
Consequences for alveolar macrophages after treatment with MWCNTs
Upload
independentCategory
view
1download
0
COX-2 Inhibition Decreases VEGFExpression and Alveolar Bone LossDuring the Progression of ExperimentalPeriodontitis in RatsThais M. Oliveira,* Vivien T. Sakai,* Maria Aparecida A.M. Machado,* Thiago J. Dionısio,†
Tania Mary Cestari,† Rumio Taga,† Sandra L. Amaral,‡ and Carlos F. Santos†
Background: Vascular endothelial growth factor (VEGF) is a macromolecule of importance in inflamma-tion that has been implicated in periodontitis. The aims of this study were to investigate VEGF expressionduring the progression of periodontal disease and to evaluate the effect of a preferential cyclooxygenase(COX)-2 inhibitor meloxicam on VEGF expression and alveolar bone loss in experimentally induced peri-odontitis.
Methods: A total of 120 Wistar rats were randomly separated into groups 1 (control) and 2 (meloxicam,3 mg/kg/day, intraperitoneally, for 3, 7, 14, or 30 days). Silk ligatures were placed at the gingival margin levelof the lower right first molar of all rats. VEGF expression was assessed by reverse transcription-polymerasechain reaction (RT-PCR), Western blot (WB), and immunohistochemical (IHC) analyses. The hemiarcadeswere processed for histopathologic analysis. RT-PCR and WB results were submitted to analysis of variance,the Tukey test, and Pearson correlation analysis (P <0.05).
Results: A reduction in alveolar bone resorption was observed in the meloxicam-treated group comparedto the control group at all periods studied. There was a positive correlation between COX-2 mRNA and VEGFmRNA in the gingival tissues and periodontal disease (R = 0.80; P = 0.026). Meloxicam significantly reducedthe increased mRNA VEGF expression in diseased tissues after 14 days of treatment (P = 0.023). Some al-terations in VEGF receptor 1 mRNA expression were observed, but these were not statistically significant.VEGF protein expression in WB experiments was significantly higher in diseased sites compared to healthysites (P <0.05). After 14 days of treatment with meloxicam, an important decrease in VEGF protein expres-sion was detected in diseased tissues (P = 0.08). Qualitative IHC analysis revealed that VEGF protein expres-sion was higher in diseased tissues and decreased in tissues from rats treated with meloxicam.
Conclusions: The present data suggest an important role for VEGF in the progression of periodontal dis-ease. Systemic therapy with meloxicam can modify the progression of experimentally induced periodontitisin rats by reducing VEGF expression and alveolar bone loss. J Periodontol 2008;79:1062-1069.
KEY WORDS
Alveolar bone loss; cyclooxygenase-2; inflammation; meloxicam; periodontal disease;vascular endothelial growth factor.
* Department of Pediatric Dentistry, Orthodontics and Community Health, Bauru School of Dentistry, University of Sao Paulo, Bauru, SP, Brazil.† Department of Biological Sciences, Bauru School of Dentistry, University of Sao Paulo.‡ Department of Physical Education, Sao Paulo State University, Sao Paulo, SP, Brazil.
doi: 10.1902/jop.2008.070411
Volume 79 • Number 6
1062

Periodontitis is an important cause of tooth lossin adults.1-3 Although multifactorial, the path-ogenesis of periodontitis involves the presence
of a plaque-retentive factor that initiates a localinflammation reaction in a predisposed host, pro-voking edema, cell influx, and the release of inflam-matory mediators.4-6 Vasodilation and the increasein vessel permeability are events commonly ob-served during inflammation that enhance the inter-stitial fluid volume in the inflamed zone of connectivetissue.4,6,7 However, there is little information con-cerning the biologic mechanisms that may regulatethese changes in tissues affected by periodontaldisease.
Several inflammatory mediators, cytokines, hor-mones, and growth factors are detected during inflam-mation.8-11 These substances directly or indirectlystimulate connective tissue resident host cells, suchas leukocytes, fibroblasts, mast cells, endothelial cells,dendritic cells, and lymphocytes.12,13 Current datasuggest that vascular endothelial growth factor (VEGF)also plays an important role in the regulation of in-flammatory periodontal disease.14-19
VEGF is a key regulator of physiologic angiogene-sis during embryogenesis, skeletal growth, and repro-ductive functions.20 It is one of the most powerfulsubstances known to induce endothelial cell growthand increase vascular permeability.21,22 VEGF in-duces endothelial cell proliferation, promotes cellmigration, and inhibits apoptosis as well as the per-meabilization of blood vessels, thus playing a centralrole in the regulation of vasculogenesis.20-22 VEGFexpression is potentiated in response to hypoxiaand by a variety of cytokines. Deregulated VEGFexpression contributes to the etiology of severaldiseases that are characterized by abnormal angio-genesis.23-25
Many factors are involved in regulating the mecha-nisms of inflammation, including VEGF, which is over-expressed in the majority of inflamed tissues and iscorrelated with poor prognosis.22 COX-2, which isan enzyme responsible for the formation of prosta-glandin E2 from arachidonic acid, regulates angio-genesis, and a COX-2 preferential inhibitor meloxicamcan modify the inflammatory processes.5,26-28 COX-2and VEGF expression are closely linked in some in-flammatory models29,30 and may play critical rolesin the regulation of periodontal disease.
Therefore, the aims of this study were to investigateVEGF expression during the progression of experi-mentally induced periodontitis in rats and to evaluatethe effects of meloxicam, a preferential COX-2 inhib-itor, on VEGF expression and alveolar bone loss. Thehypothesis tested is that meloxicam decreases VEGFexpression and alveolar bone loss.
MATERIALS AND METHODS
Animals and Induction of Periodontal DiseaseThe Institutional Experimentation Committee for An-imal Experiments, Bauru School of Dentistry, Univer-sity of Sao Paulo, approved the protocol for this study(protocol #17/2004). A total of 120 male Wistar ratsweighing 200 to 250 g were randomly separated intogroup 1 (control; 0.9% NaCl; n = 60) and group2 (meloxicam,§ 3 mg/kg/day;5 n = 60). A stock solu-tion of meloxicam in 0.9% NaCl was prepared to yielda proper concentration that would allow the adminis-tration of 0.1 ml intraperitoneally once daily duringthe induction period. The rats were sacrificed after3, 7, 14, or 30 days. After each induction period,30 animals were sacrificed: 15 in group 1 (control)and 15 in group 2 (meloxicam treated). Five animalsfrom each group were used for each experimentalanalysis (reverse transcription-polymerase chain re-action [RT-PCR], Western blot, and immunohisto-chemistry). The experimental periodontitis model inrats was used with minor modifications, as describedelsewhere.31-33 The rats were anesthetized by intra-peritoneal injection of thiopental (60 mg/kg), and asilk31-33 thread ligature was placed around the lowerright first molar in a submarginal position to induce ex-perimental periodontitis. The animals were housed intemperature-controlled rooms and received waterand food ad libitum.
Histologic ProcessingEach dentoalveolar segment contained the alveolarbone, three molars, and the gingival tissue. After fix-ation with 10% formaldehyde solution for 24 hours,the segments were decalcified in 5% EDTA solutionfor ;45 days. Samples were cut mesio-distally androutinely processed for paraffin embedding. Sections5-mm thick were obtained and stained with hematox-ylin and eosin. The site analyzed consisted of the areabetween the first and second molars where the ligaturewas maintained. Histologic analysis consisted of a 0 to3 score based on cell influx, osteoclast numbers, alve-olar process, and cementum integrity and was gradedas described by Leitao et al.,34 i.e., score 0 = absenceof or only discrete cellular infiltration and preservedalveolar process and cementum; score 1 = moderatecellular infiltration, some but minor alveolar processresorption, and intact cementum; score 2 = accentu-ated cellular infiltration and partial destruction of ce-mentum; and score 3 = accentuated cellular infiltrate,complete resorption of the alveolar process, and se-vere destruction of cementum.
§ Movatec, Boehringer Ingelheim do Brasil Quımica e Farmaceutica,Itapecirica da Serra, SP, Brazil.
J Periodontol • June 2008 Oliveira, Sakai, Machado, et al.
1063
RT-PCR Analysis to Detect VEGF andCOX-2 mRNAsFor the RT-PCR studies, frozen gingivalsamples stored in reagenti were homoge-nized with a tissue homogenizer,¶ and totalRNA was isolated by guanidinium isothiocya-natephenol-chloroform extraction.35-37 RNAwas resuspended in diethyl pyrocarbonate–treated water and treated with DNase,# ac-cording to the manufacturer’s instructions,for 15 minutes at room temperature to removeany potential genomic DNA contamination.After RNA concentration measurement on aspectrophotometer at 260 nm, it was storedat -80�C until use. First-strand cDNA synthe-sis and RT-PCR were carried out as describedin previous works by our group.35-37 Temper-ature cycling consisted of an initial denatura-tion step for 2 minutes at 96�C, followed by30 to 40 cycles of amplification.
For the constitutive expressing geneb-actin, each round consisted of denaturation for 30seconds at 95�C, annealing for 30 seconds at 60�C,and extension for 1 minute 30 seconds at 72�C. ForVEGF and COX-2 analyses, each round consisted ofdenaturation for 60 seconds at 94�C, primer anneal-ing for 30 seconds at 65�C, and extension for 60 sec-onds at 72�C. Samples were incubated for anadditional 10 minutes at 72�C for terminal elongationafter the completion of the final cycle. For each set ofprimers, RT-PCR was performed on sterile water tocheck for contamination, and for each tissue, PCR(no RT) was conducted on RNA to check for genomicDNA contamination. A 10-ml aliquot of each samplewas electrophoretically size fractionated on a 2% ag-arose gel containing ethidium bromide (0.5 mg/ml).DNA was visualized under ultraviolet light to detectthe presence of PCR amplification products at the pre-dicted sizes. The size of the PCR products was deter-mined by comparison with a 25– or 100–base pairladder.** The agarose gel containing amplificatedproducts was scanned and analyzed with a computerprogram†† to obtain numeric values that permitted asemiquantitative comparison between each target(VEGF and COX-2) and the constitutive control (b-ac-tin). The sequences of primers used in these experimentsare shown in Table 1.
Western Blot Analysis to Detect VEGFProtein ExpressionThe gingival tissue obtained from the first molarperimeter was homogenized, and protein was sus-pended in potassium buffer (10 mM) for the Westernblot procedures as described previously.38 Twentymicrograms of protein (as determined by a protein as-say kit‡‡) from each tissue and from mouse-kidney
tissue, known to express VEGF at high levels, wereseparated on a 12% denaturing polyacrylamide gel.The proteins in the gels were transferred to a nitrocel-lulose membrane, which was blocked for 2 hours atroom temperature in 5% non-fat dry milk diluted inTris-buffered saline (50 mM Tris and 750 mM NaCl,pH 8.0) with 0.08% Tween 20.§§ The blots were incu-bated overnight with a polyclonal antibody to a pep-tide derived from the human VEGF sequence(1:1,000 dilution)ii at 4�C. Washed blots were incu-bated with biotinylated goat anti-mouse secondaryantibody¶¶ at a dilution of 1:500 for 1.5 hours at roomtemperature and then were subjected to a chemilumi-nescent substrate detection system.## Membraneswere exposed to x-ray film*** for 10 minutes and de-veloped.††† For the quantitative VEGF analysis, filmwas always exposed for a period of time that ensuredthat all signals were within the linear range of the de-tection of the film. VEGF band intensity was quantifiedusing software,‡‡‡ and values were expressed as apercentage of the positive control (mouse-kidneyVEGF expression).
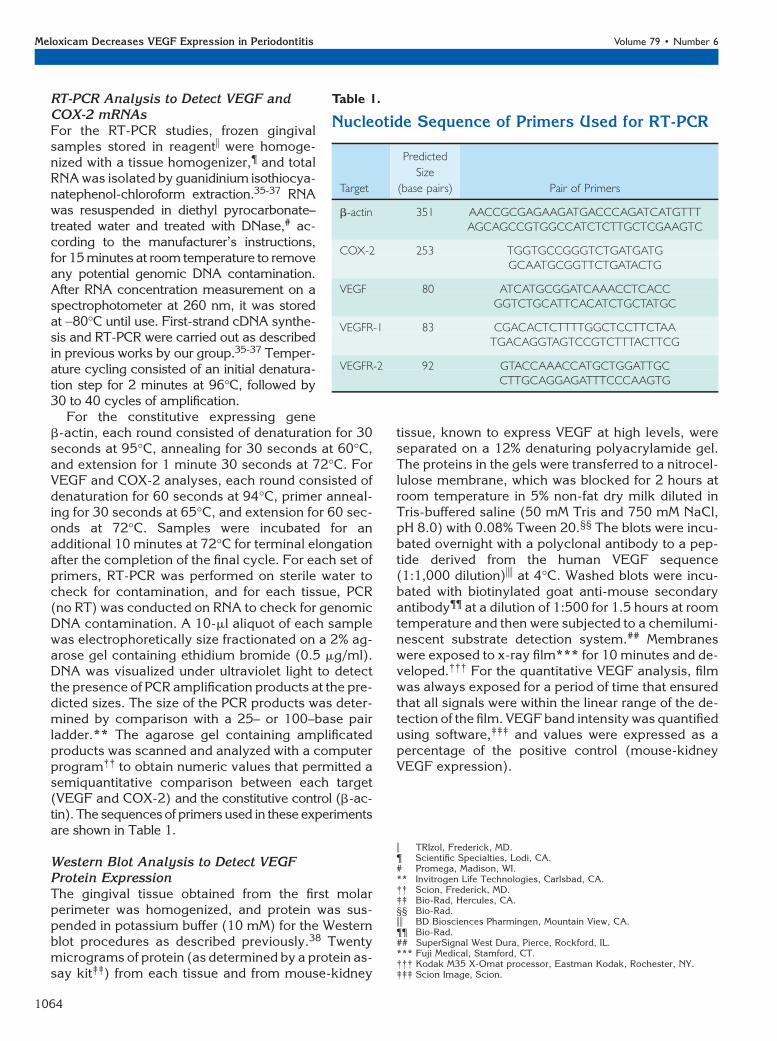
Table 1.
Nucleotide Sequence of Primers Used for RT-PCR
Target
Predicted
Size
(base pairs) Pair of Primers
b-actin 351 AACCGCGAGAAGATGACCCAGATCATGTTTAGCAGCCGTGGCCATCTCTTGCTCGAAGTC
COX-2 253 TGGTGCCGGGTCTGATGATGGCAATGCGGTTCTGATACTG
VEGF 80 ATCATGCGGATCAAACCTCACCGGTCTGCATTCACATCTGCTATGC
VEGFR-1 83 CGACACTCTTTTGGCTCCTTCTAATGACAGGTAGTCCGTCTTTACTTCG
VEGFR-2 92 GTACCAAACCATGCTGGATTGCCTTGCAGGAGATTTCCCAAGTG
i TRIzol, Frederick, MD.¶ Scientific Specialties, Lodi, CA.# Promega, Madison, WI.** Invitrogen Life Technologies, Carlsbad, CA.†† Scion, Frederick, MD.‡‡ Bio-Rad, Hercules, CA.§§ Bio-Rad.ii BD Biosciences Pharmingen, Mountain View, CA.¶¶ Bio-Rad.## SuperSignal West Dura, Pierce, Rockford, IL.*** Fuji Medical, Stamford, CT.††† Kodak M35 X-Omat processor, Eastman Kodak, Rochester, NY.‡‡‡ Scion Image, Scion.
Meloxicam Decreases VEGF Expression in Periodontitis Volume 79 • Number 6
1064
Immunohistochemical Analysis to Detect andLocalize VEGF Protein ExpressionTissue sections were deparaffinized in xylene and re-hydrated through graded concentrations of alcohol.The activity of endogenous peroxidase was blockedwith 3% hydrogen peroxide solution in methanol(0.01 M) for 30 minutes. Sections were heated in a mi-crowave oven, for two cycles of 15 minutes each, incitrate buffer. After a 20-minute cooling period atroom temperature, the slides were rinsed with Tris/phosphate buffered saline (PBS), and non-specificbinding was blocked by incubating the sections for30 minutes with blocking solution.§§§ Sections wereincubated with primary rabbit polyclonal anti-VEGFantibodyiii diluted 1:200 at 4�C with antibody di-luent¶¶¶ for 120 minutes. The sections were incubatedwith biotinylated swine anti-rabbit secondary anti-body### for 15 minutes. Sections were rinsed in PBScontaining 0.1% Triton and incubated with streptavi-din peroxidase complex**** for 15 minutes. Peroxi-dase activity was visualized with 3, 39-diaminobenzidinetetrahydrochloride solution containing 1 ml/l hydro-gen peroxide solution for 3 minutes and counter-stained with Lillie-Mayer hematoxylin for 60 seconds.Normal mouse immunoglobulin G was substitutedfor the primary antibody as a negative control. Posi-tive controls were performed on rat lung sections be-cause VEGF is abundantly expressed in alveolar andbronchial epithelium, glandular cells of the bronchi,and activated alveolar macrophages.39,40 Sectionscounterstained with hematoxylin were mounted andexamined with a light microscope. Immunohisto-chemical results were described qualitatively.
Statistical AnalysisThe Mann-Whitney test was used to compare histo-logic scoring, which was described as medians. Thedata for the RT-PCR and Western blot studies were ex-pressed as mean – SEM. The statistical significance ofdifferences in the measured values was evaluated bytwo-way analysis of variance, followed by multiplecomparisons with the Tukey test and Pearson correla-tion analysis. A difference was considered statisticallysignificant if P <0.05.
RESULTS
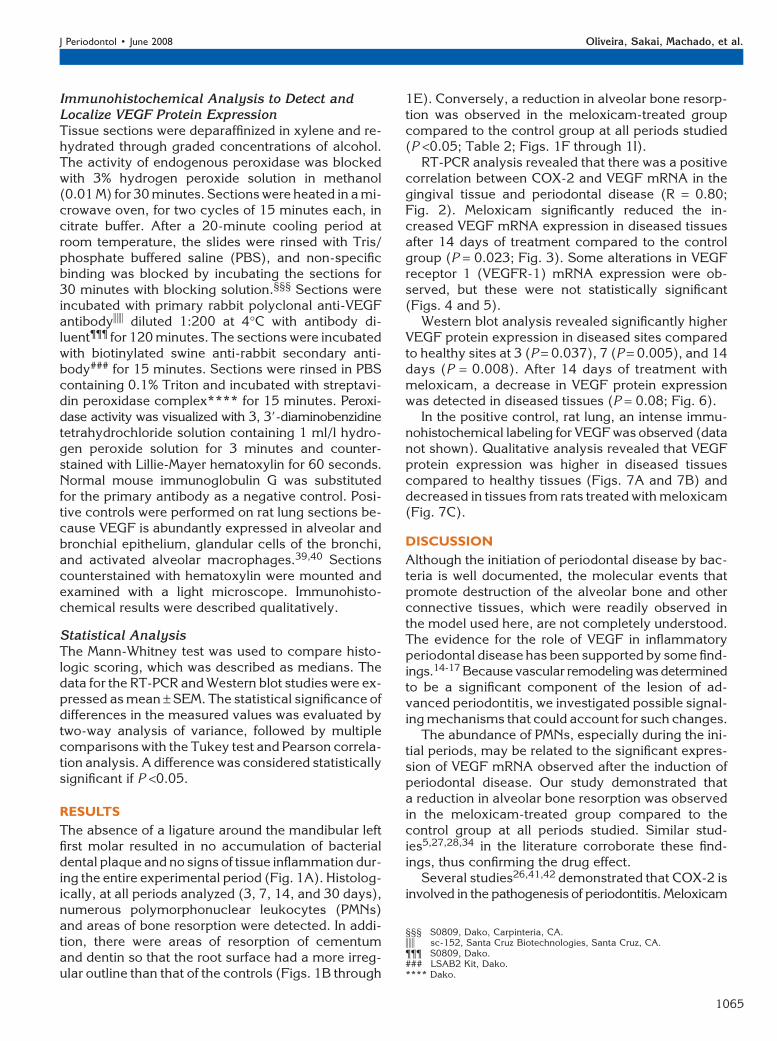
The absence of a ligature around the mandibular leftfirst molar resulted in no accumulation of bacterialdental plaque and no signs of tissue inflammation dur-ing the entire experimental period (Fig. 1A). Histolog-ically, at all periods analyzed (3, 7, 14, and 30 days),numerous polymorphonuclear leukocytes (PMNs)and areas of bone resorption were detected. In addi-tion, there were areas of resorption of cementumand dentin so that the root surface had a more irreg-ular outline than that of the controls (Figs. 1B through
1E). Conversely, a reduction in alveolar bone resorp-tion was observed in the meloxicam-treated groupcompared to the control group at all periods studied(P <0.05; Table 2; Figs. 1F through 1I).
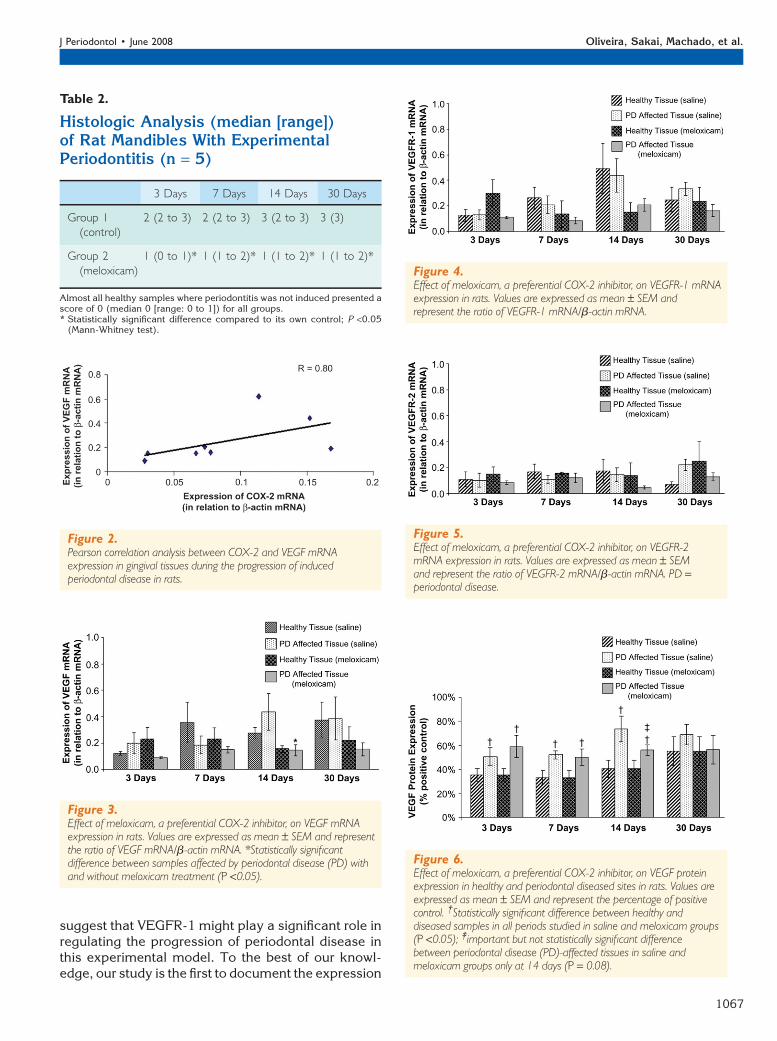
RT-PCR analysis revealed that there was a positivecorrelation between COX-2 and VEGF mRNA in thegingival tissue and periodontal disease (R = 0.80;Fig. 2). Meloxicam significantly reduced the in-creased VEGF mRNA expression in diseased tissuesafter 14 days of treatment compared to the controlgroup (P = 0.023; Fig. 3). Some alterations in VEGFreceptor 1 (VEGFR-1) mRNA expression were ob-served, but these were not statistically significant(Figs. 4 and 5).
Western blot analysis revealed significantly higherVEGF protein expression in diseased sites comparedto healthy sites at 3 (P = 0.037), 7 (P = 0.005), and 14days (P = 0.008). After 14 days of treatment withmeloxicam, a decrease in VEGF protein expressionwas detected in diseased tissues (P = 0.08; Fig. 6).
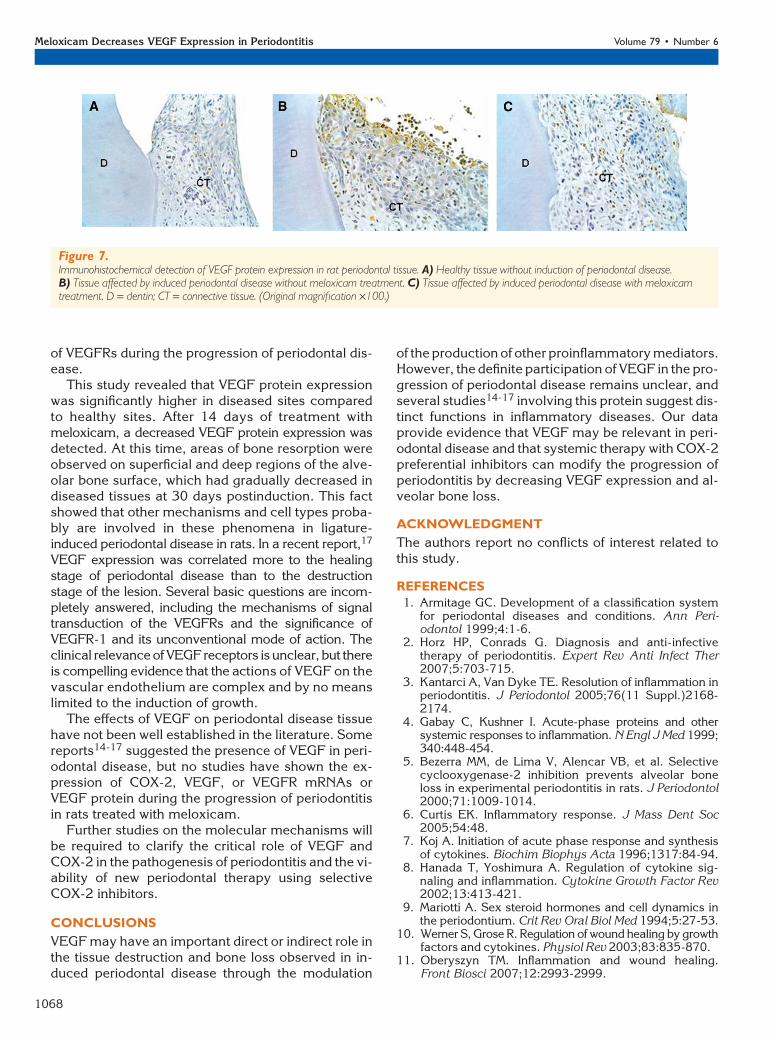
In the positive control, rat lung, an intense immu-nohistochemical labeling for VEGF was observed (datanot shown). Qualitative analysis revealed that VEGFprotein expression was higher in diseased tissuescompared to healthy tissues (Figs. 7A and 7B) anddecreased in tissues from rats treated with meloxicam(Fig. 7C).
DISCUSSION
Although the initiation of periodontal disease by bac-teria is well documented, the molecular events thatpromote destruction of the alveolar bone and otherconnective tissues, which were readily observed inthe model used here, are not completely understood.The evidence for the role of VEGF in inflammatoryperiodontal disease has been supported by some find-ings.14-17 Because vascular remodeling was determinedto be a significant component of the lesion of ad-vanced periodontitis, we investigated possible signal-ing mechanisms that could account for such changes.
The abundance of PMNs, especially during the ini-tial periods, may be related to the significant expres-sion of VEGF mRNA observed after the induction ofperiodontal disease. Our study demonstrated thata reduction in alveolar bone resorption was observedin the meloxicam-treated group compared to thecontrol group at all periods studied. Similar stud-ies5,27,28,34 in the literature corroborate these find-ings, thus confirming the drug effect.
Several studies26,41,42 demonstrated that COX-2 isinvolved in the pathogenesis of periodontitis. Meloxicam
§§§ S0809, Dako, Carpinteria, CA.iii sc-152, Santa Cruz Biotechnologies, Santa Cruz, CA.¶¶¶ S0809, Dako.### LSAB2 Kit, Dako.**** Dako.
J Periodontol • June 2008 Oliveira, Sakai, Machado, et al.
1065
is a non-steroidal anti-inflammatory drug (NSAID)that preferentially inhibits COX-2; it is a potent inhib-itor of acute exudation and cartilage destruction.43
Meloxicam was reported to be effective in preventingalveolar bone loss in experimental periodontitis in rats,with a better risk/benefit ratio than the non-selectiveCOX inhibitors.5 It also was demonstrated that pa-tients with rheumatoid arthritis using meloxicam hada lower incidence of gastrointestinal adverse eventsthan patients using piroxicam, naproxen, or indometh-acin. This finding was associated with greater COX-2selectivity for meloxicam, thus providing strong evi-dence that selective COX-2 inhibitors have a betterclinical anti-inflammatory benefit compared to tradi-tional NSAIDs.44
The VEGF family of growth factors is the focus ofintense research. VEGF has been detected in variousperiodontal tissues and saliva and was postulated toplay roles in tissue maintenance/homeostasis andwound healing.14-17 It was detectable in periodontaltissues within vascular endothelial cells, plasma cells,and macrophages and in junctional, sulcular, and gin-gival epithelium.14 Another study18 indicated that in-flammatory processes induced by the activation ofcertain cytokines (VEGF, monocyte chemoattractantprotein-1, and interleukin-8) in periodontal disease
may be relevant to host-mediated destruction inchronic periodontitis.
In the present study, a positive correlation wasobserved between COX-2 and VEGF mRNA in theprogression of periodontal disease. Meloxicam signif-icantly reduced the increased mRNA VEGF expres-sion in diseased tissues after 14 days of treatmentcompared to the control group. These data are indic-ative of the important role of VEGF in the progressionof periodontal disease and justify further studies. A re-cent study19 showed that VEGF levels in gingival cre-vicular fluid increased from health to periodontitis,and periodontal treatment resulted in a reduction intheir concentrations. These data indicate that VEGFplays a key role in periodontal disease progression.
Pharmacologic treatments can modulate the circu-lating proteins involved in VEGF signaling, includingsoluble forms of VEGFRs. This group of proteinsmay be of value as biomarkers of the pharmacologicand clinical activity of angiogenic processes in cancerand other diseases.23,45,46 With regard to VEGFR-1and -2 in our study, an alteration in VEGFR-1 mRNAexpression was observed, but this was not statisticallysignificant. These data suggest that alterations mayoccur in VEGFR-1 and -2 mRNA expression duringthe progression of periodontal disease. They also
Figure 1.Histologic analysis of rat healthy (A) and periodontally diseased tissues after 3 (B), 7 (C), 14 (D), and 30 (E) days of silk ligature periodontal diseaseinduction. F through I illustrate the reduction in inflammation and alveolar bone loss with meloxicam treatment for 3, 7, 14, and 30 days, respectively.D = dentin; C = cementum; B = bone; PL = periodontal ligament. (Hematoxylin and eosin; original magnification ·40.)
Meloxicam Decreases VEGF Expression in Periodontitis Volume 79 • Number 6
1066
suggest that VEGFR-1 might play a significant role inregulating the progression of periodontal disease inthis experimental model. To the best of our knowl-edge, our study is the first to document the expression
Table 2.
Histologic Analysis (median [range])of Rat Mandibles With ExperimentalPeriodontitis (n = 5)
3 Days 7 Days 14 Days 30 Days
Group 1(control)
2 (2 to 3) 2 (2 to 3) 3 (2 to 3) 3 (3)
Group 2(meloxicam)
1 (0 to 1)* 1 (1 to 2)* 1 (1 to 2)* 1 (1 to 2)*
Almost all healthy samples where periodontitis was not induced presented ascore of 0 (median 0 [range: 0 to 1]) for all groups.* Statistically significant difference compared to its own control; P <0.05
(Mann-Whitney test).
Figure 2.Pearson correlation analysis between COX-2 and VEGF mRNAexpression in gingival tissues during the progression of inducedperiodontal disease in rats.
Figure 3.Effect of meloxicam, a preferential COX-2 inhibitor, on VEGF mRNAexpression in rats. Values are expressed as mean – SEM and representthe ratio of VEGF mRNA/b-actin mRNA. *Statistically significantdifference between samples affected by periodontal disease (PD) withand without meloxicam treatment (P <0.05).
Figure 4.Effect of meloxicam, a preferential COX-2 inhibitor, on VEGFR-1 mRNAexpression in rats. Values are expressed as mean – SEM andrepresent the ratio of VEGFR-1 mRNA/b-actin mRNA.
Figure 5.Effect of meloxicam, a preferential COX-2 inhibitor, on VEGFR-2mRNA expression in rats. Values are expressed as mean – SEMand represent the ratio of VEGFR-2 mRNA/b-actin mRNA. PD =periodontal disease.
Figure 6.Effect of meloxicam, a preferential COX-2 inhibitor, on VEGF proteinexpression in healthy and periodontal diseased sites in rats. Values areexpressed as mean – SEM and represent the percentage of positivecontrol. †Statistically significant difference between healthy anddiseased samples in all periods studied in saline and meloxicam groups(P <0.05); ‡important but not statistically significant differencebetween periodontal disease (PD)-affected tissues in saline andmeloxicam groups only at 14 days (P = 0.08).
J Periodontol • June 2008 Oliveira, Sakai, Machado, et al.
1067
of VEGFRs during the progression of periodontal dis-ease.
This study revealed that VEGF protein expressionwas significantly higher in diseased sites comparedto healthy sites. After 14 days of treatment withmeloxicam, a decreased VEGF protein expression wasdetected. At this time, areas of bone resorption wereobserved on superficial and deep regions of the alve-olar bone surface, which had gradually decreased indiseased tissues at 30 days postinduction. This factshowed that other mechanisms and cell types proba-bly are involved in these phenomena in ligature-induced periodontal disease in rats. In a recent report,17
VEGF expression was correlated more to the healingstage of periodontal disease than to the destructionstage of the lesion. Several basic questions are incom-pletely answered, including the mechanisms of signaltransduction of the VEGFRs and the significance ofVEGFR-1 and its unconventional mode of action. Theclinical relevance of VEGFreceptors is unclear, but thereis compelling evidence that the actions of VEGF on thevascular endothelium are complex and by no meanslimited to the induction of growth.
The effects of VEGF on periodontal disease tissuehave not been well established in the literature. Somereports14-17 suggested the presence of VEGF in peri-odontal disease, but no studies have shown the ex-pression of COX-2, VEGF, or VEGFR mRNAs orVEGF protein during the progression of periodontitisin rats treated with meloxicam.
Further studies on the molecular mechanisms willbe required to clarify the critical role of VEGF andCOX-2 in the pathogenesis of periodontitis and the vi-ability of new periodontal therapy using selectiveCOX-2 inhibitors.
CONCLUSIONS
VEGF may have an important direct or indirect role inthe tissue destruction and bone loss observed in in-duced periodontal disease through the modulation
of the production of other proinflammatory mediators.However, the definite participation of VEGF in the pro-gression of periodontal disease remains unclear, andseveral studies14-17 involving this protein suggest dis-tinct functions in inflammatory diseases. Our dataprovide evidence that VEGF may be relevant in peri-odontal disease and that systemic therapy with COX-2preferential inhibitors can modify the progression ofperiodontitis by decreasing VEGF expression and al-veolar bone loss.
ACKNOWLEDGMENT
The authors report no conflicts of interest related tothis study.
REFERENCES1. Armitage GC. Development of a classification system
for periodontal diseases and conditions. Ann Peri-odontol 1999;4:1-6.
2. Horz HP, Conrads G. Diagnosis and anti-infectivetherapy of periodontitis. Expert Rev Anti Infect Ther2007;5:703-715.
3. Kantarci A, Van Dyke TE. Resolution of inflammation inperiodontitis. J Periodontol 2005;76(11 Suppl.)2168-2174.
4. Gabay C, Kushner I. Acute-phase proteins and othersystemic responses to inflammation. N Engl J Med 1999;340:448-454.
5. Bezerra MM, de Lima V, Alencar VB, et al. Selectivecyclooxygenase-2 inhibition prevents alveolar boneloss in experimental periodontitis in rats. J Periodontol2000;71:1009-1014.
6. Curtis EK. Inflammatory response. J Mass Dent Soc2005;54:48.
7. Koj A. Initiation of acute phase response and synthesisof cytokines. Biochim Biophys Acta 1996;1317:84-94.
8. Hanada T, Yoshimura A. Regulation of cytokine sig-naling and inflammation. Cytokine Growth Factor Rev2002;13:413-421.
9. Mariotti A. Sex steroid hormones and cell dynamics inthe periodontium. Crit Rev Oral Biol Med 1994;5:27-53.
10. Werner S, Grose R. Regulation of wound healing by growthfactors and cytokines. Physiol Rev 2003;83:835-870.
11. Oberyszyn TM. Inflammation and wound healing.Front Biosci 2007;12:2993-2999.
Figure 7.Immunohistochemical detection of VEGF protein expression in rat periodontal tissue. A) Healthy tissue without induction of periodontal disease.B) Tissue affected by induced periodontal disease without meloxicam treatment. C) Tissue affected by induced periodontal disease with meloxicamtreatment. D = dentin; CT = connective tissue. (Original magnification ·100.)
Meloxicam Decreases VEGF Expression in Periodontitis Volume 79 • Number 6
1068
12. Madianos PN, Bobetsis YA, Kinane DF. Generation ofinflammatory stimuli: How bacteria set up inflamma-tory responses in the gingiva. J Clin Periodontol 2005;32(Suppl. 6):57-71.
13. McCourt P. Genetic analysis of hormone signaling.Annu Rev Plant Physiol Plant Mol Biol 1999;50:219-243.
14. Booth V, Young S, Cruchley A, Taichman NS, PaleologE. Vascular endothelial growth factor in human peri-odontal disease. J Periodontal Res 1998;33:491-499.
15. Johnson RB, Serio FG, Dai X. Vascular endothelialgrowth factors and progression of periodontal dis-eases. J Periodontol 1999;70:848-852.
16. Suthin K, Matsushita K, Machigashira M, et al. En-hanced expression of vascular endothelial growthfactor by periodontal pathogens in gingival fibroblasts.J Periodontal Res 2003;38:90-96.
17. Cetinkaya BO, Keles GC, Ayas B, Sakallioglu EE,Acikgoz G. The expression of vascular endothelial growthfactor in a rat model at destruction and healing stages ofperiodontal disease. J Periodontol 2007;78:1129-1135.
18. Lee E, Yang YH, Ho YP, Ho KY, Tsai CC. Potential roleof vascular endothelial growth factor, interleukin-8and monocyte chemoattractant protein-1 in periodon-tal diseases. Kaohsiung J Med Sci 2003;19:406-415.
19. Prapulla DV, Sujatha PB, Pradeep AR. Gingival cre-vicular fluid VEGF levels in periodontal health anddisease. J Periodontol 2007;78:1783-1787.
20. Ferrara N, Gerber HP, LeCouter J. The biology ofVEGF and its receptors. Nat Med 2003;9:669-676.
21. Ferrara N. Molecular and biological properties ofvascular endothelial growth factor. J Mol Med 1999;77:527-543.
22. Ferrara N. The role of VEGF in the regulation ofphysiological and pathological angiogenesis. EXS 2005;94:209-231.
23. Neufeld G, Cohen T, Gengrinovitch S, Poltorak Z.Vascular endothelial growth factor (VEGF) and itsreceptors. FASEB J 1999;13:9-22.
24. Yamazaki Y, Morita T. Molecular and functional diver-sity of vascular endothelial growth factors. Mol Divers2006;10:515-527.
25. Ferrara N. VEGF and the quest for tumour angiogen-esis factors. Nat Rev Cancer 2002;2:795-803.
26. Morton RS, Dongari-Bagtzoglou AI. Cyclooxygenase-2is upregulated in inflamed gingival tissues. J Peri-odontol 2001;72:461-469.
27. Gurgel BC, Duarte PM, Nociti FH Jr., et al. Impact ofan anti-inflammatory therapy and its withdrawal onthe progression of experimental periodontitis in rats.J Periodontol 2004;75:1613-1618.
28. Nassar CA, Nassar PO, Nassar PM, Spolidorio LC.Selective cyclooxygenase-2 inhibition prevents boneresorption. Braz Oral Res 2005;19:36-40.
29. Gallo O, Franchi A, Magnelli L, et al. Cyclooxygenase-2pathway correlates with VEGF expression in head andneck cancer. Implications for tumor angiogenesis andmetastasis. Neoplasia 2001;3:53-61.
30. Pai R, Szabo IL, Soreghan BA, Atay S, Kawanaka H,Tarnawski AS. PGE(2) stimulates VEGF expression inendothelial cells via ERK2/JNK1 signaling pathways.Biochem Biophys Res Commun 2001;286:923-928.
31. Lohinai Z, Benedek P, Feher E, et al. Protective ef-fects of mercaptoethylguanidine, a selective inhibitorof inducible nitric oxide synthase, in ligature-inducedperiodontitis in the rat. Br J Pharmacol 1998;123:353-360.
32. Di Paola R, Marzocco S, Mazzon E, et al. Effect ofaminoguanidine in ligature-induced periodontitis inrats. J Dent Res 2004;83:343-348.
33. Gyorfi A, Fazekas A, Suba Z, Ender F, Rosivall L.Neurogenic component in ligature-induced periodon-titis in the rat. J Clin Periodontol 1994;21:601-605.
34. Leitao RF, Rocha FA, Chaves HV, et al. Locallyapplied isosorbide decreases bone resorption in ex-perimental periodontitis in rats. J Periodontol 2004;75:1227-1232.
35. Santos CF, Oliveira EB, Salgado MC, Greene AS.Molecular cloning and sequencing of the cDNA forrat mesenteric arterial bed elastase-2, an angiotensinII-forming enzyme. J Cardiovasc Pharmacol 2002;39:628-635.
36. Santos CF, Caprio MA, Oliveira EB, et al. Functionalrole, cellular source, and tissue distribution of ratelastase-2, an angiotensin II-forming enzyme. Am JPhysiol Heart Circ Physiol 2003;285:H775-H783.
37. Becari C, Sivieri DO Jr., Santos CF, Moyses MK,Oliveira EB, Salgado MC. Role of elastase-2 as anangiotensin II-forming enzyme in rat carotid artery.J Cardiovasc Pharmacol 2005;46:498-504.
38. Amaral SL, Papanek PE, Greene AS. Angiotensin IIand VEGF are involved in angiogenesis induced byshort-term exercise training. Am J Physiol Heart CircPhysiol 2001;281:H1163-H1169.
39. Tsokos M, Pufe T, Paulsen F, Anders S, Mentlein R.Pulmonary expression of vascular endothelial growth fac-tor in sepsis. Arch Pathol Lab Med 2003;127:331-335.
40. Monacci WT, Merrill MJ, Oldfield EH. Expression ofvascular permeability factor/vascular endothelial growthfactor in normal rat tissues. Am J Physiol 1993;264:C995-C1002.
41. Lohinai Z, Stachlewitz R, Szekely AD, Feher E, Dezsi L,Szabo C. Evidence for the expression of cyclooxygenase-2 enzyme in periodontitis. Life Sci 2001;70:279-290.
42. Zhang ZH, Wei SG, Francis J, Felder RB. Cardiovas-cular and renal sympathetic activation by blood-borneTNF-alpha in rat: The role of central prostaglandins.Am J Physiol Regul Integr Comp Physiol 2003;284:R916-R927.
43. Engelhardt G. Pharmacology of meloxicam, a newnon-steroidal anti-inflammatory drug with an im-proved safety profile through preferential inhibition ofCOX-2. Br J Rheumatol 1996;35(Suppl. 1):4-12.
44. Jouzeau JY, Terlain B, Abid A, Nedelec E, Netter P.Cyclooxygenase isoenzymes. How recent findings af-fect thinking about nonsteroidal anti-inflammatorydrugs. Drugs 1997;53:563-582.
45. Neufeld G, Lange T, Varshavsky A, Kessler O. Semaphorinsignaling in vascular and tumor biology. Adv Exp MedBiol 2007;600:118-131.
46. Deprimo SE, Bello CL, Smeraglia J, et al. Circulatingprotein biomarkers of pharmacodynamic activity ofsunitinib in patients with metastatic renal cell carci-noma: Modulation of VEGF and VEGF-related pro-teins. J Transl Med 2007;5:32.
Correspondence: Dr. Carlos F. Santos, Department of Bio-logical Sciences, Bauru School of Dentistry, University ofSao Paulo, Alameda Dr. Octavio Pinheiro Brisolla, 9-75,Bauru, SP, 17012-901 Brazil. Fax: 55-14-32234679;e-mail: [email protected].
Submitted July 25, 2007; accepted for publication De-cember 4, 2007.
J Periodontol • June 2008 Oliveira, Sakai, Machado, et al.
1069
Copyright © 2022 FDOKUMEN




















