Electrophysiological correlates of familiarity in recognition memory and exclusion tasks

P1: JLS
Applied Psychophysiology and Biofeedback [apb] pp1257-apbi-489566 August 19, 2004 2:43 Style file version Nov 28th, 2002
Applied Psychophysiology and Biofeedback, Vol. 29, No. 3, September 2004 ( C© 2004)
Electrophysiological Correlates of Vigilance Duringa Continuous Performance Test in Healthy Adults1
Thomas S. Bearden,2,4 Jeffrey E. Cassisi,2 and J. Noland White3
The present study evaluated patterns of electrophysiological activity associated with sus-tained vigilance in healthy adults. Quantitative electroencephalographs (QEEG) wererecorded during the performance of a Continuous Performance Test (CPT). Participantswere divided into low and high vigilance groups based upon their reaction time changes be-tween the early and late portions of the CPT. Coherence measures were calculated from theQEEG across the baseline, early CPT, and late CPT experimental conditions. Participantsin the low vigilance group had higher baseline and CPT frontal to posterior coherence inthe alpha and beta bands suggestive of a less vigilant state throughout the entire study.Additionally, the low vigilance group had a significantly greater beta 1 band coherencedrop from baseline to the initial portion of the CPT than the high vigilance group. Thecombined groups had significantly lower amounts of right hemisphere frontal to posteriorcoherence across a number of frequency bands throughout all of the phases of the studywhen compared to the homologous left hemisphere sites. These interhemispheric coherencedifferences are consistent with vigilance network theories that implicate the right frontaland parietal lobes in the maintenance of sustained attention (M. I. Posner & M. E. Raichle,1994).
KEY WORDS: vigilance; CPT; QEEG; IVA; attention.
INTRODUCTION
The maintenance of alertness and sustained attention (vigilance) is key to successfulinformation processing. Posner and Raichle (1994) postulated the existence of a vigilancenetwork consisting of the right frontal and right parietal lobes. Although many measurescan be used to assess vigilance, the Continuous Performance Test (CPT) is the most fre-quently utilized measure for the assessment of vigilance (DuPaul, Anastopoulos, Shelton,
1This study was originally published as a dissertation by Thomas Bearden in partial fulfillment of the require-ments of a Ph.D. in Clinical Psychology at Jackson State University. Dr. Cassisi was the dissertation committeechairperson.
2Department of Psychology, Jackson State University, Jackson, Mississippi.3Department of Psychology, Georgia College and State University, Milledgeville, Georgia.4Address all correspondence to Thomas S. Bearden, 1338 Chambers St. Vicksburg, Mississippi 39180; e-mail:[email protected].
175
1090-0586/04/0900-0175/0 C© 2004 Springer Science+Business Media, Inc.

P1: JLS
Applied Psychophysiology and Biofeedback [apb] pp1257-apbi-489566 August 19, 2004 2:43 Style file version Nov 28th, 2002
176 Bearden, Cassisi, and White
Guevremont, & Metevia, 1992). Numerous neuroimaging and evoked response studies havebeen conducted during CPT administration to attempt to identify the components of theattentional system activated by CPT performance, with most results confirming Posner andRaichle’s vigilance network theory (Riccio, Reynolds, & Lowe, 2001).
In addition to assessing vigilance, most CPTs also assess selective attention and re-sponse inhibition (Riccio et al., 2001). Riccio et al. stated, “the basic paradigm for the CPTinvolves selective attention or vigilance for an infrequently occurring target or relevantstimulus; the CPT paradigm is generally characterized by rapid presentation of continu-ously changing stimuli with a designated target stimulus or target pattern” (p. 18). Errorsof omission are associated with inattention and often occur when many foils are given withfew targets. Errors of commission are associated with hyperactivity and often occur whenonly a few foils are present among many targets.
A number of specific measures generated by CPTs have been utilized to assess vigilanceincluding reaction time, signal detection sensitivity (d ′), and errors of omission. Duringthe course of a CPT, reaction time typically declines and these declines are associatedwith decreased vigilance (Egan, Greenberg, & Schulman, 1961). Signal detection theorypostulates that the ratio of responses to signal and noise stimuli allows the calculation ofsensitivity (d ′), which is the ability to discriminate nontargets from targets. Decreases in (d ′)are also associated with decreased vigilance (Cohen & O’Donnell, 1993). However, not allvigilance tasks are suitable for the derivation of (d ′). Parasuraman (1979) noted that ideallythe stimulus should vary, discrimination should become more difficult, and the task shouldlast for at least 30–45 min. None of the widely utilized commercial CPT tests meet all of thesecriteria. However, all CPTs do provide measures of errors of omission. If the number of errorsof omission increases over the course of the test, or if an increase in reaction time occurs,one may conclude that a vigilance decrement has occurred (Parasuraman & Davies, 1976).
Only a few studies have attempted to correlate local measures of electroencephalo-graph (EEG) power with vigilance levels (Arruda et al., 1996; Arruda, Walker, Weiler, &Valentino, 1999; Teixeira, 1993; Valentino, Arruda, & Gold, 1993; Weiler, 1992). In a seriesof three studies, Arruda, Valentino, Weiler, and associates investigated eyes-closed QEEGpower changes between phases of an auditory CPT specifically to assess vigilance-relatedeffects (Arruda et al., 1996, 1999; Valentino et al., 1993). Because of inherent problemscomparing resting baseline to activated experimental conditions, the authors advocatedcomparing QEEG measures between good and poor performers on early and late compo-nents of a vigilance task. In their initial study, Valentino et al. recorded the QEEGs of 102undergraduate students from eight bipolar sites while they performed an auditory CPT forapproximately 11 min. They divided the CPT into early and late phases. Valentino et al. thendivided the participants into two groups based on the differences in the number of omissionerrors the participants made between the initial and late phases of the CPT. Valentino et al.only found one significant change over the latter phase of the CPT (decreased temporalbeta 2 power for the low vigilance group) that differed between the low and high vigilancegroups.
However, the groups differed on a number of resting measures as well as the pattern ofchanges between resting and the initial phase of the CPT. Valentino et al. (1993) found thelow vigilance group had greater amounts of alpha and theta power in the resting and otherexperimental conditions and a relative lack of alpha attenuation between resting and theinitial phase of the CPT. The low vigilance group’s higher resting alpha and theta power werepredictive of their higher number of omission errors than the high vigilance group on the

P1: JLS
Applied Psychophysiology and Biofeedback [apb] pp1257-apbi-489566 August 19, 2004 2:43 Style file version Nov 28th, 2002
Electrophysiological Correlates of Vigilance 177
latter portion of the CPT. The low vigilance group’s lack of alpha attenuation while engagedwith the CPT is consistent with a large body of event-related desynchronization research(ERD). Pfurtsheller and Aranibar (1977) built upon Berger’s original observation in 1929that alpha attenuates to eye-opening and during focused concentration by measuring ERDto stimuli (Berger, 1929). Additional research by Klimesch, Schimke, and Pfurtscheller(1993) has confirmed that the lower alpha ERD reflects attentional processes, whereas theupper alpha band ERD reflects stimulus-related semantic processes. These findings are allassociated with decreased vigilance and drowsiness and are consistent with Parasuraman’swork that suggests the initial level of alertness is the key factor in predicting vigilancedecrements over time (Parasuraman, 1979; Parasuraman, Mutter, & Molloy, 1991).
Unlike local EEG power, EEG coherence delineates the frequency-specific covariancebetween two electrode sites. As such, it is thought to reflect the functional coupling ofthe EEG activity between the two sites (Tucker & Roth, 1984). Coherence is the ratio ofcovariance divided by the cross products of variance and it is similar to the correlationcoefficient (Thatcher, Krause, & Hrybyk, 1986).
Coherence is defined for a frequency band ( f ) as
r2xy( f ) = (Gxy( f ))2(Gxx( f )Gyy( f ))
where Gxy( f ) is the cross-power spectral density and Gxx( f ) and Gyy( f ) are the respectiveautopower spectral densities (Thatcher et al., 1986). Coherence is independent of the EEGamplitude at each site and may be thought of as a measure of the degree of symmetrybetween two sites waveforms’ morphologies and should not be confused with amplitudeasymmetry measures (Thatcher, McAlaster, Lester, Horst, & Cantor, 1983). Thatcher et al.(1986) postulated a two-compartmental model of EEG coherence that has subsequentlybeen confirmed and extended by a number of researchers (Thatcher, 1999). Thatcher et al.demonstrated that at short (millimeter to a few centimeter) interelectrode distances the maincontributors to coherence measures are the densely-packed Golgi type II neurons that haveshort axons that do not enter the white matter. In contrast, at long interelectrode distances,the major contributors to coherence measures are the long axoned pyramidal Golgi typeI neurons that do enter the white matter and form long distance corticocortical feedbackloops. Thatcher et al. also found that anterior sites had higher coherence than posteriorsites and in concordance with the greater amount of white matter and Golgi I neurons inthe right hemisphere versus the left, that the right hemisphere had higher long distancecoherence values when measured from individuals with their eyes-closed. Additional stud-ies by Thatcher and others have revealed that among children, higher interhemisphericcoherence measures (revealing a relative lack of functional cortical differentiation) are cor-related with lower fullscale IQ scores and reading disabilities (Gasser, Jennen-Steinmetz,& Verleger, 1987; Marosi et al., 1992; Thatcher et al., 1983). Numerous clinical studieshave demonstrated that EEG coherence has important clinical utility. Ford, Goethe, andDecker (1986) found that alpha band coherence measures were superior to amplitude mea-sures for discriminating between groups of patients diagnosed with paranoid schizophrenia,dysthymia, or a major affective disorder. In addition, several researchers have found co-herence measures to be sensitive discriminators between groups of control children andchildren with ADHD (Barry, Clarke, McCarthy, & Selikowitz, 2002; Chabot & Serfontein,1996).

P1: JLS
Applied Psychophysiology and Biofeedback [apb] pp1257-apbi-489566 August 19, 2004 2:43 Style file version Nov 28th, 2002
178 Bearden, Cassisi, and White
The authors are unaware of any studies that have explored possible EEG coherencecorrelates of vigilance level during a CPT. However, as previously noted, the frontal andparietal lobes have clearly been implicated as being activated during CPTs and other vig-ilance tasks by neuroimaging and regional EEG power studies. Although neuroimagingtechniques such as PET scans or fMRIs are excellent for delineating local regional activa-tion, they are unable to assess the level of functional coupling between activated regions.The main strength of coherence measures are their ability to almost instantaneously assessfunctional coupling between regions.
The purpose of this study was to attempt to identify patterns of functional couplingbetween the frontal and posterior brain regions associated with sustained attention, thusyielding a better understanding of the electrophysiological underpinnings of the vigi-lance system. It was hoped that the use of these intrahemispheric frontal to posteriorcoherence measures would yield additional insight into Posner and Raichle’s vigilancetheories.
Three specific hypotheses were formulated based on the division of the participantsinto low and high vigilance groups and the utilization of coherence measures from fourpairs of frontal to posterior electrodes. The first hypothesis stated that all the participant’sintrahemispheric coherence patterns would differ significantly between the initial eyes-open baseline and the initial phase of the CPT, with decreases in intrahemispheric anteriorto posterior alpha 1 (8–10 Hz) band coherence as measured from F3–O1, F4–O2, F3–P3, and F4–P4 in conjunction with increased anterior to posterior beta band coherenceas measured from F3–P3 and F4–P4. The second hypothesis stated that the low and highvigilance groups’ coherence measures would differ significantly, with the low vigilancegroup demonstrating higher intrahemispheric coherence in most frequency bands. The thirdhypothesis stated that the low vigilance group would have greater numbers of baseline toinitial CPT coherence changes than the high vigilance group. An additional premise ofthe study was that differential hemispheric group effects would be observed based onvigilance neuroimaging work that implicated the right hemisphere in sustained vigilancetasks (Posner & Raichle, 1994). However, because of the mixed auditory and visual stimuliutilized with the IVA that could elicit bihemispheric processing, no formal hypothesis waspostulated.
METHOD
Participants
Participants were recruited from two locations. The first set of 21 participants wasrecruited by the third author as part of his normal control group for his dissertation research(White, 2001). These participants were recruited from undergraduate and graduate studentsfrom various courses in the College of Arts and Sciences and Department of Education atthe University of Tennessee in Knoxville, Tennessee after IRB approval. The other set of39 participants was recruited by the first author from undergraduate students from coursesin the Department of Psychology at Jackson State University in Jackson, Mississippi afterobtaining IRB approval. All participants were offered extra credit for their participation inthe study.
After inclusion criteria were applied (see Procedure) and the remaining participantswere divided into groups (see Results), a total of 28 participants remained in the study. The

P1: JLS
Applied Psychophysiology and Biofeedback [apb] pp1257-apbi-489566 August 19, 2004 2:43 Style file version Nov 28th, 2002
Electrophysiological Correlates of Vigilance 179
average age of all 28 participants was 22.6-years-old (SD = 5.8). There were no significantdifferences between data sources on age or gender.
Measures
Health History Questionnaire. The Health History Questionnaire was devised by Barkleyand Murphy (1998) for use as a screening instrument. It lists 14 types of health problemsand requests the respondent to check if they experienced the problems during childhood,in the past as an adult, or currently.
DSM-IV ADHD Symptom Checklist. The symptom checklist includes nine questions regard-ing inattentive symptoms and nine questions regarding hyperactive/impulsive symptoms(American Psychiatric Association, 1994).
Peabody Picture Vocabulary Test—3rd ed. (PPVT-III). The PPVT-III is a test of receptivevocabulary and general verbal cognitive functioning and may be used as a screener forgeneral cognitive functioning (Dunn & Dunn,1997).
Electroencephalograph Recording. The EEG was recorded from 19 scalp electrodes with alinked-ear reference utilizing an electrode cap following the international 10–20 place-ment system (Jasper, 1958). Electrode impedances were reduced at or below 10 Kohms.The raw EEG was collected with a high-pass filter of 0.5 Hz and a low-pass filter of 32 Hzand digitized with a Lexicor NeurosearchTM -24 Electroencephalograph with a samplingrate of 128 samples per second, which allowed for an epoch length of 2-s and a frequencyresolution of 0.5 Hz.
Integrated Auditory and Visual Continuous Performance Test (IVA). The IVA is a combinedvisual and auditory CPT that lasts for approximately 22-min and the main portion of thetest is divided into five sets of stimuli (Sandford & Turner, 1994). The test administrationis automated and instructions are given verbally from the computer. The test is composedof four parts: (1) Warm-up, (2) Practice, (3) Main CPT, and (4) Cool-down. The testee isinstructed to only click the mouse when he sees (on the monitor) or hears a “1” (target).They are not to click when they see or hear a “2” (foil). The main section of the IVAlasts 12.8 min and is composed of five sets (quintiles) of 100 auditory and visual stimuli.Each quintile begins with a block of 50 stimuli composed of 42 “1”s and 8 “2”s ofmixed auditory and visual presentations, which is designed to elicit errors of commissionassociated with impulsivity. The second block of each set contains 50 stimuli composedof 8 “1”s and 42 “2”s, which is designed to elicit inattentive errors of omission.
Modified Stanford Sleepiness Scale (MSSS). The Stanford Sleepiness Scale was initially de-signed to assess subtle changes in states of consciousness related to drowsiness (Dement& Carskadon, 1982). It consisted of seven statements that range from feeling wide awaketo feeling drowsy, to feeling briefly asleep. The original scale was modified and partici-pants were asked to circle the number of the statement that best described the way theyfelt during the first half, second half, and over the entire course of the IVA.
Procedure
Exclusionary criteria for participants from both data sources included: (1) history ofhead trauma with loss of consciousness, (2) history of epilepsy or seizures, (3) any medica-tion use (except for contraceptives), (4) current substance abuse (as assessed by interview),(5) a standard score of less than 85 on the PPVT-III, and (6) a possible history of ADHD as

P1: JLS
Applied Psychophysiology and Biofeedback [apb] pp1257-apbi-489566 August 19, 2004 2:43 Style file version Nov 28th, 2002
180 Bearden, Cassisi, and White
indicated by a score of 4 or greater on either the hyperactive/impulsive or inattentive symp-tom categories in the DSM-IV ADHD Symptom Checklist, and (7) left-handedness. Demo-graphic information included age, gender, and race. After these exclusions, 18 Tennesseeand 22 Mississippi participants’ data was available for the study. After group assignment,28 participants’ data was available for analysis (see Results).
Participants completed the Health History Questionnaire and were questioned regard-ing possible substance abuse. They were then administered the DSM-IV ADHD Symp-tom Checklist. Subsequently, they were assessed for general intellectual ability using thePPVT-III.
The participants then moved to a comfortable chair that had a computer monitor posi-tioned approximately 3 feet in front of them. EEG electrodes were applied using an electrodecap. Two additional electrodes were placed under the right outer canthus and over the leftouter canthus of the right and left eyes respectively to monitor eye movements to assistin subsequent artifacting of the EEG recordings. All Mississippi participants completed a5-min eyes-open baseline recording (where they stared at the monitor), a 3-min eyes-closedrecording, a 12.8 min recording during the IVA, and a 5-min posttest eyes-open base-line recording. Immediately after the last recording, participants completed the ModifiedStanford Sleepiness Scale.
The procedure for the Tennessee participants was similar to that of the Mississippi par-ticipants, but there were several differences. The eyes-closed and eyes-open baselines wererecorded at the beginning of the experiment as were the Mississippi participants’ baselineQEEGs. However, the Tennessee participants then performed two neuropsychological testsprior to performing the IVA. They also did not have a post-IVA baseline recording and werenot administered a Modified Stanford Sleepiness Scale.
RESULTS
Preparatory Steps
Group Assignment
To create a high and low vigilance group the following steps were undertaken. A dif-ference score was calculated from the mean of each participant’s rare auditory and rarevisual targets’ reaction times from the first five min of the IVA (IVA1) and the last 5-minof the IVA (IVA2). The 40 participants were then divided into 3 groups based on the mag-nitude of their IVA1–IVA2 difference scores. The low vigilance (LoVig) group members(n = 14) had negative difference scores (signifying slower reaction times during IVA2) thatwere below the 36th percentile derived from the difference scores from all 40 participants.The high vigilance (HiVig) group’s members (n = 14) had more positive difference scores(consistent with very small or no increases in IVA2 reaction times) that were above the 67thpercentile. Twelve participants whose difference scores were in the middle range, wereexcluded from further analysis. As a manipulation check for this splitting of the groups,independent t tests were utilized to assess whether the mean reaction time differences be-tween LoVig and HiVig groups were significant. There was a significant group difference,t(26) = 10.58, p < .001, on the mean rare target reaction time measure with the LoViggroup’s mean difference, M = −16.1 ms, SD = 6.1, being significantly more negative

P1: JLS
Applied Psychophysiology and Biofeedback [apb] pp1257-apbi-489566 August 19, 2004 2:43 Style file version Nov 28th, 2002
Electrophysiological Correlates of Vigilance 181
(indicative of slower IVA2 than IVA1 reaction times) than the HiVig group’s mean differ-ence, M = 3.4 ms, SD = 3.2. The LoVig group was composed of six Tennessee and eightMississippi participants, with four males and 10 females. The HiVig group was composedof five Tennessee and nine Mississippi participants, with four males and 10 females.
Once these groups were formed, group equivalence of their demographics was evalu-ated using independent t tests for continuous data and chi-square tests for categorical data.There were no significant age, gender, race, PPVT, or MSSS group differences.
Definition of Measurement Phases
The EEG waveforms from the initial eyes-open (EO1) baseline and those recordedduring the IVA were visually examined using the Lexicor NeuroLex software (LexicorMedical Technology, 1992). The IVA QEEG data was divided into two separate files (IVA1& IVA2). IVA1 was composed of the first 150 epochs (300-s) of the IVA, which correspondsto the 1st and 2nd quintiles of the test. IVA2 was composed of the last 150 epochs of theIVA, which corresponds to the 4th and 5th quintiles of the test.
Electrode Placement
Planned site comparisons based primarily on Posner and Rachile’s (1994) neuroimag-ing vigilance studies utilized coherence measures from four electrode pairs (F3–O1, F4- O2,F3–P3, & F4–P4). The two left hemisphere pairs were F3–O1 and F3–P3, which assessedcoherence from the frontal to occipital and parietal regions respectively. The two remainingpairs, F4–O2 and F4–P4, assessed coherence from the homologous right hemisphere sites.
Data Transformation
Two-s epochs that displayed artifacts were excluded from further data analysis. Aminimum of 30 epochs were utilized for additional data analysis from each of the exper-imental conditions (EO1, IVA1, & IVA2). Because of possible residual EMG artifact thatis capable of mimicking beta band activity, beta band measures were only utilized fromparasaggital frontal to parietal electrode sites (F3–P3 & F4–P4) that are less prone to EMGcontamination.
The retained epochs underwent Fast Fourier Transform (FFT) and coherence valueswere calculated between intrahemispheric electrode sites. Coherence values were generatedin the theta (4.0–7.5 Hz), alpha 1 (8.0–10 Hz), alpha 2 (10.5–12.5), beta 1 (13.0–21.0 Hz),and beta 2 (21.5–32 Hz) frequency bands. All coherence values were transformed to anormal distribution using Fisher’s z transform prior to statistical analyses (Harmony et al.,1993). Five separate repeated measures ANOVAs were conducted for each frequency bandto test the hypotheses. Group (LoVig, HiVig) was the between subjects factor and phase(EO1, IVA1, IVA2), electrode pair, and hemisphere were the within-subject factors.
Hypothesis Testing
To test the hypotheses, a series of ANOVAs were performed on each of the previouslyspecified EEG frequency bands. These took the form of a 2 (group) × 3 (phase) × 2

P1: JLS
Applied Psychophysiology and Biofeedback [apb] pp1257-apbi-489566 August 19, 2004 2:43 Style file version Nov 28th, 2002
182 Bearden, Cassisi, and White
(hemisphere) × 2 (electrode pair) repeated measures ANOVA, where group was the onlybetween-subjects factor. Phase, hemisphere, and electrode pair were within-subject factors.The α level of significance was set a priori at p < .05.
Theta band. No significant main effect, interactions, or planned comparisons were obtainedfor the theta band.
Alpha 1 band. A significant main effect for group was found with the mean alpha 1 coherenceacross all the experimental phases from the LoVig group significantly higher than theHiVig group, F(1, 26) = 4.38, p = .05 (see Table I for means). A significant main effectfor hemisphere was found with the mean coherence values from all the participants acrossall the phases significantly higher from the left hemisphere sites than those from the righthemisphere, F(1, 26) = 4.09, p = .05 (see Table IV). None of the planned comparisonsof group by phase from the alpha 1 band were significant.
Alpha 2 band. A significant main effect for group was found due to higher mean coherencevalues across all the phases from the LoVig group than the HiVig group, F(1, 26) = 5.85,p = .02 (see Table II). None of the planned comparisons of group by phase from thealpha 2 band were significant.
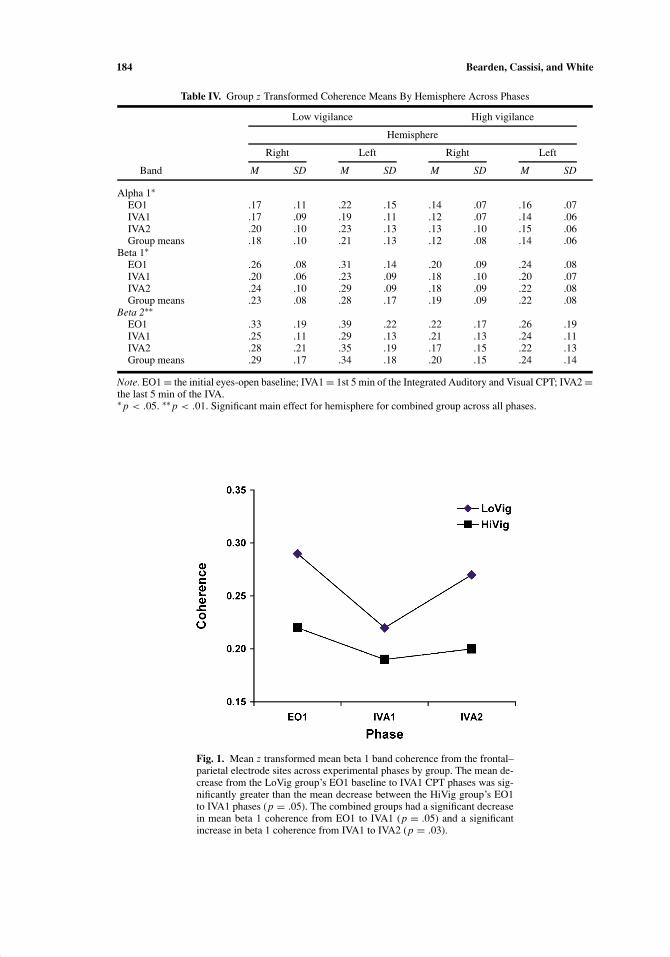
Beta 1 band. A significant main effect for group was found due to higher mean coher-ence values across all the phases from the LoVig group when compared to the HiViggroup, F(1, 26) = 4.09, p = .05 (see Table III). A significant main effect for hemi-sphere was found with the mean coherence values from all the participants across allthe phases significantly higher from the left hemisphere sites than those from the righthemisphere, F(1, 26) = 6.51, p = .02 (see Table IV). A significant main effect for phasewas also found, F(2, 26) = 6.67, p < .01 (see Table III). To explain the differences as-sociated with the main effect of phase, tests of simple main effects were run. Thesetests indicated that for all the participants, coherence values dropped from the initialeyes-open baseline phase (EO1) to the IVA1 phase, F(1, 26) = 4.09, p = .05, and thenincreased from the IVA1 phase to the IVA2 phase, F(1, 26) = 5.59, p = .03 (see Fig. 1).Because hypothesis 3 specifically addressed a phase by group effect, subsequent con-trasts were run and a significant phase by group difference was found between the EO1and IVA1 phases with the LoVig group’s mean differences between the phases being
Table I. Alpha 1: Group z Transformed Coherence Means Across Phases
Low vigilance High vigilance
Site M SD M SD
Bihemispheric meansEyes-open baseline
Frontal–parietal .28 .16 .23 .09Frontal–occipital .11 .01 .07 .05
IVA1Frontal–parietal .27 .13 .20 .09Frontal–occipital .09 .07 .05 .04
IVA2Frontal–parietal .30 .14 .22 .10Frontal–occipital .13 .09 .07 .06Group means∗ .20 .10 .14 .07
Note. IVA1 = 1st 5 min of the Integrated Auditory and Visual CPT; IVA2 =the last 5 min of the IVA.∗ p < .05. Significant main effect for group.

P1: JLS
Applied Psychophysiology and Biofeedback [apb] pp1257-apbi-489566 August 19, 2004 2:43 Style file version Nov 28th, 2002
Electrophysiological Correlates of Vigilance 183
Table II. Alpha 2: Group z Transformed Coherence Means Across Phases
Low vigilance High vigilance
Site M SD M SD
Bihemispheric meansEyes-open baseline
Frontal–parietal .23 .13 .17 .12Frontal–occipital .12 .10 .06 .03
IVA1Frontal–parietal .21 .13 .14 .09Frontal–occipital .13 .12 .06 .05
IVA2Frontal–parietal .20 .11 .17 .14Frontal–occipital .12 .12 .06 .06Group means∗ .17 .12 .11 .08
Note. IVA1 = 1st 5 min of the Integrated Auditory and Visual CPT; IVA2 =the last 5 min of the IVA.∗ p < .05. Significant main effect for group.
larger than the HiVig group’s mean phase differences, F(1, 26) = 4.23, p = .05 (seeFig. 1).
Beta 2 band. A significant main effect for hemisphere was found with the mean coherencevalues from all the participants across all the phases significantly higher from the lefthemisphere sites than those from the right hemisphere, F(1, 26) = 9.44, p < .01 (seeTable IV).
DISCUSSION
The purpose of this study was to attempt to identify patterns of functional couplingbetween the frontal and posterior brain regions associated with sustained attention, thusyielding a better understanding of the electrophysiological underpinnings of the vigilancesystem. It was hoped that the use of these intrahemispheric frontal to posterior coherencemeasures would yield additional insight into Posner and Raichle’s vigilance theories.
Previous studies that have assessed vigilance during various monotonous tasks andCPTs have utilized measures such as the number of omission errors and d ′ to quantify
Table III. Beta 1: Group z Transformed Coherence Means Across Phases
Low vigilance High vigilance
Site M SD M SD
Bihemispheric meansEyes-open baseline∗∗
Frontal–parietal .29 .11 .22 .09IVA1∗∗
Frontal–parietal .22 .08 .19 .09IVA2∗∗
Frontal–parietal .27 .10 .20 .09Group means∗ .26 .10 .20 .09
Note. IVA1 = 1st 5 min of the Integrated Auditory and Visual CPT; IVA2 =the last 5 min of the IVA.∗ p < .05. Significant main effect for group. ∗∗ p < .01. Significant main effectfor phase.
P1: JLS
Applied Psychophysiology and Biofeedback [apb] pp1257-apbi-489566 August 19, 2004 2:43 Style file version Nov 28th, 2002
184 Bearden, Cassisi, and White
Table IV. Group z Transformed Coherence Means By Hemisphere Across Phases
Low vigilance High vigilance
Hemisphere
Right Left Right Left
Band M SD M SD M SD M SD
Alpha 1∗EO1 .17 .11 .22 .15 .14 .07 .16 .07IVA1 .17 .09 .19 .11 .12 .07 .14 .06IVA2 .20 .10 .23 .13 .13 .10 .15 .06Group means .18 .10 .21 .13 .12 .08 .14 .06
Beta 1∗EO1 .26 .08 .31 .14 .20 .09 .24 .08IVA1 .20 .06 .23 .09 .18 .10 .20 .07IVA2 .24 .10 .29 .09 .18 .09 .22 .08Group means .23 .08 .28 .17 .19 .09 .22 .08
Beta 2∗∗EO1 .33 .19 .39 .22 .22 .17 .26 .19IVA1 .25 .11 .29 .13 .21 .13 .24 .11IVA2 .28 .21 .35 .19 .17 .15 .22 .13Group means .29 .17 .34 .18 .20 .15 .24 .14
Note. EO1 = the initial eyes-open baseline; IVA1 = 1st 5 min of the Integrated Auditory and Visual CPT; IVA2 =the last 5 min of the IVA.∗ p < .05. ∗∗ p < .01. Significant main effect for hemisphere for combined group across all phases.
Fig. 1. Mean z transformed mean beta 1 band coherence from the frontal–parietal electrode sites across experimental phases by group. The mean de-crease from the LoVig group’s EO1 baseline to IVA1 CPT phases was sig-nificantly greater than the mean decrease between the HiVig group’s EO1to IVA1 phases (p = .05). The combined groups had a significant decreasein mean beta 1 coherence from EO1 to IVA1 (p = .05) and a significantincrease in beta 1 coherence from IVA1 to IVA2 (p = .03).

P1: JLS
Applied Psychophysiology and Biofeedback [apb] pp1257-apbi-489566 August 19, 2004 2:43 Style file version Nov 28th, 2002
Electrophysiological Correlates of Vigilance 185
decrements in sustained attention over relatively long time periods. In this study, thosemeasures did not provide sufficient distributions for forming distinct groups over the shorttime period of the main portion of the IVA CPT (12.8 min). However, when reaction timebased differences between the early and late portions of the CPT to the rare auditory andvisual targets were utilized, distinct groupings were possible. The reaction times in responseto rare targets were used (excluding reaction times to frequent targets) because only raretargets are utilized to elicit errors of omission, which are associated with reduced vigilance.
Hypotheses
The first hypothesis stated that all the participant’s intrahemispheric coherence patternswould differ significantly between the initial eyes-open baseline and first phase of the IVA,with decreases in intrahemispheric anterior to posterior alpha 1 (8–10 Hz) band coherenceas measured from F3–O1, F4–O2, F3–P3, and F4–P4 in conjunction with increased anteriorto posterior beta band coherence as measured from F3–P3 and F4–P4. This hypothesis wasbased on numerous neuroimaging studies that have demonstrated activation of the frontaland parietal lobes during performance of CPTs (Riccio et al., 2001). The first part of thishypothesis was not confirmed because there was no significant phase effect in the plannedcomparisons of the alpha 1 band. In addition, the second part of the first hypothesis wasnot confirmed. There was a significant phase effect in the repeated measures ANOVA onthe beta 1 band. This phase effect was due to a significant decrease in the beta 1 frontal toparietal coherence means from all the participants between the EO1 to IVA1 periods. Thisdecrease in beta 1 means from EO1 to IVA1 was opposite to the hypothesized effect.
The second hypothesis stated that the low and high vigilance groups’ coherence mea-sures would differ significantly with the low vigilance group demonstrating higher intra-hemispheric coherence in most frequency bands. This hypothesis was confirmed for thealpha 1, alpha 2, and beta 1 bands, because there was a significant main effect for groupdue to the higher low vigilance group coherence means.
The third hypothesis stated that the low vigilance group would have greater numbersof baseline to initial phase of the IVA coherence changes than the high vigilance group.This hypothesis was confirmed because the low vigilance group had a significant decreasein their beta 1 coherence means from EO1 to IVA1, whereas the high vigilance group hadno significant EO1 to IVA1 changes whatsoever.
An additional premise of the study was that differential hemispheric group effectswould be observed based on vigilance neuroimaging work, neuroimaging studies duringCPTs, and QEEG power studies during CPTs that implicated the right hemisphere in sus-tained vigilance tasks (Riccio et al., 2001). A significant main effect for hemisphere wasfound for the alpha 1, beta 1, and beta 2 frequency bands. The coherence means from allof the participants were higher from the left hemisphere than the right across all of theexperimental phases.
Implications of Higher Coherence in the LoVig Group Across All Phases
The results from hypothesis two revealed that the low and high vigilance groups’coherence means differed significantly across all the experimental phases within the alphaand beta bands, with higher means from the low vigilance group. The fact that the lowvigilance participants had higher eyes-open baseline coherence means across most of the

P1: JLS
Applied Psychophysiology and Biofeedback [apb] pp1257-apbi-489566 August 19, 2004 2:43 Style file version Nov 28th, 2002
186 Bearden, Cassisi, and White
frequency bands suggests their frontal to posterior regions were functionally coupled andnot engaged in localized active processing of stimuli. As previously noted, Valentino et al.(1993) found their low vigilance group had greater amounts of alpha and theta power in theresting and other experimental conditions and a relative lack of alpha attenuation betweenresting and the initial phase of the CPT. Their low vigilance group’s lack of alpha attenuationwhile engaged in the CPT is consistent with a large body of EEG power research dating backto Berger in 1929, which details a power attenuation in conjunction with a desynchronization(also called event-related desynchronization) across all of the frequency bands during eye-opening or mental effort (Pfurtsheller & Aranibar, 1977). Further support for the idea thathigher power and higher long-range coherence values at baseline and during some mentaltasks equates with poorer mental performance comes from studies by Thatcher and othersthat revealed among children, higher interhemispheric coherence measures (revealing arelative lack of functional cortical differentiation) are correlated with lower fullscale IQscores and reading disabilities (Gasser et al., 1987; Marosi et al., 1992; Thatcher et al., 1983).Taken together, these previous studies’ coherence and power results and the coherencefindings of the present study, support Parasuraman’s (1979) contention that the initial levelof vigilance is the key factor in predicting vigilance decrements over time.
Implications of Differential Group Baseline to IVA1 Beta Findings
Another interesting result was apparent from the beta 1 band group by phase results.As is observed from Fig. 1, there was a significant difference between the low vigilancegroup’s larger beta 1 mean coherence decreases from EO1 to IVA1 versus the smaller highvigilance group’s decreases. This differential pattern of marked IVA1 beta band coherencedrops from the low vigilance participants’ high baseline values, again suggests that thelow vigilance group’s participants were initially in a nonvigilant state. When they beganperforming the IVA, their anterior to posterior beta coherence decreased. On the other hand,the high vigilance group had only a small drop from baseline to IVA1 because their anteriorto posterior beta band baseline coherence values were initially low, which is suggestive ofa more vigilant state capable of performing the localized processing necessary to respondto the IVA stimuli.
Implications of Reduced Beta Coherence During a CPT
The first hypothesis (which was not confirmed) was predicated on the premise thathigher coherence values (especially in the beta band) would occur during CPT performance.It was hypothesized the frontal and parietal lobes would increase their functional couplingto accomplish the CPT task. The frontal and parietal lobes have clearly been implicatedas being activated during CPTs by neuroimaging studies. However, neuroimaging studiesare unable to instantaneously assess functional coupling between regions as is possiblewith coherence. The present study’s results suggest that upon the initial presentation of aCPT task, increased localized processing may occur that results in decreased long rangefrontal to parietal coherence. Apparently when a novel task such as a CPT, which requiresseparate frontal and parietal operations to perform adequately, is introduced there is atleast a transitory decrease in the background level of functional coupling between theseregions. Von Stein, Rappesberger, Sarnthein, and Petsche (1999) investigated coherence

P1: JLS
Applied Psychophysiology and Biofeedback [apb] pp1257-apbi-489566 August 19, 2004 2:43 Style file version Nov 28th, 2002
Electrophysiological Correlates of Vigilance 187
changes from eyes-open baselines to pictorial, written, and auditory presentations of objects.They found that the only reliable changes across all the experimental conditions wereincreases in localized parietal and posterior temporal beta 1 band coherence. Von Steinet al. concluded that decreases in coherence between distant sites may well stem from afunctional compartmentalization of the active cortical area.
The current study’s finding of reduced right hemisphere frontal to posterior coherencefrom the combined groups in the alpha 1, beta 1, and beta 2 bands across all of the ex-perimental phases, supports the contention that reduced long range coherence equates withregional activation. Despite the mixed auditory and visual nature of the IVA CPT stimuli,the participants did have to maintain a visual focus on the monitor throughout the test tobe ready to respond to the visual stimuli. This finding of a differential right hemisphereactivation is consistent with Posner and Raichle’s vigilance theory, which postulates that theright frontal and parietal lobes are key components of the vigilance network. The findingof a significant increase in beta 1 coherence from IVA1 to IVA2 for the combined groupssuggests that as the participants became more familiar with the demands of the task, theirfrontal to parietal beta 1 coherence rose because they no longer needed to exert as muchfocused regional effort to complete the task.
Limitations
The results of this study are limited by the small sample sizes of the two groups. Anumber of results in the beta 2 band mirrored the beta 1 band findings, however, they did notreach the specified significance level (p = .06). Additional participants may have increasedthe magnitude of these differences.
Future QEEG vigilance studies utilizing CPTs should utilize larger number of coher-ence comparisons over the entire scalp. They should also examine regional power changesand attempt to correlate them with any observed coherence changes to help delineate theirfunctional significance.
The use of the IVA CPT made it more difficult to delineate reductions in vigilance asoriginally defined by Parasuraman (1979). The IVA is a widely used commercial CPT, whichby necessity is adapted for relatively short administration times. A longer task with degradedmonotonous stimuli, as recommended by Parasuraman, may have produced different groupassignments. Therefore, additional approaches to defining low and high vigilance groupsneed to be studied in the future.
REFERENCES
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.).Washington, DC: Author.
Arruda, J. E., Walker, K. A., Weiler, M. D., & Valentino, D. A. (1999). Validation of a right hemisphere vigi-lance system as measured by principal component and factor analyzed quantitative electroencephalogram.International Journal of Psychophysiology, 32, 119–128.
Arruda, J. E., Weiler, M. D., Valentino, D., Willis, W. G., Rossi, J. S., Stern, R. A., et al. (1996). A guide forapplying principal component analysis and confirmatory factor analysis to quantitative electroencephalogramdata. International Journal of Psychophysiology, 23, 63–81.
Barkley, R. A., & Murphy, K. R. (1998). Attention-deficit hyperactivity disorder: A clinical workbook (2nd ed.).New York: Guilford.
Barry, R. J., Clarke, A. R., McCarthy, R., & Selikowitz, M. (2002). EEG coherence in attention-deficit/hyperactivitydisorder: A comparative study of two DSM-IV types. Clinical Neurophysiology, 113, 579–585.
Berger, H. (1929). On the electroencephalogram in man. Archives of Psychiatry, 87, 527–570.

P1: JLS
Applied Psychophysiology and Biofeedback [apb] pp1257-apbi-489566 August 19, 2004 2:43 Style file version Nov 28th, 2002
188 Bearden, Cassisi, and White
Chabot, R. J., & Serfontein, G. (1996). Quantitative electroencephalographic profiles of children with attentiondeficit disorder. Biological Psychiatry, 40, 951–963.
Cohen, R. A., & O’Donnell, B. F. (1993). Models and mechanisms of attention: A summary. In R. A. Cohen (Ed.),The neuropsychology of attention (pp. 177–188). New York: Plenum.
Dement, W. C., & Carskadon, M. A. (1982). Current perspectives on daytime sleepiness: The issues. Sleep,5(Suppl. 2), S56–S66.
Dunn, L. M., & Dunn, L. M. (1997). Examiner’s manual for the PPVT-III. Circle Pines, MN: American GuidanceService.
DuPaul, G. J., Anastopoulos, A. D., Shelton, T. L., Guevremont, D. C., & Metevia, L. (1992). Multimethodassessment of attention deficit hyperactivity disorder: The diagnostic utility of clinic-based tests. Journal ofClinical Child Psychology, 21, 394–402.
Egan, J. P., Greenberg, G. Z., & Schulman, A. (1961). Interval of time uncertainty in auditory detection. Journalof the Acoustical Society of America, 33, 771–778.
Ford, M. R., Goethe, J. W., & Dekker, D. K. (1986). EEG coherence and power in the discrimination of psychiatricdisorders and medication effects. Biological Psychiatry, 21, 1175–1188.
Gasser, T., Jennen-Steinmetz, C., & Verleger, R. (1987). EEG coherence at rest and during a visual task in twogroups of children. Electroencephalography and Clinical Neurophysiology, 67, 151–158.
Harmony, T., Fernandz, T., Rodriguez, M., Reyes, A., Marosi, E., & Bernal, J. (1993). Test-retest reliability ofEEG spectral parameters during cognitive tasks: II coherence. International Journal of Neuroscience, 68,263–271.
Jasper, H. (1958). The ten–twenty electrode system of the International Federation. Electroencephalography andClinical Neurophysiology, 10, 371–375.
Klimesch, W., Schimke, H., & Pfurtscheller, G. (1993). Alpha frequency, cognitive load and memory performance.Brain Topography, 5(3), 241–251.
Lexicor Medical Technology. (1992). NeuroLex Software for EEG—Data Acquistion and Analysis (Version 1.2)[Computer software]. Denver, CO: Author.
Marosi. E., Harmony, T., Sanchez, L., Becker, J., Bernal, J., Reyes, A., et al. (1992). Maturation of the coher-ence of the EEG activity in normal and learning-disabled children. Electroencephalography and ClinicalNeurophysiology, 83, 350–357.
Parasuraman, R. (1979). Memory load and event rate control sensitivity decrements in sustained attention. Science,205, 924–927.
Parasuraman, R., & Davies, D. R. (1976). Decision theory analysis of response latencies in vigilance. Journal ofExperimental Psychology Humun Perception and Performance, 2, 569–582.
Parasuraman, R., Mutter, S. A., & Molloy, R. (1991). Sustained attention following mild closed-head injury.Journal of Clinical and Experimental Neuropsychology, 3(5), 789–811.
Pfurtscheller, G., & Aranibar, A. (1977). Event-related cortical synchronization detected by power measurementsof scalp EEG. Electroencephalography and Clinical Neurophysiology, 42, 817–826.
Posner, M. I., & Raichle, M. E. (1994). Images of mind. New York: Freeman.Riccio, C. A., Reynolds, C. R., & Lowe, P. A. (2001). Clinical applications of continuous performance tests.
New York: Wiley.Sandford, J. A., & Turner, A. (1994). Integrated Visual and Auditory Continuous Performance Test manual.
Richmond, VA: BrainTrain.Teixeira, L. C. H. (1993). Comparison of EEG of depressed and nondepressed college students during an attention
task. Unpublished doctoral dissertation, University of Rhode Island, Providence.Thatcher, R. W. (1999). EEG database-guided neurotherapy. In J. R. Evans & A. Abarbanel (Eds.), Introduction
to quantitative EEG and neurofeedback (pp. 29–64). New York: Academic Press.Thatcher, R. W., Krause, P. J., & Hrybyk, M. (1986). Cortico-cortical associations and EEG coherence: A two
compartmental model. Electroencephalography and Clinical Neurophysiology, 64, 123–143.Thatcher, R. W., McAlaster, R., Lester, M. L., Horst, R. L., & Cantor, D. S. (1983). Hemispheric EEG asymmetries
related to cognitive functioning in children. In A. Perecman (Ed.), Cognitive processing in the right hemisphere(pp. 125–146). New York: Academic Press.
Tucker, D. M., & Roth, D. L. (1984). Factoring the coherence matrix: Patterning of the frequency-specific covari-ance in a multichannel EEG. Psychophysiology, 21, 228–236.
Valentino, D. A., Arruda, J. E., & Gold, S. M. (1993). Comparison of QEEG and response accuracy in good vs.poorer performers during a vigilance task. International Journal of Psychophysiology, 15, 123–133.
Von Stein, A., Rappelsberger, P., Sarnthein, J., & Petsche, H. (1999). Synchronization between temporal andparietal cortex during multimodal object processing in man. Cerebral Cortex, 9, 137–150.
Weiler, M. D. (1992). A measurement model for spectral analyzed EEG. Unpublished doctoral dissertation,University of Rhode Island, Providence.
White, J. N., Jr. (2001). Neuropsychological and electrophysiological assessment of adults with Attention DeficitHyperactivity Disorder. Unpublished doctoral dissertation, The University of Tennessee, Knoxville.
Copyright © 2022 FDOKUMEN