E1–E7.
764 Arterioscler Thromb Vasc Biol. April 2006
by guest on November 25, 2013http://atvb.ahajournals.org/Downloaded from

Detailed Methods
Isolation, Labeling, and FACS of PBMCS
50-100 ml human blood was collected from healthy adult volunteers according to University of Iowa
Institutional Review Board approved protocols with informed consent as described.1 Briefly,
mononuclear cells were collected after fractionation on Histopaque 1077 (Sigma, St. Louis) per
manufacturer's instructions and washed. CD34+ PBMCs were isolated using 2 rounds of CD34+ cell
selection with an auto MACS (Miltenyi, Auburn, CA) per manufacturer’s instructions. Residual CD34-
cells were used directly or CD34-CD14+ PBMCs (hereafter referred to as CD14+ PBMCs for clarity) were
isolated by two rounds of CD14+ selection using auto MACS according to manufacturer’s instructions.
Prior to injection, cells were labeled with the vital dye, CM-DiI (Molecular Probes, Eugene, OR), as
described in some animals.2
To assess VEGFR2 expression on the freshly isolated CD14+ and CD34+ PBMCs, cells were incubated 30
min on ice with 20μg/ml anti-VEGFR2 (Abcam Cat # Ab9539, Cambridge, MA), washed twice in 1%
fetal bovine serum (FBS) in PBS then overlaid on FBS serum and pelleted. Cells were resuspended in
1% FBS in PBS and incubated 30 min with 13 μg/ml Alexa 488 anti mouse IgG then washed as above,
and resuspended in propidium iodide containing buffer at 1 x106 cells/ml in PBS for FACS.
Animals
Animal procedures were approved by the University of Iowa Animal Care and Use Committee.
Anesthesia was induced with 4% isoflurane and maintained with 0.8-1.2% isoflurane. Euthanasia was
performed by injection of 150mg/kg sodium pentobarbital.
Induction of Ischemia and Cell Treatment
Diabetes was induced with streptozotocin in 8-12 wk old HFh11nu athymic mice male mice (Jackson
Laboratories, Bar Harbor, ME) as described.3 Mice that lost more than 20% of their body weight or
appeared ill were euthanized and excluded from analysis. Three to four weeks after inducing diabetes, the
left proximal femoral artery was ligated as described.1 Two to four hours later, fresh human CD34+
PBMCs (5 x 105, n=12 or 1 x 106; n=3), CD14+ PBMCs (1 x 106, n=11), or the combination of the two (5
x 105 CD34+ and 1 x 106 CD14+; n=9) were injected intramuscularly into the ischemic limbs. (Figure 1A)
Additional mice were injected with CD34- PBMCs (1 x 106) (n=4), vehicle (n=7), or nothing (n=5).
Blood Flow Analysis
Limb blood flow restoration was assessed using scanning LASER Doppler analysis as described.1,4 Flow
was analyzed immediately before and after surgery and 2, 4, 6, 8, 10, and 12 days after surgery in the
entire limb distal to the ligation. (Figure 1A) Comparisons of blood flow over time among groups were
made by repeated measures ANOVA with Tukey’s honestly significant difference post-hoc analysis using
SPSS software (SPSS Science, Chicago, IL). P< 0.05 was considered statistically significant. Data are
presented as percent mean blood flux in the operated ischemic limb relative the unoperated control limb.
Histology, Immunolabeling, and Morphometry
Control and ischemic limb hamstrings muscles, from approximately 4mm proximal to 4mm distal of the
injection site (Figure 1A) were collected 5 days after surgery (n = 4 each group), methanol fixed, paraffin
embedded, and serially sectioned at 7 μm. Sections from 6 different equally spaced levels were used for
morphological examination and vessel density measurements. Six hematoxylin and eosin stained sections
were scored for inflammation,5 and the area of necrotic and non-necrotic muscle was estimated by tracing
using Metavue software (Universal Imaging, Downington, PA). Data were analyzed by ANOVA
followed by SNK post-hoc analysis.

To examine ischemic muscle for the presence of mouse monocyte/macrophages, additional sections of
muscle in which inflammation was present were incubated with 1μg/ml anti-mouse macrophage
galactose-specific lectin (MMGL) clone ER-MP23 (Abcam, Cambridge, MA) overnight followed by 2 h
with 10 μg/ml Alexa 488 anti-rat IgG (Molecular Probes, Eugene , OR).
To analyze vascularity, smooth muscle cells were labeled with Cy3-anti-smooth muscle actin (1:600;
Sigma, St. Louis, MO) 40 min at 37oC and the borders of muscle fibers were delineated by incubation
with rabbit anti-laminin (1:30; Sigma, St. Louis) 2 h at 37oC followed by Alexa 488 goat anti-rabbit
(Molecular Probes). Images were digitized with Image Pro software (Media Cybernetics, San Diego,
CA). Measurements were made on images of 3-5 cross-sections of the entire hamstrings muscle group
per animal in each treatment condition using a modification of a previously described method.6 The axial
ratios of vessels were used to calculate length density according to the relationship: Length density =
numerical density X a/b, where a and b are the long and short axes, respectively. Numerical density
(vessels per area), vessel diameter (external diameter), and vessels per muscle fiber were also determined.
Data were analyzed by ANOVA followed by Tukey’s honestly significant difference post-hoc test. These
sections were also examined for the presence of human CM-DI labeled cells.
Western Blot
Hamstrings muscle, (Figure 1A) from PBMC injected or uninjected ischemic limbs were collected one or
five days after induction of ischemia and snap frozen. Tissue was pulverized in liquid N2, resuspended in
lysis buffer (50mM Tris, pH 7.5, 1mM EDTA, 1% Triton, 0.9% NaCl, 1mM PMSF) clarified at 12,000 x
g for 30 min at 4oC. Clarified supernatants were used immediately or stored at -80oC until use. Protein
concentration were determined using a modified Bradford assay using Protein Assay Reagent (BioRad,
Hercules, CA).7 50 μg protein samples were separated by SDS-PAGE and transferred to PVDF (BioRad).
Membranes were blocked in 5% non-fat milk, incubated in primary antibody 2 hr at room temperature or
overnight at 4oC in blocking solution, washed 3 times in PBS with 0.05% /Tween-20, then incubated in
horseradish peroxidase conjugated secondary antibody for 1 hr at room temperature. Bands were
visualized with Super Signal (Pierce, Rockford, IL) after 3 washes in PBS with 0.05% /Tween-20.
Primary antibodies used were anti- angiopoietin-1 (1:300), angiopoietin-2 (1:200), tie-2 (1:200), VEGF
(1:2000), flk-1 (1:200), (all from Santa Cruz Biotechnology, Santa Cruz, CA), and MCP-1 (1:1500)
(eBioscience, San Diego, CA). Blots were analyzed using anti-GAPDH (1:8000) (Chemicon, Temecula,
CA) as above and data were normalized to GAPDH levels. Tissue from four to six mice in each group
was analyzed 2-4 times each. Means from each animal were compared among groups by ANOVA.
Tukey's post-hoc analysis was done with P< 0.05 considered statistically significant.
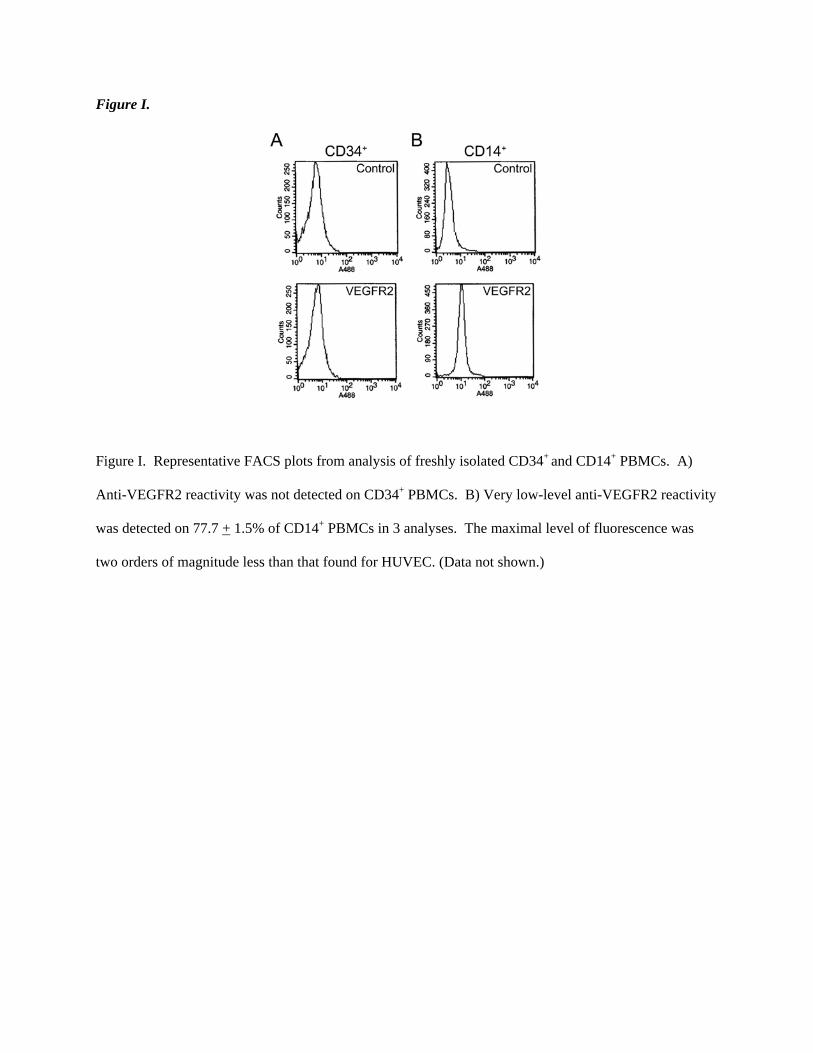
Figure I.
Figure I. Representative FACS plots from analysis of freshly isolated CD34+ and CD14+ PBMCs. A)
Anti-VEGFR2 reactivity was not detected on CD34+ PBMCs. B) Very low-level anti-VEGFR2 reactivity
was detected on 77.7 + 1.5% of CD14+ PBMCs in 3 analyses. The maximal level of fluorescence was
two orders of magnitude less than that found for HUVEC. (Data not shown.)
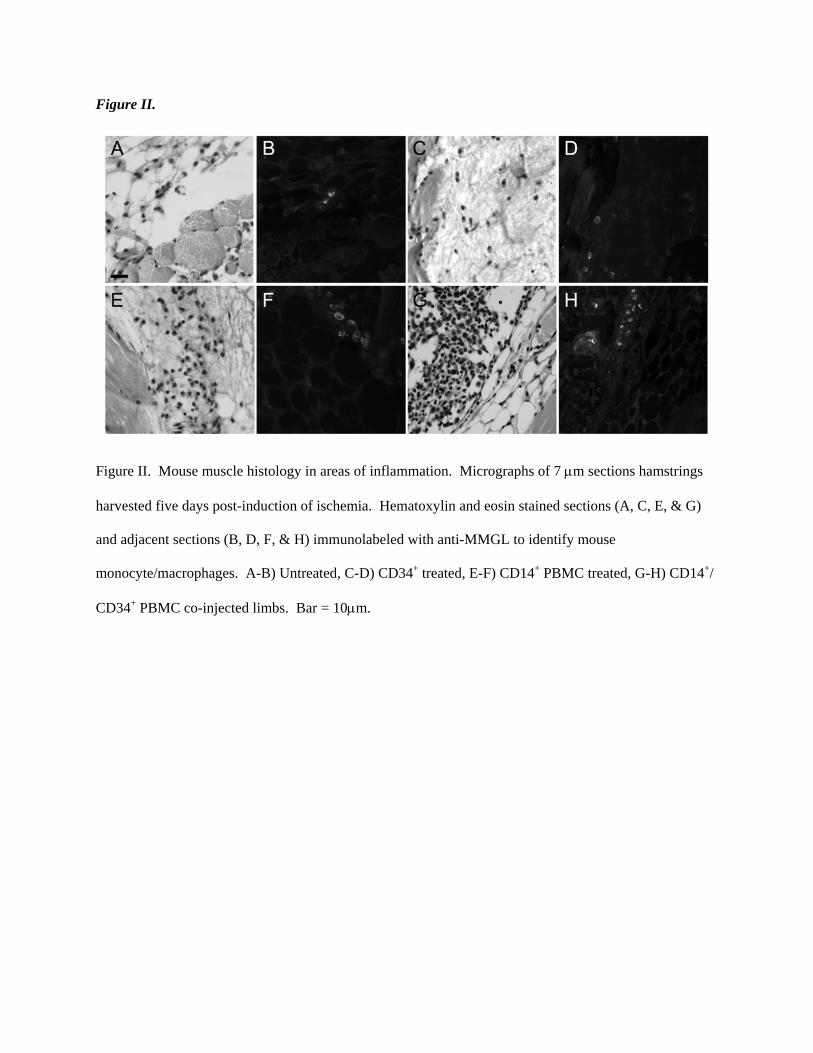
Figure II.
Figure II. Mouse muscle histology in areas of inflammation. Micrographs of 7 μm sections hamstrings
harvested five days post-induction of ischemia. Hematoxylin and eosin stained sections (A, C, E, & G)
and adjacent sections (B, D, F, & H) immunolabeled with anti-MMGL to identify mouse
monocyte/macrophages. A-B) Untreated, C-D) CD34+ treated, E-F) CD14+ PBMC treated, G-H) CD14+/
CD34+ PBMC co-injected limbs. Bar = 10μm.

Figure III.
Figure III. Schematic of aggregate arteriole density in PBMC (left) and vehicle (right) treated ischemic
muscles. The density of arterioles (black dots) is similar in viable muscle in both groups, but the amount
of viable muscle is greater in PBMC treated limbs than in vehicle controls. Aggregate arteriolar density
(arteriolar density x healthy muscle/all muscle) is greater in PBMC than vehicle treated limbs. Vehicle
treated limbs are small because of muscle loss due to necrosis.
References
1. Schatteman GC, Hanlon HD, Jiao C, Dodds SG, Christy BA. Blood-derived angioblasts
accelerate blood-flow restoration in diabetic mice. J Clin Invest. 2000;106:571-578.
2. Harraz M, Jiao C, Hanlon HD, Hartley RS, Schatteman GC. Cd34(-) blood-derived
human endothelial cell progenitors. Stem Cells. 2001;19:304-12.
3. Kunjathoor VV, Wilson DL, LeBoeuf RC. Increased atherosclerosis in streptozotocin-
induced diabetic mice. J Clin Invest. 1996;97:1767-73.
4. Couffinhal T, Silver M, Zheng LP, Kearney M, Witzenbichler B, Isner JM. Mouse model
of angiogenesis. Am J Pathol. 1998;152:1667-79.
5. Akar H, Sarac A, Konuralp C, Yildiz L, Kolbakir F. Comparison of histopathologic
effects of carnitine and ascorbic acid on reperfusion injury. Eur J Cardiothorac Surg.
2001;19:500-6.
6. Zheng W, Weiss RM, Wang X, Zhou R, Arlen AM, Lei L, Lazartigues E, Tomanek RJ.
DITPA stimulates arteriolar growth and modifies myocardial postinfarction remodeling.
Am J Physiol Heart Circ Physiol. 2004;286:H1994-2000.
7. Bradford. A Rapid and sensitive method for the quantitation of microgram quantities of
protein utilizing the principle of protein dye binding. Analytical Biochemistry.
1976;72:248-254.
Copyright © 2022 FDOKUMEN




















