
Eosinophilic Granulomatosis with Polyangiitis and Diffuse Gastrointestinal Involvement
12
ARTHRITIS & RHEUMATISM Vol. 65, No. 1, January 2013, pp 270–281 DOI 10.1002/art.37721 © 2013, American College of Rheumatology Eosinophilic Granulomatosis With Polyangiitis (Churg-Strauss) Clinical Characteristics and Long-Term Followup of the 383 Patients Enrolled in the French Vasculitis Study Group Cohort Cloe ´ Comarmond, 1 Christian Pagnoux, 1 Mehdi Khellaf, 2 Jean-Franc ¸ois Cordier, 3 Mohamed Hamidou, 4 Jean-Franc ¸ois Viallard, 5 Franc ¸ois Maurier, 6 Ste ´phane Jouneau, 7 Boris Bienvenu, 8 Xavier Pue ´chal, 9 Olivier Aumaître, 10 Guillaume Le Guenno, 11 Alain Le Quellec, 12 Ramiro Cevallos, 13 Olivier Fain, 14 Bertrand Godeau, 2 Raphae `le Seror, 15 Bertrand Dunogue ´, 1 Alfred Mahr, 1 Philippe Guilpain, 16 Pascal Cohen, 1 Achille Aouba, 1 Luc Mouthon, 1 and Loı ¨c Guillevin, 1 for the French Vasculitis Study Group Objective. Earlier studies of eosinophilic granulo- matosis with polyangiitis (Churg-Strauss) (EGPA), with limited patient numbers and followup durations, dem- onstrated that clinical presentation at diagnosis, but not outcome, differed according to antineutrophil cyto- plasmic antibody (ANCA) status. This study was under- taken to describe the main characteristics of a larger patient cohort and their long-term outcomes. Methods. A retrospective study of EGPA patients in the French Vasculitis Study Group cohort who satis- fied the American College of Rheumatology criteria and/or Chapel Hill definitions was conducted. Patient characteristics and outcomes were compared according to ANCA status and year of diagnosis. Results. We identified 383 patients diagnosed between 1957 and June 2009 (128 [33.4%] before 1997 or earlier) and followed up for a mean SD of 66.8 62.5 months. At diagnosis, their mean SD age was 50.3 15.7 years, and 91.1% had asthma (duration 9.3 10.8 years). Main manifestations included peripheral neu- ropathy (51.4%); ear, nose, and throat (ENT) signs (48.0%); skin lesions (39.7%); lung infiltrates (38.6%); Dr. Pagnoux is recipient of fellowships from the Vasculitis Clinical Research Consortium and the Toronto General Hospital/ Toronto Western Hospital Foundation/University Health Network. 1 Cloe ´ Comarmond, MD, Christian Pagnoux, MD, MPH, MSc (current address: Mount Sinai Hospital, University Health Network, Toronto, Ontario, Canada), Bertrand Dunogue ´, MD, Alfred Mahr, MD, MPH, PhD, Pascal Cohen, MD, Achille Aouba, MD, MPH, Luc Mouthon, MD, PhD, Loı ¨c Guillevin, MD: Ho ˆpital Cochin, AP-HP, and Universite ´ Paris Descartes, Paris 5, Paris, France; 2 Mehdi Khellaf, MD, Bertrand Godeau, MD, PhD: Centre Hospitalier Universitaire Henri-Mondor, AP-HP, and Universite ´ Paris-Est Cre ´teil, Cre ´teil, France; 3 Jean-Franc ¸ois Cordier, MD: Ho ˆpital Louis-Pradel, Hospices Civils de Lyon, and Universite ´ Claude-Bernard Lyon I, Lyon; 4 Mo- hamed Hamidou, MD, PhD: University Hospital Ho ˆtel-Dieu, Nantes, France; 5 Jean-Franc ¸ois Viallard, MD, PhD: Ho ˆpital Haut-Le ´ve ˆque and Universite ´ Victor Segalen–Bordeaux 2, Centre Hospitalier Uni- versitaire de Bordeaux, Bordeaux, France; 6 Franc ¸ois Maurier, MD: Centre Hospitalier Re ´gional de Metz, Metz, France; 7 Ste ´phane Jou- neau, MD, PhD: Centre Hospitalier Universitaire de Rennes, Rennes, France; 8 Boris Bienvenu, MD, PhD: Division of Internal Medicine, Centre Hospitalier Universitaire de Caen, Co ˆte de Nacre, Caen, France; 9 Xavier Pue ´chal, MD, PhD: Le Mans General Hospital, Le Mans, France; 10 Olivier Aumaître, MD, PhD: Centre Hospitalier Universitaire, Ho ˆpital Gabriel-Montpied, Clermont-Ferrand, France; 11 Guillaume Le Guenno, MD, PhD: Centre Hospitalier Universitaire Estaing, Clermont-Ferrand, France; 12 Alain Le Quellec, MD, PhD: Ho ˆpital Saint-Eloi, Centre Hospitalier Universitaire de Montpellier, Montpellier, France; 13 Ramiro Cevallos, MD, PhD: Groupe Hospita- lier Saint-Vincent, Strasbourg, France; 14 Olivier Fain, MD: Centre Hospitalier Universitaire Jean-Verdier, Bondy, France; 15 Raphae `le Seror, MD, PhD: Ho ˆpital Cochin, AP-HP, Universite ´ Paris Descartes, Paris 5, Paris, France, and Universite ´ Paris, Sud 11 and AP-HP Ho ˆpital Bice ˆtre, Le Kremlin-Bice ˆtre, France; 16 Philippe Guilpain, MD, PhD: Ho ˆpital Cochin, AP-HP, and Universite ´ Paris Descartes, Paris 5, Paris, France, and Universite ´ Montpellier 1 and Ho ˆpital Saint-Eloi, Mont- pellier, France. Drs. Comarmond and Pagnoux contributed equally to this work. Dr. Pagnoux has received consulting fees, speaking fees, and/or honoraria from Hoffmann-La Roche and Schering-Plough (less than $10,000 each). Dr. Bienvenu has received speaking fees from Octapharma and Sanofi-Aventis (less than $10,000 each). Dr. Seror has received consulting fees, speaking fees, and/or honoraria from Hoffmann-La Roche, Pfizer, and GlaxoSmithKline (less than $10,000 each). Address correspondence to Christian Pagnoux, MD, MPH, MSc, Division of Rheumatology, Mount Sinai Hospital, 60 Murray Street S-2-220, Toronto, Ontario M5G 1X5, Canada. E-mail: [email protected]. Submitted for publication January 14, 2012; accepted in revised form September 20, 2012. 270
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Eosinophilic Granulomatosis with Polyangiitis and Diffuse Gastrointestinal Involvement
ARTHRITIS & RHEUMATISMVol. 65, No. 1, January 2013, pp 270–281DOI 10.1002/art.37721© 2013, American College of Rheumatology
Eosinophilic Granulomatosis With Polyangiitis (Churg-Strauss)
Clinical Characteristics and Long-Term Followup of the383 Patients Enrolled in the French Vasculitis Study Group Cohort
Cloe Comarmond,1 Christian Pagnoux,1 Mehdi Khellaf,2 Jean-Francois Cordier,3
Mohamed Hamidou,4 Jean-Francois Viallard,5 Francois Maurier,6 Stephane Jouneau,7
Boris Bienvenu,8 Xavier Puechal,9 Olivier Aumaître,10 Guillaume Le Guenno,11
Alain Le Quellec,12 Ramiro Cevallos,13 Olivier Fain,14 Bertrand Godeau,2 Raphaele Seror,15
Bertrand Dunogue,1 Alfred Mahr,1 Philippe Guilpain,16 Pascal Cohen,1 Achille Aouba,1
Luc Mouthon,1 and Loıc Guillevin,1 for the French Vasculitis Study Group
Objective. Earlier studies of eosinophilic granulo-matosis with polyangiitis (Churg-Strauss) (EGPA), withlimited patient numbers and followup durations, dem-onstrated that clinical presentation at diagnosis, butnot outcome, differed according to antineutrophil cyto-plasmic antibody (ANCA) status. This study was under-taken to describe the main characteristics of a largerpatient cohort and their long-term outcomes.
Methods. A retrospective study of EGPA patientsin the French Vasculitis Study Group cohort who satis-fied the American College of Rheumatology criteriaand/or Chapel Hill definitions was conducted. Patient
characteristics and outcomes were compared accordingto ANCA status and year of diagnosis.
Results. We identified 383 patients diagnosedbetween 1957 and June 2009 (128 [33.4%] before 1997 orearlier) and followed up for a mean � SD of 66.8 � 62.5months. At diagnosis, their mean � SD age was 50.3 �15.7 years, and 91.1% had asthma (duration 9.3 � 10.8years). Main manifestations included peripheral neu-ropathy (51.4%); ear, nose, and throat (ENT) signs(48.0%); skin lesions (39.7%); lung infiltrates (38.6%);
Dr. Pagnoux is recipient of fellowships from the VasculitisClinical Research Consortium and the Toronto General Hospital/Toronto Western Hospital Foundation/University Health Network.
1Cloe Comarmond, MD, Christian Pagnoux, MD, MPH, MSc(current address: Mount Sinai Hospital, University Health Network,Toronto, Ontario, Canada), Bertrand Dunogue, MD, Alfred Mahr,MD, MPH, PhD, Pascal Cohen, MD, Achille Aouba, MD, MPH, LucMouthon, MD, PhD, Loıc Guillevin, MD: Hopital Cochin, AP-HP,and Universite Paris Descartes, Paris 5, Paris, France; 2Mehdi Khellaf,MD, Bertrand Godeau, MD, PhD: Centre Hospitalier UniversitaireHenri-Mondor, AP-HP, and Universite Paris-Est Creteil, Creteil,France; 3Jean-Francois Cordier, MD: Hopital Louis-Pradel, HospicesCivils de Lyon, and Universite Claude-Bernard Lyon I, Lyon; 4Mo-hamed Hamidou, MD, PhD: University Hospital Hotel-Dieu, Nantes,France; 5Jean-Francois Viallard, MD, PhD: Hopital Haut-Levequeand Universite Victor Segalen–Bordeaux 2, Centre Hospitalier Uni-versitaire de Bordeaux, Bordeaux, France; 6Francois Maurier, MD:Centre Hospitalier Regional de Metz, Metz, France; 7Stephane Jou-neau, MD, PhD: Centre Hospitalier Universitaire de Rennes, Rennes,France; 8Boris Bienvenu, MD, PhD: Division of Internal Medicine,Centre Hospitalier Universitaire de Caen, Cote de Nacre, Caen,France; 9Xavier Puechal, MD, PhD: Le Mans General Hospital, LeMans, France; 10Olivier Aumaître, MD, PhD: Centre HospitalierUniversitaire, Hopital Gabriel-Montpied, Clermont-Ferrand, France;
11Guillaume Le Guenno, MD, PhD: Centre Hospitalier UniversitaireEstaing, Clermont-Ferrand, France; 12Alain Le Quellec, MD, PhD:Hopital Saint-Eloi, Centre Hospitalier Universitaire de Montpellier,Montpellier, France; 13Ramiro Cevallos, MD, PhD: Groupe Hospita-lier Saint-Vincent, Strasbourg, France; 14Olivier Fain, MD: CentreHospitalier Universitaire Jean-Verdier, Bondy, France; 15RaphaeleSeror, MD, PhD: Hopital Cochin, AP-HP, Universite Paris Descartes,Paris 5, Paris, France, and Universite Paris, Sud 11 and AP-HP HopitalBicetre, Le Kremlin-Bicetre, France; 16Philippe Guilpain, MD, PhD:Hopital Cochin, AP-HP, and Universite Paris Descartes, Paris 5, Paris,France, and Universite Montpellier 1 and Hopital Saint-Eloi, Mont-pellier, France.
Drs. Comarmond and Pagnoux contributed equally to thiswork.
Dr. Pagnoux has received consulting fees, speaking fees,and/or honoraria from Hoffmann-La Roche and Schering-Plough (lessthan $10,000 each). Dr. Bienvenu has received speaking fees fromOctapharma and Sanofi-Aventis (less than $10,000 each). Dr. Serorhas received consulting fees, speaking fees, and/or honoraria fromHoffmann-La Roche, Pfizer, and GlaxoSmithKline (less than $10,000each).
Address correspondence to Christian Pagnoux, MD, MPH,MSc, Division of Rheumatology, Mount Sinai Hospital, 60 MurrayStreet S-2-220, Toronto, Ontario M5G 1X5, Canada. E-mail:[email protected].
Submitted for publication January 14, 2012; accepted inrevised form September 20, 2012.
270

and cardiomyopathy (16.4%). Among the 348 patientstested at diagnosis for ANCA, the 108 ANCA-positivepatients (31.0%) had significantly more frequent ENTmanifestations, peripheral neuropathy, and/or renalinvolvement, but less frequent cardiac manifestations,than the ANCA-negative patients. Vasculitis relapsesoccurred in 35.2% of the ANCA-positive versus 22.5% ofthe ANCA-negative patients (P � 0.01), and 5.6% versus12.5%, respectively, died (P < 0.05). The 5-year relapse-free survival rate was 58.1% (95% confidence interval[95% CI] 45.6–68.6) for ANCA-positive and 67.8% (95%CI 59.8–74.5) for ANCA-negative patients (P � 0.35).Multivariable analysis identified cardiomyopathy, olderage, and diagnosis during or prior to 1996 as indepen-dent risk factors for death and lower eosinophil count atdiagnosis as predictive of relapse.
Conclusion. The characteristics and long-termoutcomes of EGPA patients differ according to theirANCA status. Although EGPA relapses remain fre-quent, mortality has declined, at least since 1996.
Eosinophilic granulomatosis with polyangiitis(Churg-Strauss) (EGPA) is one of the rarest but stillpotentially life-threatening systemic necrotizing vascu-litides predominantly affecting small vessels (1–3). Sincethe first description of the disease in 1951 (4), severaldescriptive series have been published, but each in-cluded fewer than 120 patients and had limited followup(5–15). Whereas EGPA pathophysiology remains onlypartially understood, it has consistently been found that30–40% of affected patients have antineutrophil cyto-plasmic antibodies (ANCA), mainly ANCA with a peri-nuclear labeling pattern on immunofluorescence (IF),usually directed against myeloperoxidase (MPO) onenzyme-linked immunosorbent assay (ELISA) (13,16,17).Two of the most recent series, including one of 112patients described by our group, concurrently demon-strated that ANCA-positive patients differed from theirANCA-negative counterparts in that ANCA-positivepatients had a lower frequency of cardiac involvementbut more frequent renal disease and peripheral nerveinvolvement (16,17). However, and despite EGPA-related cardiomyopathy having been shown by our groupsince 1996 to carry a poor prognosis (6,18,19), along withgastrointestinal, central nervous system (CNS), and re-nal involvement, respective prognoses for patient sub-sets based on ANCA status did not differ. One possibleexplanation was the relatively short mean followupdurations of those studies, which did not exceed 3 years(mean � SD 34 � 23 months for the French VasculitisStudy Group [FVSG] analysis [17]).
Therefore, we decided to conduct a new investi-
gation of all EGPA patients with data entered into theFVSG cohort database since its initiation in 1983, in-cluding the 112 previously described patients (6,17,19),in order to further analyze their characteristics anddetermine whether longer-term outcomes differed ac-cording to ANCA status and year of diagnosis. We alsoattempted to identify potential predictors of vasculitisrelapse by using a stringent definition of relapse andanalyzing nonspecific and isolated asthma or allergicrhinitis flares separately.
PATIENTS AND METHODS
Patients. We conducted a systematic retrospectivestudy of patients with EGPA according to the AmericanCollege of Rheumatology (ACR) 1990 criteria (20) and/orChapel Hill definition (1) who had data entered into the FVSGdatabase before July 2009. (See Appendix A for members ofthe FVSG.) All patient data have been collected in the FVSGdatabase since its inception in 1983, when it was declared tothe Commission Nationale Informatique et Libertes. For pa-tients who participated in prospective therapeutic trials, writ-ten informed consent for the prospective collection and furtheranalysis of their data was obtained at enrollment. All otherpatients received oral and written information attesting to theirunrestricted rights to ask for the deletion of their data. Thediagnosis of EGPA was reassessed by the investigators (CC,CP, and LG), taking into account the entire followup period,so that those patients who were eventually diagnosed as havingother systemic eosinophilic disorders were excluded (21).Patients with insufficient data (only 1 visit and/or no clinicaldetails), concomitant human immunodeficiency virus and/orhepatitis C virus infection, cryoglobulinemia, or other systemicdiseases were also excluded.
Baseline measurements. For patients who had beenincluded in clinical trials, data were extracted from the stan-dardized record forms that have been used since 1983 forFVSG clinical trials. For other patients, medical charts wereretrieved and reviewed for demographic characteristics andclinical, biologic, radiologic, and histologic findings. Amongthe recorded and analyzed clinical manifestations, the follow-ing definitions were applied. Fever was defined as a tempera-ture of �38.5°C, weight loss as a loss of �3 kg over the 3months preceding diagnosis, and surgical abdomen as severegastrointestinal symptoms requiring intervention or at leastconsultation with a surgeon. Heart manifestations, includingcardiomyopathy, were diagnosed based on clinical findings incombination with ultrasound and electrocardiogram results(thereby corresponding to the Five-Factors Score [FFS] defi-nitions) (19). The biologic parameters studied included pro-teinuria (�0.4 gm/24 hours), serum creatinine level, C-reactiveprotein (CRP) level at diagnosis, and ANCA status (consid-ered to be positive when ANCA were detected by IF and/orELISA in the serum at diagnosis or later during the diseasecourse when they had initially tested negative). For patientswho were diagnosed as having EGPA before the disseminationof ANCA testing, these tests were run on serum samples thatwere obtained at the time of diagnosis and frozen, whenavailable. Biopsy findings were also recorded, as normal or as
EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (CHURG-STRAUSS) 271

showing evidence of vasculitis, granuloma, and/or eosinophilicinfiltrates (or necrotizing glomerulonephritis for kidney biopsyspecimens).
Disease activity and scores. Disease activity was as-sessed at diagnosis using the original 1994 Birmingham Vasc-ulitis Activity Score (BVAS) (22) and recorded in the data-base. The prognostic FFS, devised in 1996 (19) and based on5 items (severe vasculitis-related gastrointestinal involvement,CNS involvement, and/or cardiomyopathy, serum creatininelevel �140 �moles/liter, and/or proteinuria �1 gm/24 hours)was recorded, as was the revised FFS for EGPA (severevasculitis-related gastrointestinal involvement and/or cardiacinvolvement, serum creatinine level �150 �moles/liter, ageolder than 65, and/or absence of ear, nose, and throat [ENT]symptoms) (23). All scores were obtained from the FVSGdatabase or calculated retrospectively for those patients whowere diagnosed before the scoring systems were created.
Treatment procedures. Patients included in clinicaltrials were treated according to the scheduled therapeuticregimens (24–29). Others were treated with what was consid-ered to be the standard of care when they were diagnosed.Drugs used to achieve remission were recorded, as were thosegiven subsequently for maintenance or relapse, when applica-ble, and prednisone dose at last assessment, when it wasavailable.
Outcomes. Outcomes studied included relapses, termi-nation of corticosteroid treatment, deaths and their causes,and cancers occurring during followup. Relapse was pre-defined as either 1) the recurrence or worsening of a clinicalEGPA manifestation following a period of remission of �3months, or 2) the need for the addition of, or a change in,immunosuppressive drugs and/or the reinstitution of predni-sone or an increase in prednisone dosage of more than twicethe previous dosage, resulting in a total dosage of �30 mg/day.An increase in the eosinophil count without any other clinicalEGPA manifestations; or isolated asthma, sinusitis, or rhinitisexacerbations, with or without a concomitant increase ineosinophil count, were recorded when considered clinicallysignificant by the patient’s referring physician to justify anytherapeutic adjustment but were not considered a failure,recurrent EGPA manifestations, or relapse per se, and wereanalyzed separately. Remission was defined as the absence ofdisease activity attributable to EGPA vasculitis manifestations(parenchymal lung disease; peripheral nerve involvement; orskin, cardiac, CNS, renal, and/or gastrointestinal signs) for �3consecutive months, corresponding to a BVAS of 0. Accordingto this definition of remission, patients could still be receivinga specified prednisone dose for isolated asthma or rhinitis.
Statistical analysis. Patient characteristics are re-ported as the number and percentage for categorical variablesand as the mean � SD for continuous variables. Patient sub-sets were established based on ANCA status, sex, or year ofdiagnosis. For these subsets, quantitative variables were com-pared using Student’s t-test, and categorical variables werecompared using the chi-square test or Fisher’s exact test, asappropriate. Patient survival was analyzed using life tables andthe Kaplan-Meier method (30) and were compared using logrank tests (31). Survival was calculated from the time of EGPAdiagnosis to death or the last followup visit. Relapse-freesurvival was calculated from the time of EGPA diagnosis torelapse, death, or end of followup.
Main patient demographics (sex, age at diagnosis, year
of diagnosis prior to/during 1996 or after 1996, i.e. after theFFS was devised, and prior inclusion in a therapeutic trial) andclinical, biologic, and therapeutic parameters (�1 immuno-suppressant in the initial therapeutic regimen or during fol-lowup) with P � 0.20 in the univariable analysis were includedin multivariable Cox proportional hazards models to identifyindependent predictors of death or relapse. The FFS andrevised FFS were not included in the multivariable model,because their composite items had already been analyzedseparately. We used a backward stepwise procedure to deter-mine the parameters of the final model (32). Results areexpressed as hazard ratios (HRs) and 95% confidence intervals(95% CIs). The standardized incidence ratio (SIR) of cancersobserved during followup was calculated for comparison withthe expected cancer rate in the general population of France,with corresponding sex and age (expected cancer incidencerates from 1975 to 2005 were obtained from http://www.invs.sante.fr/surveillance/cancers/estimations_cancers/default.htm,and incidence rates for the years 1975 and 2005 were used forthe periods prior to 1975 and since 2005, respectively). Allstatistical analyses were conducted using Stata software version10 (StataCorp), except for the SIR calculation, which wascomputed with Pamcomp software version 1.41 (33). P valuesless than 0.05 were considered significant.
RESULTS
Patient identification and characteristics. Afterexcluding 60 patients with concomitant infections, sys-temic disease, and/or insufficient recorded data, weidentified 383 patients in the FVSG database whosatisfied the inclusion criteria and were diagnosed ashaving EGPA between March 1957 and July 2009. Nopatient was excluded because of a revised diagnosis ofanother systemic eosinophilic disorder during followup.Among these selected patients, 210 (54.8%) had beenincluded in prospective therapeutic trials (24–29), and128 (33.4%) had been diagnosed during or prior to 1996.Their demographic characteristics and main clinicalmanifestations at diagnosis are shown in Table 1.
The mean � SD age at diagnosis was 50.3 � 15.7years, and neither sex was predominant (male:femaleratio 1.08). Of the 383 patients, 376 (98.2%) were white,4 (1%) were of African or Caribbean ancestry, and 3(0.8%) were of Asian descent. At EGPA diagnosis, 349(91.1%) of the patients had asthma, which had beenpresent for a mean � SD of 9.3 � 10.8 years, andbecame manifest no more than 6 months before EGPAdiagnosis in 13 (3.4%) of them. The remaining 34patients had ENT signs and/or developed asthma within6 months following EGPA diagnosis (n � 6). The mostcommon EGPA manifestations at diagnosis includedweight loss (49.3%), mononeuritis multiplex (46.0%),nonerosive sinusitis/polyposis (41.8%), skin lesions(39.7%), and lung infiltrates (38.6%). Pleural effusionwas reported in 34 (8.9%), among whom 14 (3.7%) also
272 COMARMOND ET AL
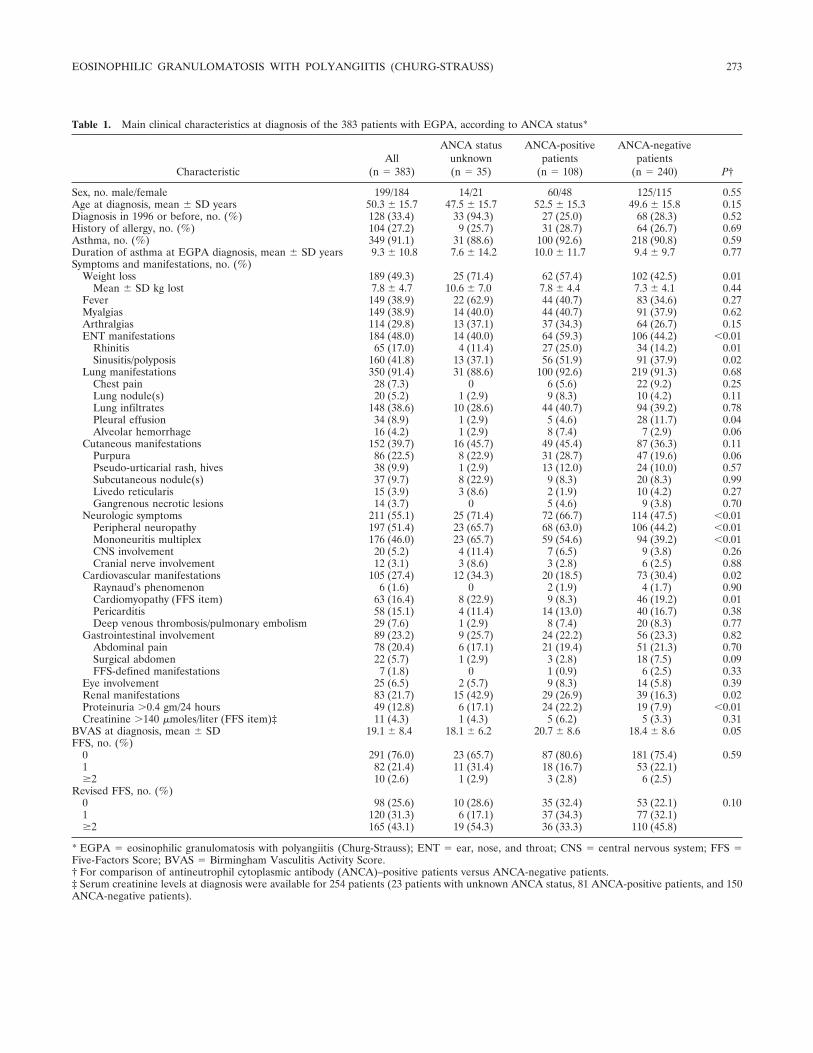
Table 1. Main clinical characteristics at diagnosis of the 383 patients with EGPA, according to ANCA status*
CharacteristicAll
(n � 383)
ANCA statusunknown(n � 35)
ANCA-positivepatients
(n � 108)
ANCA-negativepatients
(n � 240) P†
Sex, no. male/female 199/184 14/21 60/48 125/115 0.55Age at diagnosis, mean � SD years 50.3 � 15.7 47.5 � 15.7 52.5 � 15.3 49.6 � 15.8 0.15Diagnosis in 1996 or before, no. (%) 128 (33.4) 33 (94.3) 27 (25.0) 68 (28.3) 0.52History of allergy, no. (%) 104 (27.2) 9 (25.7) 31 (28.7) 64 (26.7) 0.69Asthma, no. (%) 349 (91.1) 31 (88.6) 100 (92.6) 218 (90.8) 0.59Duration of asthma at EGPA diagnosis, mean � SD years 9.3 � 10.8 7.6 � 14.2 10.0 � 11.7 9.4 � 9.7 0.77Symptoms and manifestations, no. (%)
Weight loss 189 (49.3) 25 (71.4) 62 (57.4) 102 (42.5) 0.01Mean � SD kg lost 7.8 � 4.7 10.6 � 7.0 7.8 � 4.4 7.3 � 4.1 0.44
Fever 149 (38.9) 22 (62.9) 44 (40.7) 83 (34.6) 0.27Myalgias 149 (38.9) 14 (40.0) 44 (40.7) 91 (37.9) 0.62Arthralgias 114 (29.8) 13 (37.1) 37 (34.3) 64 (26.7) 0.15ENT manifestations 184 (48.0) 14 (40.0) 64 (59.3) 106 (44.2) �0.01
Rhinitis 65 (17.0) 4 (11.4) 27 (25.0) 34 (14.2) 0.01Sinusitis/polyposis 160 (41.8) 13 (37.1) 56 (51.9) 91 (37.9) 0.02
Lung manifestations 350 (91.4) 31 (88.6) 100 (92.6) 219 (91.3) 0.68Chest pain 28 (7.3) 0 6 (5.6) 22 (9.2) 0.25Lung nodule(s) 20 (5.2) 1 (2.9) 9 (8.3) 10 (4.2) 0.11Lung infiltrates 148 (38.6) 10 (28.6) 44 (40.7) 94 (39.2) 0.78Pleural effusion 34 (8.9) 1 (2.9) 5 (4.6) 28 (11.7) 0.04Alveolar hemorrhage 16 (4.2) 1 (2.9) 8 (7.4) 7 (2.9) 0.06
Cutaneous manifestations 152 (39.7) 16 (45.7) 49 (45.4) 87 (36.3) 0.11Purpura 86 (22.5) 8 (22.9) 31 (28.7) 47 (19.6) 0.06Pseudo-urticarial rash, hives 38 (9.9) 1 (2.9) 13 (12.0) 24 (10.0) 0.57Subcutaneous nodule(s) 37 (9.7) 8 (22.9) 9 (8.3) 20 (8.3) 0.99Livedo reticularis 15 (3.9) 3 (8.6) 2 (1.9) 10 (4.2) 0.27Gangrenous necrotic lesions 14 (3.7) 0 5 (4.6) 9 (3.8) 0.70
Neurologic symptoms 211 (55.1) 25 (71.4) 72 (66.7) 114 (47.5) �0.01Peripheral neuropathy 197 (51.4) 23 (65.7) 68 (63.0) 106 (44.2) �0.01Mononeuritis multiplex 176 (46.0) 23 (65.7) 59 (54.6) 94 (39.2) �0.01CNS involvement 20 (5.2) 4 (11.4) 7 (6.5) 9 (3.8) 0.26Cranial nerve involvement 12 (3.1) 3 (8.6) 3 (2.8) 6 (2.5) 0.88
Cardiovascular manifestations 105 (27.4) 12 (34.3) 20 (18.5) 73 (30.4) 0.02Raynaud’s phenomenon 6 (1.6) 0 2 (1.9) 4 (1.7) 0.90Cardiomyopathy (FFS item) 63 (16.4) 8 (22.9) 9 (8.3) 46 (19.2) 0.01Pericarditis 58 (15.1) 4 (11.4) 14 (13.0) 40 (16.7) 0.38Deep venous thrombosis/pulmonary embolism 29 (7.6) 1 (2.9) 8 (7.4) 20 (8.3) 0.77
Gastrointestinal involvement 89 (23.2) 9 (25.7) 24 (22.2) 56 (23.3) 0.82Abdominal pain 78 (20.4) 6 (17.1) 21 (19.4) 51 (21.3) 0.70Surgical abdomen 22 (5.7) 1 (2.9) 3 (2.8) 18 (7.5) 0.09FFS-defined manifestations 7 (1.8) 0 1 (0.9) 6 (2.5) 0.33
Eye involvement 25 (6.5) 2 (5.7) 9 (8.3) 14 (5.8) 0.39Renal manifestations 83 (21.7) 15 (42.9) 29 (26.9) 39 (16.3) 0.02Proteinuria �0.4 gm/24 hours 49 (12.8) 6 (17.1) 24 (22.2) 19 (7.9) �0.01Creatinine �140 �moles/liter (FFS item)‡ 11 (4.3) 1 (4.3) 5 (6.2) 5 (3.3) 0.31
BVAS at diagnosis, mean � SD 19.1 � 8.4 18.1 � 6.2 20.7 � 8.6 18.4 � 8.6 0.05FFS, no. (%)
0 291 (76.0) 23 (65.7) 87 (80.6) 181 (75.4) 0.591 82 (21.4) 11 (31.4) 18 (16.7) 53 (22.1)�2 10 (2.6) 1 (2.9) 3 (2.8) 6 (2.5)
Revised FFS, no. (%)0 98 (25.6) 10 (28.6) 35 (32.4) 53 (22.1) 0.101 120 (31.3) 6 (17.1) 37 (34.3) 77 (32.1)�2 165 (43.1) 19 (54.3) 36 (33.3) 110 (45.8)
* EGPA � eosinophilic granulomatosis with polyangiitis (Churg-Strauss); ENT � ear, nose, and throat; CNS � central nervous system; FFS �Five-Factors Score; BVAS � Birmingham Vasculitis Activity Score.† For comparison of antineutrophil cytoplasmic antibody (ANCA)–positive patients versus ANCA-negative patients.‡ Serum creatinine levels at diagnosis were available for 254 patients (23 patients with unknown ANCA status, 81 ANCA-positive patients, and 150ANCA-negative patients).
EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (CHURG-STRAUSS) 273

had associated cardiomyopathy. Alveolar hemorrhagewas diagnosed in 16 (4.2%) of the patients, 6 of whomhad both alveolar hemorrhage (massive in only 1) andrenal manifestations. Heart, gastrointestinal tract, andkidney involvement were found in 27.4%, 23.2%, and21.7% of the patients, respectively, but only 16.4%(cardiomyopathy), 1.8% (surgical complications), and4.3% (creatinine level �140 �moles/liter) of them metFFS definitions of severe manifestations. CNS manifes-tations were present in 20 patients (5.2%), includingischemic stroke in 8 (2.1%) and hemorrhagic stroke in 2(0.5%).
As shown in Table 2, at diagnosis, �50% of thepatients had an inflammatory syndrome, and themean � SD blood eosinophil count was 7,569 � 6,428/mm3, with a maximum of 34,110/mm3. Only 10 patients(2.6%), who were taking oral prednisone for theirunderlying asthma, had blood eosinophil counts of�500/mm3 at diagnosis. Thirty-five patients (33 of whomwere diagnosed during or prior to 1996), could not betested for ANCA. Of the remaining 348 patients, 108(31.0%) were ANCA positive; 72 of them had a perinu-clear labeling pattern on IF and 68 had MPO specificityon ELISA. Eighteen of the 108 ANCA-positive patientshad a cytoplasmic labeling pattern, 4 with proteinase 3(PR3) specificity on ELISA. Three of the 108 ANCA-positive patients had both perinuclear and cytoplasmiclabeling patterns on IF, with 1 being both MPO-positive
and PR3-positive on ELISA. The remaining 15 ANCA-positive patients had atypical IF labeling patterns. Noneof the patients who were initially ANCA negative sub-sequently tested positive.
Among the 180 patients who underwent �1biopsy, 145 had histologic findings supporting a diagno-sis of EGPA (vasculitis in 61.0%, eosinophil infiltratein 61.3%, and granuloma in 33.3%). Among these 145patients, ANCA results were available for 130, and 52(40%) were ANCA positive (see Supplementary Table1, available on the Arthritis & Rheumatism web site athttp://onlinelibrary.wiley.com/journal/10.1002/(ISSN)1529-0131, for more details on these patients). Moreprecisely, 74 patients underwent nerve and muscle biop-sies and 40 underwent muscle biopsies which supportedan EGPA diagnosis in 45 patients, and 20 patients(biopsy sensitivity 61% and 50%), respectively. Ninepatients had myocardial biopsies (sensitivity 89%), 13had open lung biopsies (sensitivity 77%), 21 had trans-bronchial biopsies (sensitivity 52%), 23 had nasal orsinus mucosa biopsies (sensitivity 35%), and 85 had skinbiopsies. The skin biopsies reached 88% sensitivity, butthe main findings for the latter were nonspecific leuko-cytoclastic vasculitis, with eosinophilic infiltrates andgranulomas, in only 36% and 10%, respectively, of thosewith positive skin biopsy findings. Fourteen patients hadkidney biopsies, 12 of which showed pauci-immune
Table 2. Main biologic characteristics at diagnosis of the 383 patients with EGPA, according to ANCA status*
CharacteristicAll
(n � 383)
ANCA statusunknown(n � 35)
ANCA-positivepatients
(n � 108)
ANCA-negativepatients
(n � 240)
Creatinine, �moles/liter† 89.1 � 38.6 85.9 � 24.3 91.3 � 55.4 88.3 � 28.3Creatinine, mg/dl 1.01 � 0.44 0.97 � 0.27 1.03 � 0.63 0.99 � 0.32Estimated MDRD GFR, ml/minute/1.73 m2 83.7 � 26.8 84.6 � 26.4 88.1 � 31.7 81.1 � 23.5Estimated Cockcroft GFR, ml/minute/1.73 m2 78.4 � 24.3 73.9 � 22.9 79.7 � 25.0 78.2 � 24.1Other laboratory findings
CRP, mg/liter‡ 66.9 � 61.8 150 78.7 � 62.4 58.5 � 60.1§ESR �30 mm/first hour, no. (%)‡ 189 (56.1) 19 (54.3) 60 (58.8) 110 (55.0)Eosinophils, /mm3¶ 7,569 � 6,428 8,139 � 6,150 7,833 � 6,462 7,329 � 6,643Neutrophils, /mm3 7,427 � 3,763 7,662 � 3,292 7,916 � 3,794 7,100 � 3,810Lymphocytes, /mm3 2,046 � 1,194 1,524 � 1,239 1,777 � 789 2,238 � 1,378#Platelets, /mm3¶ 361,012 � 132,782 416,158 � 149,297 374,560 � 133,592 344,633 � 127,561
* Except where indicated otherwise, values are the mean � SD. EGPA � eosinophilic granulomatosis with polyangiitis (Churg-Strauss); MDRDGFR � Modification of Diet in Renal Disease glomerular filtration rate.† Serum creatinine levels at diagnosis were available for 254 patients (23 patients with unknown antineutrophil cytoplasmic antibody [ANCA] status,81 ANCA-positive patients, and 150 ANCA-negative patients).‡ Data on the C-reactive protein (CPR) level were available for 160 patients (1 patient with unknown ANCA status, 97 ANCA-positive patients, and62 ANCA-negative patients), and data on the erythrocyte sedimentation rate (ESR) were available for 337 patients (35 patients with unknownANCA status, 102 ANCA-positive patients, and 200 ANCA-negative patients).§ P � 0.04 versus ANCA-positive patients.¶ Complete white blood cell and platelet counts were available for 254 patients (21 patients with unknown ANCA status, 87 ANCA-positive patients,and 146 ANCA-negative patients).# P � 0.03 versus ANCA-positive patients.
274 COMARMOND ET AL

necrotizing glomerulonephritis, and 2 of which showedsegmental and focal glomerulonephritis.
Patient characteristics at diagnosis, according toANCA status, year of diagnosis, and sex. As shown inTable 1, ANCA-positive patients had significantly morefrequent ENT manifestations, peripheral nerve involve-ment, and renal disease than ANCA-negative patients;renal disease remained relatively uncommon. Con-versely, ANCA-negative patients had significantly morefrequent cardiomyopathy. The mean BVAS and CRPlevel were significantly higher in ANCA-positive pa-tients, but no other major biologic difference was foundaccording to ANCA status (Table 2). Among the pa-tients whose biopsy findings supported an EGPA diag-nosis, histologic vasculitis features were more frequentin ANCA-positive patients (77.4% versus 48.8% inANCA-negative patients, P � 0.01), while granuloma-tous and eosinophilic infiltrates were seen in 42.1%and 63.2%, respectively, of the ANCA-positive patientsversus 29.0% and 69.7%, respectively, of the ANCA-negative patients (P � 0.32 and P � 0.63, respectively).
Patients diagnosed during or prior to 1996, ascompared to those diagnosed after 1996, were youngerat diagnosis (mean � SD 48.0 � 15.7 years versus 51.8 �15.5 years; P � 0.04) and more frequently had constitu-tional symptoms, asthma (96.1% versus 88.6%; P �0.02), mononeuritis multiplex (68.0% versus 35.0%; P �0.01), cardiomyopathy (22.7% versus 13.3%; P � 0.02),and kidney disease (31.3% versus 16.9%; P � 0.01).Patients diagnosed during the two time periods hada comparable duration of asthma prior to EGPA diag-nosis, FFS distribution, mean BVAS, and frequency ofANCA positivity among those with ANCA status avail-able (28.4% versus 32.8%; P � 0.51) (see Supplemen-tary Tables 2 and 3, available on the Arthritis & Rheu-matism web site at http://onlinelibrary.wiley.com/journal/10.1002/(ISSN)1529-0131).
Compared to male patients, female patients withEGPA were significantly younger at diagnosis, had alonger duration of asthma before EGPA diagnosis, andhad less frequent renal abnormalities, although thefrequencies of biopsy-proven glomerulonephritis werecomparable for both sexes.
Treatments. Remission-induction treatment in-cluded corticosteroids for all patients and a combinationof corticosteroids and immunosuppressants for 214 pa-tients (55.9%). Throughout their entire followup, 271patients (70.8%) eventually received �1 immunosup-pressant, including cyclophosphamide for 217 (56.7%),azathioprine for 98 (25.6%), methotrexate for 26 (6.8%),and rituximab for 3 (0.8%). Eighty-five of the 92 patientswith an original FFS of �1 received �1 immunosuppres-
sant, compared to 186 of the 291 patients with an FFS of0. Fifty-four (50%) of the ANCA-positive patients re-ceived immunosuppressants as part of their inductiontherapy, and 76 (70.4%) received immunosuppressantsduring followup, which was comparable to the frequencyof immunosuppressant use in the ANCA-negative group(56.3% during induction therapy and 70.4% duringfollowup; P � 0.28 and P � 0.99, respectively).
Disease outcomes. The mean � SD duration offollowup was 66.8 � 62.5 months (median 50.5 months)and was comparable for ANCA-positive and ANCA-negative patients (64.6 � 56.2 and 65.7 � 62.2 months,respectively; P � 0.88). The duration of followup ex-ceeded 1 year from diagnosis for all of the patientsexcept those who died early. Forty-five patients (11.7%)died, including 6 ANCA-positive patients, 30 ANCA-negative patients, and 9 patients with unknown ANCAstatus (crude mortality rate 5.6% versus 12.5% [P �0.05] and 25.7%, respectively). Deaths occurred amean � SD of 50.4 � 60.1 months (median 21.4 months)after diagnosis and were attributed to cardiac events(myocardial infarction, cardiac insufficiency, or arrhyth-mia) in 14 patients (10 ANCA-negative patients), infec-tions or cancers in 5 patients each, active vasculitis orrespiratory events (severe asthma attacks and/or termi-nal chronic obstructive pulmonary disease) in 4 patientseach, and miscellaneous causes in the remaining 13patients (such as hemorrhage under anticoagulation in2 patients or food allergy–associated anaphylactic shockin 1 patient). Among the 14 fatal cardiac events, 8occurred in patients with known EGPA-related cardio-myopathy, a median of 14 months after diagnosis (range3.5–136 months), and only 5 occurred within the first 6months after diagnosis.
Vasculitis relapse occurred in 97 patients (25.3%),including 38 ANCA-positive patients, 54 ANCA-negative patients, and 5 patients with unknown ANCAstatus (relapse rates 35.2% versus 22.5% [P � 0.01] and14.3%, respectively), while 72 additional patients(18.8%) experienced asthma flares, sinusitis, and/or in-creased eosinophilia, justifying adjustments to therapy(22 ANCA-positive patients and 46 ANCA-negativepatients [20.4% versus 19.2%, respectively; P � 0.79]).Among the 280 patients for whom data on prednisoneuse at their last visit was available, 44 (15.7%) were nottaking prednisone (mean � SD duration of cortico-steroid use 65.8 � 44.5 months), with no differenceaccording to ANCA status. For the remaining 236patients, prednisone had to be continued (started 77.1 �102.2 months earlier) with a mean daily dose of 12.9 �12.5 mg at the last visit (with 62 patients taking �5mg/day, 94 taking �7.5 mg/day, and 62 taking �15
EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (CHURG-STRAUSS) 275
mg/day), which was comparable in the ANCA-positiveand ANCA-negative subgroups.
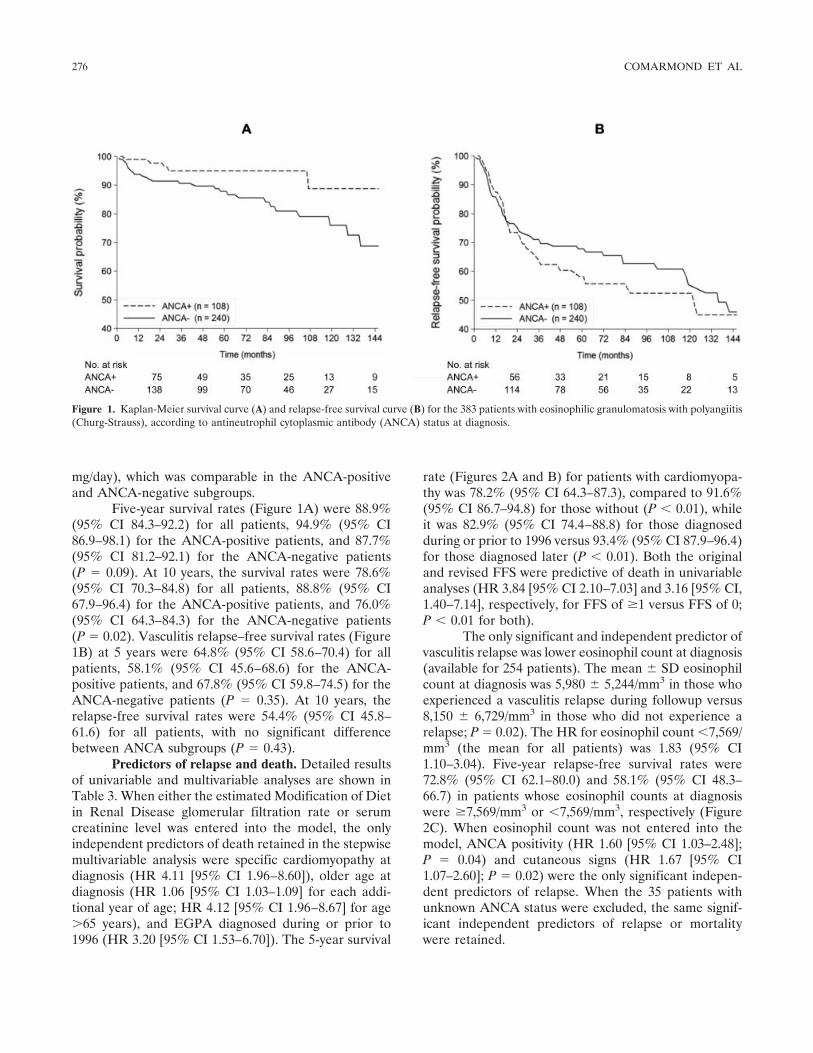
Five-year survival rates (Figure 1A) were 88.9%(95% CI 84.3–92.2) for all patients, 94.9% (95% CI86.9–98.1) for the ANCA-positive patients, and 87.7%(95% CI 81.2–92.1) for the ANCA-negative patients(P � 0.09). At 10 years, the survival rates were 78.6%(95% CI 70.3–84.8) for all patients, 88.8% (95% CI67.9–96.4) for the ANCA-positive patients, and 76.0%(95% CI 64.3–84.3) for the ANCA-negative patients(P � 0.02). Vasculitis relapse–free survival rates (Figure1B) at 5 years were 64.8% (95% CI 58.6–70.4) for allpatients, 58.1% (95% CI 45.6–68.6) for the ANCA-positive patients, and 67.8% (95% CI 59.8–74.5) for theANCA-negative patients (P � 0.35). At 10 years, therelapse-free survival rates were 54.4% (95% CI 45.8–61.6) for all patients, with no significant differencebetween ANCA subgroups (P � 0.43).
Predictors of relapse and death. Detailed resultsof univariable and multivariable analyses are shown inTable 3. When either the estimated Modification of Dietin Renal Disease glomerular filtration rate or serumcreatinine level was entered into the model, the onlyindependent predictors of death retained in the stepwisemultivariable analysis were specific cardiomyopathy atdiagnosis (HR 4.11 [95% CI 1.96–8.60]), older age atdiagnosis (HR 1.06 [95% CI 1.03–1.09] for each addi-tional year of age; HR 4.12 [95% CI 1.96–8.67] for age�65 years), and EGPA diagnosed during or prior to1996 (HR 3.20 [95% CI 1.53–6.70]). The 5-year survival
rate (Figures 2A and B) for patients with cardiomyopa-thy was 78.2% (95% CI 64.3–87.3), compared to 91.6%(95% CI 86.7–94.8) for those without (P � 0.01), whileit was 82.9% (95% CI 74.4–88.8) for those diagnosedduring or prior to 1996 versus 93.4% (95% CI 87.9–96.4)for those diagnosed later (P � 0.01). Both the originaland revised FFS were predictive of death in univariableanalyses (HR 3.84 [95% CI 2.10–7.03] and 3.16 [95% CI,1.40–7.14], respectively, for FFS of �1 versus FFS of 0;P � 0.01 for both).
The only significant and independent predictor ofvasculitis relapse was lower eosinophil count at diagnosis(available for 254 patients). The mean � SD eosinophilcount at diagnosis was 5,980 � 5,244/mm3 in those whoexperienced a vasculitis relapse during followup versus8,150 � 6,729/mm3 in those who did not experience arelapse; P � 0.02). The HR for eosinophil count �7,569/mm3 (the mean for all patients) was 1.83 (95% CI1.10–3.04). Five-year relapse-free survival rates were72.8% (95% CI 62.1–80.0) and 58.1% (95% CI 48.3–66.7) in patients whose eosinophil counts at diagnosiswere �7,569/mm3 or �7,569/mm3, respectively (Figure2C). When eosinophil count was not entered into themodel, ANCA positivity (HR 1.60 [95% CI 1.03–2.48];P � 0.04) and cutaneous signs (HR 1.67 [95% CI1.07–2.60]; P � 0.02) were the only significant indepen-dent predictors of relapse. When the 35 patients withunknown ANCA status were excluded, the same signif-icant independent predictors of relapse or mortalitywere retained.
Figure 1. Kaplan-Meier survival curve (A) and relapse-free survival curve (B) for the 383 patients with eosinophilic granulomatosis with polyangiitis(Churg-Strauss), according to antineutrophil cytoplasmic antibody (ANCA) status at diagnosis.
276 COMARMOND ET AL

Cancers. During followup, 14 malignancies werediagnosed in 13 patients (2 ANCA-positive patients, 9ANCA-negative patients, and 2 patients with un-known ANCA status; P � 0.48), 5 of whom died. Thecancer incidence did not differ significantly from thatexpected in the general population (SIR 1.15 [95% CI0.63–1.94]). There were 11 solid tumors (1 colon cancer,2 basal cell skin carcinomas, 1 bladder cancer, 1 breast
cancer, and the 5 fatal cancers [1 colon, 1 ovarian, 1 lung,and 1 gastric, and 1 glioblastoma in a man who alsohad prostate cancer]) and 3 hematologic neoplasms(1 B cell lymphoma, 1 polycythemia vera, and 1 myelo-dysplasia). Nine of these patients had received cyclo-phosphamide; 2 took immunosuppressants other thancyclophosphamide; and 2 had been treated with cortico-steroids only.
Table 3. Results of univariable and multivariable survival analyses for the risk of death or relapse in patients withEGPA*
Parameter
Univariable analysis Multivariable analysis†
HR(95% CI) P
HR(95% CI) P
Predictors of deathAge at diagnosis 1.05 (1.02–1.08) �0.01 1.06 (1.03–1.09) �0.01Sex 1.40 (0.76–2.57) 0.28Diagnosis in 1996 or before 2.40 (1.22–4.71) 0.01 3.20 (1.53–6.70) �0.01‡Inclusion in a therapeutic trial 0.89 (0.49–1.61) 0.69Asthma 2.61 (0.62–11.04) 0.19 1.35 (0.30–5.96) 0.70ENT manifestations 0.46 (0.25–0.85) 0.01 0.59 (0.29–1.20) 0.15Cutaneous manifestations 1.38 (0.75–2.52) 0.30Peripheral nerve involvement 1.09 (0.57–2.07) 0.79CNS involvement 2.61 (1.02–6.66) 0.05 1.63 (0.48–5.62) 0.44Cardiomyopathy (FFS item) 2.91 (1.57–5.39) �0.01 4.11 (1.96–8.60) �0.01Gastrointestinal involvement (FFS item) 0.96 (0.23–3.98) 0.95Serum creatinine, �moles/liter 1.01 (1.00–1.01) 0.02 1.01 (0.99–1.02) 0.05MDRD GFR estimate, ml/minute/1.73 m2 0.98 (0.97–1.00) 0.07 0.99 (0.98–1.01) 0.91Eosinophil count, /mm3 0.99 (0.99–1.01) 0.40CRP, mg/liter 1.00 (0.99–1.01) 0.37ANCA positive 0.43 (0.18–1.03) 0.06 0.47 (0.16–1.32) 0.15Immunosuppressant as initial treatment 2.12 (1.11–4.07) 0.02 1.56 (0.61–3.98) 0.36Ever received an immunosuppressant 1.32 (0.65–2.68) 0.77
Predictors of relapseAge at diagnosis 0.99 (0.98–1.01) 0.32Sex 1.41 (0.92–2.16) 0.12 1.01 (0.61–1.63) 0.99Diagnosis in 1996 or before 0.76 (0.48–1.19) 0.23Inclusion in a therapeutic trial 0.98 (0.64–1.50) 0.92Asthma 0.79 (0.41–1.53) 0.49ENT manifestations 1.04 (0.68–1.59) 0.87Cutaneous manifestations 1.59 (1.04–2.43) 0.03 1.54 (0.94–2.55) 0.09Peripheral nerve involvement 1.35 (0.85–2.13) 0.20 1.38 (0.78–2.43) 0.27CNS involvement 1.33 (0.54–3.29) 0.53Cardiomyopathy (FFS item) 1.16 (0.69–1.95) 0.58Gastrointestinal involvement (FFS item) 1.67 (0.41–6.81) 0.47Serum creatinine, �moles/liter 1.00 (0.99–1.01) 0.42MDRD GFR estimate, ml/minute/1.73 m2 1.00 (0.99–1.01) 0.41Eosinophil count, /mm3 0.99 (0.99–0.99) �0.01 0.99 (0.99–0.99) �0.01¶CRP, mg/liter 1.00 (0.99–1.01) 0.34ANCA positive 1.67 (1.08–2.60) 0.02 1.49 (0.92–2.43) 0.36Immunosuppressant as initial treatment 0.86 (0.56–1.31) 0.48Ever received an immunosuppressant 1.51 (0.91–2.49) 0.11 1.19 (0.64–2.23) 0.58
* EGPA � eosinophilic granulomatosis with polyangiitis (Churg-Strauss); ENT � ear, nose, and throat; CNS � centralnervous system; FFS � Five-Factors Score; MDRD GFR � Modification of Diet in Renal Disease glomerular filtrationrate; CRP � C-reactive protein.† All parameters with a P value of �0.20 in the univariable analysis were included in the multivariable analysis.‡ When year of diagnosis (during or prior to 1996 versus after 1996) was excluded from the model, the final parameterspredictive of death were age at diagnosis (hazard ratio [HR] 1.06 [95% confidence interval (95% CI) 1.03–1.09], P �0.01) and cardiomyopathy (HR 3.85 [95% CI 2.00–7.41], P � 0.01).¶ When eosinophil count was excluded from the model, the final parameters predictive of relapse were antineutrophilcytoplasmic antibody (ANCA) positivity (HR 1.60 [95% CI 1.03–2.48], P � 0.04) and cutaneous signs (HR 1.67 [95%CI 1.07–2.60], P � 0.02).
EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (CHURG-STRAUSS) 277

DISCUSSION
This analysis of a large cohort of EGPA patientswith followup exceeding 5 years confirms the previouslyreported differences in clinical disease presentationbased on ANCA status (16,17) and provides new infor-mation on outcomes and relapse predictors that mayhave therapeutic implications. Compared to ANCA-negative patients, ANCA-positive patients more fre-quently had clinical vasculitis manifestations, such asperipheral neuropathy or renal involvement, but lessfrequently had cardiomyopathy. Their mortality rate waslower, but the risk of relapse appeared to be slightlyhigher. Cardiomyopathy remained the main indepen-dent predictor of death in EGPA patients on multi-variable analysis.
The patients included in this study satisfied theACR classification criteria (20) and/or the Chapel Hillnomenclature definition (1). No established diagnosticcriteria for EGPA are currently available, and in theabsence of clinical or histologic evidence of vasculitis, itmay be difficult to differentiate between EGPA andother systemic eosinophilic disorders (34,21). In someANCA-negative patients, an overlap between someforms of EGPA and nonclassified systemic eosinophilicdisorders cannot be totally excluded (35,36). However,in practice, response to treatment is usually achievedbetter and faster in EGPA than in primary systemiceosinophilic disorders. Subsequent patient outcomes canalso further help to confirm or, inversely, correct theinitial diagnosis.
A pathogenic role of ANCA has not been dem-onstrated in EGPA, and only a minority of EGPApatients are indeed ANCA positive. Hence, whether
EGPA includes 2 phenotypic subsets based on ANCAstatus or whether ANCA positivity is only a surrogatemarker of more diffuse vasculitis-induced damage re-mains to be determined (35,36). We found the samedifferences in clinical presentation based on ANCAstatus as previous investigators (16,17). Despite thoseclinical differences, outcomes did not differ according toANCA status in those earlier studies (13,16,17); how-ever, their followup durations and sample sizes werelimited. Furthermore, a recurrent limitation of thoseprevious EGPA investigations is the unclear, or at leastinconsistent, definition of disease flares. Authentic vas-culitis flares, like purpura or glomerulonephritis, shouldbe analyzed separately from simple exacerbations ofasthma, ENT symptoms, or increased eosinophil counts.In addition, asthma or rhinitis exacerbations can beunderreported, depending on whether physicians con-sider them significant or not. Our results, based on morepatients, with longer followup and a more stringentdefinition of relapse, suggest that ANCA positivity isassociated with a higher risk of relapse, but a lowermortality rate (in univariable analysis). Recent resultsobtained in an Italian series of 38 patients were similar,with 46.7% of relapses occurring in ANCA-positivepatients versus 8.7% in ANCA-negative patients (37).
Eosinophilia at diagnosis did not differ accordingto ANCA status, but a lower eosinophil count wasunexpectedly identified as the main predictive factorassociated with relapse. Because eosinophilia fluctuatesbroadly and is corticosteroid sensitive and because theuse of inhaled or systemic corticosteroids for asthmaor allergic rhinitis/sinusitis at diagnosis was not system-atically recorded, this finding will have to be further
Figure 2. A and B, Kaplan-Meier survival curves for the 383 patients with eosinophilic granulomatosis with polyangiitis (Churg-Strauss) (EGPA),according to the presence of cardiomyopathy at diagnosis (A) and the year of diagnosis (before or after December 31, 1996) (B). C, Relapse-freesurvival curve for the patients with EGPA, according to the eosinophil count at diagnosis. The 7,569/mm3 threshold value corresponds to the meaneosinophil count at diagnosis in all 254 patients for whom data were available.
278 COMARMOND ET AL

analyzed in other cohorts. When the eosinophil countwas excluded from the model for relapse, ANCA posi-tivity and cutaneous signs at diagnosis were the strongestpredictors of subsequent relapses.
ANCA status was also associated with death, withANCA-positive patients having a lower mortality rate inunivariable analysis. However, in multivariable analysis,cardiomyopathy remained the main poor-prognosis fac-tor, as repeatedly reported over the past decades andincluded in the 1996 FFS (19). Other independentpoor-prognosis parameters were older age at diagnosis,which was included in the revised FFS (23), and diag-nosis during or prior to 1996, i.e., before the FFS wasdevised and used to optimize treatment and guide theneed for cyclophosphamide in patients with more severeEGPA (19,28,29,38,39). Alternative or additional hy-potheses for the better outcomes of those patientsdiagnosed after 1996 include advances in the manage-ment of cardiac insufficiency within the last decade andless frequent major organ involvement at diagnosis,although their FFS and BVAS did not differ from thoseof patients who were diagnosed earlier. In our study,most of the fatal cardiac events occurred a median of 14months after EGPA diagnosis, underlining the potentiallate consequences of cardiac damage and the impor-tance of thorough and serial cardiovascular assessments.
In the Italian study by Sinico et al (16), 52% ofthe patients, mainly those who were ANCA positive,received an immunosuppressant as part of their initialtherapeutic regimen. However, therapeutic regimens didnot differ markedly according to ANCA status in ourstudy. All of the patients in the present study receivedcorticosteroids; half of them received both cortico-steroids and an immunosuppressant at diagnosis, andtwo-thirds received both corticosteroids and an immu-nosuppressant at some point during the course of theirdisease. Importantly, most patients required long-termoral corticosteroids, with a mean daily prednisone doseof �12 mg, whereas �7.5 mg/day is the upper thresholddefining remission in the European League AgainstRheumatism recommendations for studies of systemicvasculitides (40). However, the majority of the patientswere in clinical remission with regard to vasculitis man-ifestations and needed prednisone only to controlasthma, rhinitis, or poorly specific arthralgias.
While this study has several strengths, includingits sample size, long followup duration, and the stringentdefinition of EGPA relapse, which allowed EGPA re-lapse to be distinguished from asthma exacerbations,it has some limitations. It was a partly retrospectivemulticenter study and included patients who partici-pated in therapeutic trials at some time during the
course of their vasculitis. We did not analyze in detailthe impact of each treatment separately, because thatwould have yielded the same conclusions as those re-ported for trials in which the patients had participated(28,29,38).
The sensitivity of ANCA testing methods mayvary, and not all of our patients were tested centrally. Inaddition, though not observed in the present study, ithas been reported that ANCA testing can be negative atdiagnosis and become positive only later, during a flare(13). However, the ANCA frequencies and clinical dif-ferences at diagnosis according to ANCA status thatwere observed in the present study are consistent withthose reported earlier based on other independent co-horts (16,17,37,41). Although asthma duration was sim-ilar in both ANCA status groups, we cannot exclude thepossibility that a longer time to diagnosis may also haveaffected the survival of ANCA-negative patients, whosediagnosis can be more challenging. That patients diag-nosed during or prior to 1996 had more frequent asthmaand major organ involvement than those diagnosedsubsequently might also suggest that physicians werethen less likely to enroll patients with less overt EGPAmanifestations in a study, especially before the routineuse of ANCA testing.
Finally, the definition of cardiomyopathy, forthis study, as for the FFS, remained based on easily de-tectable clinical parameters (19). Abnormalities onechocardiography, magnetic resonance imaging, or auto-nomic nervous system evaluations are frequent in EGPApatients but of still unknown prognostic value (42–48).
In summary, our analysis of a large group ofwell-defined EGPA patients with long followup dura-tions revealed that global survival has improved over thelast few decades and that, in addition to some clinicaldifferences at diagnosis, outcomes also varied dependingon ANCA status. Although ANCA-positive patients hada lower mortality rate, their risk of relapse appeared tobe higher. If confirmed in other independent patientcohorts, those findings could suggest that treatment mayhave to be adapted according to ANCA status. However,the number of ANCA-positive EGPA patients remainedrelatively low, and other prognostic parameters appearto be more important, especially cardiomyopathy. Sev-eral issues in EGPA remain to be addressed, includingthe identification of more effective therapies so that theuse of corticosteroids and conventional cytotoxic drugscan be limited or avoided.
ACKNOWLEDGMENTThe authors thank Ms Janet Jacobson for editorial
assistance.
EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (CHURG-STRAUSS) 279

AUTHOR CONTRIBUTIONS
All authors were involved in drafting the article or revising itcritically for important intellectual content, and all authors approvedthe final version to be published. Drs. Comarmond, Pagnoux, andGuillevin had full access to all of the data in the study and takeresponsibility for the integrity of the data and the accuracy of the dataanalysis.Study conception and design. Comarmond, Pagnoux, Cordier,Puechal, Aumaître, Le Guenno, Aouba, Guillevin.Acquisition of data. Comarmond, Pagnoux, Khellaf, Cordier,Hamidou, Viallard, Maurier, Jouneau, Bienvenu, Puechal, Aumaître,Le Guenno, Le Quellec, Cevallos, Fain, Godeau, Seror, Mahr, Cohen,Aouba, Mouthon, Guillevin.Analysis and interpretation of data. Comarmond, Pagnoux, Viallard,Puechal, Aumaître, Le Guenno, Cevallos, Seror, Dunogue, Guilpain,Guillevin.
REFERENCES
1. Jennette JC, Falk RJ, Andrassy K, Bacon PA, Churg J, Gross WL,et al. Nomenclature of systemic vasculitides: proposal of aninternational consensus conference. Arthritis Rheum 1994;37:187–92.
2. Eustace JA, Nadasdy T, Choi M. Disease of the month: theChurg-Strauss syndrome. J Am Soc Nephrol 1999;10:2048–55.
3. Vaglio A, Casazza I, Grasselli C, Corradi D, Sinico RA, Buzio C.Churg-Strauss syndrome. Kidney Int 2009;76:1006–11.
4. Churg J, Strauss L. Allergic angiitis and periarteritis nodosa. Am JPathol 1951;27:277–301.
5. Pagnoux C, Guilpain P, Guillevin L. Churg-Strauss syndrome.Curr Opin Rheumatol 2007;19:25–32.
6. Guillevin L, Cohen P, Gayraud M, Lhote F, Jarrousse B, CasassusP. Churg-Strauss syndrome: clinical study and long-term follow-upof 96 patients. Medicine (Baltimore) 1999;78:26–37.
7. Abu-Shakra M, Smythe H, Lewtas J, Badley E, Weber D, Key-stone E. Outcome of polyarteritis nodosa and Churg-Strausssyndrome: an analysis of twenty-five patients. Arthritis Rheum1994;37:1798–803.
8. Chumbley LC, Harrison EG Jr, DeRemee RA. Allergic granulo-matosis and angiitis (Churg-Strauss syndrome): report and analysisof 30 cases. Mayo Clin Proc 1977;52:477–84.
9. Davis MD, Daoud MS, McEvoy MT, Su WP. Cutaneous manifes-tations of Churg-Strauss syndrome: a clinicopathologic correla-tion. J Am Acad Dermatol 1997;37:199–203.
10. Della Rossa A, Baldini C, Tavoni A, Tognetti A, Neglia D,Sambuceti G, et al. Churg-Strauss syndrome: clinical and serolog-ical features of 19 patients from a single Italian centre. Rheuma-tology (Oxford) 2002;41:1286–94.
11. Gaskin G, Clutterbuck EJ, Pusey CD. Renal disease in theChurg-Strauss syndrome: diagnosis, management and outcome.Contrib Nephrol 1991;94:58–65.
12. Haas C, Le Jeunne C, Choubrac P, Durand H, Hugues FC.Churg-Strauss syndrome: retrospective study of 20 cases. BullAcad Natl Med 2001;185:1113–30. In French.
13. Keogh KA, Specks U. Churg-Strauss syndrome: clinical presenta-tion, antineutrophil cytoplasmic antibodies, and leukotriene recep-tor antagonists. Am J Med 2003;115:284–90.
14. Reid AJ, Harrison BD, Watts RA, Watkin SW, McCann BG, ScottDG. Churg-Strauss syndrome in a district hospital. QJM 1998;91:219–29.
15. Solans R, Bosch JA, Perez-Bocanegra C, Selva A, Huguet P,Alijotas J, et al. Churg-Strauss syndrome: outcome and long-termfollow-up of 32 patients. Rheumatology (Oxford) 2001;40:763–71.
16. Sinico RA, Di Toma L, Maggiore U, Bottero P, Radice A, TosoniC, et al. Prevalence and clinical significance of antineutrophilcytoplasmic antibodies in Churg-Strauss syndrome. ArthritisRheum 2005;52:2926–35.
17. Sable-Fourtassou R, Cohen P, Mahr A, Pagnoux C, Mouthon L,Jayne D, et al. Antineutrophil cytoplasmic antibodies and theChurg-Strauss syndrome. Ann Intern Med 2005;143:632–8.
18. Guillevin L, Le Thi Huong D, Godeau P, Jais P, Wechsler B.Clinical findings and prognosis of polyarteritis nodosa and Churg-Strauss angiitis: a study in 165 patients. Br J Rheumatol 1988;27:258–64.
19. Guillevin L, Lhote F, Gayraud M, Cohen P, Jarrousse B, Lortho-lary O, et al. Prognostic factors in polyarteritis nodosa andChurg-Strauss syndrome: a prospective study in 342 patients.Medicine (Baltimore) 1996;75:17–28.
20. Masi AT, Hunder GG, Lie JT, Michel BA, Bloch DA, Arend WP,et al. The American College of Rheumatology 1990 criteria for theclassification of Churg-Strauss syndrome (allergic granulomatosisand angiitis). Arthritis Rheum 1990;33:1094–100.
21. Roufosse F, Weller PF. Practical approach to the patient withhypereosinophilia. J Allergy Clin Immunol 2010;126:39–44.
22. Luqmani RA, Bacon PA, Moots RJ, Janssen BA, Pall A, Emery P,et al. Birmingham Vasculitis Activity Score (BVAS) in systemicnecrotizing vasculitis. QJM 1994;87:671–8.
23. Guillevin L, Pagnoux C, Seror R, Mahr A, Mouthon L, LeToumelin P, the French Vasculitis Study Group (FVSG). TheFive-Factor Score revisited: assessment of prognoses of systemicnecrotizing vasculitides based on the French Vasculitis StudyGroup (FVSG) cohort. Medicine (Baltimore) 2011;90:19–27.
24. Guillevin L, Cevallos R, Durand-Gasselin B, Lhote F, Jarrousse B,Callard P. Treatment of glomerulonephritis in microscopic poly-angiitis and Churg-Strauss syndrome. Indications of plasma ex-changes: meta-analysis of 2 randomized studies on 140 patients,32 with glomerulonephritis. Ann Med Interne (Paris) 1997;148:198–204.
25. Guillevin L, Fain O, Lhote F, Jarrousse B, Le Thi Huong D,Bussel A, et al. Lack of superiority of steroids plus plasmaexchange to steroids alone in the treatment of polyarteritis nodosaand Churg-Strauss syndrome: a prospective, randomized trial in 78patients. Arthritis Rheum 1992;35:208–15.
26. Guillevin L, Lhote F, Cohen P, Jarrousse B, Lortholary O,Genereau T, et al. Corticosteroids plus pulse cyclophosphamideand plasma exchanges versus corticosteroids plus pulse cyclo-phosphamide alone in the treatment of polyarteritis nodosa andChurg-Strauss syndrome patients with factors predicting poorprognosis: a prospective, randomized trial in sixty-two patients.Arthritis Rheum 1995;38:1638–45.
27. Guillevin L, Lhote F, Jarrousse B, Fain O. Treatment of polyar-teritis nodosa and Churg-Strauss syndrome: a meta-analysis of 3prospective controlled trials including 182 patients over 12 years.Ann Med Interne (Paris) 1992;143:405–16.
28. Ribi C, Cohen P, Pagnoux C, Mahr A, Arene JP, Lauque D, et al,for the French Vasculitis Study Group. Treatment of Churg-Strauss syndrome without poor-prognosis factors: a multicenter,prospective, randomized, open-label study of seventy-two patients.Arthritis Rheum 2008;58:586–94.
29. Cohen P, Pagnoux C, Mahr A, Arene JP, Mouthon L, Le Guern V,et al, for the French Vasculitis Study Group. Churg-Strausssyndrome with poor-prognosis factors: a prospective multicentertrial comparing glucocorticoids and six or twelve cyclo-phosphamide pulses in forty-eight patients. Arthritis Rheum 2007;57:686–93.
30. Kaplan E, Meier P. Non parametric estimation from incompleteobservations. Am Stat Assoc 1958;87:161–7.
31. Peto R, Pike MC. Conservatism of the approximation sigma(O-E)2-E in the logrank test for survival data or tumor incidencedata. Biometrics 1973;29:579–84.
32. Cox DR. Regression models and life-tables. J R Stat Soc Ser B1972;34:187–219.
33. Taeger D, Sun Y, Keil U, Straif K. A stand-alone Windowsapplications for computing exact person-years, standardized mor-tality ratios and confidence intervals in epidemiological studies.Epidemiology 2000;11:607–8.
280 COMARMOND ET AL

34. Lhote F. Churg-Strauss syndrome. Presse Med 2007;36:875–89. InFrench.
35. Pagnoux C. Churg-Strauss syndrome: evolving concepts. DiscovMed 2010;9:243–52.
36. Kallenberg CG. Churg-Strauss syndrome: just one disease entity?[editorial]. Arthritis Rheum 2005;52:2589–93.
37. Baldini C, Della Rossa A, Grossi S, Catarsi E, Talarico R,d’Ascanio A, et al. Churg-Strauss syndrome: outcome and long-term follow-up of 38 patients from a single Italian centre. Reuma-tismo 2009;61:118–24. In Italian.
38. Gayraud M, Guillevin L, Cohen P, Lhote F, Cacoub P, Deblois P,et al, and the French Cooperative Study Group for Vasculitides.Treatment of good-prognosis polyarteritis nodosa and Churg-Strauss syndrome: comparison of steroids and oral or pulsecyclophosphamide in 25 patients. Br J Rheumatol 1997;36:1290–7.
39. Hellmich B, Gross WL. Recent progress in the pharmacotherapyof Churg-Strauss syndrome. Expert Opin Pharmacother 2004;5:25–35.
40. Hellmich B, Flossmann O, Gross WL, Bacon P, Cohen-TervaertJW, Guillevin L, et al, on behalf of the European Vasculitis StudyGroup. EULAR recommendations for conducting clinical studiesand/or clinical trials in systemic vasculitis: focus on anti-neutrophilcytoplasm antibody-associated vasculitis. Ann Rheum Dis 2007;66:605–17.
41. Cottin V, Khouatra C, Dubost R, Glerant JC, Cordier JF. Persis-tent airflow obstruction in asthma of patients with Churg-Strausssyndrome and long-term follow-up. Allergy 2009;64:589–95.
42. Dennert RM, van Paassen P, Schalla S, Kuznetsova T, Alzand BS,Staessen JA, et al. Cardiac involvement in Churg-Strauss syn-drome. Arthritis Rheum 2010;62:627–34.
43. Bhagirath KM, Paulson K, Ahmadie R, Bhalla RS, Robinson D,Jassal DS. Clinical utility of cardiac magnetic resonance imaging inChurg-Strauss syndrome: case report and review of the literature.Rheumatol Int 2009;29:445–9.
44. Marmursztejn J, Vignaux O, Cohen P, Guilpain P, Pagnoux C,Gouya H, et al. Impact of cardiac magnetic resonance imaging forassessment of Churg-Strauss syndrome: a cross-sectional study in20 patients. Clin Exp Rheumatol 2009;27 Suppl 52:S70–6.
45. Morgan JM, Raposo L, Gibson DG. Cardiac involvement inChurg-Strauss syndrome shown by echocardiography. Br Heart J1989;62:462–6.
46. Morita H, Yokoyama I, Yamada N, Uno K, Nagai R. Usefulnessof 18FDG/13N-ammonia PET imaging for evaluation of the cardiacdamage in Churg-Strauss syndrome. Eur J Nucl Med Mol Imaging2004;31:1218.
47. Pagnoux C, Guillevin L. Cardiac involvement in small- andmedium-sized vessel vasculitides. Lupus 2005;14:718–22.
48. Pela G, Tirabassi G, Pattoneri P, Pavone L, Garini G, Bruschi G.Cardiac involvement in the Churg-Strauss syndrome. Am J Cardiol2006;97:1519–24.
APPENDIX A: FVSG MEMBERS
The following physicians, listed alphabetically by city (inFrance, except where indicated otherwise), are currently active mem-bers of the FVSG and followed up patients included in the presentstudy: J.-P. Ducroix, R. Makdassi, A. Smail (CHU, Hopital Nord,Amiens); P. Bourrier, C. Lavigne, J.-F. Subra (CHU d’Angers, An-gers); M. Bonnefoy, A. Riche (Centre Hospitalier [CH] Saint-Michel,Angouleme); R. Sable-Fourtassou (CH Robert Ballanger, Aulnay-sous-Bois); B. Redouane (CH d’Auxerre, Auxerre); B. de Wazieres,
J.-L. Dupond (CHU, Besancon); F. Goutorbes (CH de Beziers,Beziers); S. Abad, R. Dhote (CHU Avicenne, Bobigny); E. Letellier(CHU Jean-Verdier, Bondy); O. Caubet, M.-P. Moiton (CHU deBordeaux, Hopital Haut-Leveque, Bordeaux-Pessac); S. Moreau(Hopital Ambroise-Pare, Boulogne); G. Adam (CH de Bourges,Bourges); M. Roux (CH Pierre-Oudot, Bourgoin Jallieu); B. Huraultde Ligny, P. Letellier, Y. Ollivier, G. Zalcman, K. Zoulim (CHURegional Clemenceau, Caen); L. Blum, E. Pertuiset (CH Rene-Dubos,Cergy-Pontoise); E. Giraud, C. Lecomte (CH de Chambery, Cham-bery); A. Witte (CH de Chartres, Chartres); M. Humbert, C. Le Gall(CH Antoine-Beclere, Clamart); I. Delevaux, H. Marson (CHU,Hopital Gabriel-Montpied, Clermont-Ferrand); M. Ruivard (CHUEstaing, Clermont-Ferrand); V. Rieu (CHU, Hopital Hotel-Dieu,Clermont-Ferrand); L. Federici (CH Louis-Pasteur, Colmar); P. Vey-ssier (CH de Compiegne, Compiegne); P. Bartolucci, M. Michel (CHUHenri-Mondor, Creteil); P. Bielefeld, D. Bonnotte, P. Camus (CHUde Dijon, Dijon); G. Lecapitaine, A. Saraux (CH de Montmorency,Eaubonne); A. Mehdaoui (CH d’Evreux, Evreux); F. Blanc-Jouvan(CHU de Grenoble, Grenoble); R. Azarian (CH de Versailles, LeChesnay); X. Mariette (CHU du Kremlin-Bicetre, Le Kremlin-Bicetre); D. Blockmans (CHU du Gasthuisberg, Leuven, Belgium);G. Khayat (CH Notre-Dame Perpetuel Secours, Levallois-Perret);F. Maupetit (CH de Libourne, Libourne); E. Hachulla, P.-Y. Hatron,M. Lambert, D. Launay, H. Zephir (CHU Claude-Huriez, Lille);A. Sparsa, E. Vidal (CHU Dupuytren, Limoges); B. Coppere, A. Hot,G. Madoux, J. Ninet, M. Simon (CHU, Hopital Edouard-Herriot,Lyon); A.-S. Blanchet (CHU, Hopital Louis-Pradel, Lyon-Montchat);L. Kouyoumdjian (Hopital de Mantes, Mantes-la-Jolie); K. Benia(CH de Montargis, Montargis); S. Riviere (CHU, Hopital Saint-Eloi,Montpellier); J. Laederich (CH Intercommunal Andre-Gregoire,Montreuil); C. Roge (CH des Pays de Morlaix, Morlaix); F. Chabot(CHU de Nancy, Nancy); A. Neel, T. Ponge (CHU Regional Hotel-Dieu, Nantes); P. Chevalet (Hopital Bellier, Nantes); S. Kernbaum(Hopital Americain, Neuilly-sur-Seine); J.-G. Fuzibet, P. Heudier,J.-F. Quaranta, V. Queyrel, F. Sanderson (CHU de Nice, Nice); J.-F.Pouget-Abadie (CH de Niort, Niort); B. Crestani, G. Hayem, O.Lidove, T. Papo, K. Sacre (CHU Bichat–Claude-Bernard, Paris);J.-P. Arene, A. Berezne, P. Blanche, B. Christoforov, M. de Menthon,E. Foıs, C. Ginsburg, V. Le Guern, R. Scavennec (CHU Cochin,Paris); C. Le Jeunne (CHU Hotel-Dieu, Paris); M. Gayraud (InstitutMutualiste Montsouris, Paris); J.-M. Ziza (Groupe Hospitalier [GH]Diaconesses–Croix Saint-Simon, Paris); Z. Amoura, P. Cacoub,P. Cherin, D. Le Thi Huong, B. Terrier, S. Trad, B. Wechsler (GHUniversitaire Pitie-Salpetriere, Paris); J. Cabane (CHU Saint-Antoine,Paris); L. Louis, M. Rybojad (CHU Saint-Louis, Paris); J. Benichou,L. Lequen (CH de Pau, Pau); F. Caron, D. Chatellier, C. Landron,P. Roblot (CHU de Poitiers, Poitiers); P.-Y. Leberruyer (CH Robert-Debre, Reims); C. Cazalets, O. Decaux (CHU Regional Sud,Rennes); P. Delaval (CH Pontchaillou, Rennes); S. Dominique (CHUde Rouen, Rouen); F. Lhote (Hopital Delafontaine, Saint-Denis); P.Hermant (CH Intercommunal de Poissy–Saint-Germain-en-Laye,Saint-Germain-en-Laye); J.-L. Pasquali (CHU de Strasbourg, HopitalCivil, Strasbourg); M. Stern (Hopital Foch, Suresnes); P. Carli (Hopi-tal d’Instruction des Armees Sainte-Anne, Toulon); P. Bayle-Lebey,A. Cantagrel, D. Lauque, S. Ollier, J. Pourrat, R. Viraben (CHU deToulouse, Toulouse); J.-M. Besnier, B. de Toffol, E. Diot, P. Diot,M.-C. Faure (CHU Bretonneau, Tours); P.-L. Caraman (CH RegionalMetz-Thionville, Thionville); A. Fur (CH de Troyes, Troyes); P. Brun(CH de Valence, Valence); X. Kyndt, J. Mouawad, T. Quemeneur,P. Vanhille (CH de Valenciennes, Valenciennes); P. Godmer,H. Jardel (CH Bretagne Atlantique, Vannes).
EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (CHURG-STRAUSS) 281




















