Effects of 660 and 780 nm low‐level laser therapy on neuromuscular recovery after crush injury in...
10
Lasers in Surgery and Medicine 42:673–682 (2010) Effects of 660 and 780 nm Low-Level Laser Therapy on Neuromuscular Recovery After Crush Injury in Rat Sciatic Nerve Davilene Gigo-Benato, PhD, 1 * Thiago Luiz Russo, PhD, 2 Erika Harumi Tanaka, 1 Lı ´via Assis, MS, 1 Tania Fa ´ tima Salvini, PhD, 2 and Nivaldo Antonio Parizotto, PhD 1 1 Thermophototherapy Unit, Physical Therapy Department, Federal University of Sa˜o Carlos (UFSCar), Sa˜o Carlos, SP13565-905, Brazil 2 Skeletal Muscle Plasticity Unit, Physical Therapy Department, Federal University of Sa˜o Carlos (UFSCar), Sa˜o Carlos, SP 13565-905, Brazil Background and Objective: Post-traumatic nerve repair is still a challenge for rehabilitation. It is particularly important to develop clinical protocols to enhance nerve regeneration. The present study investigated the effects of 660 and 780 nm low-level laser therapy (LLLT) using different energy densities (10, 60, and 120 J/cm 2 ) on neuromuscular and functional recovery as well as on matrix metalloproteinase (MMP) activity after crush injury in rat sciatic nerve. Materials and Methods: Rats received transcutaneous LLLT irradiation at the lesion site for 10 consecutive days post-injury and were sacrificed 28 days after injury. Both the sciatic nerve and tibialis anterior muscles were analyzed. Nerve analyses consisted of histology (light microscopy) and measurements of myelin, axon, and nerve fiber cross-sectional area (CSA). S-100 labeling was used to identify myelin sheath and Schwann cells. Muscle fiber CSA and zymography were carried out to assess the degree of muscle atrophy and MMP activity, respectively. Stat- istical significance was set at 5% (P0.05). Results: Six hundred sixty nanometer LLLT either using 10 or 60 J/cm 2 restored muscle fiber, myelin and nerve fiber CSA compared to the normal group (N). Furthermore, it increased MMP-2 activity in nerve and decreased MMP-2 activity in muscle and MMP-9 activity in nerve. In contrast, 780 nm LLLT using 10 J/cm 2 decreased MMP-9 activity in nerve compared to the crush group (CR) and N; it also restored normal levels of myelin and nerve fiber CSA. Both 60 and 120 J/cm 2 decreased MMP-2 activity in muscle compared to CR and N. 780 nm did not prevent muscle fiber atrophy. Functional recovery in the irradiated groups did not differ from the non- irradiated CR. Conclusion: Data suggest that 660 nm LLLT with low (10 J/cm 2 ) or moderate (60 J/cm 2 ) energy densities is able to accelerate neuromuscular recovery after nerve crush injury in rats. Lasers Surg. Med. 42:673–682, 2010. ß 2010 Wiley-Liss, Inc. Key words: peripheral nerve repair; laser therapy; denervated muscle; rehabilitation; functional analysis INTRODUCTION Peripheral nerve injury is a common clinical event which is generally related to incapacity [1]. According to a U.S. study, 50,000 subjects suffer traumatic injury to peripheral nerves every year [2,3] representing a significant public health problem. In Brazil, a recent study classified 456 cases of nerve injury and showed that axonotmesis represents the most common nerve injury (45%) followed by neurotmesis (41%) and neuropraxia (14%), respectively [4]. The mechanisms involving nerve regeneration are well- described. When nerve fiber continuity is interrupted, the distal stump undergoes Wallerian degeneration [5]. The proximal axon stump can then regenerate along the nerve tract distal to the lesion and reach the peripheral target (muscle fibers and sensory receptors) [5]. Another tissue strongly affected by peripheral nerve injuries is skeletal muscle. Innervation is critical for muscle functionality and structural integrity [6,7]. Thus, denervation leads to a profound loss of muscle mass and inability to generate force [8,9]. The regeneration process depends on numerous changes in the extracellular matrix (ECM) [10] occurring concom- itantly in both injured nerve and denervated muscles [11 – 13]. These changes require the action of proteolytic zinc- containing enzymes called matrix metalloproteinases (MMPs), which play a critical role in the ECM reorganiza- tion. MMPs are secreted by Schwann cells, intramuscular axons, muscle satellite cells, and fibroblasts into the skeletal muscle at the neuromuscular junction (NMJ) and around muscle fibers [11,14–16]. Contract grant sponsor: Fundac ¸a ˜o de Amparo a ` Pesquisa do Estado de Sa ˜o Paulo (FAPESP); Contract grant numbers: 2006/ 52931-4, 08/03499-8. *Correspondence to: Davilene Gigo-Benato, PhD, Physical Therapy Department, Federal University of Sa ˜ o Carlos (UFSCar), Rodovia Washington Luı ´s km 235, C.P. 676—CEP 13565-905, Sa ˜o Carlos, SP, Brazil. E-mail: [email protected] Accepted 5 September 2010 Published online 15 October 2010 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/lsm.20978 ß 2010 Wiley-Liss, Inc.
Transcript of Effects of 660 and 780 nm low‐level laser therapy on neuromuscular recovery after crush injury in...

Lasers in Surgery and Medicine 42:673–682 (2010)
Effects of 660 and 780 nm Low-Level Laser Therapy onNeuromuscular Recovery After Crush Injury inRat Sciatic Nerve
Davilene Gigo-Benato, PhD,1* Thiago Luiz Russo, PhD,2 Erika Harumi Tanaka,1 Lıvia Assis, MS,1
Tania Fatima Salvini, PhD,2 and Nivaldo Antonio Parizotto, PhD1
1Thermophototherapy Unit, Physical Therapy Department, Federal University of Sao Carlos (UFSCar), Sao Carlos,SP13565-905, Brazil2Skeletal Muscle Plasticity Unit, Physical Therapy Department, Federal University of Sao Carlos (UFSCar), Sao Carlos,SP 13565-905, Brazil
Background and Objective: Post-traumatic nerverepair is still a challenge for rehabilitation. It is particularlyimportant to develop clinical protocols to enhance nerveregeneration. The present study investigated the effects of660 and 780 nm low-level laser therapy (LLLT) usingdifferent energy densities (10, 60, and 120 J/cm2) onneuromuscular and functional recovery as well as onmatrix metalloproteinase (MMP) activity after crush injuryin rat sciatic nerve.Materials and Methods: Rats received transcutaneousLLLT irradiation at the lesion site for 10 consecutive dayspost-injury and were sacrificed 28 days after injury. Boththe sciatic nerve and tibialis anterior muscles wereanalyzed. Nerve analyses consisted of histology (lightmicroscopy) and measurements of myelin, axon, and nervefiber cross-sectional area (CSA). S-100 labeling was used toidentify myelin sheath and Schwann cells. Muscle fiberCSA and zymography were carried out to assess the degreeof muscle atrophy and MMP activity, respectively. Stat-istical significance was set at 5% (P�0.05).Results: Six hundred sixty nanometer LLLT either using10 or 60 J/cm2 restored muscle fiber, myelin and nervefiber CSA compared to the normal group (N). Furthermore,it increased MMP-2 activity in nerve and decreasedMMP-2 activity in muscle and MMP-9 activity in nerve.In contrast, 780 nm LLLT using 10 J/cm2 decreasedMMP-9 activity in nerve compared to the crush group(CR) and N; it also restored normal levels of myelin andnerve fiber CSA. Both 60 and 120 J/cm2 decreased MMP-2activity in muscle compared to CR and N. 780 nm didnot prevent muscle fiber atrophy. Functional recoveryin the irradiated groups did not differ from the non-irradiated CR.Conclusion: Data suggest that 660 nm LLLT with low(10 J/cm2) or moderate (60 J/cm2) energy densities is able toaccelerate neuromuscular recovery after nerve crushinjury in rats. Lasers Surg. Med. 42:673–682, 2010.� 2010 Wiley-Liss, Inc.
Key words: peripheral nerve repair; laser therapy;denervated muscle; rehabilitation; functional analysis
INTRODUCTION
Peripheral nerve injury is a common clinical event whichis generally related to incapacity [1]. According to a U.S.study, 50,000 subjects suffer traumatic injury to peripheralnerves every year [2,3] representing a significant publichealth problem. In Brazil, a recent study classified 456cases of nerve injury and showed that axonotmesisrepresents the most common nerve injury (45%) followedby neurotmesis (41%) and neuropraxia (14%), respectively[4].
The mechanisms involving nerve regeneration are well-described. When nerve fiber continuity is interrupted, thedistal stump undergoes Wallerian degeneration [5]. Theproximal axon stump can then regenerate along the nervetract distal to the lesion and reach the peripheral target(muscle fibers and sensory receptors) [5]. Another tissuestrongly affected by peripheral nerve injuries is skeletalmuscle. Innervation is critical for muscle functionality andstructural integrity [6,7]. Thus, denervation leads to aprofound loss of muscle mass and inability to generate force[8,9].
The regeneration process depends on numerous changesin the extracellular matrix (ECM) [10] occurring concom-itantly in both injured nerve and denervated muscles [11–13]. These changes require the action of proteolytic zinc-containing enzymes called matrix metalloproteinases(MMPs), which play a critical role in the ECM reorganiza-tion. MMPs are secreted by Schwann cells, intramuscularaxons, muscle satellite cells, and fibroblasts into theskeletal muscle at the neuromuscular junction (NMJ) andaround muscle fibers [11,14–16].
Contract grant sponsor: Fundacao de Amparo a Pesquisa doEstado de Sao Paulo (FAPESP); Contract grant numbers: 2006/52931-4, 08/03499-8.
*Correspondence to: Davilene Gigo-Benato, PhD, PhysicalTherapy Department, Federal University of Sao Carlos (UFSCar),Rodovia Washington Luıs km 235, C.P. 676—CEP 13565-905, SaoCarlos, SP, Brazil. E-mail: [email protected]
Accepted 5 September 2010Published online 15 October 2010 in Wiley Online Library(wileyonlinelibrary.com).DOI 10.1002/lsm.20978
� 2010 Wiley-Liss, Inc.

Nevertheless, only a few studies have investigatedMMPs in neuromuscular diseases [11,12,14,17–19].Studies on nerve crush injury suggest that MMP-2 andMMP-9 are involved in facilitating axonal growth along theperipheral nerve via basal lamina remodeling [12,13].Thus, MMP activity can be considered a good marker forinvestigating peripheral nerve recovery.
Low-level laser therapy (LLLT) seems to be an efficienttechnique in peripheral nerve recovery, and its effective-ness has been shown over the years. A critical review of theliterature [1] found that more than 80% of the experimentalstudies carried out so far on the use of LLLT for promotingperipheral nerve repair led to a positive outcome in post-traumatic/post-operative nerve recovery, thus pointing tothis physical therapy tool as a very promising clinicalapproach for patients who suffered a nerve lesion.
In contrast, there are conflicting results on the use ofLLLT. These results may be due to the lists of technicalvariables (in particular wavelength, doses, and types ofradiation) that, if not properly adjusted, can reduce thesuccess of any therapeutic procedure [1,20]. Following theneed to establish clinical protocols for the application ofLLLT, the present study intends to further the investiga-tion into the effect of this therapy on the peripheral nerve,focusing particular attention on the choice and combina-tion of the LLLT wavelength (660 and 780 nm) and theparameters of irradiation (10, 60, and 120 J/cm2). Theeffects of such LLLT parameters were investigated bymeans of the MMP activity response and neuromuscularrecovery after sciatic nerve crush in rats. The results of thepresent study reveal important aspects of the prospects forLLLT application in patients in the future.
MATERIALS AND METHODS
Crush Injury
Adult male Wistar rats (Rattus norvegicus) weighing275 g were used in this study. Good laboratory animalpractice was observed according to the internationalstandards for animal experimentation and followingapproval by our institution’s Animal Care and EthicsCommittee. The animals were anesthetized with an intra-peritoneal injection of a premixed solution containing
ketamine (95 mg/kg) and xylazine (12 mg/kg). The skinwas shaved and cleaned with 10% povidone iodine. A 2-cm-long incision was made on the skin through a glutealapproach, and the left sciatic nerve was exposed. A non-serrated clamp, exerting a force of 54 N [21,22], was used fora period of 30 seconds to create a 3-mm-long crush injury,10 mm above the bifurcation, to achieve good reproduci-bility of the axonotmetic lesion [22]. The starting diameterof the sciatic nerve was about 1 mm. During the crush thenerve flattens to a new diameter of 2 mm, giving a finalpressure of P¼ 9 MPa. The nerves were kept moist with378C sterile saline solution throughout the surgicalintervention. After surgery, animals were housed in singlecages and fed rat chow and water ad libitum. For the first4 days, acetaminophen (13.5 mg/100 ml) was added to thewater for pain reduction.
LLLT Protocol and Experimental Design
Biostimulation was carried out using a gallium–alumi-num–arsenide laser device (TWIN LASER; MM Optics,Sao Carlos, SP, Brazil) with the following parameters:continuous radiation, wavelength: 660 or 780 nm, power:40 mW, spot area: 4 mm2, energy density at the point ofentry: 10, 60, or 120 J/cm2. The stimulation time waspredetermined by the device according to the above-described parameters. Table I describes all parameters indetail.
After the skin was shaved at the site of surgery(recognizable by the surgical scar), the radiation wasapplied transcutaneously to two points along the sciaticnerve, one above and one below the scar site, with a distanceof 2 cm between them. Applications were made daily for 10consecutive days beginning on day 1 after surgery. Theanimals were handled gently, and laser biostimulation didnot produce any painful sensation or distress to theanimals.
A total of 64 animals were randomly divided into eightgroups (n¼ 8 per group): (1) normal (N), in which theanimals received no intervention and remained free in thecage for 28 days; (2) crush (CR), in which the animals weresubmitted to the crush injury and received a simulationtreatment (placebo); (3) crushed nerve irradiated with660 nm LLLT at 10 J/cm2 (CR660 10 J); (4) crushed nerve
TABLE I. Experimental Groups and LLLT Parameters Investigated
Experimental
groups (n¼ 8)
Wavelength
(nm)
Power
(mW)
Energy density
(J/cm2)
Total energy emitted
per point (J)a
Time ON
(min)
N — — — — —
CR — — — — 1
CR660 10 J 660 40 10 4 0.3
CR660 60 J 660 40 60 24 1
CR660 120 J 660 40 120 48 2
CR780 10 J 780 40 10 4 0.3
CR780 60 J 780 40 60 24 1
CR780 120 J 780 40 120 48 2
N, normal group; CR: crush group. Note that ‘‘J’’ in the experimental groups column means‘‘J/cm2.’’aTotal energy emitted per point¼ energy density (J/cm2)� spot area.
674 GIGO-BENATO ET AL.

irradiated with 660 nm LLLT at 60 J/cm2 (CR660 60 J);(5) crushed nerve irradiated with 660 nm LLLT at120 J/cm2 (CR660 120 J); (6) crushed nerve irradiated with780 nm LLLT at 10 J/cm2 (CR780 10 J); (7) crushed nerveirradiated with 780 nm LLLT at 60 J/cm2 (CR780 60 J);(8) crushed nerve irradiated with 780 nm LLLT at120 J/cm2 (CR780 10 J). The experimental groups and theLLLT parameters are described in Table I.
The Assessment of Nerve Function Recovery
Nerve function recovery was assessed by calculating thesciatic functional index (SFI) as described by Bain et al.[23]. The animals were tested in a confined corridor 42 cmlong and 8.2 cm wide, with a dark shelter at the end. Thecorridor was lined with white paper, and ink was applied tothe hind feet of the rats with a sponge. The rats were thenallowed to walk down the corridor recording their footprintson the paper. Three measurements were taken from thefootprints: (1) the print length (PL), that is, the distancefrom the heel to the third toe; (2) the toe spread (TS), that is,distance from the first to the fifth toe; and (3) the inter-mediary toe spread (ITS), that is, distance from the secondto the fourth toe. All three measurements were taken fromthe experimental (E) and normal (N) sides. The SFI wascalculated according to the following equation:
SFI ¼ �38:3EPL�NPL
NPL
� �þ 109:5
ETS�NTS
NTS
� �
þ 13:3EITS�NITS
NITS
� ��8:8
Muscle and Nerve Evaluation
Twenty-eight days after surgery, all animals wereeuthanized with anesthetic overdose. The right sciaticnerve and the right tibialis anterior (TA) muscle werecarefully dissected to avoid mechanical injury. The musclewas then divided in half at the middle of the belly. The distalfragment was used for the histological and morphometricmeasurements. The proximal fragment was immediatelyfrozen in liquid nitrogen and stored at �808C (FormaScientific, Marietta, OH) for the zymography analysis.
Afterwards, the distal fragment was frozen in isopentanepreviously cooled in liquid nitrogen. Muscle samples wereplaced in plastic tubes and stored in a freezer at �808C.Histological serial cross-sections (10 mm), cut transverselyto the muscle’s main axis, were obtained with an HM505Ecryostat (Microm, Walldorf, Germany) at a level corre-sponding to the middle belly of the muscle. Sections werestained with Masson’s Trichrome kit for morphologicalevaluation according to manufacturer instructions (catalogno. HT15; Sigma–Aldrich, St. Louis, MO). For muscle fibermorphometry, the cross-sectional area (CSA) of 200randomly selected fibers was measured in the middle bellyof each TA muscle, using a light microscope (Axioplan 2,Carl Zeiss, Jena, Germany) equipped with a digital camera(AxioCam HRc, Carl Zeiss, Germany) and the AxioVision4.7 software (Carl Zeiss). A blind procedure was used formeasurements.
Four sciatic nerves were immediately frozen in liquidnitrogen and stored at �808C for zymography. The otherfour nerves were divided in half at the distal portion of thelesion. One part was fixed in 10% formalin for 3 hoursand then washed in phosphate buffer saline (PBS) untilembedding. The specimens were dehydrated and embeddedin paraffin and cut at 7 mm perpendicular to the main nerveaxis. For immune histochemistry, sections were incubatedovernight in a solution of rabbit polyclonal anti-S100(Sigma), which detects bovine 21 kD monomeric unitsof S-100 calcium-binding protein (dilution 1:800). Afterwashing in PBS, immunolabeling was carried out byincubating sections for 1 hour in a solution containinga secondary antibody: TRITC-conjugated anti-rabbit IgG(dilution 1:200; Dako, Milano, Italy). The sections werefinally mounted with Dako fluorescent mounting mediumand analyzed using a fluorescence microscope (Axiolab;Carl Zeiss) equipped with appropriate filter. A magnifica-tion of 100� was used.
For specificity assessment, we also carried out a‘‘morphology-based specificity test,’’ consisting of the sameimmunolabeling protocol to stain sections from normalperipheral nerve where the protein is known to be presentwith a clear localization easily detectable from a morpho-logical viewpoint. This test supported the specificity of thereagent by demonstrating that it specifically labels onlythe tissue elements where the immunogen is known to bepresent.
The other part of the divided nerve was fixed by dripping(for 5 minutes) and then immersion in a solution containing2.5% purified glutaraldehyde and 0.5% saccharose in 0.1 MSorensen phosphate buffer (pH 7.4; 48C) for 6–8 hours.Specimens were washed in a solution containing 1.5%saccharose in 0.1 M Sorensen phosphate buffer (pH 7.4)for 6–12 hours, post-fixed in 1.5% osmium tetroxide,dehydrated and then embedded in historesin according tomanufacturer instructions (Leica HistoResin; Leica, Wehr-heim, Germany). Series of 2-mm-thick semi-thin cross-sections were cut using an ultramicrotome and stained withtoluidine blue for 30 seconds. The nerve sections wereobserved under a light microscope (Axiolab; Carl Zeiss)equipped with a Carl Zeiss AxioCam HRc camera.
For morphometric analysis of the regenerated nervefibers, we used systematic random sampling and the 2D-disector method which has been previously described [24].The measurements were performed using the softwareImageJ 1.42q (Wayne Rasband, National Institutes ofHealth, US; http://rsb.info.nih.gov/ij). The variables ana-lyzed were: number of nerve fibers per field; axon, myelin,and nerve fiber CSA. Numerical data were analyzed usingMATLAB (version 7.0.1).
Zymography
Muscle and nerve extraction and zymographic analysiswere performed according to current methodology [25,26].The molecular mass of gelatinolytic activities was deter-mined by comparison to the reference protein molecularweight marker, PageRuler Prestained Protein Ladder(Fermentas Life Sciences, Burlington, ON, Canada).
EFFECTS OF LLLT ON NEUROMUSCULAR RECOVERY 675
Activity bands were identified according to their molecularweights (active-MMP-9: 85 kDa; pro-MMP-2: 72 kDa; inter-mediary-MMP-2: 64 kDa; and active-MMP-2: 57 kDa).Densitometric quantitative analysis of the total protein inthe zymography was performed using GeneTools v3.06software (Syngene, Cambridge, UK).
Statistics
Shapiro-Wilk’s W and Levene’s test were applied toevaluate the normality and homogeneity of the results,respectively. For parametric data, one-way ANOVA wasused to identify possible differences between groups. Whendifferences were observed, Tukey’s test was performed. Fornonparametric data, the Kruskal–Wallis test was per-formed followed by the Newman–Keuls test. For all tests,the significance level was set at 5% (P�0.05).
RESULTS
Walking Track Analysis
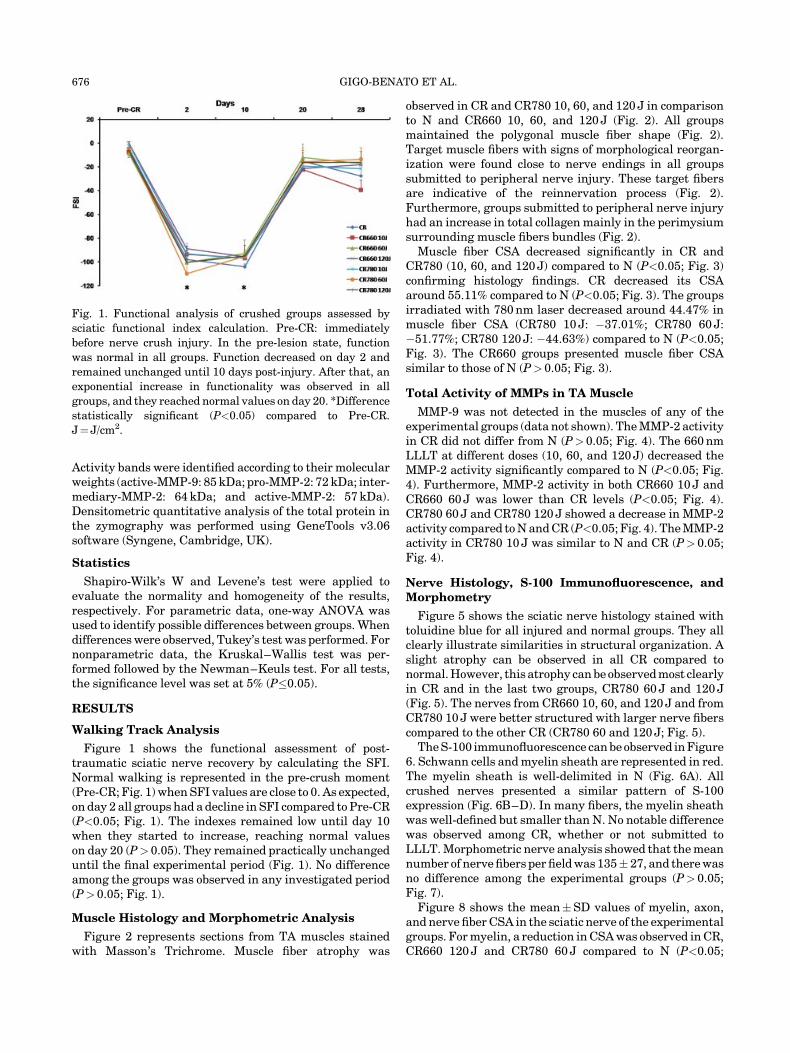
Figure 1 shows the functional assessment of post-traumatic sciatic nerve recovery by calculating the SFI.Normal walking is represented in the pre-crush moment(Pre-CR; Fig. 1) when SFI values are close to 0. As expected,on day 2 all groups had a decline in SFI compared to Pre-CR(P<0.05; Fig. 1). The indexes remained low until day 10when they started to increase, reaching normal valueson day 20 (P> 0.05). They remained practically unchangeduntil the final experimental period (Fig. 1). No differenceamong the groups was observed in any investigated period(P> 0.05; Fig. 1).
Muscle Histology and Morphometric Analysis
Figure 2 represents sections from TA muscles stainedwith Masson’s Trichrome. Muscle fiber atrophy was
observed in CR and CR780 10, 60, and 120 J in comparisonto N and CR660 10, 60, and 120 J (Fig. 2). All groupsmaintained the polygonal muscle fiber shape (Fig. 2).Target muscle fibers with signs of morphological reorgan-ization were found close to nerve endings in all groupssubmitted to peripheral nerve injury. These target fibersare indicative of the reinnervation process (Fig. 2).Furthermore, groups submitted to peripheral nerve injuryhad an increase in total collagen mainly in the perimysiumsurrounding muscle fibers bundles (Fig. 2).
Muscle fiber CSA decreased significantly in CR andCR780 (10, 60, and 120 J) compared to N (P<0.05; Fig. 3)confirming histology findings. CR decreased its CSAaround 55.11% compared to N (P<0.05; Fig. 3). The groupsirradiated with 780 nm laser decreased around 44.47% inmuscle fiber CSA (CR780 10 J: �37.01%; CR780 60 J:�51.77%; CR780 120 J: �44.63%) compared to N (P<0.05;Fig. 3). The CR660 groups presented muscle fiber CSAsimilar to those of N (P> 0.05; Fig. 3).
Total Activity of MMPs in TA Muscle
MMP-9 was not detected in the muscles of any of theexperimental groups (data not shown). The MMP-2 activityin CR did not differ from N (P> 0.05; Fig. 4). The 660 nmLLLT at different doses (10, 60, and 120 J) decreased theMMP-2 activity significantly compared to N (P<0.05; Fig.4). Furthermore, MMP-2 activity in both CR660 10 J andCR660 60 J was lower than CR levels (P<0.05; Fig. 4).CR780 60 J and CR780 120 J showed a decrease in MMP-2activity compared to N and CR (P<0.05; Fig. 4). The MMP-2activity in CR780 10 J was similar to N and CR (P> 0.05;Fig. 4).
Nerve Histology, S-100 Immunofluorescence, andMorphometry
Figure 5 shows the sciatic nerve histology stained withtoluidine blue for all injured and normal groups. They allclearly illustrate similarities in structural organization. Aslight atrophy can be observed in all CR compared tonormal. However, this atrophy can be observed most clearlyin CR and in the last two groups, CR780 60 J and 120 J(Fig. 5). The nerves from CR660 10, 60, and 120 J and fromCR780 10 J were better structured with larger nerve fiberscompared to the other CR (CR780 60 and 120 J; Fig. 5).
The S-100 immunofluorescence can be observed in Figure6. Schwann cells and myelin sheath are represented in red.The myelin sheath is well-delimited in N (Fig. 6A). Allcrushed nerves presented a similar pattern of S-100expression (Fig. 6B–D). In many fibers, the myelin sheathwas well-defined but smaller than N. No notable differencewas observed among CR, whether or not submitted toLLLT. Morphometric nerve analysis showed that the meannumber of nerve fibers per field was 135� 27, and there wasno difference among the experimental groups (P> 0.05;Fig. 7).
Figure 8 shows the mean�SD values of myelin, axon,and nerve fiber CSA in the sciatic nerve of the experimentalgroups. For myelin, a reduction in CSA was observed in CR,CR660 120 J and CR780 60 J compared to N (P<0.05;
Fig. 1. Functional analysis of crushed groups assessed by
sciatic functional index calculation. Pre-CR: immediately
before nerve crush injury. In the pre-lesion state, function
was normal in all groups. Function decreased on day 2 and
remained unchanged until 10 days post-injury. After that, an
exponential increase in functionality was observed in all
groups, and they reached normal values on day 20. *Difference
statistically significant (P<0.05) compared to Pre-CR.
J¼ J/cm2.
676 GIGO-BENATO ET AL.

Fig. 2. Histological appearance of tibialis anterior muscle after Masson’s Trichrome staining.
Note that CR and CR780 10, 60, and 120 J presented muscle fiber atrophy compared to N.
Arrowheads indicate increase in total collagen in the perimysium in all crushed groups.
Arrows show target muscle fibers indicating cytoarchitectural reorganization. Target fibers
are indicative of the reinnervation process. Asterisks (*) indicate an intramuscular nerve
termination. J¼ J/cm2. Bar¼ 100 mm.
Fig. 3. Mean cross-sectional area of tibialis anterior muscle
fibers. *P<0.05 compared to N. Note that CR and CR780 10, 60,
and 120 J did not recover normal values of muscle fiber cross-
sectional area (CSA). Groups irradiated with 660 nm LLLT
presented normal muscle fiber CSA. J¼ J/cm2.
Fig. 4. Total MMP-2 activity observed in the different
experimental groups. Representative bands of MMP-2 gelat-
inolytic activity are represented at the top of the figure. J¼ J/
cm2. *P<0.05: compared to N; {P<0.05: compared to CR. Note
the significant decrease in MMP-2 activity in CR660 10 and
60 J and also in CR780 60 and 120 J compared to N and CR.
EFFECTS OF LLLT ON NEUROMUSCULAR RECOVERY 677

Fig. 8). CR660 10 and 60 J and CR780 10 and 120 J hadmyelin CSA values similar to N (P> 0.05; Fig. 8). Axon CSAdecreased in all CR compared to N (P<0.05, Fig. 8) with nodifference among them (P> 0.05; Fig. 8). Nerve fiber CSAfollowed the changes observed in myelin, for example,CR660 10 and 60 J and CR780 20 and 120 J had valuessimilar to N (P> 0.05; Fig. 8), whereas CR, CR660 120 J andCR780 60 J were smaller than N (P<0.05; Fig. 8).
Total MMP Activity in Sciatic Nerve
After 28 days, the MMP-9 activity for CR was similar to N(P> 0.05; Fig. 9). 660 nm LLLT, regardless of the dose used,decreased MMP-9 activity in injured sciatic nerve com-pared to CR (CR660 10 J: �62%, P¼ 0.0002; CR660 60 J:�68%, P¼ 0.0001; and CR660 120 J: �39%, P¼ 0.03; Fig.9). CR780 10 J showed a significant reduction in MMP-9activity compared to N and CR (P¼ 0.02 and P¼ 0.0001,respectively; Fig. 9). Both CR780 60 and 120 J presentedthe same levels of MMP-9 activity compared to N and CR(P> 0.05; Fig. 9).
The MMP-2 activity remained unchanged in CR andCR780 10, 60, and 120 J compared to N (P> 0.05; Fig. 10).However, all groups irradiated with 660 nm LLLT hadsignificantly increased MMP-2 activity compared to N(CR660 10 J: þ81%, P¼ 0.04; CR660 60 J: þ126%,P¼ 0.003, and CR660 120 J: þ100%, P¼ 0.02) and CR(P<0.05; Fig. 10).
DISCUSSION
The present study brings new information about theeffects of different doses of LLLT on peripheral nerveregeneration and denervated muscle recovery after crushinjury. Several studies have already shown that LLLT
Fig. 5. Histological nerve sections stained with toluidine blue.
Note structural similarities among the experimental groups.
Scale bar: 40 mm2. J¼ J/cm2.
Fig. 6. Immunofluorescence analysis of S-100 performed in
sciatic nerves. Myelin sheath and Schwann cells are marked in
red. Arrowheads represent normal S-100 expression in N.
White arrows show S-100 expression in small regenerated
fibers. No difference was observed among crushed groups. Bar:
100mm2. J¼ J/cm2.
Fig. 7. Number of nerve fibers per microscopic field in different
experimental groups. There was no difference among the
groups.
678 GIGO-BENATO ET AL.

accelerates the peripheral nerve regeneration process[1,27–39]. However, no study in the last decade hasexamined the effects of LLLT irradiation on TA muscletrophism after peripheral nerve injury [38,39]. Anotherinnovative aspect of the present study was the analysis ofMMP activity in both nerve and muscle submitted to LLLT.The authors consider that the results cannot be interpretedout of their overall context given that some parametersseemed to induce better neuromuscular recovery thanothers.
The LLLT parameters chosen in the present study werebased on several scientific studies. The literature showsthat there is an increase in the use of infrared laser devices,and this is justified by its greater penetration through theskin [40]. Nevertheless, positive effects obtained fromexperimental studies used either visible [29,41,42] ornear-infrared lasers [20]. It seems that both types of LLLT
wavelengths are useful to promote nerve regeneration.Another important parameter to be considered wheninvestigating LLLT effects is energy density. Analysis ofpublished results showed that LLLT at different levels ofenergy density (ranging <10 to 150 J/cm2) are effective inpromoting nerve regeneration [1]. The same can bereported for the time of irradiation which varies from <1to 90 minutes. Therefore, these observations suggestthat LLLT has positive effects on nerve regeneration. Incontrast, there is still uncertainty regarding the bestparameter combination to consider when treating nerveinjuries. All published studies which presented good resultsin nerve regeneration used continuous LLLT, thus this typeof laser emission was used in the current study [1,27,38].
The 660 nm LLLT Accelerates NeuromuscularRecovery
Regarding muscle fiber CSA results, 660 nm LLLT with10, 60, or 120 J/cm2 seemed to be effective in acceleratingthe recovery of muscle fiber trophism in the present study.In addition, nerve morphometry showed that both myelinand nerve fiber CSA reached normal levels in CR660 10 and60 J/cm2 and also in CR780 10 and 120 J/cm2. The myelinsheath is responsible for action potential conduction alongthe axon, and its reduction causes decrease or loss in axonalfunction [43]. Nerve histology corroborated these findingsbecause these groups presented larger nerve fibers and lessconnective tissue surrounding the fibers. Furthermore,S-100, a marker of Schwann cells and myelin sheath,showed that its expression was quite similar among thecrushed groups, and myelin was not structured in the sameway as in the control groups. To elucidate these differentaspects involving muscle and nerve recovery, futurestudies should investigate electrical neurophysiologicparameters of the neuromuscular system, for example,H-reflex and M-wave, and factors related to musclereinnervation, for example, neural cell adhesion molecule(N-CAM), agrin, and acetylcholine receptor expressions.
Fig. 8. Myelin, axon, and nerve fiber cross-sectional area
(CSA) from sciatic nerve. *P<0.05 compared to N. Note that
CR660 10 and 60 J and CR780 10 and 120 J had myelin and
nerve fiber CSA values similar to N. All crushed groups had
decreased axon CSA compared to N with no difference among
them. J¼ J/cm2.
Fig. 9. Total MMP-9 activity observed in sciatic nerve of
experimental groups. Representative bands of MMP-2 gelat-
inolytic activity are presented at the top of the figure. J¼ J/cm2.
*P<0.05: compared to N; {P<0.05: compared to CR. Note that
all CR660 groups (10, 60, and 120 J) and CR780 10 J had
decreased MMP-9 activity compared to CR.
Fig. 10. Total MMP-2 activity observed in sciatic nerve of
experimental groups. Representative bands of MMP-2 gelat-
inolytic activity are presented at the top of the figure. J¼ J/cm2.
*P<0.05: compared to N and CR. Note that all groups
submitted to 660 nm LLLT regardless the dose (10, 60, and
120 J) had increased MMP-2 activity.
EFFECTS OF LLLT ON NEUROMUSCULAR RECOVERY 679

MMP-2 and -9 Activities Are Regulated Differentlyby 660 nm LLLT in Nerves and Muscles
Regarding the MMP activity results, the biologicalmeaning of its behavior due to LLLT is interpretedaccording to overall nerve and muscle results. Therefore,the authors conclude that 660 nm LLLT, especially at 10and 60 J/cm2, accelerated nerve regeneration and musclefiber reinnervation. This hypothesis can be supported bythe fact that groups irradiated with 660 nm laser recoveredmuscle fiber CSA compared to N. This recovery wasaccompanied by increased MMP-2 activity in nerve anddecreased MMP-9 and MMP-2 activities in nerve andmuscle, respectively.
During the initial phases of Wallerian degeneration,axonal cytoskeleton disintegration and myelin sheathbreakdown are highly coordinated by MMPs, especiallyMMP-9 and -2. La Fleur et al. [44] showed that high levels ofMMP-9 on days 1 and 4 after nerve crush injury are relatedto neutrophils and macrophage influx, respectively. Fur-thermore, the authors report that inflammatory cells andSchwann cells are able to secrete MMP-9. Its secretion isimportant to degrade axon and myelin debris promotingECM remodeling necessary for axonal growth. In addition,MMPs can release Schwann cells from their connectionswith basal membrane allowing their proliferation andstimulating the penetration of axon terminals throughECM [44].
Although increased MMP-9 activity is desired during theearly stage of nerve degeneration, the maintenance of highMMP-9 levels can be detrimental to tissue integrity.Beuche et al. [45] observed an increase in serum MMP-9levels in patients with amyotrophic lateral sclerosispossibly caused by peripheral nerve degeneration andmuscle denervation. MMP-9-knockout mice that under-went a spinal cord injury showed an accelerated recovery ofmotor function compared to wild-type mice [46]. Together,these results indicate that the negative regulation of MMP-9 might be important during the final stages of neuralrepair. Thus, our results suggest that LLLT may have ananti-inflammatory effect, controlling inflammatory cellinflux via MMP-9 down-regulation.
In this context, the production and degradation of ECMcomponents seems to stimulate or impair axonal growth.Gantus et al. [10] reported that laminin, fibronectin, andcollagen IV are important to support axonal growth duringthe regenerative process, forming a network of ECM to thegrowth cone. However, other ECM components, such aschondroitin sulfate proteoglycan (CSPG), are able to inhibitthis process [10].
Previous studies have shown that during the Wallerianprocess, increased MMP-2 activity in nerve is able toreorganize the basal lamina by degrading collagen type IVand allowing the axonal growth cone to move forward [44].Moreover, it is well described in the literature that MMP-2degrades CSPG [10] suggesting that the increase in MMP-2activity could be a positive indicator of axon regeneration.
Our results corroborate these findings. In the presentstudy, the groups that presented normal values of muscle
fiber and myelin CSA had the lowest values of MMP-9 andthe highest values of MMP-2 in sciatic nerve. It is alsonecessary to emphasize that these MMPs are systemati-cally regulated by tissue inhibitors of metalloproteinase(TIMP), which control the process and protect the basallamina structure [44]. Future studies should investigatethe role of LLLT not only in MMP activity in nerve andmuscle tissues but also in TIMP expression.
For the denervated skeletal muscle, the role of MMPs inthis affection is still not well-defined. Some studies haveshown that the increase in MMP-2 activity in muscles after28 days of denervation may be related not only to muscleatrophy and proliferation of connective tissue aroundmuscle fibers [25] but also to ECM remodeling, whichallows axonal growth and muscle fiber reinnervation.However, other studies show that increased MMP-2activity may be related to cycles of degeneration/regener-ation of muscle fibers. Thus, the decrease in MMP-2 activityin the muscles of the groups irradiated with 660 nm LLLTmay have been beneficial to the muscle tissue, possiblycausing less damage to the muscle fibers. Future studiesshould evaluate the behavior of these MMPs in themuscular and peripheral nervous systems at differentperiods of time to confirm the hypotheses suggested here.
780 nm LLLT Did Not Prevent Muscle Atrophy ButRegulated MMP Activity According to the EnergyDensity
Rochkind et al. [37,38] used 780 nm LLLT to treat severenerve injury in humans. They reported that LLLTaccelerated nerve regeneration and improved musclerecruitment 6 months after nerve injury [37]. The LLLTprotocol consisted of: wavelength, 780 nm; power, 250 mW;3 hours of transcutaneous irradiation to the injuredperipheral nerve (energy density, 450 J/mm2) and 2 hourson the corresponding segments of the spinal cord (energydensity, 300 J/mm2). In the present study, however, 780 nmLLLT did not prevent muscle fiber atrophy due to nervecrush injury. In addition, no changes were observed in theMMP-2 activity in nerves compared to N and CR. Never-theless, energy density at 10 J/cm2 decreased MMP-9activity and restored both myelin and fiber CSA in nervescompared to N. Furthermore, 120 J/cm2 can restore myelinand nerve fiber CSA and decrease the MMP-2 activity inmuscles compared to N values. Together, the data showedthat although it does not prevent muscle atrophy, 780 LLLTcan affect MMP activity in nerves and muscles. Futurestudies should evaluate different times of irradiation andenergy densities to verify if these molecular modificationscan accelerate neuromuscular recovery.
Neither 660 Nor 780 nm LLLT Improves FunctionalRecovery After Nerve Crush Injury
Regarding functional analysis, all experimental groupssubmitted to nerve crush injury recovered normal functionat the end of the experimental period. Such response wasexpected due to the type of nerve injury performed. Varejaoet al. [22] used the same protocol of crush injury in rat
680 GIGO-BENATO ET AL.

sciatic nerve and found that 4 weeks post-injury animalshad recovered about 80% of their function, and on the8th week, the motor recovery was complete. Followingthis premise, the authors opted to use a well-described,controlled, and reproducible model of crush injury of ratsciatic nerve [21,22,29,30,42,47–49] that allows theverification of different phases of nerve recovery. Morpho-logical findings of the present study such as target musclefibers were observed in all crushed groups suggesting thatmuscle fibers were reinnervated confirming the time set fornerve recovery after the crush.
Despite the prognosis of rapid recovery in animal models,traumatic nerve injury in humans has a recovery time ofseveral months or even years, depending on the severityand extension of the lesion [37]. Additionally, the recoverywas often incomplete, generating dysfunctions, and impair-ing daily life activities. Regarding clinical applicability, thistype of study makes an important contribution to thedevelopment of safe and effective strategies of peripheralnerve injury rehabilitation.
The functional test used in our study is widely used as it isan easy, non-invasive, and affordable procedure. However,scientists disagree as to the effectiveness of its results.Some accept the test as an appropriate tool to evaluatesciatic nerve injury. Other groups question its accuracy andsuggest that video analysis could be more precise [50–52].Nevertheless, the functional test is an additional analysisthat, combined with other analyses, can suggest how theneuromuscular recovery is progressing.
CONCLUSION
The present study demonstrated that both nerves andmuscles have a biological response according to the wave-length and dose used, that is, data support a dose-depend-ent curve. CR660 10 J and CR660 60 J presented normalvalues of muscle fiber, myelin, and nerve fiber CSA. Thesegroups also showed a decrease in MMP-2 and -9 activities inTA muscle and sciatic nerve, respectively, and an increasein MMP-2 activity in nerve. Based on the objectiveproposed, we conclude that 660 nm LLLT, especially atlow (10 J/cm2) and moderate (60 J/cm2) energy densities,accelerated neuromuscular recovery and ECM remodelingin nerve and muscle via MMP-2 and -9 regulation, however,it failed to accelerate the improvement in function afternerve crush injury in rats.
REFERENCES
1. Gigo-Benato D, Geuna S, Rochkind S. Phototherapy forenhancing peripheral nerve repair: A review of the literature.Muscle Nerve 2005;31:694–701.
2. Millesi H. Techniques for nerve grafting. Hand Clinics2000;16:73–91.
3. Evans GR. Peripheral nerve injury: A review and approach totissue engineered constructs. Anat Rec 2001;263:396–404.
4. Kouyoumdjian JA. Peripheral nerve injuries: A retrospectivesurvey of 456 cases. Muscle Nerve 2006;34:785–788.
5. Lundborg G. Nerve Injury and Repair, 2nd edition. Edin-burgh: Churchill Livingstone; 2005.
6. Ishido M, Kami K, Mitsuhiko M. In vivo expression patternsof MyoD, p21 and Rb proteins in myonuclei and satellite cellsof denervated rat skeletal muscle. Am J Physiol Cell Physiol2004;287:C484–C493.
7. Kostrominova TY, Dow DE, Dennis RG, Miller RA, FaulknerJA. Comparison of gene expression of two-month denervated,two-month stimulated-denervated and control rat skeletalmuscles. Physiol Genomics 2005;22:227–243.
8. Billington L, Carlson BM. The recovery of long-termdenervated rat muscles after marcaine treatment andgrafting. J Neurol Sci 1996;144:147–155.
9. Dow DE, Cederna PS, Hassett CA, Kostrominova TY,Faulkner JA, Dennis RG. Number of contractions to maintainmass and for force of a denervated rat muscle. Muscle Nerve2004;30:77–86.
10. Gantus MAV, Nasciutti LE, Cruz CM, Persechini PM,Martinez AMB. Modulation of extracellular matrix compo-nents by metalloproteinases and their tissue inhibitorsduring degeneration and regeneration of rat sural nerve.Brain Res 2006;1122:36–46.
11. Demestre M, Orth M, Wells GM, Gearing AJ, Hughes RA,Gregson NA. Characterization of matrix metalloproteinasesin denervated muscle. Neuropathol Appl Neurobiol 2005;31:545–555.
12. Platt CI, Krekoski CA, Ward RV, Edwards DR, Gavrilovic J.Extracellular matrix and matrix metalloproteinases in sciaticnerve. J Neurosci Res 2003;74:417–429.
13. Siebert H, Dippel N, Mader M, Weber F, Bruck W.Matrix metalloproteinase expression and inhibition aftersciatic nerve axotomy. J Neuropathol Exp Neurol 2001;60:85–93.
14. Ahtikoski AM, Tuominen H, Korpelainen JT, Takala TE,Oikarinen A. Collagen synthesis and degradation in poly-neuropathy and myopathies. Muscle Nerve 2004;30:602–608.
15. Schoser BG, Blottner D. Matrix metalloproteinases MMP-2,MMP-7 and MMP-9 in denervated human muscle. Neuro-report 1999;10:2795–2797.
16. Carmeli E, Moas M, Reznick AZ, Coleman R. Matrix metal-loproteinases and skeletal muscle: A brief review. MuscleNerve 2004;29:191–197.
17. Kherif S, Dehaupas M, Lafuma C, Fardeau M, AlameddineHS. Matrix metalloproteinases MMP-2 and MMP-9 indenervated muscle and injured nerve. Neuropathol ApplNeurobiol 1998;24:309–319.
18. Koskinen SO, Kjaer M, Mohr T, Sørensen FB, Suuronen T,Takala TE. Type IV collagen and its degradation in paralyzedhuman muscle: Effect of functional electrical stimulation.Muscle Nerve 2000;23:580–589.
19. Schoser BG, Blottner D, Stuerenburg HJ. Matrix metal-loproteinases in inflammatory myopathies: Enhanced immu-noreactivity near atrophic myofibers. Acta Neurol Scand2002;105:309–313.
20. Rochkind S, El-Ani D, Nevo Z, Shahar A. Increase of neuronalsprouting and migration using 780nm laser phototherapy asprocedure for cell therapy. Lasers Surg Med 2009;41:277–281.
21. Beer GM, Steurer J, Meyer VE. Standardizing nerve crusheswith a non-serrated clamp. J Reconstr Microsurg 2001;17:531–534.
22. Varejao AS, Cabrita AM, Meek MF, Bulas-Cruz J, Melo-PintoP, Raimondo S, Geuna S, Giacobini-Robecchi MG. Functionaland morphological assessment of a standardized rat sciaticnerve crush injury with a non-serrated clamp. J Neuro-trauma 2004;21:1652–1670.
23. Bain JR, Mackinnon SE, Hunter DA. Functional evalua-tion of complete sciatic, peroneal, and posterior tibialnerve lesions in the rat. Plast Reconstr Surg 1989;83:129–138.
24. Geuna S, Gigo-Benato D, De Catro Rodrigues A. On samplingand sampling errors in histomorphometry of peripheral nervefibers. Microsurgery 2004;24:72–76.
25. Russo TL, Peviani SM, Durigan JL, Salvini TF. Electricalstimulation increases matrix metalloproteinase-2 geneexpression but does not change its activity in denervatedrat muscle. Muscle Nerve 2008;37:593–600.
26. Peviani SM, Russo TL, Durigan JL, Vieira BS, Pinheiro CM,Galassi MS, Salvini TF. Stretching and electrical stimulationregulate the metalloproteinase-2 in rat denervated skeletalmuscle. Neurol Res 2009 (in press).
EFFECTS OF LLLT ON NEUROMUSCULAR RECOVERY 681

27. Anders JJ, Geuna S, Rochkind S. Phototherapy promotesregeneration and functional recovery of injured peripheralnerve. Neurol Res 2004;26:233–239.
28. Rochkind S, Nissan M, Razon N, Schwartz M, Bartal A.Electrophysiological effect of HeNe laser on normal andinjured sciatic nerve in the rat. Acta Neurochir 1986;83:125–130.
29. Rochkind S, Barr-Nea L, Razon N, Bartal A, Schwartz M.Stimulatory effect of He–Ne low dose laser on injured sciaticnerves of rats. Neurosurgery 1987;20:843–847.
30. Rochkind S, Nissan M, Barr-Nea L, Razon N, Schwartz M,Bartal A. Response of peripheral nerve to He–Ne laser:Experimental studies. Lasers Surg Med 1987;7:441–443.
31. Rochkind S, Nissan M, Lubart R, Avram J, Bartal A. The in-vivo-nerve response to direct low-energy-laser irradiation.Acta Neurochir 1988;94:74–77.
32. Rochkind S, Rousso M, Nissan M, Villarreal M, Barr-Nea L,Rees DG. Systemic effects of low-power laser irradiation onthe peripheral and central nervous system, cutaneouswounds, and burns. Lasers Surg Med 1989;9:174–182.
33. Rochkind S, Barr-Nea L, Volger I. Spinal cord response tolaser treatment of injured peripheral nerve. Spine 1990;15:6–10.
34. Rochkind S, Ouaknine GE. New trend in neuroscience: Low-power laser effect on peripheral and central nervous system(basic science, preclinical and clinical studies). Neurol Res1992;14:2–11.
35. Rochkind S, Nissan M, Alon M, Shamir M, Salame K. Effectsof laser irradiation on the spinal cord for the regeneration ofcrushed peripheral nerve in rats. Lasers Surg Med 2001;28:216–219.
36. Rochkind S, Drory V, Alon M, Nissan M, Ouaknine GE. Laserphototherapy (780nm), a new modality in treatment of long-term incomplete peripheral nerve injury: A randomizeddouble-blind placebo-controlled study. Photomed Laser Surg2007;25:436–442.
37. Rochkind S, Leider-Trejo L, Nissan M, Shamir MH, Khar-enko O, Alon M. Efficacy of 780-nm laser phototherapy onperipheral nerve regeneration after neurotube reconstruc-tion procedure (double-blind randomized study). PhotomedLaser Surg 2007;25:137–143.
38. Rochkind S, Geuna S, Shainberg A. Chapter 25: Photo-therapy in peripheral nerve injury: Effects on musclepreservation and nerve regeneration. Int Rev Neurobiol2009;87: 445–464.
39. Rochkind S. Phototherapy in peripheral nerve injury formuscle preservation and nerve regeneration. PhotomedLaser Surg 2009;27:219–220.
40. Tuner J, Hode L. Laser Therapy: Clinical Practice andScientific Background. Sweden: Prima Books Grangesberg;2003:380–434.
41. Hamilton GF, Robinson TK, Ray RH. The effects of helium-neon laser upon regeneration of the crushed peroneal nerve.J Orthop Sports Phys Therapy 1992;15:209–214.
42. Anders JJ, Borke RC, Woolery SK, Van De Merwe WP. Lowpower laser irradiation alters the rate of regeneration of therat facial nerve. Lasers Surg Med 1993;13:72–82.
43. Shin OHJ. Color Atlas of Nerve Biopsy Pathology. EUA: CRCPress LLC; 2005.
44. La Fleur M, Underwood JL, Rappolee DA, Werb Z. Basementmembrane and repair of injury to peripheral nerve: Defininga potential role for macrophages, matrix metalloproteinases,and tissue inhibitor of metalloproteinases-1. J Exp Med1996;184:2311–2326.
45. Beuche W, Yushchenko M, Mader M, Maliszewska M,Felgenhauer K, Weber F. Matrix metalloproteinase-9 iselevated in serum of patients with amyotrophic lateralsclerosis. Neuroreport 2000;11:3419–3422.
46. Noble LJ, Donovan F, Igarashi T, Goussev S, Werb Z. Matrixmetalloproteinases limit functional recovery after spinal cordinjury by modulation of early vascular events. J Neurosci2002;22:7526–7535.
47. Khullar SM, Brodin P, Messelt EB, Haanaes HR. The effectsof low level laser treatment on recovery of nerve conductionand motor function after compression injury in the rat sciaticnerve. Eur J Oral Sci 1995;103:299–305.
48. Bagis S, Comelekoglu U, Coskun B, Milcan A, Buyukakilli B,Sahin G, Ozisik S, Erdogan C. No effect of GA-AS (904nm)laser irradiation on the intact skin of the injured rat sciaticnerve. Lasers Med Sci 2003;18:83–88.
49. Shin DH, Lee E, Hyun JK, Lee SJ, Chang YP, Kim JW, ChoiYS, Kwon BS. Growth-associated protein-43 is elevated in theinjured rat sciatic nerve after low power laser irradiation.Neurosci Lett 2003;344:71–74.
50. Bervar M. An alternative video footprint analysis to assessfunctional loss following injury to the rat sciatic nerve. ActaChir Plast 2002;44:86–89.
51. Sarikciouglu L, Demirel BM, Utuk A. Walking track analysis:An assessment method for functional recovery after sciaticnerve injury in the rat. Folia Morphol (Warsz) 2009;68:1–7.
52. Costa LM, Simoes MJ, Maurıcio AC, Varejao AS. Chapter 7:Methods and protocols in peripheral nerve regenerationexperimental research: Part IV—Kinematic gait analysis toquantify peripheral nerve regeneration in the rat. Int RevNeurobiol 2009;87:127–139.
682 GIGO-BENATO ET AL.