Cyphering the complexity of coronary artery disease using the syntax score to predict clinical...
10
Cyphering the Complexity of Coronary Artery Disease Using the Syntax Score to Predict Clinical Outcome in Patients With Three-Vessel Lumen Obstruction Undergoing Percutaneous Coronary Intervention Marco Valgimigli, MD, PhD a , Patrick Washington Serruys, MD, PhD a, *, Keiichi Tsuchida, MD, PhD a , Sophia Vaina, MD, PhD a , Marie-Angèle Morel, BSc b , Marcel J. van den Brand, MD b , Antonio Colombo, MD d , Marie Claude Morice, MD h , Keith Dawkins, MD i , Bernard de Bruyne, MD j , Ran Kornowski, MD k , Stefano de Servi, MD e , Giulio Guagliumi, MD f , J. Wouter Jukema, MD c , Frederick W. Mohr, MD l , Arie-Pieter Kappetein, MD, PhD a , Kristel Wittebols, MSc m , Hans-Peter Stoll, MD m , Eric Boersma, PhD a , and Giovanni Parrinello, PhD g , on behalf of the ARTS II Investigators The Syntax score (SXscore) was recently developed as a comprehensive angiographic scoring system aiming to assist in patient selection and risk stratification of patients with extensive coronary artery disease undergoing contemporary revascularization. A validation of this angiographic classification scheme is lacking. We assessed its predictive value in patients who underwent percutaneous intervention (PCI) for 3-vessel disease and explored its performance in comparison with the modified lesion classification system of the Amer- ican Heart Association/American College of Cardiology. The SXscore, applied to 1,292 lesions in 306 patients who underwent PCI for 3-vessel disease in the Arterial Revascu- larization Therapies Study Part II, was 4 to 54.5, and after a median of 370 days (range 274 to 400) predicted the rate of major adverse cardiac and cerebrovascular events (hazard ratio 1.08/U increase, 95% confidence interval 1.05 to 1.11, p <0.0001), with patients in the highest SXscore tertile having a significantly higher event rate (27.9%) than patients in the lowest tertile (8.7%, hazard ratio 3.5, 95% confidence interval 1.7 to 7.4, p 0.001). By multivariable analyses, SXscore independently predicted outcome with an almost fourfold adjusted increase in the risk of major adverse cardiac and cerebrovascular events in patients with high versus low values based on the discrimination level provided by classification and regression tree analysis. Compared with the modified lesion classification scheme of the Amer- ican Heart Association/American College of Cardiology, SXscore showed a greater discrimi- nation ability (c-index 0.58 0.08 vs 0.67 0.08, respectively, p <0.001) and a better goodness of fit with the Hosmer-Lemeshow statistic. In conclusion, the SXscore is a promising tool to risk stratify outcome in patients with extensive coronary artery disease undergoing contemporary PCI. © 2007 Elsevier Inc. All rights reserved. (Am J Cardiol 2007;99:1072–1081) Dramatic changes have recently occurred in the field of percutaneous coronary intervention (PCI), which include liberal use of drug-eluting stents 1 and upfront administration of adenosine diphosphate receptor blockers, 2,3 allowing treatment of more complex and extensive lesions 4 and lower overall risk. 5 The Syntax score (SXscore) is a recently developed, comprehensive, angiographic scoring system. It merges several previously validated angiographic classifi- cations based on morphology and location of coronary ar- tery disease (CAD) within the coronary tree, aiming to assist in patient selection and risk stratification of patients with extensive coronary lumen obstruction undergoing contem- porary revascularization. 6 A validation of this angiographic classification scheme is lacking. We applied the SXscore to 1,292 lesions in 306 patients who underwent treatment for 3-vessel disease in the Arterial Revascularization Therapies Study part II (ARTS II) to examine its role in predicting short- and long-term incidences of major adverse events. Comparative predictive values of the SXscore and the mod- ified lesion classification system of the American College of a Thoraxcenter, Erasmus Medical Center, and b Cardialysis B.V., Rot- terdam, and c Leiden Univerisity Medical Center, Leiden, The Netherlands; d San Raffaele Hospital, Milan, e Ospedale Civile di Legnano, Legnano, f Ospedali Riuniti di Bergamo, Bergamo, and g Medical Statistics Unit, University of Brescia, Brescia, Italy; h Institut Cardiovasculaire Paris Sud, Massy, France; i Wessex Cardiac Unit, Southampton University Hos- pital, Southampton, United Kingdom; j Onze Lieve Vrouw Ziekenhuis, Aalst, Belgium; k Rabin Medical Center, Petach Tikva, Israel; l Department of Cardiac Surgery, Heartcenter, University of Leipzig, Leipzig, Germany; and m Cordis Corporation, Johnson & Johnson Company, Miami Lakes, Florida. Manuscript received September 13, 2006; revised manuscript received and accepted November 16, 2006. *Corresponding author: Tel: 31-10-463-5260; fax: 31-10-436-9154. E-mail address: [email protected] (P.W. Serruys). 0002-9149/07/$ – see front matter © 2007 Elsevier Inc. All rights reserved. www.AJConline.org doi:10.1016/j.amjcard.2006.11.062
Transcript of Cyphering the complexity of coronary artery disease using the syntax score to predict clinical...

Dpl
td
f
USpAoaFr
0d
Cyphering the Complexity of Coronary Artery Disease Usingthe Syntax Score to Predict Clinical Outcome in Patients
With Three-Vessel Lumen Obstruction UndergoingPercutaneous Coronary Intervention
Marco Valgimigli, MD, PhDa, Patrick Washington Serruys, MD, PhDa,*,Keiichi Tsuchida, MD, PhDa, Sophia Vaina, MD, PhDa, Marie-Angèle Morel, BScb,
Marcel J. van den Brand, MDb, Antonio Colombo, MDd, Marie Claude Morice, MDh,Keith Dawkins, MDi, Bernard de Bruyne, MDj, Ran Kornowski, MDk, Stefano de Servi, MDe,
Giulio Guagliumi, MDf, J. Wouter Jukema, MDc, Frederick W. Mohr, MDl,Arie-Pieter Kappetein, MD, PhDa, Kristel Wittebols, MScm, Hans-Peter Stoll, MDm,
Eric Boersma, PhDa, and Giovanni Parrinello, PhDg, on behalf of the ARTS II Investigators
The Syntax score (SXscore) was recently developed as a comprehensive angiographicscoring system aiming to assist in patient selection and risk stratification of patients withextensive coronary artery disease undergoing contemporary revascularization. A validationof this angiographic classification scheme is lacking. We assessed its predictive value inpatients who underwent percutaneous intervention (PCI) for 3-vessel disease and exploredits performance in comparison with the modified lesion classification system of the Amer-ican Heart Association/American College of Cardiology. The SXscore, applied to 1,292lesions in 306 patients who underwent PCI for 3-vessel disease in the Arterial Revascu-larization Therapies Study Part II, was 4 to 54.5, and after a median of 370 days (range 274to 400) predicted the rate of major adverse cardiac and cerebrovascular events (hazard ratio1.08/U increase, 95% confidence interval 1.05 to 1.11, p <0.0001), with patients in thehighest SXscore tertile having a significantly higher event rate (27.9%) than patients in thelowest tertile (8.7%, hazard ratio 3.5, 95% confidence interval 1.7 to 7.4, p � 0.001). Bymultivariable analyses, SXscore independently predicted outcome with an almost fourfoldadjusted increase in the risk of major adverse cardiac and cerebrovascular events in patientswith high versus low values based on the discrimination level provided by classification andregression tree analysis. Compared with the modified lesion classification scheme of the Amer-ican Heart Association/American College of Cardiology, SXscore showed a greater discrimi-nation ability (c-index 0.58 � 0.08 vs 0.67 � 0.08, respectively, p <0.001) and a better goodnessof fit with the Hosmer-Lemeshow statistic. In conclusion, the SXscore is a promising tool to riskstratify outcome in patients with extensive coronary artery disease undergoing contemporary
PCI. © 2007 Elsevier Inc. All rights reserved. (Am J Cardiol 2007;99:1072–1081)otodmctiepc13SsC
ramatic changes have recently occurred in the field ofercutaneous coronary intervention (PCI), which includeiberal use of drug-eluting stents1 and upfront administration
aThoraxcenter, Erasmus Medical Center, and bCardialysis B.V., Rot-erdam, and cLeiden Univerisity Medical Center, Leiden, The Netherlands;San Raffaele Hospital, Milan, eOspedale Civile di Legnano, Legnano,Ospedali Riuniti di Bergamo, Bergamo, and gMedical Statistics Unit,niversity of Brescia, Brescia, Italy; hInstitut Cardiovasculaire Parisud, Massy, France; iWessex Cardiac Unit, Southampton University Hos-ital, Southampton, United Kingdom; jOnze Lieve Vrouw Ziekenhuis,alst, Belgium; kRabin Medical Center, Petach Tikva, Israel; lDepartmentf Cardiac Surgery, Heartcenter, University of Leipzig, Leipzig, Germany;nd mCordis Corporation, Johnson & Johnson Company, Miami Lakes,lorida. Manuscript received September 13, 2006; revised manuscripteceived and accepted November 16, 2006.
*Corresponding author: Tel: 31-10-463-5260; fax: 31-10-436-9154.
iE-mail address: [email protected] (P.W. Serruys).002-9149/07/$ – see front matter © 2007 Elsevier Inc. All rights reserved.oi:10.1016/j.amjcard.2006.11.062
f adenosine diphosphate receptor blockers,2,3 allowingreatment of more complex and extensive lesions4 and lowerverall risk.5 The Syntax score (SXscore) is a recentlyeveloped, comprehensive, angiographic scoring system. Iterges several previously validated angiographic classifi-
ations based on morphology and location of coronary ar-ery disease (CAD) within the coronary tree, aiming to assistn patient selection and risk stratification of patients withxtensive coronary lumen obstruction undergoing contem-orary revascularization.6 A validation of this angiographiclassification scheme is lacking. We applied the SXscore to,292 lesions in 306 patients who underwent treatment for-vessel disease in the Arterial Revascularization Therapiestudy part II (ARTS II) to examine its role in predictinghort- and long-term incidences of major adverse events.omparative predictive values of the SXscore and the mod-
fied lesion classification system of the American College of
www.AJConline.org
Ca
M
w
nspAc
Fc
1073Coronary Artery Disease/Application of the Syntax Score
ardiology/American Heart Association (ACC/AHA) werelso explored.
ethodsStudy design and patient population: The ARTS II
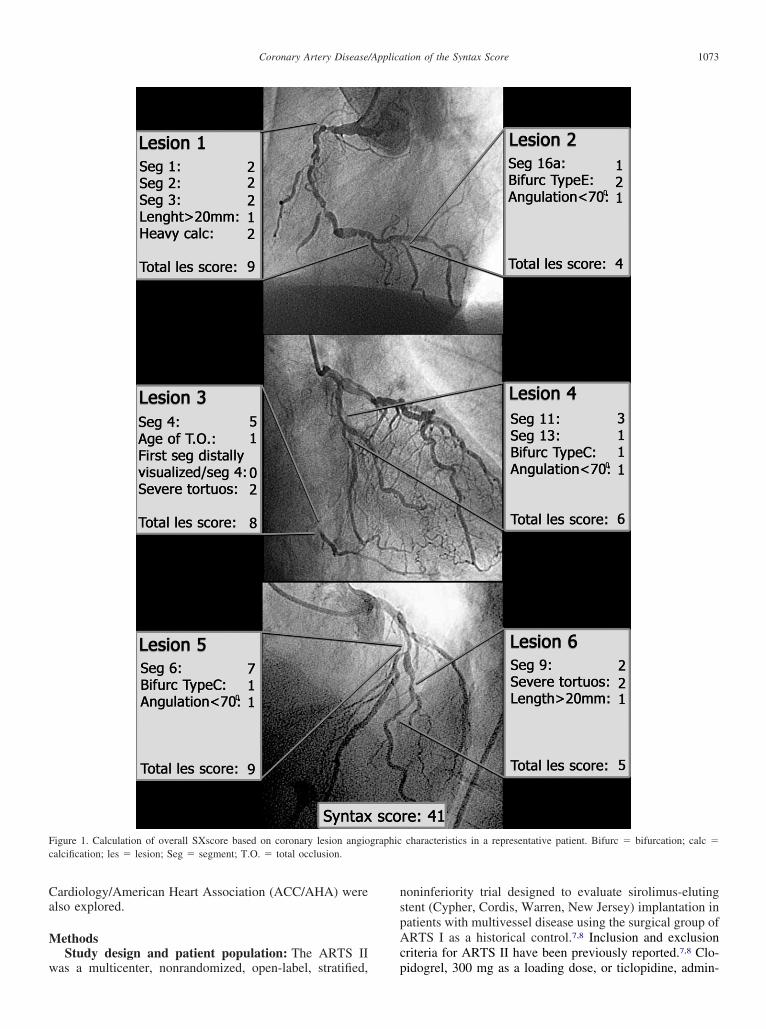
igure 1. Calculation of overall SXscore based on coronary lesion angioalcification; les � lesion; Seg � segment; T.O. � total occlusion.
as a multicenter, nonrandomized, open-label, stratified, p
oninferiority trial designed to evaluate sirolimus-elutingtent (Cypher, Cordis, Warren, New Jersey) implantation inatients with multivessel disease using the surgical group ofRTS I as a historical control.7,8 Inclusion and exclusion
riteria for ARTS II have been previously reported.7,8 Clo-
characteristics in a representative patient. Bifurc � bifurcation; calc �
graphicidogrel, 300 mg as a loading dose, or ticlopidine, admin-

it2leew�idpoi
s�oiwm
LswAFcgapocmtisaRas
TB
V
AMBD
HHCFCLPPACPCC
M
M
1074 The American Journal of Cardiology (www.AJConline.org)
stered at a dose of 500 mg, was started �24 hours beforehe procedure. Clopidogrel 75 mg/day or ticlopidine 250 mg
times a day was prescribed for �2 months after revascu-arization. Written informed consent was obtained fromach patient before enrollment. The ethics committee ofach participating site approved the study. Patients under-ent stratification by clinical site to ensure the inclusion of33% of patients with 3-vessel disease. Of 607 patients
ncluded in the ARTS II, 325 patients developed 3-vesselisease according to site investigators. For 19 of theseatients (5.8%), the diagnostic angiogram was not availabler was of poor imaging quality. Thus, 306 patients werencluded in the present analysis.
SXscore and angiographic analysis: Each coronary le-ion producing �50% luminal obstruction lumen in vessels1.5 mm was separately scored and added to provide the
verall SXscore. The SXscore was calculated using a ded-cated software that integrates (1) the number of lesionsith their specific weighting factors based on the amount of
able 1aseline characteristics of the study population
ariable
�18(n � 103)
ge (yrs) 61 � 10en 81 (79%)ody mass index (kg/m2) 28 � 4iabetes 19 (18%)Insulin dependent 5 (5%)ypertension* 67 (65%)ypercholesterolemia† 83 (81%)urrent smokers 21 (20%)amily history 49 (46%)reatinine elevation 0V ejection fraction (%) 63 � 11revious PCI 0revious myocardial infarction 29 (28%)nterior wall myocardial infarction 6 (6%)hronic obstructive pulmonary disease 1 (1%)eripheral arterial disease 10 (10%)arotid surgery 2 (2%)linical PresentationStable angina pectoris 64 (62%)Canadian Cardiovascular Society class 2.3 � 0.64Silent myocardial ischemia 6 (6%)Unstable angina pectoris 33 (32%)IIIB/IIIC 7 (7%)/1 (3%)edications at screening
Aspirin 93 (90%)� Blockers 72 (70%)Angiotensin-converting enzyme inhibitors 45 (44%)Statins 79 (77%)edications at discharge
Aspirin 102 (99%)� Blockers 77 (75%)Angiotensin-converting enzyme inhibitors 49 (48%)Statins 90 (87%)
* Defined as arterial pressure �140/90 mm Hg or antihypertensive trea† Defined as total cholesterol level �5.6 mmol/L or lipid-lowering treaLV � left ventricular.
yocardium distal to the lesion according to the score of C
eaman et al,9 and (2) the morphologic features of eachingle lesion, as previously reported6 (available at http://ww.europcronline.com/eurointervention/2nd_issue/36/).n example of SXscore calculation in 1 subject is shown inigure 1. All angiographic variables pertinent to SXscorealculation were computed by 2 of 3 experienced cardiolo-ists (MV, KT, SV) who were blinded to procedural datand clinical outcome on angiograms obtained before therocedure. In case of disagreement, the opinion of the thirdbserver was obtained and the final decision was made byonsensus. All other angiographic characteristics, includingodified ACC/AHA lesions classification computed before
he procedure and completeness of revascularization byntent, defined as successful dilation (i.e., residual diametertenosis �20%) of all intended lesions, were derived fromn angiographic core laboratory database (Cardialysis B.V.,otterdam, The Netherlands). For the purpose of statisticalnalysis, type A stenoses were coded as 1 point, type B1tenoses as 2 points, type B2 stenoses as 3 points, and type
SXscore p Value
�18–26(n � 110)
�26(n � 93)
64 � 8 66 � 10 0.0002582 (75%) 71 (76%) 0.7827 � 4 27 � 4 0.4228 (38%) 26 (28%) 0.265 (5%) 6 (6%) 0.81
78 (71%) 68 (73%) 0.4480 (72%) 68 (73%) 0.3423 (21%) 14 (15%) 0.5139 (35%) 25 (27%) 0.011 (1%) 2 (2%) 0.30
59 � 12 60 � 11 0.0440 0 —
47 (43%) 33 (35%) 0.0816 (15%) 5 (5%) 0.035 (5%) 5 (5%) 0.204 (4%) 10 (10%) 0.111 (1%) 2 (2%) 0.73
44 (40%) 57 (61%) 0.0012.20 � 0.70 2.24 � 0.73 0.90
15 (14%) 7 (8%) 0.1151 (46%) 29 (31%) 0.03
8 (7%)/5 (5%) 5 (5%)/2 (2%) 0.71
99 (90) 79 (85) 0.4289 (81) 65 (70) 0.1050 (45) 42 (45) 0.9675 (68) 64 (69) 0.32
107 (97%) 89 (96%) 0.3491 (83%) 71 (76%) 0.3359 (54%) 46 (49%) 0.6696 (87%) 79 (85%) 0.85
tment.tment.
stenoses as 4 points, as previously described.10
tp3ipdcct
picadMcQnkCawmaic
tcttomdtbsflto
atgtTevfwgsir
TA
V
DTT
PPNTMT
TTMTEBSBUP
1075Coronary Artery Disease/Application of the Syntax Score
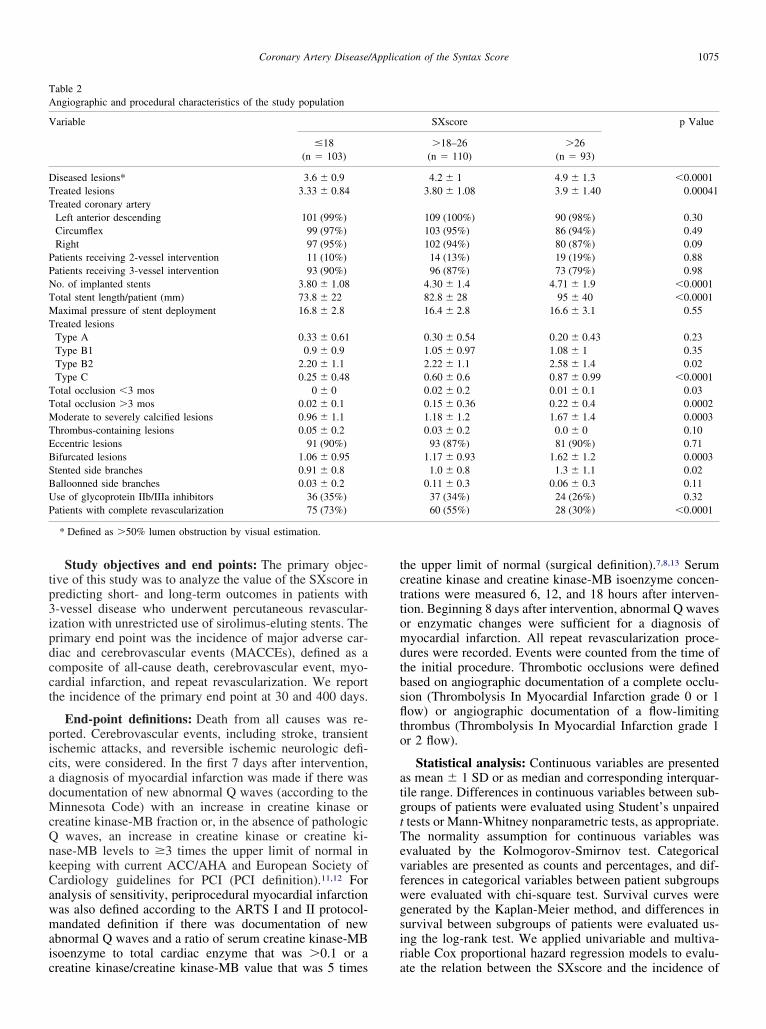
Study objectives and end points: The primary objec-ive of this study was to analyze the value of the SXscore inredicting short- and long-term outcomes in patients with-vessel disease who underwent percutaneous revascular-zation with unrestricted use of sirolimus-eluting stents. Therimary end point was the incidence of major adverse car-iac and cerebrovascular events (MACCEs), defined as aomposite of all-cause death, cerebrovascular event, myo-ardial infarction, and repeat revascularization. We reporthe incidence of the primary end point at 30 and 400 days.
End-point definitions: Death from all causes was re-orted. Cerebrovascular events, including stroke, transientschemic attacks, and reversible ischemic neurologic defi-its, were considered. In the first 7 days after intervention,diagnosis of myocardial infarction was made if there wasocumentation of new abnormal Q waves (according to theinnesota Code) with an increase in creatine kinase or
reatine kinase-MB fraction or, in the absence of pathologicwaves, an increase in creatine kinase or creatine ki-
ase-MB levels to �3 times the upper limit of normal ineeping with current ACC/AHA and European Society ofardiology guidelines for PCI (PCI definition).11,12 Fornalysis of sensitivity, periprocedural myocardial infarctionas also defined according to the ARTS I and II protocol-andated definition if there was documentation of new
bnormal Q waves and a ratio of serum creatine kinase-MBsoenzyme to total cardiac enzyme that was �0.1 or a
able 2ngiographic and procedural characteristics of the study population
ariable
�18(n � 103)
iseased lesions* 3.6 � 0.9reated lesions 3.33 � 0.84reated coronary arteryLeft anterior descending 101 (99%)Circumflex 99 (97%)Right 97 (95%)atients receiving 2-vessel intervention 11 (10%)atients receiving 3-vessel intervention 93 (90%)o. of implanted stents 3.80 � 1.08otal stent length/patient (mm) 73.8 � 22aximal pressure of stent deployment 16.8 � 2.8
reated lesionsType A 0.33 � 0.61Type B1 0.9 � 0.9Type B2 2.20 � 1.1Type C 0.25 � 0.48otal occlusion �3 mos 0 � 0otal occlusion �3 mos 0.02 � 0.1oderate to severely calcified lesions 0.96 � 1.1
hrombus-containing lesions 0.05 � 0.2ccentric lesions 91 (90%)ifurcated lesions 1.06 � 0.95tented side branches 0.91 � 0.8alloonned side branches 0.03 � 0.2se of glycoprotein IIb/IIIa inhibitors 36 (35%)atients with complete revascularization 75 (73%)
* Defined as �50% lumen obstruction by visual estimation.
reatine kinase/creatine kinase-MB value that was 5 times a
he upper limit of normal (surgical definition).7,8,13 Serumreatine kinase and creatine kinase-MB isoenzyme concen-rations were measured 6, 12, and 18 hours after interven-ion. Beginning 8 days after intervention, abnormal Q wavesr enzymatic changes were sufficient for a diagnosis ofyocardial infarction. All repeat revascularization proce-
ures were recorded. Events were counted from the time ofhe initial procedure. Thrombotic occlusions were definedased on angiographic documentation of a complete occlu-ion (Thrombolysis In Myocardial Infarction grade 0 or 1ow) or angiographic documentation of a flow-limiting
hrombus (Thrombolysis In Myocardial Infarction grade 1r 2 flow).
Statistical analysis: Continuous variables are presenteds mean � 1 SD or as median and corresponding interquar-ile range. Differences in continuous variables between sub-roups of patients were evaluated using Student’s unpairedtests or Mann-Whitney nonparametric tests, as appropriate.he normality assumption for continuous variables wasvaluated by the Kolmogorov-Smirnov test. Categoricalariables are presented as counts and percentages, and dif-erences in categorical variables between patient subgroupsere evaluated with chi-square test. Survival curves wereenerated by the Kaplan-Meier method, and differences inurvival between subgroups of patients were evaluated us-ng the log-rank test. We applied univariable and multiva-iable Cox proportional hazard regression models to evalu-
SXscore p Value
�18–26(n � 110)
�26(n � 93)
4.2 � 1 4.9 � 1.3 �0.00013.80 � 1.08 3.9 � 1.40 0.00041
109 (100%) 90 (98%) 0.30103 (95%) 86 (94%) 0.49102 (94%) 80 (87%) 0.09
14 (13%) 19 (19%) 0.8896 (87%) 73 (79%) 0.98
4.30 � 1.4 4.71 � 1.9 �0.000182.8 � 28 95 � 40 �0.000116.4 � 2.8 16.6 � 3.1 0.55
0.30 � 0.54 0.20 � 0.43 0.231.05 � 0.97 1.08 � 1 0.352.22 � 1.1 2.58 � 1.4 0.020.60 � 0.6 0.87 � 0.99 �0.00010.02 � 0.2 0.01 � 0.1 0.030.15 � 0.36 0.22 � 0.4 0.00021.18 � 1.2 1.67 � 1.4 0.00030.03 � 0.2 0.0 � 0 0.10
93 (87%) 81 (90%) 0.711.17 � 0.93 1.62 � 1.2 0.0003
1.0 � 0.8 1.3 � 1.1 0.020.11 � 0.3 0.06 � 0.3 0.11
37 (34%) 24 (26%) 0.3260 (55%) 28 (30%) �0.0001
te the relation between the SXscore and the incidence of

tjcistsc9arrfoaccwtLwrsiaTivbitSsV
R
TaTps2(wpvcS
v3ttwiccvws
drdi
TT
V
S
P
DCQTPCS
1076 The American Journal of Cardiology (www.AJConline.org)
he primary end point. In our multivariable model, we ad-usted for a broad range of potential confounders, includinglinical and angiographic characteristics that are presentedn Tables 1 and 2. To avoid data overfitting, we followed atepwise modeling approach by applying a variable selec-ion using the Akaike information criterion14 and a boot-trapped variance estimation of the final model.15 We reportrude and adjusted hazard ratios (HRs) and corresponding5% confidence intervals (CIs). Performance of the SXscorend the AHA/ACC classification scheme were studied withespect to discrimination and calibration. Discriminationefers to the ability to distinguish patients with MACCEsrom those without; it was quantified at 30 days by receiver-perating characteristics with their areas under the curvend by the c-index for contrasting long-term outcomes. The-indexes for AHA/ACC classification and SXscore wereompared by means of U statistics.16 Calibration refers tohether the predicted probability of MACCEs agrees with
he observed probability; it was measured with the Hosmer-emeshow goodness-of-fit test. All variables associatedith outcome at a p value of 0.10 in Cox proportional
egression analysis, including the AHA and SXscore, wereubjected to classification and regression tree analysis todentify the best outcome predictors, in terms of MACCEst follow-up, and develop the risk stratification model.17
his method is based on recursive partitioning analysis andnvolves the segregation of different values of classificationariables through a decision tree composed of progressiveinary splits. This approach has the advantage of uncover-ng possible interactions among predictors. All statisticalests were 2-tailed, and p values were significant at �0.05.tatistical analysis was performed with Statistica 6.1 (Stat-oft, Inc., Tulsa, Oklahoma) and R-language (R Foundation,
able 3hirty day outcome
ariable
urgical myocardial infarction definitionMACCEsDeath/cerebrovascular accident/nonfatal myocardial infarctionDeath/nonfatal myocardial infarctionNonfatal myocardial infarctionNon–Q-wave myocardial infarctionCI definitionMACCEsDeath/cerebrovascular accident/nonfatal myocardial infarctionDeath/nonfatal myocardial infarctionNonfatal myocardial infarctionNon-Q-wave myocardial infarctioneatherebrovascular accident-wave myocardial infarctionarget vessel revascularizationCIoronary artery bypass graftingubacute occlusion†
* By Fisher’s exact test.† Angiographically documented.
ienna, Austria). o
esultsSXscore and baseline or procedural characteristics:
hree hundred six patients and 1,292 lesions in total, withn average of 4.22 � 1.2 lesions per patient, were analyzed.he overall SXscore in the studied population had an ap-roximately normal distribution (p � 0.37) with a slight leftkewness; it ranged from 4 to 54.5 with mean � SD of2.7 � 8.6 (95% CI 21.8 to 23.7) and a median of 22interquartile range 16 to 28). In 4 patients, only 2 lesionsere scored because the third treated lesion in each of theseatients was judged to result in �50% lumen obstruction atisual estimation. Baseline angiographic and proceduralharacteristics of the study population stratified acrossXscore tertiles are presented in Tables 1 and 2.
Thirty-day outcome: Short-term outcome after inter-ention according to SXscore tertiles is presented in Table. No death occurred within the first 30 days. Patients inhe first SXscore tertile showed the lowest, and those in thehird tertile, the highest rate of MACCEs. This differenceas driven by reintervention and occurrence of myocardial
nfarction, particularly when the PCI definition of peripro-edural myocardial infarction was applied. One cerebrovas-ular accident and 2 angiographically confirmed subacuteessel occlusions occurred in the third SXscore tertile,hereas none of these events were observed in the first or
econd SXscore tertile.
Long-term outcome: After a median follow-up of 370ays (range 274 to 400), SXscore significantly predicted theate of MACCEs (death, cerebrovascular accident, myocar-ial infarction, or target vessel revascularization; HR 1.08/Uncrease, 95% CI 1.05 to 1.11, p �0.0001). The distribution
SXscore p Value*
18103)
�18–26(n � 110)
�26(n � 93)
0 2 (2) 7 (8) 0.0050 1 (1) 4 (4) 0.050 1 (1) 3 (3) 0.120 1 (1) 3 (3) 0.120 0 0 —
(3) 5 (5) 11 (12) 0.03(3) 3 (3) 10 (11) 0.02(3) 3 (3) 9 (10) 0.04(3) 3 (3) 9 (10) 0.04(3) 2 (2) 6 (6) 0.230 0 0 —0 0 1 (1) 0.320 1 (0) 3 (3) 0.120 1 (1) 5 (5) 0.020 0 2 (2) 0.100 1 (1) 3 (3) 0.120 0 2 (2) 0.10
�
(n �
33333
f the MACCE rate according to SXscore tertiles is shown
Fi(
1077Coronary Artery Disease/Application of the Syntax Score
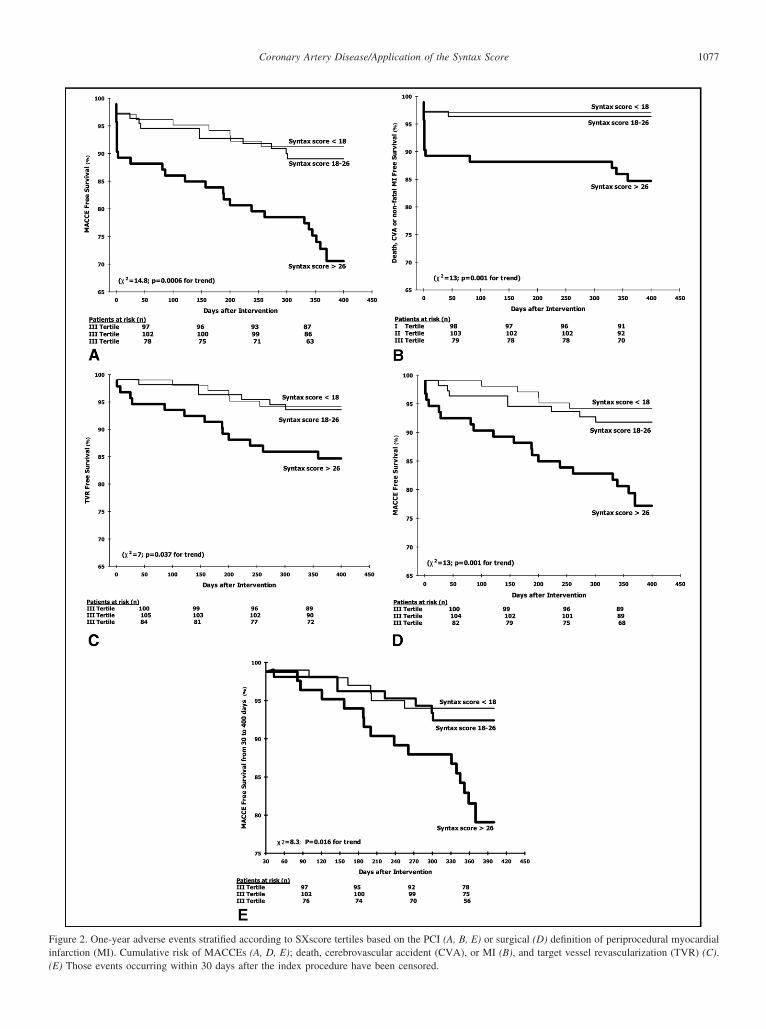
igure 2. One-year adverse events stratified according to SXscore tertiles based on the PCI (A, B, E) or surgical (D) definition of periprocedural myocardialnfarction (MI). Cumulative risk of MACCEs (A, D, E); death, cerebrovascular accident (CVA), or MI (B), and target vessel revascularization (TVR) (C).
E) Those events occurring within 30 days after the index procedure have been censored.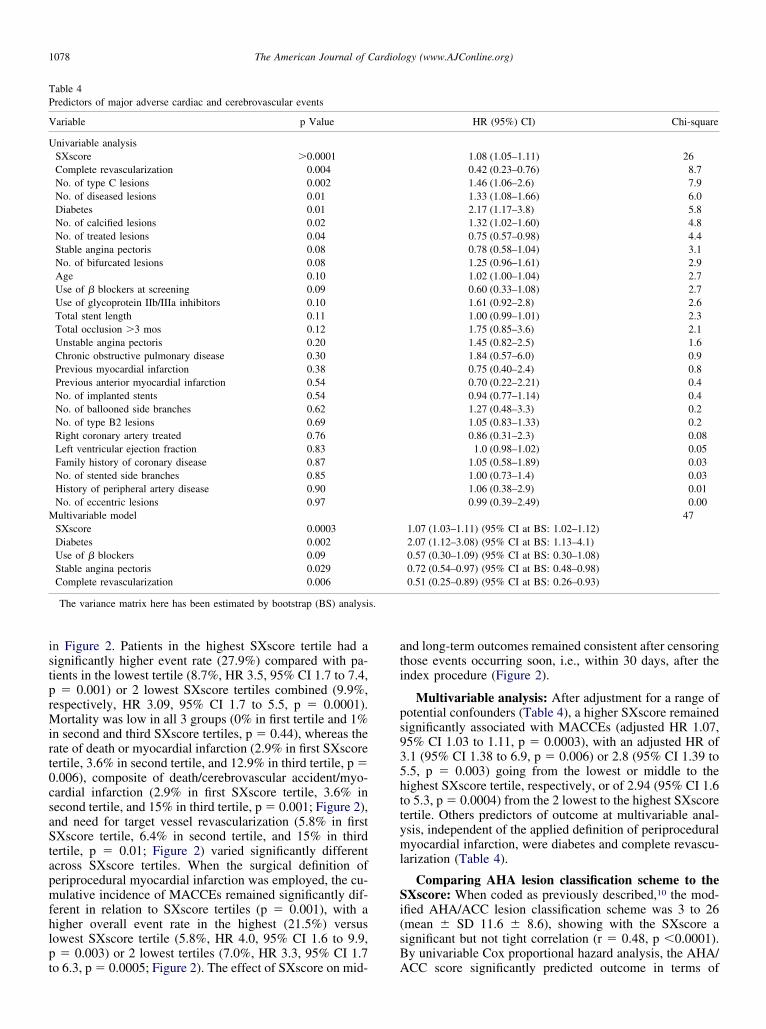
istprMirt0csaStapmfhlpt
ati
ps935httyml
Si(sB
TP
V
U
M
s.
1078 The American Journal of Cardiology (www.AJConline.org)
n Figure 2. Patients in the highest SXscore tertile had aignificantly higher event rate (27.9%) compared with pa-ients in the lowest tertile (8.7%, HR 3.5, 95% CI 1.7 to 7.4,
� 0.001) or 2 lowest SXscore tertiles combined (9.9%,espectively, HR 3.09, 95% CI 1.7 to 5.5, p � 0.0001).
ortality was low in all 3 groups (0% in first tertile and 1%n second and third SXscore tertiles, p � 0.44), whereas theate of death or myocardial infarction (2.9% in first SXscoreertile, 3.6% in second tertile, and 12.9% in third tertile, p �.006), composite of death/cerebrovascular accident/myo-ardial infarction (2.9% in first SXscore tertile, 3.6% inecond tertile, and 15% in third tertile, p � 0.001; Figure 2),nd need for target vessel revascularization (5.8% in firstXscore tertile, 6.4% in second tertile, and 15% in third
ertile, p � 0.01; Figure 2) varied significantly differentcross SXscore tertiles. When the surgical definition oferiprocedural myocardial infarction was employed, the cu-ulative incidence of MACCEs remained significantly dif-
erent in relation to SXscore tertiles (p � 0.001), with aigher overall event rate in the highest (21.5%) versusowest SXscore tertile (5.8%, HR 4.0, 95% CI 1.6 to 9.9,� 0.003) or 2 lowest tertiles (7.0%, HR 3.3, 95% CI 1.7
able 4redictors of major adverse cardiac and cerebrovascular events
ariable p Value
nivariable analysisSXscore �0.0001Complete revascularization 0.004No. of type C lesions 0.002No. of diseased lesions 0.01Diabetes 0.01No. of calcified lesions 0.02No. of treated lesions 0.04Stable angina pectoris 0.08No. of bifurcated lesions 0.08Age 0.10Use of � blockers at screening 0.09Use of glycoprotein IIb/IIIa inhibitors 0.10Total stent length 0.11Total occlusion �3 mos 0.12Unstable angina pectoris 0.20Chronic obstructive pulmonary disease 0.30Previous myocardial infarction 0.38Previous anterior myocardial infarction 0.54No. of implanted stents 0.54No. of ballooned side branches 0.62No. of type B2 lesions 0.69Right coronary artery treated 0.76Left ventricular ejection fraction 0.83Family history of coronary disease 0.87No. of stented side branches 0.85History of peripheral artery disease 0.90No. of eccentric lesions 0.97ultivariable model
SXscore 0.0003Diabetes 0.002Use of � blockers 0.09Stable angina pectoris 0.029Complete revascularization 0.006
The variance matrix here has been estimated by bootstrap (BS) analysi
o 6.3, p � 0.0005; Figure 2). The effect of SXscore on mid- A
nd long-term outcomes remained consistent after censoringhose events occurring soon, i.e., within 30 days, after thendex procedure (Figure 2).
Multivariable analysis: After adjustment for a range ofotential confounders (Table 4), a higher SXscore remainedignificantly associated with MACCEs (adjusted HR 1.07,5% CI 1.03 to 1.11, p � 0.0003), with an adjusted HR of.1 (95% CI 1.38 to 6.9, p � 0.006) or 2.8 (95% CI 1.39 to.5, p � 0.003) going from the lowest or middle to theighest SXscore tertile, respectively, or of 2.94 (95% CI 1.6o 5.3, p � 0.0004) from the 2 lowest to the highest SXscoreertile. Others predictors of outcome at multivariable anal-sis, independent of the applied definition of periproceduralyocardial infarction, were diabetes and complete revascu-
arization (Table 4).
Comparing AHA lesion classification scheme to theXscore: When coded as previously described,10 the mod-
fied AHA/ACC lesion classification scheme was 3 to 26mean � SD 11.6 � 8.6), showing with the SXscore aignificant but not tight correlation (r � 0.48, p �0.0001).y univariable Cox proportional hazard analysis, the AHA/
HR (95%) CI) Chi-square
1.08 (1.05–1.11) 260.42 (0.23–0.76) 8.71.46 (1.06–2.6) 7.91.33 (1.08–1.66) 6.02.17 (1.17–3.8) 5.81.32 (1.02–1.60) 4.80.75 (0.57–0.98) 4.40.78 (0.58–1.04) 3.11.25 (0.96–1.61) 2.91.02 (1.00–1.04) 2.70.60 (0.33–1.08) 2.71.61 (0.92–2.8) 2.61.00 (0.99–1.01) 2.31.75 (0.85–3.6) 2.11.45 (0.82–2.5) 1.61.84 (0.57–6.0) 0.90.75 (0.40–2.4) 0.80.70 (0.22–2.21) 0.40.94 (0.77–1.14) 0.41.27 (0.48–3.3) 0.21.05 (0.83–1.33) 0.20.86 (0.31–2.3) 0.08
1.0 (0.98–1.02) 0.051.05 (0.58–1.89) 0.031.00 (0.73–1.4) 0.031.06 (0.38–2.9) 0.010.99 (0.39–2.49) 0.00
471.07 (1.03–1.11) (95% CI at BS: 1.02–1.12)2.07 (1.12–3.08) (95% CI at BS: 1.13–4.1)0.57 (0.30–1.09) (95% CI at BS: 0.30–1.08)0.72 (0.54–0.97) (95% CI at BS: 0.48–0.98)0.51 (0.25–0.89) (95% CI at BS: 0.26–0.93)
CC score significantly predicted outcome in terms of

M1letltftp0rsTladAoff9tbp0Tt0r(p
rrsfi
pid3bH4vd
D
TwbriaiaschmdbcmuTicwawl
Fsd cardial
1079Coronary Artery Disease/Application of the Syntax Score
ACCEs at 400 days (1.09/U increase, 95% CI 1.01 to.17, p � 0.02), with patients in the highest AHA/ACCesion classification tertile having a significantly highervent rate (30.6%) compared with patients in the lowestertile (12.9%, HR 2.2, 95% CI 1.06 to 4.9, p � 0.03) or 2owest AHA/ACC score tertiles combined (13.7%, respec-ively, HR 2.01, 95% CI 1.11 to 3.6, p � 0.019). Whenorced into the multivariable model presented in Table 4,he AHA/ACC score failed to emerge as an independentredictor of outcome (1.001, 95% CI 0.83 to 1.06, p �.24), whereas the estimate and 95% CI for the SXscoreemained unchanged. Similarly, including the AHA/ACCcore among the univariable MACCE predictors listed inable 4 and excluding B2 or C type lesions to avoid co-
inearity in the model, the AHA/ACC score failed to emerges an independent predictor of MACCEs (irrespective of theefinition of myocardial infarction applied) based on thekaike information criterion selection process. By receiver-perating characteristics analysis, the area under the curveor MACCE rate at 30 days was higher for the SXscore thanor the AHA/ACC score (0.73, 95% CI 0.61 to 0.86 vs 0.56,5% CI 0.42 to 0.69, p � 0.02). At 400 days, the c-index forhe SXscore was higher than that for the AHA/ACC scoreased on the PCI definition (0.58 � 0.08 and 0.67 � 0.08,�0.001) and surgical definition (0.58 � 0.1 and 0.66 �
.09, p � 0.001) of periprocedural myocardial infarction.he c-index for the full model, including the SXscore and
he AHA/ACC score, was 0.73, which became 0.67 and.73 after removal of the SXscore and AHA/ACC score,espectively. The Hosmer-Lemeshow statistics were 4.5chi-square, p � 0.81) for the SXscore and 12.1 (chi-square,� 0.15) for the AHA/ACC scoring system.
Classification tree analysis: By evaluating all variableselated to 400-day MACCEs at a p value �0.10 at univa-iable Cox regression analysis (Table 4), including the AHAcore, the classification and regression tree method con-
igure 3. Binary splits based on classification and regression tree analysis.ingle discriminator between patients with and those without MACCEs depending on the applied PCI or surgical definition of periprocedural myo
rmed the SXscore as the best single discriminator between i
atients with and those without MACCEs, with a discrim-nation level of 31 or 35 according to the PCI or surgicalefinition of periprocedural myocardial infarction (Figure). When stratified into the discrimination level suggestedy classification and regression tree analysis, the adjustedR for MACCEs was 3.9 (95% CI 2 to 7.3, p �0.0001) or.5 (95% CI 2.1 to 9.6, p � 0.0001) for patients with highersus those with low SXscore based on the PCI or surgicalefinition of myocardial infarction, respectively.
iscussion
he identification of different distinct features associatedith poor prognosis in patients with CAD has been a majorreakthrough in modern medicine as an aid to allocateesources and as a tool to tailor intervention based onndividual risk. Despite a continuous effort to detect newnd progressively more sophisticated markers of prognosisn patients with CAD, implementation of unconventionalnd expensive risk stratification algorithms in the clinicaletting remains problematic. Since the earliest reports oforonary angiography, extent of coronary artery narrowingas been considered a primary and readily available deter-inant of survival in patients with CAD.18–21 Moreover,
espite continuous refinement in periprocedural antithrom-otic therapy and intracoronary devices, the extent andomplexity of CAD remain well-recognized major deter-inants of short- and long-term prognoses in patients
ndergoing percutaneous coronary revascularization.22
he AHA/ACC lesion classification scheme was proposedn 198823 and modified in 1990.10 It remains by far the mostommonly employed lesion classification system world-ide. The SXscore was recently developed in an attempt to
ssist in patient selection and risk stratification of patientsith extensive CAD undergoing revascularization6 of the
eft main coronary artery and/or the 3 main coronary arter-
ested univariable predictors of outcome, the SXscore emerged as the beste period of observation, with a discrimination level of 31 (A) or 35 (B)infarction definition, respectively.
Of all turing th
es, i.e., a subset of patients who were not or only poorly

rv
StsisppcSbsa
pcwtmepci
iS1rl
gvcsp
cAttfirwol
datvSpdonwcSi
itd
doatc“sdwtgprtwstvhwdmpialtwt
Aa
A
AA
1080 The American Journal of Cardiology (www.AJConline.org)
epresented when the AHA scoring system was created andalidated.
To obtain some insights into the performance of theXscore in this context, patients who underwent interven-
ion for 3-vessel disease as part of the ARTS II weretudied, including 306 patients and 1,292 lesions. Our find-ngs suggest that the SXscore may be a suitable tool totratify risk in early and late outcomes in this subset ofatients. Moreover, in the context of 3-vessel disease, inatients who were selected according to inclusion and ex-lusion criteria imposed by the ARTS II investigation,8 theXscore seemed to perform significantly, although slightly,etter than the modified AHA/ACC lesion classificationystem in terms of prognostic accuracy. These statementsre mainly based on the following observations.
First, the SXscore predicted the rate of MACCEs, withatients in the highest SXscore tertile showing a signifi-antly higher event rate at 30 days and 1 year comparedith patients in the lowest tertile or 2 lowest SXscore
ertiles combined. This was true for applied periproceduralyocardial infarction definitions and after censoring those
vents occurring within the first 30 days after the indexrocedure, which might be more frequently related to pro-edural success than to coronary lesion extension/complex-ty alone.
Second, after adjustment for all potential confounders,ncluding clinical presentation and lesion characteristics, theXscore remained an independent predictor of MACCEs at-year follow-up, with an almost threefold increase in theisk of events in patients in the highest versus those in the 2owest SXscore tertiles.
Third, by using a time-independent analysis, a betteroodness of fit was obtained when modeling the risk pro-ided by SXscore than that by the modified AHA lesionlassification. This implies a closer relation between ob-erved and predicted event rates when the SXscore is em-loyed.
In keeping with the previous analysis, the area under theurve for the SXscore was larger than that for the AHA/CC score for MACCEs at 30 days. Similarly, by using a
ime-dependent analysis, based on the c-index computation,he prognostic accuracy provided by the SXscore was con-rmed to be significantly higher. This was further corrobo-ated after calculating the c-index for the entire model,hich decreased from 0.73 to 0.67 after forcing the SXscoreut, but remained unaffected after exclusion of the AHAesion classification.
Fourth, the classification and regression tree is a recentlyeveloped nonparametric technique that can select frommong a large number of variables and their interactionshose that are most important in determining the outcomeariable to be explained. Based on this statistical tool, theXscore was identified as the best single predictor betweenatients with and those without MACCEs at follow-up, withiscrimination levels of 31 and 35 according to the thresh-ld set to define the occurrence of significant periproceduralecrosis. This was in keeping with the c-index analysis,hich showed a value of 0.68 for the SXscore, individually
onsidered, whereas the full model, in the absence of theXscore, computed a value of 0.67. Based on these discrim-
nation levels, the adjusted HR for MACCEs at follow-up
ncreased to 3.9 or 4.5 for patients with high compared withhose with low SXscores according to the PCI or surgicalefinition of myocardial infarction.
Most prognostic models proposed thus far have beenerived from an original dataset from a large-scale registryr a randomized, controlled trial.24 In this context, a vitalspect of prediction is to consider whether such a model isransportable to similar patients in another location.25 Theoncept is sometimes referred to as “generalizability” orvalidity,” and a model that is found to pass such a test isaid to be have been “validated.”25 The SXscore was noterived from an analysis of an original dataset. Rather, itas created by an international group of expert interven-
ional cardiologists and cardiac surgeons by merging to-ether and tailoring, based on personal expertise, severalreviously proposed CAD scoring systems.6 The presenteport is the first attempt to evaluate the predictive value ofhis recently developed angiographic scoring system. Thus,e currently face the uncommon situation in which a new
coring system is tested on a dataset that is different fromhe original, yet the new score cannot be considered fullyalidated because this is the only dataset in which the modelas been tested. As such, it remains unclear whether and tohat extent our present findings can be reproduced in aifferent group of patients with extensive CAD. Similarly,ore data are required to clarify whether the slightly better
erformance of the SXscore observed in this study justifiests use in clinical practice compared with the conventionalnd straightforward ACC/AHA classification system. Theow discriminatory capacity of the SXscore in the 2 lowestertiles was likely the reflection of a power issue, because itas similarly reproduced by comparing outcomes among
ertiles of the ACC/AHA lesion classification system.18–23
cknowledgment: We acknowledge helpful suggestionsnd editorial comments by Brian Firth, MD.
ppendix
complete list of investigators and committees of theRTS II study has been previously published.8
1. Teirstein PS. A chicken in every pot and a drug-eluting stent in everylesion. Circulation 2004;109:1906–1910.
2. Moliterno DJ, Steinhubl SR. Clopidogrel for percutaneous coronaryrevascularization: time for more pretreatment, retreatment, or both?JAMA 2005;294:1271–1273.
3. Kastrati A, von Beckerath N, Joost A, Pogatsa-Murray G, GorchakovaO, Schomig A. Loading with 600 mg clopidogrel in patients withcoronary artery disease with and without chronic clopidogrel therapy.Circulation 2004;110:1916–1919.
4. van Domburg RT, Lemos PA, Takkenberg JJ, Liu TK, van HerwerdenLA, Arampatzis CA, Smits PC, Daemen J, Venema AC, Serruys PW,Bogers AJ. The impact of the introduction of drug-eluting stents on theclinical practice of surgical and percutaneous treatment of coronaryartery disease. Eur Heart J 2005;26:675–681.
5. Loscalzo J. Clinical trials in cardiovascular medicine in an era ofmarginal benefit, bias, and hyperbole. Circulation 2005;112:3026–3029.
6. Sianos G, Morel MA, Kappetein AP, Morice MC, Colombo A,Dawkins K, van den Brand M, van Dick N, Russell ME, Mohr FW,Serruys PW. The Syntax score: an angiographic tool grading the
complexity of coronary artery disease. Eurointervention 2005;1:219–227.
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
1081Coronary Artery Disease/Application of the Syntax Score
7. Serruys PW, Lemos PA, van Hout BA. Sirolimus eluting stent im-plantation for patients with multivessel disease: rationale for the Ar-terial Revascularisation Therapies Study part II (ARTS II). Heart2004;90:995–998.
8. Serruys PW, Ong AT, Morice MC, De Bruyne B, Colombo A, MacayaC, Richardt G, Fajadet J, Hamm C, Dawkins K, et al. Arterial Revas-cularisation Therapies study part II—sirolimus-eluting stents for thetreatment of patients with multivessel de novo coronary lesions. Eu-rointervention 2005;1:147–156.
9. Leaman DM, Brower RW, Meester GT, Serruys P, van den Brand M.Coronary artery atherosclerosis: severity of the disease, severity ofangina pectoris and compromised left ventricular function. Circulation1981;63:285–299.
0. Ellis SG, Vandormael MG, Cowley MJ, DiSciascio G, Deligonul U,Topol EJ, Bulle TM. Coronary morphologic and clinical determinantsof procedural outcome with angioplasty for multivessel coronary dis-ease. Implications for patient selection. Multivessel Angioplasty Prog-nosis Study Group. Circulation 1990;82:1193–1202.
1. Smith SC Jr, Dove JT, Jacobs AK, Kennedy JW, Kereiakes D, KernMJ, Kuntz RE, Popma JJ, Schaff HV, Williams DO, et al. ACC/AHAguidelines for percutaneous coronary intervention (revision of the1993 PTCA guidelines)—executive summary: a report of the Ameri-can College of Cardiology/American Heart Association task force onpractice guidelines (committee to revise the 1993 guidelines for per-cutaneous transluminal coronary angioplasty) endorsed by the Societyfor Cardiac Angiography and Interventions. Circulation 2001;103:3019–3041.
2. Silber S, Albertsson P, Aviles FF, Camici PG, Colombo A, Hamm C,Jorgensen E, Marco J, Nordrehaug JE, Ruzyllo W, et al. Guidelines forpercutaneous coronary interventions. The Task Force for PercutaneousCoronary Interventions of the European Society of Cardiology. EurHeart J 2005;26:804–847.
3. Serruys PW, Unger F, Sousa JE, Jatene A, Bonnier HJ, SchonbergerJP, Buller N, Bonser R, van den Brand MJ, van Herwerden LA, MorelMA, van Hout BA. Comparison of coronary-artery bypass surgery andstenting for the treatment of multivessel disease. N Engl J Med 2001;344:1117–1124.
4. Sauerbrei W, Schumacher M. A bootstrap resampling procedure formodel building: application to the Cox regression model. Stat Med1992;11:2093–2109.
5. Ambler G, Brady AR, Royston P. Simplifying a prognostic model: a
simulation study based on clinical data. Stat Med 2002;21:3803–3822.6. Zhang DD, Zhou XH, Freeman DH Jr, Freeman JL. A non-parametricmethod for the comparison of partial areas under ROC curves and itsapplication to large health care data sets. Stat Med 2002;21:701–715.
7. Fonarow GC, Adams KF Jr, Abraham WT, Yancy CW, Boscardin WJ.Risk stratification for in-hospital mortality in acutely decompensatedheart failure: classification and regression tree analysis. JAMA 2005;293:572–580.
8. Ellis SG, Roubin GS, King SB III, Douglas JS Jr, Weintraub WS,Thomas RG, Cox WR. Angiographic and clinical predictors of acuteclosure after native vessel coronary angioplasty. Circulation 1988;77:372–379.
9. Holmes DR Jr, Holubkov R, Vlietstra RE, Kelsey SF, Reeder GS,Dorros G, Williams DO, Cowley MJ, Faxon DP, Kent KM, et al.Comparison of complications during percutaneous transluminal coro-nary angioplasty from 1977 to 1981 and from 1985 to 1986: theNational Heart, Lung, and Blood Institute Percutaneous TransluminalCoronary Angioplasty Registry. J Am Coll Cardiol 1988;12:1149–1155.
0. Ischinger T, Gruentzig AR, Meier B, Galan K. Coronary dissectionand total coronary occlusion associated with percutaneous translumi-nal coronary angioplasty: significance of initial angiographic morphol-ogy of coronary stenoses. Circulation 1986;74:1371–1378.
1. Meier B, Gruentzig AR, Hollman J, Ischinger T, Bradford JM. Doeslength or eccentricity of coronary stenoses influence the outcome oftransluminal dilatation? Circulation 1983;67:497–499.
2. Ross MJ, Herrmann HC, Moliterno DJ, Blankenship JC, DemopoulosL, DiBattiste PM, Ellis SG, Ghazzal Z, Martin JL, White J, Topol EJ.Angiographic variables predict increased risk for adverse ischemicevents after coronary stenting with glycoprotein IIb/IIIa inhibition:results from the TARGET trial. J Am Coll Cardiol 2003;42:981–988.
3. Ryan TJ, Faxon DP, Gunnar RM, Kennedy JW, King SB III, Loop FD,Peterson KL, Reeves TJ, Williams DO, Winters WL Jr, et al. Guide-lines for percutaneous transluminal coronary angioplasty. A report ofthe American College of Cardiology/American Heart Association TaskForce on Assessment of Diagnostic and Therapeutic CardiovascularProcedures (Subcommittee on Percutaneous Transluminal CoronaryAngioplasty). Circulation 1988;78:486–502.
4. Antman EM, Cohen M, Bernink PJ, McCabe CH, Horacek T, PapuchisG, Mautner B, Corbalan R, Radley D, Braunwald E. The TIMI riskscore for unstable angina/non–ST elevation MI: a method for prog-nostication and therapeutic decision making. JAMA 2000;284:835–842.
5. Altman DG, Royston P. What do we mean by validating a prognostic
model? Stat Med 2000;19:453–473.