
Asociación entre la severidad de la periodontitis y la ...
179
UNIVERSIDAD COMPLUTENSE DE MADRID FACULTAD DE ODONTOLOGÍA TESIS DOCTORAL Asociación entre la severidad de la periodontitis y la severidad de la artritis reumatoide MEMORIA PARA OPTAR AL GRADO DE DOCTOR PRESENTADA POR Jerián González Febles Director Mariano Sanz Alonso Madrid © Jerián González Febles, 2021
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Asociación entre la severidad de la periodontitis y la ...
UNIVERSIDAD COMPLUTENSE DE MADRID FACULTAD DE ODONTOLOGÍA
TESIS DOCTORAL
Asociación entre la severidad de la periodontitis y la severidad de la artritis reumatoide
MEMORIA PARA OPTAR AL GRADO DE DOCTOR
PRESENTADA POR
Jerián González Febles
Director
Mariano Sanz Alonso
Madrid
© Jerián González Febles, 2021
UNIVERSIDAD COMPLUTENSE DE MADRID FACULTAD DE ODONTOLOGÍA
TESIS DOCTORAL
“Asociación entre la severidad de la Periodontitis y la severidad de la Artritis Reumatoide”
MEMORIA PARA OPTAR AL GRADO DE DOCTOR
PRESENTADA POR
Jerián González Febles
DIRECTOR
Mariano Sanz Alonso

2
4

5
A mi familia y amigos

6
7
"Intelligence is the ability to adapt to change."
"Look up at the stars and not down at your feet. Try to make sense of what you see,
and wonder about what makes the universe exist. Be curious. "
Stephen Hawking

8
9
Agradecimientos
Desde que era pequeño, siempre estuve interesado en la Medicina y tenía curiosidad por como funcionaba la biología del cuerpo humano. A medida que me fui haciendo mayor, cuando visitaba a mi ortodoncista el Dr. Ruperto González Giralda, expresidente de la Federación Dental Internacional (FDI), siempre me gustó su especialidad y la profesionalidad con la ejercía su profesión. Cuando tuve qué decidir qué carrera hacer, no tuve dudas en hacer Odontología en la Universidad Complutense de Madrid, la que ha sido mi casa durante más de 10 años de mi vida. Durante ese trayecto, en cuarto de carrera conocí a dos personas que han marcado mi carrera profesional, al Dr. David Herrera y al Dr. Mariano Sanz. Su profesionalidad, su alto nivel científico y sobre todo su dedicación con el alma a la enseñanza, que determinaron que quisiera especializarme en Periodoncia.
Por ello, quisiera empezar los agradecimientos por mi tutor y director de tesis, el Profesor Mariano Sanz, no solo por como es, sino por su gran dedicación, paciencia y esfuerzo, en enseñarme en todos estos años las formas y pasión por nuestra querida especialidad. También por guiarme, por saber animarme, e incluso por ayudarme a salir de diferentes situaciones durante todos estos años. Incontables razones se podrían dar para agradecerle todo lo que ha hecho por mí.
También quisiera agradecer al Dr. Ruperto González Giralda, y al Dr. Carlos Fernández Frías, por su inestimable cariño, consejo y compañía durante muchos años, y a quienes les tengo un gran cariño.
A los reumatólgos, Beatriz Rodríguez Lozano y Federico Díaz González, y al Prof. Enrique Francisco González Dávila, con quienes he trabajado estrechamente estos años, por su inestimable ayuda y colaboración, y con los que espero seguir mi carrera investigadora durante muchos años.
Por supuesto, a toda la familia del Máster de Periodoncia de la Universidad Complutense de Madrid, profesores, alumnos, auxiliares, pero en especial a mi promoción Iñaki Suárez, Javier Sanz y sobre todo, a mi gran amiga Susy Linder, con
10
quien hemos compartido mucho camino académico juntos, creciendo, y ayudándonos el uno al otro.
También al Dr. Bascones, por su confianza y humanidad, así como también a la Dra. Berta Legido, quien en su inmensa bondad, animó a un alumno llenarse de fuerzas para poder convertir muchos de sus sueños en realidad.
Al Dr. Ion Zabalegui a quien le debo mucha de mi formación en Periodoncia, pero también por su paternal forma de enseñarme y transmitirme toda su pasión por la Periodoncia.
Al Dr. Héctor Juan Rodríguez Casanovas, amigo y compañero de profesión, quien ha demostrado una incansable capacidad de trabajo, y quien me ha enseñado a no rendirme durante muchos años.
Al Dr. Antonio Bujaldón Daza, amigo, jefe y profesor, quien, a parte de enseñarme la especialidad, comparte el día a día trabajando codo con codo en la clínica con pacientes. Su trabajo, tesón, valor e incansable espíritu de superación son ejemplo a seguir cada día que paso a su lado.
A mis amigos de la niñez, el Profesor Álvaro Hernández Díaz, y el Dr. Alberto García Hernández, quienes han sido pilares esenciales para entender la vida, vivirla y disfrutarla, y quienes me han enseñado lecciones fundamentales, que sin ellas, no hubiera llegado hasta el día de hoy.
A la Dra. Ruth Pérez Alfayate, a quien admiro y quien me ha dado su comprensión, ayuda, y cariño, acompañándome y aguantándome todo este tiempo, siendo, además, un ejemplo de tesón, inteligencia y dedicación, como especialista, investigadora y profesora de universidad, que me ha animado a dedicarle el último empujón a esta etapa de mi vida académica.
A toda mi familia, abuelos, primos, hermanos, pero sobre todo a mis padres, Julián Antonio González Hernández y Luz Petra Febles Padilla, quienes han dado toda su vida en criarme, enseñarme y animarme a cumplir todos los sueños que he
11
tenido en mi vida. Sin su ejemplo, determinación y tesón, hubiera sido imposible llegar a este momento inolvidable en mi vida.
Por último, quisiera terminar agradeciendo y dedicando este día a todas aquellas personas, que en cierto modo han influido, no sólo académicamente, sino personalmente, para ser la persona que soy hoy.

12
13
Prefacio La presente tesis doctoral se compone de los siguientes 3 estudios publicados: Estudio #1: González-Febles J, Sanz M. Periodontitis and Rheumatoid Arthritis:
What have we learned about their connection and their treatment. Perio 2000 2021: 10.1111/prd.12385
Estudio #2: Rodríguez-Lozano B, González-Febles J, Garnier-Rodríguez JL, Dadlani S, Bustabad-Reyes S, Sanz M, Sánchez-Alonso F, Sánchez-Piedra C, González-Dávila E, Díaz-González F. Association between severity of periodontitis and clinical activity in rheumatoid arthritis patients: a case-control study. Arthritis Res Ther 2019: 21: 27. 10.1186/s13075-019-1808-z
Estudio #3: González-Febles J, Rodríguez-Lozano B, Sánchez-Piedra C,
Garnier-Rodríguez J, Bustabad S, Hernández-González M, González-Dávila E, Sanz M, Díaz-González F. Association between periodontitis and anti-citrullinated protein antibodies in rheumatoid arthritis patients: a cross-sectional study. Arthritis Res Ther 2020: 22: 27. 10.1186/s13075-020-2121-6

14
15
Índice
Agradecimientos…....................................................................................................11 Prefacio…..................................................................................................................15 Índice .................................................................................................................17 Resumen ...........................................................................................................21 Abstract .............................................................................................................23 Introducción ..............................................................................................................27
Artritis Reumatoide...................................................................................................... 30
Prevalencia y Factores de riesgo asociados..................................................... 30
Diagnóstico y Anticuerpos específicos de la AR ……….………….…………34
Patogénesis de la AR........................................................................................ 38
Periodontitis ………………………………................................................................ 40
Prevalencia, Clasificación y Factores de riesgo asociados............................... 40
Implicaciones sistémicas de la periodontitis………………………................ 44
Justificación...............................................................................................................49 Hipótesis y Objetivos.................................................................................................51
Hipótesis .....................................................................................................................……51
Hipótesis general.........................................................................................................51
Hipótesis específicas ...................................................................................................51
Objetivos..................................................................................................................... ……55
Objetivo general..........................................................................................................55
Objetivos específicos...................................................................................................55
Material, Métodos y Resultados.................................................................................57 Artículo #1....................................................................................................................61
Artículo#2.....................................................................................................................89
Artículo #3..................................................................................................................111
Discusión ................................................................................................................129 Conclusiones ..........................................................................................................143 Bibliografía...............................................................................................................147

16

17
I. Resumen

18
19
Resumen Antecedentes: La periodontitis es la enfermedad crónica inflamatoria no
comunicable más prevalente en el ser humano, la cual se ha asociado, mediante mecanismos directos e indirectos, a diferentes enfermedades sistémicas como son la enfermedad cardiovascular, la diabetes o la AR. Existen diferentes estudios que muestran una gran prevalencia de periodontitis en pacientes con AR, así como otros que sugieren un rol importante de la periodontitis y bacterias periodontales en la patogénesis de la AR. Sin embargo, debido a la disparidad de las definiciones de caso de periodontitis como también muestras poblacionales insuficientes, no está bien establecida dicha relación entre la AR y la periodontitis. Del mismo modo, existe muy poca evidencia la relación entre la severidad de la periodontitis y de las diferentes variables secundarias como son la pérdida dentaria, pérdida de inserción, o la profundidad de sondaje, con el control y variaciones de la actividad de la AR, así como su probable repercusión en los títulos de ACPAs.
Objetivos: Evaluar si la periodontitis y sus variables subrogadas afectan a la expresión clínica de la AR, así como a su actividad, a los marcadores inmunológicos propios de dicha enfermedad, y estudiar las posibles implicaciones que pueda ejercer la periodontitis tanto en el diagnóstico y tratamiento de la AR.
Material y métodos: se han realizado tres publicaciones, donde en el #Estudio
1 se ha realizado una revisión de toda la literatura científica sobre la asociación epidemiológica entre ambas enfermedades, así como los mecanismos que las conectan, y todos los datos provenientes de estudios de intervención sobre si el tratamiento periodontal puede tener un impacto en la iniciación y progresión de la AR; en el #Estudio 2, se llevó a cabo un estudio de casos y controles de 187 pacientes con AR y 157 pacientes con artrosis donde se valoró la asociación entre ambas enfermedades, y si la severidad de la periodontitis se asocia a la severidad de la AR; por último, en el #Estudio 3 se evaluaron 164 pacientes con AR, con el fin de discernir el impacto y asociación de la periodontitis y sus variables subrogadas como la pérdida de inserción(PIC) o las bolsas ≥5mm, con la presencia y títulos de anti-CCP.

20
Resultados: #Estudio 1: identificamos una gran asociación entre ambas
enfermedades, donde la periodontitis puede actuar en distintas fases del desarrollo, progresión y tratamiento de la AR. #Estudio 2: demostramos una asociación estadísticamente significativa entre la periodontitis y la AR con una OR de 20,57 (IC 95% 6,02–70,27, p < 0,001), donde además observamos una asociación estadísticamente significativa entre la severidad de la periodontitis y la actividad de la AR(p < 0.001), con una OR ajustada de 2,66 (IC 95% 1,24–5,74, p = 0,012). #Estudio 3: se observó una asociación significativa entre la presencia de anti-CCP2 y la severidad de ciertos parámetros periodontales como PIC media(OR 1,483, p = 0,036), IP media (OR 1,029, p = 0,012), y el número de bolsas ≥ 5 mm (OR 1,021, p = 0,08). Los títulos altos de ACPAs se asociaron tanto con PIC media, IP media o el número de bolsas ≥ 5 mm con una OR de 1,593 (p = 0,043), 1,060 (p < 0,001), y 1,031 (p = 0,031), respectivamente. Por último, se encontró un aumento estadísticamente significativo de 4,45 U/mL de los niveles de anti-CCP2 (p = 0.002) por cada bolsa ≥ 5 mm en pacientes con AR tras ajustar a edad, género, tabaquismo, tiempo de evolución de la enfermedad y el nivel de actividad de la AR.
Conclusiones: los resultados obtenidos de los tres estudios incluidos en este trabajo, han demostrado la asociación entre la periodontitis y su severidad con la actividad clínica de la AR, su expresión clínica así como en sus diferentes variables inmunológicas, las cuales son marcadores de progresión y agresividad de la enfermedad.
21
Abstract
Background: Periodontitis is a the most prevalent non-communicable chronic inflammatory disease worldwide. This disease has been related to different systemic diseases such as Cardiovascular Disease, Diabetes or Rheumatoid Arthritis, through indirect and direct mechanisms. There are several studies that show a high prevalence of periodontitis in RA individuals, as well as there are others that suggest an important role of periodontitis and periodontopathogenic bacteria in RA pathogenesis. As consequence of the disparity of periodontitis case definitions and insufficient sample size of studies, the association between periodontitis and RA is still controversial. Similarly, there is scarce evidence of the relationship between the severity of periodontitis and its subrogate variables (clinical attachment loss (CAL) or probing pocket depth (PPD)) with the control and variations in RA clinical activity, as well as with its repercussion with ACPA titres.
Objectives: to evaluate whether periodontitis and its subrogate variables could affect the clinical expression and immunological markers of RA, as well as, the implications of periodontitis in RA diagnosis and treatment.
Material and methods: This research consisted of three publications: #Study 1: a narrative review of the entire scientific evidence of the
epidemiological association between periodontitis and RA, as well as the mechanisms that link both diseases, and the data coming from the intervention studies about the impact of periodontal treatment on the onset and progression of RA; #Study 2: a case-control study has been carried out in 187 RA patients and 157 osteoarthritis individuals as controls. This study evaluated the association between both diseases and whether periodontitis severity may be related to the severity of RA; #Study 3: to assess the impact and the association between periodontitis and its subrogate variables with the the presence and titres of anti-CCP antibodies, a cross-sectional study in 164 RA patients was performed.
Results: #Study 1: we identified a high association between both diseases,
where periodontitis may interfere in different phases of the development, progression and treatment of RA. #Study 2: we demonstrated a statistically significant association
22
between periodontitis and RA with OR of 20.57 (95%CI 6.02–70.27, p < 0.001), where the severity of periodontitis was statistically significant associated to the RA clinical activity (p < 0.001), with an adjusted OR of 2.66(95% CI 1.24–5.74, p = 0.012). #Study
3: we observed a statistically significant association between the presence anti-CCP2 antibodies and the severity of different periodontal parameters such as CAL (OR 1.483, p = 0.036), PI (OR 1.029, p = 0.012), and the number of PPD ≥ 5 mm (OR 1.021, p = 0.08). High anti-CCP2 titres were also associated with CAL, PI and the number of PPD ≥ 5 mm with an OR of 1.593 (p = 0.043), 1.060 (p < 0.001), and 1.031 (p = 0,031), respectively. Finally, a statistically significant increase 4,45 U/mL in the levels of anti-CCP2 (p = 0.002) was found for each pocket ≥ 5 mm in RA individuals after adjustment by age, gender, smoking, time of disease evolution, and the clinical activity of RA.
Conclusions: the results obtained from the three different studies included in the present work have demonstrated a strong association between periodontitis and its severity with the RA clinical activity, its clinical expression, as well as, with its different immunological markers, which, in turn, are markers of progression and disease aggressiveness.

23

24
25
II. Introducción

26

27
28
Introducción
Artritis Reumatoide
La Artritis Reumatoide (AR) es una enfermedad autoinmune crónica que cursa con inflamación y proliferación de la membrana sinovial de las articulaciones de pacientes susceptibles. Si no se trata de manera adecuada, progresa causando la destrucción del cartílago articular, lo que genera a su vez, deformidades articulares y una gran incapacidad funcional, que deriva en una disminución de la calidad de vida de dichos pacientes (1). A pesar de que la lesión principal se localiza afecta a las membranas sinoviales de articulaciones periféricas, al menos un 40% de pacientes con AR presentan manifestaciones extra-articulares de otros órganos (1), tanto específicas como no especificas, con efectos sistémicos claros como un mayor riesgo cardiovascular u otras manifestaciones inflamatorias crónicas, que reducen la calidad de vida de estos pacientes, así como su esperanza de vida(2).
Prevalencia y Factores de riesgo asociados
La AR es una enfermedad que suele comenzar a una edad relativamente temprana afectando a pacientes de entre 40 y 60 años, siendo más frecuente en mujeres, en una proporción de 3 mujeres por cada hombre (proporción 3:1) (3). Su incidencia anual en mujeres es de 36 pacientes por cada 100.000 habitantes, y de 16 por cada 100.000 habitantes en el caso de los hombres a nivel europeo (4), afectando al 0,9% de la población española (5,6). Recientemente, una revisión sistemática en la que se incluyeron 67 artículos y 742.246 pacientes estimó una prevalencia global de dicha enfermedad del 0,46% (intervalo de confianza [IC] 95% 0,39-0,54) (7), donde al seleccionar aquellos estudios con menor riesgo de sesgo, la prevalencia ascendería hasta el 0,51% (IC 95% 0,46-0,58). Sin embargo, la disparidad y cambios en la definición caso de Artritis de los estudios, como la zona geográfica o como el grado de desarrollo del país o continente de estudio, hace variar dicha prevalencia, incidiendo en la importancia en analizar todos estos factores, analizar su impacto y homogeneizar criterios diagnósticos.
A pesar de que la AR es una enfermedad crónica autoinmune causada por la combinación distintos factores de riesgo, como factores genéticos, hormonales o
29
ambientales (como las infecciones o el tabaco), su etiología es aun controvertida (3,8), dado que se desconoce qué evento específico desencadena la respuesta inmune que da lugar a la patología articular. Existe la hipótesis probable de que la interacción entre la susceptibilidad individual (factores genéticos) y la exposición a factores ambientales como el tabaco comprometen la inmunotolerancia del paciente, desencadenando la cascada inflamatoria que da lugar a la manifestación clínica de la artralgia y comienzo de la enfermedad. Una gran cantidad de estudios han tratado de identificar diversos genes específicos asociados con esta enfermedad crónica inflamatoria, donde estudios en gemelos monocigóticos y dicigóticos han demostrado que la AR presenta aproximadamente un 60% de carga hereditaria (9). Uno de los genes de susceptibilidad más estudiados (polimorfismo de un solo nucleótido, single-nucleotide polymorphism, SNP) es el epítopo compartido HLA-DRB1, el cual se ha asociado significativamente a la AR con una odds ratio (OR) de 2,88(IC 95% 2,73-3,03) (10). Otros polimorfismos relacionados con la patogénesis de la AR son aquellos relacionados con la presentación de antígenos al receptor de células T (TCR) (10), los haplotipos DR-ß *0401, DR-ß *0404, DR-ß *0101, y DR-ß *1402(11); el polimorfismo PTPN22 que codifica la proteína de tirosina fosfatasa, la cual está relacionada con la regulación de la inmunidad tanto adaptativa como innata(12,13); y los polimorfismos del alelo del receptor Fc-gamma, del receptor beta-2 adrenérgico o del subtipo 1A2 del citocromo P450(11). Recientemente, se ha relacionado un nuevo haplotipo del gen PADI4 que codifica la enzima peptidil arginina demininasa(PAD), con mayores niveles de esta enzima, aumentando de esta manera la susceptibilidad a la AR(14). No obstante, esta susceptibilidad aumentada solamente ha sido confirmada en población coreana, pero no en sujetos caucásicos (15,16).
Por otro lado, existen ciertos mecanismos epigenéticos que también han sido relacionados con la AR, entre los que se encuentran la expresión de micro-ARN, hipometilación de ADN, o la desregulación en la acetilación de histonas (17), los cuales pueden tanto interferir en la regulación de la expresión genética o aumentar la producción de citoquinas y proteínas pro-inflamatorias que darán lugar a un estado de inflamación crónica.
30
Dentro de los factores ambientales, el hábito tabáquico es el factor más significativamente asociado con la incidencia de AR, debido a no sólo su capacidad de aumentar la susceptibilidad genética a un estado pro-inflamatorio, sino también que está directamente relacionado con el aumento de la respuesta inflamatoria por parte del huésped. De hecho, pacientes fumadores presentan de 1,5 a 2 veces más riesgo de tener AR, especialmente pacientes fumadores que presentan el epítopo compartido HLA-DRB1, asociado a la AR (18,19), donde las ORs pueden variar significativamente entre 1,5-2(20) a 17,8(21). Esto se debe a que el tabaco se ha asociado a unos mayores niveles de anticuerpos anti-péptidos citrulinados (anti-citrullinated protein antibodies, ACPA), anticuerpos específicos de la AR, debido a la presencia de una mayor citrulinación de proteínas en tejidos inflamados de manera crónica, como ocurre en pacientes fumadores (22,23). Por ello, el tabaco se ha asociado a una AR más agresiva, caracterizada por la presencia de niveles de Factor Reumatoide (FR) elevados, nódulos reumatoides, y mayor reabsorción radiológica estructural (18). Recientemente, en un estudio transversal en 106 pacientes con AR se observaron una alta asociación entre el tabaquismo y el índice de tabaquismo en paquetes/año alto (>20 paquetes/año) con la presencia de ACPA (OR 2,79 IC 95% 1,12-6,97; y 8,93 IC 95% 1,95-40,82, respectivamente), y FR (OR 3,89 IC 95% 1,06-14,28; y 8,33 IC 95% 1,05-66,22, respectivamente). De hecho, un estudio de cohortes retrospectivo en 1349 sujetos con AR, se observó que los pacientes no fumadores responden mejor al tratamiento con fármacos modificadores de la enfermedad (FAMEs) tanto sintéticos como biológicos con respecto a pacientes exfumadores y fumadores (73% vs 65% and 64.1%, respectivamente; p = 0.004). En otro estudio de cohortes prospectivo en 230.732 pacientes sin AR, se investigó el efecto tanto de la presencia del tabaco como su cese a lo largo del tiempo sobre la incidencia de AR en esta cohorte de pacientes. Tras 38 años de seguimiento, se observaron que los pacientes exfumadores presentaron un ligero riesgo elevado de presentar AR seropositiva con respecto a pacientes no fumadores, donde además los pacientes exfumadores de más de 30 años que han dejado de fumar durante el periodo de estudio redujeron el riesgo de tener AR seropositiva en un 37% (Hazard Ratio 0,63, IC 95% 0,44-0,90) en comparación con aquellos que solamente dejaron de fumar durante < de 5 años. Sin embargo, cuando se estudia tanto otros factores
31
de riesgo como la periodontitis y la presencia de ciertas bacterias como Porphyromonas gingivalis en la presencia o no de AR, el tabaquismo pasa a un segundo plano, donde en un estudio transversal en pacientes con o sin periodontitis y con o sin AR, se observa que la asociación entre la presencia de P. gingivalis y la AR (OR 2,96 IC 95% 2,00-4,37) es mayor que entre la AR y el tabaquismo (OR 1,37 IC 95% 1,07-1,74) (24).
Otros factores ambientales asociados con el desarrollo de la AR son por ejemplo la exposición al polvo de sílice (Riesgo relativo, [RR], 3,43 IC 95% 2,25-5,22), u otras sustancias contaminantes como el asbestos, así como trabajadores de la industria de la madera (25). Cabe destacar, el caso del ataque terrorista del World Trade Centre en Nueva York, donde se observó una incidencia aumentada de enfermedades autoinmunes, incluida la AR, entre el personal de emergencia que actuó en dicho atentado (OR 1,13 IC 95% 1,02-1,26) (26). Por otra parte, la obesidad y el sobrepeso son factores asociados a una mayor susceptibilidad a la AR, especialmente en mujeres mayores de 55 años (Hazard Ratio[HR] 1,65 IC 95% 1,34-2,05, y 1,45 IC 95% 1,03-2,03) (27). No obstante, el consumo de alcohol o largos períodos de lactancia se asocian con una reducción del riesgo de desarrollar AR (RR 0,86, IC 95% 0,78-0,94) (20).
Otros factores como el estrés o enfermedades sistémicas como la diabetes, o la hipertensión, pueden ejercer cierto rol en el desarrollo de la AR. En un estudio transversal en China(28) en 142 pacientes con AR divididieron la muestra en pacientes que desarrollan la AR a una edad temprana AR (Young-onset Rheumatoid Arthritis, YORA) y pacientes que desarrollan la AR a una edad tardía (elderly-onset Rheumatoid Arthritis, EORA) con el fin de analizar qué factores como la edad o enfermedades sistémicas, interfieren en el desarrollo, y mortalidad de la AR. Tras el análisis de regresión, se observó que la diabetes (OR 118,10 IC 95% 3,50-3985,57) se asocia de manera independiente a un mayor daño estructural radiográfico. De hecho, la hipertensión arterial (HR 12,08 IC 95% 1,08-133,54), así como la enfermedad intersticial pulmonar (HR 85,04 IC 95% 4,11-1759,19) se asociaron a una mayor mortalidad. Recientemente, en un estudio poblacional en 3724 pacientes con AR en Suecia, intentaron estudiar el posible papel de ciertos estresores sociales como la baja capacidad de decisión en el trabajo o el escaso apoyo social como
32
factores modificadores de la AR(29). Tras el análisis de regresión logística, solamente la baja capacidad de decisión en el trabajo se asoció con el riesgo de padecer AR (OR 1,52 IC 95% 1,20-1,94), que, tras ajustar por distintos factores de confusión, no fue estadísticamente significativa (OR 1,24 IC 95% 0,93-1,63).
Estudios epidemiológicos bastante recientes han demostrado también una asociación entre ciertos patógenos infecciosos y la AR(30). Distintos microorganismos, como Porphyromonas gingivalis, Proteus mirabilis, el virus de Epstein-Barr (VEB), mycoplasma(30) así como bacterias intestinales (31-34), se han relacionado con el inicio, desarrollo y curso de la AR. En este sentido, se ha descrito un aumento de la permeabilidad intestinal debido a un cambio en la flora tanto en pacientes con AR precoz como con AR establecida. Este aumento de la permeabilidad intestinal estaría asociada a una disbiosis de la microbiota intestinal, que generaría a su vez, un aumento de la inflamación de las mucosas, asociada al desarrollo de la AR(33). En una revisión sistemática de 26 artículos que investigaron el impacto de la microbiota intestinal sobre el desarrollo de la AR(35), se identificaron tanto niveles reducidos de diferentes especies de Faecalibacterium, Streptococcus y Haemophilus, como niveles aumentados de Prevotella asociados a estadios tempranos de la AR. En este sentido, Kishikawa et. al (36) en un estudio de casos y controles en 124 pacientes, llevaron a cabo técnicas de pirosecuenciación con el fin de dilucidar el rol de la microbiota intestinal en la patogénesis de la AR. Tras el análisis filogenético, los resultados mostraron una gran abundancia de diferentes especies pertenecientes al genus Prevotella en pacientes con AR con respecto al grupo control. En otro estudio reciente, se observó una gran abundancia en los recuentos de Lachnospiraceae, Helicobacteraceae,
Ruminococcaceae, Erysipelotrichaceae y Bifidobacteriace en pacientes anti-CCP positivos sin sinovitis con respecto a controles sanos. Sin embargo, esta evidencia es muy inicial, precisando de estudios prospectivos que confirmen esta tendencia.
Diagnóstico y Anticuerpos específicos de la Artritis Reumatoide
A pesar de que el diagnóstico de la AR se basa en la sintomatología clínica y en la afectación de las articulaciones, son las variables inmunológicas las que son imprescindibles en la valoración tanto de la progresión, como de eficacia del
33
tratamiento de la AR. Tanto en el desarrollo como en la progresión de la AR, destacan la interacción de dos autoanticuerpos, característicos de dicha enfermedad: el Factor Reumatoide (FR) y los anticuerpos anti-péptidos citrulinados (ACPAs) (37-39). El Factor Reumatoide es una inmunoglobulina, principalmente Ig M, cuya aparición parece estar mediada por células T, las cuales reaccionan a un antígeno presente en los tejidos sinoviales, probablemente la proteína p205, la cual muestra secuencias peptídicas similares a las de la 3º y 4º región constante de las inmunoglobulinas. Dichas células T podrían activar a linfocitos B, que a su vez producirían factor reumatoide, mediante un proceso de “molecular mimicry” (40).
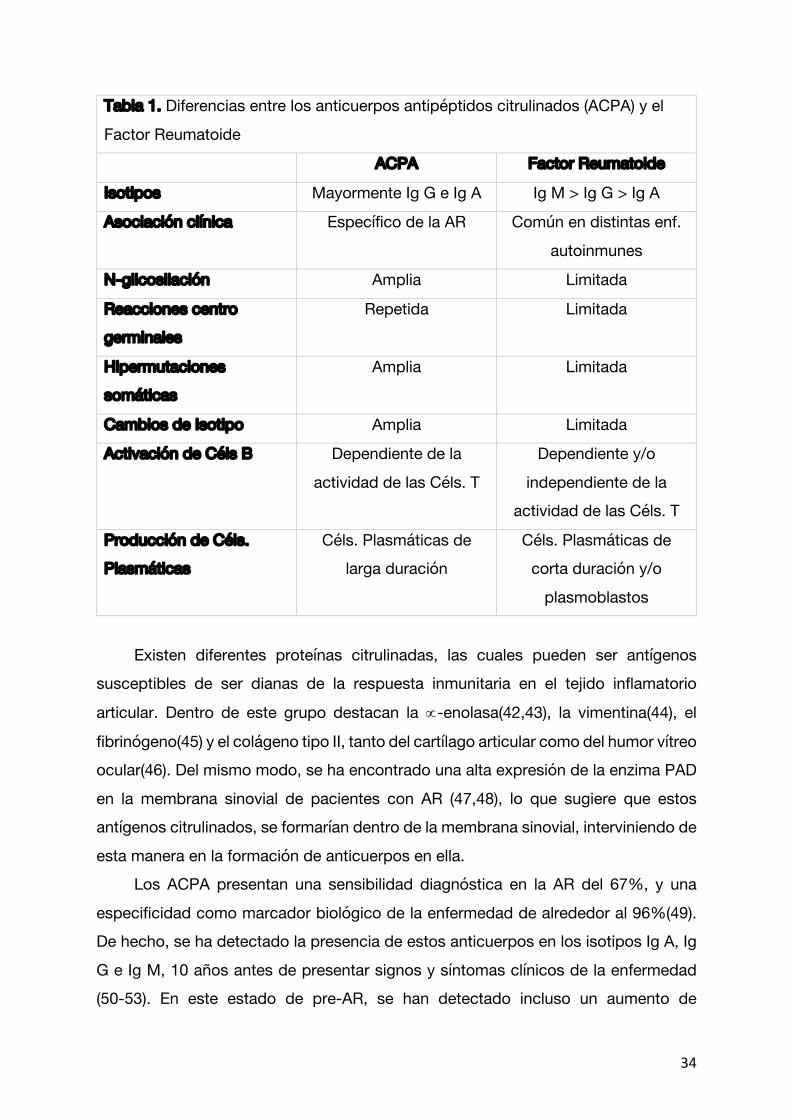
Por otro lado, los anticuerpos anti-péptidos citrulinados (ACPAs) son inmunoglobulinas, mayormente Ig G e Ig A, cuya maduración y amplia N-glicosilación va a repercutir en la alteración de las funciones de dichas inmunoglobulinas, dando lugar a la producción de células plasmáticas de larga duración, a diferencia del factor reumatoide (ver tabla 1) (41). Puesto que los isotipos principales en los ACPAs sean Ig G e Ig A, fundamentan la hipótesis del origen en mucosas, que se ha propuesto de manera extensa en la literatura científica(41).
34
Tabla 1. Diferencias entre los anticuerpos antipéptidos citrulinados (ACPA) y el Factor Reumatoide
ACPA Factor Reumatoide
Isotipos Mayormente Ig G e Ig A Ig M > Ig G > Ig A
Asociación clínica Específico de la AR Común en distintas enf. autoinmunes
N-glicosilación Amplia Limitada
Reacciones centro
germinales Repetida Limitada
Hipermutaciones
somáticas Amplia Limitada
Cambios de Isotipo Amplia Limitada
Activación de Céls B Dependiente de la actividad de las Céls. T
Dependiente y/o independiente de la
actividad de las Céls. T
Producción de Céls.
Plasmáticas Céls. Plasmáticas de
larga duración Céls. Plasmáticas de
corta duración y/o plasmoblastos
Existen diferentes proteínas citrulinadas, las cuales pueden ser antígenos
susceptibles de ser dianas de la respuesta inmunitaria en el tejido inflamatorio
articular. Dentro de este grupo destacan la µ-enolasa(42,43), la vimentina(44), el
fibrinógeno(45) y el colágeno tipo II, tanto del cartílago articular como del humor vítreo ocular(46). Del mismo modo, se ha encontrado una alta expresión de la enzima PAD en la membrana sinovial de pacientes con AR (47,48), lo que sugiere que estos antígenos citrulinados, se formarían dentro de la membrana sinovial, interviniendo de esta manera en la formación de anticuerpos en ella.
Los ACPA presentan una sensibilidad diagnóstica en la AR del 67%, y una especificidad como marcador biológico de la enfermedad de alrededor al 96%(49). De hecho, se ha detectado la presencia de estos anticuerpos en los isotipos Ig A, Ig G e Ig M, 10 años antes de presentar signos y síntomas clínicos de la enfermedad (50-53). En este estado de pre-AR, se han detectado incluso un aumento de
35
diferentes citoquinas pro-inflamatorias, al mismo tiempo que los niveles de ACPA son elevados, lo cual refleja un estado de inflamación sistémica subclínica previo a la aparición de los primeros síntomas de artralgia por parte del paciente (54). Del mismo modo, en un estudio observacional de cohortes prospectivo, en 100 pacientes ACPA positivo con síntomas músculo-esquléticos, realizaron un modelo predictivo donde valoraron el papel de distintos factores, como altos niveles de ACPAs, factor reumatoide, proteína C-reactiva (PCR), o el tabaco (55). Tras el análisis de regresión, los pacientes que presentan altos títulos de ACPA muestran 4,86 veces más riesgo de padecer artritis inflamatoria (HR 4,86 IC 95% 1,16-20,43) (55). No obstante, del mismo modo se ha demostrado que las biopsias de membranas sinoviales de pacientes ACPA positivos no se asocia directamente con la inflamación de dicha membrana (56). Sin embargo, a pesar de que no hallan cambios locales previo a la aparición clínica de los síntomas, dichos autores ponen de manifiesto que sí que se producen cambios sistémicos que preceden muchos años antes de los cambios estructurales que acompañan luego a la artralgia. Recientemente, en un estudio en 1780 familiares de primer grado de pacientes con AR, observaron que dichos familiares ACPA positivos presentaron 4 veces más riesgo de padecer AR con respecto a los ACPA negativos (HR 4,09 IC 95% 1,67-10,04, p <0,002) (57).
De manera similar, existen numerosos estudios que relacionan el daño estructural con la presencia de ACPAs (37,39,58). En un estudio en 404 pacientes con AR, relacionaron el daño estructural con la severidad de la enfermedad, la presencia del epítopo compartido HLA-DRB1 y la presencia de ACPAs (39). De hecho, la combinación de la presencia tanto de ACPAs como de factor reumatoide, ejerce un incremento en el daño estructural, tanto en el número como en el tamaño de las erosiones, en comparación con aquellos pacientes que presentan solo un tipo de anticuerpos (58). En un estudio de cohortes prospectivo reciente, se realizaron pruebas de seropositividad a ACPA en 1022 pacientes con síntomas de AR inicial (59). A 24 meses, la seropositividad a ACPA se asoció significativamente con la progresión de la actividad clínica, y radiográfica (59).
Por otro lado, se han descrito 3 procesos diferentes por le que se pueden producir auto-anticuerpos antipéptidos modificados (anti-modified protein antibodies, AMPAs). A parte de la citrulinación en la modificación de proteínas que
36
dan lugar a la formación de autoanticuerpos, también existen la carbamilación y la acetilación (38,41,60). En un modelo experimental en ratas, Kampstra et. al (60) observaron que cualquier AMPA producido por los 3 diversos procesos de formación, puede originar una respuesta mediada por células B, que a su vez se diversifica en múltiples respuestas a AMPAs, lo cual explica su gran presencia y relación con el desarrollo y progresión de la AR.
Dado que el proceso de citrulinación de proteínas por el que se forman los ACPAs, es el más frecuente y estudiado, es importante entender que es un proceso completamente dependiente de la acción de la enzima, peptidil arginina deiminasa (PAD), cuyo papel es crucial. Un subtipo de PAD, en concreto, la PAD4, se cree que es esencial para la formación de trampas extracelulares de neutrófilos (Neutrophil extracelullar traps, NETs) (61), las cuales son un mecanismo de muerte celular de los neutrófilos, que sirve además de entrelazado de fibras, que a su vez, presentan proteínas capaces de neutralizar factores de virulencia y matar bacterias(61). Existen 2 mecanismos por los cuales se produce la descondensación de la cromatina, dando lugar a la formación de las NETs: 1) el aumento de ionóforos de calcio, los cuales son potentes activadores de la PAD, lo que induce a la liberación extracelular de ADN similar a la NETosis; y 2) la hipercitrulinación de histonas producida por la PAD4, la cual provoca el desdoble de la cromatina liberando ADN a la matriz extracelular. Tanto la activación de la PAD4 y la hipercitrulinación de histonas, se han sugerido como mecanismos que conectan la producción de ROS y la descondensación de cromatina durante la NETosis (61). Sin embargo, Konig et. al (61) reflexiona en su revisión crítica del proceso de NETosis, exponiendo que no existe suficiente evidencia que sustente esta hipótesis.
Patogénesis de la Artritis Reumatoide
A pesar de los diferentes factores causales y de riesgo que intervienen en el desarrollo de la AR, la hipótesis más aceptada está relacionada con el proceso de citrulinación de proteínas, que conllevan a la formación de anticuerpos antipéptidos citrulinados (anti-citrullinated protein antiboides, ACPA), y el posterior estado de autoinmunidad del huésped.
37
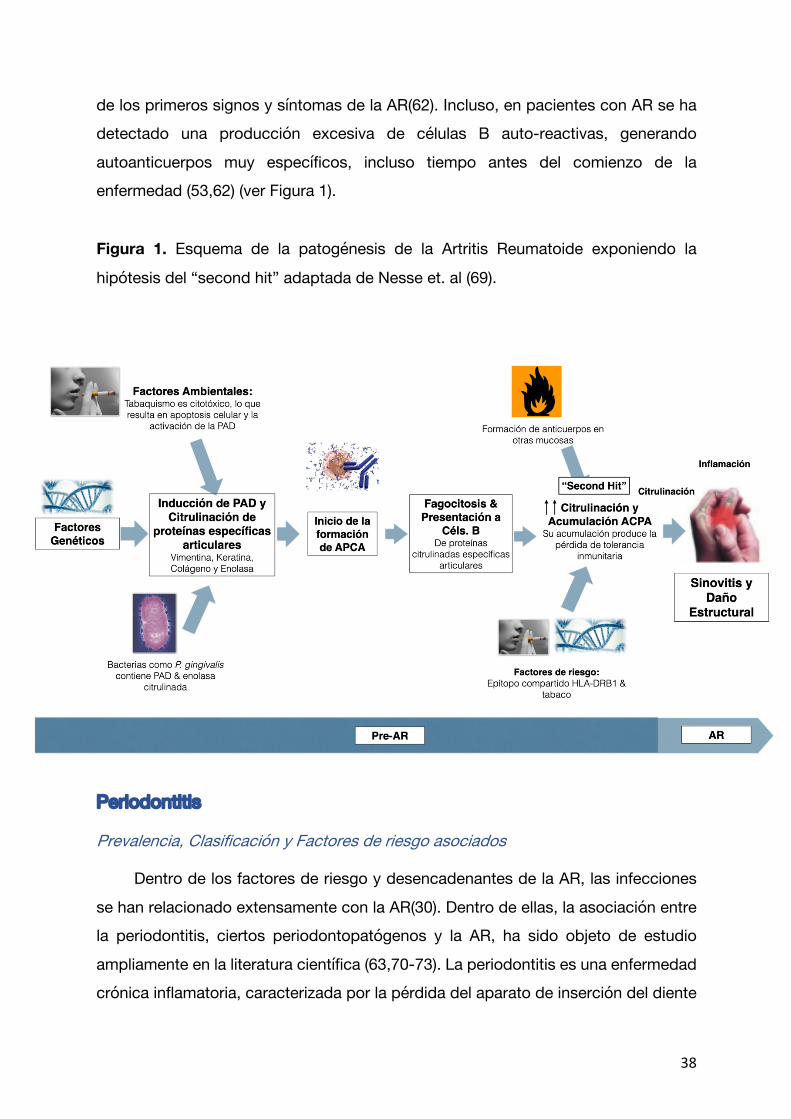
En individuos sanos, las proteínas estructurales contienen, normalmente terminaciones de arginina que son reconocidas por el sistema inmune del huésped como propias. Sin embargo, en sujetos con AR, debido a la actividad aumentada de ciertas deiminasas, en especial, de la peptidil arginina deiminasa(PAD), se produce una transformación de dichas terminaciones de arginina en citrulina, lo cual, el sistema inmune del paciente reconoce como extraño, produciendo la formación de anticuerpos citrulinados, característicos de esta enfermedad(62). Este proceso comienza con el aumento progresivo de la respuesta inmune innata y del proceso de citrulinación, seguido por el aumento de la carga de células presentadoras de antígenos (antigen-presenting cells, APC) con autoantígenos en la articulación, y la migración al sistema linfoide central. Tras ello, se produciría la presentación de antígenos a los linfocitos T, que pueden, o bien activar a los linfocitos B, o migrar nuevamente a la membrana sinovial (62). A pesar de que la citrulinación no es específica de la AR, los anticuerpos antipétidos citrulinados son específicos de la AR,
especialmente para ciertas proteínas citrulinadas, como la µ-enolasa, vimentina y
fibrinógeno. Dentro de las distintas PADs identificadas en mamíferos, solamente la PAD-2 y PAD-4 han sido asociadas a la citrulinación de proteínas en sujetos con AR(63). Recientemente, en un estudio de cohortes prospectivo a 10 años, se ha asociado la presencia de PAD-3 con una mayor actividad de la enfermedad y daño articular estructural (64). Por tanto, la acumulación de esas proteínas dentro la cápsula articular y su posterior degradación, la cual es dependiente de las PAD-2, PAD-3 PAD-4, dan lugar a la exposición de nuevos epítopos para ser reconocidos por células inmunocompetentes del sistema inmunitario en individuos con AR (64,65). Tras este proceso de citrulinación y formación de nuevos epítopos, y su reconocimiento por el sistema inmunocompetente, se da lugar a la formación de los anticuerpos antipéptidos citrulinados (ACPAs) (62), los cuales pueden ser detectados en pacientes pre-AR o susceptibles de padecer AR muchos años antes de los primeros síntomas de la enfermedad, siendo incluso asociados a una progresión más agresiva de la misma (53,55,66,67). Esta activación repetida del sistema inmune debido a dicha acumulación, en combinación con el efecto de ciertos factores ambientales (second hit o segunda agresión) (68) desencadena una serie de mecanismos que debilitan la inmunotolerancia del huésped, provocando la aparición
38
de los primeros signos y síntomas de la AR(62). Incluso, en pacientes con AR se ha detectado una producción excesiva de células B auto-reactivas, generando autoanticuerpos muy específicos, incluso tiempo antes del comienzo de la enfermedad (53,62) (ver Figura 1).
Figura 1. Esquema de la patogénesis de la Artritis Reumatoide exponiendo la
hipótesis del “second hit” adaptada de Nesse et. al (69).
Periodontitis
Prevalencia, Clasificación y Factores de riesgo asociados
Dentro de los factores de riesgo y desencadenantes de la AR, las infecciones se han relacionado extensamente con la AR(30). Dentro de ellas, la asociación entre la periodontitis, ciertos periodontopatógenos y la AR, ha sido objeto de estudio ampliamente en la literatura científica (63,70-73). La periodontitis es una enfermedad crónica inflamatoria, caracterizada por la pérdida del aparato de inserción del diente
39
(entre los que se incluye ligamento periodontal y hueso alveolar), lo que desemboca en la pérdida del diente. La periodontitis se considera la enfermedad inflamatoria crónica no transmisible más prevalente a nivel mundial (74). Su prevalencia oscila entre el 23-48% de la población mundial adulta mayor de 35 años(75), donde sus formas más severas afectan alrededor del 11,2% de la población mundial(76). En España, la prevalencia en personas trabajadoras ronda el 38,4%, donde el 7,7% de ella presenta periodontitis avanzada (77).
Durante más de 30 años, la clasificación de la periodontitis ha supuesto un gran dilema a la comunidad académica. De acuerdo a un estudio longitudinal a 15 años en trabajadores de té en Sri Lanka, Löe et.al (78) describieron 3 patrones distintos de progresión, desde periodontitis de rápida progresión a no progresiva. Debido a dichas diferencias en dichos patrones, en la clasificación de 1999, Armitage et. al(79) intentaron clasificarla, considerando dos fenotipos distintos de periodontitis, periodontitis crónica o periodontitis agresiva. Sin embargo, tanto la superposición de criterios de un fenotipo a otro, así como, la dificultad en la aplicación de dichos criterios, derivaron en el cambio en su sistema de clasificación (80). Por ello, en el último consenso de la Federación Europea de Periodoncia(EFP) y la Academia Americana de Periodoncia(AAP) en 2018, establecieron clasificar la periodontitis como una sola entidad con 4 estadios de severidad y 3 grados de progresión basándose como criterio principal la pérdida de inserción, debido a que no existe suficiente evidencia para diferenciar entre dos entidades diferentes, además de la existencia de múltiples factores de riesgo que modifican la expresión y progresión de la enfermedad(80). De hecho, en un estudio reciente en 251 pacientes con periodontitis a 21 años de seguimiento, Graetz et. al {Graetz:2019gh} intentaron comparar la adherencia de cada clasificación y su eficacia en categorizar a los pacientes con periodontitis, y de esta manera dilucidar qué sistema es capaz de describir mejor un caso de periodontitis. Tras analizar los datos, utilizando ambos sistemas, determinaron que la clasificación de 2018 reflejaba de manera adecuada y con bastante precisión las características, severidad, extensión y progresión de la periodontitis en comparación con la clasificación de 1999, confirmando de esta manera su idoneidad como sistema de clasificación de la periodontitis.
40
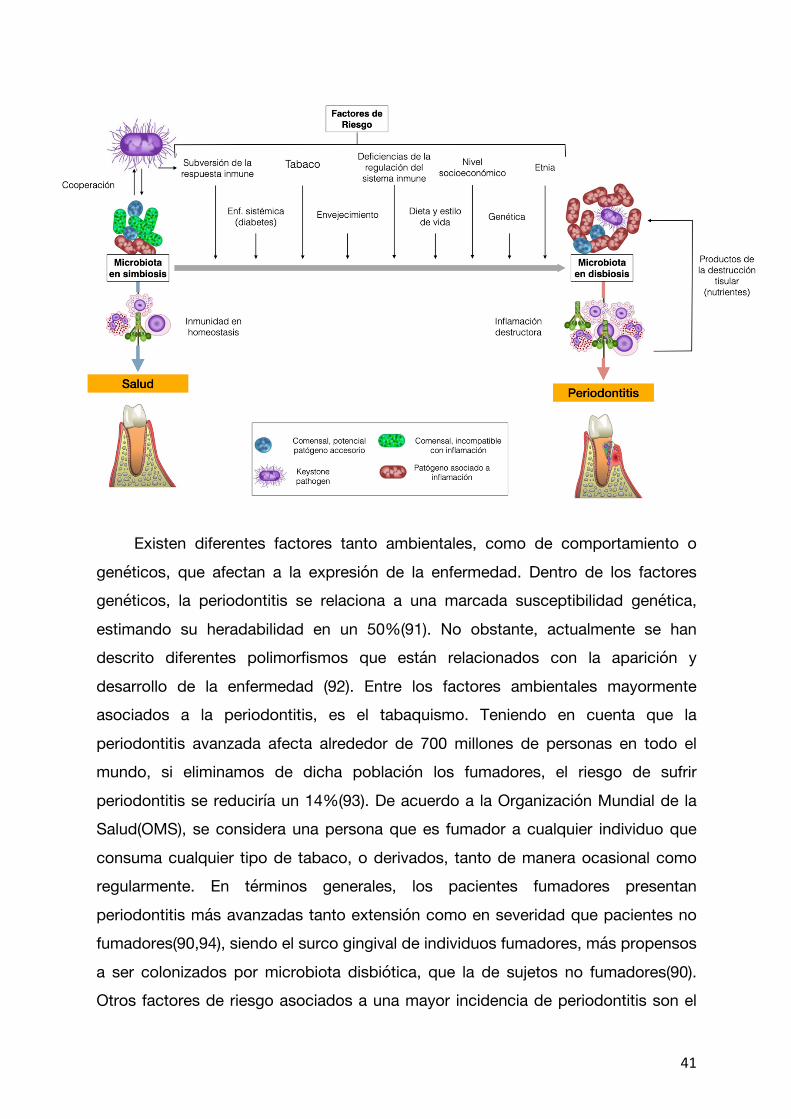
En cuanto a su etiología, el factor causal principal de la periodontitis es bacteriano, cuya flora se organiza en biofilm subgingival. Dicha estructura, ha sido objeto de estudio durante los últimos años (81). De hecho, se ha establecido el biofilm dental como una comunidad microbiana que interacciona con el huésped (81). Dichas interacciones con el huésped ocurren tanto en salud como en enfermedad. En salud, dicha comunidad microbiana se encuentra en un estado de simbiosis con el huésped, donde dichas interacciones varían en distinto grado de beneficio tanto para el biofilm como para el huésped (81). No obstante, en enfermedad, dicho estado de simbiosis, pasa a estar en disbiosis, cuyo cambio está asociado a una variación en la composición de la flora microbiana del biofilm, la cual genera una ruptura de las interacciones beneficiosas entre ambos, causando efectos dañinos al huésped, y en este caso desencadenando el inicio de la periodontitis (81-86). Dichos cambios en la composición del biofilm asociado a enfermedad están relacionados con la aparición o aumento de los recuentos de bacterias como Treponema denticola Tannerella
forsythia, Aggregatibacter actinomycetemcomitans, o Porphyromonas gingivalis, siendo esta última considerada como “key stone pathogen” (81-83,85-87). No obstante, el aumento de los recuentos y cambios en la composición microbiana van a estar determinados por el efecto de diferentes factores modificadores de la enfermedad(88)(Ver Figura 2). Figura 2. Esquema de la patogénesis de la periodontitis adaptada de Hajishengallis
et. al (89) y Buduneli et. al (90)
41
Existen diferentes factores tanto ambientales, como de comportamiento o
genéticos, que afectan a la expresión de la enfermedad. Dentro de los factores genéticos, la periodontitis se relaciona a una marcada susceptibilidad genética, estimando su heradabilidad en un 50%(91). No obstante, actualmente se han descrito diferentes polimorfismos que están relacionados con la aparición y desarrollo de la enfermedad (92). Entre los factores ambientales mayormente asociados a la periodontitis, es el tabaquismo. Teniendo en cuenta que la periodontitis avanzada afecta alrededor de 700 millones de personas en todo el mundo, si eliminamos de dicha población los fumadores, el riesgo de sufrir periodontitis se reduciría un 14%(93). De acuerdo a la Organización Mundial de la Salud(OMS), se considera una persona que es fumador a cualquier individuo que consuma cualquier tipo de tabaco, o derivados, tanto de manera ocasional como regularmente. En términos generales, los pacientes fumadores presentan periodontitis más avanzadas tanto extensión como en severidad que pacientes no fumadores(90,94), siendo el surco gingival de individuos fumadores, más propensos a ser colonizados por microbiota disbiótica, que la de sujetos no fumadores(90). Otros factores de riesgo asociados a una mayor incidencia de periodontitis son el
42
estrés, nivel socioeconómico, el envejecimiento, o deficiencias del sistema inmune(90). El envejecimiento es otro factor claramente asociado a la periodontitis, dado que a medida que aumenta la edad, existe un aumento exponencial de la pérdida de inserción (95). Por otro lado, el estrés también se ha asociado a una mayor incidencia de periodontitis, debido a que la hormona mayormente asociada con el estrés, el cortisol, está a su vez relacionado con la periodontitis. De hecho, individuos con mayor presión económica, y con una pobre respuesta frente a situaciones de estrés desarrollan mayor incidencia de periodontitis avanzadas (90).
Implicaciones Sistémicas de la Periodontitis
Otros factores que influyen en la periodontitis, y viceversa, son ciertas enfermedades sistémicas. La periodontitis no solamente se relaciona con efectos a nivel local como es la pérdida de inserción, y posterior pérdida del diente, sino además, presenta una gran repercusión sistémica, que eleva el riesgo de pacientes que la padecen de desarrollar enfermedades sistémicas como enfermedades cardiovasculares, diabetes, enfermedades pulmonares, partos prematuros, o artritits reumatoide (96-99). Tanto por un mecanismo directo como sería el paso de ciertas bacterias periodontales al torrente sanguíneo migrando hasta el órgano diana (bacteriemia); como indirecto, por el aumento de la inflamación sistémica producida por el curso de la periodontitis, la cual podría aumentar el riesgo de desarrollar o empeorar las enfermedades sistémicas anteriormente mencionadas (63,100-102). Diferentes periodontopatógenos periodontales, se han asociado con la patogénesis de diferentes enfermedades por encontrarse dichas bacterias en las lesiones específicas de cada enfermedad, como en la ateroesclerosis(103-105), Alzheimer(106,107) o Artritis Reumatoide(108-110).
Por otro lado, la periodontitis supone una extensa superficie inflamatoria, dado que un paciente con periodontitis avanzada puede presentar alrededor de 2309 mm2 de superficie inflamatoria, lo que equivale a la palma de la mano (111). De hecho, Paraskevas et. al (112) en una revisión sistemática de estudios transversales, casos y controles, y de cohortes, determina unos niveles elevados de PCR, marcador sérico de inflamación sistémica, en pacientes con periodontitis comparados con pacientes sin periodontitis. Dicha inflamación sistémica tiene un gran impacto, la cual se ha
43
relacionado con el aumento del riesgo, por ejemplo, de enfermedad arterial periférica(113), diabetes (101), partos prematuros(114), o artritis reumatoide(115). No obstante, ciertos autores enfatizan que la propia inflamación producida en dientes afectados periodontalmente, puede ser otra fuente de citrulinación de proteínas, formación de anticuerpos que induzcan a la autoinmunidad propia de la AR (69,116-121). Incluso, ciertos autores han remarcado el papel de la periodontitis en el proceso de citrulinación de proteínas, que a su vez aumenta la inflamación sistémica del paciente, relacionándose con ateroesclerosis, artritis reumatoide o Alzheimer(122).

44

45
III. Justificación
46
47
Justificación La periodontitis es la enfermedad crónica inflamatoria no comunicable más
prevalente en el ser humano. Mediante mecanismos directos e indirectos se han asociado a diferentes enfermedades sistémicas como son la enfermedad cardiovascular, diabetes o AR. Existen diferentes estudios que han puesto de relieve una gran prevalencia de periodontitis en pacientes con AR, así como otros que sugieren un rol importante de la periodontitis en la patogénesis de la AR. Sin embargo, debido a la disparidad de las definiciones de caso de periodontitis como también muestras poblacionales insuficientes, no está bien establecida dicha relación entre la AR y la periodontitis. Por otro lado, existe escasa evidencia que ponga de relieve el papel de la severidad de la periodontitis y de las diferentes variables secundarias como son la pérdida dentaria, pérdida de inserción, o la profundidad de sondaje, en el control y variaciones de la actividad de la AR, así como su probable repercusión en los títulos de ACPAs, dada su alta relación con mecanismos inflamatorios propios de la periodontitis, como el papel de ciertos patógenos periodontales en la AR.

48

49
IV. Hipótesis y Objetivos

50
51
Hipótesis y Objetivos
Hipótesis
Hipótesis general
Existe una asociación independiente entre la artritis reumatoide (AR) y la periodontitis, donde la periodontitis y sus variables subrogadas condicionarían una mayor actividad clínica de la AR, así como un aumento en los títulos séricos de ACPAs, y por tanto su papel pueda ser crucial en distintas fases del desarrollo y progresión de la AR.
Hipótesis específicas
Estudio #1:
Dada la gran cantidad de nueva evidencia adquirida en estos últimos años, la periodontitis podría interferir en distintas fases del desarrollo y progresión de la AR, lo que sugiere un importante rol tanto en el diagnóstico, pronóstico y tratamiento de la AR.
Estudio #2:
La periodontitis y sus variables subrogadas están relacionadas significativamente a la AR, donde la severidad de la periodontitis se asocia a la alta actividad clínica de la AR.
Estudio #3:
Tanto la periodontitis como sus variables subrogadas se asocian con la presencia y títulos de ACPAs en pacientes con AR.

52
53
Objetivos
Objetivo general
Evaluar si la periodontitis y sus variables subrogadas afectan a la expresión clínica de la AR, así como a su actividad, a los marcadores inmunológicos propios de dicha enfermedad, y estudiar las posibles implicaciones que pueda ejercer la periodontitis tanto en el diagnóstico y tratamiento de la AR.
Objetivos específicos
Estudio #1:
Revisar toda la evidencia emergente tanto de la asociación epidemiológica entre la AR y la periodontitis, sus mecanismos biológicos que conectan ambas enfermedades, como de la influencia del tratamiento periodontal en el inicio y progresión de la AR, y sus posibles implicaciones tanto a nivel diagnóstico como terapéutico de los pacientes con AR.
Estudio #2:
Realizar un estudio epidemiológico (casos controles) que evalúe si la periodontitis está asociada a la AR, y si la severidad de la periodontitis está correlacionada con la actividad de la AR.
Estudio #3:
Evaluar si tanto la periodontitis como sus variables subrogadas de severidad se asocian con la presencia y títulos de ACPAs en pacientes con AR.
54

55
V. Material, Métodos y
Resultados

56
57
Material, Métodos y Resultados Estudio #1: González-Febles J, Sanz M. Periodontitis and Rheumatoid Arthritis:
What have we learned about their connection and their treatment. Perio 2000. 2021;00:1-23. https://doi.org/10.1111/prd.12385
Estudio #2: Rodríguez-Lozano B, González-Febles J, Garnier-Rodríguez JL, Dadlani S, Bustabad-Reyes S, Sanz M, Sánchez-Alonso F, Sánchez-Piedra C, González-Dávila E, Díaz-González F. Association between severity of periodontitis and clinical activity in rheumatoid arthritis patients: a case-control study. Arthritis Res Ther 2019: 21: 27. https://doi.org/10.1186/s13075-019-1808-z
Estudio #3: González-Febles J, Rodríguez-Lozano B, Sánchez-Piedra C,
Garnier-Rodríguez J, Bustabad S, Hernández-González M, González-Dávila E, Sanz M, Díaz-González F. Association between periodontitis and anti-citrullinated protein antibodies in rheumatoid arthritis patients: a cross-sectional study. Arthritis Res Ther 2020: 22: 27. https://doi.org/10.1186/s13075-020-2121-6

58
59
Artículo 1

60

61
Artículo #1
Periodontitis y Artritis Reumatoide: Qué hemos aprendido de su conexión y
tratamiento.
Resumen: La Artritis Reumatoide (AR) y la periodontitis son enfermedades inflamatorias crónicas definidas, respectivamente, por la destrucción de cartílago articular y de los tejidos de soporte periodontales. A pesar de que la evidencia epidemiológica de la asociación entre ambas enfermedades sigue siendo controvertida y escasa, existen datos recientes que ponen de relieve el rol importante de ciertas bacterias periodontales como Porphyromonas gingivalis y Agreggatibacter actinomycetemcomitans en el proceso de citrulinación de proteínas, y posterior formación de auto anticuerpos, pudiendo romper la inmunotolerancia inmunitaria del paciente susceptible de padecer AR. Por ello, hemos realizado una revisión de toda la literatura científica que estudie la asociación epidemiológica entre ambas enfermedades, así como los mecanismos que las conectan, y todos los datos provenientes de estudios de intervención sobre si el tratamiento periodontal puede tener un impacto en la iniciación y progresión de la AR.

62
63
123456789
1011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
PR
D12385
Dispatch: 8-1-2021
CE: Shobana
Journal Nam
eM
anuscript No.
No. of pages: 23
PE: M
aheswari S.
Periodontology 2000. 2020;00:1–23. | 1wileyonlinelibrary.com/journal/prd
DOI: 10.1111/prd.12385
R E V I E W A R T I C L E
Periodontitis and rheumatoid arthritis: What have we learned about their connection and their treatment?
Jerián González-Febles1,2 | Mariano Sanz1,2
1Departament of Dental Clinical Specialties, Faculty of Odontology, University Complutense, Madrid, Spain2Research Group on the Aetiology and Treatment of Periodontal and Periimplant Diseases (ETEP), Faculty of Odontology, University Complutense, Madrid, Spain
CorrespondenceMariano Sanz, Department of Dental Clinical Specialties, Faculty of Odontology, University Complutense of Madrid, Plaza Ramon y Cajal, E-28040 Madrid, Spain.Email: [email protected]
1 | INTRODUC TION
Rheumatoid arthritis is an autoimmune chronic inflammatory dis-
ease that mainly affects the synovial membranes at multiple joints
leading to their inflammation, proliferation, and eventual destruc-
tion. If left untreated, it progresses to the destruction of the articu-
lar cartilage, leading to deformities and functional disability, with a
marked decline in the patient's quality of life. Even although the main
lesion is located at the synovial membranes in peripheral joints, in at
least 40% of rheumatoid arthritis patients this disease may affect
other organs, with either specific or nonspecific extra-articular in-
flammatory manifestations,1 with systemic effects, such as a higher
risk of cardiovascular disease and other noncommunicable chronic
inflammatory diseases that reduce patients’ quality of life and life
expectancy.2 This disease usually starts in relatively young individ-
uals (aged 40-60 years) and affects females more frequently, with
a 3:1 bias compared with males.3 Its annual incidence rate is about
36/100 000 for females and 16/100 000 for males4 in Europe, with a
prevalence of 0.9% in Spain.5,6 The global rheumatoid arthritis prev-
alence has been recently evaluated in a systematic review assessing
67 studies and 742 246 rheumatoid arthritis patients with an esti-
mate of 0.46% (95% confidence interval 0.39-0.54).7
The etiology of rheumatoid arthritis has not been fully elucidated,
although it is a chronic autoimmune inflammatory disease caused
by a combination of risk factors, including genetic, hormonal, and
environmental (eg, infections, smoking) factors.3,8 The autoimmune
basis of this disease is manifested by the presence of autoantibod-
ies, mainly anti-citrullinated protein antibodies. Structural proteins
contain terminal arginines recognized as self by our immune system.
However, in rheumatoid arthritis patients, the higher activity of
deaminases, mainly peptidyl arginine deiminase, are able to trans-
form arginine into citrulline, which is not recognized by our immune
system and leads to the formation of anti-citrullinated protein anti-
bodies. These specific autoantibodies can be detected in rheumatoid
arthritis patients even years before their first articular symptoms.9-11
What triggers the events leading to the autoimmune response
and the ensuing articular pathology is still controversial. It is prob-
ably the interaction between individual susceptibility (genetic fac-
tors) and exposure to environmental factors that compromises the
immunotolerance and thereby triggers this complex disease. Many
researchers have tried to identify the specific genetic traits associ-
ated with this chronic inflammatory disease, since studies in dizy-
gotic and monozygotic twins have demonstrated that about 60% of
rheumatoid arthritis pathogenesis is attributed to heritability.12 The
most studied susceptibility gene (single nucleotide polymorphism)
is the human leukocyte antigen class II histocompatibility antigen,
DRB1 beta chain 1 shared epitope, which has shown a significant
association with rheumatoid arthritis (odds ratio 2.88, 95% confi-
dence interval 2.73-3.03).13 Other single nucleotide polymorphisms
that have shown different degrees of association with rheumatoid
arthritis include those related to antigen presentation to the T-cell
receptor,13 the haplotypes DR-beta *0401, DR-beta *0404, DR-
beta *0101, and DR-beta *1402,14 the protein tyrosine phosphatase
non-receptor type 22 polymorphism encoding the protein tyrosine
phosphatase, which is involved in the regulation of the innate and
adaptive immune system,15,16 the Fc-gamma receptor allele poly-
morphism, and the beta-2 adrenergic receptor polymorphism or
subtype 1A2 cytochrome P450 polymorphism.14 Moreover, differ-
ent epigenetic processes, such as microRNA expression, DNA hypo
methylation, or a deregulation in histone acetylation,17 upregulate
© 2020 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
2
1
5 6 7
8
9
10
11
12
13
14
15
16
17
18

64
123456789
1011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
2 | GONZÁLEZ-FEBLES aNd SaNZ
gene expression and increase the release of pro-inflammatory pro-teins that lead to chronic inflammation.
A new haplotype of the gene peptidylarginine deiminase type 4 that encodes the enzyme peptidyl arginine deiminase may cause higher levels of this enzyme and a higher susceptibility to rheuma-toid arthritis.18 This higher susceptibility has been demonstrated in Korean subjects, but not in Caucasians.19,20
In regard to environmental factors, smoking is significantly associated with the incidence of rheumatoid arthritis, since it not only enhances the genetic susceptibility to inflammation, but is also directly involved in promoting an autoimmune response. In fact, subjects who smoke have a 1.5-2–fold risk of having rheumatoid arthritis, especially when also positive for an rheumatoid arthritis epitope.21,22 However, odds ratios range broadly from 1.5-223 to 17.8 (95% confidence interval 11-29).24 Tobacco consumption has been associated with higher levels of anti-citrullinated protein an-tibodies in rheumatoid arthritis patients, as explained by the higher protein citrullination occurring in chronically inflamed tissues.25,26 Furthermore, smoking has been associated with a more aggressive disease, characterized by the presence of rheumatoid factor and rheumatoid nodes, as well as higher radiologic structural damage.21
Other environmental factors associated with the development of rheumatoid arthritis are exposure to silica dust (relative risk 3.43, 95% confidence interval 2.25-5.22),27 or other pollutants, such as asbestos or wooden dust.28 It was remarkable to see the increased incidence of autoimmune diseases, including rheumatoid arthritis, among the emergency personal involved in the World Trade Center terrorist attack in New York (odds ratio 1.13, 95% confidence inter-val 1.02-1.26).29 Being overweight and obesity have been associated with susceptibility to rheumatoid arthritis, especially in women aged older than 55 years (hazard ratio 1.45, 95% confidence interval 1.03-2.03; hazard ratio 1.65, 95% confidence interval 1.34-2.05, respec-tively).30 Conversely, alcohol consumption or breastfeeding with longer duration appear to reduce the risk of developing rheumatoid arthritis (relative risk 0.86, 95% confidence interval 0.78-0.94).62,94
Recent epidemiologic studies have also shown an association between microbial infections and rheumatoid arthritis. In fact, in-fections with different microorganisms, such as Porphyromonas gin-givalis, Proteus mirabilis, Epstein–Barr virus, and mycoplasma, have shown in clinical and preclinical in vivo studies that they may con-tribute to the etiopathogenesis of rheumatoid arthritis.31
Irrespective of the causative factor, the pathogenesis of rheu-matoid arthritis is related to the citrullination process and autoim-munity. This process starts with progressive activation of the innate immune response, namely an increase in antigen-presenting cells and B cell activation, to produce the specific autoantibodies (anti-citrul-linated protein antibodies) that migrate and form immune complexes at the synovial membrane of joints.32 Even although citrullination is not specific to rheumatoid arthritis, the anti-citrullinated protein an-tibodies in rheumatoid arthritis are specific for certain citrullinated proteins, including alpha-enolase, vimentin, and fibrinogen. Of the five known mammalian peptidyl arginine deiminases, peptidyl argi-nine deiminase-2 and peptidyl arginine deiminase-4 are associated
with protein citrullination in rheumatoid arthritis.33 Accumulation of proteins, such as fibrin, within the synovium and their prolonged degradation, leads to exposure of new epitopes to immunocompe-tent cells within the synovium.34 In fact, anti-citrullinated protein antibodies may be detected in a susceptible rheumatoid arthritis pa-tient years before the appearance of the first symptoms, and anti-ci-trullinated protein antibodies are also associated with worse clinical outcomes.11,35 It is probably the accumulation of these known, and probably many unknown, environmental factors that leads to a trig-ger (the so-called second hit)36 that further weakens the immune tolerance and prompts the clinical symptomatology.32 Also, an ex-cessive production of autoreactive B cells has been detected in rheumatoid arthritis patients before clinical onset of the disease.11,32
Even although the diagnosis of rheumatoid arthritis is based on the clinical symptomatology and the joint affectation, its biologic diagnosis is critical to assessing the disease process, and also for early detection and effective therapy.37,38 Different autoantibodies have been used as part of its biologic diagnosis.39 Among them, the levels of rheumatoid factor and anti-citrullinated protein antibod-ies are clearly associated with more aggressive disease activity.11,35 These autoantibodies also demonstrate a high sensitivity (67%) and specificity (96%) in terms of disease diagnosis.40 Furthermore, the detection of anti-cyclic citrullinated peptide may precede the onset of rheumatoid arthritis clinical symptomatology by more than 10 years.41-44 Other less specific biomarkers, such as pro-in-flammatory cytokines, have also been detected in high numbers in pre-rheumatoid arthritis patients and are also associated with the early stages of the disease.45
2 | EPIDEMIOLOGIC A SSOCIATION BET WEEN PERIODONTITIS AND RHEUMATOID ARTHRITIS
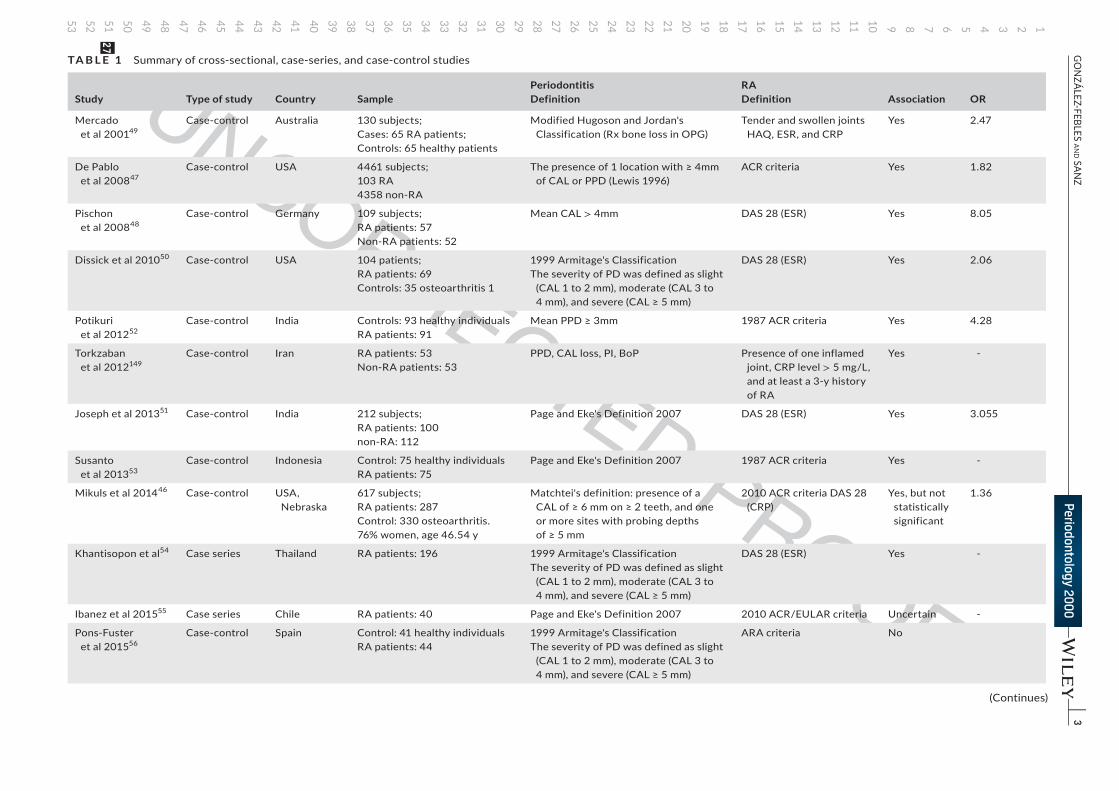
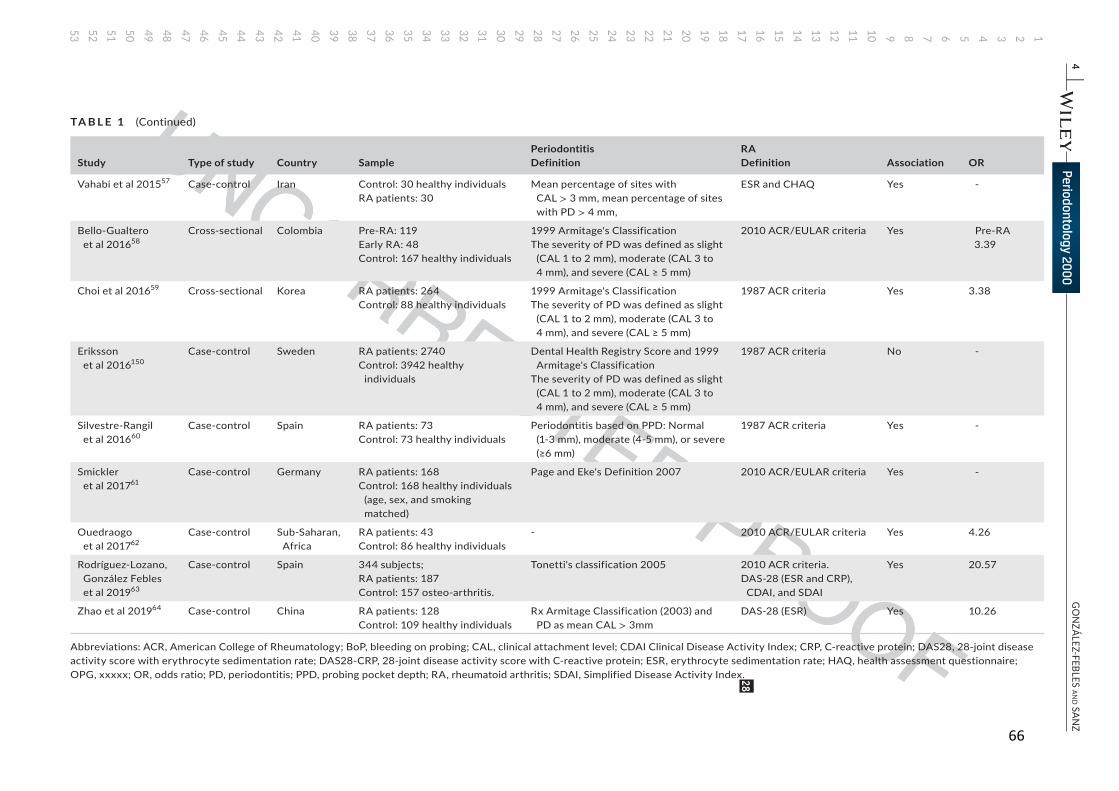
The body of evidence supporting the association between peri-odontitis and rheumatoid arthritis comes from case-control studies (Table 1). Most of these studies show a clear association between periodontitis and rheumatoid arthritis,46-64 with odds ratios rang-ing between 1.82 and 20.57 and patients with rheumatoid arthri-tis exhibiting a high prevalence of periodontitis and tooth loss. De Pablo et al47 studied 103 patients older than 60 years of age with rheumatoid arthritis from the third US National Health and Nutrition Examination Survey. The authors found that patients with rheuma-toid arthritis had an increased risk of periodontitis (odds ratio 4.1, 95% confidence interval 1.3-13.1) after adjusting for age, gender, race, and smoking. The authors also demonstrated a strong asso-ciation between edentulism and seropositive rheumatoid arthritis (odds ratio 4.5, 95% confidence interval 1.2-17). In a recent system-atic review with a meta-analysis that included 19 studies, Kaur et al65 reported a significant association between rheumatoid arthritis and surrogate variables of periodontitis, such as clinical attachment loss (odds ratio 1.17, 95% confidence interval 0.43-1.90) and tooth loss (odds ratio 2.38, 95% confidence interval 1.48-3.29).
19
20
21
22
23
2425
26
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
|
3G
ON
ZÁLEZ-FEBLES aNd SaN
Z
TA B L E 1 Summary of cross-sectional, case-series, and case-control studies
Study Type of study Country SamplePeriodontitisDefinition
RADefinition Association OR
Mercado et al 200149
Case-control Australia 130 subjects;Cases: 65 RA patients;Controls: 65 healthy patients
Modified Hugoson and Jordan's Classification (Rx bone loss in OPG)
Tender and swollen joints HAQ, ESR, and CRP
Yes 2.47
De Pablo et al 200847
Case-control USA 4461 subjects;103 RA4358 non-RA
The presence of 1 location with ≥ 4mm of CAL or PPD (Lewis 1996)
ACR criteria Yes 1.82
Pischon et al 200848
Case-control Germany 109 subjects;RA patients: 57Non-RA patients: 52
Mean CAL > 4mm DAS 28 (ESR) Yes 8.05
Dissick et al 201050 Case-control USA 104 patients;RA patients: 69Controls: 35 osteoarthritis 1
1999 Armitage's ClassificationThe severity of PD was defined as slight
(CAL 1 to 2 mm), moderate (CAL 3 to 4 mm), and severe (CAL ≥ 5 mm)
DAS 28 (ESR) Yes 2.06
Potikuri et al 201252
Case-control India Controls: 93 healthy individualsRA patients: 91
Mean PPD ≥ 3mm 1987 ACR criteria Yes 4.28
Torkzaban et al 2012149
Case-control Iran RA patients: 53Non-RA patients: 53
PPD, CAL loss, PI, BoP Presence of one inflamed joint, CRP level > 5 mg/L, and at least a 3-y history of RA
Yes -
Joseph et al 201351 Case-control India 212 subjects;RA patients: 100non-RA: 112
Page and Eke's Definition 2007 DAS 28 (ESR) Yes 3.055
Susanto et al 201353
Case-control Indonesia Control: 75 healthy individualsRA patients: 75
Page and Eke's Definition 2007 1987 ACR criteria Yes -
Mikuls et al 201446 Case-control USA, Nebraska
617 subjects;RA patients: 287Control: 330 osteoarthritis.76% women, age 46.54 y
Matchtei's definition: presence of a CAL of ≥ 6 mm on ≥ 2 teeth, and one or more sites with probing depths of ≥ 5 mm
2010 ACR criteria DAS 28 (CRP)
Yes, but not statistically significant
1.36
Khantisopon et al54 Case series Thailand RA patients: 196 1999 Armitage's ClassificationThe severity of PD was defined as slight
(CAL 1 to 2 mm), moderate (CAL 3 to 4 mm), and severe (CAL ≥ 5 mm)
DAS 28 (ESR) Yes -
Ibanez et al 201555 Case series Chile RA patients: 40 Page and Eke's Definition 2007 2010 ACR/EULAR criteria Uncertain -
Pons-Fuster et al 201556
Case-control Spain Control: 41 healthy individualsRA patients: 44
1999 Armitage's ClassificationThe severity of PD was defined as slight
(CAL 1 to 2 mm), moderate (CAL 3 to 4 mm), and severe (CAL ≥ 5 mm)
ARA criteria No
(Continues)
27
66
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
4 |
GO
NZÁLEZ-FEBLES aN
d SaNZ
Study Type of study Country SamplePeriodontitisDefinition
RADefinition Association OR
Vahabi et al 201557 Case-control Iran Control: 30 healthy individualsRA patients: 30
Mean percentage of sites with CAL > 3 mm, mean percentage of sites with PD > 4 mm,
ESR and CHAQ Yes -
Bello-Gualtero et al 201658
Cross-sectional Colombia Pre-RA: 119Early RA: 48Control: 167 healthy individuals
1999 Armitage's ClassificationThe severity of PD was defined as slight
(CAL 1 to 2 mm), moderate (CAL 3 to 4 mm), and severe (CAL ≥ 5 mm)
2010 ACR/EULAR criteria Yes Pre-RA3.39
Choi et al 201659 Cross-sectional Korea RA patients: 264Control: 88 healthy individuals
1999 Armitage's ClassificationThe severity of PD was defined as slight
(CAL 1 to 2 mm), moderate (CAL 3 to 4 mm), and severe (CAL ≥ 5 mm)
1987 ACR criteria Yes 3.38
Eriksson et al 2016150
Case-control Sweden RA patients: 2740Control: 3942 healthy
individuals
Dental Health Registry Score and 1999 Armitage's Classification
The severity of PD was defined as slight (CAL 1 to 2 mm), moderate (CAL 3 to 4 mm), and severe (CAL ≥ 5 mm)
1987 ACR criteria No -
Silvestre-Rangil et al 201660
Case-control Spain RA patients: 73Control: 73 healthy individuals
Periodontitis based on PPD: Normal (1-3 mm), moderate (4-5 mm), or severe (≥6 mm)
1987 ACR criteria Yes -
Smickler et al 201761
Case-control Germany RA patients: 168Control: 168 healthy individuals
(age, sex, and smoking matched)
Page and Eke's Definition 2007 2010 ACR/EULAR criteria Yes -
Ouedraogo et al 201762
Case-control Sub-Saharan, Africa
RA patients: 43Control: 86 healthy individuals
- 2010 ACR/EULAR criteria Yes 4.26
Rodríguez-Lozano, González Febles et al 201963
Case-control Spain 344 subjects;RA patients: 187Control: 157 osteo-arthritis.
Tonetti's classification 2005 2010 ACR criteria.DAS-28 (ESR and CRP),
CDAI, and SDAI
Yes 20.57
Zhao et al 201964 Case-control China RA patients: 128Control: 109 healthy individuals
Rx Armitage Classification (2003) and PD as mean CAL > 3mm
DAS-28 (ESR) Yes 10.26
Abbreviations: ACR, American College of Rheumatology; BoP, bleeding on probing; CAL, clinical attachment level; CDAI Clinical Disease Activity Index; CRP, C-reactive protein; DAS28, 28-joint disease activity score with erythrocyte sedimentation rate; DAS28-CRP, 28-joint disease activity score with C-reactive protein; ESR, erythrocyte sedimentation rate; HAQ, health assessment questionnaire; OPG, xxxxx; OR, odds ratio; PD, periodontitis; PPD, probing pocket depth; RA, rheumatoid arthritis; SDAI, Simplified Disease Activity Index.
TA B L E 1 (Continued)
28
123456789
1011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
| 5GONZÁLEZ-FEBLES aNd SaNZ
However, the relationship between the severity of periodontitis and rheumatoid arthritis disease activity is still controversial. Mikuls et al46 evaluated 287 patients with rheumatoid arthritis and demon-strated a statistically significant association between periodontitis and increased swollen joint counts, greater disease activity, and an-ti-cyclic citrullinated peptide antibody levels. Nevertheless, other studies did not find this association.50,66 An independent case-con-trol study carried out in Spain63 on 187 patients with rheumatoid ar-thritis and 157 control patients with osteoarthritis revealed a strong association between periodontitis and rheumatoid arthritis with an odds ratio of 20.57 (95% confidence interval 6.02-70.27; P < .001). The severity of periodontitis was significantly related to rheumatoid arthritis disease activity in an adjusted linear regression model (odds ratio 2.75, 95% confidence interval 1.28-5.93; P = .012).
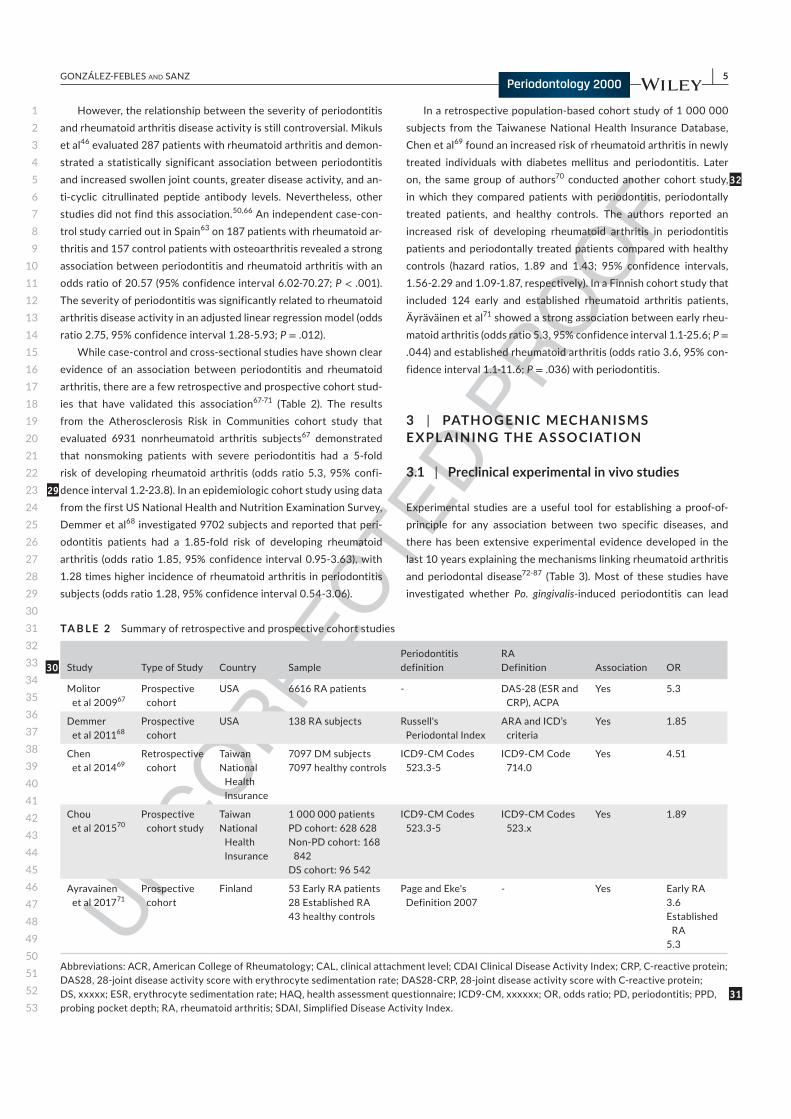
While case-control and cross-sectional studies have shown clear evidence of an association between periodontitis and rheumatoid arthritis, there are a few retrospective and prospective cohort stud-ies that have validated this association67-71 (Table 2). The results from the Atherosclerosis Risk in Communities cohort study that evaluated 6931 nonrheumatoid arthritis subjects67 demonstrated that nonsmoking patients with severe periodontitis had a 5-fold risk of developing rheumatoid arthritis (odds ratio 5.3, 95% confi-dence interval 1.2-23.8). In an epidemiologic cohort study using data from the first US National Health and Nutrition Examination Survey, Demmer et al68 investigated 9702 subjects and reported that peri-odontitis patients had a 1.85-fold risk of developing rheumatoid arthritis (odds ratio 1.85, 95% confidence interval 0.95-3.63), with 1.28 times higher incidence of rheumatoid arthritis in periodontitis subjects (odds ratio 1.28, 95% confidence interval 0.54-3.06).
In a retrospective population-based cohort study of 1 000 000 subjects from the Taiwanese National Health Insurance Database, Chen et al69 found an increased risk of rheumatoid arthritis in newly treated individuals with diabetes mellitus and periodontitis. Later on, the same group of authors70 conducted another cohort study, in which they compared patients with periodontitis, periodontally treated patients, and healthy controls. The authors reported an increased risk of developing rheumatoid arthritis in periodontitis patients and periodontally treated patients compared with healthy controls (hazard ratios, 1.89 and 1.43; 95% confidence intervals, 1.56-2.29 and 1.09-1.87, respectively). In a Finnish cohort study that included 124 early and established rheumatoid arthritis patients, Äyräväinen et al71 showed a strong association between early rheu-matoid arthritis (odds ratio 5.3, 95% confidence interval 1.1-25.6; P = .044) and established rheumatoid arthritis (odds ratio 3.6, 95% con-fidence interval 1.1-11.6; P = .036) with periodontitis.
3 | PATHOGENIC MECHANISMS E XPL AINING THE A SSOCIATION
3.1 | Preclinical experimental in vivo studies
Experimental studies are a useful tool for establishing a proof-of-principle for any association between two specific diseases, and there has been extensive experimental evidence developed in the last 10 years explaining the mechanisms linking rheumatoid arthritis and periodontal disease72-87 (Table 3). Most of these studies have investigated whether Po. gingivalis-induced periodontitis can lead
TA B L E 2 Summary of retrospective and prospective cohort studies
Study Type of Study Country SamplePeriodontitisdefinition
RADefinition Association OR
Molitor et al 200967
Prospective cohort
USA 6616 RA patients - DAS-28 (ESR and CRP), ACPA
Yes 5.3
Demmer et al 201168
Prospective cohort
USA 138 RA subjects Russell's Periodontal Index
ARA and ICD’s criteria
Yes 1.85
Chen et al 201469
Retrospective cohort
TaiwanNational
Health Insurance
7097 DM subjects7097 healthy controls
ICD9-CM Codes 523.3-5
ICD9-CM Code 714.0
Yes 4.51
Chou et al 201570
Prospective cohort study
TaiwanNational
Health Insurance
1 000 000 patientsPD cohort: 628 628Non-PD cohort: 168
842DS cohort: 96 542
ICD9-CM Codes 523.3-5
ICD9-CM Codes 523.x
Yes 1.89
Ayravainen et al 201771
Prospective cohort
Finland 53 Early RA patients28 Established RA43 healthy controls
Page and Eke's Definition 2007
- Yes Early RA3.6Established
RA5.3
Abbreviations: ACR, American College of Rheumatology; CAL, clinical attachment level; CDAI Clinical Disease Activity Index; CRP, C-reactive protein; DAS28, 28-joint disease activity score with erythrocyte sedimentation rate; DAS28-CRP, 28-joint disease activity score with C-reactive protein; DS, xxxxx; ESR, erythrocyte sedimentation rate; HAQ, health assessment questionnaire; ICD9-CM, xxxxxx; OR, odds ratio; PD, periodontitis; PPD, probing pocket depth; RA, rheumatoid arthritis; SDAI, Simplified Disease Activity Index.
29
30
31
32

68
123456789
1011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
6 | GONZÁLEZ-FEBLES aNd SaNZ
to the initiation and progression of rheumatoid arthritis.74-87 Po. gingivalis produces a specific peptidyl arginine deiminase, Po. gingi-valis peptidil-arginine deiminase,8,88 which can citrullinate human proteins and may increase the probability of greater formation of anti-cyclic citrullinated peptide. In fact, Po. gingivalis peptidil-argi-nine deiminase may citrullinate peptides that are released from Po. gingivalis gingipain-mediated degradation of fibrinogen and alpha-enolase,42 or it may promote self-citrullination.42,88-90 Hence, Po. gin-givalis peptidil-arginine deiminase, as a bacterial auto-citrullinated protein, may constitute a powerful antigen that can break the im-mune tolerance of the host by increasing the release of anti-cyclic citrullinated peptide87 and anti-cyclic citrullinated peptide-1 autoan-tibodies,91,92 thereby triggering the onset of rheumatoid arthritis clinical symptoms. A recent experimental study87 has shown that Po. gingivalis-induced periodontitis triggered seropositive anti-cyclic cit-rullinated peptide rheumatoid arthritis with systemic inflammation and increased bone erosion.
Recent laboratory studies using rheumatoid arthritis patient samples have reported that Po. gingivalis may not be the only peri-odontal bacteria with an ability to citrullinate proteins and induce anti-citrullinated protein antibodies formation.93 In fact, Konig et al94 showed that Aggregatibacter actinomycetemcomitans can induce hypercitrullination in host neutrophils, leading to anti-ci-trullinated protein antibodies formation. This is probably mediated through pore-forming leukotoxin A and can lead to membrane damage on neutrophils and uncontrolled activation of citrullina-tion enzymes, similar to Po. gingivalis peptidil-arginine deiminase in rheumatoid arthritis joints.
Other studies have shown that Tannerella forsythia,95 as well as Fusobacterium nucleatum and Po. gingivalis, may also be associated with triggering anti-cyclic citrullinated peptide antibodies in posi-tive rheumatoid arthritis patients.61 In fact, in a recent experimen-tal study,85 mice inoculated with a mix of Po. gingivalis, F. nucleatum, and A. actinomycetemcomintans showed less periodontal bone loss than mice inoculated with Po. gingivalis alone. However, when F. nucleatumor A. actinomycetemcomintans were inoculated on their own, arthritis onset and progression were both enhanced.85
Experimental studies have also examined whether rheumatoid arthritis might exacerbate periodontal destruction, but no evidence of this has been provided to date.72,73,96
3.2 | Clinical studies
Clinical studies support the experimental evidence, since they show the presence of autoantibodies in the gingival crevicular fluid of periodontitis patients88 and increased autoantibody lev-els in nonrheumatoid arthritis patients with severe periodonti-tis97,98 (Table 4). In a recent cross-sectional study in a cohort of 600 subjects, Oluwagbemigun et al99 demonstrated that in spe-cific patients with elevated systemic inflammation, higher salivary Po. gingivalis DNA was associated with elevated serum anti-cit-rullinated protein antibodies. In fact, Jenning et al100 correlated
anti-rheumatoid arthritis-Po. gingivalis peptidil-arginine deiminase (a recombinant modification of Po. gingivalis peptidil-arginine deiminase) with anti-citrullinated protein antibodies levels and in-terstitial lung disease autoantigens, suggesting an infection-based concept for induction of anti-citrullinated protein antibodiess via enzymatic mimicry.
To understand how these specific bacteria might trigger the onset of rheumatoid arthritis, it is important to understand the role of these bacteria in the development of rheumatoid arthri-tis symptoms in patients at risk. While Mikuls et al101 reported that Po. gingivalis was significantly associated with the presence of anti-cyclic citrullinated peptide antibodies in individuals at risk of rheumatoid arthritis, de Smit et al102 did not find that Po. gingi-valis antibody levels were a prognostic factor for the development of rheumatoid arthritis. However, other authors103 have reported that Po. gingivalis peptidil-arginine deiminase was specific for Po. gingivalis and no other bacteria, suggesting a specific role for Po. gingivalis in the pathogenesis of rheumatoid arthritis. Similarly, Bello-Gualtero et al58 reported that in pre-rheumatoid arthritis subjects with significant periodontal inflammation and destruc-tion, there was a significant association between anti-Po. gingi-valis IgG and anti-citrullinated protein antibodies. Furthermore, a significant association was found between Po. gingivalis-positive periodontitis patients and pre-rheumatoid arthritis patients with positive anti-cyclic citrullinated peptide titers.104
These experimental and clinical studies clearly show that the in-creased citrullination seen in periodontitis patients is probably me-diated by both bacterial Po. gingivalis peptidil-arginine deiminase and host peptidyl arginine deiminase. This may lead to the breakdown of immune tolerance and subsequent increase in the release of rheu-matoid arthritis characteristic autoantibodies, which genetically pre-dispose individuals to rheumatoid arthritis and thereby also trigger the onset of rheumatoid arthritis.
With respect to interventional studies on rheumatoid arthritis and periodontal disease, there are only limited data available.105 A study with 64 subjects—distributed into four groups: (a) healthy controls (P-RA-), (b) periodontitis patients without rheumatoid ar-thritis (P + RA−), (c) rheumatoid arthritis patients without periodon-titis (P-RA+), and (d) rheumatoid arthritis patients with periodontitis (P + RA+)—showed that periodontitis could contribute to rheuma-toid arthritis progression, but not vice versa. There is a need for well-designed studies with longer follow-up to confirm these early results.
Besides the role of periodontopathogen bacteria in citrullination, there are studies suggesting that periodontitis-induced inflammation may also play a significant role in rheumatoid arthritis pathogenesis98,106-111 (Table 5). In a cross-sectional study, Nesse et al106 demonstrated that ci-trullination is an inflammation-dependent phenomenon within periodon-tal tissues, similar to what occurs within the synovium in affected joints of rheumatoid arthritis patients. The authors indicated that periodon-titis-induced citrullination might have an important role in the etiology of rheumatoid arthritis. De Pablo et al98 also showed that the antibody response in periodontitis, compared with non-periodontitis subjects, was
33
34
35
39
40
41
45
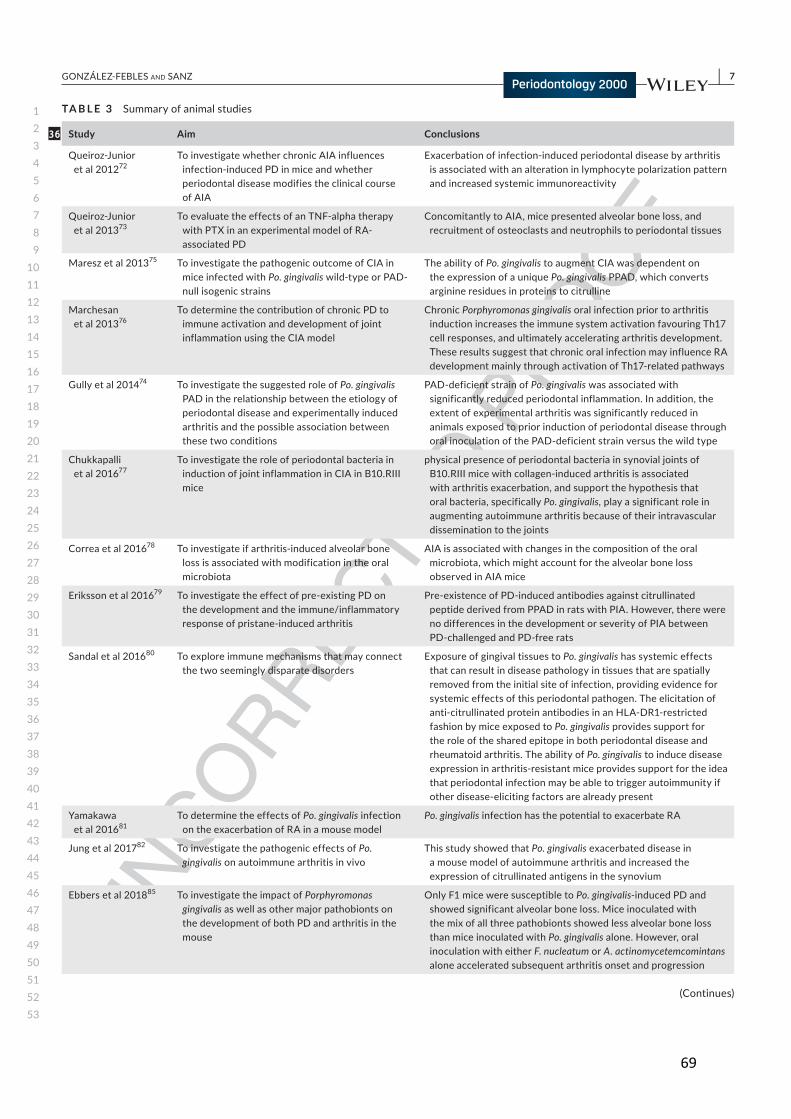
69
123456789
1011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
| 7GONZÁLEZ-FEBLES aNd SaNZ
TA B L E 3 Summary of animal studies
Study Aim Conclusions
Queiroz-Junior et al 201272
To investigate whether chronic AIA influences infection-induced PD in mice and whether periodontal disease modifies the clinical course of AIA
Exacerbation of infection-induced periodontal disease by arthritis is associated with an alteration in lymphocyte polarization pattern and increased systemic immunoreactivity
Queiroz-Junior et al 201373
To evaluate the effects of an TNF-alpha therapy with PTX in an experimental model of RA-associated PD
Concomitantly to AIA, mice presented alveolar bone loss, and recruitment of osteoclasts and neutrophils to periodontal tissues
Maresz et al 201375 To investigate the pathogenic outcome of CIA in mice infected with Po. gingivalis wild-type or PAD-null isogenic strains
The ability of Po. gingivalis to augment CIA was dependent on the expression of a unique Po. gingivalis PPAD, which converts arginine residues in proteins to citrulline
Marchesan et al 201376
To determine the contribution of chronic PD to immune activation and development of joint inflammation using the CIA model
Chronic Porphyromonas gingivalis oral infection prior to arthritis induction increases the immune system activation favouring Th17 cell responses, and ultimately accelerating arthritis development. These results suggest that chronic oral infection may influence RA development mainly through activation of Th17-related pathways
Gully et al 201474 To investigate the suggested role of Po. gingivalis PAD in the relationship between the etiology of periodontal disease and experimentally induced arthritis and the possible association between these two conditions
PAD-deficient strain of Po. gingivalis was associated with significantly reduced periodontal inflammation. In addition, the extent of experimental arthritis was significantly reduced in animals exposed to prior induction of periodontal disease through oral inoculation of the PAD-deficient strain versus the wild type
Chukkapalli et al 201677
To investigate the role of periodontal bacteria in induction of joint inflammation in CIA in B10.RIII mice
physical presence of periodontal bacteria in synovial joints of B10.RIII mice with collagen-induced arthritis is associated with arthritis exacerbation, and support the hypothesis that oral bacteria, specifically Po. gingivalis, play a significant role in augmenting autoimmune arthritis because of their intravascular dissemination to the joints
Correa et al 201678 To investigate if arthritis-induced alveolar bone loss is associated with modification in the oral microbiota
AIA is associated with changes in the composition of the oral microbiota, which might account for the alveolar bone loss observed in AIA mice
Eriksson et al 201679 To investigate the effect of pre-existing PD on the development and the immune/inflammatory response of pristane-induced arthritis
Pre-existence of PD-induced antibodies against citrullinated peptide derived from PPAD in rats with PIA. However, there were no differences in the development or severity of PIA between PD-challenged and PD-free rats
Sandal et al 201680 To explore immune mechanisms that may connect the two seemingly disparate disorders
Exposure of gingival tissues to Po. gingivalis has systemic effects that can result in disease pathology in tissues that are spatially removed from the initial site of infection, providing evidence for systemic effects of this periodontal pathogen. The elicitation of anti-citrullinated protein antibodies in an HLA-DR1-restricted fashion by mice exposed to Po. gingivalis provides support for the role of the shared epitope in both periodontal disease and rheumatoid arthritis. The ability of Po. gingivalis to induce disease expression in arthritis-resistant mice provides support for the idea that periodontal infection may be able to trigger autoimmunity if other disease-eliciting factors are already present
Yamakawa et al 201681
To determine the effects of Po. gingivalis infection on the exacerbation of RA in a mouse model
Po. gingivalis infection has the potential to exacerbate RA
Jung et al 201782 To investigate the pathogenic effects of Po. gingivalis on autoimmune arthritis in vivo
This study showed that Po. gingivalis exacerbated disease in a mouse model of autoimmune arthritis and increased the expression of citrullinated antigens in the synovium
Ebbers et al 201885 To investigate the impact of Porphyromonas gingivalis as well as other major pathobionts on the development of both PD and arthritis in the mouse
Only F1 mice were susceptible to Po. gingivalis-induced PD and showed significant alveolar bone loss. Mice inoculated with the mix of all three pathobionts showed less alveolar bone loss than mice inoculated with Po. gingivalis alone. However, oral inoculation with either F. nucleatum or A. actinomycetemcomintans alone accelerated subsequent arthritis onset and progression
(Continues)
36
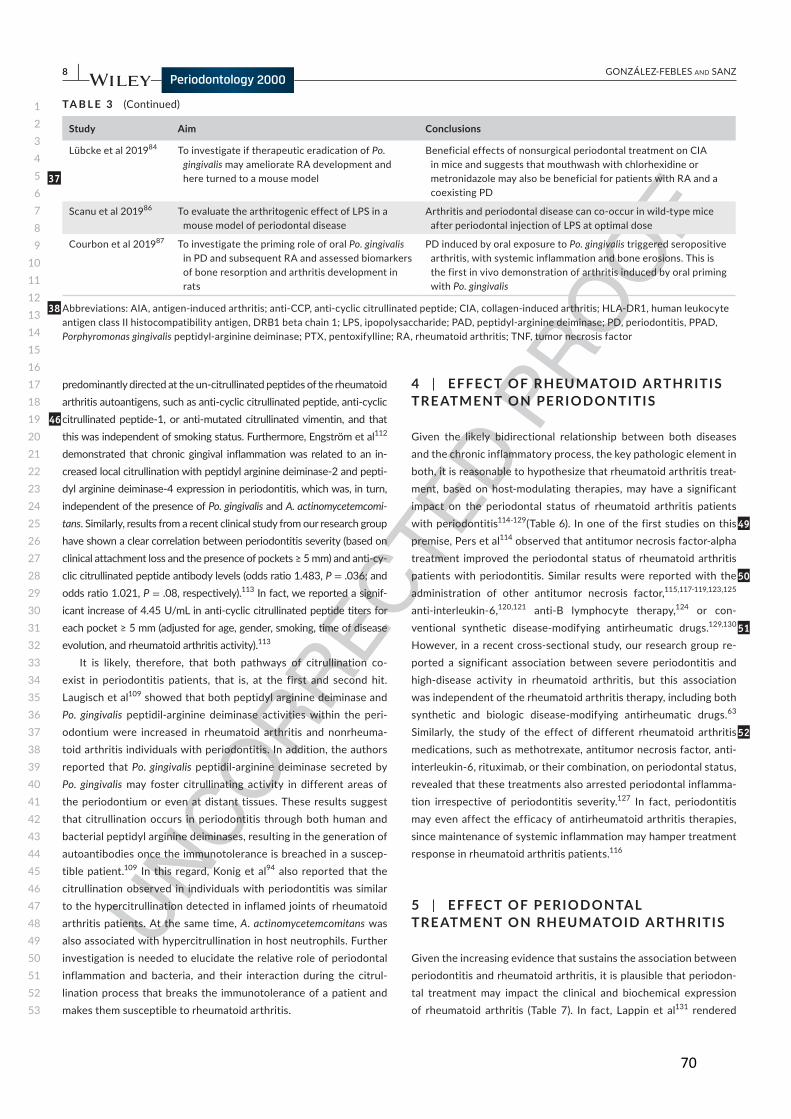
70
123456789
1011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
8 | GONZÁLEZ-FEBLES aNd SaNZ
predominantly directed at the un-citrullinated peptides of the rheumatoid
arthritis autoantigens, such as anti-cyclic citrullinated peptide, anti-cyclic
citrullinated peptide-1, or anti-mutated citrullinated vimentin, and that
this was independent of smoking status. Furthermore, Engström et al112
demonstrated that chronic gingival inflammation was related to an in-
creased local citrullination with peptidyl arginine deiminase-2 and pepti-
dyl arginine deiminase-4 expression in periodontitis, which was, in turn,
independent of the presence of Po. gingivalis and A. actinomycetemcomi-tans. Similarly, results from a recent clinical study from our research group
have shown a clear correlation between periodontitis severity (based on
clinical attachment loss and the presence of pockets ≥ 5 mm) and anti-cy-
clic citrullinated peptide antibody levels (odds ratio 1.483, P = .036; and
odds ratio 1.021, P = .08, respectively).113 In fact, we reported a signif-
icant increase of 4.45 U/mL in anti-cyclic citrullinated peptide titers for
each pocket ≥ 5 mm (adjusted for age, gender, smoking, time of disease evolution, and rheumatoid arthritis activity).113
It is likely, therefore, that both pathways of citrullination co-
exist in periodontitis patients, that is, at the first and second hit.
Laugisch et al109 showed that both peptidyl arginine deiminase and
Po. gingivalis peptidil-arginine deiminase activities within the peri-
odontium were increased in rheumatoid arthritis and nonrheuma-
toid arthritis individuals with periodontitis. In addition, the authors
reported that Po. gingivalis peptidil-arginine deiminase secreted by
Po. gingivalis may foster citrullinating activity in different areas of
the periodontium or even at distant tissues. These results suggest
that citrullination occurs in periodontitis through both human and
bacterial peptidyl arginine deiminases, resulting in the generation of
autoantibodies once the immunotolerance is breached in a suscep-
tible patient.109 In this regard, Konig et al94 also reported that the
citrullination observed in individuals with periodontitis was similar
to the hypercitrullination detected in inflamed joints of rheumatoid
arthritis patients. At the same time, A. actinomycetemcomitans was
also associated with hypercitrullination in host neutrophils. Further
investigation is needed to elucidate the relative role of periodontal
inflammation and bacteria, and their interaction during the citrul-
lination process that breaks the immunotolerance of a patient and
makes them susceptible to rheumatoid arthritis.
4 | EFFEC T OF RHEUMATOID ARTHRITIS TRE ATMENT ON PERIODONTITIS
Given the likely bidirectional relationship between both diseases
and the chronic inflammatory process, the key pathologic element in
both, it is reasonable to hypothesize that rheumatoid arthritis treat-
ment, based on host-modulating therapies, may have a significant
impact on the periodontal status of rheumatoid arthritis patients
with periodontitis114-129(Table 6). In one of the first studies on this
premise, Pers et al114 observed that antitumor necrosis factor-alpha
treatment improved the periodontal status of rheumatoid arthritis
patients with periodontitis. Similar results were reported with the
administration of other antitumor necrosis factor,115,117-119,123,125
anti-interleukin-6,120,121 anti-B lymphocyte therapy,124 or con-
ventional synthetic disease-modifying antirheumatic drugs.129,130
However, in a recent cross-sectional study, our research group re-
ported a significant association between severe periodontitis and
high-disease activity in rheumatoid arthritis, but this association
was independent of the rheumatoid arthritis therapy, including both
synthetic and biologic disease-modifying antirheumatic drugs.63
Similarly, the study of the effect of different rheumatoid arthritis
medications, such as methotrexate, antitumor necrosis factor, anti-
interleukin-6, rituximab, or their combination, on periodontal status,
revealed that these treatments also arrested periodontal inflamma-
tion irrespective of periodontitis severity.127 In fact, periodontitis
may even affect the efficacy of antirheumatoid arthritis therapies,
since maintenance of systemic inflammation may hamper treatment
response in rheumatoid arthritis patients.116
5 | EFFEC T OF PERIODONTAL TRE ATMENT ON RHEUMATOID ARTHRITIS
Given the increasing evidence that sustains the association between
periodontitis and rheumatoid arthritis, it is plausible that periodon-
tal treatment may impact the clinical and biochemical expression
of rheumatoid arthritis (Table 7). In fact, Lappin et al131 rendered
Study Aim Conclusions
Lübcke et al 201984 To investigate if therapeutic eradication of Po. gingivalis may ameliorate RA development and here turned to a mouse model
Beneficial effects of nonsurgical periodontal treatment on CIA in mice and suggests that mouthwash with chlorhexidine or metronidazole may also be beneficial for patients with RA and a coexisting PD
Scanu et al 201986 To evaluate the arthritogenic effect of LPS in a mouse model of periodontal disease
Arthritis and periodontal disease can co-occur in wild-type mice after periodontal injection of LPS at optimal dose
Courbon et al 201987 To investigate the priming role of oral Po. gingivalis in PD and subsequent RA and assessed biomarkers of bone resorption and arthritis development in rats
PD induced by oral exposure to Po. gingivalis triggered seropositive arthritis, with systemic inflammation and bone erosions. This is the first in vivo demonstration of arthritis induced by oral priming with Po. gingivalis
Abbreviations: AIA, antigen-induced arthritis; anti-CCP, anti-cyclic citrullinated peptide; CIA, collagen-induced arthritis; HLA-DR1, human leukocyte antigen class II histocompatibility antigen, DRB1 beta chain 1; LPS, ipopolysaccharide; PAD, peptidyl-arginine deiminase; PD, periodontitis, PPAD, Porphyromonas gingivalis peptidyl-arginine deiminase; PTX, pentoxifylline; RA, rheumatoid arthritis; TNF, tumor necrosis factor
TA B L E 3 (Continued)
37
38
46
49
50
51
52
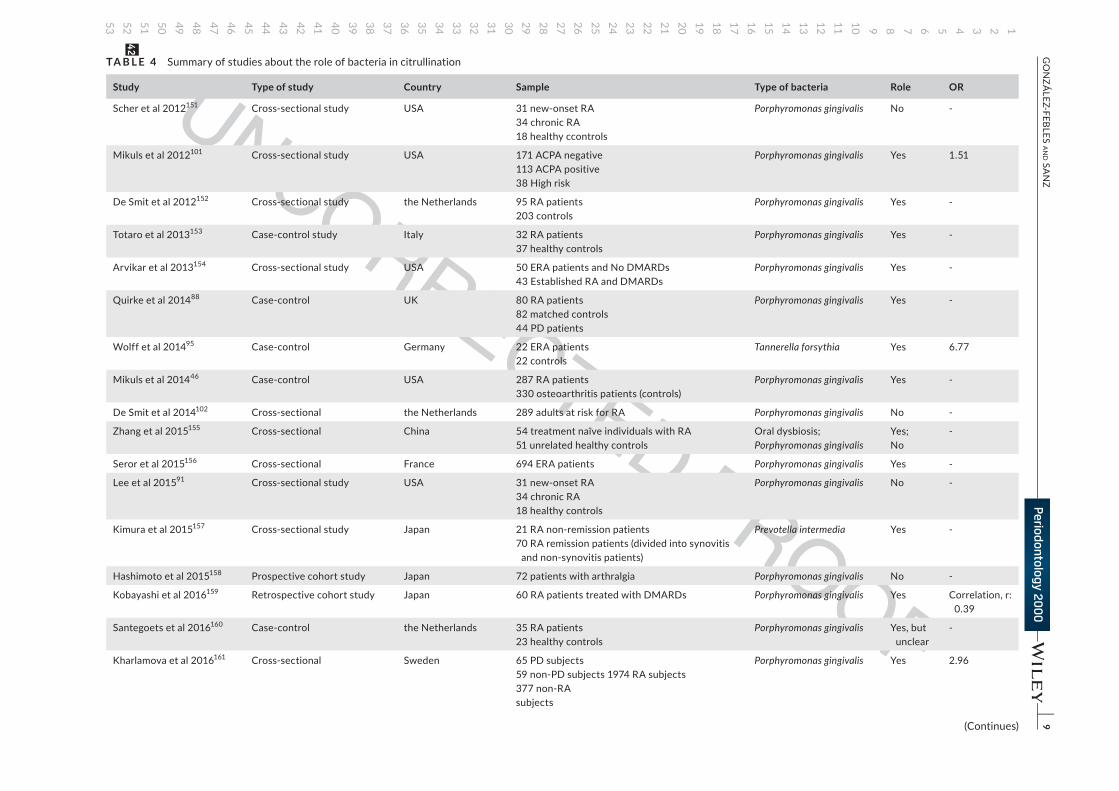
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
|
9G
ON
ZÁLEZ-FEBLES a
Nd Sa
NZ
TA B L E 4 Summary of studies about the role of bacteria in citrullination
Study Type of study Country Sample Type of bacteria Role OR
Scher et al 2012151 Cross-sectional study USA 31 new-onset RA34 chronic RA18 healthy ccontrols
Porphyromonas gingivalis No -
Mikuls et al 2012101 Cross-sectional study USA 171 ACPA negative113 ACPA positive38 High risk
Porphyromonas gingivalis Yes 1.51
De Smit et al 2012152 Cross-sectional study the Netherlands 95 RA patients203 controls
Porphyromonas gingivalis Yes -
Totaro et al 2013153 Case-control study Italy 32 RA patients37 healthy controls
Porphyromonas gingivalis Yes -
Arvikar et al 2013154 Cross-sectional study USA 50 ERA patients and No DMARDs43 Established RA and DMARDs
Porphyromonas gingivalis Yes -
Quirke et al 201488 Case-control UK 80 RA patients82 matched controls44 PD patients
Porphyromonas gingivalis Yes -
Wolff et al 201495 Case-control Germany 22 ERA patients22 controls
Tannerella forsythia Yes 6.77
Mikuls et al 201446 Case-control USA 287 RA patients330 osteoarthritis patients (controls)
Porphyromonas gingivalis Yes -
De Smit et al 2014102 Cross-sectional the Netherlands 289 adults at risk for RA Porphyromonas gingivalis No -
Zhang et al 2015155 Cross-sectional China 54 treatment naïve individuals with RA51 unrelated healthy controls
Oral dysbiosis;Porphyromonas gingivalis
Yes;No
-
Seror et al 2015156 Cross-sectional France 694 ERA patients Porphyromonas gingivalis Yes -
Lee et al 201591 Cross-sectional study USA 31 new-onset RA34 chronic RA18 healthy controls
Porphyromonas gingivalis No -
Kimura et al 2015157 Cross-sectional study Japan 21 RA non-remission patients70 RA remission patients (divided into synovitis
and non-synovitis patients)
Prevotella intermedia Yes -
Hashimoto et al 2015158 Prospective cohort study Japan 72 patients with arthralgia Porphyromonas gingivalis No -
Kobayashi et al 2016159 Retrospective cohort study Japan 60 RA patients treated with DMARDs Porphyromonas gingivalis Yes Correlation, r: 0.39
Santegoets et al 2016160 Case-control the Netherlands 35 RA patients23 healthy controls
Porphyromonas gingivalis Yes, but unclear
-
Kharlamova et al 2016161 Cross-sectional Sweden 65 PD subjects59 non-PD subjects 1974 RA subjects377 non-RAsubjects
Porphyromonas gingivalis Yes 2.96
(Continues)
42
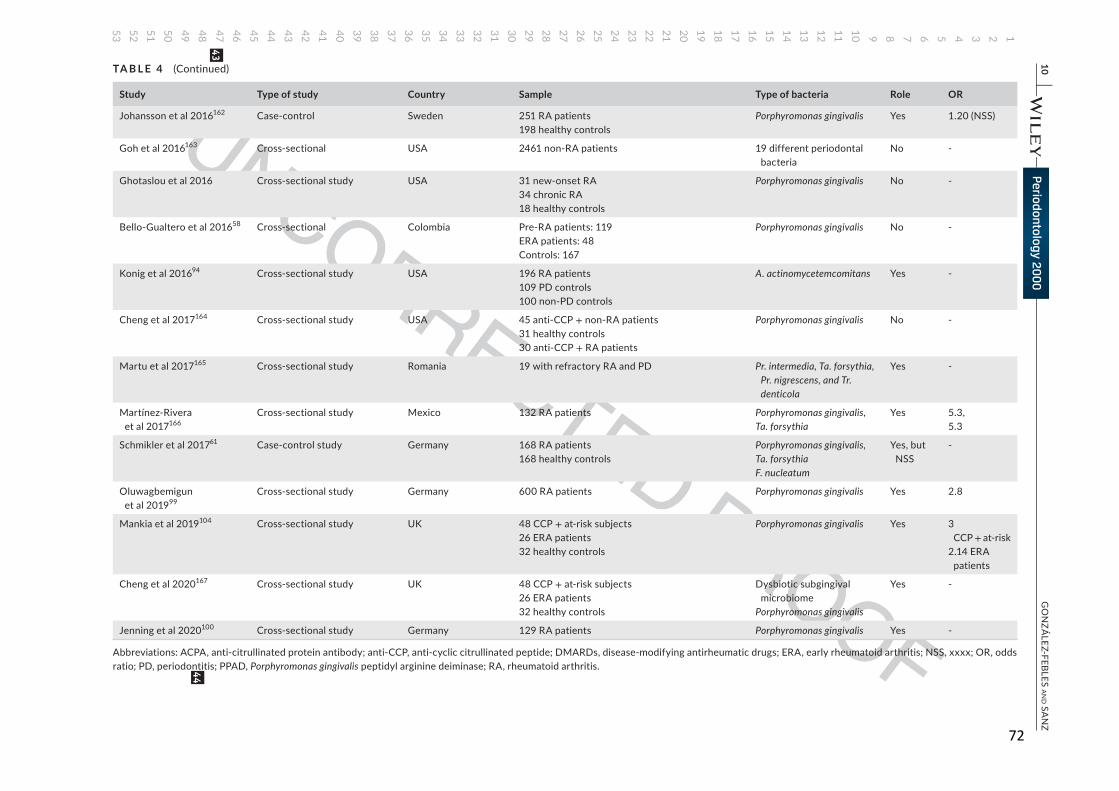
72
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
10 |
GO
NZÁ
LEZ-FEBLES aN
d SaN
Z
Study Type of study Country Sample Type of bacteria Role OR
Johansson et al 2016162 Case-control Sweden 251 RA patients198 healthy controls
Porphyromonas gingivalis Yes 1.20 (NSS)
Goh et al 2016163 Cross-sectional USA 2461 non-RA patients 19 different periodontal bacteria
No -
Ghotaslou et al 2016 Cross-sectional study USA 31 new-onset RA34 chronic RA18 healthy controls
Porphyromonas gingivalis No -
Bello-Gualtero et al 201658 Cross-sectional Colombia Pre-RA patients: 119ERA patients: 48Controls: 167
Porphyromonas gingivalis No -
Konig et al 201694 Cross-sectional study USA 196 RA patients109 PD controls100 non-PD controls
A. actinomycetemcomitans Yes -
Cheng et al 2017164 Cross-sectional study USA 45 anti-CCP + non-RA patients31 healthy controls30 anti-CCP + RA patients
Porphyromonas gingivalis No -
Martu et al 2017165 Cross-sectional study Romania 19 with refractory RA and PD Pr. intermedia, Ta. forsythia, Pr. nigrescens, and Tr. denticola
Yes -
Martínez-Rivera et al 2017166
Cross-sectional study Mexico 132 RA patients Porphyromonas gingivalis,Ta. forsythia
Yes 5.3,5.3
Schmikler et al 201761 Case-control study Germany 168 RA patients168 healthy controls
Porphyromonas gingivalis,Ta. forsythiaF. nucleatum
Yes, but NSS
-
Oluwagbemigun et al 201999
Cross-sectional study Germany 600 RA patients Porphyromonas gingivalis Yes 2.8
Mankia et al 2019104 Cross-sectional study UK 48 CCP + at-risk subjects26 ERA patients32 healthy controls
Porphyromonas gingivalis Yes 3 CCP + at-risk
2.14 ERA patients
Cheng et al 2020167 Cross-sectional study UK 48 CCP + at-risk subjects26 ERA patients32 healthy controls
Dysbiotic subgingival microbiome
Porphyromonas gingivalis
Yes -
Jenning et al 2020100 Cross-sectional study Germany 129 RA patients Porphyromonas gingivalis Yes -
Abbreviations: ACPA, anti-citrullinated protein antibody; anti-CCP, anti-cyclic citrullinated peptide; DMARDs, disease-modifying antirheumatic drugs; ERA, early rheumatoid arthritis; NSS, xxxx; OR, odds ratio; PD, periodontitis; PPAD, Porphyromonas gingivalis peptidyl arginine deiminase; RA, rheumatoid arthritis.
TA B L E 4 (Continued)
43
44

123456789
1011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
| 11GONZÁLEZ-FEBLES aNd SaNZ
nonsurgical periodontal therapy to periodontitis patients with rheu-
matoid arthritis and reported a significant decrease in anti-cyclic
citrullinated peptide and anti-Po. gingivalis antibody levels 6 months
after the therapy, suggesting a potential beneficial effect on rheu-
matoid arthritis disease activity.
A systematic review with a meta-analysis evaluated the effect
of periodontal treatment on rheumatoid arthritis subjects.132 The
five identified studies evaluated the impact of periodontal treat-
ment on both clinical and biochemical parameters associated with
rheumatoid arthritis disease activity. A significant reduction in the
erythrocyte sedimentation rate, and a tendency towards a reduction
in tumor necrosis factor-alpha levels and 28-joint disease activity
score with erythrocyte sedimentation rate, was demonstrated after
periodontal treatment. Conversely, no significant reductions in the
levels of C-reactive protein, rheumatoid factor, anti-citrullinated pro-
tein antibodies, or interleukin-6 levels were reported. Similar results
were reported in a more recent systematic review.133 Nevertheless,
the randomized controlled trials selected in both systematic reviews
represented a short follow-up period (of less than 6 months) and a
small sample size, thereby making interpretation of the data difficult.
Even although some of these interventional studies have shown a
decrease in rheumatoid arthritis disease activity after periodontal
therapy,134-140 there are also studies not reporting any impact.141-143
Similarly, in a 3-month randomized clinical trial, Monsarrat et al142
could not demonstrate a statistically significant reduction in 28-joint
disease activity score with erythrocyte sedimentation rate, although
this study had a very short follow-up, and unspecified periodon-
titis case selection and rheumatoid arthritis disease activity score
criteria.
A recent prospective case-controlled clinical intervention trial in
15 rheumatoid arthritis patients with periodontitis and 18 healthy
periodontitis patients reported a significant decrease in 28-joint
disease activity score with erythrocyte sedimentation rate and
C-reactive protein levels in the rheumatoid arthritis group 6 months
after nonsurgical periodontal therapy.144 Similarly, in another study
of 64 subjects—distributed into four groups: (a) healthy controls
(P-RA-), (b) periodontitis patients without rheumatoid arthritis
(P + RA−), (c) rheumatoid arthritis patients without periodontitis (P-RA+), and (d) rheumatoid arthritis patients with periodontitis
(P + RA+)—there was a statistically significant reduction in eryth-
rocyte sedimentation rate, C-reactive protein, anti-citrullinated pro-
tein antibodies, and 28-joint disease activity score with erythrocyte
sedimentation rate in rheumatoid arthritis patients with periodonti-
tis 1 month after periodontal treatment,105
Because of this limited yet compelling evidence, there is a need
for randomized controlled trials with larger samples sizes and lon-
ger follow-up to fully understand the impact of periodontal therapy
on the progression of rheumatoid arthritis and its effect on disease
activity. Furthermore, there is a need to evaluate the impact of re-
ducing bacterial loads, specifically the levels of Po. gingivalis and A. actinomycetemcomitans, on anti-citrullinated protein antibodies ti-
ters (Figure 1).
6 | IMPLIC ATIONS FOR PRE VENTION AND THERAPY
In an editorial article, Marotte145 discussed nonsurgical peri-
odontal treatment as a preventive and therapeutic tool in the
comprehensive treatment of the rheumatoid arthritis patient. He
concluded that good oral hygiene measures and periodontal treat-
ment should be integrated into the management of rheumatoid
arthritis, and rheumatologists should ensure that periodontal care
and long-term periodontal status evaluation is provided for these
subjects.
Since both periodontal inflammation106,113 and the presence of
high numbers of periodontal pathogenic bacteria may play a signif-
icant role in the citrullination process, which is key in rheumatoid
arthritis development104 and/or disease activity,63 preventive and
therapeutic measures to control both inflammation and microorgan-
isms seem appropriate in the management of periodontitis patients
with rheumatoid arthritis. These measures should probably be im-
plemented before rheumatoid arthritis treatment, as indicated by a
retrospective study of 54 rheumatoid arthritis patients receiving bi-
ologic disease-modifying antirheumatic drugs.146 These patients had
a significant correlation between baseline periodontal inflammation
evaluated by the periodontal inflamed surface area and rheumatoid
arthritis disease clinical activity, swollen joint counts, and the pa-
tients’ and evaluators’ global assessment. These relationships were
again demonstrated in an interventional study, where a substantial
number of subjects with severe periodontitis and rheumatoid arthri-
tis did not respond appropriately to several rounds of synthetic and
biologic disease-modifying antirheumatic drugs.147 However, in five
out of eight of those nonresponder patients, there was a good re-
sponse in 28-joint disease activity score with erythrocyte sedimen-
tation rate following nonsurgical periodontal therapy, thus indicating
that a healthy periodontal status may be important for the compre-
hensive treatment of rheumatoid arthritis.
7 | CONCLUSIONS
Periodontitis has been directly associated with rheumatoid arthri-
tis, in which the presence of both periodontal inflammation and
high numbers of periodontopathic bacteria have been associated
with the onset of rheumatoid arthritis and increased rheumatoid
arthritis disease activity. Furthermore, the presence of periodon-
tal inflammation appears to affect rheumatoid arthritis treatment
when using synthetic and biologic disease-modifying antirheu-
matic drugs, since it reduces their efficacy. On the other hand,
nonsurgical periodontal therapy seems to play a role in the con-
trol of rheumatoid arthritis disease activity, through the reduction
of C-reactive protein, erythrocyte sedimentation rate, 28-joint
disease activity score with erythrocyte sedimentation rate, and
rheumatoid arthritis disease clinical activity levels, and also by
improving the control of rheumatoid arthritis activity in patients
55
58
59
60
61 62
63
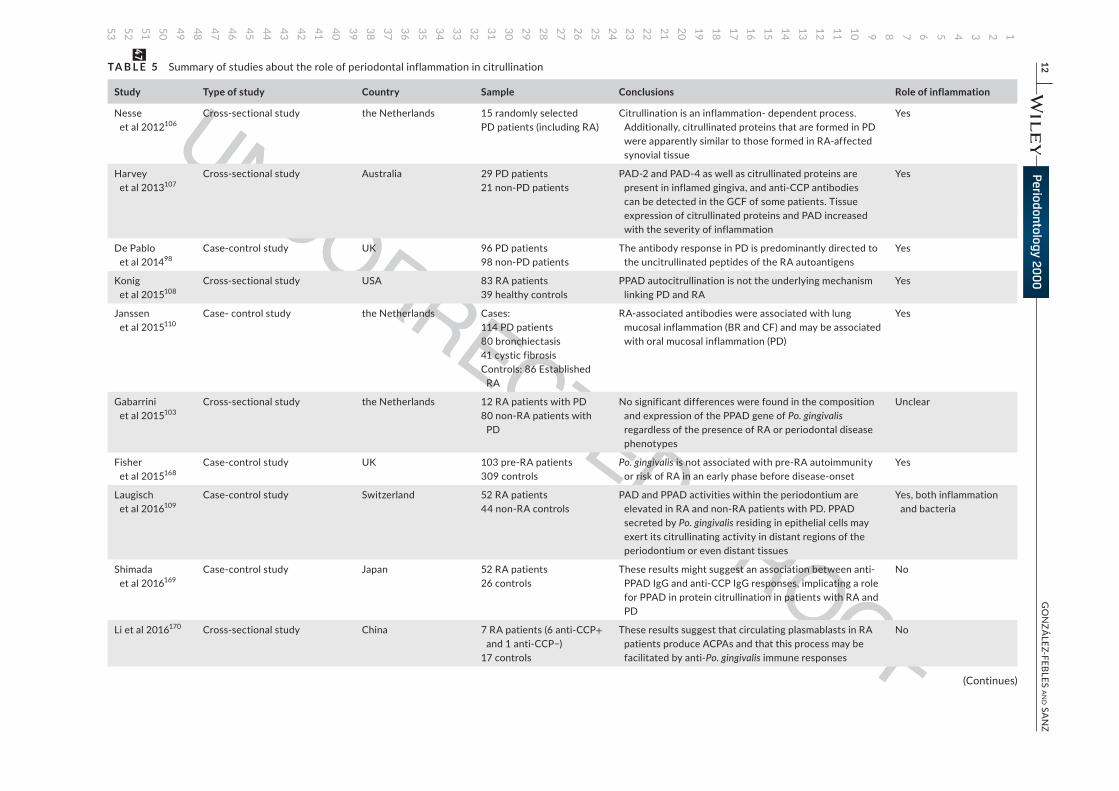
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
12 |
GO
NZÁ
LEZ-FEBLES aN
d SaN
ZTA B L E 5 Summary of studies about the role of periodontal inflammation in citrullination
Study Type of study Country Sample Conclusions Role of inflammation
Nesse et al 2012106
Cross-sectional study the Netherlands 15 randomly selectedPD patients (including RA)
Citrullination is an inflammation- dependent process. Additionally, citrullinated proteins that are formed in PD were apparently similar to those formed in RA-affected synovial tissue
Yes
Harvey et al 2013107
Cross-sectional study Australia 29 PD patients21 non-PD patients
PAD-2 and PAD-4 as well as citrullinated proteins are present in inflamed gingiva, and anti-CCP antibodies can be detected in the GCF of some patients. Tissue expression of citrullinated proteins and PAD increased with the severity of inflammation
Yes
De Pablo et al 201498
Case-control study UK 96 PD patients98 non-PD patients
The antibody response in PD is predominantly directed to the uncitrullinated peptides of the RA autoantigens
Yes
Konig et al 2015108
Cross-sectional study USA 83 RA patients39 healthy controls
PPAD autocitrullination is not the underlying mechanism linking PD and RA
Yes
Janssen et al 2015110
Case- control study the Netherlands Cases:114 PD patients80 bronchiectasis41 cystic fibrosisControls: 86 Established
RA
RA-associated antibodies were associated with lung mucosal inflammation (BR and CF) and may be associated with oral mucosal inflammation (PD)
Yes
Gabarrini et al 2015103
Cross-sectional study the Netherlands 12 RA patients with PD80 non-RA patients with
PD
No significant differences were found in the composition and expression of the PPAD gene of Po. gingivalis regardless of the presence of RA or periodontal disease phenotypes
Unclear
Fisher et al 2015168
Case-control study UK 103 pre-RA patients309 controls
Po. gingivalis is not associated with pre-RA autoimmunity or risk of RA in an early phase before disease-onset
Yes
Laugisch et al 2016109
Case-control study Switzerland 52 RA patients44 non-RA controls
PAD and PPAD activities within the periodontium are elevated in RA and non-RA patients with PD. PPAD secreted by Po. gingivalis residing in epithelial cells may exert its citrullinating activity in distant regions of the periodontium or even distant tissues
Yes, both inflammation and bacteria
Shimada et al 2016169
Case-control study Japan 52 RA patients26 controls
These results might suggest an association between anti-PPAD IgG and anti-CCP IgG responses, implicating a role for PPAD in protein citrullination in patients with RA and PD
No
Li et al 2016170 Cross-sectional study China 7 RA patients (6 anti-CCP+ and 1 anti-CCP−)
17 controls
These results suggest that circulating plasmablasts in RA patients produce ACPAs and that this process may be facilitated by anti-Po. gingivalis immune responses
No
(Continues)
47
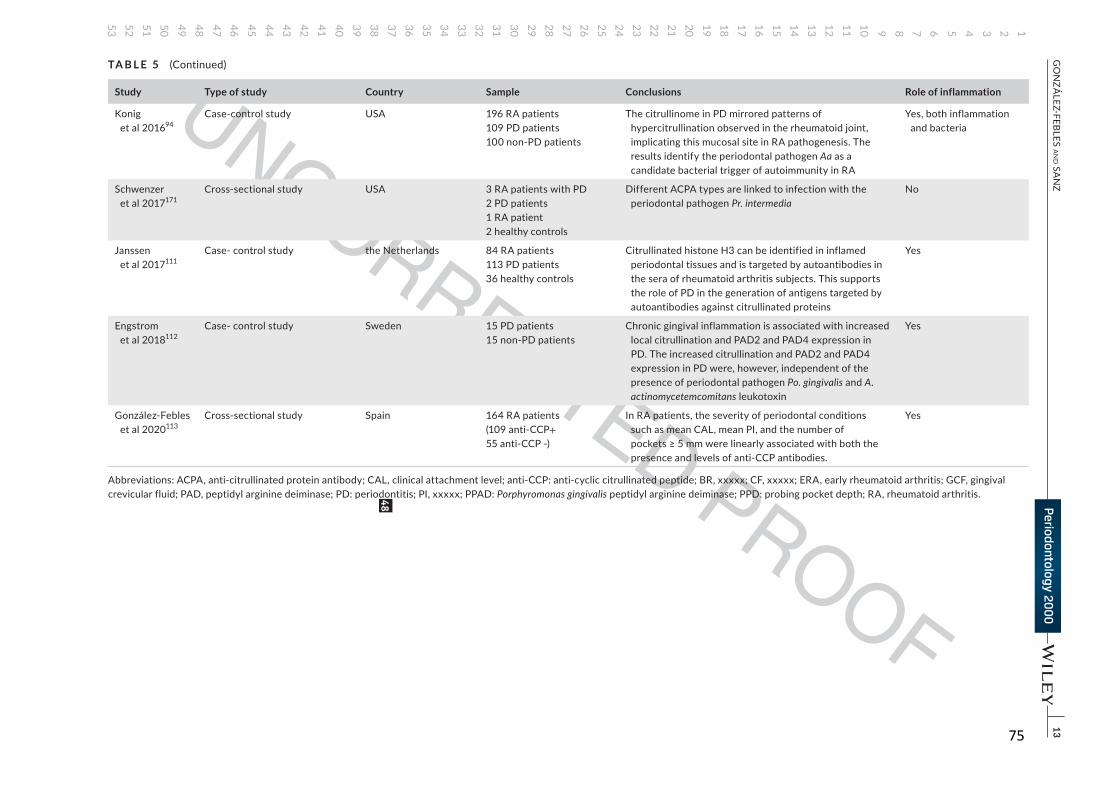
75
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
|
13G
ON
ZÁLEZ-FEBLES a
Nd Sa
NZ
Study Type of study Country Sample Conclusions Role of inflammation
Konig
et al 201694
Case-control study USA 196 RA patients
109 PD patients
100 non-PD patients
The citrullinome in PD mirrored patterns of
hypercitrullination observed in the rheumatoid joint,
implicating this mucosal site in RA pathogenesis. The
results identify the periodontal pathogen Aa as a
candidate bacterial trigger of autoimmunity in RA
Yes, both inflammation
and bacteria
Schwenzer
et al 2017171
Cross-sectional study USA 3 RA patients with PD
2 PD patients
1 RA patient
2 healthy controls
Different ACPA types are linked to infection with the
periodontal pathogen Pr. intermediaNo
Janssen
et al 2017111
Case- control study the Netherlands 84 RA patients
113 PD patients
36 healthy controls
Citrullinated histone H3 can be identified in inflamed
periodontal tissues and is targeted by autoantibodies in
the sera of rheumatoid arthritis subjects. This supports
the role of PD in the generation of antigens targeted by
autoantibodies against citrullinated proteins
Yes
Engstrom
et al 2018112
Case- control study Sweden 15 PD patients
15 non-PD patients
Chronic gingival inflammation is associated with increased
local citrullination and PAD2 and PAD4 expression in
PD. The increased citrullination and PAD2 and PAD4
expression in PD were, however, independent of the
presence of periodontal pathogen Po. gingivalis and A. actinomycetemcomitans leukotoxin
Yes
González-Febles
et al 2020113
Cross-sectional study Spain 164 RA patients
(109 anti-CCP+55 anti-CCP -)
In RA patients, the severity of periodontal conditions
such as mean CAL, mean PI, and the number of
pockets ≥ 5 mm were linearly associated with both the presence and levels of anti-CCP antibodies.
Yes
Abbreviations: ACPA, anti-citrullinated protein antibody; CAL, clinical attachment level; anti-CCP: anti-cyclic citrullinated peptide; BR, xxxxx; CF, xxxxx; ERA, early rheumatoid arthritis; GCF, gingival
crevicular fluid; PAD, peptidyl arginine deiminase; PD: periodontitis; PI, xxxxx; PPAD: Porphyromonas gingivalis peptidyl arginine deiminase; PPD: probing pocket depth; RA, rheumatoid arthritis.
TA B L E 5 (Continued)
48
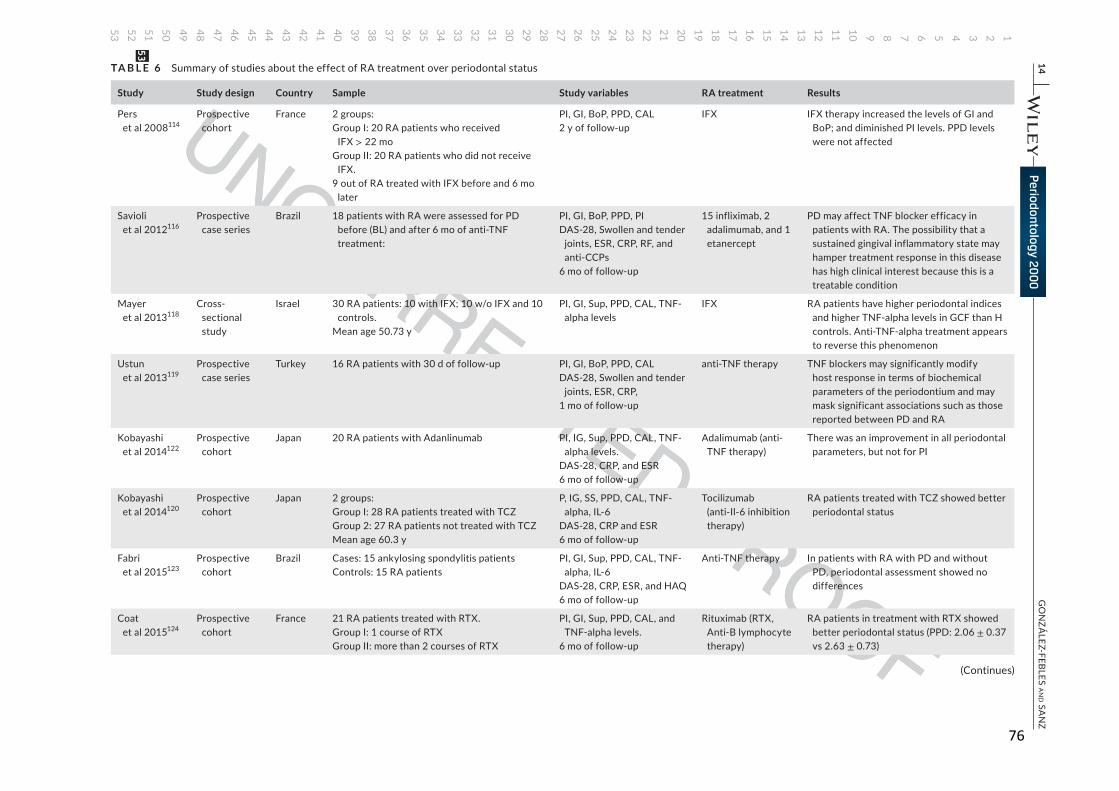
76
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
14 |
GO
NZÁ
LEZ-FEBLES aN
d SaN
ZTA B L E 6 Summary of studies about the effect of RA treatment over periodontal status
Study Study design Country Sample Study variables RA treatment Results
Pers
et al 2008114
Prospective
cohort
France 2 groups:
Group I: 20 RA patients who received
IFX > 22 mo
Group II: 20 RA patients who did not receive
IFX.
9 out of RA treated with IFX before and 6 mo
later
PI, GI, BoP, PPD, CAL
2 y of follow-up
IFX IFX therapy increased the levels of GI and
BoP; and diminished PI levels. PPD levels
were not affected
Savioli
et al 2012116
Prospective
case series
Brazil 18 patients with RA were assessed for PD
before (BL) and after 6 mo of anti-TNF
treatment:
PI, GI, BoP, PPD, PI
DAS-28, Swollen and tender
joints, ESR, CRP, RF, and
anti-CCPs
6 mo of follow-up
15 infliximab, 2
adalimumab, and 1
etanercept
PD may affect TNF blocker efficacy in
patients with RA. The possibility that a
sustained gingival inflammatory state may
hamper treatment response in this disease
has high clinical interest because this is a
treatable condition
Mayer
et al 2013118
Cross-
sectional
study
Israel 30 RA patients: 10 with IFX; 10 w/o IFX and 10
controls.
Mean age 50.73 y
PI, GI, Sup, PPD, CAL, TNF-
alpha levels
IFX RA patients have higher periodontal indices
and higher TNF-alpha levels in GCF than H
controls. Anti-TNF-alpha treatment appears
to reverse this phenomenon
Ustun
et al 2013119
Prospective
case series
Turkey 16 RA patients with 30 d of follow-up PI, GI, BoP, PPD, CAL
DAS-28, Swollen and tender
joints, ESR, CRP,
1 mo of follow-up
anti-TNF therapy TNF blockers may significantly modify
host response in terms of biochemical
parameters of the periodontium and may
mask significant associations such as those
reported between PD and RA
Kobayashi
et al 2014122
Prospective
cohort
Japan 20 RA patients with Adanlinumab PI, IG, Sup, PPD, CAL, TNF-
alpha levels.
DAS-28, CRP, and ESR
6 mo of follow-up
Adalimumab (anti-
TNF therapy)
There was an improvement in all periodontal
parameters, but not for PI
Kobayashi
et al 2014120
Prospective
cohort
Japan 2 groups:
Group I: 28 RA patients treated with TCZ
Group 2: 27 RA patients not treated with TCZ
Mean age 60.3 y
P, IG, SS, PPD, CAL, TNF-
alpha, IL-6
DAS-28, CRP and ESR
6 mo of follow-up
Tocilizumab
(anti-Il-6 inhibition
therapy)
RA patients treated with TCZ showed better
periodontal status
Fabri
et al 2015123
Prospective
cohort
Brazil Cases: 15 ankylosing spondylitis patients
Controls: 15 RA patients
PI, GI, Sup, PPD, CAL, TNF-
alpha, IL-6
DAS-28, CRP, ESR, and HAQ
6 mo of follow-up
Anti-TNF therapy In patients with RA with PD and without
PD, periodontal assessment showed no
differences
Coat
et al 2015124
Prospective
cohort
France 21 RA patients treated with RTX.
Group I: 1 course of RTX
Group II: more than 2 courses of RTX
PI, GI, Sup, PPD, CAL, and
TNF-alpha levels.
6 mo of follow-up
Rituximab (RTX,
Anti-B lymphocyte
therapy)
RA patients in treatment with RTX showed
better periodontal status (PPD: 2.06 ± 0.37
vs 2.63 ± 0.73)
(Continues)
53
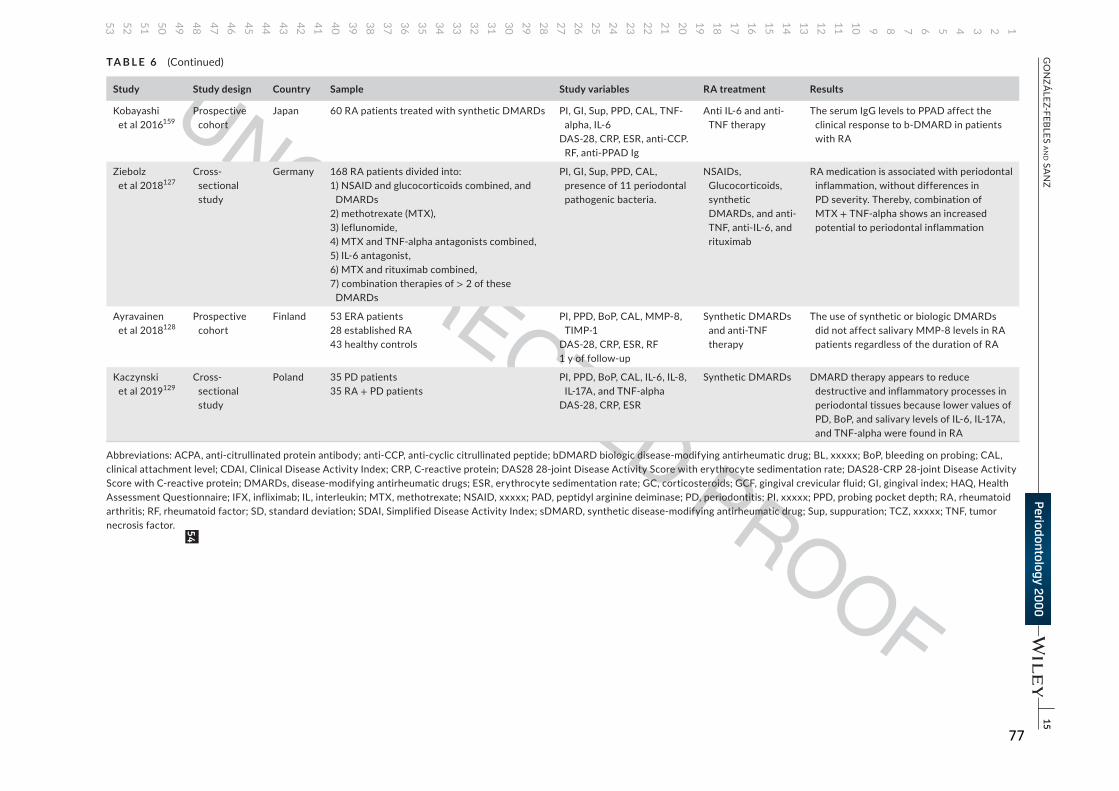
77
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
|
15G
ON
ZÁLEZ-FEBLES a
Nd Sa
NZ
Study Study design Country Sample Study variables RA treatment Results
Kobayashi et al 2016159
Prospective cohort
Japan 60 RA patients treated with synthetic DMARDs PI, GI, Sup, PPD, CAL, TNF- alpha, IL-6
DAS-28, CRP, ESR, anti-CCP. RF, anti-PPAD Ig
Anti IL-6 and anti-TNF therapy
The serum IgG levels to PPAD affect the clinical response to b-DMARD in patients with RA
Ziebolz et al 2018127
Cross-sectional study
Germany 168 RA patients divided into:1) NSAID and glucocorticoids combined, and
DMARDs2) methotrexate (MTX),3) leflunomide,4) MTX and TNF-alpha antagonists combined,5) IL-6 antagonist,6) MTX and rituximab combined,7) combination therapies of > 2 of these
DMARDs
PI, GI, Sup, PPD, CAL, presence of 11 periodontal pathogenic bacteria.
NSAIDs, Glucocorticoids, synthetic DMARDs, and anti-TNF, anti-IL-6, and rituximab
RA medication is associated with periodontal inflammation, without differences in PD severity. Thereby, combination of MTX + TNF-alpha shows an increased potential to periodontal inflammation
Ayravainen et al 2018128
Prospective cohort
Finland 53 ERA patients28 established RA43 healthy controls
PI, PPD, BoP, CAL, MMP-8, TIMP-1
DAS-28, CRP, ESR, RF1 y of follow-up
Synthetic DMARDs and anti-TNF therapy
The use of synthetic or biologic DMARDs did not affect salivary MMP-8 levels in RA patients regardless of the duration of RA
Kaczynski et al 2019129
Cross-sectional study
Poland 35 PD patients35 RA + PD patients
PI, PPD, BoP, CAL, IL-6, IL-8, IL-17A, and TNF-alpha
DAS-28, CRP, ESR
Synthetic DMARDs DMARD therapy appears to reduce destructive and inflammatory processes in periodontal tissues because lower values of PD, BoP, and salivary levels of IL-6, IL-17A, and TNF-alpha were found in RA
Abbreviations: ACPA, anti-citrullinated protein antibody; anti-CCP, anti-cyclic citrullinated peptide; bDMARD biologic disease-modifying antirheumatic drug; BL, xxxxx; BoP, bleeding on probing; CAL, clinical attachment level; CDAI, Clinical Disease Activity Index; CRP, C-reactive protein; DAS28 28-joint Disease Activity Score with erythrocyte sedimentation rate; DAS28-CRP 28-joint Disease Activity Score with C-reactive protein; DMARDs, disease-modifying antirheumatic drugs; ESR, erythrocyte sedimentation rate; GC, corticosteroids; GCF, gingival crevicular fluid; GI, gingival index; HAQ, Health Assessment Questionnaire; IFX, infliximab; IL, interleukin; MTX, methotrexate; NSAID, xxxxx; PAD, peptidyl arginine deiminase; PD, periodontitis; PI, xxxxx; PPD, probing pocket depth; RA, rheumatoid arthritis; RF, rheumatoid factor; SD, standard deviation; SDAI, Simplified Disease Activity Index; sDMARD, synthetic disease-modifying antirheumatic drug; Sup, suppuration; TCZ, xxxxx; TNF, tumor necrosis factor.
TA B L E 6 (Continued)
54
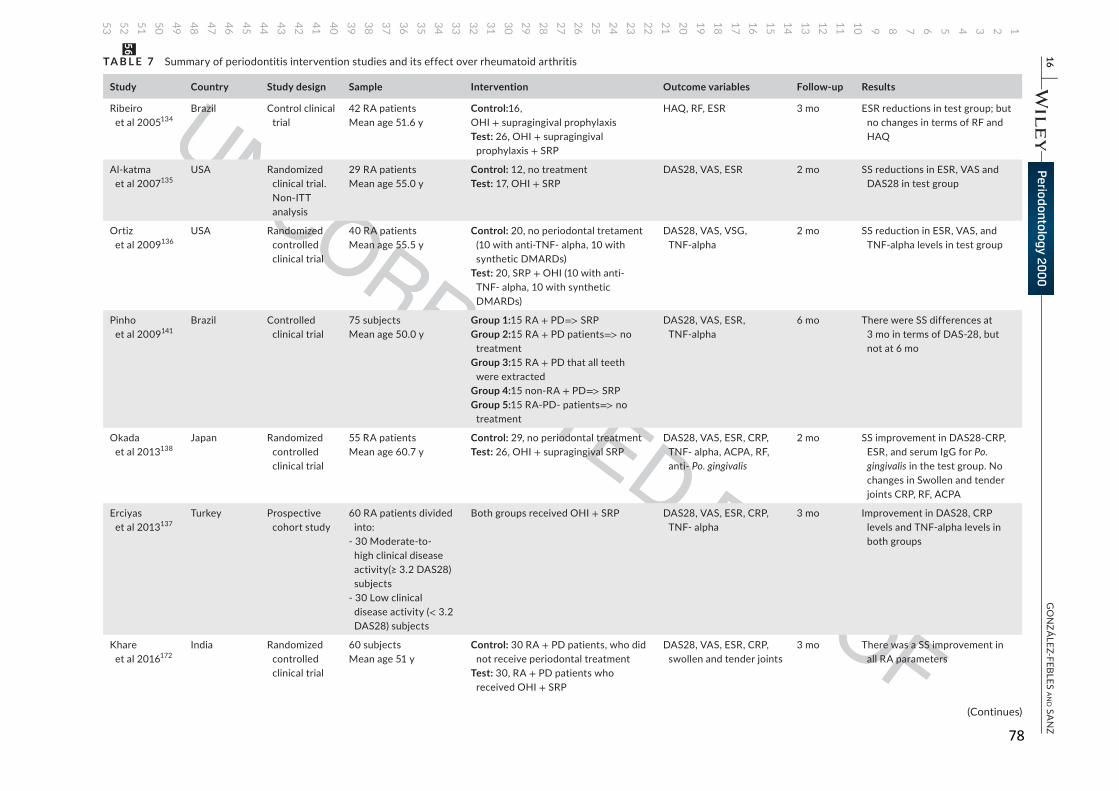
78
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
16 |
GO
NZÁ
LEZ-FEBLES aN
d SaN
ZTA B L E 7 Summary of periodontitis intervention studies and its effect over rheumatoid arthritis
Study Country Study design Sample Intervention Outcome variables Follow-up Results
Ribeiro
et al 2005134
Brazil Control clinical
trial
42 RA patients
Mean age 51.6 y
Control:16,
OHI + supragingival prophylaxis
Test: 26, OHI + supragingival
prophylaxis + SRP
HAQ, RF, ESR 3 mo ESR reductions in test group; but
no changes in terms of RF and
HAQ
Al-katma
et al 2007135
USA Randomized
clinical trial.
Non-ITT
analysis
29 RA patients
Mean age 55.0 y
Control: 12, no treatment
Test: 17, OHI + SRP
DAS28, VAS, ESR 2 mo SS reductions in ESR, VAS and
DAS28 in test group
Ortiz
et al 2009136
USA Randomized
controlled
clinical trial
40 RA patients
Mean age 55.5 y
Control: 20, no periodontal tretament
(10 with anti-TNF- alpha, 10 with
synthetic DMARDs)
Test: 20, SRP + OHI (10 with anti-
TNF- alpha, 10 with synthetic
DMARDs)
DAS28, VAS, VSG,
TNF-alpha
2 mo SS reduction in ESR, VAS, and
TNF-alpha levels in test group
Pinho
et al 2009141
Brazil Controlled
clinical trial
75 subjects
Mean age 50.0 y
Group 1:15 RA + PD=> SRP
Group 2:15 RA + PD patients=> no
treatment
Group 3:15 RA + PD that all teeth
were extracted
Group 4:15 non-RA + PD=> SRP
Group 5:15 RA-PD- patients=> no
treatment
DAS28, VAS, ESR,
TNF-alpha
6 mo There were SS differences at
3 mo in terms of DAS-28, but
not at 6 mo
Okada
et al 2013138
Japan Randomized
controlled
clinical trial
55 RA patients
Mean age 60.7 y
Control: 29, no periodontal treatment
Test: 26, OHI + supragingival SRP
DAS28, VAS, ESR, CRP,
TNF- alpha, ACPA, RF,
anti- Po. gingivalis
2 mo SS improvement in DAS28-CRP,
ESR, and serum IgG for Po. gingivalis in the test group. No
changes in Swollen and tender
joints CRP, RF, ACPA
Erciyas
et al 2013137
Turkey Prospective
cohort study
60 RA patients divided
into:
- 30 Moderate-to-
high clinical disease
activity(≥ 3.2 DAS28) subjects
- 30 Low clinical
disease activity (< 3.2
DAS28) subjects
Both groups received OHI + SRP DAS28, VAS, ESR, CRP,
TNF- alpha
3 mo Improvement in DAS28, CRP
levels and TNF-alpha levels in
both groups
Khare
et al 2016172
India Randomized
controlled
clinical trial
60 subjects
Mean age 51 y
Control: 30 RA + PD patients, who did
not receive periodontal treatment
Test: 30, RA + PD patients who
received OHI + SRP
DAS28, VAS, ESR, CRP,
swollen and tender joints
3 mo There was a SS improvement in
all RA parameters
(Continues)
56
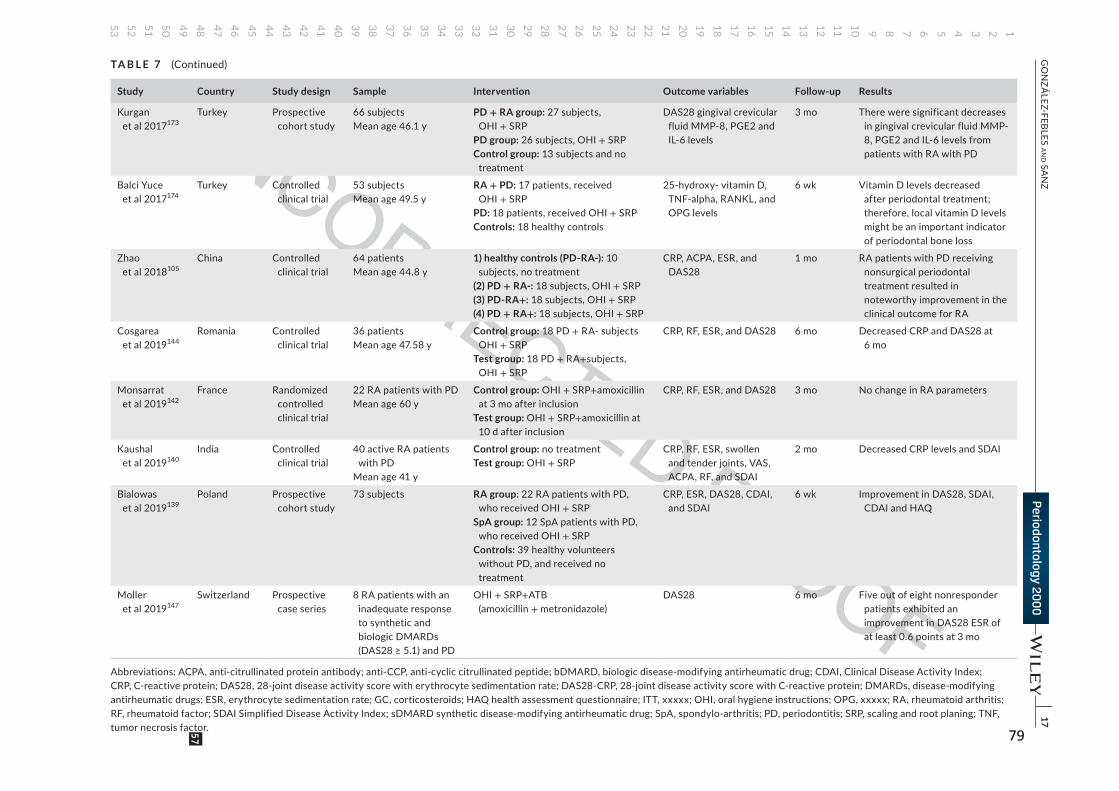
79
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
|
17G
ON
ZÁLEZ-FEBLES a
Nd Sa
NZ
Study Country Study design Sample Intervention Outcome variables Follow-up Results
Kurgan et al 2017173
Turkey Prospective cohort study
66 subjectsMean age 46.1 y
PD + RA group: 27 subjects, OHI + SRP
PD group: 26 subjects, OHI + SRPControl group: 13 subjects and no
treatment
DAS28 gingival crevicular fluid MMP-8, PGE2 and IL-6 levels
3 mo There were significant decreases in gingival crevicular fluid MMP-8, PGE2 and IL-6 levels from patients with RA with PD
Balci Yuce et al 2017174
Turkey Controlled clinical trial
53 subjectsMean age 49.5 y
RA + PD: 17 patients, received OHI + SRP
PD: 18 patients, received OHI + SRPControls: 18 healthy controls
25-hydroxy- vitamin D, TNF-alpha, RANKL, and OPG levels
6 wk Vitamin D levels decreased after periodontal treatment; therefore, local vitamin D levels might be an important indicator of periodontal bone loss
Zhao et al 2018105
China Controlled clinical trial
64 patientsMean age 44.8 y
1) healthy controls (PD-RA-): 10 subjects, no treatment
(2) PD + RA-: 18 subjects, OHI + SRP(3) PD-RA+: 18 subjects, OHI + SRP(4) PD + RA+: 18 subjects, OHI + SRP
CRP, ACPA, ESR, and DAS28
1 mo RA patients with PD receiving nonsurgical periodontal treatment resulted in noteworthy improvement in the clinical outcome for RA
Cosgarea et al 2019144
Romania Controlled clinical trial
36 patientsMean age 47.58 y
Control group: 18 PD + RA- subjects OHI + SRP
Test group: 18 PD + RA+subjects, OHI + SRP
CRP, RF, ESR, and DAS28 6 mo Decreased CRP and DAS28 at 6 mo
Monsarrat et al 2019142
France Randomized controlled clinical trial
22 RA patients with PDMean age 60 y
Control group: OHI + SRP+amoxicillin at 3 mo after inclusion
Test group: OHI + SRP+amoxicillin at 10 d after inclusion
CRP, RF, ESR, and DAS28 3 mo No change in RA parameters
Kaushal et al 2019140
India Controlled clinical trial
40 active RA patients with PD
Mean age 41 y
Control group: no treatmentTest group: OHI + SRP
CRP, RF, ESR, swollen and tender joints, VAS, ACPA, RF, and SDAI
2 mo Decreased CRP levels and SDAI
Bialowas et al 2019139
Poland Prospective cohort study
73 subjects RA group: 22 RA patients with PD, who received OHI + SRP
SpA group: 12 SpA patients with PD, who received OHI + SRP
Controls: 39 healthy volunteers without PD, and received no treatment
CRP, ESR, DAS28, CDAI, and SDAI
6 wk Improvement in DAS28, SDAI, CDAI and HAQ
Moller et al 2019147
Switzerland Prospective case series
8 RA patients with an inadequate response to synthetic and biologic DMARDs (DAS28 ≥ 5.1) and PD
OHI + SRP+ATB (amoxicillin + metronidazole)
DAS28 6 mo Five out of eight nonresponder patients exhibited an improvement in DAS28 ESR of at least 0.6 points at 3 mo
Abbreviations: ACPA, anti-citrullinated protein antibody; anti-CCP, anti-cyclic citrullinated peptide; bDMARD, biologic disease-modifying antirheumatic drug; CDAI, Clinical Disease Activity Index; CRP, C-reactive protein; DAS28, 28-joint disease activity score with erythrocyte sedimentation rate; DAS28-CRP, 28-joint disease activity score with C-reactive protein; DMARDs, disease-modifying antirheumatic drugs; ESR, erythrocyte sedimentation rate; GC, corticosteroids; HAQ health assessment questionnaire; ITT, xxxxx; OHI, oral hygiene instructions; OPG, xxxxx; RA, rheumatoid arthritis; RF, rheumatoid factor; SDAI Simplified Disease Activity Index; sDMARD synthetic disease-modifying antirheumatic drug; SpA, spondylo-arthritis; PD, periodontitis; SRP, scaling and root planing; TNF, tumor necrosis factor.
TA B L E 7 (Continued)
57
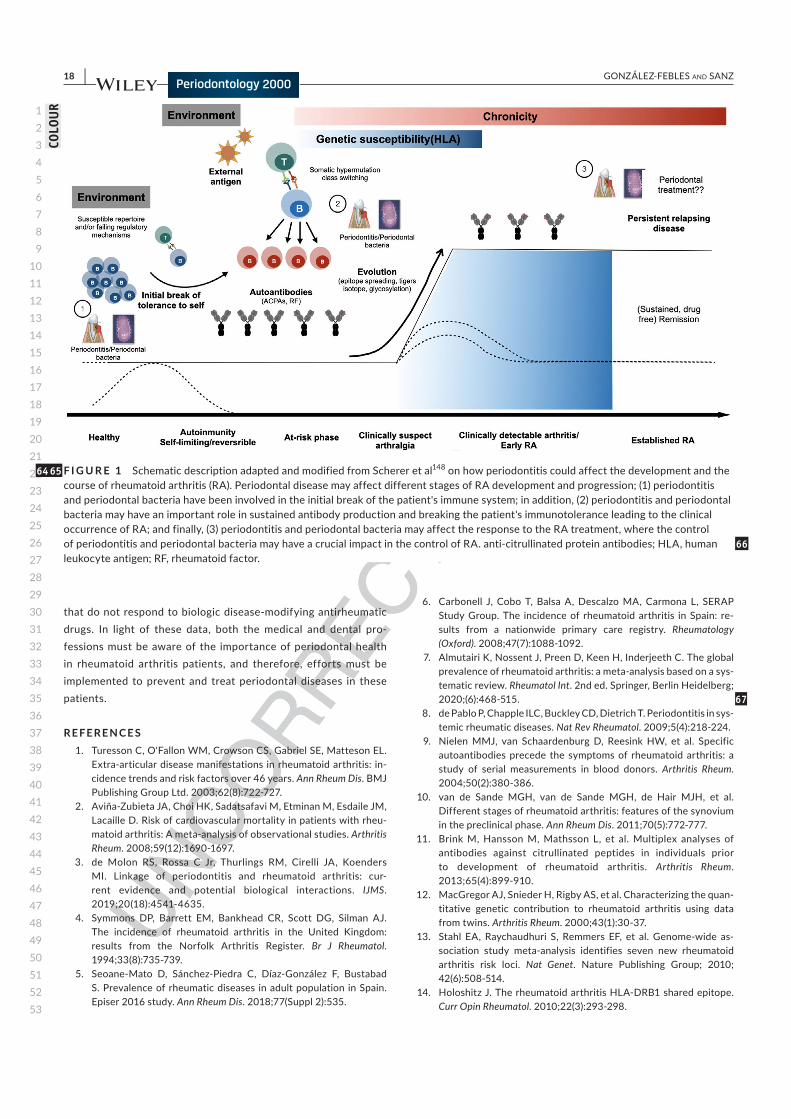
123456789
1011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
18 | GONZÁLEZ-FEBLES aNd SaNZ
that do not respond to biologic disease-modifying antirheumatic
drugs. In light of these data, both the medical and dental pro-
fessions must be aware of the importance of periodontal health
in rheumatoid arthritis patients, and therefore, efforts must be
implemented to prevent and treat periodontal diseases in these
patients.
REFERENCES 1. Turesson C, O'Fallon WM, Crowson CS, Gabriel SE, Matteson EL.
Extra-articular disease manifestations in rheumatoid arthritis: in-cidence trends and risk factors over 46 years. Ann Rheum Dis. BMJ Publishing Group Ltd. 2003;62(8):722-727.
2. Aviña-Zubieta JA, Choi HK, Sadatsafavi M, Etminan M, Esdaile JM, Lacaille D. Risk of cardiovascular mortality in patients with rheu-matoid arthritis: A meta-analysis of observational studies. Arthritis Rheum. 2008;59(12):1690-1697.
3. de Molon RS, Rossa C Jr, Thurlings RM, Cirelli JA, Koenders MI. Linkage of periodontitis and rheumatoid arthritis: cur-rent evidence and potential biological interactions. IJMS. 2019;20(18):4541-4635.
4. Symmons DP, Barrett EM, Bankhead CR, Scott DG, Silman AJ. The incidence of rheumatoid arthritis in the United Kingdom: results from the Norfolk Arthritis Register. Br J Rheumatol. 1994;33(8):735-739.
5. Seoane-Mato D, Sánchez-Piedra C, Díaz-González F, Bustabad S. Prevalence of rheumatic diseases in adult population in Spain. Episer 2016 study. Ann Rheum Dis. 2018;77(Suppl 2):535.
6. Carbonell J, Cobo T, Balsa A, Descalzo MA, Carmona L, SERAP Study Group. The incidence of rheumatoid arthritis in Spain: re-sults from a nationwide primary care registry. Rheumatology (Oxford). 2008;47(7):1088-1092.
7. Almutairi K, Nossent J, Preen D, Keen H, Inderjeeth C. The global prevalence of rheumatoid arthritis: a meta-analysis based on a sys-tematic review. Rheumatol Int. 2nd ed. Springer, Berlin Heidelberg; 2020;(6):468-515.
8. de Pablo P, Chapple ILC, Buckley CD, Dietrich T. Periodontitis in sys-temic rheumatic diseases. Nat Rev Rheumatol. 2009;5(4):218-224.
9. Nielen MMJ, van Schaardenburg D, Reesink HW, et al. Specific autoantibodies precede the symptoms of rheumatoid arthritis: a study of serial measurements in blood donors. Arthritis Rheum. 2004;50(2):380-386.
10. van de Sande MGH, van de Sande MGH, de Hair MJH, et al. Different stages of rheumatoid arthritis: features of the synovium in the preclinical phase. Ann Rheum Dis. 2011;70(5):772-777.
11. Brink M, Hansson M, Mathsson L, et al. Multiplex analyses of antibodies against citrullinated peptides in individuals prior to development of rheumatoid arthritis. Arthritis Rheum. 2013;65(4):899-910.
12. MacGregor AJ, Snieder H, Rigby AS, et al. Characterizing the quan-titative genetic contribution to rheumatoid arthritis using data from twins. Arthritis Rheum. 2000;43(1):30-37.
13. Stahl EA, Raychaudhuri S, Remmers EF, et al. Genome-wide as-sociation study meta-analysis identifies seven new rheumatoid arthritis risk loci. Nat Genet. Nature Publishing Group; 2010; 42(6):508-514.
14. Holoshitz J. The rheumatoid arthritis HLA-DRB1 shared epitope. Curr Opin Rheumatol. 2010;22(3):293-298.
F I G U R E 1 Schematic description adapted and modified from Scherer et al148 on how periodontitis could affect the development and the course of rheumatoid arthritis (RA). Periodontal disease may affect different stages of RA development and progression; (1) periodontitis and periodontal bacteria have been involved in the initial break of the patient's immune system; in addition, (2) periodontitis and periodontal bacteria may have an important role in sustained antibody production and breaking the patient's immunotolerance leading to the clinical occurrence of RA; and finally, (3) periodontitis and periodontal bacteria may affect the response to the RA treatment, where the control of periodontitis and periodontal bacteria may have a crucial impact in the control of RA. anti-citrullinated protein antibodies; HLA, human leukocyte antigen; RF, rheumatoid factor.
6465
66
67
COLO
UR
81
123456789
1011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
| 19GONZÁLEZ-FEBLES aNd SaNZ
15. Begovich AB, Carlton VEH, Honigberg LA, et al. A missense sin-gle-nucleotide polymorphism in a gene encoding a protein tyrosine phosphatase (PTPN22) is associated with rheumatoid arthritis. Am J Hum Genet. 2004;75(2):330-337.
16. Lie BA, Viken MK, Odegård S, et al. Associations between the PTPN22 1858C->T polymorphism and radiographic joint destruc-tion in patients with rheumatoid arthritis: results from a 10-year longitudinal study. Ann Rheum Dis. 2007;66(12):1604-1609.
17. Bottini N, Firestein GS. Epigenetics in rheumatoid arthritis: a primer for rheumatologists. Curr Rheumatol Rep. 2013;15(11):372-411.
18. Suzuki A, Yamada R, Chang X, et al. Functional haplotypes of PADI4, encoding citrullinating enzyme peptidylarginine deimi-nase 4, are associated with rheumatoid arthritis. Nat Genet. 2003;34(4):395-402.
19. Martinez A, Valdivia A, Pascual-Salcedo D, et al. PADI4 polymor-phisms are not associated with rheumatoid arthritis in the Spanish population. Rheumatology. 2005;44(10):1263-1266.
20. Barton A, Bowes J, Eyre S, et al. A functional haplotype of the PADI4 gene associated with rheumatoid arthritis in a Japanese population is not associated in a United Kingdom population. Arthritis Rheum. 2004;50(4):1117-1121.
21. Karlson EW, Lee IM, Cook NR, Manson JE, Buring JE, Hennekens CH. A retrospective cohort study of cigarette smoking and risk of rheumatoid arthritis in female health professionals. Arthritis Rheum. 1999;42(5):910-917.
22. Wolfe F. The effect of smoking on clinical, laboratory, and radiographic status in rheumatoid arthritis. J Rheumatol. 2000;27(3):630-637.
23. Liao KP, Alfredsson L, Karlson EW. Environmental influences on risk for rheumatoid arthritis. Curr Opin Rheumatol. 2009;21(3):279-283.
24. Pedersen M, Jacobsen S, Garred P, et al. Strong combined gene-en-vironment effects in anti-cyclic citrullinated peptide-positive rheumatoid arthritis: a nationwide case-control study in Denmark. Arthritis Rheum. 2007;56(5):1446-1453.
25. Demoruelle MK, Weisman MH, Simonian PL, et al. Brief report: airways abnormalities and rheumatoid arthritis-related autoanti-bodies in subjects without arthritis: early injury or initiating site of autoimmunity? Arthritis Rheum. 2012;64(6):1756-1761.
26. Klareskog L, Malmström V, Lundberg K, Padyukov L, Alfredsson L. Smoking, citrullination and genetic variability in the im-munopathogenesis of rheumatoid arthritis. Semin Immunol. 2011;23(2):92-98.
27. Khuder SA, Peshimam AZ, Agraharam S. Environmental risk factors for rheumatoid arthritis. Rev Environ Health. 2002;17(4):307-315.
28. Cooper GS. Occupational exposures and risk of rheumatoid ar-thritis: continued advances and opportunities for research. J Rheumatol. 2008;35(6):950-952.
29. Webber MP, Moir W, Zeig-Owens R, et al. Nested case-con-trol study of selected systemic autoimmune diseases in World Trade Center rescue/recovery workers. Arthritis Rheumatol. 2015;67(5):1369-1376.
30. Lu B, Hiraki LT, Sparks JA, et al. Being overweight or obese and risk of developing rheumatoid arthritis among women: a prospective cohort study. Ann Rheum Dis. 2014;73(11):1914-1922.
31. Li S, Yu Y, Yue Y, Zhang Z, Su K. Microbial infection and rheumatoid arthritis. J Clin Cell Immunol. 2013;4(6):174.
32. McInnes IB, Schett G. The pathogenesis of rheumatoid ar-thritis. N Engl J Med. Massachusetts Medical Society. 2011;365(23):2205-2219.
33. Bartold PM, Lopez-Oliva I. Periodontitis and rheumatoid arthritis: An update 2012–2017. Periodontol 2000. 2020; 83(1):189-212.
34. Reichert S, Haffner M, Keyßer G, et al. Detection of oral bacterial DNA in synovial fluid. J Clin Periodontol. 2013;40(6):591-598.
35. Rakieh C, Rakieh C, Nam JL, et al. Predicting the development of clinical arthritis in anti-CCP positive individuals with non-specific
musculoskeletal symptoms: a prospective observational cohort study. Ann Rheum Dis. 2015;74(9):1659-1666.
36. Golub LM, Payne JB, Reinhardt RA, Nieman G. Can systemic dis-eases co-induce (not just exacerbate) periodontitis? A hypotheti-cal “two-hit” model. Journal of Dental Research. SAGE Publications. 2006;85(2):102-105.
37. Lindqvist E, Eberhardt K, Bendtzen K, Heinegård D, Saxne T. Prognostic laboratory markers of joint damage in rheumatoid ar-thritis. Ann Rheum Dis. 2005;64(2):196-201.
38. Jansen LMA, van Schaardenburg D, van der Horst-Bruinsma I, van der Stadt RJ, de Koning MHMT, Dijkmans BAC. The predictive value of anti-cyclic citrullinated peptide antibodies in early arthri-tis. J Rheumatol. 2003;30(8):1691-1695.
39. Aletaha D, Neogi T, Silman AJ, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569-2581.
40. Whiting PF, Smidt N, Sterne JAC, et al. Systematic review: accu-racy of anti-citrullinated Peptide antibodies for diagnosing rheu-matoid arthritis. Ann Intern Med. American College of Physicians. 2010;152(7):456-464–W155–66.
41. Wegner N, Lundberg K, Kinloch A, et al. Autoimmunity to specific citrullinated proteins gives the first clues to the etiology of rheu-matoid arthritis. Immunol Rev. 2010;233(1):34-54.
42. Wegner N, Wait R, Sroka A, et al. Peptidylarginine deiminase from Porphyromonas gingivalis citrullinates human fibrinogen and !-enolase: implications for autoimmunity in rheumatoid arthritis. Arthritis Rheum. 2010;62(9):2662-2672.
43. Kokkonen H, Mullazehi M, Berglin E, et al. Antibodies of IgG, IgA and IgM isotypes against cyclic citrullinated peptide precede the develop-ment of rheumatoid arthritis. Arthritis Res Ther. 2011;13(1):R13-R10.
44. Jørgensen KT, Wiik A, Pedersen M, et al. Cytokines, autoan-tibodies and viral antibodies in premorbid and postdiagnostic sera from patients with rheumatoid arthritis: case-control study nested in a cohort of Norwegian blood donors. Ann Rheum Dis. 2008;67(6):860-866.
45. Deane KD, O'Donnell CI, Hueber W, et al. The number of elevated cytokines and chemokines in preclinical seropositive rheumatoid arthritis predicts time to diagnosis in an age-dependent manner. Arthritis Rheum. 2010;62(11):3161-3172.
46. Mikuls TR, Payne JB, Yu F, et al. Periodontitis and porphyromonas gingivalisin patients with rheumatoid arthritis. Arthritis Rheumatol. 2014;66(5):1090-1100.
47. de Pablo P, Dietrich T, McAlindon TE. Association of periodontal disease and tooth loss with rheumatoid arthritis in the US popula-tion. J Rheumatol. 2008;35(1):70-76.
48. Pischon T, Kröger J, Gülmez E, et al. Association among Rheumatoid Arthritis, oral hygiene, and periodontitis. J Periodontol. 2008;79(6):979-986.
49. Mercado FB, Marshall RI, Klestov AC, Bartold PM. Relationship between rheumatoid arthritis and periodontitis. J Periodontology. 2001;72(6):779-787.
50. Dissick A, Redman RS, Jones M, et al. Association of periodon-titis with rheumatoid arthritis: a pilot study. J Periodontol. 2010;81(2):223-230.
51. Joseph R, Rajappan S, Nath SG, Paul BJ. Association between chronic periodontitis and rheumatoid arthritis: a hospital-based case-control study. Rheumatol Int. 2013;33(1):103-109.
52. Potikuri D, Dannana KC, Kanchinadam S, et al. Periodontal disease is significantly higher in non-smoking treatment-naive rheumatoid arthritis patients: results from a case-control study. Ann Rheum Dis. 2012;71(9):1541-1544.
53. Susanto H, Nesse W, Kertia N, et al. Prevalence and severity of periodontitis in Indonesian patients with rheumatoid arthritis. J Periodontol. 2013;84(8):1067-1074.
68

82
123456789
1011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
20 | GONZÁLEZ-FEBLES aNd SaNZ
54. Khantisopon N, Louthrenoo W, Kasitanon N, et al. Periodontal disease in Thai patients with rheumatoid arthritis. Int J Rheum Dis. 2014;17(5):511-518.
55. Ibáñez SV, Ferreiro C, Contreras A, et al. Frequency and severity of periodontitis among patients with rheumatoid arthritis. Rev Med Chil. 2015;143(12):1539-1545.
56. Pons-Fuster A, Rodríguez Agudo C, Galvez Muñoz P, Saiz Cuenca E, Pina Perez FM, Lopez-Jornet P. Clinical evaluation of periodon-tal disease in patients with rheumatoid arthritis: A cross-sectional study. Quintessence Int. 2015;46(9):817-822.
57. Vahabi S, Rostamian A, Baniebrahimi G. Characteristics and rela-tionship of periodontal disease with juvenile idiopathic and rheu-matoid arthritis. Dent Res J. 2015;12(6):541-547.
58. Bello-Gualtero JM, Lafaurie GI, Hoyos LX, et al. Periodontal dis-ease in individuals with a genetic risk of developing arthritis and early rheumatoid arthritis: a cross-sectional study. J Periodontol. 2016;87(4):346-356.
59. Choi IA, Kim J-H, Kim YM, et al. Periodontitis is associated with rheumatoid arthritis: a study with longstanding rheumatoid arthri-tis patients in Korea. Korean J Intern Med. 2016;31(5):977-986.
60. Silvestre-Rangil J, Bagán L, Silvestre F-J, Bagán JV. Oral manifes-tations of rheumatoid arthritis. A cross-sectional study of 73 pa-tients. Clin Oral Investig. 2016;20(9):2575-2580.
61. Schmickler J, Rupprecht A, Patschan S, et al. Cross-sectional eval-uation of periodontal status and microbiologic and rheumatoid pa-rameters in a large cohort of patients with rheumatoid arthritis. J Periodontol. 2017;88(4):368-379.
62. Ouédraogo D-D, Tiendrébéogo J, Guiguimdé PLW, et al. Periodontal disease in patients with rheumatoid arthritis in Sub-Saharan Africa: A case-control study. Joint Bone Spine. 2017;84(1):113-114.
63. Rodríguez-Lozano B, González-Febles J, Garnier-Rodríguez JL, et al. Association between severity of periodontitis and clinical activity in rheumatoid arthritis patients: a case-control study. Arthritis Res Ther. 2019;21(1):27.
64. Zhao R, Gu C, Zhang Q, et al. Periodontal disease in Chinese pa-tients with rheumatoid arthritis: A case-control study. Oral Dis. 2019;2015(8):259074.
65. Kaur S, White S, Bartold PM. Periodontal disease and rheumatoid arthritis: a systematic review. J Dent Res. 2013;92(5):399-408.
66. Xibille-Friedmann D, Xibille-Friedmann D, Martínez-Rivera JI, et al. Periodontal disease and Clinical Activity of Rheumatoid Arthritis Patients. ACR congress. 2014.
67. Molitor JA, Alonso A, Wener MH, Michalowics BS, Gersuk VH. Moderate to severe periodontitis increases risk of rheumatoid ar-thritis in non-smokers and is associated with elevated ACPA Titers: The ARIC Study. Arthritis Rheum. 2009;60:S433.
68. Demmer RT, Molitor JA, Jacobs DR Jr, Michalowicz BS. Periodontal disease, tooth loss and incident rheumatoid arthritis: results from the First National Health and Nutrition Examination Survey and its epidemiological follow-up study. J Clin Periodontol. 2011;38(11):998-1006.
69. Chen H-H, Chen D-Y, Lin S-Y, et al. Periodontitis exposure within one year before anti-diabetic treatment and the risk of rheumatoid arthritis in diabetes mellitus patients: a population-based cohort study. Rev Bras Reumatol. 2014;54(2):124-130.
70. Chou Y-Y, Lai K-L, Chen D-Y, Lin C-H, Chen H-H. Rheumatoid ar-thritis risk associated with periodontitis exposure: a nationwide, population-based cohort study. PLoS One. 2015;10(10):e0139693.
71. Äyräväinen L, Leirisalo-Repo M, Kuuliala A, et al. Periodontitis in early and chronic rheumatoid arthritis: a prospective follow-up study in Finnish population. BMJ Open. 2017;7(1):e011916.
72. Queiroz-Junior CM, Madeira MFM, Coelho FM, et al. Experimental arthritis exacerbates Aggregatibacter actinomycetemcomitans-in-duced periodontitis in mice. J Clin Periodontol. 2012;39(7):608-616.
73. Queiroz-Junior CM, Bessoni RLC, Costa VV, Souza DG, Teixeira MM, Silva TA. Preventive and therapeutic anti-TNF-! therapy with pentoxifylline decreases arthritis and the associated periodontal co-morbidity in mice. Life Sci. 2013;93(9–11):423-428.
74. Gully N, Bright R, Marino V, et al. Porphyromonas gingivalis pepti-dylarginine deiminase, a key contributor in the pathogenesis of ex-perimental periodontal disease and experimental arthritis. Yilmaz Ö, editor. PLoS One. 2014;9(6):e100838.
75. Maresz KJ, Hellvard A, Sroka A, et al. Porphyromonas gingivalis facilitates the development and progression of destructive arthri-tis through its unique bacterial peptidylarginine deiminase (PAD). PLoS Pathog. 2013;9(9):e1003627.
76. Marchesan JT, Gerow EA, Schaff R, et al. Porphyromonas gingiva-lis oral infection exacerbates the development and severity of col-lagen-induced arthritis. Arthritis Res Ther. 2013;15(6):R186-R213.
77. Chukkapalli S, Rivera-Kweh M, Gehlot P, et al. Periodontal bacte-rial colonization in synovial tissues exacerbates collagen-induced arthritis in B10.RIII mice. Arthritis Res Ther. 2016;18(1):161-212.
78. Corrêa JD, Saraiva AM, Queiroz-Junior CM, et al. Arthritis-induced alveolar bone loss is associated with changes in the composition of oral microbiota. Anaerobe. 2016;39:91-96.
79. Eriksson K, Lönnblom E, Tour G, et al. Effects by periodontitis on pristane-induced arthritis in rats. J Transl Med. 2016;14(1):311-314.
80. Sandal I, Karydis A, Luo J, et al. Bone loss and aggravated auto-immune arthritis in HLA-DR"1-bearing humanized mice following oral challenge with Porphyromonas gingivalis. Arthritis Res Ther. 2016;18(1):249-313.
81. Yamakawa M, Ouhara K, Kajiya M, et al. Porphyromonas gingiva-lis infection exacerbates the onset of rheumatoid arthritis in SKG mice. Clin Exp Immunol. 2016;186(2):177-189.
82. Jung H, Jung SM, Rim YA, et al. Arthritic role of Porphyromonas gingivalis in collagen-induced arthritis mice. PLoS One. 2017;12(11):e0188698.
83. Corrêa JD, Fernandes GR, Calderaro DC, et al. Oral microbial dys-biosis linked to worsened periodontal condition in rheumatoid ar-thritis patients. Sci Rep. 2019;9(1):8379-8410.
84. Lübcke PM, Ebbers MNB, Volzke J, et al. Periodontal treatment prevents arthritis in mice and methotrexate ameliorates periodon-tal bone loss. Sci Rep. 2019;9(1):8128-8129.
85. Ebbers M, Lübcke PM, Volzke J, et al. Interplay between P. gingiva-lis, F. nucleatum and A. actinomycetemcomitans in murine alveolar bone loss, arthritis onset and progression. Sci Rep. 2018;8(1):15129.
86. Scanu A, Giraudo C, Galuppini F, et al. Periodontal injection of lipopolysaccharide promotes arthritis development in mice. Inflammation. 2019;42(3):1117-1128.
87. Courbon G, Rinaudo-Gaujous M, Blasco-Baque V, et al. Porphyromonas gingivalis experimentally induces periodon-tis and an anti-CCP2-associated arthritis in the rat. Ann Rheum Dis. 2019;78(5):594-599.
88. Quirke A-M, Lugli EB, Lugli EB, et al. Heightened immune re-sponse to autocitrullinated Porphyromonas gingivalis pepti-dylarginine deiminase: a potential mechanism for breaching immunologic tolerance in rheumatoid arthritis. Ann Rheum Dis. 2014;73(1):263-269.
89. McGraw WT, Potempa J, Farley D, Travis J. Purification, char-acterization, and sequence analysis of a potential virulence fac-tor from Porphyromonas gingivalis, peptidylarginine deiminase. Infection and Immunity. American Society for Microbiology Journals. 1999;67(7):3248-3256.
90. Rodríguez SB, Stitt BL, Ash DE. Expression of peptidylarginine deiminase from Porphyromonas gingivalis in Escherichia coli: enzyme purification and characterization. Arch Biochem Biophys. 2009;488(1):14-22.
91. Lee JY, Lee JY, Choi IA, et al. Association between anti-Porphy-romonas gingivalis or anti-!-enolase antibody and severity of
83
123456789
1011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
| 21GONZÁLEZ-FEBLES aNd SaNZ
periodontitis or rheumatoid arthritis (RA) disease activity in RA.
BMC Musculoskelet Disord. 2015;16:190.
92. Lundberg K, Wegner N, Yucel-Lindberg T, Venables PJ.
Periodontitis in RA—the citrullinated enolase connection. Nat Rev Rheumatol. 2010;7:1-4.
93. Sanz M, Beighton D, Curtis MA, et al. Role of microbial biofilms
in the maintenance of oral health and in the development of den-
tal caries and periodontal diseases. Consensus report of group
1 of the Joint EFP/ORCA workshop on the boundaries between
caries and periodontal disease. J Clin Periodontol. 2017;44(Suppl.
11):S5-S11.
94. Konig MF, Abusleme L, Reinholdt J, et al. Aggregatibacter actino-
mycetemcomitans-induced hypercitrullination links periodontal
infection to autoimmunity in rheumatoid arthritis. Sci Transl Med.
2016;8(369):369ra176.
95. Wolff B, Wolff B, Berger T, et al. Oral status in patients with
early rheumatoid arthritis: a prospective, case-control study.
Rheumatology (Oxford). 2014;53(3):526-531.
96. Corrêa MG, Sacchetti SB, Ribeiro FV, et al. Periodontitis increases
rheumatic factor serum levels and citrullinated proteins in gingi-
val tissues and alter cytokine balance in arthritic rats. PLoS One.
2017;12(3):e0174442.
97. Hendler A, Mulli TK, Hughes FJ, et al. Involvement of autoimmu-
nity in the pathogenesis of aggressive periodontitis. J Dent Res.
2010;89(12):1389-1394.
98. de Pablo P, Dietrich T, Chapple ILC, et al. The autoantibody rep-
ertoire in periodontitis: a role in the induction of autoimmunity
to citrullinated proteins in rheumatoid arthritis? Ann Rheum Dis.
2014;73(3):580-586.
99. Oluwagbemigun K, Yucel-Lindberg T, Dietrich T,
et al. A cross-sectional investigation into the association between
Porphyromonas gingivalis and autoantibodies to citrullinated
proteins in a German population. Ther Adv Musculoskelet Dis.
2019;11:1759720X19883152.
100. Jenning M, Marklein B, Ytterberg J, et al. Bacterial citrulli-
nated epitopes generated by Porphyromonas gingivalis in-
fection-a missing link for ACPA production. Ann Rheum Dis.
2020;79(9):1194-1202.
101. Mikuls TR, Thiele GM, Deane KD, et al. Porphyromonas gingivalis
and disease-related autoantibodies in individuals at increased risk
of rheumatoid arthritis. Arthritis Rheum. 2012;64(11):3522-3530.
102. de Smit M, de Smit M, van de Stadt LA, et al. Antibodies against
Porphyromonas gingivalis in seropositive arthralgia patients do
not predict development of rheumatoid arthritis. Ann Rheum Dis.
2014;73(6):1277-1279.
103. Gabarrini G, de Smit M, Westra J, et al. The peptidylarginine deimi-
nase gene is a conserved feature of Porphyromonas gingivalis. Sci Rep. 2015;5(1):13936-13938.
104. Mankia K, Cheng Z, Do T, et al. Prevalence of periodontal disease
and periodontopathic bacteria in anti-cyclic citrullinated protein
antibody-positive at-risk adults without arthritis. JAMA Netw Open. 2019;2(6):e195394.
105. Zhao X, Liu Z, Shu D, et al. Association of periodontitis with
rheumatoid arthritis and the effect of non-surgical periodontal
treatment on disease activity in patients with rheumatoid ar-
thritis. Med Sci Monit. International Scientific Information, Inc;
2018;24:5802-5810.
106. Nesse W, Nesse W, Westra J, et al. The periodontium of peri-
odontitis patients contains citrullinated proteins which may play a
role in ACPA (anti-citrullinated protein antibody) formation. J Clin Periodontol. 2012;39(7):599-607.
107. Harvey GP, Fitzsimmons TR, Dhamarpatni AASSK, Marchant C,
Haynes DR, Bartold PM. Expression of peptidylarginine deimi-
nase-2 and -4, citrullinated proteins and anti-citrullinated protein
antibodies in human gingiva. J Periodontal Res. 2013;48(2):252-261.
108. Konig MF, Paracha AS, Moni M, Bingham CO, Andrade F. Defining
the role of Porphyromonas gingivalis peptidylarginine deiminase
(PPAD) in rheumatoid arthritis through the study of PPAD biology.
Ann Rheum Dis. 2015;74(11):2054-2061.
109. Laugisch O, Wong A, Wong A, et al. Citrullination in the periodon-
tium-a possible link between periodontitis and rheumatoid arthri-
tis. Clin Oral Investig. 2015; 20(4): 675-683.
110. Janssen KMJ, de Smit MJ, de Smit MJ, et al. Rheumatoid arthri-
tis-associated autoantibodies in non-rheumatoid arthritis patients
with mucosal inflammation: a case-control study. Arthritis Res Ther. 2015;17:174.
111. Janssen KMJ, de Smit MJ, Withaar C, et al. Autoantibodies against
citrullinated histone H3 in rheumatoid arthritis and periodontitis
patients. J Clin Periodontol. 2017;44(6):577-584.
112. Engström M, Eriksson K, Lee L, et al. Increased citrullination and
expression of peptidylarginine deiminases independently of P. gin-
givalis and A. actinomycetemcomitans in gingival tissue of patients
with periodontitis. J Transl Med. 2018;16(1):214.
113. González-Febles J, Rodríguez-Lozano B, Sánchez-Piedra C, et al.
Association between periodontitis and anti- citrullinated protein
antibodies in rheumatoid arthritis patients: a cross- sectional
study. Arthritis Research Ther 2020;22(1):27.
114. Pers J-O, Saraux A, Pierre R, Youinou P. Anti-TNF-alpha immuno-
therapy is associated with increased gingival inflammation with-
out clinical attachment loss in subjects with rheumatoid arthritis. J Periodontol. 2008;79(9):1645-1651.
115. Han J-Y, Reynolds MA. Effect of anti-rheumatic agents on peri-
odontal parameters and biomarkers of inflammation: a sys-
tematic review and meta-analysis. J Periodontal Implant Sci. 2012;42(1):3-12.
116. Savioli C, Ribeiro ACM, Fabri GMC, et al. Persistent periodontal
disease hampers anti-tumor necrosis factor treatment response in
rheumatoid arthritis. J Clin Rheumatol. 2012;18(4):180-184.
117. Mayer Y, Balbir-Gurman A, Machtei EE. Anti-tumor necrosis fac-
tor-alpha therapy and periodontal parameters in patients with
rheumatoid arthritis. J Periodontol. 2009;80(9):1414-1420.
118. Mayer Y, Elimelech R, Balbir-Gurman A, Braun-Moscovici Y,
Machtei EE. Periodontal condition of patients with autoimmune
diseases and the effect of anti-tumor necrosis factor-! therapy.
The Journal of Periodontology. 2013;84(2):136-142.
119. Üstün K, Erciyas K, Kısacık B, et al. Host modulation in rheu-
matoid arthritis patients with TNF blockers significantly de-
creases biochemical parameters in periodontitis. Inflammation.
2013;36(5):1171-1177.
120. Kobayashi T, Okada M, Ito S, et al. Assessment of Interleukin-6 receptor
inhibition therapy on periodontal condition in patients with rheuma-
toid arthritis and chronic periodontitis. J Periodontol. 2014;85(1):57-67.
121. Kobayashi T, Yoshie H. Host responses in the link between
periodontitis and rheumatoid arthritis. Curr Oral Health Rep.
2015;2:1-8.
122. Kobayashi T, Yokoyama T, Ito S, et al. Periodontal and serum
protein profiles in patients with rheumatoid arthritis treated
with tumor necrosis factor inhibitor adalimumab. J Periodontol. 2014;85(11):1480-1488.
123. Fabri GMC, Pereira RMR, Savioli C, et al. Periodontitis response
to Anti-TNF therapy in ankylosing spondylitis. J Clin Rheumatol. 2015;21(7):341-345.
124. Coat J, Coat J, Demoersman J, et al. Anti-B lymphocyte im-
munotherapy is associated with improvement of periodontal
status in subjects with rheumatoid arthritis. J Clin Periodontol. 2015;42(9):817-823.
125. Kadkhoda Z, Amirzargar A, Esmaili Z, Vojdanian M, Akbari S.
Effect of TNF-! blockade in gingival crevicular fluid on periodon-
tal condition of patients with rheumatoid arthritis. Iran J Immunol. 2016;13(3):197-203.

84
123456789
1011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
22 | GONZÁLEZ-FEBLES aNd SaNZ
126. Domínguez-Pérez RA, Loyola-Rodríguez JP, Abud-Mendoza C, Alpuche-Solis AG, Ayala-Herrera JL, Martínez-Martínez RE. Association of cytokines polymorphisms with chronic peridonti-tis and rheumatoid arthritis in a Mexican population. Acta Odontol Scand. 2017;75(4):243-248.
127. Ziebolz D, Rupprecht A, Schmickler J, et al. Association of differ-ent immunosuppressive medications with periodontal condition in patients with rheumatoid arthritis: Results from a cross-sectional study. J Periodontol. 2018;89(11):1310-1317.
128. Äyräväinen L, Heikkinen AM, Kuuliala A, et al. Anti-rheumatic medication and salivary MMP-8, a biomarker for periodontal dis-ease. Oral Dis. 2018;24(8):1562-1571.
129. Kaczyński T, Wroński J, Głuszko P, et al. Salivary interleukin 6, in-terleukin 8, interleukin 17A, and tumour necrosis factor ! levels in patients with periodontitis and rheumatoid arthritis. Cent Eur J Immunol. Termedia. 2019;44(3):269-276.
130. Jung G-U, Han J-Y, Hwang K-G, Park C-J, Stathopoulou PG, Fiorellini JP. Effects of conventional synthetic disease-mod-ifying antirheumatic drugs on response to periodontal treat-ment in patients with rheumatoid arthritis. Biomed Res Int. 2018;2018(1):1465402-1465407.
131. Lappin DF, Apatzidou D, Quirke A-M, et al. Influence of periodontal disease, Porphyromonas gingivalis and cigarette smoking on sys-temic anti-citrullinated peptide antibody titres. J Clin Periodontol. 2013;40(10):907-915.
132. Kaur S, Bright R, Proudman SM, Bartold PM. Does periodontal treatment influence clinical and biochemical measures for rheu-matoid arthritis? A systematic review and meta-analysis. Semin Arthritis Rheum. 2014;44(2):113-122.
133. Silvestre F-J, Silvestre-Rangil J, Bagán L, Bagán JV. Effect of non-surgical periodontal treatment in patients with periodontitis and rheumatoid arthritis: A systematic review. Med Oral Patol Oral Cir Bucal. 2016;21(3):e349-e354.
134. Ribeiro J, Leão A, Novaes AB. Periodontal infection as a possi-ble severity factor for rheumatoid arthritis. J Clin Periodontol. 2005;32(4):412-416.
135. Al-Katma MK, Bissada NF, Bordeaux JM, Sue J, Askari AD. Control of periodontal infection reduces the severity of active rheumatoid arthritis. J Clin Rheumatol. 2007;13(3):134-137.
136. Ortiz P, Bissada NF, Palomo L, et al. Periodontal therapy reduces the severity of active rheumatoid arthritis in patients treated with or without tumor necrosis factor inhibitors. J Periodontol. 2009;80(4):535-540.
137. Erciyas K, Sezer U, Ustün K, et al. Effects of periodontal therapy on disease activity and systemic inflammation in rheumatoid arthritis patients. Oral Dis. 2013;19(4):394-400.
138. Okada M, Kobayashi T, Ito S, et al. Periodontal treatment de-creases levels of antibodies to Porphyromonas gingivalis and ci-trulline in patients with rheumatoid arthritis and periodontitis. J Periodontol. 2013;84(12):e74-84.
139. Białowąs K, Radwan-Oczko M, Duś-Ilnicka I, Korman L, Świerkot J. Periodontal disease and influence of periodontal treatment on disease activity in patients with rheumatoid arthritis and spondy-loarthritis. Rheumatol Int. 2019;93(Suppl 2):1045-1049.
140. Kaushal S, Singh AK, Lal N, Das SK, Mahdi AA. Effect of peri-odontal therapy on disease activity in patients of rheumatoid arthritis with chronic periodontitis. J Oral Biol Craniofac Res. 2019;9(2):128-132.
141. Pinho MDN, Oliveira RDR, Novaes AB, Voltarelli JC. Relationship between periodontitis and rheumatoid arthritis and the ef-fect of non-surgical periodontal treatment. Braz Dent J. 2009;20(5):355-364.
142. Monsarrat P, Fernandez de Grado G, Constantin A, et al. The effect of periodontal treatment on patients with rheumatoid
arthritis: The ESPERA randomised controlled trial. Joint Bone Spine. 2019;86(5):600-609.
143. Mariette X, Perrodeau E, Verner C, et al. Role of good oral hy-giene on clinical evolution of rheumatoid arthritis: a random-ized study nested in the ESPOIR cohort. Rheumatology (Oxford). 2019;3(35):70.
144. Cosgarea R, Tristiu R, Dumitru RB, et al. Effects of non-surgical periodontal therapy on periodontal laboratory and clinical data as well as on disease activity in patients with rheumatoid arthritis. Clin Oral Investig. 2019;23(1):141-151.
145. Marotte H. Non-surgical periodontal disease: A new treatment for rheumatoid arthritis? Joint Bone Spine. 2020;87(1):1-3.
146. Moe Y, Tetsuo K, Satoshi I, et al. The periodontal inflamed sur-face area is associated with the clinical response to biological disease-modifying antirheumatic drugs in rheumatoid arthritis: A retrospective study. Mod Rheumatol. 2019;30(6):990-996.
147. Möller B, Bender P, Eick S, et al. Treatment of severe periodon-titis may improve clinical disease activity in otherwise treat-ment-refractory rheumatoid arthritis patients. Rheumatology. 2019;10(16):214-223.
148. Scherer H-U, Häupl T, Burmester GR. The etiology of rheumatoid arthritis. J Autoimmun. 2020;110:102400.
149. Torkzaban P, Hjiabadi T, Basiri Z, Poorolajal J. Effect of rheumatoid arthritis on periodontitis: a historical cohort study. J Periodontal Implant Sci. 2012;42(3):67-72.
150. Eriksson K, Nise L, Kats A, et al. Prevalence of periodontitis in patients with established rheumatoid arthritis: a swedish popula-tion based case-control study. PLoS One Public Library of Science. 2016;11(5):e0155956.
151. Scher JU, Scher JU, Ubeda C, et al. Periodontal disease and the oral microbiota in new-onset rheumatoid arthritis. Arthritis Rheum. 2012;64(10):3083-3094.
152. de Smit M, Westra J, Vissink A, Doornbos-van der Meer B, Brouwer E, van Winkelhoff AJ. Periodontitis in established rheu-matoid arthritis patients: a cross-sectional clinical, microbiological and serological study. Arthritis Res Ther. 2012;14(5):R222.
153. Totaro MC, Cattani P, Ria F, et al. Porphyromonas gingivalis and the pathogenesis of rheumatoid arthritis: analysis of various compartments including the synovial tissue. Arthritis Res Ther. 2013;15(3):R66-R68.
154. Arvikar SL, Collier DS, Fisher MC, et al. Clinical correlations with Porphyromonas gingivalis antibody responses in patients with early rheumatoid arthritis. Arthritis Res Ther. 2013;15(5):R109-R112.
155. Zhang B, Khalaf H, Sirsjö A, Bengtsson T. Gingipains from the periodontal pathogen porphyromonas gingivalis play a significant role in regulation of angiopoietin 1 and angiopoi-etin 2 in human aortic smooth muscle cells. Infect Immun. 2015;83(11):4256-4265.
156. Seror R, Seror R, Le Gall-David S, et al. Association of anti-porphy-romonas gingivalis antibody titers with nonsmoking status in early rheumatoid arthritis: results from the prospective french cohort of patients with early rheumatoid arthritis. Arthritis Rheumatol. 2015;67(7):1729-1737.
157. Kimura Y, Yoshida S, Takeuchi T, et al. Periodontal pathogens par-ticipate in synovitis in patients with rheumatoid arthritis in clin-ical remission: a retrospective case-control study. Rheumatology (Oxford) 2015;54(12):2257-2263.
158. Hashimoto M, Hashimoto M, Yamazaki T, et al. Periodontitis and Porphyromonas gingivalis in preclinical stage of arthritis patients. PLoS One. 2015;10(4):e0122121.
159. Kobayashi T, Ito S, Kobayashi D, et al. Serum immunoglobulin G lev-els to porphyromonas gingivalis peptidylarginine deiminase affect clinical response to biological disease-modifying antirheumatic
85
123456789
1011121314151617181920212223242526272829303132333435363738394041424344454647484950515253
| 23GONZÁLEZ-FEBLES aNd SaNZ
drug in rheumatoid arthritis. PLoS One. Public Library of Science. 2016;11(4):e0154182.
160. Santegoets KCM, Wenink MH, Braga FAV, et al. Impaired porphy-romonas gingivalis-induced tumor necrosis factor production by dendritic cells typifies patients with rheumatoid arthritis. Arthritis Rheumatol. 2016;68(4):795-804.
161. Kharlamova N, Jiang X, Sherina N, et al. Antibodies to porphy-romonas gingivalis indicate interaction between oral infection, smoking, and risk genes in rheumatoid arthritis etiology. Arthritis Rheumatol. 2016;68(3):604-613.
162. Johansson L, Pratesi F, Brink M, et al. Antibodies directed against endogenous and exogenous citrullinated antigens pre-date the onset of rheumatoid arthritis. Arthritis Res Ther. 2016;18(1):127.
163. Goh CE, Kopp J, Papapanou PN, Molitor JA, Demmer RT. Association between serum antibodies to periodontal bacteria and rheumatoid factor in the third national health and nutrition examination survey. Arthritis Rheumatol. 2016;68(10):2384-2393.
164. Cheng Z, Do T, Mankia K, et al. The subgingival microbiomes in periodontitis and health of individuals with rheumatoid arthritis and at risk of developing rheumatoid arthritis. J Oral Microbiol. 2017; 9(sup1): 1325216.
165. Martu MA, Solomon SM, Sufaru I, et al. Study on the prevalence of periodontopathogenic bacteria in serum and subgingival bac-terial plaque in patients with rheumatoid arthritis. Rev Chim. 2017;68(8).
166. Martínez-Rivera J-I, Xibillé-Friedmann DX, González-Christen J, la Garza-Ramos de MA, Carrillo-Vázquez SM, Montiel-Hernández J-L. Salivary ammonia levels and Tannerella forsythia are associated with rheumatoid arthritis: A cross sectional study. Clin Exp Dent Res. John Wiley & Sons, Ltd. 2017;3(3):107-114.
167. Cheng Z, Do T, Mankia K, et al. Dysbiosis in the oral microbiomes of anti-CCP positive individuals at risk of developing rheumatoid arthritis. Ann Rheum Dis. 2020;1(20):216972.
168. Fisher BA, Cartwright AJ, Quirke A-M, et al. Smoking, Porphyromonas gingivalis and the immune response to citrul-linated autoantigens before the clinical onset of rheumatoid
arthritis in a Southern European nested case-control study. BMC Musculoskelet Disord. BioMed Central. 2015;16(1):331-411.
169. Shimada A, Kobayashi T, Ito S, et al. Expression of anti-Porphy-romonas gingivalis peptidylarginine deiminase immunoglobulin G and peptidylarginine deiminase-4 in patients with rheumatoid ar-thritis and periodontitis. J Periodontal Res. 2016;51(1):103-111.
170. Li S, Yu Y, Yue Y, et al. Autoantibodies from single circulating plasmablasts react with citrullinated antigens and porphyromonas gingivalis in rheumatoid arthritis. Arthritis Rheumatol. John Wiley & Sons, Ltd. 2016;68(3):614-626.
171. Schwenzer A, Quirke A-M, Marzeda AM, et al. Association of dis-tinct fine specificities of anti-citrullinated peptide antibodies with elevated immune responses to prevotella intermedia in a subgroup of patients with rheumatoid arthritis and periodontitis. Arthritis Rheumatol. Wiley-Blackwell. 2017;69(12):2303-2313.
172. Khare N, Vanza B, Sagar D, Saurav K, Chauhan R, Mishra S. Nonsurgical periodontal therapy decreases the severity of rheu-matoid arthritis: a case-control study. J Contemp Dent Pract. 2016;17(6):484-488.
173. Kurgan Ş, Fentoğlu Ö, Önder C, et al. The effects of periodontal therapy on gingival crevicular fluid matrix metalloproteinase-8, interleukin-6 and prostaglandin E2 levels in patients with rheuma-toid arthritis. J Periodontal Res. 2016;51(5):586-595.
174. Yuce HB, Gokturk O, Turkal HA, Inanir A, Benli I, Demir O. Assessment of local and systemic 25-hydroxy-vitamin D, RANKL, OPG, and TNF levels in patients with rheumatoid arthritis and periodontitis. J Oral Sci. 2017;59(3):397-404.
How to cite this article: González-Febles J, Sanz M.
Periodontitis and rheumatoid arthritis: What have we learned
about their connection and their treatment?. Periodontol 2000. 2020;00:1–23. https://doi.org/10.1111/prd.12385
69
70

86

87
Artículo 2
88
89
Artículo #2
Asociación entre la severidad de la Periodontitis y la actividad clínica de la
enfermedad en pacientes con Artritis Reumatoide: un estudio de casos y controles
Antecedentes: Numerosos estudios han observado una alta prevalencia de periodontitis en pacientes con Artritis Reumatoide(AR). Sin embargo, la evidencia tanto de la fuerza de asociación, como de su consistencia temporal y la posible relación entre la severidad de la periodontitis y la actividad clínica de la AR sigue siendo escasa. El objetivo de este estudio es investigar si la periodontitis está asociada a la AR, y si la severidad de la periodontitis está relacionada a la actividad clínica de la AR.
Métodos: En este estudio de casos y controles se incluyeron 187 pacientes diagnosticados de AR y 157 controles sanos con artrosis. La actividad y severidad de la AR se evaluó mediante registro del DAS-28, SDAI, CDAI, títulos de Factor Reumatoide y anticuerpos anti-péptidos citrulinados, la velocidad de sedimentación globular (VSG), proteína C-reactiva (PCR), la presencia de manifestaciones extra-articulares y el tipo de terapia de la AR. En el caso de la periodontitis se evaluaron el índice de placa, sangrado al sondaje, profundidad de sondaje y pérdida de inserción. Se registraron tanto variables sociodemográficas como comorbilidades como posibles factores de confusión. Tanto la exposición como la variable resultado se compararon estadísticamente mediante test paramétricos y no paramétricos, y su posible asociación se evaluó mediante un análisis de regresión calculando la odds ratio (OR) ajustada.
Resultados: se observó una asociación estadísticamente significativa entre la periodontitis y la AR con una OR de 20.57 (IC 95% 6,02–70,27, p < 0.001). Con respecto a los controles, los pacientes con AR presentaron peor estado periodontal siendo estadísticamente significativo (p < 0.001). Tras el modelo de regresión ordinal se observó una asociación estadísticamente significativa entre la severidad de la periodontitis y la actividad de la AR(p < 0.001), con una OR ajustada de 2.66 (IC 95% 1,24–5,74, p = 0,012).
90
Conclusiones: Los resultados de esta investigación muestran una asociación independiente y estadísticamente significativa entre la periodontitis y la AR, demostrando una relación estadísticamente significativa entre el nivel de actividad de la AR y la severidad de la periodontitis.
91
RESEARCH ARTICLE Open Access
Association between severity ofperiodontitis and clinical activity inrheumatoid arthritis patients: a case–control studyBeatriz Rodríguez-Lozano1, Jerián González-Febles2, Jorge Luis Garnier-Rodríguez3, Shashi Dadlani3,Sagrario Bustabad-Reyes1, Mariano Sanz4, Fernando Sánchez-Alonso5, Carlos Sánchez-Piedra5,Enrique González-Dávila6 and Federico Díaz-González1,7*
Abstract
Background: A high prevalence of periodontitis has been reported in rheumatoid arthritis (RA) patients, althoughthe strength of this association, its temporal link and the possible relationship between the severity of periodontitisand RA disease activity remain unclear. The objective of this work was to investigate whether periodontitis isassociated with RA and whether periodontitis severity is linked to RA disease activity.
Methods: This case–control study included 187 patients diagnosed with RA and 157 control patients withoutinflammatory joint disease. RA disease activity and severity were evaluated by the Disease Activity Score 28, theSimplified Disease Activity Index, the Clinical Disease Activity Index, rheumatoid factor, anti-citrullinated proteinantibody titers, the erythrocyte sedimentation rate, C-reactive protein, presence of extra-articular manifestations andtype of RA therapy. Exposure severity was assessed by the following periodontal parameters: plaque index, bleedingon probing, probing pocket depth and clinical attachment levels. Sociodemographic variables and comorbiditieswere evaluated as confounding variables. Outcome and exposure variables were compared by both parametric andnonparametric tests, and possible associations were assessed through regression analysis with a calculation for theadjusted odds ratio (OR).
Results: A significant association was demonstrated between periodontitis and RA with an adjusted OR of 20.57(95% CI 6.02–70.27, p < 0.001). Compared with controls, all parameters related to periodontal status (plaque index,bleeding on probing, probing pocket depth and clinical attachment levels) were significantly worse in RA patients(p < 0.001). Periodontitis severity was significantly associated with RA disease activity (p < 0.001), showing in anordinal logistic regression model an association between periodontal severity and disease activity with an adjustedOR of 2.66 (95% CI 1.24–5.74, p = 0.012).
Conclusion: A significant association was demonstrated between periodontitis and RA, independent of otherconfounders. This association was more evident in patients with pronounced periodontal disease and higher RAdisease activity.
Keywords: Rheumatoid arthritis, Periodontitis, Disease activity
* Correspondence: [email protected] de Reumatología, Hospital Universitario de Canarias, La Laguna,Spain7Departamento de Medicina, Facultad de Medicina, Calle Ofra s/n 38320, LaLaguna, SpainFull list of author information is available at the end of the article
© The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Rodríguez-Lozano et al. Arthritis Research & Therapy (2019) 21:27 https://doi.org/10.1186/s13075-019-1808-z

92
BackgroundRheumatoid arthritis (RA) is a systemic autoimmunechronic disease that causes inflammation and the prolif-eration of synovial membranes in di-arthrodial joints.When uncontrolled, RA destroys articular structures,resulting in functional disability, decreased quality of lifeand reduced life expectancy, mainly due to an increasedrisk of cardiovascular events [1]. RA is a multifactorialdisease of unknown etiology in which genetic suscepti-bility, environmental and hormonal factors interact incomplex ways [2]. The current understanding of RApathogenesis postulates that the activity of peptidil ar-ginine deiminase (PAD), an enzyme that transforms ar-ginine into citrulline, which causes a posttranslationalmodification in structural proteins, could be the mainevent in the early stages of RA. Although protein citrul-lination is not exclusive to RA, the formation ofanti-citrullinated protein antibodies (ACPA) is almostunique to this disease, these antibodies being a markerof aggressive RA [3, 4].Periodontitis is a chronic inflammatory disease charac-
terized by the destruction of the periodontal ligament andalveolar bone, which if untreated can lead to tooth loss.Periodontitis is considered one of the most prevalentchronic inflammatory noncommunicable diseases [5, 6].Recent epidemiological studies have highlighted the im-portant links between periodontitis and other chronic in-flammatory diseases such as diabetes or cardiovasculardisease [7, 8]. In this regard, clinical [9, 10] and epidemio-logical studies [11] have reported a high prevalence ofperiodontitis and tooth loss in RA patients, although thestrength of this association, its temporal link and the pos-sible relationship between the severity of periodontitis andRA disease activity remain unclear. Mikuls et al. [9] re-ported a statistically significant association between peri-odontitis and swollen joints, high-level disease activity andserum levels of ACPA in patients with RA. Other studies,however, were unable to find this link [12]. There is evi-dence that periodontitis and RA share genetic risk factorssuch as the HLA-DRB1 allele of the MHC class II mole-cules [13]. Similarly, environmental risk factors, such assmoking, socioeconomic status and obesity, may influenceboth diseases [2]. In spite of these well-established sharedrisk factors, some authors have explained this associationthrough the activity of some periodontal pathogens [2].Specifically, Porphyromonas gingivalis, a Gram-negative,anaerobic bacterium, by releasing a specific deaminase isable to induce protein citrullination, which through aprocess of mimicry might stimulate ACPA formation inRA patients [9, 14]. In severe periodontitis, the chronicexposure of citrullinated proteins and the subsequent de-velopment of autoantibodies could explain this reportedassociation between periodontitis and RA, but the existingevidence is still limited [15, 16].
The objective of this case–control study was to investi-gate the link between RA and periodontitis, to assesswhether RA disease activity is associated with periodon-titis severity and to determine the degree to which thisassociation is affected by shared risk factors.
Patients and methodsStudy populationRA patients (cases) were consecutively included fromthose outpatients attending the Department of Rheuma-tology of the Hospital Universitario de Canarias in Ten-erife from January to September 2016 following a designstratified by the use of biologics (see later). RA patientsaged 18 years and older fulfilling the 2010 ACR/EULARclassification criteria [17] were included and categorizedas early-onset RA (! 2 years of disease evolution) andestablished RA (> 2 years of disease evolution). Controlswere those patients matching in age suffering fromosteoarthritis or soft tissue rheumatic diseases seen cor-relatively in the rheumatology outpatient clinic of ourinstitution during the same time period. Patients havingfewer than eight teeth [12], having received periodontalor antibiotic treatment during the previous 6 months[18], with joint replacement(s), in need of antibioticprophylaxis, or being treated with cyclosporine A or an-ticonvulsants [19] were excluded.All enrolled subjects were informed about the objec-
tives and characteristics of this study and signed a writ-ten informed consent previously approved by the ethicscommittee of Hospital Universitario de Canarias.
Study variablesOutcome and exposure variablesFor all RA patients the following parameters were recorded:28-joint Disease Activity Score using the erythrocyte sedi-mentation rate (ESR) (DAS28) or C-reactive protein(DAS28-CRP) [20], the Simplified Disease Activity Index(SDAI) [21], the Clinical Disease Activity Index (CDAI)[22], the Health Assessment Questionnaire (HAQ) [23],rheumatoid factor (RF), ACPA and extra-articular manifes-tations. Patients were categorized into remission, low, mod-erate and high disease activity when at least two of theDAS28, DAS28-CRP and SDAI agreed on the level of dis-ease activity (combined index). Furthermore, in patientstreated with biologics, the RA activity was also expressed asthe mean ± SD of DAS28-CRP values obtained during the2-year period prior to the periodontal evaluation.Patients’ periodontal status was evaluated for cases
and controls using the following parameters (seeAdditional file 1): full mouth plaque index (PI) [24],bleeding on probing (BoP) [25], probing pocket depth(PPD), recession (REC), clinical attachment level (CAL) andtooth loss. Based on these parameters, patients were catego-rized into one of three case definitions of periodontitis [26]:
Rodríguez-Lozano et al. Arthritis Research & Therapy (2019) 21:27 Page 2 of 12

93
Level 0, individuals with a healthy periodontium and up toone proximal site with loss of attachment ! 3mm; Level 1,presence of proximal attachment and loss ! 3mm in ! 2nonadjacent teeth; and Level 2, presence of proximal attach-ment loss ! 5mm in ! 30% of teeth. PI and BoP were alsorecorded as percentages. In addition, when calculating thenumber of teeth, dental implants and third molars wereexcluded.The presence of comorbidities, such as diabetes melli-
tus, osteoporosis, myocardial infarction or dyslipidemia,as well as body mass index (BMI) were recorded for allpatients. In RA patients, any history of therapy with glu-cocorticoids, synthetic disease-modifying antirheumaticdrugs (sDMARDs) and bDMARDs was also recorded.Anthropometric and socioeconomic variables were
also recorded including BMI, smoking status, stress bythe Perceived Stress Scale (PSS-14) categorized into highstress yes (> 28 points) or no (" 28 points) [27, 28] andsocial welfare indicators using the Graffar Scale ques-tionnaire [29].
Study designThis was an observational, case–control study of RA pa-tients treated in a single rheumatology department whowere assessed for the presence and severity of periodon-tal disease.
Medical examinationCases were subjected to a routine medical examination.The patient’s and care provider’s global assessments ofdisease activity were based on a 100-mm visual analogscale (VAS), and the RA functional index was assessedby the HAQ. Disease activity was calculated by means ofDAS28, DAS28-CRP, SDAI and CDAI scores, and themedications used were logged from the patient files andby asking the patient during medical examination. Bloodsamples were tested for plasma RF and CRP using animmunoturbidimetric assay (Roche/cobas® 8000 ModularAnalyzer Series; Roche Diagnostics, USA) and for ACPA(anti-cyclic citrullinated peptide anti-CCP-2 by Immu-noscan CCPlus®; Euro Diagnostica), with a positive valueestablished as that exceeding 25 U/ml in both serologicaltests and 3mg/l in the CRP test.
Periodontal examinationA full oral and periodontal examination was carried outby two experienced periodontists masked to the patient’sdiagnosis. A kappa test showed 70% inter-examiner con-cordance. Queried dental visits and symptoms of oralsicca were also recorded.Full mouth PPD and CAL measurements were registered
using an UNC-15 periodontal probe (six sites per tooth),excluding third molars and implants. Full mouth periapicalX-ray scans were taken to confirm the periodontal
diagnosis when it was not clear. Although subjects were in-formed on their periodontal status and advised to seek peri-odontal therapy when appropriate, no periodontal therapywas rendered as part of this investigation.
Sample size and statistical analysesFor sample size calculation we used the DAS28 score asthe main outcome variable, with the assumption of thedifference between RA patients exposed (with periodon-titis) versus nonexposed (without periodontitis) reportedby Mikuls et al. [9]. A sample size of 166 patients wasestimated to provide 80% power to achieve statistical sig-nificance at a two-sided significance level of 0.05, and as-suming a 15% dropout rate, and therefore we included190 patients per group. Thirty percent of RA patients inour service were being treated with biologicdisease-modifying antirheumatic drugs (bDMARDs). Tomaintain this proportion, 56 biologic-treated patientswere included in our study. Descriptive statistics werepresented as means, standard deviations (SDs) and fre-quency distributions. Inter-group comparisons for thecontinuous variables were studied with a t test andone-way ANOVA with Dunnett’s post test. The Mann–Whitney U test and Kruskall–Wallis test were used fornonparametric continuous variables and a chi-squaredtest for categorical variables, using Fisher’s exact test inthe comparison of 2 ! 2 tables with expected values < 5.The degree of relationship between the categorical or-dinal variables was measured with Kendall’s tau-b correl-ation coefficient.The study of the relationship between periodontitis
(exposure) and RA (outcome) was carried out with a lo-gistic regression model examining the odds ratio (OR)and 95% confidence intervals (CIs). Additionally, thesevalues were adjusted for possible confounders (covari-ates) such as age, sex, sociodemographic index, annualdental prophylaxis, tobacco use, BMI and comorbidities.In RA patients, the relationship between periodontitisseverity (classified as Level 0 + 1 and Level 2) and RAdisease activity levels (classified as remission, low andmoderate + high) was studied with an ordinal logistic re-gression model taking into account the information fromthe previous covariates. The coefficients of the differentcovariates and factors verified the test of parallel lines (p= 0.340). The linear predictor of cumulated probabilitieswas assessed, maintaining the sign of the thresholds andchanging the sign of coefficient estimations of the differ-ent covariates [30]. A linear regression analysis was per-formed to elucidate any association between the DAS28and DAS28-CRP scores and periodontal attachment loss.Finally, the relationships between periodontitis levelsand RA treatments (one or more DMARDs, biologicsand steroids), and positivity for autoantibodies (RF andanti-CCP), were analyzed by chi-squared test.
Rodríguez-Lozano et al. Arthritis Research & Therapy (2019) 21:27 Page 3 of 12
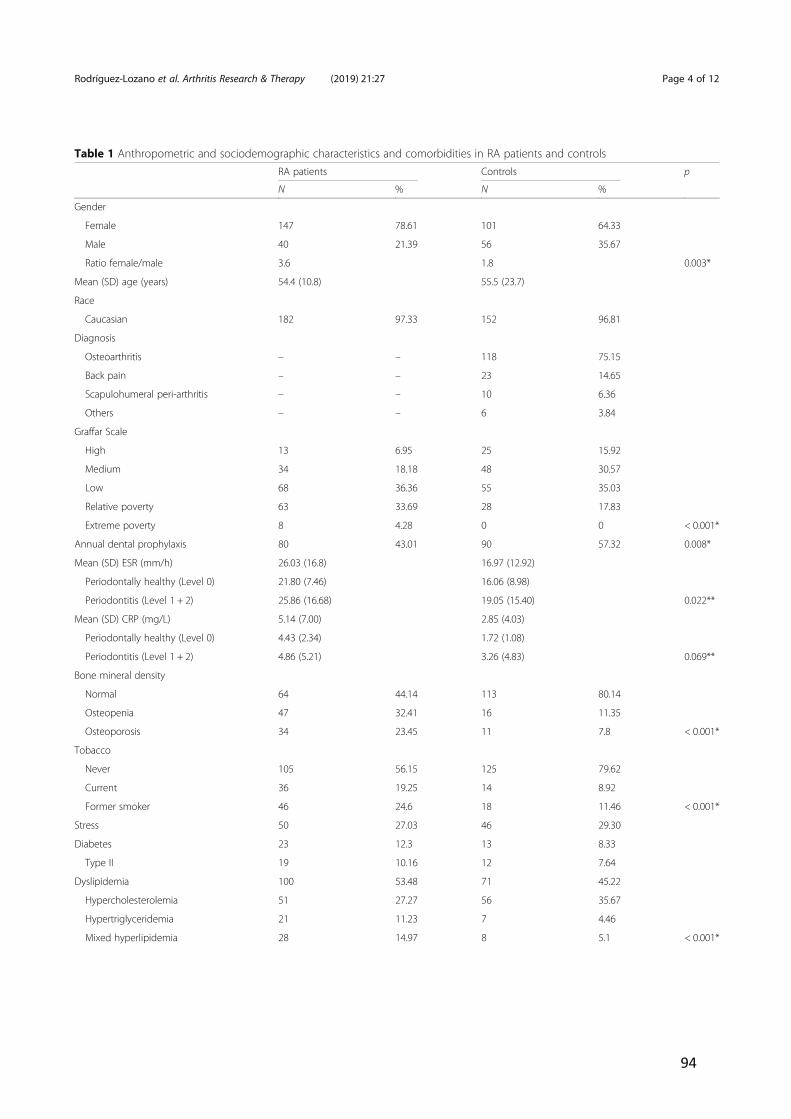
94
Table 1 Anthropometric and sociodemographic characteristics and comorbidities in RA patients and controlsRA patients Controls p
N % N %
Gender
Female 147 78.61 101 64.33
Male 40 21.39 56 35.67
Ratio female/male 3.6 1.8 0.003*
Mean (SD) age (years) 54.4 (10.8) 55.5 (23.7)
Race
Caucasian 182 97.33 152 96.81
Diagnosis
Osteoarthritis – – 118 75.15
Back pain – – 23 14.65
Scapulohumeral peri-arthritis – – 10 6.36
Others – – 6 3.84
Graffar Scale
High 13 6.95 25 15.92
Medium 34 18.18 48 30.57
Low 68 36.36 55 35.03
Relative poverty 63 33.69 28 17.83
Extreme poverty 8 4.28 0 0 < 0.001*
Annual dental prophylaxis 80 43.01 90 57.32 0.008*
Mean (SD) ESR (mm/h) 26.03 (16.8) 16.97 (12.92)
Periodontally healthy (Level 0) 21.80 (7.46) 16.06 (8.98)
Periodontitis (Level 1 + 2) 25.86 (16.68) 19.05 (15.40) 0.022**
Mean (SD) CRP (mg/L) 5.14 (7.00) 2.85 (4.03)
Periodontally healthy (Level 0) 4.43 (2.34) 1.72 (1.08)
Periodontitis (Level 1 + 2) 4.86 (5.21) 3.26 (4.83) 0.069**
Bone mineral density
Normal 64 44.14 113 80.14
Osteopenia 47 32.41 16 11.35
Osteoporosis 34 23.45 11 7.8 < 0.001*
Tobacco
Never 105 56.15 125 79.62
Current 36 19.25 14 8.92
Former smoker 46 24.6 18 11.46 < 0.001*
Stress 50 27.03 46 29.30
Diabetes 23 12.3 13 8.33
Type II 19 10.16 12 7.64
Dyslipidemia 100 53.48 71 45.22
Hypercholesterolemia 51 27.27 56 35.67
Hypertriglyceridemia 21 11.23 7 4.46
Mixed hyperlipidemia 28 14.97 8 5.1 < 0.001*
Rodríguez-Lozano et al. Arthritis Research & Therapy (2019) 21:27 Page 4 of 12
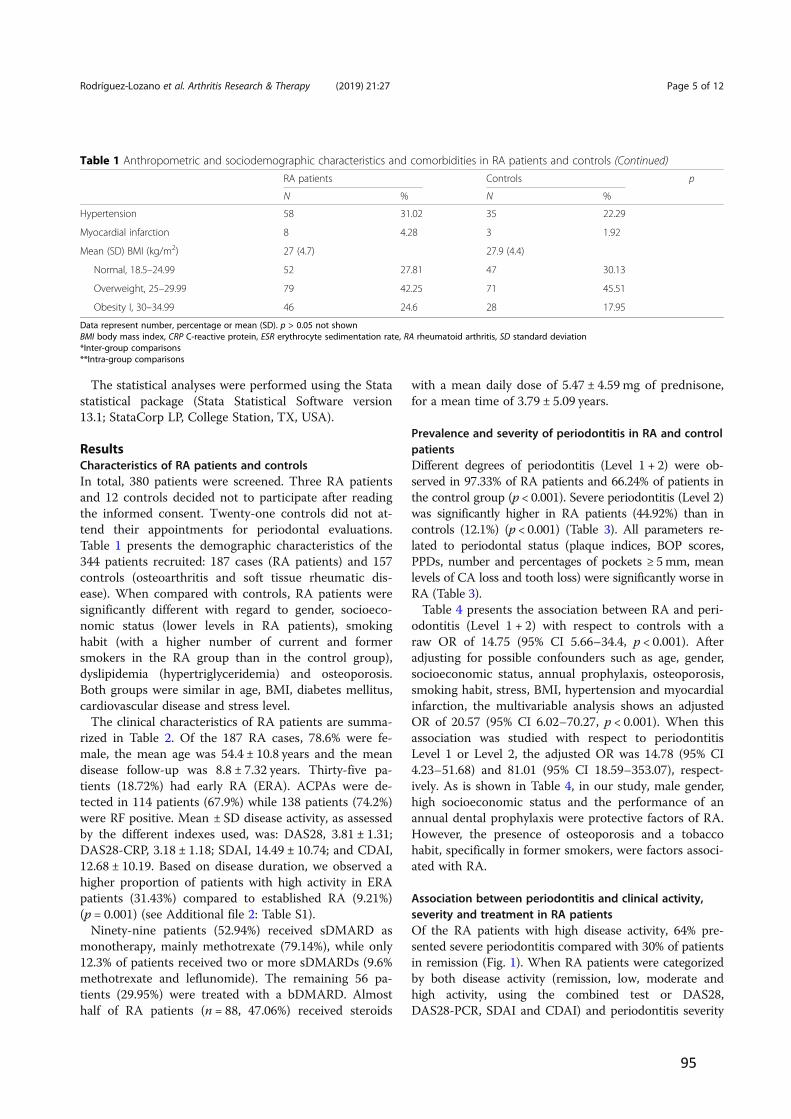
95
The statistical analyses were performed using the Statastatistical package (Stata Statistical Software version13.1; StataCorp LP, College Station, TX, USA).
ResultsCharacteristics of RA patients and controlsIn total, 380 patients were screened. Three RA patientsand 12 controls decided not to participate after readingthe informed consent. Twenty-one controls did not at-tend their appointments for periodontal evaluations.Table 1 presents the demographic characteristics of the344 patients recruited: 187 cases (RA patients) and 157controls (osteoarthritis and soft tissue rheumatic dis-ease). When compared with controls, RA patients weresignificantly different with regard to gender, socioeco-nomic status (lower levels in RA patients), smokinghabit (with a higher number of current and formersmokers in the RA group than in the control group),dyslipidemia (hypertriglyceridemia) and osteoporosis.Both groups were similar in age, BMI, diabetes mellitus,cardiovascular disease and stress level.The clinical characteristics of RA patients are summa-
rized in Table 2. Of the 187 RA cases, 78.6% were fe-male, the mean age was 54.4 ± 10.8 years and the meandisease follow-up was 8.8 ± 7.32 years. Thirty-five pa-tients (18.72%) had early RA (ERA). ACPAs were de-tected in 114 patients (67.9%) while 138 patients (74.2%)were RF positive. Mean ± SD disease activity, as assessedby the different indexes used, was: DAS28, 3.81 ± 1.31;DAS28-CRP, 3.18 ± 1.18; SDAI, 14.49 ± 10.74; and CDAI,12.68 ± 10.19. Based on disease duration, we observed ahigher proportion of patients with high activity in ERApatients (31.43%) compared to established RA (9.21%)(p = 0.001) (see Additional file 2: Table S1).Ninety-nine patients (52.94%) received sDMARD as
monotherapy, mainly methotrexate (79.14%), while only12.3% of patients received two or more sDMARDs (9.6%methotrexate and leflunomide). The remaining 56 pa-tients (29.95%) were treated with a bDMARD. Almosthalf of RA patients (n = 88, 47.06%) received steroids
with a mean daily dose of 5.47 ± 4.59 mg of prednisone,for a mean time of 3.79 ± 5.09 years.
Prevalence and severity of periodontitis in RA and controlpatientsDifferent degrees of periodontitis (Level 1 + 2) were ob-served in 97.33% of RA patients and 66.24% of patients inthe control group (p < 0.001). Severe periodontitis (Level 2)was significantly higher in RA patients (44.92%) than incontrols (12.1%) (p < 0.001) (Table 3). All parameters re-lated to periodontal status (plaque indices, BOP scores,PPDs, number and percentages of pockets ! 5mm, meanlevels of CA loss and tooth loss) were significantly worse inRA (Table 3).Table 4 presents the association between RA and peri-
odontitis (Level 1 + 2) with respect to controls with araw OR of 14.75 (95% CI 5.66–34.4, p < 0.001). Afteradjusting for possible confounders such as age, gender,socioeconomic status, annual prophylaxis, osteoporosis,smoking habit, stress, BMI, hypertension and myocardialinfarction, the multivariable analysis shows an adjustedOR of 20.57 (95% CI 6.02–70.27, p < 0.001). When thisassociation was studied with respect to periodontitisLevel 1 or Level 2, the adjusted OR was 14.78 (95% CI4.23–51.68) and 81.01 (95% CI 18.59–353.07), respect-ively. As is shown in Table 4, in our study, male gender,high socioeconomic status and the performance of anannual dental prophylaxis were protective factors of RA.However, the presence of osteoporosis and a tobaccohabit, specifically in former smokers, were factors associ-ated with RA.
Association between periodontitis and clinical activity,severity and treatment in RA patientsOf the RA patients with high disease activity, 64% pre-sented severe periodontitis compared with 30% of patientsin remission (Fig. 1). When RA patients were categorizedby both disease activity (remission, low, moderate andhigh activity, using the combined test or DAS28,DAS28-PCR, SDAI and CDAI) and periodontitis severity
Table 1 Anthropometric and sociodemographic characteristics and comorbidities in RA patients and controls (Continued)RA patients Controls p
N % N %
Hypertension 58 31.02 35 22.29
Myocardial infarction 8 4.28 3 1.92
Mean (SD) BMI (kg/m2) 27 (4.7) 27.9 (4.4)
Normal, 18.5–24.99 52 27.81 47 30.13
Overweight, 25–29.99 79 42.25 71 45.51
Obesity I, 30–34.99 46 24.6 28 17.95
Data represent number, percentage or mean (SD). p > 0.05 not shownBMI body mass index, CRP C-reactive protein, ESR erythrocyte sedimentation rate, RA rheumatoid arthritis, SD standard deviation*Inter-group comparisons**Intra-group comparisons
Rodríguez-Lozano et al. Arthritis Research & Therapy (2019) 21:27 Page 5 of 12
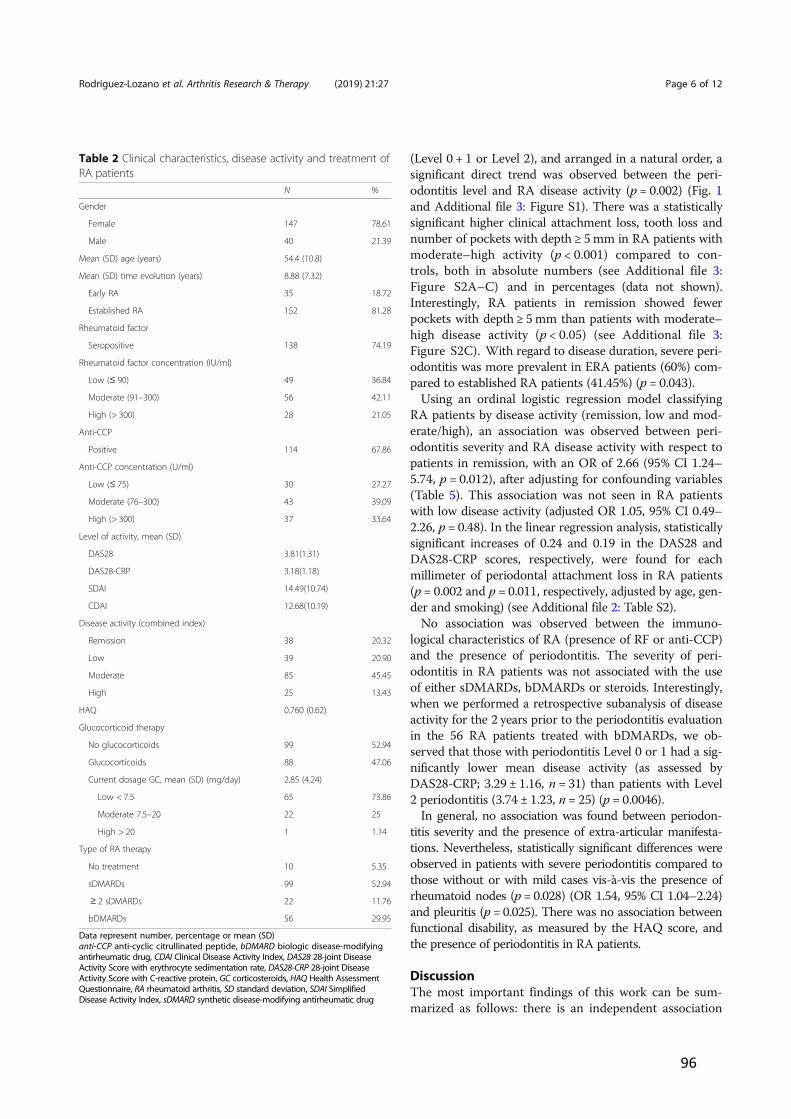
96
(Level 0 + 1 or Level 2), and arranged in a natural order, asignificant direct trend was observed between the peri-odontitis level and RA disease activity (p = 0.002) (Fig. 1and Additional file 3: Figure S1). There was a statisticallysignificant higher clinical attachment loss, tooth loss andnumber of pockets with depth ! 5mm in RA patients withmoderate–high activity (p < 0.001) compared to con-trols, both in absolute numbers (see Additional file 3:Figure S2A–C) and in percentages (data not shown).Interestingly, RA patients in remission showed fewerpockets with depth ! 5mm than patients with moderate–high disease activity (p < 0.05) (see Additional file 3:Figure S2C). With regard to disease duration, severe peri-odontitis was more prevalent in ERA patients (60%) com-pared to established RA patients (41.45%) (p = 0.043).Using an ordinal logistic regression model classifying
RA patients by disease activity (remission, low and mod-erate/high), an association was observed between peri-odontitis severity and RA disease activity with respect topatients in remission, with an OR of 2.66 (95% CI 1.24–5.74, p = 0.012), after adjusting for confounding variables(Table 5). This association was not seen in RA patientswith low disease activity (adjusted OR 1.05, 95% CI 0.49–2.26, p = 0.48). In the linear regression analysis, statisticallysignificant increases of 0.24 and 0.19 in the DAS28 andDAS28-CRP scores, respectively, were found for eachmillimeter of periodontal attachment loss in RA patients(p = 0.002 and p = 0.011, respectively, adjusted by age, gen-der and smoking) (see Additional file 2: Table S2).No association was observed between the immuno-
logical characteristics of RA (presence of RF or anti-CCP)and the presence of periodontitis. The severity of peri-odontitis in RA patients was not associated with the useof either sDMARDs, bDMARDs or steroids. Interestingly,when we performed a retrospective subanalysis of diseaseactivity for the 2 years prior to the periodontitis evaluationin the 56 RA patients treated with bDMARDs, we ob-served that those with periodontitis Level 0 or 1 had a sig-nificantly lower mean disease activity (as assessed byDAS28-CRP; 3.29 ± 1.16, n = 31) than patients with Level2 periodontitis (3.74 ± 1.23, n = 25) (p = 0.0046).In general, no association was found between periodon-
titis severity and the presence of extra-articular manifesta-tions. Nevertheless, statistically significant differences wereobserved in patients with severe periodontitis compared tothose without or with mild cases vis-à-vis the presence ofrheumatoid nodes (p = 0.028) (OR 1.54, 95% CI 1.04–2.24)and pleuritis (p = 0.025). There was no association betweenfunctional disability, as measured by the HAQ score, andthe presence of periodontitis in RA patients.
DiscussionThe most important findings of this work can be sum-marized as follows: there is an independent association
Table 2 Clinical characteristics, disease activity and treatment ofRA patients
N %
Gender
Female 147 78.61
Male 40 21.39
Mean (SD) age (years) 54.4 (10.8)
Mean (SD) time evolution (years) 8.88 (7.32)
Early RA 35 18.72
Established RA 152 81.28
Rheumatoid factor
Seropositive 138 74.19
Rheumatoid factor concentration (IU/ml)
Low (! 90) 49 36.84
Moderate (91–300) 56 42.11
High (> 300) 28 21.05
Anti-CCP
Positive 114 67.86
Anti-CCP concentration (U/ml)
Low (! 75) 30 27.27
Moderate (76–300) 43 39.09
High (> 300) 37 33.64
Level of activity, mean (SD)
DAS28 3.81(1.31)
DAS28-CRP 3.18(1.18)
SDAI 14.49(10.74)
CDAI 12.68(10.19)
Disease activity (combined index)
Remission 38 20.32
Low 39 20.90
Moderate 85 45.45
High 25 13.43
HAQ 0.760 (0.62)
Glucocorticoid therapy
No glucocorticoids 99 52.94
Glucocorticoids 88 47.06
Current dosage GC, mean (SD) (mg/day) 2.85 (4.24)
Low < 7.5 65 73.86
Moderate 7.5–20 22 25
High > 20 1 1.14
Type of RA therapy
No treatment 10 5.35
sDMARDs 99 52.94
" 2 sDMARDs 22 11.76
bDMARDs 56 29.95
Data represent number, percentage or mean (SD)anti-CCP anti-cyclic citrullinated peptide, bDMARD biologic disease-modifyingantirheumatic drug, CDAI Clinical Disease Activity Index, DAS28 28-joint DiseaseActivity Score with erythrocyte sedimentation rate, DAS28-CRP 28-joint DiseaseActivity Score with C-reactive protein, GC corticosteroids, HAQ Health AssessmentQuestionnaire, RA rheumatoid arthritis, SD standard deviation, SDAI SimplifiedDisease Activity Index, sDMARD synthetic disease-modifying antirheumatic drug
Rodríguez-Lozano et al. Arthritis Research & Therapy (2019) 21:27 Page 6 of 12
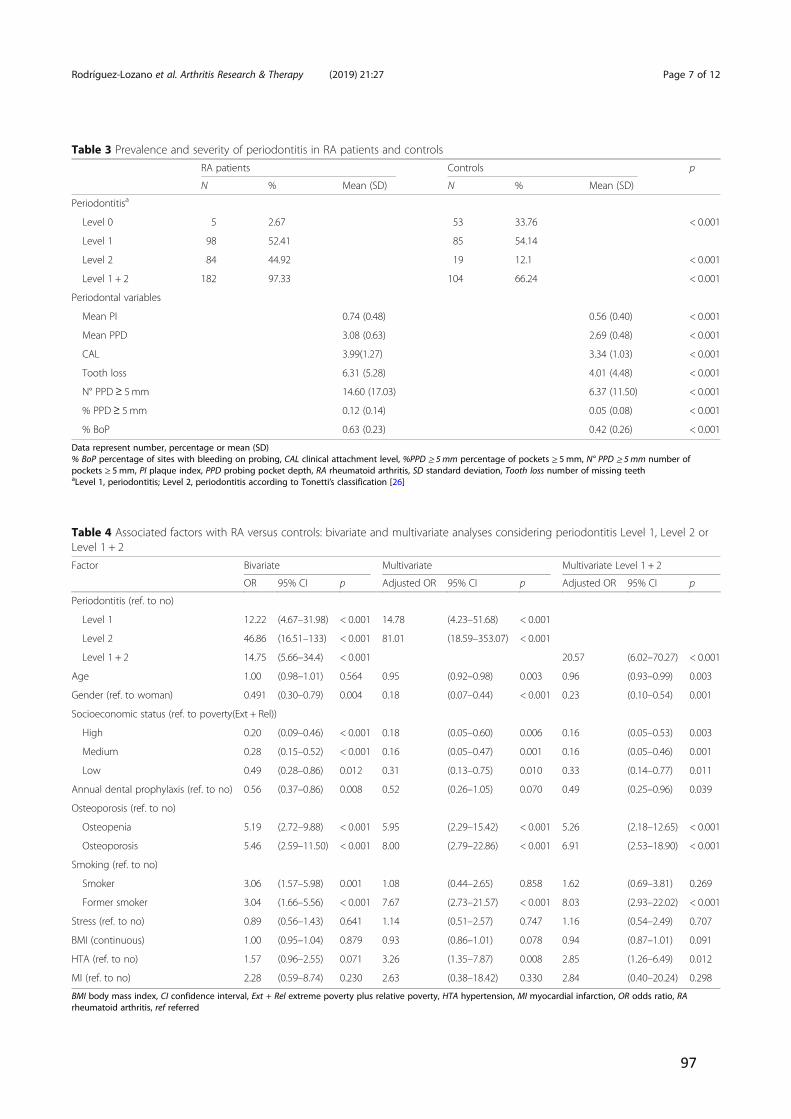
97
Table 3 Prevalence and severity of periodontitis in RA patients and controlsRA patients Controls p
N % Mean (SD) N % Mean (SD)
Periodontitisa
Level 0 5 2.67 53 33.76 < 0.001
Level 1 98 52.41 85 54.14
Level 2 84 44.92 19 12.1 < 0.001
Level 1 + 2 182 97.33 104 66.24 < 0.001
Periodontal variables
Mean PI 0.74 (0.48) 0.56 (0.40) < 0.001
Mean PPD 3.08 (0.63) 2.69 (0.48) < 0.001
CAL 3.99(1.27) 3.34 (1.03) < 0.001
Tooth loss 6.31 (5.28) 4.01 (4.48) < 0.001
N° PPD ! 5 mm 14.60 (17.03) 6.37 (11.50) < 0.001
% PPD! 5 mm 0.12 (0.14) 0.05 (0.08) < 0.001
% BoP 0.63 (0.23) 0.42 (0.26) < 0.001
Data represent number, percentage or mean (SD)% BoP percentage of sites with bleeding on probing, CAL clinical attachment level, %PPD ! 5 mm percentage of pockets ! 5 mm, N° PPD ! 5 mm number ofpockets ! 5 mm, PI plaque index, PPD probing pocket depth, RA rheumatoid arthritis, SD standard deviation, Tooth loss number of missing teethaLevel 1, periodontitis; Level 2, periodontitis according to Tonetti’s classification [26]
Table 4 Associated factors with RA versus controls: bivariate and multivariate analyses considering periodontitis Level 1, Level 2 orLevel 1 + 2Factor Bivariate Multivariate Multivariate Level 1 + 2
OR 95% CI p Adjusted OR 95% CI p Adjusted OR 95% CI p
Periodontitis (ref. to no)
Level 1 12.22 (4.67–31.98) < 0.001 14.78 (4.23–51.68) < 0.001
Level 2 46.86 (16.51–133) < 0.001 81.01 (18.59–353.07) < 0.001
Level 1 + 2 14.75 (5.66–34.4) < 0.001 20.57 (6.02–70.27) < 0.001
Age 1.00 (0.98–1.01) 0.564 0.95 (0.92–0.98) 0.003 0.96 (0.93–0.99) 0.003
Gender (ref. to woman) 0.491 (0.30–0.79) 0.004 0.18 (0.07–0.44) < 0.001 0.23 (0.10–0.54) 0.001
Socioeconomic status (ref. to poverty(Ext + Rel))
High 0.20 (0.09–0.46) < 0.001 0.18 (0.05–0.60) 0.006 0.16 (0.05–0.53) 0.003
Medium 0.28 (0.15–0.52) < 0.001 0.16 (0.05–0.47) 0.001 0.16 (0.05–0.46) 0.001
Low 0.49 (0.28–0.86) 0.012 0.31 (0.13–0.75) 0.010 0.33 (0.14–0.77) 0.011
Annual dental prophylaxis (ref. to no) 0.56 (0.37–0.86) 0.008 0.52 (0.26–1.05) 0.070 0.49 (0.25–0.96) 0.039
Osteoporosis (ref. to no)
Osteopenia 5.19 (2.72–9.88) < 0.001 5.95 (2.29–15.42) < 0.001 5.26 (2.18–12.65) < 0.001
Osteoporosis 5.46 (2.59–11.50) < 0.001 8.00 (2.79–22.86) < 0.001 6.91 (2.53–18.90) < 0.001
Smoking (ref. to no)
Smoker 3.06 (1.57–5.98) 0.001 1.08 (0.44–2.65) 0.858 1.62 (0.69–3.81) 0.269
Former smoker 3.04 (1.66–5.56) < 0.001 7.67 (2.73–21.57) < 0.001 8.03 (2.93–22.02) < 0.001
Stress (ref. to no) 0.89 (0.56–1.43) 0.641 1.14 (0.51–2.57) 0.747 1.16 (0.54–2.49) 0.707
BMI (continuous) 1.00 (0.95–1.04) 0.879 0.93 (0.86–1.01) 0.078 0.94 (0.87–1.01) 0.091
HTA (ref. to no) 1.57 (0.96–2.55) 0.071 3.26 (1.35–7.87) 0.008 2.85 (1.26–6.49) 0.012
MI (ref. to no) 2.28 (0.59–8.74) 0.230 2.63 (0.38–18.42) 0.330 2.84 (0.40–20.24) 0.298
BMI body mass index, CI confidence interval, Ext + Rel extreme poverty plus relative poverty, HTA hypertension, MI myocardial infarction, OR odds ratio, RArheumatoid arthritis, ref referred
Rodríguez-Lozano et al. Arthritis Research & Therapy (2019) 21:27 Page 7 of 12
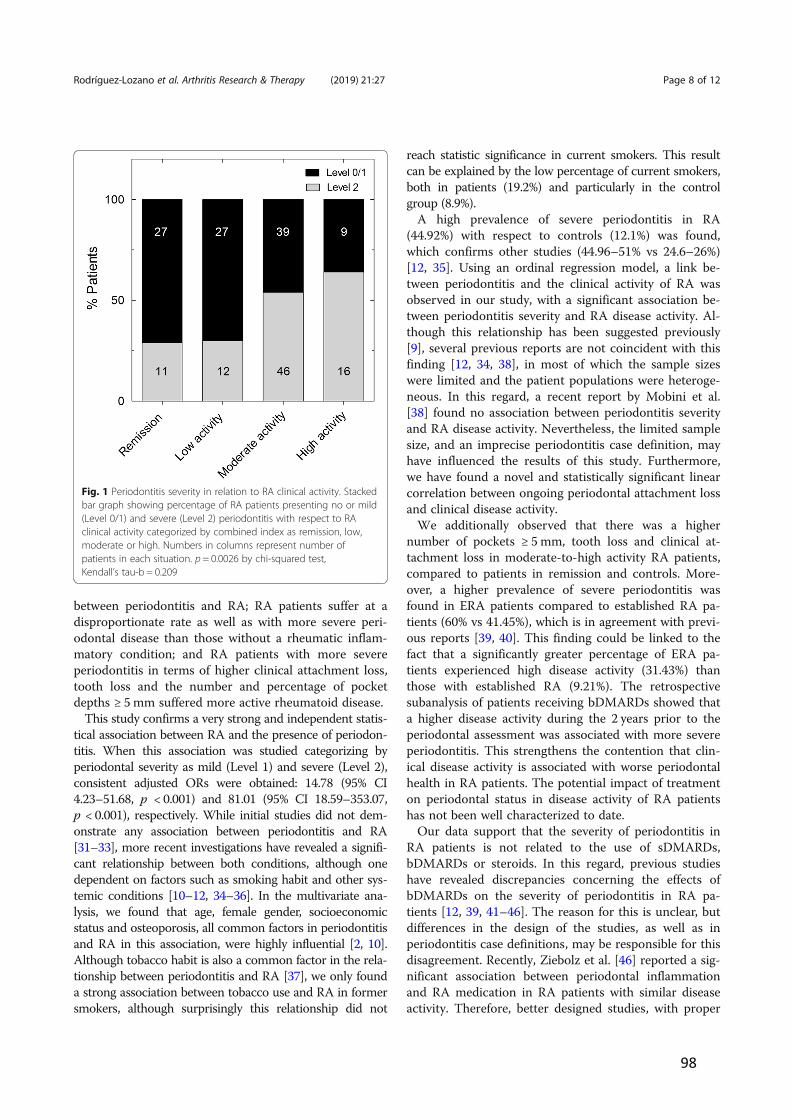
98
between periodontitis and RA; RA patients suffer at adisproportionate rate as well as with more severe peri-odontal disease than those without a rheumatic inflam-matory condition; and RA patients with more severeperiodontitis in terms of higher clinical attachment loss,tooth loss and the number and percentage of pocketdepths ! 5 mm suffered more active rheumatoid disease.This study confirms a very strong and independent statis-
tical association between RA and the presence of periodon-titis. When this association was studied categorizing byperiodontal severity as mild (Level 1) and severe (Level 2),consistent adjusted ORs were obtained: 14.78 (95% CI4.23–51.68, p < 0.001) and 81.01 (95% CI 18.59–353.07,p < 0.001), respectively. While initial studies did not dem-onstrate any association between periodontitis and RA[31–33], more recent investigations have revealed a signifi-cant relationship between both conditions, although onedependent on factors such as smoking habit and other sys-temic conditions [10–12, 34–36]. In the multivariate ana-lysis, we found that age, female gender, socioeconomicstatus and osteoporosis, all common factors in periodontitisand RA in this association, were highly influential [2, 10].Although tobacco habit is also a common factor in the rela-tionship between periodontitis and RA [37], we only founda strong association between tobacco use and RA in formersmokers, although surprisingly this relationship did not
reach statistic significance in current smokers. This resultcan be explained by the low percentage of current smokers,both in patients (19.2%) and particularly in the controlgroup (8.9%).A high prevalence of severe periodontitis in RA
(44.92%) with respect to controls (12.1%) was found,which confirms other studies (44.96–51% vs 24.6–26%)[12, 35]. Using an ordinal regression model, a link be-tween periodontitis and the clinical activity of RA wasobserved in our study, with a significant association be-tween periodontitis severity and RA disease activity. Al-though this relationship has been suggested previously[9], several previous reports are not coincident with thisfinding [12, 34, 38], in most of which the sample sizeswere limited and the patient populations were heteroge-neous. In this regard, a recent report by Mobini et al.[38] found no association between periodontitis severityand RA disease activity. Nevertheless, the limited samplesize, and an imprecise periodontitis case definition, mayhave influenced the results of this study. Furthermore,we have found a novel and statistically significant linearcorrelation between ongoing periodontal attachment lossand clinical disease activity.We additionally observed that there was a higher
number of pockets ! 5 mm, tooth loss and clinical at-tachment loss in moderate-to-high activity RA patients,compared to patients in remission and controls. More-over, a higher prevalence of severe periodontitis wasfound in ERA patients compared to established RA pa-tients (60% vs 41.45%), which is in agreement with previ-ous reports [39, 40]. This finding could be linked to thefact that a significantly greater percentage of ERA pa-tients experienced high disease activity (31.43%) thanthose with established RA (9.21%). The retrospectivesubanalysis of patients receiving bDMARDs showed thata higher disease activity during the 2 years prior to theperiodontal assessment was associated with more severeperiodontitis. This strengthens the contention that clin-ical disease activity is associated with worse periodontalhealth in RA patients. The potential impact of treatmenton periodontal status in disease activity of RA patientshas not been well characterized to date.Our data support that the severity of periodontitis in
RA patients is not related to the use of sDMARDs,bDMARDs or steroids. In this regard, previous studieshave revealed discrepancies concerning the effects ofbDMARDs on the severity of periodontitis in RA pa-tients [12, 39, 41–46]. The reason for this is unclear, butdifferences in the design of the studies, as well as inperiodontitis case definitions, may be responsible for thisdisagreement. Recently, Ziebolz et al. [46] reported a sig-nificant association between periodontal inflammationand RA medication in RA patients with similar diseaseactivity. Therefore, better designed studies, with proper
Fig. 1 Periodontitis severity in relation to RA clinical activity. Stackedbar graph showing percentage of RA patients presenting no or mild(Level 0/1) and severe (Level 2) periodontitis with respect to RAclinical activity categorized by combined index as remission, low,moderate or high. Numbers in columns represent number ofpatients in each situation. p = 0.0026 by chi-squared test,Kendall’s tau-b = 0.209
Rodríguez-Lozano et al. Arthritis Research & Therapy (2019) 21:27 Page 8 of 12
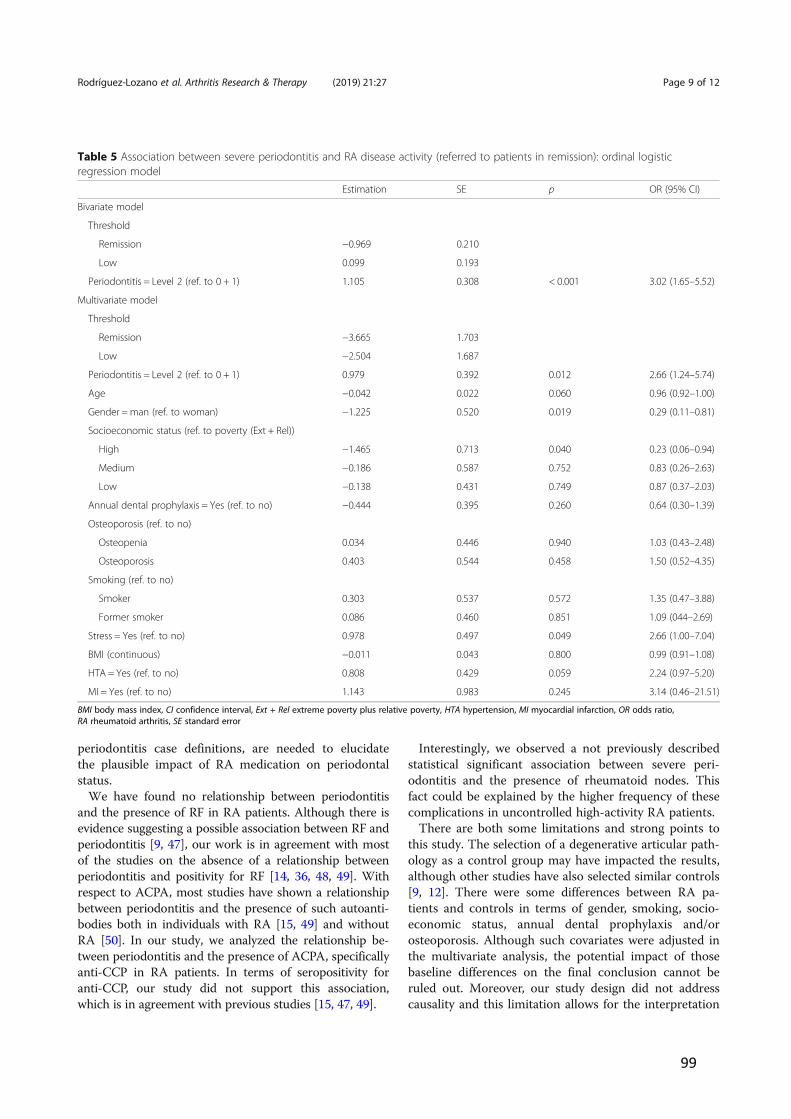
99
periodontitis case definitions, are needed to elucidatethe plausible impact of RA medication on periodontalstatus.We have found no relationship between periodontitis
and the presence of RF in RA patients. Although there isevidence suggesting a possible association between RF andperiodontitis [9, 47], our work is in agreement with mostof the studies on the absence of a relationship betweenperiodontitis and positivity for RF [14, 36, 48, 49]. Withrespect to ACPA, most studies have shown a relationshipbetween periodontitis and the presence of such autoanti-bodies both in individuals with RA [15, 49] and withoutRA [50]. In our study, we analyzed the relationship be-tween periodontitis and the presence of ACPA, specificallyanti-CCP in RA patients. In terms of seropositivity foranti-CCP, our study did not support this association,which is in agreement with previous studies [15, 47, 49].
Interestingly, we observed a not previously describedstatistical significant association between severe peri-odontitis and the presence of rheumatoid nodes. Thisfact could be explained by the higher frequency of thesecomplications in uncontrolled high-activity RA patients.There are both some limitations and strong points to
this study. The selection of a degenerative articular path-ology as a control group may have impacted the results,although other studies have also selected similar controls[9, 12]. There were some differences between RA pa-tients and controls in terms of gender, smoking, socio-economic status, annual dental prophylaxis and/orosteoporosis. Although such covariates were adjusted inthe multivariate analysis, the potential impact of thosebaseline differences on the final conclusion cannot beruled out. Moreover, our study design did not addresscausality and this limitation allows for the interpretation
Table 5 Association between severe periodontitis and RA disease activity (referred to patients in remission): ordinal logisticregression model
Estimation SE p OR (95% CI)
Bivariate model
Threshold
Remission !0.969 0.210
Low 0.099 0.193
Periodontitis = Level 2 (ref. to 0 + 1) 1.105 0.308 < 0.001 3.02 (1.65–5.52)
Multivariate model
Threshold
Remission !3.665 1.703
Low !2.504 1.687
Periodontitis = Level 2 (ref. to 0 + 1) 0.979 0.392 0.012 2.66 (1.24–5.74)
Age !0.042 0.022 0.060 0.96 (0.92–1.00)
Gender =man (ref. to woman) !1.225 0.520 0.019 0.29 (0.11–0.81)
Socioeconomic status (ref. to poverty (Ext + Rel))
High !1.465 0.713 0.040 0.23 (0.06–0.94)
Medium !0.186 0.587 0.752 0.83 (0.26–2.63)
Low !0.138 0.431 0.749 0.87 (0.37–2.03)
Annual dental prophylaxis = Yes (ref. to no) !0.444 0.395 0.260 0.64 (0.30–1.39)
Osteoporosis (ref. to no)
Osteopenia 0.034 0.446 0.940 1.03 (0.43–2.48)
Osteoporosis 0.403 0.544 0.458 1.50 (0.52–4.35)
Smoking (ref. to no)
Smoker 0.303 0.537 0.572 1.35 (0.47–3.88)
Former smoker 0.086 0.460 0.851 1.09 (044–2.69)
Stress = Yes (ref. to no) 0.978 0.497 0.049 2.66 (1.00–7.04)
BMI (continuous) !0.011 0.043 0.800 0.99 (0.91–1.08)
HTA = Yes (ref. to no) 0.808 0.429 0.059 2.24 (0.97–5.20)
MI = Yes (ref. to no) 1.143 0.983 0.245 3.14 (0.46–21.51)
BMI body mass index, CI confidence interval, Ext + Rel extreme poverty plus relative poverty, HTA hypertension, MI myocardial infarction, OR odds ratio,RA rheumatoid arthritis, SE standard error
Rodríguez-Lozano et al. Arthritis Research & Therapy (2019) 21:27 Page 9 of 12

100
of these data, either as a measure of the severity of theimpact of periodontitis on RA disease activity or, con-versely, as evidence that RA activity influences the sever-ity of periodontitis. With regard to the statistical powerand selection bias, a large sample size from the targetpopulation in different stages of disease progression andactivity was recruited, which reduced the selection bias.We adopted the case definition of periodontitis recom-mended by the European Federation of Periodontology[26], which has been extensively used in epidemiologicalstudies [51–53] and has proven its validity. We con-ducted full mouth examinations, which differs fromother similar studies that made only partial mouth eval-uations. The assessment was carried by two experiencedperiodontists and showed high inter-examiner reproduci-bility. This may have resulted in an overestimation orunderestimation of the exposure [11, 12, 14, 54]. On theother hand, we have analyzed RA disease activity bymeans of three indexes (DAS28, DAS28-CRP and SDAI)in order to avoid the high heterogeneity reported whendefining RA disease activity [10, 12, 34, 36]. This enabledus to establish the level of RA disease activity when two ofthe three used indexes agreed. Therefore, the results fromthis investigation provide a basis for further prospectiveinterventional studies that could deepen our understand-ing of the association between periodontitis and RA.
ConclusionsThis study has demonstrated a significant association be-tween RA and periodontitis, and more specifically be-tween periodontitis severity and RA disease activity. Theseresults suggest an independent relationship between se-vere periodontitis and RA in spite of common shared riskfactors and other confounding factors affecting both dis-eases. Further well-designed prospective interventionstudies are needed to elucidate how periodontitis may in-fluence the development and progression of RA.
Additional files
Additional file 1: Periodontal section. (DOC 25 kb)
Additional file 2: Table S1. Disease activity in early and established RApatients. Table S2. Linear regression model of clinical attachment leveland RA disease activity. (DOC 59 kb)
Additional file 3: Figure S1. Relationship between RA disease activityassessed by different indexes and periodontitis severity. Figure S2Periodontal parameters in patients with RA in relation to their clinicalactivity. (DOC 399 kb)
AbbreviationsACPA: Anti-citrullinated peptide antibodies; Anti-CCP: Anti-cyclic citrullinatedpeptide; bDMARD: Biologic disease-modifying antirheumatic drug; BMI: Bodymass index; BoP: Bleeding of probing; CAL: Clinical attachment level;CDAI: Clinical Disease Activity Index; CRP: C-reactive protein; DAS28: 28-jointDisease Activity Score; DMARD: Disease-modifying antirheumatic drug;ERA: Early rheumatoid arthritis; ESR: Erythrocyte sedimentation rate;HAQ: Health Assessment Questionnaire; OD: Odds ratio; PAD: Peptidil
arginine deiminase; PI: Plaque index; PPD: Proving pocket depth; PSS-14: Perceived Stress Scale; RA: Rheumatoid arthritis; REC: Recession;RF: Rheumatoid factor; SD: Standard deviation; sDMARD: Synthetic disease-modifying antirheumatic drug
AcknowledgementsThe authors would like to thank to all members of the Department ofRheumatology of Hospital Universitario de Canarias for their helpfulness inthe patients’ recruitment.
FundingThis work was partially supported by a grant from the Spanish Ministry ofHealth (Fondo de Investigaciones Sanitarias Carlos III) to F.D-G [15/01810]and cofinanced by the European Regional Development Fund. The authorsdeclare that they do not have any conflicts of interest with the design or theresults from this investigation.
Availability of data and materialsThe datasets used and/or analyzed during the current study are availablefrom the corresponding author on reasonable request.
Authors’ contributionsBR-L designed the trial, collected clinical data, interpreted results andparticipated in manuscript writing. JG-F designed the trial, collectedperiodontal data, interpreted results and participated in writing themanuscript. JLG-R collected periodontal data and interpreted results. SDcollected periodontal data and interpreted results. SB-R collected clinicaldata and interpreted results. MS participated in the trial design, andinterpreted results. FS-A interpreted results and performed statistical analysis.CS-P interpreted results and performed statistical analysis. EG-D interpretedresults and performed statistical analysis (ordinal logistic regression). FD-Gdesigned the trial, interpreted results and wrote the manuscript. All authorsrevised the final version of the manuscript.
Ethics approval and consent to participateThis study was approved by an independent ethics committee andinstitutional review board from Hospital Universitario de Canarias (Spain), andall subjects provided written informed consent.
Consent for publicationIn this manuscript individual patient data are not presented.
Competing interestsThe authors declare that they have no competing interests.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Author details1Servicio de Reumatología, Hospital Universitario de Canarias, La Laguna,Spain. 2Periodoncia, Facultad de Odontología, Universidad Complutense,Madrid, Spain. 3Clínica Dental Dr. Garnier, S/C de Tenerife, Spain. 4Grupo deInvestigación de Etiología y Tratamiento de las Enfermedades Periodontales(ETEP), Facultad de Odontología, Universidad Complutense, Madrid, Spain.5Unidad de Investigación de la Sociedad Española de Reumatología, Madrid,Spain. 6Departamento de Estadística e Investigación Operativa, Universidadde La Laguna, S/C de Tenerife, La Laguna, Spain. 7Departamento deMedicina, Facultad de Medicina, Calle Ofra s/n 38320, La Laguna, Spain.
Received: 21 July 2018 Accepted: 2 January 2019
References1. Avina-Zubieta JA, Choi HK, Sadatsafavi M, Etminan M, Esdaile JM, Lacaille D.
Risk of cardiovascular mortality in patients with rheumatoid arthritis: a meta-analysis of observational studies. Arthritis Rheum. 2008;59:1690–7.
2. de Pablo P, Chapple IL, Buckley CD, Dietrich T. Periodontitis in systemicrheumatic diseases. Nat Rev Rheumatol. 2009;5:218–24.
Rodríguez-Lozano et al. Arthritis Research & Therapy (2019) 21:27 Page 10 of 12

101
3. Brink M, Hansson M, Mathsson L, Jakobsson PJ, Holmdahl R, Hallmans G, et al.Multiplex analyses of antibodies against citrullinated peptides in individuals priorto development of rheumatoid arthritis. Arthritis Rheum. 2013;65:899–910.
4. Rakieh C, Nam JL, Hunt L, Hensor EM, Das S, Bissell LA, et al. Predicting thedevelopment of clinical arthritis in anti-CCP positive individuals with non-specific musculoskeletal symptoms: a prospective observational cohortstudy. Ann Rheum Dis. 2015;74:1659–66.
5. Eke PI, Dye BA, Wei L, Slade GD, Thornton-Evans GO, Borgnakke WS, et al.Update on prevalence of periodontitis in adults in the United States:NHANES 2009 to 2012. J Periodontol. 2015;86:611–22.
6. Carasol M, Llodra JC, Fernandez-Meseguer A, Bravo M, Garcia-Margallo MT,Calvo-Bonacho E, et al. Periodontal conditions among employed adults inSpain. J Clin Periodontol. 2016;43:548–56.
7. Tonetti MS, Van Dyke TE. Periodontitis and atherosclerotic cardiovasculardisease: consensus report of the Joint EFP/AAP Workshop on Periodontitisand Systemic Diseases. J Clin Periodontol. 2013;40 Suppl 14:S24–9.
8. Taylor JJ, Preshaw PM, Lalla E. A review of the evidence for pathogenicmechanisms that may link periodontitis and diabetes. J Periodontol. 2013;84:S113–34.
9. Mikuls TR, Payne JB, Yu F, Thiele GM, Reynolds RJ, Cannon GW, et al.Periodontitis and Porphyromonas gingivalis in patients with rheumatoidarthritis. Arthritis Rheumatol. 2014;66:1090–100.
10. de Pablo P, Dietrich T, McAlindon TE. Association of periodontal disease andtooth loss with rheumatoid arthritis in the US population. J Rheumatol.2008;35:70–6.
11. Demmer RT, Molitor JA, Jacobs DR Jr, Michalowicz BS. Periodontal disease,tooth loss and incident rheumatoid arthritis: results from the First NationalHealth and Nutrition Examination Survey and its epidemiological follow-upstudy. J Clin Periodontol. 2011;38:998–1006.
12. Dissick A, Redman RS, Jones M, Rangan BV, Reimold A, Griffiths GR, et al.Association of periodontitis with rheumatoid arthritis: a pilot study. JPeriodontol. 2010;81:223–30.
13. Marotte H, Farge P, Gaudin P, Alexandre C, Mougin B, Miossec P. Theassociation between periodontal disease and joint destruction inrheumatoid arthritis extends the link between the HLA-DR shared epitopeand severity of bone destruction. Ann Rheum Dis. 2006;65:905–9.
14. Ziebolz D, Pabel SO, Lange K, Krohn-Grimberghe B, Hornecker E, MausbergRF. Clinical periodontal and microbiologic parameters in patients withrheumatoid arthritis. J Periodontol. 2011;82:1424–32.
15. de Pablo P, Dietrich T, Chapple IL, Milward M, Chowdhury M, Charles PJ, etal. The autoantibody repertoire in periodontitis: a role in the induction ofautoimmunity to citrullinated proteins in rheumatoid arthritis? Ann RheumDis. 2014;73:580–6.
16. Hendler A, Mulli TK, Hughes FJ, Perrett D, Bombardieri M, Houri-Haddad Y,et al. Involvement of autoimmunity in the pathogenesis of aggressiveperiodontitis. J Dent Res. 2010;89:1389–94.
17. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO 3rd, et al.Rheumatoid arthritis classification criteria: an American College ofRheumatology/European League Against Rheumatism collaborativeinitiative. Arthritis Rheum. 2010. 2010;62:2569–81.
18. Herrera D, Sanz M, Jepsen S, Needleman I, Roldan S. A systematic review onthe effect of systemic antimicrobials as an adjunct to scaling and rootplaning in periodontitis patients. J Clin Periodontol. 2002;29(Suppl 3):136–59.
19. Mavrogiannis M, Ellis JS, Thomason JM, Seymour RA. The management ofdrug-induced gingival overgrowth. J Clin Periodontol. 2006;33:434–9.
20. Prevoo ML, van ‘t Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB,van Riel PL. Modified disease activity scores that include twenty-eight-jointcounts. Development and validation in a prospective longitudinal study ofpatients with rheumatoid arthritis. Arthritis Rheum. 1995;38:44–8.
21. Smolen JS, Breedveld FC, Schiff MH, Kalden JR, Emery P, Eberl G, et al. Asimplified disease activity index for rheumatoid arthritis for use in clinicalpractice. Rheumatology (Oxford). 2003;42:244–57.
22. Aletaha D, Nell VP, Stamm T, Uffmann M, Pflugbeil S, Machold K, et al. Acutephase reactants add little to composite disease activity indices forrheumatoid arthritis: validation of a clinical activity score. Arthritis Res Ther.2005;7:R796–806.
23. Pincus T, Swearingen C, Wolfe F. Toward a multidimensional HealthAssessment Questionnaire (MDHAQ): assessment of advanced activities of dailyliving and psychological status in the patient-friendly health assessmentquestionnaire format. Arthritis Rheum. 1999;42:2220–30.
24. Silness J, Loe H. Periodontal disease in pregnancy. II. Correlation betweenoral hygiene and periodontal condtion. Acta Odontol Scand. 1964;22:121–35.
25. Ainamo J, Bay I. Problems and proposals for recording gingivitis and plaque.Int Dent J. 1975;25:229–35.
26. Tonetti MS, Claffey N. Advances in the progression of periodontitis andproposal of definitions of a periodontitis case and disease progression foruse in risk factor research. Group C consensus report of the 5th EuropeanWorkshop in Periodontology. J Clin Periodontol. 2005;32(Suppl 6):210–3.
27. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. JHealth Soc Behav. 1983;24:385–96.
28. Remor E. Psychometric properties of a European Spanish version of thePerceived Stress Scale (PSS). Span J Psychol. 2006;9:86–93.
29. Graffar M. Une méthode de classification social d’ échantillons depopulation. Courier. 1956;6:455–9.
30. Agresti A. Categorical data analysis. 2nd ed. Hoboken: Wiley; 2002.31. Helminen-Pakkala E, Laine V. The relationship between periodontal findings
and articular involvement in a group of subjects suffering from rheumatoidarthritis. Proc Finn Dent Soc. 1973;69:52–5.
32. Sjostrom L, Laurell L, Hugoson A, Hakansson JP. Periodontal conditions inadults with rheumatoid arthritis. Community Dent Oral Epidemiol. 1989;17:234–6.
33. Yavuzyilmaz E, Yamalik N, Calguner M, Ersoy F, Baykara M, Yeniay I. Clinicaland immunological characteristics of patients with rheumatoid arthritis andperiodontal disease. J Nihon Univ Sch Dent. 1992;34:89–95.
34. Joseph R, Rajappan S, Nath SG, Paul BJ. Association between chronicperiodontitis and rheumatoid arthritis: a hospital-based case-control study.Rheumatol Int. 2013;33:103–9.
35. Mercado FB, Marshall RI, Klestov AC, Bartold PM. Relationship betweenrheumatoid arthritis and periodontitis. J Periodontol. 2001;72:779–87.
36. Pischon N, Pischon T, Kroger J, Gulmez E, Kleber BM, Bernimoulin JP, et al.Association among rheumatoid arthritis, oral hygiene, and periodontitis. JPeriodontol. 2008;79:979–86.
37. Potempa J, Mydel P, Koziel J. The case for periodontitis in the pathogenesisof rheumatoid arthritis. Nat Rev Rheumatol. 2017;13:606–20.
38. Mobini M, Maboudi A, Ali Mohammadpour R. Periodontitis in rheumatoidarthritis patients, abundance and association with disease activity. Med JIslam Repub Iran. 2017;31:44.
39. Ayravainen L, Leirisalo-Repo M, Kuuliala A, Ahola K, Koivuniemi R, MeurmanJH, et al. Periodontitis in early and chronic rheumatoid arthritis: aprospective follow-up study in Finnish population. BMJ Open. 2017;7:e011916.
40. Scher JU, Ubeda C, Equinda M, Khanin R, Buischi Y, Viale A, et al. Periodontaldisease and the oral microbiota in new-onset rheumatoid arthritis. ArthritisRheum. 2012;64:3083–94.
41. Kobayashi T, Okada M, Ito S, Kobayashi D, Ishida K, Kojima A, et al.Assessment of interleukin-6 receptor inhibition therapy on periodontalcondition in patients with rheumatoid arthritis and chronic periodontitis. JPeriodontol. 2014;85:57–67.
42. Coat J, Demoersman J, Beuzit S, Cornec D, Devauchelle-Pensec V, Saraux A,et al. Anti-B lymphocyte immunotherapy is associated with improvement ofperiodontal status in subjects with rheumatoid arthritis. J Clin Periodontol.2015;42:817–23.
43. Mayer Y, Balbir-Gurman A, Machtei EE. Anti-tumor necrosis factor-alphatherapy and periodontal parameters in patients with rheumatoid arthritis. JPeriodontol. 2009;80:1414–20.
44. Pers JO, Saraux A, Pierre R, Youinou P. Anti-TNF-alpha immunotherapy isassociated with increased gingival inflammation without clinical attachmentloss in subjects with rheumatoid arthritis. J Periodontol. 2008;79:1645–51.
45. Kobayashi T, Yokoyama T, Ito S, Kobayashi D, Yamagata A, Okada M, et al.Periodontal and serum protein profiles in patients with rheumatoid arthritistreated with tumor necrosis factor inhibitor adalimumab. J Periodontol.2014;85:1480–8.
46. Ziebolz D, Rupprecht A, Schmickler J, Bothmann L, Kramer J, Patschan D, etal. Association of different immunosuppressive medications withperiodontal condition in patients with rheumatoid arthritis: results from across-sectional study. J Periodontol. 2018;89:1310–7.
47. Gonzalez SM, Payne JB, Yu F, Thiele GM, Erickson AR, Johnson PG, et al.Alveolar bone loss is associated with circulating anti-citrullinated proteinantibody (ACPA) in patients with rheumatoid arthritis. J Periodontol. 2015;86:222–31.
Rodríguez-Lozano et al. Arthritis Research & Therapy (2019) 21:27 Page 11 of 12

102
48. Goh CE, Kopp J, Papapanou PN, Molitor JA, Demmer RT. Associationbetween serum antibodies to periodontal bacteria and rheumatoid factor inthe Third National Health and Nutrition Examination Survey. ArthritisRheumatol. 2016;68:2384–93.
49. Lee JY, Choi IA, Kim JH, Kim KH, Lee EY, Lee EB, et al. Association betweenanti-Porphyromonas gingivalis or anti-alpha-enolase antibody and severityof periodontitis or rheumatoid arthritis (RA) disease activity in RA. BMCMusculoskelet Disord. 2015;16:190.
50. Lappin DF, Apatzidou D, Quirke AM, Oliver-Bell J, Butcher JP, Kinane DF, etal. Influence of periodontal disease, Porphyromonas gingivalis and cigarettesmoking on systemic anti-citrullinated peptide antibody titres. J ClinPeriodontol. 2013;40:907–15.
51. Matuliene G, Pjetursson BE, Salvi GE, Schmidlin K, Bragger U, Zwahlen M, etal. Influence of residual pockets on progression of periodontitis and toothloss: results after 11 years of maintenance. J Clin Periodontol. 2008;35:685–95.
52. Schatzle M, Faddy MJ, Cullinan MP, Seymour GJ, Lang NP, Burgin W, et al.The clinical course of chronic periodontitis: V. Predictive factors inperiodontal disease. J Clin Periodontol. 2009;36:365–71.
53. Van der Velden U, Abbas F, Armand S, Loos BG, Timmerman MF, Van derWeijden GA, et al. Java project on periodontal diseases. The naturaldevelopment of periodontitis: risk factors, risk predictors and riskdeterminants. J Clin Periodontol. 2006;33:540–8.
54. Akinkugbe AA, Saraiya VM, Preisser JS, Offenbacher S, Beck JD. Bias inestimating the cross-sectional smoking, alcohol, obesity and diabetesassociations with moderate-severe periodontitis in the Atherosclerosis Riskin Communities study: comparison of full versus partial-mouth estimates. JClin Periodontol. 2015;42:609–21.
Rodríguez-Lozano et al. Arthritis Research & Therapy (2019) 21:27 Page 12 of 12
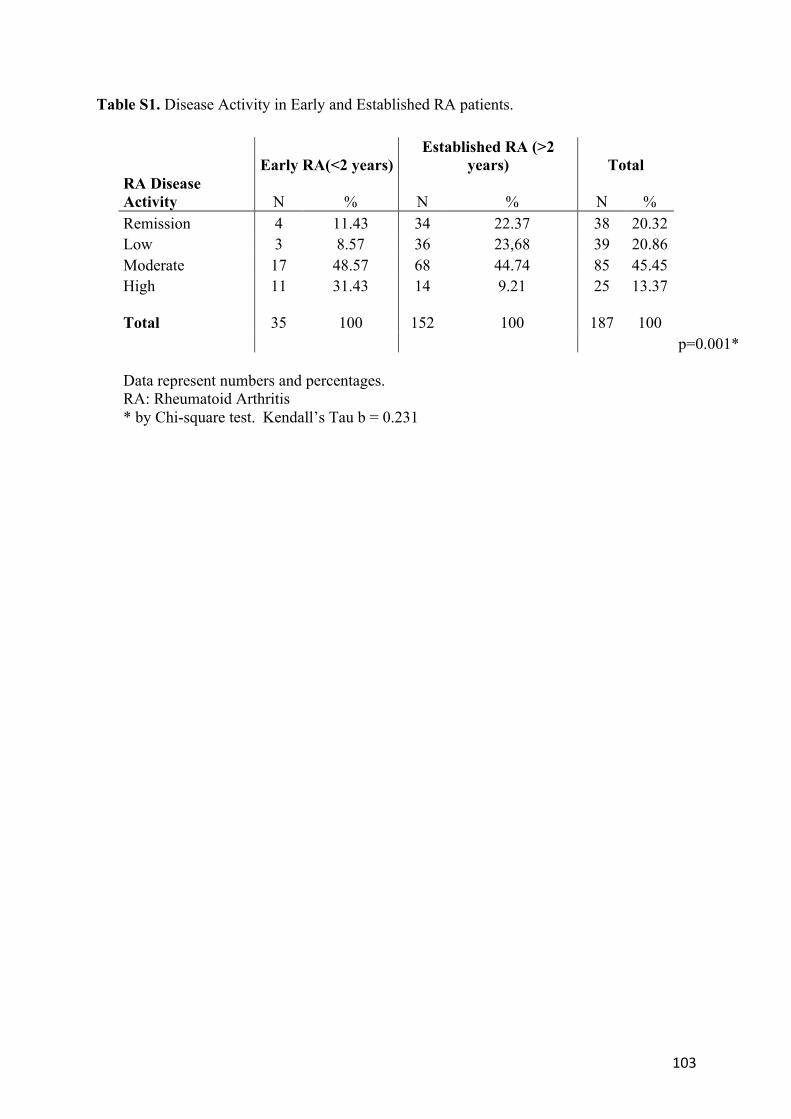
103
Table S1. Disease Activity in Early and Established RA patients.
Early RA(<2 years) Established RA (>2
years) Total
RA Disease Activity N % N % N %
Remission 4 11.43 34 22.37 38 20.32
Low 3 8.57 36 23,68 39 20.86
Moderate 17 48.57 68 44.74 85 45.45
High 11 31.43 14 9.21 25 13.37
Total 35 100 152 100 187 100
p=0.001*
Data represent numbers and percentages. RA: Rheumatoid Arthritis
* by Chi-square test. Kendall’s Tau b = 0.231
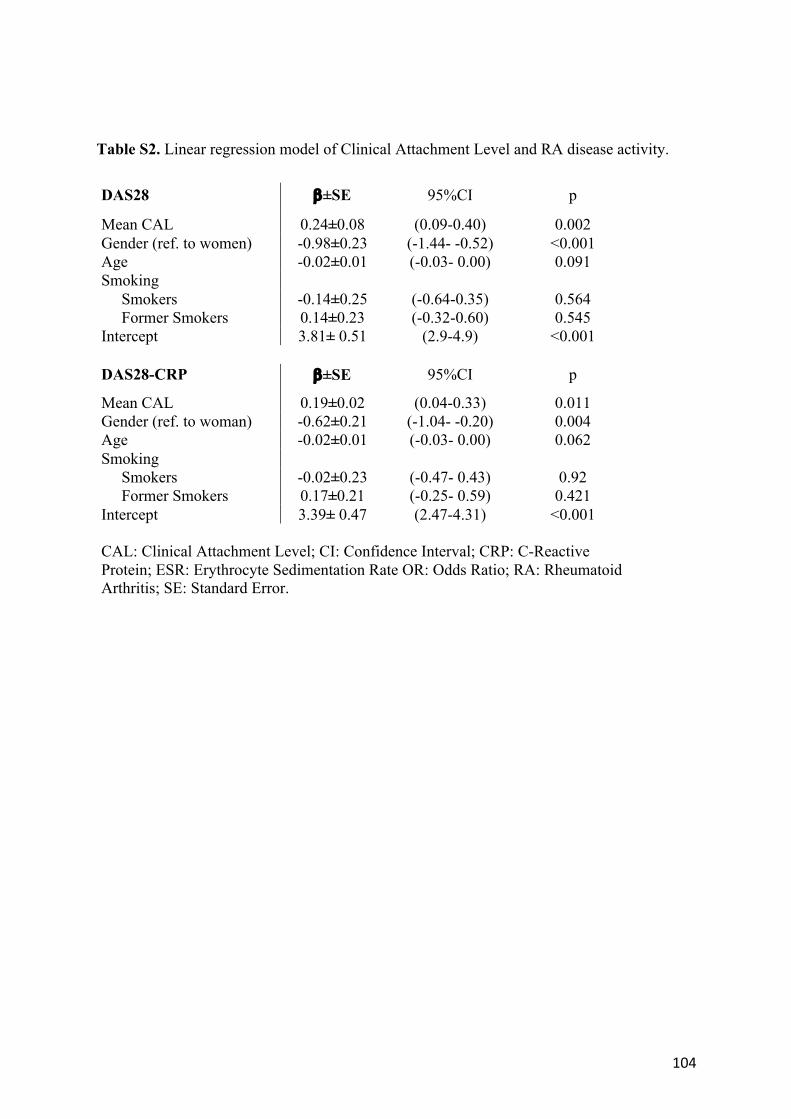
104
Table S2. Linear regression model of Clinical Attachment Level and RA disease activity.
DAS28 b±SE 95%CI p
Mean CAL 0.24±0.08 (0.09-0.40) 0.002
Gender (ref. to women) -0.98±0.23 (-1.44- -0.52) <0.001
Age -0.02±0.01 (-0.03- 0.00) 0.091
Smoking
Smokers -0.14±0.25 (-0.64-0.35) 0.564
Former Smokers 0.14±0.23 (-0.32-0.60) 0.545
Intercept 3.81± 0.51 (2.9-4.9) <0.001
DAS28-CRP b±SE 95%CI p
Mean CAL 0.19±0.02 (0.04-0.33) 0.011
Gender (ref. to woman) -0.62±0.21 (-1.04- -0.20) 0.004
Age -0.02±0.01 (-0.03- 0.00) 0.062
Smoking
Smokers -0.02±0.23 (-0.47- 0.43) 0.92
Former Smokers 0.17±0.21 (-0.25- 0.59) 0.421
Intercept 3.39± 0.47 (2.47-4.31) <0.001
CAL: Clinical Attachment Level; CI: Confidence Interval; CRP: C-Reactive
Protein; ESR: Erythrocyte Sedimentation Rate OR: Odds Ratio; RA: Rheumatoid Arthritis; SE: Standard Error.
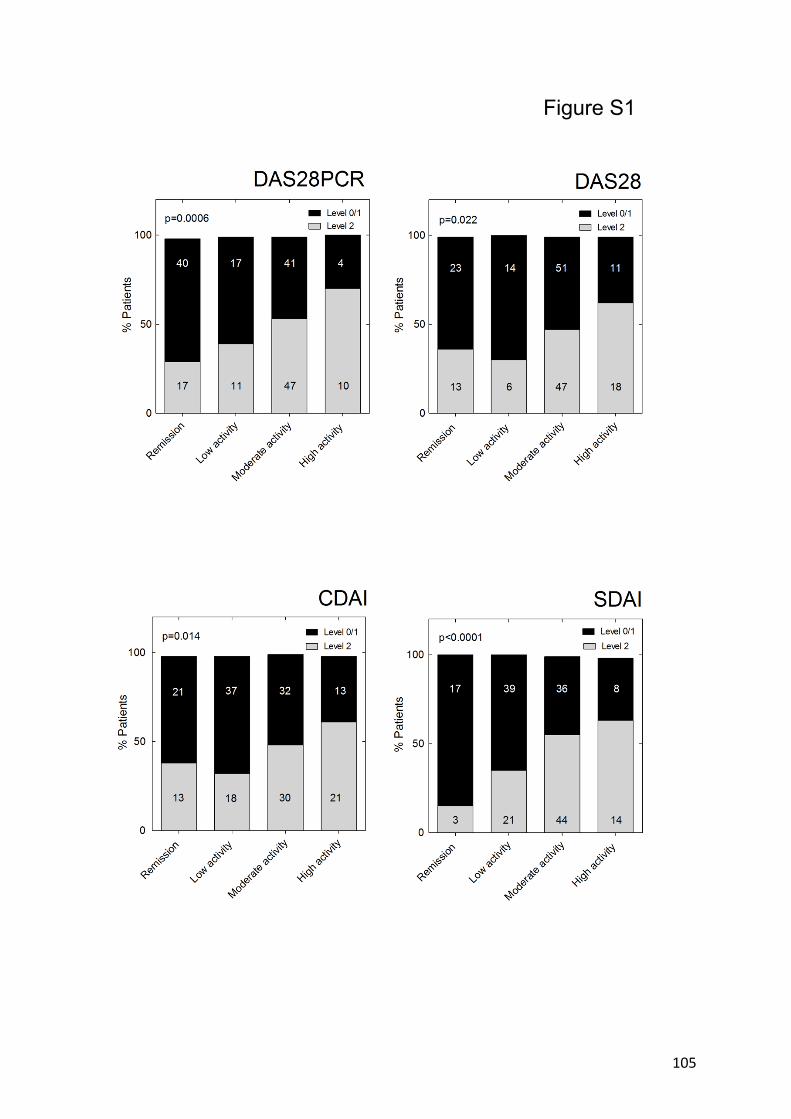
105
Figure S1

106
Figure S1. Relationship between RA disease activity assessed by different indexes and
periodontitis severity. Stacked bar graphs showing the percentage of RA patients that presented
none or mild (level 0/1) and severe (level 2) periodontitis with respect to RA disease activity
assessed by DAS28-CRP, DAS-28, SDAI and CDAI and categorized as remission, low,
moderate or high activity accordingly to threshold of each index. Numbers into columns
represent the number of patients in each situation. The four graphs show relation between RA
activity and periodontal state (all with p < 0.022 by Chi-Square test) and a linear increase in
the level 2 ratio of periodontitis (Kendall’s Tau b of 0.237, 0.168, 0.169 and 0.271 for DAS28-
CRP, DAS-28, CDAI and SDAI, respectively)
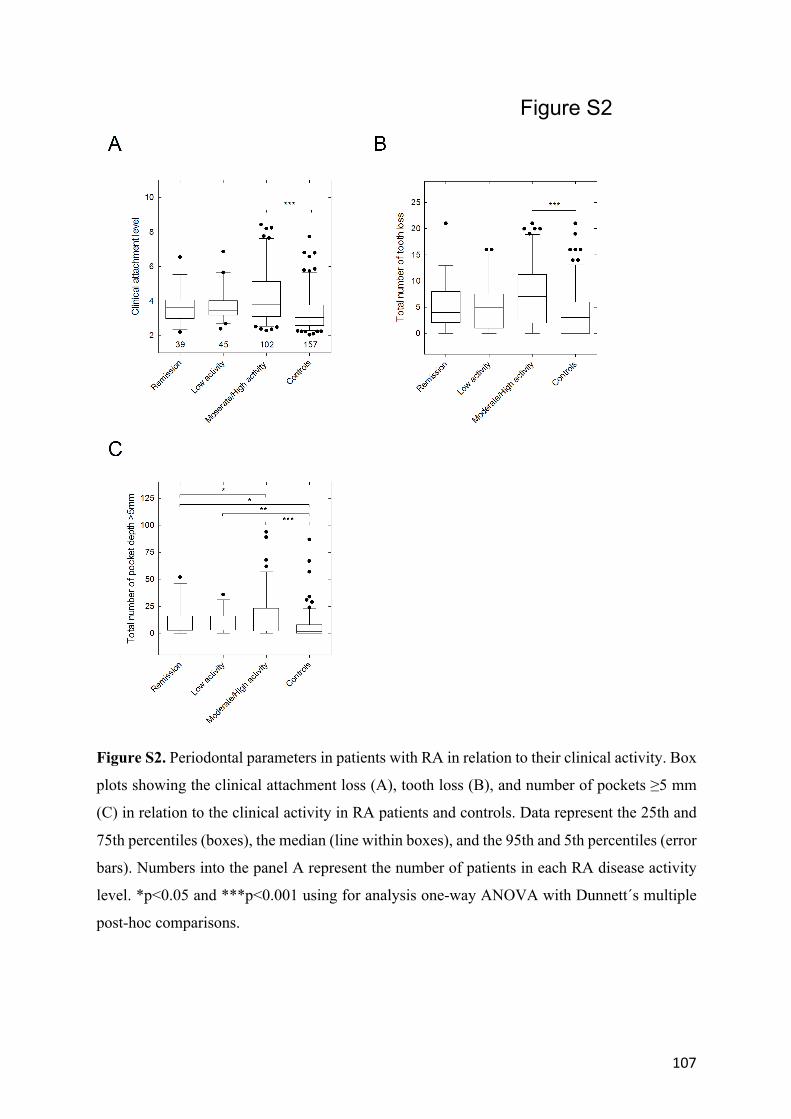
107
Figure S2
Figure S2. Periodontal parameters in patients with RA in relation to their clinical activity. Box
plots showing the clinical attachment loss (A), tooth loss (B), and number of pockets ≥5 mm
(C) in relation to the clinical activity in RA patients and controls. Data represent the 25th and
75th percentiles (boxes), the median (line within boxes), and the 95th and 5th percentiles (error
bars). Numbers into the panel A represent the number of patients in each RA disease activity
level. *p<0.05 and ***p<0.001 using for analysis one-way ANOVA with Dunnett´s multiple
post-hoc comparisons.

108

109
Artículo 3

110
111
Artículo #3
Asociación entre la periodontitis y la anticuerpos anti-péptidos citrulinados en
pacientes con Artritis Reumatoide: un estudio transversal
Antecedentes: A pesar de que existe escasa evidencia que sostiene la relación entre ciertos patógenos periodontales y los anticuerpos anti-péptidos citrulinados(ACPA), su asociación sigue siendo bastante controvertida. El objetivo de este estudio fue evaluar la relación entre la severidad de la periodontitis y la presencia de ACPAs en pacientes con AR.
Métodos: Se incluyeron 164 pacientes con AR. Se evaluaron tanto variables sociodemográficas como distintos parámetros clínicos de la AR, incluyendo títulos de ACPA(anti-CCP2). Como variables periodontales se registraron el índice de placa(IP), sangrado al sondaje(SAS), profundidad de sondaje(PS) y pérdida de inserción(PIC). Tanto la presencia como los niveles de ACPAs(variables resultado) y las variables exposición se compararon mediante test paramétricos y no paramétricos, así como su asociación se evaluó mediante el cálculo de la odds ratio(OR) ajustada.
Resultados: se observó una asociación significativa entre la presencia de anti-CCP2 y la severidad de ciertos parámetros periodontales como PIC media(OR 1,483, p = 0,036), IP media (OR 1.029, p = 0.012), y el número de bolsas ≥ 5 mm (OR 1,021, p = 0,08). Los títulos altos de ACPAs se asociaron tanto con PIC media, IP media o el número de bolsas ≥ 5 mm con una OR de 1,593 (p = 0,043), 1,060 (p < 0,001), and 1,031 (p = 0,031), respectivamente. Por último, se encontró un aumento estadísticamente significativo de 4,45 U/mL de los niveles de anti-CCP2 (p = 0.002) por cada bolsa ≥ 5 mm en pacientes con AR tras ajustar a edad, género, tabaquismo, tiempo de evolución de la enfermedad y el nivel de actividad de la AR.
Conclusiones: En pacientes con AR, la severidad de la periodontitis medida por la PIC, y el número de bolsas ≥ 5 mm se correlacionan con los niveles y presencia de anti-CCP2.
112
113
RESEARCH ARTICLE Open Access
Association between periodontitis and anti-citrullinated protein antibodies inrheumatoid arthritis patients: a cross-sectional studyJerián González-Febles1,2, Beatriz Rodríguez-Lozano3, Carlos Sánchez-Piedra4, Jorge Garnier-Rodríguez5,Sagrario Bustabad3, Martina Hernández-González5, Enrique González-Dávila6, Mariano Sanz2 andFederico Díaz-González2,7*
Abstract
Aim: The aim of this study was to evaluate the association between periodontal parameters related with theperiodontal disease severity and the presence and levels of anti-citrullinated protein antibodies (ACPAs) inrheumatoid arthritis (RA) patients.
Materials and methods: This cross-sectional study included 164 RA patients. Socio-demographics and RA diseasecharacteristics, including ELISA-detected ACPA (anti-CCP-2), were recorded. Exposure was assessed by periodontalparameters: plaque index (PI), bleeding on probing (BoP), probing pocket depth, and clinical attachment levels(CAL). Presence and levels of ACPAs (outcome) and exposure variables were compared by both parametric andnon-parametric tests and associations were evaluated by adjusted odds ratio (OR).
Results: A significant association was observed between the presence of anti-CCP antibodies and severity ofperiodontal outcomes such as the mean CAL (OR 1.483, p = 0.036), mean PI (OR 1.029, p = 0.012), and the numberof pockets ! 5 mm (OR 1.021, p = 0.08). High anti-CCP antibodies levels were associated with mean CAL, mean PI,and number of pockets ! 5mm with an OR of 1.593 (p = 0.043), 1.060 (p < 0.001), and 1.031 (p = 0.031), respectively.Furthermore, a significant increase of 4.45 U/mL in anti-CCP antibodies levels (p = 0.002) in RA patients was found foreach pocket ! 5mm after adjusting for age, gender, smoking, time of disease evolution, and RA activity.
Conclusions: In RA patients, the severity of periodontal conditions such as mean CAL, mean PI, and the number ofpockets ! 5mm were linearly associated with both the presence and levels of anti-CCP antibodies.
Keywords: ACPA, Rheumatoid factor, Severe periodontitis, Rheumatoid arthritis
© The Author(s). 2020 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
* Correspondence: [email protected] de Investigación de Etiología y Tratamiento de las EnfermedadesPeriodontales (ETEP), Facultad de Odontología, Universidad Complutense,Madrid, Spain7Departamento de Medicina Interna, Facultad de Medicina, Universidad deLa Laguna, C/Ofra s/n, 38320 La Laguna, SpainFull list of author information is available at the end of the article
González-Febles et al. Arthritis Research & Therapy (2020) 22:27 https://doi.org/10.1186/s13075-020-2121-6

114
Key messages
1) Periodontitis severity parameters such as CAL andpockets ! 5 mm are associated with anti-CCP anti-bodies levels.
2) This association was more pronounced in patientswith higher levels of these antibodies.
3) There is a linear correlation between periodontalparameters such as pockets ! 5 mm and anti-CCPtiters.
IntroductionRheumatoid arthritis (RA) is a chronic systemic auto-immune disease characterized by painful joint inflamma-tion, disability, and increased mortality [1]. Althoughknowledge of the pathogenesis underlying RA has in-creased substantially during the last decade, its etiologyis still unknown. A complex interplay of genetic, envir-onmental, and hormonal factors seem to influence thehost immune tolerance leading to the characteristicautoimmune response of RA mainly characterized by thepresence of rheumatoid factor (RF) and anti-citrullinatedprotein antibodies (ACPAs). These factors may alsoaffect the mucosal surfaces of lungs, gut, and/or theperiodontium [2, 3].While citrullination, a post-translational protein modi-
fication caused by the enzyme peptidyl arginine deimi-nase (PAD), is not an exclusive process of RA, theformation of ACPAs is mainly restricted to RA patients.In fact, evidence strongly suggests that these antibodiesare markers of more aggressive disease [4–6]. Althoughother factors may be able to induce protein citrullination[7], Porphyromonas gingivalis a key pathogen associatedwith the pathogenesis of periodontitis by inducing dys-biotic changes in the subgingival biofilm [8, 9] releases aspecific deaminase, which has been linked to proteincitrullination, thereby with potential to stimulate ACPAformation in RA patients [10, 11]. In fact, in patientswith chronic periodontitis, high levels of citrullinatedproteins have been identified within the periodontal tis-sues [12] and a recent in vivo experimental study hasdemonstrated a positive correlation between P. gingiva-lis-induced periodontitis and anti-cyclic citrullinatedpeptide (anti-CCP) antibodies levels in rats [13]. Further-more, recently published evidence suggests that the pres-ence of P. gingivalis infections may precede the clinicalonset of RA years in advance [14].Nowadays, there is solid evidence supporting an epi-
demiological association between periodontitis and RA[15–21]. Recently, our group has shown a significantand consistent association between these two diseases,mainly between severe periodontitis and RA disease ac-tivity [21]. Nonetheless, the relationship between P. gin-givalis, periodontitis, and the presence of ACPAs has
been a controversial topic. Some authors have remarkedupon the specific role of P. gingivalis in shaping auto-antibody specificity in RA patients [10, 22] independ-ently of smoking status [10]. In fact, anti-CCP antibodieshave been identified in periodontitis patients without RA[23, 24]. However, there are some studies that have notsupported this association between periodontitis, thepresence of P. gingivalis, and seropositivity for anti-CCPantibodies [10, 25, 26].It was, therefore, the main objective of this cross-
sectional study to further investigate the link betweenperiodontitis and its severity with the presence and levelsof anti-CCP antibodies in RA patients. In addition, thepossible impact of shared risk factors as tobacco habiton the presence and levels of anti-CCP antibodies wasevaluated.
MethodsStudy populationStudy subjects were consecutively included from thoseoutpatients attending the Department of Rheumatologyfrom January to September 2016. RA patients aged 18years and older who fulfilled the 2010 ACR/EULAR clas-sification criteria [27] were invited to participate. Pa-tients with less than 8 teeth [17], who had receivedperiodontal or antibiotic treatment during the previous6 months [28], who had undergone joint replacement(s),who were in need of antibiotic prophylaxis, or who werebeing treated with cyclosporine A or anticonvulsants[29] were excluded. Patients treated with oral glucocorti-coids maintained a stable dose during the month priorto their periodontal assessment and none received sys-temic treatment with these products during this period.RA patients who received intraarticular glucocorticoidsduring the month prior to evaluation were excludedfrom this study.All enrolled patients were informed about the objec-
tives and characteristics of the study and signed a writ-ten informed consent that had been previously approvedby the Ethics Committee of the Hospital Universitariode Canarias (code 2015_069). Additionally, all the studyrecordings were performed in agreement with the princi-ples of the Declaration of Helsinki.
Study designThis was an observational, cross-sectional study of RApatients treated in a single Rheumatology Departmentwho were assessed for the presence and severity ofperiodontitis.
Medical examinationAll RA patients were subjected to a routine medicalexamination. Both the patient’s and care provider’s glo-bal assessments of disease activity were based on a 100-
González-Febles et al. Arthritis Research & Therapy (2020) 22:27 Page 2 of 11

115
mm visual analog scale (VAS). Disease activity was cal-culated by means of 28-joint Disease Activity Score(DAS28), DAS28-C-reactive protein (CRP) [30], andSimplified Disease Activity Index (SDAI) [31] scores,and the medications used were logged from the medicalfiles and by asking the patient during examination. Bloodsamples were tested for plasma RF and CRP, using animmunoturbidimetric assay (Roche/cobas® 8000 ModularAnalyzer Series, Roche Diagnostics, USA), and for ACPA(anti-CCP-2) by Immunoscan CCPlus®. Euro Diagnosticawith a positive value established as that exceeding 25 U/mL in both serological tests, and 3 mg/L in the CRP test.Anti-CCP antibody levels were stratified as low (between25 and 75 U/mL), moderate (76–300 U/mL), or high (>300 U/mL).
Periodontal examinationFull oral and periodontal examinations were carried outindependently by two experienced periodontists. A kappatest showed 70% inter-examiner concordance. Full mouthprobing pocket depth (PPD) and clinical attachment level(CAL) measurements were registered using an UNC-15periodontal probe (six sites per tooth), excluding thirdmolars and implants. Although subjects were informed oftheir periodontal status and advised to seek periodontaltherapy when appropriate, no periodontal therapy wasrendered as part of this investigation.
Study variablesTo evaluate RA, the following parameters were recorded:DAS28 using the erythrocyte sedimentation rate (ESR)(DAS28) or C-reactive protein (DAS28-CRP) [30], SDAI[31], RF, and ACPA presence and titers. Patients werecategorized as being in remission, or having low, moder-ate, and high disease activity when at least two of theDAS28, DAS28-CRP, and SDAI scores were in agree-ment with the level of disease activity [21]. According tothe time of disease evolution, patients with less than 2years were classified as early RA.Patient periodontal status was assessed using the fol-
lowing parameters: Full mouth plaque index (PI) andbleeding on probing (BoP) [32] were reported as meanpercent of plaque and gingivitis, respectively [33], PPD,mean clinical attachment level (CAL), and tooth loss(dental implants and third molars were excluded). Basedon these parameters, patients were categorized usingtwo different case definition criteria for periodontitis:the 2005 Tonetti’s definition [34], which establishes 3levels—level 0, individuals with a healthy periodontium;level 1, presence of proximal attachment loss ! 3 mm in! 2 nonadjacent teeth; and level 2, presence of proximalattachment loss ! 5 mm in ! 30% of teeth—and the 2018Tonetti’s definition [35], which grades periodontitismainly based on the interdental CAL at the site of
greatest loss and also on radiographic bone loss and ontooth loss, over 5 stages—stage 0, individuals with ahealthy periodontium; stage I, initial; stage II, moderate;stage III, severe; and stage IV, advanced periodontitis.The presences of co-morbidities, such as diabetes mel-
litus, osteoporosis, myocardial infarction, or dyslipidemiawere recorded, as were anthropometric and socioeco-nomic variables. These included body mass index (BMI);smoking status (none, former and current); stress via thePerceived Stress Scale (PSS-14), categorized as highstress: yes (> 28 points) or no (" 28 points) [36, 37]; andsocial welfare indicators using the Graffar Scale Ques-tionnaire [38]. History of therapy involving glucocorti-coids, synthetic disease-modifying antirheumatic drugs(sDMARDs), and biologic DMARDs (bDMARDs) werealso recorded.
Statistical analysesDescriptive data are presented as means, standard devia-tions (SD), and frequency distributions. t test and one-way ANOVA were used in continuous variables toanalyze inter-group comparisons. Chi-square tests wereused to compare categorical variables and when ex-pected values were less than 5; the Fisher’s exact test in2 ! 2 tables was used.To study the association between the presence of peri-
odontitis (exposure) and anti-CCP antibody presence(outcome), a logistic regression model was constructedcalculating the odds by means of odds ratios (OR), and95% confidence intervals. Each analysis was adjusted forpossible confounders (covariates) such as age, sex, to-bacco use, time of disease evolution, and disease activity.In addition, a logistic regression model with the back-
ward Wald variable selection method was used toanalyze the influence of periodontal variables over thepresence of anti-CCP antibody, adjusting for the samecovariates. Hence, ROC (receiver operating characteris-tic) curves and the areas under those curves (AUC-ROC) were analyzed.In order to investigate the relationship between peri-
odontal parameters as mean PI (in %), number of pocket! 5 mm, BoP, and mean CAL (exposure) and anti-CCPantibody levels (multinomial outcome), an ordinal logis-tic regression model adjusted by age, sex, time of RAevolution, and RA disease activity and tobacco was car-ried out. Afterwards, an analysis of the covariates(ANCOVA) was performed to elucidate the associationbetween anti-CCP antibody quantification and the num-ber of pockets ! 5mm, controlling for the sameconfounders.Finally, adjusted OR calculations were carried out to de-
termine the association between tobacco consumption andperiodontitis. An ordinal logistic regression model was ap-plied to assess the relationship between periodontitis and
González-Febles et al. Arthritis Research & Therapy (2020) 22:27 Page 3 of 11

116
tobacco consumption (exposures) and anti-CCP antibodylevels (outcome), including the interactions between them.The statistical analyses were performed using the statisticalpackage SPSS 25 (IBM SPSS, Armonk, NY).
ResultsCharacteristics of RA patientsIn total, 164 RA patients, 77% women, with a mean ageof 54.1 ± 10.46 years and mean disease duration of 8.3 ±7.23 years were included in this study. Positivity for anti-CCP antibodies (> 25 UI/ml) was detected in 109 pa-tients (66.5%), being distributed according to the anti-body level titers in low (28%), moderate (42%), and high(30%). Demographic characteristics and the presence ofco-morbidities in this RA population are shown inTable 1, being described for the total RA patient popula-tion, and those with presence or absence of anti-CCPantibodies. Presence of anti-CCP antibodies was not as-sociated with age, gender, race, CRP, BMD, smoking,dyslipidemia, hypertension, BMI, or myocardial infarc-tion, while a significant association was demonstratedwith higher stress levels, ESR, and overweight. Therewas a tendency for an association between presence ofanti-CCP antibodies and reduced attendance to oral pre-ventive interventions and lower socioeconomic status.Table 2 depicts the disease characteristics in patients
with positive and negative anti-CCP antibodies. Therewere statistical differences between anti-CCP antibodynegative and positive patients in terms of RF seropositiv-ity (46% vs 87%, p < 0.001), RF titers (63 ± 90.48 vs234.5 ± 392.73, p < 0.001), DAS28 (ESR) (3.47 ± 1.31 vs3.98 ± 1.34, p = 0.023), and SDAI (12.16 ± 8.97 vs 15.77 ±11.77, p = 0.043). The same tendency was observed whendisease activity was assessed by DAS28 (CRP) (2.95 ±1.15 vs 3.30 ± 1.22, p = 0.069). However, when patientswere categorized by disease activity (remission, low,moderate, or high activity), no significant differenceswere observed between anti-CCP antibodies positive andnegative patients. Nor were any differences noted be-tween the two groups with respect to treatment withglucocorticoids, sDMARDs, or bDMARDs.
Association between the presence and levels of anti-CCPantibodies and periodontal status in RA patientsUsing the 2005 definition [34], the association betweenperiodontitis and the presence of anti-CCP antibodieswas not significant (p = 0.276), with an adjusted OR of1.228 (95% CI 0.628–2.40, p = 0.549). When the 2018definition was used [35], although the percentage of pa-tients with severe periodontitis (stage III+IV) was higherin positive, versus negative, anti-CCP antibody patients(51 vs 47%, respectively), the association between peri-odontitis and the presence of anti-CCP antibodies wasalso not significant (p = 0.370), with an adjusted OR of
1.222 (95% CI 0.628–2.379, p = 0.555); indeed, it provedquite similar to the 2005 [34] periodontitis case defin-ition. Therefore, the 2018 classification [35] of periodon-titis was used for the following comparisons.When periodontal outcome parameters were used in-
stead of case definitions, anti-CCP positive patientsshowed significantly higher CAL (4.16 ± 1.43 vs 3.72 ±0.85, p = 0.015), higher numbers (16.93 ± 19.63 vs11.64 ± 11.02, p = 0.029) and percentages of pockets ! 5mm (0.14 ± 0.16 vs 0.09 ± 0.09, p = 0.014), and highermean PI (31.0 ± 19.7 vs 22.4 ± 13.3, p < 0.001), comparedto their anti-CCP antibody negative counterparts.Regarding the severity of periodontal parameters vis-à-
vis the presence of anti-CCP antibodies, a highly signifi-cant association (p = 0.007) was observed between themean PI and anti-CCP positivity after resulting in an ad-justed OR of 1.033 (95% CI, 1.009–1.058). The mean CALalso was significantly associated with anti-CCP positivitywith an adjusted OR of 1.523 (95%CI 1.057–2.194, p =0.024). In terms of the number of pockets ! 5mm, a cleartendency for a positive association with anti-CCP positiv-ity was demonstrated (adjusted OR of 1.024 95% CI0.999–1.048, p = 0.065). After adjusting for confounders,BoP was not associated with the presence of anti-CCPantibodies. Using AUC-ROC curves, the cut-off points ofmean PI (24%) and the number of pockets ! 5mm (17)were established for a significant association with presenceof anti-CCP antibodies after adjusting for confounders,being the respective adjusted ORs of 2.33 (95% CI 1.17–4.65, p = 0.017) and 2.03 (95% CI 1.01–4.10, p = 0.048).When anti-CCP antibodies were stratified by level (low,
moderate, and high), an ordinal logistic regression modelshowed a direct association between these levels and themean CAL with an OR of 1.593 (95% CI 1.017–2.482, p =0.043) in patients with high anti-CCP antibody titers ver-sus non-anti-CCP RA patients (Table 3). Similarly, al-though with a more modest, albeit significant associationwas also demonstrated for patients with high anti-CCPantibody titers and the number of pockets ! 5mm(Table 4, Fig. 1) and the mean PI (Table S1) with adjustedORs of 1.031 (95%CI 1.003–1.062, p = 0.031) and 1.060(95% CI 1.027–1.093, p < 0.001), respectively.Using a covariance analysis (ANCOVA), a significant
increase of 4.45 U/mL (95% CI 1.60–7.29, p = 0.002) ofanti-CCP titers was found for each pocket ! 5mm in RApatients after adjusting for age, gender, smoking, time ofdisease evolution, and RA activity.
Impact of tobacco consumptionTable 1 depicts the data on tobacco consumption and itspossible association with anti-CCP titers. There were nosignificant differences (p = 0.709) between antibody-positive and antibody-negative RA patients with respectto smoking. Similarly periodontitis assessed by 2018 [35]
González-Febles et al. Arthritis Research & Therapy (2020) 22:27 Page 4 of 11
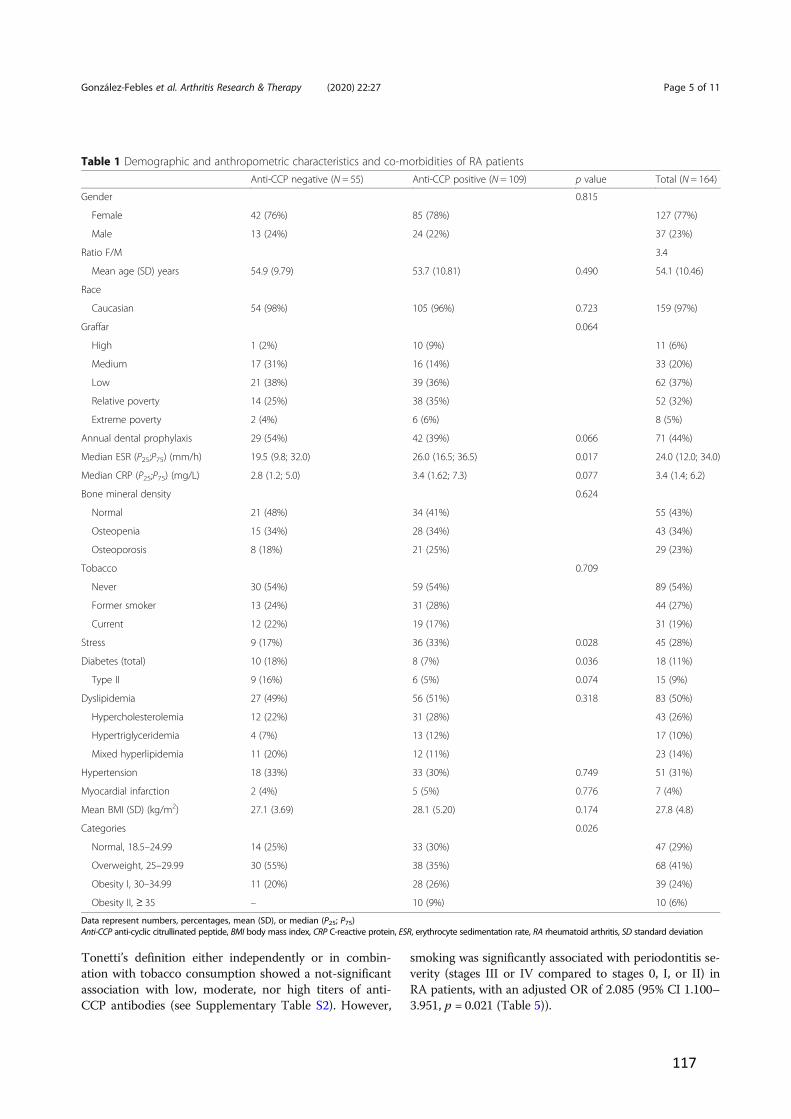
117
Tonetti’s definition either independently or in combin-ation with tobacco consumption showed a not-significantassociation with low, moderate, nor high titers of anti-CCP antibodies (see Supplementary Table S2). However,
smoking was significantly associated with periodontitis se-verity (stages III or IV compared to stages 0, I, or II) inRA patients, with an adjusted OR of 2.085 (95% CI 1.100–3.951, p = 0.021 (Table 5)).
Table 1 Demographic and anthropometric characteristics and co-morbidities of RA patientsAnti-CCP negative (N = 55) Anti-CCP positive (N = 109) p value Total (N = 164)
Gender 0.815
Female 42 (76%) 85 (78%) 127 (77%)
Male 13 (24%) 24 (22%) 37 (23%)
Ratio F/M 3.4
Mean age (SD) years 54.9 (9.79) 53.7 (10.81) 0.490 54.1 (10.46)
Race
Caucasian 54 (98%) 105 (96%) 0.723 159 (97%)
Graffar 0.064
High 1 (2%) 10 (9%) 11 (6%)
Medium 17 (31%) 16 (14%) 33 (20%)
Low 21 (38%) 39 (36%) 62 (37%)
Relative poverty 14 (25%) 38 (35%) 52 (32%)
Extreme poverty 2 (4%) 6 (6%) 8 (5%)
Annual dental prophylaxis 29 (54%) 42 (39%) 0.066 71 (44%)
Median ESR (P25;P75) (mm/h) 19.5 (9.8; 32.0) 26.0 (16.5; 36.5) 0.017 24.0 (12.0; 34.0)
Median CRP (P25;P75) (mg/L) 2.8 (1.2; 5.0) 3.4 (1.62; 7.3) 0.077 3.4 (1.4; 6.2)
Bone mineral density 0.624
Normal 21 (48%) 34 (41%) 55 (43%)
Osteopenia 15 (34%) 28 (34%) 43 (34%)
Osteoporosis 8 (18%) 21 (25%) 29 (23%)
Tobacco 0.709
Never 30 (54%) 59 (54%) 89 (54%)
Former smoker 13 (24%) 31 (28%) 44 (27%)
Current 12 (22%) 19 (17%) 31 (19%)
Stress 9 (17%) 36 (33%) 0.028 45 (28%)
Diabetes (total) 10 (18%) 8 (7%) 0.036 18 (11%)
Type II 9 (16%) 6 (5%) 0.074 15 (9%)
Dyslipidemia 27 (49%) 56 (51%) 0.318 83 (50%)
Hypercholesterolemia 12 (22%) 31 (28%) 43 (26%)
Hypertriglyceridemia 4 (7%) 13 (12%) 17 (10%)
Mixed hyperlipidemia 11 (20%) 12 (11%) 23 (14%)
Hypertension 18 (33%) 33 (30%) 0.749 51 (31%)
Myocardial infarction 2 (4%) 5 (5%) 0.776 7 (4%)
Mean BMI (SD) (kg/m2) 27.1 (3.69) 28.1 (5.20) 0.174 27.8 (4.8)
Categories 0.026
Normal, 18.5–24.99 14 (25%) 33 (30%) 47 (29%)
Overweight, 25–29.99 30 (55%) 38 (35%) 68 (41%)
Obesity I, 30–34.99 11 (20%) 28 (26%) 39 (24%)
Obesity II, ! 35 – 10 (9%) 10 (6%)
Data represent numbers, percentages, mean (SD), or median (P25; P75)Anti-CCP anti-cyclic citrullinated peptide, BMI body mass index, CRP C-reactive protein, ESR, erythrocyte sedimentation rate, RA rheumatoid arthritis, SD standard deviation
González-Febles et al. Arthritis Research & Therapy (2020) 22:27 Page 5 of 11
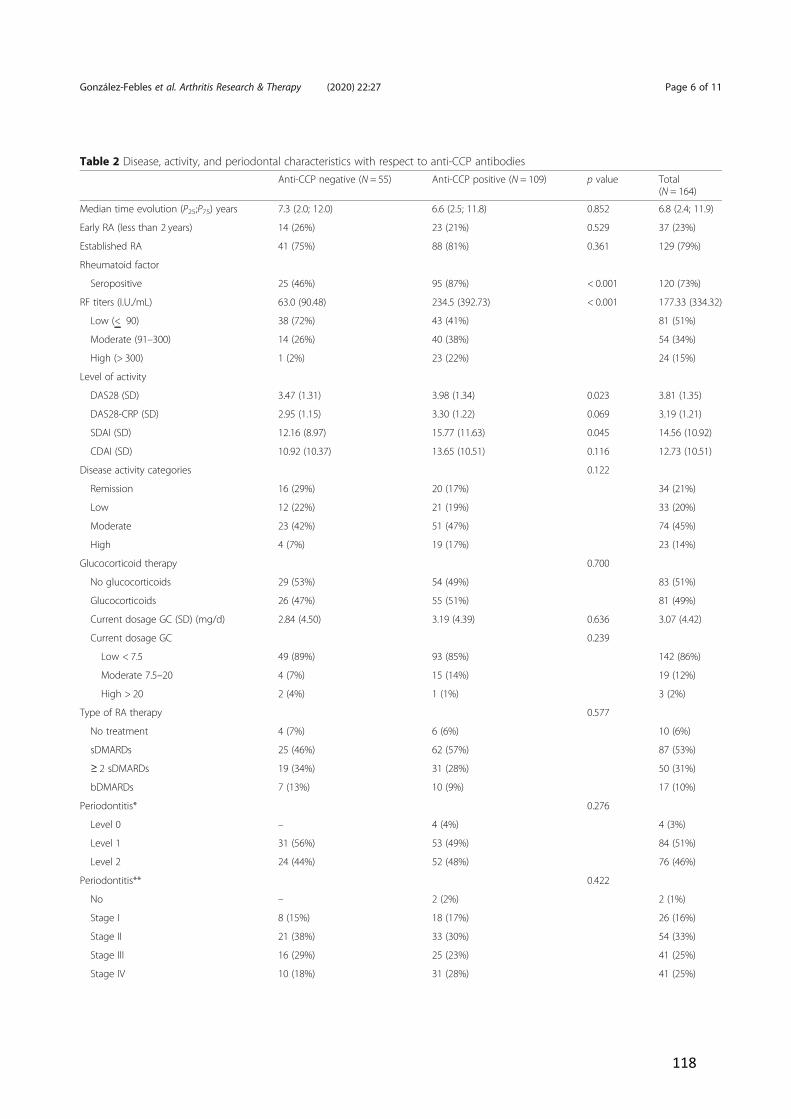
118
Table 2 Disease, activity, and periodontal characteristics with respect to anti-CCP antibodiesAnti-CCP negative (N = 55) Anti-CCP positive (N = 109) p value Total
(N = 164)
Median time evolution (P25;P75) years 7.3 (2.0; 12.0) 6.6 (2.5; 11.8) 0.852 6.8 (2.4; 11.9)
Early RA (less than 2 years) 14 (26%) 23 (21%) 0.529 37 (23%)
Established RA 41 (75%) 88 (81%) 0.361 129 (79%)
Rheumatoid factor
Seropositive 25 (46%) 95 (87%) < 0.001 120 (73%)
RF titers (I.U./mL) 63.0 (90.48) 234.5 (392.73) < 0.001 177.33 (334.32)
Low (< 90) 38 (72%) 43 (41%) 81 (51%)
Moderate (91–300) 14 (26%) 40 (38%) 54 (34%)
High (> 300) 1 (2%) 23 (22%) 24 (15%)
Level of activity
DAS28 (SD) 3.47 (1.31) 3.98 (1.34) 0.023 3.81 (1.35)
DAS28-CRP (SD) 2.95 (1.15) 3.30 (1.22) 0.069 3.19 (1.21)
SDAI (SD) 12.16 (8.97) 15.77 (11.63) 0.045 14.56 (10.92)
CDAI (SD) 10.92 (10.37) 13.65 (10.51) 0.116 12.73 (10.51)
Disease activity categories 0.122
Remission 16 (29%) 20 (17%) 34 (21%)
Low 12 (22%) 21 (19%) 33 (20%)
Moderate 23 (42%) 51 (47%) 74 (45%)
High 4 (7%) 19 (17%) 23 (14%)
Glucocorticoid therapy 0.700
No glucocorticoids 29 (53%) 54 (49%) 83 (51%)
Glucocorticoids 26 (47%) 55 (51%) 81 (49%)
Current dosage GC (SD) (mg/d) 2.84 (4.50) 3.19 (4.39) 0.636 3.07 (4.42)
Current dosage GC 0.239
Low < 7.5 49 (89%) 93 (85%) 142 (86%)
Moderate 7.5–20 4 (7%) 15 (14%) 19 (12%)
High > 20 2 (4%) 1 (1%) 3 (2%)
Type of RA therapy 0.577
No treatment 4 (7%) 6 (6%) 10 (6%)
sDMARDs 25 (46%) 62 (57%) 87 (53%)
! 2 sDMARDs 19 (34%) 31 (28%) 50 (31%)
bDMARDs 7 (13%) 10 (9%) 17 (10%)
Periodontitis* 0.276
Level 0 – 4 (4%) 4 (3%)
Level 1 31 (56%) 53 (49%) 84 (51%)
Level 2 24 (44%) 52 (48%) 76 (46%)
Periodontitis** 0.422
No – 2 (2%) 2 (1%)
Stage I 8 (15%) 18 (17%) 26 (16%)
Stage II 21 (38%) 33 (30%) 54 (33%)
Stage III 16 (29%) 25 (23%) 41 (25%)
Stage IV 10 (18%) 31 (28%) 41 (25%)
González-Febles et al. Arthritis Research & Therapy (2020) 22:27 Page 6 of 11
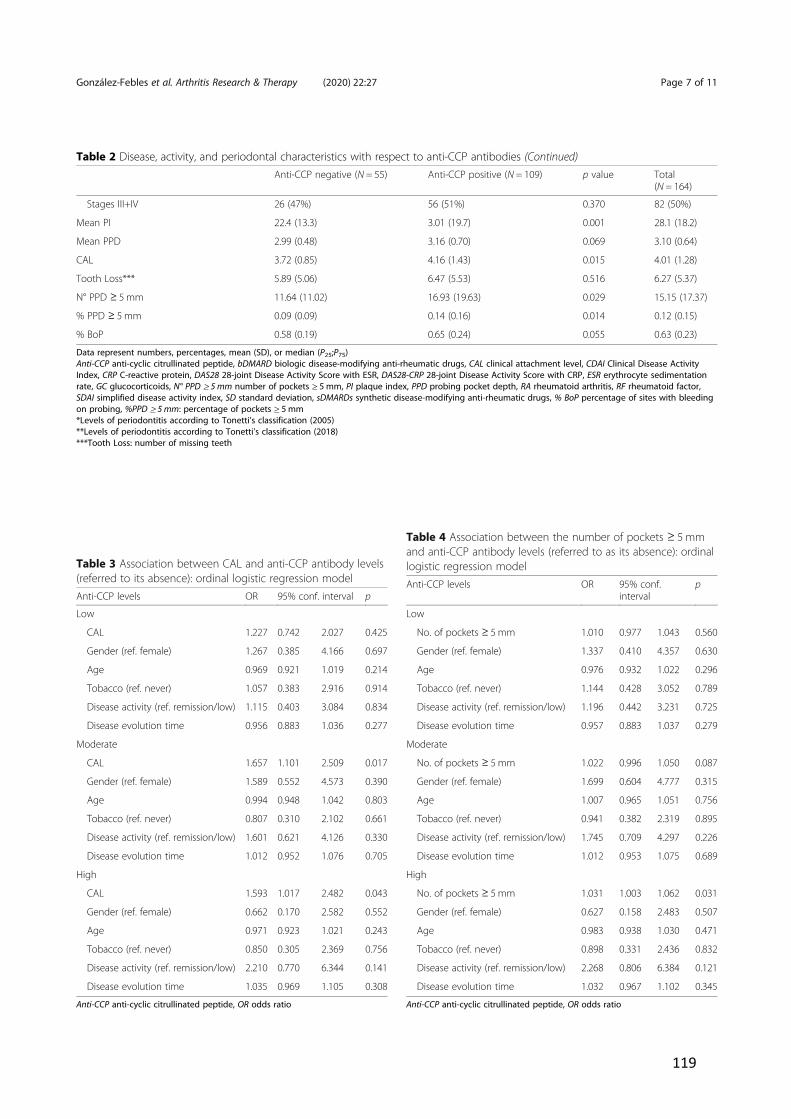
119
Table 2 Disease, activity, and periodontal characteristics with respect to anti-CCP antibodies (Continued)Anti-CCP negative (N = 55) Anti-CCP positive (N = 109) p value Total
(N = 164)
Stages III+IV 26 (47%) 56 (51%) 0.370 82 (50%)
Mean PI 22.4 (13.3) 3.01 (19.7) 0.001 28.1 (18.2)
Mean PPD 2.99 (0.48) 3.16 (0.70) 0.069 3.10 (0.64)
CAL 3.72 (0.85) 4.16 (1.43) 0.015 4.01 (1.28)
Tooth Loss*** 5.89 (5.06) 6.47 (5.53) 0.516 6.27 (5.37)
N° PPD ! 5 mm 11.64 (11.02) 16.93 (19.63) 0.029 15.15 (17.37)
% PPD ! 5 mm 0.09 (0.09) 0.14 (0.16) 0.014 0.12 (0.15)
% BoP 0.58 (0.19) 0.65 (0.24) 0.055 0.63 (0.23)
Data represent numbers, percentages, mean (SD), or median (P25;P75)Anti-CCP anti-cyclic citrullinated peptide, bDMARD biologic disease-modifying anti-rheumatic drugs, CAL clinical attachment level, CDAI Clinical Disease ActivityIndex, CRP C-reactive protein, DAS28 28-joint Disease Activity Score with ESR, DAS28-CRP 28-joint Disease Activity Score with CRP, ESR erythrocyte sedimentationrate, GC glucocorticoids, N° PPD ! 5 mm number of pockets ! 5 mm, PI plaque index, PPD probing pocket depth, RA rheumatoid arthritis, RF rheumatoid factor,SDAI simplified disease activity index, SD standard deviation, sDMARDs synthetic disease-modifying anti-rheumatic drugs, % BoP percentage of sites with bleedingon probing, %PPD ! 5 mm: percentage of pockets ! 5 mm*Levels of periodontitis according to Tonetti’s classification (2005)**Levels of periodontitis according to Tonetti’s classification (2018)***Tooth Loss: number of missing teeth
Table 3 Association between CAL and anti-CCP antibody levels(referred to its absence): ordinal logistic regression modelAnti-CCP levels OR 95% conf. interval p
Low
CAL 1.227 0.742 2.027 0.425
Gender (ref. female) 1.267 0.385 4.166 0.697
Age 0.969 0.921 1.019 0.214
Tobacco (ref. never) 1.057 0.383 2.916 0.914
Disease activity (ref. remission/low) 1.115 0.403 3.084 0.834
Disease evolution time 0.956 0.883 1.036 0.277
Moderate
CAL 1.657 1.101 2.509 0.017
Gender (ref. female) 1.589 0.552 4.573 0.390
Age 0.994 0.948 1.042 0.803
Tobacco (ref. never) 0.807 0.310 2.102 0.661
Disease activity (ref. remission/low) 1.601 0.621 4.126 0.330
Disease evolution time 1.012 0.952 1.076 0.705
High
CAL 1.593 1.017 2.482 0.043
Gender (ref. female) 0.662 0.170 2.582 0.552
Age 0.971 0.923 1.021 0.243
Tobacco (ref. never) 0.850 0.305 2.369 0.756
Disease activity (ref. remission/low) 2.210 0.770 6.344 0.141
Disease evolution time 1.035 0.969 1.105 0.308
Anti-CCP anti-cyclic citrullinated peptide, OR odds ratio
Table 4 Association between the number of pockets ! 5 mmand anti-CCP antibody levels (referred to as its absence): ordinallogistic regression modelAnti-CCP levels OR 95% conf.
intervalp
Low
No. of pockets ! 5 mm 1.010 0.977 1.043 0.560
Gender (ref. female) 1.337 0.410 4.357 0.630
Age 0.976 0.932 1.022 0.296
Tobacco (ref. never) 1.144 0.428 3.052 0.789
Disease activity (ref. remission/low) 1.196 0.442 3.231 0.725
Disease evolution time 0.957 0.883 1.037 0.279
Moderate
No. of pockets ! 5 mm 1.022 0.996 1.050 0.087
Gender (ref. female) 1.699 0.604 4.777 0.315
Age 1.007 0.965 1.051 0.756
Tobacco (ref. never) 0.941 0.382 2.319 0.895
Disease activity (ref. remission/low) 1.745 0.709 4.297 0.226
Disease evolution time 1.012 0.953 1.075 0.689
High
No. of pockets ! 5 mm 1.031 1.003 1.062 0.031
Gender (ref. female) 0.627 0.158 2.483 0.507
Age 0.983 0.938 1.030 0.471
Tobacco (ref. never) 0.898 0.331 2.436 0.832
Disease activity (ref. remission/low) 2.268 0.806 6.384 0.121
Disease evolution time 1.032 0.967 1.102 0.345
Anti-CCP anti-cyclic citrullinated peptide, OR odds ratio
González-Febles et al. Arthritis Research & Therapy (2020) 22:27 Page 7 of 11
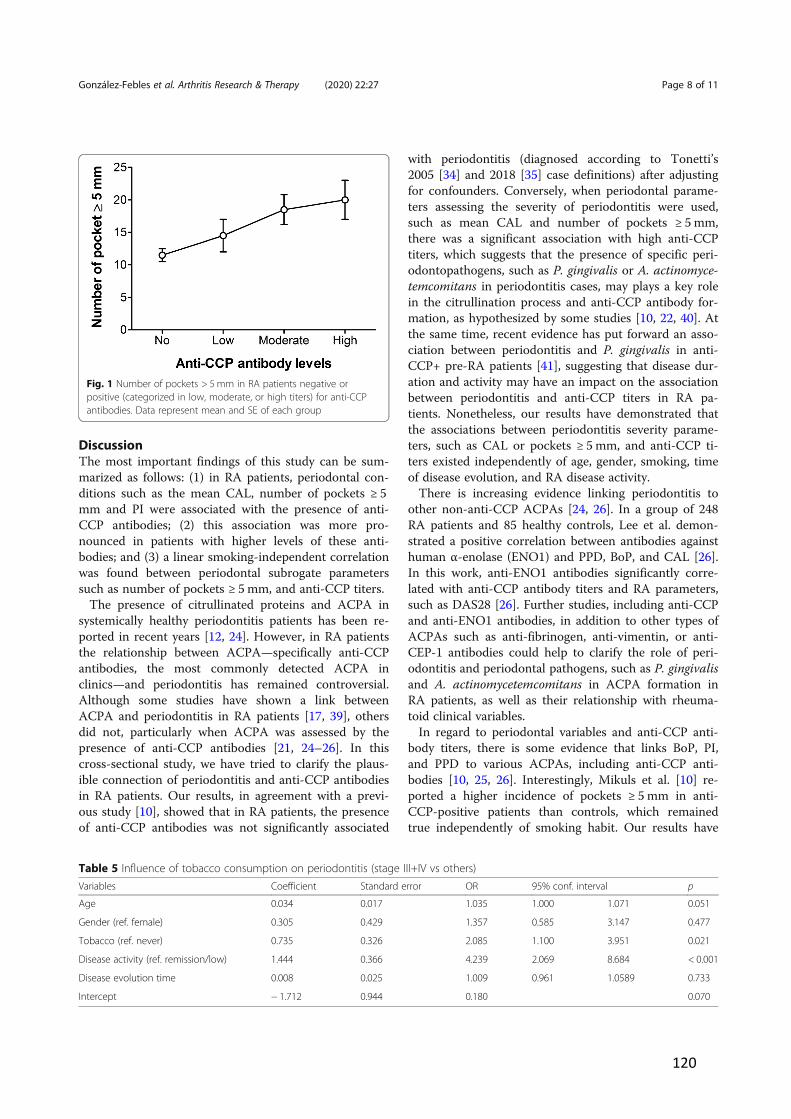
120
DiscussionThe most important findings of this study can be sum-marized as follows: (1) in RA patients, periodontal con-ditions such as the mean CAL, number of pockets ! 5mm and PI were associated with the presence of anti-CCP antibodies; (2) this association was more pro-nounced in patients with higher levels of these anti-bodies; and (3) a linear smoking-independent correlationwas found between periodontal subrogate parameterssuch as number of pockets ! 5 mm, and anti-CCP titers.The presence of citrullinated proteins and ACPA in
systemically healthy periodontitis patients has been re-ported in recent years [12, 24]. However, in RA patientsthe relationship between ACPA—specifically anti-CCPantibodies, the most commonly detected ACPA inclinics—and periodontitis has remained controversial.Although some studies have shown a link betweenACPA and periodontitis in RA patients [17, 39], othersdid not, particularly when ACPA was assessed by thepresence of anti-CCP antibodies [21, 24–26]. In thiscross-sectional study, we have tried to clarify the plaus-ible connection of periodontitis and anti-CCP antibodiesin RA patients. Our results, in agreement with a previ-ous study [10], showed that in RA patients, the presenceof anti-CCP antibodies was not significantly associated
with periodontitis (diagnosed according to Tonetti’s2005 [34] and 2018 [35] case definitions) after adjustingfor confounders. Conversely, when periodontal parame-ters assessing the severity of periodontitis were used,such as mean CAL and number of pockets ! 5 mm,there was a significant association with high anti-CCPtiters, which suggests that the presence of specific peri-odontopathogens, such as P. gingivalis or A. actinomyce-temcomitans in periodontitis cases, may plays a key rolein the citrullination process and anti-CCP antibody for-mation, as hypothesized by some studies [10, 22, 40]. Atthe same time, recent evidence has put forward an asso-ciation between periodontitis and P. gingivalis in anti-CCP+ pre-RA patients [41], suggesting that disease dur-ation and activity may have an impact on the associationbetween periodontitis and anti-CCP titers in RA pa-tients. Nonetheless, our results have demonstrated thatthe associations between periodontitis severity parame-ters, such as CAL or pockets ! 5 mm, and anti-CCP ti-ters existed independently of age, gender, smoking, timeof disease evolution, and RA disease activity.There is increasing evidence linking periodontitis to
other non-anti-CCP ACPAs [24, 26]. In a group of 248RA patients and 85 healthy controls, Lee et al. demon-strated a positive correlation between antibodies againsthuman !-enolase (ENO1) and PPD, BoP, and CAL [26].In this work, anti-ENO1 antibodies significantly corre-lated with anti-CCP antibody titers and RA parameters,such as DAS28 [26]. Further studies, including anti-CCPand anti-ENO1 antibodies, in addition to other types ofACPAs such as anti-fibrinogen, anti-vimentin, or anti-CEP-1 antibodies could help to clarify the role of peri-odontitis and periodontal pathogens, such as P. gingivalisand A. actinomycetemcomitans in ACPA formation inRA patients, as well as their relationship with rheuma-toid clinical variables.In regard to periodontal variables and anti-CCP anti-
body titers, there is some evidence that links BoP, PI,and PPD to various ACPAs, including anti-CCP anti-bodies [10, 25, 26]. Interestingly, Mikuls et al. [10] re-ported a higher incidence of pockets ! 5 mm in anti-CCP-positive patients than controls, which remainedtrue independently of smoking habit. Our results have
Fig. 1 Number of pockets > 5 mm in RA patients negative orpositive (categorized in low, moderate, or high titers) for anti-CCPantibodies. Data represent mean and SE of each group
Table 5 Influence of tobacco consumption on periodontitis (stage III+IV vs others)Variables Coefficient Standard error OR 95% conf. interval p
Age 0.034 0.017 1.035 1.000 1.071 0.051
Gender (ref. female) 0.305 0.429 1.357 0.585 3.147 0.477
Tobacco (ref. never) 0.735 0.326 2.085 1.100 3.951 0.021
Disease activity (ref. remission/low) 1.444 0.366 4.239 2.069 8.684 < 0.001
Disease evolution time 0.008 0.025 1.009 0.961 1.0589 0.733
Intercept ! 1.712 0.944 0.180 0.070
González-Febles et al. Arthritis Research & Therapy (2020) 22:27 Page 8 of 11

121
also shown significantly higher levels of mean CAL,numbers and percentages of pockets ! 5mm, mean PI,and mean PPD, in anti-CCP antibody-positive versusantibody-negative patients. Using logistic regression ana-lysis and after adjusting for confounders, we identified agradient effect in the association between mean CAL,mean PI, and the number of pockets ! 5 mm with anti-CCP antibody titers. In fact, all those periodontal param-eters reached statistical significance in patients with highanti-CCP antibody titers (> 300). In addition, usingAUC-ROC curves, we established cut-off points formean PI and the number of pockets ! 5 mm vis-à-visrisk for the presence of anti-CCP antibodies in RA pa-tients. RA patients with more than 17 pockets ! 5 mm, asituation characteristic of severe periodontitis, or a meanPI of 24% or higher, a finding that denotes poor oral hy-giene, doubles the likelihood of being anti-CCP positivethan those with periodontal parameters below thoselevels. Thus, in regard to pockets, we have established apreviously unreported linear relationship between thenumber of pockets ! 5 mm and the quantity of anti-CCPantibodies. After adjusting for age, gender, smokinghabit, time of disease evolution, and RA disease activity,we found in our group of RA patients that for every add-itional pocket ! 5mm, the concentration of anti-CCPantibodies increased by 4.45 U/ml in RA patients. Thisrelationship could reflect the potential role of P. gingiva-lis and A. actinomycetemcomitans in protein citrullina-tion and ACPA formation, due to the fact that theseperiodontal pathogens are likely present in pockets ! 5mm [42–44]. However, adequate studies using microbio-logical data are needed to correlate the presence of suchbacteria, ACPA titers, and RA clinical variables.Apart from periodontitis and presence of key periodon-
tal pathogens as sources of citrullination leading to ACPAformation [10, 13, 15, 23, 26, 40], smoking may also con-tribute to citrullination and ACPA formation [7, 45]. Like-wise, tobacco use is also a risk factor for periodontitis inboth healthy [46] and RA patients [47]. Some authors havehypothesized that the impact of smoking may be so strongthat it may mask the effects of P. gingivalis and periodon-titis on citrullination and ACPA formation in RA patients[48], although there is also data associating periodontitisand anti-CCP antibody titers, independently from tobaccoconsumption in non-RA patients [23]. Our results haveshown that tobacco use was associated with periodontitis(according to Tonetti’s case definitions) in RA patients,and at the same time, subrogate parameters of periodon-titis severity such as CAL or PPD ! 5mm were signifi-cantly associated with anti-CCP antibody titers afteradjusting by age, gender, and smoking. However, both to-bacco and periodontitis, either independently or in com-bination, did not show an association with anti-CCPantibodies titers in our series of RA patients. These results
may be explained by the lack of microbiological data inour study, due to the fact that P. gingivalis and A. actino-mycetemcomitans concentrations may play significantroles in ACPA formation, independently of tobacco con-sumption [10, 22, 40].There are some limitations in this study. The design of
our study does not address causality and the lack ofmicrobiological data does not allow for assessing thepossible association between pathogens and anti-CCP ti-ters. The correlation between periodontitis pathogens,including P. gingivalis and A. actinomycetemcomitansand anti-CCP antibodies, should be the focus of futureresearch to elucidate their impact on the pathogenesis ofRA, as has been previously mentioned. Future research,including interventional studies focused on the influenceof periodontal status and the bacteria responsible forperiodontitis on both the presence of anti-CCP anti-bodies and disease activity, would help us better under-stand the causal connections between periodontitis andRA.
ConclusionsThere is a link between anti-CCP antibody titers andperiodontitis, in which worsening periodontal condi-tions, in terms of mean CAL, mean PI, and number ofpockets > 5mm, were statistically associated with bothanti-CCP antibody positivity and higher levels of anti-CCP antibody titers. However, tobacco consumption andperiodontitis (assessed by Tonetti’s definition) does notseem to be associated with levels of anti-CCP antibodiesin our RA patient series.
Supplementary informationSupplementary information accompanies this paper at https://doi.org/10.1186/s13075-020-2121-6.
Additional file 1: Table S1. Association between mean PI and anti-CCPantibody levels (referred to its absence): ordinal logistic regression model.
Additional file 2: Table S2. Association between tobacco andperiodontitis with anti-CCP antibody levels (referred to its absence):ordinal logistic regression model.
AbbreviationsACPAs: Anti-citrullinated peptide antibodies; ANCOVA: Analysis of thecovariates; anti-CCP: Anti-cyclic citrullinated peptide; AUC-ROC: Areas underROC curves; bDMARD: Biologic disease-modifying antirheumatic drug;BMI: Body mass index; BoP: Bleeding of probing; CAL: Clinical attachmentlevel; CDAI: Clinical Disease Activity Index; CRP: C-reactive protein; DAS28: 28-joint Disease Activity Score; DMARD: Disease-modifying antirheumatic drug;ERA: Early rheumatoid arthritis; ESR: Erythrocyte sedimentation rate; OD: Oddsratio; PAD: Peptidil arginine deiminase; PI: Plaque index; PPD: Proving pocketdepth; PSS-14: Perceived Stress Scale; RA: Rheumatoid arthritis;RF: Rheumatoid factor; ROC: Receiver operating characteristic; SD: Standarddeviation; sDMARD: Synthetic disease-modifying antirheumatic drug
AcknowledgmentsThe authors would like to thank to all members of the Department ofRheumatology of Hospital Universitario de Canarias for their helpfulness inthe patients’ recruitment.
González-Febles et al. Arthritis Research & Therapy (2020) 22:27 Page 9 of 11

122
Authors’ contributionsJG-F designed the trial, collected periodontal data, interpreted results, andco-wrote the manuscript. BR-L designed the trial, collected clinical data, inter-preted results, and participated in manuscript writing. CS-P interpreted re-sults and performed statistical analysis. JLG-R collected periodontal data andinterpreted results. SB collected clinical data and interpreted results. MH-Gcollected clinical data and interpreted results. EG-D interpreted results andperformed statistical analysis (ordinal logistic regression). MS participated inthe trial design and interpreted results. FD-G designed the trial, interpretedresults, and wrote the manuscript. All authors revised the final version of themanuscript. The author(s) read and approved the final manuscript.
FundingThis work was partially supported by a grant from the Spanish Ministry ofHealth (Fondo de Investigaciones Sanitarias Carlos III) to FD-G [15/01810] andcofinanced by the European Regional Development Fund. A part of thisstudy was also supported by REUNINVES Asociación.
Availability of data and materialsThe datasets used and/or analyzed during the current study are availablefrom the corresponding author, who has the ORCID identifier 0000-0002-4139-9295, on reasonable request.
Ethics approval and consent to participateThis study was approved by an independent ethics committee andinstitutional review board from Hospital Universitario de Canarias (Spain)(code 2015_06), and all subjects provided written informed consent.
Consent for publicationIn this manuscript, individual patient data are not presented.
Competing interestsThe authors declare that they have no competing interests.
Author details1Departamento de Especialidades Odontológicas, Facultad de Odontología,Universidad Complutense, Madrid, Spain. 2Grupo de Investigación deEtiología y Tratamiento de las Enfermedades Periodontales (ETEP), Facultadde Odontología, Universidad Complutense, Madrid, Spain. 3Servicio deReumatología, Hospital Universitario de Canarias, S/C de Tenerife, Spain.4Unidad de Investigación de la Sociedad Española de Reumatología, Madrid,Spain. 5Clínica Dental Dr. Garnier, S/C de Tenerife, Spain. 6Departamento deMatemáticas, Estadística e Investigación Operativa, Universidad de La Laguna,San Cristóbal de La Laguna, Spain. 7Departamento de Medicina Interna,Facultad de Medicina, Universidad de La Laguna, C/Ofra s/n, 38320 LaLaguna, Spain.
Received: 3 September 2019 Accepted: 6 February 2020
References1. Aviña-Zubieta JA, Choi HK, Sadatsafavi M, Etminan M, Esdaile JM, Lacaille D.
Risk of cardiovascular mortality in patients with rheumatoid arthritis: a meta-analysis of observational studies. Arthritis Rheum. 2008;59:1690–7.
2. de Pablo P, Chapple ILC, Buckley CD, Dietrich T. Periodontitis in systemicrheumatic diseases. Nat Rev Rheumatol. 2009;5:218–24.
3. Potempa J, Mydel P, Koziel J. The case for periodontitis in the pathogenesisof rheumatoid arthritis. Nat Rev Rheumatol. 2017;13:606–20.
4. Brink M, Hansson M, Mathsson L, Jakobsson P-J, Holmdahl R, Hallmans G,et al. Multiplex analyses of antibodies against citrullinated peptides inindividuals prior to development of rheumatoid arthritis. Arthritis Rheum.2013;65:899–910.
5. Rakieh C, Rakieh C, Nam JL, Nam JL, Hunt L, Hunt L, et al. Predicting thedevelopment of clinical arthritis in anti-CCP positive individuals with non-specific musculoskeletal symptoms: a prospective observational cohortstudy. Ann Rheum Dis. 2015;74:1659–66.
6. Katchamart W, Koolvisoot A, Aromdee E, Chiowchanwesawakit P,Muengchan C. Associations of rheumatoid factor and anti-citrullinatedpeptide antibody with disease progression and treatment outcomes inpatients with rheumatoid arthritis. Rheumatol Int. 2015;35:1693–9.
7. Lee DM, Phillips R, Hagan EM, Chibnik LB, Costenbader KH, Schur PH.Quantifying anti-cyclic citrullinated peptide titres: clinical utility andassociation with tobacco exposure in patients with rheumatoid arthritis.Ann Rheum Dis. 2009;68:201–8.
8. Roberts FA, Darveau RP. Microbial protection and virulence in periodontaltissue as a function of polymicrobial communities: symbiosis and dysbiosis.Periodontol 2000. 2015;69:18–27.
9. Hajishengallis G. Immunomicrobial pathogenesis of periodontitis: keystones,pathobionts, and host response. Trends Immunol. 2014;35:3–11.
10. Mikuls TR, Payne JB, Yu F, Thiele GM, Reynolds RJ, Cannon GW, et al.Periodontitis and porphyromonas gingivalisin patients with rheumatoidarthritis. Arthritis Rheum. 2014;66:1090–100.
11. Ziebolz D, Pabel SO, Lange K, Krohn-Grimberghe B, Hornecker E, MausbergRF. Clinical periodontal and microbiologic parameters in patients withrheumatoid arthritis. J Periodontol. 2011;82:1424–32.
12. Nesse W, Nesse W, Westra J, Westra J, van der Wal JE, van der Wal JE, et al.The periodontium of periodontitis patients contains citrullinated proteinswhich may play a role in ACPA (anti-citrullinated protein antibody)formation. J Clin Periodontol. 2012;39:599–607.
13. Courbon G, Rinaudo-Gaujous M, Blasco-Baque V, Auger I, Caire R, Mijola L,et al. Porphyromonas gingivalis experimentally induces periodontis and ananti-CCP2-associated arthritis in the rat. Ann Rheum Dis. 2019;78:594–99.
14. Johansson L, Sherina N, Kharlamova N, Potempa B, Larsson B, Israelsson L,et al. Concentration of antibodies against Porphyromonas gingivalis isincreased before the onset of symptoms of rheumatoid arthritis. ArthritisRes Ther. 2016;18:201.
15. Mikuls TR, Thiele GM, Deane KD, Payne JB, O'Dell JR, Yu F, et al.Porphyromonas gingivalis and disease-related autoantibodies inindividuals at increased risk of rheumatoid arthritis. Arthritis Rheum.2012;64:3522–30.
16. Demmer RT, Molitor JA, Jacobs DR Jr, Michalowicz BS. Periodontal disease,tooth loss and incident rheumatoid arthritis: results from the First NationalHealth and Nutrition Examination Survey and its epidemiological follow-upstudy. J Clin Periodontol. 2011;38:998–1006.
17. Dissick A, Redman RS, Jones M, Rangan BV, Reimold A, Griffiths GR, et al.Association of periodontitis with rheumatoid arthritis: a pilot study. JPeriodontol. 2010;81:223–30.
18. de Pablo P, Dietrich T, McAlindon TE. Association of periodontal disease andtooth loss with rheumatoid arthritis in the US population. J Rheumatol.2008;35:70–6.
19. Kaur S, White S, Bartold PM. Periodontal disease and rheumatoid arthritis: asystematic review. J Dent Res. 2013;92:399–408.
20. Kim J-H, Choi IA, Lee JY, Kim K-H, Kim S, Koo K-T, et al. Periodontalpathogens and the association between periodontitis and rheumatoidarthritis in Korean adults. J Periodontal Implant Sci. 2018;48:347–59.
21. Rodríguez-Lozano B, González-Febles J, Garnier-Rodríguez JL, Dadlani S,Bustabad-Reyes S, Sanz M, et al. Association between severity ofperiodontitis and clinical activity in rheumatoid arthritis patients: a case-control study. Arthritis Res Ther. 2019;21:27.
22. de Smit M, Westra J, Vissink A, Doornbos-van der Meer B, Brouwer E, vanWinkelhoff AJ. Periodontitis in established rheumatoid arthritis patients: across-sectional clinical, microbiological and serological study. Arthritis ResTher. 2012;14:R222.
23. Lappin DF, Apatzidou D, Quirke A-M, Oliver-Bell J, Butcher JP, Kinane DF,et al. Influence of periodontal disease, Porphyromonas gingivalis andcigarette smoking on systemic anti-citrullinated peptide antibody titres. JClin Periodontol. 2013;40:907–15.
24. de Pablo P, Dietrich T, Chapple ILC, Milward M, Chowdhury M, Charles PJ,et al. The autoantibody repertoire in periodontitis: a role in the induction ofautoimmunity to citrullinated proteins in rheumatoid arthritis? Ann RheumDis. 2014;73:580–6.
25. Gonzalez SM, Payne JB, Yu F, Thiele GM, Erickson AR, Johnson PG, et al.Alveolar bone loss is associated with circulating anti-citrullinated proteinantibody (ACPA) in patients with rheumatoid arthritis. J Periodontol. 2015;86:222–31.
26. Lee JY, Lee JY, Choi IA, Choi IA, Kim J-H, Kim J-H, et al. Association betweenanti-Porphyromonas gingivalis or anti-!-enolase antibody and severity ofperiodontitis or rheumatoid arthritis (RA) disease activity in RA. BMCMusculoskelet Disord. 2015;16:190.
27. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO, et al.2010 rheumatoid arthritis classification criteria: an American College of
González-Febles et al. Arthritis Research & Therapy (2020) 22:27 Page 10 of 11
123
Rheumatology/European League Against Rheumatism collaborativeinitiative. Arthritis Rheum. 2010;62:2569–81.
28. Herrera D, Sanz M, Jepsen S, Needleman I, Roldán S. A systematic review onthe effect of systemic antimicrobials as an adjunct to scaling and rootplaning in periodontitis patients. J Clin Periodontol. 2002;29:136–59.
29. Mavrogiannis M, Mavrogiannis M, Ellis JS, Ellis JS, Thomason JM, ThomasonJM, et al. The management of drug-induced gingival overgrowth. J ClinPeriodontol. 2006;33:434–9.
30. Prevoo ML, van 't Hof MA, Kuper HH, van Leeuwen MA, van de PutteLB, van Riel PL. Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospectivelongitudinal study of patients with rheumatoid arthritis. Arthritis Rheum.1995;38:44–8.
31. Smolen JS, Breedveld FC, Schiff MH, Kalden JR, Emery P, Eberl G, et al. Asimplified disease activity index for rheumatoid arthritis for use in clinicalpractice. Rheumatology (Oxford). 2003;42:244–57.
32. Silness J, Löe H. Periodontal disease in pregnancy. II. Correlationbetween oral hygiene and periodontal condition. Acta Odontol Scand.1964;22:121–35.
33. Ainamo J, Bay I. Problems and proposals for recording gingivitis and plaque.Int Dent J. 1975;25:229–35.
34. Tonetti MS, Claffey N, Claffey N, European Workshop in Periodontologygroup C, European Workshop in Periodontology group C. Advances in theprogression of periodontitis and proposal of definitions of a periodontitiscase and disease progression for use in risk factor research. Group Cconsensus report of the 5th European Workshop in Periodontology. J ClinPeriodontol. 2005;32(Suppl 6):210–3.
35. Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis:framework and proposal of a new classification and case definition. J ClinPeriodontol. 2018;45:S149–61.
36. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. JHealth Soc Behav. 1983;24:385–96.
37. Remor E. Psychometric properties of a European Spanish version of thePerceived Stress Scale (PSS). Span J Psychol. 2006;9:86–93.
38. Graffar M. Une methode de classification sociales d’echantillons depopulation. Courrier. 1956;6:455–9.
39. Molitor JA, Alonso A, Wener MH, Michalowics BS, Gersuk VH. Moderate tosevere periodontitis increases risk of rheumatoid arthritis in non-smokersand is associated with elevated ACPA titers: The ARIC Study. ArthritisRheum. 2009;60:1160.
40. Konig MF, Abusleme L, Reinholdt J, Palmer RJ, Teles RP, Sampson K, et al.Aggregatibacter actinomycetemcomitans-induced hypercitrullination linksperiodontal infection to autoimmunity in rheumatoid arthritis. Sci TranslMed. 2016;8:369ra176.
41. Mankia K, Cheng Z, Do T, Hunt L, Meade J, Kang J, et al. Prevalence ofperiodontal disease and periodontopathic bacteria in anti-cyclic citrullinatedprotein antibody-positive at-risk adults without arthritis. JAMA Netw Open.2019;2:e195394.
42. Henderson B, Ward JM, Ready D. Aggregatibacter (Actinobacillus)actinomycetemcomitans: a triple A* periodontopathogen? Periodontol2000. 2010;54:78–105.
43. Farias BC, Souza PRE, Ferreira B, Melo RSA, Machado FB, Gusmão ES, et al.Occurrence of periodontal pathogens among patients with chronicperiodontitis. Braz J Microbiol. 2012;43:909–16.
44. Polak D, Polak D, Wilensky A, Wilensky A, Shapira L, Halabi A, et al. Mousemodel of experimental periodontitis induced by Porphyromonas gingivalis/Fusobacterium nucleatuminfection: bone loss and host response. J ClinPeriodontol. 2009;36:406–10.
45. Makrygiannakis D, Hermansson M, Nicholas AP, Zendman AJW, Eklund A,Grunewald J, et al. Smoking increases peptidylarginine deiminase 2 enzymeexpression in human lungs and increases citrullination in BAL cells. AnnRheum Dis. 2008;67:1488–92.
46. Martinez-Canut P, Llobell A, Romero A. Predictors of long-term outcomes inpatients undergoing periodontal maintenance. J Clin Periodontol. 2017;44:620–31.
47. Beyer K, Zaura E, Brandt BW, Buijs MJ, Brun JG, Crielaard W, et al.Subgingival microbiome of rheumatoid arthritis patients in relation totheir disease status and periodontal health. PLoS One. 2018;13:e0202278–18.
48. Seror R, Seror R, Le Gall-David S, Le Gall-David S, Bonnaure-Mallet M,Bonnaure-Mallet M, et al. Association of anti-porphyromonas gingivalis
antibody titers with nonsmoking status in early rheumatoid arthritis: resultsfrom the prospective French cohort of patients with early rheumatoidarthritis. Arthritis Rheumatol. 2015;67:1729–37.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
González-Febles et al. Arthritis Research & Therapy (2020) 22:27 Page 11 of 11
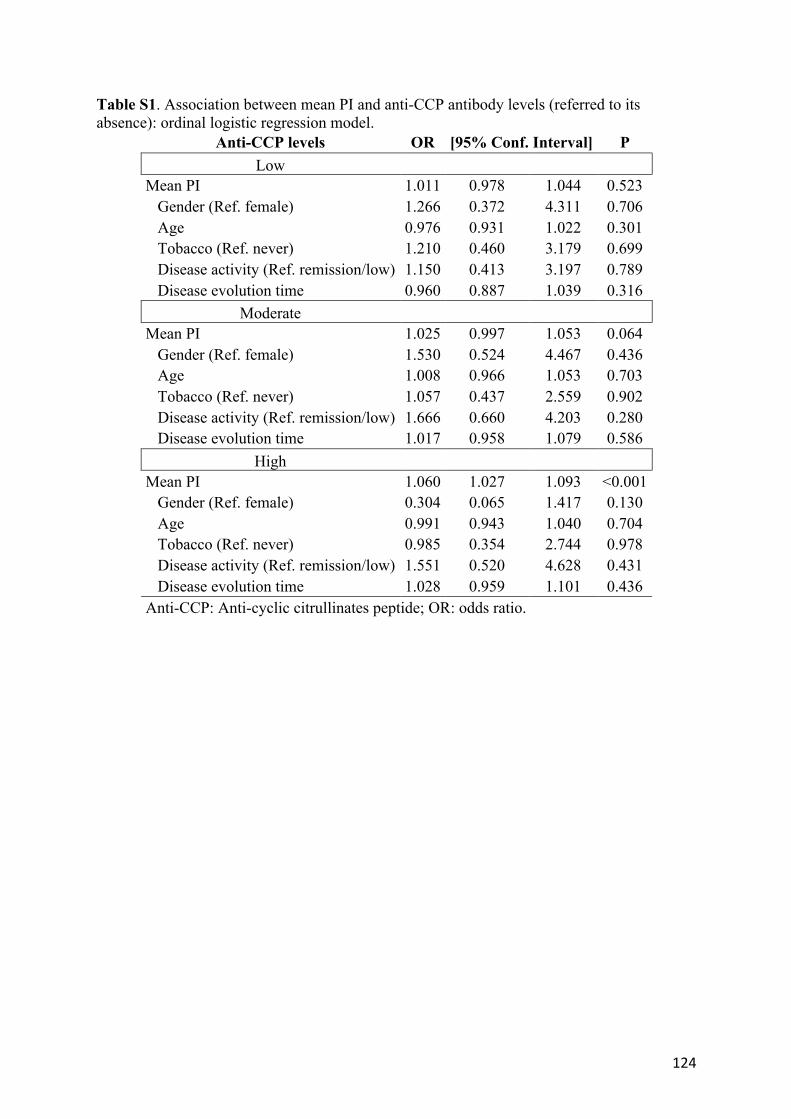
124
Table S1. Association between mean PI and anti-CCP antibody levels (referred to its absence): ordinal logistic regression model.
Anti-CCP levels OR [95% Conf. Interval] P Low
Mean PI 1.011 0.978 1.044 0.523
Gender (Ref. female) 1.266 0.372 4.311 0.706
Age 0.976 0.931 1.022 0.301
Tobacco (Ref. never) 1.210 0.460 3.179 0.699
Disease activity (Ref. remission/low) 1.150 0.413 3.197 0.789
Disease evolution time 0.960 0.887 1.039 0.316
Moderate
Mean PI 1.025 0.997 1.053 0.064
Gender (Ref. female) 1.530 0.524 4.467 0.436
Age 1.008 0.966 1.053 0.703
Tobacco (Ref. never) 1.057 0.437 2.559 0.902
Disease activity (Ref. remission/low) 1.666 0.660 4.203 0.280
Disease evolution time 1.017 0.958 1.079 0.586
High
Mean PI 1.060 1.027 1.093 <0.001
Gender (Ref. female) 0.304 0.065 1.417 0.130
Age 0.991 0.943 1.040 0.704
Tobacco (Ref. never) 0.985 0.354 2.744 0.978
Disease activity (Ref. remission/low) 1.551 0.520 4.628 0.431
Disease evolution time 1.028 0.959 1.101 0.436
Anti-CCP: Anti-cyclic citrullinates peptide; OR: odds ratio.
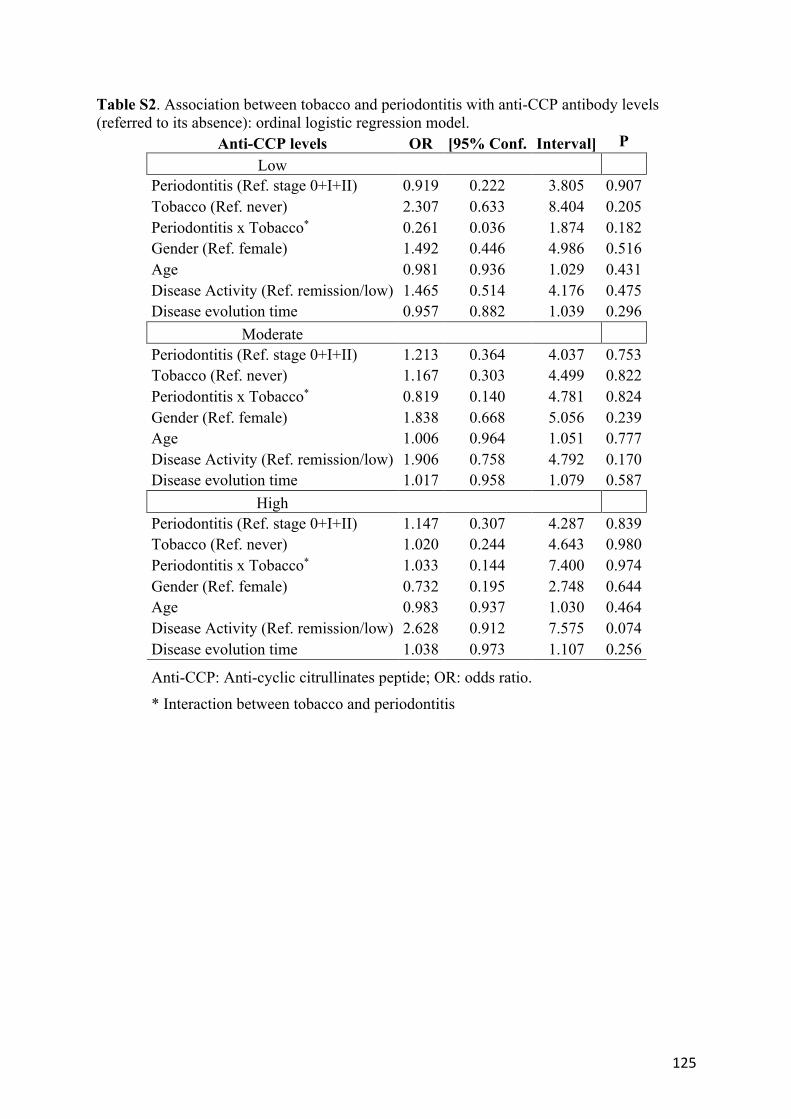
125
Table S2. Association between tobacco and periodontitis with anti-CCP antibody levels (referred to its absence): ordinal logistic regression model.
Anti-CCP levels OR [95% Conf. Interval] P Low
Periodontitis (Ref. stage 0+I+II) 0.919 0.222 3.805 0.907
Tobacco (Ref. never) 2.307 0.633 8.404 0.205
Periodontitis x Tobacco* 0.261 0.036 1.874 0.182
Gender (Ref. female) 1.492 0.446 4.986 0.516
Age 0.981 0.936 1.029 0.431
Disease Activity (Ref. remission/low) 1.465 0.514 4.176 0.475
Disease evolution time 0.957 0.882 1.039 0.296
Moderate
Periodontitis (Ref. stage 0+I+II) 1.213 0.364 4.037 0.753
Tobacco (Ref. never) 1.167 0.303 4.499 0.822
Periodontitis x Tobacco* 0.819 0.140 4.781 0.824
Gender (Ref. female) 1.838 0.668 5.056 0.239
Age 1.006 0.964 1.051 0.777
Disease Activity (Ref. remission/low) 1.906 0.758 4.792 0.170
Disease evolution time 1.017 0.958 1.079 0.587
High
Periodontitis (Ref. stage 0+I+II) 1.147 0.307 4.287 0.839
Tobacco (Ref. never) 1.020 0.244 4.643 0.980
Periodontitis x Tobacco* 1.033 0.144 7.400 0.974
Gender (Ref. female) 0.732 0.195 2.748 0.644
Age 0.983 0.937 1.030 0.464
Disease Activity (Ref. remission/low) 2.628 0.912 7.575 0.074
Disease evolution time 1.038 0.973 1.107 0.256
Anti-CCP: Anti-cyclic citrullinates peptide; OR: odds ratio.
* Interaction between tobacco and periodontitis

126

127
VI. Discusión

128
129
Discusión
Los resultados de las investigaciones incluidas en este trabajo aportan nueva evidencia en la relación entre la AR y la periodontitis, demostrando, por un lado, una significativa asociación entre ambas enfermedades, y por otro, una asociación clara entre las variables subrogadas de periodontitis y la presencia y niveles de anticuerpos específicos de la AR como son los ACPAs.
En el primer estudio (#Estudio 1(123)) se ha revisado toda la evidencia disponible sobre la asociación entre AR y periodontitis, así como las investigaciones preclínicas y clínicas que muestran los mecanismos que conectan ambas enfermedades. Con respecto a la asociación epidemiológica entre ambas enfermedades, observamos un gran número de estudios transversales y casos-control, los cuales en menor o mayor grado muestran cierta asociación entre la periodontitis y la AR (124-135)(Ver tabla 1 del #Estudio 1(123)). De hecho, en la última revisión sistemática de 19 estudios casos y controles, Kaur et. al (70) demostró una asociación significativa entre la AR y las variables subrogadas de la periodontitis, como la pérdida de inserción (OR 1,17, IC 95% 0,43-1,90) y la pérdida dentaria (OR 2,38 IC 95% 1,48-3,29). Por otro lado, aunque existen pocos estudios de cohortes tanto prospectivos como retrospectivos que hayan evaluado la relación entre ambas enfermedades (136-140)(Ver tabla 2 del #Estudio 1(123)), prácticamente todos demuestran una asociación entre ambas enfermedades. En estos estudios los pacientes con periodontitis presentan mayor riesgo de desarrollar AR, con ORs comprendidas entre 1,85 y 5,3(136-140). A pesar de ello, los resultados son muy heterogéneos, lo que se puede explicar por la disparidad en la definición de casos de periodontitis, lo que ocurre tanto en los estudios de transversales y casos-control como en los de cohortes. De ahí que en las conclusiones de nuestra revisión (#Estudio 1(123)) se ponga de relieve la necesidad de investigaciones clínicas mejor diseñadas, con una mayor muestra y una definición de caso de periodontitis validada epidemiológicamente. Por otra parte, existe no solo una asociación epidemiológica entre ambas enfermedades sino una posible relación entre la severidad de la periodontitis y de la severidad de la AR, aunque la evidencia de esta asociación está en debate. En un estudio casos -control, Mikuls et al. (127) evaluaron a 287 pacientes
130
con AR y 330 controles. Tras el análisis de los datos, los autores observaron una asociación estadísticamente significativa de la periodontitis con un recuento alto de articulaciones tumefactas, mayor actividad de la enfermedad y altos niveles de anticuerpos anti-CCP (127). Sin embargo, otros estudios con menor muestra y diferente definición de casos de periodontitis no encontraron una asociación estadísticamente significativa (141,142). Por ello, hemos puesto también de manifiesto la necesidad de estudios que exploren y confirmen la relación entre la severidad de la periodontitis y la severidad de la AR.
Con respecto a la plausibilidad biológica, hemos examinado los diferentes mecanismos que conectan ambas enfermedades (#Estudio 1 (123)), en concreto, el papel de ciertos periodontopatógenos en la citrulinación de proteínas, considerada el principal mecanismo autoinmune en la patogénesis de la AR con la formación de anticuerpos anti-peptidos citrulinados (ACPA) (63). Dichos anticuerpos son esenciales en el inicio y desarrollo de la AR, habiéndose detectado hasta 10 años antes del inicio de los primeros síntomas de artralgia (53,54). Hemos descrito dos mecanismos importantes asociados a la citrulinación de proteínas. En el primero intervienen ciertas bacterias periodonto-patógenos, en concreto, Porphyromonas
gingivalis y Agreggatibacter actinomycetemcomitans, que liberan deiminasas específicas o factores de virulencia, relacionados directamente con la hipercitrulinación de proteínas y la, ulterior formación de ACPAs (127,143-152). Por otro lado, el proceso inflamatorio crónico consecuencia de la periodontitis, puede ser otra fuente de citrulinación de proteínas, y por tanto, del proceso autoinmune con formación de auto-anticuerpos característico de la AR (69,116-121).
Con respecto al primer mecanismo, se ha demostrado que Porphyromonas gingivalis es capaz de producir una deiminasa específica, la Porphyromonas gingivalis peptidil arginina deiminasa(PPAD), con capacidad de inducir la citrulinación en proteínas humanas(117,152-154). En la evidencia experimental disponible se confirma el papel de la P. gingivalis en el desarrollo y progresión de la AR (154-159)(Ver tabla 3 del #estudio 1). De hecho, en un estudio reciente realizado en ratas wistar, Courbon et. al (154) demostraron que la periodontitis inducida por P. gingivalis se asocia con un gran aumento en los niveles de ACPAs e inflamación sistémica, así
131
como con un alto grado de daño estructural. Sin embargo, estudios recientes sugieren que P. gingivalis no es el único patógeno periodontal, capaz de producir la citrulinación de proteínas y de inducir a la formación de ACPAs. Se ha postulado que A. actinomycetemcomitans también es capaz de producir una hipercitrulinación en neutrófilos propios del huésped (147). Konig et. al (147) demostraron que dicha hipercitrulinación está mediada por la acción de la leucotoxina A(LtxA), un factor de virulencia del A. actinomycetemcomitans, el cual produce daños estructurales de la membrana de los neutrófilos, provocando, de este modo la activación descontrolada de deiminasas similares a la PPAD en las articulaciones de pacientes con AR. Otras bacterias como Tannerella forsythia(160), o Fusobacterium nucleatum(135,161) en combinación con A. actinomycetemcomitans o P. gingivalis se han asociado con un aumento de la progresión de la AR, así como con el incremento en los niveles de ACPAs. Por otro lado, a pesar de que muchos estudios experimentales han intentado investigar si la AR pudiera exacerbar la destrucción periodontal, no existe aún evidencia que demuestre tal hecho, por lo que, por el momento, se podría descartar la bi-direccionalidad de la asociación entre ambas enfermedades (155,162,163).
En relación a los estudios clínicos, la gran mayoría de las investigaciones revisadas confirman el rol de P. gingivalis en la citrulinación de proteínas y su asociación con la AR(Ver tabla 4 del #Estudio 1(123)). Entre ellos, un estudio transversal en 600 sujetos de Oluwagbemigun et. al(149) se observó una asociación estadísticamente significativa entre una alta concentración de ADN salival de P.
gingivalis y los recuentos elevados de títulos séricos de ACPAs. Recientemente, en otro estudio que evaluó 37.830 proteínas humanas del suero de 30 pacientes con AR(152), se reportó una asociación significativa entre la presencia de anti-RA-PPAD (una modificación recombinante de la PPAD) con los niveles de ACPAs y autoantígenos de la enfermedad intersticial pulmonar, lo que sugiere un concepto basado en la infección por inducción de ACPAs via “mimetismo enzimático”(“enzymatic mimicry”). No obstante, a pesar de que estos dos estudios presentan muestras amplias, la mayoría de las investigaciones son limitadas, con muestras poblacionales pequeñas, por lo que son necesarios más estudios, con muestras más amplias, que confirmen estos resultados preliminares.
132
A pesar de la numerosa evidencia sobre el papel de ciertos patógenos en la iniciación y progresión de la AR, existen autores que dan más importancia a la propia inflamación crónica inducida por la periodontitis, como fuente de citrulinación de proteínas y formación de anticuerpos, responsables del proceso autoinmune característico de la AR (69,116-121). En un estudio transversal, Nesse et. al (69) tomaron biopsias de tejido gingival en 20 pacientes con periodontitis, y 6 controles, y tejido gingival sinovial de 4 pacientes con AR y periodontitis, con el fin de valorar la presencia y localización de proteínas citrulinadas en tejido gingival con periodontitis y sin periodontitis. Tras el análisis por inmunohistoquímica y Western-blot, los autores determinaron que la citrulinación de proteínas es un fenómeno dependiente de proceso inflamatorio tanto en los tejidos periodontales como en el tejido sinovial tanto de pacientes con periodontitis como con AR. Por tanto, la inflamación producida en la periodontitis podría ser clave en el proceso de citrulinación y posterior formación de ACPAs. De Pablo et. al(117), en otro estudio en 198 pacientes con y sin periodontitis, demostraron que la respuesta inmunitaria mediada por anticuerpos en pacientes con periodontitis está dirigida a aquellos péptidos no citrulinados de los autoantígenos propios de la AR, como son los anti-CCP, anti-CEP-1 o el anti-MCV, siendo esta respuesta completamente independiente de si el paciente es fumador o no. Engstrom et. al (121) en un estudio transversal donde tomaron biopsias de tejido gingival de 30 pacientes con y sin periodontitis, demostraron que la citrulinación de proteínas o la expresión de PADs en tejido gingival, son independientes de la presencia de A. actinomycetemcomitans o P.
gingivalis, siendo mecanismos inflamatorio-dependientes. Sin embargo, cabe la posibilidad de que ambos procesos coexistan en
pacientes con periodontitis, teniendo un diferente papel dependiendo que se trate de la primera agresión “first hit” o la segunda “second hit” (68). En la figura 1 del #Estudio 1(123), hemos esquematizado 3 situaciones en las que la periodontitis y sus bacterias pudieran interactuar. La primera agresión o “first hit”, correspondería el punto #1, mientras que la segunda agresión o “second hit” correspondería al punto #2. Autores como Laugisch et. al(164) observaron que en tejidos de tanto pacientes con AR y periodontitis como en sanos con periodontitis existe actividad, tanto de la PAD humana, como de la PPAD, demostrando que tanto la citrulinación de proteínas
133
por parte de P. gingivalis, como por parte del mismo proceso inflamatorio de la periodontitis coexisten, lo que podría romper la inmunotolerancia en pacientes susceptibles y desencadenar el inicio de la enfermedad. Otros autores como Konig et. al (147), detectaron que la citrulinación que se observa en pacientes con periodontitis es similar a la hipercitrulinación en articulaciones inflamadas de pacientes con AR. Del mismo modo, dichos autores también observaron una fuerte asociación entre A. actinomycetemcomitans con la hipercitrulinación de neutrófilos del huésped. Por ello, existe la necesidad de estudios mejor diseñados, donde se investiguen tanto la acción de diferentes patógenos periodontales, como de la propia inflamación derivada de la periodontitis en el proceso de citrulinación y posterior estado hiperinflamatorio que de lugar al inicio de la AR, en pacientes susceptibles, o en pacientes con una AR precoz.
Dado que la periodontitis es un proceso inflamatorio crónico, se podría pensar que el tratamiento farmacológico de la AR, podría tener un impacto significativo en el control de la periodontitis de dichos individuos con AR. En este sentido hemos incluido tanto estudios en el que se tratan con FAMEs sintéticos como el metotrexate, como con FAMEs biológicos como por ejemplo terapia inhibitoria anti-IL 6 (Tocilizumab) o anti-TNF (Adalinumab)(ver tabla 6 del #Estudio 1(123)). A pesar de que un gran número de estudios sustentan un efecto positivo de la terapia con FAMEs sintéticos y biológicos (165-172), los pequeños tamaños muestrales limitan tener resultados con suficiente validez externa. En este sentido, en los estudios con mayor tamaño muestral(173,174) no observaron ningún efecto en el estado periodontal de pacientes en tratamiento de la AR, como en estudios prospectivos, donde, por ejemplo, Savioli et. al (175) reportaron que los pacientes con AR y periodontitis no respondían al tratamiento con terapia anti-TNF, sugiriendo que la inflamación crónica y sostenida de la periodontitis podría reducir o anular la eficacia del tratamiento farmacológico de la AR.
Por otra parte, y dado el grado de evidencia que sostiene el rol de la periodontitis en la AR, es bastante plausible que el tratamiento de la periodontitis pudiera tener un impacto significativo tanto en la expresión clínica como en las variables inmunológicas de la AR. En el #Estudio 1(123), revisamos toda la evidencia
134
disponible sobre el efecto del tratamiento periodontal en la AR (Ver Tabla 7 #Estudio 1(123)). En términos generales, la mayor parte de dichos estudios, muestran una reducción estadísticamente significativa de las variables clínicas de actividad de la AR((176-187). Sin embargo, la gran mayoría de los estudios presentan distintas definiciones de caso de periodontitis, con tamaños muestrales pequeños y con periodos cortos de seguimiento. Por ello, son necesarios estudios de intervención con mayores tamaños muestrales, mayor período de seguimiento, donde la selección de caso de periodontitis esté validada. No obstante, en un estudio de series de casos prospectivo, Moller et. al (187) seleccionaron 8 pacientes con una alta actividad de la AR (DAS28 ≥5,1), los cuales no respondían de manera adecuada al tratamiento de la AR, y que además presentaban periodontitis. Tras la evaluación inicial, trataron la periodontitis mediante raspado y alisado radicular en combinación con tratamiento antibiótico (amoxicilina + metronidazol) y los revisaron a los 6 meses. Los autores observaron que 5 de 8 pacientes mostraron una mejoría estadísticamente significativa en todos los parámetros clínicos e inmunológicos de la AR, con una reducción del DAS28 de 0,6, y con una respuesta adecuada al tratamiento de la AR. Esto pone de relieve la importancia de la selección de caso para los ensayos clínicos, dado que la selección de pacientes con AR de alta actividad con periodontitis avanzada (estadios III y IV), podría suponer un segmento interesante a estudiar y valorar los beneficios tanto para el paciente como para su manejo a nivel reumatológico.
En el segundo artículo incluido en esta tesis (#Estudio 2 (188)) se realizó un estudio de casos control, con el fin de evaluar la asociación entre la presencia de periodontitis y la AR, y si la severidad de periodontitis se relaciona con la severidad de la AR. Como mencionamos en el #Estudio 1(123), en la gran mayoría de los estudios transversales se reporta, en mayor o menor grado, relación entre ambas enfermedades. No obstante, los tamaños muestrales de dichos estudios son limitados y existe bastante disparidad en la definición de caso de periodontitis, así como en los diferentes “scores” utilizados para medir la actividad de la AR. Por ello, realizamos un estudio de casos y controles en 344 pacientes (187 pacientes con AR y 157 controles), donde utilizamos una definición de caso de periodontitis (189) validada por la EFP (Federación Europea de Periodoncia) y ampliamente utilizada en
135
estudios epidemiológicos (190-192). Del mismo modo, existen diferentes “scores” que valoran la actividad de pacientes con AR, donde los estudios suelen utilizar uno o dos para definirlo, pero no siempre usan el mismo (193). Por ello, medimos los tres índices validados (DAS28 (por VSG y PCR), SDAI y CDAI) y establecimos el grado de actividad cuando dos de los tres índices coincidían. Si observamos la figura S1 del #Estudio 2(188) se representa la severidad de la periodontitis en función de la actividad clínica tanto con el índice compuesto, como por cada índice individualmente, observando pocas variaciones entre todos, por lo que le da mayor validez externa.
Por otro lado, nuestro estudio (#Estudio 2(188)) confirma una asociación independiente entre la periodontitis y la AR. De hecho, cuando analizamos dicha asociación y categorizamos la periodontitis por niveles (nivel 1: leve, y nivel 2: moderado/avanzado) observamos de manera consistente ORs ajustadas para el nivel 1 de 14,78 (IC 95% 4,23-51,68, p<0,001) y de 81,01(IC 95% 18,59-353,07, p<0,001) para el nivel 2(Ver tabla 4 del #Estudio 2 (188)). Dichos resultados, concuerdan con una gran cantidad de estudios tanto transversales, casos y controles como de cohortes (124-128,131-141,194-199). Del mismo modo, el #Estudio 2 (188), demuestra una clara relación entre la severidad de la periodontitis y la actividad clínica de la AR. El 64% de los pacientes que presentaban alta actividad de AR, exhibían periodontitis avanzada. De hecho, pacientes con periodontitis avanzada presentaron 2,66 veces más riesgo de presentar alta actividad de AR, tras ajustar a factores de confusión como el tabaco, la edad o el género. Del mismo modo, los pacientes con AR moderada o alta actividad mostraban mayor número y porcentaje de bolsas ≥ 5mm, pérdida de inserción y pérdida dentaria con respecto a aquellos pacientes en remisión o con los controles. Esto confirma los resultados obtenidos previamente por Mikuls et. al (127), o los obtenidos recientemente por Karapetsa et. al (200), en contraposición a los obtenidos en otros estudios con tamaños muestrales reducidos, y definiciones de caso de periodontitis imprecisa(141,196,201). Por otro lado, nuestros resultados (#Estudio 2 (188)) demostraron por primera vez una correlación linear entre la actividad de la AR y variables subrogadas de la periodontitis como es la pérdida de inserción, donde encontramos un aumento de 0,24 y 0,19 del DAS28 y DAS28PCR, por cada milímetro de pérdida de inserción que
136
presentaban los pacientes con AR (p= 0,002 y p=0,011, ajustado por edad, género y tabaco). Del mismo modo, y también por primera vez, se demuestra una asociación entre la presencia de nódulos reumatoideos y la periodontitis avanzada, los cuales se asocian normalmente como complicaciones de pacientes con AR de alta actividad clínica y que no responde a bien al tratamiento. Adicionalmente, y de manera bastante interesante, observamos, a su vez, una mayor prevalencia de periodontitis severa en pacientes con AR precoz en comparación con pacientes AR establecida (60% vs 41,45%), lo cual está en concordancia con lo expuesto por estudios similares (140,143). Este hallazgo, se podría relacionar con que un porcentaje importante de pacientes con AR precoz presentan una alta o moderada actividad clínica (31,43%), con respecto a pacientes con AR establecida (9,21%).
En cuanto al impacto del tratamiento de la AR con FAMEs tanto sintéticos como biológicos sobre el estado periodontal, existe bastante controversia, como comentamos en el #Estudio 1(123). Sin embargo, nuestros datos (#Estudio 2 (188)) no muestran ningún efecto de dicho tratamiento sobre el estado periodontal de los pacientes con AR, lo cual está en concordancia con lo expuesto en el #Estudio 1(123), donde la gran mayoría de estudios que soportan un efecto positivo de la FAMEs sintéticos y biológicos (165-172), pero cuyos tamaños muestrales son bastante limitados lo cual limita sacar resultados y conclusiones con cierta validez externa.
En relación a la posible asociación entre las variables inmunológicas y la periodontitis y sus variables subrogadas, los datos obtenidos en nuestro #Estudio 2 (188) no muestran ninguna relación entre auto-anticuerpos específicos de la AR como el Factor Reumatoide o los ACPAs (en concreto, los anti-CCP2, los cuáles son los mayormente asociados con la extensión y severidad de la AR) y la periodontitis. Sin embargo, desde el punto de vista metodológico, nuestro estudio no estaba diseñado para responder a dicha pregunta, por lo que se precisan otro tipo de investigaciones con diseños experimentales adecuados.
En el tercer estudio incluido en esta tesis (#Estudio 3 (202)), dado que en nuestro #Estudio 2(188), no encontramos ninguna asociación entre las variables
137
inmnunológicas de la AR y la periodontitis y sus variables subrogadas, se realizó un estudio transversal con el objetivo de evaluar de manera más detallada la asociación entre la periodontitis y sus variables subrogadas, con la presencia y títulos de ACPA en pacientes con AR.
Tal y como se expuso en el #Estudio 1(123), existen gran cantidad de estudios que relacionan la presencia de bacterias periodontales como P. gingivalis o A.
actinomycetemcomitans con la presencia y aumento de los títulos de anti-CCP (el cual es el anticuerpo anti-péptido citrulinado más relacionado con la AR) (24,110,135,143,144,146,147,149-151,160,203-207). A pesar de que se ha observado la presencia de ACPAs en pacientes sanos con periodontitis(69,117), existen muy pocos estudios que relacionen variables subrogadas de la periodontitis con la presencia y títulos de anti-CCP en pacientes con AR. Mikuls et al (127) observaron una asociación significativa entre la presencia de periodontitis y la presencia de anti-CCP, aunque se perdía dicha asociación significativa cuando se ajustaban los datos incluyendo los pacientes anti-CCP negativos (OR ajustada 1,59, IC 95% 1,01-2,49, y OR en todos los pacientes con AR, 1,36, IC 95% 0,89-2,06). Recientemente, Karapetsa et. al (200) encontraron que pacientes con periodontitis avanzada presentaban mayor positividad a ACPA, siendo esta asociación estadísticamente significativa (p=0,029). De manera similar a los resultados de Mikuls et. al (127), el análisis de nuestros datos no demostró una asociación estadísticamente significativa entre la periodontitis y severidad de AR (anti-CCP positivos), tanto cuando la periodontitis fue definida con los criterios de Tonetti et. al(189) (OR1,228 IC 95% 0,628-2,40, p=0,549), como cuando la periodontitis fue categorizada por estadíos, siguiendo los recientes criterios de la Federación Europea de Periodoncia (EFP)(80) (OR 1,222 IC 95% 0,628-2,379, p=0,379). Curiosamente, observamos un mayor porcentaje de pacientes anti-CCP positivos con periodontitis estadio III-IV que pacientes anti-CCP negativos (51%vs 47%). En relación a las variables subrogadas de la periodontitis y su asociación con la presencia y títulos de anti-CCP, nuestros datos(#Estudio 3(202) revelan una asociación estadísticamente significativa con la pérdida de inserción (OR 1,523 IC 95% 1,057-2,194, p=0,024), y una tendencia de asociación con el número de bolsas ≥5mm (OR 1,024 IC 95% 0,999-1,048, p=0,065). De hecho, por primera vez, tras estratificar los títulos de anti-

138
CCP en títulos bajos-moderados-altos, nuestros resultados demuestran una asociación estadísticamente significativa entre la pérdida de inserción (OR 1,593 IC 95% 1,017-2,482, p=0,043) y el número de bolsas ≥5mm (OR 1,031 IC 95% 1,003-1,062, p=0,031) con títulos altos de anti-CCP. De manera adicional, y por primera vez, se ha demostrado una correlación linear entre una variable secundaria de la periodontitis, como son el número de bolsas ≥5 mm y los títulos de anti-CCP, donde se observó un incremento de 4,45 U/mL (IC 95% 1,60-7,29, p=0,002) de títulos de anti-CCP por cada bolsa ≥5mm en pacientes con AR, ajustado por edad, género, tabaquismo, tiempo de evolución de la enfermedad y actividad de la AR. Esta correlación podría ser de gran importancia, dado que podría reflejar el rol potencial de ciertas bacterias periodontales, como P. gingivalis o A. actinomycetemcomitans en la citrulinación de proteínas, dado que su presencia se asocia a bolsas profundas≥5mm (208-210) y periodontitis avanzadas. No obstante, tal y como se expuso en el #Estudio 1(123), la inflamación producida en la periodontitis podría tener también un rol en el proceso de citrulinación, por tanto, la falta de datos microbiológicos es una gran limitación que nos impide dilucidar qué factor pueda tener más peso en dicho proceso. Del mismo modo, existen datos recientes que demuestran una asociación significativa entre la periodontitis y sus variables
subrogadas, con otros anticuerpos citrulinados como es el anti-µ enolasa (anti-
ENO1) (43). Por tanto, existe la necesidad de más estudios, que analicen distintos tipos de ACPAs, como anti-CCP, anti-vimentina, anti-fibrinógeno o anti-ENO1, con el fin de esclarecer el rol de la periodontitis y bacterias periodontales en su formación y su impacto en la actividad, desarrollo y progresión de la AR.
Por otro lado, la periodontitis y la presencia de ciertos periodontopatógenos no son las únicas fuentes de citrulinación de proteínas. En este sentido, el tabaquismo es uno de los factores que mayormente contribuyen a la formación de ACPAs (211,212). Ciertos autores han planteado la hipótesis de que el impacto del tabaco es de tal magnitud que enmascararía los efectos de la periodontitis y de las bacterias periodontopatógenas como P. gingivalis, en el proceso de citrulinación y posterior formación de ACPAs(213). Sin embargo, existen datos que asocian la periodontitis con la presencia y títulos de ACPAs independientemente del consumo de tabaco en pacientes sin AR(214). Nuestros datos muestran una asociación entre el tabaquismo
139
y la periodontitis en pacientes con AR, y al mismo tiempo, una asociación independiente del tabaco, entre las variables subrogadas de la periodontitis como la pérdida de inserción o las bolsas ≥5mm con los títulos de anti-CCP, tras ajustar a edad, género y consumo de tabaco. Por tanto, el efecto del consumo tabáquico sobre la citrulinación de proteínas sería marginal con respecto a la periodontitis y sus variables subrogadas, aunque nuestro estudio presente una limitación importante, que es la falta de datos microbiológicos, que puedan dilucidar la importancia de ciertas bacterias periodontopatógenas como P. gingivalis o A.
actinomycetemcomitans, las cuales, como se describió en el #Estudio 1(123), parecen ser esenciales en la hipercitrulinación de proteínas y posterior formación de ACPAs.
Lógicamente, existen limitaciones relativas a los tres estudios presentados (#Estudio 1, #Estudio 2 y #Estudio 3 (123,188,202)). Obviando que el #Estudio 1(123) es una revisión narrativa donde integramos toda la evidencia disponible sobre la asociación entre la periodontitis y la AR, dicho estudio nos expone las diferentes limitaciones existentes en la literatura al respecto, desde la necesidad de definir adecuadamente lo que es la periodontitis en cada estudio, hasta la selección de controles con artrosis, o por ejemplo la necesidad de ampliar el tamaño muestral. Por otro lado, tanto el #Estudio 2(188) como el #Estudio 3(202) no dejan de ser estudios que no miden la causalidad de la asociación, sino que simplemente nos sirven de base para establecer un principio de asociación entre ambas enfermedades, identificando la metodología, y la selección de pacientes, para realizar posteriores estudios tanto de cohortes prospectivos como de intervención en los que se valoren de manera adecuada la causalidad de la asociación entre ambas enfermedades. Son importantes, como hemos discutido anteriormente, analizar la microbiología periodontal para establecer el posible impacto de dicho patógenos, así como también analizar diferentes tipos de ACPAs. Dado que, como hemos demostrado la asociación entre la severidad de la periodontitis con la severidad de la AR, sería importante realizar estudios de intervención donde se seleccionen pacientes con AR de moderada/alta actividad, que además presenten periodontitis estadio III/IV, los cuales son pacientes que normalmente no responden de manera adecuada al

140
tratamiento de la AR, y que el tratamiento periodontal podría jugar un papel importante en el manejo del paciente con AR.

141
VII. Conclusiones

142
143
Conclusiones
De manera general, se puede concluir que:
Los resultados obtenidos de los tres estudios incluidos en este trabajo, han demostrado la asociación clara entre la periodontitis y su severidad con la actividad clínica de la AR, su expresión clínica así como en sus diferentes variables inmunológicas, las cuales son marcadores de progresión y agresividad de la enfermedad.
Adicionalmente, nuestros datos justifican la realización de estudios mejor diseñados, con muestras más amplias, tanto de cohortes prospectivos, como de intervención, en mor de dilucidar una relación de causalidad entre ambas enfermedades, donde el manejo de la periodontitis pueda ayudar a mejorar el manejo del paciente con AR por parte del médico reumatólogo
De manera específica, se puede concluir que:
• Existe una gran asociación entre ambas enfermedades, donde la periodontitis puede actuar en distintas fases del desarrollo, progresión y tratamiento de la AR.
• Demostramos una asociación independiente y de gran magnitud entre la periodontitis y la AR, donde la severidad de la periodontitis se asocia de manera muy significativa con la actividad de la AR.
• Observamos que la severidad de la periodontitis se correlacionan con la presencia y altos títulos de ACPAs, donde a mayor pérdida de inserción o mayor cantidad de bolsas ≥5mm, mayores niveles de títulos de ACPAs.

144
145
VIII. Bibliografía

146
147
Bibliografía
1. Turesson C, O'Fallon WM, Crowson CS, Gabriel SE, Matteson EL. Extra-articular disease manifestations in rheumatoid arthritis: incidence trends and risk factors over 46 years. Ann Rheum Dis. BMJ Publishing Group Ltd; 2003 Aug;62(8):722–7.
2. Aviña-Zubieta JA, Choi HK, Sadatsafavi M, Etminan M, Esdaile JM, Lacaille D. Risk of cardiovascular mortality in patients with rheumatoid arthritis: A meta-analysis of observational studies. Arthritis Rheum. 2008 Dec 15;59(12):1690–7.
3. de Molon RS, Rossa C Jr, Thurlings RM, Cirelli JA, Koenders MI. Linkage of Periodontitis and Rheumatoid Arthritis: Current Evidence and Potential Biological Interactions. IJMS. 2019 Sep;20(18):4541–35.
4. Symmons DP, Barrett EM, Bankhead CR, Scott DG, Silman AJ. The incidence of rheumatoid arthritis in the United Kingdom: results from the Norfolk Arthritis Register. Br J Rheumatol. 1994 Aug;33(8):735–9.
5. Seoane-Mato D, Sánchez-Piedra C, Díaz-González F, Bustabad S. Prevalence of rheumatic diseases in adult population in Spain. Episer 2016 study. Ann Rheum Dis. 2018 Jun 1;77(Suppl 2):535.
6. Carbonell J, Cobo T, Balsa A, Descalzo MA, Carmona L, SERAP Study Group. The incidence of rheumatoid arthritis in Spain: results from a nationwide primary care registry. Rheumatology (Oxford). 2008 Jul;47(7):1088–92.
7. Almutairi K, Nossent J, Preen D, Keen H, Inderjeeth C. The global prevalence of rheumatoid arthritis: a meta-analysis based on a systematic review. Rheumatol Int. 2nd ed. Springer Berlin Heidelberg; 2020 Nov 11;6:468–15.
148
8. de Pablo P, Chapple ILC, Buckley CD, Dietrich T. Periodontitis in systemic rheumatic diseases. Nat Rev Rheumatol. Nature Publishing Group; 2009 Apr;5(4):218–24.
9. MacGregor AJ, Snieder H, Rigby AS, Koskenvuo M, Kaprio J, Aho K, et al. Characterizing the quantitative genetic contribution to rheumatoid arthritis using data from twins. Arthritis Rheum. John Wiley & Sons, Ltd; 2000 Jan;43(1):30–7.
10. Stahl EA, Raychaudhuri S, Remmers EF, Xie G, Eyre S, Thomson BP, et al. Genome-wide association study meta-analysis identifies seven new rheumatoid arthritis risk loci. Nat Genet. Nature Publishing Group; 2010 Jun;42(6):508–14.
11. Holoshitz J. The rheumatoid arthritis HLA-DRB1 shared epitope. Curr Opin Rheumatol. 2010 May;22(3):293–8.
12. Begovich AB, Carlton VEH, Honigberg LA, Schrodi SJ, Chokkalingam AP, Alexander HC, et al. A missense single-nucleotide polymorphism in a gene encoding a protein tyrosine phosphatase (PTPN22) is associated with rheumatoid arthritis. Am J Hum Genet. 2004 Aug;75(2):330–7.
13. Lie BA, Viken MK, Odegård S, van der Heijde D, Landewé R, Uhlig T, et al. Associations between the PTPN22 1858C->T polymorphism and radiographic joint destruction in patients with rheumatoid arthritis: results from a 10-year longitudinal study. Ann Rheum Dis. 2007 Dec;66(12):1604–9.
14. Suzuki A, Yamada R, Chang X, Tokuhiro S, Sawada T, Suzuki M, et al. Functional haplotypes of PADI4, encoding citrullinating enzyme peptidylarginine deiminase 4, are associated with rheumatoid arthritis. Nat Genet. Nature Publishing Group; 2003 Aug;34(4):395–402.
15. Martinez A, Valdivia A, Pascual-Salcedo D, Lamas JR, Fernández-Arquero M, Balsa A, et al. PADI4 polymorphisms are not associated with rheumatoid arthritis in the Spanish population. Rheumatology. 2005 Oct;44(10):1263–6.

149
16. Barton A, Bowes J, Eyre S, Spreckley K, Hinks A, John S, et al. A functional haplotype of the PADI4 gene associated with rheumatoid arthritis in a Japanese population is not associated in a United Kingdom population. Arthritis Rheum. John Wiley & Sons, Ltd; 2004 Apr;50(4):1117–21.
17. Bottini N, Firestein GS. Epigenetics in rheumatoid arthritis: a primer for rheumatologists. Curr Rheumatol Rep. Springer US; 2013 Nov;15(11):372–11.
18. Karlson EW, Lee IM, Cook NR, Manson JE, Buring JE, Hennekens CH. A retrospective cohort study of cigarette smoking and risk of rheumatoid arthritis in female health professionals. Arthritis Rheum. 1999 May;42(5):910–7.
19. Wolfe F. The effect of smoking on clinical, laboratory, and radiographic status in rheumatoid arthritis. J Rheumatol. 2000 Mar;27(3):630–7.
20. Liao KP, Alfredsson L, Karlson EW. Environmental influences on risk for rheumatoid arthritis. Curr Opin Rheumatol. 2009 May;21(3):279–83.
21. Pedersen M, Jacobsen S, Garred P, Madsen HO, Klarlund M, Svejgaard A, et al. Strong combined gene-environment effects in anti-cyclic citrullinated peptide-positive rheumatoid arthritis: a nationwide case-control study in Denmark. Arthritis Rheum. John Wiley & Sons, Ltd; 2007 May;56(5):1446–53.
22. Demoruelle MK, Weisman MH, Simonian PL, Lynch DA, Sachs PB, Pedraza IF, et al. Brief report: airways abnormalities and rheumatoid arthritis-related autoantibodies in subjects without arthritis: early injury or initiating site of autoimmunity? Arthritis Rheum. John Wiley & Sons, Ltd; 2012 Jun;64(6):1756–61.
23. Klareskog L, Malmström V, Lundberg K, Padyukov L, Alfredsson L. Smoking, citrullination and genetic variability in the immunopathogenesis of rheumatoid arthritis. 2011 Apr;23(2):92–8.
24. Kharlamova N, Jiang X, Sherina N, Potempa B, Israelsson L, Quirke A-M, et al. Antibodies to Porphyromonas gingivalis Indicate Interaction Between Oral
150
Infection, Smoking, and Risk Genes in Rheumatoid Arthritis Etiology. Arthritis Rheumatol. Wiley-Blackwell; 2016 Mar;68(3):604–13.
25. Cooper GS. Occupational exposures and risk of rheumatoid arthritis: continued advances and opportunities for research. J Rheumatol. J Rheumatol; 2008 Jun;35(6):950–2.
26. Webber MP, Moir W, Zeig-Owens R, Glaser MS, Jaber N, Hall C, et al. Nested case-control study of selected systemic autoimmune diseases in World Trade Center rescue/recovery workers. Arthritis Rheumatol. John Wiley & Sons, Ltd; 2015 May;67(5):1369–76.
27. Lu B, Hiraki LT, Sparks JA, Malspeis S, Chen C-Y, Awosogba JA, et al. Being overweight or obese and risk of developing rheumatoid arthritis among women: a prospective cohort study. Ann Rheum Dis. BMJ Publishing Group Ltd; 2014 Nov;73(11):1914–22.
28. Ke Y, Dai X, Xu D, Liang J, Yu Y, Cao H, et al. Features and Outcomes of Elderly Rheumatoid Arthritis: Does the Age of Onset Matter? A Comparative Study From a Single Center in China. Rheumatol Ther. Springer Healthcare; 2020 Dec 14;76:1245–12.
29. Hedenstierna L, Opava CH, Askling J, Jiang X, Ernestam S, Alfredsson L, et al. Social stressors and risk of rheumatoid arthritis and their relationship to known modifiable risk factors: results from the Swedish EIRA study. Scand J Rheumatol. 2021 Jan 12;64:1–5.
30. Li S, Yu Y, Yue Y, Zhang Z, Su K. Microbial Infection and Rheumatoid Arthritis. J Clin Cell Immunol. 2013 Dec;4(6).
31. Alpizar Rodriguez D, Lesker TR, Gronow A, Gilbert B, Raemy E, Lamacchia C, et al. Prevotella copri in individuals at risk for rheumatoid arthritis. Ann Rheum Dis. BMJ Publishing Group Ltd; 2019 May;78(5):590–3.
32. Alpizar Rodriguez D, Lesker TR, Gilbert B, Strowig T, Finckh A. Intestinal dysbiosis in RA development: difficulty of establishing causality. Response to:
151
“Non-causal association of gut microbiome on the risk of rheumatoid arthritis: a Mendelian randomisation study” by Inamo. Ann Rheum Dis. BMJ Publishing Group Ltd; 2019 Nov 28;:annrheumdis–2019–216637.
33. Alpizar Rodriguez D, Finckh A, Gilbert B. The Role of Nutritional Factors and Intestinal Microbiota in Rheumatoid Arthritis Development. Nutrients. Multidisciplinary Digital Publishing Institute; 2020 Dec 30;13(1):96.
34. Rooney CM, Mankia K, Mitra S, Moura IB, Emery P, Wilcox MH. Perturbations of the gut microbiome in anti-CCP positive individuals at risk of developing rheumatoid arthritis. Rheumatology (Oxford). 2020 Dec 11;50:380.
35. Chu X-J, Cao N-W, Zhou H-Y, Meng X, Guo B, Zhang H-Y, et al. The oral and gut microbiome in rheumatoid arthritis patients: a systematic review. Rheumatology (Oxford). 2020 Jan 15;388:2023.
36. Kishikawa T, Maeda Y, Nii T, Motooka D, Matsumoto Y, Matsushita M, et al. Metagenome-wide association study of gut microbiome revealed novel aetiology of rheumatoid arthritis in the Japanese population. Ann Rheum Dis. 2020 Jan;79(1):103–11.
37. Hecht C, Schett G, Finzel S. The impact of rheumatoid factor and ACPA on bone erosion in rheumatoid arthritis. Ann Rheum Dis. 2015 Jan;74(1):e4–e4.
38. Challener GJ, Jones JD, Pelzek AJ, Hamilton BJ, Boire G, de Brum-Fernandes AJ, et al. Anti-carbamylated Protein Antibody Levels Correlate with Anti-Sa (Citrullinated Vimentin) Antibody Levels in Rheumatoid Arthritis. J Rheumatol. The Journal of Rheumatology; 2016 Feb;43(2):273–81.
39. Alarcon RT, Fernandes ADRC, Laurindo IM, Bértolo MB, Pinheiro GC, Andrade LE. Characterization of cumulative joint damage patterns in patients with rheumatoid arthritis: a clinical, serological, and gene polymorphism perspective. J Rheumatol. The Journal of Rheumatology; 2015 Mar;42(3):405–12.
152
40. Bläss S, Schumann F, Hain NA, Engel JM, Stuhlmüller B, Burmester GR. p205 is a major target of autoreactive T cells in rheumatoid arthritis. Arthritis Rheum. John Wiley & Sons, Ltd; 1999 May;42(5):971–80.
41. Wu C-Y, Yang H-Y, Lai J-H. Anti-Citrullinated Protein Antibodies in Patients with Rheumatoid Arthritis: Biological Effects and Mechanisms of Immunopathogenesis. IJMS. Multidisciplinary Digital Publishing Institute; 2020 Jun 4;21(11):4015.
42. Kinloch A, Tatzer V, Wait R, Peston D, Lundberg K, Donatien P, et al. Identification of citrullinated alpha-enolase as a candidate autoantigen in rheumatoid arthritis. Arthritis Res Ther. BioMed Central; 2005;7(6):R1421–9.
43. Lee JY, Lee JY, Choi IA, Choi IA, Kim J-H, Kim J-H, et al. Association between anti-Porphyromonas gingivalis or anti-α-enolase antibody and severity of periodontitis or rheumatoid arthritis (RA) disease activity in RA. BMC Musculoskelet Disord. 2015;16:190.
44. Vossenaar ER, Després N, Lapointe E, van der Heijden A, Lora M, Senshu T, et al. Rheumatoid arthritis specific anti-Sa antibodies target citrullinated vimentin. Arthritis Res Ther. BioMed Central; 2004;6(2):R142–50.
45. Sebbag M, Moinard N, Auger I, Clavel C, Arnaud J, Nogueira L, et al. Epitopes of human fibrin recognized by the rheumatoid arthritis-specific autoantibodies to citrullinated proteins. Eur J Immunol. John Wiley & Sons, Ltd; 2006 Aug;36(8):2250–63.
46. Burkhardt H, Koller T, Engström A, Nandakumar KS, Turnay J, Kraetsch HG, et al. Epitope-specific recognition of type II collagen by rheumatoid arthritis antibodies is shared with recognition by antibodies that are arthritogenic in collagen-induced arthritis in the mouse. Arthritis Rheum. John Wiley & Sons, Ltd; 2002 Sep;46(9):2339–48.
47. De Rycke L, Nicholas AP, Cantaert T, Kruithof E, Echols JD, Vandekerckhove B, et al. Synovial intracellular citrullinated proteins colocalizing with peptidyl
153
arginine deiminase as pathophysiologically relevant antigenic determinants of rheumatoid arthritis-specific humoral autoimmunity. Arthritis Rheum. John Wiley & Sons, Ltd; 2005 Aug;52(8):2323–30.
48. Chang X, Yamada R, Suzuki A, Sawada T, Yoshino S, Tokuhiro S, et al. Localization of peptidylarginine deiminase 4 (PADI4) and citrullinated protein in synovial tissue of rheumatoid arthritis. Rheumatology. 2005 Jan;44(1):40–50.
49. Whiting PF, Smidt N, Sterne JAC, Harbord R, Burton A, Burke M, et al. Systematic review: accuracy of anti-citrullinated Peptide antibodies for diagnosing rheumatoid arthritis. Ann Intern Med. American College of Physicians; 2010 Apr 6;152(7):456–64–W155–66.
50. Wegner N, Lundberg K, Kinloch A, Fisher B, Malmström V, Feldmann M, et al. Autoimmunity to specific citrullinated proteins gives the first clues to the etiology of rheumatoid arthritis. Immunol Rev. John Wiley & Sons, Ltd; 2010 Jan;233(1):34–54.
51. Kokkonen H, Mullazehi M, Berglin E, Hallmans G, Wadell G, Rönnelid J, et al. Antibodies of IgG, IgA and IgM isotypes against cyclic citrullinated peptide precede the development of rheumatoid arthritis. Arthritis Res Ther. BioMed Central; 2011 Feb 3;13(1):R13.
52. Jørgensen KT, Wiik A, Pedersen M, Hedegaard CJ, Vestergaard BF, Gislefoss RE, et al. Cytokines, autoantibodies and viral antibodies in premorbid and postdiagnostic sera from patients with rheumatoid arthritis: case-control study nested in a cohort of Norwegian blood donors. Ann Rheum Dis. 2008 Jun;67(6):860–6.
53. Brink M, Hansson M, Mathsson L, Jakobsson P-J, Holmdahl R, Hallmans G, et al. Multiplex analyses of antibodies against citrullinated peptides in individuals prior to development of rheumatoid arthritis. Arthritis Rheum. 2013 Apr;65(4):899–910.
154
54. Deane KD, O'Donnell CI, Hueber W, Majka DS, Lazar AA, Derber LA, et al. The number of elevated cytokines and chemokines in preclinical seropositive rheumatoid arthritis predicts time to diagnosis in an age-dependent manner. Arthritis Rheum. John Wiley & Sons, Ltd; 2010 Nov;62(11):3161–72.
55. Rakieh C, Rakieh C, Nam JL, Nam JL, Hunt L, Hunt L, et al. Predicting the development of clinical arthritis in anti-CCP positive individuals with non-specific musculoskeletal symptoms: a prospective observational cohort study. Ann Rheum Dis. 2015 Sep;74(9):1659–66.
56. de Hair MJH, van de Sande MGH, Ramwadhdoebe TH, Hansson M, Landewé R, van der Leij C, et al. Features of the synovium of individuals at risk of developing rheumatoid arthritis: implications for understanding preclinical rheumatoid arthritis. Arthritis Rheumatol. 2014 Mar;66(3):513–22.
57. Bemis EA, Demoruelle MK, Seifert JA, Polinski KJ, Weisman MH, Buckner JH, et al. Factors associated with progression to inflammatory arthritis in first-degree relatives of individuals with RA following autoantibody positive screening in a non-clinical setting. Ann Rheum Dis. BMJ Publishing Group Ltd; 2021 Feb;80(2):154–61.
58. Hecht C, Englbrecht M, Rech J, Schmidt S, Araujo E, Engelke K, et al. Additive effect of anti-citrullinated protein antibodies and rheumatoid factor on bone erosions in patients with RA. Ann Rheum Dis. 2015 Dec;74(12):2151–6.
59. Boman A, Brink M, Lundquist A, Hansson M, Mathsson-Alm L, Rönnelid J, et al. Antibodies against citrullinated peptides are associated with clinical and radiological outcomes in patients with early rheumatoid arthritis: a prospective longitudinal inception cohort study. RMD Open. BMJ Specialist Journals; 2019 Sep 3;5(2):e000946–10.
60. Kampstra ASB, Dekkers JS, Volkov M, Dorjée AL, Hafkenscheid L, Kempers AC, et al. Different classes of anti-modified protein antibodies are induced on exposure to antigens expressing only one type of modification. Ann Rheum Dis. BMJ Publishing Group Ltd; 2019 Jul;78(7):908–16.
155
61. Konig MF, Andrade F. A Critical Reappraisal of Neutrophil Extracellular Traps and NETosis Mimics Based on Differential Requirements for Protein Citrullination. Front Immunol. Frontiers; 2016;7(9):461.
62. McInnes IB, Schett G. The pathogenesis of rheumatoid arthritis. N Engl J Med. Massachusetts Medical Society; 2011 Dec 8;365(23):2205–19.
63. Bartold PM, Lopez-Oliva I. Periodontitis and rheumatoid arthritis: An update 2012-2017. Periodontol 2000. 2020 Jun;83(1):189–212.
64. Lamacchia C, Courvoisier DS, Jarlborg M, Bas S, Roux-Lombard P, Möller B, et al. Predictive value of anti-CarP and anti-PAD3 antibodies alone or in combination with RF and ACPA on the severity of rheumatoid arthritis. Rheumatology (Oxford). 2021 Jan 27.
65. Badillo-Soto MA, Rodríguez-Rodríguez M, Pérez-Pérez ME, Daza-Benitez L, Bollain-Y-Goytia JJ, Carrillo-Jiménez MA, et al. Potential protein targets of the peptidylarginine deiminase 2 and peptidylarginine deiminase 4 enzymes in rheumatoid synovial tissue and its possible meaning. Eur J Rheumatol. 2016 Jun;3(2):44–9.
66. Nielen MMJ, van Schaardenburg D, Reesink HW, van de Stadt RJ, van der Horst-Bruinsma IE, de Koning MHMT, et al. Specific autoantibodies precede the symptoms of rheumatoid arthritis: a study of serial measurements in blood donors. Arthritis Rheum. John Wiley & Sons, Ltd; 2004 Feb;50(2):380–6.
67. van de Sande MGH, van de Sande MGH, de Hair MJH, de Hair MJH, van der Leij C, van der Leij C, et al. Different stages of rheumatoid arthritis: features of the synovium in the preclinical phase. Ann Rheum Dis. 2011 May;70(5):772–7.
68. Golub LM, Payne JB, Reinhardt RA, Nieman G. Can systemic diseases co-induce (not just exacerbate) periodontitis? A hypothetical “two-hit” model. Journal of Dental Research. SAGE Publications; 2006 Feb;85(2):102–5.
156
69. Nesse W, Nesse W, Westra J, Westra J, van der Wal JE, van der Wal JE, et al. The periodontium of periodontitis patients contains citrullinated proteins which may play a role in ACPA (anti-citrullinated protein antibody) formation. J Clin Periodontol. 2012 Jul;39(7):599–607.
70. Kaur S, White S, Bartold PM. Periodontal disease and rheumatoid arthritis: a systematic review. Journal of Dental Research [Internet]. 2013 Apr 16;92(5):399–408. Available from: http://eutils.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&id=23525531&retmode=ref&cmd=prlinks
71. Potempa J, Mydel P, Koziel J. The case for periodontitis in the pathogenesis of rheumatoid arthritis. Nat Rev Rheumatol. Nature Publishing Group; 2017 Oct;13(10):606–20.
72. Koziel J, Mydel P, Potempa J. The link between periodontal disease and rheumatoid arthritis: an updated review. Curr Rheumatol Rep. 2014 Mar;16(3):408.
73. Detert J, Detert J, Pischon N, Burmester GR, Burmester GR, Buttgereit F, et al. The association between rheumatoid arthritis and periodontal disease. Arthritis Res Ther. 2010;12(5):218.
74. Jepsen S, Blanco J, Buchalla W, Carvalho JC, Dietrich T, Dörfer C, et al. Prevention and control of dental caries and periodontal diseases at individual and population level: consensus report of group 3 of joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J Clin Periodontol. 3rd ed. 2017 Mar 6;44(3):S85–S93.
75. Eke PI, Dye BA, Wei L, Wei L, Slade GD, Slade GD, et al. Update on Prevalence of Periodontitis in Adults in the United States: NHANES 2009 to 2012. Journal of Periodontology. 2015 May;86(5):611–22.
157
76. Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJL, Marcenes W. Global burden of severe periodontitis in 1990-2010: a systematic review and meta-regression. Journal of Dental Research. 2014 Nov;93(11):1045–53.
77. Carasol M, Llodra JC, Fernández-Meseguer A, Bravo M, García-Margallo MT, Calvo-Bonacho E, et al. Periodontal conditions among employed adults in Spain. J Clin Periodontol. 4 ed. 2016 Jul;43(7):548–56.
78. Löe H, Anerud A, Boysen H, Morrison E. Natural history of periodontal disease in man. J Clin Periodontol. Blackwell Publishing Ltd; 1986 May 1;13(5):431–40.
79. Armitage GC, Armitage GC. Development of a classification system for periodontal diseases and conditions. Ann Periodontol. 1999 Dec;4(1):1–6.
80. Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J Clin Periodontol. 2018 Jun 20;45(Suppl 20):S149–61.
81. Sanz M, Beighton D, Curtis MA, Cury JA, Dige I, Dommisch H, et al. Role of microbial biofilms in the maintenance of oral health and in the development of dental caries and periodontal diseases. Consensus report of group 1 of the Joint EFP/ORCA workshop on the boundaries between caries and periodontal disease. J Clin Periodontol. 2017 Mar 6;44(Suppl. 11):S5–S11.
82. Marsh PD, Zaura E. Dental biofilm: ecological interactions in health and disease. J Clin Periodontol. 2017 Mar 6;44:S12–S22.
83. Marsh PD, Marsh PD, Devine DA, Devine DA. How is the development of dental biofilms influenced by the host? J Clin Periodontol. 2011 Mar;38 Suppl 11:28–35.
84. Roberts FA, Darveau RP. Microbial protection and virulence in periodontal tissue as a function of polymicrobial communities: symbiosis and dysbiosis. Periodontol 2000. 2015 Oct;69(1):18–27.
158
85. Hajishengallis G. Immunomicrobial pathogenesis of periodontitis: keystones, pathobionts, and host response. Trends Immunol. 2014 Jan;35(1):3–11.
86. Hajishengallis G. The inflammophilic character of the periodontitis-associated microbiota. Mol Oral Microbiol. 2014 Dec;29(6):248–57.
87. Hajishengallis G, Darveau RP, Curtis MA. The keystone-pathogen hypothesis. Nat Rev Microbiol. 2012 Oct;10(10):717–25.
88. Joseph S, Curtis MA. Microbial transitions from health to disease. Periodontol 2000. 2021 Mar 10.
89. Hajishengallis G, Chavakis T, Lambris JD. Current understanding of periodontal disease pathogenesis and targets for host-modulation therapy. Periodontol 2000. John Wiley & Sons, Ltd; 2020 Oct;84(1):14–34.
90. Buduneli N. Environmental factors and periodontal microbiome. Periodontol 2000. 2021 Feb;85(1):112–25.
91. Michalowicz BS, Aeppli D, Aeppli D, Virag JG, Virag JG, Klump DG, et al. Periodontal findings in adult twins. Journal of Periodontology. 1991 May;62(5):293–9.
92. Shaddox LM, Morford LA, Nibali L. Periodontal health and disease: The contribution of genetics. Periodontol 2000. John Wiley & Sons, Ltd; 2021 Feb;85(1):161–81.
93. Leite FRM, Nascimento GG, Scheutz F, López R. Effect of Smoking on Periodontitis: A Systematic Review and Meta-regression. Am J Prev Med. 2018 Jun;54(6):831–41.
94. Dietrich T, Walter C, Oluwagbemigun K, Bergmann M, Pischon T, Pischon N, et al. Smoking, Smoking Cessation, and Risk of Tooth Loss: The EPIC-Potsdam Study. Journal of Dental Research. SAGE PublicationsSage CA: Los Angeles, CA; 2015 Oct;94(10):1369–75.
159
95. Billings M, Holtfreter B, Papapanou PN, Mitnik GL, Kocher T, Dye BA. Age-dependent distribution of periodontitis in two countries: Findings from NHANES 2009 to 2014 and SHIP-TREND 2008 to 2012. J Clin Periodontol. 2018 Jun 20;45(Suppl. 18):S130–48.
96. Genco RJ, Van Dyke TE. Prevention: Reducing the risk of CVD in patients with periodontitis. Nat Rev Cardiol. Nature Publishing Group; 2010 Sep;7(9):479–80.
97. Lalla E, Papapanou PN. Diabetes mellitus and periodontitis: a tale of two common interrelated diseases. Nat Rev Endocrinol. 2011 Dec;7(12):738–48.
98. Lundberg K, Wegner N, Yucel-Lindberg T, Venables PJ. Periodontitis in RA—the citrullinated enolase connection. Nat Rev Rheumatol. Nature Publishing Group; 2010 Sep 7;:1–4.
99. Linden GJ, Lyons A, Scannapieco FA. Periodontal systemic associations: review of the evidence. Journal of Periodontology. 2013 Apr;84(4 Suppl):S8–S19.
100. Sanz M, Marco del Castillo A, Jepsen S, Gonzalez Juanatey JR, D'Aiuto F, Bouchard P, et al. Periodontitis and cardiovascular diseases: Consensus report. J Clin Periodontol. 2020 Feb 3;311(14):e318–21.
101. Sanz M, Ceriello A, Buysschaert M, Chapple I, Demmer RT, Graziani F, et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International Diabetes Federation and the European Federation of Periodontology. J Clin Periodontol. 7 ed. 2018 Feb;45(2):138–49.
102. Figuero E, Han YW, Furuichi Y. Periodontal diseases and adverse pregnancy outcomes: Mechanisms. Periodontol 2000. John Wiley & Sons, Ltd; 2020 Jun;83(1):175–88.
160
103. Kebschull M, Kebschull M, Demmer RT, Demmer RT, Papapanou PN. “Gum bug, leave my heart alone!--”epidemiologic and mechanistic evidence linking periodontal infections and atherosclerosis. Journal of Dental Research. 2010 Sep;89(9):879–902.
104. Figuero E, Figuero E, Sánchez-Beltrán M, Sánchez-Beltrán M, Cuesta-Frechoso S, Cuesta-Frechoso S, et al. Detection of periodontal bacteria in atheromatous plaque by nested polymerase chain reaction. Journal of Periodontology. 2011 Oct;82(10):1469–77.
105. Figuero E, Lindahl C, Lindahl C, Marín MJ, Marín MJ, Renvert S, et al. Quantification of periodontal pathogens in vascular, blood, and subgingival samples from patients with peripheral arterial disease or abdominal aortic aneurysms. Journal of Periodontology. 2014 Sep;85(9):1182–93.
106. Dominy SS, Lynch C, Ermini F, Benedyk M, Marczyk A, Konradi A, et al. Porphyromonas gingivalis in Alzheimer's disease brains: Evidence for disease causation and treatment with small-molecule inhibitors. Sci Adv. American Association for the Advancement of Science; 2019 Jan;5(1):eaau3333.
107. Kamer AR, Craig RG, Niederman R, Fortea J, de Leon MJ. Periodontal disease as a possible cause for Alzheimer's disease. Periodontol 2000. John Wiley & Sons, Ltd; 2020 Jun;83(1):242–71.
108. Reichert S, Haffner M, Keyßer G, Schäfer C, Stein JM, Schaller H-G, et al. Detection of oral bacterial DNA in synovial fluid. J Clin Periodontol. 2013 Jun;40(6):591–8.
109. Martinez-Martinez RE, Abud-Mendoza C, Patiño-Marin N, Rizo-Rodríguez JC, Little JW, Loyola-Rodríguez JP. Detection of periodontal bacterial DNA in serum and synovial fluid in refractory rheumatoid arthritis patients. J Clin Periodontol. John Wiley & Sons, Ltd; 2009 Dec;36(12):1004–10.
110. Totaro MC, Cattani P, Ria F, Tolusso B, Gremese E, Fedele AL, et al. Porphyromonas gingivalis and the pathogenesis of rheumatoid arthritis:
161
analysis of various compartments including the synovial tissue. Arthritis Res Ther. BioMed Central; 2013 Jun 18;15(3):R66–8.
111. Leira Y, Martín-Lancharro P, Blanco J. Periodontal inflamed surface area and periodontal case definition classification. Acta Odontol Scand. Taylor & Francis; 2018 Apr;76(3):195–8.
112. Paraskevas S, Huizinga JD, Loos BG. A systematic review and meta-analyses on C-reactive protein in relation to periodontitis. J Clin Periodontol. 2008 Apr;35(4):277–90.
113. Aoyama N, Suzuki J-I, Kobayashi N, Hanatani T, Ashigaki N, Yoshida A, et al. Periodontitis deteriorates peripheral arterial disease in Japanese population via enhanced systemic inflammation. Heart Vessels. Springer Japan; 2017 Nov;32(11):1314–9.
114. Madianos PN, Bobetsis YA, Offenbacher S. Adverse pregnancy outcomes (APOs) and periodontal disease: pathogenic mechanisms. J Clin Periodontol. 2013 Apr;40 Suppl 14:S170–80.
115. Schett G. The role of ACPAs in at-risk individuals: Early targeting of the bone and joints. Best Pract Res Clin Rheumatol. 2017 Feb;31(1):53–8.
116. Harvey GP, Fitzsimmons TR, Dhamarpatni AASSK, Marchant C, Haynes DR, Bartold PM. Expression of peptidylarginine deiminase-2 and -4, citrullinated proteins and anti-citrullinated protein antibodies in human gingiva. J Periodont Res. John Wiley & Sons, Ltd; 2013 Apr;48(2):252–61.
117. de Pablo P, Dietrich T, Chapple ILC, Milward M, Chowdhury M, Charles PJ, et al. The autoantibody repertoire in periodontitis: a role in the induction of autoimmunity to citrullinated proteins in rheumatoid arthritis? Ann Rheum Dis [Internet]. 2014 Feb 4;73(3):580–6. Available from: http://eutils.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&id=23434568&retmode=ref&cmd=prlinks
162
118. Janssen KMJ, de Smit MJ, de Smit MJ, Brouwer E, de Kok FAC, de Kok FAC, et al. Rheumatoid arthritis-associated autoantibodies in non-rheumatoid arthritis patients with mucosal inflammation: a case-control study. Arthritis Res Ther. 2015;17:174.
119. Fisher BA, Cartwright AJ, Quirke A-M, de Pablo P, Romaguera D, Panico S, et al. Smoking, Porphyromonas gingivalis and the immune response to citrullinated autoantigens before the clinical onset of rheumatoid arthritis in a Southern European nested case-control study. BMC Musculoskelet Disord. BioMed Central; 2015 Nov 4;16(1):331–11.
120. Konig MF, Bingham CO, Andrade F. PPAD is not targeted as a citrullinated protein in rheumatoid arthritis, but remains a candidate for inducing autoimmunity. Ann Rheum Dis. BMJ Publishing Group Ltd; 2015 Jan;74(1):e8–e8.
121. Engström M, Eriksson K, Lee L, Hermansson M, Johansson A, Nicholas AP, et al. Increased citrullination and expression of peptidylarginine deiminases independently of P. gingivalis and A. actinomycetemcomitans in gingival tissue of patients with periodontitis. J Transl Med. BioMed Central; 2018 Jul 31;16(1):214.
122. Olsen I, Singhrao SK, Potempa J. Citrullination as a plausible link to periodontitis, rheumatoid arthritis, atherosclerosis and Alzheimer's disease. J Oral Microbiol. 2018;10(1):1487742.
123. González-Febles J, Sanz M. Periodontitis and rheumatoid arthritis: What have we learned about their connection and their treatment? Periodontol 2000. 2021 Apr 8;00(00):1–29.
124. Mercado FB, Marshall RI, Klestov AC, Bartold PM. Relationship between rheumatoid arthritis and periodontitis. Journal of Periodontology. 2001 Jun;72(6):779–87.
163
125. de Pablo P, Dietrich T, McAlindon TE. Association of periodontal disease and tooth loss with rheumatoid arthritis in the US population. J Rheumatol. 2008 Jan;35(1):70–6.
126. Pischon T, Kröger J, Gülmez E, Kleber B-M, Bernimoulin JP, Landau H, et al. Association Among Rheumatoid Arthritis, Oral Hygiene, and Periodontitis. Journal of Periodontology. 2008 Jun;79(6):979–86.
127. Mikuls TR, Payne JB, Yu F, Thiele GM, Reynolds RJ, Cannon GW, et al. Periodontitis and Porphyromonas gingivalisin Patients With Rheumatoid Arthritis. Arthritis & Rheumatology. 2014 Apr 28;66(5):1090–100.
128. Khantisopon N, Louthrenoo W, Kasitanon N, Sivasomboon C, Wangkaew S, Sang-In S, et al. Periodontal disease in Thai patients with rheumatoid arthritis. Int J Rheum Dis. John Wiley & Sons, Ltd; 2014 Jun;17(5):511–8.
129. Ibáñez S V, Ferreiro C, Contreras A, Valenzuela L O, Giadalah N, Jara V, et al. [Frequency and severity of periodontitis among patients with rheumatoid arthritis]. Rev Med Chil. Sociedad Médica de Santiago; 2015 Dec;143(12):1539–45.
130. Pons-Fuster A, Rodríguez Agudo C, Galvez Muñoz P, Saiz Cuenca E, Pina Perez FM, Lopez-Jornet P. Clinical evaluation of periodontal disease in patients with rheumatoid arthritis: A cross-sectional study. Quintessence Int. Quintessenz Verlags-GmbH, Neue Medien, Onlineredaktion; 2015 Oct;46(9):817–22.
131. Vahabi S, Rostamian A, Baniebrahimi G. Characteristics and relationship of periodontal disease with juvenile idiopathic and rheumatoid arthritis. Dent Res J (Isfahan). 2015 Nov;12(6):541–7.
132. Bello-Gualtero JM, Lafaurie GI, Hoyos LX, Castillo DM, De-Avila J, Munevar JC, et al. Periodontal Disease in Individuals With a Genetic Risk of Developing Arthritis and Early Rheumatoid Arthritis: A Cross-Sectional Study. Journal of Periodontology. 2016 Apr;87(4):346–56.
164
133. Choi IA, Kim J-H, Kim YM, Lee JY, Kim KH, Lee EY, et al. Periodontitis is associated with rheumatoid arthritis: a study with longstanding rheumatoid arthritis patients in Korea. Korean J Intern Med. 2016 Sep;31(5):977–86.
134. Silvestre-Rangil J, Bagán L, Silvestre F-J, Bagán JV. Oral manifestations of rheumatoid arthritis. A cross-sectional study of 73 patients. Clin Oral Investig. Springer Berlin Heidelberg; 2016 Dec;20(9):2575–80.
135. Schmickler J, Rupprecht A, Patschan S, Patschan D, Müller GA, Haak R, et al. Cross-Sectional Evaluation of Periodontal Status and Microbiologic and Rheumatoid Parameters in a Large Cohort of Patients With Rheumatoid Arthritis. Journal of Periodontology. 2017 Apr;88(4):368–79.
136. Molitor JA, Alonso A, Wener MH, Michalowics BS, Gersuk VH. Moderate to severe periodontitis increases risk of rheumatoid arthritis in non-smokers and is associated with elevated ACPA Titers: The ARIC Study [Internet]. Vol. 60, Arthritis and rheumatism. 2009. p. S433.
137. Demmer RT, Molitor JA, Jacobs DR Jr., Michalowicz BS. Periodontal disease, tooth loss and incident rheumatoid arthritis: results from the First National Health and Nutrition Examination Survey and its epidemiological follow-up study. J Clin Periodontol. 2011 Sep 13;38(11):998–1006.
138. Chen H-H, Chen D-Y, Lin S-Y, Lai K-L, Chen Y-M, Chou Y-J, et al. Periodontitis exposure within one year before anti-diabetic treatment and the risk of rheumatoid arthritis in diabetes mellitus patients: a population-based cohort study. Wallace GR, editor. Revista Brasileira de Reumatologia. Rev Bras Reumatol; 2014 Mar;54(2):124–30.
139. Chou Y-Y, Lai K-L, Chen D-Y, Lin C-H, Chen H-H. Rheumatoid Arthritis Risk Associated with Periodontitis Exposure: A Nationwide, Population-Based Cohort Study. Wallace GR, editor. PLoS ONE. Public Library of Science; 2015;10(10):e0139693.
165
140. Äyräväinen L, Leirisalo-Repo M, Kuuliala A, Ahola K, Koivuniemi R, Meurman J-H, et al. Periodontitis in early and chronic rheumatoid arthritis: a prospective follow-up study in Finnish population. BMJ Open. 2017 Jan 31;7(1):e011916.
141. Dissick A, Redman RS, Jones M, Rangan BV, Reimold A, Griffiths GR, et al. Association of Periodontitis With Rheumatoid Arthritis: A Pilot Study. Journal of Periodontology. 2010 Feb;81(2):223–30.
142. Xibille-Friedmann D, Xibille-Friedmann D, Martínez-Rivera JI, Martínez-Rivera JI, Rodríguez-Amado J, Rodríguez-Amado J, et al. Periodontal disease and Clinical Activity of Rheumatoid Arthritis Patients [Internet]. ACR congress. 2014 [cited 2017 Aug 18]. Available from: http://acrabstracts.org/abstracts/periodontal-disease-and-clinical-activity-of-rheumatoid-arthritis-patients/
143. Scher JU, Scher JU, Ubeda C, Ubeda C, Equinda M, Equinda M, et al. Periodontal disease and the oral microbiota in new-onset rheumatoid arthritis. Arthritis Rheum. 2012 Oct;64(10):3083–94.
144. Mikuls TR, Thiele GM, Deane KD, Payne JB, O'Dell JR, Yu F, et al. Porphyromonas gingivalis and disease-related autoantibodies in individuals at increased risk of rheumatoid arthritis. Arthritis Rheum. 2012 Nov;64(11):3522–30.
145. Smit M, Westra J, Vissink A, Doornbos-van der Meer B, Brouwer E, van Winkelhoff A. Periodontitis in established rheumatoid arthritis patients: a cross-sectional clinical, microbiological and serological study. Arthritis Res Ther. 2012;14(5):R222–11.
146. Quirke A-M, Lugli EB, Lugli EB, Wegner N, Wegner N, Hamilton BC, et al. Heightened immune response to autocitrullinated Porphyromonas gingivalis peptidylarginine deiminase: a potential mechanism for breaching immunologic tolerance in rheumatoid arthritis. Ann Rheum Dis. 2014 Jan;73(1):263–9.
166
147. Konig MF, Abusleme L, Reinholdt J, Palmer RJ, Teles RP, Sampson K, et al. Aggregatibacter actinomycetemcomitans-induced hypercitrullination links periodontal infection to autoimmunity in rheumatoid arthritis. Sci Transl Med. 2016 Dec 14;8(369):369ra176.
148. Cheng Z, Do T, Mankia K, Meade JL, Hunt L, Nam J, et al. The subgingival microbiomes in periodontitis and health of individuals with rheumatoid arthritis and at risk of developing rheumatoid arthritis. J Oral Microbiol. Taylor & Francis; 2017 May 30.
149. Oluwagbemigun K, Yucel-Lindberg T, Dietrich T, Tour G, Sherina N, Hansson M, et al. A cross-sectional investigation into the association between Porphyromonas gingivalis and autoantibodies to citrullinated proteins in a German population. Ther Adv Musculoskelet Dis. 2019;11:1759720X19883152.
150. Mankia K, Cheng Z, Do T, Hunt L, Meade J, Kang J, et al. Prevalence of Periodontal Disease and Periodontopathic Bacteria in Anti-Cyclic Citrullinated Protein Antibody-Positive At-Risk Adults Without Arthritis. JAMA Netw Open. 2019 Jun 5;2(6):e195394.
151. Cheng Z, Do T, Mankia K, Meade J, Hunt L, Clerehugh V, et al. Dysbiosis in the oral microbiomes of anti-CCP positive individuals at risk of developing rheumatoid arthritis. Ann Rheum Dis. 2020 Oct 1;20:annrheumdis–2020–216972.
152. Jenning M, Marklein B, Ytterberg J, Zubarev RA, Joshua V, van Schaardenburg D, et al. Bacterial citrullinated epitopes generated by Porphyromonas gingivalis infection—a missing link for ACPA production. Ann Rheum Dis. BMJ Publishing Group Ltd; 2020 Sep 1;79(9):1194–202.
153. Travis J, Pike R, Imamura T, Potempa J. Porphyromonas gingivalis proteinases as virulence factors in the development of periodontitis. J Periodont Res. John Wiley & Sons, Ltd; 1997 Jan;32(1 Pt 2):120–5.
167
154. Courbon G, Rinaudo-Gaujous M, Blasco-Baque V, Auger I, Caire R, Mijola L, et al. Porphyromonas gingivalis experimentally induces periodontis and an anti-CCP2-associated arthritis in the rat. Ann Rheum Dis. 2019 May;78(5):594–9.
155. Queiroz-Junior CM, Bessoni RLC, Costa VV, Souza DG, Teixeira MM, Silva TA. Preventive and therapeutic anti-TNF-α therapy with pentoxifylline decreases arthritis and the associated periodontal co-morbidity in mice. Life Sci. 2013 Sep 17;93(9-11):423–8.
156. Gully N, Bright R, Marino V, Marchant C, Cantley M, Haynes D, et al. Porphyromonas gingivalis peptidylarginine deiminase, a key contributor in the pathogenesis of experimental periodontal disease and experimental arthritis. Yilmaz Ö, editor. PLoS ONE. Public Library of Science; 2014;9(6):e100838.
157. Maresz KJ, Hellvard A, Sroka A, Adamowicz K, Bielecka E, Koziel J, et al. Porphyromonas gingivalis facilitates the development and progression of destructive arthritis through its unique bacterial peptidylarginine deiminase (PAD). PLoS Pathog. 2013 Sep;9(9):e1003627.
158. Marchesan JT, Gerow EA, Schaff R, Taut AD, Shin S-Y, Sugai J, et al. Porphyromonas gingivalis oral infection exacerbates the development and severity of collagen-induced arthritis. Arthritis Res Ther. BioMed Central; 2013 Nov 12;15(6):R186–13.
159. Corrêa JD, Saraiva AM, Queiroz-Junior CM, Madeira MFM, Duarte PM, Teixeira MM, et al. Arthritis-induced alveolar bone loss is associated with changes in the composition of oral microbiota. Anaerobe. 2016 Jun;39:91–6.
160. Wolff B, Wolff B, Berger T, Berger T, Frese C, Frese C, et al. Oral status in patients with early rheumatoid arthritis: a prospective, case-control study. Rheumatology (Oxford). 2014 Mar;53(3):526–31.
161. Ebbers M, Lübcke PM, Volzke J, Kriebel K, Hieke C, Engelmann R, et al. Interplay between P. gingivalis, F. nucleatum and A. actinomycetemcomitans

168
in murine alveolar bone loss, arthritis onset and progression. Scientific Reports. Nature Publishing Group; 2018 Oct 11;8(1):15129.
162. Queiroz-Junior CM, Madeira MFM, Coelho FM, de Oliveira CR, Cândido LCM, Garlet GP, et al. Experimental arthritis exacerbates Aggregatibacter actinomycetemcomitans-induced periodontitis in mice. J Clin Periodontol. John Wiley & Sons, Ltd (10.1111); 2012 Jul;39(7):608–16.
163. Corrêa MG, Sacchetti SB, Ribeiro FV, Pimentel SP, Casarin RCV, Cirano FR, et al. Periodontitis increases rheumatic factor serum levels and citrullinated proteins in gingival tissues and alter cytokine balance in arthritic rats. PLoS ONE. 2017;12(3):e0174442.
164. Laugisch O, Wong A, Wong A, Sroka A, Sroka A, Kantyka T, et al. Citrullination in the periodontium-a possible link between periodontitis and rheumatoid arthritis. Clin Oral Investig. 2015 Aug 13.
165. Pers J-O, Saraux A, Pierre R, Youinou P. Anti-TNF-alpha immunotherapy is associated with increased gingival inflammation without clinical attachment loss in subjects with rheumatoid arthritis. Journal of Periodontology. 2008 Sep;79(9):1645–51.
166. Mayer Y, Balbir-Gurman A, Machtei EE. Anti-tumor necrosis factor-alpha therapy and periodontal parameters in patients with rheumatoid arthritis. Journal of Periodontology [Internet]. 2009 Sep;80(9):1414–20. Available from: http://eutils.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&id=19722791&retmode=ref&cmd=prlinks
167. Üstün K, Erciyas K, Kısacık B, Sezer U, Pehlivan Y, Öztuzcu S, et al. Host modulation in rheumatoid arthritis patients with TNF blockers significantly decreases biochemical parameters in periodontitis. Inflammation. Springer US; 2013 Oct;36(5):1171–7.
168. Kobayashi T, Okada M, Ito S, Kobayashi D, Kobayashi D, Ishida K, et al. Assessment of Interleukin-6 Receptor Inhibition Therapy on Periodontal
169
Condition in Patients With Rheumatoid Arthritis and Chronic Periodontitis. Journal of Periodontology. 2014 Jan;85(1):57–67.
169. Kobayashi T, Yokoyama T, Ito S, Kobayashi D, Yamagata A, Okada M, et al. Periodontal and serum protein profiles in patients with rheumatoid arthritis treated with tumor necrosis factor inhibitor adalimumab. Journal of Periodontology. Wiley-Blackwell; 2014 Nov;85(11):1480–8.
170. Coat J, Coat J, Demoersman J, Demoersman J, Beuzit S, Beuzit S, et al. Anti-B lymphocyte immunotherapy is associated with improvement of periodontal status in subjects with rheumatoid arthritis. J Clin Periodontol. 2015 Jul;42(9):817–23.
171. Kobayashi T, Ito S, Kobayashi D, Shimada A, Narita I, Murasawa A, et al. Serum Immunoglobulin G Levels to Porphyromonas gingivalis Peptidylarginine Deiminase Affect Clinical Response to Biological Disease-Modifying Antirheumatic Drug in Rheumatoid Arthritis. Proost P, editor. PLoS ONE. Public Library of Science; 2016;11(4):e0154182.
172. Kaczyński T, Wroński J, Głuszko P, Kryczka T, Miskiewicz A, Górski B, et al. Salivary interleukin 6, interleukin 8, interleukin 17A, and tumour necrosis factor α levels in patients with periodontitis and rheumatoid arthritis. Cent Eur J Immunol. Termedia; 2019;44(3):269–76.
173. Ziebolz D, Rupprecht A, Schmickler J, Bothmann L, Krämer J, Patschan D, et al. Association of different immunosuppressive medications with periodontal condition in patients with rheumatoid arthritis: Results from a cross-sectional study. Journal of Periodontology. Wiley-Blackwell; 2018 Nov;89(11):1310–7.
174. Äyräväinen L, Heikkinen AM, Kuuliala A, Ahola K, Koivuniemi R, Moilanen E, et al. Anti-rheumatic medication and salivary MMP-8, a biomarker for periodontal disease. Oral Diseases. 2018 Nov;24(8):1562–71.

170
175. Savioli C, Ribeiro ACM, Fabri GMC, Calich AL, Carvalho J, Silva CA, et al. Persistent periodontal disease hampers anti-tumor necrosis factor treatment response in rheumatoid arthritis. J Clin Rheumatol. 2012 Jun;18(4):180–4.
176. Ribeiro J, Leão A, Novaes AB. Periodontal infection as a possible severity factor for rheumatoid arthritis. J Clin Periodontol [Internet]. 2005 Apr;32(4):412–6. Available from: http://eutils.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&id=15811060&retmode=ref&cmd=prlinks
177. Al-Katma MK, Bissada NF, Bordeaux JM, Sue J, Askari AD. Control of periodontal infection reduces the severity of active rheumatoid arthritis. J Clin Rheumatol. 2007 Jun;13(3):134–7.
178. Ortiz P, Bissada NF, Palomo L, Han YW, Al-Zahrani MS, Panneerselvam A, et al. Periodontal therapy reduces the severity of active rheumatoid arthritis in patients treated with or without tumor necrosis factor inhibitors. Journal of Periodontology. 2009 Apr;80(4):535–40.
179. Pinho M de N, Oliveira RDR, Novaes AB, Voltarelli JC. Relationship between periodontitis and rheumatoid arthritis and the effect of non-surgical periodontal treatment. Braz Dent J. 2009;20(5):355–64.
180. Okada M, Kobayashi T, Ito S, Yokoyama T, Abe A, Murasawa A, et al. Periodontal treatment decreases levels of antibodies to Porphyromonas gingivalis and citrulline in patients with rheumatoid arthritis and periodontitis. The Journal of Periodontology. John Wiley & Sons, Ltd; 2013 Dec;84(12):e74–84.
181. Erciyas K, Sezer U, Ustün K, Pehlivan Y, Kisacik B, Senyurt SZ, et al. Effects of periodontal therapy on disease activity and systemic inflammation in rheumatoid arthritis patients. Oral Diseases. John Wiley & Sons, Ltd; 2013 May;19(4):394–400.
171
182. Khare N, Vanza B, Sagar D, Saurav K, Chauhan R, Mishra S. Nonsurgical Periodontal Therapy decreases the Severity of Rheumatoid Arthritis: A Case-control Study. J Contemp Dent Pract. 2016 Jun 1;17(6):484–8.
183. Zhao X, Liu Z, Shu D, Xiong Y, He M, Xu S, et al. Association of Periodontitis with Rheumatoid Arthritis and the Effect of Non-Surgical Periodontal Treatment on Disease Activity in Patients with Rheumatoid Arthritis. Med Sci Monit. International Scientific Information, Inc; 2018 Aug 20;24:5802–10.
184. Cosgarea R, Tristiu R, Dumitru RB, Arweiler NB, Rednic S, Sirbu CI, et al. Effects of non-surgical periodontal therapy on periodontal laboratory and clinical data as well as on disease activity in patients with rheumatoid arthritis. Clin Oral Investig. Springer Berlin Heidelberg; 2019 Jan;23(1):141–51.
185. Kaushal S, Singh AK, Lal N, Das SK, Mahdi AA. Effect of periodontal therapy on disease activity in patients of rheumatoid arthritis with chronic periodontitis. J Oral Biol Craniofac Res. 2019 Apr;9(2):128–32.
186. Białowąs K, Radwan-Oczko M, Duś-Ilnicka I, Korman L, Świerkot J. Periodontal disease and influence of periodontal treatment on disease activity in patients with rheumatoid arthritis and spondyloarthritis. Rheumatol Int. Springer Berlin Heidelberg; 2019 Nov 7;93(Suppl 2):1045–9.
187. Möller B, Bender P, Eick S, Kuchen S, Maldonado A, Potempa J, et al. Treatment of severe periodontitis may improve clinical disease activity in otherwise treatment-refractory rheumatoid arthritis patients. Rheumatology. 2019 Jul 10;16:214–3.
188. Rodríguez-Lozano B, González-Febles J, Garnier-Rodríguez JL, Dadlani S, Bustabad-Reyes S, Sanz M, et al. Association between severity of periodontitis and clinical activity in rheumatoid arthritis patients: a case-control study. Arthritis Res Ther. 2nd ed. BioMed Central; 2019 Jan 18;21(1):27.
172
189. Tonetti MS, Claffey N, Claffey N, European Workshop in Periodontology group C, European Workshop in Periodontology group C. Advances in the progression of periodontitis and proposal of definitions of a periodontitis case and disease progression for use in risk factor research. Group C consensus report of the 5th European Workshop in Periodontology. J Clin Periodontol. 2005;32 Suppl 6:210–3.
190. Matuliene G, Ash MM, Pjetursson BE, Salvi GE, Schmidlin K, Brägger U, et al. Influence of residual pockets on progression of periodontitis and tooth loss: results after 11 years of maintenance. J Clin Periodontol. 2008 Aug;35(8):685–95.
191. Schätzle M, Schätzle M, Faddy MJ, Faddy MJ, Cullinan MP, Seymour GJ, et al. The clinical course of chronic periodontitis: V. Predictive factors in periodontal disease. J Clin Periodontol. 2009 May;36(5):365–71.
192. van der Velden U, Abbas F, Abbas F, Armand S, Armand S, Loos BG, et al. Java project on periodontal diseases. The natural development of periodontitis: risk factors, risk predictors and risk determinants. J Clin Periodontol. 2006 Aug;33(8):540–8.
193. Aletaha D, Nell VPK, Stamm T, Uffmann M, Pflugbeil S, Machold K, et al. Acute phase reactants add little to composite disease activity indices for rheumatoid arthritis: validation of a clinical activity score. Arthritis Res Ther. BioMed Central; 2005;7(4):R796–806.
194. Potikuri D, Dannana KC, Kanchinadam S, Agrawal S, Kancharla A, Rajasekhar L, et al. Periodontal disease is significantly higher in non-smoking treatment-naive rheumatoid arthritis patients: results from a case-control study. Ann Rheum Dis. BMJ Publishing Group Ltd; 2012 Sep;71(9):1541–4.
195. Torkzaban P, Hjiabadi T, Basiri Z, Poorolajal J. Effect of rheumatoid arthritis on periodontitis: a historical cohort study. J Periodontal Implant Sci. 2012 Jun;42(3):67–72.
173
196. Joseph R, Rajappan S, Nath SG, Paul BJ. Association between chronic periodontitis and rheumatoid arthritis: a hospital-based case-control study. Rheumatol Int. 2013 Jan;33(1):103–9.
197. Susanto H, Nesse W, Kertia N, Soeroso J, Huijser van Reenen Y, Hoedemaker E, et al. Prevalence and severity of periodontitis in Indonesian patients with rheumatoid arthritis. The Journal of Periodontology. John Wiley & Sons, Ltd; 2013 Aug;84(8):1067–74.
198. Ouédraogo D-D, Tiendrébéogo J, Guiguimdé PLW, Nikiéma PI, Ouédraogo D, Kaboré F, et al. Periodontal disease in patients with rheumatoid arthritis in Sub-Saharan Africa: A case-control study. Joint Bone Spine. 2017 Jan;84(1):113–4.
199. Zhao R, Gu C, Zhang Q, Zhou W, Feng G, Feng X, et al. Periodontal disease in Chinese patients with rheumatoid arthritis: A case-control study. Oral Diseases. 2019 Aug 14;2015(8):259074.
200. Karapetsa D, Consensi A, Castagnoli G, Petrini M, Tonelli M, Gennai S, et al. Periodontitis in Italian patients with established rheumatoid arthritis: A cross-sectional study. Oral Diseases. John Wiley & Sons, Ltd; 2021 Mar 10.
201. Mobini M, Maboudi A, Ali Mohammadpour R. Periodontitis in rheumatoid arthritis patients, abundance and association with disease activity. Med J Islam Repub Iran. Medical Journal of The Islamic Republic of Iran (MJIRI); 2017;31(1):44–256.
202. González-Febles J, Rodríguez-Lozano B, Sánchez-Piedra C, Garnier-Rodríguez J, Bustabad S, Hernández-González M, et al. Association between periodontitis and anti-citrullinated protein antibodies in rheumatoid arthritis patients: a cross-sectional study. Arthritis Res Ther. BioMed Central; 2020 Feb 13;22(1):27.
203. de Smit M, Westra J, Vissink A, Doornbos-van der Meer B, Brouwer E, van Winkelhoff AJ. Periodontitis in established rheumatoid arthritis patients: a
174
cross-sectional clinical, microbiological and serological study. Arthritis Res Ther. 2012;14(5):R222.
204. Kimura Y, Yoshida S, Takeuchi T, Kimura M, Yoshikawa A, Hiramatsu Y, et al. Periodontal pathogens participate in synovitis in patients with rheumatoid arthritis in clinical remission: a retrospective case-control study. 2015 Dec;54(12):2257–63.
205. Johansson L, Pratesi F, Brink M, Ärlestig L, D'Amato C, Bartaloni D, et al. Antibodies directed against endogenous and exogenous citrullinated antigens pre-date the onset of rheumatoid arthritis. Arthritis Res Ther. BioMed Central; 2016 Jun 3;18(1):127.
206. Martu MA, Solomon SM, Sufaru I, Jelihovschi I, Martu S, Rezus E, et al. Study on the prevalence of periodontopathogenic bacteria in serum and subgingival bacterial plaque in patients with rheumatoid arthritis. Rev Chim. 2017 Sep;68(8).
207. Martínez-Rivera J-I, Xibillé-Friedmann DX, González-Christen J, la Garza-Ramos de MA, Carrillo-Vázquez SM, Montiel-Hernández J-L. Salivary ammonia levels and Tannerella forsythia are associated with rheumatoid arthritis: A cross sectional study. Clin Exp Dent Res. John Wiley & Sons, Ltd; 2017 Jun;3(3):107–14.
208. Henderson B, Ward JM, Ready D. Aggregatibacter (Actinobacillus) actinomycetemcomitans: a triple A* periodontopathogen? Periodontol 2000. 2010 Oct;54(1):78–105.
209. Farias BC, Souza PRE, Ferreira B, Melo RSA, Machado FB, Gusmão ES, et al. Occurrence of periodontal pathogens among patients with chronic periodontitis. Braz J Microbiol. SBM; 2012 Jul;43(3):909–16.
210. Polak D, Polak D, Wilensky A, Wilensky A, Shapira L, Halabi A, et al. Mouse model of experimental periodontitis induced by Porphyromonas gingivalis/
175
Fusobacterium nucleatuminfection: bone loss and host response. J Clin Periodontol. 2009 May;36(5):406–10.
211. Lee DM, Phillips R, Hagan EM, Chibnik LB, Costenbader KH, Schur PH. Quantifying anti-cyclic citrullinated peptide titres: clinical utility and association with tobacco exposure in patients with rheumatoid arthritis. Ann Rheum Dis. BMJ Publishing Group Ltd; 2009 Feb;68(2):201–8.
212. Makrygiannakis D, Hermansson M, Nicholas AP, Zendman AJW, Eklund A, Grunewald J, et al. Smoking increases peptidylarginine deiminase 2 enzyme expression in human lungs and increases citrullination in BAL cells. Ann Rheum Dis. 2008 Oct;67(10):1488–92.
213. Seror R, Seror R, Le Gall-David S, Le Gall-David S, Bonnaure-Mallet M, Bonnaure-Mallet M, et al. Association of Anti-Porphyromonas gingivalis Antibody Titers With Nonsmoking Status in Early Rheumatoid Arthritis: Results From the Prospective French Cohort of Patients With Early Rheumatoid Arthritis. Arthritis Rheumatol. 2015 Jul;67(7):1729–37.
214. Lappin DF, Apatzidou D, Quirke A-M, Oliver-Bell J, Butcher JP, Kinane DF, et al. Influence of periodontal disease, Porphyromonas gingivalis and cigarette smoking on systemic anti-citrullinated peptide antibody titres. J Clin Periodontol. 2013 Oct;40(10):907–15.


177

178


















![Año] El Uso del Formato de la Asociación Psicológica Americana (APA) (Actualizado de la 5a edición](https://static.fdokumen.com/doc/165x107/633581d8a1ced1126c0ad36d/ano-el-uso-del-formato-de-la-asociacion-psicologica-americana-apa-actualizado.jpg)

