
Current Clinical Applications of Ultrasound to Bone Lesions in ...
10
1997 ; 16 : 95-104 Current Clinical Applications of Ultrasound to Bone Lesions in the Extremities Department of Di agno stic Radiolo gy, Yeungnam University Co ll ege of Medicine, Taegu , Korea 1 Department of Di agnos tic Radiology, Henry Ford Hos pit al , Detroit , Michi gan, US A2 , Department of Diagnostic Radiology , Montreal General Hospital , McG ill University , Montrea l, Quebec, Canada 3 , Department of Di agno stic Radiology, New York Medical Co ll ege, Valhalla , New York , USA4 Kil-Ho Cho . M.D.' . J. Antonio Bouffa rd . M.D 2 • Rethy K. Chhem , M.D .' . & Dooh i Lee . f\1 .D. 4 =Abstract= Al though ultrasound has received little attention for bone lesions , and still limited in applying to skeletal diseases , the experie nc e is changing in where the ultrasonic evaluation of bone l esions offers us valuable information, usually with less discomfort , risk , cos 1, and time expenditure than alternative modalities. Plain radiography is undoubtedl y the basic and most important modality for bone lesions , and MR imaging has been more commonly us ed in many instances rather than ultrasound for evaluating same abnormalitie s or anatomic structures. The application of ultrasound may be helpful for additional information, and other soft tissue lesions can be excluded as the causes of pain rather than from bon e itself Authors ha ve reviewed current applications of ultra sound to peripheral bone lesions and conditions . Some of these are n ew and ha ve been used in a small series of patients While experience is being growing and additional applications may be possible with close cooperation between radiologist and the clinic ian , progress will be , in the near future , achieved in ultras onic evaluation for bone lesions . Index terms : Bone . US INTRODUCTION The ultrasonographic inability in imaging medul- lary cavity of bone has led to the mi sconception that ultrasound (US) is inadequate for the evaluation of bone disea ses [IJ . And de velopment of MR imaging, the major alternative to sonographic imaging, gives us exquisite anatomic detail , contrast resolution , and a global view of both soft-tissue and osseous structures. For the se reasons the role of ultrasonography has been relegated as a screening tool for determining whether or not a lesion is present [2J. Ultrasound is still Iimited in applying to skeletal di seases , and clini- cal applications of US in peripheral skeletal lesions is not common [3 , 4J. However, the experience is chang- ing in where the ultrasonic evaluation of bone lesions offers us valuable information, and in certain instan- ces ultra so nography ha s been employed as the princi- pal modality for evaluating a bone lesions [3-5J . Additionally, other soft tissue le sions can be excluded as the causes of pain rather than from bone itself [4]. A discussion of joint diseases and qualitative US (ultrasonic bone densitometry) is beyond the sco- pe of this essay. l : 1 99 199 : Address for repri nts : Ki 1-Ho Cho. Department of Dia gnos ti c R ad iol ogy. Co ll ege of Med i cine. Yeun gnam Uni versity 3 17 - 1. D ae myung -dong. Nam- ku . Tae gu. 7 0 5-0 3 5. Kor ea. Te l. (82-53) 620-3045 . Fax . (82 - 53) 653 - 5484 -95-
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Current Clinical Applications of Ultrasound to Bone Lesions in ...

대한초음파의학회지
1997 ; 16 : 95-104
Current Clinical Applications of Ultrasound to Bone Lesions in the Extremities
Department of Diagnostic Radiology, Yeungnam University College of Medicine, Taegu, Korea 1
Department of Diagnostic Radiology, Henry Ford Hospital, Detroit, Michigan, USA2,
Department of Diagnostic Radiology, Montreal General Hospital, McGill University, Montreal, Quebec, Canada 3 ,
Department of Diagnostic Radiology, New York Medical College, Valhalla, New York, USA4
Kil-Ho Cho. M.D.' . J . Antonio Bouffard . M.D2• Rethy K. Chhem , M.D.'. & Dooh i Lee . f\1 .D.4
=Abstract=
Although ultrasound has received little attention for bone lesions , and still limited in applying to skeletal diseases , the experience is changing in where the ultrasonic evaluation of bone lesions offers us valuable information, usually with less discomfort, risk , cos1, and time expenditure than alternative modalities. Plain radiography is undoubtedly the basic and most important modality for bone lesions , and MR imaging has been more commonly used in many instances rather than ultrasound for evaluating same abnormalities or anatomic structures . The application of ultrasound may be helpful for additional information, and other soft tissue lesions can be excluded as the causes of pain rather than from bone itself
Authors have reviewed current applications of ultrasound to peripheral bone lesions and conditions . Some of these are new and have been used in a small series of patients While experience is being growing and additional applications may be possible with close cooperation between radiologist and the clinician, progress will be, in the near future , achieved in ultrasonic evaluation for bone lesions .
Index terms : Bone. US
INTRODUCTION
The ultrasonographic inability in imaging medullary cavity of bone has led to the misconception that ultrasound (US) is inadequate for the evaluation of bone diseases [IJ . And development of MR imaging, the major alternative to sonographic imaging, gives us exquisite anatomic detail, contrast resolution, and a global view of both soft-tissue and osseous structures. For these reasons the role of ultrasonography has been relegated as a screening tool for determining whether or not a lesion is present [2J. Ultrasound is
still Iimited in applying to skeletal diseases, and clinical applications of US in peripheral skeletal lesions is not common [3, 4J. However, the experience is changing in where the ultrasonic evaluation of bone lesions offers us valuable information, and in certain instances ultrasonography has been employed as the principal modality for evaluating a partic비ar bone lesions [3-5J . Additionally, other soft tissue lesions can be excluded as the causes of pain rather than from bone itself [4]. A discussion of joint diseases and qualitative US (ultrasonic bone densitometry) is beyond the scope of this essay.
논문접수: 1997년 6 월 l 일, 수정제의 : 199 년 월 일, 수정논문접수: 199 년 월 일, 논운게재결정 : 1997년 6 월 3 일
Address for repri nts : Ki1-Ho Cho. Department of Diagnosti c Radiology. College of Medicine. Yeungnam Uni versity 3 17 - 1. Daemyung-dong. Nam-ku. Taegu. 70 5-035. Korea. Tel. (82-53) 620-3045 . Fax . (82 -53) 653 -5484
-95-
대한초음파의학회지 제 16권 제 2호 1997
TECHNICAL CONSIDERATION
The examination of bone lesions with US is very similar in the way other organs or structures of extremities are employed [1 , 3). To determine the area of interest for ultrasonic examination, the ultrasonologist should get information from clinical data and other available radiographic studies. Linear-array high-frequency transducers (usually from 5 MHz to 10 MHz or more) are the most suitable for the imag-ing of the bone lesions. On rare occasions, the 3.0 to 3.5 MHz frequency sector probe or wide-angled convex transducers have advantages in where a lesion is deeply seated in a large or muscular patient. The higher the frequency of the US waves, the better the imaging quality, but the lesser the depth of tissue penetration. Scanning planes are variable, however, orthogonal images are obtained two planes in right angles parallel and transverse to the long axis of the lesions or oblique planes. For all structures and entities being examined this multiplanar technique contributes the most information and allows three-dimensional localization and measurement of lesions Scanning the contralateral asymptomatic side of paired structures and supplementary dynamic evaluation are very useful to characterize the lesions for each patient if there is a question as to what is normal
Whenever possible, the transducer face is placed, on the region of interest, parallel to the surface of the bone to be examined so that sonologist can obtain images without anisotropic reflector artifact. However, an off-angled anisotropic artifact of tendon can be used to identify the tendon from surrounding hyper-echoic fat or other structures [4). The examiner must be careful of mechanical and technical artifacts which are well-reported in the literatures [1 , 4, 5). Applying color or power Doppler function could be informative , and be helpful to identify vessels from other structures [4).
An adequate use of acoustic coupling agent may create a gas-free pathway for US waves which makes imaging suitable. Water is the best sound-transmitting medium in the body. Therefore, the more exudative the pathology, the bet1er the imaging conditions.
US FINDINGS OF NORMAL BONE
Because bone-soft tissue interface is highly reflective, cortical bone appears normally as a smooth hyperechoic, essentially perfect specular reflector without step-off or other defect [4) . Knowledge of the
course or the canal of perforating or nutrient vessels should not be interpreted as a pathology. Posterior acoustic shadow is demonstrated because no ultrasound transrnÏssion is seen beyond the cortical bone Echoes appearing beyond the cortical surface are reverberation artifacts scat1ering off of the overlying soft tissue and highly reflective bone and soft tissue interface [1 , 4, 5).
The normal periosteum appears as a thin echogenic line parallel to the cortex, which often can not be visualized as a separate structure from the underlying bony cortex to which the periosteum is tightly attached [4). Alterations of the surface characteristics and/or vis'ualization of the periosteum may, therefore, indicate underlying pathology intrinsic or extrinsic to . bone [3).
US FINDINGS OF ABNORMAL BONE
Diseases in/or around bone can elicit periosteal reactions, and periosteum appears as hyperechoic lines which may be elevated by an underlying process such as hematoma, abscess, or tumor. Thickening of the periosteum is a nonspecific finding seen in many diseases whether they are intrinsic to bone or not [4). Conventional radiography, in the majority of cases, is the examination of choice to survey the periosteum.
Traumatic Lesions of Bone
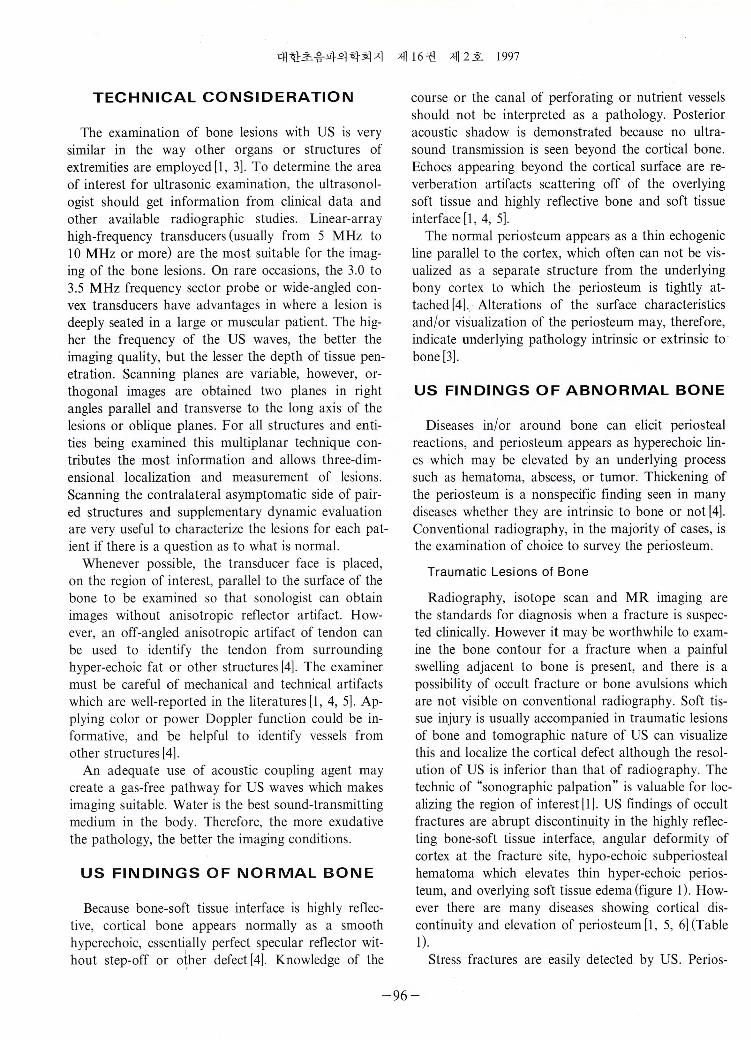
Radiography, isotope scan and MR imaging are the standards for diagnosis when a fracture is suspected clinically. However it may be worthwhile to examine the bone contour for a fracture when a painful swelling a이acent to bone is present, and there is a possibility of occult fracture or bone avulsions which are not visible on conventional radiography. Soft tissue injury is usually accompanied in traumatic lesions of bone and tomographic nature of US can visualize this and localize the cortical defect although the resolution of US is inferior than that of radiography. The technic of “ sonographic palpation" is valuable for localizing the region of interest [1). US findings of occult fractures are abrupt discontinuity in the highly re f1ecting bone-soft tissue interface, angular deformity of cortex at the fracture site, hypo-echoic subperiosteal hematoma which elevates thin hyper-echoic periosteum, and overlying soft tissue edema (figure 1). However there are many diseases showing cortical discontinuity and elevation of periosteum [1 , 5, 6) (Table
Stress fractures are easily detected by US. Perios-
-96-
조길호 등 : 사지의 골 질환에 대한 초음파검사의 임상적 이용
A B C Fig. 1. Occult green-stick Iracture 01 left libula in 3 years old . A. A plain radiograph 01 left lower leg shows questionable short transverse radiopaque line (white arrow) in distal dia-metaphysis 01 the libula. B. Longitudinal ultrasonography of right libula shows normal bone 01 which cortical line (short arrows) is cont iguous. C. Longitudinal ultrasound 01 left libula shows cortical discont inuity and ang비ar delormity at Iracture site (short arrows)
teal reaction presents as a focally thick hyper-echoic line elevated by a hyper-echoic callus overlying the cortical interruption [1 , 7J. Monitoring of fracture healing may also be evaluated with US. Callus formation appears as echoic foci at the fracture site, bridging between two fragments of bone, and increasing in volume and posterior shadowing over time [7, 8J With increasing experience, the hypervascularity or bridging callus may be characterized with power Doppler imaging.
Infectious Diseases of Bone
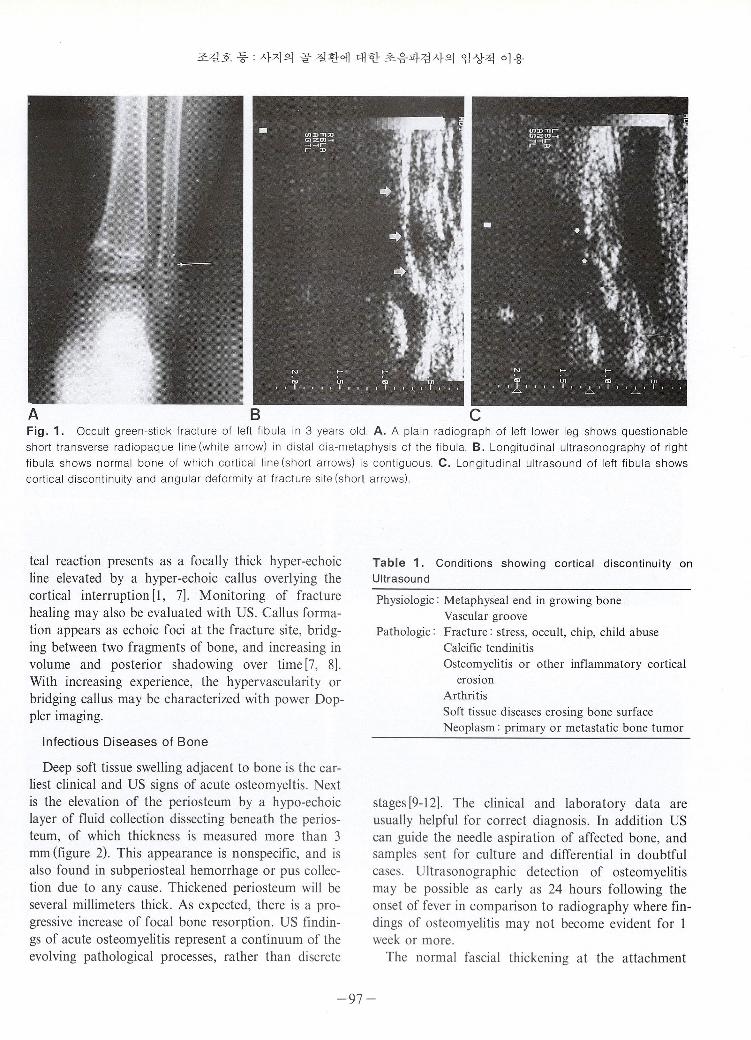
Deep soft tissue swelling adjacent to bone is the earliest c1inical and US signs of acute osteomyeltis. Next is the e1evation of the periosteum by a hypo-echoic layer of fluid collection dissecting beneath the periosteum , of which thickness is measured more than 3 mm (figure 2). This appearance is nonspecific, and is also found in subperiosteal hemorrhage or pus collection due to any cause. Thickened periosteum will be several millimeters thick. As expected, there is a progressive increase of focal bone resorption. US findings of acute osteomyelitis represent a continuum of the evolving pathological processes, rather than discrete
Table 1. Conditions showing cortical discontinuity on Ultrasound
Physiologic: κ1etaphyseal end in growing bone Vascular groove
Pathologic: Fracture: stress, occult, chip, child abuse Calcific tendinitis Osteomyelitis or other inf1ammatory cortical
erosIOn Arthritis Soft tissue diseases erosing bone surface Neoplasm : primary or metastatic bone tumor
stages [9-12J. The c1inical and laboratory data are usually helpful for correct diagnosis. In addition US can guide the needle aspiration of affected bone, and samples sent for culture and differential in doubtful cases. Ultrasonographic detection of osteomyelitis may be possible as early as 24 hours following the onset of fever in comparison to radiography where findings of osteomyelitis may not become evident for 1 week or more.
The normal fascial thickening at the attachment
-97-
대한초음파의학회지 제 16 권 제 2 호 1997
E D Fig. 2. Osteomyelitis and arthritis of left ankle in 54 years o ld. A. Axial CT scan of ankles. Left ankle shows cortical erosion
(black arrow heads) of ta lu s and lateral malleolus with circumferential fluid collection (white arrows). Right ankle is normal. 8
& C. Ultrasonograms of normal rig ht ankle. Axial views on lateral malleolus (8) and on anterior aspect to proximal talus (C)
shows normal bony cortex and soft tissue. D & E. Ultrasonograms of left ankle. Axial scans on lateral malleolus (D) and on
anterior aspect to proximal talus (E) show more than 6 mm thick (calipers) , circumferential hypoechoic pus collection (wh ite
arrows) and inflammatory thickening of subcutaneous layer (asterisks)
-98-

조길호 등 사지의 골 질환에 대한 초음파검사의 엄상적 이용
site to the bone should not be interpreted as a pathologic find ing [1]. Abscesses formed in soft tissue in osteomyelitis are usually surrounded by indistinct increased echogenicity representing perifocal inf1ammatory reaction [4]. The echogenicity of abscess cavity is variable, but typically one contains predominantly hypo-echoic f1uid often with debris seen as fine, low-Ievel echoes within the cystic area. The sonographic appearance of abscess considerably overlaps with other lesions, including hematoma, tumor, hemorrhagic cyst, and , sometimes, ganglion which may contains heterogeneous hyperechoic materials in the cyst [3] .
Chronic osteomyelitis is relatively difficult to diagnose because the bony structures, in the most cases, are changed due to infectious process, previous surgery, or combined trauma [4]. Conventional radiography and scintigraphy are not specific. US can readily demonstrate inhomogenous cortical irregularity, cortical discontinuity, periosteal change, abscess formation, and sinus fistulous tract formed in soft tissue [13]. Sonographic guidance for percutaneous needle aspiration of these masses gives us a quite easy tissue confirmation for the lesions.
Neoplastic Disease of Bone
MRI and/or CT provide c1early greater information about tumors of extremities. The role of US in tumor imaging is limited to the soft tissue component of the mass and surface change of cortical contours at the involved area. US can reveal the relationship of a mass to adjacent soft tissue structures such as muscles, nerves, vessels, bone, and intramedullary appearance of bone in the case of cortical breakdown or thinning. An aneurysmal bone cyst, for an example, may be seen on US when the cortex is suffi ciently thinned to allow beam penetration [5]. In osteochondroma, US is helpful to measure the thickness of the cartilage cap. The cartilage appears as a hypoechoic layer superficial to the highly ref1ective cortical bone echoes. Ultrasonic measurement of thickness of the cartilage cap has been proven to be very accurate, with a mean measurement error of less than 2 mm for carti lage caps less than 2 cm thick. The thickness can be c1 inically significant, since of less than 1 cm means usually a benign, that of greater than 2 cm is indicative of malignant transformation, and 1 to 2 cm is a indicator of borderline condition [14]. The thicker the cartilage cap, the more malignant the tumor. Bursa formation between the cartilage cap and adjac-
ent soft tissue may also be diagnosed. US may differentiate real osseous enlargement of tumor from a pseudotumor due to intra-tumoral hemorrhage or necrosis. US can be used to monitor recurrence of lesions by sequential examination for the resection site, especially in a patient with a metallic endoprosthesis [15, 16]. Localization for needle biopsy of an associated soft tissue mass or bone tumor with cortical thinning is safe and accurate when undertaken in detailed communication between the pathologist, the radi이
ogist, and the surgeon [17].
Ultrasound in Patients with Orthopedic Devices
In patients with external fixators, US can be used in the follow-up of the fracture healing process [18]. The scanning area is partially limited by the design of external frame so that small transducer such as intra-operative probe with a frequency of 5-7.5 MHz gives the best result. In the first phase (Iess than 2 weeks) of the fracture healing, US shows hypo-echoic area, consisting of hematoma, bone fragments, and tissue at the fracture site. In the second phase (2-4 weeks) the edges of the fragments become smooth. The hypo-echoic area becomes increasingly hyper-echoic. Small Iinear echoes suggest the formation of periosteal callus. In the third phase (3-6 weeks) fracture gap becomes more echoic, and the hyper-echoic linear echoes surrounding the hematoma at the fracture site ref1ects periosteal calcification. Small highly echogenic spots due to calcification are seen in the gap which is still penetrated by the ultrasound. In this phase radiography shows initial periosteal reaction. In the fourth phase (6-12 weeks) there is a progressive increase in echogenicity of the periosteal callus, resulting in different degrees of posterior acoustic shadowing which is an index of initial mechanical recovery [8, 18]. Ultrasound also provides information of complications involving the adjacent tissues, fistulae, and abscess
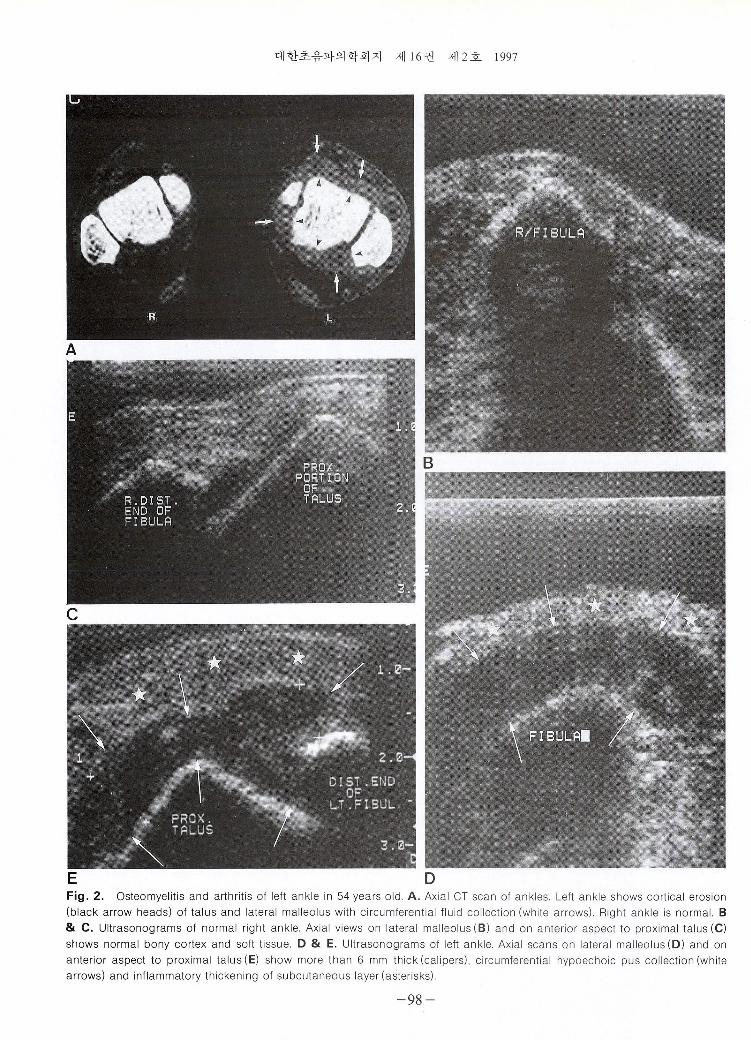
It is very important to evaluate neo-osteogenesis at the distraction site in patients who undergo leg-Iengthening procedures. The detection of new bone production determines the choice of the rate of distraction. The sensitivity of plain film in detecting new bone production relative to the size of the distraction gap is limited, and the adjustment rate for corticotomy lengthening has been largely empirica l. With US new bone formed at distraction gap can be seen as thin, echogenic strands bridging the gap between the two bony ends (figure 3). Complicating cyst formation
-99-
대한초음파의학회지 제 1 6 권 제 2호 1997
D Fig. 3 . Ultrasonic serial examinations of distraction site of tibia in bone-Iengthening procedure in 23 years old man. A & B.
Anterior longitudinal view of tibia (A) in 2 weeks of bone-Iengthening shows 12 mm distraction gap (calipers) between oste
otomy fragments (arrows) at which hypoechoic fluid collection (c) is seen. Sound transmission is seen deep to the cyst at the
osteotomy defecl. Axial image (8 ) shows the fluid (이 collected anteriorly at the osteotomy site. Needle aspiration was done. C.
Axial view in 4 weeks shows slit-like fluid collection anteriorly at the osteotomy defect (dots). Echogenic spots wi th posterior
shadowing are seen. Sou nd transmission at osteotomy defect is disappeared. D. Axial view in 8 weeks shows bony ri m (arrow
s) along the outer contour of the tibia, and the echogenic spots representing callus are increased in size and number at the
。steotomy site. No flu id col lection in/around the osteotomy site is seen
at the distraction site, which impairs bony union, is
easi1y detected with US and can be aspirated if it per
sists [1 8-20] . U1trasonography is an excellent too1 to
show the healing changes by severa1 weeks before rad
iography becomes positive.
Major complications of joint prosthesis are mech-
-100-
조길호 등 : 사지의 골 질환에 대한 초음파검사의 임상적 이용
anical loosening of the prosthesis and infection, which are clinically challenging to diagnose. On US the most specific sign of infection is the presence of extraarticular f1uid collections or abscesses. Another sign is a distention of the pseudocapsule at the prosthetic-diaphyseal junction [1 , 2이 Needle aspiration under sono-guidance enables to diagnose the nature of the f1uid collection, and it will be the standard for diagnosing an infection in orthopedic prosthesis [21]
Miscellaneous Lesions of Bone
Periosteal desmoid is a benign cortical lesion of traumatic ongm usually in growing bone, the most commonly occurring on femur at the insertion site of medial head of gastrocnemius muscle. It produces a periosteal reaction which can mimic aggressive tumor on plain film. Ultrasound shows focal hyper-echoic band displaced from the cortical line at the insertion
A B
of the muscle, and no tumor formation in soft tissue is found [22] .
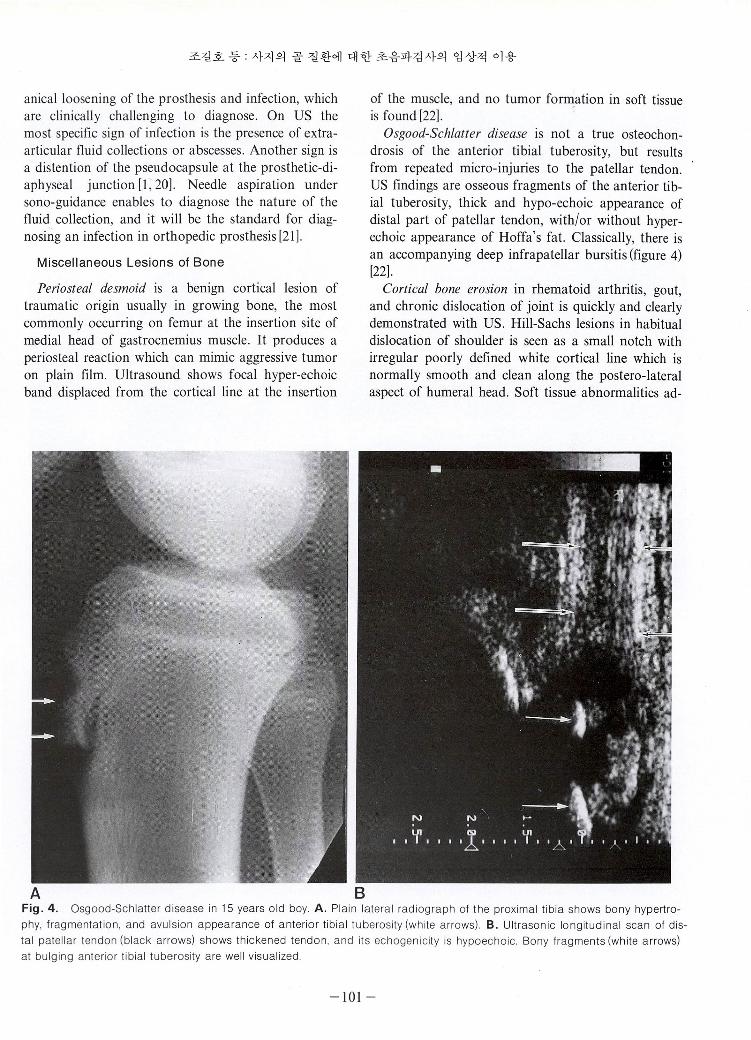
Osgood-Schlatter disease is not a true osteochondrosis of the anterior tibial tuberosity, but results from repeated micro-injuries to the patellar tendon. US findings are osseous fragments of the anterior tibial tuberosity, thick and hypo-echoic appearance of distal part of patellar tendon, with/or without hyperechoic appearance of Hoffa’s fa t. Classically, there is an accompanying deep infrapatellar bursitis (figure 4) [22].
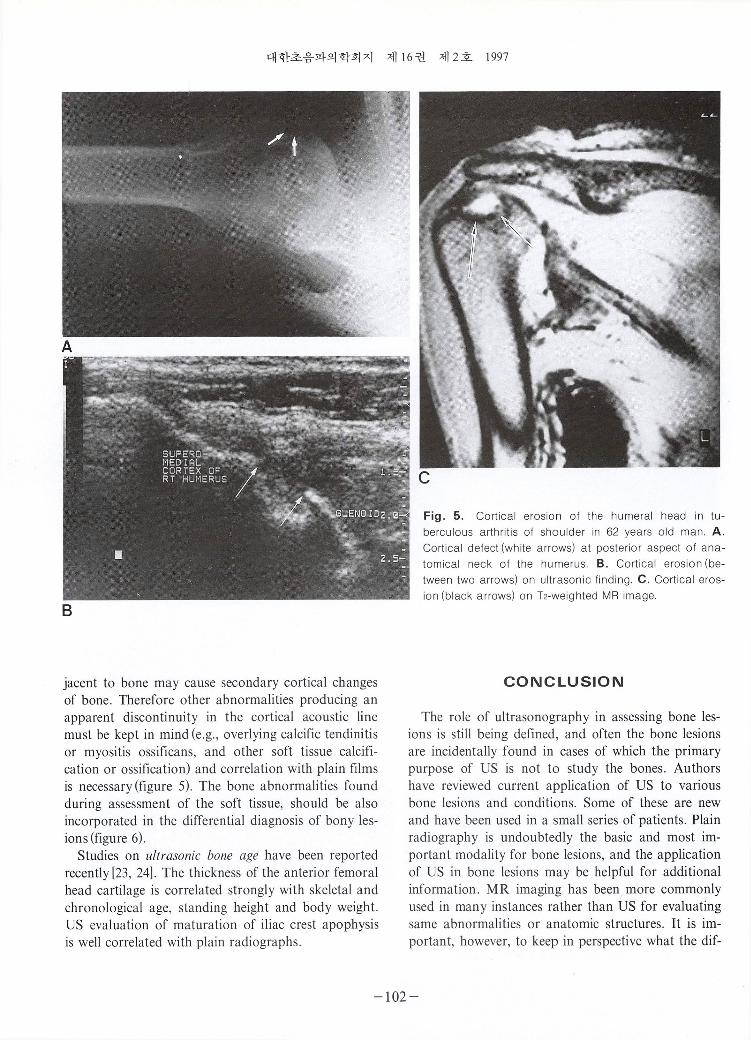
Cortical bone erosion in rhematoid arthritis, gout, and chronic dislocation of joint is quickly and cleariy demonstrated with US. Hill-Sachs lesions in habitual dislocation of shoulder is seen as a small notch with irregular poorly defined white cortical line which is normally smooth and clean along the postero-lateral aspect of humeral head. Soft tissue abnormalities ad-
Fig. 4. Osgood-Schlatter disease in 15 years old boy. A. Plain lateral radiograph 01 the proximal tibia shows bony hypertrophy , Iragmentation , and avulsion appea rance 01 anterior tibial tuberosity (white arrows). B. Ultrasonic longitudinal scan 01 distal patellar tendon (black arrows) shows thickened tendon , and its echogenicity is hypoechoic. Bony Iragments (white arrows) at bulging anterior tibial tuberosity are well visualized
-101-
대한초음파의학회지 제 16 권 제 2호 1997
B
jacent to bone may cause secondary cortical changes
of bone . Therefore other abnormalities producing an
apparent discontinuity in the cortical acoustic line
must be kept in mind (e.g. , overlying calcific tendinitis
or myositis ossificans, and other soft tissue calcifi
cation or ossification) and correlation with plain films
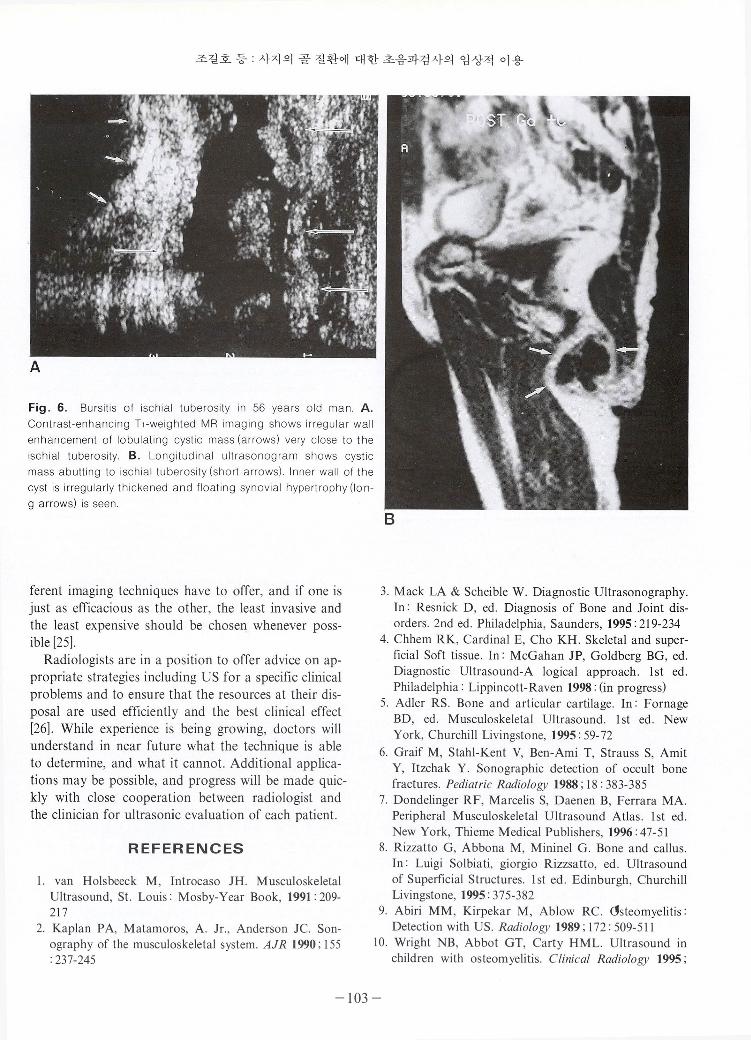
is necessary (figure 5). The bone abnormalities found
during assessment of the soft tissue, should be also
incorporated in the differential diagnosis of bony les
ions (figure 6). Studies on ultrasonic bone age have been reported
recently [23, 24]. The thickness of the anterior femoral
head cartilage is correlated strongly with skeletal and
chronological age, standing height and body weigh t. US evaluation of maturation of iliac crest apophysis
is well correlated with plain radiographs.
Fig. 5. Cortical erosion 01 the humeral head in tuberculous arthritis 01 shoulder in 62 years old man. A. Cortical delect (white arrows) at posterior aspect 01 anatomical neck 01 the humerus. B. Cortical erosion (between two arrows) on ultrasonic linding. C. Cortical erosion (black arrows) on T2-weighted MR image
CONCLUSION
The role of ultrasonography in assessing bone les
ions is still being defined, and often the bone lesions
are incidentally found in cases of which the primary
purpose of US is not to study the bones. Authors
have reviewed current application of US to various
bone lesions and conditions. Some of these are new
and have been used in a small series of patients. Plain
radiography is undoubtedly the basic and most im
portant modality for bone lesions, and the application
of US in bone lesions may be helpful for additional
information. MR imaging has been more commonly
used in many instances rather than US for evaluating
same abnormalities or anatomic structures. It is im
portant, however, to keep in perspective what the dif-
-102-
조길호 등 : 사지의 골 질환에 대한 초음파검사의 임상적 이용
Fig. 6. Bursitis 01 ischial tuberosity in 56 years old man. A. Contrast-enhancing Tl-weighted MR imaging shows irregular wall enhancement 01 lobulating cystic mass (arrows) very close to the isch ial tuberosity. B. Longitudinal ultrasonogram shows cystic mass abutting to ischial tuberosity (short arrows). Inner wall 01 the cyst is irregularly thickened and Iloating synovial hypertrophy (Ion-9 a rrows) is seen
ferent imaging techniques have to offer, and if one is just as efficacious as the other, the least invasive and the least expensive should be chosen whenever poss
ible [25] ‘
Radiologists are in a position to offer advice on appropriate strategies inciuding US for a specific clinical problems and to ensure that the resources at their disposal are used efficiently and the best clinical effect [26] . While experience is being growing, doctors will understand in near future what the technique is able to determine, and what it cannot. Additional applications may be possible, and progress will be made quickly with close cooperation between radiologist and the clinician for ultrasonic evaluation of each patient.
REFERENCES
l. van Ho1sbeeck M , Introcaso JH. M uscu1oske1eta1 U1trasound, St. Louis: Mosby-Year Book, 1991: 209-217
2. Kap1an PA, Matamoros, A. Jr., Anderson Jc. Sonography of the muscu1oske1eta1 system. AJR 1990 ‘ 155 : 237-245
B
3. Mack LA & Scheib1e W. Diagnostic U1trasonography. In: Resnick D , ed. Diagnosis of Bone and Joint disorders. 2nd ed. Phi1ade1phia, Saunders, 1995 : 219-234
4. Chhem RK, Cardina1 E, Cho KH. Ske1eta1 and superficia1 Soft tissue. In: McGahan JP, Go1dberg BG, ed. Diagnostic Ultrasound-A 10gica1 approach. 1st ed. Phi1ade1phia: Lippincott-Raven 1998: (in progress)
5. Ad1er RS. Bone and art icu1ar carti1age. In: Fornage BD, ed. Muscu1oske1eta1 U1traso und. 1 st ed. New York, Churchill Livingstone, 1995: 59- 72
6. Graif M, Stah1-Kent V, Ben-Ami T, Strauss S, Amit Y, Itzchak Y. Sonographic detection of occu1t bone fractures . Pediatric Radiology 1988; 18: 383-385
7. Donde1inger RF, Marcelis S, Daenen B, Ferrara MA. Periphera1 Muscu1oske1eta1 U1trasound Atlas. 1st ed New York, Thieme Medica1 Publi shers, 1996: 47-51
8. Rizzatto G , Abbona M, Minine1 G. Bone and callus In: Luigi Solbiati, giorgio Rizzsatto, ed. U1traso und of Superficia1 Structures. 1 st ed . Edinburgh , Churchi ll Livingstone, 1995: 375-382
9. Abiri MM , Kirpekar M , Ab10w RC. cJsteomye1itis: Detection with US. Radiology 1989 ‘ 1 72 : 509-51 1
10. Wright NB, Abbot GT, Carty HM L. U1trasound in chi1dren with osteomye1itis. Clinical Radiolo없I 1995;
-103 -
대한초음파의학회지 제 1 6 권 제 2호 1997
50: 623-627 11 . Mah ET, Lequesne GW, Gent RJ , Paterson DC.
Ultraso nic features of acute osteomyelitis in children. J Bone Joi l7l Surg ( Br) 1994; 76- B: 969-974
12 . Howard C B, Einhorn M , Daga n R, Nyska M. Ultrasound in diagnosis and management of acute haematogeno us osteomyelitis in children. J Bone Joint Surg
( Br) 1993 ; 75-B :79-82 13. Chhem RK , Kaplan PA , Dussa ult RG. Ultrasonogra
phy of the Musc ul oskeletal System RCNA 1994 ; 32(2) ‘ 275-289
14. Malghem J, Berg BV, Noel H, Maldague B. Benign Osteochondromas and exostotic chondrosarcomas: eva lua tion of cartilage cap thickness by ultrasound. Skelelal Radiology 1992 ; 2?: 33-37
15 . Garant M , Sarazin L, Cho KH , C hhem RK. Soft-tissue recurrence of osteosarcoma: ultrasound findings Canadian Association Qf Radiologisls J 1995 ; 46(4) 305-307
16. Civardi G , Livraghi T, Colombo P, Fornari F, Cavanna L, Buscarini L. Lytic bone lesions suspected for metastasis: ultrasonica ll y guided fïne-needle aspiration biopsy. J Cfin U Ilrasound 1994 ; 22(5): 307-3 11
17. Sloker DJ , Cobb JP, Pringle JAS . Needle biopsy of muscul oskeletal lesions ’ a review of 208 procedures. J
Bone Joinl Surg ( Br) 1991 ; 73-B: 498-500 18. Maffulli N, Hughes T, Fixsen JA . Ultrasonographic
=Abstract=
monito ring of limb lengthening. J Bone Joint Surg 1992 ; 74-B ’ 130-132
19. Young JWR, Kostrubiak IS, Resnik CS, Paley D. Sonographic evaluation of bone production at the distrac-tion site in Illizarov limb-lengthening procedures. AJR 1990 ; 154 : 125-128
20. Derbyshire NDJ, Simpson AHR W. A role of ultrasound in limb lengthening. British J Radiolo밍I 1992; 65: 576-580
21. va n Holsbeeck MT, Eyler WR, Sherman LS, et al. Detection of infection in loosened hip prosthesis: efficacy of sonography. AJR 1994; 163: 381-384
22. Dondelinger RF, Marcelis S, Daenen B, Ferrara MA. Peripheral M usculoskeletal Ultrasound Atlas. 1 st ed. New York, Thieme Medical Publishers, 1996 : 154
23. Castriota-Scanderbeg A, De Michell V. Ultrasound of femoral head cartilage: a new method of assessing bone age. Skeletal Radiology 1995; 24 : 197-200
24. Wagner UA, Dietrich V, Schmitt O. Determination of skeletal maturity by ultrasound: a preliminary report Skelelal Radiology 1995 ; 24: 417-420
25 . H. Theodore Harcke, Leslie E. Grisson, and Mark S Finkelstein Evaluation of the musculoskeletal system with sonography. AJR 1988 (June) ; 150 :1253-1261 , June, 1988
26. Okeefee D , Mamtora H . Ultrasound in clinical orthopaedics. J bone Joil7l Surg ( Br) 1992; 74-B: 488-494
J Korean Soc Med Ultrasound 1997; 16: 95-104
사지의 골 질환에 대한 초음파검사의 임상적 적용
조 길 호, . J. Antonio Bouffard 2 , Rethy K. Chhem 3 , Doohi Lee4
영남대학교 의과대학 진단방사선과학교실 l
Henry Ford HospitaL Detroit, Michigan , USN
Montrea1 Genera1 HospitaL McGill Uni versity , Mon treaL Quebec, Canada J
New York Medica1 College , Va1halla , New York, USN
사지의 골 질환에 대한 초음파검사는 거의 이용이 되지 않았으나 최근에 이에 대한 경험 이 많이 보고된다. 골 질환에서 단순 방사션촬영이 가장 기본적이고 중요한 검사임에는 의 성의 여지가 없고, 많은 질환에서 부가적 정보를 얻기 위해 자기공명영상을 흔히 이용한다. 단순 방사선촬영에서 관찰하기 힘든 연부조직에 대한 정보를 얻거나, 자기공명영상보다 비 용이 적게 들고, 쉽게 부가적 소견을얻을목적으로, 보다침습적 검사시행 전의 선별검사로 초음파검사가 이용된다. 저자들은 사지의 골 질환에 대한 초음파검사의 최신 임상적 적용을 문헌고찰하고자 한다.
이 중의 어떤 질환은 새로운 것이고, 대상의 수나 보고가 많지 않다. 방사선과의사와 타과의 사간의 긴밀한 협조하에 골 질환에 대한 초음파검사의 빈도와 경험 이 더 많아지면, 장차 사 지의 골 질환에 대한 초음파검사의 의의가 정럽될 것으로 기대한다.
-104-




















