
DISSERTATION ON
182
DISSERTATION ON “A STUDY TO ASSESS THE EFFECTIVENESS OF STRUCTURED TEACHING PROGRAMME ON KNOWLEDGE REGARDING CARE OF NEWBORN DURING PHOTOTHERAPY AMONG II YEAR DGNM STUDENTS AT INSTITUTE OF CHILD HEALTH AND HOSPITAL FOR CHILDREN, EGMORE , CHENNAI-08” M.Sc (NURSING) DEGREE EXAMINATION BRANCH- II CHILD HEALTH NURSING COLLEGE OF NURSING MADRAS MEDICAL COLLEGE, CHENNAI-600 003 A dissertation submitted to THE TAMIL NADU DR.M.G.R.MEDICAL UNIVERSITY, CHENNAI- 600 032 In partial fulfillment of the requirement for the award of the degree of MASTER OF SCIENCE IN NURSING OCTOBER - 2019
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of DISSERTATION ON

DISSERTATION ON
“A STUDY TO ASSESS THE EFFECTIVENESS OF
STRUCTURED TEACHING PROGRAMME ON KNOWLEDGE
REGARDING CARE OF NEWBORN DURING PHOTOTHERAPY
AMONG II YEAR DGNM STUDENTS AT INSTITUTE OF CHILD
HEALTH AND HOSPITAL FOR CHILDREN, EGMORE ,
CHENNAI-08”
M.Sc (NURSING) DEGREE EXAMINATION
BRANCH- II CHILD HEALTH NURSING
COLLEGE OF NURSING
MADRAS MEDICAL COLLEGE, CHENNAI-600 003
A dissertation submitted to
THE TAMIL NADU DR.M.G.R.MEDICAL UNIVERSITY,
CHENNAI- 600 032
In partial fulfillment of the requirement for the award of the degree of
MASTER OF SCIENCE IN NURSING
OCTOBER - 2019

“A STUDY TO ASSESS THE EFFECTIVENESS OF
STRUCTURED TEACHING PROGRAMME ON KNOWLEDGE
REGARDING CARE OF NEWBORN DURING PHOTOTHERAPY
AMONG II YEAR DGNM STUDENTS AT INSTITUTE OF CHILD
HEALTH AND HOSPITAL FOR CHILDREN , EGMORE ,
CHENNAI-08”
Examination : M.Sc (Nursing) Degree Examination
Examination Month and Year : October-2019
Branch & Course : II – CHILD HEALTH NURSING
Register Number : 301716254
Institution : COLLEGE OF NURSING,
MADRAS MEDICAL COLLEGE,
CHENNAI – 600 003.
Sd: __________________ Sd: ________________
Internal Examiner External Examiner
Date: ____________ Date: ____________
THE TAMILNADU DR.M.G.R MEDICAL UNIVERSITY,
CHENNAI – 600 032.

CERTIFICATE
This is to certify that this dissertation titled, “A STUDY TO ASSESS
THE EFFECTIVENESS OF STRUCTURED TEACHING
PROGRAMME ON KNOWLEDGE REGARDING CARE OF
NEWBORN DURING PHOTOTHERAPY AMONG II YEAR
DGNM STUDENTS AT INSTITUTE OF CHILD HEALTH AND
HOSPITAL FOR CHILDREN, EGMORE , CHENNAI-08” is a
bonafide work done by Mrs.R.REVATHY, M.Sc Nursing-II Year Student,
College of Nursing, Madras Medical College, Chennai-03 submitted to The
Tamil Nadu Dr.M.G.R. Medical University, Chennai-32 in partial fulfillment
of the university rules and regulations towards the award of the degree of
MASTER OF SCIENCE IN NURSING, BRANCH-II CHILD HEALTH
NURSING, under our guidance and supervision during academic year from
2017-2019.
Mrs.A.Thahira Begum, M.Sc (N)., MBA., M.Phil., Dr.R.Jayanthi, M.D.,F.R.C.P.(Glasg).,
Principal, Dean,
College of Nursing, Madras Medical College,
Madras Medical College, Chennai – 03.
Chennai – 03.

“A STUDY TO ASSESS THE EFFECTIVENESS OF
STRUCTURED TEACHING PROGRAMME ON KNOWLEDGE
REGARDING CARE OF NEWBORN DURING PHOTOTHERAPY
AMONG II YEAR DGNM STUDENTS AT INSTITUTE OF CHILD
HEALTH AND HOSPITAL FOR CHILDREN, EGMORE,
CHENNAI-08”.
Approved by dissertation committee on: 24.07.18
CLINICAL SPECIALITY GUIDE
Mr. A. Senthil kumaran, M.Sc (N)., Lecturer in Child Health Nursing,
College of Nursing,
Madras Medical College,
Chennai- 03.
HEAD OF THE DEPARTMENT
Mrs. A. Thahira Begum, M.Sc (N)., MBA., M.Phil.,
Principal,
College of Nursing,
Madras Medical College,
Chennai – 03.
DEAN
Dr. R. Jayanthi, M.D., FRCP(Glasg).,
Dean,
Madras Medical College,
Chennai-03.
A dissertation submitted to
THE TAMIL NADU DR.M.G.R.MEDICAL UNIVERSITY,
CHENNAI- 600 032
In partial fulfilment of the requirement for the award of the degree of
MASTER OF SCIENCE IN NURSING
OCTOBER – 2019

CERTIFICATE OF PLAGIARISM
This is to certify that the dissertation work titled, “A STUDY TO ASSESS
THE EFFECTIVENESS OF STRUCTURED TEACHING PROGRAMME ON
KNOWLEDGE REGARDING CARE OF NEWBORN DURING
PHOTOTHERAPY AMONG II YEAR DGNM STUDENTS AT INSTITUTE
OF CHILD HEALTH AND HOSPITAL FOR CHILDREN, EGMORE,
CHENNAI-08”of the candidate R.REVATHY, for the partial fulfilment of M.Sc.
Nursing programme in the branch of Child Health Nursing has been verified for
plagiarism through relevant plagiarism checker. We found that the uploaded thesis
file from introduction to conclusion pages and rewrite shows % of plagiarism(
% uniqueness) in this dissertation.
CLINICAL SPECIALITY GUIDE/ SUPERVISOR
Mr.A.Senthil Kumaran, M.Sc (N).,
Lecturer in Child Health Nursing,
College of Nursing,
Madras Medical College,
Chennai-03.
PRINCIPAL
Mrs A.Thahira Begum, M.Sc (N)., MBA., M.Phil.,
Principal,
College of Nursing,
Madras Medical College,
Chennai-03.

ACKNOWLEDGEMENT
Gratitude calls never expressed in words but this only to deep perceptions,
which make words to flow from one‟s inner heart.
First of all, I praise God Almighty, merciful and passionate, for providing me
this opportunity and granting me the capability to complete this study successfully .I
lift up my heart in gratitude to God Almighty, I feel the hand of God on me, leading
me through thick and thin heights of knowledge. It is he who granted me the grace
and the physical and mental strength behind all my efforts.
This dissertation appears in its current form due to the assistance and guidance
of many professionals and non professionals. The investigator is whole heartedly
indebted to her research advisors for their comprehensive assistance in various forms.
I express my genuine gratitude to the Institutional Ethics Committee of Madras
Medical College for giving me an opportunity to conduct this study.
I wish to express my sincere thanks to Dr.R.Jayanthi, M.D., F.R.C.P (Glasg).,
Dean. Madras Medical College, Chennai-03 for providing necessary facilities and
extending support to conduct this study.
I render my deep sense of sincere thanks to Dr.K.Jayachandran,M.D., D.C.H,
Director and Superintendent ,Institute of Child Health and Hospital for
Children,Egmore,Chennai-08,for permitting me to conduct this study at Institute of
Child Health and Hospital for Children and also, for their valuable suggestions and
guidance for this study.
I am grateful to., Head of the Department of Neonatology, Institute of Child
Health and Hospital for Children, Egmore, Chennai-08 for giving me the permission
to conduct the study among the DGNM students regarding care of newborn during
phototherapy, Institute of Child Health and Hospital for Children,Egmore,Chennai-08
for sharing her experience in providing ideas and guide me to complete this study in
useful manner.

At the very outset, I express my whole hearted gratitude to my esteemed guide
Mrs.A.Thahira Begum, M.Sc (N)., MBA., M.Phil., Principal, College of Nursing,
Madras Medical College, for her academic and professional excellence, treasured
guidance, highly instructive research mentorship, valuable suggestions, prudent
guidance, moral support and patience that has moulded me to conquer the spirit of
knowledge for sculpturing my manuscript into thesis.
I am highly indebted to Dr. R. Shankar Shanmugam, M.Sc. (N), MBA,
Ph.D., Reader, H.O.D – Department of Nursing Research, College of Nursing,
Madras Medical College, for his great support, warm encouragement, constant
guidance, thought provoking suggestions, brain storming ideas, timely insightful
decision, correction of the thesis with constant motivation and willingness to help all
the time for the fruitful outcome of this study.
I would like to express my deepest sense of gratitude to Mrs.Seetharaman
Vijayalakshmi, M.Sc.(N).,MBA., Reader, H.O.D-Child Health Nursing, College
of Nursing, Madras Medical College, for her highly instructive research mentorship,
her hard work, efforts, interest and sincerity to mould this study in a successful way.
Her easy approachability and understanding nature inspired me to laid strong
foundation in research. It is very essential to mention her wisdom and helping nature
made my research study a lively and everlasting one.
I am grateful to Mr. K. Kannan, M.Sc. (N), Nursing Tutor, Department of
Nursing Research, College of Nursing, Madras Medical College, for his valuable
guidance, suggestions, motivation, timely help and support throughout the completion
of this study.
I would like to express my deep and sincere gratitude to our respected
Dr.G.Mala, M.Sc. (N), Nursing Tutor, College of Nursing, Madras Medical
College, Chennai-03 for the approval of the study.
I am thankful to all the faculty of College of Nursing, Madras Medical College,
for their timely advice, encouragement and support.

It‟s my duty to convey my thanks to all experts, Dr.G.K.Jaikaran,MD.,
Associate Professor of Paediatric, Institute of Child Health and Hospital for Children
Egmore, Chennai, Dr.S.Madhialagan,MD., Associate Professor of Paediatric,
Institute of Child Health and Hospital for Children Egmore, Chennai,
Mrs.R.Dhanalakshmi,.M.Sc (N)., H.O.D-Child Health Nursing, Billroth College Of
Nursing, Chennai. Mrs.Nesa SathyaSatchi,.M.Sc (N)., H.O.D-Child Health Nursing,
Apollo College of Nursing, Chennai. Who validated the research tool and guided me
with valuable suggestions and corrections, constructive judgments while validating
the tool.
I owe my deepest sense of gratitude to Dr.A.Vengatesan, M.Sc., Ph.D., former
DDME (Statistics) for his suggestion and guidance in statistical analysis.
I thank Mr.S.Ravi, M.L.I.S, Librarian, College of Nursing, Madras Medical
College for his co-operation and assistance which built the sound knowledge for this
study.
I owe my great sense of gratitude to Mr.Jas Ahamed Aslam, Shajee
computers and Mr.Ramesh, B.A., MSM Xerox for their enthusiastic help and
sincere effort in typing the manuscript with valuable computer skills and also bringing
this study into a printed form.
I thank Mrs.P.Malliga.M.A. B.Ed., Headmistress, Govt.Girls Hr Sec
School, Chennai, for editing and providing certificate of English editing.
I have much pleasure of expressing my cordial appreciation and thanks to all
the students who participated in the study with interest and cooperation.
I am grateful to thank my life partner Mr.Thamodharan, for his whole
consent, encouragement, support, endless effort and love otherwise this work would
not be successfully completed.
I would be a lapse on my part if i fail to thank my daughter
Baby.T.Shamritha for her love, patience and cooperation throughout my study.

Words are beyond expressions for meticulous effort of my parent
Mr.A.Rajasekaran and Mrs.R.Bhuvaneshwari for their loving support,
encouragement, earnest prayer, which enabled me to complete the study.
I immensely extend my gratitude to thank my lovable sister Mrs.R.Gayathri,
B.E for her encouragement, constant support and timely help to finish this study
successfully.
I thank my mother in law Mrs.K.Saroja for her graceful support and all my
family members for their encouragement towards the successful completion of my
study.
I take this opportunity to thank all my Colleagues, Friends, Teaching and Non
Teaching Staff Members, Librarian and Office Staff Members of Madras Medical
College –College of Nursing for their cooperation and help rendered.
I extend my heartfelt gratitude to those who have contributed directly or
indirectly for the successful completion of this dissertation.
I thank the one above all of us, omnipresent God, for answering my prayers for
giving me strength to plod on each and every phase of my life.

ABSTRACT
Phototherapy is one of the important procedures in New born care setting.
In most infants with physiological jaundice, bilirubin levels do not rise to a
point that requires treatment. Effective treatments to decrease serum bilirubin
levels with severe jaundice include phototherapy. It is a vital procedure to save
the life of many newborns, when performed at correct time. It needs special
skills and techniques to do this procedure. The students should be specially
trained to assist the procedures tactfully. Students need to have adequate
knowledge regarding care of newborn during phototherapy in order to identify
and prevent fatal complications in neonates.
TITLE: “A study to assess the effectiveness of structured teaching
programme on knowledge regarding care of newborn during phototherapy
among II year DGNM students at ICH, Egmore , chennai-08”
OBJECTIVES: To assess the pretest knowledge of II year DGNM students
regarding care of newborn during phototherapy. To assess the post test
knowledge of II year DGNM students regarding care of newborn during
phototherapy. To compare the pre test and post test knowledge of II year
DGNM students regarding care of newborn during phototherapy. To
compare the pre test and post test knowledge of II year DGNM students
regarding care of newborn during phototherapy. To find the association
between the post-test knowledge scores of students with selected
demographic variables.
METHODS AND MATERIALS: This study was conducted with 90 samples
(students) in quantitative approach, pre experimental one group pretest posttest
design, sampling selection was done by convenient sampling technique.pre
existing knowledge was assessed by using semi structured questionnaires after
the pre test, structured teaching programme was given regarding care of

newborn during phototherapy among students after 7 days post test was
conducted by using same tool.
RESULTS: The results shows that students were gained 33.63% score on
knowledge in post test compare to pre test after structured teaching programme
and the mean difference were 3.81 by using McNamara‟s chi-square test which
is statistically significant.
CONCLUSION: Hence the structured teaching program was instructionally
effective, appropriate and feasible. It would help and guide the students to
provide care to the newborn during phototherapy.

INDEX
Chapter
No
Content Page
No.
I
INTRODUCTION 1
1.1 Background of the study 4
1.2 Need for the Study 6
1.3 Statement of the Problem 8
1.4 Objectives of the Study 9
1.5 Operational Definition 9
1.6 Assumption 10
1.7 Hypothesis 11
1.8 Limitation 12
1.9 Conceptual Framework 12
II
REVIEW OF LITERATURE 14
2.1 Review of Literature 14
III
RESEARCH METHODOLOGY 24
3.1 Research Approach 24
3.2 Study Design 24
3.3 Duration of the Study 24
3.4 Study Setting 24
3.5 Study Population 25
3.6 Sample 25
3.7 Sample Size 25
3.8 Sample Criterion
3.8.1 Inclusion Criteria
3.8.2 Exclusion Criteria
25
3.9 Sampling Technique 26
3.10 Research Variables 26

3.11 Development and Description of the Tool 26
3.11.1 Development of the Tool 26
Chapter.
No
Content
Pg.No
III
3.11.2 Description of the Tool 26
3.12 Content validity 27
3.13 Reliability of the Tool 27
3.14 Protection of Human Subjects 27
3.15 Pilot Study 28
IV ANALYSIS AND INTERPRETATION OF DATA 30
V DISCUSSION 52
VI SUMMARY,IMPLICATION,LIMITATION,
RECOMMENDATION & CONCLUSION
59
6.1 Summary of the Study 59
6.2 Findings of the Study 59
6.3 Implication of the Study 62
6.4 Limitation 64
6.5 Recommendation 64
6.6 Conclusion 65
REFERENCES 66
APPENDICES 71

LIST OF TABLES
Table
No
Title
Page
No
1.1 Statistics of Neonatal Jaundice at Institute of
Child Health and Hospital for Children, Egmore,
Chennai for the Year 2014 – 2018
5
3.1 Scoring Interpretation of knowledge score 27
4.1 Description of demographic variables of students 32
4.2 Pretest Percentage of Knowledge on Care of
Newborn during Phototherapy among Nursing
students
40
4.3 Pre test level of knowledge 41
4.4 Post test Percentage of Knowledge on Care of
Newborn during Phototherapy among Nursing
students
42
4.5 Post test level of knowledge 43
4.6 Comparison of Pre test And Post test Level of
Knowledge Score
44
4.7 Comparison of Pretest and Post test Knowledge
Score
45
4.8 Each Domain wise Pretest and Post-test
Percentage of Knowledge
46
4.9 Effectiveness of Structured teaching programme 47
4.10 Association between post test level of knowledge
and demographic variables
49
4.11 Association between students knowledge gain 52

score and their demographic variables
LIST OF FIGURES
Figure
No
Description
1.1 Mortality statistics of Neonatal Jaundice
1.2 Role of Paediatric Nurse
2.1 Conceptual framework based on Modified Kings Goal Attainment
Theory
3.1 Schematic representation of the Research Methodology
4.1 Cylindrical diagram shows distribution of sample age group
4.2 Pie diagram showing distribution of sample according to medium of
instruction in higher secondary
4.3 Bar diagram shows distribution of sample according to type of family
4.4 Bar diagram shows distribution of sample according to mother
education status
4.5 Bar diagram shows distribution of sample according to father education
status
4.6 Cylindrical diagram shows distribution of sample according to father
occupation
4.7 Cylindrical diagram shows distribution of sample according to monthly
income
4.8 Doughnut diagram shows distribution of sample according to posted in

NICU
4.9 Pie diagram shows distribution of sample according to previous
exposure on care of newborn during phototherapy.
4.10 Pre test level of knowledge score
4.11 Post test level of knowledge score
4.12 Percentage of Pre test and Post test level of knowledge
4.13 plot compares the student‟s pre test and post test knowledge score
4.14 Pretest and Post test Percentage of Knowledge Score
4.15 Multiple bar diagram shows association between the posttest level of
knowledge score and medium of instruction in higher secondary
4.16 Multiple bar diagram shows association between the posttest level of
knowledge score and NICU posting.
4.17 Multiple bar diagram shows association between the posttest level of
knowledge score and exposure on care of newborn during phototherapy
LIST OF APPENDICES
Appendix
No
Annexure
1. Certificate approval by Institutional Ethics Committee
2. Certificate of content validity by Experts
3. Letter seeking permission to conduct the study
4. Study tools (English)
Section A- Socio Demographic data of students
Section B- knowledge about care of newborn during
phototherapy
5. Structured teaching programme on care of newborn during
phototherapy
6. Informed consent form
7. Certificate for English editing
8. Photos

LIST OF ABBREVATION
ABBREVATION
EXPANSION
DF Degree of Freedom
ICH Institute of Child Health and Hospital for
Children
NS Non Significance
P Significance
SD Standard Deviation
STP Structured Teaching Programme

CHAPTER-I Introduction

CHAPTER-1
INTRODUCTION
A new baby is like the beginning of all things- wonder, hope and a dream
of possibilities.
–EdaJ.Le.Shan.
Jaundice is the accumulation of bilirubin in blood, bilirubin is
formed by breakdown of red blood cells and it is naturally removed by liver
and excreted in stool and urine. When the bilirubin is produced faster, then it
cannot be removed, it leads to increase in bilirubin level. Physiological
jaundice of the term newborn usually appears after 30 hrs. Peak level of serum
bilirubin (a maximum of 12mg/dl) is reached on the 4th
or 5th
day and icterus
disappears by 7 to 14 days. In premature babies maximum bilirubin level
reaches 12 to 15mg/dl on 5th
to 7th
day and icterus disappears by 14 days to a
month.
Jaundice appears in first days of life, it is common in newborns about
50-75% during this period, all babies have high plasmatic bilirubin than
compared with normal adults. It develops between 72 – 96 hours after birth and
usually disappears by one to two weeks after birth. In full term newborns the
level of bilirubin increases for few days, reaches high and then decreases by the
end of first week of life. In case of premature babies, it may require more time
to resolve as normal elimination mechanism mature.
Hyperbilirubinemia refers to high serum concentration in bilirubin,
treatment is according to the increase in level of bilirubin. The most commonly
used treatment for newborn jaundice is phototherapy.

Neonatal hyperbilirubinemia is a common problem in newborn and
manifest clinically as jaundice. Nearly 25-50% of all newborns and a much
higher percentage of premature babies develop hyperbilirubinemia. About 3%
of all hospital-born babies in India develop significant jaundice levels more
than 15 mg/dl.
Since the early 1970‟s, phototherapy is mainly used to treat jaundice.
Phototherapy is one of the non-invasive methods to reduce the bilirubin level
by exposing the baby skin to blue or cool white light. Light converts the
bilirubin to non – toxic water soluble compound, they are excreted in urine and
stool. Baby should be undressed expect diaper, to protect gonads. In order to
prevent chilling, an external means of maintaining normal body temperature
must be used.
The vital signs are taken at least every 4 hours to monitor the infant
temperature. Eyes are covered to prevent damage in the retina. Baby is kept
under phototherapy light at a distance of 45cm, baby position should be
changed every 2 hours or each feed for maximum exposure. Phototherapy is
stopped, bilirubin return to safe value as per protocol. Proper nursing care
should be given to the newborn during phototherapy to enhance the
effectiveness and to minimize the complication greenish stool, skin rashes and
electrolyte imbalance.
It has emerged as the most widely used tool for treating unconjugated
pathologic hyperbilirubinemia. Bilirubin absorbs light maximally at 420-490
nanometers. It gets oxidized to biliverdin with light source of this range and is
excreted in bile or to lesser extent in urine. Technique of phototherapy is now
generally opined that blue light is superior to white light although simple
sunlight is useful. Fluorescent tubes are remarkable as a potent source of blue
light. These tubes can be mounted with reflectors in frames.Baby is placed at a
distance of 18 inches below the lights. 24 -48 hours exposure is long enough to
bring down Serum bilirubin level to a safe limit. Serum bilirubin estimation is
done at intervals of 12 hours. If it is less than 11 gm/dl on two consecutive
sittings 24 hours apart, termination of phototherapy is indicated.
Phototherapy is a simple, effective, inexpensive and acceptable
procedure for the neonate in reduction of bilirubin. During phototherapy the
bilirubin molecules in the peripheral tissues are activated to biliverdin by the
absorption of light photons. Phototherapy is used to prevent the concentration
of unconjugated bilirubin in the blood from reaching the levels where neuro-
toxicity may occur. High intensity light photo chemically converts fat soluble
unconjugated bilirubin in to water soluble bilirubin that can be excreted in bile
and urine. Accurate charting is another important nursing responsibility it
includes times that phototherapy is started and stopped, proper shielding of the
eyes, types of fluorescent lamps number of lamps , distance between surface
of lamps and infant , use of phototherapy in combination with incubator or
open bassinet , photometer measurement of light intensity, occurrence of side-
effects.
Neonatal hyperbilirubinemia is the most common cause for hospital re-
admission in the first weeks of life. Bilirubin induced complication can be
prevented by instituting a neonatal jaundice protocol to identify infants at risk
for significant hyperbilirubinemia, by ensuring adequate parental education
and preparedness, and by implementing a good neonatal tracking system for
follow-up care. Hyperbirubinemia is easily treated with phototherapy, which
can be administered at home in selected infants.
Nurses play a important role in caring the newborn during
phototherapy. Nurses are the ones with the newborn for 24 hours in NICU. So,
I felt that, there is need to provide knowledge regarding care of newborn during
phototherapy among future nurses and decided to administer structured
teaching programme on care of newborn during phototherapy.

1.1 BACKGROUND OF THE STUDY
Neonatal jaundice is a transitional phenomenon affects the newborn
with consequences in first week of life.
GLOBAL STATISTICS
World Health Organization reveals the source of incidence as
hyperbilirubinemia in 50 to 60,000 neonates reported. 2% has total serum
bilirubin level over 20 mg/dl; the total serum bilirubin level in normal range
is 0.3 to 1 mg/dl. 0.15% had levels over 25mg/dl and 0.01% had over
30mg/dl.
The global burden of disease (GBD) 2016, reported that health of the
children younger than 5 years suggests that prevention of neonatal jaundice
is important in the first week of life mainly countries with highest neonatal
mortality.
Fig:1.1 MORTALITY RATE OF NEONATAL JAUNDICE

NATIONAL STATISTICS
Each year in India over 1 million newborn‟s die before they
complete their first month of life, accounting for 30% of the world‟s
neonatal death due to complication of hyperbilirubinemia. Neonatal
mortality rate is higher in rural areas. Orissa has the highest neonatal
mortality rate of 61 per 1000 live births.
INSTITUTE OF CHILD HEALTH AND HOSPITAL FOR
CHILDREN, EGMORE, CHENNAI-08
Table: 1.1 STATISTICS OF NEONATAL JAUNDICE
YEAR STATISTICS
2014 703
2015 550

2016 641
2017 520
2018 632
TOTAL CENSUS OF NEONATAL JAUNDICE IN THE YEAR
OF 2018
There is a need for creation of awareness about the care of baby in
phototherapy for future nurses. Nurses are caring the neonates during
phototherapy. So, knowledge is essential to prevent the complication and
improve the neonate‟s health status during phototherapy.
1.2 NEED FOR THE STUDY
Hyperbilirubinemia is a common cause for brain death and
encephalopathy in newborns. Over 9% of healthy term infants develop
hyperbilirubinemia with serum bilirubin levels above 15 mg/dl.
Jaundice in newborn is quite commonly affects nearly 70% of term and
80% of preterm neonates during first week of life.
A study was conducted in Postgraduate Institute of Medical
education and Research in 2012 shown that in India about 3% of all hospital
born babies develop significant jaundice with serum bilirubin level more
than 15mg/dl.
As per the National Neonatal Prenatal Database report 5% of all
neonates in India develop significant jaundice with total serum bilirubin
>15mg/dl.

The mild jaundice which appears in 30-50% of normal newborns is
usually self-limited. But in uncontrolled cases, serum indirect reacting
bilirubin concentration exceeding physiologic levels may results in acute or
chronic bilirubin encephalopathy with seizure and cerebral palsy with
hearing loss in surviving infants.
Phototherapy has been found to be effective in treating
hyperbilirubinemia in hemolytic as well as in non-hemolytic settings. It has
dramatically reduced the need for exchange transfusion. Phototherapy is the
noninvasive widely used modality for treatment of neonatal indirect
hyperbilirubinemia as it is effective and relatively safe.
On 1st Feb 2009 at Patiala, five infants including two girls were
burnt alive while five others were critically injured in a fire that broke out
due to an electric short circuit at the Government Rajindra Hospital. This
tragic accident shouldn‟t happen again, for that continuous monitoring and
nursing care is very essential in the intensive care units.
Lawrence Slater from the University of California conducted a study on
effectiveness of phototherapy on 25 term infants and showed the
hyperbilirubinemia reduced among infants after the phototherapy.
Tatil and Innet in Turkey conducted a study on effectiveness of
phototherapy on neonatal hyperbilirubinemia on 33 full term neonates with
physiological jaundice. Phototherapy was given with 6 fluorescent lamps
producing radiation with wavelength 480-520 nm with 12 microwatt/cm/nm,
total serum bilirubin checked at 24 hrs and 48hrs of phototherapy which
showed a decline in total serum bilirubin level, indicating the effectiveness
of phototherapy in treating neonatal hyperbilirubinemia. The above study
focused on the importance of phototherapy for the neonates with
hyperbilirubinemia. But certain side effects may arise in babies on
phototherapy. So we, the nurses should be careful while caring of newborns
during phototherapy.

Based on this model, as a paediatric nurse can empower and educate the
students regarding phototherapy. Paediatric nurse plays a major role in
health care settings. Nurse educator should emphasis the nursing student for
providing adequate care to the newborn in the intensive care setting. It is the
evidence based core competencies that prioritize the knowledge, skill and
attitude needed to begin practice as a professional nurse in a paediatric
intensive care setting.
Nurse educator plays a major role in importing knowledge to the nursing
students based on the role of paediatric nurse such as:
Primary care giver
Health educator
Manager
Team co ordinator and collaborator
Recreationist
Child care advocate
Nurse consultant

Fig 1.2 ROLE OF PAEDIATRIC NURSE
Nurse researcher has selected this study because neonatal
hyperbilirubinemia is one of the major health problems across the world.
With proper knowledge regarding care of newborn during phototherapy, the
complication of child can be prevented by some extent. This motivated the
investigator to undertake a study on knowledge regarding care of newborn
during phototherapy among nursing students.
1.3 STATEMENT OF THE PROBLEM
“A study to assess the effectiveness of structured teaching programme
on knowledge regarding care of newborn during phototherapy among II year
DGNM students at ICH, Egmore , chennai-08”
• Social Worker• Nurse Counselor
• Health educator• Primary Care Giver
Team Co Ordinator
and Collaborator
Manager
RecreationistChild Care Advocate
NURSE
RESEARCHER
NURSE
CONSULTANT

1.4 OBJECTIVES
The objectives of the study are to
1) To assess the pretest knowledge of II year DGNM students regarding
care of newborn during phototherapy.
2) To assess the post test knowledge of II year DGNM students regarding
care of newborn during phototherapy.
3) To compare the pre test and post test knowledge of II year DGNM
students regarding care of newborn during phototherapy.
4) To find the association between the post-test knowledge scores of
students with their selected demographic variables.
1.5 OPERATIONAL DEFINITION
Assess:
It refers to knowledge of the students about care of newborn during
phototherapy among II year DGNM students.
Effectiveness:
It refers to the significant increase in the level of knowledge of students
regarding care of newborn during phototherapy which will be measured
from the response of pre-test and post-test.
Structured teaching programme:
It refers to systematically planned teaching strategy for students posted in
pediatric wards prepared by investigator for duration of 1 hour on care of
newborn during phototherapy which includes definition, indication, mechanism
of action, care of newborn on phototherapy complications expected due to
phototherapy by using power point presentation and issued booklet regarding
care of newborn during phototherapy.

Knowledge:
It refers to the level of understanding of student‟s knowledge regarding care
of new born during phototherapy among II year DGNM students in ICH,
Chennai.
Care of newborn:
Care of newborn refers to baby under phototherapy receive eye care,
skincare, fluid requirement, maintenance of body temperature, care of
genitals, assessing dehydration, breast feeding and prevention of
complication.
Phototherapy
Phototherapy is one of the non-invasive methods to reduce the bilirubin level
by exposing the baby skin to blue or cool white light. Light converts the
bilirubin to non toxic water soluble compound, they are excreted in urine and
stool. Baby is kept under phototherapy light at a distance of 45cm.proper
nursing care should be given to the newborn during phototherapy to enhance
the effectiveness and to minimize the complication as greenish stool, skin
rashes and electrolyte imbalance.
Nursing Students
Students undergoing DGNM II Year training programme, posted at ICH,
Chennai.
1.6 RESEARCH HYPOTHESIS
The following hypothesis will be tested
H1-There will be significant difference between pre- test and post-test level of
knowledge score regarding care of newborn during phototherapy.
H2-There will be a significant association between post- test level of
knowledge and selected socio demographic variables

1.7 ASSUMPTIONS:
Students may have varying level of knowledge regarding care of
newborn during phototherapy.
Structured teaching programme may help to improve the knowledge of
students regarding care of newborn during phototherapy.
1.8 LIMITATIONS
The study is limited to Diploma Nursing students.
The study is limited to 90 samples.
The study is limited up to 4 weeks of period.

1.9 CONCEPTUAL FRAMEWORK
The investigator has adopted Imogene king‟s goal attainment
theory (2011) based upon personal and interpersonal systems including
perception, action, interaction and transaction. The investigator adopted this
basic theory for conceptual framework, which is aimed to find out the
effectiveness of structured teaching programme on level of knowledge
regarding care of newborn during phototherapy among II year DGNM students.
This involves interaction between the researcher and the students.
There are 6 major components:
PERCEPTION
It refers to student‟s representation of reality. It is non observable but it
can be interfered. Hence the investigator has the perception for the assessment
of demographic variables and pre test assessment about the level of knowledge
regarding care of newborn during phototherapy among II year DGNM students
at ICH, Egmore , chennai-08”
JUDGEMENT
The investigator found that student has inadequate knowledge regarding care of
newborn during phototherapy thus decided to give education to students, to
improve their knowledge about phototherapy.
ACTION
Action refers to the matter, energy and information that enter into the system
through its boundary. Action involves preparation of structured teaching
programme on care of newborn during phototherapy.
REACTION
The investigator‟s reaction is to set goal which is increasing the knowledge
regarding care of newborn during phototherapy.

INTERACTION
Interaction refers to the processing where the system transforms the energy
matter.
Interaction involves in introducing the structured teaching programme through
lecture method by using AV aids such as PowerPoint and information booklet
regarding care of newborn during phototherapy.
TRANSACTION
It refers to the matter, energy and information in the environment that are in an
altered state.
Transaction is the awareness among students regarding care of newborn during
phototherapy by care of eyes, skin care, and maintenance of temperature, breast
feeding and duration of exposure.
FEED BACK
It refers to the environment response to the stimuli.
Feed back is the evaluation of teaching programme by using the same semi
structured questionnaires.

Figure 2.3 CONCEPTUAL FRAMEWORK
peper Post - test
PRE - TEST ACTION INTERACTION TRANSACTION
Assessment of
learning needs
about care of
newborn during
phototherapy
among selected
demographic
variables such as
age, occupation,
income, previous
exposure in NICU
and knowledge
regarding care of
newborn during
phototherapy
Preparation of
articles for
structured
teaching
programme on
care of newborn
during
phototherapy
Introducing
structured teaching
programme
through lecture
method by using
AV aids such as
power point and
information booklet
POST - TEST
Adequate
knowledge on care
of newborn during
phototherapy
Moderate
knowledge on care
of newborn during
phototherapy
Inadequate
knowledge on care
of newborn during
phototherapy
FEED BACK
KING‟S GOAL ATTAINMENT THEORY (2011)

CHAPTER-II
REVIEW OF
LITERATURE

CHAPTER II
REVIEW OF LITERATURE
Review of literature involves the systematic identification location,
scrutiny and survey of the written materials that contain information of
research problem.
Literature review refers to activities involved in identifying and
developing a comprehensive picture of the state of knowledge on the topic.
Related literature both research and non research was explored to
broaden the understanding and gained an insight into selected problem under
study.
2.1 REVIEW OF LITERATURE:
In this study the literature reviewed is presented under the following headings:
2.1.1. Incidence and Effectiveness of phototherapy
2.1.2. Knowledge regarding phototherapy
2.1.3. Management and complication of phototherapy
2.1.1. STUDIES RELATED TO INCIDENCE AND
EFFECTIVENESS OF PHOTOTHERAPY
Abdelazeem.KS et al. (2016) were carried out a study to
assess the effectiveness of intensive phototherapy in comparison with
conventional phototherapy in reducing the need for exchange transfusion and
the duration of phototherapy for management of neonatal hyperbilirubinemia in
Neonatal Unit of Assiut University Children Hospital. The prospective study
was conducted from March 2016 to February 2017 and comprised neonates
with indirect hyperbilirubinaemia near the level of ECT who were admitted to
the Neonatal Unit. The study concludes that use of intensive phototherapy in
the treatment of indirect pathological hyperbilirubinaemia is very effective in
lowering total serum Bilirubin when its level is within 2-3 mg/dl (34-50

UMol/l) of the exchange transfusion level and it has succeeded in reducing the
frequency of exchange transfusion with its hazards and serious complications.
Saravanan.S et al. (2016) were carried out a cross sectional study
on incidence of phototherapy induced hypocalcaemia in full term normal
newborn. Samples of 198 full term jaundiced neonates were selected for the
study (113 females and 85 males) receiving phototherapy. Neonates were
completely examined, plasma and calcium level determined before and after 48
hours of phototherapy,7-15% newborn receiving phototherapy develop
hypocalcemia. As a result of the study significant decrease in serum calcium
was observed (p<0.03).the researcher concluded that phototherapy lowers
serum calcium level in term infants.
Arnold.G et al. (2014) was conducted a comparative study on
effectiveness of three LED phototherapy machine, single and double sided for
treating neonatal jaundice in low resource setting at Da Nang Hospital for
women and children Vietnam. The study population was restricted to infants
born weighing > 1500gm with diagnosed as jaundice. As a result, double sided
machine showed 54% increased in reduction of TSB, 16% reduction of length
of stay. The study confirms that increasing surface area exposure during
phototherapy and substantly decreases the duration of treatment and length of
stay in NICU.
Carolyn.G et al. (2013) carried out a descriptive study on Incidence
and risk factors for neonatal jaundice among newborns in southern Nepal.
Samples of 18,985 newborns/infants born in salahi district were selected for the
study using cluster randomized sampling, by naked eye examination jaundice
level was assessed.teh study result shows there is significant association
between difficulty feeding and increased risk factors for neonatal jaundice
(p<0.001). This study confirmed the several known risk factors for jaundice in
neonates includes birth weight, difficulty feeding and primiparity.

Thomas.B et al. (2016) were conducted a case control study on
jaundiced noted in first 24hours after birth in managed organization at northern
California Kaiser permanent medical care program.631 samples were selected
for the study by randomly selected sample. Notations of jaundice in the
medical record, timing and results of bilirubin testing ,use of phototherapy and
development of bilirubin levels of 25mg/dl or higher.teh study concludes that
jaundice noted in the medical record in the first 24hours after birth was
uncommon and often clinically significant.
Usatin.D et al. (2010) was conducted a retrospective cohort study to
assess the effect of neonatal jaundice and phototherapy on the frequency of the
first year of outpatient visits at KPMCP university of California. Group 1 never
had a documented TSB level > 12mg/dl, group 2 had a TSB level >17 and <23
mg/dl as outpatient between 48hours and 7 days of age and did not receive
phototherapy inpatient phototherapy, group 3 met criteria of group 2.the result
concludes that neonatal jaundice and inpatient phototherapy are associated with
only small increase in first year outpatient visit rates or infrequent contribution
to vulnerable child syndrome in this population.
Bertini.G et al. (2007) was conducted a study in Italy to evaluate
whether high intensity gall nitride light emitting diode (LED) phototherapy
influences trans epidermal water loss (TEWL) and cerebral hemodynamic in
preterm neonates in comparison with conventional phototherapy. Thirty-one
preterm infants were randomized for conventional (n=14) and for LED (n=17)
phototherapy. All infants were studied using a Tewameter TM 210 and cerebral
Doppler ultrasound immediately before phototherapy (time0), 30 min (time1),
1-6 (time 2), and 12-24 hours (Tim 3) after the start of phototherapy and 6-12 h
after discontinuing phototherapy (time4). The study showed that LPT doesn‟t
induce significant changes in TEWL, in peak systolic, and diastolic and mean
cerebral blood flow velocity (CBFV) and in the resistance index (RI) CPT
shows significant increase of TEWL which disappeared at time 4 when
phototherapy had stopped. This study showed that LPT, emitting light within

450-470nm spectrum for optimal bilirubin degradation can be preferable to
CPT for the therapy of hyperbilirubinemia in preterm infants.
Dgokomuljanto.S et al. (2006) study was conducted in Malaysia to
determine the addition of low-cost reflecting curtains to a standard
photography unit could increase effectiveness of phototherapy for neonatal
jaundice. 97 term newborns with uncomplicated neonatal jaundice was taken.
Phototherapy with white curtains hanging from the sides of the phototherapy
unit (study group, n = 50) was compared with single phototherapy without
curtains (control group, n = 47). Total serum bilirubin was measured after 4hr
phototherapy. The mean decrease in total serum bilirubin levels was
significantly (P<0.001) higher in study group (27.62 (25.24) M mol/l) than the
control group (4.04 (24.27) M mol/l).The duration of phototherapy was
significantly shorter in the study group (12h) than the control group. No
difference in adverse events such as hyperthermia or hypothermia weight loss,
rash, loose stools or feeding intolerance. This study showed that hanging white
curtains around phototherapy unit significantly increases efficacy of
phototherapy in the treatment of Neonatal jaundice.
2.1.2 STUDIES RELATED TO KNOWLEDGE REGARDING CARE OF
NEWBORN DURING PHOTOTHERAPY
Rajashri. B et al. (2018) conducted a quasi experimental study to
assess the effectiveness of structured teaching programme on knowledge and
practice regarding phototherapy application among student nurses in Krishna
hospital.50 students were selected for the study by purposive sampling
technique, a structured questionnaire was administered. The study findings are
pre test mean value (13.3) post test mean value (22.7) and no association
between pre test knowledge and demographic variables. Study concludes that
significant gain in knowledge score after STP to nursing students.

SM Hossain et al. (2017) conducted a cross sectional study on
knowledge regarding neonatal jaundice management among mother in a
tertiary level hospital of Dhaka city, samples of 150 mothers were selected for
the study using non – randomized purposive sampling technique .a structured
knowledge questionnaire was used to collect the data from the mothers. The
study major finding was 7.3% had excellent level knowledge regarding
neonatal jaundice, where as 40.0% had satisfactory knowledge and 34% had
poor knowledge regarding neonatal jaundice. Hence awareness should be
created among the mothers.
Adopa P et al. (2017) were conducted a case control study on
knowledge level and determinants of neonatal jaundice at Effutu Municipality
of Ghana.150 neonates were selecsted for the study 100 neonates with clinical
evident jaundice and 50 neonates without jaundice, a structured questionnaire
were used to collect demographic variables and clinical history. The study
findings are majority (54%) of neonates develop jaundice within 1-3 days,
neonatal birth weight associated with neonatal jaundice (p<0.05), prolonged
duration of labor associated with neonatal jaundice (p=0.025).
Chandrasekhar.M et al. (2017) was conducted a descriptive study to
assess the knowledge regarding neonatal jaundice and its management among
staff nurses at Mysuru.60 staff nurses were selected for the study by non-
probability convenient sampling technique. The data were collected by
structured knowledge questionnaire. The knowledge score of staff nurse ranged
from 6-28%band mean value 19.3 with (SD=4) 19.5.The research findings has
shown that nurses with more year of experience and area of working have
significant association in management of neonatal jaundice.
Ahmed.SM et al. (2017) conducted a pre experimental study on
assessment of nurse‟s knowledge and practice about neonatal
hyperbilirubinemia working in district hospitals at Minia Governorate.41 staff
nurses were selected by convenient sampling technique. Data collected by self
structured questionnaire, as a result there is a correlation between the years of
experience in NICU and year of experience in other department have high
significant p value <0.01 and training is significant p value <0.05.based on the
findings of the pretest study, majority of the nurses were competent regarding
practices related to hyperbilirubinemia.
Ghada.M et al. (2016) were conducted a quasi experimental study to
examine the effect of a designed nursing care protocol on clinical outcomes for
neonates with hyperbilirubinemia at neonatal intensive care units in Shebin El-
Kom Teaching Hospital and El Gamea El Sharea for neonates. Sample consist
of 37 nurses two work in NICU and a convenient sample (120) neonates were
selected. Instruments: three tools were used: nurses' knowledge structured
questionnaire, Nurses' practices observational checklist and Neonatal
assessment sheet. It showed significant improvement in nurses' knowledge and
practices after implementation of educational program regarding neonatal
hyperbilirubinemia. Study concluded that, implementation of the designed
nursing care protocol improved nurses' knowledge and practices regarding care
of neonates with hyperbilirubinemia on posttest than on pre test. Also, it
improved clinical outcomes of neonates with hyperbilirubinemia.
Neghabadi.FP et al. (2015).carried out a descriptive study on
auditing phototherapy related nursing care in neonatal general and ICU units
affiliated to shabid benesthi university of medical science ,Iran.120
phototherapy related nursing care delivery episodes were selected and sampling
were observed by using checklist.The checklist based on current standards. The
accordance of phototherapy related nursing care services with the current
standards in study setting was moderate (58.7%) and co-relation co-efficient is
(0.78).the study concludes that lack of knowledge about importance and
outcome of accurate phototherapy related nursing care services.
Sinmayee Kumari Devi et al. (2015) was conducted a study to
assess the Effectiveness of Video Assisted Teaching Module (VATM) on
Knowledge Regarding Care of Newborn Baby under Photo Therapy among
Female Health Workers. A quasi experimental study with pre and post test

without control group design was undertaken on 30 female health workers of
Capital Hospital, Bhubaneswar, Odisha selected by purposive sampling
technique. The data collected by multiple choice close ended questionnaire and
analyzed by using descriptive and inferential statistics. The study findings that
there is a significant difference between pre and post test knowledge was found
(t=25.48, p≤0.05). No significant association was found between post test
knowledge and demographic variable.
Rahman.J et al. (2015) conducted a pre experimental study to assess the
effectiveness of self instructional module on phototherapy knowledge and
practice among staff nurses of selected hospital, Kolkata.30 staff nurses were
selected for the study by purposive sampling technique. Data collected by
structured questionnaire. The study concludes that post test score (19.5)
knowledge,(16.8) practice is higher than pre test score. Hence the self
instructional module was effective method of importing staff nurse knowledge
and practice.
Orimadegum A.E et al. (2015) conducted a cross sectional survey of
knowledge and practice related neonatal jaundice in Ibadan,Nigeria.227
primary health workers were selected for the study, by using semi structured
questionnaire knowledge and practice was assessed. As a result of the study is
that 80.2% had poor knowledge and 46.4% engaged in wrong practices (CI =
1.03, 4.79).The researcher concludes that they need to organize regular training
programme were emphasized.
Soheila Rabiyeepoor et al. (2014) conducted a descriptive analytical
study to assess knowledge and attitude of postnatal mothers on Neonatal
jaundice in Motahari hospital.200 mothers were selected for the study by
purposive sampling technique. Data were collected by structured knowledge
questionnaire. The knowledge score was 6.65 (SD= 3.5) and attitude score was
25.9 (SD=4.48).the researcher conclude that knowledge and score was
correlated with the past experience of neonatal jaundice. An educational

programme is needed for the mothers to increase their knowledge about
neonatal jaundice.
Shrestha.S (2008) conducted a descriptive and explorative study on
knowledge and practice of nursing personnel regarding the care of neonates
under phototherapy at Paropakar Shree Rajyalaxmi Devi Hospital,
Kathmandu.50 samples were selected for the study by purposive sampling
technique .data were collected by semi structured questionnaire. The study
reveals that 56% of respondents are highly knowledgeable and 44% of
respondents are with average knowledge regarding care of baby in
phototherapy.
Ogunfowora.O et al. (2006) was carried out a pre experimental study
in Olabisi Onabanjo University in Nigeria to assess the knowledge and practice
of community health workers regarding neonatal jaundice and its
management.66 community health workers were participated and they were
interviewed by means of self administered questionnaire. The study concludes
that only 54.5% had adequate knowledge of effective treatment namely
phototherapy and exchange transfusion. Researcher recommended regular
training and workshop for the community health workers.
2.1.3 STUDIES RELATED TO MANAGEMENT AND COMPLICATION
OF PHOTOTHERAPY
Sridhar N.L et al. (2018) were conducted a study on calcium
concerns in neonates undergoing phototherapy. Study group included 50
neonates with term and late pre term neonates (35-37 weeks) receiving
phototherapy for neonatal jaundice were included in the study. At the end of
phototherapy in study group, a significant fall in calcium levels in 64% of term
and 76% of late preterm neonates was observed, but almost all expect one
remained asymptomatic.teh efficacy of phototherapy in the prevention of
treatment of hyperbilirubinemia in newborn and infants well established. The
researcher concludes that duration of phototherapy may influence the severity
of hypocalcaemia.

Venktamurthy M et al. (2016) was conducted a prospective
comparative study on effect of phototherapy on platelet count in neonatal
hyperbilirubinemia in tertiary care hospital at Karnataka. Samples of 100
neonates were selected for the study with neonates receiving phototherapy.
Before starting phototherapy platelet count was checked at 0 hours and
discontinuation of phototherapy (second sample).the first sample was
considered as control group. The study concludes that mean platelet count
(2.23 +/- 0.28 lakh) by phototherapy and (1.82 +/- 0.01 lakh) after
phototherapy. There was a decline in platelet count after phototherapy, it was
not statistically expect for low birth weight babies.
Mashal Khan et al. (2016) a cross sectional study conducted at
neonatal intensive care unit, National Institute of Child Health, Karachi. A total
of 123 term neonates with jaundice of either gender managed by phototherapy
were enrolled in the study. Duration of phototherapy was recorded. A sample
of 3ml of blood was sent to the laboratory for the serum calcium level before
initiating phototherapy and after 24 hours of phototherapy. All the data were
recorded in the proforma.Data was analyzed using SPSS version‟s value <0.05
was taken as significant. The study concludes that frequency of hypocalcaemia
is significant in the jaundiced neonates treated with phototherapy.
Olusanya B.O et al. (2009) a study was conducted in Nigeria to
establish the incidence, correlates and hearing screaming outcomes of infants
with severe neonatal jaundice. A hearing screaming was done in 5269 infants
of them 48.7% Neonatal jaundice of whom 5.5% received phototherapy and
1.9% had an exchange blood transfusion. All but two infants with severe
neonatal jaundice were exclusively breast fed. Of those who failed the hearing
test, 17.3% were treated with phototherapy and 11.3% had an exchange blood
transfusion. At least 8.9% of infants requiring phototherapy and 17.3% of those
requiring exchange blood transfusions were at risk of sensor neural hearing
loss. This study showed that severe neonatal jaundice is a significant condition
associates with modifiable risk factors in this population. Policy initiatives for

prevention, early detection followed by appropriate and timely intervention
were urgently needed to reduce the disease burden.
Mehta.S et al. (2006) was conducted a randomized control trial study
to evaluate the effectiveness of fluid supplementation in decreasing the rate of
exchange transfusion and the duration of phototherapy in term neonates with
severe no hemolytic hyperbilirubinemia, seventy four term neonates with
severe non hemolytic hyperbilirubinemia (total serum bilirubin>18mg/d to
<25mg/dl) The subjects were randomized to an extra fluid group (intravenous
fluid supplementation for 8 hours and oral supplementations for the duration of
phototherapy n=37) or a control group had (n=37). At inclusion 54 infants
(73%) had high serum osmolality, including 28 (75%) in the extra fluid group
28 (75%) in the extra fluid group and 26 (70%) in the control group. The
duration of phototherapy was also shorter in extra fluid group (5+/-18 hours
versus 73+/-31 hours). This study shows that fluid supplementation in term
neonates presenting with severe hyperbilirubinemia decrease the rate of
exchange transfusion and duration of phototherapy.
Shinwell E.S et al. (2004) study was conducted in Israel to find the
effect of position changing on bilirubin levels during phototherapy. Thirty term
infants were enrolled in the study (turned -14, supine position –16). The
blanching time was found to be approximately 150 minutes. Transcutaneous
bilirubinometer was used to determine the time required to clear the skin of
bilirubin in term infants. This study showed that infants in the supine group
showed a significantly larger drop in serum total bilirubin concentration and
required a shorter duration of phototherapy than the turned group.

CHAPTER-III
RESEARCH
METHODOLOGY

CHAPTER – III
METHODOLOGY
This chapter deals with the methodology to assess the effectiveness of
structured teaching programme on knowledge regarding care of newborn
during phototherapy among II year DGNM students at Institute of Child Health
and Hospital for Children, Egmore, Chennai-08”.
3.1 RESEARCH APPROACH
Quantitative research approach
3.2 STUDY DESIGN
Pre experimental one group pre test post test design
The research design adopted for the study is pre experimental (one group pre
test post test ) with manipulation and no randomization and no control group.
E O 1 X O2
KEY:
E – Pre experimental group
O1 – Pre assessment (Pre test)
X – Nursing intervention (Structured teaching programme)
O2 – Post assessment (Post test)
3.3 DURATION OF THE STUDY
4 weeks
3.4 STUDY SETTING
The study was conducted at the Institute of Child Health and Hospital for
Children, Egmore, Chennai-08.The Department was started in 1948, at
Government General Hospital and then upgraded in 1957 for public service. It
is an 867 bedded hospital with tertiary care centre, referral, nodal centre for

IMNCI and also the research centre. This hospital is renowned for its
excellence in medical experts, nursing care and quality diagnostic services
specifically for newborn and children. Institute of Child Health and Hospital
for Children has Departments like IMNCI, SICU, NICU and other specialities
which are rendering comprehensive care to children at and around Chennai and
for neighboring states like Andhra Pradesh etc. The rationale for selecting this
area is its feasibility and availability of adequate samples.
3.5 STUDY POPULATION
3.5.1. Target population: Students who are posted in Institute of Child Health
and Hospital for Children, during the time of study
3.5.2. Accessible population: The population available during the study time
at Institute of Child Health and Hospital for Children.
3.6 SAMPLE:
The sample comprises of II year DGNM students.
3.7 SAMPLE SIZE:
90 students who met with the inclusion criteria
3.8 SAMPLE CRITERIA
3.8.1. INCLUSION CRITERIA:
Students of II year DGNM posted in ICH.
Students of II year DGNM who are available at the time of data
collection.
Students who are willing to participate.
3.8.2. EXCLUSION CRITERIA:
Students who are studying other paramedical courses.
Students who are studying B.Sc.(N),M.Sc.(N),P.B.B.Sc(N)
3.9. SAMPLING TECHNIQUE

Sampling procedure is Non-probability convenient sampling technique
3.10. RESEARCH VARIABLES:
3.10.1. Independent variable:
The Structured teaching module on knowledge regarding care of newborn
during phototherapy
3.10.2. Dependent variable:
The knowledge of the students regarding care of newborn during
phototherapy.
3.11. DEVELOPMENT AND DESCRIPTION OF TOOLS:
3.11.1. DEVELOPMENT OF TOOLS
Structured questionnaire was developed after in-depth review of literature;
obtained opinion and content validity from medical, nursing and statistical
experts. Construction and pretesting of tool was done during pilot study and
direct assessment of students was performed during data collection.
3.11.2. DESCRIPTION OF TOOLS
SECTION I: Comprises a demographic variable of students which includes
age, medium of study, family income, education, previous exposure on
phototherapy.
SECTION II: Consists of 40 multiple choice questions to assess the
effectiveness of structured teaching programme on knowledge regarding care
of newborn during phototherapy and it has following subsection like
knowledge aspects of general information about phototherapy, nursing care of
newborn during phototherapy and side effects of phototherapy.
3.11.3. SCORING PROCEDURE:
Section A : The demographic variables were coded to assess the subject it for
statistical analysis.

Section B: The semi structured knowledge questionnaire, each correct answer
was given a score of „one‟ and the wrong answer was given a score of „zero‟
Table 3.1. INTERPRETATION OF KNOWLEDGE SCORE
SCORE INTERPRETATION
>75% Adequate knowledge
51-75% Moderate knowledge
<50% Inadequate knowledge
3.12. CONTENT VALIDITY
Content validity of the tool was obtained from 2 Medical expert and 2 Nursing
experts in the field of Child health nursing. They suggested certain
modification in the tool. The expert‟s suggestions were incorporated in the tool.
Then the tool was finalized and used for the main study.
3.13. RELIABILITY OF THE TOOL
Reliability of the tool was determined by test retest method. There was a
significant co-relation between the test and retest knowledge score according to
Karl Pearson‟s correlation coefficient the value is 0.08.This score indicates
high co relation. Hence the tool was found to be reliable to conduct the main
study.
3.14. PROTECTION OF HUMAN SUBJECTS
Obtained approval from the Institutional Ethical Committee, Madras
Medical College, Director of Institute of Child Health and Hospital for
Children, Egmore, Chennai-08 and all respondents were carefully informed
about the purpose of the study. The students were explained about the purpose
and need of the study. They were assured that their details and answers will be
used only for research purpose and kept confidentially. Written permission was
obtained from the participants before conducting the study.

3.15. PILOT STUDY:
In order to test the feasibility, relevance of the study, a pilot study was
conducted with 10 students. Convenient sampling technique was used. Before
and after structured teaching program pre and post test was conducted. Those
data were analyzed to find out the suitability of the study. The results of the
pilot study showed that there was a positive correlation between the knowledge
of the students with care of newborn during phototherapy and the investigator
found that the study was feasible.
3.16. DATA COLLECTION PROCEDURE
The study was conducted in Institute of Child Health and Hospital for
Children, after obtaining permission from the Director and Head of the
Department of NICU in Institute of Child Health and Hospital for Children,
Chennai-08. Before the data collection, the researcher introduced herself,
explained the purpose of the study to the DGNM II year students regarding
care of newborn during phototherapy. The confidential was assured and
consent was obtained from the participants. Then the students were interviewed
and educated using structured teaching module. Five to ten participants were
selected everyday and assured that at anytime they can withdraw from the
study. The period of study extended for four weeks and the data was collected
from Monday to Saturday between to 8am to 4pm. Using convenient sampling
technique, 90 samples were collected who fulfilled their selection criteria.
Pre test was conducted for 25 minutes; the structured teaching
programme was implemented on the same day for 45 minutes using
PowerPoint presentation and information booklets, which was prepared by the
researcher after consulting with the specialists. The students participated with
interest and were alert and enthusiastic. Certain points were repeated for better
understanding and doubts were cleared and given a self instructional module to
each student regarding care of newborn during phototherapy.

After seven days of interval the post test was administered to the same sample
for 25 minutes regarding the knowledge regarding care of newborn during
phototherapy, using the same questionnaire, and evaluated the effectiveness of
structured teaching programme on care of newborn during phototherapy
3.17. DATA ENTRY AND ANALYSIS
Demographic variables in categories were given in frequencies with their
percentages.
Knowledge score were given in mean and standard deviation.
Quantitative knowledge score in pre test and post-test were compared using
student‟s paired t-test.
Associations between knowledge gain score with demographic variables are
assessed using one way ANOVA F-test and t-test.
Diagram, with regression estimate were used to represent the data.

FIGURE-3.1: SCHEMATIC REPRESENTATION OF THE
RESEARCH METHODOLOGY
RESEARCH DESIGN
Pre experimental one group pre test and post test
design
STUDY SETTINGS
Institute of Child Health and Hospital for Children,
Egmore, Chennai-08
TARGET POPULATION
DGNM II Year students
SAMPLING TECHNIQUE
Convenient sampling technique
SAMPLE SIZE
90
DESCRIPTION OF THE INSTRUMENT
Semi structured questionnaire
DATA ANALYSIS
Descriptive and Inferential statistics
FINDINGS AND CONCLUSION

CHAPTER-IV
DATA ANALYSIS AND
INTERPRETATION

CHAPTER – IV
DATA ANALYSIS AND INTERPRETATION
This chapter presents the analysis and interpretation of data collected
from 90 subjects using a structured questionnaire to assess the knowledge
regarding care of newborn during phototherapy among II year DGNM students.
The data was analysed according to the objectives and hypothesis formulated
for purpose of the study using descriptive and inferential statistics.
Analysis is the process of organizing and synthesizing the data in such a way
that research questions can be answered and hypotheses tested. The purpose of
analysis is to reduce the data into an intelligible and interpretable form, so that
the relation of research problem can be studied and tested.
ORGANIZATION OF DATA
Section A: Description of frequency and percentage distribution of
demographic variables.
Section B: Assessment of pre test knowledge among nursing students with care
of newborn during phototherapy.
Section C: Assessment of post test knowledge among nursing students with
care of newborn during phototherapy.
Section D: Comparison of pre test and post test knowledge among nursing
students with care of newborn during phototherapy and effectiveness of
structured teaching programme.
Section E: Association between the post test knowledge among nursing
students with care of newborn during phototherapy with demographic
variables.

STATISTICAL ANALYSIS
Demographic variables in categories were given in frequencies with their
percentages.
Knowledge score were given in mean and standard deviation.
Quantitative knowledge score in pre test and post test were compared using
student‟s paired t-test.
Qualitative level of knowledge in pre test and post test were compared using
Stuart-Maxwell test /extended McNemar test
Association between demographic variables and knowledge score were
analysed using Pearson chi-square test
Simple bar diagram, multiple bar diagram, Pie diagram, Doughnut diagram and
Box plot were used to represent the data.
P<0.05 was considered statistically significant. All statistical test are two tailed
test.

SECTION A: DESCRIPTION OF DEMOGRAPHIC VARIABLES
OF STUDY PARTICIPANTS.
Table-4.1: Reveals distribution of demographic variables of nursing
students with care of newborn during phototherapy.
Demographic variables No. of students %
Age of the student
18-21 years
86
95.56%
21-25 years 4 4.44%
25-30 years 0 0.00%
Medium of instruction
in higher secondary
English
31
34.44%
Tamil
59 55.56%
Type of family
Nuclear
63
70.00%
Joint
20
22.22%
Extended
7 7.78%
Mothers education
Illiterate
16
17.78%
Primary 25 27.78%
Secondary education 9 10.00%
High school 25 27.78%
Higher secondary 12 13.33%
Graduate 3 3.33%

Fathers education
Illiterate
16
17.78%
Primary 24 26.67%
Secondary education 9 10.00%
High school 20 22.22%
Higher secondary 18 20.00%
Graduate 3 3.33%
Father‟s Occupation
Unemployed
9
10.00%
Unskilled worker 14 15.56%
Semiskilled worker 5 5.56%
Skilled worker 17 18.89%
Clerk, shop owner 40 44.44%
Semi profession 2 2.22%
Profession 3 3.33%
Monthly income of
the family
Below Rs. 2,091
26
28.89%
Rs .2,092 – Rs .6,213 21 23.33%
Rs .6214 – Rs .10,356 23 25.56%
Rs .10,357 – Rs
.15,535 12 13.34%
Rs .15,536 – Rs
.20,714 4 4.44%
Rs.20,715 –Rs. 41,429 2 2.22%
>Rs. 41,430 2 2.22%
Have you been posted
in NICU?
Yes
15
16.67%
No 75 83.33%

Do you have
exposure on care of
newborn during
phototherapy?
Yes
28
31.11%
No 62 68.89%
Data presented in table-4.1 shows the following:
Age: Maximum 95.56% of the students belongs to age group of 18 – 21 years,
4.44% of the students belongs to age group of 25 – 31 years.
Medium of instruction: 65.56% of the student‟s medium of instruction in
higher secondary is Tamil and 34.44% of the student‟s medium of instruction
in higher secondary is English.
Type of family system: 70% of the students were nuclear family, 22.22% of
students were joint family and 7.78% of students were extended family.
Mother education: 27.78% of the student mothers had primary and high
school education, 17.78% of the student mother is illiterate, 13.33% of the
student mother had higher education, 10% of the student‟s mothers had
secondary education and 3.33% of the student‟s mothers become graduates.
Father education: 26.67% of the student father had primary, 22.22% of the
student‟s father had high school education, 20% of the student father is higher
secondary, 17.78% of the student father become illiterate, 10% of the student‟s
fathers had secondary education and 3.33% of the student‟s fathers become
graduates.
Father occupation: 44.44% of the fathers were clerk, shop owner, 18.89% of
the fathers were skilled worker, 15.56% of the fathers were unskilled worker,
10% of the fathers were unemployed, 5.56% of the fathers were semi skilled
worker, 3.33% of the fathers were profession and 2.22% of the fathers were
semi profession.

Family income: 28.89% of subjects have family income of about (< Rs.2,091),
25.56% of subjects have family income of about (Rs.6214- Rs.10,356), 23.33%
of subjects have family income of about (Rs.2,092- Rs.6,213), 13.34% of
subjects have family income of about (Rs.10,357- Rs.15,535), 4.44% of
subjects have family income of about (Rs.15,536- Rs.20,714), 2.22% of
subjects have family income of about (Rs.20,715- Rs.41,429) and (>
Rs.41,430).
Posted in NICU: 83% of the students have not been posted in the NICU and
17% of the students have been posted in the NICU.
Previous exposure: 69% of the students not had exposure on care of newborn
during phototherapy and 31% of the students had exposure on care of newborn
during phototherapy.

Figure- 4.1: Cylindrical diagram shows distribution of sample age group
Figure-4.2: Pie diagram showing distribution of sample according to medium
of instruction in higher secondary.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
18-21 years 21-25 years 25-30 years
95.56%
4.44%0.00%
% o
f st
ud
ents
AGE DISTRIBUTION
English
34.44%
Tamil
65.56%
MEDIUM OF INSTRUCTION IN HIGHER
SECONDARY

Figure-4.3: Bar diagram shows distribution of sample according to type of
family
Figure- 4.4: Bar diagram shows distribution of sample according to mother
education status
0%
10%
20%
30%
40%
50%
60%
70%
80%
Nuclear Joint Extended
70.00%
22.22%
7.78%% of
stu
den
ts
TYPE OF FAMILY SYSTEM
0%
5%
10%
15%
20%
25%
30%
35%
40%
Illiterate Primary Secondary
education
High school Higher
secondary
Graduate
17.78%
27.78%
10.00%
27.78%
13.33%
3.33%
% o
f s
tud
ents
MOTHER EDUCATION STATUS

Figure -4.5: Bar diagram shows distribution of sample according to father
education status
Figure -4.6: Cylindrical diagram shows distribution of sample according to
father occupation
0%
5%
10%
15%
20%
25%
30%
35%
40%
Illiterate Primary Secondary
education
High school Higher
secondary
Graduate
17.78%
26.67%
10.00%
22.22%20.00%
3.33%
% of
stu
den
ts
FATHER EDUCATION
-10%
0%
10%
20%
30%
40%
50%
60%
10.00%
15.56%
5.56%
18.89%
44.44%
2.22% 3.33%% of
stu
den
ts
FATHER OCCUPATION

Figure -4.7: Cylindrical diagram shows distribution of sample according to
monthly income
Figure-4. 8: Doughnut diagram shows distribution of sample according to
posted in NICU
0%
5%
10%
15%
20%
25%
30%
35%
40%
Below Rs.
2,091
Rs .2,092 –
Rs .6,213
Rs .6214 –
Rs .10,356
Rs .10,357 –
Rs .15,535
Rs .15,536 –
Rs .20,714
Rs.20,715 –
Rs. 41,429
>Rs. 41,430
28.89%
23.33%25.56%
13.34%
4.44%2.22% 2.22%
% o
f s
tud
ents
MONTHLY INCOME OF THE FAMILY
Yes
17%
No
83%
POSTED IN NICU

Figure-4.9: Pie diagram shows distribution of sample according to previous
exposure on care of newborn during phototherapy.
Yes
31%
No
69%
PREVIOUS EXPOSURE ON CARE OF
NEWBORM
DURING PHOTOTHERAPY
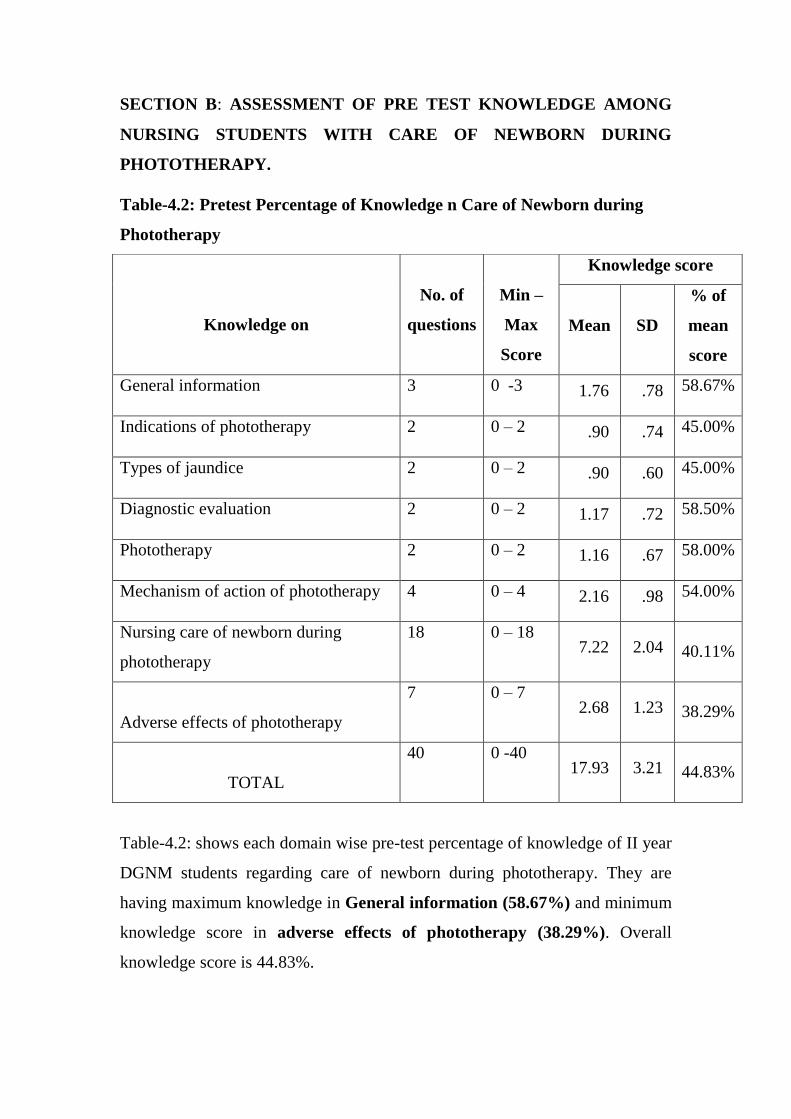
SECTION B: ASSESSMENT OF PRE TEST KNOWLEDGE AMONG
NURSING STUDENTS WITH CARE OF NEWBORN DURING
PHOTOTHERAPY.
Table-4.2: Pretest Percentage of Knowledge n Care of Newborn during
Phototherapy
Table-4.2: shows each domain wise pre-test percentage of knowledge of II year
DGNM students regarding care of newborn during phototherapy. They are
having maximum knowledge in General information (58.67%) and minimum
knowledge score in adverse effects of phototherapy (38.29%). Overall
knowledge score is 44.83%.
Knowledge on
No. of
questions
Min –
Max
Score
Knowledge score
Mean
SD
% of
mean
score
General information 3 0 -3 1.76 .78 58.67%
Indications of phototherapy 2 0 – 2 .90 .74 45.00%
Types of jaundice 2 0 – 2 .90 .60 45.00%
Diagnostic evaluation 2 0 – 2 1.17 .72 58.50%
Phototherapy 2 0 – 2 1.16 .67 58.00%
Mechanism of action of phototherapy 4 0 – 4 2.16 .98 54.00%
Nursing care of newborn during
phototherapy
18 0 – 18 7.22 2.04 40.11%
Adverse effects of phototherapy
7 0 – 7 2.68 1.23 38.29%
TOTAL
40 0 -40 17.93 3.21 44.83%

Table-4.3: Pretest Level of Knowledge
Level of knowledge No. of Students %
Inadequate knowledge 71 78.88%
Moderate knowledge 19 21.12%
Adequate knowledge 0 0.00%
Total 90 100%
Table No-4.3 Shows the level of pre-test percentage of knowledge of II year
DGNM students regarding care of newborn during phototherapy.78.88% of
students are having inadequate level of knowledge score, 21.12% of them
having moderate level of knowledge score and none of them are having
adequate level of knowledge score.

Figure-4.10: Pre Test Level of Knowledge Score
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Inadequate Moderate Adequate
78.88%
21.12%
0.00%
% o
f st
ud
ents
PRETEST LEVEL OF KNOWLEDGE SCORE

SECTION C: ASSESSMENT OF POST TEST KNOWLEDGE AMONG
NURSING STUDENTS WITH CARE OF NEWBORN DURING
PHOTOTHERAPY.
Table-4.4: Posttest Percentage of Knowledge on Care of Newborn during
Phototherapy
Table-4.4: shows each domain wise post-test percentage of knowledge of II
year DGNM students regarding care of newborn during phototherapy. They are
having maximum knowledge in General Information (90.67%) and minimum
knowledge score in Diagnostic Evaluation (81.50%). Overall knowledge
score is 84.15%.
Domains
No. of
questions
Min –
Max
score
Knowledge score
Mean SD % of
mean
score
General Information 3 0 -3 2.72 .45 90.67%
Indications Of Phototherapy 2 0 - 2 1.67 .47 83.50%
Types Of Jaundice 2 0 - 2 1.64 .48 82.00%
Diagnostic Evaluation 2 0 - 2 1.63 .48 81.50%
Phototherapy 2 0 - 2 1.70 .46 85.00%
Mechanism Of Action Of
Phototherapy
4 0 - 4 3.37 .84 84.25%
Nursing Care Of Newborn During
Phototherapy
18 0 - 18 14.92 2.40 82.89%
Adverse Effects Of Phototherapy 7 0 - 7 6.00 .92 85.71%
TOTAL 40 0 -40 33.66 3.81 84.15%

Table-4.5: Post test Level of Knowledge
Table No-4.5: shows the level of post-test percentage of knowledge of II year
DGNM students regarding care of newborn during phototherapy. None of the
students are having inadequate level of knowledge score, 17.78% of them
having moderate level of knowledge score and 82.22% of them are having
adequate level of knowledge score.
Level of knowledge No. of students %
Inadequate knowledge 0 0.00%
Moderate knowledge 16 17.78%
Adequate knowledge 74 82.22%
Total 90 100.00%

Figure-4.11: Post Test Level of Knowledge Score
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Inadequate Moderate Adequate
0.00%
17.78%
82.22%
% o
f s
tud
ents
POSTTEST LEVEL OF KNOWLEDGE SCORE

SECTION D: COMPARISON OF PRETEST AND POSTTEST LEVEL
OF KNOWLEDGE SCORE AMONG II YEAR DGNM STUDENTS
REGARDING CARE OF NEWBORN DURING PHOTOTHERAPY
Table-4.6: Comparison of Pre test And Post test Level of Knowledge Score
Level of knowledge
Pretest
Post test Extended
McNemar‟s
test n % n %
Inadequate
knowledge
71 78.88% 0 0.00% 2=81.23
P=0.001***(S)
Moderate
knowledge
19 21.12% 16 17.78%
Adequate
knowledge
0 0.00% 74 82.22%
Total 90 10.00% 90 100.00%
***very high significant at p<0.001 level
Table no 7 shows the pre-test and post test level of knowledge among students
Before STP, 78.88% of the students are having inadequate level of knowledge
score, 21.12% of them having moderate level of knowledge score and none of
them are having adequate level of knowledge score.
After STP, none of the students are having inadequate level of knowledge
score, 17.78% of them having moderate level of knowledge score and 82.22%
of them are having adequate level of knowledge score.
Level of knowledge gain score between pre-test and post-test was calculated
using Extended McNemar‟s chi-square test.

Figure-4.12: Percentage of Pre test and Post test level of knowledge
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pretest Posttest
78.88%
0.00%
21.12%17.78%
0.00%
82.22%
% o
f s
tud
ents
PRETEST AND POSTTEST LEVEL OF KNOWLEDGE SCORE
Inadequate
Moderate
Adequate

Table-4.7: Comparison of Pretest and Post test Knowledge Score
*** Very high significant at P≤0.001 DF= Degrees of Freedom
Knowledge on Pretest Post test Mean
Difference
Student‟s paired
t-test Mean SD Mean SD
1 General
Information 1.76 .78 2.72 .45 0.96
t=13.21P=0.001 ***
DF= 89 , Significant
2 Indications of
Phototherapy .90 .74 1.67 .47 0.77
t=7.75 P=0.001 ***
DF= 89 , Significant
3 Types of
Jaundice .90 .60 1.64 .48 0.74
t=9.90 P=0.001 ***
DF= 89 , Significant
4 Diagnostic
Evaluation 1.17 .72 1.63 .48 0.46
t=5.46P=0.001 ***
DF= 89 , Significant
5 Phototherapy 1.16 .67 1.70 .46 0.54
t=6.38P=0.001 ***
DF= 89 , Significant
6 Mechanism of
Action of
Phototherapy
2.16 .98 3.37 .84 1.21
t=9.26P=0.001 ***
DF= 89 , Significant
7 Nursing Care of
Newborn During
Phototherapy
7.22 2.04 14.92 2.40 7.7
t=22.80P=0.001 ***
DF= 89 , Significant
8 Adverse Effects
of Phototherapy 2.68 1.23 6.00 .92 3.32
t=20.24P=0.001 ***
DF= 89 , Significant
Total knowledge
score 17.93 3.21 33.66 3.81
15.73
t=31.12P=0.001 ***
DF= 89 , Significant

Table no-4.7 shows the comparison of Pre test and post test knowledge score
regarding care of newborn during phototherapy among II year DGNM students.
Knowledge regarding
General information: In pretest students are having 1.76 score and in posttest
they are having 2.72 score, so the difference is 0.96. This difference is large
and statistically significant difference.
Indications of phototherapy: In pretest students are having 0.90 score and in
posttest they are having 1.67 score, so the difference is 0.77. This difference is
large and statistically significant difference.
Types of jaundice: In pretest students are having 0.90 score and in posttest
they are having 1.64 score, so the difference is 0.74. This difference is large
and statistically significant difference.
Diagnostic evaluation: In pretest students are having 1.17 score and in posttest
they are having 1.63 score, so the difference is 0.46. This difference is large
and statistically significant difference.
Phototherapy: In pretest students are having 1.16 score and in posttest they are
having 1.70 score, so the difference is 0.54. This difference is large and
statistically significant difference.
Mechanism of Action of Phototherapy: In pre test students are having 2.16
score and in post test they are having 3.37 score, so the difference is 1.21. This
difference is large and statistically significant difference.
Nursing Care of Newborn During Phototherapy: In pretest students are
having 7.22 score and in post test they are having 14.92 score, so the difference
is 7.70. This difference is large and statistically significant difference.
Adverse Effects of Phototherapy: In pre test students are having 2.68 score
and in post test they are having 6.00 score, so the difference is 3.32. This
difference is large and statistically significant difference.
Total: In pre test students are having 17.93 score and in post test they are
having 33.63 score, so the difference is 15.73. This difference is large and
statistically significant difference.

On an average, students are improved their knowledge from 17.93 to
33.63 after the administration of structured teaching programme. Or we can
say, in pre test they are able to answer only 18 questions before administration
of STP, after administration of STP they are able to answer upto33 questions.
Due to STP they are able to answer 15 more questions correctly. This
difference is statistically significant. Statistical significance was calculated by
using student‟s paired „t‟test.
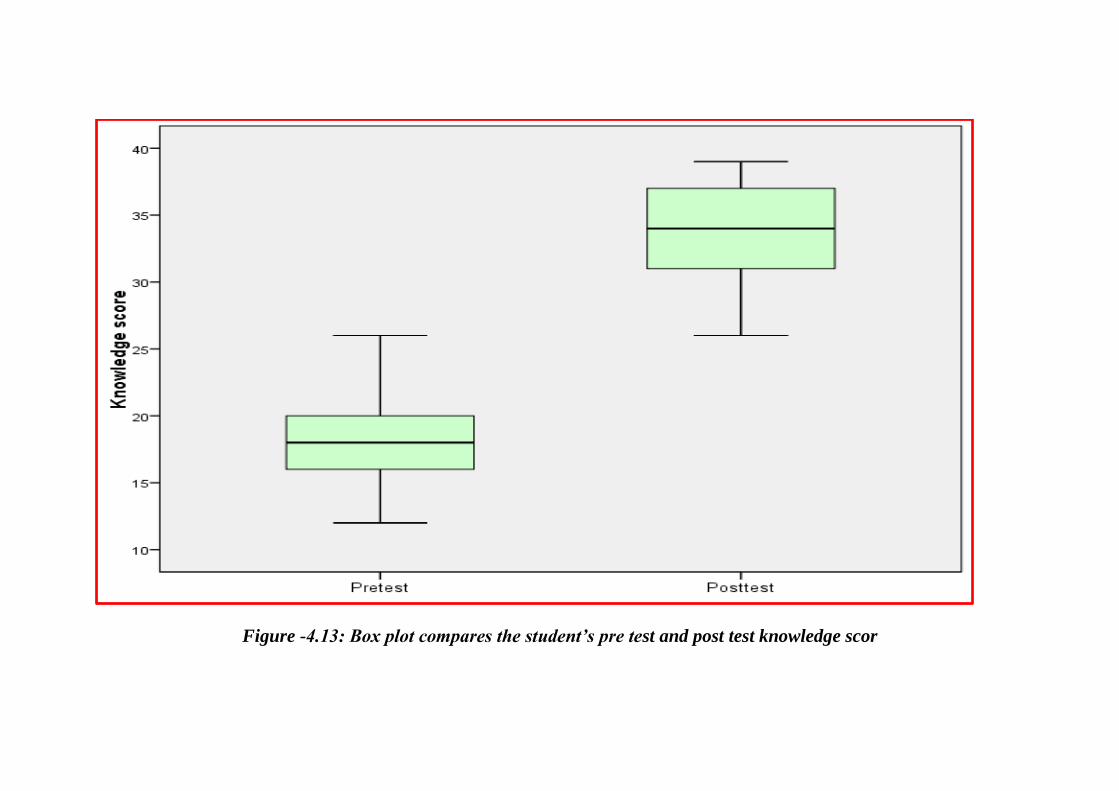
Figure -4.13: Box plot compares the student’s pre test and post test knowledge scor

Table-4.8: Each Domain wise Pretest and Post-test Percentage of
Knowledge
Table no-4.8: shows each domain wise knowledge gain score regarding care of
newborn during phototherapy among II year DGNM students at ICH, Egmore,
chennai-08. In pretest students are having 44.83% of knowledge score and in
posttest they are having 84.15%. So they gained 39.32% after structured
teaching programme
Domains
Pretest
Knowledge
Posttest
Knowledge
% of
Knowledge
Gain
General Information 58.67% 90.67% 32.00%
Indications Of Phototherapy 45.00% 83.50% 38.50%
Types Of Jaundice 45.00% 82.00% 37.00%
Diagnostic Evaluation 58.50% 81.50% 23.00%
Phototherapy 58.00% 85.00% 27.00%
Mechanism of Action of
Phototherapy 54.00% 84.25% 30.25%
Nursing Care of Newborn
During Phototherapy 40.11% 82.89% 42.78%
Adverse Effects of Phototherapy 38.29% 85.71% 47.42%
Overall 44.83% 84.15% 39.32%
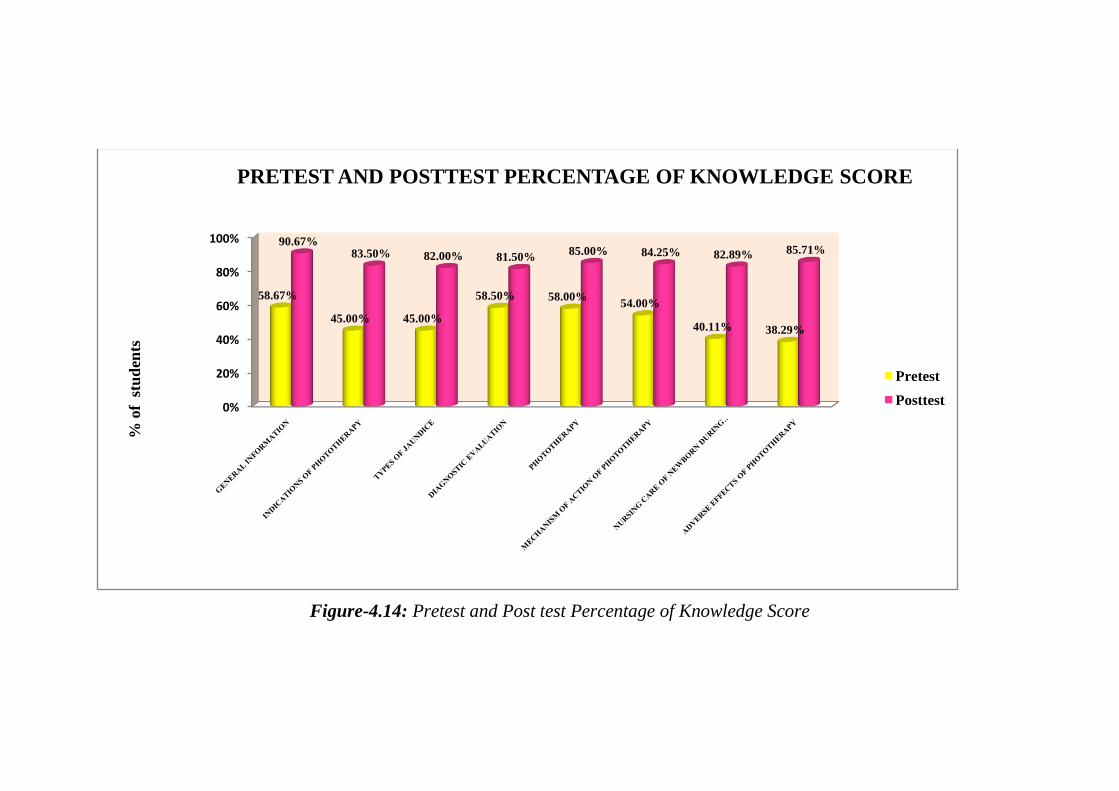
Figure-4.14: Pretest and Post test Percentage of Knowledge Score
0%
20%
40%
60%
80%
100%
58.67%
45.00% 45.00%
58.50% 58.00%54.00%
40.11% 38.29%
90.67%83.50% 82.00% 81.50%
85.00% 84.25% 82.89% 85.71%
% o
f s
tud
ents
PRETEST AND POSTTEST PERCENTAGE OF KNOWLEDGE SCORE
Pretest
Posttest

Table no-4.9: EFFECTIVENESS AND GENERALIZATION OF
STRUCTERED TEACHING PROGRAMME
Max
score
Mean score Mean Difference of
knowledge gain score
with 95% Confidence
interval
Percentage of
knowledge gain score
with 95% Confidence
interval
Pretest 40 17.93 15.72(14.71 – 16.72) 39.30 %( 36.78% –
41.80%) Posttest 40 33.66
Table no-4.9:shows the effectiveness of structured teaching programme on
knowledge regarding care of newborn during phototherapy among II year
DGNM students at ICH, Egmore , chennai-08
On an average, in posttest after having STP, students are gained 39.30% more
knowledge score than pretest score.
Differences and generalization of knowledge gain score between pretest and
posttest score was calculated using and mean difference with 95% CI and
proportion with 95% CI.

SECTION E: ASSOCIATION BETWEEN STUDENTS POSTTEST
LEVEL OF KNOWLEDGE AND THEIR DEMOGRAPHIC
VARIABLES
Table-4.10: shows association between posttest level of knowledge and
demographic variables
Demographic variables
Posttest level of knowledge score n Chi square
test Inadequate Moderate Adequate
N % n n % n n %
Age of the
student
18-21 years
0
0.00%
14
16.28%
72
83.72%
86
2=2.97
P=0.08(NS) 21-25 years 0 0.00% 2 50.00% 2 50.00% 4
25-30 years 0 0.00% 0 0.00% 0 0.00% 0
Medium of
instruction in
higher
secondary
English
0
0.00%
2
6.45%
29
93.55%
31
2=4.45
P=0.04*(S)
Tamil 0 0.00% 14 23.72% 45 76.28% 59
Type of family
Nuclear 0 0.00% 8 12.69% 55 87.31% 63 2=8.60
P=0.01**(S) Joint 0 0.00% 4 20.00% 16 80.00% 20
Extended
0 0.00% 4 57.14% 3 42.86% 7
Students
education
Illiterate 0 0.00% 2 12.50% 14 87.50% 16 2=4.01
P=0.55 (NS) Primary 0 0.00% 7 28.00% 18 72.00% 25
Secondary
education 0 0.00% 1 11.11% 8 88.89% 9
High school 0 0.00% 3 12.00% 22 88.00% 25
Higher
secondary 0 0.00% 3 25.00% 9 75.00% 12
Graduate 0 0.00% 0 0.00% 3 100.00% 3

Fathers
education
Illiterate 0 0.00% 1 6.25% 15 93.75% 16 2=6.20
P=0.29 (NS) Primary 0 0.00% 6 25.00% 18 75.00% 24
Secondary
education 0 0.00% 0 0.00% 9 100.00% 9
High school 0 0.00% 4 20.00% 16 80.00% 20
Higher
secondary 0 0.00% 5 27.78% 13 72.22% 18
Graduate 0 0.00% 0 0.00% 3 100.00% 3
Father‟s
Occupation
Unemployed
0 0.00% 2 22.22% 7 77.78% 9
2=6.20
P=0.28 (NS)
Unskilled
worker 0 0.00% 2 14.29% 12 85.71% 14
Semiskilled
worker 0 0.00% 2 40.00% 3 60.00% 5
Skilled worker 0 0.00% 1 5.88% 16 94.12% 17
Clerk, shop
owner 0 0.00% 7 17.50% 33 82.50% 40
Semi
profession 0 0.00% 0 0.00% 2 100.00% 2
Profession 0 0.00% 2 66.67% 1 33.33% 3
Monthly
income of the
family
Below Rs.
2,091 0 0.00% 3 11.54% 23 88.46% 26
2=8.91
P=0.18 (NS)
Rs .2,092 – Rs
.6,213 0 0.00% 4 19.05% 17 80.95% 21
Rs .6214 – Rs
.10,356 0 0.00% 3 13.04% 20 86.96% 23
Rs .10,357 –
Rs .15,535 0 0.00% 3 25.00% 9 75.00% 12
Rs .15,536 –
Rs .20,714 0 0.00% 1 25.00% 3 75.00% 4

Rs.20,715 –
Rs. 41,429 0 0.00% 1 50.00% 1 50.00% 2
>Rs. 41,430 0 0.00% 1 50.00% 1 50.00% 2
Have you been
posted in
NICU?
Yes 0 0.00% 0 0.00% 15 100.00% 15 2=6.55
P=0.01**
(S)
No 0 0.00% 16 21.33% 49 78.67% 75
Do you have
exposure on
care of
newborn
during
phototherapy?
Yes 0 0.00% 1 3.57% 27 96.43% 28 2=5.61
P=0.02* (S) No
0 0.00% 15 24.19% 47 75.81% 62
NS=not significant S= Significant P> 0.05 not significant *P≤0.05 significant
**P≤0.01 highly significant
Table no 10: shows the association between posttest level of knowledge and
their demographic variables.
English medium students, Nuclear family students, NICU posted students and
having exposure on care of newborn during phototherapy students are gained
more knowledge than others.
Statistical significance was calculated using chi square test.

Table -4.11: ASSOCIATION BETWEEN STUDENTS KNOWLEDGE
GAIN SCORE AND THEIR DEMOGRAPHIC VARIABLES
Demographic variables
knowledge gain score n Oneway
ANOVA
F-test/t-
test
Pretest Posttest
Gain
score=post-pre
n % n
n
% N
n
%
Age of the
student
18-21 years
17.79
3.14
32.73
3.78
14.94
4.78
86
t=1.23
P=0.22(NS) 21-25 years 21.00 3.74 33.00 4.55 12.00 2.00 4
25-30 years 0.00 0.00 0.00 0.00 0.00 0.00 0
Medium of
instruction in
higher
secondary
English
18.15
3.52
34.84
3.86
16.69
5.59
31
t=2.04
P=0.05*(S) Tamil
17.84 3.10 32.32 3.82 14.48 4.46 59
Type of
family
Nuclear
17.70
3.25
34.77
3.83
17.07
4.99
63
=3.47
P=0.04*(S) Joint 19.70 2.54 34.25 3.80 14.55 3.99 20
Extended 15.00 1.63 27.59 4.15 12.59 4.23 7
Mothers
education
Illiterate
17.50
3.74
34.31
3.68
16.81
5.21
16
F=0.92
P=0.47
(NS)
Primary 18.84 3.59 33.48 4.35 14.64 5.11 25
Secondary
education 17.00 2.45 32.44 2.46 15.44 3.47 9
High school 17.92 2.84 34.40 3.99 16.48 4.70 25
Higher
secondary 16.75 2.60 32.83 3.64 16.08 4.72 12
Graduate 20.33 2.89 32.33 2.08 12.00 4.00 3

Fathers
education
Illiterate
17.75
3.09
36.13
3.28
18.38
4.72
16
F=6.00
P=0.27
(NS)
Primary 18.29 3.10 31.87 3.63 13.58 4.48 24
Secondary
education 15.78 3.31 35.22 2.22 19.44 3.68 9
High school 18.35 3.34 33.70 3.80 15.35 4.97 20
Higher
secondary 18.17 3.28 33.22 4.19 15.06 4.18 18
Graduate 18.33 3.21 32.33 2.08 14.00 2.00 3
Father‟s
Occupation
Unemployed 17.33 4.18 33.22 4.06 15.89 5.18 9
F=0.48
P=0.82
(NS)
Unskilled
worker 17.71 2.58 33.21 3.51 15.50 4.78 14
Semiskilled
worker 19.40 1.34 33.20 5.26 13.80 5.02 5
Skilled
worker 18.76 3.77 34.76 3.49 16.00 5.34 17
Clerk, shop
owner 17.55 3.21 33.78 3.91 16.23 4.77 40
Semi
profession 20.50 2.12 34.00 1.41 13.50 .71 2
Profession 17.00 1.00 29.67 3.06 12.67 2.89 3
Monthly
income of the
family
Below Rs.
2,091 17.69 2.57 34.73 3.35 17.04 4.24 26
F=1.24
Rs .2,092 –
Rs .6,213 18.14 3.68 33.57 3.60 15.43 4.73 21
Rs .6214 –
Rs .10,356 17.87 3.58 34.00 4.09 16.13 5.19 23

Rs .10,357 –
Rs .15,535 18.50 3.99 32.58 3.50 14.08 4.64 12
P=0.29
(NS)
Rs .15,536 –
Rs .20,714 17.75 1.71 32.00 4.55 14.25 5.38 4
Rs.20,715 –
Rs. 41,429 16.00 .00 32.00 7.07 16.00 7.07 2
>Rs. 41,430 18.50 .71 28.00 2.83 9.50 3.54 2
Have you
been posted
in NICU?
Yes 17.27 2.63 35.07 3.33 17.80 3.85 15 t=2.38
P=0.02*
(S)
No 18.07 3.31 32.66 3.88 14.59 4.91 75
Do you have
exposure on
care of
newborn
during
phototherapy?
Yes 17.89 3.62 34.83 3.71 16.94 4.53 28 t=2.24
P=0.03*
(S)
No
17.95 3.04 32.44 3.87 14.49 4.94 62
NS=not significant S= Significant P> 0.05 not significant *P≤0.05 significant
**P≤0.01 highly significant
Table no12: shows the association between post-test level of knowledge and
their demographic variables.
English medium students, Nuclear family students, NICU posted students and
having exposure on care of newborn during phototherapy students are gained
more knowledge than others.
Statistical significance was calculated using chi square test.

Figure-4.15:shows association between the posttest level of knowledge score
and medium of instruction in higher secondary
Figure-4.16:shows association between posttest level of knowledge score and
type of family system
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
English Tamil
0.00% 0.00%6.45%
23.72%
93.55%
76.28%
% o
f s
tud
ents
ASSOCIATION BETWEEN POSTTEST LEVEL OF
KNOWLEDGE SCORE AND MEDIUM OF INSTRUCTION IN
HIGHER SECONDARY
Inadequate
Moderate
Adequate
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Nuclear Joint Extended
0.00% 0.00% 0.00%
12.69%20.00%
57.14%
87.31%80.00%
42.86%
% of
stu
den
ts
ASSOCIATION BETWEEN POSTTEST LEVEL OF
KNOWLEDGE SCORE AND TYPE OF FAMILY SYSTEM
Inadequate
Moderate
Adequate

Figure-4.17:shows association between the posttest level of knowledge score
and NICU posting.
Figure-4.18:shows association between the posttest level of knowledge score
and exposure on care of newborn during phototherapy
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Inadequate Moderate Adequate
0.00% 0.00%
100.00%
0.00%
21.33%
78.67%
% o
f st
ud
ents
ASSOCIATION BETWEEN STUDENTS POSTTEST
LEVEL OF KNOWLEDGE SCORE AND NICU
POSTING
Yes
No
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Yes No
0.0
0%
0.0
0%
3.5
7%
24
.19
%
96
.43
%
75
.81
%
% o
f st
ud
ents
ASSOCIATION BETWEEN POSTTEST LEVEL OF KNOWLEDGE
SCORE AND EXPOSURE ON CARE OF NEWBORN DURING
PHOTOTHERAPY
Inadequate
Moderate
Adequate

CHAPTER-V
DISCUSSION

CHAPTER-V
DISCUSSION
This chapter deals with the discussion of the results of data analyzed
based on the objectives of the study and hypotheses of the study. The purpose
of the study was designed to evaluate the effectiveness of structured teaching
programme on knowledge regarding care of newborn during phototherapy
among II year DGNM students at Institute of Child Health and Hospital for
Children, Egmore, Chennai. Non– probability convenient sampling technique
was used. The students selected for the study was 90.
The students were interviewed and educated using structured teaching
module. Five to ten participants were selected every day. Pre test was
conducted and the structured teaching programme was implemented on the
same day for 45 minutes using PowerPoint presentation and information
booklets. Post test was conducted by the researcher after seven days of interval
regarding care of newborn during phototherapy.
FINDINGS BASED ON SOCIO DEMOGRAPHIC VARIABLES
95.56% were in the age group of 18 - 21 years.
65.56% of student‟s medium of instruction is English.
70% of students belong to Nuclear family.
27.78% of the student mothers had primary and high school education.
26.67% of the student father had primary education.
28.89% students were in the income group of less than Rs.2, 091.
83% of the students not posted in NICU.
69% of the students not had exposure on care of newborn during
phototherapy.

5.1. FINDINGS BASED ON OBJECTIVES
OBJECTIVE-1: To assess the pre test knowledge on care of newborn
during phototherapy among II year DGNM students.
During pre-test score of knowledge regarding care of newborn during
phototherapy of II year DGNM students. They were having maximum
knowledge in General information (58.67%) and minimum knowledge score
in adverse effects of phototherapy (38.29%). Overall knowledge score is
44.83%.
Pre-test level of knowledge score regarding care of newborn during
phototherapy among II year DGNM students before administration of
structured teaching programme are 78.88% of students are having inadequate
level of knowledge score, 21.12% of them having moderate level of knowledge
score and none of them are having adequate level of knowledge score.
The result of the present study findings was also similar to the study
conducted by Rajashri vaishali. B et al. (2018) in which they aimed to assess
the knowledge regarding phototherapy among nursing students in Krishna
hospital at Karad, reported that majority (12%) students had poor knowledge
and 2% had good knowledge.SM.Hossain et al. (2017) conducted a study to
assess knowledge regarding neonatal jaundice among mothers in Dhaka city,
the which revealed that majority (40%) mothers had poor knowledge and
(34%) had satisfactory knowledge.Orimadegum A.E et al. (2015) carried out
a study to assess the knowledge of neonatal jaundice among health care
workers at Nigeria, the study concluded that 80% health workers were having
poor knowledge and 20% had moderate knowledge.
In General, it was observed that the nursing students are having
inadequate knowledge regarding phototherapy, which suggests that there is a
need for special attention on imparting knowledge on phototherapy to the
nursing students.

OBJECTIVE -2: To assess the post test knowledge on care of newborn
during phototherapy among II year DGNM students.
During post-test score of knowledge regarding care of newborn during
phototherapy among II year DGNM students. They were having maximum
knowledge in General Information (90.67%) and minimum knowledge score
in Diagnostic Evaluation (81.50%). Overall knowledge score is 84.15%
among nursing students.
Post test level of knowledge score regarding care of newborn during
phototherapy among II year DGNM students after administration of structured
teaching programme. In general none of the students are having inadequate
level of knowledge score, 17.78% of them having moderate level of knowledge
score and 82.22% of them are having adequate level of knowledge score.
The above study findings were supported by study conducted to assess
the knowledge regarding care of neonates under phototherapy among nursing
personnel at Kathmandu by Shreshtha (2008) ,the study findings reported
that 56% of nurses are highly knowledgeable and 44% of nurses are with
average knowledge.Ogunfowora.O (2006),carried out a study to assess the
knowledge regarding phototherapy among community health workers in
Nigeria, the researcher reported that majority (64.5%) community health
workers are having adequate knowledge regarding phototherapy and its
management. Jahanara Rahman (2015),were carried out a study to assess the
knowledge regarding Phototherapy among Staff Nurses of a Selected Hospital,
Kolkata, West Bengal, the study findings reveals that majority (66.5%) staff
nurses were having adequate knowledge regarding phototherapy.
The study findings suggest that STP is found to be effective in
improving the knowledge of the students. It is also evident that STP is effective
in empowering students with adequate knowledge and helps them in providing
quality care by preventing complications among newborn during phototherapy.

OBJECTIVE 3: To compare the pre test and post test knowledge of II
year DGNM students regarding care of newborn during phototherapy.
Knowledge regarding
General information: In pretest students are having 1.76 score and in posttest
they are having 2.72 score, so the difference is 0.96. This difference is large
and statistically significant difference.
Indications of phototherapy: In pretest students are having 0.90 score and in
posttest they are having 1.67 score, so the difference is 0.77. This difference is
large and statistically significant difference.
Types of jaundice: In pretest students are having 0.90 score and in posttest
they are having 1.64 score, so the difference is 0.74. This difference is large
and statistically significant difference.
Diagnostic evaluation: In pretest students are having 1.17 score and in posttest
they are having 1.63 score, so the difference is 0.46. This difference is large
and statistically significant difference.
Phototherapy: In pretest students are having 1.16 score and in posttest they are
having 1.70 score, so the difference is 0.54. This difference is large and
statistically significant difference.
Mechanism of Action of Phototherapy: In pre test students are having 2.16
score and in post test they are having 3.37 score, so the difference is 1.21. This
difference is large and statistically significant difference.
Nursing Care of Newborn During Phototherapy: In pretest students are
having 7.22 score and in post test they are having 14.92 score, so the difference
is 7.70. This difference is large and statistically significant difference.
Adverse Effects of Phototherapy: In pre test students are having 2.68 score
and in post test they are having 6.00 score, so the difference is 3.32. This
difference is large and statistically significant difference.
Total: In pre test students are having 17.93 score and in post test they are
having 33.63 score, so the difference is 15.73. This difference is large and
statistically significant difference.

Knowledge score, on an average, students are improved their
knowledge from 17.93 to 33.63 after the administration of structured teaching
programme. Or we can say, in pre test they are able to answer only 18
questions before administration of STP, after administration of STP they are
able to answer upto33 questions. Due to STP they are able to answer 15 more
questions correctly. This difference is statistically significant. Statistical
significance was calculated by using student‟s paired „t‟test.
Pretest percentage of knowledge score is 44.83% among nursing students
is 78.88% of students are having inadequate level of knowledge score, 21.12%
of them having moderate level of knowledge score and none of them are
having adequate level of knowledge score.
Post test level of knowledge score is 84.15% among nursing students.
Mainly none of the students are having inadequate level of knowledge score,
17.78% of them having moderate level of knowledge score and 82.22% of
them are having adequate level of knowledge score.
The results of the present study are in consistent with following studies.
Tejas pandya, et al. (2015), were conducted a study to assess the
knowledge regarding phototherapy among Nursing students in Gujarat the
researcher found that post test score (85.7%) is higher than the pre test score
(51.8%) ,the researcher proved that planned teaching program is effective to
improve the knowledge of the students. Rahman. J et al. (2015) were
conducted a study to assess the knowledge of staff nurses regarding
phototherapy in selected hospitals at Kolkata, the study findings reveals that
post test score (19.5) of staff nurses is higher than the pre test score. Sinmayee
et al. (2015), the study results indicated that there is a significant difference
between pre and post test knowledge score among female health workers.
Hence video assisted teaching module is effective in improving their
knowledge.

It is believed that self instructional module was effective method of
improving the knowledge of nursing students regarding care of newborn during
phototherapy.
Effectiveness of structured teaching programme in general
information students gained 90%,indication students gained 83%,types of
jaundice students gained 82%,diagnostic evaluation students gained
81%,phototherapy gained 85%,nursing care of newborn during
phototherapy students gained 83% and in adverse effects students gained
85% after intervention. This shows effectiveness of structured teaching
programme intervention.
The analysis revealed that there was significant difference in the level of
knowledge who received structured teaching programme. Hence hypothesis H1
stated that there is significant difference between the mean pre test and post test
knowledge regarding care of newborn during phototherapy among II year
DGNM students who received the structure teaching programme.
OBJECTIVE-4: To find the association between the post-test knowledge
scores of students with their selected demographic variables.
The association between knowledge gain score and their
demographic variables.
English medium, Nuclear family, NICU posted and having exposure on care of
newborn during phototherapy students are gained more knowledge score than
others. Statistical significance was calculated using one way analysis of
variance F-test and student independent t-test.
H2 There is a significant association between the post test knowledge score
of students with their selected demographic variables.
The study findings were showed that there is significant association
between NICU posted and previous exposure may influence the care of
newborn during phototherapy.
The results of the present study were supported by following studies.

Egube BA, et al. (2013) were conducted a study to assess
Knowledge, attitude, and practice of Neonatal jaundice and its management
among mothers attending antenatal clinic at University of Benin Teaching
Hospital, Nigeria. The study showed that 14.1% of respondents had previous
experience with NNJ. There was also an association between previous
knowledge of the respondents on NNJ and level of knowledge among the
respondents.Ahmed SM et al. (2017) conducted a study to assess the
knowledge regarding neonatal jaundice among staff nurses in Minia, the
researcher concludes that years of experience in NICU has highly significant in
management of neonatal hyperbilirubinemia.Chandrasekar. M et al. (2017)
carried out a study to assess the knowledge regarding neonatal jaundice among
staff nurses in Mysuru.The research findings has shown that nurses with more
year of experience and area of working have association in management of
neonatal jaundice.
The analysis revealed that there was significant association between
demographic variables such as English medium, nuclear family, NICU posted
and having exposure on care of newborn during phototherapy 2=6.55
P=0.01** .
The analysis revealed that there was significant association between the
knowledge regarding care of newborn during phototherapy among students
with selected demographic variables. Hence H2 was accepted.
The present study results highlight the effectiveness of STP on care of
newborn during phototherapy among II year DGNM students. It is also evident
that STP is effective in empowering students with adequate knowledge and
helps them in providing quality care by preventing complications among
newborn during phototherapy.
CHAPTER-VI
SUMMARY, IMPLICATION,
RECOMMENDATION,
LIMITATION AND
CONCLUSION

CHAPTER-VI
SUMMARY, IMPLICATION, RECOMMENDATION,
LIMITATION AND CONCLUSION
6.1 SUMMARY OF THE STUDY
Investigator undertook the study to assess the effectiveness of
structured teaching programme on knowledge regarding care of newborn
during phototherapy among II year DGNM students at the Institute of Child
Health and Hospital for children, Egmore, Chennai-08.
The conceptual framework of the study was based on the Modified
Imogene King‟s Goal Attainment Theory (2011).A pre experimental one group
pre test and post test design was used. The independent variable was the
structured teaching programme and the dependent variable was the knowledge
of the students regarding care of newborn during phototherapy.
The study period was 4 weeks from 2.2.19 to 4.3.19.Totally 90
students were selected as samples using convenient sampling technique. The
data was collected using semi structured questionnaire. Structured teaching
program and information booklet was given. The reliability of the tool was
tested by test retest method. The data analysis and interpretation were done by
using descriptive and inferential statistics.
6.2 MAJOR FINDINGS OF THE STUDY
6.2.1 Findings based on the demographic variables of the student‟s
95.56% were in the age group of 18 - 21 years.
65.56% of student‟s medium of instruction is English.
70% of students belong to Nuclear family.
27.78% of the student mothers had primary and high school education.
26.67% of the student father had primary education.
28.89% students were in the income group of less than Rs.2, 091.
83% of the students not posted in NICU.

69% of the students not had exposure on care of newborn during
phototherapy.
6.2.2 Findings based on knowledge of the students before and after
structured teaching programme:
In the pre test They are having maximum knowledge in General
information (58.67%) and minimum knowledge in adverse effects of
phototherapy (38.29%). Overall knowledge is 44.83%. Mainly 78.88%
of students are having inadequate level of knowledge, 21.12% of them
having moderate level of knowledge and none of them are having
adequate level of knowledge.
In post test They are having maximum knowledge in General
Information (90.67%) and minimum knowledge score in Diagnostic
Evaluation (81.50%). Overall knowledge score is 84.15%. Mainly
none of the students are having inadequate level of knowledge, 17.78%
are having moderate level of knowledge score and 82.22% are having
adequate level of knowledge score.
6.2.3 Findings based on comparison of pre test and post test mean
knowledge score
Knowledge regarding
General information: In pretest, students are having 1.76 score and in
posttest, they are having 2.72 score. So the difference is 0.96. This difference is
large and statistically significant.
Indications of phototherapy: In pretest, students are having 0.90 score and in
posttest they are having 1.67 score, so the difference is 0.77. This difference is
large and statistically significant.
Types of jaundice: In pretest students are having 0.90 score and in posttest
they are having 1.64 score, so the difference is 0.74. This difference is large
and statistically significant difference.

Diagnostic evaluation: In pretest students are having 1.17 score and in posttest
they are having 1.63 score, so the difference is 0.46. This difference is large
and statistically significant difference.
Phototherapy: In pretest students are having 1.16 score and in posttest they are
having 1.70 score, so the difference is 0.54. This difference is large and
statistically significant difference.
Mechanism of Action of Phototherapy: In pre test students are having 2.16
score and in post test they are having 3.37 score, so the difference is 1.21. This
difference is large and statistically significant difference.
Nursing Care of Newborn During Phototherapy: In pretest students are
having 7.22 score and in post test they are having 14.92 score, so the difference
is 7.70. This difference is large and statistically significant difference.
Adverse Effects of Phototherapy: In pre test students are having 2.68 score
and in post test they are having 6.00 score, so the difference is 3.32. This
difference is large and statistically significant difference.
Total: In pre test students are having 17.93 score and in post test they are
having 33.63 score, so the difference is 15.73. This difference is large and
statistically significant difference.
Significance of difference between pre test and post test score was
calculated by using student‟s paired „t‟test.
6.2.4 Findings based on effectiveness of structured teaching programme on
care of newborn during phototherapy among students.
In post-test, the majority of the students of about (82.22%) were having
adequate level of knowledge, (17.78%) were and none of the students having
inadequate knowledge. The overall knowledge regarding phototherapy in post
test 84.15 with standard deviation of 3.81.the improvement score of mean
value was 15.73 and „t‟ test value was 31.12 which were statistically
significant.
6.2.5 Findings based on association between post test knowledge and
demographic variables.

Association between demographic variables and post test level of
knowledge represents as, students from score. English medium (16.69), has
Nuclear family (17.07),exposure to NICU (17.8) and having exposure on care
of newborn during phototherapy (16.94).statistical significance was calculated
using Chi square test.
6.3 IMPLICATIONS OF THE STUDY
The findings of present study may be helpful for such future studies. In
this context the findings of the study has valuable implications in different
areas of nursing practice, nursing administration, nursing education and nursing
research.
6.3.1. NURSING EDUCATION
The Nurse educator can use the structured teaching module to teach the
students about care of the newborn baby under phototherapy.
The finding will help the nursing faculty to give more importance for
planning and organizing programme to improve the knowledge of
students, so that they can practice in the clinical area.
In- service educational training programs about neonatal
hyperbilirubinemia can be conducted for neonatal nurses in neonatal
intensive care units.
A standardized neonatal care protocols for neonatal hyperbilirubinemia
should be integrated into paediatric nursing curriculum.
Educational training programs for nurses should include following areas
as aseptic techniques, caring of incubator, assessing vital signs,
assessing color of newborn by Kramer's rule, measuring bilirubin level,
plotting total serum bilirubin and deciding with physician the proper
management of neonatal hyperbilirubinemia.
The nursing students should be made aware of their responsibility in the
care of newborn during phototherapy.
6.3.2. NURSING PRACTICE

This study is conducted among nursing students to assess the level of
knowledge regarding the care of newborn during phototherapy. This
study can be utilized for educating and practicing the students and help
others and give the knowledge about the phototherapy.
Ongoing in-service education programs should be designed and
implemented at neonatal intensive care units to improve nurses'
knowledge and practices on the basis of nurse's actual needs.
A standardized clinical nursing protocols and guidelines about neonatal
hyperbilirubinemia should be available in each neonatal intensive care
unit.
New staff nursing members who provide care for newborns with
hyperbilirubinemia in neonatal intensive care units should be well
oriented with each standardized international nursing care protocols to
ensure competent nursing care.
6.3.3. NURSING ADMINISTRATION
With technological advances and ever growing challenges of nursing,
the nurse administrators have responsibility to provide the nurses with
substantive educational opportunities.
Nursing administrator should provide necessary facilities and
opportunities for nursing students and staff.
In each hospital, there should be specialized units for developing
nurse‟s knowledge and practices (training unit) based on nurses needs
for practices.
The hospital administrative authority should develop up-dated
neonatology care policies and procedures for nurses and should be
annually reviewed and approved by the quality assurance committee.
Provide adequate medical and nursing supervision, guidance and
regular feed back to nurses concerning their knowledge, attitude and
performance.
Strict policies should be developed to ensure nurses adherence to
infection control rules such as hand washing and wearing gloves.

Library and internet access for all medical and nursing staff should be
established at hospitals settings and should contain the most recent
publications related to neonatal hyperbilirubinemia.
Advanced booklets and electronic media regarding clinical protocols
for neonatal hyperbilirubinemia should be available at each neonatal
intensive care unit.
6.3.4. NURSING RESEARCH
The findings can be utilized as evidence based practice in clinical
practice beneficial for paediatric nursing students and staffs.
A large scale study can be done for replication to standardize the video
assisted teaching module on care of newborn baby under phototherapy.
There is growing need for furnishing nursing research in all the areas of
care. The nurse researcher especially beginners need to enhance their
quest for knowledge. The nurse researcher may effectively use result of
available student and recommended on the importance of application of
phototherapy.
6.4. LIMITATION OF THE STUDY
This study is limited to students posted in Institute of Child Health and
Hospital for Children, Egmore.
The study is limited up to 4 weeks of period
The samples are the Students of II year DGNM.
6.5. RECOMMENDATION
On the basis of the study the following recommendations have been made for
further study:
This study could be replicated on a larger sample.
The study could be conducted in different settings to find out the
effectiveness of STP.
A study could be replicated with a control group.
A comparative study can be conducted among nursing staff and female
health workers regarding care of newborn during phototherapy.

6.6. CONCLUSION
Nurses must have holistic knowledge regarding care of newborn during
phototherapy. Nurses play a vital role in caring the newborn in NICU.The
present study had been supported by a series of other studies which confirmed
that the knowledge on care of newborn during phototherapy is important to
prevent the child from complication. Data analysis and result revealed that the
structured teaching programme on care of newborn during phototherapy was an
effective method for providing adequate knowledge to the student.

REFERENCES

REFERENCES
BOOK REFERENCES
Achar‟s (2003). TEXT BOOK OF PEDIATRICS (3rded,). New Delhi: orient
Longman publishers.
Dorothy R. Marlow, Barbara A. Redding (2002). TEXT BOOK OF
PEDIATRIC NURSING (6thed,). New Delhi. Saunders publishers.
Ghai o. piyushguptha, Paul V.K (2004) ESSENTIAL PEDIATRICS (6TH
ED,). New Delhi. GBS Publishers and distributors.
Guptesuraj, “The short book of pediatrics”, 10th
edition, Jaypee Brothers
medical publishers, New Delhi-2004.
Marilyn J. Huckleberry (2005). WONG‟S ESSENTIAL OF PEDIATRIC
NURSING (7thed,). New Delhi. Reed Elsevier India private limited.
Marlow R, Dorothy, Redding .A. Barbara, “Text Book of pediatric
Nursing”, 6th
Edition, W.B.Saunders company, Harcourt India; New
Delhi- 2001.
Meharban Singh, 2009: Essential Pediatrics for Nurses. 1st Ed. New
Delhi: Sagar Publications.
Paruldutta (2009) PEDIATRIC NURSING (2nded,). New Delhi. Brothers‟
medical publishers (P) LTD.
SurajGupte (2009). THE SHORT TEXT OF PEDIATRICS (11thed,). New
Delhi. Reed Elsevier India private limited.
Tambulwadkar R.S. (1999). PEDIATRIC NURSING (2nded,) Bombay: Vora
medical publishers.
Wong‟s “Essentials of pediatric nursing,” 7th
edition, Marilyn. J.
Hockenberry publication, Missouri,-2006.
JOURNAL REFERENCES
Abdelazeem KS, Soliman AA and Askar EAA, a study to assess the
effectiveness of intensive phototherapy in comparison with conventional
phototherapy in reducing the need for exchange transfusion:
Abdelazeem et al., J Neonatal Biology 2017, 6:3 DOI: 10.4172/2167-
0897.1000266.

AdopaP,Ephrain KD, KontorK,a study on knowledge level and
determinants of neonatal Jaundice: International Journal of
Paediatrics,2018:Vol:2,Article ID 3901505:1-9.
AlvesFilho N. Hyperbilirubinemiadorecém-nascido: condutaprática. In:
AlvesFilho N, Correa MD. Manual de Perinatologist. Rio de Janeiro
(RJ): MEDSI; 1990: 695-732.
AmanSood. Five Newborns charred to death in Patiala Hospital; [online]
available from:www.indianexpress.com/news/five-newborns.
ArnoldaG, Chien TD, Hayen A, Hoi NTX, ManingasK, Joe P, et al A
comparison of the effectiveness of three LED phototherapy machines,
single- and double-sided, for treating neonatal jaundice in a low resource
setting.PLoS ONE 13(10) . (2018):e0205432.https://doi.org/10.1371/
journal.pone.0205432.
Awasthi and Rehaman early prediction of neonatal hyperbilirubinemia.
India journal of pediatrics 2004 jan-feb;65(1):131-139
Bertini G, Perugi S, et al. Transepidermal water loss and cerebral
hemodynamic in preterm infants. Conventional Pediatrics. 2008 Jan;
167 (1): 37– 40.
Cashore W. J, Leo stern. The Management of Neonatal
Hyperbilirubinemia. Indian Journal of Pediatrics.1986; 53:587-598.
Chandrasekhar.M, VishakantamurthyD.G,Williams.S: International
Journal of Nursing Education and Research,vol.5,Issue No.3,2017:ISSN
online:2454-2660.
Dgokomuljanto.S, Quach B S, et al, NZN Neonatal Jaundice is increased
by the use of low –cost white reflecting curtains. BMJ. 2006 Jul; 28(91):
439 – 442.
Ghada.M,Ashok, Maha.I,Khalifa, Fady.M,El-Gendy, Jaklein,R.Younis:
International Journal of Novel Research in Healthcare and Nursing Vol.
3, Issue 3, pp: (62-76), Month: September - December 2016, Available
at: www.noveltyjournals.com

Khan M, Malik KA, Bai R. Hypocalcaemia in jaundiced neonates
receiving phototherapy. Pak J Med Sci. 2016;32(6):1449-1452.doi:
https://doi.org/10.12669/pjms.326.10849
Mehta S, Kumar P, Narang A. Randomized controlled trail of fluid
supplementation in term neonatal with severe hyperbilirubinemia.
Journal of pediatrics. 2006 Oct; 149 (4) : 581 –582.
Meltonk, Akinbi H T, “Neonatal jaundice. Strategies to reduce bilirubin
– induced complications.” Postgrad Med. 1999Nov; 106(6):167-168,
171-174, and 177-178.
Mohamed Ahmond SM,IOSR Journal of Nursing and Health Science,e-
ISSN:2320-1959,Vol-6,Issue-2,2017 March-April:09-16.
Monica Sari, SourabhDutta, et al. Randomized Controlled Trial of
Compact fluorescent lamp versus standard phototherapy for the
treatment of Neonatal Hyperbilirubinemia. Indian Journal of
Pediatrics.2006 Jul: 17(43); 583-585.
NeghabadiFP,ManijehNourianetal: study on auditing phototherapy
related nursing care in neonatal general and ICU units affiliated to
shabidbenesthi university of medical science
,Iran:2015,PMID;24112359.
Ogenfowora OB, Dariel OJ. Neonatal jaundice and its management:
Knowledge, attitude and practice of community health workers in
Nigeria. BMC Public Health Journal .2006 Jan; 24(6):19.
Ogunfowora.O and Daniel O.J, Neonatal Jaundice and its
Management,KAP of community health workers in Nigeria,BMC Public
Health Journal,2006 Jan:24(6);19.
Olusanya B O, Akande AA, et al. Infants with severe neonatal jaundice
in Lagos, Nigeria: incidence correlates and hearing screening outcomes.
Trop Med Int Health Journal. 2009 Mar; 14 (3):301-310.
OrimadegumA.E,Ojebiyi A.O ,a study to assess primary health workers
knowledge and practice related neonatal jaundice in Ibadan,Nigeria,Afr J
Prm Health care fam Med,2017;9(1):1-9.

Rahman.J, Ahmed.N, International Journal of Science and Research
,ISSN (online):2319-7064,vol-6,Issue-6:2017 June:1706-1710.
Rajan K, Janaki V. An Audit of Phototherapy Unit. Indian Journal of
Pediatrics.2000; 67(12):883-884.
RajashriB,vaishaliR,sangeetaP,study to assess the effectiveness of
structured teaching programme on KAP regarding phototherapy
application among student nurses in Krishna hospital,International
Journal of Health sciences and research,2018;8(9):148-153.
Ramesh A, Deoraria K. Unconjugated Hyperbilirubinemia in newborns:
Current perspective. Indian Pediatric Journal.2002 Jan 17(39):30-40.
Ramos JLA, Vaz FAC, MCK. Icterícia do recém-nascido. In: Marcondes
E. Pediatric básis. São Paulo (SP): Sarvier; 2002:466-85.
SaravananS,Raghuram A.S, Incidence of phototherapy induced
hypocalcaemia in full term normal newborn, International journal of
current medical sciences,2016 feb:vol-7,issue-2:222-224.
Scrafford Luke C,Mullany: Incidence and risk factors for neonatal
jaundice among newborns in southern Nepal.Trop.medInt
Health.2013:Nov;18 (11):1317-1328,published online 2013,sep
23,PMID:24112359.
Shinwell E S, Sciaky Y, Karplus M. Effect of position changing on
bilirubin levels during phototherapy. Journal of perinatol. 2002 Apr-
May;22 (3) : 226–229.
Shrestha.S ,a study on knowledge and practice of nursing personnel
regarding the care of neonates under phototherapy at Paropakar Shree
Rajyalaxmi Devi Hospital; Journal of Kathmandu Medical College,vol-
2,N0:2,Issue 4,April-June 2013:84-88.
SinmayeeKumari Devi and Nirupama Jena: International Journal of
Advanced Nursing Science and Practice 2015, Volume 2, Issue 1, pp.
29-35 Article ID Med-205 ISSN: 2320 – 0278.

SM Hossain, SMT Haque, MA Tarafder, conducted a study on
knowledge regarding neonatal jaundice management among mother in a
tertiary level hospital of Dhaka city,AKMMC J 2017;8(2) ;121-127.
SoheilaRabiyeepoor, ShahsanamGhibi, study to assess knowledge and
attitude of postnatal mothers on Neonatal jaundice in
MotahariHospital.Iran,Clinical Medicine Research,vol-3:2014:1-
5.doi:10.11648/j.cmr.20140301.11.
Sridhar N.L, Sreeram .S, MadooriSrinivas, a study on calcium concerns
in neonates undergoing phototherapy, International Journal of
Contemporary Paediatrics.2018 May: 988-991.
Tatil and innet in turkey conducted a study on effectiveness of
phototherapy on neonatal hyperbilirubinemia, 2015:1-9.
Thomas B Newman, LilestrandP.Gabriel j study on jaundiced noted in
first 24hours after birth in managed organization at northern California.
Arch Pediatric Adolesc Med.2002:156:1244-1250.
Usatin D, Lijestrand.P, Kuzniewicz M et al. to assess the effect of
neonatal jaundice and phototherapy on the frequency of the first year of
outpatient visits:NIH public access :2010 april:125(4):729-734.
Venktamurthy M, BalajiM.D,Reddy .K, study on effect of phototherapy
on platelet count in neonatal hyperbilirubinemia in tertiary care hospital
at Karnataka, International Journal of Contemporary Paediatrics.2016
Feb;3(1):253-255.
Viswanatha J, Desai A.B., Achars Textbook of Pediatrics 3rd
ed.
Hyderabad, Orient Longman 1995.
NET REFERENCE:
1. www.pubmed.com
2. www.google.com
3. www.medscape.com
4. www.wikipedia.com
5. www.rasp.edu.an/indexhtm

APPENDICES








SECTION-A
DEMOGRAPHIC DATA
INSTRUCTIONS: The respondents are expected to answer the following
questions by placing the (a) against the response which you feel appropriate
1. Age of the student
a) 18-21 years
b) 21-25 years
c) 25-30 years
2. Medium of instruction in higher secondary
a) English
b) Tamil
3. Type of family
a) Nuclear
b) Joint
c) Extended
4. Mothers education
a) Illiterate
b) Primary education
c) Secondary education
d) High school
e) Higher secondary
f) Graduate

5. Fathers education
a) Illiterate
b) Primary education
c) Secondary education
d) High school
e) Higher secondary
f) Graduate
6. Father‟s Occupation
a) Unemployed
b) Unskilled worker
c) Semiskilled worker
d) Skilled worker
e) Clerk, shop owner, farmer
f) Semi profession
g) Profession
7. Monthly income of the family
a) Below Rs. 2,091
b) Rs .2,092 – Rs .6,213
c) Rs .6214 – Rs .10,356
d) Rs .10,357 – Rs .15,535
e) Rs .15,536 – Rs .20,714
f) Rs.20,715 –Rs. 41,429
g) Rs. 41,430

8. Have you been posted in NICU?
a) Yes
b) No
9. Do you have exposure on care of newborn during phototherapy?
a) Yes
b) No

SECTION-B
INSTRUCTIONS: The respondents are expected to answer the following
questions by placing the (a) appropriate alphabet which you feel correct.
GENERAL INFORMATION
1. The meaning of phototherapy
a) Light therapy
b) Heliotherapy
c) Polarised light
2. The father of phototherapy
a) Louis Pasteur
b) Prof.Niels Ryberg Finsen
c) Prof.Pavlou
3. The meaning of neonatal jaundice
a) Occurs at birth
b) Occurs at any time
c) Occurs 3 or 4 days after birth in about 50% of newborns
INDICATIONS OF PHOTOTHERAPY
4. Indication for phototherapy in term baby, if the bilirubin level
a) > 17mg/dl
b) > 5mg/dl
c) > 8mg/dl

5. Phototherapy is used
a) To treat hyperbilirubinemia
b) To maintain body temperature
c) To prevent dehydration
TYPES OF JAUNDICE
6. Jaundice occurs within 48hrs after birth is called
a) Physiological jaundice
b) Pathological jaundice
c) Neonatal jaundice
7. Physiological jaundice resolves spontaneously
a) Within 2 to 4 days after birth
b) Within 8 to 10 days after birth
c) Within 10 to 14 days after birth
DIAGNOSTIC EVALUATION
8. Kramer‟s rule is used
a) To identify level of jaundice
b) To identify level of electrolytes
c) To identify level of SPO2
9. The instrument used to identify the level of jaundice
a) Icterometer
b) Transcutaneous Bilirubinometer
c) Photo probe

PHOTOTHERAPY
10. The most effective light for phototherapy
a) Fluorescent light
b) White light
c) Blue green light
11. The initiation of phototherapy is for babies
a) Less than 32 weeks of gestation
b) Less than 28 weeks of gestation
c) Less than 36 weeks of gestation
MECHANISM OF ACTION OF PHOTOTHERAPY
12. Normal total serum bilirubin level of baby
a) 0.3 – 1.0 mg/dl
b) 2mg/dl
c) 5mg/dl
13. During phototherapy, light waves converts the bilirubin
a) Lumirubin
b) Z-isomer
c) Photo voltaic
14. Mechanism of phototherapy
a) Photo oxidation effect
b) Photo voltaic effect
c) Photo energy effect

15. Elimination of bilirubin products is through
a) Urine
b) Faeces
c) Sweat
NURSING CARE OF NEWBORN DURING PHOTOTHERAPY
16. Purpose of changing position during phototherapy
a) To make the baby comfortable
b) For light to reach all the areas of the body
c) To maintain skin integrity
17. Size of the eye pad used for phototherapy
a) Size N 720
b) Size N 722
c) Size N 721
18. An important observation during phototherapy is to assess
a) Heart rate
b) Skin color
c) Conjunctiva
19. Ideal room temperature for administering phototherapy
a) 20-240c
b) 32-360c
c) 25-280c

20. The distance between phototherapy light and baby
a) 20-30cms
b) 30-45cms
c) 46-50cms
21. One of the reason to check rebound bilirubin level
a) Pigmentation of skin
b) Incase of physiological jaundice
c) Early use of phototherapy
22. Duration of phototherapy per day
a) 18 hours
b) 24 hours
c) 12 hours
23. The eye pads should be removed
a) Every 4th
hourly
b) Every 8th
hourly
c) Every 12th
hourly
24. Phototherapy light should be changed
a) Every 6 months
b) Every 3 months
c) Every 9 months

25. The number of times breast feeding can be promoted during
phototherapy
a) Every 1 hour
b) Every 4 hours
c) Every 2-3 hours
26. Purpose of covering the eyes of the newborn with eye pads
a) To prevent retinal damage
b) To prevent photo sensitivity
c) To prevent optic nerve damage
27. Daily fluid requirement of baby receiving phototherapy
a) 5 – 10 ml/kg/day
b) 10 – 15 ml/kg/day
c) 20 – 25 ml/kg/day
28. Incase of ABO incompatibility
a) Expose maximum area of skin
b) Expose minimum area of skin
c) Expose only the chest/back
29. Adverse effect of phototherapy
a) Insensible water loss
b) Extra cellular water
c) Intra cellular water

30. The amount of fluid loss for the baby
a) 25 – 50 ml/kg
b) 50-75 ml/kg
c) 75 – 100ml/kg
31. Expansion for NJCF
a) Neonatal Jaundice Condition Form
b) Neonatal Jaundice Control Form
c) Neonatal Jaundice Care Form
32. The purpose of covering genital of male baby during phototherapy
a) To prevent infertility
b) To prevent malignancy
c) To prevent hypertrophy
33. The formula to calculate insensible water loss
a) IWL= Fluid intake - Urine output + Weight gain (or) Weight loss
b) IWL= Fluid intake+ Urine output - Weight gain (or) Weight loss
c) IWL= Fluid intake+ Urine output + Weight gain
ADVERSE EFFECTS OF PHOTOTHERAPY
34. The term bronze baby syndrome denotes
a) Yellow pigmentation of skin
b) Dark grey brown pigmentation of skin
c) Bluish discoloration of skin

35. The expected colour of stool during phototherapy
a) Yellowish
b) Greenish
c) Brownish
36. Transistent skin rashes appears
a) Within 1 – 7 days
b) Within 2 – 5 days
c) Within 8 – 10 days
37. Complication of hyperbilirubinemia
a) Encephalopathy
b) Chronic kidney disease
c) Electrolyte disturbance
38. Expansion for BIND
a) Bilirubin Induced Neurologic Dysfunction
b) Bilirubin Increased Neonatal Disorder
c) Bilirubin Induced Nerve Disorder
39. Precaution measures to be taken before collecting the blood sample
a) Check the temperature
b) Turn off lights
c) Check baby condition

40. Complication of acute bilirubin encephalopathy
a) Cerebral palsy and hearing impairment
b) Seizure and blindness
c) Respiratory distress and sepsis

Key answers:
1. (a)
2. (b)
3. (c)
4. (a)
5. (a)
6. (b)
7. (b)
8. (a)
9. (b)
10. (c)
11. (b)
12. (a)
13. (a)
14. (a)
15. (a)
16. (b)
17. (a)
18. (b)
19. (c)
20. (b)
21. (c)
22. (a)
23. (a)
24. (b)
25. (c)
26. (a)
27. (c)
28. (a)
29. (a)
30. (a)
31. (b)
32. (a)
33. (a)
34. (b)
35. (b)
36. (a)
37. (a)
38. (a)
39. (b)
40. (a)
COLLEGE OF NURSING MADRAS MEDICAL COLLEGE, CHENNAI-03
STRUCTURED TEACHING PROGRAM ON
CARE OF NEWBORN DURING PHOTOTHERAPY

TOPIC : CARE OF NEWBORN DURING PHOTOTHERAPY
GROUP : DGNM II YEAR STUDENTS
PLACE OF TEACHING : NEONATAL INTENSIVE CARE UNIT
DURATION : 45 MINUTES
METHOD OF TEACHING : LECTURE CUM DISCUSSION
MEDIUM OF TEACHING : ENGLISH
TEACHING AIDS : POWERPOINT AND INFORMATION BOOKLET
RESEARCH GUIDE : MRS.S.VIJAYALAKSHMI, M.Sc (N)., READER
HOD-CHILD HEALTH NURSING, COLLEGE OF NURSING,
MADRAS MEDICAL COLLEGE, CHENNAI-03.
NAME OF THE INVESTIGATOR : R.REVATHY, M.Sc (N) II YEAR
CHILD HEALTH NURSING

CENTRAL OBJECTIVE:
At the end of the class the student will be able to acquire knowledge and understanding regarding care of newborn
during phototherapy and to develop desirable skill and attitude to practice this in all health care settings.
CONTRIBUTORY OBJECTIVE
At the end of the class, students will be able to
1. define the term neonatal hyperbilirubinemia
2. mention the causes of hyperbilirubinemia
3. describe about the diagnostic measures of neonatal jaundice
4. define the term phototherapy
5. enlist the purposes of phototherapy
6. list out the indications of phototherapy
7. specify the types of phototherapy
8. discuss the mechanism of action of phototherapy
9. explain about the care and observation during phototherapy

S.NO
TIME
SPECIFIC
OBJECTIVES
CONTENT TEACHERS
ACTIVITY
LEARNERS
ACTIVITY
AV
AIDS
EVALUATI
ON
1 min
Introduction to
the topic
INTRODUCTION:
Phototherapy is the important procedures in New born care
setting. About 1 out of 2 of term and 8 out of 10 of preterm
babies develop jaundice, which generally appears 2 to 4 days
after birth, and resolves spontaneously after 7-14 days. In
most infants with physiological jaundice bilirubin levels do
not rise to a point that requires treatment. Effective treatments
to decrease serum bilirubin levels with severe jaundice
include phototherapy. It is a vital one to save the life of many
new born when perform at correct time. It needs special skills
and techniques to do the procedures. The students should be
specially trained, to assist the procedures tactfully.
Explaining
Listening
Power
point


S.No
1.
2.
Time
2 min
3 min
Specific
objectives
define the term
neonatal hyper -
bilirubinemia
mention the
causes of hyper-
bilirubinemia
Content
DEFINITION OF NEONATAL
HYPERBILIRUBINEMIA.
It is the elevation of the bilirubin level in the newborn's
blood, which results in yellowish staining of the skin and
whites of the newborn's eyes (sclera) by pigment of bile
(bilirubin). In newborn babies, a degree of jaundice is normal.
CAUSES OF HYPERBILIRUBINEMIA
Physiological Jaundice:
Occurs in 60% of term and 80% of preterm infants.
The newborn has a high level of hemoglobin combined with a
short red cell life leading to a high rate of haemolysis whilst
the body mass bilirubin production is more than double in the
neonate. Jaundice usually occurs at 2-3 days of life and has
resolved by 7-14 days of life. 3 weeks in preterm infant.
Breastfeeding Jaundice:
Occurs in 10% of newborns when the infant does not
Teachers
activity
Explaining
Explaining
Learners
activity
Listening
Listening
Av aids
Power
point
Power
point
Evaluation
What is
neonatal
hyperbilirub
inemia?
What are
the causes
of
hyperbilirub
inemia?

S.No
Time
Specific
objectives
Content
drink enough breast milk and is similar to physiological
jaundice but is more pronounced.
Breast-Milk Jaundice:
This occurs in 1-2% of breast fed babies and is caused
by a substance that is produced in the breast milk. Jaundice
starts at 3-5 days of age and can last 3-12 weeks (occasionally
up to 16 weeks).
ABO Blood Group Incompatibility and Rhesus
Incompatibility (Haemolysis):
These can occur if the mother produces antibodies that
destroy the newborn‟s red cells, resulting in haemolysis of the
infant‟s blood. This leads to a sudden buildup of bilirubin in
the infant‟s circulation during the first 24hrs of life
Other Pathological Causes:
Sepsis, endocrine /metabolic disorders, bile duct
obstruction, G6PD deficiency.
Teachers
activity
Explaining
Learners
activity
Listening
Av aids
Power
point
Evaluation

S.No
3.
Time
4 min
Specific
objectives
describe about
the diagnostic
measures of
neonatal jaundice
Content
DIAGNOSIS OF JAUNDICE:
A serum bilirubin level will be used in conjunction with
signs and symptoms of jaundice. The serum bilirubin level
along with the gestational age and postnatal age will be
plotted on the „Treatment Threshold Graph‟. This will be
plotted by the neonatal/medical team.
It is necessary to proceed more cautiously if the serum is
above certain levels (i.e. conjugated bilirubin level greater
than 25micromol /litre) due to the potential consequences of
serious potentially. Irreversible liver disease. Pale stools / dark
urine also indicate conjugated hyperbilinaemia.
Kramer‟s rule:
Estimating the level of jaundice by simply observing the
baby‟s skin color, one can utilize cephalocaudal progression
of jaundice.
kramers divided the infant in to 5 zones, the ranges associated
with progression to the zones as follows:
Teachers
activity
Explaining
Learners
activity
Listening
Av aids
Power
point
Evaluation
What are
the
diagnostic
measures of
neonatal
jaundice?

Zone 1 2 3 4 5
SBR
UMol/L
100 150 200 250 >250
BLANCHING:
Blanching the skin of tip of nose, sternum, abdomen, palms
and soles with digital pressure. In accordance with kramer‟s
guidelines a rough estimate of the bilirubin level can be made
as follows
Area of body Level of bilirubin
Face 5mg/dl
Chest/upper abdomen 10mg/dl
Lower abdomen and thighs 12mg/dl
Arms and lower legs 15mg/dl
Palms and soles >15mg/dl
explaining
listening
Power
point

ICTEROMETER:
This is non invasive method which is more accurate and less
subjective. The tool used is a transparent plastic with 5 graded
yellow stripes of different shades corresponding to the serum
bilirubin level. It is pressed against the tip of the nose. The
color of the skin is matched with yellow stripes to obtain the
bilirubin level.
Transcutaneous bilirubinometer:
The photo probe is pressed against the skin of fore head or
sternum. When pressure is applied to the photo probe a xenon
tube generates a strobe light. This light passes through a fibre
optic filament penetrates the blanched skin and enters the
subcutaneous tissue. The intensity of the yellow color in this
light, after correcting for the haemoglobin, is measured and
instantly displayed in arbitrary unit.
Explaining
Listening
Power
point

4.
5.
6.
1 min
2 min
2 min
define the term
phototherapy
enlist the
purposes of
phototherapy
list out the
indications of
phototherapy
DEFINITION OF PHOTOTHERAPY:
A treatment for jaundice where the exposure to
ultravioletlight source converts unconjugated bilirubin
molecules into water soluble isomers that can be excreted by
the usual pathways. Blue-green light is most effective for
phototherapy as it both penetrates the skin and is aborted by
bilirubin to have the photochemical effect.
PURPOSES:
To bring down the serum bilirubin level
Treatment of Hyperbilirubinemia.
The phototherapy will help the liver to process
bilirubin, bringing your baby‟s level down to normal
INDICATIONS OF PHOTOTHERAPY:
Elevated serum bilirubin levels:
Explaining
Listening
Power
point
What is
phototherapy
What is the
purpose of
phototherapy
What is the
indication of
phototherapy

7.
3 min
specify the types
of phototherapy
Healthy term babies >17mg/dl
Preterm babies (weighting more than 1500g:>8mg/dl)
Preterm babies (weighting less than 1500g >5 mg/dl).
Severely bruising.
TYPES OF PHOTOTHERAPY:
Continuous phototherapy
Conventional phototherapy
Intensive phototherapy
Continuous phototherapy:
It is better than intermittent phototherapy. Phototherapy
should be interrupted in a newborn only during breast feeding
and nappy changes.
Conventional phototherapy:
If jaundice is non- haemolytic or rate of rise of jaundice is
slow, then one can use either conventional or fiber optic
phototherapy.
Intensive phototherapy:
In case of haemolytic or rapidly rising bilirubin or when a
Explaining
Listening
Power
point
What are the
types of
phototherapy
?

8.
7 min
discuss the
mechanism of
action of
phototherapy
conventional until is not effective, use of intensive
phototherapy is needed. This can be achieved by placing the
infant in the bili blanket and using additional overhead
phototherapy implies irradiance in the blue green spectrum
have the wavelength of approximately 425-490nm delivered
to infants surface area as possible.
MECHANISM OF ACTION:
Bilirubin is a naturally occuring molecule of the red blood
cells. It is released into blood stream .when the red blood cells
break down. This is normal and occurs often. Our livers
breakdown the bilirubin and it is excreted.
Phototherapy (light treatment) is the process of using light
to eliminate bilirubin in the blood. Your baby‟s skin and blood
absorbs these light waves. These light waves are absorbed by
your baby‟s skin and blood and change bilirubin into
products, which can pass through their system.Wavelength of
420-448nm, oxidised the bilirubin to biliverdin,a soluble
product that does not contribute to kernicterus.
Explaining
Listening
Power
Point
What is the
mechanism
of action of
phototherapy
?

The light waves convert the bilirubin to water soluble
nontoxic forms which are then easily excreted. Some
bilirubin, are present in the interstitial spaces and superficial
capillaries of the skin, subcutaneous tissues. During
phototherapy, these molecules are exposed to light. The
photons of energy are absorbed by the pigment, bilirubin. This
leads to a sequence of photochemical reactions:
1.CONFIGURATIONAL ISOMERIZATION:
Z-isomer E-isomer
Reversible as it reaches bile duct
Constitute 25% of TSB after 8-12hrs.
Excreted slowly from body.
2.STRUCTURAL ISOMERIZATION:
Bilirubin lumirubin
This reaction is directly proportional to the dose of
phototherapy. Converts 2-6% of TSB, which is excreted
Explaining
Listening
Power
point

9.
20
min
explain about the
care and
observation
during
phototherapy
rapidly from Body.
3. PHOTO OXIDATION:
Forms photo products that are excreted in the urine
CARE AND OBSERVATION DURING
PHOTOTHERAPY
1.GENERAL INSTRUCTION
Recognize the possible need for phototherapy based on
risk factors and blood testing. This will assist in the
prompt and timely detection and treatment of jaundice.
Perform a physical assessment of the infant to assess
for the presence of jaundice.
The infant should be stripped down to perform an
accurate assessment.
Where possible perform assessment in bright, natural
daylight. Artificial light can make it more difficult to
accurately assess for jaundice.
Jaundice can be detected by blanching the skin with
digital pressure.
The baby should be observed; the gums and sclera of
Explaining
Listening
Power
point
How will
you care the
baby during
phototherapy
?
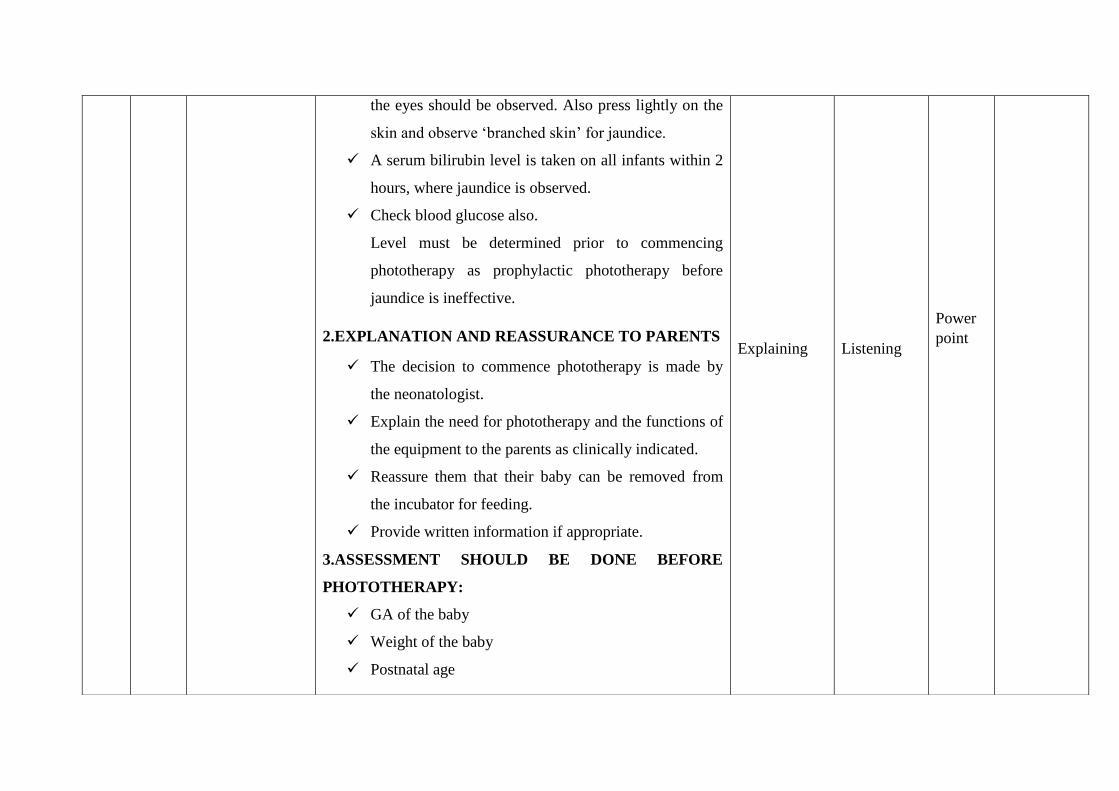
the eyes should be observed. Also press lightly on the
skin and observe „branched skin‟ for jaundice.
A serum bilirubin level is taken on all infants within 2
hours, where jaundice is observed.
Check blood glucose also.
Level must be determined prior to commencing
phototherapy as prophylactic phototherapy before
jaundice is ineffective.
2.EXPLANATION AND REASSURANCE TO PARENTS
The decision to commence phototherapy is made by
the neonatologist.
Explain the need for phototherapy and the functions of
the equipment to the parents as clinically indicated.
Reassure them that their baby can be removed from
the incubator for feeding.
Provide written information if appropriate.
3.ASSESSMENT SHOULD BE DONE BEFORE
PHOTOTHERAPY:
GA of the baby
Weight of the baby
Postnatal age
Explaining
Listening
Power
point

Types of jaundice
The level of jaundice
4.OBSERVATIONS
Neonates must be weighed on admission to the nursery
and then 2nd daily and documented as per protocol
weight-length-head circumference on the Neonatal
Weight Chart.
Monitor the infant‟s temperature more frequently
when commencing phototherapy and once stabilised,
record at least 4th hourly.
Preterm / unwell infants receiving phototherapy should
have temperature, pulse, respiration rate and oxygen
saturation monitored and documented 1- 4th hourly on
the appropriate observation chart.
The date and time phototherapy is commenced /
discontinued, the type of phototherapy device (s) and
the dose of phototherapy should be documented on the
Neonatal Jaundice Control Form.
5.ADMINISTERING PHOTOTHERAPY:
Make sure room temperature is optimum 25-280c
Remove all clothes of baby except diaper.
Explaining
Listening
Power
point
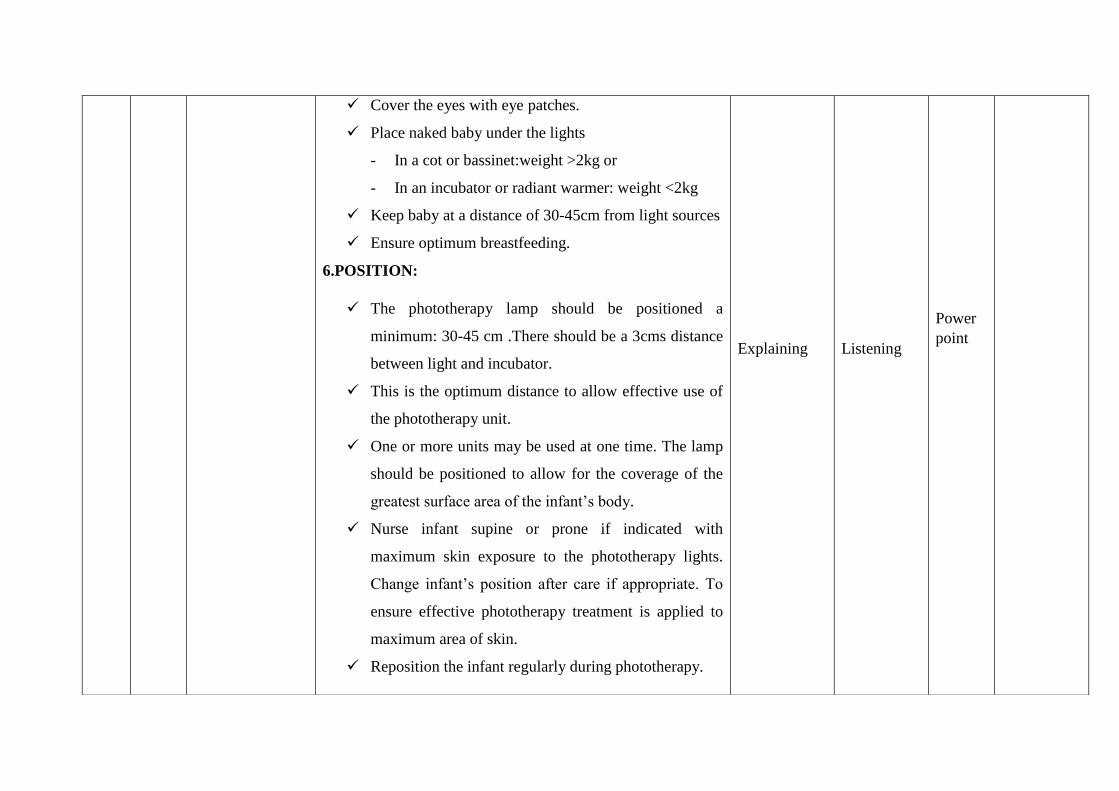
Cover the eyes with eye patches.
Place naked baby under the lights
- In a cot or bassinet:weight >2kg or
- In an incubator or radiant warmer: weight <2kg
Keep baby at a distance of 30-45cm from light sources
Ensure optimum breastfeeding.
6.POSITION:
The phototherapy lamp should be positioned a
minimum: 30-45 cm .There should be a 3cms distance
between light and incubator.
This is the optimum distance to allow effective use of
the phototherapy unit.
One or more units may be used at one time. The lamp
should be positioned to allow for the coverage of the
greatest surface area of the infant‟s body.
Nurse infant supine or prone if indicated with
maximum skin exposure to the phototherapy lights.
Change infant‟s position after care if appropriate. To
ensure effective phototherapy treatment is applied to
maximum area of skin.
Reposition the infant regularly during phototherapy.
Explaining
Listening
Power
point

7.MAINTAINING TEMPERATURE
The infant will be nursed in an incubator or radiant
warmer with only a nappy in place.
The incubator should be dressed with white linen.
The infant‟s temperature should be monitored and
recorded at least 4 hourly or more frequently as
clinically indicated.
Monitor and record incubator temperature hourly.
To ensure infant does not become cold stressed,
hypothermic or hyperthermia due to removal of
clothing or exposure to phototherapy lights.
8.DURATION OF PHOTOTHERAPY
The infant may be removed from the lights for
feeding, diaper changes and other general care but
should receive phototherapy for 18 hours every day.
Explaining
Listening
Power
point

9.BREAST FEEDING
Provide the mother who is breast feeding with the
necessary support and advice to allow her to continue
breastfeeding or to express milk if required.Frequent
feeding may help to break down the bilirubin if the
cause of the jaundice is due to breast milk or
breastfeeding.
The infant may need to be breastfed 8-12 times a day.
The newborn stomach has a capacity of 30mls
approximately. It can also promote bonding.
Feed the baby every 2-3 hours because phototherapy
causes the baby to lose fluid from the skin and have
loose stools. This may cause dehydration.
10.SKIN CARE
A more rapid response to treatment can be achieved by
exposing larger surface areas to the phototherapy light.
For infants with a rapidly rising serum bilirubin level,
for example ABO incompatibility, the maximum area
of skin should be exposed. This may require use of
Explaining
Listening
Power
point

double phototherapy and removal of the nappy.
Keep the infant clean and dry.
Cleanse skin thoroughly and change nappies when
soiled.
The registered nurse/ enrolled nurse should be
proactive with early use of barrier creams if stools are
loose and green.
Infants nursed in nappies or where the buttocks are not
directly exposed to the phototherapy may have zinc
and castor oil applied to areas of skin excoriation.
Oils and creams are not routinely applied to
phototherapy exposed skin however if LED
phototherapy is used, emollients and creams may be
used with caution (LED technology uses “cold light”).
Clean only with water. Do not apply oils or creams to
the exposed skin.
Observe the skin for rashes, dryness and excoriation.
11.RESPIRATORY MONITORING
Infants must be weighed on admission to the nursery
and 2nd
daily as per the protocol.
All infants in newborn care receiving phototherapy
Explaining
Listening
Power
point

should have a temperature, pulse, respiration rate
documented 4th
hourly.
12.EYE CARE:
There has been some speculation about an association
between neonatal phototherapy and retinopathy of
prematurity (ROP).
Eye shields (opaque) must be placed over the infant‟s
eyes at all times during phototherapy. As a prophylaxis
and to protect against retinal damage that can occur
due to irradiance from phototherapy light.
Eye pads are required for the infants comfort if
overhead white or blue fluorescent lights are used:
Size N 720(micro)<1500gm
Size N 721(small) 1500-2500gm
Size N 722(Large)>2500gm.
Ensure the eye patches are not applied too tight, as
they may apply undue pressure to the infant's delicate
eye.
Ensure the infant‟s eyes are closed when positioning
the eye shields. To prevent corneal abrasions.
Eye care should be performed 4th
hourly and eye cares

attended with normal saline and assess eyes for
drainage, oedema and evidence of infection Allow
visual stimulation at this time.
Ensure the phototherapy unit is switched off, before
removing the eye shields.
To protect against retinal damage that can occur due to
irradiance from phototherapy light .
Check baby at least every hour and see that the eye
Shields remain in place. The eye shields should not press
against the eyes.
13.FLUID REQUIREMENTS:
The requirements for fluids and electrolytes of the
newborn infant are unique. At birth, there is an excess of
extra-cellular water (ECW), and this decreases over the first
few days after birth. Furthermore, ECW at birth and
insensible water loss decrease as birth weight and gestational
age increase.
Several days after birth, fluid and electrolyte
requirements increase as the infant starts to grow. Therefore,
appropriate management of fluids and electrolytes in preterm
Explaining
Listening
Power
point

infants must take into consideration the birth weight,
gestational age and age after birth. Fluid and electrolyte
requirements are also influenced by a variety of medical
conditions that affect preterm infants.
INSENSIBLE WATER LOSS (IWL) is greatest in the
smallest and least mature infants due to high surface area to
body mass ratio and to immature, water-permeable skin.
Estimated IWL in the first few days of life are:
Phototherapy can increase IWL by 25-50%. IWL may
exceed urinary output in smaller infants but, unlike urine
output, IWL cannot be measured directly. However, IWL
must be estimated in order to plan appropriate fluid
management.
IWL can be estimated by: IWL = Fluid intake - Urine
output + weight loss (or – weight gain)
(E.g., 24-hour totals = Intake 90 mL, urine output 60 mL, and
weight loss 55 g. Therefore, IWL = 90 - 60 + 55 = 85 mL).
Monitor the infant‟s intake and output closely.
explaining
listening
Power
point

Weigh nappies to monitor output.
Maintain strict fluid balance chart.
Daily urinalysis for specific gravity or the infant may
experience poor feeding due to lethargy caused by
hyperbilirubinaemia and may require enteral feeding
for a short period.
To ensure adequate nutrition / calorie intake to
maintain enzyme activity for degeneration of bilirubin.
Phototherapy increases insensible water loss by 30
50% and poor hydration also slows bilirubin excretion.
The fluid intake may need to be increased 20ml/kg
14.MONITRING SERUM BILIRUBIN:
Obtain 6-24 hourly serum bilirubin level as determined
by age and clinical condition of the infant as clinically
indicated, following commencing phototherapy. To
monitor and evaluate the effectiveness of treatment.
NICE recommend 6 hourly testing for first 24 hours
until SBR below treatment threshold or stable / falling.
Turn off lights prior to obtaining sample. Conjugated
and unconjugated bilirubin are photo oxidized when
exposed to white or ultraviolet lights and haemolysis
Explaining
Listening
Power
point

.
can give false lower results.
WHEN TO STOP PHOTOTHERAPY
TERM BABIES:
Day <3 stop at the discretion of the consultant as the
jaundice like to be pathological.
Day > 4 : stop phototherapy for term infants with
physiological jaundice.
PRE MATUTRE BABIES:
Stop at the discretion of the consultant.
REBOUND BILIRUBIN LEVELS:
It is unnecessary to keep a baby in hospital for a
rebound bilirubin level.
If a baby does not appear visibly jaundiced 48hours
after stopping phototherapy then they do not require a
repeat bilirubin level.
Term babies who are re admitted for phototherapy
explaining
listening
Power
point

(usually between day 3-6) for physiological jaundice
do not require a routine rebound level after lights are
stopped.
Reasons to check a rebound bilirubin 24hours after
stopping phototherapy may include:
a) < 37 weeks gestation
b) Bruising
c) Early use of phototherapy (started <72 hours of
age)
Consider using trancutaneous bilirubinometer to assess the
need for further bilirubin levels to prevent unnecessary blood
tests.
YPAREHTOTOHP FO STCEFFE EDIS
emordnys ybab eznorB
it is the dark grey – brown pigmentation of skin
mucous both upper and lower limb after receiving
phototherapy for neonatal jaundice.no treatment is
required for bronze baby syndrome as the
pigmentation slowly disappears after stopping
phototherapy.
Explaining
Listening
Power
point

Greenish
era stnemevom lewob ybab,yparehtotohp gniruD
dna lamron si siht.roloc hsineerg a dna esool semitemos
.spots tnemtaert nehw pots dluohs
sehsar niks tnetsisnarT
Multiple white or yellow skin rash characterised by
erythematous of the skin that can develop in infants
after initiation of phototherapy.
Poor feeding – Infants with jaundice are often sleepy
and do not wake for feeds. Assess infant attachment
and suck and hydration on admission. Use of
expressed breast milk via bottle or intra gastric tube
may be necessary for some infants.
Temperature instability – can occur in infants under
radiant warmers or in closed care systems – monitor
closely. Now less likely to occur with the LED
phototherapy systems.
Loose stools and peri-anal excoriation – due to
transient lactose intolerance • Increased insensible
water loss – this can be managed by increasing the
daily fluid requirements if required. This is assessed
explaining
listening
Power
point

on a case by case basis.
Maternal-infant separation – otherwise well late
preterm / term infants should be managed on the
postnatal ward when appropriate and safe to do so.
hyperthermia-
Increasing metabolic rate
Dehydration
Electrolyte disturbance.
explaining
listening
Power
point

SUMMARY
So far, we discussed about the definition of phototherapy, Phototherapy is the light treatment for newborn jaundice. Newborn
jaundice is excess bilirubin in your newborn‟s blood, About the Mechanism of actions naturally occurring molecule of the red blood
cells, nursing care given to newborn in phototherapy These light waves are absorbed by your baby‟s skin and blood change bilirubin into
products, which can pass through their system, Wavelength of 420-448nm, oxidized the bilirubin, a soluble product that does not
contribute to kernicterus. Check your baby‟s blood pressure, heart rate, breathing rate, advantages of phototherapy are preventing the
needs for more invasive treatment and the serious complications, which can occur if excessive levels of bilirubin, phototherapy is a safe.
Effective method of treatment and temperature. These vital signs give healthcare providers information about your baby‟s condition.
RECAPTULIZATION:
1. What is the neonatal hyperbilirubinemia?
2. What are the causes of hyperbilirubinemia?
3. What are the diagnostic measures of neonatal jaundice?
4. What is phototherapy?
5. What is the purpose of phototherapy?
6. What is the indication of phototherapy?
7. What are the types of phototherapy?
8. What is the mechanism of action of action of phototherapy?
9. How will you care the newborn during phototherapy?

BIBLIOGRAPHY
1. Achar‟s (2003). TEXT BOOK OF PEDIATRICS (3rded,). New Delhi: orient Longman publishers.
2. Dorothy R. Marlow, Barbara A. Redding (2002). TEXT BOOK OF PEDIATRIC NURSING (6thed,). New Delhi. Saunders
publishers.
3. Ghai o. piyushguptha, Paul V.K (2004) ESSENTIAL PEDIATRICS (6TH ED,). New Delhi. GBS Publishers and distributors.
4. Marilyn J. Huckleberry (2005). WONG‟S ESSENTIAL OF PEDIATRIC NURSING (7thed,). New Delhi. Reed Elsevier India
private limited.
5. Parul dutta (2009) PEDIATRIC NURSING (2nded,). New Delhi. Brothers‟ medical publishers (P) LTD.
6. Suraj Gupte (2009). THE SHORT TEXT OF PEDIATRICS (11thed,). New Delhi. Reed Elsevier India private limited.
7. Tambulwadkar R.S. (1999). PEDIATRIC NURSING (2nded,) Bombay: Vora medical publishers

COLLEGE OF NURSING
MADRAS MEDICAL COLLEGE, CHENNAI
Information booklet ON CARE OF
NEWBORN DURING PHOTOTHERAPY

INTRODUCTION
Phototherapy is the important procedures
in New born care setting. About 1 out of 2
of term and 8 out of 10 of preterm babies
develop jaundice, which generally appears
2 to 4 days after birth, and resolves
spontaneously after 7-14 days.
Effective treatments to decrease serum
bilirubin levels with severe jaundice
include phototherapy. It is a vital one to
save the life of many new born when
perform at correct time. It needs special
skills and techniques to do the procedures.
The students should be specially trained to
assist the procedures tactfully.
HISTORY OF PHOTOTHERAPY
It was in the 19th
century that the use of
artificial light sources for phototherapy
happened.
Prof.nielsRybergFinsen is known as the
father of phototherapy.
He was the Nobel prize winner in
physiology and medicine in 1903,for his
remarkable work, since many works in the
pathway of phototherapy have been done.
NEONATAL
HYPERBILIRIUBINEMIA
It is the elevation of the bilirubin level in
the newborn‟s blood, which results in
yellowish staining of the skin and eyes
(sclera) by pigment of bile (bilirubin).
CAUSE OF HYPERBILIRUBINEMIA
Physiological Jaundice: Jaundice usually
occurs at 2-3 days of life and has resolved
by 7-14 days of life. 3 weeks in preterm
infant.
Breast-Milk Jaundice: This occurs in 1-
2% of breast fed babies and is caused by a
substance that is produced in the breast
milk. Enzyme activity in the infant‟s liver,
slows the breakdown and secretion of
bilirubin. Jaundice starts at 3-5 days of
age and can last 3-12 weeks.
ABO Blood Group Incompatibility and
Rhesus Incompatibility (Haemolysis):
These can occur if the mother produces
antibodies that destroy the newborn‟s red
cells, resulting in haemolysis of the
infant‟s blood. This leads to a sudden
build-up of bilirubin in the infant‟s
circulation during the first 24hrs of life.
DIAGNOSIS OF JAUNDICE: The
serum bilirubin level along with the
gestational age and postnatal age will be
plotted on the „Treatment Threshold
Graph”

KRAMER‟S RULE: Estimating the level
of jaundice by simply observing the baby‟s
skin color, one can utilize cephalocaudal
progression of jaundice
Zone 1 2 3 4 5
SBR
UMol/
L
100 150 200 250 >250
BLANCHING: Blanching the skin of tip
of nose, sternum, abdomen, palms and
soles with digital pressure.
ICTEROMETER:
This is non invasive method which is more
accurate and less subjective. The tool used
is a transparent plastic with 5 graded
yellow stripes of different shades
corresponding to the serum bilirubin level.
It is pressed against the tip of the nose. The
color of the skin is matched with yellow
stripes to obtain the bilirubin level.
TRANSCUTANEOUS
BILIRUBINOMETER:
The photo probe is pressed against the skin
of fore head or sternum. When pressure is
applied to the photo probe a xenon tube
generates a strobe light. This light passes
through a fiber optic filament penetrates
the blanched skin and enters the
subcutaneous tissue. The intensity of the
yellow color in this light, after correcting
for the haemoglobin, is measured and
instantly displayed in arbitrary unit.
Area of body Level of bilirubin
Face 5mg/dl
Chest/upper
abdomen
10mg/dl
Lower abdomen and
thighs
12mg/dl
Arms and lower legs 15mg/dl
Palms and soles >15mg/dl

DEFINITION OF PHOTOTHERAPY
A treatment for jaundice where the
exposure to ultravioletlight source converts
unconjugated bilirubin molecules into
water soluble isomers that can be excreted
by the usual pathways.Blue-green light is
most effective for phototherapy as it both
penetrates the skin and is aborted by
bilirubin to have the photochemical effect.
PURPOSES
To bring down the serum bilirubin
level
Treatment of Hyperbilirubinemia.
The phototherapy will help the
liver to process bilirubin, bringing
your baby‟s level down to normal.
INDICATION OF PHOTOTHERAPY
Elevated serum bilirubin levels:
Healthy term babies >17mg/dl
Preterm babies (weighting more
than 1500g:>8mg/dl)
Preterm babies (weighting less than
1500g >5 mg/dl).
Severely bruising
TYPES OF PHOTOTHERAPY
Continuous phototherapy: Phototherapy
should be interrupted in a newborn only
during breast feeding and nappy changes.
Conventional phototherapy: If jaundice
is non- haemolytic or rate of rise of
jaundice is slow, then one can use either
conventional or fiber optic phototherapy.
Intensive phototherapy: In case of
haemolytic or rapidly rising bilirubin or
when a conventional until is not effective,
use of intensive phototherapy is needed.
DIFFERENT LIGHTS USED IN
PHOTOTHERAPY
1. Micro-lite – white halogen
lightsThese should be positioned above
the infant and can deliver 10 to 30 µ
W/cm2/nm. They deliver light via a quartz
halogen bulb and have a tendency to
become quite hot so should not be
positioned closer to the infant than the
manufacturers recommendations of 52cm.
2.Fluoro-lite-2 blue and 2 white
fluorescent lights
Blue light is the most effective light for
reducing the bilirubin.

3. Ohmedabiliblanket -blue
halogen light This uses a halogen bulb directed into a
Fiberoptic mat. There is a filter that
removes the ultraviolet and infrared
components and the eventual light is a
blue-green colour.
4.Biliblankets: are not to be used on
infants less than 28 weeks gestation or
infants with broken or reduced skin
integrity.
5. MedelaBilibed – blue
fluorescent light A blue fluorescent tube is fitted into a
plastic crib with a stretched plastic cover
over the top for the baby to lie on. The
baby is dressed in the Bilicombibaby suit
and nursed on the soft plastic cover.
MECHANISM OF ACTION
Phototherapy (light treatment) is the
process of using light to eliminate bilirubin
in the blood. Your baby‟s skin and blood
absorbs these light waves. These light
waves are absorbed by your baby‟s skin
and blood and change bilirubin into
products, which can pass through their
system.
Wavelength of 420-448nm, oxidised the
bilirubin to biliverdin,a soluble product
that does not contribute to kernicterus. The
light waves convert the bilirubin to water
soluble nontoxic forms which are then
easily excreted.
During phototherapy, these molecules are
exposed to light.
The photons of energy are absorbed by the
pigment, bilirubin. This leads to a
sequence of photochemical reactions:
1. ConfigurationalIsomerisation:
Z-isomer E-isomer
Reversible as it reaches bile duct
Constitute 25% of TSB after 8-
12hrs.
Excreted slowly from body
.
2. Structural Isomerisation:
Bilirubin lumirubin
This reaction is directly
proportional to the dose of
phototherapy.
Converts 2-6% of TSB,which is
excreted rapidly from Body.
3. Photo Oxidation:
Forms photo products that are excreted
in the urine
CARE AND OBSERVATION OF
NEWBORN DURING
PHOTOTHERAPY

1. GENERAL INSTRUCTION
Recognize the possible need for
phototherapy based on risk factors and
blood testing. .
Perform a physical assessment of the
infant to assess for the presence of
jaundice.
Where possible perform assessment in
bright, natural daylight. Artificial light
can make it more difficult to accurately
assess for jaundice.
Jaundice can be detected by blanching
the skin with digital pressure.
The baby should be observed; the
gums and sclera of the eyes should be
observed.
A serum bilirubin level is taken on all
infants within 2 hours, where jaundice
is observed.
Check blood glucose also.
Level must be determined prior to
commencing phototherapy as
prophylactic phototherapy before
jaundice is ineffective.
2. EXPLANATION AND
REASSURANCE TO PARENTS
The decision to commence
phototherapy is made by the
neonatologist.
Explain the need for phototherapy to
the parents as clinically indicated.
Reassure them that their baby can be
removed from the incubator for
feeding.
Provide written information if
appropriate.
The nurse is encouraged to use
clinical judgement to facilitate a
break from phototherapy of up to 30
minutes for feeding / bonding).
Explain to the parents, type of
jaundice, the infant is being treated,
what precautions will be taken and
thatthe lights being used do not
contain ultraviolet light.
3. ASSESSMENT SHOULD BE DONE
BEFORE PHOTOTHERAPY:
GA of the baby
Weight of the baby
Postnatal age
Types of jaundice
The level of jaundice
4. OBSERVATIONS
Neonates must be weighed on
admission to the nursery and then 2nd

daily and documented on theNeonatal
Weight Chart.
Monitor the infant‟s temperature more
frequently when commencing
phototherapy and once stabilised,
record at least 4th hourly.
All infants managed with overhead
phototherapy or with eye protection in
place, need a saturationmonitor .
The date and time phototherapy is
commenced / discontinued, the type of
phototherapy device (s) and the dose of
phototherapy should be documented on
the Neonatal Jaundice Control
Form.
5. ADMINISTER PHOTOTHERAPY:
Make sure room temperature is
optimum 25-280c
Remove all clothes of baby except
diaper.
Cover the eyes with eye patches.
Place naked baby under the lights
- In a cot or bassinet:weight>2kg
or
- In an incubator or radiant
warmer: weight <2kg
Keep baby at a distance of 30-45cm
from light sources
Ensure optimum breastfeeding.
6. POSITION:
The phototherapy lamp should be
positioned a minimum: 30-45 cm
This is the optimum distance to allow
effective use of the phototherapy unit.
One or more units may be used at one
time. The lamp should be positioned to
allow for the coverage of the greatest
surface area of the infant‟s body.
Nurse infant supine or prone if
indicated with maximum skin exposure
to the phototherapy lights.
Reposition the infant regularly during
phototherapy.
7. MAINTAINING TEMPERATURE
The infant will be nursed in an
incubator or radiant warmer with only
a nappy in place.
The incubator should be dressed with
white linen.

To ensure maximum exposure of the
infant to phototherapy. A „neutral
thermal environment‟ can be achieved.
The infant‟s temperature should be
monitored and recorded at least 4
hourly.
Observe skin temperature by “warm to
touch” method.
Monitor and record incubator
temperature hourly.
If baby is hypothermic, discontinue
phototherapy and keep baby exposed
under fan. When temperature reaches
normal, restart phototherapy.
8. DURATION OF PHOTOTHERAPY
The infant may be removed from the
lights for feeding, diaper changes and
other general care but should receive
phototherapy for 18 hours every day.
If Fiberoptic blanket is used, it should
be kept next to baby‟s skin at all times.
It is not necessary to cover the eyes if
blanket alone is used.
9. BREAST FEEDING
The infant may need to be breastfed 8-
12 times a day.
The newborn stomach has a capacity of
30mls approximately. It can also
promote bonding.
Feed the baby every 2-3 hours
because phototherapy causes the baby
to lose fluid from the skin have loose
stools. This may cause dehydration.
10. SKIN CARE
A more rapid response to treatment can
be achieved by exposing larger surface
areas to the phototherapy light. For
infants with a rapidly rising serum
bilirubin level, for example ABO
incompatibility, the maximum area
of skin should be exposed.
Keep the infant clean and dry.
Cleanse skin thoroughly and change
nappies when soiled.

Infants nursed in nappies or where the
buttocks are not directly exposed to the
phototherapy may have zinc and castor
oil applied to areas of skin excoriation.
For infants less than 27 weeks, the
topical emollient when applied
sparingly may be used while the infant
is receiving phototherapy.
Clean only with water. Do not apply
oils or creams to the exposed skin.
Observe the skin for rashes, dryness
and excoriation.
11. RESPIRATORY MONITORING
Infants must be weighed on admission
to the nursery and 2nd
daily as per the
protocol.
Infants under the blue fluorescent
lights need atleast saturation
monitoring as it is difficult to assess
the infants color under these lights.
12.EYE CARE:
There has been some association
between neonatal phototherapy and
retinopathy of prematurity (ROP).
For infant comfort, eye protection
(phototherapy masks) must be used for
all babies nursed under overhead
phototherapy.
When on home phototherapy the infant
does not require eye protection.
Eye shields (opaque) must be placed
over the infant‟s eyes at all times
during phototherapy.As a prophylaxis
and to protect against retinal damage
Eye pads are required for the infants
comfort if overhead white or blue
fluorescent lights are used:
Size N 720(micro)<1500gm
Size N 721(small) 1500-2500gm
Size N 722(Large)>2500gm.
Ensure they do not slip or too tight.
Ensure the infant‟s eyes are closed
when positioning the eye shields. To
prevent corneal abrasions.
Eye care should be performed
4th
hourly and eye cares attended with
normal saline and assess eyes for
drainage, oedema and evidence of
infection.

Ensure the phototherapy unit is
switched off, before removing the eye
shields. .
Check baby at least every hour and see
that the eye Shields remain in place.
13. FLUID REQUIREMENTS:
The requirements for fluids and
electrolytes of the newborn infant are
unique. At birth, there is an excess of
extra-cellular water (ECW), and this
decreases over the first few days after
birth
INSENSIBLE WATER LOSS (IWL) is
greatest in the smallest and least
Mature infants due to high surface area
to body mass ratio and to immature,
water-permeable skin. Estimated IWL
in the first few days of life are:
IWL can be estimated by: IWL = Fluid
intake - Urine output + weight loss (or –
weight gain)
(E.g., 24-hour totals = Intake 90 mL, urine
output 60 mL, and weight loss 55 g.
Therefore, IWL = 90 - 60 + 55 = 85 mL).
14.MONITRING SERUM BILIRUBIN:
Obtain 6-24 hourly serum bilirubin
level as determined by age and clinical
condition of the infant.
To monitor and evaluate the
effectiveness of treatment. NICE
recommend 6 hourly testing for first 24
hours until SBR below treatment
threshold or stable / falling.
Turn off lights prior to obtaining
sample. Conjugate and unconjugated
bilirubin is photo oxidized when
exposed to white or ultraviolet lights
and haemolysis can give false lower
results.
REBOUND BILIRUBIN LEVELS:
It is unnecessary to keep a baby in
hospital for a rebound bilirubin level.
If a baby does not appear visibly
jaundiced 48hours after stopping
phototherapy then they do not require a
repeat bilirubin level.
Term babies who are re admitted for
phototherapy (usually between day 3-
6) for physiological jaundice do not
require a routine rebound level after
lights are stopped.
BODY WEIGHT IN INCUBATOR
<1,000
1,000-1,500
1,500-2,000
>2,000
75-100
50
25-50
25-50

Reasons to check a rebound bilirubin
24hours after stopping phototherapy
may include:
d) < 37 weeks gestation
e) Bruising
f) Early use of phototherapy
(started <72 hours of age)
COMPLICATION OF
YPAREHTOTOHP
emordnys ybab eznorB
Greenish stool
Transistent skin rashes

Poor feeding
Temperature instability
Loose stools and peri-anal
excoriation
Maternal-infant separation
hyperthermia-
Increasing metabolic rate
Dehydration
Electrolyte disturbance

GUIDED BY:
Mrs.SeetharamanVijayalakshmi, M.Sc (N).,MBA.,
Reader in Child Health Nursing,
College of Nursing,
Madras Medical College,
Chennai – 03.
Dr. R. Shankar Shanmugam, M.Sc (N), MBA., Ph.D.,
Reader in Nursing Research,
College of Nursing,
Madras Medical College,
Chennai – 03.
STUDENT INVESTIGATOR:
Mrs .R. Revathy,
M.Sc (N) II year student,
Department ofChild Health Nursing,
College of Nursing,
Madras Medical College,
Chennai – 03.

INFORMED CONSENT
TITLE: “A study to assess the Effectiveness of structured teaching programme on
knowledge regarding care of newborn during phototherapy among II year DGNM
students at Institute of Child Health and hospital for children, Egmore, Chennai-
08”.
Sample no:
Name of participant:
Name of the principal investigator: R.REVATHY
Name of the Institution : Institute of Child Health and hospital for
children, Egmore, Chennai-08
Whether the participants consent was asked: yes/no
[If the answer to the above question is yes, write the following phrase: you agree
with the manner in which consent was asked from you and given by you. You
agree to take part in this study].
[If answer to the above question is no, give reason(s):
Name and signature or thumb impression of the participant legal representative.
Name ------------------------------ Signature---------------------------
Date--------------------
Name and signature of the investigator or his representative obtaining consent:
Name ------------------------------- Signature--------------------------
Date------------------

INFORMATION TO PARTICIPANTS
TITLE OF THE STUDY :“A STUDY TO ASSESS THE
EFFECTIVENESS OF STRUCTURED TEACHING PROGRAMME ON
KNOWLEDGE REGARDING CARE OF NEWBORN DURING
PHOTOTHERAPY AMONG II YEAR DGNM STUDENTS AT
INSTITUTE OF CHILD HEALTH AND HOSPITAL FOR CHILDREN,
EGMORE, CHENNAI-08”.
Investigator : REVATHY .R
Name of the Participant :
Date :
Age/sex :
You are invited to take part in this study. The information in this document is
meant to help you decide whether or not to take part. Please feel free to ask if
you have any queries or concerns.
You are being asked to Cooperative in this study being conducted in Institute
of Child Health and Hospital for Children, Egmore, Chennai-08.
What is the Purpose of the Research (explain briefly)
` This research is conducted to evaluate to,“ A study to assess the Effectiveness
of structured teaching programme on knowledge regarding care of newborn during
phototherapy among II year DGNM students at Institute of Child Health and
hospital for children, Egmore, Chennai-08”.
We have obtained permission from the Institutional Ethics Committee.
Study Procedures
Study will be conducted after approval of ethics committee
A written formal permission will be obtained from authorities of
Institute of Child Health and Hospital for Children to conduct study.
The purpose of study will be explained to the participants.
The investigator will obtain informed consent.
The investigator will assess the knowledge regarding care of newborn
during phototherapy.
Possible benefits to other people
The result of the research may provide benefits and also empathetic care
to them by investigator.
Confidentiality of the information obtained from you
You have the right to confidentiality regarding the privacy of your
personal details. The information from this study, if published in scientific
journals or presented at scientific meetings, will not reveal your identity.
How will your decision not to participate in the study affect you?
Your decisions not to participate in this research study will not affect
your activity of daily living, medical care or your relationship with investigator
or the institution.
Can you decide to stop participating in the study once you start?
The participation in this research is purely voluntary and you have the
right to withdraw from this study at any time during course of the study
without giving any reasons.
Your Privacy in the research will be maintained throughout study. In the
event of any publications or presentation resulting from the research, no
personally identifiable information will be shared.
Signature of Investigator: Signature of Participants:
Date: Date:






















