
Dissertation (1)
177
Ti tle: Children’s views (aged 9-10) about healthy eating: Comparing two exploratory case studies (to tackle/address childhood obesity). Au thor: Khajik Sirob Yaqob Da te: September 2013 Ins titution: 1
-
Upload
oxfordbrookes -
Category
Documents
-
view
5 -
download
0
Transcript of Dissertation (1)

Ti
tle:
Children’s views (aged 9-10) about healthy eating:
Comparing two exploratory case studies (to
tackle/address childhood obesity).
Au
thor:
Khajik
Sirob Yaqob
Da
te:
September
2013
Ins
titution:
1
The Westminster Institute of Education at Oxford
Brookes University;
ʻThis dissertation is submitted in partial fulfilment
of the requirements governing the award of the
Master of Arts in Childhood Studies’.
Statement of
originality
This Dissertation is an original piece of work which
is made available for photocopying and for
interlibrary loan, with permission of the Head of
School of Education.
Signed………………………………………………………….
2
Acknowledgments
Many thanks in particular to Professor Debra McGregor for her
help and support in the evolution of this project. I am
grateful for teachers and children from the Primary school
group and local Church cohort who gave so freely of their
time. Also, I would like to express appreciation to Georgina
Glenny, Nick Swarbrick and James Bird for their assistance in
the field work without whom this project would be
insurmountable.
Abstract:
This research study was designed to explore children’s (aged
9-10) beliefs about healthy eating and what they manage to eat
healthily. It was exploratory to the way that two different
groups of children conceptualized healthy eating to compare
between them. One was at a primary school cohort and another
at a local Church group. The same questionnaire comprised of
3
14 questions was administered to children in both cohorts with
the twenty-six year 9 and 10 participants to explore how they
perceived healthy eating. Total number of children (aged 9-10)
was 26, 19 at primary school group and 7 at local Church
cohort. Both cohorts were from the same ethnicity (whitish-
British), age, gender and low-middle socioeconomic states and
different level of education of parents.
Overall, findings from primary school age group were somewhat
concerning of such a school which has been already committed
to a healthy eating policy. Although children at primary
school age group were more likely to make healthy food choices
than those of the local Church group, (77.3% vs. 47.1%) 71%
favour to eat unhealthy foods. Other concerning finding
included, the indications that 26.3% of children at the
primary school group as compared to 28.5% of those in the
local Church group thought that pasta is made from cheese and
14.2% of children at local Church cohort believed that pasta
is made from meat. 10.5% of children at primary school cohort
perceived that egg is made from Cow and 5.2% believed that
Crisps is made from plastics. The results also suggest that
children in both cohorts had a different gender food
preference for the same quality of food they favoured. Rather
surprising findings were misconceptions of healthy and
unhealthy breakfast in both cohorts. 100% of children in the
local Church group as compared to 36.8% of those at primary
school cohort had knowledge of healthy eating from their
parents. Although findings from such a small sample is not
generalizable, results suggest that children had differences
4
in their understanding of healthy eating in both cohorts and
redirection of policy and practice in the school is required.
Key Words: children’s, beliefs, healthy eating, childhood
obesity, questionnaire, local Church group, primary school
cohort, exploratory comparative research study, two case
studies.
Contents
1.0
Introduction………………………………………………………………………….............
..... 9
2.0 Literature review………………………………………………………………………. 13
2.1 Mothers´ perceptions of obesity in their
children……………………… 13
2.1.1 Factors that raised maternal concerns
about childhood obesity.. 14
2.1.2 Maternal views of contributing
factors……………… 14
2.2 Men’s understandings of obesity…………………………………. 14
2.3 Children’s understandings about their own and
other bodies’ health…. 15
5
2.4 Cognition development and relation to healthy
eating………………. 18
2.5 The relevance of breakfast………………………………………………………….
21
2.5.1 Breakfast habits through the
world…………………………………. 22
2.5.2 Food choices for
breakfast……………………………………………….. 22
2.5.3 Children’s views on what represents a
healthy breakfast…. 23
2.5.4 What is a Balanced Breakfast Model?
…………………………….. 24
2.6 Fruits and vegetables (FV) consumption,
attitudes and beliefs towards FV
And peer/parent/teacher influences on
children’s FV attitudes…… 25
2.7 Children’s diets and relation to behaviour and
performance…………. 27
2.8 Children’s views about food
origin………………………………………………… 30
6
2.9 Children’s views on foods and consumption of
selected food groups… 30
2.10 Gender differences in food
preferences………………………………………… 31
3.0 Research design and
methodology………………………………………………… 32
3.1 Development of the
question…………………………………………………… 32
3.2 Rationale for this research
question………………………………………… 33
3.3 Quantitative vs. Qualitative
research……………………………………….. 33
3.3.1 Advantages and disadvantages of
a questionnaire survey….. 34
3.3.2 Advantages of interviewing and
issues for consideration…. 35
3.3.3 Shaping a case
study…………………………………………………………. 36
3.3.4 Issues to consider when
undertaking a case study…………… 39
7
3.3.5 Types of case
study…………………………………………………………… 40
4.0 Ethics………………………………………………………………………………………………. 40
5.0 Fieldwork period……………………………………………………………………………..
42
5.1 The participating school (first
group/cohort)………………………. 42
5.1.1 The local Church group (second
case study group/cohort)… 45
5.2 Data
collection……………………………………………………………………… 46
6. Data analysis………………………………………………………………………………………
47
6.1 Results of the questionnaire
survey for children………………… 47
6.2 Descriptive data and
findings………………………………………………… 47
6.2.1 Children’s responses to the
question regarding the definition of
Healthy eating (Q1)
………………………………………………………… 47
8
6.2.2 Source of knowledge for children
about healthy eating (Q2)… 49
6.2.3 Children’s knowledge regarding
healthy snack box contents
(Q3)
…………………………………………………………… 50
6.2.4 Matters children considered when
choosing food (Q4)……. 51
6.2.5 Children’s least and most
favorite food choices (Q5) ... 53
6.2.6 Children’s understandings
regarding “5 a day” (Q6)……… 56
6.2.7 Responses of children in both
groups about the question “Why
do you think calcium is an important part of your
diet”? (Q7)… 57
6.2.8 Children’s understandings of
fish as a healthy diet (Q8)……… 58
6.2.9 Children’s beliefs about fresh
fruits and vegetables as a healthy
9
Diet (Q9)
……………………………………………………………. 59
6.2.10 Children’s views regarding
water as an important part of a
Healthy diet (Q10)
…………………………………………… 60
6.2.11 Children’s knowledge regarding
a healthy person (Q11)… 62
6.2.12 Children’s perceptions about
food origin (Q12)…………. 63
6.2.13 Children’s habits of taking
breakfast (Q13)…………………. 65
6.2.14 Children’s knowledge of
healthier food choices (Q14)……. 69
7. Discussion………………………………………….. 72
7.1 Matters for consideration in choosing
food by children (Q4)…….. 72
7.2 Gender food preferences (Q5)……………………………
74
10

7.3 Children’s knowledge regarding healthy
person (Q11)…… 76
7.4 Children’s understandings about food
origin (Q12)………… 77
7.5 Children’s habits of eating breakfast
(Q13)……………… 78
7.6 Children’s knowledge of healthier food
choices (Q14)………. 80
7.7 Source of knowledge for children about
healthy eating (Q2)…. 81
8. Limitations………………………… 82
9. Conclusions ……………………………… 83
9.1 Conclusion of study of primary school
cohort……………………………. 84
9.2 Conclusion of survey of local Church
group……………………………….. 86
References………………….. 88
11

Appendices ………………………………………….. 104
Appendix 1: Letter to parents………………. 104
Appendix 2: Letter to head………………….. 105
Appendix 3: Ethical Approval Form ………. 106
Appendix 4: Questionnaire administered to cohort 1 &
2….. 111
Appendix 5: Cover letter for questionnaire ……….. 112
Appendix 6: Interview questions (devised in
preparation for school based research)……… 114
Appendix 7: Revised questionnaire (in light of
research findings)….. 116
Appendix 8: A (research informed) example Healthy
Eating policy for primary school……………. 117
Appendix 9: Tentative suggestions for guidelines that
parents should pay attention to (School or general
guidance)…….. 120
Appendix 10: More suggestions for shaping my
dissertation…………………. 122
12
1.0 Introduction
As a qualified general practitioner, I have long been
concerned with general health issues and notoriously concerned
with children’s (aged 9-10) perception of healthy eating. My
apprehension is increasing as a result of rising incidence of
childhood obesity and type 2 diabetes. Globally, 10% of all
children and 43 million children under 5 years are either
overweight or obese (Livingstone, 2013). This statistic
indicates there is a 60 % increase in childhood obesity over
two decades. My motivation to study this, therefore, I
intended to do this research study to explore children’s views
of healthy eating and to manage their misconceptions with the
appropriate education promotion of healthy eating in the
primary school. Also to make children further appreciate the13
dangers of childhood obesity through exploration and support
of their understandings about healthy eating.
However, my main challenges lay in reconciling my different
roles as a health practitioner, future teacher and educational
researcher. As a general practitioner, I already had some
experience of paediatric food and nutrition practices, but I
wanted better understand children’s views to promote healthy
eating education programs in primary schools. As a future
health educator, I wished to support staff in their teaching
about healthy eating education who in turn can improve child's
knowledge about healthy food; and finally, as an educational
researcher, I wanted to benefit the academic community by
contributing to the scholarly debate on this topic.
Obesity is defined as “abnormal or excessive fat accumulation
that might have a negative impact on health” (WHO, 2013).
Livingstone (2013) stated that Body Mass Index (BMI) as a
person’s weight in kilograms divided by the square of his
height in meters (kg/m2). A BMI greater than or equal to 25
is overweight and a BMI greater than or equal to 30 is obese.
Childhood obesity is defined as a BMI exceeding the 85th or the
95th percentiles (Reilly et al., 2003). BMI is an international
standardized way of defining of obesity in children, and it is
a simple index of weight for height often used to classify
obesity and overweight in adults (Livingstone, 2013).
Furthermore, BMI for children is gender and age specific as
BMI varies dramatically with age and sex as body fat changes
with growth and maturity. Therefore, to measure BMI in
14

different age and sex, specific growth reference charts are
needed. For instance, those produced by WHO, International
Obesity Task Force (IOTF), the U.S. Centres for Disease
Control and Prevention (CDC), and the British 1990 Growth
Reference (UK90) Standards. However, at different ages these
criteria give somewhat various estimates of overweight and
obesity prevalence. So, when we consider the lack of
nationally representatives’ surveys that measured heights and
weights of children over time, there is really an issue to get
a good handle of the prevalence of childhood obesity.
According to Livingstone (2013), childhood obesity is one of
the serious public health challenges in the 21st century
because of the negative impacts of childhood obesity on
childhood mental and physical health. For instance, very young
children are aware of the negative views hold by the society
in addition to poor self-esteem, depression, teasing and
discrimination by peers and the psychological impact of
childhood obesity might persist into adulthood. Also, the most
serious complication of childhood obesity is type 2 diabetes
which might result in obese middle age adults and early
dementia. Once childhood obesity is established, obesity is
notoriously difficult to treat. Nevertheless, childhood
obesity and its associated co-morbidities are largely
preventable. Obesity is the result of a complex interplay of
several factors; genetic, environmental (lifestyle and
dietary), cultural, socioeconomic and psychological factors.
Livingstone (2013) stated that childhood obesity is a real
issue as approximately 30% of obese children and 70% of obese15
adolescents will go on to become obese adults. Girls are more
likely to be affected than boys. The longer a child remains
obese beyond 3 years old the more likely that obesity will
persist into adulthood. Also, childhood obesity appears to
result in premature disability and premature death. Possibly
by 2020, worldwide, 9% of all preschool children
(approximately 60 million children) will be obese; if no
significant intervention is done. However, according to the
International Association for the study of obesity (IASO,
2012) the highest Prevalence of childhood obesity is in the
USA and this is followed by the UK and Australia (IASO, world
map of childhood obesity, 2012). Globally, the rates of
obesity are increasing in all countries and till late 1970s
the rates were static and started to increase in the early
1980s (Livingstone, 2013).
Recently, Jack Johnson (2013) stressed that the NCMP (National
Childhood Measurement Program) worryingly show that across
Oxford county 7% of children (aged 4-5) and almost 16% of
children (10-11) are clinically obese.
In Livingstone (2013) terms, Obesity is a result of chronic
imbalance between energy we ingest and energy we expend and
over 100 variables might impact directly or indirectly on
energy balance. Also, Gibney (2012) suggested that:
“If we give obesity a biological complexity score of 100, then cancer will score
10 and chronic heart diseases will score 1”.
Therefore, it is evident that, an unbalanced diet, low fruit
and vegetables and low physical activity, can lead to
16
childhood obesity, abnormal behaviour and low school
performances (Wheelock, 2007, p. 17).
Paquette (2005, p. S15) suggested, however, that it is
necessary to better appreciate the public’s perceptions of
healthy eating to assess how people interpret and use health
promotion messages in their daily life. This is essential to
develop successful healthy interventions. Others (Lupton and
Chapman, 1995; Lupton, 1996; Nestle, 2002; van Dillen et al.,
2003) assured that many components of foods must be studied to
determine their healthy value, e.g., type of fat. This is as a
consequence of evolution in nutritional science over the last
century which increased the complexity of the definition of
healthy foods. Consequently, people gather information on food
and nutrition from health professionals, television, food
labels and manufactures. They have to well understand the
advantages of this information and how to apply it in their
everyday life.
According to Paquette (2005, p. 15) perceptions of healthy
eating are defined as “the public’s (children, adolescents and
adults) and health professional understandings, meanings,
views, attitudes and beliefs about healthy eating, eating for
health and healthy foods”. The public’s perceptions of healthy
eating deemed to be heavily influenced by dietary guidance,
which recommend fruit and vegetables, meat, limitation of fat,
salt and sugar, variety, moderation, fresh and balanced food
(Health Canada, 1990, 1992; Paquette, 2005, p. 16).
17
Also, healthy eating is “the consumption of a wide variety of
fresh fruit, vegetables, legumes, whole grain cereal food and
protein-rich food” (Worsley and Crawford 2004). This is
suggested by the Australian guide to Healthy Eating (Smith et
al., 1998) and The Australian Dietary Guidelines for Children
and Adolescents (NHMRC, 2003). Healthy eating is significant
for children’s growth and development and to achieve their
best educational potential (NHMRC, 2003; Journal of the
American Dietic Association, 1999, pp. 93-101). Furthermore,
food preference and eating habits established in childhood
often persist into adulthood; children are appropriate target
group to positively influence dietary habits (Nu et al., 1996;
Skinner et al., 2002; Nicklas et al., 2004). Food Preference
is a vital predictor of children’s food intake (Nu et al.,
1996; Perez-Rodrigo et al., 2003; Bere and Klepp, 2005). For
instance, children have an uncertain lower preference for
vegetables than fruit (Edwards and Hartwell, 2002; Perez-
Rodrigo et al., 2003).
Particularly, my remit focused on exploring how do children
(aged 9-10) understand healthy eating, and what they do to
attain that? I tried to develop a project that would encompass
evidence of effectiveness from all of these areas and that
could be piloted in a primary school. It was my intention
therefore that, through undertaking this area of work as a
research project, I would be able to demonstrate year 5 and 6
children’s awareness about healthy eating in a school based-
setting. Consequently inform the participant school about the
18
research outcomes and to employ them for the educational
welfare of the involved school.
Nevertheless, this study follows the following structure:
1. A review of literature relating to perception, healthy
eating, children, school-based setting, favourite food,
cognition development, attitudes and beliefs, fresh
fruits and vegetables, eating 5 a day, water, healthy
person, food origin, healthy breakfast, healthy choices
and decisions, food and gender preferences, behaviour and
performance, that informed my decision to undertake this
research field and determines the context within which
the study was ordered.
2. A synopsis of my research methodology, demonstrating the
rationale for my choices, including the discipline upon
which I am describing, the paradigm adopted, and research
methods selected.
3. A field work, an account of the steps involved throughout
the project, so that others could replicate my work, if
desired.
4. An analysis and discussion of the findings of the
research project. These are presented in chapters based
on data collection methods; but address issues raised in
the research approach such as a quite two small samples
of children (aged 9-10) were collected, just 26, from two
different groups. One from a primary school cohort and
one from a local Church group.
19
5. A conclusion, examining the wider implications for this
survey and implications for policy in school working and
for practice need to change.
2.0 Literature review
2.1 Mothers’ perception of obesity in their children:
Childhood obesity occurs within the context of the family life
and especially mothers are implicated in the rapid growth of
the prevalence of childhood obesity (Golan and Crow, 2004).
Usually mothers (Baughcum et al, 2000) influence the nature,
quality and quantity of food available to their children. They
are shaping the food related to their children’s attitudes and
behaviours, and create the family mealtime environment and
influence ceremonies around eating (Gable and Lutz, 2000;
Hodges, 2003; Golan and Crow, 2004). Furthermore, Myers and
Vargas (2000) found that only 20% of sampled mothers were
aware of overweight in their preschool children. Similarly,
(Baughcum et al, 2000) found that 35% of 200 of socially
deprived parents of preschool children were unable to identify
overweight in their preschool children.
2.11 Factors that raised maternal concerns about
childhood obesity:
Various factors might increase maternal awareness about their
children overweight, such as when their children could no
longer fit into age appropriate clothing. Other events that
20
triggered concerns like negative comments from relatives and
friends, and realizing their child in a class photo. Also,
acknowledging their child was larger than their peers were, or
being told that their child was outside percentile charts by a
paediatrician (Jackson et al., 2005).
2.12 Maternal views of contributing factors:
Some mothers believe that certain contributing factors might
contribute to childhood obesity such as family or cultural
factors, inactive lifestyle, not drinking enough water or
inadequate food chewing, genetics and slow metabolism
(Jackson, 2005). Others believe that a large infant is a
healthy infant and therefore, this is an indication of
successful mothering (Baugheum, 1998). According to (Jackson
et al., 2005), some mothers think that kids consume more than
their siblings, and they suffer lack of self-control where
food is available.
Moreover the contribution and support of parents is important
for any future intervention to prevent and manage childhood
obesity (Jackson, 2005). However, (Myers and Vargus, 2000)
indicated that it might be difficult for the paediatricians
themselves to identify childhood obesity and this is an area
to be addressed if families are to be assisted successfully.
2.2 Men’s understandings of obesity:
Weaver et al., (2008) stated that when the word obesity is
used in everyday language it does have different meaning to
the word clinical obesity. Obese people were described by men
21
ages 25-40 years old as being fat with a central obvious
distribution of the excess weight, and words like round or the
balloon are used (Weaver et al., 2008). Furthermore, others
define obesity as somebody being overweight, and not
necessarily unfit, but struggle with their breathing and
movement. For instance, men who had a BMI>25 described feeling
comfortable with how they look. Another example, men with BMI
of 36 thinks it is unhealthy to be too thin particularly in
women (Weaver et al, 2008).
(Weaver et al, 2008) found that men understand that health
issues appear because of being very heavy and that people with
high BMI could be strong and healthy. Besides, men are aware
of the complexity of issues related to weight and fitness. For
example, people of the same weight, normal or otherwise, can
have very unlike fitness levels and therefore different in
terms of health. Likewise, men realize the positive value of
physical exercise on wellbeing and they think that exercise
can counteract the ill impacts of an unhealthy diet.
Additionally, (Weaver et al, 2008) suggested that men
understand constitutes of healthy diet and many men prefer to
eat healthy eating. There was an awareness regarding policy
intervention to promote healthy eating campaigns. For example,
most men described a sensible approach to healthy eating such
as mentioning 5 portions of fruit and vegetables a day. Also,
they included references to brown rice, brown bread, avoiding
high fat, salt, sugar, and processed foods.
22
2.3 Children’s understanding about their own and
other bodies’ health:
According to Burrows (2007) primary and secondary school
students emphasized that food and exercise, across all school
settings, were expressed as vital approaches for getting
healthy apart from year group, socioeconomic context and
ethnicity. Eating fresh fruit and vegetables with good
exercise can make positive changes to one’s health status.
Primary school kids believe that eating fruit and vegetables
and/or running are the key provisions for a healthy future,
whereas older children understand health strategy is keeping
away from junk food, fizzy drink and fatty food, regular
physical exercise and eating smaller portions of food. Girls
deemed to be more aware of their health than boys and they try
to change what they eat and drink. Therefore, such gender
difference, explain the relative increase in the number of
young women in the secondary level thinking about changing
diet and exercise to minimize stress created by unhealthy diet
in the adolescent age (Drewery and Bird, 2004; Evans et al.,
2006; Wright et al., 2006).
Many children can make judgments about healthy persons simply
by looking at a person. Consequently, fitness, non-fatness,
health with size, shape, and weight, and indications that
one’s capacity to run, together with what they eat, may be
responsible for the way they look and therefore their health
(Burrows, 2007). Young children (aged 9-10) are keen to draw
these kinds of links between health and corporeal markers.
23
This notion that health can, in a sense, be read off the body
is deemed to be crucial, particularly, for physical educators’
revision (Crawford, 1980; Tinning, 1985; Shilling, 1993;
Markula, 1997).
According to Burrows (2007) some children think that being
healthy is that the state of being not too thin and not too
fat, but rather, just right. They believe that being too thin
means ill-health and they point to a main focus on obesity as
an indicator of poor health. They, also, understand that
genetics play a confounding role in the potential afforded to
people to become slim or thin or just born big or little,
therefore, not everyone is equally positioned to become the
ideal (Kirk and Colquhoun, 1989). Likewise, some children
trying out the recommended food and exercise portions and
letting out that these practices made little disparity to
their weight or size provoked a questioning of the value of
particular health essentials. For others, this understanding
that they were doing the right thing and those bodily changes
were still not taking place. This made them more concerned
about their health and their capacity to make healthy changes
in their own lives. Thus, the imperatives to eat 5 a day or
push play for 60 minutes do not essentially yield parallel
outcomes across diverse populations or even for persons within
the same household.
However, Burrows (2007) stated that skilled senior students
(aged 10-11) think that skinny people might eat junk food and
do not exercise, this does not mean that skinny people are
healthier than fat people. Also, senior children suggested24

that when kids are eating and exercising right and trying to
be healthy, they are still considered unhealthy by others.
This is because, as others suggested, their body does not
match the normative outcome of the imperatives-that is a slim
body. While, the younger children (aged 9-10) do not have
similar skills and/or experience to draw on to challenge these
consistent ideas. The senior children are more able to reject
the imperatives, stick up for their own health status, and
competently build plans to ward off other people's judgments
of their health and/or weight. This might be a developmental
phenomenon or an occasion of more attention for children in
elementary and secondary schools to providing them with
opportunities to critique orthodoxies (Gillespie and McBain,
2003; Drewery and Bird, 2004).
Moreover, a research study by Burrows (2007) revealed that
gender and age are potentially essential shaping influences on
how young children think about their own bodies and health.
This study conducted with four New Zealand schools, two
secondary and two primary, 795 students were involved in this
study to explore how the participants think and understand
their own health and that of the others. On time, “I feel good
about my body”, asked participants to choose between one of
three options, always, sometimes or rarely. Regarding
secondary school response, 67% of year 11 students responded
sometimes or rarely as compared to only 44% of the primary
school children. Also, senior girls were the most likely to
rarely feel good about their bodies. Roughly, 48% senior males
always feel good about their bodies while just 27% of the
25

girls did. Among junior children, 61% of boys always feel good
about their bodies as opposed to 51% of girls.
These findings yields marked differences in girls’ and boys’
responses and also points to links between advancing age and
increased body dissatisfaction. A marked gender and age-
related differences were clear when participants asked if they
feel happy with their current weight, and if they need to get
thinner. For example, 52% senior children boys have been
always happy with their weight as opposed to 30% of girls.
Also, 30% of boys in secondary school responded “yes” they
need to get thinner compared to 62% of girls saying “yes”. In
primary school children, just 4% gender difference responses
were derived (38% boys and 42% girls).
2.4 Cognition development and relation to healthy
eating:
A cognitive development model with four consecutive stages
developed by Jean Piaget include: sensory-motor period (0-2
years), pre-operational stage (2-7 years), concrete
operational stage (7-11 years) and the formal operational
stage (11-15 years). Along these stages, children’s thoughts
change from concrete to abstract as they grow and develop.
Children become more independent; they develop better
knowledge capacity and become more able to resolve their own
problems with better awareness for details (Delfos et al.,
2003; Flavell and Piaget, 1963; Rodder-John 1999 and Shaffer,
2003). Contento (1981) found that, children in the pre-
operational stage were unable to distinguish between food and
26
snacks, whereas those in the concrete operational stage did.
Pre-operational children thought that the ingested food did
not change in the body after being consumed. Concrete
operational children believed that food was changed by some
means in the stomach. The Pre-operational children could
refer to foods that were healthy, but they could not explain
why. Concrete operational children could tell or made the
correct connection that food made someone strong, grow and
healthy, but they could not explain why or how this occurred.
Bahn et al., (1989) stressed that, in both pre-operational and
concrete operational children, they concentrated mainly on the
quality and feature of the brand, for instance, liking the
taste or the colour of the package when they were
distinguishing the brands. Concerning preference, concrete-
operational children focused more on cognitively based
attributes, such as healthiness and adultness, than pre-
operational children. Besides, the thought of food rejection
based on distaste, danger and inappropriateness, is in line
with the growth of the child and the idea of contamination
appear gradual between the ages of 3.5 years and 12 years
(Fallon et al., 1984; Rozin et al., 1986).
However, there is a gradual emergence of different classes of
food rejections as child grown-up. Very young children of 1-
2.5 years old accept almost all kinds of edible and inedible
substances. The first rejection category to appear is
distaste; disliked products are eliminated. Secondly,
rejections based on danger appear. This means that products
are rejected because unenthusiastic consequences of ingestion27
are likely. The third refusal group is based on the idea of
what something is or where it comes from (ideational). This
class can be split into disgust, and unworthiness. Disgust
means that the association with the food product is unwilling,
whereas inappropriateness means that the food product is not
considered to be a food. It is not until the age of 7 that
children differentiate between disgust and inappropriateness
(Fallon et al., 1984; Rozin et al., 1986 and Zeinstra et al;
2007).
Others (Fallon et al., 1984; Rozin et al., 1986) suggested
that, the idea of contamination appears gradually between ages
of 3.5 and 12 years. A food is contaminated when even a trace
amount of a disgusting or inappropriate product has been or is
present in the food. This development of food rejection is in
line with the growth of the child. Also, between the ages of 2
and 7 (Rozin et al., 1986 and Delfos, 2003) children become
more independent eaters and they have to learn which foods is
edible and which foods are not.
Furthermore, the ideas children have about specific nutrients
can determine their taste, their eagerness to taste and their
whole eating experience (Oram, 1994). Consequently, these
different thoughts, perceptions and decision strategies may
significantly impact on interventions aimed at changing food
preferences and intake. Because most current approaches have
not been effective in establishing long term changes in fruit
and vegetable consumption, cognitive development may be a
promising field for achieving such changes (Zeinstra et al;
2007). Such information is crucial to know how the differences28
in cognitive development relate to children’s perceptions of
healthy eating, therefore; on the basis of the cognitive
development theories, it is expected that the number of
cognitions about healthy eating will increase as the child
matures and that these cognitions will increase in complexity
and abstraction.
In (Zeinstra et al; 2007) terms young children focus on
appearance and texture, whereas older children focus on taste
aspects. Comparable results were found by (Rose et al., 2004)
with sensory preference for meat. Others, (Szczesniak, 1972
and Oram, 1994) suggested that, for 6-7 year old children,
mouth feel characteristics were most imperative for liking,
whereas in 10-11 year old children flavour and smell were most
significant. The reduced significance of textural attributes
is due to the child's development of their teeth and jaws, and
texture is vital for disliking and liking products among the
youngest children's age groups. (Zeinstra et al; 2007) stated
that, young children could not identify the specific taste of
the product but they could tell whether they liked or dislike
the taste of the product. This study in line with the study of
Liem et al., (2004) where 4 year old children failed to
differentiate sweetness intensities during discrimination
tests but could point to their favoured solution.
(Roedder-john, 1999; Valkenburg and Cantor, 2001) found that
preoperational children focus on the most exceptional
attributes that catch the eye, whereas older children use more
functional and underlying characteristics. One characteristic
of cognitive development is a raise in the level of concept29
(Flavell and Piaget, 1963; Delfos et al., 2003). This increase
was seen in children’s improved perceptions of health and the
basic tastes, the shift in classification from concrete groups
to abstract categories, the increase of abstract relations,
and more conceptual arguments concerning healthiness. Roos
(2002) and (Zeinstra et al; 2007) stated that 9-11 year old
kids could make healthy food choices, and this is confirmed by
(Hart et al., 2002) where food nutrient and food-health links
were used between 7-11 year old children as an explanation for
the healthiness of food.
Likewise, parents play an important role in the nutrition
behaviour of children and they employ different patterns
depending on the age of the child (Fisher and Birch, 1999;
Hart et al., 2002; Bourcieret al., 2003; Wardle et al., 2005).
According to (Flavell and Piaget, 1963; Roedder-John, 1999;
and Delfos, 2003) parents use food deals or instrumental
rewarding because it is a concrete strategy for the child, for
example, (“if you eat your vegetables, you will get a candy”).
This food deal was more frequently reported by younger
children (7-8 years) compared to older children (10-11 years).
In the oldest age group, children are less egocentric, and the
instrumental rewarding appears to fit their cognitive
capacities. They have a better understanding of value, and
they can understand another’s perspective. The above subjects
are crucial to understand how cognitive development and
preferences are linked. Therefore, difference in cognitive
development are reflected in changes in attribute importance
in relation to liking and disliking foods, in children’s
30

understanding of, and reasoning about, health, and in the
child-reported parental use of strategies.
2.5 The relevance of breakfast:
In exploring the significance of breakfast, it is relevant to
find an acceptable and a unifying definition for breakfast.
Breakfast is defined as the first meal of the day, eaten
before or at the start of the daily activities within two
hours of waking, typically no later than 10:00 am, and of
caloric level between 20% and 35% of total daily energy needs
(Timlin and Pereira, 2007). Through various physiological
mechanisms, breakfast skipping might result in up-regulation
of appetite, worse overall dietary quality, and a leading
cause of obesity, diabetes and cardiovascular diseases. Also,
increased meal frequency is associated with metabolic changes
improving risk factors for chronic diseases, and reduce
appetite and energy intake (Speechly and Buffenstein, 1999;
Speechly et al., 1999) and (Farshchi et al., 2004; Farshchi et
al., 2005). Such metabolic changes are primarily related to
breakfast composition, namely high-carbohydrate, low-glycemic
index and fibre-rich foods. Consequently, regular breakfast
consumption is associated with lower risk of chronic diseases
(Pereira et al., 1998; Liese et al., 2003).
Recently, in a study involved primary and secondary school
children, BBC news (2013), stressed that “an alarming number
of children do not eat breakfast each morning” and the numbers
skipping breakfast is increasing with age. Nevertheless, 8% of
elementary children had not breakfast on that morning of the
31
research. This increased almost to a quarter (24%) of 11-14
years old and almost a third (32%) of 14-16 years old.
(Nicklas et al., 1998; Kleemola et al., 1999) suggested that
regular breakfast eaters have higher diet quality including
increased consumption of fibre, calcium, vitamin A and C,
riboflavin, zinc, iron and decreased uptake of calories, fat
and cholesterol). For children, breakfast consumption is
associated with education and better school performance
(Pollitt and Mathews, 1988; Vaisman et al., 1996; Murphy et
al., 1998). Also, breakfast has positive effects on cognitive
development and induces better academic achievement (Dye et
al., 2000). Conversely, skipping breakfast is linked with
difficulty in issue solving, short-term memory, attention, and
episodic memory in children (Pollitt et al., 1983; Vaisman et
al., 1996; Wesnes et al., 2003). According to (Giovannini et
al., 2010), therefore, recommendations to encourage regular
breakfast consumption in children include:
- Using diverse kinds of foods to support positive
experiences and learned preferences
- Teach parents to act as role models
- Hearten family breakfast attended by all family members;
- Maintenance a balance of nutrients within the day, and
within breakfast meals during the week.
2.5.1 Breakfast habits through the world:
Traditional breakfast habits usually were more viewed as a
sort of optimistic, moralizing, “good start of the day,” than
correlated to a specific scientific matter (Agostoni and32
Brighenti., 2010). In USA and Europe, 10-30% children and
adolescent are skipping breakfast, according to revision of 47
observational studies on breakfast habits (Rampersaud et al.,
2005). Although regular breakfast consumption is associated
with positive health benefits, children are more likely to
miss out breakfast than any other meal (Timlin and Pereira,
2007).
2.5.2 Food choices for breakfast:
Hanson and Chen (2007) stated that the demographic and
socioeconomic background of children and adolescents is an
objective determinant, unrelated to subjective perceptions and
taste, and deeply affect the quality of diet. However, there
are subjective situations more difficult to be quantified, for
instance 12% of total 699 thirteen-year-olds in an Australian
survey, skipped breakfast. The only statistical variable was
the gender with girls skipping at over three times the rate of
males. The reasons given for skipping breakfast were, not
being hungry in the morning, lack of time, dissatisfied with
their body shape and they have been on a diet. Therefore,
skipping breakfast in such case was just a matter of
individual choice (Shaw, 1998).
2.5.3 Children’s views on what represents a healthy
breakfast:
According to personal knowledge, thoughts and family
background, a subjective individual perception and attitudes
towards breakfast has been explored (Berg et al., 2003). This
33
study was to identify what do children think about good
breakfast (healthy vs. tasty), usual personal and parental
habits, and parents’ choices for their children breakfast
(normative breakfast). For instance, for the judgment on milk
with different fat content, there was little disagreement
between the concepts of delicious, normative, usual and
healthy compared to the broad difference between the same
concepts considering bread with varying fibre content for
example, high fibre bread and breakfast cereals are perceived
as healthy. Accordingly, parents have an essential role in
influencing breakfast choices via norms and by controlling the
availability of foods, and often children make breakfast
choices in agreement with their parents’ wishes. This suggests
that family correlates of breakfast consumption among children
and adolescents are essential to support positive breakfast
habits (Agostoni and Brighenti., 2010).
Additionally, children’s awareness on parental emphasis on
what is a good breakfast is a significant determinant (Cheng
et al., 2008; Tapper et al., 2008). Pearson et al (2009)
recognized an inverse association between socioeconomic
deprivation and skipping breakfast or consumption of an
unhealthy breakfast. Therefore, parents act as positive role
models for their children by targeting their own dietary
behaviours. Also, family structure and socio-demographic
context is necessary when designing programs to endorse
healthy breakfast habits. Touching on the relation between the
frequency of feeding breakfast and overweight, Fabritius and
Rasmussen (2008) found that frequent consumption of breakfast
34
is less protective against obesity among schoolchildren from
low socioeconomic background compared to those from higher
places. Thus, a positive parental model is a better method for
improving a child's diet than attempts at dietary control and
restriction (Scaglioni et al., (2008). Withal, as Liem et al
(2004) suggested that stronger parental control rules are
linked to a lower consumption of simple sugars in controlled
meals, and are associated with favourite for more sugary
beverages in less restricted positions.
2.5.4 What is a Balanced Breakfast Model?
According to Agostoni and Brighenti (2010) a balance breakfast
model should follow three indications:
1- To include a sufficient amount of carbohydrates,
preferably deriving from fiber-rich low-GI sources
2- To be consistent with the local dietary habits to
maintain the daily and periodical dietary allowances and
balance of micronutrient distribution;
3- To present a limited energy expenditure (ED).
A breakfast including three food items, such as a source of
milk and milk derived products (preferably low fat), cereals
(preferably whole, unrefined), and fruit (preferably fresh
fruit or natural juices with no added sugar to prevent an
increase of ED) generally meet these indications. Other
models, mainly salty breakfast models, present noticeable
imbalances of micronutrients, with high protein, high fat food
items providing lower amounts of fiber and slowly absorbed
carbohydrates, if not a marked shift in the average35
composition of the other meals of the daily diet is
implemented.
A low-GI breakfast is followed by reducing energy intake at
lunch compared with a high-GI breakfast and mainly restricted
to boys (Henry et al., 2007). This is due to enhanced fat
oxidation during physical activity after the low GI compared
to high GI test meals (Stevenson et al., 2005; 2006).
Furthermore, lower GI breakfast is associated with better
cognitive functioning in children (Wesnes et al., 2003;
Mahoney et al., 2005; Ingwersen et al., 2007). Low GI
carbohydrates have a negative impact on cognitive performance
including attention, memory, concentration, and the ability to
perform tasks through various mechanisms (Glisenan et al.,
2009). Therefore, taken together these potential benefits of a
low GI breakfast deem to indicate that this could represent an
overall positive factor to be considered as a supplementary
indicator of balance for the children’s breakfast.
2.6 Fruits and vegetables (FV) consumption, attitudes
and beliefs towards FV, and peer/parent/teacher
influence on children’s FV attitudes:
FV are fundamental elements of the perception of healthy
eating (Paquette, 2005). Eating more FV could lead to a
reduction in the consumption of high-fat, energy dense foods,
although is no direct linkage between increased FV consumption
and obesity prevalence (Gortmakeret al., 1999; Slusser et al.,
2007). FV are essential sources of a broad range of nutrients,
and it is evident that FV can prevent cardiovascular disease,
36
diabetes and some cancers (Nishida et al., 2003). Moreover, FV
can protect the child against asthma (Antova et al., 2003).
Despite the increasing evidence about the positive effects of
FV, according to the Youth Risk Behaviour Surveillance System
(YRBSS, 2007), only 20% of high school students eat five or
more FV daily (Eaton et al., 2008), and less than one fourth
among younger children consume the recommended amounts (Field
et al., 2003). According to (BBC NEWS, 2013), (77%) of primary
school children and (88%) of secondary pupils realize that
people must eat five portions of fruits and vegetables a day.
Nevertheless, 67% of primary children and 81% of secondary
pupils eat less than 5 a day.
Furthermore, (BBC NEWS, 2013) revealed that the associations
with risk of type 2 diabetes are different among individual
fruits, and greater consumption of specific whole fruits,
especially blueberries, grapes, and apples, is significantly
associated with a lower risk of type 2 diabetes, whereas
increase consumption of fruit juices has the opposite
association.
Others, (Prelip et al., 2006) revealed a slight increase in FV
consumption with no significant change in positive attitudes
towards FV, for both intervention and control groups. In this
study, there was an increase in fruit consumption from pre-
test to post-test for both the intervention and control
schools, and smaller increase in vegetable consumption in both
schools. Regardless, the FV consumption for this population
was well below the recommended 5 servings of FV a day. This
37
study (using hybrid model), a total of 1528 year 3, year 4 and
year 6 participants were included. The number of involved
primary schools was 12; nine of them were selected randomly,
as intervention schools, and 3 as control schools. A cross
sectional pre-test and post-test design was to assess the
impact of the intervention. Children completed questionnaires
to evaluate attitudes, beliefs, and behaviours at the
beginning of the school year for baseline data collection and
again at the end of the school year for post test data
collection.
The hybrid model is an accurate school based intervention
program, in which elements are planned at a district level and
then the individual schools and the teachers decide what,
when, and how to use it (Prelip et al., 2011). Moreover, the
teachers have a central potential role in affecting children’s
FV attitudes and behaviours as they were more likely to be
viewed as influential nutrition messengers and they may impart
healthy eating messages to children in the school (Prelip et
al., 2011). Therefore, I found this might be interesting to
explore with children (please see question 2, 4, 8, 9 and 10
in my questionnaire). Such questions are included specifically
to explore how year 5 and year 6 children know about healthy
eating, how they decide when choosing what to eat, and why
they think that water, fish, calcium, and fresh FV are
essential for their health.
Concerning positive influences at home about consuming FV,
there was a slight increase in the intervention group (Prelip
et al., 2006). Others (Baranowski et al., 2000 and Anderson et38
al., 2005) have documented similar findings. The latter
studies have noted the challenge of involving parents in
school-based nutrition plans and the difficulty of these
projects on impacting home consumption practices.
Consequently, the students might take this information and
positive attitudes home to their families, and this would
increase parental knowledge and attitudes towards the
importance of consuming FV for themselves, and their children
(Prelip et al., 2006). Therefore, a more structural approach;
specific homework activities engaging students with their
parents might have a greater impact on parental influence.
This might be possible only with families that value what is
happening in schools. Also, a decrease in peer influence on
children’s attitudes towards FV is much higher in the control
groups, this influence could operate through modelling, shared
activities and eating patterns.
2.7 Children’s diets and relation to behaviour and
performance:
The World Health Organization (WHO) emphasized that ” young
people who develop healthy eating habits early in life are
more likely to keep those habits as they mature, and to reduce
their future risk of chronic diseases such as cardiovascular
disease, high blood pressure, stroke, cancer, non-insulin-
dependent diabetes and osteoporosis” (Council of Europe, 2005,
p. 29).
The concept of fish as “brain food” is a shining example of
elderly wives tales passed along generations, have linked diet
39
to behaviour and performance, and is logically reliable
(Wheelock, 2007, p. 145). According to Rogers (2001), fish oil
is the primary source of omega-3 fatty acids; these acids act
as a mood stabilizer, and are advantageous in depression,
schizophrenia, dementia and aggressive and violent behaviour.
Ruxton (2004) stated that, in a number of major multinational
studies, high annual fish consumption has been associated with
lower prevalence of major depression, or higher self-reports
of mental health condition. For example, in North America and
Many European countries, the association between fish intake
and the mental status is confirmed by an increase prevalence
of reported depression in these areas. This is due to reduced
intake of fish oils (high in omega 3 fatty acids) and
increased use of vegetable oils (high in omega 6 fatty acids).
Moreover, Ruxton (2004) assured that, increasing intake of
omega-3 fatty acids are linked to potential positive health
effects related to cardiovascular disease, arthritis, brain
development and function. The omega-3 and omega-6 fatty acids
are the most plentiful in the brain cell membrane. They
increase the fluidity of neuronal membrane for neuronal
synapses essential for efficient synapses transduction.
Therefore, highly unsaturated long chain fatty acid
consumption might negatively affect mood and behaviour by
direct effect on neuronal function.
However, oily fish and seafood are rich with omega-3 fatty
acids needed by the brain while omega-6 fatty acids are more
abundant in vegetable oils, meat and dairy products. ADHD,
dyslexia, Autism and dyspraxia affect up to 20% of school age40
children and this is due to reduction in certain highly
unsaturated fatty acids (Richardson, 2003). For example, those
with ADHD have lower plasma level of omega-3 fatty acids
compared with normal children (Ruxton, 2004). Furthermore, as
Richardson (2003) suggested that, omega-3 fatty acids might
have a therapeutic effect in such mental illnesses. In
children with developmental coordination disorder, they showed
steps forward regarding the decrease in ADHD-type symptoms,
and improvement in reading and spelling (Richardson, 2003 and
Montgomery, 2005). Thus, supplementation of malnourished
children with vitamins and minerals, plus omega-3 fatty acids,
result in more than 30% decreases in antisocial behaviour
(Wheelock, 2007, p. 150).
Links have also been established pertaining to individual
nutrients, for instance, iodine supply is well recognized to
affect psychomotor and cognitive function. Therefore, eating
foods rich in iodine such as fish can protect individuals
against hypothyroidism, poor learning, ADHD and loss of memory
(Anderson and Zimmerman, 2010). Besides, in 2 years old
children with iron deficiency anaemia, lack of cognition,
attention and motivation is prominent and iron therapy has a
consistent therapeutic effect (Ruff et al, 1996 and Wheelock,
2007, p. 150). Foods rich in iron include red meat, liver,
lentils, and fruit and vegetables. Also, Mac Evilly and Kelly
(2001) suggested that, low selenium intake is associated with
greater incidence of depression and other negative mood
states. Selenium is abundant in brazil nuts, kidney, liver and
shellfish. Furthermore, thiamine and folat, as B vitamins, are
41
highly plentiful in junk food, have anti-depressive effects
(Rogers, 2001). Using certain additives such as artificial
colorants, artificial sweeteners and preservatives might lead
to ADHD (Wheelock, 2007, p. 151).
Also, the imbalance of protein and carbohydrates consumed in a
meal can negatively influence brain serotonin hormone which is
involved in the modulation of mood and behaviour. This might
lead to depression, aggression and impulsivity (Rogers, 2001).
For instance, feeling less depressed and better reaction times
are associated with carbohydrate rich/protein poor diet
(Markus et al., 1998 and Markus et al., 2000).
The brain, therefore, is sensitive to short term fluctuations
in glucose supply which is derived from the metabolism of
carbohydrates in the diet. Therefore, maintaining normal blood
glucose level is essential as glucose is needed for the
metabolism of serotonin and linked to memory, attention and
arithmetic ability (Blundell et al., 2003 and Bellisle, 2004).
However, it is evident that, child’s poor behaviour is the
consequence of eating specific food ingredients (Van de
Weyner, 2006). In particular, malnourished students had
significant improvement in behaviour after been included in a
free school breakfast program, and they showed improvements in
almost all tasks, especially in their math grades, reading and
social science (Woroby and Woroby, 1999). For instance, the
Dudes program (Tapper et al., 2003), is a healthy eating
program, which combined the peer modelling (the Food Dudes
cartoon characters in videos) and the rewards, is a successful
42

way to increase children’s consumption of fruit and
vegetables.
Therefore, children, in the primary schools, showed increase
percentage from 4% to 100% and from 1% to 87% for fruit and
vegetable consumption respectively (Wheelock, 2007, p. 193).
Such outcomes were achieved for at least six months (100% of
children were still eating fruit and 58% ate vegetables). So,
the mere presence of fruit and vegetables in the home is not
sufficient to endorse consumption and to maintain the
behavioural learning principles. Such program is regarded as
an excellent British initiative to raise children to eat at
least five helpings of fruit and vegetables daily.
Traditionally, Eastern medicine has used foods to bring about
changes in behaviour, mood and thought processes, recent
evidence suggests that diets can alter brain chemistry,
behaviour and cognitive ability (Mac Evilly and Kelly, 2001;
Blundell et al., 2003). The brain is sensitive to metabolic
changes associated with the form of meals and fasting, linked
to adequate glucose supply to the brain, and also long term
nutritional status (Bellisle, 2004). This is more significant
for children in their stage of growth and development as these
varieties might cause immediate or long term positive or
negative effects.
2.8 Children’s views about food origin:
BBC NEWS (2013) stated that nearly a third (32%) of UK primary
children deems that cheese is made from plants and 25% believe
fish fingers come from chicken or pigs. The British Nutrition43
Foundation (BNF) stated that about 10% of secondary school
pupils consider that tomatoes grow underground. This was large
survey, in which, 27,500 children (aged 5-16) were questioned
in June, 2013. Also, the survey explored ambiguity about the
source of staples such as pasta and bread among younger
pupils, with about a third of 5-8 years old believing that
they are made from meat, and 19% did not understand that
potatoes grew underground, with 10% thinking they grew on
bushes or trees.
Consequently, Roy Ballam, education program manager at BNF
called for a national agenda and management for food and
nutrition education across the UK, “especially at a time when
levels of obesity are soaring”. The study, created to coincide
with the BNFʼs healthy eating week, in which, 3000 UK schools
have signed up. Mr Ballam said aims “to begin the process of
re-engaging children with the origins of food, nutrition and
cooking, so that they grow up with a fuller understanding of
how food reaches them and what a healthy diet and lifestyle
consist of”.
2.9 Children’s views on foods and consumption of
selected food groups:
It is essential (Sharifah et al., 2013, p. 132) to assess
children’s views on foods which may influence their food
options depending on their own cultural eating patterns and
nutrient availability in their own culture. This is
significant as the information obtained might be helpful for
planning the related intervention and development of a dietary
44
assessment method and aid. For example, food frequency
questionnaire and food photographs of children. The children’s
food choice is crucial as it becomes one of the determinants
of their nutrient intake, which later can influence their
growth and maturation. Their food choices in the early stage
of life have a high possibility to be carried through into
adult life.
Zaini et al (2005) suggested that snacks and fast food
consumption can lead to childhood obesity. Furthermore,
dietary fibre might act as a protective element against
childhood overweight, as it affects food intake, digestion and
absorption of nutrients and carbohydrate metabolism (Ali et
al., 1982). Authoritative sources of dietary fiber include
fruit and vegetables, cereal and cereal products, legumes and
other whole-grain products. Besides dietary fibre, (Skinner et
al., 1999; Carruth et al., 2001) stated that dairy products
have serious potential effects on body weight in babies, and
it is important to distinguish what type of food groups really
consume by children. This is fundamental to develop
interventions to encourage them to make better health choices
and decrease the risk for chronic disease.
Moreover, children taking cereals for breakfast usually have a
lower body mass index (BMI) and lower cholesterol than those
who eat non-cereal breakfast foods. This is because breakfast
cereal is lower in fat and higher in fibre than non-breakfast
cereal and can be protective against childhood obesity
(Resnicow, 1991 and Williams, 1995).
45
Sharifah et al (2013) found that most of the (7-9 years old)
children like food because of the taste. Other reasons include
the nutrient value of the food and the attractive feature of
the food such as a nice smell and the food's texture, for
instance the crispiness. Others (Olson et al., 1981; Ricketts,
1997; Pѐrez-Rodrigo et al., 2003; Molaison et al., 2005) have
shown that the taste of food was the major limiting factor
related to consumption and regarded as a significant
determinant of children’s food choice. However, for non-
favourite food, some children dislike some types of foods when
they recognize that the food is unhealthy, for instance,
sweets as they know it can cause tooth aches or they dislike
fish as it holds heaps of bones (p. 135).
2.10 Gender Differences in Food Preferences:
The food service organizations are offered the opportunity to
look at their current offerings and policies to move towards
plummeting fat and sugar options with increasing fruit and
vegetable selections. Therefore, the food service staff should
be asking” What will kids eat?” while assessing current
policies and services (Caine-Bish and Scheule, 2009). Certain
factors are connected to food preference such as age, gender,
culture and the socioeconomic state (Logue and Smith, 1986;
Drewnowski, 1997; Turrell, 1998; Lytle et al., 2000; Wansink
et al., 2003; Westenhoefer and Cooke, 2005; Caine-Bish and
Scheule, 2007). Accordingly, it is essential to understand the
influence of these factors on children’s food preferences to
46

help develop healthy and successful menus (Caine-Bish and
Scheule, 2009).
Caine-Bish and Scheule, (2009) suggested that the food
preferences of children and adolescents varies between genders
as well as gender differences differ between primary, middle
and high school students. Thus, differences in gender and the
combination of gender and grade level are crucial to fully
appreciate children’s food preferences within the school
setting. For instance, boys as compared to the girls, have a
greater preference for pork, beef and fish in the primary
school. On the other hand, it is uncertain why the boys in
particular are less favourable to these foods in the middle
school level. Regarding girls, as compared to the boys, have a
greater preference for fruit and vegetables, sweets and
starches. However, in adult women they choose comfort foods
such as ice-cream and chocolate.
Moreover, (Caine-Bish and Scheule, 2007; Guthrie et al., 2006)
suggested that children’s food preferences can predict the
food children choose, but many of children’s top choices are
foods high in fat, sugar and calories when asked their
preferences. There are, however, many healthier food choices
that children also prefer such as grapes, strawberries and low
fat milk. Also, not only males and females would prefer
different foods, but these food preferences would change based
on their grade level with an indistinct reason.
3. Research design and methodology:
47
3.1 Development of the question:
An initial proposal question made an attempt to identify the
focus of my planned interventions, especially in terms of
establishing a clear link between the specific research
question and the related methods of date collection, an issue
I have struggled with for quite a few months. After
discussions and further thought, the question was developed
and in many respects broadened to explore the views, beliefs,
attitudes, and understandings of children (aged 9-10) about
healthy eating.
3.2 Rationale for this research question:
The question is highly topical with the high prevalence of
childhood obesity among primary school children in the UK,
coupled with the government’s agenda to reduce children’s
overweight. A number of recent national policy documents
(Livingstone, 2013; Gibney, 2012; Wheelock, 2007; Paquette,
2005; NHMRC, 2003) have stated the increasing prevalence and
the risks of childhood obesity. This makes explicit reference
to the significance of exploring children’s views about
healthy eating, with particular attention being paid to year 5
and 6 children in the primary school. However, based on
literature review, many aspects of perception of healthy
eating are closely related to the main research question.
These include how children know about healthy eating, the
influence of parents, teachers on their food choices, gender
differences and food preferences, and their views about food
origin. Moreover, the goal of this research question is to
48
explore children’s understanding about particular food groups,
and why they like certain food groups and they dislike others.
I will endeavour to explore the misconceptions in food
knowledge including the fundamental elements of healthy eating
in children (aged 9-10) in primary school.
3.3 Quantitative vs. Qualitative research:
Biggam, (2008) suggested that quantitative refers to research
that is concerned with assessing the extent of something, for
instance, the success rate of dissertation students in the USA
school of medicine. It could be more complicated than just
gaining simple quantitative information. It can involve
calculating, for pension and personal insurance purposes, the
possibility of dying before retirement for those in a given
profession (p. 86). Whereas, qualitative research links to in
depth exploratory studies, for example, why students choose a
certain module to study where the opportunity for quality
responses exists.
To explore a particular matter in depth, it is common to mix
and match both qualitative and quantitative methods,
therefore, quantitative research answers the how questions,
whereas the why questions are left to qualitative research
(Myers, 1997).
3.3.1 Advantages and disadvantages of a questionnaire
survey:
I chose to undertake a questionnaire for a number of reasons.
Menter et al., (2011, pp. 105-107) provide a list of several
49
characteristics of a questionnaire, which I will now briefly
discuss in more detail to explain why I felt this was the
appropriate method for my project:
- The need to collect large amounts of data within a
relatively short period of time.
- Although questionnaires are not essentially easy to
design, they can be easily administered.
- They can be used to explore beliefs, attitudes, views and
past behaviours. Therefore, they are flexible and a wide
range of information can be collected, although
flexibility is more a feature of an interview as once
written a questionnaire is fixed.
- Due to the focus provided by standardized questions,
there is an economy in data collection and time is not
spent on peripheral questions.
- Both closed questions, for rapid data analysis and open
questions that are more complex to analyze, can be used.
- Survey questionnaire does make larger samples possible,
and statistical techniques.
Conversely, here are some of the disadvantages of
questionnaires:
- Questionnaires, particularly self-administered ones,
could be quite challenging especially for younger
children with dyslexia. Also, writing at a level they
understand but does not confuse them is a challenge.
- It is not possible to follow up answers within
questionnaires (as we could in an interview). Therefore,
50
the responses we get are constrained by the decisions we
have made about the design of the questionnaire.
- It is relatively a mechanistic form of data gathering as
we cannot guess how confidently the respondents are
interpreting the questions and responding to them.
- They depend on the individuals’ honesty, motivation,
memory and ability to respond.
- Errors due to non-response and misinterpretation might
occur, although the subjects identified in a survey are
often a random sample. Therefore, people who choose to
respond to the survey might be different from those who
do not respond, and this can bias the findings.
Therefore, it may be easier for (9-10 years) older
children to give honest answers through an anonymous
questionnaire rather than through class discussion or
focus group where they have to look the researcher in the
eye (Menter et al., 2011, p. 106). However, children
might not feel obliged then to answer for instance
knowing the person might ʻpersuade´ the participants to
respond.
3.3.2 Advantages of interviewing and issues for
consideration:
Because of the flexible nature of the method and the
limitations can be addressed with careful planning by
complementing the approach with other methods. Also,
interviewing is responsive and can read body language and
other behaviours in response to questions. (Menter et al.,51
2011, p. 127-128) have stated many advantages of interviewing
and these include:
1. Interviewees can ask for explanation which is helpful to
collect more accurate information or might help to
realize the question need refining.
2. Interviewees can shape the research and highlight
relevant issues.
3. Interviewees can be helpful to appreciate more about the
factors influencing actions and attitudes.
4. Interviewees can provide their own views in their own
terminology. This is helpful to understand the meanings,
underpinning people’s actions and illuminate their
attitudes and rationale.
5. Because of the interactive environment of the interview,
the researcher can adapt the questions to suit responses
and gain greater insights.
However, (Menter et al., 2011, p. 128), there are certain
matters of interviewing should be considered and these
include:
1. Interviewing could be a time consuming method and costly
because of the time taken to conduct interviews and
analyze the information.
2. Sensitive topics can be difficult to discuss face to face
because of the socially interactive nature of the
interview. Therefore, it can both improve but also hamper
the gathering of information.
52
3. Differences in the level of detail across the interviews
and the interpretation of questions by the informants
might appear. This is occurring when the interviews are
conducted by more than one interviewer, each may ask
questions differently.
4. In certain cases, for example, if the researcher is
interested in a more complete understanding of a
particular issue, he might need to compare a range of
interviewees’ accounts and also triangulate with other
methods such as observation and document analysis.
5. Interviewing needs, like focus groups, skill and
awareness on behalf of the interviewer to avoid
influencing the interviewee.
3.3.3 Shaping a case study:
The chosen approach is an exploratory study that is also
comparative in nature between two different cohorts. In this
study, I am dealing with two case studies, one is the local
Church group and one is the primary school cohort, each has a
different context and background. The project has become an
opportunistic comparative case study because it focuses on the
specific instance to explore children’s views about healthy
eating of a bounded system (a department) (Cohen et al. 2007,
p. 253) and aims to provide an in-depth description focussing
on the processes involved, rather than emphasizing the final
outcomes. In Yin’s (2003) terms, it is an exploratory case
study which will aim to present “a complete exploration of a
phenomenon within its context” (p. 5).
53
This survey was administered in one primary school in west of
the Oxfordshire / UK and in one local Catholic Church in the
centre of Oxford in June 2013. Only children (aged 9-10) were
selected because younger children might find some of the
questions difficult to understand or answer on their own while
older children would be expected to be busily preparing for
the entrance examination for the secondary schools.
Nevertheless, I chose to undertake a comparative case study
for a number of rationales, children (aged 9-10), one group in
the primary school and one outside the school (social
grouping). Cohen et al., (2000, p. 182) state a list of
hallmarks of a case study, which I will now briefly consider
in more detail to elucidate the reason beyond choosing this
method:
1. ʻThe researcher is essentially involved in the case´. This was always a
concern. As already discussed, my involvement in this
research was certain. Issues of power and bias therefore
needed to be considered from the outset. I intended to
undertake both the questionnaire and interviewing the
children as focus groups. However, the school I had
arranged to go and interview children in was able to
facilitate my request as head´s permission was obtained
and enough time was available. All the interviews
questions and schedule were prepared and were ready for
processing with the children (Appendix 6).
2. ʻCase study highlights on individual actors or group of actors, and searches
for understanding their perceptions of events´. I wanted to choose a
research design where all concerned had an input into54
the project and where their understanding of the event
could contribute heavily to the outcomes, recommendation
and sustainability of the project. Furthermore, I wanted
to undertake a project that was strongly based in the
reality of school, therefore reflecting the experiences
of those involved, who were necessary to live with the
project in its entirety.
3. ʻIt is concerned with a rich and vivid description of events relevant to the
case´. It was crucial that any research undertaken could be
reachable to as many various audiences as possible:
health promotion specialist, teachers, parents, local
government officers, and so forth. As a result, it
deemed significant to choose a research method that was
inclusive for everyone, regardless of prior research
experience, and that was presented in everyday terms,
free from jargon and professional language. Choosing a
design that included a full description of the
experience as part of the research in everyday language,
reflected the many decisions that were made throughout
the process, and that detailed their influence upon the
research, seemed ideal.
4. ʻIt combines a description of events with the analysis of them´. As stated
above, this was relevant to the multi-faceted audience
that this research was aimed at.
5. ʻIt provides a sequential narrative of events imperative to the case´. As
detailed above, the research needed to be accessible to
everyone. However, it also compulsory to be influential
enough to be scrutinized by many, in particular if
55

favourable outcomes or recommendations were to be
followed up in the future.
6. ʻAn effort is made to depict the richness of the case in writing up the report´.
From the outset, I was uncertain as to what the outcome of
this study would be. Therefore, in order to capture as
much as possible, I wanted to use as many different data
collection methods as was feasibly possible. Also, for
others involved to be able to suggest and contribute
data collection methods that they believed appropriate
and felt comfortable with. However, with so many
different forms of data collection planned, I needed to
adopt a research design where all of these dissimilar
findings could be communicated. I afterwards found out
that many various styles of data collection were
certainly preferable in case studies, but it was this
initial aim of portraying the affluence of the
experience which made me enthusiastic to use it.
3.3.4 Issues to consider when undertaking a case
study:
Having made the decision to undertake an exploratory
comparative two case studies, there were a number of
characteristics of good case study design that I needed to
deem. Robson (2002) summarizes these briefly and I adhered to
all of these when planning my research design. More crucially
however, and worthy of discussion here, I felt was
necessitated to address some of the inherent weakness
56
concurrent with this form of flexible design; those of
validity and reliability.
- Validity
The accuracy of findings in fixed or quantitative designs is
usually ensured by direct replication. If an independent
investigator can confirm a finding, then it is said to be
valid. The difficulty with flexible research designs is that
identical circumstances cannot often easily be replicated. The
way to resolve this, according to Robson (2002) is to reframe
the terminology and consider ʻbeing accurate, or true, or
correctʼ (p. 170). He states that question asking, good,
listening, adaptiveness, and a grasp of the situation and a
lack of bias, (i.e. Good scientific rigor), are methods that
can be used to overcome this. These are issues I needed to
consider in my research study. ʻBeing prepared to trace the
route by which you came to your interpretation (Mason, 1996
cited in Robson, 2002 p. 171) is another approach to do this.
This was a key way that I wanted to work and so I felt sure
that I could ensure validity. I also considered the threats to
validity: description, interpretation and theory (Robson,
2002), and sought to minimize these in my research design.
-Reliability
57
ʻIn qualitative research reliability can be regarded as a fit
between what the researchers record as data and what really
occurs in the natural setting that is being researched, for
instance, the degree of accuracy and comprehensiveness of
coverageʼ (Bogdan and Biklen, 1992 cited in Cohen et al.,
2000. P. 119). As I mentioned already, my original intention
was to interview children as well as doing questionnaire.
However, due to unforeseen circumstances, and despite
preparatory discussions, the interviews were not possible to
undertake as the school that agreed to participate was so busy
and there was no enough time to undertake this study. I
intended to invite few colleagues to also become researchers,
this might make the findings more reliable as we compare and
discuss what happened. Although this cannot guarantee
reliability as they might produce completely different
findings from the same observation.
Therefore, I decided to ensure that my colleagues and I agreed
in advance the reliability of the instruments of research we
chose to use and that there were enough of them to ensure
triangulation occurred. Triangulation, plus a sufficient
number of records would hopefully prove the project findings
reliable, for instance, ensuring that there are enough
children involved in the project to ensure that the techniques
used were reliable.
3.3.5 Types of case study:
Having considered the specific issues relating to the use of
case studies and satisfied myself that this was still the most
58
appropriate form of research design for my project, I then had
to decide which type of case study to undertake. As I already
discussed, I decided to do a two exploratory comparative case
studies. A case study was described as a ʻsmall-scale version
of the real thing, a try-out of what you proposeʼ and an
opportunity to ʻlearn on the jobʼ (Robson, 2002, p. 185). An
exploratory case study is a pilot to other studies or research
questions (Basit, 2010, p. 20). Indeed, Cohen et al., (2000)
stated that exploratory case studies can actually be used
solely to generate hypothesis for larger scale research forms.
However, case studies are quick to state that this is not a
reason to devalue or disregard this type of case study as a
valid research form or to reduce it to a mere ʻpreliminaryʼ to
other studies. I was keen that my project be purposeful in its
own right, despite its dual role of also being the pilot for
further work, if only to provide ʻon-the-spotʼ satisfaction
and gratification to the school staff involved.
4. Ethics:
An essential characteristic of any research project that I
have not yet discussed clearly is ethics. Bell (1999) cites a
useful quote from Blaxter et al (1996, P.39) that succinctly
summarizes the key issues of research ethics:
ʻResearch ethics are to be comprehensible regarding the nature
of the agreement you have entered into with your research
subjects or contacts. This is why contracts can be a useful
recommendation. Ethical research involves getting the informed
consent of those that you are going to interview, question,59
observe, or take materials from. It involves reaching
agreements concerning the uses of this data, and how its
analysis will be reported and disseminated. And it is about
keeping to such agreements when they have been reached. ʼ
I considered the need for a kind of contract between myself,
as a qualified general practitioner, and the school to clarify
some of the above. I also considered the question ʻwho might
be harmed by my research? ʼ in order to generate some ʻworst-
caseʼ scenarios. I felt that by pre-emptying potential
problems, I could guarantee that the ethics contract addressed
theses issues sufficiently. Initially, it felt awkward to
think in such negative terms as someone being ʻharmedʼ by my
research, particularly with the way the project had positively
developed, the keenness that there was for the project from
all parties.
Moreover, throughout my research, I continued to be open to
both children and staff about the scope of my research study.
I intended to seek the reasonably informed consent (Cohen et
al. 2007, p. 53) of all participants including the children in
the local primary school. It assured for the participating
children that they are free to discontinue their contribution
in the project at any time without injustice to them. As I
discussed already, my original intention was to interview
children inside the school as timing and location may affect
the responses. Therefore, interview questions were arranged to
ask for the children (Appendix 6). I planned to use pseudonyms
to protect the identities of those involved. Also, respondents
to questionnaires were ensured anonymity and interviewees who60
require it were granted confidentiality (Cohen et al. 2007, p.
64). I was also aiming to show interviews records to
participants so that accounts can be checked for accuracy and
if necessary amended. Ethical approval was obtained from the
university-wide Ethics Committee at Oxford Brookes University
prior to the commencement of the study (Appendix 3). I
intended to obtain a written consent from each student’s
parent prior to his/her participation in the study.
Basit (2010, p. 56), stated that ʻsome of the most intractable
ethical problems arise from conflicts among principles and the
necessity of trading one against the other. Therefore, the
balancing of such principles in real situations is the
eventual ethical actʼ (House 1993, p. 168). I considered also
in my research to have a responsibility to meet the
requirements and to rigor (Gorard, 2003). For instance,
experimental design might be the most ethical approachable to
obtain a specific research question even where it is more
risky than other less appropriate design. (p. 173).
Furthermore, as (Basit, 2010) suggested, in my research study,
to be so gentle with the children, their gender, race, social
class, disability, ethnicity and so forth are considered when
interacting with them. The use of sexist and racist language
was avoided. We tried to create a non-hierarchical
relationship with the participants and dress appropriately for
the fieldwork (Basit, 1995).
5. Fieldwork period
61
Questionnaires (comprised of 14 questions) for children (aged
9-10) were distributed to one local primary school between 22nd
and 23rd of July 2013. Also, questionnaires were distributed to
children of the same age in a local Church group one week
later. Completed questionnaires of the children were returned
and collected via one of the teaching staff working in the
same school. Similarly, questionnaire from the local Church
group were collected via one of the Brookes staff on the 29th
of July. Both data are separately analyzed as different
background and context might influence the findings of the
research.
5.1 The participating school (first
group/cohort).
Background
The school has four grades, junior, voluntary controlled
school in the west of Oxford, Stanton Harcourt that currently
has 78 boys and girls aged range between 4-11 years on roll.
The selection of the school was opportunistic. After the
(other) school that had initially agreed to participate, for
unforeseen and unknown reasons, withdraw, there arose an
opportunity for a tutor at Brookes, who taught in the local
school to administer the questionnaire on my behalf. The
teacher there checked the questionnaire and administered it on
my behalf.
However, most of the children are from low-middle
socioeconomic state. A recent Ofsted report (2008) stated that
62
most pupils of this much smaller than average village school
are from a White British Background. The proportion of pupils
with learning difficulties and disabilities is well below
average but with increasing numbers of pupils with speech and
language problems. Numbers of pupils in each year group are
small and vary significantly from year to year. A voluntary
management committee provides a popular after-school club. The
school has achieved Healthy Schools, Eco, Active mark and
BECTA Computing Awards.
According to Ofsted report (2008), the spiritual, moral,
social and cultural development of pupils is outstanding. It
plays a significant part in their personal development and
sense of well-being. They are quick to celebrate the
achievements of others as well as their own and have a well-
developed concern for the welfare of each other.
The school is very active in village life, helping pupils
develop a strong sense of their place in the community. Their
understanding of values and beliefs in other communities
however is less well developed. The Eco club and school
council give pupils responsibilities and encourages them to
contribute to the life of the school. The Eco club, for
example, is developing in pupils a strong awareness of care
for the environment. Pupils demonstrate excellent attitudes to
learning. They have a willingness to learn which shows in the
ways they are keen to contribute to lessons, willing to take
responsibilities and eagerly take part in class discussions.
Relationships are very good and pupils say they feel safe and
confident in approaching adults for help. Their behaviour is63
excellent. They have a very good sense of a healthy lifestyle
and readily take opportunities for additional exercise at
break-times. Social skills are developed very well through
paired and group working and pupils are encouraged to become
independent in their learning.
As mentioned above, the school was already committed to
becoming a ʻHealthySchoolʼ and welcomed this research study. A
teacher working in the school was responsible for steering the
study and passing the questionnaire to the children.
Eating Environment
The school provides a safe and healthy eating environment for
pupils, staff and visitors having lunch at midday in the
school. All children are required to sit at a table for at
least 20 minutes, in order to eat their lunch. Children are
encouraged and are given the time, to try to eat most of the
food provided either by school or home. Lunchtime supervisors
or a member of staff will help any children who have any
concerns. Children help to clear up afterwards on a Rota
basis, wiping tablecloths and sweeping floors. Teachers were
the key decision maker in lunch choices, followed by parents.
The school reported nutritional value and food safety as their
top two considerations for choosing food for lunch, consistent
with parents’ wishes.
Healthy Eating Policy 64
The school agrees that healthy eating is crucial for school
education and children’s development, and has developed its
healthy eating policy. Where policy existed, it focused
primarily on school lunch followed by snacks to make explicit
the values and guidelines that underpin every aspect of food
culture in the school. Moreover, to ensure that our children
receive consistent and coherent messages about food and its
role in their long-term health in order to meet the outcomes
of the Every Child Matters legislation.
School l unches
The weekly menu is on display for the children and parents in
the assembly hall, in class areas, on the school notice board
as well as on the school web site. The menus are sent home to
parents when each new set of menus is introduced. The school
listens to the children’s opinions on the menu and adapt the
menu accordingly. All of our menus meet the new nutritional
requirements for school meals.
Free School Meals
The school recognizes the particular value of school meals to
children from low income families. The system for free school
meals is actively promoted to parents by the school and a non-
discriminatory process is emphasized.
5.1.1 The local Church group (second case study
group/cohort).
65
A supportive staff at Brookes offered an opportunistic way to
gather some empirical data for my study, so despite the good
intentions and all my plans and preparation, this was a
fallback situation. The nature of the participating cohort is
described below as these factors need to be taken into account
when interpreting the findings. However, the local Church is
the Catholic Church and is located in the centre of Oxford.
Most of the children (aged 9-10) attended this Church drawn
from nearby primary schools and they were all of whitish
British ethnicity. The children are from low- middle
socioeconomic states and most of their parents were educated
with high qualification and some of them are working in the
university.
Children (aged 9-10) were meeting in the Church on a usual
Sunday morning and all were students in the primary school.
However, I tried my utmost to get the acceptable number of
participants for my research study, and undertake both
qualitative and quantitative research methodologies. This was
my original intention and plan, and the interview questions
were all arranged in advance (Appendix 6). However, despite of
previously preliminary discussions and due to unexpected
circumstances, the interviews were not possible.
5.2 Data collection
One teacher working in the same participating school
distributed the student questionnaire to year 5 and year 6
children (aged 9-10) in one local primary school on the Friday
afternoon in June, 2013. Some of the children’s parents were
66
available and they indicated a willingness for their children
to participate in this study. The students were asked to
complete the self-administered questionnaire in a school
during a classroom session. A quite two small samples were
collected, just 26, from two different resources. One sample
from a local primary school and another was from a local
Church group. Regarding primary school cohort, no time limit
was given; the children spent about 10-15 minutes to complete
answering the questionnaire. The teacher had to clarify a few
questions and answer responses; but no direction was given in
response. The number of children was 19 in this local school,
year 5 and 6 pupils in the class (aged 9 – 10). Most of the
children (18) were either at level 4 or 5 of the national
curriculum and one child was at level 3.
The second cohort that responded to the questionnaires was
children in a local Church group in which ten questionnaires
were administered at the end of meeting, which is regular once
weekly meeting. This sample was regarded as a purposive sample
as needed responses are required for this study. A member of
Brooke’s staff first introduced himself to the children and
their teacher in the Church. He tried to explain the aim of
this research study for the children and their teacher who
were happy and welcomed the notion of the survey. The member
of Brooke’s staff administered 10 questionnaires to the
children and he was in attendance when the children filled out
the questionnaires, but did not interpret the questions for
the children, who were motivated and focussed, although one
child did not complete the whole exercise. Seven were
67

returned. Of these, two were completed by children whose
parents read with them and helped them to answer the
questions. One parent declined to let his child join the group
and answer the questions, but gave no reason for his
decision.
6. Data analysis
Descriptive statistics were used to summarize the findings of
the study and they were reported in percentages, means, and
histograms, wherever appropriate. Some percentages in the
descriptive figures might not add up to the total or 100%
because of rounding. Moreover, the sample bases for each
question might vary due to the missing answers.
6.1. Results of Questionnaire Survey for Children
A total of 46 copies of questionnaires (Appendix 4) were
administered, 36 questionnaires were administered (only 19
were returned) to children in the primary school by one
teacher. The questionnaire for the primary school group was
administered in 19th of July and collected 5 days later. Also,
10 questionnaires were administered on Sunday 28th of July to
the local Church group by one member of Brooke’s staff (only 7
were returned) and collected on Monday 29th of July 2013. A
total of 26 copies of completed questionnaire was collected
with a response rate of 92.3 % for both case studies. Of the
questionnaires, two questionnaires were not fully completed
and all were used for data analysis.
6.2 Descriptive data and Findings
68
All the data from questions of the children’s questionnaires
in the study were presented in tables, graphs, histograms, and
I will write a paragraph to explain each graph findings for
both participating groups separately.
6.2.1 Children’s responses to the question regarding
the definition of healthy eating (Q1)
Question 1 was “what does healthy eating mean to you?”
Children (aged 9-10) were asked to choose only one answer
among four options (a, b, c, and d), in which the choice (d)
was the best answer. Option (d) referred to “Healthy eating
means eating a balanced diet with good physical activity” was
the closest option for healthy eating. Other options that were
definitely not healthy eating were a) Eating more food b) Food
with high salt, sugar and fat and c) Too many calories. The
goal of this question was to explore how children do (aged 9-
10) understand and perceive the meaning of healthy eating.
Consequently, Table 1 show the number and percentage of
children correctly answered the question regarding “What does
healthy eating mean to you?” (Q1). Among the local Church
group (6 responses and one missing answer), percentage of
correct answers was 85.7% while it was 94.7% for the primary
school cohort (one missing answer among 19). The mean and SD
(standard deviation) for both case studies were 6.5, 0.70 and
18.5, 0.70 respectively. In general, an understanding of
children in both cohorts regarding the meaning of healthy
eating was very good. These responses (for example not 100%)
mean that perhaps the question was not as well clear as it
69
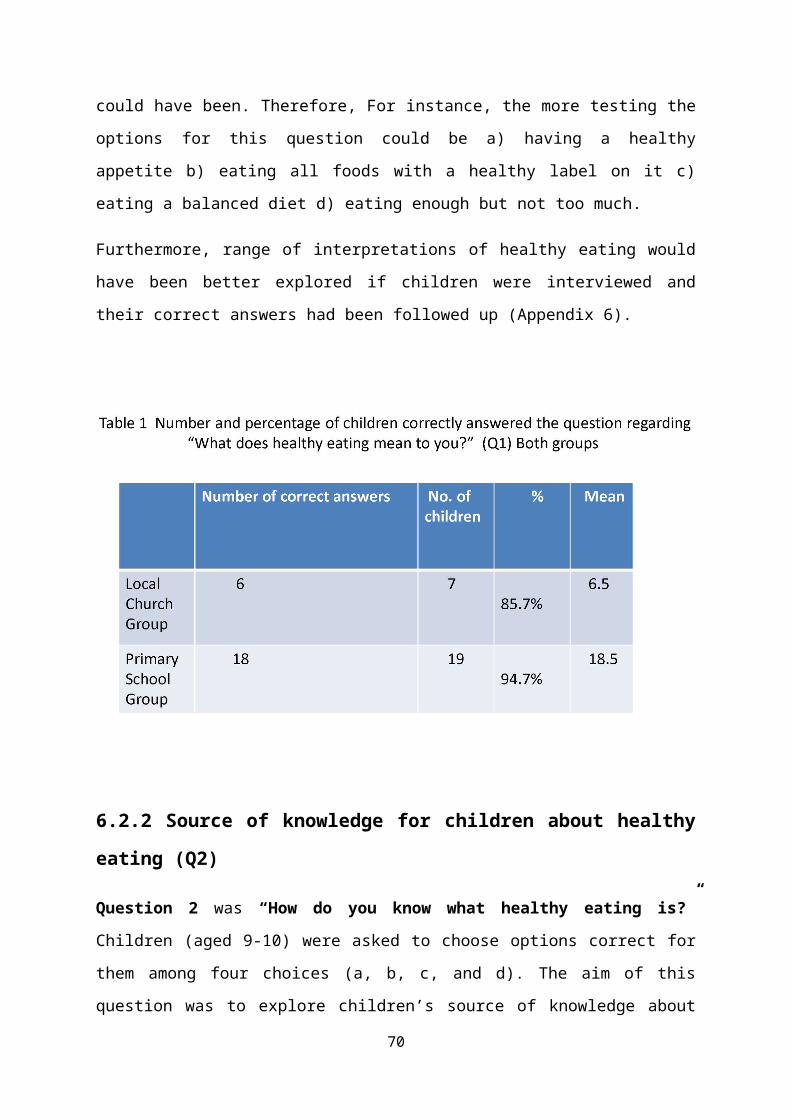
could have been. Therefore, For instance, the more testing the
options for this question could be a) having a healthy
appetite b) eating all foods with a healthy label on it c)
eating a balanced diet d) eating enough but not too much.
Furthermore, range of interpretations of healthy eating would
have been better explored if children were interviewed and
their correct answers had been followed up (Appendix 6).
6.2.2 Source of knowledge for children about healthy
eating (Q2)
Question 2 was “How do you know what healthy eating is?”
Children (aged 9-10) were asked to choose options correct for
them among four choices (a, b, c, and d). The aim of this
question was to explore children’s source of knowledge about
70
healthy eating. The options were: a) Television adverts b)
Parents told you c) Food labels/packaging d) Schools and
teachers. However, some children did not respond to only one
question, so all responses were presented as totals to provide
cumulative scores for each option.
The maximum proportion of children (100%) at local Church
group considered their parents as the main source of knowledge
for them of healthy eating as opposed to 36.8% of primary
school cohort. Also, 71.4% of children at local Church cohort
stated that they had knowledge from their schools and teachers
as compared to 36.8% at the primary school cohort. Conversely,
the highest percentage of children (42.1%) at primary school
group considered having knowledge of healthy eating from food
labels and packaging as compared to (0%) at the local Church
group. Although Television adverts were the lowest proportion
among the given options, the percentage was higher in the
local Church group (14.2%) than that at the primary school
cohort (5.2%) (Chart 1)
Such quite differences in findings between two cohorts might
suggest that parents at local Church group might do care of
their children more than those in primary school group. Or
schools of local Church cohort might have a better healthy
eating policy than those in primary school cohort. Therefore,
follow up these findings might be advantageous to further
explore the influence of parents, schools and teachers on
children’s understandings concerning source of knowledge of
healthy eating (Appendix 6).
71
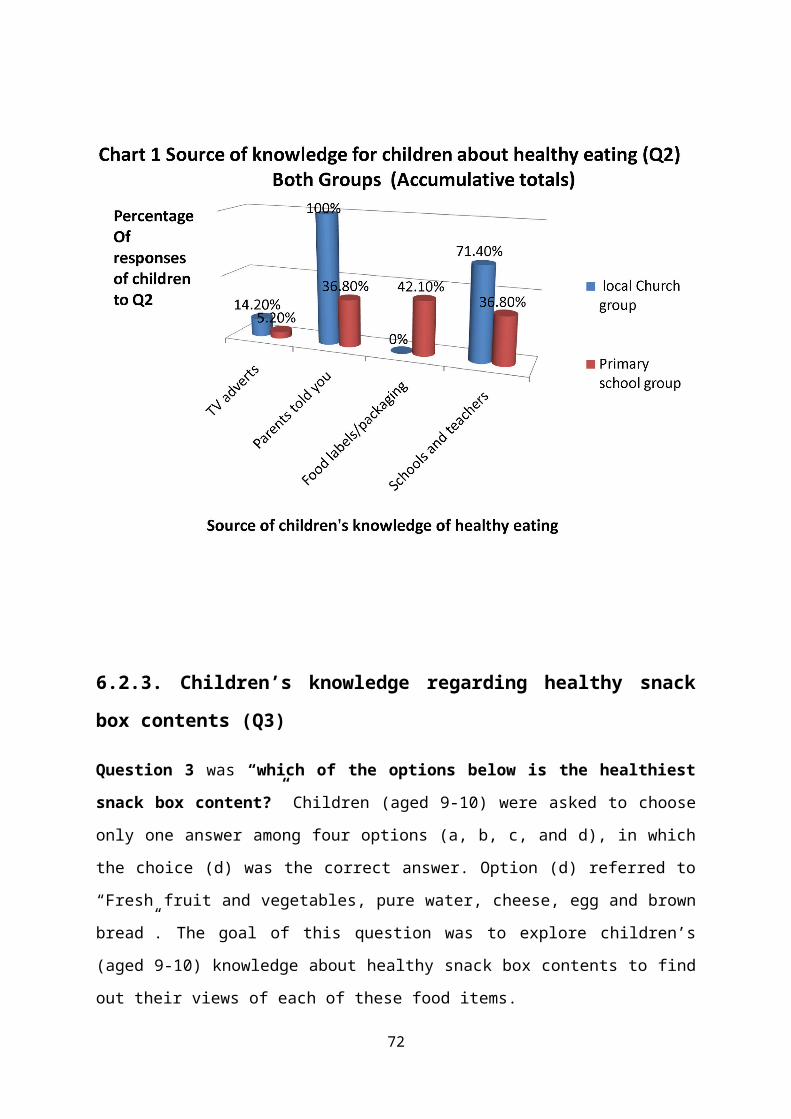
6.2.3. Children’s knowledge regarding healthy snack
box contents (Q3)
Question 3 was “which of the options below is the healthiest
snack box content?” Children (aged 9-10) were asked to choose
only one answer among four options (a, b, c, and d), in which
the choice (d) was the correct answer. Option (d) referred to
“Fresh fruit and vegetables, pure water, cheese, egg and brown
bread”. The goal of this question was to explore children’s
(aged 9-10) knowledge about healthy snack box contents to find
out their views of each of these food items.
72
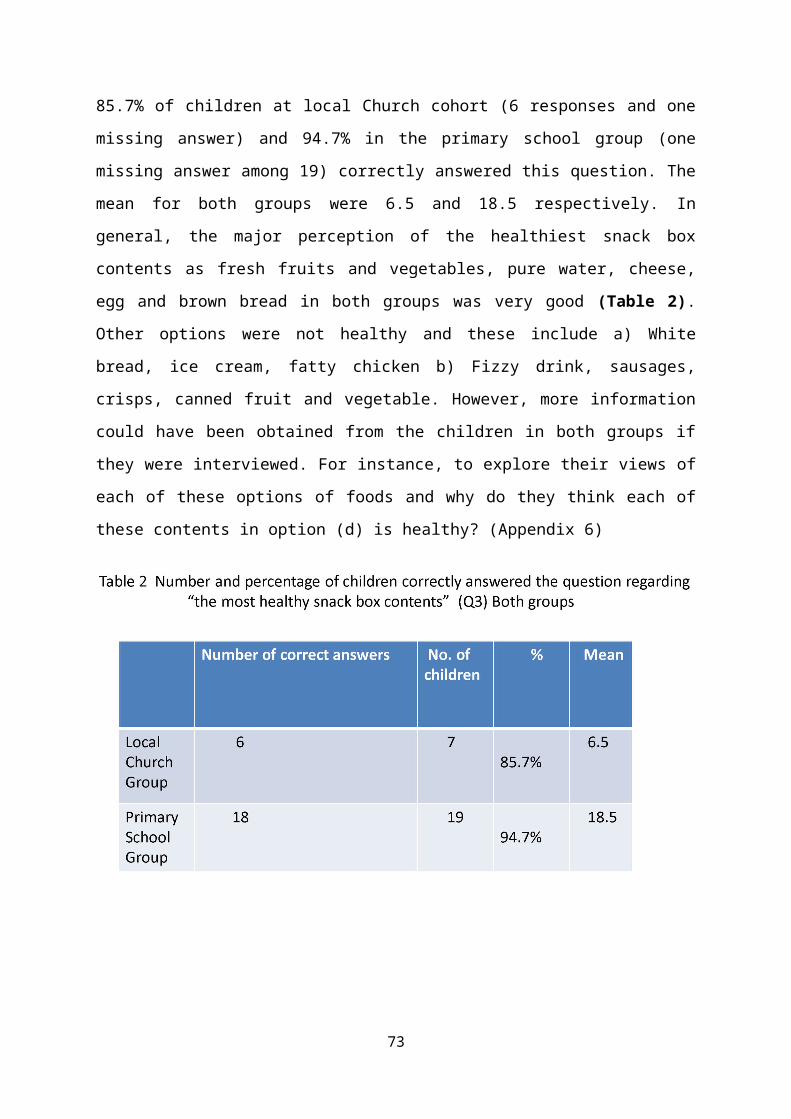
85.7% of children at local Church cohort (6 responses and one
missing answer) and 94.7% in the primary school group (one
missing answer among 19) correctly answered this question. The
mean for both groups were 6.5 and 18.5 respectively. In
general, the major perception of the healthiest snack box
contents as fresh fruits and vegetables, pure water, cheese,
egg and brown bread in both groups was very good (Table 2).
Other options were not healthy and these include a) White
bread, ice cream, fatty chicken b) Fizzy drink, sausages,
crisps, canned fruit and vegetable. However, more information
could have been obtained from the children in both groups if
they were interviewed. For instance, to explore their views of
each of these options of foods and why do they think each of
these contents in option (d) is healthy? (Appendix 6)
73
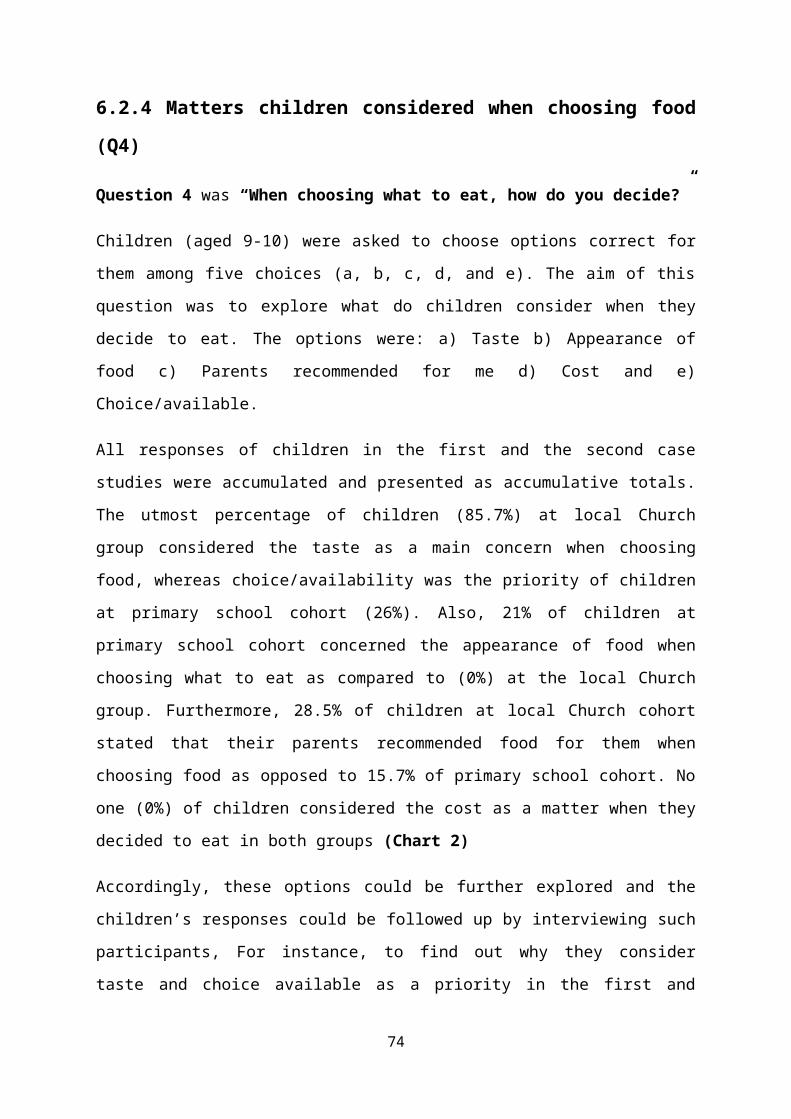
6.2.4 Matters children considered when choosing food
(Q4)
Question 4 was “When choosing what to eat, how do you decide?”
Children (aged 9-10) were asked to choose options correct for
them among five choices (a, b, c, d, and e). The aim of this
question was to explore what do children consider when they
decide to eat. The options were: a) Taste b) Appearance of
food c) Parents recommended for me d) Cost and e)
Choice/available.
All responses of children in the first and the second case
studies were accumulated and presented as accumulative totals.
The utmost percentage of children (85.7%) at local Church
group considered the taste as a main concern when choosing
food, whereas choice/availability was the priority of children
at primary school cohort (26%). Also, 21% of children at
primary school cohort concerned the appearance of food when
choosing what to eat as compared to (0%) at the local Church
group. Furthermore, 28.5% of children at local Church cohort
stated that their parents recommended food for them when
choosing food as opposed to 15.7% of primary school cohort. No
one (0%) of children considered the cost as a matter when they
decided to eat in both groups (Chart 2)
Accordingly, these options could be further explored and the
children’s responses could be followed up by interviewing such
participants, For instance, to find out why they consider
taste and choice available as a priority in the first and
74
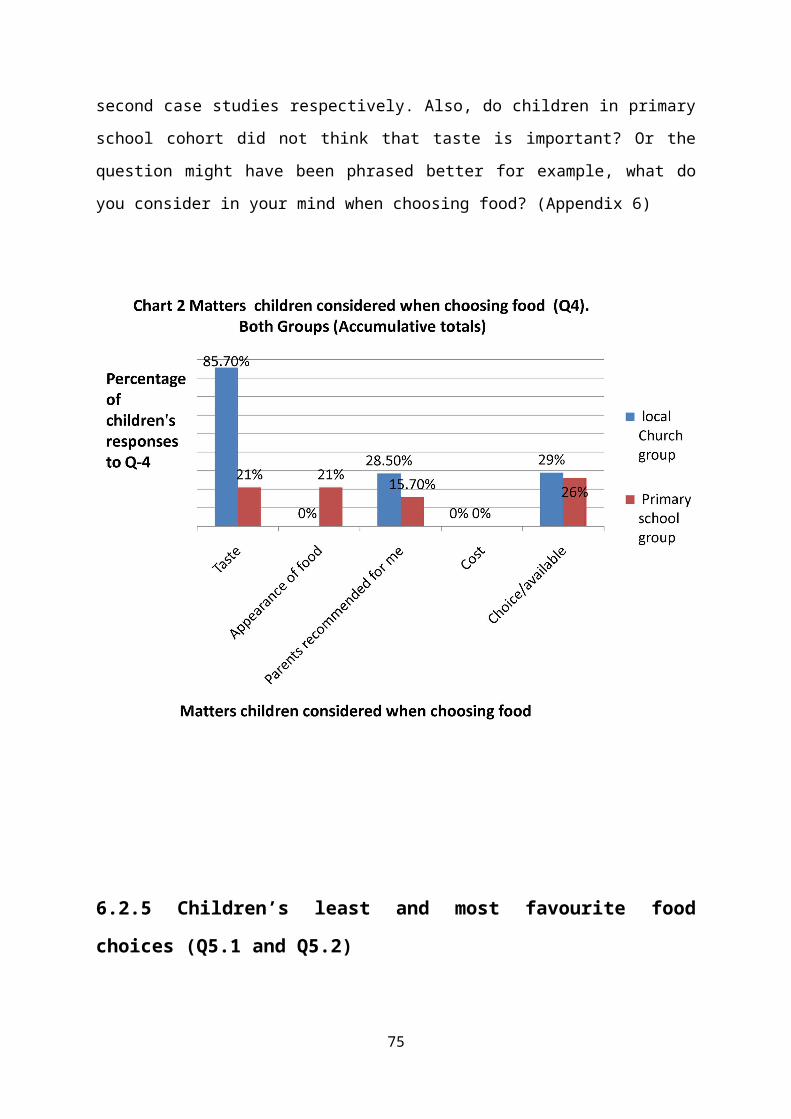
second case studies respectively. Also, do children in primary
school cohort did not think that taste is important? Or the
question might have been phrased better for example, what do
you consider in your mind when choosing food? (Appendix 6)
6.2.5 Children’s least and most favourite food
choices (Q5.1 and Q5.2)
75
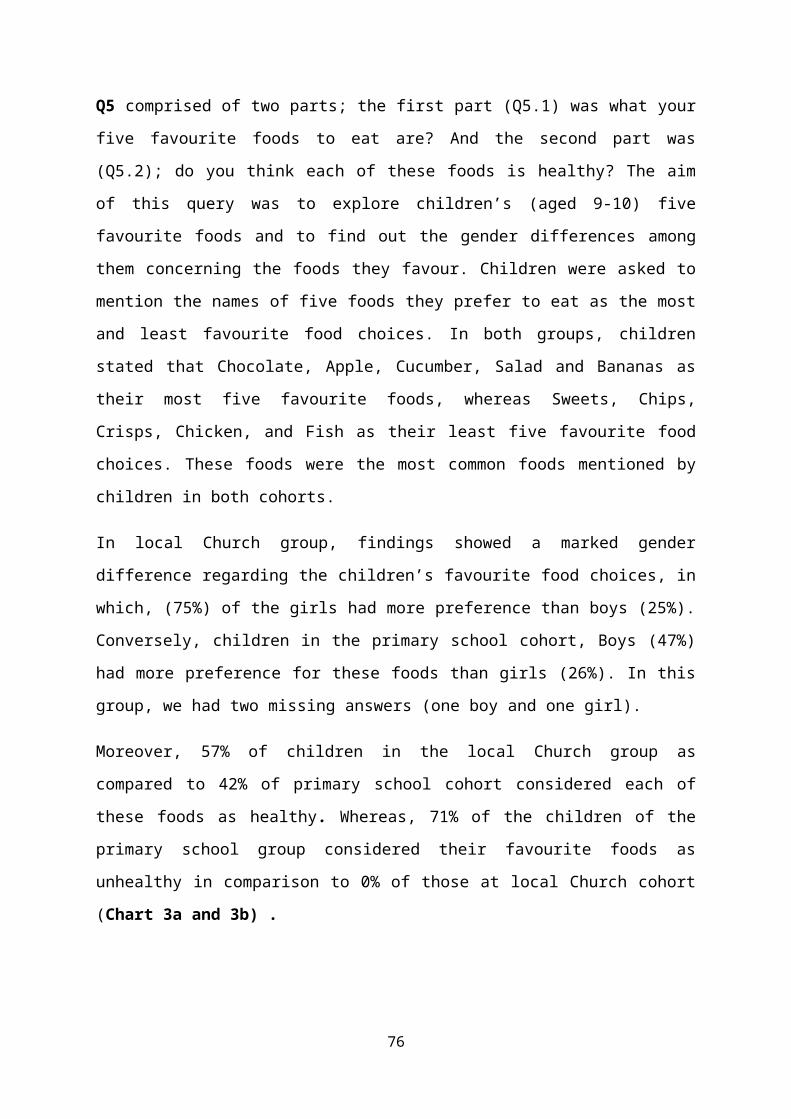
Q5 comprised of two parts; the first part (Q5.1) was what your
five favourite foods to eat are? And the second part was
(Q5.2); do you think each of these foods is healthy? The aim
of this query was to explore children’s (aged 9-10) five
favourite foods and to find out the gender differences among
them concerning the foods they favour. Children were asked to
mention the names of five foods they prefer to eat as the most
and least favourite food choices. In both groups, children
stated that Chocolate, Apple, Cucumber, Salad and Bananas as
their most five favourite foods, whereas Sweets, Chips,
Crisps, Chicken, and Fish as their least five favourite food
choices. These foods were the most common foods mentioned by
children in both cohorts.
In local Church group, findings showed a marked gender
difference regarding the children’s favourite food choices, in
which, (75%) of the girls had more preference than boys (25%).
Conversely, children in the primary school cohort, Boys (47%)
had more preference for these foods than girls (26%). In this
group, we had two missing answers (one boy and one girl).
Moreover, 57% of children in the local Church group as
compared to 42% of primary school cohort considered each of
these foods as healthy. Whereas, 71% of the children of the
primary school group considered their favourite foods as
unhealthy in comparison to 0% of those at local Church cohort
(Chart 3a and 3b) .
76
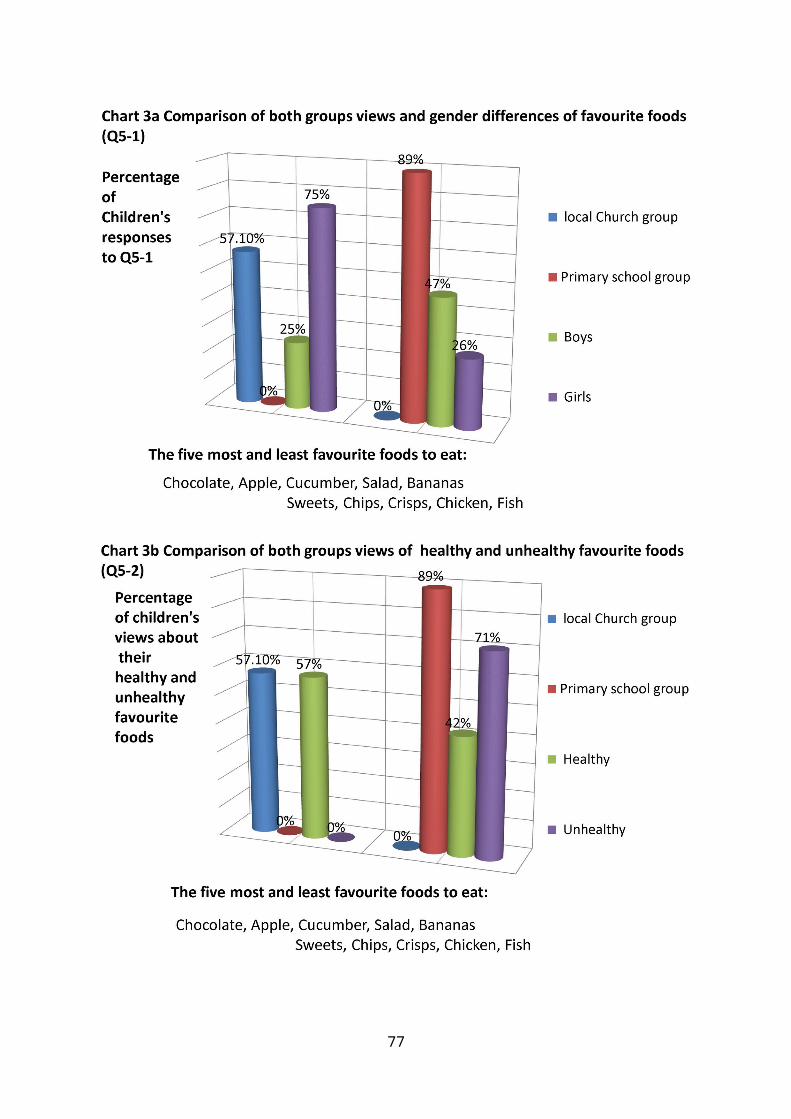
77
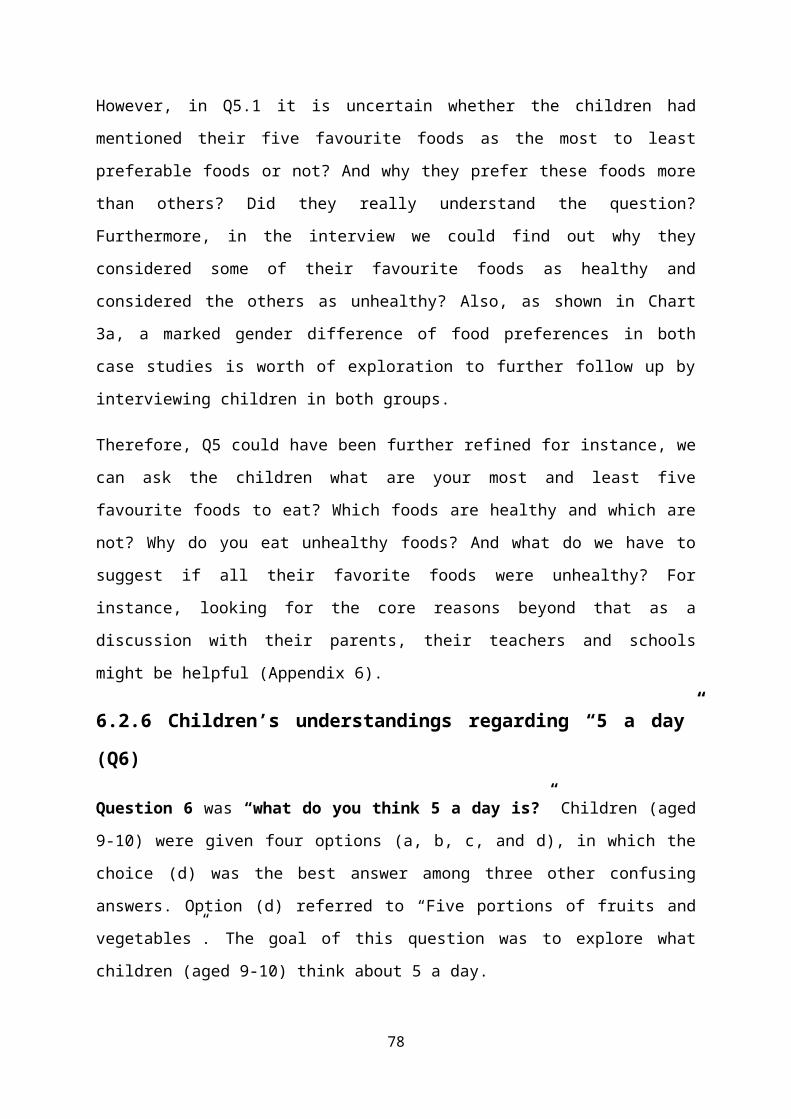
However, in Q5.1 it is uncertain whether the children had
mentioned their five favourite foods as the most to least
preferable foods or not? And why they prefer these foods more
than others? Did they really understand the question?
Furthermore, in the interview we could find out why they
considered some of their favourite foods as healthy and
considered the others as unhealthy? Also, as shown in Chart
3a, a marked gender difference of food preferences in both
case studies is worth of exploration to further follow up by
interviewing children in both groups.
Therefore, Q5 could have been further refined for instance, we
can ask the children what are your most and least five
favourite foods to eat? Which foods are healthy and which are
not? Why do you eat unhealthy foods? And what do we have to
suggest if all their favorite foods were unhealthy? For
instance, looking for the core reasons beyond that as a
discussion with their parents, their teachers and schools
might be helpful (Appendix 6).
6.2.6 Children’s understandings regarding “5 a day”
(Q6)
Question 6 was “what do you think 5 a day is?” Children (aged
9-10) were given four options (a, b, c, and d), in which the
choice (d) was the best answer among three other confusing
answers. Option (d) referred to “Five portions of fruits and
vegetables”. The goal of this question was to explore what
children (aged 9-10) think about 5 a day.
78
Accordingly, 57.1% of children in the local Church group as
compared to 89.4% of primary school cohort correctly thought
that “5 a day” means five portions of fruits and vegetables.
Also, 14.2% of children in the local Church group as opposed
to 5% in the primary school cohort perceived that “5 a day”
means five portions of fruits and five portions of vegetables.
No one (0%) in both groups thought that 5 a day mean five
portions of fruits and one portion of vegetables. Whereas, 5%
of children in the primary school and no one (0%) thought that
5 a day mean five portions of fruits and two portions of
vegetables. (Chart4)
Further information could have been explored if children were
interviewed. For instance, do you eat five portions of fruit
and vegetables a day? And why? (Appendix 6)
79
6.2.7 Responses of children in both groups about the
question “why do you think calcium is an important
part of your diet” (Q7)
Question 7 was “why do you think calcium in an important part
of your diet?” Children (aged 9-10) were asked to choose only
one answer among four options (a, b, c, and d), in which the
choice (d) was the correct answer. Option (d) referred to
“Build strong and healthy teeth and bones”. The goal of this
question was to explore children (aged 9-10) thoughts about
calcium as an important part of their diet.
85.7% of children at local Church group and 94.7% of primary
school cohort correctly answered this question. The mean for
both groups were 6.5 and 18.5 respectively. In general, the
major understanding of children about calcium as a crucial
element to build healthy bones and teeth was very good (Table
3). Also, more information could have been explored if
children were interviewed. For instance, do you know other
types of vitamins and elements which you think are healthy?
And how do you know that calcium is healthy? (Appendix 6)
80
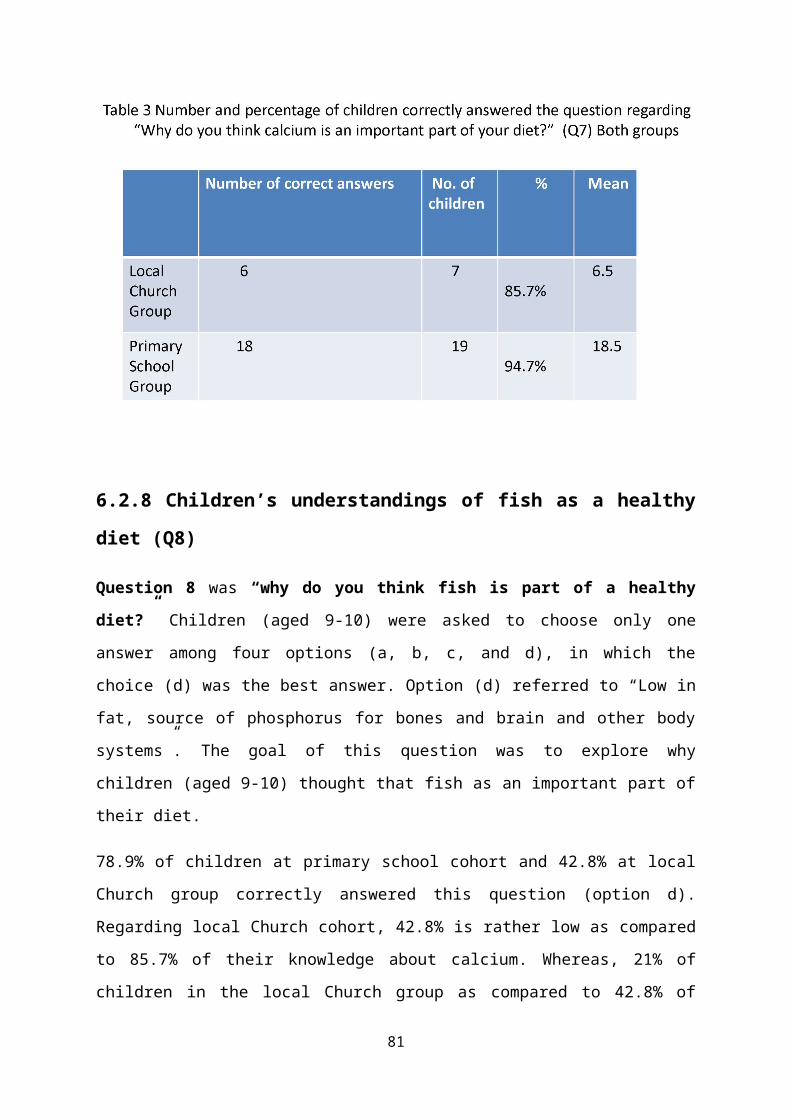
6.2.8 Children’s understandings of fish as a healthy
diet (Q8)
Question 8 was “why do you think fish is part of a healthy
diet?” Children (aged 9-10) were asked to choose only one
answer among four options (a, b, c, and d), in which the
choice (d) was the best answer. Option (d) referred to “Low in
fat, source of phosphorus for bones and brain and other body
systems”. The goal of this question was to explore why
children (aged 9-10) thought that fish as an important part of
their diet.
78.9% of children at primary school cohort and 42.8% at local
Church group correctly answered this question (option d).
Regarding local Church cohort, 42.8% is rather low as compared
to 85.7% of their knowledge about calcium. Whereas, 21% of
children in the local Church group as compared to 42.8% of
81
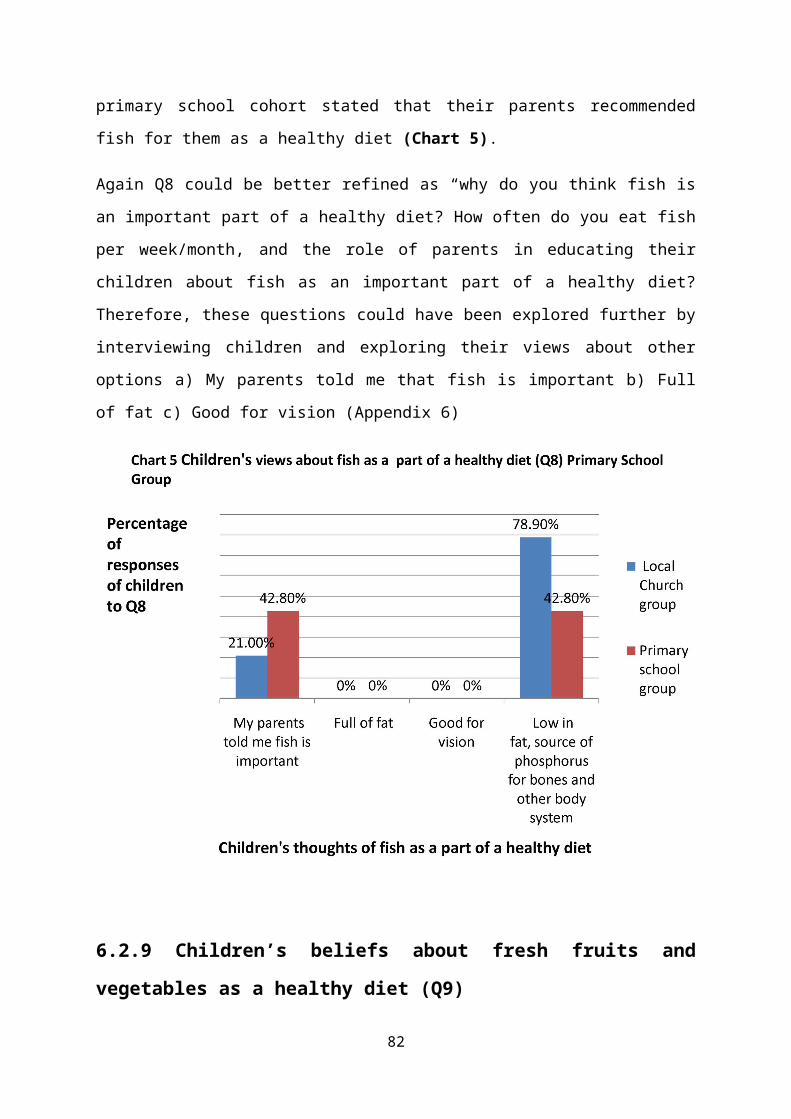
primary school cohort stated that their parents recommended
fish for them as a healthy diet (Chart 5).
Again Q8 could be better refined as “why do you think fish is
an important part of a healthy diet? How often do you eat fish
per week/month, and the role of parents in educating their
children about fish as an important part of a healthy diet?
Therefore, these questions could have been explored further by
interviewing children and exploring their views about other
options a) My parents told me that fish is important b) Full
of fat c) Good for vision (Appendix 6)
6.2.9 Children’s beliefs about fresh fruits and
vegetables as a healthy diet (Q9)
82
Question 9 was “why do you think fresh fruits and vegetables
are an important part of a healthy diet?”
Children (aged 9-10) were asked to choose only one answer
among four options (a, b, c, and d), in which the choice (d)
was the correct answer. Option (d) referred to “Source of
essential vitamins and minerals”. Other options were a) Have
beautiful colors b) Taste is good c) Always available at home.
The goal of this question was to explore why children (aged 9-
10) thought that fresh fruits and vegetables are healthy diet.
57.1% of children at local Church group and 94.7% of primary
school cohort correctly answered this question. The mean for
both local Church group and primary school cohort were 5.5 and
18.5 respectively (Table 4).
This question could have been improved such as why do you
think fresh fruits and vegetables are a significant part of a
healthy diet? And why do you think fresh is better than canned
or frozen fruits and vegetables? Which is better to eat and
why? And why do people often do not eat the fresh version?
(Appendix 6)
83
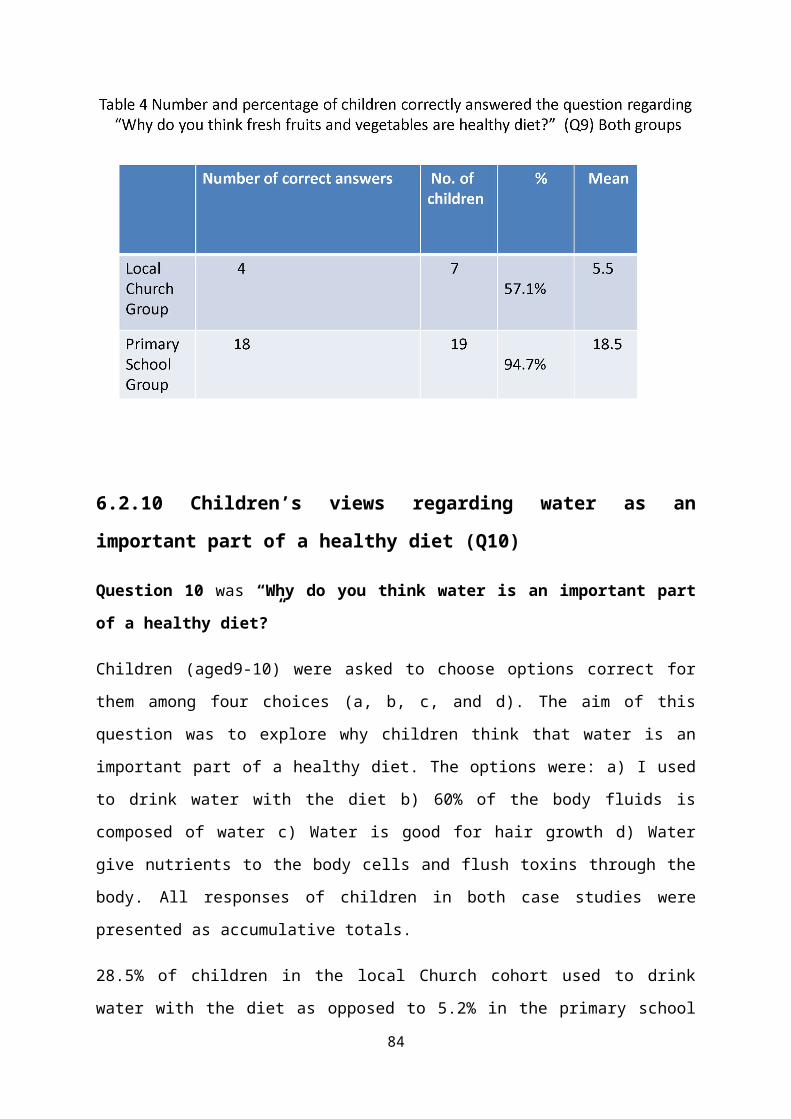
6.2.10 Children’s views regarding water as an
important part of a healthy diet (Q10)
Question 10 was “Why do you think water is an important part
of a healthy diet?”
Children (aged9-10) were asked to choose options correct for
them among four choices (a, b, c, and d). The aim of this
question was to explore why children think that water is an
important part of a healthy diet. The options were: a) I used
to drink water with the diet b) 60% of the body fluids is
composed of water c) Water is good for hair growth d) Water
give nutrients to the body cells and flush toxins through the
body. All responses of children in both case studies were
presented as accumulative totals.
28.5% of children in the local Church cohort used to drink
water with the diet as opposed to 5.2% in the primary school
84
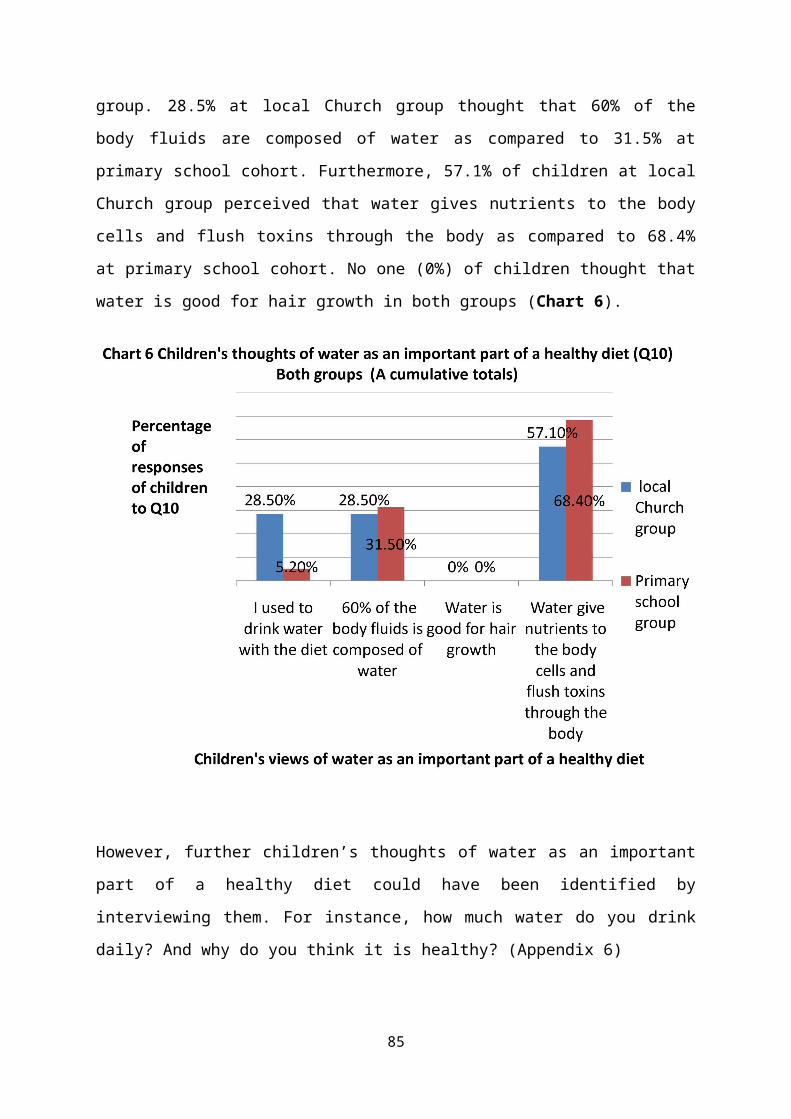
group. 28.5% at local Church group thought that 60% of the
body fluids are composed of water as compared to 31.5% at
primary school cohort. Furthermore, 57.1% of children at local
Church group perceived that water gives nutrients to the body
cells and flush toxins through the body as compared to 68.4%
at primary school cohort. No one (0%) of children thought that
water is good for hair growth in both groups (Chart 6).
However, further children’s thoughts of water as an important
part of a healthy diet could have been identified by
interviewing them. For instance, how much water do you drink
daily? And why do you think it is healthy? (Appendix 6)
85
6.2.11 Children’s knowledge regarding a healthy
person (Q11)
Question 11 was “How do you know if a person is healthy?”
Children (aged 9-10) were asked to choose options correct for
them among four choices (a, b, c, and d). The aim of this
question was to explore the children’s thoughts of a healthy
person. The options were: a) They are fit, fast and skinny b)
They look healthy not big or fat c) Good shape, no signs of
diseases, infections or obesity, and d) They are not
overweight, they do exercise, do not smoke. All responses of
children in both case studies were presented as accumulative
totals (Chart 7).
71% of children in the local Church group and 5.2% of children
at primary school cohort considered that a healthy person
looks fit, fast and skinny. Whereas, 57% of children local
Church group and only 5.2% of children at primary school
group, thought that a healthy person looks healthy not big and
fat. Moreover, 29% of children in the local Church group as
opposed to 42% of children at primary school cohort viewed
that a healthy person has good shape, no signs of diseases,
86

infections or obesity. Also, children in the both groups
relatively agreed with their understandings that a healthy
person is not overweight, do exercise and do not smoke with
57% and 58% in the first and second case studies respectively
(Chart 7).
Accordingly, the findings revealed a big difference of
children’s views in both cohorts concerning this question.
This difference perhaps could be due to the influence of their
parents, teachers and schools on their knowledge of a healthy
person. Therefore, this could have been explored further by
interviewing children in both groups. For instance, “Do you
think someone’s size or shape has anything to do with their
health?” Also, some important characteristics of a healthy
person could have been given as open questions. For instance,
fit, not overweight, good shape and signs of diseases or
infections (Appendix 6).
87
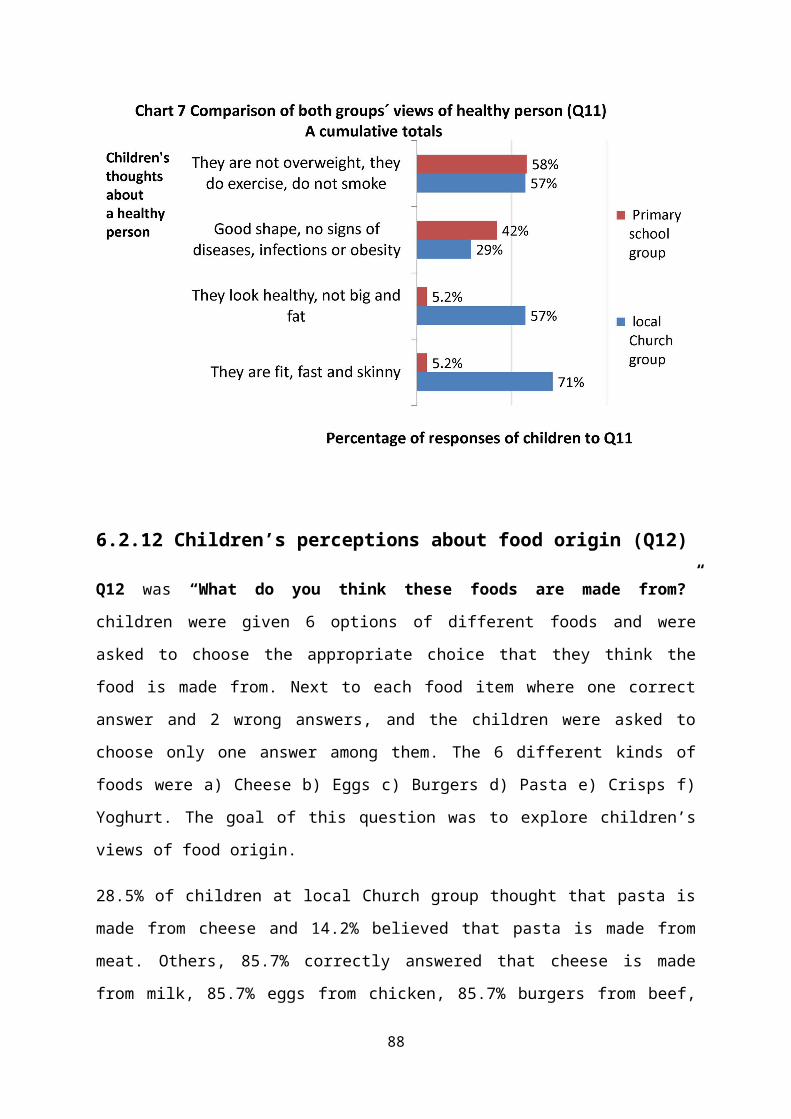
6.2.12 Children’s perceptions about food origin (Q12)
Q12 was “What do you think these foods are made from?”
children were given 6 options of different foods and were
asked to choose the appropriate choice that they think the
food is made from. Next to each food item where one correct
answer and 2 wrong answers, and the children were asked to
choose only one answer among them. The 6 different kinds of
foods were a) Cheese b) Eggs c) Burgers d) Pasta e) Crisps f)
Yoghurt. The goal of this question was to explore children’s
views of food origin.
28.5% of children at local Church group thought that pasta is
made from cheese and 14.2% believed that pasta is made from
meat. Others, 85.7% correctly answered that cheese is made
from milk, 85.7% eggs from chicken, 85.7% burgers from beef,
88

42.8% pasta from cereal, 71.4% crisps from potatoes, and 71.4%
yoghurt from milk (Table 5)
Also, 10.5% of children at primary school cohort perceived
that eggs are made from Cow, 26.3% thought that pasta is made
from cheese, and 5.2% stated that crisps are made from
plastic. Others, 94.7% correctly answered that cheese is made
from milk, 82.3% eggs from chicken, 84.2% burgers from beef,
47.3% pasta from cereal, 78.9% crisps from potatoes, and 73.6%
yoghurt from milk (Table 5). These findings revealed
children’s confusion in this small sample of children in both
groups which indicate a partial understanding of children
regarding food origin.
However, further exploration of children’s knowledge of food
origin could be maintained by interviewing them and following
up their answers to the questionnaire. For instance, “Do you
think potatoes or tomatoes grow under or above the ground?”
(Appendix 6)
89

6.2.13 Children’s habits of taking breakfast (Q13)
Question 13 comprised of two parts, the first (Q13.1) was
“Have you had your breakfast today?” with yes and no options.
Also, children were given choices of food items in case they
had their breakfast on the day of the survey. These food items
were a) Egg b) Cereal c) Milk d) Bread/Toast and e) Orange
90
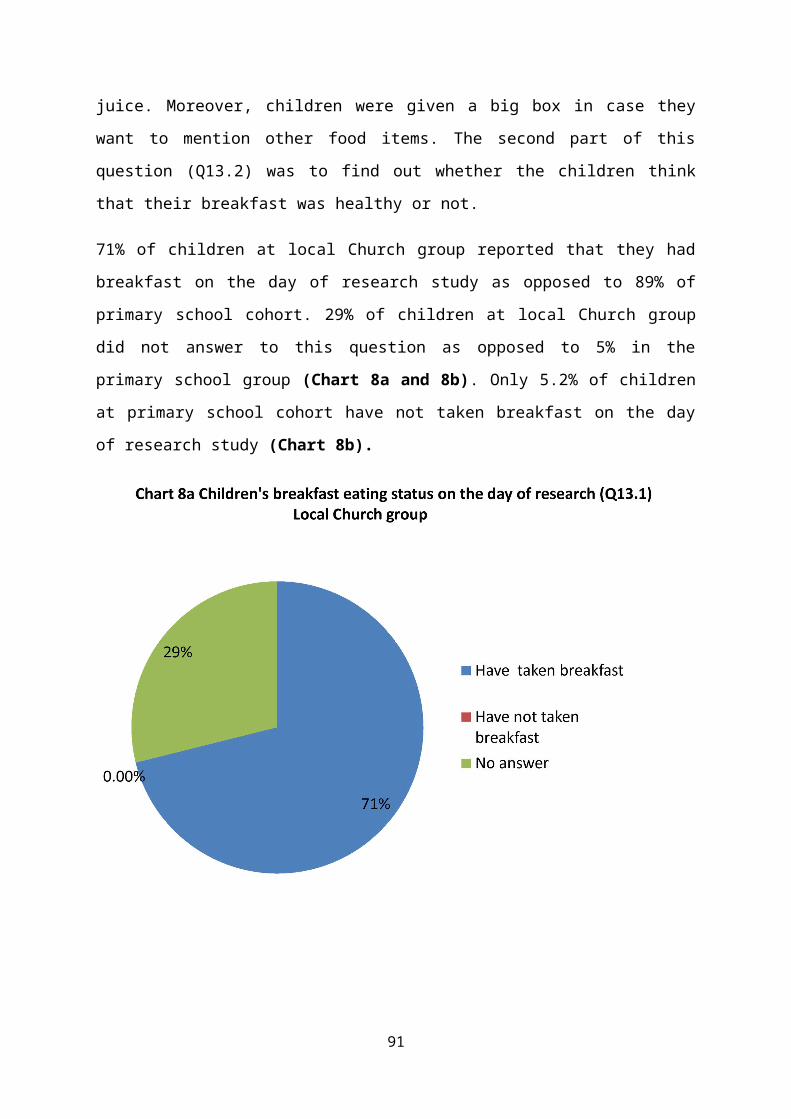
juice. Moreover, children were given a big box in case they
want to mention other food items. The second part of this
question (Q13.2) was to find out whether the children think
that their breakfast was healthy or not.
71% of children at local Church group reported that they had
breakfast on the day of research study as opposed to 89% of
primary school cohort. 29% of children at local Church group
did not answer to this question as opposed to 5% in the
primary school group (Chart 8a and 8b). Only 5.2% of children
at primary school cohort have not taken breakfast on the day
of research study (Chart 8b).
91

As shown in Chart 9, cereal was the utmost among food items
that had been consumed by the local Church group 42.8% as
compared to 47% in the primary school group on the day of the
survey. In the local Church group no one (0%) had consumed egg
on the day of survey as compared to (5.2%) at primary school
cohort. 21% of children in the local Church cohort had other
foods or drinks such as yoghurt, fruit, water, hot dogs, and
fresh fruit. Both groups had milk on the day of research with
(14.2%) and (15.7%) for the local Church group and the primary
school group respectively. Furthermore, 28.5% of children had
bread/toast in the local Church group as opposed to only
(5.2%) in the primary school cohort. Only (5.2%) of children
92
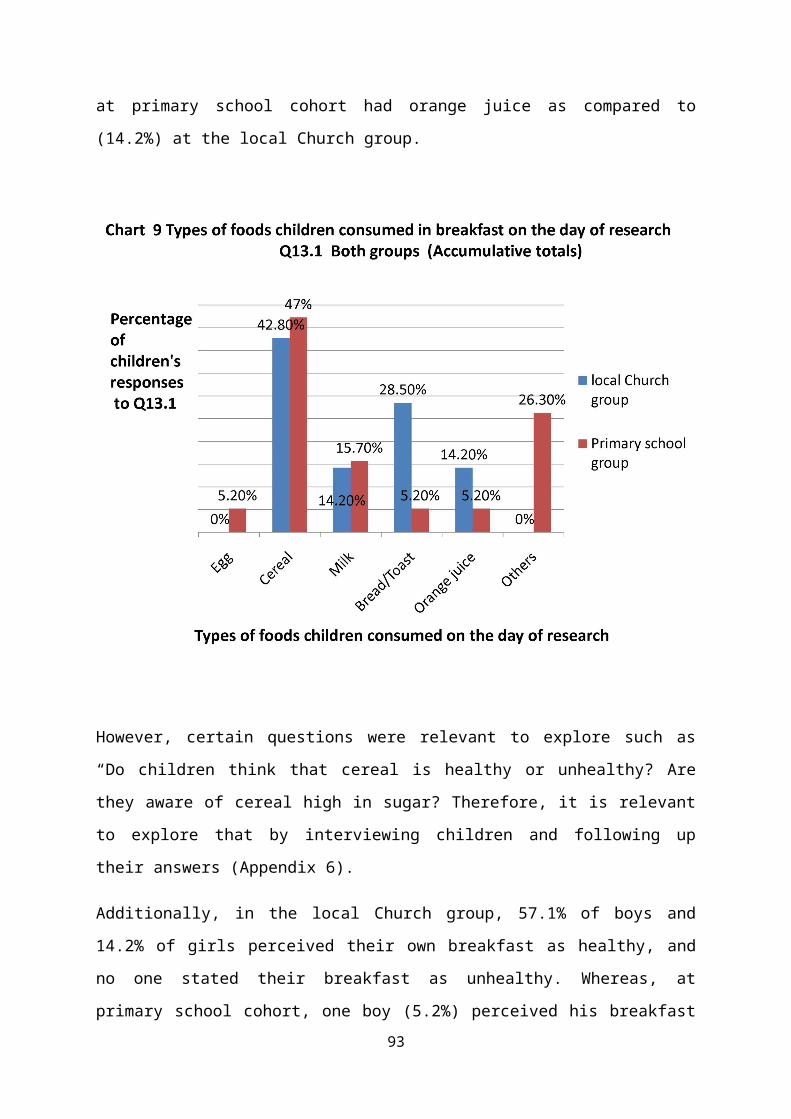
at primary school cohort had orange juice as compared to
(14.2%) at the local Church group.
However, certain questions were relevant to explore such as
“Do children think that cereal is healthy or unhealthy? Are
they aware of cereal high in sugar? Therefore, it is relevant
to explore that by interviewing children and following up
their answers (Appendix 6).
Additionally, in the local Church group, 57.1% of boys and
14.2% of girls perceived their own breakfast as healthy, and
no one stated their breakfast as unhealthy. Whereas, at
primary school cohort, one boy (5.2%) perceived his breakfast93

as mostly healthy breakfast, 31.5% girls and 26.3% boys
thought it was healthy. Only 2 boys (10.5%) and 2 girls
(10.5%) perceived their breakfast as unhealthy breakfast
(Table 6).
Therefore, it is worthy to explore why some of the children
thought their breakfast was healthy and others perceived their
breakfast as unhealthy by interviewing them and following up
their answers (Appendix 6).
6.2.14 Children’s Knowledge of healthier food choices
(Q14)
Q14 composed of 8 questions (a to h), each question had two
options, one is healthy and one is unhealthy. The aim of this94
question was to find out whether children (aged 9-10) could
make healthy food choices and could differentiate between
healthy and unhealthy food and drink options. This special
question was presented in texts and pictures to make it
attractive for children to understand this question.
Children’s were given four pairs of foods or drinks and asked
to choose the relatively healthier choices among each pair. In
local Church groups, in general, knowledge of healthy food
choices was bad (mean number of correct answers was 1.5 out of
4). Only (47.1%) could identify correctly the relatively
healthier choices among the four pairs of foods or drinks. Two
children (29%) chose both fresh and fried fruits and
vegetables as healthy foods; one child (14%) considered both
food low and high in fat as healthy, two (29%) stated that
both food low and high in salt is healthy, one (14%) chose
both boiled and fried potatoes as healthy foods, and one (14%)
regarded both brown and white bread are healthy choices
(Chart10a).
In the other cohort, at primary school group, in general,
knowledge of healthy food choices was good and better than
those at the local Church group (mean number of correct
answers was 3 out of 4. About (77.3%) could identify correctly
the relatively healthier choices among the four pairs of foods
or drinks. (24%) chose fried fruits and vegetables as healthy
foods; (6%) considered both food low and high in fat as
healthy, (24%) stated that both food low and high in salt are
healthy, (12%) considered both food low and high on sugar is
healthy, (12%) thought that both boiled and fried potatoes are95
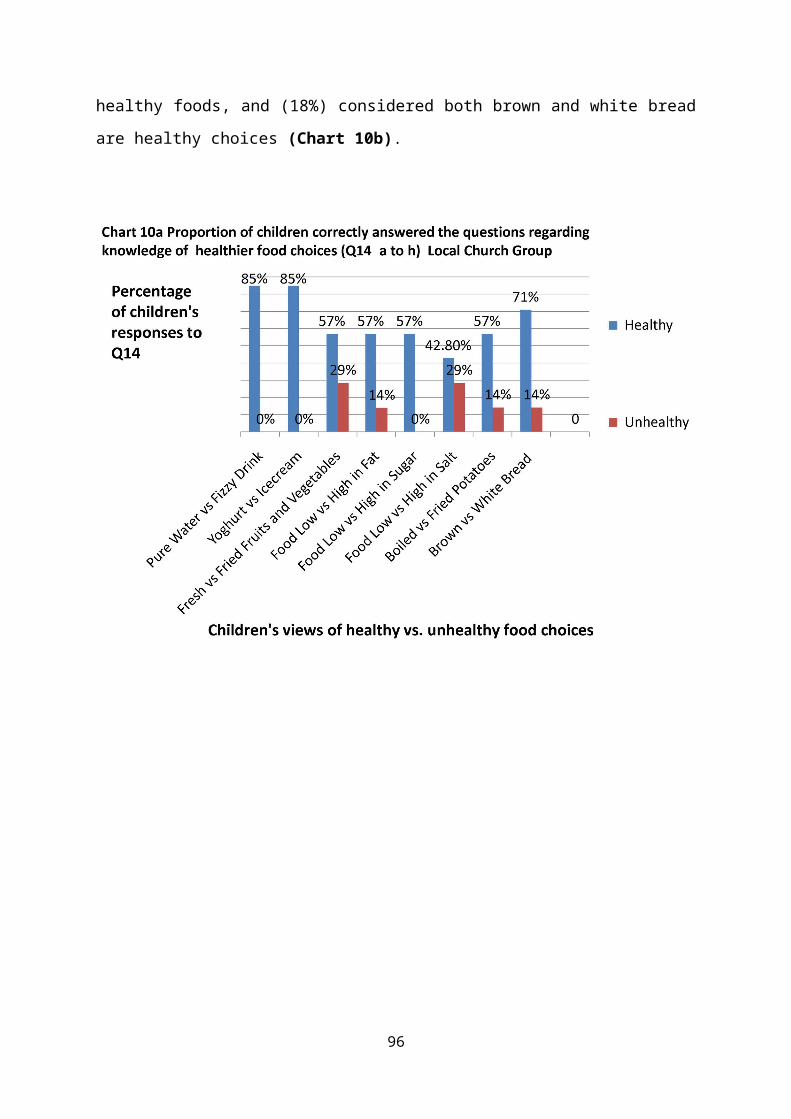
healthy foods, and (18%) considered both brown and white bread
are healthy choices (Chart 10b).
96
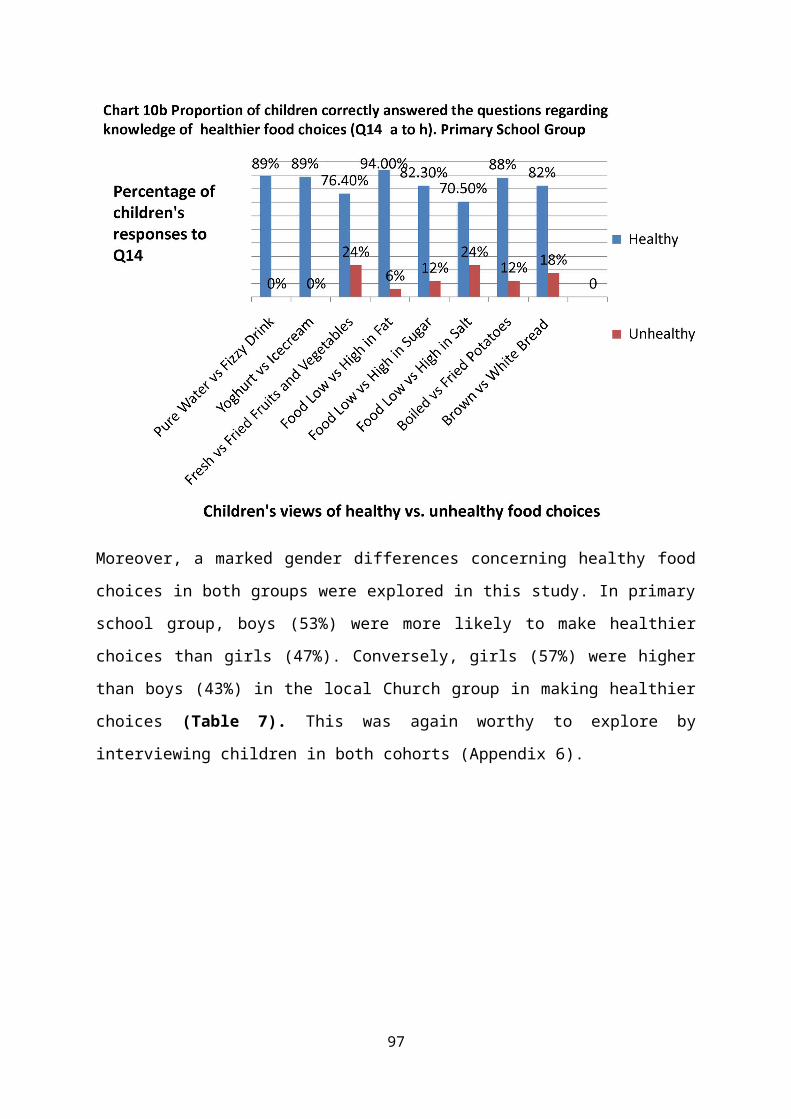
Moreover, a marked gender differences concerning healthy food
choices in both groups were explored in this study. In primary
school group, boys (53%) were more likely to make healthier
choices than girls (47%). Conversely, girls (57%) were higher
than boys (43%) in the local Church group in making healthier
choices (Table 7). This was again worthy to explore by
interviewing children in both cohorts (Appendix 6).
97

7. Discussion
Having reviewed the literatures concerned with healthy eating
and childhood obesity, and after the data results have been
presented for both cohorts, I will now highlight my discussion
for each group separately. This is because each group has a
different context and background which might influence the
research findings. Therefore, I will epitomize each group’s
findings independently so that I can argue the main
interesting issues that could be managed to address childhood
obesity and to promote healthy eating.
Findings from the current study showed lots of misconceptions
of children’s views of healthy eating; the following themes of
perceptions need to be further investigated: most importantly,
1. Matters children considered when choosing what to eat, 2.
Gender food preferences, 3. Children’s thoughts regarding a
healthy person, 4. Children’s views on Food origin, 5.
Children’s habits of taking breakfast, 6. Children’s thoughts
98

concerning healthier food choices, and 7. Source of knowledge
for children about healthy eating. I will identify and explore
each theme independently for each participating group to
epitomize children’s misconception explored in the results of
this research study.
7.1. Matters for consideration in choosing food by
children (Q4)
As I mentioned already, for this question, all responses of
children both cohorts were presented as accumulative totals.
The utmost proportion of children 85.7% at local Church group
considered the taste as a priority when choosing food as
compared to 26% at primary school cohort. In the primary
school group, (21%) of the children concerned the appearance
of food when choosing food as compared to (0%) of the local
Church cohort. Also, among the local Church group 28.5% stated
that their parents recommended food for them as opposed to
15.7% of the primary school cohort. No one (0%) considered the
cost as a matter when they decided to eat in both groups
(Chart 2).
These findings are similar to those revealed by a large cross-
sectional study in Hong Kong (DOH, 2008), despite of the
difference in cultures, socioeconomic state, ethnicity, eating
environment and quality of foods.
Moreover, our findings clearly support the cognitive
development theory which has already been mentioned in the
literature review (chapter2. 4). As we are dealing with
99
children in the concrete operational stage of development
(aged 9-10), accordingly, and as Bahn et al., (1989)
suggested, concrete operational children concentrate mainly on
the quality and characteristic of the brand, for instance,
liking the taste or the colour of the package when they were
distinguishing the brands. Young children focus on appearance
and texture, whereas older children focus on taste aspects
(Zeinstra et al; 2007).
Additionally, our findings support what already had been
suggested by Sharifa et al (2013) who found that most of the
(7-9 years old) children like food because of the taste. Also,
(Olson et al., 1981; Ricketts, 1997; Pѐrez-Rodrigo et al.,
2003; Molaison et al., 2005) have shown that the taste of food
was the major limiting factor related to consumption and
regarded as a significant determinant of children’s food
choice. Furthermore, for non-favourite food, some children
dislike some types of foods when they know that the food is
unhealthy, for instance, sweets as they know it can cause
tooth aches or they dislike fish as it contains lots of bones
(p. 135).
However, these findings are worthy to explore to find out and
follow up children’s answers such as why you prioritize taste
when choosing food, a food with taste nice is it healthy? What
about the influence of your parents on your choice, and do
they make healthy choices for their children, and how much do
children care about the appearance of food and cost? I
believe that such different children’s views could be better
100

explored by interviewing them in this critical stage of
cognitive development (Appendix 6).
Besides taste, in both groups, a surprising finding in our
study was the clear influence of the parent on children’s
decisions when choosing food. In this small sample study,
28.5% of children in the local Church group stated that their
parents recommended food for them in comparison to 15.7% of
primary school cohort. As I mentioned already, in the concrete
operational stage, children are less egocentric, and the
instrumental rewarding appears to fit their cognitive
capacities, although we did not measure the cognitive
development. Also, children have a better understanding of
value, and they can see another’s perspective, they are more
independent and self confident than younger age children
(Flavell and Piaget, 1963; Roedder-John, 1999; and Delfos,
2003). Therefore, it is relevant to explore the reasons beyond
the influence of parents on children’s decisions, in this
particular age group, when choosing food in both cohorts. For
instance, the child might have a loss of appetite or might
have abnormal growth and development (Appendix 6).
7.2 Gender food preferences (Q5)
Children in both groups had common most and least five
favourite foods. Most favourite foods were Chocolate, Apple,
Cucumber, Salad and Bananas, while the least favourite foods
were Sweets, Chips, Crisps, Chicken and Fish. As shown in
Chart 3a, the findings revealed a marked gender difference
regarding children’s five favourite food choices. That is, at
101
the local Church group, 75% of girls had more preference than
boys (25%). Conversely, at the primary school cohort, Boys 47%
had more preference for these foods as opposed to 26% of
girls.
Moreover, 57% of children in the local Church cohort,
considered each of these foods as healthy as opposed to 42% of
the primary school cohort. Despite of 71% of children at the
primary school cohort considered their five favourites as
unhealthy; they considered such foods as their favourite foods
(Chart 3b).
In local Church groups, children foods such as Pizza, Crisps,
Chicken, Chocolate, Sweets, Cake but not Fruit cake, Orange
juice, Bananas, Biscuits, Kiwi, Beef, Cucumber, Apple and
Pepper were their favourite foods. Among seven children, four
children (2 boys and 2 girls) considered each of these foods
as healthy, and three children did not answer this question (Q
5.2).
Children at the primary school cohort stated foods such as
bananas, Salad, Apple, Pasta, Pizza, pork noodles, Ice cream,
Strawberries and Chocolate, Potatoes, Carrot, Sausage, Meat,
Hotdogs, Fish, Chips, Olives, Rose berries, Cheese and Sweets
as their favourite foods. In this group, we had two missing
answers. Among 19 children in the primary school group, two
children did not answer this question (Q 5.2), 5 children
regarded these foods as healthy and 12 children considered
these foods as unhealthy.
102

However, these findings were similar to those revealed by the
department of health (DOH, 2008).
Also, boys as compared to girls, in both groups, had a greater
preference for pork, beef and fish. Whereas, girls preferred
fruit and vegetables, sweets and comfort foods such as ice-
cream and chocolate more than boys in both cohorts.
Despite of similarity of these findings to what had been
already highlighted in the literature review (Chapter 2.10),
each group of children had a different gender preference for
the same quality of food they favoured. 75% of girls at the
local Church cohort had more preference for their five
favourite foods than boys 25% as opposed to 47% boys and 26%
girls at the primary school group. This is worthy to explore
by interviewing children of different genders in both groups
to find out why they had different gender food preferences,
although they shared similar factors such as age, gender,
socioeconomic state, ethnicity and culture.
As already mentioned, such factors are connected to food
preference (Logue and Smith, 1986; Drewnowski, 1997; Turrell,
1998; Lytle et al., 2000; Wansink et al., 2003; Westenhoefer
and Cooke, 2005; Caine-Bish and Scheule, 2007). Accordingly,
it is essential to understand the influence of these factors
on children’s food preferences to help develop healthy and
successful menus (Caine-Bish and Scheule, 2009). Moreover, the
level of education of the parents is worthy to explore by
interviewing parents. However, I potentially arranged some of
the questions that were my original intention to ask children
103
to further explore and follow up the influence of their
parents and other factors on their gender preferences
(Appendix 6).
However, it was uncertain how did the children appreciate this
question? Did they consider each of their favourite foods as
healthy or unhealthy? This is relevant to find out why did
they perceive some of their favourite foods as healthy and
others as unhealthy? And if certain food was unhealthy, why
did they favour it? This finding again is worthy to explore
and follow up to further understand why in both cohorts
children had different gender food preferences which are
against studies revealed in the literature review (Chapter
2.10). Also, further research study is needed to confirm our
findings.
7.3 Children’s knowledge regarding a healthy person
(Q11)
71% of children in the local Church group thought that a
healthy person looks fit, fast and skinny as opposed to only
5.2% of children at the primary school cohort. Whereas, 57% of
children in the local Church group thought that a healthy
person looks healthy not big and fat as compared to 5.2% of
the primary school cohort. Also, 29% of children in the local
Church group perceived that a healthy person has good shape,
no signs of diseases, infections or obesity in comparison to
104

42% of the primary school group. Moreover, children in the
both groups relatively agree with that a healthy person is not
overweight, do exercise and do not smoke with 57% and 58% in
the first and second cohorts respectively (Chart 7).
Our findings support what had been already explained in the
literature review (Chapter 2.3). Accordingly, same age groups
from different contexts and background had various perceptions
of their health and others bodies’ health. These results were
similar to those found by Burrows (2007).
Certain question such as “Do you think someone’s size or shape
has anything to do with their health?” and gender
differentiation responses, are worthy to explore. For
instance, they might refer on their understandings that some
people are just born big or little. As they perceived that
genetic factors play a confounding role in the possibilities
afforded to people to become slim or thin (Kirk and Colquhoun,
1989). Such findings could have been further explored by
interviewing children (Appendix 6).
As shown in Chart 7, children’s responses represent a
conflation of fitness with non-fatness, health with size,
shape, and weight. These findings also were indications that
one’s capacity to run, together with what they eat, may be
responsible for the way they look and therefore their health.
This notion that health can, in a sense, be read off the body
is well reconsidered in physical education literature
(Crawford, 1980; Tinning, 1985; Shilling, 1993; Markula,
1997). However, this preoccupation with appearance as an
105
indicator of health is largely regarded as the preserve of
adults. The findings also indicate that children (aged 9-10)
are ready and willing to draw these kinds of links between
health and corporeal indicators as an important insight
particularly for physical educators (Burrows, 2007).
7.4 Children’s understandings about food origin (Q12)
28.5% of children at local Church cohort believed that pasta
is made from cheese and 14.2% thought that pasta is made from
meat. These results revealed children’s confusion in this
small sample of children which indicate a partial
understanding of children of food origin. Therefore, further
education about healthy eating and food origin is compulsory
for children in this group. However, 85.7% correctly answered
that cheese is made from milk, 85.7% eggs from chicken, 85.7%
burgers from beef, 42.8% pasta from cereal, 71.4% crisps from
potatoes, and 71.4% yoghurt from milk (Table 5)
In the other cohort study, 10.5% of the children of the
primary school group perceived that eggs are made from Cow,
26.3% thought that pasta is made from cheese, and 5.2% viewed
that crisps are made from plastic. These results again
revealed children’s confusion in this small sample of children
which indicate a partial understanding of children about food
origin. However, 94.7% correctly answered that cheese is made
from milk, 82.3% eggs from chicken, 84.2% burgers from beef,
47.3% pasta from cereal, 78.9% crisps from potatoes, and 73.6%
yoghurt from milk (Table 5) These findings support what had106

been previously acknowledged in the literature review (Chapter
2.8).
Moreover, the findings in this study have been similar to
those recently published by BBC NEWS (2013). However, further
exploration of children’s knowledge of food origin could have
been maintained by interviewing them. For instance, “Do you
think potatoes grow under or above the ground?” and “Have you
ever been on a farm visit?” Or do they really understand what
is plastic? Or it is the question needs to be refined?
(Appendix 6)
Again, the percentages of these findings, as compared to the
small sample of children in both cohorts, are relatively
worrying. Therefore, the data suggest that teaching children
about healthy eating and food origin must be promoted and more
focussed than before, and the policy and practice should be
re-directed. The aim must be to “start the process of re-
engaging children with the origins of food, nutrition and
cooking, so that they grow up with a fuller understanding of
how food reaches them and what a healthy diet and lifestyle
consist of” (BBC NEWS, 2013). Also, it is essential for
children to visit farms to be physically active as part of a
healthy lifestyle in addition to healthy eating.
7.5 Children’s habits of eating breakfast (Q13)
As shown in Chart 8a and 8b, 71% of children in the local
Church group had breakfast on the day of survey as opposed to
and 89% of the primary school cohort (Q13.1). Only 5.2% of the
local Church group skipped breakfast on the day of the survey.107
Besides having breakfast, Chart 9 revealed that cereal was the
highest among food items that had been consumed by the local
Church group (42.8%) and the primary school group (47%) on the
day of the survey. This is, as mentioned already, useful for
children to have a lower body mass index (BMI) and lower
cholesterol than those who eat non-cereal breakfast foods.
This is because breakfast cereal is lower in fat and higher in
fibre than non-breakfast cereal and can be protective against
childhood obesity (Resnicow, 1991 and Williams, 1995).
Although not all cereal is healthy because it might contain
high sugar and this is again worthy to find out and discuss by
interviewing children. Also the relevance of milk, egg, bread
an orange juice as a healthy breakfast, and to further explore
why some of the children in both cohorts had certain foods in
their breakfast such as yoghurt, fruit, water, hot dogs, and
fresh fruits and do they think each of these are healthy?
(Appendix 6)
Furthermore, in the local Church group, 57.1% of boys and
14.2% of girls perceived their own breakfast as healthy, and
no one stated unhealthy breakfast. Whereas, in primary school
group, one boy (5.2%) perceived his breakfast as mostly
healthy breakfast, 31.5% girls and 26.3% boys thought it was
healthy. Only 2 boys (10.5%) and 2 girls (10.5%) perceived
their breakfast as unhealthy breakfast (Table 6).
However, 71% of children at local Church group and 89% in the
primary school group stated that they had a healthy breakfast.
They were more likely to mention a large number of healthier
food options such as yoghurt, fresh fruit and vegetables than108
those who have not had breakfast or had skipped breakfast.
These findings are similar to those revealed by the Department
of Health (DH, 2008). Also our findings support what have been
already mentioned in the literature review (Chapter 2.5). For
instance, as (Nicklas et al., 1998; Kleemola et al., 1999)
suggested that regular breakfast eaters have higher diet
quality including increased consumption of fiber, calcium,
vitamin A and C, riboflavin, zinc, iron and decreased intake
of calories, fat and cholesterol).
For children, breakfast consumption is associated with
education and better school performance (Pollitt and Mathews,
1988; Vaisman et al., 1996; Murphy et al., 1998). Also,
breakfast has positive effects on cognitive development and
induces better academic achievement (Dye et al., 2000).
Conversely, skipping breakfast is linked with difficulty in
issue solving, short-term memory, attention, and episodic
memory in children (Pollitt et al., 1983; Vaisman et al.,
1996; Wesnes et al., 2003).
Again, all these issues are commendable to explore by
interviewing children in both groups. For instance, why do you
think breakfast is relevant for your health? Why do you think
your breakfast is healthy or unhealthy? Do you feel better
(more aware) in the class when you already had your breakfast?
(Appendix 6)
Moreover, it is valuable to explore the essential role of
parents in influencing breakfast choices for their children
who often make breakfast choices in agreement with their
109
parents’ wishes (Agostoni and Brighenti., 2010). Also to
explore a probable reason for skipping breakfast such as: not
being hungry in the morning, lack of time, dissatisfied with
their body shape, or being on diet particularly in girls.
7.6 Children’s Knowledge of healthier food choices
(Q14)
Our findings in Chart 10a and 10b showed that in a local
Church cohort, in general, children’s knowledge of healthy
food choices was bad (mean number of correct answers was (1.5
out of 4). Only (47.1%) could identify correctly the
relatively healthier choices among the four pairs of foods or
drinks. Whereas, among primary school group, children’s
knowledge of healthy food choices was good (mean number of
correct answers was 3 out of 4). About (77.3%) could identify
correctly the relatively healthier choices among the four
pairs of foods or drinks.
Therefore, children of the primary school group were more
likely to make healthier choices than those of the local
Church group (77.3% vs 47.1%). These findings support what had
already been mentioned in the literature review (Chapter 2.9).
However, a marked gender differences concerning healthy
choices in both groups were explored in this study. In primary
school group, boys (53%) were more likely to make healthier
choices than girls (47%). Conversely, girls (57%) were higher
than boys (43%) in making healthier choices (Table 7). These
findings were relatively similar to those found in (DH, 2008).
110
Also, children should be aware of that the associations with
risk of type 2 diabetes are different among individual fruits.
This means that a greater consumption of specific whole
fruits, particularly blueberries, grapes, and apples, is
significantly associated with a lower risk of type 2 diabetes,
whereas increase consumption of fruit juices has the opposite
association (BBC NEWS, 2013).
Moreover, by interviewing children and following up their
responses, we might explore the major limiting factor related
to food consumption and regarded as a significant determinant
of children’s food choice (Appendix 6). For instance, the
taste of the food as suggested by Olson et al (1981),
Ricketts, (1997), Pѐrez-Rodrigo et al (2003) and Molaison et
al (2005).
However, as (Zaini et al (2005) suggested that for non-
favourite food, some children dislike some types of foods when
they know that the food is unhealthy, for instance, sweets as
they know it can cause tooth aches or they dislike fish as it
contains lots of bones (p. 135). Also, as I mentioned already,
this question has a significant correlation with gender,
murders children considered when choosing food as well as
children's food preferences.
7.7 Source of knowledge for children about healthy
eating (Q2)
The maximum percentage of children 100% at local Church group
considered their parents as the main source of knowledge of
111

healthy eating and 71.4% thought that schools and teachers
were the second source. Whereas, in the primary school only
36.8% of children had their knowledge of healthy eating from
their parents and also 36.8% had from their schools and
teachers. Conversely, the highest percentage of children
(42.1%) at primary school children's group considered having
knowledge of healthy eating from food labels and packaging
whereas no one considered this source among the local Church
cohort. Also, Television adverts were the lowest proportion
among the first (14.2%) and the second (5.2%) cohorts
respectively (Chart1). These findings clearly support what
have been already mentioned in the literature review (Chapter
2.6).
These findings support the notion of influence of parents by
sending healthy eating messages to their children (Paquette,
2005). The reason might be because of that most of children in
the local Church group had qualified and educated parents.
Therefore, it is worthy to find out and follow up children’s
responses among both groups possibly by interviewing the
children, their parents and their teachers (Appendix 6).
8. Limitations
There are certain limitations in this study that should be
acknowledged; data from this study were collected using self-
administered questionnaire. Children in the primary school
group completed the questionnaire under the supervision of
teachers in a classroom setting, Whereas, those in the local
Church group did that as a social grouping in the weekly
112
Sunday meeting under the supervision of one of the Brookes’
members. Therefore, it is possible that some children might
provide socially acceptable answers that did not reflect their
true perceptions of healthy eating.
Moreover, for the purpose of reliability of this study, this
study would have been more accurate if the administered
questionnaire were cross-checked with the background
information including, the class number, gender and date of
birth for both groups. Accordingly, only the matched
questionnaire should be used to assess the associations among
the findings from the children in both groups and the school
and Church they were attending.
Concerning the primary school group, only year 5 and year 6
(aged 9-10) were included in this study. It could be argued
that they might not represent the entire primary school
population. Although data were collected in two different
settings, one school in the west of Oxford and One local
Church group in the centre of Oxford, children’s food
preferences reported in this research were likely to reflect
local and regional food preferences. Additionally, food
preferences were not measured in relationship to the
preparation or the source of the food, which may have had an
impact in the decrease in many food preferences demonstrated
in children of both sexes. It is unknown, if when rating
preferences, children reported preferences in relationship to
the food in general or the food as served at school or home.
113
Another limitation is that a small number of children
participated in this research study; therefore it is not easy
to generalize to a larger or broader population. Further
research is needed to confirm our findings.
However, several different actions were taken in this study to
ensure reliability and validity. I used to accept systematic
procedures for data collection, data handling and data
analysis. The fact that children in both cohorts were assured
that there were no wrong answers and that we did not finish
their responses for them supports validity. Major topics,
confusing and conflicting data, the analyses and
interpretations were discussed with my supervisor (Professor
Debra McGregor). Furthermore, the comparison of our findings
with other results in the literature strengthens evidence. I
have been very careful with the interpretation and I am
confident that the findings were an accurate reflection of
what the children said.
Despite these limitations, the study provided useful
information on two cohorts with two different context and
background concerning children’s knowledge, attitudes and
practices of healthy eating and the existing nutritional
environment among both case studies. The results generated
will have significant reference value for future planning of
healthy eating promotion programs in both school and local
Church groups.
As a novice researcher learning how to be systematic in the
searching for and the then synthesis of research, has proved
114

hard but an invaluable skill to develop. This was the first
piece of self-directed academic work undertaken and many
lessons have been learned along the way from my supervisor.
9. Conclusions
The insights of healthy eating continue to be a relatively
unsolved matter Because of two reasons. First, the polysemy of
“Healthy eating” has not been recognized in the past and
second reason is because of the complexity of the issue
(Gustafsson and Sidenvall, 2002). Yet, if perceptions were
found to be comparatively homogeneous across studies in varied
developed countries, age groups, genders and socioeconomic
states, more research need to be conducted to authenticate
this finding (Paquette, 2005).
Because of each cohort findings were analyzed, presented and
discussed separately, and because of that each cohort had
different context and background, therefore, each group needs
a distinct conclusion.
9.1 Conclusion of study of primary school cohort
The main confusing questions for children in this group were
Q2, Q4, Q5, Q12, Q13 and Q14. Although the school had a
healthy eating policy, maximum percentage of children (42. 1%)
stated that they had knowledge of healthy eating from food
labels and only 36.8% had their knowledge from schools and
teachers. The highest proportion 26% of children depends on
choice/availability when choosing food and no role of parents
in sending healthy eating messages was evident. A very
115
surprising finding was, although children in primary school
cohort knew that their food was unhealthy, 71% favor it. This
indicates that they had a lack of information on healthy
eating and redirection of policy and practice in the school is
compulsory. These findings were alarming of a school which has
been already committed to a healthy eating policy and had a
good sense of a healthy lifestyle (Ofsted report, 2008).
Moreover, 26.3% thought that pasta is made from cheese, 10.5%
perceived that egg is made from Caw and 5.2% believed that
Crisps is made from plastics. These findings proved that
children in the primary school cohort had a partial
understanding of knowledge of food origin. Therefore, it might
be useful for the school to sign up for the BNF´s Healthy
Eating Week program which aims “to start the process of re-
engaging children with the origins of food, nutrition and
cooking, so that they grow up with a fuller understanding of
how food reaches them and what a healthy diet and lifestyle
consist of” (BBC NEWS, 2013).
Despite of that all options given for having breakfast were
healthy, 21% of children in this group thought that their
breakfast was unhealthy (Q13). This means they had
misconceptions of which food is healthy or not which need
further efforts to be undertaken by the school. For instance,
free school breakfast programs could be added to the school
health policy and teaching children about healthy breakfast is
a good step forward. In addition, children viewed a lack of
knowledge of making healthy choices. 24% thought that fresh vs
fried fruits and vegetables, 6% believed that food low vs high116
in fat, 12% believed that food low vs sugar, 24% thought that
food low vs high in salt, 12% perceived that boiled v's fried
potatoes and 18% brown vs white bread were healthy choices.
The above analysis of children’s responses in the primary
school group, and as suggested by Burrows (2007) recommends
that there is much for physical educators to attend to
pedagogically and personally in relation to health and
physical education in schools. These findings point to a need
to equip children with strategies for making sense of both the
contradictory and normative information they are presented
with. They also need the cognitive apparatus to weigh up the
implications for themselves and others of adopting particular
health practices and the resources. This is to examine the
potential disjuncture between recommended strategies and the
embodied effects of these at the level of the individual.
Furthermore, the school provides a unique opportunity for
preventing childhood obesity and children spend a large
proportion of their time in school settings, in which children
can receive information on proper healthy eating (Elder et
al., 2010).
Moreover, food preferences differed between genders in the
primary school group. Menu offerings need to reflect the
changing preferences of children with respect to gender and
dietary recommendations for health. This school that plans
similar menus for both genders may want a look more closely at
preferences by gender and have choices that satisfy both
genders. Insight into the food preferences reported by
children (aged 9-10) with regard to gender is valuable117
information which might be used to improve the diets of
primary school children while developing lifelong healthy
eating. Also, preference data might be helpful with school
menu planning to create worthy nutrition education programs
that parallel changes being completed in the school food
service (NATALIE et al., 2009). Therefore, a greater
understanding of the implications of food quality or product
brand on the preferences and consumption of children in the
school setting also should be explored.
Additionally, the present study revealed that the children’s
preferences of food depend on several factors such as taste,
parents, schools and teachers. The involvement and support of
parents is essential to the success of any intervention aimed
at the prevention and management of overweight or obesity in
young children (Jackson et al., 2005). Therefore, in order to
promote healthy food to children the food manufacture should
produce healthier foods with good taste and an attractive
presentation which is child-friendly. Parents and teachers
should educate the children about healthier food choices, as
they might be interested in food after they know the
nutritional value of the food. Also, it is very essential to
promote the intake of fruits and vegetables, at home and
school, as snacks because they do satisfy the appetite and
they are nutritious.
Therefore, school data necessitate further efforts to be
undertaken to promote children’s awareness of healthy eating
campaigns, support of the healthy eating promotion in school,
and participation in any healthy eating activity organized by118

their school could have positive impacts on children’s views
about their healthy eating knowledge and eating habits.
Furthermore, the participating school can get benefit from a
Balanced Breakfast Model (Chapter 2.5.4) to promote eating a
healthy breakfast for their children. Thus, the food service
staff should be asking “What will kids eat?” while assessing
current policies and services (Caine-Bish and Scheule, 2009).
For future studies, it is recommended to interview children,
parents, teachers, and school canteen operators to gather
better information about the availability of foods in the
school and home environment and the children’s food choices in
both settings.
However, making suggestions about policy for schools and
guidance for parents to tackle/address obesity through
heightening healthy eating awareness is essential and could be
helpful also to further shape my dissertation (Appendix 8, 9
and 10).
9.2 Conclusion of survey of local Church group
As I mentioned already, most of the children’s parents in this
group were educated with high qualification, therefore this
might be the reason that children were very good at answering
questions Q1, Q2, Q3, Q7, and Q8.
However, certain issues were concerning particularly Q9, Q10,
Q12, and Q14 in this group need addressing to perhaps avoid
childhood obesity. Only 57% of children in this group
perceived that fresh fruit and vegetables are healthy because
119
they are sources of essential vitamins and minerals (Q9). This
percentage was low as compared to such a very small sample of
children (only 7 in number). A high proportion of children
(28%) in this cohort used to drink water with diet and thought
this was a healthy. Only 57% viewed that water is an important
part of a healthy diet because it is nutritious and antitoxic.
Also, 42.7% of children revealed partial understanding of food
origin (Q12).
Moreover, children had difficulty to make healthy choices
among certain foods such as fresh vs fried fruits (57%) and
vegetables, food low and high in fat (57%), sugar (57%) and
salt (57%), and boiled and fried potatoes (42.8%). All these
findings revealed that there were areas of partial
understanding or misconception of children in this group that
is essential to be addressed and tackled to help to avoid
childhood obesity.
However, we could have had more exploration of children’s
views in this cohort, if they had been interviewed (Appendix
6).
120

References
Agostoni, C. And Brighenti, F. (2010) Dietary Choices for
Breakfast in Children and Adolescents. Critical Reviews in Food Science
and Nutrition. 50 (2), 120-128.
Ali, R. Staub, H. Leveille, G.A. And Boyle, P.C. (1982)
Dietary fiber and obesity: a review. In: Vahouny, GV.
Kritchevsky, D. Editors. Dietary fiber in Health and Disease,
New York, NY: Plenum Press.
Anderson, A.S. Porteous, L.E.G. Foster E. Et al. (2005) The
impact of school-based nutrition education intervention on
dietary intake and cognitive and attitudinal variables
121
relating to fruits and vegetables. Public Health Nutr. 8(6): 650-
656.
Anderson, M. And Zimmerman, B. M. (2010) Influence of Iodine
Deficiency and Excess on Thyroid Function Tests. In: Anderson,
M. And Zimmerman. B. M. Thyroid Function Testing. USA: Springer US,
45-69.
Antova, T. Pattenden. S. And Nikiforov, B. et al. (2003)
Nutrition and respiratory health in children in six central
and Eastern European countries. Thorax. 58 (3), 231-236.
Baughcum, A. Chamberlin, L. Deeks, C. Powers, S. And Whitaker,
R. (2000) Maternal perceptions of
overweight preschool children. Paediatrics. 106 (6), 1380-1386.
Bellisle. (2004) Effects of diet on behavior and cognition in
children. British Journal of Nutrition. 92 (Suppl 2), S227-S232.
Blundell, J. Gumaste, D. Handley, R. And Dye, L. (2003) Diet,
behavior and cognitive functions: a psychobiological
view. Scandinavian Journal of Nutrition. 47 (2), 85-91.
Burrows, L. (2007) "Fit, Fast, and Skinny": New Zealand school
students ʻtalk´ about health. Journal of physical education in New
Zealand. 16 (1), 26-34.
Bahn, K.D. (1989) cognitively and perceptually based judgments
in children’s brand discriminations and preferences. J Bus Psychol
(Historical Archive). 4 (2), 183-197.
122
Baranowski, T. Davis, M. And Resnicow, K. et al. (2000) Gimme 5
fruits, juice, and vegetables for fun and health: outcome
evaluation. Health Educ Behav. 27 (1): 96-111.
Basit, N. T. (1995) Educational, Social and Career Aspirations
of Teenage Muslim girls in Britain: An Ethnographic Case
Study. PhD Thesis, University of Cambridge
BBC News Online (2013) Fruit consumption and risk of type 2 diabetes: results
from three prospective longitudinal cohort studies. Available at:
http://www.bmj.com/content/347/bmj.f5001 (Accessed: 20
September 2013).
BBC News Online (2013) Study reveals children's confusion. Available at:
http://www.bbc.co.uk/news/education-22730613 (Accessed: 20
September 2013).
Bell, J. (1999) Doing your research project. Buckingham: Open
University Press
Bere, E. And Klepp, K.I. (2005) Changes in accessibility and preferences
predict children’s future fruit and vegetable intake. Int J Behav Nutr Phys
Act, 2:15.
Berg, C. Jonsson, I. Conner, M. And Lissner. (2003)
Perceptions and reasons for choice of fat-and fiber-containing
foods by Swedish school children. Appetite. 40:61-7.
Blaxter, L. Hughes, C. And Tight, M. (1996) How to research.
Buckingham: Open University Press cited in Bell, J. (1999)
Doing your research project. Buckingham: Open University Press
123
Bogdan, R. G. And Biklen, S. K. (1992) (2nd Ed.) Qualitative
Research in Education. Boston, MA: Allyn and Bacon
Bourcier, E. Bowen, D. J. Meischke, H. And Moinpour, C. (2003)
Evaluation of strategies used by family food preparers to
influence healthy eating . Appetite. 41 (3), 265-272.
Caine-Bish, N. And Scheule, B. (2007) Food preferences of
school age children and adolescents in an Ohio school
district. J child Nutr Management. (2)
Caine-Bish, N. And Scheule, B. (2009) Gender Differences in
Food Preferences of School-Aged Children and
Adolescents. Journal of School Health. 79 (11), 532-540.
Carruth, B.R. And Skinner, J.D. (2001) The role of dietary
calcium and other nutrients in moderating body fat in
preschool children. Int. J. Obes. Relat.Metab.Disord. 25: 559-66.
Cheng, T. S., Tse, L. A., Yu, I. T. And Griffiths, S. (2008)
Children’s perceptions of parental attitude affecting
breakfast skipping in primary sixth-grade students. J. Sch. Health.
78: 203-8.
Cohen, I. Manion, I. And Morrison, K. (2000) (5th Ed.) Research
methods in education. London: Routledge
Cohen, L. Manion, L. And Morrison, K. (2007) (6th Ed.) Research
Methods in Education. London: Routledge. 656.
Contento, I.R. (1981) Children’s thinking about food and
eating-A Piagetian-based study . J Nutr Educ. 13 (1), S86-S90.
124
Cooke, L.J. And Wardle, J. (2005) Age and gender differences
in children’s food preferences. Br. J. Nutr. 93: 741-746.
Council of Europe (2005) (French Ed.) Eating at school-making healthy
choices. Germany: Council of Europe Publishing. 29.
Crawford, R. (1980) Healthism and the medicalisation of
everyday life. International Journal of Health Services.10, 365-388.
Delfos, M.F. (2003) (3rd Ed.) Ontwikkeling in vogelvlucht. Ontwikkeling
van kinderen en adolescenten. Lisse, Swets and Zeitlinger. 335.
Drewnowski, A. (1997) Taste preferences and food intake. Annu
Rev Nutr. 17: 237-253.
Drewery, W. And Bird, L. (2004) (2nd Ed.) Human development in
Aotearoa: A journey through life. Sydney: McGraw-Hill.
Dye, L. LIuch, A. And Blundell, J. E. (2000) Macronutrients
and mental performance. Nutrition. 16:1021-34.
Eaton, D.K. Kann, L. And Kinchen, S. et al. (2008) Youth risk
behavior surveillance-United States, 2007. Surveillance
Summaries. MMWR. 2008. 57 (4), 1-131.
Edwards, J.S. And Hartwell, H.H. (2002) Fruit and vegetables—
attitudes and knowledge of primary school children. J Hum Nutr Diet , 15
(5): 365-374.
Evans, J. Rich, E. And Allwood, R. (2006) Body pedagogies,
P/policy and gender. Paper presented at the University of
Kyoto, Japan.
125
Fabritius, K. And Rasmussen, M. (2008) Breakfast habits and
overweight in Danish school children. The role of
socioeconomic positions. Ugeskr. Laeger, 170:2559-63.
Farshchi, H.R. Taylor, M.A and MacDonald, I.A. (2004) Regular
meal frequency creates more appropriate insulin sensitivity
and lipid profiles compared with irregular meal frequency in
healthy lean women. Eur. J. Clin. Nutr. 58:1071-7.
Farshchi, H.R. Taylor, M.A and MacDonald, I.A. (2005)
Beneficial metabolic effects of regular meal frequency on
dietary thermo genesis, insulin sensitivity and fasting lipid
profiles in healthy obese women. Am J ClinNutr . 81:16-24.
Field, A.E. Austin, S.B. And Taylor, C.B. et al. (2003)
Relation between dieting and weight change among
preadolescents and adolescents. Paediatrics. 112(4):900-906.
Fisher, J.O. And Birch, L. L. (1999) Restricting access to
palatable foods affects children’s behavioral response, food
selection and intake. Am J ClinNutr . 69 (6), 1264-1272.
Flavell, J.H. And Piaget, A. (1963) The developmental psychology of
Jean Piaget. In The university series in psychology. Princeton [etc.]:[s.n.]:
McClelland DC.
Fallon, A.E. Rozin, P. And Pliner, P. (1984) The child's
conception of food: the development of food rejections with
special reference to disgust and contamination
sensitivity. Child Dev. 55 (2), 566-575.
126
Glisenan, M.B. de Bruin, E. A. And Dye, L. (2009) The
influence of carbohydrate of cognitive performance: a critical
evaluation from the perspective of glycemic load. Br. J. Nutr.
98:941-9.
Gorard, S. (2003) Quantitative Methods in Social Sciences.
London: Continuum.
Gortmaker, S.L. Cheung, L.W. And Peterson K.E. et al. (1999)
Impact of a school-based interdisciplinary intervention on
diet and physical activity among urban primary school
children: eat well and keep moving. Arch. Pediatr. Adolesc. Med. 153
(9), 975-983.
Gortmaker, S.L. Peterson, K. And Wiecha, J. et al. (1999)
Reducing obesity via a school-based interdisciplinary
intervention among youth. Arch. Pediatr. Adolesc. Med. 153 (4), 409-
418.
Guthrie, J.F. Lin, B.H. Reed, J. And Steward, H. (2006)
Understanding economic and behavioral influences on fruit and
vegetable choices. Amber Waves.3 (2).
Gable, S. And Lutz, S. (2000) Household, parent and child
contributions to childhood obesity. Family relations. 49 (3),
293-300.
Gibney, M. (2012) Fat and Sugar Taxes: Will they solve the
problem? Available at:
http://www.ucd.ie/foodandhealth/seminarseries/fatsugartaxes/
(Accessed: 21 September 2013).
127

Gillespie, L. (2003) Can physical education educates? In B. Ross & L.
Burrows (Eds.), it takes 2 feet: Teaching physical education and health in Aotearoa.
New Zealand: Palmerston North: Dunmore Press. 185-194.
Giovannini, M. Agostoni, C. And Shamir, R. (2010) The
Relevance of Breakfast: Concluding remarks . Critical Reviews in
Food Science and Nutrition. 50 (2), 129-129.
Golan, M. And Crow, S. (2004) Parents are key players in the
prevention and treatment of weight related problems. Nutrition
Reviews. 62 (1), 39-50.
Hanson, M.D. and Chen, E. (2007) Socioeconomic status and
health behaviours in adolescence: a review of the
literature. J. Behaviour. Med. 30, 263-85.
Health Canada (1990) Action towards healthy eating: Canada’s guidelines for
healthy eating and recommended strategies for implementation: the report of the
Communications/Implementation Committee. Ottawa, ON: Minister of
National Health and Welfare.
Health Canada (1992) Canada's Food Guide to Healthy Eating. Ottawa, ON:
Minister of National Health and Welfare.
Hodges, E. (2003) A primer on early childhood obesity and
parental influence. Pediatric Nursing. 29 (1), 13-16.
Hart, K.H. Bishop, J.A. And Truby, H. (2002) An investigation
into school children’s knowledge and awareness of food
and nutrition . J Hum NutrDiet . 15 (2), 129-140.
128

Henry, C.J. Lightowler, H.J. And Strik, C.M. (2007) Effects of
long term intervention with low and high glycemic index
breakfasts on food intake in children aged 8-11 years old. Br. J.
Nutr. 98 (3), 636-40.
House, E.R. (1993) Professional Evaluation: Social Impact and
Political Consequences. Newbury Park, CA: Sage.
IASO (International Association for the study of obesity)
(2012). Prevalence of Childhood obesity. Available at:
http://myemail.constantcontact.com/IASO-August-Newsletter---
International-Association-for-the-Study-of Obesity.html?
soid=1101267849538&aid=cTwikgS3-OI (Accessed: 21 September
2013).
IASO (International Association for the study of obesity)
(2012) World map of childhood obesity. Available at:
http://www.iaso.org/resources/world-map-obesity/ (Accessed: 20
September 2013).
Ingwersen, J. Defeyter, M.A. Kennedy, D.O., Wesnes, K.A. And
Scholey, A.B. (2007) A low glycemic index breakfast cereal
preferentially prevents children’s cognitive performance from
declining throughout the morning. Appetite. 49:240-4.
Journal of the American Dietetic Association (1999) “Dietary
guidance for healthy children aged 2 to 11 years”, vol. 99
Johnson, J. (2013) Childhood obesity in city tackled by new
health team fingers on the pulse! Oxford Journal. 5 Sep. p. 1
129

Jackson, D. McDonald, G. Mannix, J. Faga, P. And Firtko, A.
(2005) Mothers’ perceptions of overweight and obesity in their
children. Australian Journal of Advanced Nursing.23 (2), 8.
Kirk, D. And Colquhoun, D. (1989) Healthism and daily
physical education. British Journal of Sociology of Education. 10 (4),
417-434.
Kleemola, P. Puska, P. Vartiainen, E. Roos, E. Luoto, R. And
Ehnholm, C. (1999) The effect of breakfast cereal on diet and
serum cholesterol: a randomized trial in North
Karelia, Finland. Eur. J. Clin. Nutr. 53:716-21.
Liem, D.G. Mars, M. And de Graaf, C. (2004) Consistency of
sensory testing with 4- and 5-year-old children. Food Qual Prefer.
15 (6), 541-548.
Liem, D.G. Mars, M. And de Graaf, C. (2004) Sweet preferences
and sugar consumption of 4-and 5-year-old children: role of
parents. Appetite. 43:235-45.
Liese, A.D. Roach, A.K. Sparks, Marquart, L.D. Agostino, R.B.
Jr. and Mayer-Davis E.j. (2003) Whole-grain intake and insulin
sensitivity: the Insulin Resistance Atherosclerosis Study. Am J
ClinNutr . 78:965-71.
Livingstone, B. (2013) Dr Barbara Livingstone on Childhood
obesity. Available at: http://www.youtube.com/watch?v=PpobmbcxVKw
(Accessed: 20 September 2013).
130

Logue, A.B. And Smith, M.E. (1986) Predictors of food
preferences in adult humans. Appetite. 7 (2), 109-125.
Lytle, L.A. Seifert, S. Greenstein, J. And McGovern, P. (2000)
How children eating patterns and food choices do change over
time? Results from a cohort study. Am J Health Promot . 14 (4),
222-228.
Lupton, D. And Chapman, S. (1995) 'A healthy lifestyle might be the
death of you': discourses on diet, cholesterol control and heart disease in the press
and among the lay public. London: Social Health Illness. 17:477-94.
Lupton, D. (1996). Food, the body and the Self. London: Sage
Mac Evilly, C. And Kelly, C. (2001) Mood and Food. Nutrition
Bulletin. 26, 325-329.
Markula, P. (1997) Are fit people healthy? Health, exercise,
active living and the body in fitness discourse. Waikato Journal
of Education. 3, 21-39.
Markus, R. Panhuysen, G. Tuiten, A . Koppeschaar, H . (2000)
Effects of food on cortisol and mood in vulnerable subjects
under controllable and uncontrollable stress. Physiology and
behavior. 70, 333-342.
Markus, R. Panhuysen, G. Tuiten, A. Koppeschaar, H. Fekkas, D.
And Peters, M. (1998) Does carbohydrate-rich, protein-poor
food prevent a deterioration of mood and cognitive performance
of stress-prone subjects when subjected to a stressful
task? Appetite. 31, 49-65.
131
Murphy, J.M. Pagano, M.E. Machmani, J. Sperling, P. Kane, S.
And Kleinman, R.E. (1998) The relationship of school
breakfast and psycho social and academic functioning. Arch.
Pediatr. Adolesc. Med. 152:899-907.
Myers, S. And Vargas, Z. (2000) Parental perceptions of the
preschool obese child. Pediatric Nursing. 26 (1), 9.
Mahoney, C. R., Taylor, H. A., Kanarek, R. B. And Samuel, P.
(2005) Effect of breakfast composition on cognitive processes
in elementary school children. Physiology and behavior. 85:635-645.
Mason, J. (1996) Qualitative Researching. London: Sage cited
in Robson, C (2002) Real world research. 2nd edition. Oxford:
Blackwell
Molaison, E.F. Connell, C.L. Stuff, J.E. Yadrick, M.K. And
Bogle, M. (2005) Influences on fruit and vegetable consumption
by low income black American adolescents. J NutrEducBehav . 37:
246-51.
Myers, M. D. (1997) Qualitative research in information systems, MISQ
Discovery. Available at:
http://www.misq.org/skin/frontend/default/misq/MISQD_isworld/i
ndex.html (Accessed: 20 September 2013).
Nestle, M. (2002) Food Politics: How the food industry influences nutrition and
health. Berkeley, CA: University of California Press.
Nicklas, T.A. Myers, L. Reger, C. Beech, B. And Berenson, G.S.
(1998) Impact of breakfast consumption on nutritional adequacy
132
of the diets of young adults in Bogalusa, Louisiana. J Am Diet
Assoc . 98:1432-8.
Nicklaus, S. Boggio, V. Chabanet, C. And Issanchou, S. (2004)
A prospective study of food preferences in childhood. Food Qual Pref, 15 (7-8): 805-
818.
Nishida, C. Uauy, R. Kumanyika, S. et al. (2003) The Joint
WHO/FAO Expert Consultation on diet, nutrition and the
prevention of chronic diseases: process, product and policy
implication. Public Health Nutr. 7 (IA), 245-250.
Nu CT, MacLeod, P. And Barthelemy, J. (1996) Effects of age and
gender on adolescents’ food habits and preferences. Food Qual Pref, 7 (3-4): 251-
262.
Ofsted (Office for Standards in Education) (2008) Inspection
Report: Stanton Harcourt CofE Primary School, 21-22 May 2008.
Available from www.ofsted.gov.uk (Accessed: 19 September
2013].
Olson, C.M. And Gemmill, K.P. (1981) Association of sweet
preference and food selection among four to five year old
children. Ecol Food Nutr. 11: 145-50.
Oram, N. (1994) Children’s eating experiences could differ
from those of adults. Appetite. 22 (3), 283-287.
Paquette, M. (2005) Perceptions of Healthy Eating. Canadian
Journal of Public Health. ProQuest, 96, pg. S15.
133
Pearson, N., Biddle, S. J. H. And Gorely, T. (2009) Family
correlates of breakfast consumption among children and
adolescents. A systematic review. Appetite. 52: 1-7.
Pereira, M.A. Jacobs, D. R. Jr. Slattery, M. Hilner, J. And
Kushi, L.H. (1998) The association between whole grain intake
and fasting insulin in a bi-racial cohort of young adults: The
Cardiac Study C.V.D . Prevention. 1:231-42.
Perez-Rodrigo, C. Ribas, L. Serra-Majem, L. And Aranceta, J.
(2003) Food preferences of Spanish children and young people: the en Kid
study. Eur J CIinNutr, 57 Suppl l: S45-8.
Prelip, M. Erausquin, T. Slusser, W. et al. (2006) The role
of classroom teachers in nutrition and physical education.
California J Health Promot. 4(3): 116-127.
Prelip, M. Slusser, W. Thai, C.L. Kinsler, J. And Erausquin,
J.T. (2011) Effects of a school-based nutrition program
diffused throughout a large urban community on attitudes,
beliefs, and behaviors related to fruit and vegetable
consumption. J Sch Health. 81: 520-529.
Pollitt, E. And Mathews, R. (1988) Breakfast and cognition:
an integrative summary. Am J ClinNutr . 67:804S-13S.
Pollitt, E. Lewis, N.L. Garza, C. And Shulman, R.J. (1983)
Fasting and cognitive function. J. Psychiatr. Res. 17:169-74.
Reilly et al. (2003) Obesity in childhood and adolescence: an evidence
based clinical and public health perspectives. Available at:
134
http://www.who.int/mediacentre/factsheets/fs311/en/index.html
(Accessed: 21 September 2013).
Resnicow, K. (1991) The relationship between breakfast habits
and plasma cholesterol levels in school children. J SchHealth .
61: 81-5.
Richardson, A. And Montgomery, P. (2005) The Oxford-Durham
study: a randomized controlled trial of dietary
supplementation with fatty acids in children with
developmental coordination disorder. Paediatrics. 115 (5), 1360-
1366.
Ricketts, C.D. (1997) Fat preferences, dietary fat intake and
body composition in children. Eur. J. Clin. Nutr. 51: 778-81.
Robson, C. (2002) (2nd Ed.) Real world research. Oxford: Blackwell
Roedder-John, D. (1999) Consumer Socialization of Children: A
retrospective look at Twenty Five Years of Research. J Consum
Res. 26 (3), 183-213.
Roos, G. (2002) Our bodies are made of pizza-Food and
embodiment among children in Kentucky. Ecol Food Nutr. 41 (1), 1-
19.
Rose, G. Laing, D.G. Oram, N. And Hutchinson, I. (2004)
Sensory profiling of children aged 6 -7 and 10-11 years: a
modality approach. Food Qual Prefer. 15 (2), 597-606.
Rozin, P. Hammer, L. Oster, H. Horowitz, T. And Marmora, V.
(1986) The child's conception of food: differentiation of
135
categories of rejected substances in the 16 months to 5 year
age range. Appetite. 7 (2), 141-151.
Rampersaud, G. C. Pereira, M. A. Girard, B. L. Adams, J. And
Metz I, J. D. (2005) Breakfast habits, nutritional status,
body weight and academic performance in children and
adolescents. J. Am. Diet. Assoc. 105, 743-60.
Richardson, A. (2003) The importance of omega-3 fatty acids
for behavior, cognition and mood. . Scandinavian Journal of Nutrition.
47 (2), 92-98.
Rogers, P. (2001) A healthy body, a healthy mind: long-term
impact of diet on mood and cognitive function. Proceedings of
the NutritionSociety.60, 135-143.
Ruff, H. Markowitz, M. Bijur, P. And Rosen, J. (1996)
Relationships between blood lead levels, iron deficiency, and
cognitive development in two-year old children. Environmental
Health Perspectives.104 (2), 180-185.
Ruxton, C. Reed, S. Simpson, M. And Millington, K. (2004)
The health benefits of omega-3 polyunsaturated fatty acids : a
review of the evidence .Journal of Human Nutrition and Dietetics. 17,
449-459.
Scaglioni, S. Salvioni, M. And Galimberti, C. (2008)
Influence of parental attitudes in the development of children
eating behaviour. Br. J. Nutr. 99 (Supple 1), S22-5.
Schaffer, H.R. (2003) Introducing child psychology. UK, Oxford:
Blackwell publisher. UK Edition edition. 352.
136

Sharifah, I.S. Shamarina, S.H. And Mirnalini, K. (2013)
Assessing the children’s views on foods and consumption of
selected food groups: outcome of the focus group approach. Nutr
Res Pract. 7 (2), 132-138.
Skinner, J. Carruth, B. And Coletta, F. (1999) Does dietary
calcium have a role in body fat accumulation in young children
. Scandinavian Journal of Nutrition. 43: 45S.
Skinner, J.D. Carruth, B.R. Wendy, B. And Ziegler, P.J. (2002)
Children’s food preferences: a longitudinal analysis. J Am Diet
Assoc, 102 (11): 1638-1647.
Slusser, W.M. Cumberland, W. Browdy, B. et al. (2007) A school
salad bar increases frequency of fruit and vegetable
consumption among children living in low income
households. Public Health Nutr. 10 (12), 1490-1496.
Smith, A. Kellet, E. And Schmerlaib, Y. (1998) The Australian guide
to Healthy Eating: background information for nutrition educators, Australian
Department of Health and Aging, Canberra.
Speechly, D.P. And Buffenstein, R. (1999). Greater appetite
control associated with an increase frequency of eating in
obese males. Appetite. 33:285-97.
Speechly, D.P. Rogers, G.G. And Buffenstein, R. (1999) Acute
appetite reduction associated with an increase frequency of
eating in obese males. Int. J. Obes. Relat.Metab.Disord. 23: 1151-9.
137
Stevenson, E. J. Williams, C. Mash, L. E. Philips B. And Nute,
M. L. (2006) Influence of high carbohydrate mixed meals with
different glycemic indices on substrate utilization during
subsequent exercise in women. Am J ClinNutr. 84:354-60.
Stevenson, E. Williams, C. And Nute, M. (2005) The influence
of glycemic index of breakfast and lunch on substrate
utilization during the postprandial periods and
subsequent exercise. Br. J. Nutr. 93:885-93.
Szczesniak, A.S. (1972) Consumer awareness of and attitudes
to food texture. J Texture Stud. 3, 206-217.
Shaw, M. E. (1998) Adolescent breakfast skipping: an
Australian study. Adolescence. 33, 851-861.
Shilling, C. (1993) The body and social theory. London: Sage.
Sonja, M.E. van Dillen, Gerrit, J. Hiddink, Maria, A. Koelen,
Cees de Graaf. And Cees, M.J. Van Woerkum. (2003)
Understanding nutrition communication between health
professionals and consumers: development of a model of
nutrition awareness based on qualitative consumer research1–4.
American Journal of Clinical Nutrition. 77, 1065S-1072S.
Tapper, K. Horne, P.J. And Lowe, C.F. (2003) The Food Dudes to
the rescue! The Psychologist 16, 18-21.
Tapper, K. Murphy, S. Lynch, R. Clark. Moore, G.F. And Moore,
L. (2008) Development of a scale to measure 9-11 years olds´
attitudes towards breakfast. Eur. J. Clin. Nutr. 62:511-8.
138
Timlin, M.T. And Pereira, M.A. (2007) Breakfast frequency and
quality in the etiology of adult obesity and chronic
diseases. Nutr. Rev. 65:268-81.
Turrell, G. (1998) Socioeconomic differences in food
preferences and their influence on healthy food purchasing
choices. J Hum NutrDiet . 11 (2), 135-149.
Tinning, R. (1985) Physical education and the cult of
slenderness: A critique . The ACHPER National Journal. 107 (Autumn),
10-13.
UK. (1990) Growth charts. Available at:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1719041/
(Accessed: 20 September 2013).
USA. (2000) Growth charts. Available at:
http://www.bulimiaguide.org/summary/detail.aspx?
doc_id=9478&g=1 (Accessed: 20 September 2013).
Vaisman, N. Voet, H. Akivis, A. And Vakil, E. (1996) The
effects of breakfast timing on the cognitive function of
elementary school students. Arch. Pediatr. Adolesc. Med. 150:1089-92.
Van de Weyner, C. (2006). Nutrition, mental health and
behavior. The Food Magazine. 72, 14-15.
Valkenburg, P.M. and Cantor, J. (2001) The development of a
child into a consumer. J ApplDevPsychol . 22 (1), 61-72.
139
Weaver, F. N. Hayes, L. Nigel, Unwin, C. N. And Murtagh, J. M.
(2008) Obesity and Clinical Obesity Men’s understandings of
obesity and its relation to the risk of diabetes: A
qualitative study. Available at:
http://www.biomedcentral.com/1471-2458/8/311 (Accessed: 21
September 2013).
Wesnes, K.A. Pincock, C. Richardson, D. Helm, G. And Hails, S.
(2003) Breakfast reduces declines in attention and memory over
the morning in school children. Appetite. 41:329-31.
Wheelock, V. (2007) Healthy Eating in Schools. UK: Verner Wheelock
Associates Ltd. 256.
Wright, J.E. OFlynn, G. And Macdonald, D. (2006) Being fit and
looking healthy: Young women’s and men’s constructions of
health and fitness. Sex Roles. A Journal of Research. 54(9-10), 1-15.
Wansink, B. Cheney, M.M. And Chan, N. (2003) Exploring comfort
food preferences across age and gender. PhysiolBehav. 79: 739-
747.
Wardle, J. Carnell, L. And Cooke, L. (2005) Parental control
over feeding and children’s fruit and vegetable intake: how
are they related? J Am Diet Assoc. 105 (2), 227-232.
Westenhoefer, J. (2005) Age and gender dependent profile of
food choice. Forum Nutr. 57: 44-51.
140
WHO (World Health Organization) (1997) International Obesity Task
Force (IOTF). Available at: http://www.iaso.org/iotf/ (Accessed: 21
September 2013).
WHO (World Health Organization) (2013) Childhood obesity. Available
at:
http://www.who.int/mediacentre/factsheets/fs311/en/index.html
(Accessed: 21 September 2013).
Williams, C.L. (1995) Importance of dietary fiber in
childhood. J Am Diet Assoc. 95: 1140-6, 1149.
Woroby, J. And Woroby, H. (1999) The impact of a two-year
school breakfast program for preschool aged children on their
nutrient intake and preacademic performance. Child Study Journal 29
(2), 113-132.
Worsley, A. And Crawford, D. (2004) Children’s healthy eating: what
works, Report of the Review of Children’s Healthy Eating Interventions for the
Department of Human Services, Victoria, Melbourne.
Yin, R. (2003) (2nd Ed.) Applications of Case Study Research, London:
Sage
Zeinstra,G. G. Koelen, A. M. Kok, J. F. And Cees de Graaf.
(2007). Cognitive development and Childrens perceptions of
fruit and vegetables; a qualitative study . International Journal of
Behavioral Nutrition and Physical Activity. 4 (30), 1-11.
141
Zaini, M.Z. Lim, C.T. Low, W.Y. And Harun, F. (2005) Factors
affecting nutritional status of Malaysian primary school
children. Asia Pac J Public Health. 17 (1), 71-80.
Appendices
Appendix 1: letter to parents
Dear parents,
Childhood obesity puts children at risk of developing seriousillnesses. As a result of unhealthy diet and inactivelifestyle, we are seeing an alarming increase in childhoodobesity, i.e., almost one in five primary school children areoverweight in 2013. In addition many studies regardingchildren’s perception about healthy eating revealed children’sconfusion and misconception. For instance, cheese is made fromplants, Pasta is made from meet and crisps are made fromplastic (BBC News, June, 2013).
Therefore, I am conducting a research into Children’s ideasabout healthy eating. I would like to give your children aquestionnaire to fill in to find out what they think aboutHealthy Eating. It will take about 20 minutes for them toanswer the questions. No disadvantages or risks of taking partin this study, just time. Your child is invited to participateand complete a questionnaire to record his/her views about
142
healthy eating. The ultimate goal of this research project isto explore how do year six children make healthy choices? Howdo they think when they decide to eat? What food do theyprefer to eat and why? What does healthy eating mean to them?These are few examples involved in the questionnaire. Thisresearch project is part of my MA Childhood Studies Course atOxford Brookes University/school of education. This researchstudy will be conducted in anonymity and collected informationwill be restricted to the researcher, my supervisor and thehead teacher of the participating school. It will not affectthe academic performance or internal assessment of your child.If you have any concerns please contact my supervisor ProfDebra McGregor, [email protected], Professor in Education(Learning and Developing Pedagogy), School of Education,Faculty of Humanities and Social Sciences, Harcourt HillCampus, Oxford Brookes University, OX2 9AT, Tel : 01865488355. My contact details are: Khajik Yaqob,[email protected], student in School of Education,Faculty of Humanities and Social Sciences, Harcourt HillCampus, Oxford Brookes University, OX4 2NS, Mobile no:07753353598.
Thank you for your time,
Date 10/07/2013
Appendix 2: Letter to head teacher
Dear head teacher of St, Josephs Catholic Primary School,
I am Khajik Yaqob/ studying the MA Childhood Studies course. Iam studying for a Master degree in Oxford Brookes University/
143
school of education. I am conducting research into Children’sideas about healthy eating. I would like to give your childrena questionnaire to fill in to find out what they think aboutHealthy Eating. This is supported by focus group interviews. Iwould bring in a questionnaire for the year 6 to complete. Itwill take about 20 minutes for them to answer the questions.No disadvantages or risks of taking part in this study, justtime. I sincerely hope that you can help me to carry out thequestionnaire to year six children in your school.
A copy of the results/findings of the research will be sent tothe Head of the participating school. A full copy of thethesis will be available to borrow on request. The research ispart of the Master’s program in the Faculty of Humanities andSocial Sciences at Oxford Brookes University. Thisdissertation will be submitted to achieve that degree/award.If you have any concerns please contact my supervisor ProfDebra McGregor, [email protected], Professor in Education(Learning and Developing Pedagogy), School of Education,Faculty of Humanities and Social Sciences, Harcourt HillCampus, Oxford Brookes University, OX2 9AT, Tel : 01865488355. My contact details are: Khajik Yaqob,[email protected], student in School of Education,Faculty of Humanities and Social Sciences, Harcourt HillCampus, Oxford Brookes University, OX4 2NS, Mobile no:07753353598.
Thank you for your time
10/07/2013
144
Appendix 3: Ethical approval form
Faculty of Humanities and Social Sciences Faculty Ethics form HSS.E2
Application for ethics approval for a research project
involving human participants
Undergraduates and Foundation Degree Students:
Before completing this form, the ethics review checklist (school form
HSS.E1) should have been completed to establish whether this additional
application for ethics approval is required. If ethics approval is
required, you should complete this form, sign it and submit it to the
Faculty Research Ethics Officer, Maggie Wilson at [email protected]. A
decision form, E3 will then be returned to you by e-mail.
Master’s Students:
You should complete this form before you start your project and submit it
to your supervisor.
If he or she is unable to sign it at this stage, the form will be referred
to the Faculty Research Ethics Officer, as above, who may seek further
information and clarification from you. A decision form, E3, will then be
returned to you by e-mail.
145
All students should refer to the University Code of Practice on Ethical
Standards for Research involving Human Participants, available at
www.brookes.ac.uk/res/ethics and Faculty guidelines, which are included in
the relevant on-line module or course handbook. You should bind a copy of
the approved form in your final project or dissertation submission.
1. Name of Principal
Investigator (Student):
Khajik Yaqob
E-mail address:
2. Name of Supervisor and e-
mail address: Prof
Debra McGregor
3. Working Project Title: To
explore year 6 children’s
views about healthy eating
and what they do to eat
healthily?
4. Project Type (please
specify course and give
module number):
Master’s
project
146
Master’s
dissertation
P70899 Undergraduat
e project:
Undergraduat
e
dissertation
:Foundation
degree
project:
5. Background to and rationale
of proposed research:
The rationale of this research
project is to explore how do
children (aged 9-10) think about and
understand healthy eating, to
address Childhood obesity. As it is
evident that, unbalanced diet with
low fruit and vegetables plus low
physical activity, can lead to
childhood obesity, abnormal
behaviour and low school
performances. Moreover, obesity can
be associated with shorter life
expectancy. For instance, a 16 year
old girl with obesity, she has just
6 years to live because of her
unhealthy diet. Also, a 4 year old
girl with obesity gets bullied.
Therefore, healthy eating can
147
prevent cardiovascular disease, some
cancers and it can protect the child
against asthma. I would bring in a
questionnaire for year 6 children to
fill in to find out how they
understand healthy eating.
6. ‘Gatekeeper’ permission
If you are conducting your
research within an
organization external to
Brookes, such as a school
or company, has permission
has been obtained?
Attach a copy of the letter
or e-mail giving permission
Yes.
7 Methods of data collection:
Attach a copy of your draft
questionnaire, interview
schedule or observation
guidelines
The methodology includes
questionnaire plus focus group
interviews.
8 Participants involved in
the research:
Include the target number,
age range, source and
method of recruitment and
Only year 6 (9-10) children will be
involved as participants in this
research. The target number is 46.
This research will be recruited to
the head teacher in St. Josephs
Catholic Primary School Mrs. Tomkys
148
location of the research Sue in Headington, Headley Way, Ox3
7SX, Oxfordshire, Oxford.
9 Are participants in a
dependent relationship) as
an unequal power
relationship) with the
researcher?
If yes, what steps will you
take to ensure that
participation is entirely
voluntary and is not
influenced by this
relationship?
No
10
.
Potential benefits of the
proposed research:
The head teacher can see the results
of my study and use them to inform
what the school might do about
healthy eating.
11 Potential adverse effects
of the proposed research
and steps to be taken to
deal with them:
These are defined as risks
greater than those
encountered during normal
day to day interactions and
could include possible
psychological stress or
No disadvantages, just time.
149
anxiety
12
.
Plan for obtaining informed
consent:
Please attach copy of your
participant information
sheet and consent form
(Note consent forms are not
needed for questionnaires)
Done
13
.
Steps to be taken to ensure
confidentiality of data:
Outline steps to be taken
to ensure confidentiality,
privacy and anonymity of
data during collection and
publication of data
1- I will use pseudonyms to
protect the identities of
those involved.
2- Respondents to questionnaires
are ensured anonymity and
interviewees who require it
will be granted
confidentiality.
3- Interviews with the dealing
with the child and the school
will be re identified before
the application.
4- All data will be destroyed
once the dissertation has been
completed. In the meanwhile,
only myself as a researcher,
the head teacher and my
supervisor will see the data.
150

14 Debriefing and/or feedback
to participants
What debriefing and support
will participants receive
after the research?
How will the findings of
the research be made
available to them?
A copy of the findings/ results of
the research will be sent to the
Head of the participating school. A
full copy of the thesis will be
available to borrow on request.
15 Data storage and security
How will you ensure safe
data storage during
fieldwork and after
publication?
All the data collected will be
stored and kept in one of the
pathway protective system and this
will be checked with my supervisor
to ensure safety of the collected
data during field work and after
publication.
All materials submitted will be treated confidentially.
I have read and understood the University’s Code of Practice on Ethical
Standards for Research involving Human Participants
Signe
d:
Principal
Investigator
/Student
Khajik Yaqob
Signe Supervisor
151
d:
Prof Debra
McGregor
Date: /06/2013
Appendix 4 Sample of a questionnaire administered to
both groups
152
153
Appendix 5: Participant´s information sheet
OXFORD BROOKES UNIVERSITY
WESTMINSTER INSTITUTE OF EDUCATION
Harcourt Hill,
Oxford
OX2 9AT DATE: 24 June 2013
Direct Line for Supervisor: 01865 488355
Name: Debra McGregor
Email: [email protected]
Researcher’s name: Khajik S. Yaqob
Student No.: 12007086
Email: [email protected]
MA IN CHILDHOOD STUDIES: How do year 6 children think about and understand
Healthy Eating?
Covering letter for questionnaire
I am Khajik Yaqob/ studying the MA Childhood Studies course. Iam studying for a Master degree in Oxford Brookes University/school of education. I am conducting research into Children’sideas about healthy eating. I would like to give your childrena questionnaire to fill in to find out what they think aboutHealthy Eating. This is supported by focus group interviews.It is up to you to decide whether or not to take part. If youdo decide to take part you will be given this informationsheet to keep. If you decide to take part you are still freeto withdraw at any time and without giving a reason. Bychoosing to either take part or not take part in this studywill have no impact on children’s marks. I would bring in aquestionnaire for the year 6 to complete. It will take about20 minutes for them to answer the questions. No disadvantages
154
or risks of taking part in this study, just time. You can seethe results of my study and use them to inform what the schoolmight do about healthy eating. All data will be destroyed oncethe dissertation has been completed. In the meantime, onlyyourself as a head, myself as a researcher, and my supervisorwill see the data. Please inform me about which class can beavailable to fill in the year 6 questionnaire (date and time).A copy of the results/findings of the research will be sent tothe Head of the participating school. A full copy of thethesis will be available to borrow on request. The research ispart of the Master’s program in the Faculty of Humanities andSocial Sciences at Oxford Brookes University. Thisdissertation will be submitted to achieve that degree/award.If you have any concerns please contact my supervisor ProfDebra McGregor, [email protected], Professor in Education(Learning and Developing Pedagogy), School of Education,Faculty of Humanities and Social Sciences, Harcourt HillCampus, Oxford Brookes University, OX2 9AT, Tel : 01865488355. My contact details are: KhajikYaqob,[email protected], student in School of Education,Faculty of Humanities and Social Sciences, Harcourt HillCampus, Oxford Brookes University, OX4 2NS, Mobile no:07753353598.
Thank you for your time
24/06/2013
155
Appendix 6: Interview questions for children in local
Church cohort and primary school group.
1. What does a healthy lifestyle mean to you?
2. Do you think healthy eating is enough for a person to
live healthily?
3. What do you think of exercise and physical activity?
4. Why do you think it is difficult (the barriers) to
achieve healthy eating?
5. Why you should eat healthy food?
156

6. Do your parents often tell you about healthy eating? What
about your teachers? Was that helpful? How?
7. Do you think that your parents and school could help you
to further understand about healthy eating? How?
8. What do you think about Fresh fruit and vegetables, pure
water, cheese, egg and brown bread? Why do you think each
of these foods is significant to eat?
9. Do you have any of these foods in your snack box? And
Why?
10. Why do you think white bread, ice cream, fatty
chicken, fizzy drink, sausages, crisps, canned fruit and
vegetables are not so healthy? Do you think each of them
is good to eat?
11. Why you consider the taste when choosing foods?
What do you think about the appearance of food? Cost? And
Why?
12. What are you most and least five favorite foods to
eat? And do you think each of these foods is healthy? And
Why? And why you prefer to eat unhealthy foods? Or you
might have to eat unhealthy foods for certain reasons?
13. Do you eat five portions of fruits and vegetables a
day? And why you should eat 5 portions a day?
14. What other vitamins and minerals are healthy to eat?
Why? Which foods would you find them in? Why is it
healthy to eat calcium?
15. Do you like to eat fish and why? Do you think fish
is rich of calcium? And do you know which vitamin is
157
essential for vision? Do you know other foods which are
rich of calcium?
16. Do you think fresh is better than canned or frozen
fruits and vegetables? Which is better to eat and why?
And why do people often do not eat the fresh version?
17. How much water do you drink daily? And why do you
think it is healthy?
18. Do you think someone’s size or shape has anything
to do with their health?
19. Do you think potatoes and tomatoes grow under or
above the ground? And have you ever been on a farm visit?
Did you enjoy it? And why? Do you feel more active there?
Is that worthy for you?
20. Do you think that cereal is healthy or unhealthy?
Are you aware of cereal high in sugar? And why you like
to eat cereal? Do you think you are eating a healthy or
an unhealthy breakfast? And why?
21. Do you think boys or girls that are better in
making healthier food choices? And why? And how do you
know you eat a healthy diet?
158

Appendix 7: A revised questionnaire (in light of
research findings).
159
Appendix 8:
160
A (research informed) example Healthy Eating policy
for primary school cohort
Findings from primary school cohort were somewhat concerningof such a school which has been already committed a healthyeating policy, therefore, I would suggest a new healthy eatingpolicy for this school that could be helpful to promote andincrease children’s knowledge and awareness about healthyeating and consequently to help addressing childhood obesity.
The policy below illustrates the participating new school’scommitment to promoting healthy eating across the schoolenvironment, including teaching and the classroom, the schoolorganization, food service and the wider family community. Itwill outline a summary of the actions the school night committo achieve in the future.
The school might contribute to improving the nutrition anddecreasing the risk of lifestyle disease in our children bypromoting healthy eating and food variety in a positive way,not only in the classroom, but across the whole schoolcommunity/environment.
The following areas have been identified as the most importantfor the school to focus on:
Teachers and Curriculum School organization and Food service Parent Education
Teaching and the CurriculumWhat should the school do?
Run a curriculum on aspects of healthy eating and livingat each year level
Incorporate topics on nutrition, Childhood obesity andhealthy eating into a range of learning areas
Undertake a whole school focus during our designatedhealthy eating week in Term 1 each year
Teachers act as role models for healthy eating
161
The plan aims to: Give teachers the opportunity to update their own
knowledge of healthy food, nutrition and Childhoodobesity
Investigate further curriculum ideas and topics toinclude at each year level
Make greater use of the school market as a curriculumresource
Have Junior School Council focus some of their activitiesaround healthy living concepts
School Organization and Food Service What the school might do:
Allot eating time in class ( 25-30 minutes) Designate an allocated eating area at the junior school
for children to finish eating Year 5 and 6 children have a fruit/vegetable snack around
10.15 in class (approximately mid way point before11.35am lunch break)
Encourage and allow water bottles in class and ifpossible to provide free clean tap water in the school
Ban fizzy drinks in children’s school lunches and in theschool’s canteen
Designate and encourage water breaks during PE and sportsessions
Contact parents of children who are not supplied withlunch and if necessary provide students with food fromthe staffroom
Offer a variety of healthy food and seasonalfruit/vegetables at Before and After School Care
Offer low nutritional food on whole school hot food daysonce a term only
Free school breakfast programs should be available in thenew school healthy policy and teaching children abouthealthy breakfast is absolutely a good step forward.Furthermore, the participating school can get benefitfrom a Balanced Breakfast Model (Chapter 2.5.4) topromote eating a healthy breakfast for their children.
162
Thus, the food service staff should be asking “What willkids eat?” while assessing current policies and services
Menu offerings need to reflect the changing preferencesof children with respect to gender and dietaryrecommendations for health. This school that planssimilar menus for both genders may want a look moreclosely at preferences by gender and have choices thatsatisfy both genders. Insight into the food preferencesreported by children (aged 9-10) with regard to gender isvaluable information which might be used to improve thediets of primary school children while developinglifelong healthy eating. Also, preference data might behelpful with school menu planning to create worthynutrition education programs that parallel changes beingcompleted in the school food service. Therefore, agreater understanding of the implications of food qualityor product brand on the preferences and consumption ofchildren in the school setting also should be explored
Also the plan aims to: Introduce across the school rubbish free lunches once a
term with an emphasis on healthy eating Look at alternative fundraising options not based on low
nutritional food Investigate healthy alternatives for whole school special
hot food days Provide vegetable seeds for children to take home and
grow, then return grown vegetable to school for show andtell
Family and CommunityThe goal is to:
Promote healthy eating to families via the weeklynewsletter if possible
Inform parents of the Healthy Eating Week viathe newsletter, email, post or call
163
Discourage parents from providing foods of minimalnutritional value in school lunches via informationnights and the newsletter
An expression of interest should be placed in the FreeFruit Friday program for the junior school students
Utilize the school nurse to give informative talks toprep parents on nutrition, healthy eating and Childhoodobesity
Also to: Conduct information sessions for parents on healthy
eating practices and Childhood obesity focusing onhealthy lunchboxes and after school snacks
Include tips, simple recipes and ideas in the newsletterfor families to adopt at home if they wish
Conduct information sessions for parents on topics ofinterest related to healthy lifestyle, food origin andChildhood obesity
164

Appendix 9: Tentative suggestions for guidelines that
parents should pay attention to (School or general
guidance).
1. Also, making suggestions about guidance for parents to
tackle/address childhood obesity through heightening
healthy eating awareness is crucial and could be
supportive. Parents, teachers and cooks in the school
need further education of healthy eating as they were the
key decision maker of food choices and they should be
more aware of healthy eating, healthy lifestyle, food
origin, and making healthy choices. Also, parents at home
could help and support their children by passing healthy
eating messages to promote their children’s knowledge of
healthy eating.
2. Parents should participate, if possible, in every healthy
eating promotion program arranged by their children’s
school and to share their ideas with each other and with
the teachers and cooks. This could be helpful to maintain
a good healthy menu for their children. Particularly, as
mentioned already, the school menus are sent home to
parents when each new set of menus is introduced. Also,
the school should listen to the children’s opinions on
the menu and adapt the menu accordingly, and the menus
must meet the new nutritional requirements for school
meals.
3. Parents could give valuable information about their
children’s favorite foods to school and teachers, what do
165
they children often like or dislike eating at home, and
this might be changeable as the child grows and develops.
Accordingly, certain menus could be arranged and prepared
in school and considering the gender differences as well.
4. Parents should care about their children’s foods by
keeping in touch with their teachers and school and they
should continue informing the school about any new
condition that might happen to their children. For
instance, if the child has any medical problem such as an
allergy to specific types of foods or certain foods might
the child be not allowed to eat to avoid any future
eating complication.
5. Also, the level of education of parents has an effective
role to promote children’s knowledge and awareness about
healthy eating. It was evident in this study that parents
of children in the local Church group had a more crucial
role than those in primary school cohort by sending their
children healthy eating messages that helped them to
correctly answer the questionnaire. Therefore, parents of
children in primary school should be more aware of
healthy eating and all the issues related and to create a
healthy eating environment at home to help their children
to further understand about healthy eating and childhood
obesity.
6. Certain recommendations to encourage regular breakfast
consumption in children include:
- Using diverse kinds of foods to support positive
experiences and learned preferences
166

- Teach parents to act as role models
- Hearten family breakfast attended by all family members;
- Maintenance a balance of nutrients within the day, and
within breakfast meals during the week.
7- Finally and very recently parents and families of obese
children could have benefited from a new health service
and the scheme (Reach 4 Health Program) which has been
launched on the 6th of Sept. 2013 to help combat the
growing issue of Childhood obesity in Oxford (Oxford
Journal, 2013). Such scheme is commissioned by
Oxfordshire County Council and delivered by the trust´s
School Health Nursing service, is in direct response to
a seven year long National Childhood Measurement Program
(NCMP). Therefore, parents are set to benefit from the
scheme, which is a free weight management service for
children (aged 4-16), as it offers ongoing support to
help families make healthy changes to their lifestyles.
Moreover, the scheme is said to have an emphasis on
having fun and will include group sessions with
activities, as well as one to one support. The focus of
this ten week program will be on making healthy lifestyle
changes including healthy eating and activity and ongoing
support will be given via text and telephone once the
sessions have finished and via the all year round
activity drop-sessions, which will be held countywide.
167
Appendix 10: Reflections on ways my thesis could have
been improved.
1. As I mentioned already, self administered questionnaire
plus interviewing children in the local Church group and
primary school cohort might be the future goal for someone
who wishes to replicate or develop this research study.
2. Larger numbers and more age groups of children (not only
aged 9-10) could be included next to represent the entire
population in primary school population. Also, different
ethnicity and children from different socioeconomic status
might have various findings and conclusions.
3. Because of the goal of this research study was to explore
children’s views about healthy eating and to make
suggestions about Childhood obesity, therefore, I think the
next study should include interviewing obese children of
different age and gender to find out what and how they
think about healthy eating. This is my future intention of
my PhD degree which aims to explore further children’s
beliefs about healthy eating to help to address Childhood
obesity.
4. My future intention is to progress this study, perhaps in
my home country (Iraq, Kurdistan) to find out how do
children (aged 9-10) think about healthy eating. Also, it
is interesting to consider the religion, culture, time, and
168
food preferences, source of food and food availability, and
ethnicity and then comparing both studies could be a step
forward to further understand children’s thoughts about
healthy eating.
5. I hope to develop and improve my research study as a future
step for my PhD degree in Paediatrics and child health in
the UK, in particular, overweight and obese children (aged
9-10). The goal will be to explore obese children’s views
of healthy eating and Childhood obesity as well as the
incidence and prevalence of overweight and obese children
in the UK specifically in Oxford. This future study will be
explored and action research study to deal with real obese
children, assessing their weights and BMI. Also, trying to
explore the reasons of childhood obesity in each case and
what kinds of food do they eat.
6. However, more studies are needed to confirm the findings of
this research study.
169

170

171

172

173

174
175

176

177




















