Consulting with diverse communities for online diabetes information
42
ACCD Knowledge Portal Report from Pilot Consultations . Prepared by Dr. Margaret Mayhew November 2010.
-
Upload
independentscholar -
Category
Documents
-
view
0 -
download
0
Transcript of Consulting with diverse communities for online diabetes information
ACCD Knowledge Portal Report from Pilot Consultations .
Prepared by Dr. Margaret Mayhew
November 2010.
ACCD Knowledge Management Portal
Executive summary:
Introduction:
ACCD has been developing a comprehensive knowledge management portal since 2008.
In 2010, the ACCD undertook pilot consultation with members of key audience groups in order to determine the appeal of the portal in its current format.
Methodology:
1. Consultations Pilot consultations were undertaken with small focus groups (6-‐12 members) of each of the key target audiences for the knowledge management portal.
These consisted of:
CALD communities (from 8 community languages)
Diabetes/Healthcare partners
University Researchers
Consultations were also held with Indigenous students and the ACCD CALD advisory committee. Each group was shown a demonstration version of the portal and invited to give feedback.
2. Desktop Research A survey of a range of knowledge portals, websites and web directories in health and diabetes area was undertaken in order to have a contextual basis for recommendations.
Findings:
Content ACCD knowledge portal should aim to complement existing diabetes websites.
Information about diabetes: causes, effects, complications, prevention etc. can include a range of formats: eg FAQ’s, brief outlines leading to more details information.
There needs to be information about diagnosis, testing and high-‐risk groups.
Information about Diabetes Rates, target populations is needed.
Information needs to be reliable and verified and regularly updated
Likelihood of Use There was some ambiguity about the levels of internet access and computer use among CALD community members as opposed to health workers and researchers.
Participants argued that CALD community members have limited access to the internet, only at a library or public venue.
However, of the 61 CALD community participants consulted in this study, almost 50% reported access to broadband. However a further 29% claimed they had no internet access at all.
The most significant element of access appears in the way in which differing users access the internet and for what purposes.
All groups stated that the main factors influencing their choice to use the portal or not were if it is up to date, and if the content they require is easy and quick to find.
Some participants mentioned links to social media and other websites, and some suggested that embedding content with user generated elements (eg video clips or event notices) would also make the portal seem more attractive and relevant to a range of users.
Appearance Graphic design of the portal needs to be much less text reliant.
Existing font is too small with poor contrast and with too much text.
Text sizes should be varied and brightly coloured in order to be more attractive
Wording needs to be much simpler and as little as possible.
Portal needs to have many more images, and to use pictograms to replace text in navigation elements.
Where possible, replace text with images.
Front page needs either regular news updates or link to news page in order to indicate that portal is constantly updated.
It would be good to embed presentations, video clips and voice narrations on many pages.
Navigation Front page should be about the portal itself and mention diabetes
Front page needs to clearly flag navigation pathways for differing audience requirements (eg needing urgent advice? Health care contact details? Epidemiology info? Etc.)
Front page needs either regular news updates or link to news page in order to indicate that portal is constantly updated.
Portal needs an internal search engine/navigation tool.
Non-‐English pages need to be clearly flagged in front pages of portal
Portal needs links to other Australian Government health websites and portals eg Better Health Channel etc.
Interactivity Community members in particular would like to see more interactive components. These include links to social media, and embedded user generated content (eg blogs, discussion boards)
All groups support having interactive quizzes, games and risk calculators.
Conclusion:
The portal is currently constructed as a static single author document, consisting of a series of hotlinks to external web pages.
The issue of long-‐term maintenance and editorial of the portal has not been resolved. It is intended that the portal in its current format be hosted by Victoria University, and published by the ACCD. However, issues about intellectual property, editorial responsibility and professional reliability of content linked to the portal have yet to be resolved.
The only ACCD material on the portal consists of the maps of the diabetes epidemic in western Melbourne, as well as suburban and linguistic breakdowns for diabetes-‐related service providers. It is unclear how this information will be maintained, so that it remains relevant.
Aside from a brief text based organisational overview, there is not a great deal of information on the ACCD, or the projects, research and other work that is being conducted.
As most ACCD information is generated in the course of community based education projects, it needs to have an open-‐source, or easily accessible web-‐publishing format, in order to add reports, images, community resources and other materials.
There are currently no spaces or links to user generated content, open source publishing, social media or other interactive media formats such as: wikis, bulletin boards, youtube, blogs, calenders, FAQ’s or even inquiry forms.
Recommendations:
The overall architecture of the portal needs to be critically considered in relation to existing and future resources of the ACCD.
Back end architecture also needs to be considered, and it is recommended that this remain minimal until resources for feedback and site maintenance are ensured.
As it is, the portal has a considerable value as a web directory, but requires considerable development if it is to be launched as a fully interactive web portal. The issue of editorial responsibility for user-‐generated content still needs to resolved.
In its current format, the portal is able to be launched with a few developments:
That ACCD appoint a content manager who can ensure that portal content remains up to date.
That graphic designers be commissioned in order to increase the pictorial content of the web pages, so they are more-‐user friendly, have more pictorial content, and rely less on text.
That the portal ‘front page’ introduce the portal and direct users to relevant areas.
That community language resources be more clearly marked and linked to the portal ‘front page’
Specific Recommendations follow.
Specific Recommendations:
1. Publish a separate ‘about ACCD’ page linked to the portal. This could be established as a fixed set of pages with information (text and images) about current and recent ACCD projects, or could be linked to a separate as a blog or wiki that ACCD staff may add material to. An ACCD user content section would allow ACCD to promote events, link media coverage, upload or link new education and project materials as they are being developed.
2. Embed an email inquiry form into the ACCD page. This could also be embedded into a number of other pages as an informal Q&A, however it is unclear who would be able to respond to this.
3. Link the main ACCD page to hotlinks to: the howsyoursugar website, VU website and all ACCD Partner organisations.(using logos rather than text where possible)
4. The main portal page needs to have an accessible introduction to what the portal is, as well as a disclaimer (or links to it). It also needs a to a social media page, and the ACCD page. There should be a page of links which include the social media page, howsyoursugar website, ACCD Partner organisations, Victorian department of health better health channel, DOHA Measure Up campaign,
5. Existing ACCD materials could be uploaded onto separate pages linked to the portal. These include: blood pressure charts, BMI tables, healthy sugar ranges, food pyramid, exercise pyramid in English and 10 community languages.
6. At the moment the Portal links all diabetes pages to corresponding pages on the DA-‐Vic website. It may be good to include other Australian Government websites as well, and some video/pictorial content rather than text-‐heavy DA-‐Vic web content.
7. Diabetes info pages need clearly marked labels to CALD language pages, possibly with the use of maps or another visual ‘key’, as well as foreign language script. CALD language pages should replicate the English diabetes info pages.
8. CALD language pages have links to international (foreign language) websites but should also have links to uploaded pages of translated ACCD material.
9. Currently the portal has sorted Languages Other Than English by language only, although some languages are spoken by a wide variety of nationalities (eg Arabic). Regional maps or flags could be used as well in order to overcome some of the ambiguities in CALD identity.
10. There could be links to CALD community/health/welfare groups (most have websites) in Melbourne on each language page, with details of contact people.
11. The researcher pages – particularly on recent research projects needs to be maintained and updated in the future if it is to remain useful. Could there also be a link to the VU research repository? There should also be a page listing ACCD research projects and publications.
12. The maps of the diabetes epidemic need to be maintained if they are to remain relevant. There needs to be a more easily resourced way of doing this so there is not a 2-‐4 year turnaround between NDSS and Census figures and the publishing of rates. In addition the interactive health services pages also need to be verified and updated on a regular basis.
Draft Report Prepared by Dr. Margaret Mayhew Date: November 2011. This Report was prepared with the considerable assistance and work of the following: Margaret Hansford, Dr. Rizwana Kousar, Dr. Liping Wang, Alex Skaria, Harry Bryce.
ACCD KNOWLEDGE MANAGEMENT PORTAL 2
EXECUTIVE SUMMARY: 2
INTRODUCTION: 2 METHODOLOGY: 2 1. CONSULTATIONS 2 2. DESKTOP RESEARCH 2 FINDINGS: 2 CONTENT 2 LIKELIHOOD OF USE 3 APPEARANCE 3 NAVIGATION 3 INTERACTIVITY 4 CONCLUSION: 4 RECOMMENDATIONS: 4 SPECIFIC RECOMMENDATIONS: 5
BACKGROUND: 8
ACCD WEB PRESENCE 8 KNOWLEDGE PORTAL 8 METHODS: 9 PARTICIPANT DESCRIPTIONS 10 CALD COMMUNITY MEMBERS (N=61) 10 INDIGENOUS COMMUNITY MEMBERS (N= 6) 10 DIABETES/HEALTH ORGANISATIONS (N = 7) 10 RESEARCHERS (N = 6) 10
FINDINGS: 11
INFORMATION REQUIRED 11 KEY POINTS 11 COLLATED RESPONSES 11 MAPS OF CONSULTATIONS: 12 RELEVANCE 14 COLLATED RESPONSES 14 NAVIGATION 17 LIKELIHOOD OF USE 17 NAVIGATION 17 LIKELIHOOD OF USE 20 SUMMARY 20 COLLATION OF RESPONSES 20 MAPS OF CONSULTATIONS 21 APPEARANCE 23 SUMMARY 23 COLLATED RESPONSES 23 CONSULTATIONS MAPS 24 INTERACTIVITY 26 KEY FINDINGS 26 COLLATED RESPONSES 26 MAPS: 26 DISCUSSION: 28 SPECIFIC RECOMMENDATIONS: 30 RECOMMENDATIONS: 31 SPECIFIC RECOMMENDATIONS: 31 CONCLUSION: 33 APPENDIX 1: DEMOGRAPHIC ANALYSIS OF PARTICIPANTS 34 APPENDIX 2: QUESTIONNAIRES 38 COMMUNITY MEMBERS 38 APPENDIX 3: QUESTIONNAIRES 39 FOCUS GROUP QUESTIONS 39 APPENDIX 4: IMAGES OF KNOWLEDGE PORTAL 40
Background:
ACCD Web Presence
The Australian Community Centre, as a research centre within Victoria University, currently has a web page located at: http://www.vu.edu.au/research/centres-‐and-‐institutes/centres/australian-‐community-‐centre-‐for-‐diabetes-‐accd.
This is a fixed page, reliant on external university based web-‐editors, containing a bare minimum of information that is updated as little as possible.
The CEO of ACCD, Harry Bryce also as a personal staff page on the VU website, at http://www.vu.edu.au/about-‐vu/our-‐people/harry-‐bryce.
Individual staff members of the ACCD have contact details supplied on the internal staff directory (position, email, extension number), however there is no other internet-‐based information on ACCD or its staff.
A mapping project undertaken with Diabetes Australia-‐victoria and the National Diabetes Services Scheme went live in 2010 at http://www.diabetesepidemic.com.au/westernmelbourne/project/. This is hosted by Diabetes Australia Victoria, but has ACCD branding and a brief description of the ACCD. The hotlink to the current ACCD webpage is not currently active.
In 2009-‐2010, ACCD indigenous research staff developed an interactive website for use within indigenous communities at http://www.howsyoursugar.com.au/). This has been developed in conjunction with a range of social marketing projects in health promotion, which include photo-‐voice projects, digital story-‐telling and video development by Aboriginal communities. However, apart from a copyright statement at the base of the front page, there is no branding of the ACCD or hotlinks to the ACCD website.
Knowledge Portal
The ACCD Knowledge Portal has been a project in development since 2008.
A commissioned report prepared by Sally-‐Anne Leigh in early 2008, recommended that the ACCD establish an online presence via the development of a knowledge portal, rather than a fixed website or series of pages.
The report noted the increasing prevalence of knowledge portal systems in health promotion and community development, citing the community gateway site at: www.vicnet.net.au. The report argued that a knowledge portal would allow for a range of platforms to be linked, including user-‐generated content as well as fixed content, as well as comprehensive links to external resources.
A working party was established in 2009, comprising ACCD staff and external advisors. The terms of reference of this working party states: One of ACCD’s key functions is to develop and maintain a Knowledge Management Portal. This will be a resource that combines a research repository, consolidated sources of diabetes data and a dynamic online community-‐of-‐practice for partner organisations.
In addition a key function of the working party is to establish the baseline of diabetes prevalence in the west. This requires a more effective process for gathering and management of relevant data.
In 2009 Dr. Liping Wang was appointed as a research fellow to implement the recommendations of the working party and to research and develop the content of the knowledge portal. She initially collaborated with Diabetes Australia Victoria in developing a series of interactive maps of diabetes
prevalence in western Melbourne, as well as health organisations in Western Melbourne. Most of the data for this latter component was supplied in a separate project undertaken by RAAMPS, which was launched in conjunction with the Diabetes Australia Victoria website discussed above. In November 2009 Alex Skaria was appointed as a research assistant to Liping.
From March 2010 Liping worked on developing the Knowledge Portal content and format, using the joomla web development platform. It is intended that once it goes ‘live’, that the portal will be hosted by Victoria University. However there are still a number of ambiguities concerning the security and quality of content as well as legal responsibility for its accuracy.
This report comprises feedback from a range of stakeholders on the current format and content of the Knowledge Portal. It also includes suggestions and management issues that have been raised by a number of colleagues and stakeholders, outside of the official consultation process.
Methods:
Two major strands of consultations occurred; one, largely qualitative, consisting of focus groups with a range of stakeholders, and the second consisting of questionnaires, which were distributed and analysed with students from the Victoria University school of Marketing. The results of the latter surveys are yet to be compiled, and so this report concerns feedback from the focus group consultations.
Three types of stakeholders were identified: Community members Health Organisations Researchers
A total of 80 participants were consulted about the portal, with roughly equal gender representation. The largest stakeholder group was the community members, which included CALD community members, CALD community workers and indigenous students.
The focus groups occurred using a semi-‐structured format of five open ended questions and two facilitators. All participants were given hard copies of the questions, and asked to complete a demographic survey.(see attachment 1)
Participants were firstly asked a general question about the types of information about diabetes they would like to know.
A brief video clip was then shown to participants, illustrating the appearance of the portal and features including navigation and searching functions.
Participants were asked a series of questions, and invited to have small group discussion before reporting their feedback to the facilitators. One facilitator made notes of participants’ responses one a whiteboard, and the second facilitator summarised these notes into map diagrams using Mindjet Manager softwear. These maps were projected during the consultations and then used as the main record of the feedback.
The responses from each map were collated in tables for each question. Findings were extrapolated from the responses to each question. There was some crossover in responses to questions.
Participant Descriptions
CALD community members (N=61)
These consultations were conducted via in-‐community focus groups containing a maximum of twenty participants, as well as a focus group run during a meeting of the ACCD CALD Advisory Committee.
The following communities were targeted: African, Afghan, Bengali, Burmese, Filipino, Pakistani, Latin-‐American, Turkish, and Vietnamese.
The rationale for this selection of communities was based on: (a) high risks for and rates of diabetes in these resident communities in Australia and in their countries of origin; (b) distribution of communities that are recent through to more established settlement, and that are from a range of continents. i
Participants were recruited through existing CALD community projects including the Bilingual Health Educator project, Community Cooking Classes and the CALD advisory committee. One participant from each language group was selected as a ‘bilingual consultant’, and asked to recruit 6 participants.
Recognising the different information technology capacities at different age groups, the consultants were asked to select (one male and one female) in each of the following age groups: (1) 15-‐35 years of age; (2) 36-‐55 years of age; (3) 56 years of age and above. In some communities this was not possible (eg, those from Burma) because of recent settlement predominantly of younger people. In these cases, the number of people in accessible age range groups was increased.ii
Four consultation sessions were held with CALD community members and were conducted in English, with the consultants acting as interpreters.
Indigenous community members (N= 6) A focus group was held with Indigenous TAFE students from Victoria University during class time. This was held on the same day as the students run a community food-‐share program, in consultation with staff from Moondani Balluk who advised that this was the most appropriate source for indigenous feedback.
Diabetes/Health Organisations (N = 7) One focus group were held with staff from Western Health (with four participants), and another with staff from Baker IDI (three participants).
Researchers (N = 6) A focus groups with VU researchers was held in the place of the monthly Journal Club that is hosted by the ACCD. Three external researchers attended and three ACCD researchers attended.
Please refer to Appendix 3 for more demographic information on participants.
Findings:
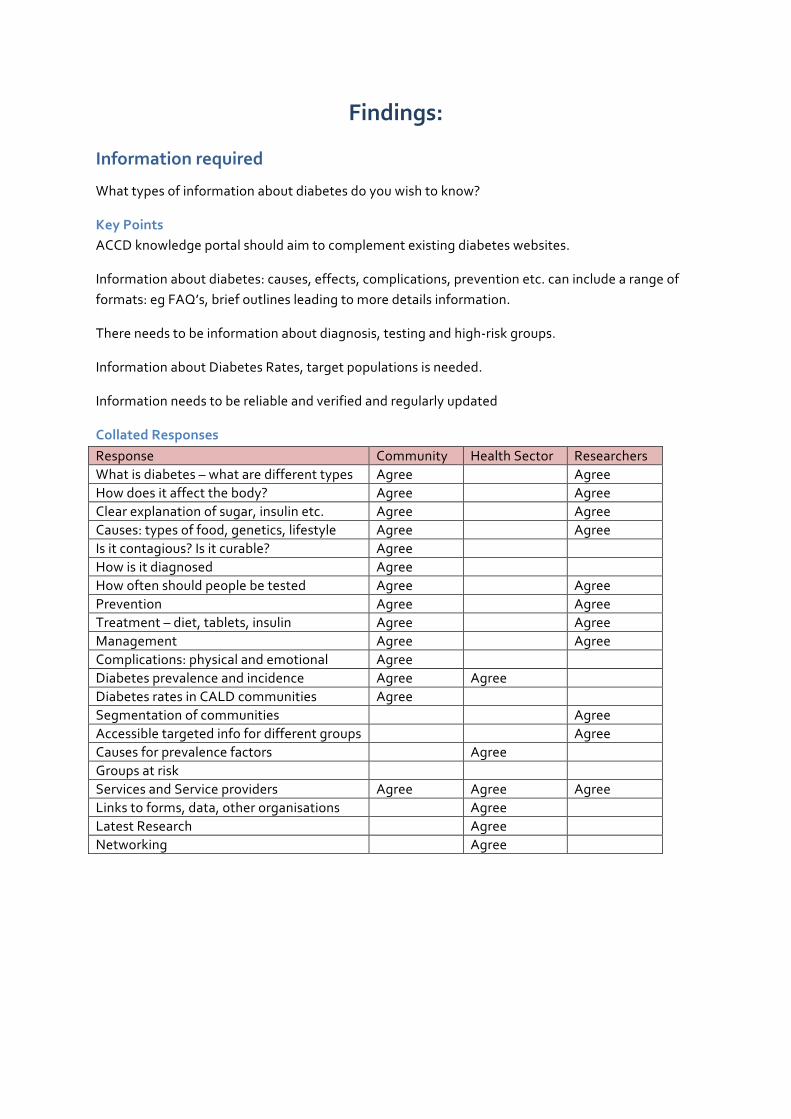
Information required
What types of information about diabetes do you wish to know?
Key Points ACCD knowledge portal should aim to complement existing diabetes websites.
Information about diabetes: causes, effects, complications, prevention etc. can include a range of formats: eg FAQ’s, brief outlines leading to more details information.
There needs to be information about diagnosis, testing and high-‐risk groups.
Information about Diabetes Rates, target populations is needed.
Information needs to be reliable and verified and regularly updated
Collated Responses Response Community Health Sector Researchers What is diabetes – what are different types Agree Agree How does it affect the body? Agree Agree Clear explanation of sugar, insulin etc. Agree Agree Causes: types of food, genetics, lifestyle Agree Agree Is it contagious? Is it curable? Agree How is it diagnosed Agree How often should people be tested Agree Agree Prevention Agree Agree Treatment – diet, tablets, insulin Agree Agree Management Agree Agree Complications: physical and emotional Agree Diabetes prevalence and incidence Agree Agree Diabetes rates in CALD communities Agree Segmentation of communities Agree Accessible targeted info for different groups Agree Causes for prevalence factors Agree Groups at risk Services and Service providers Agree Agree Agree Links to forms, data, other organisations Agree Latest Research Agree Networking Agree

Maps of consultations: Composite of CALD communities
Indigenous Students
CALD Advisory Committee
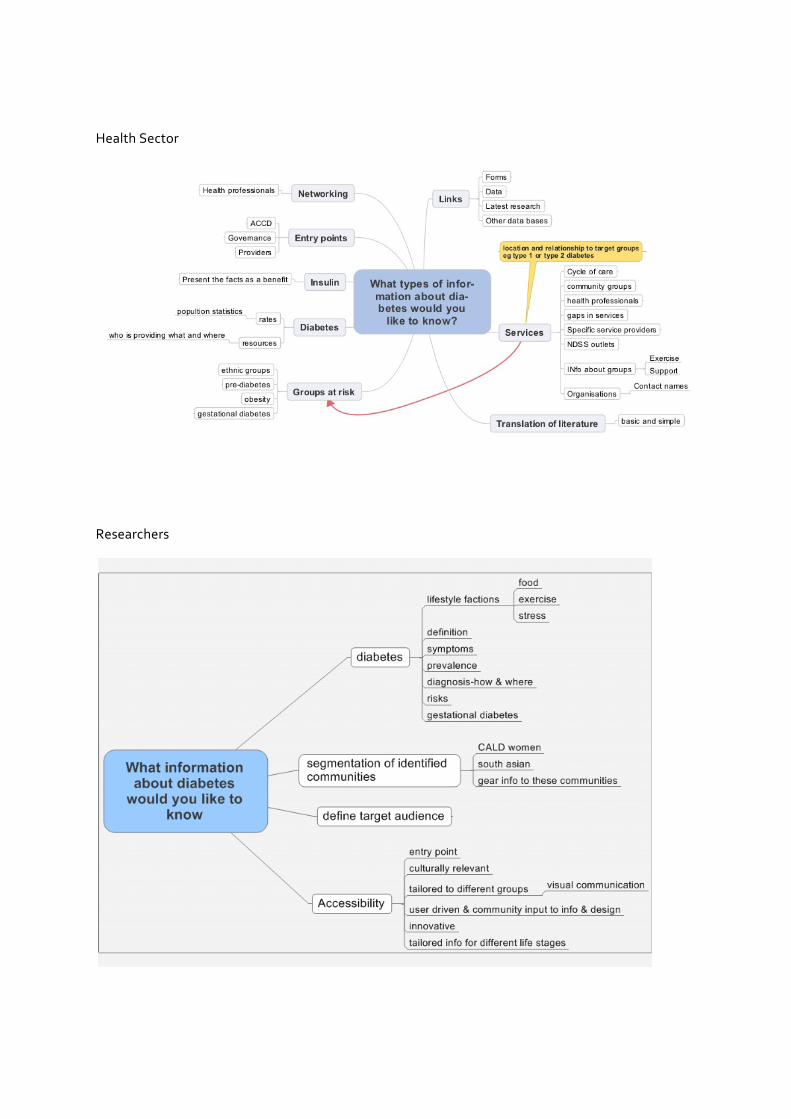
Health Sector
Researchers
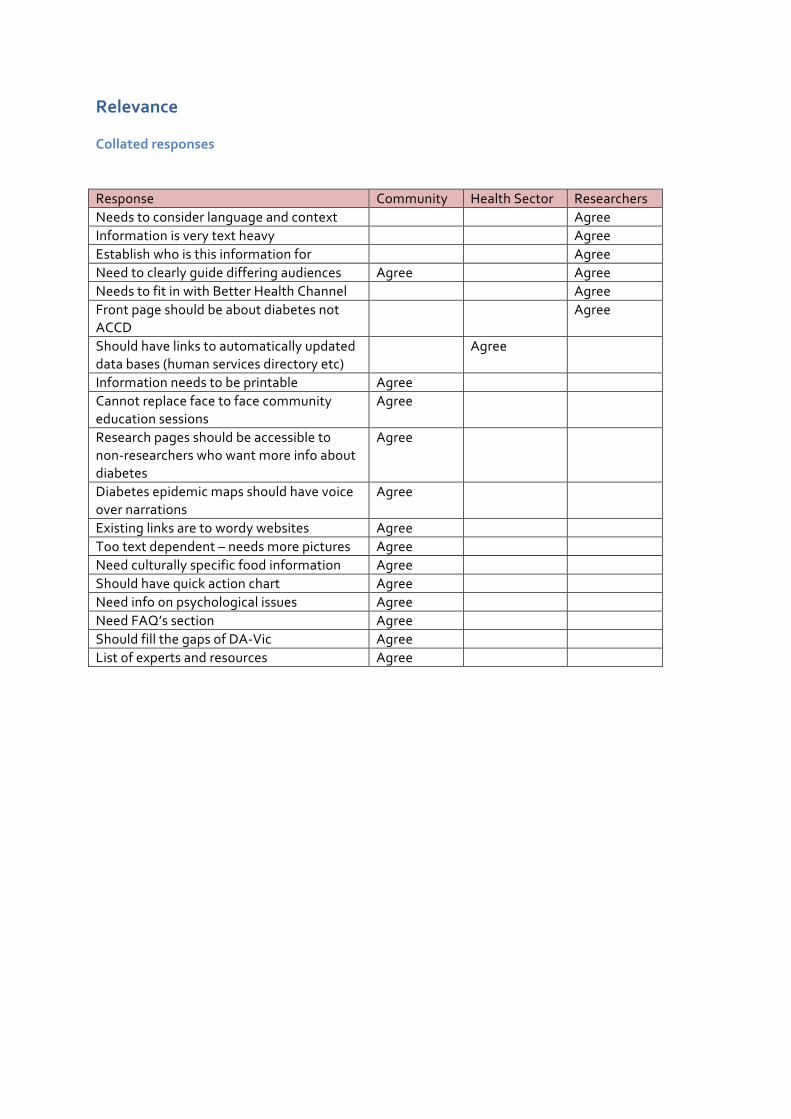
Relevance
Collated responses
Response Community Health Sector Researchers Needs to consider language and context Agree Information is very text heavy Agree Establish who is this information for Agree Need to clearly guide differing audiences Agree Agree Needs to fit in with Better Health Channel Agree Front page should be about diabetes not ACCD
Agree
Should have links to automatically updated data bases (human services directory etc)
Agree
Information needs to be printable Agree Cannot replace face to face community education sessions
Agree
Research pages should be accessible to non-‐researchers who want more info about diabetes
Agree
Diabetes epidemic maps should have voice over narrations
Agree
Existing links are to wordy websites Agree Too text dependent – needs more pictures Agree Need culturally specific food information Agree Should have quick action chart Agree Need info on psychological issues Agree Need FAQ’s section Agree Should fill the gaps of DA-‐Vic Agree List of experts and resources Agree
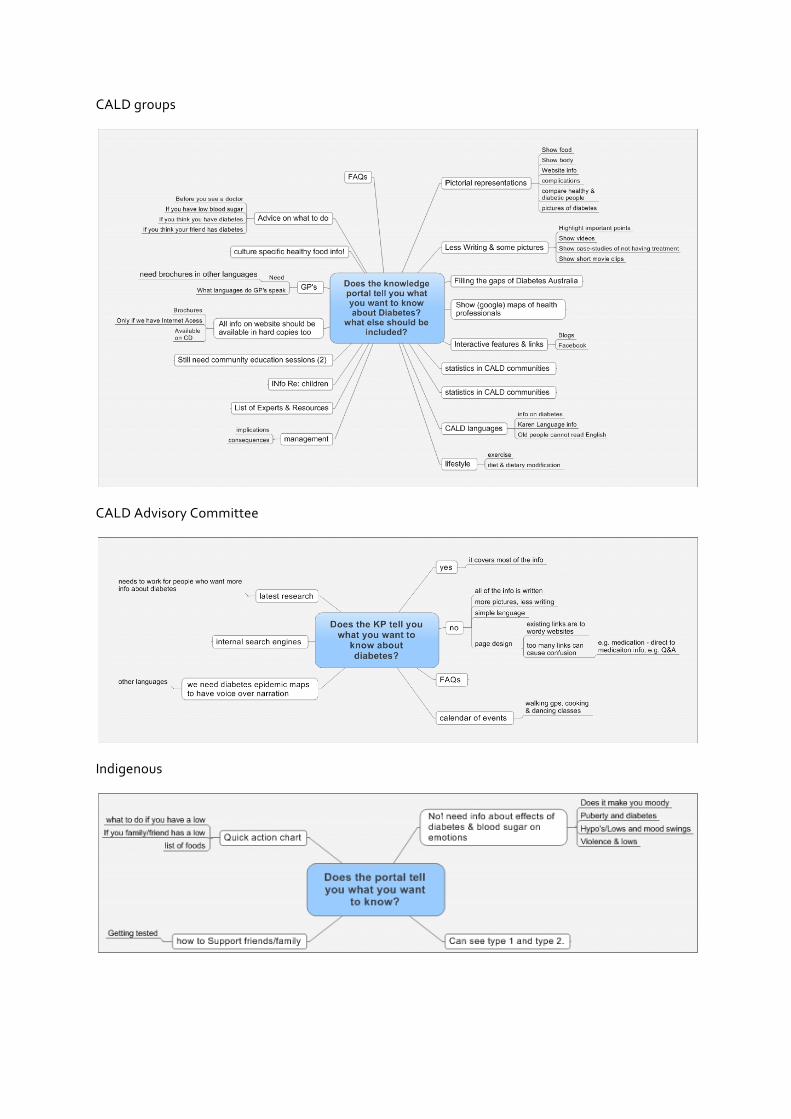
CALD groups
CALD Advisory Committee
Indigenous
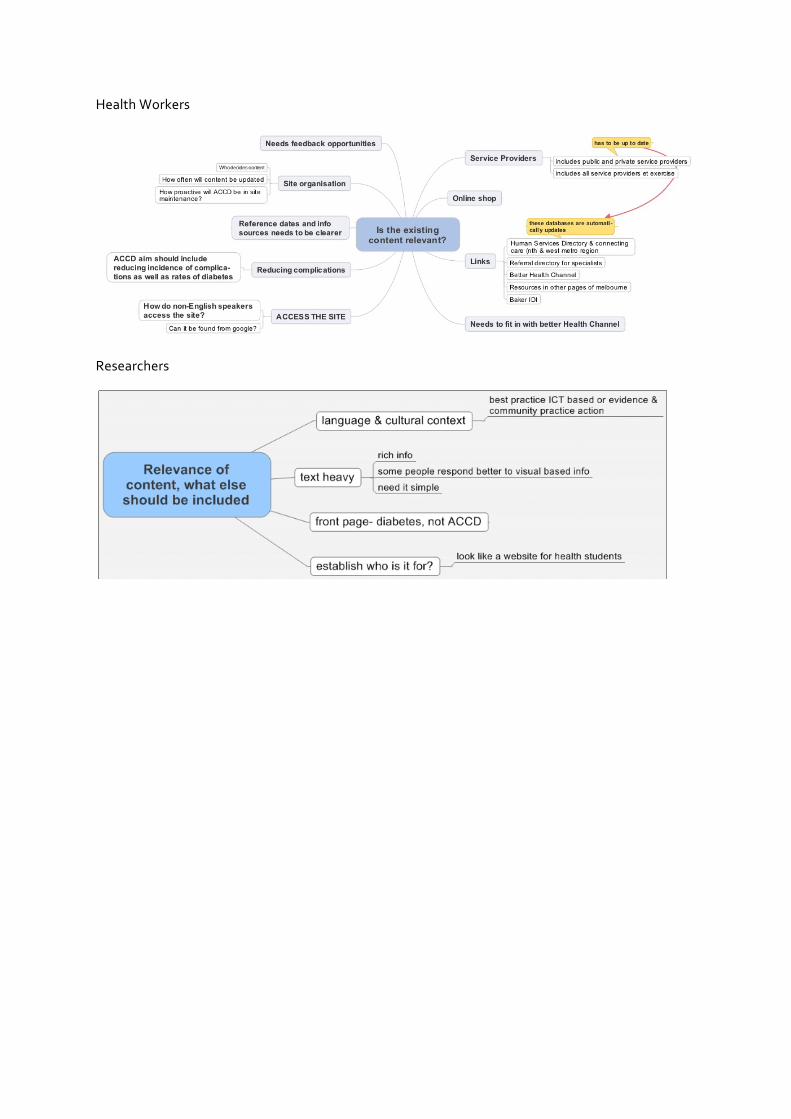
Health Workers
Researchers
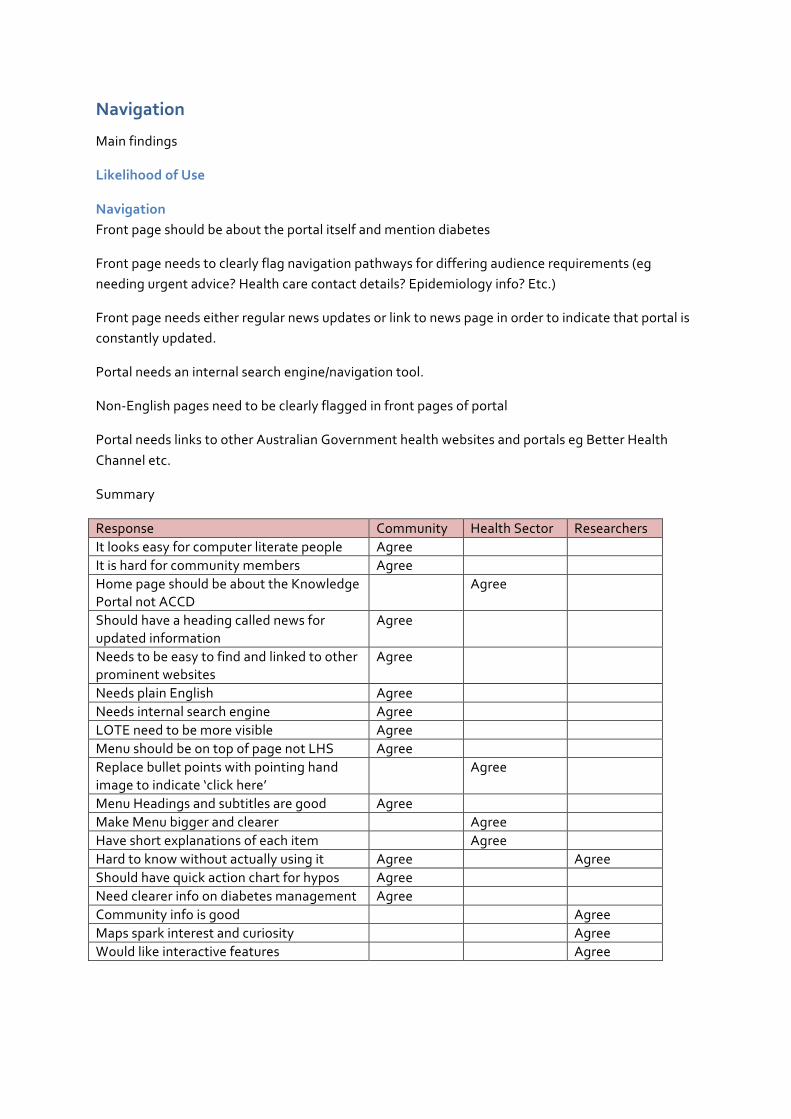
Navigation
Main findings
Likelihood of Use
Navigation Front page should be about the portal itself and mention diabetes
Front page needs to clearly flag navigation pathways for differing audience requirements (eg needing urgent advice? Health care contact details? Epidemiology info? Etc.)
Front page needs either regular news updates or link to news page in order to indicate that portal is constantly updated.
Portal needs an internal search engine/navigation tool.
Non-‐English pages need to be clearly flagged in front pages of portal
Portal needs links to other Australian Government health websites and portals eg Better Health Channel etc.
Summary
Response Community Health Sector Researchers It looks easy for computer literate people Agree It is hard for community members Agree Home page should be about the Knowledge Portal not ACCD
Agree
Should have a heading called news for updated information
Agree
Needs to be easy to find and linked to other prominent websites
Agree
Needs plain English Agree Needs internal search engine Agree LOTE need to be more visible Agree Menu should be on top of page not LHS Agree Replace bullet points with pointing hand image to indicate ‘click here’
Agree
Menu Headings and subtitles are good Agree Make Menu bigger and clearer Agree Have short explanations of each item Agree Hard to know without actually using it Agree Agree Should have quick action chart for hypos Agree Need clearer info on diabetes management Agree Community info is good Agree Maps spark interest and curiosity Agree Would like interactive features Agree
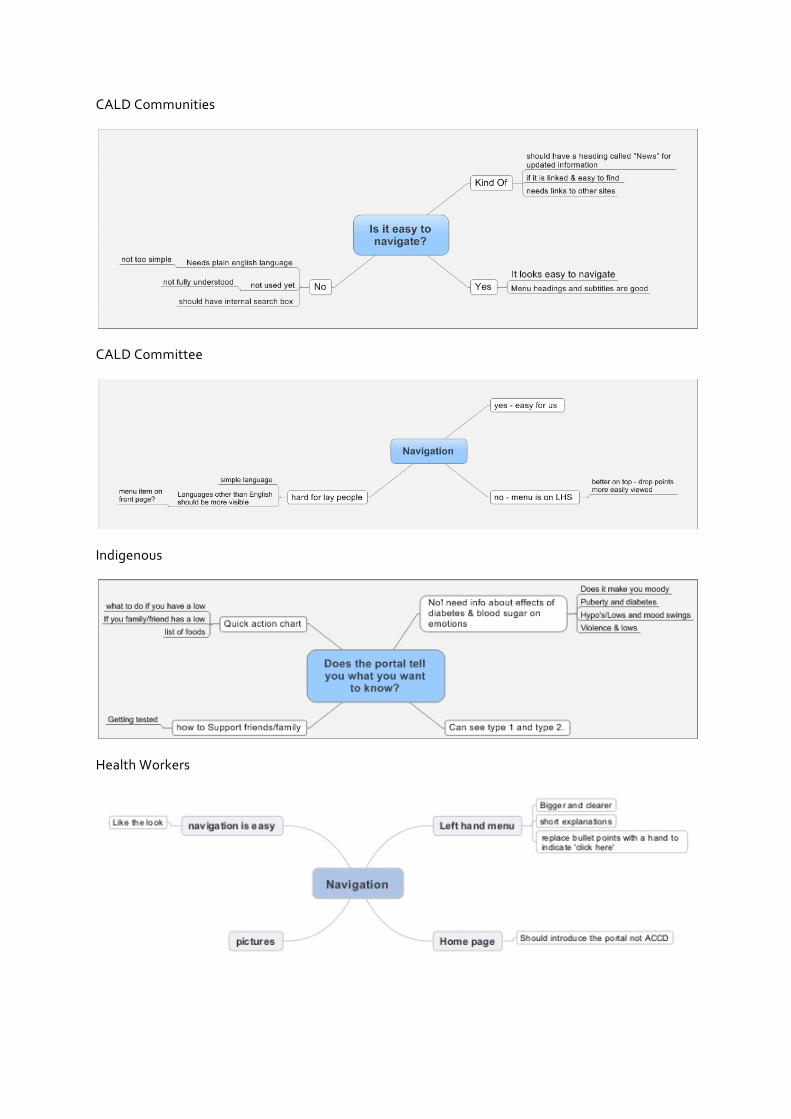
CALD Communities
CALD Committee
Indigenous
Health Workers
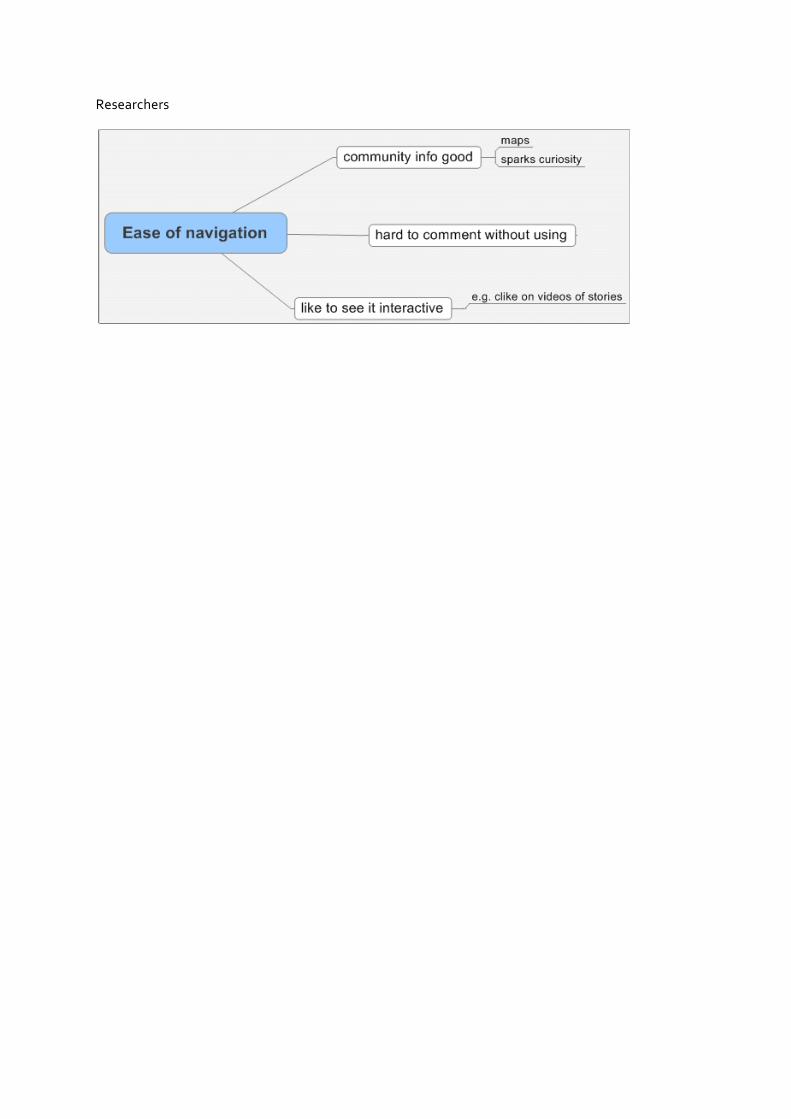
Researchers
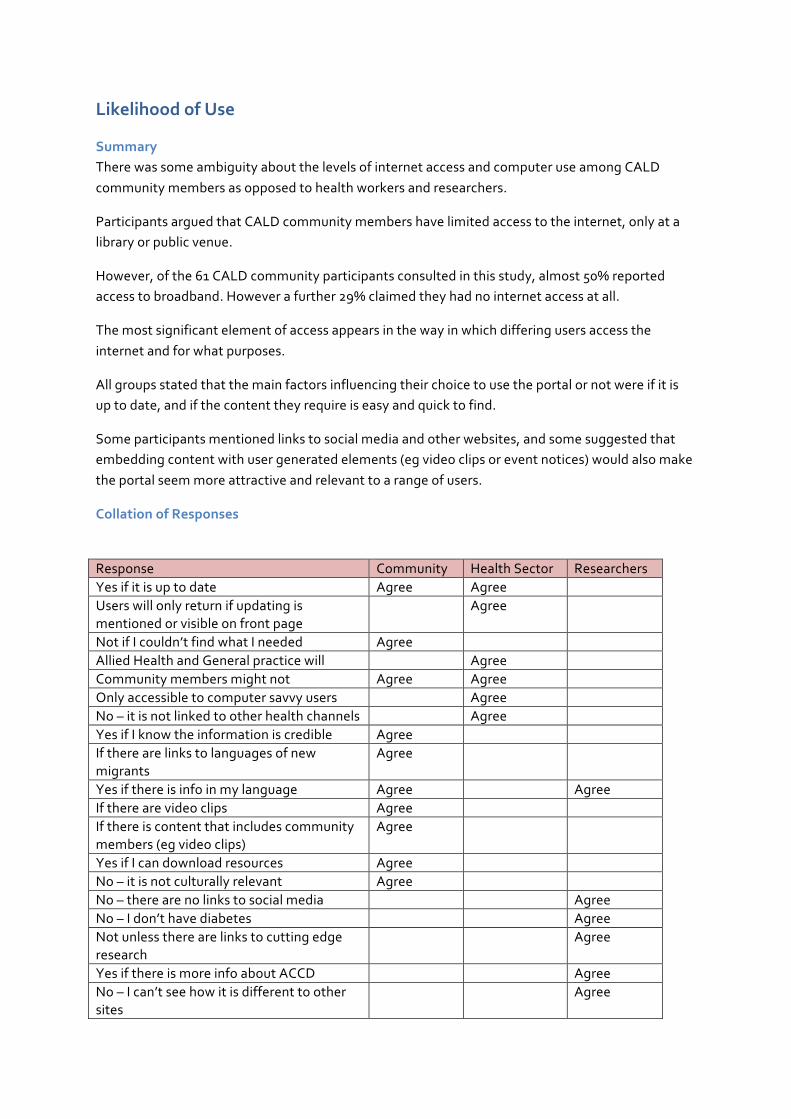
Likelihood of Use
Summary There was some ambiguity about the levels of internet access and computer use among CALD community members as opposed to health workers and researchers.
Participants argued that CALD community members have limited access to the internet, only at a library or public venue.
However, of the 61 CALD community participants consulted in this study, almost 50% reported access to broadband. However a further 29% claimed they had no internet access at all.
The most significant element of access appears in the way in which differing users access the internet and for what purposes.
All groups stated that the main factors influencing their choice to use the portal or not were if it is up to date, and if the content they require is easy and quick to find.
Some participants mentioned links to social media and other websites, and some suggested that embedding content with user generated elements (eg video clips or event notices) would also make the portal seem more attractive and relevant to a range of users.
Collation of Responses
Response Community Health Sector Researchers Yes if it is up to date Agree Agree Users will only return if updating is mentioned or visible on front page
Agree
Not if I couldn’t find what I needed Agree Allied Health and General practice will Agree Community members might not Agree Agree Only accessible to computer savvy users Agree No – it is not linked to other health channels Agree Yes if I know the information is credible Agree If there are links to languages of new migrants
Agree
Yes if there is info in my language Agree Agree If there are video clips Agree If there is content that includes community members (eg video clips)
Agree
Yes if I can download resources Agree No – it is not culturally relevant Agree No – there are no links to social media Agree No – I don’t have diabetes Agree Not unless there are links to cutting edge research
Agree
Yes if there is more info about ACCD Agree No – I can’t see how it is different to other sites
Agree
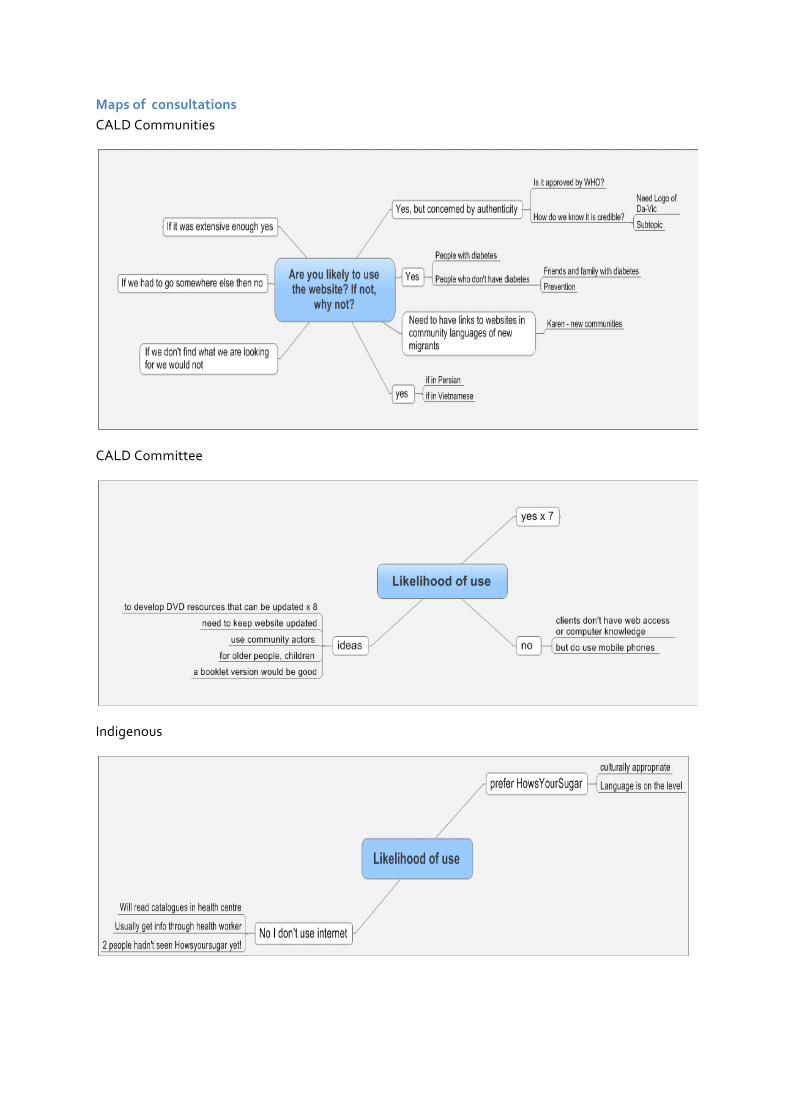
Maps of consultations CALD Communities
CALD Committee
Indigenous
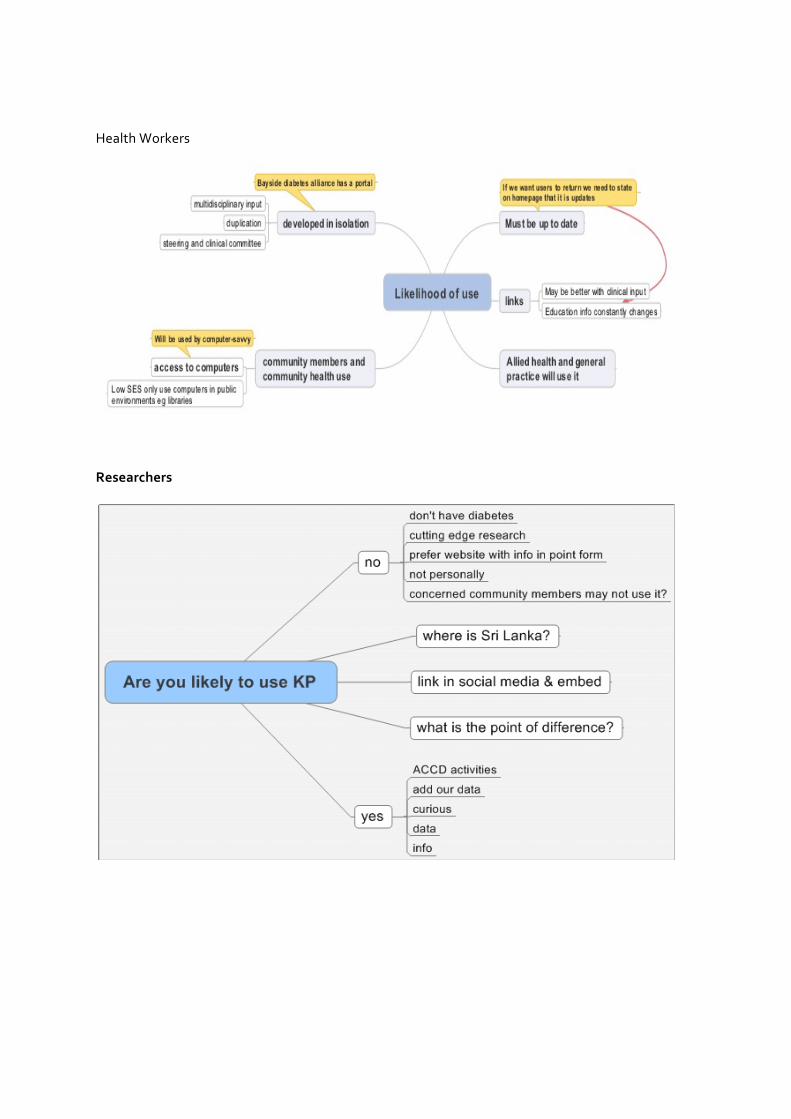
Health Workers
Researchers
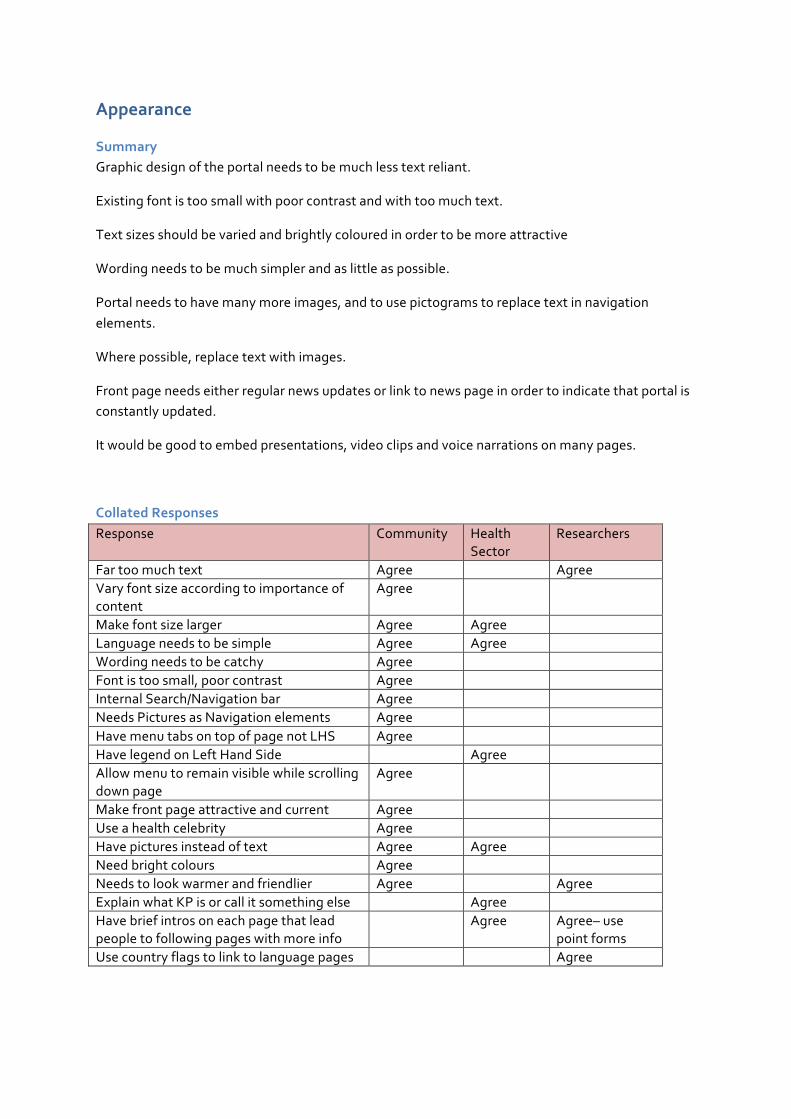
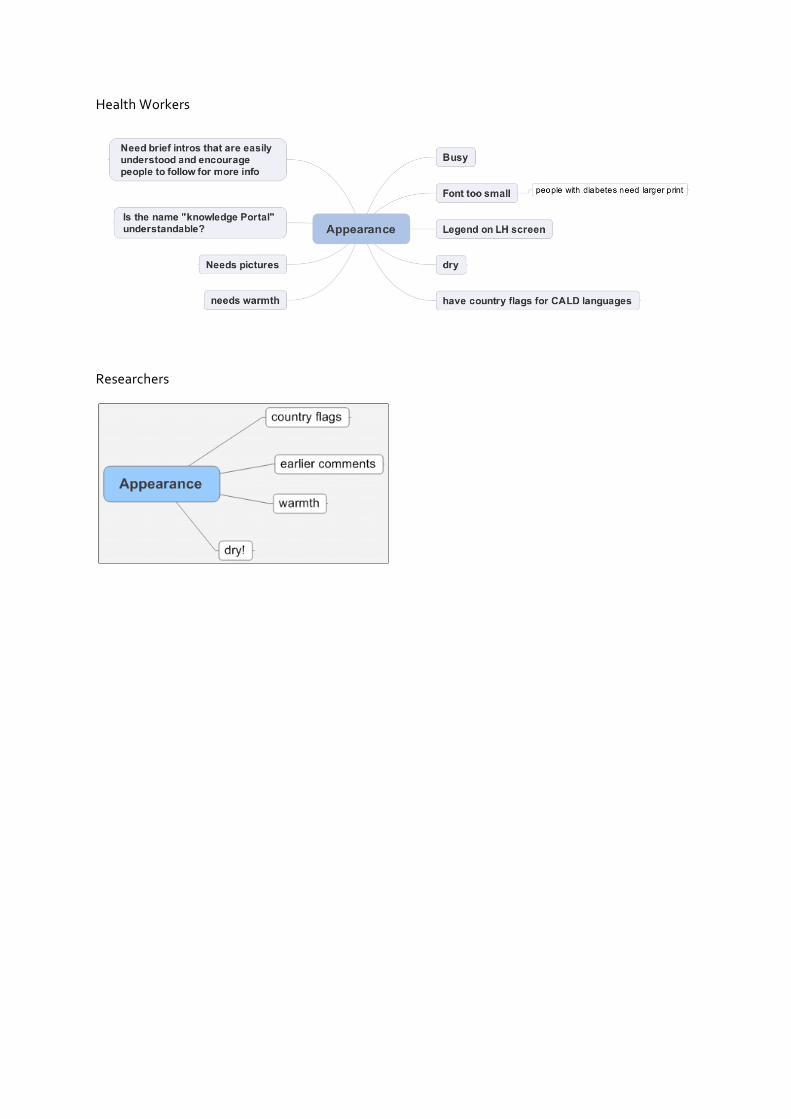
Appearance
Summary Graphic design of the portal needs to be much less text reliant.
Existing font is too small with poor contrast and with too much text.
Text sizes should be varied and brightly coloured in order to be more attractive
Wording needs to be much simpler and as little as possible.
Portal needs to have many more images, and to use pictograms to replace text in navigation elements.
Where possible, replace text with images.
Front page needs either regular news updates or link to news page in order to indicate that portal is constantly updated.
It would be good to embed presentations, video clips and voice narrations on many pages.
Collated Responses Response Community Health
Sector Researchers
Far too much text Agree Agree Vary font size according to importance of content
Agree
Make font size larger Agree Agree Language needs to be simple Agree Agree Wording needs to be catchy Agree Font is too small, poor contrast Agree Internal Search/Navigation bar Agree Needs Pictures as Navigation elements Agree Have menu tabs on top of page not LHS Agree Have legend on Left Hand Side Agree Allow menu to remain visible while scrolling down page
Agree
Make front page attractive and current Agree Use a health celebrity Agree Have pictures instead of text Agree Agree Need bright colours Agree Needs to look warmer and friendlier Agree Agree Explain what KP is or call it something else Agree Have brief intros on each page that lead people to following pages with more info
Agree Agree– use point forms
Use country flags to link to language pages Agree
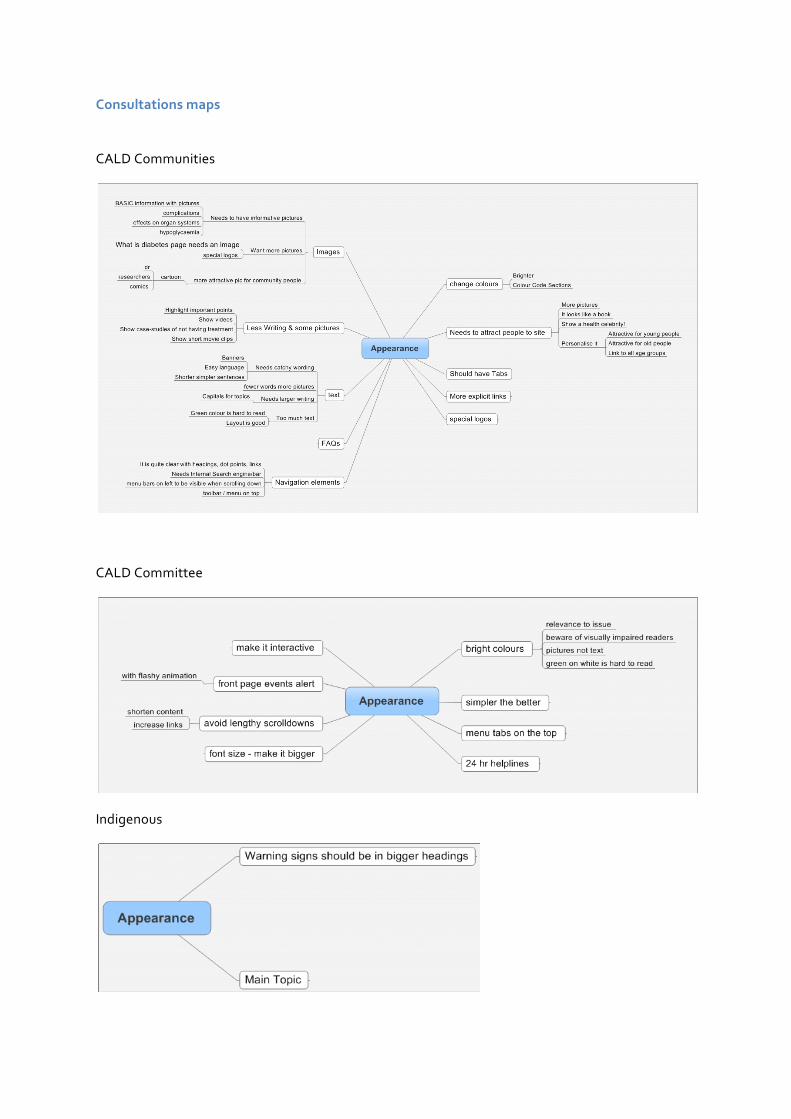
Consultations maps
CALD Communities
CALD Committee
Indigenous
Health Workers
Researchers
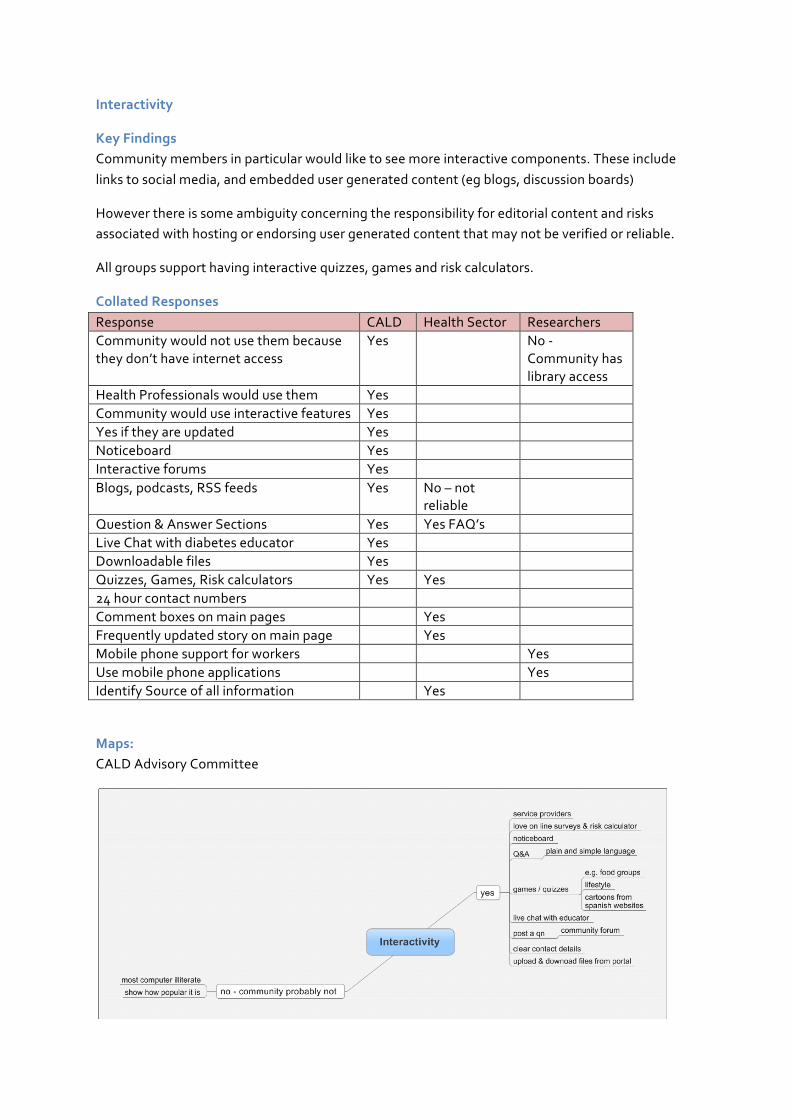
Interactivity
Key Findings Community members in particular would like to see more interactive components. These include links to social media, and embedded user generated content (eg blogs, discussion boards)
However there is some ambiguity concerning the responsibility for editorial content and risks associated with hosting or endorsing user generated content that may not be verified or reliable.
All groups support having interactive quizzes, games and risk calculators.
Collated Responses Response CALD Health Sector Researchers Community would not use them because they don’t have internet access
Yes No -‐ Community has library access
Health Professionals would use them Yes Community would use interactive features Yes Yes if they are updated Yes Noticeboard Yes Interactive forums Yes Blogs, podcasts, RSS feeds Yes No – not
reliable
Question & Answer Sections Yes Yes FAQ’s Live Chat with diabetes educator Yes Downloadable files Yes Quizzes, Games, Risk calculators Yes Yes 24 hour contact numbers Comment boxes on main pages Yes Frequently updated story on main page Yes Mobile phone support for workers Yes Use mobile phone applications Yes Identify Source of all information Yes
Maps: CALD Advisory Committee

CALD Community Members
Health Workers
Researchers
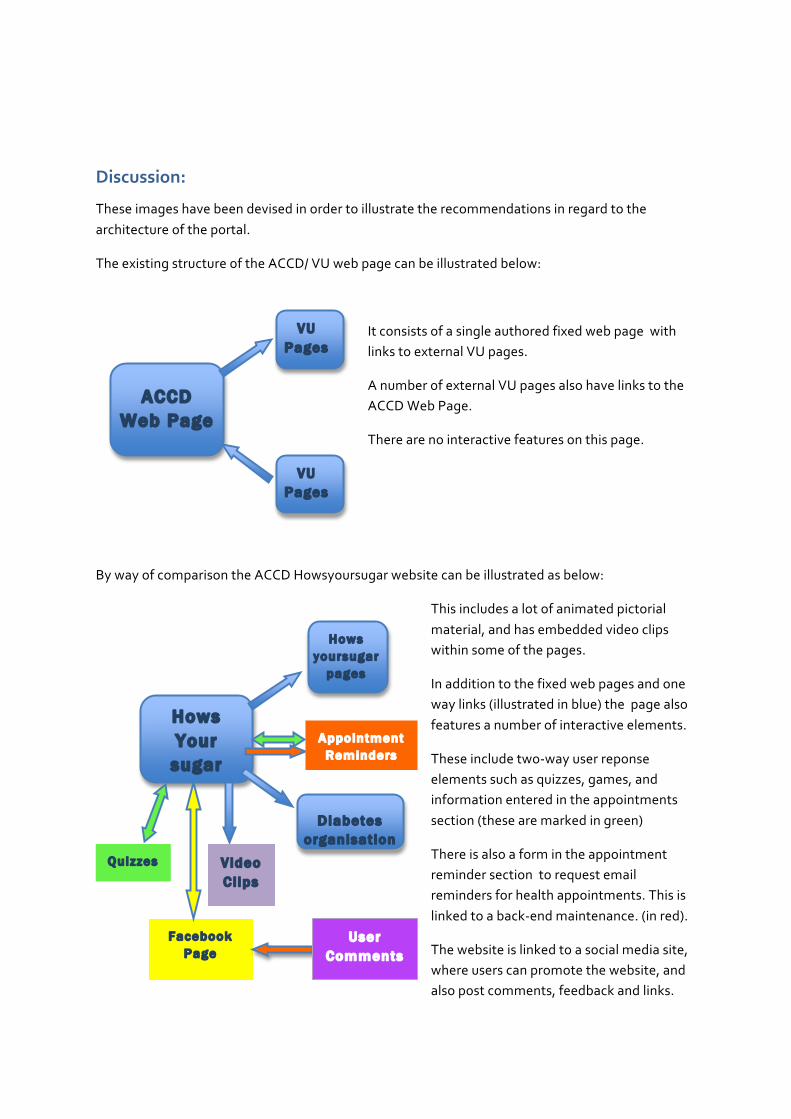
Discussion:
These images have been devised in order to illustrate the recommendations in regard to the architecture of the portal.
The existing structure of the ACCD/ VU web page can be illustrated below:
It consists of a single authored fixed web page with links to external VU pages.
A number of external VU pages also have links to the ACCD Web Page.
There are no interactive features on this page.
By way of comparison the ACCD Howsyoursugar website can be illustrated as below:
This includes a lot of animated pictorial material, and has embedded video clips within some of the pages.
In addition to the fixed web pages and one way links (illustrated in blue) the page also features a number of interactive elements.
These include two-‐way user reponse elements such as quizzes, games, and information entered in the appointments section (these are marked in green)
There is also a form in the appointment reminder section to request email reminders for health appointments. This is linked to a back-‐end maintenance. (in red).
The website is linked to a social media site, where users can promote the website, and also post comments, feedback and links.
Hows Your
sugar
Hows yoursugar
pages
Video Clips
Appointment Reminders
Facebook Page
Quizzes
Diabetes organisation
s
User Comments
ACCD Web Page
VU Pages
VU Pages
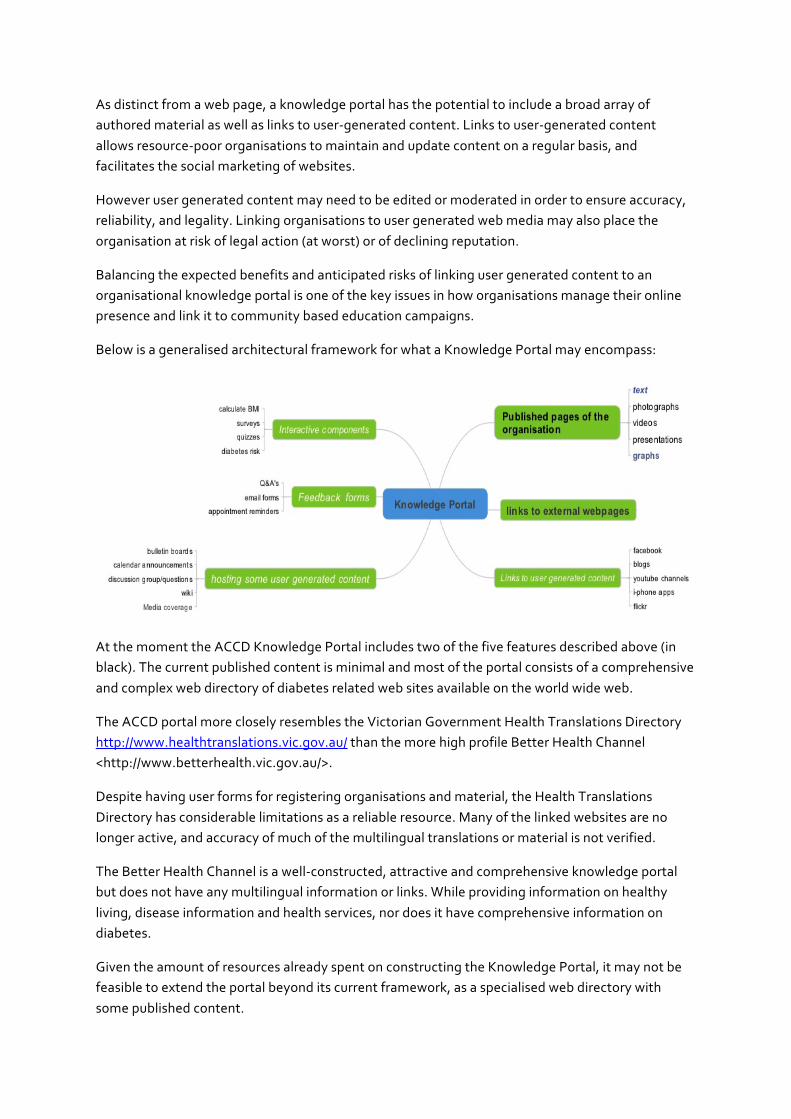
As distinct from a web page, a knowledge portal has the potential to include a broad array of authored material as well as links to user-‐generated content. Links to user-‐generated content allows resource-‐poor organisations to maintain and update content on a regular basis, and facilitates the social marketing of websites.
However user generated content may need to be edited or moderated in order to ensure accuracy, reliability, and legality. Linking organisations to user generated web media may also place the organisation at risk of legal action (at worst) or of declining reputation.
Balancing the expected benefits and anticipated risks of linking user generated content to an organisational knowledge portal is one of the key issues in how organisations manage their online presence and link it to community based education campaigns.
Below is a generalised architectural framework for what a Knowledge Portal may encompass:
At the moment the ACCD Knowledge Portal includes two of the five features described above (in black). The current published content is minimal and most of the portal consists of a comprehensive and complex web directory of diabetes related web sites available on the world wide web.
The ACCD portal more closely resembles the Victorian Government Health Translations Directory http://www.healthtranslations.vic.gov.au/ than the more high profile Better Health Channel <http://www.betterhealth.vic.gov.au/>.
Despite having user forms for registering organisations and material, the Health Translations Directory has considerable limitations as a reliable resource. Many of the linked websites are no longer active, and accuracy of much of the multilingual translations or material is not verified.
The Better Health Channel is a well-‐constructed, attractive and comprehensive knowledge portal but does not have any multilingual information or links. While providing information on healthy living, disease information and health services, nor does it have comprehensive information on diabetes.
Given the amount of resources already spent on constructing the Knowledge Portal, it may not be feasible to extend the portal beyond its current framework, as a specialised web directory with some published content.
Specific Recommendations:
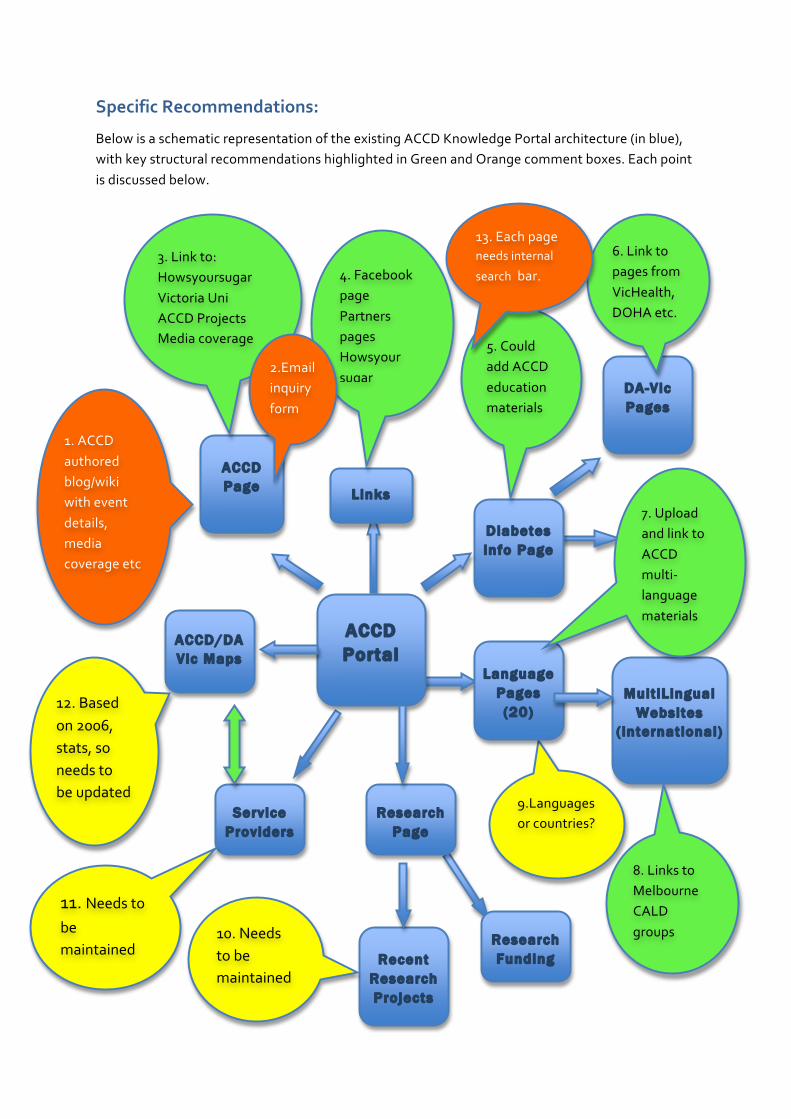
Below is a schematic representation of the existing ACCD Knowledge Portal architecture (in blue), with key structural recommendations highlighted in Green and Orange comment boxes. Each point is discussed below.
Research Page
ACCD Portal
Diabetes info Page
ACCD/DA Vic Maps
Service Providers
Language Pages (20)
Mult iLingual Websites
( international)
ACCD Page
DA-Vic Pages
Recent Research Projects
Research Funding
Links
9.Languagesor countries?
12. Based on 2006, stats, so needs to be updated
1. ACCD authored blog/wiki with event details, media coverage etc
8. Links to Melbourne CALD groups 10. Needs
to be maintained
11. Needs to
be maintained
5. Could add ACCD education materials
7. Upload and link to ACCD multi-‐language materials
4. Facebook page Partners pages Howsyour sugar
3. Link to: Howsyoursugar Victoria Uni ACCD Projects Media coverage
6. Link to pages from VicHealth, DOHA etc.
DOHA Measure Up
2.Email inquiry form
13. Each page needs internal
search bar.
Recommendations:
The overall architecture of the portal needs to be critically considered in relation to existing and future resources of the ACCD.
Back end architecture also needs to be considered, and it is recommended that this remain minimal until resources for feedback and site maintenance are ensured.
As it is, the portal has a considerable value as a web directory, but requires considerable development if it is to be launched as a fully interactive web portal. The issue of editorial responsibility for user-‐generated content still needs to resolved.
In its current format, the portal is able to be launched with a few developments:
That ACCD appoint a content manager who can ensure that portal content remains up to date.
That graphic designers be commissioned in order to increase the pictorial content of the web pages, so they are more-‐user friendly, have more pictorial content, and rely less on text.
That the portal ‘front page’ introduce the portal and direct users to relevant areas.
That community language resources be more clearly marked and linked to the portal ‘front page’
Specific Recommendations:
1. Publish a separate ‘about ACCD’ page linked to the portal. This could be established as a fixed set of pages with information (text and images) about current and recent ACCD projects, or could be linked to a separate as a blog or wiki that ACCD staff may add material to. An ACCD user content section would allow ACCD to promote events, link media coverage, upload or link new education and project materials as they are being developed.
2. Embed an email inquiry form into the ACCD page. This could also be embedded into a number of other pages as an informal Q&A, however it is unclear who would be able to respond to this.
3. Link the main ACCD page to hotlinks to: the howsyoursugar website, VU website and all ACCD Partner organisations.(using logos rather than text where possible)
4. The main portal page needs to have an accessible introduction to what the portal is, as well as a disclaimer (or links to it). It also needs a to a social media page, and the ACCD page. There should be a page of links which include the social media page, howsyoursugar website, ACCD Partner organisations, Victorian department of health better health channel, DOHA Measure Up campaign,
5. Existing ACCD materials could be uploaded onto separate pages linked to the portal. These include: blood pressure charts, BMI tables, healthy sugar ranges, food pyramid, exercise pyramid in English and 10 community languages.
6. At the moment the Portal links all diabetes pages to corresponding pages on the DA-‐Vic website. It may be good to include other Australian Government websites as well, and some video/pictorial content rather than text-‐heavy DA-‐Vic web content.
7. Diabetes info pages need clearly marked labels to CALD language pages, possibly with the use of maps or another visual ‘key’, as well as foreign language script. CALD language pages should replicate the English diabetes info pages.
8. CALD language pages have links to international (foreign language) websites but should also have links to uploaded pages of translated ACCD material.
9. Currently the portal has sorted Languages Other Than English by language only, although some languages are spoken by a wide variety of nationalities (eg Arabic). Regional maps or flags could be used as well in order to overcome some of the ambiguities in CALD identity.
10. There could be links to CALD community/health/welfare groups (most have websites) in Melbourne on each language page, with details of contact people.
11. The researcher pages – particularly on recent research projects needs to be maintained and updated in the future if it is to remain useful. Could there also be a link to the VU research repository? There should also be a page listing ACCD research projects and publications.
12. The maps of the diabetes epidemic need to be maintained if they are to remain relevant. There needs to be a more easily resourced way of doing this so there is not a 2-‐4 year turnaround between NDSS and Census figures and the publishing of rates. In addition the interactive health services pages also need to be verified and updated on a regular basis.
13. Each page of the portal should have an internal search tool eg Search inquiry box with internal engine. This would allow users to quickly find information they are seeking.

Conclusion:
The portal is currently constructed as a static single author document, consisting of a series of hotlinks to external web pages.
The issue of long-‐term maintenance and editorial of the portal has not been resolved. It is intended that the portal in its current format be hosted by Victoria University, and published by the ACCD. However, issues about intellectual property, editorial responsibility and professional reliability of content linked to the portal have yet to be resolved.
The only ACCD material on the portal consists of the maps of the diabetes epidemic in western Melbourne, as well as suburban and linguistic breakdowns for diabetes-‐related service providers. It is unclear how this information will be maintained, so that it remains relevant.
Aside from a brief text based organisational overview, there is not a great deal of information on the ACCD, or the projects, research and other work that is being conducted.
As most ACCD information is generated in the course of community based education projects, it needs to have an open-‐source, or easily accessible web-‐publishing format, in order to add reports, images, community resources and other materials.
There are currently no spaces or links to user generated content, open source publishing, social media or other interactive media formats such as: wikis, bulletin boards, youtube, blogs, calenders, FAQ’s or even inquiry forms.

Appendix 1: Demographic analysis of participants
Part A: CALD Community Members
Language Broadband None Dial-‐up Unspecified
Arab 2 2
Afghani 2 3
Bengali 3 1
English 11 1
Filipino 1 2 Burmese 6 1
Punjabi/Indian 4 3
Spanish 4 1 1 Turkish 3 4
Pakistani 3 3 1 Vietnamese 7
Sinhalese 1
Arabic-‐Nuba 1%
Dari, Persian 1%
Bengali, English 5%
Dari 1% Dari, Persian
4%
English 16%
English, Arabic, Swahili
1%
English,Filipino 1% Filipino
1% Filipino,Tagalog
1%
French,Kiswahili 1%
Karen 8%
Karen, Burma 1%
Persian 3%
Punjabi 1%
Punjabi, English 8%
Spanish 7% Spanish, English
1%
Swahili 4%
Swahili,English 1%
Turkish 9%
Urdu 9%
Vietnamese 9%
Languages
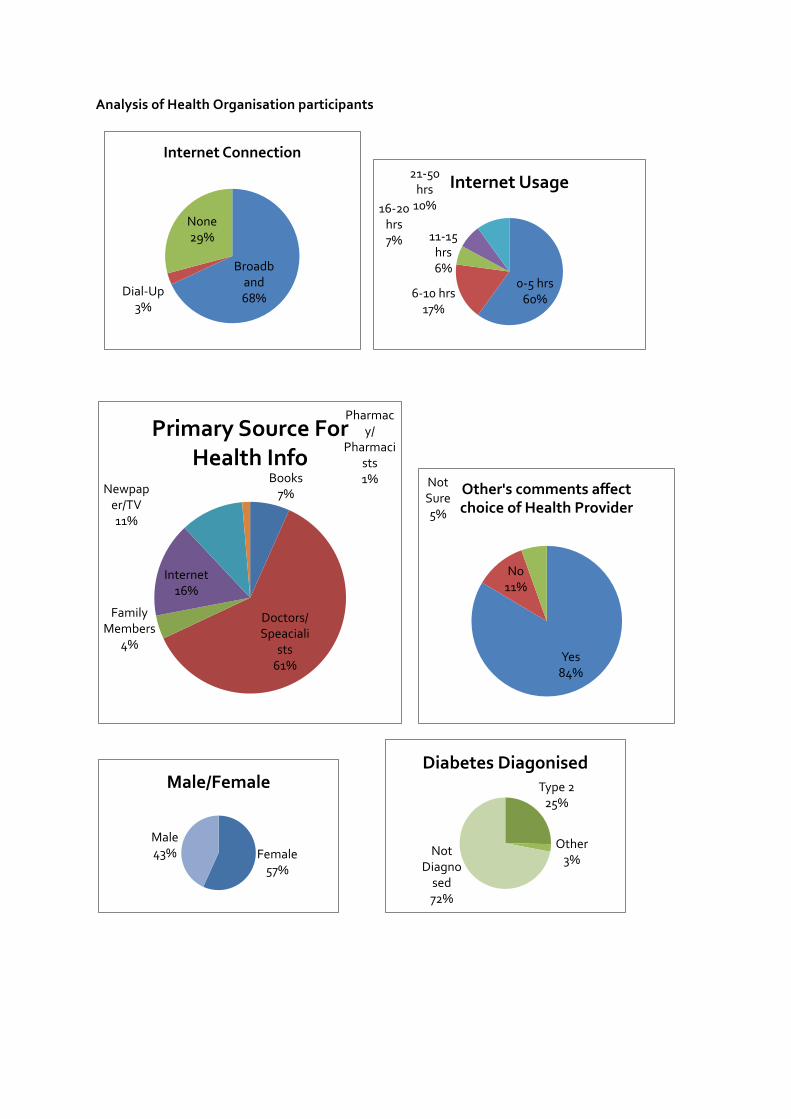
Analysis of Health Organisation participants
Broadband 68% Dial-‐Up
3%
None 29%
Internet Connection
0-‐5 hrs 60% 6-‐10 hrs
17%
11-‐15 hrs 6%
16-‐20 hrs 7%
21-‐50 hrs 10%
Internet Usage
Books 7%
Doctors/Speaciali
sts 61%
Family Members
4%
Internet 16%
Newpaper/TV 11%
Pharmacy/
Pharmacists 1%
Primary Source For Health Info
Yes 84%
No 11%
Not Sure 5%
Other's comments affect choice of Health Provider
Female 57%
Male 43%
Male/Female Type 2 25%
Other 3%
Not Diagnosed 72%
Diabetes Diagonised
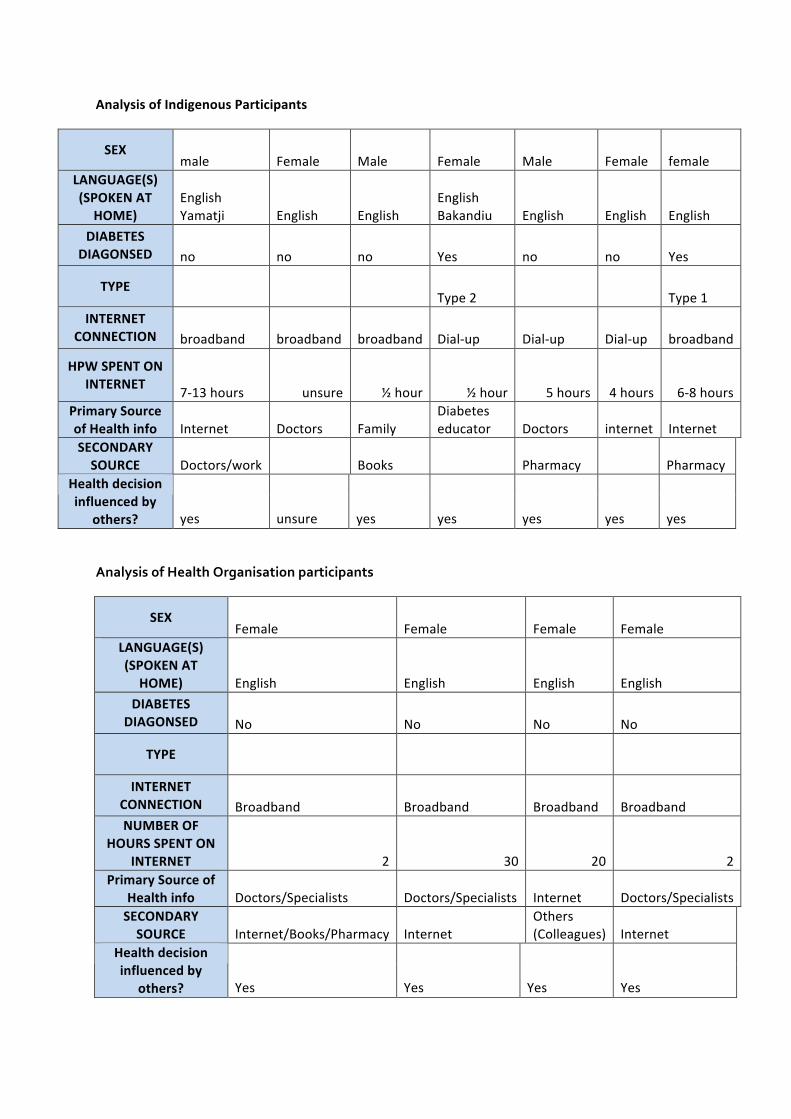
Analysis of Indigenous Participants
SEX male Female Male Female Male Female female
LANGUAGE(S) (SPOKEN AT
HOME) English Yamatji English English
English Bakandiu English English English
DIABETES DIAGONSED no no no Yes no no Yes
TYPE Type 2 Type 1
INTERNET CONNECTION broadband broadband broadband Dial-‐up Dial-‐up Dial-‐up broadband
HPW SPENT ON INTERNET
7-‐13 hours unsure ½ hour ½ hour 5 hours 4 hours 6-‐8 hours Primary Source of Health info Internet Doctors Family
Diabetes educator Doctors internet Internet
SECONDARY SOURCE Doctors/work Books Pharmacy Pharmacy
Health decision influenced by
others? yes unsure yes yes yes yes yes
Analysis of Health Organisation participants
SEX Female Female Female Female
LANGUAGE(S) (SPOKEN AT
HOME) English English English English
DIABETES DIAGONSED No No No No
TYPE
INTERNET CONNECTION Broadband Broadband Broadband Broadband NUMBER OF
HOURS SPENT ON INTERNET 2 30 20 2
Primary Source of Health info Doctors/Specialists Doctors/Specialists Internet Doctors/Specialists SECONDARY SOURCE Internet/Books/Pharmacy Internet
Others (Colleagues) Internet
Health decision influenced by
others? Yes Yes Yes Yes
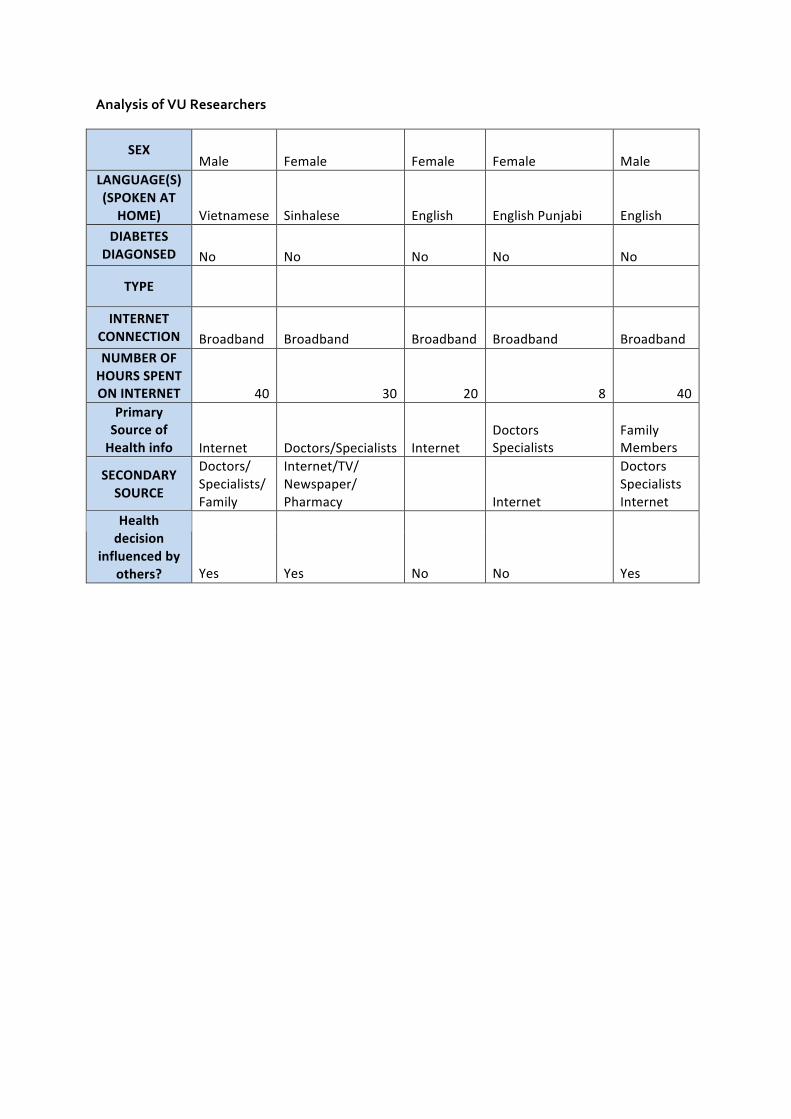
Analysis of VU Researchers
SEX Male Female Female Female Male
LANGUAGE(S) (SPOKEN AT
HOME) Vietnamese Sinhalese English English Punjabi English
DIABETES DIAGONSED No No No No No
TYPE
INTERNET CONNECTION Broadband Broadband Broadband Broadband Broadband NUMBER OF HOURS SPENT ON INTERNET 40 30 20 8 40
Primary Source of Health info Internet Doctors/Specialists Internet
Doctors Specialists
Family Members
SECONDARY SOURCE
Doctors/ Specialists/ Family
Internet/TV/ Newspaper/ Pharmacy Internet
Doctors Specialists Internet
Health decision
influenced by others? Yes Yes No No Yes
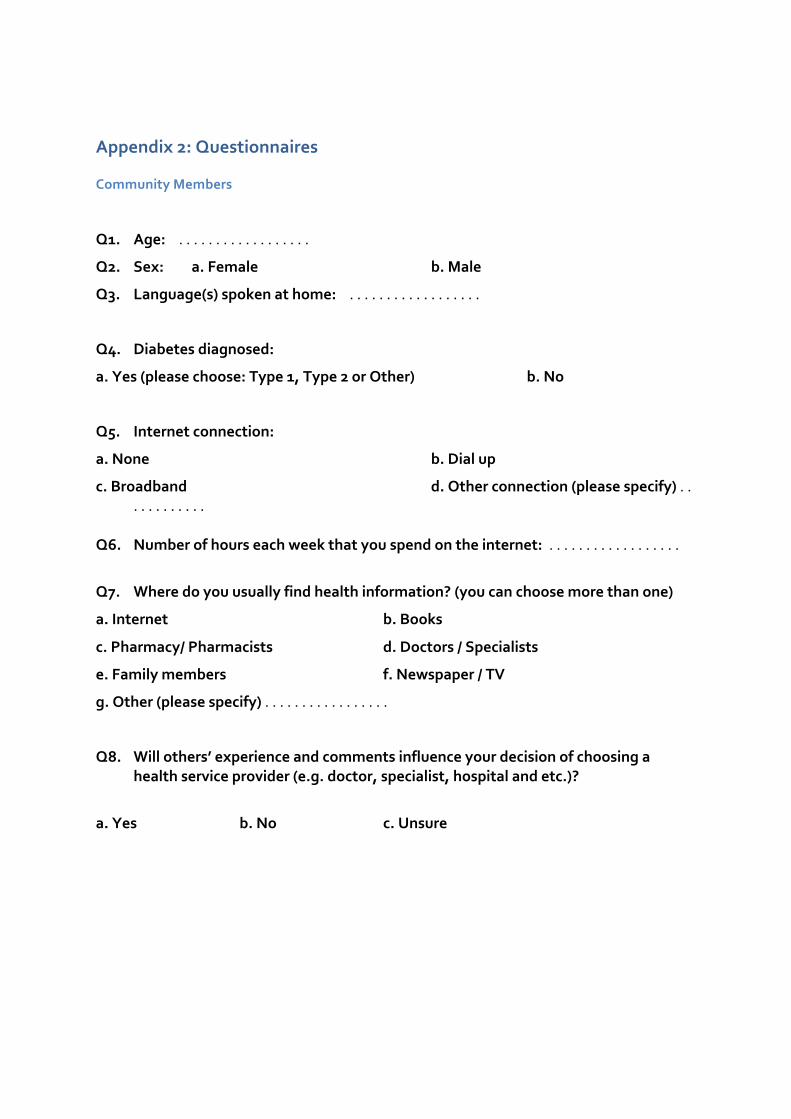
Appendix 2: Questionnaires
Community Members
Q1. Age: . . . . . . . . . . . . . . . . . .
Q2. Sex: a. Female b. Male
Q3. Language(s) spoken at home: . . . . . . . . . . . . . . . . . .
Q4. Diabetes diagnosed:
a. Yes (please choose: Type 1, Type 2 or Other) b. No
Q5. Internet connection:
a. None b. Dial up
c. Broadband d. Other connection (please specify) . . . . . . . . . . . .
Q6. Number of hours each week that you spend on the internet: . . . . . . . . . . . . . . . . . .
Q7. Where do you usually find health information? (you can choose more than one)
a. Internet b. Books
c. Pharmacy/ Pharmacists d. Doctors / Specialists
e. Family members f. Newspaper / TV
g. Other (please specify) . . . . . . . . . . . . . . . . .
Q8. Will others’ experience and comments influence your decision of choosing a health service provider (e.g. doctor, specialist, hospital and etc.)?
a. Yes b. No c. Unsure
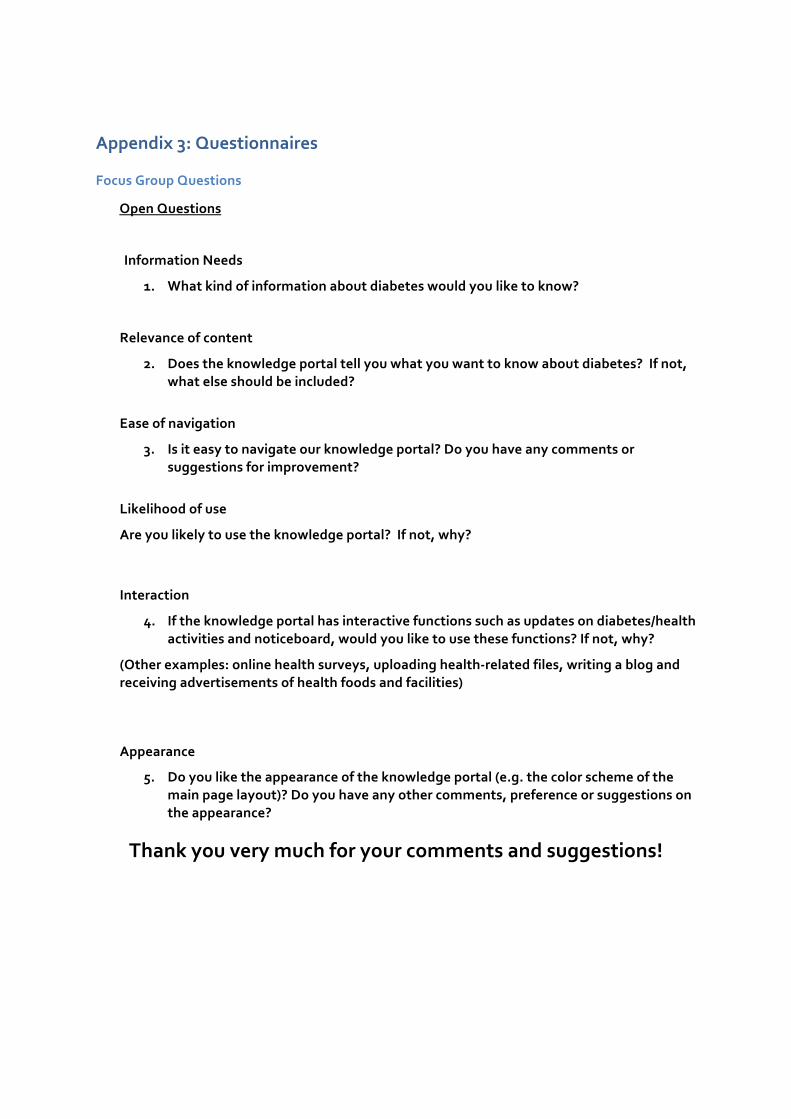
Appendix 3: Questionnaires
Focus Group Questions
Open Questions
Information Needs
1. What kind of information about diabetes would you like to know?
Relevance of content
2. Does the knowledge portal tell you what you want to know about diabetes? If not, what else should be included?
Ease of navigation
3. Is it easy to navigate our knowledge portal? Do you have any comments or suggestions for improvement?
Likelihood of use
Are you likely to use the knowledge portal? If not, why?
Interaction
4. If the knowledge portal has interactive functions such as updates on diabetes/health activities and noticeboard, would you like to use these functions? If not, why?
(Other examples: online health surveys, uploading health-‐related files, writing a blog and receiving advertisements of health foods and facilities)
Appearance
5. Do you like the appearance of the knowledge portal (e.g. the color scheme of the main page layout)? Do you have any other comments, preference or suggestions on the appearance?
Thank you very much for your comments and suggestions!
Appendix 4: Images of Knowledge Portal

i This information is adapted from the ACCD Knowledge Portal In-‐Community Consultation Plan, July 2nd 2010.
ii This information is adapted from the ACCD Knowledge Portal In-‐Community Consultation Plan, July 2nd 2010.