Inducible laryngeal obstruction: an official joint European ...
Upload
independentCategory
view
0download
0
Portal obstruction in children. L Clinical investigation and hemorrhage risk
We examined 108 children with obstruction o f the portal vein. Symptoms included sptenomegaly and
gastrointestinal tract hemorrhage. Obstruction was secondary to portal vein injury in 44 children and
was combined with congenital malformations in 17 others. Ultrasonography provided the correct
diagnosis in 36 o f the 37 children in whom it was performed. Angiography, performed in I01 children,
showed that the obstruction extended to the superior mesenteric vein in 14 children and to the entire
portal venous system in seven; intrahepatic branches were involved in half the cases. Natural
splenorenal shunts were visible in 19 children but were not elearly associated with a lower risk o f
gastrointestinal tract bleeding; in five o f 30 children, eavography displayed abnormalities o f the
inferior vena cava. Spontaneous gastrointestinal tract hemorrhage occurred in 78 children. Fiberoptie
endoscopy showed esophageal varices in 79 o f the 81 children studied, The presence o f tense varices
and congestion o f esophageal mucosa clearly augmented the risk o f bleeding. These results suggest
a simple method o f investigation based on ultrasonography for diagnosis and on endoscopy for
prognosis. Angiography should be limited to children with a history o f gastrointestinal tract bleeding
for whom a surgical portosystemic shunt is being considered. (J PEDIATIr 103:696, 1983)
F. Alvarez, M.D., O. Bernard, M.D., F. Brunelle, M.D., P. Hadehouel, M.D., M. Odi~vre, M.D., and D. Alagille, M.D. Bic~tre, France
OBSTRUCTION OF THE PORTAL VEIN is a chief cause of portal hypertension in children. ~ The greatest risk is gastrointestinal hemorrhage from esophageal varices. In view of the great progress in the management of portal hypertension in children over the past 10 years, 2 we present our experience in regard to clinical investigation and the risk of hemorrhage. Surgical management is considered in the following article.
P A T I E N T S A N D M E T H O D S
Patients. Between 1958 and 1980, extrahepatic portal obstruction was diagnosed in 108 patients. Proof of obstruction was obtained by angiography in 104 patients and by ultrasonography alone in the remaining four, who were seen during the last two years. Patients in whom portal obstruction was associated with chronic liver disease
From Unitb de Recherches d'Hbp~Otogie Infantile, I N S E R M U 56, Services d'Hbpatologie et Radiologie, Dbpartement de Pbdia- trie, Hbpital de Bic~tre.
Reprint requests: F. Alvarez, M.D., Department o f Cell Biology, New York University Medical Center, 550 First Ave., New York, N Y 10016.
or with a history of extrahepatic biliary lesions were excluded. A history of possible portal vein injury was found in 44 (41%) children (nonidiopathic group), including umbilical neonatal venous catheterization in 40, neonatal omphalitis in one, and surgical or blunt trauma in three. In the remaining 64 (59%) children, no clear history of such a
See related articles, pp. 703, 741, and 742.
lesion was recorded (idiopathic group); in this group, four children had neonatal sepsis but no overt signs of portal injury, omphalitis, or abdominal infection.
Clinical signs and symptoms. Presenting signs are shown in Table I. In retrospect, recurrent abdominal pain was also present in two children, recurrent diarrhea in five, and recurrent abdominal distention in five. On admission to the hospital (mean age 5 years 7 months, range 1 month to 15 years 2 months), 101 patients exhibited splenomegaly (five had undergone splenectomy elsewhere), and 13, moderate hepatomegaly. The liver was considered firm in one but normal in the other 12. Ascites occurred in the course of the disease in nine patients, and in each case was associ- ated with gastrointestinal tract hemorrhage, complicated
696 T h e J o u r n a l o f P E D I A T R I C S

Volume 103 Portal obstruction. I 6 9 7 Number 5
Table I. Initial signs of portal vein obstruction
Patients Mean
Age
Idiopathic group
Range
Nonidiopathic group
Mean Range
Splenomegaly 56 Gastrointestinal tract hemorrhage 50 Hemorrhoids 1 Varices on esophagogram 1
34 mo 50 mo
1 moto 13 yr 18 mo 1 m o t o 6 y r 6moto 15yr2mo 41 mo 7 m o t o 9 y r
in one by bacterial peritonitis. Various congenital malfor- mations were present in 21 (19%) children (Table II).
Biologic investigation. On admmission, liver function tests were normal in most children. The serum unconju- gated bilirubin value was slightly elevated in five of the 106 children in whom it was measured. Serum transaminase activity was high in 11 children, either on admission or later; all 11 had previously received several blood transfu- sions, and in six, hepatitis B surface antigen was positive. Hypoalbuminemia (2.5 to 3.5 gm/dl) was present in 12 of 106 patients tested; in eight, it occurred in the weeks following severe protracted gastrointestinal tract bleeding, and was associated with ascites i n five. Excretion of sulfobromophthalein sodium was abnormal in 22 of the 50 children studied. In all but one child, abnormal dye retention was present in the 15-minute sample. Thrombo- cytopenia (40,000 to 150,000 platelets/#l) was present in
64 of 102 children studied, lymphopenia (<1000 lympho- cytes/#l) in 25 of 96, and neutropenia (< 1500 neutrophils/ #1) in eight of 98. The mean age of patients with thrombo- cytopenia was 6 years 5 months, vs 3 years 10 months for those with normal platelet counts. Children with
thrombocytopenia, lymphopenia, or neutropenia common- ly exhibited marked splenomegaly. Lymphopenia and neutropen!a did not occur in the absence of thrombo-
cytopenia. Results of coagulation tests, completed in 104 children,
are shown in Table III. The factor V value was most frequently abnormal; low levels of other coagulation fac- tors were associated with low factor V values in a variable fashion. Low factor II levels were found in seven patients,
and low factor I levels in five. High fibrin split product values were found in two patients. Low levels of factor VII + X alone were never observed. During follow-up, coagulation factor levels varied, some returned to normal and others became abnormal, with no obvious correlation with splenectomy, bleeding episodes, or age of the
patient. Malabsorption secondary to celiac disease or intestinal
lymphangiectasia, both proved by jejunal biopsy, was present in two children.
Table II. Congenital malformations associated with portal vein obstruction
Idiopathic group Cardiovascular
Atrial septal defect Ventricular septal defect Pulmonic stenosis Aortic valve stenosis (two patients) Coarctation of aorta Patent ductus arteriosus Common atrioventricular canal Large cutaneous angiomas (three patients)
Urinary Posterior urethral valves Idiopathic hydronephrosis Severe hypospadias Left kidney agenesis Ureteropelvic obstruction
Biliary Moderate idiopathic dilation of bile ducts
Nonidiopathic group Aortic valve stenosis Poland syndrome Esophageal atresia Duodenal atresia
Defects found in one patient each, except when noted.
Table III. Results of coagulation tests in 104 children
~ Patients ~ f low factor Coagulation with low _ _
factor values [Mean I Range
PT (%) >60 12 56 54 to 59 II (%) >80 17 65 44 to 77 V (%) >80 27 56 32 to 75 VII + X (%) >60 3 49 30 to 58 Fibrinogen >0.25 19 0.18 0.12 to 0.23
(gm/dl)
Radiographic and other studies. Ultrasonography of the liver and portal venous system was accomplished in 37 children. Two direct signs of obstruction were present in all but one child (Fig. 1). An oblique subcostal scan showed that the porta hepatis had been replaced by an echo- generating area containing small vascular structures. Also,

6 9 8 Alvarez et al. The Journal of Pediatrics November 1983
Fig. 2. Sites of venous obstruction shown by angiography in 101 children. Number of children in whom each venous segment was obstructed is designated.
Fig. 1. Ultrasonography. A, Right subcostal scan. Porta hepatis is replaced by an echo-generating structure containing abnormal tortuous vascular structures (single arrow). Thickened lesser omentum is well demonstrated (double arrows). B, Oblique scan through long axis of portal vein, which is replaced by numerous tortuous vascular structures (arrows).
there was no normal portal vein on a scan through its axis; this finding was also associated with tortuous vascular structures. In the only child exhibiting no direct signs of portal obstruction, angiography showed that the obstruc- tion was restricted to the proximal segment of the portal vein. Indirect signs of portal hypertension were present to various degrees in all children, and included an increase in the thickness of the lesser omentum, visible on a longitudi- nal scan through the aorta or on the oblique subeostal scan, gastroesophageal vascular derivations within the lesser omentum, and naturally occurring Splenorena! shunts.
Angiograms ineluded s p l e n ~ r t o g r a p h y in 50 children, and superior mesenteric arteriography in 28 of these 50. Superior mesenteric arteriography only was performed in 51 children. No complication was recorded. Splenoportog- raphy was usually the first examination by which diagnosis
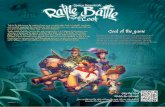
was attempted, and superior mesenterie arteriography was done when a surgical decision involving the mesenteric vein was anticipated. A scheme of the principal veins of the portal system is shown in Fig. 2. The main portal vein and one or both branches were obstructed in virtually a l l patients. In some cases, obstruction was restricted to the branches or even to one branch. Portal vein obstruction was complete or partial, in which ease the lumen was reduced to a narrow channel; Collateral veins bypassing the obstructed vein included enlarged panereaticoduodenal and biliary veins, which often reached the liver in distorted form (Fig. 3). The superior mesenterie vein was always obstructed when the splenic vein was occluded; seven patients exhibited complete obstruction o f the portal sys- tem. Natural splenogastr0renal shunts of various sizes were visible in the angiograms in 19 patients; nevertheless, 12 of them experienced gastrointestinal t rac t bleeding before or after angiography, In 79 children, the intrahepat- ie branches were visualized clearly enough for detailed study; third-order small branches were considered abnor- mal in 46 children. Abnormal intrahepatic branches were equally frequent in the nonidiopathie and idiopathic groups. Ab]aormalities consisted of abnormal segmenta- tion, irregular diameter, abnormal mode of division, and duplication of pathologic venous channels. Angiography of the inferior vena cava was performe d in 30 children and showed abnormalities in five, consisting of duplication below the renal veins in three and obstruction above the renal Veins in two, in one after umbilical vein catheteriza- tion,
Hemorrhage. Eighty six children (79%) experienced at least one episode of gastrointestinal tract bleeding. The first episode occurred spontaneously in 67 children, and after intake of aspirin in 18 or of another antiinflammatory drug in 1 child. It was manifested by Severe hematemesis (58 children), melena (19), hemorrhoidal bleeding (five), or anemia (four). Altogether, one or more episodes of
Volume 103 Portal obstruction. I 699 Number 5
Fig. 3. Venous return after injection into superior mesenteric artery. Large pancreaticoduodenal vein is opacified, bypassing portal vein obstruction, 1. Intrahepatic segmental branches are clearly abnormal. 2, Superior mesenteric vein; 3, left gastric vein; 4, remnant of portal trunk; 5, proximal splenic vein (splenectomy had been performed).
15
"6 d Z
0 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Age at first hemorrhage (years)
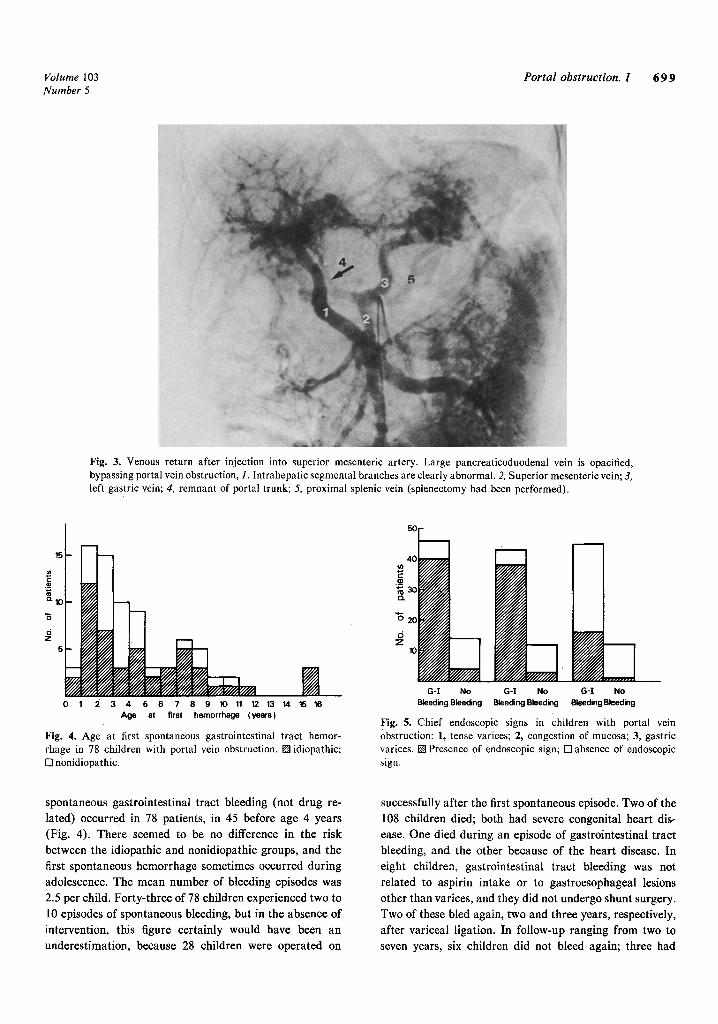
Fig. 4. Age at first spontaneous gastrointestinal tract hemor- rhage in 78 children with portal vein obstruction. []idiopathic; [] nonidiopathic.
40
2oW////A G-I No G-I No G-I No
Bleeding Bleeding Bleeding Bleeding Bleeding Bleeding
Fig. 5. Chief endoscopic signs in children with portal vein obstruction: 1, tense varices; 2, congestion of mucosa; 3, gastric varices. [] Presence of endoscopic sign; [] absence of endoscopic sign.
spontaneous gastrointestinal tract bleeding (not drug re- lated) occurred in 78 patients, in 45 before age 4 years (Fig. 4). There seemed to be no difference in the risk between the idiopathic and nonidiopathic groups, and the first spontaneous hemorrhage sometimes occurred during adolescence. The mean number of bleeding episodes was 2.5 per child. Forty-three of 78 children experienced two to 10 episodes of spontaneous bleeding, but in the absence of intervention, this figure certainly would have been an underestimation, because 28 children were operated on
successfully after the first spontaneous episode. Two of the 108 children died; both had severe congenital heart dis- ease. One died during an episode of gastrointestinal tract bleeding, and the other because of the heart disease. In eight children, gastrointestinal tract bleeding was not
related to aspirin intake or to gastroesophageal lesions other than varices, and they did not undergo shunt surgery. Two of these bled again, two and three years, respectively, after variceal ligation. In follow-up ranging from two to seven years, six children did not bleed again; three had

7110 Alvarez et al. The Journal o f Pediatrics November 1983
SPLENOMEGALY
\
PRECAUTIONS J
G-I BLEEDING
J ULTRASONOGRAPHY
ENDOSCOPY
ANGIOGRAPHY
SHUNT SURGERY
Fig, 6. Proposed method of investigation in children with portal vein obstruction.
undergone variceal ligation or gastric devascularization, one had undergone an unsuccessful mesocaval shunt else- where, and two bled only once.
Fiberoptic endoscopy of the esophagus, performed in 81 children, showed varices in 79. Varices were present either in the lower third, the lower two thirds, or along the entire length of the esophagus, but the extent was not related to the risk of bleeding. Over the past few years, the impor- tance of recording the endoscopic appearance of the varices and mucosa has become evident. Tense varices or mucosal congestion on or around the varices, or both, were present in the majority of patients who had bled before hospitalization or were to bleed later (Fig. 5). Gastric varices were found in 16 of the 56 (28%) children exam- ined. Endoscopy showed that bleeding was caused by other gastric or esophageal lesions, regardless of the presence or absence of varices, in five children (one each with gastric ulcer and diffuse ulcerative gastritis, and three with peptic esophagitis, including one with Mallory-Weiss syndrome). Of nine children who bled after aspirin intake and in whom varices were clearly visualized a few weeks or months later, eight had tense varices or congested mucosa, or both, and the remaining child had Mallory-Weiss syndrome. Among the 52 patients whose parents were instructed never to give them drugs containing aspirin, 26 experienced spontaneous
gastrointestinal tract hemorrhage; previous endoscopy in 15 of the children had shown mucosal congestion and tense varices in 14. In six children who did not undergo surgery initially, two or more endoscopies were carried out at intervals of two and one-half to seven years; five of them had tense varices or mucosal congestion, or both. Of these five, four remained unchanged and variceal tension disap- peared in one. In the sixth child, ffhO had a very small varix, a second endoscopy 2 and one-half years after the first showed that it had disappeared. A natural splenorenal shunt was visible on the initial angiogram in one of the four in whom endoscopic findings did not change and in the other two whose varices improved.
D I S C U S S I O N
Our group of children with portal vein obstruction fell into two groups, nonidiopathic and idiopathic. In the nonidiopathic group, obstruction was commonly associated with the presence of an umbilical venous catheter during the neonatal period. In the idiopathic group, two findings suggested that the problem originated during the antenatal or perinatal periods; 26% of the children in this group had associated congenital malformations, 3 and there were no differences between the tw o groups in the mean age at which the first symptoms were observed.
Splenomegaly was the major physical finding in these children, and led to the diagnosis in more than half. However, in two children, the spleen was impalpable and remained so, despite the presence of varices and gastroin- testinal tract bleeding. Ascites occurred only after bleed- ing, and was associated with hypoalbuminemia in five of nine patients. It is likely that in children who bleed, ascites results from the decrease in oncotic pressure due to hypoalbuminemia, combined with a sudden rise in portal pressure. Whenever serum albumin values were measured, they were low or slightly above the lower limit of normal.
Liver function tests are usually normal in children with portal vein obstruction. The slight increase in unconju- gated bilirubin values observed in 4% of our patients may have been caused by associated Gilbert syndrome. Abnor- malities of the sulfobromophthalein sodium retention should not be considered a sign of liver dysfunction, but a reflection of the fraction of the portal blood that does not reach the liver directly. Coagulation abnormalities were consistent with intravascular coagulation; fibrin split prod- ucts were present in a few patients, proaccelerin and fibrinogen were the factors most often reduced, and no isolated decreases in factor VII + X were observed. This argues against hepatocellular failure and is consistent with the decrease in the half-life of fibrinogen reported in portal vein obstructionAgVe therefore suggest that intravascular coagulation occurs within the veins of the portal system, outside or inside the liver, and that it may reflect an ongoing obstructive process. That splenectomy did not correct the abnormalities revealed by the coagulation tests argues against the occurrence of intravascular coagulation
only in the spleen. Q, ur data confirm that thrombocytopenia is a principal
sign .of hypersplenism. Lymphopenia is probably also directly related to hypersplenism, but when very severe and combined with hypoalbuminemia, it suggests intestinal lymphangectasia.5
Ultrasonography is a realiable noninvasive means of correctly diagnosing portal vein obstruction in children. 6-s However, it may fail when obstruction is limited to a segment of the extrahepatic portal system (e.g., the proxi-

Volume 103 Portal obstruction. 1 7 0 1 Number 5
real part of the portal vein, with a patent distal part and bifurcation) or to the very distal part of the portal vein branches, located beyond ultrasound sensitivity. In such cases, angiography may be required. 8
In most cases, angiography is now limited to children for whom a surgical portosystemic shunt is being considered, after spontaneous gastrointestinal tract bleeding. Superior mesenteric arteriography is usually preferred to splenopor- tography, because of the type of surgery currentlyprac- ticed and because it can be performed safely even when thrombocytopenia is severe. Angiography clearly indicates that obstruction in children commonly affects both extra- hepatic and intrahepatic branches of the portal vein; moreover, the abnormalities of the distal portal vein branches are very reminiscent of the lesions described in hepatoportal sclerosis in adults. 9, t0 Natural splenogastro-
renal shunts are alleged to be effective in the prevention of growth of varices and gastrointestinal tract bleeding. 11,~2
As in some of our patients, this is possible, but our results indicate that the mere presence of a natural shunt will not prevent bleeding. 13 The possibility of malformation or
thrombosis of the inferior vena cava makes the detection of its patency by angiography mandatory before attempting a surgical shunt.
We confirm that gastrointestinal tract bleeding is the major risk in childhood portal vein obstruction. ~4, ~5 Eighty
percent of our children experienced at least one episode of bleeding. In addition to hematemesis and melena, bleeding was sometimes caused by hemorrhoids. 16, ~7 Portal hyper- tension should therefore be considered in children with hemorrhoids. As reported, 14'j5 the first bleeding episode frequently occurred between 1 and 5 years of age, and bleeding tended to recur. ~7 Our low average figure of 2.5
bleeding episodes per child vs five in two other large series~5. ~8 may be due to the early shunt surgery carried out
successfully in the children reported here. High death rates from gastrointestinal tract bleeding have been re- ported)4. ~5 In our group, the only child who died during a bleeding episode also had severe congenital heart disease. In our opinion, the occurrence of death from bleeding or from posttransfusion hepatitis 19 as a consequence of repeated bleeding are two major reasons for performing shunt surgery as early as possible.
Endoscopy has become essential in the investigation of children with portal hypertension. Our results suggest that emergency endoscopy should be very useful in cases of gastrointestinal tract bleeding, because esophageal or gas-
tric lesions not directly related to varices cause bleeding in a few cases. This is important, because a surgical shunt should be considered only when endoscopy confirms that
bleeding is caused by varices. Furthermore, the presence of gastric varices in about one third of the children is another reason for confirming that bleeding varices are located in
the esophagus; bleeding gastric varices cannot be con- trolled with the Sengstaken-Blakemore tube. Our results indicate that endoscopy may, in some respects, allow
prediction of hemorrhage, because two major endoscopic signs of portal hypertension (variceal tension and conges- tion of esophageal mucosa) are closely associated with gastrointestinal tract bleeding. They were also present in most of the children who bled after aspirin ingestion, and when these signs were present, preventive measures to obviate bleeding (e.g., avoidance of aspirin-containing drugs) usually failed. We consider careful recording of these two major endoscopic signs to be very important.
Our data suggest the method of investigation shown in Fig. 6. Whether the initial symptom is splenomegaly or gastrointestinal tract bleeding, the first step in investiga- tion is ultrasonography of the portal vein, to look for signs of portal hypertension. Endoscopy is then necessary to detect the presence of varices and major signs of portal hypertension. If there has been no spontaneous gastrointes- tinal tract bleeding, the parents are given a list of aspirin-
containing drugs to be avoided, together with a Sengstak- en-Blakemore tube adapted to the size of the child, to be used in the emergency room by the physician in case of
acute bleeding. If spontaneous bleeding has already occurred, a surgical portosystemic shunt is considered and angiographic studies, including cavography, are per- formed, followed by shunt surgery.
We thank Mme. M. Dreyfus for help with revision of the manuscript.
REFERENCES
1. Alagille D, Odi6vre M: Liver and biliary tract disease in children. New York, 1979, Wiley-Flammarion, p 262.
2. Bismuth H, Franco D: Portal diversion for portal hyperten- sion in early childhood. Ann Surg 183:439, 1976.
3. Odi~vre M, Pig6 G, Alagille D: Congenital abnormalities associated with extrahepatic portal hypertension. Arch Dis Child 52:383, 1977.
4. Tytgat GN, Collen D, Verstraete M: Metabolism of fibrino- gen in cirrhosis of the liver. J Clin Invest 50:1690, 1971.
5. Choulot J J, Mercier JC, Douillet P: Cavernome porte et lymphangiectasies intestinales. Arch Fr Pediatr 36:1049, 1979.
6. Webb L J, Berger LA, Sherlock S: Grey-scale ultrasonogra- phy of the portal vein. Lancet 2:675, 1977.
7. Sassoon C, Douillet P, Cronfalt AM, Odi~vre M, Chaumont P, Doyon D: Ultrasonographic diagnosis of portal cavernoma in children: A study of twelve cases. Br J Radiol 53:1047, 1980.
8. Brunelle F, Alagille D, Pariente D, Chaumont P: An ultra- sound study of portal hypertension in children. Ann Radiol 24:121, 1981.
9. Mikkelsen WP, Edmonson HA, Piters RL, Redeker AG, Reynolds TB: Extra- and intrahepatic portal hypertension without cirrhosis (hepatoportal sclerosis). Ann Surg 162:602, 1965.
10. Boyer JL, Hales MR, Klastkin G: "Idiopathic" portal hyper-

7 II 2 Alvarez et al. The Journal of Pediatrics November 1983
tension due to occlusion of intrahepatic portal veins by organized thrombi. Medicine 53:77, 1974.
11. Alvarez F, Bernard O, Brunelle F, Hadchouel M, Leblanc A, Odi6vre M, Alagille D: Congenital hepatic fibrosis in chil- dren. J PEDIATR 99:370, 1981.
12. Wexler MJ, MacLean LD: Massive spontaneous portal- systemic shunting without varices. Arch Surg 110:995, 1975.
13. Lam KC, Juttner HU, Reynolds TB: Spontaneous portosys- temic shunt: Relationship to spontaneous encephalopathy and gastrointestinal hemorrhage. Dig Dis Sci 26:346, 1981.
14. Clatworthy HW: Extrahepatic portal hypertension. Major Probl Clin Surg 14:243, 1974.
15. Mitra SK, Kumar V, Datta DV, Rao PN, Sandhyu K, Singh GK, Sodhi JS, Pathak IC: Extrahepatic portal hypertension: A review of 70 cases. J Pediatr Surg 13:51, 1978.
16. Pinkerton JA, Holcomb GW, Foster JH: Portal hypertension in childhood. Ann Surg 175:870, 1972.
17. Grauer S, Schwartz SI: Extrahepatic portal hypertension: A retrospective analysis. Ann Surg 189:566, 1979.
18. Fonkalsrud EW, Myers NA, Robinson M J: Management of r portal hypertension in children. Ann Surg 180:487, 1974.
19. Clatworthy HW, Nahmad M, Hollabaugh RS: Presinusoidal extrahepatic portal hypertension: A review of thirty-five cases variously treated. Prog Pediatr Surg 11:125, 1978.
Copyright © 2022 FDOKUMEN