
Theory and applications of digital smear filters - University of ...
Upload
independentCategory
view
1download
0
Basic Research—Technology
Effectiveness of Different Final Irrigant Activation Protocolson Smear Layer Removal in Curved CanalsGregory Caron, DDS,* Khan Nham, DDS,† Francois Bronnec, DDS,* and Pierre Machtou, DDS*
Abstract
Introduction: A final flush with chelating agents andantiseptic irrigating solutions is needed to remove thesmear layer. The improvement of these protocols ispossible by using specific delivery and agitation tech-niques. This study examined the effect of different finalirrigation regimens and methods of activation on smearlayer removal in curved canals after root canal instru-mentation. Methodology: Mesial root canals of 50 ex-tracted mandibular molars were prepared usingProTaper rotary files (Dentsply Maillefer, Ballaigues,Switzerland) and 3% NaOCl. Teeth were then allocatedto two control groups and four experimental groups (n= 10) for final irrigation as follows: no-activation group(final rinse with a 27-gauge needle and 17% EDTA/3%NaOCl), manual-dynamic activation group (final rinse17% EDTA/3% NaOCl + gutta-percha agitation),automated-dynamic activation group (final rinse 17%EDTA/3% NaOCl + RinsEndo [Durr Dental GmbH & CoKG, Bietigheim-Bissingen, Germany]), and sonic-activation group (final rinse 17% EDTA/3% NaOCl + En-doactivator [Advanced Endodontics, Santa Barbara,CA]). All mesial roots were split with a new approachto allow visualization of every third of the canal, partic-ularly the apical third. The samples were prepared forscanning electron microscopic observation to assessthe smear layer removal. Blind scoring was performedby two calibrated observers using a five-score scale.The differences in smear layer scores between the exper-imental groups were analyzed with the Kruskal-Wallistest and the Mann-Whitney U test. The level of signifi-cance was set at p = 0.05. Results: Very high levelsof root canal cleanliness (#score 3) were found foreach test group with activation. For the middle andapical third, the no-activation group was significantlyless effective than the three other activation groups (p< 0.05). The manual-dynamic activation group (finalrinse 17%EDTA/3%NaOCl + gutta-percha agitation)and the sonic-activation group (final rinse 17%EDTA/3%NaOCl + Endoactivator) showed significantly bettersmear layer removal (p < 0.05) in comparison with theFrom the )Department of Endodontics and Restorative DentistENSCP, Paris, France.
Supported in part by the Association de formation en EndodontAddress requests for reprints to Dr Gregory Caron, 5 rue Garan
0099-2399/$0 - see front matterCopyright ª 2010 American Association of Endodontists.
doi:10.1016/j.joen.2010.03.037
JOE — Volume 36, Number 8, August 2010
other test groups in the apical third. Conclusion: Root canal cleanliness benefitsfrom solutions activation (especially sonic activation and manual-dynamic activation)in comparison with no activation during the final irrigation regimen. (J Endod2010;36:1361–1366)
Key WordsAutomated-dynamic activation, final irrigation, manual-dynamic activation, smearlayer, sonic activation
The ultimate goal of endodontic treatment is to control the microbial factor incomplex root canal anatomy, especially in the apical one third (1). This objective
is achieved by combining instrument-based preparation (manual or mechanical)with antiseptic irrigating solutions followed by three-dimensional obturation of theroot canal system. The gold standard irrigant is still sodium hypochlorite, which canbe associated with EDTA to offer bactericidal, solvent, and chelating actions all inone. This combination offsets the drawbacks of the instrument-based preparation,particularly the creation of debris (2) and the smear layer (3). The smear layer is poten-tially infected, and its removal allows more efficient penetration of intracanal medica-tions into the dentinal tubules and a better interface between the filling material and theroot canal walls (4).
The literature reports generally show that regardless of the instrumentation andirrigation techniques, the effectiveness of irrigating solutions remains limited in theapical one third of a prepared canal. This is particularly true for curved root canals(5, 6) and even on single-rooted teeth (7, 8). Therefore, the improvement ofirrigating protocols is essential during root canal treatment in order to achievebetter cleaning efficiency especially in the very complex apical area.
Currently, several techniques and systems are available and reported to improvefinal irrigation before obturation (9). Among these protocols passive ultrasonic irriga-tion has shown promising results on debris (10) and smear layer removal (11).
However, there are little published scientific data comparing the new andemerging devices and methods for disinfection with a conventional syringe irrigation.First, a fully tapered and apically trimmed nonstandardized gutta-percha master conecould be used in a well-prepared canal as a cost-effective mechanical agitator. A gentlepumping with short vertical strokes has been shown to promote disinfection (12, 13).Another recently released device, the RinsEndo irrigation system (Durr Dental GmbH &Co KG, Bietigheim-Bissingen, Germany), delivers solutions at a flush-through rate of 6.2mL/min using pressure-suction technology for intracanal activation (1.6 Hz). Thisdevice generates a mechanical action that is able to produce a hydrodynamic exchangecircuit (13, 14). Finally, the Endoactivator system (Advanced Endodontics, SantaBarbara, CA) has been purported to improve disinfection. This device uses
ry, School of Dentistry, University, Paris, France; and †Department of Surface Physico-Chemistry,
ie Appliquee.ciere 75006 Paris , France. E-mail address: [email protected].
Final Irrigant Activation Protocols for Smear Layer Removal in Curved Canals 1361

Basic Research—Technology
a cordless sonic handpiece to activate strong, highly flexible polymertips. Noncutting tips have tapers and terminal diameters that closelymatch the dimensions of the final root canal preparation (15). Mechan-ical oscillations are produced mainly at the tip of the activator witha frequency ranging from 1 to 10 kHz.The purpose of this study was to assess smear layer removal effi-ciency after using gutta-percha master cone or RinsEndo or the Endoac-tivator in comparison to conventional final irrigation using a 27-gaugeneedle. The null hypothesis was that there is no difference in smear layerremoval between final irrigation with no activation and final irrigationwith activation.
Materials and MethodsThe study was conducted on 50 freshly extracted mature human
mandibular molar teeth with two separate mesial canals. None of theteeth had received restorative or endodontic treatment before extrac-tion. After extraction, the teeth were conserved in a solution of physio-logic saline to avoid damaging the pulp tissue and then stored at 4�C(16). Each individual tooth was then photographed and x-rayed to visu-alize the root canal anatomy and confirm that each canal curved at morethan 20� (17).
After cutting a four-wall access cavity, the full lengths of the mesio-buccal and mesiolingual canals were determined when a #08 K-type filecould be visualized at the apical foramen. Both the mesial and distalroots were sealed with melted wax to close the apical foramen (18).The aim was to prevent the irrigants from escaping through the apexin order to simulate in vivo conditions (19). The two mesial root canalswere prepared using the Protaper Universal rotary files system (Dents-ply Maillefer, Ballaigues, Switzerland) following the protocol describedby Machtou and Ruddle (20) in which the apical one-third taper of thefinished preparation is approximately 10%. All the canals wereprepared so that the finished size of each apical foramen rangedbetween 0.20 mm and 0.30 mm in diameter. A medium nonstandar-dized gutta-percha master cone (Henry Schein, Melville, NY) was fittedin each canal to the full working length, and then the tooth was x-rayed.After each instrument, the expending preparation was flooded bypassively irrigating 0.5 mL of 3% sodium hypochlorite (Parcan; Septo-dont, Saint-Maur-des-Fosses, France) into the canal using a 27-gaugeneedle (Monoject; Tyco Kendall, Hampshire, UK) loosely inserted asfar as possible without binding. A #10 K-type patency file was used tomaintain apical patency and move debris into suspension followed byflushing the canal again with 0.5 mL of fresh irrigant. All procedureswere performed by the same operator (GC).
The teeth were randomly divided into four experimental groups (n= 10) and two control groups. The negative controls (n = 5) receivedno final irrigation regimen after fitting of the master cone. The positivecontrols (n = 5) were immersed for 5 minutes in a bath of 17% EDTAfollowed by an immersion for 5 minutes in a bath of 3% NaOCl after thesplitting process.
Final Irrigation ProtocolsNo-activation Group. After suctioning away the intracanal surplusof NaOCl with the 27-gauge needle, 1 mL of 17% EDTA (Largal Ultra;Septodont, Saint-Maur-des-Fosses, France) was flushed into each canaland was left in place for 1 minute per canal. All canals were then flushedwith 3 mL of 3% sodium hypochlorite, which was left in place for 30seconds per canal.
Manual-dynamic Activation Group. After suctioning away theintracanal surplus of NaOCl with the 27-gauge needle, 1 mL of 17%EDTA was flushed into each canal. This solution was activated by usinga gutta-percha cone as previously described for 1 minute in each canal.
1362 Caron et al.
The frequency of activation used was 100 push-pull strokes per minute(12). The canals were then flushed with 3 mL of a 3% solution ofsodium hypochlorite. This solution was then activated for 30 secondsper canal using the pumping master cone method.
Automated-dynamic Activation Group. After optimallypreparing the canal, surplus NaOCl was suctioned away with the27-gauge needle. Following the manufacturer’s instructions, each canalwas flushed with 1 mL of 17% EDTA using the RinsEndo system for 1minute per canal. Each canal was then flushed with 3 mL of a 3% solu-tion of sodium hypochlorite delivered via the RinsEndo system for 30seconds in each canal.
Sonic-activation Group. After optimally preparing the canal,surplus NaOCl was suctioned away with the 27-gauge needle. Each canalwas then irrigated with 1 mL of 17% EDTA using the 27-gauge needle.This intracanal solution was activated with either a red (25/04) or blue(35/04) EndoActivator tip at a speed of 10 kHz for 1 minute per canal.Each canal was then flushed with 3 mL of 3% sodium hypochlorite. Thissolution was then activated using either the red or blue EndoActivator tipfor 30 seconds per canal.
After activation, the action of the sodium hypochlorite was stoppedby syringing in 3 mL of physiologic saline solution per canal (ie, 6 mL foreach tooth in the four test groups). All the samples were then placed ina solution of physiologic saline and stored at 4�C until proceeding withthe sectioning protocol.
Sectioning of the Teeth and Preparation for SEMThe teeth were sectioned in two halves; only the mesial root was
kept for further study. Two horizontal grooves were made using a Friosdiamond-cutting disk (Microsaw; Dentsply Friadent, Mannheim,Germany) mounted on a surgical dental handpiece to separate themesial root into thirds (the apical third, the middle third, and thecoronal third). This step was performed using a surgical microscope.Colored gutta-percha cones were fitted and used as markers to bestgauge groove depth. The objective was to avoid any intrusion of thecutting disc into the canals, which would pollute the samples by splat-tering cutting debris into the root canal system. To avoid any contami-nation, coronal thirds were discarded because there was a bigger gapbetween the gutta-percha markers and the prepared walls of the canal.This gap compromised vision and increased the possibility of the cuttingdisc inadvertently introducing debris into this region of the canal.
The apical and middle one thirds of the canal were thensectioned in the longitudinal plane with a precision diamond bur(889 Model; Komet, Paris, France). A continuous supply of air wasdelivered to improve vision and cutting precision, which eliminatedthe potential of introducing debris into this region of the canal.Each third was vertically split by applying slight pressure to an enamelchisel into the longitudinal groove. Each sample was dehydrated ingraded series of ethanol solutions, critical point dried, coated withgold, and viewed with a scanning electron microscope (HitachiS2500,Verrieres-le-buisson, France) at 15 kV (Fig. 1).
SEM Evaluation and Statistical AnalysisEach fragment was first viewed at low magnification (�30) by the
operator (GC) and another trained dentist with SEM studies (KN) inorder to gain an overview of the sample. Image acquisition on themost typical zones of the sample was performed at a magnification of�1,000 to assess the presence of smear layer. The images were blindlyassessed by two practitioners with no inside knowledge of the operativeprocedures and who were fully conversant with qualitative analysis onroot canal images produced by scanning electron microscopy (PM,FB). Analysis began using the scale described in Hulsmann et al
JOE — Volume 36, Number 8, August 2010
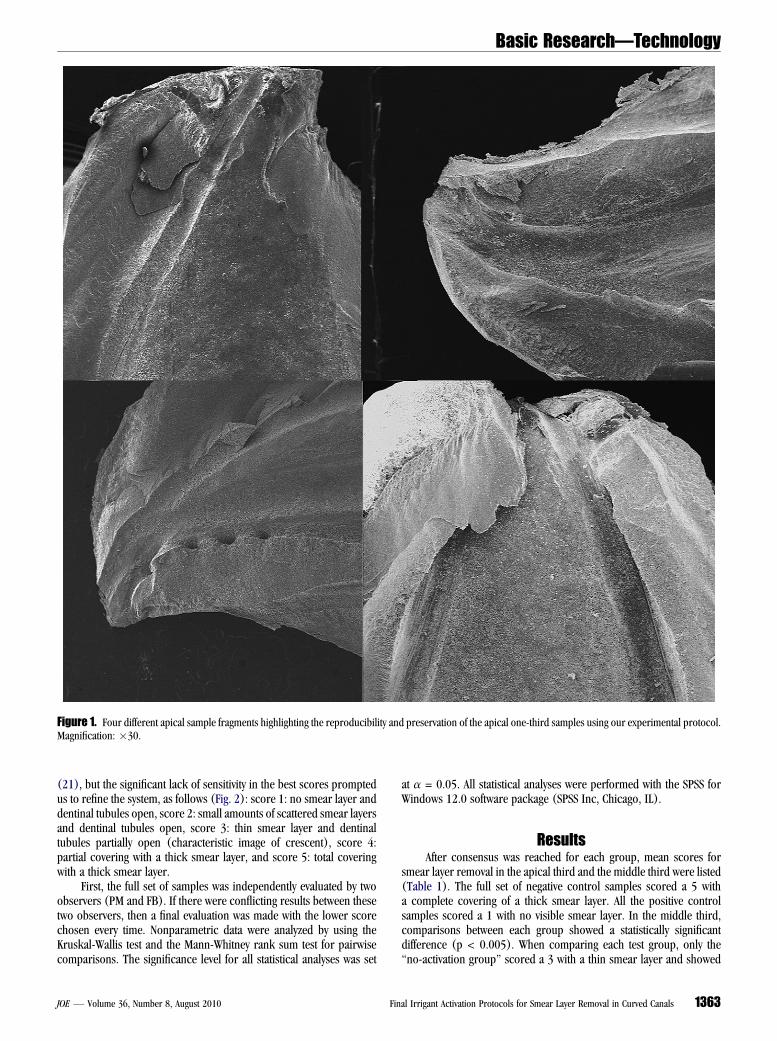
Figure 1. Four different apical sample fragments highlighting the reproducibility and preservation of the apical one-third samples using our experimental protocol.Magnification: �30.
Basic Research—Technology
(21), but the significant lack of sensitivity in the best scores promptedus to refine the system, as follows (Fig. 2): score 1: no smear layer anddentinal tubules open, score 2: small amounts of scattered smear layersand dentinal tubules open, score 3: thin smear layer and dentinaltubules partially open (characteristic image of crescent), score 4:partial covering with a thick smear layer, and score 5: total coveringwith a thick smear layer.
First, the full set of samples was independently evaluated by twoobservers (PM and FB). If there were conflicting results between thesetwo observers, then a final evaluation was made with the lower scorechosen every time. Nonparametric data were analyzed by using theKruskal-Wallis test and the Mann-Whitney rank sum test for pairwisecomparisons. The significance level for all statistical analyses was set
JOE — Volume 36, Number 8, August 2010 Fin
at a = 0.05. All statistical analyses were performed with the SPSS forWindows 12.0 software package (SPSS Inc, Chicago, IL).
ResultsAfter consensus was reached for each group, mean scores for
smear layer removal in the apical third and the middle third were listed(Table 1). The full set of negative control samples scored a 5 witha complete covering of a thick smear layer. All the positive controlsamples scored a 1 with no visible smear layer. In the middle third,comparisons between each group showed a statistically significantdifference (p < 0.005). When comparing each test group, only the‘‘no-activation group’’ scored a 3 with a thin smear layer and showed
al Irrigant Activation Protocols for Smear Layer Removal in Curved Canals 1363
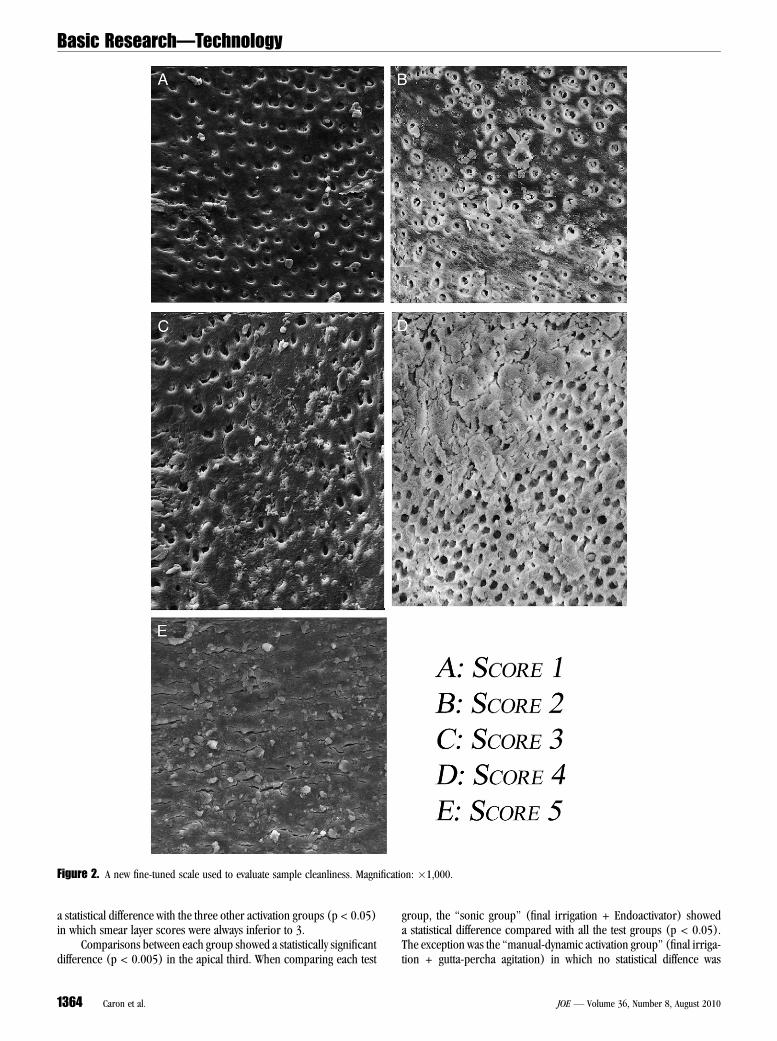
Figure 2. A new fine-tuned scale used to evaluate sample cleanliness. Magnification: �1,000.
Basic Research—Technology
a statistical difference with the three other activation groups (p < 0.05)in which smear layer scores were always inferior to 3.
Comparisons between each group showed a statistically significantdifference (p < 0.005) in the apical third. When comparing each test
1364 Caron et al.
group, the ‘‘sonic group’’ (final irrigation + Endoactivator) showeda statistical difference compared with all the test groups (p < 0.05).The exception was the ‘‘manual-dynamic activation group’’ (final irriga-tion + gutta-percha agitation) in which no statistical diffence was
JOE — Volume 36, Number 8, August 2010

TABLE 1. Mean Score � Standard Deviation Comparing the Smear Layeramong the Four Final Irrigation Regimens in the Apical and Middle Thirds
Group N Apical third Middle third
Final irrigation withoutactivation
10 3.16 �0.958 3.47�0.874
Final irrigation +Master cone
10 2.21 �1.032 2.05 �1.05
Final irrigation +Rinsendo
10 3 �1.414 2.5 �1
Final irrigation +Endoactivator
10 1.75 �0.55 1.88 �0.857
Basic Research—Technology
detected. However, only the Endoactivator group showed smear layerremoval lower than a score 2, which equates to a high level of cleanli-ness in all apical one-third samples.
DiscussionThe endodontic community is now unanimous concerning the
positive benefit of irrigation during the root canal preparation phase(22). The chemomechanical preparation should ideally result in a fullycleansed and disinfected root canal system. Literature has shown thatapical enlargement and deeper positioning of the irrigation needleare required to clean the apical third (5, 23, 24). However, very littledata exist regarding smear layer removal, especially in molar teethexhibiting curved canals where emphasis was placed on preparinga fully tapered and well-shaped canal with narrow apical diameters.
Only one recent SEM study by Khademi et al (25) has shown theimportance of the canal taper in curved canals. When the root canaltaper was 0.06 mm/mm, there was comparable smear layer removalwhen the apical diameters were between 0.30 mm and 0.40 mm. Ithas been shown that for more narrow apical diameters the taper needsto be increased to 0.10 mm/mm in order to eliminate a maximumamount of debris (26, 27).
A recent study on curved roots has shown a correlation betweencreating sufficient taper and propagation improvement of irrigants inroot canal during the shaping process (28). In the present study, allthe shaping procedures complied with the criteria of tapered canalsand maintaining apical foramen as small as practical. In funnel-shaped canals, both the tapered gutta-percha master cones and thetapered EndoActivator tips, when activated, provided cleaner resultsthan syringe delivery systems (final irrigation with no activation and Rin-sEndo).
In this study, the four-wall access cavity provided a strategic reser-voir to hold a more effective volume of irrigant for exchange during acti-vation. This is in direct contrast with many studies in which the crownhad been removed from the samples. Desirably, the irrigating solutionsare apically exchanged each time the activator system is inserted into thecanal. When the activator tip moves toward length, the reagent is dis-placed. When the activator is partially withdrawn, there is an effectiveexchange of solution into the apical one third of the canal. The efficiencyof this hydrodynamic circuit is further enhanced when combined withsonic oscillating movements. A pumping action synergisticallycombined with mechanical agitation explains the better results achievedwith the EndoActivator. Recently, Uroz-Torres et al (29) found no differ-ence in smear layer removal between the Endoactivator and conven-tional Max-I-Probe (Dentsply Rinn, Elgin, IL) irrigation using NaOCland EDTA. The difference in results is attributed to differences in theactivation protocols used. In our present study, a second activationwas performed after the final flush with NaOCl, and all apical one-third samples were shaped to 10% to enhance irrigation exchangeand efficiency (30).
JOE — Volume 36, Number 8, August 2010 Fin
So far, activation of irrigants without concomitant instrumentationof the root canal walls has been defined as passive ultrasonic irrigation(PUI) (9). PUI has been shown to be effective in removing debris (10)and smear layer in straight canals (31). Nevertheless, there are conflict-ing results about the performance of PUI in terms of smear layer elim-ination (9, 32). Even when ultrasonically driven metal canula orinstruments are precurved, there are obvious considerations andlimitations using these devices in curved canals and to length (9,33). There is always a risk of touching the walls, which wouldautomatically trigger the formation of a new undesirable smear layer.Of greater concern, contacting a dentinal wall with an activatedultrasonic instrument invites iatrogenic events. This should becontrasted with the nonmetal surfaces of the activation systems usedin this study (gutta-percha or polymer), which cannot generatea smear layer, internal ledge, or external transportation of the foramen.
It should be noted that all of the samples tested by manual-dynamicirrigation or by sonic activation yielded very little smear layer. This levelof cleanliness is an important finding because it was achieved on curvedcanals using activation systems other than metal ultrasonic files.Although these systems generate lower frequencies compared withthe ultrasonically driven files (25-30 kHz), the vertical-stroke pumpingmotion used as part of the protocol promotes dynamic coronoapicalcirculation of the irrigating solutions. The benefit of irrigant renewaland activation needs to be researched in greater detail, comparingthis irrigation dynamic with the streaming pattern observed with PUI.
Our experimental model used final irrigation times (34) and finalirrigation volumes that proved effective and efficient (35) while at thesame time avoiding peritubular and intertubular erosion. However,the timeframe given in the protocol may not be long enough for a systemsuch as RinsEndo, which may require more time to achieve the samescores as the other activation systems. During the shaping procedures,the volume of 1 mL of irrigant dispensed after the use of each file wassufficient to get a clear solution inside the pulp chamber without visibledebris.
The data gathered through this experiment are transposable toclinical practice because the experimental model proposed closelymirrors the actual conditions encountered in routine molar treatment,but results should be interpreted with precaution because of the largestandard deviation observed. One possible explanation could be thechallenge of standardizing activation procedures in complex anatomyof mandibular molars where the two mesial canals commonly commu-nicate along their lengths.
ConclusionThe experimental design implemented in this study prompted the
following observations: the activation of irrigating solutions yieldedcleaner canals compared with no activation, and a tapered activatorthat closely adapts to the dimensions of a shaped canal is the most effec-tive (ie, the master gutta-percha cone and Endoactivator). Furtherinvestigations will be required to confirm this preliminary data, partic-ularly in terms of biofilm removal and apical disinfection results.
AcknowledgmentsThe authors are grateful to Durr Dental for loaning the Rin-
sEndo device used in this experiment. The authors thank Dr C.Ruddle and Advanced Endodontics for loaning the Endoactivatordevice used in this experiment. The authors also thank Septodontfor providing the irrigating solutions Parcan and Largal Ultraused in this experiment.
al Irrigant Activation Protocols for Smear Layer Removal in Curved Canals 1365

Basic Research—Technology
References1. Nair PNR, Henry S, Cano V, et al. Microbial status of apical root canal system of
human mandibular first molars with primary apical periodontitis after ‘‘one-visit’’endodontic treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:231–52.
2. Guppy DR, Curtis RV, Pitt Ford TR. Dentine chips produced by nickel-titanium rotaryinstruments. Endod Dent Traumatol 2000;16:258–64.
3. Jeon IS, Spangberg LSW, Yoon TC, et al. Smear layer production by 3 rotary reamerswith different cutting blade designs in straight root canals: a scanning electronmicroscopic study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;96:601–7.
4. Torabinejad M, Handysides R, Khademi AA, et al. Clinical implications of the smearlayer in endodontics: a review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2002;94:658–66.
5. Sedgley CM, Nagel AC, Hall D, et al. Influence of irrigant needle depth in removingbioluminescent bacteria inoculated into instrumented root canals using real-timeimaging in vitro. Int Endod J 2005;38:97–104.
6. Senia ES, Marshall FJ, Rosen S. The solvent action of sodium hypochlorite on pulptissue of extracted teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1971;31:96–103.
7. Gambarini G, Laszkiewicz. A scanning electron microscopic study of debris andsmear layer remaining following use of GT rotary instruments. Int Endod J 2002;35:422–7.
8. Yamada RS, Armas A, Goldman M, et al. A scanning electron microscopic compar-ison of a high volume final flush with several irrigating solutions: part 3. J Endod1983;9:137–42.
9. Gu LS, Kim JR, Ling J, et al. Review of contemporary irrigant agitation techniques anddevices. J Endod 2009;35:791–804.
10. Jiang LM, Verhaagen B, Versluis M, et al. Evaluation of a sonic device designed toactivate irrigant in the root canal. J Endod 2010;36:143–6.
11. Paragliola R, Franco V, Fabiani C, et al. Final rinse optimization: influence ofdifferent agitation protocols. J Endod 2010;36:282–5.
12. Huang T-Y, Gulabivala K, Ng YL. A bio-molecular film ex-vivo model to evaluate theinfluence of canal dimensions and irrigation variables on the efficacy of irrigation.Int Endod J 2008;41:60–71.
13. McGill S, Gulabivala K, Mordan N, et al. The efficacy of dynamic irrigation usinga commercially available system (RinsEndo�) determined by removal of a collagen‘biomolecular film’ from an ex vivo model. Int Endod J 2008;42:602–8.
14. Hauser V, Braun A, Frentzen M. Penetration depth of a dye marker into dentine usinga novel hydrodynamic system (RinsEndo�). Int Endod J 2007;40. 664–52.
15. Ruddle CJ. Endodontic disinfection: tsunami irrigation. Endod Pract 2008;11:7–15.16. Gambarini G. Shaping and cleaning the root canal system: a scanning electron
microscopic evaluation of a new instrumentation and irrigation technique. J Endod1999;25:800–3.
17. Schneider SW. A comparison of canal preparations in straight and curved canals.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1971;32:271–5.
1366 Caron et al.
18. Tay FR, Gu LS, Schoeffel GJ, et al. Effect of vapor lock on root canal debridement byusing a side-vented needle for positive-pressure irrigant delivery. J Endod 2010;36:745–50.
19. Schoeffel GJ. The EndoVac method of endodontic irrigation: safety first. Dent Today2007;26:92–6.
20. Machtou P, Ruddle CJ. Advancements in the design of endodontic instruments forroot canal preparation. Alpha Omegan 2004;97:8–15.
21. Hulsmann M, Rummelin C, Schafers F. Root canal cleanliness after preparation withdifferent endodontic handpieces and hand instruments: a comparative SEM. J Endod1997;23:301–6.
22. Bystrom A, Sundqvist G. Bacteriologic evaluation of the effect of 0.5 percent sodiumhypochlorite in endodontic therapy. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1983;55:307–12.
23. Chow TW. Mechanical effectiveness of root canal irrigation. J Endod 1983;9:475–9.
24. Falk KW, Sedgley CM. The influence of preparation size on the mechanical efficacy ofroot canal irrigation in vitro. J Endod 2005;31:742–5.
25. Khademi A, Yazdizadeh M, Feizianfard M. Determination of the minimum instrumen-tation size for penetration of irrigants to the apical third of root canal systems. J En-dod 2006;32:417–20.
26. Abou-Rass M, Piccinino MV. The effectiveness of four clinical irrigation methods onthe removal of root canal debris. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1982;54:323–8.
27. Albrecht LJ, Baumgartner JC, Marshall JD. Evaluation of apical debris removal usingvarious sizes and tapers of ProFile GT Files. J Endod 2004;30:425–8.
28. Bronnec F, Bouillaguet S, Machtou P. Ex vivo assessment of irrigant penetration andrenewal during the cleaning and shaping of root canals: a digital subtraction radio-graphic study. Int Endod J 2010;43:275–82.
29. Uroz-Torres D, Gonzales-Rodriguez MP, Ferre-Luque CM. Effectiveness of the En-doactivator system in removing the smear layer after root canal instrumentation.J Endod 2010;36:308–11.
30. Yana Y. An in vivo comparative study of the penetration of sodium hypochlorite inroot canal systems during cleaning and shaping procedures using the B.U. techniqueand sonic instrumentation [masters thesis]. Boston, MA: Boston University; 1989.
31. Kuah HG, Lui JN, Tseng PS, et al. The effect of EDTA with and without ultrasonics onremoval of the smear layer. J Endod 2009;35:393–6.
32. Mayer BE, Peters OA, Barbakow F. Effects of rotary instruments and ultrasonicirri-gation on debris and smear layer scores: a scanning electron microscopic study. IntEndod J 2002;35:582–9.
33. Ahmad M, Pitt Ford TR, Crum LA. Ultrasonic debridement of root canals: acousticstreaming and its possible role. J Endod 1992;13:490–9.
34. Saito K, Webb TD, Imamura GM, et al. Effect of shortened irrigation times with 17%ethylene diamine tetra-acetic acid on smear layer removal after rotary canal instru-mentation. J Endod 2008;34:1011–4.
35. Crumpton BJ, Goodell GG, McClanahan SB. Effects on smear layer and debrisremoval with varying volumes of 17% REDTA after rotary instrumentation. J Endod2005;31:536–8.
JOE — Volume 36, Number 8, August 2010
Copyright © 2022 FDOKUMEN




















