
Clinical Characteristics of Acute Myocardial Infarction Died during Hospitalization

Human CD34+ Cells in Experimental Myocardial Infarction: Long-term Survival, Sustained Functional Improvement, andMechanism of Action
Jingxiong Wang, MD, PhD*, Sui Zhang, MD, PhD*, Brian Rabinovich, PhD, Luc Bidaut, PhD,Suren Soghomonyan, MD, PhD, Mian M. Alauddin, PhD, James A. Bankson, PhD, ElizabethShpall, MD, James T. Willerson, MD, Juri G. Gelovani, MD, and Edward T. H. Yeh, MDTexas Heart Institute at St. Luke’s Episcopal Hospital (J.X.W., J.T.W., E.T.H.Y.) and theDepartments of Cardiology (S.Z., E.T.H.Y.); Experimental Diagnostic Imaging (B.R., S.S., M.M.A.,J.G.G.); Imaging Physics (L.B., J.A.B.); and Stem Cell Transplantation & Cellular Therapy (E.S.),the University of Texas-M.D. Anderson Cancer Center, Houston, Texas, USA
AbstractRationale—Human CD34+ cells have been used in clinical trials for treatment of myocardialinfarction (MI). However, it is unknown how long the CD34+ cells persist in hearts, whether theimprovement in cardiac function is sustained, and what are the underlying mechanisms.
Objectives—We sought to track the fate of injected human CD34+ cells in the hearts of severecombined immune deficiency (SCID) mice after experimental MI, and to determine themechanisms of action.
Methods and Results—We used multimodality molecular imaging to track the fate of injectedhuman CD34+ cells in the hearts of SCID mice after experimental MI, and employed selectiveantibody blocking to determine the mechanisms of action. Bioluminescence imaging (BLI)showed that injected CD34+ cells survived in the hearts for longer than 12 months. The PET signalfrom the injected cells was detected in the wall of the left ventricle. Cardiac MRI showed that leftventricular ejection fraction was significantly improved in the treated mice compared to thecontrol mice for up to 52 weeks (P<0.05). Furthermore, treatment with anti-α4β1 showed thatgeneration of human-derived cardiomyocytes was inhibited, whereas anti-VEGF treatmentblocked the production of human-derived endothelial cells. However, the improvement in cardiacfunction was abolished only in the anti-VEGF, but not anti-α4β1, treated group.
Conclusions—Angiogenesis and/or paracrine effect, but not myogenesis, is responsible forfunctional improvement following CD34+ cells therapy.
Keywordshuman CD34+ cells; experimental myocardial infarction; molecular imaging; myogenesis;angiogenesis
Correspondence to: Edward T.H. Yeh, MD, University of Texas-M.D. Anderson Cancer Center, 1400 Pressler Blvd, Box 1451,Houston, TX 77030, USA. Phone: (713) 792-1960; Fax: (713) 745-1942; [email protected].*Jingxiong Wang and Sui Zhang contributed equally to this work.Disclosures None.This work was presented in part at the American Heart Association Scientific Sessions, Orlando, FL, November 3 7, 2007, andpublished in abstract form (Circulation. 2007;116[Suppl. II]:II-22).
NIH Public AccessAuthor ManuscriptCirc Res. Author manuscript; available in PMC 2011 June 25.
Published in final edited form as:Circ Res. 2010 June 25; 106(12): 1904–1911. doi:10.1161/CIRCRESAHA.110.221762.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Adult progenitor cells have been used to treat patients with acute myocardial infarction (MI)or chronic ischemic cardiomyopathy with variable success.1-8 Non-labeled autologousprogenitor cells were used in these clinical trials. Hence, it was hard to track the fate of thetransplanted cells in the treated hearts even post-mortem.3 In animal studies, it is easier totrack the transplanted human progenitor cells via the xenogeneic differences between thetransplanted cells and the surrounding cardiac tissues. We have injected human CD34+ cellsinto the hearts of SCID mice after experimental MI and used HLA as a marker to identifythe transplanted cells.9-11 Others have used GFP, sex mismatch, or allelic differences totrack the transplanted cells.12 Such methodology is not dynamic and requires euthanasia ofthe animals to gain a single data point. To perform non-invasive monitoring of thetransplanted cells, some laboratories have labeled the transplanted cells with iron oxidemagnetic particles or superparamagnetic nanoparticles and followed them with MRI.13-14
Activated macrophages, however, can engulf iron oxide labeled stem cells, making itdifficult to interpret the data.15 Thus, it is important to develop more reliable way to tracktransplanted cells in animal studies.
The advancement of molecular imaging techniques provides tremendous potential toidentify non-invasively the location, magnitude, and duration of cellular survival and fate ofthe transplanted cells. In principle, this approach requires the introduction of a reporter geneinto the transplanted cells. A convenient reporter is firefly-Luciferase (f-Luc), an enzymethat cleaves D-luciferin and generate photon, which can be monitored by a bioluminescencedetector.16 This method has been highly successful in small animal models because of therelatively short distance between the photon emitting cells and the detectors. However, thistechnique will not likely work in larger animals or humans because of tissue attenuation,scattering, and of the difficulty in localizing these signals inside larger bodies.
To track transplanted cells reliably in larger animals or in humans, we and others havedeveloped PET reporter gene human herpes simplex virus type 1-thymidine kinase (HSV1-tk).17 HSV1-tk is essentially nontoxic in humans, and is currently being used in clinical genetherapy protocols as a “susceptibility” gene for treatment of cancer (in combination withganciclovir). Importantly, the acquired sensitivity of HSV1-tk transduced cells toganciclovir provides an additional margin of safety because the genetically modified cellscan be easily eliminated by treatment with ganciclovir. In this study, we constructed a triplefusion (TF) reporter vector encoding for enhanced-GFP (e-GFP, for cell selection), f-Luc(for bioluminescence imaging (BLI)), and HSV1-tk (for PET imaging). Using this reporteralong with MRI and CT, we sought to determine the localization and persistence of thelabeled CD34+ cells transplanted into living animals after experimental MI. Furthermore, weinvestigated whether these transplanted cells contributed to improvement in cardiacfunction, and what are the underlying mechanisms.
The mechanisms by which the transplanted progenitor cells benefit the cardiac functionremain obscure. We have previously shown that adult human peripheral blood CD34+ cellsinjected into SCID mice transform into cardiomyocytes, endothelial cells, and smoothmuscle cells in hearts injured by experimental MI.9 We have also demonstrated that mosthuman-derived cardiomyocytes result from fusion of human CD34+ cells with mousecardiomyocytes, whereas endothelial cells are directly differentiated from human CD34+
cells.11 Furthermore, fusion of CD34+ cells with cardiomyocytes is mediated by theinteraction of VCAM-1 and α4β1, after which the fused cells re-enter the cell cycle andbecome new cardiomyocytes.10 The biological relevance of this finding is that myogenesiscan be blocked by antibodies against VCAM-1 or α4β1 but not by antibody against VEGF.On the other hand, angiogenesis can be blocked by anti-VEGF, but not by anti-α4β1antibodies. Thus, myogenesis can be distinguished from angiogenesis on the basis of
Wang et al. Page 2
Circ Res. Author manuscript; available in PMC 2011 June 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

selective antibody blockade and the relative contribution of myogenesis and angiogenesis tocardiac repair can be determined in the SCID mouse MI model.
MethodsAnimals
All animal studies were approved by the Institutional Animal Care and Use Committees ofthe University of Texas-M.D. Anderson Cancer Center. Female SCID mice (C3H, JacksonLaboratory, Bar Harbor, Maine), weighing 16 to 20 g were used.
Construction of LentivectorWe excised a TF reporter gene encoding HSV1-tk, e-GFP, and f-Luc (termed as TGL)18-19
from pBluescipt II SK+ using Sal-I and Bam-HI and ligated into pENTRIA (Invitrogen,Carlsbad, CA) generating pENTR1A-nesTGL. This vector was then recombined with a self-inactivating lentiviral destination vector encoding the human ubiquitin (hUbiq) promoteraccording to the manufacturer’s specifications (Invitrogen). Lentiviral packing,concentration and tittering were performed as previously described.20-21
Isolation and Transduction of CD34+ CellsHuman peripheral blood CD34+ cells were isolated as previously described.22 The isolatedcells were transducted with lentiviruses at a multiplicity of infection (MOI) of 50 aspreviously described.23
Induction of MI and Transplantation of Human CD34+ Cells into the MiceAfter anesthesia (3% isoflurane and oxygen) and mechanical ventilation, the left anteriordescending artery was ligated. 10 minutes later, we injected 1×106 CD34+ cells in 25 μlsaline directly into the peri-infarcted areas. Control mice were injected with saline.
In Vitro and In Vivo BLI of f-Luc Gene Expression in CD34+ CellsThe cells were serially diluted and seeded on a 24-well plate; D-luciferin (Caliper LS,Alameda, CA) was added at 1 μg/ml to the media and luminescent signal was measuredusing IVIS 200 (Caliper LS). In vivo BLI was determined 10 minutes after i.p. injection ofD-Luciferin (150 mg/kg). We manually defined regions of interest (ROI) to measure signalintensities, expressed as photons/second/cm2 × 4π (photon flux).
Small Animal MRIA 7.0 T Biospec small animal scanner (Bruker Biospin Inc., Billerica, MA) was used.Imaging gradients with 60 mm inner diameter (ID) were used with a 35 mm ID linearbirdcage-style volume resonator. T1-weighted anatomic reference images were acquiredusing a three dimension (3D) fast low-angle shot (FLASH) gradient echo sequence. Aretrospectively gated FLASH pulse sequence was used to acquire cardiac cine imagesexhibiting excellent contrast between bright blood and adjacent myocardium. To measurevolumetric left ventricular ejection fraction (LVEF), at least 6 short axis images werescanned at 1 mm interval from the apex to the base of the heart. End-diastolic (ED) and end-systolic (ES) left ventricular volumes were obtained by the biplane area length method, andpercent LVEF was calculated with the equation: [(ED − ES)/ED]/100.21
Micro-CTA micro-CT (RS-9 tabletop CT scanner, General Electric Medical Systems, London,Ontario) was used. We took 360 degree at 1-degree increments, with each projection
Wang et al. Page 3
Circ Res. Author manuscript; available in PMC 2011 June 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

consisting of a 500 msec x-ray exposure. We then used a cone-beam back-projectionreconstruction method, after normalizing and correcting the raw projection images for baddetector pixels. The CT-value grayscale from the initial reconstructed raw data was thencalibrated into Hounsfield units by sampling air, water, and bone material standardspositioned within the image’s field of view.
Micro-PETMicro-PET R4 scanner (Concorde Microsystems, Knoxville, TN) was used. PET imagingwas performed 2 hours after intravenous administration of the radiolabeled nucleosideanalog, [18F]-labeled 2’-deoxy-2’-fluoro-5-methyl-1-β-D-arabinofuranosyluracil([18F]FEAU), which was synthesized with high specific activity as previously described.24
The data acquisition, image reconstruction, and [18F]FEAU derived radioactivityquantification were performed as previously described.17
Co-registration of MRI, CT, and PET ImagesTo accurately coregister images, we used a chamber that was manufactured in-house. Weregistered PET to the reference anatomical CT through the co-registration chamber’s markerset, and this was further refined through a normalized mutual information (NMI) costfunction. We relied on an indirect MRI to CT registration process to register MRI and PETtogether. First, relatively high resolution MRI was registered to the reference CT via a NMIcost function.25-27 Independently, the diastole phase of a high planar- but low axial-resolution gated MRI data set was registered to the low resolution MRI of the same animalvia a simpler correlation cost function.26 The geometric transformations (e.g., PET to CT,CT to MRI, and MRI to gated MRI) were finally combined together to register gated MRIslices to PET images via the CT surrogate. Gated MRI slices thus provided the fine anatomydetails that permitted the exact localization of the [18F]FEAU-PET uptake in relation to themyocardium and the engraftment. After data were retrieved from the scanners, allprocessing and visualization paradigms28-29 were achieved through an ad-hoc hybridcombination of commercial platforms and in-house developments.
In Vivo Antibody Blocking of Myogenesis and AngiogenesisWe designed an experimental protocol (Figure 4A) based on our previous observation.10
Four groups of mice received anti-α4β1 or anti-VEGF antibodies or their respective isotype-matched control antibodies. The fifth group of mice received cells only, and the sixth groupreceived neither cells nor antibodies. At the end of the study, hearts were removed andcellular subsets were analyzed with FACS to ascertain the effects of antibody treatments.Antibodies were administered to the animals by i.p. injection at a concentration of 50 μg/mouse in 0.3 ml PBS 30 minutes before injected with CD34+ cells.
Preparation of Single Cell Suspension from the Heart and Cell Staining for FACS(fluorescence-activated cell sorting)
Single cell suspension was obtained by enzyme digestion. Isolated cells were washed, fixed,permeabilized, and incubated with monoclonal anti-cardiac troponin T (1:200, clone 1A11;Advanced Immunochemical), or with a polyclonal anti-VE cadherin (1:100, BenderMedSystems, CA) for 30 minutes at 4°C. The secondary antibodies were conjugated withAlexa Fluor 633 (Molecular Probes), or conjugated with Alexa Fluor 488, respectively.After three washes, all cells were incubated with anti-human HLA-ABC conjugated with PE(Cedarlane Laboratories) for 30 minutes before FACS.
Wang et al. Page 4
Circ Res. Author manuscript; available in PMC 2011 June 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Immunohistochemistry5 -micrometer serial sections were collected on slides, fixed with 3.7% paraformaldehyde(pH 7.4) at 4°C for 5 minutes, rinsed in PBS three times, and blocked at room temperaturefor 30 minutes in PBS containing 5% horse serum. Slides were then incubated with primaryantibodies at room temperature for one hour, rinsed three times, and incubated with thesecondary antibodies at room temperature for 30 minutes. The slides were rinsed in PBS 3times again and sealed with a mounting medium containing DAPI (Vector Laboratories).Antibodies used were: Anti-HLA–ABC (Cedarlane Laboratories); anti-cardiac troponin T(Abcam); anti-CD31(Abcam). Secondary antibodies (Invitrogen) were Alexa Fluor488-conjugated goat anti-mouse IgG, Alexa Fluor568 rabbit anti-rat, and Alexa Fluor 568donkey anti-rabbit.
StatisticsStudent’s t test was used to compare the means of 2 groups. When 3 or more means werecompared, 1-way ANOVA followed by multiple comparisons among means was used. Alldata collection and analyses were performed in a blinded fashion.
ResultsEfficiency of Lentiviral Transduction of CD34+ Progenitor Cells in Vitro
We used e-GFP to monitor TGL expression efficiency in transduced CD34+ cells. Theaverage transduction efficiency was 38.2 ± 4.3% at MOI of 50. A linear correlation wasobserved between transducted cell numbers and photon flux (Online Figure I).
In Vivo BLI Revealed Long-term Persistence of Transplanted CD34+ Cells after MIWe performed in vivo non-invasive BLI in SCID mice injected with TGL-expressingCD34+ cells to monitor cell localization and survival (measured as bioluminescent activity)over 12 months in living animals subjected to MI. We observed a bioluminescent signal onlyin the chest overlying the hearts (Figure 1A), suggesting that transplanted CD34+ cells didnot migrate to peripheral organs in sufficient numbers to be detected. The change in photonflux over time in hearts is shown in Figure 1B. Three days after injection, maximum photonflux was observed (2.98±0.31 ×105), this decreased to 7.20±0.13 × 104 by week 25, andmaintained at that level for greater than 1 year (Figure 1B). Photon flux was 2-3 fold higherduring the first 2 weeks after cell injection (P <0.01). This suggests that transplanted CD34+
cells had multiplied. Alternatively, the protein expression of f-Luc may have increasedfollowing transplantation. Importantly, no signal above the noise level was observed fromother organs in both the experimental and the control mice, indicating that no teratoma wasinduced by the transplantation of the transduced CD34+ cells.
Co-registration of MRI, Micro-CT, and Micro-PET Images Confirmed the Localization ofTransplanted CD34+Cells
Through the co-registration of MRI/CT/PET images (Figure 2 and Online Video I), we canprecisely localize the transplanted CD34+ cells in the peri-infarction area. PET was used tolocalize the TGL-expressing CD34+ cells using [18F]FEAU as the substrate for HSV1-tk.Phosphorylation of [18F]FEAU by HSV1-tk retained the radio-labeled PET probes inside thetransplanted CD34+ cells and can be imaged by a PET scanner. As previously reported, non-specific [18F]FEAU uptake was observed in the gallbladder and kidneys.30 As shown inOnline Video I, there was no PET signal in the cardiac region in a sham-operated mouse.However, PET signals were clearly visible in the cardiac region in a CD34+ cell transplantedmouse (Online Video II).
Wang et al. Page 5
Circ Res. Author manuscript; available in PMC 2011 June 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Improvement in Cardiac Function in Infarcted Hearts after Transplantation of CD34+ CellsWe used MRI to evaluate the therapeutic benefit of CD34+ cell transplantation into theinfarcted hearts (Figure 3 and Online Video III). ES and ED volumes, measured for up to 52weeks, were used to calculate the LVEF (Figure 3A). One day and three days after MI, thedecreases in EF were similar in both the control and cell-treated groups (Figure 3B). Theseresults suggest that our MI protocol was carried out consistently and achieved a similardegree of cardiac damage in both the control and the cell treated group. The EF began todiverge in a statistically significant way between the control and cell-treated group one weekfollowing MI and improvement in LVEF in the cell treated animals was sustained up to 52weeks.
Angiogenesis and/or Paracrine Effect is Responsible for Functional ImprovementTo the mechanism of action, we used FACS to analyze cellular subsets in the hearts 2months after MI. Figure 4B shows that between 0.78% and 0.88% of all cardiac cells in theanti-VEGF antibody and isotype control groups were HLA+/troponin T+ cells. However,anti-α4β1 antibody reduced the percentage of HLA+/troponin T+ cells to 0.13%. Thus,myogenesis was effectively blocked by the anti-α4β1 antibody but not by the anti-VEGFantibody. On the other hand, only the anti-VEGF antibody reduced the percentage of HLA+/VE-cadherin+ cells to 0.05% (Figure 4C). The FACS results were also supported byimmunohistochemical staining of cardiac sections (Online Figures II and III).
Cardiac MRI performed at the end of the study showed that the LVEF had dropped to 28%from the baseline value of 51% in the group of mice that did not receive cells (Figure 4D).However, mice that received cells had less of a drop in LVEF (from 50% to 37%). So, celltherapy produced a 10% net improvement in LVEF. In contrast, anti-α4β1 antibody did notreduce the decline in LVEF compared with the LVEF seen in isotype-matched control mice(from 50% to 36%). Interestingly, anti-VEGF antibody completely blocked theimprovement in LVEF (from 50% to 25%) seen in the CD34+ cell treatment group. Tofurther understand the effect of our treatment protocol on angiogenesis, we ascertained thenumber of CD31+ vessels in the peri-infarct zone. As shown in Online Figures IV-V, thenumber of CD31+ vessels in the anti-VEGF treated hearts was similar to the hearts that didnot receive cell therapy, whereas other groups showed a significant increase in the numberof CD31+ vessels. Thus, our results suggest that angiogenesis and/or paracrine effect, butnot myogenesis, is responsible for improving cardiac function following cell therapy.
DiscussionA variety of adult progenitor cells have been used as cellular therapy for acute MI.2Kawamoto et al. reported that CD34+ cells purified from peripheral blood mononuclear cellscan preserve myocardial integrity and function after MI.31 Using similarly prepared humanCD34+ cells in a mouse model of experimental MI, we demonstrated that transplantedCD34+ cells became cardiomyocytes, endothelial cells, and smooth muscle cells. Thus,CD34+ cells have the potential to be a clinically useful adult progenitor cells for cardiacrepair. Recently, Losordo et al. published the results of a phase I/IIa study using autologousCD34+ cells for intractable angina, showing clinical improvements in patients treated withCD34+ cells for up to 6 months.32 Our study demonstrates that human CD34+ cells persist inthe heart for up to 12 months following injection into the peri-infarct zone of SCID mice,and furthermore, the improvement in LVEF is also preserved for at least 6 months. Thus,these results suggested that transplanted CD34+ cells may similarly persist in the clinicalsetting, a finding which may correlate with myocardial repair.
Wang et al. Page 6
Circ Res. Author manuscript; available in PMC 2011 June 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
It is difficult to track the fate of injected cells in clinical studies. Hofmann et al. have labelednon purified bone marrow cells (BMC) with 2-[18F]-fluoro-2-deoxy-D-glucose ([18F]-FDG)and infused them into the infarct-related coronary artery. Fifty to 75 minutes after celltransfer, 1.3% to 2.6% of [18F]-FDG-labeled BMC were detected in the infarctedmyocardium using 3D PET imaging. Whereas after transfer of [18F]-FDG-labeled CD34-enriched cells, 14% to 39% of the total activity was detected in the infarcted myocardium.33
However, this method cannot be used to track the long-term fate of injected CD34+ cells.
Efficient expression of a given reporter is critical for in vivo tracking transplanted cellsusing live animal imaging techniques. This is particular critical for multimodality imagingusing a fusion of multiple reporter genes because the fusion tends to decrease activity ofeach reporter. Lentivirus can effectively introduce and integrate reporter genes into thegenome of CD34+ cells, achieving long-term and stable reporter gene expression. In thisstudy, we constructed lentivectors expressing the TGL reporter gene driven by humanubiquitin promoter. Remarkably, the transducted cells with these vectors survived in theinfarcted hearts for longer than 1 year. We have also confirmed that the transplanted CD34+
cells contribute to restoring cardiac function in the long-term. The profile of LVEF recoveryis comparable with results reported elsewhere.21, 34 These findings validate thatmultimodality molecular imaging is a powerful method for tracking progenitor cells in vivo.
BLI enabled us to determine the location, magnitude, survival, and especially the long termtime-spatial kinetics of the transplanted CD34+ cells. BLI, however, is not clinicallyapplicable due to several limitations (see introduction). To generate a clinically applicablemolecular imaging protocol, we included the HSV1-tk gene in the TF reporter gene and used[18F]FEAU-PET concomitant to BLI to monitor the transplanted CD34+ cells.17, 30, 35
Micro-PET imaging displayed similar tempo-spatial kinetics for HSV1-tk gene expressionas BLI. The coregistered MRI/CT/PET images provided us with detailed morphologicalpicture of CD34+ cell therapy. This paradigm can be applied clinically to track the fate ofprogenitor cell therapy in humans.
Previous studies have shown that several factors contribute to improvement in cardiacfunction, including the formation of new muscle cells and blood vessels9-11, 36 from thetransplanted cells. In addition, the secretion of cytokines from the transplanted cells canhave a paracrine effect on improving cardiac function. Here, we showed that angiogenesisand/or paracrine effect, rather than myogenesis, is responsible for the functionalimprovement. Following the injection of 1 million CD34+ cells to the peri-infarct region, wehave consistently observed that approximately 0.8% to 0.9% of total cardiac cells wereHLA+/troponin T+. One would assume that these human-derived cardiomyocytescontributed to the improvement in cardiac function following cell therapy. However, whenthe formation of the human-derived cardiomyocytes was blocked by anti-α4β1, the gain inLVEF persisted. Thus, myogenesis appears not to play a significant role in the improvementin cardiac function following CD34+ cell therapy in our model. Our finding that anti-VEGFtreatment, which abolished the formation of human-derived endothelial cells and theparacrine effect mediated by VEGF, abrogated the improvement in cardiac function furthersuggests that angiogenesis37 and/or paracrine effect38 play a critical role in the improvementin cardiac function in this murine model.
It was shown that anti-α4β1 antibody mobilizes cardiac progenitor cells from the bonemarrow to enhance cardiac repair after MI.39 Thus, anti- α4β1 antibody treatment could be adouble-edged sword that, on the one hand, blocks the formation of human-derivedcardiomyocytes but, on the other hand, recruits mouse progenitor cells from the bonemarrow to enhance cardiac repair. We think this is unlikely based on the data shown inFigure 4E. In this experiment, animals with experimentally induced MI did not receive cell
Wang et al. Page 7
Circ Res. Author manuscript; available in PMC 2011 June 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

therapy. Instead, they were treated with either anti- α4β1 or anti-VEGF antibody over a 2-month period and neither anti- α4β1 nor anti-VEGF antibody altered the drop in LVEFfollowing MI. Thus, it is unlikely that in our study the anti- α4β1 antibody enhanced theLVEF that compensated for the drop in LVEF due to blocked myogenesis.
Recently, Joseph Wu’s group has reported tracking of the fate of transplanted adipose tissue-and bone marrow-derived mesenchymal stem cells using BLI.40 However, the mesenchymalstem cells survived for less than five weeks after transplantation and did not contribute tofunctional recovery. In contrast, our current study showed that CD34+ cells persisted for upto one year and contributed to functional recovery. Furthermore, our study also providesinsights into the mechanisms of repair. Although antibody treatment may exert other effects,our FACS analysis and immunohistochemical studies suggest that our antibody treatmentprotocol can distinguish angiogenesis/paracrine effect from myogenesis, leading tomechanistic insights.
In conclusions, we co-registered MRI, micro-PET, micro-CT, and BLI images tosuccessfully obtain anatomic and functional information on CD34+ cells transplanted inmice with experimental MI. We demonstrated that BLI is capable of long term tracking oftransplanted CD34+ cells and that we can use micro-PET, micro-CT, and MRI images toaccurately localize transplanted CD34+ cells. Furthermore, we demonstrated that the long-term survival of the transplanted CD34+ cells contributed to improvement in cardiacfunction. Using selective antibody blocking, we also demonstrated that angiogeneis and/orparacrine effect accounts for the functional improvement.
Supplementary MaterialRefer to Web version on PubMed Central for supplementary material.
Novelty and Significance
What is known?• Adult stem cells have been used to treat patients suffering from myocardial
infarction or heart failure.
• CD34+ cells, one type of adult stem cells, can generate new myocardium and bloodvessels.
What new information does this article contribute?• Human CD34+ cells survived for up to one year in the mouse heart following
experimental infarction.
• Human CD34+ cells improved cardiac function after transplantation.
• Human CD34+ cells did this by forming new blood vessels or producing beneficialchemicals, but not by forming new myocardium.
SummaryAdult stem cells have been used to treat patients suffering from myocardial infarction orheart failure. However, it is not known how long these cells survive after transplantation andhow these cells improve cardiac function. To address these questions, we transplantedhuman CD34+ cells, a type of adult stem cells that can be purified from blood, into the heartof immune-deficient mice that had sustained experimental myocardial infarction. These
Wang et al. Page 8
Circ Res. Author manuscript; available in PMC 2011 June 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

CD34+ cells were labeled with reporters that allowed us to see them from outside the bodyusing cardiac imaging machines that detect light signals or positrons. We show that theinjected cells survived for up to one year in the hearts of mice and contributed toimprovement in cardiac function. We show also that the transplanted cells effected thisimprovement by forming new blood vessels or producing beneficial chemicals, but not byforming new myocardium. This study provides new insights into the mechanisms wherebyone type of adult stem cells helps to repair the heart. We expect that our results will behelpful in improving the design of clinical trials to determine the best way to provide celltherapy to patients with heart disease.
AcknowledgmentsWe thank Drs. Ryuichi Nishii and Leo G. Flores for their excellent technical assistance.
Sources of Funding This work has been supported in part by NIH R01 HL086983 (to J.G., E.T.H.Y.). Dr.Jingxiong Wang is the recipient of a Research Fellowship from the Canadian Institutes of Health Research. Dr.Edward T.H. Yeh is the McNair Scholar of the Texas Heart Institute.
References1. Assmus B, Honold J, Schachinger V, Britten MB, Fischer-Rasokat U, Lehmann R, Teupe C,
Pistorius K, Martin H, Abolmaali ND, Tonn T, Dimmeler S, Zeiher AM. Transcoronarytransplantation of progenitor cells after myocardial infarction. N Engl J Med. 2006; 355:1222–1232.[PubMed: 16990385]
2. Dimmeler S, Burchfield J, Zeiher AM. Cell-based therapy of myocardial infarction. ArteriosclerThromb Vasc Biol. 2008; 28:208–216. [PubMed: 17951319]
3. Dohmann HF, Perin EC, Takiya CM, Silva GV, Silva SA, Sousa AL, Mesquita CT, Rossi MI,Pascarelli BM, Assis IM, Dutra HS, Assad JA, Castello-Branco RV, Drummond C, Dohmann HJ,Willerson JT, Borojevic R. Transendocardial autologous bone marrow mononuclear cell injection inischemic heart failure: postmortem anatomicopathologic and immunohistochemical findings.Circulation. 2005; 112:521–526. [PubMed: 16027258]
4. Perin EC, Dohmann HF, Borojevic R, Silva SA, Sousa AL, Mesquita CT, Rossi MI, Carvalho AC,Dutra HS, Dohmann HJ, Silva GV, Belem L, Vivacqua R, Rangel FO, Esporcatte R, Geng YJ,Vaughn WK, Assad JA, Mesquita ET, Willerson JT. Transendocardial, autologous bone marrowcell transplantation for severe, chronic ischemic heart failure. Circulation. 2003; 107:2294–2302.[PubMed: 12707230]
5. Perin EC, Dohmann HF, Borojevic R, Silva SA, Sousa AL, Silva GV, Mesquita CT, Belem L,Vaughn WK, Rangel FO, Assad JA, Carvalho AC, Branco RV, Rossi MI, Dohmann HJ, WillersonJT. Improved exercise capacity and ischemia 6 and 12 months after transendocardial injection ofautologous bone marrow mononuclear cells for ischemic cardiomyopathy. Circulation. 2004;110:II213–218. [PubMed: 15364865]
6. Schachinger V, Assmus B, Britten MB, Honold J, Lehmann R, Teupe C, Abolmaali ND, Vogl TJ,Hofmann WK, Martin H, Dimmeler S, Zeiher AM. Transplantation of progenitor cells andregeneration enhancement in acute myocardial infarction: final one-year results of the TOPCARE-AMI Trial. J Am Coll Cardiol. 2004; 44:1690–1699. [PubMed: 15489105]
7. Schachinger V, Erbs S, Elsasser A, Haberbosch W, Hambrecht R, Holschermann H, Yu J, Corti R,Mathey DG, Hamm CW, Suselbeck T, Assmus B, Tonn T, Dimmeler S, Zeiher AM. Intracoronarybone marrow-derived progenitor cells in acute myocardial infarction. N Engl J Med. 2006;355:1210–1221. [PubMed: 16990384]
8. Wollert KC, Drexler H. Clinical applications of stem cells for the heart. Circ Res. 2005; 96:151–163. [PubMed: 15692093]
9. Yeh ET, Zhang S, Wu HD, Korbling M, Willerson JT, Estrov Z. Transdifferentiation of humanperipheral blood CD34+-enriched cell population into cardiomyocytes, endothelial cells, andsmooth muscle cells in vivo. Circulation. 2003; 108:2070–2073. [PubMed: 14568894]
Wang et al. Page 9
Circ Res. Author manuscript; available in PMC 2011 June 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
10. Zhang S, Shpall E, Willerson JT, Yeh ET. Fusion of human hematopoietic progenitor cells andmurine cardiomyocytes is mediated by alpha 4 beta 1 integrin/vascular cell adhesion molecule-1interaction. Circ Res. 2007; 100:693–702. [PubMed: 17303762]
11. Zhang S, Wang D, Estrov Z, Raj S, Willerson JT, Yeh ET. Both cell fusion and transdifferentiationaccount for the transformation of human peripheral blood CD34-positive cells into cardiomyocytesin vivo. Circulation. 2004; 110:3803–3807. [PubMed: 15596566]
12. Orlic D, Kajstura J, Chimenti S, Bodine DM, Leri A, Anversa P. Transplanted adult bone marrowcells repair myocardial infarcts in mice. Ann N Y Acad Sci. 2001; 938:221–229. discussion229-230. [PubMed: 11458511]
13. Arbab AS, Yocum GT, Kalish H, Jordan EK, Anderson SA, Khakoo AY, Read EJ, Frank JA.Efficient magnetic cell labeling with protamine sulfate complexed to ferumoxides for cellularMRI. Blood. 2004; 104:1217–1223. [PubMed: 15100158]
14. Hinds KA, Hill JM, Shapiro EM, Laukkanen MO, Silva AC, Combs CA, Varney TR, Balaban RS,Koretsky AP, Dunbar CE. Highly efficient endosomal labeling of progenitor and stem cells withlarge magnetic particles allows magnetic resonance imaging of single cells. Blood. 2003; 102:867–872. [PubMed: 12676779]
15. Pawelczyk E, Arbab AS, Chaudhry A, Balakumaran A, Robey PG, Frank JA. In vitro model ofbromodeoxyuridine or iron oxide nanoparticle uptake by activated macrophages from labeled stemcells: implications for cellular therapy. Stem Cells. 2008; 26:1366–1375. [PubMed: 18276802]
16. Welsh DK, Kay SA. Bioluminescence imaging in living organisms. Curr Opin Biotechnol. 2005;16:73–78. [PubMed: 15722018]
17. Tjuvajev JG, Avril N, Oku T, Sasajima T, Miyagawa T, Joshi R, Safer M, Beattie B, DiResta G,Daghighian F, Augensen F, Koutcher J, Zweit J, Humm J, Larson SM, Finn R, Blasberg R.Imaging herpes virus thymidine kinase gene transfer and expression by positron emissiontomography. Cancer Res. 1998; 58:4333–4341. [PubMed: 9766661]
18. Lois C, Hong EJ, Pease S, Brown EJ, Baltimore D. Germline transmission and tissue-specificexpression of transgenes delivered by lentiviral vectors. Science. 2002; 295:868–872. [PubMed:11786607]
19. Ponomarev V, Doubrovin M, Serganova I, Vider J, Shavrin A, Beresten T, Ivanova A, Ageyeva L,Tourkova V, Balatoni J, Bornmann W, Blasberg R, Gelovani Tjuvajev J. A novel triple-modalityreporter gene for whole-body fluorescent, bioluminescent, and nuclear noninvasive imaging. Eur JNucl Med Mol Imaging. 2004; 31:740–751. [PubMed: 15014901]
20. Rabinovich B, Li J, Wolfson M, Lawrence W, Beers C, Chalupny J, Hurren R, Greenfield B,Miller R, Cosman D. NKG2D splice variants: a reexamination of adaptor molecule associations.Immunogenetics. 2006; 58:81–88. [PubMed: 16470377]
21. van Laake LW, Passier R, Monshouwer-Kloots J, Nederhoff MG, Ward-van Oostwaard D, FieldLJ, van Echteld CJ, Doevendans PA, Mummery CL. Monitoring of cell therapy and assessment ofcardiac function using magnetic resonance imaging in a mouse model of myocardial infarction.Nat Protoc. 2007; 2:2551–2567. [PubMed: 17947998]
22. Ferrajoli A, Talpaz M, Kurzrock R, Estrov Z. Analysis of the effects of tumor necrosis factorinhibitors on human hematopoiesis. Stem Cells. 1993; 11:112–119. [PubMed: 8384506]
23. Rabinovich BA, Ye Y, Etto T, Chen JQ, Levitsky HI, Overwijk WW, Cooper LJ, Gelovani J, HwuP. Visualizing fewer than 10 mouse T cells with an enhanced firefly luciferase inimmunocompetent mouse models of cancer. Proc Natl Acad Sci U S A. 2008; 105:14342–14346.[PubMed: 18794521]
24. Alauddin MM, Conti PS, Fissekis JD. A general synthesis of [18F]-labeled 2′-deoxy-2′-fluoro-1-β-D-arabinofuranosyluracil nucleosides. J Labelled Comp Radiopharm. 2003; 46:285–289.
25. Maes F, Collignon A, Vandermeulen D, Marchal G, Suetens P. Multimodality image registrationby maximization of mutual information. IEEE Trans Med Imaging. 1997; 16:187–198. [PubMed:9101328]
26. Sonka, M.; M, MF., editors. Handbook of medical imaging - medical image processing andanalysis, SPIE. The International Society for Optical Engineering ed; 2000.
27. Studholme C, H D, Hill DLG. A normalized entropy measure for multimodality image alignment.Paper presented at: Proceedings SPIE MI’98. 1998
Wang et al. Page 10
Circ Res. Author manuscript; available in PMC 2011 June 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

28. Bidaut LM, Pascual-Marqui R, Delavelle J, Naimi A, Seeck M, Michel C, Slosman D, Ratib O,Ruefenacht D, Landis T, de Tribolet N, Scherrer JR, Terrier F. Three- to five-dimensionalbiomedical multisensor imaging for the assessment of neurological (dys) function. J DigitImaging. 1996; 9:185–198. [PubMed: 8951098]
29. Robb, RA. Three dimensional biomedical imaging. VCH Publishers, Inc.; 1995.30. Soghomonyan S, Hajitou A, Rangel R, Trepel M, Pasqualini R, Arap W, Gelovani JG, Alauddin
MM. Molecular PET imaging of HSV1-tk reporter gene expression using [18F]FEAU. Nat Protoc.2007; 2:416–423. [PubMed: 17406603]
31. Kawamoto A, Iwasaki H, Kusano K, Murayama T, Oyamada A, Silver M, Hulbert C, Gavin M,Hanley A, Ma H, Kearney M, Zak V, Asahara T, Losordo DW. CD34-positive cells exhibitincreased potency and safety for therapeutic neovascularization after myocardial infarctioncompared with total mononuclear cells. Circulation. 2006; 114:2163–2169. [PubMed: 17075009]
32. Losordo DW, Schatz RA, White CJ, Udelson JE, Veereshwarayya V, Durgin M, Poh KK,Weinstein R, Kearney M, Chaudhry M, Burg A, Eaton L, Heyd L, Thorne T, Shturman L,Hoffmeister P, Story K, Zak V, Dowling D, Traverse JH, Olson RE, Flanagan J, Sodano D,Murayama T, Kawamoto A, Kusano KF, Wollins J, Welt F, Shah P, Soukas P, Asahara T, HenryTD. Intramyocardial transplantation of autologous CD34+ stem cells for intractable angina: aphase I/IIa double-blind, randomized controlled trial. Circulation. 2007; 115:3165–3172.[PubMed: 17562958]
33. Hofmann M, Wollert KC, Meyer GP, Menke A, Arseniev L, Hertenstein B, Ganser A, Knapp WH,Drexler H. Monitoring of bone marrow cell homing into the infarcted human myocardium.Circulation. 2005; 111:2198–2202. [PubMed: 15851598]
34. Kocher AA, Schuster MD, Szabolcs MJ, Takuma S, Burkhoff D, Wang J, Homma S, EdwardsNM, Itescu S. Neovascularization of ischemic myocardium by human bone-marrow-derivedangioblasts prevents cardiomyocyte apoptosis, reduces remodeling and improves cardiac function.Nat Med. 2001; 7:430–436. [PubMed: 11283669]
35. Hajitou A, Trepel M, Lilley CE, Soghomonyan S, Alauddin MM, Marini FC 3rd, Restel BH,Ozawa MG, Moya CA, Rangel R, Sun Y, Zaoui K, Schmidt M, von Kalle C, Weitzman MD,Gelovani JG, Pasqualini R, Arap W. A hybrid vector for ligand-directed tumor targeting andmolecular imaging. Cell. 2006; 125:385–398. [PubMed: 16630824]
36. Wu SM, Chien KR, Mummery C. Origins and fates of cardiovascular progenitor cells. Cell. 2008;132:537–543. [PubMed: 18295570]
37. Dohmann HFR, Perin EC, Takiya CM, Silva GV, Silva SA, Sousa ALS, Mesquita CT, Rossi MID,Pascarelli BMO, Assis IM, Dutra HS, Assad JAR, Castello-Branco RV, Drummond C, DohmannHJF, Willerson JT, Borojevic R. Transendocardial Autologous Bone Marrow Mononuclear CellInjection in Ischemic Heart Failure: Postmortem Anatomicopathologic and ImmunohistochemicalFindings. Circulation. 2005; 112:521–526. [PubMed: 16027258]
38. Gnecchi M, He H, Liang OD, Melo LG, Morello F, Mu H, Noiseux N, Zhang L, Pratt RE, IngwallJS, Dzau VJ. Paracrine action accounts for marked protection of ischemic heart by Akt-modifiedmesenchymal stem cells. Nat Med. 2005; 11:367–368. [PubMed: 15812508]
39. Qin G, Ii M, Silver M, Wecker A, Bord E, Ma H, Gavin M, Goukassian DA, Yoon YS,Papayannopoulou T, Asahara T, Kearney M, Thorne T, Curry C, Eaton L, Heyd L, Dinesh D,Kishore R, Zhu Y, Losordo DW. Functional disruption of alpha4 integrin mobilizes bone marrow-derived endothelial progenitors and augments ischemic neovascularization. J Exp Med. 2006;203:153–163. [PubMed: 16401693]
40. van der Bogt KE, Schrepfer S, Yu J, Sheikh AY, Hoyt G, Govaert JA, Velotta JB, Contag CH,Robbins RC, Wu JC. Comparison of transplantation of adipose tissue- and bone marrow-derivedmesenchymal stem cells in the infarcted heart. Transplantation. 2009; 87:642–652. [PubMed:19295307]
Non-standard Abbreviations and Acronyms
3D three dimension
Wang et al. Page 11
Circ Res. Author manuscript; available in PMC 2011 June 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

BLI bioluminescence imaging
BMC bone marrow cells
ED end diastolic
ES end systolic
FACS fluorescence-activated cell sorting
e-GFP enhanced-GFP
FLASH fast low-angle shot
f-Luc firefly-Luciferase
HSV1-tk human herpes simplex virus type 1-thymidine kinase
HU Hounsfield units
hUbiq human ubiquitin
ID inner diameter
LVEF left ventricular ejection fraction
MI myocardial infarction
MIP maximum intensity projections
MOI multiplicity of infection
NMI normalized mutual information
ROI region of interest
TF triple fusion
TGL fused HSV1-tk, e-GFP, and f-Luc gene
[18F]-FDG 2-[18F]-fluoro-2-deoxy-D-glucose
[18F]FEAU [18F]-labeled 2’-deoxy-2’-fluoro-5-methyl-1-β-D-arabinofuranosyluracil
Wang et al. Page 12
Circ Res. Author manuscript; available in PMC 2011 June 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.Long-term BLI of TGL+-CD34+ in SCID mice. A, The bioluminescent signal in the heartwas superimposed on a photograph of a SCID mouse for the indicated time points afterCD34+ cell injection (representative mouse). B, BLI intensity in SCID mice injected withCD34+ cells is significantly higher than the mice received PBS injection over a 52-weektime period. BLI intensity was assessed by measuring the photon flux from ROI drawn overthe precordium (Data are expressed in means ± SE, n=7/group **P<0.01 and *P<0.05).
Wang et al. Page 13
Circ Res. Author manuscript; available in PMC 2011 June 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
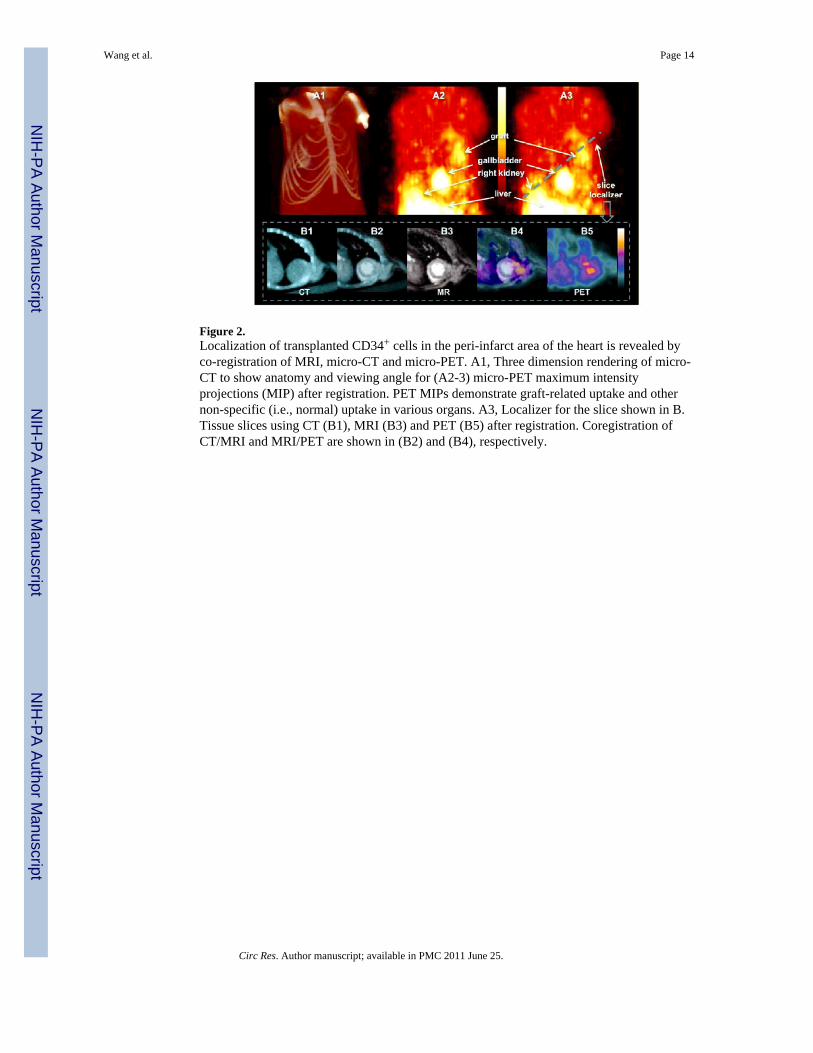
Figure 2.Localization of transplanted CD34+ cells in the peri-infarct area of the heart is revealed byco-registration of MRI, micro-CT and micro-PET. A1, Three dimension rendering of micro-CT to show anatomy and viewing angle for (A2-3) micro-PET maximum intensityprojections (MIP) after registration. PET MIPs demonstrate graft-related uptake and othernon-specific (i.e., normal) uptake in various organs. A3, Localizer for the slice shown in B.Tissue slices using CT (B1), MRI (B3) and PET (B5) after registration. Coregistration ofCT/MRI and MRI/PET are shown in (B2) and (B4), respectively.
Wang et al. Page 14
Circ Res. Author manuscript; available in PMC 2011 June 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 3.Evaluation of cardiac function using MRI. A, Representative sequential images of the ESand ED volumes from a CD34+ cell-transplanted mouse and a control mouse over 25 weeks.B, Dot graph of the LVEF in control mice versus CD34+ cell-transplanted mice over a 52-week time period. There is a significant difference between groups for LVEF at each timepoint (Data are expressed in means ± SE, n=7/group, except for week 52, NS: nosignificance; **P<0.01 and *P<0.05).
Wang et al. Page 15
Circ Res. Author manuscript; available in PMC 2011 June 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 4.In vivo antibody treatments inhibit myogenesis/angiogenesis and affect cardiac functioninduced by injection of CD34+ cells into mice after MI. A, Schematic of the experimentaldesign. All animals underwent baseline MRI scanning before the experiments. All animals,except those in the MRI control group, which were used to monitor LVEF without anyperturbation, had experimental MI on day 0. Anti-α4β1, anti-VEGF, and the respectiveisotype control antibodies were injected i.p. 30 min before MI. The heart was removed 8weeks after MI and analyzed by FACS. B, Anti-α4β1, but not anti-VEGF, antibodiesinhibited the formation of human-derived cardiomyocytes (HLA+ /troponin T+), asdetermined by FACS analysis. C, Only anti-VEGF inhibited the formation of human-derivedendothelial cells (HLA+/VE-cadherin+). D, Anti-VEGF, but not anti- α4β1, antibodiesdiminished the effect on the improvement in the LVEF caused by the injection of humanCD34+ cells. E, Treatment with anti- α4β1 or anti-VEGF antibodies did not affect LVEFfollowing MI without cell therapy (Data are expressed in means ± SE, n=4/group, **p<0.01;*p<0.05).
Wang et al. Page 16
Circ Res. Author manuscript; available in PMC 2011 June 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Copyright © 2022 FDOKUMEN




















