Abdominal Ultrasound
297
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Abdominal Ultrasound

Abdominal Ultrasound
Prelims.qxd 7/6/04 9:20 AM Page i

For Churchill Livingstone
Commissioning Editor: Dinah ThomDevelopment Editors: Kerry McGechieProject Manager: Morven DeanDesigner: Judith Wright
Prelims.qxd 7/6/04 9:20 AM Page ii

Abdominal UltrasoundHow, Why and WhenSECOND EDITION
Jane A. Bates MPhil DMU DCRLead Practitioner, Ultrasound Department, St James’s University Hospital, Leeds, UK
E D I N B U R G H L O N D O N N E W YO R K O X F O R D P H I L A D E L P H I A S T L O U I S S Y D N E Y TO R O N TO 2004
Prelims.qxd 7/6/04 9:20 AM Page iii

CHURCHILL LIVINGSTONEAn imprint of Elsevier Limited
© Harcourt Brace and Company Limited 1999© Harcourt Publishers Limited 2001© 2004, Elsevier Limited. All rights reserved.
The right of Jane Bates to be identified as author of this work has been assertedby her in accordance with the Copyright, Designs and Patents Act 1988.
No part of this publication may be reproduced, stored in a retrieval system, ortransmitted in any form or by any means, electronic, mechanical, photocopying,recording or otherwise, without either the prior permission of the publishersor a licence permitting restricted copying in the United Kingdom issued bythe Copyright Licensing Agency, 90 Tottenham Court Road, London W1T4LP. Permissions may be sought directly from Elsevier’s Health SciencesRights Department in Philadelphia, USA: phone: (+1) 215 238 7869, fax:(+1) 215 238 2239, e-mail: [email protected]. You may also complete your request on-line via the Elsevier homepage (http://www.elsevier.com),by selecting ‘Customer Support’ and then ‘Obtaining Permissions’.
First edition 1999Second edition 2004
ISBN 0 443 07243 4
British Library Cataloguing in Publication DataA catalogue record for this book is available from the British Library
Library of Congress Cataloging in Publication DataA catalog record for this book is available from the Library of Congress
NoteKnowledge and best practice in this field are constantly changing. As newresearch and experience broaden our knowledge, changes in practice, treatmentand drug therapy may become necessary or appropriate. Readers are advised tocheck the most current imformation provided (i) on procedures featured or(ii) by the manufacturer of each product to be administered, to verify therecommended dose or formula, the method and duration of administration, andcontraindications. It is the responsibility of the practitioner, relying on theirown experience and knowledge of the patient, to make diagnoses, to determinedosages and the best treatment for each individual patient, and to take allappropriate safety precautions. To the fullest extent of the law, neither thepublisher nor the authors assumes any liability for any injury and/or damage.
The Publisher
Printed in China
ThePublisher's
policy is to usepaper manufactured
from sustainable forests
Prelims.qxd 7/6/04 9:20 AM Page iv

Contents
v
Contributors vii
Preface ix
Abbreviations xi
1. Optimizing the diagnostic information 1
2. The normal hepatobiliary system 17
3. Pathology of the gallbladder and biliary tree 41
4. Pathology of the liver and portal venous system 79
5. The pancreas 121
6. The spleen and lymphatic system 137
7. The renal tract 153
8. The retroperitoneum and gastrointestinal tract 195
9. The paediatric abdomen 215
10. The acute abdomen 243
11. Interventional and other techniques 253
Bibliography and further reading 275
Index 277
Prelims.qxd 7/6/04 9:20 AM Page v

Prelims.qxd 7/6/04 9:20 AM Page vi
This page intentionally left blank

Contributors
vii
Rosemary Arthur FRCR Consultant RadiologistDepartment of X-ray & Ultrasound, The GeneralInfirmary at Leeds, Leeds, UK
Simon T. Elliott MB ChB FRCR ConsultantRadiologist Department of Radiology, FreemanHospital, Newcastle-upon-Tyne, UK
Grant M. Baxter FRCR Consultant RadiologistWestern Infirmary University NHS Trust,Glasgow, UK
Prelims.qxd 7/6/04 9:20 AM Page vii

Prelims.qxd 7/6/04 9:20 AM Page viii
This page intentionally left blank

Ultrasound continues to be one of the mostimportant diagnostic tools at our disposal. It isused by a wide range of healthcare professionalsacross many applications. This book is intended asa practical, easily accessible guide to sonographersand those learning and developing in the field ofabdominal ultrasound. The most obvious draw-backs of ultrasound diagnosis are the physical lim-itations of sound in tissue and its tremendousdependence upon the skill of the operator. Thisbook seeks to enable the operator to maximize thediagnostic information and to recognize the limi-tations of the scan.
Where possible it presents a wider, more holisticapproach to the patient, including presentingsymptoms, complementary imaging procedures
and further management options. It is not a com-prehensive account of all the pathological processeslikely to be encountered, but is intended as aspringboard from which practical skills and clinicalknowledge can develop further.
This book aims to increase the sonographer’sawareness of the contribution of ultrasound withinthe general clinical picture, and introduce thesonographer to its enormous potential.
The author gratefully acknowledges the helpand support of the staff of the UltrasoundDepartment at St James’s University Hospital,Leeds.
Leeds 2004 Jane Bates
Preface
ix
Prelims.qxd 7/6/04 9:20 AM Page ix
Abbreviations
x
ADPCDK autosomal dominant polycystic disease of the kidney
AFP alpha-fetoproteinAI acceleration indexAIDS acquired immune deficiency
syndromeAIUM American Institute for
Ultrasound in MedicineALARA as low as reasonably achievableALT alanine aminotransferaseAP anteroposteriorAPKD autosomal dominant (adult)
polycystic kidneyARPCDK autosomal recessive polycystic
disease of the kidneyAST aspartate aminotransferaseAT acceleration timeAV arteriovenousBCS Budd–Chiari syndromeCAPD continuous ambulatory
peritoneal dialysisCBD common bile ductCD common ductCF cystic fibrosisCT computed tomographyDIC disseminated intravascular
coagulationDICOM Digital Imaging and
Communications in MedicineDMSA dimercaptosuccinic acid
DTPA diethylene triaminepenta-acetic acid
EDF end-diastolic flowERCP endoscopic retrograde
cholangiopancreatographyESWL extracorporeal shock wave
lithotripsyEUS endoscopic ultrasoundFAST focused assessment with
sonography for traumaFDA Food and Drug AdministrationFPS frames per secondHA hepatic arteryHCC hepatocellular carcinomaHELLP haemolytic anaemia, elevated liver
enzymes and low platelet countHIDA hepatic iminodiacetic acidHPS hypertrophic pyloric stenosisHV hepatic veinINR international normalized ratioIOUS intraoperative ultrasoundIVC inferior vena cavaIVU intravenous urogramKUB kidneys, ureters, bladderLFT liver function testLPV left portal veinLRV left renal veinLS longitudinal sectionLUQ left upper quadrantMCKD multicystic dysplastic kidney
Prelims.qxd 7/6/04 9:20 AM Page x

ABBREVIATIONS xi
MHA middle hepatic arteryMHV middle hepatic veinMI mechanical indexMPV main portal veinMRA magnetic resonance angiographyMRA main renal arteryMRCP magnetic resonance
cholangiopancreatographyMRI magnetic resonance imagingMRV main renal veinODS output display standardPAC photographic archiving and
communicationsPACS photographic archiving and
communications systemsPBC primary biliary cirrhosisPCKD polycystic kidney diseasePCS pelvicalyceal systemPD pancreatic ductPI pulsatility indexPID pelvic inflammatory diseasePRF pulse repetition frequencyPSC primary sclerosing cholangitisPTLD post-transplant
lymphoproliferative disorderPV portal veinRAS renal artery stenosisRCC renal cell carcinomaRF radiofrequencyRHV right hepatic vein
RI resistance indexRIF right iliac fossaRK right kidneyRPV right portal veinRRA right renal arteryRRV right renal veinRUQ right upper quadrantRVT renal vein thrombosisSA splenic arterySLE systemic lupus erythematosusSMA superior mesenteric arterySV splenic veinTB tuberculosisTGC time gain compensationTHI tissue harmonic imagingTI thermal indexTIB bone-at-focus indexTIC cranial indexTIPS transjugular intrahepatic
portosystemic shuntTIS soft-tissue thermal indexTORCH toxoplasmosis, rubella,
cytomegalovirus and HIVTS transverse sectionUTI urinary tract infectionVUJ vesicoureteric junctionWRMSD work-related musculoskeletal
disordersXGP xanthogranulomatous
pyelonephritis
Prelims.qxd 7/6/04 9:20 AM Page xi
Prelims.qxd 7/6/04 9:20 AM Page xii
This page intentionally left blank

IMAGE OPTIMIZATION
Misinterpretation of ultrasound images is a signifi-cant risk in ultrasound diagnosis. Because ultrasoundscanning is operator-dependent, it is imperative thatthe sonographer has proper training in order toachieve the expected diagnostic capabilities of thetechnique. The skill of effective scanning lies in theoperator’s ability to maximize the diagnostic infor-mation available and in being able to interpret theappearances properly. This is dependent upon:
● Clinical knowledge—knowing what to look forand why, knowing how to interpret theappearances on the image and an understandingof physiological and pathological processes.
● Technical skill—knowing how to obtain themost useful and relevant images, knowledge ofartifacts and avoiding the pitfalls of scanning.
● Knowledge of the equipment being used—i.e.making the most of your machine.
The operator must use the controls to their besteffect (see Box 1.1). There are numerous ways inwhich different manufacturers allow us to makecompromises during the scanning process in orderto improve image quality and enhance diagnosticinformation.
The quality of the image can be improved by:● Increasing the frequency—at the expense of
poorer penetration (Fig. 1.1).● Increasing the line density—this may be achieved
by reducing the frame rate and/or reducing thesector angle and/or depth of field (Fig. 1.2).
Chapter 1
Optimizing the diagnosticinformation
1
CHAPTER CONTENTS
Image optimization 1The use of Doppler 2
Getting the best out of Doppler 5Choosing a machine 6Recording of images 9Safety of diagnostic ultrasound 10Medicolegal issues 12Departmental guidelines/schemes of work 13Quality assurance 13
ch01.qxd 6/30/04 5:35 PM Page 1
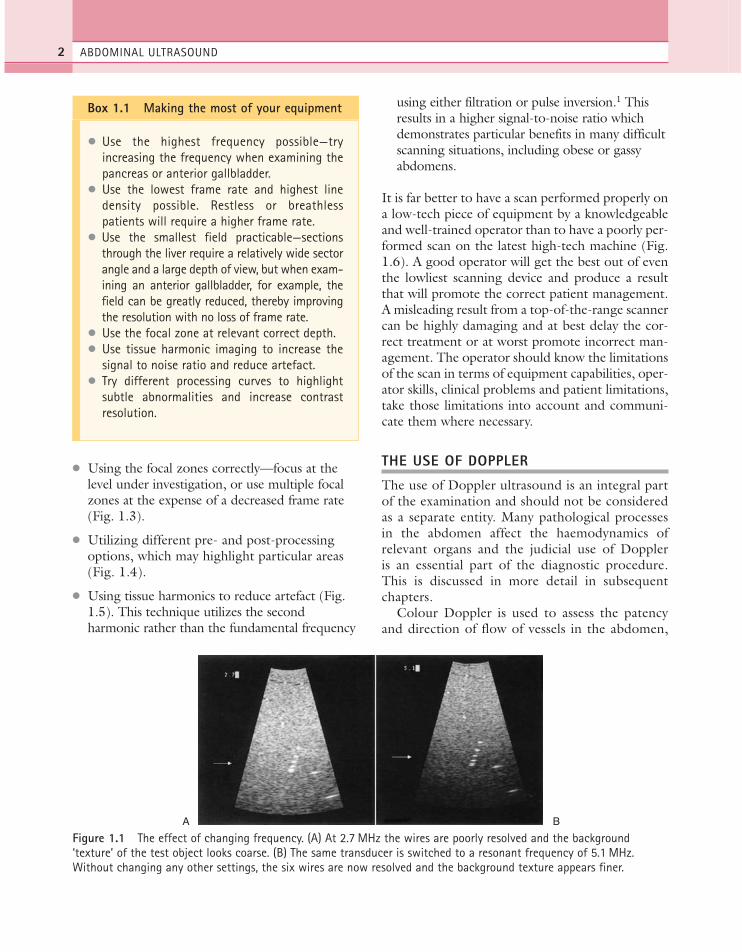
● Using the focal zones correctly—focus at thelevel under investigation, or use multiple focalzones at the expense of a decreased frame rate(Fig. 1.3).
● Utilizing different pre- and post-processingoptions, which may highlight particular areas(Fig. 1.4).
● Using tissue harmonics to reduce artefact (Fig.1.5). This technique utilizes the secondharmonic rather than the fundamental frequency
using either filtration or pulse inversion.1 Thisresults in a higher signal-to-noise ratio whichdemonstrates particular benefits in many difficultscanning situations, including obese or gassyabdomens.
It is far better to have a scan performed properly ona low-tech piece of equipment by a knowledgeableand well-trained operator than to have a poorly per-formed scan on the latest high-tech machine (Fig.1.6). A good operator will get the best out of eventhe lowliest scanning device and produce a resultthat will promote the correct patient management.A misleading result from a top-of-the-range scannercan be highly damaging and at best delay the cor-rect treatment or at worst promote incorrect man-agement. The operator should know the limitationsof the scan in terms of equipment capabilities, oper-ator skills, clinical problems and patient limitations,take those limitations into account and communi-cate them where necessary.
THE USE OF DOPPLER
The use of Doppler ultrasound is an integral partof the examination and should not be consideredas a separate entity. Many pathological processesin the abdomen affect the haemodynamics ofrelevant organs and the judicial use of Doppleris an essential part of the diagnostic procedure.This is discussed in more detail in subsequentchapters.
Colour Doppler is used to assess the patencyand direction of flow of vessels in the abdomen,
ABDOMINAL ULTRASOUND2
Figure 1.1 The effect of changing frequency. (A) At 2.7 MHz the wires are poorly resolved and the background‘texture’ of the test object looks coarse. (B) The same transducer is switched to a resonant frequency of 5.1 MHz.Without changing any other settings, the six wires are now resolved and the background texture appears finer.
Box 1.1 Making the most of your equipment
● Use the highest frequency possible—tryincreasing the frequency when examining thepancreas or anterior gallbladder.
● Use the lowest frame rate and highest linedensity possible. Restless or breathlesspatients will require a higher frame rate.
● Use the smallest field practicable—sectionsthrough the liver require a relatively wide sectorangle and a large depth of view, but when exam-ining an anterior gallbladder, for example, thefield can be greatly reduced, thereby improvingthe resolution with no loss of frame rate.
● Use the focal zone at relevant correct depth.● Use tissue harmonic imaging to increase the
signal to noise ratio and reduce artefact.● Try different processing curves to highlight
subtle abnormalities and increase contrastresolution.
A B
ch01.qxd 6/30/04 5:35 PM Page 2

OPTIMIZING THE DIAGNOSTIC INFORMATION 3
Figure 1.2 The effect of frame rate. (A) 76 frames per second (FPS). (B) 35 FPS—the resulting higher line densityimproves the image, making it sharper.
Figure 1.3 The effect of focal zone placement. (A) With the focal zone in the near field, structures in the far field arepoorly resolved. (B) Correct focal zone placement improves both axial and lateral resolution of the wires.
Figure 1.4 The effect of using post-processing options. (A) A small haemangioma in the liver merges into thebackground and is difficult to detect. (B) A post-processing option, which allocates the range of grey shades in a non-linear manner, enhances contrast resolution and improves detection of focal lesions.
A B
A B
A B
ch01.qxd 6/30/04 5:35 PM Page 3

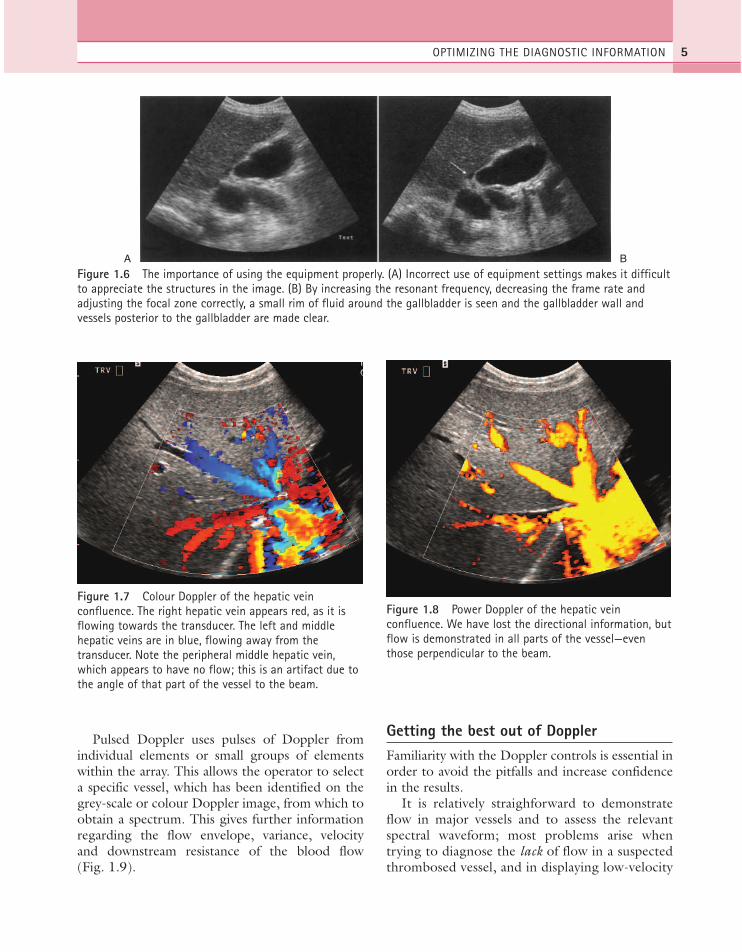
to establish the vascularity of masses or lesionsand to identify vascular disturbances, such asstenoses. Flow information is colour-coded (usu-ally red towards and blue away from the trans-ducer) and superimposed on the image. Thisgives the operator an immediate impression of avascular map of the area (Fig. 1.7). This Dopplerinformation is obtained simultaneously, oftenfrom a relatively large area of the image, at theexpense of the grey-scale image quality. The extratime taken to obtain the Doppler information foreach line results in a reduction in frame rate andline density which worsens as the colour Doppler
area is enlarged. It is advisable, therefore, to use acompact colour ‘box’ in order to maintain imagequality.
Power Doppler also superimposes Dopplerinformation on the grey-scale image, but withoutany directional information. It displays only theamount of energy (Fig. 1.8). The advantage ofthis is that the signal is stronger, allowing iden-tification of smaller vessels with lower velocityflow than colour Doppler. As it is less angle-dependent than colour Doppler it is particularlyuseful for vessels which run perpendicular to thebeam, for example the inferior vena cava (IVC).
ABDOMINAL ULTRASOUND4
A
B
Figure 1.5 The effect of tissue harmonic imaging (THI): (A) a bladder tumour in fundamental imaging mode (left) isshown with greater definition and loss of artifact in THI (right). (B) In an obese patient, cysts near the gallbladder (left)are shown in greater detail using pulse inversion tissue harmonics (right). A small nodule is demonstrated in the lowercyst.
ch01.qxd 6/30/04 5:35 PM Page 4
Pulsed Doppler uses pulses of Doppler fromindividual elements or small groups of elementswithin the array. This allows the operator to selecta specific vessel, which has been identified on thegrey-scale or colour Doppler image, from which toobtain a spectrum. This gives further informationregarding the flow envelope, variance, velocityand downstream resistance of the blood flow(Fig. 1.9).
Getting the best out of DopplerFamiliarity with the Doppler controls is essential inorder to avoid the pitfalls and increase confidencein the results.
It is relatively straighforward to demonstrateflow in major vessels and to assess the relevantspectral waveform; most problems arise whentrying to diagnose the lack of flow in a suspectedthrombosed vessel, and in displaying low-velocity
OPTIMIZING THE DIAGNOSTIC INFORMATION 5
A B
Figure 1.6 The importance of using the equipment properly. (A) Incorrect use of equipment settings makes it difficultto appreciate the structures in the image. (B) By increasing the resonant frequency, decreasing the frame rate andadjusting the focal zone correctly, a small rim of fluid around the gallbladder is seen and the gallbladder wall andvessels posterior to the gallbladder are made clear.
Figure 1.7 Colour Doppler of the hepatic veinconfluence. The right hepatic vein appears red, as it isflowing towards the transducer. The left and middlehepatic veins are in blue, flowing away from thetransducer. Note the peripheral middle hepatic vein,which appears to have no flow; this is an artifact due tothe angle of that part of the vessel to the beam.
Figure 1.8 Power Doppler of the hepatic veinconfluence. We have lost the directional information, butflow is demonstrated in all parts of the vessel—eventhose perpendicular to the beam.
ch01.qxd 6/30/04 5:35 PM Page 5
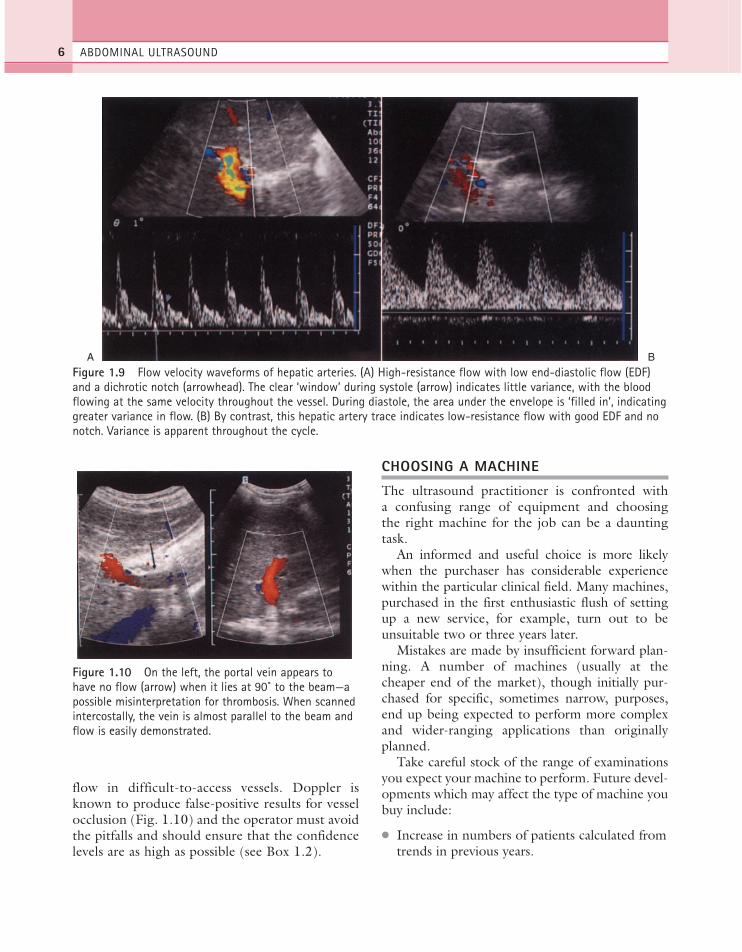
flow in difficult-to-access vessels. Doppler isknown to produce false-positive results for vesselocclusion (Fig. 1.10) and the operator must avoidthe pitfalls and should ensure that the confidencelevels are as high as possible (see Box 1.2).
CHOOSING A MACHINE
The ultrasound practitioner is confronted witha confusing range of equipment and choosingthe right machine for the job can be a dauntingtask.
An informed and useful choice is more likelywhen the purchaser has considerable experiencewithin the particular clinical field. Many machines,purchased in the first enthusiastic flush of settingup a new service, for example, turn out to beunsuitable two or three years later.
Mistakes are made by insufficient forward plan-ning. A number of machines (usually at thecheaper end of the market), though initially pur-chased for specific, sometimes narrow, purposes,end up being expected to perform more complexand wider-ranging applications than originallyplanned.
Take careful stock of the range of examinationsyou expect your machine to perform. Future devel-opments which may affect the type of machine youbuy include:
● Increase in numbers of patients calculated fromtrends in previous years.
ABDOMINAL ULTRASOUND6
A B
Figure 1.9 Flow velocity waveforms of hepatic arteries. (A) High-resistance flow with low end-diastolic flow (EDF)and a dichrotic notch (arrowhead). The clear ‘window’ during systole (arrow) indicates little variance, with the bloodflowing at the same velocity throughout the vessel. During diastole, the area under the envelope is ‘filled in’, indicatinggreater variance in flow. (B) By contrast, this hepatic artery trace indicates low-resistance flow with good EDF and nonotch. Variance is apparent throughout the cycle.
Figure 1.10 On the left, the portal vein appears tohave no flow (arrow) when it lies at 90˚ to the beam—apossible misinterpretation for thrombosis. When scannedintercostally, the vein is almost parallel to the beam andflow is easily demonstrated.
ch01.qxd 6/30/04 5:35 PM Page 6

● Increase in range of possible applications, animpending peripheral vascular service, forexample, or regional screening initiative.
● Clinical developments and changes in patientmanagement which may require more, ordifferent, ultrasound techniques, for example,medical therapies which require ultrasoundmonitoring, applications involving the use ofcontrast agents, surgical techniques which mayrequire intraoperative scanning, increases ordecreases in hospital beds, introduction of newservices and enlargement of existing ones.
● Impending political developments bygovernment or hospital management, resultingin changes in the services provided, thefunding or the catchment area.
● Other impending ultrasound developments,such as the use of contrast media or
ultrasound-guided therapies which may berequired in future.
The following points are useful to bear in mindwhen purchasing new equipment:
Probe number and design (Fig 1.11)
Consider the footprint, shape and frequenciesrequired: most modern transducers are broadbandin design, enabling the user to access a wider rangeof frequencies. This is a big advantage as this lim-its the number of probes required for a generalservice. A curved array probe is suitable for mostgeneral abdominal applications, operating in the3.5–6 MHz region. Additional higher-frequencyprobes are useful for paediatrics and for superficialstructures. A small footprint is essential if neonataland paediatric work is undertaken and a 5–8 MHzfrequency will be required.
A biopsy attachment may be needed for invasiveprocedures, and, depending on the range of workto be undertaken, linear probes, endoprobes,intraoperative probes and other designs can beconsidered.
Image quality
There are very few applications where this is not ofparamount importance and abdominal scanningrequires the very best you can afford. A machinecapable of producing a high-quality image is likely
OPTIMIZING THE DIAGNOSTIC INFORMATION 7
Box 1.2 Steps to take if you can’t detect flowwith Doppler
● Ensure the angle of insonation between thevessel and the transducer is <60˚. Colour andpulsed Doppler are highly angle-dependent.
● Ensure the Doppler gain is set at the correctlevel. (Colour and pulsed Doppler gain settingsshould be just below background noise level.)
● Ensure the Doppler power/output setting issufficient.
● Ensure the pulse repetition frequency (PRF) isset correctly. A low PRF (‘range’ or ‘scale’ set-ting) is required to pick up low-velocity flow.
● Ensure the wall thump filter setting is low. (Ifthe setting is too high, real low-velocity flowis filtered out.)
● Use power Doppler, which is more sensitiveand is not angle-dependent.
● Know the limitations of your machine.Machines differ in their ability to detect low-velocity flow.
● If in doubt, test it on a reference vessel youknow should contain flow.
Figure 1.11 Curved arrays (left and centre) suitable forabdominal scanning. A 5 MHz linear array (right) isuseful for superficial structures, e.g. gallbladder andanterior abdominal wall.
ch01.qxd 6/30/04 5:35 PM Page 7

to remain operational for much longer than onecapable of only poor quality, which will needreplacement much sooner. A poor-quality image isa false economy in abdominal scanning.
Machine capabilities and functions
The availability and ease of use of various functionsdiffer from machine to machine. Some of theimportant issues to consider when buying amachine include:
● probe selection and switching process, simulta-neous connection of several probes
● dynamic frequency capability● dynamic focusing control, number and pattern
of focal zones● functions such as beam steering, sector angle
adjustment, zoom, frame rate adjustment,trackerball controls
● time gain compensation and power outputcontrols
● cine facility—operation and size of memory● programmable presets● tissue harmonic and/or contrast harmonic
imaging● body marker and labelling functions● measurement packages—operation and display● colour/power and spectral Doppler through all
probes● Doppler sensitivity● Doppler controls—ease of use, programmable
presets● output displays● report package option.
Ergonomics
Good ergonomics contribute considerably to thesuccess of the service provided. The machine mustbe usable by various operators in all the required sit-uations. There is a significant risk of work-relatedmusculoskeletal disorders (WRMSD)2 if carefulconsideration is not given to the scanning environ-ment (see p. 12). When choosing and setting up ascanning service, forethought should be given notonly to the design of the ultrasound machine, butalso to the seating arrangements and examinationcouch. These should all be adjustable in order tofacilitate the best scanning position for the operator.
Other considerations include:
● System dimensions and steering. Therequirement for the system to be portable, forexample for ward or theatre work, or mobilefor transportation to remote clinics. Machinesused regularly for mobile work should berobust and easy to move.
● Moveable (swivel and tilt) monitor and controlpanel, including height adjustment for differentoperators and situations.
● Keyboard design, to facilitate easy use of therequired functions, without stretching ortwisting.
● Hand-held portable machines are an optionthat may be considered.
Maintenance issues
It is useful to consider the reliability record of thechosen equipment, particularly if it is to operate inout-reach clinics, or without available backup inthe case of breakdown. Contacting other users mayprove useful.
Various maintenance contract options and costsare available, including options on the replacementof probes, which should be taken into accountwhen purchasing new equipment.
Upgradeability
A machine which is potentially upgradeable has alonger, more cost-effective life and will be sup-ported by the manufacturer over a longer period oftime. Consideration should be given to future soft-ware upgrades, possible effects and costs and otheravailable options for the future, such as additionaltransducers or add-on Doppler facilities.
Links to image-recording devices
Most ultrasound machines are able to link up tomost types of imaging facility, whether it be a sim-ple black and white printer or a radiology-widephotographic archiving and communications (PAC)system. There may be costs involved, however, inlinking your new machine to your preferred imag-ing device.
ABDOMINAL ULTRASOUND8
ch01.qxd 6/30/04 5:35 PM Page 8

Equipment manufacturers now follow theDICOM standard. Digital Imaging and Commu-nications in Medicine is the industry standard fortransferring medical images and related informa-tion between computers. This facilitates compati-bility between different pieces of equipment fromdifferent manufacturers and potentially enablesthem to be linked up.
RECORDING OF IMAGES
There are no hard and fast rules about the record-ing of ultrasound scans and departmental practicesvary. It is good practice for departments to haveguidelines for taking and retaining images withinindividual schemes of work, outlining the mini-mum expected.3
The advantages of recording images are:
● They provide a record of the quality of thescan and how it has been conducted: theorgans examined, the extent of the scan, thetype and standard of equipment, the settingsused and other scanning factors. This can be aninvaluable tool in providing a medicolegaldefence.
● They provide an invaluable teaching aid.
● They help to ensure quality control withindepartments: promoting the use of goodtechnique, they can be used to ensure protocolsare followed and provide an excellent audit tool.
● They can be used to obtain a second opinionon difficult or equivocal cases and provide abasis for discussion with clinical colleagues.
The disadvantages are:
● The cost of buying, running and maintainingthe recording device or system.
● The quality of images in some cases may notaccurately reflect that of the image on theultrasound monitor.
● The scanning time must be slightly increasedto accommodate the taking of images.
● Storage and retrieval of images may be time-and space-consuming.
● Hard copy may be mislaid or lost.
● If the examination has been badly performed,the hard copy may demonstrate that too!
Generally speaking the recording of images isencouraged. It reduces the operator’s vulnerabilityto litigation and supports the ultrasound diagno-sis.4 It is only possible to record the entire exami-nation by using videotape, which is rarely practicalin larger departments. The operator must take theresponsibility for ensuring the scan has been per-formed to the required standard; any images pro-duced for subsequent discussion are onlyrepresentative of the examination and have beenchosen by the operator as an appropriate selection.If you have missed a small metastasis in the liverwhile scanning, or a gallstone in the gallbladder,you are unlikely to have included it on an image.
Choice of image-recording device depends onmany factors. Considerations include:
● image quality—resolution, grey-scale, storagelife
● capital cost of the system—including the instal-lation together with the installation of anyother necessary equipment, such as a processor
● cost of film● processing costs if applicable—this includes the
cost of chemicals, the cost of buying and main-taining a processor and possibly a chemicalmixer
● maintenance costs● reliability of the system● storage of images in terms of available space
and cost● location and size of the imaging system● other considerations
—ease of use—mobility—colour capability—ability to produce slides/teaching aids—shelf life of unused film and stored images.
Numerous methods of recording images are availableto suit all situations. Small printers, attached to ultra-sound scanners, are easy to use, cheap to buy and runand convenient if the machine is used on wards ordistant satellite units. However, systems which pro-duce hard copy, however good, are inevitably ofinferior image quality to electronic image capture.
OPTIMIZING THE DIAGNOSTIC INFORMATION 9
ch01.qxd 6/30/04 5:35 PM Page 9

Multi-system departments are tending towards net-worked systems which produce high-quality images,and can be linked to multiple machines and modali-ties. These are, of course, more expensive to purchaseand install, but are generally reliable and produceconsistent, high-quality image.
Ultimately, the goal of the filmless department isbeing realized in PACS (photographic archiving andcommunications systems). Digital imaging net-works are convenient, quick and relatively easy touse. The image quality is excellent, suffering little orno degradation in capture and subsequent retrieval,and the system can potentially be linked to a con-ventional imager should hard copy be required.
The number of workstations in the system canbe virtually unlimited, depending on the system,affording the operator the flexibility of transmit-ting images immediately to remote locations, forexample clinical meetings, outpatient clinics, etc. Itis also possible to download images from scansdone with mobile equipment, remote from themain department, on to the PACS.
Digital storage and retrieval avoid loss of filmsand afford considerable savings in time, labour andspace. Increasingly it is also possible to store movingclips—useful for dynamic studies such as thoseinvolving contrast agents and for teaching purposes.
Many systems also incorporate a patient regis-tration and reporting package, further streamliningthe ultrasound examination. Not all systems storeimages in colour and there are considerable differ-ences between the facilities available on differentsystems. The potential purchaser is advised to plancarefully for the needs of the ultrasound service.
The capital costs for PACS are high, but thesecan, to a certain extent, be offset by subsequentlylow running costs and potential savings in film,processing materials, equipment maintenance, andmanual storage and retrieval.
SAFETY OF DIAGNOSTIC ULTRASOUND
Within the field of clinical diagnostic ultrasound,it is currently accepted that there is insufficientevidence for any deleterious effects at diagnosticlevels and that the benefits to patients outweighthe risks. As new techniques and technologicaldevelopments come on to the market, new bio-physical conditions may be introduced which
require evaluation with regard to safety5 and wecannot afford to become complacent about thepossible effects. The situation remains under con-stant review.
Several international bodies continue to considerthe safety of ultrasound in clinical use. TheEuropean Federation of Societies for Ultrasound inMedicine and Biology (EFSUMB) has confirmedthe safety of diagnostic ultrasound and endorsed its‘informed’ use.6 Whilst the use of pulsed Doppler isconsidered inadvisable for the developing embryoduring the first trimester, no such exceptions arehighlighted for abdominal ultrasound.
The European Committee for UltrasoundRadiation Safety (ECURS) confirms that no dele-terious effects have yet been proven in clinicalmedicine. It recommends, however, that equip-ment is used only when designed to national orinternational safety standards and that it is usedonly by competent and trained personnel.
The World Federation for Ultrasound inMedicine and Biology (WFUMB) confirms thatthe use of B-mode imaging is not contraindicated,7concluding that exposure levels and durationshould be reduced to the minimum necessary toobtain the required diagnostic information.
Ultrasound intensities used in diagnostic ultra-sound vary according to the mode of operation.Pulsed Doppler usually has a higher level than B-mode scanning, which operates at lower intensi-ties, although there may be overlap with colour orpower Doppler.
The American Institute for Ultrasound inMedicine (AIUM) has suggested that ultrasound issafe below 100 W/cm.8 This figure refers to thespatial peak temporal average intensity (ISPTA).
The use of intensity, however, as an indicator ofsafety is limited, particularly where Doppler is con-cerned, as Doppler intensities can be considerablygreater than those in B-mode imaging. The Foodand Drug Administration (FDA) sets maximumintensity levels allowed for machine output, whichdiffer according to the application.9
Biological effects of ultrasound
Harmful effects from ultrasound have been docu-mented in laboratory conditions. These includethermal effects and mechanical effects.
ABDOMINAL ULTRASOUND10
ch01.qxd 6/30/04 5:35 PM Page 10

Thermal effects are demonstrated as a slightrise in temperature, particularly in close proximityto the transducer face, during ultrasound scanning.This local effect is usually of no significance but theoperator must be aware of the phenomenon. Themost significant thermal effects occur at bone/tis-sue interfaces and are greater with pulsed Doppler.Increases in temperature of up to 5˚C have beenproduced. Areas at particular risk are fetal bonesand the interfaces in transcranial Doppler ultra-sound scans.
Pulsed Doppler has a greater potential for heat-ing than B-mode imaging as it involves greatertemporal average intensities due to high pulse rep-etition frequency (PRF) and because the beam isfrequently held stationary over an area whileobtaining the waveform. Colour and powerDoppler usually involve a greater degree of scan-ning and transducer movement, which involves apotentially lower heating potential than withpulsed Doppler. Care must be taken to limit theuse of pulsed Doppler and not to hold the trans-ducer stationary over one area for too long.
Mechanical effects, which include cavitationand radiation pressure, are caused by stresses in thetissues and depend on the amplitude of the ultra-sound pulse. These effects are greatest around gas-filled organs, such as lungs or bowel and have, inlaboratory conditions, caused small surface bloodvessels in the lungs to rupture. Potentially, theseeffects could be a hazard when using contrastagents which contain microbubbles.
Safety indices (thermal and mechanical indices)
In order to inform users about the machine condi-tions which may potentially be harmful, mechani-cal and thermal indices are now displayed as anoutput display standard (ODS) on all equipmentmanufactured after 1998. This makes operatorsaware of the ultrasound conditions which mayexceed the limits of safety and enables them to takeavoiding action, such as reducing the power orrestricting the scanning time in that area.
In simple terms the mechanical index (MI) isrelated to amplitude and indicates how ‘big’ anultrasound pulse is, giving an indication of thechances of mechanical effects occurring. It is there-fore particularly relevant in the abdomen when
scanning gas-filled bowel or when using micro-bubble contrast agents. Gas bodies introducedby contrast agents increase the probablility ofcavitation.
The thermal index (TI) gives an indication ofthe temperature rise which might occur within theultrasound beam, aiming to give an estimate ofthe reasonable worst-case temperature rise. The TIcalculation alters, depending upon the application,giving rise to three indices: the soft-tissue thermalindex (TIS), the bone-at-focus index (TIB) andthe bone-at-surface, or cranial index (TIC). Thefirst of these is obviously most relevant for abdom-inal applications. In well-perfused tissue, such asthe liver and spleen, thermal effects are less likelydue to the cooling effect of the blood flow.
The display of safety indices is only a generalindication of the possibility of biological hazardsand cannot be translated directly into real heatingor cavitation potential.10 These ‘safety indices’ arelimited in several ways. They require the user tobe educated with respect to the implications of thevalues shown and they do not take account ofthe duration of exposure, which is particularlyimportant in assessing the risk of thermal damage.4In addition, the TI does not take account of thepatient’s temperature, and it is logical to assumethat increased caution is therefore required in scan-ning the febrile patient.
MI and TI are also unlikely to portray the opti-mum safety information during the use of contrastagents, in which, theoretically, heating effects andcavitation may be enhanced.5
Other hazards
Whilst most attention in the literature is focusedon the possible biological effects of ultrasound,there are several other safety issues which arewithin the control of the operator.
Electrical safety All ultrasound machinesshould be subject to regular quality controland should be regularly checked for any signs ofelectrical hazards. Loose or damaged wiring, forexample, is a common problem if machines areroutinely used for mobile work. Visible damage toa transducer, such as a crack in the casing, shouldprompt its immediate withdrawal from serviceuntil a repair or replacement is effected.
OPTIMIZING THE DIAGNOSTIC INFORMATION 11
ch01.qxd 6/30/04 5:35 PM Page 11

Microbiological safety It is the responsibilityof the sonographer to minimize the risks of cross-infection. Most manufacturers make recommenda-tions regarding appropriate cleaning agents fortransducers, which should be carefully followed.Sterile probe covers should be used in cases wherethere is an increased risk of infection.
Operator safety By far the most serious haz-ard of all is that of the untrained or badly trainedoperator. Misdiagnosis is a serious risk for thosenot aware of the pitfalls. Apart from the implica-tions for the patient of subsequent incorrect man-agement, the operator risks litigation which isdifficult or impossible to defend if they have hadinadequate training in ultrasound.
Work-related musculoskeletal disorders
There is increasing concern about WRMSD relatedto ultrasound scanning, as workloads increase and ithas been estimated that a significant proportion ofsonographers who practise full-time ultrasoundscanning may be affected.2 One contributing factoris the ergonomic design of the ultrasound machines,together with the position adopted by the operatorduring scanning. While more attention is now beingpaid by ultrasound manufacturers to designs whichlimit WRMSD, there are various other contributingfactors which should be taken into account whenproviding ultrasound services. Well-designed,adjustable seating for operators, adjustable patientcouches, proper staff training for manoeuvringpatients and a varied work load all contribute tominimizing the potential problems to staff.
Hand-held, portable ultrasound machines arenow available. Provided they are of sufficient func-tionality to provide the service required, they mayalso potentially limit the problems encounteredwhen manoeuvring larger scanners around hospitalwards and departments.
The safe practice of ultrasound
It is fair to say that the safety of ultrasound is lessof an issue in abdominal scanning than in obstetricor reproductive organ scanning. Nevertheless it isstill incumbent upon the operator to minimize theultrasound dose to the patient in any practicableway.
The use of X-rays is governed by the ALARAprinciple—that of keeping the radiation dose AsLow As Reasonably Achievable. Although the risksassociated with radiation are not present in the useof ultrasound, the general principle of keeping theacoustic exposure as low as possible is still goodpractice and many people still refer to ALARA inthe context of diagnostic ultrasound (see Box 1.3).
MEDICOLEGAL ISSUES
Litigation in medical practice is increasing and thefield of ultrasound is no exception to this.Although currently the majority of cases involvefirstly obstetric and secondly gynaecological ultra-sound, it is prudent for the operator to be aware ofthe need to minimize the risks of successful litiga-tion in all types of scanning procedures.
Patients have higher expectations of medicalcare than ever before and ultrasound practitionersshould be aware of the ways in which they can pro-tect themselves should a case go to court. The
ABDOMINAL ULTRASOUND12
Box 1.3 Steps for minimizing the ultrasounddose
● Ensure operators are properly trained, prefer-ably on recognized training programmes.
● Minimize the output (or power) level. Useamplification of the received echoes to manip-ulate the image in preference to increasing thetransmitted power.
● Minimize the time taken to perform the exam.● Don’t rest the transducer on the skin surface
when not scanning.● Make sure the clinical indications for the scan
are satisfactory and that a proper request hasbeen received. Don’t do unnecessary ultra-sound examinations.
● Be aware of the safety indices displayed on theultrasound machine. Limit the use of pulsedDoppler to that necessary to contribute to thediagnosis.
● Make the best use of your equipment—maxi-mize the diagnostic information by manipulat-ing the controls effectively.
ch01.qxd 6/30/04 5:35 PM Page 12
onus is upon the defendant to prove that he or sheacted responsibly and there are several helpfulguidelines which should routinely be followed (seeBox 1.4).11
The medicolegal issues surrounding ultrasoundmay be different according to whether the opera-tor is medically or non-medically qualified.Depending on their profession, operators are con-strained by codes of conduct of their respectivecolleges and/or Councils.12 Either way, the opera-tor is legally accountable for his or her professionalactions.
If non-medically qualified personnel are to per-form and report on scans (as happens in the UK,USA and Australia), this task must be properly del-egated by a medically qualified practitioner, forexample a radiologist in the case of abdominalscanning. As the role of sonographers continues toexpand, it is noteworthy that the same standard ofcare is expected from medically and non-medicallyqualified staff alike.13 To avoid liability, practition-ers must comply with the Bolam test, in which theyshould be seen to be acting in accordance withpractice accepted as proper by a responsible bodyof relevant medical people.
DEPARTMENTAL GUIDELINES/SCHEMESOF WORK
It is generally considered good and safe practice touse written guidelines for ultrasound examinations.3
These serve several purposes:
● They may be used to support a defence againstlitigation (provided, of course, that theoperator can prove he or she has followed suchguidelines).
● They serve to impose and maintain a minimumstandard, especially within departments whichmay have numerous operators of differingexperience levels.
● They serve to inform operators of currentpractice.
Guidelines should ideally be:
● Written by, and have input from, thosepractising ultrasound in the department(usually a combination of medically and non-medically qualified personnel), taking intoaccount the requirements of referringclinicians, available equipment and other localoperational issues.
● Regularly reviewed and updated to takeaccount of the latest literature and practices.
● Flexible, to allow the operator to tailor thescan to the patient’s clinical presentation andindividual requirements.
Guidelines which are too prescriptive anddetailed are likely to be ignored by operators asimpractical. The guidelines should be broadenough to allow operators to respond to differentclinical situations in an appropriate way whileensuring that the highest possible standard of scanis always performed. In cases when it is simply notpossible to adhere to departmental guidelines, thereasons should be stated on the report, for exam-ple when the pancreas cannot be demonstrated dueto body habitus or overlying bowel gas.
QUALITY ASSURANCE
The principles of quality assurance affect variousaspects of the ultrasound service offered. These
OPTIMIZING THE DIAGNOSTIC INFORMATION 13
Box 1.4 Guidelines for defensive scanning(adapted from Meire HB11)
● Ensure you are properly trained. Operatorswho have undergone approved training areless likely to make mistakes.
● Act with professionalism and courtesy. Goodcommunication skills go a long way to avoid-ing litigation.
● Use written guidelines or schemes of work.● Ensure a proper request for the examination
has been received.● A written report should be issued by the oper-
ator.● Record images to support your findings.● Clearly state any limitations of the scan which
may affect the ability to make a diagnosis.● Make sure that the equipment you use is ade-
quate for the job.
ch01.qxd 6/30/04 5:35 PM Page 13

include staff issues (such as education and training,performance and continuing professional develop-ment), patient care, the work environment (includ-ing health and safety issues) and quality assuranceof equipment. Quality assurance checks on ultra-sound equipment, unlike most other aspects of anultrasound service, involve measurable and repro-ducible parameters.
Equipment tests
After installation, a full range of equipment testsand safety checks should be carried out and theresults recorded. This establishes a baseline per-formance against which comparisons may later bemade. These tests should normally be carried outby qualified medical physicists.
It is useful to take a hard-copy image of a tissue-mimicking phantom, with the relevant settingsmarked on it. These images form a reference againstwhich the machine’s subsequent performance canbe assessed. If your machine seems to be perform-ing poorly, or the image seems to have deterioratedin some way, you will have the proof you require.
A subsequent, regular testing regime must thenbe set up, to ensure the standards of quality and
safety are maintained. This programme can be setup in conjunction with the operators and the med-ical physics department and relevant recordsshould be kept. The use of a tissue-mimickingphantom enables the sonographer to perform cer-tain tests in a reproducible and recordable manner(Fig. 1.12).
Checks should be carried out for all probes onthe machine.
Suggested equipment checks include:
● caliper accuracy● system sensitivity and penetration● axial and lateral resolution● slice thickness● grey scale● dead zone● checks on the various machine controls/func-
tions● output power● safety checks: electrical, mechanical, biological
and thermal, including a visual inspection of allprobes and leads
● imaging device checks for image quality, set-tings, dynamic range, functionality and electri-cal safety
ABDOMINAL ULTRASOUND14
A B
Figure 1.12 Tissue-mimicking phantom. (A) When using a high-frequency linear array, cross-sections of the wires inthe phantom are clearly demonstrated as small dots. (B) When using a curved array of a lower frequency, such as thatused for abdominal scanning, the lateral resolution is seen to deteriorate in the far field as the beam diverges. Thewires are displayed correctly in the near field but appear as short lines in the far field. Spacing of the wires is known,allowing caliper accuracy to be assessed.
ch01.qxd 6/30/04 5:35 PM Page 14

● biopsy guide checks● colour, power and spectral Doppler checks
(complex, requiring specialized equipment).
Some of these checks can be easily and quickly car-ried out by users in the department on a regular
basis, for example caliper checks and biopsy guidechecks. Others are more complex and may beappropriately undertaken by specialist medicalphysicists. All equipment should undergo regularservicing and any interim faults should naturally bereported.
OPTIMIZING THE DIAGNOSTIC INFORMATION 15
References1. Desser TS, Jedrzejewicz MS, Bradley C. 2000 Native
tissue harmonic imaging: basic principles and clinicalapplications. Ultrasound Quarterly 16, no. 1: 40–48.
2. Society of Radiographers. 2002 The Causes ofMuskuloskeletal Injury Amongst Sonographers in theUK. SoR, London.
3. UK Association of Sonographers. 1996 Guidelines forProfessional Working Practice. UKAS, London.
4. British Medical Ultrasound Society. 2000 Guidelinesfor the acquisition and retention of hard copyultrasound images. BMUS Bulletin 8: 2.
5. ter Haar G, Duck FA (eds). 2000 The Safe Use ofUltrasound in Medical Diagnosis. BMUS/BIR,London.
6. European Federation of Societies for Ultrasound inMedicine and Biology. 1996 Clinical safety statementfor diagnostic ultrasound. EFSUMB Newsletter 10: 2.
7. World Federation for Ultrasound in Medicine andBiology. 1998 Symposium on safety of ultrasound inmedicine: conclusions and recommendations onthermal and non-thermal mechanisms for biologicaleffects of ultrasound. Ultrasound in Medicine andBiology 24: 1–55.
8. American Institute for Ultrasound in Medicine. 1988Bioeffects and considerations for the safety ofdiagnostic ultrasound. Journal of Ultrasound inMedicine 7: Suppl.
9. Food and Drug Administration: US Department ofHealth and Human Services. 1997 Information forManufacturers Seeking Marketing Clearance ofDiagnostic Ultrasound Systems and Transducers.Center for Devices and Radiological Health Rockville,MD.
10. Duck FA. 1997 The meaning of thermal index (TI)and mechanical index (MI) values. BMUS Bulletin5: 36–40.
11. Meire HB. 1996 Editorial. Ultrasound-relatedlitigation in obstetrics and gynecology: the need fordefensive scanning. Ultrasound in Obstetrics andGynecology 7: 233–235.
12. Council for Professions Supplementary to Medicine.1995 Statement of Conduct/Code of Practice.Radiographer’s Board, London.
13. Dimond B. 2000 Red dots and radiographers’liability. Health care risk report, October. ClinicalNegligence 10–13.
ch01.qxd 6/30/04 5:35 PM Page 15

ch01.qxd 6/30/04 5:35 PM Page 16
This page intentionally left blank
INTRODUCTION
Ultrasound is the dominant first-line investigationfor an enormous variety of abdominal symptomsbecause of its non-invasive and comparativelyaccessible nature. Its success, however, in terms ofa diagnosis, depends upon numerous factors, themost important of which is the skill of the operator.
Because of their complexity and extent, the nor-mal appearances and haemodynamics of the hepato-biliary system are dealt with in this chapter, togetherwith some general upper-abdominal scanning issues.The normal appearances of the other abdominalorgans are included in subsequent relevant chapters.
It is good practice, particularly on the patient’sfirst attendance, to scan the whole of the upperabdomen, focusing particularly on the relevantareas, but also excluding or identifying any othersignificant pathology. A full abdominal surveywould normally include the liver, gallbladder, bil-iary tree, pancreas, spleen, kidneys and retroperi-toneal structures. Apart from the fact that manypathological processes can affect multiple organs, anumber of significant (but clinically occult) patho-logical processes are discovered incidentally, forexample renal carcinoma or aortic aneurysm. Athorough knowledge of anatomy is assumed at thisstage, but diagrams of upper abdominal sectionalanatomy are included in the appendix to this chap-ter for quick reference (see pp. 36–39).
It is important always to remember the opera-tor-dependent nature of ultrasound scanning (seeChapter 1); although the dynamic nature of thescan is a huge advantage over other forms of
Chapter 2
The normal hepatobiliary system
17
CHAPTER CONTENTS
Introduction 17General pointers on upper-abdominal
technique 18The liver 18
Normal appearance 18The segments of the liver 24Hepatic vasculature 25Haemodynamics of the liver 25
The gallbladder 27Normal variants of the gallbladder 29Pitfalls in scanning the gallbladder 29
Bile ducts 31Bile duct measurements 33Techniques 33
Some common referral patterns forhepatobiliary ultrasound 33Jaundice 34Abnormal liver function tests 35Other common reasons for referral 35
Appendix: Upper-abdominal anatomy 36
ch02.qxd 6/30/04 5:36 PM Page 17
imaging, the operator must continuously adjusttechnique to obtain the maximum diagnosticinformation. In any abdominal ultrasound surveythe operator assesses the limitations of the scan andthe level of confidence with which pathology canbe excluded or confirmed. The confidence limitshelp in determining the subsequent investigationsand management of the patient.
It is important, too, to retain an open mindabout the diagnosis when embarking on the scan;an operator who decides the likely diagnosis on aclinical basis may sometimes be correct but, in try-ing to fit the scan to match the symptoms, risksmissing significant pathology.
GENERAL POINTERS ON UPPER-ABDOMINAL TECHNIQUE
Scanning technique is not something that can belearnt from a book. There is absolutely no substi-tute for regular practical experience under thesupervision of a qualified ultrasound practitioner.
There are, however, some general approacheswhich help to get the best from the scanningprocedure:
● Scan in a systematic way to ensure the whole ofthe upper abdomen has been thoroughlyinterrogated. The use of a worksheet, whichindicates the structures to be examined, isadvisable when learning.1
● Always scan any organ in at least two planes,preferably at right angles to each other. Thisreduces the risk of missing pathology and helpsto differentiate artefact from true pathology.
● Where possible, scan in at least two patientpositions. It is surprising how the availableultrasound information can be enhanced byturning your patient oblique, decubitus or erect.Inaccessible organs flop into better view andbowel moves away from the area of interest.
● Use a combination of sub- and intercostalscanning for all upper-abdominal scanning. Thedifferent angles of insonation can revealpathology and eliminate artefact.
● Don’t limit yourself to longitudinal andtransverse sections. Use a variety of planes and
angulations. Trace ducts and vessels along theircourses. Use the transducer like a pair of eyes.
● Deep inspiration is useful in a proportion ofpatients, but not all. Sometimes it can makematters worse by filling the stomach with airand obscuring large areas. An intercostalapproach with the patient breathing gentlyoften has far more success.
● Positioning patients supine, particularly ifelderly or very ill, can make them breathlessand uncomfortable. Raise the patient’s head asmuch as necessary; a comfortable patient ismuch easier to scan.
● Images are a useful record of the scan and howit has been performed, but don’t make theseyour primary task. Scan first, sweepingsmoothly from one aspect of the organ to theother in two planes, then take the relevantimages to support your findings.
● Make the most of your equipment (seeChapter 1). Increase the confidence level ofyour scan by fully utilizing all the availablefacilities, using Doppler, tissue harmonics,changing transducers and frequencies andmanipulating the machine settings andprocessing options.
THE LIVER
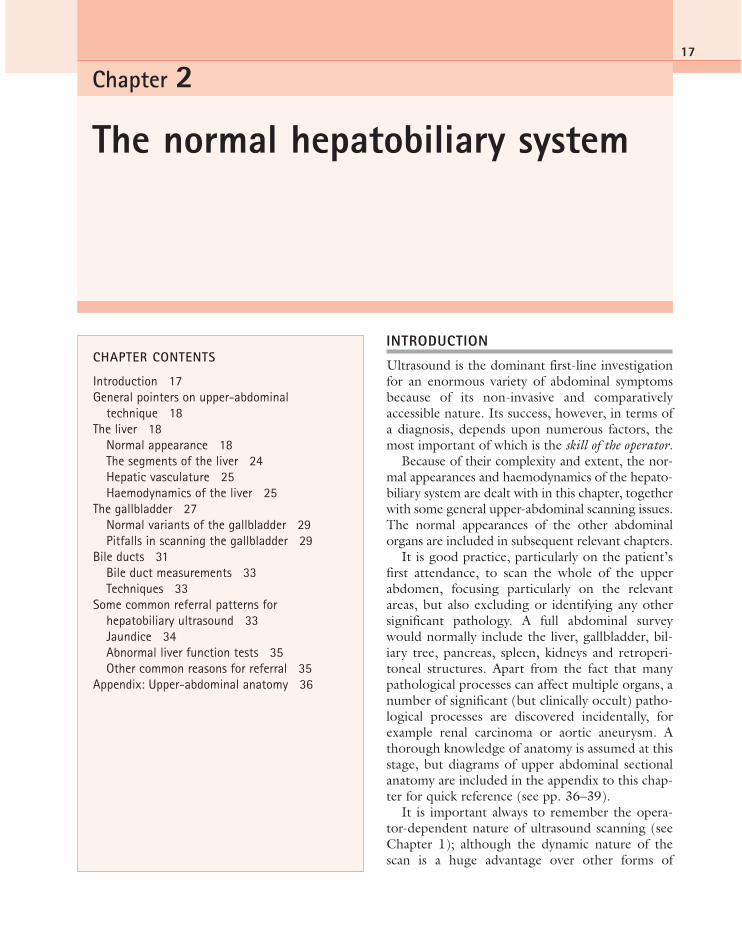
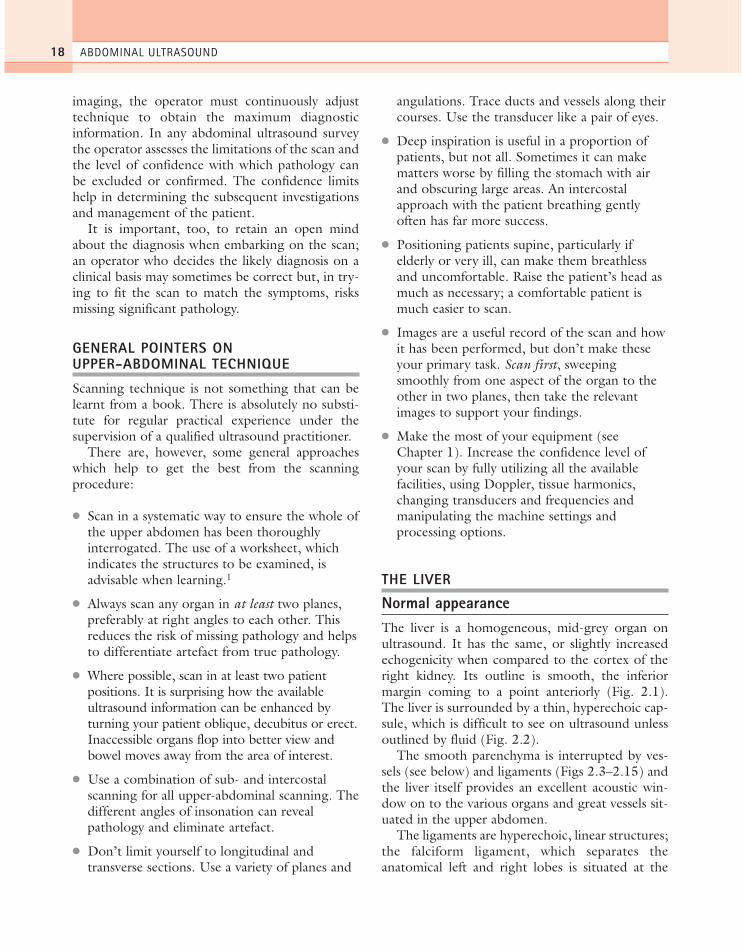
Normal appearanceThe liver is a homogeneous, mid-grey organ onultrasound. It has the same, or slightly increasedechogenicity when compared to the cortex of theright kidney. Its outline is smooth, the inferiormargin coming to a point anteriorly (Fig. 2.1).The liver is surrounded by a thin, hyperechoic cap-sule, which is difficult to see on ultrasound unlessoutlined by fluid (Fig. 2.2).
The smooth parenchyma is interrupted by ves-sels (see below) and ligaments (Figs 2.3–2.15) andthe liver itself provides an excellent acoustic win-dow on to the various organs and great vessels sit-uated in the upper abdomen.
The ligaments are hyperechoic, linear structures;the falciform ligament, which separates theanatomical left and right lobes is situated at the
ABDOMINAL ULTRASOUND18
ch02.qxd 6/30/04 5:36 PM Page 18
superior margin of the liver and is best demon-strated when surrounded by ascitic fluid. It sur-rounds the left main portal vein and is known asthe ligamentum teres as it descends towards theinfero-anterior aspect of the liver (Figs 2.9 and2.15). The ligamentum venosum separates thecaudate lobe from the rest of the liver (Fig. 2.6).
The size of the liver is difficult to quantify, asthere is such a large variation in shape betweennormal subjects and direct measurements are noto-riously inaccurate. Size is therefore usually assessedsubjectively. Look particularly at the inferior mar-gin of the right lobe which should come to a pointanterior to the lower pole of the right kidney (Fig.2.1). A relatively common variant of this is theReidel’s lobe, an inferior elongation of segment VI
on the right. This is an extension of the right lobeover the lower pole of the kidney, with a roundedmargin (Fig. 2.16), and is worth remembering as apossible cause of a palpable right upper quadrant‘mass’.
To distinguish mild enlargement from a Reidel’slobe, look at the left lobe. If this also looks bulky,with a rounded inferior edge, the liver is enlarged.A Reidel’s lobe is usually accompanied by a smaller,less accessible left lobe.
THE NORMAL HEPATOBILIARY SYSTEM 19
Figure 2.1 Longitudinal section (LS) through the rightlobe of the liver. The renal cortex is slightly lessechogenic than the liver parenchyma. LIVER
Figure 2.2 The capsule of the liver (arrows) isdemonstrated with a high-frequency (7.5 MHz) probe.
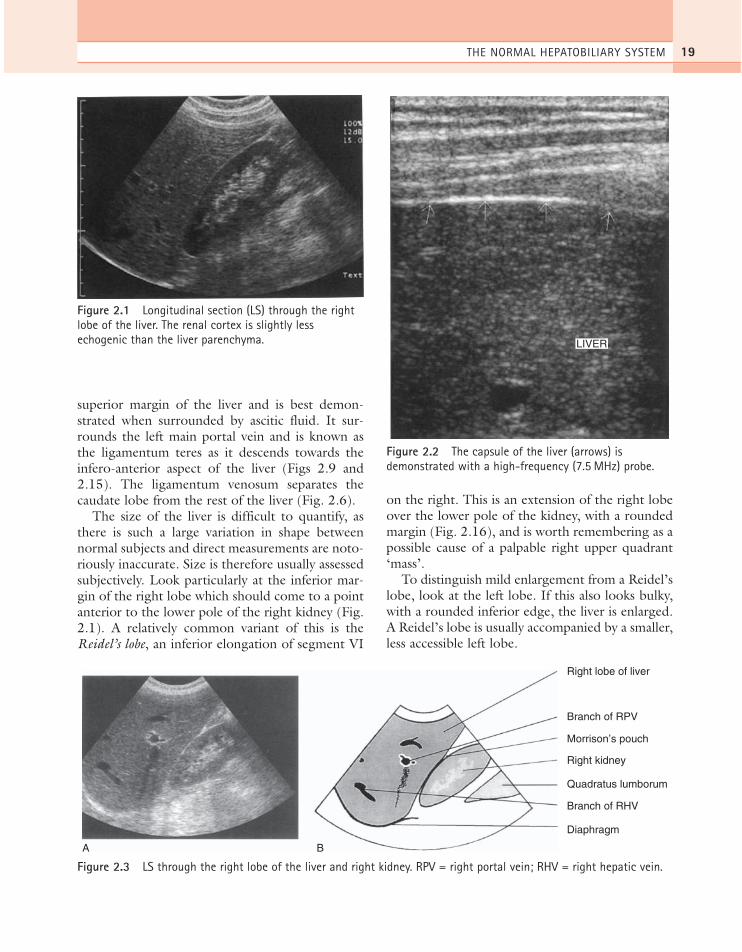
Right lobe of liver
Branch of RPV
Branch of RHV
Right kidney
Quadratus lumborum
Diaphragm
A B
Morrison’s pouch
Figure 2.3 LS through the right lobe of the liver and right kidney. RPV = right portal vein; RHV = right hepatic vein.
ch02.qxd 6/30/04 5:36 PM Page 19

ABDOMINAL ULTRASOUND20
Right lobe of liver
Right adrenal
Medial aspectright kidney
Diaphragmatic crusA B
Figure 2.4 LS, right lobe, just medial to the right kidney.
Right lobe of liver
RPV
IVC
RRA
Crus
A B
Figure 2.5 LS, right lobe, angled medially towards the inferior vena cava (IVC). RRA = right renal artery.
Left lobe of liver
LPV
Stomach
HA
Head of pancreas
Splenic vein
IVC
Ligamentumvenosum
Caudate lobeA B
Figure 2.6 LS, midline, through the left lobe, angled right towards the IVC. LPV = left portal vein; HA = hepaticartery.
ch02.qxd 6/30/04 5:36 PM Page 20

THE NORMAL HEPATOBILIARY SYSTEM 21
Left lobe of liver
Stomach
SA
Coeliac axis
Oesophagus
Aorta
A B
Body of pancreas
SV
SMA
Figure 2.7 LS through the midline. SV = splenic vein; SA = splenic artery; SMA = superior mesenteric artery.
Left lobe of liver
Stomach
Body of pancreas
SV
SMA
Aorta
Coeliac axis
A B
Figure 2.8 LS just to the left of midline.
Ligamentumteres
Stomach
Shadowingfromligament
LPV
Left lobe of liver
A B
Figure 2.9 LS, left lobe of liver.
ch02.qxd 6/30/04 5:36 PM Page 21

ABDOMINAL ULTRASOUND22
Branch of RPV
IVC
Crus
Right lobe of liver
A B
Figure 2.10 Transverse section (TS) through the liver, above the confluence of the hepatic veins.
LHV
IVC
MHV
RHV
BA
Figure 2.11 TS at the confluence of the hepatic veins (HV).
Left lobe of liver
PV
IVC
Right lobe of liver
Caudate lobe
A BFigure 2.12 TS at the porta hepatis. PV = portal vein.
ch02.qxd 6/30/04 5:36 PM Page 22
THE NORMAL HEPATOBILIARY SYSTEM 23
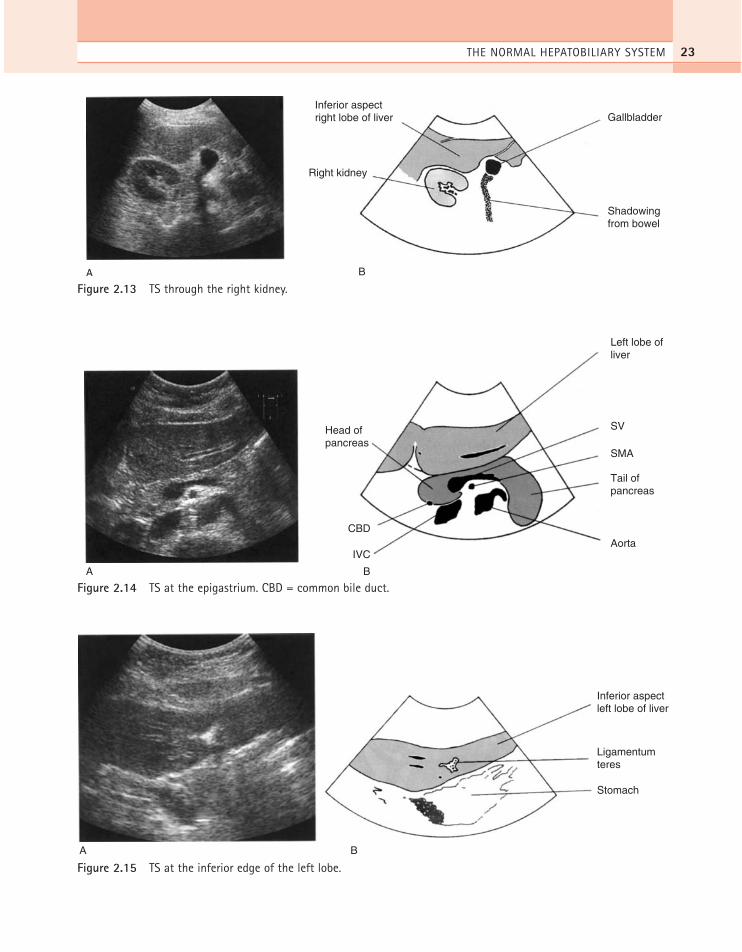
Gallbladder
Shadowingfrom bowel
Inferior aspectright lobe of liver
Right kidney
A B
Figure 2.13 TS through the right kidney.
Left lobe ofliver
SV
Aorta
Head ofpancreas
CBD
IVC
SMA
Tail ofpancreas
A B
Figure 2.14 TS at the epigastrium. CBD = common bile duct.
Inferior aspectleft lobe of liver
Ligamentumteres
Stomach
A B
Figure 2.15 TS at the inferior edge of the left lobe.
ch02.qxd 6/30/04 5:36 PM Page 23

The segments of the liverIt is often sufficient to talk about the ‘right’ or‘left’ lobes of the liver for the purposes of manydiagnoses. However, when a focal lesion is identi-fied, especially if it may be malignant, it is usefulto locate it precisely in terms of the surgical seg-
ments. This allows subsequent correlation withother imaging, such as computerized tomography(CT) or magnetic resonance imaging (MRI), andis invaluable in planning surgical procedures.
The segmental anatomy system, proposed byCouinaud in 1954,2 divides the liver into eightsegments, numbered in a clockwise direction.They are divided by the portal and hepatic veinsand the system is used by surgeons today whenplanning surgical procedures (Fig. 2.17). This sys-tem is also used when localizing lesions with CTand MRI.
Identifying the different segments on ultrasoundrequires the operator to form a mental three-dimensional image of the liver. The dynamic natureof ultrasound, together with the variation in planesof scan, makes this more difficult to do than for CTor MRI. However, segmental localization ofhepatic lesions by an experienced operator can be asaccurate with ultrasound as with MRI.3 Systematicscanning through the liver, in transverse section,identifies the main landmarks of the hepatic veins(Fig. 2.11) separating segments VII, VIII, IV andII in the superior part of the liver. As the transduceris moved inferiorly, the portal vein appears, andbelow this segments V and VI are located.
ABDOMINAL ULTRASOUND24
Figure 2.16 LS through the right lobe, demonstrating aReidel’s lobe extending below the right kidney. (Comparewith the normal liver in Figure 2.1.)
Middle hepatic vein
I
IV
V
VI
VII
VIII
II
III
Right hepatic vein
Left hepatic vein
Falciform ligament
Portal veinFigure 2.17 The surgicalsegments of the liver (afterCouinaud2).
ch02.qxd 6/30/04 5:37 PM Page 24
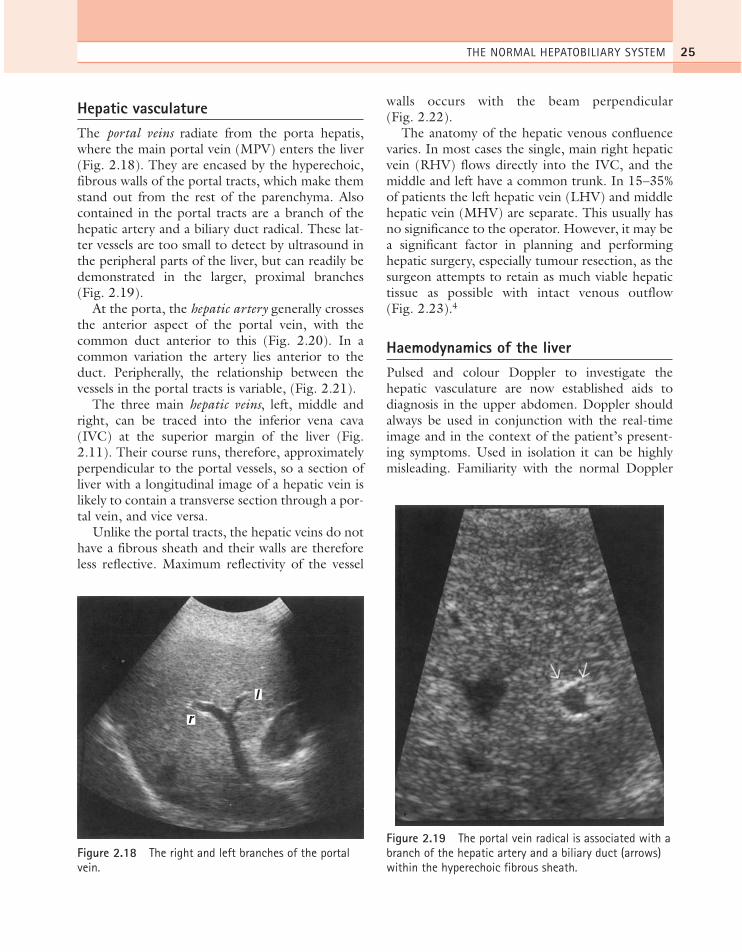
Hepatic vasculatureThe portal veins radiate from the porta hepatis,where the main portal vein (MPV) enters the liver(Fig. 2.18). They are encased by the hyperechoic,fibrous walls of the portal tracts, which make themstand out from the rest of the parenchyma. Alsocontained in the portal tracts are a branch of thehepatic artery and a biliary duct radical. These lat-ter vessels are too small to detect by ultrasound inthe peripheral parts of the liver, but can readily bedemonstrated in the larger, proximal branches(Fig. 2.19).
At the porta, the hepatic artery generally crossesthe anterior aspect of the portal vein, with thecommon duct anterior to this (Fig. 2.20). In acommon variation the artery lies anterior to theduct. Peripherally, the relationship between thevessels in the portal tracts is variable, (Fig. 2.21).
The three main hepatic veins, left, middle andright, can be traced into the inferior vena cava(IVC) at the superior margin of the liver (Fig.2.11). Their course runs, therefore, approximatelyperpendicular to the portal vessels, so a section ofliver with a longitudinal image of a hepatic vein islikely to contain a transverse section through a por-tal vein, and vice versa.
Unlike the portal tracts, the hepatic veins do nothave a fibrous sheath and their walls are thereforeless reflective. Maximum reflectivity of the vessel
walls occurs with the beam perpendicular(Fig. 2.22).
The anatomy of the hepatic venous confluencevaries. In most cases the single, main right hepaticvein (RHV) flows directly into the IVC, and themiddle and left have a common trunk. In 15–35%of patients the left hepatic vein (LHV) and middlehepatic vein (MHV) are separate. This usually hasno significance to the operator. However, it may bea significant factor in planning and performinghepatic surgery, especially tumour resection, as thesurgeon attempts to retain as much viable hepatictissue as possible with intact venous outflow(Fig. 2.23).4
Haemodynamics of the liverPulsed and colour Doppler to investigate thehepatic vasculature are now established aids todiagnosis in the upper abdomen. Doppler shouldalways be used in conjunction with the real-timeimage and in the context of the patient’s present-ing symptoms. Used in isolation it can be highlymisleading. Familiarity with the normal Doppler
THE NORMAL HEPATOBILIARY SYSTEM 25
r
l
Figure 2.18 The right and left branches of the portalvein.
Figure 2.19 The portal vein radical is associated with abranch of the hepatic artery and a biliary duct (arrows)within the hyperechoic fibrous sheath.
ch02.qxd 6/30/04 5:37 PM Page 25

spectra is an integral part of the upper-abdominalultrasound scan.
Doppler of the portal venous and hepatic vascularsystems gives information on the patency, velocityand direction of flow. The appearance of the variousspectral waveforms relates to the downstream resist-ance of the vascular bed (see Chapter 1).
The portal venous system
Colour Doppler is used to identify blood flow inthe splenic and portal veins (Figs 2.24 and 2.25).
The direction of flow is normally hepatopetal, thatis towards the liver. The main, right and left portalbranches can best be imaged by using a rightoblique approach through the ribs, so that thecourse of the vessel is roughly towards the trans-ducer, maintaining a low (< 60˚) angle with thebeam for the best Doppler signal.
The normal portal vein diameter is highly vari-able but does not usually exceed 16 mm in a rest-ing state on quiet respiration.5 The diameterincreases with deep inspiration and also in responseto food and to posture changes. An increaseddiameter may also be associated with portal hyper-tension in chronic liver disease (see Chapter 4). Anabsence of postprandial increase in diameter is alsoa sign of portal hypertension.
The normal portal vein (PV) waveform ismonophasic (Fig. 2.26) with gentle undulationswhich are due to respiratory modulation and car-diac activity. This characteristic is a sign of the nor-mal, flexible nature of the liver and may be lost insome fibrotic diseases.
The mean PV velocity is normally between 12and 20 cm per second6 but the normal range iswide. (A low velocity is associated with portal hyper-tension. High velocities are unusual, but can be dueto anastomotic stenoses in transplant patients.)
The hepatic veins
The hepatic veins drain the liver into the IVC,which leads into the right atrium. Two factorsshape the hepatic venous spectrum: the flexiblenature of the normal liver, which can easily expandto accommodate blood flow, and the close prox-imity of the right atrium, which causes a brief ‘kick’of blood back into the liver during atrial systole(Fig. 2.27). This causes the spectrum to be tripha-sic. The veins can be seen on colour Doppler to bepredominantly blue with a brief red flash duringatrial contraction. Various factors cause alterationsto this waveform: heart conditions, liver diseasesand extrahepatic conditions which compress theliver, such as ascites. Abnormalities of the hepaticvein waveform are therefore highly unspecific andshould be taken in context with the clinical picture.
As you might expect, the pulsatile nature of thespectrum decreases towards the periphery of theliver, remote from the IVC.
ABDOMINAL ULTRASOUND26
A
B
HA
HA
CDPV
CD
Figure 2.20 (A) The porta hepatis. (B) A variant with thehepatic artery anterior to the duct. CD = common duct.
ch02.qxd 6/30/04 5:37 PM Page 26

The hepatic artery
The main hepatic artery arises from the coeliac axisand carries oxygenated blood to the liver from theaorta. Its origin makes it a pulsatile vessel and therelatively low resistance of the hepatic vascular bedmeans that there is continuous forward flowthroughout the cardiac cycle (Fig. 2.28). In a nor-mal subject the hepatic artery may be elusive oncolour Doppler due to its small diameter and tortu-ous course. Use the MPV as a marker, scanning
from the right intercostal space to maintain a lowangle with the vessel. The hepatic artery is just ante-rior to this and of a higher velocity (that is, it has apaler colour of red on the colour map (Fig. 2.24)).
THE GALLBLADDER
The normal gallbladder is best visualized after fasting,to distend it. It should have a hyperechoic, thin walland contain anechoic bile (Fig. 2.29). Measure thewall thickness in a longitudinal section of the gall-bladder, with the calipers perpendicular to the wallitself. (A transverse section may not be perpendicularto the wall, and can overestimate the thickness.)
After fasting for around six hours, it should be dis-tended with bile into an elongated pear-shaped sac.The size is too variable to allow direct measurementsto be of any use, but a tense, rounded shape can indi-cate pathological, rather than physiological dilatation.
Because the size, shape and position of the gall-bladder are infinitely variable, so are the techniquesrequired to scan it. There are, however, a numberof useful pointers to maximize visualization of thegallbladder:
● Use the highest frequency possible: 5.0 MHz orhigher is especially useful for anterior gallbladders.
● Use a high line density to pick up tiny stonesor polyps (reduce the sector angle and theframe rate if possible). Make sure the focal
THE NORMAL HEPATOBILIARY SYSTEM 27
A BFigure 2.21 The relationship of the biliary duct to the portal vein varies as the vessels become more peripheral. In (A)the duct lies anterior to the LPV; in (B) the duct is posterior to the LPV.
Figure 2.22 The left hepatic vein. Vessel walls are notas reflective as portal veins; however, maximumreflectivity is produced when the beam is perpendicularto the walls, as at the periphery of this vessel.
ch02.qxd 6/30/04 5:37 PM Page 27

zone is set over the back wall of the gallbladderto maximize the chances of identifying smallstones (see Chapters 1 and 3).
● Alter the time gain compensation (TGC) toeliminate or minimize anterior artefacts and
reverberation echoes inside the gallbladder,particularly in the near field.
● Use tissue harmonic imaging to reduce artifactwithin the gallbladder and sharpen the imageof the wall (particularly in a large abdomen).
● Always scan the gallbladder in at least twoplanes (find the gallbladder’s long axis,incorporating the neck and fundus; sweep fromside to side, then transversely from neck tofundus) and two patient positions. You willalmost certainly miss pathology if you do not.
ABDOMINAL ULTRASOUND28
RHV MHVLHV
IVC
BA
Inferior RHV
Middle RHV
Figure 2.23 (A) Configuration of the hepatic venous system. (B) Inferior middle hepatic vein (arrow) arising from theIVC.
Figure 2.24 Main portal vein at the porta hepatisdemonstrating hepatopetal flow. The higher velocityhepatic artery lies adjacent to the Main portal vein (arrow).
Figure 2.25 TS through the epigastrium, demonstratingthe normal splenic vein with flow towards the liver. Notethe change from red to blue as the vessel curves awayfrom the transducer.
ch02.qxd 6/30/04 5:37 PM Page 28
● The gallbladder may be ‘folded’ (the so-calledPhrygian cap). To interrogate its contents fully,unfold it by turning the patient decubitus (rightside raised), almost prone or erect (Fig. 2.30).
● Bowel gas over the fundus can also be movedby various patient positions.
Normal variants of the gallbladderThe mesenteric attachment of the gallbladder tothe inferior surface of the liver is variable in length.This gives rise to large variations in position; at oneend of the spectrum the gallbladder, attached onlyat the neck, may be fairly remote from the liver,even lying in the pelvis; at the other the gallblad-der fossa deeply invaginates the liver and the gall-bladder appears to lie ‘intrahepatically’ enclosed onall sides by liver tissue.
The presence of a true septum in the gallbladderis rare. A folded gallbladder frequently gives theimpression of a septum but this can be distin-guished by positioning the patient to unfold thegallbladder.
Occasionally a gallbladder septum completelydivides the lumen into two parts. True gallbladderduplication is a rare entity (Fig. 2.31) and it isimportant not to mistake this for a gallbladder witha pericholecystic collection in a symptomatic
patient. Occasionally the gallbladder is absent alto-gether.
Pitfalls in scanning the gallbladderIf the gallbladder cannot be found● Check for previous surgery; a cholecystectomy
scar is usually obvious, but evidence oflaparoscopic surgery may be difficult to see inthe darkened scanning room.
● Check the patient has fasted.
THE NORMAL HEPATOBILIARY SYSTEM 29
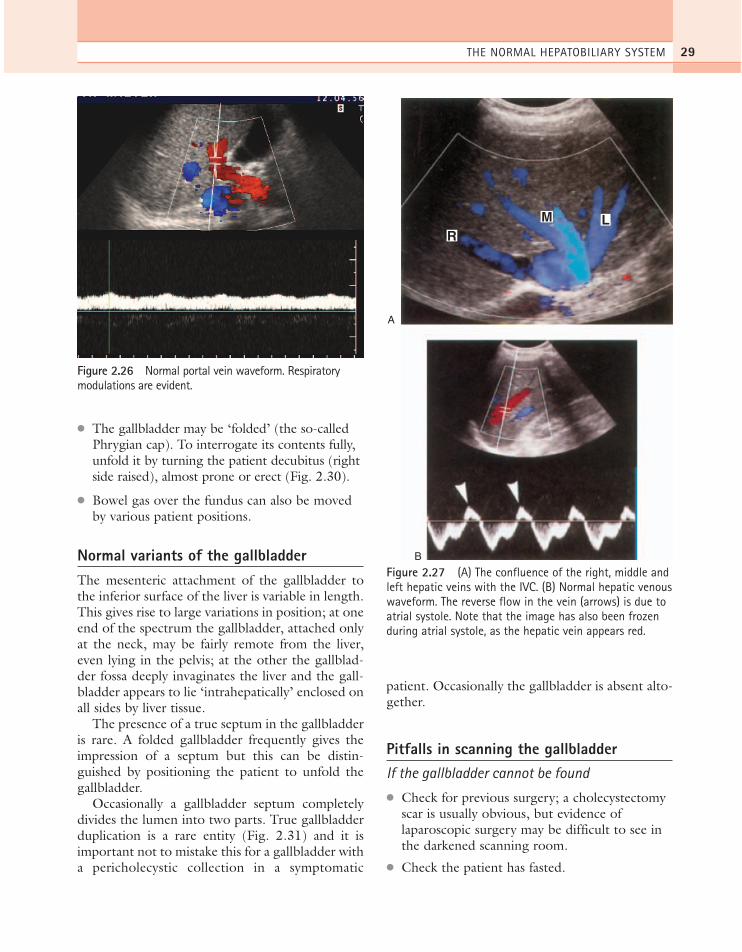
Figure 2.26 Normal portal vein waveform. Respiratorymodulations are evident.
A
RM L
B
Figure 2.27 (A) The confluence of the right, middle andleft hepatic veins with the IVC. (B) Normal hepatic venouswaveform. The reverse flow in the vein (arrows) is due toatrial systole. Note that the image has also been frozenduring atrial systole, as the hepatic vein appears red.
ch02.qxd 6/30/04 5:37 PM Page 29
● Look for an ectopic gallbladder, for examplepositioned low in the pelvis.
● Check that a near-field artefact has notobscured an anterior gallbladder, a particularproblem in very thin patients.
● Ensure the scanner frequency and settings areoptimized, find the porta hepatis and scan justbelow it in transverse section. This is the areaof the gallbladder fossa and you should see atleast the anterior gallbladder wall if thegallbladder is present (Fig. 2.32).
● A contracted, stone-filled gallbladder, producingheavy shadowing, can be difficult to identify dueto the lack of any contrasting fluid in the lumen.
Duodenum mimicking gallbladder pathology● The close proximity of the duodenum to the
posterior gallbladder wall often causes it toinvaginate the gallbladder. Maximize your machinesettings to visualize the posterior gallbladder wallseparate from the duodenum and turn the patientto cause the duodenal contents to move.
● Other segments of fluid-containinggastrointestinal tract can also cause confusion(Fig. 2.33).
Stones that don’t shadow● Ensure they are stones and not polyps by
standing the patient erect and watching them
move with gravity. (Beware—polyps on longstalks also move around.)
● The stones may be smaller than the beamwidth, making the shadow difficult to display.Make sure the focal zone is set at the back ofthe gallbladder.
● Increase the line density, if possible, byreducing the field of view.
● Scan with the highest possible frequency toensure the narrowest beam width.
● Reduce the TGC and/or power to make sureyou have not saturated the echoes distal to thegallbladder (see Chapter 3).
Beware the folded gallbladder● You may miss pathology if the gallbladder is
folded and the fundus lies underneath bowel.Always try to unfold it by positioning thepatient (Fig. 2.30).
● A fold in the gallbladder may mimic a septum.Septa are comparatively rare and have beenover-reported in the past due to the presenceof folding.
Pathology or artefact?
Sometimes the gallbladder may contain someechoes of doubtful significance, or be insufficientlydistended to evaluate accurately. A rescan, after ameal followed by further fasting, can be useful.
ABDOMINAL ULTRASOUND30
A B C
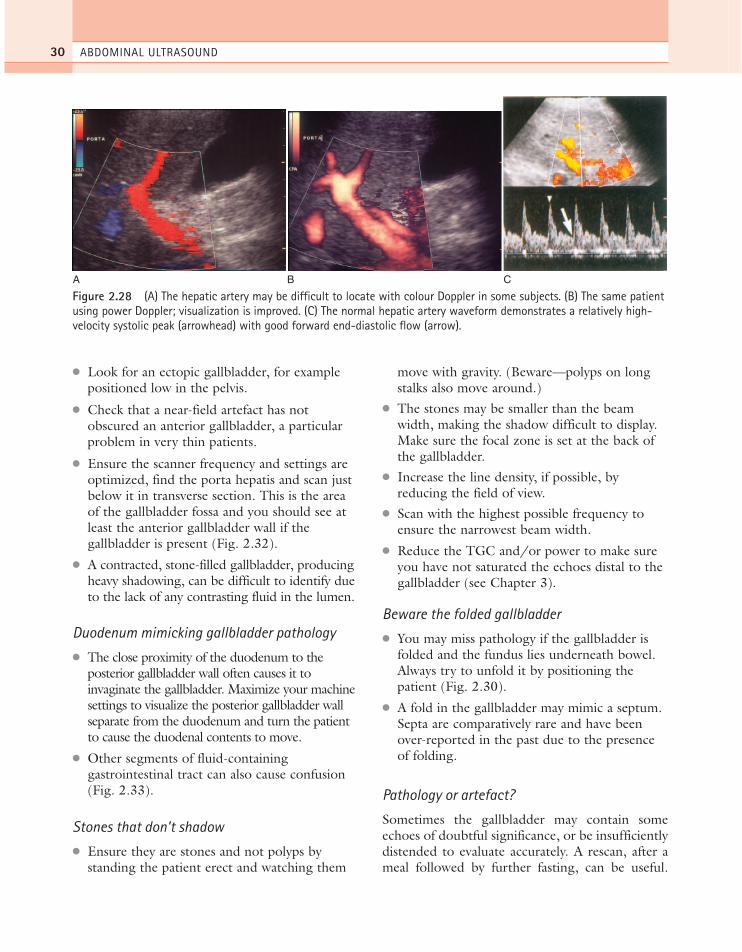
Figure 2.28 (A) The hepatic artery may be difficult to locate with colour Doppler in some subjects. (B) The same patientusing power Doppler; visualization is improved. (C) The normal hepatic artery waveform demonstrates a relatively high-velocity systolic peak (arrowhead) with good forward end-diastolic flow (arrow).
ch02.qxd 6/30/04 5:37 PM Page 30

This can flush out sludge, redistending the gall-bladder with clear bile. It may also help to clarifyany confusing appearances of adjacent bowel loops.
BILE DUCTS
The common duct can be easily demonstrated in itsintrahepatic portion just anterior and slightly to theright of the portal vein. A cross-section of the mainhepatic artery can usually be seen passing between
THE NORMAL HEPATOBILIARY SYSTEM 31
A
B
C
Figure 2.29 The gallbladder: (A) LS, (B) TS. (C) Falseappearance of wall thickening is produced (arrow) whenthe angle of scan is not perpendicular to the gallbladderwall in TS.
A
B
Figure 2.30 (A) A folded gallbladder is difficult toexamine with the patient supine. (B) Turning the patientdecubitus, right side raised, unfolds the gallbladder,enabling the lumen to be satisfactorily examined.
Figure 2.31 Double gallbladder—an incidental findingin a young woman.
ch02.qxd 6/30/04 5:37 PM Page 31

the vein and the duct (Figs 2.20A and 2.34), althougha small proportion of hepatic arteries lie anterior tothe duct (Fig. 2.20B). At this point it is usuallyreferred to as the common duct, although it may, infact, represent the right hepatic duct7 rather than
the common bile duct, because we can’t tell at whatpoint it is joined by the cystic duct.
The extrahepatic portion of the duct is less easyto see as it is often obscured by overlying duodenalgas. Good visualization of the duct usually requiresperseverance on the part of the operator. It is insuf-ficient just to visualize the intrahepatic portion ofthe duct, as early obstruction may be present witha normal-calibre intrahepatic duct and dilatation ofthe distal end. (Fig. 2.35).
ABDOMINAL ULTRASOUND32
Figure 2.32 A contracted, thick-walled gallbladderlocated in the gallbladder fossa on TS.
A
B
Figure 2.33 (A) The duodenum frequently invaginatesthe posterior wall of the gallbladder and may mimicpathology if the machine settings are not correctlymanipulated. (B) Fluid-filled stomach near thegallbladder fossa mimics a gallbladder containing astone. The real gallbladder was normal.
Figure 2.34 CBD at the porta hepatis. The lower end isfrequently obscured by shadowing from the duodenum.The duct should be measured at its widest portion.
Figure 2.35 Visualization of the lower end of the ductoften requires the operator to persevere with techniqueand patient positioning. The normal duct (calipers) isseen in the head of the pancreas.
ch02.qxd 6/30/04 5:37 PM Page 32
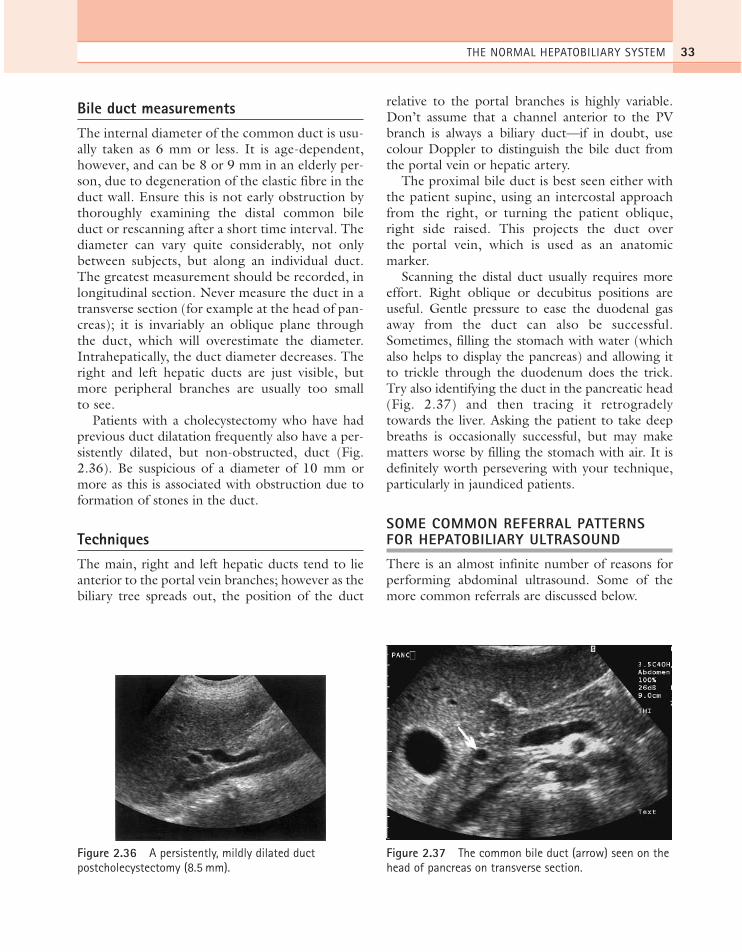
Bile duct measurementsThe internal diameter of the common duct is usu-ally taken as 6 mm or less. It is age-dependent,however, and can be 8 or 9 mm in an elderly per-son, due to degeneration of the elastic fibre in theduct wall. Ensure this is not early obstruction bythoroughly examining the distal common bileduct or rescanning after a short time interval. Thediameter can vary quite considerably, not onlybetween subjects, but along an individual duct.The greatest measurement should be recorded, inlongitudinal section. Never measure the duct in atransverse section (for example at the head of pan-creas); it is invariably an oblique plane throughthe duct, which will overestimate the diameter.Intrahepatically, the duct diameter decreases. Theright and left hepatic ducts are just visible, butmore peripheral branches are usually too smallto see.
Patients with a cholecystectomy who have hadprevious duct dilatation frequently also have a per-sistently dilated, but non-obstructed, duct (Fig.2.36). Be suspicious of a diameter of 10 mm ormore as this is associated with obstruction due toformation of stones in the duct.
TechniquesThe main, right and left hepatic ducts tend to lieanterior to the portal vein branches; however as thebiliary tree spreads out, the position of the duct
relative to the portal branches is highly variable.Don’t assume that a channel anterior to the PVbranch is always a biliary duct—if in doubt, usecolour Doppler to distinguish the bile duct fromthe portal vein or hepatic artery.
The proximal bile duct is best seen either withthe patient supine, using an intercostal approachfrom the right, or turning the patient oblique,right side raised. This projects the duct overthe portal vein, which is used as an anatomicmarker.
Scanning the distal duct usually requires moreeffort. Right oblique or decubitus positions areuseful. Gentle pressure to ease the duodenal gasaway from the duct can also be successful.Sometimes, filling the stomach with water (whichalso helps to display the pancreas) and allowing itto trickle through the duodenum does the trick.Try also identifying the duct in the pancreatic head(Fig. 2.37) and then tracing it retrogradelytowards the liver. Asking the patient to take deepbreaths is occasionally successful, but may makematters worse by filling the stomach with air. It isdefinitely worth persevering with your technique,particularly in jaundiced patients.
SOME COMMON REFERRAL PATTERNSFOR HEPATOBILIARY ULTRASOUND
There is an almost infinite number of reasons forperforming abdominal ultrasound. Some of themore common referrals are discussed below.
THE NORMAL HEPATOBILIARY SYSTEM 33
Figure 2.36 A persistently, mildly dilated ductpostcholecystectomy (8.5 mm).
Figure 2.37 The common bile duct (arrow) seen on thehead of pancreas on transverse section.
ch02.qxd 6/30/04 5:37 PM Page 33

JaundiceThis symptom is a frequent cause of referral forabdominal ultrasound. It is therefore essential forthe sonographer to have a basic understanding ofthe various mechanisms in order to maximize thediagnostic information from the ultrasound scan.The causes and ultrasound appearances of jaundiceare dealt with more fully in Chapters 3 and 4; abrief overview is included here.
Jaundice, or hyperbilirubinaemia, is an elevatedlevel of bilirubin in the blood. It is recognized bya characteristic yellow coloration of the skin andsclera of the eye, often accompanied by itching ifprolonged.
Bilirubin is derived from the haem portion ofhaemoglobin. Red blood cells are broken down inthe liver into haem and globin, releasing theirbilirubin, which is non-soluble. This is termedunconjugated bilirubin. This is then taken up bythe liver cells and converted to a water-solubleform, conjugated bilirubin, which is excreted viathe biliary ducts into the duodenum to aid fatdigestion.
By knowing which of these two types of bilirubinis present in the jaundiced patient, the cliniciancan narrow down the diagnostic possibilities. Ultrasound then further refines the diagnosis(Fig. 2.38).
ABDOMINAL ULTRASOUND34
Red blood corpuscle
Haemoglobin Haemolysis
Cirrhosis
Prehepatic
BILIRUBIN
Hepatic
Posthepatic
Hepatitis
Tumour
Ductal stones Ductal carcinoma
Pancreatic head inflammation or carcinoma
Ampulla carcinoma
Figure 2.38 Some common causes of jaundice.
ch02.qxd 6/30/04 5:37 PM Page 34

Jaundice can fall into one of two categories:
● obstructive (sometimes called posthepatic) inwhich the bile is prevented from draining outof the liver because of obstruction to thebiliary duct(s)
● non-obstructive (prehepatic or hepatic) inwhich the elevated bilirubin level is due tohaemolysis (the breakdown of the red bloodcells) or a disturbance in the mechanism ofthe liver for uptake and storage of bilirubin,such as in inflammatory or metabolic liverdiseases.
Naturally, the treatment of jaundice depends on itscause (Table 2.1). Ultrasound readily distinguishesobstructive jaundice, which demonstrates somedegree of biliary duct dilatation, from non-obstructive, which does not.
Abnormal liver function testsAltered or deranged liver function tests (LFTs) areanother frequent cause of referral for abdominalultrasound.
Biochemistry from a simple blood test is oftena primary pointer to pathology and is invariablyone of the first tests performed as it is quick andeasily accessible. Most of these markers arehighly unspecific, being associated with manytypes of diffuse and focal liver pathology. Themost frequently encountered LFTs are listed inTable 2.2.
Other common reasons for referralIn some cases, the presenting symptoms may beorgan-specific or even pathognomonic, simplifyingthe task of ultrasound diagnosis. Often, however,
THE NORMAL HEPATOBILIARY SYSTEM 35
Table 2.1 Common causes of jaundice
Non-obstructive Obstructive
Unconjugated hyperbilirubinaemia Conjugated hyperbilirubinaemia—haemolysis —stones in the biliary duct—haematoma —carcinoma of the duct, head of pancreas or ampulla—Gilbert’s disease —acute pancreatitis
—other masses which compress the common bile duct (e.g. lymph node mass)—biliary atresia
Mixed hyperbilirubinaemia—hepatitis—alcoholic liver disease—cirrhosis of all types—multiple liver metastases—drug-induced liver disease
(See Chapters 3 and 4 for further information.)
Table 2.2 Common serum liver function tests
Test Association with increased level
Bilirubin Obstructive or non-obstructive jaundice. (Differentiation can be made between conjugatedand unconjugated bilirubin)
Alkaline phosphatase Non-obstructive jaundice(ALP) (liver enzyme) Metastases
Other focal hepatic lesionsAlpha fetoprotein Hepatocellular carcinoma (HCC)Prothrombin time Malignancy
Diffuse liver disease (often with portal hypertension)
Gamma glutamyl Obstructive jaundicetransferase Alcoholic liver disease
Alanine amino- Obstructive or transferase (ALT) non-obstructive jaundice
Aspartate amino- Hepatitistransferase (AST) Viral infections(liver enzymes) Other organ failure (e.g. cardiac)
Protein Lack of protein is associated (serum albumin) with numerous liver diseases.
Low levels are associated with ascites, often due to portal hypertension
ch02.qxd 6/30/04 5:37 PM Page 35

ABDOMINAL ULTRASOUND36
the symptoms are vague and non-specific, requir-ing the sonographer to perform a comprehensiveand knowledgeable search. The non-invasivenature of ultrasound makes it ideal for the first-lineinvestigation.
Upper abdominal pain● Upper abdominal pain, the origin of which
could be linked to any of the organs, is one ofthe most frequent causes of referral. Thesonographer can narrow the possibilities downby taking a careful history (see Box 2.1).
● Is the pain focal? This may direct thesonographer to the relevant organ, for examplea thick-walled gallbladder full of stones may betender on gentle transducer pressure, pointingto acute or chronic cholecystitis, depending onthe severity of the pain.
● Bear in mind that gallstones are a commonincidental finding which may be a red herring.Always consider multiple pathologies.
● Is the pain related to any event which may givea clue? Fat intolerance might suggest a biliarycause, pain on micturition a urinary tract cause,for example.
● Is it accompanied by other symptoms such as ahigh temperature? This may be associated withan infective process such as an abscess.
● Could it be bowel-related? Generalizedabdominal pain could be due to inflammatoryor obstructive bowel conditions and knowledgeof the patient’s bowel habits is helpful.
● Has the patient had any previous surgery whichcould be significant?
Palpable right upper quadrant mass
A palpable right upper quadrant mass could be dueto a renal, hepatobiliary, bowel-related or othercause. The sonographer should gently palpate toget an idea of the size and position of the mass andwhether or not it is tender. Specifically targetingthe relevant area may yield useful and unexpectedresults, for example a Reidel’s lobe, colonic carci-noma or impacted faeces, which will help to guidethe nature of further investigations.
APPENDIX: UPPER-ABDOMINAL ANATOMY
Diagrams of sectional upper-abdominal anatomyare reproduced here for quick reference. See Box2.2 for the abbreviations used here.
Box 2.1
Always:● take a verbal history from the patient—don’t
just rely on the request card● obtain the results of any previous investiga-
tions, including previous radiology● consider the possibility of multiple pathologies
Box 2.2 Abbreviations
AO AortaCBD Common bile ductGB GallbladderGDA Gastroduodenal arteryHA Hepatic arteryHOP Head of pancreasIVC Inferior vena cavaLHV Left hepatic veinLL Left lobe of liverLPV Left portal veinLRV Left renal veinMHV Middle hepatic veinR Adr Right adrenal glandRHV Right hepatic veinRK Right kidneyRL Right lobe of liverRPV Right portal veinRRA Right renal arterySA Splenic arterySMA Superior mesenteric arterySMV Superior mesenteric veinSPL SpleenST StomachSV Splenic veinTOP Tail of pancreas
ch02.qxd 6/30/04 5:37 PM Page 36
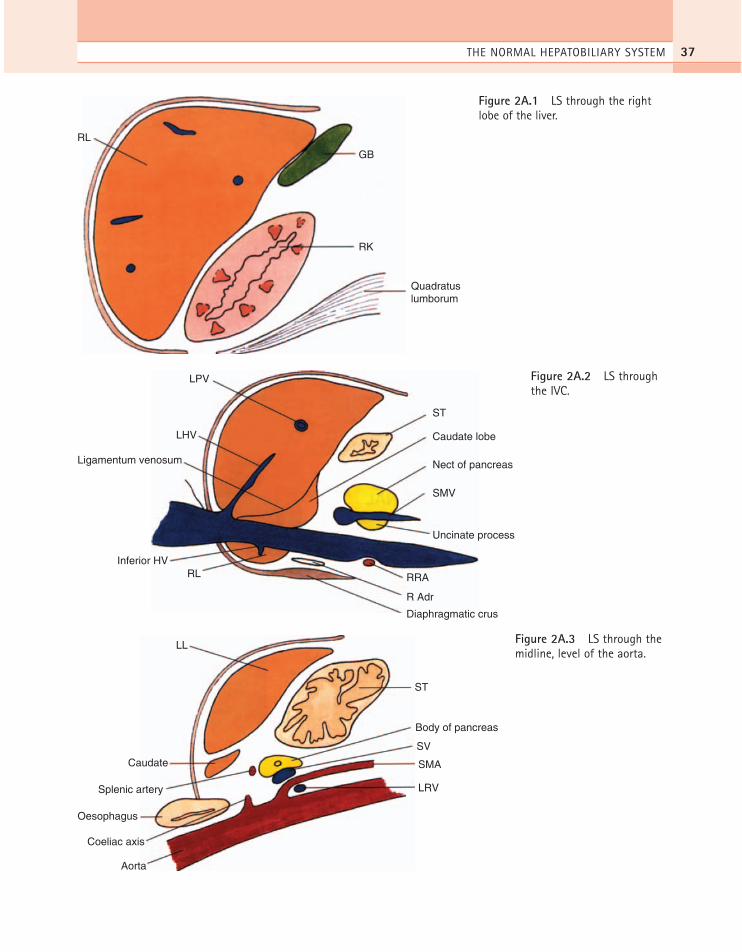
THE NORMAL HEPATOBILIARY SYSTEM 37
ST
Caudate lobe
Nect of pancreas
SMV
Uncinate process
RRARLInferior HV
Ligamentum venosum
LHV
LPV
R Adr
Diaphragmatic crus
Figure 2A.2 LS throughthe IVC.
ST
LL
Caudate
Splenic artery
Oesophagus
Coeliac axis
Aorta
Body of pancreas
SV
SMA
LRV
Figure 2A.3 LS through themidline, level of the aorta.
GB
RK
Quadratus lumborum
RL
Figure 2A.1 LS through the rightlobe of the liver.
ch02.qxd 6/30/04 5:37 PM Page 37

ABDOMINAL ULTRASOUND38
ST
Diaphragmatic crus
Spleen
Aorta
LHV
MHV
RHV
Figure 2A.5 Transverse obliquesection through the hepatic venousconfluence.
ST
Gastroduodenal artery
Head of pancreas
CBD
HA
MPV
IVC
Figure 2A.4 Longitudinal obliquesection through the CBD.
ch02.qxd 6/30/04 5:37 PM Page 38
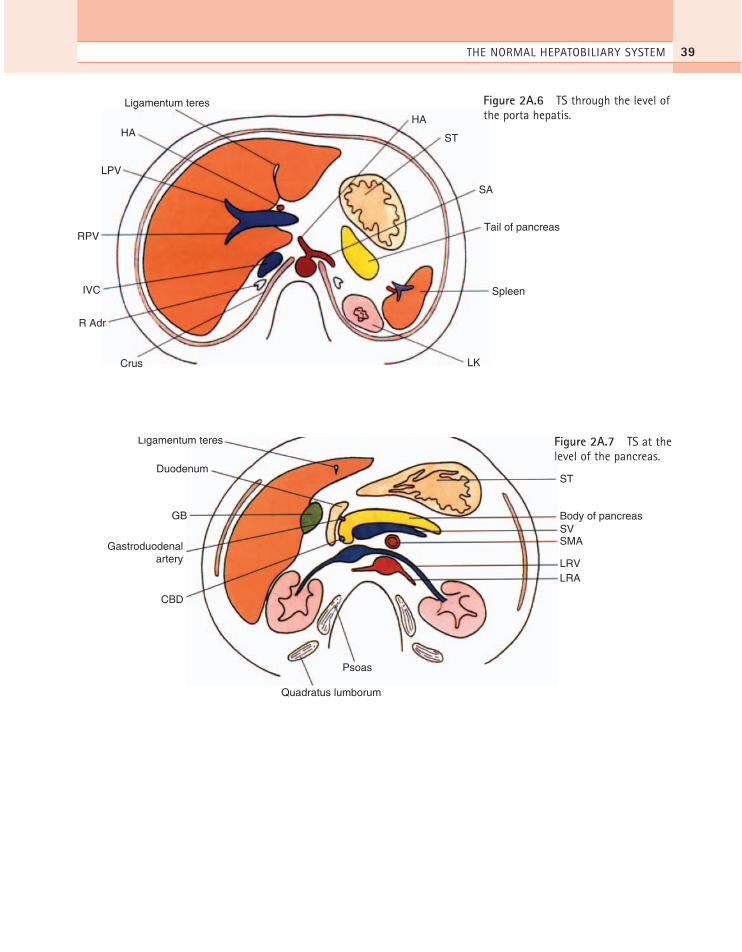
THE NORMAL HEPATOBILIARY SYSTEM 39
ST
Body of pancreasSVSMA
LRVLRA
Psoas
Ligamentum teres
Duodenum
GB
Gastroduodenalartery
CBD
Quadratus lumborum
Figure 2A.7 TS at thelevel of the pancreas.
HA
ST
SA
Tail of pancreas
Spleen
LK
Ligamentum teres
HA
LPV
RPV
IVC
R Adr
Crus
Figure 2A.6 TS through the level ofthe porta hepatis.
ch02.qxd 6/30/04 5:37 PM Page 39

ABDOMINAL ULTRASOUND40
1. UK Association of Sonographers. 2001 Guidelines forProfessional Working Standards – Ultrasound Practice.UKAS, London.
2. Couinaud C. 1954 Lobes et segments hépatiques; notesur l’architecture anatomique et chirugicale du foie.Presse Medical 62: 709.
3. Conlon RM, Bates JA. 1996 Segmental Localisation ofFocal Hepatic Lesions – A Comparison of Ultrasoundand MRI. Conference proceedings of BMUS,Edinburgh.
4. Cheng Y, Huang T, Chen C et al. 1997 Variations ofthe middle and inferior right hepatic vein: applicationin hepatectomy. Journal of Clinical Ultrasound 25:175–182.
5. Goyal AK, Pokharna DS, Sharma SK. 1990 Ultrasonicmeasurements of portal vasculature in diagnosis ofportal hypertension. Journal of Ultrasound inMedicine 9: 45.
6. Gaiani S, Bolondi L, Li Bassi S et al. 1989 Effect ofmeal on portal hemodynamics in healthy humans andin patients. Hepatology 9: 815–819.
7. Davies RP, Downey PR, Moore WR, Jeans PL, Toouli J. 1991 Contrast cholangiography versusultrasonographic measurement of the ‘extrahepatic’ bile duct: a two-fold discrepancy revisited. Journal ofUltrasound in Medicine 10: 653–657.
References
ch02.qxd 6/30/04 5:37 PM Page 40

Ultrasound is an essential first-line investigation insuspected gallbladder and biliary duct disease. It ishighly sensitive, accurate and comparatively cheapand is the imaging modality of choice.1 Gallbladderpathology is common and is asymptomatic in over13% of the population.2
CHOLELITHIASIS
The most commonly and reliably identified gall-bladder pathology is that of gallstones (see Table3.1). More than 10% of the population of the UKhave gallstones. Many of these are asymptomatic,which is an important point to remember. When
Chapter 3
Pathology of the gallbladder and biliary tree
41
CHAPTER CONTENTS
Cholelithiasis 41Ultrasound appearances 42Choledocholithiasis 45Biliary reflux and gallstone pancreatitis 47Further management of gallstones 47
Enlargement of the gallbladder 48Mucocoele of the gallbladder 48Mirizzi syndrome 48
The contracted or small gallbladder 50Porcelain gallbladder 50Hyperplastic conditions of the gallbladder wall 51
Adenomyomatosis 51Polyps 53Cholesterolosis 53
Inflammatory gallbladder disease 54Acute cholecystitis 54Chronic cholecystitis 56Acalculous cholecystitis 56Complications of cholecystitis 57
Obstructive jaundice and biliary duct dilatation 58Assessment of the level of obstruction 58Assessment of the cause of obstruction 61Management of biliary obstruction 64Intrahepatic tumours causing biliaryobstruction 64Choledochal cysts 64Cholangitis 66
Biliary dilatation without jaundice 66Postsurgical CBD dilatation 66Focal obstruction 67
Pitfalls 67Obstruction without biliary dilatation 67
Early obstruction 67Fibrosis of the duct walls 67
Other biliary diseases 67Primary sclerosing cholangitis 67Caroli’s disease 68Parasites 70
Echogenic bile 71Biliary stasis 71Haemobilia 72Pneumobilia 72
Malignant biliary disease 73Primary gallbladder carcinoma 73Cholangiocarcinoma 74Gallbladder metastases 76
ch03.qxd 6/30/04 5:40 PM Page 41

scanning a patient with abdominal pain it shouldnot automatically be assumed that, when gallstonesare present, they are responsible for the pain. It isnot uncommon to find further pathology in thepresence of gallstones and a comprehensive upper-abdominal survey should always be carried out.
Gallstones are associated with a number of con-ditions. They occur when the normal ratio ofcomponents making up the bile is altered, mostcommonly when there is increased secretion of cho-lesterol in the bile. Conditions which are associatedwith increased cholesterol secretion, and thereforethe formation of cholesterol stones, include obesity,diabetes, pregnancy and oestrogen therapy. Theincidence of stones also rises with age, probablybecause the bile flow slows down.
An increased secretion of bilirubin in the bile, asin patients with cirrhosis for example, is associatedwith pigment (black or brown) stones.
Ultrasound appearancesThere are three classic acoustic properties associ-ated with stones in the gallbladder; they are highlyreflective, mobile and cast a distal acoustic shadow.In the majority of cases, all these properties aredemonstrated (Figs 3.1–3.3).
Shadowing
The ability to display a shadow posterior to a stonedepends upon several factors:
● The reflection and absorption of sound by thestone. This is fairly consistent, regardless of thecomposition of the stone.
● The size of the stone in relation to the beamwidth. A shadow will occur when the stone
ABDOMINAL ULTRASOUND42
Table 3.1 Gallstones—clinical features
Often asymptomaticBiliary colic—RUQ pain, fatty intolerance+ve ultrasound Murphy’s sign (if inflammation is present)Recurring (RUQ) pain in chronic cholecystitisJaundice (depending on degree of obstruction)Fluctuating fever (if infection is present)
RUQ=right upper quadrant.
A
B
Figure 3.1 (A) Longitudinal section and (B) transversesection images of the gallbladder containing stones withstrong distal acoustic shadowing. Note the thickenedgallbladder wall.
Figure 3.2 Multiple tiny stones combining to form aposterior band of shadow.
ch03.qxd 6/30/04 5:40 PM Page 42
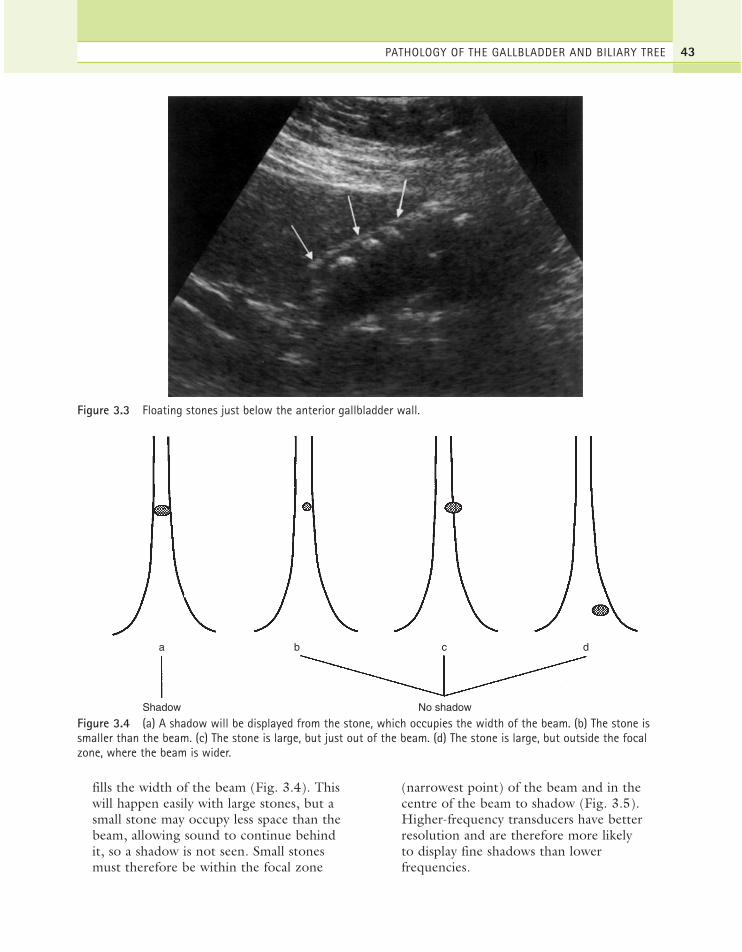
fills the width of the beam (Fig. 3.4). Thiswill happen easily with large stones, but asmall stone may occupy less space than thebeam, allowing sound to continue behind it, so a shadow is not seen. Small stones must therefore be within the focal zone
(narrowest point) of the beam and in thecentre of the beam to shadow (Fig. 3.5).Higher-frequency transducers have betterresolution and are therefore more likely to display fine shadows than lowerfrequencies.
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 43
Figure 3.3 Floating stones just below the anterior gallbladder wall.
a b c d
Shadow No shadow
Figure 3.4 (a) A shadow will be displayed from the stone, which occupies the width of the beam. (b) The stone issmaller than the beam. (c) The stone is large, but just out of the beam. (d) The stone is large, but outside the focalzone, where the beam is wider.
ch03.qxd 6/30/04 5:40 PM Page 43
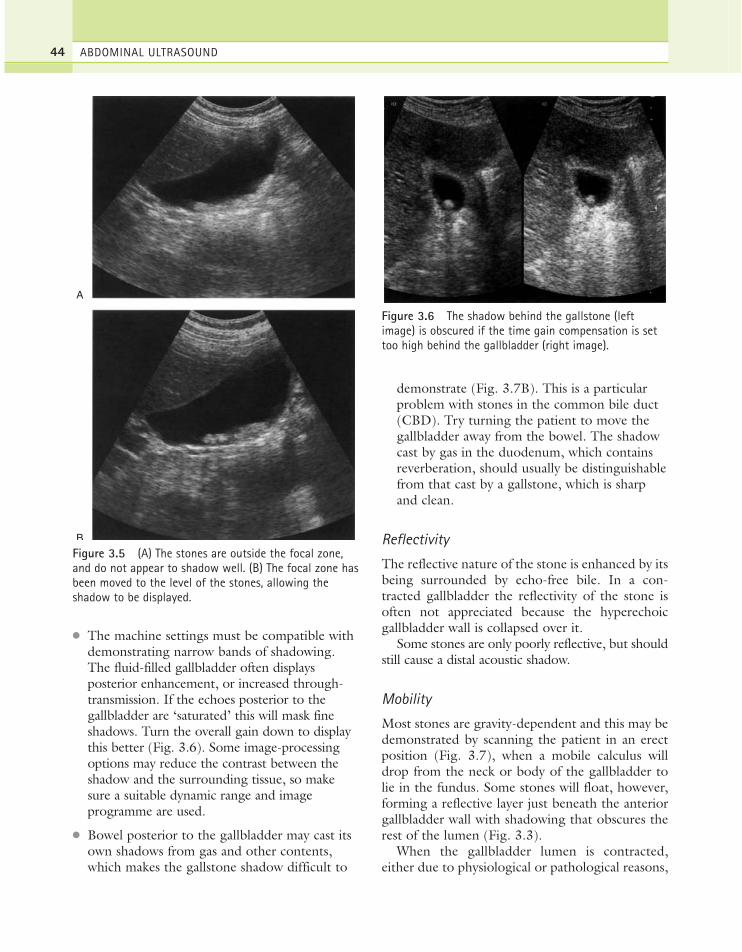
● The machine settings must be compatible withdemonstrating narrow bands of shadowing.The fluid-filled gallbladder often displaysposterior enhancement, or increased through-transmission. If the echoes posterior to thegallbladder are ‘saturated’ this will mask fineshadows. Turn the overall gain down to displaythis better (Fig. 3.6). Some image-processingoptions may reduce the contrast between theshadow and the surrounding tissue, so makesure a suitable dynamic range and imageprogramme are used.
● Bowel posterior to the gallbladder may cast itsown shadows from gas and other contents,which makes the gallstone shadow difficult to
demonstrate (Fig. 3.7B). This is a particularproblem with stones in the common bile duct(CBD). Try turning the patient to move thegallbladder away from the bowel. The shadowcast by gas in the duodenum, which containsreverberation, should usually be distinguishablefrom that cast by a gallstone, which is sharpand clean.
Reflectivity
The reflective nature of the stone is enhanced by itsbeing surrounded by echo-free bile. In a con-tracted gallbladder the reflectivity of the stone isoften not appreciated because the hyperechoicgallbladder wall is collapsed over it.
Some stones are only poorly reflective, but shouldstill cause a distal acoustic shadow.
Mobility
Most stones are gravity-dependent and this may bedemonstrated by scanning the patient in an erectposition (Fig. 3.7), when a mobile calculus willdrop from the neck or body of the gallbladder tolie in the fundus. Some stones will float, however,forming a reflective layer just beneath the anteriorgallbladder wall with shadowing that obscures therest of the lumen (Fig. 3.3).
When the gallbladder lumen is contracted,either due to physiological or pathological reasons,
ABDOMINAL ULTRASOUND44
A
B
Figure 3.5 (A) The stones are outside the focal zone,and do not appear to shadow well. (B) The focal zone hasbeen moved to the level of the stones, allowing theshadow to be displayed.
Figure 3.6 The shadow behind the gallstone (leftimage) is obscured if the time gain compensation is settoo high behind the gallbladder (right image).
ch03.qxd 6/30/04 5:40 PM Page 44

any stones present are unable to move and this isalso the case in a gallbladder packed with stones.
Occasionally a stone may become impacted in theneck, and movement of the patient is unable to dis-lodge it. Stones lodged in the gallbladder neck orcystic duct may result in a permanently contracted
gallbladder, a gallbladder full of fine echoes due toinspissated (thickened) bile (Fig. 3.8) or a distendedgallbladder due to a mucocoele (see below).
CholedocholithiasisStones may pass from the gallbladder into thecommon duct, or may develop de novo within thecommon duct. Stones in the CBD may obstructthe drainage of bile from the liver, causing obstruc-tive jaundice.
Due to shadowing from the duodenum, ductalstones are often not demonstrated with ultrasoundwithout considerable effort. Usually they are accom-panied by stones in the gallbladder and a degree ofdilatation of the CBD. In these cases the operatorcan usually persevere and demonstrate the stone atthe lower end of the duct. However, the duct may bedilated but empty, the stone having recently passed.
Stones may be seen to move up and down adilated duct. This can create a ball-valve effect sothat obstruction may be intermittent.
It is not unusual to demonstrate a stone in theCBD without stones in the gallbladder, a phenom-enon which is also well-documented followingcholecystectomy (Fig. 3.9). This may be due to asingle calculus in the gallbladder having movedinto the duct, or stone formation within the duct.
It is also important to remember that stones inthe CBD may be present without duct dilatationand attempts to image the entire common duct
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 45
A
B
Figure 3.7 (A) Supine and (B) erect viewsdemonstrating movement of the tiny stone into thefundus of the gallbladder. Note how duodenum posteriorto the gallbladder masks the shadow in the erect state.
Figure 3.8 Stone impacted in theneck of the gallbladder. The left-hand image is a TS through theneck demonstrating the impactedstone. The right-hand imagedemonstrates the dilatedgallbladder containing fine echoesfrom inspissated bile.
ch03.qxd 6/30/04 5:40 PM Page 45

ABDOMINAL ULTRASOUND46
A B
Figure 3.9 (A) A stone in a dilated common bile duct (CBD) with posterior shadowing. The gallbladder was dilatedbut did not contain stones. (B) Stone formation in the intrahepatic ducts.
A B
Figure 3.10 (A) Small stone in the CBD causing intermittent obstruction. At the time of scanning, the CBD wasnormal in calibre at 5 mm. The duct walls are irregular, consistent with cholangitis. (B) Endoscopiccholangiopancreatography (ERCP) of a stone in a normal-calibre (5 mm) duct.
with ultrasound should always be made, even if itis of normal calibre at the porta (Fig. 3.10).
Other ultrasound signs to look for are shown inTable 3.2.
Possible complications of gallstones are outlinedin Figure 3.11A. In rare cases, stones may per-forate the inflamed gallbladder wall to form a fis-tula into the small intestine or colon. A large stone
ch03.qxd 6/30/04 5:40 PM Page 46

passing into the small intestine may impact in theileum, causing intestinal obstruction (Fig. 3.11B).
Biliary reflux and gallstone pancreatitisA stone may become lodged in the distal commonbile duct near the ampulla. If the main pancreaticduct joins the CBD proximal to this, bile and pan-
creatic fluid may reflux up the pancreatic duct,causing inflammation and severe pain.
Reflux up the common bile duct may also resultin ascending cholangitis, particularly if the obstruc-tion is prolonged or repetitive. Cholangitis mayresult in dilated bile ducts with mural irregularityon ultrasound, but endoscopic retrograde cholan-giopancreatography (ERCP) is usually superior indemonstrating intrahepatic ductal changes of thisnature.
Bile reflux is also associated with anomalous cys-tic duct insertion (Fig. 3.12), which is more read-ily recognized on ERCP than ultrasound.
Further management of gallstonesERCP demonstrates stones in the duct withgreater accuracy than ultrasound, particularly atthe lower end of the CBD, which may be obscuredby duodenal gas and also allows for sphinctero-tomy and stone removal.
Laparoscopic cholecystectomy is the preferredmethod of treatment for symptomatic gallbladderdisease in an elective setting and has well-recog-nized benefits over open surgery in experienced
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 47
Table 3.2 Gallstones—other ultrasound signs tolook for
Acute or chronic cholecystitis
Complications of cholecystitis, e.g. pericholecysticcollectionStone impacted in the neck of gallbladder—mucocoele,hydropsCBD stonesBiliary obstruction—dilatation of the CBD and/orintrahepatic ductsPancreatitisOther causes of RUQ pain unrelated to stones
CBD = common bile duct.
Cholangitis hepatic abscess
Obstructive jaundice
Obstruction causing pancreatitis
Cholecysto- enteric fistula
Acute or chronic cholecystitis
A
Carcinoma
Figure 3.11 (A) The possible complication of gallstones.(Continued)
ch03.qxd 6/30/04 5:40 PM Page 47

hands. Acute cholecystitis is also increasingly man-aged by early laparoscopic surgery, with a slightlyhigher rate of conversion to open surgery than elec-tive cases.3 Laparoscopic ultrasound may be used asa suitable alternative to operative cholangiographyto examine the common duct for residual stonesduring surgery.4 Both ultrasound and cholescintig-raphy are used in monitoring postoperative biliaryleaks or haematoma (Fig. 3.13).
Other, less common options include dissolutiontherapy and extracorporeal shock wave lithotripsy(ESWL). However, these treatments are oftenonly partially successful, require careful patientselection and also run a significant risk of stonerecurrence.5
ENLARGEMENT OF THE GALLBLADDER
Because of the enormous variation in size andshape of the normal gallbladder, it is not possibleto diagnose pathological enlargement by simplyusing measurements. Three-dimensional tech-niques may prove useful in assessing gallbladdervolume6 but this is a technique which is only likelyto be clinically useful in a minority of patients withimpaired gallbladder emptying.
An enlarged gallbladder is frequently referred toas hydropic. It may be due to obstruction of thecystic duct (see below) or associated with numer-ous disease processes such as diabetes, primarysclerosing cholangitis, leptospirosis or in responseto some types of drug.
A pathologically dilated gallbladder, as opposedto one which is physiologically dilated, usuallyassumes a more rounded, tense appearance.
Mucocoele of the gallbladderIf the cystic duct is obstructed, usually by a stonewhich has failed to pass through to the CBD, thenormal flow of bile from the gallbladder is inter-rupted. Chronic cystic duct obstruction causes thebile to be replaced by mucus secreted by the liningof the gallbladder, resulting in a mucocoele. Thebiliary ducts remain normal in calibre.
If the gallbladder looks dilated, make a carefulsearch for an obstructing lesion at the neck; a stonein the cystic duct is more difficult to identify onultrasound as it is not surrounded by echo-free bile(Fig. 3.8).
Mirizzi syndromeMirizzi syndrome is a rare cause of biliaryobstruction in which the cystic duct is obstructedby a stone, which in combination with a sur-rounding inflammatory process compresses andobstructs the common hepatic duct, causing dis-tal biliary duct dilatation. This is associated with alow insertion of the cystic duct into the commonhepatic duct. Occasionally a fistula forms betweenthe hepatic duct and the gallbladder due to ero-sion of the duct wall by the stone. Ultimately thismay lead to gallstone ileus—small-bowel obstructionresulting from migration of a large stone through
ABDOMINAL ULTRASOUND48
BFigure 3.11 cont’d (B) Gallstone Ileus.
ch03.qxd 6/30/04 5:40 PM Page 48
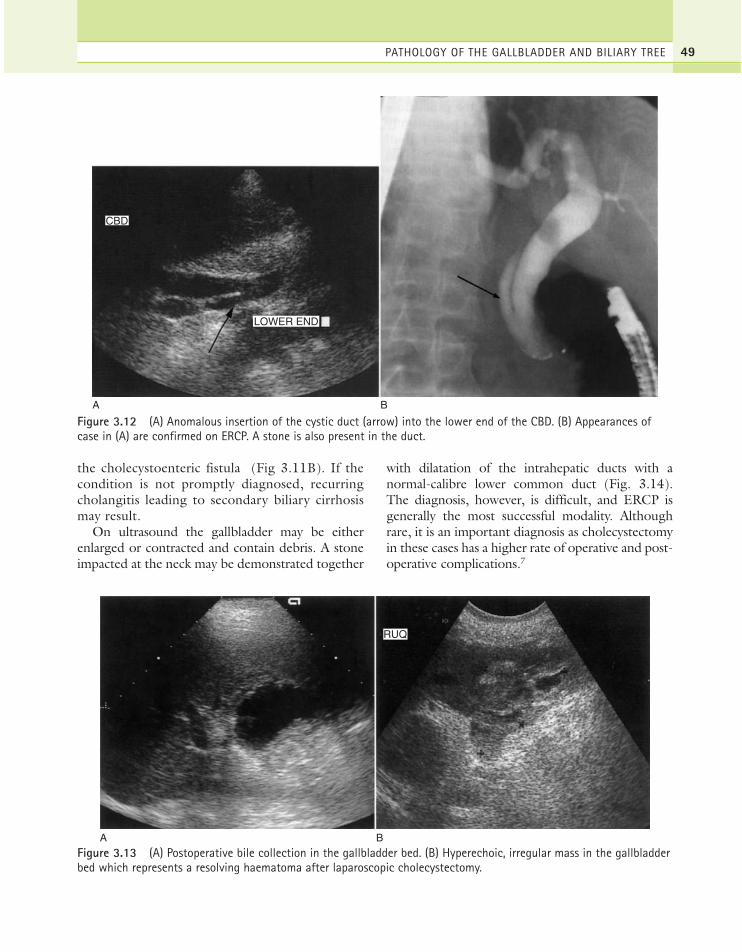
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 49
A B
CBD
LOWER END
Figure 3.12 (A) Anomalous insertion of the cystic duct (arrow) into the lower end of the CBD. (B) Appearances ofcase in (A) are confirmed on ERCP. A stone is also present in the duct.
A B
RUQ
Figure 3.13 (A) Postoperative bile collection in the gallbladder bed. (B) Hyperechoic, irregular mass in the gallbladderbed which represents a resolving haematoma after laparoscopic cholecystectomy.
the cholecystoenteric fistula (Fig 3.11B). If thecondition is not promptly diagnosed, recurringcholangitis leading to secondary biliary cirrhosismay result.
On ultrasound the gallbladder may be eitherenlarged or contracted and contain debris. A stoneimpacted at the neck may be demonstrated together
with dilatation of the intrahepatic ducts with anormal-calibre lower common duct (Fig. 3.14).The diagnosis, however, is difficult, and ERCP isgenerally the most successful modality. Althoughrare, it is an important diagnosis as cholecystectomyin these cases has a higher rate of operative and post-operative complications.7
ch03.qxd 6/30/04 5:40 PM Page 49
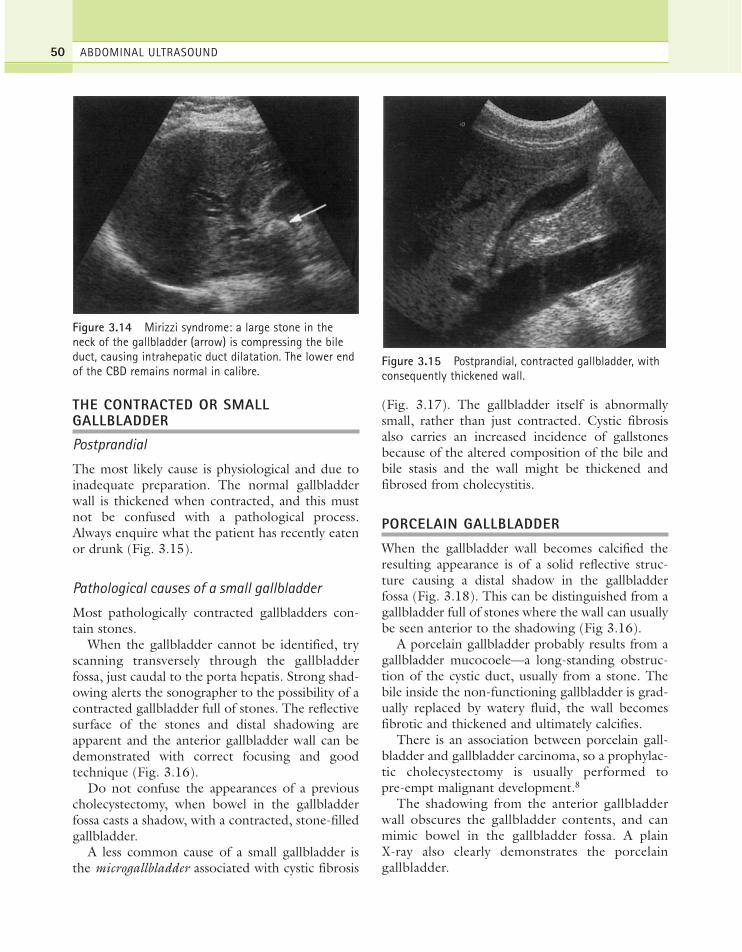
THE CONTRACTED OR SMALLGALLBLADDER
Postprandial
The most likely cause is physiological and due toinadequate preparation. The normal gallbladderwall is thickened when contracted, and this mustnot be confused with a pathological process.Always enquire what the patient has recently eatenor drunk (Fig. 3.15).
Pathological causes of a small gallbladder
Most pathologically contracted gallbladders con-tain stones.
When the gallbladder cannot be identified, tryscanning transversely through the gallbladderfossa, just caudal to the porta hepatis. Strong shad-owing alerts the sonographer to the possibility of acontracted gallbladder full of stones. The reflectivesurface of the stones and distal shadowing areapparent and the anterior gallbladder wall can bedemonstrated with correct focusing and goodtechnique (Fig. 3.16).
Do not confuse the appearances of a previouscholecystectomy, when bowel in the gallbladderfossa casts a shadow, with a contracted, stone-filledgallbladder.
A less common cause of a small gallbladder isthe microgallbladder associated with cystic fibrosis
(Fig. 3.17). The gallbladder itself is abnormallysmall, rather than just contracted. Cystic fibrosisalso carries an increased incidence of gallstonesbecause of the altered composition of the bile andbile stasis and the wall might be thickened andfibrosed from cholecystitis.
PORCELAIN GALLBLADDER
When the gallbladder wall becomes calcified theresulting appearance is of a solid reflective struc-ture causing a distal shadow in the gallbladderfossa (Fig. 3.18). This can be distinguished from agallbladder full of stones where the wall can usuallybe seen anterior to the shadowing (Fig 3.16).
A porcelain gallbladder probably results from agallbladder mucocoele—a long-standing obstruc-tion of the cystic duct, usually from a stone. Thebile inside the non-functioning gallbladder is grad-ually replaced by watery fluid, the wall becomesfibrotic and thickened and ultimately calcifies.
There is an association between porcelain gall-bladder and gallbladder carcinoma, so a prophylac-tic cholecystectomy is usually performed topre-empt malignant development.8
The shadowing from the anterior gallbladderwall obscures the gallbladder contents, and canmimic bowel in the gallbladder fossa. A plain X-ray also clearly demonstrates the porcelaingallbladder.
ABDOMINAL ULTRASOUND50
Figure 3.14 Mirizzi syndrome: a large stone in theneck of the gallbladder (arrow) is compressing the bileduct, causing intrahepatic duct dilatation. The lower endof the CBD remains normal in calibre.
Figure 3.15 Postprandial, contracted gallbladder, withconsequently thickened wall.
ch03.qxd 6/30/04 5:40 PM Page 50
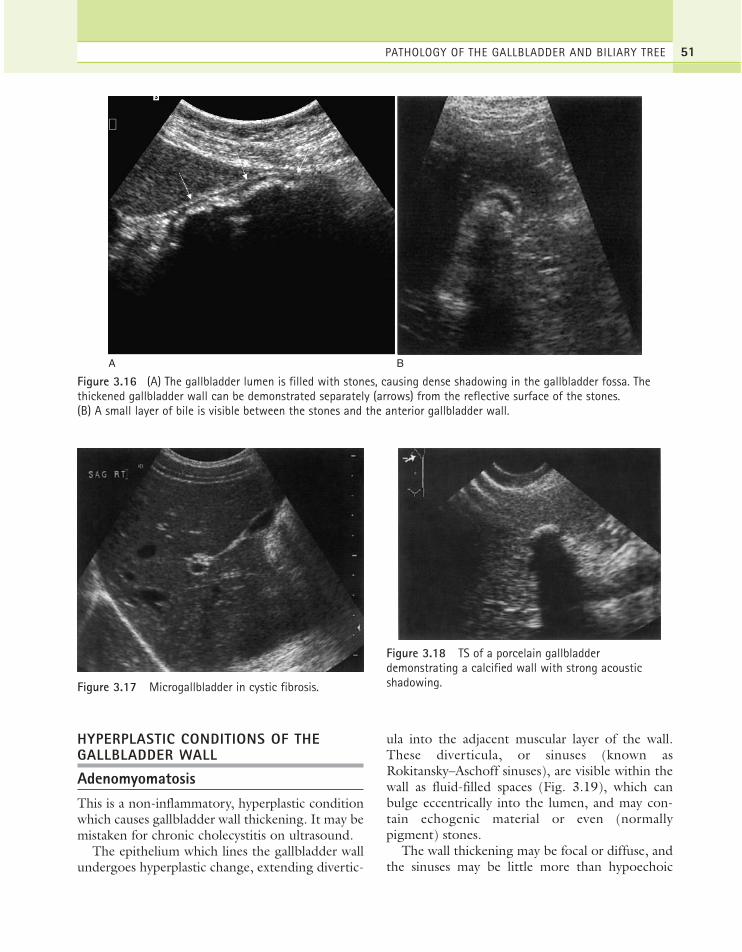
HYPERPLASTIC CONDITIONS OF THEGALLBLADDER WALL
AdenomyomatosisThis is a non-inflammatory, hyperplastic conditionwhich causes gallbladder wall thickening. It may bemistaken for chronic cholecystitis on ultrasound.
The epithelium which lines the gallbladder wallundergoes hyperplastic change, extending divertic-
ula into the adjacent muscular layer of the wall.These diverticula, or sinuses (known asRokitansky–Aschoff sinuses), are visible within thewall as fluid-filled spaces (Fig. 3.19), which canbulge eccentrically into the lumen, and may con-tain echogenic material or even (normallypigment) stones.
The wall thickening may be focal or diffuse, andthe sinuses may be little more than hypoechoic
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 51
A B
Figure 3.16 (A) The gallbladder lumen is filled with stones, causing dense shadowing in the gallbladder fossa. Thethickened gallbladder wall can be demonstrated separately (arrows) from the reflective surface of the stones.(B) A small layer of bile is visible between the stones and the anterior gallbladder wall.
Figure 3.17 Microgallbladder in cystic fibrosis.
Figure 3.18 TS of a porcelain gallbladderdemonstrating a calcified wall with strong acousticshadowing.
ch03.qxd 6/30/04 5:40 PM Page 51
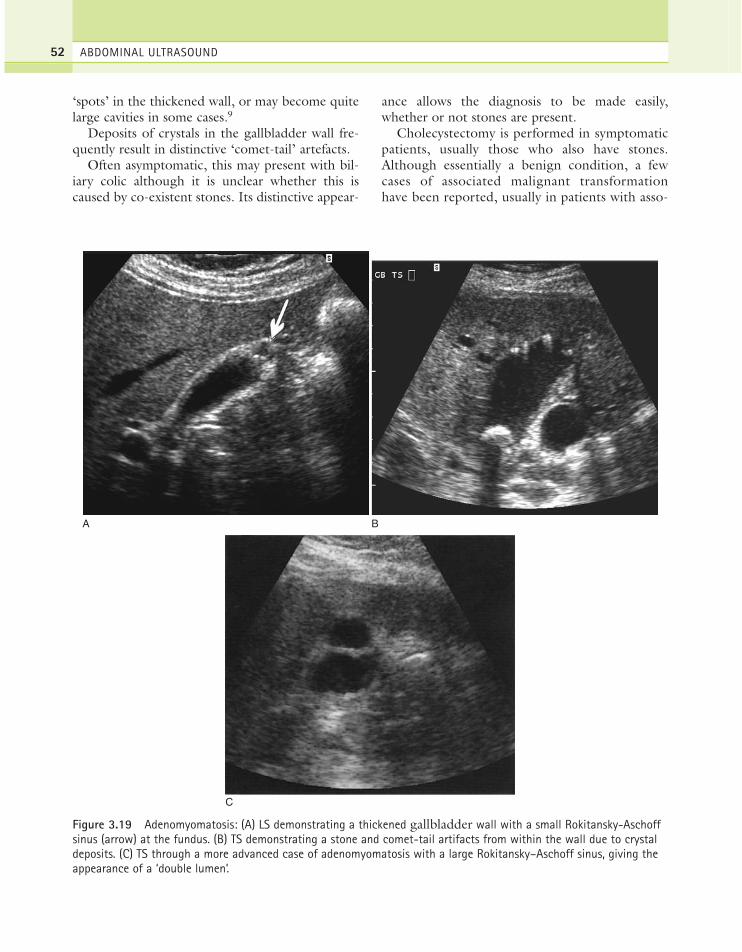
‘spots’ in the thickened wall, or may become quitelarge cavities in some cases.9
Deposits of crystals in the gallbladder wall fre-quently result in distinctive ‘comet-tail’ artefacts.
Often asymptomatic, this may present with bil-iary colic although it is unclear whether this iscaused by co-existent stones. Its distinctive appear-
ance allows the diagnosis to be made easily,whether or not stones are present.
Cholecystectomy is performed in symptomaticpatients, usually those who also have stones.Although essentially a benign condition, a fewcases of associated malignant transformationhave been reported, usually in patients with asso-
ABDOMINAL ULTRASOUND52
A B
C
Figure 3.19 Adenomyomatosis: (A) LS demonstrating a thickened gallbladder wall with a small Rokitansky-Aschoffsinus (arrow) at the fundus. (B) TS demonstrating a stone and comet-tail artifacts from within the wall due to crystaldeposits. (C) TS through a more advanced case of adenomyomatosis with a large Rokitansky–Aschoff sinus, giving theappearance of a ‘double lumen’.
ch03.qxd 6/30/04 5:40 PM Page 52

ciated anomalous insertion of the pancreaticduct.10
PolypsGallbladder polyps are usually asymptomaticlesions which are incidental findings in up to 5%of the population. Occasionally they are the causeof biliary colic. The most common type are cho-lesterol polyps. These are reflective structureswhich project into the gallbladder lumen but donot cast an acoustic shadow. Unless on a longstalk they will remain fixed on turning the patientand are therefore distinguishable from stones(Fig. 3.20).
There is an association between larger adenoma-tous gallbladder polyps and subsequent carcinoma,especially in patients over 50 years of age, so chole-cystectomy is often advised (Fig. 3.20C). Smallerpolyps of less than 1 cm in diameter may be safelymonitored with ultrasound.11 In particular, gall-bladder polyps in patients with primary sclerosingcholangitis have a much greater likelihood ofmalignancy (40–60%).12
CholesterolosisAlso known as the ‘strawberry gallbladder’, thisgets its name because of the multiple tiny noduleson the surface of the gallbladder mucosal lining.
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 53
A B
GB
C
Figure 3.20 (A) Small polyp in the gallbladder lumen—no posterior shadowing is evident. (B) A gallbladder polyp on astalk moves with different patient positions. (C) Large, fleshy gallbladder polyp.
ch03.qxd 6/30/04 5:40 PM Page 53

These nodules are the result of a build-up of lipidsin the gallbladder wall and are not usually visibleon ultrasound. However in some cases, multiplepolyps also form on the inner surface, projectinginto the lumen, and are clearly visible on ultra-sound (Fig. 3.21). Cholesterolosis may be asymp-tomatic, or may be accompanied by stones andconsequently requires surgery to alleviate symp-toms of biliary colic.
INFLAMMATORY GALLBLADDER DISEASE
Cholecystitis is usually associated with gallstones;the frictional action of stones on the gallbladderwall causes some degree of inflammation in almostall cases. The inner mucosa of the wall is injured,allowing the access of enteric bacteria. The inflam-matory process may be long-standing and chronic,acute or a combination of acute inflammation on achronic background.
Acute cholecystitisAcute inflammation of the gallbladder presentswith severe RUQ pain localized to the gallbladderarea. The pain can be elicited by (gently!) pressingthe gallbladder with the ultrasound transducer—apositive ultrasound Murphy’s sign. (This sign,although a useful pointer to acute inflammation, is
not specific and can frequently be elicited in otherconditions, such as chronic inflammatory cases.)
On ultrasound, the gallbladder wall is thickenedgreater than 2 mm. This is not in itself a specificsign (see Table 3.3), but characteristically thethickening in acute cholecystitis is symmetrical,affecting the entire wall, and there is an echo-poor‘halo’ around the gallbladder as a result of oede-matous changes (Fig. 3.22). This is not invariable,however, and focal thickening may be present, orthe wall may be uniformly hyperechoic in somecases. Pericholecystic fluid may also be present, andthe inflammatory process may spread to the adja-cent liver.
Colour or power Doppler can be helpful indiagnosing acute cholecystitis and in differentiat-ing it from other causes of gallbladder wall thick-ening. Hyperaemia in acute cholecystitis can bedemonstrated on colour Doppler around thethickened wall13 (Fig. 3.23). In a normal gallblad-der, colour Doppler flow may be seen around thegallbladder neck in the region of the cystic arterybut not elsewhere in the wall. The increased sensi-tivity of power Doppler, as opposed to colour
ABDOMINAL ULTRASOUND54
Figure 3.21 Cholesterolosis TS of the gallbladderdemonstrating multiple tiny polyps in the gallbladder.
Table 3.3 Causes of a thickened gallbladder wall
Physiological—Postprandial
Inflammatory—Acute or chronic cholecystitis—Sclerosing cholangitis—Crohn’s disease—AIDS
Adjacent inflammatory causes—Pancreatitis—Hepatitis—Pericholecystic abscesses
Non-inflammatory—Adenomyomatosis—Gallbladder carcinoma—Focal areas of thickening due to metastases or polyps—Leukaemia
Oedema—Ascites from a variety of causes, including organ
failure, lymphatic obstruction and portal hypertensionVarices
—Varices of the gallbladder wall in portal hypertension
ch03.qxd 6/30/04 5:40 PM Page 54

Doppler, does enable the operator to demonstratevascularity in the normal gallbladder wall and theoperator should be familiar with normal appear-ances for the machine in use when making thediagnosis of acute cholecystitis14 (Fig. 3.24).
Doppler can potentially distinguish acute inflam-mation from chronic disease.15 However, false-positive results can be found in cases of pancreatitisand gallbladder carcinoma and the technique doesnot add significantly to the grey-scale image.
Complications may occur if the acute inflamma-tion progresses (see below) due to infection,pericholecystic abscesses and peritonitis.
Further management of acute cholecystitis
In an uncomplicated acute cholecystitis, analgesiato settle the patient in the short term is followedby the removal of the gallbladder. Open surgery,which is increasingly reserved for the more
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 55
A B
C D
Figure 3.22 Acute cholecystitis: (A) TS of an oedematous, thickened gallbladder wall with a stone. (B) LS with athickened wall (arrows). Stones and debris are present. (C) and (D) TS and LS demonstrating pericholecystic fluid.
(Continued)
ch03.qxd 6/30/04 5:40 PM Page 55

complex cases, is giving way to the more frequentuse of laparoscopic cholecystectomy.
If unsuitable for immediate surgery, for examplein cases complicated by peritonitis, the patient ismanaged with antibiotics and/or percutaneousdrainage of pericholecystic fluid or infected bilefrom the gallbladder, usually under ultrasoundguidance. This allows the patient’s symptoms tosettle and reduces morbidity from the subsequentelective operation.16
Hepatobiliary scintigraphy has high sensitivityand specificity for evaluating patients with acutecholecystitis,17 particularly if the ultrasound exam-ination is technically difficult or equivocal and hasthe advantage of being able to demonstrate hepa-tobiliary drainage into the duodenum.
Plain X-ray is seldom used, but can confirm thepresence of gas in the gallbladder.
Chronic cholecystitisUsually associated with gallstones, chronic chole-cystitis presents with lower-grade, recurring rightupper quadrant pain. The action of stones on thewall causes it to become fibrosed and irregularlythickened, frequently appearing hyperechoic (Fig.3.25). The gallbladder is often shrunken and con-tracted, having little or no recognizable lumenaround the stones. Chronic cholecystitis may becomplicated by episodes of acute inflammation ona background of the chronic condition.
Most gallbladders which contain stones show atleast some histological degree of chronic cholecys-titis, even if wall thickening is not apparent onultrasound.
Acalculous cholecystitisInflammation of the gallbladder without stones isrelatively uncommon. A thickened, tender gall-bladder wall in the absence of any other obviouscause of thickening may be due to acalculouscholecystitis. This condition tends to be associatedwith patients who are already hospitalized and havebeen fasting, including post-trauma patients, thoserecovering from surgical procedures and diabeticpatients. It is brought about by bile stasis leadingto a distended gallbladder and subsequentlydecreased blood flow to the gallbladder. This,especially in the weakened postoperative state, canlead to infection. Because no stones are present,the diagnosis is more difficult and may be delayed.Patients with acalculous cholecystitis are thereforemore likely to have severe pain and fever by thetime the diagnosis is made, increasing the inci-dence of complications such as perforation.
The wall may appear normal on ultrasound inthe early stages, but progressively thickens (Fig.3.26). Biliary sludge is usually present and a
ABDOMINAL ULTRASOUND56
E
Figure 3.22 cont’d (E) Normal gallbladder in thepresence of ascites. Oedema may cause the wall tothicken, mimicking an inflammatory process.
Figure 3.23 Colour Doppler demonstrates hyperaemiain the thickened gallbladder wall in acute cholecystitis.
ch03.qxd 6/30/04 5:40 PM Page 56

pericholecystic abscess may develop in the laterstages. A positive Murphy’s sign may help to focuson the diagnosis, but in unconscious patients thediagnosis is a particularly difficult one.
Because patients may already be critically ill withtheir presenting disease, or following surgery, thereis a role for ultrasound in guiding percutaneouscholecystostomy at the bed-side to relieve thesymptoms.18
Chronic acalculous cholecystitis implies a recur-rent presentation with typical symptoms of biliarycolic, but no evidence of stones on ultrasound.Patients may also demonstrate a low ejection frac-tion during a cholecystokinin-stimulated hepaticiminodiacetic acid (HIDA) scan. The symptomsare relieved by elective laparoscopic cholecystec-tomy in most patients, with similar results to thosefor gallstone disease19 (although some are found tohave biliary pathology at surgery, which mightexplain the symptoms, such as polyps, choles-terolosis or biliary crystals/tiny stones in additionto chronic inflamation).
Complications of cholecystitisAcute-on-chronic cholecystitis
Patients with a long-standing history of chroniccholecystitis may suffer (sometimes repeated) attacks
of acute inflammation. The gallbladder wall is thick-ened, as for chronic inflammation, and may becomefocally thickened with both hypo- and hyperechoicregions. Stones are usually present (Fig. 3.27).
Gangrenous cholecystitis
In a small percentage of patients, acute gallbladderinflammation progresses to gangrenous cholecysti-tis. Areas of necrosis develop within the gallbladderwall, the wall itself may bleed and small abscessesform (Fig. 3.28). This severe complication of theinflammatory process requires immediate cholecys-tectomy.
The gallbladder wall is friable and may rupture,causing a pericholecystic collection and possiblyperitonitis. Inflammatory spread may be seen inthe adjacent liver tissue as a hypoechoic, ill-definedarea. Loops of adjacent bowel may become adher-ent to the necrotic wall, forming a cholecystoen-teric fistula.
The wall is asymmetrically thickened and areasof abscess formation may be demonstrated. Thedamaged inner mucosa sloughs off, forming theappearance of membranes in the gallbladder lumen.The gallbladder frequently contains infected debris
The presence of a bile leak may also be demon-strated with hepatobiliary scintigraphy, using tech-netium99, which is useful in identifying a bile
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 57
A B
Figure 3.24 Normal gallbladder wall vascularity. (A) In a normal gallbladder, colour Doppler can demonstrate thecystic artery (arrowhead) but does not demonstrate flow near the fundus. (B) Power Doppler is more sensitive and candemonstrate flow throughout the wall (arrows) in a normal gallbladder; this must not be mistaken for hyperaemia.
ch03.qxd 6/30/04 5:40 PM Page 57

collection which may otherwise be obscured bybowel on ultrasound.
Emphysematous cholecystitis
This is a form of acute gangrenous cholecystitis inwhich the inflamed gallbladder may becomeinfected, particularly in diabetic patients, with gas-forming organisms. Both the lumen and the wall ofthe gallbladder may contain air, which is highlyreflective, but which casts a ‘noisy’, less definiteshadow than that from stones. Discrete gas bub-
bles have been reported on ultrasound within thegallbladder wall20 and may also extend into theintrahepatic biliary ducts.21
The air rises to the anterior part of the gallbladder,obscuring the features behind it (Fig. 3.29). Thiseffect may mimic air-filled bowel on ultrasound.
Emphysematous cholecystitis has traditionallyhad a much higher mortality rate than other formsof cholecystitis, requiring immediate cholecystec-tomy. However, improvements in ultrasound reso-lution, and in the early clinical recognition of thiscondition, suggest that it is now being diagnosedearlier and may be managed more conservatively.The gas in the gallbladder may be confirmed on aplain X-ray (Fig. 3.30), but ultrasound is more sen-sitive in demonstrating the earlier stages.
Gallbladder empyema
Empyema is a complication of cholecystitis in whichthe gallbladder becomes infected behind anobstructed cystic duct. Fine echoes caused by pusare present in the bile (Fig. 3.31). These patients areoften very ill with a fever and acute pain. A peri-cholecystic gallbladder collection may result fromleakage through the gallbladder wall with subse-quent peritonitis. Ultrasound may be used to guidea bedside drainage in order to allow the patient’ssymptoms to settle before surgery is attempted.22
OBSTRUCTIVE JAUNDICE AND BILIARYDUCT DILATATION
Dilatation of all or part of the biliary tree is usuallythe result of proximal obstruction. Less commonlythe biliary tree may be dilated but not obstructed(Table 3.4). The most common causes of obstruc-tion are stones in the common duct or a neoplasmof the bile duct or head of pancreas.
The patient with obstructive jaundice may pres-ent with upper abdominal pain, abnormal liverfunction tests (LFTs) (see Chapter 2) and, if theobstruction is not intermittent, the sclera of theeye and the skin adopt a yellow tinge.
Assessment of the level of obstructionIt is possible for the sonographer to work outwhere the obstructing lesion is situated by observ-
ABDOMINAL ULTRASOUND58
A
B
Figure 3.25 Chronic cholecystitis. (A) A hyperechoic,irregular, thickened wall. The gallbladder contains a smallstone and thickened, echogenic bile. It was mildly tenderon scanning. (B) The wall is focally thickened anteriorly,and the gallbladder contains a large stone and a polyp inthe fundus.
ch03.qxd 6/30/04 5:40 PM Page 58

ing which parts of the biliary tree are dilated (Fig.3.32):
● Dilatation of the common bile duct (that is,that portion of the duct below the cystic ductinsertion) implies obstruction at its lower end.
● Dilatation of both biliary and pancreatic ductsimplies obstruction distally, at the head of thepancreas or ampulla of Vater. This is morelikely to be due to carcinoma of the head ofpancreas, ampulla or acute pancreatitis than astone. However, it is possible for a stone to be
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 59
A B
Figure 3.26 (A) Acalculous cholecystitis. The gallbladder wall is markedly thickened and tender on scanning.(B) Gravity-dependent sludge with a thick, oedematous wall. No stones were present.
Figure 3.27 Acute on chronic cholecystitis. A patientwith known gallstones and chronic cholecystitis presentswith an episode of acute gallbladder pain. The wall isconsiderably more thickened and hyperechoic than onprevious scans.
Figure 3.28 Gangrenous cholecystitis. The gallbladderwall is focally thickened and an intramural abscess hasformed on the anterior aspect.
ch03.qxd 6/30/04 5:40 PM Page 59

lodged just distal to the confluence of thebiliary and pancreatic ducts.
● Dilatation of the gallbladder alone (that iswithout ductal dilatation) is usually caused by,obstruction at the neck or cystic duct (Fig. 3.8).
To assess whether the gallbladder is pathologi-cally dilated may be difficult on ultrasound. Thesonographer should look at both the size and
shape; the dilated gallbladder will have a rounded,bulging shape due to the increase in pressure insideit. A gallbladder whose wall has become fibrosedfrom chronic cholecystitis due to stones will oftenlose the ability to distend, so the biliary ducts canlook grossly dilated despite the gallbladder remain-ing ‘normal’ in size, or contracted.
Early ductal obstruction
Beware very early common duct obstruction, beforethe duct becomes obviously dilated. The duct maybe mildly dilated at the lower end, just proximal to astone. Likewise intermittent obstruction by a smallstone at the lower end of the duct may be non-dilated by the time the scan is performed (Fig. 3.10).
A significant ultrasound feature in the absenceof any other identifiable findings is that of thicken-ing of the wall of the bile duct. This represents aninflammatory process in the duct wall, which maybe found in patients with small stones in a non-dilated duct, but is also associated with sclerosingcholangitis.23
It is sometimes technically difficult in somepatients (particularly those with diffuse liver dis-ease) to work out whether a tubular structure on
ABDOMINAL ULTRASOUND60
A
B
C
Figure 3.29 Emphysematous cholecystitis. (A) and (B)TS and LS with gas and debris in the gallbladder lumen.(C) Gas in the gallbladder lumen completely obscures thecontents.
Figure 3.30 X-ray demonstrating gas in the gallbladderin emphysematous cholecystitis.
ch03.qxd 6/30/04 5:40 PM Page 60
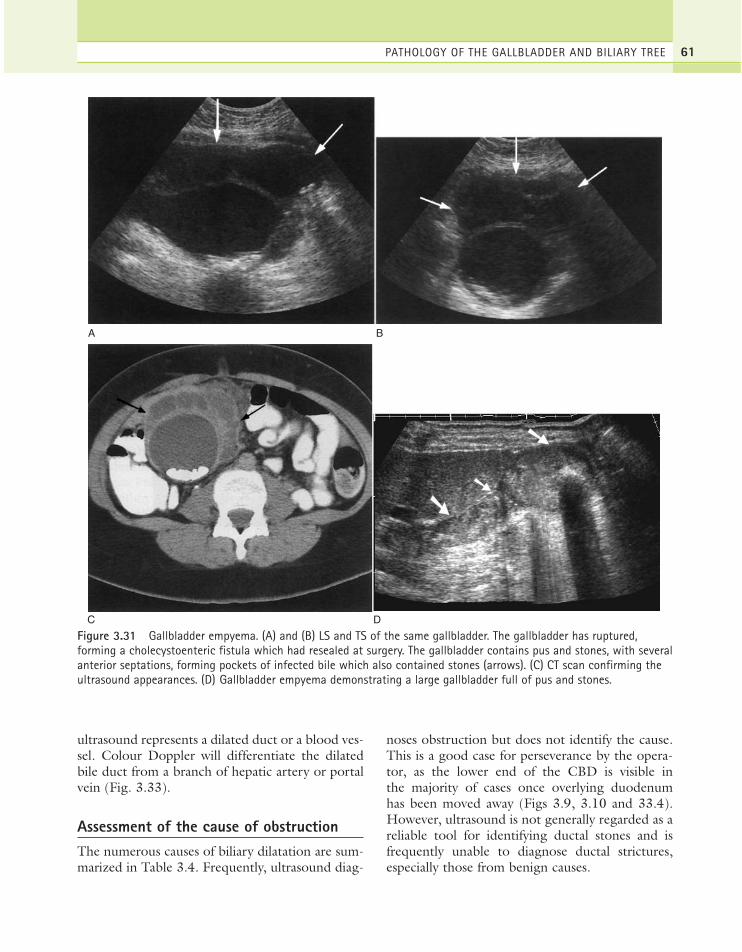
ultrasound represents a dilated duct or a blood ves-sel. Colour Doppler will differentiate the dilatedbile duct from a branch of hepatic artery or portalvein (Fig. 3.33).
Assessment of the cause of obstructionThe numerous causes of biliary dilatation are sum-marized in Table 3.4. Frequently, ultrasound diag-
noses obstruction but does not identify the cause.This is a good case for perseverance by the opera-tor, as the lower end of the CBD is visible inthe majority of cases once overlying duodenumhas been moved away (Figs 3.9, 3.10 and 33.4).However, ultrasound is not generally regarded as areliable tool for identifying ductal stones and isfrequently unable to diagnose ductal strictures,especially those from benign causes.
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 61
C D
A B
Figure 3.31 Gallbladder empyema. (A) and (B) LS and TS of the same gallbladder. The gallbladder has ruptured,forming a cholecystoenteric fistula which had resealed at surgery. The gallbladder contains pus and stones, with severalanterior septations, forming pockets of infected bile which also contained stones (arrows). (C) CT scan confirming theultrasound appearances. (D) Gallbladder empyema demonstrating a large gallbladder full of pus and stones.
ch03.qxd 6/30/04 5:40 PM Page 61

ABDOMINAL ULTRASOUND62
Figure 3.32 Sites of possible gallstone obstruction.
A B
PV
HA
LOBESAG RT
Figure 3.33 (A) Dilated biliary ducts do not demonstrate flow on colour Doppler, differentiating them from portalvessels. (B) Originally suspected as a dilated biliary tree, colour Doppler demonstrates that the ‘extra tubes’ are, in fact,dilated intrahepatic arteries in a patient with end-stage chronic liver disease with reversed portal venous flow.
ERCP, although invasive, is a more accuratemethod of examining the CBD and will often iden-tify strictures or small calculi not visible on ultra-sound. It has the advantage of a therapeutic role in
addition to its diagnostic capabilities, by allowingthe extraction of stones at the time of diagnosis. Itis associated with a small risk of complication, how-ever, and its use is therefore increasingly limited infavour of the non-invasive magnetic resonancecholangiopancreatography (MRCP) (Fig. 3.34F).MRCP has been found to be highly effective inthe diagnosis of CBD stones24 and can potentiallyavoid the use of purely diagnostic ERCP.25
Table 3.4 Causes of biliary duct dilatation
Intrinsic—Stones—Carcinoma of the ampulla of Vater—Cholangiocarcinoma—Stricture (associated with chronic pancreatitis)—Biliary atresia/choledochal cyst—Post-liver-transplantation bile duct stenosis (usually
anastomotic)—Parasites—Age-related or post-surgical mild CBD dilatation
Extrinsic—Carcinoma of the head of pancreas—Acute pancreatitis—Lymphadenopathy at the porta hepatis—Other masses at the porta, e.g. hepatic artery
aneurysm, gastrointestinal tract mass—Intra-hepatic tumours (obstruct distal segments)
Diffuse hepatic conditions—Sclerosing cholangitis—Caroli’s disease
ch03.qxd 6/30/04 5:41 PM Page 62
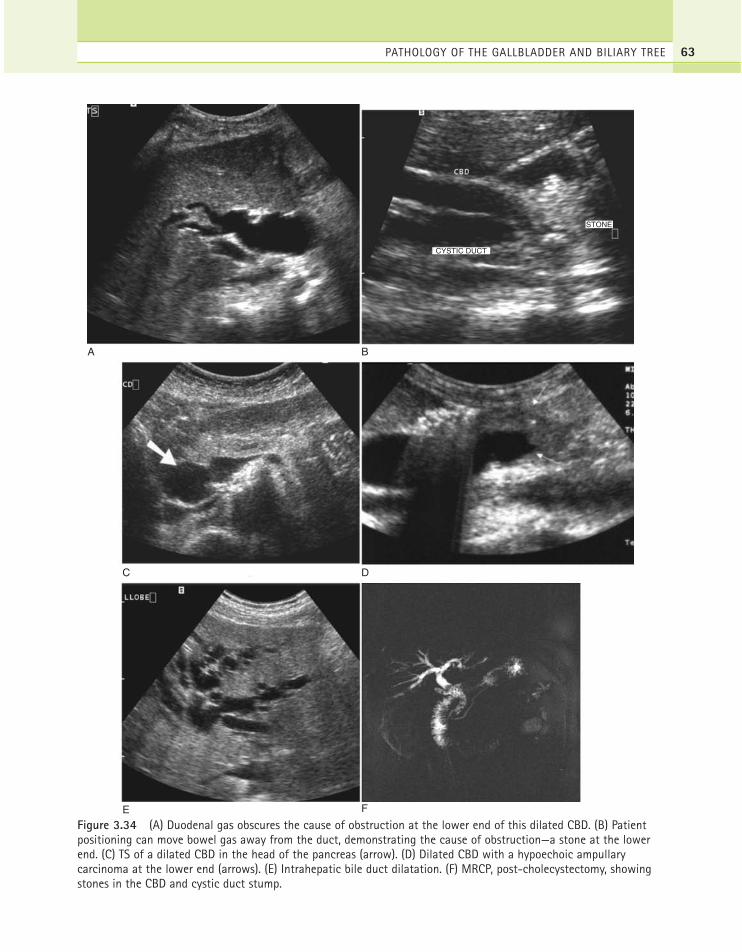
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 63
A B
D
CYSTIC DUCT
STONE
C
FE
Figure 3.34 (A) Duodenal gas obscures the cause of obstruction at the lower end of this dilated CBD. (B) Patientpositioning can move bowel gas away from the duct, demonstrating the cause of obstruction—a stone at the lowerend. (C) TS of a dilated CBD in the head of the pancreas (arrow). (D) Dilated CBD with a hypoechoic ampullarycarcinoma at the lower end (arrows). (E) Intrahepatic bile duct dilatation. (F) MRCP, post-cholecystectomy, showingstones in the CBD and cystic duct stump.
ch03.qxd 6/30/04 5:41 PM Page 63

ABDOMINAL ULTRASOUND64
CT and MRI are useful for staging purposes if theobstructing lesion is malignant. Cholangiocarci-nomas spread to the lymph nodes and to the liverand small liver deposits are particularly difficult torecognize on ultrasound if the intrahepatic biliaryducts are dilated.
In hepatobiliary scintigraphy, technetium99m-labelled derivatives of iminodiacetic acid areexcreted in the bile and may help to demonstratesites of obstruction, for example in the cystic duct,or abnormal accumulations of bile, for examplecholedochal cysts.
Courvoisier’s law, to which there are numerousexceptions, states that if the gallbladder is dilatedin a jaundiced patient, then the cause is not due toa stone in the common duct. The reason for this isthat, if stones are or had been present, then thegallbladder would have a degree of wall fibrosisfrom chronic cholecystitis which would prevent itfrom distending. In fact there are many exceptionsto this ‘law’ which include the formation of stonesin the duct, without gallbladder stones, and alsoobstruction by a pancreatic stone at the ampulla.Thus:
● Do not assume that obstructive jaundice in apatient with gallstones is due to a stone in theCBD. The jaundice may be attributable toother causes.
● Do not assume that obstructive jaundicecannot be due to a stone in the CBD if thegallbladder does not contain stones. A solitarystone can be passed into the duct from thegallbladder or stones can form within the duct.
Management of biliary obstructionManagement of biliary obstruction obviouslydepends on the cause and the severity of the con-dition. Removal of stones in the CBD may be per-formed by ERCP with sphincterotomy. Electivecholecystectomy may take place if gallstones arepresent in the gallbladder.
Laparoscopic ultrasound is a useful adjunct tosurgical exploration of the biliary tree and its accu-racy in experienced hands equals that of X-raycholangiography. It is rapidly becoming the imag-ing modality of choice to examine the ducts duringlaparoscopic cholecystectomy.26
Endoscopic ultrasound can also be used toexamine the CBD, avoiding the need for laparo-scopic exploration of the duct when performed inthe immediate preoperative stage.27
The treatment of malignant obstruction isdetermined by the stage of the disease. Accuratestaging is best performed using CT and/or MRI.If surgical removal of the obstructing lesion is nota suitable option because of local or distant spread,palliative stenting may be performed endoscopi-cally to relieve the obstruction and decompress theducts (Fig. 3.35). The patency of the stent may bemonitored with ultrasound scanning by assessingthe degree of dilatation of the ducts.
Clinical suspicion of early obstruction should beraised if the serum alkaline phosphatase is elevated,(often more sensitive in the early stages than araised serum bilirubin). In the presence of ductaldilatation on ultrasound, further imaging, such asCT or MRCP, may then refine the diagnosis.
Intrahepatic tumours causing biliaryobstructionFocal masses which cause segmental intrahepaticduct dilatation are usually intrinsic to the ductitself, for example cholangiocarcinoma.
It is also possible for a focal intrahepatic mass,whether benign or malignant, to compress anadjacent biliary duct, causing subsequent obstruc-tion of that segment. This is not, however, a com-mon cause of biliary dilatation and occurs mostusually with hepatocellular carcinomas.28 Mostliver metastases deform rather than compress adja-cent structures and biliary obstruction only occursif the metastases are very large and/or invade thebiliary tree. A hepatocellular carcinoma or metasta-tic deposit at the porta hepatis may obstruct thecommon duct by squeezing it against adjacentextrahepatic structures. Benign intrahepatic lesionsrarely cause ductal dilatation, but occasionally theirsheer size obstructs the biliary tree.
Choledochal cystsMost commonly found in children, this is associ-ated with biliary atresia, in which the distal ‘blind’end of the duct dilates into a rounded, cystic massin response to raised intrahepatic pressure.
ch03.qxd 6/30/04 5:41 PM Page 64

Choledochal cysts in adults are rare, and tend tobe asymptomatic unless associated with stones orother biliary disease. They are sometimes associatedwith an anomalous insertion of the CBD into thepancreatic duct. The mechanism of the subsequentcholedochal cyst formation is unclear, but it isthought that the common channel, which drainsinto the duodenum, is prone to reflux of pancreaticenzymes into the biliary duct. This can cause a bil-
iary stricture, with subsequent proximal dilatation ofthe duct, forming a choledochal cyst29 [Fig. 3.36].
Less commonly the dilatation is due to a non-obstructive cause in which the biliary ducts them-selves become ectatic and can form diverticula.This may be due to a focal stricture of the ductwhich causes reflux and a localized enlargement ofthe duct proximal to the stricture. (See alsoCaroli’s disease, below (Fig. 3.42.)
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 65
A B
Figure 3.35 (A) This dilated CBD is obstructed by a mass (arrows) invading the lower end. (B) ERCP demonstrates a tight, malignant stricture, and can be used to position a palliative stent. (C) Stent in the CBD of a patient with acholangiocarcinoma and malignant ascites. Decompression of the dilated biliary tree has been achieved, and ultrasoundcan be used to monitor the patency of the stent.
C
ch03.qxd 6/30/04 5:41 PM Page 65
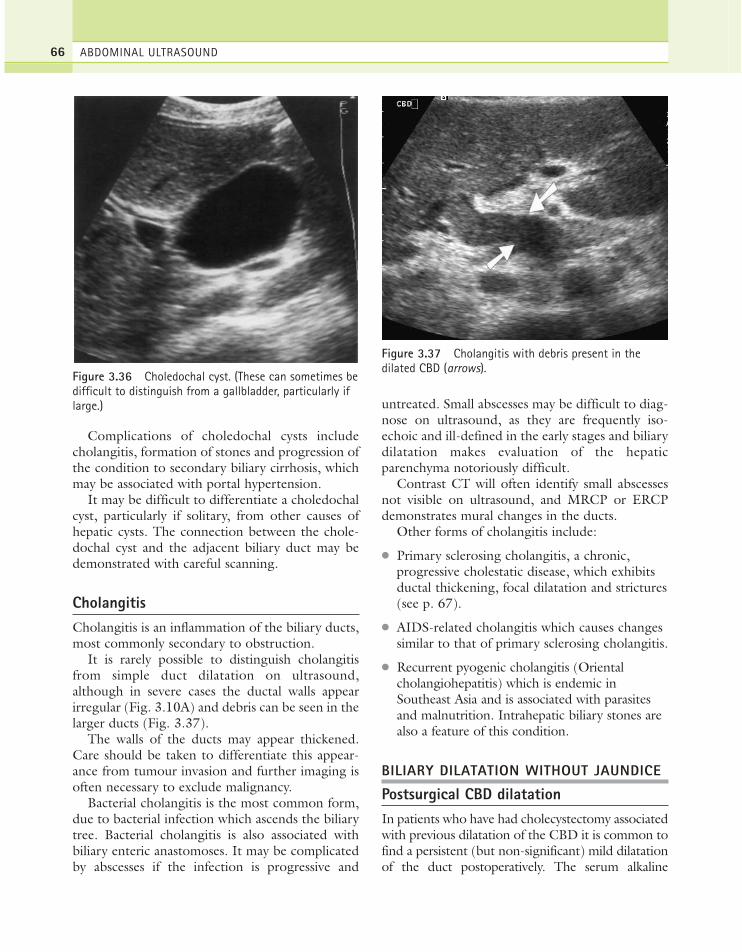
Complications of choledochal cysts includecholangitis, formation of stones and progression ofthe condition to secondary biliary cirrhosis, whichmay be associated with portal hypertension.
It may be difficult to differentiate a choledochalcyst, particularly if solitary, from other causes ofhepatic cysts. The connection between the chole-dochal cyst and the adjacent biliary duct may bedemonstrated with careful scanning.
CholangitisCholangitis is an inflammation of the biliary ducts,most commonly secondary to obstruction.
It is rarely possible to distinguish cholangitisfrom simple duct dilatation on ultrasound,although in severe cases the ductal walls appearirregular (Fig. 3.10A) and debris can be seen in thelarger ducts (Fig. 3.37).
The walls of the ducts may appear thickened.Care should be taken to differentiate this appear-ance from tumour invasion and further imaging isoften necessary to exclude malignancy.
Bacterial cholangitis is the most common form,due to bacterial infection which ascends the biliarytree. Bacterial cholangitis is also associated withbiliary enteric anastomoses. It may be complicatedby abscesses if the infection is progressive and
untreated. Small abscesses may be difficult to diag-nose on ultrasound, as they are frequently iso-echoic and ill-defined in the early stages and biliarydilatation makes evaluation of the hepaticparenchyma notoriously difficult.
Contrast CT will often identify small abscessesnot visible on ultrasound, and MRCP or ERCPdemonstrates mural changes in the ducts.
Other forms of cholangitis include:
● Primary sclerosing cholangitis, a chronic,progressive cholestatic disease, which exhibitsductal thickening, focal dilatation and strictures(see p. 67).
● AIDS-related cholangitis which causes changessimilar to that of primary sclerosing cholangitis.
● Recurrent pyogenic cholangitis (Orientalcholangiohepatitis) which is endemic inSoutheast Asia and is associated with parasitesand malnutrition. Intrahepatic biliary stones arealso a feature of this condition.
BILIARY DILATATION WITHOUT JAUNDICE
Postsurgical CBD dilatationIn patients who have had cholecystectomy associatedwith previous dilatation of the CBD it is common tofind a persistent (but non-significant) mild dilatationof the duct postoperatively. The serum alkaline
ABDOMINAL ULTRASOUND66
Figure 3.36 Choledochal cyst. (These can sometimes bedifficult to distinguish from a gallbladder, particularly iflarge.)
Figure 3.37 Cholangitis with debris present in thedilated CBD (arrows).
ch03.qxd 6/30/04 5:41 PM Page 66

phosphatase and bilirubin levels should be normal inthe absence of pathology. Because stones may befound in the duct postoperatively, it is important todifferentiate non-obstructive from truly obstructivedilatation in a symptomatic patient (Fig. 3.38). If indoubt, the patient may be rescanned at a suitableinterval to assess any increase in ductal diameter.
Focal obstructionIntrahepatic tumour, such as cholangiocarcinoma,may obstruct a segment of the biliary tree whilstthe remainder of the liver and biliary tree appearsnormal. Focal duct dilatation should trigger theoperator to examine the proximal area of dilatationfor a possible mass. Such tumours may be presentbefore jaundice is clinically apparent.
PitfallsPatients with cirrhosis and portal hypertension mayhave dilated hepatic arteries which can mimic theappearances of dilated ducts. Colour or powerDoppler will readily differentiate between these, asthe bile duct lacks a Doppler signal. Pneumobilia(air in the ducts) casts a distal acoustic shadow, andmay therefore obscure ductal dilatation.
OBSTRUCTION WITHOUT BILIARYDILATATION
Early obstructionIt is possible to scan a patient at the time of recentonset of obstruction from a stone before the ductshave had time to dilate, leading to a false-negativediagnosis. If clinical suspicion persists, a rescan isfrequently useful in these cases.
Occasionally, stones have a ball-valve effect inthe duct, causing intermittent obstruction whichmay not demonstrate ductal dilatation on theultrasound scan.
Fibrosis of the duct wallsThere are a number of chronic pathological condi-tions which cause the walls of the ducts to becomefibrotic and stiff. These include primary sclerosingcholangitis (see below), hepatitis and other chronichepatic diseases leading to cirrhosis. The liver itselfbecomes rigid and this prevents biliary dilatation.In such cases the lack of dilated bile ducts does notnecessarily imply an absence of obstruction.
OTHER BILIARY DISEASES
Primary sclerosing cholangitis (PSC)PSC is a chronic hepatobiliary disease in which thewalls of the bile ducts become inflamed, causingnarrowing. It occurs predominantly in young men(with a 2:1 male to female ratio) and is character-ized by multiple biliary strictures and bead-likedilatations of the ducts. The aetiology of PSCremains unclear but is associated with inflamma-tory bowel disorders or may be idiopathic.
Clinical features include jaundice, itching andfatigue. Some 25% of patients also have gallstones,which complicates the diagnosis. Approximately70% of patients affected also have ulcerative colitis.
It is progressive gradual fibrosis which eventu-ally obliterates the biliary tree. Untreated, thiseventually leads to hepatic failure. PSC has a strongassociation with cholangiocarcinoma, and it is this,rather than hepatic failure, which may lead todeath. In the absence of malignancy, however,hepatic transplant has a 70–90% 5-year survivalrate.30
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 67
Figure 3.38 Biliary dilatation following laparoscopiccholecystectomy, due to a surgical clip across the CBD.
ch03.qxd 6/30/04 5:41 PM Page 67

Ultrasound appearances
The ultrasound appearances in PSC may be normalor may demonstrate a coarse, hyperechoic texturethroughout the liver. Ductal strictures may causedownstream dilatation in some segments (Fig. 3.39)and in some cases there is marked biliary dilatation,but in the majority of patients the biliary ducts areprevented from dilatation by the surrounding fibro-sis and so appear unremarkable on ultrasound.MRCP is superior at demonstrating intrahepaticductal strictures. Mural thickening, particularly inthe CBD, may be demonstrated with careful, high-resolution scanning31 (Fig. 3.40).
Ultrasound also demonstrates the effects of por-tal hypertension in advanced disease. The gallblad-der may also have a thickened wall and can bedilated.32
Due to the association between PSC andcholangiocarcinoma, which may be multifocal, acareful search must be made for mass lesions.Because the ultrasound appearances may be thoseof a coarse, nodular liver texture, it is difficult toidentify small cholangiocarcinomas and colour orpower Doppler may be an advantage here (Fig.3.41). This diagnosis is an important one, becausethe patient’s prognosis and management areaffected by the presence of cholangiocarcinomata.If no masses are identified, the prognosis is goodand includes the endoscopic removal of stones torelieve symptoms, endoscopic stenting of mainduct strictures to relieve jaundice and subsequentliver transplant to pre-empt the formation of carci-noma. However, if carcinoma is already present, 5-year survival falls to 10%.
Caroli’s disease (congenital intrahepaticbiliary dilatation)This is a rare, congenital condition in which thebile ducts are irregularly dilated with diverticula-like projections. These diverticula may becomeinfected and may separate off from the biliary duct,forming choledochal cysts (Fig. 3.42).
In most cases, the entire hepatobiliary system isaffected to some degree. Sufferers may present inearly childhood, with symptoms of portal hyper-tension, 33 or may remain well until adulthood, pre-senting with cholangitis. It is generally thought to
be an autosomal recessive inherited condition andthe prognosis is poor. Medical control of associatedportal hypertension with varices can improve thequality of life.
In a few cases, the disease is confined to one ortwo segments of the liver, in which case a cure canbe effected with hepatic resection.34 The extrahep-atic biliary tree is often unaffected.
ABDOMINAL ULTRASOUND68
A
B
Figure 3.39 (A) Localized biliary dilatation due to aductal stricture in a patient with primary sclerosingcholangitis (PSC). (B) Coarse-textured liver with a dilatedCBD in PSC. A small choledochal cyst is present justanterior to the lower CBD.
ch03.qxd 6/30/04 5:41 PM Page 68
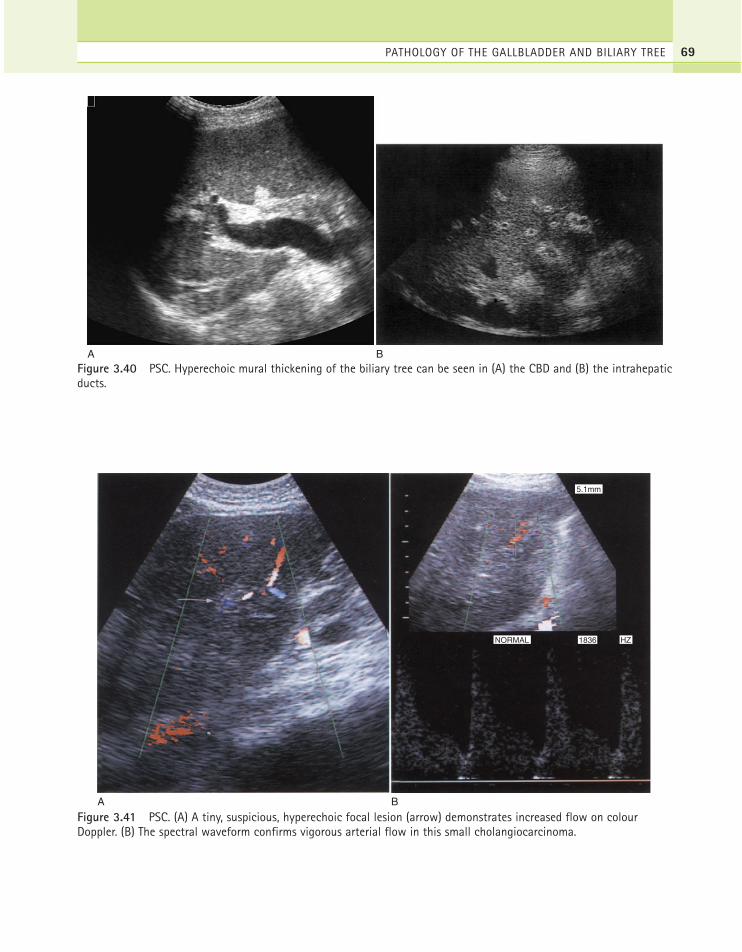
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 69
A BFigure 3.40 PSC. Hyperechoic mural thickening of the biliary tree can be seen in (A) the CBD and (B) the intrahepaticducts.
A B
NORMAL 1836 HZ
5.1mm
Figure 3.41 PSC. (A) A tiny, suspicious, hyperechoic focal lesion (arrow) demonstrates increased flow on colourDoppler. (B) The spectral waveform confirms vigorous arterial flow in this small cholangiocarcinoma.
ch03.qxd 6/30/04 5:41 PM Page 69

The ultrasound appearances are usually of wide-spread intrahepatic duct dilatation, with both sac-cular and fusiform biliary ectasia. Because it is alsoassociated with biliary stone formation, the diag-nosis is often not clear. The dilatation is also asso-ciated with cholangitis and signs of infection maybe present in the form of debris within the ducts.Sometimes, frank choledocal cysts can be located.
Advanced disease is associated with portal hyper-tension and, in some cases, cholangiocarcinoma.35
ParasitesParasitic organisms, such as the Ascaris worm andliver fluke, are extremely rare in the UK. However,they are a common cause of biliary colic in Africa,
ABDOMINAL ULTRASOUND70
A
kr
C
B D
Figure 3.42 Caroli’s disease. (A) Dilated biliary tree and ascites. (B) TS of a different patient with end-stage disease.The grossly abnormal liver texture contrasts with the right kidney. (C) A small section of focal CBD dilatation persistedin a symptomatic patient, with normal-calibre distal CBD. This was confirmed on ERCP and thought to be a dyskineticsegment, causing biliary reflux, but was later diagnosed as a mild form of Caroli’s. (D) 3D CT reconstruction of the casein (C), confirming the ultrasound appearances. Note the tiny ectatic ‘pouchings’ of the intrahepatic ducts characteristicof Caroli’s.
ch03.qxd 6/30/04 5:41 PM Page 70

the Far East and South America. The hyperechoiclinear structures in the gallbladder lumen shouldraise the sonographer’s suspicion in patients nativeto, or who have visited these countries. Impactedworms in the biliary ducts may mimic other ductalmasses.36
They are a rare cause of obstructive biliarydilatation (Fig. 3.43).
Patients may present with acute cholangitis orabdominal pain and vomiting. Endoscopic man-agement is frequently highly effective.37
ECHOGENIC BILE
Biliary stasisFine echoes in the bile within the gallbladder arenot uncommon on an ultrasound scan. This iscommonly due to the inspissation of bile followingprolonged starving, for example following surgery(Fig. 3.44). These appearances disappear after anormal diet is resumed and the gallbladder hasemptied and refilled.
It occurs when the solutes in the bile precipitate,often due to hypomotility of the gallbladder, andcan commonly be seen following bone marrowtransplantation and in patients who have under-gone prolonged periods (4–6 weeks) of total par-enteral nutrition.38
Prolonged biliary stasis may lead to inflamma-tion and/or infection, particularly in post-operative patients and those on immunosuppression(Fig. 3.44B). Its clinical course varies from com-
plete resolution to progression to gallstones.However, following the resumption of oral feed-ing, the gallbladder may contract and empty thesludge into the biliary tree causing biliary colic,acute pancreatitis and/or acute cholecystitis.39 Forthis reason, cholecystectomy may be considered insymptomatic patients with biliary sludge.
The fine echoes may form a gravity-dependentlayer and may clump together, forming ‘sludgeballs’. To avoid misdiagnosing sludge balls aspolyps, turn the patient to disperse the echoes or
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 71
Figure 3.43 Ascaris worm in the gallbladder.
A
B
Figure 3.44 (A) Inspissated bile in the normalgallbladder of a fasting patient. (B) Gravity-dependentbiliary sludge with a small stone.
ch03.qxd 6/30/04 5:41 PM Page 71
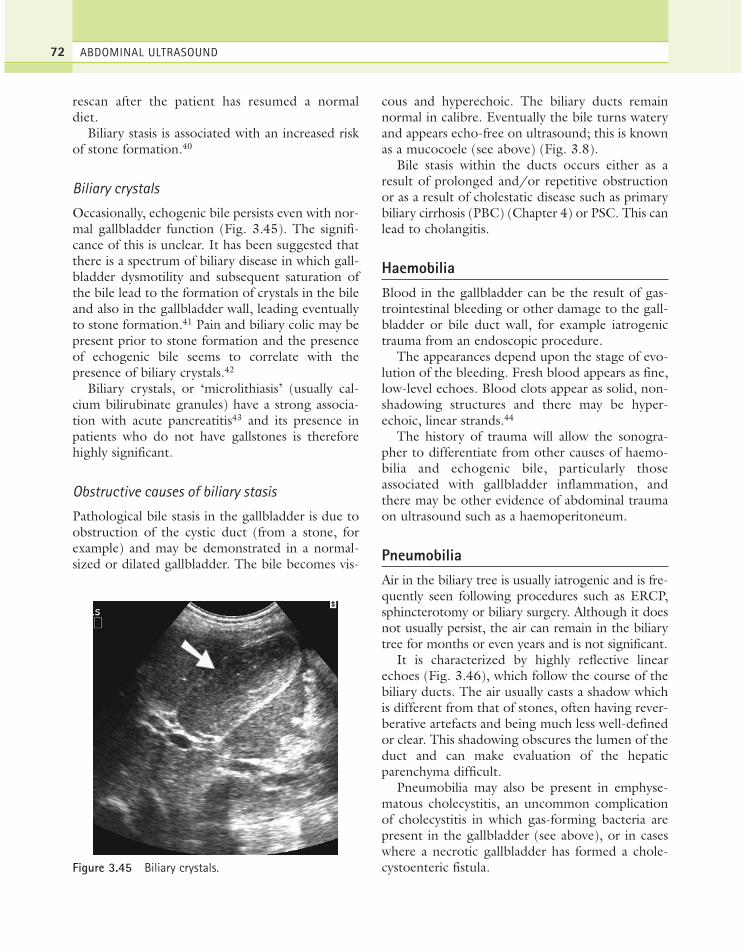
rescan after the patient has resumed a normaldiet.
Biliary stasis is associated with an increased riskof stone formation.40
Biliary crystals
Occasionally, echogenic bile persists even with nor-mal gallbladder function (Fig. 3.45). The signifi-cance of this is unclear. It has been suggested thatthere is a spectrum of biliary disease in which gall-bladder dysmotility and subsequent saturation ofthe bile lead to the formation of crystals in the bileand also in the gallbladder wall, leading eventuallyto stone formation.41 Pain and biliary colic may bepresent prior to stone formation and the presenceof echogenic bile seems to correlate with thepresence of biliary crystals.42
Biliary crystals, or ‘microlithiasis’ (usually cal-cium bilirubinate granules) have a strong associa-tion with acute pancreatitis43 and its presence inpatients who do not have gallstones is thereforehighly significant.
Obstructive causes of biliary stasis
Pathological bile stasis in the gallbladder is due toobstruction of the cystic duct (from a stone, forexample) and may be demonstrated in a normal-sized or dilated gallbladder. The bile becomes vis-
cous and hyperechoic. The biliary ducts remainnormal in calibre. Eventually the bile turns wateryand appears echo-free on ultrasound; this is knownas a mucocoele (see above) (Fig. 3.8).
Bile stasis within the ducts occurs either as aresult of prolonged and/or repetitive obstructionor as a result of cholestatic disease such as primarybiliary cirrhosis (PBC) (Chapter 4) or PSC. This canlead to cholangitis.
HaemobiliaBlood in the gallbladder can be the result of gas-trointestinal bleeding or other damage to the gall-bladder or bile duct wall, for example iatrogenictrauma from an endoscopic procedure.
The appearances depend upon the stage of evo-lution of the bleeding. Fresh blood appears as fine,low-level echoes. Blood clots appear as solid, non-shadowing structures and there may be hyper-echoic, linear strands.44
The history of trauma will allow the sonogra-pher to differentiate from other causes of haemo-bilia and echogenic bile, particularly thoseassociated with gallbladder inflammation, andthere may be other evidence of abdominal traumaon ultrasound such as a haemoperitoneum.
PneumobiliaAir in the biliary tree is usually iatrogenic and is fre-quently seen following procedures such as ERCP,sphincterotomy or biliary surgery. Although it doesnot usually persist, the air can remain in the biliarytree for months or even years and is not significant.
It is characterized by highly reflective linearechoes (Fig. 3.46), which follow the course of thebiliary ducts. The air usually casts a shadow whichis different from that of stones, often having rever-berative artefacts and being much less well-definedor clear. This shadowing obscures the lumen of theduct and can make evaluation of the hepaticparenchyma difficult.
Pneumobilia may also be present in emphyse-matous cholecystitis, an uncommon complicationof cholecystitis in which gas-forming bacteria arepresent in the gallbladder (see above), or in caseswhere a necrotic gallbladder has formed a chole-cystoenteric fistula.
ABDOMINAL ULTRASOUND72
Figure 3.45 Biliary crystals.
ch03.qxd 6/30/04 5:41 PM Page 72
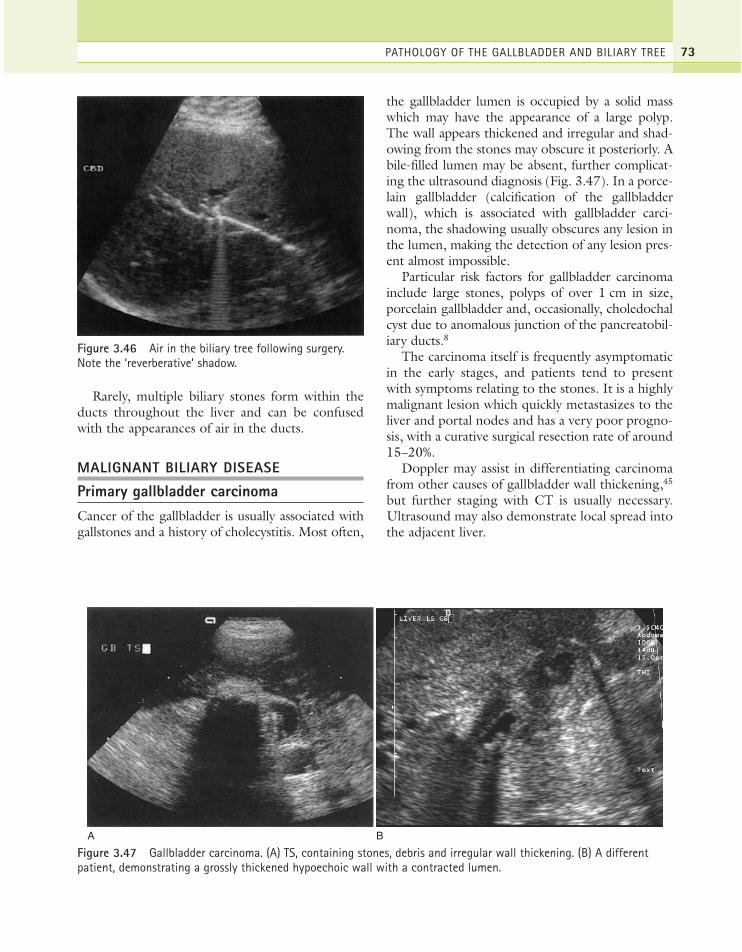
Rarely, multiple biliary stones form within theducts throughout the liver and can be confusedwith the appearances of air in the ducts.
MALIGNANT BILIARY DISEASE
Primary gallbladder carcinomaCancer of the gallbladder is usually associated withgallstones and a history of cholecystitis. Most often,
the gallbladder lumen is occupied by a solid masswhich may have the appearance of a large polyp.The wall appears thickened and irregular and shad-owing from the stones may obscure it posteriorly. Abile-filled lumen may be absent, further complicat-ing the ultrasound diagnosis (Fig. 3.47). In a porce-lain gallbladder (calcification of the gallbladderwall), which is associated with gallbladder carci-noma, the shadowing usually obscures any lesion inthe lumen, making the detection of any lesion pres-ent almost impossible.
Particular risk factors for gallbladder carcinomainclude large stones, polyps of over 1 cm in size,porcelain gallbladder and, occasionally, choledochalcyst due to anomalous junction of the pancreatobil-iary ducts.8
The carcinoma itself is frequently asymptomaticin the early stages, and patients tend to presentwith symptoms relating to the stones. It is a highlymalignant lesion which quickly metastasizes to theliver and portal nodes and has a very poor progno-sis, with a curative surgical resection rate of around15–20%.
Doppler may assist in differentiating carcinomafrom other causes of gallbladder wall thickening,45
but further staging with CT is usually necessary.Ultrasound may also demonstrate local spread intothe adjacent liver.
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 73
Figure 3.46 Air in the biliary tree following surgery.Note the ‘reverberative’ shadow.
A B
Figure 3.47 Gallbladder carcinoma. (A) TS, containing stones, debris and irregular wall thickening. (B) A differentpatient, demonstrating a grossly thickened hypoechoic wall with a contracted lumen.
ch03.qxd 6/30/04 5:41 PM Page 73

CholangiocarcinomaThis is a malignant lesion arising in the wall of thebile duct (Fig. 3.48). It is obviously easier to rec-ognize from an ultrasound point of view when itoccurs in and obstructs the common duct, as thesubsequent dilatation outlines the proximal part ofthe tumour with bile. Cholangiocarcinoma mayoccur at any level along the biliary tree and is fre-quently multifocal.
A cholangiocarcinoma is referred to as a Klatskintumour when it involves the confluence of the rightand left hepatic ducts. These lesions are often diffi-cult to detect on both ultrasound and CT. They arefrequently isoechoic, and the only clue may be theproximal dilatation of the biliary ducts (Fig. 3.49).
Although rare, the incidence of cholangiocarci-noma seems to be increasing and it is strongly asso-ciated with PSC, a disease of the biliary ductswhich predominantly affects young men (seeabove).
Multifocal cholangiocarcinoma may spread to thesurrounding liver tissue and carries a very poorprognosis for long-term survival. In a liver whosetexture is already altered by diffuse disease it may bealmost impossible to identify these lesions beforethey become large. A pattern of dilated ducts distalto the lesion is a good clue (Figs 3.50 and 3.51).
ABDOMINAL ULTRASOUND74
Figure 3.48 The distal CBD has a thickened wall(arrowheads), and the lumen is filled with tumour at thelower end. (Gallbladder anterior.)
A B
Figure 3.49 Cholangiocarcinoma. (A) Irregular mass at the porta, causing biliary obstruction—a Klatskin tumour.(B) MRI of the same patient, confirming the mass at the porta.
ch03.qxd 6/30/04 5:41 PM Page 74
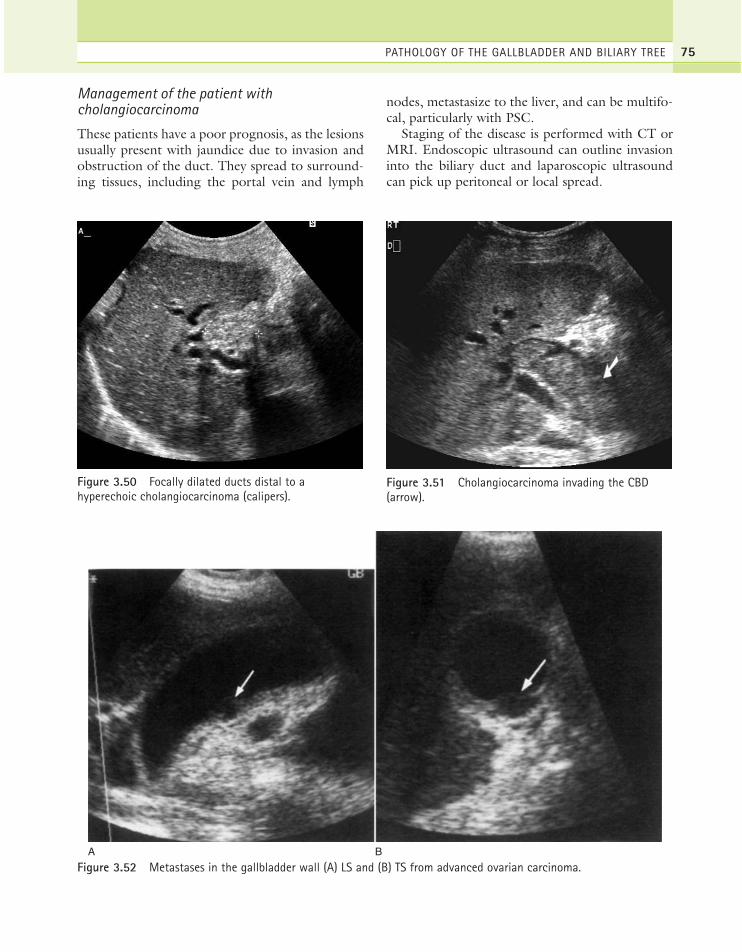
Management of the patient withcholangiocarcinoma
These patients have a poor prognosis, as the lesionsusually present with jaundice due to invasion andobstruction of the duct. They spread to surround-ing tissues, including the portal vein and lymph
nodes, metastasize to the liver, and can be multifo-cal, particularly with PSC.
Staging of the disease is performed with CT orMRI. Endoscopic ultrasound can outline invasioninto the biliary duct and laparoscopic ultrasoundcan pick up peritoneal or local spread.
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 75
Figure 3.50 Focally dilated ducts distal to ahyperechoic cholangiocarcinoma (calipers).
Figure 3.51 Cholangiocarcinoma invading the CBD(arrow).
A B
Figure 3.52 Metastases in the gallbladder wall (A) LS and (B) TS from advanced ovarian carcinoma.
ch03.qxd 6/30/04 5:41 PM Page 75

Surgical resection of the tumour is becomingmore successful in patients with single lesions.46
Palliation is frequently the only feasible option andthe insertion of a stent, either percutaneously orendoscopically, to bypass the obstructing lesionand assist drainage of the liver will relieve thesymptoms and often allows the patient to returnhome for some months.
Other treatment options, such as chemotherapy,have limited success, although transplantation isincreasingly regarded as an option in some cases.Despite improvements in treatment, only a minor-ity of patients survive beyond twelve months afterthe initial diagnosis.
Gallbladder metastasesMetastases from other primaries may occasionallybe deposited within the gallbladder wall (Fig.3.52), usually as a late presentation of the diseaseprocess. Often, other metastatic deposits, forexample in the liver and lymph nodes, may raisesuspicion of gallbladder metastases in an irregularlythickened gallbladder wall.
The ultrasound appearances are of focal thicken-ing and polyp-like lesions in the wall of the gall-bladder. This may mimic primary gallbladdercarcinoma but knowledge of a previously diagnosedprimary, for example melanoma, lung or breast car-cinoma, will point towards the diagnosis.
ABDOMINAL ULTRASOUND76
References1. Shea JA, Berlin JA, Escarce JJ et al. 1994 Revised
estimates of diagnostic test sensitivity and specificity insuspected biliary tract disease. Archives of InternalMedicine 154: 2573–2581.
2. Pandey M, Khatri AK, Sood BP et al. 1996Cholecystosonographic evaluation of the prevalence ofgallbladder disease: a university hospital experience.Clinical Imaging 20: 269–272.
3. Liu TH, Consorti ET, Mercer DW. 2002Laparoscopic cholesystectomy for acute cholecystitis:technical considerations and outcome. Seminar ofLaparoscopic Surgery 9(1): 24–31.
4. Tranter SE, Thompson MH. 2001 Potential oflaparoscopic ultrasonography as an alternative tooperative cholangiography in the detection of bileduct stones. British Journal of Surgery 88: 65–69.
5. Petroni ML, Jazrawi RP, Pazzi P et al. 2000 Riskfactors for the development of gallstone recurrencefollowing medical dissolution. The British-ItalianGallstone Study Group. European Journal ofGastroenterology and Hepatology 12: 695–700.
6. Pauletzki J, Sackman M, Holl J, Paumgartner G. 1996Evaluation of gallbladder volume and emptying with anovel three-dimensional ultrasound system: comparisonwith sum-of-cylinders and the ellipsoid methods.Journal of Clinical Ultrasound 24: 277–285.
7. Johnson LW, Sehon JK, Lee WC et al. 2001 Mirizzi’ssyndrome: experience from a multi-institutionalreview. American Surgery 67: 11–14.
8. Sheth S, Bedford A, Chopra S. 2000 Primarygallbladder cancer: recognition of risk factors and roleof prophylactic cholecystectomy. American Journal ofGastroenterology 95: 1402–1410.
9. Fowler RC, Reid WA. 1988 Ultrasound diagnosis ofadenomyomatosis of the gallbladder: ultrasonic andpathological correlation. Clinical Radiology 39:402–406.
10. Tanno S, Obara T, Maguchi H et al. 1998 Associationbetween anomalous pancreatobiliary ductal union andadenomyomatosis of the gallbladder. Journal ofGastroenterology and Hepatology 13: 175–180.
11. Myers RP, Shaffer EA, Beck PL. 2002 Gallbladderpolyps: epidemiology, natural history andmanagement. Canadian Journal of Gastroenterology16: 187–194.
12. Buckles DC, Lindor KD, Larusso NF et al. 2002 Inprimary sclerosing cholangitis, gallbladder polyps arefrequently malignant. American Journal ofGastroenterology 97: 1138–1142.
13. Schiller VL, Turner RR, Sarti DA. 1996 ColorDoppler imaging of the gallbladder wall in acutecholecystitis: sonographic–pathologic correlation.Abdominal Imaging 21: 233–237.
14. Olcott EW, Jeffrey RB, Jain KA. 1997 Power versuscolour Doppler sonography of the normal cysticartery: implications for patients with acute cholcystitis.American Journal of Roentgenology 168: 703–705.
15. Draghi F, Ferrozzi G, Calliada F et al. 2000 PowerDoppler ultrasound of gallbladder wall vascularisationin inflammation: clinical implications. EuropeanRadiology 10: 1587–1590.
16. McLoughlin RF, Patterson EJ, Mathieson JR et al.1994 Radiologically guided percutaneouscholecystostomy for acute cholecystitis: long-termoutcome in 50 patients. Canadian Association ofRadiologists Journal 45: 455–459.
ch03.qxd 6/30/04 5:41 PM Page 76

17. Shea JA, Berlin JA, Escarce JJ et al. 1994 Revisedestimates of diagnostic test sensitivity and specificity insuspected biliary tract disease. Archives of InternalMedicine 154: 2573–2581.
18. Babb RR. 1992 Acute acalculous cholecystitis: areview. Journal of Clinical Gastroenterology 15:238–241.
19. Chen PF, Nimeri A, Pham QH et al. 2001 Theclinical diagnosis of chronic acalculous cholecystitis.Surgery 130: 578–581.
20. Coffin CT, Weingardt JP, Drose JA. 1995Sonographic appearances of emphysematouscholecystitis. Journal of Diagnostic MedicalSonography 11: 204–206.
21. Konno K, Ishida H, Naganuma H et al. 2002Emphysematous cholecystitis: sonographic findings.Abdominal Imaging 27: 191–195.
22. Tseng LJ, Tsai CC, Mo LR et al. 2000 Palliativepercutaneous transhepatic gallbladder drainage ofgallbladder empyema before laparoscopiccholecystectomy. Hepatogastroenterology 47:932–936.
23. Berger J, Lindsell DRM. 1997 Case report:Thickening of the walls of non-dilated bile ducts.Clinical Radiology 52: 474–476.
24. Kim TK, Kim BS, Kim JH et al. 2002 Diagnosis ofintrahepatic duct stones: superiority of MRcholangiopancreatography over endoscopic retrogradecholangiopancreatography. American Journal ofRoentgenology 179: 429–434.
25. Calvo MM, Bujanda L, Calderon A. 2002 Role ofmagnetic resonance cholangiopancreatography inpatients with suspected choledocholithiasis. MayoClinic Proceedings 77: 407–412.
26. Tranter SE, Thompson MH. 2001 Potential oflaparoscopic ultrasonography as an alternative tooperative cholangiography in the detection ofbile duct stones. British Journal of Surgery 88:65–69.
27. Aubertin JM, Levoir D, Bouillot JL et al. 1996Endoscopic ultrasonography immediately prior tolaparoscopic cholecystectomy: a prospectiveevaluation. Endoscopy 28: 667–673.
28. Lau WY, Leung KL, Leung TWT et al. 1995Obstructive jaundice secondary to hepatocellularcarcinoma. Surgical Oncology 4: 303–308.
29. Savader SJ, Benenati JF, Venbrux AC et al. 1991Choledochal cysts: classification and cholangiographicappearance. American Journal of Roentgenology 56:327–331.
30. Martins E, Chapman RW. 1996 Sclerosingcholangitis. Current Opinion in Gastroenterology 12:466–470.
31. Majoie CBLM, Smits NJ, Phoa SSKS et al. 1995Primary sclerosing cholangitis: sonographic findings.Abdominal Imaging 20: 109–113.
32. Van de Meeberg PC, Portincasa P, Wolfhagen FHJ,Van Erpecum KJ. 1996 Increased gall bladder volumein primary sclerosing cholangitis. Gut 39: 594–599.
33. Kawarasaki H, Sato T, Sanjo K et al. 1995 Evaluationof long-term results of Caroli’s disease: 21 years’observation of a family with autosomal ‘dominant’inheritance and review of the literature. Hepato-gastroenterology 42: 175–181.
34. Benhidjeb T, Rudolph B, Muller JM. 1997 Curativepartial hepatectomy in unilobar Caroli’s syndrome –report of three cases with long-term follow-up.Digestive Surgery 14: 123–125.
35. Miller WJ, Sechtin AG, Campbell WL, Pieters PC.1995 Imaging findings in Caroli’s disease. AmericanJournal of Roentgenology 165: 333–337.
36. Ali M, Khan AN. 1996 Sonography of hepatobiliaryascariasis. Journal of Clinical Ultrasound 24: 235–241.
37. Misra SP, Dwivedi M. 2000 Clinical features andmanagement of biliary ascariasis in a non-endemicarea. Postgraduate Medicine 76: 29–32.
38. Chen EY, Nguyen TD. 2001 Gallbladder sludge.New England Journal of Medicine 345 (10): 2e.
39. Ko CW, Sekijima JH, Lee SP. 1999 Biliary sludge.Annals of Internal Medicine 131: 630–631.
40. Portincasa P, Di Ciaula A, Vendemiale G et al. 2000Gallbladder motility and cholesterol crystallization inbile from patients with pigment and cholesterolgallstones. European Journal of Clinical Investigation30: 317–324.
41. Velanovich V, Bowden T. 1997 Biliary dyskinesia andbiliary crystals: a prospective study. American Surgeon63: 69–74.
42. Wilkinson LS, Levine TS, Smith D, Chadwick SJD.1996 Biliary sludge: can ultrasound reliably detect thepresence of crystals in bile? European Journal ofGastroenterology 8: 999–1001.
43. Kohut M, Nowak A, Nowakowska-Dulawa E. 2001The frequency of bile duct crystals in patients withpresumed biliary pancreatitis. GastrointestinalEndoscopy 54: 37–41.
44. Lo HW, Yuan CY. 1994 Ultrasonic spectrum ofhaemobilia in the bile duct and gallbladder. Journal ofMedical Ultrasound 2: 77–80.
45. Futamura M. 1996 Analysis of blood flow signals inultrasonic Doppler study of gallbladder carcinoma.Japanese Journal of Medical Ultrasonics 23: 27–36.
46. Figueras J, Llado L, Valla C et al. 2000 Changingstrategies in diagnosis and management of hilarcholangiocarcinoma. Liver Transplantation 6:786–794
PATHOLOGY OF THE GALLBLADDER AND BILIARY TREE 77
ch03.qxd 6/30/04 5:41 PM Page 77
ch03.qxd 6/30/04 5:41 PM Page 78
This page intentionally left blank

Ultrasound is often the first line of investigationfor suspected liver pathology and the decision toproceed to secondary investigative procedures,such as further radiology or histology, is frequentlydetermined by the findings of the initial ultrasoundscan. Ultrasound is used in the diagnosis, stagingand monitoring of liver disorders and also con-tributes to their treatment with ultrasound-guidedinvasive procedures.
Increasingly, ultrasound is also a reliable tool formore focused, complex examinations. Developingtechnology and techniques now result in improveddiagnostic accuracy and are increasingly obviatingthe need for further radiology.
Intraoperative and laparoscopic ultrasound, usinghigh-frequency, direct-contact techniques, set thestandard for liver imaging in many cases.
BENIGN FOCAL LIVER LESIONS
Simple cystsOne of the most frequently seen liver lesions, thesimple cyst, is either congenital (from abnormaldevelopment of a biliary radicle) or acquired (fromtrauma or previous infection). It is asymptomatic,unless large enough to cause a ‘mass effect’, com-pressing and displacing adjacent structures, and is
Chapter 4
Pathology of the liver and portalvenous system
79
CHAPTER CONTENTS
Benign focal liver lesions 79Simple cysts 79Complex cysts 80Polycystic liver 81Hydatid cyst 82Abscesses 82Haematoma 84Haemangioma 85Adenoma 86Focal fatty change 87Focal nodular hyperplasia 88Granuloma 88Hepatic calcification 88
Malignant focal liver lesions 89Metastases 90Hepatocellular carcinoma 93Cholangiocarcinoma 95
Diffuse liver conditions 95Fatty infiltration 95Cirrhosis 97Portal hypertension 99Hepatitis 106Primary sclerosing cholangitis 107Budd–Chiari syndrome 107Cystic fibrosis 109Congestive cardiac disease 109Liver conditions in pregnancy 109
Liver transplants 110Indications for transplant 110Preoperative assessment 111Operative procedure 112
Postoperative assessment 113Postoperative ultrasound appearances 113
ch04.qxd 6/30/04 5:48 PM Page 79

usually an incidental finding during the ultrasoundscan. Frequently, small cysts are peripheral andtherefore more likely to be missed on ultrasoundthan CT.
The simple cyst has three acoustic properties,which are pathognomonic (see Table 4.1); it isanechoic, has a well-defined smooth capsule andexhibits posterior enhancement (increased through-transmission of sound) (Fig. 4.1).
Although theoretically it is possible to confuse asimple cyst with a choledochal cyst (see Chapter 3),the latter’s connection to the biliary tree is usuallydemonstrable on ultrasound. A radioisotopehepatic iminodiacetic acid (HIDA) scan will con-firm the biliary connection if doubt exists.
Complex cystsSome cysts may contain a thin septum, which is nota significant finding. However, cysts which containsolid nodules or thickened walls should be viewed
with suspicion (Fig. 4.2). Occasionally haemor-rhage or infection may occur in a simple cyst, giv-ing rise to low-level, fine echoes within it (Fig.4.3).
These cysts are not usually actively treated; how-ever the larger ones may be monitored with ultra-sound, particularly if symptomatic. Percutaneousaspiration of larger cysts under ultrasound guid-ance may afford temporary decompression but israrely performed as they invariably recur.Laparoscopic unroofing provides a more perma-nent solution to large, symptomatic cysts.1
ABDOMINAL ULTRASOUND80
Table 4.1 Cystic focal liver lesions—differentialdiagnoses
Simple cystAnechoic, thin capsule, Common finding, usually posterior enhancement insignificant. Consider (may contain thin septa) polycystic disease if multiple
(Rarely an AV malformationmay mimic a septated cyst—exclude by usingcolour Doppler)
Complex cystThin capsule + internal Haemorrhage or infection echoes in a cyst
Mucinous metastasisCystadenoma
Capsule thickened or Hydatid cystcomplex, may also Cystadenocarcinomacontain echoes Intrahepatic pancreatic
pseudocyst (rare)Solid/cystic lesionIrregular margin, internal Abscessechoes + debris/solid Haematomamaterial Necrotic metastasis
Cavernous haemangioma
AV = arteriovenous.
Figure 4.1 Typical simple liver cyst demonstrating aband of posterior enhancement. A smaller, bilocular cystis seen behind it.
Figure 4.2 Small cyst adjacent to the gallbladdercontaining a nodule. This was a mucinous metastasisfrom an ovarian carcinoma.
ch04.qxd 6/30/04 5:48 PM Page 80

Another uncommon cause of a cystic lesion in theliver is a cystadenoma—a benign epithelial tumour.These have the potential to turn malignant, forminga cystadenocarcinoma. Close monitoring with ultra-
sound will demonstrate a gradual increase in size,changes in the appearances of the wall of the cyst,such as thickening or papillary projections, andinternal echoes in some cases, which may arousesuspicion. A diagnostic aspiration may be performedunder ultrasound guidance, and the fluid may con-tain elevated levels of carcinoembryonic antigen ifmalignant.2 Cystadenomas are usually surgicallyremoved due to their malignant potential (Fig. 4.4).
Rarely, cystic lesions in the liver may be due toother causes. These include pancreatic pseudocyst(within an interlobular fissure) in patients withacute pancreatitis or mucin-filled metastaticdeposits in primary ovarian cancer.
An arteriovenous malformation, a rare findingin the liver, may look like a septated cystic lesion.Doppler, however, will demonstrate flow through-out the structure.
Polycystic liverThere is a fine dividing line between a liver whichcontains multiple simple cysts and polycystic liver
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 81
Figure 4.3 Large, infected hepatic cyst containing low-level echoes.
A B
Figure 4.4 (A) Large cystadenoma containing echoes and a septum. The cyst was large enough to cause obstructivejaundice—the patient’s presenting symptom. The diagnosis was made by ultrasound-guided aspiration. This cyst haddeveloped into a cystadenocarcinoma after 2 years. (B) A cystadenocarcinoma in a young woman presenting withaltered liver function tests (LFTs). The cyst contains echoes and some solid material.
ch04.qxd 6/30/04 5:48 PM Page 81

disease. The latter usually occurs with polycystickidneys, a common autosomal dominant conditionreadily recognizable on ultrasound (see Chapter 7),but may rarely affect the liver alone (Fig. 4.5).
The appearances are of multiple, often septatedcysts, of varying sizes throughout the liver. Thecumulative enhancement behind the numerouscysts imparts a highly irregular echogenicity to theliver texture and may make it extremely difficult topick up other focal lesions which may be present.
The polycystic liver is usually asymptomatic, buteasily palpable, and if the kidneys are also affectedthe abdomen can look very distended. As withcysts in the kidneys, haemorrhage or infection in acyst can cause localized pain. Treatment of thecysts by drainage is not successful and in rare caseshepatic transplant offers the only viable option inpatients with intractable symptoms.
Hydatid (echinococcal) cystHydatid disease comes from a parasite, Echinococcusgranulosus, which is endemic in the Middle East butrare in the UK. The worm lives in the alimentarytract of infected dogs, which excrete the eggs. Thesemay then be ingested by cattle or sheep and subse-quently complete their life cycle in a human.
The parasite spreads via the bloodstream to theliver, where it lodges, causing an inflammatoryreaction. The resulting cyst can be slow-growing
and asymptomatic and may be single or multiple,depending on the degree of infestation.
Although the appearances are often similar tothose of a simple cyst, the diagnosis can be made bylooking carefully at the wall and contents; thehydatid cyst has two layers to its capsule, which mayappear thickened, separated or detached on ultra-sound. Daughter cysts may arise from the inner cap-sule—the honeycomb or cartwheel appearance (Fig.4.6). Thirdly, a calcified rind around a cyst is usuallyassociated with an old, inactive hydatid lesion.
The diagnosis of hydatid, as opposed to a simplecyst, is an important one as any attempted aspira-tion may spread the parasite further by seedingalong the needle track if the operator is unaware ofthe diagnosis.
Management of hepatic hydatid cysts has tradi-tionally been surgical resection. However, consid-erable success has now been achieved usingpercutaneous ultrasound-guided aspiration withsclerotherapy.3
AbscessesClinical features of an abscess
Patients present with fever, often accompanied byright upper quadrant (RUQ) pain and vomiting.Abnormal liver function tests (LFTs) and anaemia
ABDOMINAL ULTRASOUND82
Figure 4.5 Multiple cysts in the liver. In this case thekidneys are normal. Polycystic liver is more usuallyassociated with polycystic kidney disease.
Figure 4.6 Hydatid cyst demonstrating surroundingdaughter cysts.
ch04.qxd 6/30/04 5:48 PM Page 82

can also be present. The clinical history helps thesonographer to establish the nature of the focallesion and aetiology of the abscess. Abscesses ofany type may be solitary or multiple.
Because the ultrasound appearances of abscessescan be similar to those of necrotic tumours orhaematoma, the clinical picture is of particularimportance to the sonographer.
Ultrasound appearances
Hepatic abscesses may display a variety of acousticfeatures. Their internal appearances vary consider-ably. In the very early stages there is a zone ofinfected, oedematous liver tissue which appears onultrasound as a hypoechoic, solid focal lesion. As theinfection develops, the liver tissue becomes necroticand liquefaction takes place. The abscess may stillappear full of homogeneous echoes from pus andcan be mistaken for a solid lesion, but as it pro-gresses, the fluid content may become apparent,usually with considerable debris within it. Becausethey are fluid-filled, abscesses demonstrate posteriorenhancement (Fig. 4.7A). The margins of an abscessare irregular and often ill-defined and frequentlythickened. The inflammatory capsule of the abscessmay demonstrate vascularity on colour or powerDoppler but this is not invariable and depends onequipment sensitivity and size of the lesion.
Infection with gas-forming organisms mayaccount for the presence of gas within some liverabscesses (Fig. 4.7B).
There are three main types of abscess:
● Pyogenic abscess. These form as a result ofinfection entering the liver through the portalvenous system. Most commonly, appendiceal ordiverticular abscesses are responsible, butintrahepatic abscesses are also seen inimmunosuppressed patients and followingpostoperative infection. They are frequentlymultiple, and the patient must be closelymonitored after diagnosis to prevent rapidspread. Pyogenic abscess is still considered alethal condition, which has increased in recentyears due to increasingly aggressive surgicalapproaches to many abdominal neoplasms.4
● Amoebic abscess. This is a parasitic infectionwhich is rare in the UK, but found frequently
in parts of Africa, India and the southern partsof the USA. Suspicion should be raised whenthe patient has visited these countries. It isusually contracted by drinking contaminatedwater and infects the colon, ulcerating the walland subsequently being transported to the livervia the portal venous system.
● Candidiasis abscess. This is a fungal infectionwhich may be seen in immunosuppressedpatients. It is a rare cause of abscess formationand is usually blood-borne. The resulting
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 83
A
B
Figure 4.7 (A) Early stages of a pyogenic abscess in atransplanted liver. The lesion looks quite solid, but notethe posterior enhancement. (B) The gas contained withinthis large abscess in the right lobe of the liver obscuresthe full extent of the lesion. (Large abscesses like this,which contain gas, may mimic the acoustic appearancesof normal bowel.)
(Continued)
ch04.qxd 6/30/04 5:48 PM Page 83

abscesses are likely to be small but multiple onpresentation. About 25% of infected patientsform hepatic abscesses and the infection mayspread to other sites in the abdomen.
Management of hepatic abscesses
An ultrasound-guided aspiration to obtain pus forculture is useful for identifying the responsibleorganism.
Aspiration combined with antibiotic therapy isusually highly successful for smaller abscesses andultrasound is used to monitor the resolution of theabscesses in the liver.
Ultrasound-guided drainage is used for largelesions, and surgical removal is rarely required.
Further radiology may be indicated to establishthe underlying cause and extent, for example bar-ium enema or CT, particularly if amoebic infectionis suspected.
HaematomaThe liver haematoma may have similar acousticappearances to those of an abscess, but does notshare the same clinical features. A haematoma isthe result of trauma (usually, therefore, via theAccident and Emergency department) but the
trauma may also be iatrogenic, for example follow-ing a biopsy procedure (hence the value of usingultrasound guidance to avoid major vessels in theliver) or surgery (Fig. 4.8).
The acoustic appearances depend upon the tim-ing—a fresh haematoma may appear liquid andecho-poor, but rapidly becomes more ‘solid’-looking
ABDOMINAL ULTRASOUND84
C
Figure 4.7 cont’d (C) A percutaneous drain is identifiedin a liver abscess.
A
B
Figure 4.8 (A) Intrahepatic haematoma following aroad traffic accident with rib fractures. The lesion isrelatively fresh and contains some low-level echoes. (B) 2-day-old subcapsular haematoma. The collectionbecame progressively smaller and hyperechoic as itresolved.
ch04.qxd 6/30/04 5:48 PM Page 84

and hyperechoic, as the blood clots. As it resolvesthe haematoma liquefies and may contain fibrinstrands. It will invariably demonstrate a band ofposterior enhancement and has irregular, ill-defined walls in the early stages. Later on it mayencapsulate, leaving a permanent cystic ‘space’ inthe liver, and the capsule may calcify.
Injury to the more peripheral regions may causea subcapsular haematoma which demonstrates thesame acoustic properties. The haematoma outlinesthe surface of the liver and the capsule can be seensurrounding it. This may be the cause of a palpable‘enlarged’ liver (Fig. 4.8B).
Intervention is rarely necessary and monitoringwith ultrasound confirms eventual resolution.More serious hepatic ruptures, however, causinghaemoperitoneum, usually require surgery.
HaemangiomaThese common, benign lesions are highly vascular,composed of a network of tiny blood vessels. Theymay be solitary or multiple. Most haemangiomas aresmall and found incidentally. They are rarely symp-tomatic but do cause diagnostic problems as theycan be indistinguishable from liver metastases. Theiracoustic appearances vary; the majority are hyper-echoic, rounded well-defined lesions; however,atypical hypoechoic lesions or those with mixedechogenicity cause particular diagnostic dilemmas.Larger ones can demonstrate a spectrum of reflec-tivity depending on their composition and maydemonstrate pools of blood and central areas ofdegeneration. They frequently exhibit slightlyincreased through-transmission, with posteriorenhancement, particularly if large. This is probablydue to the increased blood content compared withthe surrounding liver parenchyma (Fig. 4.9).
Because the blood within the haemangioma isvery slow-flowing, it is usually not possible todemonstrate flow with colour or power Dopplerand the lesions appear avascular on ultrasound.Microbubble contrast agents demonstrate aperipheral, globular enhancement with gradualcentripetal filling of the lesion, helping to charac-terize them and differentiate haemangioma frommalignant lesions.
When found in children, haemangiomas tend tobe large and do produce symptoms. These masses
produce shunting of blood from the aorta via themain hepatic artery and, in extreme cases, presentwith resulting cardiac failure. They are often het-erogeneous in appearance and larger vessels withinthem may be identified with Doppler. Althoughmany regress over a period of time, others mayhave to be embolized with coils under radiologicalguidance to control the symptoms.
In patients with no cause to suspect malignancy,it may be suggested that the appearances of a small,
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 85
A
B
Figure 4.9 (A) Three small haemangiomas (arrows). (B)A haemangioma is demonstrated in the anterior part ofthe right lobe of the liver.
(Continued)
ch04.qxd 6/30/04 5:49 PM Page 85

well-defined, hyperechoic mass are due to benignhaemangioma. Follow-up scans will demonstrateno appreciable change over time. However, wheredoubt exists, it is useful to refer the patient for fur-ther imaging, such as MRI scanning, to character-ize the lesion confidently.
Administration of an ultrasound contrast agent isalso useful in lesion characterization and a haeman-gioma usually demonstrates a peripheral, nodularenhancement pattern in the arterial phase, withgradual centripetal filling (Fig. 4.9C).5
AdenomaThe hepatic adenoma is a benign focal lesion con-sisting of a cluster of atypical liver cells (Fig. 4.10).Within this, there may be pools of bile or focalareas of haemorrhage or necrosis. This gives rise toa heterogeneous, patchy echotexture. The smallerones tend to be homogeneous with a smooth tex-ture. They are usually less reflective than a hae-mangioma and may have similar reflectivity to thesurrounding liver parenchyma.
Larger adenomas may contain vigorous arterialflow on Doppler, but this is not pathognomonic anddoes not differentiate it from a malignant lesion.
Clinical features
There is a particularly strong association betweenhepatic adenoma and use of the oral contraceptiveso these masses tend to present in younger women.Adenomas are also associated with glycogen stor-age disease.
They may cause pain, particularly if they haemor-rhage, and may be palpable. Surgical removal is themanagement of choice, although they occasionallyregress if the oral contraceptive is discontinued.
Ultrasound is useful in monitoring patients withglycogen storage disease for changes in the charac-
ABDOMINAL ULTRASOUND86
C
Figure 4.9 cont’d (C) On administration of microbubblecontrast agent, the lesion in (B) demonstrates peripheral,globular enhancement, with gradual centripetal filling,consistent with haemangioma.
B
A
Figure 4.10 (A) Adenoma in segment 5 in a youngwoman on the oral contraceptive pill. (B) An unusualexample of cystic degeneration in a large adenoma.
ch04.qxd 6/30/04 5:49 PM Page 86
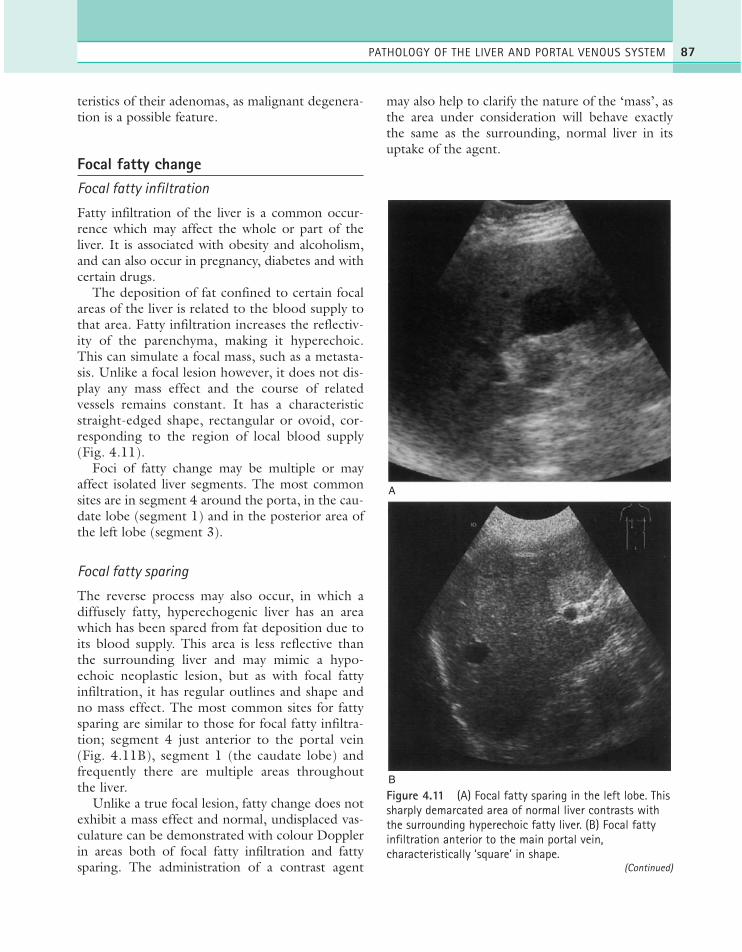
teristics of their adenomas, as malignant degenera-tion is a possible feature.
Focal fatty changeFocal fatty infiltration
Fatty infiltration of the liver is a common occur-rence which may affect the whole or part of theliver. It is associated with obesity and alcoholism,and can also occur in pregnancy, diabetes and withcertain drugs.
The deposition of fat confined to certain focalareas of the liver is related to the blood supply tothat area. Fatty infiltration increases the reflectiv-ity of the parenchyma, making it hyperechoic.This can simulate a focal mass, such as a metasta-sis. Unlike a focal lesion however, it does not dis-play any mass effect and the course of relatedvessels remains constant. It has a characteristicstraight-edged shape, rectangular or ovoid, cor-responding to the region of local blood supply(Fig. 4.11).
Foci of fatty change may be multiple or mayaffect isolated liver segments. The most commonsites are in segment 4 around the porta, in the cau-date lobe (segment 1) and in the posterior area ofthe left lobe (segment 3).
Focal fatty sparing
The reverse process may also occur, in which adiffusely fatty, hyperechogenic liver has an areawhich has been spared from fat deposition due toits blood supply. This area is less reflective thanthe surrounding liver and may mimic a hypo-echoic neoplastic lesion, but as with focal fattyinfiltration, it has regular outlines and shape andno mass effect. The most common sites for fattysparing are similar to those for focal fatty infiltra-tion; segment 4 just anterior to the portal vein(Fig. 4.11B), segment 1 (the caudate lobe) andfrequently there are multiple areas throughoutthe liver.
Unlike a true focal lesion, fatty change does notexhibit a mass effect and normal, undisplaced vas-culature can be demonstrated with colour Dopplerin areas both of focal fatty infiltration and fattysparing. The administration of a contrast agent
may also help to clarify the nature of the ‘mass’, asthe area under consideration will behave exactlythe same as the surrounding, normal liver in itsuptake of the agent.
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 87
A
B
Figure 4.11 (A) Focal fatty sparing in the left lobe. Thissharply demarcated area of normal liver contrasts withthe surrounding hyperechoic fatty liver. (B) Focal fattyinfiltration anterior to the main portal vein,characteristically ‘square’ in shape.
(Continued)
ch04.qxd 6/30/04 5:49 PM Page 87

Lipoma
The hepatic lipoma is a relatively rare, benignhepatic tumour which is very similar in nature andacoustic appearance to focal fatty change. It differsin that it is a discrete tumour of fatty depositionrather than an infiltrative process and so can exerta mass effect on surrounding vessels if large. Thefat content makes the lipoma hyperechoic com-pared to the surrounding liver tissue.
Focal nodular hyperplasiaThis is a benign tumour made up of a proliferationof liver cells with hepatocytes, Kupffer cells and bil-iary and fibrous elements. It is most commonlyfound in young women and is usually discoveredby chance, being asymptomatic. Its ultrasoundcharacteristics vary, and it may be indistinguishablefrom hepatic adenoma.
It tends to affect the caudate lobe and has theappearance of a homogeneous mass often of simi-lar echogenicity to the liver (Fig. 4.12). It presentsa diagnostic difficulty both with CT and ultra-sound, as its characteristics can vary.6 ColourDoppler shows an increased arterial flow in the
mass. The administration of an ultrasound contrastagent displays a characteristic ‘spoked-wheel’ pat-tern of arteries with a central scar.7
The diagnosis can usually be confirmed on MRIscanning (which shows a similar vascular pattern tothat of ultrasound contrast scanning) but mayoccasionally require biopsy proof. Management ofthis benign mass is usually conservative, with ultra-sound follow-up, once the diagnosis has beenestablished, but surgical resection may be necessaryin larger lesions.
GranulomaGranulomata are benign liver masses which areassociated with chronic inflammatory liver diseases.They are particularly associated with primary bil-iary cirrhosis, sarcoidosis or TB. They may be mul-tiple and small, in which case the liver often lookscoarse and hyperechoic. More often they are smalldiscrete lesions which may be hypo- or isoechoic,sometimes with a hypoechoic rim like a target, orcalcified with distal shadowing (Fig. 4.13). Theycan undergo central necrosis.
Differential diagnoses include metastases orregenerating nodules.
Hepatic calcificationCalcification occurs in the liver as a result ofsome pathological processes and may be seenfollowing infection or parasitic infestation. Itmay be focal (usually the end stage of a previ-ous abscess, haematoma or granuloma) whichusually indicates that the lesion in question is nolonger active. It may also be seen within somemetastases.
Calcification may also be linear in nature, fol-lowing the course of the portal tracts. This can beassociated with old TB or other previous parasiticinfestations.
Occasionally hepatic calcification is seen inchildren or in the fetus. This is usually not a sig-nificant finding but prenatal infection should beexcluded with a TORCH (toxoplasmosis, rubella,cytomegalovirus and HIV) screen. Calcification,which casts a strong and definite shadow, shouldbe distinguished from air in the biliary tree (Fig.3.46), which casts a reverberative shadow and is
ABDOMINAL ULTRASOUND88
C
Figure 4.11 cont’d (C) Wedge-shaped area of fattyinfiltration in the right lobe.
ch04.qxd 6/30/04 5:49 PM Page 88
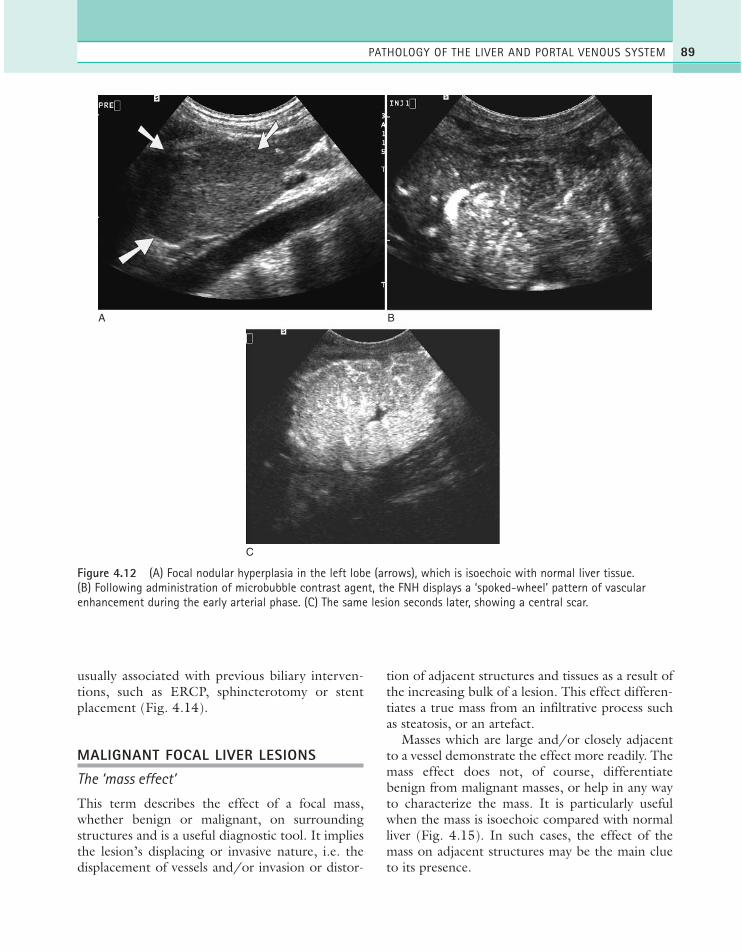
usually associated with previous biliary interven-tions, such as ERCP, sphincterotomy or stentplacement (Fig. 4.14).
MALIGNANT FOCAL LIVER LESIONS
The ‘mass effect’
This term describes the effect of a focal mass,whether benign or malignant, on surroundingstructures and is a useful diagnostic tool. It impliesthe lesion’s displacing or invasive nature, i.e. thedisplacement of vessels and/or invasion or distor-
tion of adjacent structures and tissues as a result ofthe increasing bulk of a lesion. This effect differen-tiates a true mass from an infiltrative process suchas steatosis, or an artefact.
Masses which are large and/or closely adjacentto a vessel demonstrate the effect more readily. Themass effect does not, of course, differentiatebenign from malignant masses, or help in any wayto characterize the mass. It is particularly usefulwhen the mass is isoechoic compared with normalliver (Fig. 4.15). In such cases, the effect of themass on adjacent structures may be the main clueto its presence.
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 89
A B
C
Figure 4.12 (A) Focal nodular hyperplasia in the left lobe (arrows), which is isoechoic with normal liver tissue.(B) Following administration of microbubble contrast agent, the FNH displays a ‘spoked-wheel’ pattern of vascularenhancement during the early arterial phase. (C) The same lesion seconds later, showing a central scar.
ch04.qxd 6/30/04 5:49 PM Page 89
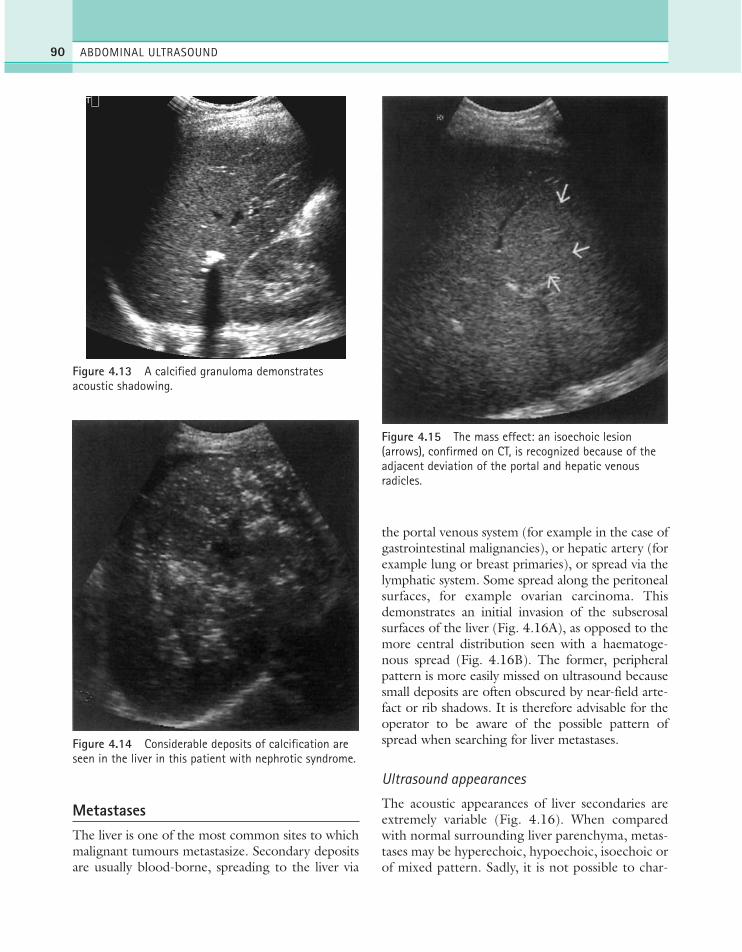
ABDOMINAL ULTRASOUND90
MetastasesThe liver is one of the most common sites to whichmalignant tumours metastasize. Secondary depositsare usually blood-borne, spreading to the liver via
the portal venous system (for example in the case ofgastrointestinal malignancies), or hepatic artery (forexample lung or breast primaries), or spread via thelymphatic system. Some spread along the peritonealsurfaces, for example ovarian carcinoma. Thisdemonstrates an initial invasion of the subserosalsurfaces of the liver (Fig. 4.16A), as opposed to themore central distribution seen with a haematoge-nous spread (Fig. 4.16B). The former, peripheralpattern is more easily missed on ultrasound becausesmall deposits are often obscured by near-field arte-fact or rib shadows. It is therefore advisable for theoperator to be aware of the possible pattern ofspread when searching for liver metastases.
Ultrasound appearances
The acoustic appearances of liver secondaries areextremely variable (Fig. 4.16). When comparedwith normal surrounding liver parenchyma, metas-tases may be hyperechoic, hypoechoic, isoechoic orof mixed pattern. Sadly, it is not possible to char-
Figure 4.13 A calcified granuloma demonstratesacoustic shadowing.
Figure 4.14 Considerable deposits of calcification areseen in the liver in this patient with nephrotic syndrome.
Figure 4.15 The mass effect: an isoechoic lesion(arrows), confirmed on CT, is recognized because of theadjacent deviation of the portal and hepatic venousradicles.
ch04.qxd 6/30/04 5:49 PM Page 90
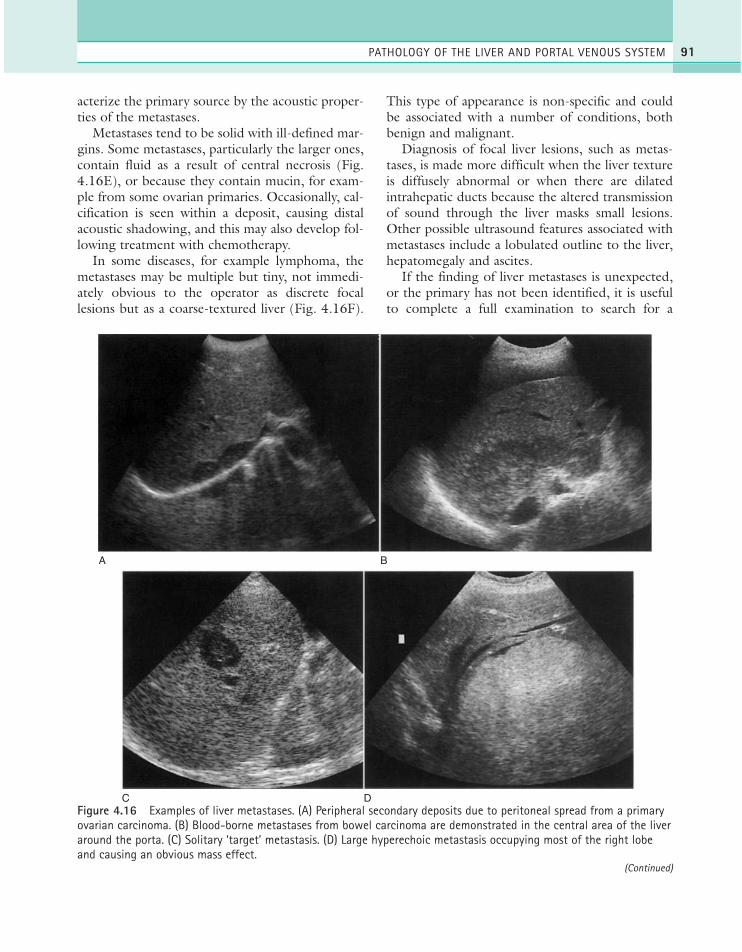
acterize the primary source by the acoustic proper-ties of the metastases.
Metastases tend to be solid with ill-defined mar-gins. Some metastases, particularly the larger ones,contain fluid as a result of central necrosis (Fig.4.16E), or because they contain mucin, for exam-ple from some ovarian primaries. Occasionally, cal-cification is seen within a deposit, causing distalacoustic shadowing, and this may also develop fol-lowing treatment with chemotherapy.
In some diseases, for example lymphoma, themetastases may be multiple but tiny, not immedi-ately obvious to the operator as discrete focallesions but as a coarse-textured liver (Fig. 4.16F).
This type of appearance is non-specific and couldbe associated with a number of conditions, bothbenign and malignant.
Diagnosis of focal liver lesions, such as metas-tases, is made more difficult when the liver textureis diffusely abnormal or when there are dilatedintrahepatic ducts because the altered transmissionof sound through the liver masks small lesions.Other possible ultrasound features associated withmetastases include a lobulated outline to the liver,hepatomegaly and ascites.
If the finding of liver metastases is unexpected,or the primary has not been identified, it is usefulto complete a full examination to search for a
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 91
A
C D
B
Figure 4.16 Examples of liver metastases. (A) Peripheral secondary deposits due to peritoneal spread from a primaryovarian carcinoma. (B) Blood-borne metastases from bowel carcinoma are demonstrated in the central area of the liveraround the porta. (C) Solitary ‘target’ metastasis. (D) Large hyperechoic metastasis occupying most of the right lobeand causing an obvious mass effect.
(Continued)
ch04.qxd 6/30/04 5:49 PM Page 91
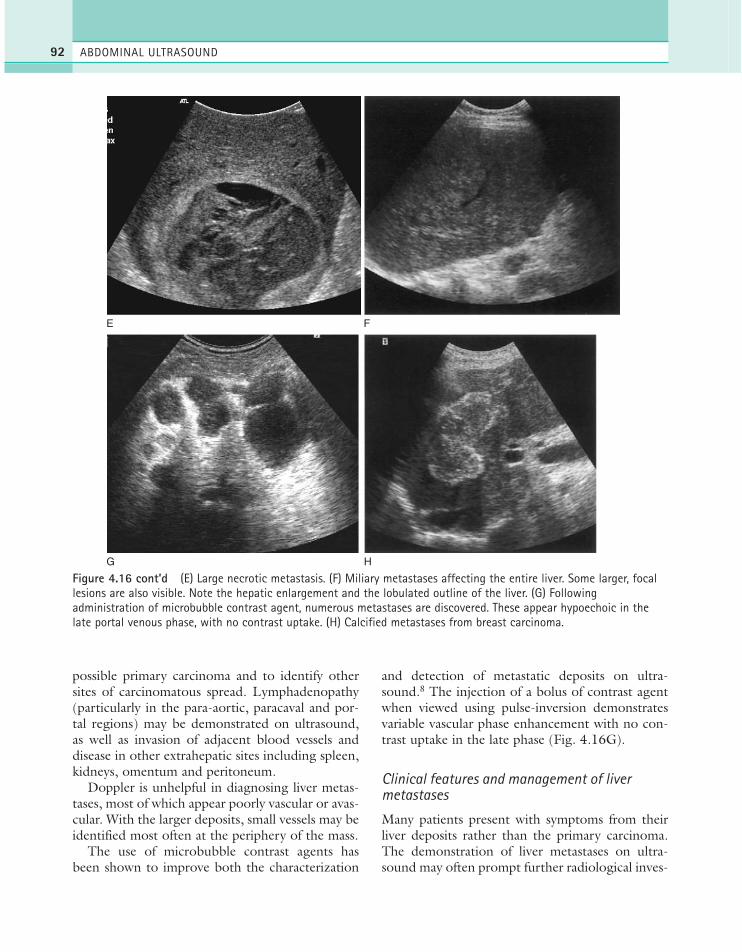
possible primary carcinoma and to identify othersites of carcinomatous spread. Lymphadenopathy(particularly in the para-aortic, paracaval and por-tal regions) may be demonstrated on ultrasound,as well as invasion of adjacent blood vessels anddisease in other extrahepatic sites including spleen,kidneys, omentum and peritoneum.
Doppler is unhelpful in diagnosing liver metas-tases, most of which appear poorly vascular or avas-cular. With the larger deposits, small vessels may beidentified most often at the periphery of the mass.
The use of microbubble contrast agents hasbeen shown to improve both the characterization
and detection of metastatic deposits on ultra-sound.8 The injection of a bolus of contrast agentwhen viewed using pulse-inversion demonstratesvariable vascular phase enhancement with no con-trast uptake in the late phase (Fig. 4.16G).
Clinical features and management of livermetastases
Many patients present with symptoms from theirliver deposits rather than the primary carcinoma.The demonstration of liver metastases on ultra-sound may often prompt further radiological inves-
ABDOMINAL ULTRASOUND92
E
G H
F
Figure 4.16 cont’d (E) Large necrotic metastasis. (F) Miliary metastases affecting the entire liver. Some larger, focallesions are also visible. Note the hepatic enlargement and the lobulated outline of the liver. (G) Followingadministration of microbubble contrast agent, numerous metastases are discovered. These appear hypoechoic in thelate portal venous phase, with no contrast uptake. (H) Calcified metastases from breast carcinoma.
ch04.qxd 6/30/04 5:49 PM Page 92

tigations for the primary. The symptoms of liverdeposits may include non-obstructive jaundice,obstructive jaundice (which may occur if a largemass is present at the porta), hepatomegaly, right-sided pain, increasing abdominal girth from ascitesand altered LFTs.
Ultrasound-guided biopsy may be useful indiagnosing the primary and complements furtherimaging such as X-rays and contrast bowelstudies.
Accurate staging of the disease is currently bestperformed with CT or MRI, which have greatersensitivity for identifying small, sub-centimetre livermetastases, peritoneal deposits and lymphadenopa-thy and which can demonstrate more accurately anyadjacent spread of primary disease.
The prognosis for most patients with livermetastases is poor, particularly if multiple, anddepends to a large extent on the origin of the pri-mary carcinoma. A regime of surgical debulking(removal of the primary carcinoma, adjacentinvaded viscera, lymphadenopathy, etc.) togetherwith chemotherapy can slow down the progress ofthe disease.
In an increasing number of cases, particularlythose with metastases from a colorectal primary,which are less aggressive and grow more slowly,long-term survival can be achieved by resectingboth the primary bowel lesion and then the liverdeposits. The smaller and fewer the liverdeposits, the better the prognosis. The success ofthis treatment has meant that tumours previouslyconsidered inoperable are now potentially cur-able. In such cases it is particularly useful tolocalize the lesions using the segmental liveranatomy prior to surgery (see Chapter 2).Intraoperative ultrasound (IOUS) is then used toconfirm the preoperative appearances and exam-ine the tumour margins to plan the line of resec-tion (Fig. 4.17).
Other methods of treatment include chemoem-bolization, and radiofrequency, microwave or laserablation often under ultrasound guidance.9 Thesuccess of these options depends upon the numberand size of the lesions, and the nature of the pri-mary. Currently, these methods are considered pal-liative, rather than curative, and are an option forpatients who are unsuitable candidates for hepaticresection. (See Chapter 11.)
Ultrasound of other relevant areas
In suspected or confirmed malignancy, the exami-nation of the abdomen may usefully include all thesites likely to be affected. While the liver is one ofthe most common sites for spread of the disease, itis also useful to examine the adrenals, spleen andkidneys, and to look for lymphadenopathy in thepara-aortic, paracaval and portal regions.
If ascites is present, deposits may sometimes bedemonstrated on the peritoneal or omental sur-faces in patients with late-stage disease.
Hepatocellular carcinoma (HCC)This primary carcinoma of the liver is more com-mon in Africa and the Far East than in the UK.Most HCCs arise in diseased livers, hence thestrong association with alcoholic cirrhosis and hep-atitis, and one of the main reasons for ultrasoundreferral in these patients is to try to exclude focalliver lesions which could represent carcinoma.HCC is also associated with metabolic disordersand drug-related liver disease.
Clinically, small tumours are asymptomatic butcause a raised serum alpha-fetoprotein (AFP). Therelationship between cirrhosis and HCC promptsscreening of such patients with AFP and ultra-sound.
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 93
Figure 4.17 Intraoperative ultrasound scandemonstrates a small metastasis (arrow) in segment 4.
ch04.qxd 6/30/04 5:49 PM Page 93

The ultrasound appearances of HCC vary fromhypo- to hyperechogenic or mixed echogenicitylesions (Fig. 4.18). It is often particularly difficultto locate small HCCs in a cirrhotic liver which isalready coarse-textured and nodular. CT and MRImay be useful in these cases.10,11
These lesions may be solitary or multifocal.Colour and spectral Doppler can demonstratevigorous flow, helping to distinguish HCCs frommetastases or haemangiomas, which demonstratelittle or no flow. All carcinomas demonstrate neo-vascularization: the formation of numerous new
blood vessels to supply the growing lesion. Thevascular characteristics of such new vessels are dif-ferent from those of the normal, established ves-sels. The lesion usually demonstrates a knot ofshort, tortuous vessels with an irregular course.Because these new vessels have a paucity ofsmooth muscle in the intima and media, theyexhibit a low resistance to blood flow, having rel-atively high end diastolic flow (EDF). They areable to multiply relatively quickly, causing arterio-venous shunting within the mass which may resultin high velocities.
ABDOMINAL ULTRASOUND94
Figure 4.18 (A) Exophytic hepatocellular carcinoma (HCC) in a patient with cirrhosis. (B) Multifocal HCCs (arrows) in acirrhotic patient. (C) A patient with chronic Budd–Chiari syndrome has a nodular liver with suspicion of a lesion near theanterior surface. (D) Administration of contrast in the same patient as (C) demonstrates increased uptake in the arterialphase, with wash-out of contrast in the late portal phase, helping to locate the lesion, and characterize it as an HCC.
A B
C D
ch04.qxd 6/30/04 5:49 PM Page 94

Increasingly, contrast ultrasound is used todetect and characterize HCCs in patients with abackground of liver disease. HCCs tend to demon-strate an early enhancement of tortuous vessels,followed by a ‘blush’ of arterial enhancement com-pared to normal liver.
CholangiocarcinomaThis primary carcinoma of the bile ducts is discussedmore fully in Chapter 3. Most commonly seenaffecting the main biliary ducts, it also occurs in theintrahepatic biliary tree where it infiltrates the sur-rounding liver parenchyma, having the appearanceof a solid mass. It may be solitary or multifocal anda clue to its location is often the focal dilatation ofducts proximal to the obstructing mass.
For a summary of solid focal liver lesions, seeTable 4.2.
DIFFUSE LIVER CONDITIONS
Diseases which diffusely affect the liver may havevery non-specific ultrasound appearances. Suspicionis usually raised following altered LFTs (seeChapter 1) and the diagnosis made histologically.
A number of diffuse liver conditions can causehepatocellular (or non-obstructive) jaundice whichis associated with increased levels of unconjugatedbile in the blood. Many of these can be demon-
strated with ultrasound, others cannot. The mainrole of ultrasound in the jaundiced patient is toexclude any obstructive cause (by the presence orabsence of biliary duct dilatation) and to search forliver metastases or signs of a diffuse liver condition(Table 4.3).
Fatty infiltration (steatosis)The process of accumulation of fat within the hepaticcells may be either focal (see above) or diffuse.
Related to various conditions such as alco-holism, obesity and diabetes, it is associated withany process which alters liver metabolism and it isreversible in many circumstances.
The acoustic properties of fat differ from those ofnormal liver tissue. The liver appears hyperechoic asthe fat globules provide interfaces which are highly
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 95
Table 4.2 Common solid focal liver lesions: differentialdiagnoses
Lesion Characteristics
BenignHaemangioma Usually hyperechoic. Common
incidental findingAdenoma Associated with oral contraceptive pillFocal fatty change No mass effectFocal nodular Uncommon, usually hyperplasia asymptomatic lesion, often found in
young womenGranuloma Associated with PBC or TB. May
calcifyRegenerating Associated with cirrhosis. Multiple nodules lesionsAbscess May appear solid in the early stages.
Look for posterior enhancement. Fever and pain
Infarct Associated with HA thrombosis in liver transplant
MalignantMetastasis Wide spectrum of possible acoustic
appearancesHepatocellular Associated with cirrhosis carcinomaCholangiocar- Associated with PBC. Proximal cinoma biliary dilatation
PBC = primary biliary cirrhosis; TB = tuberculosis.
E
Figure 4.18 cont’d (E) Tumour thrombus almostoccluding the PV in a patient with multifocal HCC.
ch04.qxd 6/30/04 5:49 PM Page 95

reflective. As the level of fat deposition increases, thelevel of echogenicity may reach that of the highlyreflective portal tract walls. This has the effect ofreducing the prominence of the portal tracts (Fig.4.19) and making the liver appear smooth andhomogeneous, with closely packed, fine echoes.
The contrast between the liver and parenchymaof the right kidney is therefore increased (a partic-ularly useful sign confirming that the correct gainsettings have been used). Hepatomegaly is also afeature, though not invariably.
Finally, the attenuation of fat is greater thanthat of normal liver tissue; this has the effect ofreduced penetration in the far field, rather as if thetime gain compensation (TGC) paddles or slopecontrol had been incorrectly set. In severe cases ofinfiltration, most of the sound is reflected back tothe transducer in the first few centimetres, creat-ing a highly reflective near-field band throughwhich the sound is unable to penetrate.
Fatty infiltration itself is not usually a signifi-cant finding; however it often occurs in conjunc-tion with other significant diffuse processes suchas cirrhosis. Its increased attenuation reduces theability of ultrasound to exclude other disease or
ABDOMINAL ULTRASOUND96
Table 4.3 Causes of non-obstructive (‘medical’)jaundice
Condition Aetiology
Haemolysis In which red cells are destroyed, releasing the haemo-globin (from which bilirubin isderived) into the surroundingtissue
Haematoma Haemolytic process
Gilbert’s disease A defect in the hepatic uptake of bilirubin
Viral hepatitis, Destruction of the liver cells by cirrhosis of all types, these diseases prevents the alcoholic or mechanism of hepatic uptake drug-induced liver and excretion of bilirubin. Both disease conjugated and unconjugated
bilirubin are present
Abscess, Multiple and/or large lesions intrahepatic prevent the take-up and malignancy excretion of bilirubin by the liver
cells
A B
Figure 4.19 (A) Fatty infiltration increases the hepato-renal contrast. The portal tracts are reduced in prominence,giving a more homogeneous appearance. (B) Attenuation of the beam by fat prevents demonstration of far-fieldstructures.
ch04.qxd 6/30/04 5:49 PM Page 96

focal lesions and therefore CT is often a usefuladjunct.
CirrhosisCirrhosis is a process associated with end-stagechronic liver disease and is not really a disease initself. It can result from a wide range of patholog-ical processes including chronic hepatitis and alco-holic disease.
Ultrasound appearances of cirrhosis
In cirrhosis bands of fibrous tissue are laid down inthe liver parenchyma between the hepatic lobules.This distorts and destroys the normal architecture ofthe liver, separating it into nodules. The process maybe micronodular, which gives a generally coarseechotexture, or macronodular in which discretenodules of 1 cm and above can be distinguished onultrasound (Fig. 4.20).
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 97
A B
C
Figure 4.20 (A) Micronodular cirrhosis in a patient with alcoholic liver disease. (B) Macronodular cirrhosis in apatient with primary biliary cirrhosis. Cirrhotic nodules are demonstrated throughout the peripheral hepatic substancewith a lobulated liver outline. Ascites is also present. (C) Monophasic ‘damped’ flow in the hepatic veins in a patientwith micronodular cirrhosis. This sign is not specific for cirrhosis and may be present under many other circumstances,including the presence of ascites.
ch04.qxd 6/30/04 5:49 PM Page 97

The hepatocellular damage which causes cirrhosisgives rise to hepatic fibrosis, a precursor of cirrhosis.The fibrosis itself may have very little effect on theultrasound appearances of the liver, but whenadvanced it is more highly reflective than normalliver tissue, giving the appearance of a ‘bright’ liveroften with a coarse texture.10 Unlike fatty change,which is potentially reversible, fibrosis is the result ofirreversible damage to the liver cells. The picture isfurther complicated by the association of fibrosiswith fatty change, which also increases theechogenicity. The acoustic attenuation properties offibrosis, however, are similar to normal liver, so theultrasound beam can penetrate to the posterior areasusing normal TGC settings. Fat, on the other hand,increases both the echogenicity and the attenuation,preventing penetration to the far field (Fig. 4.19).
The cirrhotic liver tends to shrink as the diseaseprogresses. However, it may be normal in size, ormay undergo disproportionate changes within dif-ferent lobes. In some patients the right lobe shrinks,giving rise to relative hypertrophy of the caudateand/or left lobes. This is likely to be due to thevenous drainage of the different areas of the liver.
The rigid nature of the diseased liver also causeshaemodynamic changes which can be demon-strated on spectral Doppler. The normally triphasichepatic venous waveform can become flattenedand monophasic (Fig. 4.20C). This is not neces-sarily specific to cirrhosis but is also associated withnumerous types of chronic liver disease or any con-dition, either intra- or extrahepatic, which com-presses the venous flow, such as polycystic liverdisease or the presence of ascites.12
The portal venous flow may also be compro-mised due to portal hypertension (see below) andis associated with numerous changes on ultrasoundshowing reduced velocity, reversed flow, partial ortotal thrombosis.
A compensatory increase in hepatic arterial flowto the liver may also be seen as a result of portalvenous compromise in portal hypertension.
Patients with cirrhosis are at increased risk ofdeveloping HCC, the detection of which is partic-ularly difficult in an already nodular liver. Both CTand ultrasound have a low sensitivity for detectingsmall focal lesions in cirrhotic livers.11 The use ofDoppler, contrast CT and contrast MRI continuesto improve the detection rate13 of small lesions andmany high-risk patients (i.e. those with cirrhosis)
undergo regular ultrasound screening with tumourmarkers (AFP) as a precaution.14 Small lesions con-tinue to present a diagnostic challenge, and the useof ultrasound contrast agents, and the develop-ment of MRI using iron oxide, are likely to improveboth detection and characterization of HCCs.15
Cirrhosis has numerous aetiologies:Alcoholic cirrhosis The spectrum of alcoholic
liver disease may take three forms: steatosis (alco-holic fatty liver), alcoholic hepatitis (often preced-ing cirrhosis) and finally cirrhosis. The later,chronic stages carry a worse prognosis, frequentlyassociated with portal hypertension and anincreased incidence of HCC (Fig. 4.18). Alcoholicliver disease may be halted or reversed in the earlystages in patients who discontinue alcohol intake,with subsequent nodular regeneration of hepatictissue (Fig. 4.20D). Nodular regeneration is noteasy to distinguish from frank cirrhosis or otherfocal liver lesions, such as HCC, and the use ofultrasound contrast agents, or other imaging suchas MRI may be required. Regenerating nodulesmay cause the liver to enlarge, whereas end-stagecirrhosis causes shrinkage of the liver.
Primary biliary cirrhosis (PBC) This is a pro-gressive cholestatic liver disease of unknown aetiologywhich occurs predominantly in middle-aged females.The term ‘cirrhosis’ may be rather misleading for theearly stages of this condition, which actually take theform of an inflammatory destruction of the intra-hepatic bile ducts. These early stages of cholangitisare not, strictly speaking, cirrhotic. However as thedestruction progresses, fibrotic bands form in aprocess of macronodular cirrhosis (Fig. 4.20B).
Treatment of PBC involves control of the asso-ciated symptoms of portal hypertension and pruri-tus, but its progression is inevitable. Livertransplantation now offers a successful therapeuticoption for these patients.16
Although the liver frequently looks normal onultrasound in the early stages of the disease, gall-stones, splenomegaly and lymphadenopathy can bedemonstrated in many patients.17
Secondary biliary cirrhosis This occurs as aresult of long-standing biliary obstruction. Causesusually include benign strictures or chronic stoneimpaction in the common bile duct causing pro-gressive, gradual obstruction over a period of time.This causes ascending cholangitis and jaundice. Thebile ducts may appear only mildly dilated on ultra-
ABDOMINAL ULTRASOUND98
ch04.qxd 6/30/04 5:49 PM Page 98

sound. It is also a recognized sequel of biliary atresiain children.
Other causes of cirrhosis Cirrhosis may bedrug-induced, particularly in patients on long-termtreatment or therapy.
It is also associated with many other diseases, suchas hepatitis (see p. 106) diabetes, ulcerative colitis,rheumatoid arthritis or any long-term conditions,acquired or congenital, which can affect the liver.
Congenital forms of cirrhosis exist due to meta-bolic disorders: Wilson’s disease (deposition ofcopper in the liver and kidneys), glycogen storagedisease (inability to break down glycogen to glu-cose), haemochromatosis (deposition of iron in theliver and pancreas) and others.
Clinical features and management of cirrhosis
Clinical presentation depends upon the aetiology,and may involve either chronic symptoms or anacute episode.
Pruritus, fatigue and jaundice, with steatorrhoeaand deranged LFTs (raised alkaline phosphataseand serum bilirubin in PBC, raised alanine amino-transferase [ALT] and aspartate aminotransferase[AST] in alcoholic disease) are generally present bythe later stages. This is followed by the symptomsof portal hypertension (see below), which is a poorprognostic feature associated with late-stagecirrhosis.
The process may be reversed in alcoholics whostop drinking. However the prognosis of any cir-rhotic condition is extremely poor if malignancy ispresent. In severe cases, the management revolvesaround trying to treat the symptoms of portalhypertension rather than the disease itself.
Liver transplant is now an established and highlysuccessful treatment option for PBC when thesymptoms can no longer be controlled with drugs.It is also an option for alcoholic cirrhosis, althoughthere is currently a significant incidence of post-transplant return to alcoholism.
Portal hypertensionPortal hypertension occurs when the pressure in theportal venous system is raised. This may happen as aresult of chronic liver disease, particularly in the cir-rhotic stage, when the nodular and fibrosed nature
of the parenchyma impedes the flow of blood intothe liver. It is significant because it causes numerousdeleterious effects on the patient, many of whichcan be recognized on ultrasound (Table 4.4).
Raised portal venous pressure is associated withseveral complications:
Portal vein signs Portal vein (PV) flow is influ-enced by numerous factors, including prandial state,patient position, exercise and cardiac output.18 Itsvelocity varies considerably in both cirrhotic andhealthy subjects, and it is essential to use colour andspectral Doppler to investigate the portal flow.19
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 99
Table 4.4 Summary of possible ultrasound appearances in cirrhosis
Normal May appear normal, parenchyma particularly in the early stagesChanges in texture Coarse texture (micronodular)
Irregular nodular appearance (macronodular)
Changes in Fibrosis increases the overall reflectivity echogenicity (but not the
attenuation)May be accompanied by fatty change, which increases bothechogenicity and attenuationgiving a hyper-reflective nearfield with poor penetration to theposterior liver
Changes in size Small, shrunken liverand outline Nodular, irregular surface outline
Possible disproportionate hypertrophy of left or caudatelobes
Focal lesions Increased incidence of HCCRegenerative nodules
Vascular Signs of portal hypertension:—changes in portal vein direction and velocity—possible thrombosis—varices and collaterals—increased hepatic arterial flow—flattened, monophasic hepatic venous flow on spectral Doppler(a non-specific finding)
Other signs AscitesSplenomegalyLymphadenopathy
HCC = hepatocellular carcinoma.
ch04.qxd 6/30/04 5:49 PM Page 99

The vein may appear dilated and tortuous, butnot invariably. (The normal portal vein diameterdoes not usually exceed 16 mm in a resting state;see Chapter 2).
Portal venous flow may be:
● normal in direction (hepatopetal) andvelocity.20
● reduced in velocity21 (Fig. 4.21A), < 10 cm/sec,although there is overlap with the normal range.
● damped, in which there is a lack of normalrespiratory variation of both the calibre and thewaveform of the splenic and portal veins. Thenormal spectrum has a ‘wavy’ characteristic,which may be lost.
● reversed (hepatofugal) (Fig. 4.21B). Thisindicates serious liver disease. Interestingly,patients with hepatofugal PV flow are muchless likely to suffer from bleeding varices,suggesting a type of ‘protective’ mechanismhere.
● balanced, in which both forward and reverselow velocity flow is present, a condition which may precede imminent thrombosis (Fig. 4.21C).
● thrombosed (Fig. 4.21D). Low-level echoesfrom the thrombus may be evident but withfresh thrombus the vein may appear anechoic,as in the normal vein. Although PV thrombosismost commonly results from portalhypertension in cirrhosis, there are many
ABDOMINAL ULTRASOUND100
A
B
Figure 4.21 The MPV in portal hypertension. (A) Portalvein (PV) velocity is greatly reduced. (B) Reversed PV flow inportal hypertension. Note the increased velocity of hepaticarterial flow indicated by the light colour of red justanterior to the portal vein. The patient has macronodularcirrhosis with ascites.
Box 4.1 Causes of portal vein thrombosis
Chronic liver disease—especially cirrhosis
Inflammatory—pancreatitis—acute cholecystitis—necrotizing enterocolitis
Malignancy—pancreatic tumour—gastric tumour
Coagulation disorders—may be associated with Budd–Chiari
syndrome
(Continued)
ch04.qxd 6/30/04 5:49 PM Page 100

PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 101
D
C
NORMAL
+34.9MM
1442 HZ
Figure 4.21 cont’d (C) Balanced PV flow. Alternateforward and reverse low-velocity flow on the Dopplerspectrum. The PV colour Doppler alternates red and blue.(D) PV thrombosis. The PV is dilated (arrows) and filledwith thrombus. A collateral vessel is seen anterior to this—not to be confused with the PV—as this is a sourceof false-negative ultrasound results. (E) Non-dilated,thrombosed PV (arrow) with collaterals demonstrated onpower Doppler.
E
other causes, including inflammatory ormalignant conditions which may surround,compress or invade the portal and/or splenicveins (Box 4.1). The thrombosis may be totalor partial.
● hepatopetal main PV flow with hepatofugalperipheral flow may be a sign of HCC,
requiring careful scanning to identify thelesion.
● cavernous transformation. A network ofcollateral vessels may form around athrombosed main portal vein at the porta,especially if the thrombosis is due to extrahepatic causes (for example
ch04.qxd 6/30/04 5:49 PM Page 101
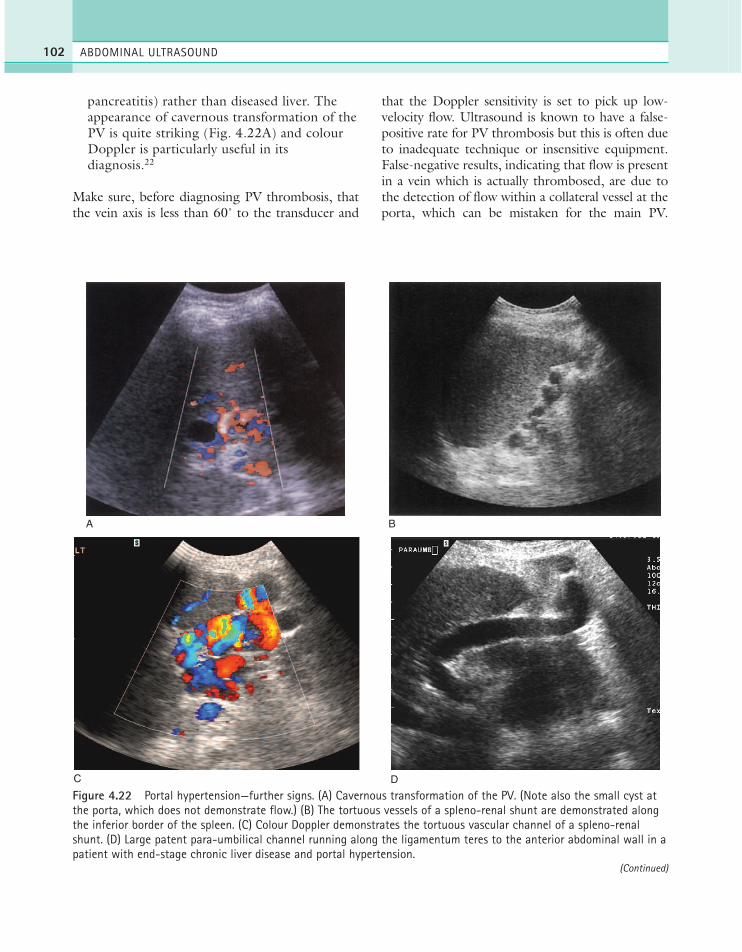
pancreatitis) rather than diseased liver. Theappearance of cavernous transformation of thePV is quite striking (Fig. 4.22A) and colourDoppler is particularly useful in itsdiagnosis.22
Make sure, before diagnosing PV thrombosis, thatthe vein axis is less than 60˚ to the transducer and
that the Doppler sensitivity is set to pick up low-velocity flow. Ultrasound is known to have a false-positive rate for PV thrombosis but this is often dueto inadequate technique or insensitive equipment.False-negative results, indicating that flow is presentin a vein which is actually thrombosed, are due tothe detection of flow within a collateral vessel at theporta, which can be mistaken for the main PV.
ABDOMINAL ULTRASOUND102
A B
C D
Figure 4.22 Portal hypertension—further signs. (A) Cavernous transformation of the PV. (Note also the small cyst atthe porta, which does not demonstrate flow.) (B) The tortuous vessels of a spleno-renal shunt are demonstrated alongthe inferior border of the spleen. (C) Colour Doppler demonstrates the tortuous vascular channel of a spleno-renalshunt. (D) Large patent para-umbilical channel running along the ligamentum teres to the anterior abdominal wall in apatient with end-stage chronic liver disease and portal hypertension.
(Continued)
ch04.qxd 6/30/04 5:49 PM Page 102
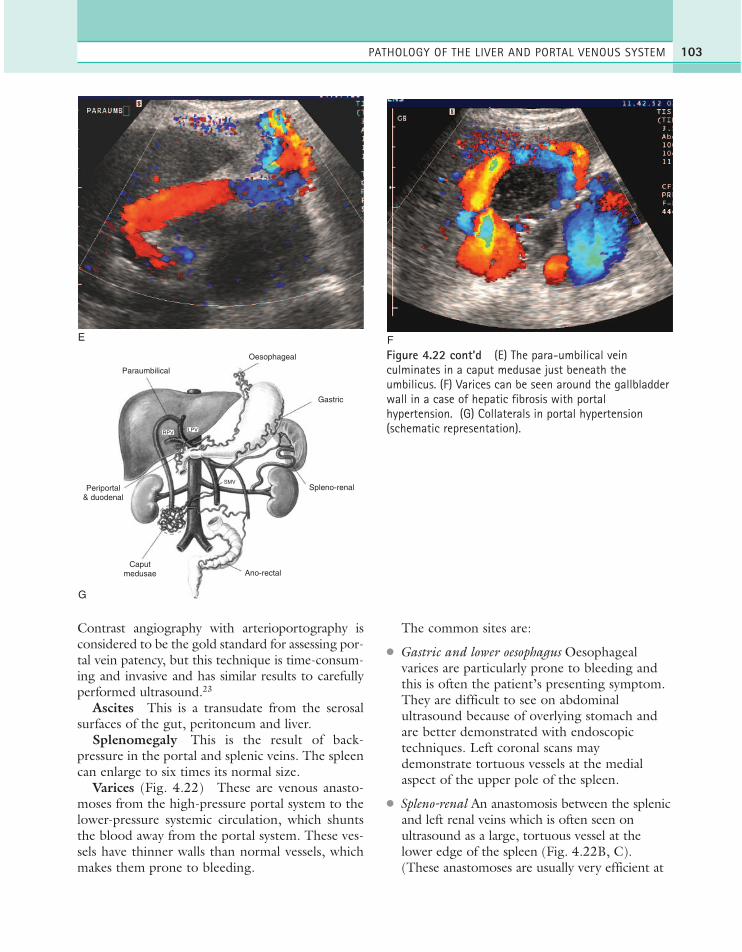
Contrast angiography with arterioportography isconsidered to be the gold standard for assessing por-tal vein patency, but this technique is time-consum-ing and invasive and has similar results to carefullyperformed ultrasound.23
Ascites This is a transudate from the serosalsurfaces of the gut, peritoneum and liver.
Splenomegaly This is the result of back-pressure in the portal and splenic veins. The spleencan enlarge to six times its normal size.
Varices (Fig. 4.22) These are venous anasto-moses from the high-pressure portal system to thelower-pressure systemic circulation, which shuntsthe blood away from the portal system. These ves-sels have thinner walls than normal vessels, whichmakes them prone to bleeding.
The common sites are:
● Gastric and lower oesophagus Oesophagealvarices are particularly prone to bleeding andthis is often the patient’s presenting symptom.They are difficult to see on abdominalultrasound because of overlying stomach andare better demonstrated with endoscopictechniques. Left coronal scans maydemonstrate tortuous vessels at the medialaspect of the upper pole of the spleen.
● Spleno-renal An anastomosis between the splenicand left renal veins which is often seen onultrasound as a large, tortuous vessel at thelower edge of the spleen (Fig. 4.22B, C).(These anastomoses are usually very efficient at
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 103
E F
Oesophageal
Gastric
Paraumbilical
Periportal& duodenal
Caputmedusae Ano-rectal
Spleno-renalSMV
G
LPVRPV
Figure 4.22 cont’d (E) The para-umbilical veinculminates in a caput medusae just beneath theumbilicus. (F) Varices can be seen around the gallbladderwall in a case of hepatic fibrosis with portalhypertension. (G) Collaterals in portal hypertension(schematic representation).
ch04.qxd 6/30/04 5:49 PM Page 103

redirecting the blood from the portal systemand so these patients have a lower incidence of gastric varices and therefore a betterprognosis.)
● Periumbilical A substantial vessel can often beseen in the liver lying in the ligamentum teres(Fig. 4.22D, E), and running down theanterior abdominal wall to a knot of vessels atthe umbilicus, the so-called ‘caput medusae’.(A patent para-umbilical channel mayoccasionally be seen in normal patients, butwith a diameter of 1 or 2 mm.)
● Porta hepatis Varices around the main portalvein itself, especially if the latter is thrombosed(see below).
● Gallbladder wall Rarely, varices form aroundthe gallbladder wall to bypass the main portalvein and feed into the intrahepatic portalbranches (Fig. 4.22F).
● Coronary vein A vessel may be seen arisingfrom the portal vein near the superior mesentericvein, directing blood in a cephalic direction.(This can sometimes be seen in normal patients.)
It is fair to say that the extent of portosystemic col-laterals is usually underestimated on ultrasound.However, a systematic approach which investigatesall the possible sites can demonstrate up to 90% ofcollaterals.20, 24 (Fig. 4.22G).
The hepatic artery This may also be anotherultrasound clue to compromised portal venousflow. The main hepatic artery may demonstrateincreased flow velocity, especially if the PV isthrombosed. This is a compensatory mechanism tomaintain the blood flow into the liver. The mainhepatic artery may appear enlarged and more obvi-ous than usual on ultrasound, and in some cases,peripheral intrahepatic arterial flow is also easilydemonstrated (Fig. 4.23).
ABDOMINAL ULTRASOUND104
A B
NORMAL 3372NORMAL 2098
HZ
+24.8MM
Figure 4.23 (A) Vigorous, high-velocity middle hepatic artery (MHA) flow in the presence of portal vein thrombosis.(B) Arterial flow is also readily demonstrated in the peripheral intrahepatic arteries.
ch04.qxd 6/30/04 5:49 PM Page 104

Management of portal hypertension
This depends on the cause and on whether the PVis still patent or not. The most pressing problem islikely to be bleeding from varices, especiallyoesophageal varices, and patients may present withmelaena or haematemasis. Management mayinvolve medical means, endoscopic techniques(either injection sclerotherapy of oesophagealvarices or banding, in which a ring is placed aroundthe base of the varix causing thrombosis), com-pression using a Sengstaken tube with an inflatedballoon, surgical or percutaneous transjugularintrahepatic portosystemic shunt (TIPS). All thesemethods are relatively temporary, and can relievepressure in the portal venous system, controllingportal hypertensive complications in order to planfurther management.
TIPS is a percutaneous method used to relievethe symptoms of portal hypertension in cirrhoticpatients. It connects the portal vein directly to theright hepatic vein with an expandable metal shunt.
A catheter and guide wire are passed, under X-raycontrol, through the jugular vein to the inferiorvena cava (IVC) and into the hepatic vein. A path-way is then forged with a needle through the liverparenchyma to join the PV with the insertion of ashunt to keep the channel open. Portal venousblood then effectively bypasses the liver, flowingstraight into the hepatic vein. This usually results inthe speedy decompression of varices and improve-ment of other symptoms of portal hypertension.
Ultrasound may be used to monitor stentpatency (Fig. 4.24). Shunt stenosis or occlusion is acommon problem, particularly in long-term shunts;this can be detected with routine postprocedureultrasound screening and treated with reinterven-tion. The most common site for a stenosis is at thejunction of the stent with the PV. The velocity ofblood flow in the shunt should be between 1 and2 m/s and this should be consistent throughout thestent. A variety of Doppler parameters can be usedto detect the malfunction of the shunt. A shuntvelocity of less than 50 cm/s is a sign of stenosis25
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 105
A B
IVCRHV
RPV
LPV
MPV PV
HA
STENT
Figure 4.24 (A) Transjugular intrahepatic portosystemic shunt (TIPS). (B) TIPS shunt in a patient with severe portalhypertension. The higher-velocity MHA is seen anterior to the shunt, which demonstrates flow from right to left of theimage.
(Continued)
ch04.qxd 6/30/04 5:50 PM Page 105

but this has not been reproducible in all institu-tions, and other factors such as a change of 50 cm/sor more from the baseline scan, a localized eleva-tion of velocity at the stenotic site (with an upperlimit of normal of up to 220 cm/s) or an increasein the velocity gradient (as the stenotic stentexhibits an increased maximum velocity and adecreased minimum velocity) are also poor prog-nostic signs.26
TIPS is regarded as a temporary measure but canconsiderably improve the patient’s condition pend-ing treatment of chronic liver disease, relievinghaemorrhage from varices, relieving intractableascites and stabilizing liver function. It is increas-ingly used as a bridge to liver transplant. It is alsoused as an alternative to surgery in patients who arepoor surgical risks, although the diversion of bloodaway from the liver can result in adversely affectedliver function and eventual encephalopathy.27
HepatitisViral hepatitis
Acute viral hepatitis may be caused by one of sev-eral viruses: A, B, C, D or E. The viruses whichcause hepatitis B, C and D may also go on tochronic disease and predispose the liver to HCC in
the later stages. Vaccines exist for A and B, but notyet for the others. Hepatitis A and E are transmit-ted via contaminated food or drink and are partic-ularly prevalent in third-world countries. HepatitisB, C and D are likely to be transmitted throughtransfusion or sexual contact.
Fulminant hepatitis, in which there is completeliver failure, is a rare complication of acute hepati-tis B.
Most patients with acute hepatitis recover com-pletely, but hepatitis B, C and D may go on todevelop chronic hepatitis. This has two forms:
● Chronic persistent hepatitis is a mild form ofinflammation limited to the portal tracts. It isusually of comparatively little clinical significanceand does not show ultrasound changes.
● Chronic active hepatitis is a more serious andaggressive form of the disease which causesdiffuse, persistent inflammation. This mayeventually lead to cirrhosis, which can beassociated with HCC.
Other causes of acute hepatitis
Acute hepatitis may also occur with many otherconditions. The most common of these are alco-holic hepatitis (see alcoholic cirrhosis, above),infectious mononucleosis, herpesvirus andcytomegalovirus.
Patients with AIDS and those who are immuno-suppressed are also particularly prone to hepatitis.
Clinical features of hepatitis
It may be asymptomatic (patients who have anti-bodies present, but who deny having had the dis-ease, must have had subclinical disease at onetime). Other signs include lethargy, nausea, vomit-ing and jaundice. The liver is enlarged and tenderin the acute phase.
The diagnosis and classification of hepatitis mustbe made histologically, ideally with an ultrasound-guided biopsy.
Ultrasound appearances of hepatitis
The liver frequently appears normal on ultrasound.In the acute stage, if ultrasound changes are pres-
ABDOMINAL ULTRASOUND106
C
HA
Figure 4.24 cont’d (C) Thrombosed TIPS shunt. Arecanalized left portal vein (LPV) (arrow) can be seenanterior to this.
ch04.qxd 6/30/04 5:50 PM Page 106

ent, the liver is slightly enlarged with a diffuselyhypoechoic parenchyma. The normally reflectiveportal tracts are accentuated in contrast (Fig.4.25A). This ‘dark liver’ appearance is non-specific,and may also occur in leukaemia, cardiac failure,AIDS and other conditions.
The inflammation may start at the portal tractsworking outwards into the surroundingparenchyma, the so-called periportal hepatitis. Insuch cases, the portal tracts become less well-defined and hyperechoic. The gallbladder wall mayalso be thickened, and some patients demonstrateportal lymphadenopathy.
If the disease progresses to the chronic stage,the liver may reduce in size, becoming nodular andcoarse in appearance (Fig. 4.25).
Primary sclerosing cholangitis (PSC)This is a primary disease of the biliary ducts, mostfrequently found in young men. Like PBC, it is acholestatic disease. It is discussed more fully inChapter 3, but is included here for reference as itmay often result in a coarse liver texture, similar tothat seen in some forms of cirrhosis, and is associ-ated with the formation of cholangiocarcinomas.
Budd–Chiari syndrome (BCS)Budd–Chiari syndrome is the name given to thesymptoms associated with partial or completeocclusion of the hepatic veins. There are numerouscauses of hepatic vein occlusion, of which the mainones are:
● congenital or acquired coagulation disorders,which may affect both the hepatic and portalveins (potentially treatable by liver transplant)
● malignancy: primary or secondary liver tumourmay invade the hepatic veins or may travel upthe IVC (for example renal carcinoma) toocclude the hepatic vein confluence
● congenital web obstructing the IVC (surgicallyremovable).
Ultrasound appearances of Budd–Chiarisyndrome
In the acute stage, the liver may enlarge. As the con-dition progresses, compensatory hypertrophy of any‘spared’ segments occurs—usually the caudate lobe,because the venous drainage from here is inferior tothe main hepatic veins. The hepatic veins may bedifficult or impossible to visualize (Fig. 4.26).
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 107
A BFigure 4.25 (A) Subtle changes of oedema in acute hepatitis: the liver is hypoechoic compared with the right kidney,mildly enlarged and has prominent portal tracts. (B) Chronic hepatitis and cirrhosis, demonstrating a coarse-textured,nodular liver.
ch04.qxd 6/30/04 5:50 PM Page 107

Dilated serpiginous collateral veins may form todirect blood away from the liver and in some casesthe portal venous flow reverses to achieve this. Thespleen also progressively enlarges and, if the diseaseis long-standing, the liver becomes cirrhotic,acquiring a coarse texture.
Ascites may also be present, particularly if thereis complete obstruction involving the IVC. Thecause of IVC obstruction may be a web, which canoccasionally be identified on ultrasound. If thecause of BCS is a coagulation disorder, the portalvenous system may also be affected by thrombosis,causing portal hypertension.
Doppler is particularly helpful in diagnosingBCS.21 The hepatic veins and IVC may be totally
or partially occluded; if partial, the waveforms maybecome flattened, losing their characteristic tripha-sic pattern. In some cases flow may be reversed inthe IVC, hepatic and/or portal veins. Ultrasoundmay miss partial hepatic vein occlusion, but the useof contrast agents in suspected cases of BCS mayimprove diagnostic accuracy.
Management of Budd–Chiari syndrome
This depends upon the cause. Both medical andsurgical treatments have mixed success. Severecoagulative disorders may have to be transplanted,although there is a significant risk of recurrence. Ifthe cause is an IVC web, this may be surgically
ABDOMINAL ULTRASOUND108
A
HV
B
RHV
MHV
C
Figure 4.26 (A) Budd–Chiari syndrome (BCS). The MHVis tortuous and strictured, and difficult to identify onultrasound. (B) Large collaterals are seen (arrows) nearthe surface of the liver in BCS. (C) Tumour thrombusfrom a renal carcinoma occludes the inferior vena cava(IVC), causing BCS.
ch04.qxd 6/30/04 5:50 PM Page 108

removed. In some patients, palliative treatmentwith percutaneous stent placement in the hepaticveins can relieve the symptoms of ascites andvarices.28 Ultrasound may assist in guiding theplacement of stents.
Cystic fibrosisCystic fibrosis, one of the most common chromo-somal abnormalities, has historically been associ-ated with the paediatric population. However,increasing success in the management of this con-dition, particularly in specialist centres, hasimproved the current median survival to 40 yearsfor a child born in the last decade.29
Ultrasound appearances
Progression of the disease means that changes inthe ultrasound appearances of the liver are moresevere in adults (Fig. 4.27) than children, in whomthe liver frequently looks normal (see Chapter 9).Progressive hepatic fibrosis in adults results in ahyperechoic and enlarged liver. Ultimately the liverbecomes coarse and nodular in appearance as thefeatures of cirrhosis become apparent. Portalhypertension is a common finding at this stagewith splenomegaly, varices, ascites and possibly PV
thrombosis (see above). Changes of fibrosis canalso be seen in the pancreas.
Congestive cardiac diseasePatients with cardiac failure frequently demon-strate dilated hepatic veins in the liver, sometimeswith a dilated IVC. Although this may give thesonographer the overall impression of hypo-echogenicity, due to the proliferation of large, an-echoic vessels, the liver texture itself tends to be ofeither normal echogenicity, or, in the later stages offailure, hyperechoic.
Mitral valve disease may be the cause of alteredwaveforms in the hepatic veins; the usual triphasicflow becomes more pronounced, with a highly pul-satile waveform (Fig. 4.28A).
The portal venous waveform may sometimes bealtered in cases of tricuspid valve regurgitation.The normally monophasic flow may become bidi-rectional (Fig. 4.28B). This phenomenon, associ-ated with congestive heart failure, also occurs incirrhosis prior to PV thrombosis. However the lat-ter ‘balanced’ flow is of very low velocity (Fig.4.21C), while that due to tricuspid regurgitation isa higher-velocity, more pulsatile waveform.
Liver conditions in pregnancyAcute fatty liver
This rare condition occurs in the third trimester ofpregnancy. Acute fatty deposition in the liver tissuecan cause abdominal pain, vomiting and jaundice.The liver may appear sonographically normal or bediffusely hyperechoic, although focal areas of fattydeposition have also been reported. Acute fattyliver tends to resolve during the first month of thepostpartum period, but may in rare cases progressto cause liver failure.
HELLP syndrome
The HELLP syndrome is a rare complication ofpregnancy occurring in up to 20% of motherswith severe pre-eclampsia.30 Haemolytic anaemia(H), elevated liver enzymes (EL) and low plateletcount (LP) cause abdominal pain, nausea andfever.
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 109
Figure 4.27 Marked changes in the liver of an adultpatient with cystic fibrosis.
ch04.qxd 6/30/04 5:50 PM Page 109

Its complications include areas of haemorrhage(either subcapsular haematoma or intraparenchy-mal bleeding), infarction or necrosis within theliver which can be identified with ultrasound orMRI scanning (Fig. 4.29).
The recognition and prompt diagnosis of acutefatty liver and HELLP syndrome reduce maternalmorbidity by enabling emergency caesarean sec-tion to be performed.
Causes of changes in liver reflectivity are listed inTable 4.5. Causes of free intraperitoneal fluid arelisted in Table 4.6.
LIVER TRANSPLANTS
Indications for transplantLiver transplantation has now become a successfultreatment for many chronic liver conditions and isalso used in the treatment of fulminant hepatic fail-ure. The range of indications has steadily increasedas surgical techniques have developed andimmunosuppression has improved (Table 4.7). Themajority of hepatic transplants (80%) are still per-formed in patients with cirrhosis and primarycholestatic disease.31
The 5-year survival rate is between 65 and 90%.32,33
This is highly dependent upon both the primary dis-ease and upon the clinical state of the patient.
Currently, seven centres in the UK perform livertransplants, totalling around 700 patients per year.
ABDOMINAL ULTRASOUND110
A
RHV
B
Figure 4.28 (A) The waveform of the hepatic vein in apatient with mitral valve disease demonstrates increasedpulsatility. (B) The portal vein has an abnormal, highlypulsatile flow waveform in this patient with tricuspidregurgitation. This is quite distinct from the low-velocity‘balanced flow’ of portal hypertension.
Figure 4.29 Liver infarct in pregnancy in a patient withHELLP syndrome.
ch04.qxd 6/30/04 5:50 PM Page 110

This figure has remained relatively stable for sometime and is dependent upon the availability ofdonor organs.
Worldwide, the most common cause for livertransplantation is hepatitis C. The indications fortransplant are now many and varied and the numberof absolute contraindications continues to dwindle,including AIDS and extrahepatic malignancy.34
Transplantation in patients with malignant liverdisease has a poorer prognosis with a lower 5-yearsurvival. However, the presence of small HCCsin patients with chronic liver disease is not acontraindication, and tumour recurrence isuncommon in these patients. Patients with largerHCCs (> 3 cm) and those with cholangiocarci-noma have a higher rate of recurrence post-trans-plant, and are generally not considered fortransplantation.
Preoperative assessmentThe ultrasound scan is one of many investigationsleading up to transplantation. The diagnosis ofliver pathology often uses ultrasound scanning as a
first line, augmented by histology and additionalcross-sectional imaging.
The role of ultrasound includes contributing to,or confirming, the initial diagnosis, assessing thedegree of severity and associated complications ofthe disease and providing guidance for biopsy. Animportant objective is also to exclude patients forwhom liver transplant is not feasible, or of littlebenefit (Table 4.8), for example those with extra-hepatic malignant disease.
The preoperative scan includes all the features ofany abdominal ultrasound survey, with the empha-sis on assessing the complications of the disease,depending upon the initial diagnosis.
In particular, the sonographer should look for:
● Portal vein thrombosis: this may be acontraindication to transplant if it is extensive,
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 111
Table 4.5 Causes of changes in liver reflectivity
Increased echogenicity—fatty infiltration (also increases attenuation)—fibrosis—cirrhosis—chronic hepatitis—cystic fibrosis
Decreased echogenicity—acute hepatitis—AIDS—leukaemia—toxic shock syndrome—can be normal, particularly in the young
Coarse or nodular texture—cirrhosis, various aetiologies—regenerating nodules—metastases/diffuse metastatic infiltration—chronic or granulomatous hepatitis—PSC, PBC—diffuse infective process, e.g. with AIDS or
immunosuppressed patients
AIDS = acquired immunodeficiency syndrome; PSC = primary scle-rosing cholangitis; PBC = primary biliary cirrhosis.
Table 4.6 Causes of free intraperitoneal fluid
Organ failure—chronic liver disease with portal hypertension—acute liver failure—renal failure—cardiac failure
MalignancyInflammatory
—acute pancreatitis—acute cholecystitis—peritonitis, TB—Crohn’s disease
Budd–Chiari syndromePostoperative
—blood, urine, bile or lymphatic fluidOrgan damage
—biliary perforation—urinary tract perforation—bowel perforation (e.g. in diverticulitis)—trauma to liver, spleen or pancreas
CAPD fluid—patients on peritoneal dialysis
Ruptured ectopic pregnancy—haemoperitoneum
Gynaecological—ruptured ovarian cyst, ovarian carcinoma, ovarian
fibroma—(Meig’s syndrome), ovarian torsion, PID
TB = tuberculosis; CAPD = continuous ambulatory peritoneal disease;PID = pelvic inflammatory disease.
ch04.qxd 6/30/04 5:50 PM Page 111
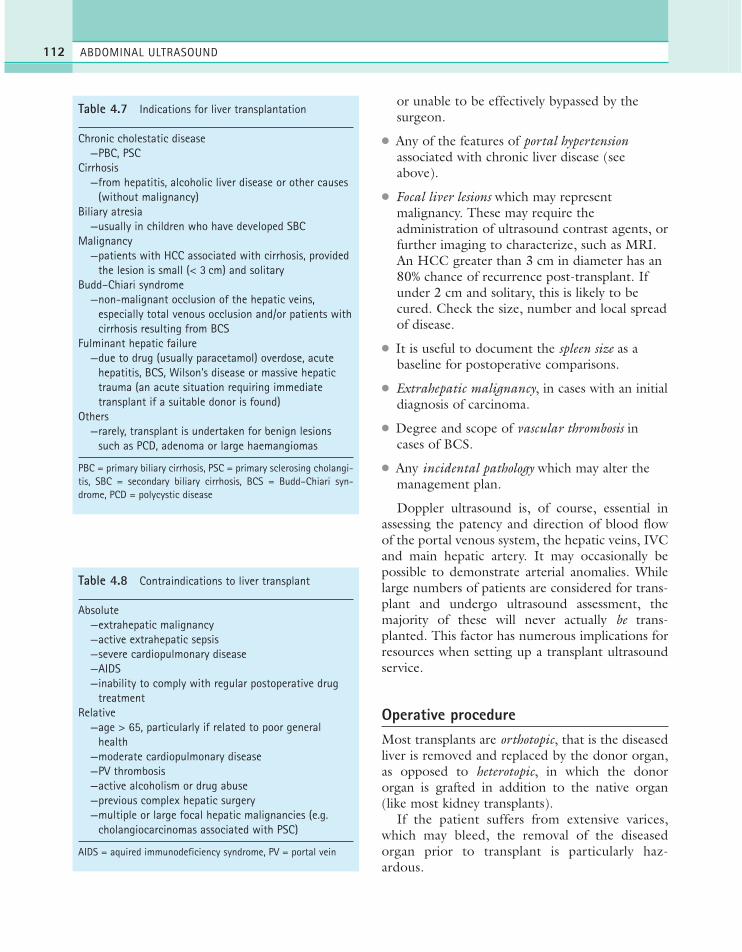
or unable to be effectively bypassed by thesurgeon.
● Any of the features of portal hypertensionassociated with chronic liver disease (seeabove).
● Focal liver lesions which may representmalignancy. These may require theadministration of ultrasound contrast agents, orfurther imaging to characterize, such as MRI.An HCC greater than 3 cm in diameter has an80% chance of recurrence post-transplant. Ifunder 2 cm and solitary, this is likely to becured. Check the size, number and local spreadof disease.
● It is useful to document the spleen size as abaseline for postoperative comparisons.
● Extrahepatic malignancy, in cases with an initialdiagnosis of carcinoma.
● Degree and scope of vascular thrombosis incases of BCS.
● Any incidental pathology which may alter themanagement plan.
Doppler ultrasound is, of course, essential inassessing the patency and direction of blood flowof the portal venous system, the hepatic veins, IVCand main hepatic artery. It may occasionally bepossible to demonstrate arterial anomalies. Whilelarge numbers of patients are considered for trans-plant and undergo ultrasound assessment, themajority of these will never actually be trans-planted. This factor has numerous implications forresources when setting up a transplant ultrasoundservice.
Operative procedureMost transplants are orthotopic, that is the diseasedliver is removed and replaced by the donor organ,as opposed to heterotopic, in which the donororgan is grafted in addition to the native organ(like most kidney transplants).
If the patient suffers from extensive varices,which may bleed, the removal of the diseasedorgan prior to transplant is particularly haz-ardous.
ABDOMINAL ULTRASOUND112
Table 4.7 Indications for liver transplantation
Chronic cholestatic disease—PBC, PSC
Cirrhosis—from hepatitis, alcoholic liver disease or other causes
(without malignancy)Biliary atresia
—usually in children who have developed SBCMalignancy
—patients with HCC associated with cirrhosis, providedthe lesion is small (< 3 cm) and solitary
Budd–Chiari syndrome—non-malignant occlusion of the hepatic veins,
especially total venous occlusion and/or patients withcirrhosis resulting from BCS
Fulminant hepatic failure—due to drug (usually paracetamol) overdose, acute
hepatitis, BCS, Wilson’s disease or massive hepatictrauma (an acute situation requiring immediatetransplant if a suitable donor is found)
Others—rarely, transplant is undertaken for benign lesions
such as PCD, adenoma or large haemangiomas
PBC = primary biliary cirrhosis, PSC = primary sclerosing cholangi-tis, SBC = secondary biliary cirrhosis, BCS = Budd–Chiari syn-drome, PCD = polycystic disease
Table 4.8 Contraindications to liver transplant
Absolute—extrahepatic malignancy—active extrahepatic sepsis—severe cardiopulmonary disease—AIDS—inability to comply with regular postoperative drug
treatmentRelative
—age > 65, particularly if related to poor generalhealth
—moderate cardiopulmonary disease—PV thrombosis—active alcoholism or drug abuse—previous complex hepatic surgery—multiple or large focal hepatic malignancies (e.g.
cholangiocarcinomas associated with PSC)
AIDS = aquired immunodeficiency syndrome, PV = portal vein
ch04.qxd 6/30/04 5:50 PM Page 112
Donor livers which are too large for the recipi-ent, for example in small children, may require cut-ting down to reduce the size. There is anincreasing trend towards a ‘split liver’ technique, inwhich the donor liver is divided to provide for tworecipients. The lack of donors has also led to thedevelopment of living-related donor transplanta-tion for paediatrics.
The transplant requires five surgical anasto-moses:
● suprahepatic vena cava● infrahepatic vena cava● hepatic artery (either end-to-end, or end-to-
side to aorta)● PV● CBD (the gallbladder is removed).
IOUS is useful for assessing the size and spreadof intrahepatic neoplastic growths and to assessvascular invasion in the recipient. Mapping of thehepatic vascular anatomy in living-related donors isalso feasible using IOUS.
IOUS with Doppler is also useful for assessingthe vascular anastomoses and establishing if portalvenous and hepatic arterial flow are adequate.
Postoperative assessmentUltrasound plays a key role in the postoperativemonitoring of liver transplant patients. Numerouscomplications are possible (Table 4.9) and many ofthese can be diagnosed with ultrasound.
The operation is generally followed by ciclosporinimmunosuppression. Blood levels of ciclosporin are aclosely monitored balancing act; too low and thegraft may reject, too high and the toxic effects ofthe drug may affect the kidneys.
Liver function is biochemically monitored forearly signs of complications. Elevated serum biliru-bin, alkaline phosphatase and/or aminotransferaselevels are present with most types of graft dysfunc-tion or complication and are investigated first withultrasound.
Renal dysfunction is a further recognized com-plication following transplant. This can be due tovarious causes, including ciclosporin nephrotoxic-ity, intraoperative hypotension or preoperativerenal failure.
Postoperative ultrasound appearancesThe vessels and vascular anastomoses
These are potential sites of complication in termsof thrombosis, stenosis, occlusion or leakage.
The hepatic artery is vital to graft success as itis the sole vascular supply to the biliary system.Most hepatic artery occlusions occur relativelysoon after operation, before a good collateral sup-ply is able to be established.
A blocked hepatic artery quickly results inischaemia with resultant hepatic necrosis and istherefore treated as an emergency requiring surgicalintervention and, frequently, retransplant. Taken incontext with the clinical picture, the patient mayproceed immediately to surgery if the ultrasounddiagnosis of occlusion is confident. If doubt exists,MRI or X-ray angiography may be performed.Ensure the artery is scanned intercostally to main-tain a low vessel-to-beam angle, and that the
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 113
Table 4.9 Postoperative liver transplant complications
Infection—hepatic abscess/general abdominal infection leading
to sepsisVascular
—anastomotic leaks → haematoma—thrombosis or stenosis → ischaemia/infarction
Biliary—bile duct stricture or stenosis leading to dilatation—bile leak → biloma
Rejection—acute episodes are common in up to 80% of patients
in the first 2 weeks and are of variable severityOther medical complications
—neurological—renal dysfunction
Recurrence of original disease—hepatitis—cholangiocarcinoma or hepatocellular carcinoma—Budd–Chiari syndrome—PSC
Post-transplant lymphoproliferative disorder (PTLD)—more common in children, PTLD is more usually
associated with immunosuppressions, occurringwithin the first year of transplant
ch04.qxd 6/30/04 5:50 PM Page 113

Doppler sensitivity and filter controls are set for lowvelocities if arterial flow is not found.
Hepatic artery thrombosis or stenosis can lead tobile duct necrosis, causing bile leaks and abscesses,or areas of infarction within the liver tissue.
Hepatic artery stenosis/thrombosis is still a rel-atively common post-transplant complication inup to 12% of adult patients. Colour Doppler ultra-sound detects between 50% and 86% of totalocclusions35 and angiography is still consideredthe gold standard although ultrasound continuesto increase its clinical value here.36 The adminis-tration of ultrasound contrast media, whilst poten-tially useful for detection of flow, is rarelynecessary in practice.
Stenosis of the artery at the site of anastomosisis detected by examining the Doppler spectrum(Fig. 4.30). The systolic upstroke tends to bedelayed (‘tardus parvus’ pattern) downstream ofthe stenosis;37 the acceleration time is increased(over 0.08 seconds) and the resistance indexdecreased (less than 55) in many cases.38 Both oreither of these indices may be affected, giving asensitivity and specificity of 81% and 60% for thediagnosis of hepatic artery stenosis with Doppler.39
The appearance of the hepatic artery waveformimmediately postoperatively is often one of a smallspike with no EDF. This is not a significant findingand will usually develop into the more familiarwaveform with forward EDF by 48 hours aftertransplantation.40
The PV anastomosis is readily demonstrated atthe porta. The waveform invariably shows turbu-lence associated with the anastomotic site (Fig.4.31A), as the diameters of the donor and recipi-ent veins invariably differ. This is not significant initself but can indicate a clinically significant steno-sis when accompanied by high velocities of greaterthan 100 cm/sec (Fig. 4.31B).
PV stenosis also causes a steadily increasing spleensize, which is why it is important to have a baselinemeasurement of the spleen. PV thrombosis shouldonly be diagnosed using the correct Doppler set-tings (low pluse repetitions frequency and optimumcolour gain) and at an angle as near parallel to thebeam as possible. In the absence of colour flow,power Doppler may be helpful in confirmingthrombosis, as it is less angle-dependent, and con-trast may be used to increase the level of confidence.
It is also possible to have a blocked main PV withpatent intrahepatic PVs, due to collateral formation.
The IVC infrahepatic anastomosis is also readilyseen on ultrasound (Fig. 4.32). Because of the
ABDOMINAL ULTRASOUND114
A
B(i)
B(ii)
Figure 4.30 (A) MHA in a liver transplant demonstratedon power Doppler, lying anterior to the MPV. (B) i, Normalhepatic artery (HA) waveform post-transplant; ii, 1 monthlater, the systolic slope shows a tardus parvus pattern.HA stenosis was confirmed with angiography.
ch04.qxd 6/30/04 5:50 PM Page 114

near-perpendicular angle of the IVC to the beam itis difficult to assess blood flow velocity in the IVC.Power Doppler is helpful in confirming patency intechnically difficult cases as it is angle-independent.Thrombosis in the IVC is a relatively rare compli-
cation of transplants, accounting for fewer than 3%of patients.
If the transplant has been performed for BCS,pay particular attention to the hepatic veins, whichshow a tendency to re-thrombose in some patients.
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 115
A
B
Figure 4.31 (A) The portal vein in a liver transplantdemonstrates a very turbulent waveform because of the surgicalanastomosis. This is not usually a significant finding. (B) MPVstenosis. A high-velocity jet is seen through the stenosis (arrow)at the site of the anastomosis. The spectral Doppler waveformexceeded the Nyquist limit at this point.
ch04.qxd 6/30/04 5:50 PM Page 115

The common bile duct
This should be carefully monitored postopera-tively. A measurement serves as a baseline fromwhich to detect small degrees of dilatation whichmay imply stenosis or obstruction. Even relativelyminor dilatation can be significant in the transplantpatient; cholestasis can precipitate ascending biliaryinfection which may subsequently form liverabscesses, a process which may be aggravated byimmunosuppression.
Biliary complications occur in up to 15% of trans-plants and most biliary complications become evi-dent during the first 3 months, although latestenosis can occur after this. Strictures commonlyoccur at the anastomosis due to scar tissue, butother, non-anastomotic strictures can result fromhepatic artery insufficiency causing ischaemia.Leakage is a comparatively rare event.
Focal lesions
Focal lesions within the parenchyma of the trans-plant liver are usually a poor prognostic indicator.Hepatic abscesses may be multiple and are oftenacoustically subtle in the early stages, with echopatterns closely similar to normal liver tissue.Other causes of focal lesions in the early postoper-
ative period may be due to infarction and are asso-ciated with interruption of the arterial supply.These can be hyper- or hypoechoic, have well-defined borders and do not exert a mass effect(Fig. 4.33).
The longer the interval between removing andtransplanting the donor liver, the greater the likeli-hood of ischaemic patches forming.
In patients who have been transplanted follow-ing cirrhosis with malignancy, recurrence of HCCmay also be a serious complication.
Post-transplant lymphoproliferative disordermay also demonstrate hypoechoic focal lesionswithin the liver, occasionally also involving thespleen and kidneys.
Fluid collections
These can frequently be demonstrated and moni-tored with ultrasound. These may representhaematoma (Fig. 4.34), seroma, loculated ascitesor biloma. It is not possible to differentiate differ-ent types of collection with ultrasound alone. Theappearances are taken in conjunction with the clin-ical features and the role of ultrasound is primarilyto monitor the gradual resolution of the collection.
It is important to determine if a collection isinfected in a clinically ill patient. This cannot be
ABDOMINAL ULTRASOUND116
Figure 4.32 The site of anastomosis in the IVC in aliver transplant.
Figure 4.33 An area of infarction in a liver transplant.
ch04.qxd 6/30/04 5:50 PM Page 116

done on the ultrasound appearances alone andguided aspiration is usually required.
Haematomas frequently resolve if left untreated.However, a large haematoma could result from ananastomotic leak requiring surgical intervention. Aleaking bile duct anastomosis is potentially a seri-ous complication which could cause peritonitis.Drainage under ultrasound guidance is a tempo-rary option but surgical repair is invariably neces-
sary. Recent recipients of liver transplants will oftenhave some free intraperitoneal fluid and a rightpleural effusion, which resolve spontaneously.
Rejection
Rejection episodes are common in the first 2 weeksafter transplantation. Graft rejection may be acute,in which case the immunosuppression is increased,or chronic following several acute episodes.Chronic rejection can only be treated by retrans-plantation. Rejection does not have any specificultrasound features on either conventional imagingor Doppler, and the diagnosis is made from a liverbiopsy following clinical suspicion.
Post-transplant malignancy
Because of the immunosuppression, patients are atgreater risk than normal for developing malig-nancy. Most of these manifest as post-transplantlymphoproliferative disorder (similar in appearanceto non-Hodgkin’s lymphoma) which can affect thelymphatics, gastrointestinal tract or other organs,including the transplanted liver.41 The most com-monly found ultrasound appearances include focal,hypoechoic liver lesions and lymphadenopathy.
Patients with malignant lesions pretransplant,such as HCC or cholangiocarcinoma, have a sig-nificant risk of recurrence after transplantation.
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 117
Figure 4.34 Subphrenic haematoma post-transplant.
References1. Moorthy K, Mihssin N, Houghton PW. 2001 The
management of simple hepatic cysts: sclerotherapy orlaparoscopic fenestration? Annals of the Royal Collegeof Surgeons of England 83: 409–414.
2. Adam YG, Nonas CJ 1995 Hepatobiliarycystadenoma. Southern Medical Journal 88:1140–1143.
3. Men S, Hekimoglu B et al. 1999 Percutaneoustreatment of hydatid cysts: an alternative to surgery.American Journal of Roentgenology 172: 83–89.
4. Huang CJ, Pitt HA, Lipsett PA et al. 1996 Pyogenichepatic abscess: changing trends over 42 years. Annalsof Surgery 223: 600–609.
5. Kim TK, Choi BI et al. 2000 Hepatic tumours:contrast agent-enhancement patterns with pulseinversion harmonic US. Radiology 216: 411–417.
6. Stephenson NJH, Gibson RN. 1995 Hepatic focalnodular hyperplasia: colour Doppler ultrasound can be diagnostic. Australasian Radiology 39:296–299.
7. Dill-Macky MJ, Burns PN, Khalili K, Wilson SR.2002 Focal hepatic masses: enhancement patternswith SH U 508A and pulse inversion US. Radiology222: 95–102.
8. Albrecht T, Hoffmann CW, Schmitz SA et al. 2001Phase-inversion sonography during the liver-specificlate phase of contrast enhancement: improveddetection of liver metastases. American Journal ofRoentgenology 176: 1191–1198.
9. Adam A. 2002 Interventional radiology in thetreatment of hepatic metastases. Cancer TreatmentReview 28: 93–99.
ch04.qxd 6/30/04 5:50 PM Page 117
10. Zweibel WJ. 1995 Sonographic diagnosis of diffuseliver disease. Seminars in Ultrasound, CT and MRI16: 8–15.
11. Shapiro RS, Katz R, Mendelson DS et al. 1996Detection of hepatocellular carcinoma in cirrhoticpatients: sensitivity of CT and ultrasound. Journal ofUltrasound in Medicine 15: 497–502.
12. Chuah SK, Changchien CS, Chiu KW et al.1995 Changes of hepatic vein waveform in chronicliver diseases. Journal of Medical Ultrasound 3:75–80.
13. Ishiguchi T, Shimamoto K, Fukatsu H et al. 1996Radiologic diagnosis of hepatocellular carcinoma.Seminars in Surgical Oncology 12: 164–169.
14. Ohtomo K, Itai Y. 1995 Imaging of hepatocellularcarcinoma. Digestive Surgery 1995; 12: 22–33.
15. Ward J, Robinson PJ. 2002 How to detecthepatocellular carcinoma in cirrhosis. EuropeanRadiology 12: 2258–2272.
16. Heathcote J. 1996 Review: treatment of primarybiliary cirrhosis. Journal of Gastroenterology andHepatology 11: 605–609.
17. Dietrich C, Leuschner M, Zeuzem S et al. 1999Perihepatic lymphadenopathy in primary biliarycirrhosis reflects progression of the disease. EuropeanJournal of Gastroenterology and Hepatology 11:747–753.
18. Kok T, van der Jagt EJ, Haagsma EB et al. 1999 Thevalue of Doppler ultrasound in cirrhosis and portalhypertension. Scandinavian Journal ofGastroenterology Supplement 230: 82–88.
19. Gorg C, Riera-Knorrenschild J, Dietrich J. 2002Pictorial review: colour Doppler ultrasound flowpatterns in the portal venous system. British Journalof Radiology 75: 919–929.
20. Zweibel WJ. 1995 Sonographic diagnosis of hepaticvascular disorders. Seminars in Ultrasound, CT andMRI 16: 34–48.
21. Wu CC, Yeh YH, Hwang MH. 1994 Observation ofportal venous flow in liver cirrhosis by Dopplerultrasound: the significance of PVH index. Journal ofMedical Ultrasound 2: 180–184.
22. Konno K, Ishida H, Uno A et al. 1996 Cavernoustransformation of the portal vein (CTPV): role ofcolor Doppler sonography in the diagnosis. EuropeanJournal of Ultrasound 3: 231–240.
23. Bach AM, Hann LE, Brown KT et al. 1996 Portalvein evaluation with US: comparison to angiographyand CT arterial portography. Radiology 201:149–154.
24. Lafortune M, Patriquin H, Pomier G et al. 1987Haemodynamic changes in portal circulation afterportosystemic shunts; use of duplex sonography in 43
patients. American Journal of Roentgenology 149:701–706.
25. Chong WK, Malisch TW, Mazer MJ. 1995Sonography of transjugular intrahepatic portosystemicshunts. Seminars in Ultrasound, CT and MRI 16:69–80.
26. Middleton WD, Teefey SA, Darcy MD. 2003 Dopplerevaluation of transjugular intrahepatic portosystemicshunts. Ultrasound Quarterly 19: 56–70.
27. Reed MH. 1995 TIPS: a liver transplant surgeon’sview. Seminars in Interventional Radiology 12:396–400.
28. Vogel J, Gorich J, Kramme E et al. 1996 Alveolarechinococcosis of the liver: percutaneous stent therapyof Budd–Chiari syndrome. Gut 39: 762–764.
29. Mahadeva R, Webb K, Westerbeek R et al. 1998Clinical outcome in relation to care in centresspecialising in cystic fibrosis: cross sectional study.British Medical Journal 316: 1771–1779.
30. Geary M. 1997 The HELLP Syndrome. BritishJournal of Obstetric and Gynaecology 104: 887–891.
31. Redvanly RD, Nelson RC, Stieber AC, Dodd GD.1995 Imaging in the preoperative evaluation of adultliver-transplant candidates: goals, merits of variousprocedures, and recommendations. American Journalof Roentgenology 164: 611–617.
32. Belle SH, Beringer KC, Murphy JB, Detre KM. 1992The Pittsburgh-UNOS liver transplant registry. In:Terasaki PI, Cecka JM eds. Clinical Transplants.UCLA Tissue Typing Laboratory, Los Angeles: 1–16.
33. Prasad KR, Lodge JP. 2001 Transplantation of theliver and pancreas. British Medical Journal 322:845–847.
34. Devlin J, O’Grady J. 2000 Indications for referral andassessment in adult liver transplantation: clinicalguidelines. BSG Guidelines in Gastroenterology, Feb.
35. Dravid VS, Shapiro NJ, Needleman L et al. 1994Arterial abnormalities following orthotopic livertransplantation: arteriographic findings andcorrelation with Doppler sonographic findings.American Journal of Roentgenology 74: 967–977.
36 Guerra L. 1996 Postoperative hepatic transplants.Review of ultrasound applications in detecting hepaticartery thrombosis. Journal of Diagnostic MedicalSonography 12: 12–17.
37. Dodd GD III, Memel DS, Zajko AB et al. 1994Hepatic artery stenosis and thrombosis in transplantrecipients: Doppler diagnosis with resistive index andsystolic acceleration time. Radiology 192: 657–661.
38. Platt JF, Yutzy GG, Bude RO et al. 1997 Use ofDoppler sonography for revealing hepatic arterystenosis in liver transplant recipients. AmericanJournal of Roentgenology 168: 473–476.
ABDOMINAL ULTRASOUND118
ch04.qxd 6/30/04 5:50 PM Page 118

39. Arundale LJ, Patel S, Irving HC. 1997 The ‘parvus-tardus’ waveform for the detection of hepatic arterycompromise in transplanted livers. Proceedings of the29th BMUS annual scientific meeting, Bournemouth,1997.
40. Holbert BL, Campbell WL, Skolnick ML. 1995Evaluation of the transplanted liver and postoperative
complications. Radiologic Clinics of North America33: 521–540.
41. Shaw AS, Ryan SM et al. 2003 Ultrasound of non-vascular complications in the post liver transplantpatient. Clinical Radiology 58: 672–680.
PATHOLOGY OF THE LIVER AND PORTAL VENOUS SYSTEM 119
ch04.qxd 6/30/04 5:50 PM Page 119
ch04.qxd 6/30/04 5:50 PM Page 120
This page intentionally left blank

THE NORMAL PANCREAS
Ultrasound techniques
Because the pancreas lies posterior to the stomachand duodenum, a variety of techniques must usuallybe employed to examine it fully. Although ultra-sound may still be considered the first line of inves-tigation, CT, MRI and/or endoscopic retrogradecholangiopancreatography (ERCP) are frequentlyrequired to augment and refine the diagnosis.
The operator must make the best use of availableacoustic windows and different patient positionsand techniques to investigate the pancreas fully.
The most useful technique is to start by scan-ning the epigastrium in transverse plane, using theleft lobe of the liver as an acoustic window. Usingthe splenic vein as an anatomical marker, the bodyof the pancreas can be identified anterior to this.The tail of pancreas is slightly cephalic to the head,so the transducer should be obliqued accordinglyto display the whole organ (Fig. 5.1).
Different transducer angulations display differ-ent sections of the pancreas to best effect:● Identify the echo-free splenic vein and the
superior mesenteric artery posterior to it. Thelatter is surrounded by an easily visible,hyperechoic fibrous sheath. The pancreas is‘draped’ over the splenic vein (Fig. 5.1).
● Where possible, use the left lobe of the liver asan acoustic window to the pancreas, anglingslightly caudally.
● The tail, which is often quite bulky, mayrequire the transducer to be angled towards
Chapter 5
The pancreas
121
CHAPTER CONTENTS
The normal pancreas 121Congenital anomalies of the pancreas 123
Pancreatitis 124Acute pancreatitis 125Chronic pancreatitis 128
Malignant pancreatic disease 128Pancreatic carcinoma 128Pancreatic metastases 133
Benign focal pancreatic lesions 133Focal fatty sparing of the pancreas 133Focal pancreatitis 133Cysts 134
Trauma of the pancreas 134Pancreatic transplant 135
ch05.qxd 7/6/04 8:49 AM Page 121
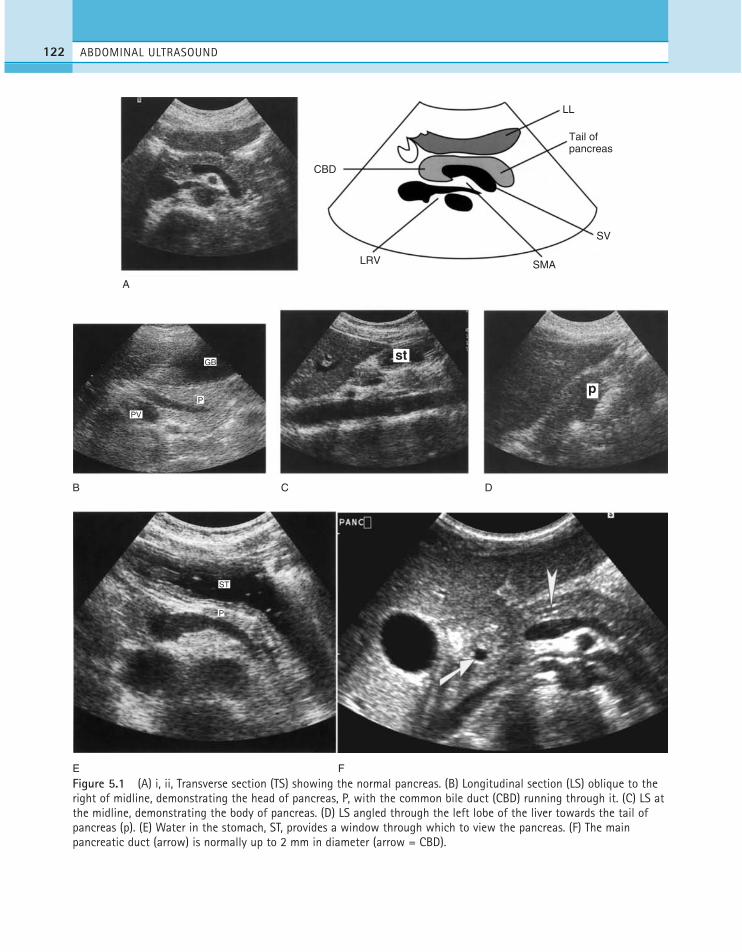
ABDOMINAL ULTRASOUND122
A
B
E
ST
PV
P
GB
P
F
C D
CBD
LRV SMA
SV
Tail of pancreas
LL
st
p
Figure 5.1 (A) i, ii, Transverse section (TS) showing the normal pancreas. (B) Longitudinal section (LS) oblique to theright of midline, demonstrating the head of pancreas, P, with the common bile duct (CBD) running through it. (C) LS atthe midline, demonstrating the body of pancreas. (D) LS angled through the left lobe of the liver towards the tail ofpancreas (p). (E) Water in the stomach, ST, provides a window through which to view the pancreas. (F) The mainpancreatic duct (arrow) is normally up to 2 mm in diameter (arrow = CBD).
ch05.qxd 7/6/04 8:49 AM Page 122

the patient’s left. The spleen also makes a goodwindow to the tail in coronal section.
If you can’t see the pancreatic head properly,turn the patient left side raised, which movesthe duodenal gas up towards the tail of thepancreas. Right side raised may demonstratethe tail better.
If these manoeuvres still fail to demonstratethe organ fully, try:—asking the patient to perform the Valsalva
manoeuvre with abdominal protrusion—scanning the patient erect—filling the stomach with a water load to
create an acoustic window through whichthe pancreas can be seen.
Ultrasound appearances
The texture of the pancreas is rather coarser thanthat of the liver. The echogenicity of the normalpancreas alters according to age. In a child oryoung person it may be quite bulky and relativelyhypoechoic when compared to the liver. In adult-hood, the pancreas is hyperechoic compared tonormal liver, becoming increasingly so in the eld-erly, and tending to atrophy (Fig. 5.2).
The pancreas does not have a capsule and itsmargins can appear rather ill-defined, becominginfiltrated with fat in later life.
These age-related changes are highly significantto the sonographer; what may be considered nor-mal in an elderly person would be abnormallyhyperechoic in a younger one, and may represent achronic inflammatory state. Conversely a hypo-echoic pancreas in an older patient may representacute inflammation, whereas the appearanceswould be normal in a young person.
The main pancreatic duct can usually be visual-ized in the body of pancreas, where its walls areperpendicular to the beam. The normal diameter is2 mm or less.
The common bile duct can be seen in the lateralportion of the head and the gastroduodenal arterylies anterolaterally. The size of the uncinate processvaries.
Pitfalls in scanning the pancreas
The normal stomach or duodenum can mimic pan-creatic pathology if the patient is insufficiently
fasted. A fluid-filled stomach can be particularlydifficult when looking for pancreatic pseudocystsin patients with acute pancreatitis. Giving thepatient a drink of water usually differentiates thegastrointestinal tract from a collection.
Epigastric or portal lymphadenopathy may alsomimic a pancreatic mass. If careful scanning andappropriate patient positioning are unable to eluci-date, CT is normally the next step.
Biochemical analysis
In many pancreatic diseases, the production of thedigestive pancreatic enzymes is compromised,either by obstruction of the duct draining the pan-creas or by destruction of the pancreatic cellswhich produce the enzymes. This can result inmalabsorption of food and/or diarrhoea.
The pancreas produces digestive enzymes, amy-lase, lipase and peptidase, which occur in traceamounts in the blood. If the pancreas is damagedor inflamed, the resulting release of enzymes intothe blood stream causes an increase in the serumamylase and lipase levels. The enzymes alsopass from the blood stream into the urine andtherefore urinalysis can also contribute to thediagnosis.
Congenital anomalies of the pancreasThe normal pancreas is the result of the fusion oftwo embryonic buds: the ventral bud arises fromthe CBD, forming the uncinate process and partof the head, and the dorsal arises from the poste-rior wall of the duodenum. Developmental anom-alies of the pancreas occur as a result of a failureof the dorsal and ventral pancreatic ducts to fuse,that is pancreas divisum. This arrangement maycause inadequate drainage of the pancreatic duct,leading to pancreatitis. A rare developmentalanomaly of the ventral bud may occur, pancreasannulare, in which pancreatic tissue encircles thebowel. In this latter case, patients can presentwith proximal small-bowel obstruction in infancy,but this may also be an incidental finding atautopsy. These relatively uncommon anomaliescannot usually be diagnosed on ultrasound.Increasingly, magnetic resonance cholangiopan-creatography (MRCP) is replacing ERCP in the
THE PANCREAS 123
ch05.qxd 7/6/04 8:49 AM Page 123
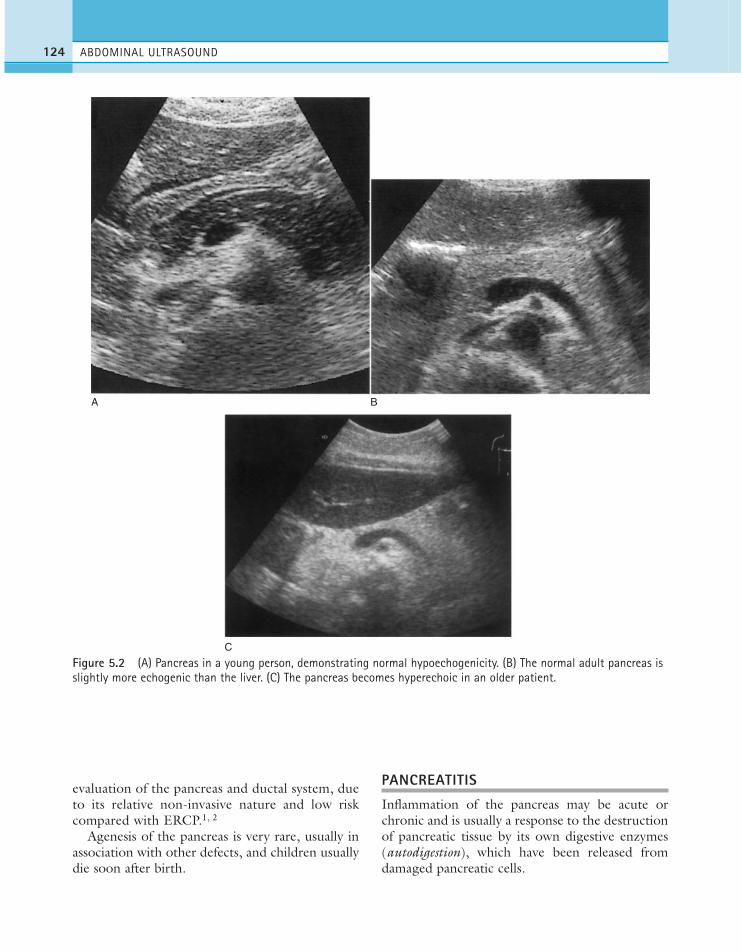
evaluation of the pancreas and ductal system, dueto its relative non-invasive nature and low riskcompared with ERCP.1, 2
Agenesis of the pancreas is very rare, usually inassociation with other defects, and children usuallydie soon after birth.
PANCREATITIS
Inflammation of the pancreas may be acute orchronic and is usually a response to the destructionof pancreatic tissue by its own digestive enzymes(autodigestion), which have been released fromdamaged pancreatic cells.
ABDOMINAL ULTRASOUND124
A B
C
Figure 5.2 (A) Pancreas in a young person, demonstrating normal hypoechogenicity. (B) The normal adult pancreas isslightly more echogenic than the liver. (C) The pancreas becomes hyperechoic in an older patient.
ch05.qxd 7/6/04 8:49 AM Page 124

Acute pancreatitisClinical features
Acute inflammation of the pancreas has a numberof possible causes (Table 5.1), but is most com-monly associated with gallstones or alcoholism.
Clinically it presents with severe epigastric pain,abdominal distension and nausea or vomiting. Inmilder cases, the patient may recover sponta-neously. If allowed to progress untreated, peritoni-tis and other complications may occur.
Biochemically, raised levels of amylase and lipase(the pancreatic enzymes responsible for the diges-tion of starch and lipids) are present in the bloodand urine. Acute inflammation causes the pancre-atic tissue to become necrosed, releasing the pan-creatic enzymes which can further destroy thepancreatic tissue and also the capillary walls, enter-ing the blood stream.
Ultrasound appearances
Mild acute pancreatitis may have no demonstrablefeatures on ultrasound, especially if the scan is per-formed after the acute episode has settled. In moresevere cases the pancreas is enlarged and hypo-
echoic due to oedema. The main duct may bedilated or prominent.
As the condition progresses, digestive enzymesleak out, forming collections or pseudocysts. Theseare most frequently found in the lesser sac, near thetail of the pancreas, but can occur anywhere in theabdomen—within the pancreatic tissue itself, any-where in the peritoneal or retroperitoneal space oreven tracking up the fissures into the liver—so afull abdominal ultrasound survey is essential oneach attendance (Fig. 5.3).
Pseudocysts are so called because they do nothave a capsule of epithelium like most cysts, but aremerely collections of fluid surrounded by adjacenttissues. A pseudocyst may appear to have a capsuleon ultrasound if it lies within a fold of peritoneum.
Pseudocysts may be echo-free, but generallycontain echoes from tissue debris and may be loc-ulated.
In a small percentage of cases, a pseudocyst ornecrotic area of pancreatic tissue may becomeinfected, forming a pancreatic abscess.
Although acute pancreatitis usually affects theentire organ, it may occur focally. This presents adiagnostic dilemma for ultrasound, as the appear-ances are indistinguishable from tumour. The clin-ical history may help to differentiate; suspicion offocal pancreatitis should be raised in patients withprevious history of chronic pancreatitis, a historyof alcoholism and normal CA 19–9 levels4 (atumour marker for pancreatic carcinoma).
The enlargement of the pancreas in acute pan-creatitis may have other consequences, for examplethe enlarged pancreatic head may obstruct thecommon bile duct, causing biliary dilatation.
Doppler ultrasound is useful in assessing associ-ated vascular complications. Prolonged andrepeated attacks of acute pancreatitis may cause thesplenic vein to become encased and compressed,causing splenic and/or portal vein thrombosis,with all its attendant sequelae (see Chapter 4) (Fig.5.3E).
Although ultrasound is used to assess the pan-creas in cases of suspected acute pancreatitis, itsmain role is in demonstrating the cause of the pan-creatitis, for example biliary calculi, in order toplan further management. The ultrasound findingof microlithiasis or sludge in the gallbladder ishighly significant in cases of suspected pancreatitis,5
THE PANCREAS 125
Table 5.1 Causes of acute pancreatitis
Biliary calculi—most common cause. Obstructs the mainpancreatic duct/papilla of Vater and may cause reflux ofbile into the pancreatic ductAlcoholism—alcohol overstimulates pancreatic secretionscausing overproduction of enzymesTrauma/iatrogenic—damage/disruption of the pancreatictissue, e.g. in a road traffic accident, or by surgery, biopsyor ESWL3
Drug-induced—a relatively uncommon cause. Some anti-cancer drugs can cause chemical injuryInfection—e.g. mumps. A rare cause of pancreatitisCongenital anomaly—duodenal diverticulum, duodenalduplication, sphincter of Oddi stenosis or choledochal cystmay obstruct the pancreatic duct, giving rise topancreatitisHereditary—a rare, autosomal dominant conditionpresenting with recurrent attacks in childhood or earlyadulthood
ESWL = extracorporeal shock wave lithotripsy.
ch05.qxd 7/6/04 8:49 AM Page 125

and has been implicated in the cause of recurrentpancreatitis.
Management of acute pancreatitis
While ultrasound is useful in demonstrating associ-ated gallstones, biliary sludge and fluid collections,CT or MRI demonstrates the complications of
acute pancreatitis with greater sensitivity and speci-ficity. Localized areas of necrotic pancreatic tissuecan be demonstrated on contrast-enhanced CT,together with vascular complications, such asthrombosis.
MRCP or CT is used to demonstrate the mainpancreatic duct and its point of insertion into thecommon bile duct. Anomalous insertions are asso-
ABDOMINAL ULTRASOUND126
A B
C D
Figure 5.3 (A) Acute pancreatitis in a patient with alcoholic liver disease. The pancreas is hypoechoic and bulky witha lobulated outline. (B) Large pseudocyst near the tail of the pancreas in acute pancreatitis. (C) Necrotic tail ofpancreas surrounded by exudate. (D) Inflammatory exudate is seen around the right kidney in acute pancreatitis.
(Continued)
ch05.qxd 7/6/04 8:49 AM Page 126
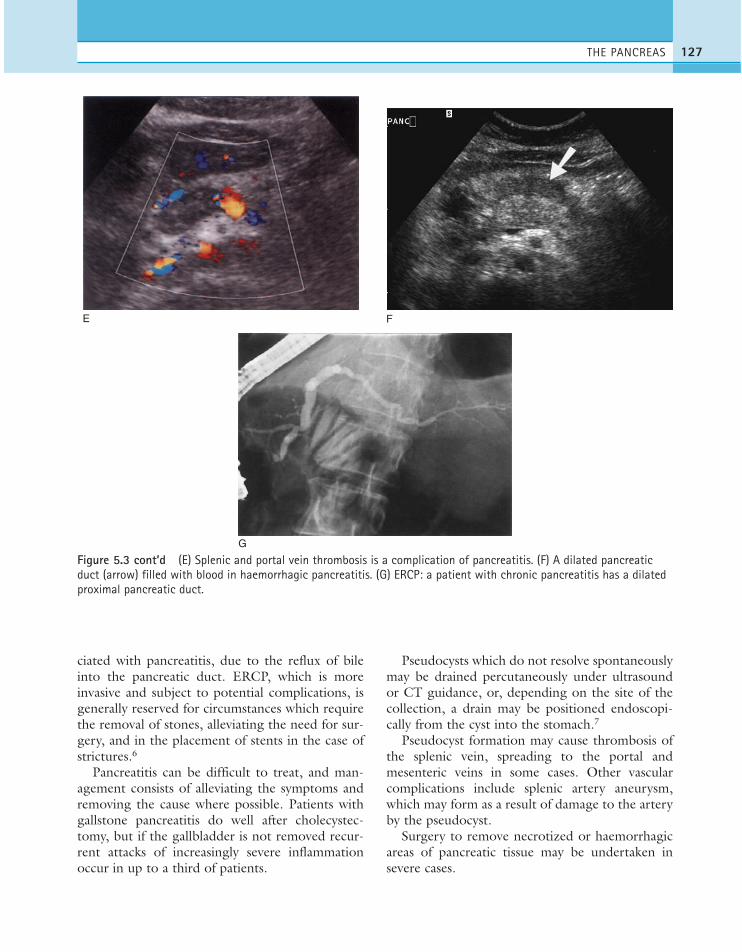
ciated with pancreatitis, due to the reflux of bileinto the pancreatic duct. ERCP, which is moreinvasive and subject to potential complications, isgenerally reserved for circumstances which requirethe removal of stones, alleviating the need for sur-gery, and in the placement of stents in the case ofstrictures.6
Pancreatitis can be difficult to treat, and man-agement consists of alleviating the symptoms andremoving the cause where possible. Patients withgallstone pancreatitis do well after cholecystec-tomy, but if the gallbladder is not removed recur-rent attacks of increasingly severe inflammationoccur in up to a third of patients.
Pseudocysts which do not resolve spontaneouslymay be drained percutaneously under ultrasoundor CT guidance, or, depending on the site of thecollection, a drain may be positioned endoscopi-cally from the cyst into the stomach.7
Pseudocyst formation may cause thrombosis ofthe splenic vein, spreading to the portal andmesenteric veins in some cases. Other vascularcomplications include splenic artery aneurysm,which may form as a result of damage to the arteryby the pseudocyst.
Surgery to remove necrotized or haemorrhagicareas of pancreatic tissue may be undertaken insevere cases.
THE PANCREAS 127
E F
G
Figure 5.3 cont’d (E) Splenic and portal vein thrombosis is a complication of pancreatitis. (F) A dilated pancreaticduct (arrow) filled with blood in haemorrhagic pancreatitis. (G) ERCP: a patient with chronic pancreatitis has a dilatedproximal pancreatic duct.
ch05.qxd 7/6/04 8:49 AM Page 127

Chronic pancreatitisPatients with acute pancreatitis are at risk ofrepeated inflammatory episodes which eventuallydevelop into chronic inflammation. The mostcommon cause is alcohol abuse. In other cases,chronic pancreatitis has a gradual onset which doesnot seem to be associated with previous acuteattacks.
The normal pancreatic tissue is progressivelyreplaced by fibrosis, which may encase the nervesin the coeliac plexus, causing abdominal pain, par-ticularly post-prandially. The patient has fattystools (steatorrhoea) due to malabsorption, asthere is a decreased capacity to produce the diges-tive enzymes.
Diagnosis of chronic pancreatitis can be diffi-cult, especially in the early stages.8 Serum enzymelevels are less elevated than in acute disease (if atall). ERCP, which detects abnormalities of the duc-tal system in the early stages, is increasingly contra-indicated due to the risk of aggravating thepancreatitis. MRCP is promising, but is limited inassessing the smaller side ducts. Endoscopic ultra-sound is currently a sensitive and accurate modal-ity in assessing both the ductal system and thepancreatic tissue.
Ultrasound appearances
The pancreas becomes abnormally hyperechoic(Fig. 5.4A). This should not be confused with thenormal increase in echogenicity with age. Thegland may be atrophied and lobulated and themain pancreatic duct is frequently dilated andectatic,9 with a beaded appearance.
Calcification may be identified in the pancreatictissue, both on ultrasound and on a plain X-ray,and there may be stones in the duct. (Generallyspeaking, strong shadows are cast from the calcificfoci, but small flecks may be too small to shadow)(Fig 5.4 B, C).
As with acute inflammation, CT is the methodof choice for demonstrating the complications ofchronic pancreatitis.
Obstruction of the duct can cause pseudocystformation, and other complications include biliaryobstruction and portal/splenic vein thrombosis.
MALIGNANT PANCREATIC DISEASE
Pancreatic carcinomaClinical features and management
Carcinoma of the pancreas is a major cause ofcancer-related death. It carries a very poor progno-sis with less than 5% 5 year survival,10 related to itslate presentation.
The presenting symptoms depend on the size ofthe lesion, its position within the pancreas and theextent of metastatic deposits. Most pancreatic car-cinomas (60%) are found in the head of the pan-creas,11 and patients present with the associatedsymptoms of jaundice due to obstruction of thecommon bile duct (Fig. 5.5). Carcinomas locatedin the body or tail of pancreas do not causeobstructive jaundice.
The majority (80%) of pancreatic cancers areductal adenocarcinomas, most of which are locatedin the head of pancreas. The rest comprise a mixedbag of less common neoplasms and endocrinetumours.
Endocrine tumours, which originate in the isletcells of the pancreas, tend to be either insulinomas(generally benign) or gastrinomas (malignant).These present with hormonal abnormalities whilethe tumour is still small and are more amenable todetection by intraoperative ultrasound than byconventional sonography.
Mucin-secreting tumours (Fig. 5.5E), whichappear predominantly cystic on ultrasound, tend tobe located in the body or tail of pancreas and fol-low a much less aggressive course than adenocarci-nomas, metastasizing late. These tumours, thoughcomparatively rare, have a much higher curativerate with surgery.12
Metastatic deposits from primary pancreaticadenocarcinoma occur early in the course of thedisease, and 80% of patients already have nodal dis-ease or distant metastases in the lungs, liver orbone by the time the diagnosis is made, whichaccounts for the poor prognosis.
Surgical removal of the carcinoma by partial pan-creaticoduodenectomy, the Whipples procedure, ispotentially curative but only 20% of patients have atumour which is potentially resectable, and the 5-year survival rate following resection is less than
ABDOMINAL ULTRASOUND128
ch05.qxd 7/6/04 8:49 AM Page 128
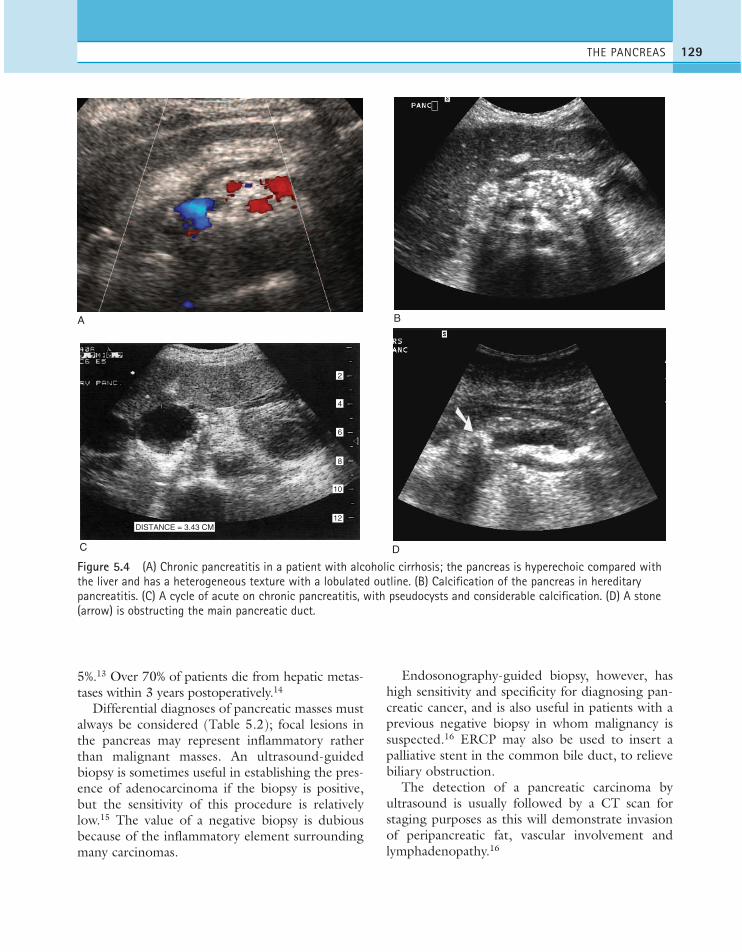
5%.13 Over 70% of patients die from hepatic metas-tases within 3 years postoperatively.14
Differential diagnoses of pancreatic masses mustalways be considered (Table 5.2); focal lesions inthe pancreas may represent inflammatory ratherthan malignant masses. An ultrasound-guidedbiopsy is sometimes useful in establishing the pres-ence of adenocarcinoma if the biopsy is positive,but the sensitivity of this procedure is relativelylow.15 The value of a negative biopsy is dubiousbecause of the inflammatory element surroundingmany carcinomas.
Endosonography-guided biopsy, however, hashigh sensitivity and specificity for diagnosing pan-creatic cancer, and is also useful in patients with aprevious negative biopsy in whom malignancy issuspected.16 ERCP may also be used to insert apalliative stent in the common bile duct, to relievebiliary obstruction.
The detection of a pancreatic carcinoma byultrasound is usually followed by a CT scan forstaging purposes as this will demonstrate invasionof peripancreatic fat, vascular involvement andlymphadenopathy.16
THE PANCREAS 129
A B
C
DISTANCE = 3.43 CM
2
4
6
8
10
12
D
Figure 5.4 (A) Chronic pancreatitis in a patient with alcoholic cirrhosis; the pancreas is hyperechoic compared withthe liver and has a heterogeneous texture with a lobulated outline. (B) Calcification of the pancreas in hereditarypancreatitis. (C) A cycle of acute on chronic pancreatitis, with pseudocysts and considerable calcification. (D) A stone(arrow) is obstructing the main pancreatic duct.
ch05.qxd 7/6/04 8:49 AM Page 129

ABDOMINAL ULTRASOUND130
A B
c
CD
E F
m
S
LK
Figure 5.5 (A) The common bile duct, c, is obstructed by a large hypoechoic solid mass at its lower end (calipers),which is a carcinoma in the head of the pancreas. (B) TS through the head of the pancreas, which is swollen by ahypoechoic adenocarcinoma (arrow). (C) The tumour in (B) displays considerable vascularity on colour Doppler. (Note thecolour sensitivity setting has been reduced to accommodate this, so eliminating low-velocity flow from the splenic vein.)(D) Tumour in the head of the pancreas (arrows), confirmed by CT. (E) Complex cystic mass in the head of the pancreas,confirmed as a cystadenocarcinoma. (F) A complex mass (m) between the spleen (S) and the left kidney is a large carcinomaof the tail of the pancreas. (Continued)
ch05.qxd 7/6/04 8:49 AM Page 130

THE PANCREAS 131
G
I
H
Figure 5.5 cont’d (G) Dilated pancreatic duct due to a carcinoma in the head (arrow). (H) Colour Doppler helps todifferentiate the dilated pancreatic duct (measured), which does not contain flow, from the splenic vein posterior tothe duct. (I) Endoscopic retrograde cholangiopancreatography (ERCP) demonstrating a long stricture of the pancreaticduct (arrow) involving the side branches, in a large pancreatic carcinoma. The CBD is compressed (arrowhead) bynodes, causing biliary dilatation. A palliative stent was inserted.
ch05.qxd 7/6/04 8:49 AM Page 131
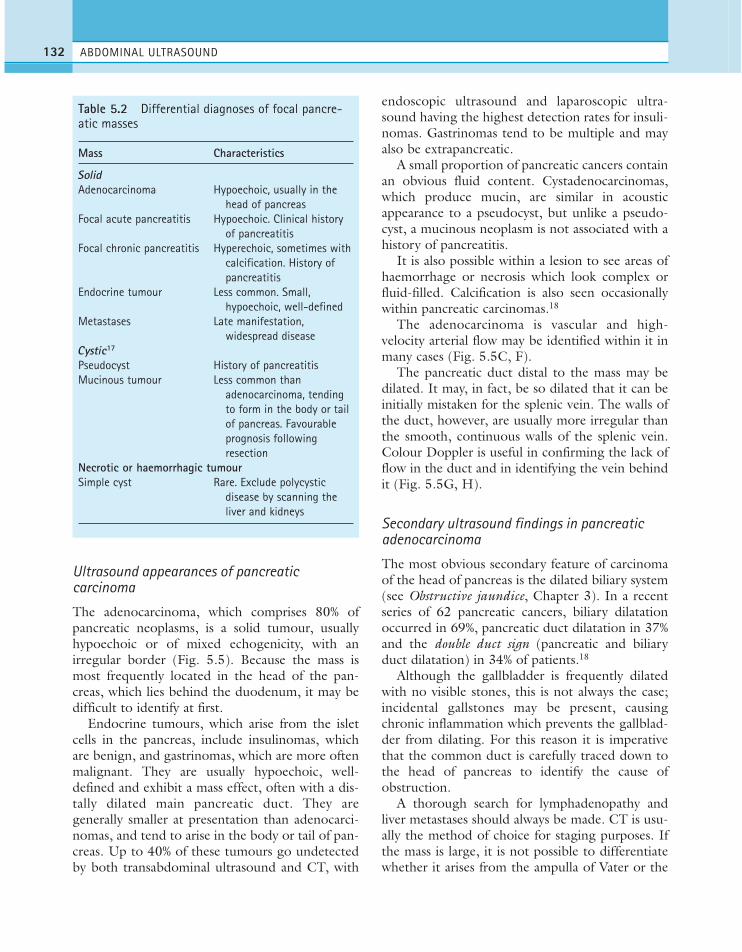
Ultrasound appearances of pancreaticcarcinoma
The adenocarcinoma, which comprises 80% ofpancreatic neoplasms, is a solid tumour, usuallyhypoechoic or of mixed echogenicity, with anirregular border (Fig. 5.5). Because the mass ismost frequently located in the head of the pan-creas, which lies behind the duodenum, it may bedifficult to identify at first.
Endocrine tumours, which arise from the isletcells in the pancreas, include insulinomas, whichare benign, and gastrinomas, which are more oftenmalignant. They are usually hypoechoic, well-defined and exhibit a mass effect, often with a dis-tally dilated main pancreatic duct. They aregenerally smaller at presentation than adenocarci-nomas, and tend to arise in the body or tail of pan-creas. Up to 40% of these tumours go undetectedby both transabdominal ultrasound and CT, with
endoscopic ultrasound and laparoscopic ultra-sound having the highest detection rates for insuli-nomas. Gastrinomas tend to be multiple and mayalso be extrapancreatic.
A small proportion of pancreatic cancers containan obvious fluid content. Cystadenocarcinomas,which produce mucin, are similar in acousticappearance to a pseudocyst, but unlike a pseudo-cyst, a mucinous neoplasm is not associated with ahistory of pancreatitis.
It is also possible within a lesion to see areas ofhaemorrhage or necrosis which look complex orfluid-filled. Calcification is also seen occasionallywithin pancreatic carcinomas.18
The adenocarcinoma is vascular and high-velocity arterial flow may be identified within it inmany cases (Fig. 5.5C, F).
The pancreatic duct distal to the mass may bedilated. It may, in fact, be so dilated that it can beinitially mistaken for the splenic vein. The walls ofthe duct, however, are usually more irregular thanthe smooth, continuous walls of the splenic vein.Colour Doppler is useful in confirming the lack offlow in the duct and in identifying the vein behindit (Fig. 5.5G, H).
Secondary ultrasound findings in pancreaticadenocarcinoma
The most obvious secondary feature of carcinomaof the head of pancreas is the dilated biliary system(see Obstructive jaundice, Chapter 3). In a recentseries of 62 pancreatic cancers, biliary dilatationoccurred in 69%, pancreatic duct dilatation in 37%and the double duct sign (pancreatic and biliaryduct dilatation) in 34% of patients.18
Although the gallbladder is frequently dilatedwith no visible stones, this is not always the case;incidental gallstones may be present, causingchronic inflammation which prevents the gallblad-der from dilating. For this reason it is imperativethat the common duct is carefully traced down tothe head of pancreas to identify the cause ofobstruction.
A thorough search for lymphadenopathy andliver metastases should always be made. CT is usu-ally the method of choice for staging purposes. Ifthe mass is large, it is not possible to differentiatewhether it arises from the ampulla of Vater or the
ABDOMINAL ULTRASOUND132
Table 5.2 Differential diagnoses of focal pancre-atic masses
Mass Characteristics
SolidAdenocarcinoma Hypoechoic, usually in the
head of pancreasFocal acute pancreatitis Hypoechoic. Clinical history
of pancreatitisFocal chronic pancreatitis Hyperechoic, sometimes with
calcification. History of pancreatitis
Endocrine tumour Less common. Small, hypoechoic, well-defined
Metastases Late manifestation, widespread disease
Cystic17
Pseudocyst History of pancreatitisMucinous tumour Less common than
adenocarcinoma, tending to form in the body or tail of pancreas. Favourable prognosis following resection
Necrotic or haemorrhagic tumourSimple cyst Rare. Exclude polycystic
disease by scanning the liver and kidneys
ch05.qxd 7/6/04 8:49 AM Page 132

head of pancreas. This differentiation, however, isusually academic at this stage.
Colour Doppler can demonstrate considerablevascularity within the mass and is also important inidentifying vascular invasion of the coeliac axis,superior mesenteric artery, hepatic, splenic and/orgastroduodenal arteries and of the portal andsplenic veins, a factor which is particularly impor-tant in assessing the suitability of the tumour forcurative resection. The recognition of involvementof peripancreatic vessels by carcinoma with colourDoppler, together with the ultrasound assessmentof compression or encasement of these vessels, hasbeen found to be highly sensitive and specific (79%and 89%) for diagnosing unresectability,19 thus theneed for further investigative procedures such asCT may be avoided, particularly in cases of largetumours.20
Pancreatic metastasesPancreatic metastases may occur from breast, lungand gastrointestinal tract primary tumours. Theyare relatively uncommon on ultrasound (Fig. 5.6),simply because they are a late manifestation inpatients who already have known, widespread dis-ease and in whom investigations are generally con-sidered unnecessary.
Widespread metastatic disease can be demon-strated on ultrasound, particularly in the liver, andthere is often considerable epigastric lym-phadenopathy, which can be confused with theappearances of pancreatic metastases on the scan.
BENIGN FOCAL PANCREATIC LESIONS
Focal fatty sparing of the pancreasThe uncinate process and ventral portion of thehead of pancreas may sometimes appear hypo-echoic in comparison with the rest of the gland(Fig. 5.7). This is due to a relative lack of fatty dep-osition and is often more noticeable in olderpatients, in whom the pancreas is normally hyper-echoic. Its significance lies in not confusing it witha focal pancreatic mass. The area of fatty sparing iswell-defined, with no enlargement or mass effect,and is regarded as a normal variation in the ultra-sound appearances. If doubt exists, CT will differ-entiate fatty sparing from true neoplasm.21
Focal pancreatitisInflammation can affect the whole, or just part ofthe gland. Occasionally, areas of hypoechoic, focalacute or chronic pancreatitis are present (seePancreatitis, above). These are invariably a diag-nostic dilemma, as they are indistinguishable onultrasound from focal malignant lesions (Fig. 5.8).Factors which point towards inflammation include
THE PANCREAS 133
Pathology of the pancreas, both benign andmalignant, can affect the adjacent vasculatureby compression, encasement or thrombosis.Doppler of the splenic, portal and superiormesenteric veins is useful in demonstrating theextent of vascular complication when pancreaticabnormalities are suspected.
Figure 5.6 Metastatic deposit from primary breastcarcinoma in the body of the pancreas (arrow).
Figure 5.7 The uncinate process is relativelyhypoechoic (arrows) because of fatty sparing.
ch05.qxd 7/6/04 8:49 AM Page 133
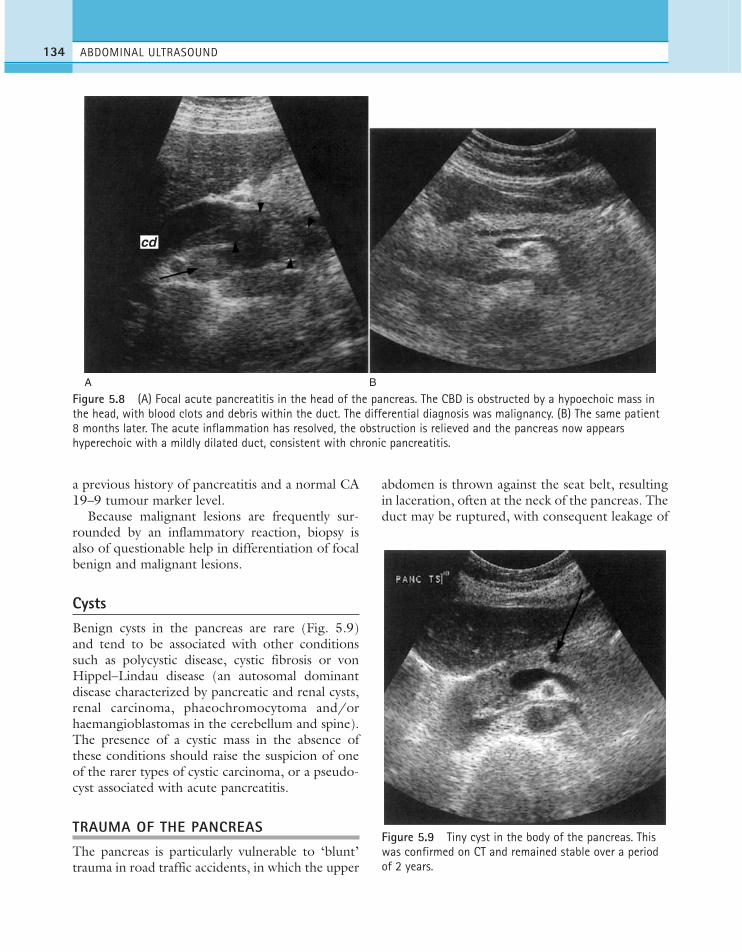
a previous history of pancreatitis and a normal CA19–9 tumour marker level.
Because malignant lesions are frequently sur-rounded by an inflammatory reaction, biopsy isalso of questionable help in differentiation of focalbenign and malignant lesions.
CystsBenign cysts in the pancreas are rare (Fig. 5.9)and tend to be associated with other conditionssuch as polycystic disease, cystic fibrosis or vonHippel–Lindau disease (an autosomal dominantdisease characterized by pancreatic and renal cysts,renal carcinoma, phaeochromocytoma and/orhaemangioblastomas in the cerebellum and spine).The presence of a cystic mass in the absence ofthese conditions should raise the suspicion of oneof the rarer types of cystic carcinoma, or a pseudo-cyst associated with acute pancreatitis.
TRAUMA OF THE PANCREAS
The pancreas is particularly vulnerable to ‘blunt’trauma in road traffic accidents, in which the upper
abdomen is thrown against the seat belt, resultingin laceration, often at the neck of the pancreas. Theduct may be ruptured, with consequent leakage of
ABDOMINAL ULTRASOUND134
A B
cd
Figure 5.8 (A) Focal acute pancreatitis in the head of the pancreas. The CBD is obstructed by a hypoechoic mass inthe head, with blood clots and debris within the duct. The differential diagnosis was malignancy. (B) The same patient8 months later. The acute inflammation has resolved, the obstruction is relieved and the pancreas now appearshyperechoic with a mildly dilated duct, consistent with chronic pancreatitis.
Figure 5.9 Tiny cyst in the body of the pancreas. Thiswas confirmed on CT and remained stable over a periodof 2 years.
ch05.qxd 7/6/04 8:49 AM Page 134

pancreatic juice into the abdominal cavity andsevere cases result in complete pancreatic transec-tion with pancreatic ascites.
The release of pancreatic enzymes triggers pan-creatitis and/or peritonitis, with the gland appear-ing enlarged and hypoechoic.
Ultrasound may be helpful in localizing a col-lection, but will not differentiate pancreatic secre-tions from haematoma. CT is the method ofchoice in cases of suspected pancreatic trauma,although even here the signs of injury can be sur-prisingly subtle considering the damage.22
PANCREATIC TRANSPLANT
In patients with insulin-dependent diabetes melli-tus with end-stage renal disease, simultaneous pan-creatic and kidney transplant is a successfultreatment which improves the quality of life andthe survival of the patients. Typically such patientsalso have severe complications, such as retinopathyand vascular disease, which may be stabilized, oreven reversed, by transplantation.
Simultaneous pancreas and kidney transplanta-tion now has a 1-year graft survival of almost 90%due to improved organ preservation techniques,surgical techniques and immunosuppression.23
The transplanted kidney is placed in the iliacfossa with the pancreas on the contralateral side.The donor kidney is transplanted in as usual, withanastomoses to the recipient iliac artery and vein.The pancreatic vessels are anastamosed to the con-tralateral iliac vessels.
The pancreatic secretions are primarily byenteric drainage, as the previous method of blad-der drainage was associated with an increasedincidence of urologic complications such asurinary tract infection, haematuria or refluxpancreatitis.24
Postoperative monitoring of the pancreatictransplant is difficult, on both clinical and imaginggrounds. No one imaging modality has provedwithout limitations and a combination of ultra-sound, CT, MRI, angiography and nuclearmedicine may be required.25 Postoperative compli-cations include thrombosis, infection, inflamma-tion, anastomotic leaks and rejection. Localizedpostoperative bleeding usually resolves sponta-neously.
Ultrasound appearances
The donor pancreas is usually situated in the iliacfossa but can be placed more centrally, particularlyif a renal transplant has also been performed.
Ultrasound is limited in its ability to assess thetransplanted pancreas, even if it can be locatedamongst the bowel loops. The lack of an adjacentreference organ, such as the liver, makes assessmentof its echogenicity subjective, and therefore subtledegrees of inflammation are difficult to detect.Fluid collections are frequently concealed beneathbowel and, when identified, their appearance isnon-specific. Contrast CT is more successful indetecting anastomotic leaks and collections, and isusually used for guided aspiration.
Colour Doppler should display perfusionthroughout the pancreas and the main vessels maybe traced to their anastomoses, depending on over-lying bowel (Fig. 5.10). Neither CT nor ultra-sound is particularly helpful in evaluating rejection,and it is difficult to differentiate transplant pancre-atitis from true rejection. The Doppler resistanceindex does not correlate with a rejection processand has not been found useful. MRI has beenfound to display more positive findings in pancre-atic rejection than other imaging modalities.
THE PANCREAS 135
Figure 5.10 The transplanted pancreas may be difficultto identify in the iliac fossa. The main artery is seen hererunning through the body of the pancreas.
ch05.qxd 7/6/04 8:49 AM Page 135

1. Brambs HJ. 1996 Developmental anomalies andcongenital disorders of the pancreas. Radiologe 36:381–388.
2. Calvo MM, Bujanda L, Calderson A et al. 2002Comparison between magnetic resonancecholangiopancreatography and ERCP for evaluationof the pancreatic duct. American Journal ofGastroenterology 97: 347–353.
3. Siech M, Boker M, Beger HG. 1996 Extracorporealshock wave lithotripsy as a cause of acute pancreatitis.Digestive Surgery 13: 210–221.
4. Yamaguchi K, Chijiiwa K, Saiki S et al. 1996 ‘Mass-forming’ pancreatitis masquerades as pancreaticcarcinoma. International Journal of Pancreatology 20:27–35.
5. Pezzilli R, Billi P, Barakat B et al. 1999 Ultrasonicevaluation of the common bile duct in biliary acutepancreatitis patients: comparison with endoscopicretrograde cholangiopancreatography. Journal ofMedical Ultrasound 18: 391–394.
6. Madhotra R, Lombard M. 2002 Endoscopicretrograde cholangiopancreatography should nolonger be used as a diagnostic test: the case against.Digestive Liver Disease 34: 375–380.
7. Gumaste VV, Pitchumoni CS. 1996 Pancreaticpseudocyst. Gastroenterologist 4: 33–43.
8. Glasbrenner B, Kahl S, Malfertheiner P. 2002 Moderndiagnostics of chronic pancreatitis. European Journalof Gastroenterology and Hepatology 14: 935–941.
9. Bolondi L, LiBassi S, Gaiani S, Barbara L. 1989Sonography of chronic pancreatitis. Radiology Clinicsof North America 27: 815–833.
10. Friedman AC, Krudy AG, Shawker TH et al. 1987Pancreatic neoplasms. In: Radiology of the Liver,Biliary Tract, Pancreas and Spleen. Williams &Wilkins, Baltimore, 735–837.
11. Damjanov I. 1996 Pancreatic neoplasms. In:Pathology for Health Related Professionals. Saunders,Philadelphia, 324–326.
12. Lichtenstein DR, Carr-Locke DL. 1995 Mucin-secreting tumours of the pancreas. GastrointestinalEndoscopy Clinics of North America 5: 237–258.
13. Cooperman AM, Kini S, Snady H et al. 2000 Currentsurgical therapy for carcinoma of the pancreas.Journal of Clinical Gastroenterology 31: 107–113.
14. Ishikawa O, Ohigashi H, Imaoka S et al. 1994 Is thelong-term survival rate improved by preoperativeirradiation prior to Whipple’s procedure foradenocarcinoma of the pancreatic head? Archives ofSurgery 129: 1075–1080.
15. Di Stasi M, Lencioni R, Solmi L et al. 1998Ultrasound-guided fine needle biopsy of pancreaticmasses: results of a multicenter study. AmericanJournal of Gastroenterology 93: 1329–1333.
16. Wieersema M. 2001 Accuracy of endoscopicultrasound in diagnosing and staging pancreaticcarcinoma. Pancreatology 1: 625–632.
17. Hammond N, Miller F, Sica G, Gore R. 2002Imaging of cystic diseases of the pancreas. RadiologyClinics of North America 40:1243–1262.
18. Yassa N, Yang J, Stein S et al. 1997 Gray-scale andcolour flow sonography of pancreatic ductaladenocarcinoma. Journal of Clinical Ultrasound 25:473–480.
19. Angeli E, Venturini M, Vanzulli A et al. 1997 ColorDoppler imaging in the assessment of vascularinvolvement by pancreatic carcinoma. AmericanJournal of Roentgenology 168: 193–197.
20. Tomiyama T, Ueno N, Tano S et al. 1996 Assessmentof arterial invasion in pancreatic cancer using colourDoppler ultrasonography. American Journal ofGastroenterology 91: 1410–1416.
21. Jacobs JE, Coleman BG, Arger PH, Langer JE. 1994Pancreatic sparing of focal fatty inflitration. Radiology190: 437–439.
22. Craig MH, Talton DS, Hauser CJ, Poole GV. 1995Pancreatic injuries from blunt trauma. AmericanSurgeon 61: 125–128.
23. Krishnamurthi V, Philosophe B, Bartlett ST. 2001Pancreas transplantation: contemporary surgicaltechniques. Urology Clinics of North America 28:833–838.
24. Sutherland DE, Gruessner RW, Dunn DL et al. 2001Lessons learned from more than 1000 pancreastransplants at a single institution. Annals of Surgery233: 463–501.
25. Pozniak MA, Propeck PA, Kelcz F, Sollinger H. 1995Imaging of pancreas transplants. Radiologic Clinics ofNorth America 33: 581–594
ABDOMINAL ULTRASOUND136
References
ch05.qxd 7/6/04 8:49 AM Page 136
THE SPLEEN—NORMAL APPEARANCESAND TECHNIQUE
The spleen normally lies posterior to the splenicflexure and stomach, making an anterior approachalmost invariably unsuccessful due to overlyingbowel gas. The spleen should therefore beapproached from the left lateral aspect: coronal andtransverse sections may be obtained with thepatient supine by using an intercostal approach.Gentle respiration is frequently more successfulthan deep inspiration, as the latter brings the lungbases downwards and may obscure a small spleenaltogether.
Lying the patient decubitus, left side raised, mayalso be successful but sometimes has the effect ofcausing the gas-filled bowel loops to rise to the leftflank, once again obscuring the spleen. A slightlyposterior approach may overcome this.
Ultrasound appearances
The normal spleen has a fine, homogeneous tex-ture, with smooth margins and a pointed inferioredge. It has similar echogenicity to the liver butmay be slightly hypo- or hyperechoic in somesubjects.
Sound attenuation through the spleen is lessthan that through the liver, requiring the operatorto ‘flatten’ the time gain compensation controls inorder to maintain an even level of echoesthroughout the organ. The main splenic arteryand vein and their branches may be demonstratedat the splenic hilum (Fig. 6.1).
Chapter 6
The spleen and lymphatic system
137
CHAPTER CONTENTS
The spleen—normal appearances and technique 137Splenomegaly 139Splenunculi 139
Malignant splenic disease 141Lymphoma 141Metastases 141Leukaemia 142
Benign splenic conditions 143Cysts 144Haemangioma 145Abscess 145Calcification 145Haemolytic anaemia 146Vascular abnormalities of the spleen 146Splenic trauma 148
Lymphatics 148
ch06.qxd 6/30/04 5:55 PM Page 137

ABDOMINAL ULTRASOUND138
A B
Figure 6.1 (A) Left coronal view of the normal spleen demonstrating the main splenic artery and vein at the hilum.(B) Transverse section (TS) demonstrating the splenic vein at the hilum. (C) By increasing the Doppler sensitivity, theintrasplenic perfusion can be demonstrated. (D) An elongated or enlarged spleen can be displayed more fully using anextended field of view. Shadowing from the ribs (arrows) is evident.
CD
The spleen provides an excellent acoustic win-dow to the upper pole of the left kidney, the leftadrenal gland and the tail of the pancreas.
Splenic variants
Spleen size and shape are both highly variable, witha gradual age-related decrease in volume. A spleniclength of below 12 cm is generally considered nor-mal, although this is subject to variation in shapeand the plane of measurement used.
Rarely, the diaphragmatic surface of the spleenmay be lobulated, or even completely septated.This appearance may give rise to diagnostic uncer-tainty, and Doppler may be helpful in establishingthe vascular supply, and differentiating this fromother masses in the left upper quadrant (LUQ), orfrom scarring or infarction in the spleen.
The spleen may lie in an ectopic position, in theleft flank or pelvis, or posterior to the left kidney. Theectopic (or wandering) spleen is situated on a longpedicle, allowing it to migrate within the abdomen.
ch06.qxd 6/30/04 5:55 PM Page 138

The significance of this rare condition is that thepedicle may twist, causing the patient to presentacutely with pain from splenic torsion. Ultrasounddemonstrates the enlarged, hypoechoic organ inthe abdomen, with the absence of the spleen in itsnormal position.
SplenomegalyEnlargement of the spleen is a highly non-specificsign associated with numerous conditions, themost common being infection, portal hyperten-sion, haematological disorders and neoplastic con-ditions (Table 6.1).
As with the liver, measurement of splenic vol-ume is usually considered inaccurate due to varia-tions in shape, and not reproducible. However, thelength of the spleen is an adequate indicator of sizefor most purposes and provides a useful baselinefor monitoring changes in disease status. Thelength of the normal adult spleen is less than12 cm.
The spleen enlarges downwards and medially.Its inferior margin becomes rounded, rather thanpointed, and may extend below the left kidney(Fig. 6.2).
Although the aetiology of splenomegaly maynot be obvious on ultrasound, the causes can benarrowed down by considering the clinical pictureand by identifying other relevant appearances inthe abdomen. Splenomegaly due to portal hyper-tension, for example, is frequently accompaniedby other associated pathology such as cirrhoticliver changes, varices (Fig. 6.2B) or ascites (seeChapter 4).
SplenunculiIn around 10% of the population, a small accessoryspleen, or splenunculus, may be located at thesplenic hilum. These small, well-defined ectopic
THE SPLEEN AND LYMPHATIC SYSTEM 139
Table 6.1 Examples of causes of splenomegaly
● Portal hypertension● Acute or chronic systemic infection, e.g. hepatitis,
AIDS, infectious mononucleosis, sepsis● Haemolytic anaemia, sickle cell disease, thalassaemia,
pernicious anaemia, spherocytosis● Malignancy—leukaemia, Hodgkin’s and non-Hodgkin’s
lymphoma, myeloproliferative disorders● Storage disorders● Immunological diseases
Figure 6.2 (A) Splenomegaly in portal hypertension.The inferior splenic margin is blunted, descending belowand medial to the left kidney. (B) Varices at the splenichilum in portal hypertension.
A
B
(Continued)
ch06.qxd 6/30/04 5:55 PM Page 139

nodules of splenic tissue (Fig. 6.2C) rarely exceed2 cm in diameter. Splenunculi enlarge under thesame circumstances as those which causesplenomegaly and may also hypertrophy in post-splenectomy patients.
The importance of recognizing these lies in dif-ferentiating them from lymph nodes, left adrenalnodules or masses in the tail of pancreas. Colour
Doppler may identify the vascular supply as beingcommon to the main spleen1 (Fig. 6.2D).
Pitfalls in scanning the spleen● In hepatomegaly, the left lobe of liver may
extend across the abdomen, indenting thespleen. This can give the appearance of a
ABDOMINAL ULTRASOUND140
C D
E
LL
S
Figure 6.2 cont’d (C) A splenunculus (arrow) at the hilum of a mildly enlarged spleen. (D) The circulation of thesplenunculus derives from the main splenic artery and drains into the main splenic vein. (E) The left lobe of the liver, LL, extends across the abdomen and above the spleen, S, in hepatomegaly, giving the appearance of a well-definedsplenic mass.
ch06.qxd 6/30/04 5:55 PM Page 140
homogeneous, intrasplenic ‘mass’ when thespleen is viewed coronally (Fig. 6.2D). Atransverse scan at the epigastrium shoulddemonstrate the extent of left hepaticenlargement and confirm its relationship to thespleen.
● Splenunculi may be mistaken for enlargedlymph nodes at the splenic hilum. ColourDoppler can confirm the vascular supply isshared by the spleen.
● The normal tail of pancreas may mimic aperisplenic mass.
● A left adrenal mass, or upper pole renal mass,may indent the spleen making it difficult toestablish the origin of the mass.
MALIGNANT SPLENIC DISEASE
LymphomaLymphoma is the most common malignant diseaseaffecting the spleen. Lymphomas comprise a num-ber of diseases, all malignant, which affect the lym-phocytes. Malignant cells can infiltrate the spleen,lymph nodes, bone marrow and thymus and canalso involve the liver, gastrointestinal tract, kidneyand other organs. Approximately 3% of malignantdiseases are lymphomas.
Splenic involvement may be found in up to 60%of lymphomas as a result of dissemination of thedisease. Primary splenic lymphoma, limited to thespleen, is very rare, and accounts for less than 1%of lymphomas. There are two main groups:Hodgkin’s and non-Hodgkin’s lymphomas.
Clinical features and management
Patients may present with a range of non-specificsymptoms which include lymph node enlargement,anaemia, general fatigue, weight loss, fever, sweat-ing and infections associated with decreased immu-nity.
If the disease has spread to other organs, thesemay produce symptoms related to the organs inquestion.
Prognosis depends upon the type of the disease,which must be determined histologically, and itsstage. Both ultrasound and CT may be used in
staging: ultrasound demonstrates splenic involve-ment with greater sensitivity than CT, and CT issuperior in demonstrating para-aortic and iliaclymph nodes.2 Bone scintigraphy and MRI are fur-ther supplementary techniques in staging.
Depending upon the type of lymphoma,chemotherapy regimes may be successful and, ifnot curative, can cause remission for lengthy peri-ods. High-grade types of lymphoma are particu-larly aggressive with a poor survival rate.
Ultrasound appearances
The range of possible ultrasound appearances inlymphoma is varied (Fig. 6.3). In many cases thespleen is not enlarged and shows no acousticabnormality. In a study of 61 patients withHodgkin’s disease involving the spleen, the organwas usually normal in size and showed no acousticabnormality in 46% of cases.3
Lymphoma may produce a diffuse splenicenlargement with normal, hypo- or hyper-echogenicity. Focal lesions may be present in up to16% of lymphomas.4,5 They tend to be hypoechoicand may be single or multiple, and of varying sizes.In larger lesions the margins may be ill-defined andthe echo contents vary from almost anechoic toheterogeneous, often with increased through-trans-mission. In such cases, they may be similar inappearance to cysts, however, the well-defined cap-sule is absent in lymphoma, which has a more indis-tinct margin.6 Smaller lesions may be hyperechoicor mixed. Tiny lymphomatous foci may affect theentire spleen, making it appear coarse in texture.
Lymphadenopathy may be present elsewhere inthe abdomen. If other organs, such as the kidneyor liver, are affected, the appearances of masslesions vary but are commonly echo-poor or ofmixed echo pattern.
A differential diagnosis of metastases should beconsidered in the presence of multiple solid hypo-echoic splenic lesions, but most cases are due tolymphoma.7
MetastasesMetastatic deposits occur in the spleen much lesscommonly than in the liver. Autopsy reports anincidence of around 10%, although a proportion of
THE SPLEEN AND LYMPHATIC SYSTEM 141
ch06.qxd 6/30/04 5:55 PM Page 141

these are microscopic and not amenable to radio-logical imaging.
The most commonly found splenic metastaseson ultrasound are from lymphoma, but may occurwith any primary cancer. Intrasplenic deposits aremore likely in later-stage disease and favourmelanoma, pulmonary, ovarian or breast primaries.
As with liver metastases, the ultrasound appear-ances vary enormously, ranging from hypo- tohyperechogenic or of mixed pattern (Fig. 6.4).They may be solitary, multiple or diffusely infiltra-tive, giving a coarse echo-pattern.8
LeukaemiaLeukaemia (literally meaning ‘white blood’, fromthe Greek) is characterized by an increased numberof malignant white blood cells. Unlike lymphoma,which affects the lymphatic system, leukaemiaaffects the circulation.
There are two main types, myeloid and lym-phoid, both of which can be either acute or chronic.
The bone marrow becomes infiltrated withmalignant cells which cause the blood to haveincreasing levels of immature blood cells.
ABDOMINAL ULTRASOUND142
A B
C
Figure 6.3 Lymphoma: (A) Small, focal lesion in a normal-sized spleen. (B) Enlarged, hyperechoic spleen with ahypoechoic focal lesion (arrow). (C) Enlarged, coarse-textured spleen containing multiple tiny lymphomatous lesions.(D) Extensive lymphadenopathy in the epigastric region.
D
ch06.qxd 6/30/04 5:55 PM Page 142
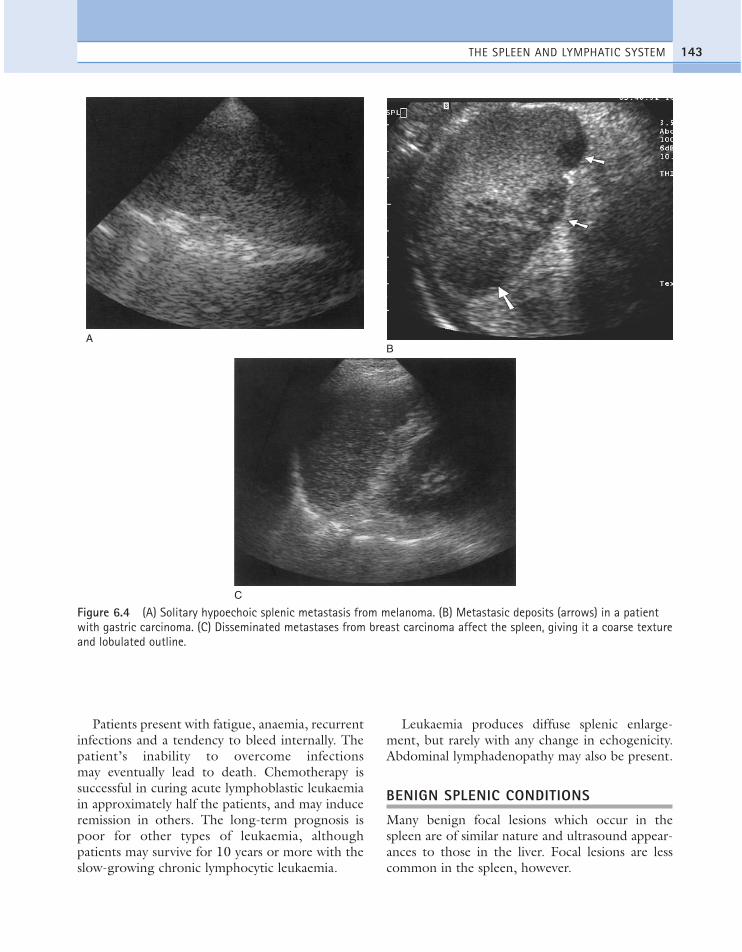
Patients present with fatigue, anaemia, recurrentinfections and a tendency to bleed internally. Thepatient’s inability to overcome infectionsmay eventually lead to death. Chemotherapy issuccessful in curing acute lymphoblastic leukaemiain approximately half the patients, and may induceremission in others. The long-term prognosis ispoor for other types of leukaemia, althoughpatients may survive for 10 years or more with theslow-growing chronic lymphocytic leukaemia.
Leukaemia produces diffuse splenic enlarge-ment, but rarely with any change in echogenicity.Abdominal lymphadenopathy may also be present.
BENIGN SPLENIC CONDITIONS
Many benign focal lesions which occur in thespleen are of similar nature and ultrasound appear-ances to those in the liver. Focal lesions are lesscommon in the spleen, however.
THE SPLEEN AND LYMPHATIC SYSTEM 143
AB
C
Figure 6.4 (A) Solitary hypoechoic splenic metastasis from melanoma. (B) Metastasic deposits (arrows) in a patientwith gastric carcinoma. (C) Disseminated metastases from breast carcinoma affect the spleen, giving it a coarse textureand lobulated outline.
ch06.qxd 6/30/04 5:55 PM Page 143

CystsSplenic cysts have a relatively low incidence, butare nevertheless the most common benign massfound in the spleen. They demonstrate the usualacoustic characteristics of well-defined capsule, nointernal echoes and posterior enhancement (Fig.6.5). Splenic cysts may occasionally be associatedwith adult polycystic disease.
Other causes of cystic lesions in the spleeninclude post-traumatic cysts (liquefied haema-toma), hydatid cysts (Echinococcus granulosusparasite) or cystic metastases (for example fromprimary ovarian carcinoma, which may containmucin).
As with hepatic cysts, haemorrhage may occur,causing LUQ pain (Fig. 6.5B). Large cysts may beresected, in order to avoid rupture.
ABDOMINAL ULTRASOUND144
A B
C D
Figure 6.5 (A) Small, simple splenic cyst. (B) Haemorrhage into a splenic cyst causes low-level echoes. (C) Largesplenic abscess in an immunosuppressed patient following hepatic transplantation. (D) This abscess, involving theentire spleen, followed a severe episode of empyema. The patient presented, following cholecystectomy, with a spikingtemperature.
ch06.qxd 6/30/04 5:55 PM Page 144
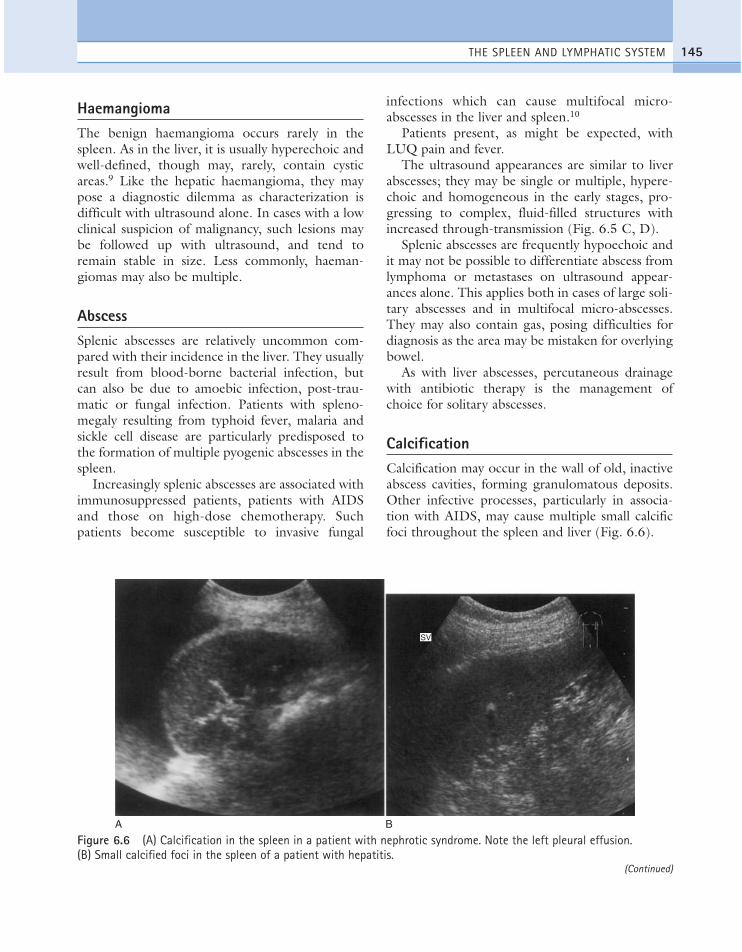
HaemangiomaThe benign haemangioma occurs rarely in thespleen. As in the liver, it is usually hyperechoic andwell-defined, though may, rarely, contain cysticareas.9 Like the hepatic haemangioma, they maypose a diagnostic dilemma as characterization isdifficult with ultrasound alone. In cases with a lowclinical suspicion of malignancy, such lesions maybe followed up with ultrasound, and tend toremain stable in size. Less commonly, haeman-giomas may also be multiple.
AbscessSplenic abscesses are relatively uncommon com-pared with their incidence in the liver. They usuallyresult from blood-borne bacterial infection, butcan also be due to amoebic infection, post-trau-matic or fungal infection. Patients with spleno-megaly resulting from typhoid fever, malaria andsickle cell disease are particularly predisposed tothe formation of multiple pyogenic abscesses in thespleen.
Increasingly splenic abscesses are associated withimmunosuppressed patients, patients with AIDSand those on high-dose chemotherapy. Suchpatients become susceptible to invasive fungal
infections which can cause multifocal micro-abscesses in the liver and spleen.10
Patients present, as might be expected, withLUQ pain and fever.
The ultrasound appearances are similar to liverabscesses; they may be single or multiple, hypere-choic and homogeneous in the early stages, pro-gressing to complex, fluid-filled structures withincreased through-transmission (Fig. 6.5 C, D).
Splenic abscesses are frequently hypoechoic andit may not be possible to differentiate abscess fromlymphoma or metastases on ultrasound appear-ances alone. This applies both in cases of large soli-tary abscesses and in multifocal micro-abscesses.They may also contain gas, posing difficulties fordiagnosis as the area may be mistaken for overlyingbowel.
As with liver abscesses, percutaneous drainagewith antibiotic therapy is the management ofchoice for solitary abscesses.
CalcificationCalcification may occur in the wall of old, inactiveabscess cavities, forming granulomatous deposits.Other infective processes, particularly in associa-tion with AIDS, may cause multiple small calcificfoci throughout the spleen and liver (Fig. 6.6).
THE SPLEEN AND LYMPHATIC SYSTEM 145
A B
SV
Figure 6.6 (A) Calcification in the spleen in a patient with nephrotic syndrome. Note the left pleural effusion. (B) Small calcified foci in the spleen of a patient with hepatitis.
(Continued)
ch06.qxd 6/30/04 5:55 PM Page 145
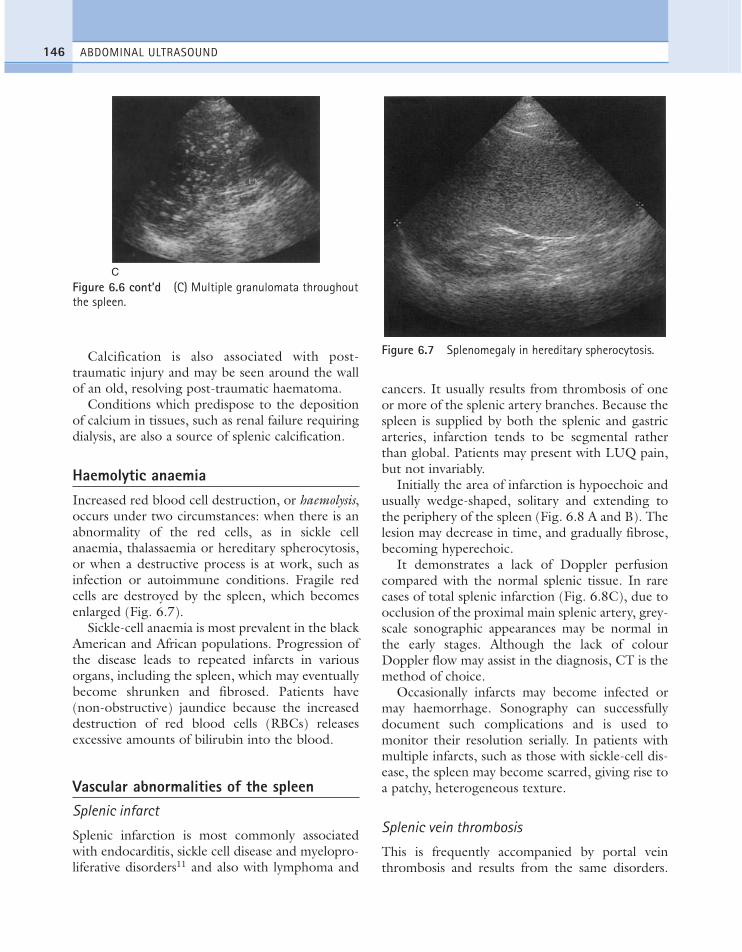
Calcification is also associated with post-traumatic injury and may be seen around the wallof an old, resolving post-traumatic haematoma.
Conditions which predispose to the depositionof calcium in tissues, such as renal failure requiringdialysis, are also a source of splenic calcification.
Haemolytic anaemiaIncreased red blood cell destruction, or haemolysis,occurs under two circumstances: when there is anabnormality of the red cells, as in sickle cellanaemia, thalassaemia or hereditary spherocytosis,or when a destructive process is at work, such asinfection or autoimmune conditions. Fragile redcells are destroyed by the spleen, which becomesenlarged (Fig. 6.7).
Sickle-cell anaemia is most prevalent in the blackAmerican and African populations. Progression ofthe disease leads to repeated infarcts in variousorgans, including the spleen, which may eventuallybecome shrunken and fibrosed. Patients have(non-obstructive) jaundice because the increaseddestruction of red blood cells (RBCs) releasesexcessive amounts of bilirubin into the blood.
Vascular abnormalities of the spleenSplenic infarct
Splenic infarction is most commonly associatedwith endocarditis, sickle cell disease and myelopro-liferative disorders11 and also with lymphoma and
cancers. It usually results from thrombosis of oneor more of the splenic artery branches. Because thespleen is supplied by both the splenic and gastricarteries, infarction tends to be segmental ratherthan global. Patients may present with LUQ pain,but not invariably.
Initially the area of infarction is hypoechoic andusually wedge-shaped, solitary and extending tothe periphery of the spleen (Fig. 6.8 A and B). Thelesion may decrease in time, and gradually fibrose,becoming hyperechoic.
It demonstrates a lack of Doppler perfusioncompared with the normal splenic tissue. In rarecases of total splenic infarction (Fig. 6.8C), due toocclusion of the proximal main splenic artery, grey-scale sonographic appearances may be normal inthe early stages. Although the lack of colourDoppler flow may assist in the diagnosis, CT is themethod of choice.
Occasionally infarcts may become infected ormay haemorrhage. Sonography can successfullydocument such complications and is used tomonitor their resolution serially. In patients withmultiple infarcts, such as those with sickle-cell dis-ease, the spleen may become scarred, giving rise toa patchy, heterogeneous texture.
Splenic vein thrombosis
This is frequently accompanied by portal veinthrombosis and results from the same disorders.
ABDOMINAL ULTRASOUND146
C
Figure 6.6 cont’d (C) Multiple granulomata throughoutthe spleen.
Figure 6.7 Splenomegaly in hereditary spherocytosis.
ch06.qxd 6/30/04 5:55 PM Page 146

The most common of these are pancreatitis andtumour thrombus. Colour and spectral Dopplerare an invaluable aid to the diagnosis, particularlywhen the thrombus is fresh and therefore echo-poor. Contrast agents may be administered ifdoubt exists over vessel patency.
Splenic vein occlusion causes splenomegaly andvarices may be identified around the splenic hilum.
Splenic artery aneurysm
These are rare, although more common thanhepatic artery aneurysms. They are only clinicallysignificant if over 2 cm in diameter, when the riskof rupture and fatal haemorrhage is present.
Colour and spectral Doppler confirm arterial flowthrough the aneurysm and help to differentiate it
THE SPLEEN AND LYMPHATIC SYSTEM 147
AB
C D
Figure 6.8 (A) Splenic infarct due to an embolus following recent liver resection. (B) Colour Doppler of the samepatient demonstrates a lack of perfusion in the infarcted area. (C) CT scan of the same patient. (D) Complete splenicinfarction. The spleen is small and hyperechoic. Considerable free fluid is present.
ch06.qxd 6/30/04 5:55 PM Page 147
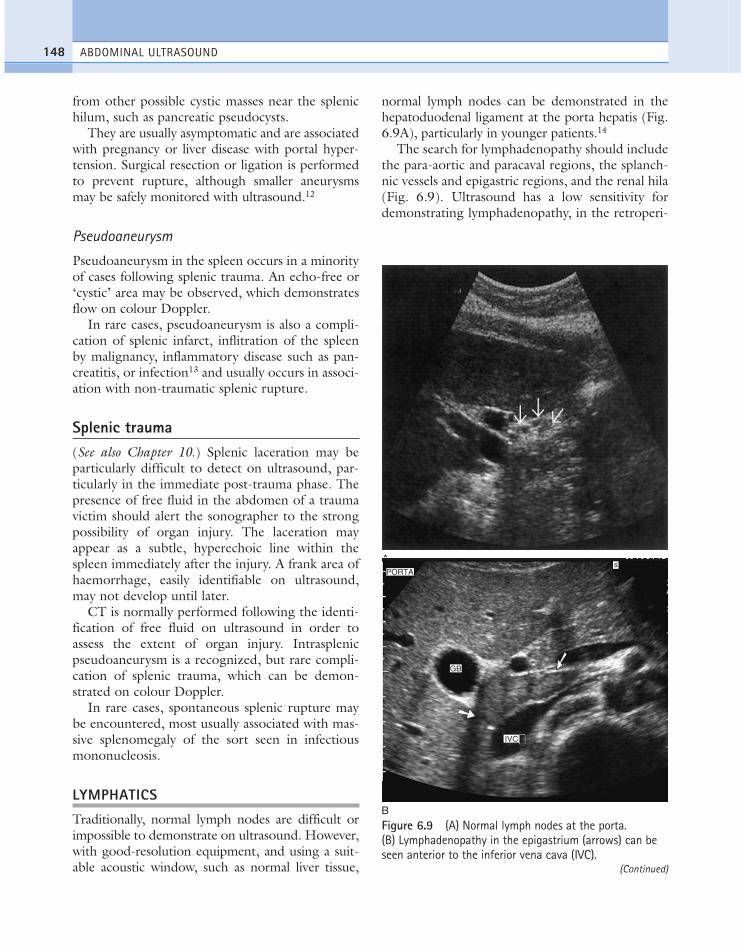
from other possible cystic masses near the splenichilum, such as pancreatic pseudocysts.
They are usually asymptomatic and are associatedwith pregnancy or liver disease with portal hyper-tension. Surgical resection or ligation is performedto prevent rupture, although smaller aneurysmsmay be safely monitored with ultrasound.12
Pseudoaneurysm
Pseudoaneurysm in the spleen occurs in a minorityof cases following splenic trauma. An echo-free or‘cystic’ area may be observed, which demonstratesflow on colour Doppler.
In rare cases, pseudoaneurysm is also a compli-cation of splenic infarct, inflitration of the spleenby malignancy, inflammatory disease such as pan-creatitis, or infection13 and usually occurs in associ-ation with non-traumatic splenic rupture.
Splenic trauma(See also Chapter 10.) Splenic laceration may beparticularly difficult to detect on ultrasound, par-ticularly in the immediate post-trauma phase. Thepresence of free fluid in the abdomen of a traumavictim should alert the sonographer to the strongpossibility of organ injury. The laceration mayappear as a subtle, hyperechoic line within thespleen immediately after the injury. A frank area ofhaemorrhage, easily identifiable on ultrasound,may not develop until later.
CT is normally performed following the identi-fication of free fluid on ultrasound in order toassess the extent of organ injury. Intrasplenicpseudoaneurysm is a recognized, but rare compli-cation of splenic trauma, which can be demon-strated on colour Doppler.
In rare cases, spontaneous splenic rupture maybe encountered, most usually associated with mas-sive splenomegaly of the sort seen in infectiousmononucleosis.
LYMPHATICS
Traditionally, normal lymph nodes are difficult orimpossible to demonstrate on ultrasound. However,with good-resolution equipment, and using a suit-able acoustic window, such as normal liver tissue,
normal lymph nodes can be demonstrated in thehepatoduodenal ligament at the porta hepatis (Fig.6.9A), particularly in younger patients.14
The search for lymphadenopathy should includethe para-aortic and paracaval regions, the splanch-nic vessels and epigastric regions, and the renal hila(Fig. 6.9). Ultrasound has a low sensitivity fordemonstrating lymphadenopathy, in the retroperi-
ABDOMINAL ULTRASOUND148
A
B
GB
sPORTA
IVC
Figure 6.9 (A) Normal lymph nodes at the porta. (B) Lymphadenopathy in the epigastrium (arrows) can beseen anterior to the inferior vena cava (IVC).
(Continued)
ch06.qxd 6/30/04 5:55 PM Page 148

THE SPLEEN AND LYMPHATIC SYSTEM 149
toneum, as bowel contents frequently obscure therelevant areas.
CT or MRI is better able to define the extent oflymphadenopathy, particularly in the pelvis.
The presence of lymphadenopathy is highlynon-specific, being associated with a wide range of
conditions including malignancy, infections andinflammatory disorders.
Benign lymphadenopathy is commonly seen inconjunction with hepatitis and other inflammatorydisorders such as pancreatitis, cholangitis andcolitis.15
C D
E(i)
E(ii)
Figure 6.9 cont’d (C) TS through the left upper quadrant (LUQ) showing lymphadenopathy at the splenic hilum of apatient with lymphoma. (D) A large hyperechoic lymph mass at the porta hepatis, causing obstructive jaundice. (E) i,Blood flow in a malignant lymph node in a patient with renal carcinoma; ii, showing a high resistance index of 0.91.
ch06.qxd 6/30/04 5:55 PM Page 149

Nodes of 1.5 cm or over are generally consid-ered pathological. Enlarged nodes are most oftenhypoechoic, rounded or oval in shape and well-defined. Larger nodes display colour or powerDoppler flow.
Less frequently nodes are hyperechoic, or maycombine to form large, lobulated masses. There issome evidence that colour Doppler may assistin differentiating benign from malignant superfi-cial nodes (Fig. 6.9E), the latter displaying asignificantly higher resistance on spectralanalysis.16,17
Lymphadenopathy at the porta may occasionallycause obstructive jaundice due to compression ofthe common bile duct.
Lymphangioma
These are benign tumours of the lymphatic ves-sels, usually diagnosed in the neonatal period oron prenatal sonography. They are predominantlycystic, frequently septated, and may be large (Fig.6.10). They can compress adjacent organs and
vessels and their severity depends to a large extentupon their location. They are most common in theneck (cystic hygroma) but can be found in variouslocations, including the abdomen,18 and are occa-sionally found in adults after a long asymptomaticperiod.
ABDOMINAL ULTRASOUND150
Figure 6.10 Lymphangioma. This large, septated cysticmass was present in the chest wall of this 2-year-old girl.
References1. Bertolotto M, Gioulis E, Ricci C et al. 1998
Ultrasound and Doppler features of accessory spleensand splenic grafts. British Journal of Radiology 71:595–600.
2. Munker R, Stengel A, Stabler A et al. 1995Diagnostic accuracy of ultrasound and computedtomography in the staging of Hodgkin’s disease:verification by laparotomy in 100 cases. Cancer 76:1460–1466.
3. Siniluoto T, Paivansalo M, Alavaikko M. 1991Ultrasonography of spleen and liver in stagingHodgkin’s disease. European Journal of Radiology13: 181–186.
4. Di-Stasi M, Cavanna L, Fornari F et al. 1995 Spleniclesions in Hodgkin’s and non-Hodgkin’s lymphomas.An ultrasonographic study. European Journal ofUltrasound 2: 117–124.
5. Gorg C, Weide R, Schwerk WB. 1997 Malignantsplenic lymphoma: sonographic patterns, diagnosisand follow-up. Clinical Radiology 52: 535–540.
6. Ishida H, Konno K, Naganuma H et al. 2001Splenic lymphoma: differentiation from splenic cystswith ultrasonography. Abdominal Imaging 26:529–532.
7. Goerg C, Schwerk WB, Goerg K. 1990 Sonographyof focal lesions of the spleen. American Journal ofRoentgenology 157: 965–966.
8. Siniluoto T Paivansalo M, Lahde S. 1989Ultrasonography of splenic metastases. ActaRadiologica 30: 463.
9. Ros PR, Moser RP, Dachman AH et al. 1987Haemangioma of the spleen: radiologic–pathologiccorrelation in ten cases. American Journal ofRoentgenology 162: 73–77.
10. Gorg C, Weide R, Schwerk WB et al. 1994Ultrasound evaluation of hepatic and splenicmicroabscesses in the immunocompromised patient:sonographic patterns, differential diagnosis andfollow-up. Journal of Clinical Ultrasound 22:525–529.
11. Georg C, Schwerk WB. 1990 Splenic infarction;sonographic pattern, diagnosis, follow-up andcomplications. Radiology 174: 803–807.
12. Mattar SG, Lumsden AB. 1995 The management ofsplenic artery aneurysms: experience with 23 cases.American Journal of Surgery 169; 580–584.
13. Gorg C, Colle J, Wied M et al. 2003 Spontaneousnontraumatic intrasplenic pseudoaneurysm: causes,
ch06.qxd 6/30/04 5:55 PM Page 150
sonographic diagnosis and prognosis. Journal ofClinical Ultrasound 31: 129–134.
14. Metreweli C, Ward S. 1995 Ultrasounddemonstration of lymph nodes in the hepatoduodenalligament (‘daisy chain nodes’) in normal subjects.Clinical Radiology 50: 99–101.
15. Gimondo P, Mirk P, Messina G, Pizzi C. 1996Abdominal lymphadenopathy in benign diseases:sonographic detection and clinical significance.Journal of Ultrasound in Medicine 15: 353–359.
16. Dong GN, Hyo KL, Hong SB et al. 1997 Differentialdiagnosis of cervical lymphadenopathy: usefulness of
colour Doppler sonography. American Journal ofRoentgenology 168: 1311–1316.
17. Min YC, Jun WL, Kyung JJ. 1995 Distinctionbetween benign and malignant causes of cervical,axillary and inguinal lymphadenopathy: value ofDoppler spectral waveform analysis. American Journalof Roentgenology 165: 981–984.
18. Schmidt M. 1995 Intra-abdominal lymphangioma.Kansas Medicine 93: 149–150.
THE SPLEEN AND LYMPHATIC SYSTEM 151
ch06.qxd 6/30/04 5:55 PM Page 151
ch06.qxd 6/30/04 5:55 PM Page 152
This page intentionally left blank
Chapter 7
The renal tract
153
CHAPTER CONTENTS
The normal renal tract 154Ultrasound technique 154Assessment of renal function 157Normal variants 158
Renal cysts and cystic disease 160Cysts 160Autosomal dominant (adult) polycystic kidneydisease 161Autosomal recessive (infantile) disease 162Acquired cystic disease 162Multicystic dysplastic kidney (MCDK) 162
Benign focal renal tumours 162Angiomyolipoma 162Adenoma 162
Malignant renal tract masses 163Renal cell carcinoma 163Transitional cell carcinoma 164Lymphoma 165Metastases 165
Pelvicalyceal system dilatation and obstructiveuropathy 166Physiological dilatation 166Obstructive uropathy 166Vesicoureteric junction 170Non-obstuctive hydronephrosis 170
Renal tract calcification 170Renal tract stones 171Nephrocalcinosis 173Hyperparathyroidism 173
Renal tract inflammation and infection 174
Pyelonephritis 174Focal pyelonephritis 175Renal abscess 175Tuberculosis (TB) 175Xanthogranulomatous pyelonephritis (XGP) 177Hydatid cysts 177
Diffuse renal disease and renal failure 177Acute tubular necrosis 177Glomerulonephritis 178Medullary sponge kidney 179Amyloid 179The renal biopsy 179
Renal vascular pathology 179Renal artery stenosis (RAS) 179Renal vein thrombosis 180Arteriovenous fistula 181Ultrasound in dialysis 181
Renal trauma 182Renal transplants 182
Normal anatomy 182Normal ultrasound and appearances 182Postoperative complications 185Renal transplant dilatation 185Rejection 185Fluid collections associated withtransplantation 186Vascular complications 187Infection 189Acute tubular necrosis 189Ciclosporin nephrotoxicity 191Renal transplant dysfunction and Dopplercorrelation 191
ch07.qxd 6/30/04 6:08 PM Page 153

THE NORMAL RENAL TRACT
Ultrasound techniqueThe right kidney is readily demonstrated throughthe right lobe of the liver. Generally a subcostalapproach displays the (more anterior) lower poleto best effect, while an intercostal approach is bestfor demonstrating the upper pole (Fig. 7.1).
The left kidney is not usually demonstrablesagittally because it lies posterior to the stomachand splenic flexure. The spleen can be used as an
acoustic window to the upper pole by scanningcoronally, from the patient’s left side, with thepatient supine or decubitus (left side raised),but, unless the spleen is enlarged, the lower polemust usually be imaged from the left side poste-riorly.
Coronal sections of both kidneys are particularlyuseful as they display the renal pelvicalyceal system(PCS) and its relationship to the renal hilum (Fig.7.2A). This section demonstrates the main bloodvessels and ureter (if dilated).
ABDOMINAL ULTRASOUND154
A B
Figure 7.1 (A) Sagittal section through the normal right kidney (RK), using the liver as an acoustic window. Thecentral echoes from the renal sinus are hyperechoic due to the fat content. The hypoechoic, triangular, medullarypyramids are demonstrated in a regular arrangement around the sinus. The cortex is of similar echogenicity to the liver.(B) TS through the hilum of the RK, demonstrating the renal vein (arrow) draining into the inferior vena cava (IVC)(arrowhead). (C) Left kidney (LK) in coronal section. The renal hilum is seen furthest from the transducer (s = spleen).(Compare this with the sagittal section of the RK in which cortex is seen all the way around the pelvicalyceal system.)(D) The renal cortex lies between the capsule and the lateral margin of the medullary pyramid (arrowheads).
C D
ch07.qxd 6/30/04 6:08 PM Page 154

As with any other organ, the kidneys must beexamined in both longitudinal and transverse(axial) planes. This usually requires a combinationof subcostal and intercostal scanning with anterior,posterior and lateral approaches. The operatormust be flexible in approach to obtain the neces-sary results.
The bladder should be filled and examined tocomplete the renal tract scan. An excessively fullbladder may cause mild dilatation of the PCS,
which will return to normal following micturi-tion.
Normal ultrasound appearances of the kidneys
The cortex of the normal kidney is slightly hypo-echoic when compared to the adjacent liverparenchyma, although this is age-dependent. Inyoung people it may be of similar echogenicity andin the elderly it is not unusual for it to be compara-
THE RENAL TRACT 155
A
B
C
p
POST MICT
Figure 7.2 (A) Coronal section through the RKdemonstrating fetal lobulations (arrows). Thepelvicalyceal system (PCS) is mildly distended due to afull bladder. (B) TS through the base of the bladder,demonstrating a left ureteric jet. (C) Longitudinalsection (LS) and TS scans through the bladder aftermicturition demonstrating an enlarged prostate (P) and asmall residual urine volume of 40 ml.
ch07.qxd 6/30/04 6:08 PM Page 155

tively hyperechoic and thin. The medullary pyramidsare seen as regularly spaced, echo-poor triangularstructures between the cortex and the renal sinus(Fig. 7.1). The tiny reflective structures often seen atthe margins of the pyramids are echoes from thearcuate arteries which branch around the pyramids.
The renal sinus containing the PCS is hyper-echoic due to sinus fat which surrounds the vessels.The main artery and vein can be readily demon-strated at the renal hilum and should not be con-fused with a mild degree of PCS dilatation.Colour Doppler can help differentiate.
The kidney develops in the fetus from a numberof lobes, which fuse. Occasionally the traces ofthese lobes can be seen on the surface of the kid-ney, forming fetal lobulations (Fig. 7.2A); thesemay persist into adulthood.
Normal ultrasound appearances of the lowerrenal tract
When the bladder is distended with urine, the wallsare thin, regular and hyperechoic. The walls mayappear thickened or trabeculated if the bladder isinsufficiently distended, making it impossible toexclude a bladder lesion.
The ureteric orifices can be demonstrated in atransverse section at the bladder base. Ureteric jetscan easily be demonstrated with colour Doppler atthis point and normally occur between 1.5 and12.4 times per minute (a mean of 5.4 jets perminute) from each side1 (Fig. 7.2B).
It is useful to examine the pelvis for other masses,e.g. related to the uterus or ovaries, which couldexert pressure on the ureters causing proximal dilata-tion. The prostate is demonstrated transabdominallyby angling caudally through the full bladder (Fig.7.2C). The investigation of choice for the prostate istransrectal ultrasound; however an approximate ideaof its size can be gained from transabdominal scan-ning. When prostatic hypertrophy is suspected, it isuseful to perform a postmicturition bladder volumemeasurement to determine the residual volume ofurine (see Measurements below).
Measurements
The normal adult kidney measures between 9 and12 cm in length. A renal length outside the normal
range may be an indication of a pathological processand measurements should therefore form part of theprotocol of renal scanning. The maximum renallength can often only be obtained from a sectionwhich includes rib shadowing. A subcostal section,which foreshortens the kidney, often underestimatesthe length and it is more accurate to measure a coro-nal or posterior longitudinal section.
The cortical thickness of the kidney is generallytaken as the distance between the capsule and themargin of the medullary pyramid (Fig. 7.2D). Thisvaries between individuals and within individualkidneys and tends to decrease with age.
The bladder volume (Fig. 7.2C) can be esti-mated for most purposes by taking the product ofthree perpendicular measurements and multiplyingby 0.56:
Bladder volume (ml) = length ¥ width ¥anteroposterior diameter (cm) ¥ 0.56
Haemodynamics
The vascular tree of the kidney can be effectivelydemonstrated with colour Doppler (Fig. 7.3). Bymanipulating the system sensitivity and using alow pulse repetition frequency (PRF), small vesselscan be demonstrated at the periphery of thekidney.
Demonstration of the extrarenal main arteryand vein with colour Doppler is most successful inthe coronal or axial section by identifying the renalhilum and tracing the artery back to the aorta orthe vein to the inferior vena cava (IVC). The bestDoppler signals, that is, the highest Doppler shiftfrequencies, are obtained when the direction ofthe vessel is parallel to the beam, and taken on sus-pended respiration. The left renal vein is readilydemonstrated between the superior mesentericartery (SMA) and aorta by scanning just below thebody of the pancreas in transverse section. Theorigins of the renal arteries may be seen arisingfrom the aorta in a coronal section [Fig. 7.3D].
The normal adult renal vasculature is of lowresistance with a fast, almost vertical systolicupstroke and continuous forward end diastolicflow. Resistance generally increases with age.2 Themore peripheral arteries are of lower velocity withweaker Doppler signals, and are less pulsatile thanthe main vessel.
ABDOMINAL ULTRASOUND156
ch07.qxd 6/30/04 6:08 PM Page 156
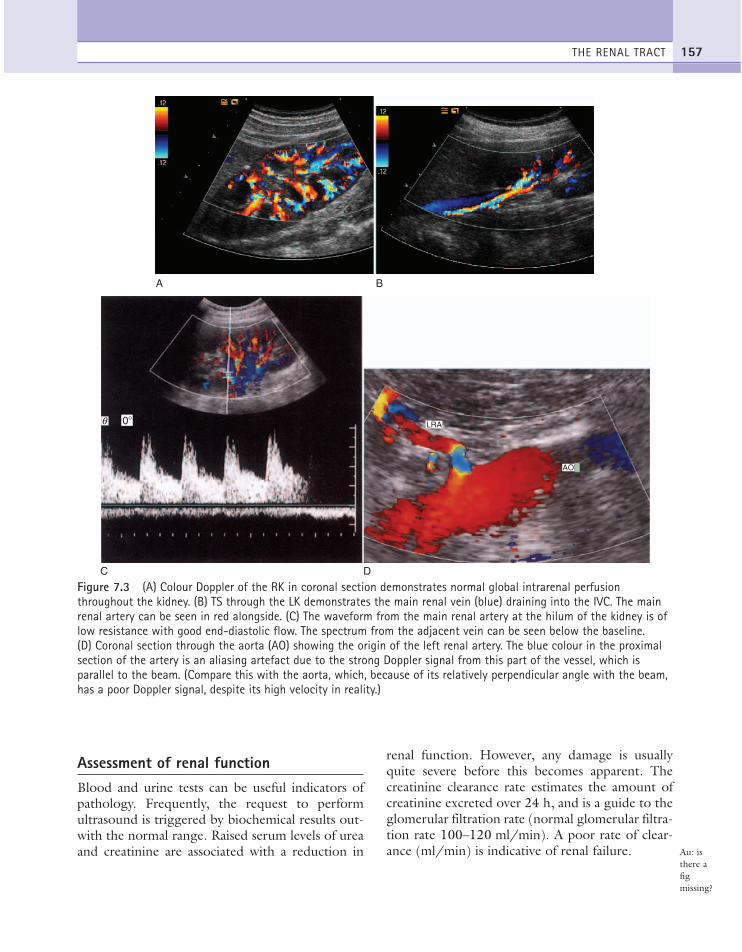
Assessment of renal functionBlood and urine tests can be useful indicators ofpathology. Frequently, the request to performultrasound is triggered by biochemical results out-with the normal range. Raised serum levels of ureaand creatinine are associated with a reduction in
renal function. However, any damage is usuallyquite severe before this becomes apparent. Thecreatinine clearance rate estimates the amount ofcreatinine excreted over 24 h, and is a guide to theglomerular filtration rate (normal glomerular filtra-tion rate 100–120 ml/min). A poor rate of clear-ance (ml/min) is indicative of renal failure.
THE RENAL TRACT 157
A B
C D
0�q
AO
LRA
Figure 7.3 (A) Colour Doppler of the RK in coronal section demonstrates normal global intrarenal perfusionthroughout the kidney. (B) TS through the LK demonstrates the main renal vein (blue) draining into the IVC. The mainrenal artery can be seen in red alongside. (C) The waveform from the main renal artery at the hilum of the kidney is oflow resistance with good end-diastolic flow. The spectrum from the adjacent vein can be seen below the baseline.(D) Coronal section through the aorta (AO) showing the origin of the left renal artery. The blue colour in the proximalsection of the artery is an aliasing artefact due to the strong Doppler signal from this part of the vessel, which isparallel to the beam. (Compare this with the aorta, which, because of its relatively perpendicular angle with the beam,has a poor Doppler signal, despite its high velocity in reality.)
Au: isthere afigmissing?
ch07.qxd 6/30/04 6:08 PM Page 157

Blood in the urine is a potentially serious signwhich should prompt investigation with ultra-sound. Frank haematuria may be a sign of renaltract malignancy. Microscopic haematuria mayreflect inflammation, infection, calculi or malig-nancy. The urine can be easily examined for pro-tein, glucose, acetone and pH using chemicallyimpregnated strips.
Radioisotope scans
Although the ultrasound scan is invaluable in assess-ing the morphology of the kidneys, it is not able toassess function. The administration of a radioactivetracer, however, reveals valuable information regard-ing renal function and an isotope scan may often beperformed in addition to ultrasound.
A diethylene triaminepenta-acetic acid (DTPA)scan, in which the isotope is intravenously injectedas a bolus, can assess renal perfusion, with furtherdata reflecting renal uptake, excretion and drainageduring later images.
A dimercaptosuccinic acid (DMSA) scan showsuptake of isotope which is proportional to func-tioning renal tissue. Relative renal function can bedetermined between kidneys and localized areas ofpoor or absent function, such as scars, are clearlydemonstrated.
Normal variantsDuplex kidneys
These occur in a spectrum of degrees, from twoseparate organs with separate collecting systems andduplex ureters, to a mild degree of separation of thePCS at the renal hilum (Fig. 7.4A). The latter ismore difficult to recognize on ultrasound, but thetwo moieties of the PCS are separated by a zone ofnormal renal cortex which invaginates the kidney, ahypertrophied column of Bertin (see below).
If duplex ureters are present (a difficult diagnosisto make on ultrasound unless dilatation is present)then a ureterocoele related to the upper moietyshould be sought at or adjacent to the bladder. Thismay cause dilatation of the affected moiety.
The main renal artery and vein may also beduplicated, which can occasionally be identifiedusing colour or power Doppler.
Ectopic kidneys
The kidney normally ascends from the pelvis into therenal fossa during its course of development. Duringthis ‘migration’ it rotates inwards so that the renalhilum faces medially. A failure of this mechanismcauses the kidney to fall short of its normal position,remaining in the pelvis, that is, a pelvic kidney. Usuallyit lies on the correct side, however occasionally it cancross to the other side, lying inferior to its normallyplaced partner—crossed renal ectopia. Frequently itmay fuse with the lower pole of the other kidney,crossed fused renal ectopia, resulting in what appearsto be a very long, unilateral organ.
Horseshoe kidneys
In the horseshoe kidney, the kidneys lie one oneach side of the abdomen but their lower poles arefused by a connecting band of renal tissue, or isth-mus, which lies anterior to the aorta and IVC (Fig.7.4). The kidneys tend to be rotated and lie withtheir lower poles medially.
It may be difficult to visualize the isthmus dueto bowel gas anterior to it but a horseshoe kidneyshould always be suspected when the operator isunable to identify the lower poles of the kidneysconfidently.
When the isthmus can be seen, it is important notto confuse it with other abdominal masses, such aslymphadenopathy. CT is occasionally performedbecause of this but normally clarifies the findings.
Extrarenal pelvis
Not infrequently, the renal pelvis projects outsidethe kidney, medial to the renal sinus. This is bestseen in a transverse section through the renalhilum. It is frequently ‘baggy’, containing anechoicurine, which is prominently demonstrated on theultrasound scan (Fig. 7.4E).
The importance of recognizing the extrarenalpelvis lies in not confusing it with dilatation of thePCS, or with a parapelvic cyst or collection.
Hypertrophied column of Bertin
The septum of Bertin is an invagination of renalcortex down to the renal sinus. It occurs at the
ABDOMINAL ULTRASOUND158
ch07.qxd 6/30/04 6:08 PM Page 158

THE RENAL TRACT 159
A
C
B
D
rk
i
lk
Figure 7.4 (A) Duplex kidney showing two separate intrarenal collecting systems (arrows). These drained into a singleureter on intravenous urogram (IVU). (B) TS through the abdomen demonstrating the fused lower poles of thehorseshoe kidney anterior to the spine. (C) Coronal section through a horseshoe kidney with the isthmus of the kidney(i) anterior to the aorta and IVC. (D) MAG3 scan demonstrating a horseshoe kidney with a poorly functioning LK andisthmus. Differential function is 86% on the right and 14% on the left.
junctions of original fetal lobulations and is presentin duplex systems (see above), dividing the twomoieties. Particularly prominent, hypertrophiedcolumns of Bertin may mimic a renal tumour. It isusually possible to distinguish between the two asthe column of Bertin does not affect the renal out-line and has the same acoustic characteristics as theadjacent cortex (Fig. 7.4F).
Colour or power Doppler can be helpful inrevealing the normal, regular vascular pattern (asopposed to the chaotic and increased blood flowpattern of malignant renal tumours). If doubt per-sists, particularly in a symptomatic patient, CT willdifferentiate tumour from a prominent column ofBertin; an isotope scan can also be helpful indemonstrating normally functioning renal tissue.
(Continued)
ch07.qxd 6/30/04 6:08 PM Page 159

Renal humps
These are areas of renal cortex, which form a bulgein the renal outline. Like the hypertrophied col-umn of Bertin, a hump may mimic a renal mass.Careful scanning can usually solve the dilemma asthe cortex remains constant in thickness. The mostusual manifestation is the splenic hump on the leftkidney, which is a flattening of the upper pole witha lateral prominence just below the margin of thespleen. Humps are basically a variation in the shapeof the kidney rather than an area of hypertrophiedtissue.
RENAL CYSTS AND CYSTIC DISEASE
CystsThe most common renal mass is a simple cystwhich can be found in up to 50% of the popula-tion, the incidence increasing with age. Most cystsare asymptomatic and may be solitary or multiple.Generally they are peripheral but may occur withinthe kidney adjacent to the renal pelvis. A parapelviccyst may be difficult to distinguish from pelvica-lyceal dilatation, a calyceal diverticulum or an extra-
renal pelvis and careful scanning is required to dif-ferentiate. A parapelvic cyst may be the cause of afilling defect on intravenous urogram (IVU) andCT can differentiate a cyst from a diverticulum ifnecessary, as the latter will fill with contrast.
Occasionally cysts can haemorrhage causing pain.Large cysts, particularly of the lower pole, may bepalpable, prompting a request for an ultrasoundscan.
Ultrasound appearances
Like cysts in any other organ, renal cysts displaythree basic characteristics: they are anechoic, havea thin, well-defined capsule and exhibit posteriorenhancement. It can be difficult to appreciate theposterior enhancement if the hyperechoic perirenalfat lies distal to the cyst; scanning from a differentangle (Fig. 7.5) may be helpful. Haemor-rhage orinfection can give rise to low-level echoes within acyst and in some cases the capsule may display cal-cification.
Whilst a solitary, simple cyst can almost certainlybe ignored, cysts with more complex acousticcharacteristics may require further investigation,
ABDOMINAL ULTRASOUND160
F
Figure 7.4 cont’d (E) TS through the RK demonstrating a baggy extrarenal pelvis. The PCS remains undilated, andthis should not be confused with hydronephrosis. (F) Hypertrophied column of Bertin (arrows).
E
ch07.qxd 6/30/04 6:08 PM Page 160

for example CT. A calcified wall may be associatedwith malignancy.
Autosomal dominant (adult) polycystickidney disease (APKD)This autosomal dominant disease has a wide spec-trum of presentation. It is normally associated withprogressive renal failure. A renal transplant offers asuccessful cure for many patients. Although insome cases APKD may cause renal failure in earlylife, it is also possible to achieve a normal life spanwith no appreciable symptoms.
In about 50% of cases, cysts are present in theliver; they are also found in the spleen and pancreasin a small proportion of patients.
Ultrasound screening for APKD is performed infamilies with a positive history, as patients may thenbe monitored and treated for hypertension. A neg-ative scan does not entirely exclude disease, especiallyin the younger patient, and multiple examinationsover years may need to be performed.
Ultrasound appearances
The disease is always bilateral, causing progres-sively enlarging kidneys with multiple cysts ofvarious sizes, many having irregular margins
(Fig. 7.6). There is often little or no demonstra-ble normal renal tissue and the kidneys maybecome so large that they visibly distend theabdomen.
APKD predisposes the patient to urinary tractinfections and some of the cysts may contain low-level echoes as a result of infection or haemorrhage.
The liver, spleen and pancreas should also beexamined on ultrasound for associated cysts. A smallbut recognized increased incidence of tumour isrecorded in patients with APKD.
THE RENAL TRACT 161
A B
Figure 7.5 (A) Simple renal cyst with posterior enhancement (arrowheads). (B) Small renal cyst containingcalcification following episodes of infection. This remained stable on follow-up.
Figure 7.6 Autosomal dominant (‘adult’) polycysticdisease. Numerous cysts of varying size are seen withinthe renal bed. No discernible renal architectrue isapparent. A cyst containing solid debris, i.e. haemorrhage(arrow), is seen.
ch07.qxd 6/30/04 6:08 PM Page 161
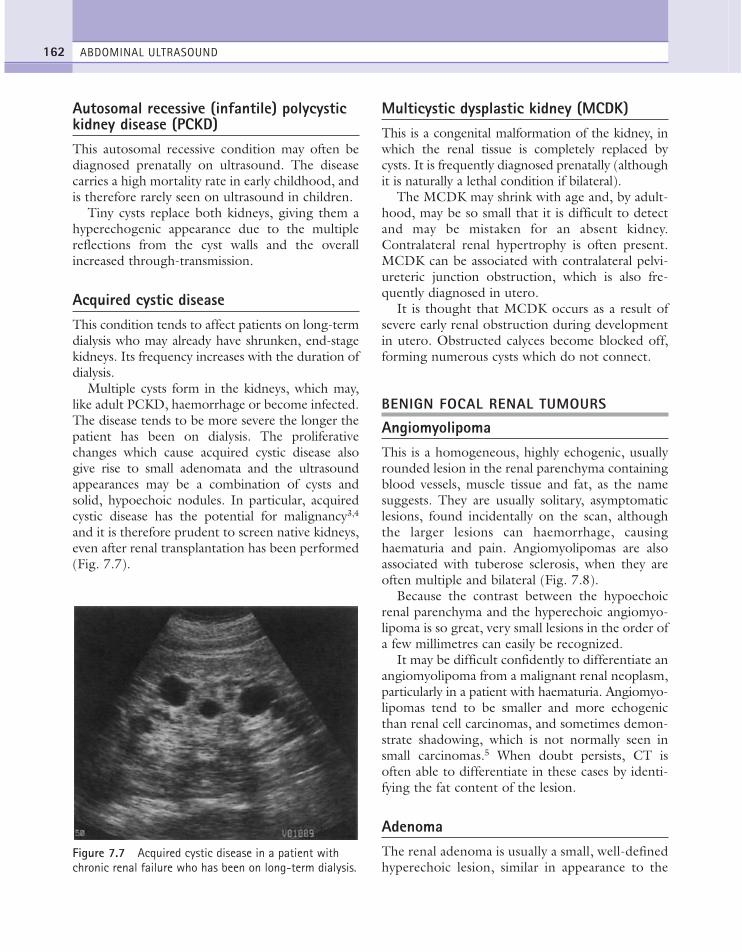
Autosomal recessive (infantile) polycystickidney disease (PCKD)This autosomal recessive condition may often bediagnosed prenatally on ultrasound. The diseasecarries a high mortality rate in early childhood, andis therefore rarely seen on ultrasound in children.
Tiny cysts replace both kidneys, giving them ahyperechogenic appearance due to the multiplereflections from the cyst walls and the overallincreased through-transmission.
Acquired cystic diseaseThis condition tends to affect patients on long-termdialysis who may already have shrunken, end-stagekidneys. Its frequency increases with the duration ofdialysis.
Multiple cysts form in the kidneys, which may,like adult PCKD, haemorrhage or become infected.The disease tends to be more severe the longer thepatient has been on dialysis. The proliferativechanges which cause acquired cystic disease alsogive rise to small adenomata and the ultrasoundappearances may be a combination of cysts andsolid, hypoechoic nodules. In particular, acquiredcystic disease has the potential for malignancy3,4
and it is therefore prudent to screen native kidneys,even after renal transplantation has been performed(Fig. 7.7).
Multicystic dysplastic kidney (MCDK)This is a congenital malformation of the kidney, inwhich the renal tissue is completely replaced bycysts. It is frequently diagnosed prenatally (althoughit is naturally a lethal condition if bilateral).
The MCDK may shrink with age and, by adult-hood, may be so small that it is difficult to detectand may be mistaken for an absent kidney.Contralateral renal hypertrophy is often present.MCDK can be associated with contralateral pelvi-ureteric junction obstruction, which is also fre-quently diagnosed in utero.
It is thought that MCDK occurs as a result ofsevere early renal obstruction during developmentin utero. Obstructed calyces become blocked off,forming numerous cysts which do not connect.
BENIGN FOCAL RENAL TUMOURS
AngiomyolipomaThis is a homogeneous, highly echogenic, usuallyrounded lesion in the renal parenchyma containingblood vessels, muscle tissue and fat, as the namesuggests. They are usually solitary, asymptomaticlesions, found incidentally on the scan, althoughthe larger lesions can haemorrhage, causinghaematuria and pain. Angiomyolipomas are alsoassociated with tuberose sclerosis, when they areoften multiple and bilateral (Fig. 7.8).
Because the contrast between the hypoechoicrenal parenchyma and the hyperechoic angiomyo-lipoma is so great, very small lesions in the order ofa few millimetres can easily be recognized.
It may be difficult confidently to differentiate anangiomyolipoma from a malignant renal neoplasm,particularly in a patient with haematuria. Angiomyo-lipomas tend to be smaller and more echogenicthan renal cell carcinomas, and sometimes demon-strate shadowing, which is not normally seen insmall carcinomas.5 When doubt persists, CT isoften able to differentiate in these cases by identi-fying the fat content of the lesion.
AdenomaThe renal adenoma is usually a small, well-definedhyperechoic lesion, similar in appearance to the
ABDOMINAL ULTRASOUND162
Figure 7.7 Acquired cystic disease in a patient withchronic renal failure who has been on long-term dialysis.
ch07.qxd 6/30/04 6:08 PM Page 162

angiomyolipoma. It is felt that adenomas are fre-quently early manifestations of renal carcinoma asdistinct from a benign lesion6 and the two may behistologically indistinguishable.
Renal adenomas are often found in associationwith a renal cell carcinoma in the same or con-tralateral kidney,7 although these are radiologicallyindistinguishable from metastases.
Because of the controversy surrounding the dis-tinction between adenomas and small renal cell
carcinomas, the management of patients with thesemasses is uncertain. Most incidentally discovered,small (less than 3 cm), parenchymal renal massesare slow-growing and may be safely monitoredwith CT or ultrasound, particularly in the elderly.8
MALIGNANT RENAL TRACT MASSES
Imaging of malignant renal masses
Ultrasound, as one of the first-line investigations inpatients with haematuria, is highly sensitive indetecting large renal masses above 2.5 cm in diam-eter and in differentiating them from renal cysts.Smaller masses may be missed with ultrasoundhowever, as they are frequently isoechoic (in 86%of cases); CT is more sensitive in small lesiondetection.
MRI also detects small renal masses more fre-quently than ultrasound but is generally reserved forpatients with equivocal CT scans as it is less widelyavailable. IVU is also known to miss small renalmasses and normally requires further characteriza-tion of any detected mass with ultrasound or CT.
Renal cell carcinoma (RCC)Adenocarcinoma is the most common type of renalmalignancy (referred to as renal cell carcinoma)occurring less commonly in the bladder and ureter.RCCs are frequently large at clinical presentation;they may occasionally be identified as an incidentalfinding in an asymptomatic patient.
Ultrasound appearances
The RCC is a (usually) large, heterogeneous masswhich enlarges and deforms the shape of the kid-ney (Fig. 7.9). The mass may contain areas of cys-tic degeneration and/or calcification. It has apredilection to spread into the ipsilateral renal veinand IVC (see also Chapter 8).
Colour Doppler usually reveals a disorganizedand increased blood flow pattern within the masswith high velocities from the arterioverous shuntswithin the carcinoma.
Smaller RCCs can be hyperechoic and may beconfused with benign angiomyolipoma. The latter
THE RENAL TRACT 163
B
CORONAL RT
A
Figure 7.8 (A) Angiomyolipoma in the RK. (B) Multiple,small angiomyolipomas in a patient with tuberose sclerosis.
ch07.qxd 6/30/04 6:08 PM Page 163
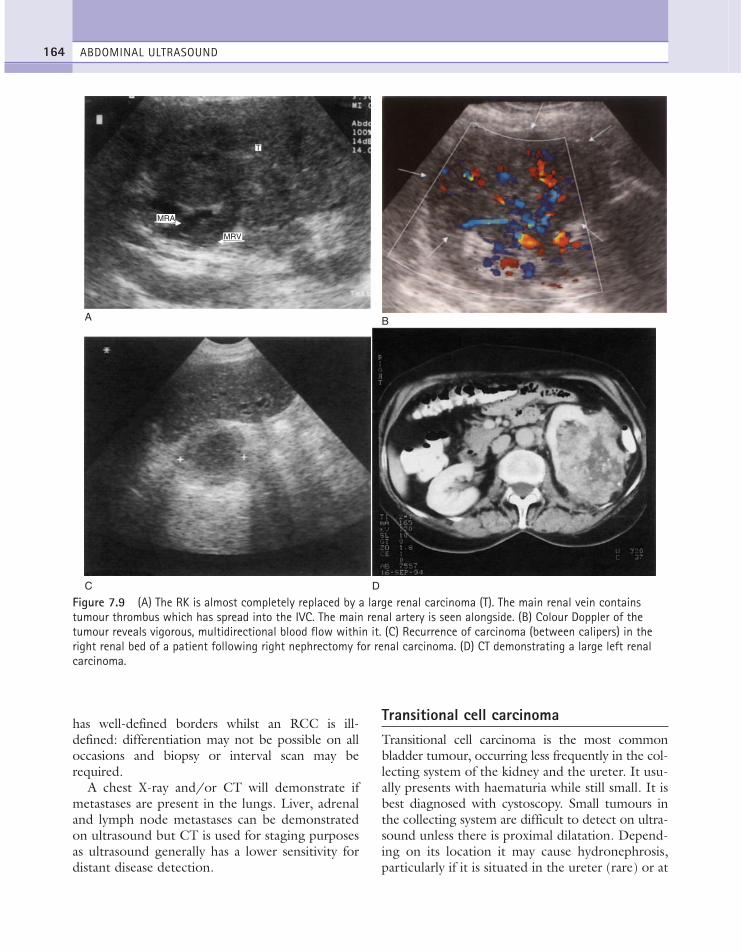
has well-defined borders whilst an RCC is ill-defined: differentiation may not be possible on alloccasions and biopsy or interval scan may berequired.
A chest X-ray and/or CT will demonstrate ifmetastases are present in the lungs. Liver, adrenaland lymph node metastases can be demonstratedon ultrasound but CT is used for staging purposesas ultrasound generally has a lower sensitivity fordistant disease detection.
Transitional cell carcinomaTransitional cell carcinoma is the most commonbladder tumour, occurring less frequently in the col-lecting system of the kidney and the ureter. It usu-ally presents with haematuria while still small. It isbest diagnosed with cystoscopy. Small tumours inthe collecting system are difficult to detect on ultra-sound unless there is proximal dilatation. Depend-ing on its location it may cause hydronephrosis,particularly if it is situated in the ureter (rare) or at
ABDOMINAL ULTRASOUND164
A
MRA
T
MRV
C D
Figure 7.9 (A) The RK is almost completely replaced by a large renal carcinoma (T). The main renal vein containstumour thrombus which has spread into the IVC. The main renal artery is seen alongside. (B) Colour Doppler of thetumour reveals vigorous, multidirectional blood flow within it. (C) Recurrence of carcinoma (between calipers) in theright renal bed of a patient following right nephrectomy for renal carcinoma. (D) CT demonstrating a large left renalcarcinoma.
B
ch07.qxd 6/30/04 6:09 PM Page 164

the vesicoureteric junction (VUJ). IVU, retrogradecystography and CT are methods of diagnosis.
Ultrasound appearances
Situated within the collecting system of the kidney,the transitional cell tumour is usually small (com-pared to the RCC), homogeneous and relativelyhypoechoic (Fig. 7.10A). Proximal renal tractdilatation may sometimes be present. Thesetumours are easy to miss on ultrasound unless thekidney is scanned very carefully, and often are,unless the case is highlighted by clinical symptomsor a high clinical index of suspicion. They can mimica hypertrophied column of Bertin (see above); CTmay differentiate in cases of doubt.
Once large, they invade the surrounding renalparenchyma and become indistinguishable fromRCC on ultrasound. They frequently spread to thebladder and the entire renal tract should be care-fully examined.
In the bladder they are potentially easier to seeas they are surrounded by urine (Fig. 7.10B).Invasion of the bladder wall can be identified onultrasound in the larger ones but biopsy is neces-sary to determine formally the level of invasion.
IVU or a retrograde cystogram are the methodsof choice for demonstrating a filling defect in thePCS (Fig. 7.11) or ureter; CT may be useful and isalso used for staging purposes.
LymphomaRenal involvement of non-Hodgkin’s orHodgkin’s lymphoma is not uncommon anddepends upon the stage of the disease. The ultra-sound appearances are highly variable and rangefrom solitary to multiple masses, usually hypo-echoic but sometimes anechoic, hyperechoic ormixed.
The masses may have increased through trans-mission of sound and may mimic complex fluidlesions such as haematoma or abscess. The clinicalhistory should help to differentiate these cases.Occasionally diffuse enlargement may occur second-ary to diffuse infiltration.
MetastasesRenal metastases from a distant primary are usuallyfound in cases of widespread metastatic disease andare frequently multiple.
THE RENAL TRACT 165
B
Figure 7.10 (A) Large, transitional cell carcinoma in the upper pole of the RK. The changes are more subtle thanthose of renal cell carcinoma, and the renal outline remains intact. (B) Transitional cell carcinoma in the bladder at theright vesicoureteric junction. Blood flow can clearly be seen within the tumour, and right renal and ureteric dilatationwas present.
A
ch07.qxd 6/30/04 6:09 PM Page 165

In such cases, the primary diagnosis is usuallyalready known and other abdominal metastases,such as liver deposits and/or lymphadenopathy, arecommonly seen on ultrasound.
Rarely, a single metastasis is seen in the kidneywithout other evidence of metastatic spread, mak-ing the diagnosis difficult (as the question arises ofwhether this could be a primary or secondarylesion). CT may identify the primary and fre-quently picks up other, smaller metastases notidentified on ultrasound.9
PELVICALYCEAL SYSTEMDILATATION AND OBSTRUCTIVEUROPATHY
Not all PCS dilatation, i.e. hydronephrosis, ispathological, or indeed obstructive, that is, therecan be dilatation without physiological obstruc-tion. Conversely, not all obstructive uropathy nec-essarily results in PCS dilatation.
Physiological dilatationMild dilatation of the renal collecting system is acommon finding, most commonly secondary to anover-distended bladder. Following micturition, thecollecting system decompresses and returns to nor-mal. An external renal pelvis (see above) is a non-obstructive ‘baggy’ dilatation of the pelvis and canbe regarded as a normal variant. The intrarenalcollecting system is normal in this situation(Fig. 7.4, D,E).
Pregnancy is another common cause of mildPCS dilatation, more frequently on the right, par-ticularly in the second and third trimester. This isthought to be due partly to pressure on the uretersfrom the advancing pregnancy and partly hor-monal. It is however wrong to assume that the kid-ney is not obstructed just because the patient ispregnant. If symptomatic, the suspicion ofobstruction in a dilated system is increased, partic-ularly if echoes are present in the PCS.
Obstructive uropathyRenal obstruction, particularly if long-standing, canirreversibly damage the kidney or kidneys, leadingeventually to renal failure. If diagnosed earlyenough, renal function can be preserved and there-fore ultrasound plays a prominent role as one of thefirst-line investigations in patients with loin pain,renal colic or micturition disorders (Table 7.1).
In the vast majority of cases, urinary tractobstruction causes dilatation of the collecting sys-tem proximal to the site of obstruction (Fig. 7.12).Whether the hydronephrosis is bilateral or unilateraland whether or not it involves the ureter(s) dependson the cause and site of the obstructing lesion.
Dilatation of the collecting system may be local-ized. Sometimes only one moiety of the kidneymay be obstructed by a stone or tumour, whilst therest of the kidney remains normal. In a duplex kid-ney, dilatation of the upper pole moiety is a com-mon occurrence due to an anomaly at the VUJ,that is, a ureterocoele.
If the obstruction is long-standing the renal cor-tex may atrophy, becoming thin. Normal thicknessof cortex is a good prognostic indicator. Functionmay be assessed with a nuclear medicine (DTPA)scan prior to further management.
ABDOMINAL ULTRASOUND166
Figure 7.11 IVU with multiple filling defects in therelatively non-dilated PCS of the RK, which representtransitional cell carcinomas.
ch07.qxd 6/30/04 6:09 PM Page 166
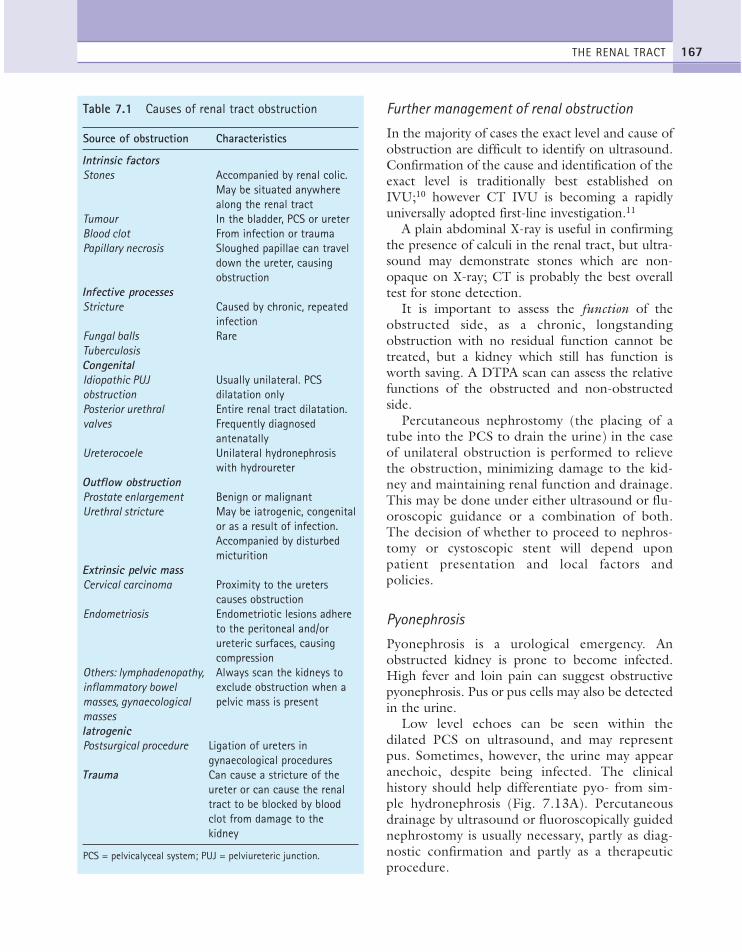
Further management of renal obstruction
In the majority of cases the exact level and cause ofobstruction are difficult to identify on ultrasound.Confirmation of the cause and identification of theexact level is traditionally best established onIVU;10 however CT IVU is becoming a rapidlyuniversally adopted first-line investigation.11
A plain abdominal X-ray is useful in confirmingthe presence of calculi in the renal tract, but ultra-sound may demonstrate stones which are non-opaque on X-ray; CT is probably the best overalltest for stone detection.
It is important to assess the function of theobstructed side, as a chronic, longstandingobstruction with no residual function cannot betreated, but a kidney which still has function isworth saving. A DTPA scan can assess the relativefunctions of the obstructed and non-obstructedside.
Percutaneous nephrostomy (the placing of atube into the PCS to drain the urine) in the caseof unilateral obstruction is performed to relievethe obstruction, minimizing damage to the kid-ney and maintaining renal function and drainage.This may be done under either ultrasound or flu-oroscopic guidance or a combination of both.The decision of whether to proceed to nephros-tomy or cystoscopic stent will depend uponpatient presentation and local factors andpolicies.
Pyonephrosis
Pyonephrosis is a urological emergency. Anobstructed kidney is prone to become infected.High fever and loin pain can suggest obstructivepyonephrosis. Pus or pus cells may also be detectedin the urine.
Low level echoes can be seen within thedilated PCS on ultrasound, and may representpus. Sometimes, however, the urine may appearanechoic, despite being infected. The clinicalhistory should help differentiate pyo- from sim-ple hydronephrosis (Fig. 7.13A). Percutaneousdrainage by ultrasound or fluoroscopically guidednephrostomy is usually necessary, partly as diag-nostic confirmation and partly as a therapeuticprocedure.
THE RENAL TRACT 167
Table 7.1 Causes of renal tract obstruction
Source of obstruction Characteristics
Intrinsic factorsStones Accompanied by renal colic.
May be situated anywherealong the renal tract
Tumour In the bladder, PCS or ureterBlood clot From infection or traumaPapillary necrosis Sloughed papillae can travel
down the ureter, causingobstruction
Infective processesStricture Caused by chronic, repeated
infectionFungal balls RareTuberculosisCongenitalIdiopathic PUJ Usually unilateral. PCS obstruction dilatation onlyPosterior urethral Entire renal tract dilatation. valves Frequently diagnosed
antenatallyUreterocoele Unilateral hydronephrosis
with hydroureterOutflow obstructionProstate enlargement Benign or malignantUrethral stricture May be iatrogenic, congenital
or as a result of infection.Accompanied by disturbed micturition
Extrinsic pelvic massCervical carcinoma Proximity to the ureters
causes obstructionEndometriosis Endometriotic lesions adhere
to the peritoneal and/orureteric surfaces, causing compression
Others: lymphadenopathy, Always scan the kidneys to inflammatory bowel exclude obstruction when a masses, gynaecological pelvic mass is presentmassesIatrogenicPostsurgical procedure Ligation of ureters in
gynaecological proceduresTrauma Can cause a stricture of the
ureter or can cause the renaltract to be blocked by bloodclot from damage to the kidney
PCS = pelvicalyceal system; PUJ = pelviureteric junction.
ch07.qxd 6/30/04 6:09 PM Page 167

Haemo-hydronephrosis
Blood within the dilated PCS may be due totrauma or other local or semilocal pathologicalprocesses such as infection or tumour. It is not usu-ally possible to determine whether obstruction is
caused by a blood clot or whether the blood is theresult of an obstructing lesion which is also causingbleeding. Renal colic as a result of obstruction by ablood clot in the absence of trauma or blooddyscrasia must naturally be thoroughly investigatedto exclude an underlying lesion.
ABDOMINAL ULTRASOUND168
A B
C D
E
RT KIDNEY
Figure 7.12 (A) Hydronephrosis of the left kidney, secondary to a large circumferential bladder tumour. (B) A uretericstent is noted within the renal pelvis of (A) (arrow); however, a moderate degree of hydronephrosis is present andhighly suggestive of partial or complete stent occlusion. (C) Moderate to marked hydronephrosis of the right kidneysecondary to a pelvic lesion. The cortical thickness is normal suggesting the obstruction is relatively recent and thatrelief of obstruction should produce a significant improvement in renal function. (D) Hydronephrosis of the rightkidney. The kidney however is small at 7.2 cm, the cortex echogenic and thinned, particularly at mid pole level.Appearances suggest this appearance is chronic. (E) TS of a left-sided hydronephrosis. Echogenic material is presentwithin the collecting system. The patient was pyrexial. Pus was drained.
ch07.qxd 6/30/04 6:09 PM Page 168

Like pyonephrosis, low-level echoes may be seenon ultrasound within the collecting system (Fig.7.13B). Although ultrasonically it is not possible todifferentiate pyo- from haemohydronephrosis, theclinical picture can be suggestive of one or the other.
Non-dilated renal obstruction
Obstruction may occasionally be present in theacute stages before renal dilatation is apparent:beware—the finding of a non-dilated PCS on ultra-sound does not exclude obstruction in any patientwith symptoms of renal colic.
Spectral Doppler is useful in diagnosing acute,early renal obstruction, before PCS dilatation devel-ops, because of the associated increase in blood flowresistance in the affected kidney (Fig. 7.14). This
causes an increase in the resistance and pulsatilityindices (RI and PI) on the obstructed side, due to areduction in diastolic flow. A raised RI in itself is anon-specific finding, not necessarily indicatingobstruction; it is known to be age-related or can beassociated with extrinsic compression of the kidney(for example by a fluid collection or mass) or withsome chronic renal diseases or vascular disorders.This can be overcome by analysing Doppler spectrafrom both kidneys and evaluating any differencebetween the two sides.
A marked difference in the RI between the kid-neys in a patient with renal colic points towardsobstruction of the kidney with the higher resist-ance.12,13 A difference in RI of greater than 6 ishighly suspicious of obstruction in a patient withrenal colic; a reduction in the RI on the affected side
THE RENAL TRACT 169
A B
Figure 7.13 (A) Pyonephrosis. Low-level echoes from pus can be seen in the dilated PCS. (Note that absence ofechoes does not exclude pyonephrosis.) (B) A hyperechoic blood clot can be seen within the collecting system of thisdilated kidney.
A B
Figure 7.14 (A) A patient with acute renal colic has a normal-looking, non-dilated RK with a raised resistance indexof 75.8. IVU subsequently confirmed early obstruction of the RK. The resistance index (RI) subsequently returned tonormal following relief of the obstruction. (B) In the same patient, the contralateral, normal kidney has a much lowerresistance index of 67.2.
ch07.qxd 6/30/04 6:09 PM Page 169

can be observed when the obstruction has beenrelieved or after the renal PCS has become dilated.
This effect often does not persist once thekidney dilates, presumably because the intrarenalpressure is relieved, which emphasizes the useof Doppler in acute cases, before dilatation hasbecome established.14 Because of the vagariesof the stage of obstruction, renal pressure, etc.the interpretation of RI should be made cautiously.
IVU will show delayed PCS opacification and isalso more useful than ultrasound in assessing thelevel of obstruction. CT IVU, as mentioned previ-ously, is more commonly fulfilling the role previ-ously held by the IVU.
Vesicoureteric junctionThe normal ureters may be identified on ultrasoundwith high-resolution equipment, as they enter thebladder. Jets of urine emerge into the bladder atthese points and can be demonstrated with colourDoppler. An absent or reduced number of jets mayindicate obstruction on that side; this finding againshould be interpreted cautiously. Ureteric jetanalysis is not routinely performed at most hospi-tals as a diagnostic test of renal obstruction.
Careful scanning at the VUJs can identify signif-icant anomalies (Figs 7.12 D, E):
● Reflux can be seen to dilate the ureterintermittently (see below).
● A ureterocoele may be diagnosed as it dilates withthe passage of urine; it may not be obvious untilthe operator has watched carefully for a fewminutes.
● Stones may become lodged at the VUJ,causing proximal dilatation.
Non-obstructive hydronephrosisNot all renal dilatation is the result of an obstruc-tive process and the kidney may frequently bedilated for other reasons.
Reflux
This is the most common cause of non-obstructiverenal dilatation, and is normally diagnosed in chil-dren. Reflux is associated with recurrent urinary
tract infections and can result in reflux nephropa-thy, in which the renal parenchyma is irretrievablydamaged.
Reflux can be distinguished from other causes ofrenal dilatation by observing the dilatation of theureters at the bladder base, due to the retrogradepassage of urine. For a more detailed considerationof the diagnosis of reflux, see Chapter 9.
Postobstructive dilatation
Dilatation of a once severely obstructed kidneymay persist. The PCS remains baggy and dilateddespite the obstruction having been relieved.
Papillary necrosis
The renal papillae, which are situated in the medullaadjacent to the calyces, are susceptible to ischaemiadue to relatively low oxygenation in the region ofthe medullary junction. This is particularly associ-ated with diabetic patients and those on long-termanti-inflammatory or analgesic medication.
The papillae tend to necrose and slough off,causing blunting of calyces on IVU. Sloughed-offpapillae may lodge in the entrance to the calyces,causing obstruction.
Papillary necrosis is difficult to detect on ultra-sound unless advanced. It appears as prominentcalyces with increased corticomedullary differenti-ation. IVU is the imaging method of choice (Fig.7.15).
Congenital megacalyces
This is a congenital condition in which the PCS isdilated due to poor development of the papillae.The calyces are normally markedly enlarged butthe cortex is normal and the ureters are of normalcalibre and not dilated.15 Occasionally this is asso-ciated with congenital megaureter in which themuscular layer of the ureter is atonic.
Differential diagnoses for fluid-filled renalmasses are summarized in Table 7.2.
RENAL TRACT CALCIFICATON
Calcification within the kidney usually occurs inthe form of stones. Smaller foci of calcium, which
ABDOMINAL ULTRASOUND170
Paediatricch?
ch07.qxd 6/30/04 6:09 PM Page 170
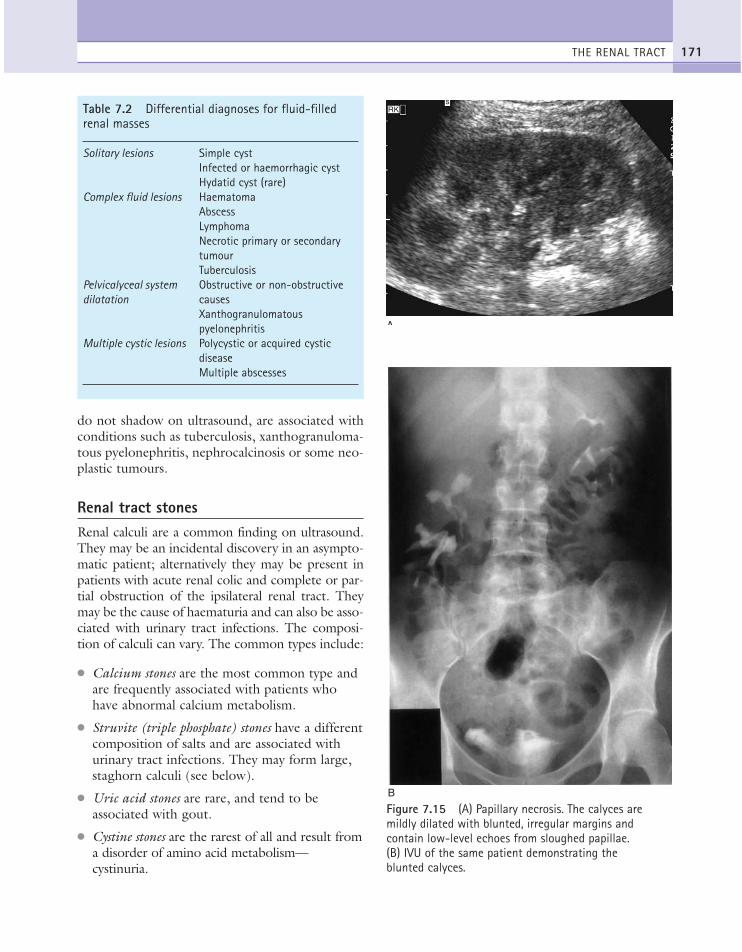
do not shadow on ultrasound, are associated withconditions such as tuberculosis, xanthogranuloma-tous pyelonephritis, nephrocalcinosis or some neo-plastic tumours.
Renal tract stonesRenal calculi are a common finding on ultrasound.They may be an incidental discovery in an asympto-matic patient; alternatively they may be present inpatients with acute renal colic and complete or par-tial obstruction of the ipsilateral renal tract. Theymay be the cause of haematuria and can also be asso-ciated with urinary tract infections. The composi-tion of calculi can vary. The common types include:
● Calcium stones are the most common type andare frequently associated with patients whohave abnormal calcium metabolism.
● Struvite (triple phosphate) stones have a differentcomposition of salts and are associated withurinary tract infections. They may form large,staghorn calculi (see below).
● Uric acid stones are rare, and tend to beassociated with gout.
● Cystine stones are the rarest of all and result froma disorder of amino acid metabolism—cystinuria.
THE RENAL TRACT 171
A
RKs
B
Figure 7.15 (A) Papillary necrosis. The calyces aremildly dilated with blunted, irregular margins andcontain low-level echoes from sloughed papillae. (B) IVU of the same patient demonstrating the blunted calyces.
Table 7.2 Differential diagnoses for fluid-filledrenal masses
Solitary lesions Simple cystInfected or haemorrhagic cystHydatid cyst (rare)
Complex fluid lesions HaematomaAbscessLymphomaNecrotic primary or secondary tumourTuberculosis
Pelvicalyceal system Obstructive or non-obstructive dilatation causes
Xanthogranulomatous pyelonephritis
Multiple cystic lesions Polycystic or acquired cystic diseaseMultiple abscesses
ch07.qxd 6/30/04 6:09 PM Page 171
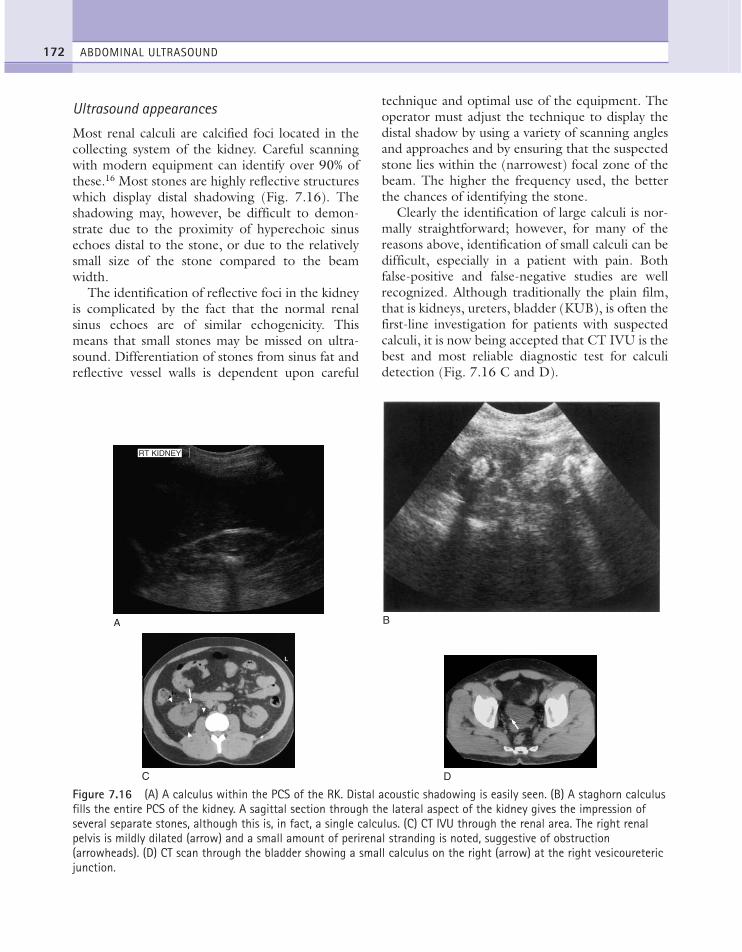
Ultrasound appearances
Most renal calculi are calcified foci located in thecollecting system of the kidney. Careful scanningwith modern equipment can identify over 90% ofthese.16 Most stones are highly reflective structureswhich display distal shadowing (Fig. 7.16). Theshadowing may, however, be difficult to demon-strate due to the proximity of hyperechoic sinusechoes distal to the stone, or due to the relativelysmall size of the stone compared to the beamwidth.
The identification of reflective foci in the kidneyis complicated by the fact that the normal renalsinus echoes are of similar echogenicity. Thismeans that small stones may be missed on ultra-sound. Differentiation of stones from sinus fat andreflective vessel walls is dependent upon careful
technique and optimal use of the equipment. Theoperator must adjust the technique to display thedistal shadow by using a variety of scanning anglesand approaches and by ensuring that the suspectedstone lies within the (narrowest) focal zone of thebeam. The higher the frequency used, the betterthe chances of identifying the stone.
Clearly the identification of large calculi is nor-mally straightforward; however, for many of thereasons above, identification of small calculi can bedifficult, especially in a patient with pain. Bothfalse-positive and false-negative studies are wellrecognized. Although traditionally the plain film,that is kidneys, ureters, bladder (KUB), is often thefirst-line investigation for patients with suspectedcalculi, it is now being accepted that CT IVU is thebest and most reliable diagnostic test for calculidetection (Fig. 7.16 C and D).
ABDOMINAL ULTRASOUND172
A
RT KIDNEY
C
B
D
Figure 7.16 (A) A calculus within the PCS of the RK. Distal acoustic shadowing is easily seen. (B) A staghorn calculusfills the entire PCS of the kidney. A sagittal section through the lateral aspect of the kidney gives the impression ofseveral separate stones, although this is, in fact, a single calculus. (C) CT IVU through the renal area. The right renalpelvis is mildly dilated (arrow) and a small amount of perirenal stranding is noted, suggestive of obstruction(arrowheads). (D) CT scan through the bladder showing a small calculus on the right (arrow) at the right vesicouretericjunction.
ch07.qxd 6/30/04 6:09 PM Page 172
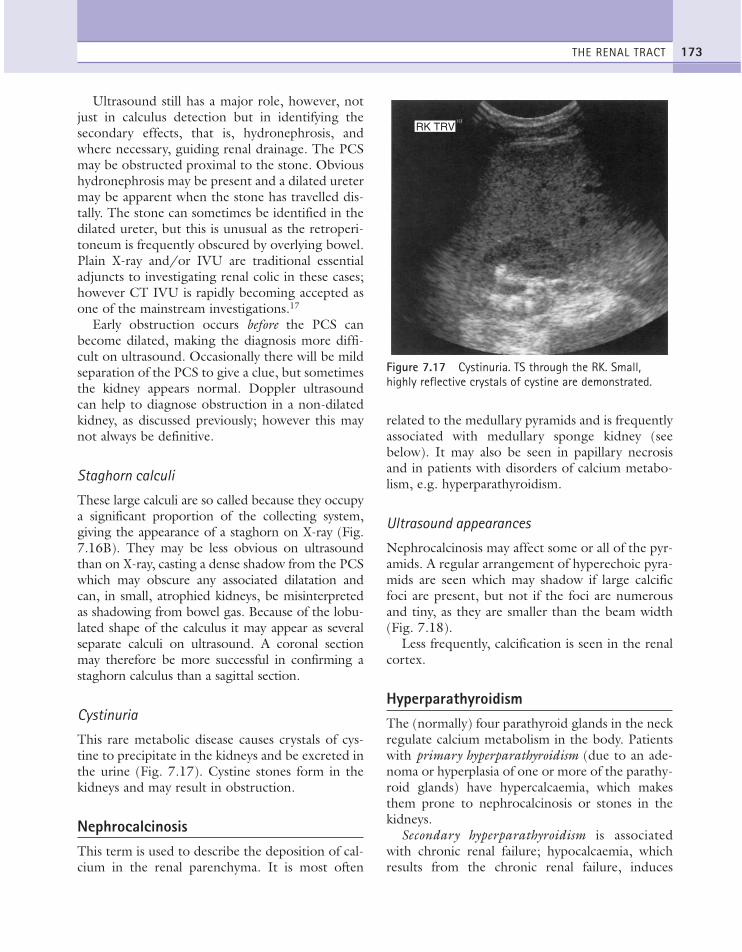
Ultrasound still has a major role, however, notjust in calculus detection but in identifying thesecondary effects, that is, hydronephrosis, andwhere necessary, guiding renal drainage. The PCSmay be obstructed proximal to the stone. Obvioushydronephrosis may be present and a dilated uretermay be apparent when the stone has travelled dis-tally. The stone can sometimes be identified in thedilated ureter, but this is unusual as the retroperi-toneum is frequently obscured by overlying bowel.Plain X-ray and/or IVU are traditional essentialadjuncts to investigating renal colic in these cases;however CT IVU is rapidly becoming accepted asone of the mainstream investigations.17
Early obstruction occurs before the PCS canbecome dilated, making the diagnosis more diffi-cult on ultrasound. Occasionally there will be mildseparation of the PCS to give a clue, but sometimesthe kidney appears normal. Doppler ultrasoundcan help to diagnose obstruction in a non-dilatedkidney, as discussed previously; however this maynot always be definitive.
Staghorn calculi
These large calculi are so called because they occupya significant proportion of the collecting system,giving the appearance of a staghorn on X-ray (Fig.7.16B). They may be less obvious on ultrasoundthan on X-ray, casting a dense shadow from the PCSwhich may obscure any associated dilatation andcan, in small, atrophied kidneys, be misinterpretedas shadowing from bowel gas. Because of the lobu-lated shape of the calculus it may appear as severalseparate calculi on ultrasound. A coronal sectionmay therefore be more successful in confirming astaghorn calculus than a sagittal section.
Cystinuria
This rare metabolic disease causes crystals of cys-tine to precipitate in the kidneys and be excreted inthe urine (Fig. 7.17). Cystine stones form in thekidneys and may result in obstruction.
NephrocalcinosisThis term is used to describe the deposition of cal-cium in the renal parenchyma. It is most often
related to the medullary pyramids and is frequentlyassociated with medullary sponge kidney (seebelow). It may also be seen in papillary necrosisand in patients with disorders of calcium metabo-lism, e.g. hyperparathyroidism.
Ultrasound appearances
Nephrocalcinosis may affect some or all of the pyr-amids. A regular arrangement of hyperechoic pyra-mids are seen which may shadow if large calcificfoci are present, but not if the foci are numerousand tiny, as they are smaller than the beam width(Fig. 7.18).
Less frequently, calcification is seen in the renalcortex.
HyperparathyroidismThe (normally) four parathyroid glands in the neckregulate calcium metabolism in the body. Patientswith primary hyperparathyroidism (due to an ade-noma or hyperplasia of one or more of the parathy-roid glands) have hypercalcaemia, which makesthem prone to nephrocalcinosis or stones in thekidneys.
Secondary hyperparathyroidism is associatedwith chronic renal failure; hypocalcaemia, whichresults from the chronic renal failure, induces
THE RENAL TRACT 173
RK TRV
Figure 7.17 Cystinuria. TS through the RK. Small,highly reflective crystals of cystine are demonstrated.
ch07.qxd 6/30/04 6:09 PM Page 173

compensatory hyperplasia of the parathyroidglands. There is a high incidence of hyperparathy-roidism secondary to chronic renal failure inpatients on dialysis; scintigraphy may demonstratethe region of increased activity and ultrasound isparticularly suitable for demonstrating theenlarged parathyroid, guiding a diagnostic aspira-tion and, if necessary, ablating the gland withethanol as an alternative to surgical removal.Alcohol ablation is generally reserved for thosepatients deemed to be a poor surgical risk.
RENAL TRACT INFLAMMATION AND INFECTION
The most common urinary tract infections are bac-terial in origin, with viral and fungal infectionsbeing comparatively rare. The diagnosis is made byurinalysis after the patient presents with symptomsof dysuria, haematuria and/or suprapubic or renalangle pain. The origin of the infection may be viathe blood stream (haematogenous) or the urethra(ascending). Ascending infections are more com-mon in women due to their short urethra.
Ultrasound is often requested, particularly inchildren, to identify any unsuspected renal pathol-ogy which may be associated with the infection,for example a duplex collecting system, pelvickidney.
Common conditions which may be identified onultrasound include renal cystic diseases, calculi,obstructive uropathy, reflux and anatomical variants.
The infection may be either acute or chronic.Ultrasound signs of renal infection may be absentaltogether, and this is the commonest scenario asthe infective episode has often been successfullytreated with antibiotics by the time the ultrasoundscan is performed.
The infection may be confined to the bladder,that is cystitis, in which case low-level echoes and/orhyperechoic debris may be identified, or may haveprogressed to the kidneys. Scarring and/or corticalthinning may be present in cases of repeated infec-tions (see Chronic pyelonephritis below).
PyelonephritisAcute pyelonephritis
Acute inflammation of the kidney rarely results inany ultrasound abnormality. Occasionally the kid-ney may be enlarged and hypoechoic, the contrastbetween the kidney and the hepatic or splenicparenchyma increasing due to oedema, but theultrasound changes are generally subtle.
The normally clear differentiation between thecortex and the medullary pyramids may becomeindistinct, but again may go unrecognized.
ABDOMINAL ULTRASOUND174
A B
Figure 7.18 (A) Nephrocalcinosis, demonstrating deposists of calcium within the renal pyramids which are too smallto cast an acoustic shadow. (B) Calcification in the renal pyramids with strong acoustic shadowing.
ch07.qxd 6/30/04 6:09 PM Page 174

CT is useful for detecting subtle inflammatorychanges within the kidney.
Chronic pyelonephritis
This chronic inflammatory state is usually theresult of frequent previous inflammatory/infectiveepisodes.
The kidney may be small and often has focalscarring present. Scar tissue has the appearance ofa hyperechoic, linear lesion which affects thesmooth renal outline and crosses the renal cortex(Fig. 7.19A). (Do not confuse focal scarring withfetal lobulation: the latter is smooth, thin, contin-uous with the capsule and forms an indentationbetween the pyramids.)
The renal cortex is frequently thin in chronicpyelonephritis and may appear abnormally hyper-echoic.
Bladder diverticula Repeated infections cancause the bladder wall to thicken and become tra-beculated. In such cases, a bladder diverticulummay form, making treatment of subsequent infec-tions particularly difficult. The diverticulum mayharbour debris or stones and may fail to emptyproperly, often enlarging as the urine refluxes intoit when the patient micturates (Fig. 7.19B).
Focal pyelonephritisThe presence of acute infection within the kidneymay progress in focal regions of the renalparenchyma. This phenomenon is particularlyassociated with diabetics.
The ultrasonic changes are subtle, as in diffusepyelonephritis, but it is possible to detect a slightchange in echogenicity when it is surrounded bynormal-looking parenchyma.
Focal pyelonephritis (sometimes called focalnephronia) may be either hypo- or hyperechoiccompared with normal renal tissue. Depending onthe size of the lesion, it may cause a mass effect,mimicking a renal tumour. The outline of the kid-ney is preserved, however (Fig. 7.19C).
The patient presents with fever and tendernesson the affected side and frequently has a historyof urinary tract infection. A focal renal mass underthese circumstances is highly suggestive of focalpyelonephritis and is also well demonstrated on
CT.18 It usually responds to antibiotic therapy andresolution of the lesion can be monitored withultrasound scans. Focal pyelonephritis can progressto form an abscess in the kidney, which can nor-mally be treated by percutaneous drainage andantibiotics.
Renal abscessA renal abscess is generally a progression of focalinflammation within the kidney (see above). Thearea liquefies and may enlarge to form a complexmass with distal acoustic enhancement. Low-levelechoes from pus may fill the abscess cavity, givingit the appearance of increased echogenicity, but itmay also be hypoechoic. The margins of theabscess may be ill-defined at first but may developa more obvious capsule as the lesion becomesestablished (Fig. 7.19F), this capsule often has aneasily identifiable thick rim. Flow may be seen inthe inflammatory capsule with colour Doppler, butnot in the liquefied centre.
A renal abscess may mimic a lymphoma as bothmay be hypoechoic on ultrasound, and both mayhave either single or multiple foci.
The abscess may be intrarenal, subcapsular orperirenal. Frequently, drainage under ultrasoundguidance is the preferred treatment; gradual reso-lution of the abscess can also be monitored withultrasound.
Tuberculosis (TB)Renal TB is an uncommon finding and a difficultdiagnosis to make on ultrasound. The subtleinflammatory changes which affect the calycesin the early stages are best demonstrated with CT.
In the later stages ultrasound may show calcificfoci and obstructed calyces as a result of thickenedinflammatory calyceal walls, calcification anddebris.
TB frequently spreads to other adjacent sites inthe abdomen, including the psoas muscle and gas-trointestinal tract.
The differential diagnosis is xanthogranuloma-tous pyelonephritis, which is often indistinguish-able from TB on ultrasound, or a necrotic renalneoplasm.
THE RENAL TRACT 175
ch07.qxd 6/30/04 6:09 PM Page 175
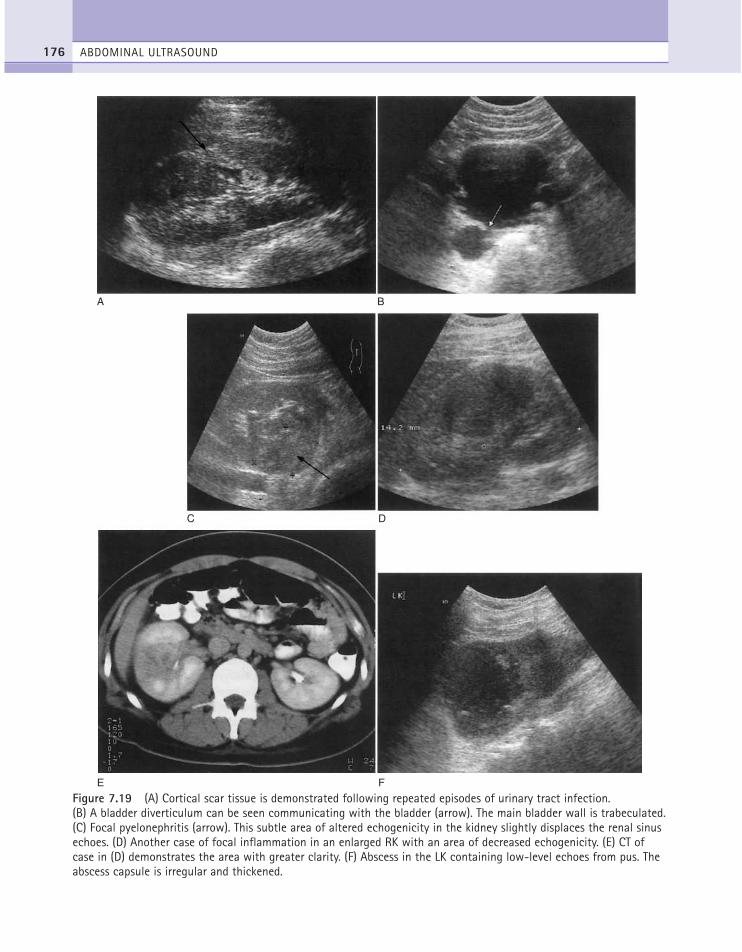
ABDOMINAL ULTRASOUND176
A B
DC
FE
Figure 7.19 (A) Cortical scar tissue is demonstrated following repeated episodes of urinary tract infection.(B) A bladder diverticulum can be seen communicating with the bladder (arrow). The main bladder wall is trabeculated.(C) Focal pyelonephritis (arrow). This subtle area of altered echogenicity in the kidney slightly displaces the renal sinusechoes. (D) Another case of focal inflammation in an enlarged RK with an area of decreased echogenicity. (E) CT ofcase in (D) demonstrates the area with greater clarity. (F) Abscess in the LK containing low-level echoes from pus. Theabscess capsule is irregular and thickened.
ch07.qxd 6/30/04 6:09 PM Page 176

Xanthogranulomatous pyelonephritis (XGP)This condition (which gets its name from the yel-low colour of the kidney) is the result of renalobstruction by calculi in the pelvicalyceal system.Frequently, a staghorn calculus is responsible.
The kidney becomes chronically infected andthe calyces enlarge and become filled with infecteddebris. The cortex may be eroded and thin (Fig.7.20).
On ultrasound, these appearances are similar toTB or to a pyonephrosis. The latter is usuallyaccompanied by a more severe, acute pain andfever whereas XGP or TB has a lower-grade,chronic pain.
CT may differentiate TB from XGP and is alsomore sensitive to extrarenal spread of disease.
Hydatid cystsThe Echinococcus parasite spends part of its lifecycle in dogs. The larvae may be transmitted tohumans through contact with dog faeces, findingtheir way to the lungs, liver and, less frequently, thekidneys.
The parasite forms a cyst which has a thickenedwall, often with smaller, peripheral daughter cysts.Frequently the main cyst contains echoes.
The condition is rare in the UK, but may bediagnosed when small, grape-like cysts are passedin the urine.
DIFFUSE RENAL DISEASE AND RENALFAILURE
Most diffuse medical renal conditions have non-spe-cific appearances on ultrasound, the kidneys oftenappearing normal in the early stages of disease.Renal failure may be acute or chronic and its causesare numerous. If acute, an increase in overall renalsize may be observed and there may be a diffusealteration in the renal echogenicity, however this canbe either hypo-or hyperechoic compared with nor-mal. Either increased or decreased corticomedullarydifferentiation may also be observed (Fig. 7.21).Although ultrasound is successful in detecting renalparenchymal disease, the acoustic changes are notspecific and the cause must usually be diagnosed his-tologically,19 ultrasound being invaluable in direct-ing the biopsy procedure.
In chronic renal failure the kidneys shrink andthe cortex thins. The end-stage kidney can be quitetiny and hyperechoic and may be difficult to dif-ferentiate from the surrounding tissues (Fig.7.21C).
Depending on the cause, either one but gener-ally both of the kidneys are affected.
Acute tubular necrosisAcute tubular necrosis is the result of ischaemia,which destroys the tubules of the kidney, resultingin acute renal failure. It occurs when there is a sud-den decrease in renal perfusion as a result of aseverely hypotensive episode, for example, cardiacarrest, massive haemorrhage, drug toxicity or sep-ticaemia.
Patients are treated temporarily by dialysis.Tubular damage is capable of regeneration once theblood supply and perfusion pressure return to nor-mal, reversing the renal failure. If suspected, it isuseful to perform a biopsy to determine the cause ofrenal failure, in order to plan further management.
On ultrasound the kidneys are normal in sizeor slightly enlarged. They may be completely nor-mal in appearance, a not uncommon finding,although in some cases the echogenicity is altered,
THE RENAL TRACT 177
Figure 7.20 Xanthogranulomatous pyelonephritis.Numerous stones have obstructed the PCS, whichcontains debris. The renal cortex is thin, and thearchitecture of the kidney is difficult to recognize.
ch07.qxd 6/30/04 6:09 PM Page 177
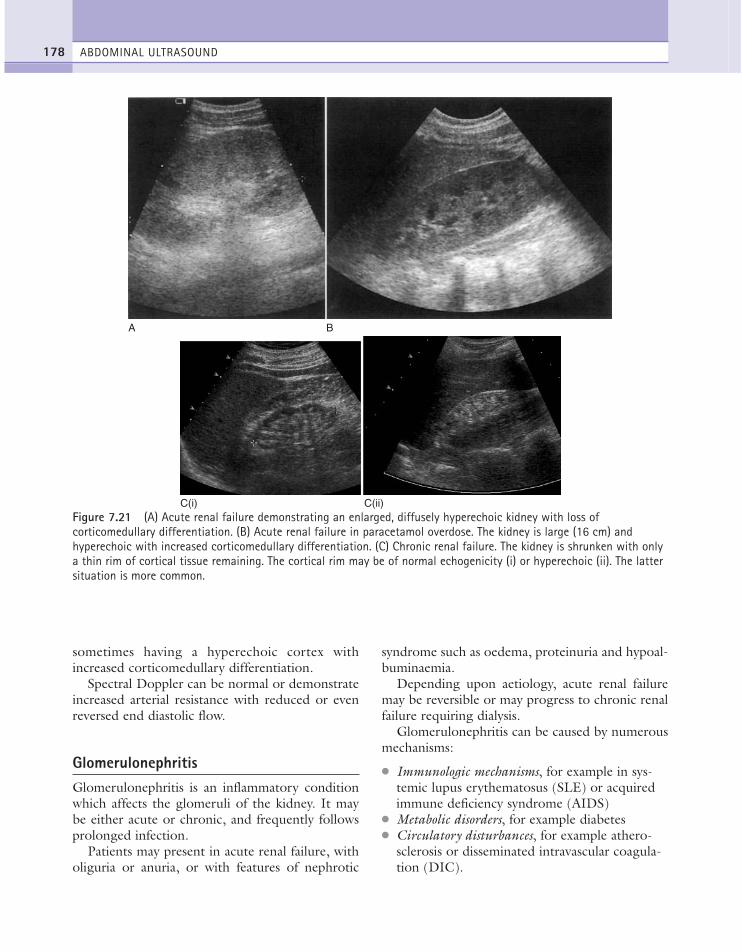
sometimes having a hyperechoic cortex withincreased corticomedullary differentiation.
Spectral Doppler can be normal or demonstrateincreased arterial resistance with reduced or evenreversed end diastolic flow.
GlomerulonephritisGlomerulonephritis is an inflammatory conditionwhich affects the glomeruli of the kidney. It maybe either acute or chronic, and frequently followsprolonged infection.
Patients may present in acute renal failure, witholiguria or anuria, or with features of nephrotic
syndrome such as oedema, proteinuria and hypoal-buminaemia.
Depending upon aetiology, acute renal failuremay be reversible or may progress to chronic renalfailure requiring dialysis.
Glomerulonephritis can be caused by numerousmechanisms:
● Immunologic mechanisms, for example in sys-temic lupus erythematosus (SLE) or acquiredimmune deficiency syndrome (AIDS)
● Metabolic disorders, for example diabetes● Circulatory disturbances, for example athero-
sclerosis or disseminated intravascular coagula-tion (DIC).
ABDOMINAL ULTRASOUND178
A B
Figure 7.21 (A) Acute renal failure demonstrating an enlarged, diffusely hyperechoic kidney with loss ofcorticomedullary differentiation. (B) Acute renal failure in paracetamol overdose. The kidney is large (16 cm) andhyperechoic with increased corticomedullary differentiation. (C) Chronic renal failure. The kidney is shrunken with onlya thin rim of cortical tissue remaining. The cortical rim may be of normal echogenicity (i) or hyperechoic (ii). The lattersituation is more common.
C(i) C(ii)
ch07.qxd 6/30/04 6:09 PM Page 178
As with acute tubular necrosis, the ultrasoundappearances are non-specific. In the acute stagesthe kidneys may be slightly enlarged; changes inthe echogenicity of the cortex may be observed. Inthe chronic stages the kidneys shrink, becomehyperechoic, lose cortical thickness and haveincreased corticomedullary differentiation.19
Medullary sponge kidneyIn medullary sponge kidney the distal tubules,which lie in the medullary pyramids, dilate. Thismay be due to a developmental anomaly but this isnot certain. In itself it is usually asymptomatic andtherefore rarely seen on ultrasound. However, thecondition is prone to nephrocalcinosis, particularlyat the outer edges of the pyramids, and stone for-mation (see above), which may cause pain andhaematuria.
AmyloidIn amyloid disease, excess protein is deposited inthe renal parenchyma, predominantly the cortex.This causes proteinuria and may progress tonephrotic syndrome (oedema, proteinuria andhypoalbuminaemia).
Amyloidosis can cause acute renal failure and isparticularly associated with long-standing rheuma-toid arthritis.
As with other diffuse renal diseases, the acutestage may cause renal enlargement and theparenchyma tends to be diffusely hyperechoic. Bythe time the chronic stage of disease has beenreached, the kidneys become shrunken andhyperechoic, in keeping with all end-stageappearances.
The renal biopsy(See Chapter 11.) Biopsy is rarely merited in end-stage renal failure, as the only treatment is dialysisor renal transplantation. Small kidneys, below 8 cmin length therefore, are almost never subjected tobiopsy.
Histology is required when the kidney is poten-tially curable, such as in cases of acute disease, orwhen a specific knowledge of aetiology is para-mount.
RENAL VASCULAR PATHOLOGY
Renal artery stenosis (RAS)Stenosis of the renal artery is due to atreroscle-rotic disease in the vast majority of patients, or tofibromuscular dysplasia of the arterial wall in theyounger, generally female patient. RAS maycause hypertension and may eventually causerenal failure. It is frequently bilateral, and isresponsible for up to 15% of patients who requirelong-term dialysis. It is associated with aorticaneurysm, neurofibromatosis or can be traumaticin origin.
Stenosis generally affects the main vessel at itsorigin and involves the aorta (ostial) or occurswithin 1 cm of its origin (non-ostial). It can occurin both native and transplanted organs. It is fre-quently bilateral.
Ultrasound appearances of RAS
If the stenosis is long-standing and/or severe, thekidney is likely to be small. Loss of renal mass isassociated with a stenosis of 60% or greater.20
However, the ultrasound appearances are oftennormal with milder grades of RAS.
Ultrasound has traditionally had a limited roleto play in the diagnosis of RAS and digital subtrac-tion angiography is still considered the gold stan-dard, although magnetic resonance angiography(MRA) is now regarded as the first-line imagingmodality of choice. However, colour and spectralDoppler techniques have greatly enhanced the use-fulness of ultrasound, particularly in experiencedhands.21
At the site of a stenosis, an increase in peak sys-tolic velocity may be found (greater than 1.5–1.8m/s) with poststenotic turbulence. Although, it isoften not technically possible confidently to exam-ine and sample the whole main renal artery andthus make a definitive diagnosis, it neverthelessremains the best Doppler technique for diagnosis.
In addition, the intrarenal vessels may showchanges on colour or power Doppler which areindicative of a downstream stenosis. Within thekidney, the perfusion may appear subjectivelyreduced in the number of vessels and velocity offlow and it may be necessary for the operator touse a low PRF value to detect blood flow. This is
THE RENAL TRACT 179
ch07.qxd 6/30/04 6:09 PM Page 179
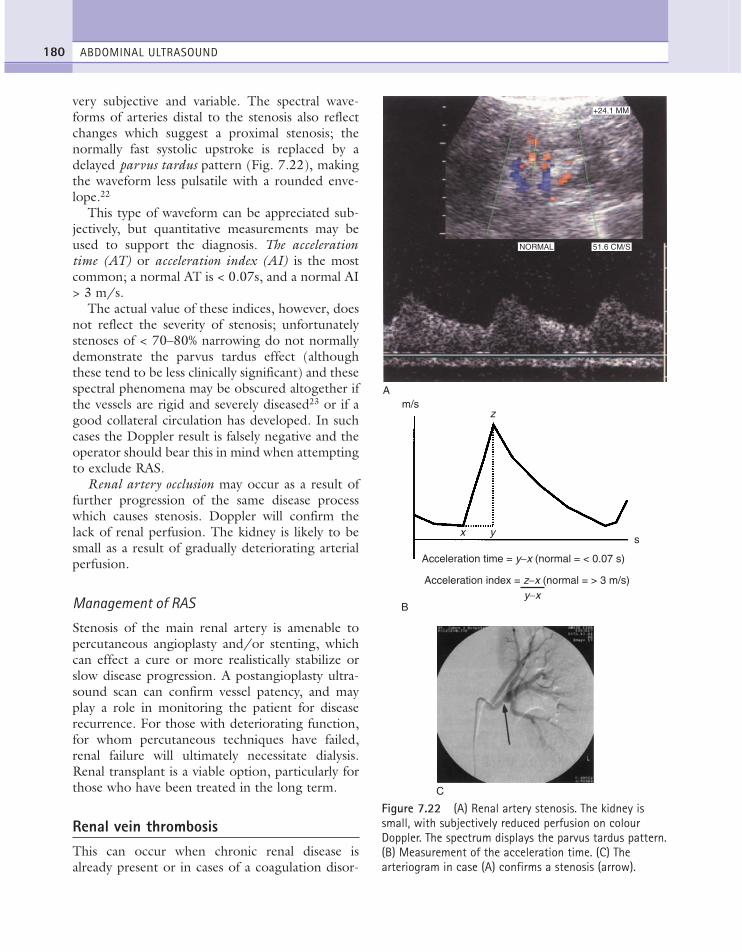
very subjective and variable. The spectral wave-forms of arteries distal to the stenosis also reflectchanges which suggest a proximal stenosis; thenormally fast systolic upstroke is replaced by adelayed parvus tardus pattern (Fig. 7.22), makingthe waveform less pulsatile with a rounded enve-lope.22
This type of waveform can be appreciated sub-jectively, but quantitative measurements may beused to support the diagnosis. The accelerationtime (AT) or acceleration index (AI) is the mostcommon; a normal AT is < 0.07s, and a normal AI> 3 m/s.
The actual value of these indices, however, doesnot reflect the severity of stenosis; unfortunatelystenoses of < 70–80% narrowing do not normallydemonstrate the parvus tardus effect (althoughthese tend to be less clinically significant) and thesespectral phenomena may be obscured altogether ifthe vessels are rigid and severely diseased23 or if agood collateral circulation has developed. In suchcases the Doppler result is falsely negative and theoperator should bear this in mind when attemptingto exclude RAS.
Renal artery occlusion may occur as a result offurther progression of the same disease processwhich causes stenosis. Doppler will confirm thelack of renal perfusion. The kidney is likely to besmall as a result of gradually deteriorating arterialperfusion.
Management of RAS
Stenosis of the main renal artery is amenable topercutaneous angioplasty and/or stenting, whichcan effect a cure or more realistically stabilize orslow disease progression. A postangioplasty ultra-sound scan can confirm vessel patency, and mayplay a role in monitoring the patient for diseaserecurrence. For those with deteriorating function,for whom percutaneous techniques have failed,renal failure will ultimately necessitate dialysis.Renal transplant is a viable option, particularly forthose who have been treated in the long term.
Renal vein thrombosisThis can occur when chronic renal disease isalready present or in cases of a coagulation disor-
ABDOMINAL ULTRASOUND180
A
NORMAL 51.6 CM/S
+24.1 MM
Figure 7.22 (A) Renal artery stenosis. The kidney issmall, with subjectively reduced perfusion on colourDoppler. The spectrum displays the parvus tardus pattern.(B) Measurement of the acceleration time. (C) Thearteriogram in case (A) confirms a stenosis (arrow).
m/s
s
Acceleration time = y−x (normal = < 0.07 s)
Acceleration index = z−x (normal = > 3 m/s)y−x
z
x y
B
C
ch07.qxd 6/30/04 6:09 PM Page 180

der with increased tendency to thrombose, forexample polycythaemia. It is frequently associatedwith nephrotic syndrome. Other associated factorsinclude the oral contraceptive pill and the use ofsteroids.24
Tumour thrombus from RCC is also prone toinvade the ipsilateral renal vein, and sometimesmay extend into the IVC and even renal artery.
Thrombus in the renal vein, whether secondaryto a malignancy or thrombocythaemia can travelup the IVC forming a source of emboli. If non-malignant, the thrombus may be successfullytreated medically and the renal function can bepreserved even if the vein is totally occluded.
Ultrasound appearances
It is often possible to see echo-poor thrombuswithin a dilated renal vein, running beside therenal artery in an axial section through the renalhilum (Fig. 7.9). Colour Doppler confirms absentvenous flow.
Perfusion within the kidney itself is reduced andthere may be a highly pulsatile arterial waveformwith reversed diastolic flow (Fig. 7.23), althoughthis is not commonly seen in the native kidney.
If the thrombus produces a total and suddenocclusion, the kidney becomes oedematous andswollen within the first 24 h. Eventually it willshrink and become hyperechoic.
Partially occluding thrombus is more difficult todiagnose as the changes in the kidney may not beapparent. However, a non-dilated renal vein withgood colour Doppler displayed throughout has ahigh negative predictive value.
Incomplete thrombosis may still demonstratevenous flow within the kidney, although the arte-rial waveforms are of lower velocity than normal,with a marked reduction in the systolic peak.25
Forward diastolic flow may be preserved at thisstage.
Arteriovenous fistulaThese lesions can occur at the site of a biopsy andare recognized on colour and spectral Doppler bylocalized vessel enlargement with turbulent, some-times high-velocity flow. A ‘pool’ of colour flow isoften present. The vein may show a regular, pul-
satile pattern and be dilated. These iatrogenic fis-tulae usually resolve spontaneously and are clini-cally insignificant. If bleeding is a clinical problemand is ongoing, recurrent and/or severe thenembolization is the treatment of choice.
Ultrasound in dialysisPatients with chronic renal failure may undergoeither haemodialysis (in which a subcutaneousarteriovenous shunt is created, often in the wrist)or continuous ambulatory peritoneal dialysis(CAPD), in which a catheter is inserted throughthe abdominal wall. Ultrasound may be used toassess the patency of the shunt or catheter, and mayidentify localized areas of infection along theCAPD tract which can be drained under ultra-sound guidance if necessary.
THE RENAL TRACT 181
NORMAL 1686 HZ
+7.8MM
Figure 7.23 Renal vein thrombosis. Small shrunkenkidney (6 cm) demonstrating hardly any perfusion, apartfrom a tiny interlobar artery with forward and reverseflow.
ch07.qxd 6/30/04 6:09 PM Page 181

Ultrasound may also be used to diagnoseacquired cystic kidney disease in long-term dialysispatients (see above).
RENAL TRAUMA
The severity of trauma to the kidney may vary sig-nificantly and therefore a range of findings can beseen with ultrasound. A direct injury can rupturethe kidney. This will result in blood and/or urineleaking out into the perinephric space. The natureof the fluid can be determined by ultrasoundguided aspiration. A large urinoma or haematomamay be drained percutaneously. The main renalvessels may also be damaged, causing lack of per-fusion (see Chapter 10).
Causes of haematuria are listed in Table 7.3.
RENAL TRANSPLANTS
Although there are a number of treatment choicesfor patients with renal failure including peritonealand haemodialysis, undoubtedly the treatment ofchoice is renal transplantation.
From the very early days of Carrel’s experimen-tal attempts at transplantation in the 1900s(resulting in the Nobel Prize of 191226), to theun-immunosuppressed allografting of the 1950s,the more successful and encouraging outcome oftwin to twin transplants,27 a better understandingof tissue rejection and the introduction of azathio-prine and steroid in 1963,28 and more specificallyciclosporin A by Calne in the 1970s,29 have all
contributed immensely to slow but positiveprogress in this field. Improvements in surgicaltechnique, newer, more effective and less toxicanti-rejection therapy, the routine use of ultra-sound in the 1970s and then Doppler a decadelater, and the development of interventional radi-ology have all combined to make this the success-ful operation and clinical outcome we now take somuch for granted.
Although many different imaging modalities areavailable, ultrasound is the single most usefulinvestigation in the postoperative monitoring ofthe transplant. Amongst its many roles, it is sensi-tive to early PCS dilatation, can be used to guidebiopsy procedures and to guide the drainage offluid collections and placement of nephrostomytubes.
An early, baseline scan is an essential part of thepostoperative management, and serial scans are tobe recommended.
Normal anatomyMost renal transplants are heterotopic, that is theyare placed in addition to the diseased, native kid-neys, which remain in situ.
The transplanted organ is usually positioned inthe iliac fossa anterior to the psoas and iliacus mus-cles. It lies outside the peritoneal cavity.
Within the UK the majority of transplanted kid-neys are cadaveric, and are harvested with theirmain vessels intact, which are then anastomosed tothe recipient iliac artery and vein.
Normal ultrasound appearancesThe transplanted kidney is particularly amenable toultrasonic investigation; its position relatively nearto the skin surface allows a high frequency trans-ducer (5 MHz) to be used for better detail. Forvisualization of the vasculature or origins of thetransplant vessels a 3.5–4.0MHz probe is normallyrequired.
The ultrasonic appearances of the transplant kid-ney are the same as expected for a native kidney,allowing for the higher resolution [Fig. 7.24]. Thetransplant kidney should be assessed in the sameway as the native organ, that is in two planes.Features to be observed include:
ABDOMINAL ULTRASOUND182
Table 7.3 Causes of haematuria
● Urinary tract infection● Stones● Neoplasm (renal cell or transitional cell carcinoma in
the kidney, ureter or bladder)● Prostatic pathology (benign hypertrophy or carcinoma)● Renal cyst haemorrhage● Papillary necrosis● Glomerulonephritis● Trauma● Tuberculosis● Renal infarct
ch07.qxd 6/30/04 6:09 PM Page 182
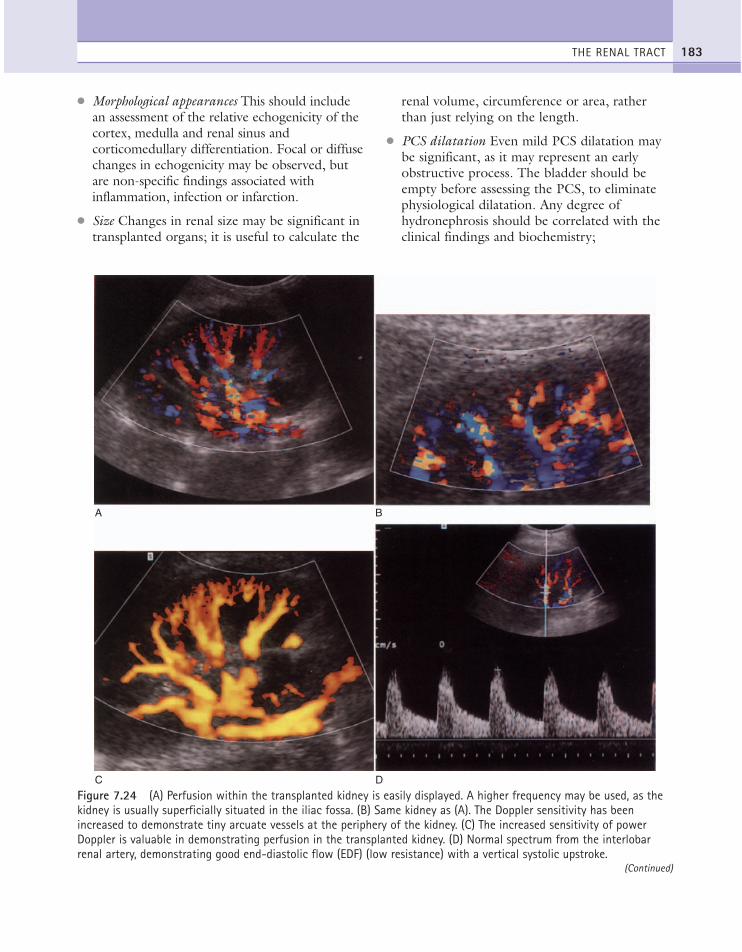
● Morphological appearances This should includean assessment of the relative echogenicity of thecortex, medulla and renal sinus andcorticomedullary differentiation. Focal or diffusechanges in echogenicity may be observed, butare non-specific findings associated withinflammation, infection or infarction.
● Size Changes in renal size may be significant intransplanted organs; it is useful to calculate the
renal volume, circumference or area, ratherthan just relying on the length.
● PCS dilatation Even mild PCS dilatation maybe significant, as it may represent an earlyobstructive process. The bladder should beempty before assessing the PCS, to eliminatephysiological dilatation. Any degree ofhydronephrosis should be correlated with theclinical findings and biochemistry;
THE RENAL TRACT 183
A B
C D
Figure 7.24 (A) Perfusion within the transplanted kidney is easily displayed. A higher frequency may be used, as thekidney is usually superficially situated in the iliac fossa. (B) Same kidney as (A). The Doppler sensitivity has beenincreased to demonstrate tiny arcuate vessels at the periphery of the kidney. (C) The increased sensitivity of powerDoppler is valuable in demonstrating perfusion in the transplanted kidney. (D) Normal spectrum from the interlobarrenal artery, demonstrating good end-diastolic flow (EDF) (low resistance) with a vertical systolic upstroke.
(Continued)
ch07.qxd 6/30/04 6:10 PM Page 183
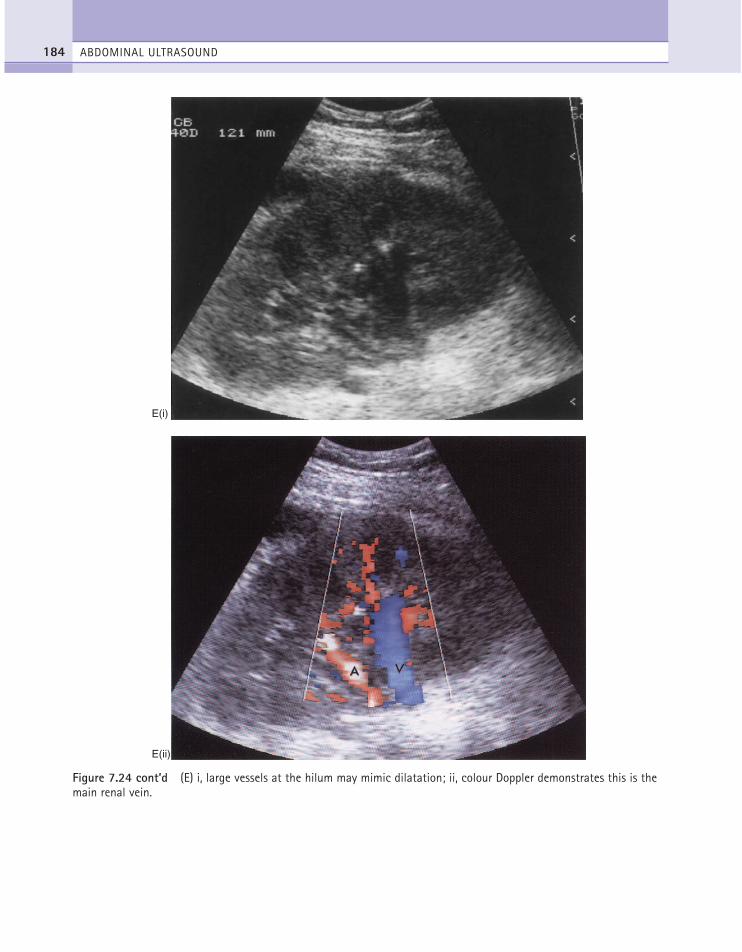
ABDOMINAL ULTRASOUND184
E(i)
E(ii)
Figure 7.24 cont’d (E) i, large vessels at the hilum may mimic dilatation; ii, colour Doppler demonstrates this is themain renal vein.
ch07.qxd 6/30/04 6:10 PM Page 184

hydronephrosis in isolation is not a reason fornephrostomy.
● Vascular anatomy The main transplant arteryand vein are anastomosed to the recipient’sexternal iliac artery and vein respectively andcan normally be visualized throughout theirlength. Overall global perfusion can be assessedwith colour Doppler and the smaller vessels atthe periphery of the kidney (Fig. 7.24) shouldbe discernible. The normal spectral Dopplerwaveform is a low-resistance waveform withcontinuous forward end diastolic flow.
● Perirenal fluid A small amount of free fluid isnot unusual postoperatively. This usually resolvesspontaneously. Fluid collections around thekidney are a common complication. They mayresolve on further scanning; drainage is onlypeformed for good clinical reasons (see below).
Postoperative complicationsUltrasound has an essential role in assessing thetransplant and makes a significant contributiontowards graft survival through the early recogni-tion of postoperative complications. Complicationsare varied and include acute rejection, uretericobstruction, vascular occlusions, perirenal fluidcollections, renal dysfunction (of various aetiolo-gies) and infection. Drug toxicity from theimmunosuppressive therapy can also compromisegraft function. Finally, in the long term, the origi-nal disease, for which transplantation was per-formed, may recur.
Complications can be divided into three maincategories: immediate postoperative complications,primary and secondary renal dysfunction.
● Immediate—non-perfusion, normally the result of an
occluded or twisted renal artery; correctionis surgical
—haematoma● Primary dysfunction
—non-perfusion (arterial occlusion), total orlobar
—acute tubular necrosis—renal vein thrombosis—obstruction
—acute or accelerated acute rejection● Secondary dysfunction
—acute rejection—ciclosporin nephrotoxicity—acute tubular necrosis—obstruction—RAS—postbiopsy fistula—infection—chronic rejection.
Renal transplant dilatationA mild degree of PCS dilatation is normal postop-eratively, due to oedema at the site of the vesi-coureteric anastomosis. This phenomenon isusually transient, and serial scans in conjunctionwith biochemistry (urea, creatinine) is normally allthat is required. More severe dilatation may beindicative of obstruction, especially if the individ-ual calyces are also dilated. A trend of increasingdilatation is a poor prognostic indicator. A ratiobetween the area of the PCS and the renal outlinein two planes, the dilatation index, has been foundto predict obstruction and differentiate obstructivefrom non-obstructive dilatation30 (Fig. 7.25).
The degree of dilatation of the PCS correlateswell with the severity of obstruction.
Obstruction of the transplant kidney may be dueto an ischaemic related stricture at the vesicouretericanastomosis, or may be the result of a blood clot orinfected debris in the ureter. Haematoma or debriswithin the PCS may appear echogenic but requiresto be differentiated from fungal balls.
Percutaneous nephrostomy is the method ofchoice to relieve obstruction.
RejectionThis can be acute or chronic. Acute rejection maybe responsible for delayed graft function whereaschronic rejection is a gradual deterioration in renalfunction that may begin any time after 3 months oftransplantation. Ongoing episodes of acute rejec-tion should raise the possibility of non-compliancewith therapy. Acute rejection cannot be differenti-ated on ultrasound from other causes of delayedfunction, particularly acute tubular necrosis, andtherefore biopsy is invariably necessary.
THE RENAL TRACT 185
ch07.qxd 6/30/04 6:10 PM Page 185
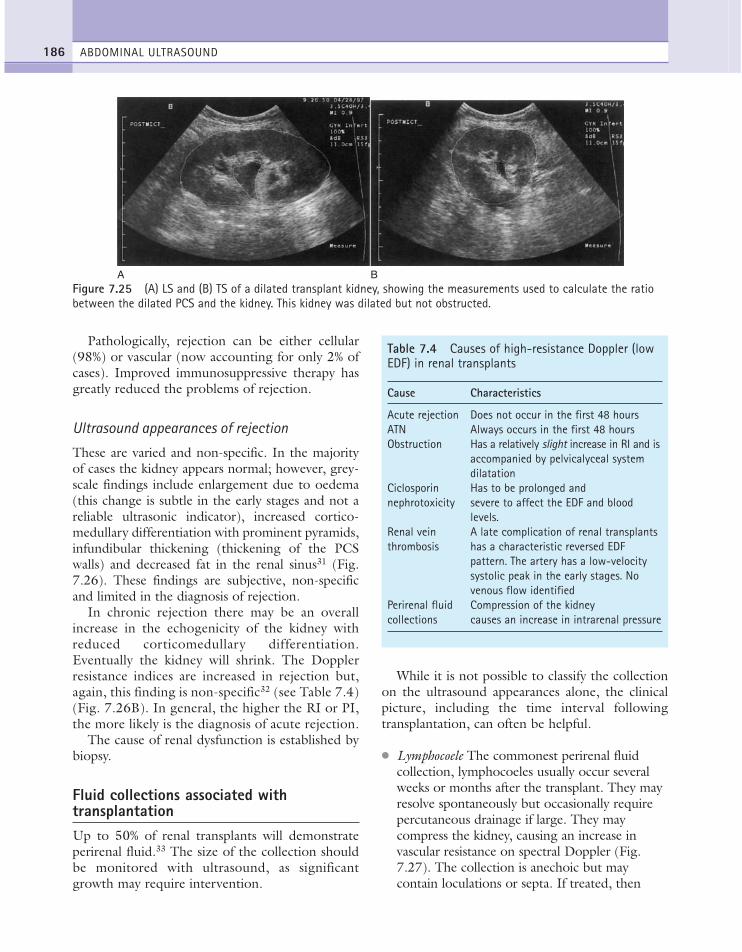
Pathologically, rejection can be either cellular(98%) or vascular (now accounting for only 2% ofcases). Improved immunosuppressive therapy hasgreatly reduced the problems of rejection.
Ultrasound appearances of rejection
These are varied and non-specific. In the majorityof cases the kidney appears normal; however, grey-scale findings include enlargement due to oedema(this change is subtle in the early stages and not areliable ultrasonic indicator), increased cortico-medullary differentiation with prominent pyramids,infundibular thickening (thickening of the PCSwalls) and decreased fat in the renal sinus31 (Fig.7.26). These findings are subjective, non-specificand limited in the diagnosis of rejection.
In chronic rejection there may be an overallincrease in the echogenicity of the kidney withreduced corticomedullary differentiation.Eventually the kidney will shrink. The Dopplerresistance indices are increased in rejection but,again, this finding is non-specific32 (see Table 7.4)(Fig. 7.26B). In general, the higher the RI or PI,the more likely is the diagnosis of acute rejection.
The cause of renal dysfunction is established bybiopsy.
Fluid collections associated withtransplantationUp to 50% of renal transplants will demonstrateperirenal fluid.33 The size of the collection shouldbe monitored with ultrasound, as significantgrowth may require intervention.
While it is not possible to classify the collectionon the ultrasound appearances alone, the clinicalpicture, including the time interval followingtransplantation, can often be helpful.
● Lymphocoele The commonest perirenal fluidcollection, lymphocoeles usually occur severalweeks or months after the transplant. They mayresolve spontaneously but occasionally requirepercutaneous drainage if large. They maycompress the kidney, causing an increase invascular resistance on spectral Doppler (Fig.7.27). The collection is anechoic but maycontain loculations or septa. If treated, then
ABDOMINAL ULTRASOUND186
A BFigure 7.25 (A) LS and (B) TS of a dilated transplant kidney, showing the measurements used to calculate the ratiobetween the dilated PCS and the kidney. This kidney was dilated but not obstructed.
Table 7.4 Causes of high-resistance Doppler (lowEDF) in renal transplants
Cause Characteristics
Acute rejection Does not occur in the first 48 hoursATN Always occurs in the first 48 hoursObstruction Has a relatively slight increase in RI and is
accompanied by pelvicalyceal systemdilatation
Ciclosporin Has to be prolonged and nephrotoxicity severe to affect the EDF and blood
levels.Renal vein A late complication of renal transplantsthrombosis has a characteristic reversed EDF
pattern. The artery has a low-velocitysystolic peak in the early stages. Novenous flow identified
Perirenal fluid Compression of the kidney collections causes an increase in intrarenal pressure
ch07.qxd 6/30/04 6:10 PM Page 186
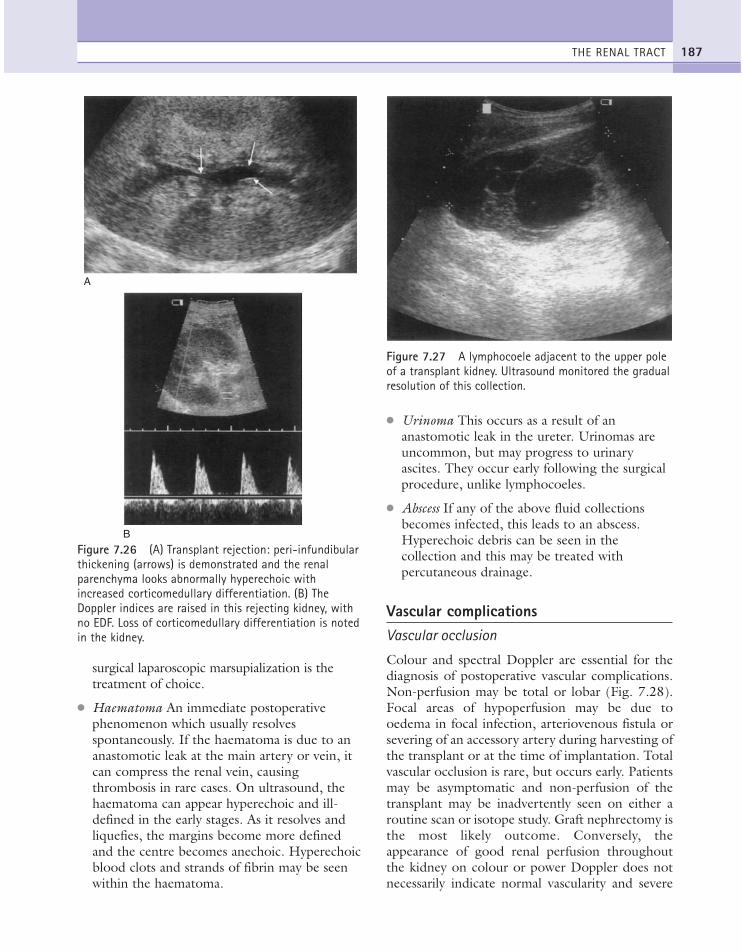
surgical laparoscopic marsupialization is thetreatment of choice.
● Haematoma An immediate postoperativephenomenon which usually resolvesspontaneously. If the haematoma is due to ananastomotic leak at the main artery or vein, itcan compress the renal vein, causingthrombosis in rare cases. On ultrasound, thehaematoma can appear hyperechoic and ill-defined in the early stages. As it resolves andliquefies, the margins become more definedand the centre becomes anechoic. Hyperechoicblood clots and strands of fibrin may be seenwithin the haematoma.
● Urinoma This occurs as a result of ananastomotic leak in the ureter. Urinomas areuncommon, but may progress to urinaryascites. They occur early following the surgicalprocedure, unlike lymphocoeles.
● Abscess If any of the above fluid collectionsbecomes infected, this leads to an abscess.Hyperechoic debris can be seen in thecollection and this may be treated withpercutaneous drainage.
Vascular complicationsVascular occlusion
Colour and spectral Doppler are essential for thediagnosis of postoperative vascular complications.Non-perfusion may be total or lobar (Fig. 7.28).Focal areas of hypoperfusion may be due tooedema in focal infection, arteriovenous fistula orsevering of an accessory artery during harvesting ofthe transplant or at the time of implantation. Totalvascular occlusion is rare, but occurs early. Patientsmay be asymptomatic and non-perfusion of thetransplant may be inadvertently seen on either aroutine scan or isotope study. Graft nephrectomy isthe most likely outcome. Conversely, theappearance of good renal perfusion throughoutthe kidney on colour or power Doppler does notnecessarily indicate normal vascularity and severe
THE RENAL TRACT 187
A
B
Figure 7.26 (A) Transplant rejection: peri-infundibularthickening (arrows) is demonstrated and the renalparenchyma looks abnormally hyperechoic withincreased corticomedullary differentiation. (B) TheDoppler indices are raised in this rejecting kidney, withno EDF. Loss of corticomedullary differentiation is notedin the kidney.
Figure 7.27 A lymphocoele adjacent to the upper poleof a transplant kidney. Ultrasound monitored the gradualresolution of this collection.
ch07.qxd 6/30/04 6:10 PM Page 187

ABDOMINAL ULTRASOUND188
A
B C
Figure 7.28 (A) Lack of perfusion in the upper pole due to rejection. (B) High-velocity jet at the site of a magneticresonance angiography stenosis. This patient had had increasing, badly controlled hypertension since his transplant.(C) The same kidney, demonstrating turbulence distal to the site of stenosis.
ch07.qxd 6/30/04 6:10 PM Page 188

vascular rejection or acute tubular necrosis can bepresent under such circumstances.34
Vascular complications can include arterial steno-sis or thrombosis, venous stenosis or thrombosis,pseudoaneurysms and arteriovenous fistulae.33
Renal artery stenosis
This generally occurs at the site of the anastomosisclose to the iliac artery but can also occur along thelength of the artery or even affect the intrarenalbranches. The patient may present with severe,difficult-to-control hypertension, graft dysfunction,or both. Alternatively the patient’s renal functionmay deteriorate following angiotensin-convertingenzyme inhibitor therapy and this is also an indica-tion of a possible underlying RAS. Careful Dopplerexamination is now the accepted first-line investi-gation in the diagnosis of RAS.
In most cases it is possible to trace the arteryback to its anastomosis with the iliac artery, usingcolour Doppler. If the site of the stenosis is identi-fied, spectral Doppler will demonstrate an increasein peak systolic velocity at the lesion, followed bypoststenotic turbulence (Fig. 7.28, B,C). This canbe difficult to pinpoint with MRA, especially ifbowel is overlying the vessel.
A delayed systolic rise (the parvus tardus wave-form) can be identified in the intrarenal spectralDoppler waveforms, as for the native kidney (seeabove). The diagnosis however is primarily madeon the peak systolic velocity within the renal artery.A value of < 2.5 m/s is normal while > 2.5 m/sconstitutes RAS. If the stenosis is severe, it may bedifficult to identify colour flow in the kidney andthe waveform may be reduced in velocity with atiny, damped trace in the main vessel.
A stenosis affecting an interlobar artery mayresult in focal, segmental changes in the kidney.
In general, contrast angiography is only used tograde and treat stenoses after a positive ultrasoundscan, or when a high index of clinical suspicion per-sists, despite a negative ultrasound.33
Renal vein thrombosis
The occlusion may be partial or complete and thevenous Doppler spectrum may therefore be absent(Fig. 7.29).
If venous thrombosis is partial, the arterial spectralwaveform becomes very pulsatile, with reverse enddiastolic flow; in the clinical setting of an oliguricpatient with a tender graft in the early postoperativeperiod, this is almost pathognomonic for RVT.
During the early stages, when thrombosis isincomplete, venous flow may be seen in the kidney,but the artery is of reduced velocity.25
The ultrasound findings of renal vein thrombosismay be indistinguishable from severe rejection; how-ever venous flow is generally unaffected in the latter.
Thrombosis is rare, occurring typically in theimmediate postoperative period.33 It may be asso-ciated with a faulty venous anastomosis, secondaryto compression of the vein, for example by a large,perivenous collection, or the patient may have anincreased thrombotic tendency for a number ofreasons.
Pseudoaneurysms and arteriovenous fistulae
These may sometimes form as a result of vasculardamage during biopsy procedures. They are usu-ally not significant and tend to resolve sponta-neously (Fig. 7.30A).
An arteriovenous fistula shows an irregular knotof vessels on colour or power Doppler with a pul-satile venous waveform and high peak and end dias-tolic velocity in the feeding artery. A large drainingvein may also be seen.
A pseudoaneurysm may appear cystic on thegrey-scale image, but will demonstrate filling oncolour Doppler with a pulsatile flow velocity wave-form (Fig. 7.30B, C). Careful biopsy techniquehelps to avoid such lesions (see Chapter 11).
InfectionThis is characterized by swelling of the uroepithe-lium, especially with fungal infections. Fungal ballsmay be visible as relatively hyperechoic structureswithin the PCS (Fig. 7.31).
Acute tubular necrosisThis may demonstrate prominent medullary pyra-mids on ultrasound, with low end diastolic flow.Reverse end diastolic flow is uncommon but rec-ognized. A biopsy is required for confirmation.
THE RENAL TRACT 189
ch07.qxd 6/30/04 6:10 PM Page 189

ABDOMINAL ULTRASOUND190
A B
C
NORMAL 2623
+ 8.7MM
Figure 7.29 Renal vein thrombosis. (A) Poor transplantperfusion, with scanty demonstration of arterial flow. (B) The same vessels demonstrate reversal of flow at theend of the cardiac cycle. (C) The bidirectional flow isdemonstrated on the spectral trace.
ch07.qxd 6/30/04 6:10 PM Page 190
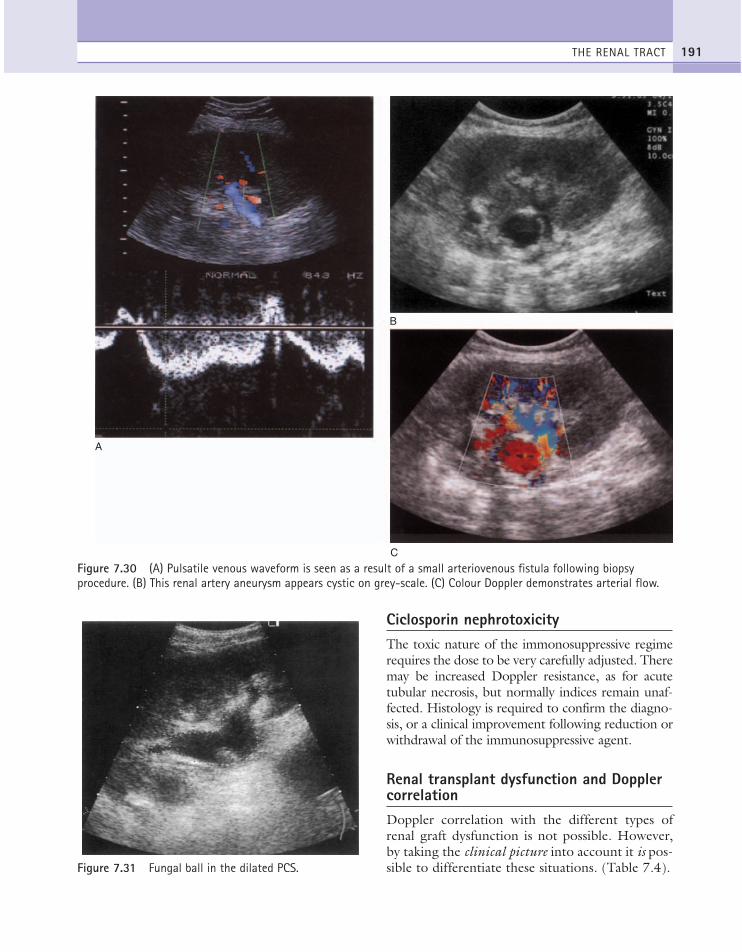
Ciclosporin nephrotoxicityThe toxic nature of the immonosuppressive regimerequires the dose to be very carefully adjusted. Theremay be increased Doppler resistance, as for acutetubular necrosis, but normally indices remain unaf-fected. Histology is required to confirm the diagno-sis, or a clinical improvement following reduction orwithdrawal of the immunosuppressive agent.
Renal transplant dysfunction and DopplercorrelationDoppler correlation with the different types ofrenal graft dysfunction is not possible. However,by taking the clinical picture into account it is pos-sible to differentiate these situations. (Table 7.4).
THE RENAL TRACT 191
A
B
C
Figure 7.30 (A) Pulsatile venous waveform is seen as a result of a small arteriovenous fistula following biopsyprocedure. (B) This renal artery aneurysm appears cystic on grey-scale. (C) Colour Doppler demonstrates arterial flow.
Figure 7.31 Fungal ball in the dilated PCS.
ch07.qxd 6/30/04 6:10 PM Page 191
1. Burge HJ, Middleton WD, McClennan BL et al.1991 Ureteral jets in healthy subjects and in patientswith unilateral ureteral calculi: comparison with colorDoppler US. Radiology 180: 437–442.
2. Brkljacic B, Drinkovic I, Delic-Brkljacic D, HebrangA. 1995 Age-related changes of renal vascularresistance in normal native kidneys: colour duplexDoppler ultrasound assessment. Radiology andOncology 29: 102–106.
3. Heinz-Peer G, Schoder M, Rand T, Mayer G,Mostbeck GH. 1995 Prevalence of acquired cystickidney disease and tumours in native kidneys of renaltransplant recipients: a prospective study. Radiology195: 667–671.
4. Levine E. 1996 Acquired cystic kidney disease.Radiologic Clinics of North America 34: 947–964.
5. Siegel CL, Middleton WD, Teefey SA, McClennanBL. 1996 Angiomyolipoma and renal cell carcinoma:US differentiation. Radiology 198: 789–793.
6. Curry NS, Schabel SI, Betsill WL. 1986 Small renalneoplasms: diagnostic imaging, pathologic featuresand clinical course. Radiology 158: 113–117.
7. Licht MR. 1995 Renal adenoma and oncocytoma.Seminars in Urologic Oncology 13: 262–266.
8. Bosniak MA, Birnbaum BA, Krinsky GA, Waisman J.1996 Small renal parenchymal neoplasms: furtherobservations on growth. Radiology 197: 589–597.
9. Jamis-Dow CA, Choyke PL, Jennings SB et al. 1996Small (< 3 cm) renal masses: detection with CT versusUS and pathologic correlation. Radiology 198:785–788.
10. Deyoe LA, Cronan JJ, Breslaw BH, Ridlen MS. 1995New techniques of ultrasound and color Doppler inthe prospective evaluation of acute renal obstruction.Do they replace the intravenous urogram? AbdominalImaging 20: 58–63.
11. Smith RC, Essenmacher KR, Rosenfield AT, ChoeKA, Glickman M. 1995 Acute flank pain: comparisonof non-contrast CT and IVU. Radiology 194:789–794.
12. Rodgers PM, Bates JA, Irving HC. 1992 IntrarenalDoppler ultrasound studies in normal and acutelyobstructed kidneys. British Journal of Radiology 65:207–212.
13. Miletic D, Fuckar Z, Sustic A et al. 1998 Resistanceand pulsatility indices in acute renal obstruction.Journal of Clinical Ultrasound 26: 79–84.
14. Hak-JL, Seung HK, Yoong KJ, Kyung MY. 1996Doppler sonographic resistive index in obstructedkidneys. Journal of Ultrasound in Medicine 15/9:613–618.
15. Cronan JJ. 1991 Contemporary concepts in imagingurinary tract obstruction. Radiologic Clinics of NorthAmerica 29: 527–542.
16. Haddad MC, Sharif HS, Shahed MS et al. 1992 Renalcolic: diagnosis and outcome. Radiology 184: 83–88.
17. Zagoria RJ, Khatod EG, Chen MYM. 2001Abdominal radiography after CT reveals urinarycalculi: a method to predict usefulness of abdominalradiography on the basis of size and CT attenuationof calculi. American Journal of Roentgenology176(5): 1117–1122.
18. Li Y, Zhang Y. 1996 Diagnosis and treatment ofacute focal bacterial nephritis. Chinese MedicalJournal 109: 168–172.
19. Page JE, Morgan SH, Eastwood JB et al. 1994Ultrasound findings in renal parenchymal disease:comparison with histological appearances. ClinicalRadiology 49: 867–870.
20. Strandness DE. 1994 Natural history of renal arterystenosis. American Journal of Kidney Disease 24:630–635.
21. Olin JW, Piedmonte MR, Young JR et al. 1995 Theutility of duplex ultrasound scanning of the renalarteries for diagnosing significant renal artery stenosis.Annals of Internal Medicine 122: 833–838.
22. Baxter GM, Aitchison F, Sheppard D et al. 1996Colour Doppler ultrasound in renal artery stenosis:intrarenal waveform analysis. British Journal ofRadiology 69/825: 810–815.
23. Bude RO, Rubin JM, Platt JF et al. 1994 Pulsustardus: its cause and potential limitations in detectionof arterial stenosis. Radiology 190: 779–784.
24. Witz M, Kantarovsky A, Morag B, Shifin EG. 1996Renal vein occlusion: a review. Journal of Urology155: 1173–1179.
25. MacLennan AC, Baxter GM, Harden P, Rowe PA.1995 Renal transplant vein occlusion: an earlydiagnostic sign? Clinical Radiology 50/4: 251–253.
26. Hamilton D. 1987 Alexis Carrel and the early days of tissue transplantation. Transplant Review 2:1–15.
27. Murray JE, Merrill JP, Harrison JH. 1958 Kidneytransplantation between seven pairs of identical twins.Annals of Surgery 148: 343–359.
28. Starzl TE. 1964 Experience in Renal Transplantation.Saunders, Philadelphia.
29. Calne RY, White DJG, Thiru S et al. 1978Ciclosporin A in patients receiving renal allograftsfrom cadaveric donors. Lancet ii: 1323–1327.
30. Kashi SH, Irving HC. 1993 Improving the evaluationof renal transplant collecting system dilatation by
ABDOMINAL ULTRASOUND192
References
ch07.qxd 6/30/04 6:10 PM Page 192
computerised ultrasound imaging digitisation. BritishJournal of Radiology 66: 1002–1008.
31. Townsend RR, Tomlanovich SJ, Goldstein RB et al.1990 Combined Doppler and morphologicsonographic evaluation of renal transplant rejection.Journal of Ultrasound in Medicine 9: 199–206.
32. Perella RR, Duerincky AJ, Tessler FN et al. 1990Evaluation of renal transplant dysfunction by duplexDoppler sonography; a prospective study and review
of the literature. American Journal of Kidney Disease15: 544–550.
33. Tublin ME, Dodd GD. 1995 Sonography of renaltransplantation. Radiologic Clinics of North America33: 447–459.
34. Hilborn MD, Bude RO, Murphy KJ et al. 1997 Renaltransplant evaluation with power Doppler sonography.British Journal of Radiology 70: 39–42.
THE RENAL TRACT 193
ch07.qxd 6/30/04 6:10 PM Page 193

ch07.qxd 6/30/04 6:10 PM Page 194
This page intentionally left blank

NORMAL ANATOMY
The peritoneum is the large sheet of serous mem-brane which lines the abdominal cavity and sur-rounds the organs. The peritoneum has several‘extensions’ which bind the organs together: themesentery, which loosely anchors the small bowelensuring it does not twist, the transverse meso-colon, which attaches the transverse colon to theposterior abdominal wall, and the greater andlesser omentum. These projections coat the visceraand form pouches, or sacs, within the peritonealcavity in which dependent fluid can collect.
The retroperitoneal space contains the kidneysand ureters, adrenal glands, pancreas and duodenalloop, great vessels and the ascending and descend-ing portions of the large bowel, including the cae-cum (Fig. 8.1).
THE ABDOMINAL AORTA
The abdominal aorta can be visualized proximallyin the midline, posterior to the left lobe of the liver.The coeliac axis and superior mesenteric artery(SMA) are easily demonstrated in longitudinal sec-tion (LS), arising from its anterior aspect (Fig.8.2).
In transverse section (TS) the coeliac axisbranches, the main hepatic and splenic arteries,may be better appreciated. Just below this level,the origin of the renal arteries is seen.
The distal abdominal aorta, which runs moreanteriorly, and bifurcation are frequently obscuredby bowel gas in sagittal section. A coronal
Chapter 8
The retroperitoneum and gastrointestinal tract
195
CHAPTER CONTENTS
Normal anatomy 195The abdominal aorta 195
Aortic aneurysm 196The inferior vena cava (IVC) 199
Pathology of the IVC 200The adrenal glands 201
Pathology of the adrenal glands 203Gastrointestinal (GI) tract 206
Oesophagus and stomach 206Appendix 206Mesenteric ischaemia 207Inflammatory bowel conditions 209Malignant tumours 210Obstruction 211
Other retroperitoneal abnormalities 212
ch08.qxd 6/30/04 6:14 PM Page 195

approach from the patient’s left side often over-comes this problem (Fig. 8.2D) and is also usefulin displaying the origin of the renal arteries.
The aorta often becomes ectatic and tortuouswith age, and it is not unusual to detect consider-able calcification of the walls (Fig. 8.2G).
Aortic aneurysmThe most frequent referral for aortic scanning is toestablish or monitor the presence of an aneurysm.The incidence of aortic aneurysm increases with
age and patients may present with a pulsatile, midabdominal mass. Patients most at risk are men aged60 or over, with an incidence of up to 9% after age75. The risk of aneurysm rupture increases withdiameter, increasing dramatically when it reaches6 cm, with a 1-year mortality of 50%.1
ABDOMINAL ULTRASOUND196
A
B
Figure 8.1 (A) Axial and (B) sagittal sections throughthe abdomen, showing the relationship of the abdominalviscera to the peritoneum (red).
A
B
C
Sa
ha
Figure 8.2 (A) Longitudinal section (LS) through theabdominal aorta, demonstrating the coeliac axis(arrowhead) and the superior mesenteric artery (SMA)(arrow). The splenic vein (SV) and body of pancreas areseen anterior to the SMA. (B) Transverse section (TS)through the proximal abdominal aorta. The coeliac axis,(C), divides into the hepatic and splenic arteries.
(Continued)
ch08.qxd 6/30/04 6:14 PM Page 196

THE RETROPERITONEUM AND GASTROINTESTINAL TRACT 197
C D
E
F GFigure 8.2 cont’d (C) TS slightly distal to (B). The right renal artery (RRA) is seen arising from the lateral aspect ofthe aorta; the left renal vein (LRV) passes anteriorly to drain into the inferior vena cava (IVC). (D) A coronal plane, fromthe patient’s left side, demonstrates the aortic bifurcation. (E) Coronal section of the aorta at the level of the renalarteries (arrows). (F) The Doppler spectrum from the aorta demonstrates a highly pulsatile waveform with reversed flowin early diastole. (G) The aorta of an elderly patient contains calcification in the walls, which causes acousticshadowing.
ch08.qxd 6/30/04 6:14 PM Page 197
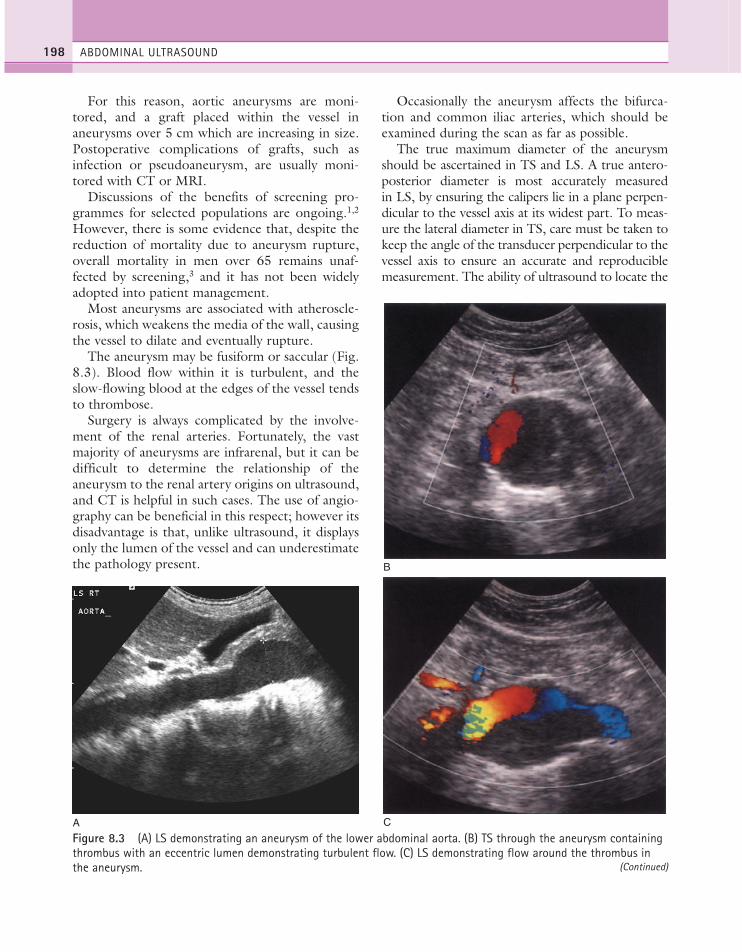
For this reason, aortic aneurysms are moni-tored, and a graft placed within the vessel inaneurysms over 5 cm which are increasing in size.Postoperative complications of grafts, such asinfection or pseudoaneurysm, are usually moni-tored with CT or MRI.
Discussions of the benefits of screening pro-grammes for selected populations are ongoing.1,2
However, there is some evidence that, despite thereduction of mortality due to aneurysm rupture,overall mortality in men over 65 remains unaf-fected by screening,3 and it has not been widelyadopted into patient management.
Most aneurysms are associated with atheroscle-rosis, which weakens the media of the wall, causingthe vessel to dilate and eventually rupture.
The aneurysm may be fusiform or saccular (Fig.8.3). Blood flow within it is turbulent, and theslow-flowing blood at the edges of the vessel tendsto thrombose.
Surgery is always complicated by the involve-ment of the renal arteries. Fortunately, the vastmajority of aneurysms are infrarenal, but it can bedifficult to determine the relationship of theaneurysm to the renal artery origins on ultrasound,and CT is helpful in such cases. The use of angio-graphy can be beneficial in this respect; however itsdisadvantage is that, unlike ultrasound, it displaysonly the lumen of the vessel and can underestimatethe pathology present.
Occasionally the aneurysm affects the bifurca-tion and common iliac arteries, which should beexamined during the scan as far as possible.
The true maximum diameter of the aneurysmshould be ascertained in TS and LS. A true antero-posterior diameter is most accurately measuredin LS, by ensuring the calipers lie in a plane perpen-dicular to the vessel axis at its widest part. To meas-ure the lateral diameter in TS, care must be taken tokeep the angle of the transducer perpendicular to thevessel axis to ensure an accurate and reproduciblemeasurement. The ability of ultrasound to locate the
ABDOMINAL ULTRASOUND198
A
B
C
Figure 8.3 (A) LS demonstrating an aneurysm of the lower abdominal aorta. (B) TS through the aneurysm containingthrombus with an eccentric lumen demonstrating turbulent flow. (C) LS demonstrating flow around the thrombus inthe aneurysm. (Continued)
ch08.qxd 6/30/04 6:14 PM Page 198

THE RETROPERITONEUM AND GASTROINTESTINAL TRACT 199
D EFigure 8.3 cont’d (D) TS and (E) LS of a dissecting aortic aneurysm. The detached intimal flap is clearly seen withinthe aortic lumen.
correct plane, regardless of vessel tortuosity, is a dis-tinct advantage over CT, which may over- or under-estimate the size of the aneurysm in an axial plane.
Complications of aortic aneurysm
Dissection of the aneurysm, in which the intimabecomes detached, is uncommon in the abdomen.Ultrasound may visualize the intimal flap and thefalse lumen created between the media and intimaoften contains slower, more turbulent or evenreversed flow. Layers of thrombus may mimic a dis-section, and colour flow Doppler is particularlyuseful in such cases.
Leakage of an aneurysm may cause retroperi-toneal haematoma, but CT is usually more reliablein detecting leaks than ultrasound.
Rupture of an aortic aneurysm is not unknownin the ultrasound department or emergencydepartment, and is accompanied by abdominalpain and severe hypotension. It is associated with ahigh mortality rate and is a surgical emergency.
Involvement of the renal arteries may causerenal artery thrombosis and subsequently smallkidney(s). Always check the kidneys at the time ofscanning to ensure they are of normal size andappearance.
THE INFERIOR VENA CAVA (IVC)
Ultrasound is highly successful in demonstratingthe proximal IVC, by using the liver as an acousticwindow, especially if the patient is turned rightanterior oblique. The distal IVC may be obscuredby overlying bowel gas and, unlike the aorta, is alsosusceptible to compression, making visualizationdifficult in some cases.
The normal IVC has thinner walls and a moreflattened profile than the aorta, and its lumen alterswith changing abdominal pressure; for example,during respiration the lumen decreases on inspira-tion, or with the Valsalva manoeuvre (Fig. 8.4). Itscourse becomes slightly anterior as it passesthrough the diaphragm, unlike the aorta whichtravels posteriorly at this point.
The main renal veins may be seen in TS, enter-ing the IVC just below the level of the pancreas(Fig. 8.2).
Haemodynamically, the blood flow spectrumfrom the IVC alters according to the distance ofthe sample volume from the right atrium (Fig. 8.4F, G). The blood flow through the IVC and prox-imal hepatic veins is pulsatile, with reverse flowduring right atrial systole. Pulsatility reduces in thedistal IVC.
ch08.qxd 6/30/04 6:14 PM Page 199
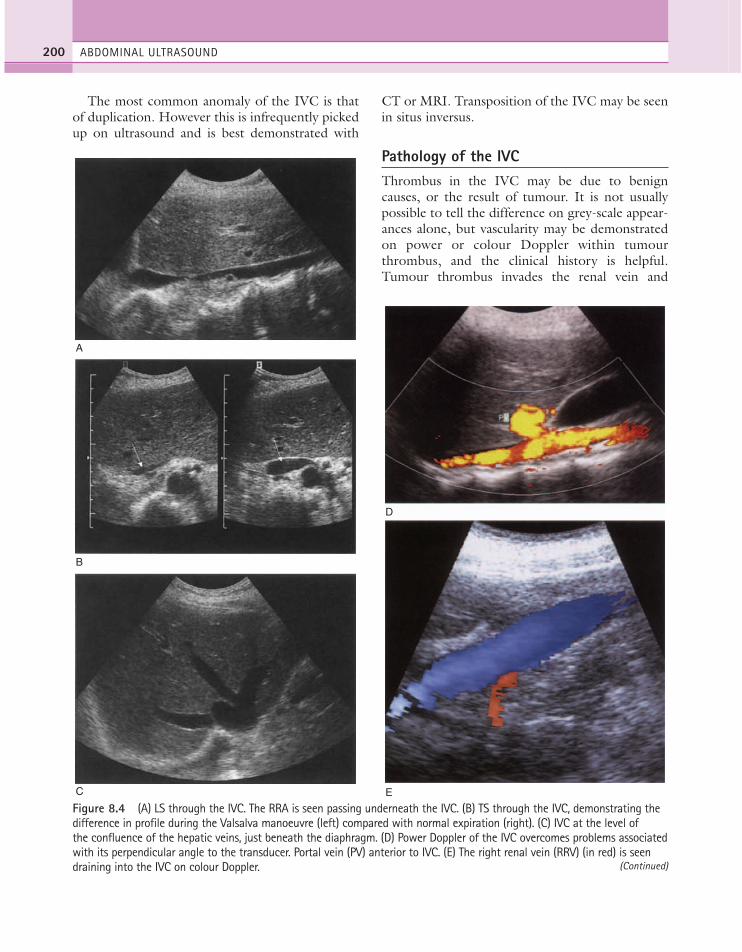
The most common anomaly of the IVC is thatof duplication. However this is infrequently pickedup on ultrasound and is best demonstrated with
CT or MRI. Transposition of the IVC may be seenin situs inversus.
Pathology of the IVCThrombus in the IVC may be due to benigncauses, or the result of tumour. It is not usuallypossible to tell the difference on grey-scale appear-ances alone, but vascularity may be demonstratedon power or colour Doppler within tumourthrombus, and the clinical history is helpful.Tumour thrombus invades the renal vein and
ABDOMINAL ULTRASOUND200
A
B
C
D
E
Figure 8.4 (A) LS through the IVC. The RRA is seen passing underneath the IVC. (B) TS through the IVC, demonstrating thedifference in profile during the Valsalva manoeuvre (left) compared with normal expiration (right). (C) IVC at the level ofthe confluence of the hepatic veins, just beneath the diaphragm. (D) Power Doppler of the IVC overcomes problems associatedwith its perpendicular angle to the transducer. Portal vein (PV) anterior to IVC. (E) The right renal vein (RRV) (in red) is seendraining into the IVC on colour Doppler. (Continued)
ch08.qxd 6/30/04 6:14 PM Page 200

enters the IVC in around 10% of renal carcinomacases. Tumour thrombus from hepatic or adrenalmasses can also invade the IVC.
Coagulation disorders, which cause Budd–Chiari syndrome (see Chapter 4) predominantlyaffect the hepatic veins, but may also involve theIVC (Fig. 8.5).
Patients may require the insertion of a caval fil-ter, which is performed under X-ray guidance, butmay be monitored for patency using ultrasoundwith Doppler.
Dilatation of the IVC is a finding commonlyassociated with congestive heart failure, and is fre-quently accompanied by hepatic vein dilatation.
Compression of the IVC by large masses is notuncommon. This may be due to retroperitonealmasses, such as a large lymph node, or liver massessuch as tumour or caudate lobe hypertrophy.Colour or power Doppler is particularly useful inconfirming patency of the vessel and differentiatingextrinsic compression from invasion. Insertion ofmetallic stents may be performed under angio-graphic control to maintain the vessel patency, par-ticularly if the compression is due to inoperablehepatic metastasis (Fig. 8.6).
Tumours of the IVC are rare. Leiomyosarcomais a primary IVC tumour, appearing as a hyper-echoic mass in the lumen of the vein.4,5 This causespartial or complete obstruction of the IVC, result-ing in Budd–Chiari syndrome. In partial occlusion,the hepatic veins and proximal IVC may be con-siderably dilated. Resection of the tumour, withrepair of the IVC, is possible provided the adjacentliver is not invaded.4
THE ADRENAL GLANDS
Normal appearances
The normal adrenal glands can be seen on ultra-sound in the vast majority of patients,6,7 if you knowwhere and how to look. Each adrenal gland is con-structed with a central fold or ridge, which pointsanteromedially, from which extend two thin ‘wings’of tissue—a medial and a lateral wing (Fig. 8.7).
The ultrasound appearances are therefore of a< shape in LS, or a thin, linear structure as thetransducer is moved medially towards the centralridge.
The wings of the gland appear hypoechoic andare no more than 2 mm in thickness.
Ultrasound technique
For the right adrenal, use the liver as an acousticwindow. Scan the upper pole of the kidney inter-costally through the liver, and angle slightly medi-ally to the kidney, where the gland can be locatedbetween the liver and the diaphragmatic crus (Fig.8.7A). Continue angling slightly medially towardsthe IVC and the central ridge of the gland is seenbehind the IVC (Fig. 8.7B).
For the left gland the spleen must be used as awindow. To avoid overlying bowel this is bestachieved with the patient supine, using a coronalsection. When the upper pole of the left kidney islocated through the spleen, the left adrenal can beseen in the small triangular area between thespleen, kidney and diaphragmatic crus (Fig.8.7D).6,7
THE RETROPERITONEUM AND GASTROINTESTINAL TRACT 201
F G
Figure 8.4 cont’d (F) Normal, pulsatile spectrum from the proximal IVC is influenced by the proximity of the rightatrium. (G) The waveform from the distal IVC is lower in velocity, less pulsatile and displays more variance.
ch08.qxd 6/30/04 6:14 PM Page 201
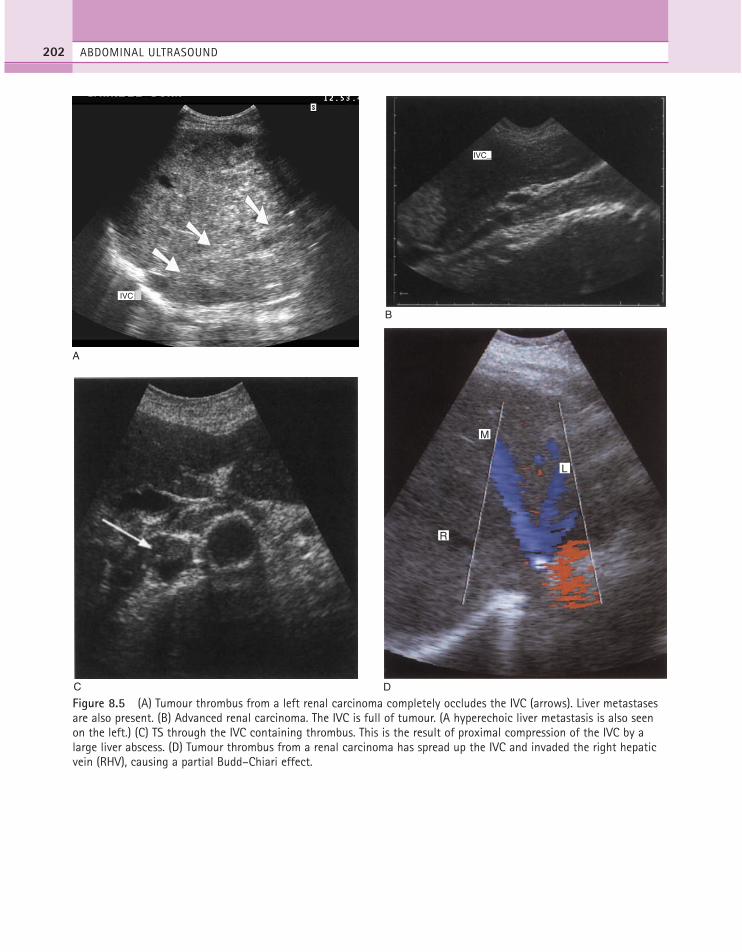
ABDOMINAL ULTRASOUND202
A
IVC
B
IVC_
C D
R
M
L
Figure 8.5 (A) Tumour thrombus from a left renal carcinoma completely occludes the IVC (arrows). Liver metastasesare also present. (B) Advanced renal carcinoma. The IVC is full of tumour. (A hyperechoic liver metastasis is also seenon the left.) (C) TS through the IVC containing thrombus. This is the result of proximal compression of the IVC by alarge liver abscess. (D) Tumour thrombus from a renal carcinoma has spread up the IVC and invaded the right hepaticvein (RHV), causing a partial Budd–Chiari effect.
ch08.qxd 6/30/04 6:15 PM Page 202
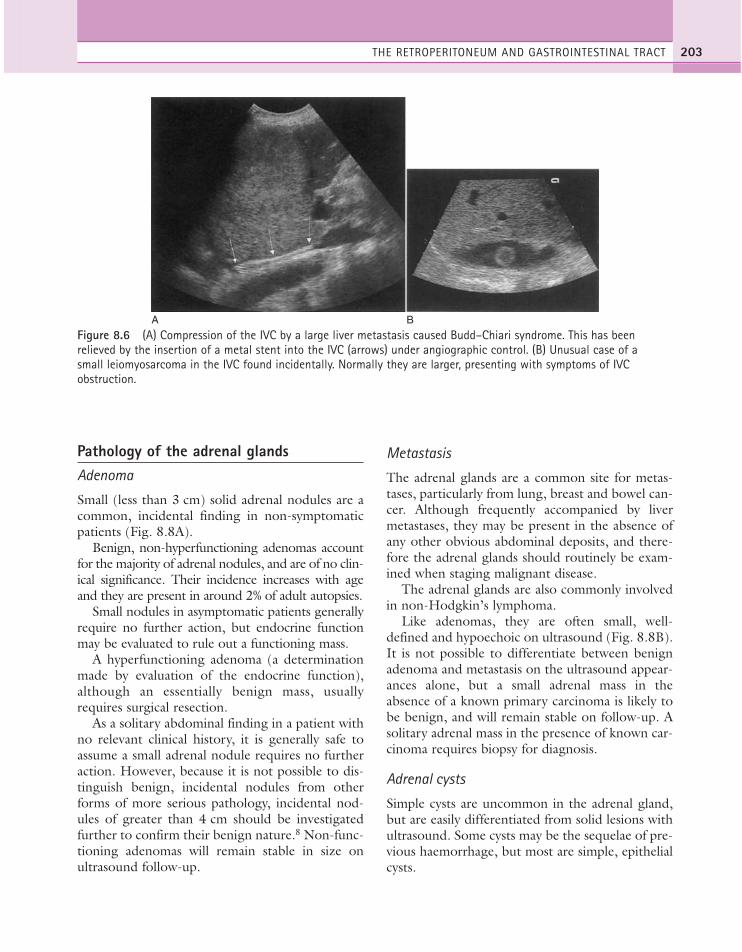
Pathology of the adrenal glandsAdenoma
Small (less than 3 cm) solid adrenal nodules are acommon, incidental finding in non-symptomaticpatients (Fig. 8.8A).
Benign, non-hyperfunctioning adenomas accountfor the majority of adrenal nodules, and are of no clin-ical significance. Their incidence increases with ageand they are present in around 2% of adult autopsies.
Small nodules in asymptomatic patients generallyrequire no further action, but endocrine functionmay be evaluated to rule out a functioning mass.
A hyperfunctioning adenoma (a determinationmade by evaluation of the endocrine function),although an essentially benign mass, usuallyrequires surgical resection.
As a solitary abdominal finding in a patient withno relevant clinical history, it is generally safe toassume a small adrenal nodule requires no furtheraction. However, because it is not possible to dis-tinguish benign, incidental nodules from otherforms of more serious pathology, incidental nod-ules of greater than 4 cm should be investigatedfurther to confirm their benign nature.8 Non-func-tioning adenomas will remain stable in size onultrasound follow-up.
Metastasis
The adrenal glands are a common site for metas-tases, particularly from lung, breast and bowel can-cer. Although frequently accompanied by livermetastases, they may be present in the absence ofany other obvious abdominal deposits, and there-fore the adrenal glands should routinely be exam-ined when staging malignant disease.
The adrenal glands are also commonly involvedin non-Hodgkin’s lymphoma.
Like adenomas, they are often small, well-defined and hypoechoic on ultrasound (Fig. 8.8B).It is not possible to differentiate between benignadenoma and metastasis on the ultrasound appear-ances alone, but a small adrenal mass in theabsence of a known primary carcinoma is likely tobe benign, and will remain stable on follow-up. Asolitary adrenal mass in the presence of known car-cinoma requires biopsy for diagnosis.
Adrenal cysts
Simple cysts are uncommon in the adrenal gland,but are easily differentiated from solid lesions withultrasound. Some cysts may be the sequelae of pre-vious haemorrhage, but most are simple, epithelialcysts.
THE RETROPERITONEUM AND GASTROINTESTINAL TRACT 203
A B
Figure 8.6 (A) Compression of the IVC by a large liver metastasis caused Budd–Chiari syndrome. This has beenrelieved by the insertion of a metal stent into the IVC (arrows) under angiographic control. (B) Unusual case of a small leiomyosarcoma in the IVC found incidentally. Normally they are larger, presenting with symptoms of IVCobstruction.
ch08.qxd 6/30/04 6:15 PM Page 203

Myelolipoma
The adrenal myelolipoma is found, uncommonly,as an incidental mass. It is highly echogenic andwell-defined, due to its fatty content (Fig. 8.8C).These are relatively rare, require no furthermanagement, and are endocrinologically non-functioning.
Phaeochromocytoma
The phaeochromocytoma is uncommon, but maybe found in up to 1% of patients with hypertension.It is a tumour arising in the chromaffin cells of theadrenal medulla (most commonly) or in autonomicnervous tissue. It may be bilateral and appears solidon ultrasound, although larger masses may have
ABDOMINAL ULTRASOUND204
A B
IVC
C
Medial wing
Lateral wing Medulla
Cortex
C D
E
RK
LK
c
Figure 8.7 (A) Right adrenal. The medial (anterior arrow) and lateral (posterior arrow) wings of the gland lie justanterior to the crus, C. (B) The medial ridge of the right adrenal (arrows) is seen anterior to the diaphragmatic crus(arrowheads) and posterior to the IVC. (C) Transverse right adrenal (arrow) between the IVC and crus (arrowheads).(D) The two hypoechoic wings of the left adrenal (arrows) can be seen in the space between the spleen, left kidney (LK)and the crus, c. (The dynamic range has been reduced to appreciate the gland better.) (E) Section through the rightadrenal gland.
ch08.qxd 6/30/04 6:15 PM Page 204
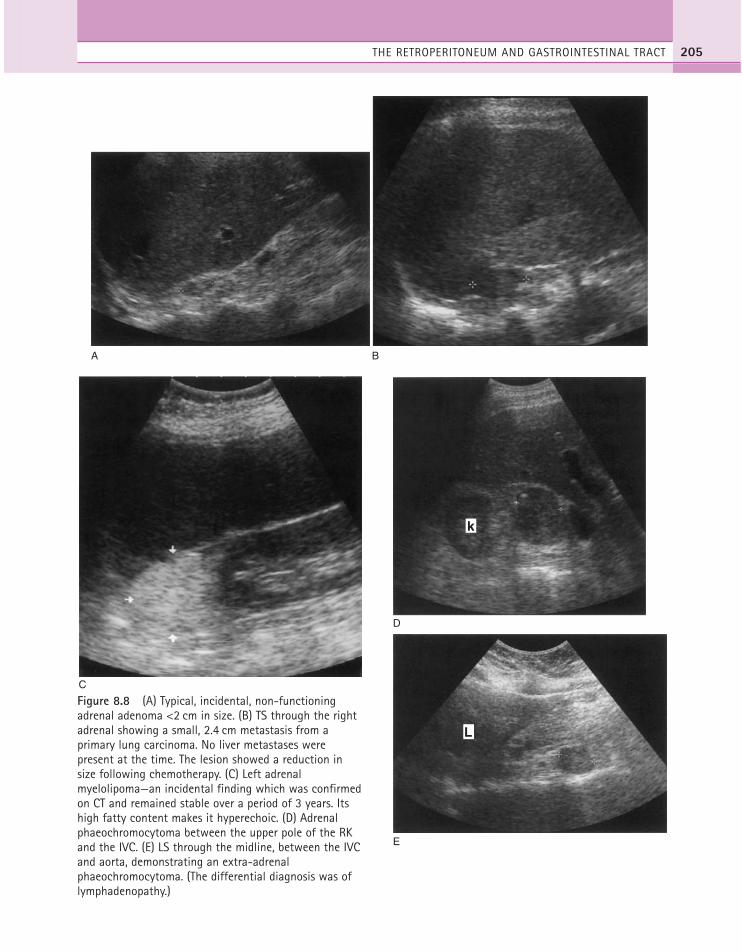
THE RETROPERITONEUM AND GASTROINTESTINAL TRACT 205
A B
C
D
k
E
L
Figure 8.8 (A) Typical, incidental, non-functioningadrenal adenoma <2 cm in size. (B) TS through the rightadrenal showing a small, 2.4 cm metastasis from aprimary lung carcinoma. No liver metastases werepresent at the time. The lesion showed a reduction insize following chemotherapy. (C) Left adrenalmyelolipoma—an incidental finding which was confirmedon CT and remained stable over a period of 3 years. Itshigh fatty content makes it hyperechoic. (D) Adrenalphaeochromocytoma between the upper pole of the RKand the IVC. (E) LS through the midline, between the IVCand aorta, demonstrating an extra-adrenalphaeochromocytoma. (The differential diagnosis was oflymphadenopathy.)
ch08.qxd 6/30/04 6:15 PM Page 205

ABDOMINAL ULTRASOUND206
areas of necrosis within them. Most are benign, but5–10% are malignant. It presents on a backgroundof episodic, severe hypertension and the urine con-tains catecholamines. (Although this is also a fea-ture of adrenal neuroblastoma, the latter ispredominantly a childhood tumour.) These lesionsshould be treated with great care—vigorous palpa-tion may precipitate a severe hypertensive episodeand biopsy should therefore be avoided.
Although most phaeochromocytomas arise in theadrenal glands, and are therefore demonstrable onultrasound, those arising in the sympathetic chainmay be obscured by bowel gas and are not possibleto exclude on ultrasound (Fig. 8.8D, E). If thereremains biochemical evidence of phaeochromo-cytoma in the presence of normal adrenal glands,a Meta-Iodobenzylguanidine isotope scan willdemonstrate increased activity in a phaeochromo-cytoma and CT scan can then be targeted to theappropriate area.
Phaeochromocytomas are also associated withvon Hippel–Lindau syndrome.
Adrenal carcinoma
Primary adrenal carcinomas are rare in the adult.They are commonly endocrinologically inactive inadults, and therefore tend to present late whenthey are quite large. They may invade the IVC andmetastasize to the liver. Surgical removal oftumours in the absence of liver metastases has agood prognosis9 and, in patients with metastases,radiofrequency ablation of the adrenal mass mayhave some benefit in prolonging survival.10
GASTROINTESTINAL (GI) TRACT
Contrast radiographic investigations, including CT,are generally accepted as the methods of choice forinvestigating diseases of the GI tract. Although ultra-sound is not considered a primary tool in the inves-tigation of bowel lesions, as the gas-filled lumenmakes visualization difficult in many cases, ultra-sound is remarkably successful in diagnosing GItract pathology in the hands of an experienced oper-ator. GI tract ultrasound can be time-consuming,but a wealth of information can be obtained with ahigh-frequency linear probe in a symptomatic
patient. Considerable diagnostic benefit has beenshown for careful, targeted, percutaneous ultrasoundof the large and small GI tract using high-frequencytransducers.11
It is important to be aware of the variable ultra-sound appearances of normal bowel, as it may beresponsible for mimicking other pathology.Normal bowel is frequently difficult to examine onultrasound as the gas-filled lumen reflects thesound, requiring careful compression techniques.Abnormal bowel is particularly accessible to ultra-sound, however. A fluid-filled lumen also makeeasy the demonstration of valvulae conniventes ofthe small bowel and haustra of the large colon.
Oesophagus and stomachThe oesophagus is not usually accessible to percuta-neous ultrasound; however, the lower end can bedemonstrated as it passes through the diaphragm inthe midline, just anterior to the aorta (Fig. 8.9A).Its normal appearances should not be confused witha mass. Occasionally, ultrasound demonstrates thethickened wall associated with an oesophageal carci-noma involving the lower oesophagus (Fig. 8.9B).
Endoscopic ultrasound (EUS), with its high fre-quency and proximity to the relevant structures, isable to demonstrate the layers of the gut wall, andto demonstrate pathology and accurately stagemalignant disease in both the oesophagus andstomach, and also to guide invasive procedures.12,13
Barium X-ray studies are still the first-line inves-tigation of choice for many potential GI tract con-ditions; however, endoscopy is regarded as thegold standard for investigating the lining of thestomach and duodenum and can be combinedwith biopsy when necessary. Although percuta-neous ultrasound has had modest success in reveal-ing stomach masses if the stomach is filled withwater,14 it can never replace endoscopy. However,if such lesions are discovered, this helps to directsubsequent radiological management (Fig. 8.10).
AppendixAcute appendicitis is a common diagnosis onadmission to the casualty department with rightlower abdominal pain. However around 15–25% of
ch08.qxd 6/30/04 6:15 PM Page 206

patients who undergo laparotomy turn out to havenormal appendices.
The use of ultrasound in the investigation ofacute abdominal pain is well established and canincrease the reliability of the diagnosis of acuteappendicitis when performed by an experiencedoperator.15
The normal appendix is difficult to locate. Ahigh-frequency (7 MHz or more) linear or curvedarray probe is useful. Gentle, graduated compres-sion may move overlying bowel. Raising thepatient’s left side may encourage bowel gas tomove away from the area of interest. The normalappendix is compressible by gentle transducerpressure, which is usually well tolerated by thepatient.
The ultrasound features of acute appendicitisinclude an enlarged, usually hypoechoic appendixgreater than 6 mm in diameter. The inflamedappendix is non-compressible. Attempted com-pression of the acutely inflamed appendix obvi-ously requires great care from the operator.Compression must be very slow and the release ofcompression must be equally as gentle. These fea-tures have a high sensitivity and specificity for acuteappendicitis (74% and 94% respectively).15 Acute
appendicitis often demonstrates hypervascularityon power Doppler.
Other causes for right iliac fassa masses inpatients presenting with pain include inflameddiverticula in patients with diverticulitis.16
Perforation of the appendix may result in ademonstrable periappendiceal fluid collection, orfree fluid plus or minus dilated loops of non-peri-staltic small bowel. The presence of an ill-definedfluid mass in the right iliac fossa of a symptomaticpatient is highly suggestive of acute appendicitiswith perforation (Fig. 8.11). This may becomeinfected, leading to peritonitis.
Occasionally, a hyper-reflective appendicolithmay be seen in the blind end of the inflamedappendix, casting an acoustic shadow.
Mesenteric ischaemiaMesenteric ischaemia is a potentially lethal condi-tion, associated with atherosclerosis of the mesen-teric vessels, which can cause bowel necrosis anddeath if left untreated. It is a difficult diagnosis tomake on clinical grounds because the symptomsare varied and non-specific, including acuteabdominal pain following meals, diarrhoea and
THE RETROPERITONEUM AND GASTROINTESTINAL TRACT 207
A B
Figure 8.9 (A) Normal oesophagus between the aorta and the left lobe of the liver—thin, hypoechoic walls with ahyperechoic lumen due to the presence of air. (B) Thickened walls of the oesophagus in a carcinoma involving thelower oesophagus.
ch08.qxd 6/30/04 6:15 PM Page 207

subsequent weight loss. Patients frequently undergoa number of comparatively invasive investigationsbefore a diagnosis is reached, and this delay increasesthe mortality and morbidity of the condition.17,18
Treatment involves restoring the blood flow viaangioplasty or surgery and, if necessary, resectingsegments of necrosed bowel.
Atherosclerosis may be demonstrated in theSMA in a number of cases. Signs of occlusion orstenosis of the SMA may be identified with colouror power Doppler19 as a filling defect within thelumen of the vessel. However, significant stenoseshave been diagnosed with Doppler in a relativelyhigh percentage (18%) of the asymptomatic, eld-erly population. The finding of a stenosis on ultra-sound, therefore, is an indication for further
imaging in symptomatic patients, rather than anabsolute indicator of mesenteric ischaemia.20
In a normal patient, the response of the SMA tofood can be demonstrated as an increase in enddiastolic flow velocities (Fig. 8.12).
Mesenteric compromise has also been associ-ated with an abnormal postprandial response;Doppler waveforms of the SMA have decreasedpeak systolic and end diastolic velocities afterfood.21
None of these ultrasound signs and appearancesare specific for mesenteric ischaemia; the mesen-tery is supplied by three arteries which cannot allbe evaluated with ultrasound and, in addition,numerous other conditions are associated withaltered SMA Doppler resistance, including inflam-
ABDOMINAL ULTRASOUND208
A
C
B
Figure 8.10 (A) LS through the epigastriumdemonstrating a gastric carcinoma (arrows). (B) TSthrough the epigastrium demonstrating a gastriccarcinoma (arrows). (C) Gastric carcinoma,presenting with altered liver function tests (LFTs).The patient had multiple liver metastases.
ch08.qxd 6/30/04 6:15 PM Page 208

matory bowel conditions, haemorrhage, elevationof venous pressure and cirrhosis.
Inflammatory bowel conditionsBoth barium studies and ultrasound have a usefulrole to play in the management of patients withinflammatory bowel disease. Diagnosis is generallymade with conventional barium X-ray studies, whileultrasound may be used to monitor disease andidentify extraluminal complications of the disease.22
Crohn’s disease is a common cause of inflamma-tion affecting the small bowel and particularly theterminal ileum. It usually presents with pain, diar-rhoea and weight loss. The terminal ileum/ileocae-cal junction is involved in the majority of cases, andthickened, hypoechoic bowel wall can often bedemonstrated in this area.16 Ultrasound may beused to identify complications of Crohn’s disease,screen patients at risk, and monitor patients forrecurrence of disease following surgery.23
Crohn’s disease affects the entire thickness of thebowel wall, and one of the common complicationsis that of intramural abscesses. These can sometimesbe seen within the thickened wall as gas-containing,highly echogenic areas. When large, they may per-forate, resulting in an ill-defined collection of pus,which may be drained percutaneously (Fig. 8.13).
Fistulae are another complication of Crohn’s,and are easier to demonstrate with contrast radio-graphy.
Ulcerative colitis affects the mucosa, rather thanthe whole wall. On ultrasound it produces a thick-ened, stratified hypoechoic wall, unlike Crohn’s, inwhich the entire thickness of the wall is affected.
A wall thickness greater than 3 mm is consid-ered abnormal. Like Crohn’s, small ulcer craterswithin the wall of the colon in ulcerative colitismay appear as hyperechoic gas-filled foci.
Inflammatory bowel diseases increase the perfu-sion of the intestine, decreasing vascular resistance.Hypervascularized bowel wall has been identified
THE RETROPERITONEUM AND GASTROINTESTINAL TRACT 209
A
APP_ENDIX
Measure
7.5L40/3.
B C
Figure 8.11 (A) Acute appendicitis with a thickened,tender wall and an abscess at the distal end.(B) Perforation of the inflamed appendix has resulted inthe presence of intraperitoneal fluid under the liver.(C) Inflamed, fluid-filled appendix containing anappendicolith.
ch08.qxd 6/30/04 6:15 PM Page 209

in both Crohn’s and ulcerative colitis24 comparedwith normal subjects. Doppler of the SMA hasrevealed an increase in flow velocities (both peaksystolic and end diastolic) and a decrease in resist-ance index in numerous types of pathologicalbowel, including Crohn’s.25 However the lack ofspecificity limits its use in clinical work.
Changes in resistance index have been found tobe related to the activity of Crohn’s disease,26
which could prove valuable in monitoring patientswith known disease.
Diverticulitis may also be recognized on ultra-sound as outpouchings from the bowel wall, mostcommonly affecting the sigmoid colon11 (Fig.8.13C). Perforation of a diverticulum may give riseto a diverticular abscess, although the presence of airmakes ultrasound limited in its evaluation of thiscondition.
Malignant tumoursThe most common site for a bowel tumour in theadult is around the caecum. It is useful to targetthis area in patients with altered bowel habit inwhom bowel carcinoma is suspected, althoughdetection with ultrasound is usually incidental.
The mass tends to be hypoechoic, or of mixedechogenicity, with a small, eccentric, gas-filledlumen. This cannot be differentiated, however,from an inflammatory mass on ultrasound. Vigo-rous Doppler flow can usually be visualized inboth inflammatory and malignant masses (Fig.8.14).
The finding of a colonic mass would normallyprompt a barium enema, to delineate the nature,extent and position of the mass, with subsequentstaging by CT if malignancy is confirmed. Theadvantage of ultrasound over barium enema is thatof displaying the tumour itself, rather than just thenarrowed lumen.
The role of ultrasound in patients with knownbowel carcinoma is to identify and document thepresence of distant metastases, particularly in theliver, as metastases from colorectal carcinoma areparticularly amenable to curative resection.
Bowel tumours should be considered in the listof differential diagnoses when the origin of a massdiscovered on ultrasound is unclear.
Endosonography may be used to detect andstage rectal cancers, although it is only able todemonstrate perirectal nodes and cannot evaluatedistant disease. Endosonography is ideal however,
ABDOMINAL ULTRASOUND210
A B
SMA
POST P
Figure 8.12 (A) Normal spectral waveform from the SMA in a fasting patient is highly pulsatile with little or no end-diastolic flow (EDF) and reverse flow in early diastole. (B) Postprandially, the waveform becomes much less pulsatile,with low resistance and good EDF.
ch08.qxd 6/30/04 6:15 PM Page 210
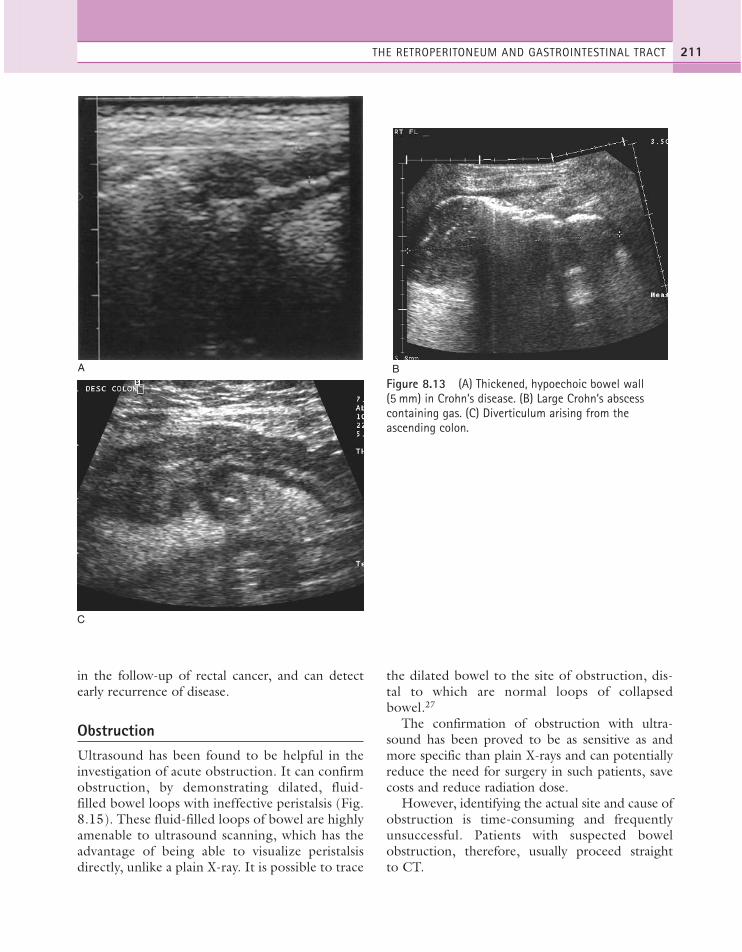
in the follow-up of rectal cancer, and can detectearly recurrence of disease.
ObstructionUltrasound has been found to be helpful in theinvestigation of acute obstruction. It can confirmobstruction, by demonstrating dilated, fluid-filled bowel loops with ineffective peristalsis (Fig.8.15). These fluid-filled loops of bowel are highlyamenable to ultrasound scanning, which has theadvantage of being able to visualize peristalsisdirectly, unlike a plain X-ray. It is possible to trace
the dilated bowel to the site of obstruction, dis-tal to which are normal loops of collapsedbowel.27
The confirmation of obstruction with ultra-sound has been proved to be as sensitive as andmore specific than plain X-rays and can potentiallyreduce the need for surgery in such patients, savecosts and reduce radiation dose.
However, identifying the actual site and cause ofobstruction is time-consuming and frequentlyunsuccessful. Patients with suspected bowelobstruction, therefore, usually proceed straightto CT.
THE RETROPERITONEUM AND GASTROINTESTINAL TRACT 211
A B
C
Figure 8.13 (A) Thickened, hypoechoic bowel wall (5 mm) in Crohn’s disease. (B) Large Crohn’s abscesscontaining gas. (C) Diverticulum arising from theascending colon.
ch08.qxd 6/30/04 6:15 PM Page 211

OTHER RETROPERITONEALABNORMALITIES
Ultrasound is successful in identifying retroperi-toneal masses, but CT and MRI are more effectiveat establishing the extent and nature of many ofthese masses, particularly those partly obscured bygas-filled bowel.
The majority of malignant retroperitonealtumours are renal or adrenal in origin. Other pri-mary tumours, apart from lymphomas, are rare,and include liposarcoma and leiomyosarcoma.These tend to be large when they present, and ofvariable/complex ultrasound appearance. Encase-ment of major vessels by tumour is a further char-acteristic of the retroperitoneal origin of the mass,together with anterior displacement of structuressuch as the pancreas, kidneys, aorta and IVC.
Ultrasound is also able to identify peritoneal andomental deposits in patients with late-stage carci-noma. These are particularly amenable to diagno-sis when surrounded by ascites (Fig. 8.16) andusually arise from gynaecological or urologicaltumours.
Benign retroperitoneal masses identifiable onultrasound include haematomas, psoas abscesses,lymphadenopathy (Fig. 8.17) and pancreaticpseudocysts.
ABDOMINAL ULTRASOUND212
Figure 8.15 Dilated, fluid-filled loops of bowel as aresult of an obstructing caecal carcinoma. Ascites is alsopresent.
A B
Figure 8.14 (A) Hypoechoic, caecal carcinoma. The eccentrically thickened bowel wall is demonstrated with a narrow,hyperechoic lumen (arrow). (B) Caecal carcinoma presenting as a mass in the right iliac fossa.
ch08.qxd 6/30/04 6:15 PM Page 212

A B
Figure 8.17 (A) Enlarged lymph node anterior to the aorta (arrow). (B) Lymphadenopathy may be the cause ofobstructive jaundice.
THE RETROPERITONEUM AND GASTROINTESTINAL TRACT 213
A
B
C
Figure 8.16 (A) Late-stage breast carcinomademonstrates abdominal ascites with a hyperechoicomental cake of metastatic deposit in the left upperquadrant (LUQ). (B) A large, irregular omental depositfrom ovarian carcinoma was palpable during the scan.(C) Retroperitoneal metastases from a teratoma.
ch08.qxd 6/30/04 6:15 PM Page 213

1. Russel JGB. 1990 Is screening for abdominal aorticaneurysms worthwhile? Clinical Radiology 41:182–184.
2. Scott RAP, Wilson NM, Ashton HA, Kay DN. 1995Influence of screening on the incidence of rupturedabdominal aortic aneurysm: 5-year results of arandomized controlled study. British Journal ofSurgery 82: 1066–1070.
3. Fisher D, Lord R. 2003 Does ultrasound screeningfor abdominal aortic aneurysm improve mortality inmen over 65? Journal of Family Practitioners 52: 272.
4. Mingoli A, Cavallaro A, Sapienza P et al. 1996International registry of inferior vena cavaleiomyosarcoma: analysis of a world series on 218patients. Anticancer Research 16: 3201–3205.
5. Singh-Panghaal S, Karcnik TJ, Wachsberg RH, BakerSR. 1997 Inferior vena caval leiomyosarcoma:diagnosis and biopsy with colour Doppler sonography.Journal of Clinical Ultrasound 25: 275–278.
6. Marchal G, Gelin J, Verbeken E et al. 1986 High-resolution real-time sonography of the adrenal glands.Journal of Ultrasound in Medicine 5: 65–68.
7. Bates JA, Irving HC. 1989 Adrenal sonography.Electro Medica 2: 70–75.
8. Kasperlik-Zaluska AA, Rosslonowska E, Slowinska-Srzednicka J et al. 1997 Incidentally discoveredadrenal mass (incidentaloma): investigation andmanagement of 208 patients. Clinical Endocrinology46: 29–37.
9. Ng L, Libertino JM. 2003 Adrenocortical carcinoma:diagnosis, evaluation and treatment. Journal ofUrology 169: 5–11.
10. Wood BJ, Abraham J, Hvizda JL et al. 2003 Radio-frequency ablation of adrenal tumours and adreno-cortical carcinoma metastases. Cancer 1: 554–560.
11. O’Malley M, Wilson S. 2003 Ultrasound ofgastrointestinal tract abnormalities with CTcorrelation. Radiographics 23: 59–72.
12. Dye CE, Waxman I. 2002 Endoscopic ultrasound.Gastroenterologic Clinics of North America 31:863–879.
13. Yong AA, Roberts SA. 2003 Interventionalendoscopic ultrasound. Clinical Radiology 58: 32–43.
14. Tous F, Busto M. 1997 Assessment of abdominalsonography in the diagnosis of tumours of thegastroduodenal tract. Journal of Clinical Ultrasound25: 243–247.
15. Zeidan BS, Wasser T, Nicholas GG. 1997Ultrasonography in the diagnosis of acuteappendicitis. Journal of the Royal College of Surgeonsof Edinburgh 42: 24–26.
16. McLoughlin RF, Downey DR, Rizkalla KS. 1996Sonography of intestinal abnormality in the right iliacfossa. American Journal of Roentgenology 167:1473–1476.
17. Deehan DJ, Heys SD, Brittenden J, Eremin O. 1995Mesenteric ischaemia: prognostic factors and influenceof delay upon outcome. Journal of the Royal Collegeof Surgeons of Edinburgh 40: 112–115.
18. Hoogenburg K, Van-Essen LH, Van Den DungenJJAM et al. 1995 Chronic mesenteric ischaemia:diagnostic challenges and treatment options. Journalof Internal Medicine 237: 293–299.
19. Danse EM, Van Beers BE, Goffette P et al. 1996Acute intestinal ischaemia due to occlusion of thesuperior mesenteric artery: detection with Dopplersonography. Journal of Ultrasound in Medicine 15:323–326.
20. Roobottom CA, Dubbins PA. 1993 Significantdisease of the celiac and superior mesenteric arteries inasymptomatic patients: predictive value of Dopplersonography. American Journal of Roentgenology 161:985–988.
21. Nichols S, Windeler H. 1995 Duplex scanning indiagnosis of mesenteric insuficiency. Journal ofDiagnostic Medical Sonographers 11: 120–127.
22. Carucci LR, Levine MS. 2002 Radiographic imagingof inflammatory bowel disease. GastroenterologyClinics of North America 31: 93–117.
23. Andreoli A, Cerro P, Flasco G. 1998 Role ofultrasonography in the diagnosis of postsurgicalrecurrence of Crohn’s disease. American Journal ofGastroenterology 93: 1117–1121.
24. Heyne R, Rickes S, Bock P et al. 2002 Non-invasiveevaluation of activity in inflammatory bowel diseaseby Doppler sonography. Zeitschrift fürGastroenterologie 40: 171–175.
25. Erden A, Cumhur T, Olcer T. 1997 Superiormesenteric artery Doppler waveform changes inresponse to inflammation of the ileocecal region.Abdominal Imaging 22: 483–486.
26. Van Oostayen JA, Wasser MNJM, Van Hogezand RAet al. 1997 Doppler sonography evaluation of superiormesenteric artery flow to assess Crohn’s disease activity:correlation with clinical evaluation, Crohn’s diseaseactivity index and alpha-1-antitrypsin clearance in feces.American Journal of Roentgenology 168: 429–433.
27. Ogata M, Mateer JR, Condon RE. 1996 Prospectiveevaluation of abdominal sonography for the diagnosisof bowel obstruction. Annals of Surgery 223:237–241.
ABDOMINAL ULTRASOUND214
References
ch08.qxd 6/30/04 6:15 PM Page 214

Ultrasound of the paediatric abdomen requiresdifferent techniques and skills from those used inthe adult. Although there are a few situations inwhich knowledge of adult pathology can beapplied to the paediatric patient, the child cannotsimply be considered a mini-version of an adult.The presenting symptoms and pathologicalprocesses in the child are generally quite differentfrom those in adults and the operator must befully aware of the special considerations of the pae-diatric patient in terms of both diagnosis and tech-nique. This chapter addresses only the mostcommon paediatric situations likely to be encoun-tered in a general department, and further special-ist paediatric reading is recommended. (See thegeneral reading list at the end of this chapter.)
Techniques
The operator can minimize any distress to thechild, and make the examination considerably eas-ier and quicker, in numerous ways.
● The ultrasound environment should be asfriendly as possible, with appropriate decorationsand toys, and should always be kept warm(nothing is more likely to make your patientuncooperative than cold gel). Minimize the timethe child spends in the scanning room by havingeverything ready first. Small children maybenefit from seeing a video of a scan beforehandand being reassured that it will not hurt.
● Most children find it reassuring to be accom-panied by their carer during the examination.
Chapter 9
The paediatric abdomen
215
CHAPTER CONTENTS
Hepatobiliary pathology 216Pancreas 220
Normal appearances 220Pathology of the pancreas 220
Urinary tract 221Normal appearances 221Anatomical variants and pathology 221
Adrenal glands 232Normal appearances 232
Gastrointestinal tract 232
ch09.qxd 6/30/04 6:17 PM Page 215

● Separate facilities, such as a dedicatedchildren’s waiting area, are preferable and morereassuring for the child.
● The equipment should incorporate a range ofhigh-frequency (5–15 MHz) transducers withsmall as well as conventional footprints. A smallcurvilinear transducer is useful for mostabdominal work and a high-frequency linearprobe is essential for bowel sonography andassessment of the acute abdomen. Transducerswith a dynamic frequency facility are anexcellent choice, as it is easy to switch to thehighest possible frequency without having tochange the transducer. The use of more thanone transducer, that is, both curvilinear andlinear, may be necessary, particularly in theassessment of the acute abdomen.
● A cine facility on the ultrasound machine isinvaluable, and cuts down scanning time.Colour Doppler is essential in the assessmentof hepatobiliary problems and the examinationof the acute abdomen.
● Generally speaking it is necessary to employ afast frame rate. (The smaller field of viewneeded for children allows the line density toremain high, maintaining adequate resolution.)
HEPATOBILIARY PATHOLOGY
Cystic fibrosis
Cystic fibrosis (CF) is a common, autosomal reces-sive multisystem disease. The main organs affectedare the lungs, liver and pancreas. Accumulation ofmucus in the bronchi rapidly leads to respiratoryproblems including infections, with a predispositionto abscess formation with destruction of the termi-nal bronchioles developing into bronchiectasis.
Pancreatic insufficiency, requiring enzyme sup-plements, is a feature of CF, with gradual fattyreplacement and subsequent fibrosis of pancreatictissue, resulting in increased echogenicity of thepancreatic parenchyma. The pancreas is generallyreduced in size. Cysts, calcification and ductaldilatation may also be found.1 Advances in themanagement of pulmonary problems associatedwith CF have led to longer survival and a subse-quent increase in the prevalence of chronic liver
disease. Annual ultrasound examination is recom-mended as sonographic changes may be identifiedin the absence of abnormality on biochemicalassessment.2 The liver may be hyperechoic andthe texture becomes coarse and nodular asfibrosis develops (Fig. 9.1). Increased periportalechogenicity may be demonstrated. Eventually cir-rhosis develops, causing portal hypertension.Assessment of the portal venous system withcolour and spectral Doppler is useful, providing abaseline with which to compare progression of thedisease.
The gallbladder is small in up to one-third ofpatients3 (Fig. 9.1E). This microgallbladder meas-ures less than 3 × 1 × 1 cm after fasting and is filledwith mucus. Up to 10% of patients with CF mayhave gallstones; cholecystitis and biliary stricturesmay occur.
Neonatal cholestasis and biliary atresia
Neonatal hepatitis and biliary atresia are the mostcommon causes of neonatal cholestasis, presentingaround the age of 4 weeks with neonatal jaundice,dark urine and pale stools. Early diagnosis of biliaryatresia and differentiation from hepatitis and othercauses of neonatal cholestasis is crucial to success-ful treatment. The aetiology of biliary atresiaremains unclear but progressive inflammation,destruction and fibrosis of the biliary tree occurs,resulting in obliteration of all or part of the bileducts and gallbladder, with the subsequent devel-opment of biliary cirrhosis.4
The ultrasonic features of neonatal hepatitis andbiliary atresia overlap. The gallbladder is generallysmall and thick-walled or absent in biliary atresia,but may occasionally appear normal,5 whereas inhepatitis the gallbladder, although often normal insize, may be difficult to visualize. The presence orabsence of a gallbladder is not a reliable sign of bil-iary atresia. In cases of biliary atresia where only thehepatic duct is atretic (that is, with a normal gall-bladder and common duct), the gallbladder canappear normal in size and contract postprandially.The liver may appear normal but in more severecases the liver parenchyma shows increasedechogenicity due to developing cirrhosis. The intra-and extrahepatic biliary tree is not dilated,although occasionally small choledochal cysts or
ABDOMINAL ULTRASOUND216
ch09.qxd 6/30/04 6:17 PM Page 216
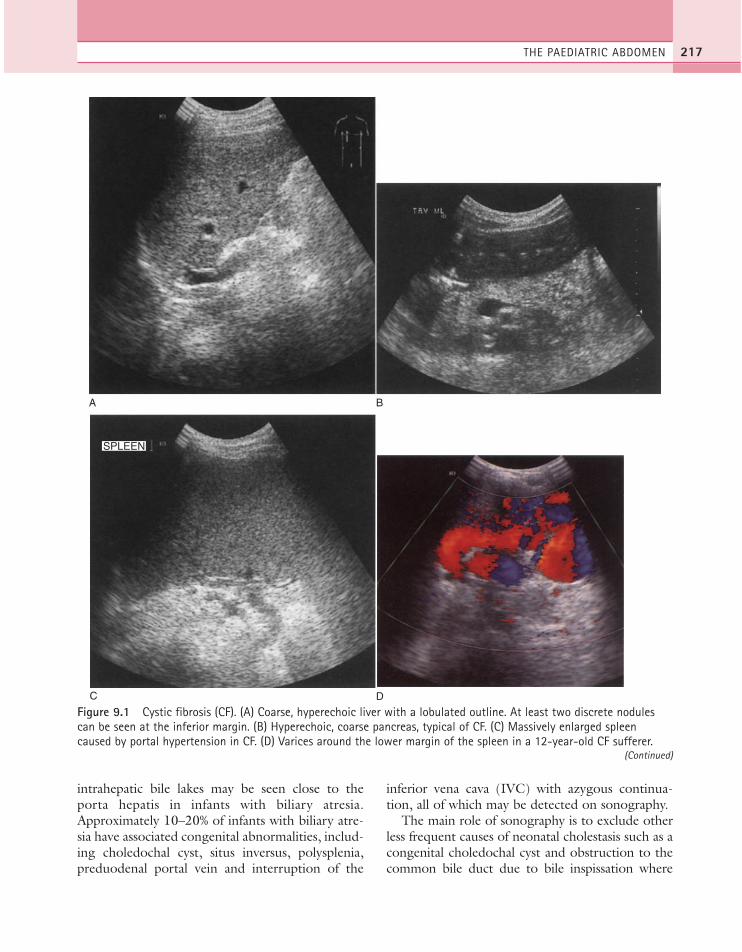
intrahepatic bile lakes may be seen close to theporta hepatis in infants with biliary atresia.Approximately 10–20% of infants with biliary atre-sia have associated congenital abnormalities, includ-ing choledochal cyst, situs inversus, polysplenia,preduodenal portal vein and interruption of the
inferior vena cava (IVC) with azygous continua-tion, all of which may be detected on sonography.
The main role of sonography is to exclude otherless frequent causes of neonatal cholestasis such as acongenital choledochal cyst and obstruction to thecommon bile duct due to bile inspissation where
THE PAEDIATRIC ABDOMEN 217
A
SPLEEN
B
C D
Figure 9.1 Cystic fibrosis (CF). (A) Coarse, hyperechoic liver with a lobulated outline. At least two discrete nodulescan be seen at the inferior margin. (B) Hyperechoic, coarse pancreas, typical of CF. (C) Massively enlarged spleencaused by portal hypertension in CF. (D) Varices around the lower margin of the spleen in a 12-year-old CF sufferer.
(Continued)
ch09.qxd 6/30/04 6:17 PM Page 217
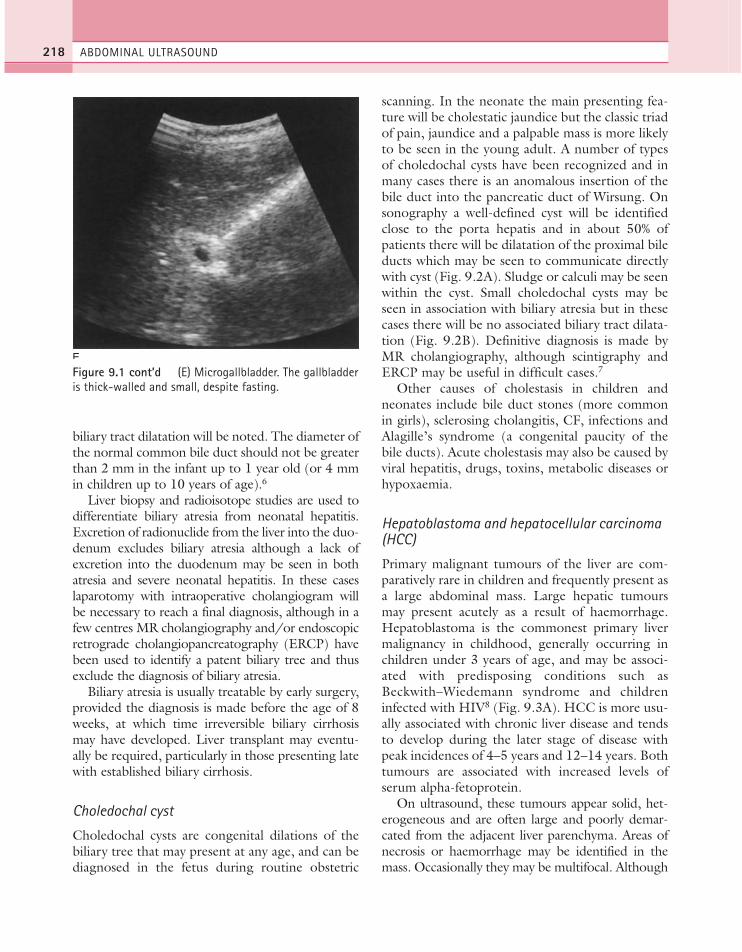
biliary tract dilatation will be noted. The diameter ofthe normal common bile duct should not be greaterthan 2 mm in the infant up to 1 year old (or 4 mmin children up to 10 years of age).6
Liver biopsy and radioisotope studies are used todifferentiate biliary atresia from neonatal hepatitis.Excretion of radionuclide from the liver into the duo-denum excludes biliary atresia although a lack ofexcretion into the duodenum may be seen in bothatresia and severe neonatal hepatitis. In these caseslaparotomy with intraoperative cholangiogram willbe necessary to reach a final diagnosis, although in afew centres MR cholangiography and/or endoscopicretrograde cholangiopancreatography (ERCP) havebeen used to identify a patent biliary tree and thusexclude the diagnosis of biliary atresia.
Biliary atresia is usually treatable by early surgery,provided the diagnosis is made before the age of 8weeks, at which time irreversible biliary cirrhosismay have developed. Liver transplant may eventu-ally be required, particularly in those presenting latewith established biliary cirrhosis.
Choledochal cyst
Choledochal cysts are congenital dilations of thebiliary tree that may present at any age, and can bediagnosed in the fetus during routine obstetric
scanning. In the neonate the main presenting fea-ture will be cholestatic jaundice but the classic triadof pain, jaundice and a palpable mass is more likelyto be seen in the young adult. A number of typesof choledochal cysts have been recognized and inmany cases there is an anomalous insertion of thebile duct into the pancreatic duct of Wirsung. Onsonography a well-defined cyst will be identifiedclose to the porta hepatis and in about 50% ofpatients there will be dilatation of the proximal bileducts which may be seen to communicate directlywith cyst (Fig. 9.2A). Sludge or calculi may be seenwithin the cyst. Small choledochal cysts may beseen in association with biliary atresia but in thesecases there will be no associated biliary tract dilata-tion (Fig. 9.2B). Definitive diagnosis is made byMR cholangiography, although scintigraphy andERCP may be useful in difficult cases.7
Other causes of cholestasis in children andneonates include bile duct stones (more commonin girls), sclerosing cholangitis, CF, infections andAlagille’s syndrome (a congenital paucity of thebile ducts). Acute cholestasis may also be caused byviral hepatitis, drugs, toxins, metabolic diseases orhypoxaemia.
Hepatoblastoma and hepatocellular carcinoma(HCC)
Primary malignant tumours of the liver are com-paratively rare in children and frequently present asa large abdominal mass. Large hepatic tumoursmay present acutely as a result of haemorrhage.Hepatoblastoma is the commonest primary livermalignancy in childhood, generally occurring inchildren under 3 years of age, and may be associ-ated with predisposing conditions such asBeckwith–Wiedemann syndrome and childreninfected with HIV8 (Fig. 9.3A). HCC is more usu-ally associated with chronic liver disease and tendsto develop during the later stage of disease withpeak incidences of 4–5 years and 12–14 years. Bothtumours are associated with increased levels ofserum alpha-fetoprotein.
On ultrasound, these tumours appear solid, het-erogeneous and are often large and poorly demar-cated from the adjacent liver parenchyma. Areas ofnecrosis or haemorrhage may be identified in themass. Occasionally they may be multifocal. Although
ABDOMINAL ULTRASOUND218
E
Figure 9.1 cont’d (E) Microgallbladder. The gallbladderis thick-walled and small, despite fasting.
ch09.qxd 6/30/04 6:17 PM Page 218

the two types of tumour are not distinguishable onultrasound, the clinical history may give a clue andultrasound-guided biopsy can be used to obtain ahistological diagnosis.
Ultrasound is useful in identifying the extent ofthe tumour and, when combined with colour flowDoppler imaging, adjacent vascular invasion can beevaluated. CT or MRI complements the ultra-sound findings and is essential for staging and
assessment of suitability for resection or transplan-tation.9 Chemotherapy may be used to shrink thetumour prior to surgery.
Rhabdomyosarcoma is a rare tumour which mayoriginate in the biliary ducts, causing biliary dilata-tion. It is indistinguishable from other livertumours on ultrasound. Rhabdomyosarcoma orig-inates from muscle cells and is the commonest typeof soft-tissue sarcoma seen in childhood, with a
THE PAEDIATRIC ABDOMEN 219
A B
B
Figure 9.2 (A) Large choledochal cyst at the porta hepatis. (B) Intrahepatic choledochal cysts in biliary atresia withno proximal biliary tract dilatation.
A B
Figure 9.3 (A) A large hepatoblastoma, containing both cystic and solid areas, occupies most of the right lobe of theliver in this 18-month-old girl. (She is undergoing chemotherapy at the time of going to press.) (B) Multiplehypoechoic haemangiomata. Hyperdynamic circulation was noted in the portal vein and hepatic artery on Doppler.These lesions spontaneously regressed, leaving only a solitary haemangioma at the time of going to press.
ch09.qxd 6/30/04 6:17 PM Page 219
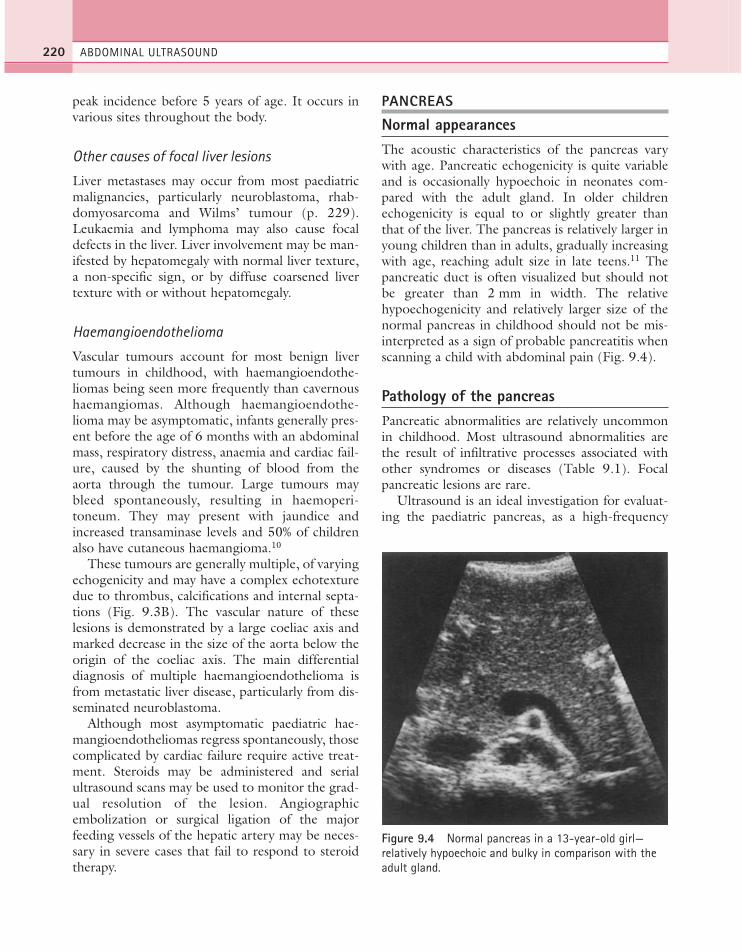
peak incidence before 5 years of age. It occurs invarious sites throughout the body.
Other causes of focal liver lesions
Liver metastases may occur from most paediatricmalignancies, particularly neuroblastoma, rhab-domyosarcoma and Wilms’ tumour (p. 229).Leukaemia and lymphoma may also cause focaldefects in the liver. Liver involvement may be man-ifested by hepatomegaly with normal liver texture,a non-specific sign, or by diffuse coarsened livertexture with or without hepatomegaly.
Haemangioendothelioma
Vascular tumours account for most benign livertumours in childhood, with haemangioendothe-liomas being seen more frequently than cavernoushaemangiomas. Although haemangioendothe-lioma may be asymptomatic, infants generally pres-ent before the age of 6 months with an abdominalmass, respiratory distress, anaemia and cardiac fail-ure, caused by the shunting of blood from theaorta through the tumour. Large tumours maybleed spontaneously, resulting in haemoperi-toneum. They may present with jaundice andincreased transaminase levels and 50% of childrenalso have cutaneous haemangioma.10
These tumours are generally multiple, of varyingechogenicity and may have a complex echotexturedue to thrombus, calcifications and internal septa-tions (Fig. 9.3B). The vascular nature of theselesions is demonstrated by a large coeliac axis andmarked decrease in the size of the aorta below theorigin of the coeliac axis. The main differentialdiagnosis of multiple haemangioendothelioma isfrom metastatic liver disease, particularly from dis-seminated neuroblastoma.
Although most asymptomatic paediatric hae-mangioendotheliomas regress spontaneously, thosecomplicated by cardiac failure require active treat-ment. Steroids may be administered and serialultrasound scans may be used to monitor the grad-ual resolution of the lesion. Angiographicembolization or surgical ligation of the majorfeeding vessels of the hepatic artery may be neces-sary in severe cases that fail to respond to steroidtherapy.
PANCREAS
Normal appearancesThe acoustic characteristics of the pancreas varywith age. Pancreatic echogenicity is quite variableand is occasionally hypoechoic in neonates com-pared with the adult gland. In older childrenechogenicity is equal to or slightly greater thanthat of the liver. The pancreas is relatively larger inyoung children than in adults, gradually increasingwith age, reaching adult size in late teens.11 Thepancreatic duct is often visualized but should notbe greater than 2 mm in width. The relativehypoechogenicity and relatively larger size of thenormal pancreas in childhood should not be mis-interpreted as a sign of probable pancreatitis whenscanning a child with abdominal pain (Fig. 9.4).
Pathology of the pancreasPancreatic abnormalities are relatively uncommonin childhood. Most ultrasound abnormalities arethe result of infiltrative processes associated withother syndromes or diseases (Table 9.1). Focalpancreatic lesions are rare.
Ultrasound is an ideal investigation for evaluat-ing the paediatric pancreas, as a high-frequency
ABDOMINAL ULTRASOUND220
Figure 9.4 Normal pancreas in a 13-year-old girl—relatively hypoechoic and bulky in comparison with theadult gland.
ch09.qxd 6/30/04 6:17 PM Page 220

probe demonstrates excellent detail. A water-baseddrink may be given to provide an acoustic window.In cases of blunt injury to the abdomen with sus-pected pancreatic damage, CT is the imagingmodality of choice in the acute situation, althoughsonography should be used during follow-up todetect the presence of a pseudocyst.
URINARY TRACT
Ultrasound is the first line of investigation in bothantenatally detected abnormalities and in sympto-matic children.
● The bladder should be scanned first, as voidingmay often occur during the examination.
● Measurements of both kidneys, either lengthor renal volume, should be taken to highlightany difference in size and to provide a baselinefor further growth comparison.
● A variety of planes can be used to view thekidneys in children. Often a posterior approachis best for obtaining an accurate bipolar length.
● Ensure that renal pelvic dilatation is notphysiological, by rescanning postmicturition.
● Measure the anteroposterior diameter of anyrenal pelvic dilatation in transverse sectionthrough the renal hilum.
● Always scan the bladder immediately aftermicturition, paying attention to the uretericorifice and looking for any ureteric or renaldilatation which may suggest reflux. Measureany residual volume.
● Colour Doppler may be helpful in identifyingthe ureteric orifice, by locating the jets of urineentering the bladder (Fig. 9.10D).
Normal appearancesAfter birth the renal cortex is relatively hyperechoiccompared to the adult kidney, in strong contrast tothe hypoechoic medullary pyramids. The outline ofthe kidney is often lobulated due to a persistentfetal lobulation. The renal pelvis is relativelyhypoechoic, as the fat deposition seen in the adultis not yet present (Fig. 9.5A).
Gradually the cortex becomes less hyperechoicwith age, the corticomedullary differentiationlessens and fat deposition in the renal sinus becomesmore evident. The outline becomes smooth,although fetal lobulations do persist in some adultkidneys.
Normal postnatal growth of the kidneys, in termsof length and volume, is closely related to the height,weight and age of the child. Charts giving normalage- and weight-related values should routinely bereferred to.12 Errors do occur in measurements ofrenal length with a potential error in the order of 1year’s growth.13 Thus follow-up measurements forrenal growth should not be undertaken at intervalsof less than 1 year.
Anatomical variants and pathologyThe duplex system
The duplex system is one of the more commoncongenital anomalies, occurring in up to 9% ofreferrals.14 It stems from aberrant budding ofthe Wolffian duct in utero, and can take a varietyof forms, from complete duplication with twokidneys, each with a separate ureter, to a partialduplication involving the kidney only. Complete
THE PAEDIATRIC ABDOMEN 221
Table 9.1 Paediatric pancreatic abnormalities
Increased echogenicityCystic fibrosis—fatty replacement of the pancreas, calcifications, ectatic
pancreatic duct, coarse texture, cystsPancreatitis—hereditary—trauma (physical abuse, road traffic accident)—congenital anomaly, e.g. choledochal cyst—drug toxicity—viral and parasitic infectionHaemochromatosis—pancreatic fibrosis, iron deposition in liver and pancreasFocal lesionsCysts—isolated congenital cyst—autosomal dominant polycystic disease—von Hippel–Lindau disease—Meckel–Gruber syndromeSolid lesions—primary pancreatic neoplasms are very rare in children
ch09.qxd 6/30/04 6:17 PM Page 221
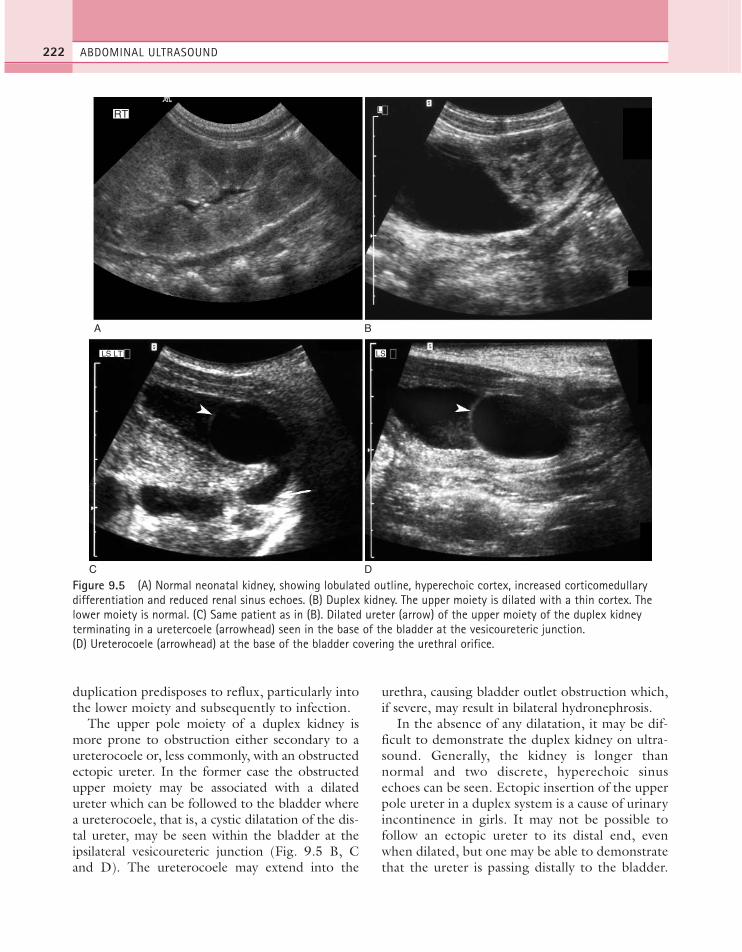
duplication predisposes to reflux, particularly intothe lower moiety and subsequently to infection.
The upper pole moiety of a duplex kidney ismore prone to obstruction either secondary to aureterocoele or, less commonly, with an obstructedectopic ureter. In the former case the obstructedupper moiety may be associated with a dilatedureter which can be followed to the bladder wherea ureterocoele, that is, a cystic dilatation of the dis-tal ureter, may be seen within the bladder at theipsilateral vesicoureteric junction (Fig. 9.5 B, Cand D). The ureterocoele may extend into the
urethra, causing bladder outlet obstruction which,if severe, may result in bilateral hydronephrosis.
In the absence of any dilatation, it may be dif-ficult to demonstrate the duplex kidney on ultra-sound. Generally, the kidney is longer thannormal and two discrete, hyperechoic sinusechoes can be seen. Ectopic insertion of the upperpole ureter in a duplex system is a cause of urinaryincontinence in girls. It may not be possible tofollow an ectopic ureter to its distal end, evenwhen dilated, but one may be able to demonstratethat the ureter is passing distally to the bladder.
ABDOMINAL ULTRASOUND222
A B
C D
RT
LS LT LS
L
Figure 9.5 (A) Normal neonatal kidney, showing lobulated outline, hyperechoic cortex, increased corticomedullarydifferentiation and reduced renal sinus echoes. (B) Duplex kidney. The upper moiety is dilated with a thin cortex. Thelower moiety is normal. (C) Same patient as in (B). Dilated ureter (arrow) of the upper moiety of the duplex kidneyterminating in a uretercoele (arrowhead) seen in the base of the bladder at the vesicoureteric junction.(D) Ureterocoele (arrowhead) at the base of the bladder covering the urethral orifice.
ch09.qxd 6/30/04 6:17 PM Page 222
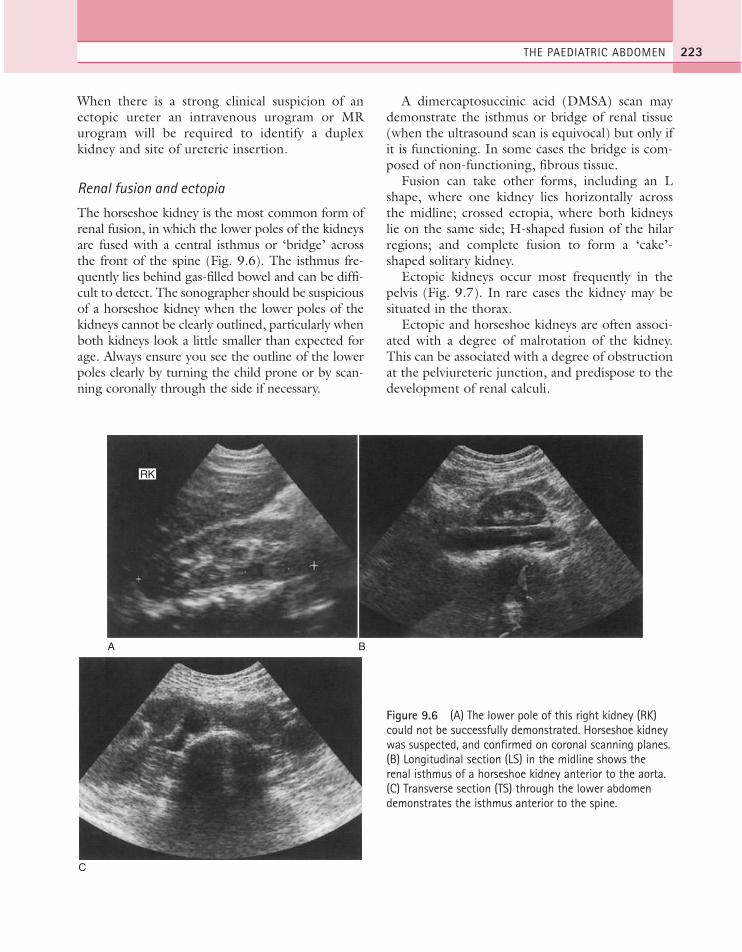
When there is a strong clinical suspicion of anectopic ureter an intravenous urogram or MRurogram will be required to identify a duplexkidney and site of ureteric insertion.
Renal fusion and ectopia
The horseshoe kidney is the most common form ofrenal fusion, in which the lower poles of the kidneysare fused with a central isthmus or ‘bridge’ acrossthe front of the spine (Fig. 9.6). The isthmus fre-quently lies behind gas-filled bowel and can be diffi-cult to detect. The sonographer should be suspiciousof a horseshoe kidney when the lower poles of thekidneys cannot be clearly outlined, particularly whenboth kidneys look a little smaller than expected forage. Always ensure you see the outline of the lowerpoles clearly by turning the child prone or by scan-ning coronally through the side if necessary.
A dimercaptosuccinic acid (DMSA) scan maydemonstrate the isthmus or bridge of renal tissue(when the ultrasound scan is equivocal) but only ifit is functioning. In some cases the bridge is com-posed of non-functioning, fibrous tissue.
Fusion can take other forms, including an Lshape, where one kidney lies horizontally acrossthe midline; crossed ectopia, where both kidneyslie on the same side; H-shaped fusion of the hilarregions; and complete fusion to form a ‘cake’-shaped solitary kidney.
Ectopic kidneys occur most frequently in thepelvis (Fig. 9.7). In rare cases the kidney may besituated in the thorax.
Ectopic and horseshoe kidneys are often associ-ated with a degree of malrotation of the kidney.This can be associated with a degree of obstructionat the pelviureteric junction, and predispose to thedevelopment of renal calculi.
THE PAEDIATRIC ABDOMEN 223
A B
RK
C
Figure 9.6 (A) The lower pole of this right kidney (RK)could not be successfully demonstrated. Horseshoe kidneywas suspected, and confirmed on coronal scanning planes. (B) Longitudinal section (LS) in the midline shows therenal isthmus of a horseshoe kidney anterior to the aorta.(C) Transverse section (TS) through the lower abdomendemonstrates the isthmus anterior to the spine.
ch09.qxd 6/30/04 6:17 PM Page 223

Renal agenesis
The kidneys form from the ureteric bud, whicharises from the pelvic area during the fifth to sixthweek of gestation. The bud undergoes numerousdivisions, forming the ureters, renal pelvis, calycesand renal tubules. Any interruption of this processmay cause renal agenesis or ectopia.
Bilateral renal agenesis is lethal and is usuallydiagnosed prenatally. The incidence of unilateralrenal agenesis is about 1:450 live births and is usu-ally prenatally detected. Ultrasound is useful inconfirming the prenatal diagnosis and excludingthe presence of an ectopic kidney. A DMSA scanconfirms the diagnosis. Renal agenesis is associatedwith VATER syndrome and with ipsilateral gynae-cological anomalies in girls.
Multicystic dysplastic kidney (MCDK)
The MCDK is generally the result of complete,early ureteric obstruction in utero before 10 weeks,and is frequently diagnosed antenatally. The result-ing kidney is non-functioning and contains cysts ofvarying sizes, separated by echogenic ‘dysplastic’renal parenchyma. In general the cysts do not com-municate but occasionally some communicationcan be seen, making differentiation from a severehydronephrosis difficult.
MCDK is usually unilateral and is considered abenign condition, although there is a slight risk of
malignancy and hypertension in later life. The kid-ney gradually involutes and often completely dis-appears (Fig. 9.8A, B). Surgical removal isunnecessary unless symptomatic due to its largesize or is associated with repeated episodes of infec-tion. Provided the contralateral kidney is normal,with good function, the prognosis is good. Thereis, however, an increased risk of associated urinarytract anomalies, such as ureterocoele, vesi-coureteric reflux or contralateral pelviureteric junc-tion obstruction, which may predispose toinfection. These can be demonstrated with ultra-sound and micturating cysto-urethrogram.
A DMSA scan differentiates MCDK, which iscompletely non-functioning, from a grosslyhydronephrotic kidney, a distinction which maysometimes be difficult to make on ultrasound.Follow-up ultrasound scanning is generally advisedin view of the slight increased risk of Wilms’tumour and to monitor the growth of the con-tralateral kidney.
Polycystic disease of the kidneys
Autosomal recessive polycystic disease of the kid-ney (ARPCDK: infantile) may be diagnosed prena-tally. Both kidneys are abnormal, being large andhyperechoic, with loss of corticomedullary differ-entiation (Fig. 9.8C). There is a spectrum of sever-ity of disease and in some cases it may present later
ABDOMINAL ULTRASOUND224
A B
b
Figure 9.7 (A) Pelvic kidney (b = bladder). (B) Dimercaptosuccinic acid (DMSA) scintigraphy shows 33% function inthe smaller, pelvic RK and 66% in the left kidney (LK).
ch09.qxd 6/30/04 6:17 PM Page 224

THE PAEDIATRIC ABDOMEN 225
in childhood with the milder, juvenile form of thedisease. Prenatally the less severe forms appear nor-mal on ultrasound. ARPCDK is associated withhepatic fibrosis and portal hypertension.
Autosomal dominant polycystic disease of the kid-ney (ADPCDK: adult) also has a wide spectrum ofseverity. Although it tends to present later in life, themore severe forms can present in childhood and canoccasionally be diagnosed prenatally. Frank cysts canusually be demonstrated on ultrasound, but may notbe detected until the second or third decade of life.The disease is also associated with cysts in the liverand pancreas, and with intracranial berry aneurysms.
Renal dilatation
Hydronephrosis is frequently detected antenatally,although the cause may be difficult to demonstrate.Dilatation is due either to obstructive uropathy, forexample vesico- or pelviureteric junction obstruction,posterior urethral valves or obstructed upper moietyof a duplex kidney (Fig. 9.9), or it may be non-obstructive, for example due to reflux (Fig. 9.10).
Postnatal ultrasound scans should be performedwhen the infant is more than 4 days old, becausethere is commonly a period of dehydration immedi-ately after birth. This may cause an obstructed orotherwise dilated kidney to appear normal for thefirst few days of life. If normal a follow-up scan is gen-erally recommended at about the age of 6 weeks.
The presence of any calyceal dilatation or uretericdilatation, as opposed to dilatation confined to therenal pelvis, is an important factor to note, indicatinga greater degree of severity. A measurement of theanteroposterior diameter of the dilated intrarenalpelvis is a useful baseline from which to compare sub-sequent follow-up scans (Fig. 9.9D). It should benoted that slight separation of the renal pelvis is anormal finding in the newborn: an anteroposteriorrenal pelvis of 5 mm is the upper limit of normal.
The presence of a baggy, extrarenal pelvis, lessthan 10 mm, without pelvicalyceal system (PCS)dilatation is usually managed conservatively usingultrasound monitoring to demonstrate any increas-ing dilatation. PCS dilatation with a renal pelvicdiameter of between 10 and 20 mm is more serious
A
+ 78
C
B
20.3 mm
Figure 9.8 (A) Multicystic dysplastic kidney. (B) This multicystic dysplastic kidney, diagnosed antenatally, has shrunkto little over 2 cm in length by the age of 1 year. (C) Large, hyperechoic kidneys in a neonate in autosomal recessivepolycystic disease.
ch09.qxd 6/30/04 6:17 PM Page 225
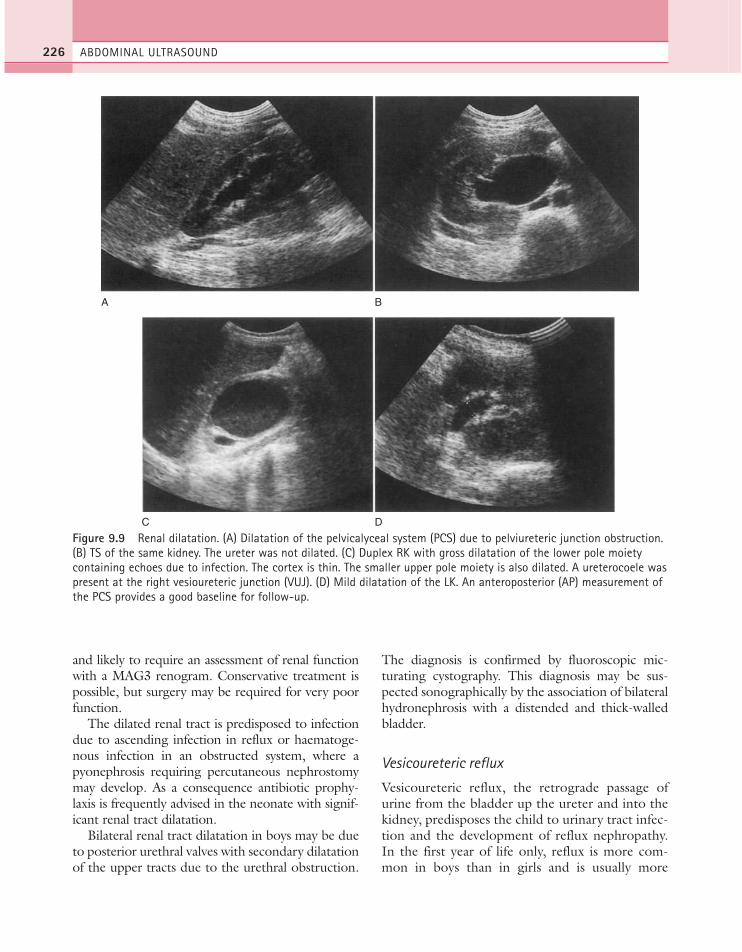
and likely to require an assessment of renal functionwith a MAG3 renogram. Conservative treatment ispossible, but surgery may be required for very poorfunction.
The dilated renal tract is predisposed to infectiondue to ascending infection in reflux or haematoge-nous infection in an obstructed system, where apyonephrosis requiring percutaneous nephrostomymay develop. As a consequence antibiotic prophy-laxis is frequently advised in the neonate with signif-icant renal tract dilatation.
Bilateral renal tract dilatation in boys may be dueto posterior urethral valves with secondary dilatationof the upper tracts due to the urethral obstruction.
The diagnosis is confirmed by fluoroscopic mic-turating cystography. This diagnosis may be sus-pected sonographically by the association of bilateralhydronephrosis with a distended and thick-walledbladder.
Vesicoureteric reflux
Vesicoureteric reflux, the retrograde passage ofurine from the bladder up the ureter and into thekidney, predisposes the child to urinary tract infec-tion and the development of reflux nephropathy.In the first year of life only, reflux is more com-mon in boys than in girls and is usually more
ABDOMINAL ULTRASOUND226
A B
DC
Figure 9.9 Renal dilatation. (A) Dilatation of the pelvicalyceal system (PCS) due to pelviureteric junction obstruction.(B) TS of the same kidney. The ureter was not dilated. (C) Duplex RK with gross dilatation of the lower pole moietycontaining echoes due to infection. The cortex is thin. The smaller upper pole moiety is also dilated. A ureterocoele waspresent at the right vesioureteric junction (VUJ). (D) Mild dilatation of the LK. An anteroposterior (AP) measurement ofthe PCS provides a good baseline for follow-up.
ch09.qxd 6/30/04 6:17 PM Page 226

THE PAEDIATRIC ABDOMEN 227
A B
C D
Figure 9.10 (A) Mild PCS dilatation due to reflux. (B) The right lower ureter is dilated (arrowheads) and urine wasseen to reflux back up the ureter, dilating the kidney. (C) Bilateral reflux (right worse than left) is observed in a TSthrough the base of the bladder. Both ureters (arrows) are seen to dilate intermittently. (D) Compare (C) with a normalpatient, in whom the vesicoureteric junctions can be identified by the presence of jets on colour Doppler. No uretericdilatation can be demonstrated either before or after micturition.
severe.15 Conversely, after the first year of lifereflux is more likely to present in girls and is oftenless severe. Vesicoureteric reflux is a commoncause of hydronephrosis antenatally, accountingfor up to 38% of all prenatal urinary tract dilata-tions, requiring ultrasound follow-up and anti-biotic prophylaxis.16,17
Reflux may either be due to a developmentalanomaly at the vesicoureteric junction, or theresult of a neurogenic bladder, partial outletobstruction or foreign bodies such as calculi andthe presence of a catheter.
Children who have had one or more episodes ofurinary tract infection should be investigated tosearch for an underlying cause and to identify evi-dence of reflux nephropathy (Tables 9.2 and 9.3).Approximately 2% of boys and 8% of girls willdevelop at least one urinary tract infection by 10years of age, requiring investigation, and in mostcentres will account for a substantial proportion ofthe paediatric sonography performed.
Reflux itself is not reliably diagnosed by ultra-sound as it is possible to have intermittent reflux inthe presence of a normal ultrasound scan, with a
(Continued)
ch09.qxd 6/30/04 6:17 PM Page 227

non-dilated urinary tract.17,18 There may be evidenceof thickening of the uroepithelium of the renal pelvisdue to intermittent renal pelvis distension. Uni- orbilateral dilatation may be present to a mild or severedegree and may involve the kidney and/or ureter(Fig. 9.10). It is important to scan the renal pelvesand ureteric orifice immediately after micturition,when intermittent dilatation due to reflux may bedemonstrated on an otherwise normal scan.
When dilatation is seen, the exact cause may beuncertain unless reflux is actually visualized, whichis rare, and micturating cystography is required.
Although most commonly performed convention-ally by fluoroscopy using iodinated contrastmedium, radionuclide cystography and morerecently contrast sonocystography have been usedas an alternative, particularly in the older child.18
The most common complication of reflux is infec-tion and most children present with at least oneepisode of urinary tract infection. This can causerenal scarring. It is important to make the diagnosisof vesicoureteric reflux and renal scarring early inorder to prescribe prophylactic antibiotics in anattempt to avoid the damaging complications causedby reflux of infected urine. The ultrasound appear-ances of scarring include a focal reduction in corticalthickness, irregular outline, interruption of or loss ofthe renal capsule echo or a disruption in the renalarchitecture. Colour flow and power Doppler mayshow triangular areas of decreased or absent bloodflow (and occasionally increased flow) and canimprove the detection rate of focal scarring onsonography.19 These signs can be difficult to demon-strate in young children’s kidneys, particularly whenhighly lobulated, and the most reliable method ofscar detection is a DMSA scan (Fig. 9.10F).
Chronic reflux nephropathy leads to failure ofrenal growth, resulting in a shrivelled, poorlyfunctioning kidney. Measurements of the maximumlength of the kidneys should be routinely performed,and can be related to age, height and weight.12 A dif-ference in renal length of more than 10% between
ABDOMINAL ULTRASOUND228
E F
POSTERIOR
Figure 9.10 cont’d (E) Small, scarred RK, due to reflux. (F) DMSA scan showing bilateral renal scarring due to reflux.Note in particular two wedge-shaped scars in the RK.
Table 9.2 Conditions associated with urinary tractinfection (UTI)
● Vesicoureteric reflux● Obstruction
—pelviureteric junction—vesicoureteric junction—posterior urethral valves—duplex kidney with obstructed moiety/ectopic ureter—ureterocoele
● Other structural anomalies—duplex and/or ectopic renal anatomy—multicystic dysplastic kidney—prune belly syndrome
● Calculi● Neurogenic bladder
ch09.qxd 6/30/04 6:17 PM Page 228
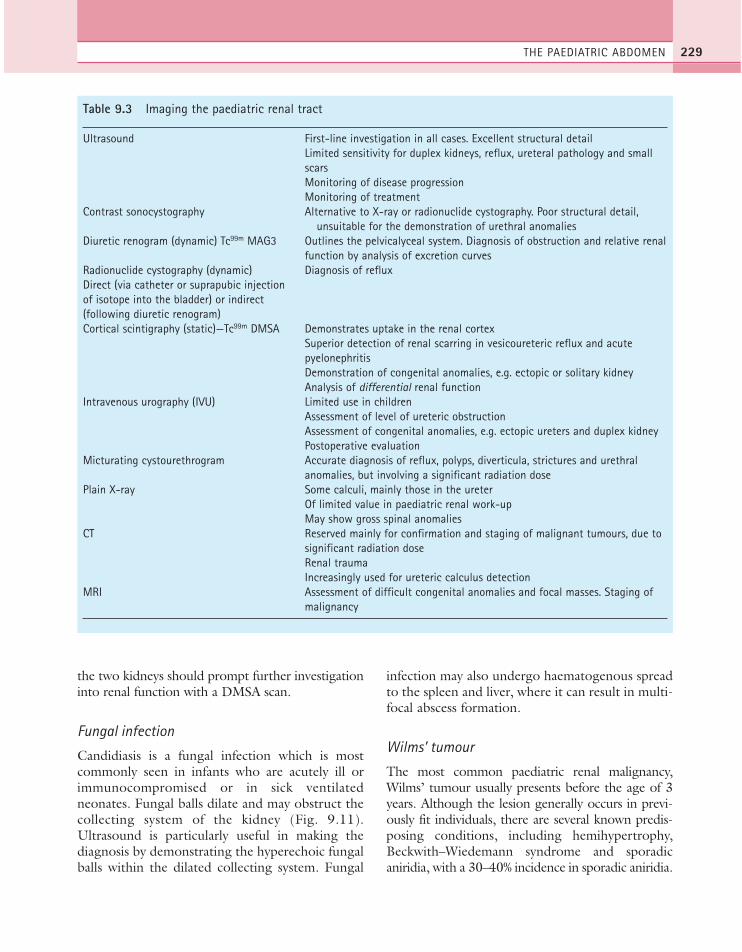
the two kidneys should prompt further investigationinto renal function with a DMSA scan.
Fungal infection
Candidiasis is a fungal infection which is mostcommonly seen in infants who are acutely ill orimmunocompromised or in sick ventilatedneonates. Fungal balls dilate and may obstruct thecollecting system of the kidney (Fig. 9.11).Ultrasound is particularly useful in making thediagnosis by demonstrating the hyperechoic fungalballs within the dilated collecting system. Fungal
infection may also undergo haematogenous spreadto the spleen and liver, where it can result in multi-focal abscess formation.
Wilms’ tumour
The most common paediatric renal malignancy,Wilms’ tumour usually presents before the age of 3years. Although the lesion generally occurs in previ-ously fit individuals, there are several known predis-posing conditions, including hemihypertrophy,Beckwith–Wiedemann syndrome and sporadicaniridia, with a 30–40% incidence in sporadic aniridia.
THE PAEDIATRIC ABDOMEN 229
Table 9.3 Imaging the paediatric renal tract
Ultrasound First-line investigation in all cases. Excellent structural detailLimited sensitivity for duplex kidneys, reflux, ureteral pathology and small scarsMonitoring of disease progressionMonitoring of treatment
Contrast sonocystography Alternative to X-ray or radionuclide cystography. Poor structural detail, unsuitable for the demonstration of urethral anomalies
Diuretic renogram (dynamic) Tc99m MAG3 Outlines the pelvicalyceal system. Diagnosis of obstruction and relative renal function by analysis of excretion curves
Radionuclide cystography (dynamic) Diagnosis of refluxDirect (via catheter or suprapubic injection of isotope into the bladder) or indirect (following diuretic renogram)Cortical scintigraphy (static)—Tc99m DMSA Demonstrates uptake in the renal cortex
Superior detection of renal scarring in vesicoureteric reflux and acute pyelonephritisDemonstration of congenital anomalies, e.g. ectopic or solitary kidneyAnalysis of differential renal function
Intravenous urography (IVU) Limited use in childrenAssessment of level of ureteric obstructionAssessment of congenital anomalies, e.g. ectopic ureters and duplex kidneyPostoperative evaluation
Micturating cystourethrogram Accurate diagnosis of reflux, polyps, diverticula, strictures and urethral anomalies, but involving a significant radiation dose
Plain X-ray Some calculi, mainly those in the ureterOf limited value in paediatric renal work-upMay show gross spinal anomalies
CT Reserved mainly for confirmation and staging of malignant tumours, due to significant radiation doseRenal traumaIncreasingly used for ureteric calculus detection
MRI Assessment of difficult congenital anomalies and focal masses. Staging of malignancy
ch09.qxd 6/30/04 6:17 PM Page 229

The tumours are large at presentation, presentingwith a palpable abdominal mass, and, less frequently,pain, haematuria and fever. About 5% of thesetumours are bilateral.20 The prognosis when unilat-eral is generally good.
The ultrasound appearances are of a relativelywell-defined heterogeneous mass, predominantlysolid but frequently with some necrotic or haem-orrhagic areas, often almost completely replacingthe kidney (Fig. 9.12). Small focal areas of calcifi-cation are seen very occasionally. A search shouldbe made for tumour invasion of the renal vein andIVC which occurs in up to 10% of cases. Tumourinvasion may extend into the right atrium.Occasionally a large, right-sided Wilms’ tumourmay compress the IVC but not invade it; colour orpower Doppler may be useful in the difficult dis-tinction between compression and invasion onultrasound. Ultrasound also identifies associatedlymphadenopathy, particularly in the para-aorticand paracaval regions, and metastatic liver disease.
In a small percentage of cases, tumour may alsobe found in the contralateral kidney. This is usuallymuch smaller than the mass on the presenting sideand may be acoustically subtle. Up to 7% of con-tralateral tumours are missed on preoperativeimaging due to their small size and the operatormust be alert to the possibility of bilateral disease.20
Occasionally a Wilms’ tumour may be found tobe predominantly cystic, having the appearances of
a large, multiloculated cystic mass. The main dif-ferential diagnosis would be of a mesonephric blas-toma occurring during the first year of life andhistology is required to establish the diagnosis.
In most cases, an ultrasound and chest radio-graph are sufficient to diagnose correctly Wilms’tumour but CT of the chest and abdomen is gen-erally used for staging, and to exclude metastaticdisease in the chest and liver.21 Percutaneousbiopsy for confirmation of histological type is gen-erally performed. CT or MRI is more sensitivethan ultrasound scanning in demonstrating smalltumours in the contralateral kidney.
Xanthogranulomatous pyelonephritis
Xanthogranulomatous pyelonephritis results fromchronic infection in an obstructed kidney and chil-dren present with a history of general malaise, low-grade fever and flank pain and may be found to beanaemic. The finding of a palpable abdominal masson examination often leads to an early diagnosis ofa possible Wilms’ tumour. On sonography the kid-ney is diffusely enlarged, with loss of the normalcorticomedullary differentiation. The presence ofcalyceal dilatation with debris and calculi in the col-lecting system and confirmation of urinary infec-tion in addition to the generalized involvement ofthe kidney helps to differentiate this conditionfrom Wilms’ tumour (Fig. 9.12B). Occasionally
ABDOMINAL ULTRASOUND230
A B
LT LT
Figure 9.11 (A) The dilated collecting system of this kidney is filled with a large, rounded fungal ball of candidiasisinfection. (B) The fungus ball is seen to disintegrate, emptying into the renal pelvis.
ch09.qxd 6/30/04 6:17 PM Page 230

CT scanning may also be helpful. The kidney willusually be found to be non-functioning on aDMSA scan and nephrectomy is required.
Renal vein thrombosis (RVT)
RVT primarily occurs in the neonatal period butmay occur in the older child, particularly in associa-tion with renal malignancy and amyloidosis.
Classically the sick neonate is noted to develop grosshaematuria in association with a palpable abdominalmass. RVT is usually unilateral but may be bilateraland is associated with acute adrenal haemorrhagewhen left-sided. Sonographically the affected kidneyis enlarged and globular and develops an inhomo-geneous echogenicity of the renal parenchyma withareas of increased echogenicity due to haemorrhage(Fig. 9.12C). Thrombus may be detected in the
THE PAEDIATRIC ABDOMEN 231
B
LT
A
C
Figure 9.12 (A) Large Wilms’ tumour arising in the left kidney and filling the left flank with a solid, heterogeneousmass. (B) Xanthogranulomatous pyelonephritis was the cause of the renal mass in this 8-year-old boy presenting withanaemia and a flank mass. (C) Renal vein thrombosis in a dehydrated neonate, showing an enlarged ‘globular’ kidneywith loss of the normal corticomedullary differentiation.
ch09.qxd 6/30/04 6:17 PM Page 231

ipsilateral renal vein and IVC and Doppler sonogra-phy shows reduced or absent blood flow in the renalvein and loss of the normal variation in the renalvein waveform. Arterial flow is also decreased. Onfollow-up the kidney may completely recover due tothe development of collateral blood flow or earlyrecanalization of the renal vein, but in severe casesthe kidney may atrophy and calcify.
ADRENAL GLANDS
Normal appearancesIn utero and postnatally, the adrenal glands arelarge, about one-third the size of the kidney, andcomposed mainly of the bulky, hypoechoic fetalcortex which makes up about 80% of the gland.The neonatal adrenal glands are easily demon-strated on ultrasound. The bulky fetal cortex issonographically apparent as a thick hypoechoiclayer surrounding the thinner, hyperechoic adre-nal medulla (Fig. 9.13A). The fetal cortex sur-rounds the smaller, permanent cortex andgradually starts to involute after birth. By the ageof 2–4 months, the adrenal glands have attainedtheir normal adult configuration of the thin,hypoechoic cortex with a tiny layer of hyperechoicadrenal medulla within.
Neuroblastoma
The neuroblastoma is a malignant tumour arisingin the sympathetic chain, most commonly theadrenal medulla. The majority of neuroblastomaspresent before the age of 4 years with a palpableabdominal mass, and many already have metas-tases at the time of presentation to the liver, bonemarrow, skin or lymph nodes. Table 9.4 lists themost frequent abdominal tumours occurring inchildhood.
The tumour is usually large on presentation,displacing the kidney downwards and laterally. Insome cases it may invade the adjacent kidney,becoming difficult to distinguish from a Wilms’tumour. Neuroblastoma is predominantly solid onultrasound, having a heterogeneous texture andfrequently containing calcification. The tumourmargins are ill-defined and infiltrate the surround-ing organs and tissues, crossing the midline and
encasing vascular structures: it may be difficult todifferentiate from lymphadenopathy (Fig. 9.13B,C and D). Nodes tend to surround and elevate theaorta and IVC.
MRI and CT are used for staging, particularly inassessing retroperitoneal spread.22 Bone scintigra-phy and MIBG scans are also useful in demon-strating metastases.
Adrenal haemorrhage
After birth, the bulky fetal cortex normally invo-lutes. Adrenal haemorrhage occurs in the neonateas a result of trauma to the vulnerable fetal cortexduring delivery or in association with perinatalasphyxia. Haemorrhage may occur in up to 2% ofbirths.23 This may be uni- or bilateral and maycause a palpable mass and abdominal pain.Ultrasound can be used to follow the resolution ofthe haemorrhage over a period of weeks; in the ini-tial stages of haemorrhage the adrenal mass ishyperechoic, gradually liquefying into a well-defined mass of mixed echo pattern and becomingcystic (Fig. 9.13 E, F). This may completely resolveover a period of some weeks leaving a normal adre-nal gland or the gland may become atrophic andcalcify. In rare cases an adrenal haemorrhage mayprogress to an abscess.24
Adrenal calcification
Calcification of the gland in babies and infants isusually the result of previous infection or haemor-rhage. Adrenal abscess cavities may calcify aftersuccessful treatment. Gross calcification in bilateral adrenal glands in association withhepatosplenomegaly in the infant indicates thelikely diagnosis of Wolman’s disease, an inbornerror of lipid metabolism that is invariably fatal.
GASTROINTESTINAL TRACT
Bowel ultrasound in paediatrics is an establishedand readily accepted investigation, replacing con-trast radiology in many cases. The range of poten-tial applications continues to increase.25 Mostgastrointestinal tract scanning in paediatrics is bestperformed with a high-frequency (15–7.5 MHz)linear or small footprint curvilinear probe.
ABDOMINAL ULTRASOUND232
ch09.qxd 6/30/04 6:17 PM Page 232
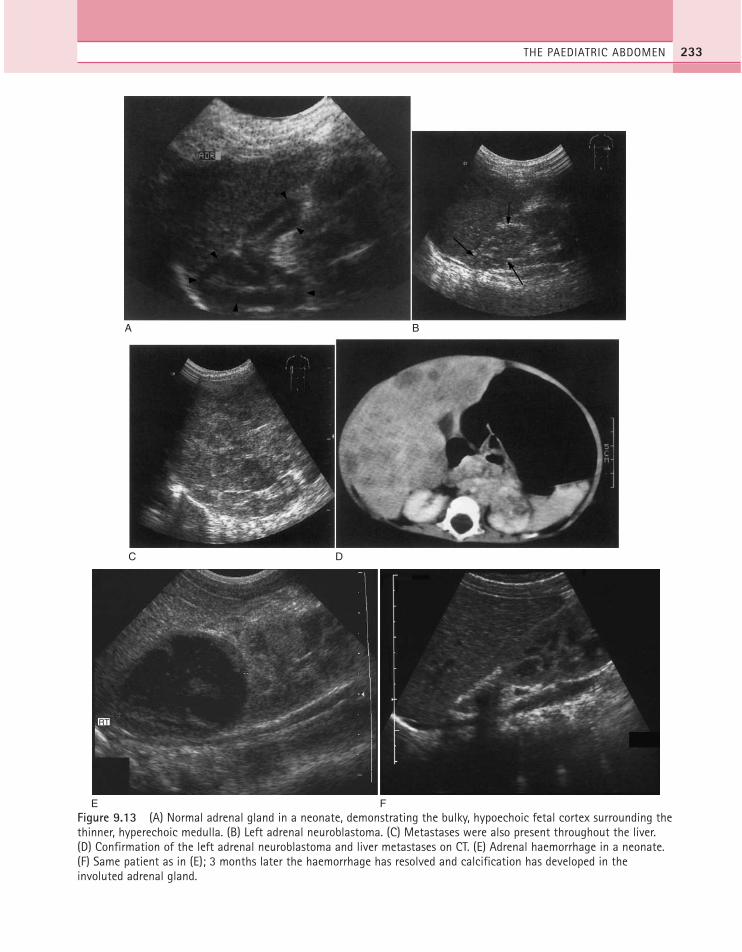
THE PAEDIATRIC ABDOMEN 233
A B
DC
Figure 9.13 (A) Normal adrenal gland in a neonate, demonstrating the bulky, hypoechoic fetal cortex surrounding thethinner, hyperechoic medulla. (B) Left adrenal neuroblastoma. (C) Metastases were also present throughout the liver. (D) Confirmation of the left adrenal neuroblastoma and liver metastases on CT. (E) Adrenal haemorrhage in a neonate.(F) Same patient as in (E); 3 months later the haemorrhage has resolved and calcification has developed in theinvoluted adrenal gland.
E F
RT
ch09.qxd 6/30/04 6:17 PM Page 233

Hypertrophic pyloric stenosis (HPS)
HPS is a condition occurring in newborn infantscommonly about 6 weeks of age when the pyloricmuscle becomes hypertrophied and elongated,restricting the passage of gastric contents, causingprojectile vomiting. Most infants with HPS arefound to have a hypochloraemic alkalosis and,when seen in association with a palpable epigastricmass the size of an olive on test feeding, the diag-nosis is clear without the need for ultrasonic imag-ing. However, ultrasound is very successful indemonstrating HPS in approximately 20% ofinfants in whom the pyloric olive cannot be pal-pated.26,27
The baby should be positioned comfortably rightside down and the stomach and pylorus identifiedusually just to the right of the midline in the low epi-gastric region. A small feed, of approximately 20–30 ml of sugared water (preferable to milk as it doesnot contain echoes which may obscure vital detail),may be used to aid visualization of the gastric antrumif the stomach is empty. A nasogastric tube may alsobe used to administer clear fluid in a controlled wayproviding that the gastric position of the tube is con-firmed prior to injection of the fluid. A small, high-frequency linear or curved linear transducer is best.
The pylorus projects into gastric lumen and isoutlined by the fluid. HPS can be confirmed by thedemonstration of:
● thickened and elongated pyloric muscle● increased but ineffective peristalsis● failure of the pylorus to relax and open
Various figures have been quoted for musclethickness in hypertrophic pyloric stenosis rangingfrom 2.5 to 5 mm but 3 mm is most commonlyaccepted28,29 (Table 9.5).
It must be stressed that the examination isdynamic and measurements of muscle thicknessmust be interpreted in conjunction with the obser-vations of gastric peristalsis and failure of thepylorus to relax normally. Sensitivity and specificityof 97% and 99% for the diagnosis of HPS have beenreported in expert hands (Fig. 9.14). If clinical sus-picion persists after a negative ultrasound, a repeatexamination after 1 or 2 days may be performed toexclude an evolving pyloric stenosis.
Intussusception
Intussusception is the invagination of a segment ofbowel into the lumen of the adjacent bowel. It is acommon paediatric emergency, especially inyounger children aged 3 months to 3 years, andtends to affect the ileocaecal region.
The child presents with abdominal pain, some-times with a palpable mass, vomiting or rectal bleed-ing. Intussusception can result in bowel necrosis andsubsequently perforation requiring surgery.
The ultrasound appearances of bowel withinbowel are characteristic. In cross-section, thebowel assumes a ‘doughnut’ configuration, withconcentric rings of bowel wall (Fig. 9.15). Dilatedloops of fluid-filled obstructed bowel may bedemonstrated proximal to the intussusception.
The use of ultrasound to diagnose this condi-tion is highly reliable,30 reducing or eliminating theneed for contrast radiology.
An air enema is most commonly used to reducethe intussusception using inflation pressures of upto 120 mmHg. Hydrostatic reduction (that is,with water/saline) under fluoroscopic or ultra-sound control is also an accepted treatment.31
ABDOMINAL ULTRASOUND234
Table 9.5 Pyloric muscle dimensions
Normal Hypertrophic pylorus pyloric stenosis
Pyloric length < 15 ≥ 16(mm)Pyloric width < 11 ≥ 11(mm)Muscle thickness < 2.5 ≥ 3(mm)
Table 9.4 Paediatric abdominal malignancies
Wilms’ tumourNeuroblastomaHepatoblastomaHepatocellular carcinomaRhabdomyosarcomaLeukaemiaLymphoma
ch09.qxd 6/30/04 6:17 PM Page 234
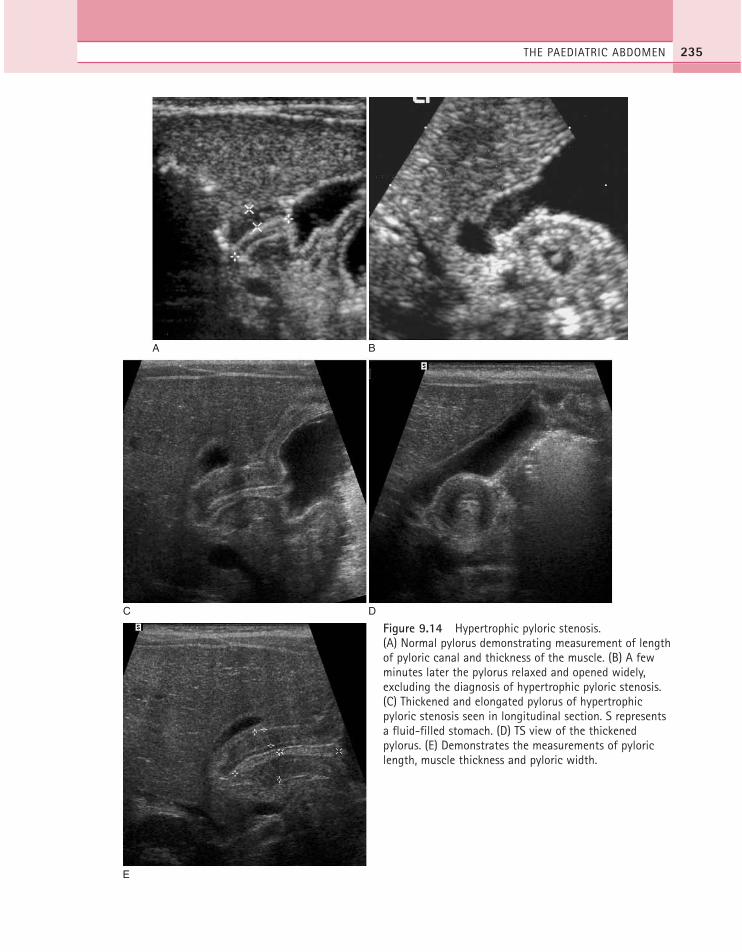
THE PAEDIATRIC ABDOMEN 235
A B
DC
E
Figure 9.14 Hypertrophic pyloric stenosis. (A) Normal pylorus demonstrating measurement of lengthof pyloric canal and thickness of the muscle. (B) A fewminutes later the pylorus relaxed and opened widely,excluding the diagnosis of hypertrophic pyloric stenosis.(C) Thickened and elongated pylorus of hypertrophicpyloric stenosis seen in longitudinal section. S representsa fluid-filled stomach. (D) TS view of the thickenedpylorus. (E) Demonstrates the measurements of pyloriclength, muscle thickness and pyloric width.
ch09.qxd 6/30/04 6:17 PM Page 235

The main contraindications to attempting a non-surgical reduction are peritonitis and free intraperi-toneal air. A number of sonographic features havebeen reported to be associated with a decreased suc-cess rate of non-surgical reduction, including a hypo-echoic rim greater than 10 mm, absent blood flow oncolour flow Doppler sonography, or a large amountof fluid trapped within the intussusception, but thesefindings are not contraindications to a careful attempt
at non-surgical reduction.32 Approximately 10% ofcases recur whether the initial intussuception wastreated surgically or non-surgically.
Midgut volvulus
Malrotation of the midgut occurs as a result of failureof normal rotation of the small bowel duringintrauterine development, resulting in a shortened
ABDOMINAL ULTRASOUND236
A
B
C
Figure 9.15 Intussusception. (A) The characteristicappearance of bowel within bowel due to anintussusception. (B) Dilated, fluid-filled loops of obstructedbowel are seen proximal to the intussusception. (C) Airenema; the intussusceptum is seen indenting into thelumen of the air-filled sigmoid colon during a successfulair enema reduction (arrow).
ch09.qxd 6/30/04 6:17 PM Page 236
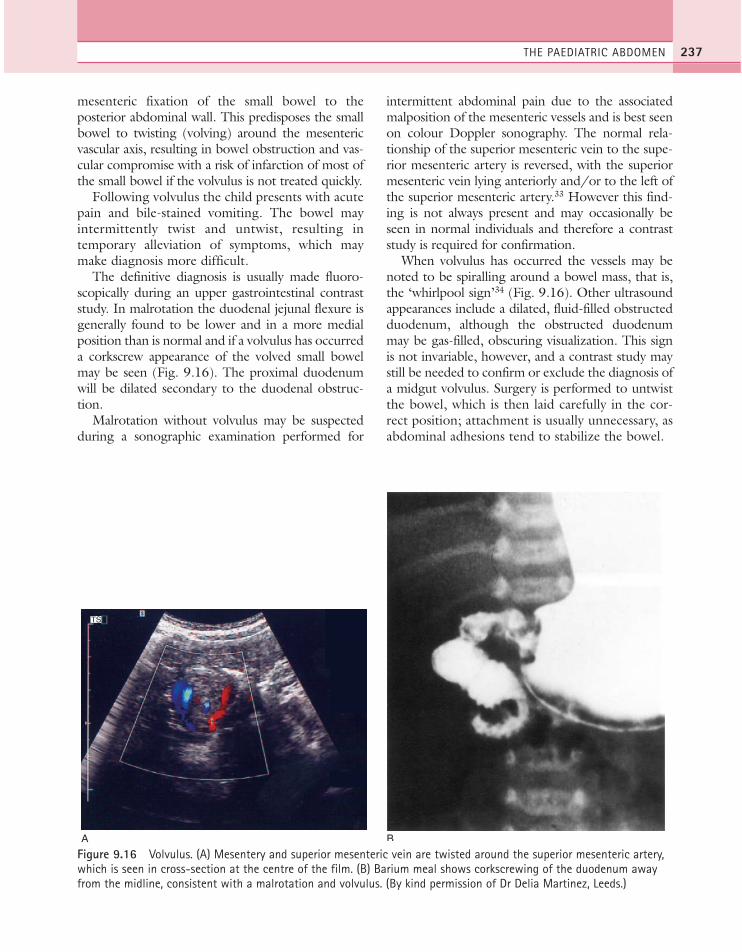
mesenteric fixation of the small bowel to theposterior abdominal wall. This predisposes the smallbowel to twisting (volving) around the mesentericvascular axis, resulting in bowel obstruction and vas-cular compromise with a risk of infarction of most ofthe small bowel if the volvulus is not treated quickly.
Following volvulus the child presents with acutepain and bile-stained vomiting. The bowel mayintermittently twist and untwist, resulting intemporary alleviation of symptoms, which maymake diagnosis more difficult.
The definitive diagnosis is usually made fluoro-scopically during an upper gastrointestinal contraststudy. In malrotation the duodenal jejunal flexure isgenerally found to be lower and in a more medialposition than is normal and if a volvulus has occurreda corkscrew appearance of the volved small bowelmay be seen (Fig. 9.16). The proximal duodenumwill be dilated secondary to the duodenal obstruc-tion.
Malrotation without volvulus may be suspectedduring a sonographic examination performed for
intermittent abdominal pain due to the associatedmalposition of the mesenteric vessels and is best seenon colour Doppler sonography. The normal rela-tionship of the superior mesenteric vein to the supe-rior mesenteric artery is reversed, with the superiormesenteric vein lying anteriorly and/or to the left ofthe superior mesenteric artery.33 However this find-ing is not always present and may occasionally beseen in normal individuals and therefore a contraststudy is required for confirmation.
When volvulus has occurred the vessels may benoted to be spiralling around a bowel mass, that is,the ‘whirlpool sign’34 (Fig. 9.16). Other ultrasoundappearances include a dilated, fluid-filled obstructedduodenum, although the obstructed duodenummay be gas-filled, obscuring visualization. This signis not invariable, however, and a contrast study maystill be needed to confirm or exclude the diagnosis ofa midgut volvulus. Surgery is performed to untwistthe bowel, which is then laid carefully in the cor-rect position; attachment is usually unnecessary, asabdominal adhesions tend to stabilize the bowel.
THE PAEDIATRIC ABDOMEN 237
A
TS
B
Figure 9.16 Volvulus. (A) Mesentery and superior mesenteric vein are twisted around the superior mesenteric artery,which is seen in cross-section at the centre of the film. (B) Barium meal shows corkscrewing of the duodenum awayfrom the midline, consistent with a malrotation and volvulus. (By kind permission of Dr Delia Martinez, Leeds.)
ch09.qxd 6/30/04 6:18 PM Page 237
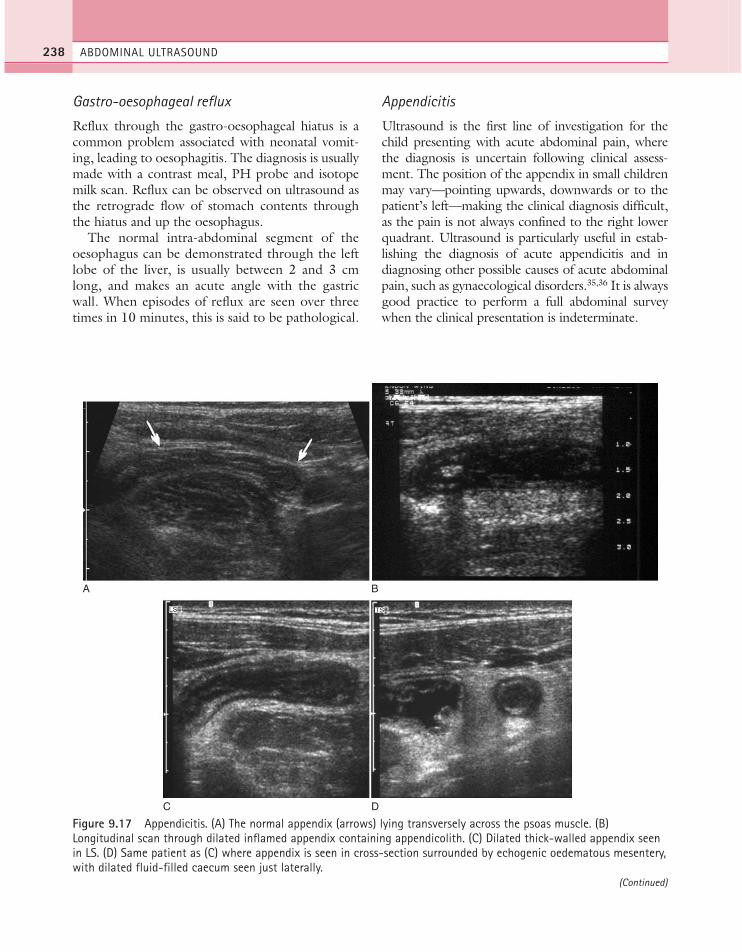
Gastro-oesophageal reflux
Reflux through the gastro-oesophageal hiatus is acommon problem associated with neonatal vomit-ing, leading to oesophagitis. The diagnosis is usuallymade with a contrast meal, PH probe and isotopemilk scan. Reflux can be observed on ultrasound asthe retrograde flow of stomach contents throughthe hiatus and up the oesophagus.
The normal intra-abdominal segment of theoesophagus can be demonstrated through the leftlobe of the liver, is usually between 2 and 3 cmlong, and makes an acute angle with the gastricwall. When episodes of reflux are seen over threetimes in 10 minutes, this is said to be pathological.
Appendicitis
Ultrasound is the first line of investigation for thechild presenting with acute abdominal pain, wherethe diagnosis is uncertain following clinical assess-ment. The position of the appendix in small childrenmay vary—pointing upwards, downwards or to thepatient’s left—making the clinical diagnosis difficult,as the pain is not always confined to the right lowerquadrant. Ultrasound is particularly useful in estab-lishing the diagnosis of acute appendicitis and indiagnosing other possible causes of acute abdominalpain, such as gynaecological disorders.35,36 It is alwaysgood practice to perform a full abdominal surveywhen the clinical presentation is indeterminate.
ABDOMINAL ULTRASOUND238
A B
TS
DC
LS
Figure 9.17 Appendicitis. (A) The normal appendix (arrows) lying transversely across the psoas muscle. (B)Longitudinal scan through dilated inflamed appendix containing appendicolith. (C) Dilated thick-walled appendix seenin LS. (D) Same patient as (C) where appendix is seen in cross-section surrounded by echogenic oedematous mesentery,with dilated fluid-filled caecum seen just laterally.
(Continued)
ch09.qxd 6/30/04 6:18 PM Page 238
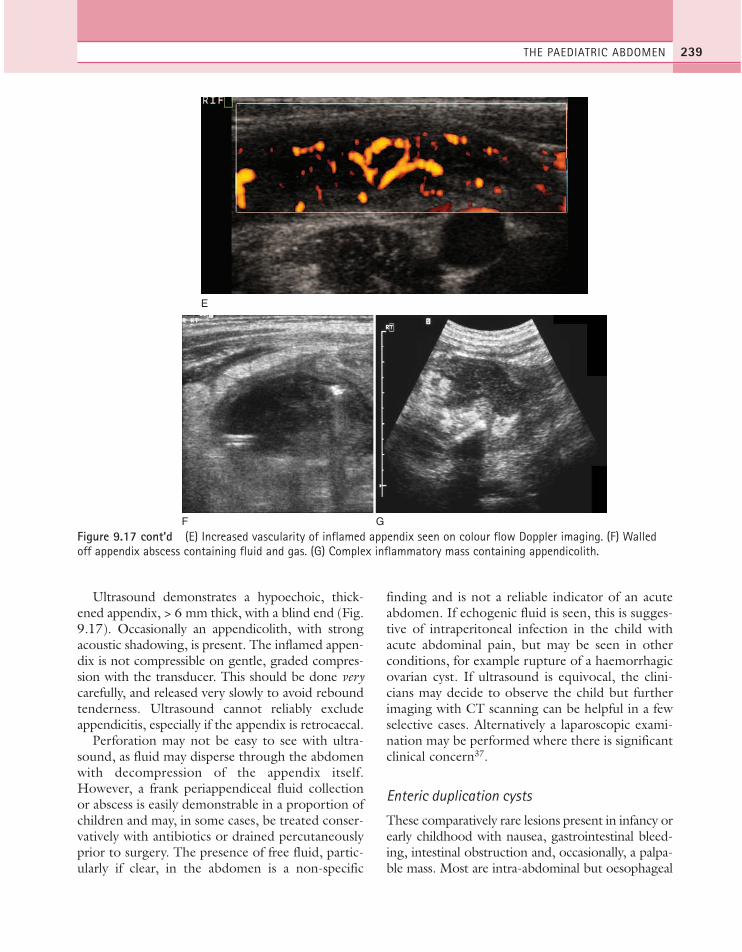
Ultrasound demonstrates a hypoechoic, thick-ened appendix, > 6 mm thick, with a blind end (Fig.9.17). Occasionally an appendicolith, with strongacoustic shadowing, is present. The inflamed appen-dix is not compressible on gentle, graded compres-sion with the transducer. This should be done verycarefully, and released very slowly to avoid reboundtenderness. Ultrasound cannot reliably excludeappendicitis, especially if the appendix is retrocaecal.
Perforation may not be easy to see with ultra-sound, as fluid may disperse through the abdomenwith decompression of the appendix itself.However, a frank periappendiceal fluid collectionor abscess is easily demonstrable in a proportion ofchildren and may, in some cases, be treated conser-vatively with antibiotics or drained percutaneouslyprior to surgery. The presence of free fluid, partic-ularly if clear, in the abdomen is a non-specific
finding and is not a reliable indicator of an acuteabdomen. If echogenic fluid is seen, this is sugges-tive of intraperitoneal infection in the child withacute abdominal pain, but may be seen in otherconditions, for example rupture of a haemorrhagicovarian cyst. If ultrasound is equivocal, the clini-cians may decide to observe the child but furtherimaging with CT scanning can be helpful in a fewselective cases. Alternatively a laparoscopic exami-nation may be performed where there is significantclinical concern37.
Enteric duplication cysts
These comparatively rare lesions present in infancy orearly childhood with nausea, gastrointestinal bleed-ing, intestinal obstruction and, occasionally, a palpa-ble mass. Most are intra-abdominal but oesophageal
THE PAEDIATRIC ABDOMEN 239
E
F G
Figure 9.17 cont’d (E) Increased vascularity of inflamed appendix seen on colour flow Doppler imaging. (F) Walledoff appendix abscess containing fluid and gas. (G) Complex inflammatory mass containing appendicolith.
ch09.qxd 6/30/04 6:18 PM Page 239
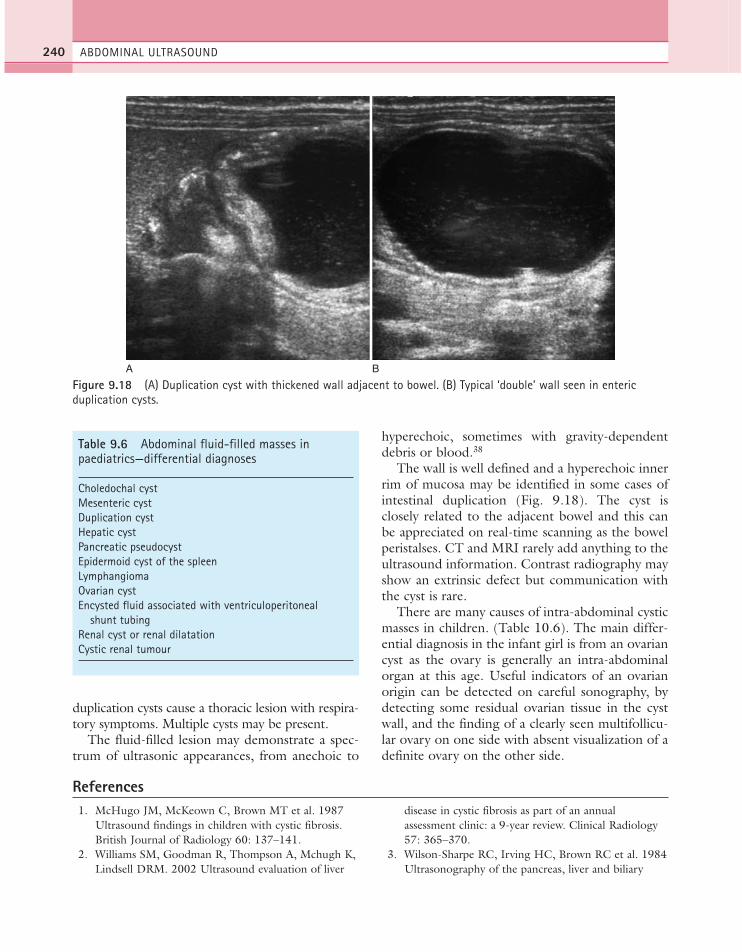
duplication cysts cause a thoracic lesion with respira-tory symptoms. Multiple cysts may be present.
The fluid-filled lesion may demonstrate a spec-trum of ultrasonic appearances, from anechoic to
hyperechoic, sometimes with gravity-dependentdebris or blood.38
The wall is well defined and a hyperechoic innerrim of mucosa may be identified in some cases ofintestinal duplication (Fig. 9.18). The cyst isclosely related to the adjacent bowel and this canbe appreciated on real-time scanning as the bowelperistalses. CT and MRI rarely add anything to theultrasound information. Contrast radiography mayshow an extrinsic defect but communication withthe cyst is rare.
There are many causes of intra-abdominal cysticmasses in children. (Table 10.6). The main differ-ential diagnosis in the infant girl is from an ovariancyst as the ovary is generally an intra-abdominalorgan at this age. Useful indicators of an ovarianorigin can be detected on careful sonography, bydetecting some residual ovarian tissue in the cystwall, and the finding of a clearly seen multifollicu-lar ovary on one side with absent visualization of adefinite ovary on the other side.
ABDOMINAL ULTRASOUND240
A B
Figure 9.18 (A) Duplication cyst with thickened wall adjacent to bowel. (B) Typical ‘double’ wall seen in entericduplication cysts.
Table 9.6 Abdominal fluid-filled masses in paediatrics—differential diagnoses
Choledochal cystMesenteric cystDuplication cystHepatic cystPancreatic pseudocystEpidermoid cyst of the spleenLymphangiomaOvarian cystEncysted fluid associated with ventriculoperitoneal
shunt tubingRenal cyst or renal dilatationCystic renal tumour
References1. McHugo JM, McKeown C, Brown MT et al. 1987
Ultrasound findings in children with cystic fibrosis.British Journal of Radiology 60: 137–141.
2. Williams SM, Goodman R, Thompson A, Mchugh K,Lindsell DRM. 2002 Ultrasound evaluation of liver
disease in cystic fibrosis as part of an annualassessment clinic: a 9-year review. Clinical Radiology57: 365–370.
3. Wilson-Sharpe RC, Irving HC, Brown RC et al. 1984Ultrasonography of the pancreas, liver and biliary
ch09.qxd 6/30/04 6:18 PM Page 240
system in cystic fibrosis. Archives of Diseases ofChildhood 59: 923–926.
4. McEvoy CF, Suchy FJ. 1996 Biliary tract disease inchildren. Pediatric Gastroenterology 43: 75–98.
5. Farrant P, Meire HB, Mieli-Vergani G. 2000Ultrasound features of the gallbladder in infantspresenting with conjugated hyperbilirubinaemia.British Journal of Radiology 73: 1154–1158.
6. Kim SH, Lim JH, Yoon HK et al. 2000 Choledochalcyst: comparison of MR and conventionalcholangiography. Clinical Radiology 55 (5): 378–383.
7. Siegel MJ. 2002 Gallbladder and biliary tract. In:Siegel M (ed.) Pediatric Sonography. LippincottWilliams & Wilkins, Philadelphia, pp. 275–304.
8. Takano H, Smith WL. 1997 Gastrointestinal tumorsof childhood. Radiologic Clinics of North America35: 1367–1389.
9. Buetow PC, Rao P, Marshall WH. 1997 Imaging ofpaediatric liver tumours. Magnetic ResonanceImaging Clinics of North America 5: 397–413.
10. Boon LM, Burrows PE, Patiel HJ et al. 1996Hepatic vascular anomalies in infancy: a twenty-sevenyear experience. Journal of Paediatrics 129:3346–3354.
11. Siegel MJ, Martin KW, Worthington JL. 1987Normal and abnormal pancreas in children: USstudies. Radiology 165: 15–18.
12. Han BK, Babcock DS. 1985 Sonographicmeasurements and appearances of normal kidneys inchildren. American Journal of Roentgenology 145:611–616.
13. Ferrer FA, McKenna PH, Bauer B, Miller SF. 1997Accuracy of renal ultrasound measurements forpredicting actual kidney size. Journal of Urology 157:2278–2281.
14. Bisset GS, Strife JL. 1987 The duplex collectingsystem in girls with urinary tract infection prevalenceand significance. American Journal of Roentgenology148: 497–500.
15. Assael BM, Guez S, Marra G et al. 1998 Congenitalreflux nephropathy: a follow-up of 108 casesdiagnosed perinatally. British Journal of Urology 82:252–257.
16. Tibballs JM, De Bruyn R. 1996 Primaryvesicoureteric reflux: how useful is postnatalultrasound? Archives of Diseases of Childhood 75:444–478.
17. Zerin JM, Ritchey ML, Chang CCH. 1993 Incidentalvesicoureteral reflux in neonates with antenatallydetected hydronephrosis and other renalabnormalities. Radiology 187: 157–160.
18. Mackenzie S. 2001 Radiological investigation ofpaediatric UTI. Imaging 13(4): 285–294.
19. Dacher JN, Pfister C, Monroc M, Eurin D, LedosseurP. 1996 Power Doppler sonographic pattern of acutepyelonephritis in children: comparison with CT.American Journal of Roentgenology 166: 1451–1455.
20. Ritchey ML, Green DM, Breslow NB et al. 1995Accuracy of current imaging modalities in thediagnosis of synchronous bilateral Wilms’ tumour: areport from the National Wilms’ Tumour StudyGroup. Cancer 75: 600–604.
21. Scott D J, Wallace WHB, Hendry GMA. 1999 Withadvances in medical imaging can the radiologistreliably diagnose Wilms’ tumours? Clinical Radiology54: 321–327.
22. Abramson SJ. 1997 Adrenal neoplasms in children.Radiologic Clinics of North America 35 (6):1415–1453.
23. Felc Z. 1995 Ultrasound in screening for neonataladrenal haemorrhage. American Journal of Perinatology12: 363–366.
24. Steffens J, Zaubitzer T, Kirsch W, Humke U. 1997Neonatal adrenal abscesses. European Journal ofUrology 31: 347–349.
25. John SD. 1999 Trends in pediatric emergencyimaging. Radiologic Clinics of North America 37:995–1007.
26. Godbole P, Sprigg A, Dickson JAS, Lin PC. 1996Ultrasound compared with clinical examination ininfantile hypertrophic pyloric stenosis. Archives ofDiseases of Childhood 75: 335–337.
27. Morrison SC. 1997 Controversies in abdominalimaging. Pediatric Clinics of North America 44:555–574.
28. Stunden RJ, LeQuesne GW, Little KE. 1986 Theimproved ultrasound diagnosis of hypertrophic pyloricstenosis. Pediatric Radiology 16: 200–205.
29. O’Keefe FN, Stansberry SD, Swischuk LE et al. 1991Antropyloric muscle thickness at ultrasound in infants:what is normal? Radiology 187: 827–830.
30. Verschelden P, Filiatrault D, Garel L et al. 1992Intussusception in children: reliability of US indiagnosis – a prospective study. Pediatric Radiology184: 741–744.
31. Chan KL, Saing H, Peh WCG et al. 1997 Childhoodintussusception: ultrasound-guided Hartmann’ssolution, hydrostatic reduction or barium enemareduction? Journal of Pediatric Surgery 32: 3–6.
32. Britton I, Wilkinson AG. 1999 Ultrasound features ofintussusception predicting outcome of air enema.Pediatric Radiology 29: 705–710.
33. Zerin JM, DiPietro MA. 1992 Superior mesentericvascular anatomy at US in patients with surgicallyproved malrotation of the midgut. Radiology 183:693–694.
THE PAEDIATRIC ABDOMEN 241
ch09.qxd 6/30/04 6:18 PM Page 241

34. Pracros P, Sann L, Genin G et al. 1992 Ultrasounddiagnosis of midgut volvulus: the ‘whirlpool’ sign.Pediatric Radiology 22: 18–20.
35. Siegal MJ. 1995 Appendicitis in childhood:usefullness of ultrasound in diagnosis. PaediatricSurgery International 10: 62–67.
36. Pena BM, Taylor GA, Fishman SJ et al. 2002 Effectof an imaging protocol on clinical outcomes amongpediatric patients with appendicitis. Pediatrics 110:1088–1093.
37. Quillan SP, Siegel MJ, Coffin CM. 1992 Acuteappendicitis in children: value of sonography indetecting perforation. American Journal ofRoentgenology 159: 1265–1268.
38. Segal SR, Sherman NH, Rosenberg HK et al. 1994 Ultrasonic features of gastrointestinalduplications. Journal of Ultrasound in Medicine 13:863–870.
ABDOMINAL ULTRASOUND242
General reading1. Carty H, Brunelle F, Shaw D, Kendall B. 1994
Imaging Children. Churchill Livingstone, Edinburgh.2. Siegel MJ. 2002 Pediatric Sonography, 3rd edn.
Lippincott/Williams & Wilkins, Philadelphia.
3. Stringer DA, Babyn PS. 2000 Pediatric GastrointestinalImaging and Intervention. BC Decker, Ontario.
ch09.qxd 6/30/04 6:18 PM Page 242
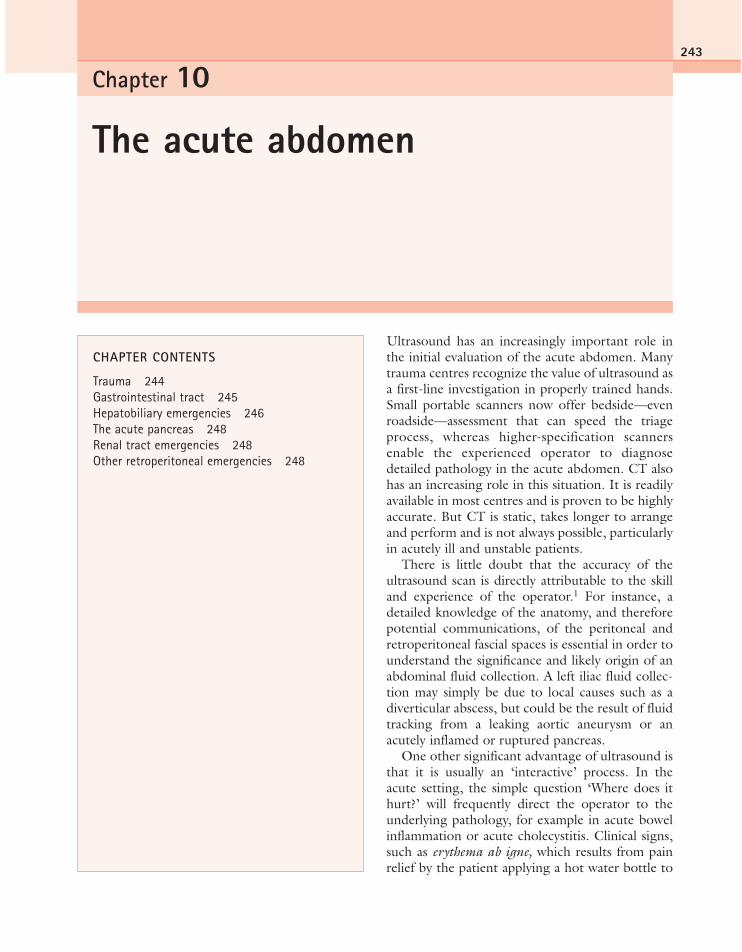
Ultrasound has an increasingly important role inthe initial evaluation of the acute abdomen. Manytrauma centres recognize the value of ultrasound asa first-line investigation in properly trained hands.Small portable scanners now offer bedside—evenroadside—assessment that can speed the triageprocess, whereas higher-specification scannersenable the experienced operator to diagnosedetailed pathology in the acute abdomen. CT alsohas an increasing role in this situation. It is readilyavailable in most centres and is proven to be highlyaccurate. But CT is static, takes longer to arrangeand perform and is not always possible, particularlyin acutely ill and unstable patients.
There is little doubt that the accuracy of theultrasound scan is directly attributable to the skilland experience of the operator.1 For instance, adetailed knowledge of the anatomy, and thereforepotential communications, of the peritoneal andretroperitoneal fascial spaces is essential in order tounderstand the significance and likely origin of anabdominal fluid collection. A left iliac fluid collec-tion may simply be due to local causes such as adiverticular abscess, but could be the result of fluidtracking from a leaking aortic aneurysm or anacutely inflamed or ruptured pancreas.
One other significant advantage of ultrasound isthat it is usually an ‘interactive’ process. In theacute setting, the simple question ‘Where does ithurt?’ will frequently direct the operator to theunderlying pathology, for example in acute bowelinflammation or acute cholecystitis. Clinical signs,such as erythema ab igne, which results from painrelief by the patient applying a hot water bottle to
Chapter 10
The acute abdomen
243
CHAPTER CONTENTS
Trauma 244Gastrointestinal tract 245Hepatobiliary emergencies 246The acute pancreas 248Renal tract emergencies 248Other retroperitoneal emergencies 248
ch10.qxd 6/30/04 6:19 PM Page 243

the symptomatic area, may also help to focus theexamination. The operator should be alert topotential clues and be prepared to step outsidestandard scanning protocols, adapting to the manypossible presentations of trauma or other acuteabdominal conditions.
Although many of the following conditions aredealt with in other relevant chapters, together withdetails of the respective ultrasound appearances,there are issues that are specific to the patient whopresents acutely.
TRAUMA
Blunt or penetrating trauma to the torso, fre-quently due to a road traffic accident (RTA) orother forms of accident or violence, is a frequentcause of referral to most accident and emergencydepartments, and forms the main indication fortrauma ultrasound. Internal organ injury as a resultof trauma is extremely difficult to assess clinically,especially as many patients are admitted uncon-scious or in a highly unstable condition. Suchtrauma patients may require emergency laparo-tomy and ultrasound has been shown to be aninvaluable tool in the triage process.2,3 This may beaccompanied by CT, which has the advantage ofbeing able to recognize other injuries which maybe present, such as bony, spinal or retroperitonealtrauma which may or may not be accessible toultrasound investigation.
A system of scanning known as FAST (focusedassessment with sonography for trauma) hasrecently become widely adopted in trauma centres.This system depends upon the proper training ofappropriate personnel, and a number of standard-ized training and accreditation programmes havebeen devised, notably by the American College ofEmergency Physicians.4 FAST scanning involves aminimum four-view examination, principally todetect the presence of fluid which may result fromthe rupture of internal organs. The four-view scanshould include the right and left flanks (for hepa-torenal space, perisplenic regions and spaces aboveand below the diaphragm), the subcostal region(to include the pericardial space) and the pelvis(retrovesical and retrouterine spaces).5
Free fluid is associated with numerous types ofinjury, which may be detected on ultrasound with
varying success. These include rupture of theliver, spleen, kidney, pancreas or bowel (Fig. 10.1).A notable limitation of sonography in the traumasituation is in detecting free fluid in the pelvis, asthe bladder is frequently empty or underfilled, andthe use of the Trendelenburg position, if possible,helps to reduce the number of false-negative resultsin this respect by allowing any free fluid to collectin the pelvis under the influence of gravity.Ultrasound is more successful in detecting freefluid than in detecting organ injury directly.6,7 Onestudy reported a 98% sensitivity for detection offluid, but only 41% of organ injuries could bedemonstrated.8 However, most of the publishedstudies have concentrated only on the presence orabsence of free fluid, rather than the comprehen-sive assessment of the abdomen by suitably quali-fied sonographers. The presence of free fluid onultrasound in a trauma situation therefore infersorgan injury requiring careful ultrasonic assess-ment, further investigation with CT or direct refer-ral for surgery depending on the state of thepatient.
Direct visualization of organ rupture is difficultunless a haematoma or other collection is seen.Laceration or contusion may be demonstrated inthe liver, kidneys or spleen, but less easily inthe pancreas and very infrequently in the bowel.A subtle change in texture may be observed by theexperienced operator, or a fine, high-reflectivitylinear band representing an organ tear. A delayedscan may demonstrate more obvious organ injurythan that apparent on an immediate post-traumaexamination. Small visceral lacerations not visibleon ultrasound may become apparent when imagedwith CT. In particular, pancreatic damage (oftendue to the sudden pressure of a seat belt across theabdomen during road accidents) may not be obvi-ous immediately post-trauma on either ultrasoundor CT.9 Damage to the pancreatic duct (Fig. 10.1E)causes leakage of pancreatic fluid into the abdomi-nal cavity, resulting in pancreatitis and possiblepseudocyst formation or peritonitis.
Free fluid may be present as the result of vessel,rather than organ, rupture. A reduction or loss ofblood flow to all or part of the relevant organ, forexample the kidney, may be demonstrated usingcolour and power Doppler ultrasound. The findingof free fluid in women should prompt a detailed
ABDOMINAL ULTRASOUND244
ch10.qxd 6/30/04 6:19 PM Page 244

scan of the pelvis where possible. Gynaecologicalmasses may rupture or haemorrhage, presentingacutely, and in women of childbearing age, ectopicpregnancy should be included in the list of differ-ential diagnoses.
When visceral trauma is treated conservatively,follow-up ultrasound may be used to monitor theresolution of any fluid collections or haematoma.
GASTROINTESTINAL TRACT
Most acute presentations of gastrointestinal tractpathology are due to obstruction or inflammation,and the ultrasound appearances of these conditionsare discussed more fully in Chapter 8. Appendicitis,and its possible complications, is one of the mostcommon reasons for referral (Fig. 10.2). Ultrasound
THE ACUTE ABDOMEN 245
A
C
B
D
Figure 10.1 (A) The presence of free fluid in a trauma patient implies organ injury, even if this cannot be successfullydemonstrated on ultrasound. CT on this patient demonstrated perforation of the bowel. (B) A patient who has beenstabbed on the right side has injury to the liver causing a subcapsular haematoma. Blood is also present in the rightchest. (C) Laceration of the spleen following a road traffic accident. Free fluid was also present in the abdomen. (D) Splenic lacerations are more obvious several hours after injury. This large splenic haematoma resolved followingconservative treatment.
(Continued)
ch10.qxd 6/30/04 6:19 PM Page 245

has a high sensitivity for acute appendicitis, partic-ularly in children.
Although the detailed assessment of the primarygastrointestinal pathology usually requires evaluationby an experienced operator with a high-frequency
linear probe, many useful indicators can be foundwith the basic curvilinear or sector abdominal scan.The presence of fluid-filled bowel segments, whichmay also show ‘overactive’ peristalsis, should alertthe operator to the possibility of acute intestinalobstruction. Such segments frequently lie proximalto the obstructing lesion, and so the point at whichthey appear to end should be the subject ofdetailed examination. Ultrasound is highly accu-rate in demonstrating obstruction. However, it isless successful in finding its cause and contrast CTor other bowel studies are usually undertakenwhen obstruction is diagnosed. With both intes-tinal obstruction and focal pain it may be necessaryto examine the hernial orifices. A small but symp-tomatic epigastric hernia often goes unnoticedunless a detailed scan of the abdominal wall isperformed.
Fluid collections such as abscesses may alsopoint to the diseased segment, for example inCrohn’s disease or acute diverticulitis. Such inflam-matory bowel conditions may well present with anestablished history which helps the operator tofocus the ultrasound examination accordingly.
Perforation of an abdominal viscus can producesmall amounts of ascites. This is usually ‘mucky’,i.e. containing particulate or gas bubble echoes,and may be localized close to the perforation site,around the duodenum or within the lesser sac.Although gas is usually regarded as an obstacle toultrasound diagnosis, recent studies have shownthat specific patterns of gas echoes can make ultra-sound more sensitive than plain radiography in thediagnosis of pneumoperitoneum.10
HEPATOBILIARY EMERGENCIES
Ultrasound scanning is invariably the first-lineinvestigation for suspected biliary tract emergen-cies. These include inflammatory conditions caus-ing right upper quadrant and epigastric pain,mostly acute cholecystitis or gallstone pancreatitis,and the various causes of obstructive jaundice(Fig. 10.3). If possible, interventional treatmentshould be delayed until a detailed imaging assess-ment of the cause of biliary obstruction has beenmade, since the presence of a biliary stent cancompromise subsequent imaging by CT, MRI orendoscopic ultrasound. Similarly, biliary stents
ABDOMINAL ULTRASOUND246
E
Figure 10.1 cont’d (E) CT demonstrating pancreaticfracture (arrow) in the tail of the pancreas following aroad traffic accident. Ultrasound was not able todemonstrate the fracture but did demonstrate free fluidfollowing the accident and also diagnoseddevascularization of the left kidney (no Doppler flowwithin the kidney) following a severed left renal artery.This is also confirmed on CT.
Figure 10.2 Appendicitis abscess.
ch10.qxd 6/30/04 6:19 PM Page 246

frequently cause bile duct wall thickening and mayintroduce gas into the biliary tree. These will pre-vent the diagnosis of cholangitis or ductal calculiwith ultrasound, and may impede detailed Dopplerinvestigation of, for example, the portal vein. Ifurgent biliary drainage is required, particularlywhen the bile is infected, this can quickly beeffected by endoscopic stent placement or sphinc-terotomy.11 These less invasive methods are replac-ing surgery as the treatment of choice in thissituation, having a lower mortality rate. Endo-scopic sphincterotomy and stone extraction havebeen found to be preferable to surgery, particularlyin cases of severe gallstone pancreatitis where
patients may be poor operative risks12 and in casesof stone-related cholangitis.
Ultrasound-guided bed-side cholecystostomymay also be useful in high-risk patients withinfected gallbladders and is an effective treatmentfor acalculous cholecystitis brought on by pro-longed postoperative fasting.
The liver itself may be acutely tender in systemicvenous congestion due to cardiac failure, acutehepatitis, or the presence of an intrahepaticabscess. The management of liver abscesses isdetermined by their size, number and cause.Ultrasound is used to guide diagnostic aspirationand drainage procedures, and most types of hepatic
THE ACUTE ABDOMEN 247
A
LIVER LS GBSTENT RUQ
B
DC
Figure 10.3 (A) An acutely tender, inflamed gallbladder containing stones and debris. (B) A patient with knowncarcinoma of the head of the pancreas has presented acutely with obstructive jaundice. Her stent (arrow) is blocked,causing intrahepatic biliary duct dilatation with cholangitis (C). (D) Large liver abscess in an acutely ill patient.
ch10.qxd 6/30/04 6:19 PM Page 247

abscess can be treated successfully using these tech-niques combined with appropriate antibiotictherapy.
THE ACUTE PANCREAS
(See also Chapter 5.) Most cases of acute pancreati-tis are suspected clinically, with raised amylase lev-els and often a history of recurrent epigastric painpointing to the diagnosis of acute pancreatitis (Fig.10.4). Although pancreatitis may be due toabdominal trauma, it is more frequently due togallstone obstruction or alcohol abuse. The pan-creas often appears normal even when acutelyinflamed, so ultrasound examination should focuson the possible causes (such as gallstones, biliarydilatation or evidence of alcoholic liver disease) andcomplications (pseudocysts, portal or splenic veinthrombosis). Many pancreatic pseudocysts are nowmanaged successfully by endoscopic ultrasound-guided transgastric drainage.13
RENAL TRACT EMERGENCIES
(See also Chapter 7.) Ultrasound is usually the first-line investigation in the assessment of acute loinpain, which in the absence of trauma is commonlydue to acute urinary tract obstruction and/or renalinfection (Fig. 10.5). Less common acute presen-
tations include renal vein thrombosis or sponta-neous haemorrhage, usually from a renal tumouror cyst.
Until recently, ultrasound and/or intravenousurography (IVU) have been the investigations ofchoice in acute renal colic due to suspected uretericcalculus, and in most UK centres the IVU is cur-rently the method of choice for demonstratingureteric obstruction (Fig. 10.5E). Low-doseunenhanced multislice CT is increasingly beingrecommended as a replacement for these twomodalities,14 but even with this technique diagnos-tic pitfalls exist.15 Abdominal ultrasound with orwithout plain radiography may still provide com-parable accuracy where CT resources are lim-ited.16,17
The main limitation of ultrasound in acuteureteric obstruction is that obstruction may bepresent in the early stages without collecting sys-tem dilatation. But the minimally dilated renalpelvis, which would normally be dismissed as unre-markable in a patient with a full bladder, shouldraise the operator’s suspicion in the patient withacute loin pain. Doppler ultrasound of the kidneysshows a higher resistance index in the obstructedkidney than in the normal side.18 Upper tractobstruction can be relieved via cystoscopy-guidedureteric stent placement. Ultrasound-guided per-cutaneous nephrostomy may be required if this isnot practicable, or if there is evidence of infection.
Renal infection with parenchymal involvement(acute pyelonephritis) may be the cause of severeacute loin pain with fever, but ultrasound examina-tion mostly shows no abnormality. Occasionallythe skilled operator using high-specification equip-ment may be able to identify segmental areas ofhigh reflectivity, showing decreased blood flowwith power Doppler. The diagnosis of this con-dition is usually based on clinical criteria, butthese segments can be demonstrated with CT ifnecessary.
OTHER RETROPERITONEAL EMERGENCIES
(See also Chapter 8.) Ultrasound has an establishedrole in identifying the presence of an abdominalaortic aneurysm, but should not be used to assesssubacute leakage or rupture. However, where rup-ture is suspected, and no previous imaging results
ABDOMINAL ULTRASOUND248
Figure 10.4 Pancreatitis with a large pseudocyst. Thepatient was acutely tender, and the cyst was drainedunder ultrasound guidance.
ch10.qxd 6/30/04 6:19 PM Page 248
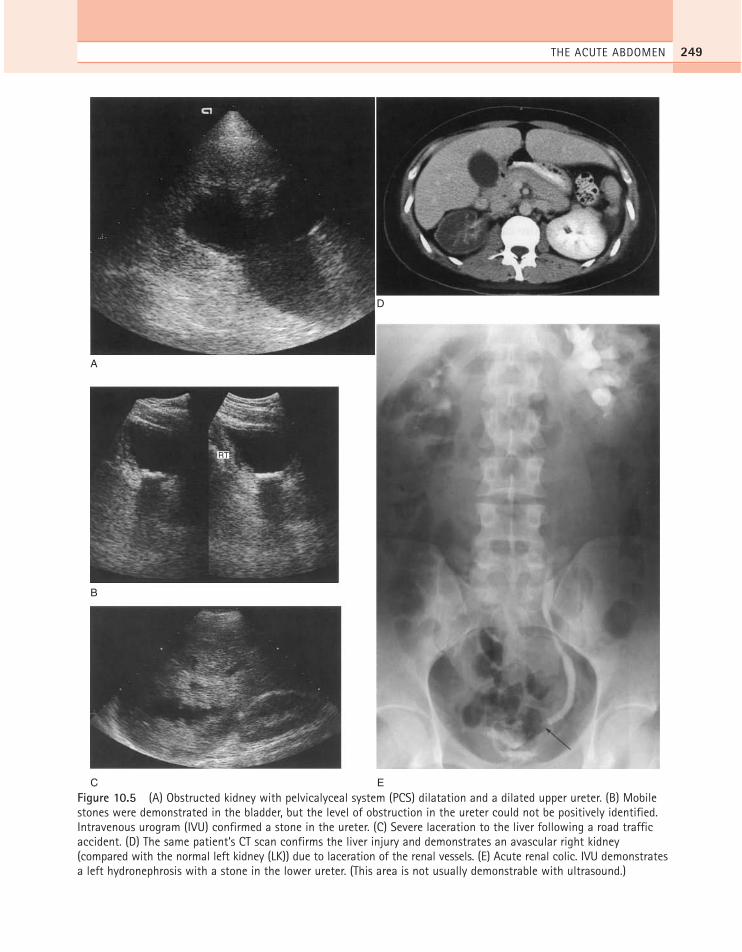
THE ACUTE ABDOMEN 249
A
B
RT
C E
D
Figure 10.5 (A) Obstructed kidney with pelvicalyceal system (PCS) dilatation and a dilated upper ureter. (B) Mobilestones were demonstrated in the bladder, but the level of obstruction in the ureter could not be positively identified.Intravenous urogram (IVU) confirmed a stone in the ureter. (C) Severe laceration to the liver following a road trafficaccident. (D) The same patient’s CT scan confirms the liver injury and demonstrates an avascular right kidney(compared with the normal left kidney (LK)) due to laceration of the renal vessels. (E) Acute renal colic. IVU demonstratesa left hydronephrosis with a stone in the lower ureter. (This area is not usually demonstrable with ultrasound.)
ch10.qxd 6/30/04 6:19 PM Page 249

are available, ultrasound can be a time-saving triagetool to exclude an aneurysm from the differentialdiagnosis of abdominal pain. Suitably trainedemergency department clinical staff can performthis quickly and successfully.19 Rupture of an aorticaneurysm is a catastrophic event, and although anurgent contrast-enhanced CT can be helpful,emergency surgery based on clinical findingsshould not be delayed by imaging investigations.
Ultrasound is also the first investigation ofchoice for demonstrating suspected psoas abscessor haematoma20 (Fig. 10.6).
ABDOMINAL ULTRASOUND250
SAG RT
Figure 10.6 A large, right-sided psoas haematoma.
References1. Forster R, Pillasch J, Zielke A. 1993 Ultrasonography
in blunt abdominal trauma: influence of the inves-tigator’s experience. Journal of Trauma 34: 264–269.
2. Porter RS, Nester BA, Dalsey WC et al. 1997 Use ofultrasound to determine the need for laparotomy intrauma patients. Annals of Emergency Medicine 29:323–330.
3. McGahan JP, Rose J, Coates TL et al. 1997 Use ofultrasonography in the patient with acute abdominaltrauma. Journal of Ultrasound in Medicine 16:653–662.
4. American College of Emergency Physicians. 1997 Useof ultrasound imaging by emergency physicians[policy statement]. Annals of Emergency Medicine30: 364–365.
5. Scalea TM, Rodriguez A, Chiu WC et al. 1999Focused assessment with sonography for trauma(FAST): results from an international consensusconference. Journal of Trauma-Injury, Infection andCritical Care 46: 466–472.
6. Bode PJ, Neizen RA, Van Vugt AB. 1993 Abdominalultrasound as a reliable indicator for conclusivelaparotomy in blunt abdominal trauma. Journal ofTrauma 34: 27–31.
7. Lentz KA, McKenney MG, Nunez DB et al. 1996Evaluating blunt abdominal trauma. Journal ofUltrasound in Medicine 15: 447–451.
8. Rothlin MA, Naf R, Amgwerd M. 1993 Ultrasoundin blunt abdominal and thoracic trauma. Journal ofTrauma 34: 488–495.
9. Craig MH, Talton DS, Hauser CJ, Poole GV. 1995Pancreatic injuries from blunt trauma. AmericanSurgeon 61: 125–128.
10. Chen SC, Wang HP, Chen WJ et al. 2002 Selectiveuse of ultrasonography for the detection ofpneumoperitoneum. Academic Emergency Medicine9: 643–645.
11. Lameris JS, Van-Overhagen H. 1995 Imaging andintervention in patients with acute right upperquadrant disease. Baillière’s Clinical Gastroenterology9: 21–36.
12. Cohen SA, Siegel JH. 1995 Biliary tract emergencies:endoscopic and medical management. Critical CareClinics 11: 273–294.
13. Norton ID, Clain JE, Wiersema MJ et al. 2001Utility of endoscopic ultrasonography in endoscopicdrainage of pancreatic pseudocysts in selectedpatients. Mayo Clinic Proceedings 76: 794–798.
14. Tack D, Sourtzis S, Delpierre I, de Maertelaer V,Gevenois PA. 2003 Low-dose unenhancedmultidetector CT of patients with suspected renal colic.American Journal of Roentgenology 180: 305–311.
15. Colistro R, Torreggiani WC, Lyburn ID et al. 2002Unenhanced helical CT in the investigation of acuteflank pain. Clinical Radiology 57: 435–441.
16. Catalano O, Nunziata A, Altei F, Siani A. 2002Suspected ureteral colic: primary helical CT versusselective helical CT after unenhanced radiography andsonography. American Journal of Roentgenology 178:379–387.
ch10.qxd 6/30/04 6:19 PM Page 250

17. Patlas M, Farkas A, Fisher D et al. 2001 Ultrasoundvs CT for the detection of ureteric stones in patientswith renal colic. British Journal of Radiology 74:901–904.
18. Rodgers PM, Bates JA, Irving HC. 1992 IntrarenalDoppler ultrasound studies in normal and acutelyobstructed kidneys. British Journal of Radiology 65:207–212.
19. Kuhn M, Bonnin RL, Davey MJ et al. 2000Emergency department ultrasound scanning forabdominal aortic aneurysm: accessible, accurate, andadvantageous. Annals of Emergency Medicine 36:219–223.
20. Monnier-Cholley L, Arrive L, Taboury J et al. 1996Non-vascular retroperitoneal emergencies. Annales deRadiologie 39: 72–77.
THE ACUTE ABDOMEN 251
ch10.qxd 6/30/04 6:19 PM Page 251

ch10.qxd 6/30/04 6:19 PM Page 252
This page intentionally left blank

The development of ultrasound-guided minimallyinvasive procedures, incorporating diagnosticbiopsy, therapeutic drainage and treatment tech-niques, has developed significantly over the lastdecade and is now accepted practice, in many cir-cumstances being used in isolation as a definitivetreatment, and in others in conjunction with otherradiological or surgical options. These minimallyinvasive methods are advantageous, with lowerpatient mortality and morbidity, increased patientacceptability, and are economically beneficial.
The relative speed and ease with which theseprocedures can be carried out have resulted in areduction of the diagnostic laparotomy and moreprompt and appropriate patient treatment. Whilstboth ultrasound and CT may be used for many ofthese procedures, in general, ultrasound is oftenthe first-line method as it is effective in the vastmajority, generally more accessible, and does notcarry a radiation risk. Clearly, the choice of tech-nique will depend upon the experience of the indi-vidual, machine availability and the site and depthof the lesion.
ULTRASOUND-GUIDED BIOPSY: GENERALCONSIDERATIONS
Percutaneous biopsy of organs, masses or focal vis-ceral lesions is an integral part of the diagnosticprocess for a large number of patients. Althoughchanges on ultrasound may confirm the suspectedclinical suspicion, that is, a bright liver may indicatefatty change, a nodular liver may suggest cirrhosisor enlarged kidneys of increased echogenicity may
Chapter 11
Interventional and othertechniques
253
CHAPTER CONTENTS
Ultrasound-guided biopsy: generalconsiderations 253Analgesia 254Methods of ultrasound guidance 255
Ultrasound-guided biopsy procedures 257Complications of ultrasound-guided biopsy 261
Ultrasound-guided drainage 261Intraoperative ultrasound 264Laparoscopic ultrasound 265Ultrasound contrast agents in the
abdomen 266The treatment of primary and secondary hepatic
tumours by percutaneous methods 268Endoscopic ultrasound 269
ch11.qxd 6/30/04 10:43 PM Page 253

suggest glomerulonephritis, imaging alone is notenough and a definitive histological diagnosis isrequired. The advantages of using ultrasound toguide such procedures are numerous:
● The needle tip is directed, in real time, alongthe biopsy path and visualized within the lesion.
● Greater precision is obtained; needle guidanceis essential for all small lesions and lesions atdepth.
● Fewer needle passes are required to obtain thedesired result.
● The best route can be utilized and vitalstructures, such as blood vessels, avoided.
● Postprocedure complications, such as haema-toma, are minimized.
● Confidence in the biopsy result, particularly anegative one, is increased due to directvisualization of the needle tip in the lesion.
● All the advantages of ultrasound over otherimaging methods apply (quick, direct vision,no radiation hazard, low cost). The limitationsdue to bone and air-filled structures also apply.
● The capability to perform bedside proceduresfor critically ill patients and to use inconjunction with other imaging techniques, forexample fluoroscopy, is advantageous.
With ultrasound the biopsy procedure is quick,safe and accurate and is therefore acceptable to thepatient. There are several accepted methods of per-forming a guided biopsy, but certain generic rulesare common to the procedure, regardless of theorgan under investigation:
● A written request form from a medicalpractitioner with the results of any previousinvestigations should be available. The reasonfor biopsy should be appropriate.
● Assessment of blood clotting status. Normallythe prothrombin time should be within 3 s ofthe control, platelet count > 75 000/ml andinternational normalized ratio (INR) < 1.3.
● Identification of possible contraindications tobiopsy, for example an uncooperative patient,coagulopathy.
● Careful explanation of the procedure to thepatient, including risks and benefits.
● Informed, written consent for the procedure.
● Procedure should be performed in a quiet andclean environment. Appropriate measuresshould be taken to preserve pre-, peri- andpostprocedure sterility.
● A prebiopsy scan to identify a suitable biopsyroute avoiding vital structures.
● Satisfactory care of the patient both during andafter the biopsy procedure with relevantobservations of vital signs. A pulse oximeterand appropriate nurse cover are nowrecommended.
● Appropriate preparation of the specimen.
● Contraindications are relative and include thebiopsy pathway, an uncooperative patient anduncorrectable coagulation and should beassessed on an individual basis.
AnalgesiaFor the vast majority of biopsy procedures localanaesthetic is administered following localizationof the biopsy site on ultrasound. Either 1% or 2%lidocaine (lignocaine) is commonly used; the vol-ume will depend upon patient build, depth oflesion and patient anxiety. Normally a short periodof time, commonly 4–5 min, is allowed to pass sothat the anaesthetic can work, after which a smallscalpel incision is made in the skin to facilitate thebiopsy needle’s introduction, with little or no dis-comfort to the patient.
In cases of, for example, simple aspiration with a22-gauge needle or smaller, local anaesthetic isnormally unnecessary.
Patients who are particularly apprehensive mayrequire preprocedure medication with a sedativesuch as diazepam or similar anxiolytic agent;however this is not common. Very occasionally intra-venous analgesia and/or sedation may be requiredduring the procedure; it is often a good idea to havean intravenous cannula in situ prior to biopsy.
The use of a general anaesthetic for children iscommon practice, to enable the procedure to becarried out quickly and accurately while the childremains still.
ABDOMINAL ULTRASOUND254
ch11.qxd 6/30/04 10:43 PM Page 254

Methods of ultrasound guidanceThere are various ways of performing ultrasound-guided procedures: organ/lesion localization(‘blind biopsy’), biopsy guide or freehand tech-nique. The choice of method depends upon theprocedure in question, equipment and the experi-ence and skill of the operator.
Blind biopsy
With this method a position on the skin surface ismarked overlying the organ or lesion to be biopsied,using ultrasound to localize. This remains accept-able for diffuse disease, when only a representativesample of liver tissue is required. Nevertheless, it isgood practice even in these situations to visualizethe needle during the procedure, and this methodof biopsy is now used less frequently.
Biopsy guidance
Most manufacturers provide a biopsy guide whichfits snugly on to the transducer head and providesa rigid pathway for the needle (Fig. 11.1). Theseare now the commonest and preferred method ofbiopsy. Previously adjustable angle biopsy guideswere available; however these offered no specificadvantages and were prone to user error. The fixedbiopsy guides contain a groove for a series of plas-tic inserts ranging from 14G to 22G size, depending
on the size of the biopsy needle. It is often pre-ferred to use one size greater than the needle, thatis a 16G insert for an 18G needle, as the needletends to move more freely. These guides are steril-ized and fitted on to the transducer, which caneither be covered by a sterile sheath or thoroughlycleaned with chlorhexidine solution. The use of asheath is highly recommended, as it maintains thesterility of the procedure, reducing the risk ofinfection, with no adverse effect on the image.
The needle pathway is displayed on the ultra-sound monitor electronically as a line or narrowsector, through which the needle passes. The oper-ator then scans in order to align the electronicpathway along the chosen route, the needle isinserted and the biopsy taken. These attachmentsshould be tested regularly to ensure the needle fol-lows the correct path (Fig. 11.2).
Freehand
A freehand approach, in which the operator scanswith one hand and introduces the needle near tothe transducer with the other, may be used forlarger or more superficial lesions. This technique iscommonly used for breast biopsy and biopsy in thehead and neck. The needle is inserted from oneend of the probe at right angles to the ultrasoundbeam; generally speaking the angle utilized is shal-low in comparison with the fixed guide systems fordeeper structures.
INTERVENTIONAL AND OTHER TECHNIQUES 255
A B
a
d
C
b
Figure 11.1 (A) Necessary component parts to perform an ultrasound-guided biopsy procedure. A series of plasticinserts (A) range in size from 14 to 22G. The appropriate insert is inserted into a fixed biopsy guide (B). The procedureis performed with sterile jelly (C) and a sterile probe cover (D) if required. (B) The assembled biopsy guide.
ch11.qxd 6/30/04 10:43 PM Page 255

Equipment and needles
The core of tissue for histological analysis isobtained with a specially designed needle consist-ing of an inner needle with a chamber or recess forthe tissue sample and an outer, cutting needlewhich moves over it—the Tru-Cut needle. Thebiopsy is obtained in two stages: first the innerneedle is advanced into the tissue, then the outercutting sheath is advanced over it and the needlewithdrawn containing the required tissue core(Fig. 11.3).
The use of a spring-loaded gun to operate theseneedles is now commonplace (Fig. 11.4). Suchdevices are designed to operate the needle withone hand; the whole needle is advanced into thetissue, just in front of the area to be biopsied. Bypressing the spring-loaded control, the inner partis rapidly advanced into the lesion, followed rapidlyby the cutting sheath over it. These needles can beobtained in a variety of sizes—generally 14, 16, 18or, less commonly, 20 gauge. Most focal lesions arebiopsied with a standard 18G needle. As a generalprinciple, as the needle advances approximately1.5–2.0 cm during biopsy, it is advisable to posi-
tion the needle tip on the edge of a lesion to obtaina good histological sample as most lesion necrosistends to be centrally located.
Such biopsy guns enable the operator to scanwith one hand and biopsy with the other, observ-ing the needle within the lesion, yielding a highrate of diagnosis with a single-pass technique1 andminimizing post-biopsy complications.
ABDOMINAL ULTRASOUND256
Figure 11.2 Testing the alignment of the biopsy guide. The electronic pathway is activated on the image, and theneedle is scanned as it is passed into a jug of water.
Figure 11.3 Biopsy needle closed (top) and open(bottom).
ch11.qxd 6/30/04 10:43 PM Page 256

As an alternative to the gun/needle combina-tion a number of ‘self-fire’ needles are available.This is essentially a single-use spring-loaded biopsyneedle. Again these come in a variety of sizes buttheir advantage is that they are easier and lighter touse than the gun/needle combination, and there-fore are easier employed in the CT situation. Mostdepartments will tend to utilize a combination ofboth.
In cases where the clinician is not familiar withultrasound techniques, appropriate guidance bya sonographer, while the clinician biopsies, ishighly successful, quick and avoids potentialcomplications.
Fine-needle histology, involving the use of nee-dles of 21 gauge or less, reduces even further thepossibility of postprocedure complications. Theseare generally not used as only small amounts of tis-sue are obtained for analysis and, as thin needles,they are apt to bend more easily, and are thereforemore difficult to see and retain within the plane ofthe scan. Biopsy of deep lesions is therefore moredifficult, if not impossible.
Fine-needle aspiration cytology
Cytology is the analysis of cells rather than the coreof tissue obtained for histology. This is generallymore difficult to interpret pathologically, as thecharacteristic architecture and intercellular rela-tionships seen in a histological sample are absent.It has the advantage, however, of allowing a finerneedle to be used. This can be passed through
structures, for example the stomach, blood vessels,en route to the site of interest, with no adverseeffects.
Fine needles for cytology are of 21 gauge orsmaller. They are of a simple design with a bev-elled, hollow core and no cutting mechanism.
The needle is introduced under ultrasoundguidance to the required position. Fragments oftissue are removed into the needle by applyingnegative (sucking) pressure with a syringe to theneedle, while moving the needle to and fro toloosen the tissue.
These can then be expelled on to a microscopeslide and smeared. The main disadvantage of thistechnique is that it requires a highly trained andspecialized pathologist to interpret the samples,whereas all trained pathologists can view histo-logical specimens. In addition, for many condi-tions, histological diagnosis is required, althoughcytology remains a useful tool in the breast andthyroid.
ULTRASOUND-GUIDED BIOPSYPROCEDURES
Liver biopsy
The most common reason for ultrasound-guidedbiopsy is for suspected metastatic disease. The liveris one of the most common sites for metastases andhistology is often required to confirm the diagno-sis, or to identify the origin of an unknown primarylesion (Figs 11.5 and 11.6).
Biopsy of other focal lesions in patients withchronic liver disease (for example, cirrhosis, hepa-titis B or C) in whom there may be suspected hepa-tocellular carcinoma and occasionally in patientswith benign disease (for example, capillary hae-mangiomas or focal nodular hyperplasia) can alsobe performed, although MRI and contrast ultra-sound are increasingly used to characterize lesions,without recourse to biopsy.
Focal lesion biopsy is generally safely and accu-rately performed with an 18G Tru-Cut needlewhich yields reliable tissue for histological analysis.In general an accuracy of 96% should be achiev-able2 (Fig. 11.7).
In addition to focal lesion biopsy anothercommon reason for liver biopsy is to assess the
INTERVENTIONAL AND OTHER TECHNIQUES 257
Figure 11.4 Spring-loaded gun designed to operate thecutting needle.
ch11.qxd 6/30/04 10:43 PM Page 257
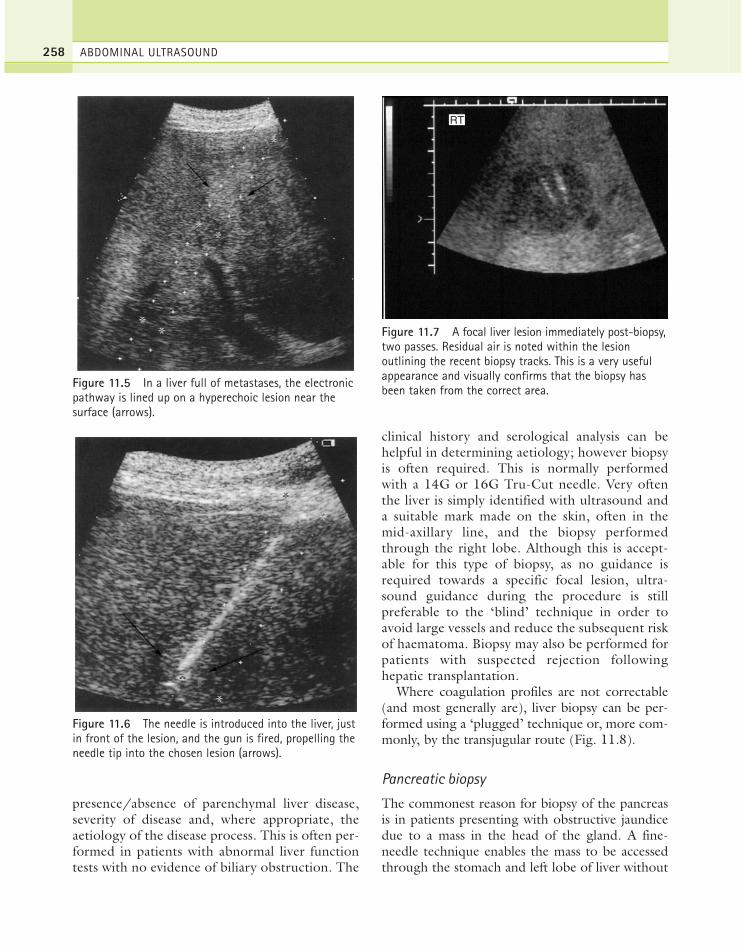
presence/absence of parenchymal liver disease,severity of disease and, where appropriate, theaetiology of the disease process. This is often per-formed in patients with abnormal liver functiontests with no evidence of biliary obstruction. The
clinical history and serological analysis can behelpful in determining aetiology; however biopsyis often required. This is normally performedwith a 14G or 16G Tru-Cut needle. Very oftenthe liver is simply identified with ultrasound anda suitable mark made on the skin, often in themid-axillary line, and the biopsy performedthrough the right lobe. Although this is accept-able for this type of biopsy, as no guidance isrequired towards a specific focal lesion, ultra-sound guidance during the procedure is stillpreferable to the ‘blind’ technique in order toavoid large vessels and reduce the subsequent riskof haematoma. Biopsy may also be performed forpatients with suspected rejection followinghepatic transplantation.
Where coagulation profiles are not correctable(and most generally are), liver biopsy can be per-formed using a ‘plugged’ technique or, more com-monly, by the transjugular route (Fig. 11.8).
Pancreatic biopsy
The commonest reason for biopsy of the pancreasis in patients presenting with obstructive jaundicedue to a mass in the head of the gland. A fine-needle technique enables the mass to be accessedthrough the stomach and left lobe of liver without
ABDOMINAL ULTRASOUND258
Figure 11.5 In a liver full of metastases, the electronicpathway is lined up on a hyperechoic lesion near thesurface (arrows).
Figure 11.6 The needle is introduced into the liver, justin front of the lesion, and the gun is fired, propelling theneedle tip into the chosen lesion (arrows).
RT
Figure 11.7 A focal liver lesion immediately post-biopsy,two passes. Residual air is noted within the lesionoutlining the recent biopsy tracks. This is a very usefulappearance and visually confirms that the biopsy hasbeen taken from the correct area.
ch11.qxd 6/30/04 10:43 PM Page 258
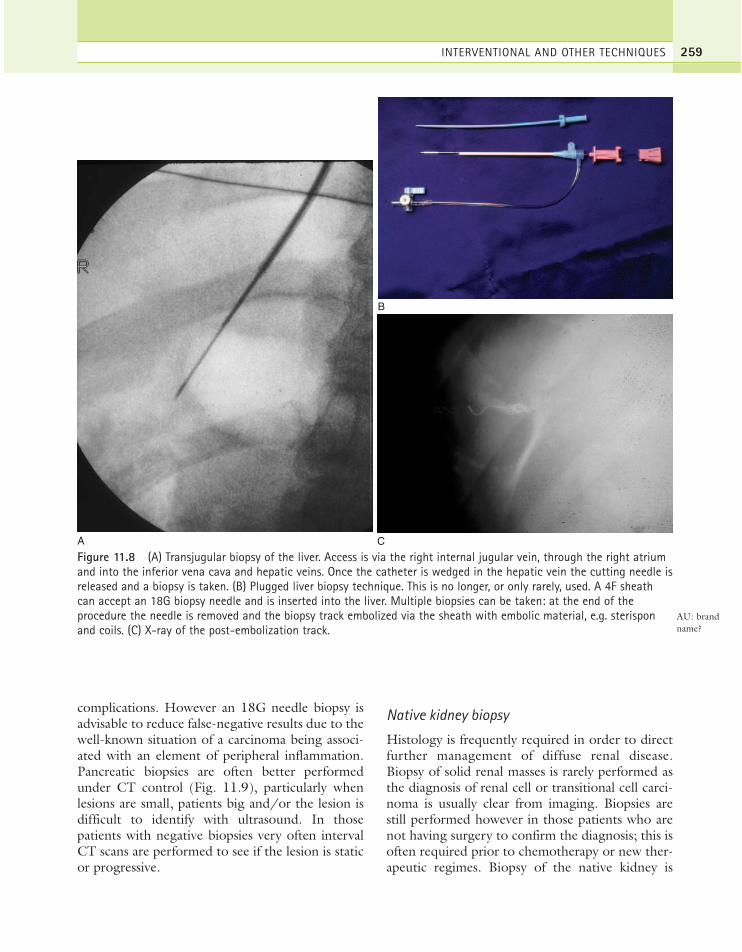
complications. However an 18G needle biopsy isadvisable to reduce false-negative results due to thewell-known situation of a carcinoma being associ-ated with an element of peripheral inflammation.Pancreatic biopsies are often better performedunder CT control (Fig. 11.9), particularly whenlesions are small, patients big and/or the lesion isdifficult to identify with ultrasound. In thosepatients with negative biopsies very often intervalCT scans are performed to see if the lesion is staticor progressive.
Native kidney biopsy
Histology is frequently required in order to directfurther management of diffuse renal disease.Biopsy of solid renal masses is rarely performed asthe diagnosis of renal cell or transitional cell carci-noma is usually clear from imaging. Biopsies arestill performed however in those patients who arenot having surgery to confirm the diagnosis; this isoften required prior to chemotherapy or new ther-apeutic regimes. Biopsy of the native kidney is
INTERVENTIONAL AND OTHER TECHNIQUES 259
A
B
C
Figure 11.8 (A) Transjugular biopsy of the liver. Access is via the right internal jugular vein, through the right atriumand into the inferior vena cava and hepatic veins. Once the catheter is wedged in the hepatic vein the cutting needle isreleased and a biopsy is taken. (B) Plugged liver biopsy technique. This is no longer, or only rarely, used. A 4F sheathcan accept an 18G biopsy needle and is inserted into the liver. Multiple biopsies can be taken: at the end of theprocedure the needle is removed and the biopsy track embolized via the sheath with embolic material, e.g. sterisponand coils. (C) X-ray of the post-embolization track.
AU: brandname?
ch11.qxd 6/30/04 10:43 PM Page 259

performed in the majority of centres under ultra-sound guidance. Contraindications to biopsyinclude hydronephrosis, which may be moreappropriately treated with catheterization ornephrostomy, or small kidneys, that is < 8 cm lon-gitudinal axis (these appearances being indicativeof chronic renal impairment). Kidneys > 9 cm canpotentially be biopsied; however other factors,including cortical thickness, age, clinical historyand the requirement for definitive diagnosis willall have a bearing on whether biopsy is performedor not. Hydronephrosis and kidney size are easilyassessable with a prebiopsy scan.
In most cases the biopsy is performed with thepatient prone over a small bolster to maximizeaccess to the kidney. The shortest route, avoidingadjacent structures, is selected; subcostally, travers-ing the cortex of the lower pole and avoiding thecollecting system and major vessels is recom-mended. With ultrasound guidance, either kidneymay be chosen and accessibility will vary betweenpatients. The depth of penetration and angle ofapproach are carefully assessed. Biopsy is normallywith a 16G needle.
The patient’s cooperation is required with sus-pending respiration at the crucial moment. This
avoids undue damage to the kidney as the needle isintroduced through the capsule. The needleshould be positioned just within the capsule priorto biopsy so that the maximum amount of corticaltissue is obtained for analysis, as the throw of theneedle may be up to 2 cm.
Renal transplant biopsy
Biopsy is a valuable tool in the postoperative man-agement of the transplant patient (Chapter 7),enabling the cause of graft dysfunction to be iden-tified, in particular differentiating acute tubularnecrosis from acute rejection. Ultrasound guidanceis essential in order to reduce complications such ashaematoma, vascular damage (which may result inarteriovenous fistula or pseudoaneurysm forma-tion) and laceration of the renal collecting system.A single-pass technique, using the spring-loadedbiopsy gun with a 16-gauge needle, is usuallysufficient for histological purposes; howevertwo passes are often required so that electronmicroscopy and immunofluorescence can also beperfomed. The procedure is well tolerated by thepatient and the complication rate low, at lessthan 5%.3
ABDOMINAL ULTRASOUND260
A B
R L R
Figure 11.9 (A) CT-guided biopsy of a pancreatic head mass. The tip of the biopsy needle (arrow) is positioned in theperiphery of the lesion so that when the biopsy is taken a good core of tissue is obtained. Note the artifact from theneedle tip. (B) CT-guided bioposy of a retroperitoneal lymph node mass (arrowheads). The mass lies adjacent to theaorta (arrow); however this is protected from the needle by the angle of approach and its relationship to the vertebralbody. CT is the preferred biopsy method of choice for deep structures within the retroperitoneum.
ch11.qxd 6/30/04 10:43 PM Page 260
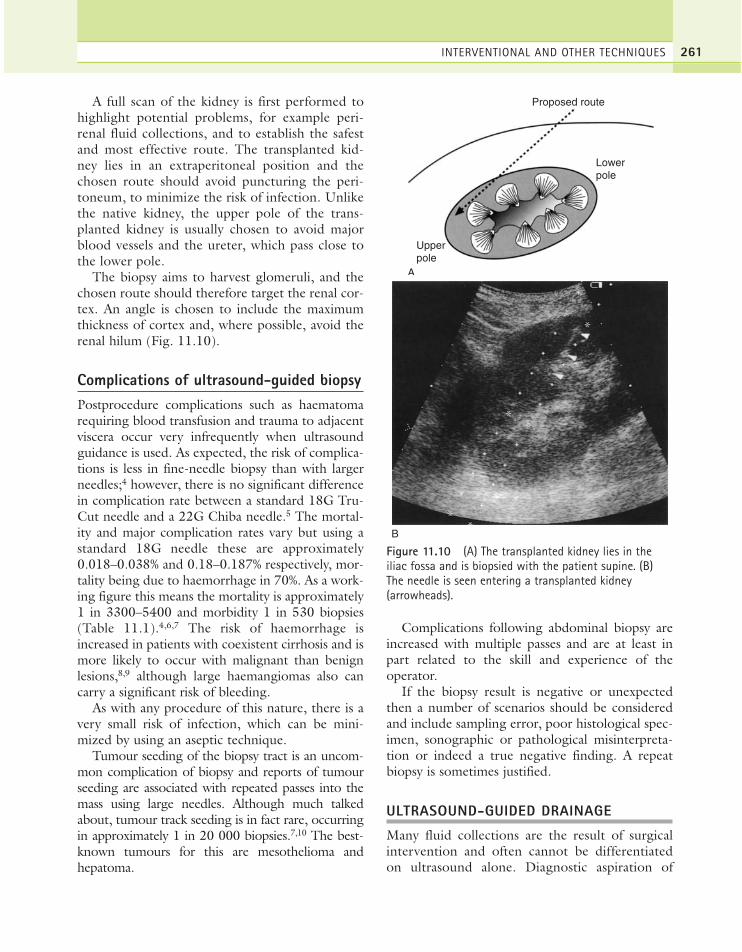
A full scan of the kidney is first performed tohighlight potential problems, for example peri-renal fluid collections, and to establish the safestand most effective route. The transplanted kid-ney lies in an extraperitoneal position and thechosen route should avoid puncturing the peri-toneum, to minimize the risk of infection. Unlikethe native kidney, the upper pole of the trans-planted kidney is usually chosen to avoid majorblood vessels and the ureter, which pass close tothe lower pole.
The biopsy aims to harvest glomeruli, and thechosen route should therefore target the renal cor-tex. An angle is chosen to include the maximumthickness of cortex and, where possible, avoid therenal hilum (Fig. 11.10).
Complications of ultrasound-guided biopsyPostprocedure complications such as haematomarequiring blood transfusion and trauma to adjacentviscera occur very infrequently when ultrasoundguidance is used. As expected, the risk of complica-tions is less in fine-needle biopsy than with largerneedles;4 however, there is no significant differencein complication rate between a standard 18G Tru-Cut needle and a 22G Chiba needle.5 The mortal-ity and major complication rates vary but using astandard 18G needle these are approximately0.018–0.038% and 0.18–0.187% respectively, mor-tality being due to haemorrhage in 70%. As a work-ing figure this means the mortality is approximately1 in 3300–5400 and morbidity 1 in 530 biopsies(Table 11.1).4,6,7 The risk of haemorrhage isincreased in patients with coexistent cirrhosis and ismore likely to occur with malignant than benignlesions,8,9 although large haemangiomas also cancarry a significant risk of bleeding.
As with any procedure of this nature, there is avery small risk of infection, which can be mini-mized by using an aseptic technique.
Tumour seeding of the biopsy tract is an uncom-mon complication of biopsy and reports of tumourseeding are associated with repeated passes into themass using large needles. Although much talkedabout, tumour track seeding is in fact rare, occurringin approximately 1 in 20 000 biopsies.7,10 The best-known tumours for this are mesothelioma andhepatoma.
Complications following abdominal biopsy areincreased with multiple passes and are at least inpart related to the skill and experience of theoperator.
If the biopsy result is negative or unexpectedthen a number of scenarios should be consideredand include sampling error, poor histological spec-imen, sonographic or pathological misinterpreta-tion or indeed a true negative finding. A repeatbiopsy is sometimes justified.
ULTRASOUND-GUIDED DRAINAGE
Many fluid collections are the result of surgicalintervention and often cannot be differentiatedon ultrasound alone. Diagnostic aspiration of
INTERVENTIONAL AND OTHER TECHNIQUES 261
Figure 11.10 (A) The transplanted kidney lies in theiliac fossa and is biopsied with the patient supine. (B)The needle is seen entering a transplanted kidney(arrowheads).
Proposed route
Lowerpole
Upperpole
A
B
ch11.qxd 6/30/04 10:43 PM Page 261

fluid collections is used to establish theirexact nature: this may include haematoma,lymphocoele, urinoma, biloma, pseudocysts andothers.
Postoperative haematomas are normally treatedconservatively and tend to resolve spontaneously.Insertion of a drain into such a collection is at highrisk of converting the collection into an abscess.
Abscess drainage
Ultrasound-guided drainage of abscesses is nowthe preferred treatment when the collection canbe visualized on ultrasound and a safe route cho-sen. These may result from postoperative infec-tion, inflammatory bowel conditions, such asCrohn’s disease or appendicitis, or other sourcesof infection, particularly in immunosuppressedpatients. Drains come in different sizes and gen-erally the thicker the pus, the larger the bore ofdrain that is required. Whilst aspiration is initiallyperformed to confirm the nature of the collec-tion, very often a drain is left in situ; togetherwith appropriate antibiotic therapy this is usuallyeffective. At the very least it normally leads to animprovement in the overall clinical condition toallow definitive treatment and can in itself be adefinitive cure.
Ultrasound is particularly useful in cases of hepaticabscesses and in draining the subphrenic, pericolicand subhepatic areas. Superficial collections, usuallyassociated with wound sites, are also readily accessi-ble to ultrasound. Collections obscured by bowel gasare best drained under CT guidance.
Gallbladder drainage
Gallbladder drainage under ultrasound control is atemporary, palliative procedure which tends to bereserved for particularly ill patients with septi-caemia, as a method of stabilizing their conditionprior to surgery. Drainage of, for example, a gall-bladder empyema buys useful time, reducing therisk of perforation and subsequent peritonitis andimproving clinical status prior to surgical removal.Although the portable nature of ultrasound allowsa bedside procedure to be performed (which is par-ticularly useful in patients under intensive therapywho cannot be moved), these procedures carry ahigh risk to the patient and full anaesthetic, nurs-ing and medical support is required.
Nephrostomy
Renal obstruction in which the pelvicalyceal systemis dilated may be alleviated by the percutaneousintroduction of a nephrostomy tube under ultra-sound guidance. This procedure relieves pressure inthe renal collecting system and avoids potential irre-versible damage to the renal parenchyma (Fig.11.11). Although the procedure may be carried outcompletely under ultrasound control, it is normallyperformed in a screening room where a combina-tion of ultrasound and X-ray screening can be usedto maximal effect.
Cyst drainage
The percutaneous treatment of renal and hepaticcysts by simple aspiration may afford only temporaryrelief as they frequently recur, but a more permanentresult may be achieved by injecting a sclerosant, forexample absolute alcohol or tetracycline into thecyst. In addition, percutaneous treatment of hydatidliver disease (traditionally avoided because of the riskof spreading parasites along the needle track andcausing further infection) has been successfully per-formed by injecting of a scolicidal agent,11 avoidingthe need for surgical removal.
Other applications include draining of pancre-atic pseudocysts and inserting a cystogastrostomytube with combined fluoroscopy and ultrasoundguidance; the cyst is allowed to drain through this
ABDOMINAL ULTRASOUND262
Table 11.1 Complications of ultrasound-guidedbiopsy
Major Number compli-of Mortality cation
Author Year biopsies rate rate
Fornari et al4 1989 10 800 1:5400 1:530Nolsoe et al6 1990 8000 1:2700 1:540Smith7 1991 16 400 1:3300 —
ch11.qxd 6/30/04 10:43 PM Page 262

tube into the stomach. This is now better doneendoscopically.12
Indirect ultrasound guidance
Not infrequently drainage of fluid, for examplefrom the pleural cavity, may be performed awayfrom the ultrasound department in the ward orclinic. Although ideally this is done under guidance
with a portable scanner, in practice excellent resultsare obtained for larger, non-loculated collections,particularly pleural effusions, by marking the skinsurface with a felt-tip marker in the main scanningdepartment to enable drainage to be safely carriedout on the ward.
The mark should be made with the patient inthe position in which drainage is to be attempted,for example sitting or decubitus right side raised,
INTERVENTIONAL AND OTHER TECHNIQUES 263
A B
C
LT
Figure 11.11 (A) Longitudinal ultrasound image of the left kidney. There is clear evidence of hydronephrosis. (B) Similar image during a nephrostomy procedure. The electronic ultrasound guide path can be easily visualized. Theguide wire (arrow) can also be seen within the renal pelvis and collecting system. (C) Longitudinal ultrasound scan ofthe left kidney immediately following nephrostomy. The collecting system remains dilated due to injected contrast. Theechogenic tips of the drainage cathether (arrow) can be visualized within the renal pelvis.
ch11.qxd 6/30/04 10:43 PM Page 263

and this information communicated to the clini-cian performing the drainage, together with thedepth from the skin surface to the fluid. The punc-ture site should be marked so that the route is per-pendicular to the skin surface. Drainage of pleuraleffusions and of ascites are the two most com-monly performed procedures using this method.
INTRAOPERATIVE ULTRASOUND (IOUS)
IOUS is increasingly used in the abdomen, inboth the diagnosis and treatment of lesions. Itsapplications are varied and its dynamic nature,mobility and high resolution make it ideal for sur-gical work.
Hepatic IOUS
The most frequent application in the abdomen isin diagnosing and locating liver metastases prior tosurgical resection. Resection of metastases, partic-ularly from colorectal tumours, is a potentialcure, but results are unsuccessful if small lesions,undetected preoperatively, are not removed atoperation.
The direct contact of the IOUS probe with theliver surface, avoiding attenuative subcutaneoustissue, enables a high-frequency (7.5 MHz) probeto be used. IOUS can demonstrate lesions toosmall to be detected on preoperative imaging, andas a result can change operative management13,14
in terms of altering the resection line to includemore tissue, removing additional hepatic seg-ments or even abandoning the operative proce-dure altogether.
A combination of surgical palpation, whichdetects small surface lesions, and IOUS, whichdetects small, deep lesions, has the highest diagnos-tic accuracy. IOUS is quick to perform in the handsof an experienced operator and its contribution tothe success of surgery is invaluable15 (Fig. 11.12).
IOUS is particularly useful when there has been adelay between preoperative imaging and surgery, asprogression of disease may have occurred duringthis interval, or when preoperative imaging is equiv-ocal (for example, differentiating tiny cystic fromsolid lesions). IOUS is often able to offer a defini-tive diagnosis and when doubt still exists guidedbiopsy under ultrasound control may be performed.
In addition to lesion detection it is able to demon-strate vascular invasion by tumour and to demon-strate clearly, in real time, the relationship of thetumour to adjacent vascular structures; this is essen-tial for planning a resection line. The greater themargin of normal tissue around the resectedtumour, the better the long-term prognosis, and amargin of greater than 1 cm normal tissue is pre-ferred. IOUS can also be used to locate deep lesionsfor ultrasound-guided biopsy or ablation.
Other applications of IOUS
There are numerous extrahepatic applications forIOUS in the abdomen, including urological, vas-cular and gastrointestinal tract scanning.
Ultrasound evaluation of the common duct forcalculi following cholecystectomy can identifysmall fragments which may not be easily palpablethrough the duct wall. Using this technique theduct is less susceptible to injury which may be asso-ciated with direct examination or the introductionof X-ray contrast agents.
Pancreatic scanning is particularly useful inidentifying small tumours of the body and tail ofpancreas for curative resection16 and in differenti-ating small pancreatic retention cysts from solidnodules.17
The treatment of tumours by percutaneous ultra-sound-guided techniques, rather than surgical resec-tion, is becoming more common. However, it maynot always be possible to achieve success percuta-neously and techniques have been developed toablate tumours during open surgery. Cryotherapy,18
in which the lesion is frozen by introducing a cryo-probe into the centre of the lesion under intraoper-ative ultrasound guidance, has been successfullyused, but is now largely superseded by radio-frequency and microwave ablation (Fig. 11.13).These techniques have resulted in long-term sur-vival in patients with hepatocellular carcinoma19 andmultiple liver metastases.20 The success of such tech-niques depends to a large extent upon patient selec-tion. Those with very large and/or multiple lesionstend to have a poor prognosis compared withpatients with smaller, well-confined disease.However these techniques continue to develop andare likely to offer hope to many patients currentlyuntreatable with conventional methods.
ABDOMINAL ULTRASOUND264
ch11.qxd 6/30/04 10:43 PM Page 264

LAPAROSCOPIC ULTRASOUND
Dedicated laparoscopic ultrasound probes may bepassed through the laparoscopic port during surgicalprocedures to investigate the liver, biliary tree,pancreas and other viscera without the need for opensurgery (Fig. 11.14).
The trend towards laparoscopic rather thanopen cholecystectomy has increased the need foraccurate laparoscopic exploration of the biliaryductal system to confirm the presence or absenceof stones. Laparoscopic ultrasound is better atdemonstrating stones in the duct and anatomicalductal variations than conventional intraoperativecholangiography.21
Laparoscopic ultrasound has also provenadvantageous in staging patients with hepatictumours for liver resection,22 demonstrating deeptumours not visible on surgical laparoscopy, or bypreoperative imaging methods and so avoiding theneed to proceed to open hepatic resection in somepatients.
Patients with pancreatic head and ampullary car-cinomas are potentially resectable in only a minorityof cases. Preoperative imaging is known to under-estimate the extent of the disease, and so manypatients traditionally undergo a staging laparotomybefore resection is attempted. However, over one-third of patients previously considered resectable
INTERVENTIONAL AND OTHER TECHNIQUES 265
A B
C D
Figure 11.12 Intraoperative ultrasound (A) Demonstrating a margin of tissue of only 2 or 3 mm between themetastasis and the hepatic vein. (B) Metastasis in segment 8, at the confluence of the hepatic veins. (C) This metastasishas started to invade the hepatic vein. (D) Tiny metastasis, not diagnosed on preoperative imaging and not surgicallypalpable. (Differential diagnosis would be of haemangioma.)
ch11.qxd 6/30/04 10:43 PM Page 265
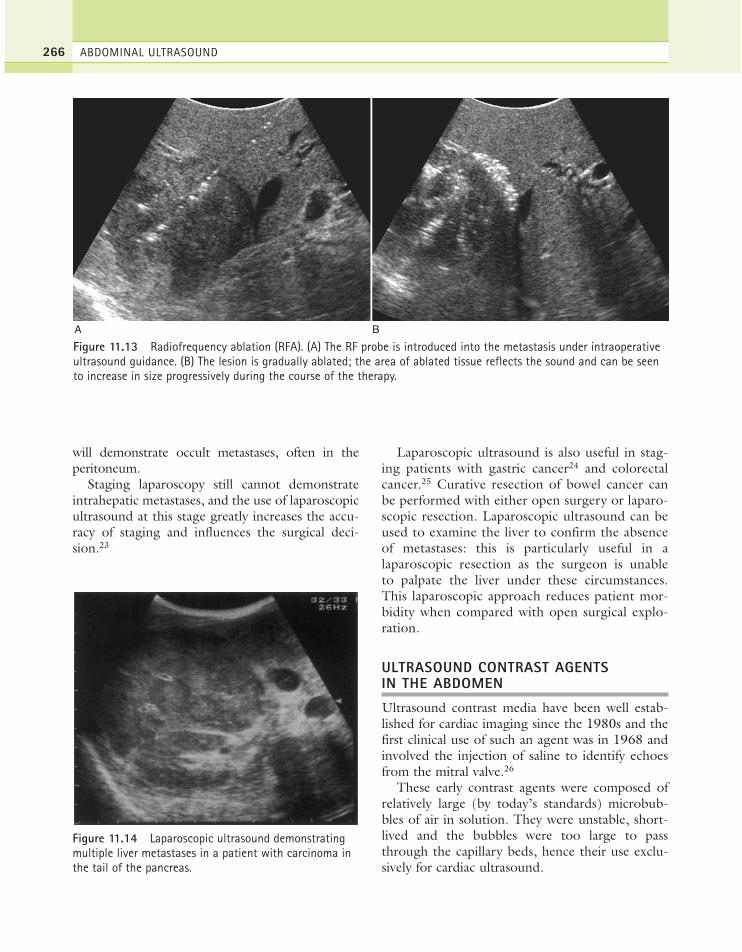
will demonstrate occult metastases, often in theperitoneum.
Staging laparoscopy still cannot demonstrateintrahepatic metastases, and the use of laparoscopicultrasound at this stage greatly increases the accu-racy of staging and influences the surgical deci-sion.23
Laparoscopic ultrasound is also useful in stag-ing patients with gastric cancer24 and colorectalcancer.25 Curative resection of bowel cancer canbe performed with either open surgery or laparo-scopic resection. Laparoscopic ultrasound can beused to examine the liver to confirm the absenceof metastases: this is particularly useful in alaparoscopic resection as the surgeon is unableto palpate the liver under these circumstances.This laparoscopic approach reduces patient mor-bidity when compared with open surgical explo-ration.
ULTRASOUND CONTRAST AGENTS IN THE ABDOMEN
Ultrasound contrast media have been well estab-lished for cardiac imaging since the 1980s and thefirst clinical use of such an agent was in 1968 andinvolved the injection of saline to identify echoesfrom the mitral valve.26
These early contrast agents were composed ofrelatively large (by today’s standards) microbub-bles of air in solution. They were unstable, short-lived and the bubbles were too large to passthrough the capillary beds, hence their use exclu-sively for cardiac ultrasound.
ABDOMINAL ULTRASOUND266
A B
Figure 11.13 Radiofrequency ablation (RFA). (A) The RF probe is introduced into the metastasis under intraoperativeultrasound guidance. (B) The lesion is gradually ablated; the area of ablated tissue reflects the sound and can be seento increase in size progressively during the course of the therapy.
Figure 11.14 Laparoscopic ultrasound demonstratingmultiple liver metastases in a patient with carcinoma inthe tail of the pancreas.
ch11.qxd 6/30/04 10:43 PM Page 266

Since those early years there have been a num-ber of developments in the field of contrast ultra-sound. Agents such as Albunex (MolecularBiosystems, San Diego, USA), consisting of albu-min-coated microbubbles, were small enough topass through the pulmonary capillaries and enterthe left side of the heart; however they were tooweak to withstand systolic pressure and could nottherefore enter the blood pool in any appreciablequantity.
A more stable suspension was then produced,consisting of small microbubbles in the order of2–5 µm which passed through the pulmonary cap-illary bed after intravenous injection, and actedas a true blood-pool agent. Called Levovist(Schering, Berlin, Germany), this is a galactose-based agent (99.9%) containing palmitic acid(0.1%) for stability, which traps air which is subse-quently released when the bubbles burst. As thefirst stable blood-pool agent it could be used forexamining the abdominal viscera and vasculature.
By coincidence, microbubbles of this size canpass through the pulmonary capillaries and res-onate at frequencies used in clinical diagnosticultrasound (1–20 MHz). This resonance causes amuch greater capacity for scattering the beam thanthat from a non-resonating particle and thus astronger signal is produced of up to 25 dB on bothgrey-scale and Doppler. The Doppler signal from acontrast-enhanced blood vessel is therefore mucheasier to identify. In addition, vessels too small tobe identified on normal grey-scale or non-enhanced Doppler scans can be identified whenusing a microbubble agent (Fig. 11.15).
Despite the use of microbubble agents, bloodflow in tiny vessels can still be difficult to detect;harmonic imaging techniques however aid detec-tion further. When insonated with ultrasound of acertain frequency, microbubbles emit a secondaryharmonic frequency twice that of the incidentwave, in addition to the primary harmonic. As thesecond peak is a purer signal, this increases the sen-sitivity, enabling smaller vessels with slow flow tobe successfully detected and distinguished fromsurrounding tissues. Many harmonic-based pulsemethods are used with contrast agents and some ofthe more popular ones include pulse and phaseinversion, for example pulse inversion is a dualpulse technique, 180º out of phase, resulting in
summation of signal from non-linear scatterers(microbubbles) and cancellation of signal fromlinear scatterers (tissue).
Potential applications of these agents includesituations in which ultrasound findings are equivo-cal or in which Doppler information is suboptimal.A contrast agent will enhance the Doppler ultra-sound signal from the blood pool and increasediagnostic confidence. This may therefore obviatethe need for other more invasive angiographicinvestigations.27 These agents therefore have thepotential to extend the applications of Dopplerultrasound in the abdomen.
With regard to the abdomen it can be useful inpatients with chronic liver disease for the investiga-tion of portal vein thrombosis. Increased sensitivityand specificity have been reported for examinationof the portal vein,28 avoiding the need for contrastangiography. In patients with hepatic transplanta-tion it is helpful in confirming hepatic artery patencyin the early postoperative period: this can be difficultto confirm with conventional imaging alone.Although it is felt intuitively that it may be of helpin the diagnosis of renal artery stenosis, the evidenceis as yet not convincing to support its routine use.
The diagnosis and characterization of hepatictumours are also improved with contrast agents asthese agents, for example, Levovist and Sonovue,are preferentially taken up by the hepatosplenicparenchyma and so focal lesions appear as fillingdefects in much the same way as CT or MRI (Fig.11.16). The exact site of accumulation within theliver is unknown but may be within the reticulo-endothelial system or liver sinusoids. There isgrowing evidence to support the differentiation oflesions within the liver, not previously possiblewith conventional ultrasound,29,30 and certainlymicrobubble agents are helpful in the diagnosis ofcapillary haemangiomas, hepatomas and focalnodular hyperplasia. How are microbubble agentsused currently? Generally an agent such as Sonovue,currently the most commonly used, which consistsof a phospholipid membrane containing perfluoro-carbon gas, is injected intravenously. Imaging, forexample in the liver, can now be performed in botha hepatic arterial and portal venous phase similar toCT. Most imaging is performed with a harmonic-based technique—pulse or phase inversion—andutilizing a low mechanical index (< 0.15) to
INTERVENTIONAL AND OTHER TECHNIQUES 267
ch11.qxd 6/30/04 10:43 PM Page 267

prolong longevity of the bubbles. Although thereis no definitive evidence as yet to support its rou-tine use, it is currently undergoing a number of tri-als comparing it with CT and MRI in the detectionof focal liver disease, and early results arefavourable.31
Other simple substances, technically consideredcontrast agents, including water or saline, are used tooutline the stomach (for example, to visualize thepancreas or to assess the nature of an epigastric mass)or the rectum. In the future, oral ultrasound contrast
agents may be developed specifically to examine thestomach or colon and to reduce bowel gas.
THE TREATMENT OF PRIMARY ANDSECONDARY HEPATIC TUMOURS BYPERCUTANEOUS METHODS
In patients with colorectal carcinoma the presenceof liver metastasis is the most accurate predictor ofsurvival. Resection of liver metastases is known toincrease the lifespan of patients, with good quality
ABDOMINAL ULTRASOUND268
A (i)
B (i) B (ii)
A (ii)
TIPS
HA
TIPPS
LAEVOVIST 300 MG/ML
Figure 11.15 (A) i, Pre-injection of contrast—no flow is demonstrated in this transjugular intrahepatic portosystemicshunt; ii, post-injection, flow is still not demonstrated, confirming the shunt to be thrombosed. (B) i, the same patient—pre-injection the hepatic artery is identified adjacent to the shunt; ii, post-injection: without altering the settings,greatly enhanced arterial Doppler signals are demonstrated from even the most peripheral hepatic arteries.
(continued)
ch11.qxd 6/30/04 10:43 PM Page 268
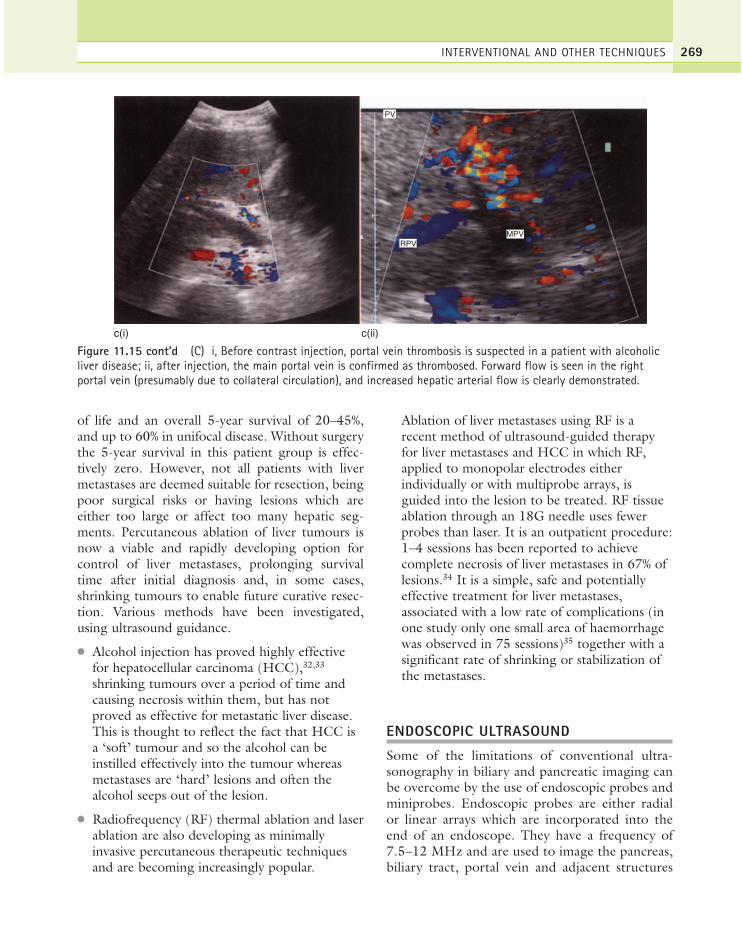
of life and an overall 5-year survival of 20–45%,and up to 60% in unifocal disease. Without surgerythe 5-year survival in this patient group is effec-tively zero. However, not all patients with livermetastases are deemed suitable for resection, beingpoor surgical risks or having lesions which areeither too large or affect too many hepatic seg-ments. Percutaneous ablation of liver tumours isnow a viable and rapidly developing option forcontrol of liver metastases, prolonging survivaltime after initial diagnosis and, in some cases,shrinking tumours to enable future curative resec-tion. Various methods have been investigated,using ultrasound guidance.
● Alcohol injection has proved highly effectivefor hepatocellular carcinoma (HCC),32,33
shrinking tumours over a period of time andcausing necrosis within them, but has notproved as effective for metastatic liver disease.This is thought to reflect the fact that HCC isa ‘soft’ tumour and so the alcohol can beinstilled effectively into the tumour whereasmetastases are ‘hard’ lesions and often thealcohol seeps out of the lesion.
● Radiofrequency (RF) thermal ablation and laserablation are also developing as minimallyinvasive percutaneous therapeutic techniquesand are becoming increasingly popular.
Ablation of liver metastases using RF is arecent method of ultrasound-guided therapyfor liver metastases and HCC in which RF,applied to monopolar electrodes eitherindividually or with multiprobe arrays, isguided into the lesion to be treated. RF tissueablation through an 18G needle uses fewerprobes than laser. It is an outpatient procedure:1–4 sessions has been reported to achievecomplete necrosis of liver metastases in 67% oflesions.34 It is a simple, safe and potentiallyeffective treatment for liver metastases,associated with a low rate of complications (inone study only one small area of haemorrhagewas observed in 75 sessions)35 together with asignificant rate of shrinking or stabilization ofthe metastases.
ENDOSCOPIC ULTRASOUND
Some of the limitations of conventional ultra-sonography in biliary and pancreatic imaging canbe overcome by the use of endoscopic probes andminiprobes. Endoscopic probes are either radialor linear arrays which are incorporated into theend of an endoscope. They have a frequency of7.5–12 MHz and are used to image the pancreas,biliary tract, portal vein and adjacent structures
INTERVENTIONAL AND OTHER TECHNIQUES 269
c(i) c(ii)
RPV
PV
MPV
Figure 11.15 cont’d (C) i, Before contrast injection, portal vein thrombosis is suspected in a patient with alcoholicliver disease; ii, after injection, the main portal vein is confirmed as thrombosed. Forward flow is seen in the rightportal vein (presumably due to collateral circulation), and increased hepatic arterial flow is clearly demonstrated.
ch11.qxd 6/30/04 10:43 PM Page 269

within 5–6 cm of the probe. Radial probes may beused in the preoperative staging of a number ofdiseases, including oesophageal, gastric, pancre-atic and lung cancer, whilst linear array probes areused for interventional procedures such as fine-needle aspiration analysis of mediastinal lymphnodes, solid organ assessment, for example pan-creas, occasionally liver, adrenals, pseudocystdrainage and coeliac plexus neurolysis.
Endoscopic ultrasound is more sensitive and spe-cific than spiral CT, MRI or transabdominal ultra-sound in the detection of small pancreatic massesand its diagnostic ability can be further enhancedby the use of endoscopic ultrasonically guided fine-needle aspiration cytology36 and biopsy.
It may also detect early changes of pancreatitiswhich are not visible on endoscopic netrogradecholangiopancreatography (ERCP), and one of its
ABDOMINAL ULTRASOUND270
A
C D
B
Figure 11.16 (A) Conventional ultrasound of the liver showing no abnormality. (B) Pulse inversion mode followingintravenous Levovist injection showing a focal lesion (arrow) i.e. metastasis in the same patient as Fig. 16a. (C)Conventional grey-scale scan of the liver. A number of metastases were seen throughout the liver. One in the left lobehas been arrowed. (D) Pulse inversion mode with intravenous Levovist in the same patient as (C). The metastasis seenon the unenhanced grey-scale image can still be seen (arrow); however, easily discernible additional lesions are nowalso appreciated.
ch11.qxd 6/30/04 10:43 PM Page 270

main uses is in staging pancreatic tumours, pre-dicting their resectability, identifying small lymphnode metastases and assessing vascular invasion.37
It is particularly accurate in identifying small pan-creatic insulinomas,38 often difficult or impossibleto identify on conventional cross-sectional imagingdespite a documented biochemical abnormality,and thus guiding subsequent surgical procedures.Endoscopic ultrasound is also used in the detectionof biliary calculi, particularly in the normal-calibrecommon bile duct, with a much higher accuracythan other imaging techniques and without thepotential additional risks of ERCP.39
Further, less-established uses of endoscopicultrasound include gastrointestinal examinations,in which invasion of gastric lesions into andthrough the wall of the stomach can be assessed,40
anal ultrasound, which is used to visualize thesphincter muscles in cases of sphincter dysfunction,the staging of colorectal carcinomas and thedemonstration of bowel wall changes in inflamma-tory bowel conditions.41
The miniprobe has a higher frequency (20–30MHz) and may be passed down a conventionalendoscope. It therefore has the advantage of a one-stage gastrointestinal tract endoscopy/ERCP,rather than requiring a separate procedure. It maybe inserted into the common duct of the biliarytree to assess local tumour invasion and to clarify
the extent and/or nature of small lesions alreadyidentified by other imaging methods. It showsremarkable accuracy in the detection of commonbile duct tumours and other biliary tract diseasewhen compared with other imaging modalities.42
It may be used in the staging of oesophageal andgastric cancer, and is especially useful when a tightoesophageal stricture prevents the passage of theendoscope.41 The layers of the oesophageal or gas-tric wall and the extent of tumour invasion can beaccurately assessed.
The miniprobe is also used in patients with sus-pected pancreatic carcinoma, for example in patientswith a negative CT but who have irregularity of thepancreatic duct on contrast examination. The probecan be passed into the pancreatic duct during ERCPto detect small lesions, assess the extent of thetumour and predict resectability.43 It is superior toconventional endoscopic ultrasound in the detec-tion of the smaller, branch tumour nodules, and canalso detect local retroperitoneal or vascular invasionin areas adjacent to the probe.
The use of endoscopic ultrasound is currentlylimited to a few specialist centres. A steep learningcurve together with the expense of the equipmentis likely to restrict its widespread use; however, asits applications expand and its value becomesproven, it is likely to become a more routine inves-tigation at many centres.41
INTERVENTIONAL AND OTHER TECHNIQUES 271
References1. Ishii C, Yamada T, Irie T et al. 1996 Clinical
evaluation of renal biopsy using automated biopsygun under ultrasonography. Journal of ClinicalRadiology 41: 233–236.
2. Reading CC, Charboneau JW, James EM, Hunt MR.1988 Sonographically guided percutaneous biopsy ofsmall (3 cm or less) masses. American Journal ofRoentgenology 151(1): 189–92.
3. Wilczek HE. 1990 Percutaneous needle biopsy of therenal allograft. Transplant 50: 790–797.
4. Fornari F, Civardi G, Cavanna L et al. 1989Complications of ultrasonically guided fine needleabdominal biopsy: results of a multicenter Italianstudy and review of the literature. ScandinavianJournal of Gastroenterology 24: 949–955.
5. Martino CR, Haaga JR, Bryan PJ et al. 1984 CTguided liver biopsies: eight years’ experience. Work inprogress. Radiology 152(3): 755–757.
6. Nolsoe C, Nielsen L, Torp-Pedersen S et al. 1990Major complications and deaths due to interventionalultrasonography: a review of 8000 cases. Journal ofClinical Ultrasound 18: 179–184.
7. Smith EH. 1991 Complications of percutaneousabdominal fine needle biopsy. Radiology 178: 253–258.
8. Di Stasi M, Buscarini L, Bolondi L et al. 1995Ultrasound-guided fine-needle liver biopsy: a multi-centre survey of pre-procedure evaluation practicesand complication rates. Journal of InterventionalRadiology 10: 43–48.
9. Livraghi T, Lazzaroni S, Civelli L et al. 1997 Riskconditions and mortality rate of abdominal fine needlebiopsy. Journal of Interventional Radiology 12: 57–64.
10. Ryd W, Hagmar B, Eriksson O. 1983 Local tumourcell seeding by fine needle aspiration biopsy. ActaPathologica Microbiologica Immunologica Scandinavica 91: 17–21.
ch11.qxd 6/30/04 10:43 PM Page 271

11. Salama H, Abdel-Wahab MF, Strickland GT. 1995Diagnosis and treatment of hepatic hydatid cysts withthe aid of echo-guided percutaneous cyst puncture.Clinical Infectious Diseases 21: 1372–1376.
12. Yong AA, Roberts SA. 2003 Interventional endoscopicultrasound. Clinical Radiology 58(1): 32–43.
13. Solomon MJ, Stephen MS, Gallinger S, White GH.1994 Does intraoperative ultrasonography changesurgical decision making during liver resection?American Journal of Surgery 168: 307–310.
14. Fortunato L, Claor M, Hoffman J et al. 1995 Is CTportography (CTAP) really useful in patients withliver tumours who undergo intraoperativeultrasonography (IOUS)? American Surgery 61:560–565.
15. Bates JA, Conlon RM. 1995 Intraoperativeaultrasound in hepatic resection. In: Paterson A andPrice R (eds) Current Topics in Radiography.Saunders, London.
16. Correnti S, Liverani A, Antoni G et al. 1996Intraoperative ultrasonography for pancreaticinsulinomas. Hepato-Gastroenterology 43: 207–211.
17. Kubota K, Noie T, Sano K et al. 1997 Impact ofintraoperative ultrasonography on surgery for cysticlesions of the pancreas. World Journal of Surgery 21:2–77.
18. Morris DL, Ross WB. 1996 Australian experience ofcryoablation of liver tumours: metastases. Surgical andOncologic Clinics of North America 5: 391–397.
19. Sato M, Watanabe Y, Ueda S et al. 1996 Microwavecoagulation therapy for hepatocellular carcinoma.Gastroenterology 110: 1507–1514.
20. Ogawa M, Shibata T, Takami M et al. 1995 Long-term survival in two cases of multiple liver metastasessuccessfully treated with intraoperative ultrasound-guided microwave tumour coagulation (MTC).Japanese Journal of Cancer Chemotherapy 22:1679–1683.
21. Rothlin MA, Schob O, Schlumpf R, Largiader F. 1996Laparoscopic ultrasonography during cholecystectomy.British Journal of Surgery 83: 1512–1516.
22. John TG, Greig JD, Crosbie JL et al. 1995 Superiorstaging of liver tumours with laparoscopy andlaparoscopic ultrasound. Annals of Surgery 220:711–719.
23. John TG, Greig JD, Carter DC, Garden OJ. 1995Carcinoma of the pancreatic head and periampullaryregion: tumour staging with laparoscopy andlaparoscopic ultrasonography. Annals of Surgery 221:156–164.
24. Conlon KC, Karpeh MS Jr. 1996 Laparoscopy andlaparoscopic ultrasound in the staging of gastriccancer. Seminars on Oncology 23: 347–351.
25. Marchesa P, Milsom JW, Hale JC et al. 1996Intraoperative laparoscopic liver ultrasonography forstaging of colorectal cancer: an initial experience.Diseases of the Colon and Rectum 39 (Suppl.)(S73–S78).
26. Gramiak R, Shah PM. 1968 Echocardiography of theaortic root. Investigative Radiology 3: 356–366.
27. Schlief R. 1996 Developments in echo-enhancingcontrast agents. Clinical Radiology 51 (Suppl. 1): 5–7.
28. Braunschweig R, Stern W, Dabidian A et al. 1993Contrast-enhanced colour Doppler studies of livervessels. Abstract. Echocardiography 10: 674.
29. Cosgrove D. 1996 Ultrasound contrast enhancementof tumours. Clinical Radiology 51 (Suppl. 1): 44–49.
30. Leen E, Mcardle CA. 1996 Ultrasound contrastagents in liver imaging. Clinical Radiology 51 (Suppl. 1):35–39.
31. Harvey CJ, Pilcher JM, Eckersley RJ et al. 2002Advances in ultrasound. Clinical Radiology 57(3):157–177.
32. Livraghi T, Giorgio A, Marin G et al. 1995Hepatocellular carcinoma and cirrhosis in 746patients: long-term results of percutaneous ethanolinjection. Radiology 197: 101–108.
33. Ohnishi K, Ohyama N, Ito S, Fujiwara K. 1994 Smallhepatocellular carcinoma: treatment with US-guidedintratumoral injection of acetic acid. Radiology 193:747–752.
34. Rossi S, Di Stasi M, Buscarini E et al. 1996Percutaneous RF interstitial thermal ablation in thetreatment of hepatic cancer. American Journal ofRoentgenology 167: 673–759.
35. Solbiati L, Ierace T, Goldberg SN et al. 1997Percutaneous US-guided radio-frequency tissueablation of liver metastases. Treatment and follow-upin 16 patients. Radiology 202: 195–203.
36. Cahn M, Chang K, Nguyen P. 1996 Impact ofendoscopic ultrasound with fine needle aspiration onthe surgical management of pancreatic cancer.American Journal of Surgery 172: 470–472.
37. Tio TL, Sie LH, Kallimanis G et al. 1996 Staging ofampullary and pancreatic carcinoma: comparisonbetween endosonography and surgery.Gastrointestinal Endoscopy 44: 706–713.
38. Pitre J, Soubrane O, Palazzo L, Chapuis Y. 1996Endoscopic ultrasonography for the preoperativelocalisation of insulinoma. Pancreas 13: 55–60.
39. Amouyal P, Amouyal G, Levy P et al. 1994 Diagnosisof choledocholithiasis by endoscopic ultrasonography.Gastroenterology 106: 1062–1067.
40. Wojtowycz AR, Spirt BA, Kaplan DS, Roy AK. 1995Endoscopic ultrasonography of the gastrointestinaltract. Ultrasound Quarterly 13: 139–152.
ABDOMINAL ULTRASOUND272
ch11.qxd 6/30/04 10:43 PM Page 272

41. McLean A, Fairclough P. Review: Endoscopicultrasound—current applications. Clinical Radiology51: 83–98.
42. Gillams AR, Lees WR. 1996 Recent developments inbiliary tract imaging. Gastrointestinal EndoscopyClinics of North America 6: 1–15.
43. Taki T, Goto H, Naitoh Y et al. 1997 Diagnosis ofmucin-producing tumour of the pancreas with anintraductal sonographic system. Journal of Ultrasoundin Medicine 16: 1–6.
INTERVENTIONAL AND OTHER TECHNIQUES 273
ch11.qxd 6/30/04 10:43 PM Page 273
ch11.qxd 6/30/04 10:43 PM Page 274
This page intentionally left blank

Allan P, Dubbins P, Pozniak M, McDicken N. 2000Clinical Doppler Ultrasound. Churchill Livingstone,Edinburgh.
Bisset RAL, Khan AN. 2002 Differential Diagnosis inAbdominal Ultrasound. Baillière Tindall, London.
Brooke JR, Ralls PW. 1995 Sonography of the Abdomen.Raven Press, New York.
Carty H, Brunelle F, Shaw D, Kendall B. 1994 ImagingChildren. Churchill Livingstone, Edinburgh.
Damjanov I. 1996 Pathology for the Health-RelatedProfessions. Saunders, Philadelphia.
Gebel M. 1999 Ultrasound in Gastroenterology andHepatology. Blackwell Science, Berlin.
Lees WR, Lyons EA. 1996 Invasive Ultrasound. MartinDunitz.
Meire H, Cosgrove D, Dewbury K, Farrant P. 2001Clinical Ultrasound—Abdominal and GeneralUltrasound, 2nd edn. Churchill Livingstone,Edinburgh.
Williams P. 1999 Gray’s Anatomy. Elsevier, Edinburgh.
Bibliography and further reading
275
Biblio.qxd 6/30/04 5:34 PM Page 275

Biblio.qxd 6/30/04 5:34 PM Page 276
This page intentionally left blank

A
Abdomen, acutegastrointestinal tract, 245–6hepatobiliary emergencies, 246–8other retroperitoneal emergencies,
248–50pancreas, acute, 248renal tract emergencies, 248trauma, 244–5use of ultrasound, 243–4
Abdominal aorta, 195–9, 196Abdominal aortic aneurysms, 248Abscesses
appendicitis, 246, 246drainage of, 262hepatic, 82–4, 84, 95, 96, 116,
247psoas, 250renal, 175, 176, 187splenic, 145
Acalculous cholecystitis, 59Acquired cystic disease, 162, 162Acquired immunodeficiency
syndrome (AIDS), 111, 139Acute abdomen see Abdomen, acuteAcute appendicitis, 209Acute cholecystitis, 59, 246Acute diverticulitis, 246Acute fatty liver, 109Acute hepatitis, 106, 107Acute pancreas, 248Acute tubular necrosis (ATN),
177–8, 189, 260Acute ureteric obstruction, 248Adenocarcinomas, 130, 132Adenomas, 86, 86–7, 95, 162–3,
203, 205
Adenomyomatosis, 51–3, 52Adrenal glands, 201–6, 204, 232,
233Adrenal haemorrhage, 232, 233Agenesis, renal, 224Air in the biliary tree, 72–3, 73Alagille’s syndrome, 218Alcoholic cirrhosis, 98, 129Alcoholic-induced liver disease, 96,
97, 125, 126, 248Alcoholism, 125American Institute for Ultrasound in
Medicine (AIUM), 10Amoebic abscess, 83Amyloid, 179Anaemia, 82–3, 109–10, 139, 146Analgesia, 254Aneurysms
aortic, 196–9, 198, 199, 248renal artery, 191splenic artery, 147–8
Angiomyolipoma, 162, 163Aorta, 38, 213Aortic aneurysms, 196–9, 199, 248Appearances, ultrasound
adrenal glands, 201Budd–Chiari syndrome, 107–9cirrhosis, 97–9hepatic metastases, 90–2hepatitis, 106–7hepatocellular carcinoma, 94kidneys, 155normal spleen, 137–9, 138normal transplanted kidney,
182–5pancreas, 123pancreatic carcinoma, 132pancreatic transplant, 135pancreatitis, 125
renal artery stenosis (RAS),179–80
renal calculi, 172–3renal cell carcinoma (RCC),
163–4renal cysts, 160–1splenic lymphoma, 141
Appendicitis, 209, 238, 238–9, 239,245–6, 246
Appendix, 206–7, 209Arrays, 7Artefacts, 30Arteriovenous fistulae, 181, 189, 191Artery aneurysm, splenic, 147–8Artery stenosis, renal (RAS), 179–80,
180, 187–9, 188Ascaris worm, 70, 71Ascites, 103, 212, 213Atresia, biliary, 112, 216–18Atrial systole, 29Autosomal dominant polycystic
kidney disease (APKD), 161–2Autosomal recessive disease (PCKD),
162Autosomal recessive polycystic disease
of the kidneys (ARPCDK),224–5
B
Beckwith–Wiedemann syndrome,218, 229
Benign focal liver lesions, 79–89Benign focal pancreatic lesions,
133–4Benign focal renal tumours, 162–3Benign splenic conditions, 143–8Bile, 49, 71
Index
277
Index.qxd 6/30/04 6:21 PM Page 277
Bile ducts, 31–3see also Common bile duct (CBD)
Biliaryatresia, 112, 216–18, 219biliary tree, 17calculi, 125colic, 52, 70crystals, 72, 72dilatation, 248dilation without jaundice, 66–7obstruction, 246reflux, 47sludge, 56stasis, 71–2see also Bile ducts; Gallbladder
Bilirubin, 34–5Biochemical analysis, pancreas, 123Biological effects of ultrasound, 10–11Biopsy attachments, 7Biopsy, renal, 179, 259–61Biopsy, ultrasound-guided see
Ultrasound-guided biopsyBladder
diverticulum, 175, 176paediatric, 221tumour, 4
Blind biopsy, 255Blood clot, renal, 167, 168–9Blood in the gallbladder, 72Blood tests for renal function, 157Bone-at-focus index (TIB), 11Bone-at-surface index (TIC), 11Bowels
carcinoma, 91gas in, 29, 63, 223malignant tumours in the, 210–11perforation of the, 245problems in the, 36rupture of the, 244
Breast carcinoma, 143, 213Budd–Chiari syndrome (BCS)
free intraperitoneal fluid, 111indications for liver
transplantation, 112liver metastasis, 203management of, 108–9risk of thrombosis, 115ultrasound appearances of, 107–8,
108with suspected liver lesion, 94
C
Caecal carcinoma, 212, 212Calcification
adrenal, 232, 233hepatic, 88–9, 90
pancreatic, 128, 129, 132renal tract, 170–4splenic, 145, 145–6
Calcium stones, 171Candidiasis, 229, 230Candidiasis abscess, 83–4CAPD fluid, 111Capillary haemangiomas, 257Carcinomas
adenocarcinoma, 130, 132adrenal, 206bowel, 36, 91, 212, 212breast, 143, 213cervical, 167cholangiocarcinoma, 64, 67, 68,
74, 75, 95colorectal, 268–9, 271cystadenocarcinoma, 130, 132gallbladder, 50, 73, 73gastric, 208hepatocellular carcinoma (HCC)
(see Main entry)lung, 205oesophagus, 207ovarian, 75, 80, 81, 90, 111pancreatic, 128–33, 131, 247, 266,
271renal, 134, 163–5, 164, 202transitional cell carcinoma, 164–5,
165, 166Cardiac failure, 111Caroli’s diesease, 68–70, 70Cervical carcinoma, 167Chemotherapy, 91Children see Paediatric abdomenCholangiocarcinomas, 64, 67, 68,
74, 75, 95Cholangitis, 66, 66, 70, 247, 247Cholecystectomy
acalculous cholecystitis, treatmentfor, 247
bile duct measurements, 33, 33choledocholithiasis, 45gallstones, management of, 47, 52laparoscopic, 56, 67scar, 29
Cholecystitisacalculous, 56–7, 59, 247acute, 54–6, 55, 59, 111, 246chronic, 56, 59complications of, 47, 57–8emphysematous, 60
Cholecystokinin-stimulated hepaticiminodiacetic acid (HIDA)scan, 57
Choledochal cysts, 64–6, 66, 68–70,218, 219
Choledocholithiasis, 45–7
Cholelithiasis see GallstonesCholestasis, 110, 112, 216–18, 218Cholesterolosis, 53–4, 54Choosing a machine, 6–9Chronic cholecystitis, 59Chronic liver disease, 257
see also specific diseaseCiclosporin nephrotoxicity, 191Cirrhosis
alcoholic, 98, 129and chronic hepatitis, 107and hepatocellular carcinoma
(HCC), 94causes of non-obstructive
jaundice, 96increased echogenicity, 111liver biopsy in patients with, 257,
261liver transplants, 110, 112micronodular, 97ultrasound appearances, 97–9
Coarse texture of the liver, 111Colic, acute renal, 249Colitis, ulcerative, 209Colonic carcinoma, 36Colonic mass, 210Colorectal carcinoma, 268–9, 271Colour Doppler
diagnosing cholecystitis, 54dilated bile duct, 61hepatic vein, 5pancreatic duct, 131pancreatic transplant, 135portal venous system, 26, 101renal tract, 155–6, 157thermal effects of, 11use of, 2–4
Common bile duct (CBD)cysts, 64–6, 66, 68–70, 218, 219dilated, 58–67, 59, 62, 65, 66–7normal, 25, 27, 31–3, 32obstructed, 130postoperative ultrasound
appearances, 116stones in, 45–7, 46, 218see also Gallbladder
Complex cysts, 80–1, 81Complications, post operative renal
transplant, 185Computed tomography (CT) scan,
167, 212, 229, 232, 244, 246,259
Congenital anomalies of thepancreas, 123–4
Congenital intrahepatic biliarydilation, 68–70
Congenital megacalyces, 170Congestive cardiac disease, 109
278 INDEX
Index.qxd 6/30/04 6:21 PM Page 278

Continuous ambulatory peritonealdialysis (CAPD), 181–2
Contracted gallbladder, 49–50, 50Contrast agents, 266–8, 268, 269Contrast sonocystography, 229Cortical scintigraphy, 229Cranial index (TIC), 11Crohn’s disease, 111, 209, 211, 246Cryotherapy, 264, 266Cyst drainage, 262–3Cystadenocarcinomas, 130, 132Cystadenomas, 81, 81Cystic disease, 160–2Cystic duct, 49Cystic duct obstruction, 48, 50Cystic fibrosis (CF)
changes in liver reflectivity, 111cholestasis, 218cysts, 134gallstones, 50general information, 216increased echogenicity, 221microgallbladder, 51ultrasound appearances, 109, 109,
217Cystine stones, 171Cystinuria, 173, 173Cysts
adrenal, 203choledochal, 218, 219enteric duplication, 239–40, 240hepatic, 79–81, 80, 81, 82hydatid, 82in children, 221in obese patients, 4ovarian, 111pancreatic, 132, 134, 134renal, 160–1, 161splenic, 144, 144
Cytology, 257
D
Deep inspiration, 18Defensive scanning, guidelines for, 13Departmental guidelines, 13Design of machines, 7Dialysis, ultrasound in, 181–2Diethylene triaminepenta-acetic acid
(DTPA) scan, 158, 167Diffuse liver conditions, 95–110Dilation
PCS, 166renal, 225–6, 226renal transplant, 185
Dimer capto succinic acid (DMSA)scan, 223
Dissolution therapy, 48Diuretic renogram, 229Diverticulitis, 210, 211, 246Doppler
cirrhosis, 98correlation, 189detecting flow, 7hepatic metastases, 92kidneys, 248pancreatitis, 125sensitivity, 114spectra, 26use of, 2–6, 18using microbubble agents, 267see also Colour Doppler; Power
DopplerDouble gallbladder, 31Drainage, ultrasound-guided, 261–4Drug-induced liver disease, 96Drug-induced pancreatitis, 125Duodenal gas, 63Duodenum, 30, 32Duplex kidneys, 158, 159, 221–3,
222, 225
E
Echogenic bile, 71–3Echogenicity, 111, 124, 221Ectopic gallbladder, 30Ectopic kidneys, 158, 223Ectopic pregnancy, 111Electrical safety, 11Emphysematous cholecystitis, 58, 60Empyema, 58, 61Endocrine tumour, 132Endometriosis, 167Endoscopic retrograde
cholangiopancreatography(ERCP), 47, 62
Endoscopic ultrasound, 64, 246,269–71
Endosonography, 210Enlargement of the gallbladder, 48–9Enlargement of the spleen, 109, 139,
139, 140, 146Enteric duplication cysts, 239–40,
240Epigastrium, 28, 29, 208Equipment for biopsy, 255, 256–7Equipment tests, 14–15Ergonomics of machines, 8European Committee for Ultrasound
Radiation Safety (ECURS), 10European Federation of Societies for
Ultrasound in Medicine andBiology (EFSUMB), 10
Extracorporeal shock wave lithotripsy(ESWL), 48
Extrarenal pelvis, 158, 160
F
Faeces, impacted, 36Failure, renal, 111, 177–9Fasting, 27, 29Fatty infiltration, 87, 88, 95–7, 96,
111Fatty sparing, 87, 87–8Fever, 82–3Fibrosis, 67, 111Field, size of, 2Fine needle aspiration cytology, 257Fistulae, 209Flow
detection with Doppler, 7in major vessels, 5–6velocity waveforms, 6
Fluid collections, transplantation,186–7
Focal fatty change, 87–8, 87–8, 95Focal fatty sparing of the pancreas,
133Focal lesions, 116Focal liver lesions, 24, 112Focal nodular hyperplasia, 88, 89, 95,
257Focal obstruction, 67Focal pancreatitis, 133–4Focal zone, 2, 3, 5, 44Focused Assessment with
Sonography for Trauma(FAST), 244
Folded gallbladder, 29, 30, 31Fracture, pancreatic, 246Frame rate, 2, 3, 5Free fluid detection, 244, 245Free intraperitoneal fluid, 111Freehand biopsy, 255Frequency
changing, 2increasing the, 1, 5range of, 7settings for gallbladder, 2, 27, 30
Fundamental imaging mode, 4Fungal balls, 167, 191, 229, 230Fungal infections, 229
G
Gallbladderbiliary dilation without jaundice,
66–7
279INDEX
Index.qxd 6/30/04 6:21 PM Page 279

Gallbladder (Continued)blood in the, 72carcinoma, 50, 73, 73cholecystitis (see Main entry)cholelithiasis, 41–8contracted or small, 49–50, 50double, 31drainage of, 262echogenic bile, 71–3ectopic, 30enlargement of the, 48–9folded, 29, 30, 31frequency settings for, 2, 5, 27, 30full abdominal survey, 17hyperplastic conditions of the
wall, 51–4in children, 216in the obese patient, 4inflammatory gallbladder disease,
54–8introduction, 27–9malignant biliary disease, 73–6metastases, 76microgallbladder, 50, 51, 216, 217mucocoele, 48normal variants of the, 29obstruction without biliary
dilation, 67obstructive jaundice and biliary
duct dilation, 58–66other biliary diseases, 67–71pitfalls in scanning the, 29–31polyps, 28porcelain, 50, 51removal (see Cholecystectomy)septum, 29stones (see Gallstones)strawberry, 53–4, 54ultrasound appearances, 31, 32
Gallstonesabdominal pain, 36, 248chronic cholecystitis, 56clinical features, 41–2gallstone pancreatitis, 47, 246general information, 42–5in the common bile duct, 45–7small gallbladder, 50ultrasound appearances, 42, 51
Gangrenous cholecystitis, 57–8, 59Gas, bowel, 29, 63, 212, 223Gastric carcinoma, 208Gastrinomas, 128Gastro-oesophageal reflux, 238Gastrointestinal tract
acute presentations of, 245–6appendix, 206–7inflammatory bowel conditions,
209–10
malignant tumours, 210mesenteric ischaemia, 207–9obstruction, 211oesophagus and stomach, 206paediatric, 232–40
Gilbert’s disease, 96Glomerulonephritis, 178–9Glycogen storage disease, 99Granulomatas, 88, 90, 95, 146Guidance, biopsy, 255Guidelines, departmental, 13
H
Haemangioblastomas, 134Haemangioendotheliomas, 220Haemangiomas, 3, 85–6, 85–6, 95,
145Haemangiomatas, 219Haematomas
complications of biopsy, 258, 261hepatic, 84, 84–5, 96, 116psoas, 250, 250renal, 187subcapsular, 245subphrenic, 117
Haematuria, 182Haemo-hydronephrosis, 168–9Haemobilia, 72Haemochromatosis, 99, 221Haemodynamics, 25–7, 155–6Haemolysis, 96Haemolytic anaemia, 139, 146Haemorrhage, 232, 233, 248, 261Haemorrhagic tumour, 132Harmful effects of ultrasound, 10–12HELLP syndrome, 109–10, 110Hepatic see LiverHepatitis, 106–7, 107, 111, 139,
216, 257Hepatobiliary system
bile ducts, 31–3common referral patterns, 33–6gallbladder, 27–31hepatobiliary emergencies, 246–8hepatobiliary pathology: paediatric
abdomen, 216–20introduction, 17–18liver, 18–27upper-abdominal anatomy, 36–9upper-abdominal technique, 18see also Bile ducts; Liver
Hepatoblastomas, 218–20, 219, 234Hepatocellular carcinoma (HCC)
biopsy procedures, 257general information, 93–5hepatobiliary pathology, 218–20
in a patient with cirrhosis, 94, 95,98
treatment of, 269viral hepatitis, 106
Hepatomas, 261Hepatomegaly, 220Hippel–Lindau disease, 134Hodgkin’s lymphoma, 139, 165Horseshoe kidneys, 158, 159, 223,
223Hydatid cysts, 82, 82, 177Hydronephrosis, 168, 168–9, 170,
225–6, 263Hyperaemia, 54, 56Hyperparathyroidism, 173–4Hyperplastic conditions of the gall
bladder wall, 51–4Hypertension, portal see Portal
hypertensionHypertrophic pyloric stenosis (HPS),
234, 235Hypervascularized bowel, 210Hypotrophied column of Bertin,
158–9
I
Image optimization, 1–2Image quality, 1–2, 7–8Images, recording of, 9–10Imaging the paediatric renal tract,
229Impacted faeces, 36Impacted gallstones, 45, 45Incorrect use of equipment, 5Increasing the frequency, 1Indirect ultrasound guidance,
263–4Infarction of the spleen, 146, 147Infection, renal tract, 174–7, 189Inferior vena cava (IVC), 199–201,
200, 201Inflammation
gastrointestinal tract, 245–6renal tract, 174–7
Inflammatory bowel conditions,209–10
Inflammatory gallbladder disease,54–8
Inspiration, deep, 18Inspissated bile, 71, 71Insulin-dependent diabetes, 135Insulinomas, 128Intercostal scanning, 18Intrahepatic tumours, 64, 67Intraoperative ultrasound (IOUS),
113, 264, 265
280 INDEX
Index.qxd 6/30/04 6:21 PM Page 280
Intravenous urography (IVU), 229,248
Intussusception, 234–6, 236
J
Jaundicecommon causes of, 34general information, 34–5neonatal, 216non-obstructive, 93, 96obstructive, 58–67, 213, 246,
247, 258
K
Kidneysabscesses, 175, 176, 187acute renal colic, 249agenesis, 224aneurysms, renal artery, 191autosomal dominant polycystic
kidney disease (APKD), 161–2autosomal recessive polycystic
disease of the kidneys(ARPCDK), 224–5
benign focal renal tumours,162–3
biopsy, 179, 259–61calcification of, 170–4carcinoma, 134, 163–5, 164, 202cysts and cystic disease, 160–2,
161devascularization of the, 246diffuse renal disease and renal
failure, 177–9dilation, 185, 225–6, 226disease, 135duplex kidneys, 158, 159, 222,
225ectopic kidneys, 158, 223failure, 111, 177–9full abdominal survey, 17function tests, 157horseshoe kidneys, 158, 159, 223,
223inflammation and infection,
174–7, 189malignant renal tract masses,
163–6measurements of, 155medullary sponge kidney, 179metastases, 165–6multicystic dysplastic kidney
(MCDK), 162, 224, 225normal, 154, 154–60
obstruction of the, 166–7,169–70, 249
PCS dilation and obstructiveuropathy, 166–70
pelvic kidney, 224renal artery stenosis (RAS),
179–80, 180, 187–9, 188renal cell carcinoma (RCC),
163–4renal fusion, 223renal humps, 160renal tract emergencies, 224, 248renal transplants, 182–91renal vein thrombosis (RVT) (see
Main entry)rupture of the, 244stones, 167, 171–3, 172transplant biopsy, 260–1, 261transplants, 182–91, 183, 184trauma, 182vascular pathology, 179–82
Klatskin tumour, 74, 74
L
Laparoscopic cholecystectomy, 56Laparoscopic ultrasound, 48, 64,
265–6, 266Laser ablation, 269Legal issues, 12–13Leukaemia, 111, 139, 142–3, 220,
234Line density, 1, 2Links to image-recording devices,
8–9Lipomas, 88Litigation, 12–13Liver
abscesses, 82–4, 84, 95, 96, 116,247
acute fatty liver, 109alcohol-induced liver disease, 96,
97, 125, 126, 248anatomy, 36, 37benign focal liver lesions, 78–9,
79–89calcification, 88–9, 90chronic liver disease, 257cirrhosis (see Main entry)conditions in pregnancy, 109–10diffuse liver conditions, 95–110drug-induced liver disease, 96failure of the, 111full abdominal survey, 17haematoma, 84–5haemodynamics of, 25–7hepatic abscess, 247
hepatic artery (HA), 6, 27, 30,104, 113
hepatic biopsy, 257–8, 258, 259hepatic venous system, 5, 28, 38jaundice, 34, 34–5liver fluke, 70liver function tests (LFTs), 35, 58,
82–3liver transplants, 110–17malignant focal liver lesions,
89–95mass, 89, 90metastases (see Hepatic under
Metastases)normal appearances, 18–24,
18–24polycystic, 81–2rupture of the, 244segments of, 24, 24texture of the, 111transplants
indications for, 110–11operative procedure, 112–13postoperative assessment, 113postoperative ultrasound
appearances, 113–17preoperative assessment,
111–12tumours, treatment of, 268–9use of equipment, 2, 3vasculature, 25see also Cirrhosis
Lung cancer, 270Lymph nodes, enlarged, 213Lymphadenopathy, 92, 132, 149,
149, 213Lymphangiomas, 150, 150Lymphatics, 148, 148–50, 149Lymphocoele, 187, 187Lymphomas
hepatic, 220Hodgkin’s, 139, 165in children, 234metastases, 91non-Hodgkin’s, 139, 165, 203renal, 165splenic, 141, 142
Lymphoproliferative disorder, 116
M
Magnetic resonancecholangiopancreatography(MRCP), 62
Magnetic resonance imaging (MRI),212, 229, 232, 246
Maintenance of machines, 8
281INDEX
Index.qxd 6/30/04 6:21 PM Page 281

Malignant biliary disease, 73–6Malignant focal liver lesions, 89–95Malignant obstruction, 64Malignant renal tract masses, 163–6Malignant splenic disease, 141–3Malignant tumours, bowel, 210–11Management of gallstones, 47Mass
colonic, 210hepatic, 89, 90malignant renal tract, 163–6retroperitoneal, 212see also specific condition
Measurements of the bile duct, 33Measurements of the kidneys, 155Mechanical effects of ultrasound, 11Mechanical Index (MI), 11Meckel–Gruber syndrome, 221Medicolegal issues, 12–13Medullary sponge kidney, 179Meig’s syndrome, 111Melanomas, 143Mesenteric ischaemia, 207–9Mesotheliomas, 261Metastases
adrenal gland, 203, 233gallbladder, 76hepatic
biopsy, 257, 258causes of, 203, 220changes in liver reflectivity, 111clinical features and
management, 90–2examples of, 91, 93intraoperative ultrasound,
264laparascopic ultrasound, 266multiple, 208necrotic, 92ultrasound appearances, 90–2
pancreatic, 132, 133, 133renal, 165–6retroperitoneal, 213splenic, 141–2, 143
Microbiological safety, 12Microbubble agents, 267Microgallbladder, 50, 51, 216, 217Microlithiasis, 72, 72Micturating cystourethrogram, 229Midgut volvulus, 236–7, 237Minimizing the ultrasound dose,
12–13Mirizzi syndrome, 48–9, 50Misinterpretation, 1Mobility, gallstones, 44, 45Mononucleosis, 139Mucinous tumour, 132Mucocoele of the gallbladder, 48
Multicystic dysplastic kidney(MCDK), 162, 224, 225
Murphy’s sign, 54, 57Myelolipomas, 204, 205
N
Necrotic tumour, 132Needles, biopsy, 256, 256–7Neonatal cholestasis, 216–18Neonatal hepatitis, 216Neonatal jaundice, 216Nephrocalcinosis, 173, 174Nephrostomy, 262, 263Nephrotic syndrome, 90Neuroblastomas, 232, 234Nodular texture of the liver, 111Non-Hodgkin’s lymphoma, 139,
165, 203Non-obstructive hydronephrosis, 170
O
Obese patients, 4Obstruction
biliary, 246gastrointestinal tract, 245–6intestinal, 211non dilated renal, 169–70of the pancreatic duct, 128pelvi-ureteric junction, 226renal, 166–7, 249urinary tract, 248without biliary dilation, 67
Obstructive jaundice, 58–67, 213,246, 247, 258
Oedema, 187Oesophagus, 206, 207Operator safety, 12Operator skill, 17Oral contraceptives, 86Organ damage, 111Organ failure, 111Output Display Standard (ODS), 11Ovarian carcinoma, 75, 80, 81, 90,
111Ovarian cyst, 111Ovarian fibroma, 111
P
Paediatric abdomensadrenal glands, 232gastrointestinal tract, 232–40hepatobiliary pathology, 216–20
pancreas, 220, 220–1techniques, 215–16urinary tract, 221–32
Pain, upper abdominal, 36see also Abdomen, acute
Palpable right upper quadrant mass,36
Pancreasacute, 248anatomy, 37, 39benign focal pancreatic lesions,
133–4biochemical analysis, 123biopsy, 258–9, 260calcification, 128, 129, 132congenital anomalies, 123–4cysts, 132, 134, 134focal fatty sparing, 133fracture of, 246frequency settings, 2full abdominal survey, 17malignant pancreatic disease,
128–33metastases, 132, 133, 133normal, 121–4, 122paediatric, 220, 220–1pancreatic carcinoma, 128–33,
131, 247, 266, 271pancreatic ducts, 59, 128, 131pancreatic transplant, 135pancreatitis
acute, 81, 111, 126, 248endoscopic ultrasound, 270focal, 132, 133–4gallstone, 47, 246general information, 124–8paediatric, 221
rupture of the, 244techniques, ultrasound, 121–3transplants, 135trauma of the, 125, 134–5
Papillary necrosis, 167, 170, 171Parasites, 70–1, 82Pelvic kidney, 224Pelvicalyceal system (PCS) dilation
and obstructive uropathy,166–70
Percutaneous drain, 84Perforated appendix, 209Pericholecystic abscess, 56–7Peritoneum, 195
see also RetroperitoneumPeritonitis, 111Pernicious anaemia, 139Phaeochromocytomas, 134, 204–6,
205Photographic archiving
communications (PAC), 8, 10
282 INDEX
Index.qxd 6/30/04 6:21 PM Page 282
Phrygian cap, 29Pneumobilia, 72–3, 73Polycystic disease, 134, 144, 161,
224–5Polycystic liver, 81–2Polyps, 53, 53, 54Polyps, gallbladder, 28Porcelain gallbladder, 50, 51Portal hypertension
free intraperitoneal fluid, 111general information, 99–105management of, 105–6splenomegaly in, 139, 139, 217ultrasound appearances, 100, 102
Portal veinanastomosis, 114flow, 99–103liver transplants, 115portal venous system, 24, 24, 25,
25, 26, 27thrombosis, 111–12, 127, 248
Positioning the patient, 18Post-processing options, 3Postoperative bile collection, 49Postsurgical CBD dilation, 66–7Power Doppler
diagnosing cholecystitis, 54general information, 4liver transplant, 114of the hepatic vein confluence, 5thermal effects of, 11
Pre-eclampsia, 109–10Pregnancy, liver conditions in,
109–10Primary biliary cirrhosis (PBC), 97,
98, 111, 112Primary gallbladder carcinoma, 73,
73Primary sclerosing cholangitis
(PSC), 67–8, 68, 69, 107,111, 112
Probe number, 7Processing options, 2Prostate enlargement, 167Pseudoaneurysm, 148, 189Pseudocysts, 125, 126, 132, 248,
248Psoas abscesses, 250Pulsed Doppler, 5, 11Pyelonephritis, 174–5, 176, 248Pyogenic abscess, 83, 83Pyonephrosis, 167, 169, 169
Q
Quality assurance, 13–15Quality of the image, 1–2
R
Radio frequency (RF) thermalablation, 269
Radioisotope scans, 158Radionuclide cystography, 229Recording of images, 9–10Rectal cancers, 210Referral patterns for hepatobiliary
ultrasound, 33–9Reflectivity, 44, 111Reflux, 170, 225, 227, 238Reidel’s lobe, 36Rejection, transplant, 117, 185–6,
186Renal cell carcinoma (RCC), 163–4Renal tract see KidneysRenal vein thrombosis (RVT)
causes of renal tract obstruction,167
general information, 180–1, 191hydronephrosis, 168–9in neonates, 231, 231–2ultrasound appearances, 181, 190
Retroperitoneumabdominal aorta, 195–9adrenal glands, 201–6gastrointestinal tract, 206–11inferior vena cava, 199–201normal anatomy of, 195other abnormalities in, 212–13
Rhabdomyosarcomas, 219–20, 234Rokitansky–Aschoff sinuses,
51, 52Rupture, organ, 244
S
Safety indices, 11Safety of diagnostic ultrasound,
10–12Schemes of work, 13Sclerosing cholangitis, 60, 218Secondary biliary cirrhosis, 98–9Sepsis, 139Septum, gallbladder, 29Shadowing, gallstones, 42–4, 42–4Sickle cell disease, 139, 146Simple cysts, 79–80, 80Skills of the operator, 17Small gallbladder, 49–50Small spleen, 139–40Soft tissue thermal index (TIS), 11Spectral Doppler, 115, 169Spectral waveform, 5–6Spherocytosis, 139, 146Sphincter dysfunction, 271
Spleenabscess, 145benign splenic conditions, 143–8calcification, 145, 145–6cysts, 144, 144enlarged paediatric, 217full abdominal survey, 17haemangioma, 145laceration of, 245lymphoma, 141, 142malignant splenic disease,
141–3metastases, 141–2, 143normal, 137–9, 138rupture of the, 244small accessory spleen, 139–40splenic artery aneurysm, 147–8splenic infarction, 146, 147splenic vein thrombosis, 127,
146–7, 248splenomegaly, 103, 139, 139, 140,
146splenunculi, 139–41trauma, 148
Staghorn calculi, 173Steatosis, 95–7Stenosis, 114Stomach, 206Stones
bladder, 249gallbladder, 28, 30, 247 (see also
Gallstones)renal, 167, 171–3, 172struvite, 171
Strawberry gallbladder, 53–4, 54Stricture, renal tract, 167Struvite stones, 171Sub-scanning, 18
T
Techniques, ultrasoundadrenal glands, 201bile ducts, 33paediatric abdomen, 215–16pancreas, 121–3renal tract, 154–7upper-abdominal, 18
Teratomas, 213Thalassaemia, 139, 146Thermal effects of ultrasound, 11Thermal Index (TI), 11Thin patients, 30Thrombosis
misinterpretation of results, 6portal vein, 100, 101, 111–12,
127
283INDEX
Index.qxd 6/30/04 6:21 PM Page 283

Thrombosis (Continued)renal vein thrombosis (RVT)
causes of renal tractobstruction, 167
general information, 180–1,189
hydronephrosis, 168–9in neonates, 231, 231–2ultrasound appearances, 181,
190splenic, 127, 248thrombosed vessels, 5–6
Time gain compensation (TGC), 28,96
Tissue Harmonic Imaging, 2, 4, 18,28
Tissue-mimicking phantom, 14TORCH screen, 88Toxic shock syndrome, 111Transitional cell carcinomas, 164–5,
165, 166Transjugular intrahepatic
portosystemic shunt (TIPS),105, 105–6, 106
Transplantshepatic, 110–17pancreatic, 135renal, 182–91, 183, 184
Traumaabdomen, 244–5pancreatic, 125, 134–5renal, 182splenic, 148
Tuberculosis, 111, 167, 175Tuberose sclerosis, 163Tubular necrosis, acute (ATN),
177–8, 189
Tumoursbladder, 4hepatic, 268–9malignant bowel, 210–11renal, 167tumour seeding, 261vascular, 220see also specific tumour
U
Ulcerative colitis, 209Ultrasound contrast agents, 266–8,
268, 269Ultrasound-guided biopsy
complications, 261general considerations, 253–7procedures, 257–61
Ultrasound-guided drainage, 261–4Upgradability of machines, 8Upper-abdominal anatomy, 36–9,
36–9Upper-abdominal technique, 18Ureteric obstruction, 248Urethral stricture, 167Uric acid stones, 171Urinary tract, 221–32, 248
see also KidneysUrine tests for renal function, 157Urinomas, 187
V
Varices, 103
Vascular abnormalities of the spleen,146–8
Vascular occlusion, 187Vascular pathology, renal, 179–82Vascular tumours, 220VATER syndrome, 224Veins see specific veinVesico-ureteric junction, 170Vesicoureteric reflux, 226–9Vessel occlusion, 6, 6Viral hepatitis, 96, 106Volvulus, 236–7, 237Von Hippel–Lindau disease, 221
W
Wilms’ tumour, 220, 229–30,230–1, 231, 234
Wilson’s disease, 99Work-related musculoskeletal
disorders (WRMSD), 8, 12World Federation for Ultrasound in
Medicine and Biology(WFUMB), 10
X
X-ray, 229Xanthogranulomatous pyelonephritis
(XGP), 177, 177, 230–1, 231
284 INDEX
Index.qxd 6/30/04 6:21 PM Page 284