cp dissertation paper
87
DECLARATION I, Cyprien HABINSHUTI a student of University of Rwanda, Huye Campus, College of Business and Economics, School of Economics, Department of Applied Statistics, hereby declare that the work done and presented in this dissertation entitled “ASSESSEMENTOF THE IMPACT OF HIV/AIDS COUNSELING SERVICES ON RURAL AREA POPULATION” is my own work and has not been presented anywhere for any academic qualification. Any reference in terms of books or any other written and electronic materials made concerning other people’s work are indicated in the references. Signature: ………………………… Date: ………………………………………. Name of Student: Cyprien HABINSHUTI Supervisor signature: ……………………… Date: ………………………………. Name of Supervisor: Dr Dieu Donne MUHOZA i
-
Upload
umutarapolytech -
Category
Documents
-
view
4 -
download
0
Transcript of cp dissertation paper

DECLARATIONI, Cyprien HABINSHUTI a student of University of Rwanda, Huye
Campus, College of Business and Economics, School of Economics,
Department of Applied Statistics, hereby declare that the work
done and presented in this dissertation entitled “ASSESSEMENTOF
THE IMPACT OF HIV/AIDS COUNSELING SERVICES ON RURAL AREA
POPULATION” is my own work and has not been presented anywhere
for any academic qualification. Any reference in terms of books
or any other written and electronic materials made concerning
other people’s work are indicated in the references.
Signature: ………………………… Date: ……………………………………….
Name of Student: Cyprien HABINSHUTI
Supervisor signature: ……………………… Date: ……………………………….
Name of Supervisor: Dr Dieu Donne MUHOZA
i

DEDICATION
ii
I dedicate my dissertation
work:
To Almighty Powerful God
To my family and my friends,A special feeling of gratitude to my loving relatives: Adrien
MUHIGIRWAFather Pie NEMEYAMAHOROMy loving Aunt M. Jeanne
IRAGUHA,
Grandmother whose words of encouragement are still in my ears, to my esteem friends:
Augustin NSHUTI IYAMUREMYE andValentine IMANISHIMWE.
I also dedicate this dissertation to my parents who
give me way of live.I will always appreciate all
they have done.

AcknowledgementThis laborious work would not have been a success without such
intervention: moral, financial support, ideas and guidance from
various persons to whom I would like to thank.
Firstly, I thank God for protecting me during this work and wholemy life. This work is the greatest effort result provided bydifferent people to whom I appreciate.
My sincere thanking is addressed to the Dean of School of
economics, Dr Dieu Donne MUHOZA who, for his demonstrations,
elaboration of new concepts and clarification of concepts not
well understood and for his unfailing help by proper guidance,
effective comments and with a good support
I am very grateful to him for giving me the benefits of his
experience and suggestions.
I actually thank the Head of RANGO health center who for hispermission to data collection,
Great thanks also to the Heads of Department of Applied
Statistics Prof. Sai Kumar CHINTALAPUDI and Mr. Charles RURANGAiii
I dedicate my dissertation
work:
To Almighty Powerful God
To my family and my friends,A special feeling of gratitude to my loving relatives: Adrien
MUHIGIRWAFather Pie NEMEYAMAHOROMy loving Aunt M. Jeanne
IRAGUHA,
Grandmother whose words of encouragement are still in my ears, to my esteem friends:
Augustin NSHUTI IYAMUREMYE andValentine IMANISHIMWE.
I also dedicate this dissertation to my parents who
give me way of live.I will always appreciate all
they have done.

for the interventions allowed this research to be carried out
smoothly and under good conditions
I really accord my deepest gratitude to all of my family members
because of their advices, love, endless patience, care, and
constant encouragement, financial and moral support they gave me
when it was most required.
My Special thanks to my colleagues we shared the experience andto all my classmates in the department of Applied Statistics fortheir collaboration during our studies.
In general, I thank all people participated near or far so that Icould accomplish my intended task in the convenient time andspace.
Cyprien HABINSHUTI
Signnature……………………, date………………
ContentsDECLARATION..........................................................i
DEDICATION..........................................................ii
Acknowledgement....................................................iii
List of abbreviations..............................................vii
LIST OF TABLES......................................................ix
iv

LIST OF FIGURES......................................................x
Abstract............................................................xi
CHAPTER I: GENERAL INTRODUCTION......................................1
I.1 Background......................................................1
1.2 Back ground to the study........................................1
1.3 Problem statement...............................................3
1.4 Objectives of The study.........................................4
1.4.1 General Objectives..........................................4
1.4.2 Specific objectives.........................................4
1.4 Research Questions..............................................4
1.5 Research hypothesis.............................................4
1.6 Scope of the Study..............................................4
1.7. Arrangement of the study.......................................5
CHAPTER TWO: LITERATURE RIVIEW.......................................6
II.0. DEFINITION OF KEY TERMS.......................................7
II.1.The History of HIV/AIDS........................................7
II.2. Definition of HIV/AIDS globally...............................7
II.3. HIV/AIDS STATUS...............................................8
II.3.1. HIV/AIDS Status all over the World........................8
II.3.2. HIV/AIDS status in EAST Africa............................9
II.3 .3. HIV/AIDS status in Rwanda...............................11
II.4. Health services regarding HIV/AIDS alleviation in Rwanda.....11
v

II.5. Rwanda’ strategies to reduce the increment of HIV/AIDS among Rwandans...........................................................12
CHAPTER THREE.......................................................14
RESEARCH METHODOLOGY................................................14
3.1. Introduction..................................................14
3.2 Research Design................................................14
3 .2.1 .The analytical research..................................14
3.3. Study Area....................................................14
3.4. Study Population..............................................15
3.5. Sampling techniques...........................................15
3.5.0. Sample size...............................................15
3.5.1 Sample size calculation....................................15
3.5.2. Purposive sampling........................................17
3.6. Techniques of Sample selection................................17
3.6. Source of Data................................................18
3.6.1. Primary data..............................................18
3.6.2. Secondary Data............................................19
3.7. Techniques of Data collection.................................19
3.8. Research instruments..........................................19
3.8.1. Questionnaire.............................................19
3.8.2. Interview.................................................19
3.8.3. Observation...............................................19
3.9. Data processing and analysis..................................20
vi

3.9.1. Editing...................................................20
3.9.2. Coding....................................................20
3.9.3. Tabulation................................................20
3.10. Limitations of the study.....................................21
CHAPTER IV: ANALYSIS AND DISCUSSION OF FINDINGS....................22
4.0. Introduction..................................................22
4.1. The structure and number of focusing population...............24
Figure 4.1 The figure below showing the distribution of HIV/AIDS status among male and female.......................................25
4.2. Social demographic characteristics............................25
4.2.1 HIV+ and HIV- of clients to counselors within their age and education levels.................................................27
4.2.2 Occupation of population who access to counseling services. 28
4.3. Characteristics of Service Providers interviewed..............29
4.4 The data analysis and data presentation........................32
4.4.1 The analysis and interpretation..............................34
CHAPTER V: RECOMMENDATION AND CONCLUSIONS...........................36
5.1. Introduction..................................................36
5.2 Conclusion.....................................................37
5.3 Recommendation.................................................38
Bibliography........................................................40
QUESTIONNAIRES......................................................41
vii

List of abbreviations5 C: Consent, Confidentiality, Counseling, Correct
AIDS: Acquired Immune Deficiency Syndrome
ARS: acute retroviral syndrome
ART: antiretroviral therapy
CDC: Disease Control and Prevention
CSS: Care and Support Services
EGPAF: Elizabeth Glaser Pediatric AIDS Foundation
H1: The alternative hypothesis
HIV/AIDS: Human Immunodeficiency Virus for Acquired ImmuneDeficiency Syndrome
HIV: Human Immunodeficiency Virus
HIV-: Human Immunodeficiency Virus negative
HIV+: Human Immunodeficiency Virus positive
Ho: The null hypothesis
HSCP: HIV Clinical Services Program
MIYCN: Maternal Infant and Young Child Nutrition
MOH: Ministry of Health
viii

NGO: Non-governmental Organization
NUDIPU: National Union of Disabled Persons of Uganda
PEP: Post- exposure prophylaxis
PEPFAR: President’s Emergency Plan for AIDS Relief
PIT: Provider Initiated Testing
PLHIV: People Living with HIV
PMTCT: Prevention of Mother-to-Child Transmission
RBC: Rwanda biomedical center
RSPA: Rwanda Service Provision Assessment
SIV: simian immunodeficiency virus
SPSS: statistical package for social sciences
STIs: sexually transmitted infections
TB: tuberculosis
UNAIDS: Joint United Nations Program on HIV/AIDS
USAID: United State Agency for International Development
USAID: United States Agency for International Development
VCT: Voluntary Counseling and Testing
WHO: World Health Organization
ix
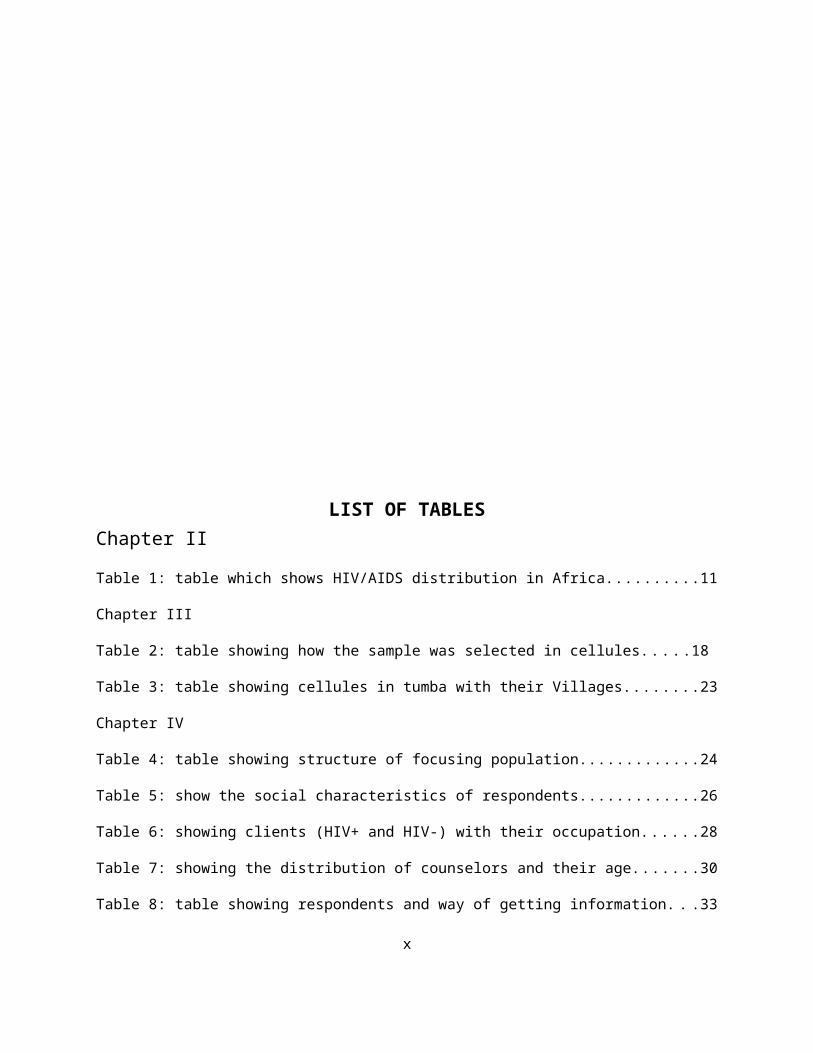
LIST OF TABLESChapter II
Table 1: table which shows HIV/AIDS distribution in Africa..........11
Chapter III
Table 2: table showing how the sample was selected in cellules.....18
Table 3: table showing cellules in tumba with their Villages........23
Chapter IV
Table 4: table showing structure of focusing population.............24
Table 5: show the social characteristics of respondents.............26
Table 6: showing clients (HIV+ and HIV-) with their occupation......28
Table 7: showing the distribution of counselors and their age.......30
Table 8: table showing respondents and way of getting information. . .33
x
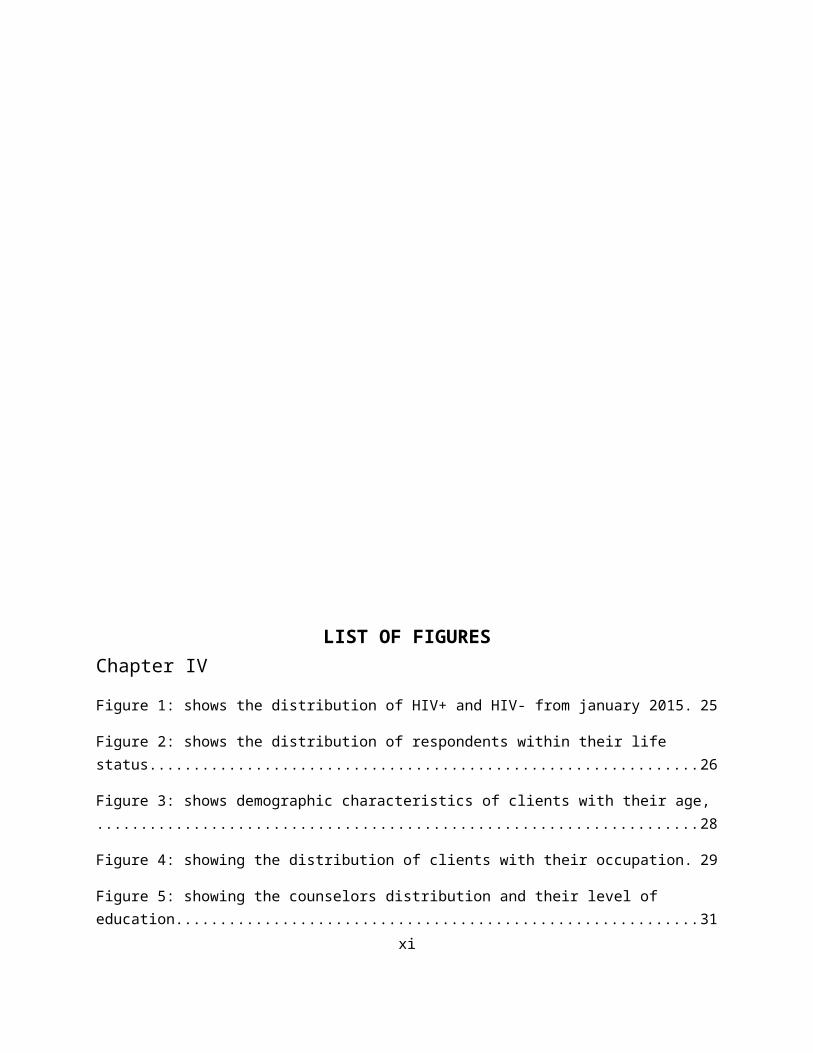
LIST OF FIGURESChapter IV
Figure 1: shows the distribution of HIV+ and HIV- from january 2015. 25
Figure 2: shows the distribution of respondents within their life status..............................................................26
Figure 3: shows demographic characteristics of clients with their age,....................................................................28
Figure 4: showing the distribution of clients with their occupation. 29
Figure 5: showing the counselors distribution and their level of education...........................................................31
xi

figure 6: showing counselors distribution and their gender..........32
Figure 7: figure showing respondents and means of information.......34
ABSTRACT
Persons with or at risk for human immunodeficiency virus (HIV)
infection need client-centered counseling and information about
the disease. One of the best opportunities to provide counseling
xii

and information is during an HIV testing encounter. New testing
guidelines from the Centers for Disease Control and Prevention
encourage less counseling before and after testing. We review the
evidence regarding voluntary counseling and testing (VCT).
There is clear endorsement in peer-reviewed scientific
information for VCT as part of an evidence-based bundle of
interventions to prevent HIV infection. For persons who test
seropositive, VCT has an impact, but it is hard to uncouple the
impact of counseling from that of testing. For persons who test
seronegative, counseling has a beneficial impact on risk
behaviors and sexually transmitted disease incidence and costs
very little to implement.
This study investigated the different ways through which
counseling was constructed for clients. To access HIV/AIDS
counselling services in Huye District. The counseling impact was
investigated through four different ways. First, it was examine
the extent to which the institutions deriver services to the
people in need. Secondly it was through to find out the
characteristics of people living with the infection of HIV/AIDS
in community. Thirdly, it was through to evaluate whether the
counseling services have an effect on life of the infected
persons and non-infected. Fourth, it was through to find the
challenge faced by infected persons and institutions in charge of
counseling services.
xiii

A cross- sectional study design was used for collection of data.
The study was conducted in one health center (RANGO Health
center) that under the control of KABUTARE Hospital. Five (5)
cellules of Tumba sector were selected, where the health center
locate, and are namely (Rango B, Gitwa, Cyimana, Cyarwa, Mpare).
These cellules are the base to select the respondents used in
primary data collection of this study.
The results of the study revealed that 11counselors showed that
they do not give the counseling on HIV/AIDS and other 7counselors
they do in case of client in need. To access on the services
4HIV- clients used television, 2 HIV+ newspaper or billboards,
4news or schools, 26 HIV- used news and schools, 7counselors try
to give the information on HIV/AIDS by public talk, 2HIV+ clients
used public talk, 9HIV- clients used public talk as a means of
information.
The study recommended that in order to empower counseling
services, there was need to create and maintain situations. The
sensitization should maid to people in need of HIV/AIDS services
using counselors and giving them time in public meeting. The
hospital also must provide training support to the counselors on
the way they care clients. The hospital should also give to
counselors the facility in order to perform their work as best
they can.
xiv

CHAPTER I: GENERAL INTRODUCTION
I.1 BackgroundIn many countries the people living with HIV/AIDS experience asituation of discrimination from others, such kind of situationand its levels of discrimination continue to broom to peopleliving with HIV, it will lead to harm and increase in stigmaamong those affected people.
Many international level studies conducted on HIV/AIDSprevalence and services delivery had shown that people in need,should not access to the services., some organizations cannotdeliver appropriate services needed by affected people (WHO,NUDIPU 2003).
In fact the extent to which people with Human Immune DeficiencyVirus counseling or care services is questionable, still they arehighly affected to HIV/AIDS infection. Most people might besubjected to poverty, discrimination, and stigmatization. This study aimed to examine how services are being to be drawn inmultiple activities for people living with HIV/AIDS relatively toaccess HIV/AIDS counseling services in Rwanda especially HuyeDistrict.
1.2 Back ground to the studyMany international working groups, including representative fromthe World Health Organization (WHO), the United National Programon HIV/AIDS (UNAIDS), the United Agency for InternationalDevelopment (USAID), and other entities such as NGOs thatimplement HIV/AIDS services, has developed common indicators formeasuring the quality of HIV/AIDS services provided through theformal health sector such that Capacity to provide basic servicesfor HIV/AIDS, Capacity to provide advanced services for HIV/AIDS,
1

Availability of recordkeeping systems for monitoring HIV/AIDScare and support, Capacity to provide services for prevention ofmother-to-child transmission (PMTCT) of HIV and Availability ofyouth-friendly services.Services and resources provision interventions in community maybe assumed that people meet similarities of inequality and commonneeds for being access to the needed services. In any communitydifferences arise and people are categorized within those livingwith HIV/AIDS prevalence. Service and resource provisioninstitutions as No-Government institution (NGO’s), Government andprivate institutions (WHO, 1999). They include those who providecounseling, Testing, care and other governance support to thepopulation living with HIV/AIDS prevalence.
Some services like counseling are accessed by few personincluding AIDS patients due to stigmatization and their socialunit club in the community rural and urban population are alike,infected and non-infected, currently access the pervasive andpopular HIV/AIDS counseling services and treatment. Out ofexpectation, it is highly probable that people live with HIV/AIDSexperience the discrimination event in Rwandan community.
Rwanda has been considered one of the African countries mostaffected by the HIV/AIDS epidemic. The first case of HIV/AIDS inRwanda was seen at the Centre Hospitalier de Kigali in 1983. Theinfection spread rapidly and widely throughout the country. TheHIV/AIDS epidemic has devastated the economy and the health caresystem of the country. It is estimated that 49,000 people diedeach year because of AIDS and related conditions, and as of 2003,an estimated 260,000 children had been orphaned by AIDS, thoughthe real figure could be much higher. AIDS cases occupy 60percent of all hospital beds (ROR and WJCF, 2003).
Rwanda survey on services provision of 2007 shows that More thanhalf (55%) of all facilities offer care and support services
2
(CSS), which is defined as any care for HIV/AIDS-relatedillnesses (e.g. opportunistic infections) or provision ofcounseling or social support services for people living withHIV/AIDS. Three-quarters of government-assisted facilities offerCSS compared to only half of government facilities and 27% ofprivate, NGO, and community facilities
Most HIV/AIDS services in the country are concentrated inhospitals; however, there are only 42 hospitals. As not allRwandans have easy access to hospitals, expanding HIV testing andprovision of ART to other facilities may lead to an increase inaccess to care.
The health care on HIV/AIDS relate to Voluntary ConfidentialCounseling and Testing in Rwanda that the survey defines afacility as having an HIV testing system or offering counselingand testing if: (1) before and/or after HIV testing ,Clients arecounseled on the prevention of HIV, the meaning of the test,transmission of the virus, living with HIV/AIDS, care andsupport, and other aspects of the condition; and (2) clients areoffered an HIV test conducted within the facility or by anaffiliated lab, or the facility has a system for referringclients to an external testing site and receives test resultsback from that external site in order to follow up clients aftertesting. A facility that simply refers clients elsewhere,expecting the other location to counsel and follow up on testresults, is not defined as having an HIV testing system oroffering HIV counseling and testing.
Rwanda Care and support services (CSS) Care and support servicesinclude any services that are directed towards improving the lifeof an HIV-infected person. These most often include treatment foropportunistic infections and illnesses that are commonlyassociated with or worsened by HIV infection, such astuberculosis (TB), sexually transmitted infections (STIs), and
3

malaria. Care and support services also may include palliativecare and socioeconomic and psychological support services (RSPA2007 final report).
The African situation revealed that HIV/AIDS pandemic wasspreading in heterosexual intercourse, while propagated bycultural practices such as marriage and polygamy. HIV/AIDScounseling services and treatment were few and unaffordable andtherefore available to only those who were economically empowered(Barnet, 1992). In Rwanda the extreme fatality of HIV/AIDSdeserved emergency establishment of counseling and treatmentcenters which began in 2009, with the Ministry of Healthspearheading Centers for Disease Control and Prevention (CDC)-Rwanda began transitioning the management of clinical servicesfrom international NGOs to the Rwanda MOH. A Transition TaskForce was created under the joint leadership of the Rwanda MOH,making HIV/AIDS counseling services accessible to both men andwomen, (UNAIDS, 2001).
Health care providers are on the forefront of preventing HIVtransmission and caring for people already infected. Post-exposure prophylaxis should be made more widely available tohealth care providers. PEP along with proper infection preventionpractices can keep health care providers safe from inadvertentinfection with HIV/AIDS
Worldwide, voluntary counseling and testing (VCT) is nowrecognized as an important element of HIV/AIDS prevention, careand support programmes and services, and indeed an entry pointfor the control of HIV transmission (Republic of Eritrea, 2005).HIV/AIDS counseling services presently offered include Freestanding counseling and testing services, Integrated counselingand testing services, and Post-test counseling services (WHO,2002).
4
1.3 Problem statementIt has stated that at international level that institutions couldnot give the appropriate services in need by affected people andthose who are rejected (WHO, 1999). The research identificationin this study is to study whether the services and resources areequally distributed or accessed. By taking reference on otherresearch conducted, some studies had shown that institutionsdeliver services and resources in unequal way (NUDIPU), the levelby which people affected access to the resources and services itis not known. As the infection new cases continues to be observedthis will lead to poverty due to an increase in number ofHIV/AIDS infection, this also lead to stigmatization anddiscrimination among people that will affect the services andresources accessibility.
The affected people may meet the problem of non-accessibility tothe services and resources especially in counseling and treatmenton HIV/AIDS when the issue of restriction arises due socialbehavior or stigmatization among the community people.
1.4 Objectives of The study
1.4.1 General ObjectivesThe overall objective of the research is to evaluate how servicesoffered to people infected and non-infected living with HIV/AIDSinfected people throughout the access of HIV/AIDS in a given areaof Huye District.
1.4.2 Specific objectivesThe study objectives are:
5

1. To examine the extent to which the institutions deriverservices to the people in need.
2. To find out the characteristics of people living with HIV/AIDSinfection in community.
3. To evaluate whether the counseling services have an effect onlife of the infected persons and partners of infected persons.
4. To find the challenge faced by infected persons andinstitutions in charge of counseling services.
1.4 Research QuestionsIn the following the foregoing the specific objectives, theresearch will seek to answer the following questions:
1. How institutions in charge of services deriver those serviceswhere it is required?
2. What are the working capacities or characteristics of peopleliving with HIV/AIDS?
3. What are the effects of counseling services on life ofinfected people?
4. What are the challenge faced by infected person andinstitution in charge of counseling services?
1.5 Research hypothesisThere is a positive impact of counseling services on infected andnon-infected people.
1.6 Scope of the StudyThe study is entailed to examine the effect of counseling
services on infected alongside non-infected person while
accessing services in Huye district, Tumba sector within Rango
6

Health Center. It seeks to know the extent to which the
counseling services providers bring the effect to both infected
and non-infected.
1.7. Arrangement of the studyThis first chapter provided a highlight of the background to the
study, research problem and purpose of the study, objectives,
research questions, scope and the significance of the study. The
second chapter is concerned with the review of related literature
and the theoretical framework and conceptualization of the study.
The third chapter outlined how the study was carried out,
indicating the research design, the methods that were employed
in the study, how the selection of study population, sample size
and sampling procedures, data collection methods, data analysis,
presentation and ethical consideration to be applied. The
fourth chapter will be dealing with the discussion on the
research findings under form of presentation of analysis done
about the research. The fifth chapter will provide the summary,
conclusions drawn from the study and gave recommendations for all
interested people
7
CHAPTER TWO
LITERATURE RIVIEW
This chapter presents the analysis of mentioned literature on the
multiplicity of people living with HIV/AIDS and the services of
HIV Testing and Counseling. The aims of this analysis are to see
the contribution of counseling services and to highlight the gaps
and weaknesses existing on both infected and non-infected people.
This literature review focuses on themes of the study which
include multiplicity of differences, Institutionalized
difference norms and practices, services inequalities as
constructed by society and family, institutions/organizations,8

Rules and Norms, unequal delivery of HIV/AIDS of Counseling
services and exclusion and restriction from recognition.
History shows that HIV Testing and counseling services have
helped millions of people learn their HIV status and for those
testing positive, learn about options for long term care and
treatment. In 2012, an estimate of 118 million people in 124 low-
and middle-income countries received HIV testing and counseling
in the past 12 months and learned their test result (by WHO).
HIV testing should be voluntary and the right to decline
testing should be recognized. Mandatory or coerced testing by
a health-care provider, authority or by a partner or family
member is not acceptable as it undermines good public health
practice and infringes on human rights.
Some countries have introduced, or are considering, self-
testing as an additional option. HIV self-testing is a process
whereby a person who wants to know his or her HIV status
collects a specimen, performs a test and interprets the test
results in private. HIV self-testing does not provide a
definitive diagnosis; instead, it is a screening test for HIV.
All testing and counseling services must include the 5 C’s
recommended by WHO: informed Consent, Confidentiality,
Counseling, Correct test results and linkage to Care,
treatment and other services.
9

While every nation has in some way been affected by this
pandemic, it is in Africa that the grip of HIV and AIDS has been,
by far the deadliest. Twenty-eight million people in Africa are
living with HIV/AIDS and Southern Africa has the Highest HIV
adult prevalence in the world. Well over two thirds of the
HIV/AIDS related Deaths (S18million, or 72%) are from Africa
(World Bank, 2002), although infection rates in individual
countries such South Africa, Botswana, Malawi and Swaziland are
much higher.
II.0. DEFINITION OF KEY TERMS
II.1.The History of HIV/AIDS Scientists identified a type of chimpanzee in West Africa as the
source of HIV infection in humans. They believe that the
chimpanzee version of the immunodeficiency virus (called simian
immunodeficiency virus, or SIV) most likely was transmitted to
humans and mutated into HIV when humans hunted these chimpanzees
for meat and came into contact with their infected blood. Studies
show that HIV may have jumped from apes to humans as far back as
the late 1800s. Over decades, the virus slowly spread across
Africa and later into other parts of the world. We know that the
virus has existed in the United States since at least the mid- to
late 1970s.
II.2. Definition of HIV/AIDS globallyHIV disease has a well-documented progression. Untreated, HIV is
almost universally fatal because it eventually overwhelms the10

immune system—resulting in acquired immunodeficiency syndrome
(AIDS). HIV treatment helps people at all stages of the disease,
and treatment can slow or prevent progression from one stage to
the next.
A person can transmit HIV to others during any of these stages
three,
Acute infection: Within 2 to 4 weeks after infection with HIV,
you may feel sick with flu-like symptoms. This is called acute
retroviral syndrome (ARS) or primary HIV infection, and it’s the
body’s natural response to the HIV infection. (Not everyone
develops ARS, however—and some people may have no symptoms.)
During this period of infection, large amounts of HIV are being
produced in your body. The virus uses important immune system
cells called CD4 cells to make copies of itself and destroys
these cells in the process. Because of this, the CD4 count can
fall quickly. Your ability to spread HIV is highest during this
stage because the amount of virus in the blood is very high.
Eventually, your immune response will begin to bring the amount
of virus in your body back down to a stable level. At this point,
your CD4 count will then begin to increase, but it may not return
to pre-infection levels.
Clinical latency (inactivity or dormancy): This period is
sometimes called asymptomatic HIV infection or chronic HIV
infection. During this phase, HIV is still active, but reproduces
11

at very low levels. You may not have any symptoms or get sick
during this time. People who are on antiretroviral therapy (ART)
may live with clinical latency for several decades. For people
who are not on ART, this period can last up to a decade, but some
may progress through this phase faster. It is important to
remember that you are still able to transmit HIV to others during
this phase even if you are treated with ART, although ART greatly
reduces the risk. Toward the middle and end of this period, your
viral load begins to rise and your CD4 cell count begins to drop.
As this happens, you may begin to have symptoms of HIV infection
as your immune system becomes too weak to protect you.
AIDS (acquired immunodeficiency syndrome): This is the stage of
infection that occurs when your immune system is badly damaged
and you become vulnerable to infections and infection-related
cancers called opportunistic illnesses. When the number of your
CD4 cells falls below 200 cells per cubic millimeter of blood
(200 cells/mm3), you are considered to have progressed to AIDS.
(Normal CD4 counts are between 500 and 1,600 cells/mm3.) You can
also be diagnosed with AIDS if you develop one or more
opportunistic illnesses, regardless of your CD4 count. Without
treatment, people who are diagnosed with AIDS typically survive
about 3 years. Once someone has a dangerous opportunistic
illness, life expectancy without treatment falls to about 1 year.
People with AIDS need medical treatment to prevent death.
12

II.3. HIV/AIDS STATUS
II.3.1. HIV/AIDS Status all over the WorldSince the beginning of the epidemic, almost 78 million peoplehave been infected with the HIV virus and about 39 million peoplehave died of HIV. Globally, 35.0 million, the 33.2 to 37.2million people were living with HIV with the end of 2013. Anestimated 0.8% of adults aged 15–49 years worldwide are livingwith HIV, within this situation, the burden of the epidemiccontinues to vary considerably between countries and regions.Sub-Saharan Africa remains most severely affected, with nearly 1in every 20 adults living with HIV and accounting for nearly 71%of the people living with HIV worldwide.
II.3.2. HIV/AIDS status in EAST AfricaIn generally sub-Saharan Africa contains only about 11 percent ofthe Earth's population; the region is the world's epicenter ofHIV/AIDS. The numbers are daunting. Adult HIV prevalence is 1.2percent worldwide (0.6 percent in North America), but it is 9.0percent in sub-Saharan Africa. UNAIDS estimates that at the endof 2001, there were 40 million people living with HIV/AIDS, 28.5million of them from sub-Saharan African. Five million adults andchildren became newly infected with HIV in 2001, 3.5 million ofthem from sub-Saharan Africa. Three million people died fromAIDS-related causes in 2001, and 2.2 million of these deaths wereamong sub-Saharan Africans.2 (July 2002)
AIDS is now the leading cause of death in sub-Saharan Africa.(Worldwide, AIDS is the fourth leading cause of death). Lifeexpectancy at birth has plummeted in many African countries,wiping out the gains made since independence. The combinationof high birth rates and high AIDS mortality among adults,including many parents, has meant that more than 90 percent ofchildren who have been orphaned as a consequence of theHIV/AIDS epidemic are in this region.
13

These statistics disguise an important part of the story,however. Most of the worst affected countries form an "AIDSbelt" in eastern and southern Africa. This belt consists ofabout 16 countries3 and stretches from Djibouti and Ethiopiadown the east side of the continent through South Africa.These countries constitute only a little more than 4 percentof the world's population but account for more than 50 percentof HIV infections worldwide.
According to UNAIDS, all the worst affected countries (withprevalence rates over 20 percent) are contiguous to oneanother in the lower part of the continent. These includeSouth Africa, Lesotho, Swaziland, Botswana, Namibia, Zambia,and Zimbabwe. Botswana, Lesotho, Swaziland, and Zimbabwe haveprevalence rates above 30 percent.
Elsewhere, Somalia, Eritrea, Djibouti, and Sudan have littleor no data, and Madagascar remains an interesting case.Despite tourism, an active commercial sex trade, and highrates of other sexually transmitted infections (STIs), anddespite being separated from the African mainland by only 60kms of water, adult HIV prevalence remains below 1 percent.
Though having overall adult prevalence rates lower than in theeastern and southern parts of the continent, the middle partof Africa is undergoing a serious and generalized HIV/AIDSepidemic. Among the countries in the region, the DemocraticRepublic of Congo, Chad, and Equatorial Guinea show adult HIVprevalence rates under 5 percent. Angola has been war-torn andchaotic for so long that it is difficult to know exactly whatis transpiring with the epidemic there. However, UNAIDS placesthe adult prevalence rate at 5.5 percent. Elsewhere in theregion, UNAIDS reports prevalence rates of 7.2 percent in theCongo, 11.8 percent in Cameroon, and 12.9 percent in theCentral African Republic. Many of the worst affected countriesin middle Africa have the highest rates of other STIs on thecontinent.
14

Further north in the AIDS belt, Mozambique, Malawi, Burundi,Rwanda, Kenya, Tanzania, and Ethiopia all have adultprevalence rates in the 6-15 percent range. Adult prevalencein Uganda is estimated to be around 5 percent. Uganda is theone country in the region that has probably achieved alongstanding decline in HIV prevalence. Prevalence in Ugandamay have peaked in the 12-13 percent range in the early 1990sbefore the onset of this decline.
In fact, HIV prevalence in East Africa is generally moderate tohigh, and second behind southern Africa. However, generalprevalence has been in decline for the past two decades. Forexample, Kenya has seen its HIV prevalence drop from a high of 14percent to nearly 6 percent. Uganda and Tanzania also haveprevalence over 5 percent, with the lowest seen in Madagascar(0.5 percent) and Mauritius (1.2 percent).
Despite of this progress, there are new areas of concern with HIVprevalence on the rise among vulnerable groups including peoplewho inject drugs (PWIDs), prisoners and uniformed services (suchas the armed forces and the police)
Table below shows Estimated Number of People in the African “AIDSBelt” especially in eastern Africa Living with HIV/AIDS, end of 2001.
Total Adults andChildren
Total Women(15-49)
Adults (15-49)rate (%)
GlobalTotal
40 million 18.5 million 1.2
Ethiopia 2.1 million 1.1 million 6.4
Uganda 600,000 280,000 5.0
15

Kenya 2.5 million 1.4 million 15.0
Tanzania 1.5 million 750,000 7.8
Rwanda 500,000 250,000 8.9
Burundi 390,000 190,000 8.3
Mozambique
1.1 million 630,000 13.0
Malawi 850,000 440,000 15.0
Botswana 330,000 170,000 38.8
Swaziland 170,000 89,000 33.4
Lesotho 360,000 180,000 31.0
SouthAfrica
5.0 million 2.7 million 20.1
Table 1: table which shows HIV/AIDS distribution in Africa
Source: UNAIDS, Report on the Global HIV/AIDS Epidemic: July 2002.
II.3 .3. HIV/AIDS status in RwandaRwanda’s population and health care system have suffered from theHIV epidemic due to lack of infrastructures. The first case ofHIV/AIDS was seen at the Centre Hospitalier in Kigali in 1983.Since then, the infection has spread throughout the country. Anestimated 49,000 people have died each year due to HIV infection
16

and related conditions, and HIV infection cases occupy 60% of allhospital beds.
II.4. Health services regarding HIV/AIDS alleviation in RwandaImmunization coverage has stalled since 2000, with the percentageof children receiving all vaccines remaining at 75%, thoughfalling in urban areas. Sustained sensitization campaigns in therural areas may explain why rural rates of immunization are nowhigher than urban.
HIV prevalence is estimated at 3% of adults. A national campaignwas Conducted to reduce perceptions about the stigma of HIV andthe accompanying discrimination and there are now 234 healthcenters with Voluntary Counseling and Testing (VCT), andtreatment of PLHIV has increased (72% of pregnant PLHIV areestimated to receive a complete course of ARVs). However,concern remains in several areas including: low condomutilization among youth and groups at higher risk of HIVexposure, the rural versus urban ratio of HIV prevalence andincreasing transmission amongst married couples and the culturalnorms associated with this. Thus, Rwanda must strive to take thenecessary precautionary steps now so that increasing rates ofinfection do not erode the impressive gains made in the last fiveyears (Rwanda poverty reduction 2008-2012)
Services and resources provision interventions in community maybe assumed that people meet similarities of inequality and commonneeds for being access to the needed services. In any communitydifferences arise and people are categories within those livingwith HIV/AIDS prevalence. Service and resource provisioninstitutions as No-Government institution (NGO’s), Government andprivate institutions (WHO, 1999). They include those who providecounseling, Testing, care and other governance support to thepopulation living with HIV/AIDS prevalence.
17

II.5. Rwanda’ strategies to reduce the increment of HIV/AIDS among Rwandans Rwanda implements the program of reducing HIV/AIDS prevalenceamong Rwandans in accordance of Elizabeth Glaser Pediatric AIDSFoundation (EGPAF) program and its focus in Rwanda.The Elizabeth Glaser Pediatric AIDS Foundation (EGPAF) began itssupport for HIV clinical services in Rwanda in 2001 withtechnical and financial support to the Treatment and ResearchAIDS Center (today known as the Rwanda Biomedical Center [RBC])for scale-up of Rwanda’s prevention of mother-to-childtransmission of HIV (PMTCT) program. The HIV Clinical ServicesProgram (HSCP), funded by the U.S. Agency for InternationalDevelopment (USAID) and the President’s Emergency Plan for AIDSRelief (PEPFAR) began in June 2007. Under the HCSP, EGPAF was thelead PEPFAR technical partner in the Eastern Province of Rwanda,working closely with Rwandan governmental institutions at thedistrict level, the Ministry of Health (MOH), other partners, andlocal organizations.
EGPAF/Rwanda’s HIV program was developed to respond to Rwanda’sdevelopment vision for its health programs, which is comprised ofa strategic plan (Rwanda Vision 2020), the Economic Developmentand Poverty Reduction Strategy (EDPRS), and other health sectorstrategies. The program also is aligned with donor mandates andbilateral accords such as the partnership framework between theU.S. and Rwandan Governments that focuses on HIV/AIDS prevention;care and treatment; quality of care; health systems strengthening(HSS); and transitioning of financial and technical managementcapacity to local institutions.EGPAF/Rwanda assists in implementing comprehensive, integratedHIV clinical services at the site and central levels, providingtechnical expertise to health institutions to build theircapacity to maintain high-quality HIV services in theirdistricts. These include:
Prevention of Mother-to-Child Transmission of HIV (PMTCT)18

Voluntary Counseling and Testing (VCT) Provider Initiated Testing (PIT) Care and Treatment services Support for tuberculosis screening and testing Maternal Infant and Young Child Nutrition (MIYCN) Maternal and Child Health / Family Planning / Sexual and
Gender-Based Violence / Water and Sanitation (all supplementedwith funding from USAID)
EGPAF/Rwanda is committed to sustainable, locally-owned programs,and works closely with the MOH, districts, and health facilitiesto address priorities and build local staff capacity. To thisend, EGPAF/Rwanda offers grants, mentorship, and training todistricts, health facilities, and community members.
The United States Agency for International Development (USAID) isthe foreign assistance agency of the United States Government.USAID supports $150 million of development assistance annually toRwanda, with programs in health, economic development, education,and democracy and governance.
Rwanda has stepped up efforts to prevent new HIV infections toachieve the 2015 global target of zero new infections andgovernment has put in place several initiatives to ensure a 0%record of new infections by 2015- such as the circumcisioncampaign, we would reduce new infections by 50%.
Other areas of focus have been seen in containing the HIVincidents that lead to new infections mainly in some targetgroups like the commercial sex workers of whom the HIV/AIDSprevalence is 51% and campaigns to ensure a reasonable reductionin the transmission of Mother to Child Infections.
Rwanda’s HIV/AIDS prevalence is 3% an equivalent of about 400,000people from 7% in 2002 when the government set up measures to
19
address the issue of HIV/Aids at a large scale by involvingcommunities and local leaders.
CHAPTER THREE
RESEARCH METHODOLOGY
3.1. IntroductionThis chapter indicates an explanation of the methodology that
will be used in the study ; the research design, the study
population, sample size and sampling methods and procedures, data
collection methods, data analysis and dissemination, ethical
consideration and study limitations. Kenneth D. Bailley (1978:
83) defines the methodology as the set of methods and principles
that are used when studying a particular kind of work. A method
is composed of all intellectual process in orderly system or
arrangements that enable a researcher to reach an aspect of
knowledge by using various techniques.
20
3.2 Research DesignResearch design focuses on an outline, plan or strategyspecifying the procedure to be used in investigating the researchproblem. (Christensen, 199:269). The researcher collects relevantdata needed to test the researcher hypothesis. The design of thestudy is analytical in nature.
3 .2.1 .The analytical researchAccording to (Jill and Roger Hussey, 1997: 11) the analytical
research design is continuation of the descriptive research. The
researcher goes beyond merely describing the characteristics to
analyzing and explaining why and how it is happening. Thus, this
research aims to understand the use of accounting ratios by
measuring causal relation among them in decision making.
This study will adopt a cross sectional study design that will
use qualitative and quantitative methods to collect required data
outcomes so as to come up with recommendations that will address
the research problem. It is cross-sectional because it
encourages in investigating the positive change on rural
population who seek to access HIV/AIDS counseling services at
this point in time in selected sector in Huye District.
3.3. Study AreaThe selected sector for the study is found in Huye district. Thecriteria for selection of these institutions will be based onability to have population who get HIV/AIDS services and/orcounseling services by one of medical institutions found in HuyeDistrict.
21

3.4. Study PopulationGrinnell and Williams, 1990: 118, said that, «a population can be
defined as the totality of persons or objects with which a study
is concerned». The study population is from several selected
households in Tumba sector that whoever has access on HIV/AIDS
services. Mainly the research will be concerning the people who
are beneficiaries of HIV/AIDS delivered services for improving
their lives.
They are targeted because they are deemed knowledgeable and
expected to provide relevant information concerning to access on
HIV/AIDS counseling services. Population that is supposed to
access on those services in Tumba sector is estimated to be 1479
while service respondents of interest are 65 in 5 cellule; in
choosing this targeted population some criteria have been
followed.
The first criterion for choosing my sample population has been
availability and willingness to answer my questions. However, in
the selection of my subjects I had to take into consideration the
availability of my population of the study. As far as the latter
is concerned, Cohen and Manion (1994:77) explain that the
researcher handpicks cases to be included in his sample
population on the basis of his judgment of their typicality. The
second criterion has been the fact that the population to be
questioned is located around the residence. The representativity
of my sample has also been taken into account. 22

3.5. Sampling techniques
3.5.0. Sample sizeThe research will use 65 respondents who are including in 5cellules with33 villages of all those cellule, it mean at least 2respondents for every village 1 in one village of mpare cellule.The total respondents is 65, this sample is selected because theyare more knowledgeable about the study it means they have beenselected basing on the information they have.
3.5.1 Sample size calculationThe question then is, how large of a sample is required to infer
research findings back to a population?
Standard textbook authors and researchers offer tested methods
that allow studies to take full advantage of statistical
measurements, which in turn give researchers the upper hand in
determining the correct sample size. Sample size is one of the
four inter-related features of a study design that can influence
the detection of significant differences, relationships or
interactions (Peers, 1996)
As a part of this discussion, considerations for the appropriate
use of Cochran’s (1977) sample size formula for both continuous
and categorical data will be presented.
Cochran (1977) addressed this issue by stating that “One method
of determining sample size is to specify margins of error for the
items that are regarded as most vital to the survey.
Cochran’s (1977) formula uses two key factors:
23

1. The risk the researcher is willing to accept in the study,
commonly called the margin of error, or the error the
researcher is willing to accept
2. The alpha level, the level of acceptable risk the researcher
is willing to accept that the true margin of error exceeds
the acceptable margin of error i.e., the probability that
differences revealed by statistical analyses really do not
exist.
Alpha Level: The alpha level used in determining sample size in
most educational research studies is either .05 or .01 (Ary,
Jacobs, & Razavieh, 1996)
In general, an alpha level of .05 is acceptable for most
research.
An alpha level of .10 or lower may be used if the researcher is
more interested in identifying marginal relationships,
differences or other statistical phenomena as a precursor to
further studies.
Cochran’s sample size formula for continuous data is presented
here along with the explanations as to how these decisions were
made:
Where t: value for selected alpha level of
0.05 from t-student table
(P)(q): estimate of variance in the
24

Population
P: percentage picking a choice, expressed as
decimal (0.5 used for
Sample size needed)
and q=1-p
D: acceptable margin of error for mean
being estimated, so
the confidence interval, in decimals (0.05 level
of significance) or
error researcher is willing to except).
No: the sample size
For our study we have population of 1479
Level of significance
α=0.1
T=1.645
P=0.5
= =67.650625
Required sample size according to Cochran’s formula:
= = =64.69
Where N: population size (population of interest).
25

Many researchers could benefit from a real-life primer on the
tools needed to properly conduct research, including, but not
limited to, sample size selection. This manuscript will describe
common procedures for determining sample size for simple random
and systematic random samples. It will also discuss alternatives
to these formulas for special situations. This manuscript is not
intended to be a totally inclusive treatment of other sample size
issues and techniques. Rather, this manuscript will address
sample size issues that have been selected as a result of
observing problems in published manuscripts. (James E Bartlett)
3.5.2. Purposive samplingThis will be used to select the respondents from key persons from
the local residence which are the villages of Tumba sector. This
is because of their participation in HIV/AIDS counseling
services. So, they have the necessary information needed by the
researcher. Also, purposive sampling will be used in order to
obtain the more accurate data.
3.6. Techniques of Sample selectionA sample is a part of population, which is deliberately selected
for the purpose of investigating the population. It involves the
determination of the sample size from the targeted population.
Therefore, purposive sampling will be applied to the local
beneficiaries; it will help the researcher to get reliable
information, because all population are not informed about
26

HIV/AIDS counseling services, only informants people are
considered by the researcher.
The total population of interest in Tumba sector 1489
people .Therefore, the sample size is 65 respondents. All these
selected population are concerned with the research and are aware
HIV/AIDS counseling services. This means that, they are selected
purposively.
Table 3.1: Sample selection
Categoryofpopulation
Name ofcellule
Totalnumberincellule
Sampleselectedofbeneficiaries
Sampleofcounselors
Basisofselection
Technique used
HIV/AIDSCounselingservices’beneficiaries
Total
1. RangoB
14 10 4 Theyarenearthecounselingservicesplaceandhavesomeinformationon thedeliveredservices
Purposivesampling
2. Gitwa 10 6 43.Cyimana
10 7 3
4.Cyarwa
10 8 2
5. Mpare 13 10 4
27

Table 2: table showing how the sample was selected in cellules
Source: Primary data, April, 2015
In this study, participants were selected basing upon Yamanemethod where every population must be selected based on thecharacter of interest and the condition of being selected or mustbe the desired population have typical characteristicsnecessary to provide information but rare and very difficult tolocate and recruit for a study. The sampling will be done frompopulation whoever had the HIV/AIDS Services and take servicesfrom one of the hospital in Huye District.
3.6. Source of Data
3.6.1. Primary dataThe primary data according to Bailley (1987:2) are eye witness
accounts written by people who experienced a particular event or
behavior.
3.6.2. Secondary Data Secondary data is information that has been collected for a
purpose other than your current research project but has some
relevance and utility for your research.
3.7. Techniques of Data collection To collect relevant information and appropriate data required for
the study, the researcher used documentary analysis, observation,
interview and questionnaire as research instruments
28

3.8. Research instruments
3.8.1. Questionnaire Kakinda (1990:25) defines Questionnaire as a set of related
questions designed to collect information from a respondent. This
was employed in obtaining views and opinions with individual
respondents. In this research English questionnaire was used and
translated into Kinyarwanda version.
3.8.2. Interview This is intended to add quality that provided by the
questionnaire. Face-to-face interview will be conducted with the
help of the interview schedule during data collection. Structured
and non-structured interview were used. Under unstructured
interview, the respondents were given the subject of the whole
issue in general and the respondents were asked to relict the
information without any bias. The interview will be used
especially to the leaders of beneficiaries ‘cooperative .On the
other hand, the structured interview schedule the respondents are
given answers from which they would choose. The researcher used
both structured and unstructured interviews, in order to avoid
limitations in their responses.
3.8.3. Observation The researcher used the Observation technique in data collection,
which is the primary technique for collecting data. Observation
29

most commonly involves sight or visual data collection via other
senses such as hearing, touching and smelling.
3.9. Data processing and analysis “Data processing is concerned with classifying responses into
meaningful categories called codes”(Roth, 1989: 58). It consists
of editing, schedules and coding the responds. The data
processing begins with editing, coding and finally ended with
tabulation. Nachmias (1976: 143) assert that, data processing is
a link between data collection and data analysis. It involves the
transformation of the observation gathered from the fields into
the system of categories and the transformation of these
categories into codes and amenable to quantitative analysis and
tabulation.
Not all data can be presented in their entity. The variables to
be presented are those most central to the goals of the study;
generally variables include specifically in the research
questions (Bailey, 1978: 321). The researcher will have
technically processed data before performing proper analysis so
as to become more meaningful for interpretation. Data processing
will be done in accordance with general and specific objectives
of the research study. The data will be analyzed by using
computer program SPSS and Microsoft excel.
30

3.9.1. EditingEditing is the process of going through the questionnaire to
ensure that the `skip patterns' were followed and required
questions are filled out according to Daniel and Gates (1991:
387), Editing involves the inspection and if necessary,
connections of each questionnaire or observation form; the basic
purpose of editing is to impose some minimum quality standards on
the raw data (Churchill, 1992:608).
3.9.2. CodingMoses and Kalton (1971: 415), states that the purpose of coding
in the survey is to classify the answers acquired were coded and
tallies used to determine the frequencies of each response and
according to Churchill (1992: 612), coding is the procedure by
which data are categorized. It involves the categorization of
similar responses according to their different categories.
3.9.3. Tabulation Tabulation refers to the part of technical process on
statistical analysis of data that involves counting to determine
the number cases that fall into various categories according to
Selltiz et al. (1965: 406-407), Tables with corresponding
calculations will be used to indicate the frequency of particular
answers. Percentages also will be used to express the data in a
ratio form. For making the data easily and clearly understood,
each table will be followed by small explanation of the nature of
relationship indicated in the table.31

3.10. Limitations of the studyThe scope of this study has been continuously narrowed downbecause of many factors, namely:
The time constraint; such a study normally requires enoughtime without any interruption but it is requires to do twooverlapping activities (to study and conducting researchlike this one.
By far the most limiting factor to the effective conduct of
the research work, the financial resources will not enable
us to make a thorough collection and analysis of data as we
expect.
During this study, the expected constraints are not many.
Even though there are there the effort will be applied so as
to reach the best success of this study
32

CHAPTER IV
ANALYSIS AND DISCUSSION OF FINDINGS
4.0. IntroductionThis chapter provides the analysis and discussion of research
findings collected in the study conducted during the period
between April and May, 2015. The study tends to show how the
counseling services impact lives of population of rural area who
access to HIV/AIDS Counseling services in selected health
institution in Huye District.
First, the study seeks to examine the level to which
institutional rules and norms take people who try to access
HIV/AIDS counseling services. Secondly, the study set out to
examine the extent to which the structural positioning of HIV+
persons in society and how they access to HIV/AIDS counseling
services.
Thirdly, the study intended to analyze the extent to which the
interaction between rural population and HIV/AIDS counseling
service providers create and reinforce with different way in
access to and control over resources.
As said above, this analysis is based on the information (primary
source) from one of many heath centers under the control of
KABUTE hospital. The health center used is counselors from
33

different 5 cellules and 33 villages, each village it has 3
counselors.
In fact the total number of counselors that supervised by RANGO
heath center are almost 99 counselors. The table below shows the
total number of villages in TUMBA sector where those counselors
belong.
Name of the
cellule
Villages’names
1. RANGO B Ntangarugero, Akakanyamanza, Akabeza, Kigarama,
Byimana, Urugwiro, Impuhwe
2. GITWA Rebero, Rimba, Berwa, Agasenyi, Nyarurembo
3 .CYIMANA Amahoro, Ubumwe, Ubwiyunge, Abizerwa, Akamuhoza
4. CYARWA Agasengasenge, Kabeza, Mukoni, Agateme, Agahora,
Kigarama,
Taba, Icyili, Agasharu
5. MPARE Akabuga, Rwanyanza, Runyinya, Musange,
Akarugirinka,
Kigarama, Agasharu.
Table 3: table showing cellules in tumba with their Villages
Source: Primary sources
34

Rango health center is one among many health centers under the
control of KABUTARE Hospital and the one with program of VCT
(Voluntary Counseling and Testing) and PMTCT (Prevention of
Mother-to-Child Transmission). Those two services are concerned
with HIV/AIDS counseling and testing.
Hereafter the photo of the RANGO heath center hall that they use
when they are providing services to the clients.
The photo of RANGO Health Center hall.
4.1. The structure and number of focusing populationThe specific objective of the study was to examine the extent to
which the structural positioning of HIV+ in society affects their
access to HIV/AIDS counseling services.
In the context of this study, positioning is defined as placement
in society of a homogeneous Category of persons with similar35

defining characteristics, whether socially, culturally,
economically or otherwise. The number of population of interest
was delivered by data manager of the health center in order to
facilitate us in our study. Hereafter a table showing the total
population who participate in services related to HIV/AIDS
(counseling, voluntary testing,….. )
sex January February March Aprilmale HIV+ 5 3 0 5
HIV- 106 208 42 220femal
e
HIV+ 3 3 3 7HIV- 263 233 63 206
Total
population
tested
377 447 108 437
Table 4: table showing structure of focusing population
This table shows how population access on HIV/AIDS services in
Rango Health center from the beginning of the year 2015 up to
April of this year.
Those given numbers of 1370 respondents derived in the above
table, 99 counselors were added on the population of interest as
the service providers and more knowledgeable in those services.
36

Figure 4.1The figure below showing the distribution of HIV/AIDS status among male and female.
Figure 1: shows the distribution of HIV+ and HIV- from January 2015
Source: primary source
From the graphic above and based on the primary given by RANGO
health center, in January the men were more HIV+ than women (5
males and 3 females were HIV+), in February both male and female
they equate (3 males and 3 females), in March the number of
female HIV+ were higher that men (0 male and 3 female), in April
the number of HIV+ female increase by 4 and HIV+ male increased
by 5(5male and 7 female. With those number the female are tend to
be more HIV+ than men.
As our study is the assessment of counseling on HIV/AIDS, it
couldn’t be possible to explore the whole population because of
time limits and the costs, the sampling method have been applied
to select a population representative (sample).
37

4.2. Social demographic characteristics The analysis and associated discussion of findings starts with
description and analysis of demographic characteristics in this
study in order to provide background information that was
considered essential for purposes of making reliable
interpretation and conclusions on population of interest in this
study.
The primary information of this section were derived from
materials used (questionnaires) that were filled with
intervention of service providers, and different responses
obtained from people who were being given the services by service
provider in the first part of materials in order to provide
background information about their occupation, age, sex, levels
of education, in addition to their marital status. A total of 65
Respondents were interviewed of whom eighteen (18) and on who
don’t gave information, in fact 19 were service providers
(counselors) all are HIV-, nine (9) of clients are HIV+, thirty
eight (38) of them are HIV- clients. The SPSS graphic below
shows all distribution of our population.
38
Frequency Percent
ValidPercent Cumulative Percent
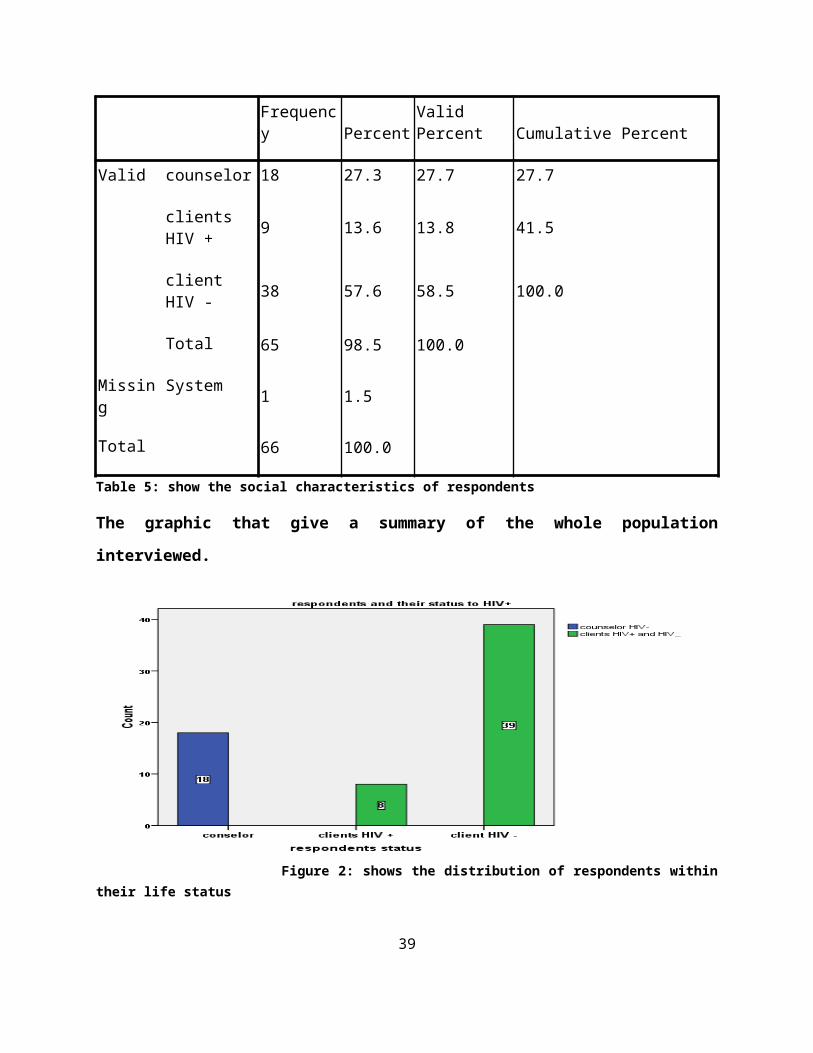
Valid counselor 18 27.3 27.7 27.7
clientsHIV + 9 13.6 13.8 41.5
clientHIV - 38 57.6 58.5 100.0
Total 65 98.5 100.0
Missing
System 1 1.5
Total 66 100.0
Table 5: show the social characteristics of respondents
The graphic that give a summary of the whole population
interviewed.
Figure 2: shows the distribution of respondents withintheir life status
39

This figure above shows the status of all respondents, counselors
and their clients.
4.2.1 HIV+ and HIV- of clients to counselors within their age andeducation levelsHIV+ and HIV- interviewed were from the population of interest in
HUYE district from rural area that around the district.
Table 4.3.1 this the summary table of clients in HIV/AIDS
consoling
Count
respondents status
Total
clients
HIV +
client HIV
-
age 11-20 2 2 4
21-30 2 29 31
31-40 2 8 10
50- 2 0 2
Total 8 39 47
Table: table showing clients and their age
40

Figure 3: shows demographic characteristics ofclients with their age,
Findings in Table 4.1 and its graph show a summary of the
selected sample of 65 respondents and; 47 is clients and 8 HIV
positive and 39 HIV negative. The graph below shows it very nicer
4.2.2 Occupation of population who access to counseling services
Table 4.4.2 table showing occupation of population who access to
counseling services
41

Count
working status
public
sector
private
sector
unemploy
ed Total
respondent
s status
clients
HIV +0 0 8 8
client
HIV -6 7 26 39
Total 6 7 34 47
Table 6: showing clients (HIV+ and HIV-) with their occupation
42

Figure 4: showing the distribution of clients with theiroccupation
Table 4.4.2 and the corresponding graph show the occupation of
clients to counselors respondents who were involved in this study.
These included clients of( HIV+ and HIV-), clients of HIV+ are
eight all are unemployed, clients with HIV- are thirty nine(39)
with six(6) of public sector, seven(7) of private sector and twenty
six(26) of unemployed level.
4.3. Characteristics of Service Providers interviewedThis study was conducted in one of Huye District institutions
which give counseling services to people in need. The findings
that are used come from visited institution of KABUTARE Hospital,
as counseling centers or organization supposed to offer
43

counseling services to all categories of people including HIV+
and HIV negative.
Service providers interviewed from the institutions where the
research was conducted included counselors, co-ordinator HIV/AIDS
programme and editor.
Counselors constituted great contribution the services provision
by Service providers. The respondents interviewed of whom only
27.7% were counselors as well as all could use sign language and
their status of life.
Further, service providers were requested to provide their
educational background levels in order to establish their ability
population with HIV+ no HIV+ as they seek to access HIV/AIDS
counseling services. Below is Tables 4.3.0 and 4.3.1 summarizing
the sex and levels of education of the respondent service
providers (counselors).
Table 4.3.0 table of numbers of counselors and their education
levels
44

Count
respondents status
counselor Total
education
levels
primary 11 11
secondar
y7 7
Total 18 18
Table 7: showing the distribution of counselors and their age
Figure 5: showing the counselors distribution and their level of education
Results showed that service providers who attained either a
primary or secondary school are 11 for primary school and
7attained secondary school. Findings further showed that most of
the respondent service providers attained primary school.
45

They were well familiar with the society, honest and understood
the questions that were asked in the questionnaires. Their
responses and information given was therefore consideredreliable.
Table 4.3.1table showing number of counselor and
their gender
Count
Respondents status
counselor Total
sex male 4 4
female 14 14
Total 18 18
46

Figure 6: showing counselors distribution andtheir gender
4.4 The data analysis and data presentationResults above showed that service providers who participated in
the research were male and female. With 14 females and 4 males,
Findings further showed that most of the respondent service
providers were female.
Being female for the majority of these service providers was
probably an extension of their way of improving their
participation in public services from the private to public
sphere.
47

Table 4.4.1 Characteristics of respondents by the means of
informationCount
information status
nocounselingaboutHIV
television
Newspaper
,billboards
news,schools
publictalk(counselor) Total
respondentsstatus
counselor 11
00 0 7 18
clientsHIV + 0 1 2 4 2 9
clientHIV - 0 3 0 26 9 38
Total 11 4 2 30 18 65
48

Table 8: table showing respondents and way of getting information
Figure 7: figure showing respondents and means ofinformation
The table 4.2.1 above and its graph show a summary of the 65
respondents, and how they managed to access on the information in
order to be a part of servicers whether (clients or counselors)
or how services providers treat the clients by means of
information.
The results reveal that 11counselors showed that they do not give
the counseling on HIV/AIDS and other they do. To access on the
services 4HIV- clients used television, 2 HIV+ newspaper or
billboards, 4HIV+ used news or information from their schools, 26
HIV- used news and schools, 7counselors try to give the
information on HIV/AIDS by public talk, 2HIV+ clients used public
talk, 9HIV- clients used public talk as a means of information.
49

4.4.1 The analysis and interpretation
Step 1: set the hypothesis
Ho: the number of clients depends on the counseling information
from providers (counselors)
H1: the number of clients depends on the counseling information
from providers (counselors)
Step2: level of significance (α=0.05)
Step3: calculation
Chi-square of independence has been used and finds the results in
the table below
50

Chi-Square Tests
Value df
Asymp.Sig.(2-sided)
Pearson Chi-Square 56.349a 8 .000
LikelihoodRatio 60.063 8 .000
Linear-by-LinearAssociation
13.787 1 .000
N of ValidCases 65
P-value is 0.000
step4: compare p-value and the level of significance.
Reject Ho; if P-value<level of significance
Otherwise fail to reject Ho.
step5: conclusion
As p-value (0.000) is less than level of significance (α=0.05),
we reject the null hypothesis in favor of alternative hypothesis.
As conclusion, at level of significance of 0.05 we infer that the
number of population in services or clients does not depends on51

the information or counseling from the service providers, but it
depends on others sources of information.
CHAPTER V
DISCUSSION OF FINDINGS, CONCLUSION AND RECOMMENDATIONS
5.1. Introduction
This chapter presents summary and conclusions derived from the
study and subsequent recommendations. In addition, the chapter
points out each specific objective and its relevance conclusion.
The general objective of the study was to evaluate how servicesdrawn to people infected and non-infected living with HIV/AIDSinfected people throughout the access of HIV/AIDS counseling in agiven area of Huye District. Specifically for populations ofTumba sector as indicated in Chapter 1 section 1.4.1.
The specific objectives were. To examine the extent to which theinstitutions deriver services to the people in need, To find outthe characteristics of people living with the infection ofHIV/AIDS in community; To evaluate whether the counselingservices have effect on life of the infected persons and non-infected; To find the challenge faced by infected persons andinstitutions in charge of counseling services.
The study was conducted in Huye District in many health centersunder the control of KABUTARE hospital, Rango health center, thisis specifically for services of VTC and PMTCT where generallythey are serving communities irrespective as indicated in thefindings.
52

The study employed the use of both quantitative and qualitativemethods, observation and case studies to enrich the findings. Thefindings of the study were based on a sample population of sixty-five (67) respondents. The study relied on Institutional theoryand Social relations Framework which generally argue thatindividuals and social groups, where people who need otherservices are not interested.
The first objective sets out .How institutions in charge ofservices deriver those services where it is required. As normsand regulations used by those institution, they derive theservices to people who pretend to get based on their will.
The second objective was to find out the characteristics ofpeople living with HIV/AIDS, in fact people living with HIV/AIDSmost of them are like isolated and live as to die tomorrow.Generally, discriminatory actins revealed as inequality asconstructed by society and family, institutions making HIV+ evenmore unequal in society by the means of being served asparticular client.
The Third objective was to the effect of counseling services onlife of infected people, the Findings revealed that communicationbarrier was advanced as an immense challenge followed by HIV+ notbeing accessible. In addition the level of education and feel notcomfortable when consulting the counselors because clients do notwish their status be know by anybody else. Those issue also wasconsidered as the prime hindering factor for HIV+ or HIV-‘saccess to HIV/AIDS counseling services.
The fourth objective was to know the challenge faced by infectedperson and institution in charge of counseling services, thefindings revealed that most of clients faced some challengeswhile accessing the HIV/AIDS services, like the means ofcommunication to counselors, no consultancy office for
53

counselors, most of counselors are women. Generally, based on thestudy clients in HIV/AIDS showed that the means of accessing toservices is difficult due to many challenges that they had facedand stated above.
Generally, to be a part of services clients is not mainly due tocounseling services and information rather than other mainchannels of information arise in research as means ofcommunication; news, newspaper, billboards, meetings and publictalk,… The key source of information used by clients is publictalks and news as big number of respondents approved it.
5.2 Discussion of findings
Persons with or at risk for human immunodeficiency virus (HIV)
infection need client-centered counseling and information about
the disease. One of the best opportunities to provide counseling
and information is during an HIV testing encounter. New testing
guidelines from the Centers for Disease Control and Prevention
encourage less counseling before and after testing. We review the
evidence regarding voluntary counseling and testing (VCT).
The study of U.S national library of Medicine of evaluation the
efficiency of rural health centers in Rwanda in delivering the
three key human immunodeficiency virus/acquired immunodeficiency
syndrome services: Antiretroviral Treatment(ART), Prevention of
Mother-To-Child Transmission(PMTCT), and voluntary counseling and
testing(VCT) using data envelopment analysis, and assesses the
impact of community-based health insurance (CBHI) and
performance-based financing on improving the delivery of the
three services. Results show that health centers average
54

efficiency of 78%, and despite the observed variation, the
performance increased by 15.6% from 2006 through 2007. When the
services are examined separately, each 1% growth of CBHI use was
associated with 3.7% more prevention of mother-to-child
transmission and 2.5% more voluntary counseling and testing
services. Although more health centers would have been needed to
evaluate performance-based financing, we found that high use of
CBHI in Rwanda was an important contributor to improving human
immunodeficiency virus/acquired immunodeficiency syndrome
services in rural health centers in Rwanda.( By.)
In my findings, 16.9% of respondents who are counselors confess
that no counseling on HIV/AIDS they give, 27.7% of respondents
(7counselors, 2HIV+, 9HIV-) infer that counseling or information
on HIV/AIDS services is done in public talk, 46.2% of respondents
confess that they knew information from news and schools (26HIV-,
4HIV+), 3.1% in newspaper, billboards means (2HIV+cliens), 6.2%
of respondents they knew information from television (4HIV-
clients).
As the above research showed the results Voluntary Testing and
counseling on HIV/AIDS and how must be associated with testing to
efficacy of its contribution. The findings from their research
showed that voluntary testing and counseling contributes 2.5% in
services efficiency. This support positively my findings revealed
that counseling itself doesn’t contributes to the decision of
clients to be part of clients HIV/AIDS services where only 16.9%
55
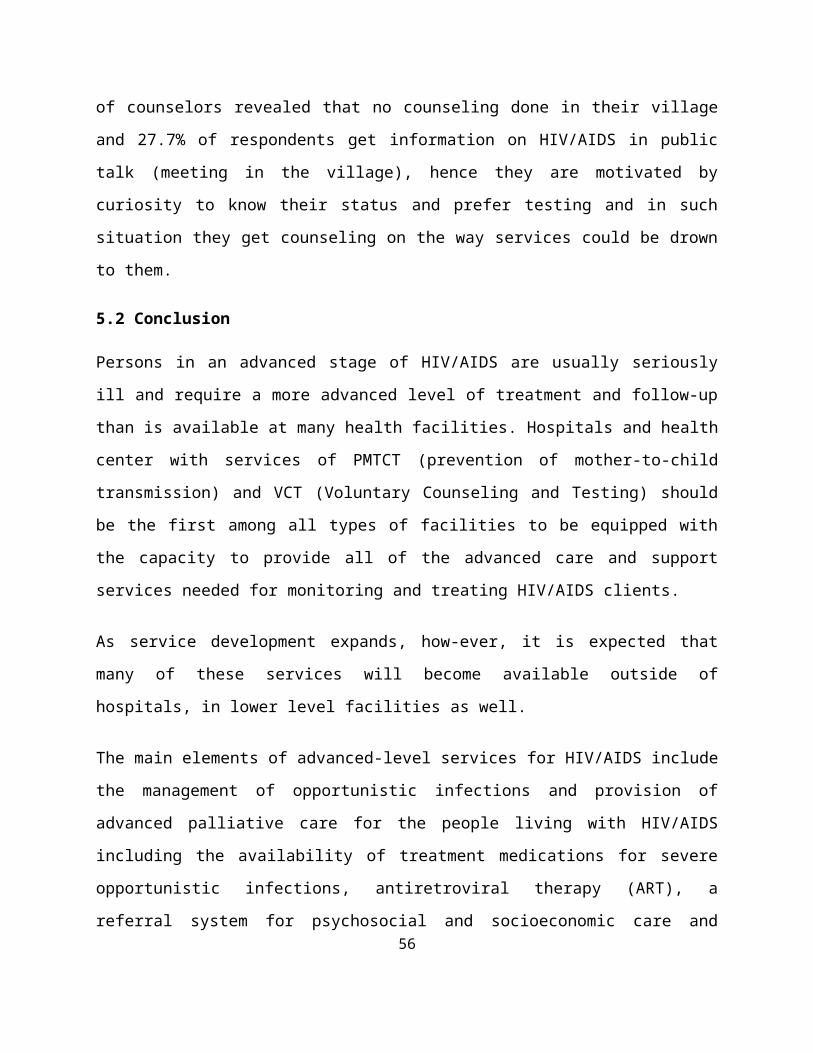
of counselors revealed that no counseling done in their village
and 27.7% of respondents get information on HIV/AIDS in public
talk (meeting in the village), hence they are motivated by
curiosity to know their status and prefer testing and in such
situation they get counseling on the way services could be drown
to them.
5.2 Conclusion
Persons in an advanced stage of HIV/AIDS are usually seriously
ill and require a more advanced level of treatment and follow-up
than is available at many health facilities. Hospitals and health
center with services of PMTCT (prevention of mother-to-child
transmission) and VCT (Voluntary Counseling and Testing) should
be the first among all types of facilities to be equipped with
the capacity to provide all of the advanced care and support
services needed for monitoring and treating HIV/AIDS clients.
As service development expands, how-ever, it is expected that
many of these services will become available outside of
hospitals, in lower level facilities as well.
The main elements of advanced-level services for HIV/AIDS include
the management of opportunistic infections and provision of
advanced palliative care for the people living with HIV/AIDS
including the availability of treatment medications for severe
opportunistic infections, antiretroviral therapy (ART), a
referral system for psychosocial and socioeconomic care and56

support services, conditions to support home care services,
counseling and have a good way of information for the clients.
Care management throughout and across these disciplines is
essential. However, as we have described, much of this service
provision and all of the care coordination are not reimbursable
by insurers. The findings revealed that 26 of HIV- clients get
information from news and schools, 9 of HIV- clients in Public
talk, 4 HIV+ clients in news and schools, 2 HIV+ clients in
public talk, 2 HIV+ clients newspaper and billboards, 7 of
counselors in public talk and 11 confess that no counseling given
about HIV/AIDS, it is done only for voluntary to the services.
5.3 Recommendation
After data collection, analysis and reviewing the findings,
research come up taking account counseling as positive way of
sensitization of people to HIV/AIDS services. To support the
decision makers, the research point out the following
recommendation:
To KABUTARE Hospital of Rwanda
Researcher recommends sensitizing people on HIV/AIDS services
using counselors and giving them time in public meeting. The
hospital also must provide training support to the counselors on
how the way they may care the clients. The hospital should also
57

give to counselors the facility in order to perform their work as
best they can.
To Counselors
Researcher recommends the counselors to be aware of the
population and have enough capacity to handle issue related to
HIV/AIDS services and advise the clients to consult medical care
as well as possible. The counselors should use the total
confidence that people given them.
To clients
The researcher recommends the clients to have continuous
dialogues and discuss how they may consult medical doctor and
take into accounts the advice that they got from their doctor and
follow them.
Researcher recommends also Member of households (clients)
intervention with its great important as it gives couples an
opportunity to confidentially discuss risk of HIV infection and
be assisted to learn HIV status for purpose of prevention, care
and treatment.
To other researcher
Researcher recommends to other researcher to expand the advocacy
and show the reality as HIV and AIDS present multi-dimensional
challenges to individuals, families and communities. These58

challenges may present as feeling of hopelessness, rejection and
stigma at various levels of the community.
Many concepts out of the conceptual framework in this study could
not be examined. Therefore, it is recommended that for further
study it would be desirable to include some additional variables
such as factors associated with counseling belief and its
consideration by the community, attitude and behavior regarding
hospital based deliveries, and factors associated with health
care providers, in order to capture the whole aspect that may
influence delivery status of the clients.
Bibliography1. (http://www.ubuzimabwacu.com/urusobe-rw%e2%80%99ubuzima/5837/usaid-
impressed-rwandas-progress-fighting hiv/ )23th March 26, 2015, 10h00.
2. http://mak.ac.ug/documents/Makfiles/theses/Nantumbwe_Miriam_Ssebuliba.pdf. (2006/ HD14/ 6380U). MULTIPLICITYOF DISCRIMINATION. NANTUMBWE MIRIAM SEBULIBA FAITH.
3. http://study.com/academy/lesson/secondary-data-in-marketing-research-definition-sources-collection.html Accessed on 25 march,2015 at 1:49.
4. http://www.statistics.gov.rw/system/files/user_uploads/files/survey-reports/RSPA%202007%20FINAL%20REPORT-ENGLISH_0.pdf.(sempter 2008, p 204/205). Rwanda services provision assessment. nationalinstitute of statistics of rwanda.
59

5. http://www.statistics.gov.rw/system/files/user_uploads/files/survey-reports/RSPA%202007%20FINAL%20REPORT-ENGLISH_0.pdf.(septempber 2008, p 203). rwanda services provision report. NationalInstitute of Statistics of Rwanda.
6. James E Bartlett, I. Determining Appropriate Sample Size in Survey Research.http://www.opalco.com/wp-content/uploads/2014/10/Reading-Sample-Size.pdf.
7. James E. Bartlett, I.http://www.opalco.com/wp-content/uploads/2014/10/Reading-Sample-Size.pdf. JoeW. Kotrlik,.
8. (2008-2012). Rwanda poverty reduction 2008-2012).
9. (http://www.statistics.gov.rw/system/files/user_uploads/files/survey-reports/RSPA%202007%20FINAL%20REPORT-ENGLISH_0.pdf, sempter 2008, p 204/205)
10. http://www.pedaids.org/ by 26th march 205 at 17h57.
11. (July 2002.). Report on the Global HIV/AIDS Epidemic. UNAIDS, Report onthe Global HIV/AIDS Epidemic.
12. (september 2008).http://www.statistics.gov.rw/system/files/user_uploads/files/survey-reports/RSPA%202007%20FINAL%20REPORT-ENGLISH_0.pdf. national institute ofstatistics.
13. cochran.http://www.opalco.com/wp-content/uploads/2014/10/Reading-Sample-Size.pdf.
14.(http://cid.oxfordjournals.org/content/45/Supplement_4/
S240.long
15.http://www.nlm.nih.gov
60

Appendices
QUESTIONNAIRESQUESTIONNAIRE FOR COUNSELLOR
RESEARCH TOPIC: “THE IMPACT OF HIV/AIDS COUNSELING SERVICES ONTHE POPULATION OF RURAL AREA”
RESEARCH’S PREPARATOR: Cyprien HABINSHUTI
QUESTIONNAIRE NO……………..
I am working as a student in University of Rwanda, College of
Business and Economics, School of Economics, Department of
Applied Statistics and I have to write a research paper.
In this respect, I am carrying out a study on “the impact of
HIV/AIDS counseling services on the population of rural area.
This research is intended to provide information that will be
useful in examining how HIV/AIDS counseling services on the
population of rural area is constructed through multiple actions
as they try to access HIV/AIDS counseling services in selected
sector ……………...
This questionnaire is to facilitate the collection of data from
sector with population who access HIV/AIDS counseling services.
You are requested to provide information in order to facilitate
the study. All the information you have given will be kept with
high confidentiality.
61

Thank you for your good cooperation!!!
Respondent demographic characteristics,
1. Respondent status: (a) Counselors………… (b) Clients (HIV+
……………
(C) HIV - ) …………………….. (d) Partner of HIV+………………………..
2. Age of Respondent.............................
3. Sex...................
Female Male
4. Marital Status.......................
Single Married separated
widower
5. Working status
Private sector Public sector
unemployed
6. Educational level
None Primary level Secondary level
Undergraduate and above
7. Date of completing
form..........................................................
Section A: the structure of access of HIV/AIDS counseling
Services.
8. What type of services does the institution offer to the
clients?
62

.................................................................
.................................................................
....................
.................................................................
.................................................................
..........
9. Does the institution provide favorable services regularly?
Yes………. No……….
If Yes, What does it specify?
.................................................................
.................................................................
....................
10. have you ever attend any training to handle counseling
services and related issue?
Yes.......................
No....................
If not, please explain how you manage to be a part of consoling
services providers?
.................................................................
.................................................................
....................
.................................................................
.................................................................
..........
11. Do you think all organization’s service providers have any
formal qualifications in HIV/AIDS counseling? 63

Yes …………… No
………………………..
12. How often do populations seek counseling services in your
organization a week?
Time a week responseOnce twiceSeveral time
QUESTIONNAIRE FOR CLIENTS
RESEARCH TOPIC: “THE IMPACT OF HIV/AIDS COUNSELING SERVICES ONTHE POPULATION OF RURAL AREA”
RESEARCH’S PREPARATOR: Cyprien HABINSHUTI
QUESTIONNAIRE NO……………..
I am working as a student in University of Rwanda, College of
Business and Economics, School of Economics, Department of
Applied Statistics and I have to write a research paper.
In this respect, I am carrying out a study on “the impact of
HIV/AIDS counseling services on the population of rural area.
This research is intended to provide information that will be
useful in examining how HIV/AIDS counseling services on the64

population of rural area is constructed through multiple actions
as they try to access HIV/AIDS counseling services in selected
sector ……………...
This questionnaire is to facilitate the collection of data from
sector with population who access HIV/AIDS counseling services.
You are requested to provide information in order to facilitate
the study.
All the information you have given will be kept with high
confidentiality.
Thank you for your good cooperation!!!
Respondent demographic characteristics,
1. Id number of
respondent.......................................................
..............
2. Age of Respondent.............................
3. Sex...................
Female Male
4. Marital Status.......................
Single Married separated
widower
5. Working status
Private sector Public sector
unemployed
6. Educational level
Primary level Secondary level
Undergraduate and above65

7. Date of completing
form..........................................................
CLIENTS SECTION
Section B: Society impacts on infected population.
1. How does society react to population infected?
……………………………………………………………………………………………
2. To what extent did you manage to get information to be a
part of counseling services clients of the institution you
belong to?
Method responseTelevisionNews papers, posters, billboardsInformation, education, training
and cooperative By interview
3. Do you belong to any HIV+ affected cooperative?
Yes No
If yes go to question 4, if not go to question 6
4. Which kind of help do you get from the cooperative?
- …………………………………………………………..…………………………………….
…………………………………………………………………………………………………
5. Are you satisfied with the services offered by the
cooperative?66

Period Response excellent (as you
want)good (ordinary=
ibisanzwe)No good (bitari
byiza cyane)
.
6. What is the general attitude of the counselors towards you?
………………………………………………………………………………………
7. What problems do you encounter when you visit HIV/AIDS
Counseling services?
………………………………………………………………………………
………………………………………………………………………………
………………………………………………………………………………
8. can education level affect the use of the services?
Yes No
9. If yes, what is the most education level affect the use?
Education level respons
ePrimary
67

secondaryUniversity and
high learning
and above
10. Are the services offered by your organization show a
great importance to the beneficiaries?
1) Yes ……………
2) No....................................
INSANGANYA Y’UBUSHAKASHATSI: KUREBA ICYO UBUJYANAMA KUNDWARA YA SIDA BWAFASHIJE ABATURAGE BO MUBYARO.
UTEGURA UBUSHAKASHATSI: Cyprien HABINSHUTIUBUSHAKASHATSI NO: ………………
Nitwa HABINSHUTI Cyprien, Ndi umunyeshuri muri kaminuza y’u Rwanda, ishuri ry’ubukungu n’icunga mutungo, ishami ry’icunga mutungo, agashami k’ibarurishamibare nkaba ndimo kwandika igitabonkuko biteganywa namategeko yakaminuza.
68

Ni muri urwo rwego ndimo gukora ubushashatsi kureba icyo ubujyanama ku ndwara ya sida bwafashije abaturage bo hirya y,umujyi nabomucyaro, bityo bikaba bizamfasha kunoza no kurangiza neza amasomo yanjye. Ibazwa ryateguwe rizadufasha kubona amakuru ngenderwaho mukureba koko niba hari impinduka nziza ubujyanama bwazaniye abaturage muri rusange.Amakuru yatanzwe abikwana ubunyanga mugayo. Murakoze kubufatanye bwanyu!
Ibiranga umufatanya bikorwa.1. Numero y’usubiza……………2. Imyanka…………….3. igitsina
Gabo Gore4. imimerere rusange
Ingaragu yarashatse umupfakazi yatandukanye nuwo bashakanye bitemewe namategeko
5. Aho akora Umukozi wa leta ibigo byigenga ntakora
6. Amashuri yizeAbanza ayisumbuye kaminuza ntiyize 7. Itariki amakuru yatangiweho……………………
Igika cya kabiri: uko umuryango rusange ufata ababananubwandu bw’agakoko gatera SIDA (Abagenerwa bikorwa).
1. Nigute sosiyesi (society) ifata ababana na gakoko gatera SIDA?………………………………………………………………………………………………………………………………………………………………..
2. Ni mubuhe buryo mwamenye amakuru kugira mufate icyemezo cyo kubaumugenerwa bikorwa muri serivisi?
Uburyo bwakoreshejwe igisubizo
69

Insakaza mashusho(television)Ibinyamakuru, inzandiko, amatangazoAmakuru, ishuru, amahugurwaIbiganiro, ubujyanama
3. Hari ishyirahamwe(cooperative) ry’ababana n’ubwandu bwa gakoko gatera virisi ya SIDA ubarizwamo?Yego oya
Niba ari yego, jya kukibazo cya 4, niba ari oya jya kuri 6
4. Ni ubuhe bufasha ishyirahamwe (cooperative) ryaba ribagenera?…………………………………………………………………………………………………………………………………………………………………………………………
5. Ese ubufasha ishyirahamwe(cooperative) ribaha buhagaze bute?ubufasha igisubizoBwiza cyaneIbisanzweButari bwiza cyane
6. Mubona abajyanama babakira gute?............................................................................................................................................................................................................................................................................................
7. Ni ibihe bibazo muhuranabyo mugihe muhabwa izo serivizi?.......................................................................................................................................................................................................................................................................................................
70

...........................................................
...........................................................
.............8. Ese mubona amashuri umuntu yize hari uruhare afite
mukubahiriza serivi muhabwa/yego oya Niba ari yego, komeza nicya 9, niba ari oya komeza nicya 10.
9. Ni ikihe cyiciro cyamashuri kigiramo uruhare runini/Icyiciro cy’amashuri igisubizoAbanzaAyisumbuyekaminuza
10. Hari umumaro mubona serivisi muhabwa yabamariye ?1) Yego……………..2) Oya……………..
INSANGANYA Y’UBUSHAKASHATSI: KUREBA ICYO UBUJYANAMA KU NDWARA YASIDA BWAFASHIJE ABATURAGE BO MUBYARO.
UTEGURA UBUSHAKASHATSI: Cyprien HABINSHUTIUBUSHAKASHATSI NO: ………………
Nitwa HABINSHUTI Cyprien, Ndi umunyeshuri muri kaminuza y’u Rwanda, ishuri ry’ubukungu n’icunga mutungo, ishami ry’icunga mutungo, agashami k’ibarurishamibare nkaba ndimo kwandika igitabonkuko biteganywa namategeko yakaminuza.
Ni muri urwo rwego ndimo gukora ubushashatsi bugamije kureba icyoubujyanama ku ndwara ya sida bwafashije abaturage bo hirya y’imijyi n’ibyaro, bityo bikaba bizamfasha kunoza no kurangiza neza amasomo yanjye.
Ibazwa ryateguwe rizadufasha kubona amakuru ngenderwaho mukureba koko niba hari impinduka nziza ubujyanama bwazaniye abaturage babugenewe muri rusange.
Amakuru yatanzwe abikwana ubunyanga mugayo.71
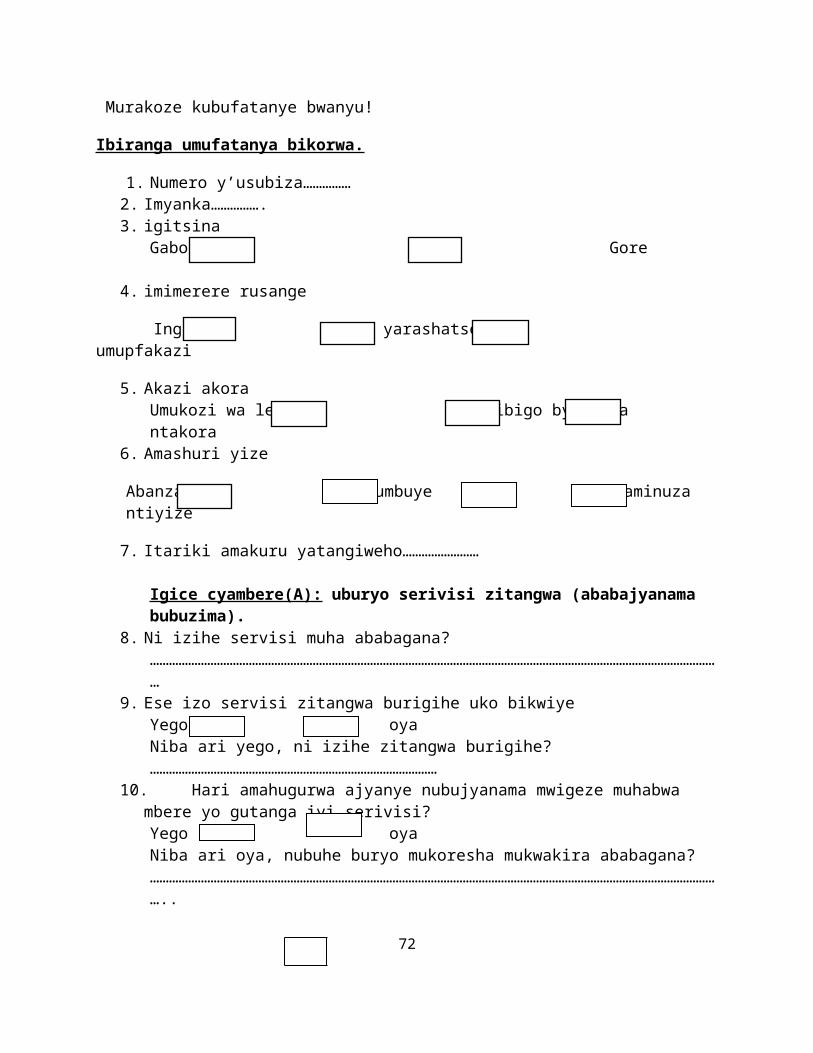
Murakoze kubufatanye bwanyu!
Ibiranga umufatanya bikorwa.
1. Numero y’usubiza……………2. Imyanka…………….3. igitsina
Gabo Gore
4. imimerere rusange
Ingaragu yarashatse umupfakazi
5. Akazi akora Umukozi wa leta ibigo byigenga ntakora
6. Amashuri yize
Abanza ayisumbuye kaminuza ntiyize
7. Itariki amakuru yatangiweho……………………
Igice cyambere(A): uburyo serivisi zitangwa (ababajyanama bubuzima).
8. Ni izihe servisi muha ababagana?………………………………………………………………………………………………………………………………………………………………
9. Ese izo servisi zitangwa burigihe uko bikwiyeYego oya Niba ari yego, ni izihe zitangwa burigihe?………………………………………………………………………………
10. Hari amahugurwa ajyanye nubujyanama mwigeze muhabwa mbere yo gutanga iyi serivisi?Yego oya Niba ari oya, nubuhe buryo mukoresha mukwakira ababagana?………………………………………………………………………………………………………………………………………………………………..
72

11. Ese abakozi bose bikigo baba bafite ubumenyi kubujyanama kundwara ya SIDA?Yego oya
12. Ni kangahe mucyumweru mwakira ababagana?
Inshuro k’umweru igisubizo
rimwe
kabiri
Inshuro nyinshi
73