
Airway Involvement in Wegener's Granulomatosis
21
Airway Involvement in Wegener’s Granulomatosis Vlassis S. Polychronopoulos, MD a,b , Udaya B.S. Prakash, MD b , Jason M. Golbin, DO, MS b , Eric S. Edell, MD b , Ulrich Specks, MD b, * a Third Pulmonary Department, Sismanaglion General Hospital, Athens, Greece b Division of Pulmonary and Critical Care Medicine, Mayo Clinic, Rochester, MN 55905, USA Wegener’s granulomatosis is characterized by necrotizing granulomatous inflammation and necrotizing vasculitis affecting predominantly small arteries, arterioles, capillaries, and venules [1–4]. Larger vessels are rarely affected. The disease has a predilection for the upper respiratory tract, lungs, and kidneys, but any organ can be involved. The spectrum of disease ranges from limited disease affecting the nasal and paranasal tract to aggressive multisystem inflammation leading to multiple organ damage and failure [5,6]. Immunosuppressive therapy has improved the prognosis from being universally fatal with a median survival of 5 months to a treatable, chroni- cally relapsing disease with a median survival of 21.7 years (95% confidence interval, 15.6–27.86 years) after diagnosis [6,7]. The etiology of the disease remains unknown. Its response to immunosuppressive therapy and the pres- ence of antineutrophil cytoplasmic antibodies (ANCA) in most patients sug- gest autoimmune mechanisms of pathogenesis [8]. In contrast to the well-described pulmonary parenchymal involvement of Wegener’s granulomatosis, the lower airway (tracheobronchial) disease manifestations are less well recognized by clinicians. Consequently, mild dis- ease of the airways is easily missed. Airway involvement usually occurs in conjunction with disease manifestations elsewhere, but occasionally it may be the only manifestation of the disease [9]. Early in the course of the disease symptoms from active inflammatory lesions of the airways may be absent or very subtle. Frequently, they are insidious in onset and sometimes * Corresponding author. E-mail address: [email protected] (U. Specks). 0889-857X/07/$ - see front matter Ó 2007 Elsevier Inc. All rights reserved. doi:10.1016/j.rdc.2007.09.004 rheumatic.theclinics.com Rheum Dis Clin N Am 33 (2007) 755–775
-
Upload
veltechuniv -
Category
Documents
-
view
3 -
download
0
Transcript of Airway Involvement in Wegener's Granulomatosis
Rheum Dis Clin N Am 33 (2007) 755–775
Airway Involvement in Wegener’sGranulomatosis
Vlassis S. Polychronopoulos, MDa,b,Udaya B.S. Prakash, MDb, Jason M. Golbin, DO, MSb,
Eric S. Edell, MDb, Ulrich Specks, MDb,*aThird Pulmonary Department, Sismanaglion General Hospital, Athens, Greece
bDivision of Pulmonary and Critical Care Medicine, Mayo Clinic,
Rochester, MN 55905, USA
Wegener’s granulomatosis is characterized by necrotizing granulomatousinflammation and necrotizing vasculitis affecting predominantly smallarteries, arterioles, capillaries, and venules [1–4]. Larger vessels are rarelyaffected. The disease has a predilection for the upper respiratory tract, lungs,and kidneys, but any organ can be involved. The spectrum of disease rangesfrom limited disease affecting the nasal and paranasal tract to aggressivemultisystem inflammation leading to multiple organ damage and failure[5,6]. Immunosuppressive therapy has improved the prognosis from beinguniversally fatal with a median survival of 5 months to a treatable, chroni-cally relapsing disease with a median survival of 21.7 years (95% confidenceinterval, 15.6–27.86 years) after diagnosis [6,7]. The etiology of the diseaseremains unknown. Its response to immunosuppressive therapy and the pres-ence of antineutrophil cytoplasmic antibodies (ANCA) in most patients sug-gest autoimmune mechanisms of pathogenesis [8].
In contrast to the well-described pulmonary parenchymal involvement ofWegener’s granulomatosis, the lower airway (tracheobronchial) diseasemanifestations are less well recognized by clinicians. Consequently, mild dis-ease of the airways is easily missed. Airway involvement usually occurs inconjunction with disease manifestations elsewhere, but occasionally it maybe the only manifestation of the disease [9]. Early in the course of the diseasesymptoms from active inflammatory lesions of the airways may be absentor very subtle. Frequently, they are insidious in onset and sometimes
* Corresponding author.
E-mail address: [email protected] (U. Specks).
0889-857X/07/$ - see front matter � 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.rdc.2007.09.004 rheumatic.theclinics.com

756 POLYCHRONOPOULOS et al
misdiagnosed as asthma or other common airway diseases. This may resultin significant delays in arriving at the correct diagnosis [10]. Tracheobron-chial disease manifestations may also occur after remission has beenachieved with appropriate immunosuppressive therapy, and the airway dis-ease may proceed to airway scarring and stenosis [11].
There is a relative paucity of published information on various tracheo-bronchial manifestations of Wegener’s granulomatosis. Many of the reportsare based on single cases or small case series. Since the publication of theauthors’ experience with tracheobronchial manifestations of Wegener’sgranulomatosis in 51 patients [9], additional insights on this topic havebeen gained at their institution and other medical centers. This article pro-vides a comprehensive review of the diagnosis and management of the infra-glottic tracheobronchial disease manifestations.
Clinical presentation and differential diagnosis
The ease with which the diagnosis of Wegener’s granulomatosis is madedepends on the clinical presentation. When the patient presents with typicaland well-defined features of Wegener’s granulomatosis and corroboratingblood test abnormalities including positive ANCA serology, the diagnosisis readily apparent. The difficulty arises when clinical features are subtleor nonspecific, and several key elements in the diagnosis are either absentor not easily discernible.
Tracheobronchial involvement is usually associated with disease affectingthe supraglottic structures, pulmonary parenchyma, and other organ sys-tems [9,11,12]. Airway involvement is found in 15% to 55% of patientswith Wegener’s granulomatosis [9,11,13,14]. On rare occasions, however,airway involvement may be the only or the presenting feature of Wegener’sgranulomatosis. In such cases a positive ANCA test result can point to theright diagnosis, but ANCA are undetectable in about 20% of patients withWegener’s granulomatosis limited to the respiratory tract [15].
Patients younger than 30 years of age are more prone to develop airwayinvolvement. In one report on 158 patients with Wegener’s granulomatosis,23 patients were younger than 20 years of age, and 11 of them (approxi-mately 50%) developed upper tracheal involvement [16]. Women also aremore likely to develop airway disease than men [13,17]. One report has sug-gested that pregnancy may contribute both to the relapse of Wegener’s gran-ulomatosis and the occurrence of tracheal stenosis [18].
The common symptoms caused by tracheobronchial Wegener’s granulo-matosis include hoarseness, cough, hemoptysis, dyspnea, stridor, andwheezing [9,11,19]. Hoarseness and cough are not as frequent as dyspneaand wheezing, the former symptoms being reported in less than 10% of pa-tients with airway stenosis caused by Wegener’s granulomatosis [9]. Hemop-tysis is a common symptom in Wegener’s granulomatosis and has severalanatomic sources including cavitated pulmonary parenchymal lesions,
757AIRWAY INVOLVEMENT IN WEGENER’S GRANULOMATOSIS
alveolar hemorrhage, bronchiectasis, and expectoration of blood aspiratedfrom supraglottic airways, the last two being uncommon sources of hemop-tysis in Wegener’s granulomatosis.
Progressive respiratory difficulty with stridor can be the first manifesta-tion of airway involvement and may be sudden or progressive. Subglotticstenosis is the most common cause of stridor in Wegener’s granulomatosis.Conversely, the differential diagnosis in any patient with stridor shouldinclude Wegener’s granulomatosis of the upper airways. When stridor isthe first manifestation of the disease, differential diagnoses include foreignbody aspiration, trauma, acute paralysis of vocal cords, papillomatosis,and malignancy.
If cough, wheezing, and dyspnea are the main symptoms considerable de-lay in diagnosing Wegener’s granulomatosis may result from patients beingmisdiagnosed as asthmatics. Involvement of nasal passages and paranasalsinuses is common in Wegener’s granulomatosis. The resultant symptomsmay also be erroneously attributed to asthma complex. In a large cohort(N ¼ 701) of patients with Wegener’s granulomatosis, up to 15% of patientsindicated that their first symptoms had initially been attributed to asthma[10]. Substantial delays (sometimes years) in the diagnosis have beenreported in patients in whom airway symptoms were not accompanied byother more severe disease manifestations, such as glomerulonephritis[10,20]. For these reasons, it is essential for physicians to consider Wegener’sgranulomatosis in patients with airway symptoms who are initially thoughtto have asthma, but are not promptly responding to optimal asthma therapy[11,17]. Moreover, it is important to reiterate that slowly progressive airwaydisease occurs in a significant number of patients with documented Wege-ner’s granulomatosis who have been optimally treated with immunosuppres-sive agents and are considered to be in remission [21].
Physiologic features
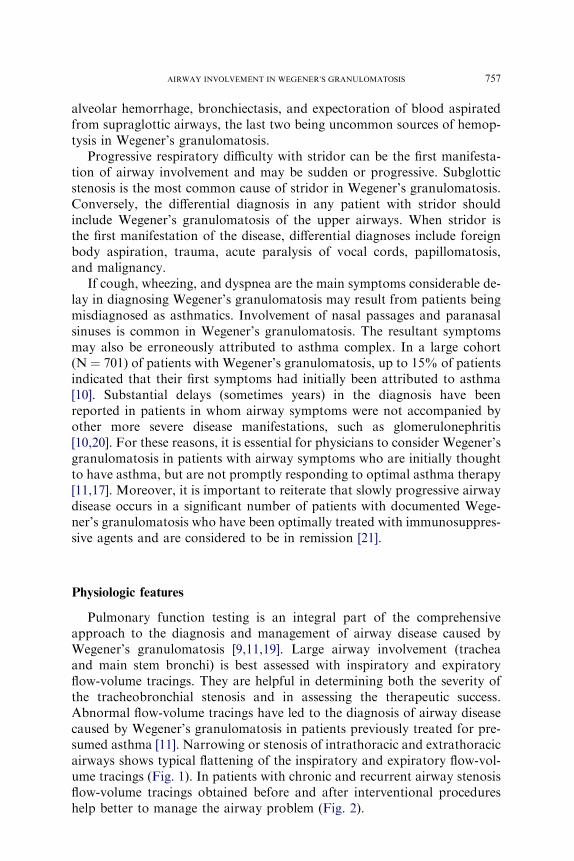
Pulmonary function testing is an integral part of the comprehensiveapproach to the diagnosis and management of airway disease caused byWegener’s granulomatosis [9,11,19]. Large airway involvement (tracheaand main stem bronchi) is best assessed with inspiratory and expiratoryflow-volume tracings. They are helpful in determining both the severity ofthe tracheobronchial stenosis and in assessing the therapeutic success.Abnormal flow-volume tracings have led to the diagnosis of airway diseasecaused by Wegener’s granulomatosis in patients previously treated for pre-sumed asthma [11]. Narrowing or stenosis of intrathoracic and extrathoracicairways shows typical flattening of the inspiratory and expiratory flow-vol-ume tracings (Fig. 1). In patients with chronic and recurrent airway stenosisflow-volume tracings obtained before and after interventional procedureshelp better to manage the airway problem (Fig. 2).
758 POLYCHRONOPOULOS et al
In addition to the flow-volume tracings, spirometric analysis of flowrates, lung volumes, and other parameters of lung function help determinethe presence or absence of obstructive airways disease. Obstructive diseaseof smaller airways occurs in patients with Wegener’s granulomatosis. Themechanisms responsible include diffuse or localized areas of bronchialluminal compromise, bronchiectasis, peribronchial scarring, and broncho-malacia. When smaller airways (lobar, segmental, or subsegmental) areinvolved, many physiologic abnormalities typical of chronic obstructivepulmonary disease are seen. A study of 22 patients with Wegener’s granu-lomatosis found that forced expiratory volume in 1 second and maximal ex-piratory flow were reduced in more than 50% of patients with airwayinvolvement [22]. Pulmonary function testing in another group of 41 pa-tients observed that 24% of patients had pulmonary symptoms and thesame percent of patients exhibited reduced diffusing capacity for carbonmonoxide, whereas forced expiratory volume in 1 second was reduced inonly 10% [23]. Reductions in lung volumes and diffusing capacity for car-bon monoxide are more likely to be caused by pulmonary parenchymalinvolvement.
Pulmonary function and flow-volume tracings are not uniformly abnor-mal in all patients with airway disease caused by Wegener’s granulomatosis.Pulmonary function test abnormalities and their severity depend on the ex-tent of compromise of the airway lumina. Particularly early in the diseaseprocess, when active inflammation has not yet caused significant scarringor stenosis, even severe tracheobronchial inflammation may be reflectedonly in subtle abnormalities of the flow-volume tracing. Furthermore,
Fig. 1. Flow-volume tracings in a patient with significant midtracheal stenosis (inset) show typ-
ical features of a fixed major airway obstruction with flattening of both the inspiratory and
expiratory flow-volume curves. Interrupted lines show predicted normal tracing.
759AIRWAY INVOLVEMENT IN WEGENER’S GRANULOMATOSIS
with mild degrees of tracheal stenosis or main stem bronchial narrowingflow-volume tracings may appear near-normal.
Imaging studies
Chest radiographs combined with CT of the chest demonstrate abnor-malities during the course of the disease in 85% of patients with Wegener’sgranulomatosis. The abnormal findings include lung nodules (often cavi-tated); consolidation; ground glass opacification; and less often pleural dis-ease, mediastinal lymphadenopathy, and interstitial processes [24]. Eventhough airway involvement occurs in approximately 50% of patients withWegener’s granulomatosis [14], these findings are less frequently appreciatedradiographically [12,24,25]. Large airway involvement by Wegener’s granu-lomatosis may consist of focal or elongated segments of stenosis, and intra-luminal and extraluminal soft tissue masses or thickening with or withoutlobar or segmental atelectasis [24,26]. In patients with significant airway dis-ease, airway narrowing as depicted by CT can be extensive. Other findings
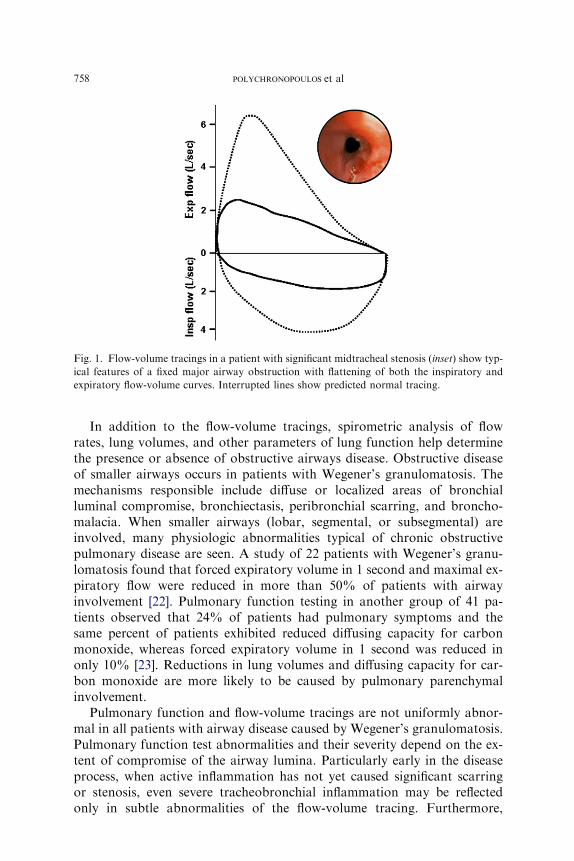
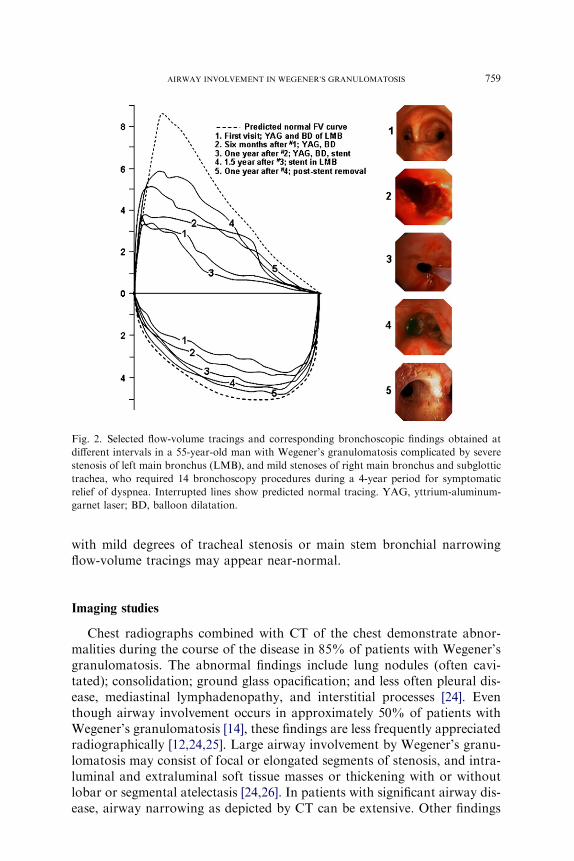
Fig. 2. Selected flow-volume tracings and corresponding bronchoscopic findings obtained at
different intervals in a 55-year-old man with Wegener’s granulomatosis complicated by severe
stenosis of left main bronchus (LMB), and mild stenoses of right main bronchus and subglottic
trachea, who required 14 bronchoscopy procedures during a 4-year period for symptomatic
relief of dyspnea. Interrupted lines show predicted normal tracing. YAG, yttrium-aluminum-
garnet laser; BD, balloon dilatation.
760 POLYCHRONOPOULOS et al
include calcification and thickening of the tracheal rings [24]. In one reporton 30 patients with Wegener’s granulomatosis, large airways were found tobe abnormal in nine (30%) patients, and bronchial wall thickening in thesegmental and subsegmental bronchi was discovered in 22 (73%) patients[27]. The airway lesions showed complete or partial improvement with treat-ment. In this series of patients, bronchiectasis was found in four (13%)patients [27]. Bronchial abnormalities, including bronchiectasis and peri-bronchial thickening of the small airways, have been reported in approxi-mately 40% of cases [28–30].
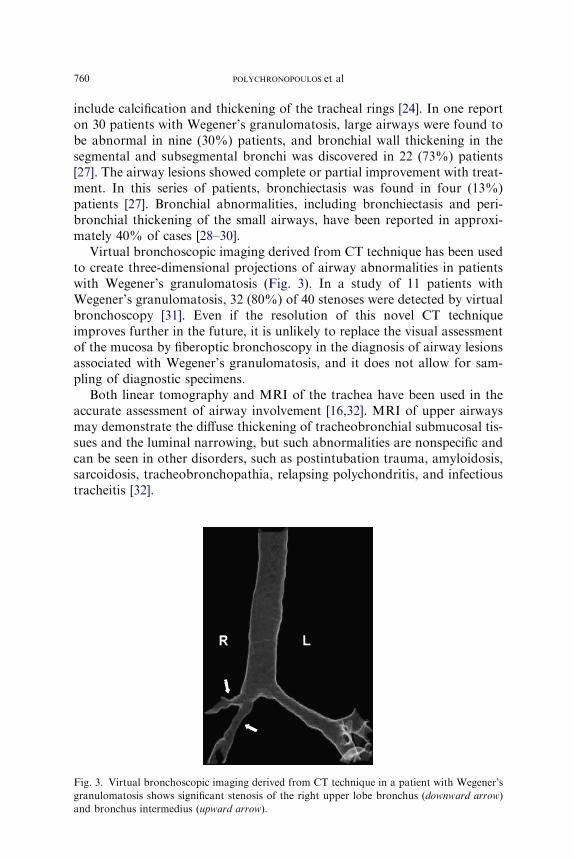
Virtual bronchoscopic imaging derived from CT technique has been usedto create three-dimensional projections of airway abnormalities in patientswith Wegener’s granulomatosis (Fig. 3). In a study of 11 patients withWegener’s granulomatosis, 32 (80%) of 40 stenoses were detected by virtualbronchoscopy [31]. Even if the resolution of this novel CT techniqueimproves further in the future, it is unlikely to replace the visual assessmentof the mucosa by fiberoptic bronchoscopy in the diagnosis of airway lesionsassociated with Wegener’s granulomatosis, and it does not allow for sam-pling of diagnostic specimens.
Both linear tomography and MRI of the trachea have been used in theaccurate assessment of airway involvement [16,32]. MRI of upper airwaysmay demonstrate the diffuse thickening of tracheobronchial submucosal tis-sues and the luminal narrowing, but such abnormalities are nonspecific andcan be seen in other disorders, such as postintubation trauma, amyloidosis,sarcoidosis, tracheobronchopathia, relapsing polychondritis, and infectioustracheitis [32].
Fig. 3. Virtual bronchoscopic imaging derived from CT technique in a patient with Wegener’s
granulomatosis shows significant stenosis of the right upper lobe bronchus (downward arrow)
and bronchus intermedius (upward arrow).

761AIRWAY INVOLVEMENT IN WEGENER’S GRANULOMATOSIS
The imaging procedures are helpful in the overall assessment of pulmo-nary involvement by Wegener’s granulomatosis. The clinical applicabilityof imaging in the management of airway involvement is limited.
Bronchoscopy
Endoscopic visualization of the airways remains the major diagnosticprocedure in the evaluation, diagnosis, and management of airway diseasein Wegener’s granulomatosis. The various airway abnormalities are listedin Table 1, and Table 2 summarizes the most important case series reportsfocusing on airway pathology in Wegener’s granulomatosis. The supraglot-tic airways can be assessed by examining the nasal passages and obtainingtissue biopsies for histologic documentation of the disease. Laryngoscopypermits detailed examination of oropharynx, nasopharynx, epiglottic, glot-tis, and larynx. Bronchoscopy is the most important diagnostic procedure inthe assessment of location and the degree of airway involvement below thevocal cords, the nature of luminal abnormalities, and the feasibility of bron-choscopic therapy to restore functional airway patency. Bronchoscopy isalso used for diagnostic tissue sampling, and it is valuable in the evaluationof the efficacy of both pharmacologic and interventional therapy of the air-way involvement in Wegener’s granulomatosis.
The symptoms related to airway disease from Wegener’s granulomatosismay remain undiagnosed or misdiagnosed until clinical suspicion promptsbronchoscopy. Similarly, a cursory bronchoscopy can easily overlook subtlechanges in the airways, particularly in the subglottic trachea. The bronchos-copist should be cognizant of the possibility of Wegener’s granulomatosisaffecting the tracheobronchial tree and carefully examine the airway lumenand describe the abnormalities. If suspicious mucosal abnormalities aredetected, adequate tissue samples should be obtained for histologic docu-mentation of the diagnosis. A significant number of patients with knownand treated airway disease from Wegener’s granulomatosis require repeated,periodic, bronchoscopies for the re-evaluation of airway lumen and to detectlocalized disease recurrence. Ideally, the findings should be recorded in thereport and by photographic documentation.
The following paragraphs provide more detailed information regardingthe types of airway involvement, bronchoscopic findings, and managementoptions to treat symptomatic airway involvement.
Types of airway involvement
Airway involvement is present in 15% to 55% of patients with Wegener’sgranulomatosis [11,13,14,33–37]. Because the airway manifestations in thisdisease are varied, it is difficult to classify them in any specific manner.The following discussions encompass the common and uncommon airway

762 POLYCHRONOPOULOS et al
abnormalities encountered in this disease (see Tables 1 and 2). The type andseverity of symptoms are dependent on a variety of factors, including thespecific nature of the lesion, the extent of airway luminal involvement andits location, and the sequelae airway obstruction.
Mucosal abnormalities
In Wegener’s granulomatosis, mucosal abnormalities can occur any-where in the tracheobronchial tree; they are usually patchy in distributionand may occur as isolated lesions. The most common airway abnormality
Table 1
Types of airway abnormalities described in Wegener’s granulomatosis
Supraglottic airways
Nasal passages Mucosal ulceration
Hemorrhagic mucosal lesions
Crusting of mucosa
Nose Saddle nose deformity
Sinuses Sinusitis
Ears Otitis media
Oropharynx Gingivitis
Ulceration and hemorrhage
Epiglottis Ulceration and hemorrhage
Edema
Granuloma
Glottis and larynx Edema
Ulceration and hemorrhage
Stenosisa
Granuloma
Nodules and masses
Trachea and bronchi Mucosal edema and erythema
Ulceration and hemorrhage
Cobble-stone mucosa
Nodule and mass (pseudotumor)
Polyps and pseudopolyps
Submucosal tunnels
Luminal synechial bands
Membrane formation
Mucosal lattice
Stenotic (transluminal)
Stenosis (subglottic)a
Simple (localized)
Complex (multiple)
Stenosis (tracheobronchial)a
Simple (localized)
Complex (multiple)
Necrosis of airway
Cartilaginous deformities
Tracheobronchomalacia
Tracheoesophageal fistula
a Large airway stenosis can be reversible or fixed.
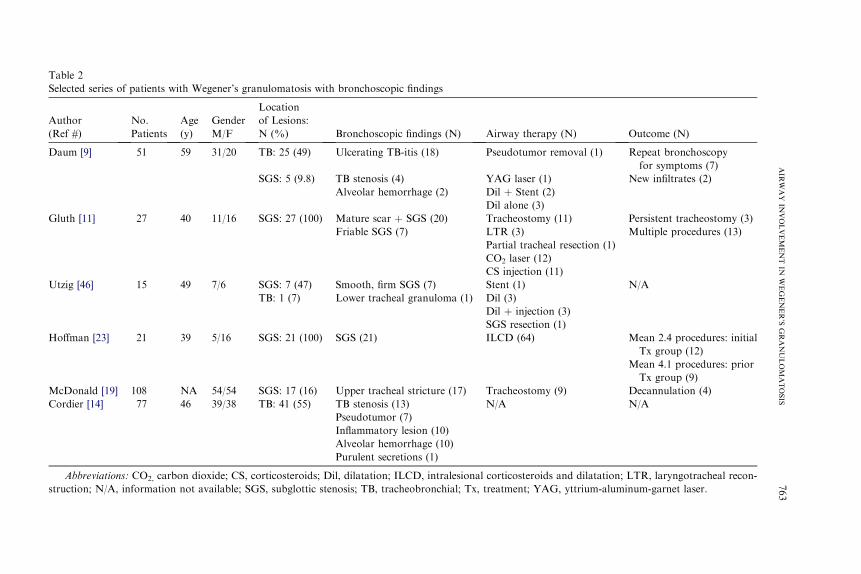
Table 2
Selected series of patients with Wegener’s granulomatosis with bronchoscopic findings
A
( erapy (N) Outcome (N)
D or removal (1) Repeat bronchoscopy
for symptoms (7)
r (1) New infiltrates (2)
nt (2)
(3)
G omy (11) Persistent tracheostomy (3)
Multiple procedures (13)
cheal resection (1)
(12)
on (11)
U N/A
ction (3)
tion (1)
H ) Mean 2.4 procedures: initial
Tx group (12)
Mean 4.1 procedures: prior
Tx group (9)
M omy (9) Decannulation (4)
C N/A
roids and dilatation; LTR, laryngotracheal recon-
s YAG, yttrium-aluminum-garnet laser.
763
AIR
WAY
INVOLVEMENT
INWEGENER’S
GRANULOMATOSIS
uthor
Ref #)
No.
Patients
Age
(y)
Gender
M/F
Location
of Lesions:
N (%) Bronchoscopic findings (N) Airway th
aum [9] 51 59 31/20 TB: 25 (49) Ulcerating TB-itis (18) Pseudotum
SGS: 5 (9.8) TB stenosis (4) YAG lase
Alveolar hemorrhage (2) Dil þ Ste
Dil alone
luth [11] 27 40 11/16 SGS: 27 (100) Mature scar þ SGS (20) Tracheost
Friable SGS (7) LTR (3)
Partial tra
CO2 laser
CS injecti
tzig [46] 15 49 7/6 SGS: 7 (47) Smooth, firm SGS (7) Stent (1)
TB: 1 (7) Lower tracheal granuloma (1) Dil (3)
Dil þ inje
SGS resec
offman [23] 21 39 5/16 SGS: 21 (100) SGS (21) ILCD (64
cDonald [19] 108 NA 54/54 SGS: 17 (16) Upper tracheal stricture (17) Tracheost
ordier [14] 77 46 39/38 TB: 41 (55) TB stenosis (13) N/A
Pseudotumor (7)
Inflammatory lesion (10)
Alveolar hemorrhage (10)
Purulent secretions (1)
Abbreviations: CO2, carbon dioxide; CS, corticosteroids; Dil, dilatation; ILCD, intralesional corticoste
truction; N/A, information not available; SGS, subglottic stenosis; TB, tracheobronchial; Tx, treatment;
764 POLYCHRONOPOULOS et al
in Wegener’s granulomatosis consists of mucosal edema, erythema, thick-ening, and granularity of mucosal surface. Shallow mucosal ulcers maybe interspersed throughout the tracheobronchial tree. Ulcerated lesionsare responsible for hemoptysis, but the extent of hemoptysis is not asvoluminous as sometimes associated with cavitated lesions and alveolarhemorrhage. In patients with ulcerating tracheobronchial lesions, theinflammation is often associated with the narrowing of tracheal or bron-chial lumen [9]. Cobble-stoning of the mucosa is also the result of activeinflammation. It is very likely that prolonged mucosal inflammation fol-lowed by fibrosis is responsible for the eventual formation of bronchialstenosis.
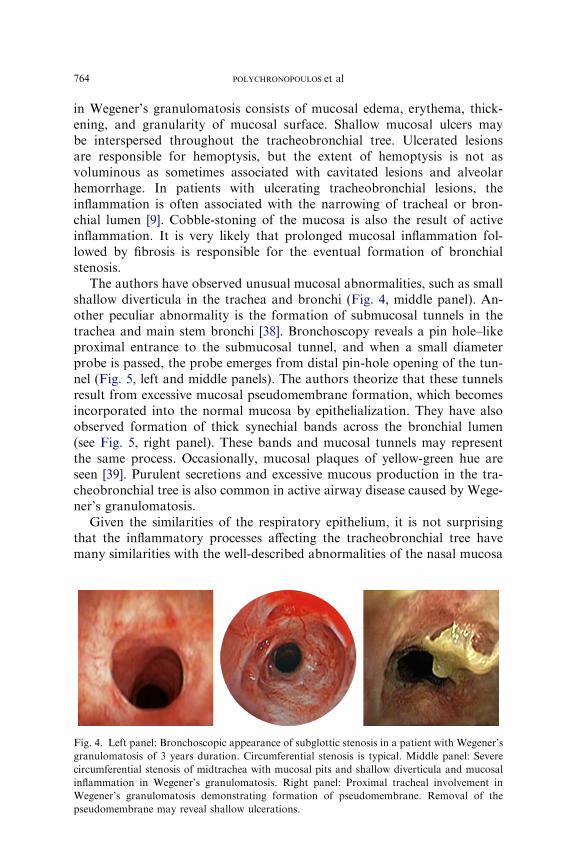
The authors have observed unusual mucosal abnormalities, such as smallshallow diverticula in the trachea and bronchi (Fig. 4, middle panel). An-other peculiar abnormality is the formation of submucosal tunnels in thetrachea and main stem bronchi [38]. Bronchoscopy reveals a pin hole–likeproximal entrance to the submucosal tunnel, and when a small diameterprobe is passed, the probe emerges from distal pin-hole opening of the tun-nel (Fig. 5, left and middle panels). The authors theorize that these tunnelsresult from excessive mucosal pseudomembrane formation, which becomesincorporated into the normal mucosa by epithelialization. They have alsoobserved formation of thick synechial bands across the bronchial lumen(see Fig. 5, right panel). These bands and mucosal tunnels may representthe same process. Occasionally, mucosal plaques of yellow-green hue areseen [39]. Purulent secretions and excessive mucous production in the tra-cheobronchial tree is also common in active airway disease caused by Wege-ner’s granulomatosis.
Given the similarities of the respiratory epithelium, it is not surprisingthat the inflammatory processes affecting the tracheobronchial tree havemany similarities with the well-described abnormalities of the nasal mucosa
Fig. 4. Left panel: Bronchoscopic appearance of subglottic stenosis in a patient with Wegener’s
granulomatosis of 3 years duration. Circumferential stenosis is typical. Middle panel: Severe
circumferential stenosis of midtrachea with mucosal pits and shallow diverticula and mucosal
inflammation in Wegener’s granulomatosis. Right panel: Proximal tracheal involvement in
Wegener’s granulomatosis demonstrating formation of pseudomembrane. Removal of the
pseudomembrane may reveal shallow ulcerations.

765AIRWAY INVOLVEMENT IN WEGENER’S GRANULOMATOSIS
in Wegener’s granulomatosis. Furthermore, many of the mucosal abnormal-ities described previously are not specific for Wegener’s granulomatosis.Similar findings can be encountered in airway involvement in acute infec-tious or noninfectious tracheobronchitis, submucosal spread of malignancy,endobronchial sarcoidosis, tracheobronchial amyloidosis, and fungaltracheobronchitis.
Masses and polyps
Wegener’s granulomatosis can cause tracheal or bronchial mass lesions,which have also been referred to as ‘‘inflammatory pseudotumor’’ [9].Such lesions mimic malignancy and call for optimal biopsy specimens to es-tablish Wegener’s granulomatosis as the cause [9]. Case reports of trachealmass protruding into the airway lumen have been described [40]. Polypoidlesions and mucosal projections into the airway lumen also occur and mimicmalignancy (Fig. 6). These lesions may ulcerate and cause hemoptysis. The
Fig. 5. Submucosal tunnel in the trachea of a patient with Wegener’s granulomatosis. The left
panel reveals a pin-hole like proximal entrance to the submucosal tunnel, and the middle panel
shows a probe passed through the aperture emerging from the distal opening of the tunnel.
Right panel: Thick synechial band across the bronchial lumen in a patient with Wegener’s
granulomatosis.
Fig. 6. Left panel: A polypoid lesion in the distal main bronchus in a patient with Wegener’s
granulomatosis. These lesions are friable and usually reveal granulation tissue on histologic
analysis. Middle panel: Distal tracheal mass-like lesion (inflammatory pseudotumor) caused
by Wegener’s granulomatosis. Right panel: The airway obstruction required rigid broncho-
scopic insertion of a silicone stent to provide symptomatic relief.
766 POLYCHRONOPOULOS et al
tracheobronchial luminal masses can be present at the time of presentationof the disease or at the time of relapse [41]. They are generally a reflection ofactive disease. On rare occasions, rapidly proliferative tissue growth maylead to acute laryngotracheal airway obstruction and death [42]. Biopsy ofthese lesions may show characteristic histopathologic features of Wegener’sgranulomatosis, various degrees of fibrosis, or granulation tissue [36,42].
Subglottic stenosis
Subglottic stenosis is the most frequent airway manifestation in Wege-ner’s granulomatosis (see Fig. 4, left panel). Depending on the acuity of on-set and the degree of airway compromise, it can be life threatening.Subglottic stenosis may occur at initial presentation or later in the courseof the disease. When the airway obstruction is caused by fibrotic scarring(damage occurring in the process of healing inflammation) rather than byactive inflammation, it develops independently of other features of Wege-ner’s granulomatosis and is unresponsive to systemic immunosuppressivetherapy [43].
The reported frequency of subglottic stenosis has ranged from 8.5% to50% of patients [44,45]. The numbers derived from reports focusing on air-way manifestations of Wegener’s granulomatosis are difficult to interpretbecause of highly variable selection bias. For instance, in the Mayo Clinicseries of 51 patients with Wegener’s granulomatosis, subglottic stenosiswas found in 10%, but only patients who had undergone bronchoscopywere included, thus not including those subglottic stenosis detected on lar-yngoscopy [9]. In two other studies subglottic stenosis, tracheobronchitis,and tracheal or bronchial narrowing were identified at bronchoscopy in55% and 59% of patients, respectively [14,25]. In a group of 108 patientswith Wegener’s granulomatosis, direct laryngoscopy in 17 patients showedsubglottic stenosis in all [19]. In another group of 15 patients with Wegener’sgranulomatosis, eight had tracheal involvement and all but one showed in-volvement of the subglottic area [46].
Information derived from large cohorts of patients with Wegener’s gran-ulomatosis does not provide more clarity. Among the 158 patients with We-gener’s granulomatosis seen at the National Institute of Health, 25 (16%)had subglottic stenosis, but the degree of inflammatory activity is not spec-ified [16]. Among the 180 patients enrolled with newly diagnosed or relaps-ing disease into the Wegener’s granulomatosis etanercept trial, 8.3% haddocumented active subglottic inflammation at the time of enrollment [47].A subsequent analysis of damage in this cohort found that 17.8% had sub-glottic stenosis scored as a damage item at completion of the trial, but it isnot stated how many of the patients enrolled with a relapse already had sub-glottic stenosis as a damage item scored at enrollment [48].
Based on individual personal observations and the interpretation of theliterature the following concept emerges. Subglottic (tracheobronchial)

767AIRWAY INVOLVEMENT IN WEGENER’S GRANULOMATOSIS
inflammation is a common feature at the time of active disease. At this stageerythematous, edematous, and friable mucosa and ulcerations can be de-tected, and the lesions are typically circumferential. In most cases symptomsare mild or absent because the vocal cords are usually not affected, and theairway is not compromised. Consequently, the early inflammatory lesionsmay remain undetected, unless specifically looked for. If the inflammationis not treated and if fibrotic scarring occurs during the resolution of in-flammation, significant compromise of the airway lumen develops, causingstridor and dyspnea (see Fig. 4, left panel). In the absence of persistentactive inflammation, the development of subglottic stenosis should not bemisinterpreted to indicate failure of immunosuppressive therapy. Serial pul-monary function tests and inspiratory and expiratory flow-volume tracingsmay aid in follow-up of patients with subglottic inflammation and stenosis(see Fig. 2).
Subglottic involvement can occasionally be an isolated finding [49]. Insuch patients the attribution of this lesion to underlying Wegener’s granulo-matosis may only be possible with a diagnostic biopsy specimen or a positiveANCA test result. In the absence of evidence for Wegener’s granulomatosisin other organs, other causes of isolated subglottic stenosis should be ex-cluded. These include postintubation stenosis, idiopathic subglottic stenosis,postinfectious stenosis, hypocomplementemic urticarial vasculitis, andextrinsic compression [50,51].
Tracheobronchial stenosis
Similar inflammatory processes described for the subglottic region canoccur at any level of the tracheobronchial tree and lead to stenoses. Thesecan be simple (a localized tracheal segmental stenosis) or complex (multipletracheal segmental stenoses with luminal distortion). Most of the trachealand bronchial stenoses are circumferential, and the mucosa in the stenoticsegment and just above and below reveals mucosal thickening (see Fig. 4,middle panel). In acute and active disease, the stenotic area may exhibiterythematous and edematous mucosa, with formation of pseudomembraneand ulceration (see Fig. 4, right panel). Tracheal stenosis produces symp-toms similar to those in patients with subglottic stenosis. If stenosis isaccompanied by significant mucosal inflammation and ulceration, hemopty-sis occurs. Excessive instrumentation and biopsy may lead to hemorrhage,but this is usually easily controlled.
In isolated cases of tracheal stenosis caused by Wegener’s granulomato-sis, the following causes of focal stenosis should be excluded: postintubationstenosis; postinfectious stenosis; posttransplantation stenosis; and varioussystemic diseases that may also involve the airways and lead to focal stenosisincluding Crohn’s disease, sarcoidosis, and Behcet’s syndrome. In therare event of diffuse tracheal involvement, other diseases more likely tocause diffuse tracheal disease, such as relapsing polychondritis,
768 POLYCHRONOPOULOS et al
tracheobronchopathia osteochondroplastica, tracheobronchial amyloidosis,and papillomatosis, need to be excluded [39].
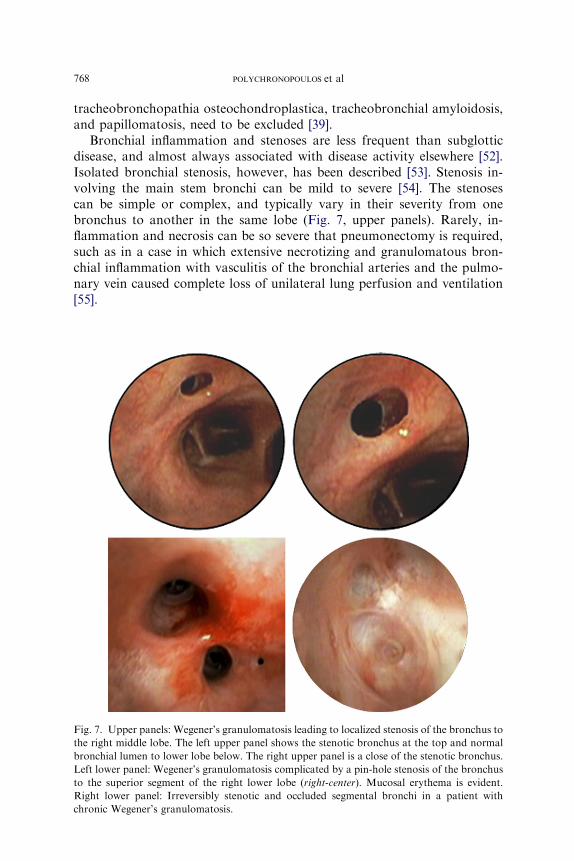
Bronchial inflammation and stenoses are less frequent than subglotticdisease, and almost always associated with disease activity elsewhere [52].Isolated bronchial stenosis, however, has been described [53]. Stenosis in-volving the main stem bronchi can be mild to severe [54]. The stenosescan be simple or complex, and typically vary in their severity from onebronchus to another in the same lobe (Fig. 7, upper panels). Rarely, in-flammation and necrosis can be so severe that pneumonectomy is required,such as in a case in which extensive necrotizing and granulomatous bron-chial inflammation with vasculitis of the bronchial arteries and the pulmo-nary vein caused complete loss of unilateral lung perfusion and ventilation[55].
Fig. 7. Upper panels: Wegener’s granulomatosis leading to localized stenosis of the bronchus to
the right middle lobe. The left upper panel shows the stenotic bronchus at the top and normal
bronchial lumen to lower lobe below. The right upper panel is a close of the stenotic bronchus.
Left lower panel: Wegener’s granulomatosis complicated by a pin-hole stenosis of the bronchus
to the superior segment of the right lower lobe (right-center). Mucosal erythema is evident.
Right lower panel: Irreversibly stenotic and occluded segmental bronchi in a patient with
chronic Wegener’s granulomatosis.

769AIRWAY INVOLVEMENT IN WEGENER’S GRANULOMATOSIS
Symptoms of patients with bronchial inflammation or stenosis may in-clude cough; wheezing (often localized or asymmetric); and dyspnea (ifthe mainstem bronchi or multiple segments are affected). As in patientswith tracheal stenosis, hemoptysis is more likely in acute inflammatory dis-ease with significant mucosal involvement, ulceration, and nodular or polyp-oid changes.
Lesions occurring in the lobar or segmental bronchi lead to concentricnarrowing of the lumen, which becomes progressively more severe (seeFig. 7). In patients with chronic and active Wegener’s granulomatosisinvolving the bronchial tree, bronchoscopy may demonstrate early stagesof the stenotic process in the form of thin semitranslucent membranescovering the bronchial lumen. Most of the severely narrowed bronchibecome irreversibly occluded from fibrotic scarring (see Fig. 7, right lowerpanel).
Other airway abnormalities
Wegener’s granulomatosis affecting the airways occasionally leads to tra-cheomalacia or bronchomalacia [9]. Even though CT imaging has shownbronchiectasis in patients with Wegener’s granulomatosis, significant clini-cal features of bronchiectasis are described only occasionally [56,57]. Anunusual case of Wegener’s granulomatosis presenting as paratracheal medi-astinal lesion with tracheal wall invasion, which responded dramatically tocorticosteroid treatment, has been described [58]. Cases of right middle lobesyndrome and acquired tracheoesophageal fistula caused by Wegener’sgranulomatosis have also been described [59,60].
Histology
In a report on pathologic features in 87 open lung biopsies from 67patients with Wegener’s granulomatosis, the following were detected inthe airways: bronchial or bronchiolar lesions including acute and chronicbronchiolitis (51% and 64%); follicular bronchiolitis (28%); and bronchio-litis obliterans (31%). Bronchial stenosis was found in three specimens [36].In contrast to open-lung biopsy, bronchoscopic tissue sampling of tracheo-bronchial luminal abnormalities reveals typical histologic features of Wege-ner’s granulomatosis only in a minority of cases. In previously reportedexperience, biopsies of tracheobronchial mucosa in 17 patients with Wege-ner’s granulomatosis showed changes diagnostic of the disease in only threepatients with an additional seven patients showing features that were inter-preted as supportive of the diagnosis in the given clinical context [9]. Simi-larly, biopsy of mass-like lesions and polypoid lesions in the airways ofpatients with active disease may reveal typical features of Wegener’s granu-lomatosis. In many cases, however, the tissue analysis reveals granulationtissue or nonspecific inflammation.
770 POLYCHRONOPOULOS et al
Management
Treatment of airway disease in Wegener’s granulomatosis can be broadlyclassified into medical and nonmedical types.
PharmacologicGlucocorticoids (systemic, topical, intralesional)Cytotoxic agentsAntibioticsImmunomodulatorsOthers
NonpharmacologicAirway debridement (laser, electrocautery, and so forth)Airway dilatationStent insertionLaryngotracheoplastyResection or reanastomosis of stenotic segmentsTracheostomy
Many patients respond well to appropriate medical therapy, with resolu-tion of the airway disease. In a significant number of patients, however,tracheobronchial stenosis occurs, persists, or recurs, despite prolonged im-munosuppressive therapy. This group of patients requires nonmedical (in-terventional) approaches for the relief of their symptoms.
Medical
The general principles of medical therapy for Wegener’s granulomatosisapply also to patients who have tracheobronchial involvement. The severityof disease governs the choice of the initial remission induction regimen. If thedisease severity is judged to be life threatening or putting an affected organ atrisk for irreversible damage, glucocorticoids in combination with cyclophos-phamide remains the treatment of choice. In less severe cases, methotrexateis the preferred alternative to cyclophosphamide. Successful remission in-duction is followed by less aggressive remission maintenance therapy witheither methotrexate or azathioprine. Regardless of the severity of otherorgan manifestations, severe tracheobronchial disease should initially betreated with the combination of oral glucocorticoids and cyclophosphamide.Methotrexate should only be considered as remission induction agent if thereis no compromise of airway lumen, and the bronchoscopically apparent‘‘inflammatory burden’’ is mild or affected isolated segmental bronchi.
In addition, in the authors’ practice patients with documented tracheo-bronchial disease are treated with high-dose inhaled glucocorticoids, suchas fluticasone, 440 to 880 mg twice daily. Inhaled glucocorticoid therapy isusually initiated when the oral glucocorticoid dose has been tapered to dailydoses less than 30 mg. The role of intralesional injection of long-actingglucocorticoids is described later.
771AIRWAY INVOLVEMENT IN WEGENER’S GRANULOMATOSIS
Nonmedical
The management of subglottic disease in Wegener’s granulomatosisremains a therapeutic dilemma. This complication often occurs indepen-dently of other features of active Wegener’s granulomatosis and is fre-quently unresponsive to systemic immunosuppressive therapy. Almost allnonmedical therapies consist of invasive procedures aimed at mechanicallyrelieving the airway obstruction. The types of treatments have included in-tralesional injection of corticosteroids; balloon dilatation; mechanical sub-glottic dilation (bouginage); laser ablation; intraluminal stent placement;tracheostomy; and surgical resection and reanastomosis [12,19,43,44,61–64]. Some of these procedures must be repeated to provide symptomaticrelief. In patients with critical airway stenosis that is unresponsive to medi-cal and dilatational therapies, tracheostomy provides long-term relief. Inone series of 27 patients with Wegener’s granulomatosis and subglottic ste-nosis, 11 (41%) underwent tracheotomy and 13 (48%) required multiplesurgical procedures [11].
Tracheostomy has been recommended as the first-line surgical treatmentin the presence of airway obstruction [17]. This recommendation should betempered with assessment of the severity of respiratory distress. It has beensuggested that airway manipulation be minimal or avoided during diseaseactivity because this may aggravate upper airway obstruction [11]. If clinicalevaluation does not indicate the need for urgent tracheostomy, appropriateimmunosuppressive therapy first should be administered. Induction of re-mission with glucocorticoids and cytotoxic agents, however, does not alwaysprevent the progression of subglottic stenosis. Patients with known activesubglottic inflammation need to be observed and followed carefully.
Intralesional long-acting corticosteroid injection combined with luminaldilatation has been used to treat subglottic stenosis caused by Wegener’sgranulomatosis [13,44,46,65]. Among 21 patients who underwent 64 proce-dures, methylprednisolone acetate was injected directly into the stenoticsegment, followed by microsurgical lysis of the stenotic ring and serialdilatation with Maloney bougies or Fogarty catheter balloon [13]. Theprocedure was repeated at a later date if restenosis occurred. The meanfollow-up was 40.6 months. In patients without luminal scarring from pre-vious procedures, a mean of 2.4 procedures were required at mean intervalsof 11.6 months to maintain subglottic patency; complications included twocases of pneumothorax [13]. More recently, some laryngologists have alsolocally injected mitomycin C because of its antifibrotic properties, but theoutcomes of this approach have not been formally assessed.
Bronchoscopic intervention to treat airway involvement in Wegener’sgranulomatosis is an important therapeutic option for patients with signif-icant or progressive airway symptoms. Bronchoscopic applications includemechanical debulking of endoluminal masses and tissue, rigid broncho-scopic dilatation of major airway stenosis, flexible bronchoscopic balloon
772 POLYCHRONOPOULOS et al
dilatation laser ablation, and endoluminal stent insertion (see Figs. 2 and 6,right panel) [9]. Successful bronchoscopic dilatation of airway stenosiscaused by Wegener’s granulomatosis has been reported in a small numberof patients [66]. Many patients require repeated therapeutic interventionsbecause of recurrent airway stenosis. Of all the bronchoscopic interventions,silicone stents seem to provide the most long-lasting symptomatic relief [9].Insertion of these stents requires expertise in rigid bronchoscopy. Becausethere is no consensus regarding the optimal type of bronchoscopic therapyfor the airway disease caused by Wegener’s granulomatosis, each caseshould be evaluated on an individual basis and suitable therapy selected.Ideally, manipulations of the airways in patients with Wegener’s granuloma-tosis should only be performed at specialized centers with extensive experi-ence with both the disease and interventional bronchoscopy.
Extensive surgical options are not recommended in patients with activedisease. In appropriate cases, resection and anastomosis have been success-fully performed [46,62]. Among 158 patients with Wegener’s granulomatosisseen at the National Institutes of Health, 25 (16%) had subglottic stenosisand their symptoms varied from minimal to life-threatening. Sixteen(80%) of 20 patients with fixed subglottic stenosis required surgical inter-vention, including manual dilations, carbon-dioxide laser resections, andlaryngotracheoplasty with and without microvascular reconstruction [16].Following resection of the stenotic lesion, disease reactivation can occurin the remaining subglottis and may lead to dehiscence of anastomotic sitesand recurrent stenosis [19]. In unusual cases of severe airway involvement,such as bronchial necrosis, treatment has required pneumonectomy [55,67].
Anecdotal patients with Wegener’s granulomatosis have been treatedwith external beam radiation therapy for severe airway inflammation[34,68]. This form of treatment is not routinely used, however, and cannotbe recommended.
Summary
Wegener’s granulomatosis affects the tracheobronchial tree in more thanhalf of the patients with the disease. The airway involvement can be an iso-lated presentation, part of the fully developed multisystem disease, ora chronic complication of progressive disease or disease in remission. Symp-toms are dependent on the degree of airway narrowing and may includewheezing, dyspnea, cough, and hemoptysis. The severity can vary frommild wheezing and dyspnea to life-threatening stridor. Clinical features, pul-monary function test, imaging studies, and bronchoscopy are helpful in thediagnosis and management of airway complications in patients with Wege-ner’s granulomatosis. Bronchoscopic findings include mucosal inflamma-tion, ulceration and hemorrhage, formation of pseudomembrane, mucosaltunneling, luminal masses, simple or complex airway stenosis, and tracheo-bronchomalacia. Therapeutic options for the treatment of airway
773AIRWAY INVOLVEMENT IN WEGENER’S GRANULOMATOSIS
involvement caused by Wegener’s granulomatosis include pharmacologicagents, bronchoscopic interventions, and surgical techniques.
References
[1] Wegener F. On generalised septic vessel diseases. Thorax 1987;42:918–9.
[2] Godman GC, Churg J. Wegener’s granulomatosis: pathology and review of the literature.
AMA Arch Path 1954;58:533–53.
[3] Leavitt RY, Fauci AS, Bloch DA, et al. The American College of Rheumatology 1990
criteria for the classification ofWegener’s granulomatosis. Arthritis Rheum 1990;33:1101–7.
[4] Jennette JC, FalkRJ, AndrassyK, et al. Nomenclature of systemic vasculitides: the proposal
of an international consensus conference. Arthritis Rheum 1994;37:187–92.
[5] Hoffman GS, Kerr GS, Leavitt RY, et al. Wegener granulomatosis: an analysis of 158
patients. Ann Intern Med 1992;116:488–98.
[6] Reinhold-Keller E, Beuge N, Latza U, et al. An interdisciplinary approach to the care of
patients with Wegener’s granulomatosis: long-term outcome in 155 patients. Arthritis
Rheum 2000;43(5):1021–32.
[7] Walton EW. Giant-cell granuloma of the respiratory tract (Wegener’s granulomatosis).
Br Med J 1958;2:265–70.
[8] Hewins P, Tervaert JW, Savage CO, et al. Is Wegener’s granulomatosis an autoimmune dis-
ease? Curr Opin Rheumatol 2000;12(1):3–10.
[9] Daum TE, Specks U, Colby TV, et al. Tracheobronchial involvement in Wegener’s granu-
lomatosis. Am J Respir Crit Care Med 1995;151(2 Pt 1):522–6.
[10] Abdou NI, Kullman GJ, Hoffman GS, et al. Wegener’s granulomatosis: survey of 701
patients inNorthAmerica.Changes in outcome in the 1990s. JRheumatol 2002;29(2):309–16.
[11] Gluth MB, Shinners PA, Kasperbauer JL. Subglottic stenosis associated with Wegener’s
granulomatosis. Laryngoscope 2003;113(8):1304–7.
[12] Shapshay SM, Valdez TA. Bronchoscopic management of benign stenosis. Chest Surg Clin
N Am 2001;11(4):749–68.
[13] HoffmanGS, Thomas-Golbanov CK, Chan J, et al. Treatment of subglottic stenosis, due to
Wegener’s granulomatosis, with intralesional corticosteroids and dilation. J Rheumatol
2003;30(5):1017–21.
[14] Cordier JF, Valeyre D, Guillevin L, et al. Pulmonary Wegener’s granulomatosis: a clinical
and imaging study of 77 cases. Chest 1990;97(4):906–12.
[15] Lee AS, Finkielman JD, Peikert T, et al. Agreement of anti-neutrophil cytoplasmic antibody
measurements obtained from serum and plasma. Clin Exp Immunol 2006;146(1):15–20.
[16] Lebovics RS, Hoffman GS, Leavitt RY, et al. The management of subglottic stenosis in
patients with Wegener’s granulomatosis. Laryngoscope 1992;102(12 Pt 1):1341–5.
[17] Alaani A,HoggRP,DrakeLeeAB.Wegener’s granulomatosis and subglottic stenosis: man-
agement of the airway. Journal of Laryngology & Otology 2004;118(10):786–90.
[18] Pauzner R, Mayan H, Hershko E, et al. Exacerbation of Wegener’s granulomatosis during
pregnancy: report of a case with tracheal stenosis and literature review. J Rheumatol 1994;
21(6):1153–6.
[19] McDonald TJ, Neel HB III, DeRemee RA. Wegener’s granulomatosis of the subglottis and
the upper portion of the trachea. Ann Otol Rhinol Laryngol 1982;91(6 Pt 1):588–92.
[20] D’Cruz DP, Baguley E, Asherson RA, et al. Ear, nose, and throat symptoms in subacute
Wegener’s granulomatosis. BMJ 1989;299(6696):419–22.
[21] Boubenider SA, Akhtar M, Alfurayh O, et al. Late recurrence of Wegener’s granulomatosis
presenting as tracheal stenosis in a renal transplant patient. Clin Transplant 1994;8(1):5–9.
[22] RosenbergDM,Weinberger SE, Fulmer JD, et al. Functional correlates of lung involvement
in Wegener’s granulomatosis: use of pulmonary function tests in staging and follow-up. Am
J Med 1980;69(3):387–94.

774 POLYCHRONOPOULOS et al
[23] Koldingsnes W, Jacobsen EA, Sildnes T, et al. Pulmonary function and high-resolution CT
findings five years after disease onset in patients with Wegener’s granulomatosis. Scand
J Rheumatol 2005;34(3):220–8.
[24] Sheehan RE, Flint JD,Muller NL. Computed tomography features of the thoracic manifes-
tations of Wegener granulomatosis. J Thorac Imaging 2003;18(1):34–41.
[25] Kuhlman JE,HrubanRH,FishmanEK.Wegener granulomatosis: CT features of parenchy-
mal lung disease. J Comput Assist Tomogr 1991;15(6):948–52.
[26] Aberle DR, GamsuG, LynchD. Thoracic manifestations ofWegener granulomatosis: diag-
nosis and course. Radiology 1990;174(3 Pt 1):703–9.
[27] Lee KS, Kim TS, Fujimoto K, et al. Thoracic manifestation of Wegener’s granulomatosis:
CT findings in 30 patients. Eur Radiol 2003;13(1):43–51.
[28] Foo SS, Weisbrod GL, Herman SJ, et al. Wegener granulomatosis presenting on CT with
atypical bronchovasocentric distribution. J Comput Assist Tomogr 1990;14(6):1004–6.
[29] Papiris SA,ManoussakisMN,Drosos AA, et al. Imaging of thoracicWegener’s granuloma-
tosis: the computed tomographic appearance. Am J Med 1992;93(5):529–36.
[30] Maskell GF, Lockwood CM, Flower CD. Computed tomography of the lung in Wegener’s
granulomatosis. Clin Radiol 1993;48(6):377–80.
[31] Summers RM, Aggarwal NR, Sneller MC, et al. CT virtual bronchoscopy of the central air-
ways in patients with Wegener’s granulomatosis. Chest 2002;121(1):242–50.
[32] Park KJ, Bergin CJ, Harrell J. MR findings of tracheal involvement in Wegener’s granulo-
matosis. AJR Am J Roentgenol 1998;171(2):524–5.
[33] MaguireR, FauciAS,Doppman JL, et al. Unusual radiographic features ofWegener’s gran-
ulomatosis. AJR Am J Roentgenol 1978;130(2):233–8.
[34] Eagleton LE, Rosher RB, Hawe A, et al. Radiation therapy and mechanical dilation of en-
dobronchial obstruction secondary to Wegener’s granulomatosis. Chest 1979;76(5):609–10.
[35] HellmannD, Laing T, Petri M, et al. Wegener’s granulomatosis: isolated involvement of the
trachea and larynx. Ann Rheum Dis 1987;46(8):628–31.
[36] Travis WD, Hoffman GS, Leavitt RY, et al. Surgical pathology of the lung in Wegener’s
granulomatosis: review of 87 open lung biopsies from 67 patients. Am J Surg Pathol 1991;
15(4):315–33.
[37] Amin R. Endobronchial involvement in Wegener’s granulomatosis. Postgrad Med J 1983;
59(693):452–4.
[38] Prakash UBS. Bronchoscopy. In: Gold WM,Murray JF, Nadel JA, editors. Atlas of proce-
dures in respiratory medicine. Philadelphia: WB Saunders; 2002. p. 214–65.
[39] Prince JS,DuhamelDR,LevinDL, et al.Nonneoplastic lesions of the tracheobronchial wall:
radiologic findings with bronchoscopic correlation. Radiographics 2002;22:S215–30.
[40] BohlmanME, Ensor RE, Goldman SM. Primary Wegener’s granulomatosis of the trachea:
radiologic manifestations. South Med J 1984;77(10):1318–9.
[41] Yilmaz A, Damadoglu E, Aksoy F, et al. A relapsing case of Wegener’s granulomatosis pre-
senting as an endobronchial mass. Tuberk Toraks 2006;54(1):56–60.
[42] Matt BH.Wegener’s granulomatosis, acute laryngotracheal airway obstruction and death in
a 17-year-old female: case report and review of the literature. Int J Pediatr Otorhinolaryngol
1996;37(2):163–72.
[43] Strange C, Halstead L, BaumannM, et al. Subglottic stenosis in Wegener’s granulomatosis:
development during cyclophosphamide treatment with response to carbon dioxide laser
therapy. Thorax 1990;45(4):300–1.
[44] Langford CA, Sneller MC, Hallahan CW, et al. Clinical features and therapeutic manage-
ment of subglottic stenosis in patients with Wegener’s granulomatosis. Arthritis Rheum
1996;39(10):1754–60.
[45] ScreatonNJ, Sivasothy P, Flower CD, et al. Tracheal involvement inWegener’s granuloma-
tosis: evaluation using spiral CT. Clin Radiol 1998;53(11):809–15.
[46] Utzig MJ, Warzelhan J, Wertzel H, et al. Role of thoracic surgery and interventional bron-
choscopy in Wegener’s granulomatosis. Ann Thorac Surg 2002;74(6):1948–52.

775AIRWAY INVOLVEMENT IN WEGENER’S GRANULOMATOSIS
[47] Stone JH. Limited versus severe Wegener’s granulomatosis: baseline data on patients in the
Wegener’s granulomatosis etanercept trial. Arthritis Rheum 2003;48(8):2299–309.
[48] Seo P, Min YI, Holbrook JT, et al. Damage caused by Wegener’s granulomatosis and its
treatment: prospective data from the Wegener’s Granulomatosis Etanercept Trial
(WGET). Arthritis Rheum 2005;52(7):2168–78.
[49] GuerreroM,Gall E, Tilahun E, et al.Wegener’s granulomatosis presenting as subglottic ste-
nosis. J Clin Rheumatol 2001;7(2):91–6.
[50] Valdez TA, Shapshay SM. Idiopathic subglottic stenosis revisited. Ann Otol Rhinol Lar-
yngol 2002;111(8):690–5.
[51] Chen HJ, Bloch KJ. Hypocomplementemic urticarial vasculitis, Jaccoud’s arthropathy, val-
vular heart disease, and reversible tracheal stenosis: a surfeit of syndromes. J Rheumatol
2001;28(2):383–6.
[52] Hervier B, Pagnoux C, Renaudin K, et al. Stenoses endobronchiques au cours de la granu-
lomatose de Wegener. Revue de Medecine Interne 2006;27(6):453–7.
[53] Hirsch MM, Houssiau FA, Collard P, et al. A rare case of bronchial stenosis in Wegener’s
granulomatosis: dramatic response to intravenous cyclophosphamide and oral cotrimoxa-
zole. J Rheumatol 1992;19(5):821–4.
[54] StavngaardT,Mortensen J.Wegener’s granulomatosis causingmain stembronchial stenosis
and large perfusion-ventilation defects. Clin Nucl Med 2002;27(6):440–1.
[55] Schneider P, Grone J, Braun J, et al. Wegener’s granulomatosis presenting as necrosis of the
left mainstem bronchus. Asian Cardiovasc Thorac Ann 2002;10(3):277–9.
[56] Woywodt A, Goebel U. Bronchial stenosis and extensive bronchiectasis due to Wegener’s
granulomatosis. Nephron 2000;85(4):366–7.
[57] Sitara D, Hoffbrand BI. Chronic bronchial suppuration and antineutrophil cytoplasmic an-
tibody (ANCA) positive systemic vasculitis. Postgrad Med J 1990;66(778):669–71.
[58] Song YH, Kim TH, Lee IH, et al. Wegener’s granulomatosis presenting as mediastinal soft
tissue mass invading the tracheal wall. Clin Rheumatol 2000;19(6):495–8.
[59] Lee SJ, BerryGJ, Husari AW.Wegener’s granulomatosis presenting as rightmiddle lobe ob-
struction. Chest 1993;103(5):1623–4.
[60] Conces DJ Jr, Kesler KA, Datzman M, et al. Tracheoesophageal fistula due to Wegener
granulomatosis. J Thorac Imaging 1995;10(2):126–8.
[61] Watters K, Russell J. Subglottic stenosis in Wegener’s granulomatosis and the nitinol stent
[see comment]. Laryngoscope 2003;113(12):2222–4.
[62] Herridge MS, Pearson FG, Downey GP. Subglottic stenosis complicating Wegener’s gran-
ulomatosis: surgical repair as a viable treatment option. J Thorac Cardiovasc Surg 1996;
111(5):961–6.
[63] Eliachar I, Chan J, Akst L. New approaches to the management of subglottic stenosis in
Wegener’s granulomatosis. Cleve Clin J Med 2002;69:SII149–51.
[64] Sheski FD, Mathur PN. Long-term results of fiberoptic bronchoscopic balloon dilation in
the management of benign tracheobronchial stenosis. Chest 1998;114(3):796–800.
[65] Stappaerts I, Van Laer C, Deschepper K, et al. Endoscopic management of severe subglottic
stenosis in Wegener’s granulomatosis. Clin Rheumatol 2000;19(4):315–7.
[66] Mayse ML, Greenheck J, Friedman M, et al. Successful bronchoscopic balloon dilation of
nonmalignant tracheobronchial obstruction without fluoroscopy. Chest 2004;126(2):634–7.
[67] Chandran PK, First MR, Weiss MA, et al. Wegener’s granulomatosis: prolonged pa-
tient survival after pneumonectomy and renal transplantation. Am J Nephrol 1982;
2(6):325–9.
[68] Neviani CB, Carvalho Hde A, Hossamu C, et al. Radiation therapy as an option for upper
airway obstruction due to Wegener’s granulomatosis. Otolaryngol Head Neck Surg 2002;
126(2):195–6.




















