
Complete_thesis.pdf - the University of Groningen research ...
207
University of Groningen Moving forward to achieve universal health coverage in Indonesia Wasir, Riswandy DOI: 10.33612/diss.124431881 IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2020 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Wasir, R. (2020). Moving forward to achieve universal health coverage in Indonesia. University of Groningen. https://doi.org/10.33612/diss.124431881 Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 08-01-2022
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Complete_thesis.pdf - the University of Groningen research ...
University of Groningen
Moving forward to achieve universal health coverage in IndonesiaWasir, Riswandy
DOI:10.33612/diss.124431881
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2020
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Wasir, R. (2020). Moving forward to achieve universal health coverage in Indonesia. University ofGroningen. https://doi.org/10.33612/diss.124431881
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 08-01-2022

Moving Forward to Achieve Universal Health Coverage in Indonesia | 1
Moving Forward to Achieve Universal Health Coverage in Indonesia
Progress and Challenges
Riswandy Wasir

2 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Moving Forward to Achieve Universal Health Coverage in Indonesia
Progress and Challenges
Author : Riswandy Wasir
Cover design : Kihajar (graphic design) and Riswandy Wasir (concept)
Layout : Kihajar
Printing : Masagena Printing
ISBN (book) : 978-94-034-2694-5
ISBN (electronic version) : 978-94-034-2695-2
The work presented in this thesis was funded by DIKTI Scholarship, the Ministry of
Research, Technology and Higher Education of Republic of Indonesia and the University of
Groningen, the Netherlands. This thesis was conducted within Research Institute for Health
Research (SHARE). Printing of this thesis was financially supported by University Medical
Center Groningen (UMCG), university of Groningen, and the University Library of the
University of Groningen
Copyright © Riswandy Wasir, Groningen 2020.
All rights reserved. No part of this thesis may be reproduced or transmitted in any form by
any means, electronically or mechanically by photocopying, recording, or otherwise, without
written permission of the author. The copyright of previously published articles of this thesis
remains with the publishers or journals

Moving Forward to Achieve Universal Health Coverage in Indonesia | 3
\
…to my beloved family, respectful teachers, and kind friends

4 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Paranymphs
Muh. Akbar Bahar
Sylvi Irawati

Moving Forward to Achieve Universal Health Coverage in Indonesia | 5
Moving Forward to Achieve Universal Health Coverage
in Indonesia
Progress and challenges
PhD thesis
to obtain the degree of PhD at the
University of Groningen
on the authority of the
Rector Magnificus Prof. C. Wijmenga
and in accordance with
the decision by the College of Deans.
This thesis will be defended in public on
Wednesday 13 May 2020 at 9.00 hours
by
Riswandy Wasir
born on 12 January 1988
in Makassar, Indonesia

6 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Supervisors
Prof. E. Buskens
Prof. M.J. Postma
Co-supervisor
Dr. W. Goettsch
Assessment Committee
Prof. K. Taxis
Prof. A.K. Mantel
Prof. S.A. Reijneveld

Moving Forward to Achieve Universal Health Coverage in Indonesia | 7
TABLE OF CONTENTS
Chapter 1 General Introduction .................................................................... 9
Chapter 2 Use of medicine pricing and reimbursement policies for universal
health coverage in Indonesia ........................................................ 19
Chapter 3 The implementation of health technology assessment (HTA) in
medicine pricing and reimbursement policies in Indonesia:
insights from multiple stakeholders .............................................. 69
Chapter 4 Trends and projection of health financing for universal health
coverage in Indonesia ................................................................... 111
Chapter 5 Long term risk of incidence of cardiovascular events in Asian
Populations: Systematic review and Meta-Analysis of
Population-Based Cohort Studies ................................................. 131
Chapter 6 Discussion and future perspective ................................................. 167
Addendum Summary ....................................................................................... 183
Samenvatting ................................................................................ 187
Ringkasan ..................................................................................... 193
Acknowledgement ....................................................................... 197
PhD Portofolio .............................................................................. 201
About the Author .......................................................................... 204
Tentang Penulis ............................................................................ 205
Research Institute for Health Research (SHARE) ......................... 206

8 | Moving Forward to Achieve Universal Health Coverage in Indonesia

Moving Forward to Achieve Universal Health Coverage in Indonesia | 9
Chapter 1
GENERAL INTRODUCTION
10 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Concept of universal health coverage
The united nations have committed to achieve universal health coverage (UHC) as
part of the sustainable development goals (SDGs) by 2030[1]. The world health
organizations (WHO) states that UHC has been achieved in a country when all
people and communities can use the promotive, preventive, curative, rehabilitative
and palliative health services they need, of sufficient quality to be effective, while
also ensuring that the use of these services does not expose the user to financial
hardship[2-4]. In order for countries to move towards achieving UHC, a
comprehensive health benefits package needs to be outlined, i.e., a set of healthcare
services that can feasibly be financed and provided by the agency of UHC.
Furthermore, out-of-pocket (OOP) payments, direct payments made by individuals
to health care provider at the time of service use should be reduced or eliminated
[5,6]. The WHO outlines that UHC is achieved by a country when OOP expenditures
fall below 20% of total healthcare expenditures. Furthermore, the WHO urged that
government spending on healthcare should be at least 4% of gross domestic product
(GDP) to achieve UHC[5,7,8].
Indonesia’s health system transformation towards UHC
As a member of the United Nations, Indonesia is also aiming to achieve UHC. The
concept of UHC is in line with the Indonesian constitution or Undang-Undang
Dasar 1945, article 28. Health is a basic right of every individual, and all citizens
are entitled to health services including the poor. In 2004, the government legalized
a national social security system (SJSN) law, which became the basis to regulate the
provision of health insurance for all Indonesian people. Since then, between 2004
and 2013, there were several state-owned insurance companies proffered by the
government of Indonesia. They were Asuransi Kesehatan (Askes, for civil servants),
Asuransi Sosial Angkatan Bersenjata (Asabri, for military personnel), Jaminan
Sosial Tenaga Kerja (Jamsostek, social security program for labourers), Jaminan
Kesehatan Masyarakat (Jamkesmas, for poor and near poor), Jaminan Kesehatan
Daerah (Jamkesda, for poor and near poor in several provinces)[9]. The
implementation of various kinds of social health insurances were among the efforts
1
Chapter One

Moving Forward to Achieve Universal Health Coverage in Indonesia | 11
of the Indonesian government to provide health protection to all Indonesian people.
It was noted, however, that the fragmented health insurance schemes made health
care spending and quality of healthcare services difficult to control. In addition,
between 2002 and 2013, the OOP payments still were the dominant resource,
comprising over 50% of total health expenditures. Thus, back then UHC still
appeared a distant goal for Indonesia[10].
Therefore, at the beginning of 2014, a transformation of the health
insurance system was initiated in Indonesia. All the fragmented health insurances
were integrated into a new national health insurance, which is known as Jaminan
Kesehatan Indonesia-Kartu Indonesia Sehat (JKN-KIS). In this new system, a new
health insurance provider, which is called Badan Penyelenggara Jaminan Sosial-
Kesehatan (BPJS-Kesehatan) was also introduced. Also, the government of
Indonesia officially announced their plan to achieve UHC by 2020 through the JKN-
KIS[11].
In parallel with the introduction of JKN-KIS, several new medicine policies
were implemented as well. First, the national formulary was launched as a medicine
reimbursement policy, and also as health benefits packages for medicines on the
JKN-KIS. The formulary provides a list of medicines covered by the BPJS-
Kesehatan. All the medicines listed in the national formulary should be available in
the healthcare facilities. Second, a so-called e-Catalogue was introduced as a
medicine pricing policy. This provides lists of medicines with specifications, prices,
and suppliers. All healthcare facilities are obliged to purchase medicines, especially
medicines listed in the national formulary, through the e-Catalogue. In addition, a
few months after the launch of the national formulary and the e-Catalogue, the
Ministry of Health established the health technology assessment committee to assess
the potential of medicines that should be included or excluded from the national
formulary and the e-Catalogue. The introduction of several new medicine policies
was expected to support the JKN-KIS program in terms of reducing or eliminating
OOP payments, and subsequently help achieving UHC in Indonesia[10-17].
1
General Introduction

12 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Challenges for the JKN-KIS to achieve UHC by 2020
Indonesia is the fourth most populous and the largest archipelagic country in the
world, with 252 million inhabitants spread over 17.744 islands in 2014[18]. Providing
universal healthcare access to the whole society by 2020 was an ambitious goal of
the Indonesian government. With a large population and relying on one insurance
provider in the JKN-KIS program, Indonesia will run the largest single-payer system
in the world.
Challenges on medicines management
The high proportion of OOPs for medical bills was the main motive for the UHC
declaration at the World Health Assembly meeting in 2005. In addition, the WHO
highly recommends to the low middle-income countries (LMICs) to eliminate
unnecessary spending on medicines for achieving UHC. This is due to the fact that
the proportion of OOPs in healthcare spending for medicines is high, ranging
between 50% and 90% in LMICs. Moreover, medicine expenditure accounted for up
to 67% of total health expenditure[19-21].
As a low middle-income country, reducing OOPs for medicines and
eliminating sources of inefficiency in medicines procurement are major challenges
for Indonesia to achieve UHC. Before the implementation of the JKN-KIS, most
OOP payments in healthcare were for medicines. The price of one type of medicine
also varies in the same area. In addition, the medicines formulary provided by the
previous health insurances, such as Askes, Jamkesmas, Jamkesda, were also lacking
an evidence base [22-24].
Challenges for the health financing system
Health financing is a core function of health systems concerned with the
mobilization, accumulation, and allocation of financial resources to cover the cost of
health needs of the people, individually and collectively [25]. Health financing is
instrumental and intrinsic for countries like Indonesia to move forward towards
UHC. As a single-payer, BPJS-Kesehatan not only collects health budgets for the
sustainability of the JKN-KIS program, but also ensures that budgets are allocated in
line with the UHC target[11].
1
Chapter One
Moving Forward to Achieve Universal Health Coverage in Indonesia | 13
Prior to the implementation of the JK-KIS, Indonesia already was facing
the challenge of increasing health expenditure at the national level. Between 1995
and 2014, instead of relying on government healthcare financing, Indonesia was
dominated by OOP expenditures[26]. In order to accelerate progress towards UHC
and meeting its population coverage target by 2020, the government of Indonesia
have had to manage their health financing system to ensure that the available
resources would meet financial demands in the communities.
Challenges concerning the epidemiological condition
Already before the implementation of the JKN-KIS, efforts made by the Indonesian
government to make Indonesian people healthier indeed have shown significant
progress. This may be concluded from the increasing life expectancy of Indonesian
people by 6 years, i.e., from 63 years in 1990 to 69 years by 2014[27]. Notably, this
raises a new demographic situation in Indonesia, and the JKN-KIS faces a new
challenge. With an ageing population the proportional mortality due to NCDs
increased from 37% in 1990 to 73% in 2014, which have in the meantime become
the main cause of death in Indonesia[28]. The rising burden of chronic non-
communicable diseases in low and middle-income countries (LMICs), like
Indonesia, has major implications for the ability of these countries to achieve UHC.
Over 60 percent of people living with NCDs have experienced catastrophic health
expenditures, which is spending on health care that exceeds a certain proportion of a
household‘s income[26].
Cardiovascular diseases (CVDs) are the leading cause of death and
disability among NCDs. CVDs account for 37% of deaths in Indonesia[27]. As the
biggest disease burden CVD also represents a high financial risk in BPJS-
Kesehatan[26]. It is critical to consider how underlying trends in epidemiology will
impact the scheme‘s expenditures, and its overall financial sustainability. It would
appear that the BPJS-Kesehatan should find sufficient resources to cover the entire
population and indeed achieve UHC by 2020.
1
General Introduction

14 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Gaps of knowledge
In moving forward towards achieving UHC, the JKN-KIS program might
exploit several opportunities that exist for improving the efficiency, effectiveness,
and sustainability of the health system. The role of new medicines policies, the e-
Catalogue and the national formulary, should be fully utilized to support the JKN-
KIS for achieving UHC in Indonesia. The use of the e-Catalogue could homogenize
medicine price in the same region and help to improve effectiveness, efficiency, and
transparency in medicines procurement. The use of national formulary should ensure
the availability of good quality, efficacious, and affordable medicines. These
medicine policies should help Indonesia to reduce OOP payments, especially for
medicines. Furthermore, the use of health technology assessment should also be
implemented in the process of medicines selection on the e-Catalogue and the
national formulary to increase the evidence base and minimize unnecessary
spending. Furthermore, estimating future health spending, and possible sources for
funding is vital for effective health policy. With reliable spending forecasts, decision
makers may adjust long term planning and process. As JKN-KIS continues to
scaleup toward UHC, critical policy decisions are required to increase revenue,
rationalize healthcare expenditure, and anticipate any future deficits to ensure the
scheme is managed sustainably. Looking at the future burden of disease in Indonesia
will help the Indonesia to wisely spending their resources on health.
Unfortunately, there are no studies that report the extent of the progress of
the national formulary, e-Catalogue and the health technology assessment since their
implementation together with the JKN-KIS program in 2014. In addition, detailed
information on the trends of health financing in Indonesia is needed to report the
JKN-KIS‘ financial status. Next characteristics of its design, key arrangements
affecting choices for financial sustainability, key trends in revenues and
expenditures affecting its future financial position, and potential policy actions to
improve its future sustainability are needed. Finally, a detailed study on the future
burden of disease is necessary to make appropriate planning in providing access and
financial protection to all Indonesian people. All these aspects are aimed to be at
least partly covered with this thesis.
1
Chapter One

Moving Forward to Achieve Universal Health Coverage in Indonesia | 15
Thesis objectives
The general aim of this thesis is to evaluate the implementation of UHC in
Indonesia. A number of key issues, and progress of the JKN-KIS program toward
UHC are describing in chapter 2,3, and 4. In chapter 2, we assess the utilization of
the e-Catalogue and the national formulary as medicine pricing and reimbursement
policies for UHC in Indonesia. In chapter 3, we assess the implementation of HTA
in the use of the e-Catalogue and the NF. In chapter 4, we describe the trend and
project the health financing system in Indonesia. Furthermore, in chapter 5, we
estimate the long-term (>10 years) CVD burden, as well as underlying risk factors in
Asian populations. Chapter 6 presents an overview, general discussion, implications
and future perspectives related to the findings of the studies presented in this thesis.
1
General Introduction

16 | Moving Forward to Achieve Universal Health Coverage in Indonesia
References
1. Kieny MP, Bekedam H, Dovlo D,
et al. Strengthening health systems
for universal health coverage and
sustainable development. Bull
World Health Organ.
2017;95(7):537-539.
2. Kutzin J, Witter S, Jowett M,
Bayarsaikhan D. Developing a
national health financing strategy:
A reference guide.geneva: World
health organization; (health
financing guidance no 3). . 2017.
3. World Health Organization.
Tracking universal health coverage:
2017 global monitoring report.
World Health Organization and
International Bank for
Reconstruction and Development/
The World Bank. 2017.
4. World Health Organization.
Tracking universal health
coverage: First global monitoring
report. World Health Organization;
2015.
5. World Health Organization. The
world health report: Health systems
financing: The path to universal
coverage: Executive summary. .
2010.
6. World Health Organization. World
health statistics 2016: Monitoring
health for the SDGs sustainable
development goals. World Health
Organization; 2016.
7. Jowett M, Brunal MP, Flores G,
Cylus J. Spending targets for
health: No magic number. World
Health Organization; 2016.
8. World Health Organization. Health
financing strategy for the asia
pacific region (2010-2015). Manila:
WHO Regional Office for the
Western Pacific; 2009.
9. Pisani E, Olivier Kok M, Nugroho
K. Indonesia's road to universal
health coverage: A political
journey. Health Policy Plan.
2017;32(2):267-276.
10. Wasir R, Irawati S, Makady A, et
al. Use of medicine pricing and
reimbursement policies for
universal health coverage in
indonesia. PloS one.
2019;14(2):e0212328.
11. Menteri Kesehatan Republik
Indonesia. Peraturan menteri
kesehatan republik indonesia
1
Chapter One

Moving Forward to Achieve Universal Health Coverage in Indonesia | 17
nomor 28 tahun 2014 tentang
pedoman pelaksanaan program
jaminan kesehatan nasional. ; 2014.
12. Menteri Kesehatan Republik
Indonesia. Peraturan menteri
kesehatan republik indonesia
nomor 48 tahun 2013 tentang
petunjuk pelaksanaan pengadaan
obat dengan prosedur E-
purchasing berdasarkan E-
catalogue. ; 2013.
13. Menteri Kesehatan Republik
Indonesia. Peraturan menteri
kesehatan republik indonesia
nomor 63 tahun 2014 tentang
pengadaan obat berdasarkan
katalog elektronik (E-catalogue). ;
2014.
14. Menteri Kesehatan Republik
Indonesia. Keputusan menteri
kesehatan republik indonesia nomor
HK.02.02/ menkes/ 523/ 2015
tentang formularium nasional. .
2015.
15. Menteri Kesehatan Republik
Indonesia. Keputusan menteri
kesehatan republik indonesia nomor
171/ menkes/ SK/ IV/ 2014 tentang
komite penilaian teknologi
kesehatan. . 2014.
16. Menteri Kesehatan Republik
Indonesia. Keputusan menteri
kesehatan RI no.
HK.02.02/menkes/422/2016
tentang komite penilaian teknologi
kesehatan. . 2016.
17. Wasir R, Irawati S, Makady A, et
al. The implementation of HTA in
medicine pricing and
reimbursement policies in
indonesia: Insights from multiple
stakeholders. PLoS One.
2019;14(11):e0225626.
18. Kemenkes R. Profil kesehatan
indonesia tahun 2014. Jakarta:
Kemenkes RI. 2015.
19. Rickwood S, Kleinrock M, Nunez-
Gaviria M, Sakhrani S, Aitken M.
The global use of medicines:
Outlook through 2017. IMS
Institute for Healthcare
Informatics. 2013:5.
20. Bigdeli M, Laing R, Tomson G.
Medicines and universal health
coverage: Challenges and
opportunities. . 2015.
21. Tangcharoensathien V, Patchara-
narumol W, Ir P, et al. Health-
financing reforms in southeast asia:
Challenges in achieving universal
1
General Introduction
18 | Moving Forward to Achieve Universal Health Coverage in Indonesia
coverage. The Lancet. 2011;377
(9768):863-873.
22. Van Doorslaer E, O'Donnell O,
Rannan-Eliya RP, et al. Paying out-
of-pocket for health care in asia:
Catastrophic and poverty impact.
Erasmus University, Rotterdam and
IPS, Colombo. 2005.
23. Sparrow R, Suryahadi A, Widyanti
W. Social health insurance for the
poor: Targeting and impact of
indonesia's askeskin programme.
Soc Sci Med. 2013;96:264-271.
24. Niëns L, Brouwer W. Measuring
the affordability of medicines:
Importance and challenges. Health
Policy. 2013;112(1-2):45-52.
25. World Health Organization. The
world health report 2000: Health
systems: Improving performance.
World Health Organization; 2000.
26. Mahendradhata Y, Laksono
Trisnantor, Shita Listyadewi, et al.
The republic of indonesia health
system review. . 2017;Vol. 7 No. 1
Asia Pacific Observatory on Health
Systems and Policies(World Health
Organization).
27. Mboi N, Murty Surbakti I,
Trihandini I, et al. On the road to
universal health care in indonesia,
1990-2016: A systematic analysis
for the global burden of disease
study 2016. Lancet. 2018.
28. World Health Organization.
Noncommunicable diseases:
Progress monitor 2017. . 2017.
1
Chapter One
Moving Forward to Achieve Universal Health Coverage in Indonesia | 19
Chapter 2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia
Use of medicine policy for universal health
coverage in Indonesia
Riswandy Wasir
Sylvi Irawati
Amr Makady
Maarten Postma
Wim Goettsch
Erik Buskens
Talitha Feenstra
This chapter is based on the published manuscript:
Wasir R, Irawati S, Makady A, Postma M, Goettsch W, Buskens E, et al. (2019) Use
of medicine pricing and reimbursement policies for universal health coverage in
20 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Abstract
Objectives
This study aimed to define the problems of the current use of the e-Catalogue and
the national formulary (NF)—two elements of medicine pricing and reimbursement
policies in Indonesia for achieving universal health coverage (UHC)—by examining
the knowledge and attitudes of stakeholders. Specifically, to investigate (1) the
perceived challenges involved in the further implementation of the e-Catalogue and
the NF, (2) reasons of prescribing medicines not listed in the NF, and (3) possible
improvements in the acceptance and use of the e-Catalogue and the NF.
Methods
Semi-structured interviews were conducted with stakeholders (policymakers,
healthcare providers, a pharmaceutical industry representative, and experienced
patients) to collect the qualitative data. The data was analysed using directed content
analysis, following the guidelines of the COnsolidated criteria for REporting
Qualitative studies (COREQ) in reporting the findings.
Results
Interestingly, 20 of 45 participants decided to withdraw from the interview due to
their lack of knowledge of the e-Catalogue and the NF. All 25 stakeholders who
fully participated in this research were in favor of the e-Catalogue and the NF.
However, interviewees identified a range of challenges. A major challenge was the
lack of harmonization between the lists of medicines in the e-Catalogue and the NF.
Several system and personal reasons for prescribing medicines not listed in the NF
were identified. Important reasons were a lack of incentives for physicians as well as
a lack of transparent and evidence-based methods of selection for the medicines to
be listed in the NF.
2
Chapter two

Moving Forward to Achieve Universal Health Coverage in Indonesia | 21
Conclusions
The e-Catalogue and the NF have not been fully utilized for achieving UHC in
Indonesia. Some possible improvements suggested were harmonization of medicines
listed in the e-Catalogue and the NF, restructuring incentive programs for
prescribing NF medicines, and increasing the transparency and evidence-based
approach for selection of medicines listed in the e-Catalogue and the NF.
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia
22 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Introduction
Many countries strive for universal health coverage (UHC), a concept recommended
by the World Health Organization (WHO) to ensure that all people have access to
health services they need without suffering financial hardship. One of the goals of
UHC is to eliminate out-of-pocket payments (OOPs), a direct payment made by an
individual to healthcare providers at the time of service use[1,2]. OOPs can be a great
catastrophe for the family of a sick individual[3]. In low middle-income countries
(LMICs), the proportion of OOPs in healthcare spending for medicines is high,
ranging from 50% to 90%[4]. Moreover, medicine expenditure accounted for up to
67% of total health expenditure[5]. Appropriate policies are needed to reduce OOPs
on medicines and to control medicine expenditure[6]. Furthermore, in order to move
towards UHC, WHO has recommended to incorporate health technology assessment
(HTA) to establish policies on medicines. The WHO defines HTA as the systematic
evaluation of properties, effects and/or impacts of health technologies and
interventions[7]. HTA is a critical component of evidence-based policy decision
making[8,9].
In line with the global trends, Indonesia also makes a concerted effort to
achieve UHC. Prior to 2014, Indonesians were supported by several social health
insurances. The three biggest social health insurances were Asuransi
Kesehatan (Askes, for civil servants and the military), Jaminan Kesehatan
Masyarakat (Jamkesmas, for poor and near poor), and Jaminan Sosial Tenaga
Kerja (Jamsostek, social security program for labourers). Notably, the fragmented
health insurance schemes made health care spending and service quality difficult to
control. Regarding medicines, previous studies have reported a large number of
different medicine formularies existed with an unclear evidence-base[10]. In addition,
OOPs were still dominant[11,12], e.g. the OOP in total was 49% in 2013[13].
In 2014, the Government of Indonesia introduced a new health insurance
scheme, known as Jaminan Kesehatan Nasional–Kartu Indonesia Sehat (JKN-KIS),
which was managed by Indonesia‘s National Healthcare Security Agency,
namely Badan Penyelenggara Jaminan Sosial–Kesehatan (BPJS-Kesehatan). JKN-
KIS was the result of a merger of pre-existing social health insurance schemes.
2
Chapter two

Moving Forward to Achieve Universal Health Coverage in Indonesia | 23
Furthermore, the Ministry of Health (MOH) introduced several new medicine
policies for supporting the implementation of the JKN-KIS program.
First, the e-Catalogue is a national medicine pricing policy and exists since
2013. The MOH proposes medicines, usually at the substance level (e.g.
paracetamol), with specifications (dosage and types e.g. tablet, liquid, capsules) to
LKPP (Lembaga Kebijakan Pengadaan Barang Jasa Pemerintah/ National Public
Procurement Agency). Then, LKPP writes a tender for supply at a national scale and
selects the preferred suppliers. As a result, the e-Catalogue provides a list of
medicines with specifications, prices, and suppliers. All healthcare facilities are
obliged to purchase medicines through the e-Catalogue. Nevertheless, healthcare
facilities are allowed to perform their own tender for medicines that they need and
are not listed in the e-Catalogue[14–16].
Second, the national formulary (NF) is a medicine reimbursement policy. It
provides a list of medicines covered by BPJS-Kesehatan. The MOH has established
the NF committee that is in charge of compiling the list of medicines in the NF. All
healthcare facilities and healthcare professionals may propose medicines to be
included in the NF. These medicines are then selected by the NF committee using
several criteria among which efficacy, safety, marketing authorization, and benefit-
risk ratio. In the NF, international non-proprietary names (INN) are used. The first
NF was cmpiled in 2013 referring to formularies used in the previous health
insurances in Indonesia and the last edition of the Indonesian essential medicines
list. The list of medicines in the NF is revised at least every two years. The last
revision was in 2017. All medicines listed in the NF should be available in the
healthcare facilities. The director of the hospital and the hospital‘s medical
committee should approve when healthcare facilities prescribe medicines not listed
in the NF. Notably, the approved medicine is not reimbursed by BPJS-
Kesehatan[15,17,18], which implies either OOPs or payment from the hospital is
needed.
Third, the use of HTA was introduced to assess new medicines which
might have potential to be included in the e-Catalogue and the NF. The assessment
is to be conducted by the HTA committee. This committee was formed by the MOH
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia

24 | Moving Forward to Achieve Universal Health Coverage in Indonesia
in April 2014, then renewed in 2016[19,20]. The current HTA committee consists of
eight senior health scientists and one employee of the MOH. They are supported by
a technical staff (thirteen clinicians, two MOH employees, one engineer, and four
secretaries). Currently, the main task of the HTA committee is to develop their
program. The guidelines of the JKN-KIS state that the HTA committee is
responsible for providing recommendations to the MOH regarding the list of
healthcare services, including medicines, which are covered by the BPJS-Kesehatan.
This implies the HTA committee is responsible for advice regarding the NF[15,20,21].
The Indonesian healthcare system since the implementation of the JKN-
KIS shows several positive changes. Healthcare facilities seldom perform their own
tender for procuring medicines[14]. Furthermore, instead of different formularies for
each insurance scheme, there is a single NF. The MOH introduced the e-Catalogue
and the NF, expecting that they would improve effectiveness, efficiency, and
transparency in medicines procurement, as well as ensure the availability of good
quality, efficacious, and affordable medicines[16,22]. Thus, this should help Indonesia
to achieve UHC.
However, problems regarding the practical use of the e-Catalogue and the
NF have been reported. For instance, it was found that many public healthcare
facilites rarely use the e-Catalogue to procure medicines[23]. Moreover, of all
medicines prescribed in 2015, up to 40% were not listed in the NF[24]. This may
explain the increase of OOPs in 2015 to 50%[13]. Out of these, 70% were found to be
OOPs for medicines[25], which obviously contrasts the philosophy of UHC. The
obstacles hindering medicine pricing and reimbursement policies in Indonesia are
far from clear and need to be investigated.
This research aims to shed light on the current use of the e-Catalogue and
the NF by examining the knowledge and attitudes of stakeholders regarding the
JKN-KIS program, especially concerning the e-Catalogue and the NF. Therefore,
this research will investigate (1) the perceived challenges involved in the further
implementation of the e-Catalogue and the NF, (2) the reasons behind the
prescription of medicines not listed in the NF, and (3) possible improvements in the
acceptance and use of the e-Catalogue and the NF.
2
Chapter two

Moving Forward to Achieve Universal Health Coverage in Indonesia | 25
Methods
Semi-structured interviews were conducted to collect information about the
perception of stakeholders regarding the JKN-KIS program, the e-Catalogue, and the
NF. This study followed the reporting guidelines of the COnsolidated criteria for
REporting Qualitative studies (COREQ)[26] to ensure good quality. The COREQ
checklist provides guidance for explicit and comprehensive reporting of qualitative
studies.
Recruitment of participants
A purposive sampling method was used to recruit the stakeholders[27]. The following
stakeholders in the healthcare system were approached to participate: policymakers
(WHO members, NF committee, HTA committee, and JKN-KIS Agency),
pharmaceutical industry, healthcare providers (physicians and pharmacists), and
experienced patients. The stakeholders should have at least 5 years of relevant work
experience. Experienced patients were selected based on the duration of their health
insurance in Indonesia (at least 5 years) and their routine use of medicines (at least 5
years). In order to ensure that these patient criteria were met, participants were
recruited from the BPJS-Kesehatan‘s chronic disease management program
(Program pelayanan penyakit kronis, Prolanis)[28]. The selection criteria of at least 5
years of experience for stakeholders was used to ensure that they could explain the
healthcare system of Indonesia during and before the implementation of the new
medicine policies.
A rough estimation of participants needed for attaining saturation was then
made. A total of at least twenty-two stakeholders were aimed at. This was based on
at least two representatives for each group of policy makers, at least two
pharmaceutical industry representatives, at least four interviewees from each group
of healthcare providers, and at least four patients. The reason for having more
interviewees in the groups of healthcare providers and patients was our interest in
the practical issues of the e-Catalogue and the NF, for instance prescribing
medicines not listed in the NF.
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia
26 | Moving Forward to Achieve Universal Health Coverage in Indonesia
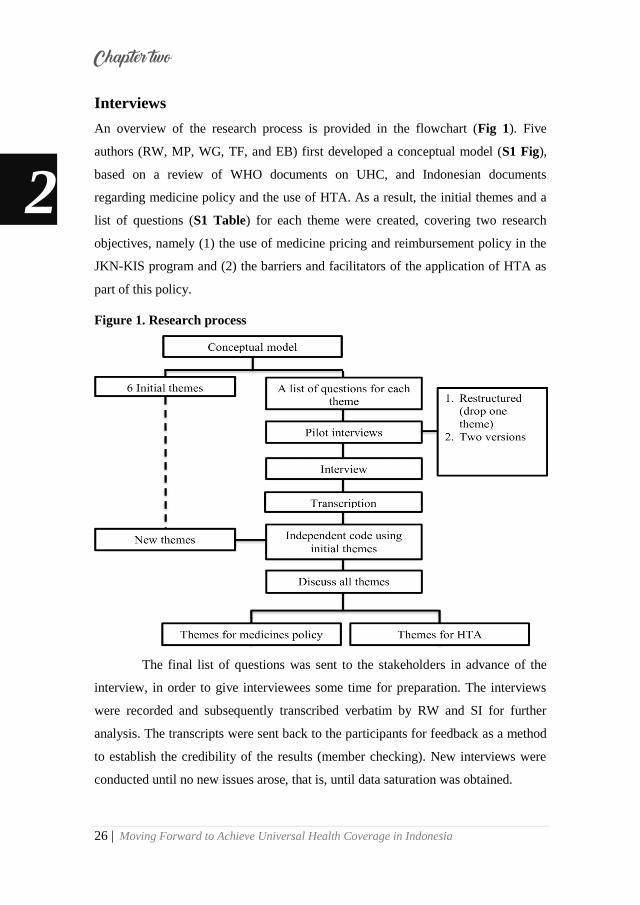
Interviews
An overview of the research process is provided in the flowchart (Fig 1). Five
authors (RW, MP, WG, TF, and EB) first developed a conceptual model (S1 Fig),
based on a review of WHO documents on UHC, and Indonesian documents
regarding medicine policy and the use of HTA. As a result, the initial themes and a
list of questions (S1 Table) for each theme were created, covering two research
objectives, namely (1) the use of medicine pricing and reimbursement policy in the
JKN-KIS program and (2) the barriers and facilitators of the application of HTA as
part of this policy.
Figure 1. Research process
The final list of questions was sent to the stakeholders in advance of the
interview, in order to give interviewees some time for preparation. The interviews
were recorded and subsequently transcribed verbatim by RW and SI for further
analysis. The transcripts were sent back to the participants for feedback as a method
to establish the credibility of the results (member checking). New interviews were
conducted until no new issues arose, that is, until data saturation was obtained.
2
Chapter two
Moving Forward to Achieve Universal Health Coverage in Indonesia | 27
Data analysis
Directed content analysis was conducted to systematically organize the qualitative
data into a structured format[29] using MAXQDA version 12.3.2. The two
Indonesian-speaking authors (RW and SI) read each transcript carefully. They then
coded the transcripts independently using the initial themes. The codes were
compared, and the non-fitting items were discussed. Texts that did not fit into one of
the initial themes and were mentioned by several interviewees were coded as new
themes. These new themes were then discussed with the research team (RW, SI,
MP, AM, WG TF, and EB) to ensure consensus. RW and SI then checked saturation
by theme. Saturation was reached when no new information was generated.
For the current study, four initial themes related to medicine policy were
analyzed, namely, (1) the development of medicine policy and national health
insurance, (2) medicine policy for UHC, (3) stakeholders‘ perspective and (4)
prescribing medicines not listed in the NF. The two remaining initial themes were
left aside. The first of these, barriers and promoting factors of HTA, was analyzed in
a separate study focusing on HTA. We skipped the final initial theme from the
interviews, since eliciting the interviewees‘ ideas regarding what conditions had the
largest burden of disease and the amount of expenditure for medications, was
impossible, as explained under interviews above.
Ethical considerations
Written informed consent (S2 File) was obtained from all participants. Before the
interviews, all participants were aware/understood that their participation was
voluntary and that they were free to stop the interview at any time. All participants
consented to review the verbatim transcript of their interview. The research plan and
the interviews to be conducted were reviewed by the University Medical Center
Groningen (UMCG) ethical review board, who deemed the study non-intrusive, and
subsequently provided a formal waiver statement, i.e., the study would not need
regular ethical approval.
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia

28 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Results
Participants
Aiming at about 22 final participants, a total of 51 different individuals were
approached during the recruitment process (S2 Table). Out of this number, 45
agreed to participate in this research. However, 9 withdrew after receiving list of
questions; 7 decided to stop their interviews before they were finished, since they
experienced difficulties in answering the questions and were not confident about
their answers; and 4 had no time for an interview, leaving a final number of 25
participants. This means that the remaining interviewed persons were, to a certain
degree, a select group with better knowledge than most stakeholders.
Classification of the twenty-five participants can be seen in Table 1.
Participants included policy makers (WHO members, HTA Committee, NF
Committee, JKN-KIS Agency), a medicine supplier (pharmaceutical industry),
healthcare providers (physician and pharmacist), and users (patients). On average,
the policymakers, the representative from the pharmaceutical industry and
healthcare providers had a work experience of 26 years, with 14 years as the
minimum. Furthermore, all patients interviewed had been enrolled in health
insurance in Indonesia for an average of 11 years at the time of interview.
2
Chapter two

Moving Forward to Achieve Universal Health Coverage in Indonesia | 29
Table 1: Classification of participants involved in the study
Participants Gender Age
(years)
Work
experience
(years)
Years using
public health
insurance
Policy makers
WHO Member Male 50 25 -
HTA Committee Female 53 28 -
HTA Committee Male 55 30 -
NF Committee Male 56 31 -
JKN-KIS Agency Female 51 26 -
JKN-KIS Agency Female 46 21 -
Medicine supplier
Pharmaceutical Industry Male 54 29 -
Healthcare Providers
Physician Male 58 33 -
Physician Male 59 34 -
Physician Male 66 41 -
Physician Male 44 19 -
Physician Male 51 26 -
Physician Female 54 29 -
Pharmacist Female 53 28 -
Pharmacist Male 50 25 -
Pharmacist Male 39 14 -
Pharmacist Male 42 17 -
Pharmacist Female 51 26 -
Pharmacist Female 40 19 -
Users
Patients Male 53 - 8
Patients Male 63 - 13
Patients Female 59 - 10
Patients Male 57 - 8
Patients Female 63 - 12
Patients Male 63 - 13
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia
30 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Interviews and analysis of transcripts
Semi-structured interviews were conducted with stakeholders between August 2016
and April 2017 by RW. Interviews were conducted face to face (16 participants) or
through video calls (9 participants) in locations comfortable to the participants. One
of the interviewees invited her colleague to answer the questions together. One
interview was conducted in English, while all others were in Bahasa. The average
time spent on each interview was about an hour. All predetermined codes were
covered by the interview results to a sufficient degree.
Several texts from the transcripts could not be coded into one of the five
initial themes (S1 Table), and were mentioned many times by different stakeholders.
Therefore, 18 new themes identified by RW and SI were discussed with AM, WG,
MP, TF, and EB to reach a consensus. Overall, 24 final themes were identified from
the transcripts, of which 17 (S3 Table) were used in this study while the 7 remaining
themes were left for further research and concerned HTA. The 17 themes in the
current research were categorized into 5 topics, which were given overarching
names (Fig 2).
2
Chapter two

Moving Forward to Achieve Universal Health Coverage in Indonesia | 31
Figure 2. Clustering the themes
Attitude towards JKN-KIS program
Attitude towards the e-Catalogue
Knowledge of JKN-KIS program
Knowledge of medicine policy before the JKN-KIS program
Knowledge of the JKN-
KIS program, the e-
Catalogue and the NF
Knowledge of medicine policy in the JKN-KIS program
Attitude towards the
JKN-KIS program, the
e-Catalogue and the NF
Attitude towards NF
Challenges for both the e-Catalogue and the NF
Challenges for the e-Catalogue
The challenges of
further implementation
of the e-Catalogue and
the NF
Challenges for the NF
Experience prescribing medicines not in the NF
Attitude towards prescribing medicines not in the NF
Reason for prescribing medicines not in the NF Prescribing medicines
not listed in the NF
Non-NF medicine most often prescribed
NF Medicines most often unavailable
LIST OF THEMES
TOPIC LIST
Recommendation to improve the e-Catalogue and the NF
Recommendation to avoid prescribing medicines not in the NF
Possible solutions for
optimizing the use of
the e-Catalogue and the
NF
Knowledge of the development of the e-Catalogue and the NF
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia

32 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Topic 1: Knowledge of the JKN-KIS program, the e-Catalogue and the NF
Among these 25 stakeholders, only patients had limited knowledge of the JKN-KIS
program, the e-Catalogue, and the NF. The other stakeholders could explain the
JKN-KIS program, the e-Catalogue, and the NF. Thus, to obtain accurate
information from the patients for the next theme, the interviewer explained the JKN-
KIS program to the patients, as well as the role and development of the e-Catalogue
and the NF, based on the guidelines of medicines policies in Indonesia[14,16,22].
Topic 2: Attitude towards the JKN-KIS program, the e-Catalogue, and the NF
All stakeholders endorsed the aim of the JKN-KIS program to achieve UHC by
2020 and approved of the existence of the e-Catalogue and the NF. However, they
emphasized that there were still some challenges to optimizing the implementation
of these policies.
“Yes, I agree. Why Universal Health Coverage by 2020, I hope it can be
achieved next year (2017).” [Patient 3]
―I agree with the existence of the e-Catalogue and the NF. However, the
development and the implementation of these policies still need to be optimized.‖ [Physician 3]
Topic 3: The challenges of further implementation of the e-Catalogue and the NF
One challenge for both the e-Catalogue and the NF that almost all stakeholders
mentioned was the lack of harmonization between the list of medicines in the e-
Catalogue and the NF. Some medicines in the NF are not listed in the e-Catalogue
and vice versa. As a result, some NF medicines were in limited supply and difficult
to provide and some were not even available at healthcare facilities. Furthermore,
lack of harmonization between the e-Catalogue and the NF implied that healthcare
facilities did not always use the e-Catalogue to procure medicines. Consequently,
the prices of medicines were higher than needed.
―If there were NF medicines that should be provided by the healthcare facilities,
but these medicines were not in the e-Catalogue, this confused the medicine
procurement committee, which would then have to spend time obtaining the
standard price of the NF medicine. The price of medicines that has been listed in the e-Catalogue is much cheaper than previous price‖ [Physician 2]
2
Chapter two

Moving Forward to Achieve Universal Health Coverage in Indonesia | 33
In fact, the Indonesian government allows the procurement of NF
medicines not listed in the e-Catalogue with the approval of the hospital‘s medical
committee. However, approval often takes a long time.
―To get claims from BPJS-Kesehatan, we ask the approval of the medical
committee to help set the price. We usually wait for unpredictable lengths of time. It takes a long time to get approval.‖ [Pharmacist 6]
A second challenge for both the e-Catalogue and the NF was the presence
of a poor distribution system of medicines in combination with the geographical
conditions of Indonesia. It is not easy to distribute NF medicines in a short period of
time to all locations in Indonesia. This was mentioned in various ways by many
participants.
“Our country is vast. Distributing medicines in Jakarta will be different from
distributing in Papua; the difficulties of distribution in Papua are great. Maybe
the medicine is available, but it gets there too late. If the healthcare provider
does not put the RKO (Plan of Medicine Needs) online, the pharmaceutical
industry cannot anticipate demand. Now the pharmaceutical industry is trying to anticipate but it is too late.‖ [Policymaker 4]
A challenge mentioned primarily by healthcare providers was that of the
low price of medicines in the e-Catalogue. Consequently, some pharmaceutical
industries were unable to provide NF medicines to healthcare facilities. If the
pharmaceutical industry is pressed to provide the medicine at a low price, the quality
of the medicine may also be lower. This is possible since no agency is responsible
for controlling the good manufacturer practices (GMP) of pharmaceutical industry
after they won the tender.
―The price of the medicine set in the e-Catalogue is too low. So, they (the
pharmaceutical industry) reduce their operating expenses. It is feared that
economizing on operational expenses will put the quality of the medicines at
risk.‖ [Pharmacist 4]
“The requirement to take part on a tender of medicines on the e-Catalogue is
very simple. The most important thing is to have a GMP certificate. However,
no one checked the pharmaceutical industry after they won tender.”
[Pharmaceutical Industry]
However, participants also stated that the low price of medicine in the e-
Catalogue is caused by the pharmaceutical industry itself. Pharmaceutical firms bid
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia
34 | Moving Forward to Achieve Universal Health Coverage in Indonesia
low prices in order to win tenders and obtain the right to distribute medicines
throughout Indonesia. Moreover, BPJS-Kesehatan was not involved in price-setting
even though it is stated in the National Social Security System (SJSN) Law.
―The price now deemed too low by the pharmaceutical industry is actually a
result of competition among pharmaceutical firms regarding the supply of NF
medicines through the e-Catalogue. So even though the estimated price was
first set quite high – for example, paracetamol per tablet is set at a price of 70
rupiahs – because of the competition, an offer made was far below the price of
70. The goal of these firms is to win the tender.‖ [Pharmaceutical Industry]
―BPJS-Kesehatan is currently losing its power because of the tariff-setting by
the Ministry of Health. In the National Social Security System (SJSN) Law, it is
clear that the BPJS-Kesehatan is mandated to develop health system services
and set prices and tariffs.‖ [Policymaker 5]
Finally, it was observed that the NF was not the only reimbursement policy
considered. For example, several hospitals have developed their own formularies.
Such formularies list additional medicines not on the NF medicine list.
―A hospital formulary is required by every hospital in Indonesia. The hospital
formulary partially refers to the NF. For additional medicines not listed in the
NF, patients do not have to pay, as long as the patients are participants in the
JKN-KIS program and have the approval of the General Director of the
Hospital. Those medicines will be subsidized by the hospitals.‖ [Pharmacist 2]
The various challenges for further implementation of the e-Catalogue and
the NF, mentioned in the interviews, are summarized in Table 2 and are categorized
by policy types.
2
Chapter two

Moving Forward to Achieve Universal Health Coverage in Indonesia | 35
Table 2. Implementation challenges of the e-Catalogue and the NF
Policies Challenges
e-Catalogue The price of medicines is set too low.
National Formulary A lack of harmonization with other
prescription guidelines (hospital
formularies and standard treatment
guidelines).
e-Catalogue and National Formulary 1. A lack of harmonization between
the list of medicines in the e-
Catalogue and the NF;
2. A poor distribution system for
medicines and the geographical
conditions of Indonesia.
Topic 4: Prescribing medicines not listed in the NF
All stakeholders were aware of the practice of prescribing medicines not listed in the
NF. All physicians have prescribed medicines not listed in the NF, while all patients
and other stakeholders have obtained prescriptions not listed in the NF.
―Yes. Of course. There were still many prescriptions for medicines not in the NF; even I have prescribed medicines not listed in the NF.” [Physician 5].
Almost all stakeholders were opposed to the prescription of medicines not
listed in the NF. However, despite this reluctance, the stakeholders mentioned
several reasons to explain this practice. Tables 3 and 4 list the main reasons
mentioned as well as the underlying explanations.
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia

36 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Table 3. Reasons for prescriptions of medicines not listed in the NF in
relation to the healthcare system
Reasons Causes
Unavailability of NF medicines in the
healthcare facilities.
1. A lack of harmonization between
the list of medicines in the e-
Catalogue and the NF;
2. A poor distribution system;
3. The price of medicines in the e-
Catalogue is too low;
Some important medicines are not listed
in the NF.
1. Failure to negotiate the prices
with the pharmaceutical industry;
2. Some importance medicines
have not yet been registered in
Indonesia;
The existence of other prescription
guidelines.
The regulation of pharmaceutical
service standards in hospitals requires
a hospital formulary and standard
treatment guidelines
2
Chapter two
Moving Forward to Achieve Universal Health Coverage in Indonesia | 37
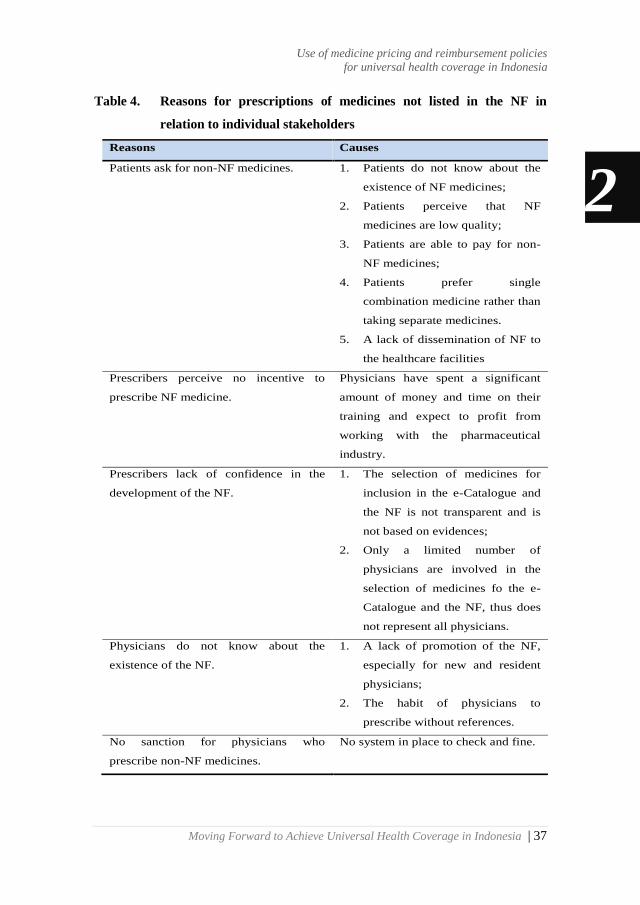
Table 4. Reasons for prescriptions of medicines not listed in the NF in
relation to individual stakeholders
Reasons Causes
Patients ask for non-NF medicines. 1. Patients do not know about the
existence of NF medicines;
2. Patients perceive that NF
medicines are low quality;
3. Patients are able to pay for non-
NF medicines;
4. Patients prefer single
combination medicine rather than
taking separate medicines.
5. A lack of dissemination of NF to
the healthcare facilities
Prescribers perceive no incentive to
prescribe NF medicine.
Physicians have spent a significant
amount of money and time on their
training and expect to profit from
working with the pharmaceutical
industry.
Prescribers lack of confidence in the
development of the NF.
1. The selection of medicines for
inclusion in the e-Catalogue and
the NF is not transparent and is
not based on evidences;
2. Only a limited number of
physicians are involved in the
selection of medicines fo the e-
Catalogue and the NF, thus does
not represent all physicians.
Physicians do not know about the
existence of the NF.
1. A lack of promotion of the NF,
especially for new and resident
physicians;
2. The habit of physicians to
prescribe without references.
No sanction for physicians who
prescribe non-NF medicines.
No system in place to check and fine.
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia

38 | Moving Forward to Achieve Universal Health Coverage in Indonesia
The unavailability of NF medicines in healthcare facilities and its causes
has been discussed above. Examples of several NF medicines that often prescribed
but not available in healthcare facilities according to participating healthcare
providers were ceftriaxone, cefotaxime, furosemide, metronidazole, lansoprazole,
omeprazole, and paracetamol.
Medicines missing from the NF are another explanation for non-NF
prescriptions. The list of non-NF medicines often prescribed in healthcare facilities
according to healthcare providers and policymakerswere acetylcholine, amdixal,
flexpen, flunarizine, glyceryl guaicolate, lincomycin, neurodex, novomix,
pantoprazole, and piracetam.
―Glyceryl guaiacolate is an important medicine for a coughing pregnant
woman. This medicine is not in the NF, but its use is important. So, I still prescribe it if there are pregnant women who have a cough.‖ [Physician 5]
Among these many reasons, the most interesting might be those relating to
physicians‘ perspective, since they write the prescriptions. Most of the physicians
interviewed mentioned that their personal reason for prescribing medicines not listed
in the NF was the lack of (financial) incentive.
―Pity the doctor, once they were free to prescribe and get a bonus. Now they are
limited by the NF. Many people insist on going to medical school, because
hopefully, they will earn high salaries in the future. They will have paid
expensive tuition fees, studied diligently, and lived less sociably because there
was no time. But now their income is going to be limited. Pity the doctor, their individual rights were rescinded, for the benefit of society.‖ [Physician 1]
Another reason mentioned by many physicians was lack of confidence in
the development of the e-Catalogue and the NF.
―I think the NF medicines were not selected on the basis of recent scientific
evidences. I still suspect the selection of medicines was based on other
considerations as well. For example, the pharmaceutical industry intervened so
that certain medicines were included in the NF. In my opinion, at this time, the
NF committee has not been able to account for the selection of medicines in the
NF scientifically, because HTA is not yet running.‖ [Physician 5]
―The physicians disagreed with the list of NF medicines. Well, these complaints
are usually from senior physicians who were not involved in drawing up the
NF.‖ [Physician 6]
2
Chapter two

Moving Forward to Achieve Universal Health Coverage in Indonesia | 39
In contrast to this, one of the policymakers stated that the list of medicines
in the NF has, only to a certain degree, been selected based on evidences.
―The medicine proposed by physicians for the NF must be supported by
scientific evidence, so that the proposal is accountable, not just a proposal.‖
[Policymaker 4]
Topic 5: Possible solutions for optimizing the use of the e-Catalogue and the NF
Some possible solutions were suggested by stakeholders to overcome the challenges
of the e-Catalogue and the NF. Many participants (14 out of 25) recommended
harmonizing the list of medicines in the e-Catalogue and the NF. Moreover, the
selection of medicines needed to be transparent and evidence-based.
―The government should harmonize all the medicines policies in the JKN-KIS
system such as the NF, e-Catalogue, and also other medicine policies such as
hospital formularies, standard treatment guidelines and Indonesian Case Base
Groups (INA-CBGs)‖ [Pharmacist 5]
“The selection of medicines in the e-Catalogue and the NF should be
transparent and reflect the latest scientific evidence. Therefore, HTA should be
implemented.‖ [Physician 5]
A second possible solution suggested was to apply rewards and
punishments for prescribers in order to avoid prescriptions of medicines not listed in
the NF. Almost all physicians and some policymakers mentioned this.
“A bonus should be given to the physicians if they prescribe NF medicines, and
consequently, the physicians will become more motivated. Furthermore, penalties
can also be issued if the physicians prescribe medicines that are not in the NF.”
[Physician 1]
A third possible solution proposed was to have at least one distributor of
NF medicines in all provinces in Indonesia, or alternatively, to have more than one
industry providing each type of NF medicines. Some pharmacists and policymakers
mentioned this.
―There is a need for an alternative provider to the one who won the tender in
the e-Catalogue, so that the price of more than one potential provider can be
included for the same medicine. Thus, healthcare facilities would have
alternatives when one of the pharmaceutical providers is unable to provide NF
medicines.‖ [Pharmacist 4]
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia
40 | Moving Forward to Achieve Universal Health Coverage in Indonesia
A fourth possible solution recommended was to disseminate the list of NF
medicines to patients. Furthermore, the list of NF medicines needed to be extended.
Almost all patients and some policymakers mentioned this.
―Every patient should receive a list of NF medicines, thus consequently being
made aware of whether the medicine being administered to the patient is listed
in the NF or not. The patient can then also ask for an NF medicine if his/her
medicine is not included in the list of free medicines.‖ [Patient 6]
―The list of NF medicines should be expanded, so that all medicines would be free to the patients.‖ [Patient 4]
A fifth possible solution was to ensure the quality of the list of medicines in
the e-Catalogue and the NF. This possible solution was mentioned by the
representative of the pharmaceutical industry.
―Determining the winning bidder for NF medicines should not only be based on
price and production capacity. There must be some kind of pre-qualification.
There should be an audit to ascertain the quality of the medicines, which can be
conducted using the WHO pre-qualification process.‖ [Pharmaceutical
Industry]
Another possible solution from policymakers was to encourage patients to
report to the BPJS-Kesehatan when obtaining a prescription of medicines not listed
in the NF.
―Patients should give feedback on prescribed medicines not listed in the NF. In
every health facility, there was a BPJS-Kesehatan office. So, if there is a
complaint from the patient, we will confirm this with the doctor and pharmacist.‖ [Policymaker 6]
2
Chapter two
Moving Forward to Achieve Universal Health Coverage in Indonesia | 41
Discussion
All the stakeholders interviewed were in favour of the e-Catalogue and the NF.
However, many healthcare providers and patients had limited knowledge of the role
and the existence of the e-Catalogue and the NF. Interviewees identified a range of
challenges preventing optimal implementation. The challenges mentioned were
related to the general structure of the healthcare system as well as to individual
behaviour. The stakeholders had the following suggestions for improvement: (1)
The list of medicines in the e-Catalogue and the NF should be harmonized to
accelerate the procurement of NF medicines and to facilitate the availability of NF
medicines in healthcare facilities; (2) The procedure for selecting medicines in the
NF and setting their prices in the e-Catalogue should be made more transparent and
evidence-based in order to convince stakeholders to use them; (3) Physicians could
be rewarded for prescribing NF medicines or sanctioned for writing prescriptions for
medicines not listed in the NF; (4) More dissemination of information concerning
the NF could be targeted to all citizens.
The suggestion to harmonize the e-Catalogue and the NF is related to the
current confusion caused by a lack of harmony. For medicines on the NF, but not
listed in the e-Catalogue, healthcare facilities need to find a reference price.
However, the price must be in accordance with the maximum claims of the BPJS-
Kesehatan. If healthcare facilities procure medicines at higher prices, healthcare
facilities can lose money. Furthermore, the existence of individual hospital
formularies adds to the confusion. Medicines that are not listed in the NF can be
listed in a hospital formulary. A hospital formulary is needed for hospital
accreditation[30,31]. Hence, here we see policies are not in harmony. Similar problems
were noticed in other LMIC countries, e.g. Namibia, with different advices between
different national bodies causing problems[32].
Lack of harmony was indicated by many interviewees. Therefore, the
authors have compared both lists systematically. We found that in 2013[33], there
were 519 substances of medicines with 923 specifications in the NF, and 374 of the
specifications were not listed in the 2018 e-Catalogue. In 2015[34], 562 substances of
medicines with 983 specifications were in the NF, and 359 of specifications were
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia

42 | Moving Forward to Achieve Universal Health Coverage in Indonesia
not listed in the e-Catalogue. In 2017[35], 586 substances of medicines with 1031
specifications were in the NF, and 380 were not listed in the e-Catalogue. The e-
Catalogue listed 1076 specifications of medicines[36]. This highlight that the problem
of lack of harmony was stable over time.
The current study identifies reasons for prescribing medicines not listed in
the NF. A full list of the reasons for these non-NF prescriptions can be found in the
results section. A first important reason is that physicians are not convinced by the
listings in the NF, since the selection process was perceived as neither transparent
nor evidence-based. The requirements linked to the successful implementation of a
NF include transparency and an evidence-based selection process of the
medicines[37]. Physicians trust in formularies is a key area[38]. One way to
accomplish this might be the use of HTA, as also suggested by some interviewees.
HTA has been used by many organisations in Economic Co-operation and
Development (OECD) countries to select the medicines to be included in their
NFs[39,40]. Furthermore, HTA can also facilitate the setting of reasonable prices for
medicines[41]. Thailand is one of the Southeast Asian countries which is now
successfully using HTA for selecting medicines in their medicine pricing and
reimbursement list[6,42]. An HTA committee in Indonesia does exist, however, it is
still in its early stages of development. Other Southeast Asian countries, such as the
Philippines, Malaysia and Vietnam are also still in the early stages of HTA
development[43-46].
A second important reason for prescribing non-NF medicines is the lack of
incentives for the healthcare providers, particularly, the physicians who prescribe the
medicines. A previous study suggested that providing incentives to the stakeholders
could reduce the number of medicines not listed in the formularies[47]. Maybe the
Indonesian government could rethink their policy regarding incentives for all
stakeholders. The current regulations of Indonesia vis-à-vis rewards and
punishments for healthcare professionals do not touch on this aspect of the
prescription of medicines listed in the NF. Moreover, such clauses reward and
punish only those physicians working in primary healthcare, not physicians working
in hospitals[48]. In some countries, pay-for-performance schemes for providers have
2
Chapter two

Moving Forward to Achieve Universal Health Coverage in Indonesia | 43
been set up. Such schemes could financially reward physicians for achieving
healthcare system targets[49,50]. The literature discusses various methods to influence
physicians‘ prescribing, including incentives. Other methods consist of educational,
organizational, and regulatory approaches[51,52].
The fourth suggestion to disseminate the NF to all healthcare facilities is
equally important and touches upon the educational approach. Mostly patients had
this suggestion since they were not aware of the existence of the NF. A previous
study also suggested the quality of care to patients may be compromised by the
lacking availability of some essential policy documents in the healthcare
facilities[53]. Medicines listed in the NF are free of charge to patients. If patients are
better aware of the list of medicines, they may avoid to use non-NF medicines.
Therefore, this also can help to reduce OOPs, in particular for medicines.
Though a variety of stakeholders were interviewed in this study, this does
not automatically mean that all stakeholders were represented. This research
contained interviews with a specific group of patients, namely, those from Prolanis.
The main reason for this was that participants from this group were relatively easy to
find and recruit. Furthermore, we knew that at the time of the interviews, they had
been taking medication since before the implementation of the JKN-KNS program
in 2014, and therefore were able to provide informed views. This research
highlighted a variety of barriers, facilitators and solutions which were mentioned by
patients and professionals until saturation was reached. However, although more
participants (25) were interviewed than the number of participants aimed at (22),
this study did not manage to achieve two interviewees for each subgroup of
stakeholders. Notably, only one WHO member, member of NF committee, and
pharmaceutical industry representative were interviewed. Therefore, all policy
makers were combined into one category. Nonetheless, the interviewees attained
were relatively experienced. In particular, the representative of pharmaceutical
industry interviewed was a leader in several pharmaceutical associations in
Indonesia.
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia

44 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Conducting semi-structured interviews allowed the researchers to obtain
detailed information about personal feelings, perceptions and opinions from the
participants without any influences from other group members. Moreover, all
ambiguities could be clarified, and incomplete answers were completely followed
up. Several steps were taken to ensure good research practice during the data
compilation and analysis stages. The sampling process used to select participants
and the interview guide were compared with recommendations published in the
COREQ[26]. Transcripts were coded independently by two authors and all
discrepancies were resolved by consensus.
Some suggestions for policy improvement mentioned by the interviewees
could facilitate the improvement of the e-Catalogue and the NF, specifically
avoiding writing prescriptions for medicines not listed in the NF and setting
reasonable prices in the e-Catalogue. These results could prove relevant to other
countries striving to achieve UHC, particularly for the countries which are
experiencing similar problems regarding the implementation of a medicine pricing
and reimbursement policy.
2
Chapter two

Moving Forward to Achieve Universal Health Coverage in Indonesia | 45
Conclusions
In conclusion, the e-Catalogue and the NF as medicine pricing and reimbursement
policies of Indonesia have not been fully utilized to support the JKN-KIS program‘s
aim of achieving UHC. The main challenge identified by the interviewees was the
lack of harmonization between the lists of medicines in the e-Catalogue and the NF.
Important reasons mentioned for prescribing medicines not listed in the NF included
a lack of incentives for physicians as well as a lack of transparent and evidence-
based selection methods for the medicines to be included in the NF. Possible
improvements to the use of e-Catalogue and the NF were discussed. First, the list of
medicines in the e-Catalogue and the NF could be harmonized. Second, the current
incentive program for providers could be altered to provide more rewards for
prescribing NF medicines while more education on the NF would be worthwhile.
Finally, the procedure for selecting medicines in the NF and setting their prices in
the e-Catalogue could be made more transparent and evidence-based in order to
convince stakeholders to use them.
Acknowledgments
The authors would like to thank all stakeholders who participated in this study.
2 2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia

46 | Moving Forward to Achieve Universal Health Coverage in Indonesia
References
1. World Health Organization. The
world health report: health systems
financing: the path to universal
coverage: executive summary.
2010.
2. World Health Organization. World
health statistics 2016: monitoring
health for the SDGs sustainable
development goals.: World Health
Organization; 2016.
3. Cameron A, Ewen M, Ross-Degnan
D, Ball D, Laing R. Medicine
prices, availability, and
affordability in 36 developing and
middle-income countries: a
secondary analysis. The lancet
2009;373(9659):240-249.
4. Bigdeli M, Laing R, Tomson G.
Medicines and universal health
coverage: challenges and
opportunities. 2015.
5. Rickwood S, Kleinrock M, Nunez-
Gaviria M, Sakhrani S, Aitken M.
The global use of medicines:
outlook through 2017. IMS Institute
for Healthcare Informatics 2013:5.
6. Wirtz VJ, Hogerzeil HV, Gray AL,
Bigdeli M, De Joncheere CP, Ewen
MA, et al. Essential medicines for
universal health coverage. The
Lancet 2017;389(10067):403-476.
7. World Health Organization. Health
Technology Assessment, HTA,
WHO Definition (EB 134/30).
Access on January 5, 2019; .
8. Chalkidou K, Marten R, Cutler D,
Culyer T, Smith R,
Teerawattananon Y, et al. Health
technology assessment in universal
health coverage. Lancet 2013 Dec
21;382(9910): e48-9.
9. Angelis A, Lange A, Kanavos P.
Using health technology assessment
to assess the value of new
medicines: results of a systematic
review and expert consultation
across eight European countries.
The European Journal of Health
Economics 2018;19(1):123-152.
10. Holloway KA. Pharmaceuticals in
Health Care Delivery. Mission
Report 2011;30.
11. Soonman Kwon, Sujin Kim,
Boyoung Jeon, Youn Jung.
Pharmaceutical Policy and
Financing in Asia-Pacific
2 2
Chapter two

Moving Forward to Achieve Universal Health Coverage in Indonesia | 47
Countries.: OECD Korea Policy
Centre, Graduate School of Public
Health, Seoul National University
(WHO Collaborating Centre for
Health System and Financing);
2014.
12. Diack A, Seiter A, Hawkins L,
Dweik IS. Assessment of
governance and corruption in the
pharmaceutical sector: Lessons
learned from low- and middle-
income countries. 2010.
13. World Health Organization. Global
Health Expenditure Database.
access on October 29, 2018.
14. Menteri Kesehatan Republik
Indonesia. Peraturan Menteri
Kesehatan Republik Indonesia
Nomor 48 Tahun 2013 tentang
Petunjuk Pelaksanaan Pengadaan
Obat dengan Prosedur E-
Purchasing berdasarkan E-
Catalogue.; 2013.
15. Menteri Kesehatan Republik
Indonesia. Peraturan Menteri
Kesehatan Republik Indonesia
Nomor 28 Tahun 2014 Tentang
Pedoman Pelaksanaan Program
Jaminan Kesehatan Nasional.;
2014.
16. Menteri Kesehatan Republik
Indonesia. Peraturan Menteri
Kesehatan Republik Indonesia
Nomor 63 Tahun 2014 tentang
Pengadaan Obat Berdasarkan
Katalog Elektronik (E-catalogue).;
2014.
17. Kemetrian Kesehatan Republik
Indonesia. Pedoman Penerapan
Formularium Nasional. 2015.
18. Dirjen Binfar dan Alkes Kemenkes
RI. Keputusan Dirjen Binfar Nomor
HK. 02. 03/ III/ 1346/ 2014
Tentang Pedoman Penerapan
Formularium Nasiona. 2014.
19. Menteri Kesehatan Republik
Indonesia. Keputusan Menteri
Kesehatan Republik Indonesia
Nomor 171/ Menkes/ SK/ IV/ 2014
tentang Komite Penilaian
Teknologi Kesehatan. 2014.
20. Menteri Kesehatan Republik
Indonesia. Keputusan Menteri
Kesehatan RI No. HK. 02. 02/
Menkes/ 422/ 2016 tentang Komite
Penilaian Teknologi Kesehatan.
2016.
21. Presiden Republik Indonesia.
Peraturan Presiden Republik
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia

48 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Indonesia Nomor 12 Tahun 2013
tentang Jaminan Kesehatan.; 2013.
22. Menteri Kesehatan Republik
Indonesia. Pedoman Penerapan
Formularium Nasional.; 2015.
23. Niken Ariati. Tata Kelola Obat di
Era Sistem Jaminan Kesehatan
Nasional. 2017.
24. Dirjen Binfar dan Alkes Kemenkes
RI. Implementasi Formularium
nasional dalam Pelaksanaan
Jaminan Kesehatan nasional. 2015.
25. Hidayat B, Mundiharno, Nemec J,
Rabovskaja V, Rozanna C, Spatz J.
Out-of-Pocket Payments in the
National Health Insurance of
Indonesia. 2015.
26. Tong A, Sainsbury P, Craig J.
Consolidated criteria for reporting
qualitative research (COREQ): a
32-item checklist for interviews and
focus groups. International journal
for quality in health care
2007;19(6):349-357.
27. Mays N, Pope C. Qualitative
research: Observational methods in
health care settings. BMJ 1995 Jul
15;311(6998):182-184.
28. BPJS Kesehatan. Panduan Praktis
Prolanis (Program Pengelolaan
Penyakit Kronis). 2014.
29. Hsieh H, Shannon SE. Three
approaches to qualitative content
analysis. Qual Health Res
2005;15(9):1277-1288.
30. Menteri Kesehatan Republik
Indonesia. Keputusan Menteri
Kesehatan Nomor 1197/ Menkes/
SK/ X/ 2004, Standar Pelayanan
Farmasi di Rumah Sakit. 2004.
31. Menteri Kesehatan Republik
Indonesia. Peraturan Menteri
Kesehatan Nomor 58 Tahun 2014,
Formularium Rumah Sakit. 2014.
32. Kibuule D, Mubita M, Naikaku E,
Kalemeera F, Godman BB, Sagwa
E. An analysis of policies for
cotrimoxazole, amoxicillin and
azithromycin use in Namibia's
public sector: Findings and
therapeutic implications. Int J Clin
Pract 2017;71(2): e12918.
33. Menteri Kesehatan Republik
Indonesia. Keputusan Menteri
Kesehatan Republik Indonesia
Nomor 328/Menkes/IX/ 2013
tentang Formularium Nasional.
2013.
2
Chapter two
Moving Forward to Achieve Universal Health Coverage in Indonesia | 49
34. Menteri Kesehatan Republik
Indonesia. Keputusan Menteri
Kesehatan Republik Indonesia
Nomor HK.02.02/ Menkes/ 523/
2015 tentang Formularium
Nasional. 2015.
35. Menteri Kesehatan Republik
Indonesia. Keputusan Menteri
Kesehatan Republik Indonesia
Nomor HK. 01. 07/ Menkes/ 659/
2017 tentang Formularium
Nasional. 2017.
36. Lembaga Kebijakan Pengadaan
Barang dan Jasa Pemerintah
(LKPP). Katalog Produk Obat
2018. Access on January 5, 2019; .
37. Nguyen TA, Knight R, Roughead
EE, Brooks G, Mant A. Policy
options for pharmaceutical pricing
and purchasing: issues for low-and
middle-income countries. Health
Policy Plan 2014;30(2):267-280.
38. Gustafsson LL, Wettermark B,
Godman B, Andersén‐Karlsson E,
Bergman U, Hasselström J, et al.
The ‗wise list‘–a comprehensive
concept to select, communicate and
achieve adherence to
recommendations of essential drugs
in ambulatory care in Stockholm.
Basic & clinical pharmacology &
toxicology 2011;108(4):224-233.
39. Whyte P, Hall C. The Role of
Health Technology Assessment in
Medicine Pricing and
Reimbursement. Pharmaceutical
Pricing Policies and
Interventions.Geneva: WHO 2013.
40. Hawkins L. WHO/HAI Project on
Medicine Prices and Availability
Review Series on Pharmaceutical
Pricing Policies and Interventions.
World Health Organization and
Health Action International 2011.
41. World Health Organization. WHO
guideline on country
pharmaceutical pricing policies.:
World Health Organization; 2015.
42. Jongudomsuk P, Samrit
Srithamrongsawat, Walaiporn
Patcharanarumol, Supon
Limwattananon, Supasit
Pannarunothai, Patama
Vapatanavong, et al. The Kingdom
of Thailand Health System Review.
2015(Manila: WHO Regional
Office for the Western Pacific).
43. Babar Z. Pharmaceutical Policy in
Countries with Developing
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia
50 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Healthcare Systems.: Springer
International Publishing AG; 2017.
44. Jaafar S, Kamaliah Mohd Noh,
Khairiyah Abdul Muttalib, Nour
Hanah Othman, Judith Healy,
Kalsom Maskon, et al. Malaysia
health system review. 2013.
45. Ministry of Health Malaysia.
Malaysian National Medicines
Policy 2nd Edition (Dasar Ubat
Nasional (DUNas) Edisi Kedua.
2012.
46. Nguyen TA, Vitry A, Roughead
EE. Pharmaceutical Policy in
Vietnam. Pharmaceutical Policy in
Countries with Developing
Healthcare Systems: Springer;
2017. p. 75-94.
47. Huskamp HA, Deverka PA, Epstein
AM, Epstein RS, McGuigan KA,
Frank RG. The effect of incentive-
based formularies on prescription-
drug utilization and spending. N
Engl J Med 2003;349(23):2224-
2232.
48. Menteri Kesehatan Republik
Indonesia. Peraturan Menteri
Kesehatan Republik Indonesia
Nomor 30 Tahun 2014 tentang
Standar Pelayanan Kefarmasian di
Puskesmas. 2014.
49. Doran T, Fullwood C, Gravelle H,
Reeves D, Kontopantelis E, Hiroeh
U, et al. Pay-for-performance
programs in family practices in the
United Kingdom. N Engl J Med
2006;355(4):375-384.
50. Leach M. Patients' views of pay for
performance in primary care. Br J
Gen Pract 2012 Jun;62(599):293.
51. Godman B, Wettermark B, van
Woerkom M, Fraeyman J, Alvarez-
Madrazo S, Berg C, et al. Multiple
policies to enhance prescribing
efficiency for established medicines
in Europe with a particular focus on
demand-side measures: findings
and future implications. Frontiers in
pharmacology 2014; 5:106.
52. Wettermark B, Godman B,
Jacobsson B, Haaijer-Ruskamp FM.
Soft regulations in pharmaceutical
policy making. Applied health
economics and health policy
2009;7(3):137-147.
53. Mashalla YJ, Sepako E, Setlhare V,
Chuma M, Bulang M, Massele AY.
Availability of guidelines and
policy documents for enhancing
2
Chapter two

Moving Forward to Achieve Universal Health Coverage in Indonesia | 51
performance of practitioners at the
Primary Health Care (PHC)
facilities in Gaborone, Tlokweng
and Mogoditshane, Republic of
Botswana. Journal of Public Health
and Epidemiology 2016;8(8):127-
135.
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia

52 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Supporting Information
S1 Fig. Conceptual framework
Explanation of conceptual framework:
Many countries aim to reform their national health insurance to reach universal
health coverage. Nowadays, 58 countries are using universal health coverage
besides Indonesia. Before 2014, various health insurance schemes covered health
insurance for Indonesian society. As of 2014, all these schemes were integrated
and organized under one agency called BPJS-Kesehatan. The main goal of this
insurance is to achieve universal health coverage by 2019. The problem with
BPJS-Kesehatan was budgetary constraints, with the highest expenditure being
pharmaceuticals. The national formulary was used to organize medicines. HTA
has not yet been applied in the national formulary, while many UHC countries
do.
2
Chapter two
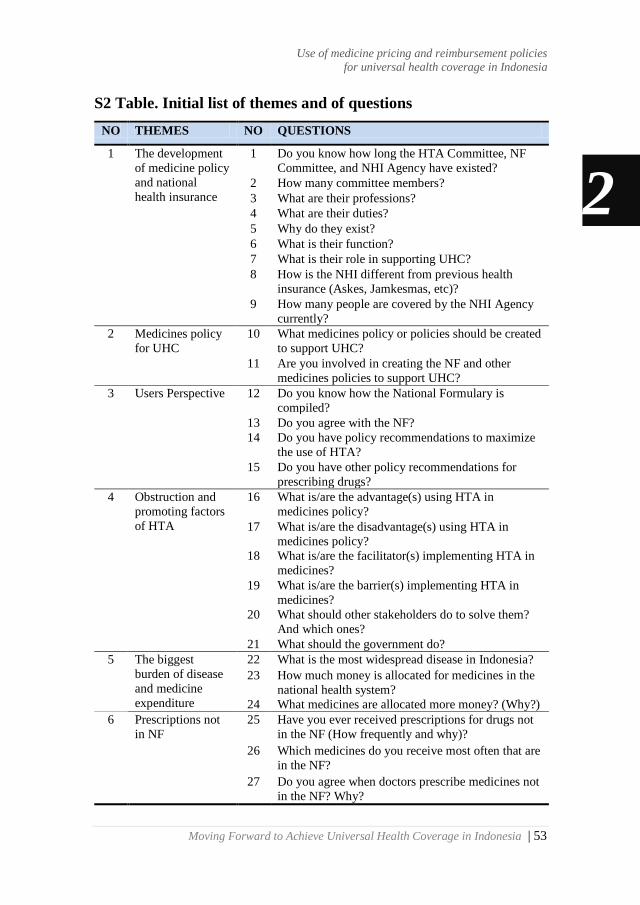
Moving Forward to Achieve Universal Health Coverage in Indonesia | 53
S2 Table. Initial list of themes and of questions
NO THEMES NO QUESTIONS
1 The development
of medicine policy
and national
health insurance
1 Do you know how long the HTA Committee, NF
Committee, and NHI Agency have existed?
2 How many committee members?
3 What are their professions?
4 What are their duties?
5 Why do they exist?
6 What is their function?
7 What is their role in supporting UHC?
8 How is the NHI different from previous health
insurance (Askes, Jamkesmas, etc)?
9 How many people are covered by the NHI Agency
currently?
2 Medicines policy
for UHC
10 What medicines policy or policies should be created
to support UHC?
11 Are you involved in creating the NF and other
medicines policies to support UHC?
3 Users Perspective 12 Do you know how the National Formulary is
compiled?
13 Do you agree with the NF?
14 Do you have policy recommendations to maximize
the use of HTA?
15 Do you have other policy recommendations for
prescribing drugs?
4 Obstruction and
promoting factors
of HTA
16 What is/are the advantage(s) using HTA in
medicines policy?
17 What is/are the disadvantage(s) using HTA in
medicines policy?
18 What is/are the facilitator(s) implementing HTA in
medicines?
19 What is/are the barrier(s) implementing HTA in
medicines?
20 What should other stakeholders do to solve them?
And which ones?
21 What should the government do?
5 The biggest
burden of disease
and medicine
expenditure
22 What is the most widespread disease in Indonesia?
23 How much money is allocated for medicines in the
national health system?
24 What medicines are allocated more money? (Why?)
6 Prescriptions not
in NF
25 Have you ever received prescriptions for drugs not
in the NF (How frequently and why)?
26 Which medicines do you receive most often that are
in the NF?
27 Do you agree when doctors prescribe medicines not
in the NF? Why?
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia

54 | Moving Forward to Achieve Universal Health Coverage in Indonesia
S3 File. Final list of questions
List of Questions for participants (excluding patients)
1. What do you know about the JKN-KIS program? Which points can you
explain:
a. Implementing Agency;
b. When executed;
c. Implementation goals;
d. Other personal information according to participants?
2. As far as you know, what public health insurance programs have been
implemented prior to the implementation of the JKN-KIS program?
a. Implementing Agency;
b. The policy/program that they imposed to control medicines?
3. Do you know why all public health insurance programs are integrated into
JKN-KIS?
4. What are the medicine policies/programs imposing on the JKN-KIS?
a. The role or the functions of the policies
b. What are the policy-making processes?
c. Are you involved in the policy-making process?
d. Who is involved in the policy-making process?
e. Do you agree with the program/policies?
f. Do you think there is/are stakeholder(s) harmed by that policy? For
example, doctors, pharmacists, the pharmaceutical industry, patients, etc.
g. Do you think the policy is based on the latest scientific evidence?
h. In your opinion, are there any other policy proposals that should be
applied?
Key terms:
GOI = Government of Indonesia
HTA = Health Technology Assessment
JKN-KIS = a National Health Insurance scheme of Indonesia UHC = Universal Health Coverage 2
Chapter two
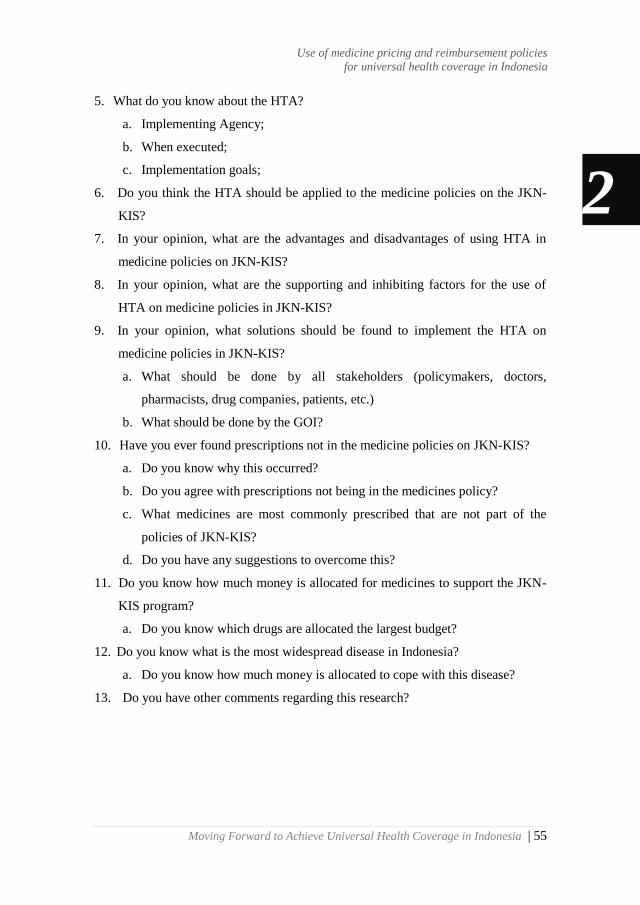
Moving Forward to Achieve Universal Health Coverage in Indonesia | 55
5. What do you know about the HTA?
a. Implementing Agency;
b. When executed;
c. Implementation goals;
6. Do you think the HTA should be applied to the medicine policies on the JKN-
KIS?
7. In your opinion, what are the advantages and disadvantages of using HTA in
medicine policies on JKN-KIS?
8. In your opinion, what are the supporting and inhibiting factors for the use of
HTA on medicine policies in JKN-KIS?
9. In your opinion, what solutions should be found to implement the HTA on
medicine policies in JKN-KIS?
a. What should be done by all stakeholders (policymakers, doctors,
pharmacists, drug companies, patients, etc.)
b. What should be done by the GOI?
10. Have you ever found prescriptions not in the medicine policies on JKN-KIS?
a. Do you know why this occurred?
b. Do you agree with prescriptions not being in the medicines policy?
c. What medicines are most commonly prescribed that are not part of the
policies of JKN-KIS?
d. Do you have any suggestions to overcome this?
11. Do you know how much money is allocated for medicines to support the JKN-
KIS program?
a. Do you know which drugs are allocated the largest budget?
12. Do you know what is the most widespread disease in Indonesia?
a. Do you know how much money is allocated to cope with this disease?
13. Do you have other comments regarding this research?
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia
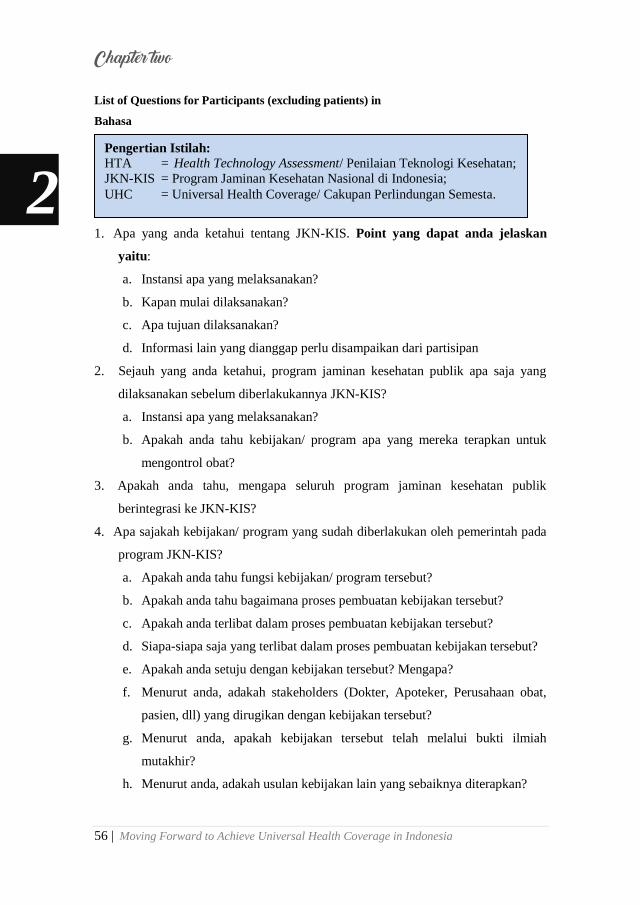
56 | Moving Forward to Achieve Universal Health Coverage in Indonesia
List of Questions for Participants (excluding patients) in
Bahasa
1. Apa yang anda ketahui tentang JKN-KIS. Point yang dapat anda jelaskan
yaitu:
a. Instansi apa yang melaksanakan?
b. Kapan mulai dilaksanakan?
c. Apa tujuan dilaksanakan?
d. Informasi lain yang dianggap perlu disampaikan dari partisipan
2. Sejauh yang anda ketahui, program jaminan kesehatan publik apa saja yang
dilaksanakan sebelum diberlakukannya JKN-KIS?
a. Instansi apa yang melaksanakan?
b. Apakah anda tahu kebijakan/ program apa yang mereka terapkan untuk
mengontrol obat?
3. Apakah anda tahu, mengapa seluruh program jaminan kesehatan publik
berintegrasi ke JKN-KIS?
4. Apa sajakah kebijakan/ program yang sudah diberlakukan oleh pemerintah pada
program JKN-KIS?
a. Apakah anda tahu fungsi kebijakan/ program tersebut?
b. Apakah anda tahu bagaimana proses pembuatan kebijakan tersebut?
c. Apakah anda terlibat dalam proses pembuatan kebijakan tersebut?
d. Siapa-siapa saja yang terlibat dalam proses pembuatan kebijakan tersebut?
e. Apakah anda setuju dengan kebijakan tersebut? Mengapa?
f. Menurut anda, adakah stakeholders (Dokter, Apoteker, Perusahaan obat,
pasien, dll) yang dirugikan dengan kebijakan tersebut?
g. Menurut anda, apakah kebijakan tersebut telah melalui bukti ilmiah
mutakhir?
h. Menurut anda, adakah usulan kebijakan lain yang sebaiknya diterapkan?
Pengertian Istilah:
HTA = Health Technology Assessment/ Penilaian Teknologi Kesehatan;
JKN-KIS = Program Jaminan Kesehatan Nasional di Indonesia;
UHC = Universal Health Coverage/ Cakupan Perlindungan Semesta. 2
Chapter two
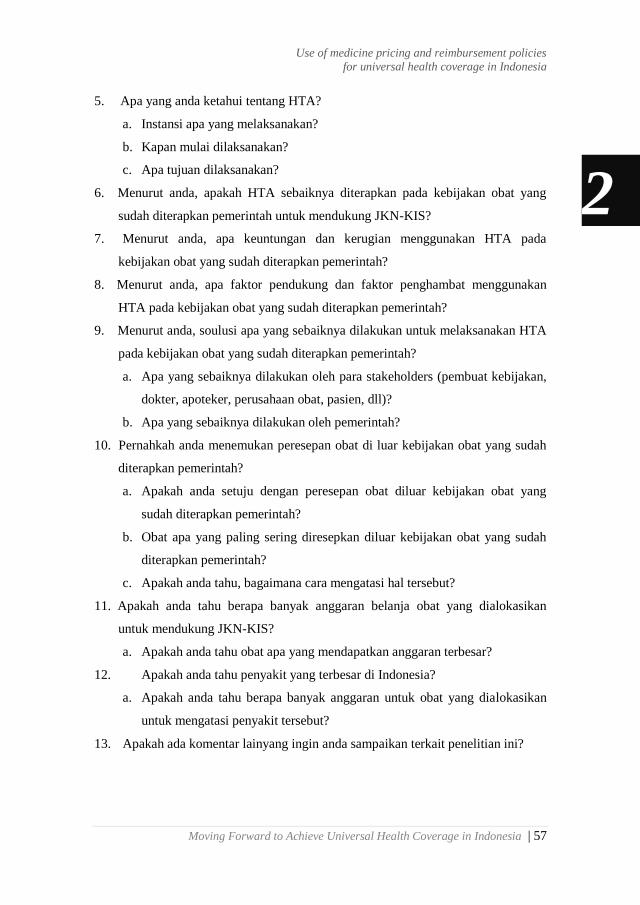
Moving Forward to Achieve Universal Health Coverage in Indonesia | 57
5. Apa yang anda ketahui tentang HTA?
a. Instansi apa yang melaksanakan?
b. Kapan mulai dilaksanakan?
c. Apa tujuan dilaksanakan?
6. Menurut anda, apakah HTA sebaiknya diterapkan pada kebijakan obat yang
sudah diterapkan pemerintah untuk mendukung JKN-KIS?
7. Menurut anda, apa keuntungan dan kerugian menggunakan HTA pada
kebijakan obat yang sudah diterapkan pemerintah?
8. Menurut anda, apa faktor pendukung dan faktor penghambat menggunakan
HTA pada kebijakan obat yang sudah diterapkan pemerintah?
9. Menurut anda, soulusi apa yang sebaiknya dilakukan untuk melaksanakan HTA
pada kebijakan obat yang sudah diterapkan pemerintah?
a. Apa yang sebaiknya dilakukan oleh para stakeholders (pembuat kebijakan,
dokter, apoteker, perusahaan obat, pasien, dll)?
b. Apa yang sebaiknya dilakukan oleh pemerintah?
10. Pernahkah anda menemukan peresepan obat di luar kebijakan obat yang sudah
diterapkan pemerintah?
a. Apakah anda setuju dengan peresepan obat diluar kebijakan obat yang
sudah diterapkan pemerintah?
b. Obat apa yang paling sering diresepkan diluar kebijakan obat yang sudah
diterapkan pemerintah?
c. Apakah anda tahu, bagaimana cara mengatasi hal tersebut?
11. Apakah anda tahu berapa banyak anggaran belanja obat yang dialokasikan
untuk mendukung JKN-KIS?
a. Apakah anda tahu obat apa yang mendapatkan anggaran terbesar?
12. Apakah anda tahu penyakit yang terbesar di Indonesia?
a. Apakah anda tahu berapa banyak anggaran untuk obat yang dialokasikan
untuk mengatasi penyakit tersebut?
13. Apakah ada komentar lainyang ingin anda sampaikan terkait penelitian ini?
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia

58 | Moving Forward to Achieve Universal Health Coverage in Indonesia
A List of Questions for Patients
1. Do you know about JKN-KIS, which is part of BPJS-Kesehatan? Could you
explain briefly it?
2. Are you a participant in JKN-KIS?
3. When were you be a participant in JKN-KIS?
4. What health insurance did you use before JKN-KIS?
5. For how long were you a participant in that insurance?
6. Are you currently taking any medication?
a. When was the last time you took the drugs?
b. What drugs did you take?
7. Did you also take that medicine when using your previous insurance?
8. Do you feel a difference when taking medication of JKN-KIS compared with
medication of your previous health insurance?
a. Which one is cheaper?
b. Which are more efficacious?
c. Which one do you like, and think is better?
9. Is there a difference, do you feel, in terms of service between JKN-KIS and your
previous health insurance?
a. Are there differences when seeing doctors?
b. Is there a difference when conducting laboratory checks or other checks?
10. Do you know about UHC? Could you explain briefly what you know?
a. Do you agree with the GOI‘s target of reaching UHC in 2019?
b. Do you think it can be achieved?
c. Are there any suggestions from you in order to achieve the UHC?
11. Do you know about NF? Could you explain briefly about that?
a. Do you know how NF is created?
Key terms:
GOI = Government of Indonesia
HTA = Health Technology Assessment
JKN-KIS = a National Health Insurance scheme of Indonesia
UHC = Universal Health Coverage
NF = National Formulary 2
Chapter two

Moving Forward to Achieve Universal Health Coverage in Indonesia | 59
b. Do you agree with NF?
c. What medications do you often receive which are in NF?
d. Have you ever received prescriptions not in the NF? How often? Why?
e. Do you agree with prescriptions not in the NF? Why?
f. Do you have a policy recommendation in prescriptions?
12. Do you know about HTA? Could you explain briefly what you know?
a. Do you think the HTA can be used for medicines policy in Indonesia?
b. In your opinion, what is the advantage of using HTA in determining the
choice of medicines?
c. In your opinion, what are the disadvantages of using HTA in determining
the choice of medicines?
d. In your opinion, what are the promoting factors in implementing an HTA
for drug selection?
e. In your opinion, what are the obstacles in implementing an HTA for drug
selection?
f. In your opinion, what should be done by stakeholders to resolve this?
g. In your opinion, what should the government do?
13. Do you have suggestions for improving medicines policy?
14. Do you have other comments related to this research?
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia
60 | Moving Forward to Achieve Universal Health Coverage in Indonesia
A List of Questions for Patients in Bahasa
1. Apakah anda tahu tentang jaminan kesehatan nasional yang dikelola oleh BPJS-
Kesehatan? Bisakah anda Jelaskan sedikit tentang hal itu?
2. Apakah anda anggota BPJS-Kesehatan?
3. Kapan anda mulai menjadi anggota BPJS-Kesehatan?
4. Asuransi apa yang anda gunakan sebelum menjadi anggota BPJS-Kesehatan ?
5. Berapa lama anda menjadi anggota asuransi tersebut?
6. Apakah anda mengkonsumsi obat saat ini?
a. Kapan terakhir kali anda mengkonsumsi obat?
b. Obat apa?
7. Apakah obat tersebut juga anda konsumsi dengan menggunakan asuransi yang
sebelumnya?
8. Apakah ada perbedaan yang anda rasakan ketika menggunakan obat dari BPJS
dengan obat dari asuransi anda sebelumnya?
a. Yang mana yang lebih murah?
b. Yang mana yang lebih berkhasiat?
c. Yang mana yang anda suka dan anggap lebih baik?
9. Apakah ada perbedaan yang anda rasakan dari sisi pelayanan pada Asuransi
BPJS dan Asuransi yang anda gunakan sebelumnya?
a. Apakah ada perbedaan ketika bertemu dengan dokter?
b. Apakah ada perbedaan ketika melakukan cek laboratorium atau
pemeriksaan lainnya?
10. Apakah anda tahu tentang Univeral Health Coverage (UHC)/ Jaminan kesehatan
secara menyeluruh? Bisakah anda Jelaskan sedikit tentang hal itu?
a. Apakah anda sependapat dengan pemerintah Indonesia yang ingin
mencapai UHC di tahun 2019?
b. Apakah anda pikir itu bisa dicapai?
c. Apakah ada saran dari anda untuk mencapai UHC tersebut?
11. Apakah anda tahu tentang Formularium Nasional (Fornas)?
a. Apakah anda tahu bagaimana Fornas dibuat?
b. Apakah anda setuju dengan Formularium Nasional?
2
Chapter two
Moving Forward to Achieve Universal Health Coverage in Indonesia | 61
c. Obat apa yang sering anda terima yang ada di dalam Fornas?
d. Pernakah anda menerima obat di luar Fornas? Seberapa sering? Kenapa?
e. Apakah anda setuju ketika dokter menuliskan obat diluar formularium
nasional? Kenapa?
f. Apakah anda memiliki rekomendasi kebijakan dalam penulisan obat?
12. Apakah anda tahu tentang Health Technology Assessment (HTA) / Penilaian
Teknologi Kesehatan? Bisakah anda Jelaskan sedikit tentang hal itu?
a. Menurut anda, apakah HTA dapat digunakan untuk kebijakan obat di
Indonesia?
b. Menurut anda, apa keuntungan menggunakan HTA dalam menentukan
pilihan obat?
c. Menurut anda, apa kerugian menggunakan HTA dalam menentukan
pemilihan obat?
d. Menurut anda, apa faktor pendukung dalam menjalankan HTA pada
pemilihan obat?
e. Menurut anda, apa faktor penghambat dalam menjalankan HTA pada
pemilihan obat?
f. Apa yang harus dilakukan oleh pemangku kebijakan untuk menyelesaikan
itu?
g. Menurut anda, apa yang harus dilakukan oleh pemerintah?
13. Apakah anda memiliki saran untuk meningkatkan kebijakan obat?
14. Apakah anda memiliki saran untuk penelitian ini?
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia
62 | Moving Forward to Achieve Universal Health Coverage in Indonesia
S4 File. Informed consent
Lembar penjelasan dan persetujuan kepada partisipan
Peluang dan tantangan kebijakan obat pada program JKN-KIS untuk mencapai
Cakupan Perlindungan Semesta / Universal Health Coverage (UHC)
Saya Riswandy Wasir, Mahasiswa Program Pascasarjana (S3) Departemen
Epidemiologi, Univerity Medical Center Groningen (UMCG), University of
Groningen, Netherlands. Saat ini saya sedang melakukan penelitian yang berjudul
―peluang dan tantangan kebijakan obat pada program JKN-KIS untuk mencapai
cakupan perlindungan semesta‖.
Pemerintah Indonesia telah menerapkan skema asuransi kesehatan nasional
(JKN-KIS) yang terintegrasi dimulai pada tahun 2014. Asuransi kesehatan yang
dikelolah oleh BPJS-Kesehatan dimaksudkan sebagai pengganti seluruh asuransi
kesehatan publik sebelumnya. Peta jaminan kesehatan nasional yang dirilis oleh
pemerintah menyatakan bahwa program JKN-KIS diupayakan mencapai cakupan
perlindungan semseta/ Universal Health Coverage (UHC) pada tahun 2019.
Organisasi Kesehatan Dunia/ World Health Organization (WHO) menyatakan
bahwa bukan hanya kepesertaan yang menjadi indikator tercapainya cakupan
perlindungan semesta, tetapi juga kualitas pelayanan.
Berbagai upaya telah dilakukan oleh pemerintah dan para pemangku
kebijakan untuk meningkatkan mutu pelayanan JKN-KIS. Pada sektor obat,
pemerintah Indonesia telah menerapkan formularium nasional. Manfaat Fornas yaitu
sebagai acuan penetapan penggunaan obat dalam JKN-KIS, serta meningkatkan
penggunaan obat yang rasional, dapat juga mengendalikan mutu dan biaya
pengobatan, serta mengoptimalkan pelayanan kepada pasien Namun, Hasil evaluasi
awal yang dilakukan oleh Direktorat Jenderal Bina Farmasi dan Alat Kesehatan
(Dirjen Binfar dan Alkes) memperlihatkan bahwa kesesuaian obat yang digunakan
di rumah sakit dengan formularium nasional berkisar antara 60 – 86 %. Hal ini
memperlihatkan bahwa masih ditemukan cost-sharing, suatu kondisi dimana peserta
JKN-KIS harus mengeluarkan biaya untuk pembayaran pelayanan kesehatan
2
Chapter two
Moving Forward to Achieve Universal Health Coverage in Indonesia | 63
termasuk obat. Salah satu Indikator tercapainya cakupan perlindungan semesta
(UHC) menurut WHO adalah tidak adanya cost-sharing.
Kami, melakukan penelitian ini untuk mengidentifikasi peluang dan
tantangan kebijakan obat pada program JKN-KIS untuk mencapai cakupan
perlindungan semesta. Penelitian ini akan melibatkan beberapa pemangku
kepentingan yang dianggap memiliki peran dalam membuat kebijakan,
mengimplementasikan serta merasakan dampak dari kebijakan tersebut antara lain
sebagai berikut:
No Partisipan Peran
1 Organisasi Kesehatan Dunia (WHO) Pembuat Kebijakan skala Internasional
2 Komite HTA Pembuat kebijakan skala nasional
3 Komite Formularium Nasional Pembuat kebijakan skala nasional
4 BPJS-Kesehatan Penyelenggara JKN-KIS dan Pembayar
5 Perusahaan Farmasi Pemasok obat
6 Dokter Penyedia pelayanan kesehatan
7 Apoteker Penyedia pelayanan kesehatan
8 Pasien Peserta JKN-KIS/ Pengguna
Penelitian akan dilaksanakan dengan metode wawancara bebas terpimpin
(semi-structured interview). Daftar pertanyaan, surat kesediaan berpartisipasi
(informed consent), dan pedoman wawancara akan diberikan oleh peneliti kepada
partisipan sehari sebelum wawancara atau pada waktu yang telah ditentukan
bersama. Durasi waktu pada saat melaksanakan wawancara mendalam yaitu sekitar
1 (satu) jam.
A. Kesukarelaan untuk ikut penelitian
Bapak/ Ibu/ Saudara bebas memilih keikutsertaan dalam penelitian ini tanpa ada
paksaan. Bila bapak/ ibu/ saudara sudah memutuskan untuk ikut dapat juga
mengundurkan diri setiap saat tanpa dikenai denda ataupun sanksi apapun.
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia

64 | Moving Forward to Achieve Universal Health Coverage in Indonesia
B. Prosedur Penelitian
Apabila Bapak/ Ibu/ Saudara bersedia berpartisipasi dalam penelitian ini,
diminta menandatangani lembar persetujuan ini rangkap dua, satu untuk Bapak/
Ibu/ Saudara simpan, dan satu untuk peneliti. Prosedur selanjutnya adalah :
1. Penelitian akan dilaksanakan dengan metode wawancara terpimpin (semi-
structured Interview) sesuai dengan kesepakatan dan kenyamanan bapak/
ibu/ saudara menggunakan alat perekam.
2. Peneliti akan mentranskrip hasil wawancara setelah melaksanakan
interview dengan partisipan.
3. Hasil transkrip akan diperlihatkan kembali kepada partisipan untuk
mengklarifikasi hasil wawancara.
4. Hasil transkrip yang telah disepakati antara peneliti dan partisipan akan
diproses oleh peneliti beserta tim peneliti lainnya untuk kemudian dijadikan
data kualitatif yang akan di publikasi.
C. Kewajiban partisipan
Sebagai partisipan, Bapak/Ibu/Saudara berkewajiban mengikuti aturan atau
petunjuk penelitian seperti yang tertulis di atas. Bila ada yang belum jelas,
Bapak/ Ibu/ Saudara bisa bertanya lebih lanjut kepada peneliti.
D. Risiko
Penelitian ini tidak menyebabkan risiko yang berbahaya, karena peneliti tidak
melakukan intervensi apapun. Risiko ketidaknyamanan atau dampak yang
mungkin akan diterima yaitu merasa bosan dengan banyaknya
pertanyaan- pertanyaan dari peneliti dan kerugian waktu selama
diwawancarai oleh peneliti.
E. Manfaat dan Keuntungan
Manfaat dan keuntungan yang bapak/ ibu/ saudara dapatkan adalah kesempatan
dan kebebasan untuk menjelaskan mengenai apa yang anda rasakan terhadap
kebijakan obat pada program JKN-KIS. Penelitian ini nantinya akan diupayakan
menjadi masukan terhadap pengambil kebijakan dalam meningkatkan sektor
kesehatan nasional.
2
Chapter two

Moving Forward to Achieve Universal Health Coverage in Indonesia | 65
F. Kerahasiaan
Semua informasi yang berkaitan dengan identitas partisipan akan dirahasiakan
dan hanya akan diketahui oleh peneliti. Data hasil penelitian akan disimpan
dan didokumentasikan oleh peneliti serta hanya digunakan untuk
kepentingan ilmiah. Hasil penelitian akan dipublikasikan tanpa identitas
partisipan.
G. Kompensasi
Bapak/ ibu/ saudara akan mendapatkan souvenir sebagai wujud terima kasih
peneliti atas partisipasinya dalam penelitian ini.
H. Informasi Tambahan
Bapak/ ibu/ saudara diberi kesempatan untuk menanyakan semua hal yang
belum jelas sehubungan dengan penelitian ini. Bila sewaktu-waktu terjadi
kekeliruan atau membutuhkan penjelasan lebih lanjut, Bapak/ ibu/ saudara
dapat menghubungi Riswandy Wasir pada no HP: +62-81225835007 atau
bisa juga dengan mengirimkan email: [email protected]
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia

66 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Persetujuan keikutsertaan dalam penelitian
(informed consent)
Saya yang bertandatangan dibawah ini:
Nama :........................................................................
Alamat : .......................................................................
Nomor Hp : .......................................................................
E-mail : .......................................................................
Umur : .......................................................................
Pekerjaan : .......................................................................
Pendidikan Terakhir : .......................................................................
Peran partisipan :
1. Anggota Organisasi Kesehatan Dunia / World Health Organization (WHO)
2. Komite Penilaian Teknologi Kesehatan / Health Technology Assessment
(HTA)
3. Komite Formularium Nasional
4. Instansi Penyelenggara Asuransi Kesehatan Nasional
5. Perusahaan Farmasi
6. Dokter
7. Apoteker
8. Pasien
Menyatakan bahwa, semua penjelasan tersebut telah disampaikan kepada saya
sebagai partisipan dan semua pertanyaan saya telah dijawab oleh peneliti.
Saya mengerti bahwa bila memerlukan penjelasan, saya dapat menanyakan
kepada saudara Riswandy Wasir sebagai peneliti utama.
Dengan menandatangani formulir ini, saya setuju untuk ikut serta dalam penelitian
ini
Tanggal: Tanggal:
Tanda Tangan Partisipan Tanda Tangan Peneliti
Nama Jelas: …………………………….
Nama Jelas: Riswandy Wasir
2
Chapter two
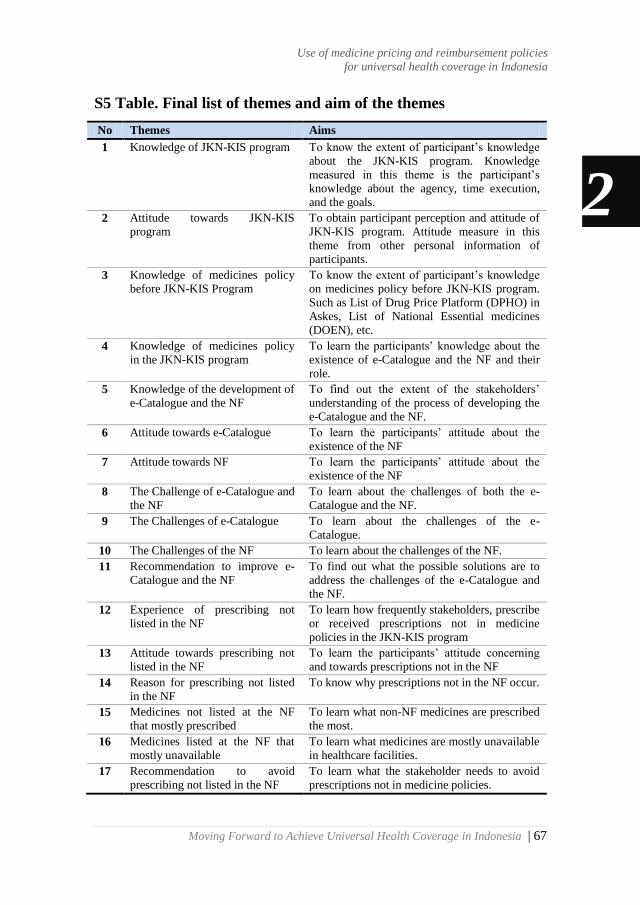
Moving Forward to Achieve Universal Health Coverage in Indonesia | 67
S5 Table. Final list of themes and aim of the themes
No Themes Aims
1 Knowledge of JKN-KIS program To know the extent of participant‘s knowledge
about the JKN-KIS program. Knowledge
measured in this theme is the participant‘s
knowledge about the agency, time execution,
and the goals.
2 Attitude towards JKN-KIS
program
To obtain participant perception and attitude of
JKN-KIS program. Attitude measure in this
theme from other personal information of
participants.
3 Knowledge of medicines policy
before JKN-KIS Program
To know the extent of participant‘s knowledge
on medicines policy before JKN-KIS program.
Such as List of Drug Price Platform (DPHO) in
Askes, List of National Essential medicines
(DOEN), etc.
4 Knowledge of medicines policy
in the JKN-KIS program
To learn the participants‘ knowledge about the
existence of e-Catalogue and the NF and their
role.
5 Knowledge of the development of
e-Catalogue and the NF
To find out the extent of the stakeholders‘
understanding of the process of developing the
e-Catalogue and the NF.
6 Attitude towards e-Catalogue To learn the participants‘ attitude about the
existence of the NF
7 Attitude towards NF To learn the participants‘ attitude about the
existence of the NF
8 The Challenge of e-Catalogue and
the NF
To learn about the challenges of both the e-
Catalogue and the NF.
9 The Challenges of e-Catalogue To learn about the challenges of the e-
Catalogue.
10 The Challenges of the NF To learn about the challenges of the NF.
11 Recommendation to improve e-
Catalogue and the NF
To find out what the possible solutions are to
address the challenges of the e-Catalogue and
the NF.
12 Experience of prescribing not
listed in the NF
To learn how frequently stakeholders, prescribe
or received prescriptions not in medicine
policies in the JKN-KIS program
13 Attitude towards prescribing not
listed in the NF
To learn the participants‘ attitude concerning
and towards prescriptions not in the NF
14 Reason for prescribing not listed
in the NF
To know why prescriptions not in the NF occur.
15 Medicines not listed at the NF
that mostly prescribed
To learn what non-NF medicines are prescribed
the most.
16 Medicines listed at the NF that
mostly unavailable
To learn what medicines are mostly unavailable
in healthcare facilities.
17 Recommendation to avoid
prescribing not listed in the NF
To learn what the stakeholder needs to avoid
prescriptions not in medicine policies.
2
Use of medicine pricing and reimbursement policies
for universal health coverage in Indonesia

68 | Moving Forward to Achieve Universal Health Coverage in Indonesia
S6
Ta
ble
. O
ver
vie
w o
f re
cru
itm
en
t p
roce
ss
Ty
pes
of
sta
keh
old
ers
Sen
d l
ette
r
Res
po
nd
s In
terv
iew
s
Ca
nce
l a
fter
rece
ivin
g l
ist
of
qu
esti
on
s
Sto
p t
he
inte
rvie
w
No
tim
es
av
ail
ab
le
No
t
resp
on
se
WH
O m
em
ber
s 2
2
1
0
0
1
0
HT
A c
om
mit
tee
3
2
2
0
0
0
1
NF
co
mm
itte
e
3
1
1
0
0
0
2
NH
I A
gen
cy
3
3
2
0
0
1
0
Phar
mac
euti
cal
Ind
ust
ry
4
3
1
0
0
2
1
Ph
ysi
cian
s 1
2
10
6
1
3
0
2
Phar
mac
ist
15
15
6
5
4
0
0
Pat
ients
9
9
6
3
0
0
0
To
tal
51
45
25
9
7
4
6
2
Chapter two

Moving Forward to Achieve Universal Health Coverage in Indonesia | 69
Chapter 3
The implementation of health technology assessment (HTA) in
medicine pricing and reimbursement policies in Indonesia: insights
from multiple stakeholders
The implementation of HTA in Indonesia
Riswandy Wasir
Sylvi Irawati
Amr Makady
Maarten Postma
Wim Goettsch
Talitha Feenstra
Erik Buskens
This chapter is based on the published manuscript:
Wasir R, Irawati S, Makady A, Postma M, Goettsch W, Feenstra T, et al. (2019) The
implementation of HTA in medicine pricing and reimbursement policies in
Indonesia: Insights from multiple stakeholders. PLoS ONE 14(11): e0225626.
https://doi.org/10.1371/journal.pone.0225626

70 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Abstract
Objectives
This study aimed to identify the barriers and facilitators to improve the use of health
technology assessment (HTA) for the selection of medicines listed in the e-
Catalogue and the national formulary in Indonesia.
Methods
Semi-structured interviews were conducted to collect qualitative data. Purposive
sampling was used to recruit the stakeholders consisting of policymakers, a
pharmaceutical industry representative, healthcare providers, and patients. The data
were analyzed using directed content analysis and following the COnsolidated
criteria for REporting Qualitative studies (COREQ).
Results
The twenty-five participants interviewed agreed with the use of HTA for supporting
the e-Catalogue and the national formulary and perceived the advantages of HTA
implementation outweighed the disadvantages. Barriers mentioned were a lack of
capability of local human resources, financial incentives, a clear framework and
insufficient data. Strategies suggested to overcome the barriers were establishing
(inter)national networks to build up capacity, setting up departments of HTA in
several universities in Indonesia, and introducing a clear HTA framework.
Facilitators mentioned were the ambition to achieve universal health coverage, the
presence of legal frameworks to implement HTA in the e-Catalogue and the national
formulary, and the demands for appropriate medicine policies.
Conclusions
Several barriers are currently hampering broad implementation of HTA in medicine
pricing and reimbursement policy in Indonesia. Solutions to these issues appear
feasible and important facilitators exist.
3
Chapter three

Moving Forward to Achieve Universal Health Coverage in Indonesia | 71
Introduction
The 2015 transition from Millennium Development Goals to Sustainable
Development Goals has triggered a shift in global health from service-specific
targets to broader health system goals[1]. Target 3.8 of the Sustainable Development
Goals explicitly states to achieve Universal Health Coverage (UHC)[2]. UHC will be
accomplished when all people receive the healthcare services they need of sufficient
quality and without suffering financial hardship. Therefore, the presence of UHC
ideally will reduce or eliminate the proportion of out-of-pocket payments from
healthcare expenditures[3]. Out-of-pocket payment, a direct payment to the
healthcare providers at the time of service use, can drive an individual or a
household below the poverty line[4]. In low middle-income countries (LMICs), the
proportion of out-of-pocket payments in healthcare expenditures is still high,
particularly for medicines, the number ranges from 50% to 90 %[5].
Appropriate medicine policies combined with an implementation of health
technology assessment (HTA) can facilitate countries to reduce the out-of-pocket
payments for medicines on their way towards UHC. For instance, the United
Kingdom (UK) and Thailand, as one of the oldest and the newest UHC examples
respectively, have shown that the implementation of HTA supports their medicine
policies[6]. Furthermore, the World Health Organization (WHO) highly recommends
the use of HTA to facilitate the creation of a list of medicines in the medicine benefit
package[7]. The WHO defines HTA as the systematic evaluation of properties,
effects and/or impacts of health technologies and interventions[8]. HTA is a critical
component of evidence-based policy decision making[7,9].
In response to target 3.8 of the Sustainable Development Goals, the
Government of Indonesia launched a new national health insurance system, which is
called Jaminan Kesehatan Nasional – Kartu Indonesia Sehat (JKN-KIS) in 2014.
The JKN-KIS aims to achieve UHC by 2020 and is managed by Indonesia‘s
National Healthcare Security Agency, namely Badan Penyelenggara Jaminan Sosial
Kesehatan (BPJS-Kesehatan)[10,11]. Additionally, several new medicine policies were
introduced separately by the Ministry of Health to support the JKN-KIS. First, the e-
Catalogue was introduced as a national medicine pricing policy. The e-Catalgue
3
2
The implementation of health technology assessment (HTA) in Indonesia
72 | Moving Forward to Achieve Universal Health Coverage in Indonesia
provides a list of medicines with specifications, prices, and suppliers. Second, the
national formulary was compiled as a list of medicines covered by the BPJS-
Kesehatan[12]. The e-Catalogue and the national formulary have their own respective
responsible committees, which were both established in 2013, a year before the
implementation of the JKN-KIS. Although the e-Catalogue and the national
formulary were established separately, in practice these policies are interrelated.
Indonesian healthcare facilities can reimburse medicines listed in the national
formulary based on its prices listed in the e-Catalogue[12-14].
According to the national health insurance guidelines of Indonesia, an HTA
approach should be used to select a health technology or intervention, including
medicines, which will be covered by the BPJS-Kesehatan. This implies that HTA
should be used in further developing the e-Catalogue and the national formulary. As
a way forward, both may build on the guideline on the implementation of HTA in
particular for medicines that the Department of Pharmacy and Medical Devices in
the Ministry of Health of Indonesia introduced in 2013[15]. In detail, the national
health insurance recommended that the use of HTA is developed and performed by
an HTA committee installed by the Ministry of Health[12].
Indeed in 2014, several months after the implementation of the JKN-KIS,
the Ministry of Health formed the HTA committee. The committee had eight senior
health scientists and six employees of the Ministry of Health, and was supported by
14 secretaries. The tasks of the committee were establishing a policy concept,
guidelines, and the HTA committee itself to regulate the implementation of HTA[16].
In 2016, the HTA committee was reformed. The current HTA committee is
composed of eight senior health scientists, one employee of the Ministry of Health,
and supported by four secretaries. A technical staff with thirteen clinicians, two
Ministry of Health employees, and one technician is now added to support the HTA
committee tasks. Their current tasks are to define a guideline for HTA
implementation, to establish the HTA committee and their work plan, to build a
relationship with HTA committees in other countries, to assess the technologies or
interventions covered by BPJS-Kesehatan, and to disseminate the results of their
assessments[17].
3
Chapter three

Moving Forward to Achieve Universal Health Coverage in Indonesia | 73
However, although the HTA guideline was published in 2013 and the HTA
committee had been installed in 2014, HTA has not been used in the development of
the e-Catalogue and the national formulary. This might be one of the reasons why
the use of the e-Catalogue and the national formulary could not help to reduce out-
of-pocket payments for medicines in Indonesia[18]. In 2014, the out-of-pocket
payments comprised approximately half of the total health expenditure in Indonesia,
and it has remained at a similar level since[19]. The proportion of out-of-pocket
payments for medicines was 70% in recent years[20]. Furthermore, over the same
period, the Ministry of Health reported that up to 40% of prescribed medicines were
not listed in the NF[21]. Relevant stakeholders were interviewed to provide a better
understanding of how to improve the implementation of HTA in Indonesia, with
particular attention for suggestions on and barriers perceived regarding the use of
HTA in revising the e-Catalogue and the national formulary.
3
2
The implementation of health technology assessment (HTA) in Indonesia
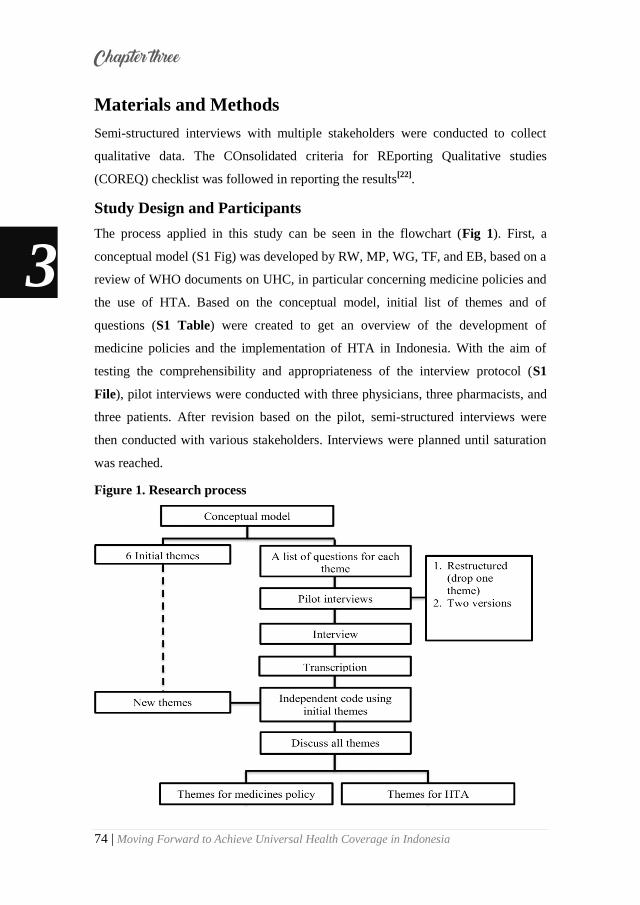
74 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Materials and Methods
Semi-structured interviews with multiple stakeholders were conducted to collect
qualitative data. The COnsolidated criteria for REporting Qualitative studies
(COREQ) checklist was followed in reporting the results[22].
Study Design and Participants
The process applied in this study can be seen in the flowchart (Fig 1). First, a
conceptual model (S1 Fig) was developed by RW, MP, WG, TF, and EB, based on a
review of WHO documents on UHC, in particular concerning medicine policies and
the use of HTA. Based on the conceptual model, initial list of themes and of
questions (S1 Table) were created to get an overview of the development of
medicine policies and the implementation of HTA in Indonesia. With the aim of
testing the comprehensibility and appropriateness of the interview protocol (S1
File), pilot interviews were conducted with three physicians, three pharmacists, and
three patients. After revision based on the pilot, semi-structured interviews were
then conducted with various stakeholders. Interviews were planned until saturation
was reached.
Figure 1. Research process
3
2
Chapter three

Moving Forward to Achieve Universal Health Coverage in Indonesia | 75
A purposive sampling method was used to recruit stakeholders, which
consisted of policymakers, medicine suppliers, healthcare providers, and patients in
various places of Indonesia. Recruitment criteria were: stakeholders (policy makers,
healthcare provider, industry representative) should have at least 5 years of relevant
work experience. Physicians were not selected based on their specialization, because
HTA would be implemented in the development of the national formulary, which is
used by all healthcare providers regardless of their specialization. Both
pharmaceutical industries approached produced medicines and medical devices and
were responsible for distributing medicine to the healthcare facilities. Patients were
selected based on the duration of their health insurance in Indonesia (at least 5 years)
and their routine use of medicines (at least 5 years). In order to ensure that these
patient criteria were met, participants were recruited from the BPJS-Kesehatan‘s
chronic disease management program (Program pelayanan penyakit kronis,
Prolanis).
A priory estimation of the number of participants required to reach
saturation was made. We estimated that at least twenty-two stakeholders should be
approached based on at least two representatives for each group of policy makers,
i.e., at least two pharmaceutical industry representatives, at least four interviewees
from each group of healthcare providers, and at least four patients. The reason for
having more interviewees in the groups of healthcare providers and patients was our
interest in the practical issues of the implementation of medicine policy and the
difficulties reported for applying HTA for selecting medicine in the medicine
policy. Potential participants were approached by email, phone and visit.
Data analysis
All interviews were audiotaped and then transcribed. The transcripts were
independently coded by two authors (RW, SI) using MAXQDA version 12.3.2.
Directed content analysis [23] was applied to systematically structure the content of
the transcripts. The codes were compared, and in case of disagreements, items were
discussed with AM, WG, MP, TF, and EB to reach a consensus. Twenty four themes
were identified during coding process. The themes were then divided into two
categories. The first concerned medicine pricing and reimbursement policy [18] and
3
2
The implementation of health technology assessment (HTA) in Indonesia
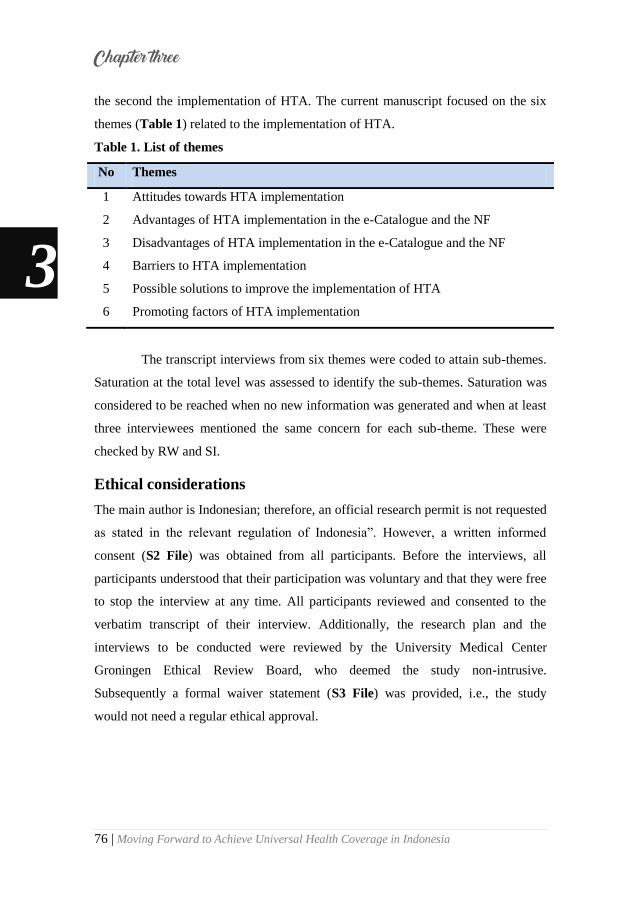
76 | Moving Forward to Achieve Universal Health Coverage in Indonesia
the second the implementation of HTA. The current manuscript focused on the six
themes (Table 1) related to the implementation of HTA.
Table 1. List of themes
No Themes
1 Attitudes towards HTA implementation
2 Advantages of HTA implementation in the e-Catalogue and the NF
3 Disadvantages of HTA implementation in the e-Catalogue and the NF
4 Barriers to HTA implementation
5 Possible solutions to improve the implementation of HTA
6 Promoting factors of HTA implementation
The transcript interviews from six themes were coded to attain sub-themes.
Saturation at the total level was assessed to identify the sub-themes. Saturation was
considered to be reached when no new information was generated and when at least
three interviewees mentioned the same concern for each sub-theme. These were
checked by RW and SI.
Ethical considerations
The main author is Indonesian; therefore, an official research permit is not requested
as stated in the relevant regulation of Indonesia‖. However, a written informed
consent (S2 File) was obtained from all participants. Before the interviews, all
participants understood that their participation was voluntary and that they were free
to stop the interview at any time. All participants reviewed and consented to the
verbatim transcript of their interview. Additionally, the research plan and the
interviews to be conducted were reviewed by the University Medical Center
Groningen Ethical Review Board, who deemed the study non-intrusive.
Subsequently a formal waiver statement (S3 File) was provided, i.e., the study
would not need a regular ethical approval.
3
2
Chapter three

Moving Forward to Achieve Universal Health Coverage in Indonesia | 77
Results
Participants
Aiming at about 22 final participants, a total of 51 (S2 Table) different individuals
were approached during the recruitment process. Out of this number, 45 agreed to
participate in this research. However, 9 withdrew after receiving the list of
questions; another 7 decided to stop their interviews before they were finished, since
they experienced difficulties in answering the questions, and were not confident
about their answer; Furthermore 4 had no time for an interview, leaving a final
number of 25 participants. Notably, this was more than initially aimed at.
Twenty-five participants participated in this research (Table 2). They were
policy makers (WHO members, HTA Committee, NF Committee and National
Health Insurance Agency), a medicine supplier (a pharmaceutical industry
representative), healthcare providers (physicians and pharmacists), and users
(patients). All participants had the Indonesian nationality, except the WHO
members. The policymakers, the pharmaceutical industry representative and
healthcare providers each have more than 20 years of work experience in the
Indonesian healthcare system. Furthermore, all interviewed patients had been
enrolled in health insurance in Indonesia for an average of 11 years at the time of
interview.
3
2
The implementation of health technology assessment (HTA) in Indonesia

78 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Table 2. Classification of participants involved
Participants Gender Age
(Years)
Work
experience
(Yes)
Years using
public health
insurance
Professional
location
Policymakers
WHO Members Male 50 25 NA Geneva
HTA Committee Female 53 28 28 Jakarta
HTA Committee Male 55 30 30 Jakarta
NF Committee Male 56 31 31 Yogyakarta
JKN-KIS Agency Female 51 26 26 Jakarta
JKN-KIS Agency Female 46 21 21 Jakarta
Medicine Supplier
Pharmaceutical Industry Male 54 29 29 Jakarta
Healthcare Providers
Physician Male 58 33 33 Lombok
Physician Male 59 34 34 Makassar
Physician Male 66 41 41 Makassar
Physician Male 44 19 19 Surabaya
Physician Male 51 26 26 Jakarta
Physician Female 54 29 29 Yogyakarta
Pharmacist Female 53 28 28 Jakarta
Pharmacist Male 50 25 25 Manado
Pharmacist Male 39 14 14 Kendari
Pharmacist Male 42 17 17 Yogyakarta
Pharmacist Female 51 26 26 Lombok
Pharmacist Female 40 19 19 Makassar
Users
Patient Male 53 NA 8 Makassar
Patient Male 63 NA 13 Makassar
Patient Female 59 NA 10 Makassar
Patient Male 57 NA 8 Makassar
Patient Female 63 NA 12 Makassar
Patient Male 63 NA 13 Makassar
3
2
Chapter three

Moving Forward to Achieve Universal Health Coverage in Indonesia | 79
Interviews and analysis of transcripts
Semi-structured interviews were conducted face to face with 16 participants and
through video calls with 9 participants between August 2016 and April 2017. One
interview was conducted in English, while all others were in Bahasa Indonesia. The
average time spent on each interview was circa one hour.
Transcripts from the themes for HTA were checked to obtain sub-themes
(S3 Table). For all six themes, more than three interviewees mentioned the same
concern on each sub-theme. It means that saturation could be confirmed at the total
level. In table S3 we summarize the answers by respondent group, to make it easier
for readers to understand the main concerns of each stakeholder group. The
complete statement per theme can be found at raw materials (S4 Table).
Findings per theme
Theme 1: Attitudes towards HTA implementation
All stakeholders demonstrated positive attitudes towards applying HTA to the
development of the e-Catalogue and the NF. The main reason expressed for this
attitude was the necessity of having appropriate medicine policies to support the
JKN-KIS program in achieving UHC, in particular, reducing out-of-pocket
payments for medicines. Moreover, participants perceived the advantages would
outweigh the disadvantages.
“If the HTA is applied to the NF or e-Catalogue I am very amenable. This will definitely be very good and provide great benefits” [Physician 5]
Theme 2: Advantages of HTA implementation in the e-Catalogue and the NF
Stakeholders recognized that the main advantage of HTA is to provide scientific
evidence for decision makers to assess the value of a medicine. Additionally, the
participants identified various other benefits when HTA would be implemented in
the e-Catalogue and the NF.
“The money allocated for the health sector is limited, especially for medicines.
So, we can convince the government that more money should be allocated for
medicines” [Policymaker 6]
3
2
The implementation of health technology assessment (HTA) in Indonesia

80 | Moving Forward to Achieve Universal Health Coverage in Indonesia
The pharmaceutical industry representative mentioned that HTA would
provide a ground for fair pricing in the e-Catalogue. Thus, pharmaceutical industries
would not arbitrarily adapt their prices.
“HTA can provide the rational price for bidding the medicines. Now, the
pharmaceutical industry can bid the medicines as low as possible”
[Pharmaceutical Industry]
The policy makers, healthcare providers, and patients mentioned the use of
HTA would reassure all stakeholders that the medicines listed in the NF were the
best choice of medication. This would convince the government to allocate the
money for providing the medicines listed in the NF, the physicians to prescribe the
medicines listed in the NF, and also the patients to consume the medicines listed in
the NF.
“The advantage is that we may not doubt anymore about taking the medicine listed in the NF” [Patient 1]
Theme 3: Disadvantages of HTA implementation in the e-Catalogue and the NF
Among all interviewees, only a few could mention disadvantages of HTA
implementation in the e-Catalogue and the NF. The most frequently mentioned
disadvantage was the cost of developing the e-Catalogue and the NF probably would
increase, in particular to pay HTA experts. In addition, complicated bureaucracy and
lengthy processes for renewing the medicines listed in the e-Catalogue and the NF
were also mentioned by the policy makers and healthcare providers.
“People could say that this is too heavy or too bureaucratic, you need an excessively lengthy process for this” [Policymaker 1]
Theme 4: Barriers to HTA implementation
The participants identified various barriers that are currently hampering the
implementation of HTA. The first barrier mentioned by all stakeholder categories,
except the patients, was a lack of capability and a lack of capacity of local human
resources. The reasons for this as explained by several interviewees were that HTA
is a new science in Indonesia, and a lack of HTA departments, training and
associations.
3
2
Chapter three

Moving Forward to Achieve Universal Health Coverage in Indonesia | 81
“The science of HTA is still very new in Indonesia. Honestly, there are still
many health workers and maybe including me who do not understand the
application.”[Pharmacist 5]
A second barrier mentioned by all categories of stakeholders, except the
pharmaceutical industry representative, was a lack of incentives. The stakeholders
considered that currently little resources are available for paying the HTA experts,
holding HTA seminars, and performing HTA research.
“There is a significant financial problem for the experts, since the HTA
Committee still depends on the state budget and the standard fees established
by the Ministry of Finance must be adhered to. We cannot give the fee
according to their (HTA experts) expertise because there is a maximum salary that can be awarded when using the state budget”. [Policymaker 3]
A third barrier mentioned by the policy makers pharmaceutical industry
representative and healthcare providers was a lack of a clear framework of how to
implement using HTA results in the medicine policy, in particular in the e-Catalogue
and the NF. These interviewees mentioned that a clear framework is needed since
multiple professions have to cooperate to initiate HTA, perform HTA, assess and
appraise HTA results, and translate findings into policy advise.
“We do not yet have a clear path of how to apply HTA. Moreover, HTA
requires a variety of professions. This will create a conflict of interest. If there
are no clear guidelines, all will be based on the point of view of each profession”. [Pharmaceutical Industry]
A fourth barrier mentioned by the policy makers and healthcare providers
was insufficient data for conducting HTA studies. The HTA committee members
interviewed perceived the insufficient data was caused by difficulties to access data
on the national scale. National data gathering is managed by the JKN-KIS agency.
The JKN-KIS agency representative explained that the insufficient data was caused
by unclarities regarding the data needed for conducting HTA studies. Furthermore,
the health care providers also mentioned that the healthcare registry data, for
instance, individual patient data, have not been integrated in the national scale.
“The number of provinces in Indonesia makes it difficult to integrate all the
data that could be used for HTA studies, so, we still need time to collect the
data needed by the HTA researchers” [Policymaker 6]
3
2
The implementation of health technology assessment (HTA) in Indonesia
82 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Theme 5: Possible solutions to improve the implementation of HTA
The participants provided a variety of possible solutions to address the barriers
hampering the implementation of HTA. The policy makers indicated a necessity to
establish a good network to build up the capacity. For instance, students and
researchers could be endorsed to conduct HTA studies using Indonesian data.
Currently, the Ministry of Health only depends on the state budget to establish the
HTA committee and to build the capacity. Pharmaceutical industries could be
encouraged to provide additional means.
“The government must obtain alternative funding instead of depending on the
state budget to implement HTA. I think the pharmaceutical industry can
actually be asked to provide additional income in order to finance experts or researchers of HTA studies”. [Policymaker 2]
The pharmaceutical industry representative suggested the creation of a clear
framework for performing HTA implementation. The healthcare providers
recommended that the government would provide more training and seminars to
improve the capability of human resources regarding HTA. The healthcare
professionals similarly suggested opening more HTA departments in universities in
Indonesia. Finally, patients expected the government and all stakeholders to have a
good collaboration in terms of introducing the implementation of HTA in Indonesia.
“The government through the health ministry should establish guidelines to
have a clear path to implement HTA” [Pharmaceutical Industry]
“The government should encourage universities to open HTA departments. So,
we can learn the topics of HTA in a good curriculum”. [Pharmacist 1]
I hope all stakeholders can work together and find a good solution to start the
implementation of HTA in Indonesia”. [Patient 6]
Theme 6: Promoting factors for the implementation of HTA
The participants identified several promoting factors for the implementation of
HTA. First of all, the main factor mentioned by all stakeholder‘s category was that
the JKN-KIS aims to achieve UHC. Several stakeholders perceived that the use of
HTA is suitable for countries that are on their way to implement UHC. A second
promoting factor mentioned was that the use of HTA is already in the regulation for
3
2
Chapter three

Moving Forward to Achieve Universal Health Coverage in Indonesia | 83
implementing JKN-KIS, in particular to select medicines which will be covered by
the BPJS-Kesehatan. Therefore, the use of HTA is mandatory in developing the list
of medicines in the e-Catalogue and the NF. A third promoting factor was the use of
the current e-Catalogue and the NF without HTA implementation have not helped
sufficiently to reduce out-of-pocket payments for medicines.
"The supporting factor is that we are implementing an international scale
program, which is Universal Health Coverage. The HTA program is highly
recommended World Health Organization for countries implementing UHC
program.” [Physician 6]
“The regulation of Indonesia stated that HTA should be conducted for
selecting the healthcare services needed. Indonesia is lucky since it has a legal
aspect, whereas Vietnam does not have this. In some European countries it is
also not present”. [Policymaker 2]
“We need a list of medications which were well selected at the NF. This was to
avoid the doctors prescribed medicines not listed in the NF and also to prevent
patients from spending money because they have to buy medicines that are not covered by BPJS Kesehatan”. [Pharmacist 5]
3
2
The implementation of health technology assessment (HTA) in Indonesia

84 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Discussion
This study provides insight into the current implementation of HTA in Indonesia in
the development of the e-Catalogue and the National Formulary as medicines
policies, as perceived by multiple stakeholders. To the best of our knowledge, no
previous interview-based studies on this topic were performed in South East Asia.
All interviewees showed a positive attitude towards the application of HTA to the e-
Catalogue and the NF. The interviewees expected HTA could optimize the use of
the e-Catalogue and the NF to reduce out-of-pocket payments and, subsequently, to
achieve UHC in Indonesia. Furthermore, the stakeholders identified the advantages
of applying HTA to both the e-Catalogue and the NF were greater than the
disadvantages. However, interviewees mentioned that the application of HTA has
the potential to increase costs for the development of the e-Catalogue and the NF.
Specifically, this study clarifies the barriers, possible solutions, and facilitators of
HTA implementation.
Interestingly, some interviewees perceived that the use of HTA would
increase the cost for developing the e-Catalogue and the NF. However, other
participants mentioned that the use of HTA for the e-Catalogue and the NF could
improve efficiency. Our previous study[18] has revealed that the e-Catalogue and the
NF have not been fully utilized in the healthcare facilities and were often ignored by
stakeholders. This implies that unnecessary spendings have been allocated for
producing these two medicine policies. For the e-Catalogue, HTA might support the
setting of minimum prices as one of the problems mentioned was that the final
tendered prices of medicines were too low and might jeopardize quality and
distribution of medicines. Such prices would then reflect reasonable price levels for
each medicine, in terms of costs per quality adjusted life years gained[24]. In
addition, interviewees mentioned that the use of HTA in the NF might help to
provide transparency and evidence for selecting medicines listed in the NF, and that
this could improve its acceptance and use by stakeholders. Several LMICs aiming to
achieve UHC have to consider a way to limit or choose the available healthcare
services and HTA is one of the tools to support reimbursement package decision
making. Many exemplary countries, such as Thailand, China, and Australia show
3
2
Chapter three

Moving Forward to Achieve Universal Health Coverage in Indonesia | 85
how the use of HTA is helpful in selecting the medicines listed in their medicine
reimbursement list. Thus, a more effective way of achieving UHC is achieved[6].
Several barriers to implement HTA were identified and reported in the
results. The two most important barriers mentioned were a lack of local human
resources and a lack of financial incentives. Previous studies[25] based on surveys
stated that these barriers were the major barriers in 19 LMICs, including Vietnam as
Indonesia's neighboring country. In addition, for other neighboring countries, such
as Philipines and Malaysia, capacity building and financial incentives were also
identified as significant barriers for implementing HTA in their medicine policies[26-
28]. In the current study, the interviewees offered several possible solutions to
overcome these obstacles. An interesting solution suggested by the NHI agency was
that the HTA committee could establish a network with other countries that have a
well-established system, and with international HTA organizations. In response to
financial barriers, the authors support a solution suggested by the HTA committee
that the Government of Indonesia could provide an alternative funding instead of
depending on the state budget. The interviewees recognized the need of HTA but
also wondered how it should be funded. We think the implementation as achieved
by the HTA committee of Thailand may serve as an example. The Committee
obtains funding from the Thai Health Promotion Foundation, an institution
established by the Ministry of Health of Thailand to collect health funding through
two percents surcharge levied on the excise tax of alcohol and tobacco. This
institution also obtains its funding from pharmaceutical companies and international
HTA agencies[29].
The main important factor mentioned to support HTA implementation in
the e-Catalogue and the NF was a mandate in the Presidential Decree[30], which
stated that the development of medicine policies must be based on the HTA study.
This implies the HTA must be applied in the e-Catalogue and the NF development.
Based on a previous international study[31], this implication can lead to a continuous
development of the capacity building for local human resources.
Conducting interviews allowed the researcher to obtain detailed
information about personal feelings, perceptions and opinions from the participants
3
2
The implementation of health technology assessment (HTA) in Indonesia

86 | Moving Forward to Achieve Universal Health Coverage in Indonesia
indepedently from other group members. Moreover, all ambiguities and incomplete
answers could be clarified and followed up. Several steps were taken to ensure a
good research practice during the data compilation and analysis stages. The
sampling processs used to select participants and the interview guide were compared
with recommendations published in the COREQ[22].
Though a variety of stakeholders were interviewed in this study, not all
groups of stakeholders were equally large and it turned out hard to find industry
representatives willing to participate. Notably, only one pharmaceutical industry
representative agreed to participate. Nonetheless, the interviewee was relatively
experienced and was a leader in several pharmaceutical associations in Indonesia.
While saturation was reached at the level of the total group, it could not be
ensured for smaller groups of stakeholders, namely industry and policy makers.
Also, this research contained interviews with a specific group of patients, namely
from the Prolanis. The main reason for this was that participants from this group
were relatively easy to find and recruit. These patients affiliated to the Prolanis
group were considered as being able to provide more information than other patients
since they had already routinely consumed medicines and had actively used public
health insurance in Indonesia for a significant time period. It is relevant to note that
quite a few people did not feel comfortable to participate or withdrew their consent
after having seen the questions for the interview. This may indicate that a substantial
part of stakeholders is not very familiar with the concepts discussed during the
interviews and/or considers the topics as hard to discuss.
Recognizing the current barriers and facilitators identified to apply HTA in
the development of the e-Catalogue and the national formulary could assist decision
makers in developing a blueprint for the further implementation of HTA in
Indonesia. This could also be relevant for international policymakers in other LMICs
with similar characteristics and ambition to achieve UHC.
3
2
Chapter three

Moving Forward to Achieve Universal Health Coverage in Indonesia | 87
Conclusions
Several barriers are currently hampering the implementation of HTA to support
medicine pricing and reimbursement policies in Indonesia. However, solutions for
these issues are under consideration and facilitators do exist. The major barriers to
the implementation of HTA are a lack of capacity of local human resources and a
lack of (financial) incentives. Possible solutions to address these issues would be to
establish a network with other countries that have a well-established system, and
with international HTA organizations. A major opportunity to support the
implementation of HTA in the e-Catalogue and the NF is the existing legal
framework to implement HTA in medicine policies of the JKN-KIS program in
Indonesia.
Acknowledgments
The authors would like to thank all stakeholders who participated in this study.
3
2
The implementation of health technology assessment (HTA) in Indonesia

88 | Moving Forward to Achieve Universal Health Coverage in Indonesia
References
1. Sachs JD. From millennium
development goals to sustainable
development goals. Lancet.
2012;379(9832):2206-2211.
2. Kieny MP, Bekedam H, Dovlo D,
Fitzgerald J, Habicht J, Harrison G,
et al. Strengthening health systems
for universal health coverage and
sustainable development. Bull
World Health Organ.
2017;95(7):537-539.
3. World Health Organization.
Tracking universal health
coverage: First global monitoring
report. World Health Organization;
2015.
4. Khan JA, Ahmed S, Evans TG.
Catastrophic healthcare
expenditure and poverty related to
out-of-pocket payments for
healthcare in bangladesh—an
estimation of financial risk
protection of universal health
coverage. Health Policy Plan.
2017;32(8):1102-1110.
5. Bigdeli M, Laing R, Tomson G.
Medicines and universal health
coverage: Challenges and
opportunities. . 2015.
6. Yoongthong W, Hu S, Whitty JA,
Wibulpolprasert S, Sukantho K,
Thienthawee W, et al. National
drug policies to local formulary
decisions in thailand, china, and
australia: Drug listing changes and
opportunities. Value Health.
2012;15(1 Suppl):S126-31.
7. Chalkidou K, Marten R, Cutler D,
Culyer T, Smith R,
Teerawattananon Y, et al. Health
technology assessment in universal
health coverage. Lancet.
2013;382(9910):e48-9.
8. World Health Organization.
Health technology assessment,
HTA, WHO definition (EB
134/30). . Updated Access on
January 5, 2019.
9. Angelis A, Lange A, Kanavos P.
Using health technology
assessment to assess the value of
new medicines: Results of a
systematic review and expert
consultation across eight european
countries. The European Journal of
Health Economics.
2018;19(1):123-152.
10. Republik Indonesia. Undang-
undang republik indonesia nomor
3
2
3
2
Chapter three
Moving Forward to Achieve Universal Health Coverage in Indonesia | 89
24 tahun 2011 tentang badan
penyelenggara jaminan sosial. ;
2011.
11. Mundiharno TH. Peta jalan
menuju jaminan kesehatan
nasional 2012-2019. ; 2012.
12. Menteri Kesehatan Republik
Indonesia. Peraturan menteri
kesehatan republik indonesia
nomor 28 tahun 2014 tentang
pedoman pelaksanaan program
jaminan kesehatan nasional. ;
2014.
13. Kemetrian Kesehatan Republik
Indonesia. Pedoman penerapan
formularium nasional. . 2015.
14. Menteri Kesehatan Republik
Indonesia. Peraturan menteri
kesehatan republik indonesia
nomor 63 tahun 2014 tentang
pengadaan obat berdasarkan
katalog elektronik (E-catalogue). ;
2014.
15. Kementrian Kesehatan R.
Pedoman penerapan kajian
farmakoekonomi. Direktorat
Jendral Bina Kefarmasian dan Alat
Kesehatan, Jakarta. 2013.
16. Menteri Kesehatan Republik
Indonesia. Keputusan menteri
kesehatan republik indonesia
nomor 171/ menkes/ SK/ IV/ 2014
tentang komite penilaian teknologi
kesehatan. . 2014.
17. Menteri Kesehatan Republik
Indonesia. Keputusan menteri
kesehatan RI no.
HK.02.02/menkes/422/2016
tentang komite penilaian teknologi
kesehatan. . 2016.
18. Wasir R, Irawati S, Makady A,
Postma M, Goettsch W, Buskens E,
et al. Use of medicine pricing and
reimbursement policies for
universal health coverage in
indonesia. PloS one.
2019;14(2):e0212328.
19. World Health Organization.
Global health expenditure database.
. access on October 29, 2018.
20. Hidayat B, Mundiharno, Nemec J,
Rabovskaja V, Rozanna C, Spatz J.
Out-of-pocket payments in the
national health insurance of
indonesia. . 2015.
21. Dirjen Binfar dan Alkes
Kemenkes RI. Implementasi
formularium nasional dalam
pelaksanaan jaminan kesehatan
nasional. . 2015.
22. Tong A, Sainsbury P, Craig J.
Consolidated criteria for reporting
3
2
The implementation of health technology assessment (HTA) in Indonesia

90 | Moving Forward to Achieve Universal Health Coverage in Indonesia
qualitative research (COREQ): A
32-item checklist for interviews
and focus groups. International
journal for quality in health care.
2007;19(6):349-357.
23. Hsieh H, Shannon SE. Three
approaches to qualitative content
analysis. Qual Health Res.
2005;15(9):1277-1288.
24. World Health Organization. WHO
guideline on country
pharmaceutical pricing policies.
World Health Organization; 2015.
25. Babigumira JB, Jenny AM,
Bartlein R, Stergachis A, Garrison
Jr LP. Health technology
assessment in low‐and
middle‐income countries: A
landscape assessment. Journal of
Pharmaceutical Health Services
Research. 2016;7(1):37-42.
26. Jaafar S, Kamaliah Mohd Noh,
Khairiyah Abdul Muttalib, Othman
NH, Healy J, Maskon K, et al.
Malaysia health system review. .
2013.
27. Babar Z. Pharmaceutical policy in
countries with developing
healthcare systems. Springer
International Publishing AG; 2017.
28. Nguyen TA, Vitry A, Roughead
EE. Pharmaceutical policy in
vietnam. In: Pharmaceutical policy
in countries with developing
healthcare systems. Springer;
2017:75-94.
29. Teerawattananon Y, Tantivess S,
Yothasamut J, Kingkaew P,
Chaisiri K. Historical development
of health technology assessment in
thailand. Int J Technol Assess
Health Care. 2009;25(S1):241-252.
30. Presiden Republik Indonesia.
Peraturan presiden republik
indonesia nomor 12 tahun 2013
tentang jaminan kesehatan. ; 2013.
31. Kaló Z, Gheorghe A, Huic M,
Csanádi M, Kristensen FB. HTA
implementation roadmap in central
and eastern european countries.
Health Econ. 2016;25(S1):179-
192.
3
2
Chapter three

Moving Forward to Achieve Universal Health Coverage in Indonesia | 91
Supporting Information
S1 Fig. Conceptual framework
Explanation of conceptual framework:
Many countries aim to reform their national health insurance to reach universal
health coverage. Nowadays, 58 countries are using universal health coverage
besides Indonesia. Before 2014, various health insurance schemes covered health
insurance for Indonesian society. As of 2014, all these schemes were integrated
and organized under one agency called BPJS-Kesehatan. The main goal of this
insurance is to achieve universal health coverage by 2019. The problem with
BPJS-Kesehatan was budgetary constraints, with the highest expenditure being
pharmaceuticals. The national formulary was used to organize medicines. HTA
has not yet been applied in the national formulary, while many UHC countries
do.
3
2
The implementation of health technology assessment (HTA) in Indonesia

92 | Moving Forward to Achieve Universal Health Coverage in Indonesia
S1 Table. Initial list of themes and of questions
NO THEMES NO QUESTIONS
1 The development
of medicine policy
and national
health insurance
1 Do you know how long the HTA Committee, NF
Committee, and NHI Agency have existed?
2 How many committee members?
3 What are their professions?
4 What are their duties?
5 Why do they exist?
6 What is their function?
7 What is their role in supporting UHC?
8 How is the NHI different from previous health
insurance (Askes, Jamkesmas, etc)?
9 How many people are covered by the NHI Agency
currently?
2 Medicines policy
for UHC
10 What medicines policy or policies should be created
to support UHC?
11 Are you involved in creating the NF and other
medicines policies to support UHC?
3 Users Perspective 12 Do you know how the National Formulary is
compiled?
13 Do you agree with the NF?
14 Do you have policy recommendations to maximize
the use of HTA?
15 Do you have other policy recommendations for
prescribing drugs?
4 Obstruction and
promoting factors
of HTA
16 What is/are the advantage(s) using HTA in
medicines policy?
17 What is/are the disadvantage(s) using HTA in
medicines policy?
18 What is/are the facilitator(s) implementing HTA in
medicines?
19 What is/are the barrier(s) implementing HTA in
medicines?
20 What should other stakeholders do to solve them?
And which ones?
21 What should the government do?
5 The biggest
burden of disease
and medicine
expenditure
22 What is the most widespread disease in Indonesia?
23 How much money is allocated for medicines in the
national health system?
24 What medicines are allocated more money? (Why?)
6 Prescriptions not
in NF
25 Have you ever received prescriptions for drugs not
in the NF (How frequently and why)?
26 Which medicines do you receive most often that are
in the NF?
27 Do you agree when doctors prescribe medicines not
in the NF? Why?
3
2
Chapter three
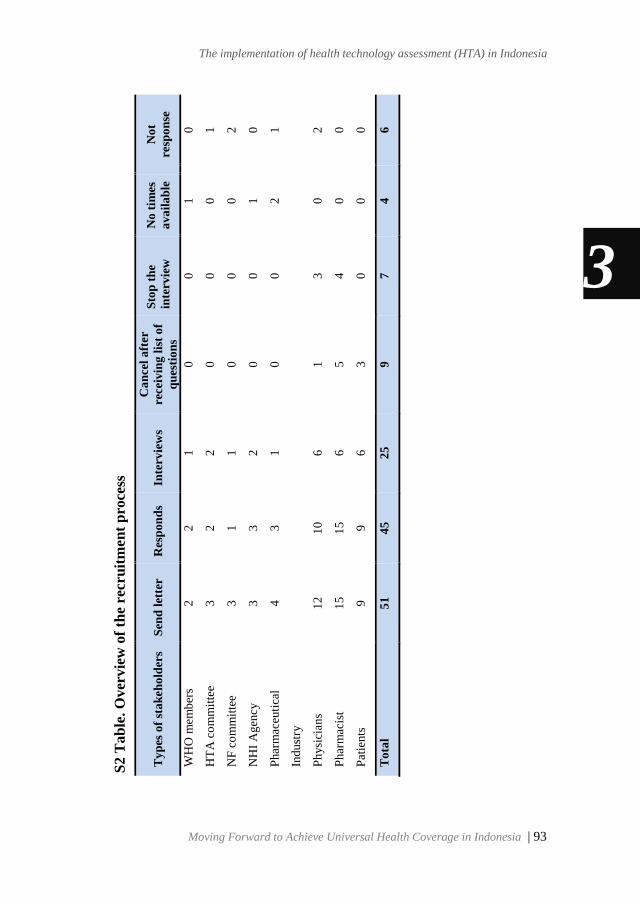
Moving Forward to Achieve Universal Health Coverage in Indonesia | 93
S6
Ta
ble
. O
ver
vie
w o
f re
cru
itm
en
t p
roce
ss
Ty
pes
of
sta
keh
old
ers
Sen
d l
ette
r
Res
po
nd
s In
terv
iew
s
Ca
nce
l a
fter
rece
ivin
g l
ist
of
qu
esti
on
s
Sto
p t
he
inte
rvie
w
No
tim
es
av
ail
ab
le
No
t
resp
on
se
WH
O m
em
ber
s 2
2
1
0
0
1
0
HT
A c
om
mit
tee
3
2
2
0
0
0
1
NF
co
mm
itte
e
3
1
1
0
0
0
2
NH
I A
gen
cy
3
3
2
0
0
1
0
Phar
mac
euti
cal
Ind
ust
ry
4
3
1
0
0
2
1
Ph
ysi
cian
s 1
2
10
6
1
3
0
2
Phar
mac
ist
15
15
6
5
4
0
0
Pat
ients
9
9
6
3
0
0
0
To
tal
51
45
25
9
7
4
6
S2 T
ab
le. O
ver
vie
w o
f th
e re
cru
itm
ent
pro
cess
3
2
The implementation of health technology assessment (HTA) in Indonesia

94 | Moving Forward to Achieve Universal Health Coverage in Indonesia
3
2
Chapter three
Moving Forward to Achieve Universal Health Coverage in Indonesia | 95
S4. Table. Raw materials
Raw material can be found in this link below:
https://doi.org/10.1371/journal.pone.0225626.s005
or in this quick response code below
3
2
The implementation of health technology assessment (HTA) in Indonesia
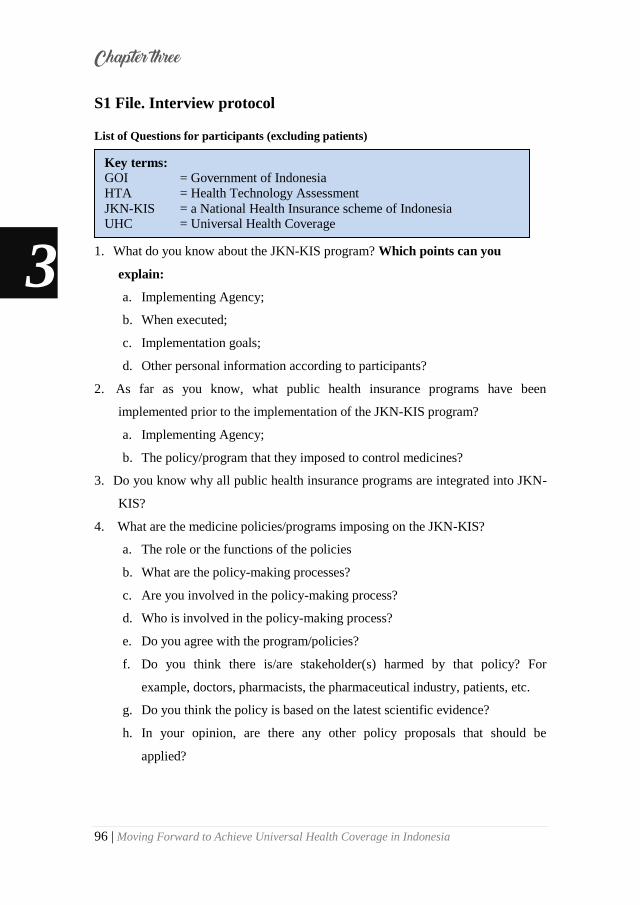
96 | Moving Forward to Achieve Universal Health Coverage in Indonesia
S1 File. Interview protocol
List of Questions for participants (excluding patients)
1. What do you know about the JKN-KIS program? Which points can you
explain:
a. Implementing Agency;
b. When executed;
c. Implementation goals;
d. Other personal information according to participants?
2. As far as you know, what public health insurance programs have been
implemented prior to the implementation of the JKN-KIS program?
a. Implementing Agency;
b. The policy/program that they imposed to control medicines?
3. Do you know why all public health insurance programs are integrated into JKN-
KIS?
4. What are the medicine policies/programs imposing on the JKN-KIS?
a. The role or the functions of the policies
b. What are the policy-making processes?
c. Are you involved in the policy-making process?
d. Who is involved in the policy-making process?
e. Do you agree with the program/policies?
f. Do you think there is/are stakeholder(s) harmed by that policy? For
example, doctors, pharmacists, the pharmaceutical industry, patients, etc.
g. Do you think the policy is based on the latest scientific evidence?
h. In your opinion, are there any other policy proposals that should be
applied?
Key terms:
GOI = Government of Indonesia
HTA = Health Technology Assessment
JKN-KIS = a National Health Insurance scheme of Indonesia UHC = Universal Health Coverage
3
2
Chapter three

Moving Forward to Achieve Universal Health Coverage in Indonesia | 97
5. What do you know about the HTA?
a. Implementing Agency;
b. When executed;
c. Implementation goals;
6. Do you think the HTA should be applied to the medicine policies on the JKN-
KIS?
7. In your opinion, what are the advantages and disadvantages of using HTA in
medicine policies on JKN-KIS?
8. In your opinion, what are the supporting and inhibiting factors for the use of
HTA on medicine policies in JKN-KIS?
9. In your opinion, what solutions should be found to implement the HTA on
medicine policies in JKN-KIS?
a. What should be done by all stakeholders (policymakers, doctors,
pharmacists, drug companies, patients, etc.)
b. What should be done by the GOI?
10. Have you ever found prescriptions not in the medicine policies on JKN-KIS?
a. Do you know why this occurred?
b. Do you agree with prescriptions not being in the medicines policy?
c. What medicines are most commonly prescribed that are not part of the
policies of JKN-KIS?
d. Do you have any suggestions to overcome this?
11. Do you know how much money is allocated for medicines to support the JKN-
KIS program?
a. Do you know which drugs are allocated the largest budget?
12. Do you know what is the most widespread disease in Indonesia?
a. Do you know how much money is allocated to cope with this disease?
13. Do you have other comments regarding this research?
3
2
The implementation of health technology assessment (HTA) in Indonesia

98 | Moving Forward to Achieve Universal Health Coverage in Indonesia
List of Questions for Participants (excluding patients) in
Bahasa
1. Apa yang anda ketahui tentang JKN-KIS. Point yang dapat anda jelaskan
yaitu:
a. Instansi apa yang melaksanakan?
b. Kapan mulai dilaksanakan?
c. Apa tujuan dilaksanakan?
d. Informasi lain yang dianggap perlu disampaikan dari partisipan
2. Sejauh yang anda ketahui, program jaminan kesehatan publik apa saja yang
dilaksanakan sebelum diberlakukannya JKN-KIS?
a. Instansi apa yang melaksanakan?
b. Apakah anda tahu kebijakan/ program apa yang mereka terapkan untuk
mengontrol obat?
3. Apakah anda tahu, mengapa seluruh program jaminan kesehatan publik
berintegrasi ke JKN-KIS?
4. Apa sajakah kebijakan/ program yang sudah diberlakukan oleh pemerintah pada
program JKN-KIS?
a. Apakah anda tahu fungsi kebijakan/ program tersebut?
b. Apakah anda tahu bagaimana proses pembuatan kebijakan tersebut?
c. Apakah anda terlibat dalam proses pembuatan kebijakan tersebut?
d. Siapa-siapa saja yang terlibat dalam proses pembuatan kebijakan tersebut?
e. Apakah anda setuju dengan kebijakan tersebut? Mengapa?
f. Menurut anda, adakah stakeholders (Dokter, Apoteker, Perusahaan obat,
pasien, dll) yang dirugikan dengan kebijakan tersebut?
g. Menurut anda, apakah kebijakan tersebut telah melalui bukti ilmiah
mutakhir?
h. Menurut anda, adakah usulan kebijakan lain yang sebaiknya diterapkan?
Pengertian Istilah:
HTA = Health Technology Assessment/ Penilaian Teknologi Kesehatan;
JKN-KIS = Program Jaminan Kesehatan Nasional di Indonesia;
UHC = Universal Health Coverage/ Cakupan Perlindungan Semesta.
3
2
Chapter three

Moving Forward to Achieve Universal Health Coverage in Indonesia | 99
5. Apa yang anda ketahui tentang HTA?
a. Instansi apa yang melaksanakan?
b. Kapan mulai dilaksanakan?
c. Apa tujuan dilaksanakan?
6. Menurut anda, apakah HTA sebaiknya diterapkan pada kebijakan obat yang
sudah diterapkan pemerintah untuk mendukung JKN-KIS?
7. Menurut anda, apa keuntungan dan kerugian menggunakan HTA pada
kebijakan obat yang sudah diterapkan pemerintah?
8. Menurut anda, apa faktor pendukung dan faktor penghambat menggunakan
HTA pada kebijakan obat yang sudah diterapkan pemerintah?
9. Menurut anda, soulusi apa yang sebaiknya dilakukan untuk melaksanakan HTA
pada kebijakan obat yang sudah diterapkan pemerintah?
a. Apa yang sebaiknya dilakukan oleh para stakeholders (pembuat kebijakan,
dokter, apoteker, perusahaan obat, pasien, dll)?
b. Apa yang sebaiknya dilakukan oleh pemerintah?
10. Pernahkah anda menemukan peresepan obat di luar kebijakan obat yang sudah
diterapkan pemerintah?
a. Apakah anda setuju dengan peresepan obat diluar kebijakan obat yang
sudah diterapkan pemerintah?
b. Obat apa yang paling sering diresepkan diluar kebijakan obat yang sudah
diterapkan pemerintah?
c. Apakah anda tahu, bagaimana cara mengatasi hal tersebut?
11. Apakah anda tahu berapa banyak anggaran belanja obat yang dialokasikan
untuk mendukung JKN-KIS?
a. Apakah anda tahu obat apa yang mendapatkan anggaran terbesar?
12. Apakah anda tahu penyakit yang terbesar di Indonesia?
a. Apakah anda tahu berapa banyak anggaran untuk obat yang dialokasikan
untuk mengatasi penyakit tersebut?
13. Apakah ada komentar lainyang ingin anda sampaikan terkait penelitian ini?
3
2
The implementation of health technology assessment (HTA) in Indonesia

100 | Moving Forward to Achieve Universal Health Coverage in Indonesia
A List of Questions for Patients
1. Do you know about JKN-KIS, which is part of BPJS-Kesehatan? Could you
explain briefly it?
2. Are you a participant in JKN-KIS?
3. When were you be a participant in JKN-KIS?
4. What health insurance did you use before JKN-KIS?
5. For how long were you a participant in that insurance?
6. Are you currently taking any medication?
a. When was the last time you took the drugs?
b. What drugs did you take?
7. Did you also take that medicine when using your previous insurance?
8. Do you feel a difference when taking medication of JKN-KIS compared with
medication of your previous health insurance?
a. Which one is cheaper?
b. Which are more efficacious?
c. Which one do you like, and think is better?
9. Is there a difference, do you feel, in terms of service between JKN-KIS and
your previous health insurance?
a. Are there differences when seeing doctors?
b. Is there a difference when conducting laboratory checks or other checks?
10. Do you know about UHC? Could you explain briefly what you know?
a. Do you agree with the GOI‘s target of reaching UHC in 2019?
b. Do you think it can be achieved?
c. Are there any suggestions from you in order to achieve the UHC?
11. Do you know about NF? Could you explain briefly about that?
a. Do you know how NF is created?
Key terms:
GOI = Government of Indonesia
HTA = Health Technology Assessment
JKN-KIS = a National Health Insurance scheme of Indonesia
UHC = Universal Health Coverage
NF = National Formulary
3
2
Chapter three

Moving Forward to Achieve Universal Health Coverage in Indonesia | 101
b. Do you agree with NF?
c. What medications do you often receive which are in NF?
d. Have you ever received prescriptions not in the NF? How often? Why?
e. Do you agree with prescriptions not in the NF? Why?
f. Do you have a policy recommendation in prescriptions?
12. Do you know about HTA? Could you explain briefly what you know?
a. Do you think the HTA can be used for medicines policy in Indonesia?
b. In your opinion, what is the advantage of using HTA in determining the
choice of medicines?
c. In your opinion, what are the disadvantages of using HTA in determining
the choice of medicines?
d. In your opinion, what are the promoting factors in implementing an HTA
for drug selection?
e. In your opinion, what are the obstacles in implementing an HTA for drug
selection?
f. In your opinion, what should be done by stakeholders to resolve this?
g. In your opinion, what should the government do?
13. Do you have suggestions for improving medicines policy?
14. Do you have other comments related to this research?
3
2
The implementation of health technology assessment (HTA) in Indonesia

102 | Moving Forward to Achieve Universal Health Coverage in Indonesia
A List of Questions for Patients in Bahasa
1. Apakah anda tahu tentang jaminan kesehatan nasional yang dikelola oleh BPJS-
Kesehatan? Bisakah anda Jelaskan sedikit tentang hal itu?
2. Apakah anda anggota BPJS-Kesehatan?
3. Kapan anda mulai menjadi anggota BPJS-Kesehatan?
4. Asuransi apa yang anda gunakan sebelum menjadi anggota BPJS-Kesehatan ?
5. Berapa lama anda menjadi anggota asuransi tersebut?
6. Apakah anda mengkonsumsi obat saat ini?
a. Kapan terakhir kali anda mengkonsumsi obat?
b. Obat apa?
7. Apakah obat tersebut juga anda konsumsi dengan menggunakan asuransi yang
sebelumnya?
8. Apakah ada perbedaan yang anda rasakan ketika menggunakan obat dari BPJS
dengan obat dari asuransi anda sebelumnya?
a. Yang mana yang lebih murah?
b. Yang mana yang lebih berkhasiat?
c. Yang mana yang anda suka dan anggap lebih baik?
9. Apakah ada perbedaan yang anda rasakan dari sisi pelayanan pada Asuransi
BPJS dan Asuransi yang anda gunakan sebelumnya?
a. Apakah ada perbedaan ketika bertemu dengan dokter?
b. Apakah ada perbedaan ketika melakukan cek laboratorium atau
pemeriksaan lainnya?
10. Apakah anda tahu tentang Univeral Health Coverage (UHC)/ Jaminan kesehatan
secara menyeluruh? Bisakah anda Jelaskan sedikit tentang hal itu?
a. Apakah anda sependapat dengan pemerintah Indonesia yang ingin
mencapai UHC di tahun 2019?
b. Apakah anda pikir itu bisa dicapai?
c. Apakah ada saran dari anda untuk mencapai UHC tersebut?
11. Apakah anda tahu tentang Formularium Nasional (Fornas)?
a. Apakah anda tahu bagaimana Fornas dibuat?
b. Apakah anda setuju dengan Formularium Nasional?
3
2
Chapter three

Moving Forward to Achieve Universal Health Coverage in Indonesia | 103
c. Obat apa yang sering anda terima yang ada di dalam Fornas?
d. Pernakah anda menerima obat di luar Fornas? Seberapa sering? Kenapa?
e. Apakah anda setuju ketika dokter menuliskan obat diluar formularium
nasional? Kenapa?
f. Apakah anda memiliki rekomendasi kebijakan dalam penulisan obat?
12. Apakah anda tahu tentang Health Technology Assessment (HTA) / Penilaian
Teknologi Kesehatan? Bisakah anda Jelaskan sedikit tentang hal itu?
a. Menurut anda, apakah HTA dapat digunakan untuk kebijakan obat di
Indonesia?
b. Menurut anda, apa keuntungan menggunakan HTA dalam menentukan
pilihan obat?
c. Menurut anda, apa kerugian menggunakan HTA dalam menentukan
pemilihan obat?
d. Menurut anda, apa faktor pendukung dalam menjalankan HTA pada
pemilihan obat?
e. Menurut anda, apa faktor penghambat dalam menjalankan HTA pada
pemilihan obat?
f. Apa yang harus dilakukan oleh pemangku kebijakan untuk menyelesaikan
itu?
g. Menurut anda, apa yang harus dilakukan oleh pemerintah?
13. Apakah anda memiliki saran untuk meningkatkan kebijakan obat?
14. Apakah anda memiliki saran untuk penelitian ini?
The implementation of health technology assessment (HTA) in Indonesia
3
2

104 | Moving Forward to Achieve Universal Health Coverage in Indonesia
S2 File. Informed consent
Lembar penjelasan dan persetujuan kepada partisipan
Peluang dan tantangan kebijakan obat pada program JKN-KIS untuk mencapai
Cakupan Perlindungan Semesta / Universal Health Coverage (UHC)
Saya Riswandy Wasir, Mahasiswa Program Pascasarjana (S3) Departemen
Epidemiologi, Univerity Medical Center Groningen (UMCG), University of
Groningen, Netherlands. Saat ini saya sedang melakukan penelitian yang berjudul
―peluang dan tantangan kebijakan obat pada program JKN-KIS untuk mencapai
cakupan perlindungan semesta‖.
Pemerintah Indonesia telah menerapkan skema asuransi kesehatan nasional
(JKN-KIS) yang terintegrasi dimulai pada tahun 2014. Asuransi kesehatan yang
dikelolah oleh BPJS-Kesehatan dimaksudkan sebagai pengganti seluruh asuransi
kesehatan publik sebelumnya. Peta jaminan kesehatan nasional yang dirilis oleh
pemerintah menyatakan bahwa program JKN-KIS diupayakan mencapai cakupan
perlindungan semseta/ Universal Health Coverage (UHC) pada tahun 2019.
Organisasi Kesehatan Dunia/ World Health Organization (WHO) menyatakan
bahwa bukan hanya kepesertaan yang menjadi indikator tercapainya cakupan
perlindungan semesta, tetapi juga kualitas pelayanan.
Berbagai upaya telah dilakukan oleh pemerintah dan para pemangku
kebijakan untuk meningkatkan mutu pelayanan JKN-KIS. Pada sektor obat,
pemerintah Indonesia telah menerapkan formularium nasional. Manfaat Fornas yaitu
sebagai acuan penetapan penggunaan obat dalam JKN-KIS, serta meningkatkan
penggunaan obat yang rasional, dapat juga mengendalikan mutu dan biaya
pengobatan, serta mengoptimalkan pelayanan kepada pasien Namun, Hasil evaluasi
awal yang dilakukan oleh Direktorat Jenderal Bina Farmasi dan Alat Kesehatan
(Dirjen Binfar dan Alkes) memperlihatkan bahwa kesesuaian obat yang digunakan
di rumah sakit dengan formularium nasional berkisar antara 60 – 86 %. Hal ini
memperlihatkan bahwa masih ditemukan cost-sharing, suatu kondisi dimana peserta
JKN-KIS harus mengeluarkan biaya untuk pembayaran pelayanan kesehatan
Chapter three
3
2
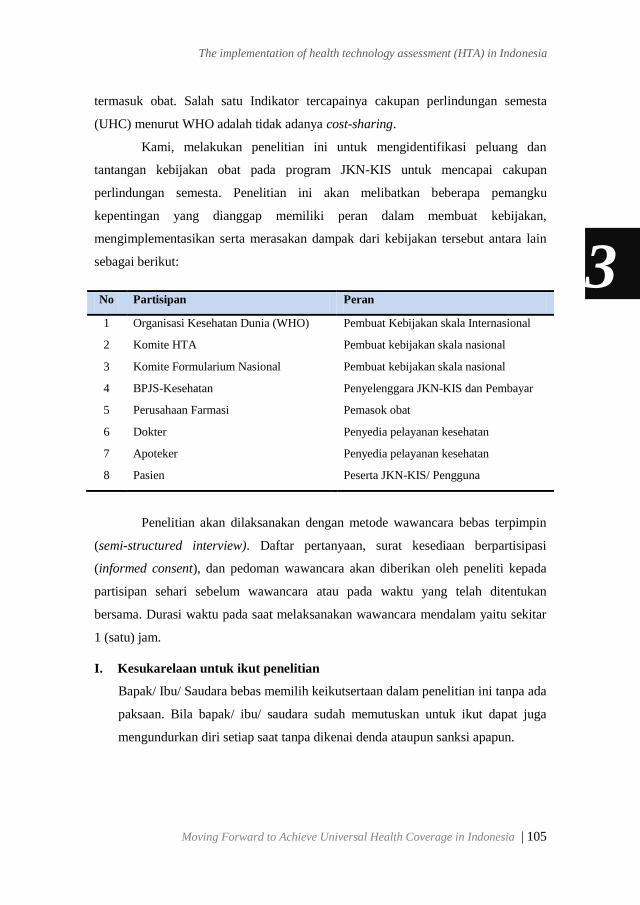
Moving Forward to Achieve Universal Health Coverage in Indonesia | 105
termasuk obat. Salah satu Indikator tercapainya cakupan perlindungan semesta
(UHC) menurut WHO adalah tidak adanya cost-sharing.
Kami, melakukan penelitian ini untuk mengidentifikasi peluang dan
tantangan kebijakan obat pada program JKN-KIS untuk mencapai cakupan
perlindungan semesta. Penelitian ini akan melibatkan beberapa pemangku
kepentingan yang dianggap memiliki peran dalam membuat kebijakan,
mengimplementasikan serta merasakan dampak dari kebijakan tersebut antara lain
sebagai berikut:
No Partisipan Peran
1 Organisasi Kesehatan Dunia (WHO) Pembuat Kebijakan skala Internasional
2 Komite HTA Pembuat kebijakan skala nasional
3 Komite Formularium Nasional Pembuat kebijakan skala nasional
4 BPJS-Kesehatan Penyelenggara JKN-KIS dan Pembayar
5 Perusahaan Farmasi Pemasok obat
6 Dokter Penyedia pelayanan kesehatan
7 Apoteker Penyedia pelayanan kesehatan
8 Pasien Peserta JKN-KIS/ Pengguna
Penelitian akan dilaksanakan dengan metode wawancara bebas terpimpin
(semi-structured interview). Daftar pertanyaan, surat kesediaan berpartisipasi
(informed consent), dan pedoman wawancara akan diberikan oleh peneliti kepada
partisipan sehari sebelum wawancara atau pada waktu yang telah ditentukan
bersama. Durasi waktu pada saat melaksanakan wawancara mendalam yaitu sekitar
1 (satu) jam.
I. Kesukarelaan untuk ikut penelitian
Bapak/ Ibu/ Saudara bebas memilih keikutsertaan dalam penelitian ini tanpa ada
paksaan. Bila bapak/ ibu/ saudara sudah memutuskan untuk ikut dapat juga
mengundurkan diri setiap saat tanpa dikenai denda ataupun sanksi apapun.
3
2
The implementation of health technology assessment (HTA) in Indonesia

106 | Moving Forward to Achieve Universal Health Coverage in Indonesia
J. Prosedur Penelitian
Apabila Bapak/ Ibu/ Saudara bersedia berpartisipasi dalam penelitian ini,
diminta menandatangani lembar persetujuan ini rangkap dua, satu untuk Bapak/
Ibu/ Saudara simpan, dan satu untuk peneliti. Prosedur selanjutnya adalah :
5. Penelitian akan dilaksanakan dengan metode wawancara terpimpin (semi-
structured Interview) sesuai dengan kesepakatan dan kenyamanan bapak/
ibu/ saudara menggunakan alat perekam.
6. Peneliti akan mentranskrip hasil wawancara setelah melaksanakan
interview dengan partisipan.
7. Hasil transkrip akan diperlihatkan kembali kepada partisipan untuk
mengklarifikasi hasil wawancara.
8. Hasil transkrip yang telah disepakati antara peneliti dan partisipan akan
diproses oleh peneliti beserta tim peneliti lainnya untuk kemudian dijadikan
data kualitatif yang akan di publikasi.
K. Kewajiban partisipan
Sebagai partisipan, Bapak/Ibu/Saudara berkewajiban mengikuti aturan atau
petunjuk penelitian seperti yang tertulis di atas. Bila ada yang belum jelas,
Bapak/ Ibu/ Saudara bisa bertanya lebih lanjut kepada peneliti.
L. Risiko
Penelitian ini tidak menyebabkan risiko yang berbahaya, karena peneliti tidak
melakukan intervensi apapun. Risiko ketidaknyamanan atau dampak yang
mungkin akan diterima yaitu merasa bosan dengan banyaknya
pertanyaan- pertanyaan dari peneliti dan kerugian waktu selama
diwawancarai oleh peneliti.
M. Manfaat dan Keuntungan
Manfaat dan keuntungan yang bapak/ ibu/ saudara dapatkan adalah kesempatan
dan kebebasan untuk menjelaskan mengenai apa yang anda rasakan terhadap
kebijakan obat pada program JKN-KIS. Penelitian ini nantinya akan diupayakan
menjadi masukan terhadap pengambil kebijakan dalam meningkatkan sektor
kesehatan nasional.
3
2
Chapter three
Moving Forward to Achieve Universal Health Coverage in Indonesia | 107
N. Kerahasiaan
Semua informasi yang berkaitan dengan identitas partisipan akan dirahasiakan
dan hanya akan diketahui oleh peneliti. Data hasil penelitian akan disimpan
dan didokumentasikan oleh peneliti serta hanya digunakan untuk
kepentingan ilmiah. Hasil penelitian akan dipublikasikan tanpa identitas
partisipan.
O. Kompensasi
Bapak/ ibu/ saudara akan mendapatkan souvenir sebagai wujud terima kasih
peneliti atas partisipasinya dalam penelitian ini.
P. Informasi Tambahan
Bapak/ ibu/ saudara diberi kesempatan untuk menanyakan semua hal yang
belum jelas sehubungan dengan penelitian ini. Bila sewaktu-waktu terjadi
kekeliruan atau membutuhkan penjelasan lebih lanjut, Bapak/ ibu/ saudara
dapat menghubungi Riswandy Wasir pada no HP: +62-81225835007 atau
bisa juga dengan mengirimkan email: [email protected]
3
2
The implementation of health technology assessment (HTA) in Indonesia

108 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Persetujuan keikutsertaan dalam penelitian
(informed consent)
Saya yang bertandatangan dibawah ini:
Nama :........................................................................
Alamat : .......................................................................
Nomor Hp : .......................................................................
E-mail : .......................................................................
Umur : .......................................................................
Pekerjaan : .......................................................................
Pendidikan Terakhir : .......................................................................
Peran partisipan :
9. Anggota Organisasi Kesehatan Dunia / World Health Organization (WHO)
10. Komite Penilaian Teknologi Kesehatan / Health Technology Assessment
(HTA)
11. Komite Formularium Nasional
12. Instansi Penyelenggara Asuransi Kesehatan Nasional
13. Perusahaan Farmasi
14. Dokter
15. Apoteker
16. Pasien
Menyatakan bahwa, semua penjelasan tersebut telah disampaikan kepada saya
sebagai partisipan dan semua pertanyaan saya telah dijawab oleh peneliti.
Saya mengerti bahwa bila memerlukan penjelasan, saya dapat menanyakan
kepada saudara Riswandy Wasir sebagai peneliti utama.
Dengan menandatangani formulir ini, saya setuju untuk ikut serta dalam penelitian
ini
Tanggal: Tanggal:
Tanda Tangan Partisipan Tanda Tangan Peneliti
Nama Jelas: …………………………….
Nama Jelas: Riswandy Wasir
3
2
Chapter three

Moving Forward to Achieve Universal Health Coverage in Indonesia | 109
S3 File. A formal waiver statements
3
2
The implementation of health technology assessment (HTA) in Indonesia

110 | Moving Forward to Achieve Universal Health Coverage in Indonesia
3
2
Chapter three

Moving Forward to Achieve Universal Health Coverage in Indonesia | 111
Chapter 4
Trends and projection of health financing for
universal health coverage in Indonesia
Riswandy Wasir,
Maarten Postma
Jurjen Van der Schans
Ali Gufron Mukti
Erik Buskens
Submitted

112 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Abstract
Objectives
Universal Health Coverage (UHC) is part of the sustainable development goals
(SDGs) that should be achieved by 2030. The World Health Organization (WHO)
proposed several health financing goals for countries aiming for UHC: out-of-
pocket (OOP) payments should be less than 20% of total health expenditures (THE),
voluntary healthcare payment schemes should not surpass a maximum of 10 % of
THE, and, finally, governmental healthcare schemes should represent at least 4% of
the gross domestic product (GDP). In 2014, Indonesia introduced, Jaminan
Kesehatan Nasional-Kartu Indonesia Sehat (JKN-KIS), a national health insurance,
aiming for UHC by 2020. This study assesses the progress of Indonesia‘s health
financing towards UHC.
Methods:
Data from the period of 2000–2016 on population, GDP and health financing of
Indonesia were extracted from the Indonesian central bureau of statistics, ministry of
health of Indonesia, national health accounts of Indonesia and WHO global health
expenditure database. Developments of Indonesia‘s health financing by schemes and
revenue schemes were assessed. Then trends in health financing by schemes were
extrapolated. Linear extrapolation was applied to estimate population size, GDP, and
health expenditures through 2030. Comparisons with the foreseen UHC targets were
displayed.
Results:
Between 2000 and 2016 OOP payments still dominated health financing of
Indonesia. From 2014 to 2016, government schemes increased and OOP schemes
decreased. Based on extrapolation of trends we predict government spending to
increase, and the household OOP scheme to decrease until 2030. Notably, the target
for achieving OOP below 20% will not be achieved by 2020. This most likely will
take five more years. Meanwhile, we also estimate the government expenditure
schemes to remain less than 2% of GDP for considerably longer.
4
2
Chapter four

Moving Forward to Achieve Universal Health Coverage in Indonesia | 113
Conclusions:
JKN-KIS may a cornerstone for Indonesia to achieve UHC according to the WHO
targets. By 2030, the targets of reducing household OOP payments below 20% and
reducing voluntary healthcare payment to 10% appear feasible to achieve given de
funds required will be made available. However, the target of government schemes
as high a 4% of GDP may be a challenging target.
4
2
Health financing system for universal health coverage in Indonesia

114 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Introduction
In 2015 the commitment to achieve universal health coverage (UHC) as part of the
sustainable development goals by 2030 was agreed by all member states of the
United Nations[1]. UHC is defined by all people in a society being able to obtain the
high-quality health services that they need, without the possibility that the cost of
paying for these services at the time of use will push them into severe financial
hardship[2]. Appropriate health financing systems are required for achieving UHC in
a country. The system should provide prepaid pooled resources to make sure that the
households do not experience financial difficulties while or after obtaining health
services[3]. Many countries committed to achieving UHC are reviewing, analyzing,
and modifying their health financing arrangements[4,5].
In 2017, the Organization for Economic Co-operation and Development
(OECD), Eurostat and the World Health Organization (WHO) produced a system of
health accounts (SHA) 2011 to provide a framework of health financing schemes. In
moving forward to achieving UHC, SHA 2011 could facilitate countries for
understanding and assessing their health expenditure. According to WHO, targets of
health expenditure for achieving UHC are that (1) the household out-of-pocket
(OOP) schemes should be below 20% of the total health expenditure (THE); (2) the
voluntary healthcare payment schemes should not surpass a maximum of 10 % of
THE; and (3) the government schemes and compulsory contributory healthcare
financing schemes should at least reach 4% of GDP[6-8].
Indonesia is one of the countries of the United Nations which is currently
striving to achieve UHC. Indonesia‘s constitution or Undang-Undang Dasar 1945,
article 28 states that health is a basic right of every individual, and that all citizens
are entitled to health services including the least affluent. Between 2000 and 2014,
there were several social health insurances offered by the government of Indonesia.
These were Asuransi Kesehatan (Askes, for civil servants and the military), Jaminan
Sosial Tenaga Kerja (Jamsostek, social security program for laborers, Jaminan
Kesehatan Masyarakat (Jamkesmas, for poor and near-poor), and Jaminan
Kesehatan Daerah (Jamkesda, for poor and near poor in several provinces)[9,10].
4
2
Chapter four

Moving Forward to Achieve Universal Health Coverage in Indonesia | 115
Because the different schemes were difficult to manage and lead to unequal
access, on the first of January 2014 all the social health insurances were merged into
one single national health insurance, which is known as Jaminan Kesehatan
Nasional-Kartu Indonesia Sehat (JKN-KIS). Through the JKN-KIS program, the
Indonesian government has officially stated its commitment to achieve UHC by
2020. The Badan Penyelenggara Jaminan Sosial Kesehatan (BPJS-Kesehatan) is a
new public health insurance provider created by the Indonesian government to
implement the JKN-KIS program. As a single payer, BPJS Kesehatan plays a role in
collecting a prepaid pool from the government, private firms, and households into a
single national pool[11,12].
Understanding current and future trajectories of health financing is vital for
Indonesia to assess their progress towards UHC. Notably, it remains unclear whether
Indonesia has organized its health financing system in line with the UHC targets.
Overall, this study aims to assess the progress of the health financing system in
Indonesia. Trends of health financing schemes prior to and after the implementation
of JKN-KIS are described. Furthermore, projection of health financing schemes is
also made through 2030, i.e., in line with the target of achieving UHC set in SDGs
agenda.
4
2
Health financing system for universal health coverage in Indonesia

116 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Methods
Data sources
The historical data of Indonesia between 2000 and 2016 were extracted from multiple
sources. Data on Indonesian health financing systems, gross domestic product (GDP),
and number of the population, were obtained from the Indonesian central bureau of
statistics, ministry of health of Indonesia, national health account of Indonesia, and the
global health expenditure database. The data on health financing and GDP were reported
in current US dollars. Exchange rates are adjusted per year.
In this study, components of health financing data were collected by
following the SHA 2011 revised edition framework[13]. In this framework,
components of health financing are categorized by schemes and by revenues. Health
financing by schemes are structural components of health care financing systems.
Health financing schemes comprise four components: (1) government schemes and
compulsory contributory healthcare financing schemes, which has two sub
components: government and social health insurance schemes; (2) voluntary
healthcare payment schemes, which has three sub components: voluntary health
insurance, non-profit organization, and enterprise financing schemes; (3) household
OOP schemes; (4) rest of the world (non-resident) schemes.
Health financing by revenues are the sources of revenues of health
financing by schemes. Health financing by revenues comprises of six components:
(1) transfer from government domestic revenue, which has three components:
internal transfer and grants, transfer by government on behalf of specific groups,
other transfers from government domestic revenues; (2) transfer distributed by
government from foreign origin; (3) social insurance contribution; (4) voluntary
prepayment; (5) Other domestic revenues from four sources, namely, household,
corporations, non-profit organization, and unspecified sources; (6) direct foreign
transfer.
The sources of health financing by schemes and by revenues is presented in
table 1. The funds for health financing by schemes may come from one or more
health financing source[13].
4
2
Chapter four
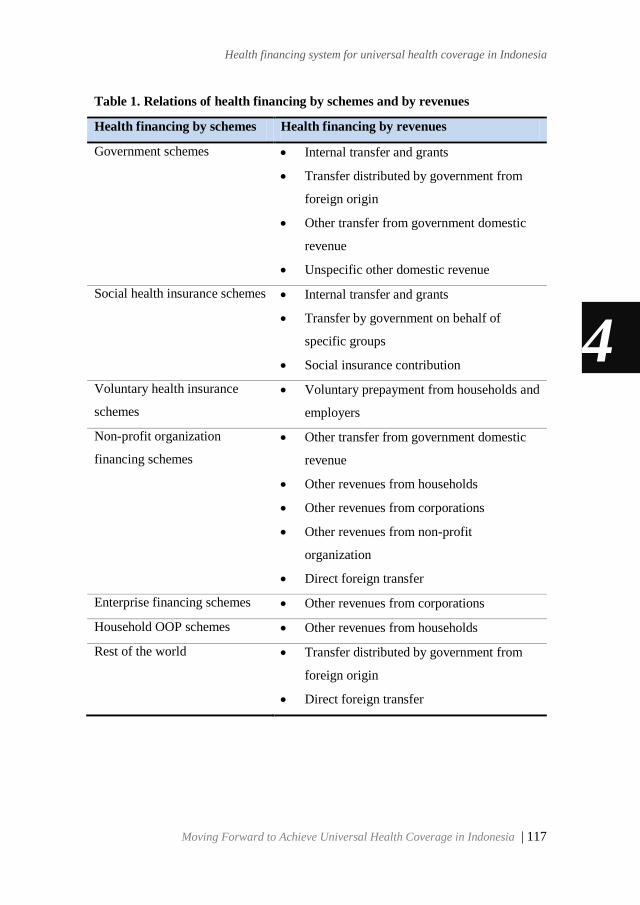
Moving Forward to Achieve Universal Health Coverage in Indonesia | 117
Table 1. Relations of health financing by schemes and by revenues
Health financing by schemes Health financing by revenues
Government schemes Internal transfer and grants
Transfer distributed by government from
foreign origin
Other transfer from government domestic
revenue
Unspecific other domestic revenue
Social health insurance schemes Internal transfer and grants
Transfer by government on behalf of
specific groups
Social insurance contribution
Voluntary health insurance
schemes
Voluntary prepayment from households and
employers
Non-profit organization
financing schemes
Other transfer from government domestic
revenue
Other revenues from households
Other revenues from corporations
Other revenues from non-profit
organization
Direct foreign transfer
Enterprise financing schemes Other revenues from corporations
Household OOP schemes Other revenues from households
Rest of the world Transfer distributed by government from
foreign origin
Direct foreign transfer
4
2
Health financing system for universal health coverage in Indonesia

118 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Describing trend of Indonesia’s health financing
A time trend analysis using MS. Excel was used to describe trend of health
financing by schemes and by revenue in Indonesia prior to and after the
implementation of the JKN-KIS program. The expenditures of each component of
health financing by schemes and by revenues are calculated in each year from 2000
to 2016.
Projection of Indonesia’s health financing
The projection of Indonesia‘s health financing was obtained using time trends of
health financing by schemes only. This is because health financing by schemes is the
key and these make up the structural components of the health financing system.
There have been no political interventions that directly affect health financing by
schemes, although health financing by revenues depends on political decisions.
The time trend of four components of health financing by schemes were
extended using linear extrapolation through 2030, i.e., the year set by the SDGs‘
agenda. Considering the year of JKN-KIS implementation in 2014 and the data
available until 2017, the observed years for the extrapolation were 2014 through
2016. Notably, the observed years for the proportion of GDP of Indonesia are
extrapolated from 2000 through 2016 since there have not been relevant policy
changes for defining Indonesia's GDP during this period.
Assessment of Indonesia’s health financing towards UHC
For the initial assessment the proportions of the three components of health
financing by schemes, (1) household OOP schemes; (2) voluntary healthcare
payments schemes; and (3) the government schemes and compulsory contributory
healthcare financing schemes, were calculated for each year. These proportions were
obtained by dividing their yearly amount by total expenditures of health financing
schemes in the pertaining year. Total yearly expenditures of health financing
through the various schemes is obtained by accumulating all expenditures of health
financing. Finally, the initial targets of UHC by WHO SDGs were used to assess
Indonesia‘s progress towards sustainable health financing.
4
2
Chapter four

Moving Forward to Achieve Universal Health Coverage in Indonesia | 119
Results
Trend of Indonesia’s health financing
Indonesia‘s health financing by schemes
Figure 1 shows trend of health financing by schemes between 2000 and 2016 in
Indonesia. Overall, it can be clearly seen that expenditures of all components on
health financing by schemes increased every year. Household OOP schemes
dominated the health financing by schemes during seventeen years. This scheme
reached a peak, with $15.021 billion, in 2011, which was the period before the
implementation of the JKN-KIS. Expenditure on social health insurance schemes
doubled, amounting to $3.955 billion in 2014, in the first year of JKN-KIS
implementation. Then this figure continued to increase and reached a peak in 2016,
with $5.378 billion. Expenditure of enterprise financing schemes was higher than
two other voluntary healthcare payment schemes. Expenditures within of the ‗rest of
the world‘ financing schemes or non-residents was the smallest and only found
between 2000 and 2006. These expenditures were not on record afterward.
Figure 1. Trend of Indonesia’s health financing by schemes between 2000 and
2016
4
2
Health financing system for universal health coverage in Indonesia

120 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Indonesia‘s health financing by revenue
Figure 2 shows the trend of health financing by revenues between 2000 and 2016 in
Indonesia. Overall, it can be clearly seen that domestic revenues from household
dominated the health financing of Indonesia during the seventeen years. Internal
transfer and grants were the second highest revenue of health financing in all
periods. After the implementation of the JKN-KIS, this revenue increased
consistently and reached a peak, with $8.1 billion in 2016. In contrast, revenues
from corporations and NPISH consistently decreased during the JKN-KIS
implementation. Interestingly, revenues from social insurance increased
significantly in the beginning of the JKN-KIS implementation from $2.2 billion in
2013 to $3.7 billion in 2014, however, in the next two years this revenue decreased.
There were three revenues of health financing contributing only in 2015 and 2016.
They were revenues from (1) government transfer on behalf of specific group; (2)
government transfer from other domestic; and (3) unspecific domestic revenue.
Figure 2. Trend of Indonesia’s health financing by revenues between 2000 and
2016
4
2
Chapter four
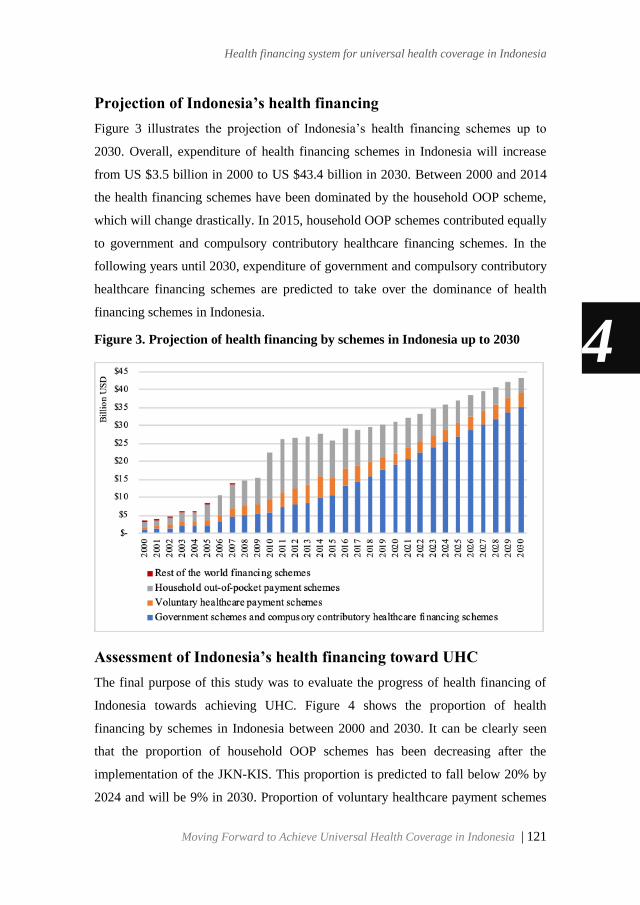
Moving Forward to Achieve Universal Health Coverage in Indonesia | 121
Projection of Indonesia’s health financing
Figure 3 illustrates the projection of Indonesia‘s health financing schemes up to
2030. Overall, expenditure of health financing schemes in Indonesia will increase
from US $3.5 billion in 2000 to US $43.4 billion in 2030. Between 2000 and 2014
the health financing schemes have been dominated by the household OOP scheme,
which will change drastically. In 2015, household OOP schemes contributed equally
to government and compulsory contributory healthcare financing schemes. In the
following years until 2030, expenditure of government and compulsory contributory
healthcare financing schemes are predicted to take over the dominance of health
financing schemes in Indonesia.
Figure 3. Projection of health financing by schemes in Indonesia up to 2030
Assessment of Indonesia’s health financing toward UHC
The final purpose of this study was to evaluate the progress of health financing of
Indonesia towards achieving UHC. Figure 4 shows the proportion of health
financing by schemes in Indonesia between 2000 and 2030. It can be clearly seen
that the proportion of household OOP schemes has been decreasing after the
implementation of the JKN-KIS. This proportion is predicted to fall below 20% by
2024 and will be 9% in 2030. Proportion of voluntary healthcare payment schemes
4
2
Health financing system for universal health coverage in Indonesia
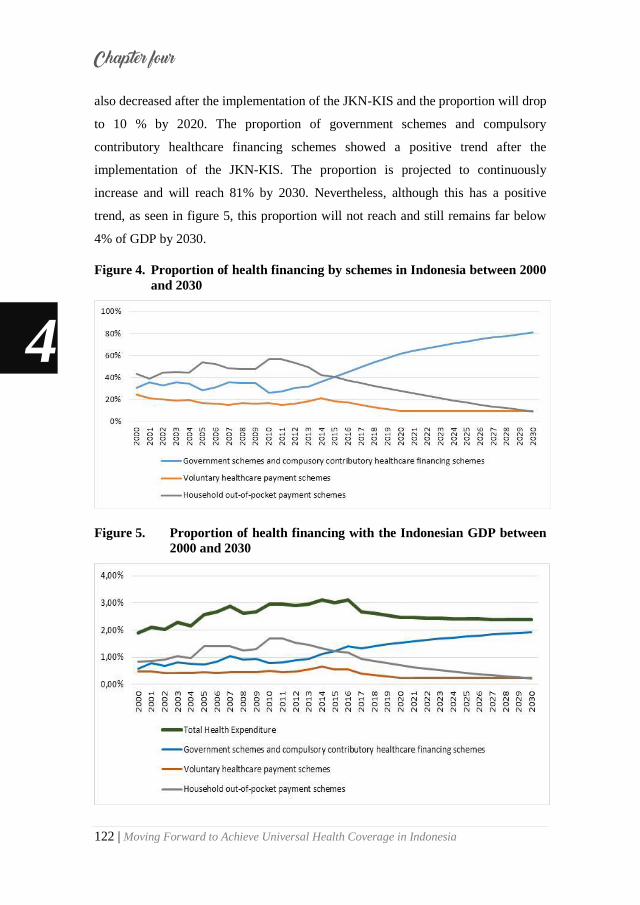
122 | Moving Forward to Achieve Universal Health Coverage in Indonesia
also decreased after the implementation of the JKN-KIS and the proportion will drop
to 10 % by 2020. The proportion of government schemes and compulsory
contributory healthcare financing schemes showed a positive trend after the
implementation of the JKN-KIS. The proportion is projected to continuously
increase and will reach 81% by 2030. Nevertheless, although this has a positive
trend, as seen in figure 5, this proportion will not reach and still remains far below
4% of GDP by 2030.
Figure 4. Proportion of health financing by schemes in Indonesia between 2000
and 2030
Figure 5. Proportion of health financing with the Indonesian GDP between
2000 and 2030
4
2
Chapter four
Moving Forward to Achieve Universal Health Coverage in Indonesia | 123
Discussion
We set out this study with the aim of assessing Indonesia‘s health financing
progress. Interestingly, in the results we found that the targets for achieving UHC by
2020 will not be attained. The target for reducing household OOP schemes below 20
% will probably be reached by 2024. The target for reducing voluntary healthcare
payment at 10% may be achieved by 2021. Importantly, these first two targets may
still be achieved well before the SDGs in 2030. However, the government schemes
and compulsory contributory health financing schemes will most likely fall
considerably below 4% of GDP by 2020. This last target will remain a challenge for
Indonesia to achieve by 2030.
Prior to the implementation of the JKN-KIS (between 2000 and 2013), we
found that OOP schemes and revenues from household dominated Indonesia‘s
health financing. A previous study, 14 observing health financing of Indonesia in the
perspective of revenues found similar results. These results are consistent with the
WHO report 15 which found OOP to dominate health expenditure in low-middle-
income countries. It would appear that financial protection for health in Indonesia
was low before the implementation of the JKN-KIS. One of the problems that is
ensuing from this issue, is that OOP for healthcare can cause individuals and
communities to go bankrupt and pushing them into poverty[16,17].
An interesting finding in this study is that after the implementation of the
JKN-KIS in 2014 expenditure of social health insurance schemes increased quite
significantly from $2.0 billion (8,52% of THE) in 2013 to US $4.0 billion (14,25%
of THE) by 2014. In the same period, the trend of OOP schemes by household
decreased to US$ 1.5 billion (7% of THE). Both trends mark important changes in
health financing in Indonesia. These results indicate that the JKN-KIS has the
intended impact of health financing in Indonesia since the JKN-KIS reduced
household OOP schemes at the expense of increased social health insurance
schemes. Other high and middle income countries that have achieved UHC, such as
the Netherlands, the United Kingdom, and Thailand, have shown that the OOP by
household decrease at the expensed of increased social health insurances[3].
4
2
Health financing system for universal health coverage in Indonesia

124 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Surprisingly, we noted that the expenditures of social health insurance
schemes are not equal with their revenues since the implementation of the JKN-KIS.
This is different from the situation before the implementation of the JKN-KIS, i.e.,
there used to be a balancing between expenditure and sources of social health
insurances. This is corroborated by the evidence from several newspapers[18-20]
broadcasting that BPJS-Kesehatan was experiencing deficits since the first year of
implementation up to now. Based on the BPJS-Kesehatan report, the accumulation
of deficit of the JKN-KIS up to December 2018 was US $2.5 billion[21]. Our review
found that there are four main possible causes. Firstly, the use of social health
insurance benefits doubled compare to the era before the JKN-KIS[22-24]. Secondly,
the premium paid by members of the JKN-KIS is low, probably caused by not
setting the premium amount according to the actuarial analysis, a method used to
calculate the social health insurance contributions[25-27]. Thirdly, premium
collectability is not optimal among the self-enrolled members (17% of JKN-KIS
participants). Of all self-enrolled members, only 57% routinely pay their
contribution. Moreover, 23% of self-enrolled members register when becoming ill
and stop paying the contribution after treatment has been obtained [28,29]. Fourthly,
JKN-KIS expenditures are dominated by disorders requiring long-term and even
lifetime use of medications[14,21,30-32].
It is important to note that the expenditure of government and compulsory
contributory health financing schemes are predicted to increase by 2.5 times in 2030
compared to 2014. Hence, the deficit of the JKN-KIS should be addressed soon to
stabilize revenue and ensure financial sustainability of the JKN-KIS. This will be a
new challenge for the Indonesian government, but, if managed to do so, the goal for
achieving UHC could be maintained. Several countries heading towards UHC, such
as Korea and Taiwan, experienced similar deficits in the initial period of
implementing UHC. Government subsidies for health and raising premium rates
periodically are the policies used to address these deficits[33-39]. The Indonesian
government might also consider applying these policies since under the Indonesian
Social Security Law[40] the government was mandated to finance any deficit and
4
2
Chapter four

Moving Forward to Achieve Universal Health Coverage in Indonesia | 125
revise the premium tariff every two years. Moreover, premium of BPJS-Kesehtan
has not been revised since 2016[27,41].
Strengths of this study are that the SHA 2011 revised edition framework
allowed for this study to investigate health financing in Indonesia in a more
comprehensive way by looking from the perspective of financing schemes and
revenues. Investigating health financing using frameworks described by SHA 2011
revised edition is the new approach not only useful for Indonesia. Many countries
also, particularly southeast Asian and low middle-income countries have also
reported their health financing not to be in line with SHA 2011 revised edition
framework. Health financing by schemes could help for the assessment of universal
health coverage assessment. Whereas, revenues of health financing schemes could
provide better understanding to facilitate the policy makers to arrange the allocation
of health funding. Therefore, this research will provide information to the
government to develop or revise appropriate policies to improve the health financing
system in Indonesia and to achieve UHC.
However, the results of this study should be considered in the context of
possible limitations. In this study, the projections of Indonesia‘s health financing is
extrapolated up to 2030. There will clearly be opportunities for new and revised
policies within a 10-year period towards the target SDGs. Revised policies could
obviously have an impact on the projected results. The current results assume that
policy and intentions to fund will not change in the next decade. In addition, we
assumed linear extrapolation to be predictive of the future trend of healthcare
financing. Furthermore, the observed years used for extrapolation was only three
years (2014, 2015, and 2016) since up to now data on health financing in Indonesia
after implementation of the JKN-KIS was only available on these years.
Additionally, our projection did not consider ageing population which might cause
changes in expenditure patterns. All these limitations could cause our predictions on
healthcare financing to diverge from the actual expenditure. However, it is likely
that the trend will remain positive, and the predictions are a first indication for
policy makers in Indonesia.
4
2
Health financing system for universal health coverage in Indonesia

126 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Conclusions
JKN-KIS is contributing to achieve UHC in Indonesia according to the WHO
targets. Firstly, the target for reducing household OOP payments below 20% will not
be achieved by 2020. It might be achieved by 2024. Secondly, the target for
reducing voluntary healthcare payment at 10% will probably be achieved by 2021.
These two targets are still well before 2030 SDGs. Notably, the government
schemes expenditure as 4% share of GDP remains a challenging target for achieving
until 2030 SDGs.
4
2
Chapter four

Moving Forward to Achieve Universal Health Coverage in Indonesia | 127
References
1. Kieny MP, Bekedam H, Dovlo D,
et al. Strengthening health systems
for universal health coverage and
sustainable development. Bull
World Health Organ.
2017;95(7):537-539.
2. Kutzin J, Witter S, Jowett M,
Bayarsaikhan D. Developing a
national health financing strategy:
A reference guide.geneva: World
health organization; (health
financing guidance no 3). . 2017.
3. Global Burden of Disease Health
Financing Collaborator Network.
Trends in future health financing
and coverage: Future health
spending and universal health
coverage in 188 countries, 2016-
40. Lancet. 2018;391(10132):1783-
1798.
4. Kutzin J. Health financing for
universal coverage and health
system performance: Concepts and
implications for policy. Bull World
Health Organ. 2013;91:602-611.
5. World Health Organization.
Arguing for universal health
coverage. . 2013.
6. Jowett M, Brunal MP, Flores G,
Cylus J. Spending targets for
health: No magic number. World
Health Organization; 2016.
7. World Health Organization. Health
financing strategy for the asia
pacific region (2010-2015).
Manila: WHO Regional Office for
the Western Pacific; 2009.
8. World Health Organization. The
world health report: Health systems
financing: The path to universal
coverage: Executive summary. .
2010.
9. Pisani E, Olivier Kok M, Nugroho
K. Indonesia's road to universal
health coverage: A political
journey. Health Policy Plan.
2017;32(2):267-276.
10. Wasir R, Irawati S, Makady A, et
al. The implementation of HTA in
medicine pricing and
reimbursement policies in
indonesia: Insights from multiple
stakeholders. PLoS One.
2019;14(11):e0225626.
11. Wasir R, Irawati S, Makady A, et
al. Use of medicine pricing and
reimbursement policies for
4
2
Health financing system for universal health coverage in Indonesia

128 | Moving Forward to Achieve Universal Health Coverage in Indonesia
universal health coverage in
indonesia. PloS one.
2019;14(2):e0212328.
12. Peraturan Presiden R. Perpres RI
no. 12 tahun 2013, tentang jaminan
kesehatan. . 2013.
13. OECD, Eurostat, World Health
Organization. A system of health
accounts 2011. . 2017.
14. Mahendradhata Y, Laksono
Trisnantor, Shita Listyadewi, et al.
The republic of indonesia health
system review. . 2017;Vol. 7 No. 1
Asia Pacific Observatory on Health
Systems and Policies(World Health
Organization).
15. World Health Organization. Public
spending on health: A closer look
at global trends. . 2018.
16. Nundoochan A, Thorabally Y,
Monohur S, Hsu J. Impact of out of
pocket payments on financial risk
protection indicators in a setting
with no user fees: The case of
mauritius. International journal for
equity in health. 2019;18(1):63.
17. Hailemichael Y, Hanlon C,
Tirfessa K, et al. Catastrophic
health expenditure and
impoverishment in households of
persons with depression: A cross-
sectional, comparative study in
rural ethiopia. BMC Public Health.
2019;19(1):930.
18. The Jakarta Post. Higher healthcare
premiums 'urgent', BPJS kesehatan
pleads as finances bleed. . 2019.
19. IDN Financials. BPJS kesehatan
deficit hits rp 7 trilion as of june
2019, 2019.
20. Nikkei Asian Review. Indonesia
struggles to pay for huge universal
health care program. . 2019.
21. BPJS Kesehatan. Laporan
pengelolaan program dan laporan
keuangan jaminan sosial kesehatan
tahun 2018. . 2019.
22. Erlangga D, Ali S, Bloor K. The
impact of public health insurance
on healthcare utilisation in
indonesia: Evidence from panel
data. International journal of
public health. 2019;64(4):603-613.
23. Rolindrawan D. The impact of
BPJS health implementation for the
poor and near poor on the use of
health facility. Procedia-Social and
Behavioral Sciences.
2015;211:550-559.
4
2
Chapter four
Moving Forward to Achieve Universal Health Coverage in Indonesia | 129
24. Maharani C, Afief DF, Weber D,
Marx M, Loukanova S. Primary
care physicians‘ satisfaction after
health care reform: A cross-
sectional study from two cities in
central java, indonesia. BMC health
services research. 2019;19(1):290.
25. Susanty A, Puspitasari NB,
Wicaksono PA, Pungky PPA.
Choosing the benefit package from
the BPJS program: Findings from
CHAT experiment. International
Journal of Healthcare
Management. 2016;9(3):201-209.
26. Hidayat B, Mundiharno NJ,
Rabovskaja V, Rozanna C, Spatz J.
Financial sustainability of the
national health insurance in
indonesia: A first year review.
Policy brief.Jakarta: the
Indonesian-German Social
Protection Programme. 2015.
27. Prabhakaran et al. Financial
sustainability of indonesia’s
jaminan kesehatan nasional:
Performance, prospects, and policy
options. Washington, DC:
Palladium, Health Policy Plus, and
Jakarta, Indonesia: Tim Nasional
Percepatan Penanggulangan
Kemiskinan (TNP2K); 2019.
28. Agustina R, Dartanto T, Sitompul
R, et al. Universal health coverage
in indonesia: Concept, progress,
and challenges. The Lancet.
2019;393(10166):75-102.
29. Dartanto T, Halimatussadiah A,
Rezki JF, et al. Why do informal
sector workers not pay the
premium regularly? evidence from
the national health insurance
system in indonesia. Applied health
economics and health policy.
2019:1-16.
30. BPJS Kesehatan. Laporan
pengelolaan program dan laporan
keuangan 2015. . 2016.
31. BPJS Kesehatan. Laporan
pengelolaan program dan laporan
keuangan jaminan sosial kesehatan
tahun 2016. . 2017.
32. Tandon A, Pambudi ES, Harimurti
P, et al. Indonesia health financing
system assessment: Spend more,
spend right, spend better. World
Bank; 2016.
33. Lee JC. Health care reform in south
korea: Success or failure? Am J
Public Health. 2003;93(1):48-51.
34. Kang MS, Jang HS, Lee M, Park E.
Sustainability of korean national
4
2
Health financing system for universal health coverage in Indonesia

130 | Moving Forward to Achieve Universal Health Coverage in Indonesia
health insurance. J Korean Med
Sci. 2012;27(Suppl):S21-S24.
35. Kwon S. Thirty years of national
health insurance in south korea:
Lessons for achieving universal
health care coverage. Health Policy
Plan. 2008;24(1):63-71.
36. Lu JR, Hsiao WC. Does universal
health insurance make health care
unaffordable? lessons from taiwan.
Health Aff. 2003;22(3):77-88.
37. Huang SK, Tsai SL, Hsu MT.
Ensuring the sustainability of the
taiwan national health insurance. J
Formos Med Assoc. 2014;113(1):1-
2.
38. Davis K, Huang AT. Learning from
taiwan: Experience with universal
health insurance. Ann Intern Med.
2008;148(4):313-314.
39. Cheng T. Reflections on the 20th
anniversary of taiwan‘s single-
payer national health insurance
system. Health Aff.
2015;34(3):502-510.
40. Republik Indonesia. Undang-
undang republik indonesia nomor
40 tahun 2004 tentang sistem
jaminan sosial nasional. Timur
Putra Mandiri; 2004.
41. Deloitte. Ensuring the
sustainability of JKN-KIS for the
indonesian people. . 2019.
4
2
Chapter four
Moving Forward to Achieve Universal Health Coverage in Indonesia | 131
Chapter 5
Long term risk of incidence of cardiovascular events in
Asian Populations: Systematic review and Meta-Analysis of
Population-Based Cohort Studies
Riswandy Wasir
Sylvi Irawati
Amand Floriaan Schmidt
Atiqul Islam
Talitha Feenstra
Erik Buskens
Bob Wilffert
Eelko Hak
This chapter is based on the published manuscript:
Sylvi Irawati, Riswandy Wasir, Amand Floriaan Schmidt, Atiqul Islam, Talitha
Feenstra, Erik Buskens, Bob Wilffert & Eelko Hak (2019) Long-term incidence and
risk factors of cardiovascular events in Asian populations: systematic review and
meta-analysis of population-based cohort studies, Current Medical Research and
Opinion, 35:2, 291-299, DOI: 10.1080/03007995.2018.1491149
132 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Abstract
Background:
Scientific studies on cardiovascular disease (CVD) burden and risk factors are
predominantly based on short-term risk in Westerner populations, and such
information may not be applicable to Asian populations, especially over the longer
term. This review aims to estimate the long-term (>10 years) CVD burden, including
coronary heart disease (CHD) and stroke, as well as associated risk factors in Asian
populations.
Methods:
PubMed, Embase and Web of Science were systematically searched, and hits
screened on: Asian adults, free of CVD at baseline; cohort study design (follow-up
>10 years). Primary outcomes were fatal and non-fatal CVD events. Pooled
estimates and between-study heterogeneity were calculated using random effects
models, Q and I 2 statistics.
Results:
Overall, 32 studies were eligible for inclusion (follow-up: 11–29 years). The average
long-term rate of fatal CVD is 3.68 per 1000 person-years (95% CI 2.84–4.53), the
long-term cumulative risk 6.35% (95% CI 4.69%–8.01%, mean 20.13 years) and the
cumulative fatal stroke/CHD risk ratio 1.5:1. Important risk factors for long-term
fatal CVD (RR, 95% CI) were male gender (1.49, 1.36–1.64), age over 60/65 years
(7.55, 5.59–10.19) and current smoking (1.68, 1.26–2.24). High non-HDL-c, and b-
and c-tocopherol serum were associated only with CHD (HR 2.46 [95% CI 1.29–
4.71] and 2.47 [1.10–5.61] respectively), while stage 1 and 2 hypertensions were
associated only with fatal stroke (2.02 [1.19–3.44] and 2.89 [1.68–4.96]
respectively).
5
2
Chapter five

Moving Forward to Achieve Universal Health Coverage in Indonesia | 133
Conclusions:
Over a 10 year þ follow-up period Asian subjects had a higher risk of stroke than
CHD. Contrary to CVD prevention in Western countries, strategies should also
consider stroke instead of CHD only
5
2
Long term risk of incidence of cardiovascular events in Asian Populations

134 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Introduction
Despite declining trends in fatal cardiovascular disease (CVD), coronary heart
disease (CHD) and stroke remain a significant cause of death and morbidity
worldwide[1,2]. Owing to the fact that most CVD events are not fatal anymore, the
prevalence and burden of CVD is increasing further. To prevent or postpone CVD
occurrence, high-risk subjects need to be identified earlier, allowing for early
targeting of modifiable risk factors and treatments with (personalized) preventive
medications[3–6]. This is especially true for Asian countries where more than half of
the world‘s population resides, and where CVD death is on the rise[7,8]. Most studies
on Asian populations have traditionally focused on the occurrence and risk factors of
CVD within a short-term period (10 years)[9,10]. This may underestimate a long-term
CVD risk (>10 year follow-up), especially when detrimental behavioral and
environmental factors may occur earlier in life and continue to go unmanaged[11–14].
Furthermore, the majority of this research also stems from ―developed‖ Western
countries[15–17], where the risk of CHD is approximately four times higher than of
stroke[18,19]. This focus on CHD may not appropriately translate to CVD prevention
in Asians. The current review aims to estimate the long-term CVD burden and risk
factors.
5
2
Chapter five
Moving Forward to Achieve Universal Health Coverage in Indonesia | 135
Methods
Study design
The protocol for this review was registered with PROSPERO (Reference
CRD42016042939). This report was written based on a MOOSE checklist[20].
Search strategy
A search strategy was developed by S.I., E.H., B.W. and librarians (K.S., S.W.)
(supplemental online material). S.I. conducted the search through PubMed, Embase
and Web of Science on 12 July 2016. A web-based reference manager, RefWorks,
was used to identify and eliminate duplicate studies. Predetermined inclusion criteria
were applied in title/abstract and full-text screenings by S.I. and R.W.
independently. Authors of the original studies were contacted to obtain any required
information. In both screenings, the interrater agreement for study inclusion was
assessed using Cohen‘s kappa (Œ). Any disagreements between review authors were
resolved by discussion. A third review author (E.H. or B.W.) was consulted when no
agreement was reached after discussion.
Study selection
To obtain long-term incidence rates in the general population, only cohort studies
were included. All types of review, meta-analyses, randomized controlled trials,
cross-sectional studies, case series, case reports, editorials, letters and commentaries
were excluded. We focused on Asian healthy adults (aged 18 years) from the general
population. Subjects were free from CVD, i.e. had no history of myocardial
infarction (MI) or stroke, at the start of the study. Only studies with a follow-up
period of more than 10 years were included. Studies investigating only males or
females, participants with a specific condition or disease, or occupational based
cohort were excluded.
The primary outcomes of interest were fatal and non-fatal CVD events.
Secondary outcomes included any CHD and stroke incidences, fatal CHD, fatal
stroke, and all-cause mortality. Only studies which defined their outcomes similarly
5
2
Long term risk of incidence of cardiovascular events in Asian Populations
136 | Moving Forward to Achieve Universal Health Coverage in Indonesia
or using the International Statistical Classification of Diseases (ICD) from the World
Health Organization (WHO) were included.
Data extraction, risk of bias assessment and statistical analysis
To describe absolute risks, both rates and proportion with a 95% confidence interval
(CI) were calculated for each outcome. The measure of association between risk
factors and each outcome was presented as a pooled relative risk (RR), also with
95% CI. Forest plots were created using Microsoft Office Excel 2010[21] and Review
Manager (RevMan) version 5.3 (2014). Publications using the same existing data set
were consolidated into a single record, with data preferentially extracted based on
the longest period of follow-up. S.I. extracted data while R.W. and A.I. checked the
correctness of the process. The risk of bias of the included studies was assessed by
S.I. and R.W. independently using the Risk of Bias Assessment tool for Non-
randomized Studies (RoBANS) (supplemental online material)[22]. Disagreements
were resolved by discussion. A third review author (E.H.) was consulted when no
agreement was reached after discussion.
In both descriptive and analytic meta-analyses, we used a random-effects
model to calculate the pooled estimates[23]. Heterogeneity across studies was
evaluated using the Q-test (p value .10 used as a cut-off point) and the I 2 statistic
with 95% CI[24–26]. When I2 was >50%, studies were subdivided based on the study
duration.
5
2
Chapter five
Moving Forward to Achieve Universal Health Coverage in Indonesia | 137
Results
Study identification, study characteristics and risk of bias
assessment
Of 1705 initial titles and abstracts, 1546 were excluded. After reviewing 159 full
texts, 32 studies were included in the meta-analysis[27–58] (Figure 1, Supplemental
Online Material Table SI). The strength of interrater agreement after both
title/abstract and full-text screenings was satisfactory (agreement 92%, Cohen‘s
kappa 0.43; 79%, 0.55, respectively). Most studies were from Japan (21 studies),
followed by Taiwan (5), China (3), Israel (2) and Singapore (1). The duration of
followup ranged from 11 to 29 years. Of 32 studies, 27 studies had started following
their participants since the 1980s or 1990s, four since the 1960s or 1970s and only
one since 2000. The participants‘ age ranged from 18 to 92 years. Of these studies,
the risk of bias in one or more domains in 10 and 18 studies were considered high
and unclear, respectively (Supplemental Online Material Table SII).
5
2
Long term risk of incidence of cardiovascular events in Asian Populations

138 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Figure 1. Study selection flow
5
2
Chapter five

Moving Forward to Achieve Universal Health Coverage in Indonesia | 139
Primary outcomes: fatal and non-fatal cardiovascular disease
events
The ―average‖ (pooled-estimate) long-term rate of fatal CVD in the Asian
populations was 3.68 per 1000 person-years (95% CI 2.84–4.53) (Figure 2). Studies
from Singapore, Japan and Taiwan, all of which started their follow-up in the 1980s
or 1990s, contributed to this number. Only the fatal CVD rate in Singapore (4.67
[4.52–4.81]) was above the average and the highest estimate. The average
cumulative fatal CVD over mean 20.13 years was 6.35% (95% CI 4.69%–8.01%)
(Supplemental Online Material Figure FI). The highest cumulative fatal CVD was
found in Taiwan, at 7.18% (95% CI 6.58%–7.77%) over mean 22.5 years, which
was also the longest period of follow-up.
Figure 2. Long-term (>10 years) rate of fatal cardiovascular disease in the
Asian populations. Figure created using a tool from Someka.net.
5
2
Long term risk of incidence of cardiovascular events in Asian Populations

140 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Secondary outcomes: any coronary heart disease and stroke
incidences, fatal coronary heart disease, fatal stroke, and all-cause
mortality
The average long-term incidence rate of any stroke was higher than fatal and non-
fatal coronary events (3.14 per 1000 person-years [95% CI 2.12–4.16] vs. 1.51
[0.84–2.18]) (Table 1). The estimates for fatal and non-fatal coronary events were
drawn from studies in the East-Asian populations (Japan and China) while those for
any stroke events were only from Japan. Compared to the average estimates and to
the Chinese, the Japanese had a higher incidence rate of fatal and non-fatal coronary
events. However, in Japan itself, both the incidence rate and cumulative incidence of
any stroke were higher than fatal and non-fatal coronary events, even after excluding
a study started in the 1960s[57] when the incidence of any stroke was still very high
(3.14 per 1000 person-years [95% CI 2.12–4.16] vs. 1.72 [0.00–3.64]; 3.92% [3.35–
4.48] vs. 2.23% [0.00–4.69]).
Table 1. Long-term risk of fatal and non-fatal coronary and any stroke events
in the Asian populations.
5
2
Chapter five

Moving Forward to Achieve Universal Health Coverage in Indonesia | 141
The long-term fatal rate of subcomponents of CVD was derived from three
countries: Singapore, Taiwan and Japan (Table 2). Overall, the average long-term
rate of fatal stroke was higher than fatal CHD (1.46 per 1000 person-years [95% CI
1.18–1.75] vs. 1.03 [0.26–1.81]). Singapore had above-average rates for fatal CHD
(2.56 per 1000 person-years [2.45–2.66]) while Taiwan had them for fatal stroke
(1.8 per 1000 person-years [1.57–2.02]). This was also reflected in between-country
comparisons. Singapore had the highest rate for fatal CHD and Taiwan had the
lowest. In contrast, when the rate of fatal stroke was considered, the rank was the
exact opposite. Specifically, the rate and cumulative estimate of fatal stroke in Japan
and Taiwan were higher than those of CHD. The risks were opposite in Singapore.
Table 2. Long-term risk of fatal coronary heart disease and fatal stroke in the
Asian population
The average long-term rate of all-cause mortality was 11.31 per 1000
person-years (95% CI 7.49–15.12) from Japan (five studies) and Taiwan (one
study). Compared to the average, the risk in Japanese (10.87 [6.69–15.04]) was
below while in Taiwanese (13.52 [12.91–14.13]) was above. The same pattern was
5
2
Long term risk of incidence of cardiovascular events in Asian Populations

142 | Moving Forward to Achieve Universal Health Coverage in Indonesia
found in long-term cumulative all-cause mortality (Supplemental Online Material
Table SIII).
Risk factors for long-term fatal and non-fatal cardiovascular
disease events
Of the individual studies included in this review (Supplemental Online Material
Table SI), risk factors of fatal CVD were still dominated by traditional variables
such as: smoking[29,52], hypertension[30,50,51], overweight and obesity[31]. There was a
synergistic effect between current smokers and each of these factors: hypertension,
obesity and metabolic syndrome, which modified their effects on fatal CVD[29,52].
Risk factors associated with long-term risks of fatal CHD and stroke were different,
except for the use of incense (aromatic sticks release fragrant smoke when burned)
in Singapore (HR 1.13 [95% CI 1.01–1.26] and 1.24 [1.06–1.45] for fatal CHD and
fatal stroke, respectively)[47]. Risk factors associated only with fatal CHD were non-
fasting non-HDL-c 189 mg/dL (vs. 150 mg/dL)[32], and b- and c-tocopherol serum
(HR 2.46 [95% CI 1.29–4.71] and 2.47 [1.10–5.61], respectively)[34]. On the
contrary, compared to normal blood pressure, stage 1 and 2 hypertension were
significantly associated only with fatal stroke (HR 2.02 [95% CI 1.19–3.44] and
2.89 [1.68–4.96], respectively)[51]. Several protective factors also appeared to have
contradictory effects on fatal CHD and fatal stroke. Non-fasting HDL-c 60–79
mg/dL (vs. 40–59 mg/dL) and high intake of fruit and vegetables were protective
only against fatal CHD (HR 0.38 [95% CI 0.19–0.75] and 0.57 [0.37–0.87],
respectively)[28,46] while b-carotene serum, high intake of fruit, and per 10 mg/m3
increase in particulate matter levels were only protective against fatal stroke (HR
0.60 [95% CI 0.37–0.98], 0.72 [0.54–0.95], 0.69 [0.59–0.82], respectively)[34,44,46].
Male gender, older age and current smokers were risk factors for fatal CVD
(RR 1.49 [95% CI 1.36–1.64], 7.55 [5.59–10.19], 1.68 [1.26–2.24], respectively)
(Figure 3). The risk of males compared to females in developing fatal CHD was
higher than that in fatal stroke (RR 1.77 [95% CI 1.60–1.96] vs. 1.46 [1.28–1.68]).
Additionally, the risk of suffering a fatal stroke among elderly compared to middle-
aged people was higher than that of fatal CHD (RR 7.36 [95% CI 5.72–9.47] vs.
5.96 [4.17–8.52]).
5
2
Chapter five

Moving Forward to Achieve Universal Health Coverage in Indonesia | 143
Figure 3. Meta-analysis of long-term risk factors for fatal and non-fatal
cardiovascular disease, fatal coronary heart disease, fatal stroke, and
all-cause mortality in the Asian populations.
Sensitivity and subgroup analysis
We conducted sensitivity analysis and subdivided studies based on duration of
follow-up which resulted in non-significant heterogeneities (Supplemental Online
Material Figure FII and FIII). Over a >20 year follow-up, the cumulative fatal stroke
was higher than fatal CHD (4.18% [95% CI 3.48%–4. 89%] vs. 1.57% [1.01–2.14]).
The risks of suffering fatal CHD and fatal stroke were twice as high among males
compared to females in a 15/20 year follow-up. However, in the longer term, the
risk of fatal stroke was slightly lower than of fatal CHD among males compared to
females (RR 1.34 [95% CI 1.23–1.46] vs. 1.52 [1.04–2.22]).
5
2
Long term risk of incidence of cardiovascular events in Asian Populations
144 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Discussion
This study explored the risk of (non)-fatal CVD in Asian populations without prior
CVD with follow-up of more than 10 years. Previously, the Asia-Pacific Cohort
Study Collaboration (APCSC) and the Evidence for Cardiovascular Prevention from
Observational Cohorts in Japan Study (EPOCH-JAPAN) metaanalyses focused on
CVD after a shorter follow-up period (10 years)[10,59,60]. The APCSC included cohort
studies mainly from China and Japan and single cohorts from Thailand, South Korea
and Hong Kong while EPOCH-JAPAN only included Japanese cohorts[9,59].
Our study extends findings from these earlier studies to a 10 year þ follow-
up, where the average long-term cumulative incidence of fatal CVD, both in the
Asian population as a whole (6.35% [95% CI 4.69%–8.01%], mean follow-up 20.00
years) and in Japanese alone (5.93% [3.68–8.23], mean follow-up 19.60 years) was
around two times larger than the short-term risk found in APCSC (3.52% [3.47%–
3.58%], median follow-up 6.1 years)10 and in EPOCH-JAPAN (2.89% [2.76–3.02],
mean follow-up 10.2 years)[60].
Our analysis appears to support the assumption that the cumulative risk of
long-term fatal CVD increases non-exponentially over time. A former study
suggested that the 20 year risk of hard CHD should be at least twice the 10 year risk
using a Framingham score approximation[61]. However, in the latter study, this
―naïve‖ approach was proven to underestimate the true risk because it overlooked
aging as an important factor of CVD. The most close estimation of longterm risk
was a model which took competing risk of nonCVD death into account[62]. From two
individual studies included in our review, the 20 year and lifetime risks of CHD and
stroke (competing-risk adjusted) did not always increase linearly or exponentially in
the Japanese. The most rapid increase of the 20 year and lifetime risks for both
events compared to the 10 year risks occurred in the youngest index age group (45
years) and the leaps of increase were getting smaller as index ages were getting
older[55,56]. The long-term risk of CVD also varied depending on gender and the
burden of CVD risk factor(s)[55,56,58].
The average long-term cumulative incidence of subcomponents of CVD in
the Asian populations was higher than the short-term risk, six times for fatal CHD
5
2
Chapter five
Moving Forward to Achieve Universal Health Coverage in Indonesia | 145
(1.61% [95% CI 0.42%–2.81%] vs. 0.27% [0.25–0.28]) and four times for fatal
stroke (2.42% [1.83–3.02] vs. 0.57% [0.55–0.59])[10]. However, in Japan, the risk
was only almost two times higher than the short-term risk for both events (fatal
CHD: 1.14% [0.65–1.64] vs. 0.58% [0.52–0.63], fatal stroke: 2.22% [1.16–3.29] vs.
1.36% [1.27–1.45])[60]. Consistent with the short-term risk, the longterm risk of fatal
stroke in the Asian population was also larger than that of fatal CHD. In our study,
the long-term fatal stroke/CHD ratio was lower than the short-term ratio in Asians
(1.5:1 vs. 2:1) similar to the Japanese (2:1)[10,60]. Western subjects had an opposite
fatal stroke/CHD ratio after both short-term (1:3)[10] and long-term periods (e.g.
around 1:4 in men and 1:2 in women, index age of 45 years with 2 major CVD risk
factors)[18]. The relative importance of fatal stroke over fatal CHD on the long-term
risk of fatal CVD in different populations was previously reported by Ancel Keys
and coinvestigators from the Seven Countries Study. Started 60 years ago in 1958,
the study involved 16 cohorts of 12,763 men aged 40–59 years in seven countries.
Of the 16 cohorts, one originated from the US, two were from Finland (eastern and
western), one from the Netherlands (Zutphen), three from Italy (Crevalcore,
Montegiorgio and Rome), two from Croatia (Dalmatia and Slavonia), three from
Serbia (Velika Krsna, Zrenjanin and Belgrade), two from Greece (Crete and Corfu)
and two from Japan (Tanushimaru and Ushibuka)[63–65]. The 25 year age-adjusted
stroke death rates in the US (36 per 1000) and most of Europe (Finland, Greece,
Italy, Netherlands, Belgrade; range: 38–77 per 1000) were lower than Japan (83 and
107 per 1000), Serbia (94 and 119 per 1000) and Croatia (83 and 113 per 1000)[63].
In contrast, the 25 year age-adjusted CHD death rates in the US and Europe (range:
118–202 per 1000), except in Dalmatia, were higher than Japan (45 and 63 per
1000) and Greece (46 and 95 per 1000).
This 25 year data from Japan was largely in agreement with our data,
although there was a population difference and a large time difference between our
included studies and this Seven Countries Study. Although the variety of
investigated populations, especially with regard to Asians, was limited to Japan, the
study still highlights different contributors to fatal CVD in different populations.
The different pattern of CVD burden between Asian and Western populations might
5
2
Long term risk of incidence of cardiovascular events in Asian Populations

146 | Moving Forward to Achieve Universal Health Coverage in Indonesia
be translated into different risk factors which potentially require a different approach
to the CVD prevention.
We only found a few short-term and no long-term followup studies
investigating any possible differences between the two populations. In a short-term
study (mean 4 years), among other factors (SBP, total cholesterol [TC], body mass
index [BMI], diabetes and current smoking), only triglyceride (TG) was
significantly different between the two populations (p < .05), with a stronger
association with fatal CHD in Westerners (HR 1.66 [95% CI 1.33–2.07]) than in
Asians (1.26 [1.12–1.41]). Interestingly, for subtypes of stroke, SBP was the only
factor differing significantly between the two populations with a stronger association
in Asians than in Westerners (fatal cerebral infarction: HR 1.44 [95% CI 1.35–1.54]
vs. 1.36 [1.17–1.57]; fatal cerebral hemorrhage: 1.72 [1.63–1.82] vs. 1.49 [1.31–
1.70])[66].
Based on individual studies included in our review, these same factors have
different effects on developing CHD and stroke over a long-term period, e.g. non-
fasting non-HDL-c 189 mg/dL and HDL-c 60–79 mg/dL were associated only with
long-term fatal CHD (HR 2.46 [95% CI 1.29–4.71] and 0.38 [0.19–0.75],
respectively) while stage 1 and 2 hypertensions were associated only with long-term
fatal stroke (HR 2.02 [1.19–3.44] and 2.89 [1.68–4.96], respectively). In shortterm
studies in Asian Pacific subjects, a lower level of one standard deviation (15.6
mg/dL) of HDL-c was associated only with fatal or non-fatal CHD (HR not clearly
reported)[67]. However, hypertension was significantly associated with short-term
risk of both fatal and non-fatal CHD, cerebral infarction, and cerebral hemorrhage
(HR 2.47 [95% CI 2.16–2.82], 3.99 [3.32–4.80] and 9.26 [7.25–11.82])[68].
To summarize, three points are worth mentioning: 1) the risk of stroke is
higher than CHD over a long-term period in Asians, 2) the limited evidence
available showed a significant contribution of hypertension to the risk of developing
CHD and stroke over a short-term period but only to the risk of stroke over a long-
term period in Asians, and 3) the risk factors of developing CHD and stroke over a
short-term period are different between Asians and Westerners while no evidence is
available on the comparison of risk factors over a long-term period between the two
5
2
Chapter five

Moving Forward to Achieve Universal Health Coverage in Indonesia | 147
populations. These points suggest that a different approach to CVD prevention may
be needed. It is also worth noticing that most of the studies included and discussed
here, both short-term and long-term studies, were conducted mainly in East Asian
regions and in an era when the use of cardiovascular preventive medications was not
highly promoted. Thus, this finding also reflects the lack of epidemiologic studies on
CVD in other Asian regions, especially in lower-middle income countries, where
CVD deaths take place the most.
The strengths of this review lie in its use of a comprehensive search
strategy to include studies from all Asian countries and selection of only studies
with more than 10 years of follow-up and with participants free of CVD at baseline,
which enabled long-term absolute risk estimation. Prior studies relied on country
death registries without specifying whether participants had already suffered from
CVD at baseline[69,70].
Given the moderate to substantial degree of study heterogeneity (I 2 ¼
50%–90%), we had to stratify our analyses. Another limitation is the difference in
the start and end dates of the observation periods of the included studies. Those
limitations were addressed by exploring regional and temporal variations, presenting
the pooled estimate from studies started at the same period, and subgrouping studies
based on duration of follow-up. Unavailable data for events in specific age groups
also limits the standardization of (non)-fatal CVD rates which may overestimate or
underestimate the burden depending on the structure of the study populations. The
focus on English publications is another limitation; however, it is unclear whether
language restriction may result in bias[71,72], for example some Asian countries
explicitly publish research in English only[73]. Due to the limited number of studies,
it was not possible to formally address publication bias. We could only pool risk
estimates for limited CVD risk factors because of the small number of studies
investigating the same risk factors and the unavailability of individual participant
data.
5
2
Long term risk of incidence of cardiovascular events in Asian Populations

148 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Conclusion
The long-term fatal CVD risk was almost double that of the reported short-term risk.
Unlike Western populations, in the long term stroke risk remained larger than CHD
risk. Male gender, older age and current smoking were important risk factors for
long-term fatal CVD. Factors like non-HDL-c and HDL-c had different effects on
long-term CHD and stroke, with hypertension being a more important predictor of
longterm stroke risk than of short-term risk. Since most studies, even short-term
studies, were from East Asian countries, there is limited information on both short-
term and longterm burden, and risk factors of CVD, in other Asian countries. The
different pattern of CVD risk and risk factors in Asian populations compared to
Westerners asks for a different approach towards prevention.
5
2
Chapter five

Moving Forward to Achieve Universal Health Coverage in Indonesia | 149
Transparency
Declaration of funding
This work was supported by LPDP and DIKTI scholarships from the Ministry of
Finance and the Ministry of Research, Technology and Higher Education of the
Republic of Indonesia, respectively. The LPDP and DIKTI had no direct role in
research design, data collection, analysis and interpretation, or manuscript writing
and publication. Author contributions: All authors were involved in study design,
interpretation, review and final approval of the manuscript. Additionally, S.I.
conducted search and study selection, data extraction, risk of bias assessment, data
analysis, and prepared the first draft of the manuscript. R.W. conducted study
selection, confirmed the correctness of data extraction and risk of bias assessment.
A.F.S. provided advice in the data interpretation and important intellectual content
in the draft of the manuscript. A.I. confirmed the correctness of data extraction and
provided statistical advice. T.F. provided advice in the data analysis and important
intellectual content in the draft of the manuscript. E.B. provided important
intellectual content in the draft of the manuscript. B.W. resolved disagreements in
study selection and provided important intellectual content in the draft of the
manuscript. E.H. resolved disagreements in study selection and risk of bias
assessment, and provided important intellectual content in the data analysis and the
draft of the manuscript.
Declaration of financial/other relationships
S.I., R.W., A.F.S., A.I., T.F., E.B., B.W. and E.H. have disclosed that they have no
significant relationships with or financial interests in any commercial companies
related to this study or article. CMRO peer reviewers on this manuscript have no
relevant financial or other relationships to disclose.
5
2
Long term risk of incidence of cardiovascular events in Asian Populations

150 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Acknowledgements
We would like to thank Karin Sijtsma for her contribution to developing the search
strategy and Sjoukje van der Werf for her contribution to checking the
appropriateness of the search strategy. We also would like to thank several authors
of the included studies (Pao-Hwa Lin, WoonPuay Koh and Ying Wang) for their
contribution to providing complementary data for the meta-analysis.
Data availability statement
The data that support the findings of this study are available from the corresponding
author, Sylvi Irawati, upon reasonable request.
5
2
Chapter five
Moving Forward to Achieve Universal Health Coverage in Indonesia | 151
References
1. GBD 2013 Mortality and Causes of
Death Collaborators. Global,
regional, and national age-sex
specific all-cause and cause-specific
mortality for 240 causes of death,
1990–2013: a systematic analysis for
the Global Burden of Disease Study
2013. Lancet 2015;385:117-71
2. GBD 2015 Mortality and Causes of
Death Collaborators. Global,
regional, and national life
expectancy, all-cause mortality, and
cause-specific mortality for 249
causes of death, 1980–2015: a
systematic analysis for the Global
Burden of Disease Study 2015.
Lancet 2016;388:1459-544
3. Goff DJ, Lloyd-Jones DM, Bennett
G, et al. 2013 ACC/AHA guideline
on the assessment of cardiovascular
risk: a report of the American
College of Cardiology/American
Heart Association Task Force on
Practice Guidelines. Circulation
2014;129(25 Suppl 2):S49-73
4. World Health Organization.
Prevention of Cardiovascular
Disease: Guidelines for Assessment
and Management of Cardiovascular
Risk. Geneva: WHO Press, 2007
5. Piepoli MF, Hoes AW, Agewall S,
et al. 2016 European Guidelines on
cardiovascular disease prevention in
clinical practice. Eur Heart J
2016;37:2315-81
6. JBS3 Board. Joint British Societies‘
consensus recommendations for the
prevention of cardiovascular disease
(JBS3). Heart 2014;100:ii1-67
7. Worldometers.info. Worldometers.
Dover, Delaware, USA, 2017.
Available at:
http://www.worldometers.info/world
-population/asiapopulation/ [Last
accessed 28 August 2017]
8. World Health Organization. Health
statistics and information systems:
estimates for 2000–2015. 2017. p. 2.
Available at:
http://www.who.int/healthinfo/globa
l_burden_disease/estimates/en/
index1.html [Last accessed 28
August 2017]
9. Woodward M, Barzi F, Martiniuk A,
et al. Cohort profile: the Asia Pacific
Cohort Studies Collaboration. Int J
Epidemiol 2006;35: 1412-16
10. Woodward M, Huxley R, Ueshima
H, et al. The Asia Pacific Cohort
Studies Collaboration: a decade of
5
2
Long term risk of incidence of cardiovascular events in Asian Populations

152 | Moving Forward to Achieve Universal Health Coverage in Indonesia
achievements. Glob Heart
2012;7:343-51
11. Bleakley C, Millar A, Harbinson M,
et al. Lifetime risk of cardiovascular
disease: the next generation in risk
prediction. Can J Cardiol
2013;29:147-50
12. Di Castelnuovo A, Costanzo S,
Persichillo M, et al. Distribution of
short and lifetime risks for
cardiovascular disease in Italians.
Eur J Prev Cardiol 2012;19:723-30
13. Kuh D, Hardy R, Hotopf M, et al. A
review of lifetime risk factors for
mortality. Br Actuar J 2009;15:17-
64
14. Lloyd-Jones DM. Short-term versus
long-term risk for coronary artery
disease: implications for lipid
guidelines. Curr Opin Lipidol
2006;17:619-25
15. Liu J, Hong Y, D‘Agostino RB, et
al. Predictive value for the Chinese
population of the Framingham CHD
risk assessment tool compared with
the Chinese Multi-provincial Cohort
Study. JAMA 2004;291:2591
16. Maharani A, Tampubolon G. Unmet
needs for cardiovascular care in
Indonesia. PLoS One 2014;9:1-10
17. Asia Pacific Cohort Studies
Collaboration. Cardiovascular risk
prediction tools for populations in
Asia. J Epidemiol Community Heal
2007;61:115-21
18. Berry JD, Dyer A, Cai X, et al.
Lifetime risks of cardiovascular
disease. N Engl J Med
2012;366:321-9
19. Go AS, Mozaffarian D, Roger VL,
et al. Heart disease and stroke
statistics – 2013 update: a report
from the American Heart
Association. Circulation
2013;127:e6-245
20. Stroup DF, Berlin JA, Morton S, et
al. MOOSE statement: meta-analysis
of observational studies in
epidemiology: a proposal for
reporting. JAMA 2000;283:2008-12
21. Neyeloff JL, Fuchs SC, Moreira LB.
Meta-analyses and forest plots using
a Microsoft Excel spreadsheet: step-
by-step guide focusing on
descriptive data analysis. BMC Res
Notes 2012;5:52
22. Kim SY, Park JE, Lee YJ, et al.
Testing a tool for assessing the risk
of bias for nonrandomized studies
showed moderate reliability and
promising validity. J Clin Epidemiol
2013;66:408-14
5
2
Chapter five
Moving Forward to Achieve Universal Health Coverage in Indonesia | 153
23. Lau J, Ioannidis JPA, Schmid CH.
Summing up evidence: one answer
is not always enough. Lancet
1998;351:123-7
24. Higgins JP, Thompson SG, Deeks
JJ, Altman DG. Measuring
inconsistency in meta-analyses. BMJ
2003;327:557-60
25. Higgins JPT, Thompson SG.
Quantifying heterogeneity in a
metaanalysis. Stat Med
2002;21:1539-58
26. Higgins J, Green S, editors.
Cochrane handbook for systematic
reviews of interventions version
5.1.0. Updated March 2011. The
Cochrane Collaboration. 2011.
Available at: http://training.
cochrane.org/handbook [Last
accessed 28 August 2017]
27. Brunner D, Weisbort J, Meshulam
N, et al. Relation of serum total
cholesterol and high-density
lipoprotein cholesterol percentage to
the incidence of definite coronary
events: twenty-year follow-up of the
donolo-Tel Aviv prospective
coronary artery disease study. Am J
Cardiol 1987;59:1271-6
28. Hirata A, Okamura T, Sugiyama D,
et al. The relationship between very
high levels of serum high-density
lipoprotein cholesterol and cause-
specific mortality in a 20-year
follow-up study of Japanese general
population. J Atheroscler Thromb
2016;23:800-9
29. Hozawa A, Okamura T, Murakami
Y, et al. Joint impact of smoking and
hypertension on cardiovascular
disease and all-cause mortality in
Japan: NIPPON DATA80, a 19-year
follow-up. Hypertens Res
2007;30:1169-75
30. Hsu PF, Cheng HM, Wu CH, et al.
High short-term blood pressure
variability predicts long-term
cardiovascular mortality in untreated
hypertensives but not in
normotensives. Am J Hypertens
2016;29:806-13
31. Hwang LC, Chen SC, Chen CJ.
Increased risk of mortality from
overweight and obesity in middle-
aged individuals from six
communities in Taiwan. J Formos
Med Assoc 2011;110:290-8
32. Ito T, Arima H, Fujiyoshi A, et al.
Relationship between nonhigh-
density lipoprotein cholesterol and
the long-term mortality of
cardiovascular diseases: NIPPON
5
2
Long term risk of incidence of cardiovascular events in Asian Populations
154 | Moving Forward to Achieve Universal Health Coverage in Indonesia
DATA 90. Int J Cardiol
2016;220:262-7
33. Ito Y, Kurata M, Suzuki K, et al.
Cardiovascular disease mortality and
serum carotenoid levels: a Japanese
population-based followup study. J
Epidemiol 2006;16:154-60
34. Ito Y, Suzuki K, Ishii J, et al. A
population-based follow-up study on
mortality from cancer or
cardiovascular disease and serum
carotenoids, retinol and tocopherols
in Japanese inhabitants. Asian
Pacific J Cancer Prev 2006;7:533-46
35. Kubo M, Hata J, Doi Y, et al.
Secular trends in the incidence of
and risk factors for ischemic stroke
and its subtypes in Japanese
population. Circulation
2008;118:2672-8
36. Lin PH, Yeh WT, Svetkey LP, et al.
Dietary intakes consistent with the
DASH dietary pattern reduce blood
pressure increase with age and risk
for stroke in a Chinese population.
Asia Pac J Clin Nutr 2013;22:482-91
37. Lin YS, Liu PH, Wu LS, et al. Major
adverse cardiovascular events in
adult congenital heart disease: a
population-based follow-up study
from Taiwan. BMC Cardiovasc
Disord 2014;14:38
38. Liu J, Wang W, Wang M, et al.
Impact of diabetes, high
triglycerides and low HDL
cholesterol on risk for ischemic
cardiovascular disease varies by
LDL cholesterol level: a 15-year
follow-up of the Chinese Multi-
provincial Cohort Study. Diabetes
Res Clin Pract 2012;96:217-24
39. Livshits G, Weisbort J, Meshulam
N, et al. Multivariate analysis of the
twenty-year follow-up of the
Donolo-Tel Aviv Prospective
Coronary Artery Disease Study and
the usefulness of high density
lipoprotein cholesterol percentage.
Am J Cardiol 1989;63:676-81
40. Matsumoto M, Ishikawa S, Kajii E.
Cumulative effects of weather on
stroke incidence: a multi-community
cohort study in Japan. J Epidemiol
2010;20:136-42
41. Miyagawa N, Miura K, Okuda N, et
al. Long-chain n-3 polyunsaturated
fatty acids intake and cardiovascular
disease mortality risk in Japanese: a
24-year follow-up of NIPPON
DATA80. Atherosclerosis
2014;232:384-9
42. Nagai K, Sairenchi T, Irie F, et al.
5
2
Chapter five

Moving Forward to Achieve Universal Health Coverage in Indonesia | 155
Relationship between estimated
glomerular filtration rate and
cardiovascular mortality in a
Japanese cohort with long-term
follow-up. PLoS One 2016;11:1-11
43. Nakamura Y, Okuda N, Okamura T,
et al. Low-carbohydrate diets and
cardiovascular and total mortality in
Japanese: a 29-year follow-up of
NIPPON DATA80. Br J Nutr
2014;112:916-24
44. Nishiwaki Y, Michikawa T,
Takebayashi T, et al. Long-term
exposure to particulate matter in
relation to mortality and incidence of
cardiovascular disease: the JPHC
Study. J Atheroscler Thromb
2013;20:296-309
45. Oki I, Nakamura Y, Okamura T, et
al. Body mass index and risk of
stroke mortality among a random
sample of Japanese adults: 19-year
follow-up of NIPPON DATA80.
Cerebrovasc Dis 2006;22:409-15
46. Okuda N, Miura K, Okayama A, et
al. Fruit and vegetable intake and
mortality from cardiovascular
disease in Japan: a 24-year follow-
up of the NIPPON DATA80 Study.
Eur J Clin Nutr 2015;69:482-8
47. Pan A, Clark ML, Ang LW, et al.
Incense use and cardiovascular
mortality among Chinese in
Singapore: the Singapore Chinese
Health Study. Environ Health
Perspect 2014;122:1279-84
48. Ren J, Grundy SM, Liu J, et al.
Long-term coronary heart disease
risk associated with very-low-
density lipoprotein cholesterol in
Chinese: the results of a 15-Year
Chinese Multi-Provincial Cohort
Study (CMCS). Atherosclerosis
2010;211:327-32
49. Saito I, Konishi M, Iso H, et al.
Impact of weight change on specific-
cause mortality among middle-aged
Japanese individuals. J Epidemiol
Community Health 2009;63:447-54
50. Takagi S, Saitoh S, Nakano M, et al.
Relationship between blood pressure
level and mortality rate: an 18-year
study conducted in two rural
communities in Japan. J Hypertens
2000;18:139-44
51. Takashima N, Ohkubo T, Miura K,
et al. Long-term risk of BP values
above normal for cardiovascular
mortality: a 24-year observation of
Japanese aged 30 to 92 years. J
Hypertens 2012;30:2299-306
52. Takashima N, Miura K, Hozawa A,
5
2
Long term risk of incidence of cardiovascular events in Asian Populations

156 | Moving Forward to Achieve Universal Health Coverage in Indonesia
et al. Population attributable fraction
of smoking and metabolic syndrome
on cardiovascular disease mortality
in Japan: a 15-year follow up of
NIPPON DATA90. BMC Public
Health 2010;10:306
53. Tanno K, Sakata K, Ohsawa M, et
al. Associations of ikigai as a
positive psychological factor with
all-cause mortality and causespecific
mortality among middle-aged and
elderly Japanese people: findings
from the Japan Collaborative Cohort
Study. J Psychosom Res
2009;67:67-75
54. Tsai MS, Li YF, Lin CL, et al.
Long-term risk of acute coronary
syndrome in patients with
cholangitis: a 13-year nationwide
cohort study. Eur J Intern Med
2014;25:444-8
55. Turin TC, Okamura T, Afzal AR, et
al. Hypertension and lifetime risk of
stroke. J Hypertens 2016;34:116-22
56. Turin TC, Okamura T, Afzal AR, et
al. Impact of hypertension on the
lifetime risk of coronary heart
disease. Hypertens Res
2016;39:548-51
57. Ueda K, Hasuo Y, Kiyohara Y, et al.
Intracerebral hemorrhage in a
Japanese community, Hisayama:
incidence, changing pattern during
long-term follow-up, and related
factors. Stroke 1988;19:48-52
58. Wang Y, Liu J, Wang W, et al.
Lifetime risk for cardiovascular
disease in a Chinese population: the
Chinese Multi-Provincial Cohort
Study. Eur J Prev Cardiol
2015;22:380-8
59. Murakami Y. Meta-analyses using
individual participant data from
cardiovascular cohort studies in
Japan: current status and future
directions. J Epidemiol 2014;24:96-
101
60. Fujiyoshi A, Ohkubo T, Miura K, et
al. Blood pressure categories and
long-term risk of cardiovascular
disease according to age group in
Japanese men and women.
Hypertens Res 2012;35:947-53
61. Grundy S, Pasternak R, Greenland
P, et al. Assessment of
cardiovascular risk by use of
multiple-risk-factor assessment
equations: a statement for healthcare
professionals from the American
Heart Association and the American
College of Cardiology. Circulation
1999;100:1481-92
5
2
Chapter five

Moving Forward to Achieve Universal Health Coverage in Indonesia | 157
62. Pencina MJ, D‘Agostino RB, Larson
MG, et al. Predicting the 30- year
risk of cardiovascular disease: the
Framingham heart study. Circulation
2009;119:3078-84
63. Menotti A, Jacobs DR, Blackburn H,
et al. Twenty-five-year prediction of
stroke deaths in the seven countries
study: the role of blood pressure and
its changes. Stroke 1996;27:381-7
64. Menotti A, Keys A, Kromhout D, et
al. Inter-cohort differences in
coronary heart disease mortality in
the 25-year follow-up of the seven
countries study. Eur J Epidemiol
1993;9:527-36
65. Keys A, Aravanis C, Blackburn
HW, et al. Epidemiological studies
related to coronary heart disease:
characteristics of men aged 40–59 in
seven countries. Acta Med Scand
Suppl 1966;460:1-392
66. Woodward M, Huxley H, Lam TH,
et al. A comparison of the
associations between risk factors and
cardiovascular disease in Asia and
Australasia. Eur J Cardiovasc Prev
Rehabil 2005;12:484-91
67. Woodward M, Barzi F, Feigin V, et
al. Associations between high-
density lipoprotein cholesterol and
both stroke and coronary heart
disease in the Asia Pacific region.
Eur Heart J 2007;28: 2653-60
68. Arima H, Murakami Y, Lam TH, et
al. Effects of prehypertension and
hypertension subtype on
cardiovascular disease in the
AsiaPacific region. Hypertension
2012;59:1118-23
69. Ueshima H, Sekikawa A, Miura K,
et al. Cardiovascular disease and risk
factors in Asia: a selected review.
Circulation 2008;118:2702-9
70. Ohira T, Iso H. Cardiovascular
disease epidemiology in Asia. Circ J
2013;77:1646-52
71. Bown MJ, Sutton AJ. Quality
control in systematic reviews and
meta-analyses. Eur J Vasc Endovasc
Surg 2010;40:669-77
72. Morrison A, Moulton K, Clark M, et
al. English-language restriction
when conducting systematic review-
based meta-analyses: systematic
review of published studies. Ottawa:
Canadian Agency for Drugs and
Technologies in Health, 2009
73. Meneghini R, Packer AL. Is there
science beyond English? EMBO
Rep 2007;8:112-16
5
2
Long term risk of incidence of cardiovascular events in Asian Populations

158 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Supplemental online material
Search strategy
PubMed®
#1 "Asia"[Mesh] OR Asia*[tiab] OR Arab[tiab] OR Arabs[tiab] OR
Arabia*[tiab] OR Saudi*[tiab] OR Persian*[tiab] OR Palestinian*[tiab] OR
Bangladesh[tiab] OR Bengali*[tiab] OR Bahrain*[tiab] OR Bahrani*[tiab]
OR Bhutan*[tiab] OR Brunei*[tiab] OR Cambodia*[tiab] OR Khmer*[tiab]
OR China[tiab] OR Chinese[tiab] OR Beijing[tiab] OR Hong Kong[tiab] OR
Macau[tiab] OR Mongol*[tiab] OR Tibet*[tiab] OR India*[tiab] OR
Dravidian*[tiab] OR Maldiv*[tiab] OR Indonesia*[tiab] OR Iran*[tiab] OR
Iraq*[tiab] OR Israel*[tiab] OR Bukhar*[tiab] OR Jew*[tiab] OR
Japan*[tiab] OR Jordan*[tiab] OR Korea*[tiab] OR Kuwait*[tiab] OR
Lao*[tiab] OR Leban*[tiab] OR Malay*[tiab] OR Myanmar[tiab] OR
Burm*[tiab] OR Nepal*[tiab] OR Oman*[tiab] OR Pakistan*[tiab] OR
Philippine*[tiab] OR Filipin*[tiab] OR Qatar*[tiab] OR Russia*[tiab] OR
Dungan[tiab] OR Hui[tiab] OR Kazakh*[tiab] OR Kyrg*[tiab] OR
Kirghiz[tiab] OR Siberia*[tiab] OR Uzbek*[tiab] OR Turk*[tiab] OR
Uyghur*[tiab] OR Singapore*[tiab] OR Sri Lanka*[tiab] OR Sinhalese[tiab]
OR Syria*[tiab] OR Taiwan*[tiab] OR Tajik*[tiab] OR Thai*[tiab] OR
Timor-Leste[tiab] OR Vietnam*[tiab] OR Yemen*[tiab] OR Kurd*[tiab] OR
Tatar*[tiab] OR Karakalpak*[tiab] OR Bashkir*[tiab] OR Altay[tiab] OR
Altai*[tiab] OR Pashtun*[tiab] OR Pathan*[tiab] OR Afghan*[tiab] OR
Hazara*[tiab] OR Aima*[tiab] OR Nuristan*[tiab] OR Mord*[tiab]
#2 "Risk "[Mesh] OR risk*[tiab] OR associat*[ti] OR relat*[ti] OR factor*[ti]
OR predict*[ti]
#3 "Cohort Studies"[Mesh:noexp] OR cohort*[tiab]
#4 "Cardiovascular Diseases"[Mesh] OR cardiovasc*[ti] OR heart[ti] OR
cardiac[ti] OR myocard*[ti] OR "Cerebrovascular Disorders"[Mesh] OR
cerebrovasc*[ti] OR stroke*[ti]
5
2
Chapter five

Moving Forward to Achieve Universal Health Coverage in Indonesia | 159
#5 longterm[tiab] OR long-term[tiab] OR longerterm[tiab] OR longer-term[tiab]
OR lifetime[tiab] OR life-time[tiab] OR long-time[tiab] OR longtime[tiab]
OR followed-up[ti] OR follow-up[ti]
#6 #1 AND #2 AND #3 AND #4 AND #5
#7 #6 Filters: English
Embase®
#1 'asia'/exp OR arab:ab,ti OR arabs:ab,ti OR arabia*:ab,ti OR saudi*:ab,ti OR
persian*:ab,ti OR palestinian*:ab,ti OR bangladesh:ab,ti OR bengali*:ab,ti
OR bahrain*:ab,ti OR bahrani*:ab,ti OR bhutan*:ab,ti OR brunei*:ab,ti OR
cambodia*:ab,ti OR khmer*:ab,ti OR china:ab,ti OR chinese:ab,ti OR
beijing:ab,ti OR 'hong kong':ab,ti OR macau:ab,ti OR mongol*:ab,ti OR
tibet*:ab,ti OR india*:ab,ti OR dravidian*:ab,ti OR maldiv*:ab,ti OR
indonesia*:ab,ti OR iran*:ab,ti OR iraq*:ab,ti OR israel*:ab,ti OR
bukhar*:ab,ti OR jew*:ab,ti OR japan*:ab,ti OR jordan*:ab,ti OR
korea*:ab,ti OR kuwait*:ab,ti OR lao*:ab,ti OR leban*:ab,ti OR malay*:ab,ti
OR myanmar:ab,ti OR burm*:ab,ti OR nepal*:ab,ti OR oman*:ab,ti OR
pakistan*:ab,ti OR philippine*:ab,ti OR filipin*:ab,ti OR qatar*:ab,ti OR
russia*:ab,ti OR dungan:ab,ti OR hui:ab,ti OR kazakh*:ab,ti OR kyrg*:ab,ti
OR kirghiz:ab,ti OR siberia*:ab,ti OR uzbek*:ab,ti OR turk*:ab,ti OR
uyghur*:ab,ti OR singapore*:ab,ti OR 'sri lanka':ab,ti OR 'sri lankan':ab,ti
OR 'sri lankans':ab,ti OR sinhalese:ab,ti OR syria*:ab,ti OR taiwan*:ab,ti OR
tajik*:ab,ti OR thai*:ab,ti OR 'timor leste':ab,ti OR vietnam*:ab,ti OR
yemen*:ab,ti OR kurd*:ab,ti OR tatar*:ab,ti OR karakalpak*:ab,ti OR
bashkir*:ab,ti OR altay:ab,ti OR altai*:ab,ti OR pashtun*:ab,ti OR
pathan*:ab,ti OR afghan*:ab,ti OR hazara*:ab,ti OR aima*:ab,ti OR
nuristan*:ab,ti OR mord*:ab,ti
#2 'risk'/exp OR risk*:ab,ti OR associat*:ti OR relat*:ti OR factor*:ti OR
predict*:ti
#3 'cohort analysis'/exp OR cohort*:ab,ti
5
2
Long term risk of incidence of cardiovascular events in Asian Populations
160 | Moving Forward to Achieve Universal Health Coverage in Indonesia
#4 'cardiovascular disease'/exp OR cardiovasc*:ti OR heart:ti OR cardiac:ti OR
myocard*:ti OR 'cerebrovascular disease'/exp OR cerebrovasc*:ti OR
stroke*:ti
#5 longterm:ab,ti OR 'long term':ab,ti OR longerterm:ab,ti OR 'long-term':ab,ti
OR lifetime:ab,ti OR 'life time':ab,ti OR 'long time':ab,ti OR longtime:ab,ti
OR 'followed up':ti OR 'follow up':ti
#6 #1 AND #2 AND #3 AND #4 AND #5
#7 #6 AND [english]/lim
#8 #7 AND ([article]/lim OR [article in press]/lim OR [review]/lim)
Web of ScienceTM
#1 TS=(Asia* OR Arab OR Arabs OR Arabia* OR Saudi* OR Persian* OR
Palestinian* OR Bangladesh OR Bengali* OR Bahrain* OR Bahrani* OR
Bhutan* OR Brunei* OR Cambodia* OR Khmer* OR China OR Chinese
OR Beijing OR "Hong Kong" OR Macau OR Mongol* OR Tibet* OR India*
OR Dravidian* OR Maldiv* OR Indonesia* OR Iran* OR Iraq* OR Israel*
OR Bukhar* OR Jew* OR Japan* OR Jordan* OR Korea* OR Kuwait* OR
Lao* OR Leban* OR Malay* OR Myanmar OR Burm* OR Nepal* OR
Oman* OR Pakistan* OR Philippine* OR Filipin* OR Qatar* OR Russia*
OR Dungan OR Hui OR Kazakh* OR Kyrg* OR Kirghiz OR Siberia* OR
Uzbek* OR Turk* OR Uyghur* OR Singapore* OR "Sri Lanka" OR "Sri
Lankan" OR "Sri Lankans" OR Sinhalese OR Syria* OR Taiwan* OR Tajik*
OR Thai* OR Timor-Leste OR Vietnam* OR Yemen* OR Kurd* OR Tatar*
OR Karakalpak* OR Bashkir* OR Altay OR Altai* OR Pashtun* OR
Pathan* OR Afghan* OR Hazara* OR Aima* OR Nuristan* OR Mord*)
#2 TOPIC: (Risk*) OR TITLE: (associat* OR relat* OR factor* OR predict*)
#3 TOPIC: (Cohort*) OR TITLE: (associat* OR relat* OR factor* OR predict*)
#4 TS=(cardiovasc* OR cerebrovasc*) OR TI=(heart OR cardiac OR myocard*
OR stroke*)
5
2
Chapter five

Moving Forward to Achieve Universal Health Coverage in Indonesia | 161
#5 TS=("longterm" OR "long-term" OR "longerterm" OR "longer-term" OR
"lifetime" OR "life-time" OR "longtime" OR "long-time") OR
TI=("followed-up") OR TI=("follow-up")
#6 #1 AND #2 AND #3 AND #4 AND #5
#7 #6 Refined by: DOCUMENT TYPES: (ARTICLE OR REVIEW) AND
LANGUAGES: (ENGLISH)
5
2
Long term risk of incidence of cardiovascular events in Asian Populations
162 | Moving Forward to Achieve Universal Health Coverage in Indonesia
The Risk of Bias Assessment tool for Non-randomized Studies
(RoBANS)
1. Domain selection participant
Were the exposure and comparison groups selected from the same
populations (i.e. the exposure group did not differ from the control group
with respect to study period or study centre, or historical control group was
used)? Was the absence of outcomes among the study participants confirmed
at the start of the study?
‗Low risk‘ of bias: exposure and control groups are the same population
group (identical institution and period), and the absence of outcomes among
the study participants was confirmed at the start of the study.
‗High risk‘ of bias:
- The exposure and control groups were selected from different
population groups (e.g. the intervention group differs from the control
group with respect to study period or study centre, or historical control
groups were used).
- The presence of outcomes among the study participants was not
confirmed at the start of the study.
‗Unclear risk‘ of bias: it is uncertain whether the selection of participants
resulted in a ‗high risk‘ or a ‗low risk‘ of bias.
2. Domain confounding variables
Were the major confounding variable factors adequately confirmed and
considered during the design phase (e.g. through matching, participation
restriction or other methods) OR analysis phase (e.g. through stratification,
propensity score approaches, statistical adjustments or other methods)?
‗Low risk‘ of bias:
- The major confounding variables were adequately confirmed and
considered during the design phase (e.g. through matching, participation
restriction or other methods).
5
2
Chapter five

Moving Forward to Achieve Universal Health Coverage in Indonesia | 163
- The major confounding variables were adequately confirmed and
accounted for during the analysis phase (e.g. through stratification,
propensity score approaches, statistical adjustments or other methods).
‗High risk‘ of bias:
- The major confounding variables were not considered.
- Although the existence of major confounding variables was confirmed,
these variables were not adequately considered during the design and
analysis phases.
‗Unclear risk‘ of bias: it is uncertain whether the confounding variables
resulted in a ‗high risk‘ or a ‗low risk‘ of bias.
3. Domain measurement of exposure
Was the data obtained from trustworthy sources (e.g. medical records) OR
structured interviews?
‗Low risk‘ of bias: exposure data were described using at least one of the
methods listed below:
- Data were obtained from trustworthy sources, such as medical records.
- Data were obtained from structured interviews.
‗High risk‘ of bias: any one of the following conditions:
- Data were obtained through self-reported methods.
- A clear case of interviewer bias: a situation in which the characteristics
of the investigators causes the study data to be standardized in a manner
that affects the study results. This phenomenon can be reduced through
the training of investigators.
- A clear case of recall bias: a situation in which the respondents‘ degree
of recall can affect the study results.
‗Unclear risk‘ of bias: it is uncertain whether the exposure measurement
resulted in a ‗high risk‘ or a ‗low risk‘ of bias.
4. Domain blinding of outcome assessments
Were outcome assessments blinded OR if blinding was not present, can its
absence be judged to have had no effect on the outcome measurements?
‗Low risk‘ of bias: any one of the following conditions:
5
2
Long term risk of incidence of cardiovascular events in Asian Populations
164 | Moving Forward to Achieve Universal Health Coverage in Indonesia
- The outcome assessments were blinded.
- Although blinding was not present, its absence was judged to have no
effect on the outcome measurements.
‗High risk‘ of bias: blinding was not performed or incomplete, and this lack
of appropriate blinding appears likely to have affected the outcome
measurements.
‗Unclear risk‘ of bias: it is uncertain whether the blinding of the outcome
assessments resulted in a ‗high risk‘ or a ‗low risk‘ of bias.
5. Domain incomplete outcome data
Was there no missing data? If there was missing data, were the causes of any
missing data considered to be relevant to the study outcomes? If there was
missing data, was the quantity of the missing data a product of similar
developments in the exposure and control groups and were the causes of
these developments similar?
‗Low risk‘ of bias: any one of the following conditions:
- There are no missing data.
- The causes of any missing data are considered to be relevant to the study
outcomes (i.e. censoring does not create a bias in the survival data).
- The quantity of missing data was a product of similar developments in
both the intervention (exposure) and the control groups, and the causes of
these developments are similar.
‗High risk‘ of bias: any one of the following conditions:
- The missing data could affect the study outcome. These effects may be
attributed to the differences in the missing data between the intervention
(exposure) group and the control group, or the effects may be caused by
the absence of important measurements.
‗Unclear risk‘ of bias: it is uncertain whether the incomplete outcome data
resulted in a ‗high risk‘ or a ‗low risk‘ of bias.
5
2
Chapter five

Moving Forward to Achieve Universal Health Coverage in Indonesia | 165
6. Domain selective outcome reporting
Was the experimental protocol available and were the predefined
primary/secondary outcomes described as planned? In the absence of the
experimental protocol, were all the expected outcomes included in the study
descriptions?
‗Low risk‘ of bias: any one of the following conditions:
- The experimental protocol was available and the predefined
primary/secondary outcomes were described as planned.
- All the expected outcomes were included in the study descriptions (even
in the absence of the experimental protocols).
‗High risk‘ of bias: any one of the following conditions:
- The predefined primary outcomes were not fully reported.
- The outcomes were not reported in accordance with the previously
defined standards.
- There were primary outcomes that were not pre-specified in the study (in
addition to outcomes with clear explanations, such as unexpected adverse
effects).
- The existence of incomplete reporting regarding the primary outcome of
interest.
- The absence of reports on important outcomes that would be expected to
be reported for studies in related fields.
‗Unclear risk‘ of bias: it is uncertain whether the selective outcome reporting
resulted in a ‗high risk‘ or a ‗low risk‘ of bias. Most of the studies examined
were classified in this category.
5
2
Long term risk of incidence of cardiovascular events in Asian Populations

166 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Supplemental materials
Other suplemental online materials can be found in this link below:
https://www.tandfonline.com/doi/suppl/10.1080/03007995.2018.1491149?scroll=to
p
or in this quick response code below
5
2
Chapter five
Moving Forward to Achieve Universal Health Coverage in Indonesia | 167
Chapter 6
GENERAL DISCUSSION

168 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Overview
With the studies described in this thesis we aim to evaluate the progress of the
Jaminan Kesehatan Nasional-Kartu Indonesia Sehat (JKN-KIS) towards universal
health coverage (UHC) since the it‘s implementation in 2014. In this chapter, we
will provide an update on the three key challenges JKN-KIS has encountered, i.e.,
medicines management, health financing system, and the epidemiological situation.
Furthermore, we will provide future a perspective, and present the implications of
our findings.
Medicines management during the implementation of the JKN-KIS
The e-catalogue and the national formulary (NF) are two policy instruments
regulating medicine pricing and reimbursement in support of JKN-KIS to achieve
UHC. Ideally, the e-Catalogue would help improve effectiveness, efficiency, and
transparency. Additionally, the NF would help ensure the availability of good
quality, efficacious, and affordable medicines, which subsequently should reduce
out-of pocket payment (OOP) for medicines. However, a year after the
implementation of the JKN KIS, many public healthcare facilities still rarely used
the e-Catalogue, and 40% of all medicines prescribed were not listed in the NF.
Importantly, 70% of OOP expenditures in Indonesia were for medicines in 2015[1-3].
To understand the slow implementation of both instruments we first undertook a
qualitative study.
In chapter 2, we performed a semi-structured interview with stakeholders to
identify the problems with the e-Catalogue and the NF. We found that the lack of
harmonization between medicines listed in the e-Catalogue and the NF was a major
issue. This triggered us to systematically compare the NF medicines published in
2013, 2015, and 2017 with the e-Catalogue 2018 version[4-6]. We found that indeed
41% in 2013, 37% in 2015, and 37% in 2017 of NF medicines were not listed in the
2018 e-Catalogue version. This indicates a continuing lack of harmonization
between the e-Catalogue and the NF. Furthermore, we also identified several
reasons for prescribing medicines that are not listed in the NF. The most important
6
2
Chapter six
Moving Forward to Achieve Universal Health Coverage in Indonesia | 169
reason was that physicians perceived the selection process of the NF as neither
transparent nor evidence-based[7].
In addition, in 2014, several months after the implementation of the JKN-
KIS the health technology assessment (HTA) committee was installed by the
Indonesia‘s Ministry of Health[8,9]. Ideally, this committee would have provided the
transparency and evidence base for the e-Catalogue and the NF in line with the
guidelines of the JKN-KIS implementation[10]. However, HTA has as yet not been
part of the development of the e-Catalogue and the NF. Barriers of HTA
implementation for the e-Catalogue and the NF that we found in chapter 3
concerned a lack of human resources, a lack of financial incentives, a lack of a clear
framework and insufficient data. The first two barriers represent the most important
obstacles. Reasons for the lack of human resources were that HTA is a new science
in Indonesia, and only few HTA departments exist, formal training is not nationally
provided, and an official association is missing in Indonesia. Clearly, financial
resources would be needed to pay the HTA experts, to organize HTA seminars, and
conduct HTA research[11]. Subsequently, we looked into the health insurance
coverage and data regarding healthcare expenditures.
Health financing system during the implementation of the JKN-KIS
The Badan Penyelenggara Jaminan Sosial Kesehatan (BPJS-Kesehatan) is a new
public health insurance provider implementing the JKN-KIS program. As a single
payer, the BPJS-Kesehatan plays a role in collecting a prepaid pool from the
government, private firms, and households into a single national reserve[12].
Furthermore, the most important role of the BPJS-Kesehatan is to ensure that budget
is allocated in line with the UHC targets[13-15]. In chapter 4, we assess health
financing in Indonesia towards UHC. We found that the target for achieving UHC
by 2020 will likely not be attained. The target of reducing household OOP schemes
to below 20 % may be reached by 2024. The target for reducing voluntary healthcare
payment to less than 10% may already be achieved by 2021. The government
schemes and compulsory contributory health financing schemes, however, will still
remain far away from 4% of GDP by 2020.
6
2
General Discussion

170 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Notably, we did find that the JKN-KIS has contributed to moving the health
financing in Indonesia towards the UHC targets. Before the JKN-KIS
implementation, between 2000 and 2013, OOP schemes and revenues from
household dominated Indonesia‘s health financing. Then, after the JKN-KIS had
been implemented, we found that the expenditure of social health insurance schemes
increased quite significantly from US $2.0 billion (8.52% of total health
expenditure) in 2013 to US $4.0 billion (14.25% of total health expenditure) by
2014. In the same period, the trend of OOP schemes by household decreased by US$
1.5 billion (7% of total health expenditure).
However, we also found that the expenditures of social health insurances
schemes were higher than its revenues since the implementation of the JKN-KIS. This is
different from the situation before the implementation of the JKN-KIS, i.e., there used to
be a balance between expenditures and resources from social health insurances. Our
findings corroborate the signals from several newspapers[16-18] that broadcasted that
BPJS-Kesehatan was experiencing deficits from the first year of implementation onward.
The BPJS-Kesehatan reported that the accumulation of the JKN-KIS‘ deficit up to
December 2018 was US $2.5 billion[19]. Based on our review, we found four main
possible causes of deficits. Firstly, the utilization of social health insurance benefits
doubled compare to the era prior to the JKN-KIS[20-22]. Secondly, the premium paid by
members of the JKN-KIS is low, probably caused by not setting the premium amount
according to the actuarial analysis, which is the most common method used to calculate
the social health insurance contributions[23-25]. Thirdly, premium collectability has not
been optimal among the self-enrolled members (17% of JKN-KIS participants). Of all
self-enrolled members, only 57% routinely pay their contribution. Moreover, 23% of
self-enrolled members only register when becoming ill, and stop paying the contribution
after treatment has been obtained[26,27]. Fourthly, expenditures of the JKN-KIS are
dominated by chronic disorders that might otherwise bankrupt individuals, such as
cardiovascular, diabetic, and cancer. These required prolonged hospitalization and high
cost treatment[19,28-31].
The latter was part of further studies on the demographic and epidemiological
perspectives of Indonesia.
6
2
Chapter six
Moving Forward to Achieve Universal Health Coverage in Indonesia | 171
Epidemiological conditions during the implementation of the JKN-KIS
While striving to achieve UHC by 2020, BPJS-Kesehatan is facing demographic and
epidemiological changes in Indonesia. After the implementation of the JKN-KIS,
life expectancy of Indonesian people increased from 69 years in 2014 to 71 years in
2017[32]. Notably, an ageing population implies that the prevalence of non-
communicable diseases increases. Especially cardiovascular diseases (CVDs)
increased from 2013 to 2018. For instance, stroke rose from 7% to 10.9%, and
hypertension from 25.8% to 34.1% [33,34]. Moreover, the most frequently used JKN-
KIS benefits packages since the first year of implementation has been for CVDs.
From January to August 2018, the BPJS-Kesehatan spent US $1.1 billion for CVDs
treatment. The latter represents two thirds of the eight chronic diseases with high
cost[35].
With the high prevalence of CVDs and the largest proportional financial
burden to the BPJS-Kesehatan, the government of Indonesia urgently needs to
develop a new approach to curb the emergence of CVDs. Prevention and addressing
the risk factors of CVDs could avoid or delay the incidence and prevalence of
CVDs[36,37]. In chapter 5, we estimated the long-term CVDs burden and risk factors
in Asian populations through a systematic review. The most important results were
that male sex, older age, and current smoking are the most prominent risk factors for
long-term CVDs in the Asian populations[38]. It is clear that only smoking can be
influenced through various interventions. Unfortunately, in our systematic review,
we did not find studies from Indonesia. Despite the unavailability of information
regarding long term risk of CVDs in Indonesia, this result might be used as a
reference. Clearly, Indonesia needs to recognize and identify people with additional
risk factors for CVDs that may potentially be influenced through the government
policies.
6
2
General Discussion

172 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Future perspective
As noted above the progress of JKN-KIS is such that UHC will not be achieved by
2020. Partly, this seems to have been caused by inefficient use of resources. Hence,
several policy options for promoting efficiency and eliminating waste during the
implementation of the JKN-KIS are necessary. In this part we encourage policy
options that government of Indonesia could implement to improve efficiency.
Furthermore, we propose further research to support and improve the progress of
UHC in Indonesia.
Policy options for improving UHC in Indonesia
It has been identified that the e-Catalogue and the NF have not been fully utilized to
support the aim of the JKN-KIS to achieve UHC. Hence, in order to avoid
unnecessary spending on medicines during the implementation of the JKN-KIS we
suggest the government of Indonesia to improve the harmonization between the e-
Catalogue and the NF. Several studies have explained that the asynchroneous
policies on medicine pricing and reimbursement lead to unnecessary spending on
medicines [39-41]. Furthermore, we also suggest to provide transparency and an
evidence-base in developing the e-Catalogue and the NF. Thus, a reasonable price in
the e-Catalogue may be negotiated while avoiding prescription of medicines not
listed in the NF.
As we explained in chapter 2, and 3, as supported by several studies, that
the use of HTA might facilitate transparency in the e-Catalogue and the NF [42,43,44].
Although several barriers currently hampering the implementation of HTA in the
development of the e-Catalogue and the NF, the existence of an Indonesian
Presidential Decree[45] may force the Indonesian government to utilize HTA in the
development of the e-Catalogue and the NF. Also, it would be beneficial for
Indonesia to establish a network with other neigbouring countries that have a well-
established system, and with international HTA organizations to learn how to
establish a national HTA process[11].
With respect to the deficit of the BPJS-Kesehatan that we found in chapter
4, the government of Indonesia should prioritize further use of HTA to ensure the
6
2
Chapter six

Moving Forward to Achieve Universal Health Coverage in Indonesia | 173
financial sustainability of the JKN-KIS program. Also, several adjacent policies
must be put in place to resolve most common and relevant causes of deficit.
Notably, here we will offer possible solutions of the possible causes of deficits that
we identified above.
Firstly, regarding the increasing utilization of JKN-KIS benefit packages,
we propose to extensively review the claim system and subsidized group data. In the
claim system, several frauds, such as unnecessary treatment, phantom and repeated
billing were found at the primary and secondary health providers[46-48]. For example,
in the subsidized groups data, there seem to be some people who do have ability to
pay included in the data, and entries of some poor people were not included in the
data. This is also caused by the subsidized group data that have not been updated
since 2008[25]. Secondly, regarding the low JKN-KIS premium income we suggest to
set the premium to be in line to the actuarial analysis. The national social security
council and several institutions have provided actuarial calculations for setting the
JKN-KIS premium, but so far it has never been used when revising the BPJS-
Kesehatan premium[23-25]. Thirdly, regarding a lack of contribution from the self-
enrolled members, we proposed to improve public awareness and BPJS-Kesehatan
system. For the public awareness, all individuals should be obliged to register for
JKN-KIS memberships. In 2018, 24 % of Indonesian population had not been
enrolled to the BPJS-Kesehatan. Furthermore, the self-enrolled members of BPJS-
Kesehatan should become full and regular contributors They should contribute
regularly either healthy or sick. In case they are unable to pay their contributions due
to financial hardship, they could join to the subsidized groups of the JKN-KIS[26,27].
Importantly, several reasons for self-enrolled members not paying the contribution
were attributable to failing of the BPJS-Kesehatan system itself. These were as a
lack of information on membership payment method, a lack of comprehensive
knowledge of JKN-KIS‘s benefit package, and dissatisfaction with the workforce of
healthcare services[27]. Therefore, we propose to improve BPJS-Kesehatan
infrastructure, particularly the payment method, to massively increase insurance
literacy to the societies, and finally to improve health professional capacity.
6
2
General Discussion

174 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Fourthly, considering the dominance of chronic disorders that might
bankrupt individuals as well as the BPJS-Kesehatan as such, we propose to improve
preventive programs instead of spending all resources on curative care. In particular
for CVDs we confirmed that smoking is the key risk factor that may be modified in
Asia[38]. Especially since Indonesia has the highest prevalence of smoking in the
world, with 34% overall prevalence in adults, and 65% in adult men this appears an
essential first risk factor to address. The high prevalence of smoking particularly
among people living in poverty, increases their vulnerability[33,49]. Hence, we
recommend to increase the cost of cigarette and tobacco taxes to ultimately reduce
the prevalence of CVDs, and the financial burden on the JKN-KIS. Several countries
have shown that raising the price of cigarettes and tobacco reduces smoking, and
subsequently the prevalence and incidence of CVDs[50].
Further research for improving UHC
In this thesis, we have identifiede the main challenges currently faced by Indonesia in its
efforts to achieve UHC, along with strategies to face these challenges. Notably, there is
still a lot of research needed to deal with medicines management, healthcare financing,
and curbing chronic disease in Indonesia. Further research for improving UHC in
Indonesia is obviously needed. First of all, it is important to assess the demographics of
the JKN-KIS claim data. This information will trigger further research that can improve
efficiency in the JKN-KIS program. For instance, we could compare the claims data of
the JKN-KIS with the data on the disease burden of Indonesia. The results may indicate
whether treatment and expenditure are appropriately used. Furthermore, from the claim
data we might try and estimate the balance between costs and effects of medicines or
treatments in one disease. The most cost-effective medicines or treatment should be
prioritized in the e-Catalogue and the NF. However, currently the claims data of the
JKN-KIS are not available. Availability of these BPJS-Kesehatan data should be
enhanced to trigger research and help the BPJS-Kesehatan to improve efficiency, and
maintain the goal of achieving UHC. Several UHC countries, such as the Netherlands,
the UK, South Korea, Taiwan, Japan, and Thailand, have shown that providing claims
data to the academia and researchers helps these countries for maintaining and
optimizing their UHC [51-54].
6
2
Chapter six

Moving Forward to Achieve Universal Health Coverage in Indonesia | 175
Implications
This thesis comes at a crucial time for recognizing the progress of the JKN-KIS in
moving forward towards UHC. Strategies presented in this thesis, i.e., harmonizing
the e-Catalogue and the NF, and utilizing HTA in the e-Catalogue and the NF could
facilitate the Indonesian government to improve efficiency and avoid unnecessary
expenditure on medicines. Furthermore, recognizing deficit and also its causes
would help to ensure financial sustainability of the JKN-KIS and maintain the goal
for UHC. In addition, identifying and addressing the modifiable risk factors of
CVDs would in the future relieve the government of catastrophic diseases, which is
currently the highest financial burden within the JKN-KIS. Such studies might also
provide comprehensive information and guidance to other countries aiming to
achieve and maintain UHC. Especially, low middle-income countries have similar
issues with high medicine expenditures, dominant OOP payments, and increasing
NCDs [55,56].
6
2
General Discussion
176 | Moving Forward to Achieve Universal Health Coverage in Indonesia
References
1. Niken Ariati. Tata kelola obat di era
sistem jaminan kesehatan nasional. .
2017.
2. Dirjen Binfar dan Alkes Kemenkes
RI. Implementasi formularium
nasional dalam pelaksanaan jaminan
kesehatan nasional. . 2015.
3. Hidayat B, Mundiharno, Nemec J,
Rabovskaja V, Rozanna C, Spatz J.
Out-of-pocket payments in the
national health insurance of
indonesia. . 2015.
4. Menteri Kesehatan Republik
Indonesia. Keputusan menteri
kesehatan republik indonesia nomor
328/menkes/IX/ 2013 tentang
formularium nasional. . 2013.
5. Menteri Kesehatan Republik
Indonesia. Keputusan menteri
kesehatan republik indonesia nomor
HK.02.02/ menkes/ 523/ 2015
tentang formularium nasional. .
2015
6. Menteri Kesehatan Republik
Indonesia. Keputusan menteri
kesehatan republik indonesia nomor
HK. 01. 07/ menkes/ 659/ 2017
tentang formularium nasional. .
2017.
7. Wasir R, Irawati S, Makady A, et al.
Use of medicine pricing and
reimbursement policies for universal
health coverage in indonesia. PloS
one. 2019;14(2):e0212328.
8. Menteri Kesehatan Republik
Indonesia. Keputusan menteri
kesehatan republik indonesia nomor
171/ menkes/ SK/ IV/ 2014 tentang
komite penilaian teknologi
kesehatan. . 2014.
9. Menteri Kesehatan Republik
Indonesia. Keputusan menteri
kesehatan RI no.
HK.02.02/menkes/422/2016 tentang
komite penilaian teknologi
kesehatan. . 2016.
10. Menteri Kesehatan Republik
Indonesia. Peraturan menteri
kesehatan republik indonesia nomor
28 tahun 2014 tentang pedoman
pelaksanaan program jaminan
kesehatan nasional. ; 2014.
11. Wasir R, Irawati S, Makady A, et al.
The implementation of HTA in
medicine pricing and reimbursement
6
2
Chapter six

Moving Forward to Achieve Universal Health Coverage in Indonesia | 177
policies in indonesia: Insights from
multiple stakeholders. PLoS One.
2019;14(11):e0225626.
12. Peraturan Presiden R. Perpres RI no.
12 tahun 2013, tentang jaminan
kesehatan. . 2013.
13. Jowett M, Brunal MP, Flores G,
Cylus J. Spending targets for health:
No magic number. World Health
Organization; 2016.
14. World Health Organization. Health
financing strategy for the asia
pacific region (2010-2015). Manila:
WHO Regional Office for the
Western Pacific; 2009.
15. World Health Organization. The
world health report: Health systems
financing: The path to universal
coverage: Executive summary. .
2010.
16. The Jakarta Post. Higher healthcare
premiums 'urgent', BPJS kesehatan
pleads as finances bleed. . 2019.
17. IDN Financials. BPJS kesehatan
deficit hits rp 7 trilion as of june
2019
18. Nikkei Asian Review. Indonesia
struggles to pay for huge universal
health care program. . 2019.
19. BPJS Kesehatan. Laporan
pengelolaan program dan laporan
keuangan jaminan sosial kesehatan
tahun 2018. . 2019.
20. Erlangga D, Ali S, Bloor K. The
impact of public health insurance on
healthcare utilisation in indonesia:
Evidence from panel data.
International journal of public
health. 2019;64(4):603-613.
21. Rolindrawan D. The impact of BPJS
health implementation for the poor
and near poor on the use of health
facility. Procedia-Social and
Behavioral Sciences. 2015;211:550-
559.
22. Maharani C, Afief DF, Weber D,
Marx M, Loukanova S. Primary care
physicians‘ satisfaction after health
care reform: A cross-sectional study
from two cities in central java,
indonesia. BMC health services
research. 2019;19(1):290.
23. Susanty A, Puspitasari NB,
Wicaksono PA, Pungky PPA.
Choosing the benefit package from
the BPJS program: Findings from
CHAT experiment. International
Journal of Healthcare Management.
2016;9(3):201-209.
6
2
General Discussion

178 | Moving Forward to Achieve Universal Health Coverage in Indonesia
24. Hidayat B, Mundiharno NJ,
Rabovskaja V, Rozanna C, Spatz J.
Financial sustainability of the
national health insurance in
indonesia: A first year review.
Policy brief.Jakarta: the
Indonesian-German Social
Protection Programme. 2015.
25. Prabhakaran et al. Financial
sustainability of indonesia’s
jaminan kesehatan nasional:
Performance, prospects, and policy
options. Washington, DC:
Palladium, Health Policy Plus, and
Jakarta, Indonesia: Tim Nasional
Percepatan Penanggulangan
Kemiskinan (TNP2K); 2019.
26. Agustina R, Dartanto T, Sitompul R,
et al. Universal health coverage in
indonesia: Concept, progress, and
challenges. The Lancet.
2019;393(10166):75-102.
27. Dartanto T, Halimatussadiah A,
Rezki JF, et al. Why do informal
sector workers not pay the premium
regularly? evidence from the
national health insurance system in
indonesia. Applied health economics
and health policy. 2019:1-16.
28. BPJS Kesehatan. Laporan
pengelolaan program dan laporan
keuangan 2015. . 2016.
29. BPJS Kesehatan. Laporan
pengelolaan program dan laporan
keuangan jaminan sosial kesehatan
tahun 2016. . 2017.
30. Tandon A, Pambudi ES, Harimurti
P, et al. Indonesia health financing
system assessment: Spend more,
spend right, spend better. World
Bank; 2016.
31. Mahendradhata Y, Laksono
Trisnantor, Shita Listyadewi, et al.
The republic of indonesia health
system review. . 2017;Vol. 7 No. 1
Asia Pacific Observatory on Health
Systems and Policies(World Health
Organization).
32. The World Bank,. World bank
database. . Updated 2019. Accessed
02/27, 2020.
33. Kemenkes R. Riset kesehatan dasar
(riskesdas) 2013. Kemenkes
RI.Jakarta. 2013.
34. Kemenkes R. Hasil utama
RISKESDAS 2018.
35. Deloitte. Ensuring the sustainability
of JKN-KIS for the indonesian
people. . 2019.
6
2
Chapter six
Moving Forward to Achieve Universal Health Coverage in Indonesia | 179
36. World Health Organization.
Prevention of cardiovascular
disease. World Health Organization;
2007.
37. Maharani A, Sujarwoto, Praveen D,
Oceandy D, Tampubolon G, Patel
A. Cardiovascular disease risk factor
prevalence and estimated 10-year
cardiovascular risk scores in
indonesia: The SMARThealth
extend study. PLoS One.
2019;14(4):e0215219.
38. Irawati S, Wasir R, Floriaan
Schmidt A, et al. Long-term
incidence and risk factors of
cardiovascular events in asian
populations: Systematic review and
meta-analysis of population-based
cohort studies. Curr Med Res Opin.
2019;35(2):291-299.
39. Acosta A, Ciapponi A, Aaserud M,
et al. Pharmaceutical policies:
Effects of reference pricing, other
pricing, and purchasing policies.
Cochrane Database of Systematic
Reviews. 2014(10).
40. Hu J, Mossialos E. Pharmaceutical
pricing and reimbursement in china:
When the whole is less than the sum
of its parts. Health Policy.
2016;120(5):519-534.
41. Vogler S, Paris V, Ferrario A, et al.
How can pricing and reimbursement
policies improve affordable access
to medicines? lessons learned from
european countries. Applied health
economics and health policy.
2017;15(3):307-321.
42. Vella Bonanno P, Bucsics A,
Simoens S, et al. Proposal for a
regulation on health technology
assessment in europe–opinions of
policy makers, payers and
academics from the field of HTA.
Expert review of
pharmacoeconomics & outcomes
research. 2019;19(3):251-261.
43. Paolucci F, Redekop K, Fouda A,
Fiorentini G. Decision making and
priority setting: The evolving path
towards universal health coverage.
Applied health economics and
health policy. 2017;15(6):697-706.
44. Ngorsuraches S, Meng W, Kim B,
Kulsomboon V. Drug
reimbursement decision-making in
thailand, china, and south korea.
6
2
General Discussion
180 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Value in Health. 2012;15(1):S120-
S125.
45. Presiden Republik Indonesia.
Peraturan presiden republik
indonesia nomor 12 tahun 2013
tentang jaminan kesehatan. ; 2013.
46. Ekawati FM, Claramita M, Hort K,
Furler J, Licqurish S, Gunn J.
Patients‘ experience of using
primary care services in the context
of indonesian universal health
coverage reforms. Asia Pacific
family medicine. 2017;16(1):4.
47. Santoso B, Hendrartini J, Rianto
BUD, Trisnantoro L. System for
detection of national healthcare
insurance fraud based on computer
application. Public Health of
Indonesia. 2018;4(2):46-56.
48. Fathurrohman N, Dewi A. Potential
fraud in the primary healthcare.
Jurnal Medicoeticolegal dan
Manajemen Rumah Sakit.
2018;7(3):196-204.
49. Kusumawardani N, Tarigan I,
Suparmi ea, Schlotheuber A. Socio-
economic, demographic and
geographic correlates of cigarette
smoking among indonesian
adolescents: Results from the 2013
indonesian basic health research
(RISKESDAS) survey. Global
health action. 2018;11(sup1):54-62.
50. Kalkhoran S, Benowitz NL, Rigotti
NA. Reprint of: Prevention and
treatment of tobacco use: JACC
health promotion series. J Am Coll
Cardiol. 2018;72(23 Part B):2964-
2979.
51. Wammes JJG, Tanke M, Jonkers W,
Westert GP, Van der Wees P,
Jeurissen PP. Characteristics and
healthcare utilisation patterns of
high-cost beneficiaries in the
netherlands: A cross-sectional
claims database study. BMJ Open.
2017;7(11):e017775-2017-017775.
52. Tanaka H, Tomio J, Sugiyama T,
Kobayashi Y. Process quality of
diabetes care under favorable access
to healthcare: A 2-year longitudinal
study using claims data in japan.
BMJ Open Diabetes Research and
Care. 2016;4(1):e000291.
53. Seo HJ, Oh I, Yoon S. A
comparison of the cancer incidence
rates between the national cancer
registry and insurance claims data in
korea. Asian Pacific Journal of
6
2
Chapter six
Moving Forward to Achieve Universal Health Coverage in Indonesia | 181
Cancer Prevention.
2012;13(12):6163-6168.
54. World Health Organization.
Universal health coverage: Moving
towards better health: Action
framework for the western pacific
region. . 2016.
55. Reeves A, Gourtsoyannis Y, Basu S,
McCoy D, McKee M, Stuckler D.
Financing universal health
coverage—effects of alternative tax
structures on public health systems:
Cross-national modelling in 89 low-
income and middle-income
countries. The Lancet.
2015;386(9990):274-280.
56. Lagomarsino G, Garabrant A,
Adyas A, Muga R, Otoo N. Moving
towards universal health coverage:
Health insurance reforms in nine
developing countries in africa and
asia. The Lancet.
2012;380(9845):933-943.
6
2
General Discussion
182 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Addendum

Moving Forward to Achieve Universal Health Coverage in Indonesia | 183
SUMMARY
All countries in the United Nations (UN) has committed to achieving
universal health coverage (UHC) as part of the sustainable development goals by
2030. The World Health Organization (WHO) states that UHC has been achieved by
a country when all people and communities can use the promotive, preventive,
curative, rehabilitative and palliative health services they need, of sufficient quality
to be effective, while also ensuring that the use of these services does not expose the
user to financial hardship. The WHO outlines that UHC is achieved by a country
when out-of-pocket (OOP) expenditure falls below 20% of total healthcare
expenditures. Furthermore, the WHO urged that government spending on healthcare
should be at least 4% of a country‘s gross domestic product (GDP) to achieve UHC.
As a member of the UN, Indonesia is aiming to achieve UHC. This goal is
increasingly supported with the Indonesian constitution or Undang-Undang Dasar
1945, article 28. Health is a basic right of every individual, and all citizens are
entitled to health services including those living in poverty. At the beginning of
2014, the government of Indonesia officially announced its plan to achieve UHC by
2020 through a new national health insurance, which is known as Jaminan
Kesehatan Nasional-Kartu Indonesia Sehat (JKN-KIS). This program is managed
by a new health insurance program, which is called Badan Penyelenggara Jaminan
Sosial-Kesehatan (BPJS-Kesehatan). The JKN-KIS was the result of a merger of
pre-existing social health insurance schemes. The fragmented health insurance
schemes made health care spending and quality of healthcare services difficult to
control.
Prior to the JKN-KIS implementation, there were several unresolved issues
concerning medicine management, health financing system, and the epidemiological
situation in Indonesia. In medicine management, the proportion of OOPs for
medicines was high, accounting for over 50% of total health expenditures.
Furthermore, medicine expenditure accounted for 67% of total health expenditure.
With respect to health financing, the government of Indonesia experienced
difficulties in increasing health expenditure at the national level. Instead of relying

184 | Moving Forward to Achieve Universal Health Coverage in Indonesia
on government healthcare financing, Indonesia was dominated by OOP
expenditures. Regarding the epidemiological situation, the ageing population lead
the proportional mortality due to non-communicable diseases almost doubled from
37% in 1990 to 73% in 2014. Of all non-communicable diseases, cardiovascular
diseases (CVDs) are the leading cause of deaths and disability.
The main objective of this thesis was to evaluate the progress of the JKN-
KIS in moving forward to achieve UHC in Indonesia. In particular, it set out to
provide comprehensive findings on how the JKN-KIS has encountered three key
challenges on medicine management, health financing, and epidemiological
situation. In Chapter 1, we will briefly explain the concept of UHC according to the
WHO. This is followed by an explanation of the Indonesia‘s health system
transformation towards UHC, and the potential challenges for achieving UHC by
2020. Furthermore, the gaps in knowledge and the thesis objectives are presented.
In Chapter 2, we performed semi structured interviews to identify the
problems of the e-Catalogue and the National Formulary (NF). These are the two
new policy instruments that were introduced to regulate medicine pricing and
reimbursement during the implementation of the JKN-KIS. Ideally, the e-Catalogue
would help improve effectiveness, efficiency, and transparency on procuring
medicine on healthcare facilities. While the NF would help ensure the availability of
good quality, efficacious and affordable medicines. Therefore, these policies should
help the JKN-KIS to control the medicine expenditure and reduce OOPs for
medicines, which subsequently to achieve UHC. However, a year after the
implementation, many public healthcare facilities only rarely used the e-catalogue
for medicine procurement, and 40% of all medicines prescribed were not listed in
the NF. We found that the major issue was the lack of harmonization between
medicine listed in the e-Catalogue and the NF. Then, the most important reasons for
prescribing medicines outside the NF was a lack of transparency and evidence base
in the development of the NF.
In Chapter 3, we identified the barriers and facilitators of implementing
health technology assessment (HTA) in the development of the e-Catalogue and the
NF. The HTA committee was installed by the Indonesia‘s Ministry of Health several
Moving Forward to Achieve Universal Health Coverage in Indonesia | 185
months after the implementation of the JKN-KIS. Ideally, the committee would have
provided the transparency and evidence base of the e-Catalogue and the NF in line
with the guidelines of the JKN-KIS implementation. However, HTA has not been
part of the development of the e-Catalogue and the NF. Several barriers of HTA
implementation in the e-Catalogue and the NF were a lack of capacity, a lack of
financial incentives, a lack of a clear framework and insufficient data. The first two
barriers represent the most important obstacles. Reasons for the lack of capacity
were that HTA is a new science in Indonesia, and only few HTA departments exist,
formal training is not nationally provided, and an official association is missing in
Indonesia. Furthermore, financial resources would be needed to pay the HTA
experts, to organize HTA seminars, and conduct HTA research.
In Chapter 4, we assess health financing in Indonesia towards UHC. This is
to understand whether Indonesia has organized its health financing system in line
with the UHC targets. Trends of health financing prior to and after the
implementation of the JKN-KIS are described. Furthermore, the projection of health
financing schemes is also extended through 2030, as the year of sustainable
development goals agenda. We found that the target for achieving UHC by 2020
will not be attained. The target for reducing household OOP schemes below 20 %
may be reached by 2024. The target for reducing voluntary healthcare payment to
less than 10% may be achieved by 2021. Importantly, the government schemes and
compulsory contributory health financing schemes will remain far away from 4% of
the GDP by 2020. Furthermore, we also found that in the first year of the JKN-KIS
implementation, the expenditure of the BPJS-Kesehatan increased significantly from
$2.0 billion (8.52% of THE) to US $4.0 billion (14.25% of THE). This resulted in
the OOP schemes by household decreasing to US$ 1.5 billion (7% of THE).
Increasing social health insurance expenditures and reducing OOP is the right
progress for achieving UHC. However, we found that the revenues of the BPJS-
Kesehatan was insufficient for fulfilling their expenditure. This led the BPJS-
Kesehatan to continuously develop a deficit since the first-year of implementation.
In Chapter 5, we estimate the long-term CVD burden and risk factors in
Asian populations through a systematic review. The most important results for the

186 | Moving Forward to Achieve Universal Health Coverage in Indonesia
objective of the thesis was that the male sex, old age, and smooking status are the
most prominent risk factors for long-term fatal CVD in the Asian population. In our
systematic review we did not find studies from Indonesia in line with the inclusion
criteria of our studies (cohort studies, Asian healthy above 18 years, free from
CVDs, 10-year follow-up period). Notably, our inclusion criteria could obtain long-
term incidence rate in the general population. Given the unavailability of
information regarding long term risk factors of long-term fatal CVD in Indonesia,
this result could be used as a reference to recognize that smoking is the modifying
risk factor of CVDs. Therefore, this can be influenced through various interventions
to reduce the mortality of CVDs in Indonesia and to reduce the financial burden of
the BPJS-Kesehatan.
In Chapter 6, we present the general discussion of this thesis. We start with
an overview of how the JKN-KIS has encountered the three key main challenges.
Then, the future perspective will offer policy options to address the challenges and
suggestions for further research needed for improving UHC. We will then explain
how this thesis gives possible guidance to Indonesia and other countries. Finally, the
conclusion of this thesis is that JKN-KIS is the cornerstone for Indonesia to achieve
UHC in line with WHO targets. However, improving efficiency and raising financial
resources for health are crucial for the JKN-KIS to address several challenges that
are currently hampering the efforts being made to achieve UHC.

Moving Forward to Achieve Universal Health Coverage in Indonesia | 187
SAMENVATTING
De Verenigde Naties hebben toegezegd om in 2030 universele
gezondheidsdekking (UHC) te bereiken als onderdeel van de doelstellingen voor
duurzame ontwikkeling. De Wereldgezondheidsorganisatie (WHO) stelt dat UHC is
bereikt in een land waar alle mensen en gemeenschappen gebruik kunnen maken van
preventieve, genezende, revaliderende en palliatieve gezondheidsdiensten die zij
nodig hebben, van voldoende kwaliteit zijn om doeltreffend te zijn, en er
tegelijkertijd voor te zorgen dat het gebruik van deze diensten de gebruiker niet
blootstelt aan financiële moeilijkheden. De WHO schetst dat UHC wordt bereikt
door een land wanneer de eigen uitgaven (OOP) onder 20% van de totale uitgaven
voor gezondheidszorg dalen. Bovendien drong de WHO erop aan dat de
overheidsuitgaven voor gezondheidszorg ten minste 4% van het bruto binnenlands
product bedragen om UHC te bereiken.
Als lid van de Verenigde Naties streeft Indonesië naar UHC. Dit doel wordt
in toenemende mate ondersteund door de Indonesische grondwet of Undang-Undang
Dasar 1945, artikel 28. Gezondheid is een basisrecht van elk individu en alle burgers
hebben recht op gezondheidsdiensten, inclusief de armen. Begin 2014 kondigde de
Indonesische regering officieel haar plan aan om UHC tegen 2020 te bereiken via
een nieuwe nationale ziektekostenverzekering, die bekend staat als Jaminan
Kesehatan Nasional-Kartu Indonesia Sehat (JKN-KIS). Dit programma wordt
beheerd door een nieuw zorgverzekeringsprogramma, genaamd Badan
Penyelenggara Jaminan Sosial-Kesehatan (BPJS-Kesehatan). De JKN-KIS was het
resultaat van een fusie van reeds bestaande sociale ziektekostenverzekeringen. Door
de gefragmenteerde ziektekostenverzekeringen waren de uitgaven voor de
gezondheidszorg en de kwaliteit van de gezondheidszorg moeilijk te controleren.
Voorafgaand aan de implementatie van JKN-KIS zijn er verschillende
onopgeloste kwesties op het gebied van medicijnbeheer, gezondheidsfinanciering en
epidemiologische situatie in Indonesië. Bij medicijnbeheer is het aandeel van OOP's
voor geneesmiddelen hoog, tot meer dan 50% van de totale gezondheidsuitgaven.
Bovendien waren de geneesmiddelenuitgaven goed voor 67% van de totale
188 | Moving Forward to Achieve Universal Health Coverage in Indonesia
gezondheidsuitgaven. Met betrekking tot gezondheidsfinanciering ondervond de
regering van Indonesië moeilijkheden bij het verhogen van de gezondheidsuitgaven
op nationaal niveau. In plaats van te vertrouwen op overheidsfinanciering voor de
gezondheidszorg, werd Indonesië gedomineerd door OOP-uitgaven. Wat de
epidemiologische situatie betreft, leidt een vergrijzende bevolking ertoe dat de
proportionele sterfte als gevolg van niet-overdraagbare ziekten bijna is verdubbeld
van 37% in 1990 tot 73% in 2014. Van alle niet-overdraagbare ziekten zijn hart- en
vaatziekten de belangrijkste doodsoorzaak en oorzaak van invaliditeit.
Het hoofddoel van dit proefschrift is het evalueren van de voortgang van de
JKN-KIS om UHC in Indonesië te bereiken. Met name om een uitgebreide
beschrijving te geven over hoe de JKN KIS drie belangrijke uitdagingen op het
gebied van medicijnbeheer, gezondheidsfinanciering en epidemiologische situatie is
tegengekomen. In hoofdstuk 1 zullen we het concept van UHC kort uitleggen
volgens de WHO. Gevolgd door uitleg over de transformatie van het Indonesische
gezondheidssysteem naar UHC en de potentiële uitdagingen om UHC tegen 2020 te
bereiken. Verder worden daar de kenniskloof en de doelstellingen van de diverse
studies gepresenteerd.
In hoofdstuk 2 hebben we een semi-gestructureerd interview uitgevoerd
om de problemen van de e-Catalogus en het Nationaal Formularium (NF) te
identificeren. Dit zijn de twee nieuwe beleidsinstrumenten die de prijsstelling en
vergoeding van geneesmiddelen regelen tijdens de implementatie van de JKN-KIS.
In het ideale geval zou de e-catalogus de doeltreffendheid, efficiëntie en
transparantie van de aankoop van medicijnen in zorginstellingen helpen verbeteren.
OOk het NF zou bijdragen tot de beschikbaarheid van goede, effectieve en
betaalbare geneesmiddelen. Daarom zou dit beleid de JKN-KIS moeten helpen om
de uitgaven voor geneesmiddelen te beheersen en de OOP voor geneesmiddelen te
verminderen, om uiteindelik UHC te bereiken. Een jaar na de implementatie
gebruikten veel openbare zorginstellingen de e-catalogus echter slechts zelden voor
het verkrijgen van medicijnen en 40% van alle voorgeschreven medicijnen was niet
opgenomen in de NF. We ontdekten dat het belangrijkste probleem het gebrek aan
harmonisatie was tussen de medicijnen die in de e-Catalogus en het NF staan
Addendum

Moving Forward to Achieve Universal Health Coverage in Indonesia | 189
vermeld. De belangrijkste redenen voor het voorschrijven van geneesmiddelen
buiten het NF waren dan ook een gebrek aan transparantie en evidence-base bij de
ontwikkeling van het NF.
In Hoofdstuk 3 identificeerden we de belemmeringen en facilitator van het
implementeren van health technology assessment (HTA) bij de ontwikkeling van de
e-Catalog en het NF. De HTA-commissie werd enkele maanden na de implementatie
van de JKN-KIS geïnstalleerd door het Indonesische ministerie van
Volksgezondheid. Idealiter zou de commissie de transparantie en bewijsbasis van de
e-Catalog en de NF hebben geleverd in overeenstemming met de richtlijnen van de
implementatie van JKN-KIS. HTA heeft echter geen deel uitgemaakt van de
ontwikkeling van de e-catalogus en de NF. Verschillende belemmeringen voor de
implementatie van HTA in de e-catalogus en de NF waren een gebrek aan capaciteit,
een gebrek aan financiële prikkels, een gebrek aan een duidelijk kader en
onvoldoende gegevens. De eerste twee belemmeringen vormen de belangrijkste
obstakels. Redenen voor het gebrek aan capaciteit waren dat HTA een nieuwe
wetenschap is in Indonesië en dat er maar weinig HTA-afdelingen zijn, dat er geen
nationale opleiding wordt gegeven en dat er in Indonesië een officiële vereniging
ontbreekt. Bovendien zouden financiële middelen nodig zijn om de HTA-experts te
betalen, HTA-seminars te organiseren en HTA-onderzoek uit te voeren.
In hoofdstuk 4 beoordelen we gezondheidsfinanciering in Indonesië
richting UHC. Dit is om te begrijpen of Indonesië zijn systeem voor
gezondheidsfinanciering heeft georganiseerd in overeenstemming met de UHC-
doelstellingen. Trends van gezondheidsfinanciering voor en na de implementatie van
de JKN-KIS worden beschreven. Bovendien wordt de prognose van
financieringsregelingen voor de gezondheidszorg ook verlengd tot 2030, als agenda
voor het jaar van doelstellingen voor duurzame ontwikkeling. We stelden vast dat de
doelstelling om UHC tegen 2020 te halen niet gehaald zal worden. De doelstelling
om de OOP-regelingen voor huishoudens onder de 20% te verminderen, kan tegen
2024 worden bereikt. De doelstelling om de vrijwillige betaling voor
gezondheidszorg tot minder dan 10% te verminderen, kan tegen 2021 worden
bereikt. Belangrijk is dat de overheidsregelingen en verplichte bijdragende
Samenvatting

190 | Moving Forward to Achieve Universal Health Coverage in Indonesia
regelingen voor gezondheidsfinanciering nog steeds ver weg blijven van 4% van het
BBP tegen 2020. Verder ontdekten we ook dat in het eerste jaar van de
implementatie van JKN-KIS de uitgaven van de BPJS-Kesehatan stegen van $ 2,0
miljard (8,52% van totale uitgaven gezondheidszorg) tot $ 4,0 miljard (14,25%). Dit
leidde ertoe dat de OOP-regelingen per huishouden afnamen tot US $ 1,5 miljard
(7%). Het verhogen van de uitgaven voor sociale verzekeringen en het verminderen
van OOP is de juiste koers voor het bereiken van UHC. We ontdekten echter dat de
inkomsten van de BPJS-Kesehatan niet voldoende waren om hun uitgaven te
dekken. Dit leidde ertoe dat de BPJS-Kesehatan sinds de implementatie in het eerste
jaar voortdurend een tekort ontwikkelde.
In hoofdstuk 5 schatten we de CVD-belasting op lange termijn en
risicofactoren in Aziatische populaties door middel van een systematische review.
De belangrijkste resultaten waren dat mannelijk geslacht, oudere leeftijd en het
huidige roken de meest prominente risicofactoren zijn voor fatale HVZ op lange
termijn bij de Aziatische bevolking. In onze systematische review vonden we studies
uit Indonesië niet in overeenstemming met de inclusiecriteria van onze studies
(cohortstudies, Aziatisch gezond boven 18 jaar, vrij van HVZ, 10 jaar follow-up
periode). Onze bevindingen ewaren dat op langer termijn een stijgende incidentie te
verwachten is. Aangezien er geen informatie beschikbaar is over de risicofactoren
op lange termijn van fatale HVZ in Indonesië, kan dit resultaat worden gebruikt als
een referentie om te erkennen dat roken de wijzigende risicofactor van CVD's is. Dit
kan worden beïnvloed door verschillende interventies om de mortaliteit van hart- en
vaatziekten in Indonesië te verminderen en de financiële last van de BPJS-
Kesehatan te verminderen.
In hoofdstuk 6 presenteren we de algemene discussie van dit proefschrift.
We beginnen met het overzicht om te beschrijven hoe JKN-KIS de drie belangrijkste
uitdagingen is tegengekomen. Vervolgens biedt het toekomstperspectief
beleidsopties om de uitdagingen aan te gaan; en verder onderzoek nodig om UHC te
verbeteren. Vervolgens leggen we uit hoe dit proefschrift mogelijk richting geeft aan
Indonesië en andere landen. Ten slotte is de conclusie van dit proefschrift dat JKN-
KIS de hoeksteen is voor Indonesië om UHC te bereiken in overeenstemming met
Addendum

Moving Forward to Achieve Universal Health Coverage in Indonesia | 191
de WHO-doelen. Het verbeteren van de efficiëntie en het verhogen van financiële
middelen voor de gezondheid zijn echter noodzakelijk voor de JKN-KIS om
verschillende uitdagingen aan te pakken die momenteel de verwezenlijking van
UHC belemmeren.
Samenvatting

192 | Moving Forward to Achieve Universal Health Coverage in Indonesia
RINGKASAN
Negara yang tergabung dalam Perserikatan Bangsa-Bangsa (PBB) telah
berkomitmen untuk mencapai cakupan kesehatan universal (UHC) sebagai bagian
dari tujuan pembangunan berkelanjutan 2030. Organisasi kesehatan dunia (WHO)
menyatakan bahwa UHC tercapai di suatu negara ketika semua masyarakatnya dapat
mendapatkan pelayanan kesehatan berupa promotif, preventif, kuratif, rehabilitatif
dan paliatif, dengan kualitas yang tinggi, tanpa membuat masyarakat terpapar
kesulitan membayar ketika menerima pelayanan tersebut. WHO menjelaskan
indikator UHC tercapai oleh suatu negara ketika pembiayaan kesehatan dari kantong
masyarakat (OOP) turun di bawah 20% dari total pembiayaan kesehatan suatu
negara. WHO juga mendesak setiap negara yang ingin mencapai UHC agar
pembiayaan kesehatan dari pemerintah harus mencapai setidaknya 4% dari produk
domestik bruto.
Sebagai anggota dari PBB, Indonesia bertujuan untuk mencapai UHC.
Pencapaian target UHC semakin didukung oleh Undang-Undang Dasar 1945, pasal
28, yaitu kesehatan adalah hak dasar setiap individu, dan semua warga negara
berhak atas layanan kesehatan termasuk orang miskin. Pada awal 2014, pemerintah
Indonesia secara resmi mengumumkan rencana mereka untuk mencapai UHC
sebelum tahun 2020 melalui asuransi kesehatan nasional baru, yang dikenal sebagai
Jaminan Kesehatan Nasional-Kartu Indonesia Sehat (JKN-KIS). Program ini
dikelola oleh program asuransi kesehatan baru, yang disebut Badan Penyelenggara
Jaminan Sosial-Kesehatan (BPJS-Kesehatan). JKN-KIS adalah hasil dari
penggabungan skema asuransi kesehatan sosial yang sudah ada sebelumnya. Skema
asuransi kesehatan yang terfragmentasi membuat pengeluaran perawatan kesehatan
dan kualitas layanan kesehatan sulit dikendalikan.
Sebelum pelaksanaan JKN-KIS, ada beberapa masalah kesehatan yang
belum terselesaikan, yaitu pada manajemen obat-obatan, pembiayaan kesehatan, dan
situasi epidemiologis di Indonesia. Dalam manajemen obat-obatan, proporsi OOP
untuk obat-obatan tinggi, berkisar lebih dari 50% dari total pengeluaran kesehatan.
Selanjutnya, pengeluaran obat-obatan mencapai 67% dari total pengeluaran
Moving Forward to Achieve Universal Health Coverage in Indonesia | 193
kesehatan. Mengenai pembiayaan kesehatan, pemerintah Indonesia mengalami
kesulitan untuk meningkatkan pengeluaran kesehatan di tingkat nasional. Alih-alih
mengandalkan pembiayaan kesehatan dari pemerintah, Indonesia didominasi oleh
pembiayaan kesehatan dari masyarakat. Dalam hal situasi epidemiologis, angka
harapan hidup yang meningkat menyebabkan proporsi orang meninggal karena
penyakit tidak menular mencapai hampir dua kali lipat, yaitu dari 37% pada tahun
1990 menjadi 73% pada tahun 2014. Dari semua penyakit tidak menular, penyakit
kardiovaskular adalah penyebab utama kematian dan kecacatan.
Tujuan tesis ini adalah untuk mengevaluasi perkembangan JKN-KIS dalam
melangkah menuju pencapaian UHC di Indonesia. Terutama, untuk memberikan
temuan komprehensif tentang bagaimana JKN KIS telah menghadapi tiga tantangan
utama pada manajemen obat-obatan, pembiayaan kesehatan, dan situasi
epidemiologis. Dalam bab 1, kami menjelaskan secara singkat mengenai konsep
UHC menurut WHO. Kemudian, penjelasan tentang transformasi sistem kesehatan
Indonesia menuju UHC, dan tantangan potensial mereka untuk mencapai UHC
sebelum tahun 2020. Selanjutnya, gap terhadap pengetahuan dan tujuan tesis
disajikan pada bab 1.
Dalam bab 2, kami melakukan wawancara semi terstruktur untuk
mengidentifikasi masalah e-katalog dan formularium nasional (fornas). Ini adalah
dua instrumen kebijakan baru yang mengatur penentuan harga dan penggantian
biaya obat selama implementasi JKN-KIS. Idealnya, e-katalog membantu
meningkatkan efektivitas, efisiensi, dan transparansi dalam pengadaan obat-obatan
pada fasilitas kesehatan. Sementara fornas membantu memastikan ketersediaan obat-
obatan yang berkualitas baik, manjur dan terjangkau. Oleh karena itu, kebijakan ini
seharusnya membantu JKN-KIS untuk mengontrol pengeluaran obat-obatan dan
mengurangi OOP untuk obat-obatan, sehingga dapat mencapai UHC. Namun,
setahun setelah implementasi, banyak fasilitas kesehatan umum jarang
menggunakan e-katalog untuk pengadaan obat-obatan, dan 40% dari semua obat
yang diresepkan tidak terdaftar dalam fornas. Kami menemukan bahwa masalah
utama adalah kurangnya harmonisasi antara obat-obatan yang tercantum dalam e-
katalog dan fornas. Kemudian, alasan utama dokter ketika meresepkan obat-obatan
Addendum
194 | Moving Forward to Achieve Universal Health Coverage in Indonesia
di luar fornas adalah kurangnya transparansi dan basis bukti dalam pengembangan
fornas.
Dalam Bab 3, kami mengidentifikasi faktor penghambat dan pendukung
penerapan penilaian teknologi kesehatan (HTA) dalam mengembangkan e-katalog
dan fornas. Komite HTA ditunjuk oleh Menteri Kesehatan Indonesia beberapa bulan
setelah implementasi JKN-KIS. Idealnya, komite HTA dapat menyediakan bukti
ilmiah dan transparansi pengembangan e-katalog dan fornas sesuai dengan pedoman
pelaksanaan JKN-KIS. Namun, HTA belum menjadi bagian dari pengembangan e-
katalog dan fornas. Beberapa hambatan implementasi HTA dalam e-katalog dan
fornas adalah kurangnya kapasitas, kurangnya insentif keuangan, kurangnya
kerangka kerja yang jelas dan data yang tidak mencukupi. Dua hambatan pertama
merupakan hambatan yang paling utama. Alasan kurangnya kapasitas karena HTA
adalah ilmu baru di Indonesia, dan hanya sedikit departemen HTA yang tersedia,
pelatihan formal tidak disediakan secara nasional, dan asosiasi resmi tidak ada di
Indonesia. Selanjutnya, sumber daya keuangan akan diperlukan untuk membayar
para ahli HTA, untuk mengatur seminar HTA, dan melakukan penelitian HTA.
Dalam bab 4, kami melakukan penilaian terhadap pembiayaan kesehatan
UHC di Indonesia. Ini untuk memahami apakah Indonesia telah mengatur sistem
pembiayaan kesehatannya sesuai dengan target UHC. Tren pembiayaan kesehatan
sebelum dan sesudah implementasi JKN-KIS dijelaskan pada bab ini. Selain itu,
proyeksi skema pembiayaan kesehatan juga dibuat hingga 2030, target tahun
pencapaian tujuan pembangunan berkelanjutan. Kami menemukan bahwa target
untuk mencapai UHC sebelum tahun 2020 tidak akan tercapai. Target untuk
mengurangi skema OOP < 20% dapat dicapai pada tahun 2024. Target untuk
mengurangi pembiayaan kesehatan privat < 10% dapat dicapai pada tahun 2021.
Yang paling utama adalah skema pembiyaan kesehatan pemerintah masih akan jauh
dari 4% PDB sebelum tahun 2020. Selanjutnya, kami juga menemukan bahwa pada
tahun pertama implementasi JKN-KIS, pengeluaran BPJS-Kesehatan meningkat
secara signifikan dari US $ 2,0 miliar (8,52% dari THE) menjadi US $ 4,0 miliar
(14,25% dari THE). Hal ini menyebabkan skema OOP oleh rumah tangga menurun
menjadi US $ 1,5 miliar (7% dari THE). Meningkatkan pengeluaran asuransi
Ringkasan

Moving Forward to Achieve Universal Health Coverage in Indonesia | 195
kesehatan sosial dan mengurangi OOP adalah kemajuan yang tepat untuk mencapai
UHC. Namun, kami menemukan bahwa pendapatan BPJS-Kesehatan tidak cukup
memadai untuk memenuhi pengeluaran mereka. Hal ini membuat BPJS-Kesehatan
terus mengembangkan defisit sejak implementasi tahun pertama.
Dalam Bab 5, kami memperkirakan beban penyakit kardiovaskular (CVD)
jangka panjang dan faktor risiko pada populasi Asia melalui tinjauan sistematis.
Hasil yang paling penting adalah bahwa jenis kelamin laki-laki, usia yang lebih tua,
dan perokok adalah faktor risiko yang paling menonjol untuk CVD jangka panjang
pada populasi Asia. Dalam tinjauan sistematis ini, kami tidak menemukan studi dari
Indonesia sesuai dengan kriteria inklusi studi kami (studi kohort, orang Asia yang
sehat di atas 18 tahun, bebas dari CVD, 10 tahun masa tindak lanjut). Khususnya,
kriteria inklusi kami dapat memperoleh tingkat insiden jangka panjang pada
populasi umum. Mengingat tidak tersedianya informasi mengenai faktor risiko
jangka panjang dari CVD fatal jangka panjang di Indonesia, hasil ini dapat
digunakan sebagai referensi untuk mengetahui bahwa perokok adalah faktor risiko
CVD yang dapat dirubah. Oleh karena itu, ini dapat dipengaruhi melalui berbagai
intervensi untuk mengurangi angka kematian akibat CVD di Indonesia dan untuk
mengurangi beban keuangan BPJS-Kesehatan.
Dalam bab 6, kami menyajikan diskusi umum dari tesis ini. Kami mulai
dengan ikhtisar untuk menggambarkan bagaimana JKN-KIS telah menghadapi tiga
tantangan utama utama. Kemudian, pada perspektif masa depan, kami akan
menawarkan opsi kebijakan untuk mengatasi tantangan, dan penelitian lebih lanjut
diperlukan untuk meningkatkan UHC. Kemudian kami akan menjelaskan bagaimana
tesis ini memberikan panduan yang memungkinkan untuk Indonesia dan negara-
negara lain. Akhirnya, kesimpulan dari tesis ini adalah bahwa JKN-KIS adalah
landasan bagi Indonesia untuk mencapai UHC yang sejalan dengan target WHO.
Namun, meningkatkan efisiensi dan meningkatkan sumber daya keuangan untuk
kesehatan adalah keharusan bagi JKN-KIS untuk mengatasi beberapa tantangan
yang saat ini menghambat pencapaian UHC di Indonesia.
Addendum

196 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Acknowledgement
“Feed two birds with one seed”, this proverb might describe me during the period I
was pursuing my PhD, marrying my love, and raising my kids in the last four years.
Therefore, I would like to send my greatest gratitude to Allah, the Almighty, who
mercifully bestows upon me health, strength, determination, and patience to
encounter these monumental occasions in the same period. I really enjoyed
experiencing these remarkable moments simultaneously because of precious support
from many parties. Hence, I would like to sincerely express my gratitude in these
pages to all people and institutions for their contributions during my tremendous journey.
To start, I would like to pay my special regards to my supervisors, and co-
supervisors. Mostly, I would like to thank you for your flexibility and for allowing
me to develop my research ideas. I realize my research, especially in data collection,
was costly, time consuming, and ambitious. But, your financial assistance, followed by your comprehensive supervision, made my goals achievable.
Prof. Erik Buskens, you are the one who contributed in all stages of my PhD
trajectory. I am really grateful because you always provided me the opportunity to
confide both my academic and personal matters. Your intelligent advice, and
especially wise encouragements you delivered to me during our weekly meetings
always increased my confidence. Most importantly, I was always glad to receive
your feedback on manuscripts, cover letters for the journals, and so on. Sentences
will change like written by a highly professional writer. One unforgettable moment
was when preparing my oral presentation for attending ISPOR 2018 conference. I
am indebted since you helped me to create a professional slide set and speech.
Lastly, I sincerely appreciate the availability of your time for me, even though you recently were in mourning for your father's death.
Prof. Maarten Postma, you are the first person that I encountered in Groningen. I
remember when nominated as a DIKTI scholarship awardee. Then, I was required to
to submit a letter of acceptance as soon as possible. In three days, you helped me to
obtain it. Furthermore, my fortune was that you gave me another desk in PTEE
instead of just the one in Epidemiology. This allowed me to meet with other
forgoing Indonesians, expecting they could help me to avoid becoming homesick
and familiarize me with the Dutch culture. Most importantly, I am glad to your
creative solutions in dealing with my academic and personal matters. So, thank you
very much for giving me a chance as your PhD student, helping me to get started on
PhD, and always providing me meaningful ways to accomplish my PhD journey.
Dr. Wim Goettsch, I remember the first time we met at the Dutch National Health
Care Institute in Diemen. You provided me an important reference to develop a
framework for my first and second research project. You also connected me to Amr
Makady, to help me analyze the qualitative data and run the qualitative study tool.
So, thank you for collaborating on my two studies and for accepting to be my co-
promoter in your busy time. Collaborating with the special advisor HTA at the

Moving Forward to Achieve Universal Health Coverage in Indonesia | 197
Dutch National Health care Institute will be certainly worthwhile, and great for my future networking.
Dr. Talitha Feenstra, the first two years of my PhD journey were the most difficult
period. Lucky me to have you as my daily supervisor in these days. You
passionately explained me several basic research skills, such as searching references
in PubMed, writing reports to the supervisors, and scheduling my research project.
Your strict and intensive supervision helped me to be a disciplined and independent
researcher for the next two years of my PhD period. So, thank you very much for the valuable technical skills that you provided to me.
I would like to express my profound gratitude to my research collaborators: Prof.
Ali Ghufron Mukti, Silvy Irawati, Jurjen Van der Schans, and Amr Makady, for their analytical assistances, and meaningful feedback on my manuscripts.
I would also thank the assessment committee: Prof. Menno Reijneveld, Prof.
Katja Taxis, and Prof. Aukje Mantel for providing me their valuable time, particularly during the COVID 19 pandemic to read and appraise my thesis.
I am also truly thankful to the staff of the Epidemiology Department: Erwin, Aukje,
Lizette, and Gerben, and the staff of PTEE unit in the Pharmacy Department: Jannie, Bert, and, Hugo, for their practical and technical support.
I also thank my friends and colleagues in the PTEE unit: Prof. Bob Wilffert, Prof.
Eelko Hak, Abraham, Mas Adjie, Mbak Afifah, Kak Akbar, Christian, Mas
Didik, Eva, Kak Ira, Mas Ivan, Jurjen, Mas Khairul, Linda, Mbak Lusi, Mbak
Neily, Nynke, Pepijn, Pieter, Qi, Simon, Mbak Sofa, Mbak Sylvi, Taichi, Tanja,
Mbak Tia, Kak Ury, Yuan; in the Patient-Centered HTA Unit: Paul, Thea, Henk,
Maarten, Karin, Sander, Koen, Ariuntuya, Ahmed, Kaying; and in the
Epidemiology Department: Omar, Pato, Reinder, Katri; you all brightened my
PhD journey through scientific talks in our group meetings, and spontaneous conversation on any occasion.
I would like to express my deepest thanks to Kak Ury for provoking me to pursue
my PhD at the University of Groningen, teaching me life skills, portraying me the Dutch academic atmosphere, and sharing your badminton techniques to me.
I would like to send my sincere thanks to Kak Akbar for being a big brother to me
in Groningen and allowing me to have chitchat every time. Most importantly, your
wife Andis, and son Abdullah, have become close friends for my wife and children.
I and my family are now counting down the days for a lot of wonderful moments we
will create in Makassar.
My deepest gratitude also goes to Pak Asmoro and family as well as Kak Habibie
and family for accompanying my wife while delivering my second kids in the
UMCG Hospital. At that time I was also expected to deliver my presentation in the study group meeting and then pick my family up at the airport thereafter.
Addendum

198 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Being a thousand miles from home to pursue my PhD and build my new sweet
household feels easier with all friendship from the Indonesian student association in
Groningen and the Groningen Indonesian Moslem community. Therefore, I would
like to sincerely thanks them all who made Groningen become my second home.
Budhe Nunung-Pakde Zaid, Oom Herman-Budhe Arie, Oom Weno-Uwak Asiyah,
Oom Archie-Tante Mary. Mas Didik Setiawan and family, Mas Amak and family,
Mas Zaki Almuzakki and Family, Mas Surya and Family, Mas Ali Syariati and
Family, Mas Mega and Family, Mas Joko and family, Mas Azkario, Mbak May,
Mbak Dina, Mas Adhyatmika and family, Mas Kuswanto and Family, Bli Kadek
and Family, Mas Zainal and Family, Mas Azis and family, Mbak Nur Qomariah,
Mas Fajar and family, Mas Khairul and family, Mas Ivan and family, Mas Yudi
and Family, Mbak Nuriel, Mas Ristiono and family, Mas Didin and family, Mas
Latief and family, Mas Krisna and family, Mas Hegar and family, Mas Azkamuji
and family, Mas Luthfi, Mas Guntur, Mas Yoga, Mas Ade and family, Mas Agung
and family, Mas Fika and family, Mas Chalis and family, Mas Afif, Mas Bhimo,
Mbak Inda and Family, Mas Umar Djalins, Mas Ajie Mahar, Mas Fean, Mas
Lana and family, Mas Ali Abdurrahman and family, Adzkia, Ibu Neno Purba,
Fathki, Stephanie, Yessaya, Kinanti, Inez, Sarah, Afra, Laras, Mas Rifki, Kang
Angga, Mas Romy and family, Kang Deny and all my Indonesian friends who could not be listed in this acknowledgement.
I also credit my house landlord, Mr. Sulaiman Surie for providing me a house for
living with my family which is close to the UMCG. This helps me to be flexible to do my work and check my little family during lunchtime.
I would also like to express my deepest gratitude to those who have provided me
motivation and their sincere prayers for my PhD life: Bapak Anies Rasyid
Baswedan (Governor of DKI Jakarta), Bapak Prof. Nurdin Abdullah (Governor of
South Sulawesi), Bapak Syahrul Yasin Limpo (Indonesia‘s Minister of
Agriculture), Bapak Agus Arifin Nu'mang (ex-vice governor of South Sulawesi),
Bapak Aksa Mahmud, Bapak AGH Sanusi Baco, and all people attending at my salvation event to start my PhD trajectory.
Finally, I wish to express my deepest gratitude to my beloved family for giving me
extraordinary motivation. The unforgettable moments when you all repeatedly drove
me to the airport accompanied by your heartfelt tears. These moments continuously
crossed to my mind in all my activities in Groningen. Hence, I dedicate this thesis to all of you and hopefully, this answers all your prayers and wishes.
To my parents (Bapak and Mama): Prof. Wasir Thalib and Ummu Kalsum, as
well as my parent in law (Papa and Ibu): Prof. Sidin Ali and Hafsah Usman, I
consider myself nothing without you. Thank you so much for your endless love,
sincere unceasing prayer, moral and financial support to me. Most importantly, I pay
my deepest gratitude for helping me to take care of my wife, son, and daughter in
the last year of my PhD. So that I only pay attention to my PhD journey without any obstacle in the way.
Acknowledgement

Moving Forward to Achieve Universal Health Coverage in Indonesia | 199
To my siblings: Kak Rika Fatimah Wasir, Kak Rizqurrachman Wasir, Rina
Wahyuni Wasir; my brother and sister in law: Kak Ikrar Sakti Yusuf, Kak
Wahida Masrah, Andi Agung Yasser, My nephews, and nieces: Iffat, Dzakiyah,
Adzkia, Fakhri, Farzan, Rafassya, Radeva. My wife‘s siblings (also in law): Kak
Risna Sari, Kak Irwan Rais, Kak Tri hastiti Fiskawarni, Kak Zulhajji Hamid;
and my wife‘s nephews, and nieces: Sadam, Zaky, Fildzah, Fairah, I am very
pleased for your time to take care of Bapak and Mama, as well as Papa and Ibu when I was not in Indonesia.
To my beloved wife, Fadilah Aulia Rahma, accepting me as your husband in the
first year of my PhD, and, subsequently, living with me in Groningen was a
remarkable moment in my life. As a youngest and carefree child of Papa and Ibu,
with a strong determination to be a doctor, I never thought you would actualy leave
your comfort zone and your ideals. Most importantly, you were willing to give birth
to our kids in Groningen, without being accompanied by extended family, as is
common in Indonesia. Amazingly, in addition to fulltime caring for our two kids,
you provided me delicious foods and tidied my clothes up every day to ensure my
nutrition and appearance during my research work. So, thank you very much for
devoting your quality time, and your career to allow me to pursue my PhD, and
raising our kids. I owe you everything. Therefore, I dedicate this thesis and of course the rest of my life to you.
To my kids, Muhammad Mikail Davian Riswandy and Mikhayla Maritza
Riswandy, your smiles and funny reactions always relieve my stress and booster my
spirit to write my manuscripts. Importantly, you both foster my self-awareness to
make the best use of time during Pursuing my PhD. So, thank you for providing
quality time for me during my PhD Journey and for expressing to me that I should
obtain value in every single activity. I apologize for leaving you both for a while in Indonesia. Surely, we will have our quality time again.
Ministry of research and higher education, thank you for providing me a DIKTI
scholarship. Without your funding I would not have been able to develop my scientific competence and discoveries in four years.
Last but not least, I am grateful to all people who contributed to my PhD projects
that cannot be listed one by one in this acknowledgment. Thank you very much!
Groningen, April 2020
Riswandy Wasir
Addendum

200 | Moving Forward to Achieve Universal Health Coverage in Indonesia
PHD PORTOFOLIO
Personalia
Name : Riswandy Wasir
Gender : Male
Place and Date of Birth : Makassar, 12 January 1988
Nationality : Indonesian
E-mail : [email protected]
Department of PhD : Epidemiology, University Medical Center Groningen
PhD Period : December 2015-Mei 2020 (4 years, 6 months)
Promotors : Prof. Dr. Erik Buskens
Prof. Dr. Maarten Postma
Co-Promotors : Dr. Wim Goettsch
List of Publications
Wasir R, Irawati S, Makady A, Postma MJ, Goettsch W, Feenstra T, Buskens E
(2018). Use of medicine policies for universal health coverage in Indonesia. Value
in Health, 21(3), S1, October, 2018. DOI: https://doi.org/10.1016/j.jval.2018.09.004
Wasir R, Irawati S, Makady A, Postma MJ, Goettsch W, Feenstra T, Buskens E
(2018). Barriers to and facilitators of the application of health technology
assessment in medicine pricing and reimbursement policies in Indonesia. Value in
Health, Volume 21, S184, October, 2018. DOI:
https://doi.org/10.1016/j.jval.2018.09.1099
S Irawati S, R Wasir R, Schimdt AF, Islam A, Feenstra T, Buskens E, Wilfert B, E
Hak (2019). Long term risk of incidence of cardiovascular events in Asian
Populations. Systematic review and Meta-Analysis of Population-Based Cohort
Studies. Current Medical research and opinion, 35(2), 291-299. DOI:
https://doi.org/10.1080/03007995.2018.1491149
Wasir R, Irawati S, Makady A, Postma MJ, Goettsch W, Buskens E, Feenstra T
(2019). Use of medicine pricining and reimbursement policies for universal health
coverage in Indonesia. PloS ONE, 14(2), [e0212328]. February, 2019 DOI:
https://doi.org/10.1371/journal.pone.0212328
Wasir R, Irawati S, Makady A, Postma MJ, Goettsch W, Feenstra T, Buskens E
(2019). The implementation of HTA in medicine pricing and reimbursement policies
in Indonesia: Insight from multiple stakeholders. PloS ONE, 14(11), [e022565626].
November, 2019 DOI: https://doi.org/10.1371/journal.pone.0225626
Moving Forward to Achieve Universal Health Coverage in Indonesia | 201
Wasir R, Postma MJ, van der Schans J, Mukti AG, Buskens E (2019).
Implementation of universal health coverage in Indonesia. Value in Health, 22(3),
S782, November, 2019. DOI: https://doi.org/10.1016/j.jval.2019.09.2024
Wasir R, Postma MJ, van der Schans J, Mukti AG, Buskens E. Trends and projection of
health financing for universal health coverage in Indonesia. (Submitted)
Irawati S, Wasir R, Bahar MA, Hak E, Wilffert, B, Taxis K, Postma MJ, Buskens
E, The burden of cardiovascular disease and trend of claim reimbursement for statin
prescription in Indonesia after the implementation of the National Health Insurance
(Jaminan Kesehatan Nasional, JKN) 2014-2016 (In preparation)
Wasir R, Postma MJ, van der Schans J, Buskens E. Health and economic
implications of national treatment coverage for cardiovascular disease in Indonesia:
an estimation of the return on investment on statin (In preparation)
Scientific Conferenes
Wasir R, Feenstra T, Postma MJ, Goettsch W, Buskens E. The role of a health
technology assessment in medicine policy to enable universal health coverage in low
middle-income countries: Indonesia as a reference case. The 3rd InaHEA conference,
July 28-30th, 2016, Yogyakarta, Indonesia. (Poster presentation).
Wasir R, Irawati S, Makady A, Postma MJ, Goettsch W, Feenstra T, Buskens E
(2018). Use of medicine pricing and reimbursement policies for universal health
coverage in Indonesia. International Society for Pharmacoeconomics and Outcomes
Research (ISPOR) Europe 2018, New Perspective for improving 21st Century health
system. 10-14 November 2018, Barcelona, Spain. (Oral Presentation)
Wasir R, Irawati S, Makady A, Postma MJ, Goettsch W, Feenstra T, Buskens E
(2018). Use of medicine pricing and reimbursement policies for universal health
coverage in Indonesia. International Society for Pharmacoeconomics and Outcomes
Research (ISPOR) Europe 2018, Student research spotlight. 10-14 November 2018,
Barcelona, Spain. New Perspective for improving 21st Century health system. 10-14
November 2018, Barcelona, Spain. (Poster Presentation)
Wasir R, Irawati S, Makady A, Postma MJ, Goettsch W, Feenstra T, Buskens E
(2018). Barriers to and facilitators of the application of health technology
assessment in medicine pricing and reimbursement policies in Indonesia.
International Society for Pharmacoeconomics and Outcomes Research (ISPOR)
Europe 2018, New Perspective for improving 21st Century health system. 10-14
November 2018, Barcelona, Spain. (Poster Presentation)
Wasir R. Experience on the first event of ISPOR student research spotlight.
Webinar Presidents Teleconference. November 2018. (Panelists)
Wasir R, Postma MJ, van der Schans J, Mukti AG, Buskens E. Trend and
Projection on financial protection for universal health coverage in Indonesia. The
Addendum

202 | Moving Forward to Achieve Universal Health Coverage in Indonesia
13th Post Graduate Forum on Health System and Health Policy. Medical specialist
within the Health System in Asia: A perspective on production and utilization. 19-20
July 2019, Yogyakarta, Indonesia. (Poster Presentation)
Wasir R, Postma MJ, van der Schans J, Mukti AG, Buskens E. Implementation of
universal health coverage in Indonesia. International Society for Pharmacoeconomics
and Outcomes Research (ISPOR) Europe 2019. Digital transformation of Healthcare. 2-
6 November 2019, Copenhagen, Denmark. (Poster Presentation)
Awards Nominations
Top outcomes research at International Society for Pharmacoeconomics and
Outcomes Research (ISPOR) Europe 2018, New Perspective for improving 21st
Century health system. 10-14 November 2018, Barcelona, Spain
Top-3 Poster Prize at the 13th Post Graduate Forum on Health System and Health
Policy. Medical specialist within the Health System in Asia: A perspective on
production and utilization. 19-20 July 2019, Yogyakarta, Indonesia
PhD level courses taken
Courses Year Workload
Academic Writing 2016 2 ECTS
PhD Introductory Event 2016 1 ECTS
Pharmacoeconomics 2016 5 ECTS
Qualitative Data Collection and Analysis 2016 5 ECTS
Ethics of Research and Scientific Integrity for Researchers 2017 2,5 ECTS
Managing your PhD 2017 2 ECTS
Presentation Skills 2018 2 ECTS
Publishing in English 2018 2 ECTS
Budget Impact Analysis I: A 6-Step Approach at ISPOR
Europe, Barcelona, Spain
2018 5 hours
Budget Impact Analysis II: Application and Design Issues at
ISPOR Europe, Barcelona, Spain
2018 5 hours
Introduction to Modelling at ISPOR Europe, Copenhagen,
Denmark
2019 5 hours
Statistical Methods for Health Economics and Outcomes
Research at ISPOR Europe, Copenhagen, Denmark
2019 5 hours
Bayesian Analysis: Overview and Applications at ISPOR
Europe, Copenhagen, Denmark
2019 10 hours
PhD Portofolio
Moving Forward to Achieve Universal Health Coverage in Indonesia | 203
About the Author
Riswandy Wasir was born on January 12th, 1988 in
Makassar, South Sulawesi, Indonesia. He is the third
son of four children from Ayahanda Prof. Dr. H. M.
Wasir Thalib, MS and Ibunda Dra. Hj. Ummu Kalsum
Ali Tadjo. His primary, secondary and tertiary school
was obtained in Makassar, which are respectively in
SD Negeri Kompleks IKIP, SMP Negeri 6 and SMA
Negeri 3. He obtained a Bachelor of Pharmacy at
Universitas Muslim Indonesia (UMI), a Pharmacist
certificate at Universitas Islam Indonesia (UII) and a Master of Public Health at the
University of Gadjah Mada (UGM). In December 2015, He started his PhD
trajectory at the unit of Patient-Centered Health Technology Assessment (HTA),
Epidemiology Department, University Medical Center of Groningen (UMCG),
University of Groningen, Groningen, the Netherlands under the supervision of Prof.
Dr. Erik Buskens, Prof. Dr. Maarten Postma and Dr. Wim Goettsch. His PhD project
focused on the health policy strategies to enable countries (in particular Indonesia)
to achieve universal health coverage as part of the sustainable development goals.
His study is funded by the Ministry of Research, Technology and Higher Education
of the Republic of Indonesia under the scheme of DIKTI scholarship. During his
PhD trajectory, he has published his studies in international peer-reviewed journals
and also actively presented his studies at international conferences. One of his
studies was nominated for top outcomes research at the International Society for
Pharmacoeconomics and Outcomes Research (ISPOR) Europe 2018, in Barcelona,
Spain. He was also awarded a top-3 poster prize at the 13th Post Graduate Forum on
Health System and Health Policy, in Yogyakarta, Indonesia. Currently, he continues
his career as a lecturer and researcher at the Sekolah Tinggi Ilmu Farmasi (STIFA)
Makassar, Makassar, South Sulawesi, Indonesia. His research interests are in the
areas of universal health coverage and health policy, particularly in policies in
medicine management. He married his beloved wife Fadilah Aulia Rahma, a
youngest and carefree child of Prof. Dr. H. M. Sidn Ali, M.Pd and Dra. Hj. Hafsah
Usman, M.Pd. The marriage of Riswandy and Fadilah has been blessed with two
beloved children, Muhammad Mikail Davian Riswandy and Mikhayla Maritza
Riswandy. Their kids were both born in Groningen in the period of pursuing a PhD
of Riswandy Wasir.
Addendum

204 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Tentang Penulis
Riswandy Wasir lahir pada 12 Januari 1988 di
Makassar, Sulawesi Selatan, Indonesia. Dia adalah
putra ketiga dari empat bersaudara dari pasangan
Ayahanda Prof. Dr. H. M. Wasir Thalib, MS dan
Ibunda Dra. Hj. Ummu Kalsum Ali Tadjo. Sekolah
dasar, menengah pertama dan menengah atas diperoleh
di Makassar, yang masing-masing di SD Negeri
Kompleks IKIP, SMP Negeri 6 dan SMA Negeri 3. Ia
memperoleh gelar Sarjana Farmasi di Universitas
Muslim Indonesia (UMI), sertifikat Apoteker di
Universitas Islam Indonesia (UII) dan Magister
Kesehatan Masyarakat di Universitas Gadjah Mada (UGM). Pada Desember 2015,
dia memulai perjalanan PhD-nya di Unit Patient-Centered Health Technology
Assessment (HTA), Epidemiology Department, University Medical Center of
Groningen (UMCG), University of Groningen, Groningen, Belanda di bawah
pengawasan Prof. Dr. Erik Buskens, Prof. Dr. Maarten Postma dan Dr. Wim
Goettsch. Proyek PhD-nya berfokus pada strategi kebijakan kesehatan untuk
memungkinkan negara, khususnya Indonesia, untuk mencapai cakupan kesehatan
universal (Universal Health Coverage, UHC), yang merupakan bagian dari tujuan
pembangunan berkelanjutan. Studinya didanai oleh Kementerian Riset, Teknologi,
dan Pendidikan Tinggi, Republik Indonesia di bawah skema beasiswa DIKTI.
Selama perjalanan PhD, dia telah menerbitkan beberapa artikel di jurnal
internasional bereputasi tinggi dan juga aktif mempresentasikan penelitiannya di
konferensi internasional. Salah satu penelitianya dinobatkan sebagai penelitian
dengan luaran terbaik pada International Society for Pharmacoeconomics and
Outcomes Research (ISPOR) Europe 2018, di Barcelona, Spanyol. Dia juga
dianugerahi sebagai presenter poster terbaik ke 3 di Post Graduate Forum on Health
System and Health Policy ke 13, di Yogyakarta, Indonesia. Saat ini, dia melanjutkan
karirnya sebagai dosen dan peneliti di Sekolah Tinggi Ilmu Farmasi (STIFA)
Makassar, Makassar, Sulawesi Selatan, Indonesia. Minat penelitiannya adalah di
bidang universal health coverage dan kebijakan kesehatan, terutama dalam
kebijakan manajemen obat-obatan. Dia menikahi gadis pujaan hatinya Fadilah Aulia
Rahma, putri bungsu yang riang dari Prof. Dr. H. M. Sidn Ali, M.Pd dan Dra. Hj.
Hafsah Usman, M.Pd. Pernikahan Riswandy dan Fadilah telah dikaruniai dua anak
kesayangan, Muhammad Mikail Davian Riswandy dan Mikhayla Maritza Riswandy.
Anak-anak mereka berdua lahir di Groningen ketika Riswandy Wasir sedang
mengejar gelar PhDnya.
PhD Portofolio

Moving Forward to Achieve Universal Health Coverage in Indonesia | 205
Research Institute SHARE
This thesis is published within the Research Institute SHARE (Science in
Healthy Ageing and healthcaRE) of the University Medical Center Groningen /
University of Groningen.
Further information regarding the institute and its research can be obtained from our internet
site: http://www.share.umcg.nl/
More recent theses can be found in the list below. (supervisors are between brackets)
2020
Renting N
Clinical workplace learning today; how competency frameworks inform
clinical workplace learning (and how they do not)
(prof ROB Gans, prof ADC Jaarsma, prof JCC Borlefs)
Kramer T
How to develop a Grand Slam winner…; physical and psychological skills in
Dutch junior tennis players
(dr MT Elferink-Gemser, prof C Visscher, dr BCH Huijgen)
Raven D
Where‘s the need? The use of specialist mental health services in adolescence
and young adulthood
(prof AJ Oldehinkel, prof RA Schoevers, dr F Jörg)
Stoter IK
Staying on track; the road to elite performance in 1500 m speed skating
(dr MT Elferink-Gemser, prof C Visscher, prof FJ Hettinga)
Silva Lagos LA
Gestational diabetes mellitus and fetoplacental vasculature alterations;
exploring the role of adenosine kinase in endothelial (dys)function
(dr MM Faas, prof T Plösch, prof P de Vos, prof L Sobrevia)
Reints R
On the design and evaluation of adjustable footwear for the prevention of
diabetic foot ulcers
(prof ir GJ Verkerke, porf K Postema, dr JM Hijmans)
Bekhuis E
A body-mind map; epidemiological and clinical aspects of the relation between
somatic, depressive and anxiety symptomatology
(prof JGM Rosmalen, prof RA Schroevers, dr L Boschloo)
Havinga PJ
Breaking the cycle? Intergenerational transmission of depression/anxiety and
opportunaties for intervention
(prof RA Schoevers, prof CA Hartman, dr L Boschloo)
Geer SJ van der
Trismus in head and neck cancer patients
(prof PU Dijkstra, prof JLN Rodenburg, dr H Reintsema)
206 | Moving Forward to Achieve Universal Health Coverage in Indonesia
Salavati N
Preconception environmental factors and placental morphometry in relation to
pregnancy outcome
(prof JJHM Erwich, prof RM van der Beek, dr MK Bakker, dr SJ Gordijn)
Fels IMJ van der
Movement, cognition and underlying brain functioning in children
(dr E Hartman, prof C Visscher, prof RJ Bosker, dr J Smith)
Braaksma P
Moving matters for children with developmental coordination
(prof R Dekker, prof CK van der Sluis, dr MM Schoemaker, dr I Stuive)
Akkerman M
Functioning beyong pediatric burns
(prof LHV van der Woude, dr LJ Mouton, dr MK Nieuwenhuis)
Buurke TJW
Adaptive control of dynamic balance in human walking
(dr CJC Lamoth, prof LHV van der Woude, dr AR den Otter)
Bos GJFJ
Physical activity and physical fitness in children with chronic conditions
(prof PU Dijkstra, prof JHB Geertzen)
Heugten P van
Talent in international business defined: implications and applications for
honours education
(prof ADC Jaarsma, dr MVC Wolfensberger, dr M Heijne-Pennninga)
Kranenburg HA
Adverse effects following cervical manual physical therapy techniques
(prof CP van der Schans, dr MA Schmidt, dr GJR Luijckx)
Lameijer CM
Perspectives on outcome following hand and wrist injury in non-osteoporotic
patients
(prof CK van der Sluis, prof HJ ten Duis, dr M El Moumni)
2019
Nijholt W
Gaining insight in factors associated with successful ageing: body composition, nutrition, and
cognition
(prof CP van der Schans, dr JSM Hobbelen, dr H Jager-Wittenaar)
Schaap FD
Dementia Care Mapping in the care for elderly people with an intellectual disability and
dementia
(prof SA Reijneveld, dr EJ Finnema, dr GJ Dijkstra)
For earlier theses visit our website




















