
Comparative proteomic analysis of whole saliva from chronic periodontitis patients
8
Comparative proteomic analysis of whole saliva from chronic periodontitis patients Lorena Da Rós Gonçalves a,b , Márcia Regina Soares c,f, ⁎ , Fábio C.S. Nogueira c , Carlos Garcia c , Danielle Resende Camisasca a , Gilberto Domont c,f , Alfredo C.R. Feitosa d , Denise de Abreu Pereira a , Russolina B. Zingali e,f , Gilda Alves a, ⁎ a Laboratório de Genética Aplicada, Instituto Nacional de Câncer, INCA, Rio de Janeiro, Brazil b Departamento de Genética, Universidade Federal do Rio de Janeiro, UFRJ, Rio de Janeiro, Brazil c Departamento de Bioquímica, Instituto de Química, Universidade Federal do Rio de Janeiro, UFRJ, Rio de Janeiro, Brazil d Faculdade de Odontologia, Instituto de Ciências da Saúde, Universidade Federal do Espírito Santo, UFES, Espírito Santo, Brazil e Laboratório de Hemóstase e Venenos e Unidade de Espectrometria de Massas e Proteômica, Instituto de Biquímica Médica, Programa de Biologia Estrutural, UFRJ, Rio de Janeiro, Brazil f Rede proteômica do Rio de Janeiro, RJ, Brazil ARTICLE INFO ABSTRACT Article history: Received 15 January 2010 Accepted 19 February 2010 Chronic periodontal disease is a chronic inflammatory process affecting tooth supporting tissues in the presence of pathogenic bacterial biofilm. There is some evidence for changes in the protein composition of whole saliva from chronic periodontitis patients, but there have been no studies using a proteomic approach. Hence, the aim of this study was to compare the protein profiles of unstimulated whole saliva from patients with periodontitis and healthy subjects by two complementary approaches (2D-gel electrophoresis and liquid chromatography). Protein spots of interest were analyzed by MALDI-TOF-TOF, and the data was complemented by an ESI-Q-TOF experiment. The analyses revealed that subjects with periodontal disease have increased amounts of blood proteins (serum albumin and hemoglobin) and immunoglobulin, and they have a lower abundance of cystatin compared to the control group. A higher number of protein spots were observed in the periodontitis group, of which most were identified as alpha-amylase. This higher number of alpha-amylase variants seems to be caused by hydrolysis by cysteine proteases under such inflammatory conditions. This approach gives novel insights into alterations of salivary protein in presence of periodontal inflammation and may contribute to the improvement of periodontal diagnosis. © 2010 Elsevier B.V. All rights reserved. Keywords: Saliva Proteomic 2-D electrophoresis Periodontitis 1. Introduction Saliva is a body fluid essential for the health of the oral cavity. Whole saliva is a complex mixture of oral fluids including secretions of the major and minor salivary glands; constitu- ents of non-salivary origin derived from gingival crevicular fluid, expectorated bronchial secretions, serum and blood cells from oral wounds, bacteria and bacterial products, desqua- mated epithelial cells and food debris. Its composition is therefore a complex hypotonic aqueous solution containing JOURNAL OF PROTEOMICS 73 (2010) 1334 – 1341 ⁎ Corresponding authors. Brown is to be contacted at Laboratório de Genética Aplicada, Instituto Nacional de Câncer, (INCA)-HCI, Praça Cruz Vermelha, 23-6° andar, Rio de Janeiro, CEP:20230-130, RJ, Brazil. Tel.: + 55 21 2506 6622. Soares, Departamento de Bioquímica, Instituto de Química, UFRJ Av. Athos da Silveira, 149, Cidade Universitária, CEP:21941-909, Rio de Janeiro, RJ, Brazil. Tel.: +55 21 2562 7355. E-mail addresses: [email protected] (M.R. Soares), [email protected] (G. Alves). 1874-3919/$ – see front matter © 2010 Elsevier B.V. All rights reserved. doi:10.1016/j.jprot.2010.02.018 available at www.sciencedirect.com www.elsevier.com/locate/jprot
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Comparative proteomic analysis of whole saliva from chronic periodontitis patients

J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 1 3 3 4 – 1 3 4 1
ava i l ab l e a t www.sc i enced i r ec t . com
www.e l sev i e r . com/ loca te / j p ro t
Comparative proteomic analysis of whole saliva from chronicperiodontitis patients
Lorena Da Rós Gonçalvesa,b, Márcia Regina Soaresc,f,⁎, Fábio C.S. Nogueirac, Carlos Garciac,Danielle Resende Camisascaa, Gilberto Domontc,f, Alfredo C.R. Feitosad,Denise de Abreu Pereiraa, Russolina B. Zingalie,f, Gilda Alvesa,⁎aLaboratório de Genética Aplicada, Instituto Nacional de Câncer, INCA, Rio de Janeiro, BrazilbDepartamento de Genética, Universidade Federal do Rio de Janeiro, UFRJ, Rio de Janeiro, BrazilcDepartamento de Bioquímica, Instituto de Química, Universidade Federal do Rio de Janeiro, UFRJ, Rio de Janeiro, BrazildFaculdade de Odontologia, Instituto de Ciências da Saúde, Universidade Federal do Espírito Santo, UFES, Espírito Santo, BrazileLaboratório de Hemóstase e Venenos e Unidade de Espectrometria de Massas e Proteômica, Instituto de Biquímica Médica,Programa de Biologia Estrutural, UFRJ, Rio de Janeiro, BrazilfRede proteômica do Rio de Janeiro, RJ, Brazil
A R T I C L E I N F O
⁎ Corresponding authors. Brown is to be contCruz Vermelha, 23-6° andar, Rio de Janeiro, CEde Química, UFRJ Av. Athos da Silveira, 149,
E-mail addresses: [email protected] (M.R.
1874-3919/$ – see front matter © 2010 Elsevidoi:10.1016/j.jprot.2010.02.018
A B S T R A C T
Article history:Received 15 January 2010Accepted 19 February 2010
Chronic periodontal disease is a chronic inflammatory process affecting tooth supportingtissues in the presence of pathogenic bacterial biofilm. There is some evidence for changesin the protein composition of whole saliva from chronic periodontitis patients, but therehave been no studies using a proteomic approach. Hence, the aim of this study was tocompare the protein profiles of unstimulated whole saliva from patients with periodontitisand healthy subjects by two complementary approaches (2D-gel electrophoresis and liquidchromatography). Protein spots of interest were analyzed by MALDI-TOF-TOF, and the datawas complemented by an ESI-Q-TOF experiment. The analyses revealed that subjects withperiodontal disease have increased amounts of blood proteins (serum albumin andhemoglobin) and immunoglobulin, and they have a lower abundance of cystatincompared to the control group. A higher number of protein spots were observed in theperiodontitis group, of whichmost were identified as alpha-amylase. This higher number ofalpha-amylase variants seems to be caused by hydrolysis by cysteine proteases under suchinflammatory conditions. This approach gives novel insights into alterations of salivaryprotein in presence of periodontal inflammation andmay contribute to the improvement ofperiodontal diagnosis.
© 2010 Elsevier B.V. All rights reserved.
Keywords:SalivaProteomic2-D electrophoresisPeriodontitis
1. Introduction
Saliva is a body fluid essential for the health of the oral cavity.Whole saliva is a complex mixture of oral fluids includingsecretions of the major and minor salivary glands; constitu-
acted at Laboratório de GP:20230-130, RJ, Brazil. TeCidade Universitária, CEPSoares), [email protected]
er B.V. All rights reserved
ents of non-salivary origin derived from gingival crevicularfluid, expectorated bronchial secretions, serumand blood cellsfrom oral wounds, bacteria and bacterial products, desqua-mated epithelial cells and food debris. Its composition istherefore a complex hypotonic aqueous solution containing
enética Aplicada, Instituto Nacional de Câncer, (INCA)-HCI, Praçal.: +55 21 2506 6622. Soares, Departamento de Bioquímica, Instituto:21941-909, Rio de Janeiro, RJ, Brazil. Tel.: +55 21 2562 7355.v.br (G. Alves).
.

1335J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 1 3 3 4 – 1 3 4 1
proteins, peptides, enzymes, hormones, sugars, lipids, growthfactors and a variety of other compounds. Many salivaryprotein components have been studied and some differenceson protein profiles identified by proteomic approaches havebeen associated with systemic diseases such as breast cancer[1], Sjögren's syndrome [2,3], diabetes mellitus [4], cysticfibrosis [5], diffuse systemic sclerosis [6] and oral pathologiessuch as oral lichen planus [7], oral cancer [8], dental caries [9]and generalized aggressive periodontitis [10].
Periodontal diseases reflect the interplay between apathogenic bacterial biofilm present on the root surface/periodontal pocket and host-derived inflammatory cells andmolecules from periodontal tissue. This process results in lossof connective tissue and bone support and is a major cause oftooth loss in adults. According to the American Academy ofPeriodontology, three types of periodontitis are currentlyrecognized, namely chronic periodontitis, aggressive period-ontitis and periodontitis associated with systemic disease.Chronic periodontitis, which is themost prevalent in adults, isa destructive disease frequently found in the presence of localfactors and subgingival calculus [11]. The diagnosis of activephases of chronic periodontitis and the identification ofpatients at risk for active disease represents a challenge forboth clinical investigators and clinicians. Clinical and radio-graphic assessment of periodontal disease remains the basisfor patient evaluation, which is subject to considerablemeasurement error and often poorly tolerated by patients.Many studies have focused on finding possible compounds insaliva that could be associated with the presence and/orseverity of chronic periodontitis, such as enzymes (alkalinephosphatase, aminopeptidases, collagenase, elastase, ester-ase, and lysozyme), immunoglobulins (IgA, IgG, and IgM),other proteins (cystatins, fibronectin, and lactoferrin), growthfactors (vascular endothelial growth factor and plateletactivating factor), ions (calcium) and hormones (cortisol)(for a review see [12]).
In this study, thedifferences in protein profiles ofwhole salivafrom patients with chronic periodontitis were compared to thosefrom a control group by two-dimensional gel electrophoresis andliquid chromatography followed by mass spectrometry.
2. Material and methods
2.1. Patient selection
Patients seeking treatment in the School of Dentistry of theFederal University of Espírito Santo (UFES) Brazil wererecruited on August 2008. To participate in this study,individuals signed an informed consent to a research protocolthat had been reviewed and approved by the UFES EthicsCommittee. All study subjects were systemically healthy.Subjects were excluded from the study if they were nursing orpregnant, smoked, drank alcohol, had received periodontaltreatment in the last 2 years or taken antibiotics in the previousyear. Clinical parameters were recorded with a North Carolinaperiodontal probe (UNC-15, Hu-Friedy, Chicago, IL) and includedprobing pocket depth (PPD), clinical attachment level (CAL) andbleeding on probing (BOP). Chronic periodontitis was diagnosedin patients older than 35 years of age, who had six sites BOP on
different teeth with PPD≥6 mm and CAL>5 mm. Controlsubjects had <10% of sites BOP and PPD<3mm. Each group(control and periodontitis) consisted of 10 individuals (5 femaleand 5 male) and their mean age±SD was 35.6±9.5 and 45±5.1,respectively.
2.2. Sample collection and processing
Volunteers were asked to rest for 15 min before saliva collection(at morning, 2 h after tooth brushing), sitting in an uprightposition and were asked not to speak until saliva collectionended. Unstimulated whole saliva samples were immediatelykept on ice and were then centrifuged at 14,000×g for 15 min at4 °C to remove insoluble materials, cell debris and foodremnants. The supernatant of each sample was collected and1 mM EDTA (Sigma, St. Louis, MO, USA) and 1 mM PMSF (Sigma,St. Louis, MO, USA) were added to inhibit proteases. Proteinconcentration was determined according to Lowry assay usingthe Bio-Rad DC Protein Assay (Bio-Rad, Hercules, CA, USA).Supernatants were frozen at −70 °C until analysis.
2.3. Sample preparation and 2D gel electrophoresis
Protein (100 μg) wasmixed from each subject (n=10) for a totalof 1 mg of protein. This was precipitated with 1 mL of coldacetone/0.2% DTT (w/v) overnight and centrifuged at 14,000×gfor 30 min at 4 °C. The pellets were washed three times withcold acetone (90% v/v) containing 0.02%DTT. Pellets were thensolubilized in 340 μL rehydration solution (8 MUrea, 2%CHAPS,0.5% IPG buffer, DTT 18 mM, 0.002% bromophenol blue(BPB)).IEF was carried out in the first dimension on precast 18 cmImmobilineDryStrips, pH3–10 L (GEHealthcare) in an Ettan IPGPhor unit as described by the manufacturer (GE Healthcare)and focused in 5 steps (60 V, 720 Vh; 200 V, 200 Vh; 500 V,500 Vh; 1000 V, 1000 Vh;and 8000 V, 32,000 Vh). The tempera-ture was maintained at 20 °C. For the second dimension, eachstripwas incubated for 15 min first in 10 mL of 50 mMTris–HClbuffer pH 8.8, 6 M urea, 30% v/v glycerol, 2% w/v SDS, 0.002%bromophenol blue (BPB), 65 mM DTT, and then in the samebuffer solution containing 135 mM iodoacetamide instead ofDTT. Strips were then rinsed in Tris-glycine buffer, transferredto a homogeneous 12% SDS-polyacrylamide gel and 5 μL ofBench Mark protein ladder (Invitrogen) was added at top rightposition of the gel. Finally, gel strips were overlaid with 0.5%(w/v) agarose in running buffer containing BPB. Gels wererun on Ettan DALTsix system (GE Healthcare) at 2.5 W/gel for30 min and 100 W for six gels until the end of the run. Thegels were fixed and then stainedwith Coomassie Brilliant BlueG-250 (Sigma, St. Louis, MO, USA). All experiments were donein triplicate and all sample gels were electrophoresed underthe identical conditions in the first and second dimension.
2.4. Gel image and statistical analysis imaging processing
All gels were digitized at 300 dpi and 16 bits depth resolution byan ImageScanner (Amersham Biosciences) using LabScansoftware (Amersham Biosciences). ImageMaster 2D Platinumsoftware (Amersham Biosystem) was used for image analysis.Proteins loaded on gels were normalized between replicates topartially quantify spot intensities and to minimize analytical

1336 J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 1 3 3 4 – 1 3 4 1
variation among gels. To analyze protein intensity, triplicate 2Dgels of the periodontitis groupwere compared to control gels aswell as to each other. At least 5 well-defined landmarks wereused for matching gels. Spots exhibiting a greater than 2-foldchange in their normalized volumebetween two sample groupsand present in at least five of the six replicate gels of each groupwere submitted for statistical analysis. Statistical significancewas estimated through theStudent's t-test using SPSS software-version 11 (SPSS Inc., Chicago, IL, USA) and p<0.05 wasconsidered significant. Spots that exhibited a statistical differ-ence were selected for mass spectrometry identification.
2.5. In-gel digestion
Protein spots were excised from gels and washed with 25mMammonium bicarbonate in 50% acetonitrile overnight at roomtemperature to destain the proteins. They were then dehydratedin 100% acetonitrile for 10min and dried completely in a Speed-Vac centrifuge (Savant, Minnesota, USA). Gel fragments wereallowed to reswell in 10 μL of the digestion buffer containingtrypsin (Promega, modified sequencing grade) at a final concen-tration 10 ng/μL in 25mM ammonium bicarbonate. The gelfragments were digested with trypsin for 20 h at 37 °C. Theresulting tryptic peptides were extracted from the gel pieces byincubatingwith 50 μL of 50%acetonitrile in 5% trifluoroacetic acidtwice for 15min, first with agitation and then with sonication.Supernatants were transferred, pooled and concentrated to neardryness in a Speed-Vac centrifuge. Each samplewas then dilutedwith 10 μL of Milli-Q water in 0.1% trifluoroacetic acid.
2.6. MALDI-TOF/TOF mass spectrometry analysis
Roughly 0.4 μL of the solution of extracted peptides wasmixed with an equal volume of CHCA matrix solution(10 mg/mlα-cyano-4-hydroxycinnamic acid (Aldrich,Milwaukee,WI) in 50% acetonitrile/0.1% trifluoroacetic acid) and left to dry.Data for protein identifications were obtained from 4700 Proteo-mics Analyzer (Applied Biosystems, Foster City, CA). BothMS andMS/MS data were acquired with a neodymium-doped yttriumaluminum garnet (Nd:YAG) laser with a 200-Hz repetition rate.Typically, 1600 shots were accumulated for spectra in MS modewhile 2400 shots were accumulated for spectra in MS/MS mode.MSandMS/MSmass spectrawere acquired in reflectormode andinternallycalibratedwith trypsinautolysispeptides.Uptoeightofthe most intense ion signals with signal to noise ratio above 30were selected as precursors for MS/MS acquisition. Externalcalibration in MS mode was performed using a mixture offour peptides: des-Arg1-Bradykinin (m/z=904.468), angiotensin I(m/z=1296.685), Glu1-fibrinopeptide B (m/z=1570.677), and ACTH(18–39) (m/z=2465.199). MS/MS spectra were externally calibratedusing known fragment ion masses observed in the MS/MSspectrum of angiotensin I.
2.7. Enzymatic digestion for LC-ESI-MS experiments andwhole saliva peptide ultrafiltrate preparations
An aliquot of pooled whole saliva (1 mg/mL) from eachgroup was ultrafiltered in two types of Microcon concentra-tors(YM-10K and YM-3K, Millipore, Billerica, MA, USA) to enrichwhole saliva into three fractions (fraction 1, salivary peptides
<3 kDa; fraction 2, enriched proteins and peptides between 3and 10 kDa, and fraction 3 with enriched proteins >10 kDa).From 1 mL of whole saliva sample, approximately 500 µLfraction 1, 100 µL fraction 2, and 100 µL fraction 3were obtained.All fractionswere treatedwith 10mMDTT for 30min, thenwith50 mMiodoacetamide for 30min in the dark. Trypsin (1 µg/50 µgprotein) was then added to the sample for overnight trypticdigestionat37 °C.All sampleswere concentrated inaSpeed-Vaccentrifuge to produce a 20 μL final volume of Digested Ultrafil-trate Sample (DUFs).
2.8. Analysis of DUFs by nLC-Q-TOF
The DUFs were loaded on a Waters® nanoACQUITY UPLC®System (Waters, Milford, MA) with a Waters Opti-Pak C18 trapcolumn coupled to Q-Tof Ultima® (Waters, Milford, MA). Thedigested protein was fractionated and desalted by liquidchromatography (LC) on line to electrospray ionization quad-rupole time-of-flight mass spectrometry (ESI-Q-TOF). 3.0 µL ofsample was injected on a nanoEase C18 150 mm×75 µmcolumn (Waters, Milford, MA) at a flow rate of 0.6 µL/min andeluted with a linear gradient (10 to 50%) of acetonitrilecontaining 0.1% formic acid. The ESI voltage was set at 3.5 kVusingametal needle, the source temperaturewas80 °C and thecone voltage was 100 V. The instrument control and dataacquisition was conducted by MassLynx data system (Version4.0, Waters) and experiments were performed by scanningfrom a mass-to-charge ratio (m/z) of 200 to 2000 using a scantime of 1 s applied during the whole chromatographic process.A maximum of 3 ions with charge states of 2, 3 or 4 wereselected for MS/MS from a single MS survey. Adduct masses ofNa+ and K+ were automatically excluded. Collision-induceddissociation (CID)MS/MS spectrawere obtained using argon asthe collision gas at a pressure of 13 psi and the collision voltagewas varied between 18 and 45 V depending on the mass of theprecursor. The reference ion used was the mono charged ionm/z 588.8692 of phosphoric acid.Mass spectra corresponding toeach signal from the total ion current (TIC) chromatogramwere averaged, allowing an accurate molecular mass determi-nation. Exact mass MS/MS was automatically determinedusing the Q-Tof's LockSpray™ (Waters, Milford, MA, USA).
2.9. Database searching
Data were processed using Data Explorer® Software (version4.0, Applied Biosystems) for matrix-assisted laser desorptionionization (MALDI-TOF-TOF) analysis and ProteinLynx Globalserver (version 2.0, Waters) for ESI-Q-TOF analysis. Proteinswere identified by correlation of tandem mass spectra to theNCBInr proteins and MSDB database, using the MASCOTonline software (www.matrixscience.com). The first analysisconsidered all taxonomies and a second analysis was restrict-ed to Homo sapiens to remove the redundancy of proteinidentifications. One missed cleavage per peptide was allowedand an initial peptide mass tolerance of ±0.3 Da was used forMALDI-TOF-TOF analysis and ±0.1 Da for ESI-Q-TOF analysis.Cysteines were assumed to be carbamidomethylated andvariable modification of methionine (oxidation) was allowed.ForMALDI-TOF-TOF identifications, at least two peptideswererequired to match for each protein.
1337J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 1 3 3 4 – 1 3 4 1
2.10. Caititu analysis
Peptides sequence from some alpha-amylase spots of specialinterest were localized in the primary structure of this protein(gi| 178585; NCBI database) and a graphic representation wasgenerated by the CAITITU software version 2.0.0.1.9 [13].
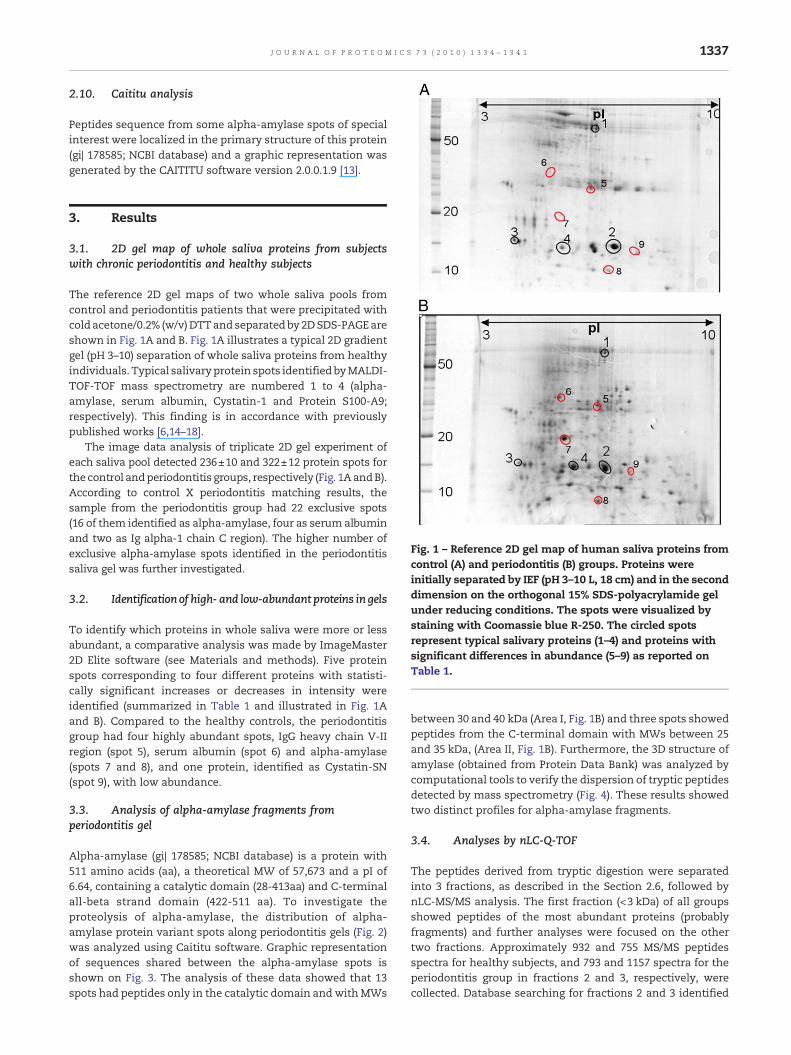
Fig. 1 – Reference 2D gel map of human saliva proteins fromcontrol (A) and periodontitis (B) groups. Proteins wereinitially separated by IEF (pH 3–10 L, 18 cm) and in the seconddimension on the orthogonal 15% SDS-polyacrylamide gelunder reducing conditions. The spots were visualized bystaining with Coomassie blue R-250. The circled spotsrepresent typical salivary proteins (1–4) and proteins withsignificant differences in abundance (5–9) as reported onTable 1.
3. Results
3.1. 2D gel map of whole saliva proteins from subjectswith chronic periodontitis and healthy subjects
The reference 2D gel maps of two whole saliva pools fromcontrol and periodontitis patients that were precipitated withcoldacetone/0.2% (w/v)DTTand separatedby2DSDS-PAGEareshown in Fig. 1A and B. Fig. 1A illustrates a typical 2D gradientgel (pH 3–10) separation of whole saliva proteins from healthyindividuals. Typical salivaryprotein spots identified byMALDI-TOF-TOF mass spectrometry are numbered 1 to 4 (alpha-amylase, serum albumin, Cystatin-1 and Protein S100-A9;respectively). This finding is in accordance with previouslypublished works [6,14–18].
The image data analysis of triplicate 2D gel experiment ofeach saliva pool detected 236±10 and 322±12 protein spots forthe control andperiodontitis groups, respectively (Fig. 1AandB).According to control X periodontitis matching results, thesample from the periodontitis group had 22 exclusive spots(16 of them identified as alpha-amylase, four as serum albuminand two as Ig alpha-1 chain C region). The higher number ofexclusive alpha-amylase spots identified in the periodontitissaliva gel was further investigated.
3.2. Identification of high- and low-abundant proteins in gels
To identify which proteins in whole saliva were more or lessabundant, a comparative analysis was made by ImageMaster2D Elite software (see Materials and methods). Five proteinspots corresponding to four different proteins with statisti-cally significant increases or decreases in intensity wereidentified (summarized in Table 1 and illustrated in Fig. 1Aand B). Compared to the healthy controls, the periodontitisgroup had four highly abundant spots, IgG heavy chain V-IIregion (spot 5), serum albumin (spot 6) and alpha-amylase(spots 7 and 8), and one protein, identified as Cystatin-SN(spot 9), with low abundance.
3.3. Analysis of alpha-amylase fragments fromperiodontitis gel
Alpha-amylase (gi| 178585; NCBI database) is a protein with511 amino acids (aa), a theoretical MW of 57,673 and a pI of6.64, containing a catalytic domain (28-413aa) and C-terminalall-beta strand domain (422-511 aa). To investigate theproteolysis of alpha-amylase, the distribution of alpha-amylase protein variant spots along periodontitis gels (Fig. 2)was analyzed using Caititu software. Graphic representationof sequences shared between the alpha-amylase spots isshown on Fig. 3. The analysis of these data showed that 13spots had peptides only in the catalytic domain andwithMWs
between 30 and 40 kDa (Area I, Fig. 1B) and three spots showedpeptides from the C-terminal domain with MWs between 25and 35 kDa, (Area II, Fig. 1B). Furthermore, the 3D structure ofamylase (obtained from Protein Data Bank) was analyzed bycomputational tools to verify the dispersion of tryptic peptidesdetected by mass spectrometry (Fig. 4). These results showedtwo distinct profiles for alpha-amylase fragments.
3.4. Analyses by nLC-Q-TOF
The peptides derived from tryptic digestion were separatedinto 3 fractions, as described in the Section 2.6, followed bynLC-MS/MS analysis. The first fraction (<3 kDa) of all groupsshowed peptides of the most abundant proteins (probablyfragments) and further analyses were focused on the othertwo fractions. Approximately 932 and 755 MS/MS peptidesspectra for healthy subjects, and 793 and 1157 spectra for theperiodontitis group in fractions 2 and 3, respectively, werecollected. Database searching for fractions 2 and 3 identified

Table 1 – Statistical data of proteins with different abundance among groups analyzed by MALDI-TOF-TOF.
Spot Protein name NCBI number Sequence coverage (%) Score Matched peptides p-value ⁎ Folds in
Periodontitis group vs. healthy group5 Ig heavy chain V-III region gi|106482 17 100 3 p<0.01 ↑4.546 Serum Albumin gi|28592 12 277 6 p<0.05 ↑2.177 Alpha-amylase gi|178585 14 282 5 p<0.05 ↑1.138 Alpha-amylase gi|178585 4 70 2 p<0.01 ↑2.589 Cystatin-SN precursor (Cystatin-1) gi|118188 51 322 6 p<0.1 ↓1.29
⁎ p-value was calculated according to the Student's t-test. Peptide score was calculated as 10*Log(P), where Pwas the probability of the observedmatch to be a random event.
1338 J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 1 3 3 4 – 1 3 4 1
32 and 14 proteins from healthy subjects and 20 and 49proteins from the saliva of the periodontitis group.
Table 2 shows proteins that were identified with a score ofgreater than 50. The majority of the detected peptidescorrespond toalpha-amylaseor serumalbumin inall fractions.Prolactin and transferrin/serotransferrin were also found in allgroups. In this analysis, the MS/MS spectra of hemoglobinpeptides were frequently present in the fraction from theperiodontitis group, while the control group hadmore cystatinpeptides. It is also significant that immunoglobulin was moreextensively detected in saliva from periodontitis patients.
4. Discussion
Chronic periodontitis is a biofilm-induced infection caused bycomponents of pathogenic oral microbiota. Host inflammatory-immunologic responses are responsible for periodontal tissuedamage that can progress to a tooth loss. Saliva is a fluid that canbe easily collected and contains locally and systemically derivedmarkers of periodontal diseases. Although many studies havefocused on possible alterations of salivary protein components,this is the first to use a proteomic approach. In the present study,the protein profile of unstimulated whole saliva from patientswith chronic periodontitis was compared with that from healthy
Fig. 2 – 2D gel map of saliva from the periodontitis groupshowing specific spots identified as alpha-amylase. Spotswere grouped according to the MS/MS identification ofpeptides in the catalytic domain (Area I) and C-terminal(Area II) regions of the alpha-amylase sequence.
subjectsby twocomplementaryexperimental approaches (2D-gelelectrophoresis and liquid chromatography). The analysesrevealed an increased amount of blood proteins (hemoglobinand serum albumin) and immunoglobulin, and a lower abun-dance of cystatin in the periodontitis group compared to thecontrol group. The periodontis group also had ahigher number ofprotein spots, most of them identified as alpha-amylase.
By using 2D SDS-PAGE and liquid chromatography separa-tion approaches coupled with MS/MS identifications, thecomposition of the salivary proteins was obtained in acomplementary fashion. The identification of several spotscorresponding to the same protein demonstrated the ability of2-DE to detect post-translational modifications such as glyco-sylation, truncation and phosphorylation. The results of 2-DEcomparative analysis allowed the visual identification of ahigher number of alpha-amylase fragments and a characteristicclustering of these fragments into two areas in the periodontitisgroup. The ultrafiltration step in conjunction to nLC-MS/MSprovides additional information about differences in proteinprofile between groups that were also obtained from 2-DEexperiments. These differences are discussed below in detail.
4.1. Immunoglobulins
Compared to the healthy saliva group, the periodontitis salivagroup showed a higher abundance of Ig heavy chain V-III region(2-DE analysis; spot 5) and also 2 exclusive spots of this protein.The analyses of fractions 2 and 3 indicated that differentpeptides from this class of protein were founded in diseasedgroups. These results are in agreement with previous studies[19,20] that found an increased concentration of IgG in salivaderived from gingival crevicular fluid or a positive correlationbetween IgA concentration (from plasma cells in the parotidgland) and the severity of inflammation [21]. Hence, IgA2 andIgG levels were higher in the proteomic profiles of wholeunstimulated saliva obtained from generalized aggressiveperiodontitis patients than in healthy control subjects [22].
4.2. Hemoglobin and albumin
The results of this study showed a higher abundance of serumalbumin in diseased group saliva compared to control group(spot 6 and 10, respectively, 2-DE analysis). Analysis of DUFs bynLC-Q-TOF indicated the presence of peptides from hemoglo-bin in the diseased group (Table 2), which is consistent withthe increased number of red blood cells (spontaneousbleeding) found in periodontal inflammation [23].
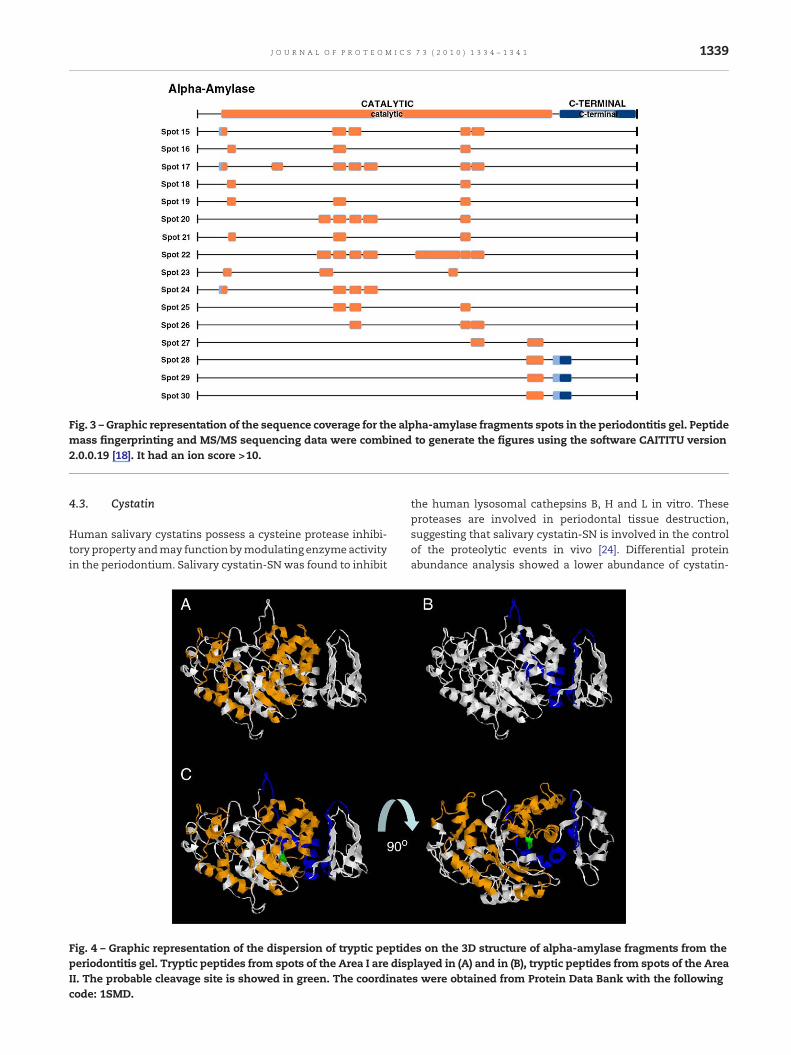
Fig. 3 – Graphic representation of the sequence coverage for the alpha-amylase fragments spots in the periodontitis gel. Peptidemass fingerprinting and MS/MS sequencing data were combined to generate the figures using the software CAITITU version2.0.0.19 [18]. It had an ion score >10.
1339J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 1 3 3 4 – 1 3 4 1
4.3. Cystatin
Human salivary cystatins possess a cysteine protease inhibi-tory property andmay functionbymodulating enzymeactivityin the periodontium. Salivary cystatin-SNwas found to inhibit
Fig. 4 – Graphic representation of the dispersion of tryptic peptidperiodontitis gel. Tryptic peptides from spots of the Area I are dispII. The probable cleavage site is showed in green. The coordinatecode: 1SMD.
the human lysosomal cathepsins B, H and L in vitro. Theseproteases are involved in periodontal tissue destruction,suggesting that salivary cystatin-SN is involved in the controlof the proteolytic events in vivo [24]. Differential proteinabundance analysis showed a lower abundance of cystatin-
es on the 3D structure of alpha-amylase fragments from thelayed in (A) and in (B), tryptic peptides from spots of the Areas were obtained from Protein Data Bank with the following

Table 2 – List of proteins from nLC-MS/MS experiments.
Proteins NCBInumber
Control Periodontitis
3–10 kDa >10 kDa 3–10 kDa >10 kDa
Alpha-amylase gi|178585 40/13 85/10 38/11 107/11Alpha-2-macroglobulin gi|112911 – 1/1 ⁎ – 5/3Apolipoprotein APO-A1 gi|119587681 – 2/2 – 8/6Carbonic anhydrase 6 gi|179732 – 2/2 – 3/2Cystatin-S gi|30366 12/4 33/4 4/3 5/2Cystatin-SA gi|235948 5/3 17/3 – 4/2Cystatin-SN gi|118188 17/5 33/5 8/3 7/2Hemoglobin subunit alpha gi|122440 – 1/1 ⁎ 9/3 3/3Hemoglobin subunit beta gi|122698 – – 9/5 54/32Ig alpha-1 chain C region gi|113584 2/1 ⁎ 1/1 ⁎ 2/1 ⁎ 6/4Ig alpha-2 chain C region gi|70058 – – – 5/3Ig kappa chain region gi|306958 – 2/2 – 1/1 ⁎
Immunoglobulin gamma heavy chain gi|23683338 – – – 4/3immunoglobulin kappa light chain gi|3169770 – – – 8/3Immunoglobulin J chain gi|400044 – – – 2/2Keratin, type II cytoskeletal 1 gi|1346343 – – 1/1 ⁎ –Keratin, type I cytoskeletal 10 gi|251757513 – – 1/1 ⁎ –Lipocalin 1 precursor gi|4504963 – – – 3/2Mucin 5-B gi|11275568 – 4/3 – 5/4Poly-Ig receptor gi|514366 – – – 4/2Prolactin-induced protein gi|4505821 10/4 42/1 – 3/2Proline-rich protein 3 gi|21264497 9/2 – 2/1 ⁎ –Protein S100-A9 gi|4506773 – 1/1 ⁎ – –Serum albumin gi|28592 48/14 20/9 68/13 33/17Thioredoxin gi|55957946 – – – 2/2Transferrin/serotransferrin gi|553788 2/1 ⁎ 4/3 3/1 ⁎ 6/4Zymogen granule protein 16 homolog B gi|94536866 – – 1/1 ⁎ 4/3
⁎ Ion score>50.
1340 J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 1 3 3 4 – 1 3 4 1
SN (spot 8) in the periodontitis group, and nLC-Q-TOF analysisshowed that cystatins were more commonly found in thecontrol group compared to the periodontitis group. Previousstudies demonstrated a higher activity of total cystatin inwhole and parotid saliva of periodontitis patients in compar-ison to healthy subjects suggesting a response of the salivaryglands to an inflammatory condition of the oral cavity [23,25–27]. However, Baron et al. [27] showed that the concentration ofcystatin-SN was depleted in the periodontally diseasedpatients, but was still present in sufficient quantities to actas an effective physiological cysteine protease inhibitor ofcathepsinsHandL.Huang [18] also found significant decreasesin the levels of cystatins in saliva from patients with bleedingoral cavities as analyzed by 2-DE electrophoresis and massspectrometry. Moreover, Aguirre et al. [28] showed no signif-icant differences in the levels and activity of salivary cystatinswhen comparing periodontally healthy and diseased indivi-duals. Finally, our results indicate that these proteins may bereduced in saliva from periodontitis patients.
4.4. Alpha-amylase
In the gels of periodontis patients, 17 spots were identified asalpha-amylase, the majority containing peptides in thecatalytic domain (Area I) or in C-terminal region (Area II).Hirtz et al. [29] analyzed the alpha-amylase redundant spotson 2-D gels of salivary proteins and identified more than 140protein spots of alpha-amylase. These spots were neitheraffected by the omission of protease inhibitors during the
collect and storage nor by prolonged storage, even at roomtemperature, indicating that degradations occurred in the oralcavity, despite the natural abundance of protease inhibitors insaliva like cystatins. However, no studies have investigatedthe relationship between salivary alpha-amylase isoforms orproteolysis and periodontal disease. Our results suggest thathigher alpha-amylase proteolysis in the periodontitis group,as shown by 2D electrophoresis, is probably due to anincreased specific protease activity in these patients. Thedecreased level of cystatin in this group suggests that cysteineproteases may be involved in this cleavage.
4.5. Prolactin-induced protein
Prolactin-induced protein is also an extra-parotid glycoproteinassociated with secretory cell differentiation and used in thediagnostic evaluation of the salivary gland [30]. Decreasedlevels of this protein were found in saliva from bleeding oralcavities [18], but no further studies have correlated thisalteration in saliva with periodontal disease. Our dataindicates that prolactin may be reduced in saliva from theperiodontitis group.
5. Conclusion
The proteomic profile of whole saliva from chronic period-ontitis patients studied by 2D-electrophoresis and comple-mented by nL-Q-TOF analyses showed differences compared

1341J O U R N A L O F P R O T E O M I C S 7 3 ( 2 0 1 0 ) 1 3 3 4 – 1 3 4 1
to the healthy control group. Increased levels of some bloodproteins (spontaneous bleeding) and from inflammation(immunoglobulin) were observed in the diseased group.Moreover, this study has identified a novel higher and specificproteolysis of alpha-amylase in periodontitis patients, prob-ably due to cleavage by cysteine proteases. This is supportedby the finding that levels of cystatinwere also reduced in thesepatients, which is currently being further investigated in ourlaboratory using other methodologies. Finally, a proteomicapproach may be important in understanding changes inprotein composition of saliva in the presence of periodontalalterations and to improve periodontal diagnosis.
Acknowledgments
The authors thank Vanessa Sandim, Rodrigo Santana, PatríciaR. Guimarães and Ana Lúcia O. Carvalho for their technicalsupport. We also thank the Brazilian Synchrotron LightLaboratory (LNLS) for the use of its Mass Spectrometry facility.This work was supported by grants from Fundação CarlosChagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro(FAPERJ). All experiments were supported by Rede Proteômicado Rio de Janeiro and INCA/Ministério da Saúde. Da Rós, L. isrecipient of graduation fellowship from Coordenação deAperfeiçoamento de Pessoal de Nível Superior (CAPES).
R E F E R E N C E S
[1] Streckfus CF, Mayorga-Wark O, Arreola D, Edwards C, Bigler L,Dubinsky WP. Breast cancer related proteins are present insaliva and are modulated secondary to ductal carcinoma insitu of the breast. Cancer Invest 2008;1:1–9.
[2] Giusti L, Baldini C, Bazzichi L, Ciregia F, Tonazzini I, Mascia G,et al. Proteome analysis of whole saliva: a new tool forrheumatic diseases—the example of Sjögren's syndrome.Proteomics 2007;7:1634–43.
[3] Peluso G, De Santis M, Inzitari R, Fanali C, Cabras T, Messana I,et al. Proteomic study of salivary peptides and proteins inpatients with Sjögren's syndrome before and after pilocarpinetreatment. Arthritis Rheum 2007;56:2216–22.
[4] Rao PV, Reddy AP, Lu X, Dasari S, Krishnaprasad A, Biggs E,et al. Proteomic identification of salivary biomarkers of type-2diabetes. J Proteome Res 2009;8:239–45.
[5] Minarowski Ł, Sands D, Minarowska A, Karwowska A,Sulewska A, Gacko M, et al. Thiocyanate concentration insaliva of cystic fibrosis patients. Folia Histochem Cytobiol2008;46:245–6.
[6] Giusti L, Bazzichi L, Baldini C, Ciregia F,MasciaG,GiannacciniG,et al. Specific proteins identified in whole saliva from patientswith diffuse systemic sclerosis. J Rheumatol 2007;34:2063–9.
[7] Yang LL, Liu XQ, Liu W, Cheng B, Li MT. Comparative analysisof whole saliva proteomes for the screening of biomarkers fororal lichen planus. Inflamm Res 2006;55:405–7.
[8] Hu S, Yu T, Xie Y, Yang Y, Li Y, Zhou X, et al. Discovery of oralfluid biomarkers for humanoral cancer bymass spectrometry.Cancer Genomics Proteomics 2007;4:55–64.
[9] Mungia R, Cano SM, Johnson DA, Dang H, Brown JP.Interaction of age and specific saliva component output oncaries. Aging Clin Exp Res Dec 2008;20:503–8.
[10] Giannobile WV, Beikler T, Kinney JS, Ramseier CA, Morelli T,Wong DT. Saliva as a diagnostic tool for periodontal disease:
current state and future directions. Periodontol 2000 2009;50:52–64.
[11] Flemming T. Periodontitis. Ann Periodontol 1999;4:32–6.[12] Kaufman E, Lamster IB. Analysis of saliva for periodontal
diagnosis—a review. J Clin Periodontol 2000;27:453–65.[13] Carvalho PC, Junqueira M, Valente RH, Domont GB. Caititu: a
tool to graphically represent peptide sequence coverage anddomain distribution. J Proteomics 2008;27:486–9.
[14] Fleissig Y, Deutsch O, Reichenberg E, Redlich M, Zaks B,Palmon A, et al. Different proteomic protein patterns in salivaof Sjögren's syndrome patients. Oral Dis 2009;15:61–8.
[15] Walz A, Stühler K, Wattenberg A, Hawranke E, Meyer HE,Schmalz G, et al. Proteome analysis of glandular parotid andsubmandibular-sublingual saliva incomparison towholehumansaliva by two-dimensional gel electrophoresis. Proteomics2006;6:1631–9.
[16] Hu S, Xie Y, Ramachandran P, Ogorzalek Loo RR, Li Y, Loo JA,et al. Large-scale identification of proteins in human salivaryproteome by liquid chromatography/mass spectrometry andtwo-dimensional gel electrophoresis-mass spectrometry.Proteomics 2005;5:1714–28.
[17] Vitorino R, Lobo MJ, Ferrer-Correira AJ, Dubin JR, Tomer KB,Domingues PM, et al. Identification of human whole salivaprotein components using proteomics. Proteomics 2004;4:1109–15.
[18] Huang CM. Comparative proteomic analysis of human wholesaliva. Arch Oral Biol 2004;49:951–62.
[19] Wilton JM, Curtis MA, Gillett IR, Griffiths GS, Maiden MF,Sterne JA, et al. Detection of high-risk groups and individualsfor periodontal diseases: laboratory markers from analysis ofsaliva. J Clin Periodontol Sep 1989;16:475–83.
[20] Shapiro L, Goldman H, Bloom A. Sulcular exudate flow ingingival inflammation. J Periodontol Jun 1979;50:301–4.
[21] Güven O, De Visscher JG. Salivary IgA in periodontal disease.J Periodontol May 1982;53(5):334–5.
[22] Wu Y, Shu R, Luo L-J, Ge L-H, Xie Y-F. Initial comparison ofproteomic profiles of whole unstimulated saliva obtainedfrom generalized aggressive periodontitis patients andhealthy control subjects. J Periodont Res 2009;44:636–44.
[23] Henskens YMC, van der Velden U, Veerman EC, et al. Protein,albumin and cystatin concentrations in saliva of healthysubjects and of patients with gingivitis and periodontitis.J Periodont Res 1993;28:43–8.
[24] Dickinson DP. Salivary (SD-type) cystatins: over one billionyears in the making—but to what purpose? Crit Rev Oral BiolMed 2002;13:485–508.
[25] Henskens YM, Veerman EC, Mantel MS, van der Velden U,Nieuw Amerongen AV. Cystatins S and C in human wholesaliva and in glandular salivas in periodontal health anddisease. J Dent Res 1994;73:1606–14.
[26] Henskens YM, van den Keijbus PA, Veerman EC, Van derWeijden GA, Timmerman MF, Snoek CM, et al. Proteincomposition of whole and parotid saliva in healthy andperiodontitis subjects. Determination of cystatins, albumin,amylase and IgA. J Periodontal Res 1996;31:57–65.
[27] Baron AC, Gansky SA, Ryder MI, Featherstone JD. Cysteineprotease inhibitory activity and levels of salivary cystatins inwhole saliva of periodontally diseased patients. J PeriodontalRes 1999;34:437–44.
[28] Aguirre A, Testa-Weintraub LA, Banderas JA, Dunford R,LevineMJ. Levels of salivary cystatins in periodontally healthyand diseased older adults. Arch Oral Biol 1992;35:355–61.
[29] Hirtz C, Chevalier F, Centeno D, Egea JC, Rossignol M,Sommerer N, et al. Complexity of the human whole salivaproteome. J Physiol Biochem 2005;61:469–80.
[30] Haagensen Jr DE, Dilley WG, Mazoujian G, Wells Jr SA. Reviewof GCDFP-15. An apocrine marker protein. Ann N Y Acad Sci1990;586:161–73.




















